Regionalizing Acute Regionalizing Acute Stroke Care to Stroke Care to Specialized Centers: Specialized Centers: Hype or Help? Hype or Help? Lee H. Schwamm, MD Lee H. Schwamm, MD Professor of Neurology, Professor of Neurology, Harvard Medical Harvard Medical School School Director, TeleStroke & Acute Stroke Director, TeleStroke & Acute Stroke Services, Services, Massachusetts General Hospital Massachusetts General Hospital Chair Chair , , National Steering Committee, National Steering Committee, AHA/ASA AHA/ASA GWTG GWTG QCOR 2010

Regionalizing Acute Stroke Care to Specialized Centers: Hype or Help? Lee H. Schwamm, MD Professor of Neurology, Harvard Medical School Director, TeleStroke.
Dec 23, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Regionalizing Acute Stroke Regionalizing Acute Stroke Care to Specialized Centers: Care to Specialized Centers:
Hype or Help?Hype or Help?
Lee H. Schwamm, MDLee H. Schwamm, MD
Professor of Neurology, Professor of Neurology, Harvard Medical SchoolHarvard Medical SchoolDirector, TeleStroke & Acute Stroke Services, Director, TeleStroke & Acute Stroke Services,
Massachusetts General HospitalMassachusetts General HospitalChairChair, , National Steering Committee, National Steering Committee, AHA/ASA GWTG AHA/ASA GWTG
QCOR 2010

DisclosuresDisclosures
FederalFederalNIH (IMS3, MR RESCUE) NIH (IMS3, MR RESCUE)
Industry Clinical Trial Steering Committees Industry Clinical Trial Steering Committees Lundbeck (DIAS4), CoAxia (Flo24)Lundbeck (DIAS4), CoAxia (Flo24)
OtherOtherStroke Systems Consultant to MA DPH, CDC, Stroke Systems Consultant to MA DPH, CDC,
TJCTJCDirector TeleStroke Program at MGHDirector TeleStroke Program at MGH

Over my dead body!
Phil, you and I both know the American public needs
regionalization of acute stroke care

PrimaryStroke Center
CompStrokeCenter
tPA CapableHospitals
Emergency Stabilization Facilities
Field Response and Triage
Paradigm forGeographicRegionalization
Limited?Advanced

“Make the right diagnosis so you can get me to the right place in the right amount of time”

Comp StrokeCenter
Primary StrokeCenter
tPA CapableCenter

Easy to get inEasy to get in Hard to get outHard to get out
Ideal set of evidence-based Ideal set of evidence-based conditions for regionalizationconditions for regionalization
Patients can be identified in pre-hospital settingPatients can be identified in pre-hospital setting When rapidly achieved, patients benefit from an When rapidly achieved, patients benefit from an
intervention or an environment of careintervention or an environment of care More benefit at centers with specific resources More benefit at centers with specific resources
(eg, cath lab) or expertise (eg, trauma team)(eg, cath lab) or expertise (eg, trauma team) Variability in capability (infrastructure) or Variability in capability (infrastructure) or
performance (benefit or harm) across hospitalsperformance (benefit or harm) across hospitals Improved performance is generalizableImproved performance is generalizable Reallocation of patients is feasible, acceptable to Reallocation of patients is feasible, acceptable to
patients, and will lead to the improved outcomepatients, and will lead to the improved outcome

National Recommendations already National Recommendations already endorse acute stroke ROCendorse acute stroke ROC
Stroke 2005;36(3):690-703; Circulation 2005;111(8):1078-91

Acute Stroke ROC already in place in Acute Stroke ROC already in place in certain local and regional service areascertain local and regional service areas

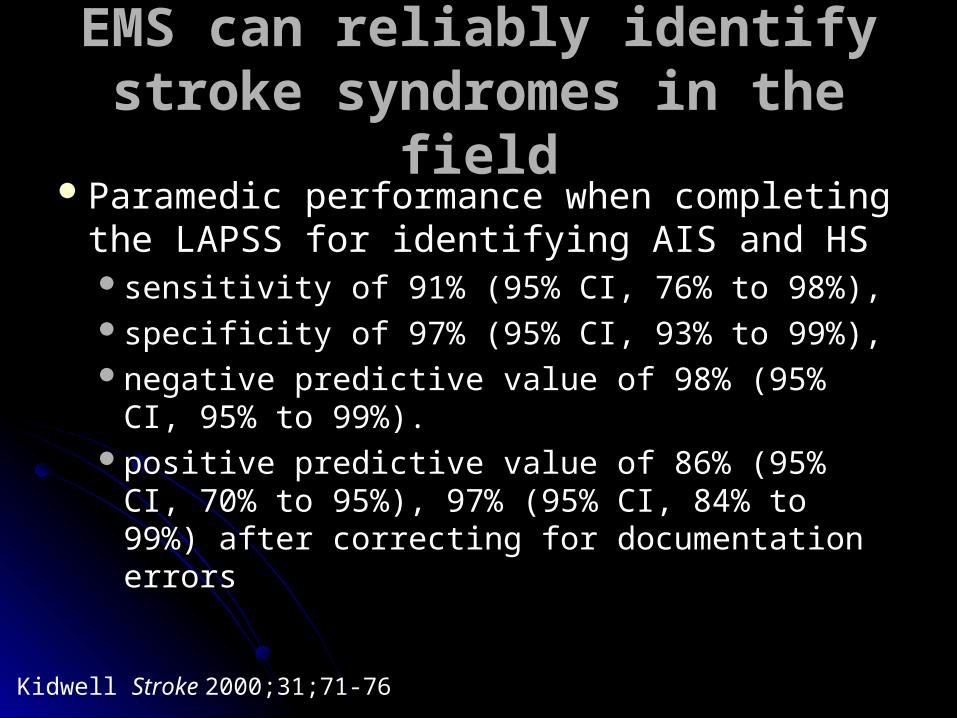
Why Stroke Regionalization?Why Stroke Regionalization? Patients can be identified by stroke screensPatients can be identified by stroke screens Patient benefit occurs with IV tPA (1A), catheter-Patient benefit occurs with IV tPA (1A), catheter-
based reperfusion (1B) or stroke units (1A)based reperfusion (1B) or stroke units (1A) More benefit expected at centers with high More benefit expected at centers with high
volume (SAH) or expertise (stroke teams, INR)volume (SAH) or expertise (stroke teams, INR) Variability in capability (INR, tPA use) or Variability in capability (INR, tPA use) or
performance (sICH rates) across hospitalsperformance (sICH rates) across hospitals Improved performance is generalizable (GWTG)Improved performance is generalizable (GWTG) Reallocation of patients is feasible, acceptable to Reallocation of patients is feasible, acceptable to
patients, and will lead to the improved outcome patients, and will lead to the improved outcome (depends on how much triage you’re planning)(depends on how much triage you’re planning)

Albers GW et al. Chest. 1998;119:683S-698S.Albers GW. Personal communication. February 27, 2003.Rosamond WD et al. Stroke. 1999;30:736-743.
Cardioembolic (20%)Lacunar (25%)(small vessel disease)
Ischemic Stroke (80%) Hemorrhagic Stroke (20%)
Subarachnoid Hemorrhage (30%)
Cryptogenic (30%)
Atherothrombotic CerebrovascularDisease (20%)
IntracerebralHemorrhage (70%)
Cerebrovascular Disease: Cerebrovascular Disease: Stroke TypesStroke Types
?

Various public education and first-Various public education and first-responder screening toolsresponder screening tools
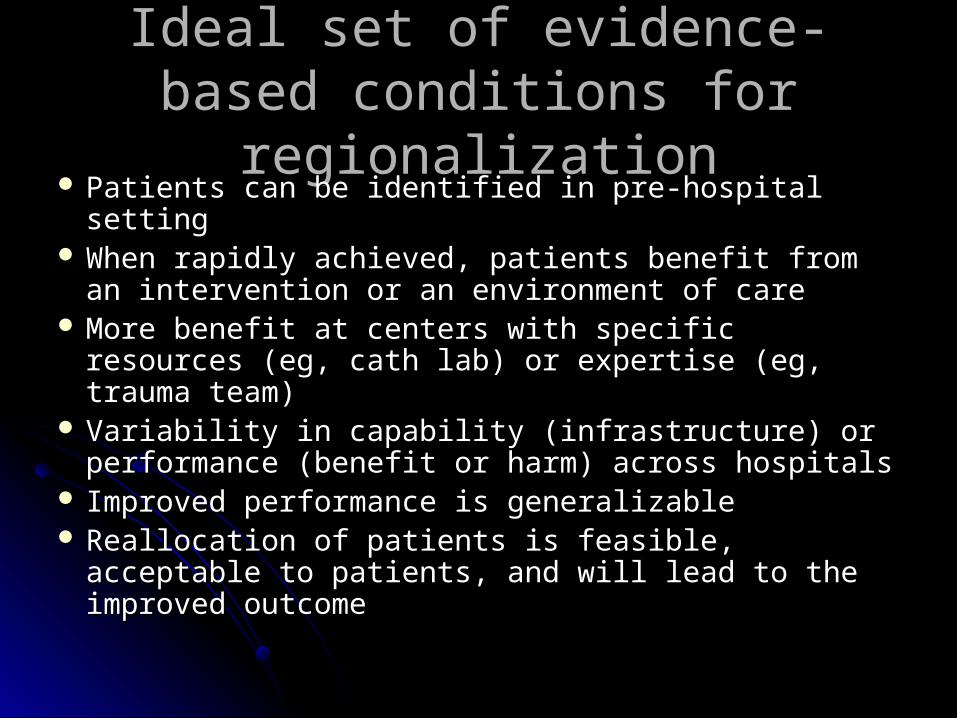
EMS can reliably identify stroke EMS can reliably identify stroke syndromes in the fieldsyndromes in the field
Paramedic performance when completing Paramedic performance when completing the LAPSS for identifying AIS and HS the LAPSS for identifying AIS and HS sensitivity of 91% (95% CI, 76% to 98%), sensitivity of 91% (95% CI, 76% to 98%), specificity of 97% (95% CI, 93% to 99%), specificity of 97% (95% CI, 93% to 99%), negative predictive value of 98% (95% CI, negative predictive value of 98% (95% CI,
95% to 99%).95% to 99%).positive predictive value of 86% (95% CI, 70% positive predictive value of 86% (95% CI, 70%
to 95%), 97% (95% CI, 84% to 99%) after to 95%), 97% (95% CI, 84% to 99%) after correcting for documentation errorscorrecting for documentation errors
Kidwell Stroke 2000;31;71-76
Why Stroke Regionalization?Why Stroke Regionalization? Patients can be identified by stroke screensPatients can be identified by stroke screens Patient benefit occurs with IV tPA (1A), catheter-Patient benefit occurs with IV tPA (1A), catheter-
based reperfusion (1B) or stroke units (1A)based reperfusion (1B) or stroke units (1A) More benefit expected at centers with high More benefit expected at centers with high
volume (SAH) or expertise (stroke teams, INR)volume (SAH) or expertise (stroke teams, INR) Variability in capability (INR, tPA use) or Variability in capability (INR, tPA use) or
performance (sICH rates) across hospitalsperformance (sICH rates) across hospitals Improved performance is generalizable (GWTG)Improved performance is generalizable (GWTG) Reallocation of patients is feasible, acceptable to Reallocation of patients is feasible, acceptable to
patients, and will lead to the improved outcome patients, and will lead to the improved outcome (depends on how much triage you’re planning)(depends on how much triage you’re planning)
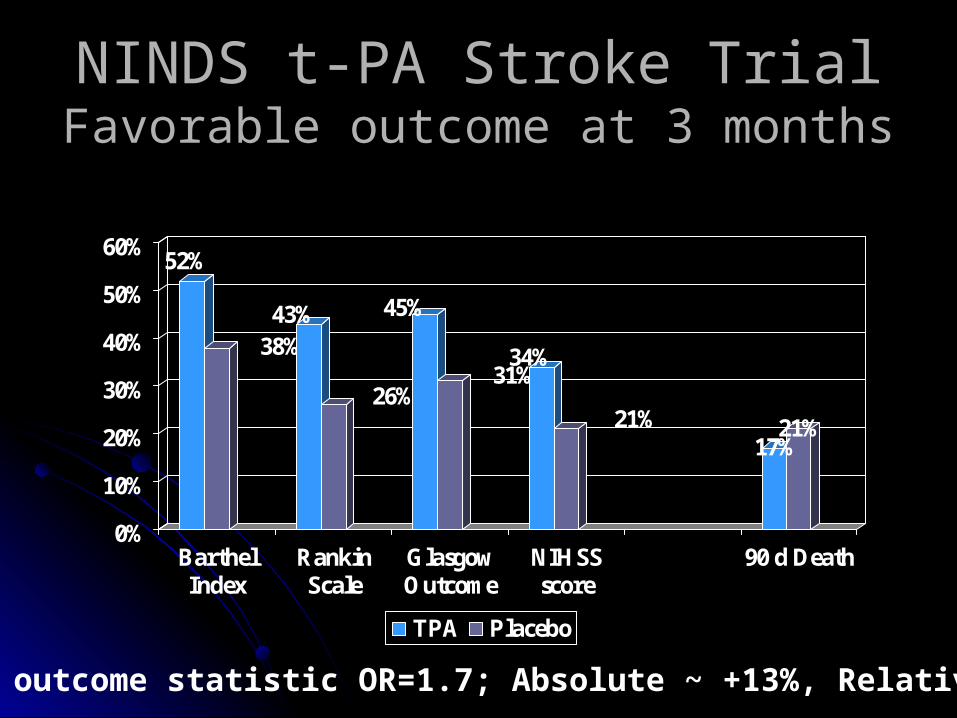
NINDS t-PA Stroke TrialNINDS t-PA Stroke TrialFavorable outcome at 3 monthsFavorable outcome at 3 months
52%
38%43%
26%
45%
31%34%
21%17%
21%
0%
10%
20%
30%
40%
50%
60%
BarthelIndex
RankinScale
GlasgowOutcome
NIHSSscore
90 d Death
TPA Placebo
Global outcome statistic OR=1.7; Absolute ~ +13%, Relative 30%
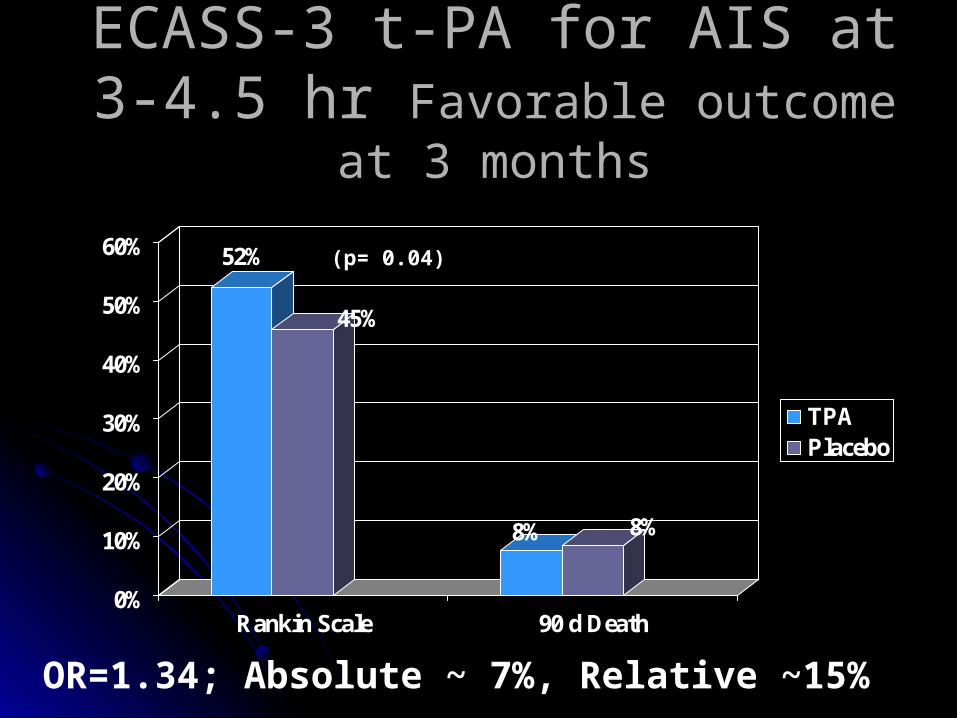
ECASS-3 t-PA for AIS at 3-4.5 hr ECASS-3 t-PA for AIS at 3-4.5 hr Favorable outcome at 3 monthsFavorable outcome at 3 months
52%
45%
8% 8%
0%
10%
20%
30%
40%
50%
60%
Rankin Scale 90 d Death
TPAPlacebo
OR=1.34; Absolute ~ 7%, Relative ~15%
(p= 0.04)

IV tPA is Beneficial 0-4.5 hrIV tPA is Beneficial 0-4.5 hr
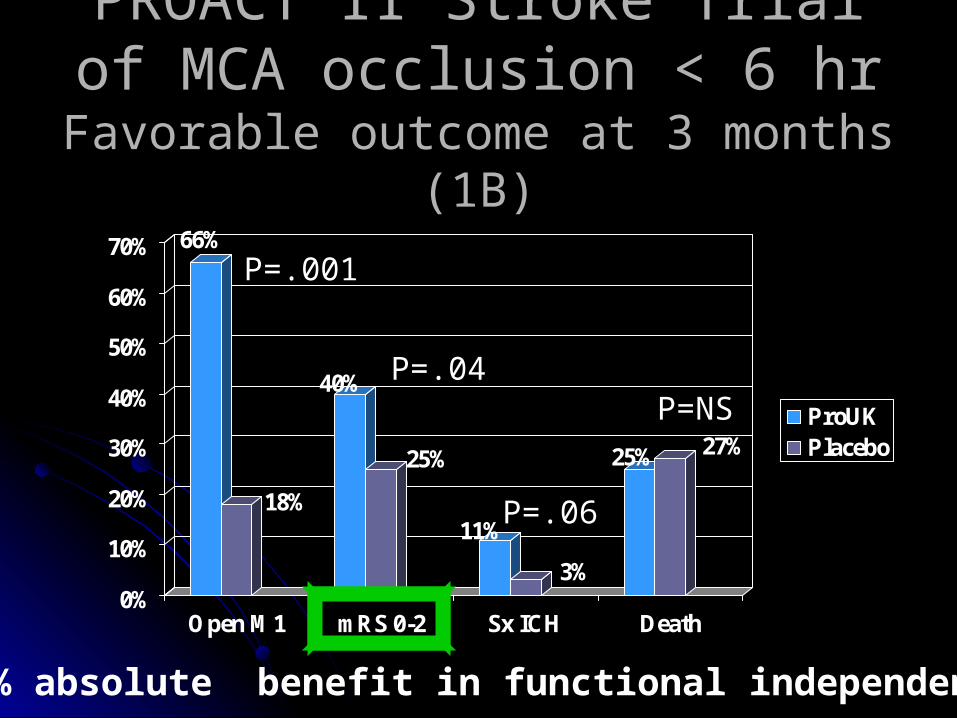
PROACT II Stroke TrialPROACT II Stroke Trialof MCA occlusion < 6 hrof MCA occlusion < 6 hr
Favorable outcome at 3 months (1B)Favorable outcome at 3 months (1B)66%
18%
40%
25%
11%
3%
25% 27%
0%
10%
20%
30%
40%
50%
60%
70%
Open M1 mRS 0-2 Sx ICH Death
ProUKPlacebo
15% absolute benefit in functional independence
P=.001
P=.04
P=.06
P=NS

Comparisons of Efficacy Comparisons of Efficacy TrialsTrials Pts RxPts Rx To Prevent a MajorTo Prevent a Major
CEACEA for Sx ICAfor Sx ICA 66 1 Stroke 1 Stroke
IA Lysis (0-6h)IA Lysis (0-6h) 77 1 Stroke1 Stroke
IV tPA (0-3h)IV tPA (0-3h) 88 1 Stroke 1 Stroke
IV tPA (3-4.5 h) IV tPA (3-4.5 h) 1414 1 Stroke1 Stroke
Stroke UnitsStroke Units 1818 1 Stroke or Death1 Stroke or Death
CEA for Asx ICA CEA for Asx ICA 15-2015-20 1 Stroke1 Stroke
Oral Anticoag AFOral Anticoag AF 2020 1 Stroke /yr1 Stroke /yr
IV tPA in AMIIV tPA in AMI 2626 1 Death from MI1 Death from MI
NASCET (n=659); PROACT; NINDS (n=624); ECASS3; BMJ 1997; ACAS; BAATAF; Lancet 1994
Why Stroke Regionalization?Why Stroke Regionalization? Patients can be identified by stroke screensPatients can be identified by stroke screens Patient benefit occurs with IV tPA (1A), catheter-based Patient benefit occurs with IV tPA (1A), catheter-based
reperfusion (1B) or stroke units (1A)reperfusion (1B) or stroke units (1A) More benefit expected w/ operators (CEA) or centers More benefit expected w/ operators (CEA) or centers
with high volume (SAH) or expertise (stroke teams, INR)with high volume (SAH) or expertise (stroke teams, INR) Variability in capability (INR, tPA use) or performance Variability in capability (INR, tPA use) or performance
(sICH rates) across hospitals(sICH rates) across hospitals Improved performance is generalizable (GWTG)Improved performance is generalizable (GWTG) Reallocation of patients is feasible, acceptable to Reallocation of patients is feasible, acceptable to
patients, and will lead to the improved outcome patients, and will lead to the improved outcome (depends on how much triage you’re planning)(depends on how much triage you’re planning)

Better Outcomes at High Volume Better Outcomes at High Volume Centers for Care of Aneurysmal SAHCenters for Care of Aneurysmal SAH
Bardach Stroke 2002;33;1851-1856

Surgeon CEA volume (low, med, high) Surgeon CEA volume (low, med, high) vs. in-hospital mortality, stroke or LOSvs. in-hospital mortality, stroke or LOS
J Am Coll Surg. 2002 Dec;195(6):814-21.
National Inpatient Sample 1996-1997 in 35,821 patients who underwent CEA

Why Stroke Regionalization?Why Stroke Regionalization? Patients can be identified by stroke screensPatients can be identified by stroke screens Patient benefit occurs with IV tPA (1A), catheter-Patient benefit occurs with IV tPA (1A), catheter-
based reperfusion (1B) or stroke units (1A)based reperfusion (1B) or stroke units (1A) More benefit expected at centers with high More benefit expected at centers with high
volume (SAH) or expertise (stroke teams, INR)volume (SAH) or expertise (stroke teams, INR) Variability in performance (sICH rates) or Variability in performance (sICH rates) or
capability (INR, tPA use) across hospitalscapability (INR, tPA use) across hospitals Improved performance is generalizable (GWTG)Improved performance is generalizable (GWTG) Reallocation of patients is feasible, acceptable to Reallocation of patients is feasible, acceptable to
patients, and will lead to the improved outcome patients, and will lead to the improved outcome (depends on how much triage you’re planning)(depends on how much triage you’re planning)

Marked variations in IV tPA by hospital type, in Ontario, from 2002/03 vs. 2004/05
Courtesy of Moira Kapral
All Ischemic Strokes
Ischemic Strokes <2.5 hr
What’s different about stroke?What’s different about stroke?“Stuff vs. Eyeballs”“Stuff vs. Eyeballs”
TraumaTrauma Blood bank, OR, trauma service, imagingBlood bank, OR, trauma service, imaging
Decompression sickness or Air embolismDecompression sickness or Air embolism Hyperbaric Chamber Hyperbaric Chamber
STEMISTEMI IV thrombolysis: EKG/Trop (+test), IV, EMS/ED MD PCI: Cath lab, cardiologist, CCU, anesthesia (?)PCI: Cath lab, cardiologist, CCU, anesthesia (?)
Acute Stroke Acute Stroke IV tPA: CT (-test), ED MD, IV +/- stroke expertise for
a clinical basis for diagnosis and prediction of outcome
IAT: Biplane, INR/ES, NICU, anesthesia (?)IAT: Biplane, INR/ES, NICU, anesthesia (?)
b-ii.
b-i.
a.
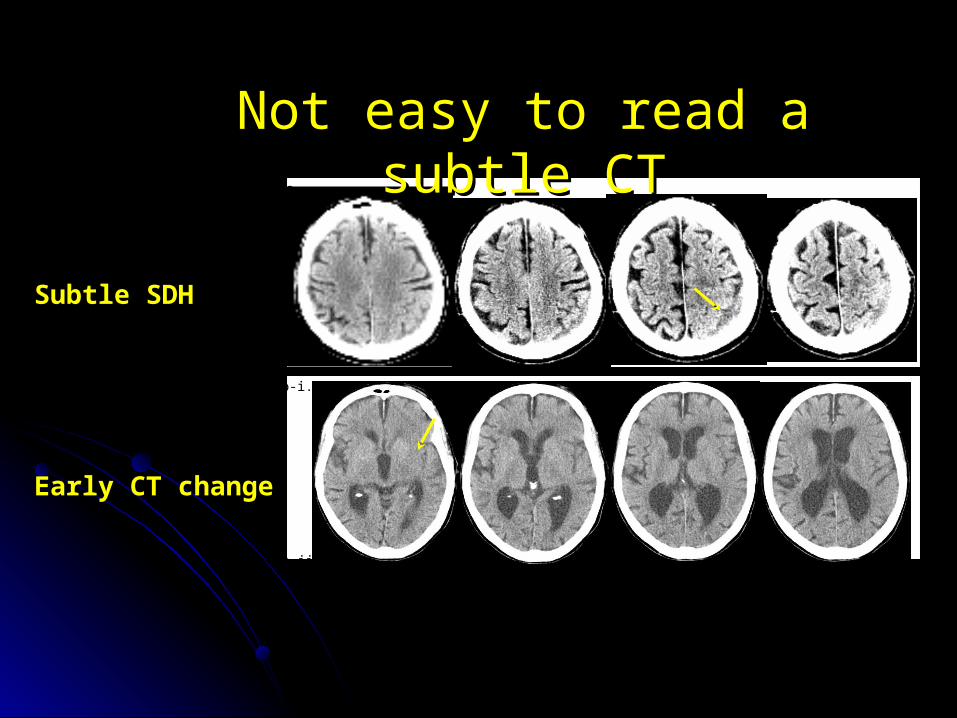
Not easy to read a subtle CTNot easy to read a subtle CT
Subtle SDH
Early CT change
The impact of external forces on The impact of external forces on provider tolerance for medical provider tolerance for medical
uncertainty at the bedsideuncertainty at the bedside
Low volume centers struggleLow volume centers struggle 1997-1998, 3948 patients at 29 hospitals in 1997-1998, 3948 patients at 29 hospitals in
ClevelandCleveland 1.8% received IV tPA. 1.8% received IV tPA. 15.7% (8.1%-26.4%) had SICH 15.7% (8.1%-26.4%) had SICH In-hospital mortality was 15.7% In-hospital mortality was 15.7% 50% (37.8%-62.2%) had protocol deviations50% (37.8%-62.2%) had protocol deviations
After training and protocol implementation After training and protocol implementation supervised by the Cleveland Clinic in 1999supervised by the Cleveland Clinic in 1999 18.8% of patients received IV tPA 18.8% of patients received IV tPA SICH rate was 6.4%.SICH rate was 6.4%. protocol deviations occurred in 19.1% of patientsprotocol deviations occurred in 19.1% of patients
Katzan JAMA. 2000;283:1151-1158 and JAMA. 2000;283:1151-1158 and Stroke 2003;34;799-800

Fancy Stuff: Fancy Stuff: Dissolve or Remove ClotsDissolve or Remove Clots
MCA occluded Device placed Clot removed
post 15 mins
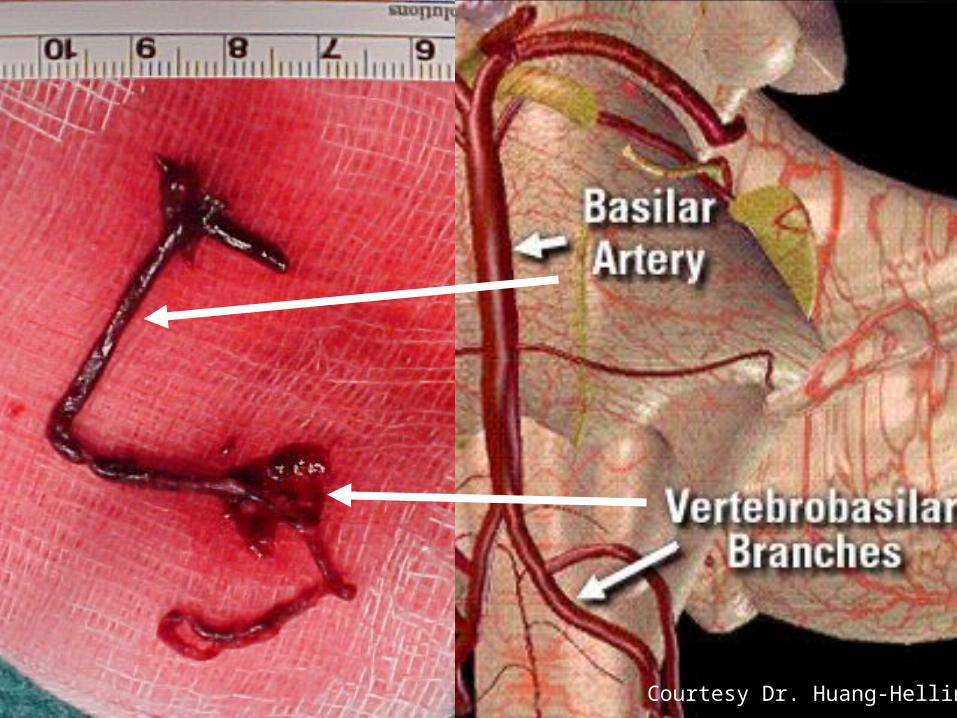
Courtesy Dr. Huang-Hellinger
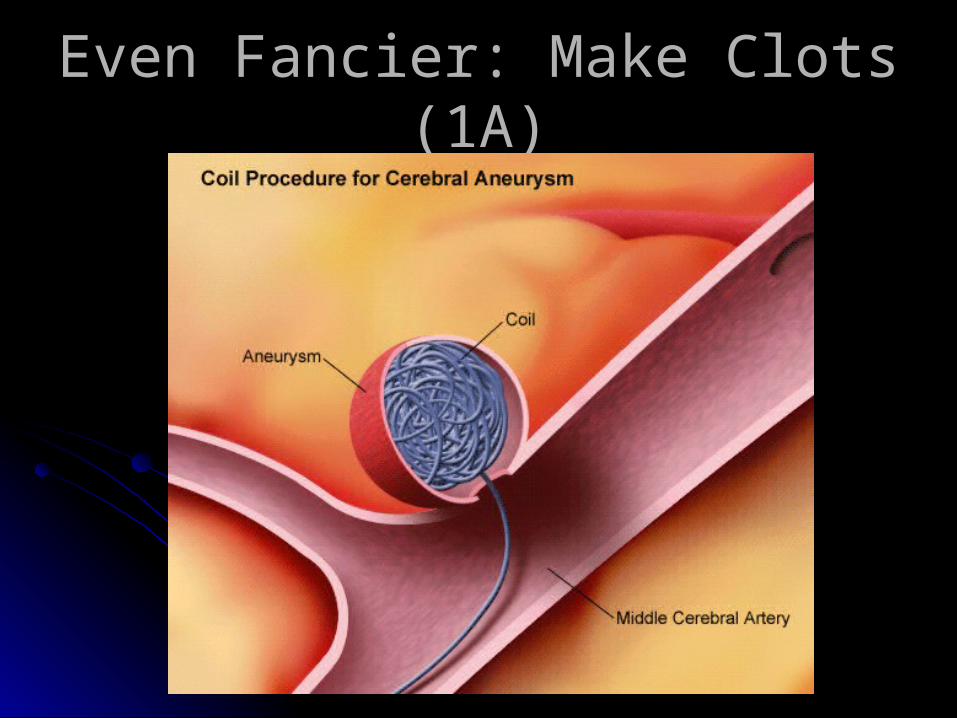
Even Fancier: Make Clots (1A)Even Fancier: Make Clots (1A)
Why Stroke Regionalization?Why Stroke Regionalization? Patients can be identified by stroke screensPatients can be identified by stroke screens Patient benefit occurs with IV tPA (1A), catheter-Patient benefit occurs with IV tPA (1A), catheter-
based reperfusion (1B) or stroke units (1A)based reperfusion (1B) or stroke units (1A) More benefit expected at centers with high More benefit expected at centers with high
volume (SAH) or expertise (stroke teams, INR)volume (SAH) or expertise (stroke teams, INR) Variability in capability (INR, tPA use) or Variability in capability (INR, tPA use) or
performance (sICH rates) across hospitalsperformance (sICH rates) across hospitals Improved performance is generalizable (GWTG)Improved performance is generalizable (GWTG) Reallocation of patients is feasible, acceptable to Reallocation of patients is feasible, acceptable to
patients, and will lead to the improved outcome patients, and will lead to the improved outcome (depends on how much triage you’re planning)(depends on how much triage you’re planning)

Quality Improvement from 2003-2009 in AHAQuality Improvement from 2003-2009 in AHA“Get With the Guidelines-Stroke”“Get With the Guidelines-Stroke”
0%
20%
40%
60%
80%
100%
Baseline YR1 YR2 YR3 YR4 YR5
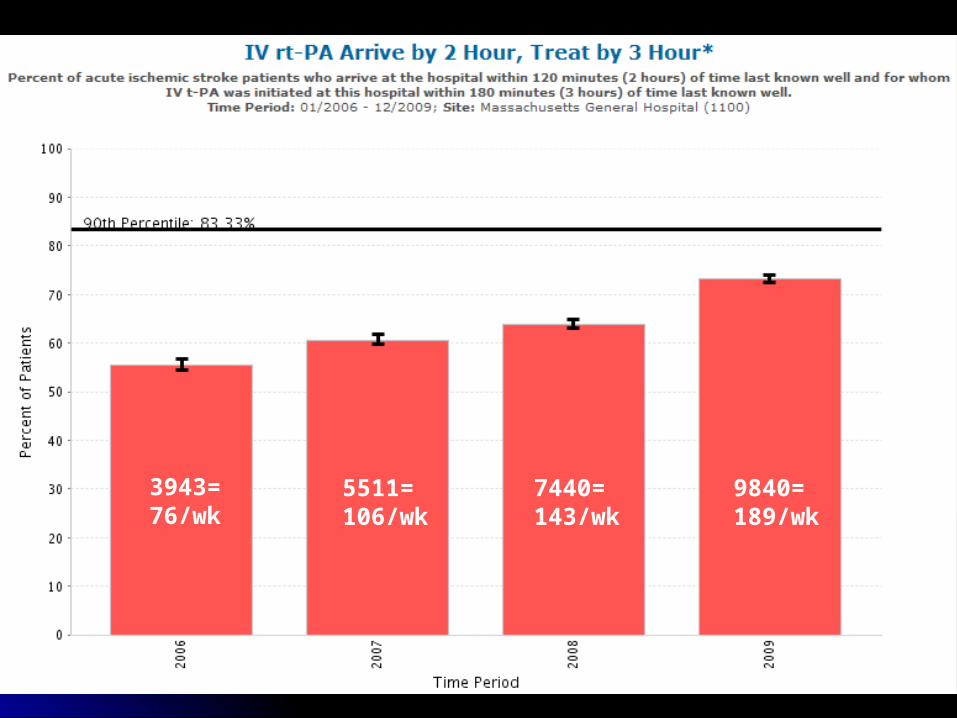
3943=76/wk
5511=106/wk
7440=143/wk
9840=189/wk

CT (18)
RI (5)
GWTG Stroke Hospitals in Every State1,272 Stroke Contracts Last updated: 6/11/2009
WA(28)
OR(18)
CA(88)
ID(1)
NV(9)
MT(4)
WY(2)
CO(37)
NM(3)
ND(2)
SD(3)
NE (10)
KS(6)
OK(9)
TX(78)
MN(13)
IA(16)
MO(22)
AR(8)
LA(15)
WI(61) MI
(42)
UT(10)
AZ(17)
IL(45)
IN(23)
KY(16)
TN (26)
MS(12)
AL(16)
GA(58)
FL(115)
SC(11)
NC(19)
VA(28)
OH(44)
WV(5)
PA(83)
NY(110)
MD (35)
ME(6)
VT (1)
NH (4)
NJ (39)
MA (60)
DE (4)
DC (4)
1-9
10-19
20-49
50-99
>100
# of Hospitals
Median Beds 300; Major or minor Teaching, 51%
Stroke Discharges <100, 30%; 101-300, 54%; >300, 16%

All triage in America is LocalAll triage in America is Local
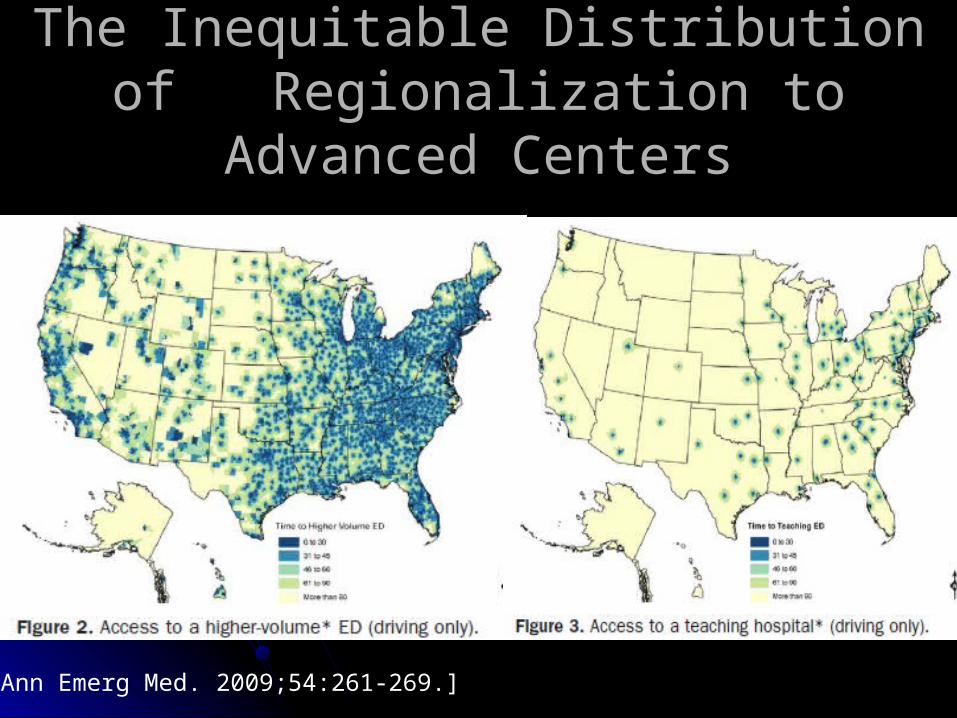
The Inequitable Distribution of The Inequitable Distribution of Regionalization to Advanced CentersRegionalization to Advanced Centers
[Ann Emerg Med. 2009;54:261-269.]
Time lost in transit is brain lost in transitTime lost in transit is brain lost in transit

Virtual Regionalization Brings Virtual Regionalization Brings High-Volume Providers to PatientsHigh-Volume Providers to Patients
Spoke Hospital
Hub Hospital
Real Time Audio and Video with full far-end camera controls
Digital Imaging
Remote MD
MD / Fellow / Resident “In-House”
Nurse
Transfer

Comparison of TeleStroke to Conventional Care Comparison of TeleStroke to Conventional Care at a Regional (CA) and Urban (TX) Centerat a Regional (CA) and Urban (TX) Center
Stroke Center
Patient
PopulationSample
Symptom-to-Door
(min)
Door-to-Consult
(min)
Consult-to-Needle
(min)
Symptom-to-Needle
(min)
MGH
(TeleS)Rural
Received tPA(n=6) 36 70 36 = 142
REACH
(TeleS)Rural
Received tPA (n=12) 71 45 18 = 134
TEMPiS
(TeleS)Rural
Received tPA
(n=106) 65 15 61 = 141
Ontario*
(Tx-tPA)Rural
Received tPA (n=23) 34 89 49 = 173
Houston
(Conv)Urban
Received tPA
(n=269) 67 70 = 137
Chapman Stroke. 2000;31:2920-2924

shipship & drip & drip vs. drip & ship

Distribution of TeleStroke Hospitals in Massachusetts
MGH& BWH
21 hospitals in Network6 hospitals Considering------------------------------66 tPA-Capable Centers
Regionalization of Stroke Regionalization of Stroke Thrombolysis in MA (2005 -)Thrombolysis in MA (2005 -)
On site inspection by DPH with mandatory quality On site inspection by DPH with mandatory quality and safety data submision and safety data submision
As of July 2005 when re-routing began, 56/72 As of July 2005 when re-routing began, 56/72 (78%) hospitals had already gained licensure(78%) hospitals had already gained licensure
Licensed hospitals were more likely than non-Licensed hospitals were more likely than non-licensed hospitals to be licensed hospitals to be larger (259 ± 174 v 103 ± 81 beds, p=0.004) larger (259 ± 174 v 103 ± 81 beds, p=0.004) urban (93% v 44%, p<0.001)urban (93% v 44%, p<0.001) teaching (60% v 18%, p=0.02)teaching (60% v 18%, p=0.02)

Effect of DPH PSS on tPA use Effect of DPH PSS on tPA use among eligible patientsamong eligible patients
Variable Pre-PSS (%) Post-PSS (%) P Value
IV tPA when Onset to ED Arrival < 2 hr
40.0 63.7 .0004
IV tPA when Onset to ED Arrival < 3 hr
31.2 53.3 .0001
reason for no IV tPA
83.4 92.0 .0003
Data before re-routing (PrePSSr: 2004-Q4 to 2005-Q2) were compared to after re-routing (PostPSSr: 2005-Q3 to 2006-Q2) by means of Chi-square or Fisher’s exact test.
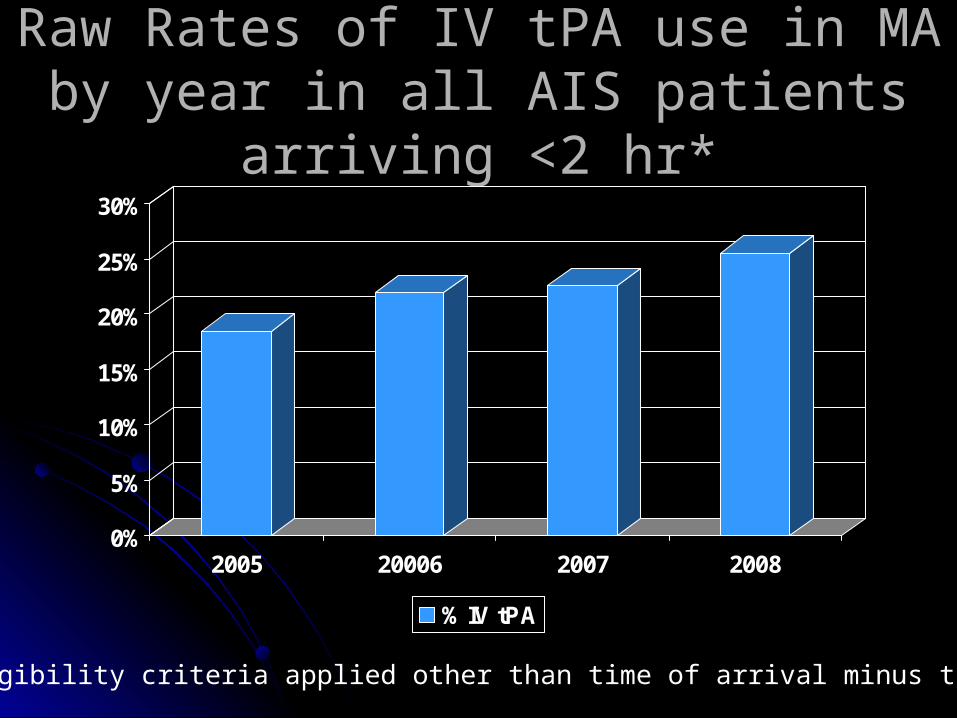
Raw Rates of IV tPA use in MA by year Raw Rates of IV tPA use in MA by year in all AIS patients arriving <2 hr*in all AIS patients arriving <2 hr*
0%
5%
10%
15%
20%
25%
30%
2005 20006 2007 2008
% IV tPA
*No eligibility criteria applied other than time of arrival minus time of LSW

The MGH TeleStroke Experience:The MGH TeleStroke Experience:Rates of IV-tPA Treatment by Consult TypeRates of IV-tPA Treatment by Consult Type
TeleStroke (TS) vs. In House/Phone Only (ASL)
Yr TS tPA %tPA ASL tPA %tPA2004 10 3 30.0% 257 38 14.8%2005 33 16 48.5% 482 65 13.5%2006 83 28 33.7% 481 59 12.3%2007 98 40 40.8% 512 63 12.3%2008 146 47 32.2% 572 75 13.1%2009 247 96 38.9% 935 114 12.2%Total 617 230 37.3% 3239 414 12.8%
Overall tPA Rate in 2009 = 17%
Why Stroke Regionalization?Why Stroke Regionalization? Patients can be identified by stroke screensPatients can be identified by stroke screens Patient benefit occurs with IV tPA (1A), catheter-based Patient benefit occurs with IV tPA (1A), catheter-based
reperfusion (1B) or stroke units (1A)reperfusion (1B) or stroke units (1A) More benefit expected at centers with high volume More benefit expected at centers with high volume
(SAH) or expertise (stroke teams, INR)(SAH) or expertise (stroke teams, INR) Variability in capability (INR, tPA use) or performance Variability in capability (INR, tPA use) or performance
(sICH rates) across hospitals(sICH rates) across hospitals Improved performance is generalizable (GWTG)Improved performance is generalizable (GWTG) Smart triage and early treatment initiation via Smart triage and early treatment initiation via
telemedicine with escalation of care environment for telemedicine with escalation of care environment for patients requiring tertiary care is feasible, acceptable to patients requiring tertiary care is feasible, acceptable to patients, and will lead to the improved outcomespatients, and will lead to the improved outcomes

World Leaders Embrace Acute Stroke Care Regionalization.
Middle East Declares Lasting Peace
Tea Party Suffers Stunning Nov. Losses
Related Documents