Regional Interdependence Utilizing Dynamic Hip Control and Strengthening as a Treatment for Plantar Fasciitis Capstone Presentation: December 2016 Author: Zac Lynch East Tennessee State University

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Regional Interdependence Utilizing Dynamic Hip
Control and Strengthening as a Treatment for
Plantar Fasciitis
Capstone Presentation: December 2016
Author: Zac Lynch
East Tennessee State University

Outline
Introduction and overview of the case report
Current best evidence
Case description
Examination
Differential diagnosis and impression
Intervention
Outcome
Discussion and review
References

Introduction1,2
Plantar fasciitis
Sedentary vs active injuries
Long distance runner with signs and symptoms of right-sided
plantar fasciitis
Proximal impairment, distal pain

Current Evidence – Martin, et al.2
• Joint and soft tissue
mobilization
• Passive fascia stretching
• Gastrocnemius and soleus
stretching
• Anti-excessive pronation
therapeutic taping
• Medial arch support for heel
strike maintenance
• Night splints
• Phonophoresis
• Shoe rotation
• Strengthening and movement
correction

Current Evidence – Young, et al.3
Posterior talocrural joint mobilization
Subtalar joint distraction mobilization and manipulation
Triceps surae stretching
Plantar fascia stretching
Self AP mobilization at home

Current Evidence4,5,6
Rathleff, et al.
High-load progressive
strength training
performed every second
day. Consisted of
unilateral heel raises with
a towel inserted under the
toes.
Cole, et al.
One article stated that custom-made splints help promote maintenance of range of motion.
Chien-Tsung Tsai, et al.
Kinesiotaping in comparison to standardized stretching and strengthening of the ankle and foot.

Current Evidence – Urovitz, et al.7
Systematic review reported that home based exercises
focused on stretching the calf muscles, plantar fascia, flexor
hallicus longus, and Achilles tendon proved to be a superior
treatment option for short and long term effects of plantar
fasciitis
This review compared exercises to control group therapy,
exercises with a custom orthoses, foot insoles and exercise
therapy, calcaneal taping, iontophoresis

Limitations to “Current Evidence”
Pathoanatomic pendulum
Lack of movement based, performance based evaluations such as
FMS, MDT systems
Interventions focused on the painful region
CPG briefly mention treating the hip for biomechanical deviations
Passive treatments
Poor injury prevention education, lack of prophylaxis

Case Description

Examination
NPRS
4/10 currently and consistently
6/10 exacerbation during running
Subjective
Jumping, running increased symptoms
Ice massage, anti-inflammatory OTC medication briefly eased symptoms
Painful areas and body chart
Goals
Return to running without pain

Examination
Vital Signs
Blood Pressure (mmHg)
130/82
Heart Rate (BPM)
59
Body Mass Index
25.33
Oxygen Saturation (%)
98

Examination
Palpation
Increased muscle tone at distal right Triceps Surae
Tenderness medial slip and origin of right plantar fascia
Posterior Tibialis at level of Medial Mallelous
Achilles Tendon – midportion and insertion
Range of Motion

Examination
Strength

Examination
Neurological and Edema Assessment
Special Tests

Examination
Observational Gait
Analysis
Functional Strength
and Motor Control
Testing
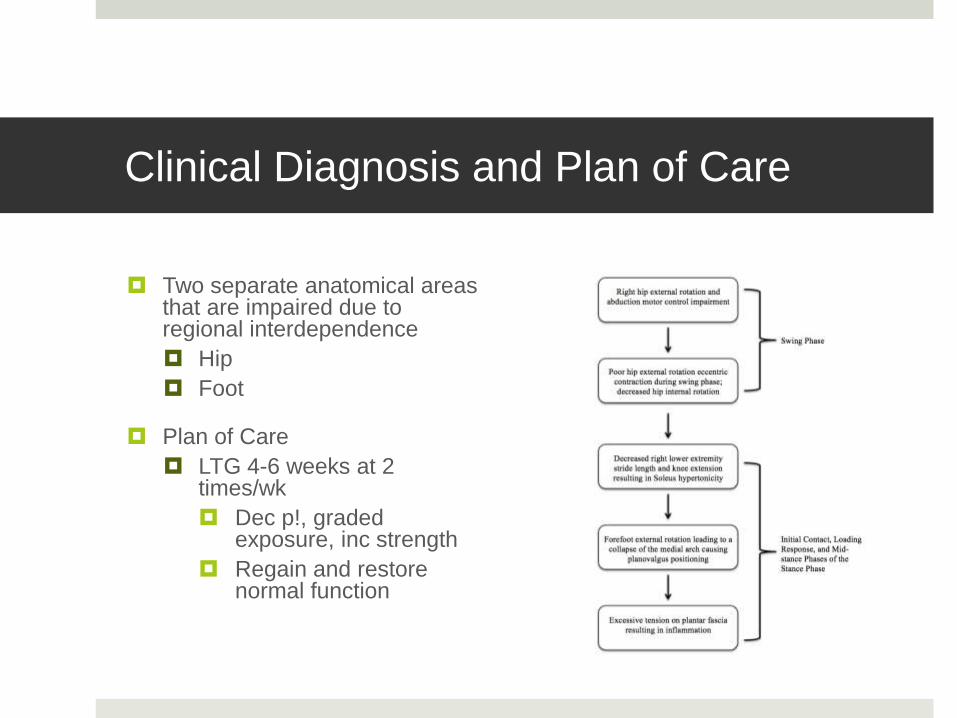
Clinical Diagnosis and Plan of Care
Two separate anatomical areas that are impaired due to regional interdependence
Hip
Foot
Plan of Care
LTG 4-6 weeks at 2 times/wk
Dec p!, graded exposure, inc strength
Regain and restore normal function

Intervention8,9
Passive Modalities
Phonophoresis – Medial slip of plantar fascia at the origin
US gel + Dexamethasone Phosphate (0.4%) with a setting of 3.3 MHz, 1.0W/cm, 50% pulsed at 5 minutes
Applied prior to exercise in order to allow medication to promote anti-inflammatory effects during therapeutic movements
Cryotherapy to right ankle and foot
15 minutes application for short term pain relief
Applied after treatment in order to avoid a decrease in nerve conduction velocity prior to movement

Intervention10-12
Manual Therapy
Joint Mobilization
Talocrural
Mobilization with Movement
CKC dorsiflexion technique with strap
Passive Range of Motion
Knee extension and ankle dorsiflexion
Intervention13-15
Strengthening
Eccentric strengthening for hip external rotation
Manually resisted side-lying hip external rotation
Hip abduction strengthening for distal mechanical correction
Concentric and eccentric lower extremity exercise in order to provide stability and motor control during dynamic movements

Intervention2,16
Stretching
Gastrocnemius
Soleus
Hamstrings

Exe
rcis
e D
osa
ge

Exercise Dosage

Outcomes
D/C after 8 treatment sessions
Improvement in strength and ROM to that of contralateral LE
Improvement in proper mechanics during gait analysis and running
Decrease in resting high muscle tone
The patient ran a half marathon two days prior to discharge. Reported no pain, stiffness, or restriction before/during/after the race
Discussion2,17-21
CPGs interventions suggested:
Manual therapy of the lower extremity, being joint mobilization/soft tissue mobilization
Stretching of plantar fascia, gastrocnemius, soleus
Anti-pronation taping of the ankle and foot
Orthoses to support medial longitudinal arch of the foot
Night splints to prevent morning stiffness
Low-level laser therapy
Phonophoresis
Rocker-bottom shoe fabrication with implementation of a foot orthosis
Rotation of shoes during the work week
Education about weight loss
Strengthening and movement correction of muscles correlated to weight bearing forces and pronation control

Discussion2,17-21
As we utilized many of the interventions recommended in the current CPG for plantar fasciitis, we also utilized a treatment philosophy called REGIONAL INTERDEPENDENCE in order to facilitate improvement of plantar fasciitis signs and symptoms, and also underlying pathology
Our approach encompassed strengthening and the promotion of motor control exercises of the right side hip in order to control movement in the sagittal and frontal plane and correct abnormal movement at the knee and the foot

Discussion2,17-21
Regional Interdependence - a theoretical model structured on
improvements of sport specific movements rather than just
treating the presenting complaint, pain
Impairments of right hip external rotation and abduction motor
control lead to the patient compensating with knee valgus
positioning during the weight acceptance phase, and forceful
pronation of the right foot during weight acceptance through
the mid-foot and heel-off portions of the gait cycle

Discussion2,17-21
This case report suggests that the regional interdependence
model is appropriate for treating anatomical areas related to,
but not in the same region as the chief complaint

Limitations2
Lack of use of patient reported outcome measures
Suggestions from CPG:
Foot Function Index
Foot Health Status Questionnaire
Foot and Ankle Ability Measure
Lower Extremity Functional Scale

Conclusion
Regional interdependence was utilized in order to identify and manage contributions of weakness and motor control issues in the proximal hip that led to plantar fasciitis signs and symptoms
Improvement in pain and performance of the patient’s recreational activities
D/C with no pain, improved display of dynamic movements and high intensity running
Further research is warranted to clarify the regional interdependence correlation to ipsilateral hip impairment and distal foot plantar fasciitis
References
1. Thompson JV, Saini SS, Reb CW, et a.. Diagnosis and Management of Plantar Fasciitis. J Am Osteopath Assoc2014;114(12):900-901. doi: 10.7556/jaoa.2014.177.
2. Martin RL, Davenport TE, Reischl SF, et al. Heel pain-plantar fasciitis: revision 2014. J Orthop Sports Phys Ther. 2014;44(11):A1-33.
3. Young B, Walker MJ, Strunce J et al. A combined treatment approach emphasizing impairment-based manual physical therapy for plantar heal pain: a case series. JOSPT. 2004;34:725-733.
4. Rathleff MS, Mølgaard CM, Fredberg U, et al. High-load strength training improves outcome in patients with plantar fasciitis: A randomized controlled trial.
5. Cole C, Seto C, Gazewood J. Plantar fasciitis: evidence-based review of diagnosis and therapy. Am FamPhysician. 2005 Dec 1;72(11):2237-42.
6. Chien-Tsung Tsai et al., Effects of Short-Term Treatment with kinesiotaping for Plantar fasciitis, Journal of Musculoskeletal Pain, March 2010, Vol. 18, No. 1, Pages 71-80.
7. Urovitz EP, Birk-Urovitz A, Birk-Urovitz E. Endoscopic plantar fasciotomy in the treatment of chronic heel pain. Can J Surg. 2008 Aug;51(4):281-3

References
8. Landrum EL, Kelln CB, Parente WR, et al. Immediate Effects of Anterior-to-Posterior Talocrural Joint Mobilization after Prolonged Ankle Immobilization: A Preliminary Study. J Man Manip Ther. 2008;16(2):100-5
9. Deshpande MM, Patil CB. Heel pain and phonophoresis. J Indian Med Assoc. 2010;108(6):365.
10. Jerrold S. Petrofsky, Michael S. Laymon, Faris Alshammari, et al. Evidence Based use of Heat, Cold and NSAIDS for Plantar Fasciitis. Clinical Research on Foot & Ankle. 2014.
11. Landrum EL, Kelln CB, Parente WR, et al. Immediate Effects of Anterior-to-Posterior Talocrural Joint Mobilization after Prolonged Ankle Immobilization: A Preliminary
11. Vicenzino B, Branjerdporn M, Teys P, et al. Initial changes in posterior talar glide and dorsiflexion of the ankle after mobilization with movement in individuals with recurrent ankle sprain. J Orthop Sports Phys Ther. 2006;36(7):464-71.
12. Landrum EL, Kelln CB, Parente WR, et al. Immediate Effects of Anterior-to-Posterior Talocrural Joint Mobilization after Prolonged Ankle Immobilization: A Preliminary Study. J Man Manip Ther. 2008;16(2):100-5.
13. Nakagawa TH, Muniz TB, Baldon Rde M, et al. The effect of additional strengthening of hip abductor and lateral rotator muscles in patellofemoral pain syndrome: a randomized controlled pilot study. Clin Rehabil. 2008;22(12):1051-60.

References
14. Woitzik E, Jacobs C, Wong JJ, et al. The effectiveness of exercise on recovery and clinical outcomes of soft tissue injuries of the leg, ankle, and foot: A systematic review by the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. Man Ther. 2015;20(5):633-45.
15. Andreasen J, Mølgaard CM, Christensen M, et al. Exercise therapy and custom-made insoles are effective in patients with excessive pronation and chronic foot pain-a randomized controlled trial. Foot (Edinb). 2013;23(1):22-8.
16. Radford JA, Landorf KB, Buchbinder R, et al. Effectiveness of calf muscle stretching for the short-term treatment of plantar heel pain: a randomised trial. BMC Musculoskelet Disord. 2007;8:36.
17. Sueki DG, Cleland JA, Wainner RS. A regional interdependence model of musculoskeletal dysfunction: research, mechanisms, and clinical implications. J Man Manip Ther. 2013;21(2):90-102.
18. Cashman GE. The effect of weak hip abductors or external rotators on knee valgus kinematics in healthy subjects: a systematic review. J Sport Rehabil. 2012;21(3):273-84.
19. Bolgla LA, Malone TR. Plantar fasciitis and the windlass mechanism: a biomechanical link to clinical practice. J Athl Train. 2004;39(1):77-82.
20. Bialosky JE, Bishop MD, George SZ. Regional interdependence: a musculoskeletal examination model whose time has come. J Orthop Sports Phys Ther. 2008;38(3):159-60.
21. Mcdevitt A, Young J, Mintken P, et al. Regional interdependence and manual therapy directed at the thoracic spine. J Man Manip Ther. 2015;23(3):139-46.
Related Documents