Opinions expressed by CE authors are their own and may not reflect those of Dentistry Today. Mention of specific product names does not infer endorsement by Dentistry Today. Information contained in CE articles and courses is not a substitute for sound clinical judgment and accepted standards of care. Participants are urged to contact their state dental boards for continuing education requirements. Rico Short, DMD Upon successful completion of this CE activity, 2 CE credit hours may be awarded A Peer-Reviewed CE Activity by Course Number: 183 Regenerative Endodontics: Clinical Review and Case Reports Dentistry Today, Inc, is an ADA CERP Recognized Provider. ADA CERP is a service of the American Dental Association to assist dental professionals in indentifying quality providers of continuing dental education. ADA CERP does not approve or endorse individ- ual courses or instructors, nor does it imply acceptance of credit hours by boards of den- tistry. Concerns or complaints about a CE provider may be directed to the provider or to ADA CERP at ada.org/goto/cerp. Approved PACE Program Provider FAGD/MAGD Credit Approval does not imply ac- ceptance by a state or provincial board of dentistry or AGD endorsement. June 1, 2012 to May 31, 2015 AGD PACE approval number: 309062 CONTINUING EDUCATION

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Opinions expressed by CE authors are their own and may not reflect those of Dentistry Today. Mention of specific product names does
not infer endorsement by Dentistry Today. Information contained in CE articles and courses is not a substitute for sound clinical judgment
and accepted standards of care. Participants are urged to contact their state dental boards for continuing education requirements.
Rico Short, DMD
Upon successful completion of this CE activity, 2 CE credit hours may be awarded
A Peer-Reviewed CE Activity by
Course Number: 183
Regenerative Endodontics:Clinical Review and Case Reports
Dentistry Today, Inc, is an ADA CERP Recognized Provider. ADA CERP is a service of theAmerican Dental Association to assist dental professionals in indentifying qualityproviders of continuing dental education. ADA CERP does not approve or endorse individ-ual courses or instructors, nor does it imply acceptance of credit hours by boards of den-tistry. Concerns or complaints about a CE provider may be directed to the provider or toADA CERP at ada.org/goto/cerp.
Approved PACE ProgramProvider FAGD/MAGD CreditApproval does not imply ac-ceptance by a state orprovincial board of dentistryor AGD endorsement. June 1, 2012 to May 31, 2015 AGD PACEapproval number: 309062
CONTINUING EDUCATION

Regenerative endodontic procedures (REPs) represent aparadigm shift for the treatment of necrotic pulps in immature permanent teeth, ranging from traditional
barrier formation utilizing calcium hydroxide or mineral trioxideaggregate (MTA), to a biologically based treatment for root maturation. REPs capture the ability to use stem cells that reside
naturally in and around the tooth to extend the life of the tooth.In particular, periradicular tissues of immature teeth are rich inblood supply and contain stem cells that have the potential fortissue regeneration.1 These stem cells may be the next break-through technology which may allow clinicians to grow humanteeth in the foreseeable future. In fact, a Harvard-led team in May2014 successfully used low-powered lasers to activate stem cellsand stimulate the growth of teeth in rats and human dental tissue in a laboratory setting. The results were published in thejournal Science Translational Medicine.2 Titanium dental implantsmay one day be considered “archaic,” such as silver cones or retrograde amalgams are now considered out of date by manyclinicians, teachers, and researchers.
WHAT IS REGENERATIVE ENDODONTICS?Regeneration is the process of renewal, restoration, and growth
1
CONTINUING EDUCATION
Regenerative Endodontics: Clinical Review andCase Reports
Dr. Short graduated from Morris BrownCollege in 1995 as valedictorian with a BSdegree. He attended the Medical Collegeof Georgia School of Dentistry to attain a DMD degree in 1999. In 2002, heearned his postdoctorate degree in endodontics from Nova Southeastern Uni-versity. Dr. Short became a board-certifiedendodontist in 2009, a status which only25% of endodontists achieve. He is aDiplomate of the American Board of Endodontics, and his private practice, ApexEndodontics PC, is located in Smryna, Ga.He is an expert consultant to the GeorgiaBoard of Dentistry and an assistant clinicalprofessor at the Georgia Regents Univer-
sity School of Dentistry. In addition, he has lectured nationally. Dr. Shorthas received several prestigious awards and accolades throughout his career and volunteers at various nonprofit organizations in his community,such as The Ben Massell Dental Clinic, which provides free dental care tothose in need. Dr. Short has authored a book, Getting to the Root of YourProblem: 365 Days of Inspirational Thinking. As an Affordable Care Act(ACA) correspondent in oral healthcare, Dr. Short is currently part of apanel that corresponds with White House government officials dealing withhealthcare issues and the ACA. He was also recognized as one of the Top40 Dentists Under 40 in America by Incisal Edge Magazine. He can bereached at (678) 503-0790 or via email at [email protected].
Disclosure: Dr. Short reports no disclosures.
Learning Objectives: After reading this article, the individual will learn:(1) principles of regenerative endodontics in the treatment of imma-ture necrotic permanent teeth, and (2) clinical protocol for treating im-mature necrotic permanent teeth with regenerative endodontics.
About the Author
Effective Date: 03/01/2015 Expiration Date: 03/01/2018
Regenerative endodontics procedures are based on thebest available data at this time.
Case Selection: Tooth No. ______l Tooth with necrotic pulp and an immature apex or openapex
l Pulp space not needed for post/core, final restorationl Compliant patient
Informed Consentl Two (or more) appointmentsl Use of antimicrobial(s) l Possible adverse effects: staining of crown/root, lack ofresponse to treatment, pain/infection, root fracture
l Alternatives: MTA apexification, no treatment, extraction(when deemed nonsalvageable)
l Permission to enter information into the American Association of Endodontics database (optional) via thewebsite aae.org
l Follow-ups necessary to track healing until completion
There is not a 100% success rate with this procedure. However, it is the best current technique and technology we have available in efforts to save this tooth.
X (patient signature)__________________________________
Date______________
Table 1. Informed Consent for Regenerative Procedures(Sample Addendum)

that makes genomes, cells, or organisms resilient to naturalfluctuations or events that cause disturbance or damage.3Every species, from bacteria to humans, is capable of regenera-tion. Regeneration can either be complete where the new tissueis the same as the lost tissue, or incomplete where fibrosis occurs after the necrotic tissue is removed.4 In regenerative en-dodontics, the goal is for the pulp to “revitalize” or “regenerate”new tissue so that root maturation can occur in the absence ofdisease and the patient’s tooth can return to function, form,and aesthetics. The management of immature permanent teeth with
pulpal disease can be very challenging for the clinician. For example, it is difficult to properly debride, clean, and shape
thin dentinal walls, which can result in cervical fracture.5 Anextraction or fracture will present a restorative and aestheticproblem, especially if the patient is young, due to the fact thatthe bone is too immature for an implant.Regenerative endodontics in its original state began with
Ostby6 in 1961 with limited success. During the last decade, ithas been redefined as “biologically based procedures designedto replace damaged structures, including dentin and root structures, as well as cells of the pulp-dentin complex.”7Another term many use to describe regenerative endodonticsis revascularization, which can result in thickening of dentinalwalls and continued root development in immature teeth withnecrotic pulps.8
2
CONTINUING EDUCATION
Regenerative Endodontics: Clinical Review and Case Reports
Figure 1a. Apexifica-tion with white mineraltrioxide aggregate(MTA) on tooth No. 8.Preoperative radio -graph of tooth No. 8shows necrotic pulpwith open apex due totrauma.
Figure 1b. Tooth No. 8 accessed witha size 90 hand file toshow open apex andthin walls.
Figure 1c. Calcium hydroxide USP placed insidecanal and sealed with Cavit Temporary Filling Material Refill (3M ESPE).
a b c
Figure 1f. White MTA (DENTSPLY Tulsa Dental Specialties) was placed inside canal as final obturation material to complete apexification.
f
Figure 1d. Calcium hydroxide washed outafter 3 months andhad to be repacked. Itwas repacked every 3months for 13 months.
Figure 1e. Calcified barrier was formedafter 13 months, evident with a size140 hand file.
d
e
Figure 1g. One-year recall showing tooth still stable and healing.Note the thin walls,which could easily result in fractures in thefuture. However, tooth isstill stable after 8years.
g

When Should Regenerative Endodontics be Considered?1.Necrotic pulp and immature or open apex2. Young patient3.Very thin dentinal walls4. Cannot achieve a predictable apical seal with conven-
tional endodontics5. Presence of pathology with very large apical foramen.
What are the Key Components of Regenerative Endodontics?
In order for the regenerative endodontic technique to be effective,the following 3 key components are needed:
1. Stem cells
2. Scaffolds3. Growth factors.Stem cells are undifferentiated cells that continuously divide.
There are 2 main types: embryonic and postnatal (adult). Anadult stem cell can divide and create another identical cell, butthe capacity for differentiation into other cell types is limited.There are several types of adult stem cells that have been isolated from teeth: (1) dental pulp stem cells, (2) stem cellsfrom human deciduous teeth, (3) periodontal ligament stemcells, (4) dental follicle progenitor stem cells, and (5) stem cellsfrom apical papilla (SCAPs). The most current stem cells usedin REPs are the SCAPs due to their location in Hertwig’s epithelial root sheath.9
3
CONTINUING EDUCATION
Regenerative Endodontics: Clinical Review and Case Reports
First Appointmentl Diagnose case properly (necrotic pulp with open or immature apex)l Local anesthesia (with or without vasoconstrictor), rubber dam isolation, accessl Copious, gentle irrigation with 20 mL 3% sodium hypochlorite with side-vented syringe 2 mm from the apexl Rinse with 5 mL of sterile salinel Irrigate with 10 mL 0.12% chlorhexidine gluconate with sided-vented syringel Dry canal with large paper pointl Place calcium hydroxide (injectable) inside canal with sterile cotton pelletl Seal with cotton pellet and 3 to 4 mm of temporary restorative material (such as Cavit Temporary Filling Material Refill [3M ESPE])l Dismiss patient for 4 weeks to allow the calcium hydroxide time to disinfect the canal
Second Appointmentl Assess response from patient from initial treatment; no signs or symptoms of remaining infectionl If swelling or sinus tract remains, repeat the first appointment procedurel If patient is asymptomatic, anesthetize with 3% mepivicaine without vasoconstrictor, rubber dam isolation, accessl Copious, gentle irrigation with 20 mL 17% ethylenediaminetetraacetic acid with side-vented syringe followed by sterile salinel Dry canal with large paper pointl Create bleeding into the canal space by over-instrumenting or poking the bone with a sterile endodontic file (this forms theblood clot, which acts as a scaffold to bring the stem cells up into the canal space)
l Stop bleeding 3 mm from cemento-enamel junction with sterile cotton pellet and remove the cotton pelletl Place 3 to 4 mm of EndoSequence Root Repair Material (Brasseler USA), or white mineral trioxide aggregate (MTA)(DENTSPLY Tulsa Dental Specialties) on top of blood clot very lightly (note: MTA is now known to create a discolored tooth inthis technique, which is discussed later in this article)
l Restore with composite or glass ionomer
Follow-Up Evaluationl First follow-up in one monthl Tooth should be asymptomatic and functionall The 6- to 12-month follow-up: radiographic evaluation (resolution of periapical radiolucency starting and may see increaseddentinal wall thickness)
l The 12- to 24-month follow-up: radiographic evaluation (increased dentinal wall thickness, radiographic healing more evident,and increased root length and width)
Table 2. Regenerative Endodontic Technique

4
CONTINUING EDUCATION
Regenerative Endodontics: Clinical Review and Case Reports
Figure 2a. A 9-year-old malewith a necrotic pulp, largeperiapical lesion, and imma-ture root with blunderbussapex on tooth No. 20. Nohistory of trauma. Possiblecase of dens evaginatus.There is no conventional endodontic therapy that willcause the root to continue toform in length, width, andstrength. These cases willrequire the regenerative endodontic procedure for a better outcome than apexification.
a
Figure 2b. Anesthetize, access, irrigate, dry, and place calcium hydrox-ide (injectable UltraCal XS Calcium Hydroxide Paste [Ultradent Products])according to first appointment treat-ment protocol (see Table 2). Temporizewith Cavit. No endodontic files are in-volved for cleaning and shaping.
b
Figure 2f. The 8-month recallon tooth No. 20 showingroot elongation and apicalclosure starting to occur.
f
Figure 2g. Dark staining ofcrown after 8-month recallon tooth No. 20 due to thewhite MTA. (EndoSequenceRoot Repair Material [Bras-seler USA] can be used asa barrier and will not stainthe crown.)
g
Figure 2h. Clinical view oftooth No. 20 with dark colorstaining after 8-month recallusing MTA and composite.
h
Figure 2i. One-year recallshowing complete apical closure and an intact periodontal ligament ontooth No. 20.
i
Figure 2j. The 2-year recall on tooth No. 20 showing absence of pathology and intact periodontal ligament.
j
CASE 1
Scaffolds are “ladders” that provide support for cell organi-zation, proliferation, and vascularization.10Dentin, blood clots,and platelet-rich plasma have been used to provide scaffolds inREPs. However, there are many other types of natural or syn-thetic materials available. The most common and readily avail-able scaffold is the blood clot that is formed during the REPs.11
Growth factors are proteins that bind to receptors on the celland act as signals to induce cellular proliferation and/or differ-entiation. Examples in the pulp and dentin complex are bonemorphogenic protein, transforming growth factor-beta, and
fibroblastic growth factor. Current REPs utilize growth factorsalready found in platelets from the blood and dentin.7
Regenerative Endodontic Therapy Versus ApexificationIn the past, long-term calcium hydroxide was used to induceapexification of the immature tooth with pulpal necrosis. Oncean apical barrier was formed, obturation material such as warmgutta-percha or MTA would be placed in the root canal system.12 While the success rate of calcium hydroxide was approximately 95%, there were several problems associated
Figure 2c. Clinicalview of tooth No.20 with Cavit inplace. Note normal color ofenamel at thispoint.
c
Figure 2d. One-month recallshowing positive healing withsome calcium hydroxide stillin place.
d
Figure 2e. Completion ontooth No. 20 after one monthwith white MTA and compositefollowing second appointmenttreatment protocol (see Table2). A file is used to poke thebone and stimulate a bloodclot to bring the stem cells upinto the once-necrotic pulpchamber. The MTA is used asa barrier, not as an obturationmaterial.
e
5
CONTINUING EDUCATION
Regenerative Endodontics: Clinical Review and Case Reports
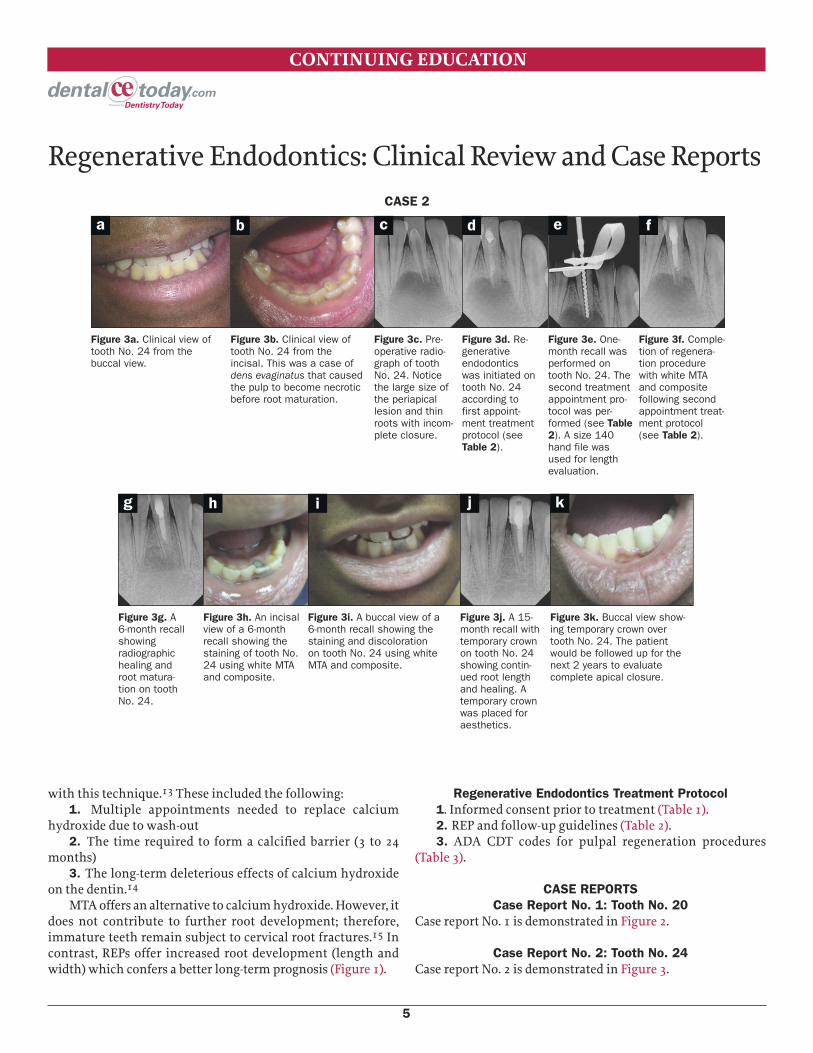
Figure 3a. Clinical view oftooth No. 24 from the buccal view.
a
Figure 3b. Clinical view oftooth No. 24 from the incisal. This was a case ofdens evaginatus that causedthe pulp to become necroticbefore root maturation.
b
Figure 3c. Pre-operative radio -graph of toothNo. 24. Noticethe large size ofthe periapical lesion and thinroots with incom-plete closure.
c
Figure 3d. Re-generative endodonticswas initiated ontooth No. 24 according tofirst appoint-ment treatmentprotocol (seeTable 2).
d
Figure 3e. One-month recall wasperformed ontooth No. 24. Thesecond treatmentappointment pro-tocol was per-formed (see Table2). A size 140hand file wasused for lengthevaluation.
e
Figure 3f. Comple-tion of regenera-tion procedurewith white MTAand composite following secondappointment treat-ment protocol(see Table 2).
f
Figure 3g. A6-month recallshowing radiographichealing androot matura-tion on toothNo. 24.
g
Figure 3h. An incisalview of a 6-month recall showing thestaining of tooth No.24 using white MTAand composite.
h
Figure 3i. A buccal view of a6-month recall showing thestaining and discolorationon tooth No. 24 using whiteMTA and composite.
i
Figure 3j. A 15-month recall withtemporary crownon tooth No. 24showing contin-ued root lengthand healing. Atemporary crownwas placed foraesthetics.
j
Figure 3k. Buccal view show-ing temporary crown overtooth No. 24. The patientwould be followed up for thenext 2 years to evaluate complete apical closure.
k
CASE 2
with this technique.13 These included the following:1. Multiple appointments needed to replace calcium
hydroxide due to wash-out2. The time required to form a calcified barrier (3 to 24
months)3. The long-term deleterious effects of calcium hydroxide
on the dentin.14MTA offers an alternative to calcium hydroxide. However, it
does not contribute to further root development; therefore, immature teeth remain subject to cervical root fractures.15 Incontrast, REPs offer increased root development (length andwidth) which confers a better long-term prognosis (Figure 1).
Regenerative Endodontics Treatment Protocol1. Informed consent prior to treatment (Table 1).2. REP and follow-up guidelines (Table 2).3. ADA CDT codes for pulpal regeneration procedures
(Table 3).
CASE REPORTSCase Report No. 1: Tooth No. 20
Case report No. 1 is demonstrated in Figure 2.
Case Report No. 2: Tooth No. 24Case report No. 2 is demonstrated in Figure 3.

Case Report No. 3: Tooth No. 9Case report No. 3 is demonstrated in Figure 4.
DISCUSSIONThe success rate of regenerative endodontics is relatively highif the procedure is done properly and the patient is compliant.Some studies show a success rate of up to 90%.7 The majorityof human case studies have shown good clinical outcomes forimmature permanent teeth with pulpal necrosis REPs.16 In addition, a positive response to cold and/or electric pulp tests
have occurred in some cases.17 The rate of root maturogenesisis variable because of unique individual immune systems.18 Aresorbable matrix such as CollaCote (Zimmer Dental) could beplaced over the blood clot so material can lay against it, but isnot essential for repair.19The 3 most important treatment factors in regenerative
endodontics are: (1) disinfection of the root canal canal, (2) establishing bleeding to create a blood clot to carry the stemcells inside the canal, and (3) a bacteria-tight seal of the accessopening.16 One of the main disinfectant agents in regenerative
6
CONTINUING EDUCATION
Regenerative Endodontics: Clinical Review and Case Reports
Figure 4a. Pre -operative radio -graph on toothNo. 9 of a 7-year-old patient withhistory of trauma.The pulp wasnecrotic with anopen apex. Acomposite placed by a general dentist had dis-lodged.
a
Figure 4b. Clinical view of toothNo. 9 crown fracture restored withcomposite. Note stable color oftooth No. 9. Tooth No. 8 was intruded because of trauma.
b
Figure 4c. Regenerative endodontics wasinitiated accord-ing to first appointmenttreatment proto-col on tooth No. 9(see Table 2).
c
Figure 4d. Endo -Sequence Root RepairMaterial was used instead of white MTAon tooth No. 9 to minimize staining.
d
Figure 4e. Open jar ofthe EndoSequenceRoot Repair Material.
e
Figure 4f. EndoSequenceRoot Repair Material wasused instead ofwhite MTA fol-lowing secondappointmenttreatment proto-col on tooth No.9 (see Table 2).
f
Figure 4g. A 6-month recallshowing improvedhealing and rootmaturation ontooth No. 9.Tooth was restored withcomposite.
g
Figure 4h. Clinical view of 6-month recall showing nostaining on tooth No. 9using EndoSequence RootRepair Material. White MTAhad usually stained by 6 to8 months.
h
Figure 4i. A 10-month recallshowing increased rootlength and healing on toothNo. 9. Tooth No.8 has now naturallyerupted into itsnormal position.
i
Figure 4j. A 10-month recallshowing stable color and novisible staining. The patientwould continue to be followedfor the next 24 months untilfull root maturation could becomplete.
j
CASE 3

therapy is sodium hypochlorite, due to its ability to removenecrotic and organic tissue from the root canal.11 It is dilutedto 3% in order to reduce toxicity to the stem cells.20 When irrigating, the side-vented needle should be introduced into theroot canal to a point 2 mm short of the apical foramen, veryslowly to prevent a sodium hypochlorite accident in the peri-apical tissue. Initial sodium hypochlorite irrigation is followedby 5 mL of sterile saline to prevent possible interaction withchlorhexidine. Chlorhexidine is recommended because of itsantimicrobial activity and long-term substantiveness interact-ing with dentin. It should not be used alone because it has notissue dissolution capabilities.Historically, research with antibiotics showed that a com-
bination of metronidazole, minocycline, and cipro floxacincould be effective against common endodontic patho gens (alsoknown as triple antibiotic paste).17 However, minocycline cancause staining of the dentin which can create an aesthetic issueas reported by Kim et al,21 and triple antibiotic paste can betoxic to living tissue in such a high concentration.22 Further-more, if a patient does not know he or she is allergic to any ofthese antibiotics, there is a potential for anaphylactic shock. Latest research has shown that calcium hydroxide can be
used as the intracanal medicament, which will properly disin-fect the canal space and stimulate proliferation of SCAPs with-out causing any severe allergic reactions or staining.22 Calciumhydroxide also acts as a physiochemical barrier, which preventsproliferation of residual micro-organisms inside the canal andhelps to prevent reinfection of micro-organisms from the oralcavity.20Calcium hydroxide should not be placed with a lentulospiral. Instead, it should be placed with a syringe-tip carrier andthen tamped down gently with a moistened cotton pellet.The use of 17% ethylenediaminetetraacetic acid (EDTA) is
recommended at the second appointment to promote survivalof the stem cells and assist with adhesion of the stem cells on
the dentin.20 EDTA is a chelating agent and decalcifies the surface of the root canal dentin to expose its collagen fibers, promoting differentiation of the stem cells which is vital in theregenerative procedure.23Several studies have shown that white MTA can cause stain-
ing after REPs.24 Blood contamination was shown to exacerbatethe color change using white MTA,25which happens due to theblood clot which forms the scaffold of the regenerative proce-dure. In addition, the sodium hypochlorite contacts the bis-muth oxide in the white MTA and causes dark brown, nearlyblack discoloration.26 A new root repair material by BrasselerUSA called EndoSequence BC Root Repair Material Fast SetPutty has shown similar results as the MTA for root maturationwith less staining and shortened set time. The putty is completelydevoid of heavy metals such as bismuth oxide, which has beenshown to cause discoloration.26 In addition, Biodentine bySeptodont has shown similar efficacy as MTA for positive bioactivity and biocompatibility in promoting dental pulp stemcell proliferation,27 and can possibly be used in REPs.
CONCLUSIONThroughout decades, there have been significant changes in theclinical management of infected immature permanent teeth,dating back to the 1960s in work by Ostby.6 In the 2000s, Banchsand Trope11 reported an alternative treatment to revasculariza-tion by introducing the use of triple antibiotic pastes. Like alldental procedures, these procedures are subject to change asmore research and case studies are published, including bettermaterials and technology. Regenerative endodontics is one of the most exciting devel-
opments in dentistry, and endodontics is at the cutting edge ofthe technology. Knowledge of pulp biology, intracanal medica-ments, and dental trauma lays the framework in which this pro-cedure should be understood in order to perform it properly andsuccessfully. A working knowledge of biological and mechani-cal skill is required to attain the highest results in order to makeregenerative endodontics a success in clinical practice.
References1. Hargreaves KM, Diogenes A, Teixeira FB. Treatment options: biological basis of re-
generative endodontic procedures. J Endod. 2013;39(suppl 3):S30-S43.2. Arany PR, Cho A, Hunt TD, et al. Photoactivation of endogenous latent transforming
growth factor–ß1 directs dental stem cell differentiation for regeneration. Sci TranslMed. May 28, 2014;238(6):238ra69. DOI: 10.1126/scitranslmed.3008234.
3. Carlson BM. Principles of Regenerative Biology. Philadelphia, PA: Academic Press;2007:400.
4. Complete regeneration. In: Min S, Wang SW, Orr W, eds. Graphic General Pathology.Shantou, China: Shantou University Medical College; 2006.
5. Cvek M. Prognosis of luxated non-vital maxillary incisors treated with calcium hydrox-ide and filled with gutta-percha. A retrospective clinical study. Endod Dent Traumatol.1992;8:45-55.
6. Ostby BN. The role of the blood clot in endodontic therapy: an experimental histo-
7
CONTINUING EDUCATION
Regenerative Endodontics: Clinical Review and Case Reports
First Phase of Treatment: D3351 (debridement and place-ment of antibacterial medication)
Interim Phase (repeat of first phase, if necessary): D3352(interim medication replacement)
Final Phase: D3354 (pulpal regeneration [completion of re-generative treatment in an immature permanent tooth with anecrotic pulp]; does not include final restoration)
Table 3. ADA Code on Dental Procedures and Nomenclature (CDT Codes) for Pulpal Regeneration Procedures

logical study. Acta Odontol Scand. 1961;19:324-353.7. Murray PE, Garcia-Godoy F, Hargreaves KM. Regenerative endodontics: a review of
current status and a call for action. J Endod. 2007;33:377-390.8. Bose R, Nummikoski P, Hargreaves K. A retrospective evaluation of radiographic out-
comes in immature teeth with necrotic root canal systems treated with regenerativeendodontic procedures. J Endod. 2009;35:1343-1349.
9. Sedgley CM, Botero TM. Dental stem cells and their sources. Dent Clin North Am.2012;56:549-561.
10.Bohl KS, Shon J, Rutherford B, et al. Role of synthetic extracellular matrix in devel-opment of engineered dental pulp. J Biomater Sci Polym Ed. 1998;9:749-764.
11.Banchs F, Trope M. Revascularization of immature permanent teeth with apical perio -dontitis: new treatment protocol? J Endod. 2004;30:196-200.
12.Frank AL. Therapy for the divergent pulpless tooth by continued apical formation. JAm Dent Assoc. 1966;72:87-93.
13.Webber RT. Apexogenesis versus apexification. Dent Clin North Am. 1984;28:669-697.
14.Andreasen JO, Farik B, Munksgaard EC. Long-term calcium hydroxide as a root canaldressing may increase risk of root fracture. Dent Traumatol. 2002;18:134-137.
15.El-Meligy OA, Avery DR. Comparison of apexification with mineral trioxide aggregateand calcium hydroxide. Pediatr Dent. 2006;28:248-253.
16.Law AS. Considerations for regeneration procedures. J Endod. 2013;39(suppl3):S44-S56.
17.Sato I, Ando-Kurihara N, Kota K, et al. Sterilization of infected root canal dentine bytopical application of a mixture of ciprofloxacin, metronidazole and minocycline in
situ. Int Endod J. 1996;29:118-124.18.Nagy MM, Tawfik HE, Hashem AA, et al. Regenerative potential of immature perma-
nent teeth with necrotic pulps after different regenerative protocols. J Endod.2014;40:192-198.
19.Kahler B, Mistry S, Moule A, et al. Revascularization outcomes: a prospective analy-sis of 16 consecutive cases. J Endod. 2014;40:333-338.
20.Siqueira JF Jr, Lopes HP. Mechanisms of antimicrobial activity of calcium hydroxide:a critical review. Int Endod J. 1999;32:361-369.
21.Kim JH, Kim Y, Shin SJ, et al. Tooth discoloration of immature permanent incisor as-sociated with triple antibiotic therapy: a case report. J Endod. 2010;36:1086-1091.
22.Ruparel NB, Teixeira FB, Ferraz CC, et al. Direct effect of intracanal medicaments onsurvival of stem cells of the apical papilla. J Endod. 2012;38:1372-1375.
23.Trevino EG, Patwardhan AN, Henry MA, et al. Effect of irrigants on the survival ofhuman stem cells of the apical papilla in a platelet-rich plasma scaffold in humanroot tips. J Endod. 2011;37:1109-1115.
24.Petrino JA, Boda KK, Shambarger S, et al. Challenges in regenerative endodontics:a case series. J Endod. 2010;36:536-541.
25.Felman D, Parashos P. Coronal tooth discoloration and white mineral trioxide aggre-gate. J Endod. 2013;39:484-487.
26.Camilleri J. Color stability of white mineral trioxide aggregate in contact with hypochlo-rite solution. J Endod. 2014;40:436-440.
27.Luo Z, Kohli MR, Yu Q, et al. Biodentine induces human dental pulp stem cell differ-entiation through mitogen-activated protein kinase and calcium-/calmodulin-depen-dent protein kinase II pathways. J Endod. 2014;40:937-942.
8
CONTINUING EDUCATION
Regenerative Endodontics: Clinical Review and Case Reports
POST EXAMINATION QUESTIONS
1. Complete regeneration is where new tissue is the same as thelost tissue. Incomplete regeneration is where fibrosis occurs afternecrotic tissue is removed.
a. The first statement is true, the second is false.b. The first statement is false, the second is true.c. Both statements are true.d. Both statements are false.
2. Another term many use to describe regenerative endodontics isrevascularization.
a. True.b. False.
3. When should regenerative endodontics be considered?a. Necrotic pulp and immature or open apex.b. Young patient.c. Very thin dentinal walls.d. All of the above.
4. The key component(s) of regenerative endodontics is/are:a. Stem cells.b. Scaffolds.c. Growth factors. d. All of the above.
5. The most current type of stem cells used in regenerative endodontics is:
a. Dental pulp stem cells.b. Stem cells from apical papilla.c. Stem cells from human deciduous teeth.d. Dental follicle progenitor stem cells.
6. The most common and readily available scaffold for use in regenerative endodontic procedures (REPs) is:
a. Dentin.b. Platelet-rich plasma.c. Blood clot.d. None of the above.
7. Growth factors in the pulp and dentin complex include:a. Bone morphogenic protein.b. Transforming growth factor-beta.c. Fibroblastic growth factor.d. All of the above.
8. One of the main disinfectant agents in regenerative therapy issodium hypochlorite. It is diluted to 6% in order to reduce toxicityto stem cells.
a. The first statement is true, the second is false.b. The first statement is false, the second is true.c. Both statements are true.d. Both statements are false.
9
CONTINUING EDUCATION
POST EXAMINATION INFORMATION
To receive continuing education credit for participation in this educational activity, you must complete the program post examination and receive a score of 70% or better.
Traditional Completion Option:You may fax or mail your answers with payment to Dentistry Today (see Traditional Completion Information on following page).All information requested must be provided in order to process the program for credit. Be sure to complete your “Payment,”“Personal Certification Information,” “Answers,” and “Evaluation” forms. Your exam will be graded within 72 hours of receipt.Upon successful completion of the post-exam (70% or higher), a letter of completion will be mailed to the address provided.
Online Completion Option:Use this page to review the questions and mark your answers. Return to dentalcetoday.com and sign in. If you have not pre-viously purchased the program, select it from the “Online Courses” listing and complete the online purchase process. Oncepurchased, the program will be added to your User History page where a Take Exam link will be provided directly across fromthe program title. Select the Take Exam link, complete all the program questions and Submit your answers. An immediategrade report will be provided. Upon receiving a passing grade, complete the online evaluation form. Upon submitting the form, your Letter of Completion will be provided immediately for printing.
General Program Information:Online users may log in to dentalcetoday.com any time in the future to access previously purchased programs and view orprint letters of completion and results.
Regenerative Endodontics: Clinical Review and Case Reports

9. This chelating agent promotes differentiation of stem cells, whichis vital in the regenerative procedure.
a. MTA.b. Calcium hydroxide.c. 17% ethylenediaminetetraacetic acid.d. None of the above.
10. In REPs, calcium hydroxide acts as a physiochemical barrieragainst micro-organisms. It should be placed into the canal witha lentulo spiral.
a. The first statement is true, the second is false.b. The first statement is false, the second is true.c. Both statements are true.d. Both statements are false.
10
CONTINUING EDUCATION
Regenerative Endodontics: Clinical Review and Case Reports

CONTINUING EDUCATION
Regenerative Endodontics: Clinical Review and Case Reports PROGRAM COMPLETION INFORMATION
If you wish to purchase and complete this activity traditionally (mail or fax) rather than online, you must provide the information requested below. Please be sure toselect your answers carefully and complete the evaluationinformation. To receive credit you must answer at least 7 of the 10 questions correctly.Complete online at: dentalcetoday.com
TRADITIONAL COMPLETION INFORMATION:Mail or fax this completed form with payment to:
Dentistry TodayDepartment of Continuing Education100 Passaic AvenueFairfield, NJ 07004
Fax: 973-882-3622
PAYMENT & CREDIT INFORMATION:
Examination Fee: $40.00 Credit Hours: 2.0
Note: There is a $10 surcharge to process a check drawn on any bank other than a US bank. Should you have additional questions, please contact us at (973) 882-4700.
o I have enclosed a check or money order.
o I am using a credit card.
My Credit Card information is provided below.
o American Express o Visa o MC o Discover
Please provide the following (please print clearly):
Exact Name on Credit Card
Credit Card # Expiration Date
Signature
PROGRAM EVAUATION FORMPlease complete the following activity evaluation questions.
Rating Scale: Excellent = 5 and Poor = 0
Course objectives were achieved.
Content was useful and benefited your clinical practice.
Review questions were clear and relevant to the editorial.
Illustrations and photographs were clear and relevant.
Written presentation was informative and concise.
How much time did you spend reading the activity and completing the test?
What aspect of this course was most helpful and why?
What topics interest you for future Dentistry Today CE courses?
ANSWER FORM: COURSE #: 183Please check the correct box for each question below.
1. o a o b o c o d 6. o a o b o c o d
2. o a o b 7. o a o b o c o d
3. o a o b o c o d 8. o a o b o c o d
4. o a o b o c o d 9. o a o b o c o d
5. o a o b o c o d 10. o a o b o c o d
PERSONAL CERTIFICATION INFORMATION:
Last Name (PLEASE PRINT CLEARLY OR TYPE)
First Name
Profession / Credentials License Number
Street Address
Suite or Apartment Number
City State Zip Code
Daytime Telephone Number With Area Code
Fax Number With Area Code
E-mail Address
/
Dentistry Today, Inc, is an ADA CERP RecognizedProvider. ADA CERP is a service of the American DentalAssociation to assist dental professionals in indentifyingquality providers of continuing dental education. ADACERP does not approve or endorse individual coursesor instructors, nor does it imply acceptance of credithours by boards of dentistry. Concerns or complaintsabout a CE provider may be directed to the provider orto ADA CERP at ada.org/goto/cerp.
Approved PACE Program ProviderFAGD/MAGD Credit Approval doesnot imply acceptance by a state orprovincial board of dentistry or AGDendorsement. June 1, 2012 to May 31, 2015 AGD PACE approvalnumber: 309062
11
Related Documents











