Reflections on Reflections on previous rounds’ previous rounds’ proposals proposals Laksami Suebsaeng Laksami Suebsaeng WHO/SAERO WHO/SAERO

Reflections on previous rounds’ proposals Laksami Suebsaeng WHO/SAERO.
Dec 27, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Reflections on previous Reflections on previous rounds’ proposalsrounds’ proposals
Laksami SuebsaengLaksami SuebsaengWHO/SAEROWHO/SAERO

AIDS in Asia AIDS in Asia
An estimated 8.6 million people were living with An estimated 8.6 million people were living with HIV/AIDS in 2006HIV/AIDS in 2006960,000 newly infected individuals960,000 newly infected individualsApproximately 630,000 people died from AIDS-Approximately 630,000 people died from AIDS-related illnesses. related illnesses. Although the number of people receiving ART Although the number of people receiving ART has increased more than three-fold since 2003, has increased more than three-fold since 2003, reaching an estimated 235,000 people by June reaching an estimated 235,000 people by June 2006, this only represents16% of the total 2006, this only represents16% of the total number of people in need of ART in Asia.number of people in need of ART in Asia.

SE Asia – HIV/AIDS
Has the second highest burden of HIV in the world. Although the overall adult HIV prevalence in the Region is less than 1%, the total burden in terms of absolute number of affected people is huge due to a large population base. By the end of 2006, there were an estimated 7.2 million people living with HIV in SEAR. This includes 0.77 million new infections in 2006. Approximately half a million persons died of AIDS during 2006

HIV remains concentrated and uncontrolled in populations engaged in high-risk behaviors, such as, SWs, IDUs, and MSM.
In countries with long standing epidemics such as Thailand and India, HIV is now spreading from high-risk populations to their male clients and then to their monogamous spouses. Thus, women are being increasingly affected.
Further, a high burden of STIs effects the HIV epidemic.
Social factors such as poverty, low literacy and widespread stigma provide an adverse setting for spread of HIV.
Moreover, health systems in many Member States are weak.
These place constraints on expansion of prevention, treatment and care services.

TuberculosisTuberculosis
Southeast Asia: With an estimated three million new cases of TB each year, this is the world's hardest-hit region.

Tuberculosis control: progress and Tuberculosis control: progress and long-term planninglong-term planning
Progress: good to excellentFocussed attention needed on: HSS, sustainability and quality, partnerships including community involvement, and impact evaluation and researchAddressing newer challenges: Drug resistance, TB-HIV, fighting complacencyBuilding technical and managerial capacity at country level a key priority

MalariaMalariaFocus has been on malaria in Africa
Big burden of malaria in Asia: 100 million cases annually; affecting all age groups; repeated attacks common; monotherapy prevalent; drug resistance expanding; outbreaks occurring frequently
Need to scale up evidence-based, local-specific prevention and treatment interventions using multi-sectoral and integrated approach
Prevention based on ecological, environmental and behavioural determinants and treatment using appropriate/effective combination therapies

Region Number of people receiving ARVsRegion Number of people receiving ARVs
East Africa East Africa 115,000 115,000Southern Africa Southern Africa 109,000109,000East Asia & the Pacific East Asia & the Pacific 73,000 73,000West and Central Africa West and Central Africa 45,000 45,000Latin America & the Caribbean Latin America & the Caribbean 28,000 28,000South Asia South Asia 9,000 9,000Eastern Europe & Central Asia 3,000Eastern Europe & Central Asia 3,000North Africa & the Middle East 2,000North Africa & the Middle East 2,000
Total 384,000Total 384,000

GFATM-supportedGFATM-supported
Results of Global Fund-supported programs for the major indicators show millions are receiving lifesaving services, results are doubling each year and Global Fund targets for 2006 have been met or exceeded.
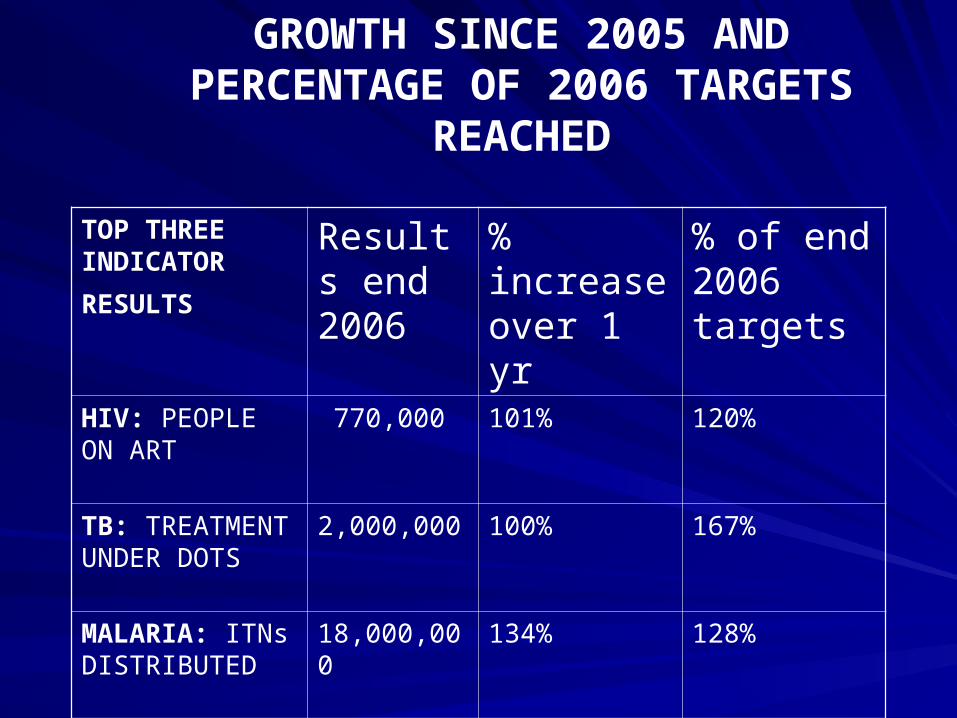
GROWTH SINCE 2005 AND PERCENTAGE OF 2006 TARGETS
REACHED
TOP THREE INDICATOR
RESULTS
Results end 2006
% increase over 1 yr
% of end 2006 targets
HIV: PEOPLE ON ART
770,000 101% 120%
TB: TREATMENT UNDER DOTS
2,000,000 100% 167%
MALARIA: ITNs DISTRIBUTED
18,000,000 134% 128%

TBTB
Global Fund grants are helping to Global Fund grants are helping to detect detect 5 million additional cases5 million additional cases of of infectious tuberculosis infectious tuberculosis
cure cure 3 million people3 million people through the through the internationally approved DOTS treatment internationally approved DOTS treatment strategy strategy
24,000 new treatments24,000 new treatments of multi-drug of multi-drug resistant tuberculosis resistant tuberculosis

MalariaMalaria
finance finance 109 million bed nets109 million bed nets to protect to protect families from transmission of malaria, thus families from transmission of malaria, thus becoming the largest financier of becoming the largest financier of insecticide-treated bed nets in the world insecticide-treated bed nets in the world
deliver deliver 264 million artemisinin-based 264 million artemisinin-based combination drug treatmentscombination drug treatments for for resistant malaria resistant malaria

Thailand:Thailand:
The Global Fund supports 70 to 80 percent of The Global Fund supports 70 to 80 percent of the investment in laboratory infrastructure, CD4 the investment in laboratory infrastructure, CD4 count and viral load machines, and 25 percent of count and viral load machines, and 25 percent of the CD4 count and viral load reagents. the CD4 count and viral load reagents. The Global Fund supports procurement of ARV The Global Fund supports procurement of ARV drugs that cover 25 percent of the national ART drugs that cover 25 percent of the national ART program. program. The Global Fund also supports the provincial The Global Fund also supports the provincial data coordinators for M&E and care programs data coordinators for M&E and care programs for PLWHAs in 140 hospitals.for PLWHAs in 140 hospitals.

Approved funding by RegionApproved funding by Region
East Africa $2.59 billion
Southern Africa $2.08 billion
West and Central Africa $1.91 billion
East Asia and the Pacific $1.55 billion
South Asia $1.07 billion
Eastern Europe and Central Asia $1.90 billion
Latin America and the Caribbean $0.85 billion
North Africa and the Middle East $0.76 billion
Total $12.7 billion in 126 countries

Distribution of funding after 6 Distribution of funding after 6 roundsrounds

Distribution of funding after 6 Distribution of funding after 6 roundsrounds

Round 6 – SE Asia and PacificRound 6 – SE Asia and PacificCambodia Malaria 13,148,613 31,191,393
China HIV/AIDS 5,812,875 14,395,715
Malaria 7,047,932 16,808,186
Indonesia Malaria 27,727,920 57,965,100
Lao PDR HIV/AIDS 3,418,698 8,978,927
Malaria 1,726,701 4,099,092
PNG TB 5,007,912 20,869,303
Philippines HIV/AIDS 7,474,964 18,434,190
Malaria 16,297,659 22,344,786
Thailand TB 7,726,769 19,627,001
Vietnam HIV/AIDS 10,219,180 28,771,590
TB 1,614,335 10,638,357
REGION TOTALS: 236,390,316 643,082,770

Round 6 – South AsiaRound 6 – South Asia
Bangladesh HIV/AIDS 13,998,844 40,002,452
Malaria 18,587,179 39,062,586
Bhutan HIV/AIDS 1,812,825 3,596,325
TB 884,690 1,773,135
India HIV/AIDS 75,954,670 259,211,574
TB 9,072,464 24,271,555
Maldives HIV/AIDS 2,655,685 4,865,956
Sri Lanka HIV/AIDS 1,009,760 1,884,360
TB 5,190,641 14,291,187
REGION TOTALS: 236,390,316 643,082,770

Most common strengths of proposals submitted to GF – comments of TRP
round 3-6
The proposal was clear, well organised and well-documented; the strategy was sound. e.g. Bhutan (H), Cambodia (H), Lao PDR (M), Maldives (H)
The proposal demonstrated complementarity – i.e., it built on existing activities, including national strategic plans, and/or it built on earlier programmes financed by the Global Fund. e.g. Cambodia (M)

There was good involvement of partners (including NGOs and other sectors) in the implementation plan. e.g. Bhutan (H), India (H), East Timor (H)
The proposal contained a good situational analysis.
There was a strong political commitment to implement the programme. e.g. Bhutan (T)

Other strengths identified fairly frequently:
Programme targeted high-risk groups and vulnerable populations, e.g. Bangladesh (M), Sri Lanka (H)
Demonstrated sustainability – i.e., national budgets were identified to help sustain the activities once Global Fund support terminates. Demonstrated good co-funding.
M&E plan was solid, e.g. Bhutan (H)
Budget was well detailed, well presented and reasonable, e.g. Nepal (T), PNG (T).
Proposal reflected comments made by the TRP during earlier rounds of funding.
Good collaboration between HIV and TB.
Realistic with respect to what could be accomplished, and/or had a limited and concentrated focus.

More strengths:The PR is a strong organisation, with experience managing similar programmes, e.g. Laos, Thailand
The CCM was strong and had wide sectoral representation.
The proposal was developed through a transparent, participatory process, e.g. China (H)
Included capacity building measures and identified technical support needs, e.g. Indonesia (T)
Built on lessons learned and best practices, India (H)
Contained innovative strategies, some of which could lead to best practices.
Had a strong human rights focus.
Contained solid strategies for procurement and supply management (PSM), e.g. PNG (T)

The following strengths began to emerge during Round 6:
The proposal described solid strategies for managing the programme, e.g. India (T)
The proposal contained solid indicators and targets.
The proposal identified the SRs, and/or provided a good description of the process for identifying the SRs, e.g. Lao (H)
The proposal contained a strong section on health systems strengthening (HSS), e.g. India (T)

Weaknesses identified most often: Narrative description of the programme was inadequate, insufficient, unclear or questionable information on one or more of the following: the rationale, the strategic approach, the objectives, the activities, the indicators, the targets and the expected outcomes.
Budget information was inaccurate, questionable and/or not sufficiently detailed.
Did not demonstrate complementarity or additionality; it was not clear how the programme related or added to existing programmes, including programmes funded by the GF through earlier grants.
Did not contain a good situational (i.e., gap) analysis.

Other weaknesses identified frequently:
Some of the proposed approaches or activities were inappropriate.
There were problems concerning the PR or CCM.
Programme was too ambitious; some or all of the goals, objectives and targets were not realistic.
The use of partners (including NGOs) in the implementation of the programme was inadequate or unclear.
Did not focus sufficiently on vulnerable groups.

M&E plan was inadequate.
Plan for PSM was inadequate.
Failed to adequately address issues of capacity building and technical
Failed to address weaknesses identified by the TRP for proposals submitted in earlier rounds of funding.

More weaknesses:Insufficient attention was paid to human rights issues.
Budget was imbalanced; too much or too little was allocated to one or more sectors or activities. Demonstrated insufficient co-funding.
Proposal development process was not sufficiently transparent or inclusive.
There were either no joint activities or insufficient joint activities involving TB and HIV;
The treatment, care and support component of the proposal was missing or inadequate.
Failed to demonstrate absorptive capacity.
Information on sustainability was lacking.
How health systems will be strengthened is not well explained.

Following weaknesses started to emerge in Round 6:
Lack of information concerning problems with previous Global Fund grants.
Failed to make the case for additional funding over and above that received from earlier grants.
Insufficient information on how the project would be coordinated.

Health system
Stewardship
Financing
Human resources
Technologies and infrastructure
Information and
knowledge
Service delivery
Stewardship Financing
Human resourcesTechnologies and
infrastructure Information and knowledge
Service delivery
Stewardship Financing
Human resourcesTechnologies and
infrastructure Information and knowledge
Service deliveryStewardship Financing
Human resourcesTechnologies and
infrastructure Information and knowledge
Service delivery
HIV/AIDS control programme
Malaria control programme
TB control programme

Possible areas where GF Possible areas where GF resources may be used for HSDresources may be used for HSD
Primary Health Care infrastructure and service Primary Health Care infrastructure and service deliverydelivery
Laboratory, blood safety, Laboratory, blood safety,
Drug procurement, logistics managementDrug procurement, logistics management
Human resource development and managementHuman resource development and management
Linking with the Private sectorLinking with the Private sector
Strengthening health information systemsStrengthening health information systems
Surveillance monitoring and evaluationSurveillance monitoring and evaluation

Health System ComponentHealth System Component
Not limited to health sector: may include Not limited to health sector: may include education, workplace . But it must:education, workplace . But it must:– Demonstrate a clear benefit in the fight Demonstrate a clear benefit in the fight
against AIDS, tuberculosis and/or malariaagainst AIDS, tuberculosis and/or malaria– Show that it is a necessary prerequisite to Show that it is a necessary prerequisite to
scaling up against any or all of the three scaling up against any or all of the three diseases diseases
– Describe how it will have positive system-wide Describe how it will have positive system-wide effects. effects.


DOTS combines five elements: political DOTS combines five elements: political commitment, microscopy services, drug commitment, microscopy services, drug supplies, surveillance and monitoring supplies, surveillance and monitoring systems, and use of highly efficacious systems, and use of highly efficacious regimes with direct observation of regimes with direct observation of treatment treatment

GUIDING PRINCIPLESGUIDING PRINCIPLES
Focusing on sustainability after GF projects are overConcentrating on cross -cutting aspects of health systems that benefit the fight against AIDS, tuberculosis and/or malaria Building on existing health systems and infrastructure to scale up service delivery for the 3 diseasesStrengthening partnerships between the public sector, private sector, and NGOs

What’s new about the new Stop TB
Strategy?
Sustaining quality DOTS
Additional interventions
– Address TB/HIV & MDR-TB
– Contribute to health system strengthening
– Engage all care providers
– Empower patients and communities
– Enable and promote operational research

Translating the strategy into action
Member countries are requested to:
– Support the full implementation of the Regional Plan
2006-2015 aimed at achieving the TB related MDGs
– Develop long and medium-term plans based on the
new strategy, adapted to country-specific contexts
– Sustain adequate financing through domestic and
external funding, in line with WHA 58 resolution:
“Sustainable financing for TB prevention and control”

Implementation at country level
Build capacity: ensure adequate skilled personnel and
infrastructure, including for laboratories
Strengthen surveillance and monitoring systems
Scale up public and private partnerships at all levels
Accelerate interventions to prevent drug-resistance and
enhance collaboration with AIDS programmes
Augment significantly advocacy, communication and
social mobilization approaches
Strengthen delivery of TB services through primary health
care systems

WHO’s role?WHO’s role?To help governments through:To help governments through:
Support for mobilising funds from Global Fund (and Support for mobilising funds from Global Fund (and others)others)
Ensuring that health system development is an integral Ensuring that health system development is an integral part of GF proposals.part of GF proposals.
Bringing together people and build networks of national Bringing together people and build networks of national institutions and WHO collaborating centres, which institutions and WHO collaborating centres, which contribute to common health system goalscontribute to common health system goals
Facilitating cross-country support and interaction in Facilitating cross-country support and interaction in assessment and policy analysisassessment and policy analysis

WHO SEARO Support
Facilitating GFATM Regional technical meetings
Briefing/communication on GFATM Board, SEAR Constituency and Task Force meetings
Proposal development/mock TRP
Technical support missions
Facilitating mobilization of other sources of funds where GFATM support is not there

Related Documents











