1. Wilding IR, Davis SS, Pozzi F, Furlani P, Gazzaniga A. Enteric coated timed release systems for colonic targeting. Int J Pharm. 1994;111:99-102. 2. Niwa K, Takaya T, Morimoto T, Takada I. Preparation and evaluation of a time controlled release capsule made of ethyl cellulose for colon delivery of drugs. J Drug Target. 1995;3:83-89. 3. Gazzaniga A, Iamartino P, Maffione G, Sangalli ME. Oral delayed- release system for colonic specific delivery. Int J Pharm. 1994;2(108):77-83. 4. Gazzaniga A, Sangalli ME, Giordano F. Oral chronotopic & Mac226: drug delivery systems: achievement of time and/or site specifity. Eur J Biopharm. 1994;40(4):246-250. 1. Wilding IR, Davis SS, Bakhshaee M, Stevens HNE, Sparrow RA, Brennan J. Gastrointestinal transit and systemic absorption of captopril from a pulsed-release formulation. Pharm Res.1992;9:654- 657. 2. Saeger H, Virley P. Pulsincap& Mac226: Pulsed-Release Dosage Form. Product information from Scherer DDS, Ltd; 2004. 3. Binns J, Stevens HNE, McEwen J, Pritchard G, Brewer FM, Clarke A, Johnson ES, McMillan I. The tolerability of multiple oral doses of Pulsincap & Mac226 capsules in healthy volunteers. J Control Rel. 1996;38:151-158. 4. Kr? I, Bodmeier R. Pulsatile drug release from an insoluble capsule body controlled by an erodible plug. Pharm Res. 1998;15(3):474-481. 5. Kr? I, Bodmeier R. Evaluation of an enzyme-containing capsular shaped pulsatile drug delivery system. Pharm Res. 1999;16(9):1424- 1429. 6. Crison JR, Siersma PR, Taylor MD, Amidon GL. Programmable oral release technology, Port Systems & Mac226: a novel dosage form for time and site specific oral drug delivery. Proceed Intern Symp Control Rel Bioact Mater. 1995;22:278-279. 1. Conte U, Colombo P, La Manna A, Gazzaniga A. A new ibuprofen pulsed release oral dosage form. Drug Dev Ind Pharm. 1989;15(14- 16):2583-2596. 1. Bussemer T, Bodmeier R. Pulsatile drug release from coated capsules. AAPS Pharm Sci. 1999;1(4 suppl):434 (1999). 1. Ueda Y, Hata T, Yamaguchi H, Ueda S, Kotani M. Time Controlled Explosion System and Process for Preparation for the Same. US Patent No. 4,871,549;1989. 2. Ueda Y, Hata T, Yamaguchi H, Kotani M, Ueda S. Development of a novel drug release system, time-controlled explosion system (TES). Part 1: concept and design. J Drug Targeting. 1994;2:35-44.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1. Wilding IR, Davis SS, Pozzi F, Furlani P, Gazzaniga A. Enteric coated timed release systems for colonic targeting. Int J Pharm. 1994;111:99-102.
2. Niwa K, Takaya T, Morimoto T, Takada I. Preparation and evaluation of a time controlled release capsule made of ethyl cellulose for colon delivery of drugs. J Drug Target. 1995;3:83-89.
3. Gazzaniga A, Iamartino P, Maffione G, Sangalli ME. Oral delayed-release system for colonic specific delivery. Int J Pharm. 1994;2(108):77-83.
4. Gazzaniga A, Sangalli ME, Giordano F. Oral chronotopic & Mac226: drug delivery systems: achievement of time and/or site specifity. Eur J Biopharm. 1994;40(4):246-250.
1. Wilding IR, Davis SS, Bakhshaee M, Stevens HNE, Sparrow RA, Brennan J. Gastrointestinal transit and systemic absorption of captopril from a pulsed-release formulation. Pharm Res.1992;9:654-657.
2. Saeger H, Virley P. Pulsincap& Mac226: Pulsed-Release Dosage Form. Product information from Scherer DDS, Ltd; 2004.
3. Binns J, Stevens HNE, McEwen J, Pritchard G, Brewer FM, Clarke A, Johnson ES, McMillan I. The tolerability of multiple oral doses of Pulsincap & Mac226 capsules in healthy volunteers. J Control Rel. 1996;38:151-158.
4. Kr? I, Bodmeier R. Pulsatile drug release from an insoluble capsule body controlled by an erodible plug. Pharm Res. 1998;15(3):474-481.
5. Kr? I, Bodmeier R. Evaluation of an enzyme-containing capsular shaped pulsatile drug delivery system. Pharm Res. 1999;16(9):1424-1429.
6. Crison JR, Siersma PR, Taylor MD, Amidon GL. Programmable oral release technology, Port Systems & Mac226: a novel dosage form for time and site specific oral drug delivery. Proceed Intern Symp Control Rel Bioact Mater. 1995;22:278-279.
1. Conte U, Colombo P, La Manna A, Gazzaniga A. A new ibuprofen pulsed release oral dosage form. Drug Dev Ind Pharm. 1989;15(14-16):2583-2596.
1. Bussemer T, Bodmeier R. Pulsatile drug release from coated capsules. AAPS Pharm Sci. 1999;1(4 suppl):434 (1999).
1. Ueda Y, Hata T, Yamaguchi H, Ueda S, Kotani M. Time Controlled Explosion System and Process for Preparation for the Same. US Patent No. 4,871,549;1989.
2. Ueda Y, Hata T, Yamaguchi H, Kotani M, Ueda S. Development of a novel drug release system, time-controlled explosion system (TES). Part 1: concept and design. J Drug Targeting. 1994;2:35-44.
3. Ueda S, Yamaguchi H, Kotani M, Kimura S, Tokunaga Y, Kagayama A, Hata T. Development of a novel drug release system, time-controlled explosion system (TES). Part II: design of multiparticulate TES and in vitro drug release properties. Chem Pharm Bull. 1994;42(2):359-363.
4. Ueda S, Ibuki R, Kimura S, Murata S, Takahashi T, Tokunaga Y, Hata T. Development of a novel drug release system, time controlled explosion system (TES). Part III: relation between lag time and membrane thickness. Chem Pharm Bull. 1994;42(2):364-367.
5. Evaluation of gastro-resistance pulse release delivery system ( Pulsincap ) in human
Clive G. Wilson; Massoud Bakhshaee; Howard N. E. Stevens; Alan C. Perkins; Malcolm Frier; Elaine P. Blackshaw; Julie S. Binns Drug Delivery, 1521-0464, Volume 4, Issue 3, 1997, Pages 201 – 2061. Krishnaiah, Y.S.R., Bhaskar Reddy, P.R. and Satyanarayana, V., Int. J. Pharm.,
2002, 236, 43. 2. Samanta, M.K., Suresh, N.V. and Suresh, B., Indian J. Pharm. Sci., 2000, 62,
102. 3. Sarasija, S. and Hota, A., Indian J. Pharm. Sci., 2000, 62, 1. 4. Gandhi, R., Kaul, C.L. and Panchagnula, R., PSTT, 1999, 2, 160.
5. Seshasayana, A., Sreenivasa Rao, B., Prasanna Raju, Y. and Ramana Murthy, K.V., Indian J. Pharm. Sci., 2001,63, 337.
6. Indian Pharmacopoeia, Vol. I, Ministry of Health, Govt. of India, 1996,488.
Colon Targeted Delivery Systems of Metronidazole Based on Osmotic Technology: Development and EvaluationKumar, P. and Singh, S. and Mishra, B.CHEMICAL \& PHARMACEUTICAL BULLETIN. 2008; 56(9): 1234-1242 [Pubmed]
Gurny, R., Junginger, H.E. and Peppas, N., Eds., In; Pulsatile Drug Delivery: Current Application and Future Trends, Wissenschefliche Verlagsgesellschaft,
Stuttgart, Germany, 1993, 36.
Lemmer, B., J. Pharm. Pharmacol. , 1999, 51, 887.
Chourasia, M.K. and Jain, S.K., J. Pharm. Pharm. Sci., 2003, 6, 33. Mc Neill, M.E., Rashid, A. and Stevens, H.N.E., GBPatent No., GB2230442,
1993. Bakshee, M., Burns, J.S., Stevens, H.N.E. and Miller, C.J., Pharm Re, 1992, 9
(Suppl), F230. Hebden, J.M., Wilson, C.G., Spiller, R.C., GilChrist P.J., BlackShaw P.E., Frier, M.
and Perkins, A.C., Pharm. Res., 1999, 16, 1087. Burns, J.S., Stevens, H.N.E., McEwen, J., Pritchard, G., Brewer, F.M., Clarke, A.,
Johnsons, E.S. and McMillan, I., J. Control. Release, 1996, 38, 151. Stevens, H.N.E., Rashid, A. and Bakshee, M., US Patent No., US5474784, 1995.
Ross, A.C.; Macrae, R.J.; Walther, M.; Stevens, H.N.E. J. Pharm. Pharmcol., 2000,
52, 903.
Krogel, I. and Bodmeier, R., Pharm. Res., 1998, 15, 474. Stevens, H.N.E., Ross, A.C. and Johnson, J.R., J. Pharm. Pharmcol. , 2000, 52,
S41. Soutar, S., Stevens, H.N.E., Mahony, B.O., Bakshee, M., Perkins, A.C., Grattan, T. and Wilson, C.G., Proc. Int. Symp. Control Release Bioact. Mater., 2001, 28,
790. Crison, J.R., Siersna, P.R., Taylor, M.D. and Amidon, G.L., Proc. Int. Symp.

Control Release Bioact. Mater., 1995, 22, 278.
Linkwitz, A., Magruder, J.A., Merrill, S., US Patent No., US5318558, 1994. Gazzaniga, A., Ianartino, P., Maffione, G. and Sangalli, M.E., Int. J. Pharm., 1994,
2, 77. Gazzaniga, A.; Sangalli, M.E.; Giordano, F.; Eur J. Biopharm. Pharm., 1994, 40,
246. Gazzaniga, A., Busetti, C., Moro, L., Crimella, T., Sangalli, M.E. and Giordano, F.,
Proc. Int. Symp. Control Release Bioact. Mater., 1995, 22, 242.
Polli, S., Busetti, C. and Moro, L., EP Patent No., EP0572942, 1993. Sangalli, M.E., Maroni, A., Zema, L., Busetti, C., Gazzaniga, A. and Giordano, F., J.
Control. Release, 2001, 73, 103.
Midha, K.K.; Teicher , M.H. US Patent No., US6217904, 2001 . Dittigen, M.; Fricke, S.; Timpe, C.; Gercke, H.; Eichardt, A. US Patent No., US
6117450, 2000.
Pope, D.G.; Royce, A.E. US Patent No., US473958, 1988 Sungthongjeen, S., Puttipipakhachorn, S., Paeratakul, O., Dashevsky, A. and
Bodmeier, R., J. Control. Release, 2004, 95, 147. Bussemer, T., Dashevsky, A. and Bodimeier, R., J. Control. Release, 2003, 93,
331.
Bussemer, T., Bodmeier, R., Int. J. Pharm. , 2003, 267, 59.
Bechgaard, H.; Ladefoged, K. J. Pharm. Pharmacol, 1978, 30, 690.
Guo, X. PhD thesis, The University of Texas, Austin, 1996.
Chen ,C.M., US Patent No., US5260068, 1993.
Bai. US Patent No., US 5840329, 1998.
Dethlefsen, U. and Repgas, R., Med Klinik , 1985, 80, 44 . Urwitz, H., Karim, A. and Burns, H.S., J. of Clinical PharmEvaluation of an Enzyme-Containing Capsular Shaped Pulsatile Drug Delivery System
Ina Krögel1 and Roland Bodmeier1
(1) College of Pharmacy, Freie Universität Berlin, Kelchstr. 31, 12169 Berlin, GermanyAbstract Purpose. To develop an enzymatically-controlled pulsatile drug release system based on an impermeable capsule body, which contains the drug and is closed by an erodible pectin/pectinase-plug. Methods. The plug was prepared by direct compression of pectin and pectinase in different ratios. In addition to the disintegration times of the plugs, the lag times and the release profiles of the pulsatile system were determined as a function of pectin:enzyme ratio, the pH of the surrounding medium, and the addition of buffering or chelating agents.Results. The disintegration time of the plug, respectively the lag time prior to the drug release was controlled by the pectin:enzyme ratio and the plug weight. The inclusion of a buffering agent within the plug lead to a plug disintegration independent of the surrounding pH. The addition of Na-EDTA hindered the formation of non-soluble calcium pectinate in the presence of calcium ions in the environment. The addition of effervescent agents to the capsule content resulted in a rapid emptying of the capsule content after plug degradation.Conclusions. A pulsatile drug delivery system based on an erodible pectin plug containing a pectinolytic enzyme was developed. The drug release was controlled by the enzymatic degradation and dissolution of pectin.
controlled drug release - enzymatically-controlled drug release - oral drug delivery - pectin - pulsatile drug release
Roland BodmeierEmail: [email protected]
Fulltext Preview (Small, Large)
SummaryExpert Opinion on Drug DeliveryApril 2009, Vol. 6, No. 4, Pages 441-452 , DOI 10.1517/17425240902895972
Multiple-pulse drug delivery systems: setting a new paradigm for infectious disease therapy
Nitin Saigal , Sanjula Baboota , Alka Ahuja & Javed Ali † Faculty of Pharmacy, Department of Pharmaceutics, Jamia Hamdard, Hamdard Nagar, New Delhi 110 062, India +91 9811 312247; +91 11 2605 9663; [email protected]
† Author for correspondence
Background: Pulsatile drug delivery of actives based on the body's biological rhythms came into sight as a novel and emerging concept in the field of drug delivery. The concept of late has given birth to another field of research worth exploring: multiple-pulse drug delivery. Objective: Delivering a drug in multiple pulses has been applied to antibiotics for effective and patient compliant drug delivery. Delivering antibiotics in divided pulses results in better annihilation of microbes, as it prevents them going into a resistant/dormant stage and developing biological tolerance. The concept appears to have potential, and on 16 March 2009 MiddleBrook™ Pharmaceuticals, Inc. will launch the first of such once-daily product based on their proprietary pulsatile drug delivery technology, PULSYS™. Methods: This review focuses on the rationale, possible strategies and technologies employed for multiple-pulse delivery, as well as current status and future trends. Conclusion: The concept is in its infancy and promises great potential in the fight against microbial resistance; many approved formulations based on similar approaches with new and improved therapeutic paradigms are anticipated in the near future.
Howard N. E. Stevens , , a, Clive G. Wilsona, Peter G. Wellinga, Massoud
Bakhshaeeb, Julie S. Binnsb, Alan C. Perkinsc, Malcolm Frierc, Elaine P.
Blackshawc, Margaret W. Framed, Don J. Nicholsd, Michael J. Humphreyd and
Steve R. Wicksd

a Department of Pharmaceutical Sciences, University of Strathclyde, 27 Taylor Street,
Glasgow G4 0NR, UK
b Scherer DDS Ltd, Clydebank, UK
c Department of Medical Physics, Queen's Medical Centre, Nottingham, UK
d Pfizer Central Research, Sandwich, UK
Received 8 January 2001;
revised 17 December 2001;
accepted 10 January 2002.
Available online 30 January 2002.
Abstract
Pulsincap™ formulations designed to deliver a dose of drug following a 5-h delay were
prepared to evaluate the capability of the formulation to deliver dofetilide to the lower
gastrointestinal (GI) tract. By the expected 5-h release time, the preparations were well
dispersed throughout the GI tract, from stomach to colon. Plasma analysis permitted drug
absorption to be determined as a function of GI tract site of release. Dofetilide is a well-
absorbed drug, but showed a reduction in observed bioavailability when delivered from
the Pulsincap™ formulations, particularly at more distal GI tract sites. Dispersion of the
drug from the soluble excipient used in this prototype formulation relies on a passive
diffusion mechanism and the relevance of this factor to the reduced extent and
consistency of absorption from the colon is discussed. In these studies the effects of the
degree of dispersion versus the site of dispersion could not be ascertained; nevertheless
the scintigraphic analysis demonstrated good in vitro–in vivo correlation for time of
release from Pulsincap™ preparations. The combination of scintigraphic and
pharmacokinetic analysis permits identification of the site of drug release from the
dosage form and pharmacokinetic parameters to be studied in man in a non-invasive
manner.
Author Keywords: Pulsatile release; Site-release; Gamma scintigraphy;
Pharmacokinetics; Dofetilide; Pulsincap™
Article Outline
1. Introduction
2. Materials and methods 2.1. Preparation of radiolabelled Pulsincap™ dosage forms 2.2. Study design 2.3. Study protocol 2.4. Data analysis
3. Results and discussion 3.1. In vivo study 3.2. Pharmacokinetic analysis 3.3. Correlation of pharmacokinetic and scintigraphic assessment4. Discussion References
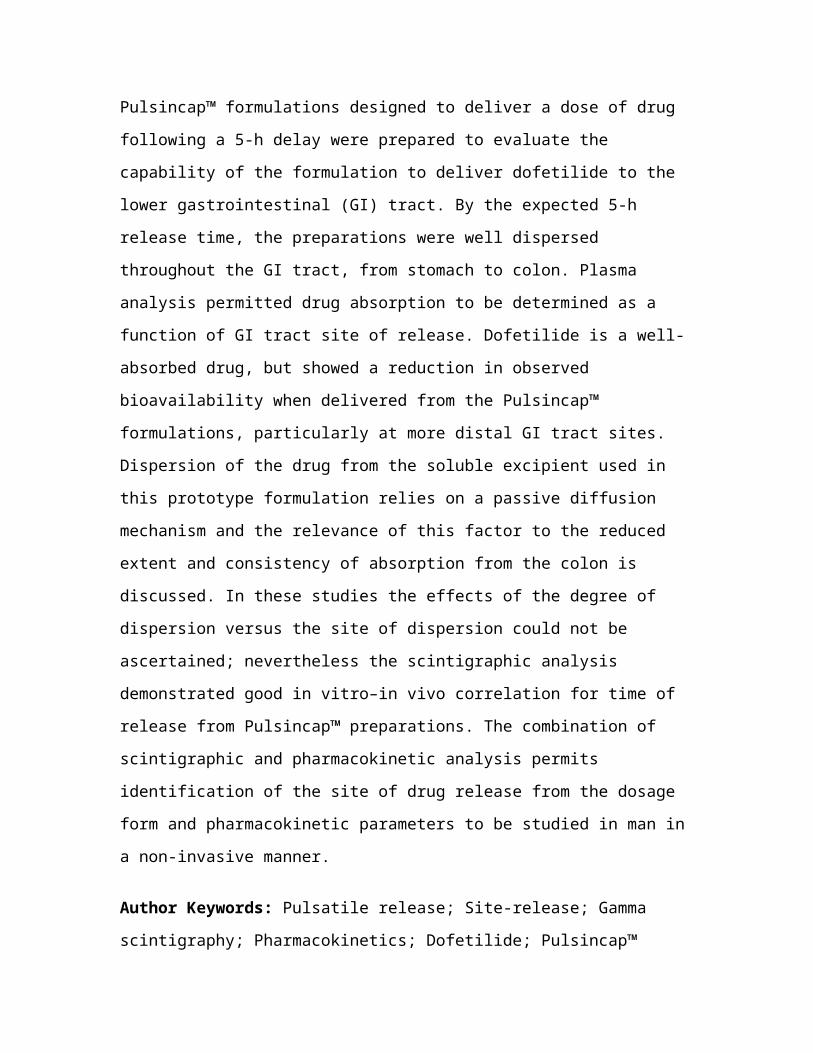
Fig. 1. Configuration of Pulsincap™ used in the study.
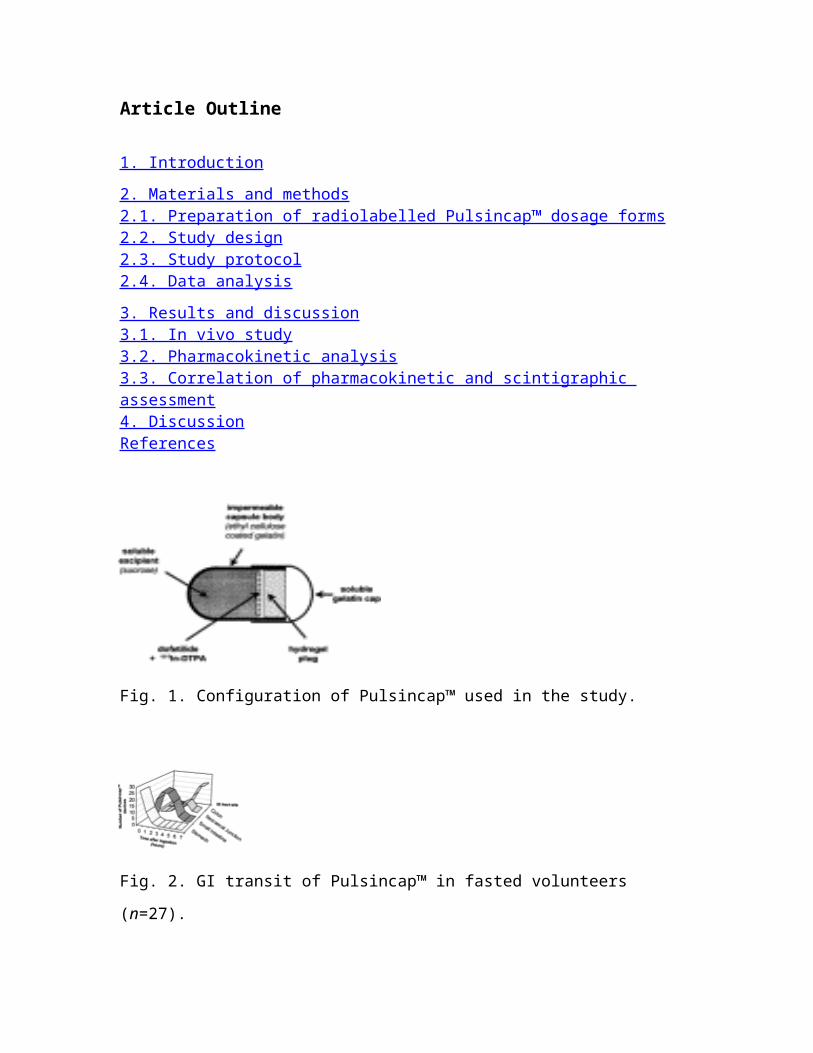
Fig. 2. GI transit of Pulsincap™ in fasted volunteers (n=27).
Fig. 3. Pharmacokinetic profile, GI transit and scintigraphic release in one subject.
Fig. 4. Dofetilide plasma profiles in a single subject with Pulsincap™ doses released in
small intestine (normalised for time 0=time of first appearance of drug in plasma).
Table 1. Mean (±S.D.) pharmacokinetic parameter values from individual plasma
dofetilide profiles following 1.0 mg solution oral dose (n=10)
r=Correlation coefficient between actual dofetilide plasma profiles and computer
generated profiles based on one compartment pharmacokinetic model.
Table 2. Pharmacokinetic parameter values (±S.D.) for Pulsincap™ formulations as a
function of dose of dofetilide and site of release in the GI tract
Table 3. Dofetilide bioavailability as a function of GI tract site for solution and
Pulsincap™ formulations
Corresponding author. Tel.: +44-141-548-2441; fax: +44-141-552-6443; email:
International Journal of PharmaceuticsVolume 236, Issues 1-2, 2 April 2002, Pages 27-34 Enteric coated timed release systems for colonic targeting
I.R. Wilding , a, S.S. Davisa, F. Pozzib, P. Furlanib and A. Gazzanigab
aPharmaceutical Profiles Ltd, 2 Faraday Building, Highfields Science Park, University
Boulevard, Nottingham NG7 2QP, UK
bZambon Group SpA, Via Lillo del Duca 10, 20091 Bresso Milano, Italy
Received 15 June 1994; accepted 27 June 1994. Available online 4 November 2002.
Abstract
The gastrointestinal transit and disintegration characteristics of an enteric coated timed
release formulation were investigated in a group of six healthy volunteers using the
technique of gamma scintigraphy. The mean in vivo tablet disintegration time was
approx. 10 h post-dose and 7.5 h after gastric emptying which was in excellent agreement
with that predicted from in vitro methodology. The anatomical site of release ranged from
the caecum to the descending colon and once the onset of disintegration had been
detected by scintigraphy, the time for complete break up was typically in the region of
45–60 min. The enteric coated Time Clock® system therefore provides for a
pharmaceutical preparation capable of drug delivery to the colon.
Keywords: Timed release; Enteric coating; Gamma scintigraphy; Colon targeting
Evaluation of Pulsincap™ to provide regional delivery of dofetilide to the human GI tract
Howard N. E. Stevens , , a, Clive G. Wilsona, Peter G. Wellinga, Massoud
Bakhshaeeb, Julie S. Binnsb, Alan C. Perkinsc, Malcolm Frierc, Elaine P. Blackshawc,
Margaret W. Framed, Don J. Nicholsd, Michael J. Humphreyd and Steve R. Wicksd
a Department of Pharmaceutical Sciences, University of Strathclyde, 27 Taylor Street,
Glasgow G4 0NR, UK
b Scherer DDS Ltd, Clydebank, UK
c Department of Medical Physics, Queen's Medical Centre, Nottingham, UK
d Pfizer Central Research, Sandwich, UK
Received 8 January 2001; revised 17 December 2001; accepted 10 January 2002. Available online 30 January 2002.
Abstract
Pulsincap™ formulations designed to deliver a dose of drug following a 5-h delay were
prepared to evaluate the capability of the formulation to deliver dofetilide to the lower
gastrointestinal (GI) tract. By the expected 5-h release time, the preparations were well
dispersed throughout the GI tract, from stomach to colon. Plasma analysis permitted drug
absorption to be determined as a function of GI tract site of release. Dofetilide is a well-
absorbed drug, but showed a reduction in observed bioavailability when delivered from
the Pulsincap™ formulations, particularly at more distal GI tract sites. Dispersion of the
drug from the soluble excipient used in this prototype formulation relies on a passive
diffusion mechanism and the relevance of this factor to the reduced extent and
consistency of absorption from the colon is discussed. In these studies the effects of the
degree of dispersion versus the site of dispersion could not be ascertained; nevertheless
the scintigraphic analysis demonstrated good in vitro–in vivo correlation for time of
release from Pulsincap™ preparations. The combination of scintigraphic and
pharmacokinetic analysis permits identification of the site of drug release from the
dosage form and pharmacokinetic parameters to be studied in man in a non-invasive
manner.
Author Keywords: Pulsatile release; Site-release; Gamma scintigraphy;
Pharmacokinetics; Dofetilide; Pulsincap™
Article Outline
1. Introduction2. Materials and methods
2.1. Preparation of radiolabelled Pulsincap™ dosage forms 2.2. Study design 2.3. Study protocol 2.4. Data analysis
3. Results and discussion3.1. In vivo study 3.2. Pharmacokinetic analysis 3.3. Correlation of pharmacokinetic and scintigraphic assessment
4. DiscussionReferences
1. Introduction
For most immediate release drug formulations, absorption is complete by the time the
swallowed dose has reached the colon and the extent of absorption in the distal gut is of
little consequence. The situation is markedly different when oral sustained or delayed
release formulations are employed, where the extent of absorption is more susceptible to
regional differences in drug absorption and gut transit times. Using scintigraphic
techniques, many studies have demonstrated quantitative differences in the extent and
rate of absorption as the formulation arrives in the distal small intestine and proximal
colon (Wilson and Olsson).
It follows from these observations that a prerequisite for the development of sustained
release dosage form for a specific drug, is a knowledge of the extent of absorption of that
drug throughout the length of the gastrointestinal (GI) tract. In the past, various
experimental methods have been employed to investigate drug absorption in man which
have often involved invasive intubation techniques (Barr; Chan and Vidon) or complex
formulation assemblies ( Gardner et al., 1997).
It has been appreciated for a long time that the intubation process itself can disturb the
normal physiological function of the GI tract and cause any resulting drug absorption
data to be questioned (Read et al., 1983). The formulation approaches employed to date
can be loosely categorised as being either engineering-based or adaptations of classical
formulation technology. The engineering-based systems, which generally rely on an
external stimulus to trigger release from the device, include the HF capsule ( Antonin,
1993), the telemetric capsule ( Lambert et al., 1991) and the Intellisite® capsule (
Gardner and Parr).
The HF capsule has been widely used to study drug absorption (Fuhr; Harder and Staib)
but suffers from the disadvantages that it is only suitable for liquid drug formulations and
requires the use of X-ray to follow GI transit. The Lambert telemetric capsule appears to
be too complex to have gained acceptance, however Intellisite® has been widely
employed and has the advantage that it can be tracked through the GI tract using non-
invasive gamma scintigraphy. It is reported to be suitable for carrying both liquid and
solid formulations, although its consistency in releasing solid drug formulations in the
low-fluid environment of the distal GI tract has been questioned (personal
communication, M.J. Humphrey) and Intellisite is now being superseded by an improved
design, the Enterion Capsule ( Connor et al., 2001).
The most commonly employed formulation systems rely on time-dependent mechanisms
to provoke drug release from capsule devices using gamma scintigraphic techniques to
visualise the site of release. An early prototype capsule device comprised a water
permeable hydrogel capsule in which the internal cavity contained a mixture of drug with
an expanding material; the contents being sealed inside the capsule by a hydrogel plug
(Rashid, 1990). Water diffused through the hydrogel wall inducing swelling of the
contents and expulsion of the plug, causing drug to be released predictably in the colon
after a 5-h mouth to colon transit period ( Wilding et al., 1992).
The Pulsincap™ device (McNeil et al., 1994) (P-CAP) comprises an impermeable
capsule body containing a drug formulation sealed in the capsule with a hydrogel
polymer plug. The plug expands in water or GI tract fluid and slowly exits the capsule
body, releasing the capsule contents after a defined time-delay determined by the length
of the hydrogel plug ( Binns et al., 1993). It has been employed in human studies for
colon targeting ( Bakhshaee; Binns; Wilson; Hebden and Hebden) in timed-release
modes as well as gastroresistant configurations. An alternative version of P-CAP, in
which the hydrogel plug is replaced by an eroding tablet, has been described ( Stevens;
Kr and Ross).
In contrast to the inherent variability associated with the gastric emptying of single unit
dosage forms, transit through the small intestine is reproducible at about 3–4 h (Wilson
and Washington, 1988). With a dosage form releasing purely on a time-basis, it would be
expected to be variably distributed within the GI tract, and thereby permit assessment of
regional absorption from a range of sites. In this study we have used a 5-h delay P-CAP
to deliver dofetilide to different sites in the GI tract, employing scintigraphy and
pharmacokinetic analysis to evaluate its performance in providing regional drug delivery.
Dofetilide was used as the experimental drug, being a weak base (pKa 7.0) with moderate
lipophilicity (log D 0.96 at pH 7.4) and exhibiting linear pharmacokinetics and complete
bioavailability after conventional oral administration (Smith et al., 1992). Dofetilide is a
potent cardiovascular drug and its regional absorption had not previously been explored
and was of interest in the context of future formulation strategies. Three doses were
investigated in the study in order to investigate whether the kinetics of absorption from
distal sites were linearly related to dose.
2. Materials and methods
2.1. Preparation of radiolabelled Pulsincap™ dosage forms
All P-CAP components were supplied by Scherer DDS Ltd and consisted of size 0 gelatin
capsule bodies coated with ethylcellulose (95%) and diethylphthalate (5%). The hydrogel
polymer plug was prepared as rods by cross-linking polyethylene glycol (PEG molecular
weight 8000) using 1,2,6-hexanetriol and dicyclohexylmethane-4,4-diisocyanate. The
cross-linking reaction was catalysed by ferric chloride and the polymer washed in
butylated hydroxyanisole solution (0.025%) before being cut into plugs of appropriate
dimensions to afford a 4–5 h in vitro release time. The devices were assembled in the
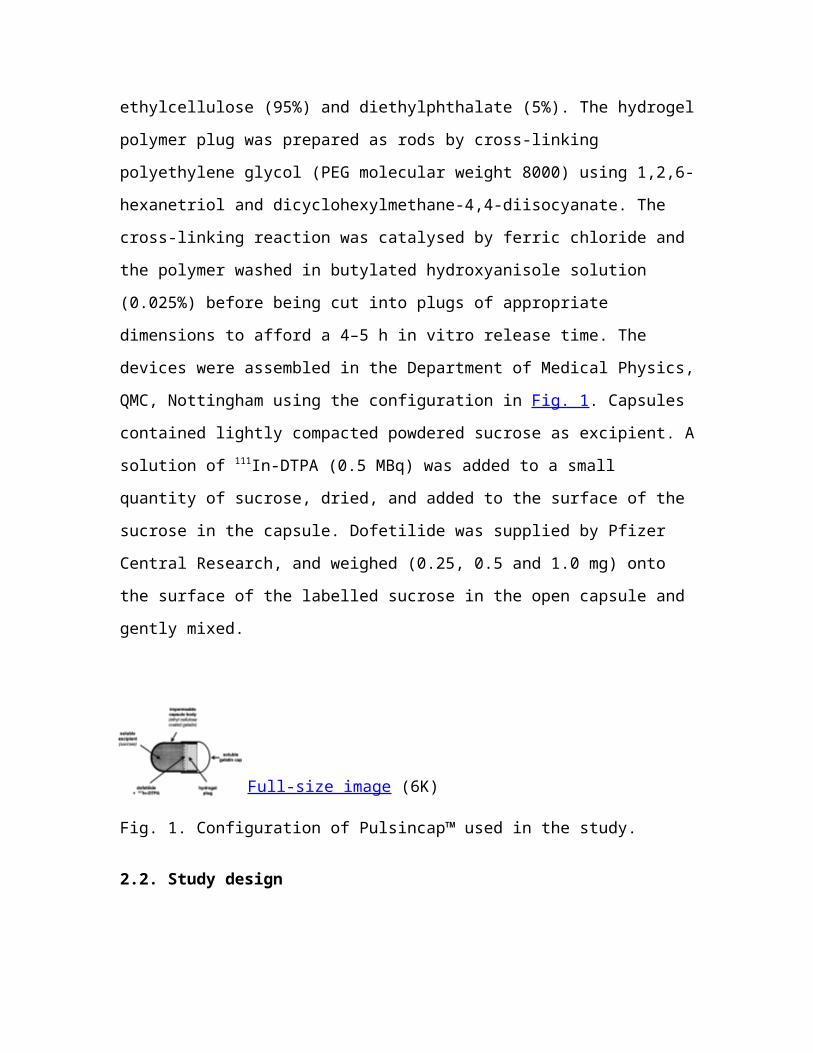
Department of Medical Physics, QMC, Nottingham using the configuration in Fig. 1.
Capsules contained lightly compacted powdered sucrose as excipient. A solution of 111In-
DTPA (0.5 MBq) was added to a small quantity of sucrose, dried, and added to the
surface of the sucrose in the capsule. Dofetilide was supplied by Pfizer Central Research,
and weighed (0.25, 0.5 and 1.0 mg) onto the surface of the labelled sucrose in the open
capsule and gently mixed.
Full-size image (6K)
Fig. 1. Configuration of Pulsincap™ used in the study.
2.2. Study design
An open, four-way crossover study in which male fasted subjects were dosed on four
occasions with an interval of 7 days between dosing. In addition to the three doses of
dofetilide administered from P-CAP, each subject also received dofetilide (1 mg) as a
solution. Eleven subjects entered the study. The study conformed to the Declaration of
Helsinki and the protocol was reviewed and approved by the local ethics committee at the
University of Nottingham Medical School. ARSAC approval was obtained prior to
initiation of the study.
2.3. Study protocol
On the study day, volunteers arrived in the Department of Medical Physics, QMC, having
fasted from 21:00 h the previous evening. Anterior and posterior markers containing a
small amount of 111In label were taped to the abdomen of each volunteer, above the
hepatic flexure, to allow accurate alignment of sequential images. Between 7.30 and 9.00
a.m., each volunteer ingested either a P-CAP with 240 ml water or a solution of 1 mg
dofetilide dissolved in the same volume of water. Using a single headed gamma camera
fitted with a medium energy collimator, serial anterior and posterior static scintigraphic
images of 30 s duration were taken immediately following administration and at 15 min
intervals around the expected time of drug release as well as at longer intervals
throughout the day. The subjects remained fasted until the first meal at 4 h post dosing,
followed by a second standard meal at dose+11 h.
Following each imaging interval a blood sample (5 ml) was taken from a forearm vein,
plasma was separated, and dofetilide concentrations in plasma were determined by
validated radioimmunoassay (Walker et al., 1991). The analytical method was chosen for
unchanged dofetilide and response was linearly related to dofetilide concentrations in
plasma with a lower limit of detection of 50 pg/ml, with inter-assay variability ranging
from 5–18% over the assay range.
2.4. Data analysis
From the scintigraphic analysis, the time of gastric emptying, arrival at the ileocaecal
junction and entry into the colon were recorded. The time of capsule opening, as
determined by spreading of radiolabel in the GI tract contents, was determined by
examination of the scintiscans. Pharmacokinetic parameter values (Cmax, Tmax, AUC(0–48 h))
and elimination T1/2 from the solution dose of dofetilide were determined by fitting
individual plasma data sets to the pharmacokinetic one-compartmental model with first
order drug input and output using software WinNonlin Version 3. Following the P-CAP
0.25, 0.5 and 1.0 mg doses, plasma dofetilide profiles did not lend themselves to
pharmacokinetic modelling and pharmacokinetic parameter values were determined
directly from observed data.
3. Results and discussion
3.1. In vivo study
Eight subjects completed the study receiving all four treatments. One subject received the
1.0 mg solution dose only, and one subject the solution and 0.25 mg P-CAP doses only.
One subject received just the 0.25 and 0.5 mg P-CAP doses.
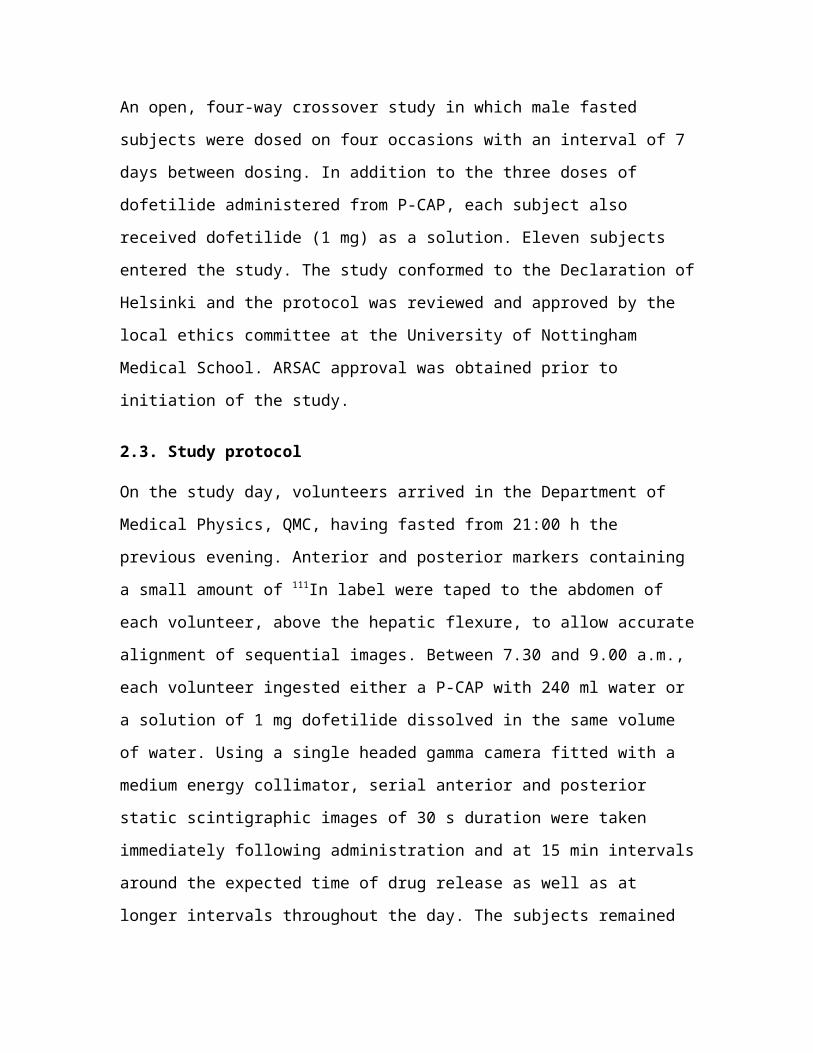
GI transit rate data are summarised in Fig. 2. Gastric emptying of the P-CAP
formulations was generally rapid, although one capsule remained in the stomach for the
duration of the study. Small intestinal transit, arrival at the ileocaecal junction, and entry
into the colon compared favourably with literature values for non-disintegrating
formulations. Site of release of drug and scintigraphic marker into the GI tract varied,
with one capsule being retained in the stomach and the others being distributed along
different regions of the GI tract (small intestine (9), ileocaecal junction (7) and colon
(10)).
Full-size image (6K)
Fig. 2. GI transit of Pulsincap™ in fasted volunteers (n=27).
3.2. Pharmacokinetic analysis
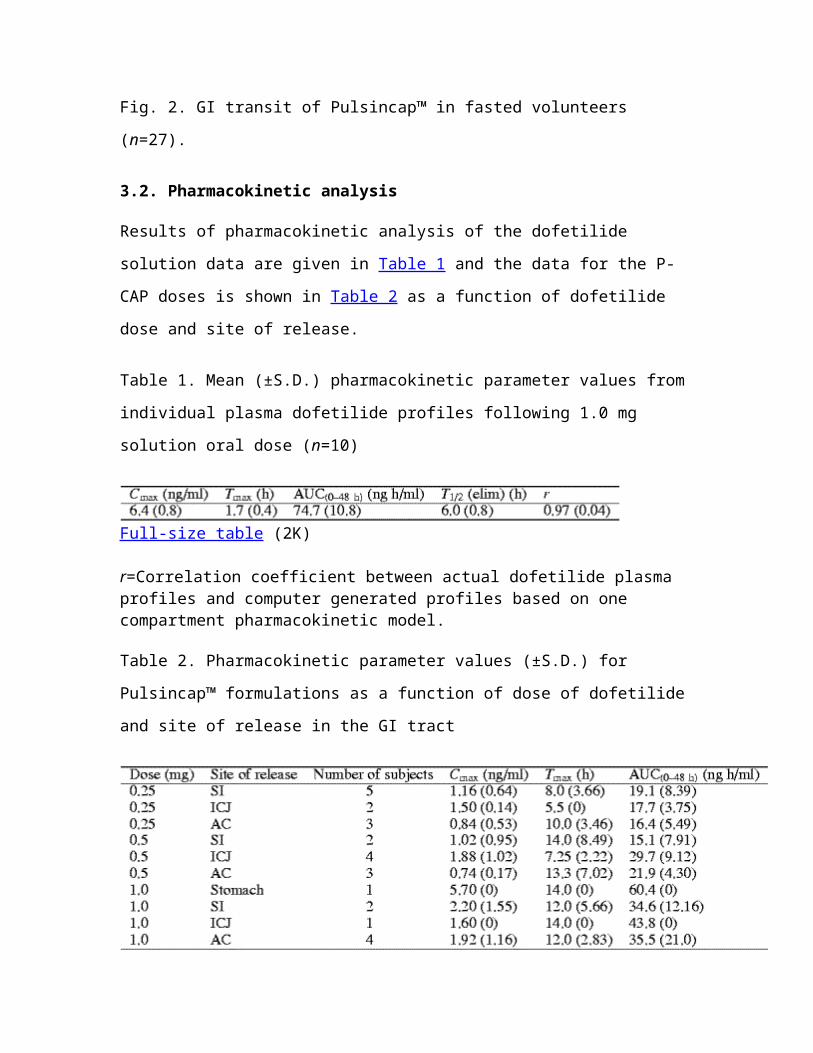
Results of pharmacokinetic analysis of the dofetilide solution data are given in Table 1
and the data for the P-CAP doses is shown in Table 2 as a function of dofetilide dose and
site of release.
Table 1. Mean (±S.D.) pharmacokinetic parameter values from individual plasma
dofetilide profiles following 1.0 mg solution oral dose (n=10)
Full-size table (2K)
r=Correlation coefficient between actual dofetilide plasma profiles and computer generated profiles based on one compartment pharmacokinetic model.

Table 2. Pharmacokinetic parameter values (±S.D.) for Pulsincap™ formulations as a
function of dose of dofetilide and site of release in the GI tract
Full-size table (11K)
An excellent fit was obtained by the ascribed one compartment open model with first
order absorption and elimination to individual plasma data sets following the solution 1.0
mg dose. The mean correlation coefficient of goodness of fit of observed data to model
values was 0.97. Following the solution dose, a mean peak dofetilide concentration of 6.4
ng/ml was obtained at 1.7 h. There was no absorption lag-time. Elimination of dofetilide
from plasma, after peak plasma levels have been reached, occurred with a half-life of 6 h.
The mean AUC(0–48 h) was 75 ng h/ml.
Plasma concentrations following P-CAP doses were consistently lower than from the 1
mg solution dose. The expected lag-time of approximately 5 h occurred before dofetilide
could be detected at a measurable concentration in plasma. Subsequent absorption of
dofetilide was generally prolonged with mean Tmax values in the range 5.5–14 h being
determined (Table 2). Both the Cmax and AUC(0–48 h) were related to the dofetilide P-CAP
doses administered, but were not dose proportional.
Inter-individual variability in plasma dofetilide levels was similar from solution and P-
CAP treatments. Among pharmacokinetic parameters, variability in Cmax, Tmax were
similar from solution and P-CAP, but variability in AUC(0–48 h) values tend to be greater
for the P-CAP administrations (Table 1 and Table 2).
3.3. Correlation of pharmacokinetic and scintigraphic assessment
Dispersion of the marker was easy to ascertain in sequential scintigraphic images
although since blood sampling and imaging are not carried out simultaneously, there is
naturally a small time shift error of no more than ±0.25 h associated with measurements.
Good concordance was noted for the observed release of activity in 24/27 subjects
available for analysis, with a mean scintigraphic release time of 5.3±1.5 h. In three
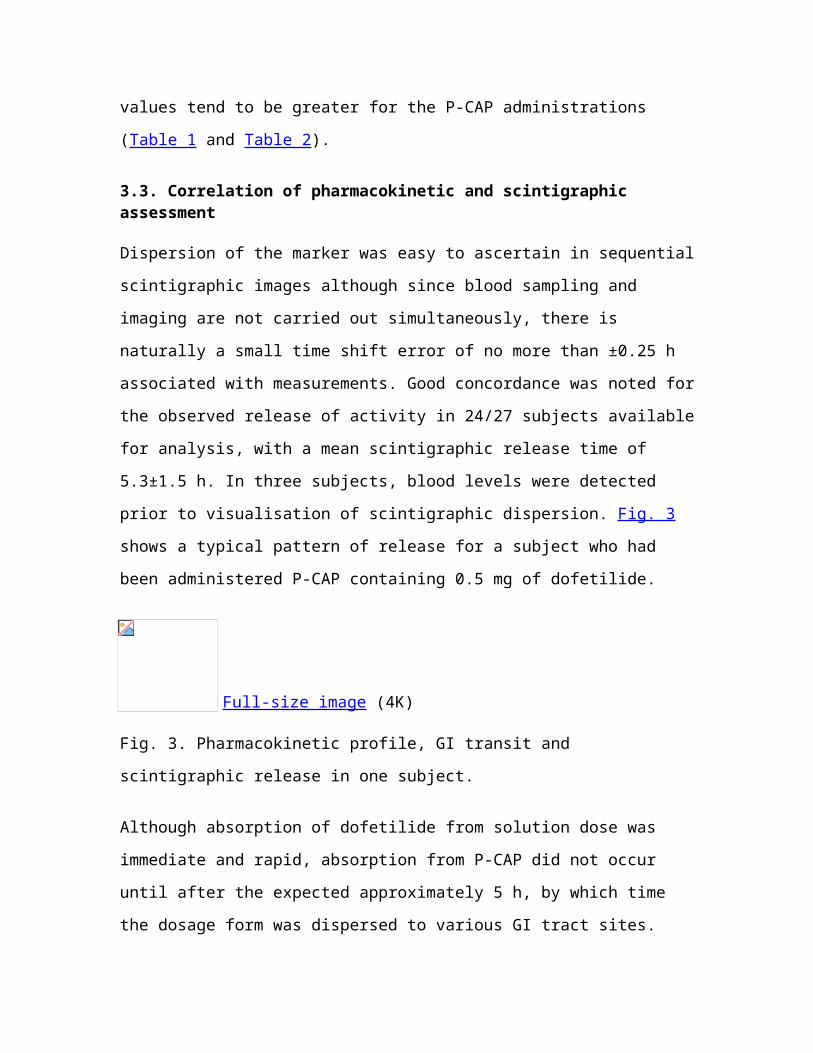
subjects, blood levels were detected prior to visualisation of scintigraphic dispersion. Fig.
3 shows a typical pattern of release for a subject who had been administered P-CAP
containing 0.5 mg of dofetilide.
Full-size image (4K)
Fig. 3. Pharmacokinetic profile, GI transit and scintigraphic release in one subject.
Although absorption of dofetilide from solution dose was immediate and rapid,
absorption from P-CAP did not occur until after the expected approximately 5 h, by
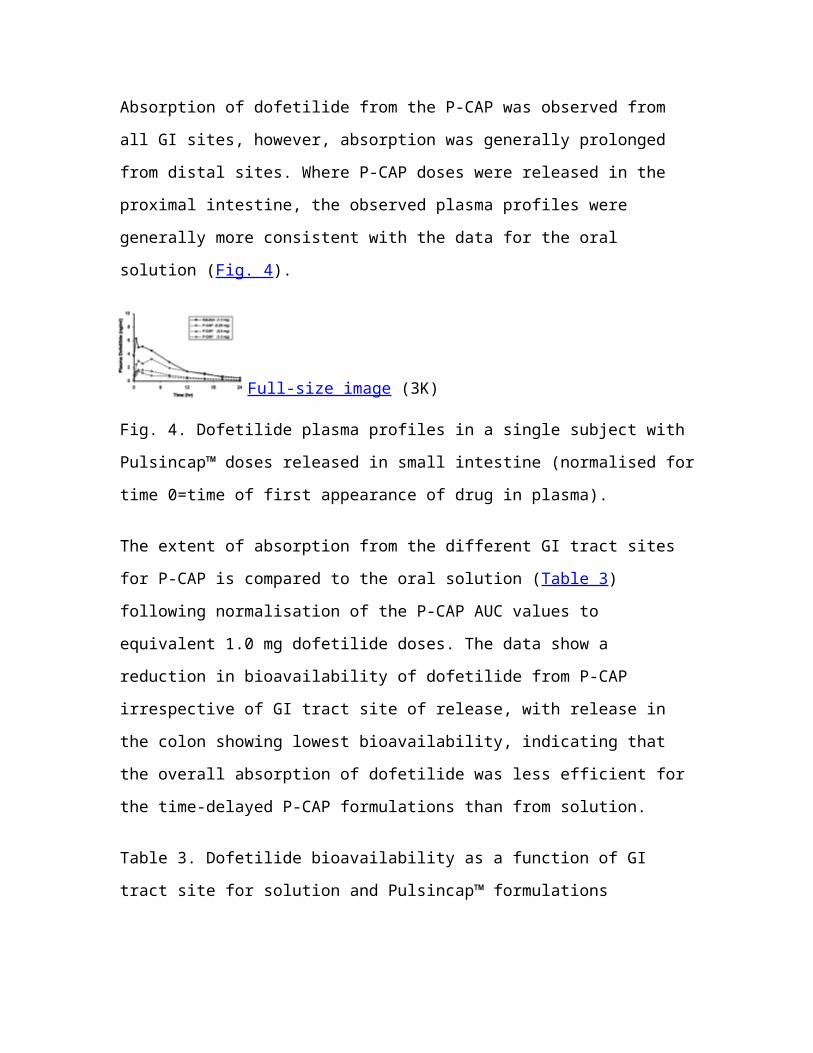
which time the dosage form was dispersed to various GI tract sites. Absorption of
dofetilide from the P-CAP was observed from all GI sites, however, absorption was
generally prolonged from distal sites. Where P-CAP doses were released in the proximal
intestine, the observed plasma profiles were generally more consistent with the data for
the oral solution (Fig. 4).
Full-size image (3K)
Fig. 4. Dofetilide plasma profiles in a single subject with Pulsincap™ doses released in
small intestine (normalised for time 0=time of first appearance of drug in plasma).
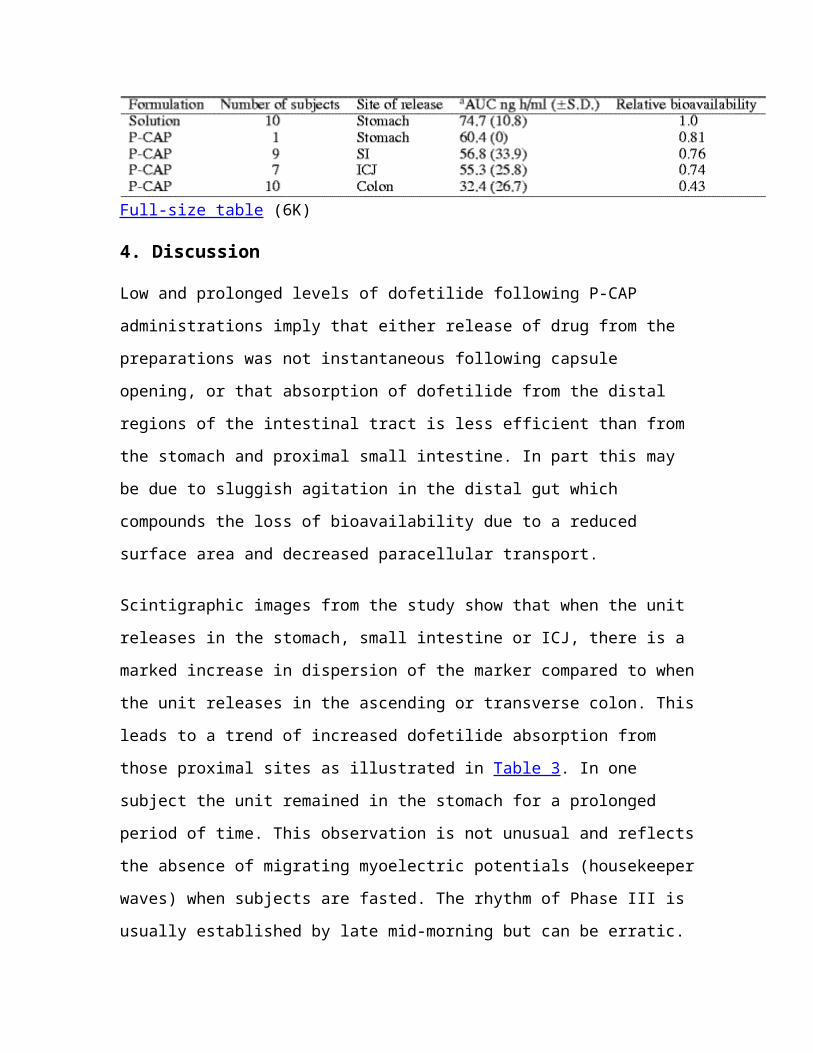
The extent of absorption from the different GI tract sites for P-CAP is compared to the
oral solution (Table 3) following normalisation of the P-CAP AUC values to equivalent
1.0 mg dofetilide doses. The data show a reduction in bioavailability of dofetilide from P-
CAP irrespective of GI tract site of release, with release in the colon showing lowest
bioavailability, indicating that the overall absorption of dofetilide was less efficient for
the time-delayed P-CAP formulations than from solution.
Table 3. Dofetilide bioavailability as a function of GI tract site for solution and
Pulsincap™ formulations
Full-size table (6K)
4. Discussion
Low and prolonged levels of dofetilide following P-CAP administrations imply that
either release of drug from the preparations was not instantaneous following capsule
opening, or that absorption of dofetilide from the distal regions of the intestinal tract is
less efficient than from the stomach and proximal small intestine. In part this may be due
to sluggish agitation in the distal gut which compounds the loss of bioavailability due to a
reduced surface area and decreased paracellular transport.
Scintigraphic images from the study show that when the unit releases in the stomach,
small intestine or ICJ, there is a marked increase in dispersion of the marker compared to
when the unit releases in the ascending or transverse colon. This leads to a trend of
increased dofetilide absorption from those proximal sites as illustrated in Table 3. In one
subject the unit remained in the stomach for a prolonged period of time. This observation
is not unusual and reflects the absence of migrating myoelectric potentials (housekeeper
waves) when subjects are fasted. The rhythm of Phase III is usually established by late
mid-morning but can be erratic. The subsequent intake of a lunchtime meal will prevent
the emptying of large non-disintegrating objects, such as the size 0 capsule employed in
this study.
The drug formulation employed in this study comprises dofetilide distributed onto a
soluble excipient that becomes exposed to GI tract fluid after the capsule opens. As fluid
enters, dofetilide may dissolve and either empty rapidly from the capsule resulting in a
high Cmax and a short Tmax (e.g. at upper GI tract sites where motility and fluid volume is
maximised and viscosity minimised) or, alternatively, may diffuse further into the
capsule and become dispersed throughout the sucrose excipient and released only
progressively, resulting in a lower Cmax and a prolonged Tmax (e.g. at lower GI tract sites
where motility is reduced and fluid is less available and more viscous). In other studies
with P-CAP preparations, in contrast to the soluble excipient fill employed here, the use
of rapidly expansive excipient fills have been shown to be highly effective in expelling
drug from the opened capsule (Stevens et al., 1999).
With the P-CAP configuration evaluated in this study it is possible that in the colon there
is insufficient water to cause rapid dissolution and additionally the sluggish stirring
provided by the haustral movements may limit dispersion of the fill. Similarly, the
importance and difficulties surrounding the dissolution process in the low-fluid
environment within the colon have been highlighted by Takaya et al. (1998) with studies
on rupturable capsule formulations.
In other studies with the P-CAP dosing form, we set out to deliver more distally and in
order to accomplish this the unit was modified by attaching the drug formulation to the
back of the hydrogel plug such that it was pulled out during plug ejection. This approach
allowed the mapping of regional differences in quinine absorption (Hebden et al., 1999b)
and to investigate the effects of manipulating lumenal water on quinine absorption in the
colon ( Hebden et al., 1999a). These data, like those presented in the present study show
that pulse delivery more distally may result in a diminution in the extent of absorption.
However, whether this arises because of reduced permeability of the drugs concerned in
the colon or of impeded dispersion from the formulation, remains to be determined.
In spite of these reservations, the data obtained from the study in human volunteers
demonstrate that the Pulsincap™ delivery system has a role as a convenient probe device
and is capable of providing time-delayed release of drug substance within the GI tract.
Utilising this approach coupled with gamma scintigraphy, pharmacokinetic parameters
can be explored from a range of GI tract sites in man in a non-invasive manner.
References
Antonin, 1993. K.H. Antonin , Other methods in studying colonic drug absorption. In:
P.R. Bieck, Editor, Colonic Drug Absorption and Metabolism, Marcel Dekker, New York
(1993), pp. 89–107.
Bakhshaee et al., 1992. M. Bakhshaee, J.S. Binns, H.N.E. Stevens and C.J. Miller ,
Pulsatile drug delivery to the colon monitored by gamma scintigraphy. Pharm. Res. 9
suppl. (1992), p. F230.
Barr et al., 1994. W.H. Barr, E.M. Zola, E.L. Chandler, S.M. Hwang, A.V. Tendolkar, R.
Shamburek, B. Parker and M.D. Hilty , Differential absorption of amoxicillin from the
human small and large intestine. Clin. Pharmacol. Ther. 56 (1994), pp. 279–285. Full
Text via CrossRef | View Record in Scopus | Cited By in Scopus (40)
Binns et al., 1993. J.S. Binns, M. Bakhshaee, C.J. Miller and H.N.E. Stevens ,
Application of a pH independent PEG based hydrogel to afford pulsatile drug delivery.
Proc. Int. Symp. Control. Rel. Bioact. Mater. 20 (1993), pp. 226–227. View Record in
Scopus | Cited By in Scopus (0)
Binns et al., 1996. J.S. Binns, H.N.E. Stevens, J. McEwan, G. Pritchard, F.M. Brewer, A.
Clarke, E.S. Johnson and I. McMillan , The tolerability of multiple oral doses of
Pulsincap™ capsules in healthy volunteers. J. Control. Rel. 38 (1996), pp. 151–158.
Article | PDF (513 K) | View Record in Scopus | Cited By in Scopus (16)
Chan et al., 1994. K.K.H. Chan, A. Buch, R.D. Glazer, V.A. John and W.H. Barr , Site-
differential gastrointestinal absorption of benazepril hydrochloride in healthy volunteers.
Pharm. Res. 11 (1994), pp. 432–437. Full Text via CrossRef | View Record in Scopus |
Cited By in Scopus (16)
Connor et al., 2001. A.L. Connor, H.A. Wray, B. Voith, U. Voight, J. Nagelschmitz, J.
Kuhlmann and I.R. Wilding , Using the Enterion capsule to investigate the absorption of
Faropenem Daloxate delivered in particulate form from different sites of the
gastrointestinal tract. AAPS Pharm. Sci. 3 3 (2001), p. s5125.
Fuhr et al., 1994. U. Fuhr, A.H. Staib, S. Harder, K. Becker, D. Liermann, G.
Schollnhammer and I.S. Rod , Absorption of ipsapirone along the human gastrointestinal
tract. Brit. J. Clin. Pharmacol. 38 (1994), pp. 83–86. View Record in Scopus | Cited By
in Scopus (13)
Gardner et al., 1997. D. Gardner, R. Casper, F. Leith and I.R. Wilding , Non-invasive
methodology for assessing regional drug absorption from the gastrointestinal tract.
Pharm. Technol. Eur. 9 (1997), pp. 46–53.
Harder et al., 1990. S. Harder, U. Fuhr, D. Beermann and A.H. Staib , Ciprofloxacin
absorption in different regions of the human gastrointestinal tract. Investigations with the
hf-capsule. Brit. J. Clin. Pharmacol. 30 (1990), pp. 35–39. View Record in Scopus |
Cited By in Scopus (36)
Hebden et al., 1999a. J.M. Hebden, P.J. Gilchrist, A.C. Perkins, C.G. Wilson and R.C.
Spiller , Stool water content and colonic drug absorption: contrasting effects of lactulose
and codeine. Pharm. Res. 16 (1999a), pp. 1254–1259. Full Text via CrossRef | View
Record in Scopus | Cited By in Scopus (15)
Hebden et al., 1999b. J.M. Hebden, C.G. Wilson, R.C. Spiller, P.J. Gilchrist, P.E.
Blackshaw, M. Frier and A.C. Perkins , Regional differences in quinine absorption from
the undisturbed human colon assessed using a timed release delivery system. Pharm. Res.
16 (1999b), pp. 1087–1092. Full Text via CrossRef | View Record in Scopus | Cited By
in Scopus (20)
Krögel and Bodmeier, 1998. I. Krögel and R. Bodmeier , Pulsatile drug release from an
insoluble capsule body controlled by an erodible plug. Pharm. Res. 15 (1998), pp. 474–
481. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (37)
Lambert et al., 1991. A. Lambert, F. Vaxman, F. Crenner, T. Wittmann and J.F. Grenier ,
Autonomous telemetric capsule to explore the small bowel. Med. Biol. Eng. Comput. 29
(1991), pp. 191–196. Full Text via CrossRef | View Record in Scopus | Cited By in
Scopus (17)
McNeil et al., 1994. McNeil, M.E., Rashid, A., Stevens, H.N.E., 1994. Drug dispensing
device. US Patent 5 342 624.
Olsson et al., 1995. B. Olsson, Z.G. Wagner, P. Mansson and G. Ragnarsson , A gamma
scintigraphic study of the absorption of morphine from controlled-release tablets. Int. J.
Pharm. 119 (1995), pp. 223–229. Article | PDF (503 K) | View Record in Scopus |
Cited By in Scopus (7)
Parr et al., 1999. A.F. Parr, E.P. Sandefer, P. Wissel, M. McCartney, C. McClain, U.Y.
Ryo and G.A. Digenis , Evaluation of the feasibility and use of a prototype remote drug
delivery capsule (RDDC) for non-invasive regional drug absorption studies in the GI tract
of man and beagle dog. Pharm. Res. 16 (1999), pp. 266–271. Full Text via CrossRef |
View Record in Scopus | Cited By in Scopus (10)
Rashid, 1990. Rashid, A., 1990. Dispensing Device. European Patent 0 384 642.
Read et al., 1983. N.W. Read, M.N. Aljanabi, T.E. Bates and D.C. Barber , Effect of
gastrointestinal intubation on the passage of a solid meal through the stomach and small
intestine in humans. Gastroenterology 84 (1983), pp. 1568–1572. View Record in Scopus
| Cited By in Scopus (68)
Ross et al., 2000. A.C. Ross, R.J. MacRae, M. Walther and H.N.E. Stevens ,
Chronopharmaceutical drug delivery from a pulsatile capsule device based on
programmable erosion. J. Pharm. Pharmacol. 52 (2000), pp. 909–916.
Smith et al., 1992. D.A. Smith, H.S. Rasmussen, D.A. Stopher and D.K. Walker ,
Pharmacokinetics and metabolism of dofetilide in mouse, rat, dog and man. Xenobiotica
22 (1992), pp. 709–719. Full Text via CrossRef | View Record in Scopus | Cited By in
Scopus (44)
Staib et al., 1989. A.H. Staib, D. Beerman, S. Harder, U. Fuhr and D. Liermann ,
Absorption differences of ciprofloxacin along the human gastrointestinal tract determined
using a remote control drug delivery device (HF-capsule). Am. J. Med. 87 (1989), pp.
66S–69.
Stevens et al., 1995. Stevens, H.N.E., Rashid, A., Bakhshaee, M., 1995. Drug Dispensing
Device. US Patent 5 474 784.
Stevens et al., 1999. Stevens, H.N.E., Rashid, A., Bakhshaee, M., Binns, J.S., Miller,
C.J., 1999. Expulsion of material from a delivery device. US Patent 5 897 874.
Takaya et al., 1998. T. Takaya, K. Niwa, M. Muraoka, I. Ogita, N. Nagai, R. Yano, G
Kimura, Y Yoshikawa, H Yoshikawa and K. Takada , Importance of dissolution process
on systemic availability of drugs delivered by colon delivery system. J. Control. Release
50 1–3 (1998), pp. 112–122.
Vidon et al., 1989. N. Vidon, A. Pfeiffer, J. Godbillon, M. Rongier, S. Gauron, J. Hirtz,
J.J. Bernier and J.P. Bidois , Evaluation of the gastric absorption and emptying of drugs
under various pH conditions using a simple intubation method: application to diclofenac.
Brit. J. Clin. Pharmacol. 28 (1989), pp. 121–124. View Record in Scopus | Cited By in
Scopus (11)
Walker et al., 1991. D.K. Walker, G.W. Herne, J.E. Arrowsmith, P.E. Cross, M.B. Kaye,
D.A. Smith, D.A. Stopher and W. Wild , Measurement of the class III antiarrhythmic
agent UK-68 798 in plasma by radioimmunoassay. J. Pharm. Biomed. Ann. 9 (1991), pp.
141–149. Abstract | PDF (565 K) | View Record in Scopus | Cited By in Scopus (13)
Wilding et al., 1992. I.R. Wilding, S.S. Davis, M. Bakhshaee, H.N.E. Stevens, R.A.
Sparrow and J. Brennan , Gastrointestinal transit and systemic absorption of captopril
from a pulsed-release formulation. Pharm. Res. 9 (1992), pp. 654–657. Full Text via
CrossRef | View Record in Scopus | Cited By in Scopus (55)
Wilson and Washington, 1988. C.G. Wilson and N. Washington , Assessment of
disintegration and dissolution of dosage forms in vivo using gamma scintigraphy. Drug
Dev. Ind. Pharm. 14 (1988), pp. 211–271.
Wilson et al., 1991. C.G. Wilson, N. Washington, J.L. Greaves, C. Washington, I.R.
Wilding, T. Hoadley and E.E. Sims , Predictive modelling of the behaviour of a
controlled-release buflomedil HCl formulation using scintigraphic and pharmacokinetic
data. Int. J. Pharm. 72 (1991), pp. 79–86. Abstract | PDF (587 K) | View Record in
Scopus | Cited By in Scopus (13)
Wilson et al., 1997. C.G. Wilson, M. Bakhshaee, H.N.E. Stevens, A.C. Perkins, M. Frier,
P.E. Blackshaw and J.S. Binns , An evaluation of a gastro-resistant pulsed release
delivery system (Pulsincap) in man. Drug Delivery 4 (1997), pp. 201–206. Full Text via
CrossRef
Corresponding author. Tel.: +44-141-548-2441; fax: +44-141-552-6443; email:
International Journal of PharmaceuticsVolume 236, Issues 1-2, 2 April 2002, Pages 27-34 Formulation parameters affecting the performance of coated gelatin capsules with pulsatile release profiles
T. Bussemer and R. Bodmeier ,
College of Pharmacy, Freie Universität Berlin, Kelchstr. 31, 12169, Berlin, Germany
Received 7 April 2003; revised 15 July 2003; accepted 31 July 2003. ; Available online 16 October 2003.
Abstract
The objective of this study was to develop and evaluate a rupturable pulsatile drug
delivery system based on soft gelatin capsules with or without a swelling layer and an
external water-insoluble but -permeable polymer coating, which released the drug after a
lag time (rupturing of the external polymer coating). The swelling of the gelatin capsule
itself was insufficient to rupture the external polymer coating, an additional swelling
layer was applied between the capsule and the polymer coating. Croscarmellose sodium
(Ac-Di-Sol) was more effective as a swelling agent than low and high molecular weight
hydroxypropylmethyl cellulose (HPMC; E5 or K100M). Brittle polymers, such as ethyl
cellulose (EC) and cellulose acetate propionate (CAPr), led to a better rupturing and
therefore more complete drug release than the flexible polymer coating, Eudragit RS. The
lag time of the release system increased with higher polymer coating levels and decreased
with the addition of a hydrophilic pore-former, HPMC E5 and also with an increasing
amount of the intermediate swelling layer. The water uptake of the capsules was linear
until rupture and was higher with CAPr than with EC. Soft gelatin capsule-based systems
showed shorter lag times compared to hard gelatin capsules because of the higher
hardness/filling state of the soft gelatin capsules. The swelling pressure was therefore
more directed to the external polymer coating with the soft gelatin capsules. Typical
pulsatile drug release profiles were obtained at lower polymer coating levels, while the
release was slower and incomplete at the higher coating levels. CAPr-coated capsules
resulted in a more complete release than EC-coated capsules.
Author Keywords: Gelatin capsules; Lag time; Mechanical properties; Oral drug
delivery; Polymeric films; Pulsatile release; Swelling agents
Article Outline
1. Introduction
2. Materials and methods2.1. Preparation of polymer films 2.2. Mechanical properties of polymer films in the dry and wet state 2.3. Preparation of the pulsatile release soft gelatin capsules 2.4. Lag time and drug release 2.5. Water uptake studies 2.6. Hardness of the pulsatile release soft gelatin capsules
3. Results and discussionReferences
1. Introduction
Most oral extended release drug delivery systems (DDS) release the drug continuously in
a linear or non-linear fashion. Pulsatile drug release profiles are interesting for the
treatment of several diseases including hypertension, bronchial asthma, myocardial
infarction, angina pectoris, rheumatic disease, and ulcer disease ([Bussemer et al., 2001
and Ritschel and Forusz, 1994]). Pulsatile release DDS allow the adaptation of drug
therapies to chronopharmacological needs ( [Lemmer, 1991 and Lemmer, 1999]).
Pulsatile drug release was obtained with drug-containing cores layered with erodible
coatings, which released the drug after erosion of the coating ([Gazzaniga et al., 1994]).
Alternatively, rupturable dosage forms, such as the time-explosion system, were
investigated, whereby pellets with a swellable hydroxypropylcellulose layer were coated
with a water-insoluble polymer layer, which ruptured after a lag-time and then released
the drug ( [Ueda et al., 1994a, Ueda et al., 1994b and Ueda et al., 1994c]). However, the
drug loading of pellets is limited and liquid fillings are not possible.
Various capsule-shaped pulsatile delivery systems have been described using
insoluble/impermeable and hard capsule halves with swellable plugs, e.g. the Pulsincap
system ([Binns et al., 1996, McNeill et al., 1990 and Wilding et al., 1992]). One
drawback of this system was the use of a non-approved plug material, which was
overcome, e.g. by the use of erodible plugs ( [Krogel and Bodmeier, 1998]) or
biocompatible materials ( [Krogel and Bodmeier, 1999a and Krogel and Bodmeier,
1999b]; [Tsume et al., 2000]). The manufacturing process was still difficult and was
conducted manually.
Capsules are pharmaceutically elegant dosage forms offering an improved drug stability,
because the content is tightly enclosed by the capsule shell and thus protected from
oxygen, moisture and light, and also from physiological fluids until the drug is released.
Hard capsules are usually filled with solid materials ([Fahrig and Hofer, 1998]), but some
drugs require a liquid formulation for solubility or bioavailability reasons ( [Savio et al.,
1998]). The filling of semisolids or liquids into hard gelatin capsules is possible
( [Bowtle, 1998 and Stegemann, 1999]).
A pulsatile delivery system based on hard gelatin capsules with a solid content has been
recently described ([Bussemer et al., 2003a]). The capsules were coated with a swelling
layer followed by an external polymer coating, which ruptured after a certain lag time,
induced by the water uptake/swelling pressure of the swelling layer.
The objective of this study was to develop and evaluate a soft gelatin capsule-based
pulsatile release system for the delivery of liquid drug contents. The performance was
compared to the pulsatile hard capsules.
2. Materials and methods
Ammonio methacrylate copolymer type B, USP 25 (Eudragit® RS, Röhm Pharma,
Darmstadt, Germany), ethyl cellulose (EC; Ethocel® Standard 10, Dow Chemical
Company, Midland, MI, USA), cellulose acetate propionate (CAPr; CAP 504-0.2,
Eastman Chemical Company, Kingsport, TN, USA), hydroxypropylmethyl cellulose
(HPMC; Methocel® E5 or K100M, Colorcon, Orpington, UK), triethyl citrate (TEC;
Morflex, Greensboro, NC, USA), croscarmellose sodium (Ac-Di-Sol®, FMC, Newark,
DE, USA), polyvinyl pyrrolidone (Kollidon® 30, BASF, Ludwigshafen, Germany), soft
gelatin capsules (length 12.6 mm, width 8 mm, filled with 50 mg methylene blue in PEG
400) (R.P. Scherer, Eberbach, Germany).
All other reagents were of analytical grade and were used without further purification.
2.1. Preparation of polymer films
Polymer films were produced by casting of 10% (w/w) polymer solutions in 90 vol.%
ethanol onto a Teflon plate using a casting knife (Multicator 411, Erichsen, Hemer,
Germany). After drying for 24 h under a special cover to reduce solvent evaporation in
order to obtain smooth homogeneous film surfaces, the films were removed and the film
thickness was measured at five points with a thickness gauge Minitest 600 (Erichsen,
Hemer, Germany).
2.2. Mechanical properties of polymer films in the dry and wet state
Polymer film samples of 6.5 cm×6.7 cm were fixed in a special Teflon holder with
several holes (n=3). The holder with the film was then immersed into 0.1 N HCl at 37 °C.
The puncture strength of films was measured with an Instron 4466 (Instron Wolpert,
Darmstadt, Germany). A metal probe, diameter 5 mm, length 15 cm, was driven with a
speed of 5 mm/min through a hole either in the dry state (initial puncture strength) or
after 60 min on films immersed in the release medium. Force (N)–displacement (mm)
curves were recorded with an Instron load cell. The following parameters were
calculated:
Modulus=slopeoftheforce–displacementcurvebeforefilmbreak
A detailed description of the puncture
test has been described ([Bodmeier and Paeratakul, 1993 and Bodmeier and Paeratakul,
1994]).
2.3. Preparation of the pulsatile release soft gelatin capsules
Pulsatile capsules were prepared by layering of a 12% (w/w) suspension of Ac-Di-Sol in
a 4% (w/w) solution of Kollidon 30 in isopropanol onto soft gelatin capsules in a GC-300
Glatt drum coater (swelling layer) (prewarming of capsules at 40 °C for 10 min, spray
nozzle diameter 1.2 mm, atomizing air pressure 0.8 bar, air flow rate 110 m3/h, inlet air
temperature 40 °C, product temperature 25–28 °C, spray rate 10–12 g/min, rotational pan
speed 15 rpm, post-coating drying at 35 °C for 10 min). In a second step, the polymer
coating was applied from a 4% (w/w) polymer solution in 90 vol.% ethanol. With HPMC
as a pore former, EC was first dissolved in 96 vol.% ethanol, then HPMC was dispersed,
and finally water was added slowly under stirring until a clear solution was obtained. The
EC solutions were applied in the GC-300 Glatt drum coater under the conditions
described above.
2.4. Lag time and drug release
The lag time was determined by visual observation of the pulsatile capsules in a USP 25
paddle apparatus (medium: phosphate buffer USP, pH 7.4, 37 °C, rotation speed
100 rpm) and was defined as the time point, when the outer coating ruptured (n=5). The
amount of methylene blue released was studied by withdrawing 3 ml samples at
predetermined time points. The samples were measured after appropriate dilution with a
Shimadzu UV-2101PC UV-Vis scanning spectrophotometer (Shimadzu Europe,
Duisburg, Germany) at a wavelength of 663 nm.
2.5. Water uptake studies
At predetermined time points after exposure of the pulsatile capsules to phosphate buffer
USP, pH 7.4 (37 °C, 50 ml-flask, shaker-incubator at 50 rpm), the capsules were
carefully blotted with tissue paper to remove the surface water and then were weighed
with an analytical balance (n=3). Water uptake was calculated as follows:
2.6. Hardness of the pulsatile release soft gelatin capsules
Capsules, optionally after incubation in phosphate buffer USP, pH 7.4 at 37 °C, were
fixed on a metal plate. A metal probe connected to the Instron 4466 was positioned on the
surface of the capsules. The metal probe was then moved downward at a constant speed
of 5 mm/min. The maximum force was the force when the coating of the capsule cracked.
It was defined as the hardness of the capsules.
3. Results and discussion
Preliminary studies were needed to select a suitable polymer for the polymer coating of
the pulsatile capsules. The outer polymer coating has to be water-permeable and has to
rupture completely after the lag time. Besides the water permeability ([Rhodes and
Porter, 1998]), the mechanical properties of the coating are therefore an important
characteristic of the system. The mechanical properties of polymer films, which were
prepared by casting from ethanolic solutions, were investigated in the dry and the wet
state ( Table 1). The mechanical parameters—puncture strength, modulus, strain and
energy—decreased after incubation of the films in the medium. This could be explained
by the uptake of water, which acted as a plasticizer ([Bodmeier and Paeratakul, 1993 and
Tho et al., 1999]). The Eudragit RS-film was very flexible and soft, as indicated by a high
strain (elongation) and a low modulus in both the dry and wet state. The EC films had a
much lower strain with a higher modulus. The most brittle film was an EC/HPMC-
combination as indicated by its low puncture strength accompanied with a low strain and
low energy required to rupture the film. The mechanical properties of CAPr-containing
films could not be investigated in this study. CAPr formed very brittle films, which could
not be removed from the Teflon plates without breakage. However, since the mechanical
properties of CAPr films were described as brittle ( [Edgar et al., 2001, Sand, 1990 and
Schauber et al., 1999]), it was included in the coating experiments.
Table 1. Mechanical properties of polymeric films, cast from ethanolic solutions
Full-size table (14K)
Not-found: mean.
In a first coating experiment, soft gelatin capsules were coated with Eudragit RS. The
coated capsules significantly increased in volume after incubation in the release medium
(Fig. 1). A big oil droplet was visible inside the capsule, the rest of the capsule was filled
with water. The swollen capsules were also very soft. Because of the flexibility of the
Eudragit RS coating, the coated capsules ruptured only slightly with very small cracks
and did not rupture completely. No significant drug release was determined. Eudragit RS
was therefore not suitable as a coating in this application. The less flexible and more
brittle polymers, EC and CAPr, were evaluated for future coatings. Both polymers are
soluble in ethanol and were directly sprayed on the soft gelatin capsules.
Full-size image (12K)
Fig. 1. Eudragit RS-coated soft gelatin capsules. Left: original capsule in the dry state;
right: capsule after 4 h of incubation in the release medium (phosphate buffer, pH 7.4).
EC- or CAPr-coated soft gelatin capsules did not expand much in size and did therefore also not rupture sufficiently. Only small amounts of the dye, methylene blue, which served as a model drug, was released from the capsules. In addition, the slope of the lag
time-coating level profile was relatively steep, which indicated a high sensitivity in the lag time to small changes in the coating level, as shown for an EC/HPMC 80:20-combination (Fig. 2). The lag time prior to drug release increased with increasing coating level (thickness of the polymeric coating). The lag time was lower for plasticizer-free systems compared to capsules coated with EC/HPMC plasticized with 20% (w/w) TEC. The plasticizer-containing coating was more flexible and resisted an increasing inner pressure for a longer time.
Full-size image (5K)
Fig. 2. Lag time of coated soft gelatin capsules without swelling layer.
The swelling forces developed by the soft gelatin capsule shell were not strong enough to rupture the outer polymer coating completely in order to assure a rapid and complete drug release. Therefore, an additional swelling layer was introduced between the capsule shell and the polymer coating. After contact with release media, the water penetrates through the polymeric coating, the swelling layer hydrates and swells and finally ruptures the outer coating completely. The gelatin shell then disintegrates and releases the drug rapidly.
Various excipients were tested as possible swelling layers. The application of HPMC E5
as a swelling layer reduced the lag time (Fig. 3), but did not improve the rupture behavior
enough, the capsules were still incompletely ruptured. The higher molecular weight
HPMC K100M resulted in an increase in the lag time because it built a strong gel, which
retarded the water uptake, thus prolonging the swelling and rupturing process.
Full-size image (5K)
Fig. 3. Lag time of coated soft gelatin capsules with HPMC swelling layer. Polymer
coating: EC/HPMC (80:20), 20% TEC, swelling layer: HPMC E5 or K100M, 6–
9 mg/cm2.
Next, the highly swellable superdisintegrant, Ac-Di-Sol (croscarmellose sodium), was
tested. Ac-Di-Sol was chosen because it showed the best swelling performance in a series of superdisintegrants ([Bussemer et al., 2003b]). Ac-Di-Sol was not soluble in organic solvents, it was therefore sprayed from an ethanolic suspension, containing Kollidon 30 (PVP) as a dissolved binder. The resulting swelling layer was mechanically stable towards attrition.
The Ac-Di-Sol-based swelling layer resulted in good rupturing of the polymer coating.
Increasing the amount of swelling layer resulted in reduced lag times at the same external
polymer coating level (Fig. 4). As expected, the lag time also increased with increasing
coating level because of a reduced permeability of the EC coating for the release medium
and the increased mechanical resistance. The extent of rupturing of the outer polymer
coating in general decreased at higher polymer coating levels because of the increased
mechanical strength of the external polymer coating.
Full-size image (5K)
Fig. 4. Lag time of coated soft gelatin capsules with an Ac-Di-Sol swelling layer.
Polymer coating: EC/HPMC (80:20), 20% TEC, swelling layer: Ac-Di-Sol:Kollidon 30
(75:25).
The water permeability of the outer EC layer can be varied by the inclusion of a low molecular weight HPMC. Increasing the HPMC E5 amount in the external coating decreased the lag time (Fig. 5). The water influx increased due to the formation of water-filled channels in the EC-membrane ([Gunder et al., 1995 and Hjartstam and Hjertberg, 1998]). Water reached the swelling layer faster and the expansion of the swelling layer was accelerated, thus shortening the lag time prior to rupture. Additionally, the puncture strength as well as the energy, necessary to rupture the film, also decreased with increasing HPMC content ( Table 1). The lag time-coating level profile became flatter, indicating a lower sensitivity of the lag time to variations in the coating level and therefore an improved robustness of the system.
Full-size image (6K)
Fig. 5. Lag time of soft gelatin capsules as a function of EC/HPMC ratio. Polymer
coating: EC/HPMC, different ratios, 20% TEC, swelling layer: Ac-Di-Sol:Kollidon 30
(75:25), 26.9 mg/cm2.
The trends in the results observed with EC were also obtained with CAPr, another cellulose-based polymer (Fig. 6). The lag time increased with the use of the plasticizer TEC due to the higher flexibility of the coating and it decreased with the addition of the pore-former HPMC. When compared to EC, the lag times were shorter with CAPr, probably because of the higher water permeability of this polymer. For example, at a HPMC level of 40%, the lag phase was very short with CAPr.
Full-size image (7K)
Fig. 6. Lag time of CAPr-coated soft gelatin capsules. Polymer coating: different CAPr-
formulations, swelling layer: Ac-Di-Sol:Kollidon 30 (75:25), 23.7–27.9 mg/cm2.
Water uptake studies on the coated capsules confirmed the higher water permeability of the CAPr coatings compared to the EC coatings (Fig. 7). The curves showed an almost linear water uptake until the polymer coating ruptured. The rate of water uptake decreased with increasing polymer coating level. In all cases, the maximum water uptake was very similar, and was between 11.4 and 11.8% (w/w) for the EC/HPMC-combination (Fig. 7A) and between 12.4 and 14.2% (w/w) for the CAPr/HPMC-combination ( Fig. 7B). The maximum water uptake value was slightly higher at the higher coating level because of the higher mechanical resistance of the thicker coatings.
Full-size image (10K)
Fig. 7. Water uptake of coated soft gelatin capsules. Polymer coating: (A) EC/HPMC
(80:20), 20% TEC; (B) CAPr:HPMC (80:20), 20% TEC, swelling layer: Ac-Di-
Sol:Kollidon 30 (75:25), 26.9 mg/cm2.
Alternatively to soft gelatin capsules, which are primarily used for the delivery of liquids, hard gelatin capsules were also investigated in this study. The structure of the delivery
system was the same in both cases, a soft or hard gelatin capsule core, a swelling layer and a layer of a water-insoluble but -permeable polymer coating.
The lag time was longer with hard gelatin than with soft gelatin capsules at the same
coating level, both having the same composition of the swelling and coating layer (Fig.
8). The reason for the shorter lag times with the soft gelatin capsules resides in the
different degree of fillings of hard and soft gelatin capsules. Soft gelatin capsules are
completely filled with liquid, the pressure developed by the swelling layer is therefore
directed primarily towards the outer polymer layer. In comparison, hard gelatin capsules
are not completely filled with powder, there is air inside the capsule. The pressure of the
swelling layer is therefore also directed towards the capsule core and not exclusively
towards the outer coating. More water has therefore to be taken up by the hard gelatin
capsules resulting in longer lag times at the same coating level. This was also confirmed
with hardness data of soft and hard gelatin capsules (Fig. 9). Soft gelatin capsules were
approximately four times harder than the hard capsules (values at time 0). The hardness
of the soft gelatin capsules declined with increasing incubation time, while the hardness
of the hard gelatin capsules could not be detected in the wet state, because the wet
capsules were squeezed under the moving punch without giving a measurable signal. As
mentioned above, the higher hardness of soft gelatin capsules was caused by the higher
thickness of the gelatin shell as well as by the complete filling and the absence of air
when compared with hard gelatin capsules.
Full-size image (8K)
Fig. 8. Comparison of lag times of coated hard (HGC) and soft gelatin capsules (SGC).
Polymer coating: CAPr with and without HPMC, 20% TEC, swelling layer: Ac-Di-
Sol:Kollidon 30 (75:25), 21.2 mg/cm2.
Full-size image (4K)Fig. 9. Hardness of soft and hard gelatin capsules after incubation in the release medium (phosphate buffer, pH 7.4).
Fig. 10 shows the drug release of individual soft gelatin capsules coated with EC/HPMC (60:40), plasticized with 20% TEC. The formulation with a low coating level of 3.2 mg/cm2 showed distinct pulsatile release profiles, with a rapid and complete drug release after the lag time. However, at a higher coating level, the drug release was not complete. The capsules did not rupture completely, only smaller cracks were visible. This was caused by the higher mechanical resistance of the thicker coatings. This behavior seemed to be more a problem with the soft gelatin capsules than with hard gelatin capsules ([Bussemer et al., 2003a]) because of the thicker gelatin shell, which had a longer disintegration time when the outer polymeric coating was still partially present, even after it was ruptured. One solution for a better rupturing could also be the use of a thicker swelling layer providing a higher swelling pressure.
Full-size image (10K)
Fig. 10. Drug release from coated soft gelatin capsules as a function of ethyl cellulose
coating level. Polymer coating: EC/HPMC (60:40), 20% TEC, swelling layer: Ac-Di-
Sol:Kollidon 30 (75:25), 23.2 mg/cm2.
With CAPr, the drug release profiles were similar (Fig. 11). Again, at low coating levels, corresponding to lag times up to 3 h, the release was rapid after rupture of the polymer coating. With higher coating levels, the release rate was reduced and in some cases it was incomplete. However, the CAPr-coated capsules performed better than the EC-coated capsules. Another reason for the slow in vitro release could be the lower agitation and the absence of peristaltic movement and destructive forces in the dissolution apparatus, which are present under in vivo conditions and which would result in a more complete drug release after rupturing.
Full-size image (23K)
Fig. 11. Drug release from coated soft gelatin capsules as a function of cellulose acetate
propionate coating level. Polymer coating: (A) CAPr, (B) CAPr, 20% TEC, (C)
CAPr:HPMC (80:20), 20% TEC, swelling layer: Ac-Di-Sol:Kollidon 30 (75:25),
26.7 mg/cm2.
In conclusion, a pulsatile release system based on soft gelatin capsules, was developed with pulsatile drug release profiles, whereby the lag time was primarily controlled by amount and composition of the swelling layer and the coating layer, which affected the swelling pressure of the swelling layer and the water permeability and mechanical properties of the external polymer coating.
References
Binns et al., 1996. J. Binns, H.N.E. Stevens, J. McEwen, G. Pritchard, F.M. Brewer, A.
Clarke, J.E. Stewart and I. McMillan, The tolerability of multiple oral doses of Pulsincap
capsules in healthy volunteers. J. Control. Rel. 38 (1996), pp. 151–158. Article |
PDF (513 K) | View Record in Scopus | Cited By in Scopus (16)
Bodmeier and Paeratakul, 1993. R. Bodmeier and O. Paeratakul, Dry and wet strength of
polymeric films prepared from an aqueous colloidal polymer dispersion, Eudragit RS30d.
Int. J. Pharm. 96 (1993), pp. 129–138. Abstract | PDF (810 K) | View Record in
Scopus | Cited By in Scopus (44)
Bodmeier and Paeratakul, 1994. R. Bodmeier and O. Paeratakul, Mechanical properties
of dry and wet cellulosic and acrylic films prepared from aqueous colloidal polymer
dispersions used in the coating of solid dosage forms. Pharm. Res. 11 (1994), pp. 882–
888. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (93)
Bowtle, 1998. W.J. Bowtle, Liquid filling of hard gelatine capsules: a new technology for
alternative formulations. Pharm. Tech. Eur. 10 (1998), pp. 84–90. View Record in
Scopus | Cited By in Scopus (7)
Bussemer et al., 2001. T. Bussemer, I. Otto and R. Bodmeier, Pulsatile drug-delivery
systems. Crit. Rev. Ther. Drug Carrier Syst. 18 (2001), pp. 433–458. View Record in
Scopus | Cited By in Scopus (55)
Bussemer et al., 2003a. Bussemer, T., Dashevsky, A., Bodmeier, R., 2003a. A pulsatile
drug delivery system based on rupturable coated hard gelatin capsule. J. Control. Rel., in
press.
Bussemer et al., 2003b. T. Bussemer, N.A. Peppas and R. Bodmeier, Evaluation of the
swelling, hydration and rupturing properties of the swelling layer of a rupturable pulsatile
drug delivery system. Eur. J. Pharm. Biopharm. 56 (2003b), pp. 261–270. Article |
PDF (537 K) | View Record in Scopus | Cited By in Scopus (24)
Edgar et al., 2001. K.J. Edgar, C.M. Buchanan, J.S. Debenham, P.A. Rundquist, B.D.
Seiler, M.C. Shelton and D. Tindall, Advances in cellulose ester performance and
application. Prog. Polym. Sci. 26 (2001), pp. 1605–1688. Article | PDF (844 K) |
View Record in Scopus | Cited By in Scopus (130)
Fahrig and Hofer, 1998. Fahrig, W., Hofer, U., 1998. Die Kapsel, Wiss. Verlagsges.
GmbH, Stuttgart, Germany.
Gazzaniga et al., 1994. A. Gazzaniga, M.E. Sangalli and F. Giordano, Oral chronotopic
drug delivery systems: achievement of time and/or site specifity. Eur. J. Pharm.
Biopharm. 40 (1994), pp. 246–250. View Record in Scopus | Cited By in Scopus (47)
Gunder et al., 1995. W. Gunder, B.H. Lippold and B.C. Lippold, Release of drugs from
ethyl cellulose microcapsules (diffusion pellets) with pore formers and pore fusion. Eur.
J. Pharm. Sci. 3 (1995), pp. 203–214. Abstract | PDF (738 K) | View Record in
Scopus | Cited By in Scopus (27)
Hjartstam and Hjertberg, 1998. J. Hjärtstam and T. Hjertberg, Swelling of pellets coated
with a composite film containing ethyl cellulose and hydroxypropyl methylcellulose. Int.
J. Pharm. 161 (1998), pp. 23–28. Article | PDF (1219 K) | View Record in Scopus |
Cited By in Scopus (17)
Krogel and Bodmeier, 1998. I. Krögel and R. Bodmeier, Pulsatile drug release from an
insoluble capsule body controlled by an erodible plug. Pharm. Res. 15 (1998), pp. 474–
481. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (37)
Krogel and Bodmeier, 1999a. I. Krögel and R. Bodmeier, Evaluation of an enzyme-
containing capsular shaped pulsatile drug delivery system. Pharm. Res. 16 (1999a), pp.
1424–1429. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (13)
Krogel and Bodmeier, 1999b. I. Krögel and R. Bodmeier, Floating or pulsatile drug
delivery systems based on coated effervescent cores. Int. J. Pharm. 187 (1999b), pp.
175–184. Article | PDF (143 K) | View Record in Scopus | Cited By in Scopus (48)
Lemmer, 1991. B. Lemmer, Ciradian rhythms and drug delivery. J. Control. Rel. 16
(1991), pp. 63–74. Abstract | PDF (1040 K) | View Record in Scopus | Cited By in
Scopus (64)
Lemmer, 1999. B. Lemmer, Chronopharmacokinetics: implications for drug treatment. J.
Pharm. Pharmacol. 51 (1999), pp. 887–890. Full Text via CrossRef | View Record in
Scopus | Cited By in Scopus (49)
McNeill et al., 1990. McNeill, M.E., Rashid, A., Stevens, H.N.E., 1990. Dispensing
device. WO Patent 90/09168 (1900).
Rhodes and Porter, 1998. C.T. Rhodes and S.C. Porter, Coatings for controlled-release
drug delivery systems. Drug Deliv. Ind. Pharm. 24 (1998), pp. 1139–1154. Full Text via
CrossRef | View Record in Scopus | Cited By in Scopus (16)
Ritschel and Forusz, 1994. W.A. Ritschel and H. Forusz, Chronopharmacology: a review
of drugs studies. Meth. Find. Exp. Clin. Pharmacol. 16 (1994), pp. 57–75. View Record
in Scopus | Cited By in Scopus (26)
Sand, 1990. I.D. Sand, The dependence of properties of cellulose acetate propionate on
molecular weight and the level of plasticizer. J. Appl. Polym. Sci. 40 (1990), pp. 943–
952. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (3)
Savio et al., 1998. D. Savio, P.C. Harrasser and G. Basso, Softgel capsule technology as
an enhancer device for the absorption of natural principles in humans. Arzneim.-
Forsch./Drug Res. 48 (1998), pp. 1104–1106. View Record in Scopus | Cited By in
Scopus (14)
Schauber et al., 1999. T. Schauber, S. De Vos, W. Huhn, B. Rieger and M. Moeller,
Phase behavior and mechanical properties of blends of cellulose propionate and an
alternating propene–carbon monoxide copolymer. Macromol. Chem. Phys. 200 (1999),
pp. 574–579. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (6)
Stegemann, 1999. S. Stegemann, Liquid and semi solid formulation in hard gelatin
capsules. Swiss Pharm. 21 (1999), pp. 21–28.
Tho et al., 1999. I. Tho, P. Schultz, T. Waaler and P. Kleinebudde, Mechanical properties
of dry and wet free polymer films. Proc. Int. Symp. Control. Rel. Bioact. Mater. Boston,
USA 26 (1999), p. 996.
Tsume et al., 2000. Y. Tsume, J.M. Hilfinger, C.A. Siersma, J. Kim and G.L. Amidon,
An oral controlled release system for small animals: in vivo testing of the port system
capsule. AAPS Pharm. Sci. 2000 AAPS Ann. Meet. Suppl. 2 (2000), p. 4038.
Ueda et al., 1994a. S. Ueda, T. Hata, H. Yamaguchi, M. Kotani and Y. Ueda,
Development of a novel drug release system, time-controlled explosion system (TES). I.
Concept and design. J. Drug Target. 2 (1994a), pp. 35–44. Full Text via CrossRef | View
Record in Scopus | Cited By in Scopus (51)
Ueda et al., 1994b. S. Ueda, H. Yamaguchi, M. Kotani, S. Kimura, Y. Tokunaga, A.
Kagayama and T. Hata, Development of a novel drug release system, time-controlled
explosion system (TES). II. Design of multiparticulate TES and in vitro drug release
properties. Chem. Pharm. Bull. 42 (1994b), pp. 359–363. View Record in Scopus | Cited
By in Scopus (34)
Ueda et al., 1994c. S. Ueda, T. Hata, H. Yamaguchi, M. Kotani and Y. Ueda,
Development of a novel drug release system, time-controlled explosion system (TES).
III. Relation between lag time and membrane thickness. Chem. Pharm. Bull. 42 (1994c),
pp. 364–367. View Record in Scopus | Cited By in Scopus (25)
Wilding et al., 1992. I.R. Wilding, S.S. Davis, M. Bakhshaee, H.N.E. Stevens, R.A.
Sparrow and J. Brennan, Gastrointestinal transit and systemic absorption of captopril
from a pulsed-release formulation. Pharm. Res. 9 (1992), pp. 654–657. Full Text via
CrossRef | View Record in Scopus | Cited By in Scopus (55)
Corresponding author. Tel.: +49-30-838-50643; fax: +49-30-838-50692.
International Journal of PharmaceuticsVolume 267, Issues 1-2, 28 November 2003, Pages 59-68
Mechanisms of dissolution of frusemide/PVP solid dispersions C. Dohertya and P. York , a
aPostgraduate School of Studies in Pharmacy, University of Bradford U.K.
Received 21 April 1986;
revised 30 June 1986;
accepted 21 July 1986.
Available online 5 November 2002.
Abstract
With a discriminating intrinsic dissolution apparatus the dissolution rates and profiles of frusemide-
polyvinylpyrrolidone (PVP) mix and solid dispersion systems (10–100% w/w frusemide) have been
examined together with scanning electron photomicrographs (SEM) of the dissolution surfaces of
compressed discs before and after dissolution. Solid dispersion systems exhibited higher dissolution rates
than corresponding mixes and untreated frusemide. The peak intrinsic dissolution rate, found for both mix
and dispersion systems containing 40% w/w frusemide, was attributed to a balance of two opposing factors.
In mix systems a dissolution-promoting effect of soluble complex formation with PVP is balanced by a
viscosity-related retarding effect of increasing PVP content in the diffusion layer. In dispersion systems a
large dissolution-promoting effect of the X-ray amorphous state of the drug at the 40% drug level produces a
highly supersaturated diffusion layer demonstrated in time/solubility profiles which is also balanced by the
increasing PVP content in the diffusion layer. These findings were further supported by the observed
dependence of the dissolution rate on the molecular weight and related solution viscosity of the PVP used to
form the X-ray amorphous solid dispersion and mechanical mix, in high polymer content systems. In
addition, a filming effect over dissolved compact faces shown by SEM, when the drug level was 40% w/w or
less was attributed to a PVP layer covering the dissolving face and the change from a crystalline drug-
controlled dissolution mechanism to a polymer controlled system.
Keywords: Solid dispersion; Mechanisms of dissolution; Amorphous state; Supersaturation phenomena;
Soluble complex; PVP retarding effect
Correspondence: P. York, Postgraduate School of Studies in Pharmacy, University of Bradford, Bradford,
West Yorkshire BD7 1DP, U.K..
International Journal of PharmaceuticsVolume 34, Issue 3, January 1987, Pages 197-205
Related Documents










