I I Reduction of thrombotic and hemorrhagic complications after stent implantation Manuel Pan, MD, a Jos~ Su~rez de Lezo, MD, a Francisco Velasco, MD, b Miguel Romero, MD, a Alfonso Medina, MD, c Jos~ Segura, MD, a Enrique Hern~ndez, MD, c Djordje Pavlovic, MD, ~ Francisco Melian, MD, c Arsenio Gallardo, MD, a Ricardo Zayas, MD, a Martin Ruiz, MD, a and Antonio Torres, MD b CSrdoba and Las Palmas de Gran Canaria, Spain This study compared two consecutive antithrombotic strat- egies after Palmaz-Schatz stent implantation and involved 918 patients. Patients treated between May 1991 and May 1994 (group 1; n = 379) received aspirin, dipyridamole, and intravenous unfractionated heparin until oral anticoagula- tion was effective. Between June 1994 and August 1995, 539 patients (group 2) were treated for 1 month with subcutane- ous low-molecular-weight heparin (Fragmin), ticlopidine, and aspirin. There were no differences between the groups in terms of sex, clinical condition, vessel diameter, and se- verity and location of stenosis. Patients in group 1 were younger than those in group 2 (4% were >70 years old com- pared with 12%, respectively; p < 0.01). Group I patients had more frequent unplanned stenting (48% vs 18%, respec- tively; p < 0.01) and fewer endoprostheses in the same artery than those in group 2 (1.1 ± 0.5 vs 1.2 ± 0.5, respectively; p < 0.01). Among group 2 patients, there was a significant reduction in thrombotic and hemorrhagic complications compared with group 1 patients. No subacute thrombosis occurred in patients in group 2 in contrast with a 5.8% inci- dence in patients in group 1 (p < 0.01). in addition, a lower incidence of groin and systemic bleeding was observed in patients in group 2 compared with patients in group I (2.6% vs 15%, respectively; p < 0.01). The association of low-mo- lecular-weight heparin and antiplatelets provides a simpler antithrombotic strategy in patients treated with intracoro- nary stents and reduces the incidence of stent thrombosis and hemorrhagic complications. Our findings suggest that this antithrombotic regimen may prevent or completely avoid stent thrombosis. (Am Heart J 1996;132:1119-26.) The Palmaz-Schatz stent has proven to be an effec- tive method for the treatment of coronary heart dis- ease. 1"3 Because of the thrombogenicity of the de- vice's metallic structure, an anticoagulation regimen is required until the inner surface of the stent is From athe Department of Cardiology and %he Department of Hematology, Hospital Reina Sofia, and from %he Department of Cardiology, Hospital del Pino. Received for publication Jan. 23, 1995; accepted May 30, 1996. Reprint requests: Manuel Pan, MD, Servicio de Cardiolog~a~ Hospital Re- ina Sofia, Avda, Men~ndez Pidal s/n, 14004-CSrdoba, Spain. Copyright © 1996 by Mosby-Year Book, Inc. 0002-8703/96/$5.00 + 0 411/75868 completely covered by endothelial cells. Since its in- troduction into clinical practice, a vigorous anticoag- ulation treatment including aspirin, dipyridamole, intravenous heparin, and subsequent oral anticoag- ulation has been recommended. 1-3 However, even with the use of appropriate treatment, hemorrhagic and thrombotic complications may still arise.l6 Some authors have proposed that the use of anticoagulants can be reduced when the device is deployed correctly and an optimal angiographic and ultrasound result is obtained. 7-9 We hypothesized that a better antithrombotic strategy, rather than changes to the technique itself, might reduce complications. Consequently, we changed our anticoagulation protocol in May 1994; intravenous unfractionated heparin, oral anticoagu- lation agents, and dipyridamole were replaced with low-molecular-weight heparin and ticlopidine. In the current study, these two antithrombotic strategies were compared in 918 consecutive patients. METHODS Patients. Between May 1991 and August 1995, 918 con- secutive patients with coronary heart disease were treated with Palmaz-Schatz stent implantation. Between May 1991 and May 1994, 379 patients (group 1) received aspi- rin 150 mg/day, dipyridamole 300 mg/day, and intrave- nous unfractionated heparin until oral anticoagulation was effective. This treatment was maintained for 3 months. Between June 1994 and February 1995, 539 consecutive patients (group 2) were treated for i month with subcuta- neous low-molecular-weight heparin (Fragmin), anti-fac- tor Xa 10,000 IU/day, ticlopidine 500 mg/day, and aspirin 150 rag/day. Aspirin administration was maintained in- definitely in both groups. All patients had evidence of my- ocardial ischemia, either spontaneous or induced by exer- cise. In 4 patients in group 2, ticlopidine treatment was discontinued because of collateral side effects. The rate of complications was assessed during hospital- ization and during the 3-month period in which the anti- thrombotic regimen was administered. After discharge a clinical follow-up was established with a first revision in 1119

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

I I
Reduction of thrombotic and hemorrhagic complications after stent implantation
Manuel Pan, MD, a Jos~ Su~rez de Lezo, MD, a Francisco Velasco, MD, b Miguel Romero, MD, a
Alfonso Medina, MD, c Jos~ Segura, MD, a Enrique Hern~ndez, MD, c Djordje Pavlovic, MD, ~
Francisco Melian, MD, c Arsenio Gallardo, MD, a Ricardo Zayas, MD, a Martin Ruiz, MD, a and
Antonio Torres, MD b CSrdoba and Las Palmas de Gran Canaria, Spain
This study compared two consecutive antithrombotic strat- egies after Palmaz-Schatz stent implantation and involved 918 patients. Patients treated between May 1991 and May 1994 (group 1; n = 379) received aspirin, dipyridamole, and intravenous unfractionated heparin until oral anticoagula- tion was effective. Between June 1994 and August 1995, 539 patients (group 2) were treated for 1 month with subcutane- ous low-molecular-weight heparin (Fragmin), ticlopidine, and aspirin. There were no differences between the groups in terms of sex, clinical condition, vessel diameter, and se- verity and location of stenosis. Patients in group 1 were younger than those in group 2 (4% were >70 years old com- pared with 12%, respectively; p < 0.01). Group I patients had more frequent unplanned stenting (48% vs 18%, respec- tively; p < 0.01) and fewer endoprostheses in the same artery than those in group 2 (1.1 ± 0.5 vs 1.2 ± 0.5, respectively; p < 0.01). Among group 2 patients, there was a significant reduction in thrombotic and hemorrhagic complications compared with group 1 patients. No subacute thrombosis occurred in patients in group 2 in contrast with a 5.8% inci- dence in patients in group 1 (p < 0.01). in addition, a lower incidence of groin and systemic bleeding was observed in patients in group 2 compared with patients in group I (2.6% vs 15%, respectively; p < 0.01). The association of low-mo- lecular-weight heparin and antiplatelets provides a simpler antithrombotic strategy in patients treated with intracoro- nary stents and reduces the incidence of stent thrombosis and hemorrhagic complications. Our findings suggest that this antithrombotic regimen may prevent or completely avoid stent thrombosis. (Am Heart J 1996;132:1119-26.)
The Palmaz-Schatz stent has proven to be an effec- tive method for the t reatment of coronary heart dis- ease. 1"3 Because of the thrombogenicity of the de- vice's metallic structure, an anticoagulation regimen is required until the inner surface of the stent is
From athe Department of Cardiology and %he Department of Hematology, Hospital Reina Sofia, and from %he Department of Cardiology, Hospital del Pino.
Received for publication Jan. 23, 1995; accepted May 30, 1996.
Reprint requests: Manuel Pan, MD, Servicio de Cardiolog~a~ Hospital Re- ina Sofia, Avda, Men~ndez Pidal s/n, 14004-CSrdoba, Spain. Copyright © 1996 by Mosby-Year Book, Inc. 0002-8703/96/$5.00 + 0 411/75868
completely covered by endothelial cells. Since its in- troduction into clinical practice, a vigorous anticoag- ulation t reatment including aspirin, dipyridamole, intravenous heparin, and subsequent oral anticoag- ulation has been recommended. 1-3 However, even with the use of appropriate treatment, hemorrhagic and thrombotic complications may still arise.l6 Some authors have proposed that the use of anticoagulants can be reduced when the device is deployed correctly and an optimal angiographic and ultrasound result is obtained. 7-9
We hypothesized that a better antithrombotic strategy, rather than changes to the technique itself, might reduce complications. Consequently , we changed our anticoagulation protocol in May 1994; intravenous unfractionated heparin, oral anticoagu- lation agents, and dipyridamole were replaced with low-molecular-weight heparin and ticlopidine. In the current study, these two antithrombotic strategies were compared in 918 consecutive patients.
METHODS Patients. Between May 1991 and August 1995, 918 con-
secutive patients with coronary heart disease were treated with Palmaz-Schatz stent implantation. Between May 1991 and May 1994, 379 patients (group 1) received aspi- rin 150 mg/day, dipyridamole 300 mg/day, and intrave- nous unfractionated heparin until oral anticoagulation was effective. This treatment was maintained for 3 months. Between June 1994 and February 1995, 539 consecutive patients (group 2) were treated for i month with subcuta- neous low-molecular-weight heparin (Fragmin), anti-fac- tor Xa 10,000 IU/day, ticlopidine 500 mg/day, and aspirin 150 rag/day. Aspirin administration was maintained in- definitely in both groups. All patients had evidence of my- ocardial ischemia, either spontaneous or induced by exer- cise. In 4 patients in group 2, ticlopidine treatment was discontinued because of collateral side effects.
The rate of complications was assessed during hospital- ization and during the 3-month period in which the anti- thrombotic regimen was administered. After discharge a clinical follow-up was established with a first revision in
1119

December 1996 1120 Pan et al. American Head Journal
Table I. Baseline characteristics of the 918 patients
Group 1 Group 2 (n = 379) (n = 539) p Value
Age (yr) 56 ± 9 57 _+ 10 NS Patients >70 yr old 15 (4%) 66 (12%) <0.01 Sex: men/women 326 (86%)/53 (14%) 463 (86%)/76 (14%) NS Unstable clinical condition 239 (63%) 355 (66%) NS Unplanned indication for stent 183 (48%) 97 (18%) <0.01 Previous myocardial infarction 219 (58%). 284 (52%) NS Previous PTCA 65 (17%) 55 (10%) <0.01 Ejection fraction 54 ± 10 54 _+ 12 NS
NS, Not statistically significant; PTCA, percutaneous transluminal coronary angiop]asty at stented segment.
the outpatient clinic 4 to 6 months after the stent implan- tation.
Technique. The technique used for stent deployment has been described in detail. 1°12 All patients were receiv- ing medical treatment with aspirin and antianginal drugs. Written informed consent was obtained from all patients. During the procedure, all patients received a 15,000 IU bolus dose of intravenous unfractionated heparin. No sheathed delivery system was used for deployment. The stents were always mounted and crimped onto a low-pro- file balloon catheter and deployed at the target segment. The stent was expanded with a balloon pressure of at least 10 to 12 atm to reach a size slightly greater than the ves- sel diameter. The technique remained basically unchanged throughout the study period. The stented segment was postdilated in both groups of patients if the first selected balloon diameter was visually underestimated, if the bal- loon burst during deployment, or if residual stenosis was observe d angiographically or by intravascular ultrasound after the stent implantation.
Intravascular ultrasound was used to document the stent implantation in 127 (12.4%) of 1018 treafed vessels. In group 1, a continuous infusion of unfractionated hepa- rin was maintained until oral anticoagulation was effec- tive, whereas in group 2, low-molecular-weight heparin and anti-factor Xa 10,000 IU/day were administered start- ing the day before stent implantation in patients undergo- ing elective procedures or in the laboratory in patients with unplanned indications for the procedure.
Definition of subacute stent thrombosis. Subacute stent thrombosis was assumed when occlusive thrombus formation was visualized angiographically within the stented vessel segment or when clinical symptoms and electrocardiographic changes revealed acute myocardial infarction of the related territory after the first 24 hours and before 1 month after the stent implantation.
Anticoagulation monitoring. The activated clotting time was measured in the catheterization laboratory after he- parinization. An activated clotting time greater than 300 seconds was considered adequate to start the procedure. In group 1, a routine coagulation analysis was performed ev- ery day after the stent implantation, and the perfusion of unfractionated heparin was adjusted according to the ac- tivated partial thromboplastin time, which was main-
tained at approximately three times the control value. Oral anticoagulation was considered to be effective when the international normalized ratio was between 2.5 and 3.5. In group 2, after the procedure was fnished, no further coag- ulation studies were considered necessary.
Angiographic analysis. Digital quantitative coronary angiography was performed in every patient. Each stented lesion was quantified in the view that best showed the most severe stenosis. The minimal lumen diameter was mea- sured and the percentage of stenosis obtained in all instances. Angiography was repeated in 359 patients 7 -+ 4 months after stent deployment. Restenosis was defined as greater than 50% stenosis at follow-up.
Statistics. Data are expressed as means _+ SD. A Stu- dent-Fisher unpaired t test was used to compare quantita- tive data from patients in the two groups. The chi-square or Fisher exact test was used to compare qualitative vari- ables. A value ofp < 0.05 was considered statistically sig- nificant.
RESULTS Patient characteristics at baseline and immediate re-
sults. Baseline clinical da ta are shown in Table I. Pa- t ients in group 1 were younger t h a n those in group 2 (4% vs 12%, respectively, were >70 years old), and more pat ients in group 1 had undergone a previous balloon angioplas ty t h a n those in group 2; however, the proport ion of unp lanned s ten t ing was h igher in group 1 t h a n in group 2. Regarding causes of un- p lanned s tent implantat ion, there were no statist ical differences between groups. The incidence of occlu- sive dissection or abrup t closure versus the incidence of a suboptimal angioplas ty resul t was 50 (27%) ver- sus 133 (73%), respectively, in group 1 and 17 (18%) versus 80 (82%), respectively, in group 2 (difference not statist ically significant). The remain ing vari- ables did not show significant differences between the two groups.
Table II summar izes baseline angiographic char- acteristics of t h e 1018 s tented vessels. Some addi- t ional differences between the groups were observed. Lesions in pat ients in group 2 were longer and

Volume 132, Number 6 American Heart Journal Pan et al. 1121
Tab le I I . Angiographic and procedural data (n = 1018 stented vessels)
Group 1 Group 2 (n = 389) (n = 629) p Value
Stented vessel NS Left anterior 186 (48%) 316 (50%)
descending artery
Circumflex 51 (13%) 106 (17%) artery
Right coronary 130 (33%) 179 (28%) artery
Left main 2 (0.5%) 9 (2%) coronary artery
Saphenous vein 20 (5%) 19 (3%) graft
Reference vessel 3.30 _+ 0.47 3.31 ± 0.51 NS diameter (ram)
Vessel diameter <3 76 (19%) 135 (21%) NS mm
Minimal lumen 0.49 ± 0.39 0.54 ± 0.49 NS diameter (mm)
Lesions with 79 (20%) 99 (16%) NS intraluminal filling defects
Lesion length 10 ± 5 11 ± 5 p < 0.01 (mm)
Lesions longer 17 (4%) 42 (7%) NS than 20 mm
Number of stents 1.1 _+ 0.5 1.2 ± 0.5 p < 0.01 per vessel
IVUS assessment 49 (12.5%) 78 (12.4%) NS of stent implantation
[VUS, Intravascular ultrasound; NS, not statistically significant.
requi red a g r ea t e r n u m b e r of s t en t s per vessel to cover the ent i re d iseased segment . The re were no differences be tween the groups in t e r m s of vessel di- ame te r , the sever i ty and location of stenosis, and the use of i n t r a v a s c u l a r u l t r a sound to documen t the s t en t implan ta t ion . No signif icant differences re- ga rd ing the ini t ial r esu l t were observed be tween the groups. Af ter s t en t implan ta t ion , the m i n i m a l l u m e n d i a m e t e r inc reased f rom 0.49_+ 0.39 m m to 3.1_+0.56 m m ( p < 0 . 0 1 ) in group 1 and f rom 0.54 _+ 0.49 m m to 3.21 _+ 0.6 m m (p < 0.01) in group 2.
C o m p l i c a t i o n s
S u b a c u t e t h r o m b o s i s . None of the 539 pa t i en t s in- cluded in group 2 fulfilled the cr i te r ia for subacu te s t en t th rombos i s as defined. By contras t , this com- pl icat ion was d iagnosed in 22 pa t i en t s in group i and occurred 1 to 20 days a f t e r s t en t implan ta t ion . The difference in the r a t e of subacu te th rombos i s r a t e groups i and 2 was s ta t i s t ica l ly s ignif icant even
Table ]]]. Complications
Group 1 Group 2 (n = 379) (n = 539) p Value
Subacute thrombosis 22 (5.8%) 0 Systemic bleeding 30 (7.9%) 2 (0.4% Groin bleeding 27 (7.1%) 12 (2.2% Groin surgery 9 (2.3%) 3 (0.5% Hospital stay (days) 16 -+ 15 6 -+ 4 Mortality
Related to 5 (1.3%) 0 thrombotic or hemorrhagic complications
Unrelated to 5 (1.3%) 4 (0.7% thrombotic or hemorrhagic complications
Total 10 (2.6%) 4 (0.7%)
<0.01 <0.01 <0.05 <0.05 <0.05
<0.05
NS
<0.05
w h e n the compar i son was pe r fo rmed wi th consider- a t ion of the type of indication. In pa t i en t s wi th u n p l a n n e d indicat ions for the procedure, subacu te th rombos i s occurred in 12 (7%) of 171 pa t i en t s in group 1 versus 0 of 97 pa t i en t s in group 2 (p < 0.01). Similar ly, in pa t i en t s wi th p l anned indicat ions this complicat ion occurred in 10 (5%) of 186 pa t i en t s in group 1 ve r sus 0 of 442 pa t i en t s in group 2 (p < 0.01).
Subacu te s t en t th rombos i s was t r ea t ed in one of severa l ways. E leven pa t i en t s were medica l ly t r ea t ed (3 received in t r avenous thromboly t ic agents); how- ever, 2 of these pa t i en t s died and 4 had an acute my- ocardial infarction. In 10 pa t ien ts , rescue mechan i - cal recana l iza t ion and balloon ang iop las ty were a t t empted ; in 8 pa t i en t s ini t ial recana l iza t ion was successful, bu t 2 requi red e m e r g e n c y bypass su rgery and 1 of these 2 pa t i en t s died. Three pa t i en t s who u n d e r w e n t recana l iza t ion h a d ear ly clinical recur- rence, and a second rescue procedure was pe r fo rmed (Fig. 1). Final ly, 1 pa t i en t u n d e r w e n t emergency surgery , wi thou t previous reca the te r iza t ion , 6 days a f t e r s t en t implan ta t ion .
H e m o r r h a g i c c o m p l i c a t i o n s . Table I I I lists the complicat ions observed in the two groups. Sys temic b leeding occurred in 30 pa t i en t s in group 1 and in 2 pa t i en t s in group 2. There were severa l origins of the sys temic hemor rhage .
1. The u p p e r gas t ro in tes t ina l t r ac t was the origin of h e m o r r h a g e in 10 pa t ien ts , all of w h o m requi red blood t ransfus ion . In 8 of them, b leeding was man i fe s t before d ischarge f rom the hospi ta l and in 2 pa t i en t s was man i fe s t wi th in 2 mon th s a f te r s ten t p lacement . In 7 pa t i en t s the h e m o r r h a g e was controlled a f te r t r a n s i e n t suppress ion of an- t icoagula t ion and subsequen t t h e r a p y adjust-

December 1996 1122 Pan et al. American Heart Journal
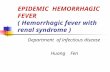
Fig. 1. Serial angiographic observations of patient in group I who had repeat subacute thrombosis despite appropriate anticoagulation. 1, Before stent deployment; 2, after stent deployment; 3, subacute stent thrombosis 10 days after deployment (international normalized ratio = 2.6); 4, after mechanical recanal- ization; 5, second stent thrombosis on day 20 (international normalized ratio = 2.7); 6, final result after balloon angioplasty and local delivery of thrombolytic agents. Arrow, Coronary thrombosis at level of stent.
ment. One patient underwent elective coronary surgery after withdrawal of all anticoagnlation therapy; another patient required endoscopy and sclerosis of the bleeding site; and a third patient underwent gastric surgery.
2. Rectal hemorrhage occurred in 1 patient, who had rectal bleeding 14 days after stent implantation. Anticoagulant agents had to be withdrawn, and this patient had a non-Q-wave myocardial infarc- tion.
3. Intracranial hemorrhage was observed in two pa- tients. One died of acute myocardial infarction after the withdrawal of anticoagnlation therapy, and the second was discharged with neurologic sequelae.
4. Urinary hemorrhage also was observed: 7 pa- tients had hematuria, which was successfully controlled by intravenous fluid infusion and the implantation of a bladder catheter for continuous washing.
5. Retroperitoneal hemorrhage occurred in 7 pa- tients. Five of these patients had a favorable out- come with bed rest and blood transfusion, 1 required surgery, and another patient died as the result of acute renal and multiorgan failure.
6. Metrorrhagia developed in 1 patient; it was con- trolled after blood transfusion and adjustment of anticoagulation therapy.
7. In 4 patients the origin of the bleeding (significant decrease in hematocrit) could not be definitively established; however, all 4 patients had a favor- able outcome.
Groin bleeding, including hemorrhage, hematoma, or pseudoaneurysm, occurred in 27 (7.1%) patients in
group I and in 12 (2.2%) patients in group 2 (p < 0.05). Although groin bleeding was not considered to be a major complication, groin surgery was required in 2.3% of patients in group 1 and 0.5% of patients in group 2, a factor that contributed to a longer hospi- tal stay in group 1 (Table III). When we compared bleeding complications between patients with planned stent indications and those with unplanned indications, there was a slight difference (8% vs 11.4%, respectively), with no statistical significance.
Hospital mortality. The rate of mortality related to subacute stent thrombosis or hemorrhagic complica- tions in the two groups is listed in Table III. There were no significant differences between the groups in mortal i tynot related to these complications. Causes of in-hospital mortality were as follows: in group 1, three patients died of acute coronary occlusion (with- in the first 24 hours or in the hemodynamic labora- tory); one died a sudden death 9 days after the stent implantation; and one died after coronary bypass surgery. In group 2, one patient (who was 79 years 01d) died of acute renal failure; one patient had car- diogenic shock before the procedure, and the shock did not revert despite a successful angiographic re- sult; one died ofelectromechanical dissociation (with- out chest pain) 8 days after the stent implantation; and one died of gastric perforation.
Late results. An angiographic reevaluation was performed in 259 patients in group 1 after 8 +-5 months of follow-up after stent implantation and in 100 patients in group 2 after 5 +- 2 months of follow- up. At follow-up, no significant differences were ob- served between the two groups in terms of residual stenosis (40% _+ 30% in group i vs 38% -+ 35% in group 2) or minimal lumen diameter (2 +_ 1 mm in

Volume 132, Number 6
American Heart Journal P a n et al. 1123
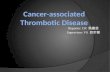
Fig. 2. Coronary angiography of patient in group 2 who had early (36 to 48 hours) clinical recurrence af- ter stent implantation. 1, Before stent deployment; 2, after stent deployment; 3, angiography 48 hours later (limiting flow dissection proximal to stent was observed without thrombotic complications despite initial suboptimal result); 4, final result after second stent implantation covering proximal dissection.
group 1 vs 1.99_+ 1.26 mm in group 2). When restenosis was considered as a binary variable (>50% stenosis), no significant differences were found be- tween the groups: 80 (31%) of 259 patients in group I and 33 (33%) of 100 patients in group 2 fulfilled this restenosis criterion.
DISCUSSION
Debate about the use of antithrombotic regimens after stent implantation continues. Initial recom- mendations arising from the first investigation 1 were made on the basis of a regimen of intravenous unfractionated heparin, dipyridamole, aspirin, and warfarin, which does not protect the patient against subacute stent thrombosis completely. Indeed this complication occurs in approximately 5% to 16% of treated patients. 1, 3-6 In addition, hemorrhagic com- plications have been described, despite frequent use of hematologic determinations. 1, 4, 13 However, some researchers in Italy 7-9 and in France 14 have sug- gested that oral anticoagulation may not be neces- sary if stent deployment is guided by intracoronary ultrasound to reach complete stent expansion.
We hypothesized that regardless of the technique used and in addition to proper stent expansion, the antithrombotic strategy should play an important role in decreasing the Complication rate. Accordingly, we modified our anticoagulation protocol in May 1994, a change that led to a significant decrease in complications. A dramatic elimination ofstent throm- bosis was observed, and the incidence of hemorrhagic complications decreased. Although Colombo et al. 9
described a low incidence of subacute stent throm- bosis when only antiplatelets were used, our strategy completely avoided this complication in a group of 539 consecutive patients. Furthermore, an excellent immediate result with no other flow-limiting lesions is not always possible after stent implantation; thus intraluminal filling defects, long dissections par- tially covered by the stents, or some degree of resid- ual stenosis (Fig. 2) may be observed after the proce- dure. In our study, the new regimen was maintained in all patients in group 2, even in those in whom ul- trasound guidance was not used and in those who had a higher risk for subacute stent thrombosis or hemorrhagic tendency.
Because the change in antithrombotic strategy was based mainly in the substitution of two phar: macologic agents and the continued used of aspirin, it is difficult to derive clear explanations on the clin- ical effect obtained with the selected drug combina- tion, and therefore each agent should be considered separately.
Low-molecular-weight heparin. Unfractionated hep- arin is a heterogeneous mixture of linear anionic polyelectrolytes of various chain lengths. It has been demonstrated that an inverse relation exists be- tween anticoagulant activity and molecular weight. Thus the lower the molecular weight, the higher the anti-factor Xa activity and the lower the thrombin inhibition capacity. Low-molecular-weight heparin has a high affinity for antithrombin III and produces a marked inhibition of kallikrein, factor Xa, and fac- tor XIIal Furthermore, compared with unfraction-

December 1996 1124 Pan et al. American Heart Journal
Jun/91.Dec/91 '='~ 4an/gg~un/92 n=2..~.~_Y Jul/92-Dec/92 ~ n=35 Jan/gS.;un/gs i ~ JulR3-Oec/93 n:
n=147 Jan/94-May/94 ~
Jan/95-Aug/g5 n:287 0% 20% 40% 60% 80% 100%
Subacute thrombosis ~mYes ~No )
Change of anti~rombotic
Fig. 3. Incidence of subacute stent thrombosis. This complication occurred at similar rates throughout 3-year period before introduction of new antithrombotic regimen, despite increasing experience of opera- tors, and was eliminated after introduction of new strategy, n, Number of patients treated by stent implantation.
ated heparin, low-molecular-weight heparin pro- duces only a slight increase in the activated partial thromboplastin and thrombin time. The efficiency of heparin is related to anti-factor Xa activity, and the risk of bleeding is associated with an increase in ac- tivated partial thromboplastin time. Therefore it can be expected that low-molecular-weight heparin would reduce the risk of bleeding while maintaining its antithrombotic capacity. 15, 1~ This beneficial ef- fect has been demonstrated in the prophylaxis of thromboembolic disease 17 and more recently in the t rea tment of unstable angina and silent ischemia, zs
The reduced incidence of thrombotic complications described in our study also may be explained by two additional properties of low-molecular-weight hepa- rin: a degree offibrinolytic Capacity and a low degree of neutralization by platelet factor 4.19 The latter seems to be of particular relevance because vascular manipulation (such as stent implantation) produces platelet activation and the release of platelet factor 4, which has a high antiheparin activity. Hence, the lower level of neutralization of low-molecular-weight heparin by platelet factor 4 leads to the higher anti- thrombotic capacity of low-molecular-weight hepa- rin.
Antiplatelets. The antiaggregation effect of these drugs has been proposed and has been used fre- quently to prevent thrombosis during and after cor- onary interventions. Several studies have demon- strated the benefit of aspirin and dipyridamole 2°, 21 in patients undergoing coronary operations. A]-
though the ideal dosage of aspirin has been ques- tioned, 22 its preventive use seems universally ac- cepted for most coronary interventions. However, the mechanisms of action of other antiplatelet drugs are not completely understood. Ticlopidine appears to decrease the ability of adenosine diphosphate to pro- duce the changes in the glycoprotein IIb/IIIa recep- tor that are responsible for developing a high- affinity ligand binding site. 23 Dipyridamole inhibits platelet function by inhibiting cyclic nucleotide phos- phodiesterase and increasing the levels of cyclic adenosine monophosphate in platelets. 24
Hypothetical considerations. Our study patients re- ceiving the mildest antithrombotic regimen had no incidence of 'thrombotic complications and fewer hemorrhagic complications, bu t because we com- pared the combination of several antithrombotic agents the proportional beneficial effect of each iso- lated drug cannot be determined. However, it may be hypothesized that a strong antithrombotic regimen with unfractionated heparin and subsequent oral anticoagulation may persistently inhibit thrombus formation and, as a consequence, delay the comple- tion of neointimal coverage of the stent. In fact, se- rial angioscopic observations 25 in patients treated With intracoronary stents have shown that this pro- cess may require even months if the anticoagulation therapy is maintained. On the contrary, if the initial bolus of unfractionated heparin is not continued by intravenous infusion, a thrombotic layer may rapidly cover the stent wires. 26 The thrombolytic and anti-

Volume 132, Number 6
American Heart Journal P a n et al. 1125
thrombin III effects of low-molecular-weight heparin and the antiplatelet effect of ticlopidine and aspirin may mainta in this covering as a thin layer, provid- ing a favorable condition for fast organization and formation of neoendothelium, processes that may explain the absence of subacute thrombosis.
Our findings seem to agree with the excellent re- sults reported by a recent study in which after the stent implantation no patient received intravenous unfractionated heparin, and the transition to oral anticoagulation was made by the administration of low-molecular-weight h e p a r i n S Thus although there is not general acceptance of the addition of low-molecular-weight heparin to antiplatelet agents after a coronary stent implantation, 2s, 29 this combi- nation may be of benefit for several reasons. First, the addition of low-molecular-weight heparin does not increase the risk of bleeding but antithrombotic capacity is maintained. Second, some of the studies that recommend the use of antiplatelets alone 2s re- fer to a population of patients with optimal results after stent implantation and exclude patients with suboptimal results or those whom the operator believed required anticoagulation. Third, in patients who have severe collateral side effects from aspirin or ticlopidine, low-molecular-weight heparin would remain a worthy pharmacologic support against subacute stent thrombosis.
Study limitations, First, our study compares two strategies in consecutive groups of patients, and therefore the effect of a learning curve in the success of stent implantation may have influenced the re- sults. However, the incidence of subacute stent thrombosis was similar during the 3-year period be- fore the introduction of the new antithrombotic reg- imen (Fig. 3) suggesting that greater experience of the operators did not affect the frequency of subacute stent thrombosis. Second, some baseline differences between groups did exist. However, some of these differences (longer lesions and larger stented surface areas) could even have favored stent thrombosis in patients in group 2. In addition, group 2 comprised patients who were treated consecutively with stent implantation in our laboratory during an uninter- rupted period of 15 months. All patients who received a stent during this period were treated with the new regimen, even patients considered to be at high risk of subacute stent thrombosis (because of thrombus- containing lesions, lesions located in smaller vessels, or diffuse lesions or dissections requiring two or more additional stents). No patients in group 2 crossed over to the unfractionated heparin-coumadin regi- men. Finally, our study was not randomized. Al- though further randomized studies may be carried
out by other groups, the observed dramatic decrease in the complication rate in our patients in group 2 provided ethical reasons for not undertaking a pro- spective randomized comparison.
Conclusions. We conclude that the antithrombotic strategy using low-molecular-weight heparin, ticlo- pidine, and aspirin leads to a reduction in thrombotic and hemorrhagic complications after stent implan- tation. This strategy seems to represent an improve- ment over the previous, widely accepted regimen of unfractionated heparin, aspirin, and dipyridamole.
REFERENCES
1. Schatz RA, Balm DS, Leon M, Ellis SG, Goldberg S, Hirshfeld JW, et al. Clinical experience with the Palmaz-Schatz coronary stent: initial results of multicenter study. Circulation 1991;83:148-61.
2. Serl~ys PW, Jaegere P, Kiemeneij F, Macaya C, Rutsch W, Heyndrickx G, et al., for the Benestent Study Group. A comparison of balloon ex- pandable stent implantation with balloon angioplasty in patients with coronary artery disease. N Engl J Med 1994;331:489-95.
3. Fischman DL, LeSn MB, Balm DS, Schatz RA, Savage MP, Penn I, et al. A randomized comparision of coronary-stent placement and ballon angioplasty in the treatment of coronary artery disease. N Engl J Med 1994;331:496-501.
4. Herrmann HC, Buchbinder M, Clemen MW, Fischman D, Goldberg S, Leon MB, et ak Emergent use of balloon-expandable coronary artery stenting for failed percutaneous transluminal coronary angioplasty. Circulation 1992;86:g12-9.
5. Haude M, Erbel R, Issa H, Straub U, Rupprecht HJ, Treese N, et al. Snbacute thrombotic complications after intracoronary implantation of Palmaz-Schatz stents. Am Heart J 1993;126:15-22.
6. Diaz L, Fajadet J, Cassagneau, Robert G, Marco J. Early outcome and angiographic predictors of subacute closure in Palmaz-Schatz coronary stenting. Rev Esp Cardiot 1994;47:747-53.
7. Goldberg SL, Colombo A, Nakamura S, Almagor Y, Maiello L, Tobis JM. Benefit ofintracoronary ultrasound in the deployment of Palmaz- Schatz stents. J Am Coll Cardiol 1994;24:996-1003.
8. Nakamura S, Colombo A, Gaglione A, Almagor Y, Goldberg SL, Maiello L, et al. Intracoronary ultrasound observations during stent implanta- tion. Circulation 1994;89:2026-34.
9. Colombo A, Hall P, Nakamura S, Almagor Y, Maiello L, Martini G, et al. Intracoronary stenting without anticoagulation accomplished with intravascular ultrasound guidance. Circulation 1995;91:1676-88.
10. Pan M, Medina A, Romero M, Su~rez de Lezo J, Hern~ndez E, Pavlovic DJ, et al. Peripheral stent recovery after failed intracoronary delivery. Cathet Cardiovasc Diagn 1992;27:230-3.
11. Medina A, Melian F, Suelrez de Lezo J, Pan M, Romero M, Hern~ndez E, et al. Effectiveness of coronary stenting for the treatment of chronic total occlusion in angina pectoris. Am J Cardiol 1994;73:1222-4.
12. Pan M, Medina A, Su~rez de Lezo J, Romero M, Meli~n F, Pavlovic D J, eta]. Follow-up patency of side branches covered by an intracoronary Palmaz-Schatz stent. Am Heart J 1995;129:436-40.
13. Carrozza JP, Kuntz RE, Levine MJ Pomerantz RM, Fishman RF, Mansour M, et al. Angiegraphic and clinical outcome ofintracoronary stenting: immediate and long-term results from a large single-center experience. J Am Coll Cardiol 1992;20:328-37.
14. Morice MC, Zemour G, Benvediste E, Biron Y, Bourdonnec C, Faivre R, et al. Intracoronary stenting without coumarin: one month results of a French multicenter study. Cathet Cardiovasc Diagn 1995;35:1-8.
15. Hirsh J. Low molecular weight heparin. Thromb Haemost 1993; 70:204-7.
16. Barrowcliffe TW, Johnson EA, Thomas DP. Low molecular weight heparin. Chichester (UK): J Wiley & Sons, 1992.
17. Kakkar V. Prevention of venous thrombosis and pulmonary embolism. Am J CardioI 1990;65:50C-4C.
18. Gurfiz~el EP, Manos EJ, Mejall RI, Cerda MA, Duroto EA, Garcia CN, eta]. Low molecular weight heparin versus regular heparin or aspirin

December 1996 1126 Pan et al. American Heart Journal
in the treatment of unstable angina and silent ischemia. J Am Cell Cardiol 1995;26:313-8.
19. Bendetowicz AV, Kai H, Knebel R, Caplain H, Hemker HC, Lindhout T, et al. The effect of subcutaneous injection of unfractionated and low molecular and low molecular weight heparin on thrombin generation in platelet rich plasma: a study in human volunteers. Thromb Haemost 1994;72:705-12.
20. Schwartz L, Bourassa MG, Lesperance J, Aldridge HE, Kazin F, Sal- vatori VA, et al. Aspirin and dipyridamol in the prevention of resteno- sis after percutaneous transluminal coronary angioplasty. N Engl J Med 1988;318:1714-9.
21. Sanz G, Pajaron A, Alegria E, Coello I, Cardena M, Fournier JA, et aL, and the Grupo Espafiol para el Seguimiento del Injerto Coronario (GE- SIC). Prevention of early aortocoronary bypass occlusion by low-dose aspirin and dipyridamole. Circulation 1990;82:765-73.
22. Fuster V, Jang IK. Role of platelet-inhibitor agents in coronary artery disease. In: Topol EJ, editor. Textbook of interventional cardiology. Philadelphia: WB Saunders, 1994:3-22.
23. Hardisty RM, Powling MJ, Nokes TJC. The action of ticlopidine on hu- man platelets: studies on aggregationl secretion, calcium mobilization and membrane glyceproteins. Thromb Haemost 1990;64:150-6.
24. Fitzgerald GA. Drug therapy: dipyridamole. N Engl J Med 1987;316: 1247-57.
25. 25. Ueda Y, Nanto S, Komamura K, Kodama tC Neontimal coverage of stents in human coronary arteries observed by angioscopy. J Am Cell Cardiol 1994;23:341-6.
26. Andrew JC, Laird JR, Farb A, Kufs W, Wortham DC, Virmani R. Mor- phologic characteristies of lesion formation and time course of smooth muscle cell proliferation in a proliferative restenosis model. J Am Cell Cardiol 1994;24:1398-405.
27. Fernandez Avil~s F, Alonso JJ, Duran JM, Gimeno F, Mufioz JC, Fu- ente L, et al. Subacute occlusion, bleeding complications, hospital stay and restenosis after Palmaz-Schatz coronary stenting under a new an- tithrombotic regimen. J Am Cell Cardiol 1996;27:22-9.
28. Hall P, Nakamura S, Maiello L, Itoh A, Blengino S, Martini G, et al. A randomized comparison of combined ticlopidine and aspirin therapy versus aspirin therapy alone after successful intravascular ultrasound- guided stent implantation. Circulation 1996;93:215-22.
29. Sch6mig A, Neumann FJ, Kastrati A, Schfihlen H, Blasini R, Had- amitzky M, et al. A randomized comparison of antiplatelet and antico- agulant therapy after the placement of coronary-artery stents. N Engl J Med 1996;334:1084-9.
Related Documents