Reducing infection rates through optimal healthcare design Janet Brintnell Tracey Herlihey Chantal Trudel

Reducing infection rates through optimal healthcare design: How you can change your environment to positively impact patient safety outcomes
Jan 21, 2018
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Reducing infection rates through optimal healthcare design
Janet BrintnellTracey HerliheyChantal Trudel

Reducing infection rates through optimal healthcare designHow you can change your environment to positively impact patient safety outcomes
Chantal Trudel1,2, Dr. Sue Cobb1, Dr. Kathryn Momtahan3,4, Janet Brintnell3 and Ann Mitchell31Human Factors Research Group, Faculty of Engineering , University of Nottingham, 2School of Industrial Design, Faculty of Engineering , Carleton University, 3The Ottawa Hospital, 4Ottawa Hospital Research Institute
Tracey Herlihey, PhD Cpsychol. National Investigator, Healthcare Safety Investigation Branch, NHS, UK
Two Case Studies A human factors study in personal protective equipmentHuman factors/design considerations in IPAC to support neonatal care

Reducing infection rates through optimal healthcare design
Tracey A. Herlihey PhD@traceyherlihey


http://fortune.com/2014/11/11/california-nurses-go-on-strike-over-lack-of-ebola-preparedness/
“The union is asking for optimal personal protective equipment for nurses and other caregivers who interact with potential Ebola patients. This includes full‐body hazmat suits that protect against blood and viral penetration, as well as air purifying respirators approved by the National Institute for Occupational Safety and Health.”
Preparedness and PPE

Participants and Environment
N = 82• Nurses• Respiratory therapists• Anaesthetists• Intensive care unit
physicians• Occupational health and
safety• Infection prevention and
control• Environmental service
providers• Security
4 academic hospitals in Toronto:

Materials tested

Materials tested

Procedure
Two human factors specialists independently observed, recorded, and documented actions and dialogue.
Each session lasted for 90 minutes from orientation to final debrief and questionnaire.

Results: 23 PPE design flaws

Results: Environment designEquipment layout and availability• Healthcare workers unknowingly stepped
between “clean” and “dirty” zones• Cleaning materials and disposal bins were
not always easily accessible• Lack of equipment to allow a visual
contamination check• Seating provided for PPE removal increased
contamination risk
Physical environment: • Environment did not facilitate effective
communication between HCWs• Size of doffing area had a significant impact
on doffing safety


Environment re-design
Design features: 1. Hand rails2. Windows3. Disposal bins; positioning;
size; colour coding4. Mirror; affixed; location5. High visibility zones, buffers
and chevrons6. Restricted doffing space7. Secured disinfectant hand
sanitizer; height and placement considerations

MethodologyParticipants:N=72 representative users of PPE
Procedure: • 36 pairs: Primary and a Secondary• Brief orientation• Application of chocolate pudding• Follow institutional protocol
Data collection: • Objective observational data• Subjective questionnaire feedback

Findings
Secured disinfectant wipes and hand sanitizer
Inclusion of mirror
Hand rails
Restricted doffing area
Some features were liked by participants and improved doffing safety, some did not have their intended effects, and others caused additional unforeseen safety issues

Findings

Findings
Require further iterations:X Contamination spread from PPE
to disposal binsX Shoe cover removal was
complicated by placement of hand rail
X Placement of mirrors affected doffing safety
X Windows did not facilitate communication
X Position of Secondary significantly affected doffing safety

Evaluations with representative users
conducting representative tasks are imperative
for revealing system design issues prior to
implementation.
Conclusions

Reducing infection rates through optimal healthcare design
Janet BrintnellChantal Trudel

http://dx.doi.org/10.1080/00140139.2017.1330967
Original study:The Value of Pre‐Design Inquiry to Understand and Improve Infection Prevention and Control (IPAC) in a Neonatal Intensive Care Unit (NICU) – Findings from a Thematic Analysis
Approved by the: Ottawa Health Science Network Research Ethics Board (OHSN‐REB) protocol # 20140854‐01H & University of Nottingham Research Ethics Board

Considerations in infection prevention and control (IPAC)• In Canada every year, more than 200,000 patients get a hospital acquired infection
(HAI), more than 8,000 die as a result.1• Health care tasks involve frequent contact, circulation among people and objects ‐
opportunities for transmitting infections2• Transmission risks are invisible making the risks challenging to visualize. 3
Janet BrintnellChantal Trudel January 16, 2018

IPAC considerations specific to neonatal intensive care
Neonates are particularly vulnerable:• low birth weight, underlying illness, immature immune systems, greater skin permeability2
NICU ‘best practice’ advocates: • 5 moments of hand hygiene;• adequate space;• workflow to reduce transmission risks; and• cleaning/disinfecting protocols.2
Rates of HAIs vary in Canadian NICUs even after adjusting for known risk factors suggesting variations may be due to differences in clinical practice.4
4Khalid et al. (2005). Variations in rates of nosocomial infection among Canadian neonatal intensive care units may be practice‐related. BMC Pediatrics 5(22).
Janet BrintnellChantal Trudel January 16, 2018

Janet BrintnellChantal Trudel January 16, 2018
Basic protocol for routine practice. The 4 moments of hand hygiene required on all patients at all times..
Hand hygiene (general)
5Trudel, Cobb, Momtahan, Brintnell & Mitchell (2018). Graphic adapted with the permission of Public Health Ontario.

Hand hygiene in NICUsProtocol for routine practice in NICUs ‐ 5 moments of hand hygiene. 2
General Hand HygieneMoments NICU Hand HygieneMoments
Four Moments' of hand hygiene from Ontario's Just Clean Your Hands Program (Ontario, Ministry of Health and Long‐Term Care, 2008) compared to 'Five Moments' of hand hygiene for Neonatal Intensive Care Units (Ontario, PIDAC, 2012).
Four moments of hand hygiene performed:
1.before initial contact with patient or environment
2. before performing aseptic procedure
3. after care involving bodily fluid
4. after contact with patient or their environment
Four moments of hand hygiene performed:
1.before initial contact with patient or environment
1a. before each entry into the infantisolette/warmer that holds the neonate
2. before performing aseptic procedure
3. after care involving bodily fluid
4. after contact with patient or their environment
Janet BrintnellChantal Trudel January 16, 2018

Are these basic protocols easy to do in reality?Everything here has been designed…does the design fit the requirements of IPAC?
Janet BrintnellChantal Trudel January 16, 2018

Other Factors Influencing IPACNICU IPAC study focused primarily on ‘Control of the Environment’ 2
Janet BrintnellChantal Trudel January 16, 2018

Infectious complications in neonates remain challenging despiteimprovements in technology6 and extensive guidelines/literature in IPAC.
Why is this and how might design be involved?
Janet BrintnellChantal Trudel January 16, 2018

How can we study this?
It can be difficult for people to explain what they do7, especially in complex work like healthcare. Study was based on research frameworks used in people/human‐centred design8• active involvement of multidisciplinary front‐line staff to define problem and solutions• thorough documentation of work, interactions and requirements to support safety, workflow• used design suggestions/ideas as ‘probes’ to develop a deeper understanding of issues
Janet BrintnellChantal Trudel January 16, 2018

Study Design
Janet BrintnellChantal Trudel January 16, 2018

Scope of Study and Stakeholders• studied 81 healthcare workers, predominantly nurses, N=81• routine care, bloodwork, TPN, tracheal intubation, lumbar puncture,
housekeeping, supply stocking, rounds• 50 hours naturalistic observation covering 24hr work cycle• training in NICU hand hygiene practice• stakeholder planning and feedback meetings
Janet BrintnellChantal Trudel January 16, 2018

Track complexing interactions among people and design
Example of Template Used for Naturalistic Observation and Coding
Data from Planning, Naturalistic Observation and Feedback Meetings:• 497 photos of environment, products, workflow, interactions• sketches of the environment with relevant dimensions• documentation of supply use at bedside from 19 individual shifts • ~ 46,000 words of observation documentation and codes (~ 80 pages)• ~ 5000 words of stakeholder meeting notes and codes• ~ 3000 words of researcher memos
Janet BrintnellChantal Trudel January 16, 2018

How can we reduce risk?
What is really needed at the bedside?Documented ‘actual’ supply use in 19 cases (one shift per case from low to high acuity patients) to understand supply use at the bedside, what can be reduced/eliminated.

Janet BrintnellChantal Trudel January 16, 2018
Barriers in IPAC – frontline perspectives on design
Nurse E ‐ “It would be better if the Purell was closer to the isolette since the equipment around is always ringing off.”
Nurse B ‐ “We’re constantly turning off alarms. But they’re programmed to go off too often.”
Researcher – Can you talk about your work, the design of the bedside and IPAC?Nurse I ‐ “Certainly the drawers, my goodness”... “we reach and grab” ... “it should be readily available”...

First Stages of Coding & Thematic Analysis• key issues identified and
shared with front‐line staff
Janet BrintnellChantal Trudel January 16, 2018

Janet BrintnellChantal Trudel January 16, 2018
How can we test/evaluate our understanding of the issues healthcare workers are experiencing?
• illustrations showed potential strategies for improvement to ‘test’ ideas and help collect more feedback from front‐line workers

Janet BrintnellChantal Trudel January 16, 2018
Findings: Designs lack critical features which may help break chain of pathogen transmission.

Janet BrintnellChantal Trudel January 16, 2018
Findings: Designs and layouts require frequent touch/contact.

Janet BrintnellChantal Trudel January 16, 2018
Findings: Designs require physical and/or cognitive effort to navigate, use or maintain.

Janet BrintnellChantal Trudel January 16, 2018
Findings: Designs create or lead to spatial constraints and crowding and inadvertent contact.

Janet BrintnellChantal Trudel January 16, 2018
Findings: Designs lack provision for cognitive aids that may decrease dependence on memory to support IPAC. Environment lacks critical spaces (e.g. at point of care) to place cognitive aids.

Findings from Thematic Analysis ‐Key design‐related issues influencing IPAC are interconnected.
Aspects of one design may be undermining the benefits of another design. Therefore, a systems design approach is needed to remediate issues.
Designs lack critical features which may help break chain of pathogen transmission.
Designs and layouts require frequent touch/contact.
Designs require physical and/or cognitive effort to navigate, use or maintain.
Designs create or lead to spatial constraints and crowding and inadvertent contact.
Designs lack provision for cognitive aids that may decrease dependence on memory to support IPAC. Environment lacks critical
spaces to place cognitive aids.
Janet BrintnellChantal Trudel January 16, 2018

Key recommendationsDesign is contributing to latent conditions that may compromise the best intentions of health care workers to practice infection prevention safely.
• Design cues needed to understand/visualize high risk transmission surfaces and zones. Cues need to be tested with variety of front‐line staff. 3,5
• Challenges with transmission risks between people, items, surfaces and zones may become even more pronounced within a context that lacks of cues, has spatial constraints, excessive physical and cognitive exertion, and time pressures on health care workers. Context and work needs to be designed holistically with this reality in mind. 5,9
• Managing, accessing and isolating supplies from other surfaces can reduce waste and decrease the likelihood of using overstock supplies on infants.5,10
• Touchless design features are needed at point‐of‐care and latent/unobvious areas to complete tasks safely (e.g. eliminate handles, open access to supplies, voice‐based or other modalities for user interfaces). 5
• More attention is needed on ‘cognitive aids’ in the design of the environment and products to strengthen our understanding of infection prevention and associated risks of unsafe behavior. 5
Janet BrintnellChantal Trudel January 16, 2018

Janet BrintnellChantal Trudel January 16, 2018
NICU IPAC Design Exploration Guide (excerpt)

Current NICU initiatives in IPAC• satellite nursery (5 beds) to keep infant numbers in main NICU to max. of 18/19 ‐ provides RNs
with more workspace and family space• removing millwork at bedsides (drawers, shelves) and adding centralized cart in each room• bedside will have clean counter and second “portable” work surface to separate clean/soiled • working group studying workflow and how to facilitate 5 moments of hand hygiene• in process with MOH to get funding for larger renovation• working with parent groups to incorporate their feedback on design• raising awareness (e.g. World Prematurity Day – Building the Future)• recognition from IPAC department for sustained good practice
Janet BrintnellChantal Trudel January 16, 2018
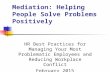
0
1
2
3
Num
ber o
f Cases
Month
NICU Central Line Associated Blood Stream Infections (CLABSI)April 2015 ‐ October 2017
Change Changes to Rolled out
Nurses started Review

For more information on the NICU IPAC study, please feel free to contact:
Chantal [email protected]
Janet [email protected]
1Canada. Public Health Agency of Canada. (2013). The Chief Public Health Officer’s Report on the State of Public Health in Canada, 2013. Infectious Disease—The Never‐ending Threat, retrieved on February 2nd 2016 from http://www.phac‐aspc.gc.ca/cphorsphc‐respcacsp/2013/infections‐eng.php2Ontario. Ontario Agency for Health Protection and Promotion, Provincial Infectious Diseases Advisory Committee (PIDAC). (2012). Best Practices for Infection Prevention and Control in Perinatology. Toronto: Queen's Printer for Ontario.3Sax, H. & Clack, L. (2015). Mental models: a basic concept for human factors design in infection prevention. Journal of Hospital Infection, 89, 335‐339.4Khalid, A.; McMillan, D.D; Andrews, W.; Pendray, M.; Qiu, Z.; Karuri, S.; Lee, S,K,; Canadian Neonatal Network. (2005). Variations in rates of nosocomial infection among Canadian neonatal intensive care units may be practice‐related. BMC Pediatrics 5(22).5Trudel, C., Cobb, S., Momtahan, K., Brintnell, A., & Mitchell, A. 2017. Human Factors Considerations in Designing for Infection Prevention and Control in Neonatal Care –Findings from a Pre‐Design Inquiry. Ergonomics 61(1), 169‐184. DOI: 10.1080/00140139.2017.1330967 6Pessoa‐Silva, C.L., Hugonnet, S., Pfister, R., Touveneau, S. Dharan, S., Posfay‐Barbe, K., & Pittet, D. (2007). Reduction of Health Care ‐ Associated Infection Risk in Neonates by Successful Hand Hygiene Promotion. Pediatrics, 120(2), e382 ‐e390. 7Rogers, Y., Sharp, H., & Preece, J. (2012) Interaction Design ‐ beyond human computer interaction (3rd ed.). UK: John Wiley & Sons Ltd.8Earthy, J., Jones, B.S., & Bevan, N. (2001). The improvement of human‐centred processes – facing the challenge and reaping the benefit of ISO 13407. International Journal of Human‐Computer Studies, 55, 553‐585.9Huslage, K., Rutala, W.A., Sickbert‐Bennett, E., & Weber, D.J. (2010). A quantitative approach to defining "high‐touch" surfaces in hospitals. Infection Control and Hospital Epidemiology 31(8), 850‐853. 10Morrow, J., Hunt, S., Rogan, V., Cowie, K., Kopacz, J., Keeler, C., Billick, M.B., & Kroh, M. (2013). Canadian Journal of Nursing Leadership 26(Spec No 2013), 17‐26..
Sources/references for images:http://scrubbing.in/neonatal‐intensive‐care‐what‐to‐expect/goo.gl/wB1afa
Related Documents