Reducing Care Fragmentation: PRESENTATION ON COORDINATING CARE MacColl Institute for Healthcare Innovation Group Health Research Institute

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Reducing Care Fragmentation:PRESENTATION ON COORDINATING CARE
MacColl Institute for Healthcare InnovationGroup Health Research Institute
Raise your hand if the following are not rare events in your practice:
• You don’t know the people to whom you are referring patients.
• Specialists complain about the information you send with a referral.
• You don’t hear back from a specialist after a consultation.• Your patient complains that the specialist didn’t seem to
know why s/he was there.• A referral doesn’t answer your question.• Your patient doesn’t come back to see you after a
consultation.• A specialist duplicates tests you have already performed.• You are unaware that your patient was seen in the ER.• You were unaware that your patient was hospitalized.
The Good Old Days
Current Fragmentation of Care
• Patients experience and clinicians operate in “silos” of care.
• Referral networks are large1 and often depersonalized.
1 Pham HH, O'Malley AS, Bach PB, Saiontz-Martinez C, Schrag D. Primary care physicians' links to other physicians through Medicare patients: the scope of care coordination. Ann Intern Med. Feb 17 2009;150(4):236-242.

Patients Report Experiencing Poor Coordination
Source: Commonwealth Fund Survey of Public Views of the U.S. Health Care System, 2008.
Percent U.S. adults reported in past two years:
No one contacted you about test results, or you had to call repeatedly to get results
Test results/medical records were not available at the time of appointment
Your primary care doctor did not receive a report back from a specialist
Any of the above
25
21
19
15
13
47
0 20 40 60
Doctors failed to provide important medical information to other doctors or nurses you think should have it
Your specialist did not receive basic medical information from your primary care doctor

37
7582
6168
62
76
0
25
50
75
100
AUS CAN GER NETH NZ UK US
Commonwealth Survey of PCPs
Percent reporting that they receive information back for “almost all” referrals (80% or more) to Other Doctors/Specialists:
Source: 2006 Commonwealth Fund International Health Policy Survey of Primary Care Physicians.
Clinicians Also Report Fragmented Care
• 63% of primary care providers and 35% of specialists are dissatisfied with their current referral process– 25% of the time, primary care providers report
receiving no information from specialists after their patient’s visit
– 68% of the time, specialists report receiving no information from primary care before referral visits
Source: Gandhi TK, Sittig DF, Franklin M, Sussman AJ, Fairchild DG, Bates DW. Communication breakdown in the outpatient referral process. J Gen Intern Med. Sep 2000;15(9):626-631. .

How often do you get the information you need after referral?
What do you think your patients would say about their experience?
Why work on Care Coordination?
Safety & quality
Practice environment
Patient experience
Resources

The Patient-centered Medical HomeKey Features:
1. Engaged leadership
2. Quality improvement strategy
3. Empanelment
4. Patient-centered interactions
5. Organized, evidence-based care
6. Care coordination
7. Enhanced access
8. Continuous, team-based health relationships
Defining Care Coordination
The deliberate organization of patient care activities between two or more participantsinvolved in a patient’s care to facilitate theappropriate delivery of health care services. (McDonald, 2007)
+ ++
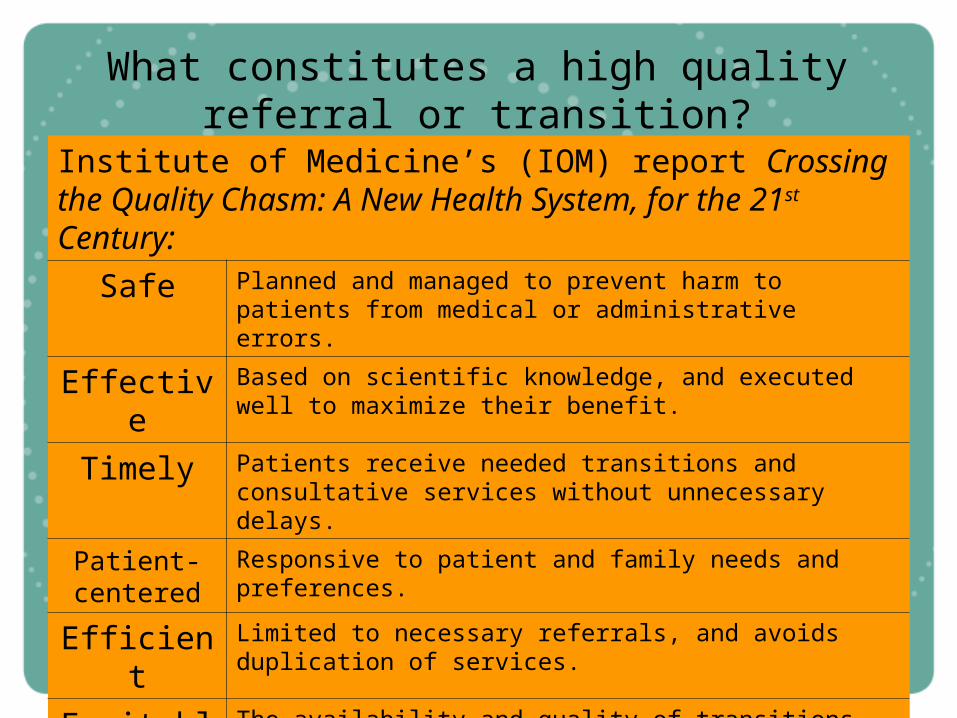
What constitutes a high quality referral or transition?
Institute of Medicine’s (IOM) report Crossing the Quality Chasm: A New Health System, for the 21st Century:
Safe Planned and managed to prevent harm to patients from medical or administrative errors.
Effective Based on scientific knowledge, and executed well to maximize their benefit.
Timely Patients receive needed transitions and consultative services without unnecessary delays.
Patient-centered
Responsive to patient and family needs and preferences.
Efficient Limited to necessary referrals, and avoids duplication of services.
Equitable The availability and quality of transitions and referrals should not vary by the personal characteristics of patients.

The Care Coordination Model
Key Changes
Assume accountability
Provide patient support
Build relationships & agreements
Develop connectivity
#1 Assume Accountability
• Decide as a primary care clinic to improve care coordination.
• Develop a referral/transition tracking system.
#2 Provide Patient Support
• Organize the practice team to support patients and families during referrals and transitions.
• Referral coordinator:– Tracks all referrals and transitions– Provides patient (and family) with
information about referral– Addresses barriers to referrals– Follows up on missed
appointments
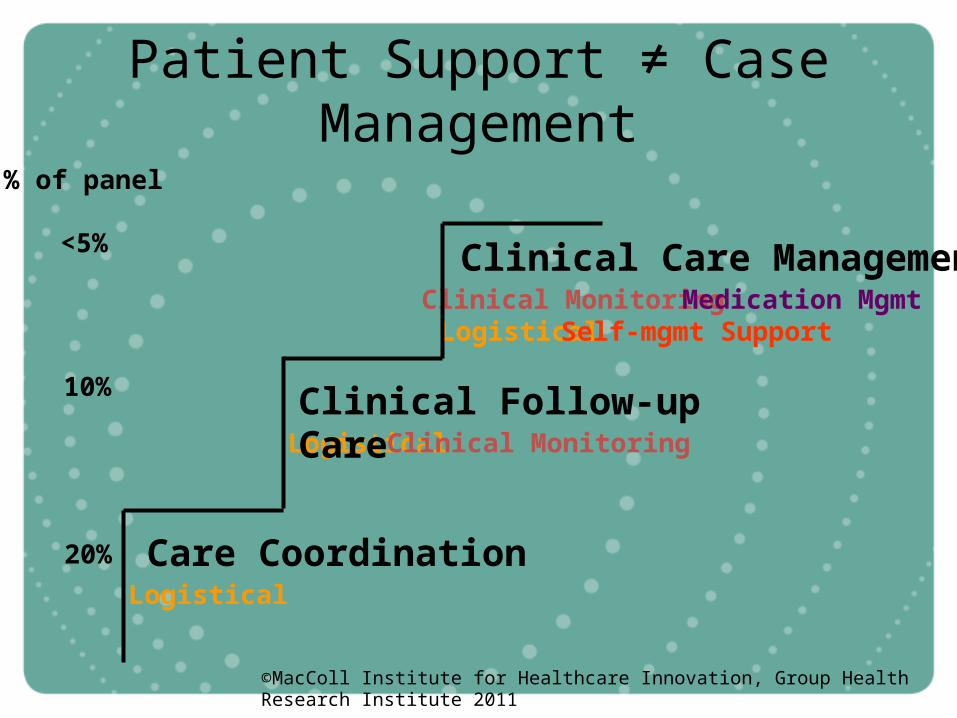
Patient Support ≠ Case Management
Clinical Care Management
Logistical
Logistical
LogisticalClinical Monitoring
% of panel
<5%
10%
20% Care Coordination
Clinical Follow-up Care
Medication Mgmt
©MacColl Institute for Healthcare Innovation, Group Health Research Institute 2011
Self-mgmt Support
Clinical Monitoring

#3 Build Relationships & Agreements
• Identify, develop and maintain relationships with key specialist groups, hospitals and community agencies.
• Develop agreements with these key groups and agencies.
• Lessons learned:– Talk through the process for a
“typical” patient case– Focus on the system and not the
people

Where might you start?
Community Agencies?Tracking & following up on lab/imagining results;
Identification & tracking of linkages to community resources.
Medical Specialists?Guidelines for referral, prior tests, and information;
Expectations about future care and specialist-to-specialist referral;Expectations for information back to PCMH.
EDs/ Hospitals?Notification of visit/admission and discharge;
Medication reconciliation after transition;Involvement of PCMH in post-discharge care.
#4 Develop Connectivity
• Develop and implement an information transfer system.
• Key elements of system:– Integrates information needs and
expectations (per agreements)– Assures that information
transmits to correct destination– Key milestones in the referral
process can be tracked– Referring clinicians and
consultants can communicate with each other
Electronic Referral (e-referral) Systems
• Web-based, and may or not be connected to EMR.• Effectiveness depends on consultants or hospitals
participating.• Can embed referral guidelines and other elements of
agreements.• Can monitor completion of referrals and return of
information to the PCMH.• Users of e-referral systems often gravitate to
experimenting with e-consultations.
Why make care coordination a priority?
• Patients and families are frustrated by fragmented “silos” in health care.
• Poor hand-offs lead to delays and miscommunications in care that may be dangerous to health.
• There is enormous waste associated with unnecessary referrals, duplicate testing, unwanted and unnecessary specialist to specialist referral.
• Primary care practice will be more rewarding.


www.improvingchroniccare.org
Check out our toolkit at:
Related Documents











