Int. J. Gynecol. Obstet., 1988, 26: 93-103 International Federation of Gynecology & Obstetrics Recurrent endometriosis following hysterectomy and oophorectomy: the role of residual ovarian fragments W.P. Dmowski, E. Radwanska and N. Rana Section of Reproductive Endocrinology/Infertility, Rush Medical College, Chicago, Illinois (USA) 93 (Received August 18th, 1986) (Revised and accepted November 15th, 1986) Abstract Seven women with recurrent endome- triosis after definitive surgery were evalu- ated. Plasma estradiol, FSH and LH indicated that recurrence was stimulated by residual ovarian fragments in six and pseu- dopregnancy regimen in one. Surgical treat- ment in two women was followed in one by hypertrophy of another ovarian frag- ment and reactivation of endometriosis as demonstrated by serial endocrine and ul- trasonographic studies. Three patients re- sponded well to hormonal treatment; one required pelvic irradiation. We conclude that: (1) small ovarian fragments may hy- pertrophy under increased gonadrotropin stimulation, become functional and stimu- late recurrence of endometriosis; (2) resec- tion of one such fragment may be fol- lowed by reactivation of another. Keywords: Recurrent endometriosis; Defini- tive surgery; Residual ovarian fragments. Introduction Endometriosis is an enigmatic disease affecting women as well as females of sev- eral species of primates. Although many aspects of this disease are incompletely understood, it is well known that prolifera- tion and spread of endometriosis are stimu- lated by the cyclic secretion of ovarian 0020-7292/88/%03.50 0 1988 International Federation of Gynecology&Obstetrics Published and Printed in Ireland estradiol and progesterone. In the absence of ovarian hormones endometriosis under- goes regression [2]. It is therefore generally accepted that endometriosis should not recur following definitive surgery, i.e. hys- terectomy and bilateral oophorectomy. Occasional reports to the contrary have not been fully explained from the pathophysiol- ogic point of view and there is no agreement as to the best therapeutic approach in such cases [ll]. Seven women with recurrent endome- triosis after definitive surgery were evaluated. This report describes clinical and laboratory findings in these cases and their responses to different therapeutic modalities. Patients and methods Between 1978 and 1985 seven women with suspected recurrence of endometriosis after definitive surgery were evaluated, Clin- ical data on these patients are summarized in Table I. All seven had previously undergone repeated operations (mean 4.1) for histologically confirmed endometriosis. In four (cases 1, 2, 4, 6) bilateral salpingo- oophorectomy (BSO) had been performed at the time of total abdominal hysterectomy (TAH). In the other three (cases 3, 5, 7) ovarian tissue had been intentionally pre- served at the time of TAH (both ovaries in case 5; one ovary in case 7; and ovarian fragment in case 3). After TAH, all seven had been operated again for recurrent Clinical and Clinical Research Article

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Int. J. Gynecol. Obstet., 1988, 26: 93-103 International Federation of Gynecology & Obstetrics
Recurrent endometriosis following hysterectomy and oophorectomy: the role of residual ovarian fragments
W.P. Dmowski, E. Radwanska and N. Rana Section of Reproductive Endocrinology/Infertility, Rush Medical College, Chicago, Illinois (USA)
93
(Received August 18th, 1986) (Revised and accepted November 15th, 1986)
Abstract
Seven women with recurrent endome- triosis after definitive surgery were evalu- ated. Plasma estradiol, FSH and LH indicated that recurrence was stimulated by residual ovarian fragments in six and pseu- dopregnancy regimen in one. Surgical treat- ment in two women was followed in one by hypertrophy of another ovarian frag- ment and reactivation of endometriosis as demonstrated by serial endocrine and ul- trasonographic studies. Three patients re- sponded well to hormonal treatment; one required pelvic irradiation. We conclude that: (1) small ovarian fragments may hy- pertrophy under increased gonadrotropin stimulation, become functional and stimu- late recurrence of endometriosis; (2) resec- tion of one such fragment may be fol- lowed by reactivation of another.
Keywords: Recurrent endometriosis; Defini- tive surgery; Residual ovarian fragments.
Introduction
Endometriosis is an enigmatic disease affecting women as well as females of sev- eral species of primates. Although many aspects of this disease are incompletely understood, it is well known that prolifera- tion and spread of endometriosis are stimu- lated by the cyclic secretion of ovarian
0020-7292/88/%03.50 0 1988 International Federation of Gynecology&Obstetrics Published and Printed in Ireland
estradiol and progesterone. In the absence of ovarian hormones endometriosis under- goes regression [2]. It is therefore generally accepted that endometriosis should not recur following definitive surgery, i.e. hys- terectomy and bilateral oophorectomy. Occasional reports to the contrary have not been fully explained from the pathophysiol- ogic point of view and there is no agreement as to the best therapeutic approach in such cases [ll].
Seven women with recurrent endome- triosis after definitive surgery were evaluated. This report describes clinical and laboratory findings in these cases and their responses to different therapeutic modalities.
Patients and methods
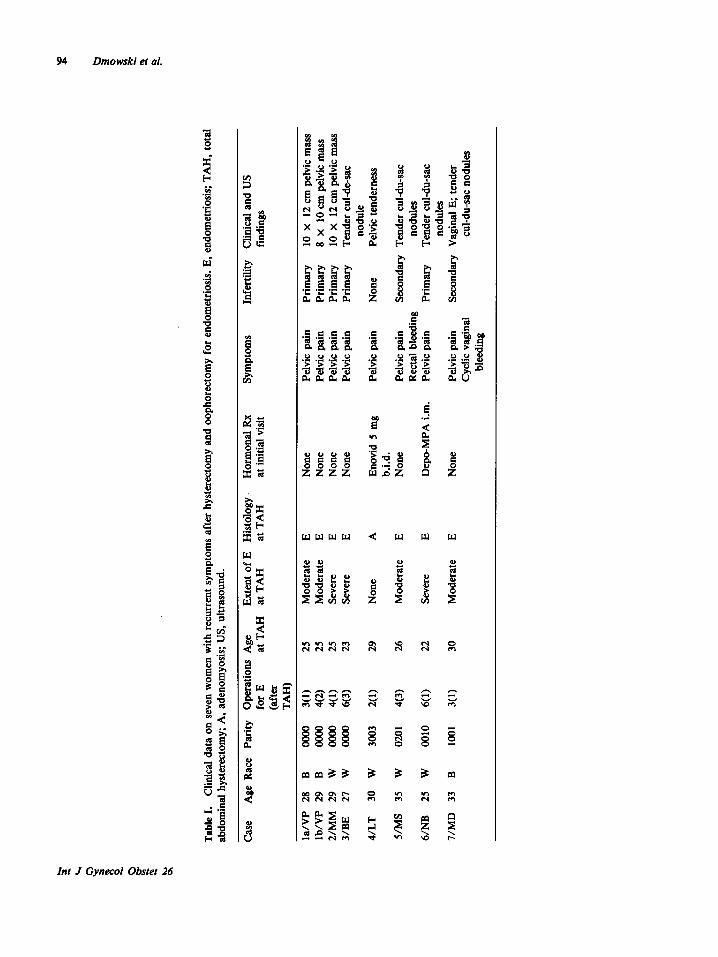
Between 1978 and 1985 seven women with suspected recurrence of endometriosis after definitive surgery were evaluated, Clin- ical data on these patients are summarized in Table I. All seven had previously undergone repeated operations (mean 4.1) for histologically confirmed endometriosis. In four (cases 1, 2, 4, 6) bilateral salpingo- oophorectomy (BSO) had been performed at the time of total abdominal hysterectomy (TAH). In the other three (cases 3, 5, 7) ovarian tissue had been intentionally pre- served at the time of TAH (both ovaries in case 5; one ovary in case 7; and ovarian fragment in case 3). After TAH, all seven had been operated again for recurrent
Clinical and Clinical Research Article
Tabl
e I.
C
linic
al d
ata
on s
even
wom
en w
ith r
ecur
rent
sy
mpt
oms
afte
r hy
ster
ecto
my
and
ooph
orec
tom
y fo
r en
dom
etrio
sis.
E, e
ndom
etrio
sis;
TA
H.
tota
l ab
dom
inal
hy
ster
ecto
my;
A
, ad
enom
yosi
s;
US,
ultr
asou
nd.
Cas
e A
ge
Rac
e Pa
rity
Ope
ratio
ns
Age
Ex
tent
of
E
His
tolo
gy.
Hor
mon
al
Rx
Sym
ptom
s In
ferti
lity
Clin
ical
and
US
for
E at
TA
H
at T
AH
at
TA
H
at i
nitia
l vi
sit
findi
ngs
(afte
r TA
I-I)
la/V
P 28
B
00
00
3(l)
25
Mod
erat
e E
Non
e Pe
lvic
pa
in
Prim
ary
10 X
12
cm
pel
vic
mas
s lb
/VP
29
B
0000
4(
2)
25
Mod
erat
e E
Non
e Pe
lvic
pai
n Pr
imar
y 8
x 10
cm
pel
vic
mas
s 2/
MM
29
W
oo
o0
4(l)
25
Seve
re
E N
one
Pelv
ic p
ain
Prim
ary
10 X
12
cm p
elvi
c m
ass
3/B
E 27
W
00
00
6(3)
23
Se
vere
E
Non
e Pe
lvic
pai
n Pr
imar
y Te
nder
cu
l-de-
sac
nodu
le
4/LT
30
W
30
03
2(l)
29
Non
e A
En
ovid
5
mg
Pelv
ic p
ain
Non
e Pe
lvic
ten
dern
ess
b.i.d
. 5/
MS
35
W
0201
4(
3)
26
Mod
erat
e E
Non
e Pe
lvic
pai
n Se
cond
ary
Tend
er c
ul-d
u-sa
c R
ecta
l bl
eedi
ng
nodu
les
6/N
B
25
W
0010
6(
l) 22
Se
vere
E
Dep
o-M
PA
i.m.
Pelv
ic p
ain
Prim
ary
Tend
er
cul-d
u-sa
c no
dule
s 7/
MD
33
B
10
01
3(l)
30
Mod
erat
e E
Non
e Pe
lvic
pai
n Se
cond
ary
Vag
inal
E;
tend
er
Cyc
lic v
agin
al
cul-d
u-sa
c no
dule
s bl
eedi
ng
Endometriosis after TAH, BSO 95
endometriosis and two (cases 3 and 5) had undergone three separate surgical proce- dures each. At the time of referral both ovaries allegedly had been removed in all seven.
Surgical and pathology reports and histo- logic slides of all surgical specimens were reviewed and an attempt was made to clas- sify the extent of endometriosis at the time of TAH into mild, moderate and severe cat- egories [l]. In all cases there was micros- copic evidence of endometriosis. Interestingly, only adenomyosis and not endometriosis was detected in the first surgi- cal specimen of case 4. The second opera- tion, however, demonstrated endometriosis of the bowel and pelvic wall. In patients 2, 3, 5 and 7, who had undergone multiple ovarian resections, the aggregate of ovarian tissue removed during these procedures in each patient significantly exceeded the size of the normal ovaries. The case in point is patient 3 whose right ovary removed at the age of 23 measured 3 x 2.7 x 1.5 cm, while the aggregate of left ovarian tissue removed during that and subsequent procedures measured 14.5 x 7.7 x 6.2 cm.
All patients were referred because of recurrence of symptoms and suspected recurrence of endometriosis. All complained of pelvic and abdominal pains; one (case 7) continued monthly vaginal bleeding in spite of prior hysterectomy; and another (case 5) complained of irregular rectal bleeding. Two patients were on hormonal treatment for suppression of endometriosis; one with mes- tranol 0.075 mg and norethynodrel 5 mg (Enovid 5 mg) BID (case 4) and the other with depo-medroxyprogesterone acetate (Depo-Provera, Depo-MPA) injections (case 6). Four of the remaining five patients who were not on exogenous hormones at the time of referral had no menopausal symp- toms in spite of prior oophorectomy. One (case 5) had just discontinued estrogen replacement and complained of frequent hot flashes, night sweats, and other vasomotor disturbances.
All patients underwent physical examina- tion, pelvic ultrasonography and endocrinological evaluation prior to the selection of treatment. Plasma FSH, LH and estradiol (E,) levels were ‘measured using specific radioimmunoassay techniques in all patients after discontinuation of exo- genous hormones (except case 6). Hormonal studies were repeated as indicated during subsequent management.
Results
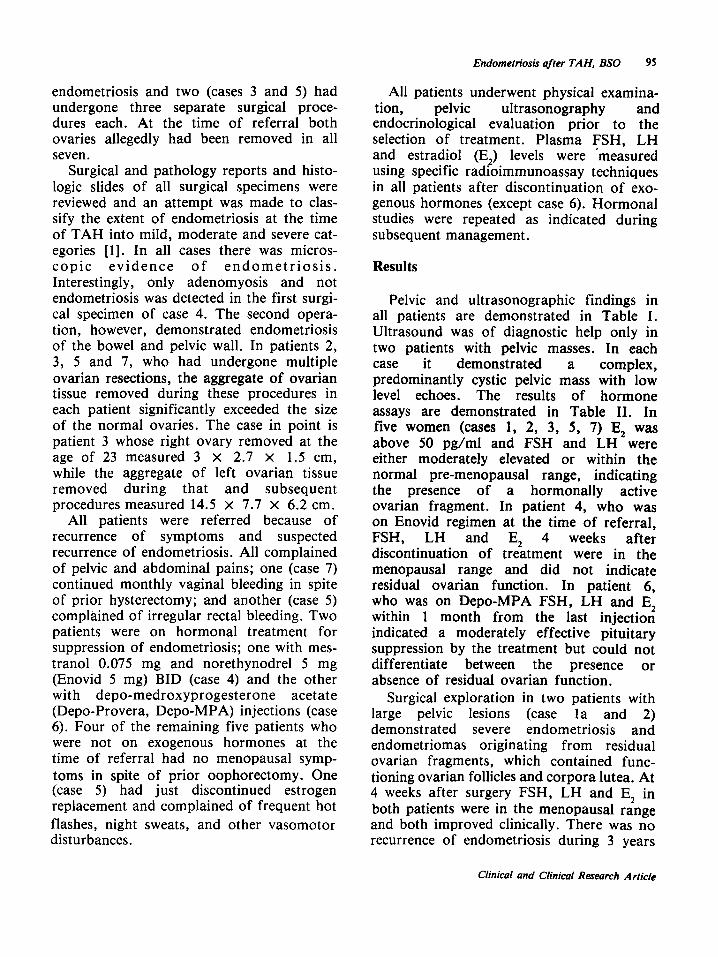
Pelvic and ultrasonographic findings in all patients are demonstrated in Table I. Ultrasound was of diagnostic help only in two patients with pelvic masses. In each case it demonstrated a complex, predominantly cystic pelvic mass with low level echoes. The results of hormone assays are demonstrated in Table II. In five women (cases 1, 2, 3, 5, 7) E, was above 50 pg/ml and FSH and LH were either moderately elevated or within the normal pre-menopausal range, indicating the presence of a hormonally active ovarian fragment. In patient 4, who was on Enovid regimen at the time of referral, FSH, LH and E, 4 weeks after discontinuation of treatment were in the menopausal range and did not indicate residual ovarian function. In patient 6, who was on Depo-MPA FSH, LH and E, within 1 month from the last injection indicated a moderately effective pituitary suppression by the treatment but could not differentiate between the presence or absence of residual ovarian function.
Surgical exploration in two patients with large pelvic lesions (case la and 2) demonstrated severe endometriosis and endometriomas originating from residual ovarian fragments, which contained func- tioning ovarian follicles and corpora lutea. At 4 weeks after surgery FSH, LH and E, in both patients were in the menopausal range and both improved clinically. There was no recurrence of endometriosis during 3 years
Clinical and Clinical Research Article
96 Dmowski et al.
Table II. Endocrine data indicating the cause of endometriosis recurrence after definitive surgery.
Case FSH LH Estradiol Diagnosis mIU/ml) (mIU/ml) (pglml)
la/VP 29.5 42.6 50 Residual ovarian function lb/VP 16.7 12.9 309 Residual ovarian function 2/MM 3.2 8.9 136 Residual ovarian function 3/BE 27.0 14.0 87 Residual ovarian function 4/LT 168.0 140.0 18 Menopausal status, recurrence
secondary to exogenous steroids S/MS 40.5 41.6 142 Residual ovarian function 6/NBa 40.7 22.8 11 Inconclusive; effect of exogenous steroids 7/MD 27.6 33.8 227 Residual ovarian function
‘On Depo-MPA.
of follow-up in one (case 2), while in the other reactivation of another ovarian frag- ment and recurrence of endometriosis 6 months after surgery was demonstrated by serial endocrine and ultrasound examinations. Pertinent clinical data and dynamics of ovarian fragment reactivation in the latter case are presented below as a case report.
Three patients (cases 3, 5, 7) with residual ovarian activity and recurrent endometriosis but without endometriomas were treated medically. Patient 7 on Depo-MPA had suppression of E, levels, arrest of vaginal bleeding and symptomatic improvement. P,atient 5 also on Depo-MPA improved ini- tially but, the effect was inconsistent. Because of frequent exacerbations of symptoms during 2 years of follow-up she was given radiation therapy to the pelvis in the dose of 3000 rad in 17 treatments, which effectively destroyed residual ovarian frag- ment(s) as indicated by a fall in E, below 10 pg/ml and a rise in FSH and LH. Patient 3, who had mild symptoms and minimal findings was managed symptomatically with analgesics and methyltestosterone 2.5 mg/ day. Twelve months later, her FSH was 187 mIU/ml, LH 198 mIU/ml and E, 25 pg/ml, indicating that the last ovarian remnant ceased to function. Patient 6, was continued on Depo-MPA with good clinical results.
Patient 4, developed severe menopausal symptoms after discontinuation of pseudo- pregnancy and was treated symptomatically. She had no further evidence of endome- triosis recurrence.
Case report VP was a 28-year-old black nulligravida
with severe pelvic pains and suspected recur- rence of endometriosis (Table I, Case la). At 21 she had undergone resection of symp- tomatic endometriosis. Four years later, TAH, BSO were performed for moderately extensive, symptomatic disease. According to the pathology report the ovaries were normal in size but had “lacerated” surfaces. There were multiple endometriotic implants on the uterus, ovaries and tubes. Menopau- sal symptoms did not appear after TAH, BSO but symptoms of endometriosis improved. Eight months later recurrent, symptomatic endometriosis was again demon- strated. The patient was placed on ethinyl estradiol 0.5 mg and norgestrel 0.5 mg (Ovral), one tablet daily. She did not improve and was referred for consultation a month after discontinuation of therapy.
At the time of initial visit there were mul- tiple tender pelvic nodules and a 10 x 12 cm cystic, exquisitely tender, pelvic mass, bulging through the vaginal vault and loca- ted somewhat to the left of the midline.
Int J Gyilecol Obstet 26
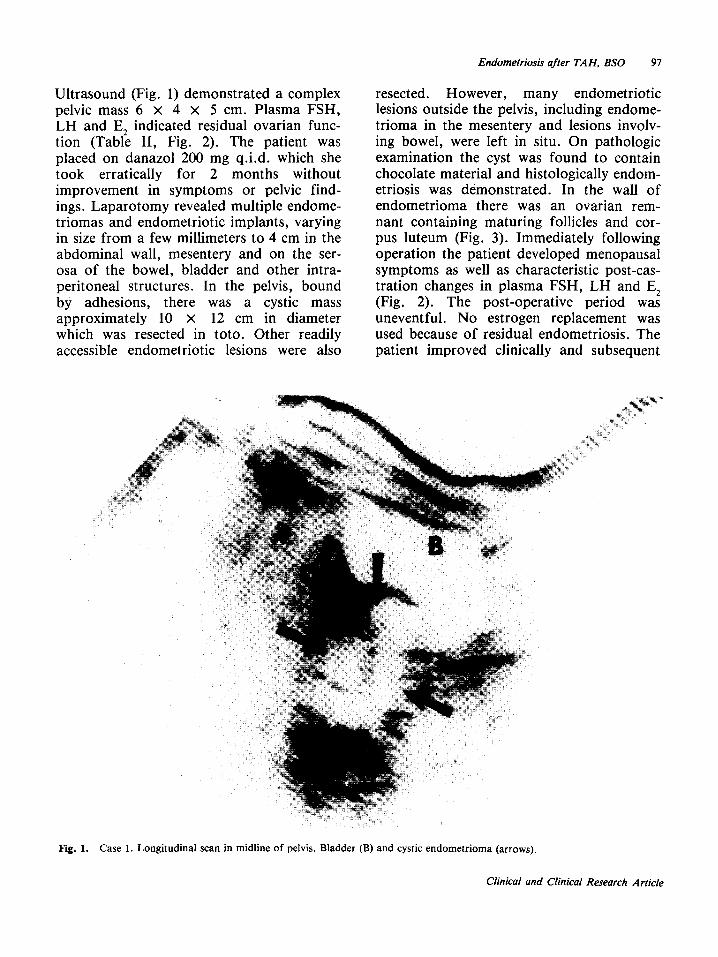
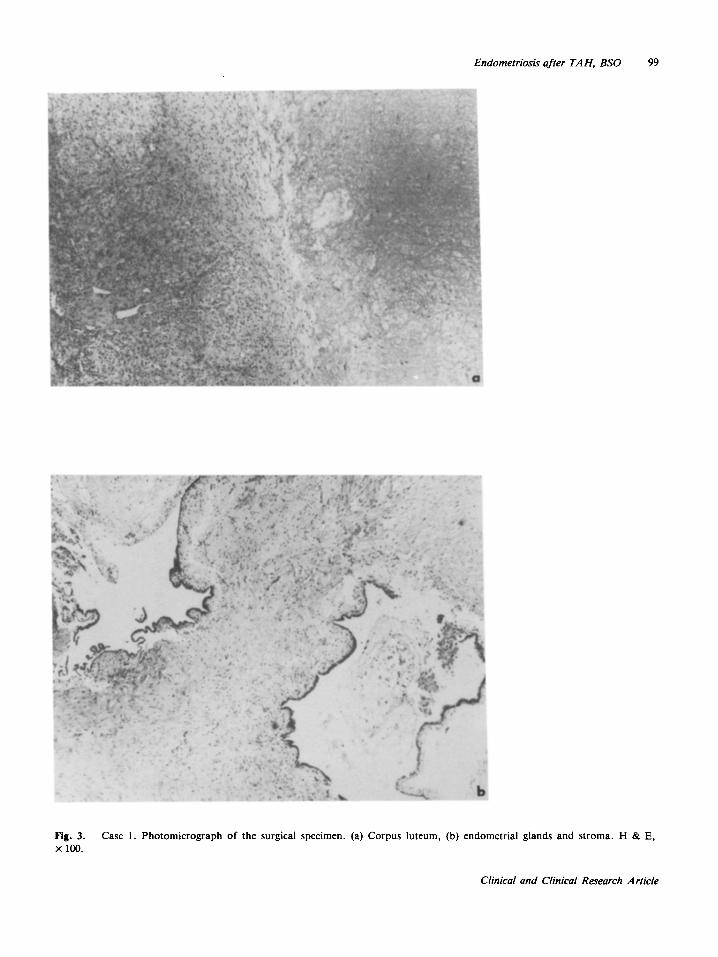
Ultrasound (Fig. 1) demonstrated a complex resected. However, many endometriotic pelvic mass 6 x 4 x 5 cm. Plasma FSH, lesions outside the pelvis, including endome- LH and E, indicated residual ovarian func- trioma in the mesentery and lesions involv- tion (Table II, Fig. 2). The patient was ing bowel, were left in situ. On pathologic placed on danazol 200 mg q.i.d. which she examination the cyst was found to contain took erratically for 2 months without chocolate material and histologically endom- improvement in symptoms or pelvic find- etriosis was demonstrated. In the wall of ings. Laparotomy revealed multiple endome- endometrioma there was an ovarian rem- triomas and endometriotic implants, varying nant containing maturing follicles and cor- in size from a few millimeters to 4 cm in the pus luteum (Fig. 3). Immediately following abdominal wall, mesentery and on the ser- operation the patient developed menopausal osa of the bowel, bladder and other intra- symptoms as well as characteristic post-cas- peritoneal structures. In the pelvis, bound tration changes in plasma FSH, LH and E, by adhesions, there was a cystic mass (Fig. 2). The post-operative period was approximately 10 x 12 cm in diameter uneventful. No estrogen replacement was which was resected in toto. Other readily used because of residual endometriosis. The accessible endometriotic lesions were also patient improved clinically and subsequent
Endometriosis after TAH. BSO 97
Fig. 1. Case 1. Longitudinal scan in midline of pelvis. Bladder (B) and cystic endometrioma (arrows).
Clinical and Clinical Research Article
98 Dmowski et al.
FSH LH
mlU/ml
Ion
r SW
I >lUU
T
4
-zoo pa/ml
-1ao
-180
-1m
-100
-150
-140
-130
-120
-110
-100
- so
- 80
- 70
-80
-50
- 40
-Jo
_m
_ 10
I
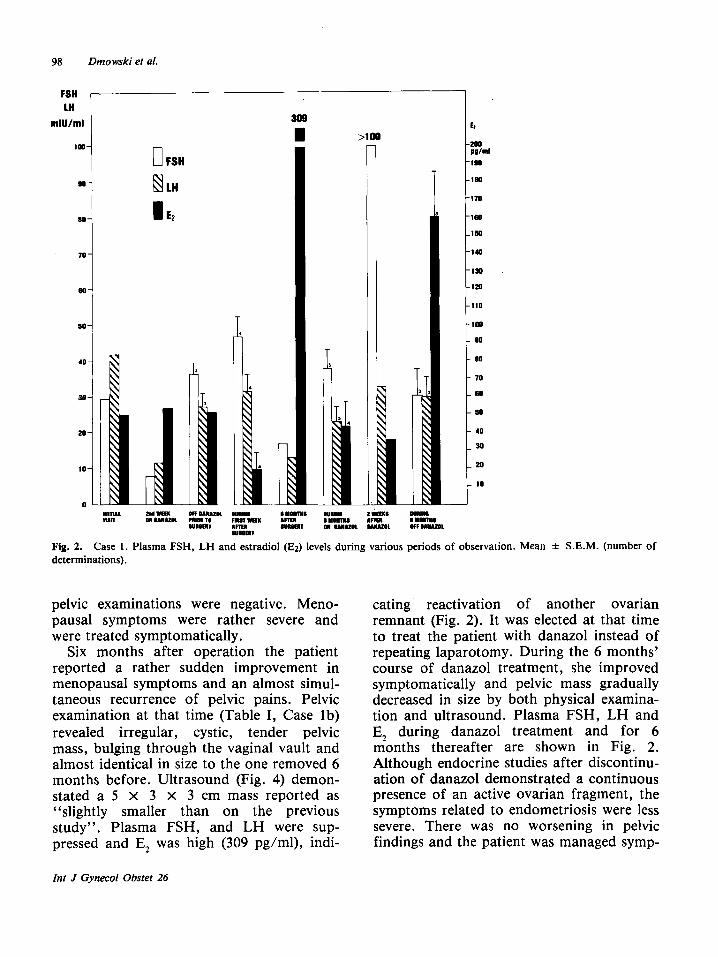
Fig. 2. Case 1. Plasma FSH, LH and estradiol (Ez) levels during various periods of observation. Mean + S.E.M. (number of determinations).
pelvic examinations were negative. Meno- pausal symptoms were rather severe and were treated symptomatically.
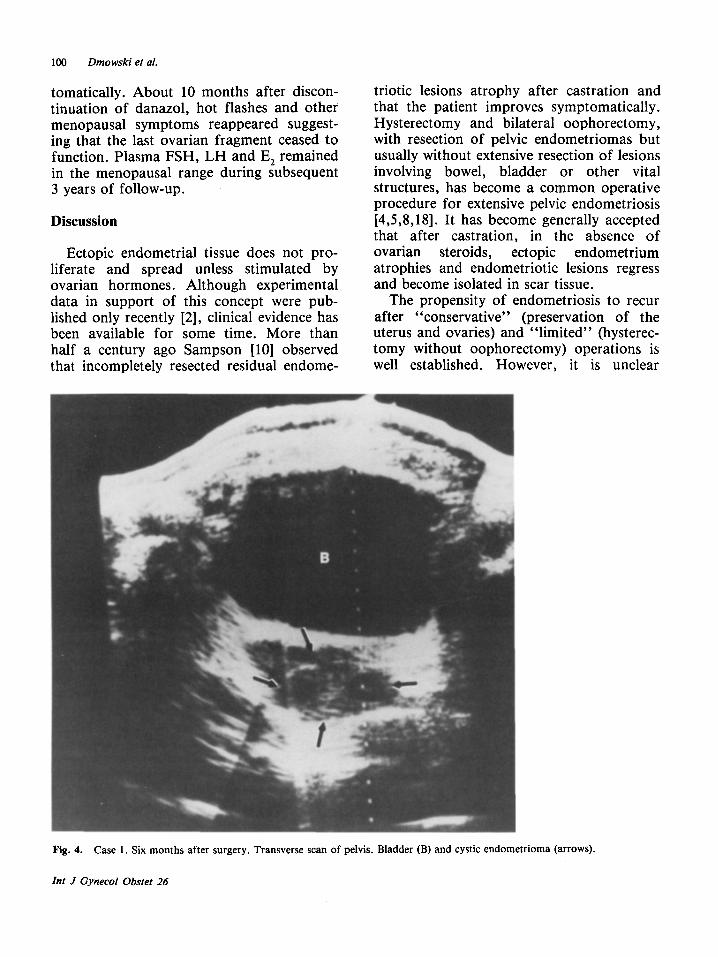
Six months after operation the patient reported a rather sudden improvement in menopausal symptoms and an almost simul- taneous recurrence of pelvic pains. Pelvic examination at that time (Table I, Case lb) revealed irregular, cystic, tender pelvic mass, bulging through the vaginal vault and almost identical in size to the one removed 6 months before. Ultrasound (Fig. 4) demon- stated a 5 x 3 x 3 cm mass reported as “slightly smaller than on the previous study”. Plasma FSH, and LH were sup- pressed and E, was high (309 pg/ml), indi-
eating reactivation of another ovarian remnant (Fig. 2). It was elected at that time to treat the patient with danazol instead of repeating laparotomy. During the 6 months’ course of danazol treatment, she improved symptomatically and pelvic mass gradually decreased in size by both physical examina- tion and ultrasound. Plasma FSH, LH and E, during danazol treatment and for 6 months thereafter are shown in Fig. 2. Although endocrine studies after discontinu- ation of danazol demonstrated a continuous presence of an active ovarian fragment, the symptoms related to endometriosis were less severe. There was no worsening in pelvic findings and the patient was managed symp-
Int J Gynecol Obstet 26
Endometriosis after TAH, BSO 99
Fig. 3. Case 1. Photomicrograph of the surgical specimen. (a) Corpus luteum, (b) endometrial glands and stroma. H & E, x loo.
Clinical and Clinical Research Article
100 Dmowski et al.
tomatically. About 10 months after discon- tinuation of danazol, hot flashes and other menopausal symptoms reappeared suggest- ing that the last ovarian fragment ceased to function. Plasma FSH, LH and E, remained in the menopausal range during subsequent 3 years of follow-up.
Discussion
Ectopic endometrial tissue does not pro- liferate and spread unless stimulated by ovarian hormones. Although experimental data in support of this concept were pub- lished only recently [2], clinical evidence has been available for some time. More than half a century ago Sampson [lo] observed that incompletely resected residual endome-
triotic lesions atrophy after castration and that the patient improves symptomatically. Hysterectomy and bilateral oophorectomy, with resection of pelvic endometriomas but usually without extensive resection of lesions involving bowel, bladder or other vital structures, has become a common operative procedure for extensive pelvic endometriosis [4,5,8,18]. It has become generally accepted that after castration, in the absence of ovarian steroids, ectopic endometrium atrophies and endometriotic lesions regress and become isolated in scar tissue.
The propensity of endometriosis to recur after “conservative” (preservation of the uterus and ovaries) and “limited” (hysterec- tomy without oophorectomy) operations is well established. However, it is unclear
Fig. 4. Case 1. Six months after surgery. Transverse scan of pelvis. Bladder (B) and cystic endometr
Int J Gynecol Obstet 26
ioma (arrows).
Endometriosis after TAH, BSO 101
whether such recurrence is a “de novo” process or recurrence from residual lesions. It is also unclear what is the frequency of such recurrence. According to some reports, it is as low as 1% to 2.5% within several years after the initial surgery [9,13,18] or it may be as high as 85% according to others [6]. It seems certain that variables associated with patient selection, surgical technique, extent of the disease, etc. are the cause of discrepancies in reported rates of recurrence. However, it is also possible that some women may be in a higher risk cate- gory. If endometriosis develops as a result of a deficiency in the immune system, as suggested by some studies [3,16] women with a more pronounced defect may have a higher risk of recurrence.
After definitive surgery, recurrence of endometriosis may be anticipated if ovarian fragments were unintentionally left in situ. Reactivation of the disease is secondary to the cyclic estrogens and progesterone secreted by such fragments. Several reports describing reactivation of residual ovarian fragments after oophorectomy, the so called “ovarian remnant syndrome” have been published [7,14,17]. The syndrome is uncommon and is probably underdiagnosed but seems to occur more frequently in women who had undergone repeated ovarian surgery [7] as was the case in all our patients. It has been suggested that ovarian fragments may be active hormonally and their presence may be indicated by the incomplete post-castration rise in plasma gonadotropins and persistence of low-nor- mal plasma E, levels [7]. However, the mechanisms responsible for reactivation of ovarian fragments have not been fully docu- mented and the level as well as the duration of the endocrine activity of such fragments and especially their ability to reactivate pel- vic endometriosis has not been studied. There is a single report of a patient with recurrent endometriosis after TAH, BSO, in whom ovarian fragment was subsequently identified at the time of surgery [12].
However, the patient was not evaluated endocrinologically prior to surgery and the recurrence was attributed to the estrogen replacement therapy.
In five of the seven women studied in this report, persistence of a hormonally active ovarian fragment after bilateral oophorec- tomy was demonstrated endocrinologically and in two of these, also histologically. Plasma E, in all five was about 50 pg/ml and in some instances above 300 pg/ml. Plasma E, levels reaching above 300 pg/ml are compatible with the normal pre-ovula- tory peak, normal follicular development and cyclic secretion of ovarian steroids. Cyclic E, and progesterone secretion by residual ovarian fragments was further sug- gested by the presence of recent corpora lutea in both patients who underwent surgi- cal exploration. FSH and LH in all five were either moderately elevated (cases la, 3, 5, 7) or were within the normal premeno- pausal range, (cases lb, 2). Normal or close to normal FSH levels also suggest normal ovarian follicular function and normal feed- back mechanisms.
FSH, LH and E, concentrations in all our patients reflected dynamic relationships in the hypothalamo-pituitary-ovarian function. Serial changes in FSH, LH and E, observed in case 1 are quite interesting in this respect (Fig. 2). They demonstrate well the dynamic process of the reactivation of ovarian frag- ments. It appears that the rise in FSH and LH to menopausal levels on two separate occasions (after surgery and after danazol) was followed by reactivation of ovarian fol- licular activity as evidenced by the subse- quent increase in E, levels. Normal E, and progesterone secretion were then able to suppress FSH and LH to the normal repro- ductive range, as indicated by hormone con- centrations 6 months after surgery.
Considering the concentration and size of primordial follicles in the ovarian cortex of young women and their ability to produce steroids and enlarge under gonadotropin stimulation, it is understandable why even
Clinical and Clinical Research Article
102 Dmowski et al.
small ovarian fragments left adherent to the bowel, ureter or pelvic organs, can hyper- trophy and function hormonally. It is well known that in laboratory animals, following unilateral castration, the contralateral ovary undergoes compensatory hypertrophy and that the extent of this hypertrophy is a func- tion of the increased gonadotropin stimula- tion [15]. It seems quite apparent that the same type of “compensatory hypertrophy” takes place in the residual ovarian frag- ments. The total amount of ovarian tissue removed on several separate occasions in each of our patients, except case 4, exceeded substantially the size of the normal ovaries.
The “life span” of the residual ovarian fragments depends most likely on their size and, more specifically, on the number of ovarian follicles they contain. The duration of their function may vary from a few months (case 3) to several years (cases lb and 5). Thus, expectant management, at least in selected cases, may be of value. However, as demonstrated by case 1, fol- lowing functional exhaustion or even surgi- cal removal of one such fragment, another one may become reactivated.
The frequency with which endometriosis recurs after definitive surgery is uncertain. The condition is uncommon and probably underdiagnosed. Many patients with recur- rence of symptoms after definitive surgery are diagnosed as having “pelvic adhesions” or other gynecologic conditions. If the symptoms are more severe, the patient is often placed on hormonal therapy to sup-
press “recurrent endometriosis”, as were all our patients at one time or another, and specifically cases 4 and 6. However, since hormonal therapy, especially that with estrogens and progestogens can maintain residual disease [2], it is of clinical impor- tance to demonstrate not only the recur- rence but also its cause. Gynecologic history, review of histologic slides, physical examination, ultrasound and laparoscopy are all of diagnostic help. However, only the measurements of FSH, LH and E, con-
centrations will establish whether endogen- ous ovarian hormones are the cause of such recurrence.
Hormonal treatment of endometriosis is based on suppression of ovarian steroids. Therefore, the presence of ovarian hor- mones in circulation should be demon- strated prior to the initiation of therapy. Patient LT (case 4) because of “pelvic symptoms” was placed on pseudopregnancy regimen within weeks after definitive sur- gery. No attempt was made at that time to demonstrate the level of her endogenous estrogens and gonadotropins. It is quite likely that subsequent appearance of endom- etriosis was stimulated by mestranol, a strongly estrogenic component of Enovid 5 mg given b.i.d. Upon discontinuation of the regimen, endocrine studies demonstrated no evidence of residual ovarian activity. Fur- thermore, discontinuation of exogenous steroids was followed by gradual regression of symptoms. In patient NB (Case 6) there was also no endocrine evidence of residual ovarian activity. However, surgically con- firmed recurrence of the disease, in the absence of exogenous steroids, suggested endogenous hormonal stimulation.
Recurrent endometriosis may be effec- tively treated surgically as in case 2. Surgical exploration and localization of residual ovarian fragments are facilitated by the presence of pelvic endometriomas which frequently contain ovarian tissue in their wall. In the absence of endometriomas, ovarian fragments may not be readily identi- fiable and dissection may be difficult. The surgical results are good if complete removal of the ovarian tissue has been accomplished. If difficulties are anticipated in the localization of the ovarian fragment, or if surgery is contraindicated the patient may be treated medically.
Pseudopregnancy regimen is probably a poor choice of treatment for recurrent endometriosis. The estrogenic component is known to stimulate endometrial proliferation and therefore may cause wors-
Int J Gynecol Obstet 26
ening of the symptoms. Danazol or progestogens alone, such as Depo-MPA, seem to be a better choice of therapy. In case lb, danazol treatment was associated with suppression of FSH, LH and E, and with symptomatic improvement and regres- sion in the size of pelvic endometrioma. Similar results were obtained with Depo- MPA injections in cases 5, 6 and 7. If symptoms associated with the recurrence are mild and the disease is less extensive, as in case 3, expectant management and sympto- matic treatment may be appropriate. In patients with severe symptoms and more extensive disease, who do not respond to the medical treatment and are not good candidates for surgery, irradiation of the pelvis in order to destroy residual ovarian tissue, may be considered.
References
Acosta AA, Buttram VC Jr, Franklin RR, Besch PK: A proposed classification of pelvic endometriosis. Obstet Gynecol 42: 19, 1973. Dizerega GA, Barber DL, Hodgen GD: Endometriosis: role of ovarian steroids in initiation maintenance and suppression. Fertil Steril 33: 649, 1980. Dmowski WP, Steele RW, Baker GF: Deficient cellular immunity in endometriosis. Am J Obstet Gynecol 141: 377, 1981. Gray LA: The management of endometriosis involving the bowel. Clin Obstet Gynecol 9: 309, 1966. Gray LA: Surgical treatment of endometriosis. Clin Obstet Gynecol 3: 472, 1960. Hammond CB, Rock JA, Parker RT: Conservative treatment of endometriosis: the effects of limited surgery
7
8
9
10
11
12
13
14
15
16
17
18
Endometriosis after TAH, BSO 103
and hormonal psuedopregnancy. Fertil Steril 27: 756, 1976. Nelson DC, Avant GR: Ovarian remnant syndrome. S Med J 75: 757, 1982. Ranney B: Endometriosis. III. Complete operations. Reasons, sequelae, treatment. Am J Obstet Gynecol 109: 1137, 1971. Ranney B: Discussion of Schenken RS, Malinak LR: Reoperation after initial treatment of endometriosis with conservative surgery. Am J Obstet Gynecol 131: 416, 1978. Sampson JA: Intestinal adenomas of the endometrial type. Arch Surg 5: 217, 1922. Schram JD: Endometriosis after “pelvic cleanout”. S Med J 71: 1419, 1978. Scully RE, Galdabini JJ, McNeely BU: Case records of the Massachusetts General Hospital, Case 23-1980. N Engl J Med 302: 1354, 1980. Sheets JL, Symmonds RE, Banner EA: Conservative surgical management of endometriosis. Obstet Gynecol 23: 625, 1964. Shemwell R, Weed J: Ovarian remnant syndrome. Obstet Gynecol36: 299, 1970. Shipley EG: Anti-gonadotropic steroids, inhibition of ovulation and mating. In Methods in Hormone Research, Vol 2, (ed RI Dorfman), pp 179-274. Aca- demic Press, New York, 1962. Steele RW, Dmowski WP, Marmer DJ: Immunological aspects of human endometriosis. Am J Reprod Immu- no1 6: 33, 1984. Symmonds R, Pettit P: Ovarian remnant syndrome. Obstet Gynecol 54: 174, 1979. Williams TJ: The role of surgery in the management of endometriosis. Mayo Clin Proc 50: 198, 1975.
Address for reprints:
W. Paul Dmowski, MD, PLD Rush Medical College 600 South Paulina Chicago, IL 60612, USA
Clinical and Clinical Research Article
Related Documents











