Mayo Clin Proc. 2001;76:958-960 958 © 2001 Mayo Foundation for Medical Education and Research Case Report Recurrence of Susac Syndrome (Retinocochleocerebral Vasculopathy) After Remission of 18 Years GEORGE W. PETTY, MD; ERIC L. MATTESON, MD; BRIAN R. YOUNGE, MD; THOMAS J. MCDONALD, MD; AND CHRISTOPHER P. WOOD, MD From the Division of Cerebrovascular Diseases (G.W.P.), Division of Rheumatology and Internal Medicine (E.L.M.), Department of Ophthal- mology (B.R.Y.), Department of Otorhinolaryngology (T.J.M.), and De- partment of Radiology (C.P.W.), Mayo Clinic, Rochester, Minn. This study was supported in part by grants NS37752 and NS06663 from the National Institute of Neurological Disorders and Stroke, Bethesda, Md, and Research to Prevent Blindness, Inc, New York, NY. Address reprint requests and correspondence to George W. Petty, MD, Division of Cerebrovascular Diseases, Mayo Clinic, 200 First St SW, Rochester, MN 55905. Susac syndrome (retinocochleocerebral vasculopathy) is a syndrome of unknown pathogenesis. The triad of multifocal encephalopathy, visual loss, and hearing loss is caused by microangiopathy of the brain, retina, and cochlea. The ill- ness tends to be monophasic, and to our knowledge, recur- rence after years of remission has not been reported. We describe a 51-year-old woman with symptoms, signs, and brain magnetic resonance imaging findings consistent with recurrence of Susac syndrome 18 years after remission. Clinicians should be aware of the possibility of late recur- rence of Susac syndrome when evaluating patients with a distant history of the syndrome who present with com- plaints referable to the brain, retina, and cochlea. Mayo Clin Proc. 2001;76:958-960 S usac syndrome (retinocochleocerebral vasculopathy) is characterized by acute or subacute onset of the triad of multifocal encephalopathic symptoms and signs, visual loss, and hearing loss caused by a microangiopathy involv- ing the brain, retina, and cochlea. 1 Case reports and reviews have emphasized that the illness tends to be monophasic and self-limited, without recurrence after remission. 2-5 Herein, we describe a patient in whom Susac syndrome recurred 18 years after remission. REPORT OF A CASE The patient’s original illness was described by MacFadyen et al. 6 In 1981, a 31-year-old pregnant woman developed numbness in the extremities, segmental visual loss, diplo- pia, lethargy, memory loss, change in personality, dysar- thria, ataxia, tinnitus, and hearing loss. Retinal arteriolar occlusions, bilateral, low-frequency sensorineural hearing loss, increased cerebrospinal fluid protein level, and bilat- eral electroencephalographic delta activity were docu- mented. She received corticosteroid treatment, which was tapered and discontinued after visual improvement was documented in August 1982. Despite persistent mild memory loss, imbalance, dysar- thria, deafness in the left ear, severe hearing loss in the right ear, and segmental visual loss in the left eye, she was suc- cessfully employed as a health care worker. She could not recall any new symptoms referable to Susac syndrome after 1982. In 1999, she began estrogen replacement therapy. In August 2000, the patient had scintillating visual sco- tomas; on 1 occasion they were followed by a persistent visual field deficit in the right eye. In September 2000, nausea, vomiting, vertigo, and ataxia developed suddenly. She subsequently experienced poor concentration, fatigue, tinnitus, and increased hearing loss in the right ear. Brain magnetic resonance imaging (MRI) without con- trast demonstrated small punctate foci of increased T2 signal in the periventricular white matter, corpus callosum, basal ganglia, thalami, cerebral peduncles, pons, brachium pontis, and cerebellum. Cerebrospinal fluid examination demon- strated a slight increase of the protein level to 63 mg/dL, no pleocytosis, normal glucose level, and no oligoclonal bands. IgG anticardiolipin antibody was negative, IgM anti- cardiolipin antibody was reported positive, and rheumatoid factor was increased slightly (40 U, with normal to 30 U). Treatment was initiated with pulse methylprednisolone, 1 g/d for 5 days, and then prednisone, 60 mg/d, azathio- prine, 100 mg/d, and clopidogrel, 75 mg/d. The patient’s hearing and imbalance improved. When the patient was evaluated at Mayo Clinic in No- vember 2000, her mental status examination demonstrated only mild deficits in calculations. She had dysarthria and mild dysnomia. Ophthalmoscopic examination demon- strated pallor of the optic disks and evidence of past retinal arteriolar occlusions. Visual field examination demonstrated segmental defects inferiorly in the right eye and centrally and nasally in the left eye. The Babinski response was present on the left and equivocal on the right. Tandem gait was im- paired, and there was appendicular ataxia on the left. For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Recurrence of Susac Syndrome (Retinocochleocerebral Vasculopathy) After Remission of 18 Years
Sep 15, 2022
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Recurrence of Susac Syndrome (Retinocochleocerebral Vasculopathy) After Remission of 18 YearsRecurrence of Susac Syndrome Mayo Clin Proc, September 2001, Vol 76958
Mayo Clin Proc. 2001;76:958-960 958 © 2001 Mayo Foundation for Medical Education and Research
Case Report
Recurrence of Susac Syndrome (Retinocochleocerebral Vasculopathy) After Remission of 18 Years
GEORGE W. PETTY, MD; ERIC L. MATTESON, MD; BRIAN R. YOUNGE, MD; THOMAS J. MCDONALD, MD; AND CHRISTOPHER P. WOOD, MD
From the Division of Cerebrovascular Diseases (G.W.P.), Division of Rheumatology and Internal Medicine (E.L.M.), Department of Ophthal- mology (B.R.Y.), Department of Otorhinolaryngology (T.J.M.), and De- partment of Radiology (C.P.W.), Mayo Clinic, Rochester, Minn.
This study was supported in part by grants NS37752 and NS06663 from the National Institute of Neurological Disorders and Stroke, Bethesda, Md, and Research to Prevent Blindness, Inc, New York, NY.
Address reprint requests and correspondence to George W. Petty, MD, Division of Cerebrovascular Diseases, Mayo Clinic, 200 First St SW, Rochester, MN 55905.
Susac syndrome (retinocochleocerebral vasculopathy) is a syndrome of unknown pathogenesis. The triad of multifocal encephalopathy, visual loss, and hearing loss is caused by microangiopathy of the brain, retina, and cochlea. The ill- ness tends to be monophasic, and to our knowledge, recur- rence after years of remission has not been reported. We describe a 51-year-old woman with symptoms, signs, and
brain magnetic resonance imaging findings consistent with recurrence of Susac syndrome 18 years after remission. Clinicians should be aware of the possibility of late recur- rence of Susac syndrome when evaluating patients with a distant history of the syndrome who present with com- plaints referable to the brain, retina, and cochlea.
Mayo Clin Proc. 2001;76:958-960
Susac syndrome (retinocochleocerebral vasculopathy) is characterized by acute or subacute onset of the triad
of multifocal encephalopathic symptoms and signs, visual loss, and hearing loss caused by a microangiopathy involv- ing the brain, retina, and cochlea.1 Case reports and reviews have emphasized that the illness tends to be monophasic and self-limited, without recurrence after remission.2-5
Herein, we describe a patient in whom Susac syndrome recurred 18 years after remission.
REPORT OF A CASE The patient’s original illness was described by MacFadyen et al.6 In 1981, a 31-year-old pregnant woman developed numbness in the extremities, segmental visual loss, diplo- pia, lethargy, memory loss, change in personality, dysar- thria, ataxia, tinnitus, and hearing loss. Retinal arteriolar occlusions, bilateral, low-frequency sensorineural hearing loss, increased cerebrospinal fluid protein level, and bilat- eral electroencephalographic delta activity were docu- mented. She received corticosteroid treatment, which was tapered and discontinued after visual improvement was documented in August 1982.
Despite persistent mild memory loss, imbalance, dysar- thria, deafness in the left ear, severe hearing loss in the right
ear, and segmental visual loss in the left eye, she was suc- cessfully employed as a health care worker. She could not recall any new symptoms referable to Susac syndrome after 1982. In 1999, she began estrogen replacement therapy.
In August 2000, the patient had scintillating visual sco- tomas; on 1 occasion they were followed by a persistent visual field deficit in the right eye. In September 2000, nausea, vomiting, vertigo, and ataxia developed suddenly. She subsequently experienced poor concentration, fatigue, tinnitus, and increased hearing loss in the right ear.
Brain magnetic resonance imaging (MRI) without con- trast demonstrated small punctate foci of increased T2 signal in the periventricular white matter, corpus callosum, basal ganglia, thalami, cerebral peduncles, pons, brachium pontis, and cerebellum. Cerebrospinal fluid examination demon- strated a slight increase of the protein level to 63 mg/dL, no pleocytosis, normal glucose level, and no oligoclonal bands. IgG anticardiolipin antibody was negative, IgM anti- cardiolipin antibody was reported positive, and rheumatoid factor was increased slightly (40 U, with normal to 30 U).
Treatment was initiated with pulse methylprednisolone, 1 g/d for 5 days, and then prednisone, 60 mg/d, azathio- prine, 100 mg/d, and clopidogrel, 75 mg/d. The patient’s hearing and imbalance improved.
When the patient was evaluated at Mayo Clinic in No- vember 2000, her mental status examination demonstrated only mild deficits in calculations. She had dysarthria and mild dysnomia. Ophthalmoscopic examination demon- strated pallor of the optic disks and evidence of past retinal arteriolar occlusions. Visual field examination demonstrated segmental defects inferiorly in the right eye and centrally and nasally in the left eye. The Babinski response was present on the left and equivocal on the right. Tandem gait was im- paired, and there was appendicular ataxia on the left.
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.
Mayo Clin Proc, September 2001, Vol 76 Recurrence of Susac Syndrome 959
Audiometry demonstrated bilateral, low-frequency sen- sorineural hearing loss, greater on the left than the right.
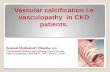
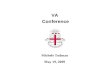
Brain MRI, including gadolinium, demonstrated moder- ate punctate-to-confluent T2 foci in periventricular cere- bral white matter, corpus callosum, basal ganglia, thalami, left midbrain, cerebral peduncle, pons, brachium pontis, and cerebellum (Figure 1). The same structures had mul- tiple, tiny enhancing foci (Figure 2).
The following laboratory tests yielded normal find- ings: complete blood cell count, erythrocyte sedimenta- tion rate, lupus anticoagulant, anticardiolipin antibodies to IgG and IgM, serum chemistry panel, lipid panel, ho- mocysteine, serum protein immunofixation electrophore- sis, creatine kinase, angiotensin-converting enzyme, α- galactosidase, cryoglobulins, anti–double-stranded DNA, rheumatoid factor, C3 and C4 complement, antineutro-
phil cytoplasmic antibodies, anticentromere antibody, C- reactive protein, antinuclear antibody, hepatitis B and C, human immunodeficiency virus, and syphilis serology. Chest radiographic, electrocardiographic, transesoph- ageal echocardiographic, and carotid ultrasonographic findings were unremarkable.
Azathioprine and estrogen replacement therapy were discontinued. The patient received a series of 5 plasma exchanges, clopidogrel treatment was continued, and pred- nisone was tapered. She had a single generalized seizure in December 2000 and was treated with phenytoin, 200 mg/d.
In February 2000, she complained of increasing imbal- ance. Findings on cerebral spinal fluid examination and cerebral angiography were normal. Treatment with phenytoin was discontinued, and she was started on clobazam, 20 mg/d.
When last evaluated at Mayo Clinic in June 2001, she was taking prednisone, 25 mg/d, clopidogrel, 75 mg/d, and clobazam, 20 mg/d. Results of neurologic, ophthalmologic, and audiometric tests were unchanged compared with ex- aminations of November 2000, and brain MRI demonstrated persistent T2 abnormalities but no gadolinium enhancement.
DISCUSSION To our knowledge, this report is the first to document the recurrence of Susac syndrome after remission. Except for infrequent patients who have had a stuttering or progres- sive course,3,7 nearly all reported patients have had mono- phasic, self-limited illness, with varying residual disability after remission, and none has had recurrence after remis- sion.2,3,8 Recurrence in our patient at age 51 years after 18 years of remission expands the clinical spectrum of Susac syndrome, not only by documenting that some patients may have late recurrence but by supporting the recent observation that the disease is not necessarily limited to young adults.9 Clinicians should be aware of the possibility of late recurrence when counseling patients with this syn- drome and when evaluating patients with a distant history of the syndrome who present with new complaints refer- able to the brain, retina, and cochlea.
Since the original description of the syndrome by Susac et al1 in 1979, fewer than 100 patients have been reported with this distinct clinical syndrome.1-5,7-9 The disease is likely underdiagnosed. Many patients with Susac syn- drome mistakenly receive another diagnosis, such as mul- tiple sclerosis, migraine, lupus erythematosus, Ménière disease, cardioembolic stroke, and even schizophrenia.3
The most common manifestations of brain involvement in Susac syndrome are related to problems with cognition, memory, behavior, and affect, as well as dizziness, ataxia, dysarthria, and bilateral corticospinal tract dysfunction.3,5,8
These manifestations correspond to the characteristic mul-
Figure 1. Axial T2 images demonstrating scattered foci of in- creased T2 signal in both basal ganglia, right thalamus, corpus callosum, and cerebral white matter.
Figure 2. Coronal T1 images after intravenous administration of gadolinium demonstrating small, scattered, enhancing foci both infratentorially and supratentorially, some of which correspond with the foci of abnormal T2 signal.
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.
Recurrence of Susac Syndrome Mayo Clin Proc, September 2001, Vol 76960
tiple, small, punctate areas of T2 signal increase and con- trast enhancement seen in both the cerebral gray matter and white matter on MRI (Figures 1 and 2).3 Visual loss, usu- ally segmental field defects in 1 eye or both eyes, is due to retinal arteriolar occlusions or narrowing visible on oph- thalmologic examination.3 Low- to mid-frequency senso- rineural hearing loss on audiometry has been attributed to microvascular infarction of the cochlear apex.4 Some pa- tients with Susac syndrome have constitutional symptoms, arthralgias, and myalgias,10 as well as pathologic microvas- cular changes on muscle biopsy, without frank arthritis or myopathy, suggesting that the disease may be a systemic illness with a predilection for producing encephalopathic, visual, and auditory symptoms either because of selective vulnerability of the brain, retina, and cochlea or because microvascular occlusions in these organs are more likely to produce striking symptoms that command the attention of patients and their physicians than do less eloquent organs.3
The pathogenesis of Susac syndrome is unknown. Brain and muscle biopsy specimens show small infarcts with some minimal perivascular lymphocytic infiltration, but not necro- tizing vasculitis.3 No procoagulant state has been docu- mented consistently. Rarely, as in our patient, the IgM anti- phospholipid antibody isotype has been positive,10 but the IgG isotype associated with thromboembolism and results of detailed functional coagulation tests have been negative in most patients tested.3 Similarly, some patients with Susac syndrome have nonspecific low-titer antinuclear antibody or rheumatoid factor tests but no definite connective tissue disease.1,3,6 The onset of symptoms during pregnancy3,6 or hormone replacement therapy (as in our patient’s recur- rence) could indicate a hormonal influence on pathogenesis, but this could be a coincidence because of the apparent predilection for the disease to afflict women. Coincidence could also account for the association of the onset of symp- toms with a preceding viral-like illness in some patients.3
Because of the clinical course and small number of cases reported, efficacy of the various treatments that have
been attempted in Susac syndrome has been difficult to assess.2,3,5,8 Most patients have received immunosuppres- sive therapy. We chose to discontinue azathioprine treat- ment and institute plasma exchange in addition to cortico- steroid treatment in our patient, because plasma exchange is relatively less toxic, and 2 patients with Susac syndrome evaluated at our institution during the past 2 years have had cessation of new symptoms following this treatment. How- ever, we have no proof of the efficacy of plasma exchange or any other treatment for Susac syndrome.
The authors thank John O. Susac, MD, for recommending referral of this patient to Mayo Clinic.
REFERENCES 1. Susac JO, Hardman JM, Selhorst JB. Microangiopathy of the brain
and retina. Neurology. 1979;29:313-316. 2. Susac JO. Susac’s syndrome: the triad of microangiopathy of the
brain and retina with hearing loss in young women. Neurology. 1994;44:591-593.
3. Petty GW, Engel AG, Younge BR, et al. Retinocochleocerebral vasculopathy. Medicine (Baltimore). 1998;77:12-40.
4. Monteiro ML, Swanson RA, Coppeto JR, Cuneo RA, DeArmond SJ, Prusiner SB. A microangiopathic syndrome of encephalopathy, hearing loss, and retinal arteriolar occlusions. Neurology. 1985; 35:1113-1121.
5. O’Halloran HS, Pearson PA, Lee WB, Susac JO, Berger JR. Microangiopathy of the brain, retina, and cochlea (Susac syn- drome): a report of five cases and a review of the literature. Oph- thalmology. 1998;105:1038-1044.
6. MacFadyen DJ, Schneider RJ, Chisholm IA. A syndrome of brain, inner ear and retinal microangiopathy. Can J Neurol Sci. 1987; 14:315-318.
7. Bogousslavsky J, Gaio JM, Caplan LR, et al. Encephalopathy, deafness and blindness in young women: a distinct retino- cochleocerebral arteriolopathy? J Neurol Neurosurg Psychiatry. 1989;52:43-46.
8. Papo T, Biousse V, Lehoang P, et al. Susac syndrome. Medicine (Baltimore). 1998;77:3-11.
9. Barker RA, Anderson JR, Meyer P, Dick DJ, Scolding NJ. Microangiopathy of the brain and retina with hearing loss in a 50 year old woman: extending the spectrum of Susac’s syndrome. J Neurol Neurosurg Psychiatry. 1999;66:641-643.
10. Nicolle MW, McLachlan RS. Microangiopathy with retinopathy, encephalopathy, and deafness (RED-M) and systemic features. Semin Arthritis Rheum. 1991;21:123-128.
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.
Recurrence of Susac Syndrome (Retinocochleocerebral Vasculopathy) After Remission of 18 Years
REPORT OF A CASE
Mayo Clin Proc. 2001;76:958-960 958 © 2001 Mayo Foundation for Medical Education and Research
Case Report
Recurrence of Susac Syndrome (Retinocochleocerebral Vasculopathy) After Remission of 18 Years
GEORGE W. PETTY, MD; ERIC L. MATTESON, MD; BRIAN R. YOUNGE, MD; THOMAS J. MCDONALD, MD; AND CHRISTOPHER P. WOOD, MD
From the Division of Cerebrovascular Diseases (G.W.P.), Division of Rheumatology and Internal Medicine (E.L.M.), Department of Ophthal- mology (B.R.Y.), Department of Otorhinolaryngology (T.J.M.), and De- partment of Radiology (C.P.W.), Mayo Clinic, Rochester, Minn.
This study was supported in part by grants NS37752 and NS06663 from the National Institute of Neurological Disorders and Stroke, Bethesda, Md, and Research to Prevent Blindness, Inc, New York, NY.
Address reprint requests and correspondence to George W. Petty, MD, Division of Cerebrovascular Diseases, Mayo Clinic, 200 First St SW, Rochester, MN 55905.
Susac syndrome (retinocochleocerebral vasculopathy) is a syndrome of unknown pathogenesis. The triad of multifocal encephalopathy, visual loss, and hearing loss is caused by microangiopathy of the brain, retina, and cochlea. The ill- ness tends to be monophasic, and to our knowledge, recur- rence after years of remission has not been reported. We describe a 51-year-old woman with symptoms, signs, and
brain magnetic resonance imaging findings consistent with recurrence of Susac syndrome 18 years after remission. Clinicians should be aware of the possibility of late recur- rence of Susac syndrome when evaluating patients with a distant history of the syndrome who present with com- plaints referable to the brain, retina, and cochlea.
Mayo Clin Proc. 2001;76:958-960
Susac syndrome (retinocochleocerebral vasculopathy) is characterized by acute or subacute onset of the triad
of multifocal encephalopathic symptoms and signs, visual loss, and hearing loss caused by a microangiopathy involv- ing the brain, retina, and cochlea.1 Case reports and reviews have emphasized that the illness tends to be monophasic and self-limited, without recurrence after remission.2-5
Herein, we describe a patient in whom Susac syndrome recurred 18 years after remission.
REPORT OF A CASE The patient’s original illness was described by MacFadyen et al.6 In 1981, a 31-year-old pregnant woman developed numbness in the extremities, segmental visual loss, diplo- pia, lethargy, memory loss, change in personality, dysar- thria, ataxia, tinnitus, and hearing loss. Retinal arteriolar occlusions, bilateral, low-frequency sensorineural hearing loss, increased cerebrospinal fluid protein level, and bilat- eral electroencephalographic delta activity were docu- mented. She received corticosteroid treatment, which was tapered and discontinued after visual improvement was documented in August 1982.
Despite persistent mild memory loss, imbalance, dysar- thria, deafness in the left ear, severe hearing loss in the right
ear, and segmental visual loss in the left eye, she was suc- cessfully employed as a health care worker. She could not recall any new symptoms referable to Susac syndrome after 1982. In 1999, she began estrogen replacement therapy.
In August 2000, the patient had scintillating visual sco- tomas; on 1 occasion they were followed by a persistent visual field deficit in the right eye. In September 2000, nausea, vomiting, vertigo, and ataxia developed suddenly. She subsequently experienced poor concentration, fatigue, tinnitus, and increased hearing loss in the right ear.
Brain magnetic resonance imaging (MRI) without con- trast demonstrated small punctate foci of increased T2 signal in the periventricular white matter, corpus callosum, basal ganglia, thalami, cerebral peduncles, pons, brachium pontis, and cerebellum. Cerebrospinal fluid examination demon- strated a slight increase of the protein level to 63 mg/dL, no pleocytosis, normal glucose level, and no oligoclonal bands. IgG anticardiolipin antibody was negative, IgM anti- cardiolipin antibody was reported positive, and rheumatoid factor was increased slightly (40 U, with normal to 30 U).
Treatment was initiated with pulse methylprednisolone, 1 g/d for 5 days, and then prednisone, 60 mg/d, azathio- prine, 100 mg/d, and clopidogrel, 75 mg/d. The patient’s hearing and imbalance improved.
When the patient was evaluated at Mayo Clinic in No- vember 2000, her mental status examination demonstrated only mild deficits in calculations. She had dysarthria and mild dysnomia. Ophthalmoscopic examination demon- strated pallor of the optic disks and evidence of past retinal arteriolar occlusions. Visual field examination demonstrated segmental defects inferiorly in the right eye and centrally and nasally in the left eye. The Babinski response was present on the left and equivocal on the right. Tandem gait was im- paired, and there was appendicular ataxia on the left.
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.
Mayo Clin Proc, September 2001, Vol 76 Recurrence of Susac Syndrome 959
Audiometry demonstrated bilateral, low-frequency sen- sorineural hearing loss, greater on the left than the right.
Brain MRI, including gadolinium, demonstrated moder- ate punctate-to-confluent T2 foci in periventricular cere- bral white matter, corpus callosum, basal ganglia, thalami, left midbrain, cerebral peduncle, pons, brachium pontis, and cerebellum (Figure 1). The same structures had mul- tiple, tiny enhancing foci (Figure 2).
The following laboratory tests yielded normal find- ings: complete blood cell count, erythrocyte sedimenta- tion rate, lupus anticoagulant, anticardiolipin antibodies to IgG and IgM, serum chemistry panel, lipid panel, ho- mocysteine, serum protein immunofixation electrophore- sis, creatine kinase, angiotensin-converting enzyme, α- galactosidase, cryoglobulins, anti–double-stranded DNA, rheumatoid factor, C3 and C4 complement, antineutro-
phil cytoplasmic antibodies, anticentromere antibody, C- reactive protein, antinuclear antibody, hepatitis B and C, human immunodeficiency virus, and syphilis serology. Chest radiographic, electrocardiographic, transesoph- ageal echocardiographic, and carotid ultrasonographic findings were unremarkable.
Azathioprine and estrogen replacement therapy were discontinued. The patient received a series of 5 plasma exchanges, clopidogrel treatment was continued, and pred- nisone was tapered. She had a single generalized seizure in December 2000 and was treated with phenytoin, 200 mg/d.
In February 2000, she complained of increasing imbal- ance. Findings on cerebral spinal fluid examination and cerebral angiography were normal. Treatment with phenytoin was discontinued, and she was started on clobazam, 20 mg/d.
When last evaluated at Mayo Clinic in June 2001, she was taking prednisone, 25 mg/d, clopidogrel, 75 mg/d, and clobazam, 20 mg/d. Results of neurologic, ophthalmologic, and audiometric tests were unchanged compared with ex- aminations of November 2000, and brain MRI demonstrated persistent T2 abnormalities but no gadolinium enhancement.
DISCUSSION To our knowledge, this report is the first to document the recurrence of Susac syndrome after remission. Except for infrequent patients who have had a stuttering or progres- sive course,3,7 nearly all reported patients have had mono- phasic, self-limited illness, with varying residual disability after remission, and none has had recurrence after remis- sion.2,3,8 Recurrence in our patient at age 51 years after 18 years of remission expands the clinical spectrum of Susac syndrome, not only by documenting that some patients may have late recurrence but by supporting the recent observation that the disease is not necessarily limited to young adults.9 Clinicians should be aware of the possibility of late recurrence when counseling patients with this syn- drome and when evaluating patients with a distant history of the syndrome who present with new complaints refer- able to the brain, retina, and cochlea.
Since the original description of the syndrome by Susac et al1 in 1979, fewer than 100 patients have been reported with this distinct clinical syndrome.1-5,7-9 The disease is likely underdiagnosed. Many patients with Susac syn- drome mistakenly receive another diagnosis, such as mul- tiple sclerosis, migraine, lupus erythematosus, Ménière disease, cardioembolic stroke, and even schizophrenia.3
The most common manifestations of brain involvement in Susac syndrome are related to problems with cognition, memory, behavior, and affect, as well as dizziness, ataxia, dysarthria, and bilateral corticospinal tract dysfunction.3,5,8
These manifestations correspond to the characteristic mul-
Figure 1. Axial T2 images demonstrating scattered foci of in- creased T2 signal in both basal ganglia, right thalamus, corpus callosum, and cerebral white matter.
Figure 2. Coronal T1 images after intravenous administration of gadolinium demonstrating small, scattered, enhancing foci both infratentorially and supratentorially, some of which correspond with the foci of abnormal T2 signal.
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.
Recurrence of Susac Syndrome Mayo Clin Proc, September 2001, Vol 76960
tiple, small, punctate areas of T2 signal increase and con- trast enhancement seen in both the cerebral gray matter and white matter on MRI (Figures 1 and 2).3 Visual loss, usu- ally segmental field defects in 1 eye or both eyes, is due to retinal arteriolar occlusions or narrowing visible on oph- thalmologic examination.3 Low- to mid-frequency senso- rineural hearing loss on audiometry has been attributed to microvascular infarction of the cochlear apex.4 Some pa- tients with Susac syndrome have constitutional symptoms, arthralgias, and myalgias,10 as well as pathologic microvas- cular changes on muscle biopsy, without frank arthritis or myopathy, suggesting that the disease may be a systemic illness with a predilection for producing encephalopathic, visual, and auditory symptoms either because of selective vulnerability of the brain, retina, and cochlea or because microvascular occlusions in these organs are more likely to produce striking symptoms that command the attention of patients and their physicians than do less eloquent organs.3
The pathogenesis of Susac syndrome is unknown. Brain and muscle biopsy specimens show small infarcts with some minimal perivascular lymphocytic infiltration, but not necro- tizing vasculitis.3 No procoagulant state has been docu- mented consistently. Rarely, as in our patient, the IgM anti- phospholipid antibody isotype has been positive,10 but the IgG isotype associated with thromboembolism and results of detailed functional coagulation tests have been negative in most patients tested.3 Similarly, some patients with Susac syndrome have nonspecific low-titer antinuclear antibody or rheumatoid factor tests but no definite connective tissue disease.1,3,6 The onset of symptoms during pregnancy3,6 or hormone replacement therapy (as in our patient’s recur- rence) could indicate a hormonal influence on pathogenesis, but this could be a coincidence because of the apparent predilection for the disease to afflict women. Coincidence could also account for the association of the onset of symp- toms with a preceding viral-like illness in some patients.3
Because of the clinical course and small number of cases reported, efficacy of the various treatments that have
been attempted in Susac syndrome has been difficult to assess.2,3,5,8 Most patients have received immunosuppres- sive therapy. We chose to discontinue azathioprine treat- ment and institute plasma exchange in addition to cortico- steroid treatment in our patient, because plasma exchange is relatively less toxic, and 2 patients with Susac syndrome evaluated at our institution during the past 2 years have had cessation of new symptoms following this treatment. How- ever, we have no proof of the efficacy of plasma exchange or any other treatment for Susac syndrome.
The authors thank John O. Susac, MD, for recommending referral of this patient to Mayo Clinic.
REFERENCES 1. Susac JO, Hardman JM, Selhorst JB. Microangiopathy of the brain
and retina. Neurology. 1979;29:313-316. 2. Susac JO. Susac’s syndrome: the triad of microangiopathy of the
brain and retina with hearing loss in young women. Neurology. 1994;44:591-593.
3. Petty GW, Engel AG, Younge BR, et al. Retinocochleocerebral vasculopathy. Medicine (Baltimore). 1998;77:12-40.
4. Monteiro ML, Swanson RA, Coppeto JR, Cuneo RA, DeArmond SJ, Prusiner SB. A microangiopathic syndrome of encephalopathy, hearing loss, and retinal arteriolar occlusions. Neurology. 1985; 35:1113-1121.
5. O’Halloran HS, Pearson PA, Lee WB, Susac JO, Berger JR. Microangiopathy of the brain, retina, and cochlea (Susac syn- drome): a report of five cases and a review of the literature. Oph- thalmology. 1998;105:1038-1044.
6. MacFadyen DJ, Schneider RJ, Chisholm IA. A syndrome of brain, inner ear and retinal microangiopathy. Can J Neurol Sci. 1987; 14:315-318.
7. Bogousslavsky J, Gaio JM, Caplan LR, et al. Encephalopathy, deafness and blindness in young women: a distinct retino- cochleocerebral arteriolopathy? J Neurol Neurosurg Psychiatry. 1989;52:43-46.
8. Papo T, Biousse V, Lehoang P, et al. Susac syndrome. Medicine (Baltimore). 1998;77:3-11.
9. Barker RA, Anderson JR, Meyer P, Dick DJ, Scolding NJ. Microangiopathy of the brain and retina with hearing loss in a 50 year old woman: extending the spectrum of Susac’s syndrome. J Neurol Neurosurg Psychiatry. 1999;66:641-643.
10. Nicolle MW, McLachlan RS. Microangiopathy with retinopathy, encephalopathy, and deafness (RED-M) and systemic features. Semin Arthritis Rheum. 1991;21:123-128.
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.
Recurrence of Susac Syndrome (Retinocochleocerebral Vasculopathy) After Remission of 18 Years
REPORT OF A CASE
Related Documents