CLINICAL STUDY Recovery of empathetic function following resection of insular gliomas Xingchao Wang • Xiaosi Gu • Jin Fan • Shiwei Wang • Fu Zhao • Patrick R. Hof • Pinan Liu • Zhixian Gao Received: 2 July 2013 / Accepted: 19 January 2014 Ó Springer Science+Business Media New York 2014 Abstract The insular cortex is located deep within the Sylvian fissure between multi-functional and structurally- compressed cerebral structures, and has been suggested to play an important role in both basic sensorimotor and complex social-emotional functions. Such structural and functional complexity presents a challenge for neurosur- geons to remove tumors within the insula safely. It has therefore not yet been documented how neurosurgical resection of insular gliomas would impact social-emotional functions. In this study, we examined empathy, a high-level social-emotional function, in four patients with localized insular gliomas pre- and post-operatively. The patients completed an empathy-for others pain task in which they viewed another person’s hand or foot in painful or non- painful situations and made judgments about either pain (explicit empathy) or laterality of the hand or foot (implicit empathy). They also completed questionnaires assessing general emotional processing and personality. Deficits in both explicit and implicit empathetic pain processing were found in patients before the operations. However, the operations significantly improved their empathetic ability after surgery, accompanied by unchanged personality traits. These results confirmed previous findings that the insula plays a critical role for empathetic pain perception. Importantly, the current results suggest that surgical resection is not only a suitable treatment for insular glio- mas for clinical consideration, but also effective in improving high-level functions such as empathetic pain perception. Keywords Cognitive function Empathic processing Insular gliomas Outcome Surgery Electronic supplementary material The online version of this article (doi:10.1007/s11060-014-1380-y) contains supplementary material, which is available to authorized users. X. Wang S. Wang P. Liu (&) Z. Gao (&) Department of Neurosurgery, Beijing Tiantan Hospital, Capital Medical University, Beijing 100050, China e-mail: [email protected] Z. Gao e-mail: [email protected] X. Gu Wellcome Trust Centre for Neuroimaging, University College London, London WC1N 3BG, UK X. Gu Virginia Tech Carilion Research Institute, Roanoke, VA 24016, USA J. Fan Department of Psychology, Queens College, The City University of New York, Flushing, NY 11367, USA J. Fan Department of Psychiatry, Icahn School of Medicine at Mount Sinai, New York, NY 10029, USA J. Fan P. R. Hof Fishberg Department of Neuroscience, Icahn School of Medicine at Mount Sinai, New York, NY 10029, USA J. Fan P. R. Hof Friedman Brain Institute, Icahn School of Medicine at Mount Sinai, New York, NY 10029, USA F. Zhao P. Liu Department of Neural Reconstruction, Beijing Neurosurgery Institute, Capital Medical University, Beijing 100050, China 123 J Neurooncol DOI 10.1007/s11060-014-1380-y

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CLINICAL STUDY
Recovery of empathetic function following resection of insulargliomas
Xingchao Wang • Xiaosi Gu • Jin Fan •
Shiwei Wang • Fu Zhao • Patrick R. Hof •
Pinan Liu • Zhixian Gao
Received: 2 July 2013 / Accepted: 19 January 2014
� Springer Science+Business Media New York 2014
Abstract The insular cortex is located deep within the
Sylvian fissure between multi-functional and structurally-
compressed cerebral structures, and has been suggested to
play an important role in both basic sensorimotor and
complex social-emotional functions. Such structural and
functional complexity presents a challenge for neurosur-
geons to remove tumors within the insula safely. It has
therefore not yet been documented how neurosurgical
resection of insular gliomas would impact social-emotional
functions. In this study, we examined empathy, a high-level
social-emotional function, in four patients with localized
insular gliomas pre- and post-operatively. The patients
completed an empathy-for others pain task in which they
viewed another person’s hand or foot in painful or non-
painful situations and made judgments about either pain
(explicit empathy) or laterality of the hand or foot (implicit
empathy). They also completed questionnaires assessing
general emotional processing and personality. Deficits in
both explicit and implicit empathetic pain processing were
found in patients before the operations. However, the
operations significantly improved their empathetic ability
after surgery, accompanied by unchanged personality
traits. These results confirmed previous findings that the
insula plays a critical role for empathetic pain perception.
Importantly, the current results suggest that surgical
resection is not only a suitable treatment for insular glio-
mas for clinical consideration, but also effective in
improving high-level functions such as empathetic pain
perception.
Keywords Cognitive function � Empathic processing �Insular gliomas � Outcome � Surgery
Electronic supplementary material The online version of thisarticle (doi:10.1007/s11060-014-1380-y) contains supplementarymaterial, which is available to authorized users.
X. Wang � S. Wang � P. Liu (&) � Z. Gao (&)
Department of Neurosurgery, Beijing Tiantan Hospital, Capital
Medical University, Beijing 100050, China
e-mail: [email protected]
Z. Gao
e-mail: [email protected]
X. Gu
Wellcome Trust Centre for Neuroimaging, University College
London, London WC1N 3BG, UK
X. Gu
Virginia Tech Carilion Research Institute, Roanoke, VA 24016,
USA
J. Fan
Department of Psychology, Queens College, The City University
of New York, Flushing, NY 11367, USA
J. Fan
Department of Psychiatry, Icahn School of Medicine at Mount
Sinai, New York, NY 10029, USA
J. Fan � P. R. Hof
Fishberg Department of Neuroscience, Icahn School of Medicine
at Mount Sinai, New York, NY 10029, USA
J. Fan � P. R. Hof
Friedman Brain Institute, Icahn School of Medicine at Mount
Sinai, New York, NY 10029, USA
F. Zhao � P. Liu
Department of Neural Reconstruction, Beijing Neurosurgery
Institute, Capital Medical University, Beijing 100050, China
123
J Neurooncol
DOI 10.1007/s11060-014-1380-y

Introduction
The insular cortex is a complex structure located in the depth
of the Sylvian fissure at the junction of the frontal, parietal,
and temporal lobes, and has intricate connectivity with sur-
rounding cerebral structures [1, 2]. The insula participates in
many basic sensorimotor processes including gustation,
olfaction, motor integration, control of cardiovascular tone,
and speech [3]. The insula is also involved in high-level
social and emotional functions [4, 5] and has been proposed
to represent an important neural substrate for subjective
awareness [6, 7]. For instance, the insula is considered to be
critical for empathy, the ability to understand and share
others’ affective states [8, 9]. Previous studies using func-
tional magnetic resonance imaging (fMRI) and behavioral
tests have demonstrated that the insula, particularly the
anterior insular cortex (AIC), is activated when subjects
observe others in pain, suggesting that AIC is essential for
empathetic pain perception [10, 11].
The insula can be affected by various disease conditions,
of which gliomas are the most common [12, 13]. The
resection of insular gliomas remains a challenge for neu-
rosurgeons because of the region’s unique anatomical
location and difficulty of access [14]. Although successful
resection of insular tumors with minimal long-term mor-
bidity has been achieved with the development of advanced
surgical tools and skills over the past two decades, such
operations can affect multiple complex neurocognitive
functions, ranging from language to social-emotional pro-
cessing [15, 16]. On the other hand, cytoreduction of the
tumor surgically relieving the involvement of the sur-
rounding normal brain structure could alleviate associated
neurological deficits. However, due to the rarity of focal
surgical resection, only a handful of studies have explored
the impact of insula surgery on high-level functions and
behaviors [11]. Traditional clinical assessments using
structural brain imaging or surveys of quality of life do not
inform on a patient’s high-level functioning, especially
those functions dependent on the insula. Additionally,
patients with insular gliomas experience a prolonged and
slowly progressive clinical course compared to similar
tumors in other locations [17]. Insular gliomas are associ-
ated with longer periods of overall survival and progres-
sion-free survival [18]. It is therefore important to assess
changes in high-level functions in these patients to evaluate
long-term outcome of insular glioma operations.
Empathy is critical for effective social interactions and
has gained increasing interest in neuroscience [8, 19, 20].
The critical role of the insula in empathetic functions
makes empathy an important test case for high-level social-
emotional functions in insular glioma patients. To inves-
tigate the surgical impact on higher-level social-emotional
functions in patients with insular gliomas, we assessed
empathy pre- and post-operatively in four patients with
insular gliomas, in comparison to 18 matched normal
controls (NC), using the empathy for others pain (EOP)
task. The EOP provides a reliable assessment for empa-
thetic pain processing involving the insula [9]. We pre-
dicted that patients with insular gliomas would show
deficits in empathetic pain processing pre-operatively, and
that surgical reduction of the tumor mass with preserved
portions of functional insula, would at least partially restore
these functions.
Materials and methods
Participants
Insular glioma patients
Five insular patients met our inclusion criteria (see Supple-
mentary Materials for detailed information). However, one
patient presented dyskinesia for precise movement of the
right arm, and had to be excluded due to inability to operate a
computer mouse for task response selection 3 months post-
operatively (the incomplete dataset for this excluded patient
is provided in the Supplementary Materials). Consequently,
only results for the other four patients with unilateral insular
gliomas are reported (see Table 1 for all participants’ char-
acteristics). Among the four patients, three had right (P1, P2,
and P4) and one had left (P3) insular lesions, and all the
gliomas were Grade II or III pathologically (Table 1). Pre-
and postoperative head MRI scans of insular lesions are
shown in Fig. 1. Each patient was assessed pre-operatively
and 3 months postoperatively.
Normal controls
Eighteen neurologically intact individuals participated in
the study as NC. They were recruited from local commu-
nities in Beijing and were matched with the patients by age,
gender, education, and ethnicity (Table 1). They were
assessed twice, and the assessments were set 3 months
apart to match the time lag between testing sessions in the
patients. Then data from these two testing sessions were
compared with the patients’ pre- and postoperative results
separately.
Tasks and Assessments (see Supplementary Materials
for detailed information about these assessments).
Empathy for others pain (EOP)
Experimental stimuli and procedures were the same as
those described in a previous study [9] (also see Fig. 2).
Briefly, participants viewed color photographs on a
J Neurooncol
123

computer screen showing another person’s left or right
hand or foot in painful or non-painful situations. There
were two types of tasks: in the task pain (TP) sessions, the
subjects were instructed to judge whether or not the person
in the photograph was suffering from pain; in the task
laterality (TL) sessions, they were instructed to judge the
laterality of the hand or foot (left or right). Accuracy and
reaction time (RT) were recorded.
General neurological evaluation
The Karnofsky performance score (KPS) and routine
neurological examination [21] were performed longitudi-
nally to provide a brief, but accurate report of the neuro-
logical status of a patient at a given time. Moreover, the
mini-mental state examination (MMSE) [22] and the short
form beck depression inventory (BDI-SF) [23, 24] were
used to assess the differences in general cognitive and
emotional abilities between the IC and NC groups.
Personality assessments
Davis [25] interpersonal reactivity index (IRI), the 20-item
Toronto Alexithymia Scale (TAS-20) [26] and the 30-Item
Short Version NEO-Five-Factor Inventory (NEO-FFI-30)
[27] were administered to assess general personality traits
in patients with insular gliomas pre- and postoperatively.
Data analysis
Accuracy and RT were analyzed for the four experimental
conditions (TP-pain, TP-no pain, TL-pain, TL-no pain) in
EOP. Participants’ sensitivity to pain and laterality was
measured by discrimination index d’ and decision bias was
measured by bias index b using signal detection theory
(SDT) [28]. SDT is a method to discern between signal and
noise, assuming the perceiver has an internal distribution of
signal and noise. In the context of TP, d’ is the distance
between the mean of the probability distribution for ‘‘pain’’
(target) and the mean of the probability distribution for ‘‘no
pain’’ (noise), measured in units of standard deviation. b,
which represents the position of the subject’s criterion, is
the ratio of the height of the ‘‘pain’’ (signal) distribution to
the ‘‘no pain’’ (noise) distribution for the value of thresh-
old. In TL, d’ is the distance between the mean of the
probability distribution for ‘‘left’’ (signal) and the mean of
the probability distribution for ‘‘right’’ (noise), measured in
units of standard deviation. b is the ratio of the height of
the ‘‘left’’ (signal) distribution to the ‘‘right’’ (noise) dis-
tribution for the value of threshold. For TL, d’ and b for
‘pain’ and ‘no pain’ conditions were calculated separately,
then the differences between conditions were tested.
Therefore, the d’ and b difference scores in TL representTa
ble
1P
arti
cip
ant
char
acte
rist
ics
Les
ion
late
rali
ty
Ch
ron
icit
y
(mo
nth
s)
Ag
e
(yea
rs)
Sex
Han
d-
nes
s
Ed
uca
tio
n
(yea
rs)
KP
Sp
re/
po
st
MM
SE
pre
/po
stB
DI
pre
/po
stH
isto
pat
ho
log
yM
edic
atio
ns
pre
/po
st
P1
R3
28
fR
99
0/9
02
6/2
54
/7A
stro
cyto
ma
no
/yes
P2
R3
28
fR
16
90
/10
02
7/2
90
/1A
stro
cyto
ma
no
/yes
P3
L3
48
fR
58
0/9
02
3/2
41
1/7
Oli
go
den
dro
gli
om
an
o/y
es
P4
R3
51
mR
15
90
/10
03
0/2
70
/1A
nap
last
ico
lig
od
end
rog
lio
ma
no
/yes
NC
N/A
N/A
43
±6
.61
0f/
8m
R1
2±
2.4
N/A
28
±1
.7/2
9±
1.4
2±
3.0
/2±
1.5
N/A
no
/no
pv
alu
eN
/AN
/A0
.30
00
.30
6N
/A0
.39
4N
/A0
.24
8/0
.06
10
.34
2/0
.14
8N
/AN
/A
Dat
aar
esh
ow
nas
mea
n±
stan
dar
dd
evia
tio
n.
All
pat
ien
tsu
nd
erw
ent
the
max
imal
safe
rese
ctio
no
fth
eir
insu
lar
gli
om
as(r
esec
tio
nv
olu
me[
95
%).
Th
ep
val
ue
isd
eriv
edfr
om
the
test
bet
wee
np
atie
nts
gro
up
san
dN
Cb
yn
on
par
amet
ric
bo
ots
trap
pin
gm
eth
od
Lle
ft,
Rri
gh
t,B
bil
ater
al,
ffe
mal
e,m
man
,P
1,
P2
,P
3an
dP
4ar
ep
atie
nts
wit
hin
sula
rg
lio
mas
,N
Cn
euro
log
ical
lyin
tact
con
tro
ls,
KP
SK
arn
ofs
ky
per
form
ance
sco
re,
ate
stto
qu
anti
fyca
nce
r
pat
ien
ts’
gen
eral
wel
l-b
ein
gan
dac
tiv
itie
so
fd
aily
life
[21],
MM
SE
min
i-m
enta
lst
atu
sex
amin
atio
n,a
test
for
cog
nit
ive
imp
airm
ent
[22
],B
DI
sho
rtfo
rmo
fth
eB
DI,
am
easu
reo
fb
asel
ine
mo
od
[24
],C
hro
nic
ity
the
tim
ele
ng
thb
etw
een
the
last
inte
rven
tio
nd
ate
and
test
ing
dat
e,A
ge
the
age
atth
efi
rst
test
ing
dat
e,P
re/P
ost
the
resu
lts
of
firs
tan
dse
con
das
sess
men
tsfo
rN
C,
and
pre
-/
po
sto
per
ativ
ere
sult
sfo
rth
ep
atie
nts
,M
edic
ati
on
sit
incl
ud
esan
ti-e
pil
epti
cd
rug
s(D
epak
in,
20
0m
gT
idp
.o.,
con
tin
uo
us
for
2w
eek
s,n
ose
izu
res,
sto
pp
ing
trea
tmen
tg
rad
ual
lyan
dle
avin
ga
med
icat
ion
-fre
ep
erio
do
f2
mo
nth
sb
efo
rep
ost
op
erat
ive
asse
ssm
ent)
and
sho
rtte
rmtr
eatm
ent
usi
ng
low
-do
sed
exam
eth
aso
ne
afte
rsu
rger
yte
mp
ora
rily
for
pre
ven
tin
gb
rain
edem
a(1
0m
g,B
id,
i.v
.fo
r2
day
s,5
mg
,B
id,
i.v
.fo
r2
day
s,5
mg
,Q
d,
i.v
.fo
r2
day
san
d0
.75
mg
,T
id,
p.o
.fo
r3
day
s)
J Neurooncol
123
the interference effect of pain on laterality judgment. The
mean RT under TP [(RTTP-pain ? RTTP-no pain)/2] and TL
[(RTTL-pain ? RTTL-no pain)/2] and cost of pain in RT
(additional time-consuming for processing the pain
information) under TP (RTTP-pain - RTTP-no pain) and TL
(RTTL-pain - RTTL-no pain) were calculated as well.
The nonparametric bootstrapping method was used to
assess the probability of observing a difference between
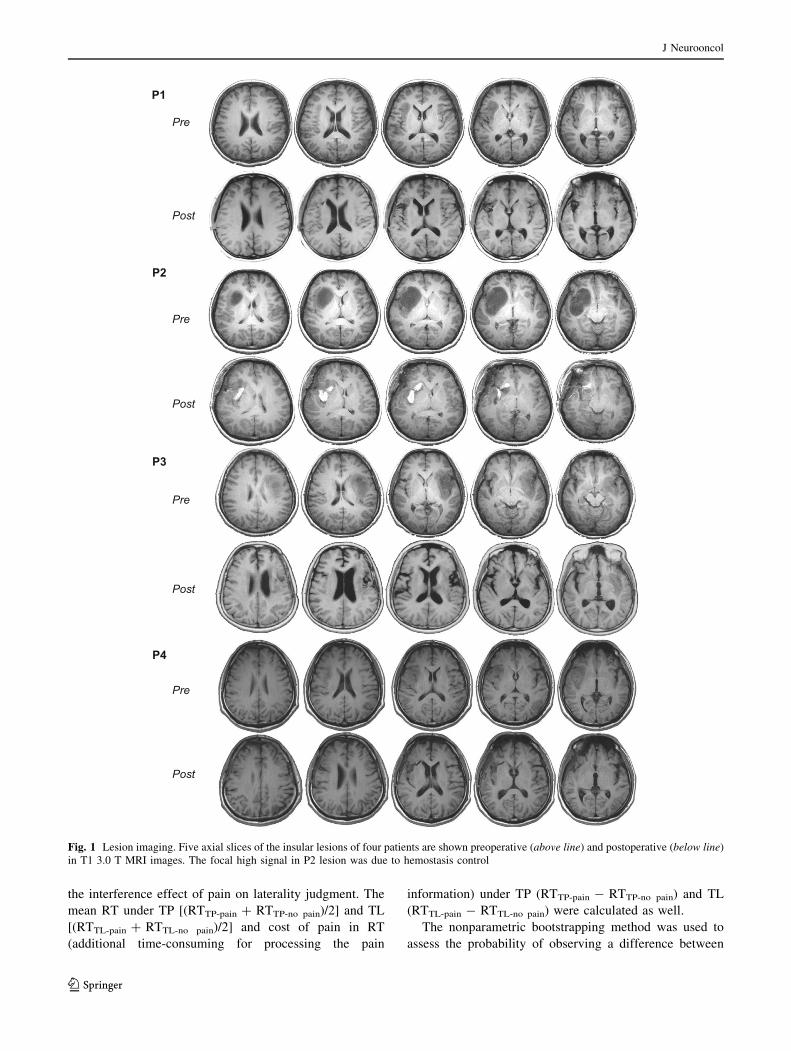
Fig. 1 Lesion imaging. Five axial slices of the insular lesions of four patients are shown preoperative (above line) and postoperative (below line)
in T1 3.0 T MRI images. The focal high signal in P2 lesion was due to hemostasis control
J Neurooncol
123

insular and control groups [29, 30] (see Supplementary
Materials for detailed information about these procedures),
due to the small sample size of the patient group, and the
fact that our dataset does not meet the assumptions required
to perform parametric tests.
Results
Clinical assessments
The pre- and postoperative MMSE scores of the patients
were similar to the NC (Table 1). The NC showed stable
BDI scores without depression, and the BDI of patients
showed mild, non-significant increase postoperatively.
Patients showed moderate improvement in KPS scores
after surgery. Only P3 had speech deficits and contralateral
hemiparesis identified during routine neurological exami-
nation immediately after surgery and these symptoms
improved substantially 3 months postoperatively. The
other patients did not show any neurological dysfunction
postoperatively.
Preoperative deficits and postoperative improvement
in explicit empathetic pain processing associated
with insular gliomas
For explicit empathetic pain processing under TP, preoper-
ative insular glioma patients showed a significantly smaller
d0 than NC (p = 0.044; Fig. 3a), indicating diminished
ability to discriminate painful from non-painful stimuli.
Postoperatively, the reassessed d’ of patients did not show
significant difference compared to results of the second
testing session of NC (p = 0.161; Fig. 3a), indicating sig-
nificant improvement in sensitivity to others’ pain.
However, there was no significant dissimilarity between
patients and controls in b during pain judgment preopera-
tively (p = 0.221; Fig. 3b). Although there were some
fluctuations among individual patients’ b scores, the post-
operative group difference between patients and NC for pain
judgment was again not significant (p = 0.138; Fig. 3b).
The response speed of patients during explicit empathetic
pain judgment did not show significant differences either in
mean RT [(RTTP-pain ? RTTP-no pain)/2] (p = 0.185; Fig. 3c)
or cost of pain RT (RTTL-pain - RTTL-no pain) (p = 0.307;
Fig. 3d) compared to NC preoperatively. Postoperatively,
group differences in cost of pain RT (p = 0.265; Fig. 3d)
and overall RT (p = 0.184; Fig. 3c) under TP between
patients and NC were also not significant. Our results
demonstrate significant post-operative improvement in dis-
crimination accuracy of others’ pain (indexed by d’), and no
significant change in other behavioral indices during explicit
empathetic processing in insular patients.
Preoperative deficits and postoperative improvement
in implicit empathetic pain processing associated
with insular gliomas
Implicit empathetic processing was examined by assessing
the interference effect of empathetic pain on laterality
Rig
htLe
ft
Painful Non-painfulFig. 2 Sample stimuli of the
experimental stimulus set.
Participants were instructed to
choose between ‘‘non-painful’’
and ‘‘painful’’ for the TP, and
‘‘left’’ and ‘‘right’’ for the TL
through button press within a
time window of 4,000 ms
(2,500 ms of stimulus display
and 1,500 ms of fixation)
J Neurooncol
123

judgment (d0TL-painful - d0TL-non-painful). The negative
scores of NC subjects (Fig. 4a) suggest that they performed
worse on the TL-painful than on the TL-non-painful con-
dition and that pain interfered with laterality judgment.
However, preoperative patients had significant greater
positive d’ difference scores compared to NC (p = 0.004;
Fig. 4a), indicating that empathetic pain did not interfere
with laterality judgment, and they performed better on the
TL-painful than on the TL-non-painful condition. These
results suggest that insular gliomas disrupted not only
explicit but also implicit processing of empathetic pain
preoperatively. When the interference effect of empathetic
pain on laterality judgment was reassessed postoperatively,
NC scores remained negative. Interestingly, the difference
in d’ scores of patients changed from positive preopera-
tively to negative postoperatively, indicating a typical
normal interference effect of pain on laterality judgment
after surgery (p = 0.385 compared to NC; Fig. 4a). These
results suggest that implicit sensitivity to others’ pain was
restored in insular patients postoperatively.
In addition, there were no significant preoperative
(p = 0.324; Fig. 4b) and postoperative (p = 0.335; Fig. 4b)
differences in interference effect of empathy for pain
on decision bias compared to NC. Neither preoperative
nor postoperative mean RT [(RTTL-pain ? RTTL-no pain)/2]
(preoperative p = 0.351 and postoperative p = 0.247;
Fig. 4c) and RT cost of pain (RTTL-pain-RTTL-no pain; pre-
operative p = 0.161 and postoperative p = 0.196; Fig. 4d)
during laterality judgment differed significantly from
controls.
Personality assessments
General personality traits were examined pre- and post-
operatively using three questionnaires (i.e. IRI, TAS-20,
NEO-FFI-30). Only the Neuroticism (N) subscale of NEO-
FFI-30 revealed a significant difference in patients com-
pared to NC in both examinations, indicating that the
patients were more neurotic (preoperative p = 0.030 and
postoperative p = 0.026; Fig. S1).
Discussion
Preoperative functional impairment in patients
with insular gliomas
The impaired sensitivity in empathetic pain processing
observed in insular glioma patients preoperatively support
the notion that insular tumors affect high-level functions
0.0
0.5
1.0
1.5
2.0
2.5
3.0
NC P1 P2 P3 P40.0
1.0
2.0
3.0
4.0
NC P1 P2 P3 P4
0.0
200.0
400.0
600.0
800.0
1000.0
1200.0
1400.0
NC P1 P2 P3 P4
mea
n R
T(m
s)
-400.0
-350.0
-300.0
-250.0
-200.0
-150.0
-100.0
-50.0
0.0
50.0
100.0
150.0
NC P1 P2 P3 P4co
st o
f pai
n in
RT
(m
s)
5.0
6.0 (the second time)
Patient (after surgery)
(the first time)
before surgery)
NC
Patient (
NCa b
c d
Fig. 3 Behavioral performance
on TP. a Presurgically, insular
glioma patients had significantly
smaller d’ (p = 0.044)
compared with NC, indicating
reduced discrimination accuracy
in empathetic pain processing.
After surgery, there was no
significant difference
(p = 0.161) between the
patients’ and retested NC
results. b For the patients group,
neither preoperative
(p = 0.221) nor postoperative
(p = 0.138) decision bias
indexed by b showed significant
alteration during TP compared
to NC. c Neither patients’
preoperative (p = 0.185) nor
postoperative (p = 0.184) mean
RT showed significant
difference compared to NC.
d RT cost of pain did not show
significant differences pre-
(p = 0.307) and postoperatively
(p = 0.265) between patients
and NC. Error bars represent
95 % CI
J Neurooncol
123

and that the insula plays an important role in empathetic
abilities. Studies have shown that both low- and high-grade
gliomas can cause neurocognitive impairments in memory,
attention, and executive function [31, 32], and that these
disturbances might be attributed to both tumor and treat-
ment side effects [33–35]. In addition, tumor location may
impact cognitive functions in different ways. For instance,
frontal and temporal lobe lesions impair social behavior
[36], but in the case of insular tumors, deficits in empathy
were evident preoperatively in our patients.
The insula serves a major role in emotional awareness
[6]. Deficits in explicit and implicit empathetic pain pro-
cessing have been associated with focal AIC lesions as
shown in our previous study [11]. Because insular gliomas
not only damage normal insular structure but also affect
surrounding brain regions [37], we propose that the com-
bination of the tumor itself and tumor-related increase in
intracranial pressure have a critical impact on AIC func-
tion, resulting in empathetic processing deficits. Further-
more, this behavioral deficit observed in preoperative
insular glioma patients may be due to the failure of
the insula to integrate sensory information with abstract
representation of subjective feelings and emotional
awareness [11].
Mechanisms underlying postoperative recovery
of empathetic function
The pre- and postoperative comparisons demonstrated that
empathy could be improved by surgery in insular glioma
patients. The restoration of empathy in these four patients
can be attributed to the reduction of the tumor mass with
proper protection of the normal surrounding tissue. Per-
ilesional plasticity is an important compensatory mecha-
nism in glioma patients for postoperative improvement of
cognitive deficits [38, 39]. In this study, however, because
of the AIC is an important structure for empathy [2, 40],
plasticity in perilesional tissues might have been insuffi-
cient to maintain normal empathetic function, but preser-
vation of parts of the AIC could explain the recovery of
empathy for pain. It is also important to note that although
the patients took anti-epileptic medications and steroids
right after their surgeries, they were reassessed 3 months
postoperatively, long after they had stopped taking these
medications. Therefore, we believe that these drugs had no
direct influence on the outcome of our study.
It is also noteworthy that there are individual differences
in empathetic processing pre- and postoperatively. Youn-
ger age and smaller tumor size may indicate a relatively
-0.8
-0.6
-0.4
-0.2
0.0
0.2
0.4
0.6
0.8
1.0
NC P1 P2 P3 P4 -8.0
-6.0
-4.0
-2.0
0.0
2.0
4.0
6.0
8.0
10.0
NC P1 P2 P3 P4
0.0
200.0
400.0
600.0
800.0
1000.0
1200.0
1400.0
1600.0
NC P1 P2 P3 P4
mea
n R
T (
ms)
0.0
20.0
40.0
60.0
80.0
100.0
120.0
140.0
NC P1 P2 P3 P4co
st o
f pai
n in
RT
(m
s)
(the second time)
Patient (after surgery)
(the first time)
(before surgery)
NC
Patient
NC
a b
c d
Fig. 4 Behavioral performance
on TL. a Insular glioma patients
group had greater scores of d’
difference on TL task
preoperatively (p = 0.004), but
not postoperatively (p = 0.385).
b Patients showed no significant
difference in interference effect
of pain on TL decision bias pre-
(p = 0.324) and postoperatively
(p = 0.335). c Patients showed
no significant difference
compared to NC in mean RT
during laterality judgment pre-
(p = 0.351) and postoperatively
(p = 0.247). d Neither
preoperative (p = 0.161) nor
postoperative (p = 0.196) RT
cost of pain during TL showed
significant alteration between
patients group and results from
both NC assessments. Error
bars represents 95 % CI
J Neurooncol
123

stable neurocognitive status and a significant postoperative
improvement of the cognitive deficits, as seen in P1. With
the same young age but a much larger glioma, however, P2
still showed the best empathetic performance (highest d’
and the d’ difference closest to NC). P2’s tumor expansion
did not invade the whole insula, and the preserved portions
of the AIC may have helped to maintain P2’s normal
functional state. Owing to the older age of P3, the large
tumor size, its extensive invasion of the AIC, and its
location in the dominant (left) hemisphere, P3 had the most
severe empathetic deficits (the smallest d’ and difference in
d’ compared to NCs). This is not surprising and is con-
sistent with our understanding of the characteristics of
glioma prognosis. Although P4 suffered from a small
tumor in the AIC, the older age and higher grade of the
glioma may have caused a more destructive progression
[32] and contribute to greater preoperative empathetic
deficits with only moderate recovery.
Clinical considerations
Neurocognitive function outcomes in brain surgery patients
have become an important consideration for neurosurgeons.
Assessments and reassessments of high-level neurocognitive
functions may inform surgeons about the changes in those
functions longitudinally and help guiding clinical manage-
ment [41–43]. Previous clinical studies have revealed that
the most common functional alterations in insular gliomas
patients after surgery were transient deficits in speech and
motor functions [17, 38]. It was concluded that insula
patients were not preferentially vulnerable to neurocognitive
decline after surgery compared to patients with lesions in
neighboring brain regions [44]. Our study provides longi-
tudinal evidence supporting the sensitivity of high level
insular functions to surgical impact. We demonstrate that
insular gliomas are associated with empathy deficits and that
appropriate surgical procedures may help mitigate these
deficits. Moreover, surgeries do not necessarily lead to
additional cognitive disability, supporting the safety and
efficacy of such insular glioma surgeries.
In the current study, we did not use awake craniotomy
and cortical mapping during surgery. Experience with
topographic anatomy and surgery can also ensure the out-
come and safety of surgery. Our protocols suggest that
determining the boundary of tumor accurately to protect
surrounding healthy brain tissues is crucial for operative
outcome. Ultimately, our findings suggest it is important to
assess the neurocognitive status of glioma patients using
sophisticated neuropsychological examinations, especially
for cortical regions like the insula. We show that technical
and anatomical challenges are always the most critical
factors for insular surgery outcomes. To date, surgical
treatment remains the most effective method for insular
patients not only for maximal cytoreduction and accurate
diagnosis, but also for the protection of social-emotional
functions.
Acknowledgments This research was supported by National Sci-
ence and Technology Support Program of the 12th 5-year of China
(Grant Number: 2012BAI12B03) to P. L, by Natural Science Foun-
dation of Beijing (Grant Number: 7112049) to P. L and by National
Science Foundation of China (Grant Number: 81328008) to J. F and
Z. G. J. F was supported by National Institute of Health (NIH) Grants
R21MH083164. P. R. H was supported by The James S. McDonnell
Foundation (Grant 22002078).
Conflict of interest The authors declare they have no conflict of
interest.
References
1. Naidich TP, Kang E, Fatterpekar GM, Delman BN, Gultekin SH,
Wolfe D, Ortiz O, Yousry I, Weismann M, Yousry TA (2004)
The insula: anatomic study and MR imaging display at 1.5 T.
AJNR 25:222–232
2. Gu X, Hof PR, Friston KJ, Fan J (2013) Anterior insular cortex
and emotional awareness. J Comp Neurol 521:3371–3388.
doi:10.1002/cne.23368
3. Stephani C, Fernandez-Baca Vaca G, Maciunas R, Koubeissi M,
Luders HO (2011) Functional neuroanatomy of the insular lobe.
Brain Struct Funct 216:137–149. doi:10.1007/s00429-010-0296-3
4. Butti C, Hof PR (2010) The insular cortex: a comparative per-
spective. Brain Struct Funct 214:477–493. doi:10.1007/s00429-
010-0264-y
5. Menon V, Uddin LQ (2010) Saliency, switching, attention and
control: a network model of insula function. Brain Struct Funct
214:655–667. doi:10.1007/s00429-010-0262-0
6. Craig AD (2009) How do you feel–now? The anterior insula and
human awareness. Nat Rev Neurosci 10:59–70. doi:10.1038/
nrn2555
7. Craig AD (2010) The sentient self. Brain Struct Funct
214:563–577. doi:10.1007/s00429-010-0248-y
8. Singer T, Seymour B, O’Doherty J, Kaube H, Dolan RJ, Frith CD
(2004) Empathy for pain involves the affective but not sensory
components of pain. Science 303:1157–1162. doi:10.1126/sci
ence.1093535
9. Gu X, Liu X, Guise KG, Naidich TP, Hof PR, Fan J (2010)
Functional dissociation of the frontoinsular and anterior cingulate
cortices in empathy for pain. J Neurosci 30:3739–3744. doi:10.
1523/JNEUROSCI.4844-09.2010
10. Singer T, Lamm C (2009) The social neuroscience of empathy.
Ann NY Acad Sci 1156:81–96. doi:10.1111/j.1749-6632.2009.
04418.x
11. Gu X, Gao Z, Wang X, Liu X, Knight RT, Hof PR, Fan J (2012)
Anterior insular cortex is necessary for empathetic pain percep-
tion. Brain 135:2726–2735. doi:10.1093/brain/aws199
12. Hentschel SJ, Lang FF (2005) Surgical resection of intrinsic
insular tumors. Neurosurgery 57:176–183
13. Signorelli F, Guyotat J, Elisevich K, Barbagallo GM (2010)
Review of current microsurgical management of insular gliomas.
Acta Neurochir (Wien) 152:19–26. doi:10.1007/s00701-009-
0450-y
14. Yasargil MG, von Ammon K, Cavazos E, Doczi T, Reeves JD,
Roth P (1992) Tumours of the limbic and paralimbic systems.
Acta Neurochir (Wien) 118:40–52
J Neurooncol
123

15. Jones CL, Ward J, Critchley HD (2010) The neuropsychological
impact of insular cortex lesions. J Neurol Neurosurg Psychiatry
81:611–618. doi:10.1136/jnnp.2009.193672
16. Xie C, Bai F, Yu H, Shi Y, Yuan Y, Chen G, Li W, Chen G,
Zhang Z, Li SJ (2012) Abnormal insula functional network is
associated with episodic memory decline in amnestic mild cog-
nitive impairment. Neuroimage 63:320–327. doi:10.1016/j.neu
roimage.2012.06.062
17. Sanai N, Polley MY, Berger MS (2010) Insular glioma resection:
assessment of patient morbidity, survival, and tumor progression.
J Neurosurg 112:1–9. doi:10.3171/2009.6.JNS0952
18. Smith JS, Chang EF, Lamborn KR, Chang SM, Prados MD, Cha
S, Tihan T, Vandenberg S, McDermott MW, Berger MS (2008)
Role of extent of resection in the long-term outcome of low-grade
hemispheric gliomas. J Clin Oncol 26:1338–1345. doi:10.1200/
JCO.2007.13.9337
19. Preston SD, de Waal FB (2002) Empathy: its ultimate and
proximate bases. Behav Brain Sci 25:1–20
20. Caruana F, Jezzini A, Sbriscia-Fioretti B, Rizzolatti G, Gallese V
(2011) Emotional and social behaviors elicited by electrical
stimulation of the insula in the macaque monkey. Current Biol
21:195–199. doi:10.1016/j.cub.2010.12.042
21. Yates JW, Chalmer B, McKegney FP (1980) Evaluation of
patients with advanced cancer using the Karnofsky performance
status. Cancer 45:2220–2224
22. Folstein MF, Folstein SE, McHugh PR (1975) Mini-mental state.
A practical method for grading the cognitive state of patients for
the clinician. J Psychiatr Res 12:189–198
23. Vath R, Miranda M, Becker J, Gibson S (1972) Attempted val-
idation of a pragmatic classification of depression. Psychol Rep
30:287–290
24. Knight RG (1984) Some general population norms for the short
form beck depression inventory. J Clin Psychol 40:751–753
25. Davis MH (1983) Measuring individual differences in empathy:
evidence for a multidimensional approach. J Pers Soc Psychol
44:113–126
26. Bagby RM, Taylor GJ, Parker JD (1994) The Twenty-item Tor-
onto Alexithymia Scale–II. Convergent, discriminant, and con-
current validity. J Psychosom Res 38:33–40
27. Korner A, Geyer M, Roth M, Drapeau M, Schmutzer G, Albani
C, Schumann S, Brahler E (2008) Personality assessment with the
NEO-Five-Factor Inventory: the 30-Item-Short-Version (NEO-
FFI-30). Psychother Psychosom Med Psychol 58:238–245.
doi:10.1055/s-2007-986199
28. Stanislaw H, Todorov N (1999) Calculation of signal detection
theory measures. Behav Res Methods Instrum Comput 31:137–149
29. Hasson U, Avidan G, Deouell LY, Bentin S, Malach R (2003)
Face-selective activation in a congenital prosopagnosic subject.
J Cogn Neurosci 15:419–431. doi:10.1162/089892903321593135
30. Mooney CZ, Duval RD (1993) Bootstrapping: a nonparametric
approach to statistical inference. Sage, Newbury Park
31. Olson JD, Riedel E, DeAngelis LM (2000) Long-term outcome of
low-grade oligodendroglioma and mixed glioma. Neurology
54:1442–1448
32. Bosma I, Vos MJ, Heimans JJ, Taphoorn MJ, Aaronson NK,
Postma TJ, van der Ploeg HM, Muller M, Vandertop WP, Slot-
man BJ, Klein M (2007) The course of neurocognitive func-
tioning in high-grade glioma patients. Neuro-oncology 9:53–62.
doi:10.1215/15228517-2006-012
33. Tucha O, Smely C, Preier M, Lange KW (2000) Cognitive def-
icits before treatment among patients with brain tumors. Neuro-
surgery 47:324–333
34. Klein M, Heimans JJ, Aaronson NK, van der Ploeg HM, Grit J,
Muller M, Postma TJ, Mooij JJ, Boerman RH, Beute GN, Os-
senkoppele GJ, van Imhoff GW, Dekker AW, Jolles J, Slotman
BJ, Struikmans H, Taphoorn MJ (2002) Effect of radiotherapy
and other treatment-related factors on mid-term to long-term
cognitive sequelae in low-grade gliomas: a comparative study.
Lancet 360:1361–1368
35. Douw L, Klein M, Fagel SS, van den Heuvel J, Taphoorn MJ,
Aaronson NK, Postma TJ, Vandertop WP, Mooij JJ, Boerman
RH, Beute GN, Sluimer JD, Slotman BJ, Reijneveld JC, Heimans
JJ (2009) Cognitive and radiological effects of radiotherapy in
patients with low-grade glioma: long-term follow-up. Lancet
Neurol 8:810–818. doi:10.1016/S1474-4422(09)70204-2
36. Gallagher HL, Happe F, Brunswick N, Fletcher PC, Frith U, Frith
CD (2000) Reading the mind in cartoons and stories: an fMRI
study of ‘theory of mind’ in verbal and nonverbal tasks. Neuro-
psychologia 38:11–21
37. Kahana MJ (2006) The cognitive correlates of human brain
oscillations. J Neurosci 26:1669–1672. doi:10.1523/JNEUR
OSCI.3737-05c.2006
38. Duffau H, Taillandier L, Gatignol P, Capelle L (2006) The insular
lobe and brain plasticity: lessons from tumor surgery. Clin Neurol
Neurosurg 108:543–548. doi:10.1016/j.clineuro.2005.09.004
39. Duffau H, Capelle L, Denvil D, Sichez N, Gatignol P, Lopes M,
Mitchell MC, Sichez JP, Van Effenterre R (2003) Functional
recovery after surgical resection of low grade gliomas in eloquent
brain: hypothesis of brain compensation. J Neurol Neurosurg
Psychiatry 74:901–907
40. Sterzer P, Kleinschmidt A (2010) Anterior insula activations
in perceptual paradigms: often observed but barely under-
stood. Brain Struct Funct 214:611–622. doi:10.1007/s00429-
010-0252-2
41. Meyers CA, Hess KR, Yung WK, Levin VA (2000) Cognitive
function as a predictor of survival in patients with recurrent
malignant glioma. J Clin Oncol 18:646–650
42. Armstrong CL, Goldstein B, Shera D, Ledakis GE, Tallent EM
(2003) The predictive value of longitudinal neuropsychologic
assessment in the early detection of brain tumor recurrence.
Cancer 97:649–656. doi:10.1002/cncr.11099
43. Giovagnoli AR (2012) Investigation of cognitive impairments in
people with brain tumors. J Neurooncol 108:277–283. doi:10.
1007/s11060-012-0815-6
44. Wu AS, Witgert ME, Lang FF, Xiao L, Bekele BN, Meyers CA,
Ferson D, Wefel JS (2011) Neurocognitive function before and
after surgery for insular gliomas. J Neurosurg 115:1115–1125.
doi:10.3171/2011.8.JNS11488
J Neurooncol
123
Related Documents











