Reconstruction of goat tibial defects using an injectable tricalcium phosphate/ chitosan in combination with autologous platelet-rich plasma Long Bi 1 , Wenjun Cheng 1 , Hongbin Fan 1 , Guoxian Pei * Institute of Orthopaedics & Traumatology, Xijing Hospital, The Fourth Military Medical University, Xi’an, 710032, People’s Republic of China article info Article history: Received 16 October 2009 Accepted 9 January 2010 Available online 8 February 2010 Keywords: Platelet-rich plasma Tricalcium phosphate Chitosan Bone regeneration abstract Injectable scaffolds held great promise for the reconstruction of bone defects. We prepared an injectable composite named PTC by combining TCP/chitosan (TC) with platelet-rich plasma (PRP). The objective of this study was to investigate the composite’s mechanical and biological properties. First, we found that the introduction of PRP in TC showed no adverse effect on mechanical strength and that there were no significant differences in compressive strength between PTC and TC (P > 0.05). In cell culture experi- ments, both cell count and alkaline phosphatase (ALP) activity measurements of PTC were higher than those of TC. The high levels of Cbfa1 and TGF-b were detected early in PTC-induced MSCs by reverse transcriptase polymerase chain reaction. Bone formation following expression of collagen type I, osteocalcin, osteonectin and calcium nodules was also observed in PRP-induced MSCs. Finally, this composite was injected into the tibial bone defect in a goat model, and its ability to induce bone regeneration was observed. Sixteen weeks after the implantation of this composite, the tibial defects had completely recuperated, with significantly better formation of mature bone and less residual material than in the control. These results demonstrate that our composite, with its concomitant mechanical strength, biocompatibility, and osteoinductive properties, has significant potential as an injectable material for the treatment of bone defects. Ó 2010 Elsevier Ltd. All rights reserved. 1. Introduction Current progress in tissue engineering research has revealed tremendous potential and new perspectives for the treatment of bone defects. Reintroduction of in vitro expanded cells, such as osteoblasts, bone marrow stromal cells or mesenchymal stem cells, in a state that guarantees their differentiation into functional bone matrix-producing cells, is now widely considered a potential alternative to autogenous bone grafting with a most promising future [1]. To support the growth and osteogenic differentiation of these cells, a suitable scaffold is necessary. At present, two different types of scaffolds are used in tissue engineering for the growth and adhesion of cells, namely, scaffolds made from solid, prefabricated materials and scaffolds made from materials that are injectable and hardened in situ [2]. Solid and prefabricated materials were first introduced as potential scaffolds for the repair of segmental bone defects and yielded many satisfactory results in animal experiments [3,4]. However, with the increasing application of solid material in clin- ical practice, surgeons find that bone defects are diverse in shape and that solid material can seldom mold to the cavity completely. Moreover, it is hard to make materials fit a bone defect on the operating table when they have been prefabricated [2,5]. In order to fill the cavity, small granules of solid material have to be prepared and used, which makes internal fixation more difficult, especially in cases with massive defects. Injectable scaffolds hold great promise for the reconstruction of bone defects because they offer some advantages over solid materials for certain indications. First, injectable materials can take the shape of the cavity into which they are placed and can thus fill irregular defects. Second, problems with cell adhesion and growth factor delivery are overcome because, under the proper conditions, the materials can be easily incorporated into the solution by mixing prior to the injection [6,7]. Thirdly, the application of injectable materials could shorten the surgical operation time, minimize the damaging effects of large muscle retraction, reduce the size of the scars and lessen postoperative pain, allowing patients to achieve rapid recovery in a cost-effective manner. Recently, with the increasing popularity of minimally invasive techniques, injectable scaffolds have been greatly encouraged [8,9]. * Corresponding author. Tel.: þ86 2984775289. E-mail address: [email protected] (G. Pei). 1 These authors contributed equally to this work. Contents lists available at ScienceDirect Biomaterials journal homepage: www.elsevier.com/locate/biomaterials 0142-9612/$ – see front matter Ó 2010 Elsevier Ltd. All rights reserved. doi:10.1016/j.biomaterials.2010.01.038 Biomaterials 31 (2010) 3201–3211

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

lable at ScienceDirect
Biomaterials 31 (2010) 3201–3211
Contents lists avai
Biomaterials
journal homepage: www.elsevier .com/locate/biomateria ls
Reconstruction of goat tibial defects using an injectable tricalcium phosphate/chitosan in combination with autologous platelet-rich plasma
Long Bi 1, Wenjun Cheng 1, Hongbin Fan 1, Guoxian Pei*
Institute of Orthopaedics & Traumatology, Xijing Hospital, The Fourth Military Medical University, Xi’an, 710032, People’s Republic of China
a r t i c l e i n f o
Article history:Received 16 October 2009Accepted 9 January 2010Available online 8 February 2010
Keywords:Platelet-rich plasmaTricalcium phosphateChitosanBone regeneration
* Corresponding author. Tel.: þ86 2984775289.E-mail address: [email protected] (G. Pei).
1 These authors contributed equally to this work.
0142-9612/$ – see front matter � 2010 Elsevier Ltd. Adoi:10.1016/j.biomaterials.2010.01.038
a b s t r a c t
Injectable scaffolds held great promise for the reconstruction of bone defects. We prepared an injectablecomposite named PTC by combining TCP/chitosan (TC) with platelet-rich plasma (PRP). The objective ofthis study was to investigate the composite’s mechanical and biological properties. First, we found thatthe introduction of PRP in TC showed no adverse effect on mechanical strength and that there were nosignificant differences in compressive strength between PTC and TC (P> 0.05). In cell culture experi-ments, both cell count and alkaline phosphatase (ALP) activity measurements of PTC were higher thanthose of TC. The high levels of Cbfa1 and TGF-b were detected early in PTC-induced MSCs by reversetranscriptase polymerase chain reaction. Bone formation following expression of collagen type I,osteocalcin, osteonectin and calcium nodules was also observed in PRP-induced MSCs. Finally, thiscomposite was injected into the tibial bone defect in a goat model, and its ability to induce boneregeneration was observed. Sixteen weeks after the implantation of this composite, the tibial defects hadcompletely recuperated, with significantly better formation of mature bone and less residual materialthan in the control. These results demonstrate that our composite, with its concomitant mechanicalstrength, biocompatibility, and osteoinductive properties, has significant potential as an injectablematerial for the treatment of bone defects.
� 2010 Elsevier Ltd. All rights reserved.
1. Introduction
Current progress in tissue engineering research has revealedtremendous potential and new perspectives for the treatment ofbone defects. Reintroduction of in vitro expanded cells, such asosteoblasts, bone marrow stromal cells or mesenchymal stem cells,in a state that guarantees their differentiation into functional bonematrix-producing cells, is now widely considered a potentialalternative to autogenous bone grafting with a most promisingfuture [1].
To support the growth and osteogenic differentiation of thesecells, a suitable scaffold is necessary. At present, two different typesof scaffolds are used in tissue engineering for the growth andadhesion of cells, namely, scaffolds made from solid, prefabricatedmaterials and scaffolds made from materials that are injectable andhardened in situ [2].
Solid and prefabricated materials were first introduced aspotential scaffolds for the repair of segmental bone defects and
ll rights reserved.
yielded many satisfactory results in animal experiments [3,4].However, with the increasing application of solid material in clin-ical practice, surgeons find that bone defects are diverse in shapeand that solid material can seldom mold to the cavity completely.Moreover, it is hard to make materials fit a bone defect on theoperating table when they have been prefabricated [2,5]. In order tofill the cavity, small granules of solid material have to be preparedand used, which makes internal fixation more difficult, especially incases with massive defects.
Injectable scaffolds hold great promise for the reconstruction ofbone defects because they offer some advantages over solidmaterials for certain indications. First, injectable materials can takethe shape of the cavity into which they are placed and can thus fillirregular defects. Second, problems with cell adhesion and growthfactor delivery are overcome because, under the proper conditions,the materials can be easily incorporated into the solution by mixingprior to the injection [6,7]. Thirdly, the application of injectablematerials could shorten the surgical operation time, minimize thedamaging effects of large muscle retraction, reduce the size of thescars and lessen postoperative pain, allowing patients to achieverapid recovery in a cost-effective manner. Recently, with theincreasing popularity of minimally invasive techniques, injectablescaffolds have been greatly encouraged [8,9].

L. Bi et al. / Biomaterials 31 (2010) 3201–32113202
Candidates for injectable materials include natural polymers,synthetic polymers and inorganic materials [2]. Due to their simi-larity to human bone, inorganic powders such as hydroxyapatite(HA) and tricalcium phosphate (TCP) are popular applicationmaterials. However, the key disadvantage of these biomaterials isbrittleness, which renders mechanical support and cell ingrowthdifficult [10]. In order to improve their properties, other injectablematerials like chitosan, gelatin and collagen are introduced intothese inorganic materials [9,11]. Chitosan, a copolymer of N-ace-tylglucosamine and glucosamine, is well known for its interestingbiological properties, such as biocompatibility and bioresorbability[12–14]. Therefore, the composite made of TCP and chitosan (i.e.,TCP/chitosan) has been prepared for bone tissue regenerationpurposes [12,15,16].
To improve the osteogenic potential of scaffolds such as TCP,chitosan or TCP/chitosan, growth factors (GFs) are usually intro-duced. GFs can influence the chemotaxis, differentiation, prolifer-ation and synthetic activity of bone cells, thereby regulatingphysiological bone reconstruction and remodeling [17]. NumerousGFs, such as bone morphogenetic proteins (BMPs), platelet-derivedgrowth factor (PDGF), transforming growth factor-b (TGF-b), andinsulin-like growth factors (IGFs), have a stimulating effect on bonedefect healing [17,18]. It is expected that the biological effect ofmultiple GFs on the enhancement of tissue regeneration and repairis greater than that of a single GF. Platelet-rich plasma (PRP)contains a number of these growth factors [PDGF, TGF-b, IGF, basicfibroblast growth factor (bFGF) and vascular endothelial growthfactor (VEGF)] in its natural composition and has relevance inclinical tissue engineering applications [19]. Because it can be usedautogenously, it poses no risk of transmissible diseases. Further-more, PRP can easily be obtained on the day of surgery fromautogenous whole blood, by two centrifugation steps [20,21].
In this study, we prepared an injectable composite by combiningTCP/chitosan (TC) with PRP. We hypothesized that the introductionof PRP will improve the osteogenic potential of TC withoutdamaging its mechanical strength. In order to test this hypothesis,PRP derived from goats was used to modify TC, and the mechanicalstrength was detected. Subsequently, goat marrow stromal cellswere cultured with this PRP-modified TCP/chitosan (PTC)composite, and their proliferation and differentiation were evalu-ated by cell count, scanning electron micrograph (SEM) observa-tion, alkaline phosphatase (ALP) activity measurement, calciumnodule staining and reverse transcriptase polymerase chain reac-tion (RT-PCR). Finally, we specifically evaluated the osteogenicability of PTC by injecting this composite into a cavity defect in goattibia, using histological and radiological methods.
2. Materials and methods
2.1. Preparation of platelet-rich plasma (PRP)
Blood samples were obtained from five healthy Chinese yellow goats (all theanimal experiments were conducted according to the Chinese regulations of AnimalWelfare and permission granted by the Ethical committee of the Fourth MilitaryMedical University). PRP was prepared using two centrifugation techniques, aspreviously reported [22]. Briefly, goats were anaesthetized, and 20 ml of wholeblood was drawn from each subject into tubes containing 4 ml of acid citratedextrose (the solution served as an anticoagulant). An aliquot was removed fromeach tube to determine the platelet count by an automated hematology analyzer(Nikon, Japan). The tubes were then spun in a laboratory centrifugation apparatus(Beckman Avanti J25, German) at 4 �C for 15 min at 800 rpm, and all plasma wastransferred to new tubes to be further centrifuged at 4 �C for 15 min at 2000 rpm.The supernatant plasma was discarded, and the approximately 1.2 ml of remainingplasma and precipitated platelets was designated PRP. Platelet counts were alsoperformed for samples of PRP. All the procedures were performed under sterileconditions. The levels of growth factors secreted from PRP and whole blood weremeasured with commercial enzyme-linked immunosorbent assay (ELISA) kit(Cusabio Biotech Co. Ltd., China), according to the manufacturer’s instructions.
2.2. Preparation of PRP-modified TCP/chitosan composite
The chitosan used in this study was a solution of chitosan containing citric acidand glucose (chitosan powder from Bio Life Science & Technology Co. Ltd., China).The degree of deacetylation was 94%, quantified with ninhydrin as describedpreviously [23]. The molecular weight was 680,000 Da. The three components weremixed at a weight ratio of 2:25:20 (chitosan/citric acid/glucose) and dissolved indistilled water. The final mass fraction of chitosan was 2% in the solution. The meanparticle size of b-tricalcium phosphate powder (TCP, from Bio-lu Bio MaterialsCompany Ltd., China) was 6.70 mm (measured by laser particle analyzer) aftermilling for 8 h.
The composite was prepared as follows. First, chitosan solution and TCP powderwere mixed at a ratio of 10:6 (ml:g) in 20 ml sterile injection syringes. Five minuteslater, 1 ml of PRP was added into the mixture. As soon as the PRP was activated bybovine thrombin and calcium chloride (at a ratio of 1 ml PRP to 100 IU bovinethrombin and 1 ml 10% calcium chloride solution), the final composite (PRP-modi-fied TCP/chitosan, PTC for short) was immediately injected into circular molds ofdifferent sizes to make cylinders and disks for mechanical testing and cell culture.Cylinders and disks of TCP/chitosan (TC) at a ratio of 10:6 (ml:g) were prepared ascontrol.
2.3. Mechanical testing
Cylinders of 10-mm diameter and 20-mm height (n¼ 5) were used formechanical testing. Mechanical testing was performed after the specimens wereprepared and left at room temperature for 1, 3 and 7 days. The mechanical propertiesof the specimens were analyzed in a materials testing machine (MTS-858, MTSSystem Inc, USA) by compression in the axial direction at a deformation rate of10 mm/min until failure. The compressive strength was calculated by S¼ Fmax/A,where Fmax is the maximum load on the load-deformation curve and A is the cross-sectional area of each specimen.
2.4. Preparation of goat marrow stroma cells (MSCs)
Marrow-derived MSCs were isolated from the same goat as used for PRPisolation. MSCs were cultured using the method described by Liu et al. [9]. Wecollected 2 ml bone marrow aspirates from the ileum of each goat. Nucleated cellswere isolated with a density gradient and resuspended in Dulbecco’s modifiedEagle’s medium (DMEM, Hyclone, USA) containing 10% fetal calf serum (Hyclone,USA) and 1% penicillin/streptomycin. The cells were plated in 25 cm2 culture flasksand incubated in a humidified atmosphere of 95% air and 5% CO2 at 37 �C. Non-adherent cells were discarded after 2 days, and adherent cells were cultured forfurther expansion. When cultured cells became near-confluent, cells were detachedby 0.25 wt% trypsinization (Type XI; Sigma Chemical, USA) in 0.1 M PBS and reseededonto new plates at 1/3 density for continued passage. The medium was changedevery 2 or 3 days.
Third-passage cell subcultures were used in the following experiments. Uponreaching 90% confluence, cells adhering to the flasks were detached. For scanningelectron microscope (SEM) observation, 5�104 cells were added to each well ofa 24-well plate. Each well contained a disk (10-mm diameter and 2-mm thickness)of either PTC or TC. For the evaluation of osteogenic differentiation, disks of both PTCand TC were placed into the wells of a 6-well plate containing 8 ml of medium(DMEM supplemented with 10% FBS). Cells cultured in an osteogenic medium (OM,consisting of DMEM supplemented with 10% FBS, 10�8
M DEX, 10�3M b-glycerol
phosphate, and 50 mg/ml L-ascorbic acid) were used as positive controls. Cellscultured without disks and OM were used as blank controls.
2.5. SEM observation
After being cultured for 3 days and 6 days, five disks from each group wereremoved from the plates and gently washed with PBS. The cells on the disks werefixed with 3% glutaraldehyde in PBS for 24 h at 4 �C. After being thoroughly washedwith PBS, the specimens were dehydrated in a graded series of alcohol (30–100%).After the disks were dehydrated twice in each ethanol concentration (15 min eachtime), they were freeze dried, sputter-coated with gold, and examined under SEM(S-3000N, Hitachi, Japan).
2.6. MSC proliferation assay
The number of MSCs on the disks was determined at 1, 7 and 14 days. Briefly, atthese predetermined times, five disks from each group were gently washed with PBSto remove unattached cells. The adherent cells were removed from the disks byincubation for 5 min in 2 ml trypsin. Then, the suspension was collected andcentrifuged at 100 rpm for 10 min. The sediment cells were resuspended in freshmedium. Fifty microliters of this cell suspension was combined with an equalamount of 0.4% (wt./vol.) trypan blue (Sigma, USA) and counted by a hemocytometerunder phase-contrast light microscopy.

Table 2Growth factor concentrations in PRP and circulating plasma (n¼ 5, mean� s).
PDGF-BB(ng/ml)
TGF-b1(ng/ml)
bFGF(pg/ml)
VEFG(pg/ml)
Circulatingplasma
5.52� 0.32 18.06� 2.26 23.46� 2.60 31.72� 5.92
PRP 25.74� 3.32* 128.88� 13.03* 81.15� 5.01* 161.53� 17.06*
*P< 0.05.
L. Bi et al. / Biomaterials 31 (2010) 3201–3211 3203
2.7. Alkaline phosphatase (ALP) activity
ALP activity was determined at 7 and 14 days of culturing as described inRef. [11]. Briefly, after the medium was removed, five disks from each group weretransferred to a new well plate. Then, 0.5 ml of Triton X-100 was added to each well.A cell scraper was used to remove MSCs from each disk. After the cells were washedby PBS they were used for ALP activity determination. The samples were thenprocessed through two freeze–thaw cycles (�80 �C and room temperature, 45 mineach) to rupture the cell membranes and extract the proteins and DNA from thecells. A p-nitrophenyl phosphate (pNPP) liquid substrate system (Nanjing Jiancheng,China) was used to analyze the ALP concentration of the cells on each disk. Fivemilliliters of each cell lysate solution was added to 195 ml of pNPP substrate andincubated in the dark at room temperature for 1 min. The absorbance was read usinga plate reader (Molecular Devices, USA) at 405 nm and normalized to the PicoGreenassay [23]. DNA was quantified using the PicoGreen Kit (Invitrogen, USA) followingstandard protocols. Briefly, 100 ml of each cell lysate solution was added to 100 ml ofPicoGreen reagent and incubated in the dark at room temperature for 5 min. Theabsorbance was read at an excitation/emission of 480–520 nm on the plate reader.
2.8. Calcium nodule staining
The mineralization of matrix was determined by alizarin red staining on the19th day. Cells cultured in PTC or TC dissolution products were fixed in 70% ethanoland stained with 1% alizarin red for 2 min. Cells were then washed with distilledwater and viewed under the light microscope. To determine the extent of miner-alization of cells cultured directly on the disks, nodules were trypsinized from thesurface and then fixed and stained as above. This was done because calcium ispresent in the material, making it difficult to visualize true positive staining [24].
2.9. Reverse transcriptase-PCR (RT-PCR)
Osteoblasts differentiated from MSCs were isolated using TRIzol reagent (Invi-trogen, USA) to obtain total RNA. Then, 1 mg of total RNA was reversibly transcribedto cDNA using 25 mM Tris–HCl (pH 8.3), 5 mM MgCl2, 50 mM KCl, 2 mM DTT, 1 mM
dNTP each, 40 mg/ml primer dT15 and 200 U/ml AMV reverse transcriptase in a finalvolume of 25 ml. Then the suspension was incubated for 40 min at 42 �C. Reversetranscription was terminated by heating at 95 �C for 5 min; 5% cDNA was used as thetemplate for PCR. These reactions were performed in 10 mM Tris–HCl (pH 8.3),1.5 mM MgCl2, 50 mM KCl, 0.2 mM each dNTP, 0.5 mM each primer, and 1.25 U of Taqpolymerase in final reaction volume of 50 ml. The primer details are summarized inTable 1. The PCR reaction was performed at 94 �C for 45 s, 60 �C for 45 s, and 72 �Cfor 1 min, for 30 cycles. The PCR products were analyzed on 1% agarose gel andstained by ethidium bromide.
2.10. Osseous defects repaired by different materials in goat models
Twenty-seven Chinese yellow goats, male, 10–12 months old with a meanweight of 40 kg (38–42 kg) were used. Food and water was withdrawn 12 h beforeinduction of anesthesia. Medetomidine (5 mg/kg intramuscularly) served as pre-medication before induction of anesthesia with atropine (0.5 mg/kg) and ketamine(2 mg/kg). Anesthesia was maintained by intravenous ketamine drip. As peri- andpostoperative infection prophylaxis, penicillin and gentamycin were administered at12 h intervals for 3 days. Animals were placed in lateral recumbency and wereoperated on alternately on the left or right posterior limb. A cavity-like (volumetric)defect of 12 mm in diameter was made perpendicularly to the bone axis into themedial plateaus of bilateral tibia from each goat. The drill cavities were carefullywashed to eliminate bone debris and dried before they were filled with differentmaterials. All the goats were divided in three groups: PTC, TC and blank control (thedefects were left empty without any filling material). Closure of fasciae, subcuta-neous tissue and skin was routinely done using resorbable sutures. A splint bandagewas used to protect the operated limbs for up to 3 weeks with weekly bandagechanges.
After surgery, the animals were placed in a suspension device for supervisedrecovery. Animals were held in this manner for up to 4 weeks to avoid spontaneousfractures. Three animals from each group were sacrificed after observation periodsof 4, 8 and 16 weeks. The mediolateral radiographs were compared with the
Table 1Description of the primers.
Gene Sense primer
Cbfa1 GATGACACTGCCACCTCTGAOsteocalcin ATGAGAGCCCTCACACTCCTCCollagen type I GATGGATTCCAGTTCGAGTATGOsteonectin AGTAGGGCCTGGATCTTCTTTGF-b1 CGCGTGCTAATGGTGGAAAGAPDH GTCAGTGGTGGACCTGACCT
postoperative radiographs and used to assess new bone formation. At the pre-determined period, the defects were macroscopically evaluated for new boneformation and signs of inflammation. Then a band saw was used to prepare the bonesamples, and the defects with an additional 2 mm of surrounding tissue weredissected from the host bone. All the harvested samples were fixed in a 4% para-formaldehyde solution buffered by 0.1 M phosphate (pH 7.2) for 3–5 days. Theharvested samples were dehydrated in graded series of alcohol (8–100%) andembedded in polymethyl methacrylate (PMMA) without decalcification. Thinsections of 200 mm thickness were cut using a microtome (SP1600, Leica, Germany).Then, the sections were polished to a thickness of about 40–50 mm using a specialgrinding machine (EXAKT Micro-Grinding System, Germany). Five sections of thecentral part in each sample were used for histomorphometric analysis. The Van-Gieson stained sections were examined under light microscopy (DMLA, Leica). Thearea of the newly formed bone (NB) and the residual material (RM) were quanti-tatively evaluated using the Image tool V3.0 software (Uthscsa, USA). The NB (%) andRM (%) were calculated as reference [25].
2.11. Statistical analysis
Statistical analyses were performed using SPSS software, version 12.0 (SPSS Inc,USA). The data were presented as the mean� SD, and levels were compared by thenon-parametric Mann–Whitney U test or Student’s t-test. P values less than 0.05were considered significant.
3. Results
3.1. Platelet counts and growth factor levels
Platelet counts of the whole blood from goat yielded a meanvalue of 226.6�17.1�103/ml, ranging from 212 to 256�103/ml. Themean platelet count for PRP was 1205�118� 103/ml, ranging from1074 to 1324�103/ml. These values confirmed the presence ofa sufficient concentration of platelets during the PRP preparationprocess. The platelet counts of PRP in all samples were almost morethan fivefold of baseline blood platelet counts [mean:531.9� 36.3%; range: 495–573%]. Analysis of growth factorconcentrations in PRP samples and circulating plasma samplesusing ELISA revealed that levels of growth factors were significantlyhigher in PRP samples (Table 2).
3.2. Mechanical testing
The compressive strength of PTC or TC increased from 1 to 7days, and there were no significant differences in terms ofcompressive strength between the two materials (P> 0.05) (Fig. 1).
3.3. SEM observation
Both TC and PTC exhibited three-dimensional structures thatcontained plentiful granules. On the surface of TC, the granules
Antisense primer PCR Product (bp)
GACTGGCGGGGTGTAAGTAA 171CGTAGAAGCGCCGATAGGC 291GTTTGGGTTGCTTGTCTGTTTG 479CTGCTTCTCAGTCAGAAGGT 575CAGCCGGTTGCTGAGGTATC 231AGGGGAGATTCAGTGTGGTG 391
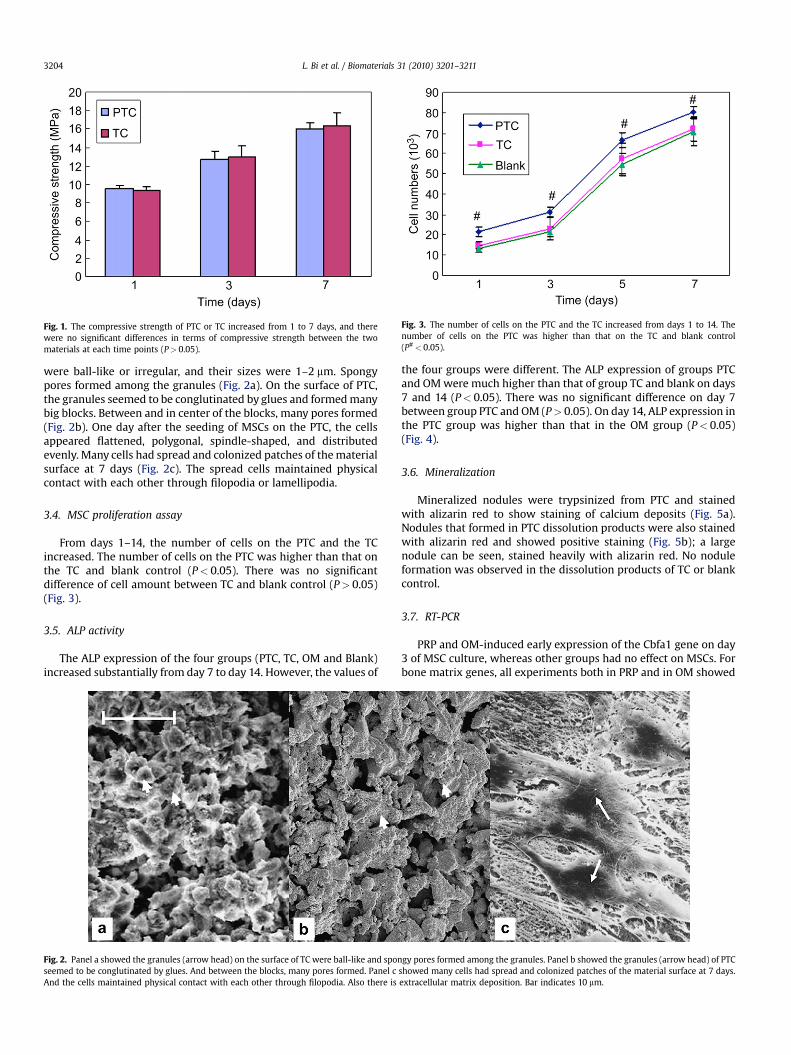
Fig. 1. The compressive strength of PTC or TC increased from 1 to 7 days, and therewere no significant differences in terms of compressive strength between the twomaterials at each time points (P> 0.05).
Fig. 3. The number of cells on the PTC and the TC increased from days 1 to 14. Thenumber of cells on the PTC was higher than that on the TC and blank control(P#< 0.05).
L. Bi et al. / Biomaterials 31 (2010) 3201–32113204
were ball-like or irregular, and their sizes were 1–2 mm. Spongypores formed among the granules (Fig. 2a). On the surface of PTC,the granules seemed to be conglutinated by glues and formed manybig blocks. Between and in center of the blocks, many pores formed(Fig. 2b). One day after the seeding of MSCs on the PTC, the cellsappeared flattened, polygonal, spindle-shaped, and distributedevenly. Many cells had spread and colonized patches of the materialsurface at 7 days (Fig. 2c). The spread cells maintained physicalcontact with each other through filopodia or lamellipodia.
3.4. MSC proliferation assay
From days 1–14, the number of cells on the PTC and the TCincreased. The number of cells on the PTC was higher than that onthe TC and blank control (P< 0.05). There was no significantdifference of cell amount between TC and blank control (P> 0.05)(Fig. 3).
3.5. ALP activity
The ALP expression of the four groups (PTC, TC, OM and Blank)increased substantially from day 7 to day 14. However, the values of
Fig. 2. Panel a showed the granules (arrow head) on the surface of TC were ball-like and sponseemed to be conglutinated by glues. And between the blocks, many pores formed. Panel cAnd the cells maintained physical contact with each other through filopodia. Also there is
the four groups were different. The ALP expression of groups PTCand OM were much higher than that of group TC and blank on days7 and 14 (P< 0.05). There was no significant difference on day 7between group PTC and OM (P> 0.05). On day 14, ALP expression inthe PTC group was higher than that in the OM group (P< 0.05)(Fig. 4).
3.6. Mineralization
Mineralized nodules were trypsinized from PTC and stainedwith alizarin red to show staining of calcium deposits (Fig. 5a).Nodules that formed in PTC dissolution products were also stainedwith alizarin red and showed positive staining (Fig. 5b); a largenodule can be seen, stained heavily with alizarin red. No noduleformation was observed in the dissolution products of TC or blankcontrol.
3.7. RT-PCR
PRP and OM-induced early expression of the Cbfa1 gene on day3 of MSC culture, whereas other groups had no effect on MSCs. Forbone matrix genes, all experiments both in PRP and in OM showed
gy pores formed among the granules. Panel b showed the granules (arrow head) of PTCshowed many cells had spread and colonized patches of the material surface at 7 days.extracellular matrix deposition. Bar indicates 10 mm.
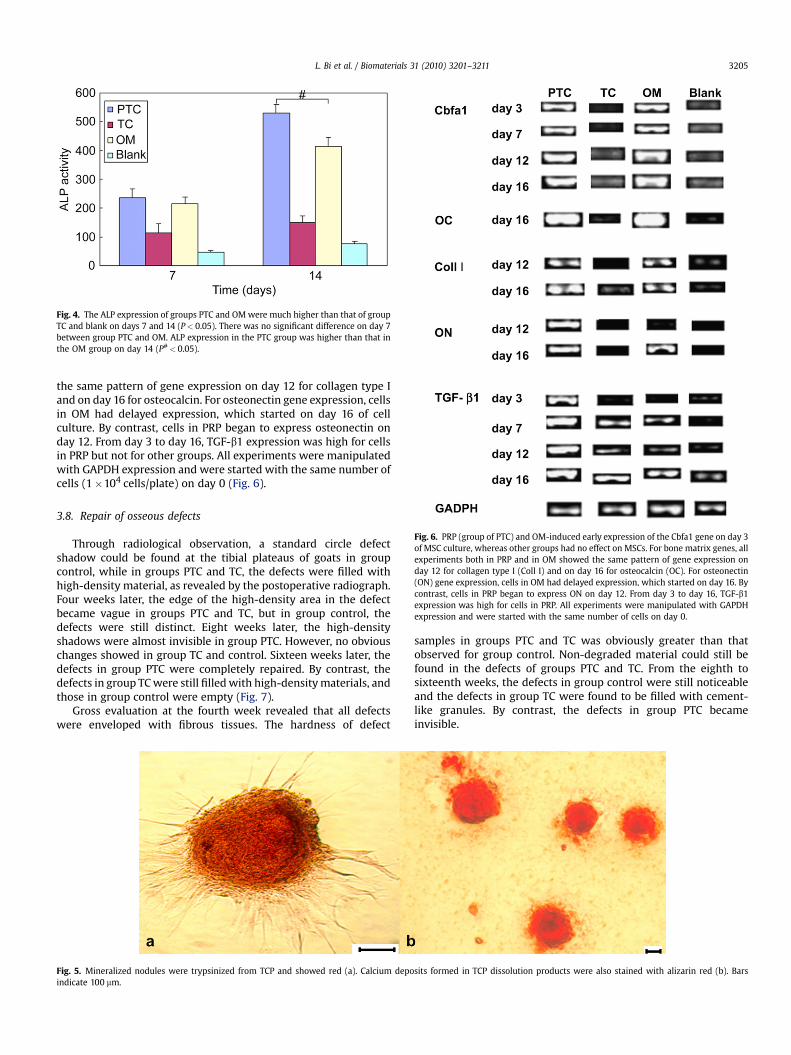
Fig. 4. The ALP expression of groups PTC and OM were much higher than that of groupTC and blank on days 7 and 14 (P< 0.05). There was no significant difference on day 7between group PTC and OM. ALP expression in the PTC group was higher than that inthe OM group on day 14 (P#< 0.05).
Fig. 6. PRP (group of PTC) and OM-induced early expression of the Cbfa1 gene on day 3of MSC culture, whereas other groups had no effect on MSCs. For bone matrix genes, allexperiments both in PRP and in OM showed the same pattern of gene expression onday 12 for collagen type I (Coll I) and on day 16 for osteocalcin (OC). For osteonectin(ON) gene expression, cells in OM had delayed expression, which started on day 16. Bycontrast, cells in PRP began to express ON on day 12. From day 3 to day 16, TGF-b1expression was high for cells in PRP. All experiments were manipulated with GAPDHexpression and were started with the same number of cells on day 0.
L. Bi et al. / Biomaterials 31 (2010) 3201–3211 3205
the same pattern of gene expression on day 12 for collagen type Iand on day 16 for osteocalcin. For osteonectin gene expression, cellsin OM had delayed expression, which started on day 16 of cellculture. By contrast, cells in PRP began to express osteonectin onday 12. From day 3 to day 16, TGF-b1 expression was high for cellsin PRP but not for other groups. All experiments were manipulatedwith GAPDH expression and were started with the same number ofcells (1�104 cells/plate) on day 0 (Fig. 6).
3.8. Repair of osseous defects
Through radiological observation, a standard circle defectshadow could be found at the tibial plateaus of goats in groupcontrol, while in groups PTC and TC, the defects were filled withhigh-density material, as revealed by the postoperative radiograph.Four weeks later, the edge of the high-density area in the defectbecame vague in groups PTC and TC, but in group control, thedefects were still distinct. Eight weeks later, the high-densityshadows were almost invisible in group PTC. However, no obviouschanges showed in group TC and control. Sixteen weeks later, thedefects in group PTC were completely repaired. By contrast, thedefects in group TC were still filled with high-density materials, andthose in group control were empty (Fig. 7).
Gross evaluation at the fourth week revealed that all defectswere enveloped with fibrous tissues. The hardness of defect
Fig. 5. Mineralized nodules were trypsinized from TCP and showed red (a). Calcium depoindicate 100 mm.
samples in groups PTC and TC was obviously greater than thatobserved for group control. Non-degraded material could still befound in the defects of groups PTC and TC. From the eighth tosixteenth weeks, the defects in group control were still noticeableand the defects in group TC were found to be filled with cement-like granules. By contrast, the defects in group PTC becameinvisible.
sits formed in TCP dissolution products were also stained with alizarin red (b). Bars
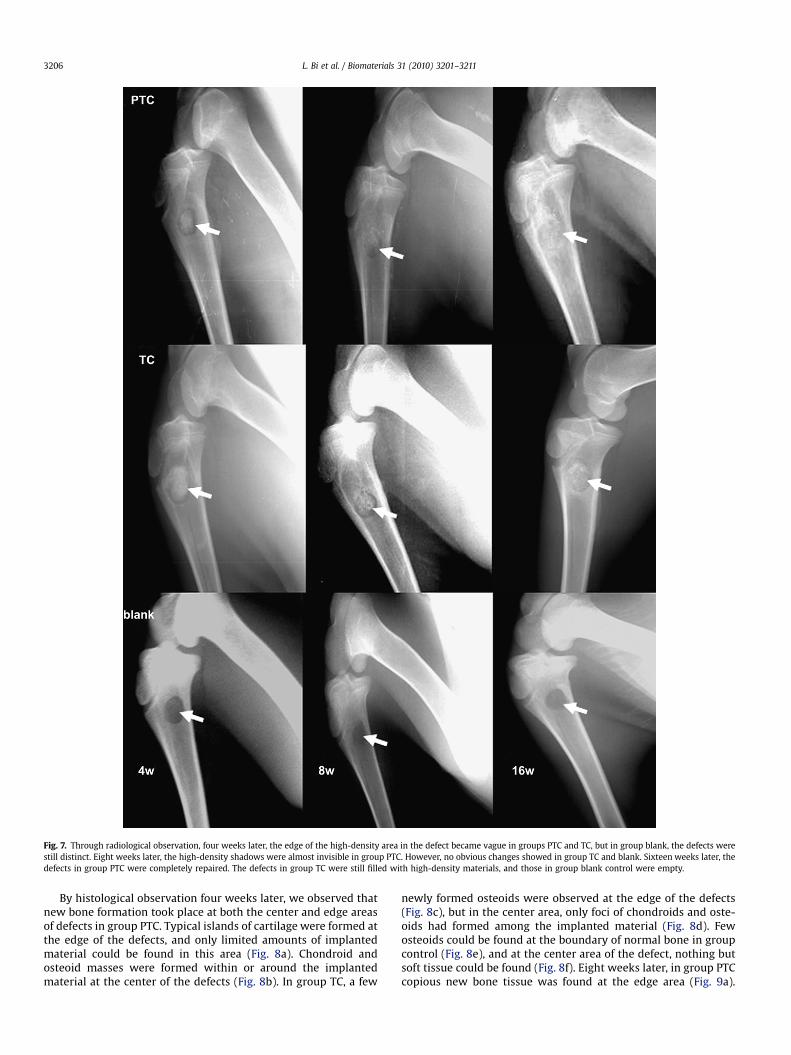
Fig. 7. Through radiological observation, four weeks later, the edge of the high-density area in the defect became vague in groups PTC and TC, but in group blank, the defects werestill distinct. Eight weeks later, the high-density shadows were almost invisible in group PTC. However, no obvious changes showed in group TC and blank. Sixteen weeks later, thedefects in group PTC were completely repaired. The defects in group TC were still filled with high-density materials, and those in group blank control were empty.
L. Bi et al. / Biomaterials 31 (2010) 3201–32113206
By histological observation four weeks later, we observed thatnew bone formation took place at both the center and edge areasof defects in group PTC. Typical islands of cartilage were formed atthe edge of the defects, and only limited amounts of implantedmaterial could be found in this area (Fig. 8a). Chondroid andosteoid masses were formed within or around the implantedmaterial at the center of the defects (Fig. 8b). In group TC, a few
newly formed osteoids were observed at the edge of the defects(Fig. 8c), but in the center area, only foci of chondroids and oste-oids had formed among the implanted material (Fig. 8d). Fewosteoids could be found at the boundary of normal bone in groupcontrol (Fig. 8e), and at the center area of the defect, nothing butsoft tissue could be found (Fig. 8f). Eight weeks later, in group PTCcopious new bone tissue was found at the edge area (Fig. 9a).

Fig. 8. At 4 weeks, in group PTC typical islands of cartilage (arrow) were formed at the edge of the defects (a). Chondroid and osteoid masses (red indicated by arrow) were formedwithin or around the implanted material (black and purple indicated by arrow head) at the center of the defects (b). In group TC, a few newly formed osteoids were observed at theedge of the defects (c), but in the center area, only foci of chondroids and osteoids had formed among the implanted material (d). Few osteoids could be found at the boundary andcenter of normal bone in group blank control (e,f) (Van-Gieson staining, bars indicate 100 mm).
L. Bi et al. / Biomaterials 31 (2010) 3201–3211 3207
There was obvious creeping substitution in the center area withthe graft disorganized, largely resorbed and combined with theformation of new bone (Fig. 9b). In group TC, only a few new boneshad formed at the edge and center of the defects (Fig. 9c and d). Ingroup control, the center zone of the defect was still filled withsoft tissue, and the newly formed osteoids at the edge of defectsbecame raritas (Fig. 9e and f). Sixteen weeks later, plenty of wovenbone and lamellar bone were identified in most of the specimens,and the defects were completely repaired with little residualmaterial observed in group PTC (Fig. 10a and b). By contrast, ingroup TC, the defects were filled with abundant non-degradedmaterial: only limited newly formed bone tissue could be detectedat both center and edge areas (Fig. 10c and d). In group control, thesoft tissue in the center of the defects became dense and fibrotic.We observed no evidence of new bone formation at the edge ofthe defect, and the circumscription of the edge was regular (Fig. 10e and f). The NB (%) of PTC was significantly higher than that of TC(P< 0.05). On the contrary, the RM (%) of PTC was significantlylower than that of TC (P< 0.05) (Fig. 11).
4. Discussion
The concept of tissue engineering is based on three pillars: cells,scaffolds and growth factors (GFs) [26]. Genetic engineering tech-nology has led to the production and commercialization ofrecombinant human GFs such as BMP-2, and BMP-7 have alsobecome available in the U.S. and Europe for clinical application inspecific indications. However, the application of recombinant GFsfaces many difficulties: most recombinant GFs have been producedfrom Escherichia coli through in vitro refolding of inclusion bodies.The refolding procedure is complicated, the overall yield is low, andthe cost is extremely high. Because of the above drawbacks, theclinical application of recombinant GFs is limited [27]. Notably,platelets are a readily available source of autologous GFs. Platelet-rich plasma (PRP) may represent a medium containingconcentrated amounts of GFs in a form that is easy to handle inregenerative sites. Furthermore, PRP has been utilized in fracturerepair as a method for improving fusion or union rates, based on thepioneering work of Marx et al. [20]. However, results using PRP to
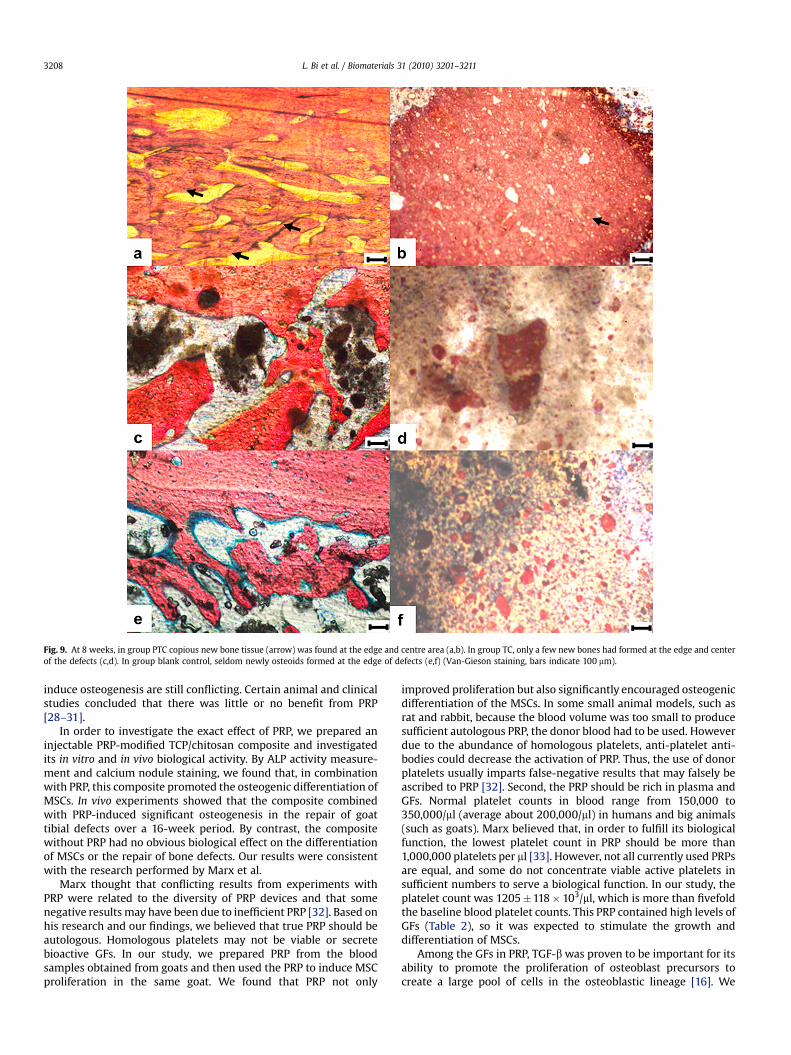
Fig. 9. At 8 weeks, in group PTC copious new bone tissue (arrow) was found at the edge and centre area (a,b). In group TC, only a few new bones had formed at the edge and centerof the defects (c,d). In group blank control, seldom newly osteoids formed at the edge of defects (e,f) (Van-Gieson staining, bars indicate 100 mm).
L. Bi et al. / Biomaterials 31 (2010) 3201–32113208
induce osteogenesis are still conflicting. Certain animal and clinicalstudies concluded that there was little or no benefit from PRP[28–31].
In order to investigate the exact effect of PRP, we prepared aninjectable PRP-modified TCP/chitosan composite and investigatedits in vitro and in vivo biological activity. By ALP activity measure-ment and calcium nodule staining, we found that, in combinationwith PRP, this composite promoted the osteogenic differentiation ofMSCs. In vivo experiments showed that the composite combinedwith PRP-induced significant osteogenesis in the repair of goattibial defects over a 16-week period. By contrast, the compositewithout PRP had no obvious biological effect on the differentiationof MSCs or the repair of bone defects. Our results were consistentwith the research performed by Marx et al.
Marx thought that conflicting results from experiments withPRP were related to the diversity of PRP devices and that somenegative results may have been due to inefficient PRP [32]. Based onhis research and our findings, we believed that true PRP should beautologous. Homologous platelets may not be viable or secretebioactive GFs. In our study, we prepared PRP from the bloodsamples obtained from goats and then used the PRP to induce MSCproliferation in the same goat. We found that PRP not only
improved proliferation but also significantly encouraged osteogenicdifferentiation of the MSCs. In some small animal models, such asrat and rabbit, because the blood volume was too small to producesufficient autologous PRP, the donor blood had to be used. Howeverdue to the abundance of homologous platelets, anti-platelet anti-bodies could decrease the activation of PRP. Thus, the use of donorplatelets usually imparts false-negative results that may falsely beascribed to PRP [32]. Second, the PRP should be rich in plasma andGFs. Normal platelet counts in blood range from 150,000 to350,000/ml (average about 200,000/ml) in humans and big animals(such as goats). Marx believed that, in order to fulfill its biologicalfunction, the lowest platelet count in PRP should be more than1,000,000 platelets per ml [33]. However, not all currently used PRPsare equal, and some do not concentrate viable active platelets insufficient numbers to serve a biological function. In our study, theplatelet count was 1205�118� 103/ml, which is more than fivefoldthe baseline blood platelet counts. This PRP contained high levels ofGFs (Table 2), so it was expected to stimulate the growth anddifferentiation of MSCs.
Among the GFs in PRP, TGF-b was proven to be important for itsability to promote the proliferation of osteoblast precursors tocreate a large pool of cells in the osteoblastic lineage [16]. We
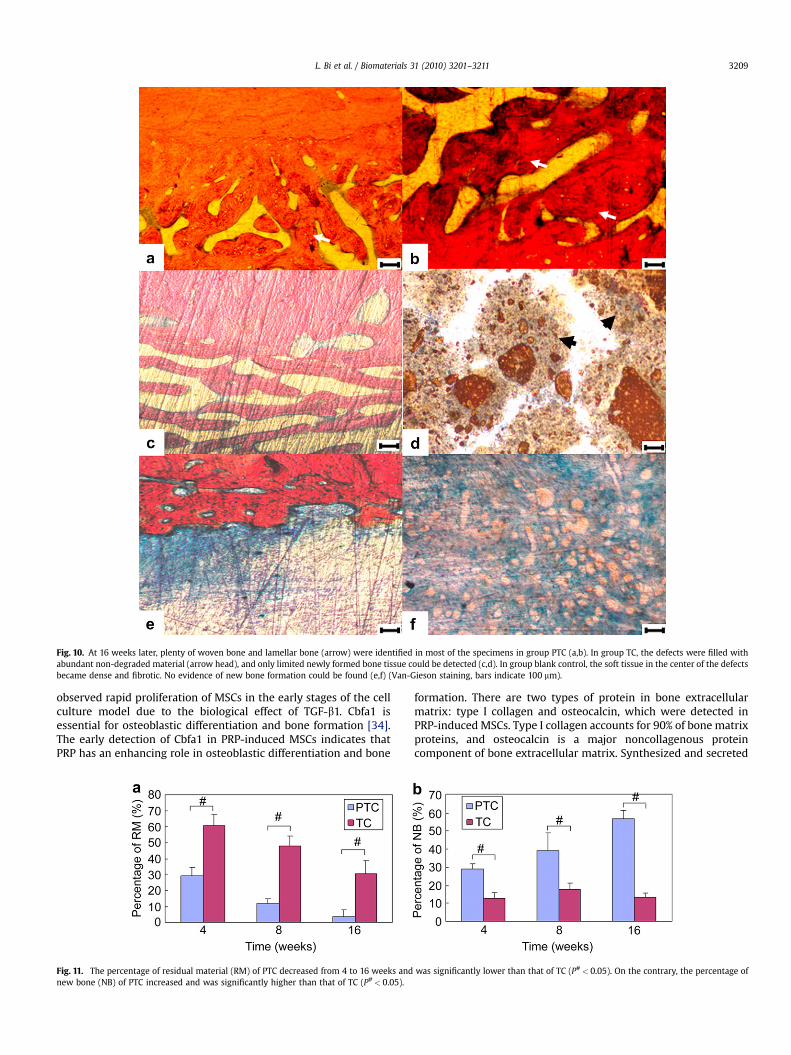
Fig. 10. At 16 weeks later, plenty of woven bone and lamellar bone (arrow) were identified in most of the specimens in group PTC (a,b). In group TC, the defects were filled withabundant non-degraded material (arrow head), and only limited newly formed bone tissue could be detected (c,d). In group blank control, the soft tissue in the center of the defectsbecame dense and fibrotic. No evidence of new bone formation could be found (e,f) (Van-Gieson staining, bars indicate 100 mm).
L. Bi et al. / Biomaterials 31 (2010) 3201–3211 3209
observed rapid proliferation of MSCs in the early stages of the cellculture model due to the biological effect of TGF-b1. Cbfa1 isessential for osteoblastic differentiation and bone formation [34].The early detection of Cbfa1 in PRP-induced MSCs indicates thatPRP has an enhancing role in osteoblastic differentiation and bone
Fig. 11. The percentage of residual material (RM) of PTC decreased from 4 to 16 weeks andnew bone (NB) of PTC increased and was significantly higher than that of TC (P#< 0.05).
formation. There are two types of protein in bone extracellularmatrix: type I collagen and osteocalcin, which were detected inPRP-induced MSCs. Type I collagen accounts for 90% of bone matrixproteins, and osteocalcin is a major noncollagenous proteincomponent of bone extracellular matrix. Synthesized and secreted
was significantly lower than that of TC (P#< 0.05). On the contrary, the percentage of

L. Bi et al. / Biomaterials 31 (2010) 3201–32113210
exclusively by osteoblasts in the late stage of maturation, osteo-calcin is considered to be an indicator of osteoblast differentiation[35]. Osteonectin is a glycoprotein abundantly expressed in boneundergoing active remodeling [36]. We found evidence of boneformation such as expression of type I collagen and osteocalcin, aswell as early expression of osteonectin in PRP-induced cells ratherthan OM-induced cells. The ability of cells to produce mineralizedmatrix and nodules is important with regard to the development ofmaterials for bone regeneration. Alizarin red is a common histo-chemical technique used to detect calcium deposits in mineralizedtissues and cultures [24]. In our study, numerous alizarin red-positive nodules were observed, demonstrating extensive osteo-genic differentiation of MSCs and indirectly supporting activationof GFs in our PRP.
The realization of optimal conditions for cell growth andattachment, GF presentation and release requires a suitabledelivery carrier [27]. In the present study, the release of GFs fromthe TCP/chitosan may be highly beneficial for enhancing MSCproliferation and differentiation. TCP is a biodegradable materialand is believed to have osteoconductivity and biocompatibility[37]. Chitosan has high viscosity in solution, and its viscosityduring the liquid phase could be greatly increased by cross-linkingit with citric acid. The moldability and in situ self-hardeningability of chitosan make it a desirable material for oral and plasticsurgery. It has been reported that calcium phosphate-containingcarboxylic acid hardens rapidly, forming an insoluble matrix bychelation. Citric acid (C6H8O7) has three carboxyl groups and onehydroxyl group that could improve the mechanical properties andbiocompatibility of TCP [9]. In order to determine whether theintroduction of PRP could influence the mechanical properties ofthe TCP/chitosan composite, we compared the compressivestrength of PRP-modified TCP/chitosan and pure TCP/chitosan.Our results showed no significant difference in compressivestrength between the two groups, which demonstrated that theintroduction of PRP did not negatively affect mechanicalproperties.
Our in vivo findings further documented that this PRP-modifiedTCP/chitosan has potential as an injectable material for theregeneration of bone defects. With the PRP combination, thecavity-like defect in goat tibia was completely repaired by thiscomposite in sixteen weeks. Moreover, this composite showedimpressive degradation properties, and our results indicate aninverse relationship between the percentage of residual material(RM) and new bone (NB) formation in the preexisting defect(Fig. 11). Importantly, this material is injectable: it can take theshape of the cavity into which it is placed and can thus fill irreg-ular defects.
5. Conclusion
The introduction of PRP into TCP/chitosan can improve thebiocompatibility and osteoinductivity of TCP/chitosan withoutcompromising its mechanical strength or injectability. With itsgood biological characteristics, such as mechanical strength,biocompatibility, and osteoinductivity, this PRP-modified TCP/chi-tosan can be used as an injectable material for the repair andregeneration of bone defects in moderate stress-bearing orthopedicapplications.
Acknowledgement
This study was supported by Chinese Ministry of Science andTechnology (973 Program No. 2009CB930003), NSF of China (GrantNo.u0732003 and No. 30901532).
Appendix
Figures with essential colour discrimination. Many of the figuresin this article have parts that are difficult to interpret in black andwhite. The full colour images can be found in the on-line version, atdoi:10.1016/j.biomaterials.2010.01.038.
References
[1] Hofmann A, Ritz U, Verrier S, Eglin D, Alini M, Fuchs S, et al. The effect ofhuman osteoblasts on proliferation and neo-vessel formation of humanumbilical vein endothelial cells in a long-term 3D co-culture on polyurethanescaffolds. Biomaterials 2008;29:4217–26.
[2] Tessmar JK, Gopferich AM. Matrices and scaffolds for protein delivery in tissueengineering. Adv Drug Deliv Rev 2007;59:274–91.
[3] Yoshikawa H, Tamai N, Murase T, Myoui A. Interconnected porous hydroxy-apatite ceramics for bone tissue engineering. J R Soc Interface 2009;6:S341–8.
[4] Liu G, Zhao L, Zhang W, Cui L, Liu W, Cao Y. Repair of goat tibial defects withbone marrow stromal cells and beta-tricalcium phosphate. J Mater Sci MaterMed 2008;19:2367–76.
[5] Khan Y, Yaszemski MJ, Mikos AG, Laurencin CT. Tissue engineering of bone:material and matrix considerations. J Bone Joint Surg Am 2008;90:S36–42.
[6] Kretlow JD, Klouda L, Mikos AG. Injectable matrices and scaffolds for drugdelivery in tissue engineering. Adv Drug Deliv Rev 2007;59:263–73.
[7] Jayabalan M, Shalumon KT, Mitha MK. Injectable biomaterials for minimallyinvasive orthopedic treatments. J Mater Sci Mater Med 2009;20:1379–87.
[8] Bensaıd W, Triffitt JT, Blanchat C, Oudina K, Sedel L, Petite H. A biodegradablefibrin scaffold for mesenchymal stem cell transplantation. Biomaterials2003;24:2497–502.
[9] Liu H, Li H, Cheng W, Yang Y, Zhu M, Zhou C. Novel injectable calcium phos-phate/chitosan composites for bone substitute materials. Acta Biomater2006;2:557–65.
[10] Petite H, Viateau V, Bensaıd W, Meunier A, de Pollak C, Bourguignon M, et al.Tissue-engineered bone regeneration. Nat Biotechnol 2000;18:959–63.
[11] Moreau JL, Xu HH. Mesenchymal stem cell proliferation and differentiation onan injectable calcium phosphate–chitosan composite scaffold. Biomaterials2009;30:2675–82.
[12] Abarrategi A, Moreno-Vicente C, Ramos V, Aranaz I, Sanz Casado JV, Lopez-Lacomba JL. Improvement of porous beta-TCP scaffolds with rhBMP-2 chi-tosan carrier film for bone tissue application. Tissue Eng Part A2008;14:1305–19.
[13] Ohara N, Hayashi Y, Yamada S, Kim SK, Matsunaga T, Yanagiguchi K, et al. Earlygene expression analyzed by cDNA microarray and RT-PCR in osteoblastscultured with water-soluble and low molecular chitooligosaccharide. Bioma-terials 2004;25:1749–54.
[14] Matsunaga T, Yanagiguchi K, Yamada S, Ohara N, Ikeda T, Hayashi Y. Chitosanmonomer promotes tissue regeneration on dental pulp wounds. J BiomedMater Res A 2006;76:711–20.
[15] Lin LC, Chang SJ, Kuo SM, Chen SF, Kuo CH. Evaluation of chitosan/beta-tri-calcium phosphate microspheres as a constituent to PMMA cement. J MaterSci Mater Med 2005;16:567–74.
[16] Lee JY, Seol YJ, Kim KH, Lee YM, Park YJ, Rhyu IC, et al. Transforming growthfactor (TGF)-beta1 releasing tricalcium phosphate/chitosan microgranules asbone substitutes. Pharm Res 2004;21:1790–6.
[17] Kasten P, Vogel J, Geiger F, Niemeyer P, Luginbuhl R, Szalay K. The effect ofplatelet-rich plasma on healing in critical-size long-bone defects. Biomaterials2008;29:3983–92.
[18] Bostrom MP, Saleh KJ, Einhorn TA. Osteoinductive growth factors in preclinicalfracture and long bone defects models. Orthop Clin North Am 1999;30:647–58.
[19] Kiuru J, Viinikka L, Myllyla G, Personen K, Perheentupa J. Cytoskeleton-dependent release of human platelet epidermal growth factor. Life Sci1991;49:1997–2003.
[20] Marx RE, Carlson ER, Eichstaedt RM, Schimmele SR, Strauss JE, Georgeff KR.Platelet rich plasma: growth factor enhancement for bone grafts. Oral SurgOral Med Oral Pathol Oral Radiol Endod 1998;85:638–46.
[21] Kawase T, Okuda K, Wolff LF, Yoshie H. Platelet-rich plasma-derived fibrin clotformation stimulates collagen synthesis in periodontal ligament and osteo-blastic cells in vitro. J Periodontol 2003;74:858–64.
[22] Ishida K, Kuroda R, Miwa M, Tabata Y, Hokugo A, Kawamoto T, et al. The regener-ative effects of platelet-rich plasma on meniscal cells in vitro and its in vivoapplication with biodegradable gelatin hydrogel. Tissue Eng 2007;13:1103–12.
[23] Laurencin CT, Ambrosio AM, Borden MD, Cooper Jr JA. Tissue engineering:orthopedic applications. Annu Rev Biomed Eng 1999;1:19–46.
[24] Gough JE, Jones JR, Hench LL. Nodule formation and mineralisation of humanprimary osteoblasts cultured on a porous bioactive glass scaffold. Biomaterials2004;25:2039–46.
[25] Ohsawa K, Neo M, Okamoto T, Tamura J, Nakamura T. In vivo absorption ofporous apatite- and wollastonite-containing glass-ceramic. J Mater Sci MaterMed 2004;15:859–64.
[26] Nair MB, Varma HK, John A. Platelet-rich plasma and fibrin glue-coatedbioactive ceramics enhance growth and differentiation of goat bone marrow-derived stem cells. Tissue Eng Part A 2009;15:1619–31.

L. Bi et al. / Biomaterials 31 (2010) 3201–3211 3211
[27] Bertoldi C, Pinti M, Zaffe D, Cossarizza A, Consolo U, Ceccherelli GB. Morphologic,histochemical, and functional analysis of platelet-rich plasma activity on skeletalcultured cells. Transfusion; 2009 [Epub ahead of print PMID: 19413738].
[28] Froum SJ, Wallace SS, Tarnow DP, Cho SC. Effect of platelet-rich plasma onbone growth and osseointegration in human maxillary sinus grafts: threebilateral case reports. Int J Periodontics Restorative Dent 2002;22:45–53.
[29] Aghaloo TL, Moy PK, Freymiller EG. Evaluation of platelet-rich plasma incombination with freeze-dried bone in the human cranium. A pilot study. ClinOral Implants Res 2005;16:250–7.
[30] Carreon LY, Glassman SD, Anekstein Y, Puno RM. Platelet gel (AGF) fails toincrease fusion rates in instrumented posterolateral fusions. Spine2005;30:E243–E246, [discussion E247].
[31] Ranly DM, Lohmann CH, Andreacchio D, Boyan BD, Schwartz Z. Platelet-richplasma inhibits demineralized bone matrix-induced bone formation in nudemice. J Bone Joint Surg Am 2007;89:139–47.
[32] Marx RE. Platelet-rich plasma: evidence to support its use. J Oral MaxillofacSurg 2004;62:489–96.
[33] Marx RE. Platelet-rich plasma (PRP): what is PRP and what is not PRP?Implant Dent 2001;10:225–8.
[34] Street J, Lenehan B. Vascular endothelial growth factor regulates osteoblastsurvival – evidence for an autocrine feedback mechanism. J Orthop Surg Res2009;4:19.
[35] Stein GS, Lian JB, Stein JL, Van Wijnen AJ, Montecino M. Transcriptionalcontrol of osteoblast growth and differentiation. Physiol Rev 1996;76:593–629.
[36] Delany AM, Canalis E. Basic fibroblast growth factor destabilizes osteonectinmRNA in osteoblasts. Am J Physiol 1998;274:C734–40.
[37] Dong J, Uemura T, Shirasaki Y, Tateishi T. Promotion of bone formation usinghighly pure porous beta-TCP combined with bone marrow-derived osteo-progenitor cells. Biomaterials 2002;23:4493–502.
Related Documents






![Science Manuscript Template · Web viewbone formation with autologous adipose stem cells and β-tricalcium phosphate granules [36]. It has been demonstrated that BMMSCs promote cartilage](https://static.cupdf.com/doc/110x72/5eaf134ba3fe5a5ff51cd9c6/science-manuscript-web-view-bone-formation-with-autologous-adipose-stem-cells-and.jpg)




