RDSC 233 Mid-term Review llowing slides highlight the information covered through the lon. erminology from the units eview questions with answers ndex of pathology from each unit echnique factors from each unit mages

RDSC 233 Mid-term Review The following slides highlight the information covered through the unit on the colon. 1. Terminology from the units 2. Review.
Dec 25, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

RDSC 233 Mid-term Review
The following slides highlight the information covered through the unit onthe colon.
1. Terminology from the units2. Review questions with answers 3. Index of pathology from each unit 4. Technique factors from each unit5. Images

Chest:nasogastric (NG) tubeendotracheal (ET) tubeSOBdyspneaangina sputumhemoptysis fibrile/afibrileaspirationchronic/acuteheart mummerhyaline membrane diseaseempyemathoracocentesispneumonectomyralesinterstitium pulmonary edemasubcutaneous emphysema
Kerely B linescardiomegaly neoplasmbenignmalignantcrepitantsitus inversustracheostomy
Abdomen: distentionflatulenceflank stripesmassarteriosclerosisfree airair fluid levelsanomalyfecal stasisperitonitisadhesionsvolvulusintussusceptionaerophagiaeructationvena cava filterpulmonary embolism
Single contrast colon: catharticpurgativeproctologyproctoscopycolonoscopySims positionguaiac testoccult bloodfamilialsepsisseptacemia
UGI: non per os (NPO)contraindicationfistulacollodial suspensionMIN/Vhematemesisretrogastric spacemotility seriesenteroclysisintubationvalsalva maneuverrefluxtrendelenburg positionasymptomaticMenkel’s diverticulum
Air contrast colon: stenosed (stenosis)adenomasessilevillouspedunculatedcarcinomacytologicdifferentiatedmetastasisenteritisinflammatory bowel diseasecolitis

Quiz Questions
Name the 9 regionsof the abdomenand pelvis
2
1 4
3
5
7
8
6 9

What can be visualized
10. Spleen 11. Gallbladder12. Adrenal glands13. Stomach 14. Veins15. kidneys16. Colon (gas)17. bladder18. Pancreas19. Ureters Liver Y N NSm. Bowel Y Y N
Y ( if needed to see) or N
Gas? Urine?

What is normally visible
10. Spleen Y N N
11. Gallbladder N N N
12. Adrenal glands N N N
13. Stomach Y Y N
14. Veins N N N
15. kidneys Y N N
16. Colon (gas) Y Y N
17. bladder Y N Y
18. Pancreas N N N
19. Ureters N N N
Y ( if needed to see) or N
Gas? Urine?
Abdomen Positioning
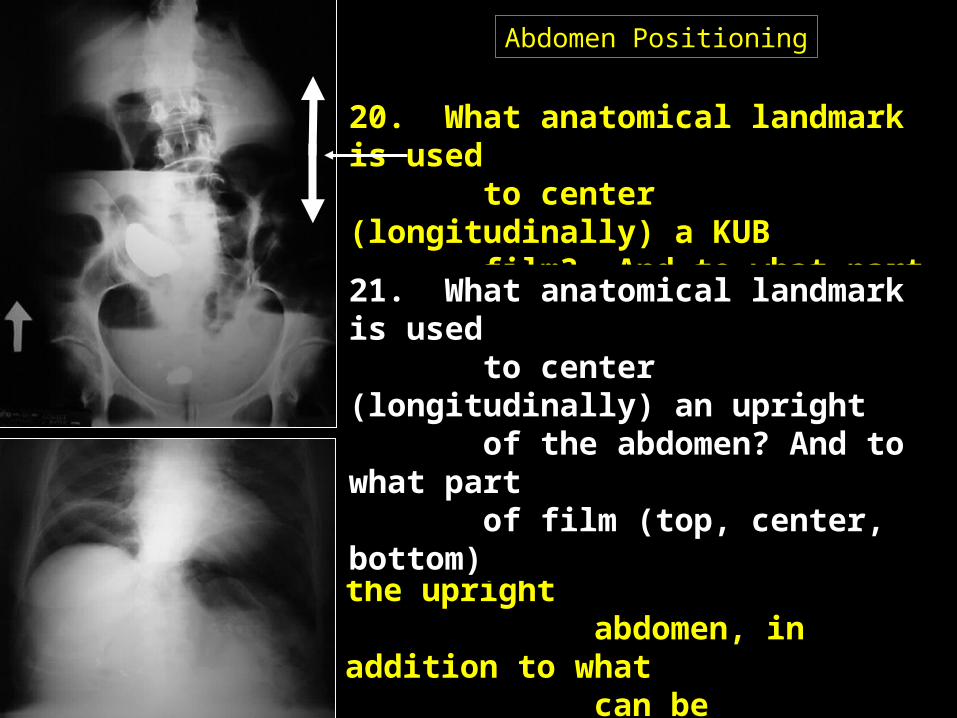
20. What anatomical landmark is used to center (longitudinally) a KUB film? And to what part of film (top, center, bottom)
22-24. What 3 conditions can be demonstrated on the upright abdomen, in addition to what can be demonstrated on the supine KUB? (Two are shown here).
21. What anatomical landmark is used to center (longitudinally) an upright of the abdomen? And to what part of film (top, center, bottom)

Abdomen Positioning
20. What anatomical landmark is used to center (longitudinally) a KUB film? And to what part of
film (top, center, bottom) Iliac Crest, center
22-24. What 3 conditions can be demonstrated on the upright abdomen, in addition to what can be demonstrated on the supine KUB? (Two are shown here).
Air fluid levelsFree air in the abdomen (pneumoperitoneum)
Ptosis
21. What anatomical landmark is used to center (longitudinally) an upright of the abdomen? And to what part of film (top, center, bottom)
Axilla, top
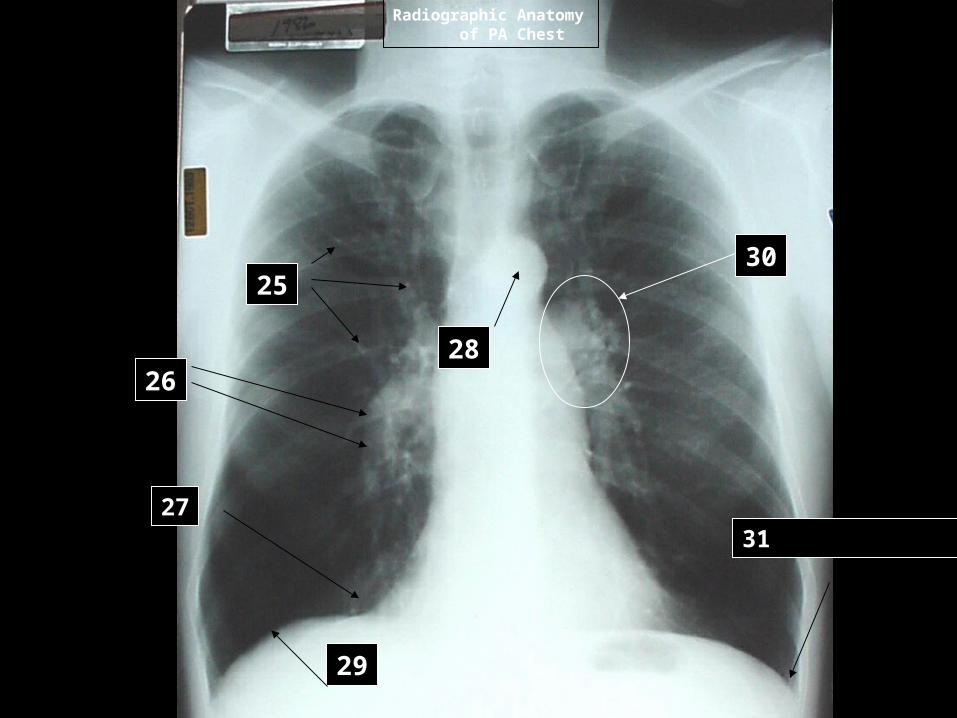
Radiographic Anatomy of PA Chest
29
3127
25
2628
30
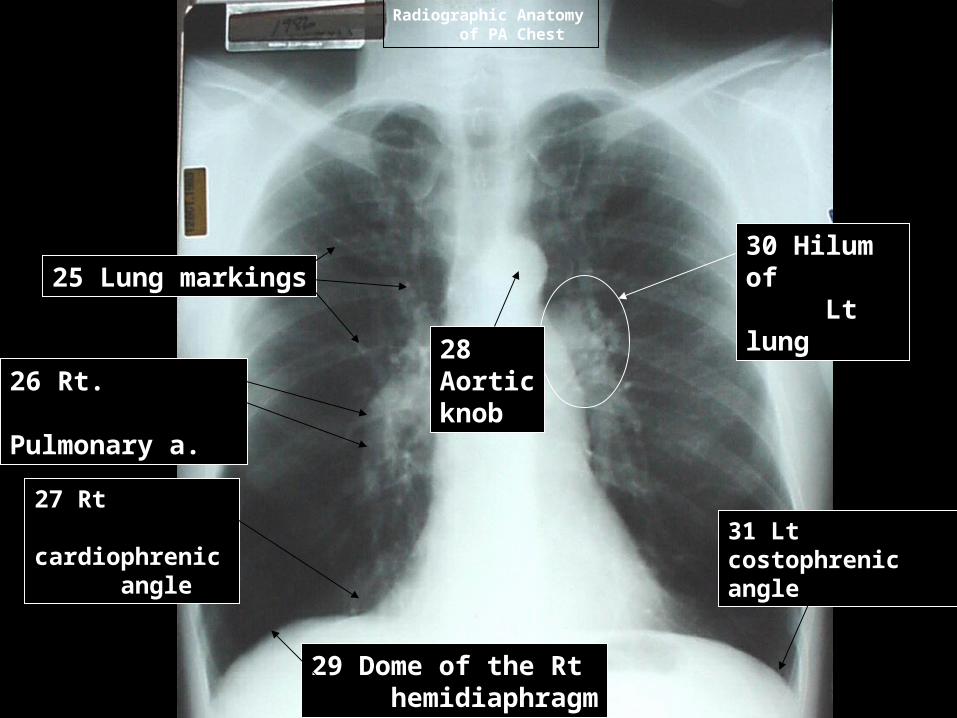
Radiographic Anatomy of PA Chest
29 Dome of the Rt hemidiaphragm
31 Lt costophrenic angle
27 Rt cardiophrenic angle
25 Lung markings
26 Rt. Pulmonary a.
28Aorticknob
30 Hilum of Lt lung
Define:
32. dyspnea33. angina34. sputum35. fibrile
Short answer:
36. How many ribs must be demonstrated on an inspiration PA CXR, and is it anterior or posterior ribs that are counted?
1
Define:
32. dyspnea – difficulty breathing 33. angina – chest pain (lt arm, neck) 34. sputum – pus/debris from deep in bronchial tree & alveoli 35. fibrile - fever
Short answer:
36. How many ribs must be demonstrated on an inspiration PA CXR, and is it anterior or posterior ribs that are counted? 10, posterior
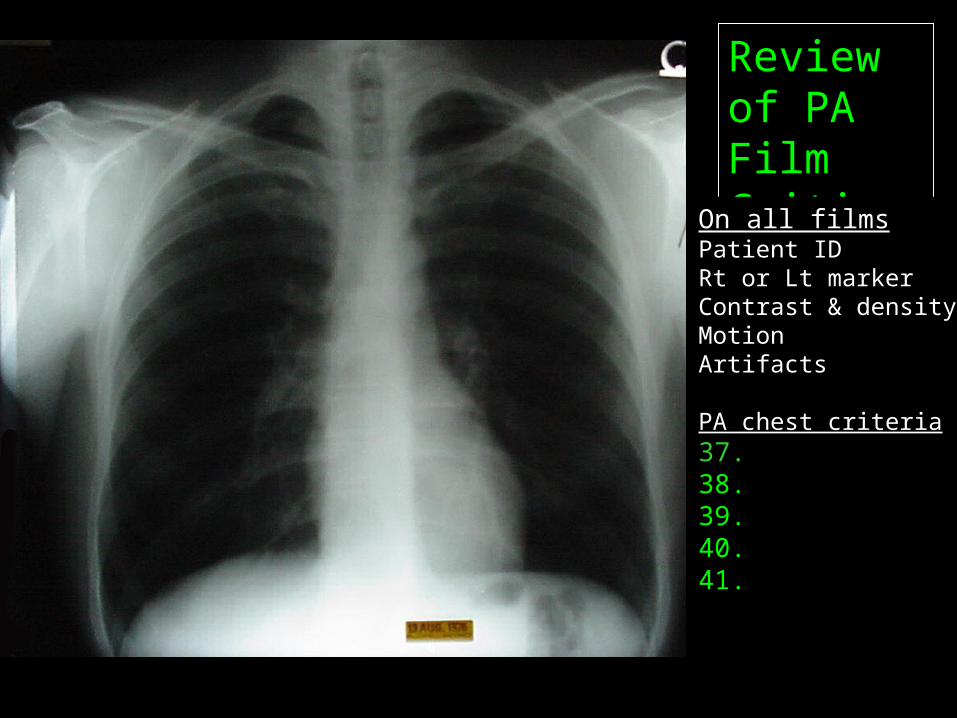
Review of PA Film CritiqueOn all filmsPatient IDRt or Lt markerContrast & densityMotionArtifacts
PA chest criteria37. 38. 39. 40. 41.

Review of PA Film CritiqueOn all filmsPatient IDRt or Lt markerContrast & densityMotionArtifacts
PA chest criteria37. Clipping38. Inspiration39. Rotation40. Scapula free of lung fields41. Penetration of mediastinum
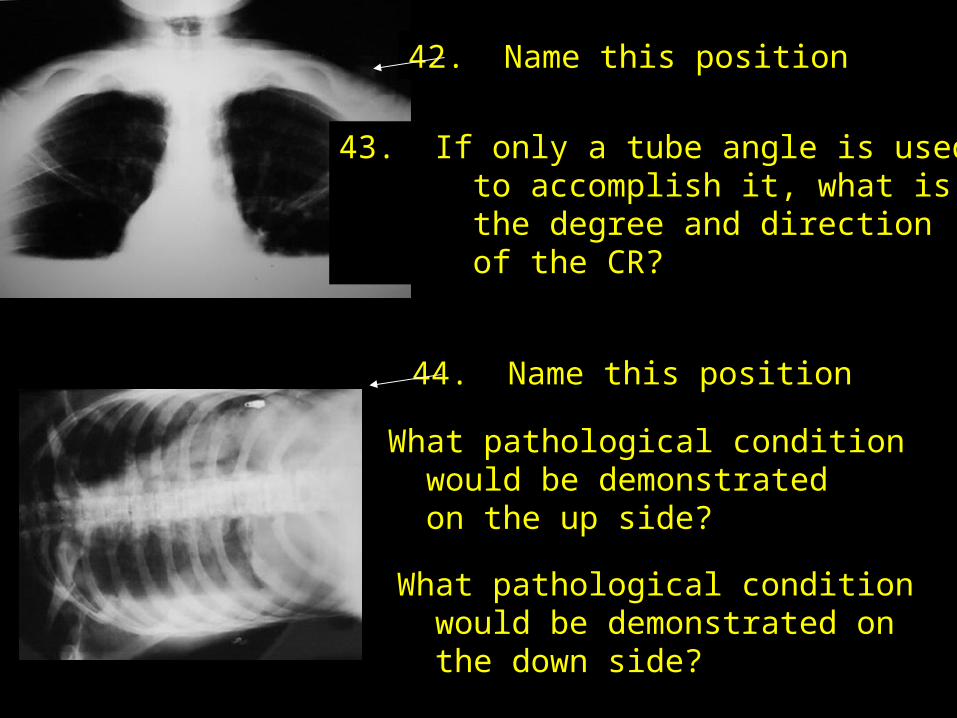
42. Name this position
43. If only a tube angle is used to accomplish it, what is the degree and direction of the CR?
45. What pathological condition would be demonstrated on the up side?
46. What pathological condition would be demonstrated on the down side?
44. Name this position

42. Name this position Apical lordotic (lordotic chest)
43. If only a tube angle is used to accomplish it, what is the degree and direction of the CR? 15-200 cephalad
45. What pathological condition would be demonstrated on the up side? Pneumothorax
46. What pathological condition would be demonstrated on the down side? Pleural effusion
44. Name this position (Rt) lateral decubitus
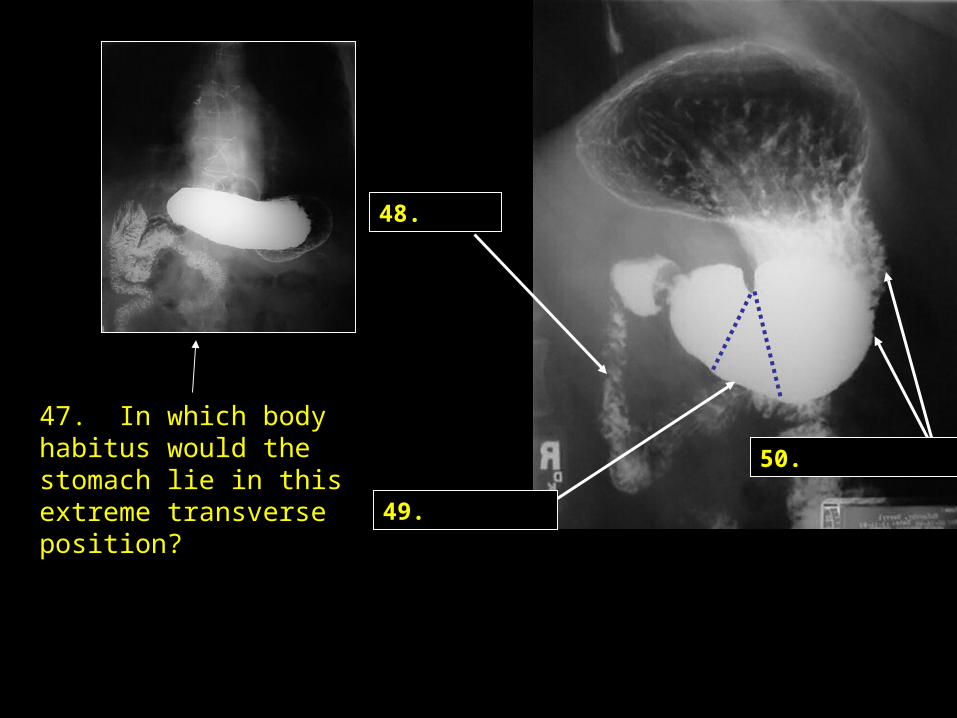
47. In which body habitus would the stomach lie in this extreme transverse position?
48.
50.
49.
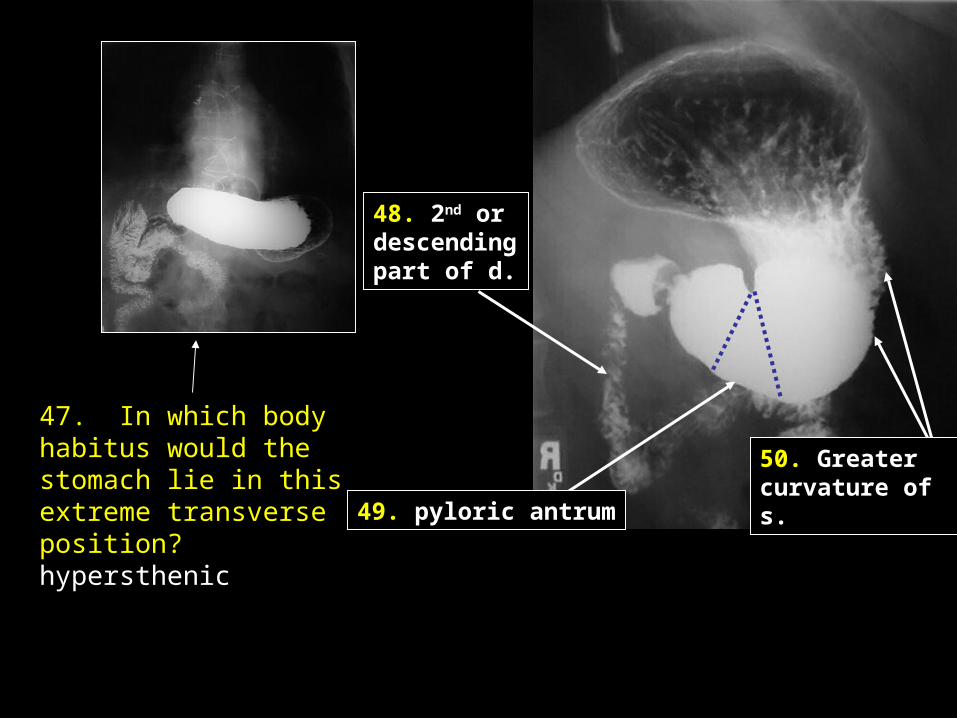
47. In which body habitus would the stomach lie in this extreme transverse position? hypersthenic
48. 2nd or descendingpart of d.
50. Greater curvature of s.
49. pyloric antrum
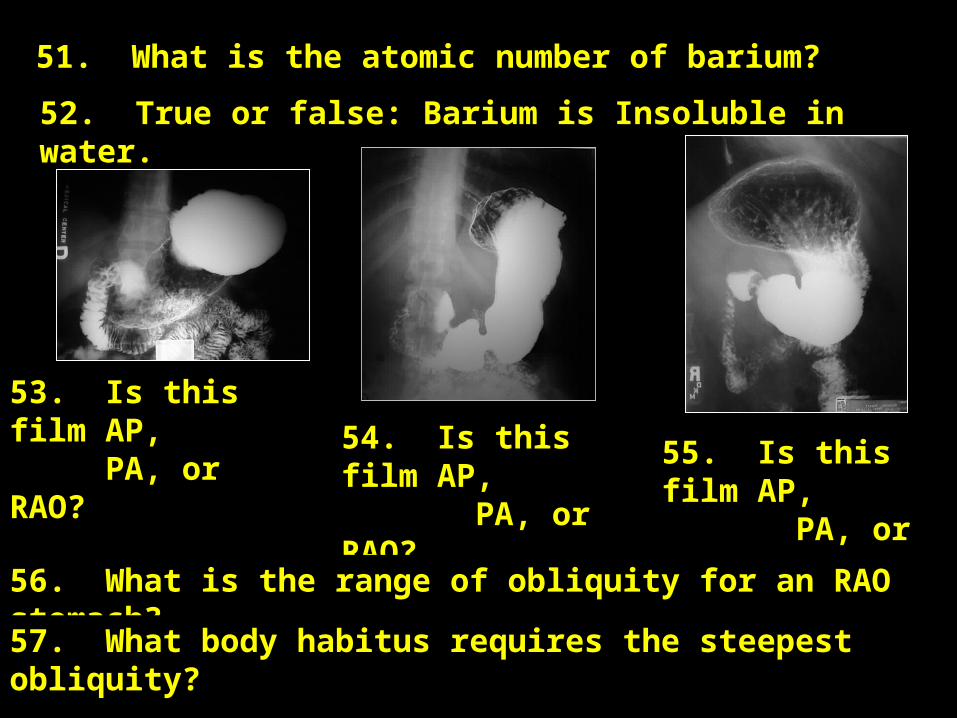
51. What is the atomic number of barium?
52. True or false: Barium is Insoluble in water.
53. Is this film AP, PA, or RAO?
54. Is this film AP, PA, or RAO?
55. Is this film AP, PA, or RAO?
56. What is the range of obliquity for an RAO stomach?
57. What body habitus requires the steepest obliquity?
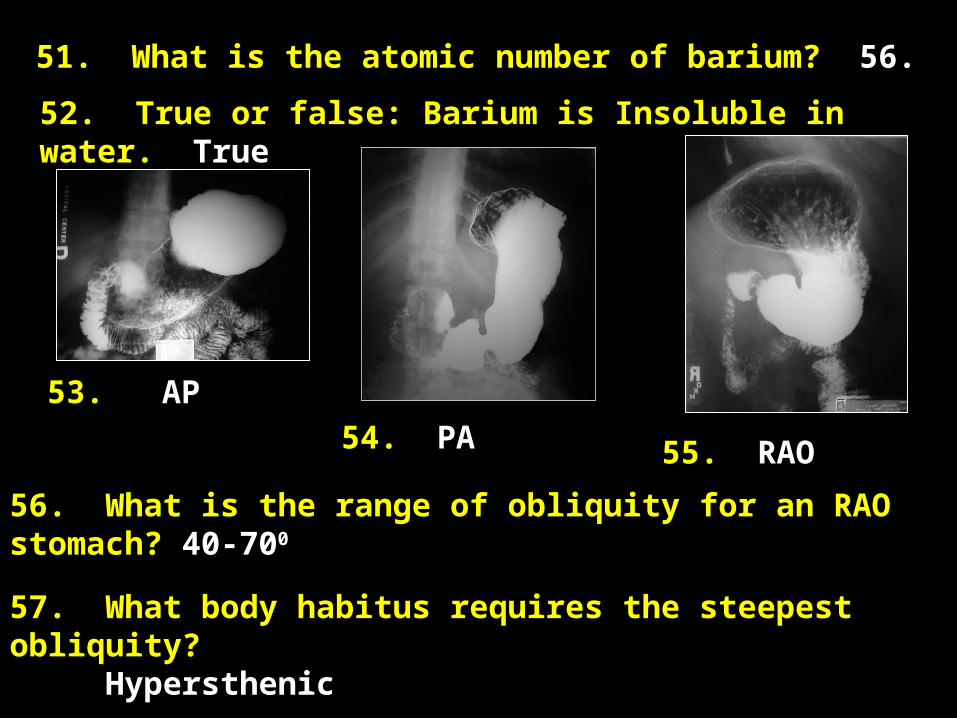
51. What is the atomic number of barium? 56.
52. True or false: Barium is Insoluble in water. True
53. AP
54. PA 55. RAO
56. What is the range of obliquity for an RAO stomach? 40-700
57. What body habitus requires the steepest obliquity? Hypersthenic

58. “Rule out MI” is sometimes given as the reason for an UGI. What is an MI?
59. What UGI projection best demonstrates the retrogastric space?
60. What is the range of obliquity for the LPO position of the stomach?
61. Name one reason that barium would be contraindicated for use in the GI tract.
62. The spot film shown here is generally taken as the film of what examination?

58. “Rule out MI” is sometimes given as the reason for an UGI. What is an MI? Myocardial infarction, or heat attack.
59. What UGI projection best demonstrates the retrogastric space? Rt lateral
60. What is the range of obliquity for the LPO position of teh stomach? 30-600
61. Name one reason that barium would be contraindicated for use in the GI tract. Perforated bowel, post surgical, or, obstruction
62. The spot film shown here is generally taken as the film of what examination? Small bowel series (SBS) Small bowel follow through (SBFT) Motility series
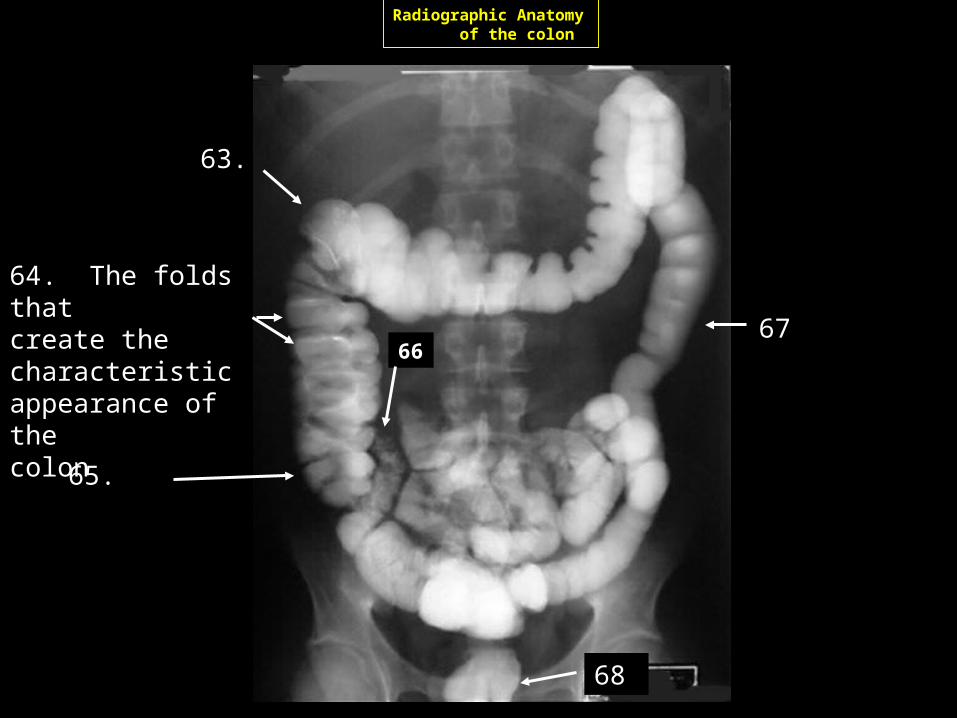
Radiographic Anatomy of the colon
65.
63.
67
68
64. The folds that create the characteristicappearance of the colon
66

Radiographic Anatomy of the colon
65. Cecum
63. Hepatic (Rt. colic) flexure
67. Descending c.
68. Rectum
64. Haustra (haustral folds, haustrations)
66. Terminal ileum
69. Other than laxative, what other name is given a medicinal preparation that stimulates the bowel to evacuate, and is so used for a bowel prep? (2 possibilities)
70. What is the name of the position used for enema tip insertion?
71. Is this position a steep RAO, LAO, RPO, or LPO?
72. Approximately how high above the table should be barium bag be hanging?
73. The terms septic and sepsis refer to: a. infection b. wall or division between parts c. toxic chemicals d. gangrene

69. Other than laxative, what other name is given a medicinal preparation that stimulates the bowel to evacuate, and is so used for a bowel prep? (2 possibilities) Cathartic or purgative
70. What is the name of the position used for enema tip insertion? Sims
71. Is this position a steep RAO, LAO, RPO, or LPO? LAO
72. Approximately how high above the table should be barium bag be hanging? 2 feet
73. The terms septic and sepsis refer to: a. infection b. wall or division between parts c. toxic chemicals d. gangrene
74. Septacemia
75. Ileostomy, jejunostomy, colostomy
76. Stoma
77. Resection
78. Anastomosis
79. Glucagon

74. Septacemia – Pathogenic microorganisms in the blood.
75. Ileostomy, jejunostomy, colostomy – ostomy = a surgically formed fistula, most commonly between intestine and the abdominal wall. (vs. otomy = surgical incision, vs. ectomy = removal)
76. Stoma – A mouth like artificial opening between two body cavities, or a passageway between a cavity and a body surface
77. Resection – partial excision of a part.
78. Anastomosis – natural or surgical connection between two tubular structures.
79. Glucagon – Hormone secreted by alpha cells of pancreas that stimulates liver to change stored glycogen to glucouse. Parentaral administration relaxes smooth muscles of alimentary tract.
Mass
Institutional colon
Pneumoperitoneum
Significant Pathologies or Pathologic Indicators of the abdomen
and their
Radiographic Appearances
Ascites
Ileus
Aneurysm
Pleural Effusion
Pneumothorax
Significant Pathologiesof the lungs, thorax, and mediastinal structures
and their
Radiographic Appearances
Pneumoconiosis
Atelectasis
Granulomatous disease
Congestive heart failure(CHF)
COPD (Bronchitis and emphysema)

Thoracic stomach
Diverticula
Ulcerations
Significant Pathologiesof the upper gastrointestinal tract
and their
Radiographic Appearances
Diverticulosis
Abdominal hernias
Tape worms
Significant Pathologiesof the colon
and their
Radiographic Appearances
Polyps
Colorectal Cancer
Chron’s disease
Intussusception
Institutional colon
Exposure Factors
From the “Rules of Thumb”
Based on: 3 phase, 100 RS film, 12:1 grid, 40” SID
Frontal
(2 x cm) + 35 =kVp @ 50 mAs
Abdomen/Pelvis
Lateral (4x frontal)
(AP + 10 kVp @ 100 mAs Oblique (AP + 40% - 60% of frontal technique

Exposure Factors
From the “Rules of Thumb”
Based on: 3 phase, 100 RS film, 40” SID
Maternal Abdomen
What is required in terms of kVp and mAs?
High kVp (110 or higher), low mAs.
On occasion a radiograph of the pregnant abdomen is ordered during labor, to checkfor a breech presentation.
Every radiology department should have at least one high speed film/screen system for this purpose.
Exposure Factors
From the “Rules of Thumb”
Based on: 3 phase, 400 RS film, 40” SID
Calculate a maternal abdomen technique for a 35 cm measurement
2. 40 mAs / 4 = 12.5 mAs (film speed)
3. 15% of 105 = 16.5 =
1. (2 x 35) + 35 = 105 kVp @ 50 mAs
Answer 121 kVp @ 6 mAs
Critique critera: For presentation, only gross anatomy need be visualized. Maternal abdomen films are rarelyrepeated.
Exposure Factors
From the “Rules of Thumb”
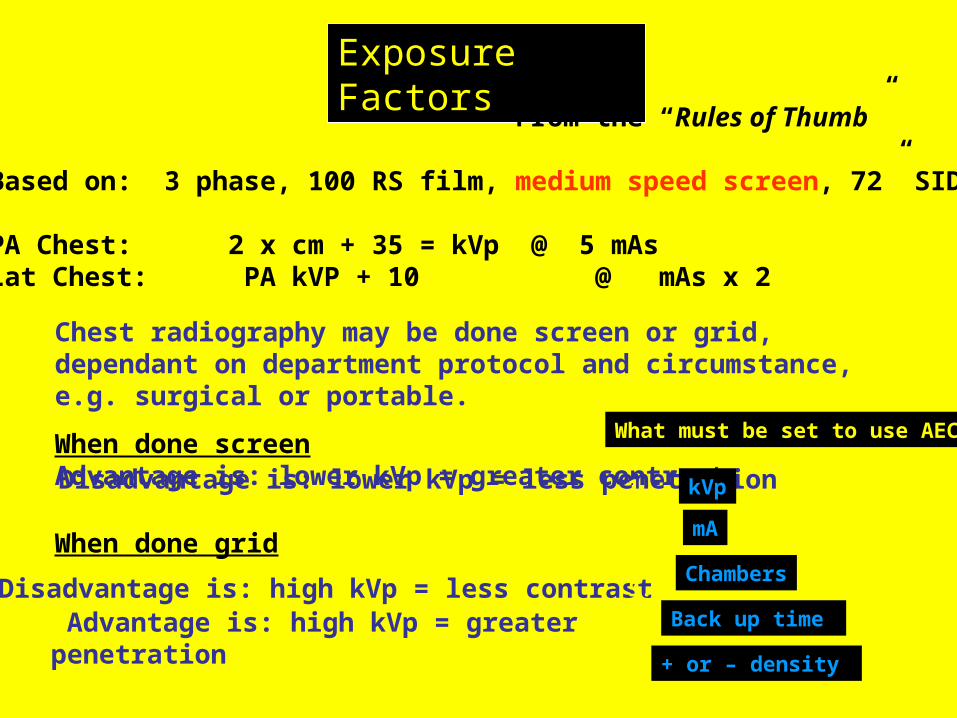
Based on: 3 phase, 100 RS film, medium speed screen, 72” SID
PA Chest: 2 x cm + 35 = kVp @ 5 mAsLat Chest: PA kVP + 10 @ mAs x 2
Chest radiography may be done screen or grid, dependant on department protocol and circumstance, e.g. surgical or portable.
When done screenAdvantage is: lower kVp = greater contrastDisadvantage is: lower kVp = less penetration
When done grid
Advantage is: high kVp = greater penetration Disadvantage is: high kVp = less contrast
What must be set to use AEC?
kVp1.2.3.4.5.
mA
Chambers
Back up time
+ or – density

Exposure Factors
From the “Rules of Thumb”
Based on: 3 phase, 100 RS film, medium speed screen, 72” SID
Compute a technique for a double contrast, and single contrastUGI for a 26 cm abdomen in an AP position, using 400 RS system
1. (2 x 26) + 35 = 87 kVP @ 50 mAs
2. 50 mAs / 4 (RS) = 87 kVp @ 12.5 mAs (Double contrast)
3. 87 + 13 = 100 kVp @ 6 mAs (Single Contrast)
Now put the patient in an RAO (single contrast)
Up AP technique by 40 – 60 % = 108 kVp at 6 mAs
Now put the patient in a right lateral (double contrast)
Up AP kVp by 10, double mAs = 97 kVp @ 25 mAs

Exposure Factors
From the “Rules of Thumb”
Based on: 3 phase, 100 RS film, 40” SID, 12:1 grid
Colon: Use computation for abdomen, except, kVp above 100 for barium
Problem: For a patient with an AP diameter of 25 cm at the level of the umbilicus, using a 400 RS screen/film combination, what techniques would be used for: AP Oblique Axial sigmoid views & Lateral rectum
Exposure Factors
From the “Rules of Thumb”
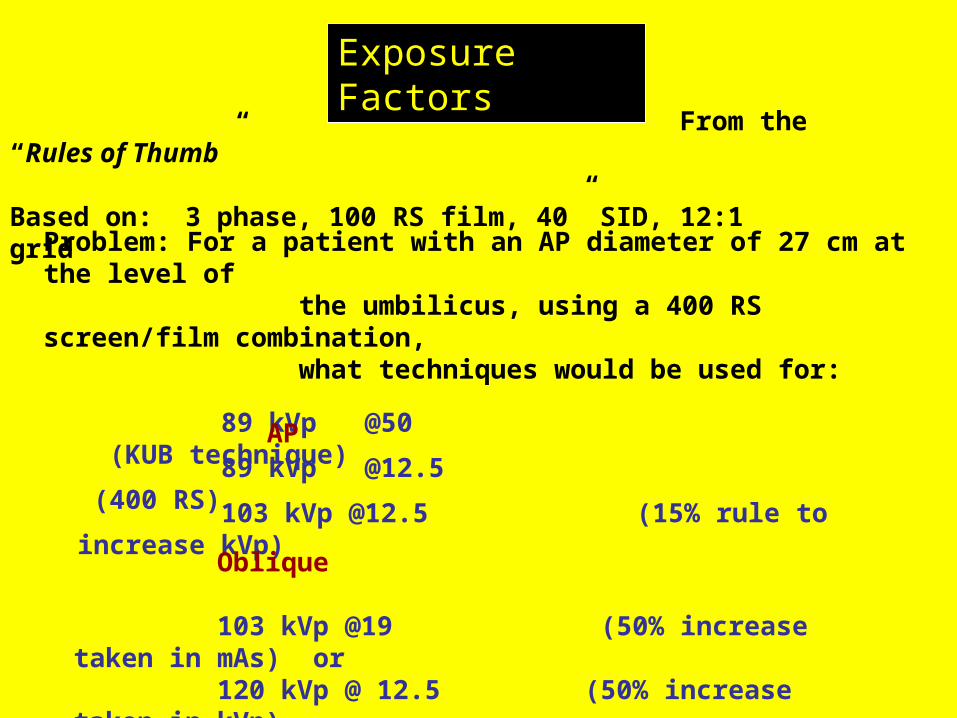
Based on: 3 phase, 100 RS film, 40” SID, 12:1 grid
89 kVp @50 (KUB technique)
Problem: For a patient with an AP diameter of 27 cm at the level of the umbilicus, using a 400 RS screen/film combination, what techniques would be used for: AP
89 kVp @12.5 (400 RS)
103 kVp @12.5 (15% rule to increase kVp)
Oblique
103 kVp @19 (50% increase taken in mAs) or 120 kVp @ 12.5 (50% increase taken in kVp)

Exposure Factors
From the “Rules of Thumb”
Based on: 3 phase, 100 RS film, 40” SID, 12:1 grid
Lateral rectum
103 kVp @ 12.5 50 (AP technique)118 kVp @ 25 mAs (2 x kVp and 2 x mAs) Note: for a KUB the kVp rule was increase by 10, but that was in the 70-80 kVp range to start with.
Problem: For a patient with an AP diameter of 27 cm at the level of the umbilicus, using a 400 RS screen/film combination, what techniques would be used for:
Axial sigmoid is same as oblique technique
103 kVp @19 (50% increase taken in mAs) or 120 kVp @ 12.5 (50% increase taken in kVp)
Exposure Factors
From the “Rules of Thumb”
AEC is sometimes used for barium studies, and is usually successful.
When using AEC for barium studies the centering of thechamber or chambers over solid barium or solid air will lead tofilms that are too light or too dark.
Using multiple results in an average of the densities sampled, andlessens the possibility of error.
Plus and minus density may be needed for some views

Related Documents











