POST CONFERENCE PRESENTATION TAYLOR XENOS, STUDENT RN

RDS
Dec 11, 2015
Adapted from Lecture
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

POST CONFERENCE PRESENTATION TAYLOR XENOS, STUDENT RN

ETIOLOGY
∴ Complex respiratory disease related to immaturity of lung tissue ∴ Manifested by signs of severe respiratory distress
• Beginning at or within few hrs. of birth • Worsens over 24-72 hrs.

RISK FACTORS
∴ Prematurity <34 wks. • Immature respiratory system • Decreased pulmonary surfactant
∴ Maternal diabetes • Persistently high ♀ blood sugars or macrosomic infant result in early delivery
∴ Spontaneous birth ∴ Maternal/fetal stress during delivery ∴ Cesarean delivery
• Lung fluid not expectorated ∴ Asphyxia, acidosis, MAS + sepsis

PATHOPHYSIOLOGY
∴ Lack of surfactant in lungs • Decrease in surface tension to allow alveoli to remain open when air is exhaled
∴ Leads to atelectasis (partial or complete collapse of lung), labored breathing, respiratory acidosis + hypoxemia
∴ Blood flow to lungs decrease ∴ Alveoli become necrotic ∴ Capillaries are damaged ∴ Lungs become noncompliant or “stiff”
DIAGNOSIS
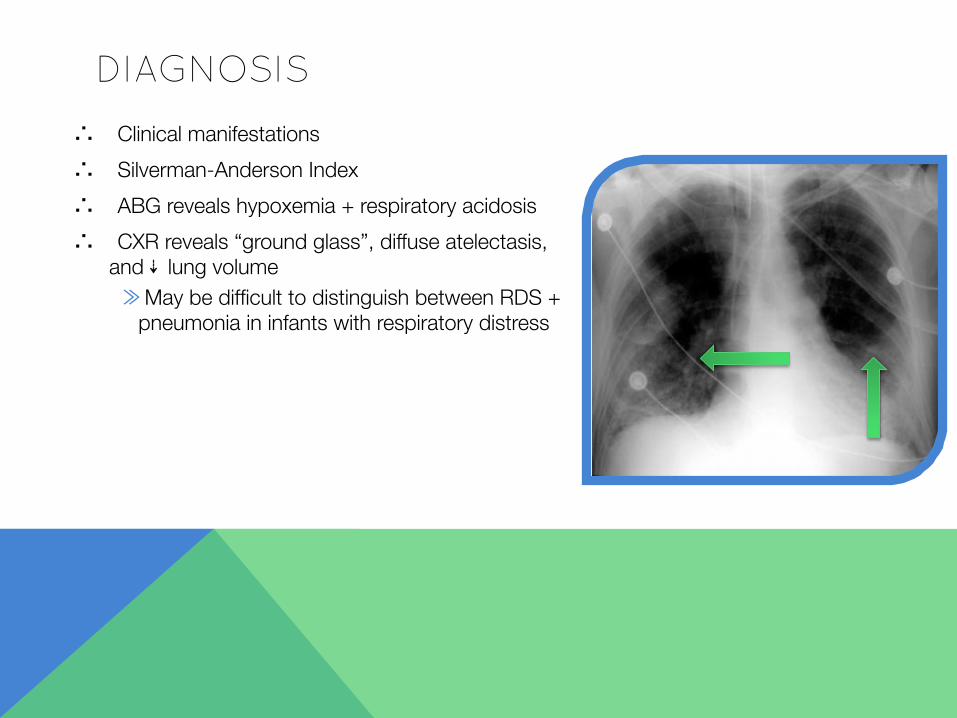
∴ Clinical manifestations ∴ Silverman-Anderson Index ∴ ABG reveals hypoxemia + respiratory acidosis ∴ CXR reveals “ground glass”, diffuse atelectasis, "
and ⇣ lung volume ≫ May be difficult to distinguish between RDS +
pneumonia in infants with respiratory distress

CLINICAL MANIFESTATIONS
∴ Tachypnea 80-120 breaths/min.
∴ Dyspnea
∴ Pronounced intercostal or substernal retractions
∴ Fine respiratory crackles
∴ Audible expiratory grunt
∴ Flaring of external nares
∴ Cyanosis or pallor
Clinical Manifestations of RDS • Tachypnea • Dyspnea • Pronounced intercostal or !
substernal retractions • Fine inspiratory crackles • Audible expiratory grunt • Flaring of the external nares • Cyanosis or pallor
☞ Not all infants born with RDS manifest these "characteristics. Extremely-low-birth-weight infants may"
have respiratory failure and shock at birth d/t "physiologic immaturity

TREATMENT
∴ Administer surfactant as ordered ∴ Institute thermoregulation ∴ Prevent hypotension ∴ Prevent hypovolemia ∴ Correct respiratory acidosis with
ventilator support ∴ Correct metabolic acidosis by
administering sodium bicarbonate
NURSING INTERVENTIONS ∴ Continuous monitoring + close observation ∴ Obtain necessary specimens for lab ∴ Continuous pulse oximetry ∴ Pharmacologic interventions ∴ Provide oxygen therapy ∴ Suction as indicated (not endotracheal) ∴ Maintain thermoregulation ∴ Provide parenteral nutrition ∴ Avoid oral feedings ∴ Cluster nursing activities ∴ Education of parent(s)/caregivers ∴ Provide emotional support ∴ Utilize Silverman-Anderson Index

SIL
VER
MA
N-A
ND
ERS
ON
IN
DEX

SILVERMAN-ANDERSON INDEX (CONT.)
∴ Performed in addition to frequent APGAR ∴ Normal infants have a cumulative score close to 0 ∴ Severely depressed infants score close to 10

CLINICAL OUTCOMES
∴ Room air or oxygen saturation >90% ∴ Respiratory rate <60 breaths/min. ∴ Blood pH >7.35
RESOURCES
∴ http://www.ceu.org/cecourses/981117/ch11b.htm ∴ http://emedicine.medscape.com/article/165139-treatment ∴ http://learnpediatrics.com/files/2010/07/RespiratoryDistress.pdf
Related Documents




![RDS 323 Restorative Dental Sciences [ RDS]](https://static.cupdf.com/doc/110x72/6235ee36aafa9c66c73cc0cf/rds-323-restorative-dental-sciences-rds.jpg)






