AUGUST 1998, VOL 68, NO 2 Valente Trainor 9 Rational Suicide Among Patients Who Are T e r ~ n a l l y Ill nd-of-life decisions, specifically euthanasia and assisted suicide, are among the most con- troversial and confusing social and clinical practice issues.’ Regardless of individual or organizational stances on assisted suicide, it is likely to be legalized. When assisted suicide becomes legal, it will have a profound effect on nurses and nursing practice. Nurses, therefore, need to examine the issues involved. Suicidal patients experience undue suffering and require therapeutic nursing intervention. Advances in medical technolo- gy have increased the average American’s life span; however, people who live longer also face life threatening and degenerative diseases that can diminish quality of life. Medical technology and laws to protect sanctity of life unintentionally may prolong life regardless of the costs or the patient’s wish for death.* Patients complain that few physi- cians ask about their preferences for cardiopul- monary resuscitation (CPR), and less than 42% of physicians discuss advance directives with patient^.^ This difficulty in discussing end-of-life preferences often increases patients’ fears. Physicians and ABSTRACT patients each expect the other to initiate discussion of end-of-life issues, and so both remain silent. Dying patients experience “a great deal of vig- orous medical intervention and pain,” but whether patients agree to such intervention is ~ n c l e a r . ~ Research suggests that too many Americans die alone and in pain and receive aggressive medical treatments not justified by likely benefits.’ Deeply held ethical positions divide society and profession- als.6 Surveys indicate growing interest in and support for physician aid in dying.’ Data show that 74% of Americans surveyed believe that society should sanction withdrawal of life support for patients who are terminally ill to allow patients more control over active means to end life.8 Laws and codes that oblige health care profes- sionals to protect life and to refrain from assisting death currently face substantive challenge and cri- tique.9 The aggressive pursuit of curing illness and prolonging life create ethical dilemmas for health professionals when the painful illness or harmful treatment outweighs the benefits of curative thera- pies. Physicians and nurses debate what, constitutes reasonable medical criteria for no treatment or no intervention. Such dilemmas often are comulicated ~~ Patients’ end-of-life decisions challenge nurses. Often, aggres- sive, life-prolonging strategies create ethical dilemmas for nurses when patients decide to stop treatment. In Oregon, assisted suicide is legal and will have a profound effect on nursing practice. When a patient considers suicide, nurses need to examine the patient‘s mental health, symptom management, and rational decision-making ability. Evaluation of suicide risk is a priority. Nurses need to recog- nize that medical and psychological symptoms often trigger thoughts of suicide, but prompt treatment of pain and symptoms also reduces suicide risk. Ethical issues and guidelines for manage- ment of patients considering suicide and evaluation of rationality are presented. AORN J 68 (August 1998) 252-264. by professionals’ discomfort with talking with patients about their end-of-life preferences and by growing pressure for patient par- ticipation in end-of-life decisions. Professionals often lack education and skill in evaluating patients’ suicide risk and ability to make rational decisions about suicide. lo Researchers assert that nurses need to be knowledgeable about the legal, professional, and moral SHARON M. VALENTE, RN; DONNA TRAINOR, RN 252 AORN JOURNAL

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
AUGUST 1998, VOL 68, NO 2 Valente Trainor 9
Rational Suicide Among Patients Who Are Ter~nally Ill
nd-of-life decisions, specifically euthanasia and assisted suicide, are among the most con- troversial and confusing social and clinical practice issues.’ Regardless of individual or organizational stances on assisted suicide, it is
likely to be legalized. When assisted suicide becomes legal, it will have a profound effect on nurses and nursing practice. Nurses, therefore, need to examine the issues involved. Suicidal patients experience undue suffering and require therapeutic nursing intervention. Advances in medical technolo- gy have increased the average American’s life span; however, people who live longer also face life threatening and degenerative diseases that can diminish quality of life. Medical technology and laws to protect sanctity of life unintentionally may prolong life regardless of the costs or the patient’s wish for death.* Patients complain that few physi- cians ask about their preferences for cardiopul- monary resuscitation (CPR), and less than 42% of physicians discuss advance directives with patient^.^ This difficulty in discussing end-of-life preferences often increases patients’ fears. Physicians and
A B S T R A C T
patients each expect the other to initiate discussion of end-of-life issues, and so both remain silent.
Dying patients experience “a great deal of vig- orous medical intervention and pain,” but whether patients agree to such intervention is ~ n c l e a r . ~ Research suggests that too many Americans die alone and in pain and receive aggressive medical treatments not justified by likely benefits.’ Deeply held ethical positions divide society and profession- als.6 Surveys indicate growing interest in and support for physician aid in dying.’ Data show that 74% of Americans surveyed believe that society should sanction withdrawal of life support for patients who are terminally ill to allow patients more control over active means to end life.8
Laws and codes that oblige health care profes- sionals to protect life and to refrain from assisting death currently face substantive challenge and cri- tique.9 The aggressive pursuit of curing illness and prolonging life create ethical dilemmas for health professionals when the painful illness or harmful treatment outweighs the benefits of curative thera- pies. Physicians and nurses debate what, constitutes
reasonable medical criteria for no treatment or no intervention. Such dilemmas often are comulicated
~~
Patients’ end-of-life decisions challenge nurses. Often, aggres- sive, life-prolonging strategies create ethical dilemmas for nurses when patients decide to stop treatment. In Oregon, assisted suicide is legal and will have a profound effect on nursing practice. When a patient considers suicide, nurses need to examine the patient‘s mental health, symptom management, and rational decision-making ability. Evaluation of suicide risk is a priority. Nurses need to recog- nize that medical and psychological symptoms often trigger thoughts of suicide, but prompt treatment of pain and symptoms also reduces suicide risk. Ethical issues and guidelines for manage- ment of patients considering suicide and evaluation of rationality are presented. AORN J 68 (August 1998) 252-264.
by professionals’ discomfort with talking with patients about their end-of-life preferences and by growing pressure for patient par- ticipation in end-of-life decisions. Professionals often lack education and skill in evaluating patients’ suicide risk and ability to make rational decisions about suicide. lo
Researchers assert that nurses need to be knowledgeable about the legal, professional, and moral
S H A R O N M . V A L E N T E , R N ; D O N N A T R A I N O R , R N
252 AORN JOURNAL

AUGUST 1998, VOL 68, NO 2 Valente Trainor
implications of assisted suicide because future laws may vary from state to state.”
The following hypothetical situation illustrates nurses’ dilemma. Imagine you are caring for Dr S, a 65-year-old physician who expected a typical recov- ery in the intensive care unit (ICU) after open heart surgery; however, she failed ventilator weaning parameters, developed a fever, and subsequently, was diagnosed with pneumonia. Though her heart healed, Dr S still could not meet weaning parameters and required medication to treat her depression. A tracheostomy was planned, but Dr S remained dependent on oxygen. Her quality of life was unac- ceptable to her, and she did not want to live if she were dependent on oxygen. Dr S did not want to live with such fatigue, negativity, and poor quality of life. She asked ICU staff members if she could die with a barbiturate overdose and without oxygen. This situa- tion challenges health care team members to exam- ine the legal, moral, and ethical issues of the patient’s request.
In this article, the authors review the literature and discuss assessment, intervention, and ethical issues involved with suicide and assisted suicide. Practice guidelines highlight assessment of a suicidal patient and identify criteria for evaluating rational suicide. The purpose of this article is to outline the nurse’s role in detection, evaluation, and prevention of suicide, and in evaluation, referral, and advocacy for a rational patient who requests assisted suicide. Nurses should emphasize improving palliative care and treating depression because these interventions improve quality of life and often decrease the risk of suicide. Nurses also should examine their profes- sional role and responsibility as advocates when rational patients request assisted suicide.
UlERAillRE REVIEW Most of the research about withdrawing life
support for critically ill patients has focused on the patient’s preferences for intensive care or withdraw- ing therapy, on ethical concerns, and on factors influencing withdrawal of life support.12 Clearly, limited variables have been investigated and scant research has examined the nurse’s role or participa- tion in these decisions. Some physicians and nurses support legalizing giving aid to patients who request help in dying, and some nurses report they have engaged in euthanasia or assisted suicide both with and without a physician’s order.I3 One researcher invited 1,600 critical care nurse subscribers to Nurs-
ing to report family member, surrogate, or physician requests for euthanasia or assisted suicide.14 Of the 852 respondents who practiced exclusively in inten- sive care, 141 (ie, 17%) reported receiving requests for euthanasia or assisted suicide, 129 (ie, 16%) reported they engaged in such practices, and an addi- tional 35 (ie, 4%) reported hastening a patient’s death by only pretending to give life-sustaining treat- ment ordered by a physician. Several problems in this study may confound the conclusions.
This study has the typical limitations of a volun- teer sample and self-report data. Nonrespondent bias may occur in a volunteer sample when those who are concerned or upset about the study or disturbed about the implication of participating in a study on assisted suicide or euthanasia might not participate (eg, nurses may overreport participation in euthana- sia). Self-report data may be biased by subjects who underreport or overreport their behavior or who mis- understand the questions. Inaccuracies also may occur when facts are distorted by memory or percep- tion. For example, if a patient who is terminally ill dies after a nurse administers morphine for pain, the nurse incorrectly may label this assisted suicide or euthanasia. Also, confusion occurs when respon- dents are asked to report requests for assisted suicide or euthanasia from such diverse sources. It is possi- ble that nurses reported requests from their own fam- ily members.
Nurses’ responses to their own family members may differ from their professional responses. Giving high doses of opiates was cited as the most common method of euthanasia; however, many nurses do not differentiate administering medication ihtended to control pain that may facilitate death from euthanasia. Nurses and their professional organizations ques- tioned the reliability and validity of the study that led to these results and the implication that some nurses seem “to deliberately give lethal overdoses of med- ication and . . . they practice at the limits of their auth~rity.”’~ Other researchers found that patients have asked nurses to hasten death by withdrawing treatment and also by active euthanasia.I6 In this sur- vey, 82% of Australian nurses called for guidelines for withholding and withdrawing treatment.
Disagreement in the literature about terms and definitions complicates the debate about the profes- sional’s response to patients’ requests for suicide. Ancient Greeks defined and the Netherlands cur- rently defines euthanasia as a good or gentle death;” however, current definitions of a good
253 AORN JOURNAL
AUGUST 1998, VOL 68, NO 2 Valente Trainor
death may reflect personal, cultural, religious, and historical differences. Euthanasia is the deliberate action to cause another individual’s death and may be subdivided into active, passive, and voluntary acts.I8 Assisted suicide means providing someone with the means to end his or her life without acting as the direct agent of death.19 The American Nurses Association (ANA) asserts that withholding or withdrawing life-sustaining treatment can be acceptable ethically, and that providing medica- tions with the intent to promote comfort and relieve suffering should not be confused with giving med- ications with intent to end life (ie, euthanasia).20 Some nurses, however, fear that providing adequate pain relief or educating a patient to avoid a lethal dose of medication might be viewed as assisting the patient to die.21 Some nurses who gave high doses of pain relievers to terminally ill patients have been called murderers by their colleagues.22
ASSESSMENT Examining a patient’s mental health needs, sui-
cide risk, and rational decision-making ability pro- vides a foundation for care and suicide risk reduc- tion. It also provides evidence for the rationality of end-of-life decisions. Nurses’ rapport, support, knowledge, and empathy powerfully strengthen patients’ coping strategies and enhance assessment of suicidal intent. Evaluation of suicide risk and clues is a priority, particularly after the patient is medically stable.
Most people provide clues before they commit suicide; they see no option to intolerable misery except suicide. At the same time, even those who are termi- nally ill also hope something might happen to relieve their suffering and often hope to be rescued from their impulses. Treatment of pain and symptoms reduces suicide risk because critically ill patients’ symptoms often trigger thoughts of suicide.23 Though it may seem unlikely, critically ill patients have committed suicide despite their fatigue, illness, or sedation. Com- plications, delayed recovery after surgery, and treat- ment failure often precipitate depression, hopeless- ness, and suicidal ideas that require monitoring.2d. Crit- ical care nurses often serve as the guardian of the patient’s mental health, particularly when specialists focus on narrow physical parameters.
In the hypothetical example of Dr S, the cardiac surgeon believed Dr S was fine because her heart was healing; however, the nurse evaluated and docu- mented the symptoms of major depression and rec-
ommended psychiatric referral and treatment. In addition, the nurse recommended ongoing monitor- ing of suicide risk. The nurse’s duty is to evaluate and document the symptoms of major depression and suicide risk, indicate a nursing diagnosis (eg, inadequate coping due to depression), and advocate for treatment or referral.25 Other important actions include improving symptom management and advo- cating for an evaluation of rational suicide. The nurse also may restrict the suicidal patient’s autono- my to prevent imminent harm, particularly when the patient lacks rational thinking or impulse control. Dr S’s nurse needed persistence and negotiation skills to convince the cardiac surgeon to reexamine his belief that Dr S’s postoperative recovery was fine.
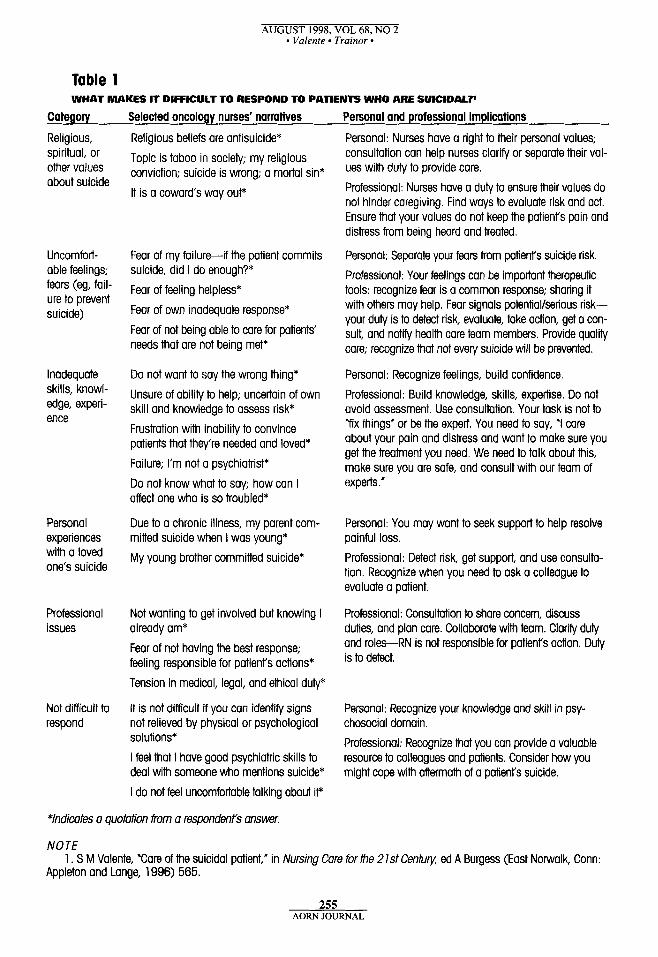
Assessment facilitates case finding, referral, effective treatment, and suicide prevention that can reduce premature death by suicide. Nurses’ fiist goals for a suicidal patient involve evaluation and suicide prevention. If a patient’s choice of suicide is deter- mined to be rational, advocacy for the patient’s autonomy becomes important. Consultation; treat- ment of depression, pain, or symptoms; and therapeu- tic interventions may dispel suicidal intent effective- ly. Nurses encounter several challenges in responding to patients who are suicidal (Table 1). Nurses report that they struggle with their religious and spiritual values, uncomfortable feelings and fears, inadequate skills and knowledge, personal experiences with a loved one’s suicide, and the weight of professional responsibility. Eligibility for assisted suicide should require that a patient be terminally ill with an incur- able condition that is causing irremediable, intolera- ble suffering. Patients should identify when suffering or pain is intolerable, and nurses should verify that patients are informed about all palliative care options and have accurate data about their diseages. Safe- guards should ensure that a patient’s choice is volun- tary. Safeguards for voluntary choice include
documentation of clear mental status, repeated request for assisted suicide over time, and a nondirective interview to evaluate whether the patient feels coerced and to examine motives.
In the worst case scenario, a nurse who is caring for a patient who is terminally ill and confused may be ordered to give a dose of opiates to the patient who is not expected to live. Imagine that an ICU physician ordered the overdose of opiates but failed to document the rationale and discuss this course of action with family members, the patient, or the nurse. When the nurse questions the order and
254 AORN JOURNAL
AUGUST 1998, VOL 68, NO 2 * Valente - Trainor 9
Table 1 WHAT MAKES IT DIFFICULT TO RESPOND TO PATIENTS WHO ARE SUICIDAL?'
Category Selected oncology nurses' narratives Personal and professional implications
Religious, spiritual, or other values about suicide
Uncomfort- able feelings; fears (eg, fail- ure to prevent suicide)
Inadequate skills, knowl- edge, experi- ence
Personal experiences with a loved one's suicide
Professional issues
Not difficult to respond
Religious beliefs are antisuicide* Topic is taboo in society; my religious conviction; suicide is wrong; a mortal sin* It is a cowards way out*
Fear of my failure-if the patient commits suicide, did I do enough?* Fear of feeling helpless* Fear of own inadequate response* Fear of not being able to care for patients' needs that are not being met*
Do not want to say the wrong thing* Unsure of ability to help; uncertain of own skill and knowledge to assess risk* Frustration with inability to convince patients that they're needed and loved* Failure; I'm not a psychiatrist* Do not know what to say; how can I affect one who is so troubled*
Due to a chronic illness, my parent com- mitted suicide when I was young* My young brother committed suicide*
Not wanting to get involved but knowing I already am* Fear of not having the best response; feeling responsible for patienrs actions* Tension in medical, legal, and ethical duty*
It is not difficult if you can identify signs not relieved by physical or psychological solutions* I feel that I have good psychiatric skills to deal with someone who mentions suicide* I do not feel uncomfortable talking about iV
Personal: Nurses have a right to their personal values; consultation can help nurses clarify or separate their val- ues with duty to provide core. Professional: Nurses have a duty to ensure their values do not hinder caregiving. Find ways to evaluate risk and act. Ensure that your values do not keep the patient's pain and distress from being heard and treated.
Personal: Separate your fears from patient's suicide risk. Professional: Your feelings can be important therapeutic tools: recognize fear is a common response; sharing it with others may help. Fear signals potentiaVserious risk- your duty is to detect risk, evaluate, take action, get a con- sult, and notify health care team members. Provide quality care; recognize that not every suicide will be prevented.
Personal: Recognize feelings, build confidence. Professional: Build knowledge, skills, expertise. Do not avoid assessment. Use consultotion. Your task is not to Yix things' or be the expert. You need to say, 'I care about your pain and distress and want to make sure you get the treatment you need. We need to talk about this, make sure you are safe, and consult with our team of experts.'
Personal: You may want to seek support to help resolve painful loss. Professional: Detect risk, get support, and use consulta- tion. Recognize when you need to ask a colleague to evaluate a patient.
Professional: Consultation to share concern, discuss duties, and plan care. Collaborate with team. Clarify duly and roles-RN is not responsible for patient's action. Duly is to detect.
Personal: Recognize your knowledge and skill in psy- chosocial domain. Professional: Recognize that you can provide a valuable resource to colleagues and patients. Consider how you might cope with aftermath of a patient's suicide.
*Indicates a quotation from a respondents answer.
NOTE
Appleton and Lange, 1996) 565. 1 . S M Valente, 'Care of the suicidal patient," in Nursing Cafe for the 2 1st Centuv ed A Burgess (East Norwalk, Conn:
255 AOFW JOURNAL
AUGUST 1998, VOL 68, NO 2 Valente 9 Trainor
objects to the lethal dose, ICU team members may report that this is best and follow the patient’s wishes. The nurse faces difficult choices:
to refuse to administer the opiates, to request consultation, to confer with supervisors, and to resist pressure from col- leagues.
The nurse may decide to refrain from giving the patient the medication during his or her shift, but may return the next day and learn that the patient did receive the opiates and subsequently died. This scenario attests to the difficulty of collaborative care planning and discussing end-of- life decisions. In these situations, health care professionals struggle to do the right thing and to weigh the patient’s wishes with ICU team members’ beliefs about what is best for the patient.
RATIONAL DECISIONS ABOVC SUICIDE
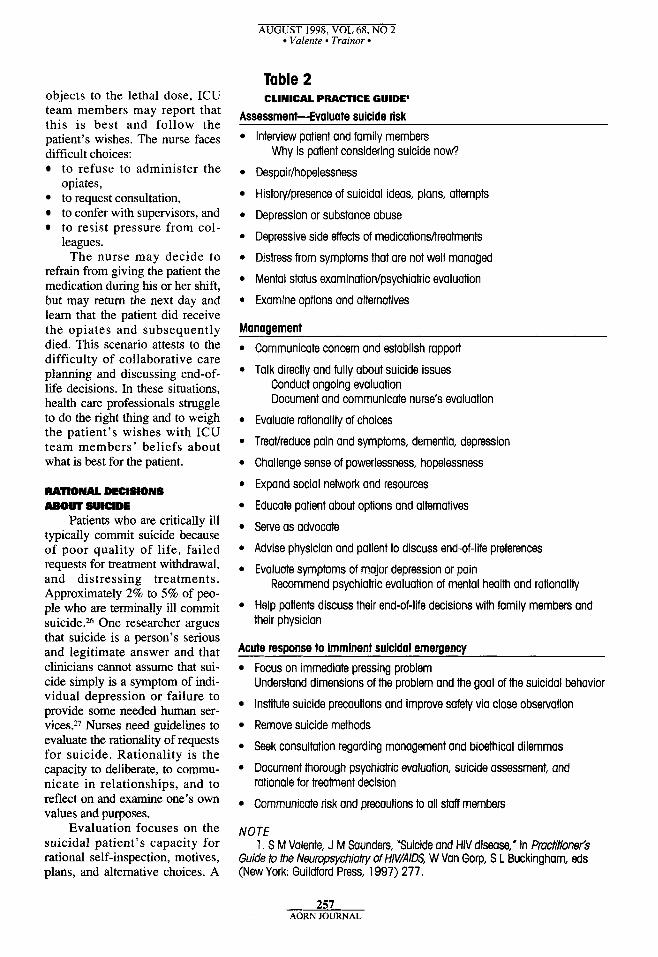
Patients who are critically ill typically commit suicide because of poor quality of life, failed requests for treatment withdrawal, and distressing treatments. Approximately 2% to 5% of peo- ple who are terminally ill commit suicide.26 One researcher argues that suicide is a person’s serious and legitimate answer and that clinicians cannot assume that sui- cide simply is a symptom of indi- vidual depression or failure to provide some needed human ser- vices?’ Nurses need guidelines to evaluate the rationality of requests for suicide. Rationality is the capacity to deliberate, to commu- nicate in relationships, and to reflect on and examine one’s own values and purposes.
Evaluation focuses on the suicidal patient’s capacity for rational self-inspection, motives, plans, and alternative choices. A
Table 2 CLINICAL PRACTICE GUIDE’
Assessment-Evaluate suicide risk Interview patient and family members
Despair/hopelessness
Histon//presence of suicidal ideas, plans, attempts
Depression or substance abuse
Depressive side effects of medicationshreatments
Distress from symptoms that are not well managed
Mental status examinatian/psychiatric evaluation
Examine options and alternatives
Why is patient considering suicide n o w
Management a
0
a
a
0
0
a
0
a
a
a
Communicate concern and establish rappori
Talk directly and fully about suicide issues Conduct ongoing evaluation Document and communicate nurse’s evaluation
Evaluate rationality of choices
TreaVreduce pain and symptoms, dementia, depression
Challenge sense of powerlessness, hopelessness
Expand social network and resources
Educate patient about options and alternatives
Serve as advocate
Advise physician and patient to discuss end-of-life preferences
Evaluate symptoms of major depression or pain Recommend psychiatric evaluation of mental health and rationality
Help patients discuss their end-of-life decisions with family members and their physician
Acute resDonse to imminent suicidal emeraencv Focus on immediate pressing problem Understand dimensions of the problem and the goal of the suicidal behavior
Institute suicide precautions and improve safety via close observation
Remove suicide methods
Seek consultation regarding management and biaethical dilemmas
Document thorough psychiatric evaluation, suicide assessment, and rationale for treatment decision
Communicate risk and precautions to all staff members
NOTE 1 . S M Valente, J M Saunders, ‘Suicide and HIV disease,” in Pmctitionefs
Guide to the Neuropsychiuty of HMAIDS, W Van Gorp, S L Buckingham, eds (New York: Guildford Press, 1997) 277.
257 AORN JOURNAL

AUGUST 1998, VOL 68, NO 2 Valente Trainor
patient’s degree of agitation, disorientation, major depression, and poor reality orientation may impair rational decisions. When these conditions are present in a patient who is suicidal, the nurse should recom- mend a psychiatric evaluation and treatment. The nurse also needs to talk with the patient about thoughts and plans that led to the choice of suicide and explore whether the patient feels pressured to choose suicide. Questions should be nonjudgmental, open ended, and ask about suicide.
Why choose suicide now? What prevented suicide before? Do you (the patient) want help or hope someone else will decide?28
Determining decisional capacity and clear men- tal status may be particularly difficult when the patient is facing death and grieving losses. Medica- tions, illness, and ambivalence may reduce the patient’s insight, ability to communicate, skills, or thinking; therefore, a formal psychiatric evaluation is useful (Table 2).
Rational decisions reflect careful planning and consideration of adequate information (eg, complete and accurate medical facts); preparations (eg, wills, funeral arrangements); effect on others; treatmefits; and alternatives (eg, durable power of attorney, advance directives). Nurses should investigate the plan, anticipated date, method and means for suicide, and the expected outcomes (eg, death, rescue) and contrast this decision with the person’s culture, val- ues, and beliefs. Discussion between nurses and patients also should focus on anticipation of the con- sequences of the suicide on loved ones and whether the person intends to inform loved ones of this plan. One goal is to encourage a thorough consideration of alternatives and palliative care options.
Rational decisions should be free from coer- cion, and all options should be examined.29 A dis- cussion of the precipitants, options, goals, intended outcome, and motives for suicide provides evidence of mental clarity and voluntary choice. If possible, nurses should suggest treatment options. For exam- ple, if the patient believes suicide is a better option to burdening his or her family, the nurse can inform the patient about home care or hospice services. Patients appreciate education about symptoms and illness trajectory that reduces misconceptions and fears. Any delay in recovery or progress prompts people to fear the worst. Hence, failure to meet weaning parameters may provoke the idea that a patient will be dependent on a ventilator inde-
finitely. This conclusion may not be true. Consultation may help nurses weigh the evi-
dence of rational thinking. The prevailing criteria for rational suicide among adults with a terminal illness include
rational considerations, understandable motives, careful planning, review of alternatives, *
absence of coercion, and recognition of conseq~ences.3~
Nurses need to document findings, collaborate with health care team members, advocate for the patient, and use consultation about ethical and legal duties.
Rational requests for suicide or assisted suicide pose difficulties because few practice guidelines exist, professional duties may confliat, and ethical dilemmas are ~hallenging.~] Many nurses would understand the feelings of a colleague who reported the following.
I know I should sound the alarm when the patient is suicidal, but when the patient has end-stage cancer and unrelieved pain, I also feel obliged to be an advocate. I can under- stand the patient’s wish to die with dignity.32
Nurses also experience distress when aggressive medical care continues although the patient has requested withdrawal of treatment. Nurses struggle to decide what is right for the patient, family mem- bers, and the critical care setting. Though most ethi- cal codes advise health care professionals, to refuse participation in assisted suicide, survey data suggest that many nurses desire better guidelines for end-of- life care.33
I ” T N ) N S Palliative care for dying patients is critically
important and depends on competent assessment. Palliative care is treatment of aversive physical, psy- chiatric, and existential symptoms of people who are dying. Poorly managed symptoms should not pro- vide the motivation for suicide. Nurses need to improve pain and symptom management and advo- cate for referral and treatment of depression or other mental health disorders. Often patients appreciate education about the physical and biochemical causes of depression or anxiety that occur with physical ill- ness. Another intervention involves helping patients consider options to improve their quality of life
258 AORN JOURNAL
AUGUST 1998, VOL 68, NO 2 Valente Trainor
Nurses may encounter
conflicts in their obligations
to respect autonomy and to
safeguard life.
through spiritual or other interventions. Education, accurate facts, and options provide
other avenues to suicide prevention. Information can help patients realize that suicide may not be the only way out of their suffering. Patients appreciate leam- ing how to talk about end-of-life preferences. Both patients and physicians need to know that they need to initiate end-of-life discussions. Suicidal thoughts may emerge when patients do not know the facts of their situations or the options (eg, hospice care, with- drawal of treatment).
Nurses need to overcome communication barri- ers and improve discussions with patients about deci- sions at the end of life. Patients need encouragement to express their wishes, and physicians need to be asked to explain their plan of care, ask patients about end-of-life decisions, and respond to patients’ con- c e r n ~ . ~ ~ Nurses can facilitate this discussion by offer- ing to be present, by encouraging advance directives, or by documenting the patient’s concerns and wishes. When a patient’s preferences are documented, physi- cians need guidance to act on these wishes.35
In another worst case scenario, surgeons failed to consider a patient’s end-of-life preferences. They also failed to inform family members that the patient with disseminated intravascular coagulation was not recovering from surgery and was nearing death. The surgeons offered hopeful comments that they would manage her symptoms of anemia, nau- sea, and infection. Nurses became distressed when surgeons refused to share the news of her deteriorat- ing condition with family members and feared the patient would die and family members would have no warning. Nurses called an outside nursing con- sultant who talked with surgeons briefly. The nurs- ing consultant then met with the patient’s husband at 9 AM to tell him that his wife’s death appeared
near. The consultant helped the husband call family members together to say good-bye, support each other, and make final arrangements. By 2 PM that afternoon, family members had convened, spent time with the patient, and were saying good-bye. By 3 PM, the patient was comatose, and she died later that evening. The ICU nurses’ intervention permit- ted the patient to die peacefully, surrounded by her family members and loved ones. Their concern that family members be notified was essential in facili- tating family members’ grief.
The difficulty of physicidpatient discussions about end-of-life issues often causes nurses to be the liaisons who facilitate patient/physician communica- tion, particularly when patients see physicians only briefly during rounds. Nurses need to negotiate with physicians to overcome barriers that interfere with communication. In one example, a critical care patient was depressed when surgeons repeatedly promised to extubate but failed to do so and failed to talk with the patient about their decision not to extu- bate. The physicians held rounds outside the patient’s room and did not share the reason for the change in plans with the patient. Effective nursing interventions included reflecting with the patient about how diffi- cult waiting was and how distressing the ventilator was and insisting that physicians talk with the patient.
Nurses can use several strategies to help patients broach sensitive topics, including dying, and share these with loved ones and physicians. Referrals to pastoral care, clinical nurse specialists, social workers, and others for social support also are beneficial. Nurses’ presence and active listening help patients and family members with their strug- gle with death issues. Patients appreciate nurses who understand their distress and recognize that no one feels suicidal without suffering and good rea- son. Family members appreciate guidance to call other family members or loved ones together, to say good-bye, to arrange for resources (eg, priest, rabbi), and to make funeral arrangements. One researcher recommends that ICU nurses voice and document concerns when a postoperative terminally ill patient’s wishes for withdrawing treatment (eg, ventilator) are ignored and when stressful or ineffec- tive treatments are continued.36 The researcher also encourages nurses to be mindful of the rational patient’s wishes and to advocate so these wishes are considered respectfully. Improving palliation and the quality of care generally requires changes in the hospital’s organization and culture and active sup-
260 AORN JOURNAL

AUGUST 1998, VOL 68, NO 2 Valente Truinor
port of hospital leaders.37 Nurses can provide pow- erful transformational leaders to accomplish these goals.
ETHIcm ISSUES Nurses may encounter conflicts in their obliga-
tions to respect autonomy and to safeguard life. In one case, for example, Mr J was a patient with a chronic autoimmune disorder with respiratory com- plications and became dependent on a ventilator after elective surgery for bladder repair. His request for assisted suicide and ventilator withdrawal caused dis- tress among ICU staff members. Some staff members argued for respecting Mr J’s autonomy and others argued that their role was to sound the alarm and pre- vent suicide. Nurses sometimes complain they have limited power over medical treatment decisions when the patient’s wishes to stop treatment are ignored (eg, a gastrostomy tube is inserted despite a terminally ill patient’s request to withdraw treatment).
A review of bioethical principles and a bioethics consultant or committee may help resolve the con- f l i ~ t . ~ ~ Consultation can provide important emotion- al, educational, legal, and ethical support. Ethical principles direct the clinician to benefit others or do good (beneficence); to prevent evil or harm (non- maleficence); and to respect the patient’s freedom to determine his or her own destiny (autonomy). Benef- icence is in force when health care providers initiate CPR when patients have documented requests for no CPR. A good example of nonmaleficence is the nurse’s request that painful or distressing treatments be withdrawn when the patient is dying. Autonomy exists when a person can act intentionally with understanding and informed decision making. Health care professionals demonstrate paternalism when they believe that they are the sole arbiter of what is good for the patient (eg, continuing to use a ventila- tor when the patient has requested its withdrawal). Paternalistic interventions (eg, providing food after inserting a gastrostomy tube for a terminally ill patient who wants food and fluid withheld) restrict autonomy and should be used with informed consent or when patients are unable to meet criteria for act- ing rationally.
Research suggests that respect for autonomy and the person’s right to die may prompt some nurs- es to support suicide or to participate in assisted sui- ~ ide .~9 Before taking action, nurses need to review the legal and ethical guidelines for practice and rec- ognize that assisting suicide currently is illegal in all
states, except Oregon. No law permits nurses to assist with suicide. Even when a state legalizes physician-assisted suicide, this does not automatical- ly give legal sanctions for nurses.
Other ethical guidelines come from feminism, situation ethics, rights and responsibilities, and car- ing. Another conflict occurs when professional duties conflict with personal values and beliefs (eg, religion, values, culture). Some nurses report their religion for- bids suicide, and they may conclude incorrectly that they cannot talk with patients about suicide. Nurses need to take precautions to avoid judging patients or imposing value judgments on others.4O Nurses are entitled to respect their own personal beliefs and val- ues and also are obliged to have the knowledge and skill to competently evaluate and treat patients. In the authors’ study of the difficulties nurses encounter with suicidal patients, nurses commented about dis- tress and their inability to talk with suicidal patients because suicide conflicted with their religious or other values. Consultation with a religious or spiritual advisor may be beneficial for health care profession- als who believe their religious values hinder their ability to evaluate and refer suicidal patients.
Nurses have a duty to care for suicidal patients. If a nurse’s religious values forbid suicide and the nurse feels unable to evaluate and care for the suici- dal patient, several choices require consideration. If the hospital offers professionals the opportunity to decline caregiving to avoid situations of ethical con- flict, the nurse can select this option when the patient admits to suicidal considerations. Otherwise, the nurse will find consultation helpful to reexamine conflicting obligations to meet the duty of Care.
The ANA guidelines outline duties for assess- ment, intervention, advocacy, counseling, and patient care.41 The California Nurses Association Ethics Committee writes that
suicide i s a mode of death that involves undue suffering in most instances. When possible, nurses should strive to relieve conditions that produce suffering and engage in a broad range of suicide prevention activities. Nurses do not act in a manner that assists patients to commit suicide.”
Encouraging or participating in suicide are contrary to the essence of nursing. Some nurses believe that this approach to suicide prevention gives inade- quate guidance-they feel overwhelmed by the
261 AORN JOURNAL

AUGUST 1998, VOL 68, NO 2 * Valente Trainor
need to resolve all the patient’s problems or they lack experience in suicide prevention.
When Oregon legalized physician-assisted sui- cide, the Oregon Nurses Association established guidelines for nurses who choose to be involved, for those who choose not to be involved, and for improved palliative care. Guidelines were estab- lished for conscientious objectors and for those whose moral and ethical stance allowed them to pro- vide care to a patient who has chosen assisted sui- cide. Regardless of a nurse’s moral and ethical stance, nurses cannot
administer lethal medication to cause death, breach confidentiality of patients exploring assist- ed suicide, subject patients or family members to unwarranted judgmental complaints or actions because of the patient’s exploration of assisted suicide, subject peers or health care team members to unwarranted judgmental comments because of their decision to care for a patient who chose assisted suicide, and abandon or refuse to provide comfort and safety measures to the patient.43
These helpful guidelines are similar to nurses’ duties when abortion became legal.44 Some people believe that legalizing assisted suicide will become a slip- pery slope because legalizing an act under specific circumstances may be broadened to permit that act for larger populations.
Patients who are terminally ill, however, pro- claim their right to die with dignity when they face overwhelming pain and unacceptable quality of life, and they ask nurses to advocate for death with digni-
NOTES 1. N Coyle, “The euthanasia and
physician-assisted suicide debate: Issues for nursing,” Oncology Nurs- ing Forum 19 (August 1992) suppl 4 1 -46.
2. T Quill, “Doctor, I want to die. Will you help me?” Journal of the American Medical Association 270 (Aug 18, 1993) 870-873.
3. S L Isaacs, J R Knickman, eds, To Improve Health and Health Care: The Robert Wood Johnson Founda- tion Anthology, first ed (San Francis- CO: JOSS~Y Bass, 1997) 21-186.
4. Ibid. 5 . L J Schneidennan et al, “Atti-
ty. Some 2.3 million Americans die yearly in the United States; evidence shows too many die without pain relief or palliative ~are .4~ Nurses who find the current guidelines insufficient will appreciate the value of political action approaches to respond to these current clinical and ethical challenges.&
Critical care and perioperative nurses are chal- lenged to examine the issues-n one hand, we must prevent suicide and safegmrd life by evaluating and treating patients and by assuring them of effective palliative care and psychiatric treatment. Our patients deserve education and high quality nursing care that respects their autonomy and wishes. On the other hand, when a terminally ill patient has received effec- tive palliative care, education about options, and treatment, the patient may decide to withdraw or refuse treatment and to request assisted dying. We need to examine the ways a patriarchal system focused on continued curative strategies may burden a patient who wishes to die without intrusive technol- ogy. As nurses, we cannot afford to bypass reflection on these issues. We must examine our responsibility as advocates for our patients, particularly when they cannot speak for themselves. This task is not easy or simple, but it is part of the essence of nursing. A
Sharon M. Valente, RN, PhD, FAAN, is an assistant professor in the Department of Nursing at the University of Southern California, Los Angeles.
Donna Trainor, RN, BSN, is a graduate student in the Department of Nursing at the University of California, Los Angeles.
tudes of seriously ill patients toward treatment that involves high costs and burdens on others,” Journal of Clini- cal Ethics 5 (Summer 1994) 109- 112.
6. Committee on Physician- Assisted Death of the American Association of Suicidology, “Report of the committee on physician-assist- ed suicide and euthanasia,” Suicide and Life Threatening Behavior 26 (1996) suppl 1-19; A M Capron, “Legalizing physician-aided death,” Cambridge Quarterly of Healthcare Ethics 3 (Winter 1996) 10-23.
7. L Slome et al, “Physicians’ attitudes toward assisted suicide in
AIDS,” Journal of Acquired Immune Deficiency Syndrome 5 no 7 (1992) 7 12-7 18.
8. B Lo, “Improving care near the end of life. Why is it so hard?’ Journal of the American Medical Association 274 (November 1995) 1634- 1636.
9. Capron, “Legalizing physician- aided death,” 10-23.
10. B Bongar, Suicide: Guide- lines for Assessment, Management, and Treatment (New York: Oxford University Press, 1992) 127-186; S M Valente, J M Saunders, M Grant, “Oncology nurses’ knowledge and misconceptions about suicide,”
262 AORN JOURNAL
AUGUST 1998, VOL 68, NO 2 Valente Trainor
Cancer Practice 2 (May/June 1994)
11. B J Daly et al, “Assisted sui- cide: Implications for nurses and nursing,” Nursing Outlook 45 (Sep- tember/October 1997) 209-214.
12. N A Christakis, D A Asch, “Physician characteristics associated with decisions to withdraw life sup- port,” American Journal of Public Health 85 (March 1995) 367-372.
13. J G Anderson, D P Caddell, “Attitudes of medical professionals toward euthanasia,” Social Science Medicine 37 (July 1993) 105-1 14; D A Asch, “The role of critical care nurses in euthanasia and assisted sui- cide,” The New England Journal of Medicine 334 (May 23, 1996) 1374- 1379; C A Stevens, R Hassan, “Nurs- es and management of death, dying and euthanasia,” Medicine and Lao 13no5/6(1994)541-554; CA Stevens, R Hassan, “Management of death, dying and euthanasia: Attitudes and practices of medical practitioners in south Australia,” Journal of Med- ical Ethics 20 (March 1994) 41-46; A Young et al, “Oncology nurses’ atti- tudes regarding voluntary physician- assisted dying for competent, termi- nally ill patients,” Oncology Nursing Forum 20 (April 1993) 445-451.
14. Anderson, Caddell, “Attitudes of medical professionals toward euthanasia,” 105-1 14.
15. Asch, “The role of critical care nurses in euthanasia and assisted sui- cide,” 1377.
16. Stevens, Hassan, “Nurses and management of death, dying and euthanasia,” 541-554; Stevens, Has- san, “Management of death, dying and euthanasia: Attitudes and prac- tices of medical practitioners in south Australia,’’ 41-46.
17. M P Battin, A G Lipman, “lntroduction,” in Drug Use in Assist- ed Suicide and Euthanasia (Bing- hamton, NY: Hawarth Press, Pharma- ceutical Products Press, 1996) 1-10.
18. American Nurses Association, “Position statement on assisted sui- cide,” in Compendium of ANA Posi- tion Statements (Washington, DC: American Nurses Association, 1996);
209-216. American Nurses Association, “Posi- tion statement on active euthanasia, 1994,” in Compendium of ANA Posi- tion Statements (Washington, DC: American Nurses Association, 1996).
19. L L Curtin, “Nurses take a stand on assisted suicide,’’ Nursing Management 26 (May 1995) 71-76.
Position Statement on Assisted Sui- cide (Washington, DC: American Nurses Association, 1996).
21. S M Valente, J M Saunders, “Case consultation: Assisted suicide and euthanasia,” Journal of Pharma- ceutical Care in Pain & Symptom Control 4 no 1-2 (1996) 291-334.
22. Ibid. 23. J M Saunders, S M Valente,
“The withdrawn response,” in Psy- chological Aspects of Critical Care Nursing, B Riegel, D Ehrenreich, eds (Rockville, M d Aspen Publishers, Inc, 1989) 92-108; J G Alspach, Instructor’s Resource Manual for the AACN Core Curriculum for Critical Care Nursing, fourth ed (Philadel- phia: W B Saunders, 1992) 200-201.
24. Ibid. 25. Valente, Saunders, “Case con-
20. American Nurses Association,
sultation: Assisted suicide and euthanasia,” 291-334; Saunders, Valente, “The withdrawn response,” in Psychological Aspects of Critical Care Nursing, 92-108; Alspach, Instructor’s Resource Manual for the AACN Core Curriculum for Critical Care Nursing, 200-201.
26. S Jamison, “AIDS and assisted suicide,” Hemlock Quarterly 48 (July
27. H E Moody, “‘Rational sui- cide’ on the grounds of old age?” Journal of Geriatric Psychiatry 24 no 2 (1991) 261-277.
28. M P Battin, Ethical Issues in Suicide (Englewood Cliffs, NJ: Pren- tice Hall, 1995) 131-154.
29. Jamison, “AIDS and assisted suicide,’’ 4-6; Moody, “Rational suicide on the ground of old age?”
30. Jamison, “AIDS and assisted suicide,” 4-6; Moody, “Rational sui- cide on the ground of old age?“ 26 1 - 277; Battin, Ethical Issues in Suicide,
1992) 4-6.
261-277.
198-226; J Werth, “Commentary in S Valente & J Saunders. Case consulta- tion: Assisted suicide and euthana- sia,” Journal of Pharmaceutical Care in Pain and Symptom Control 4 no 1- 2 (1996) 291-300, K Siegel, “Psy- chosocial aspects of rational suicide,” American Journal of Psychotherapy
31. Valente, Saunders, “Case con- sultation: Assisted suicide and euthanasia,” 291-334; Battin, Ethical Issues in Suicide, 198-227.
32. S M Valente, S Saunders, “National survey of oncology nurses’ attitudes and knowledge,” unpub- lished data.
management of death, dying and euthanasia,” 541-554.
34. Isaacs, Knickman, eds, To Improve Health and Health Care, 21-186; Lo, “Improving care near the end of life. Why is it so hard?’ 1634- 1636.
35. Isaacs, Knickman, eds, To Improve Health and Health Care,
40 (July 1986) 405-418.
33. Stevens, Hassan, “Nurses and
21 - 186. 36. Lo, “Improving care near the
end of life. Why is it so hard?’ 1634- 1636.
37. Ibid. 38. Battin, Ethical Issues in Sui-
cide, 26-74; Werth, “Commentary in S Valente & J Saunders. Case con- sultation: Assisted suicide and euthanasia,” 291-300, Siegel, “Psy- chosocial aspects of rational sui- cide,” 405-418.
nurses’ misconceptions about sui- cide,” 209-216; Valente, Saunders, “Case consultation: Assisted suicide and euthanasia,” 291-334.
40. C C Cassell, D E Meier, “Morals and moralism in the debate over euthanasia and assisted sui- cide,” The New England Journal of Medicine 323 (Sept 13, 1990) 750- 752; S M Valente, J M Saunders, “Managing depression among peo- ple with HIV disease,” Journal of Association of Nurses AIDS Care 8 (JanuaryPebruary 1997) 51-67; A J Davis et al, “Nurses’ attitudes toward active euthanasia,” Nursing
39. Valente, Saunders, “Oncology
263 AORN JOURNAL
AUGUST 1998, VOL 68, NO 2 Valente Traznor
Outlook 43 (JulylAugust 1995) 174-179.
41. American Nurses Association, “Position statement on assisted sui- cide,” in Compendium of ANA Posi- tion Statements (Washington, DC: American Nurses Association, 1996)
42. California Nurses Association, 82-88.
Position Statement on Suicide (Sacra- mento: California Nurses Associa- tion, 1989).
43. Oregon Nurses Association, Death with Dignity Act Position Statement (Portland Oregon Nurses Association, 1995).
44. American Nurses Association, “Oregon Nurses Association position
statement (1995),” in Compendium of ANA Position Statements (Washing- ton, DC: American Nurses Associa- tion, 1996).
45. Isaacs, Knickman, eds, To Improve Health and Health Care, 2 1 - 186.
46. Davis et al, “Nurses’ attitudes toward active euthanasia,” 174-179.
Environmental Health in Nursing Education and Practice The University of Maryland School of Nursing (Baltimore) has been awarded a $1.3 million grant designed to integrate and enhance environmental health content in nursing education and practice. The core curriculum will prepare nurses to identify and investigate environmental health problems, including exposure to waterborne pfiesteria, lead paint or workplace toxins, lack of vector control, handling of hazardous materials, and the environ- mental health consequences of natural disasters.
According to the university’s dean, nurses
must be prepared to examine environmental factors that are affecting the health of their patients. The grant is an important step toward developing a cadre of nurse leaders in the environ- mental health field and elevating the health status of communities.
Kellogg Foundation Awards $1.3 Million to University of Maryland School of Nursing to Develop Environmental Health Curriculum (news release, Ba/timore, Md: University of Marylancl April 15, 1998) 1-2.
Contact Hours Available at Occupational Hazards Conference The International Council of Nurses and the Ameri- can Nurses Association are sponsoring the intema- tional conference, “Caring for Those Who Care: Occupational Hazards to Health Care Workers.” The conference, which will be held Aug 25 to 26,1998, at the Hyatt Regency Washington Hotel in Washington, DC, is geared toward nurses and all health care work- ers because of their exposure to numerous occupa- tional hazards. The conference has been granted 13.6 continuing nursing education credit hours by both organizations. Objectives of the conference are to
exchange scientific information on the current
status of issues related to health care worker safety and health, infectious diseases, and the environment; describe strategies that organizations and individ- ual workers can use in dealing with safety and health issues; and promote communication and collaboration about health and safety among nurses and scientists from around the world.
For detailed information, call (800) 349-9909 and request document ICO (426). Information also is available online at www.nursingworld.org.
264 AORN JOURNAL
Related Documents

![Terminally Differentiated SH-SY5Y Cells Provide a Model [887035]](https://static.cupdf.com/doc/110x72/577c832e1a28abe054b3f104/terminally-differentiated-sh-sy5y-cells-provide-a-model-887035.jpg)









