Rapid Sequence Rapid Sequence Intubation Intubation Putting It All Together Putting It All Together New Hampshire New Hampshire Division of Fire Standards & Division of Fire Standards & Training and Training and Emergency Medical Services Emergency Medical Services

Rapid Sequence Intubation Putting It All Together New Hampshire Division of Fire Standards & Training and Emergency Medical Services.
Dec 19, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Rapid Sequence Rapid Sequence IntubationIntubation
Putting It All TogetherPutting It All Together
New HampshireNew Hampshire
Division of Fire Standards & Training andDivision of Fire Standards & Training andEmergency Medical ServicesEmergency Medical Services
“One pound of knowledge takes ten pounds of common sense to apply it.”

“To Intubate or not to Intubate?” 6 questions to ask:
Can the patient maintain an airway? Can the patient protect this airway? Is the patient appropriately ventilating? Is the patient appropriately oxygenating? Is the patient’s condition likely to
deteriorate? Is the scene appropriate: safety, moving
the patient while apneic

Purpose of this Presentation:
FAMILIARIZE Medications used for RSI
RSI Procedure
RECOGNIZE RSI: “When” and “When not” to perform
ANTICIPATE Back-up plan
“Murphy’s Law”

What is “RSI” ?
“RSI is the near-simultaneous administration of
neuromuscular blocking agents and sedative-
hypnotic drugs in order to facilitate oral intubation
of a patient with the least likelihood of trauma,
aspiration, hypoxia and other physiologic
complications.”

Why use RSI?
Maximize probability of a successful intubation
RSI:
84.2-100% success rate
(US Air Medical Programs, Sand Diego CA (Ochs, Ann. Emerg. Med, 2002) and Washington state trial (Wayen &
Friedland, Prehospital Emerg. Care, 1999)
Blind NTI:
72.2% success rate (medical)
66.7% success rate (trauma)
Minimize adverse physiologic effects

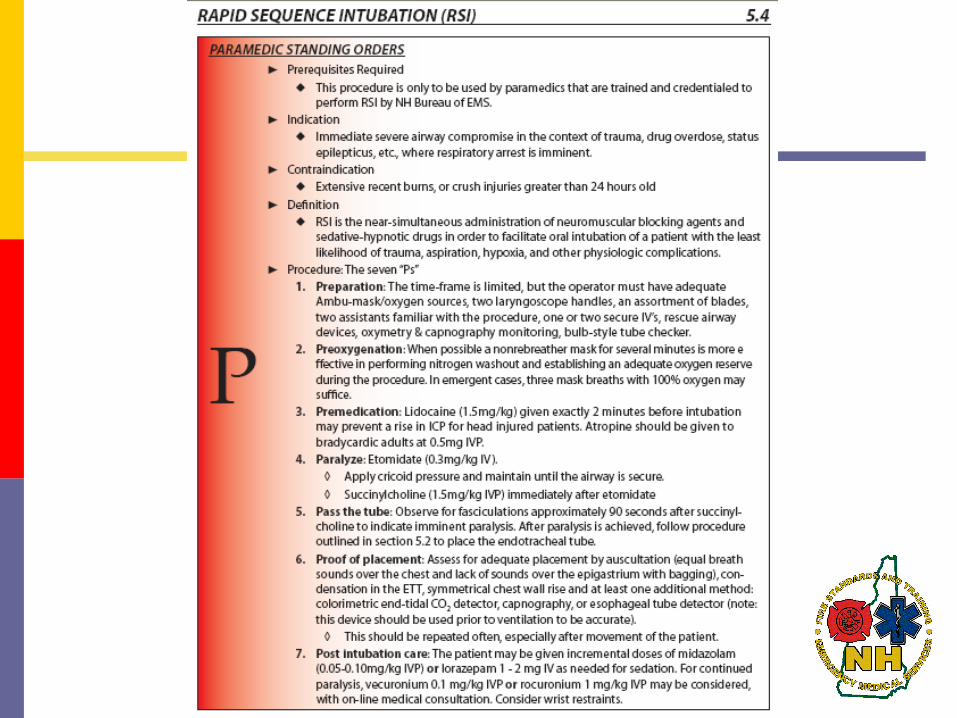
Indication
“Immediate severe airway compromise in the context of trauma, drug overdose, status epilepticus, etc. where respiratory arrest is imminent.”

Examples of RSI Indications
Conditions requiring oxygenation/ventilation control or positive pressure ventilation: Traumatic brain injury with ALOC Severe thoracic trauma (flail chest, pulmonary
contusions with hypoxemia) Clinical condition expected to deteriorate
Unconscious or ALOC with potential for or actual airway compromise or vomiting
And patient has…… A clenched jaw An active gag reflex

Contraindication “Extensive burns or crush injuries greater than
24 hours old.”
Other situations where RSI may not be the best choice:
Spontaneous breathing with adequate ventilation and oxygenation i.e. Ability to maintain an effective airway by less
invasive means Operator concern that both intubation and BVM
ventilation may not be successful due to: Major laryngeal trauma Upper airway obstruction Distorted facial or airway anatomy
Operator unfamiliarity with the medications used
The patient is a candidate for CPAP
Complications Increased intracranial pressure Increased intraocular pressure Increased intragastric pressure Aspiration due to decreased gag reflex Malignant hyperthermia Dysrythmias Hypoxemia Airway trauma Failure to intubate / failure to ventilate DEATH

3 Major Assumptions of RSI
1. The patient has a full stomach
2. The operator can secure an airwayFailure = DEATH for the patientDO NOT take away what you cannot give back!
3. The operator can resuscitate the patientEquipment & Knowledge readily available
Preparation is the KEY
for an organized,
smooth intubation
Remember the 7 P’s!!
IFEndotracheal Intubation Endotracheal Intubation
fails, you must have a back-up plan...
RSI Procedure: The Seven P’s
1. Preparation2. Preoxygenation3. Premedication4. Paralyze 5. Pass the tube6. Proof of placement7. Post intubation care

1. Preparation
A two-part process:
Assess the risks
Prepare the equipment

Assess the Risks

Difficult Airways - Assess the Risks
“The difficult airway is something one anticipates; the failed airway is something one experiences.”
-Walls 2002

How do you know if your patient is going to be difficult to intubate…
…and does it really matter?

Identifying a potentially difficult airway is essential to preparing and developing a strategy for successful ETI and also preparing an alternate plan in the event of a failed ETI.

Some Predictors of a Difficult Airway
C-spine immobilized trauma patient
Protruding tongue Short, thick neck Prominent upper
incisors (“buckteeth”) Receding mandible High, arched palate Beard or facial hair
Dentures Limited jaw opening Limited cervical mobility Upper airway conditions Face, neck, or oral trauma Laryngeal trauma Airway edema or
obstruction Morbidly obese

Additional Predictors:Medical History
Joint disease Acromegaly Thyroid or major neck
surgeries Tumors, known
abnormal structures Genetic anomalies Epiglottitis
Previous problems in surgery
Diabetes Pregnancy Obesity Pain issues

Objectives Identify 4 areas of airway difficulty
Difficult to ventilate with a BVM Difficult laryngoscopy Difficult to intubate Difficult to perform cricothyrotomy
Predict a difficult airway using the following mnemonics: MOANS LEMONS DOA
Difficult to Bag (MOANS)
Mask Seal Obesity or Obstruction Age > 55 No Teeth Stiff

Difficult Laryngoscopy & Intubation
LEMONSLook ExternallyEvaluate 3-3-2 Mallampati ScoreObstructionNeck MobilityScene and Situation

Difficult Cricothyrotomy
DOA Disruption or Distortion Obstruction Access Problems
If you can’t bag and can’t cric, they’re DOA
Disruption / Distortion
Distortion Surgeries Radiation Therapy Scarring Burns
Disruption / Distortion
Disruption Hanging Crush Injuries Penetrating Trauma Other Soft Tissue Trauma
Burns Laceration
Obstructions
Hematoma Abscess Tumor
Tumors can also create distortions & extra bleeding

Access Issues
Obesity Halo Short neck SC Emphysema Bushy beard Flexion deformity of the spine

So, give me some good news:The 3-3-2 Rule Bottom of Jaw/Chin to Neck >
3 fingers Jaw/Palate > 3 fingers wide Mouth opens > 2 fingers wide
Any single indicator has poor specificityAny single indicator has poor specificity

Mallampati Classification
Increased success/ease Decreased Increased success/ease Decreased success/easesuccess/ease
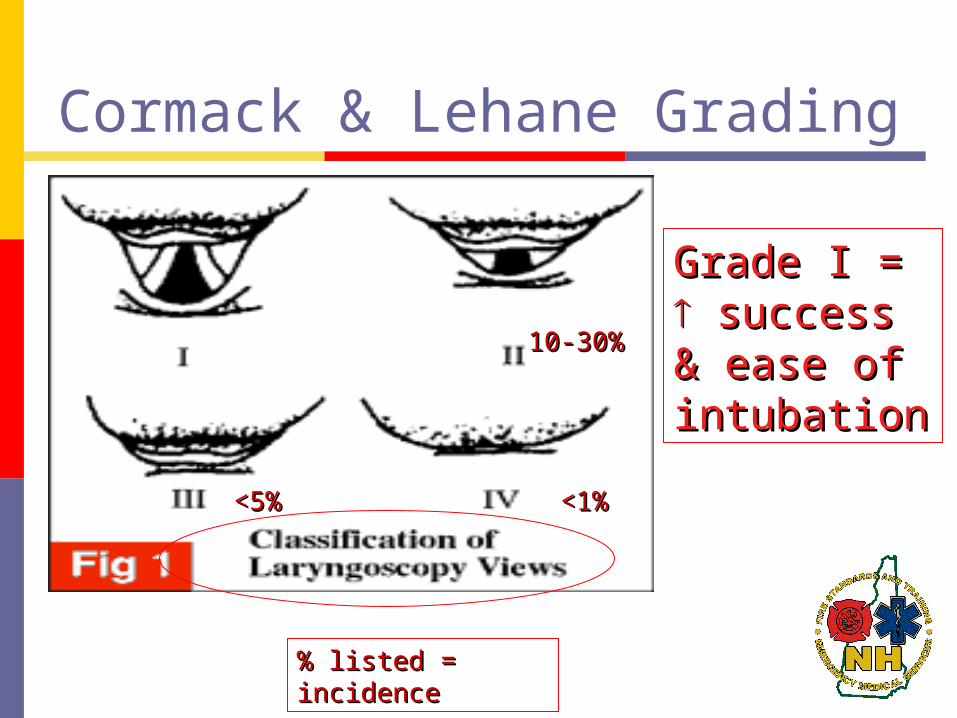
Cormack & Lehane Grading
Grade I = Grade I = success & ease success & ease of intubationof intubation
% listed = % listed = incidenceincidence
<1<1%%
<5%<5%
10-30%10-30%


Always have a back-up plan.
Plans “A”, “B”, and “C” Know the answers before you begin
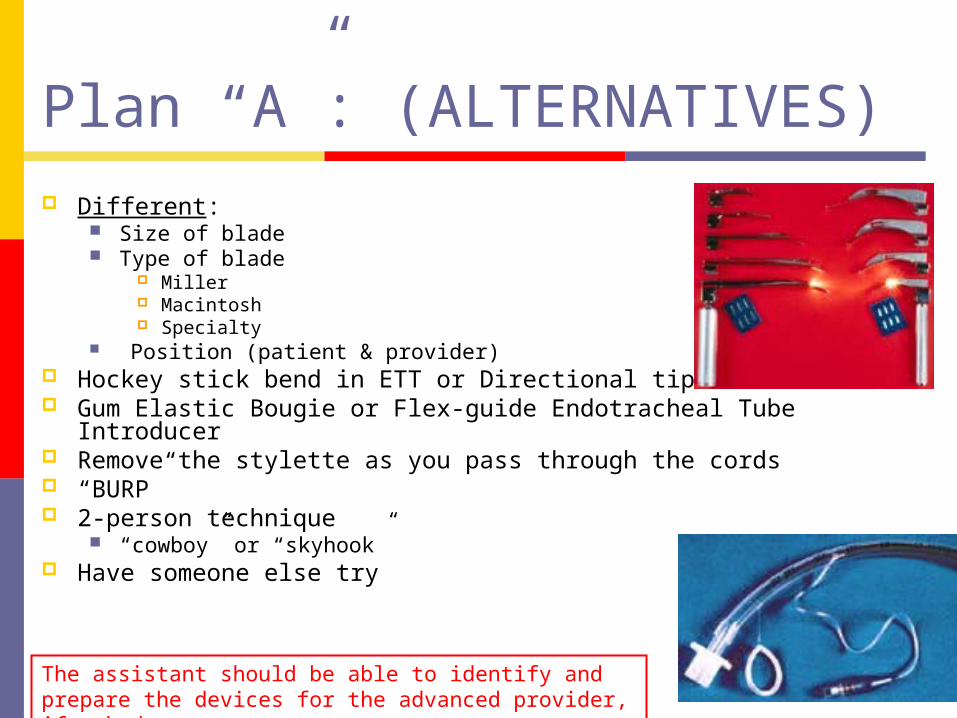
Plan “A”: (ALTERNATIVES) Different:
Size of blade Type of blade
Miller Macintosh Specialty
Position (patient & provider) Hockey stick bend in ETT or Directional tip ETT Gum Elastic Bougie or Flex-guide Endotracheal Tube
Introducer Remove the stylette as you pass through the cords “BURP” 2-person technique
“cowboy” or “skyhook” Have someone else try
The assistant should be able to identify and prepare the devices for the advanced provider, if asked.
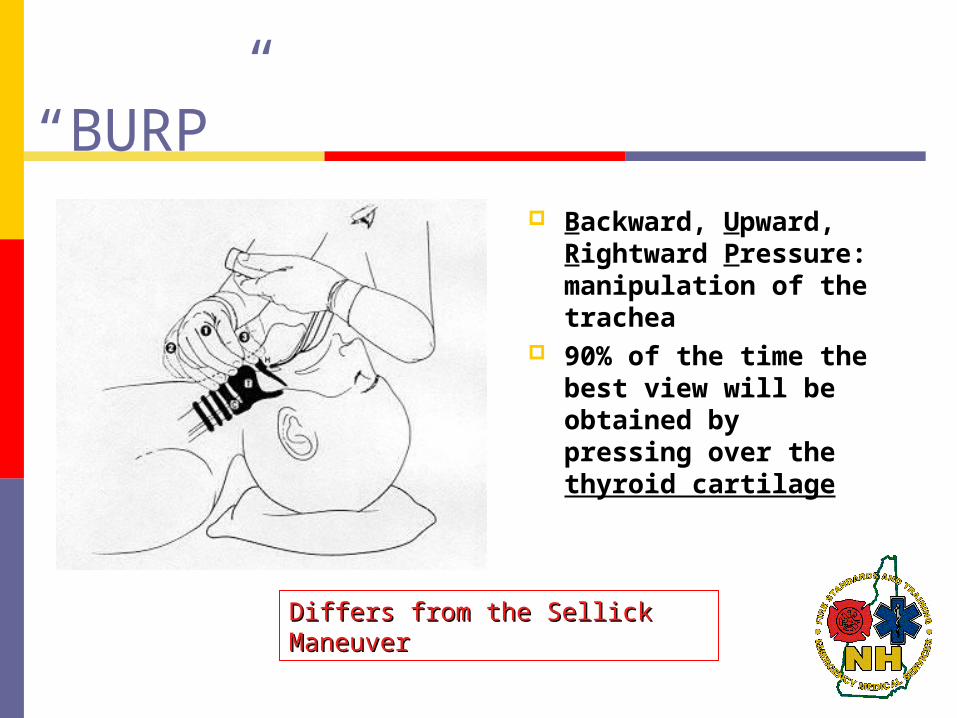
“BURP” Backward, Upward,
Rightward Pressure: manipulation of the trachea
90% of the time the best view will be obtained by pressing over the thyroid cartilage
Differs from the Sellick Differs from the Sellick ManeuverManeuver

Plan “B”: (BVM and BACKUP AIRWAY Techniques )
Can you ventilate with a BVM?
(Consider two NPA’s and an OPA, + Cricoid pressure w/
gentle ventilation)
Gum Elastic Bougie
Combitube
KING – LT-D
LMA?

What do we do when faced with a “Can’t Intubate Can’t Ventilate” situation?
Plan “C”: (CRIC) Needle, Surgical Last resort…
The assistant should be able to identify and prepare the cricothyrotomy devices for the advanced provider, if asked.

Always expect the unexpected!
RSI Procedure: The Seven P’s
1. Preparation - CONTINUED2. Preoxygenation3. Premedication4. Paralyze 5. Pass the tube6. Proof of placement7. Post intubation care
1. Preparation
A two-part process:
Assess the risks
Prepare the equipment
Prepare the Equipment
Prepare the Equipment
Adequate Ambu-mask/oxygen sources/suction 2 laryngoscope handles Assortment of blades Assortment of ET tubes, stylette, syringe Two assistants familiar with the procedure 1-2 secure IV lines All pharmaceutical agents needed for the
procedure Back-up plan and rescue airway devices Oximetry and capnography monitoring Bulb-style tube checker

Monitor the Patient
Cardiac monitor Monitor for dysrythmias
bradycardia, tachycardia, ectopy
Blood Pressure monitoring (manual or NIBP) Monitor for hypo- or hypertension
Pulse oximetry Monitor for hypoxia
Capnography Monitor for hypo- or hypercarbia

RSI Procedure: The Seven P’s
1. Preparation - CONTINUED2. Preoxygenation3. Premedication4. Paralyze 5. Pass the tube6. Proof of placement7. Post intubation care

2. Preoxygenation
Pre-oxygenate with 100% O2 via non-rebreather mask for at least 3-5 minutes Replaces the patient’s functional residual capacity (FRC)
of the lung with oxygen “Nitrogen Washout”
If done properly, this will permit as much as 3-4 minutes of apnea before hypoxia develops
In emergent cases, three mask breaths with 100% oxygen may have to suffice.
Assistant: Will most likely be responsible for the preoxygenation of your patient.

2. Preoxygenation
Resist the use of positive pressure ventilation (PPV). Use only if the patient is not ventilating adequately. PPV leads to gastric distention regurgitation
aspiration If PPV is necessary, utilize cricoid pressure Place NG/OG if prolonged use of BVM

Rapid Sequence Intubation
Medications

Note about Medications
Medications are ONLY to be drawn, prepared, and administered by paramedics.
The Basic or Intermediate Assistance cannot prepare RSI Medications, as they are not protocoled for their use.
RSI Procedure: The Seven P’s
1. Preparation - CONTINUED2. Preoxygenation3. Premedication4. Paralyze 5. Pass the tube6. Proof of placement7. Post intubation care

3. Premedication
These medications are given 2 minutes prior to intubation to reduce/blunt the patient’s physiologic responses to the subsequent intubation
Possible physiologic responses include: Bradycardia Tachycardia Hypertension Hypoxia Increased intracranial and intraocular pressures Cough and gag reflexes

Lidocaine
Dose: 1.5 mg/kg IVP When: At least 2 minutes
prior to intubation Why: May prevent a rise in
ICP in TBI patients
Assistant: Will not see any major change in patient.
Lidocaine
Lidocaine for head injuries, non-traumatic head bleeds and asthma patients (Tight head, tight chest)
Takes 3 minutes to work, so may not be worthwhile if time is critical……..
Use your judgment

Atropine Dose: 0.5 mg IVP When: Prior to intubation
for bradycardic adults Why: Given to prevent
worsening bradycardia From Succs, vagal
stimulation during direct visualization, and hypoxia
Assistant: Will not see any major change in patient.
RSI Procedure: The Seven P’s
1. Preparation - CONTINUED2. Preoxygenation3. Premedication4. Paralyze 5. Pass the tube6. Proof of placement7. Post intubation care

4. Paralyze
A three step process:
Induction
Cricoid Pressure
Paralytic

Induction with Etomidate
Hypnotic induction agent No analgesic properties
Dose: 0.3 mg/kg IV Onset: 30-60 seconds Duration: 3-5 minutes Should always be given prior to paralytic
Assistant: Will see the patient become less responsive; more relaxed.

Cricoid Pressure
Also known as “Sellick’s Maneuver”
Should be automatic Begin just as Etomidate is administered
Maintained until ETT placement is confirmed and tube is secure (cuff inflated)
Used to occlude the esophagus and prevent passive regurgitation common with Succs
If patient starts to actively vomit – RELEASE! and suction oropharnyx.
Otherwise, can lead to esophageal rupture
Assistant: This an important role for you!
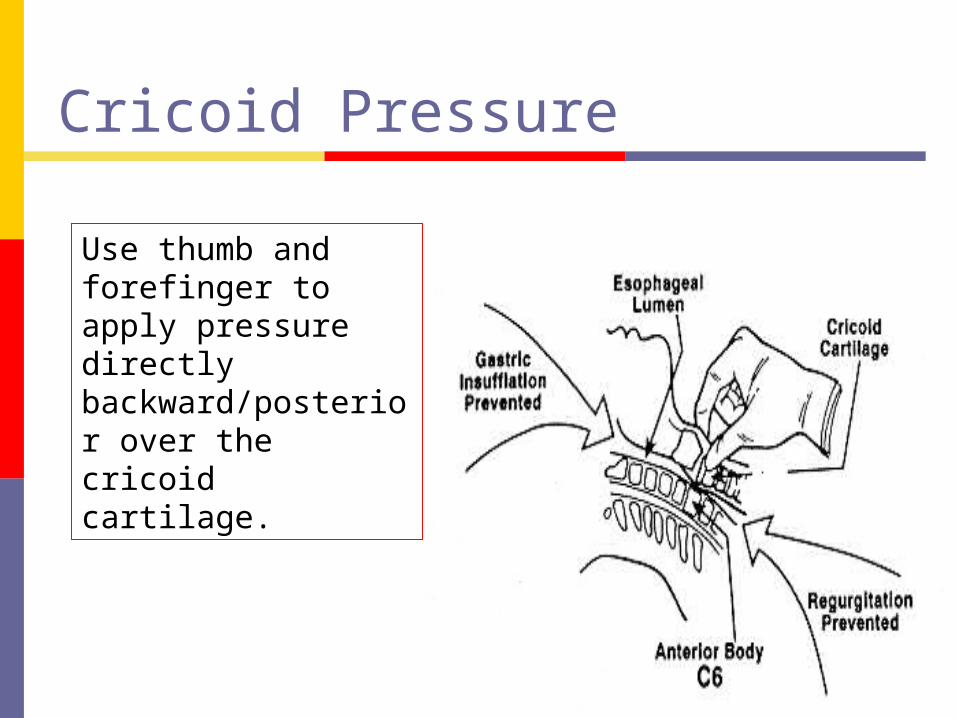
Cricoid Pressure
Use thumb and forefinger to apply pressure directly backward/posterior over the cricoid cartilage.
Cricoid Pressure
The patient MAY become apneic shortly after receiving Etomidate, and will be completely paralyzed 30-60 seconds after Succinylcholine
An assistant MUST perform cricoid pressure at the first sign of sedation and continue until the airway is secure

Anectine (Succinylcholine)SCh or “Succs” The only depolarizing paralytic in clinical
use Benefits:
Rapid onset Short duration
Will cause “fasciculations”

Fasciculations
Muscular twitching involving the simultaneous contraction of contiguous groups of muscle fibers
Merriam-Webster Dictionary

Succinylcholine Dose: 1.5mg/kg IV
When: Immediately after Etomidate
Onset: rapid, usually 30-90 secs
Duration: short acting, 3-5 mins
Assistant: You will likely see the patient go through a brief period of fasciculations followed by complete flaccidity,as the patient become paralyzed.

Contraindications
Severe burns > 24 hours old
Massive crush injuries >8 hours old
Spinal cord injury >3 days old
Penetrating eye injuries Narrow angle glaucoma
Hx of malignant hyperthermia patient or family
Pseudocholinesterase deficiency
Neuromuscular disease patient or family
Hyperkalemia May precipitate fatal
hyperkalemia!

Complications
Cardiovascular Effects Minimal in adults
Muscle Pain From the fasciculations
Hyperkalemia Not a significant issue in the acute period Should be considered in patients with known
hyperkalemia, acute renal failure

Complications
Increased intraocular pressure May be a concern for those with penetrating
globe injuries – theoretically can lead to expulsion of intraocular contents
No documented cases found Defasciculating dose of a non-depolarizing
neuromuscular blocker and lidocaine pretreatment may abolish this complication

Complications
Increased intracranial pressure Controversial May be a concern for those with suspected
traumatic brain injury Lidocaine administration is thought to blunt the
ICP spike

Complications
Increased intragastric pressure Passive regurgitation from fasciculations Importance of Cricoid Pressure / Sellick’s
maneuver

Complications
Malignant Hyperthermia Very rare condition – 1:15,000 Patient experiences a rapid increase of
temperature, metabolic acidosis, rhabdomyolysis, and DIC
Treatment includes administration of Dantrolene and external means of temp. reduction

Complications
Prolonged paralysis In patients with:
A deficiency of pseudocholinesterase Certain meds: magnesium, lithium, quinidine Cocaine
Masseter muscle rigidity

RSI Procedure: The Seven P’s
1. Preparation - CONTINUED2. Preoxygenation3. Premedication4. Paralyze 5. Pass the tube6. Proof of placement7. Post intubation care
5. Pass the Tube
Intubation is performed when there is full relaxation of the airway muscles About 90 seconds after Succs
If intubation fails, maintain cricoid pressure and ventilate with BVM
After patient is reoxygenated, reattempt or move to a different airway adjunct
Assistant: You are still performing the cricoid pressure at this point.

Direct Visualization…

Hold manual in-line axial stabilization (MIAS)
Suspected Cervical Injury?

Pass the Tube
COMPLICATIONS: If you miss or are unable to intubate after 30
seconds…… Ventilate with BVM / high flow O2 with cricoid
pressure maintained Make ONE more attempt to intubate If still unsuccessful – continue BVM / Cricoid pressure Secure Airway with backup device (CombiTube, LMA
or King-LT-D)
Assistant: The advanced provider may ask you to perform the “BURP” maneuver to better visualize the cord.

If Unable
If unable to intubate, unable to secure the airway with backup device, and unable to maintain an SpO2 of >90% with a BVM
Contact Med Control Consider surgical airway:
Surgical Cric Commercial Cric. Device Needle Cric

RSI Procedure: The Seven P’s
1. Preparation - CONTINUED2. Preoxygenation3. Premedication4. Paralyze 5. Pass the tube6. Proof of placement7. Post intubation care

6. Proof of Placement
OBJECTIVE Direct visualization
BEST CXR (in hospital) Pulse oximetry Capnography CO2 detectors
Easy Cap - colormetric Self-inflating bulb
SUBJECTIVE Absence of abdominal
sounds while ambu- bagged
Mist in the tube Bilateral breath sounds Rise/fall in chest
Confirm placement using at least 3 methods, including capnography waveform.
Assistant: Be familiar with the set-up and/or assembly of the various confirmation devices as you will likely be called upon to connect them.
SpO2 (Pulse Oximetry)
Provides quick estimate of PaO2
Often referred to as an additional vital sign
Non-invasive

Waveform Capnometry Number of important applications
Monitor & Confirm ETT placement Useful to document adequacy of ventilation
during mechanical ventilation Limitations:
For patients with impaired pulmonary function or hemodynamic instability
Assistant: Become familiar with the appropriate waveform for a properly ventilated patient.
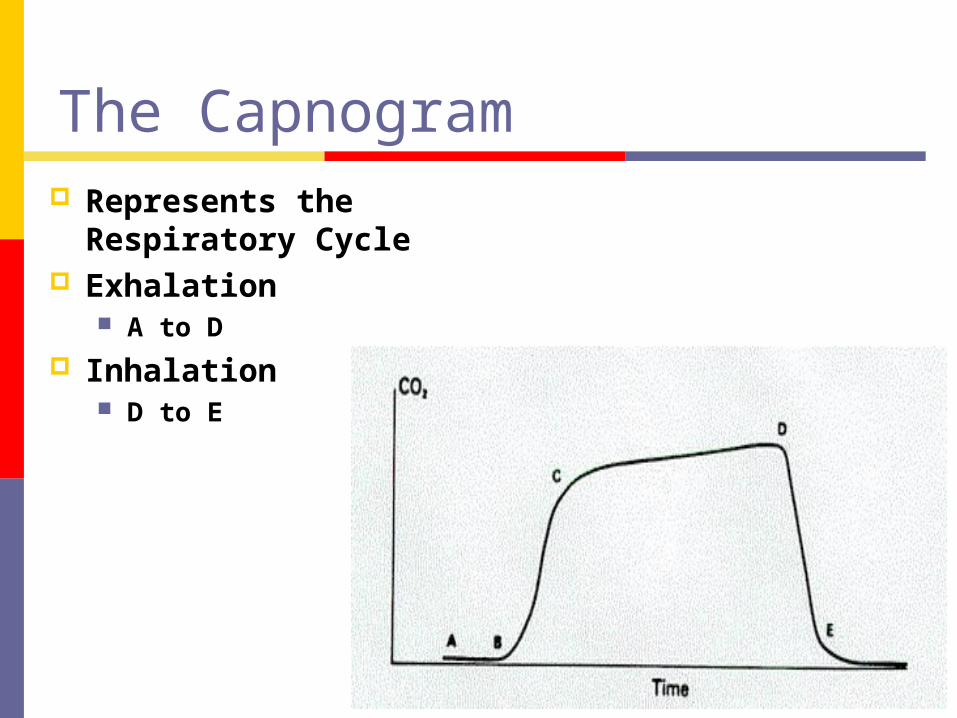
The Capnogram Represents the
Respiratory Cycle Exhalation
A to D Inhalation
D to E

Waveform Capnometry
Prerequisite Requirement
Becoming a standard of care
Easy to Use Good measure of
Pulmonary Perfusion
Relates well to PaCO2
Does have limitations

After confirming placement:
Secure airway device Immobilize the head Verify correct placement each time the
patient is moved Document appropriately
Assistant: Again, be familiar with these steps and be able to perform.

RSI Procedure: The Seven P’s
1. Preparation - CONTINUED2. Preoxygenation3. Premedication4. Paralyze 5. Pass the tube6. Proof of placement7. Post intubation care
7. Post Intubation Care
Medicate: Sedation
midazolam (0.05-0.1 mg/kg IVP) or lorazepam (1-2 mg IV) fentanyl (25-100 mcg may be considered prn)
Paralysis (with online medical control) vecuronium (0.1 mg/kg IVP) or rocuronium (1 mg/kg IVP)
Consider wrist restraints

Midazolam & Lorazepam
Benzodiazepines Provide sedation, amnesia, and
anticonvulsant properties No analgesia
Midazolam: Faster onset, shorter duration than lorazepamLorazepam: may be the preferred agent due to its longer action duration
Pay close attention to the patient’s level of consciousness. Should the patient at anytime show any signs/symptoms of discomfort (movement, increase heart rate, increased blood pressure) consider further sedation.

Sedation Assessment
Sign/symptoms Movement Increase in heart rate Increase in blood pressure Decrease in SpO2 Changes in muscle tone Facial muscle tension

Midazolam (Versed)
Dose: 0.05-0.1 mg/kg IVP Rapid onset – 1-2 minutes Single dose duration: 15-20 minutes
Midazolam
Duration: 1-4 hours Hepatic clearance Decreased dose needed (longer half life)
Obese Geriatric CHF Hepatic or renal insufficiency

Lorazepam (Ativan)
Post-RSI sedation: Lorazepam 1-2 mg IV push q 5 min prn
Titrate to keep patient sedated and SBP >90 Onset: 5 minutes Duration: 6-8 hours, dose dependant

Fentanyl
Class Anesthetic Induction /
Maintenance Narcotic
25-100 mcg may be considered prn

Fentanyl
Opioid agonist Dampens sympathetic (catecholamine)
response Does not release histamine May cause stiff chest in doses >500mcg Caution in hypotension / hypovolemia

Vecuronium & Rocuronium Non-Depolarizing
Paralytics Provide paralysis, but
NO sedation, amnesia, or analgesia properties
Vecuronium (Norcuron)
Considered safe without many contraindications
May be used in most patients including cardiovascular, pulmonary, and neurological emergencies
Must be reconstituted from powdered form
Vecuronium
Dose: 0.1mg/kg IVP Repeat/maintenance dose: 0.01 mg/kg Onset: 2-3 minutes Duration: approx. 20-30 minutes
Vecuronium
Metabolized by the liver and kidneys Use with caution in patients with liver
failure May have 2x the recovery time
Patients with renal or hepatic failure will need less medication to maintain paralysis
Does not cause hypotension or tachycardia

Rocuronium (Zemuron)
Very similar properties to Vecuronium
Does not need to be mixed, can be stored at room temp for 60 days
Less vagolytic properties

Rocuronium
Onset: 30-60 seconds Fastest onset of all non-depolarizing NMBs Dose related
Dose: 1 mg/kg IVP Duration: 20-75 minutes Repeat/maintenance dose is the same as
the initial dose


Review:Sequence of Administration
Time -5 minutes Preoxygenation
Time -2 minutes Premedication
Time -0 minutes Sellick Maneuver,
Induction Agent,
Paralytic
Time +1 minutes Intubation
Medication Sequence
Oxygen Lidocaine and/or Atropine if indicated Etomidate Cricoid Pressure Succinylcholine INTUBATION Lorazepam / Fentanyl prn Rocuronium or Vecuronium prn

IMPORTANT REMINDERS!!
Always remember (and suggest) the use of sedatives before giving paralytics, and allow them to take effect
Sedatives and paralytics do not have any analgesic properties, evaluate patient response and possible need for analgesia vital signs, skin signs

R a p id S e qu en ce In tu b a tion
L o ra zep a m IV F e n tan yl IV
IN T U B A T E !
S u cc in ylch o line
S e llic ks M a n e u ver - B U R P
E to m id a te IV
L id oca ine IV if in d ica ted
P re -o xyg e na te p a tie n t1 0 0% O 2 fo r 5 m inu tes
N R M a sk o r B V M

“Failed Airway”Worst case scenario:

Know Your Options!!!& Don’t hesitate to use them!

Failed AirwayUnable to intubate
(including blind devices) and unable to ventilate with a BVM and maintain an Sp02 > 90 %.

Rescue Airway Management
Have a back-up plan Algorithmic approach
BVM Gum Elastic Bougie Laryngeal Mask Airway (LMA) Esophageal Tracheal Combitube King-LT-D
Assistant: Be familiar with the set-up and/or assembly of the various backup devices as you will likely be called upon to assist with them.

BVM
Can you obtain a good mask seal? Adequate chest rise & fall? Adequate oxygenation & ventilation?
Assistant: You will most likely be performing this skill.

Gum Elastic Bougie (GEB) or Flex-guide (FG) Endotracheal Tube Introducer
First introduced in 1949 Useful in failed intubation with Grade III or Grade IV
laryngoscopic view Might be helpful in the immobilized trauma patient Has been found to reduce the incidence of failed intubation
96% success rate On average, use if an FG instead of a stylet only requires
10 seconds longer to perform intubation Providers must receive training in the use if the FG

LMA Good temporizing
measure Multiple sizes Aspiration likely if
vomiting occurs Pre-Hospital use
unproven/unpublished Risk of aspiration

Combitube
Especially suited for… Patients with difficult anatomy Reduced access spaces Reduced illumination (bright light)

King-LT-D

Failed Airway Management
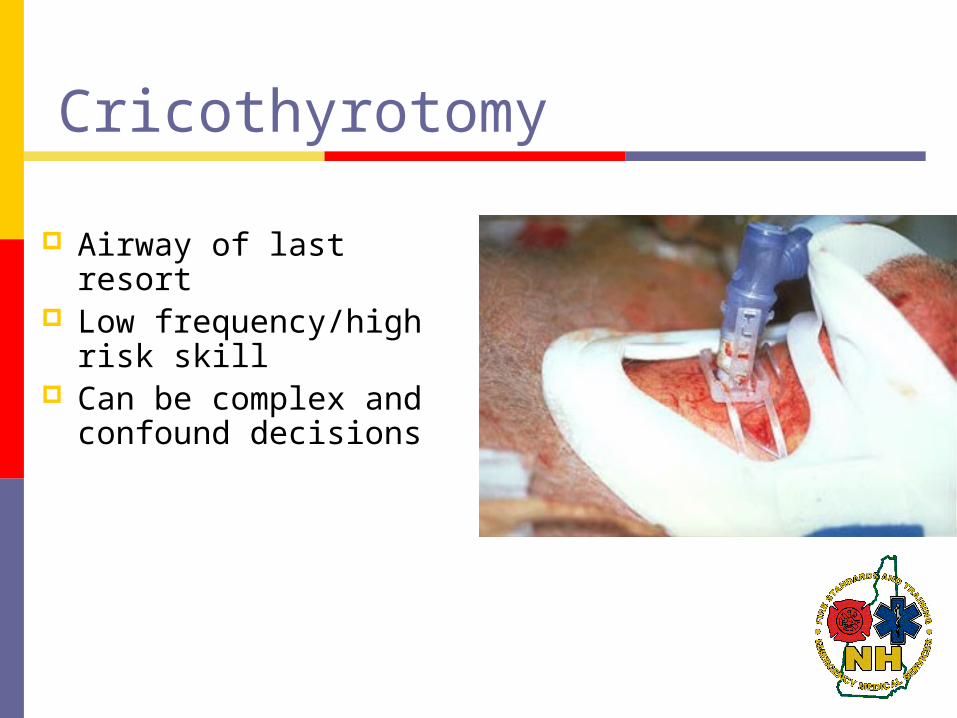
Cricothyrotomy
Airway of last resort Low frequency/high
risk skill Can be complex and
confound decisions

Cricothyrotomy
Relatively contraindicated by anatomic disruption of the cricothyroid region of the airway (Lack of landmarks)

Final Thoughts on the“Failed Airway”
In all cases of a failed airway, the operator must continually assess the adequacy of oxygenation and ventilation
7% of all trauma patients will require intubation

Additional Documentation Items
Why was the decision made to RSI
Pre & Post O2 and CO2 levels
Airway Grading/scales
Unsuccessful Attempts
Case Studies

Case 1
67 y/o female “code blue” – in asystole. PLAN?

Case 2
72 y/o female with Hx fever, productive cough and progressive dyspnea. Lethargic, perioral cyanosis. RR 34 and labored, HR 114, BP 117/76. Lung sounds equal with scattered rhonchi. PLAN?
Case 3
41 y/o female with c/o “asthma attacks” x20 minutes. Severe respiratory distress. RR 32, HR 127, BP 160/92. Bilateral I/E wheezes. Within 10 minutes, she becomes lethargic and her RR slows. PLAN?

Case 4
46 y/o male with a Hx of EtOH and drug abuse. Presents with “had a seizure” per bystanders. Pt is responsive to pain, but does not follow commands or answer questions. RR 18, HR 109, BP 120/80. Within minutes, he has 2 episodes of vomiting and “gurgling respirations”. PLAN?

Case 5
25 y/o male with GSW to abdomen. Pt is intoxicated, decreased LOC, minimal gag reflex. RR 8-10, HR 120, BP 100/80. PLAN?

Case 6
87 y/o male MVC, high-speed, unrestrained. Patient gasping for air, able to talk, c/o right side CP. RR 32, HR 120, BP 186/92. Multiple deformities to face and chin. Ecchymosis and swelling to neck and anterior chest. Large flail segment to ant/lat chest. Decreased BS on the right. No stridor, but some gurgling in throat. PLAN?
References
Marx: Rosen's Emergency Medicine: Concepts and Clinical Practice, 5th ed., Copyright © 2002 Mosby, Inc.
Miller: Miller's Anesthesia, 6th ed., Copyright © 2005 Elsevier
Roberts: Clinical Procedures in Emergency Medicine, 4th ed., Copyright © 2004 Elsevier
Related Documents