Original Contribution Rapid induction of hypothermia with a small volume aortic flush during cardiac arrest in pigs ☆,☆☆ Wolfgang Weihs DVM a , Danica Krizanac MD a , Fritz Sterz MD a, ⁎ , Gerald Hlavin b , Andreas Janata MD a , Wolfgang Sipos DVM c , Michael Holzer MD a , Udo M. Losert DVM d , Wilhelm Behringer MD a a Department of Emergency Medicine, Medical University of Vienna, Vienna, Austria b Center for Medical Statistics, Informatics and Intelligent Systems, Section of Medical Statistics, Medical University of Vienna, Vienna, Austria c Clinical Department for Farm Animals and Herd Management, University of Veterinary Medicine, Vienna, Austria d Core Centre of Biomedical Research, Medical University of Vienna, Vienna, Austria Received 2 January 2011; revised 9 February 2011; accepted 6 March 2011 Abstract Purpose: The induction of deep cerebral hypothermia (15°C) via large-volume cold (4°C) saline aortic flush during cardiac arrest and resuscitation with cardiopulmonary bypass improves neurologic outcome in pigs. We hypothesized that induction of mild cerebral hypothermia (33°C) via smaller volume and resuscitation without bypass will improve survival and neurologic outcome after 15 minutes of cardiac arrest as compared with conventional resuscitation attempts. Basic Procedures: Twenty-four pigs (29-38 kg) underwent ventricular fibrillation cardiac arrest for 15 minutes. Conventional resuscitation (n = 8) was compared with hypothermic (4°C, n = 8) and normothermic (38.5°C, n = 8) aortic flush (30 mL/kg) at the beginning of resuscitation efforts, with defibrillation attempts 2 minutes later. Outcomes after 9 days were compared. Main Findings: In the hypothermic flush group, brain temperature decreased from 38.3°C ± 0.5°C to 33°C ± 0.5°C within 277 ± 112 seconds. We observed considerably higher mean coronary perfusion pressures in the normothermic and hypothermic flush groups (hypothermic vs conventional, P = .023; normothermic vs conventional, P = .041). Three animals of each flush group, compared with none of the conventional group, achieved restoration of spontaneous circulation (P = .2); and 3 pigs of the hypothermic flush group and 2 pigs of the normothermic flush group survived to 9 days without differences in neurologic outcome. Principal Conclusion: A smaller volume, cold saline aortic flush during prolonged cardiac arrest rapidly induces mild cerebral hypothermia to 33°C and improves coronary perfusion pressure but does not result in a significant improvement in outcome as compared with conventional resuscitation attempts. © 2012 Elsevier Inc. All rights reserved. www.elsevier.com/locate/ajem ☆ The work was performed at the Core Centre of Biomedical Research, Medical University of Vienna, WaehringerGuertel 18-20, 1090 Vienna, Austria. ☆☆ The study was made possible through generous support from a Supplementary Assignment of the Austrian Council for Development of Research and Technology (BMBWK GZ: 11.100/6-VII/1/2002 3.6.2002). The authors have no conflict of interest to disclose. ⁎ Corresponding author. Universitätsklinik für Notfallmedizin, Medizinische Universität Wien, WaehringerGuertel 18-20/6D, 1090 Vienna, Austria. Tel.: +43 1 40400 1964; fax: +43 1 40400 1965. E-mail address: [email protected] (F. Sterz). 0735-6757/$ – see front matter © 2012 Elsevier Inc. All rights reserved. doi:10.1016/j.ajem.2011.03.002 American Journal of Emergency Medicine (2012) 30, 643–650

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

www.elsevier.com/locate/ajem
American Journal of Emergency Medicine (2012) 30, 643–650
Original Contribution
Rapid induction of hypothermia with a small volume aorticflush during cardiac arrest in pigs☆,☆☆
Wolfgang Weihs DVMa, Danica Krizanac MDa, Fritz Sterz MDa,⁎, Gerald Hlavin b,Andreas Janata MDa, Wolfgang Sipos DVMc, Michael Holzer MDa,Udo M. Losert DVMd, Wilhelm Behringer MDa
aDepartment of Emergency Medicine, Medical University of Vienna, Vienna, AustriabCenter for Medical Statistics, Informatics and Intelligent Systems, Section of Medical Statistics,Medical University of Vienna, Vienna, AustriacClinical Department for Farm Animals and Herd Management, University of Veterinary Medicine, Vienna, AustriadCore Centre of Biomedical Research, Medical University of Vienna, Vienna, Austria
Received 2 January 2011; revised 9 February 2011; accepted 6 March 2011
AbstractPurpose: The induction of deep cerebral hypothermia (15°C) via large-volume cold (4°C) saline aorticflush during cardiac arrest and resuscitation with cardiopulmonary bypass improves neurologic outcomein pigs. We hypothesized that induction of mild cerebral hypothermia (33°C) via smaller volume andresuscitation without bypass will improve survival and neurologic outcome after 15 minutes of cardiacarrest as compared with conventional resuscitation attempts.Basic Procedures: Twenty-four pigs (29-38 kg) underwent ventricular fibrillation cardiac arrest for 15minutes. Conventional resuscitation (n = 8) was compared with hypothermic (4°C, n = 8) andnormothermic (38.5°C, n = 8) aortic flush (30 mL/kg) at the beginning of resuscitation efforts, withdefibrillation attempts 2 minutes later. Outcomes after 9 days were compared.Main Findings: In the hypothermic flush group, brain temperature decreased from 38.3°C ± 0.5°C to33°C ± 0.5°C within 277 ± 112 seconds. We observed considerably higher mean coronary perfusionpressures in the normothermic and hypothermic flush groups (hypothermic vs conventional, P = .023;normothermic vs conventional, P = .041). Three animals of each flush group, compared with none ofthe conventional group, achieved restoration of spontaneous circulation (P = .2); and 3 pigs of thehypothermic flush group and 2 pigs of the normothermic flush group survived to 9 days withoutdifferences in neurologic outcome.Principal Conclusion: A smaller volume, cold saline aortic flush during prolonged cardiac arrest rapidlyinduces mild cerebral hypothermia to 33°C and improves coronary perfusion pressure but does notresult in a significant improvement in outcome as compared with conventional resuscitation attempts.© 2012 Elsevier Inc. All rights reserved.
☆ The work was performed at the Core Centre of Biomedical Research, Medical University of Vienna, WaehringerGuertel 18-20, 1090 Vienna, Austria.☆☆ The study was made possible through generous support from a Supplementary Assignment of the Austrian Council for Development of Research and
Technology (BMBWK GZ: 11.100/6-VII/1/2002 3.6.2002). The authors have no conflict of interest to disclose.⁎ Corresponding author. Universitätsklinik für Notfallmedizin, Medizinische Universität Wien, WaehringerGuertel 18-20/6D, 1090 Vienna, Austria.
Tel.: +43 1 40400 1964; fax: +43 1 40400 1965.E-mail address: [email protected] (F. Sterz).
0735-6757/$ – see front matter © 2012 Elsevier Inc. All rights reserved.doi:10.1016/j.ajem.2011.03.002

644 W. Weihs et al.
1. Introduction
Normovolemic cardiac arrest with global cerebral ische-mia is a major health problem [1]. Mild therapeutichypothermia (32°C-34°C) induced after successful resusci-tation improves survival and neurologic recovery [2,3].Earlier induction of hypothermia might further improveoutcome [4,5]. The concept of induction of hypothermiaduring cardiac arrest, just before the start of reperfusion, wasintroduced for trauma victims who may rapidly exsanguinateto death [6-10] and has also been investigated fornormovolemic cardiac arrest [11-14]. In previous studies,we demonstrated the feasibility of rapidly inducing deepcerebral hypothermia (15°C) with a cold (4°C) aortic salineflush in a normovolemic cardiac arrest pig model. However,just using physiologic saline did not lower brain temperature.Therefore, it was necessary to add vasopressors to the flushsolution [15], which also improved outcome [16]. Theinduction of deep cerebral hypothermia required large flushvolume (200 mL/kg), necessitating drainage of the rightatrium and resuscitation with cardiopulmonary bypass [16].In a recent study with a bypass cooling system to avoidvolume overload, we found that a 30°C brain temperaturetended to result in better outcomes as compared with lowertemperatures [17]. The use of cardiopulmonary bypass in theout-of-hospital setting might be challenging; thus, wesought for a model for rapid induction of mild cerebralhypothermia and resuscitation without the need forcardiopulmonary bypass. In this study, we hypothesizedthat mild cerebral hypothermia (33°C) induced with asmaller volume (30 mL/kg), cold (4°C) saline aortic flushduring cardiac arrest, before the start of reperfusion willimprove survival and neurologic outcome after 15 minutesof cardiac arrest as compared with conventional resuscita-tion attempts. To differentiate the effect of mild hypother-mia from volume effect, we added a group withnormothermic (38.5°C) aortic flush.
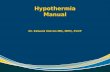
Fig. 1 Aortic flush balloon catheter and flush-pump system. BC,balloon catheter in aortic arch; P, roller pump.
2. Methods
The experimental protocol was approved by ourinstitutional animal investigation committee. Female pigs(Piétrain × Large White breed) weighing 29 to 38 kg afteradaptation to the new environment were put on a fast, withfree access to water, 12 hours before the experiment. Afterpremedication with midazolam, acepromazine, atropine,enrofloxacin, and piritramide, anesthesia was induced withpropofol [18]. Then, the pigs were intubated with anendotracheal tube and mechanically ventilated. To main-tain anesthesia during preparation, propofol (20 mg/kg perhour intravenous [IV]) and bolus of piritramide (30 mgIV) were given. Brain temperature probes (genericthermocouple probe; Biosys, Vienna, Austria) wereinserted into the right and left frontal lobes (1-cm right
and left of the sagittal suture, respectively, and 1 cm infront of the coronal suture) via burr holes to a depth of 2.0cm; the lower of the 2 temperatures was defined as thebrain temperature. Baseline brain temperature was main-tained at 38.5°C ± 0.2°C with a heating blanket or fans. Acatheter was placed in the left brachial artery to monitorarterial pressures and for blood sampling. A pulmonaryartery catheter was inserted via the right jugular vein bythe Seldinger technique to monitor blood temperature,central venous pressure, and pulmonary artery pressureand to allow administration of medications and infusions.A balloon catheter (length, 50 cm; 12F, prototype Joline;Joline GmbH & Co, Hechingen, Germany) was insertedinto the left femoral artery via cutdown and advanced intothe thoracic aorta to 47.5 cm from insertion in all animals,with the balloon above the diaphragm (Fig. 1). Afterfinalizing the preparation, 50-IU/kg heparin was adminis-tered intravenously and randomization was performed byusing envelopes. Ventricular fibrillation (VF) cardiacarrest was induced with an external current impulse of90 V and 60 Hz that was 2 seconds in duration. Abruptreduction of blood pressure and VF electrocardiogramreadings confirmed the arrest. At the same time, theendotracheal tube was disconnected from the ventilatorand all medication stopped.

645Aortic flush during cardiac arrest
2.1. Experimental protocol
2.1.1. Conventional resuscitation groupAfter 15 minutes of VF, advanced cardiac life support was
started with mechanical chest compressions with a thumperdevice (Thumper, type 1000; Michigan Instruments, GrandRapids, MI) at a rate of 90 per minute, mechanical ventilation(15 per minute), catecholamines (adrenaline 0.04 mg/kgevery 4 minutes, vasopressin 0.4 IU/kg every 8 minutes; viathe pulmonary artery catheter), and NaHCO3 1 mmol/kg at 10minutes of chest compressions in a group of 8 animals(conventional resuscitation group) (Fig. 2). Chest compres-sions were performed for 30 minutes in all animals;defibrillation attempts were performed every 2 minutes.The coronary perfusion pressure (CoPP) during chestcompressions was calculated using a data acquisition system(Dasylab; Dasytec, Amherst, NH) [19].
2.1.2. “Flush” groupsAfter 15 minutes of VF, a bolus of adrenaline 0.04 mg/kg
was given, and vasopressin 0.6 IU/kg was administeredthrough the balloon catheter into the thoracic aorta, followedby a cold (4°C) (n = 8) or normothermic (38.5°C) (n = 8)saline flush of 30 mL/kg, delivered with a roller pump(Stoeckert Instruments, Munich, Germany) at the maximalflow rate possible of approximately 1.2 L/min. The flushcontained adrenaline 0.012 mg/kg, vasopressin 0.18 IU/kg,and heparin 7.5 IU/kg. After the aortic flush was appliedthrough the balloon catheter, chest compressions andmechanical ventilation commenced. The balloon wasdeflated immediately, and the catheter was removed.Medications followed the same protocol as in the conven-tional resuscitation group (Fig. 2).
The cold flush group was kept in mild hypothermia afterthe flush, with the help of a surface cooling blanket
Fig. 2 Experimental protocol. CPR indicates cardiopulmon
(Emcools-pad; Emergency Medical Cooling Systems AG,Pfaffstätten, Austria) that was attached to the body surface ifblood temperature rose higher than 34°C. In the conventionaland normothermic flush groups, mild hypothermia (34.5°C ±0.2°C) was initiated after restoration of spontaneouscirculation by applying the Emcools-pad to the chest,abdomen, and neck. The blanket was removed when thetarget temperature was reached. After restoration ofspontaneous circulation, the cannulas were removed, andthe animals were transferred to a step-down unit.
2.2. Intensive care
Controlled ventilation was continued for 20 hours withthe FIO2 adjusted to keep the PaO2 between 13.2 and 20 kPaand the respiration rate adjusted to keep the PaCO2 between4.7 and 5.2 kPa. Sedation and analgesia were maintainedwith propofol 12 mg/kg per hour and piritramide 7.5 mgevery 6 hours. Heparin 50 IU/kg was given every 12 hoursbeginning from restoration of spontaneous circulation untilpigs were able to stand and move around independently.Mild therapeutic hypothermia was continued for 16 hourswith warming blankets or fans and Emcools-pads if needed.Standard respiratory and general intensive care includedairway suctioning, periodic deep lung inflations, positionchange (rotation), and well-balanced fluid management. Forinfection prophylaxis, enrofloxacin 5 mg/kg was admin-istered every 24 hours. Rewarming was begun 16 hoursafter restoration of spontaneous circulation at a rate of1°C/h. Neuromuscular blockade was started after achievingrestoration of spontaneous circulation with rocuronium0.09 mL/kg per hour and was stopped at 18 hours, andsedation and analgesia were discontinued at 20 hours.Extubation was performed as soon as possible after end ofsedation, depending on the individual progress of each
ary resuscitation; Epi, epinephrine; Vaso, vasopressin.

Table 1 Physiologic variables at baseline
Conventional (n = 8) Cold flush (n = 8) Normothermic flush (n = 8)
Heart rate (beats/min) 108.3 ± 15.4 95.6 ± 7.3 102.0 ± 14.0Mean arterial pressure (mm Hg) 69.4 ± 4.9 75.1 ± 2.6 75.4 ± 6.9pH 7.465 ± 0.018 7.4613 ± 0.031 7.476 ± 0.042Pao2 (mm Hg) 136.4 ± 8.4 138.8 ± 5.6 139.6 ± 7.0Paco2 (mm Hg) 39.0 ± 2.4 38.8 ± 1.6 38.3 ± 2.2Hematocrit (%) 22.6 ± 1.1 23.7 ± 1.7 23.1 ± 0.9Base excess (mEq/L) 4.0 ± 1.1 3.8 ± 1.6 4.4 ± 2.4Serum sodium (mmol/L) 136.3 ± 1.8 136.4 ± 1.5 136.3 ± 1.6Serum potassium (mmol/L) 4.3 ± 0.2 4.1 ± 0.3 4.1 ± 0.2Blood glucose (mg/dL) 99.6 ± 7.9 102.1 ± 9.1 103.3 ± 8.0Blood lactate (mmol/L) 1.3 ± 0.3 1.1 ± 0.2 0.9 ± 0.2
Data are given as means ± SD.
646 W. Weihs et al.
animal. When the pigs awoke, they were transferred to a stallfor continuous observation and life support by techniciansand critical care physicians. Seizures, opisthotonus, runningmovements, exhaustive hyperventilation, and signs ofdiscomfort were controlled with bolus of midazolam 0.4mg/kg and propofol 20 mg. If signs of pain were present,piritramide 7.5 mg IV was given every 6 hours.
2.3. Outcome evaluation
To evaluate functional outcome, neurologic deficit scores(NDS) and overall performance categories (OPC) [20] weredeveloped for pigs based on the NDS and OPC scales used indogs [21]. The final evaluation on day 9 was independentlyrecorded by blinded investigators and agreed upon by teammembers [22].
2.4. Statistical analysis
Metric data are reported as mean with SD. To compareOPC scores between the groups, a Kruskal-Wallis rank sumtest was performed. For group comparisons of OPC scores,we defined pigs that died before the final evaluation at 9days as OPC 5. For restoration of spontaneous circulation,
Table 2 Physiologic variables at 13 minutes after start of resuscitatio
Conventional (n = 8) Cold
pH 7.420 ± 0.216 7.30Pao2 (mm Hg) 212.6 ± 163.2 192Paco2 (mm Hg) 50.8 ± 41.7 49Hematocrit (%) 25.4 ± 2.6 20Base excess (mEq/L) 7.8 ± 14.6 -1Serum sodium (mmol/L) 146.9 ± 10.2 146Serum potassium (mmol/L) 7.7 ± 1.5 5Blood glucose (mg/dL) 311.3 ± 182.6 268Blood lactate (mmol/L) 12.1 ± 1.9 10
Data are given as means ± SD.
the analysis was based on Fisher exact test. We computedthe “mean CoPP” from start of chest compressions untilrestoration of spontaneous circulation and used for analysisthe time between 900 to 1500 seconds after cardiac arrest.Mean CoPP was compared between the groups by analysisof variance and subsequent pairwise t tests. Significancewas accepted for 2-sided P b .05. All calculations wereperformed with R: A language and environment forstatistical computing (R Foundation for Statistical Comput-ing, Vienna Austria).
3. Results
Of 25 female pigs, one died during preparation because ofa rupture of the femoral artery during insertion of the ballooncatheter. The 24 reported experiments (n = 8 in each studygroup) were performed according to the 3 protocols detailedin the Methods section. The pigs weighed 33 ± 3 kg in theconventional resuscitation group, 32 ± 2 kg in the cold flushgroup, and 33 ± 2 kg in the normothermic flush group. Therewere no group differences in baseline extracerebral physi-ologic variables important for cerebral recovery (Table 1).Variables in all groups were within physiologically
n
flush (n = 8) Normothermic flush (n = 8) P
5 ± 2.983 7.249 ± 0.373 .463.3 ± 134.1 188.0 ± 156.8 .952.4 ± 21.1 77.6 ± 44.8 .176.5 ± 8.5 21.4 ± 1.8 .003.7 ± 3.6 4.4 ± 17.4 .489.4 ± 59.8 147.8 ± 9.6 .966.8 ± 2.6 8.1 ± 2.3 .096.6 ± 182.0 148.0 ± 82.8 .215.3 ± 4.4 10.1 ± 1.6 .092

647Aortic flush during cardiac arrest
acceptable ranges. Extracerebral physiologic variables mea-sured 13 minutes after the start of resuscitation are shown inTable 2. Brain temperatures, blood temperatures, and CoPPsup to 45 minutes of cardiac arrest are shown in Fig. 3. In thecold flush group, the flush decreased brain temperatures from38.3°C ± 0.5°C to 33°C ± 0.5°C within 277 ± 112 seconds(Fig. 3B). Three animals in the normothermic and 3 in thecold flush groups achieved restoration of spontaneouscirculation, compared with none in the conventionalresuscitation group. This difference, however, was notstatistically significant. In the normothermic flush group,one animal achieved restoration of spontaneous circulation
Fig. 3 Temperatures (°C) and coronary perfusion pressures (CoPP, mresuscitation group (0), hypothermic flush group (1), and normothermic fl(pulmonary artery).
within the first countershock, whereas one animal needed 3and another needed 8 shocks. In the cold flush group, oneanimal needed one shock, one animal needed 3 shocks andone needed 8 shocks. Clinically noticeable lung edema wasobserved in 2 animals of the normothermic flush groupduring the resuscitation phase. We observed considerablyhigher mean CoPP values in the normothermic and cold flushgroups as compared with the conventional resuscitationgroup (analysis of variance, P = .046; cold vs conventional,P = .023; normothermic vs conventional, P = .041). Nosignificant difference in mean CoPP was found between thenormothermic and cold flush groups (P = .831).
m Hg) during 45 minutes of cardiac arrest for the conventionalush group (2). A, CoPP. B, brain temperature. C, blood temperature

Fig. 4 Outcome in final evaluation at day 9. Overall performancecategories (OPC, 1-5); each dot represents one pig. ROSC,restoration of spontaneous circulation.
648 W. Weihs et al.
Survival to 9 days after cardiac arrest was achieved in 3pigs in the cold flush group and in 2 pigs in the normothermicflush group. In the normothermic flush group, one pig died 3hours after restoration of spontaneous circulation due to heartfailure. Because our end point was final OPC at day 9, thispig was considered OPC 5 for statistical analysis. Final OPCand NDS are presented in Fig. 4.
4. Discussion
A smaller volume, cold (4°C) saline aortic flush duringprolonged cardiac arrest rapidly induces mild cerebralhypothermia to 33°C and improves coronary perfusionpressure but does not result in a significant improvement insurvival and neurologic outcome as compared with conven-tional resuscitation attempts. A normothermic (38.5°C) flushwith the same volume had similar but less strong effects oncoronary perfusion pressure and outcome as compared withthe cold flush.
None of the animals in the conventional resuscitationgroup were successfully resuscitated. However, in both flushgroups, more animals survived, thus indicating a generalpositive impact of the flush treatment due to improvedcoronary perfusion pressure. Even so, the initial restorationof spontaneous circulation rate was disappointing, may bedue to the heart not being capable of dealing with suchamounts of fluids in its early recovering phase and may bedue to the delay in commencing chest compressions until theend of the flush application. The idea behind delaying thecommencement of chest compressions 1 minute until the endof the flush application was that ischemic tissues, especiallyin the brain, might have been better protected againstreperfusion damage, for example, the potential harmfulreoxygenation cascade with the flush before the start ofreflow. In addition, the systemic blood dilution might haveimproved microcirculatory reflow and decreased levels ofthe mediators of the systemic inflammatory response
syndrome [23]. The 30-mL/kg ice-cold saline flush incombination with catecholamines applied through an arterialballoon catheter was able to reach mild hypothermia atexactly 33°C ± 0.5°C within seconds. The few survivinganimals in the cold flush group showed satisfying neurologicoutcomes, but most of the animals could not be resuscitated,which made it impossible to compare neurologic outcomesbetween hypothermic and normothermic groups in whichmost of the animals died because of heart failure.
In a previous pig study, we induced deep cerebralhypothermia (15°C) by 200 mL/kg cold saline flush [16]after 15 minutes of cardiac arrest, which resulted insuccessful resuscitation of 5 of 6 animals. In that study[16], the animals underwent a 20-minute period of cold stasiswithout chest compressions, followed by resuscitation withcardiopulmonary bypass. In a subsequent study, Janata et al[24] combined the period of cold stasis with chestcompressions to disperse hypothermia in the body, followedby resuscitation with cardiopulmonary bypass. With thismethod, all of the 8 pigs were resuscitated after 15 minutes ofcardiac arrest with good neurologic outcome. In a subsequentstudy [17], we induced 3 different brain temperatures after 15minutes of cardiac arrest by cooling with an extracorporealcooling system to avoid volume overload: surprisingly, abrain temperature of 30°C had a trend to better outcome ascompared with 24°C and 18°C. In the current study, weinvestigated the effect of a smaller volume aortic flush toinduce only mild hypothermia, which would not needcardiopulmonary bypass for rewarming and resuscitation.Without cardiopulmonary bypass, only 3 pigs in the coldaortic flush group could be resuscitated, but all 3 pigsshowed good neurologic outcome. We speculate that, in thisstudy, the imitating factor for overall good outcome wasresuscitability of the heart rather than brain damage. The coldflush, as used in this study, decreased brain temperature toonly 33°C. Whether a slightly larger flush volume might beable to improve resuscitability without volume overload, andthus improving neurologic outcome, remains speculative andwill be the subject of future studies.
Yu et al [25] compared 2 groups of pigs, in whichnasopharyngeal or IV cooling was induced after 15 minutesof untreated VF cardiac arrest. Nasopharyngeal coolingwithout the use of cardiopulmonary bypass for resuscitationresulted in the same rate of spontaneous circulation ascompared with our previous studies [17,26], in which weused cardiopulmonary bypass for resuscitation. In the samestudy, Yu et al [25] showed that coronary perfusion pressurewas significantly higher in the study group with nasopha-ryngeal cooling as compared with IV cooling, which couldbe explained by local cooling in the brain, inducingneurocardiac reflexes for beneficial cardiovascular responses[27]. In our study, the cold flush seems to have a beneficialinfluence on coronary perfusion pressure when comparedwith the normothermic flush. Especially at the end of theresuscitation period, a higher coronary perfusion pressurewas seen in the cold flush group compared with the

649Aortic flush during cardiac arrest
normothermic flush group (Fig. 3). Higher coronaryperfusion pressure resulted in a better resuscitation rate;however, not all animals could be resuscitated. We speculatethat the use of cardiopulmonary bypass would enableresuscitation of all animals, as demonstrated in our previousstudies with similar cardiac arrest durations.
The most significant limitation of this work is the clinicalscenario on which it is modeled. The time needed for vesselaccess and, thereby, application of flush volume wouldfurther prolong the anoxia time. However, the aim of thisstudy was to investigate the feasibility of induction of mildhypothermia during cardiac arrest, before reperfusion, andthe effect on resuscitability and outcome as compared withstandard resuscitation attempts with comparable cardiacarrest no-flow times. Another significant limitation of thestudy is the sample size and, thus, potential for type 1 error. Ifflush groups were combined and compared with conven-tional resuscitation, rate of restoration of spontaneouscirculation was 38% (6/16) vs 0% (0/8) (P = .06).Vasopressor support in both groups did not follow thetraditional advanced cardiac life support algorithm. We havechosen to use a combination of vasopressin and epinephrineduring chest compressions, which, in pigs, has shown to besuperior to vasopressor alone [28]. In addition, different totaldoses of epinephrine and vasopressin were used in the 2groups. The flush groups received a bolus of epinephrine andvasopressin as part of the flush before start of resuscitation,which seems to be needed to successfully reduce braintemperature and, therefore, is a condition sine qua non for theflush [15]. It cannot be ruled out that the higher total dose ofepinephrine used in the flush groups influenced outcome. Ablinded design was not feasible because of the design of thestudy with chest compressions performed only in the controlgroup; however, evaluation of neurologic outcome was byblinded investigators.
The results of this study show that a smaller volume (30mL/kg), cold (4°C) saline aortic flush during prolongedcardiac arrest rapidly induces mild cerebral hypothermia to33°C and improves coronary perfusion pressure but does notresult in a significant improvement in outcome as comparedwith conventional resuscitation attempts. A normothermic(38.5°C) flush with the same volume had similar effects oncoronary perfusion pressure and outcome as compared withthe cold flush. Further studies are needed to determineoptimal flush volume and flush temperature for resuscitationafter prolonged cardiac arrest without the need forcardiopulmonary bypass.
Acknowledgments
The authors gratefully acknowledge the help of all thenurses, laboratory technicians, nightshift students, andanimal keepers of the Core Centre of Biomedical Research,Medical University of Vienna, Vienna, Austria.
References
[1] Atwood C, Eisenberg MS, Herlitz J, Rea TD. Incidence of EMS-treated out-of-hospital cardiac arrest in Europe. Resuscitation 2005;67:75-80.
[2] Holzer M, Cerchiari E, Martens P, et al. Mild therapeutic hypothermiato improve the neurologic outcome after cardiac arrest. N Engl J Med2002;346:549-56.
[3] Bernard SA, Gray TW, Buist MD, et al. Treatment of comatosesurvivors of out-of-hospital cardiac arrest with induced hypothermia.N EnglJ Med 2002;346:557-63.
[4] Kamarainen A, Virkkunen I, Tenhunen J, et al. Prehospital therapeutichypothermia for comatose survivors of cardiac arrest: a randomizedcontrolled trial. Acta Anaesthesiol Scand 2009;53:900-7.
[5] Wolff B, Machill K, Schumacher D, et al. Early achievement of mildtherapeutic hypothermia and the neurologic outcome after cardiacarrest. Int J Cardiol 2009;133:223-8.
[6] Bellamy R, Safar P, Tisherman SA, et al. Suspended animation fordelayed resuscitation. Crit Care Med 1996;24:S24-47.
[7] Behringer W, Safar P, Wu X, et al. Survival without brain damage afterclinical death of 60-120 mins in dogs using suspended animation byprofound hypothermia. Crit Care Med 2003;31:1523-31.
[8] Wu X, Drabek T, Tisherman SA, et al. Emergency preservation andresuscitation with profound hypothermia, oxygen, and glucose allowsreliable neurological recovery after 3 h of cardiac arrest from rapidexsanguination in dogs. J Cereb Blood Flow Metab 2008;28:302-11.
[9] Alam HB, Casas F, Chen Z, et al. Development and testing of portablepump for the induction of profound hypothermia in a swine model oflethal vascular injuries. J Trauma 2006;61:1321-9.
[10] Drabek T, Stezoski J. Garman RH, et al:Exsanguination cardiac arrestin rats treated by 60 min, but not 75 min, emergency preservation anddelayed resuscitation is associated with intact outcome. Resuscitation2007;75:114-23.
[11] Busto R, Dietrich WD, Globus MY, et al. Small differences inintraischemic brain temperature critically determine the extent ofischemic neuronal injury. J Cereb Blood Flow Metab 1987;7:729-38.
[12] Minamisawa H, Smith ML, Siesjo BK. The effect of mildhyperthermia and hypothermia on brain damage following 5, 10,and 15 minutes of forebrain ischemia. Ann Neurol 1990;28:26-33.
[13] Dietrich WD, Busto R, Alonso O, et al. Intraischemic but notpostischemic brain hypothermia protects chronically following globalforebrain ischemia in rats. J Cereb Blood Flow Metab 1993;13:541-9.
[14] Abella BS, Zhao D, Alvarado J, et al. Intra-arrest cooling improvesoutcomes in a murine cardiac arrest model. Circulation 2004;109:2786-91.
[15] Janata A, Holzer M, Bayegan K, et al. Rapid induction of cerebralhypothermia by aortic flush during normovolemic cardiac arrest inpigs. Crit Care Med 2006;34:1769-74.
[16] Janata A, Bayegan K, Weihs W, et al. Emergency preservation andresuscitation improve survival after 15 minutes of normovolemiccardiac arrest in pigs. Crit Care Med 2007;35:2785-91.
[17] Weihs W, Krizanac D, Sterz F, et al. Outcome after resuscitation usingcontrolled rapid extracorporeal cooling to a brain temperature of 30degrees C, 24 degrees C and 18 degrees C during cardiac arrest in pigs.Resuscitation 2010;81:242-7.
[18] Kurita T, Morita K, Kazama T, Sato S. Comparison of isoflurane andpropofol-fentanyl anaesthesia in a swine model of asphyxia. Br JAnaesth 2003;91:871-7.
[19] Holzer M, Sterz F, Behringer W, et al. Endothelin-1 elevates regionalcerebral perfusion during prolonged ventricular fibrillation cardiacarrest in pigs. Resuscitation 2002;55:317-27.
[20] Sipos M, Holzer M, Bayegan K. A novel highly observer-independentneurologic examination procedure for pigs in a model for cardiac arrestresuscitation. WienTierarztl Monat 2008;95:28-38.
[21] Safar P. Long-term animal outcome models for cardiopulmonary-cerebral resuscitation research. Crit Care Med 1985;13:936-40.

650 W. Weihs et al.
[22] Schratter A, Holzer M, Sterz F, et al. New conventional long-termsurvival normovolemic cardiac arrest pig model. Resuscitation2011;82:90-6.
[23] Sipos W, Duvigneau C, Sterz F, et al. Changes in interleukin-10mRNA expression are predictive for 9-day survival of pigs in anemergency preservation and resuscitation model. Resuscitation2010;81:603-8.
[24] Janata A, Weihs W, Schratter A, et al. Cold aortic flush and chestcompressions enable good neurologic outcome after 15 mins of ventric-ular fibrillation in cardiac arrest in pigs. Crit Care Med 2010;38:1637-43.
[25] Yu T, Barbut D, Ristagno G, et al. Survival and neurologicaloutcomes after nasopharyngeal cooling or peripheral vein cold
saline infusion initiated during cardiopulmonary resuscitation in aporcine model of prolonged cardiac arrest. Crit Care Med 2010;38:916-21.
[26] Janata A, Bayegan K, Sterz F, et al. Limits of conventional therapiesafter prolonged normovolemic cardiac arrest in swine. Resuscitation2008;79:133-8.
[27] Davis AM, Natelson BH. Brain-heart interactions. The neurocardiol-ogy of arrhythmia and sudden cardiac death. Tex Heart Inst J 1993;20:158-69.
[28] Wenzel V, Lindner KH. Employing vasopressin during cardiopulmo-nary resuscitation and vasodilatory shock as a lifesaving vasopressor.Cardiovasc Res 2001;51:529-41.
Related Documents






![Therapeutic Hypothermia in Traumatic Brain Injurycdn.intechopen.com/pdfs/42406/InTech-Therapeutic... · 80 Therapeutic Hypothermia in Brain Injury hypothermia [13-50]. In addition,](https://static.cupdf.com/doc/110x72/5e902d36c9c187069d5dbc10/therapeutic-hypothermia-in-traumatic-brain-80-therapeutic-hypothermia-in-brain-injury.jpg)