Randomized Trial of Early Developmental Intervention on Outcomes in Children after Birth Asphyxia in Developing Countries Waldemar A. Carlo, MD 1,2 , Shivaprasad S. Goudar, MD, MHPE 3 , Omrana Pasha, MBBS, MSPH 4 , Elwyn Chomba, MD 2,5 , Jan L. Wallander, PhD 6 , Fred J. Biasini, PhD 1 , Elizabeth M. McClure, MEd 7 , Vanessa Thorsten, MPH 7 , Hrishikesh Chakraborty, DrPH 7,8 , Dennis Wallace, PhD 7 , Darlene L. Shearer, PhD 9 , Linda L. Wright, MD 10 , and the Brain Research to Ameliorate Impaired Neurodevelopment-Home-Based Intervention Trial Committee and the National Institute of Child Health and Human Development Global Network for Women’s and Children’s Health Research Investigators* Objective To determine if early developmental intervention (EDI) improves developmental abilities in resuscitated children. Study design This was a parallel group, randomized controlled trial of infants unresponsive to stimulation who received bag and mask ventilation as part of their resuscitation at birth and infants who did not require any resus- citation born in rural communities in India, Pakistan, and Zambia. Intervention infants received a parent- implemented EDI delivered with home visits by parent trainers every other week for 3 years starting the first month after birth. Parents in both intervention and control groups received health and safety counseling during home visits on the same schedule. The main outcome measure was the Mental Development Index (MDI) of the Bayley Scales of Infant Development, 2nd edition, assessed at 36 months by evaluators unaware of treatment group and resus- citation history. Results MDI was higher in the EDI (102.6 9.8) compared with the control resuscitated children (98.0 14.6, 1- sided P = .0202), but there was no difference between groups in the nonresuscitated children (100.1 10.7 vs 97.7 10.4, P = .1392). The Psychomotor Development Index was higher in the EDI group for both the resuscitated (P = .0430) and nonresuscitated children (P = .0164). Conclusions This trial of home-based, parent provided EDI in children resuscitated at birth provides evidence of treatment benefits on cognitive and psychomotor outcomes. MDI and Psychomotor Development Index scores of both nonresuscitated and resuscitated infants were within normal range, independent of early interven- tion. (J Pediatr 2013;162:705-12). F ailure to initiate or sustain spontaneous breathing at birth, also called birth asphyxia, 1 is a leading cause of perinatal mor- tality, neonatal encephalopathy, intellectual disability, cerebral palsy, and other childhood neurodevelopmental disor- ders, 2,3 particularly in low- and middle-income countries (LMIC). 4 Birth asphyxia accounts for about 23% of the 3.5 million neonatal deaths that occur each year worldwide, 98% of which occur in LMIC. 5 About 30% of infants who survived following birth asphyxia in LMIC had abnormal neurologic examinations at 2 months, accounting for 50% of the infants referred for an abnormal neurologic examination at this age. 4 An esti- mated 1 million children who survive birth asphyxia each year develop problems such as learning difficulties, cerebral palsy, and other disabilities. 6 Birth asphyxia is estimated to result in a loss of over 41 million disability adjusted life years, one of the leading causes for all ages worldwide. 7 Mortality and morbidity from birth asphyxia disproportionately affect more infants in LMIC. About 6%-10% of all infants fail to initiate or sustain spontaneous breathing at birth and need some assistance to establish normal breathing. 8,9 Resuscitation at birth decreases fresh stillbirths 10 and early neonatal mortality. 9,11,12 Although From the 1 University of Alabama at Birmingham, Birmingham, AL; 2 Center for Infectious Disease Research in Zambia, Lusaka, Zambia; 3 KLE University’s Jawaharlal Nehru Medical College, Belgaum, India; 4 Aga Kahn University Medical College, Karachi, Pakistan; 5 University of Zambia, Lusaka, Zambia; 6 University of California, Merced, Merced, CA; 7 RTI International, Durham, NC; 8 University of South Carolina, Columbia, SC; 9 Western Kentucky University, Bowling Green, KY; and 10 Eunice Kennedy Shriver National Institute of Child Health and Human Development, Bethesda, MD *A list of members of the Brain Research to Ameliorate Impaired Neurodevelopment-Home-Based Intervention Trial Committee and the National Institute of Child Health and Human Development Global Network for Women and Children’s Health Research Investigators is available at www.jpeds.com (Appendix). Funded by Eunice Kennedy Shriver National Institute of Child Health and Human Development Global Network for Women’s and Children’s Health Research and the National Institute of Neurological Disorders and Stroke (HD43464, HD42372, HD40607, and HD40636), the Fo- garty International Center (TW006703), the Perinatal Health and Human Development Research Program, and the Children’s of Alabama Centennial Scholar Fund of the University of Alabama at Birmingham. W.C. is on the Mednax Board of Directors. The other authors declare no conflicts of interest. Registered at ClinicalTrials.gov: NCT00639184. 0022-3476/$ - see front matter. Copyright ª 2013 Mosby Inc. All rights reserved. http://dx.doi.org/10.1016/j.jpeds.2012.09.052 ASQ Ages and Stages Questionnaire, 2nd edition ASQ:SE Ages and Stages Questionnaire: Social-Emotional BSID-II Bayley Scales of Infant Development, 2nd edition BSID-III Bayley Scales of Infant Development, 3rd edition EDI Early developmental intervention LMIC Low- and middle-income countries MDI Mental Development Index PDI Psychomotor Development Index WHO World Health Organization 705

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Randomized Trial of Early Developmental Intervention on Outcomesin Children after Birth Asphyxia in Developing Countries
Waldemar A. Carlo, MD1,2, Shivaprasad S. Goudar, MD, MHPE3, Omrana Pasha, MBBS, MSPH4, Elwyn Chomba, MD2,5,
Jan L. Wallander, PhD6, Fred J. Biasini, PhD1, Elizabeth M. McClure, MEd7, Vanessa Thorsten, MPH7,
Hrishikesh Chakraborty, DrPH7,8, Dennis Wallace, PhD7, Darlene L. Shearer, PhD9, Linda L. Wright, MD10, and the Brain
Research to Ameliorate Impaired Neurodevelopment-Home-Based Intervention Trial Committee and the National Institute
of Child Health and Human Development Global Network for Women’s and Children’s Health Research Investigators*
Objective To determine if early developmental intervention (EDI) improves developmental abilities in resuscitatedchildren.Study design This was a parallel group, randomized controlled trial of infants unresponsive to stimulation whoreceived bag and mask ventilation as part of their resuscitation at birth and infants who did not require any resus-citation born in rural communities in India, Pakistan, and Zambia. Intervention infants received a parent-implemented EDI delivered with home visits by parent trainers every other week for 3 years starting the first monthafter birth. Parents in both intervention and control groups received health and safety counseling during home visitson the same schedule. The main outcome measure was the Mental Development Index (MDI) of the Bayley Scalesof Infant Development, 2nd edition, assessed at 36 months by evaluators unaware of treatment group and resus-citation history.Results MDI was higher in the EDI (102.6 � 9.8) compared with the control resuscitated children (98.0 � 14.6, 1-sided P = .0202), but there was no difference between groups in the nonresuscitated children (100.1 � 10.7 vs97.7� 10.4, P = .1392). The Psychomotor Development Index was higher in the EDI group for both the resuscitated(P = .0430) and nonresuscitated children (P = .0164).Conclusions This trial of home-based, parent provided EDI in children resuscitated at birth provides evidenceof treatment benefits on cognitive and psychomotor outcomes. MDI and Psychomotor Development Indexscores of both nonresuscitated and resuscitated infants were within normal range, independent of early interven-tion. (J Pediatr 2013;162:705-12).
Failure to initiate or sustain spontaneous breathing at birth, also called birth asphyxia,1 is a leading cause of perinatal mor-tality, neonatal encephalopathy, intellectual disability, cerebral palsy, and other childhood neurodevelopmental disor-ders,2,3 particularly in low- and middle-income countries (LMIC).4 Birth asphyxia accounts for about 23% of the
From the 1University of Alabama at Birmingham,Birmingham, AL; 2Center for Infectious DiseaseResearch in Zambia, Lusaka, Zambia; 3KLE University’sJawaharlal Nehru Medical College, Belgaum, India; 4AgaKahn University Medical College, Karachi, Pakistan;5University of Zambia, Lusaka, Zambia; 6University ofCalifornia, Merced, Merced, CA; 7RTI International,Durham, NC; 8University of South Carolina, Columbia,SC; 9Western Kentucky University, Bowling Green, KY;and 10Eunice Kennedy Shriver National Institute of ChildHealth and Human Development, Bethesda, MD
*A list of members of the Brain Research to AmeliorateImpaired Neurodevelopment-Home-Based InterventionTrial Committee and the National Institute of Child Healthand Human Development Global Network for Womenand Children’s Health Research Investigators is availableat www.jpeds.com (Appendix).
3.5 million neonatal deaths that occur each year worldwide, 98% of which occurin LMIC.5 About 30% of infants who survived following birth asphyxia in LMIChad abnormal neurologic examinations at 2 months, accounting for 50% of theinfants referred for an abnormal neurologic examination at this age.4 An esti-mated 1 million children who survive birth asphyxia each year develop problemssuch as learning difficulties, cerebral palsy, and other disabilities.6 Birth asphyxiais estimated to result in a loss of over 41 million disability adjusted life years, oneof the leading causes for all ages worldwide.7 Mortality and morbidity from birthasphyxia disproportionately affect more infants in LMIC.
About 6%-10% of all infants fail to initiate or sustain spontaneous breathing atbirth and need some assistance to establish normal breathing.8,9 Resuscitation atbirth decreases fresh stillbirths10 and early neonatal mortality.9,11,12 Although
Funded by Eunice Kennedy Shriver National Institute ofChild Health and Human Development Global Networkfor Women’s and Children’s Health Research and theNational Institute of Neurological Disorders and Stroke(HD43464, HD42372, HD40607, and HD40636), the Fo-garty International Center (TW006703), the PerinatalHealth and HumanDevelopment Research Program, andthe Children’s of AlabamaCentennial Scholar Fund of theUniversity of Alabama at Birmingham. W.C. is on theMednax Board of Directors. The other authors declare noconflicts of interest.
Registered at ClinicalTrials.gov: NCT00639184.
0022-3476/$ - see front matter. Copyright ª 2013 Mosby Inc.
All rights reserved. http://dx.doi.org/10.1016/j.jpeds.2012.09.052
ASQ Ages and Stages Questionnaire, 2nd edition
ASQ:SE Ages and Stages Questionnaire: Social-Emotional
BSID-II Bayley Scales of Infant Development, 2nd edition
BSID-III Bayley Scales of Infant Development, 3rd edition
EDI Early developmental intervention
LMIC Low- and middle-income countries
MDI Mental Development Index
PDI Psychomotor Development Index
WHO World Health Organization
705

THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 162, No. 4
neonatal resuscitation training programs for perinatal healthcare providers are standard in high- income countries, theseprograms have had limited penetration in many LMIC, inpart because of the concern of saving infants at risk for neuro-developmental disorders.
It has been estimated that more than 200 of the approxi-mately 700 million children under 5 years of age fail to reachtheir potential for cognitive development.13 Programs ofearly developmental intervention (EDI) use structured expe-riences in an attempt to prevent or limit impaired cognitivefunction early in life. Positive effects of EDI have been dem-onstrated in numerous controlled trials,14-16 but few studieshave been conducted in infants with birth asphyxia and inLMIC. Although modifiable biologic and psychosocial riskfactors and possible interventions have been determined,17
a panel of international experts recommended trials to deter-mine effective and scalable parental EDI strategies with largerand more diverse patient populations using strategies of out-reach to disadvantaged children.16 Furthermore, the mosteffective EDI programs appear to be those that provide directlearning experiences to children and families, are targetedtoward younger and disadvantaged children, are of longerduration, high quality, and high intensity, and are integratedwith family support and health and nutrition counseling,16
but there is no consensus on whether or not EDI programsshould be recommended for these patients in LMIC.
Methods
The current trial, the Brain Research to Ameliorate ImpairedNeurodevelopment: Home-based Intervention Trial (regis-tered at ClinicalTrials.gov: NCT00639184), was designed totest the primary hypothesis that a well designed16 home-based, parent-implemented early intervention programimproves cognitive abilities as indicated by a higher MentalDevelopmental Index (MDI) at 36 months on the BayleyScales of Infant Development, 2nd edition (BSID-II) amonga group of infants who received bag and mask ventilation aspart of their resuscitation but did not have severe encepha-lopathy during the neonatal period compared with a controlgroup. To enable comparison, a group of infants from thesame communities who did not require resuscitation at birthwere also randomized concurrently to the same interventionor control home visits.
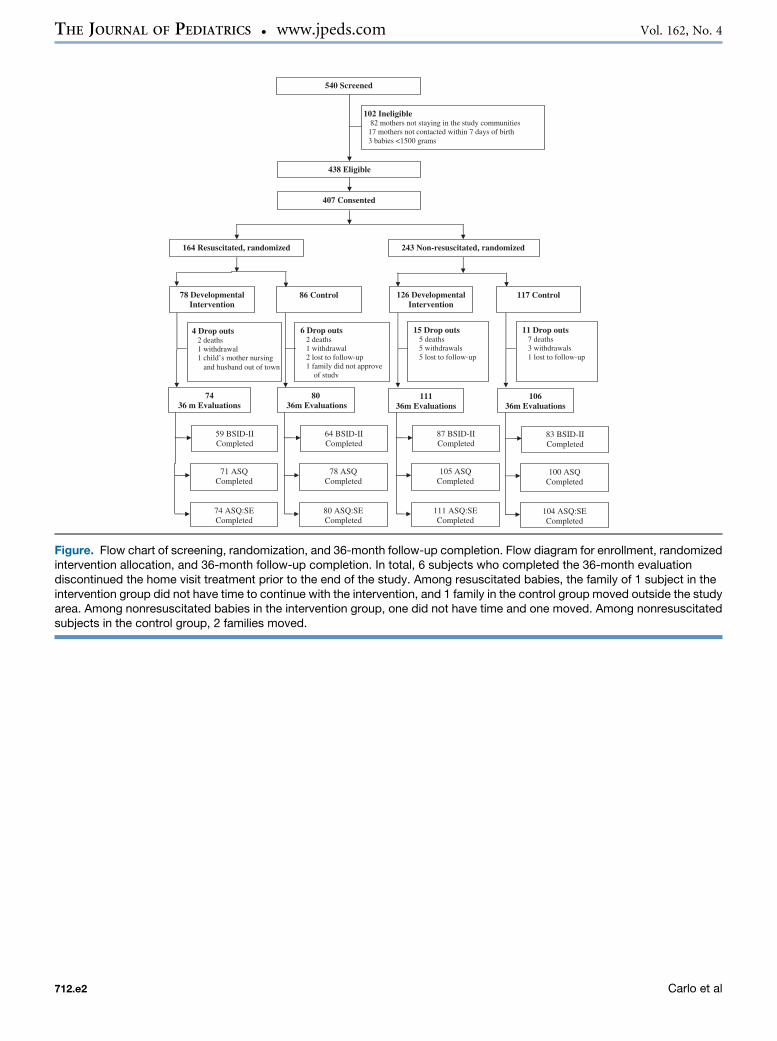
This parallel design randomized controlled trial was im-plemented in 2 populations: (1) infants with birth asphyxiaunresponsive to stimulation and the initial steps of resuscita-tion who received bag and mask ventilation; and (2) infantswho did not require any resuscitation. Infants in each cohortwere randomized individually to 1 of 2 trial conditions (EDIplus health and safety counseling or control that includedhealth and safety counseling only) using 1:1 concealed paral-lel allocation, matched for country and chronological timeusing variable block sizes to assure allocation concealment(Figure; available at www.jpeds.com). There were nochanges in trial design or outcome measures followingcommencement of enrollment other than home visits were
706
continued every other week between 12 and 36 months ofage instead of the planned every fourth week visits toincrease the intensity of the intervention. The trial wasapproved by the institutional review boards at theUniversity of Alabama at Birmingham, Research TriangleInstitute International, and each participating clinical site.Details on the trial design have been published.18
Infants who received bag and mask ventilation for resus-citation at birth, in rural, poor communities in 3 sites in In-dia, Pakistan, and Zambia during and immediatelyfollowing the First Breath Trial10 were screened for enroll-ment into this trial. Birth asphyxia was defined as the inabil-ity to initiate or sustain spontaneous breathing at birthusing the World Health Organization (WHO) definition.1
Infants were ineligible if they met any of the following ex-clusion criteria: (1) the birth weight was less than 1500 gat birth; (2) their neurologic examination at 7 days was se-verely abnormal (grade III by Ellis classification)19; (3) themother was <15 years of age or unable/unwilling to partic-ipate; or (4) the mother was not planning to stay in thestudy communities for the following 3 years. Infants withbirth asphyxia (resuscitated) and infants without birth as-phyxia or other perinatal complications (nonresuscitated)matched for country and chronological time born from Jan-uary 2007 through June 2008 were randomly selected duringthe 7-day follow-up visit after birth from infants enrolled inthe First Breath Trial.10 A list of potential enrollees was dis-tributed to the investigators in each country to obtain con-sent for the trial. Written informed consent was obtainedduring the second week after birth following the 7-day neu-rologic assessment and before randomization.
Intervention ProceduresA home-based, parent-implemented EDI model was selectedto strengthen parent-child interaction. The Partners forLearning20 curriculum and supplemental materials wereused by parent trainers to introduce playful interactive learn-ing activities depicted on cards given andmodeled to the par-ents during home visits using the Portage Model.21 Partnersfor Learning covers a full spectrum of competences, organizedinto the 4 areas: (1) cognitive and fine motor; (2) social andself-help; (3) gross motor; and (4) language skills. Investiga-tors at each research site selected EDI parent trainers (highschool graduates in 2 sites and 4-year graduates after highschool in 1 site) who were trained in an initial 5-day work-shop at each research site. A second workshop was conductedbefore participating children began to reach 18months of ageto adapt the approach to children up to 36 months. Eachparent-child pair was assigned to the same trainer through-out the trial whenever possible. Home visits were conductedevery other week from enrollment (at 1-2 weeks) through 36months. During each visit, the trainer presented 1 or 2 playfulinteractive learning activities using cards. Each activity tar-geted a developmentally appropriate competence. The parentpracticed the activity in the presence of the trainer who pro-vided feedback to the parents. The activity cards were leftwith the parents who were encouraged to apply the targeted
Carlo et al

April 2013 ORIGINAL ARTICLES
activities by integrating them into daily life with the childuntil the next home visit. Cycles of use allowed the parentsto implement several activities and move on to new activitiesas the child mastered each competence. The trainer intro-duced new activities to match and enhance the child’s devel-opmental competences. The trainers used a log book torecord their impressions about each visit. To review progresswith the activities, the trainers were supervised with observa-tions during actual home visits and constructive feedbackwas provided. Adherence to the intervention was measuredby home visits completed on schedule within its assigned2-week window following the preceding visit and parental re-port of frequency of implementation of the activities betweenhome visits.
Control ProceduresParents in both the control and intervention groups receivedhealth and safety counseling during every home visit. Healthand safety counseling content was based on the WHO healtheducation curriculum,22 which included breast feeding,nutrition, hygiene, safety in the home and community,awareness of danger signs, management of diarrhea, andwell-child checkups and vaccinations. The health and safetycounseling was provided by both the intervention and con-trol trainers who had participated in a 5-day training con-ducted separately from the EDI training at each research site.
Outcome MeasuresThe primary outcome measure was the BSID-II MDI.23 Sec-ondary outcome measures included the Psychomotor Devel-opment Index (PDI) of the BSID-II, the Ages and StagesQuestionnaire, 2nd edition (ASQ),24 the Ages and StagesQuestionnaire: Social-Emotional (ASQ:SE), and healthdata. The BSID-II was selected as the main outcome measurefor this trial because it had been used extensively in a numberof LMIC. The BSID-II underwent extensive pre-testing ateach site to verify validity in the local context, and a few itemswere slightly modified to make it more culturally appropriate(eg, image of a sandal instead of a shoe). The BSID-II was ad-ministered directly to each child in the appropriate languageusing standard material. The ASQ, which is a screening toolpreviously used in LMIC,25 was used to assess parent-reported child development observed in the home environ-ment in the domains of communication, gross motor andfine motor, problem solving, and personal-social develop-ment using age-specific forms. To remove issues of literacy,the ASQ was administered in an interview format with theparent. Health data were collected on weight, height, headcircumference, breastfeeding, diet, immunization status,hearing and vision impairment, and childhood illnesses. As-sessments of outcomes occurred when the children were 12,24, and 36 months of age and were performed by evaluatorstrained in 4-day workshops before each yearly evaluation.The evaluators were familiar with local language and cultureand unaware of the participants’ resuscitation history andtreatment group. Study evaluators made every attempt tosuccessfully evaluate the children on or shortly after thechild’s third birthday. If an evaluation could not be
Randomized Trial of Early Developmental Intervention on OutcomDeveloping Countries
completed because of severe behavioral problems uncharac-teristic of the child or an acute illness, the evaluation was re-scheduled and the child was retested when possible. Outcomeevaluation data at 36 months are presented here.
Sample SizeTo test the hypothesis that the EDI improves the MDI on theBSID-II, at least 40 children in each of the 4 groups had tohave completed the intervention and 3-year assessment (as-suming a 5% significance level, a power of 90%, a differencebetween the groups on the BSID-II of 10 points favoring theearly development group, and a SD of 15 using a 1-tailedtest). Because of high attrition and missing values in our pilottrial of 80 infants (24% lost to follow-up, 20% withdrew, and4% died),4 at least 60 infants (a minimum of 20 per site) wererequired to be enrolled in each of the 4 groups.
Data Collection and ManagementMaternal and neonatal data were collected by trained birthattendants who were supervised by community coordinatorsas part of the First Breath Trial.10 In addition, data on familydemographics and resources were collected at enrollment inthe trial through the administration of a modified WorldBank tool in a structured interview and included maternalage, education (none/illiterate, none but literate/primaryschool, at least some secondary school), family assets, andhome living standard. The presence of 11 family assets (eg,radio, television, refrigerator, bicycle) were tallied as a FamilyResources Index. A Home Living Standard Index was calcu-lated based on status regarding 7 indicators (eg, home build-ing material, number of rooms, water source). Data on eachvisit were collected by the parent trainers. The data weretransmitted electronically to the data coordinating center atRTI International. Data edits and inter- and intra-form con-sistency checks were performed. Adverse events were re-ported to the Data Monitoring Committee, whichmonitored the study progress and made reports and recom-mendations for continuation of the trial.
Statistical AnalysesDescriptive statistics were generated for monitoring enroll-ment and retention, completion of home visits, and comple-tion of the 36-month evaluation. For the ASQ and ASQ:SE,only subjects who completed the evaluation within themanual-specified windows of 34-39 months for the ASQand 34-41 months for the ASQ:SE were included in theseanalyses. Mean differences in 36-month evaluation outcomeswere determined between the 2 treatment groups for each re-suscitation cohort using t tests. All subjects included in theanalyses were assigned the treatment to which they were ran-domized. Additionally, an exploratory analysis combiningthe resuscitated and nonresuscitated children was performedto assess differences in 36-month evaluation outcomes bytreatment group (ie, intervention vs control). This post-hocanalysis was based on general linear models. Althougha 1-sided t test (alpha = 0.05) as specified by the protocolwas employed to test the primary outcome, differences be-tween the means for all other continuous measures were
es in Children after Birth Asphyxia in 707
Table
II.Thirty-six-m
onth
BSID-IIscoresandother
majorneurodevelopmentaloutcomes
bytreatm
ent
Resuscitated
Nonresuscitated
Com
bined
Earlyintervention
andhealth
care
coun
seling
Healthcare
counseling
only(control)
MD(95%
CI)/
RR(95%
CI)
Earlyintervention
andhealth
care
coun
seling
Healthcare
coun
seling
only(control)
MD(95%
CI)/
RR(95%
CI)
Earlyintervention
andhealth
care
coun
seling
Healthcare
coun
seling
only(control)
MD(95%
CI)/
RR(95%
CI)
36-m
oBSID-IIevaluation
completeN
5964
8783
146
147
MDIm
ean�
SD
102.6�
9.8
98.0�
14.6
4.63
(0.93,N)
100.1�
10.7
97.7�
10.4
2.41
(�0.79,5.62)
101.1�
10.4
97.8�
12.4
3.30
(0.67,5.93)
PDIm
ean�
SD
108.7�
12.0
103.3�
17.0
5.41
(0.17,10.65)
105.4�
15.3
99.3�
17.4
6.08
(1.13,11.03)
106.7�
14.1
101.0�
17.3
5.69
(2.06,9.31)
MDI<
85n/N(%)
2/59
(3.4)
7/64
(10.9)
0.31
(0.07,1.43)
3/87
(3.4)
8/83
(9.6)
0.36
(0.10,1.30)
5/146(3.4)
15/147
(10.2)
0.34
(0.13,0.90)
MDI<
70n/N(%)
1/59
(1.7)
4/64
(6.3)
0.27
(0.03,2.36)
2/87
(2.3)
0/83
(0.0)
-3/146(2.1)
4/147(2.7)
0.76
(0.17,3.32)
PDI<
85n/N(%)
3/59
(5.1)
7/64
(10.9)
0.46
(0.13,1.72)
5/87
(5.7)
12/83(14.5)
0.40
(0.15,1.08)
8/146(5.5)
19/147
(12.9)
0.42
(0.19,0.94)
PDI<
70n/N(%)
1/59
(1.7)
3/64
(4.7)
0.36
(0.04,3.38)
4/87
(4.6)
7/83
(8.4)
0.55
(0.17,1.79)
5/146(3.4)
10/147
(6.8)
0.50
(0.18,1.44)
MD,meandifference;RR,relativerisk.
One-sided
ttestand
meandifference
CIw
ereappliedtotesttheprimaryhypothesisthattheinterventiongroupwillimprovetheBSID-IIM
DIat36monthscomparedwith
thecontrolgroup
amongresuscitatedinfants.Tw
o-sidedttestsandmeandifference
CIswere
appliedtotheBSID-IIMDIscoresam
ongthenonresuscitatedinfantsandtheBSID-IIPDIscores
amongtheresuscitatedandnonresuscitatedinfants.
THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 162, No. 4
tested using a 2-sided t test (alpha = 0.05). Point and intervalestimates of relative risk were calculated using standardlarge-sample formulae for categorical measures. Differencesin categorical measures were tested using c2 and Fisher exacttests.
Cutoff values indicating moderate delay (score <85) andsevere delay (score <70) for the BSID-II were set at 1 and 2SDs from the instrument standardized mean (100 � 15points). Standard cutoffs24 for each ASQ developmental do-main were used to distinguish children requiring a referralfor further neurodevelopmental evaluation from those oper-ating within normal range.
Results
The infants enrolled in this trial were derived from a total of 540births screened (Figure). Of these, 438 were eligible and 407(93%) were consented; 36 (9%) infants were not assessed at36 months because of death (n = 16), withdrawal (n = 10),loss to follow-up (n = 8), or other reasons (n = 2) with lossescomparable across treatment arms within resuscitationcohorts. Six subjects who completed the 36-month evaluationdiscontinued the home visit treatment prior to the end of thestudy but their data were included in all analyses. Maternaland infant characteristics were similar in the intervention andcontrol group (Table I; available at www.jpeds.com) exceptfor a higher rate of prenatal care in the control groupnonresuscitated infants. Adherence to the home visits throughthe 36-month evaluation was 96.3% and 97.8% in the earlyintervention and control groups, respectively. Among theintervention group, parent report of adherence to theimplementation of the intervention activities over the 3 yearsof the study among those who completed the 36-monthevaluation was an average of 62.1% of the days amongresuscitated infants and 61.5% of the days amongnonresuscitated infants. This equates to practicing theintervention activities an average of 4.3 days per week in bothgroups.
The BSID-II MDI and PDI scores were successfully mea-sured in 123 resuscitated and 170 nonresuscitated childrenfor a total of 293/371 (79%) of the 36-month evaluations.Two children who scored within normal limits for the 12-and 24-month evaluations did not successfully completethe 36-month BSID-II evaluation. Additionally, evaluationsdone by 1 evaluator were excluded from the BSID-II analysis(n = 76) because the evaluator consistently scored the chil-dren much lower than the other evaluators. Specifically, theevaluator’s mean MDI score was 13 points lower than thenext lowest evaluator and 17 points lower than the overallmeanMDI. The 76 evaluations were evenly distributed acrossthe treatment groups by resuscitation status. The demo-graphics of the 76 children did not differ from evaluationscompleted by other evaluators at the affected clinical site.The primary outcome was computed both with and withoutthe evaluator’s records to confirm that removing the datafrom this evaluator did not change the determination oftreatment effect.
708 Carlo et al
Table
III.
Thirty-six-m
onth
ages
andstages
questionnairesscoresbytreatm
entgroup
Resuscitated
Nonresuscitated
Com
bined
Earlyintervention
andhealth
care
counseling
Healthcare
counselingonly
(control)
MD(95%
CI)/RR
(95%
CI)
Earlyintervention
andhealth
care
counseling
Healthcare
counseling
only(control)
MD(95%
CI)/RR
(95%
CI)
Earlyintervention
andhealth
care
counseling
Healthcare
counseling
only(control)
MD(95%
CI)/RR
(95%
CI)
36-m
oevaluationcompleteN
7480
111
106
185
186
Evaluatedwithinwindow(34-39
mo)N
7178
105
100
176
178
ASQtotalscore
Mean�
SD
253.7�
41.5
239.0�
63.2
14.75(�
2.44,31.93)
246.3�
53.4
241.5�
49.8
4.83
(�9.40,19.07)
249.3�
49.0
240.4�
55.9
8.92
(�2.07,19.91)
Median(25percentile-75
percentile)
258.0(236.0,288.0)
256.0(228.0,279.0)
264.0(230.0,280.0)
257.0(212.0,280.0)
262.5(233.5,283.0)
256.5(215.0,280.0)
ASQdomainreferralscore
Com
munication(#
38.7)n/N(%)
2/71
(2.8)
8/78
(10.3)
0.27
(0.06,
1.25)
9/105(8.6)
5/100(5.0)
1.71
(0.59,
4.94)
11/176
(6.3)
13/178
(7.3)
0.86
(0.39,
1.86)
Gross
motor
(#35.7)n/N(%)
8/71
(11.3)
12/78(15.4)
0.73
(0.32,
1.69)
15/105
(14.3)
16/100
(16.0)
0.89
(0.47,
1.71)
23/176
(13.1)
28/178
(15.7)
0.83
(0.50,
1.38)
Fine
motor
(#30.7)n/N(%)
9/71
(12.7)
18/78(23.1)
0.55
(0.26,
1.14)
23/105
(21.9)
22/100
(22.0)
1.00
(0.59,
1.67)
32/176
(18.2)
40/178
(22.5)
0.81
(0.53,
1.23)
Problem
solving(#
38.6)n/N(%)
18/71(25.4)
19/78(24.4)
1.04
(0.60,
1.82)
26/105
(24.8)
29/100
(29.0)
0.85
(0.54,
1.34)
44/176
(25.0)
48/178
(27.0)
0.93
(0.65,
1.32)
Personalsocial(#
38.7)n/N(%)
8/71(11.3)
18/78(23.1)
0.49
(0.23,
1.05)
21/105
(20.0)
19/100
(19.0)
1.05
(0.60,
1.84)
29/176
(16.5)
37/178
(20.8)
0.79
(0.51,
1.23)
ASQ:SEtotalscore
Evaluatedwithinwindow(33-41
mo)N
7480
111
104
185
184
Mean�
SD
30.8
�21.1
35.1
�32.3
�4.25(�
12.88,
4.38)
32.7
�21.1
32.3
�19.3
0.49
(�4.95,5.93)
32.0
�21.1
33.5
�25.7
�1.51(�
6.32,3.31)
Median(25percentile-75
percentile)
25.0
(15.0-45.0)
30.0
(15.0-45.0)
35.0
(15.0-50.0)
30.0(20.0-45.0)
30.0
(15.0-45.0)
30.0
(15.0-45.0)
Referralscore
(>59.0)n/N(%)
8/74
(10.8)
8/80
(10.0)
1.08
(0.43,
2.73)
9/111(8.1)
10/104
(9.6)
0.84
(0.36,
1.99)
17/185
(9.2)
18/184
(9.8)
0.94
(0.50,
1.76)
April 2013 ORIGINAL ARTICLES
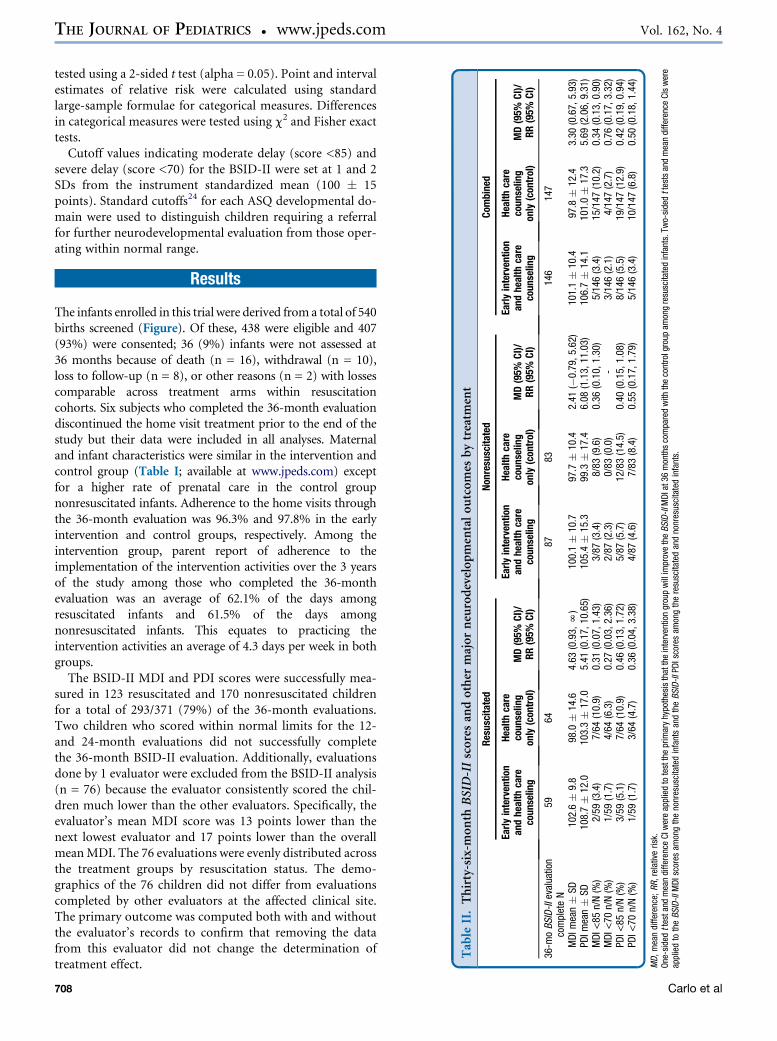
The primary outcome measure, MDI at 36 months,among the 123 resuscitated children with a successfulBSID-II evaluation was 102.6 � 9.8 in the early interventiongroup and 98.0 � 14.6 in the control group for a mean dif-ference and corresponding 95% CI of 4.63 (0.93, N) (1-sided P = .0202) (Table II). Including the records fromthe excluded evaluator resulted in a statistically significanttreatment effect of slightly lesser magnitude (mean MDIscore of 98.3 � 13.0 in the early intervention group and94.2 � 15.6 in the control group; mean difference (95%CI) 4.05 (0.18,N), 1-sided P = .0425). Among the 170 non-resuscitated children with a successful BSID-II, MDI was100.1 � 10.7 in the early intervention group and97.7 � 10.4 in the control group (P = .1392). A linearmodel that included effects for treatment, resuscitationcohort, and their interaction showed no evidence ofa differential treatment effect across the 2 cohorts(interaction P = .4158). A reduced model that included the2 main effects showed small, nonsignificant differences ofresuscitation cohort (resuscitated = 100.3 � 1.0 [adjustedmean � SE], nonresuscitated = 98.9 � 0.86 [P = .3238])and a significant treatment effect (intervention arm =101.3 � 0.94, control arm = 97.9 � 0.93 [P = .0131]).
The treatment effect remained beneficial after controllingfor potential confounders including study site, maternal de-mographics, socioeconomic status, characteristics of thechild’s birth, and the child’s demographics. The resultswere comparable with the unadjusted results (105.2 � 4.9for the intervention arm and 101.4 � 4.8 for the controlarm [P = .0143]) with both arms well within the normalrange. The child’s resuscitation status remained unassociatedwith MDI score in this model (101.2 � 5.1 for resuscitatedinfants and 105.4 � 5.5 for nonresuscitated infants[P = .3669]). For the combined group, MDI was higher inthe early intervention children (101.1 � 10.4) comparedwith the control children (97.8 � 12.4), P = .0141.
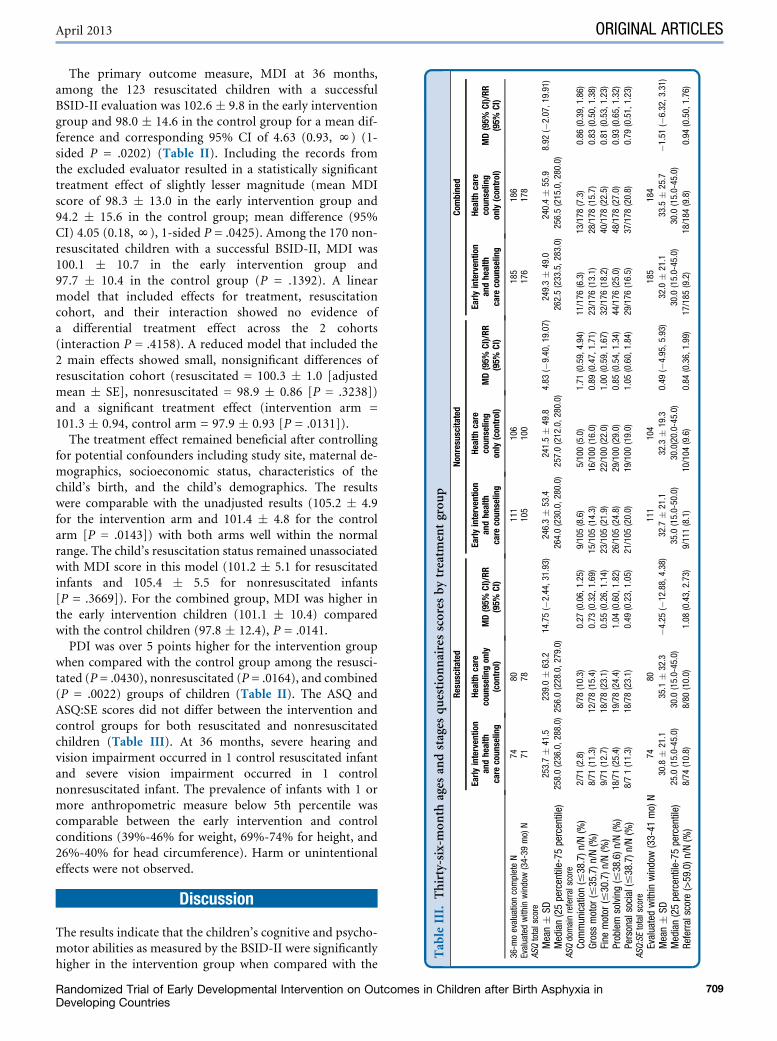
PDI was over 5 points higher for the intervention groupwhen compared with the control group among the resusci-tated (P = .0430), nonresuscitated (P = .0164), and combined(P = .0022) groups of children (Table II). The ASQ andASQ:SE scores did not differ between the intervention andcontrol groups for both resuscitated and nonresuscitatedchildren (Table III). At 36 months, severe hearing andvision impairment occurred in 1 control resuscitated infantand severe vision impairment occurred in 1 controlnonresuscitated infant. The prevalence of infants with 1 ormore anthropometric measure below 5th percentile wascomparable between the early intervention and controlconditions (39%-46% for weight, 69%-74% for height, and26%-40% for head circumference). Harm or unintentionaleffects were not observed.
Discussion
The results indicate that the children’s cognitive and psycho-motor abilities as measured by the BSID-II were significantlyhigher in the intervention group when compared with the
Randomized Trial of Early Developmental Intervention on Outcomes in Children after Birth Asphyxia inDeveloping Countries
709

THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 162, No. 4
control group. This trial tested an EDI program started soonafter birth in children in LMIC at high risk for developmentaldisorders. The intervention was integrated with family sup-port and nutritional and health education as recommen-ded.16 The effect size (4.6 points in MDI), though smallerthan hypothesized, was comparable with that observed ina large trial of children with various perinatal disorders inIndia (3 points in MDI)26 but substantially smaller thanthat of a similar trial in children with birth asphyxia in China(14 points in MDI).27 The diversity of participants enrolledin the current multi-country trial and the similar effect sizeto the Indian trial suggest that EDI may be effective but thebenefits are relatively small. It is possible that the controlvisits every 2 weeks resulted in some benefits, reducing theeffect size.
The study population consisted of survivors of birth as-phyxia from a large multi-country trial in which training ofbirth attendants in neonatal resuscitation and other essentialnewborn care knowledge and skills reduced stillbirths andperinatal mortality.10 Training of midwives with the same ed-ucational program reduced neonatal and perinatal mortalityin a large multicenter study in a low-income country.11 It isreassuring that the current trial shows that the overwhelmingmajority of the resuscitated infants did not have an increasedrate of neurodevelopmental impairment at 36 months andthat the mean BSID-II scores in survivors were in the normalrange, indicating that resuscitation increased unimpairedsurvivors. Since the time of study inception, the BSID-IIhas largely been replaced by the Bayley Scales of Infant Devel-opment, 3rd edition (BSID-III). The BSID-III covers similarskills and abilities as the BSID-II at 36 months. However,even though the average BSID-II results approximate 100,if we had used the new BSID-III our study may have resultedin higher scores as reported by others.28
A limitation of this study is that the role of the parenttrainer in the intervention was not as intense as in otherintervention studies conducted in high income coun-tries.14,15,29 To integrate the developmental intervention pro-gram with other family support and nutrition and healthcounseling, it was implemented through the parents. It ispossible that parental adherence was less intense than desir-able but the activities were practiced on average more than50% of the days throughout the 3 years of the intervention.We do not have independent observations of the quality ofthe implementation of the intervention at home but dataon frequency of practice of the activities were collected pro-spectively during each home visit. The intervention lastedonly 3 years, and it is possible that a longer interventionmay be necessary.
Another limitation is that infants were evaluated at 3 yearswhen neurodevelopmental indicators may be less predictiveof long-term outcomes than later evaluations. Although out-comes may improve from infancy to school age,30,31 studieshave found that individual stability of scores is only moderateto high.32 It is possible that larger benefits may be observed atschool age or that more survivors will have problems thatmanifest during childhood and adulthood.33,34 Follow-up
710
of 636 former low birth weight infants who participated ina multi-center early (first 3 years) intervention trial showedsome persistent benefits at 18 years.35 Thus, larger studiesand longer follow-up to school age are needed. The controlgroup received health and safety counseling every 2 weeks,and it is possible they received some benefits from the trial,which reduced the effect size. However, although this is thelargest trial of early intervention in infants with birth as-phyxia in LMIC, the small effects of the intervention wouldrequire a larger sample size to confirm the effectiveness notedin the combined group in this trial. The high prevalence ofinfants with anthropometric measures below the 5th percen-tile may be attributable in part to the low socioeconomic sta-tus of these families in comparison with the reference groupof theWHO study, which was purposely designed to producestandards among healthy children living under conditionslikely to favor the achievement of their full genetic growthpotential.36
Because the definition of birth asphyxia varies markedlybetween studies, a comparison of results may be difficult.The current study used the inclusive WHO definition ofbirth asphyxia: failure to establish spontaneous breathingat birth that includes neonatal respiratory depression.1
Thus, the high incidence of survivors with normal outcomeis not surprising. With moderate severity of birth asphyxia,there is an increased risk of mortality, and the survivors areat increasing risk of neurodevelopmental impairment.33,34
With the most severe birth asphyxia, mortality and morbid-ity increased substantially.37,38 Thus, although birthasphyxia is a major cause of mortality and disability, the de-gree of birth asphyxia markedly influences the long-termoutcome. The high rate of mild to moderate asphyxiamay be because of the effectiveness of the First Breath Trialintervention as well as the high early mortality attributableto asphyxia in this population.10 This trial documents thatthe overwhelming majority of infants with mild to moder-ate degrees of birth asphyxia in LMIC are likely to have in-tact survival.Even though programs for early intervention are common
in high income countries, trials to assess the effect of EDI forinfants following birth asphyxia have not been conducted toour knowledge. A relatively small single center randomizedcontrolled trial (n = 64) in infants who survived birth as-phyxia in China showed an increase (14 points) in MDI(105 � 15 in the early intervention group vs 91 � 11 in thecontrol group, P < .001).27 The effect size was about 1 SD,which is a relatively large effect compared with the effects re-ported in a meta-analysis.38 Similar to our study, the inter-vention was provided by the parents but contacts withtrainers occurred less often than in our trial (monthly duringthe first year and every 2 months during the second year). Atrial of early intervention in infants at risk for impairment inIndia included 665 infants, 218 of whom had mild or moder-ate birth asphyxia.26 For the group as a whole, MDI wasslightly higher in the EDI group than in the control group(83 � 14 vs 80 � 13, P < .005) but was low in both groupsoverall. Data were not reported separately for infants with
Carlo et al

April 2013 ORIGINAL ARTICLES
birth asphyxia, but the overall effect size was comparable withthat observed in the current trial.
In summary, the current trial of an EDI program imple-mented through parents from soon after birth to 3 years ofage in infants with birth asphyxia provides evidence of a treat-ment benefit on cognitive and psychomotor outcomes. BothMDI and PDI improved by approximately 5 points in theEDI group compared with the health and safety counselingcontrol group. Survivors of mild or moderate birth asphyxiahad neurodevelopmental outcomes in the normal ranges. Areview that addresses the role of interventions in childrenwith early developmental difficulties was published byWHO.39 The current trial used methods as proposed bythis consensus of experts, including advancing policy, useof common international approaches, increasing local capac-ity, empowering caregivers, and conducting research in low-resource income settings. Furthermore, the current trialdocumented benefits in children at low-risk for neurodeve-lopmental difficulties. n
Submitted for publication Mar 21, 2012; last revision received Aug 29, 2012;
accepted Sep 27, 2012.
Reprint requests: Waldemar A. Carlo, MD, University of Alabama at
Birmingham, 1700 6th Avenue South: 176F Suite 9380, Birmingham, AL
35233-7335. E-mail: [email protected]
References
1. WHO. Basic newborn resuscitation: A practical guide. Geneva: World
Health Organization; 1997.
2. Pierrat V, Haouari N, Liska A, Thomas D, Subtil D, Truffert P. Preva-
lence, causes, and outcome at 2 years of age of newborn encephalopa-
thy: population based study. Arch Dis Child-Fetal Neonat Ed 2005;90:
257-61.
3. Al-Macki N, Miller SP, Hall N, Shevell M. The spectrum of abnormal
neurologic outcomes subsequent to term intrapartum asphyxia. Pediatr
Neurol 2009;41:399-405.
4. Halloran DR, McClure E, Chakraborty H, Chomba E, Wright LL,
Carlo WA. Birth asphyxia survivors in a developing country. J Perinatol
2009;29:243-9.
5. Black RE, Cousens S, Johnson HL, Lawn JE, Rudan I, Bassani DG, et al.
Global, regional, and national causes of childmortality in 2008: a system-
atic analysis. Lancet 2010;375:1969-87.
6. WorldHealth Organization. TheWorld Health Report 2005.Make every
mother and child count. Geneva: WHO Press, World Health Organiza-
tion; 2005. Available at: http://www.who.int/whr/2005/en/index.html.
Accessed October 15, 2012.
7. World Health Organization. The global burden of disease: 2004 update.
Geneva: WHO Press, World Health Organization; 2008. Available at:
http://www.searo.who.int/0AB96CCE-162B-403C-AE11-B4B679673F20/
LinkFiles/Reports_GBD_report_2004update_full.pdf. Accessed August
28, 2012.
8. Perlman JM, Risser R. Cardiopulmonary resuscitation in the delivery
room. Associated clinical events. Arch Pediatr Adolesc Med 1995;149:
20-5.
9. Deorari AK, Paul VK, Singh M, Vidyasagar D. Impact of education and
training on neonatal resuscitation practices in 14 teaching hospitals in
India. Ann Trop Paediatr 2001;21:29-33.
10. Carlo WA, Goudar SS, Jehan I, Chomba E, Tshefu A, Garces A, et al.
Newborn-care training and perinatal mortality in developing countries.
N Engl J Med 2010;362:614-23.
11. Carlo WA, McClure EM, Chomba E, Chakraborty H, Hartwell T,
Harris H, et al. Newborn care training for midwives and neonatal and
Randomized Trial of Early Developmental Intervention on OutcomDeveloping Countries
perinatal mortality rates in a developing country. Pediatrics 2010;126:
1064-71.
12. Lee AC, Cousens S, Wall SN, Niermeyer S, Darmstadt GL, Carlo WA,
et al. Neonatal resuscitation and immediate newborn assessment and
stimulation for the prevention of neonatal deaths: a systematic review,
meta-analysis and Delphi estimation of mortality effect. BMC Public
Health 2011;2(Suppl 3):S12.
13. Grantham-McGregor S, Cheung YB, Cueto S, Glewwe P, Richter L,
Strupp B, International Child Development Steering Group. Child de-
velopment in developing countries. Lancet 2007;369:60-70.
14. Sweet MA, Appelbaum MI. Is home visiting an effective strategy? A
meta-analytic review of home visiting programs for families with young
children. Child Dev 2004;75:1435-56.
15. Maulik PK, Darmstadt GL. Community-based interventions to optimize
early child development in low resource settings. J Perinatol 2009;29:
531-42.
16. Engle PL, Black MM, Behrman JR, Cabral de Mello M, Gertler PJ,
Kapiriri L, et al. Strategies to avoid the loss of developmental potential
in more than 200 million children in the developing world. Lancet
2007;369:229-42.
17. Walker SP, Wachs TD, Gardner JM, Lozoff B, Wasserman GA, Pollitt E,
et al. Child development: risk factors for adverse outcomes in developing
countries. Lancet 2007;369:145-57.
18. Wallander JL, McClure E, Biasini F, Goudar SS, Pasha O, Chomba E,
et al. Brain research to ameliorate impaired neurodevelopment-home-
based intervention trial (BRAIN-HIT). BMC Pediatrics 2010;10:27.
19. Ellis M, Manandhar DS, Manandhar N, Wyatt J, Bolam AJ, Costello AM.
Stillbirths andneonatal encephalopathy inKathmandu,Nepal: an estimate
of the contribution of birth asphyxia to perinatal mortality in a low-
income urban population. Paediatr Perinat Epidemiol 2000;14:39-52.
20. Sparling JJ, Lewis IS. Partners for learning: Birth to 24 months. Lewis-
ville, NC: Kaplan Press; 1984.
21. Shearer DE, Shearer DL. The portage project: an international home ap-
proach to early intervention for young children and their families. In:
Roopnarine J, Johnson JE, eds. Approaches to early childhood educa-
tion. 5th ed. New York: Prentice Hall; 2008.
22. WorldHealthOrganization. Integratedmanagement of childhood illnesses
(IMCI)-an illustrated guide to improve family and community practices.
South-East Asia Region. WHO Press, World Health Organization; 2009.
Available at: http://www.searo.who.int/LinkFiles/IMCI_-An_illustrated_
Guide_intro.pdf. Accessed October 15, 2012.
23. Bayley N. Bayley scales of infant development: Manual. New York: Psy-
chological Corporation; 1993.
24. Squires J, Potter L, Bricker D. The ASQ’s user’s guide for the ages and
stages questionnaires: A parent-completed, child monitoring system.
Baltimore, MD: Brooks; 1999.
25. Tsai HLA, McClelland MM, Pratt C, Squires J. Adaptation of the
36-month ages and stages questionnaire in Taiwan: results froma prelim-
inary study. J Early Interv 2006;28:213-4.
26. Nair MK, Philip E, Jeyasselan L, George B, Matthews S, Padma K. Effect
of child development centre model early stimulation among at-risk
babies-a randomized controlled trial. Indian Pediatr Suppl 2009;46:
s20-6.
27. Bao X, Sun S, Yu R, Sun J. Early intervention improves intellectual de-
velopment in asphyxiated newborn infants. Intervention of Asphyxiated
Newborn Infants Cooperative Research Group. Chin Med J (Engl) 1997;
110:875-88.
28. Ramey CT, Bryant DM, Wasik BH, Sparling JJ, Fendt KH, LaVange LM.
Infant health and development program for low birth weight, premature
infants: program elements, family participation, and child intelligence.
Pediatrics 1992;89:454-65.
29. Marlow N, Wolke D, Bracewell MA, Samara M, EPICure Study Group.
Neurologic and developmental disability at six years of age after ex-
tremely preterm birth. N Engl J Med 2005;352:9-19.
30. Hack M, Taylor HG, Drotar D, Schluchter M, Cartar L, Wilson-
Costello D, et al. Poor predictive validity of the Bayley scales of infant
development for cognitive function of extremely low birth weight chil-
dren at school age. Pediatrics 2005;116:333-41.
es in Children after Birth Asphyxia in 711

THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 162, No. 4
31. Johnson S, Fawke J, Hennessy E, Rowell V, Thomas S, Wolke D, et al.
Neurodevelopmental disability through 11 years of age in children
born before 26 weeks of gestation. Pediatrics 2009;124:e249-57.
32. Thorngren-Jerneck K, Herbst A. Low 5-minute Apgar score: a popula-
tion-based register study of 1 million term births. Obstet Gynecol
2001;98:65-70.
33. Odd DE, Lewis G, Whitelaw A, Gunnell D. Resuscitation at birth and
cognition at 8 years of age: a cohort study. Lancet 2009;373:1615-22.
34. McCormickMC, Brooks-Gunn J, Buka SL, Goldman J, Yu J, SalganikM,
et al. Early intervention in low birth weight premature infants: results at
18 years of age for the infant health and development program. Pediat-
rics 2006;117:771-80.
35. World Health Organization. The WHO Multicentre Growth Reference
Study. Available at: http://www.who.int/childgrowth/mgrs/en/ Accessed
July 17, 2012.
36. Laptook AR, Shankaran S, Ambalavanan N, Carlo WA, McDonald SA,
Higgins RD, et al. Outcome of term infants using Apgar scores at
50 Years Ago in THE JOURNAL OF PEDIATRICS
712
10 minutes following hypoxic-ischemic encephalopathy. Pediatrics
2009;124:1619-26.
37. Edwards AD, Brocklehurst P, Gunn AJ, Halliday H, Juszczak E,
Levene M, et al. Neurological outcomes at 18 months of age after mod-
erate hypothermia for perinatal hypoxic ischemic encephalopathy: syn-
thesis and meta-analysis of trial data. BMJ 2010;340:c363-9.
38. Spittle AJ, Orton J, Doyle LW, Boyd R. Early developmental intervention
programs post hospital discharge to prevent motor and cognitive im-
pairments in preterm infants. Cochrane Database Syst Rev 2007;18:
CD005495.
39. World Health Organization. Maternal, newborn, child and adolescent
health: Developmental difficulties in early childhood: Prevention, early
identification, assessment and intervention in low- and middle-income
countries: A review. Geneva: WHO Press, World Health Organization;
2012. Available at: http://www.who.int/maternal_child_adolescent/
documents/development_difficulties_early_childhood/en/. Accessed
September 12, 2012.
The Incidence of Murmurs in Healthy Premature Infants during Their First18 Months of LifeWalsh SZ. J Pediatr 1963;62:480-3
Heart murmurs are common in normal newborn infants. It is estimated that at least 50% of all normal newbornswill have a heart murmur during the first few months of life. The majority of these murmurs are so called in-
nocent murmurs and do not reflect pathology. These murmurs also may be caused by peripheral arterial pulmonarystenosis or a very small ventricular defect. Both these murmurs will disappear with the infant’s growth and are notcause for concern. These full term infants have normal cardiovascular systems and are seldom referred to a cardiologistfor evaluation. However, if the baby is premature a patent ductus arteriosus or other significant heart disease may bepresent and further evaluation may be indicated. Usually, these infants will have an echocardiogram to confirm thediagnosis. In 1963, clinicians knew that full term infants frequently had innocent murmurs but the incidence ofsuch murmurs in infants weighing less than 2000 g was unknown.
Walsh followed 82 healthy premature infants for the first 18 months of their lives and found that 82% hadmurmursat some point. Four percent of these infants had significant congenital heart disease, which is a higher incidence thanthat found in full term infants. This was the first study that followed premature infants for heart disease in this fashionand alerted clinicians to the fact that although the majority of these infants have innocent murmurs, some do havesignificant heart disease. Today, a simple echocardiogram can rule out a significant diagnosis in this population.
Reginald Washington, MDRocky Mountain Hospital for Children
Denver, Coloradohttp://dx.doi.org/10.1016/j.jpeds.2012.10.052
Carlo et al
Appendix
Brain Research to Ameliorate Impaired Neurodevelopment-Home-Based Intervention Trial investigators include:Jawaharlal Nehru Medical College, Belgaum, India: RoopaM. Bellad, Sangappa M. Dhaded, Niranjana S. Mahant-shetti, Bhalachandra S. Kodkany, and Shivaprasad S.Goudar; Aga Khan University, Karachi, Pakistan: OmranaPasha and Zahid Abbasi; University of Zambia, Lusaka,Zambia: Elwyn Chomba; University of Alabama at Bir-mingham, Birmingham, Alabama: Waldemar A. Carloand Fred J. Biasini; Research Triangle Institute, Durham,North Carolina: Hrishikesh Chakraborty, Elizabeth M.McClure, Dennis Wallace, and Vanessa Thorsten; Christi-ana Care, Wilmington, Delaware: Richard J. Derman;Drexel University, Philadelphia, Pennsylvania: Robert L.Goldenberg; Western Kentucky University, Bowling Green,Kentucky: Darlene Shearer; University of California,Merced, California: Jan Wallander; and National Institutesof Child and Human Development, Rockville, Maryland:Linda L. Wright.
Eunice Kennedy Shriver National Institute of Child Healthand Human Development Global Network for Women’s andChildren’s Health Research Investigators include: Universityof Alabama at Birmingham, Birmingham, Alabama:Waldemar A. Carlo; University Teaching Hospital, Lusaka,Zambia: Elwyn Chomba; Center for Disease Research inZambia, Lusaka, Zambia: Albert Manasyan; ChristianaCare, Wilmington, Delaware: Richard J. Derman; KLE Uni-versity’s Jawaharlal Nehru Medical College, Belgaum, India:Shivaprasad Goudar and Bhalchandra S. Kodkany; DrexelUniversity, Philadelphia, Pennsylvania: Robert Goldenberg;Aga Khan University Medical College, Karachi, Pakistan:Omrana Pasha; Research Triangle Institute, Durham, NorthCarolina: Beth McClure, Dennis Wallace, and VanessaThorsten.
April 2013 ORIGINAL ARTICLES
Randomized Trial of Early Developmental Intervention on Outcomes in Children after Birth Asphyxia inDeveloping Countries
712.e1
102 Ineligible 82 mothers not staying in the study communities 17 mothers not contacted within 7 days of birth 3 babies <1500 grams
164 Resuscitated, randomized
4 Drop outs 2 deaths 1 withdrawal 1 child’s mother nursing and husband out of town
6 Drop outs 2 deaths 1 withdrawal 2 lost to follow-up 1 family did not approve of study
243 Non-resuscitated, randomized
438 Eligible
540 Screened
7436 m Evaluations
86 Control
11 Drop outs 7 deaths 3 withdrawals 1 lost to follow-up
15 Drop outs 5 deaths 5 withdrawals 5 lost to follow-up
80 36m Evaluations
11136m Evaluations
10636m Evaluations
407 Consented
78 Developmental Intervention
71 ASQCompleted
74 ASQ:SE Completed
59 BSID-II Completed
100 ASQCompleted
104 ASQ:SE Completed
83 BSID-II Completed
78 ASQCompleted
80 ASQ:SE Completed
64 BSID-II Completed
105 ASQCompleted
111 ASQ:SE Completed
87 BSID-II Completed
117 Control 126 Developmental Intervention
Figure. Flow chart of screening, randomization, and 36-month follow-up completion. Flow diagram for enrollment, randomizedintervention allocation, and 36-month follow-up completion. In total, 6 subjects who completed the 36-month evaluationdiscontinued the home visit treatment prior to the end of the study. Among resuscitated babies, the family of 1 subject in theintervention group did not have time to continue with the intervention, and 1 family in the control group moved outside the studyarea. Among nonresuscitated babies in the intervention group, one did not have time and one moved. Among nonresuscitatedsubjects in the control group, 2 families moved.
THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 162, No. 4
712.e2 Carlo et al
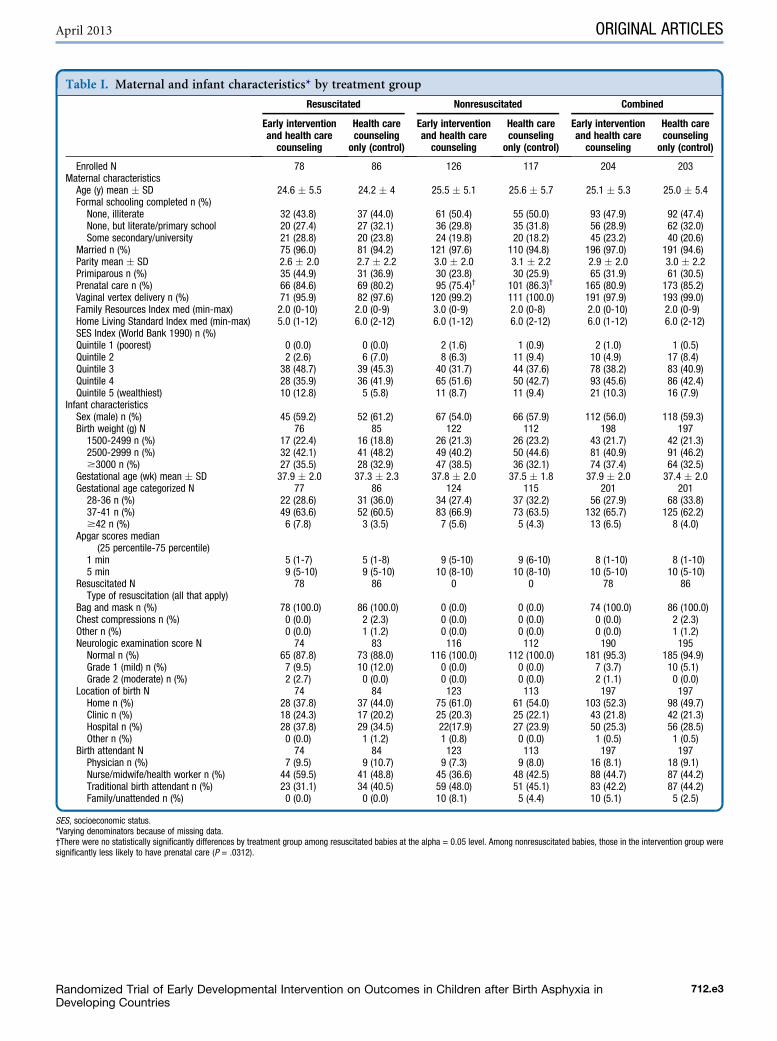
Table I. Maternal and infant characteristics* by treatment group
Resuscitated Nonresuscitated Combined
Early interventionand health carecounseling
Health carecounselingonly (control)
Early interventionand health carecounseling
Health carecounselingonly (control)
Early interventionand health carecounseling
Health carecounselingonly (control)
Enrolled N 78 86 126 117 204 203Maternal characteristicsAge (y) mean � SD 24.6 � 5.5 24.2 � 4 25.5 � 5.1 25.6 � 5.7 25.1 � 5.3 25.0 � 5.4Formal schooling completed n (%)
None, illiterate 32 (43.8) 37 (44.0) 61 (50.4) 55 (50.0) 93 (47.9) 92 (47.4)None, but literate/primary school 20 (27.4) 27 (32.1) 36 (29.8) 35 (31.8) 56 (28.9) 62 (32.0)Some secondary/university 21 (28.8) 20 (23.8) 24 (19.8) 20 (18.2) 45 (23.2) 40 (20.6)
Married n (%) 75 (96.0) 81 (94.2) 121 (97.6) 110 (94.8) 196 (97.0) 191 (94.6)Parity mean � SD 2.6 � 2.0 2.7 � 2.2 3.0 � 2.0 3.1 � 2.2 2.9 � 2.0 3.0 � 2.2Primiparous n (%) 35 (44.9) 31 (36.9) 30 (23.8) 30 (25.9) 65 (31.9) 61 (30.5)Prenatal care n (%) 66 (84.6) 69 (80.2) 95 (75.4)† 101 (86.3)† 165 (80.9) 173 (85.2)Vaginal vertex delivery n (%) 71 (95.9) 82 (97.6) 120 (99.2) 111 (100.0) 191 (97.9) 193 (99.0)Family Resources Index med (min-max) 2.0 (0-10) 2.0 (0-9) 3.0 (0-9) 2.0 (0-8) 2.0 (0-10) 2.0 (0-9)Home Living Standard Index med (min-max) 5.0 (1-12) 6.0 (2-12) 6.0 (1-12) 6.0 (2-12) 6.0 (1-12) 6.0 (2-12)SES Index (World Bank 1990) n (%)Quintile 1 (poorest) 0 (0.0) 0 (0.0) 2 (1.6) 1 (0.9) 2 (1.0) 1 (0.5)Quintile 2 2 (2.6) 6 (7.0) 8 (6.3) 11 (9.4) 10 (4.9) 17 (8.4)Quintile 3 38 (48.7) 39 (45.3) 40 (31.7) 44 (37.6) 78 (38.2) 83 (40.9)Quintile 4 28 (35.9) 36 (41.9) 65 (51.6) 50 (42.7) 93 (45.6) 86 (42.4)Quintile 5 (wealthiest) 10 (12.8) 5 (5.8) 11 (8.7) 11 (9.4) 21 (10.3) 16 (7.9)
Infant characteristicsSex (male) n (%) 45 (59.2) 52 (61.2) 67 (54.0) 66 (57.9) 112 (56.0) 118 (59.3)Birth weight (g) N 76 85 122 112 198 197
1500-2499 n (%) 17 (22.4) 16 (18.8) 26 (21.3) 26 (23.2) 43 (21.7) 42 (21.3)2500-2999 n (%) 32 (42.1) 41 (48.2) 49 (40.2) 50 (44.6) 81 (40.9) 91 (46.2)$3000 n (%) 27 (35.5) 28 (32.9) 47 (38.5) 36 (32.1) 74 (37.4) 64 (32.5)
Gestational age (wk) mean � SD 37.9 � 2.0 37.3 � 2.3 37.8 � 2.0 37.5 � 1.8 37.9 � 2.0 37.4 � 2.0Gestational age categorized N 77 86 124 115 201 201
28-36 n (%) 22 (28.6) 31 (36.0) 34 (27.4) 37 (32.2) 56 (27.9) 68 (33.8)37-41 n (%) 49 (63.6) 52 (60.5) 83 (66.9) 73 (63.5) 132 (65.7) 125 (62.2)$42 n (%) 6 (7.8) 3 (3.5) 7 (5.6) 5 (4.3) 13 (6.5) 8 (4.0)
Apgar scores median(25 percentile-75 percentile)
1 min 5 (1-7) 5 (1-8) 9 (5-10) 9 (6-10) 8 (1-10) 8 (1-10)5 min 9 (5-10) 9 (5-10) 10 (8-10) 10 (8-10) 10 (5-10) 10 (5-10)
Resuscitated N 78 86 0 0 78 86Type of resuscitation (all that apply)
Bag and mask n (%) 78 (100.0) 86 (100.0) 0 (0.0) 0 (0.0) 74 (100.0) 86 (100.0)Chest compressions n (%) 0 (0.0) 2 (2.3) 0 (0.0) 0 (0.0) 0 (0.0) 2 (2.3)Other n (%) 0 (0.0) 1 (1.2) 0 (0.0) 0 (0.0) 0 (0.0) 1 (1.2)Neurologic examination score N 74 83 116 112 190 195
Normal n (%) 65 (87.8) 73 (88.0) 116 (100.0) 112 (100.0) 181 (95.3) 185 (94.9)Grade 1 (mild) n (%) 7 (9.5) 10 (12.0) 0 (0.0) 0 (0.0) 7 (3.7) 10 (5.1)Grade 2 (moderate) n (%) 2 (2.7) 0 (0.0) 0 (0.0) 0 (0.0) 2 (1.1) 0 (0.0)
Location of birth N 74 84 123 113 197 197Home n (%) 28 (37.8) 37 (44.0) 75 (61.0) 61 (54.0) 103 (52.3) 98 (49.7)Clinic n (%) 18 (24.3) 17 (20.2) 25 (20.3) 25 (22.1) 43 (21.8) 42 (21.3)Hospital n (%) 28 (37.8) 29 (34.5) 22(17.9) 27 (23.9) 50 (25.3) 56 (28.5)Other n (%) 0 (0.0) 1 (1.2) 1 (0.8) 0 (0.0) 1 (0.5) 1 (0.5)
Birth attendant N 74 84 123 113 197 197Physician n (%) 7 (9.5) 9 (10.7) 9 (7.3) 9 (8.0) 16 (8.1) 18 (9.1)Nurse/midwife/health worker n (%) 44 (59.5) 41 (48.8) 45 (36.6) 48 (42.5) 88 (44.7) 87 (44.2)Traditional birth attendant n (%) 23 (31.1) 34 (40.5) 59 (48.0) 51 (45.1) 83 (42.2) 87 (44.2)Family/unattended n (%) 0 (0.0) 0 (0.0) 10 (8.1) 5 (4.4) 10 (5.1) 5 (2.5)
SES, socioeconomic status.*Varying denominators because of missing data.†There were no statistically significantly differences by treatment group among resuscitated babies at the alpha = 0.05 level. Among nonresuscitated babies, those in the intervention group weresignificantly less likely to have prenatal care (P = .0312).
April 2013 ORIGINAL ARTICLES
Randomized Trial of Early Developmental Intervention on Outcomes in Children after Birth Asphyxia inDeveloping Countries
712.e3
Related Documents