MAJOR ARTICLE Randomized Trial of Artesunate-Amodiaquine, Atovaquone-Proguanil, and Artesunate- Atovaquone-Proguanil for the Treatment of Uncomplicated Falciparum Malaria in Children Rachida Tahar, 1,4 Talleh Almelli, 1 Camille Debue, 1 Vincent Foumane Ngane, 4 Joseph Djaman Allico, 2,5,6 Solange Whegang Youdom, 4 and Leonardo K. Basco 3,4,a 1 Unité Mixte de Recherche 216 Mère et Enfant Face aux Infections Tropicales, Institut de Recherche pour le Développement (IRD), Unité de formation et de recherche de Pharmacie, Paris, 2 Unité de Recherche Neurobiologie et Développement, Unité Propre de Recherche 3294, Centre National de la Recherche Scientifique, Université Paris-Sud XI, Orsay, and 3 Unité de Recherche 198, Unité de Recherche des Maladies Infectieuses et Tropicales Emergentes, IRD, Faculté de Médecine La Timone, Aix-Marseille Université, Marseille, France; 4 Laboratoire de Recherche sur le Paludisme, Organisation de Coordination pour la lutte contre les Endémies en Afrique Centrale, Yaoundé, Cameroon; 5 Laboratoire de Pharmacodynamie Biochimique, Unité de Formation et de Recherche Biosciences, Université de Cocody, and 6 Département de Biochimie, Institut Pasteur de Côte d’Ivoire, Abidjan, Côte d’Ivoire Background. Artemisinin-based combination therapies (ACTs) are recommended for the treatment of acute un- complicated falciparum malaria in many malaria-endemic countries. Despite the emergence of artemisinin resis- tance, few alternative non-ACTs, including atovaquone-proguanil, are currently available. Methods. Plasmodium falciparum–infected Cameroonian children ≤5 years old (n = 338) were randomly as- signed to artesunate-amodiaquine, atovaquone-proguanil, or artesunate-atovaquone-proguanil treatment groups and followed for 28 days, according to the standard World Health Organization protocol. In vitro response to ato- vaquone and cytochrome b sequence of clinical isolates were determined. Results. Eight late failures and 16 failures (8 late and 8 early failures) were observed after artesunate- amodiaquine and atovaquone-proguanil therapies, respectively. Most late failures were due to reinfections. Artesunate- atovaquone-proguanil was not associated with any failure. After correction by genotyping, per-protocol analysis showed no difference in the efficacy of 3 drugs. However, the proportion of atovaquone-proguanil–treated patients with positive smears on day 3 was much higher (36.0%; P < .05) than that of the artesunate-amodiaquine (2.9%) and artesunate-atovaquone-proguanil (1.0%) groups. In vitro response and cytochrome b sequence did not indicate atovaquone resistance. Conclusions. Atovaquone-proguanil was characterized by a slow blood schizontocidal action and resulted in early treatment failure in a few patients. Artesunate-atovaquone-proguanil was a highly effective alternative treat- ment. Clinical Trials Registration. UMIN000003813. Keywords. drug resistance; Plasmodium falciparum; cytochrome b; artemisinin; molecular epidemiology. Artemisinin-based combination therapies (ACTs) are the current drugs of choice for the treatment of acute uncomplicated Plasmodium falciparum malaria in many parts of the world where malaria is endemic. Artesunate-amodiaquine (ASAQ) and artemether- lumefantrine have been adopted for first- or second- line treatment in many sub-Saharan African countries, including Cameroon. Although these 2 ACTs are highly effective and rapidly acting and resistance has not been Received 8 February 2014; accepted 30 May 2014. a Present affiliation: Unité de Parasitologie, Institut de Recherche Biomédicale des Armées, Ancienne Base Aérienne 217, Brétigny-sur-Orge, France. Correspondence: Leonardo K. Basco, MD, PhD, Unité de Parasitologie, Institut de Recherche Biomédicale des Armées, Ancienne Base Aérienne 217, 91223 Brétigny- sur-Orge, France ([email protected]). The Journal of Infectious Diseases © The Author 2014. Published by Oxford University Press on behalf of the Infectious Diseases Society of America. All rights reserved. For Permissions, please e-mail: [email protected]. DOI: 10.1093/infdis/jiu341 Atovaquone-Proguanil Treatment for Malaria • JID • 1 Journal of Infectious Diseases Advance Access published July 15, 2014 at Université Descartes Paris 5 on September 19, 2014 http://jid.oxfordjournals.org/ Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

M A J O R A R T I C L E
Randomized Trial of Artesunate-Amodiaquine,Atovaquone-Proguanil, and Artesunate-Atovaquone-Proguanil for the Treatment ofUncomplicated Falciparum Malaria in Children
Rachida Tahar,1,4 Talleh Almelli,1 Camille Debue,1 Vincent Foumane Ngane,4 Joseph Djaman Allico,2,5,6
Solange Whegang Youdom,4 and Leonardo K. Basco3,4,a
1Unité Mixte de Recherche 216 Mère et Enfant Face aux Infections Tropicales, Institut de Recherche pour le Développement (IRD), Unité de formation etde recherche de Pharmacie, Paris, 2Unité de Recherche Neurobiologie et Développement, Unité Propre de Recherche 3294, Centre National de laRecherche Scientifique, Université Paris-Sud XI, Orsay, and 3Unité de Recherche 198, Unité de Recherche des Maladies Infectieuses et TropicalesEmergentes, IRD, Faculté de Médecine La Timone, Aix-Marseille Université, Marseille, France; 4Laboratoire de Recherche sur le Paludisme,Organisation de Coordination pour la lutte contre les Endémies en Afrique Centrale, Yaoundé, Cameroon; 5Laboratoire de Pharmacodynamie Biochimique,Unité de Formation et de Recherche Biosciences, Université de Cocody, and 6Département de Biochimie, Institut Pasteur de Côte d’Ivoire, Abidjan,Côte d’Ivoire
Background. Artemisinin-based combination therapies (ACTs) are recommended for the treatment of acute un-complicated falciparum malaria in many malaria-endemic countries. Despite the emergence of artemisinin resis-tance, few alternative non-ACTs, including atovaquone-proguanil, are currently available.
Methods. Plasmodium falciparum–infected Cameroonian children ≤5 years old (n = 338) were randomly as-signed to artesunate-amodiaquine, atovaquone-proguanil, or artesunate-atovaquone-proguanil treatment groupsand followed for 28 days, according to the standard World Health Organization protocol. In vitro response to ato-vaquone and cytochrome b sequence of clinical isolates were determined.
Results. Eight late failures and 16 failures (8 late and 8 early failures) were observed after artesunate-amodiaquine and atovaquone-proguanil therapies, respectively. Most late failures were due to reinfections. Artesunate-atovaquone-proguanil was not associated with any failure. After correction by genotyping, per-protocol analysisshowed no difference in the efficacy of 3 drugs. However, the proportion of atovaquone-proguanil–treated patientswith positive smears on day 3 was much higher (36.0%; P < .05) than that of the artesunate-amodiaquine (2.9%) andartesunate-atovaquone-proguanil (1.0%) groups. In vitro response and cytochrome b sequence did not indicateatovaquone resistance.
Conclusions. Atovaquone-proguanil was characterized by a slow blood schizontocidal action and resulted inearly treatment failure in a few patients. Artesunate-atovaquone-proguanil was a highly effective alternative treat-ment.
Clinical Trials Registration. UMIN000003813.
Keywords. drug resistance; Plasmodium falciparum; cytochrome b; artemisinin; molecular epidemiology.
Artemisinin-based combination therapies (ACTs)are the current drugs of choice for the treatment ofacute uncomplicated Plasmodium falciparum malariain many parts of the world where malaria is endemic.Artesunate-amodiaquine (ASAQ) and artemether-lumefantrine have been adopted for first- or second-line treatment in many sub-Saharan African countries,including Cameroon. Although these 2 ACTs are highlyeffective and rapidly acting and resistance has not been
Received 8 February 2014; accepted 30 May 2014.aPresent affiliation: Unité de Parasitologie, Institut de Recherche Biomédicale des
Armées, Ancienne Base Aérienne 217, Brétigny-sur-Orge, France.Correspondence: Leonardo K. Basco, MD, PhD, Unité de Parasitologie, Institut de
Recherche Biomédicale des Armées, Ancienne Base Aérienne 217, 91223 Brétigny-sur-Orge, France ([email protected]).
The Journal of Infectious Diseases© The Author 2014. Published by Oxford University Press on behalf of the InfectiousDiseases Society of America. All rights reserved. For Permissions, please e-mail:[email protected]: 10.1093/infdis/jiu341
Atovaquone-Proguanil Treatment for Malaria • JID • 1
Journal of Infectious Diseases Advance Access published July 15, 2014 at U
niversité
Descartes Paris 5 on Septem
ber 19, 2014http://jid.oxfordjournals.org/
Dow
nloaded from
documented in the African continent [1, 2], both of these drugcombinations have some limitations. There has been some con-cern with the wide-scale use of amodiaquine in a highly chloro-quine-resistant area because of possible cross-resistance andtoxicity related to repeated intake of the drug, and amodiaquineis associated with minor but common adverse effects, such asasthenia and pruritus [3]. Artemether-lumefantrine is well tol-erated, but the requirements for twice daily doses for 3 days andcoadministration with fatty food to improve lumefantrine ab-sorption may compromise patient compliance. Other ACTs rec-ommended by the World Health Organization (WHO) [1],including artesunate-sulfadoxine-pyrimethamine, artesunate-mefloquine, and dihydroartemisinin-piperaquine, are less com-monly used in Africa today. Moreover, resistance to artemisininderivatives is emerging and has become an ominous reality inSoutheast Asia [4–6], requiring a continuous effort to developand evaluate the clinical efficacy of alternative drugs to treatmultidrug-resistant malaria.
Atovaquone-proguanil (ATPG) is a highly efficacious non-ACT drug for multidrug-resistant P. falciparum. Atovaquoneis a ubiquinone analogue that selectively inhibits cytochromeb, reduces mitochondrial membrane potential, and inhibitspyrimidine biosynthesis [7–10]. Proguanil, a biguanide, exertsa synergistic schizontocidal action with atovaquone and en-hances atovaquone-mediated collapse of the mitochondrialmembrane potential [11, 12]. Earlier studies with ATPG showedits safety, tolerance, and high prophylactic efficacy and cure ratein several epidemiological settings [13–15]. At present, ATPG isone of the drugs of choice for both chemoprophylaxis of non-immune temporary visitors traveling to areas where multidrugresistance has been reported and treatment of imported cases ofacute uncomplicated P. falciparum infections in many industri-alized countries where malaria is not endemic [16–19]. In con-trast, the use of ATPG by local populations in malaria-endemiccountries has been largely limited because of its prohibitive costand the availability of alternative antimalarial drugs.
In the African continent, most of the clinical studies ofATPG were performed in the 1990s, in Kenya, Gabon, Zambia,and Malawi [20–28]. There is little recent information on itsefficacy in African children, who constitute the most vulnera-ble population affected by malaria. Moreover, none of theprevious studies of ATPG conducted in Africa involved com-parison with an ACT, and artesunate was not coadministeredwith ATPG. Artesunate-ATPG (AS-ATPG) was found to besafe, well tolerated, and highly effective in Thai subjects, in-cluding children <5 years old and pregnant women [29–31].The aims of the present study were to compare the efficacyof ASAQ, ATPG, and AS-ATPG in Cameroonian childrenaged ≤5 years. P. falciparum isolates from patients treatedwith ATPG or AS-ATPG were analyzed for in vitro responseto atovaquone and underwent analysis of DNA sequences ofthe gene encoding cytochrome b.
PATIENTS, MATERIALS, AND METHODS
PatientsClinical studies were conducted at Nlongkak Catholic mission-ary dispensary (Yaoundé, Cameroon) in 2008–2009. Malariatransmission occurs throughout the year in Yaoundé. The ento-mological inoculation rate varies from 3 to 34 infective bites perperson per year [32–34]. Symptomatic patients with acute un-complicated malaria were enrolled, after free and informed con-sent was received from the parents or legal guardians, if thefollowing inclusion criteria were met: age between 6 monthsold and 5 years, fever at the time of consultation (measuredrectal temperature, ≥38.0°C), and parasite density of ≥2000asexual P. falciparum parasites/µL of blood, without otherPlasmodium species [35]. In addition, because of limiteddata on the safety of ATPG for treatment in children weighing<5 kg [17, 18, 26], a lower limit for body weight was set at 5.0 kg.Patients with symptoms associated with concomitant infectiousdiseases, severe malnutrition, or any general danger signs ofsevere and complicated malaria as defined by the WHO wereexcluded [35].
After informed consent was obtained, capillary blood wascollected by finger prick in a capillary tube for hematocrit mea-surement, and approximately 50–100 µL of capillary blood wasimbibed onto Whatman 3MM filter paper (GE Healthcare LifeSciences, Vélizy-Villacoublay, France) to store parasite DNA.The study protocol was reviewed and approved by the Camer-oonian National Ethics Committee and the Cameroonian Min-istry of Public Health. Clinical guidelines of the Institut deRecherche pour le Développement (France) were followed inthe conduct of this clinical research.
Treatment and Follow-UpThis was an open-label, randomized study on the efficacy of 3antimalarial drugs: ASAQ, ATPG, and AS-ATPG. Two subtrialswere conducted sequentially. Patients were randomly assignedto one of the 2 treatment groups in each subtrial: ASAQ vsATPG-1 and ATPG-2 vs AS-ATPG. Noncoformulated ASAQwas used for precise dose calculations based on the individualpatient’s body weight. Amodiaquine (AQ; Camoquin 200 mgamodiaquine base tablet or 10 mg amodiaquine base/mLsyrup; Pfizer Afrique de l’Ouest, Dakar, Senegal) was adminis-tered at a standard dose of 10 mg base/kg body weight on days0, 1, and 2. Artesunate (AS; Arinate 100 mg tablets; Dafra Phar-ma, Oud-Turnhout, Belgium) was administered at a total doseof 12 mg/kg body weight (4 mg/kg body weight on days 0, 1,and 2). ATPG (Malarone pediatric dose formulation, 62.5 mgatovaquone + 25 mg proguanil hydrochloride; GlaxoSmithK-line, Bad Oldesloe, Germany) was administered at a oncedaily dose of 20 mg/kg body weight/day for atovaquone and8 mg/kg body weight/day for proguanil for 3 days. All antima-larial drugs were administered simultaneously and once daily
2 • JID • Tahar et al
at UniversitÃ
© D
escartes Paris 5 on September 19, 2014
http://jid.oxfordjournals.org/D
ownloaded from
on days 0, 1, and 2. Each dose of antimalarial drug was admin-istered under supervision at the dispensary or during home vis-its. Paracetamol (10 mg/kg body weight) was administered to allpatients 3 times daily for fever and headache. Patients were fol-lowed up on days 1, 2, 3, 7, 14, 21, and 28 [35]. Hematocrit mea-surement was performed on day 0 and repeated on day 14.Patients who did not respond to the assigned drug were treatedwith oral quinine (25 mg base/kg body weight/day for 5 days) orartemether-lumefantrine.
The primary treatment outcome was determined on day 28and classified into one of the following categories: early treat-ment failure, late clinical failure, late parasitological failure, oradequate clinical and parasitological response [35]. Treatmentfailure refers to one of the following outcomes: early treatmentfailure, late clinical failure, or late parasitological failure. Ade-quate clinical and parasitological response is synonymouswith treatment success. The secondary outcomes were the pro-portion of patients who cleared parasitemia on or before day 3and hematocrit improvement on day 14.
In Vitro AssaysIn vitro drug susceptibility of fresh clinical isolates to atova-quone was determined by the [3H]hypoxanthine incorporationmethod [36, 37]. A venous blood sample (5 mL) was collectedinto ethylenediaminetetraacetic acid–coated tubes for in vitro
assays from patients aged 3–5 years with parasitemia ≥0.1%and assigned to the ATPG or AS-ATPG group.
Polymerase Chain Reaction (PCR) Analysis, Sequencing,and GenotypingParasite DNAwas extracted from filter papers, using the Chelexmethod [38].A 565–base pair fragment of the P. falciparummi-tochondrial cytochrome b gene was amplified as described inour earlier study [36], and DNA sequence was determined bydirect sequencing of the PCR products.
Genotypes of paired pretreatment and recurrent parasiteson or after day 7 were determined to distinguish between recru-descence (ie, reappearance of the same parasite population asthat of pretreatment sample) and reinfection (ie, appearanceof different parasite populations). Genotyping was based on3 polymorphic markers—merozoite surface antigen-1 (msa1),merozoite surface antigen-2 (msa2), and glutamine-rich protein(glurp)—as recommended by the WHO [39].
Data AnalysisBased on the PCR-uncorrected failure rate of 20% after ASAQtreatment observed at the same study site in 2005 [40], ATPG,with or without artesunate, was assumed to reduce the failurerate to <5%. The approximate total sample size for comparingproportions and detecting the difference, with a 0.05 2-sided
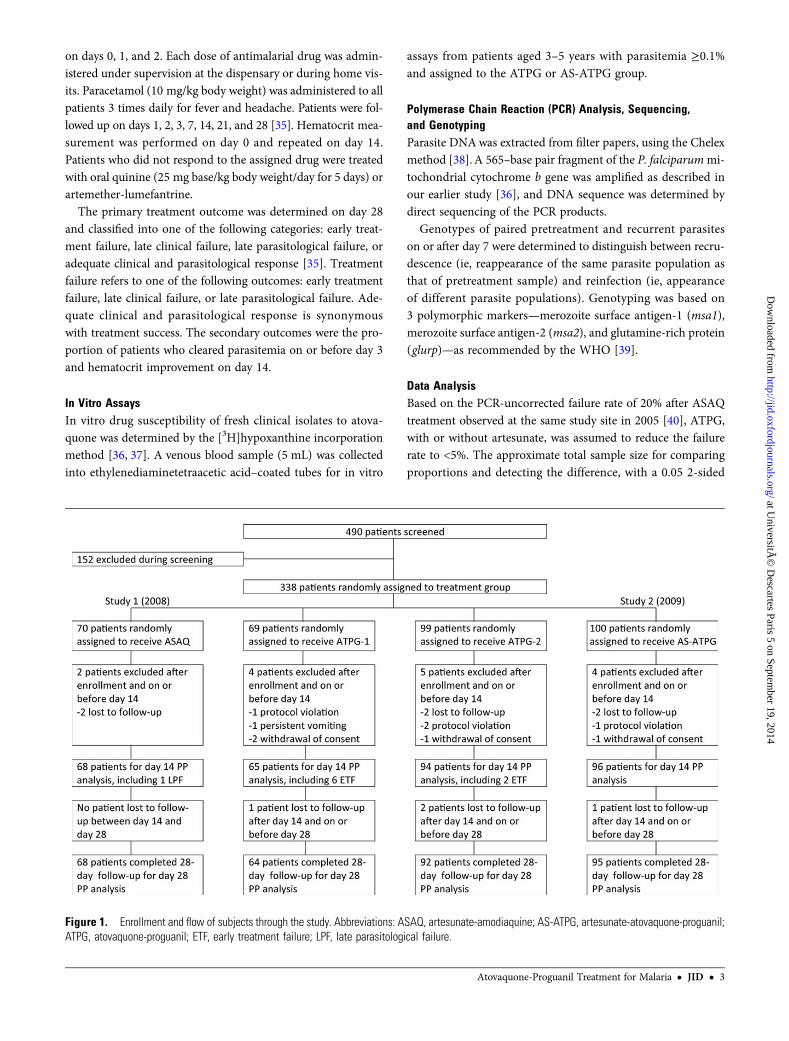
Figure 1. Enrollment and flow of subjects through the study. Abbreviations: ASAQ, artesunate-amodiaquine; AS-ATPG, artesunate-atovaquone-proguanil;ATPG, atovaquone-proguanil; ETF, early treatment failure; LPF, late parasitological failure.
Atovaquone-Proguanil Treatment for Malaria • JID • 3
at UniversitÃ
© D
escartes Paris 5 on September 19, 2014
http://jid.oxfordjournals.org/D
ownloaded from

significance level and 80% power, in 2 treatment arms was 150patients.
Continuous variables were compared using the unpaired orpaired t test. Proportions were arranged in a 2 × 2 contingencytable and compared using the Fisher exact test. Logistic regres-sion analysis was used to determine the adjusted odds ratios(ORs) for risk factors associated with positive smears on day 3and to estimate associations between the day 3 secondary out-come measure and pretreatment variables. All statistical testswere 2-sided, and the level of statistical significance was fixedat a P value of <.05. SigmaStat 3.5 (Systat Software, Point Rich-mond, CA) and Stata 11 (StataCorp, College Station, TX)software were used for these analyses.
The primary end points were determined on day 28 andtransformed to binary categorical variables. Both intention-to-treat (ITT) and per-protocol (PP) analyses of the percentage ofACPR were performed. A fixed-effect model of meta-analysiswas used to analyze dichotomous data, calculate the Peto OR,and compare treatment effect [41]. Data were analyzed usingthe meta-analysis package of software R (version 2.8.1; R Foun-dation for Statistical Computing) and Review Manager 5.2.6software (Nordic Cochrane Center, Cochrane Collaboration,Copenhagen, Denmark, 2012).
Kaplan–Meier survival analysis was performed to calculatethe probability of the time to treatment failure during the28-day follow-up period. Pairs of survival curves were com-pared using the log-rank test. Survival curves were plottedand analyzed using Prism 4.0 (GraphPad Software, La Jolla,CA) software.
Parasite growth of individual clinical isolates in the presenceof various concentrations of atovaquone was expressed as thepercentage of parasite growth in drug-free control wells andplotted against the logarithmic values of drug concentrations.The 50% inhibitory concentration (IC50), defined as the drugconcentration corresponding to 50% of the uptake of [3H]hypo-xanthine measured in the drug-free control wells, was deter-mined by a nonlinear regression analysis using Prism 4.0.Data were expressed as geometric mean IC50 values and 95%confidence intervals (CIs).
Recrudescent parasites after ATPG treatment failure havebeen characterized by Y268S, Y268N, or Y268C substitutionsin cytochrome b [42–47]. Moreover, a recrudescent isolateTM93-C1088 obtained from a Thai patient after treatmentwith atovaquone-pyrimethamine and other P. falciparumclones that have been selected during in vitro culture by step-wise exposure to increasing concentration of atovaquone
Table 1. Baseline Clinical and Parasitological Characteristics by Treatment Group, Intention-to-Treat Analysis
Characteristic ASAQ (n = 70) ATPG-1 (n = 69) ATPG-2 (n = 99) AS-ATPG (n = 100)
Male sex 27 29 57 47Age, mo
Mean ± SD 35.9 ± 16.2 34.4 ± 17.2 34.3 ± 15.1 30.2 ± 16.4
Range 6–60 6–60 7–60 5–60Weight, kg
Mean ± SD 14.4 ± 3.9 13.9 ± 4.0 14.3 ± 3.6 13.7 ± 4.1
Range 7.2–25 6.5–22 7.1–25 7.0–26Rectal temperature, °C
Mean ± SD 38.9 ± 0.8 38.8 ± 0.8 38.7 ± 0.7 39.0 ± 0.8
Range 38.0–41.0 38.0–41.0 38.0–41.0 38.0–40.9Days since symptom onset, no.,mean ± SD
3.8 ± 2.2 3.5 ± 2.0 3.2 ± 1.9 3.3 ± 2.4
Reported self-medication for currentfebrile episode, patients, %
Antimalarial druga 4.3 0 0 1.0
Antipyretic drug 50.0 58.0 49.5 53.0
Parasitemia, asexual parasites/µL bloodGeometric mean (95% CI) 38 600 (28 600–52 000) 35 100 (26 200–46 900) 38 400 (30 700–48 000) 38 700 (31 200–48 000)
Range 2120–230 000 2020–207 000 2400–319 000 2010–415 000
Parasitemia >200 000/µL, patients, % 5.7 1.4 5.1 4.0Hematocrit, %
Mean ± SD 29.0 ± 5.0 29.2 ± 5.5 29.5 ± 5.4 28.7 ± 5.2
Range 17–38 16–43 15–41 15–43
There was statistically no significant difference (P > .05) in all comparisons between the artesunate-amodiaquine (ASAQ) and atovaquone-proguanil (ATPG-1)treatment groups and between the ATPG-2 and artesunate-atovaquone-proguanil (AS-ATPG) treatment groups.
Abbreviation: CI, confidence interval.a A total of 4 patients reported self-medication with amodiaquine monotherapy (n = 3) or oral quinine (n = 1) within 2 weeks before consultation.
4 • JID • Tahar et al
at UniversitÃ
© D
escartes Paris 5 on September 19, 2014
http://jid.oxfordjournals.org/D
ownloaded from
displayed the following amino acid substitutions, either singlyor in combination: M133I, L271F, K272R, P275T, G280D,L283I, and V284K [45, 48]. Mutant cytochrome b alleles weredefined on the basis of these amino acid changes.
RESULTS
A total of 338 children were enrolled (Figure 1). The base-line clinical and laboratory characteristics of the ITT popula-tion were not different (P > .05) between the study groups(Table 1). A total of 19 study participants had no outcomedata: 10 were lost to follow-up, and 9 were excluded after enroll-ment for protocol violation, persistent vomiting, or withdrawalof consent.
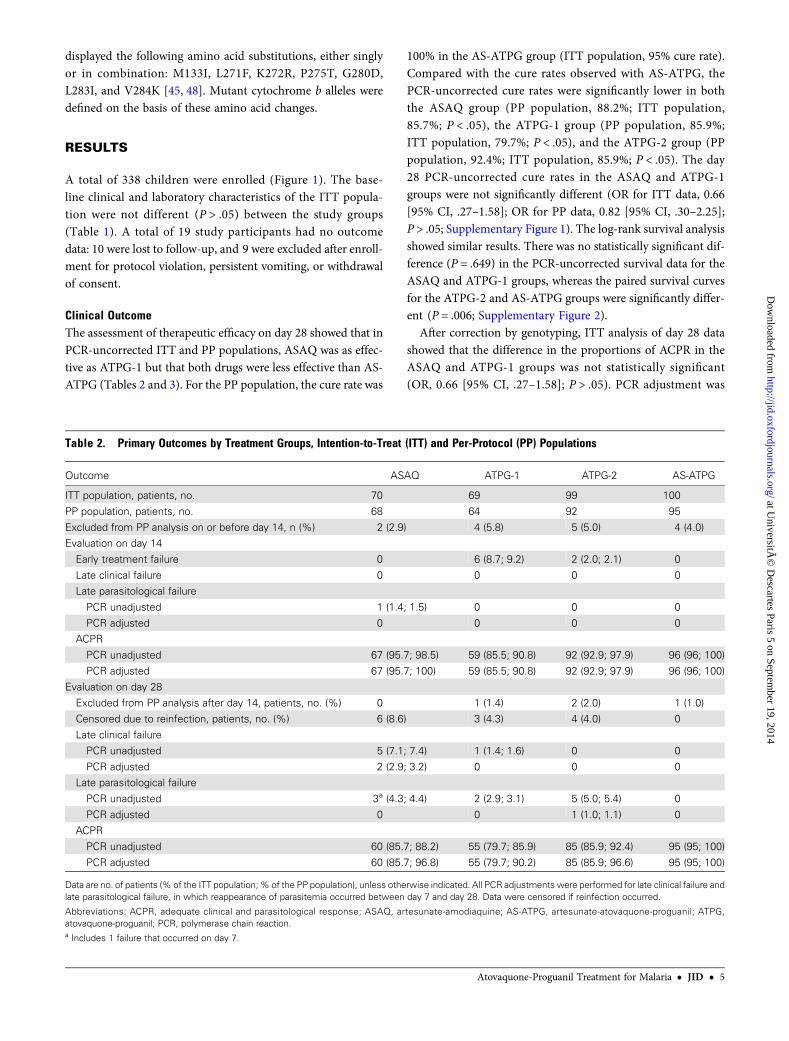
Clinical OutcomeThe assessment of therapeutic efficacy on day 28 showed that inPCR-uncorrected ITT and PP populations, ASAQ was as effec-tive as ATPG-1 but that both drugs were less effective than AS-ATPG (Tables 2 and 3). For the PP population, the cure rate was
100% in the AS-ATPG group (ITT population, 95% cure rate).Compared with the cure rates observed with AS-ATPG, thePCR-uncorrected cure rates were significantly lower in boththe ASAQ group (PP population, 88.2%; ITT population,85.7%; P < .05), the ATPG-1 group (PP population, 85.9%;ITT population, 79.7%; P < .05), and the ATPG-2 group (PPpopulation, 92.4%; ITT population, 85.9%; P < .05). The day28 PCR-uncorrected cure rates in the ASAQ and ATPG-1groups were not significantly different (OR for ITT data, 0.66[95% CI, .27–1.58]; OR for PP data, 0.82 [95% CI, .30–2.25];P > .05; Supplementary Figure 1). The log-rank survival analysisshowed similar results. There was no statistically significant dif-ference (P = .649) in the PCR-uncorrected survival data for theASAQ and ATPG-1 groups, whereas the paired survival curvesfor the ATPG-2 and AS-ATPG groups were significantly differ-ent (P = .006; Supplementary Figure 2).
After correction by genotyping, ITT analysis of day 28 datashowed that the difference in the proportions of ACPR in theASAQ and ATPG-1 groups was not statistically significant(OR, 0.66 [95% CI, .27–1.58]; P > .05). PCR adjustment was
Table 2. Primary Outcomes by Treatment Groups, Intention-to-Treat (ITT) and Per-Protocol (PP) Populations
Outcome ASAQ ATPG-1 ATPG-2 AS-ATPG
ITT population, patients, no. 70 69 99 100
PP population, patients, no. 68 64 92 95
Excluded from PP analysis on or before day 14, n (%) 2 (2.9) 4 (5.8) 5 (5.0) 4 (4.0)Evaluation on day 14
Early treatment failure 0 6 (8.7; 9.2) 2 (2.0; 2.1) 0
Late clinical failure 0 0 0 0Late parasitological failure
PCR unadjusted 1 (1.4; 1.5) 0 0 0
PCR adjusted 0 0 0 0ACPR
PCR unadjusted 67 (95.7; 98.5) 59 (85.5; 90.8) 92 (92.9; 97.9) 96 (96; 100)
PCR adjusted 67 (95.7; 100) 59 (85.5; 90.8) 92 (92.9; 97.9) 96 (96; 100)Evaluation on day 28
Excluded from PP analysis after day 14, patients, no. (%) 0 1 (1.4) 2 (2.0) 1 (1.0)
Censored due to reinfection, patients, no. (%) 6 (8.6) 3 (4.3) 4 (4.0) 0Late clinical failure
PCR unadjusted 5 (7.1; 7.4) 1 (1.4; 1.6) 0 0
PCR adjusted 2 (2.9; 3.2) 0 0 0Late parasitological failure
PCR unadjusted 3a (4.3; 4.4) 2 (2.9; 3.1) 5 (5.0; 5.4) 0
PCR adjusted 0 0 1 (1.0; 1.1) 0ACPR
PCR unadjusted 60 (85.7; 88.2) 55 (79.7; 85.9) 85 (85.9; 92.4) 95 (95; 100)
PCR adjusted 60 (85.7; 96.8) 55 (79.7; 90.2) 85 (85.9; 96.6) 95 (95; 100)
Data are no. of patients (% of the ITT population; % of the PP population), unless otherwise indicated. All PCR adjustments were performed for late clinical failure andlate parasitological failure, in which reappearance of parasitemia occurred between day 7 and day 28. Data were censored if reinfection occurred.
Abbreviations: ACPR, adequate clinical and parasitological response; ASAQ, artesunate-amodiaquine; AS-ATPG, artesunate-atovaquone-proguanil; ATPG,atovaquone-proguanil; PCR, polymerase chain reaction.a Includes 1 failure that occurred on day 7.
Atovaquone-Proguanil Treatment for Malaria • JID • 5
at UniversitÃ
© D
escartes Paris 5 on September 19, 2014
http://jid.oxfordjournals.org/D
ownloaded from
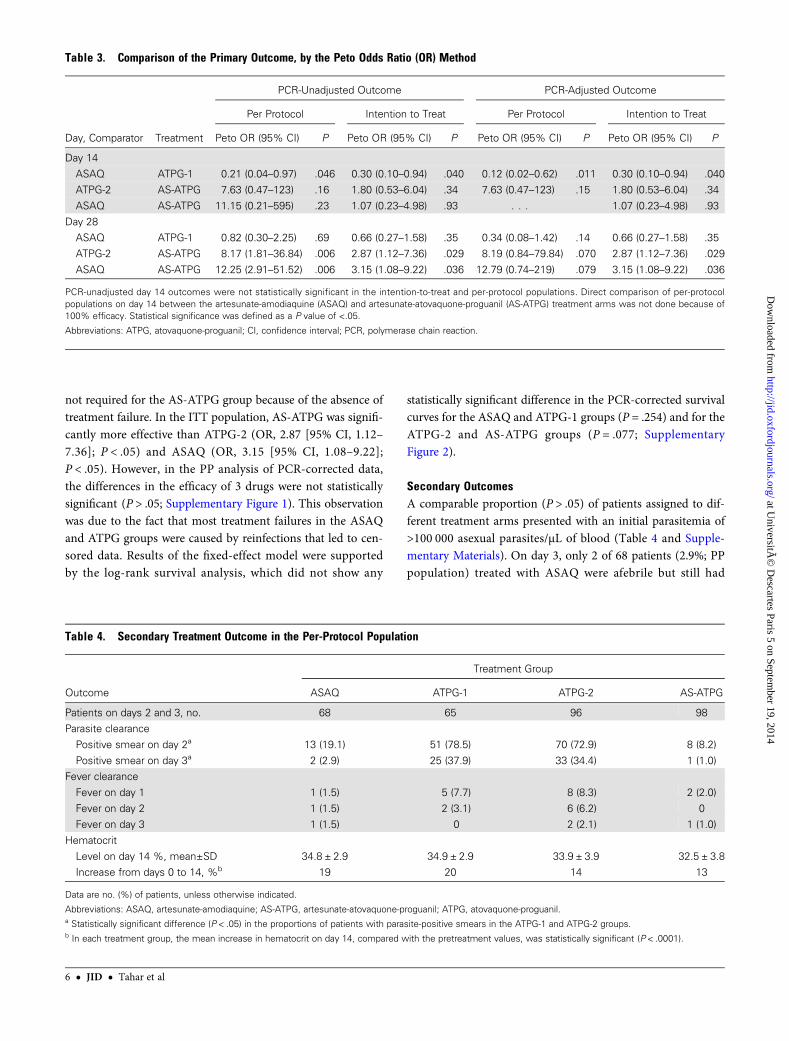
not required for the AS-ATPG group because of the absence oftreatment failure. In the ITT population, AS-ATPG was signifi-cantly more effective than ATPG-2 (OR, 2.87 [95% CI, 1.12–7.36]; P < .05) and ASAQ (OR, 3.15 [95% CI, 1.08–9.22];P < .05). However, in the PP analysis of PCR-corrected data,the differences in the efficacy of 3 drugs were not statisticallysignificant (P > .05; Supplementary Figure 1). This observationwas due to the fact that most treatment failures in the ASAQand ATPG groups were caused by reinfections that led to cen-sored data. Results of the fixed-effect model were supportedby the log-rank survival analysis, which did not show any
statistically significant difference in the PCR-corrected survivalcurves for the ASAQ and ATPG-1 groups (P = .254) and for theATPG-2 and AS-ATPG groups (P = .077; SupplementaryFigure 2).
Secondary OutcomesA comparable proportion (P > .05) of patients assigned to dif-ferent treatment arms presented with an initial parasitemia of>100 000 asexual parasites/µL of blood (Table 4 and Supple-mentary Materials). On day 3, only 2 of 68 patients (2.9%; PPpopulation) treated with ASAQ were afebrile but still had
Table 3. Comparison of the Primary Outcome, by the Peto Odds Ratio (OR) Method
Day, Comparator Treatment
PCR-Unadjusted Outcome PCR-Adjusted Outcome
Per Protocol Intention to Treat Per Protocol Intention to Treat
Peto OR (95% CI) P Peto OR (95% CI) P Peto OR (95% CI) P Peto OR (95% CI) P
Day 14
ASAQ ATPG-1 0.21 (0.04–0.97) .046 0.30 (0.10–0.94) .040 0.12 (0.02–0.62) .011 0.30 (0.10–0.94) .040ATPG-2 AS-ATPG 7.63 (0.47–123) .16 1.80 (0.53–6.04) .34 7.63 (0.47–123) .15 1.80 (0.53–6.04) .34
ASAQ AS-ATPG 11.15 (0.21–595) .23 1.07 (0.23–4.98) .93 . . . 1.07 (0.23–4.98) .93
Day 28ASAQ ATPG-1 0.82 (0.30–2.25) .69 0.66 (0.27–1.58) .35 0.34 (0.08–1.42) .14 0.66 (0.27–1.58) .35
ATPG-2 AS-ATPG 8.17 (1.81–36.84) .006 2.87 (1.12–7.36) .029 8.19 (0.84–79.84) .070 2.87 (1.12–7.36) .029
ASAQ AS-ATPG 12.25 (2.91–51.52) .006 3.15 (1.08–9.22) .036 12.79 (0.74–219) .079 3.15 (1.08–9.22) .036
PCR-unadjusted day 14 outcomes were not statistically significant in the intention-to-treat and per-protocol populations. Direct comparison of per-protocolpopulations on day 14 between the artesunate-amodiaquine (ASAQ) and artesunate-atovaquone-proguanil (AS-ATPG) treatment arms was not done because of100% efficacy. Statistical significance was defined as a P value of <.05.
Abbreviations: ATPG, atovaquone-proguanil; CI, confidence interval; PCR, polymerase chain reaction.
Table 4. Secondary Treatment Outcome in the Per-Protocol Population
Outcome
Treatment Group
ASAQ ATPG-1 ATPG-2 AS-ATPG
Patients on days 2 and 3, no. 68 65 96 98Parasite clearance
Positive smear on day 2a 13 (19.1) 51 (78.5) 70 (72.9) 8 (8.2)
Positive smear on day 3a 2 (2.9) 25 (37.9) 33 (34.4) 1 (1.0)Fever clearance
Fever on day 1 1 (1.5) 5 (7.7) 8 (8.3) 2 (2.0)
Fever on day 2 1 (1.5) 2 (3.1) 6 (6.2) 0Fever on day 3 1 (1.5) 0 2 (2.1) 1 (1.0)
Hematocrit
Level on day 14 %, mean±SD 34.8 ± 2.9 34.9 ± 2.9 33.9 ± 3.9 32.5 ± 3.8Increase from days 0 to 14, %b 19 20 14 13
Data are no. (%) of patients, unless otherwise indicated.
Abbreviations: ASAQ, artesunate-amodiaquine; AS-ATPG, artesunate-atovaquone-proguanil; ATPG, atovaquone-proguanil.a Statistically significant difference (P < .05) in the proportions of patients with parasite-positive smears in the ATPG-1 and ATPG-2 groups.b In each treatment group, the mean increase in hematocrit on day 14, compared with the pretreatment values, was statistically significant (P < .0001).
6 • JID • Tahar et al
at UniversitÃ
© D
escartes Paris 5 on September 19, 2014
http://jid.oxfordjournals.org/D
ownloaded from

parasite-positive smears. Among 98 patients (PP population)treated with AS-ATPG and followed up on day 3, only 1 childstill had a parasite-positive smear on day 3, but this patient wasafebrile from day 1 onward. These observations suggest thatthese 2 ACTs rapidly clear fever and parasitemia in a large ma-jority of patients before day 3, even in patients presenting withhigh initial parasitemias.
In contrast to the rapid parasite clearance after ACTs, 58 of161 patients (36.0%) treated with ATPG (25 from the ATPG-1group and 33 from the ATPG-2 group; PP populations) stillpresented with parasite-positive smears on day 3 (P < .001,compared to the ASAQ and AS-ATPG groups). Among these58 patients, the geometric mean parasitemia on day 3 was 222asexual parasites/µL (95% CI, 163–303 asexual parasites/µL;range, 36–4530 asexual parasites/µL). By day 7, with the excep-tion of 3 patients who were also febrile and required rescuetreatment on day 3 for early treatment failure (Table 5), 55 of58 patients had parasite-negative smears. Logistic regressionanalysis failed to identify a factor (ie, age, sex, weight, body tem-perature, or hematocrit) that may predict a delayed parasitolog-ical response on day 3.
Pretreatment hematocrit values were available for all 338 en-rolled patients. Day 14 hematocrit values were available for 323patients (ITT population, 95.6%). In each treatment group,there was a statistically significant (P < .001) increase in hemat-ocrit from day 0 to day 14. Among all treatment groups, themean increase in hematocrit was between 13% and 20%.
In Vitro and Molecular AssaysThe in vitro activity of atovaquone was determined in 65 iso-lates. The geometric mean IC50 of 55 pretreatment clinical iso-lates with interpretable data was 1.32 nM (95% CI, 1.06–1.65nM; range, 0.184–5.30 nM). The cytochrome b sequence was
determined in isolates from all patients treated with ATPG orAS-ATPG. No mutation was found.
DISCUSSION
The present study confirmed our earlier findings that ASAQ iswell tolerated and rapidly effective in clearing fever and parasi-temia in young Cameroonian children. Young African childrenaged <5 years constitute the largest and most vulnerable popu-lation that bears most of the global malaria burden in terms ofmorbidity and mortality, primarily because of inadequate levelof acquired immunity. Children with symptomatic malaria re-quire rapid and accurate diagnosis, followed by rapidly acting,effective treatment to prevent the progression of the disease to-ward potentially fatal, severe, and complicated malaria. ASAQand other ACTs fulfill this requirement for rapid clearance offever and parasitemia.
Recent clinical studies have suggested that the best availablemeans to detect early signs of decline in artemisinin efficacy isthe time to attain 50% of the pretreatment parasitemia [6]. Themain disadvantage of this measure is the requirement for aclose, 6–8-hour monitoring of parasitemia during the first 48hours of treatment. For retrospective analysis of clinical data,the best available secondary outcome to evaluate the artemisi-nin efficacy is the proportion of patients who have parasite-pos-itive smears on day 3 [35].Our previous studies of the efficacy ofASAQ conducted between 2005 and 2007 in young children inYaoundé have shown that a small minority of patients (2 of 206[0.97%]) remain smear positive on day 3 [40]. Likewise, otherACTs evaluated in young children resulted in rapid fever andparasite clearance. By contrast, amodiaquine monotherapyand amodiaquine-sulfadoxine-pyrimethamine combination re-sulted in higher proportions of positive smears (8 of 62 patients
Table 5. Evolution of Body Temperature and Parasitemia in 8 Patients Responding With Early Treatment Failure After Atovaquone-Proguanil Treatment
Patient Code Age in mo; Sex Weight, kgDay 0
Hematocrit, %
Rectal Temperature, °CParasitemia, Asexual
Parasites/µL
Day 0 Day 1 Day 2 Day 3 Day 0 Day 2 Day 3
NKO-43/1 11; M 9.6 33 40.9 38.0 38.0 38.3 42 900 25 800 117
NKO-36/2 30; M 10.0 25 39.8 38.1 38.9 38.5 36 300 10 200 240
NKO-58/2 7; M 8.1 19 39.0 37.0 36.9 38.4 20 400 4350 833NKO-103/1 15; M 7.6 36 38.5 36.5 37.7 37.1 18 600 74 900 0
NKO-60/1 59; F 18.0 32 38.0 36.7 36.2 37.3 40 900 45 200 4530
NKO-129/1 24; F 16.0 26 38.8 36.8 37.3 37.1 149 000 175 000 370NKO-112/1 48; F 15.0 29 39.0 36.8 36.6 36.0 86 200 86 400 866
NKO-138/1 10; M 8.4 30 41.0 37.0 37.3 36.0 7000 12 800 109
Two subsets of patients fulfilled one of the 4 criteria of early treatment failure: (1) fever (rectal temperature, ≥38.0°C) and positive parasitemia on day 3 (patientsNKO-43/1, NKO-36/2, and NKO-58/2) or (2) parasitemia on day 2 higher than the initial parasitemia on day 0, with or without fever on day 2 (patients NKO-103/1, NKO-60/1, NKO-129/1, NKO-112/1, and NKO-138/1).
Atovaquone-Proguanil Treatment for Malaria • JID • 7
at UniversitÃ
© D
escartes Paris 5 on September 19, 2014
http://jid.oxfordjournals.org/D
ownloaded from

[12.9%] and 9 of 65 patients [13.8%], respectively; PP analysis).Based on this criterion of day-3 parasite clearance, ATPG per-formed poorly (58 of 161 patients [36.0%] with positive smears;PP analysis), as compared with ACTs and even amodiaquinemonotherapy and amodiaquine-sulfadoxine-pyrimethamine.The slow action of ATPG in clearing parasitemia is one of itsmajor disadvantages that may also explain some of the casesof early treatment failure observed with this drug.
In an earlier study conducted in Gabon [26], early treatmentfailure due to a rebound parasitemia resulting in a parasitecount on day 2 that was higher than that on day 0 was observedin one pediatric patient after treatment with ATPG, but theblood smear of this patient became negative for parasites onday 3 without any additional treatment. In the present study,8 cases of early treatment failure were observed amongATPG-treated patients. Three patients had fever and parasite-mia on day 3 and required rescue treatment on day 3. Five pa-tients were classified as experiencing early treatment failure,based on the parasitological criterion of parasitemia on day 2higher than that on day 0, with or without fever, and were cen-sored on day 2. However, because of the delay in determiningparasitemia by independent microscopists, these 5 patients,who did not manifest any sign of clinical aggravation andwere afebrile on days 1, 2, and 3, were followed beyond day 2without rescue treatment. Two of these patients were aparasite-mic on days 7, 14, and 21 and afebrile from day 1 to day 21 buton day 28 had recurrent P. falciparum parasitemia and fever. Al-ternative treatment was administered on day 28. Genotypingdemonstrated that, in both cases, reappearance of parasitemiaon day 28 was due to reinfection. Three additional patients clas-sified as experiencing early treatment failure were afebrile fromday 1 onward and had parasite-negative smears from day 7 today 28. These patients were followed until day 28 and did notrequire any alternative treatment. These latter cases illustratethat the criterion of early treatment failure (ie, parasitemia onday 2, with or without fever, that was greater than parasitemiaon day 0) may not always predict clinical failure. Although thiscriterion may overestimate early treatment failure for slow-acting drugs, it is necessary to ensure patients’ safety and welfarein a standardized protocol for drug studies.
There were 16 late treatment failures occurring on or afterday 7: 8 were in the ASAQ group, 8 were in the ATPG-1 andATPG-2 combined groups, and none were in the AS-ATPGgroup. Only 2 of 8 failures occurring in the ASAQ groupwere due to recrudescence; the other 6 failures were due to re-infection. In the combined ATPG-1 and ATPG-2 groups, 7 of 8failures were due to reinfection, while 1 failure was attributableto recrudescence, which was not associated with any mutationin cytochrome b. Therefore, most late failures were reclassifiedas new infections and censored in the ASAQ, ATPG-1, andATPG-2 arms. The clinical observation was in agreementwith the high in vitro activity of atovaquone and the absence
of mutations, particularly in codon 268 of the cytochrome bgene. Moreover, mutant codon 268 is rarely found in Africa[49, 50].
In the present study, comparison of the tolerability profilewas not planned since it was assessed in several earlier studies[20–27]. Most individual adverse events reported by the pa-tients’ parents or legal guardians, such as headache, fever, my-algia, arthralgia, abdominal pain, gastrointestinal disorders,asthenia, loss of appetite, nausea, dizziness, vomiting, andcough, were present at enrollment and persisted during thefirst 2–3 days of follow-up. Formal links of these signs andsymptoms with drug intake, rather than being the consequencesof malarial disease, are difficult to establish, particularly becausea large majority of parents reported disappearance of these signsand symptoms on or before day 7. No serious adverse effect wasobserved with any of the 3 drugs evaluated in the present study.
In summary, ATPG was characterized by a slow blood schiz-ontocidal action resulting in parasite-positive smears on day 3and early treatment failure in some patients. ASAQ and ATPGwere generally effective but were associated with reinfections,mostly occurring between day 14 and day 28. One of the limit-ing factors of artesunate-atovaquone-proguanil is the unavail-ability of a coformulated product, which may compromisepatient compliance unless treatment is supervised. However, ar-tesunate-atovaquone-proguanil was a highly effective alterna-tive treatment that was not associated with any recrudescenceor reinfection during the 28-day follow-up period.
Supplementary Data
Supplementary materials are available at The Journal of Infectious Diseasesonline (http://jid.oxfordjournals.org). Supplementary materials consist ofdata provided by the author that are published to benefit the reader. Theposted materials are not copyedited. The contents of all supplementarydata are the sole responsibility of the authors. Questions or messages regard-ing errors should be addressed to the author.
Notes
Acknowledgments. We thank all children and their parents or legalguardians, for taking part in this study; and the medical staff of NlongkakCatholic missionary dispensary in Yaoundé, Cameroon, for participating inthe recruitment of patients.Financial support. This work was supported by the French Agence Na-
tionale de la Recherche (grant ANR-08-MIE-024).Potential conflicts of interest. All authors: No reported conflicts.All authors have submitted the ICMJE Form for Disclosure of Potential
Conflicts of Interest. Conflicts that the editors consider relevant to the con-tent of the manuscript have been disclosed.
References
1. World Health Organization. Global malaria programme. guidelines forthe treatment of malaria. 2nd ed. Geneva, Switzerland: World HealthOrganization, 2010.
2. Maiga AW, Fofana B, Sagara I, et al. No evidence of delayed parasiteclearance after oral artesunate treatment of uncomplicated falciparummalaria in Mali. Am J Trop Med Hyg 2012; 87:23–8.
8 • JID • Tahar et al
at UniversitÃ
© D
escartes Paris 5 on September 19, 2014
http://jid.oxfordjournals.org/D
ownloaded from

3. Olliaro P, Nevill C, LeBras J, et al. Systematic review of amodiaquinetreatment in uncomplicated malaria. Lancet 1996; 348:1196–201.
4. Noedl H, Se Y, Schaecher K, Smith BL, Socheat D, Fukuda MM; Arte-misinin Resistance in Cambodia 1 (ARC1) Study Consortium. Evidenceof artemisinin-resistant malaria in western Cambodia. N Engl J Med2008; 359:2619–20.
5. Dondorp AM, Nosten F, Yi P, et al. Artemisinin resistance in Plasmo-dium falciparum malaria. N Eng J Med 2009; 361:455–67.
6. Amaratunga C, Sreng S, Suon S, et al. Artemisinin-resistant Plasmodi-um falciparum in Pursat province, western Cambodia: a parasite clear-ance rate study. Lancet Infect Dis 2012; 12:851–8.
7. Hammond DJ, Burchell JR, PudneyM. Inhibition of pyrimidine biosyn-thesis de novo in Plasmodium falciparum by 2-(4-t-4-butylcyclohexyl)-3-hydroxy-1,4-naphthoquinone in vitro. Mol Biochem Parasitol 1985;14:97–109.
8. Fry M, Pudney M. Site of action of the antimalarial hydroxynaphtho-quinone, 2-[trans-4-(4′-chlorphenyl)cyclohexyl]-3-hydroxy-1,4-naph-thoquinone (566C80). Biochem Pharmacol 1992; 43:1545–53.
9. Hudson AT. Atovaquone – a novel broad-spectrum anti-infective drug.Parasitol Today 1993; 9:66–8.
10. Srivastava IK, Rottenberg H, Vaidya AB. Atovaquone, a broad spectrumantiparasitic drug, collapses mitochondrial membrane potential in amalarial parasite. J Biol Chem 1997; 272:3961–6.
11. Canfield CJ, Pudney M, Gutteridge WE. Interactions of atovaquonewith other antimalarial drugs against Plasmodium falciparum in vitro.Exp Parasitol 1995; 80:373–81.
12. Srivastava IK, Vaidya AB. A mechanism for the synergistic antimalarialaction of atovaquone and proguanil. Antimicrob Agents Chemother1999; 43:1334–9.
13. Looareesuwan S, Viravan C, Kyle Webster H, Kyle DE, Hutchinson DB,Canfield CJ. Clinical studies of atovaquone, alone or in combinationwith other antimalarial drugs, for treatment of acute uncomplicated ma-laria in Thailand. Am J Trop Med Hyg 1996; 54:62–6.
14. Looareesuwan S, Chulay JD, Canfield CJ, Hutchinson DB. Malarone(atovaquone and proguanil hydrochloride): A review of its clinical de-velopment for treatment of malaria. Malarone Clinical Trials StudyGroup. Am J Trop Med Hyg 1999; 60:533–41.
15. McKeage K, Scott LJ. Atovaquone/proguanil. A review of its use for theprophylaxis of Plasmodium falciparummalaria. Drugs 2003; 63:596–623.
16. Boggild AK, Parise ME, Lewis LS, Kain KC. Atovaquone-proguanil: re-port from the CDC expert meeting on malaria chemoprophylaxis (II).Am J Trop Med Hyg 2007; 76:208–23.
17. Griffith KS, Lewis LS, Mali S, Parise ME. Treatment of malaria in theUnited States: A systematic review. JAMA J Am Med Assoc 2007;297:2264–77.
18. Askling HH, Bruneel F, Burchard G, et al. Management of importedmalaria in Europe. Malar J 2012; 11:328.
19. World Health Organization. International travel and health. Geneva,Switzerland: World Health Organization, 2012.
20. Radloff PD, Philipps J, Nkeyi M, Hutchinson D, Kremsner PG. Atova-quone and proguanil for Plasmodium falciparummalaria. Lancet 1996;347:1511–4.
21. Lell B, Luckner D, Ndjave M, Scott T, Kremsner PG. Randomised pla-cebo-controlled study of atovaquone plus proguanil for malaria prophy-laxis in children. Lancet 1998; 351:709–13.
22. Shanks GD, Gordon DM, Klotz FW, et al. Efficacy and safety of atova-quone/proguanil as suppressive prophylaxis for Plasmodium falciparummalaria. Clin Infect Dis 1998; 27:494–9.
23. Anabwani G, Canfield CJ, Hutchinson DBA. Combination atovaquoneand proguanil hydrochloride vs. halofantrine for treatment of acutePlasmodium falciparum malaria in children. Pediatr Infect Dis J 1999;18:456–61.
24. MulengaM, Sukwa TY, Canfield CJ, Hutchinson DBA. Atovaquone andproguanil versus pyrimethamine/sulfadoxine for the treatment of acutefalciparum malaria in Zambia. Clin Ther 1999; 21:841–52.
25. Sukwa TY, Mulenga M, Chisaka N. A randomized, double blind, place-bo-controlled field trial to determine the efficacy and safety of Malarone
(atovaquone/proguanil) for the prophylaxis of malaria. Am J Trop MedHyg 1999; 60:521–5.
26. Borrmann S, Faucher JF, Bagaphou T, et al. Atovaquone and proguanilversus amodiaquine for the treatment of Plasmodium falciparummalar-ia in African infants and young children. Clin Infect Dis 2003;37:1441–7.
27. Mulenga M, Malunga F, Bennett S, et al. A randomised, double-blind,placebo-controlled trial of atovaquone-proguanil vs sulphadoxine-pyri-methamine in the treatment of malarial anaemia in Zambian children.Trop Med Int Health 2006; 11:1643–52.
28. Laufer MK, Thesing PC, Dzinjalamala FK, et al. A longitudinal trialcomparing chloroquine as monotherapy or in combination with artesu-nate, azithromycin or atovaquone-proguanil to treat malaria. PLoSONE 2012; 7:e42284.
29. Van Vugt M, Leonardi E, Phaipun L, et al. Treatment of uncomplicatedmultidrug-resistant falicparum malaria with artesunate-atovaquone-proguanil. Clin Infect Dis 2002; 35:1498–504.
30. McGready R, Keo NK, Villegas L, White NJ, Looareesuwan S, Nosten F.Artesunate-atovaquone-proguanil rescue treatment of multidrug-resis-tant Plasmodium falciparum malaria in pregnancy: a preliminary re-port. Trans R Soc Trop Med Hyg 2003; 97:592–4.
31. McGready R, Ashley EA, Moo E, et al. A randomized comparison ofartesunate-atovaquone-proguanil versus quinine in treatment for un-complicated falciparum malaria during pregnancy. J Infect Dis 2005;192:846–53.
32. Fondjo E, Robert V, Le Goff G, Toto JC, Carnevale P. Le paludisme ur-bain à Yaoundé (Cameroun). 2. Etude entomologique dans deux quar-tiers peu urbanisés. Bull Soc Pathol Exot 1992; 85:57–63.
33. Manga L, Fondjo E, Carnevale P, Robert V. Importance of low disper-sion of Anopheles gambiae (Diptera: Culicidae) on malaria transmissionin hilly towns in south Cameroon. J Med Entomol 1993; 30:936–8.
34. Van der Kolk M, Tebo AE, Nimpaye H, Ngo Ndombol D, SauerweinRW, Eling WMC. Transmission of Plasmodium falciparum in urbanYaoundé, Cameroon, is seasonal and age-dependent. Trans R SocTrop Med Hyg 2003; 97:375–9.
35. World Health Organization. Global malaria programme. methods forsurveillance of antimalarial drug efficacy. Geneva, Switzerland: WorldHealth Organization, 2009.
36. Basco LK. Molecular epidemiology of malaria in Cameroon. XVII.Baseline monitoring of atovaquone-resistant Plasmodium falciparumby in vitro drug assays and cytochrome b gene sequence analysis. AmJ Trop Med Hyg 2003; 69:179–83.
37. Basco LK. Field application of in vitro assays for the sensitivity ofhuman malaria parasites to antimalarial drugs. Geneva, Switzerland:World Health Organization, 2007.
38. Kain KC, Lanar DE. Determination of genetic variation within Plasmo-dium falciparum by using enzymatically amplified DNA from filterpaper disks impregnated with whole blood. J Clin Microbiol 1991;29:1171–4.
39. World Health Organization. Methods and techniques for clinical trialson antimalarial drug efficacy: genotyping to identify parasite popula-tions. Geneva, Switzerland: World Health Organization, 2008.
40. Whegang SY, Tahar R, Foumane VN, et al. Efficacy of non-artemisinin-and artemisinin-based combination therapies for uncomplicated falcip-arum malaria in Cameroon. Malar J 2010; 9:56.
41. Yusuf S, Peto R, Lewis J, Collins R, Sleight P. Beta blockade during andafter myocardial infarction: an overview of the randomized trials. ProgCardiovasc Dis 1985; 27:335–71.
42. Fivelman QL, Butcher GA, Adagu IS, Warhurst DC, Pasvol G. Malaronetreatment failure and in vitro confirmation of resistance of Plasmodiumfalciparum isolate from Lagos, Nigeria. Malar J 2002; 1:1.
43. Farnert A, Linkberg J, Gil P, et al. Evidence of Plasmodium falciparummalaria resistance to atovaquone and proguanil hydrochloride: case re-ports. Br Med J 2003; 326:628–9.
44. Schwartz E, Bujanover S, Kain KC. Genetic confirmation of atovaquone-proguanil-resistant Plasmodium falciparum malaria acquired by a non-immune traveller to east Africa. Clin Infect Dis 2003; 37:450–1.
Atovaquone-Proguanil Treatment for Malaria • JID • 9
at UniversitÃ
© D
escartes Paris 5 on September 19, 2014
http://jid.oxfordjournals.org/D
ownloaded from

45. Schwöbel B, Alifrangis M, Salanti A, Jelinek T. Different muta-tion patterns of atovaquone resistance to Plasmodium falciparum invitro and in vivo: rapid detection of codon 268 polymorphisms inthe cytochrome b as potential in vivo resistance marker. Malar J2003; 2:5.
46. Kuhn S, Gill MJ, Kain KC. Emergence of atovaquone-proguanil resis-tance during treatment of Plasmodium falciparum malaria acquiredby a non-immune North American traveller to West Africa. Am JTrop Med Hyg 2005; 72:407–9.
47. Musset L, Bouchaud O, Matheron S, Massias L, Le Bras J. Clinicalatovaquone-proguanil resistance of Plasmodium falciparum associatedwith cytochrome b codon 268 mutations. Microbes Infect 2006;8:2599–604.
48. Korsinczky M, Chen NH, Kotecka B, Saul A, Rieckmann K, Cheng Q.Mutations in Plasmodium falciparum cytochrome b that are associatedwith atovaquone resistance are located at a putative drug-binding site.Antimicrob Agents Chemother 2000; 44:2100–8.
49. Wichmann O, Muehlberger N, Jelinek T, et al. European Network onSurveillance of Imported Infectious Diseases. Screening for mutationsrelated to atovaquone/proguanil resistance in treatment failures andother imported isolates of Plasmodium falciparum in Europe. J InfectDis 2004; 190:1541–6.
50. Musset L, Pradines B, Parzy D, Durand R, Bigot P, Le Bras J. Apparentabsence of atovaquone/proguanil resistance in 477 Plasmodium falcip-arum isolates from untreated French travellers. J Antimicrob Chemo-ther 2006; 57:110–5.
10 • JID • Tahar et al
at UniversitÃ
© D
escartes Paris 5 on September 19, 2014
http://jid.oxfordjournals.org/D
ownloaded from
Related Documents











