ORIGINAL COMMUNICATION Randomized controlled trial of physical activity, cognition, and walking in multiple sclerosis Brian M. Sandroff • Rachel E. Klaren • Lara A. Pilutti • Deirdre Dlugonski • Ralph H. B. Benedict • Robert W. Motl Received: 23 October 2013 / Revised: 22 November 2013 / Accepted: 24 November 2013 Ó Springer-Verlag Berlin Heidelberg 2013 Abstract The present study adopted a randomized con- trolled trial design and examined the effect of a physical activity behavioral intervention on cognitive and walking performance among persons with MS who have mild or moderate disability status. A total of 82 MS patients were randomly allocated into intervention or wait-list control conditions. The intervention condition received a theory- based program for increasing physical activity behavior that was delivered via the Internet, and one-on-one video chat sessions with a behavior-change coach. Participants completed self-report measures of physical activity and disability status, and underwent the oral Symbol Digit Modalities Test (SDMT) and 6-minute walk (6MW) test before and after the 6-month period. Analysis using mixed- model ANOVA indicated a significant time 9 condi- tion 9 disability group interaction on SDMT scores (p = 0.02, partial-g 2 = 0.08), such that persons with mild disability in the intervention condition demonstrated a clinically meaningful improvement in SDMT scores (*6 point change). There was a further significant time 9 condition interaction on 6MW distance (p = 0.02, partial-g 2 = 0.07), such that those in the intervention condition demonstrated an increase in 6MW distance rel- ative to those in the control group. The current study supports physical activity as a promising tool for managing cognitive impairment and impaired walking performance in persons with MS, and suggests that physical activity might have specific effects on cognition and non-specific effects on walking performance in this population. Keywords Multiple sclerosis Á Cognition Á Physical activity Á Walking Introduction Slowed cognitive processing speed (CPS) is common, debilitating, and difficult to manage in persons with mul- tiple sclerosis (MS) [1]. Researchers have recently advo- cated for physical activity as a behavioral approach for managing slowed CPS in MS [2]. This is based, in part, on cross-sectional evidence of an association between ambu- latory-based physical activity and measures of CPS in MS [3, 4], and evidence of physical activity intervention effects on cognitive outcomes in older adults [5]. There is further evidence of coupling between walking performance and CPS in MS [6, 7], perhaps based on co-occurring damage in eloquent neural tracts sub-serving both domains of function. Physical activity has improved walking perfor- mance outcomes in clinical trials of MS [8]. Collectively, this suggests the possibility of physical activity benefits for CPS in MS. The present study involved secondary outcomes from a randomized controlled trial (RCT) and examined the effi- cacy of a physical activity behavioral intervention for improving CPS and walking performance among persons with MS. The primary goal of the RCT involved examining disability status as a moderator of an established behavioral intervention [9–12] for increasing physical activity over a 6-month period among persons with MS. The current paper B. M. Sandroff Á R. E. Klaren Á L. A. Pilutti Á D. Dlugonski Á R. W. Motl (&) Department of Kinesiology and Community Health, University of Illinois at Urbana-Champaign, 233 Freer Hall, 906 South Goodwin Ave., Urbana, IL 61801, USA e-mail: [email protected] R. H. B. Benedict Department of Neurology, SUNY Buffalo School of Medicine, Buffalo, NY, USA 123 J Neurol DOI 10.1007/s00415-013-7204-8

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
ORIGINAL COMMUNICATION
Randomized controlled trial of physical activity, cognition,and walking in multiple sclerosis
Brian M. Sandroff • Rachel E. Klaren •
Lara A. Pilutti • Deirdre Dlugonski •
Ralph H. B. Benedict • Robert W. Motl
Received: 23 October 2013 / Revised: 22 November 2013 / Accepted: 24 November 2013
� Springer-Verlag Berlin Heidelberg 2013
Abstract The present study adopted a randomized con-
trolled trial design and examined the effect of a physical
activity behavioral intervention on cognitive and walking
performance among persons with MS who have mild or
moderate disability status. A total of 82 MS patients were
randomly allocated into intervention or wait-list control
conditions. The intervention condition received a theory-
based program for increasing physical activity behavior
that was delivered via the Internet, and one-on-one video
chat sessions with a behavior-change coach. Participants
completed self-report measures of physical activity and
disability status, and underwent the oral Symbol Digit
Modalities Test (SDMT) and 6-minute walk (6MW) test
before and after the 6-month period. Analysis using mixed-
model ANOVA indicated a significant time 9 condi-
tion 9 disability group interaction on SDMT scores
(p = 0.02, partial-g2 = 0.08), such that persons with mild
disability in the intervention condition demonstrated a
clinically meaningful improvement in SDMT scores (*6
point change). There was a further significant
time 9 condition interaction on 6MW distance (p = 0.02,
partial-g2 = 0.07), such that those in the intervention
condition demonstrated an increase in 6MW distance rel-
ative to those in the control group. The current study
supports physical activity as a promising tool for managing
cognitive impairment and impaired walking performance
in persons with MS, and suggests that physical activity
might have specific effects on cognition and non-specific
effects on walking performance in this population.
Keywords Multiple sclerosis � Cognition � Physical
activity � Walking
Introduction
Slowed cognitive processing speed (CPS) is common,
debilitating, and difficult to manage in persons with mul-
tiple sclerosis (MS) [1]. Researchers have recently advo-
cated for physical activity as a behavioral approach for
managing slowed CPS in MS [2]. This is based, in part, on
cross-sectional evidence of an association between ambu-
latory-based physical activity and measures of CPS in MS
[3, 4], and evidence of physical activity intervention effects
on cognitive outcomes in older adults [5]. There is further
evidence of coupling between walking performance and
CPS in MS [6, 7], perhaps based on co-occurring damage
in eloquent neural tracts sub-serving both domains of
function. Physical activity has improved walking perfor-
mance outcomes in clinical trials of MS [8]. Collectively,
this suggests the possibility of physical activity benefits for
CPS in MS.
The present study involved secondary outcomes from a
randomized controlled trial (RCT) and examined the effi-
cacy of a physical activity behavioral intervention for
improving CPS and walking performance among persons
with MS. The primary goal of the RCT involved examining
disability status as a moderator of an established behavioral
intervention [9–12] for increasing physical activity over a
6-month period among persons with MS. The current paper
B. M. Sandroff � R. E. Klaren � L. A. Pilutti � D. Dlugonski �R. W. Motl (&)
Department of Kinesiology and Community Health, University
of Illinois at Urbana-Champaign, 233 Freer Hall, 906 South
Goodwin Ave., Urbana, IL 61801, USA
e-mail: [email protected]
R. H. B. Benedict
Department of Neurology, SUNY Buffalo School of Medicine,
Buffalo, NY, USA
123
J Neurol
DOI 10.1007/s00415-013-7204-8

examined the efficacy of this physical activity behavioral
intervention for improving CPS and walking performance
in persons with MS. Importantly, we included a measure of
physical activity only as a manipulation check for the
intervention, and CPS and walking performance represent
the foci of this paper. We included the measure of walking
performance as a confirmation of previous beneficial
effects of physical activity in MS [8] and, in particular, as a
control for possible null intervention effects on CPS. We
hypothesized that the behavioral intervention would result
in increases in physical activity, and improved CPS and
walking performance. We hypothesized that the effect for
CPS would be larger in those with mild neurological dis-
ability than in those with moderate disability, and that
walking performance would improve following the inter-
vention, regardless of disability. Such hypotheses were
based on preliminary evidence that the magnitude of the
association between physical activity and CPS was stronger
in persons with mild MS disability compared with persons
with moderate MS disability [13], and that the association
of physical activity and 6-minute walk (6MW) perfor-
mance did not differ based on disability status in persons
with MS [14].
Methods
Participants
Prospective participants were contacted by a flyer that was
distributed amongst patients in the North American
Research Committee on Multiple Sclerosis (NARCOMS)
registry and a database from previous studies conducted in
our laboratory over the past 5 years. There were 511 par-
ticipants who initially expressed interest and who were
contacted via phone by the project coordinator for study
description and screening of inclusion/exclusion criteria.
The inclusion criteria involved: (a) definite diagnosis of
MS based on physician verification; (b) relapse-free for the
past 30 days; (c) ability to walk with or without an assistive
device; (d) age between 18 and 64 years; (e) willingness
and ability to complete in-person cognitive and functional
assessments; (f) physical inactivity defined as \60 min of
physical activity per week; (g) low risk for contraindica-
tions of physical activity indicated by no more than a single
‘‘yes’’ response on the Physical Activity Readiness Ques-
tionnaire (PAR-Q; [15]); and (h) physician’s approval for
participation. Those not meeting such criteria were exclu-
ded. The final sample included 82 participants who were
randomly assigned to intervention (n = 41) or waitlist
control (n = 41) conditions. The sample size was deter-
mined based on a power analysis for detecting a differential
pattern of change in physical activity as a function of
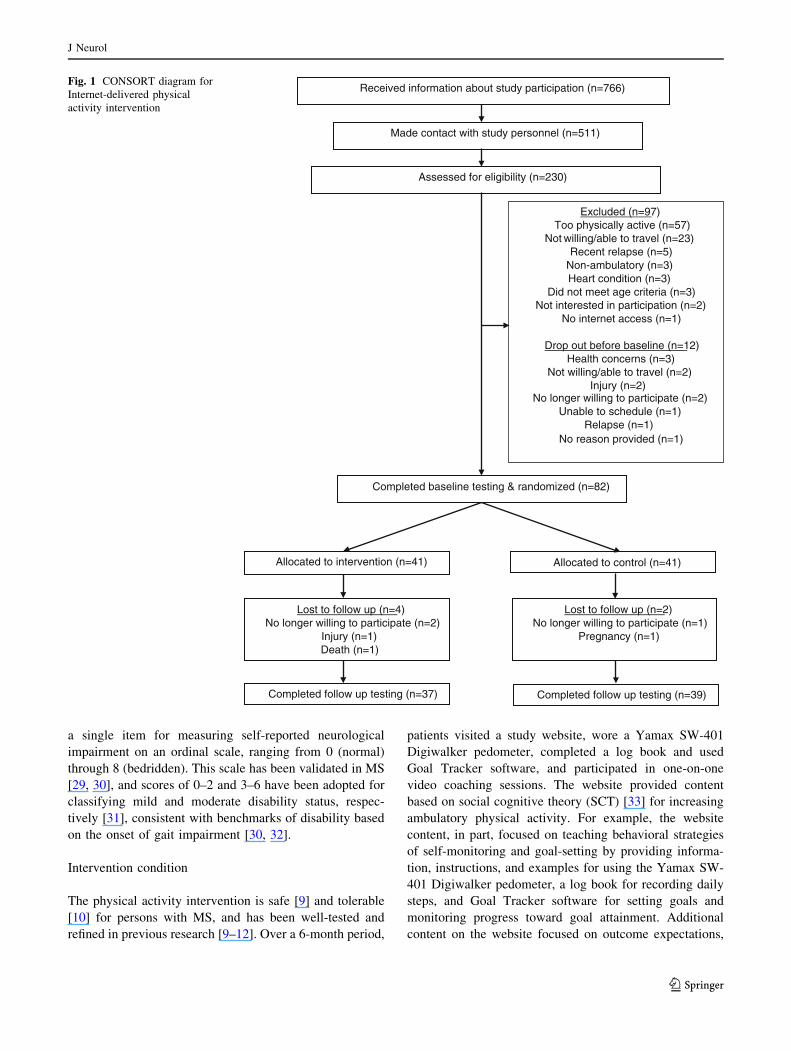
disability status. Participant flow through recruitment and
enrollment is included in the Consolidated Standards of
Reporting Trials (CONSORT) diagram (Fig. 1).
Measures
CPS
The oral version of the Symbol Digit Modalities Test
(SDMT) [16, 17] was administered in accordance with our
previous research [18]. Participants were presented with a
page showing symbols paired with single-digit numbers in
a key. The task was to voice the correct numbers for
unpaired symbols as rapidly as possible for 90 s. Responses
were recorded by the examiner. The outcome measure was
the number of correct responses provided in 90 s [19].
Walking performance
The 6MW was administered as a measure of endurance
walking performance in MS [20]. Participants were
instructed to walk as fast and as far as possible in a single
corridor with 180� turns for 6 min. One researcher fol-
lowed *1 m behind the participant with a measuring
wheel (Stanley MW50, New Briton, CT) and recorded the
total distance traveled (m). We recognize that following
behind the participant with a distance-measuring wheel
might bias 6MW performance, but this protocol is common
and well-established in research involving ambulatory
outcomes in persons with MS [14, 21], and ensures the
most accurate measurement of distance walked during the
test.
Physical activity
Physical activity was measured using the abbreviated
International Physical Activity Questionnaire (IPAQ) [22]
that has been well-validated in MS research [23–27]. The
abbreviated IPAQ is a self-report inventory that measures
the frequency of vigorous, moderate, and walking physical
activity during a 7-day period. The respective frequencies
for vigorous, moderate, and walking were multiplied by 8,
4, and 3.3 metabolic equivalents (METs), respectively.
This results in a measure of overall physical activity with
scores that range between 0 and 117, with higher scores
indicating more physical activity.
Disability status
The patient-determined disease steps (PDDS) scale [28]
was included as a self-report measure of disability status.
The PDDS was developed as an inexpensive surrogate for
the Expanded Disability Status Scale (EDSS) and contains
J Neurol
123
a single item for measuring self-reported neurological
impairment on an ordinal scale, ranging from 0 (normal)
through 8 (bedridden). This scale has been validated in MS
[29, 30], and scores of 0–2 and 3–6 have been adopted for
classifying mild and moderate disability status, respec-
tively [31], consistent with benchmarks of disability based
on the onset of gait impairment [30, 32].
Intervention condition
The physical activity intervention is safe [9] and tolerable
[10] for persons with MS, and has been well-tested and
refined in previous research [9–12]. Over a 6-month period,
patients visited a study website, wore a Yamax SW-401
Digiwalker pedometer, completed a log book and used
Goal Tracker software, and participated in one-on-one
video coaching sessions. The website provided content
based on social cognitive theory (SCT) [33] for increasing
ambulatory physical activity. For example, the website
content, in part, focused on teaching behavioral strategies
of self-monitoring and goal-setting by providing informa-
tion, instructions, and examples for using the Yamax SW-
401 Digiwalker pedometer, a log book for recording daily
steps, and Goal Tracker software for setting goals and
monitoring progress toward goal attainment. Additional
content on the website focused on outcome expectations,
Assessed for eligibility (n=230)
Excluded (n=97)Too physically active (n=57)
Not willing/able to travel (n=23)Recent relapse (n=5)
Non-ambulatory (n=3)Heart condition (n=3)
Did not meet age criteria (n=3)Not interested in participation (n=2)
No internet access (n=1)
Drop out before baseline (n=12) Health concerns (n=3)
Not willing/able to travel (n=2)Injury (n=2)
No longer willing to participate (n=2)Unable to schedule (n=1)
Relapse (n=1)No reason provided (n=1)
Completed baseline testing & randomized (n=82)
Completed follow up testing (n=37)
Allocated to intervention (n=41) Allocated to control (n=41)
Received information about study participation (n=766)
Made contact with study personnel (n=511)
Lost to follow up (n=4)No longer willing to participate (n=2)
Injury (n=1)Death (n=1)
Lost to follow up (n=2)No longer willing to participate (n=1)
Pregnancy (n=1)
Completed follow up testing (n=39)
Fig. 1 CONSORT diagram for
Internet-delivered physical
activity intervention
J Neurol
123

self-efficacy, and facilitators/barriers for physical activity
consistent with SCT. The website materials were delivered
in a titrated manner over the 6-month period such that new
content became available seven times during the first
2-month period, four times during the second 2-month
period, and twice during the final 2 months of the
intervention.
The behavioral intervention further involved weekly,
one-on-one behavioral coaching sessions via SkypeTM. The
sessions were semi-scripted and based on principles of
supportive accountability (i.e., encouraging participants to
wear the pedometer daily and monitor behavioral change
and goal attainment throughout the 6-month intervention).
The coaching sessions each consisted of a review of goal-
setting and progress toward goal attainment, as well as
discussion of strategies and facilitators of behavioral
change based on SCT and current website content. During
the 6-month intervention, there were 15 scheduled Sky-
peTM coaching sessions, which decreased in frequency over
the intervention; seven sessions occurred in the first
2 months, six in the second 2 months, and only two in the
final 2 months.
Control condition
We utilized a wait-list control in this RCT. Participants in
this condition completed the study measures before and
after the 6-month period, and then received the intervention
as described above once the study reached completion.
Procedures
The study procedures were approved by a university
institutional review board, and all participants provided
signed informed consent and physician’s clearance before
enrollment into the study. Participants initially provided
demographic/clinical information, completed the SDMT,
PDDS, IPAQ, and lastly the 6MW during a 1-h testing
session in the laboratory. The order of assessments per
testing session was intentionally standardized to minimize
cognitive and physical fatigue. All testing was adminis-
tered by laboratory personnel who were not blinded to
condition (i.e., intervention or control), as the funding
permitted limited support for study personnel necessary for
blinding. We adopted a very focused, stratified randomi-
zation process, as participants were initially grouped based
on disability (i.e., mild and moderate), then within each
disability group, matched into pairs based on physical
activity data, and randomly assigned into intervention or
wait-list control conditions using a random numbers gen-
erator and allocation by a person who was uninvolved in
testing and intervention delivery [34]. All participants
received notification of group assignment and instructions
for participation through email and United States Postal
Service. The participants completed the same assessments
in the laboratory immediately following the 6-month
intervention period, and received $50 remuneration for
completing each testing session. The payment was not
linked with completion of the intervention.
Data analysis
All analyses were conducted using SPSS Statistics 21
(SPSS Inc., Chicago, IL, USA). Data are presented in text
and tables as mean (standard deviation), unless otherwise
noted. We initially compared the demographic and clinical
characteristics between the disability groups by conditions
using two-way ANOVA and chi-squared tests. Only par-
ticipants who completed follow-up testing were included in
subsequent analyses (i.e., completers analysis). The effect
of the behavioral intervention on CPS and 6MW was
examined using three-way mixed-model ANOVA with
condition (intervention or control) and disability status
(mild or moderate disability) as between-subjects factors
and time as a within-subjects factor. We chose this analysis
because the primary aim of the current study was to
examine the differential effects of the intervention on CPS
and walking performance in persons with mild and mod-
erate disability. We expressed the overall effect sizes from
the ANOVA as partial eta-squared, with values of 0.01,
0.06, and 0.14 interpreted as small, moderate, and large,
respectively. We further computed effect sizes for the
change over time per group as Cohen’s d [35], interpreted
as small, moderate, and large based on criteria of 0.2, 0.5,
and 0.8, respectively. Lastly, we conducted Spearman’s
rank-order correlations (q) for the associations among
changes in physical activity, CPS, and 6MW distance,
respectively, in the intervention condition.
Results
Participant characteristics: comparability
between disability and condition
We randomized 41 persons per condition, and 39 individ-
uals (95.1 %) completed follow-up testing in the control
group, whereas 37 persons (90.2 %) completed follow-up
testing in the intervention group (Fig. 1). A total of 76
persons with MS were included in the data analyses.
Demographic and clinical characteristics of the samples per
condition by disability group are reported in Table 1. We
conducted two-way ANOVAs for examining baseline dif-
ferences in age, body mass index (BMI), MS duration, and
PDDS; we also conducted chi-squared difference tests for
gender and MS type (relapsing vs. progressive MS).
J Neurol
123
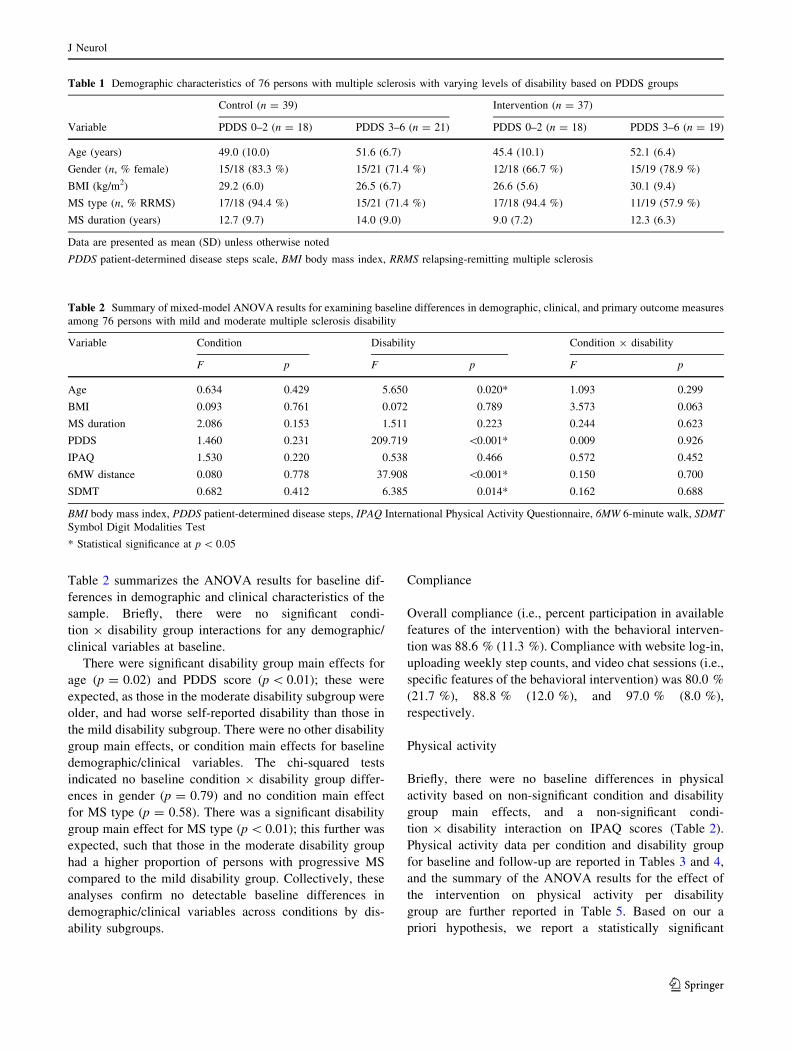
Table 2 summarizes the ANOVA results for baseline dif-
ferences in demographic and clinical characteristics of the
sample. Briefly, there were no significant condi-
tion 9 disability group interactions for any demographic/
clinical variables at baseline.
There were significant disability group main effects for
age (p = 0.02) and PDDS score (p \ 0.01); these were
expected, as those in the moderate disability subgroup were
older, and had worse self-reported disability than those in
the mild disability subgroup. There were no other disability
group main effects, or condition main effects for baseline
demographic/clinical variables. The chi-squared tests
indicated no baseline condition 9 disability group differ-
ences in gender (p = 0.79) and no condition main effect
for MS type (p = 0.58). There was a significant disability
group main effect for MS type (p \ 0.01); this further was
expected, such that those in the moderate disability group
had a higher proportion of persons with progressive MS
compared to the mild disability group. Collectively, these
analyses confirm no detectable baseline differences in
demographic/clinical variables across conditions by dis-
ability subgroups.
Compliance
Overall compliance (i.e., percent participation in available
features of the intervention) with the behavioral interven-
tion was 88.6 % (11.3 %). Compliance with website log-in,
uploading weekly step counts, and video chat sessions (i.e.,
specific features of the behavioral intervention) was 80.0 %
(21.7 %), 88.8 % (12.0 %), and 97.0 % (8.0 %),
respectively.
Physical activity
Briefly, there were no baseline differences in physical
activity based on non-significant condition and disability
group main effects, and a non-significant condi-
tion 9 disability interaction on IPAQ scores (Table 2).
Physical activity data per condition and disability group
for baseline and follow-up are reported in Tables 3 and 4,
and the summary of the ANOVA results for the effect of
the intervention on physical activity per disability
group are further reported in Table 5. Based on our a
priori hypothesis, we report a statistically significant
Table 1 Demographic characteristics of 76 persons with multiple sclerosis with varying levels of disability based on PDDS groups
Control (n = 39) Intervention (n = 37)
Variable PDDS 0–2 (n = 18) PDDS 3–6 (n = 21) PDDS 0–2 (n = 18) PDDS 3–6 (n = 19)
Age (years) 49.0 (10.0) 51.6 (6.7) 45.4 (10.1) 52.1 (6.4)
Gender (n, % female) 15/18 (83.3 %) 15/21 (71.4 %) 12/18 (66.7 %) 15/19 (78.9 %)
BMI (kg/m2) 29.2 (6.0) 26.5 (6.7) 26.6 (5.6) 30.1 (9.4)
MS type (n, % RRMS) 17/18 (94.4 %) 15/21 (71.4 %) 17/18 (94.4 %) 11/19 (57.9 %)
MS duration (years) 12.7 (9.7) 14.0 (9.0) 9.0 (7.2) 12.3 (6.3)
Data are presented as mean (SD) unless otherwise noted
PDDS patient-determined disease steps scale, BMI body mass index, RRMS relapsing-remitting multiple sclerosis
Table 2 Summary of mixed-model ANOVA results for examining baseline differences in demographic, clinical, and primary outcome measures
among 76 persons with mild and moderate multiple sclerosis disability
Variable Condition Disability Condition 9 disability
F p F p F p
Age 0.634 0.429 5.650 0.020* 1.093 0.299
BMI 0.093 0.761 0.072 0.789 3.573 0.063
MS duration 2.086 0.153 1.511 0.223 0.244 0.623
PDDS 1.460 0.231 209.719 \0.001* 0.009 0.926
IPAQ 1.530 0.220 0.538 0.466 0.572 0.452
6MW distance 0.080 0.778 37.908 \0.001* 0.150 0.700
SDMT 0.682 0.412 6.385 0.014* 0.162 0.688
BMI body mass index, PDDS patient-determined disease steps, IPAQ International Physical Activity Questionnaire, 6MW 6-minute walk, SDMT
Symbol Digit Modalities Test
* Statistical significance at p \ 0.05
J Neurol
123
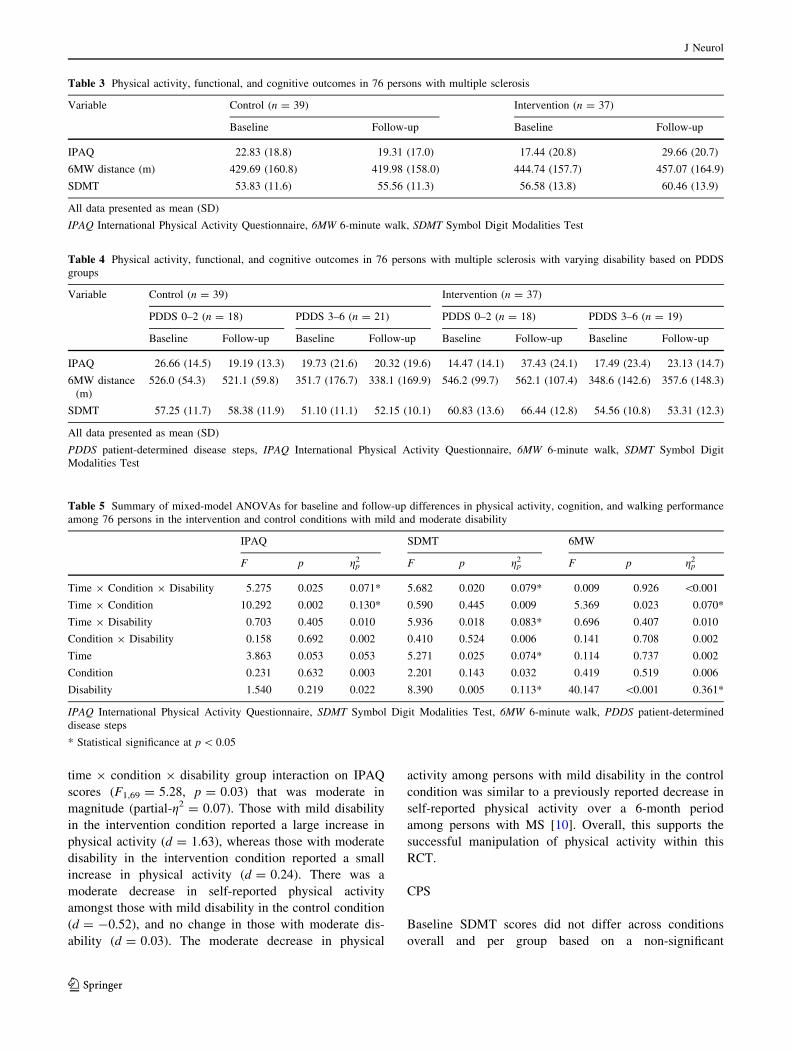
time 9 condition 9 disability group interaction on IPAQ
scores (F1,69 = 5.28, p = 0.03) that was moderate in
magnitude (partial-g2 = 0.07). Those with mild disability
in the intervention condition reported a large increase in
physical activity (d = 1.63), whereas those with moderate
disability in the intervention condition reported a small
increase in physical activity (d = 0.24). There was a
moderate decrease in self-reported physical activity
amongst those with mild disability in the control condition
(d = -0.52), and no change in those with moderate dis-
ability (d = 0.03). The moderate decrease in physical
activity among persons with mild disability in the control
condition was similar to a previously reported decrease in
self-reported physical activity over a 6-month period
among persons with MS [10]. Overall, this supports the
successful manipulation of physical activity within this
RCT.
CPS
Baseline SDMT scores did not differ across conditions
overall and per group based on a non-significant
Table 3 Physical activity, functional, and cognitive outcomes in 76 persons with multiple sclerosis
Variable Control (n = 39) Intervention (n = 37)
Baseline Follow-up Baseline Follow-up
IPAQ 22.83 (18.8) 19.31 (17.0) 17.44 (20.8) 29.66 (20.7)
6MW distance (m) 429.69 (160.8) 419.98 (158.0) 444.74 (157.7) 457.07 (164.9)
SDMT 53.83 (11.6) 55.56 (11.3) 56.58 (13.8) 60.46 (13.9)
All data presented as mean (SD)
IPAQ International Physical Activity Questionnaire, 6MW 6-minute walk, SDMT Symbol Digit Modalities Test
Table 4 Physical activity, functional, and cognitive outcomes in 76 persons with multiple sclerosis with varying disability based on PDDS
groups
Variable Control (n = 39) Intervention (n = 37)
PDDS 0–2 (n = 18) PDDS 3–6 (n = 21) PDDS 0–2 (n = 18) PDDS 3–6 (n = 19)
Baseline Follow-up Baseline Follow-up Baseline Follow-up Baseline Follow-up
IPAQ 26.66 (14.5) 19.19 (13.3) 19.73 (21.6) 20.32 (19.6) 14.47 (14.1) 37.43 (24.1) 17.49 (23.4) 23.13 (14.7)
6MW distance
(m)
526.0 (54.3) 521.1 (59.8) 351.7 (176.7) 338.1 (169.9) 546.2 (99.7) 562.1 (107.4) 348.6 (142.6) 357.6 (148.3)
SDMT 57.25 (11.7) 58.38 (11.9) 51.10 (11.1) 52.15 (10.1) 60.83 (13.6) 66.44 (12.8) 54.56 (10.8) 53.31 (12.3)
All data presented as mean (SD)
PDDS patient-determined disease steps, IPAQ International Physical Activity Questionnaire, 6MW 6-minute walk, SDMT Symbol Digit
Modalities Test
Table 5 Summary of mixed-model ANOVAs for baseline and follow-up differences in physical activity, cognition, and walking performance
among 76 persons in the intervention and control conditions with mild and moderate disability
IPAQ SDMT 6MW
F p gp2 F p gp
2 F p gp2
Time 9 Condition 9 Disability 5.275 0.025 0.071* 5.682 0.020 0.079* 0.009 0.926 \0.001
Time 9 Condition 10.292 0.002 0.130* 0.590 0.445 0.009 5.369 0.023 0.070*
Time 9 Disability 0.703 0.405 0.010 5.936 0.018 0.083* 0.696 0.407 0.010
Condition 9 Disability 0.158 0.692 0.002 0.410 0.524 0.006 0.141 0.708 0.002
Time 3.863 0.053 0.053 5.271 0.025 0.074* 0.114 0.737 0.002
Condition 0.231 0.632 0.003 2.201 0.143 0.032 0.419 0.519 0.006
Disability 1.540 0.219 0.022 8.390 0.005 0.113* 40.147 \0.001 0.361*
IPAQ International Physical Activity Questionnaire, SDMT Symbol Digit Modalities Test, 6MW 6-minute walk, PDDS patient-determined
disease steps
* Statistical significance at p \ 0.05
J Neurol
123
condition 9 disability interaction and condition main
effect. There was a significant disability group main effect
(p = 0.01) for baseline SDMT scores; this was expected,
as persons in the moderate disability group had worse
cognitive performance than those in the mild disability
group (Table 2). SDMT data per condition and disability
group for baseline and follow-up are reported in Tables 3
and 4, and the ANOVA results summarizing the effect of
the intervention on CPS are further reported in Table 5.
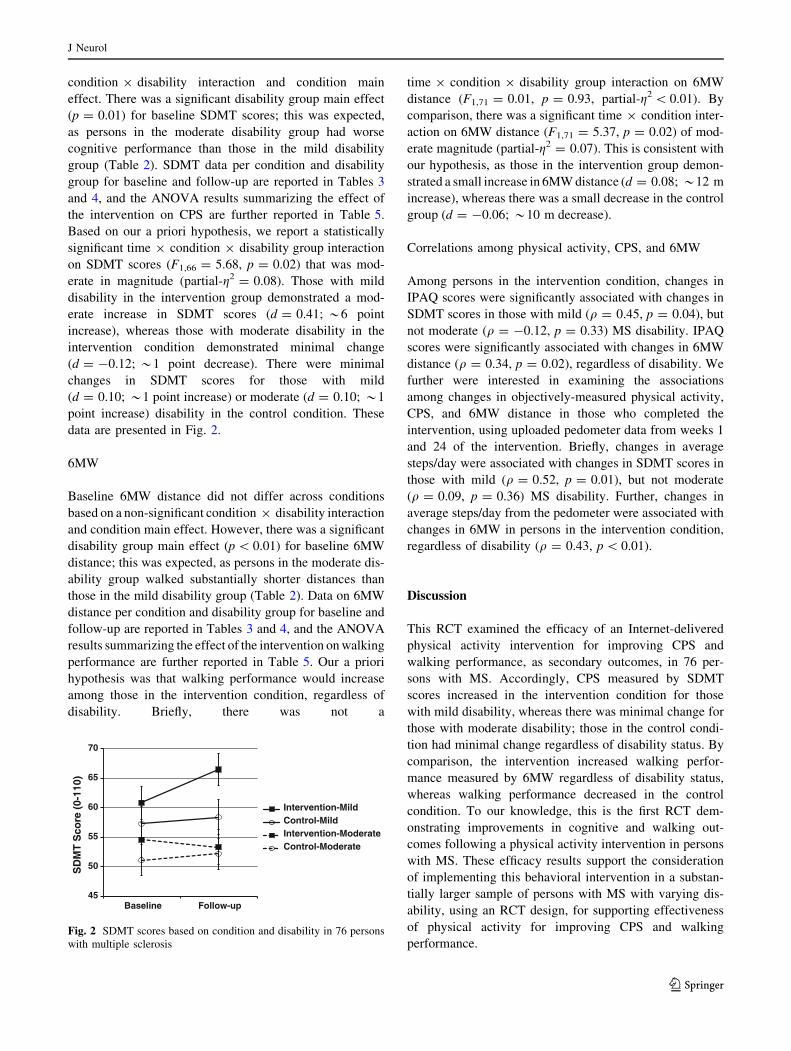
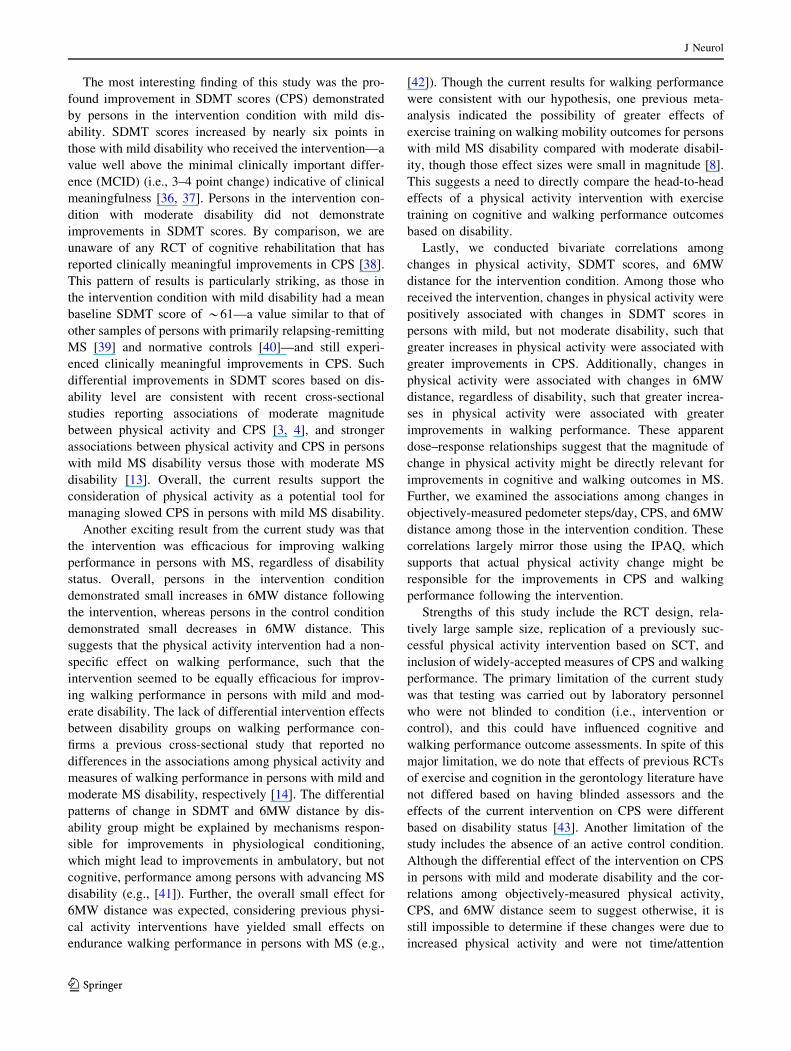
Based on our a priori hypothesis, we report a statistically
significant time 9 condition 9 disability group interaction
on SDMT scores (F1,66 = 5.68, p = 0.02) that was mod-
erate in magnitude (partial-g2 = 0.08). Those with mild
disability in the intervention group demonstrated a mod-
erate increase in SDMT scores (d = 0.41; *6 point
increase), whereas those with moderate disability in the
intervention condition demonstrated minimal change
(d = -0.12; *1 point decrease). There were minimal
changes in SDMT scores for those with mild
(d = 0.10; *1 point increase) or moderate (d = 0.10; *1
point increase) disability in the control condition. These
data are presented in Fig. 2.
6MW
Baseline 6MW distance did not differ across conditions
based on a non-significant condition 9 disability interaction
and condition main effect. However, there was a significant
disability group main effect (p \ 0.01) for baseline 6MW
distance; this was expected, as persons in the moderate dis-
ability group walked substantially shorter distances than
those in the mild disability group (Table 2). Data on 6MW
distance per condition and disability group for baseline and
follow-up are reported in Tables 3 and 4, and the ANOVA
results summarizing the effect of the intervention on walking
performance are further reported in Table 5. Our a priori
hypothesis was that walking performance would increase
among those in the intervention condition, regardless of
disability. Briefly, there was not a
time 9 condition 9 disability group interaction on 6MW
distance (F1,71 = 0.01, p = 0.93, partial-g2 \ 0.01). By
comparison, there was a significant time 9 condition inter-
action on 6MW distance (F1,71 = 5.37, p = 0.02) of mod-
erate magnitude (partial-g2 = 0.07). This is consistent with
our hypothesis, as those in the intervention group demon-
strated a small increase in 6MW distance (d = 0.08; *12 m
increase), whereas there was a small decrease in the control
group (d = -0.06; *10 m decrease).
Correlations among physical activity, CPS, and 6MW
Among persons in the intervention condition, changes in
IPAQ scores were significantly associated with changes in
SDMT scores in those with mild (q = 0.45, p = 0.04), but
not moderate (q = -0.12, p = 0.33) MS disability. IPAQ
scores were significantly associated with changes in 6MW
distance (q = 0.34, p = 0.02), regardless of disability. We
further were interested in examining the associations
among changes in objectively-measured physical activity,
CPS, and 6MW distance in those who completed the
intervention, using uploaded pedometer data from weeks 1
and 24 of the intervention. Briefly, changes in average
steps/day were associated with changes in SDMT scores in
those with mild (q = 0.52, p = 0.01), but not moderate
(q = 0.09, p = 0.36) MS disability. Further, changes in
average steps/day from the pedometer were associated with
changes in 6MW in persons in the intervention condition,
regardless of disability (q = 0.43, p \ 0.01).
Discussion
This RCT examined the efficacy of an Internet-delivered
physical activity intervention for improving CPS and
walking performance, as secondary outcomes, in 76 per-
sons with MS. Accordingly, CPS measured by SDMT
scores increased in the intervention condition for those
with mild disability, whereas there was minimal change for
those with moderate disability; those in the control condi-
tion had minimal change regardless of disability status. By
comparison, the intervention increased walking perfor-
mance measured by 6MW regardless of disability status,
whereas walking performance decreased in the control
condition. To our knowledge, this is the first RCT dem-
onstrating improvements in cognitive and walking out-
comes following a physical activity intervention in persons
with MS. These efficacy results support the consideration
of implementing this behavioral intervention in a substan-
tially larger sample of persons with MS with varying dis-
ability, using an RCT design, for supporting effectiveness
of physical activity for improving CPS and walking
performance.
45
50
55
60
65
70
Baseline Follow-up
SD
MT
Sco
re (
0-11
0)
Intervention-MildControl-MildIntervention-ModerateControl-Moderate
Fig. 2 SDMT scores based on condition and disability in 76 persons
with multiple sclerosis
J Neurol
123
The most interesting finding of this study was the pro-
found improvement in SDMT scores (CPS) demonstrated
by persons in the intervention condition with mild dis-
ability. SDMT scores increased by nearly six points in
those with mild disability who received the intervention—a
value well above the minimal clinically important differ-
ence (MCID) (i.e., 3–4 point change) indicative of clinical
meaningfulness [36, 37]. Persons in the intervention con-
dition with moderate disability did not demonstrate
improvements in SDMT scores. By comparison, we are
unaware of any RCT of cognitive rehabilitation that has
reported clinically meaningful improvements in CPS [38].
This pattern of results is particularly striking, as those in
the intervention condition with mild disability had a mean
baseline SDMT score of *61—a value similar to that of
other samples of persons with primarily relapsing-remitting
MS [39] and normative controls [40]—and still experi-
enced clinically meaningful improvements in CPS. Such
differential improvements in SDMT scores based on dis-
ability level are consistent with recent cross-sectional
studies reporting associations of moderate magnitude
between physical activity and CPS [3, 4], and stronger
associations between physical activity and CPS in persons
with mild MS disability versus those with moderate MS
disability [13]. Overall, the current results support the
consideration of physical activity as a potential tool for
managing slowed CPS in persons with mild MS disability.
Another exciting result from the current study was that
the intervention was efficacious for improving walking
performance in persons with MS, regardless of disability
status. Overall, persons in the intervention condition
demonstrated small increases in 6MW distance following
the intervention, whereas persons in the control condition
demonstrated small decreases in 6MW distance. This
suggests that the physical activity intervention had a non-
specific effect on walking performance, such that the
intervention seemed to be equally efficacious for improv-
ing walking performance in persons with mild and mod-
erate disability. The lack of differential intervention effects
between disability groups on walking performance con-
firms a previous cross-sectional study that reported no
differences in the associations among physical activity and
measures of walking performance in persons with mild and
moderate MS disability, respectively [14]. The differential
patterns of change in SDMT and 6MW distance by dis-
ability group might be explained by mechanisms respon-
sible for improvements in physiological conditioning,
which might lead to improvements in ambulatory, but not
cognitive, performance among persons with advancing MS
disability (e.g., [41]). Further, the overall small effect for
6MW distance was expected, considering previous physi-
cal activity interventions have yielded small effects on
endurance walking performance in persons with MS (e.g.,
[42]). Though the current results for walking performance
were consistent with our hypothesis, one previous meta-
analysis indicated the possibility of greater effects of
exercise training on walking mobility outcomes for persons
with mild MS disability compared with moderate disabil-
ity, though those effect sizes were small in magnitude [8].
This suggests a need to directly compare the head-to-head
effects of a physical activity intervention with exercise
training on cognitive and walking performance outcomes
based on disability.
Lastly, we conducted bivariate correlations among
changes in physical activity, SDMT scores, and 6MW
distance for the intervention condition. Among those who
received the intervention, changes in physical activity were
positively associated with changes in SDMT scores in
persons with mild, but not moderate disability, such that
greater increases in physical activity were associated with
greater improvements in CPS. Additionally, changes in
physical activity were associated with changes in 6MW
distance, regardless of disability, such that greater increa-
ses in physical activity were associated with greater
improvements in walking performance. These apparent
dose–response relationships suggest that the magnitude of
change in physical activity might be directly relevant for
improvements in cognitive and walking outcomes in MS.
Further, we examined the associations among changes in
objectively-measured pedometer steps/day, CPS, and 6MW
distance among those in the intervention condition. These
correlations largely mirror those using the IPAQ, which
supports that actual physical activity change might be
responsible for the improvements in CPS and walking
performance following the intervention.
Strengths of this study include the RCT design, rela-
tively large sample size, replication of a previously suc-
cessful physical activity intervention based on SCT, and
inclusion of widely-accepted measures of CPS and walking
performance. The primary limitation of the current study
was that testing was carried out by laboratory personnel
who were not blinded to condition (i.e., intervention or
control), and this could have influenced cognitive and
walking performance outcome assessments. In spite of this
major limitation, we do note that effects of previous RCTs
of exercise and cognition in the gerontology literature have
not differed based on having blinded assessors and the
effects of the current intervention on CPS were different
based on disability status [43]. Another limitation of the
study includes the absence of an active control condition.
Although the differential effect of the intervention on CPS
in persons with mild and moderate disability and the cor-
relations among objectively-measured physical activity,
CPS, and 6MW distance seem to suggest otherwise, it is
still impossible to determine if these changes were due to
increased physical activity and were not time/attention
J Neurol
123

effects. Another potential limitation includes the use of the
IPAQ as a self-report measure of physical activity, as the
scores might change based on the demand characteristics of
the intervention. However, we report that among persons in
the intervention condition, changes in objectively-mea-
sured physical activity were differentially associated with
changes in SDMT scores based on disability status, and
that changes in steps/day were associated with changes in
6MW distance regardless of disability. This is consistent
with previous studies that have demonstrated improve-
ments in objectively-measured physical activity with the
Internet-delivered intervention [10–12], suggesting that the
change in physical activity is real rather than a demand
characteristic. An additional limitation of this study
includes the use of the PDDS as a self-report measure of
disability rather than an EDSS score generated by a neu-
rologist as an approach for generating disability groups.
Such groups might not purely reflect MS disability, as other
factors such as cognitive impairment could influence PDDS
scores, although the PDDS has been reported to be valid
based on a strong correlation with the physician-adminis-
tered EDSS [28, 29]. The final limitation involves includ-
ing the SDMT (CPS) as the only cognitive outcome
measure, and future research should test the effectiveness
of this intervention on other domains of cognition (e.g.,
executive control, learning and memory).
Conclusions
This RCT reports that: (a) SDMT scores increased in the
intervention condition as a function of disability, and this
change was clinically meaningful and moderate in mag-
nitude for individuals with mild disability; (b) 6MW
distance increased in the intervention condition, and this
did not occur as a function of disability; and (c) greater
increases in physical activity were associated with faster
CPS and better walking performance in the intervention
condition. Collectively, such exciting results largely
support the development of a similar RCT in a sub-
stantially larger sample of persons with MS, using blin-
ded assessors and perhaps an attention control condition,
to examine the effectiveness and generalizability of this
Internet-delivered physical activity intervention on cog-
nitive and walking outcomes in this population. The
current study provides the first direct support from an
RCT of physical activity as a promising tool for man-
aging slowed CPS and impaired walking performance in
persons with MS.
Acknowledgments This study was funded by a grant from the
National Multiple Sclerosis Society, Grant Number PP1695, awarded
to the last author.
Conflicts of interest The authors declare that they have no conflicts
of interest.
Ethical statement The study procedures were approved by a uni-
versity institutional review board with guiding Ethical Principles and
Guidelines for the Protection of Human Subjects for Research (i.e.,
Belmont Report) and in accordance with Department of Health and
Human Services policy and the Common Rule.
References
1. Benedict RHB, Zivadinov R (2011) Risk factors for and man-
agement of cognitive dysfunction in multiple sclerosis. Nat Rev
Neurosci 7(6):332–342
2. Motl RW, Sandroff BM, Benedict RHB (2011) Cognitive dys-
function and multiple sclerosis: developing a rationale for con-
sidering the efficacy of exercise training. Mult Scler 201117(9):
1034–1040
3. Motl RW, Gappmaier E, Nelson K, Benedict RHB (2011)
Physical activity and cognitive function in multiple sclerosis.
J Sport Exerc Psychol 33(5):734–741
4. Sandroff BM, Dlugonski D, Pilutti LA, Pula JH, Benedict RHB,
Motl RW (2014) Physical activity is associated with cognitive
processing speed in persons with multiple sclerosis. Mult Scler
Relat Disord 3(1):123–128
5. Ratey JJ, Loehr JE (2011) The positive impact of physical
activity on cognition during adulthood: a review of underlying
mechanisms, evidence and recommendations. Rev Neurosci
22(2):171–185
6. Benedict RHB, Holtzer R, Motl RW, Foley FW, Kaur S, Ho-
jnacki D, Weinstock-Guttman B (2011) Upper and lower
extremity motor function and cognitive impairment in multiple
sclerosis. J Int Neuropsychol Soc 17(4):643–653
7. D’Orio VL, Foley FW, Armentano F, Picone MA, Kim S, Holtzer
R (2012) Cognitive and motor functioning in patients with mul-
tiple sclerosis: neuropsychological predictors of walking speed
and falls. J Neurol Sci 316:42–46
8. Snook EM, Motl RW (2009) Effect of exercise training on
walking mobility in multiple sclerosis: a meta-analysis. Neuro-
rehabil Neural Repair 23(2):108–116
9. Motl RW, Dlugonski D, Wojcicki TR, McAuley E, Mohr DC
(2011) Internet intervention for increasing physical activity in
persons with multiple sclerosis. Mult Scler 17(1):116–128
10. Dlugonski D, Motl RW, Mohr DC, Sandroff BM (2012) Internet-
delivered behavioral intervention to increase physical activity in
persons with multiple sclerosis: sustainability and secondary
outcomes. Psychol Health Med 17(6):636–651
11. Dlugonski D, Motl RW, McAuley E (2011) Increasing physical
activity in multiple sclerosis: replicating Internet intervention
effects using objective and self-report outcomes. J Rehabil Res
Dev 48(9):1129–1136
12. Motl RW, McAuley E, Dlugonski D (2012) Reactivity in baseline
accelerometer data from a physical activity behavioral interven-
tion. Health Psychol 31(2):172–175
13. Sandroff BM, Pilutti LA, Dlugonski D, Motl RW (2013) Physical
activity and information processing speed in persons with multiple
sclerosis: a prospective study. Ment Health Phys Act 6(3):205–211
14. Motl RW, Pilutti L, Sandroff BM, Dlugonski D, Sosnoff JJ, Pula
JH (2013) Accelerometry as a measure of walking behavior in
multiple sclerosis. Acta Neurol Scand 127(6):384–390
15. Thomas S, Reading J, Shephard RJ (1992) Revision of the
physical activity readiness questionnaire (PAR-Q). Can J Sport
Sci 17(4):338–345
J Neurol
123

16. Smith A (1982) Symbol digit modalities test: manual. Western
Psychological Services, Los Angeles
17. Rao SM, Leo GJ, Bernarndin L, Unverzagt F (1991) Cognitive
dysfunction in multiple sclerosis. I. Frequency, patterns, and
prediction. Neurology 41:685–691
18. Benedict RH, Smerbeck A, Parikh R, Rodgers J, Cadavid D,
Erlanger D (2012) Reliability and equivalence of alternate forms
for the Symbol Digit Modalities Test: implications for multiple
sclerosis clinical trials. Mult Scler 18(9):1320–1325
19. Benedict RH, Walton MK (2012) Evaluating cognitive outcome
measures for MS clinical trials: what is a clinically meaningful
change? Mult Scler 18(12):1673–1679
20. Goldman MD, Marrie RA, Cohen JA (2008) Evaluation of the
six-minute walk in multiple sclerosis subjects and healthy con-
trols. Mult Scler 14(3):383–390
21. Wetzel JL, Fry DK, Pfalzer LA (2011) Six-minute walk test for
persons with mild or moderate disability from multiple sclerosis:
performance and explanatory factors. Physiother Can
63(2):166–180
22. Craig CL, Marshall AL, Sjostrom M et al (2003) International
physical activity questionnaire: 12-country reliability and valid-
ity. Med Sci Sports Exerc 35:1381–1395
23. Sandroff BM, Dlugonski D, Weikert M, Suh Y, Balantrapu S,
Motl RW (2012) Physical activity and multiple sclerosis: new
insights regarding inactivity. Acta Neurol Scand 126(4):256–262
24. Gosney JL, Scott JA, Snook EM, Motl RW (2007) Physical
activity and multiple sclerosis: validity of self-report and objec-
tive measures. Fam Community Health 30:144–150
25. Motl RW, McAuley E, Snook EM, Scott JA (2006) Validity of
physical activity measures in ambulatory individuals with mul-
tiple sclerosis. Disabil Rehabil 28:1151–1156
26. Weikert M, Motl RW, Suh Y, McAuley E, Wynn D (2009)
Accelerometry in persons with multiple sclerosis: measurement
of physical activity or walking mobility? J Neurol Sci 260:6–11
27. Snook EM, Motl RW, Gliottoni RC (2009) The effect of walking
mobility on the measurement of physical activity using acceler-
ometry in multiple sclerosis. Clin Rehabil 23:248–258
28. Hadjimichael O, Kerns RD, Rizzo MA, Cutter G, Vollmer T
(2007) Persistent pain and uncomfortable sensations in persons
with multiple sclerosis. Pain 127(1–2):35–41
29. Learmonth YC, Motl RW, Sandroff BM, Pula JH, Cadavid D
(2013) Validation of patient determined disease steps (PDDS)
scale scores in persons with multiple sclerosis. BMC Neurol
13(1):37
30. Marrie RA, Goldman M (2007) Validity of performance scales
for disability assessment in multiple sclerosis. Mult Scler
13(9):1176–1182
31. Marrie RA, Cutter G, Tyry T, Vollmer T, Campagnolo D (2006)
Does multiple sclerosis-associated disability differ between
races? Neurology 66(8):1235–1240
32. Confavreux C, Vukusic S (2006) Natural history of multiple
sclerosis: a unifying concept. Brain 129:606–616
33. Bandura A (2004) Health promotion by social cognitive means.
Health Educ Behav 31:143–164
34. Donner A, Klar N (1994) Cluster randomization trials in epidemi-
ology: theory and application. J Stat Plan Inference 42(1–2):37–56
35. Cohen J (1988) Statistical power analysis for the behavioral
sciences, 2nd edn. Lawrence Erlbaum Associates, Hillsdale
36. Morrow SA, Drake A, Zivadinov R, Munschauer F, Weinstock-
Guttman B, Benedict RHB (2010) Predicting loss of employment
over three years in multiple sclerosis: clinically meaningful
cognitive decline. Clin Neuropsychol 24:1131–1145
37. Morrow SA, Jurgensen S, Forrestal F, Munchauer FE, Benedict
RH (2011) Effects of acute relapses on neuropsychological status
in multiple sclerosis patients. J Neurol 258(9):1603–1608
38. Stuifbergen AK, Becker H, Perez F, Morison J, Kullberg V, Todd
A (2012) A randomized controlled trial of a cognitive rehabili-
tation intervention for persons with multiple sclerosis. Clin
Rehabil 26(10):882–893
39. Glanz BI, Healy BC, Hviid LE, Chitnis T, Weiner HL (2012)
Cognitive deterioration in patients with early multiple sclerosis: a
5-year study. J Neurol Neurosurg Psychiatry 83(1):38–43
40. Drake AS, Weinstock-Guttman B, Morrow SA, Hojnacki D,
Munschauer FE, Benedict RHB (2010) Psychometrics and nor-
mative data for the Multiple Sclerosis Functional Composite:
replacing the PASAT with the Symbol Digit Modalities Test.
Mult Scler 16:228–237
41. Motl RW, Goldman MD, Benedict RH (2010) Walking impair-
ment in patients with multiple sclerosis: exercise training as a
treatment option. Neuropsychiatr Dis Treat 6:767–774
42. Hebert JR, Corboy JR, Manago MM, Schenkman M (2011)
Effects of vestibular rehabilitation on multiple sclerosis-related
fatigue and upright postural control: a randomized controlled
trial. Phys Ther 91(8):1166–1183
43. Smith PJ, Blumenthal JA, Hoffman BM, Cooper H, Strauman TA,
Welsh-Bohmer K, Browndyke JN, Sherwood A (2010) Aerobic
exercise and neurocognitive performance: a meta-analytic review
of randomized controlled trials. Psychosom Med 72(3):239–252
J Neurol
123
Related Documents











