R di th L h R di th L h Radiotherapy Lymphomas Radiotherapy Lymphomas Mary Gospodarowicz MD Mary Gospodarowicz MD Princess Margaret Hospital Princess Margaret Hospital University of Toronto, Toronto, Canada University of Toronto, Toronto, Canada

Radiotherapy Lymphomas
Oct 19, 2014
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

R di th L hR di th L hRadiotherapy LymphomasRadiotherapy Lymphomas
Mary Gospodarowicz MDMary Gospodarowicz MDPrincess Margaret HospitalPrincess Margaret Hospital
University of Toronto, Toronto, CanadaUniversity of Toronto, Toronto, Canada

Changing Landscape in LymphomaChanging Landscape in LymphomaChanging Landscape in LymphomaChanging Landscape in Lymphoma
•• 90% of cases in adults90% of cases in adults•• median age median age -- 64 yrs64 yrs
•• 2008 Statistics2008 StatisticsUSUS CanadaCanada
•• 66 120 new cases 7 00066 120 new cases 7 000•• 19 160 deaths19 160 deaths 3 1003 100•• 19 160 deaths19 160 deaths 3 1003 100
•• @ 500 000 people living with lymphoma@ 500 000 people living with lymphoma•• 90% B90% B--cellcell90% B90% B cell cell
•• @ 40% DLBCL@ 40% DLBCL•• 10% T10% T--cell cell

RT in NonRT in Non Hodgkin L mphomaHodgkin L mphomaRT in NonRT in Non--Hodgkin LymphomaHodgkin Lymphoma•• ChallengesChallengesChallengesChallenges
–– Only 4 Only 4 -- 6% of all cancers6% of all cancers–– Numerous distinct disease entitiesNumerous distinct disease entitiesNumerous distinct disease entitiesNumerous distinct disease entities
•• Mycosis fungoides Mycosis fungoides •• Primary brain lymphomaPrimary brain lymphomay y py y p•• Gastric MALTGastric MALT•• Burkitt’sBurkitt’s
–– Changing outcomesChanging outcomes–– Little level 1 evidence to guide practiceLittle level 1 evidence to guide practice

Radiation Therapy in CancerRadiation Therapy in CancerRadiation Therapy in CancerRadiation Therapy in Cancer•• Local therapyLocal therapy•• Local therapyLocal therapy
–– Proven most effective agent in Proven most effective agent in idi l l t t lidi l l t t lproviding local tumour controlproviding local tumour control
–– Proven capable of curing localized Proven capable of curing localized disease in most cancers disease in most cancers
–– Compensates for diagnostic ambiguityCompensates for diagnostic ambiguityp g g yp g g y•• ‘histology agnostic’ ‘histology agnostic’
–– Few contraindicationsFew contraindicationsFew contraindicationsFew contraindications

Radiation Therapy in CancerRadiation Therapy in CancerRadiation Therapy in CancerRadiation Therapy in Cancer•• Local therapyLocal therapy•• Local therapyLocal therapy
•• Proven most effective agent in providing Proven most effective agent in providing local tumour controllocal tumour controllocal tumour controllocal tumour control
•• Proven capable of curing localized disease Proven capable of curing localized disease in most cancersin most cancersin most cancers in most cancers
•• Compensates for diagnostic ambiguityCompensates for diagnostic ambiguity•• ‘histology agnostic’‘histology agnostic’histology agnostic histology agnostic
•• Few contraindicationsFew contraindications

RT in L mphomasRT in L mphomasRT in LymphomasRT in LymphomasObj ti f RTObj ti f RT•• Objective of RTObjective of RT–– Almost always to achieve local controlAlmost always to achieve local control
•• Outcomes of interestOutcomes of interest–– Pattern of failure Pattern of failure
•• Local controlLocal control•• Overall failure rateOverall failure rate
–– SurvivalSurvival–– ToxicityToxicity

Stage I&II Follicular Lymphoma 1967Stage I&II Follicular Lymphoma 1967--9999
Stage IStage I--II II -- 668 pts668 pts
Stage I&II Follicular Lymphoma 1967Stage I&II Follicular Lymphoma 1967 9999
•• Stage IStage I--II RT alone II RT alone -- 460 pts460 pts–– median followmedian follow--up up -- 12.5 yrs12.5 yrsed a o oed a o o upup 5 y s5 y s
•• rangerange -- up to 32 yrsup to 32 yrs•• TreatmentTreatment –– IF RT 30IF RT 30--35 Gy35 GyTreatment Treatment IF RT 30IF RT 30 35 Gy35 Gy•• RelapseRelapse
distantdistant 89 %89 %•• distant distant -- 89 %89 %•• distant + local distant + local -- 6 %6 %•• isolated local relapseisolated local relapse -- 5%5%•• isolated local relapse isolated local relapse -- 5%5%
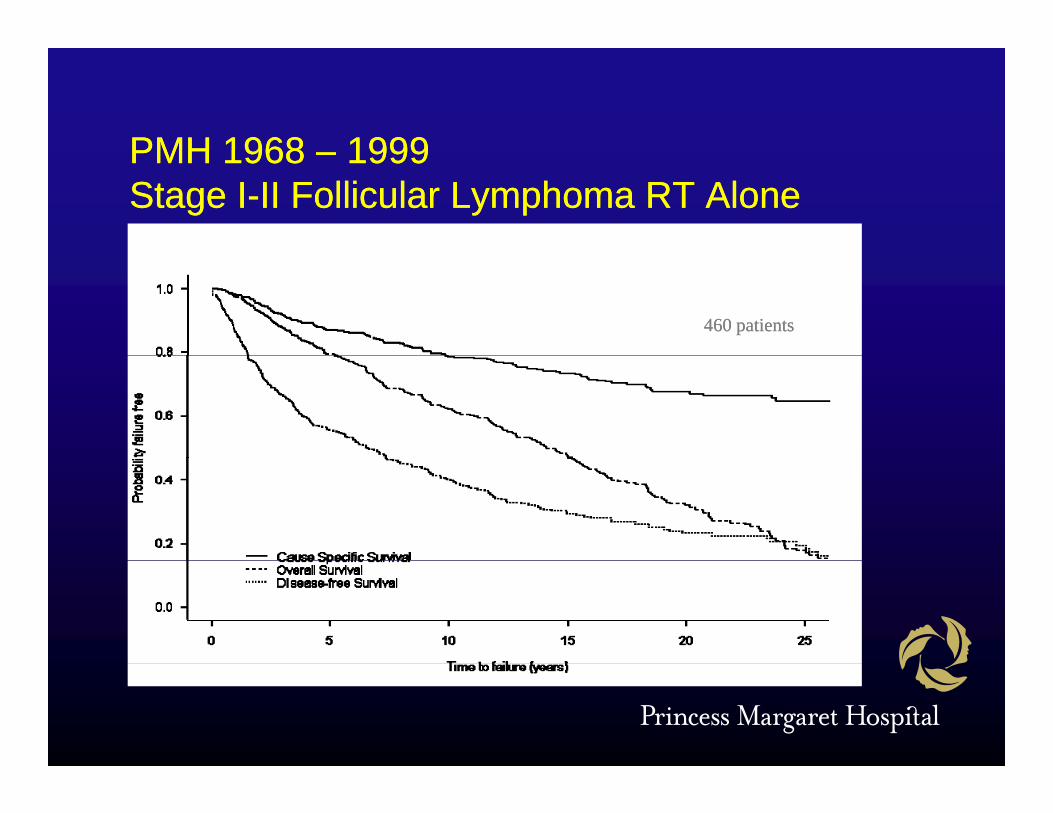
PMH 1968PMH 1968 19991999PMH 1968 PMH 1968 –– 1999 1999 Stage IStage I--II Follicular Lymphoma RT AloneII Follicular Lymphoma RT Alone
460 patients460 patients

PMH 1968 PMH 1968 –– 1999 1999 St ISt I II F lli l L h RT AlII F lli l L h RT AlStage IStage I--II Follicular Lymphoma RT AloneII Follicular Lymphoma RT Alone
70
80 No relapseRelapse
50
60
Age
30
40
0 5 10 15 20 25 30 35
20
Ti l f llTime to relapse or follow-up

Stage I-II MZL PMH 1989-2004
MALT 1989 MALT 1989 -- 20042004166 t t t d ith RT166 t t t d ith RT•• 166 pts treated with RT166 pts treated with RT
•• median followmedian follow--up 7.6 yrs (0.6 up 7.6 yrs (0.6 –– 16.2)16.2)•• median age 60 yrs median age 60 yrs (23(23--93)93)•• F : M = 2 : 1F : M = 2 : 1F : M 2 : 1F : M 2 : 1•• stage Istage I 148 (89%) 148 (89%)
t IIt II 18 (11%)18 (11%)•• stage IIstage II 18 (11%)18 (11%)

Stage I-II MZL PMH 1989-2004
Presenting SitesPresenting SitesOrbit and adnexaOrbit and adnexa 70 (42%)70 (42%) Skin & soft tissuesSkin & soft tissues 44Salivary glandSalivary gland 28 (17%)28 (17%) BreastBreast 44St hSt h 22 (13%)22 (13%) R tR t 11StomachStomach 22 (13%)22 (13%) RectumRectum 11ThyroidThyroid 21 (13%) 21 (13%) Meninges Meninges 11Other head & neck*Other head & neck* 66 ThymusThymus 11Other head & neckOther head & neck 66 ThymusThymus 11Lung Lung 44BladderBladder 44
**nasopharynx nasopharynx -- 3, 3, maxillarymaxillary sinus sinus -- 11larynx larynx -- 1, Hypopharynx 1, Hypopharynx -- 11

Stage I/II MALT lymphoma Stage I/II MALT lymphoma -- RelapseRelapseg y pg y p pp
Relapse Stomach/Thyroid (n=43)
2 yrs: 13/31 (52%) 5 yrs: 25/31 (81%)> 5 yrs: 6/31 (19%)
Other sites (n=123)
10-year RFRThyroid 95%
y ( )
Stomach 100%Salivary gland 68%Orbit 67%

Stage I/IIE MALT lymphomaStage I/IIE MALT lymphoma -- SurvivalSurvivalStage I/IIE MALT lymphoma Stage I/IIE MALT lymphoma SurvivalSurvival
10 yr RFR 77%
— 10 yr OS - 87%
--- 10 yr CSS - 98%
…. 10 yr RFR- 77%
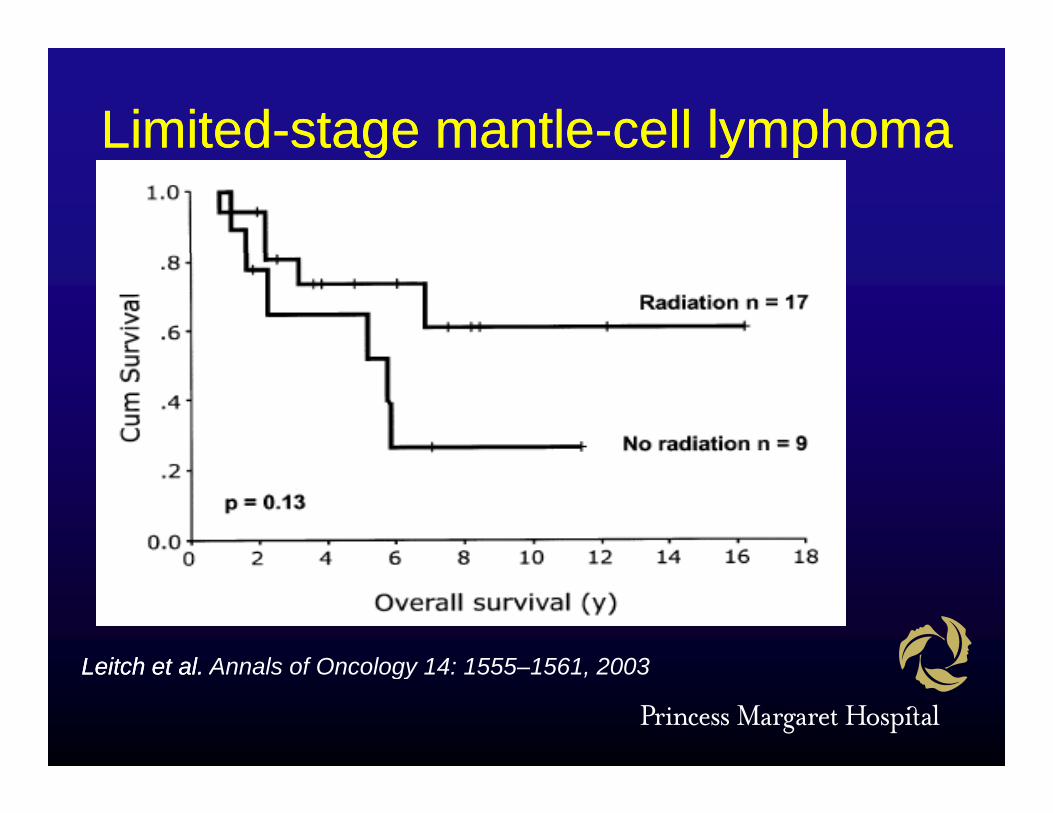
LimitedLimited--stage mantlestage mantle--cell lymphomacell lymphomagg y py p
Leitch et alLeitch et al Annals of Oncology 14: 1555 1561 2003Leitch et al. Leitch et al. Annals of Oncology 14: 1555–1561, 2003

Int J Radiat Oncol Biol Phys 65: 1185 91 2006Int J Radiat Oncol Biol Phys 65: 1185–91, 2006
Localized DLBCLLocalized DLBCLLocalized DLBCLLocalized DLBCLHeterogeneous diseaseHeterogeneous diseaseHeterogeneous diseaseHeterogeneous disease
Phenotypic, molecular characteristicsPhenotypic, molecular characteristicsNodal vs extranodal presentationsNodal vs extranodal presentationsNodal vs. extranodal presentationsNodal vs. extranodal presentationsStage I vs. II (II localized vs.. extensive)Stage I vs. II (II localized vs.. extensive)BB symptomssymptomsBB--symptomssymptomsLDHLDHA d f t tA d f t tAge and performance statusAge and performance statusComorbidityComorbidity

Spectrum of Localized DLBLSpectrum of Localized DLBLSpectrum of Localized DLBLSpectrum of Localized DLBL

PMH Experience 1984PMH Experience 1984 20032003PMH Experience 1984 PMH Experience 1984 --20032003600 patients with stage I600 patients with stage I--IIIIAge 15 Age 15 -- 91 91 median median -- 57 yrs57 yrsFollowFollow--up 0.4 up 0.4 –– 22 yrs22 yrs median median -- 10.1 yrs10.1 yrsyy yyStage IStage I -- 317317 BB--symptoms symptoms -- 6464Stage IIStage II -- 283283 Extranodal Extranodal -- 354354ggChemo 3/4 courses Chemo 3/4 courses -- 233233Chemo 5/6 coursesChemo 5/6 courses -- 336336Chemo 5/6 courses Chemo 5/6 courses 336336median RT dose median RT dose –– 35 Gy35 Gyprepre--rituximabrituximabprepre rituximabrituximab

Overall SurvivalOverall SurvivalOverall SurvivalOverall Survival
PMH DLBCL PMH DLBCL –– CMT 1984CMT 1984--20032003

Survival by ageSurvival by ageSurvival by ageSurvival by age
PMH DLBCL PMH DLBCL –– CMT 1984CMT 1984--20032003

Probability of Local RelapseProbability of Local RelapseProbability of Local RelapseProbability of Local Relapse
PMH DLBCL PMH DLBCL –– CMT 1984CMT 1984--20032003

CHOP nonCHOP non--respondersrespondersppProbability of Death from LymphomaProbability of Death from Lymphoma
PMH DLBCL PMH DLBCL –– CMT 1984CMT 1984--20032003
Rituximab EraRituximab EraRit i bRit i b d ll i t d d t thd ll i t d d t thRituximab Rituximab gradually introduced to the gradually introduced to the management of all DLBCLmanagement of all DLBCLOutcomes improvedOutcomes improvedRole of RT questionedRole of RT questionedqqNo level 1 evidence No level 1 evidence
For the benefit of RTFor the benefit of RTFor the benefit of RTFor the benefit of RTFor the lack of benefit of RTFor the lack of benefit of RT


Practice Practice G id liG id liGuidelinesGuidelines

T/NKT/NK--cell Nasal Lymphomacell Nasal LymphomaT/NKT/NK cell Nasal Lymphomacell Nasal Lymphoma
Note: Non-randomized comparisonNote: Non randomized comparison
RT n=18RT n=18RT n=18RT n=18
CMT n=61CMT n=61
Cheung et al, IJRBOP 2002; 54: 182-90

IELSG Testis LymphomaIELSG Testis LymphomaIELSG Testis LymphomaIELSG Testis LymphomaKaplan-Meier survival estimates
Actuarial risk of contralateral testicular failureby prophylactic scrotal RT
(l k t t 0 0027)
1.00
(log rank test, p=0.0027)
No scrotal XRT0 50
0.75
No scrotal XRT
0.25
0.50
Prophylactic XRT
0.00
PFS0 10 20 30

RTRT -- RefractoryRefractory--Recurrent DLBCLRecurrent DLBCLRT RT RefractoryRefractory Recurrent DLBCLRecurrent DLBCL
Martens et al, IJROBP 64: 1183Martens et al, IJROBP 64: 1183--7, 20067, 2006

Int J Radiat Oncol Biol Phys, 51:148–155, 2001

Austral Radiol 50:222–7, 2006

RO Practice in LymphomasRO Practice in LymphomasRO Practice in LymphomasRO Practice in Lymphomas•• Change in radiation oncology practiceChange in radiation oncology practiceg gy pg gy p
–– Target volume rather than nodal region Target volume rather than nodal region treatedtreated
–– GTV, CTB, PTV defined and treatedGTV, CTB, PTV defined and treated–– Most practice in adjuvant settingMost practice in adjuvant setting
N GTV CTVN GTV CTV d dd d•• No GTV, CTV nonNo GTV, CTV non--standardstandard–– Need to monitor and report RT relevant Need to monitor and report RT relevant
outcomesoutcomesoutcomesoutcomes•• Local controlLocal control•• Patterns of relapsePatterns of relapse

RT PlanningRT Planning
R i ti lRequires optimal pre-chemotherapyimagingimaging

Current StandardCurrent StandardCurrent StandardCurrent Standard•• Target Target -- post chemotherapy CTVpost chemotherapy CTV•• Dose and fractionationDose and fractionation
3030 35 Gy in 1535 Gy in 15 20 fractions20 fractions–– 30 30 –– 35 Gy in 1535 Gy in 15--20 fractions20 fractions•• 3D CRT / IMRT 3D CRT / IMRT
–– protect normal tissuesprotect normal tissues•• CT planningCT planning•• CT planningCT planning•• Image guidance as requiredImage guidance as required


Role of RTRole of RTAll trials show improved local controlAll trials show improved local controlVery safe treatmentVery safe treatment
Minimal acute and late severe toxicityMinimal acute and late severe toxicityModern techniques Modern techniques –– lower acute toxicitylower acute toxicity
Best local therapy cannot improveBest local therapy cannot improveBest local therapy cannot improve Best local therapy cannot improve distant disease controldistant disease controlIf systemic therapy results in 100% localIf systemic therapy results in 100% localIf systemic therapy results in 100% local If systemic therapy results in 100% local control control –– no need for RTno need for RT

C rrent contro ersiesC rrent contro ersiesCurrent controversiesCurrent controversiesL li d f lli l l hL li d f lli l l h•• Localized follicular lymphomaLocalized follicular lymphoma–– Curable with RT or just very slow natural Curable with RT or just very slow natural
hi thi thistoryhistory•• MALTMALT
–– Role of RT in rare presentationsRole of RT in rare presentations–– Need to learn more about the natural Need to learn more about the natural
historyhistory

C rrent contro ersiesC rrent contro ersiesCurrent controversiesCurrent controversiesL li d DLBCLL li d DLBCL•• Localized DLBCLLocalized DLBCL–– Is RT needed in RIs RT needed in R--CHOP eraCHOP era
•• Does it add to the chemotherapyDoes it add to the chemotherapy–– Must conduct studies that include optimal Must conduct studies that include optimal
chemotherapy and ask RT questionchemotherapy and ask RT questionchemotherapy and ask RT question chemotherapy and ask RT question •• Extranodal lymphomasExtranodal lymphomas
–– Differences btwn EN and N presentationsDifferences btwn EN and N presentations

C rrent contro ersiesC rrent contro ersiesCurrent controversiesCurrent controversiesR l f RT i FDG PETR l f RT i FDG PET•• Role of RT in FDG PET eraRole of RT in FDG PET era–– Assessment of response to chemotherapy Assessment of response to chemotherapy
i idi id t t t FDG PETt t t FDG PETusing midusing mid--treatment FDG PETtreatment FDG PET–– Post chemotherapy PET assessed Post chemotherapy PET assessed
response as selection factor for RTresponse as selection factor for RTresponse as selection factor for RTresponse as selection factor for RT•• Role of RT in PET +ve and PET Role of RT in PET +ve and PET ––ve casesve cases•• Patterns of failures in above situationsPatterns of failures in above situations•• Patterns of failures in above situationsPatterns of failures in above situations

FutureFutureFutureFuture•• Biologic imagingBiologic imagingg g gg g g
•• Disease extentDisease extent•• Response Response pp•• Selection for adjuvant treatmentSelection for adjuvant treatment
•• Role of precision RTRole of precision RT•• Role of precision RTRole of precision RT•• Molecular disease characteristicsMolecular disease characteristics
D fi iti f di titiD fi iti f di titi•• Definition of disease entitiesDefinition of disease entities•• Impact on the managementImpact on the management
Related Documents











