Radiographic follow-up of 84 operatively treated scapula neck and body fractures Peter A. Cole a, *, Erich M. Gauger b , Diego A. Herrera c , Jack Anavian d , Ivan S. Tarkin e a University of Minnesota/Regions Hospital, 640 Jackson Street, St. Paul, MN 55101, USA b University of Minnesota, 640 Jackson Street, St. Paul, MN 55101, USA c University of Alabama, 1530 3rd Avenue South, FOT 1203, Birmingham, AL 35294-3412, USA d Brown University, Box G-A1, Providence, RI 02912, USA e University of Pittsburgh, 3471 Fifth Avenue, Suite 1010, Pittsburgh, PA 15213, USA Introduction The majority of scapula fractures have been managed non- operatively with immobilisation followed by early range of motion and progressive strengthening as symptoms allow. 1–7 This approach has been largely accepted due to favourable outcomes when used for minimally to moderately displaced scapula fractures, which occur in the majority of patients. However, unstable or highly displaced fractures of the glenoid neck and intra-articular fractures have the potential to lead to shoulder imbalance, instability, chronic pain, weakness, stiffness, deformity and early arthrosis. 8–16 Non-operative studies have rarely provided fracture displace- ment and patterns, making conclusions regarding which patients may benefit from surgical fixation difficult to interpret. 1,4,12,17–19 Furthermore, indications for surgery in published series of operative patients represent a mix of poorly defined radiographic measurements. Explicit surgical indications in the literature include the unstable shoulder girdle based on multiple disruptions of the superior shoulder suspensory complex (SSSC), 20–22 ‘med- ialisation’ (medial/lateral (M/L) displacement) 10–25 mm, 11,23,24 Injury, Int. J. Care Injured 43 (2012) 327–333 A R T I C L E I N F O Article history: Accepted 30 September 2011 Keywords: Scapula fractures Operative Open reduction internal fixation Trauma A B S T R A C T Background: Certain scapula fractures may warrant surgical management to restore shoulder anatomy and promote optimal function. The purpose of this study is to determine the early radiographic follow- up of open reduction internal fixation (ORIF) for displaced, scapular fractures involving the glenoid neck and body. Methods: Eighty-four patients with a scapula body or neck fracture (with or without articular involvement) underwent ORIF between 2002 and 2010 at a single level I trauma centre. This study represents a retrospective review of data prospectively collected into a dedicated scapula fracture database. All patients met at least one of the following operative criteria: 20 mm medial/lateral (M/L) displacement (lateral border offset), 458 of angular deformity on a scapular-Y X-ray, the combination of angulation 308 plus M/L displacement 15 mm, double disruptions of the superior shoulder suspensory complex both displaced 10 mm, glenopolar angle (GPA) 228 and open fractures. Eighty- eight percent (74/84) had sufficient follow-up defined as at least 6 months. Measured outcomes included rates of scapula union and malunion, as well as surgical complications and re-operations. Results: All fractures were caused by high-energy trauma with 24 (29%) resulting from motor-vehicle collisions. Associated injuries occurred in 94% of patients, most commonly involving the chest (70%) and ipsilateral shoulder girdle (43%). Forty-eight patients had M/L displacement as an operative indication with a mean displacement of 25.7 mm (range = 20–40). Thirty-eight (45%) had 2 operative indications. A single surgeon performed ORIF in all patients using a posterior approach. Five patients also required an anterior (deltopectoral) approach. The fixation strategy included lateral and vertebral border stabilisation with dynamic compression and reconstruction plates, respectively. Union was achieved in all cases. There were three cases of malunion based on a GPA difference >108 from the uninjured shoulder. Re-operations included removal of hardware (seven patients) and manipulation under anaesthesia (three patients). There were no infections or wound dehiscence. Conclusions: ORIF for displaced scapula fractures is a relatively safe and effective procedure for restoration of anatomy and promotion of union. Level of evidence: Therapeutic study, level IV. ß 2011 Elsevier Ltd. All rights reserved. * Corresponding author. Tel.: +1 651 254 2815; fax: +1 651 254 1519. E-mail addresses: [email protected] (P.A. Cole), [email protected] (E.M. Gauger), [email protected] (D.A. Herrera), [email protected] (J. Anavian), [email protected] (I.S. Tarkin). Contents lists available at SciVerse ScienceDirect Injury jo ur n al ho m epag e: ww w.els evier .c om /lo cat e/inju r y 0020–1383/$ – see front matter ß 2011 Elsevier Ltd. All rights reserved. doi:10.1016/j.injury.2011.09.029

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Injury, Int. J. Care Injured 43 (2012) 327–333
Radiographic follow-up of 84 operatively treated scapula neck and body fractures
Peter A. Cole a,*, Erich M. Gauger b, Diego A. Herrera c, Jack Anavian d, Ivan S. Tarkin e
a University of Minnesota/Regions Hospital, 640 Jackson Street, St. Paul, MN 55101, USAb University of Minnesota, 640 Jackson Street, St. Paul, MN 55101, USAc University of Alabama, 1530 3rd Avenue South, FOT 1203, Birmingham, AL 35294-3412, USAd Brown University, Box G-A1, Providence, RI 02912, USAe University of Pittsburgh, 3471 Fifth Avenue, Suite 1010, Pittsburgh, PA 15213, USA
A R T I C L E I N F O
Article history:
Accepted 30 September 2011
Keywords:
Scapula fractures
Operative
Open reduction internal fixation
Trauma
A B S T R A C T
Background: Certain scapula fractures may warrant surgical management to restore shoulder anatomy
and promote optimal function. The purpose of this study is to determine the early radiographic follow-
up of open reduction internal fixation (ORIF) for displaced, scapular fractures involving the glenoid neck
and body.
Methods: Eighty-four patients with a scapula body or neck fracture (with or without articular
involvement) underwent ORIF between 2002 and 2010 at a single level I trauma centre. This study
represents a retrospective review of data prospectively collected into a dedicated scapula fracture
database. All patients met at least one of the following operative criteria: �20 mm medial/lateral (M/L)
displacement (lateral border offset), �458 of angular deformity on a scapular-Y X-ray, the combination of
angulation �308 plus M/L displacement �15 mm, double disruptions of the superior shoulder
suspensory complex both displaced �10 mm, glenopolar angle (GPA) �228 and open fractures. Eighty-
eight percent (74/84) had sufficient follow-up defined as at least 6 months. Measured outcomes included
rates of scapula union and malunion, as well as surgical complications and re-operations.
Results: All fractures were caused by high-energy trauma with 24 (29%) resulting from motor-vehicle
collisions. Associated injuries occurred in 94% of patients, most commonly involving the chest (70%) and
ipsilateral shoulder girdle (43%). Forty-eight patients had M/L displacement as an operative indication
with a mean displacement of 25.7 mm (range = 20–40). Thirty-eight (45%) had �2 operative indications.
A single surgeon performed ORIF in all patients using a posterior approach. Five patients also required an
anterior (deltopectoral) approach. The fixation strategy included lateral and vertebral border
stabilisation with dynamic compression and reconstruction plates, respectively. Union was achieved
in all cases. There were three cases of malunion based on a GPA difference >108 from the uninjured
shoulder. Re-operations included removal of hardware (seven patients) and manipulation under
anaesthesia (three patients). There were no infections or wound dehiscence.
Conclusions: ORIF for displaced scapula fractures is a relatively safe and effective procedure for
restoration of anatomy and promotion of union.
Level of evidence: Therapeutic study, level IV.
� 2011 Elsevier Ltd. All rights reserved.
Contents lists available at SciVerse ScienceDirect
Injury
jo ur n al ho m epag e: ww w.els evier . c om / lo cat e/ in ju r y
Introduction
The majority of scapula fractures have been managed non-operatively with immobilisation followed by early range of motionand progressive strengthening as symptoms allow.1–7 This approachhas been largely accepted due to favourable outcomes when used forminimally to moderately displaced scapula fractures, which occur in
* Corresponding author. Tel.: +1 651 254 2815; fax: +1 651 254 1519.
E-mail addresses: [email protected] (P.A. Cole),
[email protected] (E.M. Gauger), [email protected] (D.A. Herrera),
[email protected] (J. Anavian), [email protected] (I.S. Tarkin).
0020–1383/$ – see front matter � 2011 Elsevier Ltd. All rights reserved.
doi:10.1016/j.injury.2011.09.029
the majority of patients. However, unstable or highly displacedfractures of the glenoid neck and intra-articular fractures have thepotential to lead to shoulder imbalance, instability, chronic pain,weakness, stiffness, deformity and early arthrosis.8–16
Non-operative studies have rarely provided fracture displace-ment and patterns, making conclusions regarding which patientsmay benefit from surgical fixation difficult to interpret.1,4,12,17–19
Furthermore, indications for surgery in published series ofoperative patients represent a mix of poorly defined radiographicmeasurements. Explicit surgical indications in the literatureinclude the unstable shoulder girdle based on multiple disruptionsof the superior shoulder suspensory complex (SSSC),20–22 ‘med-ialisation’ (medial/lateral (M/L) displacement) 10–25 mm,11,23,24

P.A. Cole et al. / Injury, Int. J. Care Injured 43 (2012) 327–333328
angular deformity 25–458,11,23,24 shortening >25 mm as definedby Jones et al.24 (a measure of medialisation of the glenoid),displaced fracture of the glenoid with intra-articular step-off orgap between 2 and 10 mm, 20–30% involvement of the articularsurface or instability of the glenohumeral joint.1,9,23,25–29 Whilstthere are multiple published papers using different operativeapproaches and fixation techniques for scapula fractures,24,28,30–35
all have been recorded in small, retrospective case series providinglimited evidence for safe and effective surgery.4,5,11,19–
22,24,25,27,29,36–39
The purpose of this study is to provide an overview of thepatient demographics, radiographic fracture characteristics,operative indications and an assessment of radiographic resultsfor operatively treated scapula fractures involving the glenoidneck and body including rates of union, malunion andcomplications.
Patients and methods
A database was established in 2002 to enroll all patientsprospectively, specifically for scapula fractures meeting definedoperative indications. Patients were enrolled under InstitutionalReview Board approval. For the purpose of this study, the databasewas used to analyse the early surgical experience of open reductioninternal fixation (ORIF) of scapula body and/or glenoid neckfractures that were operated on within 21 days of injury. Strictradiographic criteria were used to determine candidacy for ORIF.
A single examiner (EMG) reviewed all radiographs, includinginjury three-dimensional (3D) computed tomography (CT) scansfor the purpose of classification, measuring displacement as well aseventual deformity (Fig. 1). Fracture patterns were classifiedaccording to the AO/OTA fracture classification system.40 Onlyextra-articular (type 14-A3 and C1) and intra-articular (C2 and C3)fractures of the scapula body and/or neck were included. Isolatedprocess (A1 and A2) and articular fractures (B1, B2 and B3) werenot included.
Scapula neck, body and associated process fractures werefurther defined according to the Ada and Miller classificationsystem,11 which is an anatomic classification system based on theradiographic analysis of 116 cases in their landmark series from1991. Multiple classification schemes were chosen because nosingle system allows for classification of the pathology that arisesin this cohort of fractures.
Nonunion was defined as a persistent fracture line present onany radiograph after 8 weeks, or failure of fixation. Malunion isdefined as a healed fracture with persistent deformity of theglenoid in relation to the scapula body. Malunion was determinedusing four parameters: displacement >0.5 cm on the AP X-ray (M/L displacement) or scapular-Y X-ray (translation), angulardeformity on a scapular-Y radiograph or a glenopolar angle(GPA) �108 difference from the contralateral shoulder (obtainedper protocol for preoperative comparison and planning). The GPAis described as an angle between a line drawn from the inferior tothe superior glenoid, and from the superior glenoid to the nadir ofthe inferior angle of the scapula, as measured on an AP X-ray (or3D CT view of the shoulder). Double lesions of the SSSC requiredthat both lesions be displaced greater than 1 cm. Double lesionsinclude any two of the following structures in the osseo-ligamentous ring defined by Goss41: glenoid neck, coracoid,coracoclavicular ligaments, clavicle, AC joint and acromion. Allother complications were recorded including return to surgery forhardware irritation or early manipulation under anaesthesia forstiffness.
Postoperative follow-up visits were scheduled at 7–14 days,and 6, 12 and 24 weeks after surgery, as well as 12, 18 and 24months.
Results
From February 2002 to January 2010, 537 patients with scapulafractures presented to either the senior author’s clinic or the level Itrauma centre, of whom 138 met the criteria for surgery. Seventy-four (54%) were referred with surgical indications, not comingdirectly through the emergency room; thus, the rate of surgicalintervention for scapula fracture patients presenting to this level Itrauma centre acutely was 13.6%. Thirty-four patients underwentORIF >3 weeks after injury, a subgroup previously reported.23 Fivepatients were operated on for a scapula malunion >90 days afterinjury, and were not included in this analysis.39 An additional 15patients were treated for an isolated intra-articular glenoid fractureand/or process fractures without fixation of the scapula body and/orglenoid neck, leaving 84 patients (68 males and 16 females) in thecohort for this study. The mean age was 45 years (range = 18–76).The mean postoperative follow-up time for patients having at least 6months follow-up was 23.5 months (range = 6–70). Ten patients hadinsufficient follow-up (<6 months) for the final analysis ofradiographs and complications, making a follow-up rate of 88%(74/84). Four of the 10 patients excluded due to ‘insufficient follow-up’ had returned to clinic for at least a 3-month postoperative examand were deemed radiographically and clinically healed at that timewith no complications.
The most prevalent mechanism of injury was a motorcyclecollision occurring in 24 (29%) patients followed by motor-vehiclecollision in 19 (23%) patients. Other mechanisms of injury includedfall from a height in 10 (12%), bicycle collision in six (7%), ATVaccident in five (6%), pedestrian versus motor vehicle accident andfall from horse in four (5%) each, motocross in three (4%),snowmobiling in two (2%) and sports and other accidents in theremaining seven. Associated injuries were common (Table 1), with79 (94%) patients sustaining at least one additional injury. Fifty-sixpatients (67%) had at least one rib fracture, 38 (45%) a haemo/pneumothorax and 28 (33%) had a clavicle fracture. A traumaticbrain injury was sustained in 22 (26%), though only one patientexperienced persistent central neurological deficit. Only fivepatients had an isolated scapula fracture.
Suprascapular nerve injury was documented in 12 cases. Injurywas noted on electromyography (EMG) and nerve conductionstudies in six patients preoperatively (presenting �2 weeks postinjury) and six more confirmed postoperatively in cases where aninjured nerve was noted intra-operatively. The nerve was exploredand noted to be injured in eight patients, with two having a franktraumatic laceration. In the remaining four cases, partial tears wereappreciated with the nerve incarcerated in the fracture site and attimes encased in a callus. In fact, fracture patterns in this subgroupof patients with nerve injury involved the spinoglenoid notch inthree patients and both the suprascapular and spinoglenoid notchin six patients. Overall, the mean time elapsed from the date ofinjury to the date of surgery was 11 days (range = 0–21 days).
Isolated extra-articular fracture (AO/OTA 14-A3, 14-C1) pat-terns of the scapula neck and/or body occurred in 64 cases,whereas additional intra-articular fractures (14-C2, 14-C3) (Table2) occurred in 20 patients. According to the Ada and Miller andrevised AO/OTA classification, 52 and 16 patients, respectively, hadmultiple assignments to a certain fracture type. Thirty-fivepatients (42%) had multiple disruptions of the SSSC,41 including29 double. Six had a third lesion, an acromioclavicular disruption inaddition to a clavicle fracture.
M/L displacement of the lateral border, sometimes referred toas medialisation, was the only operative indication in 48 patients,with a mean of 25.7 mm (range = 20–40) (Table 3). Angulardeformity was the only operative indication in four patients with amean of 50.38 (range = 46–63). Thirteen patients had an operativeindication of angular deformity and M/L displacement with a mean
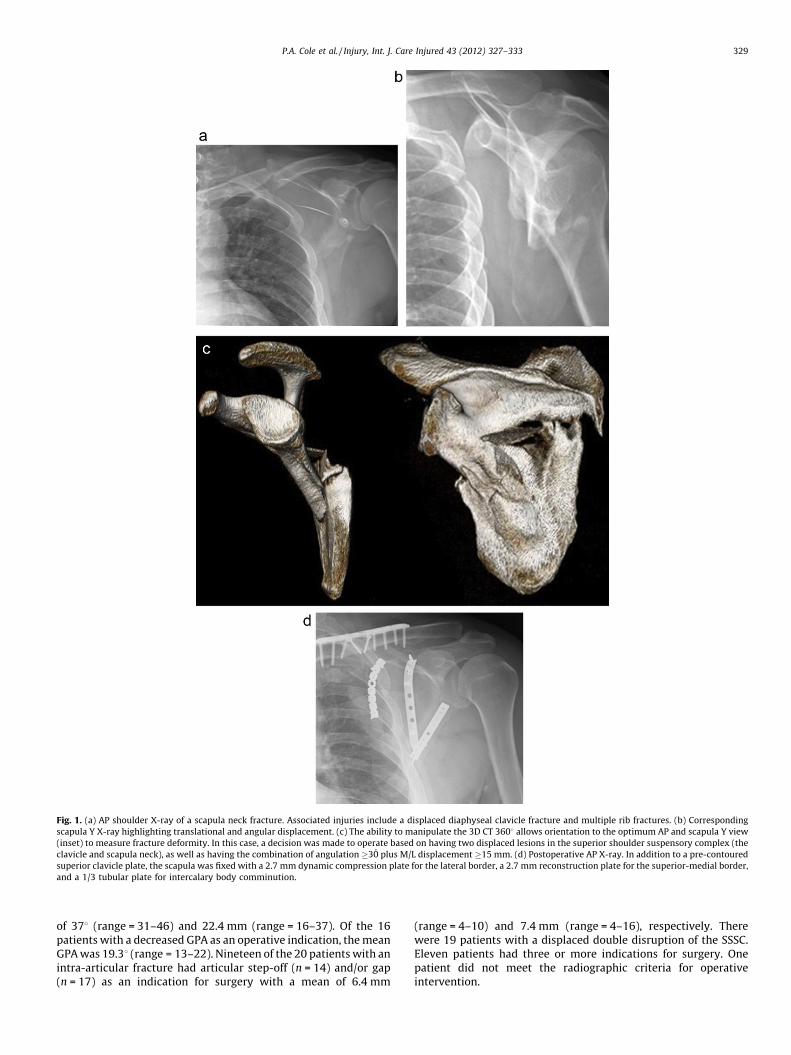
Fig. 1. (a) AP shoulder X-ray of a scapula neck fracture. Associated injuries include a displaced diaphyseal clavicle fracture and multiple rib fractures. (b) Corresponding
scapula Y X-ray highlighting translational and angular displacement. (c) The ability to manipulate the 3D CT 3608 allows orientation to the optimum AP and scapula Y view
(inset) to measure fracture deformity. In this case, a decision was made to operate based on having two displaced lesions in the superior shoulder suspensory complex (the
clavicle and scapula neck), as well as having the combination of angulation �30̊ plus M/L displacement �15 mm. (d) Postoperative AP X-ray. In addition to a pre-contoured
superior clavicle plate, the scapula was fixed with a 2.7 mm dynamic compression plate for the lateral border, a 2.7 mm reconstruction plate for the superior-medial border,
and a 1/3 tubular plate for intercalary body comminution.
P.A. Cole et al. / Injury, Int. J. Care Injured 43 (2012) 327–333 329
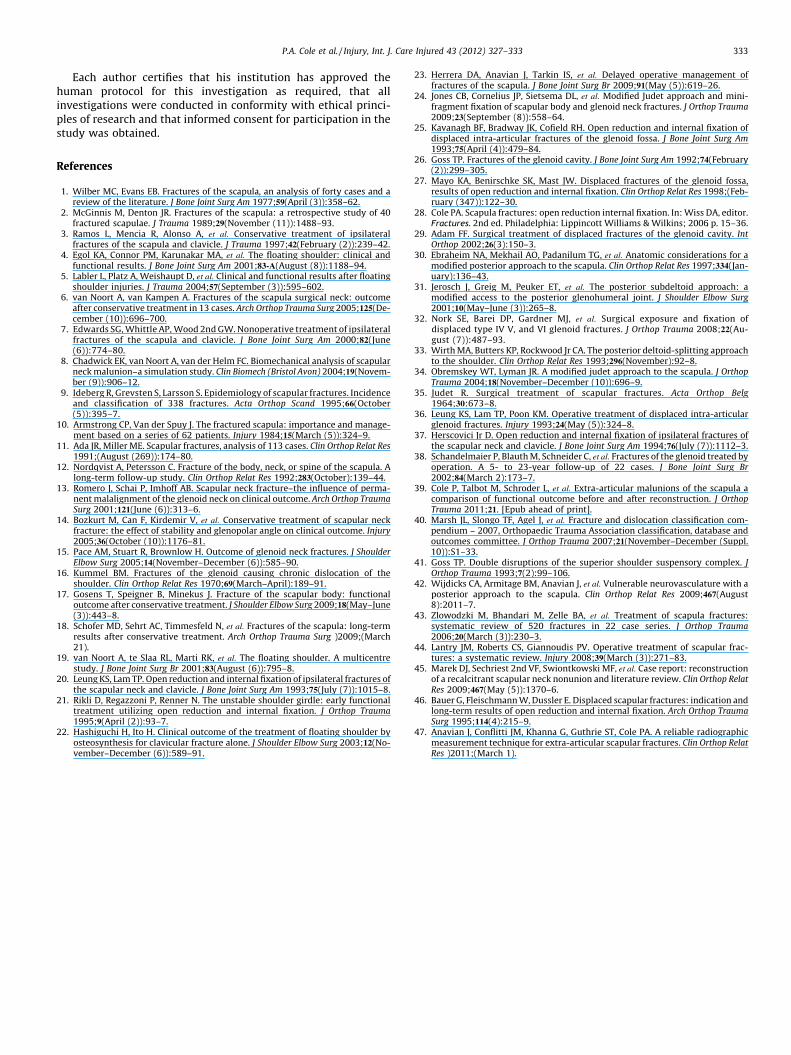
of 378 (range = 31–46) and 22.4 mm (range = 16–37). Of the 16patients with a decreased GPA as an operative indication, the meanGPA was 19.38 (range = 13–22). Nineteen of the 20 patients with anintra-articular fracture had articular step-off (n = 14) and/or gap(n = 17) as an indication for surgery with a mean of 6.4 mm
(range = 4–10) and 7.4 mm (range = 4–16), respectively. Therewere 19 patients with a displaced double disruption of the SSSC.Eleven patients had three or more indications for surgery. Onepatient did not meet the radiographic criteria for operativeintervention.
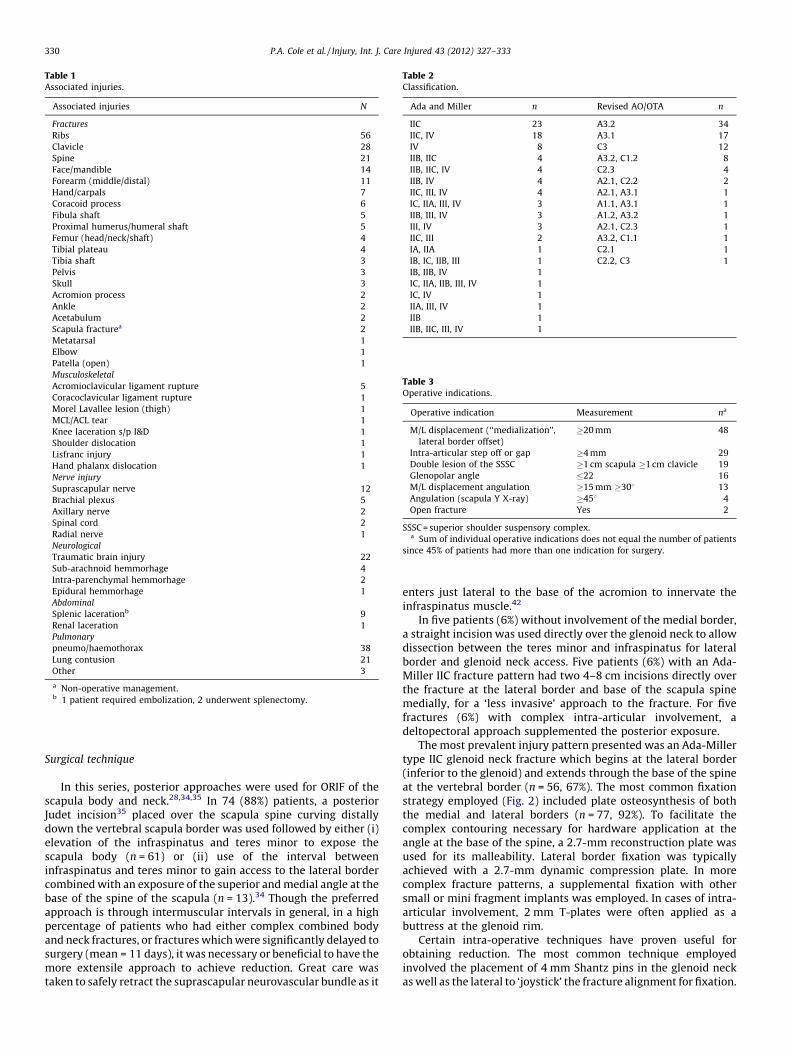
Table 1Associated injuries.
Associated injuries N
Fractures
Ribs 56
Clavicle 28
Spine 21
Face/mandible 14
Forearm (middle/distal) 11
Hand/carpals 7
Coracoid process 6
Fibula shaft 5
Proximal humerus/humeral shaft 5
Femur (head/neck/shaft) 4
Tibial plateau 4
Tibia shaft 3
Pelvis 3
Skull 3
Acromion process 2
Ankle 2
Acetabulum 2
Scapula fracturea 2
Metatarsal 1
Elbow 1
Patella (open) 1
Musculoskeletal
Acromioclavicular ligament rupture 5
Coracoclavicular ligament rupture 1
Morel Lavallee lesion (thigh) 1
MCL/ACL tear 1
Knee laceration s/p I&D 1
Shoulder dislocation 1
Lisfranc injury 1
Hand phalanx dislocation 1
Nerve injury
Suprascapular nerve 12
Brachial plexus 5
Axillary nerve 2
Spinal cord 2
Radial nerve 1
Neurological
Traumatic brain injury 22
Sub-arachnoid hemmorhage 4
Intra-parenchymal hemmorhage 2
Epidural hemmorhage 1
Abdominal
Splenic lacerationb 9
Renal laceration 1
Pulmonary
pneumo/haemothorax 38
Lung contusion 21
Other 3
a Non-operative management.b 1 patient required embolization, 2 underwent splenectomy.
Table 2Classification.
Ada and Miller n Revised AO/OTA n
IIC 23 A3.2 34
IIC, IV 18 A3.1 17
IV 8 C3 12
IIB, IIC 4 A3.2, C1.2 8
IIB, IIC, IV 4 C2.3 4
IIB, IV 4 A2.1, C2.2 2
IIC, III, IV 4 A2.1, A3.1 1
IC, IIA, III, IV 3 A1.1, A3.1 1
IIB, III, IV 3 A1.2, A3.2 1
III, IV 3 A2.1, C2.3 1
IIC, III 2 A3.2, C1.1 1
IA, IIA 1 C2.1 1
IB, IC, IIB, III 1 C2.2, C3 1
IB, IIB, IV 1
IC, IIA, IIB, III, IV 1
IC, IV 1
IIA, III, IV 1
IIB 1
IIB, IIC, III, IV 1
Table 3Operative indications.
Operative indication Measurement na
M/L displacement (‘‘medialization’’,
lateral border offset)
�20 mm 48
Intra-articular step off or gap �4 mm 29
Double lesion of the SSSC �1 cm scapula �1 cm clavicle 19
Glenopolar angle �22 16
M/L displacement angulation �15 mm �308 13
Angulation (scapula Y X-ray) �458 4
Open fracture Yes 2
SSSC = superior shoulder suspensory complex.a Sum of individual operative indications does not equal the number of patients
since 45% of patients had more than one indication for surgery.
P.A. Cole et al. / Injury, Int. J. Care Injured 43 (2012) 327–333330
Surgical technique
In this series, posterior approaches were used for ORIF of thescapula body and neck.28,34,35 In 74 (88%) patients, a posteriorJudet incision35 placed over the scapula spine curving distallydown the vertebral scapula border was used followed by either (i)elevation of the infraspinatus and teres minor to expose thescapula body (n = 61) or (ii) use of the interval betweeninfraspinatus and teres minor to gain access to the lateral bordercombined with an exposure of the superior and medial angle at thebase of the spine of the scapula (n = 13).34 Though the preferredapproach is through intermuscular intervals in general, in a highpercentage of patients who had either complex combined bodyand neck fractures, or fractures which were significantly delayed tosurgery (mean = 11 days), it was necessary or beneficial to have themore extensile approach to achieve reduction. Great care wastaken to safely retract the suprascapular neurovascular bundle as it
enters just lateral to the base of the acromion to innervate theinfraspinatus muscle.42
In five patients (6%) without involvement of the medial border,a straight incision was used directly over the glenoid neck to allowdissection between the teres minor and infraspinatus for lateralborder and glenoid neck access. Five patients (6%) with an Ada-Miller IIC fracture pattern had two 4–8 cm incisions directly overthe fracture at the lateral border and base of the scapula spinemedially, for a ‘less invasive’ approach to the fracture. For fivefractures (6%) with complex intra-articular involvement, adeltopectoral approach supplemented the posterior exposure.
The most prevalent injury pattern presented was an Ada-Millertype IIC glenoid neck fracture which begins at the lateral border(inferior to the glenoid) and extends through the base of the spineat the vertebral border (n = 56, 67%). The most common fixationstrategy employed (Fig. 2) included plate osteosynthesis of boththe medial and lateral borders (n = 77, 92%). To facilitate thecomplex contouring necessary for hardware application at theangle at the base of the spine, a 2.7-mm reconstruction plate wasused for its malleability. Lateral border fixation was typicallyachieved with a 2.7-mm dynamic compression plate. In morecomplex fracture patterns, a supplemental fixation with othersmall or mini fragment implants was employed. In cases of intra-articular involvement, 2 mm T-plates were often applied as abuttress at the glenoid rim.
Certain intra-operative techniques have proven useful forobtaining reduction. The most common technique employedinvolved the placement of 4 mm Shantz pins in the glenoid neckas well as the lateral to ‘joystick’ the fracture alignment for fixation.
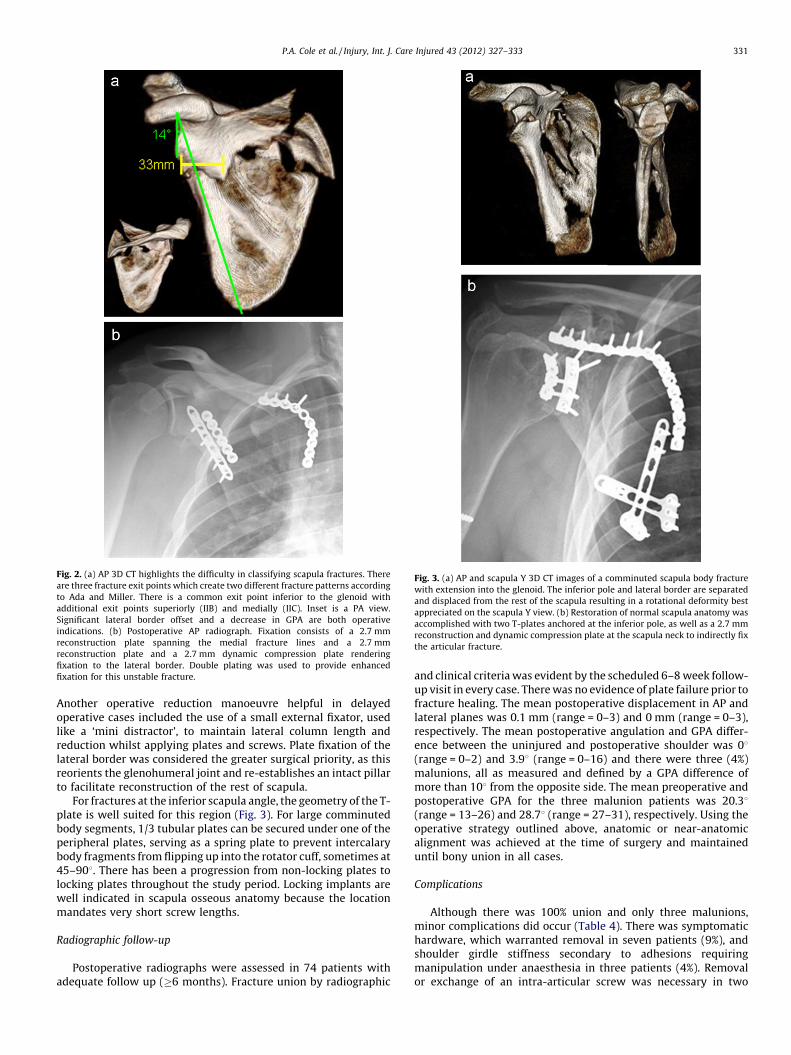
Fig. 2. (a) AP 3D CT highlights the difficulty in classifying scapula fractures. There
are three fracture exit points which create two different fracture patterns according
to Ada and Miller. There is a common exit point inferior to the glenoid with
additional exit points superiorly (IIB) and medially (IIC). Inset is a PA view.
Significant lateral border offset and a decrease in GPA are both operative
indications. (b) Postoperative AP radiograph. Fixation consists of a 2.7 mm
reconstruction plate spanning the medial fracture lines and a 2.7 mm
reconstruction plate and a 2.7 mm dynamic compression plate rendering
fixation to the lateral border. Double plating was used to provide enhanced
fixation for this unstable fracture.
Fig. 3. (a) AP and scapula Y 3D CT images of a comminuted scapula body fracture
with extension into the glenoid. The inferior pole and lateral border are separated
and displaced from the rest of the scapula resulting in a rotational deformity best
appreciated on the scapula Y view. (b) Restoration of normal scapula anatomy was
accomplished with two T-plates anchored at the inferior pole, as well as a 2.7 mm
reconstruction and dynamic compression plate at the scapula neck to indirectly fix
the articular fracture.
P.A. Cole et al. / Injury, Int. J. Care Injured 43 (2012) 327–333 331
Another operative reduction manoeuvre helpful in delayedoperative cases included the use of a small external fixator, usedlike a ‘mini distractor’, to maintain lateral column length andreduction whilst applying plates and screws. Plate fixation of thelateral border was considered the greater surgical priority, as thisreorients the glenohumeral joint and re-establishes an intact pillarto facilitate reconstruction of the rest of scapula.
For fractures at the inferior scapula angle, the geometry of the T-plate is well suited for this region (Fig. 3). For large comminutedbody segments, 1/3 tubular plates can be secured under one of theperipheral plates, serving as a spring plate to prevent intercalarybody fragments from flipping up into the rotator cuff, sometimes at45–908. There has been a progression from non-locking plates tolocking plates throughout the study period. Locking implants arewell indicated in scapula osseous anatomy because the locationmandates very short screw lengths.
Radiographic follow-up
Postoperative radiographs were assessed in 74 patients withadequate follow up (�6 months). Fracture union by radiographic
and clinical criteria was evident by the scheduled 6–8 week follow-up visit in every case. There was no evidence of plate failure prior tofracture healing. The mean postoperative displacement in AP andlateral planes was 0.1 mm (range = 0–3) and 0 mm (range = 0–3),respectively. The mean postoperative angulation and GPA differ-ence between the uninjured and postoperative shoulder was 08(range = 0–2) and 3.98 (range = 0–16) and there were three (4%)malunions, all as measured and defined by a GPA difference ofmore than 108 from the opposite side. The mean preoperative andpostoperative GPA for the three malunion patients was 20.38(range = 13–26) and 28.78 (range = 27–31), respectively. Using theoperative strategy outlined above, anatomic or near-anatomicalignment was achieved at the time of surgery and maintaineduntil bony union in all cases.
Complications
Although there was 100% union and only three malunions,minor complications did occur (Table 4). There was symptomatichardware, which warranted removal in seven patients (9%), andshoulder girdle stiffness secondary to adhesions requiringmanipulation under anaesthesia in three patients (4%). Removalor exchange of an intra-articular screw was necessary in two

Table 4Complications.
Subsequent procedures related to scapula n
Hardware removal – scapula 7
Manipulation under anaesthesia 3
Intra-articular screw removal 2
Removal of exostosis 2
Subsequent procedures unrelated to scapula n
Hardware removal – clavicle 5
Reconstruction of clavicle nonunion after removal of hardware 1
Complications requiring no additional procedure n
Malunion 3
Scapula refracture – retained hardware, nondisplaced 1
Scapula refracture after removal of hardware, displaced 1
P.A. Cole et al. / Injury, Int. J. Care Injured 43 (2012) 327–333332
patients early postoperatively, though all patients had appropriatemotion with no adverse sequelae in follow-up. The use of intra-operative fluoroscopy was not routinely used except in certainintra-articular glenoid fractures. There were no intra-operativecomplications or postoperative infections.
Discussion
The purpose of this study was to investigate the patientdemographics, fracture characteristics, operative indications andradiographic results for operatively treated fractures involving thescapular neck and body, including rates of union, malunion andcomplications.
Our findings indicate that displaced unstable scapula fracturesinvolving the neck and body of the scapula can be managed withORIF safely and effectively. We believe that surgical restoration ofscapula anatomy after highly displaced glenoid neck fractures isimportant for re-establishing function; this agrees with the reportof Chadwick et al.,8 who concluded that changes in the workinglength of the muscles crossing the shoulder, especially the rotatorcuff complex, would lead to loss of arm function in patients withscapular malunion. Anatomic restoration of scapula morphologywas achieved at the time of surgery with both extensile and limitedposterior approaches, and fracture union was achieved in 100% ofthe patients.
Our union rate mimics that of the published literature on thetopic, as no previous surgical series to our knowledge reports asingle nonunion as an outcome of surgery.43,44 There has only beena single reported case of nonunion after operative treatment of ascapula fracture described by our group in a patient referred fortreatment of the nonunion.45 Possible reasons for such aremarkable union rate, across the literature, is that the optimalenvironment for healing exists with a robust blood supply andmuscular envelope. Even in the event that the infraspinatus flap iselevated during surgery, the subscapularis muscle is leftcompletely undisturbed. Our chosen surgical tactic which includesthe goal of fixation of all fracture lines exiting the bony perimeter(lateral, acromial and vertebral borders) may also help to explainthe absence of nonunion and low rate of malunion in this series.
Based on the method of using 3D CT for diagnostic purposes,these fractures warranted two or more assignments of classifica-tion according to the Miller and Ada system11 (62% of the time),and according to the AO-OTA system40 (19% of the time). Thisshortcoming of the current classification schemes does not evenaccount for the ipsilateral clavicle or AC joint dislocation, whichmay be yet another drawback since it is believed that such doublelesions are associated with different prognoses and treatmentimplications.
We report a secondary surgical procedure rate of 16% related tothe scapula, comparable to what has been reported in theliterature;43 however, all were minor and recoverable. We report
no infections, likely resulting from the same reason that we believeunion rates to be high – excellent blood supply; however, this mayalso be promoted by use of drains placed under the muscle flap andcopious irrigation alongside vigilant haemostasis. Furthermore, wealways waited for abrasions inside the surgical field to resolve priorto surgery. The possibility of iatrogenic nerve injury is certainlypresent, but would be difficult to quantify due to the inability toobtain an accurate physical exam of suprascapular and axillarynerve function perioperatively due to pain. Posterior rotator cuffdysfunction after extensile or limited posterior approaches forscapular fracture needs to be rigorously studied as it has only beenreported in 0.9% of cases.38,44,46 External rotation strength has beenreported to be less in patients treated by operation versusconservative measures.1 Certainly, in fracture patterns involvingthe suprascapular and spinoglenoid notches, injury to thesuprascapular nerve is a reported consequence.
We acknowledge limitations in our study that may preventgeneralisation of the findings. First, these results reflect theexperience of a single surgeon with keen interest in the topic. It ispossible that other approaches to ORIF of scapula fractures mayyield different results, better or worse. However, our results doseem to closely align with the collective literature on the topic as itregards high rates of union and low rates of malunion andinfection. Second, though operative indications were well-definedin this study, the method of measuring displacement andangulation of scapula fractures has only recently been validated.47
Our experience indicates that accuracy in determining displace-ment and angulation is enhanced with strict use of 3D CT scans.
In addition, the focus of this study is intra-operative andperioperative results, limited to the review of surgical parameters,radiographic results in the early postoperative period, as well asunion, malunion and complications. At this early juncture, it is notappropriate to report functional outcomes by objective measuressuch as strength and range of motion, or subjective measuresassessed by validated outcomes instruments. Future reportsincluding rigorous analysis of these patient outcomes are clearlyneeded. Regarding assessment of fracture healing, we believe thereported time interval (�6 months) is adequate for the scapulabased on reported experience. One report from our institution onthe delayed management of scapula fractures between 21 and 57days documented abundant callus by 3 weeks as well as a findingof lack of inter-fragment mobility during operative repair in allcases.23 Furthermore, clinical healing has been apparent in theexperience of surgeons who follow this injury based on the highfunction and lack of pain in patients with this injury in the 2-monthinterval.
Finally, this is a retrospective review of prospectively collecteddata with no comparative cohort of similar patients treated non-operatively, which is the basis of new studies currently underway.
The data presented in this report are only the first step indetermining the overall results of ORIF of scapular fractures. Futurestudies including critical functional analysis must focus oncorrelating fracture patterns and displacement, fixed and unfixed,with strength and function so that surgeons can better understandthe subsets of injured patients who may benefit from operativeintervention. In conclusion, ORIF of scapula fractures is a safe andeffective procedure for restoring scapula anatomy and promotingfracture union.
Conflict of interest statement
One or more of the authors (PAC) has received funding fromSynthes, Inc, West Chester, PA, USA and Zimmer, Warsaw, IN, USA.This funding source did not play a role in the investigation.
This investigation took place at Regions Hospital. This is thecorresponding author’s (PAC) institution.
P.A. Cole et al. / Injury, Int. J. Care Injured 43 (2012) 327–333 333
Each author certifies that his institution has approved thehuman protocol for this investigation as required, that allinvestigations were conducted in conformity with ethical princi-ples of research and that informed consent for participation in thestudy was obtained.
References
1. Wilber MC, Evans EB. Fractures of the scapula, an analysis of forty cases and areview of the literature. J Bone Joint Surg Am 1977;59(April (3)):358–62.
2. McGinnis M, Denton JR. Fractures of the scapula: a retrospective study of 40fractured scapulae. J Trauma 1989;29(November (11)):1488–93.
3. Ramos L, Mencia R, Alonso A, et al. Conservative treatment of ipsilateralfractures of the scapula and clavicle. J Trauma 1997;42(February (2)):239–42.
4. Egol KA, Connor PM, Karunakar MA, et al. The floating shoulder: clinical andfunctional results. J Bone Joint Surg Am 2001;83-A(August (8)):1188–94.
5. Labler L, Platz A, Weishaupt D, et al. Clinical and functional results after floatingshoulder injuries. J Trauma 2004;57(September (3)):595–602.
6. van Noort A, van Kampen A. Fractures of the scapula surgical neck: outcomeafter conservative treatment in 13 cases. Arch Orthop Trauma Surg 2005;125(De-cember (10)):696–700.
7. Edwards SG, Whittle AP, Wood 2nd GW. Nonoperative treatment of ipsilateralfractures of the scapula and clavicle. J Bone Joint Surg Am 2000;82(June(6)):774–80.
8. Chadwick EK, van Noort A, van der Helm FC. Biomechanical analysis of scapularneck malunion–a simulation study. Clin Biomech (Bristol Avon) 2004;19(Novem-ber (9)):906–12.
9. Ideberg R, Grevsten S, Larsson S. Epidemiology of scapular fractures. Incidenceand classification of 338 fractures. Acta Orthop Scand 1995;66(October(5)):395–7.
10. Armstrong CP, Van der Spuy J. The fractured scapula: importance and manage-ment based on a series of 62 patients. Injury 1984;15(March (5)):324–9.
11. Ada JR, Miller ME. Scapular fractures, analysis of 113 cases. Clin Orthop Relat Res1991;(August (269)):174–80.
12. Nordqvist A, Petersson C. Fracture of the body, neck, or spine of the scapula. Along-term follow-up study. Clin Orthop Relat Res 1992;283(October):139–44.
13. Romero J, Schai P, Imhoff AB. Scapular neck fracture–the influence of perma-nent malalignment of the glenoid neck on clinical outcome. Arch Orthop TraumaSurg 2001;121(June (6)):313–6.
14. Bozkurt M, Can F, Kirdemir V, et al. Conservative treatment of scapular neckfracture: the effect of stability and glenopolar angle on clinical outcome. Injury2005;36(October (10)):1176–81.
15. Pace AM, Stuart R, Brownlow H. Outcome of glenoid neck fractures. J ShoulderElbow Surg 2005;14(November–December (6)):585–90.
16. Kummel BM. Fractures of the glenoid causing chronic dislocation of theshoulder. Clin Orthop Relat Res 1970;69(March–April):189–91.
17. Gosens T, Speigner B, Minekus J. Fracture of the scapular body: functionaloutcome after conservative treatment. J Shoulder Elbow Surg 2009;18(May–June(3)):443–8.
18. Schofer MD, Sehrt AC, Timmesfeld N, et al. Fractures of the scapula: long-termresults after conservative treatment. Arch Orthop Trauma Surg )2009;(March21).
19. van Noort A, te Slaa RL, Marti RK, et al. The floating shoulder. A multicentrestudy. J Bone Joint Surg Br 2001;83(August (6)):795–8.
20. Leung KS, Lam TP. Open reduction and internal fixation of ipsilateral fractures ofthe scapular neck and clavicle. J Bone Joint Surg Am 1993;75(July (7)):1015–8.
21. Rikli D, Regazzoni P, Renner N. The unstable shoulder girdle: early functionaltreatment utilizing open reduction and internal fixation. J Orthop Trauma1995;9(April (2)):93–7.
22. Hashiguchi H, Ito H. Clinical outcome of the treatment of floating shoulder byosteosynthesis for clavicular fracture alone. J Shoulder Elbow Surg 2003;12(No-vember–December (6)):589–91.
23. Herrera DA, Anavian J, Tarkin IS, et al. Delayed operative management offractures of the scapula. J Bone Joint Surg Br 2009;91(May (5)):619–26.
24. Jones CB, Cornelius JP, Sietsema DL, et al. Modified Judet approach and mini-fragment fixation of scapular body and glenoid neck fractures. J Orthop Trauma2009;23(September (8)):558–64.
25. Kavanagh BF, Bradway JK, Cofield RH. Open reduction and internal fixation ofdisplaced intra-articular fractures of the glenoid fossa. J Bone Joint Surg Am1993;75(April (4)):479–84.
26. Goss TP. Fractures of the glenoid cavity. J Bone Joint Surg Am 1992;74(February(2)):299–305.
27. Mayo KA, Benirschke SK, Mast JW. Displaced fractures of the glenoid fossa,results of open reduction and internal fixation. Clin Orthop Relat Res 1998;(Feb-ruary (347)):122–30.
28. Cole PA. Scapula fractures: open reduction internal fixation. In: Wiss DA, editor.Fractures. 2nd ed. Philadelphia: Lippincott Williams & Wilkins; 2006. p. 15–36.
29. Adam FF. Surgical treatment of displaced fractures of the glenoid cavity. IntOrthop 2002;26(3):150–3.
30. Ebraheim NA, Mekhail AO, Padanilum TG, et al. Anatomic considerations for amodified posterior approach to the scapula. Clin Orthop Relat Res 1997;334(Jan-uary):136–43.
31. Jerosch J, Greig M, Peuker ET, et al. The posterior subdeltoid approach: amodified access to the posterior glenohumeral joint. J Shoulder Elbow Surg2001;10(May–June (3)):265–8.
32. Nork SE, Barei DP, Gardner MJ, et al. Surgical exposure and fixation ofdisplaced type IV V, and VI glenoid fractures. J Orthop Trauma 2008;22(Au-gust (7)):487–93.
33. Wirth MA, Butters KP, Rockwood Jr CA. The posterior deltoid-splitting approachto the shoulder. Clin Orthop Relat Res 1993;296(November):92–8.
34. Obremskey WT, Lyman JR. A modified judet approach to the scapula. J OrthopTrauma 2004;18(November–December (10)):696–9.
35. Judet R. Surgical treatment of scapular fractures. Acta Orthop Belg1964;30:673–8.
36. Leung KS, Lam TP, Poon KM. Operative treatment of displaced intra-articularglenoid fractures. Injury 1993;24(May (5)):324–8.
37. Herscovici Jr D. Open reduction and internal fixation of ipsilateral fractures ofthe scapular neck and clavicle. J Bone Joint Surg Am 1994;76(July (7)):1112–3.
38. Schandelmaier P, Blauth M, Schneider C, et al. Fractures of the glenoid treated byoperation. A 5- to 23-year follow-up of 22 cases. J Bone Joint Surg Br2002;84(March 2):173–7.
39. Cole P, Talbot M, Schroder L, et al. Extra-articular malunions of the scapula acomparison of functional outcome before and after reconstruction. J OrthopTrauma 2011;21. [Epub ahead of print].
40. Marsh JL, Slongo TF, Agel J, et al. Fracture and dislocation classification com-pendium – 2007, Orthopaedic Trauma Association classification, database andoutcomes committee. J Orthop Trauma 2007;21(November–December (Suppl.10)):S1–33.
41. Goss TP. Double disruptions of the superior shoulder suspensory complex. JOrthop Trauma 1993;7(2):99–106.
42. Wijdicks CA, Armitage BM, Anavian J, et al. Vulnerable neurovasculature with aposterior approach to the scapula. Clin Orthop Relat Res 2009;467(August8):2011–7.
43. Zlowodzki M, Bhandari M, Zelle BA, et al. Treatment of scapula fractures:systematic review of 520 fractures in 22 case series. J Orthop Trauma2006;20(March (3)):230–3.
44. Lantry JM, Roberts CS, Giannoudis PV. Operative treatment of scapular frac-tures: a systematic review. Injury 2008;39(March (3)):271–83.
45. Marek DJ, Sechriest 2nd VF, Swiontkowski MF, et al. Case report: reconstructionof a recalcitrant scapular neck nonunion and literature review. Clin Orthop RelatRes 2009;467(May (5)):1370–6.
46. Bauer G, Fleischmann W, Dussler E. Displaced scapular fractures: indication andlong-term results of open reduction and internal fixation. Arch Orthop TraumaSurg 1995;114(4):215–9.
47. Anavian J, Conflitti JM, Khanna G, Guthrie ST, Cole PA. A reliable radiographicmeasurement technique for extra-articular scapular fractures. Clin Orthop RelatRes )2011;(March 1).
Related Documents











