RADIOACTIVE ABLATION IN THYROID CANCERS DR SAQIB AMAD SHAH PG 2 ND YEAR DEPTT OF RADIATION ONCOLOGY skims MODERATOR:-DR TANVEER AHMAD

Radioactive ablation in thyriod cancers
Jul 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

RADIOACTIVE ABLATION IN THYROID CANCERS
DR SAQIB AMAD SHAH
PG 2ND YEAR DEPTT OF RADIATION ONCOLOGY skims
MODERATOR-DR TANVEER AHMAD
PHYSIOLOGY
Discovery
bull William Stewart Halsted
bull Late 19th Century
bull Prominent American Surgeon
US EU Japan
Estimated Thyroid Cancer Incidence in 2012
0
5000
10000
15000
20000
25000
30000
35000
40000
An
nu
al In
cid
ence
LAC
~62000
~53000
~18000
~6000
Global Incidence of Thyroid Cancer was gt 312000 in 20121
LAC = Latin America and Caribbean1 GLOBOCAN 2012 International Agency for Research on Cancer httpglobocaniarcfr2 Sherman Lancet 2003361501-5113 Eustatia-Rutten et al J Clin Endocrinol Metab 200691313-319
bull Thyroid cancer is the most common form of endocrine malignancy1
bull DTC representsgt 90 of all thyroid carcinomas2
bull The prognosis of patients with DTC is generally good due to tumor biology and efficacy of the initial surgery and 131I therapy3
NCI indicates that thyroid cancer is most commonendocrine cancer and about 60220 new cases in2013 thyroid cancers where registered and theyformed about 36 of all new cancers in INDIA
National cancer institute SEER stat act sheet2013
In kashmir there where about 161 cases of ca thyroidregistered in department of nuclear medicine andRCC out of 3394 cases about 05 of all cancers inyear 2013
Causes and Risk Factors for thyroid carcinoma
bull Geneticsndash Abnormal RET oncogene may cause MTCndash MEN 2A 2B Syndrome
bull Family Historyndash Gardnerrsquos Syndrome and FAP increase risk for Papillary Ca
bull Radiation Exposurendash Radiation therapy to Head or Neck(010 GyAFTER 5 yrs 2
risk of annual risk of developing ca thyriod) ndash Exposure to Radioactive Iodine during childhood or other
radioactive substances (Chernobyl) uarr risk for particularly Papillary carcinoma
ndash The risk of radiation-induced thyroid carcinoma is greater in females certain Jewish populations and patients with a
family history of thyroid carcinoma
Preston et al2007radia res
Causes and Risk Factors
bull Chronic Iodine deficiency uarr risk for Follicular carcinomaanaplatic ca as well as radiation induced thyriodcancer
Cardis E et al Risk of thyroid cancerj nat cancer
bull Genderndash Female gt Males(2-3X)
bull Agebull More common at young adults with 15-24 years of age it
forms 75-10 of cancers with peak incidence age of 49Bleyer A Viny A Barr R Cancer in 15- to 29-year-olds by primary site Oncologist 2006
ndash MTC usually diagnosed after 60
bull Racendash White race gt Black race
Siegel R Ma J Zou Z Jemal A Cancer statistics 2014
PRESENTATIONEVALUATION IN DTC
bull Palpable nodule or cervical node enlargement(solitary nodulecommon prsesntation of DTC)
bull Dysneafixed growthincreasing swelling of nodulevocal cordpalsycervical lap with thyroid nodulestridor neurologicalcompromise
bull Investigaionsbull TSHbull USG NECKbull FNACbull MRIbull NUCLEAR SCANSbull MOLECULAR TESTINGbull CXRAYVOCAL CORD MOBILITY
DEVITA TEXT BOOK OF ONCOLOGY
PATHOLOGICAL CLASSIFICATION OF THYROID CANCERS ON BASIS OF CELL OF ORGIN
)FOLLICULAR EPITHELIAL CELLSbull A-DIFFERENTIATED THYROID CANCERS
1 Papillary and its variants(80-90)bull classicbull papillary microcarcinimabull Encapsulated variantbull Follicular variant bull Aggressive variants(diffuse scleroting tall cell columner cell)2 Follicular cancers (15-30)bull A) classicalbull B) hurthle cell variant bull B-POORLY DIFFERENTIATED THYRIOD CANCERS
1insular carcinomabull C-UNDIFFERENTIATED THYRIOD CANCER(anaplastic))PARA FOLLICULAR CELL ORGINbull A) MCTbull Perez and Bradys text book of radiation oncology
CLASSIFICATION ON BASIS OF ABLITY TO CONCENTRATE RAI
A USUALLY CONCENTRATE RAI
CLASSICAL PAPILLARY CARCINOMA
ENCAPSULATED PC
FOLLICULAR VARIANT
FOLLICULAR CARCINOMA
B FREQUENTLY DO NOT CONCENTRATE RAI
TALL CELLCOLUMNER CALL
HURTHLE CELL
INSULAR CA
C NEVER CONCENTRATE RAI
ANAPLASTIC THYRIOD CA
MEDULLARY CA
Perez and Bradys text book of radiation oncology
0 1084 62 12 14
0
20
40
60
80
100
Surv
iva
l
Stage I
Stage II
Stage III
Stage IV
DTC Initial Disease Stage Predicts OVERALL SURVIVAL
Years
75 of all
tumors
25 of all
tumors
plt0001
Jonklaas J et al Thyroid 2006 16(12) 1229-1242
NCCN and ATA guidelines for the treatment of differentiated thyroid cancer (DTC)
Initial treatmentbull Total thyroidectomy except in patients with unifocal microcarcinoma (individualized
to patient and extent of disease)12
Postoperative treatmentbull Radioactive iodine (131I) (RAI) therapy12
Follow-up treatmentbull Levothyroxine to suppress TSH levels to lt 01mUL12
Recurrent or metastatic disease treatmentbull Local therapy (re-operation external radiation)bull Systemic therapy
ndash RAI therapyndash patients with refractory advanced disease
bull chemotherapy (limited efficacy and considerable toxicity)12
bull participation in clinical trials with small molecule tyrosine kinase inhibitors is recommended12
1 NCCN Clinical Practice Guidelines in Oncology Thyroid Carcinoma V12010 2 Cooper DS et al Thyroid 200991167-214
NCCN = National Comprehensive Cancer Network
ATA = American Thyroid Association
IODINE ISOTOPES
I-131 1-125 I-123
SLIDE
Decays by e-capture with t12of 60 days into lowenergy state Te-125producesauger electrons of50-350 kevLess photon fluxfor scanning andless energy forabilation
Decays by e- captureinto te-123 with t12of 133 hrs sosuitable for 24 hourdiagnostic testhigh photon efluxthan i-131radiation burden tothyriod os lt1 thanby 131
IODINE -131bull Introduced by Seidlin et al in 1946
I-131 decays with a half life of 802 days with betamius and gamma emissions This nuclide of iodinehas 78 neutrons in its nucleus while the only stablenuclide 127I has 74 On decaying 131I most expends itsof decay energy by transforming into thestable 131Xe in two steps with gamma decay(364 kev)following rapidly after beta decay(250- 800kev)131I is available for oral ingestion as sodium iodine
radionucleotide Physical t12 Emax(MEV) LET(kevum) Appx cell diameter
Maximum range in tissue
Iodine-131
Iodine-125
Iodine -123
80 DAYS
601 days
1322 hours
081
035
015
02
4-26
10-230
lt1
20mm
2-500nm
PHYSICAL BIOLOGICAL AND EFFECTIVE HALF LIFE OF I-131
PHYSICAL t12 Biological t12 Effective t12
THYROID TISSUE
EXTRA THYRIOD TISSUE
8 days
8 days
80 days
12 days
73 days
8 hours
GOALS OF RIA IN DIFFERENTIATED CANCERS
bull 1)Thyroid reminant ablation
bull 2)Adjuvant therapy for residual micriscopic disease
bull RAI targets remaining thyroid cancer cells in thyriodbed occult lymph node and distant mets
bull Ablation of remaining thyroid tissue facalitates useof TG as sensitive and specific marker for persistantdisease after primary therapy
bull Rx wbs after RAI ablation provides crutialinformation about prognosis and furthermanagement
bull Sherma SI Lancet 2003
MD anderson experience
bull 1599 patient outcome analysis for various treatment for differentiated thyroid Ca
bull 46 had radioiodine therapybull Treatment with radioiodine was the single most
powerful prognostic indicator for increased DFS (plt 0001)
bull Its use significantly increased the survival both standard and high risk group
bull Adult patients females with intrathyroidal papillary carcinoma treated with TT + RAI between 20-59yrs ndashbest prognosis
bull J Clin Endocrinol Metab 1992 Sep75(3)714-20
bull 1004 dtc- Followed up with
ndash RAI ndash 151
ndash thyroid hormone alone 755
ndash no postoperative medical therapy -98
Tumor recurrence ~ threefold lower p lt 0001in RAI vs other treatment
Fewer patients developed distant metastases (p lt 0002)
Significantly more pronounced in tgt=15cm
Mazzaferri EL et al Thyroid remnant 131I ablation for papillary and follicular thyroid carcinoma Thyroid 1997 Apr7(2)265-71
ATA GUIDELINES
bull Distant metsgross ETE regardless of tumor sizeprimarysize gt4cm even in absence of high risk features
bull Follicular and hurthle cell variants are considered high riskand these patients are always recommended RAI ablationexcept with small unifocal FCs (lt2cm) with capsular invasiononly(no vasular invasion)
bull For 1-4cm size RAI is used for lymph node mets or highrisk features like agegt45 intra thyriod vascularinvasionmultifocal diseaseaggressive variants(tallcellcolummner cell or insular carcinoma)
bull RAI is not used for PTCS lt1cm unifocal and with out highrisk features OR when all foci in multifocal disease is in1cm focus
bull In a study assessing outcomes in 1004 patients with differentiated thyroid carcinoma tumor recurrence was about 3-fold higher in patients either treated with thyroid hormone alone or given no postoperative medical therapy when compared with patients who underwent postoperative thyroid remnant ablation with 131I (P lt 001)
bull Moreover fewer patients developed distant metastases (P lt 002) after thyroid remnant 131I ablation than after other forms of postoperative treatment However this effect is observed only in patients with primary tumors 15 cm or more in diameter Mazzaferri EL Thyroid remnant 131I ablation for papillary andfollicular thyroid carcinoma
low risk group with i-131 abilationStudy showed that remnant ablation had less of a therapeutic effect perhaps because more extensive locoregional surgery had been done Hay ID Papillary thyroid carcinoma Endocrinol Metab Clin North
bull Rising incidence of second cancers in patients with low-risk (T1N0) thyroid cancer who receive radioactive iodine therapy
bull CONCLUSIONS-The increased risk of a SPM in patients with low-risk (T1N0) WDTC along with a lack of data demonstrating improved survival outcomes with adjuvant RAI( IYER NG etal 2013cancer)
bull Impact on overall survival of radioactive iodine in low-risk differentiated thyroid cancer patients
bull CONCLUSION-With a long-term follow-up of 103 yr we failed to prove any survival benefit of RAI after surgery in a large cohort of low-risk DTC patients(SCHTWATZC et alJ Clin Endocrinol Metab 2012 May)
MAJOR FACTORS IMPACTING DECISION MAKING IN RADIOIODINE REMNANT ABLATION
ADMINSTRATION OF I-131
bull As liquid solution or in capsulesbull Each capsule accounts for 50 micro
curiebull Capsules safer than liquid- less
radioactivity released into air during handling
bull Also result in less oral mucosal irritation
bull Simultaneous ingestion large amounts of water attenuates radiation dose emitted to gastric wall
bull Rapidly and completely absorbed in the upper intestine
PATIENT PREPRATIONS1)Low iodine diet(lt50ugday) for 2 wks before and 2 days afterRAI(saltbreat and dairy products to be avoided)it has been seen doublesthe RAI uptake and lower rates of measuarable Tg levels after RAI(SAWAKAEM et al2012THYRIOD)2)Avoid iodinated contast in all DCT patients patient should have delay in RAItherapy for 3-6 months followed by measurement of urinary iodine levels (lt150ugml measured after collecting 24 hour urine and patient should be on iodine freediet gt7 days)3)Stop thyroxine repelacement therapy six weeks before RAI thepapy in case r-TSHis used stop 3-4 days before RAI therapy4)09 mg r-TSH can b used twice (2 days before and one day after) I-131(not to beused in cardiovascular diseasepara tracheal massspinal mets and inchildrenefficacy not studied in children)( studies show equal results with tshreplacement vs r-TSH)TSWNG et AL 1998CANCER5)Lithium carbonate 20mgkgday for 7 days usually 5 days before RAI ablation(measure serum lithium concentration on 4th 5th day of therapy which should be06-12 megml in its narrow theurpatic range)lithium decreases iodine exit fromthyriod cells increasing biological t12 by 50-90 with out interfering with iodineuptakeno studies have shown improved out comes with lithuimContraindicated in psychiatric problemsdementiaseizuresrenal and hepaticinsufficiencydiureticnsaidCCB intakehypohypernatremiahellip
Cancer vs normal cells
bull Metabolism of radioiodine in papillary and follicular carcinoma is profoundly altered when compared with normal thyroid tissue
bull Several defects are present in cancer tissuendash iodine uptake via the sodium-iodide symporter
(NIS) is always decreased and is undetectable in about a third of patients
ndash Iodine organification is markedly reduced
ndash Effective half-life of iodine in tumor tissue is always shorter
bull Tissues that often take up iodine and can be misconstrued as metastases include the
ndash salivary glands in the mouth
ndash esophagus (as a result of swallowing radioactive saliva)
ndash thymus gland
ndash breasts in some women
ndash liver stomach colon bladder
I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

PHYSIOLOGY
Discovery
bull William Stewart Halsted
bull Late 19th Century
bull Prominent American Surgeon
US EU Japan
Estimated Thyroid Cancer Incidence in 2012
0
5000
10000
15000
20000
25000
30000
35000
40000
An
nu
al In
cid
ence
LAC
~62000
~53000
~18000
~6000
Global Incidence of Thyroid Cancer was gt 312000 in 20121
LAC = Latin America and Caribbean1 GLOBOCAN 2012 International Agency for Research on Cancer httpglobocaniarcfr2 Sherman Lancet 2003361501-5113 Eustatia-Rutten et al J Clin Endocrinol Metab 200691313-319
bull Thyroid cancer is the most common form of endocrine malignancy1
bull DTC representsgt 90 of all thyroid carcinomas2
bull The prognosis of patients with DTC is generally good due to tumor biology and efficacy of the initial surgery and 131I therapy3
NCI indicates that thyroid cancer is most commonendocrine cancer and about 60220 new cases in2013 thyroid cancers where registered and theyformed about 36 of all new cancers in INDIA
National cancer institute SEER stat act sheet2013
In kashmir there where about 161 cases of ca thyroidregistered in department of nuclear medicine andRCC out of 3394 cases about 05 of all cancers inyear 2013
Causes and Risk Factors for thyroid carcinoma
bull Geneticsndash Abnormal RET oncogene may cause MTCndash MEN 2A 2B Syndrome
bull Family Historyndash Gardnerrsquos Syndrome and FAP increase risk for Papillary Ca
bull Radiation Exposurendash Radiation therapy to Head or Neck(010 GyAFTER 5 yrs 2
risk of annual risk of developing ca thyriod) ndash Exposure to Radioactive Iodine during childhood or other
radioactive substances (Chernobyl) uarr risk for particularly Papillary carcinoma
ndash The risk of radiation-induced thyroid carcinoma is greater in females certain Jewish populations and patients with a
family history of thyroid carcinoma
Preston et al2007radia res
Causes and Risk Factors
bull Chronic Iodine deficiency uarr risk for Follicular carcinomaanaplatic ca as well as radiation induced thyriodcancer
Cardis E et al Risk of thyroid cancerj nat cancer
bull Genderndash Female gt Males(2-3X)
bull Agebull More common at young adults with 15-24 years of age it
forms 75-10 of cancers with peak incidence age of 49Bleyer A Viny A Barr R Cancer in 15- to 29-year-olds by primary site Oncologist 2006
ndash MTC usually diagnosed after 60
bull Racendash White race gt Black race
Siegel R Ma J Zou Z Jemal A Cancer statistics 2014
PRESENTATIONEVALUATION IN DTC
bull Palpable nodule or cervical node enlargement(solitary nodulecommon prsesntation of DTC)
bull Dysneafixed growthincreasing swelling of nodulevocal cordpalsycervical lap with thyroid nodulestridor neurologicalcompromise
bull Investigaionsbull TSHbull USG NECKbull FNACbull MRIbull NUCLEAR SCANSbull MOLECULAR TESTINGbull CXRAYVOCAL CORD MOBILITY
DEVITA TEXT BOOK OF ONCOLOGY
PATHOLOGICAL CLASSIFICATION OF THYROID CANCERS ON BASIS OF CELL OF ORGIN
)FOLLICULAR EPITHELIAL CELLSbull A-DIFFERENTIATED THYROID CANCERS
1 Papillary and its variants(80-90)bull classicbull papillary microcarcinimabull Encapsulated variantbull Follicular variant bull Aggressive variants(diffuse scleroting tall cell columner cell)2 Follicular cancers (15-30)bull A) classicalbull B) hurthle cell variant bull B-POORLY DIFFERENTIATED THYRIOD CANCERS
1insular carcinomabull C-UNDIFFERENTIATED THYRIOD CANCER(anaplastic))PARA FOLLICULAR CELL ORGINbull A) MCTbull Perez and Bradys text book of radiation oncology
CLASSIFICATION ON BASIS OF ABLITY TO CONCENTRATE RAI
A USUALLY CONCENTRATE RAI
CLASSICAL PAPILLARY CARCINOMA
ENCAPSULATED PC
FOLLICULAR VARIANT
FOLLICULAR CARCINOMA
B FREQUENTLY DO NOT CONCENTRATE RAI
TALL CELLCOLUMNER CALL
HURTHLE CELL
INSULAR CA
C NEVER CONCENTRATE RAI
ANAPLASTIC THYRIOD CA
MEDULLARY CA
Perez and Bradys text book of radiation oncology
0 1084 62 12 14
0
20
40
60
80
100
Surv
iva
l
Stage I
Stage II
Stage III
Stage IV
DTC Initial Disease Stage Predicts OVERALL SURVIVAL
Years
75 of all
tumors
25 of all
tumors
plt0001
Jonklaas J et al Thyroid 2006 16(12) 1229-1242
NCCN and ATA guidelines for the treatment of differentiated thyroid cancer (DTC)
Initial treatmentbull Total thyroidectomy except in patients with unifocal microcarcinoma (individualized
to patient and extent of disease)12
Postoperative treatmentbull Radioactive iodine (131I) (RAI) therapy12
Follow-up treatmentbull Levothyroxine to suppress TSH levels to lt 01mUL12
Recurrent or metastatic disease treatmentbull Local therapy (re-operation external radiation)bull Systemic therapy
ndash RAI therapyndash patients with refractory advanced disease
bull chemotherapy (limited efficacy and considerable toxicity)12
bull participation in clinical trials with small molecule tyrosine kinase inhibitors is recommended12
1 NCCN Clinical Practice Guidelines in Oncology Thyroid Carcinoma V12010 2 Cooper DS et al Thyroid 200991167-214
NCCN = National Comprehensive Cancer Network
ATA = American Thyroid Association
IODINE ISOTOPES
I-131 1-125 I-123
SLIDE
Decays by e-capture with t12of 60 days into lowenergy state Te-125producesauger electrons of50-350 kevLess photon fluxfor scanning andless energy forabilation
Decays by e- captureinto te-123 with t12of 133 hrs sosuitable for 24 hourdiagnostic testhigh photon efluxthan i-131radiation burden tothyriod os lt1 thanby 131
IODINE -131bull Introduced by Seidlin et al in 1946
I-131 decays with a half life of 802 days with betamius and gamma emissions This nuclide of iodinehas 78 neutrons in its nucleus while the only stablenuclide 127I has 74 On decaying 131I most expends itsof decay energy by transforming into thestable 131Xe in two steps with gamma decay(364 kev)following rapidly after beta decay(250- 800kev)131I is available for oral ingestion as sodium iodine
radionucleotide Physical t12 Emax(MEV) LET(kevum) Appx cell diameter
Maximum range in tissue
Iodine-131
Iodine-125
Iodine -123
80 DAYS
601 days
1322 hours
081
035
015
02
4-26
10-230
lt1
20mm
2-500nm
PHYSICAL BIOLOGICAL AND EFFECTIVE HALF LIFE OF I-131
PHYSICAL t12 Biological t12 Effective t12
THYROID TISSUE
EXTRA THYRIOD TISSUE
8 days
8 days
80 days
12 days
73 days
8 hours
GOALS OF RIA IN DIFFERENTIATED CANCERS
bull 1)Thyroid reminant ablation
bull 2)Adjuvant therapy for residual micriscopic disease
bull RAI targets remaining thyroid cancer cells in thyriodbed occult lymph node and distant mets
bull Ablation of remaining thyroid tissue facalitates useof TG as sensitive and specific marker for persistantdisease after primary therapy
bull Rx wbs after RAI ablation provides crutialinformation about prognosis and furthermanagement
bull Sherma SI Lancet 2003
MD anderson experience
bull 1599 patient outcome analysis for various treatment for differentiated thyroid Ca
bull 46 had radioiodine therapybull Treatment with radioiodine was the single most
powerful prognostic indicator for increased DFS (plt 0001)
bull Its use significantly increased the survival both standard and high risk group
bull Adult patients females with intrathyroidal papillary carcinoma treated with TT + RAI between 20-59yrs ndashbest prognosis
bull J Clin Endocrinol Metab 1992 Sep75(3)714-20
bull 1004 dtc- Followed up with
ndash RAI ndash 151
ndash thyroid hormone alone 755
ndash no postoperative medical therapy -98
Tumor recurrence ~ threefold lower p lt 0001in RAI vs other treatment
Fewer patients developed distant metastases (p lt 0002)
Significantly more pronounced in tgt=15cm
Mazzaferri EL et al Thyroid remnant 131I ablation for papillary and follicular thyroid carcinoma Thyroid 1997 Apr7(2)265-71
ATA GUIDELINES
bull Distant metsgross ETE regardless of tumor sizeprimarysize gt4cm even in absence of high risk features
bull Follicular and hurthle cell variants are considered high riskand these patients are always recommended RAI ablationexcept with small unifocal FCs (lt2cm) with capsular invasiononly(no vasular invasion)
bull For 1-4cm size RAI is used for lymph node mets or highrisk features like agegt45 intra thyriod vascularinvasionmultifocal diseaseaggressive variants(tallcellcolummner cell or insular carcinoma)
bull RAI is not used for PTCS lt1cm unifocal and with out highrisk features OR when all foci in multifocal disease is in1cm focus
bull In a study assessing outcomes in 1004 patients with differentiated thyroid carcinoma tumor recurrence was about 3-fold higher in patients either treated with thyroid hormone alone or given no postoperative medical therapy when compared with patients who underwent postoperative thyroid remnant ablation with 131I (P lt 001)
bull Moreover fewer patients developed distant metastases (P lt 002) after thyroid remnant 131I ablation than after other forms of postoperative treatment However this effect is observed only in patients with primary tumors 15 cm or more in diameter Mazzaferri EL Thyroid remnant 131I ablation for papillary andfollicular thyroid carcinoma
low risk group with i-131 abilationStudy showed that remnant ablation had less of a therapeutic effect perhaps because more extensive locoregional surgery had been done Hay ID Papillary thyroid carcinoma Endocrinol Metab Clin North
bull Rising incidence of second cancers in patients with low-risk (T1N0) thyroid cancer who receive radioactive iodine therapy
bull CONCLUSIONS-The increased risk of a SPM in patients with low-risk (T1N0) WDTC along with a lack of data demonstrating improved survival outcomes with adjuvant RAI( IYER NG etal 2013cancer)
bull Impact on overall survival of radioactive iodine in low-risk differentiated thyroid cancer patients
bull CONCLUSION-With a long-term follow-up of 103 yr we failed to prove any survival benefit of RAI after surgery in a large cohort of low-risk DTC patients(SCHTWATZC et alJ Clin Endocrinol Metab 2012 May)
MAJOR FACTORS IMPACTING DECISION MAKING IN RADIOIODINE REMNANT ABLATION
ADMINSTRATION OF I-131
bull As liquid solution or in capsulesbull Each capsule accounts for 50 micro
curiebull Capsules safer than liquid- less
radioactivity released into air during handling
bull Also result in less oral mucosal irritation
bull Simultaneous ingestion large amounts of water attenuates radiation dose emitted to gastric wall
bull Rapidly and completely absorbed in the upper intestine
PATIENT PREPRATIONS1)Low iodine diet(lt50ugday) for 2 wks before and 2 days afterRAI(saltbreat and dairy products to be avoided)it has been seen doublesthe RAI uptake and lower rates of measuarable Tg levels after RAI(SAWAKAEM et al2012THYRIOD)2)Avoid iodinated contast in all DCT patients patient should have delay in RAItherapy for 3-6 months followed by measurement of urinary iodine levels (lt150ugml measured after collecting 24 hour urine and patient should be on iodine freediet gt7 days)3)Stop thyroxine repelacement therapy six weeks before RAI thepapy in case r-TSHis used stop 3-4 days before RAI therapy4)09 mg r-TSH can b used twice (2 days before and one day after) I-131(not to beused in cardiovascular diseasepara tracheal massspinal mets and inchildrenefficacy not studied in children)( studies show equal results with tshreplacement vs r-TSH)TSWNG et AL 1998CANCER5)Lithium carbonate 20mgkgday for 7 days usually 5 days before RAI ablation(measure serum lithium concentration on 4th 5th day of therapy which should be06-12 megml in its narrow theurpatic range)lithium decreases iodine exit fromthyriod cells increasing biological t12 by 50-90 with out interfering with iodineuptakeno studies have shown improved out comes with lithuimContraindicated in psychiatric problemsdementiaseizuresrenal and hepaticinsufficiencydiureticnsaidCCB intakehypohypernatremiahellip
Cancer vs normal cells
bull Metabolism of radioiodine in papillary and follicular carcinoma is profoundly altered when compared with normal thyroid tissue
bull Several defects are present in cancer tissuendash iodine uptake via the sodium-iodide symporter
(NIS) is always decreased and is undetectable in about a third of patients
ndash Iodine organification is markedly reduced
ndash Effective half-life of iodine in tumor tissue is always shorter
bull Tissues that often take up iodine and can be misconstrued as metastases include the
ndash salivary glands in the mouth
ndash esophagus (as a result of swallowing radioactive saliva)
ndash thymus gland
ndash breasts in some women
ndash liver stomach colon bladder
I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

Discovery
bull William Stewart Halsted
bull Late 19th Century
bull Prominent American Surgeon
US EU Japan
Estimated Thyroid Cancer Incidence in 2012
0
5000
10000
15000
20000
25000
30000
35000
40000
An
nu
al In
cid
ence
LAC
~62000
~53000
~18000
~6000
Global Incidence of Thyroid Cancer was gt 312000 in 20121
LAC = Latin America and Caribbean1 GLOBOCAN 2012 International Agency for Research on Cancer httpglobocaniarcfr2 Sherman Lancet 2003361501-5113 Eustatia-Rutten et al J Clin Endocrinol Metab 200691313-319
bull Thyroid cancer is the most common form of endocrine malignancy1
bull DTC representsgt 90 of all thyroid carcinomas2
bull The prognosis of patients with DTC is generally good due to tumor biology and efficacy of the initial surgery and 131I therapy3
NCI indicates that thyroid cancer is most commonendocrine cancer and about 60220 new cases in2013 thyroid cancers where registered and theyformed about 36 of all new cancers in INDIA
National cancer institute SEER stat act sheet2013
In kashmir there where about 161 cases of ca thyroidregistered in department of nuclear medicine andRCC out of 3394 cases about 05 of all cancers inyear 2013
Causes and Risk Factors for thyroid carcinoma
bull Geneticsndash Abnormal RET oncogene may cause MTCndash MEN 2A 2B Syndrome
bull Family Historyndash Gardnerrsquos Syndrome and FAP increase risk for Papillary Ca
bull Radiation Exposurendash Radiation therapy to Head or Neck(010 GyAFTER 5 yrs 2
risk of annual risk of developing ca thyriod) ndash Exposure to Radioactive Iodine during childhood or other
radioactive substances (Chernobyl) uarr risk for particularly Papillary carcinoma
ndash The risk of radiation-induced thyroid carcinoma is greater in females certain Jewish populations and patients with a
family history of thyroid carcinoma
Preston et al2007radia res
Causes and Risk Factors
bull Chronic Iodine deficiency uarr risk for Follicular carcinomaanaplatic ca as well as radiation induced thyriodcancer
Cardis E et al Risk of thyroid cancerj nat cancer
bull Genderndash Female gt Males(2-3X)
bull Agebull More common at young adults with 15-24 years of age it
forms 75-10 of cancers with peak incidence age of 49Bleyer A Viny A Barr R Cancer in 15- to 29-year-olds by primary site Oncologist 2006
ndash MTC usually diagnosed after 60
bull Racendash White race gt Black race
Siegel R Ma J Zou Z Jemal A Cancer statistics 2014
PRESENTATIONEVALUATION IN DTC
bull Palpable nodule or cervical node enlargement(solitary nodulecommon prsesntation of DTC)
bull Dysneafixed growthincreasing swelling of nodulevocal cordpalsycervical lap with thyroid nodulestridor neurologicalcompromise
bull Investigaionsbull TSHbull USG NECKbull FNACbull MRIbull NUCLEAR SCANSbull MOLECULAR TESTINGbull CXRAYVOCAL CORD MOBILITY
DEVITA TEXT BOOK OF ONCOLOGY
PATHOLOGICAL CLASSIFICATION OF THYROID CANCERS ON BASIS OF CELL OF ORGIN
)FOLLICULAR EPITHELIAL CELLSbull A-DIFFERENTIATED THYROID CANCERS
1 Papillary and its variants(80-90)bull classicbull papillary microcarcinimabull Encapsulated variantbull Follicular variant bull Aggressive variants(diffuse scleroting tall cell columner cell)2 Follicular cancers (15-30)bull A) classicalbull B) hurthle cell variant bull B-POORLY DIFFERENTIATED THYRIOD CANCERS
1insular carcinomabull C-UNDIFFERENTIATED THYRIOD CANCER(anaplastic))PARA FOLLICULAR CELL ORGINbull A) MCTbull Perez and Bradys text book of radiation oncology
CLASSIFICATION ON BASIS OF ABLITY TO CONCENTRATE RAI
A USUALLY CONCENTRATE RAI
CLASSICAL PAPILLARY CARCINOMA
ENCAPSULATED PC
FOLLICULAR VARIANT
FOLLICULAR CARCINOMA
B FREQUENTLY DO NOT CONCENTRATE RAI
TALL CELLCOLUMNER CALL
HURTHLE CELL
INSULAR CA
C NEVER CONCENTRATE RAI
ANAPLASTIC THYRIOD CA
MEDULLARY CA
Perez and Bradys text book of radiation oncology
0 1084 62 12 14
0
20
40
60
80
100
Surv
iva
l
Stage I
Stage II
Stage III
Stage IV
DTC Initial Disease Stage Predicts OVERALL SURVIVAL
Years
75 of all
tumors
25 of all
tumors
plt0001
Jonklaas J et al Thyroid 2006 16(12) 1229-1242
NCCN and ATA guidelines for the treatment of differentiated thyroid cancer (DTC)
Initial treatmentbull Total thyroidectomy except in patients with unifocal microcarcinoma (individualized
to patient and extent of disease)12
Postoperative treatmentbull Radioactive iodine (131I) (RAI) therapy12
Follow-up treatmentbull Levothyroxine to suppress TSH levels to lt 01mUL12
Recurrent or metastatic disease treatmentbull Local therapy (re-operation external radiation)bull Systemic therapy
ndash RAI therapyndash patients with refractory advanced disease
bull chemotherapy (limited efficacy and considerable toxicity)12
bull participation in clinical trials with small molecule tyrosine kinase inhibitors is recommended12
1 NCCN Clinical Practice Guidelines in Oncology Thyroid Carcinoma V12010 2 Cooper DS et al Thyroid 200991167-214
NCCN = National Comprehensive Cancer Network
ATA = American Thyroid Association
IODINE ISOTOPES
I-131 1-125 I-123
SLIDE
Decays by e-capture with t12of 60 days into lowenergy state Te-125producesauger electrons of50-350 kevLess photon fluxfor scanning andless energy forabilation
Decays by e- captureinto te-123 with t12of 133 hrs sosuitable for 24 hourdiagnostic testhigh photon efluxthan i-131radiation burden tothyriod os lt1 thanby 131
IODINE -131bull Introduced by Seidlin et al in 1946
I-131 decays with a half life of 802 days with betamius and gamma emissions This nuclide of iodinehas 78 neutrons in its nucleus while the only stablenuclide 127I has 74 On decaying 131I most expends itsof decay energy by transforming into thestable 131Xe in two steps with gamma decay(364 kev)following rapidly after beta decay(250- 800kev)131I is available for oral ingestion as sodium iodine
radionucleotide Physical t12 Emax(MEV) LET(kevum) Appx cell diameter
Maximum range in tissue
Iodine-131
Iodine-125
Iodine -123
80 DAYS
601 days
1322 hours
081
035
015
02
4-26
10-230
lt1
20mm
2-500nm
PHYSICAL BIOLOGICAL AND EFFECTIVE HALF LIFE OF I-131
PHYSICAL t12 Biological t12 Effective t12
THYROID TISSUE
EXTRA THYRIOD TISSUE
8 days
8 days
80 days
12 days
73 days
8 hours
GOALS OF RIA IN DIFFERENTIATED CANCERS
bull 1)Thyroid reminant ablation
bull 2)Adjuvant therapy for residual micriscopic disease
bull RAI targets remaining thyroid cancer cells in thyriodbed occult lymph node and distant mets
bull Ablation of remaining thyroid tissue facalitates useof TG as sensitive and specific marker for persistantdisease after primary therapy
bull Rx wbs after RAI ablation provides crutialinformation about prognosis and furthermanagement
bull Sherma SI Lancet 2003
MD anderson experience
bull 1599 patient outcome analysis for various treatment for differentiated thyroid Ca
bull 46 had radioiodine therapybull Treatment with radioiodine was the single most
powerful prognostic indicator for increased DFS (plt 0001)
bull Its use significantly increased the survival both standard and high risk group
bull Adult patients females with intrathyroidal papillary carcinoma treated with TT + RAI between 20-59yrs ndashbest prognosis
bull J Clin Endocrinol Metab 1992 Sep75(3)714-20
bull 1004 dtc- Followed up with
ndash RAI ndash 151
ndash thyroid hormone alone 755
ndash no postoperative medical therapy -98
Tumor recurrence ~ threefold lower p lt 0001in RAI vs other treatment
Fewer patients developed distant metastases (p lt 0002)
Significantly more pronounced in tgt=15cm
Mazzaferri EL et al Thyroid remnant 131I ablation for papillary and follicular thyroid carcinoma Thyroid 1997 Apr7(2)265-71
ATA GUIDELINES
bull Distant metsgross ETE regardless of tumor sizeprimarysize gt4cm even in absence of high risk features
bull Follicular and hurthle cell variants are considered high riskand these patients are always recommended RAI ablationexcept with small unifocal FCs (lt2cm) with capsular invasiononly(no vasular invasion)
bull For 1-4cm size RAI is used for lymph node mets or highrisk features like agegt45 intra thyriod vascularinvasionmultifocal diseaseaggressive variants(tallcellcolummner cell or insular carcinoma)
bull RAI is not used for PTCS lt1cm unifocal and with out highrisk features OR when all foci in multifocal disease is in1cm focus
bull In a study assessing outcomes in 1004 patients with differentiated thyroid carcinoma tumor recurrence was about 3-fold higher in patients either treated with thyroid hormone alone or given no postoperative medical therapy when compared with patients who underwent postoperative thyroid remnant ablation with 131I (P lt 001)
bull Moreover fewer patients developed distant metastases (P lt 002) after thyroid remnant 131I ablation than after other forms of postoperative treatment However this effect is observed only in patients with primary tumors 15 cm or more in diameter Mazzaferri EL Thyroid remnant 131I ablation for papillary andfollicular thyroid carcinoma
low risk group with i-131 abilationStudy showed that remnant ablation had less of a therapeutic effect perhaps because more extensive locoregional surgery had been done Hay ID Papillary thyroid carcinoma Endocrinol Metab Clin North
bull Rising incidence of second cancers in patients with low-risk (T1N0) thyroid cancer who receive radioactive iodine therapy
bull CONCLUSIONS-The increased risk of a SPM in patients with low-risk (T1N0) WDTC along with a lack of data demonstrating improved survival outcomes with adjuvant RAI( IYER NG etal 2013cancer)
bull Impact on overall survival of radioactive iodine in low-risk differentiated thyroid cancer patients
bull CONCLUSION-With a long-term follow-up of 103 yr we failed to prove any survival benefit of RAI after surgery in a large cohort of low-risk DTC patients(SCHTWATZC et alJ Clin Endocrinol Metab 2012 May)
MAJOR FACTORS IMPACTING DECISION MAKING IN RADIOIODINE REMNANT ABLATION
ADMINSTRATION OF I-131
bull As liquid solution or in capsulesbull Each capsule accounts for 50 micro
curiebull Capsules safer than liquid- less
radioactivity released into air during handling
bull Also result in less oral mucosal irritation
bull Simultaneous ingestion large amounts of water attenuates radiation dose emitted to gastric wall
bull Rapidly and completely absorbed in the upper intestine
PATIENT PREPRATIONS1)Low iodine diet(lt50ugday) for 2 wks before and 2 days afterRAI(saltbreat and dairy products to be avoided)it has been seen doublesthe RAI uptake and lower rates of measuarable Tg levels after RAI(SAWAKAEM et al2012THYRIOD)2)Avoid iodinated contast in all DCT patients patient should have delay in RAItherapy for 3-6 months followed by measurement of urinary iodine levels (lt150ugml measured after collecting 24 hour urine and patient should be on iodine freediet gt7 days)3)Stop thyroxine repelacement therapy six weeks before RAI thepapy in case r-TSHis used stop 3-4 days before RAI therapy4)09 mg r-TSH can b used twice (2 days before and one day after) I-131(not to beused in cardiovascular diseasepara tracheal massspinal mets and inchildrenefficacy not studied in children)( studies show equal results with tshreplacement vs r-TSH)TSWNG et AL 1998CANCER5)Lithium carbonate 20mgkgday for 7 days usually 5 days before RAI ablation(measure serum lithium concentration on 4th 5th day of therapy which should be06-12 megml in its narrow theurpatic range)lithium decreases iodine exit fromthyriod cells increasing biological t12 by 50-90 with out interfering with iodineuptakeno studies have shown improved out comes with lithuimContraindicated in psychiatric problemsdementiaseizuresrenal and hepaticinsufficiencydiureticnsaidCCB intakehypohypernatremiahellip
Cancer vs normal cells
bull Metabolism of radioiodine in papillary and follicular carcinoma is profoundly altered when compared with normal thyroid tissue
bull Several defects are present in cancer tissuendash iodine uptake via the sodium-iodide symporter
(NIS) is always decreased and is undetectable in about a third of patients
ndash Iodine organification is markedly reduced
ndash Effective half-life of iodine in tumor tissue is always shorter
bull Tissues that often take up iodine and can be misconstrued as metastases include the
ndash salivary glands in the mouth
ndash esophagus (as a result of swallowing radioactive saliva)
ndash thymus gland
ndash breasts in some women
ndash liver stomach colon bladder
I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

US EU Japan
Estimated Thyroid Cancer Incidence in 2012
0
5000
10000
15000
20000
25000
30000
35000
40000
An
nu
al In
cid
ence
LAC
~62000
~53000
~18000
~6000
Global Incidence of Thyroid Cancer was gt 312000 in 20121
LAC = Latin America and Caribbean1 GLOBOCAN 2012 International Agency for Research on Cancer httpglobocaniarcfr2 Sherman Lancet 2003361501-5113 Eustatia-Rutten et al J Clin Endocrinol Metab 200691313-319
bull Thyroid cancer is the most common form of endocrine malignancy1
bull DTC representsgt 90 of all thyroid carcinomas2
bull The prognosis of patients with DTC is generally good due to tumor biology and efficacy of the initial surgery and 131I therapy3
NCI indicates that thyroid cancer is most commonendocrine cancer and about 60220 new cases in2013 thyroid cancers where registered and theyformed about 36 of all new cancers in INDIA
National cancer institute SEER stat act sheet2013
In kashmir there where about 161 cases of ca thyroidregistered in department of nuclear medicine andRCC out of 3394 cases about 05 of all cancers inyear 2013
Causes and Risk Factors for thyroid carcinoma
bull Geneticsndash Abnormal RET oncogene may cause MTCndash MEN 2A 2B Syndrome
bull Family Historyndash Gardnerrsquos Syndrome and FAP increase risk for Papillary Ca
bull Radiation Exposurendash Radiation therapy to Head or Neck(010 GyAFTER 5 yrs 2
risk of annual risk of developing ca thyriod) ndash Exposure to Radioactive Iodine during childhood or other
radioactive substances (Chernobyl) uarr risk for particularly Papillary carcinoma
ndash The risk of radiation-induced thyroid carcinoma is greater in females certain Jewish populations and patients with a
family history of thyroid carcinoma
Preston et al2007radia res
Causes and Risk Factors
bull Chronic Iodine deficiency uarr risk for Follicular carcinomaanaplatic ca as well as radiation induced thyriodcancer
Cardis E et al Risk of thyroid cancerj nat cancer
bull Genderndash Female gt Males(2-3X)
bull Agebull More common at young adults with 15-24 years of age it
forms 75-10 of cancers with peak incidence age of 49Bleyer A Viny A Barr R Cancer in 15- to 29-year-olds by primary site Oncologist 2006
ndash MTC usually diagnosed after 60
bull Racendash White race gt Black race
Siegel R Ma J Zou Z Jemal A Cancer statistics 2014
PRESENTATIONEVALUATION IN DTC
bull Palpable nodule or cervical node enlargement(solitary nodulecommon prsesntation of DTC)
bull Dysneafixed growthincreasing swelling of nodulevocal cordpalsycervical lap with thyroid nodulestridor neurologicalcompromise
bull Investigaionsbull TSHbull USG NECKbull FNACbull MRIbull NUCLEAR SCANSbull MOLECULAR TESTINGbull CXRAYVOCAL CORD MOBILITY
DEVITA TEXT BOOK OF ONCOLOGY
PATHOLOGICAL CLASSIFICATION OF THYROID CANCERS ON BASIS OF CELL OF ORGIN
)FOLLICULAR EPITHELIAL CELLSbull A-DIFFERENTIATED THYROID CANCERS
1 Papillary and its variants(80-90)bull classicbull papillary microcarcinimabull Encapsulated variantbull Follicular variant bull Aggressive variants(diffuse scleroting tall cell columner cell)2 Follicular cancers (15-30)bull A) classicalbull B) hurthle cell variant bull B-POORLY DIFFERENTIATED THYRIOD CANCERS
1insular carcinomabull C-UNDIFFERENTIATED THYRIOD CANCER(anaplastic))PARA FOLLICULAR CELL ORGINbull A) MCTbull Perez and Bradys text book of radiation oncology
CLASSIFICATION ON BASIS OF ABLITY TO CONCENTRATE RAI
A USUALLY CONCENTRATE RAI
CLASSICAL PAPILLARY CARCINOMA
ENCAPSULATED PC
FOLLICULAR VARIANT
FOLLICULAR CARCINOMA
B FREQUENTLY DO NOT CONCENTRATE RAI
TALL CELLCOLUMNER CALL
HURTHLE CELL
INSULAR CA
C NEVER CONCENTRATE RAI
ANAPLASTIC THYRIOD CA
MEDULLARY CA
Perez and Bradys text book of radiation oncology
0 1084 62 12 14
0
20
40
60
80
100
Surv
iva
l
Stage I
Stage II
Stage III
Stage IV
DTC Initial Disease Stage Predicts OVERALL SURVIVAL
Years
75 of all
tumors
25 of all
tumors
plt0001
Jonklaas J et al Thyroid 2006 16(12) 1229-1242
NCCN and ATA guidelines for the treatment of differentiated thyroid cancer (DTC)
Initial treatmentbull Total thyroidectomy except in patients with unifocal microcarcinoma (individualized
to patient and extent of disease)12
Postoperative treatmentbull Radioactive iodine (131I) (RAI) therapy12
Follow-up treatmentbull Levothyroxine to suppress TSH levels to lt 01mUL12
Recurrent or metastatic disease treatmentbull Local therapy (re-operation external radiation)bull Systemic therapy
ndash RAI therapyndash patients with refractory advanced disease
bull chemotherapy (limited efficacy and considerable toxicity)12
bull participation in clinical trials with small molecule tyrosine kinase inhibitors is recommended12
1 NCCN Clinical Practice Guidelines in Oncology Thyroid Carcinoma V12010 2 Cooper DS et al Thyroid 200991167-214
NCCN = National Comprehensive Cancer Network
ATA = American Thyroid Association
IODINE ISOTOPES
I-131 1-125 I-123
SLIDE
Decays by e-capture with t12of 60 days into lowenergy state Te-125producesauger electrons of50-350 kevLess photon fluxfor scanning andless energy forabilation
Decays by e- captureinto te-123 with t12of 133 hrs sosuitable for 24 hourdiagnostic testhigh photon efluxthan i-131radiation burden tothyriod os lt1 thanby 131
IODINE -131bull Introduced by Seidlin et al in 1946
I-131 decays with a half life of 802 days with betamius and gamma emissions This nuclide of iodinehas 78 neutrons in its nucleus while the only stablenuclide 127I has 74 On decaying 131I most expends itsof decay energy by transforming into thestable 131Xe in two steps with gamma decay(364 kev)following rapidly after beta decay(250- 800kev)131I is available for oral ingestion as sodium iodine
radionucleotide Physical t12 Emax(MEV) LET(kevum) Appx cell diameter
Maximum range in tissue
Iodine-131
Iodine-125
Iodine -123
80 DAYS
601 days
1322 hours
081
035
015
02
4-26
10-230
lt1
20mm
2-500nm
PHYSICAL BIOLOGICAL AND EFFECTIVE HALF LIFE OF I-131
PHYSICAL t12 Biological t12 Effective t12
THYROID TISSUE
EXTRA THYRIOD TISSUE
8 days
8 days
80 days
12 days
73 days
8 hours
GOALS OF RIA IN DIFFERENTIATED CANCERS
bull 1)Thyroid reminant ablation
bull 2)Adjuvant therapy for residual micriscopic disease
bull RAI targets remaining thyroid cancer cells in thyriodbed occult lymph node and distant mets
bull Ablation of remaining thyroid tissue facalitates useof TG as sensitive and specific marker for persistantdisease after primary therapy
bull Rx wbs after RAI ablation provides crutialinformation about prognosis and furthermanagement
bull Sherma SI Lancet 2003
MD anderson experience
bull 1599 patient outcome analysis for various treatment for differentiated thyroid Ca
bull 46 had radioiodine therapybull Treatment with radioiodine was the single most
powerful prognostic indicator for increased DFS (plt 0001)
bull Its use significantly increased the survival both standard and high risk group
bull Adult patients females with intrathyroidal papillary carcinoma treated with TT + RAI between 20-59yrs ndashbest prognosis
bull J Clin Endocrinol Metab 1992 Sep75(3)714-20
bull 1004 dtc- Followed up with
ndash RAI ndash 151
ndash thyroid hormone alone 755
ndash no postoperative medical therapy -98
Tumor recurrence ~ threefold lower p lt 0001in RAI vs other treatment
Fewer patients developed distant metastases (p lt 0002)
Significantly more pronounced in tgt=15cm
Mazzaferri EL et al Thyroid remnant 131I ablation for papillary and follicular thyroid carcinoma Thyroid 1997 Apr7(2)265-71
ATA GUIDELINES
bull Distant metsgross ETE regardless of tumor sizeprimarysize gt4cm even in absence of high risk features
bull Follicular and hurthle cell variants are considered high riskand these patients are always recommended RAI ablationexcept with small unifocal FCs (lt2cm) with capsular invasiononly(no vasular invasion)
bull For 1-4cm size RAI is used for lymph node mets or highrisk features like agegt45 intra thyriod vascularinvasionmultifocal diseaseaggressive variants(tallcellcolummner cell or insular carcinoma)
bull RAI is not used for PTCS lt1cm unifocal and with out highrisk features OR when all foci in multifocal disease is in1cm focus
bull In a study assessing outcomes in 1004 patients with differentiated thyroid carcinoma tumor recurrence was about 3-fold higher in patients either treated with thyroid hormone alone or given no postoperative medical therapy when compared with patients who underwent postoperative thyroid remnant ablation with 131I (P lt 001)
bull Moreover fewer patients developed distant metastases (P lt 002) after thyroid remnant 131I ablation than after other forms of postoperative treatment However this effect is observed only in patients with primary tumors 15 cm or more in diameter Mazzaferri EL Thyroid remnant 131I ablation for papillary andfollicular thyroid carcinoma
low risk group with i-131 abilationStudy showed that remnant ablation had less of a therapeutic effect perhaps because more extensive locoregional surgery had been done Hay ID Papillary thyroid carcinoma Endocrinol Metab Clin North
bull Rising incidence of second cancers in patients with low-risk (T1N0) thyroid cancer who receive radioactive iodine therapy
bull CONCLUSIONS-The increased risk of a SPM in patients with low-risk (T1N0) WDTC along with a lack of data demonstrating improved survival outcomes with adjuvant RAI( IYER NG etal 2013cancer)
bull Impact on overall survival of radioactive iodine in low-risk differentiated thyroid cancer patients
bull CONCLUSION-With a long-term follow-up of 103 yr we failed to prove any survival benefit of RAI after surgery in a large cohort of low-risk DTC patients(SCHTWATZC et alJ Clin Endocrinol Metab 2012 May)
MAJOR FACTORS IMPACTING DECISION MAKING IN RADIOIODINE REMNANT ABLATION
ADMINSTRATION OF I-131
bull As liquid solution or in capsulesbull Each capsule accounts for 50 micro
curiebull Capsules safer than liquid- less
radioactivity released into air during handling
bull Also result in less oral mucosal irritation
bull Simultaneous ingestion large amounts of water attenuates radiation dose emitted to gastric wall
bull Rapidly and completely absorbed in the upper intestine
PATIENT PREPRATIONS1)Low iodine diet(lt50ugday) for 2 wks before and 2 days afterRAI(saltbreat and dairy products to be avoided)it has been seen doublesthe RAI uptake and lower rates of measuarable Tg levels after RAI(SAWAKAEM et al2012THYRIOD)2)Avoid iodinated contast in all DCT patients patient should have delay in RAItherapy for 3-6 months followed by measurement of urinary iodine levels (lt150ugml measured after collecting 24 hour urine and patient should be on iodine freediet gt7 days)3)Stop thyroxine repelacement therapy six weeks before RAI thepapy in case r-TSHis used stop 3-4 days before RAI therapy4)09 mg r-TSH can b used twice (2 days before and one day after) I-131(not to beused in cardiovascular diseasepara tracheal massspinal mets and inchildrenefficacy not studied in children)( studies show equal results with tshreplacement vs r-TSH)TSWNG et AL 1998CANCER5)Lithium carbonate 20mgkgday for 7 days usually 5 days before RAI ablation(measure serum lithium concentration on 4th 5th day of therapy which should be06-12 megml in its narrow theurpatic range)lithium decreases iodine exit fromthyriod cells increasing biological t12 by 50-90 with out interfering with iodineuptakeno studies have shown improved out comes with lithuimContraindicated in psychiatric problemsdementiaseizuresrenal and hepaticinsufficiencydiureticnsaidCCB intakehypohypernatremiahellip
Cancer vs normal cells
bull Metabolism of radioiodine in papillary and follicular carcinoma is profoundly altered when compared with normal thyroid tissue
bull Several defects are present in cancer tissuendash iodine uptake via the sodium-iodide symporter
(NIS) is always decreased and is undetectable in about a third of patients
ndash Iodine organification is markedly reduced
ndash Effective half-life of iodine in tumor tissue is always shorter
bull Tissues that often take up iodine and can be misconstrued as metastases include the
ndash salivary glands in the mouth
ndash esophagus (as a result of swallowing radioactive saliva)
ndash thymus gland
ndash breasts in some women
ndash liver stomach colon bladder
I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

NCI indicates that thyroid cancer is most commonendocrine cancer and about 60220 new cases in2013 thyroid cancers where registered and theyformed about 36 of all new cancers in INDIA
National cancer institute SEER stat act sheet2013
In kashmir there where about 161 cases of ca thyroidregistered in department of nuclear medicine andRCC out of 3394 cases about 05 of all cancers inyear 2013
Causes and Risk Factors for thyroid carcinoma
bull Geneticsndash Abnormal RET oncogene may cause MTCndash MEN 2A 2B Syndrome
bull Family Historyndash Gardnerrsquos Syndrome and FAP increase risk for Papillary Ca
bull Radiation Exposurendash Radiation therapy to Head or Neck(010 GyAFTER 5 yrs 2
risk of annual risk of developing ca thyriod) ndash Exposure to Radioactive Iodine during childhood or other
radioactive substances (Chernobyl) uarr risk for particularly Papillary carcinoma
ndash The risk of radiation-induced thyroid carcinoma is greater in females certain Jewish populations and patients with a
family history of thyroid carcinoma
Preston et al2007radia res
Causes and Risk Factors
bull Chronic Iodine deficiency uarr risk for Follicular carcinomaanaplatic ca as well as radiation induced thyriodcancer
Cardis E et al Risk of thyroid cancerj nat cancer
bull Genderndash Female gt Males(2-3X)
bull Agebull More common at young adults with 15-24 years of age it
forms 75-10 of cancers with peak incidence age of 49Bleyer A Viny A Barr R Cancer in 15- to 29-year-olds by primary site Oncologist 2006
ndash MTC usually diagnosed after 60
bull Racendash White race gt Black race
Siegel R Ma J Zou Z Jemal A Cancer statistics 2014
PRESENTATIONEVALUATION IN DTC
bull Palpable nodule or cervical node enlargement(solitary nodulecommon prsesntation of DTC)
bull Dysneafixed growthincreasing swelling of nodulevocal cordpalsycervical lap with thyroid nodulestridor neurologicalcompromise
bull Investigaionsbull TSHbull USG NECKbull FNACbull MRIbull NUCLEAR SCANSbull MOLECULAR TESTINGbull CXRAYVOCAL CORD MOBILITY
DEVITA TEXT BOOK OF ONCOLOGY
PATHOLOGICAL CLASSIFICATION OF THYROID CANCERS ON BASIS OF CELL OF ORGIN
)FOLLICULAR EPITHELIAL CELLSbull A-DIFFERENTIATED THYROID CANCERS
1 Papillary and its variants(80-90)bull classicbull papillary microcarcinimabull Encapsulated variantbull Follicular variant bull Aggressive variants(diffuse scleroting tall cell columner cell)2 Follicular cancers (15-30)bull A) classicalbull B) hurthle cell variant bull B-POORLY DIFFERENTIATED THYRIOD CANCERS
1insular carcinomabull C-UNDIFFERENTIATED THYRIOD CANCER(anaplastic))PARA FOLLICULAR CELL ORGINbull A) MCTbull Perez and Bradys text book of radiation oncology
CLASSIFICATION ON BASIS OF ABLITY TO CONCENTRATE RAI
A USUALLY CONCENTRATE RAI
CLASSICAL PAPILLARY CARCINOMA
ENCAPSULATED PC
FOLLICULAR VARIANT
FOLLICULAR CARCINOMA
B FREQUENTLY DO NOT CONCENTRATE RAI
TALL CELLCOLUMNER CALL
HURTHLE CELL
INSULAR CA
C NEVER CONCENTRATE RAI
ANAPLASTIC THYRIOD CA
MEDULLARY CA
Perez and Bradys text book of radiation oncology
0 1084 62 12 14
0
20
40
60
80
100
Surv
iva
l
Stage I
Stage II
Stage III
Stage IV
DTC Initial Disease Stage Predicts OVERALL SURVIVAL
Years
75 of all
tumors
25 of all
tumors
plt0001
Jonklaas J et al Thyroid 2006 16(12) 1229-1242
NCCN and ATA guidelines for the treatment of differentiated thyroid cancer (DTC)
Initial treatmentbull Total thyroidectomy except in patients with unifocal microcarcinoma (individualized
to patient and extent of disease)12
Postoperative treatmentbull Radioactive iodine (131I) (RAI) therapy12
Follow-up treatmentbull Levothyroxine to suppress TSH levels to lt 01mUL12
Recurrent or metastatic disease treatmentbull Local therapy (re-operation external radiation)bull Systemic therapy
ndash RAI therapyndash patients with refractory advanced disease
bull chemotherapy (limited efficacy and considerable toxicity)12
bull participation in clinical trials with small molecule tyrosine kinase inhibitors is recommended12
1 NCCN Clinical Practice Guidelines in Oncology Thyroid Carcinoma V12010 2 Cooper DS et al Thyroid 200991167-214
NCCN = National Comprehensive Cancer Network
ATA = American Thyroid Association
IODINE ISOTOPES
I-131 1-125 I-123
SLIDE
Decays by e-capture with t12of 60 days into lowenergy state Te-125producesauger electrons of50-350 kevLess photon fluxfor scanning andless energy forabilation
Decays by e- captureinto te-123 with t12of 133 hrs sosuitable for 24 hourdiagnostic testhigh photon efluxthan i-131radiation burden tothyriod os lt1 thanby 131
IODINE -131bull Introduced by Seidlin et al in 1946
I-131 decays with a half life of 802 days with betamius and gamma emissions This nuclide of iodinehas 78 neutrons in its nucleus while the only stablenuclide 127I has 74 On decaying 131I most expends itsof decay energy by transforming into thestable 131Xe in two steps with gamma decay(364 kev)following rapidly after beta decay(250- 800kev)131I is available for oral ingestion as sodium iodine
radionucleotide Physical t12 Emax(MEV) LET(kevum) Appx cell diameter
Maximum range in tissue
Iodine-131
Iodine-125
Iodine -123
80 DAYS
601 days
1322 hours
081
035
015
02
4-26
10-230
lt1
20mm
2-500nm
PHYSICAL BIOLOGICAL AND EFFECTIVE HALF LIFE OF I-131
PHYSICAL t12 Biological t12 Effective t12
THYROID TISSUE
EXTRA THYRIOD TISSUE
8 days
8 days
80 days
12 days
73 days
8 hours
GOALS OF RIA IN DIFFERENTIATED CANCERS
bull 1)Thyroid reminant ablation
bull 2)Adjuvant therapy for residual micriscopic disease
bull RAI targets remaining thyroid cancer cells in thyriodbed occult lymph node and distant mets
bull Ablation of remaining thyroid tissue facalitates useof TG as sensitive and specific marker for persistantdisease after primary therapy
bull Rx wbs after RAI ablation provides crutialinformation about prognosis and furthermanagement
bull Sherma SI Lancet 2003
MD anderson experience
bull 1599 patient outcome analysis for various treatment for differentiated thyroid Ca
bull 46 had radioiodine therapybull Treatment with radioiodine was the single most
powerful prognostic indicator for increased DFS (plt 0001)
bull Its use significantly increased the survival both standard and high risk group
bull Adult patients females with intrathyroidal papillary carcinoma treated with TT + RAI between 20-59yrs ndashbest prognosis
bull J Clin Endocrinol Metab 1992 Sep75(3)714-20
bull 1004 dtc- Followed up with
ndash RAI ndash 151
ndash thyroid hormone alone 755
ndash no postoperative medical therapy -98
Tumor recurrence ~ threefold lower p lt 0001in RAI vs other treatment
Fewer patients developed distant metastases (p lt 0002)
Significantly more pronounced in tgt=15cm
Mazzaferri EL et al Thyroid remnant 131I ablation for papillary and follicular thyroid carcinoma Thyroid 1997 Apr7(2)265-71
ATA GUIDELINES
bull Distant metsgross ETE regardless of tumor sizeprimarysize gt4cm even in absence of high risk features
bull Follicular and hurthle cell variants are considered high riskand these patients are always recommended RAI ablationexcept with small unifocal FCs (lt2cm) with capsular invasiononly(no vasular invasion)
bull For 1-4cm size RAI is used for lymph node mets or highrisk features like agegt45 intra thyriod vascularinvasionmultifocal diseaseaggressive variants(tallcellcolummner cell or insular carcinoma)
bull RAI is not used for PTCS lt1cm unifocal and with out highrisk features OR when all foci in multifocal disease is in1cm focus
bull In a study assessing outcomes in 1004 patients with differentiated thyroid carcinoma tumor recurrence was about 3-fold higher in patients either treated with thyroid hormone alone or given no postoperative medical therapy when compared with patients who underwent postoperative thyroid remnant ablation with 131I (P lt 001)
bull Moreover fewer patients developed distant metastases (P lt 002) after thyroid remnant 131I ablation than after other forms of postoperative treatment However this effect is observed only in patients with primary tumors 15 cm or more in diameter Mazzaferri EL Thyroid remnant 131I ablation for papillary andfollicular thyroid carcinoma
low risk group with i-131 abilationStudy showed that remnant ablation had less of a therapeutic effect perhaps because more extensive locoregional surgery had been done Hay ID Papillary thyroid carcinoma Endocrinol Metab Clin North
bull Rising incidence of second cancers in patients with low-risk (T1N0) thyroid cancer who receive radioactive iodine therapy
bull CONCLUSIONS-The increased risk of a SPM in patients with low-risk (T1N0) WDTC along with a lack of data demonstrating improved survival outcomes with adjuvant RAI( IYER NG etal 2013cancer)
bull Impact on overall survival of radioactive iodine in low-risk differentiated thyroid cancer patients
bull CONCLUSION-With a long-term follow-up of 103 yr we failed to prove any survival benefit of RAI after surgery in a large cohort of low-risk DTC patients(SCHTWATZC et alJ Clin Endocrinol Metab 2012 May)
MAJOR FACTORS IMPACTING DECISION MAKING IN RADIOIODINE REMNANT ABLATION
ADMINSTRATION OF I-131
bull As liquid solution or in capsulesbull Each capsule accounts for 50 micro
curiebull Capsules safer than liquid- less
radioactivity released into air during handling
bull Also result in less oral mucosal irritation
bull Simultaneous ingestion large amounts of water attenuates radiation dose emitted to gastric wall
bull Rapidly and completely absorbed in the upper intestine
PATIENT PREPRATIONS1)Low iodine diet(lt50ugday) for 2 wks before and 2 days afterRAI(saltbreat and dairy products to be avoided)it has been seen doublesthe RAI uptake and lower rates of measuarable Tg levels after RAI(SAWAKAEM et al2012THYRIOD)2)Avoid iodinated contast in all DCT patients patient should have delay in RAItherapy for 3-6 months followed by measurement of urinary iodine levels (lt150ugml measured after collecting 24 hour urine and patient should be on iodine freediet gt7 days)3)Stop thyroxine repelacement therapy six weeks before RAI thepapy in case r-TSHis used stop 3-4 days before RAI therapy4)09 mg r-TSH can b used twice (2 days before and one day after) I-131(not to beused in cardiovascular diseasepara tracheal massspinal mets and inchildrenefficacy not studied in children)( studies show equal results with tshreplacement vs r-TSH)TSWNG et AL 1998CANCER5)Lithium carbonate 20mgkgday for 7 days usually 5 days before RAI ablation(measure serum lithium concentration on 4th 5th day of therapy which should be06-12 megml in its narrow theurpatic range)lithium decreases iodine exit fromthyriod cells increasing biological t12 by 50-90 with out interfering with iodineuptakeno studies have shown improved out comes with lithuimContraindicated in psychiatric problemsdementiaseizuresrenal and hepaticinsufficiencydiureticnsaidCCB intakehypohypernatremiahellip
Cancer vs normal cells
bull Metabolism of radioiodine in papillary and follicular carcinoma is profoundly altered when compared with normal thyroid tissue
bull Several defects are present in cancer tissuendash iodine uptake via the sodium-iodide symporter
(NIS) is always decreased and is undetectable in about a third of patients
ndash Iodine organification is markedly reduced
ndash Effective half-life of iodine in tumor tissue is always shorter
bull Tissues that often take up iodine and can be misconstrued as metastases include the
ndash salivary glands in the mouth
ndash esophagus (as a result of swallowing radioactive saliva)
ndash thymus gland
ndash breasts in some women
ndash liver stomach colon bladder
I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

Causes and Risk Factors for thyroid carcinoma
bull Geneticsndash Abnormal RET oncogene may cause MTCndash MEN 2A 2B Syndrome
bull Family Historyndash Gardnerrsquos Syndrome and FAP increase risk for Papillary Ca
bull Radiation Exposurendash Radiation therapy to Head or Neck(010 GyAFTER 5 yrs 2
risk of annual risk of developing ca thyriod) ndash Exposure to Radioactive Iodine during childhood or other
radioactive substances (Chernobyl) uarr risk for particularly Papillary carcinoma
ndash The risk of radiation-induced thyroid carcinoma is greater in females certain Jewish populations and patients with a
family history of thyroid carcinoma
Preston et al2007radia res
Causes and Risk Factors
bull Chronic Iodine deficiency uarr risk for Follicular carcinomaanaplatic ca as well as radiation induced thyriodcancer
Cardis E et al Risk of thyroid cancerj nat cancer
bull Genderndash Female gt Males(2-3X)
bull Agebull More common at young adults with 15-24 years of age it
forms 75-10 of cancers with peak incidence age of 49Bleyer A Viny A Barr R Cancer in 15- to 29-year-olds by primary site Oncologist 2006
ndash MTC usually diagnosed after 60
bull Racendash White race gt Black race
Siegel R Ma J Zou Z Jemal A Cancer statistics 2014
PRESENTATIONEVALUATION IN DTC
bull Palpable nodule or cervical node enlargement(solitary nodulecommon prsesntation of DTC)
bull Dysneafixed growthincreasing swelling of nodulevocal cordpalsycervical lap with thyroid nodulestridor neurologicalcompromise
bull Investigaionsbull TSHbull USG NECKbull FNACbull MRIbull NUCLEAR SCANSbull MOLECULAR TESTINGbull CXRAYVOCAL CORD MOBILITY
DEVITA TEXT BOOK OF ONCOLOGY
PATHOLOGICAL CLASSIFICATION OF THYROID CANCERS ON BASIS OF CELL OF ORGIN
)FOLLICULAR EPITHELIAL CELLSbull A-DIFFERENTIATED THYROID CANCERS
1 Papillary and its variants(80-90)bull classicbull papillary microcarcinimabull Encapsulated variantbull Follicular variant bull Aggressive variants(diffuse scleroting tall cell columner cell)2 Follicular cancers (15-30)bull A) classicalbull B) hurthle cell variant bull B-POORLY DIFFERENTIATED THYRIOD CANCERS
1insular carcinomabull C-UNDIFFERENTIATED THYRIOD CANCER(anaplastic))PARA FOLLICULAR CELL ORGINbull A) MCTbull Perez and Bradys text book of radiation oncology
CLASSIFICATION ON BASIS OF ABLITY TO CONCENTRATE RAI
A USUALLY CONCENTRATE RAI
CLASSICAL PAPILLARY CARCINOMA
ENCAPSULATED PC
FOLLICULAR VARIANT
FOLLICULAR CARCINOMA
B FREQUENTLY DO NOT CONCENTRATE RAI
TALL CELLCOLUMNER CALL
HURTHLE CELL
INSULAR CA
C NEVER CONCENTRATE RAI
ANAPLASTIC THYRIOD CA
MEDULLARY CA
Perez and Bradys text book of radiation oncology
0 1084 62 12 14
0
20
40
60
80
100
Surv
iva
l
Stage I
Stage II
Stage III
Stage IV
DTC Initial Disease Stage Predicts OVERALL SURVIVAL
Years
75 of all
tumors
25 of all
tumors
plt0001
Jonklaas J et al Thyroid 2006 16(12) 1229-1242
NCCN and ATA guidelines for the treatment of differentiated thyroid cancer (DTC)
Initial treatmentbull Total thyroidectomy except in patients with unifocal microcarcinoma (individualized
to patient and extent of disease)12
Postoperative treatmentbull Radioactive iodine (131I) (RAI) therapy12
Follow-up treatmentbull Levothyroxine to suppress TSH levels to lt 01mUL12
Recurrent or metastatic disease treatmentbull Local therapy (re-operation external radiation)bull Systemic therapy
ndash RAI therapyndash patients with refractory advanced disease
bull chemotherapy (limited efficacy and considerable toxicity)12
bull participation in clinical trials with small molecule tyrosine kinase inhibitors is recommended12
1 NCCN Clinical Practice Guidelines in Oncology Thyroid Carcinoma V12010 2 Cooper DS et al Thyroid 200991167-214
NCCN = National Comprehensive Cancer Network
ATA = American Thyroid Association
IODINE ISOTOPES
I-131 1-125 I-123
SLIDE
Decays by e-capture with t12of 60 days into lowenergy state Te-125producesauger electrons of50-350 kevLess photon fluxfor scanning andless energy forabilation
Decays by e- captureinto te-123 with t12of 133 hrs sosuitable for 24 hourdiagnostic testhigh photon efluxthan i-131radiation burden tothyriod os lt1 thanby 131
IODINE -131bull Introduced by Seidlin et al in 1946
I-131 decays with a half life of 802 days with betamius and gamma emissions This nuclide of iodinehas 78 neutrons in its nucleus while the only stablenuclide 127I has 74 On decaying 131I most expends itsof decay energy by transforming into thestable 131Xe in two steps with gamma decay(364 kev)following rapidly after beta decay(250- 800kev)131I is available for oral ingestion as sodium iodine
radionucleotide Physical t12 Emax(MEV) LET(kevum) Appx cell diameter
Maximum range in tissue
Iodine-131
Iodine-125
Iodine -123
80 DAYS
601 days
1322 hours
081
035
015
02
4-26
10-230
lt1
20mm
2-500nm
PHYSICAL BIOLOGICAL AND EFFECTIVE HALF LIFE OF I-131
PHYSICAL t12 Biological t12 Effective t12
THYROID TISSUE
EXTRA THYRIOD TISSUE
8 days
8 days
80 days
12 days
73 days
8 hours
GOALS OF RIA IN DIFFERENTIATED CANCERS
bull 1)Thyroid reminant ablation
bull 2)Adjuvant therapy for residual micriscopic disease
bull RAI targets remaining thyroid cancer cells in thyriodbed occult lymph node and distant mets
bull Ablation of remaining thyroid tissue facalitates useof TG as sensitive and specific marker for persistantdisease after primary therapy
bull Rx wbs after RAI ablation provides crutialinformation about prognosis and furthermanagement
bull Sherma SI Lancet 2003
MD anderson experience
bull 1599 patient outcome analysis for various treatment for differentiated thyroid Ca
bull 46 had radioiodine therapybull Treatment with radioiodine was the single most
powerful prognostic indicator for increased DFS (plt 0001)
bull Its use significantly increased the survival both standard and high risk group
bull Adult patients females with intrathyroidal papillary carcinoma treated with TT + RAI between 20-59yrs ndashbest prognosis
bull J Clin Endocrinol Metab 1992 Sep75(3)714-20
bull 1004 dtc- Followed up with
ndash RAI ndash 151
ndash thyroid hormone alone 755
ndash no postoperative medical therapy -98
Tumor recurrence ~ threefold lower p lt 0001in RAI vs other treatment
Fewer patients developed distant metastases (p lt 0002)
Significantly more pronounced in tgt=15cm
Mazzaferri EL et al Thyroid remnant 131I ablation for papillary and follicular thyroid carcinoma Thyroid 1997 Apr7(2)265-71
ATA GUIDELINES
bull Distant metsgross ETE regardless of tumor sizeprimarysize gt4cm even in absence of high risk features
bull Follicular and hurthle cell variants are considered high riskand these patients are always recommended RAI ablationexcept with small unifocal FCs (lt2cm) with capsular invasiononly(no vasular invasion)
bull For 1-4cm size RAI is used for lymph node mets or highrisk features like agegt45 intra thyriod vascularinvasionmultifocal diseaseaggressive variants(tallcellcolummner cell or insular carcinoma)
bull RAI is not used for PTCS lt1cm unifocal and with out highrisk features OR when all foci in multifocal disease is in1cm focus
bull In a study assessing outcomes in 1004 patients with differentiated thyroid carcinoma tumor recurrence was about 3-fold higher in patients either treated with thyroid hormone alone or given no postoperative medical therapy when compared with patients who underwent postoperative thyroid remnant ablation with 131I (P lt 001)
bull Moreover fewer patients developed distant metastases (P lt 002) after thyroid remnant 131I ablation than after other forms of postoperative treatment However this effect is observed only in patients with primary tumors 15 cm or more in diameter Mazzaferri EL Thyroid remnant 131I ablation for papillary andfollicular thyroid carcinoma
low risk group with i-131 abilationStudy showed that remnant ablation had less of a therapeutic effect perhaps because more extensive locoregional surgery had been done Hay ID Papillary thyroid carcinoma Endocrinol Metab Clin North
bull Rising incidence of second cancers in patients with low-risk (T1N0) thyroid cancer who receive radioactive iodine therapy
bull CONCLUSIONS-The increased risk of a SPM in patients with low-risk (T1N0) WDTC along with a lack of data demonstrating improved survival outcomes with adjuvant RAI( IYER NG etal 2013cancer)
bull Impact on overall survival of radioactive iodine in low-risk differentiated thyroid cancer patients
bull CONCLUSION-With a long-term follow-up of 103 yr we failed to prove any survival benefit of RAI after surgery in a large cohort of low-risk DTC patients(SCHTWATZC et alJ Clin Endocrinol Metab 2012 May)
MAJOR FACTORS IMPACTING DECISION MAKING IN RADIOIODINE REMNANT ABLATION
ADMINSTRATION OF I-131
bull As liquid solution or in capsulesbull Each capsule accounts for 50 micro
curiebull Capsules safer than liquid- less
radioactivity released into air during handling
bull Also result in less oral mucosal irritation
bull Simultaneous ingestion large amounts of water attenuates radiation dose emitted to gastric wall
bull Rapidly and completely absorbed in the upper intestine
PATIENT PREPRATIONS1)Low iodine diet(lt50ugday) for 2 wks before and 2 days afterRAI(saltbreat and dairy products to be avoided)it has been seen doublesthe RAI uptake and lower rates of measuarable Tg levels after RAI(SAWAKAEM et al2012THYRIOD)2)Avoid iodinated contast in all DCT patients patient should have delay in RAItherapy for 3-6 months followed by measurement of urinary iodine levels (lt150ugml measured after collecting 24 hour urine and patient should be on iodine freediet gt7 days)3)Stop thyroxine repelacement therapy six weeks before RAI thepapy in case r-TSHis used stop 3-4 days before RAI therapy4)09 mg r-TSH can b used twice (2 days before and one day after) I-131(not to beused in cardiovascular diseasepara tracheal massspinal mets and inchildrenefficacy not studied in children)( studies show equal results with tshreplacement vs r-TSH)TSWNG et AL 1998CANCER5)Lithium carbonate 20mgkgday for 7 days usually 5 days before RAI ablation(measure serum lithium concentration on 4th 5th day of therapy which should be06-12 megml in its narrow theurpatic range)lithium decreases iodine exit fromthyriod cells increasing biological t12 by 50-90 with out interfering with iodineuptakeno studies have shown improved out comes with lithuimContraindicated in psychiatric problemsdementiaseizuresrenal and hepaticinsufficiencydiureticnsaidCCB intakehypohypernatremiahellip
Cancer vs normal cells
bull Metabolism of radioiodine in papillary and follicular carcinoma is profoundly altered when compared with normal thyroid tissue
bull Several defects are present in cancer tissuendash iodine uptake via the sodium-iodide symporter
(NIS) is always decreased and is undetectable in about a third of patients
ndash Iodine organification is markedly reduced
ndash Effective half-life of iodine in tumor tissue is always shorter
bull Tissues that often take up iodine and can be misconstrued as metastases include the
ndash salivary glands in the mouth
ndash esophagus (as a result of swallowing radioactive saliva)
ndash thymus gland
ndash breasts in some women
ndash liver stomach colon bladder
I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

Causes and Risk Factors
bull Chronic Iodine deficiency uarr risk for Follicular carcinomaanaplatic ca as well as radiation induced thyriodcancer
Cardis E et al Risk of thyroid cancerj nat cancer
bull Genderndash Female gt Males(2-3X)
bull Agebull More common at young adults with 15-24 years of age it
forms 75-10 of cancers with peak incidence age of 49Bleyer A Viny A Barr R Cancer in 15- to 29-year-olds by primary site Oncologist 2006
ndash MTC usually diagnosed after 60
bull Racendash White race gt Black race
Siegel R Ma J Zou Z Jemal A Cancer statistics 2014
PRESENTATIONEVALUATION IN DTC
bull Palpable nodule or cervical node enlargement(solitary nodulecommon prsesntation of DTC)
bull Dysneafixed growthincreasing swelling of nodulevocal cordpalsycervical lap with thyroid nodulestridor neurologicalcompromise
bull Investigaionsbull TSHbull USG NECKbull FNACbull MRIbull NUCLEAR SCANSbull MOLECULAR TESTINGbull CXRAYVOCAL CORD MOBILITY
DEVITA TEXT BOOK OF ONCOLOGY
PATHOLOGICAL CLASSIFICATION OF THYROID CANCERS ON BASIS OF CELL OF ORGIN
)FOLLICULAR EPITHELIAL CELLSbull A-DIFFERENTIATED THYROID CANCERS
1 Papillary and its variants(80-90)bull classicbull papillary microcarcinimabull Encapsulated variantbull Follicular variant bull Aggressive variants(diffuse scleroting tall cell columner cell)2 Follicular cancers (15-30)bull A) classicalbull B) hurthle cell variant bull B-POORLY DIFFERENTIATED THYRIOD CANCERS
1insular carcinomabull C-UNDIFFERENTIATED THYRIOD CANCER(anaplastic))PARA FOLLICULAR CELL ORGINbull A) MCTbull Perez and Bradys text book of radiation oncology
CLASSIFICATION ON BASIS OF ABLITY TO CONCENTRATE RAI
A USUALLY CONCENTRATE RAI
CLASSICAL PAPILLARY CARCINOMA
ENCAPSULATED PC
FOLLICULAR VARIANT
FOLLICULAR CARCINOMA
B FREQUENTLY DO NOT CONCENTRATE RAI
TALL CELLCOLUMNER CALL
HURTHLE CELL
INSULAR CA
C NEVER CONCENTRATE RAI
ANAPLASTIC THYRIOD CA
MEDULLARY CA
Perez and Bradys text book of radiation oncology
0 1084 62 12 14
0
20
40
60
80
100
Surv
iva
l
Stage I
Stage II
Stage III
Stage IV
DTC Initial Disease Stage Predicts OVERALL SURVIVAL
Years
75 of all
tumors
25 of all
tumors
plt0001
Jonklaas J et al Thyroid 2006 16(12) 1229-1242
NCCN and ATA guidelines for the treatment of differentiated thyroid cancer (DTC)
Initial treatmentbull Total thyroidectomy except in patients with unifocal microcarcinoma (individualized
to patient and extent of disease)12
Postoperative treatmentbull Radioactive iodine (131I) (RAI) therapy12
Follow-up treatmentbull Levothyroxine to suppress TSH levels to lt 01mUL12
Recurrent or metastatic disease treatmentbull Local therapy (re-operation external radiation)bull Systemic therapy
ndash RAI therapyndash patients with refractory advanced disease
bull chemotherapy (limited efficacy and considerable toxicity)12
bull participation in clinical trials with small molecule tyrosine kinase inhibitors is recommended12
1 NCCN Clinical Practice Guidelines in Oncology Thyroid Carcinoma V12010 2 Cooper DS et al Thyroid 200991167-214
NCCN = National Comprehensive Cancer Network
ATA = American Thyroid Association
IODINE ISOTOPES
I-131 1-125 I-123
SLIDE
Decays by e-capture with t12of 60 days into lowenergy state Te-125producesauger electrons of50-350 kevLess photon fluxfor scanning andless energy forabilation
Decays by e- captureinto te-123 with t12of 133 hrs sosuitable for 24 hourdiagnostic testhigh photon efluxthan i-131radiation burden tothyriod os lt1 thanby 131
IODINE -131bull Introduced by Seidlin et al in 1946
I-131 decays with a half life of 802 days with betamius and gamma emissions This nuclide of iodinehas 78 neutrons in its nucleus while the only stablenuclide 127I has 74 On decaying 131I most expends itsof decay energy by transforming into thestable 131Xe in two steps with gamma decay(364 kev)following rapidly after beta decay(250- 800kev)131I is available for oral ingestion as sodium iodine
radionucleotide Physical t12 Emax(MEV) LET(kevum) Appx cell diameter
Maximum range in tissue
Iodine-131
Iodine-125
Iodine -123
80 DAYS
601 days
1322 hours
081
035
015
02
4-26
10-230
lt1
20mm
2-500nm
PHYSICAL BIOLOGICAL AND EFFECTIVE HALF LIFE OF I-131
PHYSICAL t12 Biological t12 Effective t12
THYROID TISSUE
EXTRA THYRIOD TISSUE
8 days
8 days
80 days
12 days
73 days
8 hours
GOALS OF RIA IN DIFFERENTIATED CANCERS
bull 1)Thyroid reminant ablation
bull 2)Adjuvant therapy for residual micriscopic disease
bull RAI targets remaining thyroid cancer cells in thyriodbed occult lymph node and distant mets
bull Ablation of remaining thyroid tissue facalitates useof TG as sensitive and specific marker for persistantdisease after primary therapy
bull Rx wbs after RAI ablation provides crutialinformation about prognosis and furthermanagement
bull Sherma SI Lancet 2003
MD anderson experience
bull 1599 patient outcome analysis for various treatment for differentiated thyroid Ca
bull 46 had radioiodine therapybull Treatment with radioiodine was the single most
powerful prognostic indicator for increased DFS (plt 0001)
bull Its use significantly increased the survival both standard and high risk group
bull Adult patients females with intrathyroidal papillary carcinoma treated with TT + RAI between 20-59yrs ndashbest prognosis
bull J Clin Endocrinol Metab 1992 Sep75(3)714-20
bull 1004 dtc- Followed up with
ndash RAI ndash 151
ndash thyroid hormone alone 755
ndash no postoperative medical therapy -98
Tumor recurrence ~ threefold lower p lt 0001in RAI vs other treatment
Fewer patients developed distant metastases (p lt 0002)
Significantly more pronounced in tgt=15cm
Mazzaferri EL et al Thyroid remnant 131I ablation for papillary and follicular thyroid carcinoma Thyroid 1997 Apr7(2)265-71
ATA GUIDELINES
bull Distant metsgross ETE regardless of tumor sizeprimarysize gt4cm even in absence of high risk features
bull Follicular and hurthle cell variants are considered high riskand these patients are always recommended RAI ablationexcept with small unifocal FCs (lt2cm) with capsular invasiononly(no vasular invasion)
bull For 1-4cm size RAI is used for lymph node mets or highrisk features like agegt45 intra thyriod vascularinvasionmultifocal diseaseaggressive variants(tallcellcolummner cell or insular carcinoma)
bull RAI is not used for PTCS lt1cm unifocal and with out highrisk features OR when all foci in multifocal disease is in1cm focus
bull In a study assessing outcomes in 1004 patients with differentiated thyroid carcinoma tumor recurrence was about 3-fold higher in patients either treated with thyroid hormone alone or given no postoperative medical therapy when compared with patients who underwent postoperative thyroid remnant ablation with 131I (P lt 001)
bull Moreover fewer patients developed distant metastases (P lt 002) after thyroid remnant 131I ablation than after other forms of postoperative treatment However this effect is observed only in patients with primary tumors 15 cm or more in diameter Mazzaferri EL Thyroid remnant 131I ablation for papillary andfollicular thyroid carcinoma
low risk group with i-131 abilationStudy showed that remnant ablation had less of a therapeutic effect perhaps because more extensive locoregional surgery had been done Hay ID Papillary thyroid carcinoma Endocrinol Metab Clin North
bull Rising incidence of second cancers in patients with low-risk (T1N0) thyroid cancer who receive radioactive iodine therapy
bull CONCLUSIONS-The increased risk of a SPM in patients with low-risk (T1N0) WDTC along with a lack of data demonstrating improved survival outcomes with adjuvant RAI( IYER NG etal 2013cancer)
bull Impact on overall survival of radioactive iodine in low-risk differentiated thyroid cancer patients
bull CONCLUSION-With a long-term follow-up of 103 yr we failed to prove any survival benefit of RAI after surgery in a large cohort of low-risk DTC patients(SCHTWATZC et alJ Clin Endocrinol Metab 2012 May)
MAJOR FACTORS IMPACTING DECISION MAKING IN RADIOIODINE REMNANT ABLATION
ADMINSTRATION OF I-131
bull As liquid solution or in capsulesbull Each capsule accounts for 50 micro
curiebull Capsules safer than liquid- less
radioactivity released into air during handling
bull Also result in less oral mucosal irritation
bull Simultaneous ingestion large amounts of water attenuates radiation dose emitted to gastric wall
bull Rapidly and completely absorbed in the upper intestine
PATIENT PREPRATIONS1)Low iodine diet(lt50ugday) for 2 wks before and 2 days afterRAI(saltbreat and dairy products to be avoided)it has been seen doublesthe RAI uptake and lower rates of measuarable Tg levels after RAI(SAWAKAEM et al2012THYRIOD)2)Avoid iodinated contast in all DCT patients patient should have delay in RAItherapy for 3-6 months followed by measurement of urinary iodine levels (lt150ugml measured after collecting 24 hour urine and patient should be on iodine freediet gt7 days)3)Stop thyroxine repelacement therapy six weeks before RAI thepapy in case r-TSHis used stop 3-4 days before RAI therapy4)09 mg r-TSH can b used twice (2 days before and one day after) I-131(not to beused in cardiovascular diseasepara tracheal massspinal mets and inchildrenefficacy not studied in children)( studies show equal results with tshreplacement vs r-TSH)TSWNG et AL 1998CANCER5)Lithium carbonate 20mgkgday for 7 days usually 5 days before RAI ablation(measure serum lithium concentration on 4th 5th day of therapy which should be06-12 megml in its narrow theurpatic range)lithium decreases iodine exit fromthyriod cells increasing biological t12 by 50-90 with out interfering with iodineuptakeno studies have shown improved out comes with lithuimContraindicated in psychiatric problemsdementiaseizuresrenal and hepaticinsufficiencydiureticnsaidCCB intakehypohypernatremiahellip
Cancer vs normal cells
bull Metabolism of radioiodine in papillary and follicular carcinoma is profoundly altered when compared with normal thyroid tissue
bull Several defects are present in cancer tissuendash iodine uptake via the sodium-iodide symporter
(NIS) is always decreased and is undetectable in about a third of patients
ndash Iodine organification is markedly reduced
ndash Effective half-life of iodine in tumor tissue is always shorter
bull Tissues that often take up iodine and can be misconstrued as metastases include the
ndash salivary glands in the mouth
ndash esophagus (as a result of swallowing radioactive saliva)
ndash thymus gland
ndash breasts in some women
ndash liver stomach colon bladder
I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

PRESENTATIONEVALUATION IN DTC
bull Palpable nodule or cervical node enlargement(solitary nodulecommon prsesntation of DTC)
bull Dysneafixed growthincreasing swelling of nodulevocal cordpalsycervical lap with thyroid nodulestridor neurologicalcompromise
bull Investigaionsbull TSHbull USG NECKbull FNACbull MRIbull NUCLEAR SCANSbull MOLECULAR TESTINGbull CXRAYVOCAL CORD MOBILITY
DEVITA TEXT BOOK OF ONCOLOGY
PATHOLOGICAL CLASSIFICATION OF THYROID CANCERS ON BASIS OF CELL OF ORGIN
)FOLLICULAR EPITHELIAL CELLSbull A-DIFFERENTIATED THYROID CANCERS
1 Papillary and its variants(80-90)bull classicbull papillary microcarcinimabull Encapsulated variantbull Follicular variant bull Aggressive variants(diffuse scleroting tall cell columner cell)2 Follicular cancers (15-30)bull A) classicalbull B) hurthle cell variant bull B-POORLY DIFFERENTIATED THYRIOD CANCERS
1insular carcinomabull C-UNDIFFERENTIATED THYRIOD CANCER(anaplastic))PARA FOLLICULAR CELL ORGINbull A) MCTbull Perez and Bradys text book of radiation oncology
CLASSIFICATION ON BASIS OF ABLITY TO CONCENTRATE RAI
A USUALLY CONCENTRATE RAI
CLASSICAL PAPILLARY CARCINOMA
ENCAPSULATED PC
FOLLICULAR VARIANT
FOLLICULAR CARCINOMA
B FREQUENTLY DO NOT CONCENTRATE RAI
TALL CELLCOLUMNER CALL
HURTHLE CELL
INSULAR CA
C NEVER CONCENTRATE RAI
ANAPLASTIC THYRIOD CA
MEDULLARY CA
Perez and Bradys text book of radiation oncology
0 1084 62 12 14
0
20
40
60
80
100
Surv
iva
l
Stage I
Stage II
Stage III
Stage IV
DTC Initial Disease Stage Predicts OVERALL SURVIVAL
Years
75 of all
tumors
25 of all
tumors
plt0001
Jonklaas J et al Thyroid 2006 16(12) 1229-1242
NCCN and ATA guidelines for the treatment of differentiated thyroid cancer (DTC)
Initial treatmentbull Total thyroidectomy except in patients with unifocal microcarcinoma (individualized
to patient and extent of disease)12
Postoperative treatmentbull Radioactive iodine (131I) (RAI) therapy12
Follow-up treatmentbull Levothyroxine to suppress TSH levels to lt 01mUL12
Recurrent or metastatic disease treatmentbull Local therapy (re-operation external radiation)bull Systemic therapy
ndash RAI therapyndash patients with refractory advanced disease
bull chemotherapy (limited efficacy and considerable toxicity)12
bull participation in clinical trials with small molecule tyrosine kinase inhibitors is recommended12
1 NCCN Clinical Practice Guidelines in Oncology Thyroid Carcinoma V12010 2 Cooper DS et al Thyroid 200991167-214
NCCN = National Comprehensive Cancer Network
ATA = American Thyroid Association
IODINE ISOTOPES
I-131 1-125 I-123
SLIDE
Decays by e-capture with t12of 60 days into lowenergy state Te-125producesauger electrons of50-350 kevLess photon fluxfor scanning andless energy forabilation
Decays by e- captureinto te-123 with t12of 133 hrs sosuitable for 24 hourdiagnostic testhigh photon efluxthan i-131radiation burden tothyriod os lt1 thanby 131
IODINE -131bull Introduced by Seidlin et al in 1946
I-131 decays with a half life of 802 days with betamius and gamma emissions This nuclide of iodinehas 78 neutrons in its nucleus while the only stablenuclide 127I has 74 On decaying 131I most expends itsof decay energy by transforming into thestable 131Xe in two steps with gamma decay(364 kev)following rapidly after beta decay(250- 800kev)131I is available for oral ingestion as sodium iodine
radionucleotide Physical t12 Emax(MEV) LET(kevum) Appx cell diameter
Maximum range in tissue
Iodine-131
Iodine-125
Iodine -123
80 DAYS
601 days
1322 hours
081
035
015
02
4-26
10-230
lt1
20mm
2-500nm
PHYSICAL BIOLOGICAL AND EFFECTIVE HALF LIFE OF I-131
PHYSICAL t12 Biological t12 Effective t12
THYROID TISSUE
EXTRA THYRIOD TISSUE
8 days
8 days
80 days
12 days
73 days
8 hours
GOALS OF RIA IN DIFFERENTIATED CANCERS
bull 1)Thyroid reminant ablation
bull 2)Adjuvant therapy for residual micriscopic disease
bull RAI targets remaining thyroid cancer cells in thyriodbed occult lymph node and distant mets
bull Ablation of remaining thyroid tissue facalitates useof TG as sensitive and specific marker for persistantdisease after primary therapy
bull Rx wbs after RAI ablation provides crutialinformation about prognosis and furthermanagement
bull Sherma SI Lancet 2003
MD anderson experience
bull 1599 patient outcome analysis for various treatment for differentiated thyroid Ca
bull 46 had radioiodine therapybull Treatment with radioiodine was the single most
powerful prognostic indicator for increased DFS (plt 0001)
bull Its use significantly increased the survival both standard and high risk group
bull Adult patients females with intrathyroidal papillary carcinoma treated with TT + RAI between 20-59yrs ndashbest prognosis
bull J Clin Endocrinol Metab 1992 Sep75(3)714-20
bull 1004 dtc- Followed up with
ndash RAI ndash 151
ndash thyroid hormone alone 755
ndash no postoperative medical therapy -98
Tumor recurrence ~ threefold lower p lt 0001in RAI vs other treatment
Fewer patients developed distant metastases (p lt 0002)
Significantly more pronounced in tgt=15cm
Mazzaferri EL et al Thyroid remnant 131I ablation for papillary and follicular thyroid carcinoma Thyroid 1997 Apr7(2)265-71
ATA GUIDELINES
bull Distant metsgross ETE regardless of tumor sizeprimarysize gt4cm even in absence of high risk features
bull Follicular and hurthle cell variants are considered high riskand these patients are always recommended RAI ablationexcept with small unifocal FCs (lt2cm) with capsular invasiononly(no vasular invasion)
bull For 1-4cm size RAI is used for lymph node mets or highrisk features like agegt45 intra thyriod vascularinvasionmultifocal diseaseaggressive variants(tallcellcolummner cell or insular carcinoma)
bull RAI is not used for PTCS lt1cm unifocal and with out highrisk features OR when all foci in multifocal disease is in1cm focus
bull In a study assessing outcomes in 1004 patients with differentiated thyroid carcinoma tumor recurrence was about 3-fold higher in patients either treated with thyroid hormone alone or given no postoperative medical therapy when compared with patients who underwent postoperative thyroid remnant ablation with 131I (P lt 001)
bull Moreover fewer patients developed distant metastases (P lt 002) after thyroid remnant 131I ablation than after other forms of postoperative treatment However this effect is observed only in patients with primary tumors 15 cm or more in diameter Mazzaferri EL Thyroid remnant 131I ablation for papillary andfollicular thyroid carcinoma
low risk group with i-131 abilationStudy showed that remnant ablation had less of a therapeutic effect perhaps because more extensive locoregional surgery had been done Hay ID Papillary thyroid carcinoma Endocrinol Metab Clin North
bull Rising incidence of second cancers in patients with low-risk (T1N0) thyroid cancer who receive radioactive iodine therapy
bull CONCLUSIONS-The increased risk of a SPM in patients with low-risk (T1N0) WDTC along with a lack of data demonstrating improved survival outcomes with adjuvant RAI( IYER NG etal 2013cancer)
bull Impact on overall survival of radioactive iodine in low-risk differentiated thyroid cancer patients
bull CONCLUSION-With a long-term follow-up of 103 yr we failed to prove any survival benefit of RAI after surgery in a large cohort of low-risk DTC patients(SCHTWATZC et alJ Clin Endocrinol Metab 2012 May)
MAJOR FACTORS IMPACTING DECISION MAKING IN RADIOIODINE REMNANT ABLATION
ADMINSTRATION OF I-131
bull As liquid solution or in capsulesbull Each capsule accounts for 50 micro
curiebull Capsules safer than liquid- less
radioactivity released into air during handling
bull Also result in less oral mucosal irritation
bull Simultaneous ingestion large amounts of water attenuates radiation dose emitted to gastric wall
bull Rapidly and completely absorbed in the upper intestine
PATIENT PREPRATIONS1)Low iodine diet(lt50ugday) for 2 wks before and 2 days afterRAI(saltbreat and dairy products to be avoided)it has been seen doublesthe RAI uptake and lower rates of measuarable Tg levels after RAI(SAWAKAEM et al2012THYRIOD)2)Avoid iodinated contast in all DCT patients patient should have delay in RAItherapy for 3-6 months followed by measurement of urinary iodine levels (lt150ugml measured after collecting 24 hour urine and patient should be on iodine freediet gt7 days)3)Stop thyroxine repelacement therapy six weeks before RAI thepapy in case r-TSHis used stop 3-4 days before RAI therapy4)09 mg r-TSH can b used twice (2 days before and one day after) I-131(not to beused in cardiovascular diseasepara tracheal massspinal mets and inchildrenefficacy not studied in children)( studies show equal results with tshreplacement vs r-TSH)TSWNG et AL 1998CANCER5)Lithium carbonate 20mgkgday for 7 days usually 5 days before RAI ablation(measure serum lithium concentration on 4th 5th day of therapy which should be06-12 megml in its narrow theurpatic range)lithium decreases iodine exit fromthyriod cells increasing biological t12 by 50-90 with out interfering with iodineuptakeno studies have shown improved out comes with lithuimContraindicated in psychiatric problemsdementiaseizuresrenal and hepaticinsufficiencydiureticnsaidCCB intakehypohypernatremiahellip
Cancer vs normal cells
bull Metabolism of radioiodine in papillary and follicular carcinoma is profoundly altered when compared with normal thyroid tissue
bull Several defects are present in cancer tissuendash iodine uptake via the sodium-iodide symporter
(NIS) is always decreased and is undetectable in about a third of patients
ndash Iodine organification is markedly reduced
ndash Effective half-life of iodine in tumor tissue is always shorter
bull Tissues that often take up iodine and can be misconstrued as metastases include the
ndash salivary glands in the mouth
ndash esophagus (as a result of swallowing radioactive saliva)
ndash thymus gland
ndash breasts in some women
ndash liver stomach colon bladder
I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU
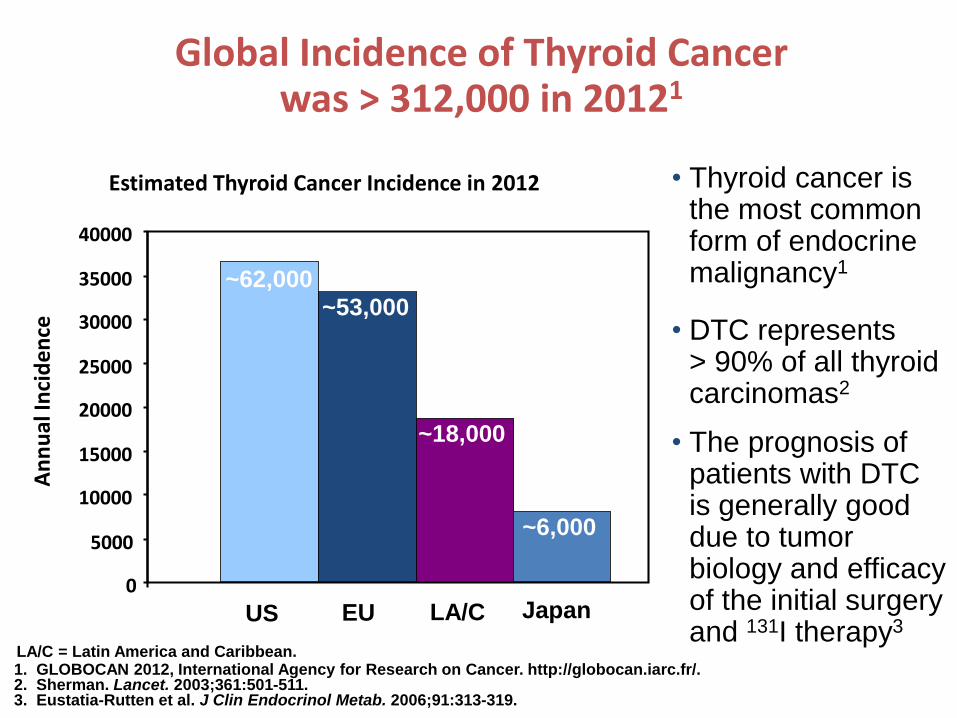
DEVITA TEXT BOOK OF ONCOLOGY
PATHOLOGICAL CLASSIFICATION OF THYROID CANCERS ON BASIS OF CELL OF ORGIN
)FOLLICULAR EPITHELIAL CELLSbull A-DIFFERENTIATED THYROID CANCERS
1 Papillary and its variants(80-90)bull classicbull papillary microcarcinimabull Encapsulated variantbull Follicular variant bull Aggressive variants(diffuse scleroting tall cell columner cell)2 Follicular cancers (15-30)bull A) classicalbull B) hurthle cell variant bull B-POORLY DIFFERENTIATED THYRIOD CANCERS
1insular carcinomabull C-UNDIFFERENTIATED THYRIOD CANCER(anaplastic))PARA FOLLICULAR CELL ORGINbull A) MCTbull Perez and Bradys text book of radiation oncology
CLASSIFICATION ON BASIS OF ABLITY TO CONCENTRATE RAI
A USUALLY CONCENTRATE RAI
CLASSICAL PAPILLARY CARCINOMA
ENCAPSULATED PC
FOLLICULAR VARIANT
FOLLICULAR CARCINOMA
B FREQUENTLY DO NOT CONCENTRATE RAI
TALL CELLCOLUMNER CALL
HURTHLE CELL
INSULAR CA
C NEVER CONCENTRATE RAI
ANAPLASTIC THYRIOD CA
MEDULLARY CA
Perez and Bradys text book of radiation oncology
0 1084 62 12 14
0
20
40
60
80
100
Surv
iva
l
Stage I
Stage II
Stage III
Stage IV
DTC Initial Disease Stage Predicts OVERALL SURVIVAL
Years
75 of all
tumors
25 of all
tumors
plt0001
Jonklaas J et al Thyroid 2006 16(12) 1229-1242
NCCN and ATA guidelines for the treatment of differentiated thyroid cancer (DTC)
Initial treatmentbull Total thyroidectomy except in patients with unifocal microcarcinoma (individualized
to patient and extent of disease)12
Postoperative treatmentbull Radioactive iodine (131I) (RAI) therapy12
Follow-up treatmentbull Levothyroxine to suppress TSH levels to lt 01mUL12
Recurrent or metastatic disease treatmentbull Local therapy (re-operation external radiation)bull Systemic therapy
ndash RAI therapyndash patients with refractory advanced disease
bull chemotherapy (limited efficacy and considerable toxicity)12
bull participation in clinical trials with small molecule tyrosine kinase inhibitors is recommended12
1 NCCN Clinical Practice Guidelines in Oncology Thyroid Carcinoma V12010 2 Cooper DS et al Thyroid 200991167-214
NCCN = National Comprehensive Cancer Network
ATA = American Thyroid Association
IODINE ISOTOPES
I-131 1-125 I-123
SLIDE
Decays by e-capture with t12of 60 days into lowenergy state Te-125producesauger electrons of50-350 kevLess photon fluxfor scanning andless energy forabilation
Decays by e- captureinto te-123 with t12of 133 hrs sosuitable for 24 hourdiagnostic testhigh photon efluxthan i-131radiation burden tothyriod os lt1 thanby 131
IODINE -131bull Introduced by Seidlin et al in 1946
I-131 decays with a half life of 802 days with betamius and gamma emissions This nuclide of iodinehas 78 neutrons in its nucleus while the only stablenuclide 127I has 74 On decaying 131I most expends itsof decay energy by transforming into thestable 131Xe in two steps with gamma decay(364 kev)following rapidly after beta decay(250- 800kev)131I is available for oral ingestion as sodium iodine
radionucleotide Physical t12 Emax(MEV) LET(kevum) Appx cell diameter
Maximum range in tissue
Iodine-131
Iodine-125
Iodine -123
80 DAYS
601 days
1322 hours
081
035
015
02
4-26
10-230
lt1
20mm
2-500nm
PHYSICAL BIOLOGICAL AND EFFECTIVE HALF LIFE OF I-131
PHYSICAL t12 Biological t12 Effective t12
THYROID TISSUE
EXTRA THYRIOD TISSUE
8 days
8 days
80 days
12 days
73 days
8 hours
GOALS OF RIA IN DIFFERENTIATED CANCERS
bull 1)Thyroid reminant ablation
bull 2)Adjuvant therapy for residual micriscopic disease
bull RAI targets remaining thyroid cancer cells in thyriodbed occult lymph node and distant mets
bull Ablation of remaining thyroid tissue facalitates useof TG as sensitive and specific marker for persistantdisease after primary therapy
bull Rx wbs after RAI ablation provides crutialinformation about prognosis and furthermanagement
bull Sherma SI Lancet 2003
MD anderson experience
bull 1599 patient outcome analysis for various treatment for differentiated thyroid Ca
bull 46 had radioiodine therapybull Treatment with radioiodine was the single most
powerful prognostic indicator for increased DFS (plt 0001)
bull Its use significantly increased the survival both standard and high risk group
bull Adult patients females with intrathyroidal papillary carcinoma treated with TT + RAI between 20-59yrs ndashbest prognosis
bull J Clin Endocrinol Metab 1992 Sep75(3)714-20
bull 1004 dtc- Followed up with
ndash RAI ndash 151
ndash thyroid hormone alone 755
ndash no postoperative medical therapy -98
Tumor recurrence ~ threefold lower p lt 0001in RAI vs other treatment
Fewer patients developed distant metastases (p lt 0002)
Significantly more pronounced in tgt=15cm
Mazzaferri EL et al Thyroid remnant 131I ablation for papillary and follicular thyroid carcinoma Thyroid 1997 Apr7(2)265-71
ATA GUIDELINES
bull Distant metsgross ETE regardless of tumor sizeprimarysize gt4cm even in absence of high risk features
bull Follicular and hurthle cell variants are considered high riskand these patients are always recommended RAI ablationexcept with small unifocal FCs (lt2cm) with capsular invasiononly(no vasular invasion)
bull For 1-4cm size RAI is used for lymph node mets or highrisk features like agegt45 intra thyriod vascularinvasionmultifocal diseaseaggressive variants(tallcellcolummner cell or insular carcinoma)
bull RAI is not used for PTCS lt1cm unifocal and with out highrisk features OR when all foci in multifocal disease is in1cm focus
bull In a study assessing outcomes in 1004 patients with differentiated thyroid carcinoma tumor recurrence was about 3-fold higher in patients either treated with thyroid hormone alone or given no postoperative medical therapy when compared with patients who underwent postoperative thyroid remnant ablation with 131I (P lt 001)
bull Moreover fewer patients developed distant metastases (P lt 002) after thyroid remnant 131I ablation than after other forms of postoperative treatment However this effect is observed only in patients with primary tumors 15 cm or more in diameter Mazzaferri EL Thyroid remnant 131I ablation for papillary andfollicular thyroid carcinoma
low risk group with i-131 abilationStudy showed that remnant ablation had less of a therapeutic effect perhaps because more extensive locoregional surgery had been done Hay ID Papillary thyroid carcinoma Endocrinol Metab Clin North
bull Rising incidence of second cancers in patients with low-risk (T1N0) thyroid cancer who receive radioactive iodine therapy
bull CONCLUSIONS-The increased risk of a SPM in patients with low-risk (T1N0) WDTC along with a lack of data demonstrating improved survival outcomes with adjuvant RAI( IYER NG etal 2013cancer)
bull Impact on overall survival of radioactive iodine in low-risk differentiated thyroid cancer patients
bull CONCLUSION-With a long-term follow-up of 103 yr we failed to prove any survival benefit of RAI after surgery in a large cohort of low-risk DTC patients(SCHTWATZC et alJ Clin Endocrinol Metab 2012 May)
MAJOR FACTORS IMPACTING DECISION MAKING IN RADIOIODINE REMNANT ABLATION
ADMINSTRATION OF I-131
bull As liquid solution or in capsulesbull Each capsule accounts for 50 micro
curiebull Capsules safer than liquid- less
radioactivity released into air during handling
bull Also result in less oral mucosal irritation
bull Simultaneous ingestion large amounts of water attenuates radiation dose emitted to gastric wall
bull Rapidly and completely absorbed in the upper intestine
PATIENT PREPRATIONS1)Low iodine diet(lt50ugday) for 2 wks before and 2 days afterRAI(saltbreat and dairy products to be avoided)it has been seen doublesthe RAI uptake and lower rates of measuarable Tg levels after RAI(SAWAKAEM et al2012THYRIOD)2)Avoid iodinated contast in all DCT patients patient should have delay in RAItherapy for 3-6 months followed by measurement of urinary iodine levels (lt150ugml measured after collecting 24 hour urine and patient should be on iodine freediet gt7 days)3)Stop thyroxine repelacement therapy six weeks before RAI thepapy in case r-TSHis used stop 3-4 days before RAI therapy4)09 mg r-TSH can b used twice (2 days before and one day after) I-131(not to beused in cardiovascular diseasepara tracheal massspinal mets and inchildrenefficacy not studied in children)( studies show equal results with tshreplacement vs r-TSH)TSWNG et AL 1998CANCER5)Lithium carbonate 20mgkgday for 7 days usually 5 days before RAI ablation(measure serum lithium concentration on 4th 5th day of therapy which should be06-12 megml in its narrow theurpatic range)lithium decreases iodine exit fromthyriod cells increasing biological t12 by 50-90 with out interfering with iodineuptakeno studies have shown improved out comes with lithuimContraindicated in psychiatric problemsdementiaseizuresrenal and hepaticinsufficiencydiureticnsaidCCB intakehypohypernatremiahellip
Cancer vs normal cells
bull Metabolism of radioiodine in papillary and follicular carcinoma is profoundly altered when compared with normal thyroid tissue
bull Several defects are present in cancer tissuendash iodine uptake via the sodium-iodide symporter
(NIS) is always decreased and is undetectable in about a third of patients
ndash Iodine organification is markedly reduced
ndash Effective half-life of iodine in tumor tissue is always shorter
bull Tissues that often take up iodine and can be misconstrued as metastases include the
ndash salivary glands in the mouth
ndash esophagus (as a result of swallowing radioactive saliva)
ndash thymus gland
ndash breasts in some women
ndash liver stomach colon bladder
I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

PATHOLOGICAL CLASSIFICATION OF THYROID CANCERS ON BASIS OF CELL OF ORGIN
)FOLLICULAR EPITHELIAL CELLSbull A-DIFFERENTIATED THYROID CANCERS
1 Papillary and its variants(80-90)bull classicbull papillary microcarcinimabull Encapsulated variantbull Follicular variant bull Aggressive variants(diffuse scleroting tall cell columner cell)2 Follicular cancers (15-30)bull A) classicalbull B) hurthle cell variant bull B-POORLY DIFFERENTIATED THYRIOD CANCERS
1insular carcinomabull C-UNDIFFERENTIATED THYRIOD CANCER(anaplastic))PARA FOLLICULAR CELL ORGINbull A) MCTbull Perez and Bradys text book of radiation oncology
CLASSIFICATION ON BASIS OF ABLITY TO CONCENTRATE RAI
A USUALLY CONCENTRATE RAI
CLASSICAL PAPILLARY CARCINOMA
ENCAPSULATED PC
FOLLICULAR VARIANT
FOLLICULAR CARCINOMA
B FREQUENTLY DO NOT CONCENTRATE RAI
TALL CELLCOLUMNER CALL
HURTHLE CELL
INSULAR CA
C NEVER CONCENTRATE RAI
ANAPLASTIC THYRIOD CA
MEDULLARY CA
Perez and Bradys text book of radiation oncology
0 1084 62 12 14
0
20
40
60
80
100
Surv
iva
l
Stage I
Stage II
Stage III
Stage IV
DTC Initial Disease Stage Predicts OVERALL SURVIVAL
Years
75 of all
tumors
25 of all
tumors
plt0001
Jonklaas J et al Thyroid 2006 16(12) 1229-1242
NCCN and ATA guidelines for the treatment of differentiated thyroid cancer (DTC)
Initial treatmentbull Total thyroidectomy except in patients with unifocal microcarcinoma (individualized
to patient and extent of disease)12
Postoperative treatmentbull Radioactive iodine (131I) (RAI) therapy12
Follow-up treatmentbull Levothyroxine to suppress TSH levels to lt 01mUL12
Recurrent or metastatic disease treatmentbull Local therapy (re-operation external radiation)bull Systemic therapy
ndash RAI therapyndash patients with refractory advanced disease
bull chemotherapy (limited efficacy and considerable toxicity)12
bull participation in clinical trials with small molecule tyrosine kinase inhibitors is recommended12
1 NCCN Clinical Practice Guidelines in Oncology Thyroid Carcinoma V12010 2 Cooper DS et al Thyroid 200991167-214
NCCN = National Comprehensive Cancer Network
ATA = American Thyroid Association
IODINE ISOTOPES
I-131 1-125 I-123
SLIDE
Decays by e-capture with t12of 60 days into lowenergy state Te-125producesauger electrons of50-350 kevLess photon fluxfor scanning andless energy forabilation
Decays by e- captureinto te-123 with t12of 133 hrs sosuitable for 24 hourdiagnostic testhigh photon efluxthan i-131radiation burden tothyriod os lt1 thanby 131
IODINE -131bull Introduced by Seidlin et al in 1946
I-131 decays with a half life of 802 days with betamius and gamma emissions This nuclide of iodinehas 78 neutrons in its nucleus while the only stablenuclide 127I has 74 On decaying 131I most expends itsof decay energy by transforming into thestable 131Xe in two steps with gamma decay(364 kev)following rapidly after beta decay(250- 800kev)131I is available for oral ingestion as sodium iodine
radionucleotide Physical t12 Emax(MEV) LET(kevum) Appx cell diameter
Maximum range in tissue
Iodine-131
Iodine-125
Iodine -123
80 DAYS
601 days
1322 hours
081
035
015
02
4-26
10-230
lt1
20mm
2-500nm
PHYSICAL BIOLOGICAL AND EFFECTIVE HALF LIFE OF I-131
PHYSICAL t12 Biological t12 Effective t12
THYROID TISSUE
EXTRA THYRIOD TISSUE
8 days
8 days
80 days
12 days
73 days
8 hours
GOALS OF RIA IN DIFFERENTIATED CANCERS
bull 1)Thyroid reminant ablation
bull 2)Adjuvant therapy for residual micriscopic disease
bull RAI targets remaining thyroid cancer cells in thyriodbed occult lymph node and distant mets
bull Ablation of remaining thyroid tissue facalitates useof TG as sensitive and specific marker for persistantdisease after primary therapy
bull Rx wbs after RAI ablation provides crutialinformation about prognosis and furthermanagement
bull Sherma SI Lancet 2003
MD anderson experience
bull 1599 patient outcome analysis for various treatment for differentiated thyroid Ca
bull 46 had radioiodine therapybull Treatment with radioiodine was the single most
powerful prognostic indicator for increased DFS (plt 0001)
bull Its use significantly increased the survival both standard and high risk group
bull Adult patients females with intrathyroidal papillary carcinoma treated with TT + RAI between 20-59yrs ndashbest prognosis
bull J Clin Endocrinol Metab 1992 Sep75(3)714-20
bull 1004 dtc- Followed up with
ndash RAI ndash 151
ndash thyroid hormone alone 755
ndash no postoperative medical therapy -98
Tumor recurrence ~ threefold lower p lt 0001in RAI vs other treatment
Fewer patients developed distant metastases (p lt 0002)
Significantly more pronounced in tgt=15cm
Mazzaferri EL et al Thyroid remnant 131I ablation for papillary and follicular thyroid carcinoma Thyroid 1997 Apr7(2)265-71
ATA GUIDELINES
bull Distant metsgross ETE regardless of tumor sizeprimarysize gt4cm even in absence of high risk features
bull Follicular and hurthle cell variants are considered high riskand these patients are always recommended RAI ablationexcept with small unifocal FCs (lt2cm) with capsular invasiononly(no vasular invasion)
bull For 1-4cm size RAI is used for lymph node mets or highrisk features like agegt45 intra thyriod vascularinvasionmultifocal diseaseaggressive variants(tallcellcolummner cell or insular carcinoma)
bull RAI is not used for PTCS lt1cm unifocal and with out highrisk features OR when all foci in multifocal disease is in1cm focus
bull In a study assessing outcomes in 1004 patients with differentiated thyroid carcinoma tumor recurrence was about 3-fold higher in patients either treated with thyroid hormone alone or given no postoperative medical therapy when compared with patients who underwent postoperative thyroid remnant ablation with 131I (P lt 001)
bull Moreover fewer patients developed distant metastases (P lt 002) after thyroid remnant 131I ablation than after other forms of postoperative treatment However this effect is observed only in patients with primary tumors 15 cm or more in diameter Mazzaferri EL Thyroid remnant 131I ablation for papillary andfollicular thyroid carcinoma
low risk group with i-131 abilationStudy showed that remnant ablation had less of a therapeutic effect perhaps because more extensive locoregional surgery had been done Hay ID Papillary thyroid carcinoma Endocrinol Metab Clin North
bull Rising incidence of second cancers in patients with low-risk (T1N0) thyroid cancer who receive radioactive iodine therapy
bull CONCLUSIONS-The increased risk of a SPM in patients with low-risk (T1N0) WDTC along with a lack of data demonstrating improved survival outcomes with adjuvant RAI( IYER NG etal 2013cancer)
bull Impact on overall survival of radioactive iodine in low-risk differentiated thyroid cancer patients
bull CONCLUSION-With a long-term follow-up of 103 yr we failed to prove any survival benefit of RAI after surgery in a large cohort of low-risk DTC patients(SCHTWATZC et alJ Clin Endocrinol Metab 2012 May)
MAJOR FACTORS IMPACTING DECISION MAKING IN RADIOIODINE REMNANT ABLATION
ADMINSTRATION OF I-131
bull As liquid solution or in capsulesbull Each capsule accounts for 50 micro
curiebull Capsules safer than liquid- less
radioactivity released into air during handling
bull Also result in less oral mucosal irritation
bull Simultaneous ingestion large amounts of water attenuates radiation dose emitted to gastric wall
bull Rapidly and completely absorbed in the upper intestine
PATIENT PREPRATIONS1)Low iodine diet(lt50ugday) for 2 wks before and 2 days afterRAI(saltbreat and dairy products to be avoided)it has been seen doublesthe RAI uptake and lower rates of measuarable Tg levels after RAI(SAWAKAEM et al2012THYRIOD)2)Avoid iodinated contast in all DCT patients patient should have delay in RAItherapy for 3-6 months followed by measurement of urinary iodine levels (lt150ugml measured after collecting 24 hour urine and patient should be on iodine freediet gt7 days)3)Stop thyroxine repelacement therapy six weeks before RAI thepapy in case r-TSHis used stop 3-4 days before RAI therapy4)09 mg r-TSH can b used twice (2 days before and one day after) I-131(not to beused in cardiovascular diseasepara tracheal massspinal mets and inchildrenefficacy not studied in children)( studies show equal results with tshreplacement vs r-TSH)TSWNG et AL 1998CANCER5)Lithium carbonate 20mgkgday for 7 days usually 5 days before RAI ablation(measure serum lithium concentration on 4th 5th day of therapy which should be06-12 megml in its narrow theurpatic range)lithium decreases iodine exit fromthyriod cells increasing biological t12 by 50-90 with out interfering with iodineuptakeno studies have shown improved out comes with lithuimContraindicated in psychiatric problemsdementiaseizuresrenal and hepaticinsufficiencydiureticnsaidCCB intakehypohypernatremiahellip
Cancer vs normal cells
bull Metabolism of radioiodine in papillary and follicular carcinoma is profoundly altered when compared with normal thyroid tissue
bull Several defects are present in cancer tissuendash iodine uptake via the sodium-iodide symporter
(NIS) is always decreased and is undetectable in about a third of patients
ndash Iodine organification is markedly reduced
ndash Effective half-life of iodine in tumor tissue is always shorter
bull Tissues that often take up iodine and can be misconstrued as metastases include the
ndash salivary glands in the mouth
ndash esophagus (as a result of swallowing radioactive saliva)
ndash thymus gland
ndash breasts in some women
ndash liver stomach colon bladder
I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

CLASSIFICATION ON BASIS OF ABLITY TO CONCENTRATE RAI
A USUALLY CONCENTRATE RAI
CLASSICAL PAPILLARY CARCINOMA
ENCAPSULATED PC
FOLLICULAR VARIANT
FOLLICULAR CARCINOMA
B FREQUENTLY DO NOT CONCENTRATE RAI
TALL CELLCOLUMNER CALL
HURTHLE CELL
INSULAR CA
C NEVER CONCENTRATE RAI
ANAPLASTIC THYRIOD CA
MEDULLARY CA
Perez and Bradys text book of radiation oncology
0 1084 62 12 14
0
20
40
60
80
100
Surv
iva
l
Stage I
Stage II
Stage III
Stage IV
DTC Initial Disease Stage Predicts OVERALL SURVIVAL
Years
75 of all
tumors
25 of all
tumors
plt0001
Jonklaas J et al Thyroid 2006 16(12) 1229-1242
NCCN and ATA guidelines for the treatment of differentiated thyroid cancer (DTC)
Initial treatmentbull Total thyroidectomy except in patients with unifocal microcarcinoma (individualized
to patient and extent of disease)12
Postoperative treatmentbull Radioactive iodine (131I) (RAI) therapy12
Follow-up treatmentbull Levothyroxine to suppress TSH levels to lt 01mUL12
Recurrent or metastatic disease treatmentbull Local therapy (re-operation external radiation)bull Systemic therapy
ndash RAI therapyndash patients with refractory advanced disease
bull chemotherapy (limited efficacy and considerable toxicity)12
bull participation in clinical trials with small molecule tyrosine kinase inhibitors is recommended12
1 NCCN Clinical Practice Guidelines in Oncology Thyroid Carcinoma V12010 2 Cooper DS et al Thyroid 200991167-214
NCCN = National Comprehensive Cancer Network
ATA = American Thyroid Association
IODINE ISOTOPES
I-131 1-125 I-123
SLIDE
Decays by e-capture with t12of 60 days into lowenergy state Te-125producesauger electrons of50-350 kevLess photon fluxfor scanning andless energy forabilation
Decays by e- captureinto te-123 with t12of 133 hrs sosuitable for 24 hourdiagnostic testhigh photon efluxthan i-131radiation burden tothyriod os lt1 thanby 131
IODINE -131bull Introduced by Seidlin et al in 1946
I-131 decays with a half life of 802 days with betamius and gamma emissions This nuclide of iodinehas 78 neutrons in its nucleus while the only stablenuclide 127I has 74 On decaying 131I most expends itsof decay energy by transforming into thestable 131Xe in two steps with gamma decay(364 kev)following rapidly after beta decay(250- 800kev)131I is available for oral ingestion as sodium iodine
radionucleotide Physical t12 Emax(MEV) LET(kevum) Appx cell diameter
Maximum range in tissue
Iodine-131
Iodine-125
Iodine -123
80 DAYS
601 days
1322 hours
081
035
015
02
4-26
10-230
lt1
20mm
2-500nm
PHYSICAL BIOLOGICAL AND EFFECTIVE HALF LIFE OF I-131
PHYSICAL t12 Biological t12 Effective t12
THYROID TISSUE
EXTRA THYRIOD TISSUE
8 days
8 days
80 days
12 days
73 days
8 hours
GOALS OF RIA IN DIFFERENTIATED CANCERS
bull 1)Thyroid reminant ablation
bull 2)Adjuvant therapy for residual micriscopic disease
bull RAI targets remaining thyroid cancer cells in thyriodbed occult lymph node and distant mets
bull Ablation of remaining thyroid tissue facalitates useof TG as sensitive and specific marker for persistantdisease after primary therapy
bull Rx wbs after RAI ablation provides crutialinformation about prognosis and furthermanagement
bull Sherma SI Lancet 2003
MD anderson experience
bull 1599 patient outcome analysis for various treatment for differentiated thyroid Ca
bull 46 had radioiodine therapybull Treatment with radioiodine was the single most
powerful prognostic indicator for increased DFS (plt 0001)
bull Its use significantly increased the survival both standard and high risk group
bull Adult patients females with intrathyroidal papillary carcinoma treated with TT + RAI between 20-59yrs ndashbest prognosis
bull J Clin Endocrinol Metab 1992 Sep75(3)714-20
bull 1004 dtc- Followed up with
ndash RAI ndash 151
ndash thyroid hormone alone 755
ndash no postoperative medical therapy -98
Tumor recurrence ~ threefold lower p lt 0001in RAI vs other treatment
Fewer patients developed distant metastases (p lt 0002)
Significantly more pronounced in tgt=15cm
Mazzaferri EL et al Thyroid remnant 131I ablation for papillary and follicular thyroid carcinoma Thyroid 1997 Apr7(2)265-71
ATA GUIDELINES
bull Distant metsgross ETE regardless of tumor sizeprimarysize gt4cm even in absence of high risk features
bull Follicular and hurthle cell variants are considered high riskand these patients are always recommended RAI ablationexcept with small unifocal FCs (lt2cm) with capsular invasiononly(no vasular invasion)
bull For 1-4cm size RAI is used for lymph node mets or highrisk features like agegt45 intra thyriod vascularinvasionmultifocal diseaseaggressive variants(tallcellcolummner cell or insular carcinoma)
bull RAI is not used for PTCS lt1cm unifocal and with out highrisk features OR when all foci in multifocal disease is in1cm focus
bull In a study assessing outcomes in 1004 patients with differentiated thyroid carcinoma tumor recurrence was about 3-fold higher in patients either treated with thyroid hormone alone or given no postoperative medical therapy when compared with patients who underwent postoperative thyroid remnant ablation with 131I (P lt 001)
bull Moreover fewer patients developed distant metastases (P lt 002) after thyroid remnant 131I ablation than after other forms of postoperative treatment However this effect is observed only in patients with primary tumors 15 cm or more in diameter Mazzaferri EL Thyroid remnant 131I ablation for papillary andfollicular thyroid carcinoma
low risk group with i-131 abilationStudy showed that remnant ablation had less of a therapeutic effect perhaps because more extensive locoregional surgery had been done Hay ID Papillary thyroid carcinoma Endocrinol Metab Clin North
bull Rising incidence of second cancers in patients with low-risk (T1N0) thyroid cancer who receive radioactive iodine therapy
bull CONCLUSIONS-The increased risk of a SPM in patients with low-risk (T1N0) WDTC along with a lack of data demonstrating improved survival outcomes with adjuvant RAI( IYER NG etal 2013cancer)
bull Impact on overall survival of radioactive iodine in low-risk differentiated thyroid cancer patients
bull CONCLUSION-With a long-term follow-up of 103 yr we failed to prove any survival benefit of RAI after surgery in a large cohort of low-risk DTC patients(SCHTWATZC et alJ Clin Endocrinol Metab 2012 May)
MAJOR FACTORS IMPACTING DECISION MAKING IN RADIOIODINE REMNANT ABLATION
ADMINSTRATION OF I-131
bull As liquid solution or in capsulesbull Each capsule accounts for 50 micro
curiebull Capsules safer than liquid- less
radioactivity released into air during handling
bull Also result in less oral mucosal irritation
bull Simultaneous ingestion large amounts of water attenuates radiation dose emitted to gastric wall
bull Rapidly and completely absorbed in the upper intestine
PATIENT PREPRATIONS1)Low iodine diet(lt50ugday) for 2 wks before and 2 days afterRAI(saltbreat and dairy products to be avoided)it has been seen doublesthe RAI uptake and lower rates of measuarable Tg levels after RAI(SAWAKAEM et al2012THYRIOD)2)Avoid iodinated contast in all DCT patients patient should have delay in RAItherapy for 3-6 months followed by measurement of urinary iodine levels (lt150ugml measured after collecting 24 hour urine and patient should be on iodine freediet gt7 days)3)Stop thyroxine repelacement therapy six weeks before RAI thepapy in case r-TSHis used stop 3-4 days before RAI therapy4)09 mg r-TSH can b used twice (2 days before and one day after) I-131(not to beused in cardiovascular diseasepara tracheal massspinal mets and inchildrenefficacy not studied in children)( studies show equal results with tshreplacement vs r-TSH)TSWNG et AL 1998CANCER5)Lithium carbonate 20mgkgday for 7 days usually 5 days before RAI ablation(measure serum lithium concentration on 4th 5th day of therapy which should be06-12 megml in its narrow theurpatic range)lithium decreases iodine exit fromthyriod cells increasing biological t12 by 50-90 with out interfering with iodineuptakeno studies have shown improved out comes with lithuimContraindicated in psychiatric problemsdementiaseizuresrenal and hepaticinsufficiencydiureticnsaidCCB intakehypohypernatremiahellip
Cancer vs normal cells
bull Metabolism of radioiodine in papillary and follicular carcinoma is profoundly altered when compared with normal thyroid tissue
bull Several defects are present in cancer tissuendash iodine uptake via the sodium-iodide symporter
(NIS) is always decreased and is undetectable in about a third of patients
ndash Iodine organification is markedly reduced
ndash Effective half-life of iodine in tumor tissue is always shorter
bull Tissues that often take up iodine and can be misconstrued as metastases include the
ndash salivary glands in the mouth
ndash esophagus (as a result of swallowing radioactive saliva)
ndash thymus gland
ndash breasts in some women
ndash liver stomach colon bladder
I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

0 1084 62 12 14
0
20
40
60
80
100
Surv
iva
l
Stage I
Stage II
Stage III
Stage IV
DTC Initial Disease Stage Predicts OVERALL SURVIVAL
Years
75 of all
tumors
25 of all
tumors
plt0001
Jonklaas J et al Thyroid 2006 16(12) 1229-1242
NCCN and ATA guidelines for the treatment of differentiated thyroid cancer (DTC)
Initial treatmentbull Total thyroidectomy except in patients with unifocal microcarcinoma (individualized
to patient and extent of disease)12
Postoperative treatmentbull Radioactive iodine (131I) (RAI) therapy12
Follow-up treatmentbull Levothyroxine to suppress TSH levels to lt 01mUL12
Recurrent or metastatic disease treatmentbull Local therapy (re-operation external radiation)bull Systemic therapy
ndash RAI therapyndash patients with refractory advanced disease
bull chemotherapy (limited efficacy and considerable toxicity)12
bull participation in clinical trials with small molecule tyrosine kinase inhibitors is recommended12
1 NCCN Clinical Practice Guidelines in Oncology Thyroid Carcinoma V12010 2 Cooper DS et al Thyroid 200991167-214
NCCN = National Comprehensive Cancer Network
ATA = American Thyroid Association
IODINE ISOTOPES
I-131 1-125 I-123
SLIDE
Decays by e-capture with t12of 60 days into lowenergy state Te-125producesauger electrons of50-350 kevLess photon fluxfor scanning andless energy forabilation
Decays by e- captureinto te-123 with t12of 133 hrs sosuitable for 24 hourdiagnostic testhigh photon efluxthan i-131radiation burden tothyriod os lt1 thanby 131
IODINE -131bull Introduced by Seidlin et al in 1946
I-131 decays with a half life of 802 days with betamius and gamma emissions This nuclide of iodinehas 78 neutrons in its nucleus while the only stablenuclide 127I has 74 On decaying 131I most expends itsof decay energy by transforming into thestable 131Xe in two steps with gamma decay(364 kev)following rapidly after beta decay(250- 800kev)131I is available for oral ingestion as sodium iodine
radionucleotide Physical t12 Emax(MEV) LET(kevum) Appx cell diameter
Maximum range in tissue
Iodine-131
Iodine-125
Iodine -123
80 DAYS
601 days
1322 hours
081
035
015
02
4-26
10-230
lt1
20mm
2-500nm
PHYSICAL BIOLOGICAL AND EFFECTIVE HALF LIFE OF I-131
PHYSICAL t12 Biological t12 Effective t12
THYROID TISSUE
EXTRA THYRIOD TISSUE
8 days
8 days
80 days
12 days
73 days
8 hours
GOALS OF RIA IN DIFFERENTIATED CANCERS
bull 1)Thyroid reminant ablation
bull 2)Adjuvant therapy for residual micriscopic disease
bull RAI targets remaining thyroid cancer cells in thyriodbed occult lymph node and distant mets
bull Ablation of remaining thyroid tissue facalitates useof TG as sensitive and specific marker for persistantdisease after primary therapy
bull Rx wbs after RAI ablation provides crutialinformation about prognosis and furthermanagement
bull Sherma SI Lancet 2003
MD anderson experience
bull 1599 patient outcome analysis for various treatment for differentiated thyroid Ca
bull 46 had radioiodine therapybull Treatment with radioiodine was the single most
powerful prognostic indicator for increased DFS (plt 0001)
bull Its use significantly increased the survival both standard and high risk group
bull Adult patients females with intrathyroidal papillary carcinoma treated with TT + RAI between 20-59yrs ndashbest prognosis
bull J Clin Endocrinol Metab 1992 Sep75(3)714-20
bull 1004 dtc- Followed up with
ndash RAI ndash 151
ndash thyroid hormone alone 755
ndash no postoperative medical therapy -98
Tumor recurrence ~ threefold lower p lt 0001in RAI vs other treatment
Fewer patients developed distant metastases (p lt 0002)
Significantly more pronounced in tgt=15cm
Mazzaferri EL et al Thyroid remnant 131I ablation for papillary and follicular thyroid carcinoma Thyroid 1997 Apr7(2)265-71
ATA GUIDELINES
bull Distant metsgross ETE regardless of tumor sizeprimarysize gt4cm even in absence of high risk features
bull Follicular and hurthle cell variants are considered high riskand these patients are always recommended RAI ablationexcept with small unifocal FCs (lt2cm) with capsular invasiononly(no vasular invasion)
bull For 1-4cm size RAI is used for lymph node mets or highrisk features like agegt45 intra thyriod vascularinvasionmultifocal diseaseaggressive variants(tallcellcolummner cell or insular carcinoma)
bull RAI is not used for PTCS lt1cm unifocal and with out highrisk features OR when all foci in multifocal disease is in1cm focus
bull In a study assessing outcomes in 1004 patients with differentiated thyroid carcinoma tumor recurrence was about 3-fold higher in patients either treated with thyroid hormone alone or given no postoperative medical therapy when compared with patients who underwent postoperative thyroid remnant ablation with 131I (P lt 001)
bull Moreover fewer patients developed distant metastases (P lt 002) after thyroid remnant 131I ablation than after other forms of postoperative treatment However this effect is observed only in patients with primary tumors 15 cm or more in diameter Mazzaferri EL Thyroid remnant 131I ablation for papillary andfollicular thyroid carcinoma
low risk group with i-131 abilationStudy showed that remnant ablation had less of a therapeutic effect perhaps because more extensive locoregional surgery had been done Hay ID Papillary thyroid carcinoma Endocrinol Metab Clin North
bull Rising incidence of second cancers in patients with low-risk (T1N0) thyroid cancer who receive radioactive iodine therapy
bull CONCLUSIONS-The increased risk of a SPM in patients with low-risk (T1N0) WDTC along with a lack of data demonstrating improved survival outcomes with adjuvant RAI( IYER NG etal 2013cancer)
bull Impact on overall survival of radioactive iodine in low-risk differentiated thyroid cancer patients
bull CONCLUSION-With a long-term follow-up of 103 yr we failed to prove any survival benefit of RAI after surgery in a large cohort of low-risk DTC patients(SCHTWATZC et alJ Clin Endocrinol Metab 2012 May)
MAJOR FACTORS IMPACTING DECISION MAKING IN RADIOIODINE REMNANT ABLATION
ADMINSTRATION OF I-131
bull As liquid solution or in capsulesbull Each capsule accounts for 50 micro
curiebull Capsules safer than liquid- less
radioactivity released into air during handling
bull Also result in less oral mucosal irritation
bull Simultaneous ingestion large amounts of water attenuates radiation dose emitted to gastric wall
bull Rapidly and completely absorbed in the upper intestine
PATIENT PREPRATIONS1)Low iodine diet(lt50ugday) for 2 wks before and 2 days afterRAI(saltbreat and dairy products to be avoided)it has been seen doublesthe RAI uptake and lower rates of measuarable Tg levels after RAI(SAWAKAEM et al2012THYRIOD)2)Avoid iodinated contast in all DCT patients patient should have delay in RAItherapy for 3-6 months followed by measurement of urinary iodine levels (lt150ugml measured after collecting 24 hour urine and patient should be on iodine freediet gt7 days)3)Stop thyroxine repelacement therapy six weeks before RAI thepapy in case r-TSHis used stop 3-4 days before RAI therapy4)09 mg r-TSH can b used twice (2 days before and one day after) I-131(not to beused in cardiovascular diseasepara tracheal massspinal mets and inchildrenefficacy not studied in children)( studies show equal results with tshreplacement vs r-TSH)TSWNG et AL 1998CANCER5)Lithium carbonate 20mgkgday for 7 days usually 5 days before RAI ablation(measure serum lithium concentration on 4th 5th day of therapy which should be06-12 megml in its narrow theurpatic range)lithium decreases iodine exit fromthyriod cells increasing biological t12 by 50-90 with out interfering with iodineuptakeno studies have shown improved out comes with lithuimContraindicated in psychiatric problemsdementiaseizuresrenal and hepaticinsufficiencydiureticnsaidCCB intakehypohypernatremiahellip
Cancer vs normal cells
bull Metabolism of radioiodine in papillary and follicular carcinoma is profoundly altered when compared with normal thyroid tissue
bull Several defects are present in cancer tissuendash iodine uptake via the sodium-iodide symporter
(NIS) is always decreased and is undetectable in about a third of patients
ndash Iodine organification is markedly reduced
ndash Effective half-life of iodine in tumor tissue is always shorter
bull Tissues that often take up iodine and can be misconstrued as metastases include the
ndash salivary glands in the mouth
ndash esophagus (as a result of swallowing radioactive saliva)
ndash thymus gland
ndash breasts in some women
ndash liver stomach colon bladder
I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

NCCN and ATA guidelines for the treatment of differentiated thyroid cancer (DTC)
Initial treatmentbull Total thyroidectomy except in patients with unifocal microcarcinoma (individualized
to patient and extent of disease)12
Postoperative treatmentbull Radioactive iodine (131I) (RAI) therapy12
Follow-up treatmentbull Levothyroxine to suppress TSH levels to lt 01mUL12
Recurrent or metastatic disease treatmentbull Local therapy (re-operation external radiation)bull Systemic therapy
ndash RAI therapyndash patients with refractory advanced disease
bull chemotherapy (limited efficacy and considerable toxicity)12
bull participation in clinical trials with small molecule tyrosine kinase inhibitors is recommended12
1 NCCN Clinical Practice Guidelines in Oncology Thyroid Carcinoma V12010 2 Cooper DS et al Thyroid 200991167-214
NCCN = National Comprehensive Cancer Network
ATA = American Thyroid Association
IODINE ISOTOPES
I-131 1-125 I-123
SLIDE
Decays by e-capture with t12of 60 days into lowenergy state Te-125producesauger electrons of50-350 kevLess photon fluxfor scanning andless energy forabilation
Decays by e- captureinto te-123 with t12of 133 hrs sosuitable for 24 hourdiagnostic testhigh photon efluxthan i-131radiation burden tothyriod os lt1 thanby 131
IODINE -131bull Introduced by Seidlin et al in 1946
I-131 decays with a half life of 802 days with betamius and gamma emissions This nuclide of iodinehas 78 neutrons in its nucleus while the only stablenuclide 127I has 74 On decaying 131I most expends itsof decay energy by transforming into thestable 131Xe in two steps with gamma decay(364 kev)following rapidly after beta decay(250- 800kev)131I is available for oral ingestion as sodium iodine
radionucleotide Physical t12 Emax(MEV) LET(kevum) Appx cell diameter
Maximum range in tissue
Iodine-131
Iodine-125
Iodine -123
80 DAYS
601 days
1322 hours
081
035
015
02
4-26
10-230
lt1
20mm
2-500nm
PHYSICAL BIOLOGICAL AND EFFECTIVE HALF LIFE OF I-131
PHYSICAL t12 Biological t12 Effective t12
THYROID TISSUE
EXTRA THYRIOD TISSUE
8 days
8 days
80 days
12 days
73 days
8 hours
GOALS OF RIA IN DIFFERENTIATED CANCERS
bull 1)Thyroid reminant ablation
bull 2)Adjuvant therapy for residual micriscopic disease
bull RAI targets remaining thyroid cancer cells in thyriodbed occult lymph node and distant mets
bull Ablation of remaining thyroid tissue facalitates useof TG as sensitive and specific marker for persistantdisease after primary therapy
bull Rx wbs after RAI ablation provides crutialinformation about prognosis and furthermanagement
bull Sherma SI Lancet 2003
MD anderson experience
bull 1599 patient outcome analysis for various treatment for differentiated thyroid Ca
bull 46 had radioiodine therapybull Treatment with radioiodine was the single most
powerful prognostic indicator for increased DFS (plt 0001)
bull Its use significantly increased the survival both standard and high risk group
bull Adult patients females with intrathyroidal papillary carcinoma treated with TT + RAI between 20-59yrs ndashbest prognosis
bull J Clin Endocrinol Metab 1992 Sep75(3)714-20
bull 1004 dtc- Followed up with
ndash RAI ndash 151
ndash thyroid hormone alone 755
ndash no postoperative medical therapy -98
Tumor recurrence ~ threefold lower p lt 0001in RAI vs other treatment
Fewer patients developed distant metastases (p lt 0002)
Significantly more pronounced in tgt=15cm
Mazzaferri EL et al Thyroid remnant 131I ablation for papillary and follicular thyroid carcinoma Thyroid 1997 Apr7(2)265-71
ATA GUIDELINES
bull Distant metsgross ETE regardless of tumor sizeprimarysize gt4cm even in absence of high risk features
bull Follicular and hurthle cell variants are considered high riskand these patients are always recommended RAI ablationexcept with small unifocal FCs (lt2cm) with capsular invasiononly(no vasular invasion)
bull For 1-4cm size RAI is used for lymph node mets or highrisk features like agegt45 intra thyriod vascularinvasionmultifocal diseaseaggressive variants(tallcellcolummner cell or insular carcinoma)
bull RAI is not used for PTCS lt1cm unifocal and with out highrisk features OR when all foci in multifocal disease is in1cm focus
bull In a study assessing outcomes in 1004 patients with differentiated thyroid carcinoma tumor recurrence was about 3-fold higher in patients either treated with thyroid hormone alone or given no postoperative medical therapy when compared with patients who underwent postoperative thyroid remnant ablation with 131I (P lt 001)
bull Moreover fewer patients developed distant metastases (P lt 002) after thyroid remnant 131I ablation than after other forms of postoperative treatment However this effect is observed only in patients with primary tumors 15 cm or more in diameter Mazzaferri EL Thyroid remnant 131I ablation for papillary andfollicular thyroid carcinoma
low risk group with i-131 abilationStudy showed that remnant ablation had less of a therapeutic effect perhaps because more extensive locoregional surgery had been done Hay ID Papillary thyroid carcinoma Endocrinol Metab Clin North
bull Rising incidence of second cancers in patients with low-risk (T1N0) thyroid cancer who receive radioactive iodine therapy
bull CONCLUSIONS-The increased risk of a SPM in patients with low-risk (T1N0) WDTC along with a lack of data demonstrating improved survival outcomes with adjuvant RAI( IYER NG etal 2013cancer)
bull Impact on overall survival of radioactive iodine in low-risk differentiated thyroid cancer patients
bull CONCLUSION-With a long-term follow-up of 103 yr we failed to prove any survival benefit of RAI after surgery in a large cohort of low-risk DTC patients(SCHTWATZC et alJ Clin Endocrinol Metab 2012 May)
MAJOR FACTORS IMPACTING DECISION MAKING IN RADIOIODINE REMNANT ABLATION
ADMINSTRATION OF I-131
bull As liquid solution or in capsulesbull Each capsule accounts for 50 micro
curiebull Capsules safer than liquid- less
radioactivity released into air during handling
bull Also result in less oral mucosal irritation
bull Simultaneous ingestion large amounts of water attenuates radiation dose emitted to gastric wall
bull Rapidly and completely absorbed in the upper intestine
PATIENT PREPRATIONS1)Low iodine diet(lt50ugday) for 2 wks before and 2 days afterRAI(saltbreat and dairy products to be avoided)it has been seen doublesthe RAI uptake and lower rates of measuarable Tg levels after RAI(SAWAKAEM et al2012THYRIOD)2)Avoid iodinated contast in all DCT patients patient should have delay in RAItherapy for 3-6 months followed by measurement of urinary iodine levels (lt150ugml measured after collecting 24 hour urine and patient should be on iodine freediet gt7 days)3)Stop thyroxine repelacement therapy six weeks before RAI thepapy in case r-TSHis used stop 3-4 days before RAI therapy4)09 mg r-TSH can b used twice (2 days before and one day after) I-131(not to beused in cardiovascular diseasepara tracheal massspinal mets and inchildrenefficacy not studied in children)( studies show equal results with tshreplacement vs r-TSH)TSWNG et AL 1998CANCER5)Lithium carbonate 20mgkgday for 7 days usually 5 days before RAI ablation(measure serum lithium concentration on 4th 5th day of therapy which should be06-12 megml in its narrow theurpatic range)lithium decreases iodine exit fromthyriod cells increasing biological t12 by 50-90 with out interfering with iodineuptakeno studies have shown improved out comes with lithuimContraindicated in psychiatric problemsdementiaseizuresrenal and hepaticinsufficiencydiureticnsaidCCB intakehypohypernatremiahellip
Cancer vs normal cells
bull Metabolism of radioiodine in papillary and follicular carcinoma is profoundly altered when compared with normal thyroid tissue
bull Several defects are present in cancer tissuendash iodine uptake via the sodium-iodide symporter
(NIS) is always decreased and is undetectable in about a third of patients
ndash Iodine organification is markedly reduced
ndash Effective half-life of iodine in tumor tissue is always shorter
bull Tissues that often take up iodine and can be misconstrued as metastases include the
ndash salivary glands in the mouth
ndash esophagus (as a result of swallowing radioactive saliva)
ndash thymus gland
ndash breasts in some women
ndash liver stomach colon bladder
I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

IODINE ISOTOPES
I-131 1-125 I-123
SLIDE
Decays by e-capture with t12of 60 days into lowenergy state Te-125producesauger electrons of50-350 kevLess photon fluxfor scanning andless energy forabilation
Decays by e- captureinto te-123 with t12of 133 hrs sosuitable for 24 hourdiagnostic testhigh photon efluxthan i-131radiation burden tothyriod os lt1 thanby 131
IODINE -131bull Introduced by Seidlin et al in 1946
I-131 decays with a half life of 802 days with betamius and gamma emissions This nuclide of iodinehas 78 neutrons in its nucleus while the only stablenuclide 127I has 74 On decaying 131I most expends itsof decay energy by transforming into thestable 131Xe in two steps with gamma decay(364 kev)following rapidly after beta decay(250- 800kev)131I is available for oral ingestion as sodium iodine
radionucleotide Physical t12 Emax(MEV) LET(kevum) Appx cell diameter
Maximum range in tissue
Iodine-131
Iodine-125
Iodine -123
80 DAYS
601 days
1322 hours
081
035
015
02
4-26
10-230
lt1
20mm
2-500nm
PHYSICAL BIOLOGICAL AND EFFECTIVE HALF LIFE OF I-131
PHYSICAL t12 Biological t12 Effective t12
THYROID TISSUE
EXTRA THYRIOD TISSUE
8 days
8 days
80 days
12 days
73 days
8 hours
GOALS OF RIA IN DIFFERENTIATED CANCERS
bull 1)Thyroid reminant ablation
bull 2)Adjuvant therapy for residual micriscopic disease
bull RAI targets remaining thyroid cancer cells in thyriodbed occult lymph node and distant mets
bull Ablation of remaining thyroid tissue facalitates useof TG as sensitive and specific marker for persistantdisease after primary therapy
bull Rx wbs after RAI ablation provides crutialinformation about prognosis and furthermanagement
bull Sherma SI Lancet 2003
MD anderson experience
bull 1599 patient outcome analysis for various treatment for differentiated thyroid Ca
bull 46 had radioiodine therapybull Treatment with radioiodine was the single most
powerful prognostic indicator for increased DFS (plt 0001)
bull Its use significantly increased the survival both standard and high risk group
bull Adult patients females with intrathyroidal papillary carcinoma treated with TT + RAI between 20-59yrs ndashbest prognosis
bull J Clin Endocrinol Metab 1992 Sep75(3)714-20
bull 1004 dtc- Followed up with
ndash RAI ndash 151
ndash thyroid hormone alone 755
ndash no postoperative medical therapy -98
Tumor recurrence ~ threefold lower p lt 0001in RAI vs other treatment
Fewer patients developed distant metastases (p lt 0002)
Significantly more pronounced in tgt=15cm
Mazzaferri EL et al Thyroid remnant 131I ablation for papillary and follicular thyroid carcinoma Thyroid 1997 Apr7(2)265-71
ATA GUIDELINES
bull Distant metsgross ETE regardless of tumor sizeprimarysize gt4cm even in absence of high risk features
bull Follicular and hurthle cell variants are considered high riskand these patients are always recommended RAI ablationexcept with small unifocal FCs (lt2cm) with capsular invasiononly(no vasular invasion)
bull For 1-4cm size RAI is used for lymph node mets or highrisk features like agegt45 intra thyriod vascularinvasionmultifocal diseaseaggressive variants(tallcellcolummner cell or insular carcinoma)
bull RAI is not used for PTCS lt1cm unifocal and with out highrisk features OR when all foci in multifocal disease is in1cm focus
bull In a study assessing outcomes in 1004 patients with differentiated thyroid carcinoma tumor recurrence was about 3-fold higher in patients either treated with thyroid hormone alone or given no postoperative medical therapy when compared with patients who underwent postoperative thyroid remnant ablation with 131I (P lt 001)
bull Moreover fewer patients developed distant metastases (P lt 002) after thyroid remnant 131I ablation than after other forms of postoperative treatment However this effect is observed only in patients with primary tumors 15 cm or more in diameter Mazzaferri EL Thyroid remnant 131I ablation for papillary andfollicular thyroid carcinoma
low risk group with i-131 abilationStudy showed that remnant ablation had less of a therapeutic effect perhaps because more extensive locoregional surgery had been done Hay ID Papillary thyroid carcinoma Endocrinol Metab Clin North
bull Rising incidence of second cancers in patients with low-risk (T1N0) thyroid cancer who receive radioactive iodine therapy
bull CONCLUSIONS-The increased risk of a SPM in patients with low-risk (T1N0) WDTC along with a lack of data demonstrating improved survival outcomes with adjuvant RAI( IYER NG etal 2013cancer)
bull Impact on overall survival of radioactive iodine in low-risk differentiated thyroid cancer patients
bull CONCLUSION-With a long-term follow-up of 103 yr we failed to prove any survival benefit of RAI after surgery in a large cohort of low-risk DTC patients(SCHTWATZC et alJ Clin Endocrinol Metab 2012 May)
MAJOR FACTORS IMPACTING DECISION MAKING IN RADIOIODINE REMNANT ABLATION
ADMINSTRATION OF I-131
bull As liquid solution or in capsulesbull Each capsule accounts for 50 micro
curiebull Capsules safer than liquid- less
radioactivity released into air during handling
bull Also result in less oral mucosal irritation
bull Simultaneous ingestion large amounts of water attenuates radiation dose emitted to gastric wall
bull Rapidly and completely absorbed in the upper intestine
PATIENT PREPRATIONS1)Low iodine diet(lt50ugday) for 2 wks before and 2 days afterRAI(saltbreat and dairy products to be avoided)it has been seen doublesthe RAI uptake and lower rates of measuarable Tg levels after RAI(SAWAKAEM et al2012THYRIOD)2)Avoid iodinated contast in all DCT patients patient should have delay in RAItherapy for 3-6 months followed by measurement of urinary iodine levels (lt150ugml measured after collecting 24 hour urine and patient should be on iodine freediet gt7 days)3)Stop thyroxine repelacement therapy six weeks before RAI thepapy in case r-TSHis used stop 3-4 days before RAI therapy4)09 mg r-TSH can b used twice (2 days before and one day after) I-131(not to beused in cardiovascular diseasepara tracheal massspinal mets and inchildrenefficacy not studied in children)( studies show equal results with tshreplacement vs r-TSH)TSWNG et AL 1998CANCER5)Lithium carbonate 20mgkgday for 7 days usually 5 days before RAI ablation(measure serum lithium concentration on 4th 5th day of therapy which should be06-12 megml in its narrow theurpatic range)lithium decreases iodine exit fromthyriod cells increasing biological t12 by 50-90 with out interfering with iodineuptakeno studies have shown improved out comes with lithuimContraindicated in psychiatric problemsdementiaseizuresrenal and hepaticinsufficiencydiureticnsaidCCB intakehypohypernatremiahellip
Cancer vs normal cells
bull Metabolism of radioiodine in papillary and follicular carcinoma is profoundly altered when compared with normal thyroid tissue
bull Several defects are present in cancer tissuendash iodine uptake via the sodium-iodide symporter
(NIS) is always decreased and is undetectable in about a third of patients
ndash Iodine organification is markedly reduced
ndash Effective half-life of iodine in tumor tissue is always shorter
bull Tissues that often take up iodine and can be misconstrued as metastases include the
ndash salivary glands in the mouth
ndash esophagus (as a result of swallowing radioactive saliva)
ndash thymus gland
ndash breasts in some women
ndash liver stomach colon bladder
I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

IODINE -131bull Introduced by Seidlin et al in 1946
I-131 decays with a half life of 802 days with betamius and gamma emissions This nuclide of iodinehas 78 neutrons in its nucleus while the only stablenuclide 127I has 74 On decaying 131I most expends itsof decay energy by transforming into thestable 131Xe in two steps with gamma decay(364 kev)following rapidly after beta decay(250- 800kev)131I is available for oral ingestion as sodium iodine
radionucleotide Physical t12 Emax(MEV) LET(kevum) Appx cell diameter
Maximum range in tissue
Iodine-131
Iodine-125
Iodine -123
80 DAYS
601 days
1322 hours
081
035
015
02
4-26
10-230
lt1
20mm
2-500nm
PHYSICAL BIOLOGICAL AND EFFECTIVE HALF LIFE OF I-131
PHYSICAL t12 Biological t12 Effective t12
THYROID TISSUE
EXTRA THYRIOD TISSUE
8 days
8 days
80 days
12 days
73 days
8 hours
GOALS OF RIA IN DIFFERENTIATED CANCERS
bull 1)Thyroid reminant ablation
bull 2)Adjuvant therapy for residual micriscopic disease
bull RAI targets remaining thyroid cancer cells in thyriodbed occult lymph node and distant mets
bull Ablation of remaining thyroid tissue facalitates useof TG as sensitive and specific marker for persistantdisease after primary therapy
bull Rx wbs after RAI ablation provides crutialinformation about prognosis and furthermanagement
bull Sherma SI Lancet 2003
MD anderson experience
bull 1599 patient outcome analysis for various treatment for differentiated thyroid Ca
bull 46 had radioiodine therapybull Treatment with radioiodine was the single most
powerful prognostic indicator for increased DFS (plt 0001)
bull Its use significantly increased the survival both standard and high risk group
bull Adult patients females with intrathyroidal papillary carcinoma treated with TT + RAI between 20-59yrs ndashbest prognosis
bull J Clin Endocrinol Metab 1992 Sep75(3)714-20
bull 1004 dtc- Followed up with
ndash RAI ndash 151
ndash thyroid hormone alone 755
ndash no postoperative medical therapy -98
Tumor recurrence ~ threefold lower p lt 0001in RAI vs other treatment
Fewer patients developed distant metastases (p lt 0002)
Significantly more pronounced in tgt=15cm
Mazzaferri EL et al Thyroid remnant 131I ablation for papillary and follicular thyroid carcinoma Thyroid 1997 Apr7(2)265-71
ATA GUIDELINES
bull Distant metsgross ETE regardless of tumor sizeprimarysize gt4cm even in absence of high risk features
bull Follicular and hurthle cell variants are considered high riskand these patients are always recommended RAI ablationexcept with small unifocal FCs (lt2cm) with capsular invasiononly(no vasular invasion)
bull For 1-4cm size RAI is used for lymph node mets or highrisk features like agegt45 intra thyriod vascularinvasionmultifocal diseaseaggressive variants(tallcellcolummner cell or insular carcinoma)
bull RAI is not used for PTCS lt1cm unifocal and with out highrisk features OR when all foci in multifocal disease is in1cm focus
bull In a study assessing outcomes in 1004 patients with differentiated thyroid carcinoma tumor recurrence was about 3-fold higher in patients either treated with thyroid hormone alone or given no postoperative medical therapy when compared with patients who underwent postoperative thyroid remnant ablation with 131I (P lt 001)
bull Moreover fewer patients developed distant metastases (P lt 002) after thyroid remnant 131I ablation than after other forms of postoperative treatment However this effect is observed only in patients with primary tumors 15 cm or more in diameter Mazzaferri EL Thyroid remnant 131I ablation for papillary andfollicular thyroid carcinoma
low risk group with i-131 abilationStudy showed that remnant ablation had less of a therapeutic effect perhaps because more extensive locoregional surgery had been done Hay ID Papillary thyroid carcinoma Endocrinol Metab Clin North
bull Rising incidence of second cancers in patients with low-risk (T1N0) thyroid cancer who receive radioactive iodine therapy
bull CONCLUSIONS-The increased risk of a SPM in patients with low-risk (T1N0) WDTC along with a lack of data demonstrating improved survival outcomes with adjuvant RAI( IYER NG etal 2013cancer)
bull Impact on overall survival of radioactive iodine in low-risk differentiated thyroid cancer patients
bull CONCLUSION-With a long-term follow-up of 103 yr we failed to prove any survival benefit of RAI after surgery in a large cohort of low-risk DTC patients(SCHTWATZC et alJ Clin Endocrinol Metab 2012 May)
MAJOR FACTORS IMPACTING DECISION MAKING IN RADIOIODINE REMNANT ABLATION
ADMINSTRATION OF I-131
bull As liquid solution or in capsulesbull Each capsule accounts for 50 micro
curiebull Capsules safer than liquid- less
radioactivity released into air during handling
bull Also result in less oral mucosal irritation
bull Simultaneous ingestion large amounts of water attenuates radiation dose emitted to gastric wall
bull Rapidly and completely absorbed in the upper intestine
PATIENT PREPRATIONS1)Low iodine diet(lt50ugday) for 2 wks before and 2 days afterRAI(saltbreat and dairy products to be avoided)it has been seen doublesthe RAI uptake and lower rates of measuarable Tg levels after RAI(SAWAKAEM et al2012THYRIOD)2)Avoid iodinated contast in all DCT patients patient should have delay in RAItherapy for 3-6 months followed by measurement of urinary iodine levels (lt150ugml measured after collecting 24 hour urine and patient should be on iodine freediet gt7 days)3)Stop thyroxine repelacement therapy six weeks before RAI thepapy in case r-TSHis used stop 3-4 days before RAI therapy4)09 mg r-TSH can b used twice (2 days before and one day after) I-131(not to beused in cardiovascular diseasepara tracheal massspinal mets and inchildrenefficacy not studied in children)( studies show equal results with tshreplacement vs r-TSH)TSWNG et AL 1998CANCER5)Lithium carbonate 20mgkgday for 7 days usually 5 days before RAI ablation(measure serum lithium concentration on 4th 5th day of therapy which should be06-12 megml in its narrow theurpatic range)lithium decreases iodine exit fromthyriod cells increasing biological t12 by 50-90 with out interfering with iodineuptakeno studies have shown improved out comes with lithuimContraindicated in psychiatric problemsdementiaseizuresrenal and hepaticinsufficiencydiureticnsaidCCB intakehypohypernatremiahellip
Cancer vs normal cells
bull Metabolism of radioiodine in papillary and follicular carcinoma is profoundly altered when compared with normal thyroid tissue
bull Several defects are present in cancer tissuendash iodine uptake via the sodium-iodide symporter
(NIS) is always decreased and is undetectable in about a third of patients
ndash Iodine organification is markedly reduced
ndash Effective half-life of iodine in tumor tissue is always shorter
bull Tissues that often take up iodine and can be misconstrued as metastases include the
ndash salivary glands in the mouth
ndash esophagus (as a result of swallowing radioactive saliva)
ndash thymus gland
ndash breasts in some women
ndash liver stomach colon bladder
I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

radionucleotide Physical t12 Emax(MEV) LET(kevum) Appx cell diameter
Maximum range in tissue
Iodine-131
Iodine-125
Iodine -123
80 DAYS
601 days
1322 hours
081
035
015
02
4-26
10-230
lt1
20mm
2-500nm
PHYSICAL BIOLOGICAL AND EFFECTIVE HALF LIFE OF I-131
PHYSICAL t12 Biological t12 Effective t12
THYROID TISSUE
EXTRA THYRIOD TISSUE
8 days
8 days
80 days
12 days
73 days
8 hours
GOALS OF RIA IN DIFFERENTIATED CANCERS
bull 1)Thyroid reminant ablation
bull 2)Adjuvant therapy for residual micriscopic disease
bull RAI targets remaining thyroid cancer cells in thyriodbed occult lymph node and distant mets
bull Ablation of remaining thyroid tissue facalitates useof TG as sensitive and specific marker for persistantdisease after primary therapy
bull Rx wbs after RAI ablation provides crutialinformation about prognosis and furthermanagement
bull Sherma SI Lancet 2003
MD anderson experience
bull 1599 patient outcome analysis for various treatment for differentiated thyroid Ca
bull 46 had radioiodine therapybull Treatment with radioiodine was the single most
powerful prognostic indicator for increased DFS (plt 0001)
bull Its use significantly increased the survival both standard and high risk group
bull Adult patients females with intrathyroidal papillary carcinoma treated with TT + RAI between 20-59yrs ndashbest prognosis
bull J Clin Endocrinol Metab 1992 Sep75(3)714-20
bull 1004 dtc- Followed up with
ndash RAI ndash 151
ndash thyroid hormone alone 755
ndash no postoperative medical therapy -98
Tumor recurrence ~ threefold lower p lt 0001in RAI vs other treatment
Fewer patients developed distant metastases (p lt 0002)
Significantly more pronounced in tgt=15cm
Mazzaferri EL et al Thyroid remnant 131I ablation for papillary and follicular thyroid carcinoma Thyroid 1997 Apr7(2)265-71
ATA GUIDELINES
bull Distant metsgross ETE regardless of tumor sizeprimarysize gt4cm even in absence of high risk features
bull Follicular and hurthle cell variants are considered high riskand these patients are always recommended RAI ablationexcept with small unifocal FCs (lt2cm) with capsular invasiononly(no vasular invasion)
bull For 1-4cm size RAI is used for lymph node mets or highrisk features like agegt45 intra thyriod vascularinvasionmultifocal diseaseaggressive variants(tallcellcolummner cell or insular carcinoma)
bull RAI is not used for PTCS lt1cm unifocal and with out highrisk features OR when all foci in multifocal disease is in1cm focus
bull In a study assessing outcomes in 1004 patients with differentiated thyroid carcinoma tumor recurrence was about 3-fold higher in patients either treated with thyroid hormone alone or given no postoperative medical therapy when compared with patients who underwent postoperative thyroid remnant ablation with 131I (P lt 001)
bull Moreover fewer patients developed distant metastases (P lt 002) after thyroid remnant 131I ablation than after other forms of postoperative treatment However this effect is observed only in patients with primary tumors 15 cm or more in diameter Mazzaferri EL Thyroid remnant 131I ablation for papillary andfollicular thyroid carcinoma
low risk group with i-131 abilationStudy showed that remnant ablation had less of a therapeutic effect perhaps because more extensive locoregional surgery had been done Hay ID Papillary thyroid carcinoma Endocrinol Metab Clin North
bull Rising incidence of second cancers in patients with low-risk (T1N0) thyroid cancer who receive radioactive iodine therapy
bull CONCLUSIONS-The increased risk of a SPM in patients with low-risk (T1N0) WDTC along with a lack of data demonstrating improved survival outcomes with adjuvant RAI( IYER NG etal 2013cancer)
bull Impact on overall survival of radioactive iodine in low-risk differentiated thyroid cancer patients
bull CONCLUSION-With a long-term follow-up of 103 yr we failed to prove any survival benefit of RAI after surgery in a large cohort of low-risk DTC patients(SCHTWATZC et alJ Clin Endocrinol Metab 2012 May)
MAJOR FACTORS IMPACTING DECISION MAKING IN RADIOIODINE REMNANT ABLATION
ADMINSTRATION OF I-131
bull As liquid solution or in capsulesbull Each capsule accounts for 50 micro
curiebull Capsules safer than liquid- less
radioactivity released into air during handling
bull Also result in less oral mucosal irritation
bull Simultaneous ingestion large amounts of water attenuates radiation dose emitted to gastric wall
bull Rapidly and completely absorbed in the upper intestine
PATIENT PREPRATIONS1)Low iodine diet(lt50ugday) for 2 wks before and 2 days afterRAI(saltbreat and dairy products to be avoided)it has been seen doublesthe RAI uptake and lower rates of measuarable Tg levels after RAI(SAWAKAEM et al2012THYRIOD)2)Avoid iodinated contast in all DCT patients patient should have delay in RAItherapy for 3-6 months followed by measurement of urinary iodine levels (lt150ugml measured after collecting 24 hour urine and patient should be on iodine freediet gt7 days)3)Stop thyroxine repelacement therapy six weeks before RAI thepapy in case r-TSHis used stop 3-4 days before RAI therapy4)09 mg r-TSH can b used twice (2 days before and one day after) I-131(not to beused in cardiovascular diseasepara tracheal massspinal mets and inchildrenefficacy not studied in children)( studies show equal results with tshreplacement vs r-TSH)TSWNG et AL 1998CANCER5)Lithium carbonate 20mgkgday for 7 days usually 5 days before RAI ablation(measure serum lithium concentration on 4th 5th day of therapy which should be06-12 megml in its narrow theurpatic range)lithium decreases iodine exit fromthyriod cells increasing biological t12 by 50-90 with out interfering with iodineuptakeno studies have shown improved out comes with lithuimContraindicated in psychiatric problemsdementiaseizuresrenal and hepaticinsufficiencydiureticnsaidCCB intakehypohypernatremiahellip
Cancer vs normal cells
bull Metabolism of radioiodine in papillary and follicular carcinoma is profoundly altered when compared with normal thyroid tissue
bull Several defects are present in cancer tissuendash iodine uptake via the sodium-iodide symporter
(NIS) is always decreased and is undetectable in about a third of patients
ndash Iodine organification is markedly reduced
ndash Effective half-life of iodine in tumor tissue is always shorter
bull Tissues that often take up iodine and can be misconstrued as metastases include the
ndash salivary glands in the mouth
ndash esophagus (as a result of swallowing radioactive saliva)
ndash thymus gland
ndash breasts in some women
ndash liver stomach colon bladder
I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

GOALS OF RIA IN DIFFERENTIATED CANCERS
bull 1)Thyroid reminant ablation
bull 2)Adjuvant therapy for residual micriscopic disease
bull RAI targets remaining thyroid cancer cells in thyriodbed occult lymph node and distant mets
bull Ablation of remaining thyroid tissue facalitates useof TG as sensitive and specific marker for persistantdisease after primary therapy
bull Rx wbs after RAI ablation provides crutialinformation about prognosis and furthermanagement
bull Sherma SI Lancet 2003
MD anderson experience
bull 1599 patient outcome analysis for various treatment for differentiated thyroid Ca
bull 46 had radioiodine therapybull Treatment with radioiodine was the single most
powerful prognostic indicator for increased DFS (plt 0001)
bull Its use significantly increased the survival both standard and high risk group
bull Adult patients females with intrathyroidal papillary carcinoma treated with TT + RAI between 20-59yrs ndashbest prognosis
bull J Clin Endocrinol Metab 1992 Sep75(3)714-20
bull 1004 dtc- Followed up with
ndash RAI ndash 151
ndash thyroid hormone alone 755
ndash no postoperative medical therapy -98
Tumor recurrence ~ threefold lower p lt 0001in RAI vs other treatment
Fewer patients developed distant metastases (p lt 0002)
Significantly more pronounced in tgt=15cm
Mazzaferri EL et al Thyroid remnant 131I ablation for papillary and follicular thyroid carcinoma Thyroid 1997 Apr7(2)265-71
ATA GUIDELINES
bull Distant metsgross ETE regardless of tumor sizeprimarysize gt4cm even in absence of high risk features
bull Follicular and hurthle cell variants are considered high riskand these patients are always recommended RAI ablationexcept with small unifocal FCs (lt2cm) with capsular invasiononly(no vasular invasion)
bull For 1-4cm size RAI is used for lymph node mets or highrisk features like agegt45 intra thyriod vascularinvasionmultifocal diseaseaggressive variants(tallcellcolummner cell or insular carcinoma)
bull RAI is not used for PTCS lt1cm unifocal and with out highrisk features OR when all foci in multifocal disease is in1cm focus
bull In a study assessing outcomes in 1004 patients with differentiated thyroid carcinoma tumor recurrence was about 3-fold higher in patients either treated with thyroid hormone alone or given no postoperative medical therapy when compared with patients who underwent postoperative thyroid remnant ablation with 131I (P lt 001)
bull Moreover fewer patients developed distant metastases (P lt 002) after thyroid remnant 131I ablation than after other forms of postoperative treatment However this effect is observed only in patients with primary tumors 15 cm or more in diameter Mazzaferri EL Thyroid remnant 131I ablation for papillary andfollicular thyroid carcinoma
low risk group with i-131 abilationStudy showed that remnant ablation had less of a therapeutic effect perhaps because more extensive locoregional surgery had been done Hay ID Papillary thyroid carcinoma Endocrinol Metab Clin North
bull Rising incidence of second cancers in patients with low-risk (T1N0) thyroid cancer who receive radioactive iodine therapy
bull CONCLUSIONS-The increased risk of a SPM in patients with low-risk (T1N0) WDTC along with a lack of data demonstrating improved survival outcomes with adjuvant RAI( IYER NG etal 2013cancer)
bull Impact on overall survival of radioactive iodine in low-risk differentiated thyroid cancer patients
bull CONCLUSION-With a long-term follow-up of 103 yr we failed to prove any survival benefit of RAI after surgery in a large cohort of low-risk DTC patients(SCHTWATZC et alJ Clin Endocrinol Metab 2012 May)
MAJOR FACTORS IMPACTING DECISION MAKING IN RADIOIODINE REMNANT ABLATION
ADMINSTRATION OF I-131
bull As liquid solution or in capsulesbull Each capsule accounts for 50 micro
curiebull Capsules safer than liquid- less
radioactivity released into air during handling
bull Also result in less oral mucosal irritation
bull Simultaneous ingestion large amounts of water attenuates radiation dose emitted to gastric wall
bull Rapidly and completely absorbed in the upper intestine
PATIENT PREPRATIONS1)Low iodine diet(lt50ugday) for 2 wks before and 2 days afterRAI(saltbreat and dairy products to be avoided)it has been seen doublesthe RAI uptake and lower rates of measuarable Tg levels after RAI(SAWAKAEM et al2012THYRIOD)2)Avoid iodinated contast in all DCT patients patient should have delay in RAItherapy for 3-6 months followed by measurement of urinary iodine levels (lt150ugml measured after collecting 24 hour urine and patient should be on iodine freediet gt7 days)3)Stop thyroxine repelacement therapy six weeks before RAI thepapy in case r-TSHis used stop 3-4 days before RAI therapy4)09 mg r-TSH can b used twice (2 days before and one day after) I-131(not to beused in cardiovascular diseasepara tracheal massspinal mets and inchildrenefficacy not studied in children)( studies show equal results with tshreplacement vs r-TSH)TSWNG et AL 1998CANCER5)Lithium carbonate 20mgkgday for 7 days usually 5 days before RAI ablation(measure serum lithium concentration on 4th 5th day of therapy which should be06-12 megml in its narrow theurpatic range)lithium decreases iodine exit fromthyriod cells increasing biological t12 by 50-90 with out interfering with iodineuptakeno studies have shown improved out comes with lithuimContraindicated in psychiatric problemsdementiaseizuresrenal and hepaticinsufficiencydiureticnsaidCCB intakehypohypernatremiahellip
Cancer vs normal cells
bull Metabolism of radioiodine in papillary and follicular carcinoma is profoundly altered when compared with normal thyroid tissue
bull Several defects are present in cancer tissuendash iodine uptake via the sodium-iodide symporter
(NIS) is always decreased and is undetectable in about a third of patients
ndash Iodine organification is markedly reduced
ndash Effective half-life of iodine in tumor tissue is always shorter
bull Tissues that often take up iodine and can be misconstrued as metastases include the
ndash salivary glands in the mouth
ndash esophagus (as a result of swallowing radioactive saliva)
ndash thymus gland
ndash breasts in some women
ndash liver stomach colon bladder
I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU
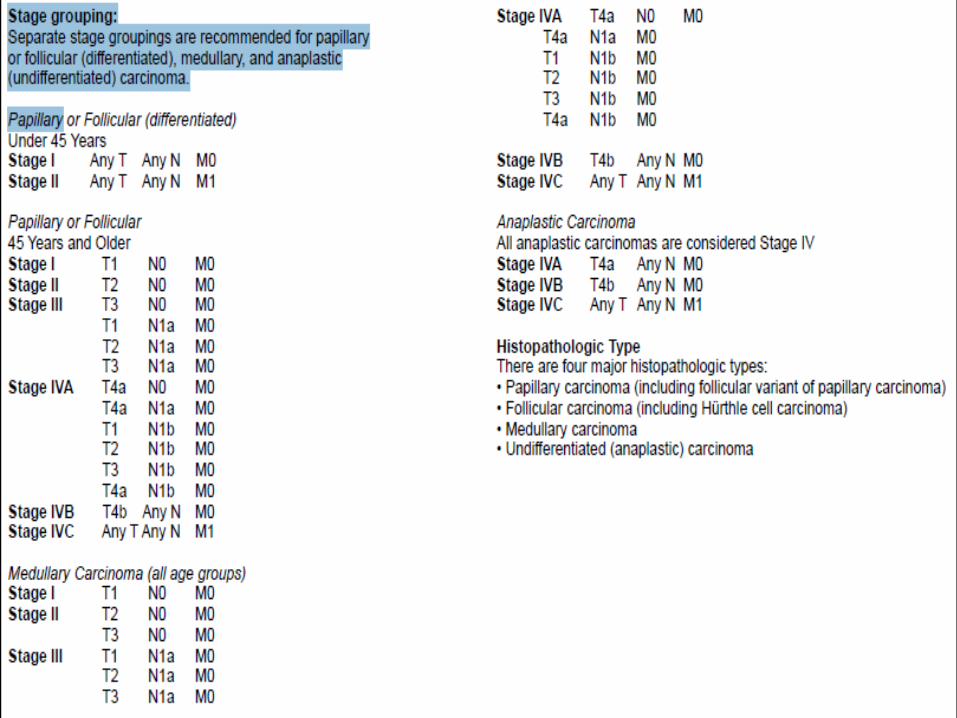
MD anderson experience
bull 1599 patient outcome analysis for various treatment for differentiated thyroid Ca
bull 46 had radioiodine therapybull Treatment with radioiodine was the single most
powerful prognostic indicator for increased DFS (plt 0001)
bull Its use significantly increased the survival both standard and high risk group
bull Adult patients females with intrathyroidal papillary carcinoma treated with TT + RAI between 20-59yrs ndashbest prognosis
bull J Clin Endocrinol Metab 1992 Sep75(3)714-20
bull 1004 dtc- Followed up with
ndash RAI ndash 151
ndash thyroid hormone alone 755
ndash no postoperative medical therapy -98
Tumor recurrence ~ threefold lower p lt 0001in RAI vs other treatment
Fewer patients developed distant metastases (p lt 0002)
Significantly more pronounced in tgt=15cm
Mazzaferri EL et al Thyroid remnant 131I ablation for papillary and follicular thyroid carcinoma Thyroid 1997 Apr7(2)265-71
ATA GUIDELINES
bull Distant metsgross ETE regardless of tumor sizeprimarysize gt4cm even in absence of high risk features
bull Follicular and hurthle cell variants are considered high riskand these patients are always recommended RAI ablationexcept with small unifocal FCs (lt2cm) with capsular invasiononly(no vasular invasion)
bull For 1-4cm size RAI is used for lymph node mets or highrisk features like agegt45 intra thyriod vascularinvasionmultifocal diseaseaggressive variants(tallcellcolummner cell or insular carcinoma)
bull RAI is not used for PTCS lt1cm unifocal and with out highrisk features OR when all foci in multifocal disease is in1cm focus
bull In a study assessing outcomes in 1004 patients with differentiated thyroid carcinoma tumor recurrence was about 3-fold higher in patients either treated with thyroid hormone alone or given no postoperative medical therapy when compared with patients who underwent postoperative thyroid remnant ablation with 131I (P lt 001)
bull Moreover fewer patients developed distant metastases (P lt 002) after thyroid remnant 131I ablation than after other forms of postoperative treatment However this effect is observed only in patients with primary tumors 15 cm or more in diameter Mazzaferri EL Thyroid remnant 131I ablation for papillary andfollicular thyroid carcinoma
low risk group with i-131 abilationStudy showed that remnant ablation had less of a therapeutic effect perhaps because more extensive locoregional surgery had been done Hay ID Papillary thyroid carcinoma Endocrinol Metab Clin North
bull Rising incidence of second cancers in patients with low-risk (T1N0) thyroid cancer who receive radioactive iodine therapy
bull CONCLUSIONS-The increased risk of a SPM in patients with low-risk (T1N0) WDTC along with a lack of data demonstrating improved survival outcomes with adjuvant RAI( IYER NG etal 2013cancer)
bull Impact on overall survival of radioactive iodine in low-risk differentiated thyroid cancer patients
bull CONCLUSION-With a long-term follow-up of 103 yr we failed to prove any survival benefit of RAI after surgery in a large cohort of low-risk DTC patients(SCHTWATZC et alJ Clin Endocrinol Metab 2012 May)
MAJOR FACTORS IMPACTING DECISION MAKING IN RADIOIODINE REMNANT ABLATION
ADMINSTRATION OF I-131
bull As liquid solution or in capsulesbull Each capsule accounts for 50 micro
curiebull Capsules safer than liquid- less
radioactivity released into air during handling
bull Also result in less oral mucosal irritation
bull Simultaneous ingestion large amounts of water attenuates radiation dose emitted to gastric wall
bull Rapidly and completely absorbed in the upper intestine
PATIENT PREPRATIONS1)Low iodine diet(lt50ugday) for 2 wks before and 2 days afterRAI(saltbreat and dairy products to be avoided)it has been seen doublesthe RAI uptake and lower rates of measuarable Tg levels after RAI(SAWAKAEM et al2012THYRIOD)2)Avoid iodinated contast in all DCT patients patient should have delay in RAItherapy for 3-6 months followed by measurement of urinary iodine levels (lt150ugml measured after collecting 24 hour urine and patient should be on iodine freediet gt7 days)3)Stop thyroxine repelacement therapy six weeks before RAI thepapy in case r-TSHis used stop 3-4 days before RAI therapy4)09 mg r-TSH can b used twice (2 days before and one day after) I-131(not to beused in cardiovascular diseasepara tracheal massspinal mets and inchildrenefficacy not studied in children)( studies show equal results with tshreplacement vs r-TSH)TSWNG et AL 1998CANCER5)Lithium carbonate 20mgkgday for 7 days usually 5 days before RAI ablation(measure serum lithium concentration on 4th 5th day of therapy which should be06-12 megml in its narrow theurpatic range)lithium decreases iodine exit fromthyriod cells increasing biological t12 by 50-90 with out interfering with iodineuptakeno studies have shown improved out comes with lithuimContraindicated in psychiatric problemsdementiaseizuresrenal and hepaticinsufficiencydiureticnsaidCCB intakehypohypernatremiahellip
Cancer vs normal cells
bull Metabolism of radioiodine in papillary and follicular carcinoma is profoundly altered when compared with normal thyroid tissue
bull Several defects are present in cancer tissuendash iodine uptake via the sodium-iodide symporter
(NIS) is always decreased and is undetectable in about a third of patients
ndash Iodine organification is markedly reduced
ndash Effective half-life of iodine in tumor tissue is always shorter
bull Tissues that often take up iodine and can be misconstrued as metastases include the
ndash salivary glands in the mouth
ndash esophagus (as a result of swallowing radioactive saliva)
ndash thymus gland
ndash breasts in some women
ndash liver stomach colon bladder
I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

bull 1004 dtc- Followed up with
ndash RAI ndash 151
ndash thyroid hormone alone 755
ndash no postoperative medical therapy -98
Tumor recurrence ~ threefold lower p lt 0001in RAI vs other treatment
Fewer patients developed distant metastases (p lt 0002)
Significantly more pronounced in tgt=15cm
Mazzaferri EL et al Thyroid remnant 131I ablation for papillary and follicular thyroid carcinoma Thyroid 1997 Apr7(2)265-71
ATA GUIDELINES
bull Distant metsgross ETE regardless of tumor sizeprimarysize gt4cm even in absence of high risk features
bull Follicular and hurthle cell variants are considered high riskand these patients are always recommended RAI ablationexcept with small unifocal FCs (lt2cm) with capsular invasiononly(no vasular invasion)
bull For 1-4cm size RAI is used for lymph node mets or highrisk features like agegt45 intra thyriod vascularinvasionmultifocal diseaseaggressive variants(tallcellcolummner cell or insular carcinoma)
bull RAI is not used for PTCS lt1cm unifocal and with out highrisk features OR when all foci in multifocal disease is in1cm focus
bull In a study assessing outcomes in 1004 patients with differentiated thyroid carcinoma tumor recurrence was about 3-fold higher in patients either treated with thyroid hormone alone or given no postoperative medical therapy when compared with patients who underwent postoperative thyroid remnant ablation with 131I (P lt 001)
bull Moreover fewer patients developed distant metastases (P lt 002) after thyroid remnant 131I ablation than after other forms of postoperative treatment However this effect is observed only in patients with primary tumors 15 cm or more in diameter Mazzaferri EL Thyroid remnant 131I ablation for papillary andfollicular thyroid carcinoma
low risk group with i-131 abilationStudy showed that remnant ablation had less of a therapeutic effect perhaps because more extensive locoregional surgery had been done Hay ID Papillary thyroid carcinoma Endocrinol Metab Clin North
bull Rising incidence of second cancers in patients with low-risk (T1N0) thyroid cancer who receive radioactive iodine therapy
bull CONCLUSIONS-The increased risk of a SPM in patients with low-risk (T1N0) WDTC along with a lack of data demonstrating improved survival outcomes with adjuvant RAI( IYER NG etal 2013cancer)
bull Impact on overall survival of radioactive iodine in low-risk differentiated thyroid cancer patients
bull CONCLUSION-With a long-term follow-up of 103 yr we failed to prove any survival benefit of RAI after surgery in a large cohort of low-risk DTC patients(SCHTWATZC et alJ Clin Endocrinol Metab 2012 May)
MAJOR FACTORS IMPACTING DECISION MAKING IN RADIOIODINE REMNANT ABLATION
ADMINSTRATION OF I-131
bull As liquid solution or in capsulesbull Each capsule accounts for 50 micro
curiebull Capsules safer than liquid- less
radioactivity released into air during handling
bull Also result in less oral mucosal irritation
bull Simultaneous ingestion large amounts of water attenuates radiation dose emitted to gastric wall
bull Rapidly and completely absorbed in the upper intestine
PATIENT PREPRATIONS1)Low iodine diet(lt50ugday) for 2 wks before and 2 days afterRAI(saltbreat and dairy products to be avoided)it has been seen doublesthe RAI uptake and lower rates of measuarable Tg levels after RAI(SAWAKAEM et al2012THYRIOD)2)Avoid iodinated contast in all DCT patients patient should have delay in RAItherapy for 3-6 months followed by measurement of urinary iodine levels (lt150ugml measured after collecting 24 hour urine and patient should be on iodine freediet gt7 days)3)Stop thyroxine repelacement therapy six weeks before RAI thepapy in case r-TSHis used stop 3-4 days before RAI therapy4)09 mg r-TSH can b used twice (2 days before and one day after) I-131(not to beused in cardiovascular diseasepara tracheal massspinal mets and inchildrenefficacy not studied in children)( studies show equal results with tshreplacement vs r-TSH)TSWNG et AL 1998CANCER5)Lithium carbonate 20mgkgday for 7 days usually 5 days before RAI ablation(measure serum lithium concentration on 4th 5th day of therapy which should be06-12 megml in its narrow theurpatic range)lithium decreases iodine exit fromthyriod cells increasing biological t12 by 50-90 with out interfering with iodineuptakeno studies have shown improved out comes with lithuimContraindicated in psychiatric problemsdementiaseizuresrenal and hepaticinsufficiencydiureticnsaidCCB intakehypohypernatremiahellip
Cancer vs normal cells
bull Metabolism of radioiodine in papillary and follicular carcinoma is profoundly altered when compared with normal thyroid tissue
bull Several defects are present in cancer tissuendash iodine uptake via the sodium-iodide symporter
(NIS) is always decreased and is undetectable in about a third of patients
ndash Iodine organification is markedly reduced
ndash Effective half-life of iodine in tumor tissue is always shorter
bull Tissues that often take up iodine and can be misconstrued as metastases include the
ndash salivary glands in the mouth
ndash esophagus (as a result of swallowing radioactive saliva)
ndash thymus gland
ndash breasts in some women
ndash liver stomach colon bladder
I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

ATA GUIDELINES
bull Distant metsgross ETE regardless of tumor sizeprimarysize gt4cm even in absence of high risk features
bull Follicular and hurthle cell variants are considered high riskand these patients are always recommended RAI ablationexcept with small unifocal FCs (lt2cm) with capsular invasiononly(no vasular invasion)
bull For 1-4cm size RAI is used for lymph node mets or highrisk features like agegt45 intra thyriod vascularinvasionmultifocal diseaseaggressive variants(tallcellcolummner cell or insular carcinoma)
bull RAI is not used for PTCS lt1cm unifocal and with out highrisk features OR when all foci in multifocal disease is in1cm focus
bull In a study assessing outcomes in 1004 patients with differentiated thyroid carcinoma tumor recurrence was about 3-fold higher in patients either treated with thyroid hormone alone or given no postoperative medical therapy when compared with patients who underwent postoperative thyroid remnant ablation with 131I (P lt 001)
bull Moreover fewer patients developed distant metastases (P lt 002) after thyroid remnant 131I ablation than after other forms of postoperative treatment However this effect is observed only in patients with primary tumors 15 cm or more in diameter Mazzaferri EL Thyroid remnant 131I ablation for papillary andfollicular thyroid carcinoma
low risk group with i-131 abilationStudy showed that remnant ablation had less of a therapeutic effect perhaps because more extensive locoregional surgery had been done Hay ID Papillary thyroid carcinoma Endocrinol Metab Clin North
bull Rising incidence of second cancers in patients with low-risk (T1N0) thyroid cancer who receive radioactive iodine therapy
bull CONCLUSIONS-The increased risk of a SPM in patients with low-risk (T1N0) WDTC along with a lack of data demonstrating improved survival outcomes with adjuvant RAI( IYER NG etal 2013cancer)
bull Impact on overall survival of radioactive iodine in low-risk differentiated thyroid cancer patients
bull CONCLUSION-With a long-term follow-up of 103 yr we failed to prove any survival benefit of RAI after surgery in a large cohort of low-risk DTC patients(SCHTWATZC et alJ Clin Endocrinol Metab 2012 May)
MAJOR FACTORS IMPACTING DECISION MAKING IN RADIOIODINE REMNANT ABLATION
ADMINSTRATION OF I-131
bull As liquid solution or in capsulesbull Each capsule accounts for 50 micro
curiebull Capsules safer than liquid- less
radioactivity released into air during handling
bull Also result in less oral mucosal irritation
bull Simultaneous ingestion large amounts of water attenuates radiation dose emitted to gastric wall
bull Rapidly and completely absorbed in the upper intestine
PATIENT PREPRATIONS1)Low iodine diet(lt50ugday) for 2 wks before and 2 days afterRAI(saltbreat and dairy products to be avoided)it has been seen doublesthe RAI uptake and lower rates of measuarable Tg levels after RAI(SAWAKAEM et al2012THYRIOD)2)Avoid iodinated contast in all DCT patients patient should have delay in RAItherapy for 3-6 months followed by measurement of urinary iodine levels (lt150ugml measured after collecting 24 hour urine and patient should be on iodine freediet gt7 days)3)Stop thyroxine repelacement therapy six weeks before RAI thepapy in case r-TSHis used stop 3-4 days before RAI therapy4)09 mg r-TSH can b used twice (2 days before and one day after) I-131(not to beused in cardiovascular diseasepara tracheal massspinal mets and inchildrenefficacy not studied in children)( studies show equal results with tshreplacement vs r-TSH)TSWNG et AL 1998CANCER5)Lithium carbonate 20mgkgday for 7 days usually 5 days before RAI ablation(measure serum lithium concentration on 4th 5th day of therapy which should be06-12 megml in its narrow theurpatic range)lithium decreases iodine exit fromthyriod cells increasing biological t12 by 50-90 with out interfering with iodineuptakeno studies have shown improved out comes with lithuimContraindicated in psychiatric problemsdementiaseizuresrenal and hepaticinsufficiencydiureticnsaidCCB intakehypohypernatremiahellip
Cancer vs normal cells
bull Metabolism of radioiodine in papillary and follicular carcinoma is profoundly altered when compared with normal thyroid tissue
bull Several defects are present in cancer tissuendash iodine uptake via the sodium-iodide symporter
(NIS) is always decreased and is undetectable in about a third of patients
ndash Iodine organification is markedly reduced
ndash Effective half-life of iodine in tumor tissue is always shorter
bull Tissues that often take up iodine and can be misconstrued as metastases include the
ndash salivary glands in the mouth
ndash esophagus (as a result of swallowing radioactive saliva)
ndash thymus gland
ndash breasts in some women
ndash liver stomach colon bladder
I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

bull In a study assessing outcomes in 1004 patients with differentiated thyroid carcinoma tumor recurrence was about 3-fold higher in patients either treated with thyroid hormone alone or given no postoperative medical therapy when compared with patients who underwent postoperative thyroid remnant ablation with 131I (P lt 001)
bull Moreover fewer patients developed distant metastases (P lt 002) after thyroid remnant 131I ablation than after other forms of postoperative treatment However this effect is observed only in patients with primary tumors 15 cm or more in diameter Mazzaferri EL Thyroid remnant 131I ablation for papillary andfollicular thyroid carcinoma
low risk group with i-131 abilationStudy showed that remnant ablation had less of a therapeutic effect perhaps because more extensive locoregional surgery had been done Hay ID Papillary thyroid carcinoma Endocrinol Metab Clin North
bull Rising incidence of second cancers in patients with low-risk (T1N0) thyroid cancer who receive radioactive iodine therapy
bull CONCLUSIONS-The increased risk of a SPM in patients with low-risk (T1N0) WDTC along with a lack of data demonstrating improved survival outcomes with adjuvant RAI( IYER NG etal 2013cancer)
bull Impact on overall survival of radioactive iodine in low-risk differentiated thyroid cancer patients
bull CONCLUSION-With a long-term follow-up of 103 yr we failed to prove any survival benefit of RAI after surgery in a large cohort of low-risk DTC patients(SCHTWATZC et alJ Clin Endocrinol Metab 2012 May)
MAJOR FACTORS IMPACTING DECISION MAKING IN RADIOIODINE REMNANT ABLATION
ADMINSTRATION OF I-131
bull As liquid solution or in capsulesbull Each capsule accounts for 50 micro
curiebull Capsules safer than liquid- less
radioactivity released into air during handling
bull Also result in less oral mucosal irritation
bull Simultaneous ingestion large amounts of water attenuates radiation dose emitted to gastric wall
bull Rapidly and completely absorbed in the upper intestine
PATIENT PREPRATIONS1)Low iodine diet(lt50ugday) for 2 wks before and 2 days afterRAI(saltbreat and dairy products to be avoided)it has been seen doublesthe RAI uptake and lower rates of measuarable Tg levels after RAI(SAWAKAEM et al2012THYRIOD)2)Avoid iodinated contast in all DCT patients patient should have delay in RAItherapy for 3-6 months followed by measurement of urinary iodine levels (lt150ugml measured after collecting 24 hour urine and patient should be on iodine freediet gt7 days)3)Stop thyroxine repelacement therapy six weeks before RAI thepapy in case r-TSHis used stop 3-4 days before RAI therapy4)09 mg r-TSH can b used twice (2 days before and one day after) I-131(not to beused in cardiovascular diseasepara tracheal massspinal mets and inchildrenefficacy not studied in children)( studies show equal results with tshreplacement vs r-TSH)TSWNG et AL 1998CANCER5)Lithium carbonate 20mgkgday for 7 days usually 5 days before RAI ablation(measure serum lithium concentration on 4th 5th day of therapy which should be06-12 megml in its narrow theurpatic range)lithium decreases iodine exit fromthyriod cells increasing biological t12 by 50-90 with out interfering with iodineuptakeno studies have shown improved out comes with lithuimContraindicated in psychiatric problemsdementiaseizuresrenal and hepaticinsufficiencydiureticnsaidCCB intakehypohypernatremiahellip
Cancer vs normal cells
bull Metabolism of radioiodine in papillary and follicular carcinoma is profoundly altered when compared with normal thyroid tissue
bull Several defects are present in cancer tissuendash iodine uptake via the sodium-iodide symporter
(NIS) is always decreased and is undetectable in about a third of patients
ndash Iodine organification is markedly reduced
ndash Effective half-life of iodine in tumor tissue is always shorter
bull Tissues that often take up iodine and can be misconstrued as metastases include the
ndash salivary glands in the mouth
ndash esophagus (as a result of swallowing radioactive saliva)
ndash thymus gland
ndash breasts in some women
ndash liver stomach colon bladder
I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

bull Rising incidence of second cancers in patients with low-risk (T1N0) thyroid cancer who receive radioactive iodine therapy
bull CONCLUSIONS-The increased risk of a SPM in patients with low-risk (T1N0) WDTC along with a lack of data demonstrating improved survival outcomes with adjuvant RAI( IYER NG etal 2013cancer)
bull Impact on overall survival of radioactive iodine in low-risk differentiated thyroid cancer patients
bull CONCLUSION-With a long-term follow-up of 103 yr we failed to prove any survival benefit of RAI after surgery in a large cohort of low-risk DTC patients(SCHTWATZC et alJ Clin Endocrinol Metab 2012 May)
MAJOR FACTORS IMPACTING DECISION MAKING IN RADIOIODINE REMNANT ABLATION
ADMINSTRATION OF I-131
bull As liquid solution or in capsulesbull Each capsule accounts for 50 micro
curiebull Capsules safer than liquid- less
radioactivity released into air during handling
bull Also result in less oral mucosal irritation
bull Simultaneous ingestion large amounts of water attenuates radiation dose emitted to gastric wall
bull Rapidly and completely absorbed in the upper intestine
PATIENT PREPRATIONS1)Low iodine diet(lt50ugday) for 2 wks before and 2 days afterRAI(saltbreat and dairy products to be avoided)it has been seen doublesthe RAI uptake and lower rates of measuarable Tg levels after RAI(SAWAKAEM et al2012THYRIOD)2)Avoid iodinated contast in all DCT patients patient should have delay in RAItherapy for 3-6 months followed by measurement of urinary iodine levels (lt150ugml measured after collecting 24 hour urine and patient should be on iodine freediet gt7 days)3)Stop thyroxine repelacement therapy six weeks before RAI thepapy in case r-TSHis used stop 3-4 days before RAI therapy4)09 mg r-TSH can b used twice (2 days before and one day after) I-131(not to beused in cardiovascular diseasepara tracheal massspinal mets and inchildrenefficacy not studied in children)( studies show equal results with tshreplacement vs r-TSH)TSWNG et AL 1998CANCER5)Lithium carbonate 20mgkgday for 7 days usually 5 days before RAI ablation(measure serum lithium concentration on 4th 5th day of therapy which should be06-12 megml in its narrow theurpatic range)lithium decreases iodine exit fromthyriod cells increasing biological t12 by 50-90 with out interfering with iodineuptakeno studies have shown improved out comes with lithuimContraindicated in psychiatric problemsdementiaseizuresrenal and hepaticinsufficiencydiureticnsaidCCB intakehypohypernatremiahellip
Cancer vs normal cells
bull Metabolism of radioiodine in papillary and follicular carcinoma is profoundly altered when compared with normal thyroid tissue
bull Several defects are present in cancer tissuendash iodine uptake via the sodium-iodide symporter
(NIS) is always decreased and is undetectable in about a third of patients
ndash Iodine organification is markedly reduced
ndash Effective half-life of iodine in tumor tissue is always shorter
bull Tissues that often take up iodine and can be misconstrued as metastases include the
ndash salivary glands in the mouth
ndash esophagus (as a result of swallowing radioactive saliva)
ndash thymus gland
ndash breasts in some women
ndash liver stomach colon bladder
I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

MAJOR FACTORS IMPACTING DECISION MAKING IN RADIOIODINE REMNANT ABLATION
ADMINSTRATION OF I-131
bull As liquid solution or in capsulesbull Each capsule accounts for 50 micro
curiebull Capsules safer than liquid- less
radioactivity released into air during handling
bull Also result in less oral mucosal irritation
bull Simultaneous ingestion large amounts of water attenuates radiation dose emitted to gastric wall
bull Rapidly and completely absorbed in the upper intestine
PATIENT PREPRATIONS1)Low iodine diet(lt50ugday) for 2 wks before and 2 days afterRAI(saltbreat and dairy products to be avoided)it has been seen doublesthe RAI uptake and lower rates of measuarable Tg levels after RAI(SAWAKAEM et al2012THYRIOD)2)Avoid iodinated contast in all DCT patients patient should have delay in RAItherapy for 3-6 months followed by measurement of urinary iodine levels (lt150ugml measured after collecting 24 hour urine and patient should be on iodine freediet gt7 days)3)Stop thyroxine repelacement therapy six weeks before RAI thepapy in case r-TSHis used stop 3-4 days before RAI therapy4)09 mg r-TSH can b used twice (2 days before and one day after) I-131(not to beused in cardiovascular diseasepara tracheal massspinal mets and inchildrenefficacy not studied in children)( studies show equal results with tshreplacement vs r-TSH)TSWNG et AL 1998CANCER5)Lithium carbonate 20mgkgday for 7 days usually 5 days before RAI ablation(measure serum lithium concentration on 4th 5th day of therapy which should be06-12 megml in its narrow theurpatic range)lithium decreases iodine exit fromthyriod cells increasing biological t12 by 50-90 with out interfering with iodineuptakeno studies have shown improved out comes with lithuimContraindicated in psychiatric problemsdementiaseizuresrenal and hepaticinsufficiencydiureticnsaidCCB intakehypohypernatremiahellip
Cancer vs normal cells
bull Metabolism of radioiodine in papillary and follicular carcinoma is profoundly altered when compared with normal thyroid tissue
bull Several defects are present in cancer tissuendash iodine uptake via the sodium-iodide symporter
(NIS) is always decreased and is undetectable in about a third of patients
ndash Iodine organification is markedly reduced
ndash Effective half-life of iodine in tumor tissue is always shorter
bull Tissues that often take up iodine and can be misconstrued as metastases include the
ndash salivary glands in the mouth
ndash esophagus (as a result of swallowing radioactive saliva)
ndash thymus gland
ndash breasts in some women
ndash liver stomach colon bladder
I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

ADMINSTRATION OF I-131
bull As liquid solution or in capsulesbull Each capsule accounts for 50 micro
curiebull Capsules safer than liquid- less
radioactivity released into air during handling
bull Also result in less oral mucosal irritation
bull Simultaneous ingestion large amounts of water attenuates radiation dose emitted to gastric wall
bull Rapidly and completely absorbed in the upper intestine
PATIENT PREPRATIONS1)Low iodine diet(lt50ugday) for 2 wks before and 2 days afterRAI(saltbreat and dairy products to be avoided)it has been seen doublesthe RAI uptake and lower rates of measuarable Tg levels after RAI(SAWAKAEM et al2012THYRIOD)2)Avoid iodinated contast in all DCT patients patient should have delay in RAItherapy for 3-6 months followed by measurement of urinary iodine levels (lt150ugml measured after collecting 24 hour urine and patient should be on iodine freediet gt7 days)3)Stop thyroxine repelacement therapy six weeks before RAI thepapy in case r-TSHis used stop 3-4 days before RAI therapy4)09 mg r-TSH can b used twice (2 days before and one day after) I-131(not to beused in cardiovascular diseasepara tracheal massspinal mets and inchildrenefficacy not studied in children)( studies show equal results with tshreplacement vs r-TSH)TSWNG et AL 1998CANCER5)Lithium carbonate 20mgkgday for 7 days usually 5 days before RAI ablation(measure serum lithium concentration on 4th 5th day of therapy which should be06-12 megml in its narrow theurpatic range)lithium decreases iodine exit fromthyriod cells increasing biological t12 by 50-90 with out interfering with iodineuptakeno studies have shown improved out comes with lithuimContraindicated in psychiatric problemsdementiaseizuresrenal and hepaticinsufficiencydiureticnsaidCCB intakehypohypernatremiahellip
Cancer vs normal cells
bull Metabolism of radioiodine in papillary and follicular carcinoma is profoundly altered when compared with normal thyroid tissue
bull Several defects are present in cancer tissuendash iodine uptake via the sodium-iodide symporter
(NIS) is always decreased and is undetectable in about a third of patients
ndash Iodine organification is markedly reduced
ndash Effective half-life of iodine in tumor tissue is always shorter
bull Tissues that often take up iodine and can be misconstrued as metastases include the
ndash salivary glands in the mouth
ndash esophagus (as a result of swallowing radioactive saliva)
ndash thymus gland
ndash breasts in some women
ndash liver stomach colon bladder
I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

PATIENT PREPRATIONS1)Low iodine diet(lt50ugday) for 2 wks before and 2 days afterRAI(saltbreat and dairy products to be avoided)it has been seen doublesthe RAI uptake and lower rates of measuarable Tg levels after RAI(SAWAKAEM et al2012THYRIOD)2)Avoid iodinated contast in all DCT patients patient should have delay in RAItherapy for 3-6 months followed by measurement of urinary iodine levels (lt150ugml measured after collecting 24 hour urine and patient should be on iodine freediet gt7 days)3)Stop thyroxine repelacement therapy six weeks before RAI thepapy in case r-TSHis used stop 3-4 days before RAI therapy4)09 mg r-TSH can b used twice (2 days before and one day after) I-131(not to beused in cardiovascular diseasepara tracheal massspinal mets and inchildrenefficacy not studied in children)( studies show equal results with tshreplacement vs r-TSH)TSWNG et AL 1998CANCER5)Lithium carbonate 20mgkgday for 7 days usually 5 days before RAI ablation(measure serum lithium concentration on 4th 5th day of therapy which should be06-12 megml in its narrow theurpatic range)lithium decreases iodine exit fromthyriod cells increasing biological t12 by 50-90 with out interfering with iodineuptakeno studies have shown improved out comes with lithuimContraindicated in psychiatric problemsdementiaseizuresrenal and hepaticinsufficiencydiureticnsaidCCB intakehypohypernatremiahellip
Cancer vs normal cells
bull Metabolism of radioiodine in papillary and follicular carcinoma is profoundly altered when compared with normal thyroid tissue
bull Several defects are present in cancer tissuendash iodine uptake via the sodium-iodide symporter
(NIS) is always decreased and is undetectable in about a third of patients
ndash Iodine organification is markedly reduced
ndash Effective half-life of iodine in tumor tissue is always shorter
bull Tissues that often take up iodine and can be misconstrued as metastases include the
ndash salivary glands in the mouth
ndash esophagus (as a result of swallowing radioactive saliva)
ndash thymus gland
ndash breasts in some women
ndash liver stomach colon bladder
I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

Cancer vs normal cells
bull Metabolism of radioiodine in papillary and follicular carcinoma is profoundly altered when compared with normal thyroid tissue
bull Several defects are present in cancer tissuendash iodine uptake via the sodium-iodide symporter
(NIS) is always decreased and is undetectable in about a third of patients
ndash Iodine organification is markedly reduced
ndash Effective half-life of iodine in tumor tissue is always shorter
bull Tissues that often take up iodine and can be misconstrued as metastases include the
ndash salivary glands in the mouth
ndash esophagus (as a result of swallowing radioactive saliva)
ndash thymus gland
ndash breasts in some women
ndash liver stomach colon bladder
I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

bull Tissues that often take up iodine and can be misconstrued as metastases include the
ndash salivary glands in the mouth
ndash esophagus (as a result of swallowing radioactive saliva)
ndash thymus gland
ndash breasts in some women
ndash liver stomach colon bladder
I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

I-131 DOSIMETRY SYSTEMSYSTEM DESCRIPTION TYPICAL DOSES COMMENT
EMPERICAL METHOD
DOSIMETRY GUIDEDTECHNIQUE
TUMOR SITE DOSIOMETRY
EVERY ONE IN PROGNOSTIC GROUP GETS SAME DOSE
CALCULATES UPPER LIMIT OF SAFE BLOOD AND WHOLE BODY DOSES OF I-131
PRESCRIBES DOSE THAT DELIVERS A SET MINIMUM ABSORBED DOSE TO TARGET TISSUE
30-50 mCI FOR REMINANT ABLATION OF BED100-175 FOR STANDARD RISK PATIENTS30-50 MCI MORE FOR HIGHER RISK 200 MCI FOR DISTANT METS
WHOLE BLOOD LIMIT SET AT 2GY WITH TOTAL BODY RETENTION lt120 mCI AT 48 HOURS
TARGET DOSE-300GY TO THYRIOD REMINANT(80 SUCCESS RATE)80-120 GY TO NODAL OR SOFT TISSUE METASTASIS(80 SUCCESS RATE)
MOST SIMPLE AND WIDELY USEDN0T BASED ON IODINE MeTABOLISM
prescribes dose that will result in minimunacceptable bone narrow toxicityRequires measuring counts at 22448 and 72 hrs of RAI adminstration
TECHNIQUE FOR WHOLE BLOOD DOSIOMETRY WITH ADDED FOCAL MEASUREMENTS
HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

HiLo trial
bull Multicentric study in UK
ndash Comparing low dose vs high dose radio iodine
ndash Thyrotropin alpha vs thyroid hormone withdrawal
bull Inclusion Criteria
ndash stage T1 to T3N0N+ but no distant metastasis
ndash total thyroidectomy with or without central lymph-node dissection
bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

bull Primary end point ndash success rate for ablation -defined as both a
negative scan (lt01 uptake over the thyroid bed) and a thyroglobulin level of less than 20 ng per milliliter at 6 to 9 months
ndash One of these criteria used if other not available
bull Secondary end pointsndash were the number of days of hospitalization
adverse events during ablation and 3 months after ablation
Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

Results
bull Ablation was successful inndash 182 214 patients (850) in low-dose radioiodine vs
ndash 184 207 patients (889) in the high dose groups
ndash Success rates were also similar in thyrotropin alfa vsthyroid hormone withdrawal
bull Adverse events were 21 in the low-dose group versus 33 in the high-dose group (P=0007)
bull More patients in the high-dose group than in the low-dose group were hospitalized for at least 3 days (363 vs 130 Plt0001)
Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

Selumetinib produces clinically meaningful increases in iodine uptake and retention in a subgroup of patients with
thyroid cancer that is refractory to radioiodine the effectiveness may be greater in patients with RAS-mutant
disease
Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer
Ho AL1 Grewal RK Leboeuf R Sherman EJ Pfister DG Deandreis D Pentlow KS Zanzonico PB HaqueS Gavane S Ghossein RA Ricarte-Filho JCDomiacutenguez JM Shen R Tuttle RM Larson SM Fagin JA
POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

POST TREATMENT SCAN
bull When 131I therapy is given whole-body 131I imaging should beperformed several days later to document 131I uptake by the tumor
bull Post-treatment whole-body 131I imaging should be done primarilybecause up to 25 of images show lesions that may be clinicallyimportant which were not detected by the diagnostic imaging
bull Post-treatment imaging was most likely to reveal clinically important newinformation in patients younger than 45 years who had received 131Itherapy in the past Conversely in older patients and patients who had notpreviously received 131I therapy post-treatment imaging rarely yieldednew information that altered the patientrsquos prognosis
bull Clinical utility of posttreatment radioiodine scans in the management of patients with thyroidcarcinomaSherman etAL Clin Endocrinol Metab 1994
bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

bull Pulmonary metastases may be found only after administering therapeutic doses of 131I and obtaining whole-body imaging within a few days of treatment In a study of 283 patients treated with 100 mCi (3700 MBq) of 131I 64 had lung and bone metastases detected after treatment that had been suspected based on high serum Tgconcentrations alone but had not been detected after 2-mCi (74 MBq) diagnostic imaging
bull Schlumberger M et al Long-term results of treatment of 283 patients with lung and bone metastases fromdifferentiated thyroid carcinoma J Clin Endocrinol Metab 1986
Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

Stunning effect
bull Stunning is defined as a reduction in uptake of the 131I therapy dose induced by a pretreatment diagnostic activity
bull Occurs most prominently with higher activities (5ndash10 mCi) of 131I with increasing time between the diagnostic dose and therapy
bull Does not occur if the treatment dose is given within 72 hours of the scanning dose
DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

DIAGNOSTIC SCAN
bull To avoid or reduce the stunning effect the following have beensuggested 1) the use of 123I or small (2 or 3 mCi) doses of 131Iandor 2) a shortened interval (le 72 hours) between the diagnostic131I dose and the therapy dose
bull Some experts recommend that diagnostic 131I imaging be avoidedcompletely with decisions based on the combination of tumor stageand serum Tg
bull Other experts advocate that whole-body 131I diagnostic imagingmay alter therapy for example 1) when unsuspected metastasesare identified or 2) when an unexpectedly large remnant isidentified that requires additional surgery
bull Thus NCCN Panel Members disagreed about using diagnostic totalbody 131I imaging before postoperative RAI which is reflected inthe category 2B recommendation for imaging Note that diagnosticimaging is usedless often for patients at low risk
Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

Maintainence therapy
bull Tsh is trophic harmone that stumulates growth of cells derived from thyriod follicular epitheliumso tshsupression is done optimal serum levels of TSH have not been defined because of a lack of specific data
bull For patients with known residual carcinoma (or those at high risk for recurrence) the recommended TSH level is below 01 mUL For patients at low risk and for those patients with an excellent response to initial therapy who are in remission the recommended TSH level is either slightly below or slightly above the reference range
Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

Side effects of TSH supressionbull The risk and benefit of TSH-suppressive therapy must be balanced
for each individual patient because of the potential toxicitiesassociated with TSH-suppressive doses of levothyroxine includingcardiac tachyarrhythmias (especially in the elderly) bonedemineralization (particularly in post-menopausal women) andfrank symptoms of thyrotoxicosisAn adequate daily intake ofcalcium (1200 mgday) and vitamin D (1000 unitsday) isrecommended for patients whose TSH levels are chronically
suppressedbull McGriff NJ Csako G Gourgiotis L et al Effects of thyroidhormone suppression therapy on
adverse clinical outcomes in thyroidcancer Ann Med 2002
bull The average dosage needed to attain serum TSH levels in the euthyroid range is higher inpatients who have been treated for thyroid carcinoma (211mcgkg per day) than in thosepatients with spontaneously occurring primary hypothyroidism (162 mcgkg per day)
Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

Long-term cardiovascular mortality in patients with differentiatedthyroid carcinomama an observational study Klein Hesselink EN et al
The risk of cardiovascular and all-cause mortality is increased in patients with DTCindependent of age sex and cardiovascular risk factors A lower TSH level isassociated with increased cardiovascular mortality supporting the currentEuropean Thyroid Association and the American Thyroid Association guidelines oftempering TSH suppression in patients with low risk of cancer recurrenceFurthermore patients with DTC may benefit from assessment and treatment ofcardiovascular risk factors
Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

Follow upbull Serum Tg determinations neck ultrasound anti thyriod antibodies and
whole-body 131Iimaging detect recurrent or residual disease in mostpatients who have undergone total thyroid ablationIn contrast neitherserum Tg nor whole-body 131I imaging is specific for thyroid carcinoma inpatients who have not undergone thyroidectomy and remnant ablationWhen initial ablative therapy has been completed serum Tg should bemeasured periodically
bull Using current Tg assays patients with measurable serum Tg levels during TSHsuppression and those with stimulated Tg levels more than 2 ngmL are likely tohave residualrecurrent disease that may be localized in almost 50 promptly andin an additional 30 over the next 3 to 5 years About 6 of patients withdetectable serum Tg levels (which are lt 2 ngmL after stimulation) will haverecurrences over the next 3 to 5 years whereas only about 2 of patients withcompletely undetectable serum Tg after stimulation will have recurrences over thenext 3 to 5 years A serum Tg of 20 ngmL or higher obtained 72 hours after thelast rhTSH injection indicates that thyroid tissue or thyroid carcinoma presentregardless of the whole-body imaging findings
bull Spencer CA Lopresti JS Measuring thyroglobulin in patients with differentiated thyroid cancer Nat Clin Pract Endocrinol Metab 2008
SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

SIDE EFFECT
To be discussed with informed consent
TEMPORARY
Neck swellingedema 24-48 hrs
bull More if there is substantial mass of thyroid left behind
bull Responds well to steroids
bull Rarely may need tracheostomy may develop thyroid storm
bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

bull Nausea Loss of taste or dysgeusia- often last few days
bull Sialadenitis-pain and enlargement of salivary glands rarely progress to chronic xerostomiandash Prophylaxis -ingestion of large quantities of fluids
sialogogues- lemon juice or chewing gum
bull Permenant complications
bull Teratogenicity - recommended that conception be delayed for 1 y after therapeutic administrations of I131
bull MENSTRUAL CYCLE DISTURBANCES(LONG TERM EARLY MENOPAUSE
WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

WITH ADMINSTRATION OF gt200mCI(TEMPORARY ONLY)bull Bone marrow supressionbull Facial nerve weaknessbull StomatitisWITH ADMINSTRATION OF CUMULATIVE LIFE TIME DOSE OF gt500 MciTEMPORARY
epistaxisalopeciaconjuctivitispneumoniaPERMENANTbull BMSsalivary and nasolacremal duct obstructionchronic eye
diseasePfibrosis(in wide spread lung mets)neurological sequlae(in wide spread brain mets)
WITH ADMINSTRATION FOR LARGE REMINANT THYRIODbull TEMPORARY-thyrioditisthyrotoxicosisbull PERMENANT-recurrent laryngeal nerve palsy
bull Data from potential side effects and complications of i-131 therapyAmdur rjmazzaferi et al Essentials of thyriod 2005
PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

PATIENT MANAGEMENT AFTER I-131 THERAPY
In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

In patient i-131 therapy indicationswhereRSO is to be informed
1-PROPOSED DOSE ISa )gt200mcib)Total effective dose gt05 rem to adults family memberor care giver or gt01 rem to pregnant women or childrenof general public2patient is unable to follow oralwritten consent due tomultiple factors likea)Incontinence issuesb)Requires help of devices like PDfolleys catetherfeedingcatethersc)Coaginitive psychiatric disordersd)Housingtravelling issue
You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU

You are still you despite what your body chooses to beyou are not the disease hellipsurvivor of thyriod cancer
THANK YOU
Related Documents




![Research Paper Rictor ablation in BMSCs inhibits bone ...Bone is the most common site for breast cancer metastasis [1, 2]. Breast cancers that detach from the primary tumor can enter](https://static.cupdf.com/doc/110x72/611dff71a00ea9282c0b4764/research-paper-rictor-ablation-in-bmscs-inhibits-bone-bone-is-the-most-common.jpg)






