12/9/2009 1 R. Angelo de Claro, MD f Division of Hematology University of Washington No conflicts of interest.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

12/9/2009
1
R. Angelo de Claro, MDfDivision of Hematology
University of Washington
No conflicts of interest.

12/9/2009
2
AML in the elderly
Drug approval process
Analysis of Recent NDAs:
Mylotarg, Zarnestra, Clolar, Onrigin
Discussion

12/9/2009
3
AML Incidence per 100,000 (2002‐2006)
http://seer.cancer.gov/csr/1975_2006/browse_csr.php?section=13&page=sect_13_table.10.html
The US Population is Aging
350 < 65 years
100
150
200
250
300 > 65 years
US Bureau of the Census. 1996.
0
50
1950 1990 2030
8.1% 12.7% 20.0%

12/9/2009
4
Median Survival
80%
100%
Overall 30%
65-74 Years 44%
ReceivedChemo
3.9
1.4
2.4
Survival (months)
20%
40%
60%
Per
cen
t S
urv
ivin
g
2.2
65 74 Years 44%
75-84 Years 24%
85+ Years 6%
0%
0 3 6 9 12 15 18 21 24
Number of Months Following Diagnosis
Menzin J et al, Arch Intern Med 2002 Jul 22;162(14):1597‐603.
M.D. Anderson AML Data (provided by E. Estey)

12/9/2009
5
Cytogenetics (1=favorable/interm 2=unknown orCytogenetics (1=favorable/interm, 2=unknown or 5=unfavorable points)
De novo vs. secondary (1 or 3 points)
Age (1=60‐64,2=65‐69,3=70‐74,4=75+)
Performance status (0,1,2,3,4)
WBC (1=<10,2=10‐49,3=50‐99,4= ≥100)
Risk group 4‐6 points best7‐8 points intermediate 9+ points worst
Wheatley K et al, Br J Haematol 2009 Jun;145(5):598‐605.
Wheatley K et al, Br J Haematol 2009 Jun;145(5):598‐605.

12/9/2009
6
Adult AML
AML Genetic AML Normal Karyotype
Falini B et al, Blood 2007 Feb 1;109(3):874‐85.
Heterogeneity
Tallman MS et al, Blood, Aug 2005; 106: 1154‐1163 and update.

12/9/2009
7
Safety (FD&C Act 1938)Safety (FD&C Act 1938)
Efficacy (1962 Amendment)
Substantial evidence
Demonstrated in adequate and well‐controlled studies
Specific Indication
Defined patient population
http://www.fda.gov/downloads/AboutFDA/CentersOffices/CDER/ucm120865.pdf

12/9/2009
8
Regular Approval
Clinical benefit (longer or “better” life) OR
Established surrogate for clinical benefit
Accelerated approval (Subpart H, 1992)
Surrogate endpoint reasonably likely to predictclinical benefitclinical benefit
in AML, durable complete response*
http://www.fda.gov/downloads/AboutFDA/CentersOffices/CDER/ucm120865.pdfFleming TR, Health Aff (Millwood) 2005 Jan‐Feb;24(1):67‐78.*Appelbaum FR et al, Blood 2007 Mar 1;109(5):1810‐6.

12/9/2009
9
Serious or life‐threatening diseaseSerious or life threatening disease
Drug provides benefit over available therapy
Surrogate endpoint reasonably likely to predict clinical benefit
Subsequent confirmation of clinical benefit isSubsequent confirmation of clinical benefit is required (post‐approval commitment)
http://www.fda.gov/downloads/AboutFDA/CentersOffices/CDER/ucm120865.pdf
Induction Consolidation Post‐Consolidation
Daunomycin Mylotarg x 3 cycles
Ara-C+ Mylotarg
DaunomycinA C
Complete Remission Disease‐Free Survival
Ara-C
No Therapy
http://www.fda.gov/ohrms/DOCKETS/ac/05/briefing/2005‐4191B1_04_01‐Wyeth‐Mylotarg.pdf

12/9/2009
10
Core of 13 voting members
4‐year terms
Convened 4 times per year, 1‐2 days per session, 1 drug/biologic = ½ day session
ODAC decisions are strongly taken into consideration however are non‐binding.
http://www.fda.gov/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/OncologicDrugsAdvisoryCommittee
21 CFR 14.5(a)
Mylotarg Zarnestra Clolar Onrigin
Study Design single arm single arm single arm single arm
Proposed Indication
1st relapse First‐line First‐line First‐lineIndication
p
Population CD33+ AML AML inage 75 or65 with MDS
AML inage 60
with 1 of the ff:
• age 70• PS 2
AML inage 60
with 1 of the ff:
• age 70• PS 2
• AHD• Int/Unfavkaryotype
•Unfavkaryotype•Card/Pulm/ Liver comorbidity
http://www.fda.gov/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/OncologicDrugsAdvisoryCommittee

12/9/2009
11
Mylotarg Zarnestra Clolar Onrigin
Primary Endpoint
CR, CRp CR CR, CRp CR, CRp
Complete Remission (CR)• Normal marrow morphology on light microscopy with less than 5% blasts• No peripheral blasts• Recovery of peripheral blood counts with ANC 1000 and platelets 100K
CRi (CR with incomplete recovery)• fulfill requirements for CR except for recovery of peripheral counts to• fulfill requirements for CR except for recovery of peripheral counts to required level
CRp (CR with incomplete platelet recovery)• subset of CRi where recovery of platelets < 100K
*Appelbaum FR et al, Blood 2007 Mar 1;109(5):1810‐6.
Mylotarg Study
CR(n=23)
CRp(n=19)
logrank = 0.7
Sievers EL et al, J Clin Oncol. 2001 Jul 1;19(13):3244‐54.

12/9/2009
12
CR
CR (n=1,328)
( 41)
p = 0.0001
CRp (n=41)
M.D. Anderson patients with AML1980‐2004
Walter RB et al, J Clin Oncol (submitted).
Mylotarg Zarnestra Clolar Onrigin
Primary Endpoint
CR, CRp CR CR, CRp CR, CRp
n = 142 136 112 140
CR 16%[11‐23]
11%[7‐18]
38%[29‐47]
27%[20‐35]
CRp 13%[8‐20]
n.d. 8% 7%[4‐13][8 20] [4 13]
Accelerated Approval * * Approved for modified indication.

12/9/2009
13
90
100
All Patients
50
40
30
20
60
70
80 Censored
All Patients
Median 164 days
Pat
ien
ts (
%)
0
10
0 100 200 300 400 600 700500 1000800 900
Number of patients136 68 31 19 13 10 4 3 1 0 0
Days
http://www.fda.gov/ohrms/dockets/ac/05/slides/2005‐4138‐Index.htm

12/9/2009
14
Median survival: 40.7 wks (95CI, 28.3‐53.0 wks)
http://www.fda.gov/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/OncologicDrugsAdvisoryCommittee
• “In general, approval of new drugs for initial
treatment of AML is based on results of
randomized controlled trials.
• It will be difficult to interpret the results of this
trial without a control; we recommend that you
conduct a randomized controlled study.”
pre‐sNDA meeting for Clofarabine, 12/4/07
http://www.fda.gov/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/OncologicDrugsAdvisoryCommittee

12/9/2009
15
Cytotoxic Therapy with Curative Intent
p = 0.054
Mengis C et al, J Clin Oncol. 2003 November 1; 21(21):3933‐9.
Patient populationAge 70AML, de novo or secondaryNo previous chemo
Overall Survival
No previous chemoECOG PS 0‐2
n = 457
CR rate = 8%
Harousseau JL et al, Blood 2009 Aug 6;114(6):1166‐73.
12/9/2009
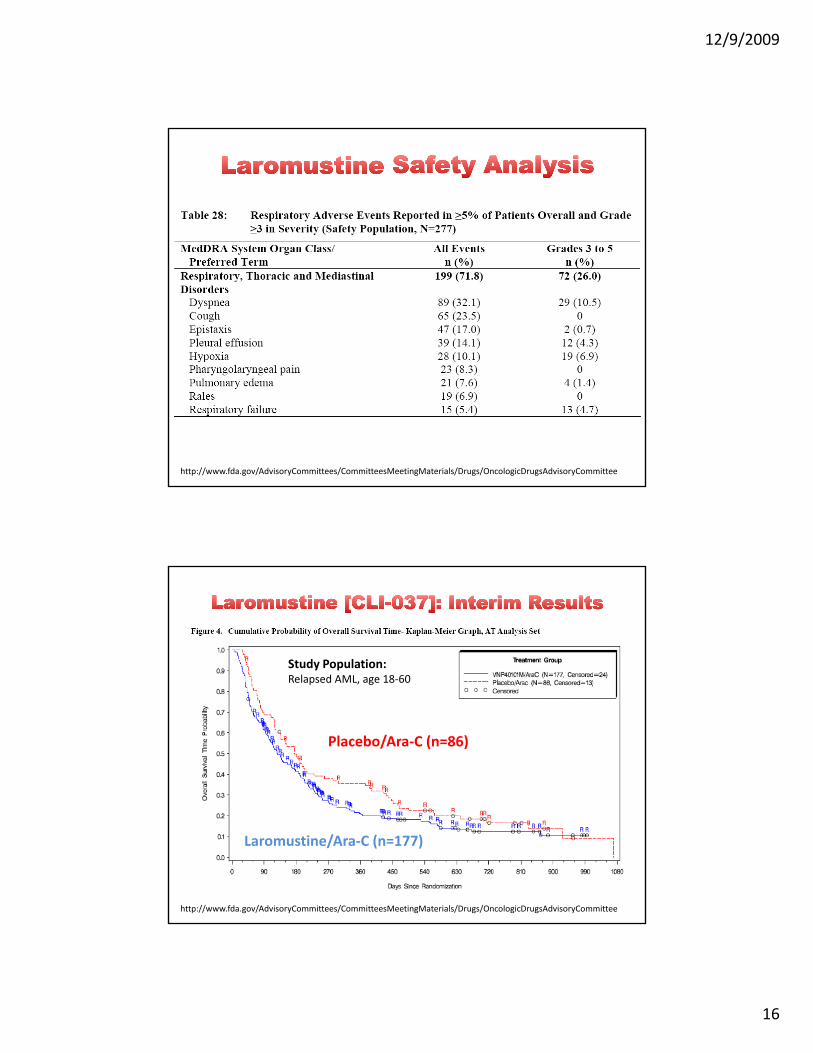
16
http://www.fda.gov/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/OncologicDrugsAdvisoryCommittee
Study Population:Relapsed AML, age 18‐60
Placebo/Ara‐C (n=86)
http://www.fda.gov/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/OncologicDrugsAdvisoryCommittee
Laromustine/Ara‐C (n=177)

12/9/2009
17
Mylotarg Zarnestra Clolar Onrigin
Study Design single arm single arm single arm single arm
Proposed Indication
1st relapse First‐line First‐line First‐lineIndication
p
Population CD33+ AML AML inage 75 or65 with MDS
AML inage 60
with 1 of the ff:
• age 70• PS 2
AML inage 60
with 1 of the ff:
• age 70• PS 2
• AHD• Int/Unfavkaryotype
•Unfav karyotype•Card/Pulm/ Liver comorbidity
http://www.fda.gov/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/OncologicDrugsAdvisoryCommittee
too sick to receiveother therapy?
Mylotarg Zarnestra Clolar Onrigin
Population CD33+ AML AML inage 75 or65 with MDS
AML inage 60
with 1 of the ff:
AML inage 60
with 1 of the ff:
MDS• age 70• PS 2• AHD• Int/Unfavkaryotype
• age 70• PS 2•Unfavkaryotype•Card/Pulm/ Liver comorbidity
7+3 salvage % received[% eligible]
7% 21%[25‐41%]
?[30%]
HSCT salvage 11%
http://www.fda.gov/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/OncologicDrugsAdvisoryCommittee

12/9/2009
18
Randomized clinical trial
Inclusion Criteria
previously untreated AML or RAEB with IPI1.5
age 60 years
WHO PS 0‐2
Löwenberg B et al, N Engl J Med 2009 Sep 24;361(13):1235‐48.

12/9/2009
19
Treatment
Cycle 1: Daunorubicin 45 vs 90 mg/m2 D1‐3 + cytarabine 200 mg/m2 CIV D1‐7
Cycle 2: Cytarabine 1 gm/m2 IV D1‐6
If in CR after cycle 2If in CR after cycle 2,
(optional) allo‐SCT if with HLA‐matched donor
Randomization to (1) mylotarg 6 mg/m2 x 3 cycles OR (2) observation
Löwenberg B et al, N Engl J Med 2009 Sep 24;361(13):1235‐48.
C ti l E l t dConventional(n=411)
Escalated(n=402)
Age 70 26% 27%
PS 2 10% 10%
Secondary AML 18% 23%
CytogeneticsCytogeneticsUnfavorable + Very Unfavorable*
11 + 13% 9 + 12%
*Very unfavorable risk: a monosomal karyotype, defined by the presence of twoautosomal monosomies or one autosomal monosomy in combination with at least onestructural abnormality other than core binding factor

12/9/2009
20
Complete Remission Rate % Conventional Escalated
Overall 54 2 64 2
Age 70 52 5 60 5
PS 1 or 2 51 3 58 3
Unfavorable cytogenetics 48 8 66 8
Very Unfavorable cytogenetics 28 6 42 7
Löwenberg B et al, N Engl J Med 2009 Sep 24;361(13):1235‐48.

12/9/2009
21
Mortality and morbidity in patients receiving encainide, flecainide, or placebo.receiving encainide, flecainide, or placebo. The Cardiac Arrhythmia Suppression Trial
(CAST)
DS Echt, PR Liebson, LB Mitchell, RW Peters, D Obias‐Manno, AH B k D A b A B k L F i d HL G d t lBarker, D Arensberg, A Baker, L Friedman, HL Greene, and et al
Echt DS et al, N Engl J Med 1991 Mar 21;324(12):781‐8.

12/9/2009
22
Clinical equipoise means that there is
i t i t h th tgenuine uncertainty over whether or not
the treatment will be beneficial.
uncertainty among expert medical community rather
than in the investigator
thi l j tifi ti f d i ti i li i l t i lethical justification for randomization in clinical trials
Freedman B, N Engl J Med 1987 Jul 16;317(3):141‐5.

12/9/2009
23
FDA approval = Marketing approval
Insurance coverageAdvertising
Return of Investment

12/9/2009
24
1999: IND filed by MDACC,
eventually licensed to Bioenvision
2001: Co‐development agreement
ILEXBioenvision
G
2004: Genzyme
acquires ILEX for
US$1B
2007: Genzyme
acquires Bioenvision
for US$350MGenzyme for US$350M
Other Interesting Facts:2007 Genzyme Revenue US$4.6B2007 FDA Budget US$2.0B
Resource burden
need more patientsneed more patients
longer accrual time
more expensive
Physician discomfort with randomization
ff t ti t’ tiaffects patient’s perceptions

12/9/2009
25
Adaptive randomization
Baseline adaptive (biased coin urn design) versusBaseline adaptive (biased coin, urn design) versus
response adaptive (play‐the‐winner, two‐armed‐bandit)
less statistical power with unbalanced arms
Zelen Design
randomization before informed consent [? IRB approval]
Seamless Phase II/III Design
? Acceptance by FDA
Randomized control trials in elderly AML are feasible, however are more resource‐intensive.
If clinical equipoise is present, then randomization is ethically acceptable.
Recent FDA actions strongly favor use of randomized control trials in non‐relapsed/ refractory settingsrefractory settings.
Reduces bias (selection, volunteer, etc.)
Balances patient heterogeneity
Allows for adequate interpretation of efficacy and safety data

12/9/2009
26
Eli Estey
Tom Fleming
Related Documents










