Quitting by Gradual Smoking Reduction Using Nicotine Gum A Randomized Controlled Trial Saul Shiffman, PhD, Stuart G. Ferguson, PhD, Kenneth R. Strahs, PhD Background: Many smokers express a desire to quit smoking by gradually reducing the number of cigarettes they smoke until they stop completely. This study tested the efficacy of nicotine gum in facilitating cessation through gradual reduction. Design: This was a multi-center, placebo-controlled, double-blind RCT of 2- and 4-mg nicotine gum versus placebo. Setting/ participants: 3297 smokers who were interested in quitting gradually. Intervention: Subjects were instructed to gradually reduce their smoking while increasing their gum use over the course of up to 8 weeks. Once they had achieved initial abstinence (no smoking for 24 hours), gum was to be used in accordance with the current FDA-approved directions for cessation. The study was conducted under over-the-counter conditions, with no counseling provided. Continuous abstinence was assessed after 28 days and 6 months. Secondary measures of smoking reduction were also assessed. Analyses were conducted in 1999 –2000 and 2007–2008. Main outcome measures: Smokers on active gum were significantly more likely to achieve initial cessation (2 mg: OR1.42; 4 mg: OR1.90); 28-day continuous abstinence (2 mg: OR2.01; 4 mg: OR4.66); and continuous abstinence at 6 months (2 mg: OR1.80; 4 mg: OR5.96). During the reduction phase, active gum aided smoking reduction, and participants who reduced their smoking were more likely to achieve abstinence. Conclusions: These findings demonstrate that smokers who wish to quit smoking by gradual reduction can increase their success by using nicotine gum to facilitate reduction and cessation. (Am J Prev Med 2009;36(2):96 –104) © 2009 American Journal of Preventive Medicine Introduction H alf of all smokers who do not quit will die due to tobacco-related disease. 1 Most smokers want to quit smoking, and each year many try without success. 2,3 Nicotine dependence hampers smokers’ ability to quit 4 : the success level for unaided quit attempts is only about 3%. 5,6 Treatment with nicotine replacement therapy (NRT) consistently increases success in smoking cessation. 7 However, the use of NRT has been restricted to abrupt quitting, when smokers stop smoking all at once and simultaneously start using NRT. Yet, as many as 66% of smokers prefer to quit by gradual reduction, 8,9 and about 33% of U.S. smokers who attempt to quit use the gradual method. 10 Smokers who want to quit by grad- ual reduction, rather than abruptly, perceive them- selves as more dependent and less successful at quit- ting. 10 Moreover, smokers who state an intention to quit by gradual reduction are less motivated to quit and only half as likely to actually even make a quit effort, 11 so inducing them to make a concerted quit attempt and helping them quit may increase quitting success. Thus, allowing NRT use as a support to gradual quitting may increase its public health impact. 12 In addition to being attractive to smokers, the con- cept of gradually reducing smoking as a means of quitting has substantial conceptual appeal: it allows smokers to change their behavior gradually and benefit from “small wins” along the way, helps break the behavioral bonds between smoking and particular situ- ations, 13 and may reduce nicotine dependence prior to quitting. 14 Unfortunately, although studies using highly structured behavioral reduction methods have shown clinical promise, 15,16 outcomes of simpler behavioral reduction methods have proved disappointing. 17 It has From Pinney Associates, Inc., and the University of Pittsburgh (Shiff- man, Ferguson), Pittsburgh, Pennsylvania; and GlaxoSmithKline Consumer Healthcare (Strahs), Parsippany, New Jersey Address correspondence and reprint requests to: Saul Shiffman, PhD, Pinney Associates, 201 North Craig Street, Suite 320, Pittsburgh PA 15213. E-mail: [email protected]; cc: gbittner@ pinneyassociates.com. 96 Am J Prev Med 2009;36(2) 0749-3797/09/$–see front matter © 2009 American Journal of Preventive Medicine. All rights reserved. doi:10.1016/j.amepre.2008.09.039

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
QNAS
B
D
Sp
I
Mom
C
I
Hwsq
cHqssa
FmC
PPp
9
uitting by Gradual Smoking Reduction Usingicotine GumRandomized Controlled Trial
aul Shiffman, PhD, Stuart G. Ferguson, PhD, Kenneth R. Strahs, PhD
ackground: Many smokers express a desire to quit smoking by gradually reducing the number ofcigarettes they smoke until they stop completely. This study tested the efficacy of nicotinegum in facilitating cessation through gradual reduction.
esign: This was a multi-center, placebo-controlled, double-blind RCT of 2- and 4-mg nicotine gumversus placebo.
etting/articipants:
3297 smokers who were interested in quitting gradually.
ntervention: Subjects were instructed to gradually reduce their smoking while increasing their gum useover the course of up to 8 weeks. Once they had achieved initial abstinence (no smokingfor 24 hours), gum was to be used in accordance with the current FDA-approved directionsfor cessation. The study was conducted under over-the-counter conditions, with nocounseling provided. Continuous abstinence was assessed after 28 days and 6 months.Secondary measures of smoking reduction were also assessed. Analyses were conducted in1999–2000 and 2007–2008.
ainutcomeeasures:
Smokers on active gum were significantly more likely to achieve initial cessation (2 mg:OR�1.42; 4 mg: OR�1.90); 28-day continuous abstinence (2 mg: OR�2.01; 4 mg:OR�4.66); and continuous abstinence at 6 months (2 mg: OR�1.80; 4 mg: OR�5.96).During the reduction phase, active gum aided smoking reduction, and participants whoreduced their smoking were more likely to achieve abstinence.
onclusions: These findings demonstrate that smokers who wish to quit smoking by gradual reductioncan increase their success by using nicotine gum to facilitate reduction and cessation.(Am J Prev Med 2009;36(2):96–104) © 2009 American Journal of Preventive Medicine
gustqoshai
cqsfbaqsc
ntroduction
alf of all smokers who do not quit will die dueto tobacco-related disease.1 Most smokers wantto quit smoking, and each year many try
ithout success.2,3 Nicotine dependence hampersmokers’ ability to quit4: the success level for unaideduit attempts is only about 3%.5,6
Treatment with nicotine replacement therapy (NRT)onsistently increases success in smoking cessation.7
owever, the use of NRT has been restricted to abruptuitting, when smokers stop smoking all at once andimultaneously start using NRT. Yet, as many as 66% ofmokers prefer to quit by gradual reduction,8,9 andbout 33% of U.S. smokers who attempt to quit use the
rom Pinney Associates, Inc., and the University of Pittsburgh (Shiff-an, Ferguson), Pittsburgh, Pennsylvania; and GlaxoSmithKlineonsumer Healthcare (Strahs), Parsippany, New JerseyAddress correspondence and reprint requests to: Saul Shiffman, PhD,
inney Associates, 201 North Craig Street, Suite 320, Pittsburgh
rA 15213. E-mail: [email protected]; cc: [email protected].
6 Am J Prev Med 2009;36(2)© 2009 American Journal of Preventive Medicine. All rights reserv
radual method.10 Smokers who want to quit by grad-al reduction, rather than abruptly, perceive them-elves as more dependent and less successful at quit-ing.10 Moreover, smokers who state an intention touit by gradual reduction are less motivated to quit andnly half as likely to actually even make a quit effort,11
o inducing them to make a concerted quit attempt andelping them quit may increase quitting success. Thus,llowing NRT use as a support to gradual quitting mayncrease its public health impact.12
In addition to being attractive to smokers, the con-ept of gradually reducing smoking as a means ofuitting has substantial conceptual appeal: it allowsmokers to change their behavior gradually and benefitrom “small wins” along the way, helps break theehavioral bonds between smoking and particular situ-tions,13 and may reduce nicotine dependence prior touitting.14 Unfortunately, although studies using highlytructured behavioral reduction methods have shownlinical promise,15,16 outcomes of simpler behavioral
eduction methods have proved disappointing.17 It has0749-3797/09/$–see front mattered. doi:10.1016/j.amepre.2008.09.039

btrwacIsnhN
eairh6HNwscptttoswintpiddgmanrt
M
P
Pmwtuawops
whdssP
mvodcIav
P
AhsbPstvatdtWapAitaeubt
mn(aaptcifapprrt�aca5
F
een suggested that as smokers reduce their smoking,hey encounter increasing withdrawal symptoms, makingeduction progressively more difficult and interferingith cessation.17 Accordingly, NRT may be useful inssisting cessation by gradual reduction, as it reducesraving and withdrawal18,19 and promotes abstinence.7
ndeed, clinical reports20 have suggested that NRT-aidedmoking cessation by gradual reduction has promise, buto clinical trial of NRT for cessation by gradual reductionas been reported. This study evaluates the efficacy ofRT in assisting quitting by gradual reduction.Several studies have shown that NRT can help smok-
rs who do not want to quit to reduce their smoking,21
nd some studies find that initiating reduction alsoncidentally increases cessation.22 Based on these data,egulators in the United Kingdom and other countriesave approved extended use of NRT for reduction over–9 months by smokers not interested in quitting.23
owever, there has not been a trial testing whetherRT might help smokers who are trying to quit butish to do so by gradual reduction. This article de-
cribes a randomized double-blind placebo-controlledlinical trial to test the efficacy of nicotine gum (versuslacebo) in assisting cessation through gradual reduc-ion. The reduce-to-quit (RTQ) approach consisted ofwo treatment phases—a reduction phase and a cessa-ion/maintenance phase. During the reduction phasef treatment, designed to achieve initial abstinence,mokers gradually increased the use of nicotine gumhile simultaneously decreasing smoking. Once partic-
pants achieved abstinence, they entered the mainte-ance phase of the study and used nicotine gum in the
raditional way to promote continued abstinence. Therimary outcome measure was abstinence from smok-
ng, but the analysis also assessed smoking reductionuring the reduction phase of the study. The study wasesigned to evaluate the contribution of active nicotineum to the efficacy of the entire treatment regime as itight be offered in practice, not to focus just on the
ddition of a reduction phase to a standard course oficotine gum. Hence, participants were assigned toeceive active or placebo treatment over the entirereatment course.
ethods
articipants
articipants were recruited using print and radio advertise-ents for smokers interested in quitting by gradual reductionithin 30 days. Prospects called one of 27 study sites across
he U.S. Inclusion criteria were: interest in quitting smokingsing gradual reduction within 30 days, aged �18 years,bility to understand English, and capable of providingritten informed consent. Exclusion criteria included: use ofther nicotine-containing products (e.g., pipes, cigars), bu-ropion (Zyban or Wellbutrin) or NRT within 30 days of
tudy entry; smoking of any substance other than cigarettes tebruary 2009
ithin 30 days of study entry; history of heart disease, recenteart attack, or irregular heartbeat; being an insulin-dependentiabetic; involvement in another clinical study, being in theame household as another participant, or being related totudy site staff; working during the night hours (i.e., 11:00M–7:00 AM, to ensure that daytime carbon monoxide [CO]easurements reflected smoking); being unable to attend
isits before 2:00 PM (to ensure CO levels reflected smoking);r being pregnant or nursing or likely to become pregnanturing the study. All participants supplied written informedonsent prior to being enrolled. This study was approved byRBs at each of the study sites. (An online appendix isvailable at www.ajpm-online.net listing the 27 Principal In-estigators and their affiliations.)
rocedure
fter providing consent, participants completed a smokingistory questionnaire and a timeline follow-back24 of dailymoking during the preceding 2 weeks; they also had theirreath tested for CO (an indicator of smoke intake25).articipants started treatment the next day. At subsequenttudy visits (2, 4, and 8 weeks later), participants reportedheir cigarette and gum consumption since the previous studyisit, and provided CO samples. Study visits were scheduledfter 2:00 PM so that CO would be near steady state.26 At six ofhe 27 study sites, participants who smoked �25 cigarettes peray (CPD) at baseline provided a blood sample for serumhiocyanate (SCN) analysis at the baseline, Week-2, and
eek-4 visits. Unlike CO, which has a short half-life, SCN hasrelatively long half-life (approximately 1 week27), thus
roviding a measure of longer-term exposure to tobacco.lthough, as with CO, SCN levels can be affected by other
nputs, SCN is regarded as a good marker of longer-termobacco exposure.27 At each visit, subjects were asked aboutdverse events, and the onset and offset dates of any adversevents were recorded. An adverse event was defined as anynintended change (including physical, psychological, orehavioral changes) from the subject’s pretreatment condi-ion, whether considered related to treatment or not.
Study visits were used to monitor for participants’ achieve-ent of initial abstinence. Participants who reported absti-ence for at least a day, as verified by CO at �10 ppmaverage of two measurements), were considered to havechieved initial abstinence. Because 8 weeks was consideredn adequate time to reduce smoking and achieve abstinence,articipants who did not achieve initial abstinence after thisime were excused from the remainder of the study andounted as treatment failures in subsequent analyses. Partic-pants who achieved initial abstinence were scheduled for aollow-up visit 28–35 days after their first day of abstinence tossess 28-day continuous abstinence. At this follow-up visit,articipants reported their smoking and gum usage since therevious visit and were specifically asked about their current andecent smoking status to ascertain outcome. Participants whoeported continuous abstinence (not even a puff) were subjecto confirmation by two CO readings, with an average reading of10 ppm verifying abstinence. (Participants who achieved initial
bstinence but did not at first maintain 28 days of abstinenceould schedule another 28-day follow-up visit if they againchieved another 24-hour period of abstinence—16.9% [85/04] of participants who achieved initial abstinence had more
han one 28-day follow-up visit.)Am J Prev Med 2009;36(2) 97
wsogcaraaaow
T
CtmsFUaab“wOglwsthtuccfwwPs
S
T(btgnesf9
eiopna
Arrstuora
ptnatpaBceu
RP
IisgoadtThpg
T6c22(tptawp
O2nb
wi
9
Participants with verified 28-day continuous abstinenceere counted as successes on the primary outcome and
cheduled for a follow-up visit 6 months from the beginningf treatment, at which time they reported on their smoking,um use, and adverse events. Participants who reportedontinuous abstinence (not even a puff) since the 28-daybstinence evaluation were subject to confirmation by two COeadings, with an average reading of �10 ppm verifyingbstinence. Participants who did not demonstrate 28-daybstinence were not scheduled for 6-month follow-up visitsnd were counted as treatment failures at 6 months. Through-ut, participants who did not participate in follow-up visitsere counted as treatment failures.
reatment
onsistent with use of an over-the-counter (OTC) medica-ion, participants self-selected their study gum dosage (2 or 4
g) after reviewing the labels for both doses, which toldmokers of �25 CPD to select the 4-mg dose (per current U.S.ood and Drug Administration [FDA]–approved labeling).sing a 1:1 computer-generated randomization scheme, bal-
nced across study sites and generated separately for the 2-nd 4-mg groups, participants were randomized on a double-lind basis to receive active or placebo gum (NicoretteOriginal” flavor) and were given 420 pieces of gum withhich to initiate treatment. The study was run in a simulatedTC setting: Instructions on quitting and the use of nicotine
um were obtained from only a printed user’s guide andabel. Absolutely no instruction, counseling, or interventionas provided by study personnel. The materials instructed
mokers to start reducing by not smoking for the first hour ofhe day and instead using a single piece of gum during thatour. On each subsequent day, participants were to extend
heir abstinence by adding an additional hour of abstinence,sing one additional piece of gum. Once smokers had quitompletely (for 24 hours), they were to use the gum in a manneronsistent with the current FDA-approved labeling for theollowing 12 weeks: one piece every 1–2 hours for the first 6eeks of treatment; one piece every 2–4 hours for the next 3eeks; and then one piece every 4–8 hours for a final 3 weeks.articipants were then permitted to use the gum “as needed totay smoke-free” for an additional 12 weeks.
tatistical Analysis
he primary endpoint was 28-day continuous abstinencewhich was the basis on which other NRT indications haveeen evaluated by the U.S. FDA28). Active and placeboreatment arms were compared, separately for 2- and 4-mgum. Reduction in smoking, achievement of initial absti-ence (24 hours), and abstinence at 6 months were alsoxamined. Cochran–Mantel–Haenszel tests controlled fortudy site; analyses pooling 2- and 4-mg groups also controlledor dose (as fixed effects). Results are presented as ORs with5% CIs.Analysis of variance was used in the analyses of reduction to
xamine change from baseline to Week 2 in average CPD andn CO concentration. (By a priori plan, the analysis focusedn the first 2 weeks of treatment because, as the reductionhase went on, more and more participants achieved absti-ence or withdrew from the study and were thus lost to
nalyses of reduction per se, potentially biasing the analyses.) n8 American Journal of Preventive Medicine, Volume 36, Num
dditionally, successful reduction—defined as a self-reportededuction of �50% in smoking level verified by a �25%eduction in CO levels (this measure was constructed to assessignificant reduction in cigarette smoking because retrospec-ively reported smoking level is subject to error and CO is oftensed to validate self-reports of smoking)—was analyzed as anutcome of treatment and as a mediator of cessation. Finally,eductions in SCN among smokers in the 4-mg gum group werenalyzed.
Differences between active and placebo conditions in theroportions of subjects experiencing adverse events wereested, by dose. To identify effects of concomitant smoking andicotine gum use on adverse events, the investigators identifieds high-concomitant participants those who were in the upperwo thirds for both smoking (CPD) and gum use (pieceser day). To test whether concomitant smoking and use ofctive gum increased the likelihood of adverse events, areslow–Day test was used to determine whether high-con-omitant smoking had greater influence on the likelihood ofxperiencing an adverse event on active versus placebo gumsers.
esultsarticipant Characteristics and Disposition
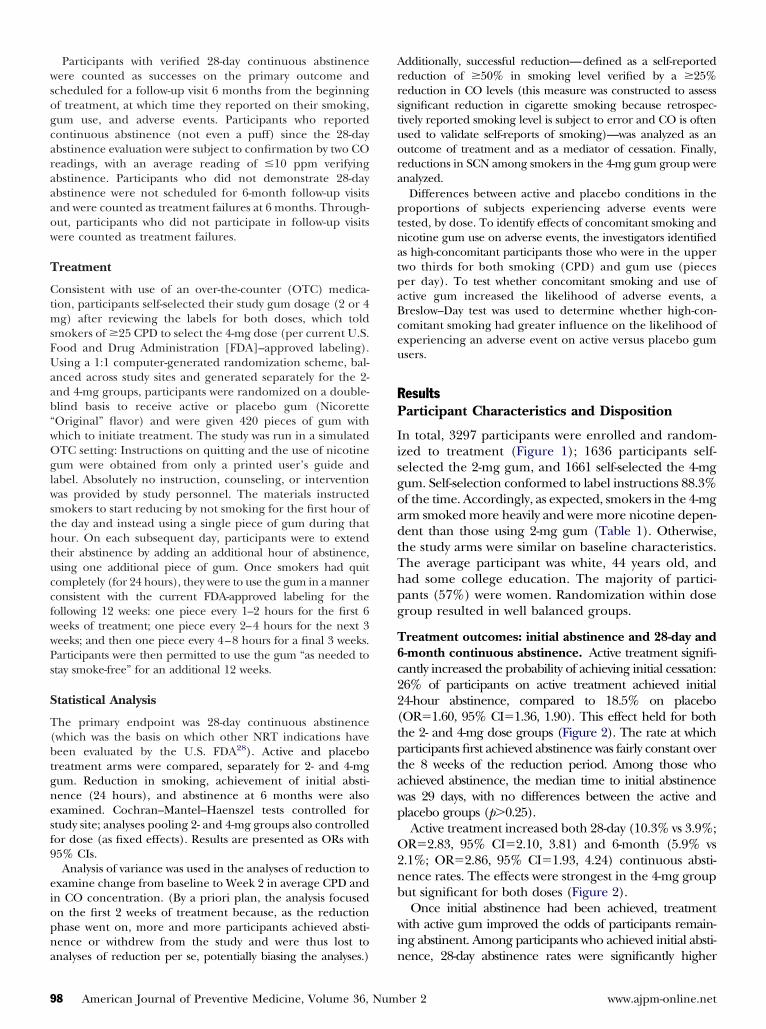
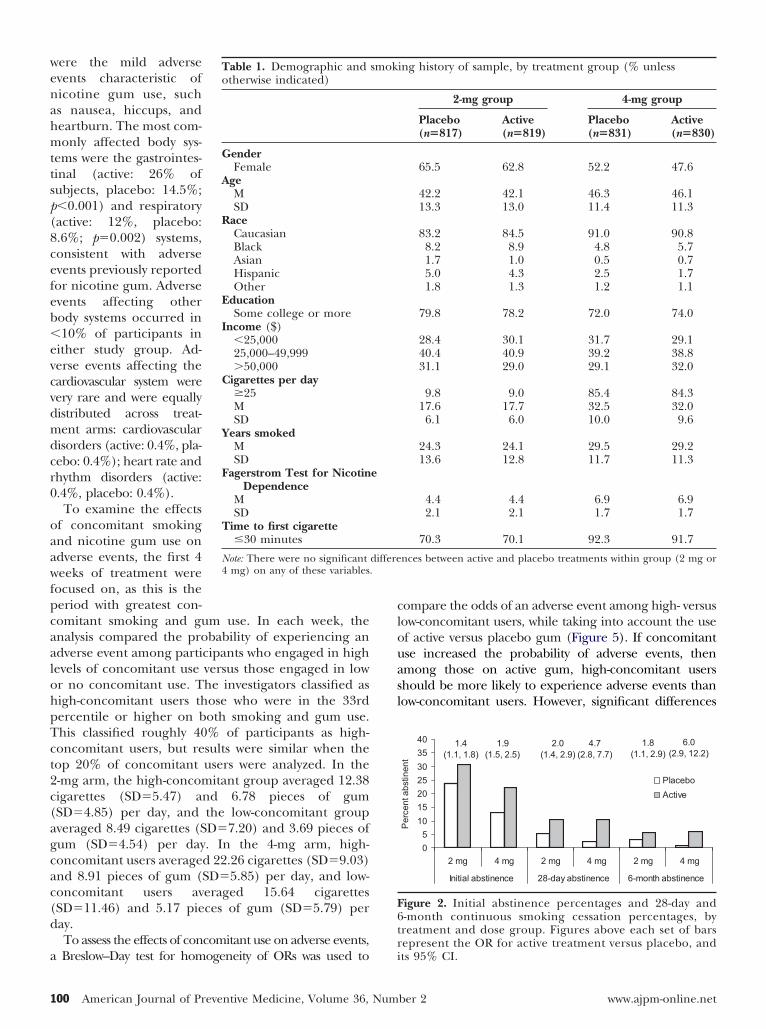
n total, 3297 participants were enrolled and random-zed to treatment (Figure 1); 1636 participants self-elected the 2-mg gum, and 1661 self-selected the 4-mgum. Self-selection conformed to label instructions 88.3%f the time. Accordingly, as expected, smokers in the 4-mgrm smoked more heavily and were more nicotine depen-ent than those using 2-mg gum (Table 1). Otherwise,he study arms were similar on baseline characteristics.he average participant was white, 44 years old, andad some college education. The majority of partici-ants (57%) were women. Randomization within doseroup resulted in well balanced groups.
reatment outcomes: initial abstinence and 28-day and-month continuous abstinence. Active treatment signifi-antly increased the probability of achieving initial cessation:6% of participants on active treatment achieved initial4-hour abstinence, compared to 18.5% on placeboOR�1.60, 95% CI�1.36, 1.90). This effect held for bothhe 2- and 4-mg dose groups (Figure 2). The rate at whicharticipants first achieved abstinence was fairly constant over
he 8 weeks of the reduction period. Among those whochieved abstinence, the median time to initial abstinenceas 29 days, with no differences between the active andlacebo groups (p�0.25).Active treatment increased both 28-day (10.3% vs 3.9%;R�2.83, 95% CI�2.10, 3.81) and 6-month (5.9% vs
.1%; OR�2.86, 95% CI�1.93, 4.24) continuous absti-ence rates. The effects were strongest in the 4-mg grouput significant for both doses (Figure 2).Once initial abstinence had been achieved, treatment
ith active gum improved the odds of participants remain-ng abstinent. Among participants who achieved initial absti-
ence, 28-day abstinence rates were significantly higherber 2 www.ajpm-online.net
av2aC6tOOO
S
Arshodsiat
li
pwtrr
saaiplvts
A
Dpeepo2
Ffsa
eb
saac
fd
e
p
F
mong those randomized to active gum treatment (38.8%s 21.1%; OR�2.29, 95% CI�1.62, 3.25), with both the-mg (33.3% vs 22.6%; OR�1.79, 95% CI�1.14, 2.79)nd the 4-mg gum (46.2% vs 18.4%; OR�3.36, 95%I�1.88, 5.99). Similarly, among this subset of participants,-month abstinence rates were significantly higher amonghose on active gum treatment (overall: 22.3% vs 11.5%;R�2.07, 95% CI�1.36, 3.17; 2 mg: 18.3% vs 13.3%;R�1.45, 95% CI�0.85, 2.49; 4 mg: 27.7% vs 8.3%;R�3.58, 95% CI�1.71, 7.53).
moking Reduction
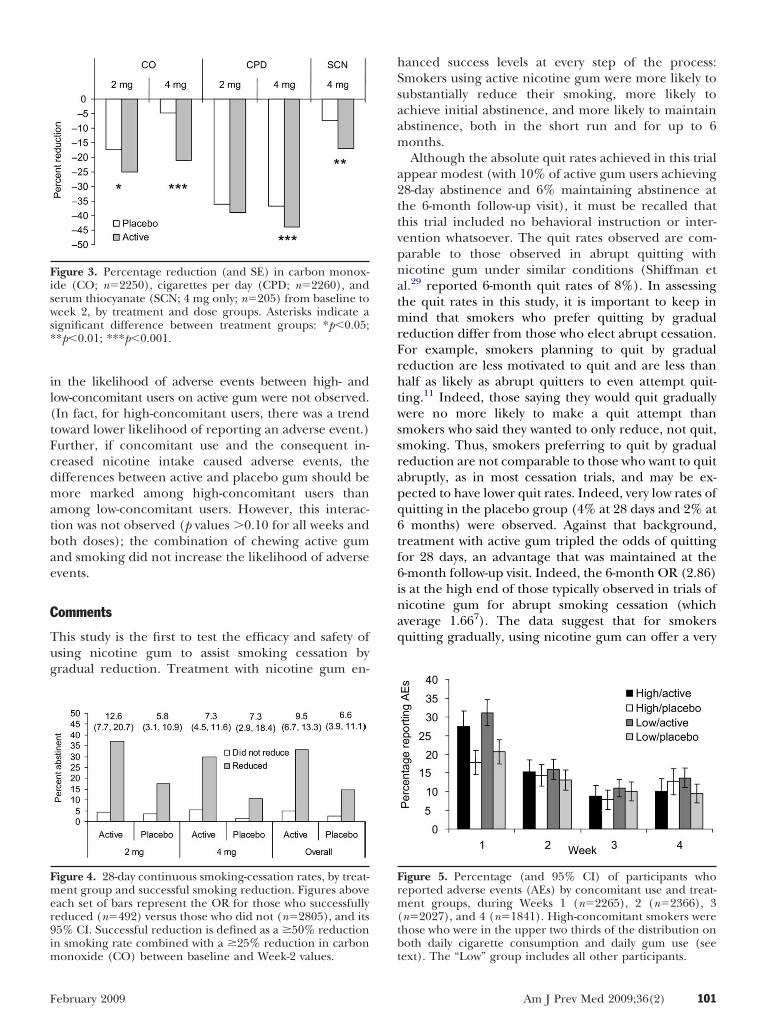
fter 2 weeks in the study, smokers on active treatmenteported greater reductions in number of cigarettesmoked than those on placebo treatment (Figure 3);owever, the difference between treatment groups wasnly significant in the 4-mg group. Participants ran-omized to active treatment (both doses) demon-trated significantly greater reductions in CO, indicat-ng reduced smoke intake. Finally, in the 4-mg group,ctive treatment resulted in significantly greater reduc-ions in SCN.
Participants using active gum were significantly moreikely to achieve successful reduction (�50% in smok-
6923 screened
3297 enrolled
817 placebo
45 succeededb
150 failed148 terminatedc
2 discontinuedd
40 completed5 did not completee
2 mgn=1636
195 succeeded622 failed
819 active
86 succeeded166 failed
159 terminated7 discontinued
75 completed11 did not complete
252 succeeded567 failed
8
21 s88 fa
18 c3 d
109 s722 fa
Self-selected group
Randomly allocated
24-hour abstinence
28-day abstinence
6-month follow-up
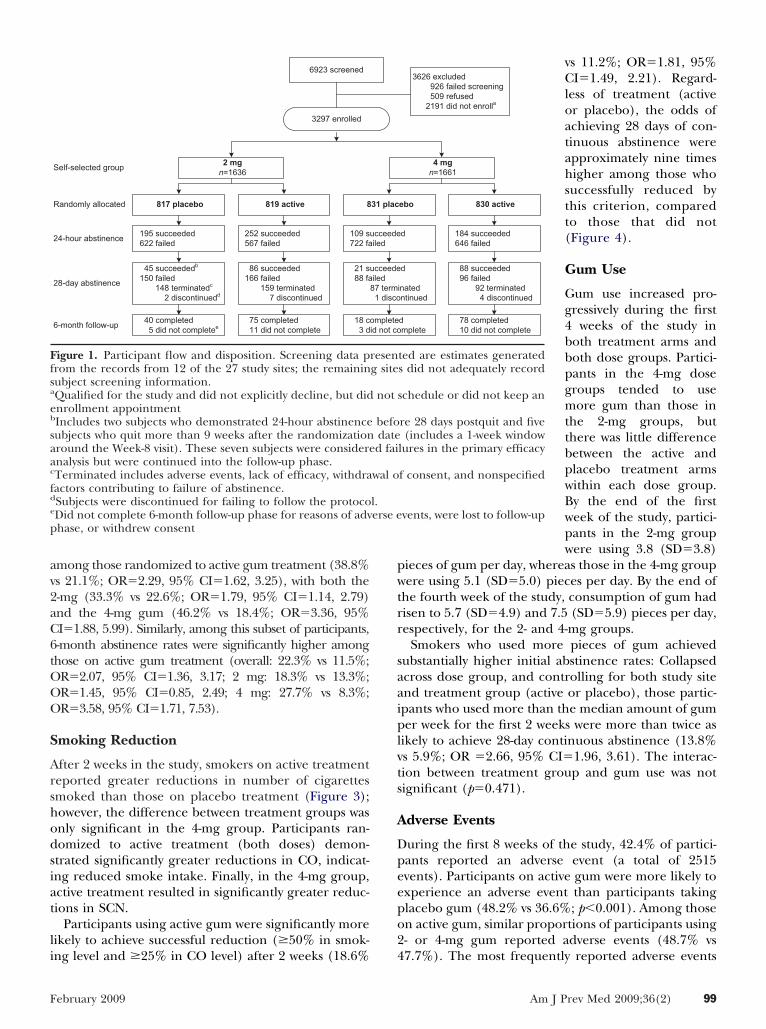
igure 1. Participant flow and disposition. Screening data prom the records from 12 of the 27 study sites; the remaininubject screening information.Qualified for the study and did not explicitly decline, but didnrollment appointmentIncludes two subjects who demonstrated 24-hour abstinenceubjects who quit more than 9 weeks after the randomizationround the Week-8 visit). These seven subjects were considerenalysis but were continued into the follow-up phase.Terminated includes adverse events, lack of efficacy, withdraactors contributing to failure of abstinence.Subjects were discontinued for failing to follow the protocoDid not complete 6-month follow-up phase for reasons of advhase, or withdrew consent
ng level and �25% in CO level) after 2 weeks (18.6% 4
ebruary 2009
vs 11.2%; OR�1.81, 95%CI�1.49, 2.21). Regard-less of treatment (activeor placebo), the odds ofachieving 28 days of con-tinuous abstinence wereapproximately nine timeshigher among those whosuccessfully reduced bythis criterion, comparedto those that did not(Figure 4).
Gum Use
Gum use increased pro-gressively during the first4 weeks of the study inboth treatment arms andboth dose groups. Partici-pants in the 4-mg dosegroups tended to usemore gum than those inthe 2-mg groups, butthere was little differencebetween the active andplacebo treatment armswithin each dose group.By the end of the firstweek of the study, partici-pants in the 2-mg groupwere using 3.8 (SD�3.8)
ieces of gum per day, whereas those in the 4-mg groupere using 5.1 (SD�5.0) pieces per day. By the end of
he fourth week of the study, consumption of gum hadisen to 5.7 (SD�4.9) and 7.5 (SD�5.9) pieces per day,espectively, for the 2- and 4-mg groups.
Smokers who used more pieces of gum achievedubstantially higher initial abstinence rates: Collapsedcross dose group, and controlling for both study sitend treatment group (active or placebo), those partic-pants who used more than the median amount of gumer week for the first 2 weeks were more than twice as
ikely to achieve 28-day continuous abstinence (13.8%s 5.9%; OR �2.66, 95% CI�1.96, 3.61). The interac-ion between treatment group and gum use was notignificant (p�0.471).
dverse Events
uring the first 8 weeks of the study, 42.4% of partici-ants reported an adverse event (a total of 2515vents). Participants on active gum were more likely toxperience an adverse event than participants takinglacebo gum (48.2% vs 36.6%; p�0.001). Among thosen active gum, similar proportions of participants using- or 4-mg gum reported adverse events (48.7% vs
3626 excluded926 failed screening509 refused
2191 did not enrolla
4 mgn=1661
ebo
d
inatedntinued
dmplete
d
830 active
88 succeeded96 failed
92 terminated4 discontinued
78 completed10 did not complete
184 succeeded646 failed
ted are estimates generateds did not adequately record
schedule or did not keep an
re 28 days postquit and five(includes a 1-week window
lures in the primary efficacy
f consent, and nonspecified
vents, were lost to follow-up
31 plac
ucceedeiled
87 term1 disco
ompleteid not co
ucceedeiled
reseng site
not
befodated fai
wal o
l.erse e
7.7%). The most frequently reported adverse events
Am J Prev Med 2009;36(2) 99
wenahmttsp(8cefeb�evcvdmdcr0
oaawfpcaalohpTct2c(agcac(d
a
clouasl
F6tr
1
ere the mild adversevents characteristic oficotine gum use, suchs nausea, hiccups, andeartburn. The most com-only affected body sys-
ems were the gastrointes-inal (active: 26% ofubjects, placebo: 14.5%;�0.001) and respiratoryactive: 12%, placebo:.6%; p�0.002) systems,onsistent with adversevents previously reportedor nicotine gum. Adversevents affecting otherody systems occurred in10% of participants in
ither study group. Ad-erse events affecting theardiovascular system wereery rare and were equallyistributed across treat-ent arms: cardiovascular
isorders (active: 0.4%, pla-ebo: 0.4%); heart rate andhythm disorders (active:.4%, placebo: 0.4%).To examine the effects
f concomitant smokingnd nicotine gum use ondverse events, the first 4eeks of treatment were
ocused on, as this is theeriod with greatest con-omitant smoking and gum use. In each week, thenalysis compared the probability of experiencing andverse event among participants who engaged in highevels of concomitant use versus those engaged in lowr no concomitant use. The investigators classified asigh-concomitant users those who were in the 33rdercentile or higher on both smoking and gum use.his classified roughly 40% of participants as high-oncomitant users, but results were similar when theop 20% of concomitant users were analyzed. In the-mg arm, the high-concomitant group averaged 12.38igarettes (SD�5.47) and 6.78 pieces of gumSD�4.85) per day, and the low-concomitant groupveraged 8.49 cigarettes (SD�7.20) and 3.69 pieces ofum (SD�4.54) per day. In the 4-mg arm, high-oncomitant users averaged 22.26 cigarettes (SD�9.03)nd 8.91 pieces of gum (SD�5.85) per day, and low-oncomitant users averaged 15.64 cigarettesSD�11.46) and 5.17 pieces of gum (SD�5.79) peray.To assess the effects of concomitant use on adverse events,
Table 1. Demographic andotherwise indicated)
GenderFemale
AgeMSD
RaceCaucasianBlackAsianHispanicOther
EducationSome college or more
Income ($)�25,00025,000–49,999�50,000
Cigarettes per day�25MSD
Years smokedMSD
Fagerstrom Test for NicotinDependence
MSD
Time to first cigarette�30 minutes
Note: There were no significant4 mg) on any of these variables.
Breslow–Day test for homogeneity of ORs was used to i
00 American Journal of Preventive Medicine, Volume 36, Num
ompare the odds of an adverse event among high- versusow-concomitant users, while taking into account the usef active versus placebo gum (Figure 5). If concomitantse increased the probability of adverse events, thenmong those on active gum, high-concomitant usershould be more likely to experience adverse events thanow-concomitant users. However, significant differences
0
5
10
15
20
25
30
35
40
2 mg 4 mg 2 mg 4 mg 2 mg 4 mg
Initial abstinence 28-day abstinence 6-month abstinence
Per
cent
abs
tinen
t
Placebo
Active
2.0 (1.4, 2.9)
4.7 (2.8, 7.7)
1.8(1.1, 2.9)
6.0 (2.9, 12.2)
1.4 (1.1, 1.8)
1.9(1.5, 2.5)
igure 2. Initial abstinence percentages and 28-day and-month continuous smoking cessation percentages, byreatment and dose group. Figures above each set of barsepresent the OR for active treatment versus placebo, and
ing history of sample, by treatment group (% unless
2-mg group 4-mg group
Placebo(n�817)
Active(n�819)
Placebo(n�831)
Active(n�830)
65.5 62.8 52.2 47.6
42.2 42.1 46.3 46.113.3 13.0 11.4 11.3
83.2 84.5 91.0 90.88.2 8.9 4.8 5.71.7 1.0 0.5 0.75.0 4.3 2.5 1.71.8 1.3 1.2 1.1
79.8 78.2 72.0 74.0
28.4 30.1 31.7 29.140.4 40.9 39.2 38.831.1 29.0 29.1 32.0
9.8 9.0 85.4 84.317.6 17.7 32.5 32.0
6.1 6.0 10.0 9.6
24.3 24.1 29.5 29.213.6 12.8 11.7 11.3
4.4 4.4 6.9 6.92.1 2.1 1.7 1.7
70.3 70.1 92.3 91.7
nces between active and placebo treatments within group (2 mg or
smok
e
differe
ts 95% CI.
ber 2 www.ajpm-online.net
il(tFcdmatbae
C
Tug
hSsaam
a2ttvpnatmrFrhtwssrapq6tf6inaq
Fisws*
Fmer9im
Frm(tb
F
n the likelihood of adverse events between high- andow-concomitant users on active gum were not observed.In fact, for high-concomitant users, there was a trendoward lower likelihood of reporting an adverse event.)urther, if concomitant use and the consequent in-reased nicotine intake caused adverse events, theifferences between active and placebo gum should beore marked among high-concomitant users than
mong low-concomitant users. However, this interac-ion was not observed (p values �0.10 for all weeks andoth doses); the combination of chewing active gumnd smoking did not increase the likelihood of adversevents.
omments
his study is the first to test the efficacy and safety ofsing nicotine gum to assist smoking cessation byradual reduction. Treatment with nicotine gum en-
igure 3. Percentage reduction (and SE) in carbon monox-de (CO; n�2250), cigarettes per day (CPD; n�2260), anderum thiocyanate (SCN; 4 mg only; n�205) from baseline toeek 2, by treatment and dose groups. Asterisks indicate a
ignificant difference between treatment groups: *p�0.05;*p�0.01; ***p�0.001.
igure 4. 28-day continuous smoking-cessation rates, by treat-ent group and successful smoking reduction. Figures above
ach set of bars represent the OR for those who successfullyeduced (n�492) versus those who did not (n�2805), and its5% CI. Successful reduction is defined as a �50% reductionn smoking rate combined with a �25% reduction in carbon
onoxide (CO) between baseline and Week-2 values. t
ebruary 2009
anced success levels at every step of the process:mokers using active nicotine gum were more likely toubstantially reduce their smoking, more likely tochieve initial abstinence, and more likely to maintainbstinence, both in the short run and for up to 6onths.Although the absolute quit rates achieved in this trial
ppear modest (with 10% of active gum users achieving8-day abstinence and 6% maintaining abstinence athe 6-month follow-up visit), it must be recalled thathis trial included no behavioral instruction or inter-ention whatsoever. The quit rates observed are com-arable to those observed in abrupt quitting withicotine gum under similar conditions (Shiffman etl.29 reported 6-month quit rates of 8%). In assessinghe quit rates in this study, it is important to keep in
ind that smokers who prefer quitting by gradualeduction differ from those who elect abrupt cessation.or example, smokers planning to quit by gradualeduction are less motivated to quit and are less thanalf as likely as abrupt quitters to even attempt quit-
ing.11 Indeed, those saying they would quit graduallyere no more likely to make a quit attempt than
mokers who said they wanted to only reduce, not quit,moking. Thus, smokers preferring to quit by gradualeduction are not comparable to those who want to quitbruptly, as in most cessation trials, and may be ex-ected to have lower quit rates. Indeed, very low rates ofuitting in the placebo group (4% at 28 days and 2% atmonths) were observed. Against that background,
reatment with active gum tripled the odds of quittingor 28 days, an advantage that was maintained at the-month follow-up visit. Indeed, the 6-month OR (2.86)s at the high end of those typically observed in trials oficotine gum for abrupt smoking cessation (whichverage 1.667). The data suggest that for smokersuitting gradually, using nicotine gum can offer a very
igure 5. Percentage (and 95% CI) of participants whoeported adverse events (AEs) by concomitant use and treat-ent groups, during Weeks 1 (n�2265), 2 (n�2366), 3
n�2027), and 4 (n�1841). High-concomitant smokers werehose who were in the upper two thirds of the distribution onoth daily cigarette consumption and daily gum use (see
ext). The “Low” group includes all other participants.Am J Prev Med 2009;36(2) 101

sitqw
itetadsumwtat
tsnodscmrs�rawi
isnipnbtnbwstwrtaipr
aNsoarOmamq
aighwrttsww2Flirtct
cNbtrapbimmasi
csgwaudt
1
ubstantial advantage. Interestingly, in a nonrandom-zed population study, Cheong et al.10 similarly foundhat using medication was associated with success inuitting by gradual reduction (OR�2.6), consistentith the findings from this RCT.The reduce-to-quit (RTQ) approach described here
s not the only approach using an NRT-assisted reduc-ion phase to promote cessation. The RTQ approachngages smokers who are ready to quit on a relativelyime-limited program of structured reduction explicitlyimed at a quitting endpoint. A contrasting approach,escribed as “cut down to quit” (CDTQ),30 encouragesmokers who are not currently interested in quitting tose NRT for reduction over a period of up to 12onths. Meta-analysis30 suggested that this approachas efficacious but less cost effective than abrupt cessa-
ion. In any case, the RTQ and CDTQ approachesddress different populations with different proposi-ions, making results difficult to compare.
Treatment with active nicotine gum facilitated reduc-ions in reported smoking and biochemical markers ofmoke exposure. Although use of active 2-mg gum didot show significantly greater reductions in self-reportsf cigarettes smoked, it did yield significantly greaterrops in CO, demonstrating greater reductions inmoke intake. Smokers on placebo gum may haveompensated for some of their reductions by smokingore intensely,31 whereas treatment with nicotine gum
educed the use of this compensation. Indeed, a mea-ure of biochemically verified reduction, requiring a50% reduction in cigarettes smoked and a �25%
eduction in CO level, showed significant effects forctive treatment in both doses. Assays based on SCN,hich has a longer half-life than CO, confirmed signif-
cant reductions in those using 4-mg gum.Many purely behavioral approaches to reducing smok-
ng have been tested previously (e.g., keeping a strictchedule, elimination of least-favored cigarettes).32 It isot known which procedures are optimal for promot-
ng reduction. In this study, smokers were instructed torogressively increase their gum use while simulta-eously decreasing their smoking on an hour-by-hourasis.20 However, the pattern of gum use observed inhe study, and the fact that smokers in the study did notecessarily achieve abstinence after 16 days (as woulde expected if they followed the regimen and added aaking hour of abstinence each day), suggests that
mokers did not strictly follow the hour-by-hour instruc-ion. Further research is needed in order to determinehether alternate procedures more effectively promoteeduction and cessation. However, it is clear that par-icipants benefited from having 8 weeks to establishbstinence, as new participants continued to achievenitial abstinence each week throughout this 8-weekeriod. This suggests that allowing a longer period for
eduction might have led to higher quit rates. s02 American Journal of Preventive Medicine, Volume 36, Num
Process analyses shed light on the ways in whichctive treatment helped smokers achieve abstinence.icotine gum was expected to help smokers reduce
moking effectively, and thus to promote achievementf initial abstinence. Indeed, the analysis showed thatctive treatment with nicotine gum promoted smokingeduction, which, in turn, promoted initial cessation.nce smokers achieved initial abstinence, active treat-ent with nicotine gum promoted maintenance of
bstinence for 28 days–6 months. Thus, active treat-ent provided a benefit at each step in the process of
uitting by gradual reduction.As noted by Shiffman et al.,33 achievement of initial
bstinence is an important but often ignored key stepn successful quitting. In this study of quitting byradual reduction, achieving initial cessation for 24ours appeared to be the greatest hurdle—treatmentith active gum helped increase the proportion whoeached that milestone by 37%, from 19% (on placebo)o 26%. This demonstrates the contribution of activereatment during the reduction phase in bringingmokers to the point of quitting. After initial cessationas achieved, active treatment further demonstrated itsell known ability to sustain abstinence, increasing8-day abstinence by 40%, from 28% (placebo) to 39%.urther work is needed on behavioral and pharmaco-
ogic treatment regimens to increase achievement ofnitial quitting in the context of gradual reductionegimens. It is possible that a more structured approacho cessation, or selection of smokers who are moreommitted to complete cessation, would yield substan-ially higher initial quit rates.
The data suggest that behavioral as well as pharma-ologic processes are at work in determining success.otably, whereas other studies have demonstrated aenefit of more NRT use in the active group only,34 inhis study, smokers who used more gum early in theeduction phase were more likely to achieve 28-daybstinence, regardless of whether they used active orlacebo gum. This could reflect nonspecific behavioralenefits of just chewing gum (chewing gum and candy
s often recommended for quitting35), or it could be aarker distinguishing those smokers who were moreotivated and prepared to make greater efforts to
chieve and maintain abstinence. In either case, thisuggests the importance of behavioral processes, evenn the context of pharmacologic treatment.
Nicotine gum has been used safely for cessation inlinical trials and in actual use for over 20 years.7 Thistudy was unique in directing that smokers use nicotineum while still smoking, for up to 8 weeks. The resultsere reassuring: Adverse events were generally mildnd were consistent with those seen with nicotine gumsed for abrupt quitting. Moreover, there was no evi-ence of increased risk among smokers who engaged inhe most concomitant smoking and gum use. Even
mokers who smoked an average of 18 CPD along withber 2 www.ajpm-online.net

sbctsiulmNl
tqsssgpaatom
wirrtitttstbteihtn
TH(fTFsDdhrt
B
pd(c
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
F
even pieces of 4-mg nicotine gum (more than is usedy the typical quitter36) did not experience an in-reased likelihood of adverse events. Nicotine regula-ion mechanisms37 likely limited exposure, causingmoking to decline as nicotine intake from the gumncreased. The safety of concomitant smoking and NRTse seen in this study is consistent with analyses of
ong-time users of nicotine gum38 and with a study ofyocardial perfusion during concomitant smoking andRT use.39 Using nicotine gum while smoking carries
ittle to no incremental risk.The study’s limitations include a lack of highly de-
ailed data about how subjects used nicotine gum touit and a lack of detailed information regardingubjects who were screened out of participation. Thetudy also did not include some groups of smokers,uch as those with cardiovascular disease, who may be atreater risk for adverse events; thus, the adverse eventrofile described in the study cannot be generalized toll smokers. The study’s strengths include a very largend diverse sample, studied under real-world condi-ions with no counseling or instruction; detailed datan cigarette and gum consumption; and biochemicaleasures of smoke exposure.This is the first study to demonstrate that smokers
anting to quit by gradual reduction can substantiallyncrease their success by using nicotine gum to facilitateeduction and cessation. Nicotine gum helped smokerseduce smoking, achieve initial abstinence, and main-ain abstinence. The advantage of active NRT treatments particularly evident for heavy smokers treated withhe 4-mg nicotine gum, for which treatment increasedhe odds of quitting for 6 months sixfold. This expandsreatment options for the substantial proportion ofmokers who prefer quitting gradually,8 who have rela-ively low chances of quitting, and who have heretoforeeen implicitly excluded from the use of NRT to helphem quit. Offering this new way to use NRT maynhance the appeal and reach of a treatment thatncreases success, and thereby have positive publicealth impact. Given the ongoing extraordinary health
oll from smoking, consideration should be given toovel approaches that increase success in quitting.
his study was supported by SmithKline Beecham Consumerealthcare, now GlaxoSmithKline Consumer Healthcare
GSKCH), which markets nicotine replacement medicationsor smoking cessation. Dr. Strahs is employed by GSKCH.hrough their work at Pinney Associates, Drs. Shiffman anderguson serve as consultants to GSKCH on matters related tomoking control and/or nicotine replacement medications.r. Shiffman also has a financial interest in a venture toevelop new nicotine replacement medications. The authorsad full access to all of the data in the study and takeesponsibility for the integrity of the data and the accuracy ofhe data analysis.
The authors wish to thank Mark Sembower and Gina
ittner for their assistance with analyzing the data and2
ebruary 2009
reparing the manuscript for publication. The authors owe aebt of gratitude to the 27 study-site Principal Investigatorslisted in an online appendix at www.ajpm-online.net) whoollected the data.
eferences1. Peto R. Smoking and death: the past 40 years and the next 40. BMJ
1994;309:937–9.2. CDC. Cigarette smoking among adults—United States, 2000. MMWR
2002;51:642–5.3. Shiffman S, Brockwell SE, Pillitteri JL, Gitchell JG. Use of smoking-
cessation treatments in the United States. Am J Prev Med 2008;34:102–11.4. Fiore MC. Treating tobacco use and dependence: an introduction to the
U.S. Public Health Service Clinical Practice Guideline. Respir Care2000;45:1196–9.
5. Garvey AJ, Bliss RE, Hitchcock JL, Heinold JW, Rosner B. Predictors ofsmoking relapse among self-quitters: a report from the Normative AgingStudy. Addict Behav 1992;17:367–77.
6. Hughes JR, Gulliver SB, Fenwick JW, et al. Smoking cessation amongself-quitters. Health Psychol 1992;11:331–4.
7. Silagy C, Lancaster T, Stead L, Mant D, Fowler G. Nicotine replacementtherapy for smoking cessation. Cochrane Database Syst Rev 2004(3):CD000146.
8. Hughes JR, Callas PW, Peters EN. Interest in gradual cessation. NicotineTob Res 2007;9:671–5.
9. Shiffman S, Hughes JR, Ferguson SG, Pillitteri JL, Gitchell JG, Burton SL.Smokers’ interest in using nicotine replacement to aid smoking reduction.Nicotine Tob Res 2007;9:1177–82.
0. Cheong Y, Yong HH, Borland R. Does how you quit affect success? Acomparison between abrupt and gradual methods using data from theInternational Tobacco Control Policy Evaluation Study. Nicotine Tob Res2007;9:801–10.
1. Peters EN, Hughes JR, Callas PW, Solomon LJ. Goals indicate motivation toquit smoking. Addiction 2007;102:1158–63.
2. Shiffman S, Gitchell J, Pinney JM, Burton SL, Kemper KE, Lara EA. Publichealth benefit of over-the-counter nicotine medications. Tob Control1997;6:306–10.
3. Rose JE, Behm FM. Extinguishing the rewarding value of smoke cues:pharmacological and behavioral treatments. Nicotine Tob Res 2004;6:523–32.
4. Carpenter MJ, Hughes JR, Keely JP. Effect of smoking reduction on latercessation: a pilot experimental study. Nicotine Tob Res 2003;5:155–62.
5. Cinciripini PM, Lapitsky LG, Wallfisch A, Mace R, Nezami E, Van VunakisH. An evaluation of a multicomponent treatment program involvingscheduled smoking and relapse prevention procedures: initial findings.Addict Behav 1994;19:13–22.
6. Cinciripini PM, Lapitsky L, Seay S, Wallfisch A, Kitchens K, Van Vunakis H.The effects of smoking schedules on cessation outcome: can we improve oncommon methods of gradual and abrupt nicotine withdrawal? J ConsultClin Psychol 1995;63:388–99.
7. Levinson BL, Shapiro D, Schwartz GE, Tursky B. Smoking elimination bygradual reduction. Behavior Therapy 1971;2:477–87.
8. West R, Shiffman S. Effect of oral nicotine dosing forms on cigarettewithdrawal symptoms and craving: a systematic review. Psychopharmacol-ogy (Berl) 2001;155:115–22.
9. Shiffman S, Ferguson SG, Gwaltney CJ, Balabanis MH, Shadel WG. Reductionof abstinence-induced withdrawal and craving using high-dose nicotine re-placement therapy. Psychopharmacology (Berl) 2006;184:637–44.
0. Cooper T, Clayton R. New hope for heavy smokers: the cooper/claytonmethod for stop smoking. Lexington: SBC Publishers, 1988.
1. Hughes JR, Carpenter MJ. The feasibility of smoking reduction: an update.Addiction 2005;100:1074–89.
2. Fagerstrom KO. Can reduced smoking be a way for smokers not interestedin quitting to actually quit? Respiration 2005;72:216–20.
3. Committee on Safety of Medicines and Healthcare Products RegulatoryAgency (CSMHPRA). Report of the committee on safety of medicinesworking group on nicotine replacement therapy 2006. London, CSM &MHRSA. www.mhra.gov.uk.
4. Brown R, Burgess E, Sales S, Whitely J, Evans D, Miller I. Reliability andvalidity of a smoking timeline follow-back interview. Psychol Addict Behav1998;12:101–12.
5. Shields PG. Tobacco smoking, harm reduction, and biomarkers. J NatlCancer Inst 2002;94:1435–44.
Am J Prev Med 2009;36(2) 103

2
2
2
2
3
3
3
3
3
3
3
3
3
3
1
6. Benowitz NL, Kuyt F, Jacob P III. Circadian blood nicotine concentrationsduring cigarette smoking. Clin Pharmacol Ther 1982;32:758–64.
7. Junge B. Changes in serum thiocyanate concentration on stopping smok-ing. Br Med J (Clin Res Ed) 1985;291:22.
8. U.S. Food and Drug Administration. Transcript of the Joint Meeting of theNon-prescription Drugs Advisory Committee and the Drug Abuse AdvisoryCommittee of the Food and Drug Administration.
9. Shiffman S, Rolf CN, Hellebusch SJ, et al. Real-world efficacy ofprescription and over-the-counter nicotine replacement therapy. Addic-tion 2002;97:505–16.
0. Wang D, Connock M, Barton P, Fry-Smith A, Aveyard P, Moore D. Cutdown to quit with nicotine replacement therapies in smoking cessation: asystematic review of effectiveness and economic analysis. Health TechnolAssess. 2008;12:iii–iv, ix–xi, 1–135.
1. Hammond D, Fong GT, Cummings KM, Hyland A. Smoking topography,brand switching, and nicotine delivery: results from an in vivo study. CancerEpidemiol Biomarkers Prev 2005;14:1370–5.
2. Schwartz JL. Review and evaluation of smoking cessation methods: the
United StatesPrinting Offic04 American Journal of Preventive Medicine, Volume 36, Num
3. Shiffman S, Scharf DM, Shadel WG, et al. Analyzing milestones in smokingcessation: illustration in a nicotine patch trial in adult smokers. J ConsultClin Psychol 2006;74:276–85.
4. Shiffman S. Use of more nicotine lozenges leads to better success inquitting smoking. Addiction 2007;102:809–14.
5. Abrams DB, Niaura R, Brown RA, Emmons KM, Goldstein MG, Monti PM.Tobacco dependence treatment handbook: a guide to best practices. NewYork: Guilford Press, 2003.
6. Shiffman S, Paty JA, Rohay JM, Di Marino ME, Gitchell J. The efficacy ofcomputer-tailored smoking cessation material as a supplement to nicotinepolacrilex gum therapy. Arch Intern Med 2000;160:1675–81.
7. Nemeth-Coslett R, Henningfield JE. Effects of nicotine chewing gum oncigarette smoking and subjective and physiologic effects. Clin PharmacolTher 1986;39:625–30.
8. Murray RP, Bailey WC, Daniels K, et al. Safety of nicotine polacrilex gumused by 3,094 participants in the Lung Health Study. Lung Health StudyResearch Group. Chest 1996;109:438–45.
9. Mahmarian JJ, Moye LA, Nasser GA, et al. Nicotine patch therapy in
uced myocardial and Canada, 1978–1985. Washington DC: U.S. Governmente, 1987.smoking cessation reduces the extent of exercise-indischemia. J Am Coll Cardiol 1997;30:125–30.
What’s new online?Visit www.ajpm-online.net today to find out how you can search 400 top medical andhealth sciences journals online, including Medline.
ber 2 www.ajpm-online.net
A
S
WSS
REE
SSB
DCA
MTP
PUH
CCO
TTT
DOP
DUM
FUL
LRH
SMD
LIS
SHW
RUC
JLO
MLL
SUO
HRL
ECP
NGMB
SII
JVM
TSE
KRG
GH
ppendix
tudy-Site Principal Investigators
anda D. Angueira, MDciman Biomedical Researchan Antonio TX
obert Bettis, MDdmonds Family Medicine Clinicdmonds WA
tephen A. Braden, MDciman Biomedical Researchryan TX
avid Brown, MDommunity Clinical Research, Inc.ustin TX
ichael Cassar, MDKL Research, Inc.aramus NJ
aul Cinciripini, PhDT MD Anderson Cancer Centerouston TX
linton N. Corder, PhD, MDOR Clinical Researchklahoma City OK
homas Fiel, DOempe Primary Care Associatesempe AZ
avid Gonzales, PhDregon Health Sciences Universityortland OR
orothy Hatsukami, PhDniversity of Minnesotainneapolis MN
. Charles Hiller, MDniversity of Arkansas for Medical Sciencesittle Rock AR
arysa Hun, MDesearch Testing Laboratories, Inc.untington NY
harad Lakhanpal, MDetroplex Clinical Research
allas TX Sawrence V. Larsen, PhDntermountain Clinical Researchalt Lake City UT
amuel Lederman, MDill Top Research, Inc.est Palm Beach FL
obin Mermelstein, PhDniversity of Illinois at Chicagohicago IL
ohn S. Muchmore, MDynn Health Science Instituteklahoma City OK
itch Nides, PhDA Smoking Research Centeros Angeles CA
tephen Rennard, MDniversity of Nebraska Medical Centermaha NE
arvey Resnick, MD/D Clinical Research, Inc.ake Jackson TX
rnie Riffer, MDentral Phoenix Medical Clinichoenix AZ
ancy Rigotti, MDeneral Internal Medicine Unitassachusetts General Hospitaloston MA
id Rosenblatt, MD, FACPrvine Clinical Research Centerrvine CA
oseph Salvatore, MDista Medical Research, Inc.esa AZ
eresa S. Sligh, MDciman Biomedical Researchuless TX
evin Tack, MDesearch Testing Laboratories, Inc.reat Neck NY
erald Wolfley, MDill Top Research
cottsdale AZ
Am J Prev Med 2009;36(2) 104.e1
Related Documents











