C o p y r i g h t b y N o t f o r Q u i n t e s s e n c e Not for Publication 285 Eur J Oral Implantol 2010;3(4):285–296 RANDOMISED CONTROLLED CLINICAL TRIAL Luigi Canullo, DDS Private practice, Rome, Italy Isabella Bignozzi, DDS “Sapienza” University of Rome, Italy Roberto Cocchetto MD, DDS Private practice, Verona, Italy, and University of Chieti, Italy Maria Paola Cristalli, DDS, PHD “Sapienza” University of Rome, Italy Giuliano Iannello Data Analyst Rome, Italy Correspondence to: Luigi Canullo Via Nizza, 46 00198 Rome, Italy Tel/Fax: +39 06 8411980 Email: [email protected] Luigi Canullo, Isabella Bignozzi, Roberto Cocchetto, Maria Paola Cristalli, Giuliano Iannello Immediate positioning of a definitive abutment versus repeated abutment replacements in post-extractive implants: 3-year follow-up of a randomised multicentre clinical trial Key words bone preservation, definitive abutment, dental implant, immediate loading, platform switching Purpose: The aim of this randomised clinical trial was to evaluate the influence of restoration on marginal bone loss (MBL) using immediately definitive abutments (one abutment–one time concept) versus provisional abutments later replaced by definitive abutments. Materials and methods: In three private clinics, 32 patients with 32 hopeless maxillary premolars were selected for post-extractive implant-supported immediate restoration and randomised to provisional abutment (PA) and definitive abutment (DA) groups, 16 sites in each group. After tooth extraction, 7 patients had to be excluded for buccal wall fracture at tooth extraction or lack of sufficient primary implant stability (< 35 Ncm). The remaining 25 patients (10 PA, 15 DA) received a post-extractive wide-diameter implant. Immediately after insertion, the PA group were immediately restored using a platform-switched provisional titanium abutment. In the DA group, definitive platform-switched tita- nium abutments were tightened. In both groups, provisional crowns were adapted, avoiding occlusal contacts. All implants were definitively restored after 3 months. In the PA group, a traditional impres- sion technique with coping transfer was adopted, dis/reconnecting abutments several times; in the DA group, metal prefabricated copings were used and final restorations were seated, avoiding abutment disconnection. Digital standardised periapical radiographs using a customised film holder were recorded at baseline (T 0 = implant insertion), final restoration (T 1 = 3 months later), and at 18-month (T 2 ) and 3-year (T 3 ) follow-ups. The MBL was evaluated with a computerised measuring technique and digital subtraction radiography (DSR) software was used to evaluate radiographic density. Results: At the 3-year follow-up a success rate of 100% in both groups was reported. In the PA group, peri-implant bone resorption was 0.36 mm at T 1 , 0.43 mm at T 2 , and 0.55 mm at T 3 . In the DA group, peri-implant bone resorption was 0.35 mm at T 1 , 0.33 mm at T 2 , and 0.34 mm at T 3 . Statistically significant lower bone losses were found at T 2 (0.1 mm) and T 3 (0.2 mm) for the DA group. At T 3 , significantly higher DSR values around implant necks were recorded in the DA group (72 ± 5.0) when compared with the PA group (52 ± 9.5). Conclusions: The current trial suggests that the ‘one abutment–one time’ concept might be a pos- sible additional strategy in post-extraction immediately restored platform-switched single implants to further minimise peri-implant crestal bone resorption, although a 0.2 mm difference may not have any clinical effect. Additional clinical trials with larger groups of patients should be performed to bet- ter investigate this hypothesis.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
� 285
Eur J Oral Implantol 2010;3(4):285–296
RANDOMISED CONTROLLED CLINICAL TRIAL
Luigi Canullo, DDSPrivate practice, Rome, Italy
Isabella Bignozzi, DDS“Sapienza” University of Rome, Italy
Roberto Cocchetto MD, DDSPrivate practice, Verona, Italy,and University of Chieti, Italy
Maria Paola Cristalli, DDS, PHD“Sapienza” University of Rome, Italy
Giuliano IannelloData AnalystRome, Italy
Correspondence to:Luigi CanulloVia Nizza, 4600198 Rome, ItalyTel/Fax: +39 06 8411980Email: [email protected]
Luigi Canullo, Isabella Bignozzi, Roberto Cocchetto, Maria Paola Cristalli, Giuliano Iannello
Immediate positioning of a definitive abutment versus repeated abutment replacements in post-extractive implants: 3-year follow-up of a randomised multicentre clinical trial
Key words bone preservation, definitive abutment, dental implant, immediate loading, platform switching
Purpose: The aim of this randomised clinical trial was to evaluate the influence of restoration on marginal bone loss (MBL) using immediately definitive abutments (one abutment–one time concept) versus provisional abutments later replaced by definitive abutments.Materials and methods: In three private clinics, 32 patients with 32 hopeless maxillary premolars were selected for post-extractive implant-supported immediate restoration and randomised to provisional abutment (PA) and definitive abutment (DA) groups, 16 sites in each group. After tooth extraction, 7 patients had to be excluded for buccal wall fracture at tooth extraction or lack of sufficient primary implant stability (< 35 Ncm). The remaining 25 patients (10 PA, 15 DA) received a post-extractive wide-diameter implant. Immediately after insertion, the PA group were immediately restored using a platform-switched provisional titanium abutment. In the DA group, definitive platform-switched tita-nium abutments were tightened. In both groups, provisional crowns were adapted, avoiding occlusal contacts. All implants were definitively restored after 3 months. In the PA group, a traditional impres-sion technique with coping transfer was adopted, dis/reconnecting abutments several times; in the DA group, metal prefabricated copings were used and final restorations were seated, avoiding abutment disconnection. Digital standardised periapical radiographs using a customised film holder were recorded at baseline (T0 = implant insertion), final restoration (T1 = 3 months later), and at 18-month (T2) and 3-year (T3) follow-ups. The MBL was evaluated with a computerised measuring technique and digital subtraction radiography (DSR) software was used to evaluate radiographic density.Results: At the 3-year follow-up a success rate of 100% in both groups was reported. In the PA group, peri-implant bone resorption was 0.36 mm at T1, 0.43 mm at T2, and 0.55 mm at T3. In the DA group, peri-implant bone resorption was 0.35 mm at T1, 0.33 mm at T2, and 0.34 mm at T3. Statistically significant lower bone losses were found at T2 (0.1 mm) and T3 (0.2 mm) for the DA group. At T3, significantly higher DSR values around implant necks were recorded in the DA group (72 ± 5.0) when compared with the PA group (52 ± 9.5).Conclusions: The current trial suggests that the ‘one abutment–one time’ concept might be a pos-sible additional strategy in post-extraction immediately restored platform-switched single implants to further minimise peri-implant crestal bone resorption, although a 0.2 mm difference may not have any clinical effect. Additional clinical trials with larger groups of patients should be performed to bet-ter investigate this hypothesis.
Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Canullo et al Definitive abutments versus repeated abutment replacement286 �
Eur J Oral Implantol 2010;3(4):285–296
� Introduction
Although buccal bone resorption occurs after tooth extraction1,2, the literature suggests that post-extrac-tive immediately restored implants can achieve opti-mal aesthetic outcomes3,4. However, preservation of peri-implant hard and soft tissues is a challenge5.
Different strategies are used to minimise bone resorption, such as graft materials6-8. Immediate pro-visional crowns are used to shape peri-implant soft tissues in an attempt to maintain interdental papil-lae9. At the same time, to reduce marginal bone loss (MBL) after post-extraction of immediately restored implants, the ‘platform switching’ concept10,11 has been suggested. Preservation of peri-implant crestal bone level may occur using an abutment with a smaller diameter than the implant12,13. From a bio-logical point of view, the presence of a non-matching, smaller diameter abutment is thought to move the implant–abutment microgap with its inflammatory cell infiltrate away from crestal bone, and to spread the biological width on the horizontal plane14,15. At the same time, better occlusal stress distribution has been advocated as a biomechanical advantage. Reduced bone strain around the implant cervical region might favourably influence marginal bone preservation16,17.
The platform-switching configuration used in post-extraction immediately restored implants has shown good clinical results regarding marginal bone preservation, when compared with implants restored using matching diameter abutments18.
Another factor that may affect peri-implant tis-sue stability is repeated abutment dis/reconnections, which are required in restorative procedures from provisional to final crown. Apical re-establishment of biological width and hard and soft tissue vertical loss may occur19. Thus, an immediate restoration with a provisional abutment could jeopardise the advan-tages of platform switching. Therefore, the use of a definitive immediately tightened abutment could be an additional strategy to preserve marginal bone.
The aim of the present clinical trial was to evalu-ate in maxillary premolar sites the influence on peri-implant marginal bone levels of immediate, platform-switched restorations using only defini-tive abutments, versus provisional abutments later disconnected and replaced by definitive abutments.
� Materials and methods
The present study was a multicentre randomised clinical trial of parallel group design and is reported according to the CONSORT Statement (http://www.consort-statement.org).
� Study design and patient selection
From September 2005 to December 2006, three private dental centres (Rome 1, Rome 2 and Verona,Italy) selected patients fulfilling the follow-ing inclusion criteria:• patient older than 18 years• requiring a single implant in premolar areas of
the maxilla• full mouth plaque score (FMPS) and full mouth
bleeding score (FMBS) < 25%• presence of opposing natural teeth• presence of adjacent teeth• radiographic and clinical appearance of intact
alveolar bone walls• presence at least of 4 mm of bone beyond the
root apex.
Implant sites that showed dehiscence or fenestra-tion at the moment of extraction and hopeless teeth affected by periodontal disease were not included. Exclusion criteria were:• patients with chronic systemic diseases• patient smoking > 10 cigarettes per day• pregnant or lactating females• teeth with acute infection at the sites• teeth with interproximal space narrower than 9 mm• teeth with clinical or radiographic appearance of
interproximal or buccal bone defects.
The tissue biotype of patients was assessed as thin or thick according to following criteria20:• thin tissue – a periodontal probe placed into the
labial gingival sulcus could be seen through the gingival tissue
• thick tissue – a periodontal probe placed into the labial gingival sulcus could not be seen through the gingival tissue.
Before the surgical procedure, patients were ran-domised into test and control groups. The randomi-
Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Canullo et al Definitive abutments versus repeated abutment replacement � 287
Eur J Oral Implantol 2010;3(4):285–296
sation list was provided by a statistician unaware of the study protocol using a random number genera-tor utility. The surgeon was informed of the alloca-tion of each patient shortly before tooth extraction, by unsealing a closed envelope; therefore allocation was not concealed.
A priori power analysis was carried out during the planning stage of the study in order to determine the appropriate sample size that would allow per-formance of robust statistics on the MBL. To detect a difference of 0.2 mm (standard deviation [SD] 0.157)18 between the two groups with a two-sided 5% significance level and a power of 80%, a sample size of 32 patients per group was necessary.
Before the surgical procedure, a full mouth pro-fessional prophylaxis appointment was scheduled. All patients were informed about the procedure and signed a consent form. The present study was performed following the principles outlined in the Declaration of Helsinki on experimentation involving human subjects.
� Clinical procedures
Patients received a single dose of 2 g of amoxycillin and clavulanic acid (Augmentin 1 g, GlaxoSmith-Kline, Verona, Italy) 1 h prior to surgery21. The tooth
extractions were performed in an atraumatic way, without raising a flap, using a periotome.
Extraction sites were thoroughly debrided and, when the buccal bone wall was reached undam-aged, 13-mm Global Implants (Sweden & Martina, Padua, Italy) with a platform diameter of 5.5 mm were inserted22. For these implants, the whole surface of the root-shaped implant is sand-blasted and acid-etched except for 0.3 mm of the machined neck surface. The surface roughness was 0.0771/μm2 (developed sur-face area ration [Sdr] 149.24%). Micro-threads in the coronal portion and a double internal abutment connection system were present.
The edge of the implant platform was placed at the margin of the buccal bone wall. To obtain adequate primary stability, implants had to achieve an initial insertion torque value from 32 to 45 Ncm.
When the distance between the implant and the neighbouring bone walls exceeded 1 mm, it was recorded and filled with nano-structured hydroxy-apatite (Sintlife, Faenza, Italy). A collagen disc (Ging-istat, Gaba-Vebas, Milan, Italy) was positioned over the implanted material. The rationale for this proce-dure was to maintain the graft material in situ and to prevent particle leakage23.
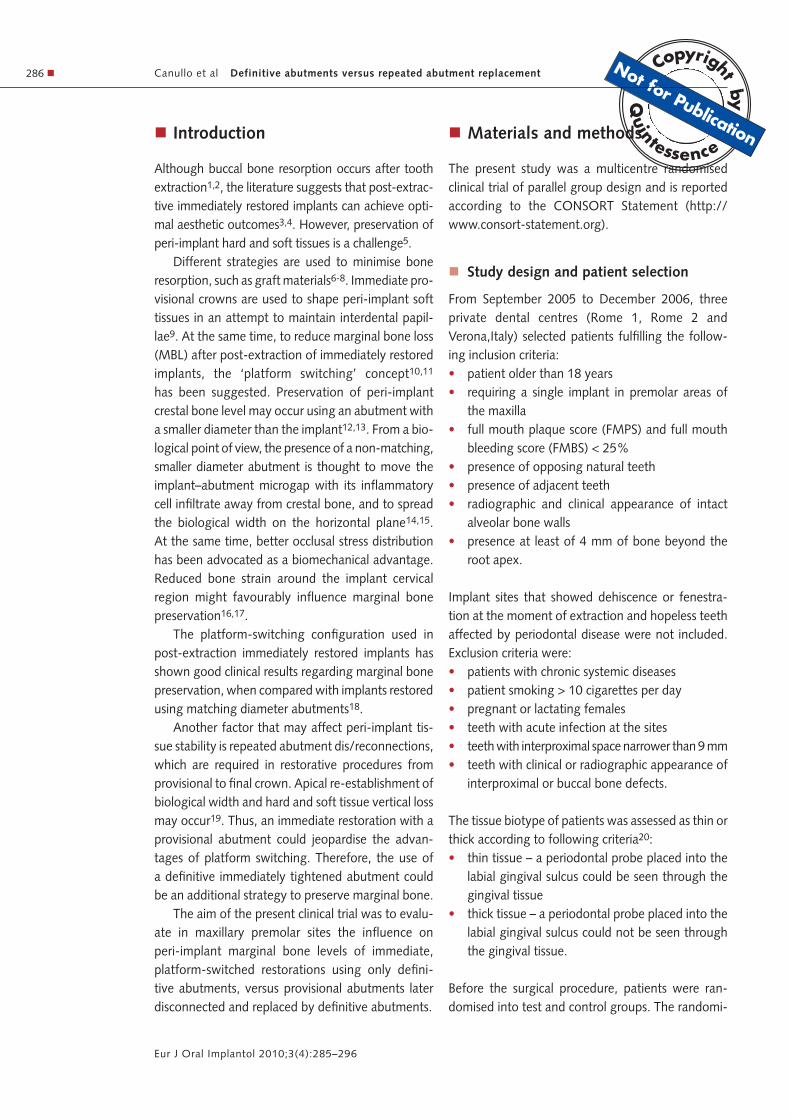
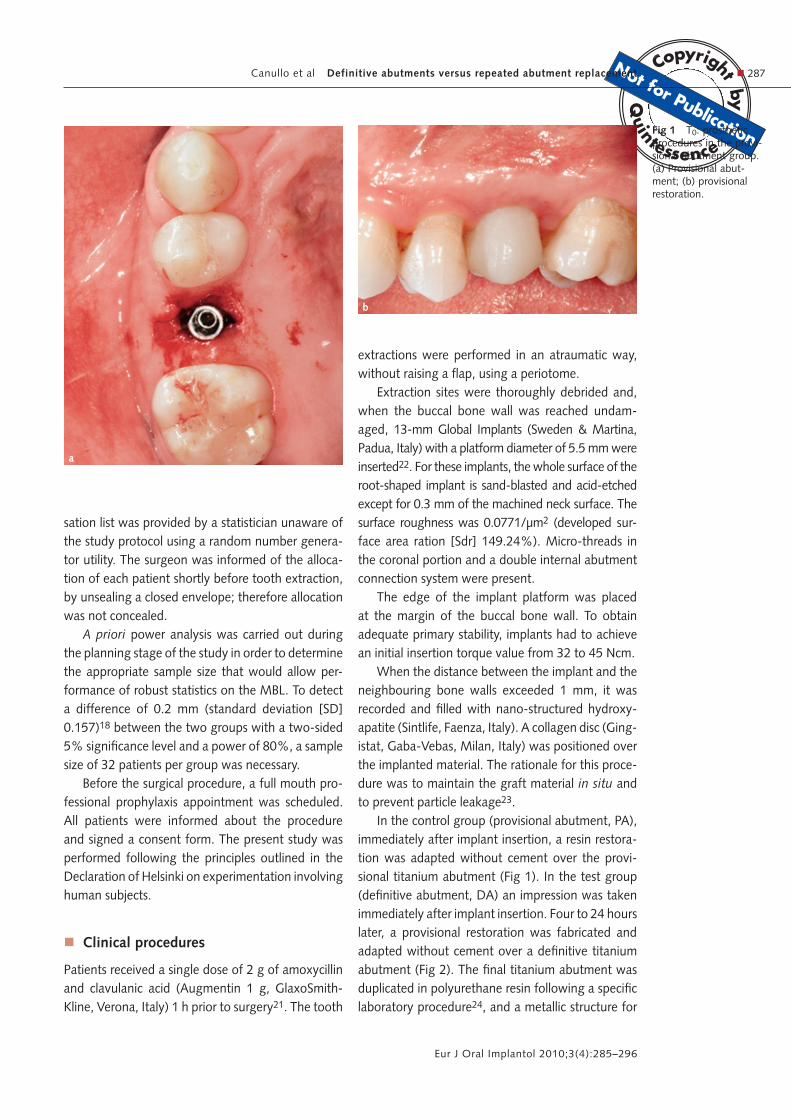
In the control group (provisional abutment, PA), immediately after implant insertion, a resin restora-tion was adapted without cement over the provi-sional titanium abutment (Fig 1). In the test group (definitive abutment, DA) an impression was taken immediately after implant insertion. Four to 24 hours later, a provisional restoration was fabricated and adapted without cement over a definitive titanium abutment (Fig 2). The final titanium abutment was duplicated in polyurethane resin following a specific laboratory procedure24, and a metallic structure for
a
b
Fig 1 T0: prosthetic procedures in the provi-sional abutment group. (a) Provisional abut-ment; (b) provisional restoration.
Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Canullo et al Definitive abutments versus repeated abutment replacement288 �
Eur J Oral Implantol 2010;3(4):285–296
the final porcelain-fused-to-metal (PFM) restoration was fabricated.
Both definitive and provisional titanium abut-ments had a diameter of 3.8 mm (1.7 mm narrower than the implant platform in diameter) and were screwed at 20 Ncm.
Provisional restorations were contoured for opti-mal marginal fit. The margin of the crown was placed 1.5 mm below the gingival margin. The chamfer was selected as the finish line for the abutment. The immediate restoration was fabricated the same day, relying on soft tissue stability according to findings
b
a
Fig 2 T0: prosthetic procedures in the defini-tive abutment group. (a) Intra-operative impression with a cop-ing transfer. (b) Healing abutment and sutures maintaining in situ graft material and collagen disc during the techni-cal procedure. (c) Soft tissues after 4 to 24 h after implant insertion. (d) Definitive abutment. (e) Finished provisional restoration after suture removal.
c
d e
Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Canullo et al Definitive abutments versus repeated abutment replacement � 289
Eur J Oral Implantol 2010;3(4):285–296
of previous studies25,26. Occlusal centric and eccen-tric contacts were not permitted on the provisional restorations, and 200 μm articulating paper was used following the guidelines for immediate non-func-tional loading27.
Digital periapical standardised radiographs with the paralleling technique were also taken using a Rinn XCP film holder (Dentsply Rinn, Elgin, IL, USA), customised and adapted on adjacent non-restored canines by means of polyvinylsiloxane polymerised in contact with its occlusal surface. Exposure parameters were conducted according to the manufacturer’s recommendations, by standard clinical protocols. These radiographs were used as baseline for the following radiographic evalu-ations.
Patients were instructed to have a soft diet and to avoid chewing in the treated area until the time of final restoration. Oral hygiene in the surgical site was limited to soft brushing for the first 2 weeks, and regular brushing in the rest of the mouth. Rinses with 0.12% chlorhexidine gluconate were prescribed for 2 weeks. Thereafter, conventional brushing and flossing were permitted.
After 1 week, provisional restorations were removed, the maturation of soft peri-implant tis-sue was evaluated and the provisional crowns
were bonded with provisional cement (Temp Bond, KerrHawe, Bioggio, Switzerland).
� Final crown delivery
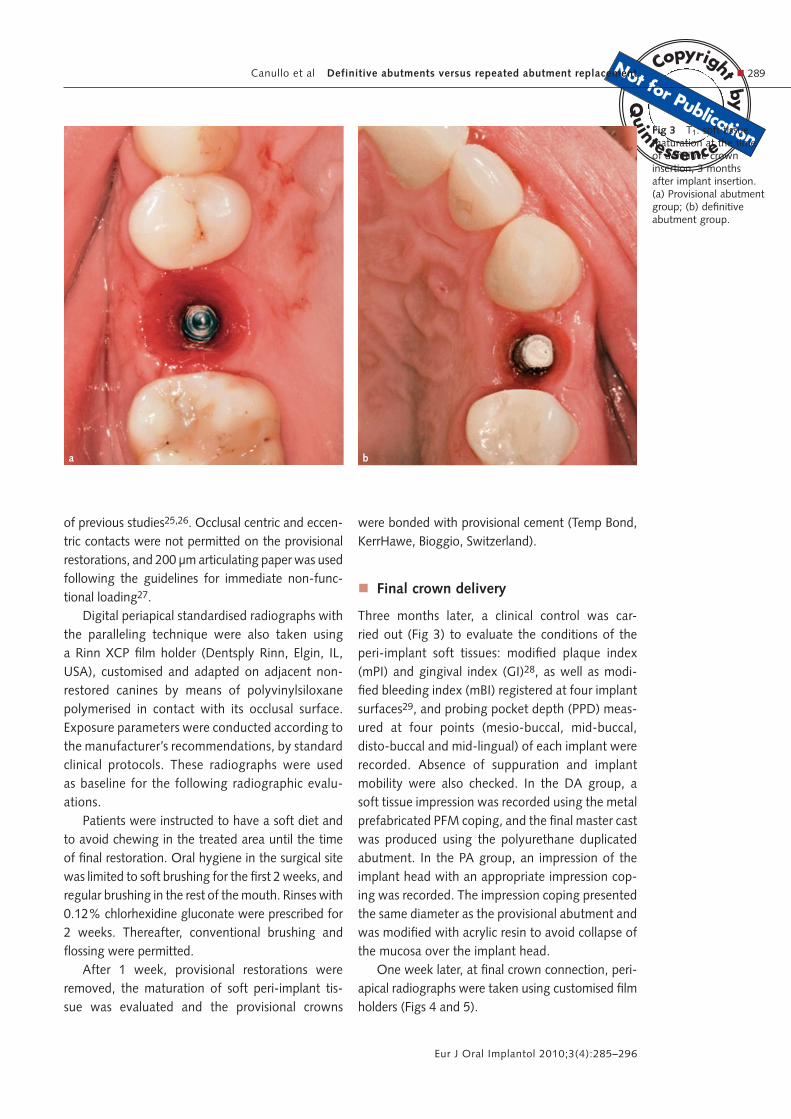
Three months later, a clinical control was car-ried out (Fig 3) to evaluate the conditions of the peri-implant soft tissues: modified plaque index (mPI) and gingival index (GI)28, as well as modi-fied bleeding index (mBI) registered at four implant surfaces29, and probing pocket depth (PPD) meas-ured at four points (mesio-buccal, mid-buccal, disto-buccal and mid-lingual) of each implant were recorded. Absence of suppuration and implant mobility were also checked. In the DA group, a soft tissue impression was recorded using the metal prefabricated PFM coping, and the final master cast was produced using the polyurethane duplicated abutment. In the PA group, an impression of the implant head with an appropriate impression cop-ing was recorded. The impression coping presented the same diameter as the provisional abutment and was modified with acrylic resin to avoid collapse of the mucosa over the implant head.
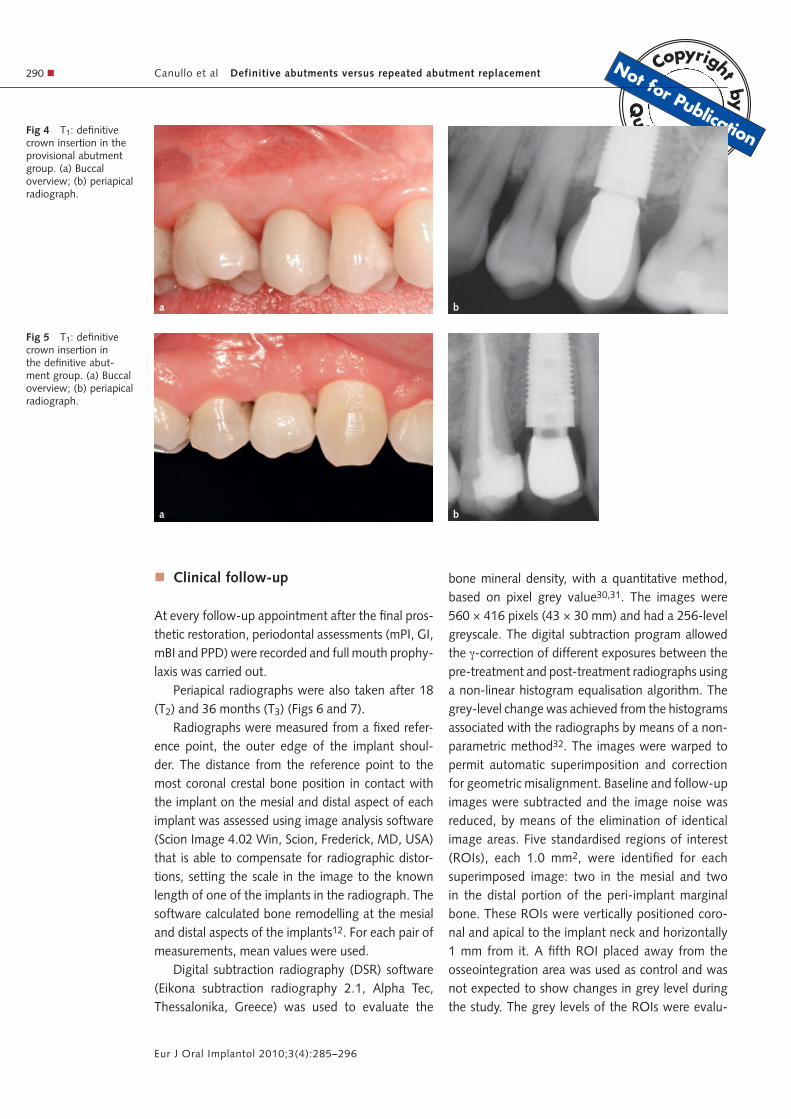
One week later, at final crown connection, peri-apical radiographs were taken using customised film holders (Figs 4 and 5).
a b
Fig 3 T1: soft tissue maturation at the time of definitive crown insertion, 3 months after implant insertion. (a) Provisional abutment group; (b) definitive abutment group.
Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Canullo et al Definitive abutments versus repeated abutment replacement290 �
Eur J Oral Implantol 2010;3(4):285–296
� Clinical follow-up
At every follow-up appointment after the final pros-thetic restoration, periodontal assessments (mPI, GI, mBI and PPD) were recorded and full mouth prophy-laxis was carried out.
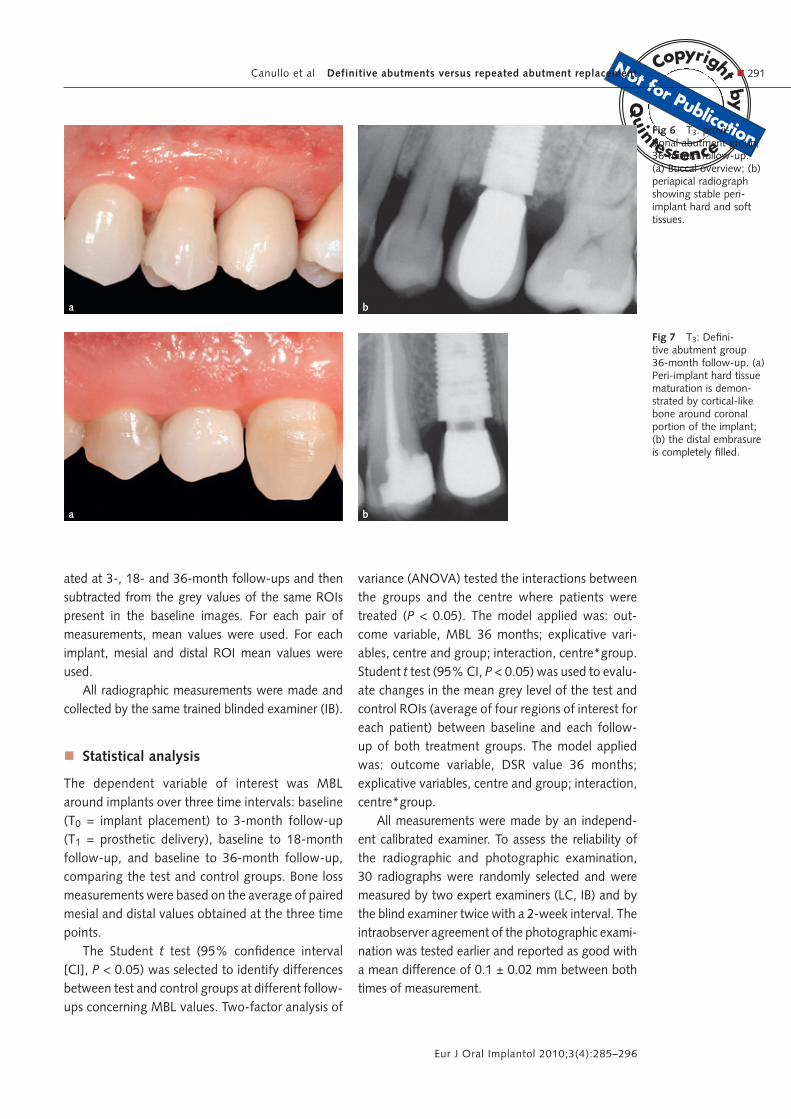
Periapical radiographs were also taken after 18 (T2) and 36 months (T3) (Figs 6 and 7).
Radiographs were measured from a fixed refer-ence point, the outer edge of the implant shoul-der. The distance from the reference point to the most coronal crestal bone position in contact with the implant on the mesial and distal aspect of each implant was assessed using image analysis software (Scion Image 4.02 Win, Scion, Frederick, MD, USA) that is able to compensate for radiographic distor-tions, setting the scale in the image to the known length of one of the implants in the radiograph. The software calculated bone remodelling at the mesial and distal aspects of the implants12. For each pair of measurements, mean values were used.
Digital subtraction radiography (DSR) software (Eikona subtraction radiography 2.1, Alpha Tec, Thessalonika, Greece) was used to evaluate the
bone mineral density, with a quantitative method, based on pixel grey value30,31. The images were 560 × 416 pixels (43 × 30 mm) and had a 256-level greyscale. The digital subtraction program allowed the �-correction of different exposures between the pre-treatment and post-treatment radiographs using a non-linear histogram equalisation algorithm. The grey-level change was achieved from the histograms associated with the radiographs by means of a non-parametric method32. The images were warped to permit automatic superimposition and correction for geometric misalignment. Baseline and follow-up images were subtracted and the image noise was reduced, by means of the elimination of identical image areas. Five standardised regions of interest (ROIs), each 1.0 mm2, were identified for each superimposed image: two in the mesial and two in the distal portion of the peri-implant marginal bone. These ROIs were vertically positioned coro-nal and apical to the implant neck and horizontally 1 mm from it. A fifth ROI placed away from the osseointegration area was used as control and was not expected to show changes in grey level during the study. The grey levels of the ROIs were evalu-
a b
Fig 4 T1: definitive crown insertion in the provisional abutment group. (a) Buccal overview; (b) periapical radiograph.
a b
Fig 5 T1: definitive crown insertion in the definitive abut-ment group. (a) Buccal overview; (b) periapical radiograph.
Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Canullo et al Definitive abutments versus repeated abutment replacement � 291
Eur J Oral Implantol 2010;3(4):285–296
ated at 3-, 18- and 36-month follow-ups and then subtracted from the grey values of the same ROIs present in the baseline images. For each pair of measurements, mean values were used. For each implant, mesial and distal ROI mean values were used.
All radiographic measurements were made and collected by the same trained blinded examiner (IB).
� Statistical analysis
The dependent variable of interest was MBL around implants over three time intervals: baseline (T0 = implant placement) to 3-month follow-up (T1 = prosthetic delivery), baseline to 18-month follow-up, and baseline to 36-month follow-up, comparing the test and control groups. Bone loss measurements were based on the average of paired mesial and distal values obtained at the three time points.
The Student t test (95% confidence interval [CI], P < 0.05) was selected to identify differences between test and control groups at different follow-ups concerning MBL values. Two-factor analysis of
variance (ANOVA) tested the interactions between the groups and the centre where patients were treated (P < 0.05). The model applied was: out-come variable, MBL 36 months; explicative vari-ables, centre and group; interaction, centre*group. Student t test (95% CI, P < 0.05) was used to evalu-ate changes in the mean grey level of the test and control ROIs (average of four regions of interest for each patient) between baseline and each follow-up of both treatment groups. The model applied was: outcome variable, DSR value 36 months; explicative variables, centre and group; interaction, centre*group.
All measurements were made by an independ-ent calibrated examiner. To assess the reliability of the radiographic and photographic examination, 30 radiographs were randomly selected and were measured by two expert examiners (LC, IB) and by the blind examiner twice with a 2-week interval. The intraobserver agreement of the photographic exami-nation was tested earlier and reported as good with a mean difference of 0.1 ± 0.02 mm between both times of measurement.
a b
a b
Fig 6 T3: provi-sional abutment group, 36-month follow-up. (a) Buccal overview; (b) periapical radiograph showing stable peri-implant hard and soft tissues.
Fig 7 T3: Defini-tive abutment group 36-month follow-up. (a) Peri-implant hard tissue maturation is demon-strated by cortical-like bone around coronal portion of the implant; (b) the distal embrasure is completely filled.
Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Canullo et al Definitive abutments versus repeated abutment replacement292 �
Eur J Oral Implantol 2010;3(4):285–296
� ResultsThirty-two patients fulfilled inclusion criteria and were enrolled in the study. After tooth extrac-tion, four patients assigned to the PA group were excluded for buccal bone fracture. At implant inser-tion, two patients assigned to the PA group and one to the DA group were excluded because of a lack of primary implant stability. The remaining 25 patients (10 in Rome 1, 7 in Rome 2, 8 in Verona), 15 in the DA group and 10 in the PA group, were followed for the entire duration of the study.
The mean age, the reason for extraction, the biotype and the position of the implant site are sum-marised in Table 1.
A bucco-oral jumping distance that exceeded 1 mm was detected in 23 out of 25 (14 for test and 9 for control group) patients, and was filled with nanostructured hydroxyapatite. No mesial or distal bone defect larger than 1 mm was reported.
All surgical interventions and postoperative heal-ing periods were without any serious complications or side effects. In the first postoperative day, some patients showed a moderate swelling without expe-riencing pain. After 1 week, no inflammation symp-toms were detectable.
At the clinical examinations, all 25 implants remained stable, and no signs of pain, suppuration or peri-implant infection were registered throughout the study period.
Periodontal parameters showed minimal variabil-ity at the different follow-up periods for both groups (Table 2).
� Radiographic results
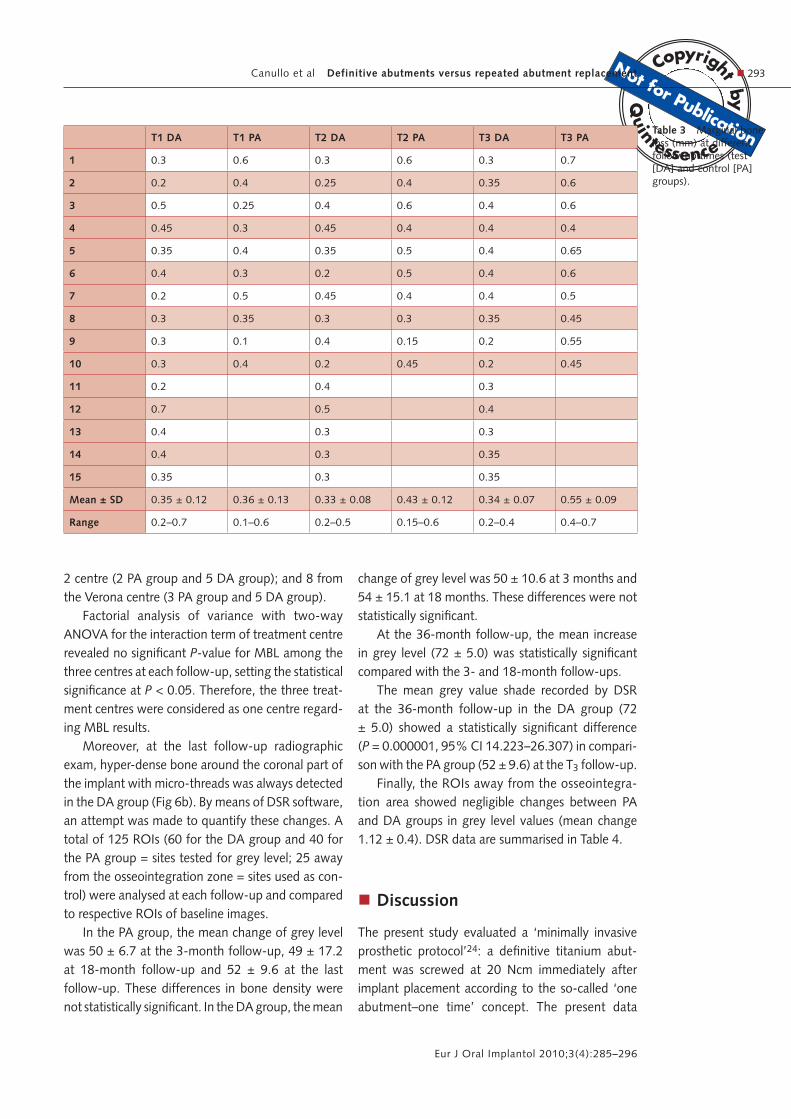
At baseline, interproximal radiographs revealed no bone defect around implants in both groups. After 3 months from baseline (T1, final crown delivery), the postoperative interproximal radiographs revealed an average bone loss of 0.35 mm (range 0.2 to 0.7 mm, SD 0.12 mm) in the DA group, and 0.36 (range 0.1 to 0.6, SD 0.13 mm) in the PA group (Table 3). After 18 months from baseline (T2), the periapical radiograph showed 0.33 mm of bone remodelling (range 0.2 to 0.5 mm, SD 0.08 mm) in the DA group, and 0.43 mm (range 0.15 to 0.60 mm, SD 0.12 mm) in the PA group. The post-operative radiographs at the last follow-up (T3, 36 months after baseline) confirmed an average bone loss of 0.34 mm (range 0.2 to 0.4 mm, SD 0.07 mm) in the DA group, and 0.55 (range 0.4 to 0.7 mm, SD 0.09 mm) in the PA group (Table 3).
A statistically significant difference between groups was found at T2 (borderline, P = 0.051, 95% CI 0.004–1.871) and T3 (P = 0.000001, 95% CI 1.302–2.784).
No statistically significant difference was found in the control and test groups for MBL between all follow-ups (paired-samples t test, P = 0.05).
The 25 patients who reached this stage of the study were distributed as follows according to the group assignment (PA or DA) and to the recruiting centre: 10 from the Rome 1 centre (5 assigned to the DA group and 5 to the PA group); 7 from the Rome
PA group DA group
Patients included in group (n)
10 15
Age at implant insertion (years)
55 ± 13.5 51 ± 7.7
Thick biotype 6 (60%) 7 (46%)
Female 3 (30%) 6 (40%)
Teeth extracted for root fracture
3 (30%) 5 (33.3%)
Teeth extracted for endo-dontic failure/caries
7 (70%) 10 (66.6%)
Table 1 Characteristics of patients included in the test (DA) and control (PA) groups.
T1 DA T1 PA T2 DA T2 PA T3 DA T3 PA
GI 0.68 ± 0.07 0.71 ± 0.06 0.98 ± 0.12 1.02 ± 0.9 0.76 ± 0.09 0.98 ± 0.11
mPI 1.14 ± 0.08 1.16 ± 0.07 1.53 ± 0.11 1.69 ± 0.1 1.34 ± 0.21 1.67 ± 0.3
mBI 0.41 ± 0.09 0.37 ± 0.04 0.67 ± 0.08 0.56 ± 0.12 0.55 ± 0.13 0.61 ± 0.08
PD (mm) 2.77 ± 0.28 2.79 ± 0.31 2.79 ± 0.24 2.82 ± 0.33 2.75 ± 0.07 2.80 ± 0.21
GI, gingival index; mBI, modified bleeding index; mPI, modified plaque index; PD, probing depth
Table 2 Periodontal parameters at different follow-up times (test [DA] and control [PA] groups).
Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Canullo et al Definitive abutments versus repeated abutment replacement � 293
Eur J Oral Implantol 2010;3(4):285–296
2 centre (2 PA group and 5 DA group); and 8 from the Verona centre (3 PA group and 5 DA group).
Factorial analysis of variance with two-way ANOVA for the interaction term of treatment centre revealed no significant P-value for MBL among the three centres at each follow-up, setting the statistical significance at P < 0.05. Therefore, the three treat-ment centres were considered as one centre regard-ing MBL results.
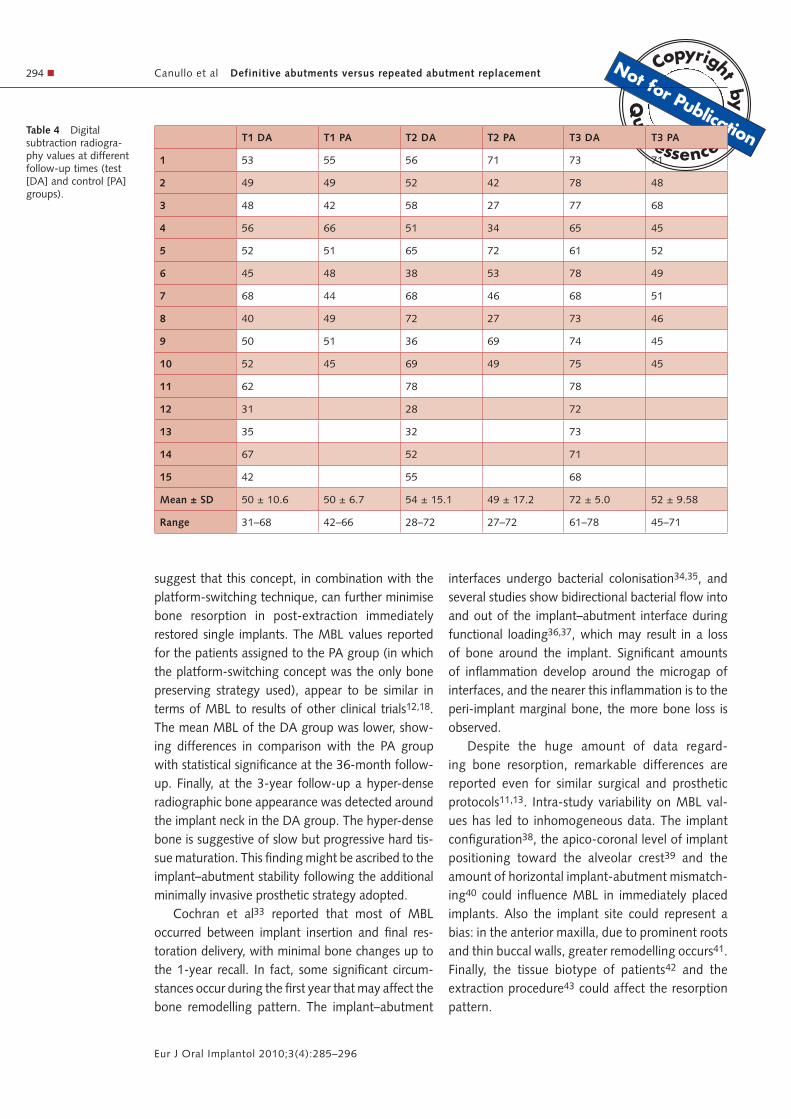
Moreover, at the last follow-up radiographic exam, hyper-dense bone around the coronal part of the implant with micro-threads was always detected in the DA group (Fig 6b). By means of DSR software, an attempt was made to quantify these changes. A total of 125 ROIs (60 for the DA group and 40 for the PA group = sites tested for grey level; 25 away from the osseointegration zone = sites used as con-trol) were analysed at each follow-up and compared to respective ROIs of baseline images.
In the PA group, the mean change of grey level was 50 ± 6.7 at the 3-month follow-up, 49 ± 17.2 at 18-month follow-up and 52 ± 9.6 at the last follow-up. These differences in bone density were not statistically significant. In the DA group, the mean
change of grey level was 50 ± 10.6 at 3 months and 54 ± 15.1 at 18 months. These differences were not statistically significant.
At the 36-month follow-up, the mean increase in grey level (72 ± 5.0) was statistically significant compared with the 3- and 18-month follow-ups.
The mean grey value shade recorded by DSR at the 36-month follow-up in the DA group (72 ± 5.0) showed a statistically significant difference (P = 0.000001, 95% CI 14.223–26.307) in compari-son with the PA group (52 ± 9.6) at the T3 follow-up.
Finally, the ROIs away from the osseointegra-tion area showed negligible changes between PA and DA groups in grey level values (mean change 1.12 ± 0.4). DSR data are summarised in Table 4.
� Discussion
The present study evaluated a ‘minimally invasive prosthetic protocol’24: a definitive titanium abut-ment was screwed at 20 Ncm immediately after implant placement according to the so-called ‘one abutment–one time’ concept. The present data
T1 DA T1 PA T2 DA T2 PA T3 DA T3 PA
1 0.3 0.6 0.3 0.6 0.3 0.7
2 0.2 0.4 0.25 0.4 0.35 0.6
3 0.5 0.25 0.4 0.6 0.4 0.6
4 0.45 0.3 0.45 0.4 0.4 0.4
5 0.35 0.4 0.35 0.5 0.4 0.65
6 0.4 0.3 0.2 0.5 0.4 0.6
7 0.2 0.5 0.45 0.4 0.4 0.5
8 0.3 0.35 0.3 0.3 0.35 0.45
9 0.3 0.1 0.4 0.15 0.2 0.55
10 0.3 0.4 0.2 0.45 0.2 0.45
11 0.2 0.4 0.3
12 0.7 0.5 0.4
13 0.4 0.3 0.3
14 0.4 0.3 0.35
15 0.35 0.3 0.35
Mean ± SD 0.35 ± 0.12 0.36 ± 0.13 0.33 ± 0.08 0.43 ± 0.12 0.34 ± 0.07 0.55 ± 0.09
Range 0.2–0.7 0.1–0.6 0.2–0.5 0.15–0.6 0.2–0.4 0.4–0.7
Table 3 Marginal bone loss (mm) at different follow-up times (test [DA] and control [PA] groups).
Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Canullo et al Definitive abutments versus repeated abutment replacement294 �
Eur J Oral Implantol 2010;3(4):285–296
suggest that this concept, in combination with the platform-switching technique, can further minimise bone resorption in post-extraction immediately restored single implants. The MBL values reported for the patients assigned to the PA group (in which the platform-switching concept was the only bone preserving strategy used), appear to be similar in terms of MBL to results of other clinical trials12,18. The mean MBL of the DA group was lower, show-ing differences in comparison with the PA group with statistical significance at the 36-month follow-up. Finally, at the 3-year follow-up a hyper-dense radiographic bone appearance was detected around the implant neck in the DA group. The hyper-dense bone is suggestive of slow but progressive hard tis-sue maturation. This finding might be ascribed to the implant–abutment stability following the additional minimally invasive prosthetic strategy adopted.
Cochran et al33 reported that most of MBL occurred between implant insertion and final res-toration delivery, with minimal bone changes up to the 1-year recall. In fact, some significant circum-stances occur during the first year that may affect the bone remodelling pattern. The implant–abutment
interfaces undergo bacterial colonisation34,35, and several studies show bidirectional bacterial flow into and out of the implant–abutment interface during functional loading36,37, which may result in a loss of bone around the implant. Significant amounts of inflammation develop around the microgap of interfaces, and the nearer this inflammation is to the peri-implant marginal bone, the more bone loss is observed.
Despite the huge amount of data regard-ing bone resorption, remarkable differences are reported even for similar surgical and prosthetic protocols11,13. Intra-study variability on MBL val-ues has led to inhomogeneous data. The implant configuration38, the apico-coronal level of implant positioning toward the alveolar crest39 and the amount of horizontal implant-abutment mismatch-ing40 could influence MBL in immediately placed implants. Also the implant site could represent a bias: in the anterior maxilla, due to prominent roots and thin buccal walls, greater remodelling occurs41. Finally, the tissue biotype of patients42 and the extraction procedure43 could affect the resorption pattern.
T1 DA T1 PA T2 DA T2 PA T3 DA T3 PA
1 53 55 56 71 73 71
2 49 49 52 42 78 48
3 48 42 58 27 77 68
4 56 66 51 34 65 45
5 52 51 65 72 61 52
6 45 48 38 53 78 49
7 68 44 68 46 68 51
8 40 49 72 27 73 46
9 50 51 36 69 74 45
10 52 45 69 49 75 45
11 62 78 78
12 31 28 72
13 35 32 73
14 67 52 71
15 42 55 68
Mean ± SD 50 ± 10.6 50 ± 6.7 54 ± 15.1 49 ± 17.2 72 ± 5.0 52 ± 9.58
Range 31–68 42–66 28–72 27–72 61–78 45–71
Table 4 Digital subtraction radiogra-phy values at different follow-up times (test [DA] and control [PA] groups).

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Canullo et al Definitive abutments versus repeated abutment replacement � 295
Eur J Oral Implantol 2010;3(4):285–296
In 23 out of 25 patients, graft material was inserted to fill the gap between the implant and the inner buccal bone wall. According to Ferrus et al44, this procedure could improve the aesthetic outcome.
Berglundh et al45, using an experimental model, reported that the soft tissue barrier adjacent to non-submerged titanium implants looks com-pletely structured within 6 weeks postoperatively. However, after this time point, between implant placement and final restoration delivery, there is repeated dis/reconnection of components such as cover screws, healing abutments, impression cop-ings and provisional abutments. These manipula-tions could not only spread bacterial contamina-tion over peri-implant tissues34,35, but also disrupt soft tissue attachment. According to Abrahamsson et al19, dis- and reconnections of prosthetic com-ponents can compromise the epithelial barrier and result in apical shifting of connective tissue attach-ment. Consequently, additional marginal bone resorption could occur due to re-establishment of proper biological width.
Furthermore, additional crestal bone loss could occur due to possible micro-movements between the implant and abutment during the provisional res-toration phase46. Hence there is a biologic rationale for the use of a single, definitive abutment at an earlier stage of prosthetic treatment.
The major limitations of the present study were the limited sample size and the inclusion of only maxillary premolars, which limit generalisation of the results, and the lack of allocation concealment, i.e. patients should have been definitively included in the study and randomised after implant place-ment.
� Conclusions
Within the limitations of the present study, and despite the statistically significant difference in peri-implant MBL of 0.2 mm observed 3 years after implant placement favouring the ‘one time–one abutment’ concept, no clinically visible differences could be observed in post-extraction immediately restored platform-switched implants. More ran-domised clinical trials are needed to properly inves-tigate this matter.
� Acknowledgements
The authors have no financial interest, either directly or indirectly, in the products listed in the study. The authors greatly appreciate the skills and commitment of Dr Audrenn Gautier and Dr Henry Canullo in their supervision of the study.
� References1. Araújo MG, Sukekava F, Wennström JL, Lindhe J. Ridge
alterations following implant placement in fresh extraction sockets: an experimental study in the dog. J Clin Periodontol 2005;32:645-652.
2. Araújo MG, Lindhe J. Dimensional ridge alterations follow-ing tooth extraction. An experimental study in the dog. J Clin Periodontol 2005;32:212-218.
3. Glauser R, Zembic A, Hämmerle CH. A systematic review of marginal soft tissue at implants subjected to immediate loading or immediate restoration. Clin Oral Implants Res 2006;17(Suppl 2):82-92.
4. Chen ST, Wilson TG Jr, Hämmerle CH. Immediate or early placement of implants following tooth extraction: review of biologic basis, clinical procedures, and outcomes. Int J Oral Maxillofac Implants 2004;19(Suppl):12-25.
5. De Rouck T, Collys K, Cosyn J. Single-tooth replacement in the anterior maxilla by means of immediate implanta-tion and provisionalization: a review. Int J Oral Maxillofac Implants 2008;23:897-904.
6. Wang HL, Kiyonobu K, Neiva RF. Socket augmentation: rationale and technique. Implant Dent 2004;13:286-296.
7. Darby I, Chen ST, Buser D. Ridge preservation tech-niques for implant therapy. Int J Oral Maxillofac Implants 2009;24(Suppl):260-271.
8. Ackermann KL. Extraction site management using a natural bone mineral containing collagen: rationale and retro-spective case study. Int J Periodontics Restorative Dent 2009;29:489-497.
9. Al-Harbi SA, Edgin WA. Preservation of soft tissue contours with immediate screw-retained provisional implant crown. J Prosthet Dent 2007;98:329-332.
10. Canullo L, Rasperini G. Preservation of peri-implant soft and hard tissues using platform switching of implants placed in immediate extraction sockets: a proof-of-concept study with 12- to 36-month follow-up. Int J Oral Maxillofac Implants 2007;22:995-1000.
11. Calvo-Guirado JL, Ortiz-Ruiz AJ, López-Marí L, Delgado-Ruiz R, Maté-Sánchez J, Bravo Gonzalez LA. Immediate maxillary restoration of single-tooth implants using platform switching for crestal bone preservation: a 12-month study. Int J Oral Maxillofac Implants 2009;24:275-281.
12. Prosper L, Redaelli S, Pasi M, Zarone F, Radaelli G, Gherlone EF. A randomized prospective multicenter trial evaluating the platform-switching technique for the preven-tion of post-restorative crestal bone loss. Int J Oral Maxil-lofac Implants 2009;24:299-308.
13. Luongo R, Traini T, Guidone PC, Bianco G, Cocchetto R, Celletti R. Hard and soft tissue responses to the platform-switching technique. Int J Periodontics Restorative Dent 2008;28:551-557.
14. Cappiello M, Luongo R, Di Iorio D, Bugea C, Cocchetto R, Celletti R. Evaluation of peri-implant bone loss around plat-form-switched implants. Int J Periodontics Restorative Dent 2008;28:347-355.

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Canullo et al Definitive abutments versus repeated abutment replacement296 �
Eur J Oral Implantol 2010;3(4):285–296
15. Degidi M, Iezzi G, Scarano A, Piattelli A . Immediately load-ed titanium implant with a tissue-stabilizing/maintaining design (‘beyond platform switch’) retrieved from man after 4 weeks: a histological and histomorphometrical evaluation. A case report. Clin Oral Implants Res 2008;19:276-282.
16. Maeda Y, Miura J, Taki I, Sogo M. Biomechanical analysis on platform switching: is there any biomechanical rationale? Clin Oral Implants Res 2007;18:581-584.
17. Schrotenboer J, Tsao YP, Kinariwala V, Wang HL. Effect of microthreads and platform switching on crestal bone stress levels: a finite element analysis. J Periodontol 2008;79: 2166-2172.
18. Canullo L, Goglia G, Iurlaro G, Iannello G. Short-term bone level observations associated with platform switching in immediately placed and restored single maxillary implants: a preliminary report. Int J Prosthodont 2009;22:277-282.
19. Abrahamsson I, Berglundh T, Lindhe J. The mucosal bar-rier following abutment dis/reconnection. An experimental study in dogs. J Clin Periodontol 1997;24:568-572.
20. Müller HP, Heinecke A, Schaller N, Eger T. Masticatory mucosa in subjects with different periodontal phenotypes. J Clin Periodontol 2000;27:621-626.
21. Esposito M, Grusovin MG, Loli V, Coulthard P, Worthing-ton HV. Does antibiotic prophylaxis at implant placement decrease early implant failures? A Cochrane systematic review. Eur J Oral Implantol 2010;3:101-110.
22. Touati B, Guez G. Immediate implantation with provisionali-zation: from literature to clinical implications. Pract Proced Aesthet Dent 2002;14:699-707.
23. Shimoji S, Miyaji H, Sugaya T, Tsuji H, Hongo T, Nakatsuka M, Uz Zaman K, Kawanami M. Bone perforation and placement of collagen sponge facilitate bone augmentation. J Perio-dontol 2009;80:505-511.
24. Cocchetto R, Resch I, Castagna M, Vincenzi G, Celletti R. The abutment duplication technique (ADT): a novel protocol for cementable implant supported restorations. Int J Perio-dontics Restorative Dent 2010;30:415-424.
25. Degidi M, Nardi D, Piattelli A. Peri-implant tissue and radio-graphic bone levels in the immediately restored single-tooth implant: a retrospective analysis. J Periodontol 2008;79: 252-259.
26. Canullo L, Iurlaro G, Iannello G. Double-blind randomized controlled trial study on post-extraction immediately restored implants using the switching platform concept: soft tissue response. Preliminary report. Clin Oral Implants Res 2009;20:414-420.
27. Degidi M, Piattelli A, Gehrke P, Felice P, Carinci F. Five-year outcome of 111 immediate nonfunctional single restora-tions. J Oral Implantol 2006;32:277-285.
28. Mombelli A, Lang NP. Clinical parameters for the evaluation of dental implants. Periodontol 2000 1994;4:81-88.
29. Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone heal-ing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. Int J Periodontics Restorative Dent 2003;23:313-323.
30. Hwang YJ, Fien MJ, Lee SS, Kim TI, Seol YJ, Lee YM, Ku Y, Rhyu IC, Chung CP, Han SB. Effect of scaling and root planing on alveolar bone as measured by subtraction radi-ography. J Periodontol 2008;79:1663-1669.
31. de Morais JA, Trindade-Suedam IK, Pepato MT, Marcanto-nio E Jr, Wenzel A, Scaf G. Effect of diabetes mellitus and
insulin therapy on bone density around osseointegrated dental implants: a digital subtraction radiography study in rats. Clin Oral Implants Res 2009;20:796-801.
32. Ruttimann UE, Webber RL, Schmidt E. A robust digital method for film contrast correction in subtraction radiogra-phy. J Periodontal Res 1986;21:486-495.
33. Cochran DL, Nummikoski PV, Schoolfield JD, Jones AA, Oates TW. A prospective multicenter 5-year radiographic evaluation of crestal bone levels over time in 596 dental implants placed in 192 patients. J Periodontol 2009;80: 725-733.
34. Jansen VK, Conrads G, Richter EJ. Microbial leakage and marginal fit of the implant–abutment interface. Int J Oral Maxillofac Implants 1997;12:527-540.
35. Callan DP, Cobb CM, Williams KB. DNA probe identifica-tion of bacteria colonizing internal surfaces of the implant–abutment interface: a preliminary study. J Periodontol 2005;76:115-120.
36. Steinebrunner L, Wolfart S, Bössmann K, Kern M. In vitro evaluation of bacterial leakage along the implant-abutment interface of different implant systems. Int J Oral Maxillofac Implants 2005;20:875-881.
37. Broggini N, McManus LM, Hermann JS, Medina R, Schenk RK, Buser D, Cocharan DL. Peri-implant inflamma-tion defined by the implant–abutment interface. J Dent Res 2006;85:473-478.
38. Sanz M, Cecchinato D, Ferrus J, Pjetursson EB, Lang NP, Jan L. A prospective, randomized-controlled clinical trial to evaluate bone preservation using implants with different geometry placed into extraction sockets in the maxilla. Clin Oral Implants Res 2010;21:13–21.
39. Caneva M, Salata LA, de Souza SS, Baffone G, Lang NP, Botticelli D. Influence of implant positioning in extraction sockets on osseointegration: histomorphometric analyses in dogs. Clin Oral Implants Res 2010;21:43-49.
40. Canullo L, Fedele GR, Iannello G, Jepsen S. Platform switching and marginal bone-level alterations: the results of a randomized-controlled trial. Clin Oral Implants Res 2010;21:115–121.
41. Huynh-Ba G, Pjetursson BE, Sanz M, Cecchinato D, Ferrus J, Lindhe J, Lang NP. Analysis of the socket bone wall dimen-sions in the upper maxilla in relation to immediate implant placement. Clin Oral Implants Res 2010;21:37-42.
42. Evans CD, Chen ST. Esthetic outcomes of immediate implant placements. Clin Oral Implants Res 2008;19:73-80.
43. Becker W, Goldstein M, Becker BE, Sennerby L, Kois D, Hujoel P. Minimally invasive flapless implant placement: follow-up results from a multicenter study. J Periodontol 2009;80:347-352.
44. Ferrus J, Cecchinato D, Pjetursson EB, Lang NP, Sanz M, Lindhe J. Factors influencing ridge alterations following immediate implant placement into extraction sockets. Clin Oral Implants Res 2010;21:22–29.
45. Berglundh T, Abrahamsson I, Welander M, Lang NP, Lindhe J. Morphogenesis of the peri-implant mucosa: an experimental study in dogs. Clin Oral Implants Res 2007;18:1-8.
46. Hermann JS, Schoolfield JD, Schenk RK, Buser D, Cochran DL. Influence of the size of the microgap on crestal bone changes around titanium implants. A histometric evaluation of unloaded non-submerged implants in the canine mandi-ble. J Periodontol 2001;72:1372-1383.
Related Documents







![Research Article Interacting Quintessence Dark Energy ...downloads.hindawi.com/journals/ahep/2014/878092.pdfoftheuniverse[ ]. It was shown that the polytropic gas model in the presence](https://static.cupdf.com/doc/110x72/609c5c11a47319470725b94b/research-article-interacting-quintessence-dark-energy-oftheuniverse-it-was.jpg)



