QUICK GUIDE TO Central Venous Access

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

QUICK GUIDE TO
Central VenousAccess
QU
ICK
GU
IDE
TO
Cen
tral Ven
ous A
ccess
Edwards Lifesciences LLC · One Edwards Way · Irvine, CA USA 92614Phone: 949.250.2500 · 800.424.3278 · Fax: 949.250.2275 · www.edwards.com
Edwards Lifesciences S.A. · Ch. du Glapin 6 · 1162 Saint-Prex · Switzerland Phone 41.21.823.4300
Edwards Lifesciences (Canada) Inc. · 1290 Central Pkwy West, Suite 300Mississauga, Ontario · Canada L5C 4R3 · Phone 905.566.4220 · 800.268.3993
Edwards Lifesciences Japan · 2-8 Rokubancho Chiyoda-ku, Tokyo 102-0085 · Japan · Phone 81.3.5213.5700
02 ED CVC Quick Guide CoverF 8/28/02 3:10 PM Page 1

Edwards Lifesciences, Edwards, the stylized E logo, Advanced VenousAccess (AVA), AVA 3Xi, AVA HF, AMC THROMBOSHIELD and Vantexare trademarks of Edwards Lifesciences Corporation. CCOmbo,Intro-Flex, Multi-Med, and Swan-Ganz are trademarks of EdwardsLifesciences Corporation and are registered in the US Patent andTrademark Office.
Interlink is a trademark of Baxter International Inc., registered in theU.S. Patent and Trademark Office. Oligon is a trademark ofImplemed, Inc.
© 2002 Edwards Lifesciences LLC. All rights reserved. 1098-6/99-CC
02 ED CVC Quick Guide CoverF 7/22/05 11:37 AM Page 2
EDITORS
Marsha Halfman, RN, MSNCritical Care ConsultantScottsdale, AZ
QUICK GUIDE TO
Central VenousAccess
Sandra Reiner, RN, BSN, CICInfection Control CoordinatorNorthwestern Memorial HospitalChicago, IL

TA
BL
E O
F C
ON
TE
NT
S
i
Table of Contents
O V E R V I E W
Historical Perspective 1
Indications for Use 1
Types of Central Venous Access Devices 2
Catheter Specifics 2
Polyurethane 2
Number of Lumens 3
Flow Characteristics 3
Length 4
Coatings 4
Other Considerations 5
CVC Port Designation 6
Port Color Designation 6
Introducers as a Central Line 6
French Catheter Size Conversion 7
I N S E R T I O N A N D R E M O VA L
Insertion Sites 9
Sites: Advantages and Disadvantages 1 0
Seldinger Technique 1 3
Patient Preparation 1 4
Patient Position 1 5
The Circulation System 1 7
Clinical Considerations: Insertion 1 8
Insertion Complications 2 0
Air Embolism 2 1
Arterial Puncture 2 1
Arrhythmias 2 2
Pneumothorax 2 2
Malpositioned Catheters 2 2
Cardiac Tamponade 2 3
Clinical Responsibilities: Complications 2 4
Delayed Complications 2 5
Thrombosis 2 5
Catheter Occlusion 2 6
Infection 2 7
Infection: Diagnosis 3 0
Clinical Responsibilities: Delayed Complications 3 1
Catheter Exchange 3 1
Clinical Responsibilities: Catheter Exchange 3 3
CVC Removal 3 3
Clinical Considerations: Catheter Removal 3 4
S I T E M A I N T E N A N C E
Site Care 3 6
Site Inspection 3 6
Site Cleansing 3 7
Dressings 3 9
Other Considerations 4 0
Clinical Considerations: Dressing Change 4 1
N E E D L E S T I C K I N J U R I E S
Hepatitis B 4 2
Hepatitis C 4 2
HIV 4 2
Safe Needle/Needleless Systems 4 3
B L O O D S A M P L I N G
Blood Conservation 4 5
Draw Methods 4 5
Discard Volume 4 7
CVC Catheter Volume 4 8
Chemistry Studies 4 8
Hematology Studies 4 9
Blood Cultures 4 9
Coagulation Studies 5 0
Clinical Considerations: Blood Sampling 5 1
Normal Reference Ranges for Laboratory Blood Tests 5 3
F L U S H I N G ( I N T E R M I T T E N T )
Positive Pressure Flushing 5 4
Saline vs. Heparin 5 4
Concentration 5 5
Flush Volume 5 6
Clinical Considerations: Flushing 5 6
TA
BL
E O
F C
ON
TE
NT
S
iiTable of Contents continued on page iii

TA
BL
EO
FC
ON
TE
NT
S
iii
I N F U S I O N T H E R A P Y
Fluid Administration 5 7
IV Delivery System 5 7
In-Line Filters 5 8
Stopcocks 5 9
Piggyback Systems 5 9
Medication Administration 6 0
Drug Incompatibility 6 1
Other Considerations 6 1
Nitroglycerin Administration 6 2
Blood Administration 6 3
Administration of TPN 6 3
Clinical Considerations: IV Administration 6 5
Frequently Used Drugs in Critical Care 6 6
M O N I T O R I N G C E N T R A L V E N O U S P R E S S U R E
Fluid Challenge Guideline Chart 7 5
Physiologic Rationale 7 6
Mechanical Cardiac Cycle Phases 7 7
CVP Interpretation 8 4
Clinical Assessment 8 4
Manometric vs. Electronic Measurement 8 6
CVP Monitoring Set-up 8 6
Pressure Monitoring System 8 6
-Frequency Response 8 8
-Calibration 8 9
-Zero Reference 8 9
Patient Position 9 1
Port Site 9 2
Respiratory Influences 9 2
Infection Control 9 4
-Troubleshooting Pressure Monitoring Systems 9 5
TA
BL
EO
FC
ON
TE
NT
S
WAV E F O R M A N A LY S I S
Normal CVP Waveform 9 6
Electrical-Mechanical Cardiac Cycle 9 7
Abnormal Waveform Analysis 9 7
Arrhythmias 9 7
Tricuspid Regurgitation 9 9
Tricuspid Stenosis 9 9
Right Ventricular Infarction 9 9
Pericardial Constriction/Cardiac Tamponade 1 0 0
Abnormal Waveform Chart 1 0 1
E D WA R D S L I F E S C I E N C E S C E N T R A L V E N O U SA C C E S S P R O D U C T S
Advanced Venous Access (AVA) Devices 1 0 6
AVA HF 1 0 6
AVA 3Xi 1 0 7
Central Venous Catheters (CVC) 1 0 9
Vantex CVC with Oligon Material 1 0 9
Vantex Average Flow Rates 1 1 1
Vantex Average Lumen Volume 1 1 2
Multi-Med CVC 1 1 2
Multi-Med CVC Average Flow Rates 1 1 4
Multi-Med CVC Average Lumen Volumes 1 1 5
Suture Loop/Box Clamp 1 1 6
Intro-Flex Percutaneous Sheath Introducers 1 1 7
C D C G U I D E L I N E
Prevention of Intravascular Device-Related Infections 1 2 0
R E F E R E N C E S 1 2 5
B I B L I O G R A P H Y 1 2 9
iv

OV
ER
VIE
W
1
Historical PerspectiveEarly attempts to access the central venous circuit occurred
in the early 1900s. Reports first described catheters advancedinto the central circulation using the cubital and femoral veins.In 1929, Werner Forssmann actually advanced a 4 F ureteralcatheter into his own heart through a widebore needle in his leftcubital fossa. He then proceeded up several flights of stairs toRadiology to document this event. In 1956, Forssmann and others were awarded the Nobel Prize for Medicine for their workin advancing venous access techniques.
Aubaniac first described his 10-year experience with the use of subclavian catheters for the rapid infusion of resuscitationfluids in military casualties in 1952. However, it was not untilWilson et al reported on the advantages of measurement of central venous pressure in the maintenance of optimal bloodvolume nearly a decade later that interest in the use of centralvenous catheters really took off. The rapid development andwide use of central venous catheters were further enhanced bythe landmark papers by Dudrick et al on the value of total parenteral nutrition.
Indications for Use – Central VenousAccess Devices■ Rapid fluid administration – for example, in cases of:
- multiple trauma - burns- extensive abdominal surgery- sepsis
■ Administration of IV fluids requiring dilution within the central circulation to avoid vascular damage (i.e.,chemotherapy, total parenteral nutrition)
■ Administration of vasoactive and/or incompatible drugs■ Frequent blood sampling (in patients without an arterial line)
and/or blood administration therapies■ Chronically ill patients in whom peripheral IV access is limited■ Central venous pressure (CVP) monitoring for assessment of
intravascular fluid status■ Measurement of oxygen saturation levels in blood returning to
the heart (SsvcO2)■ Monitoring and access for either pre- or post- pulmonary artery
catheter insertion (same insertion site)
Indications for Use – Central VenousAccess Devices (continued)
Contraindications include patients with:■ Recurrent sepsis■ Hypercoaguable state where catheter could serve as a focus for
septic or bland thrombus formation
Types of Central Venous Access DevicesA central venous catheter is, by definition, a catheter whose tip
resides in the central circulation. There are various types ofthese catheters, but, for the purpose of this guide, we will focuson the short-term (< 30 days) IV access catheters that are madeby various manufacturers, including Edwards Lifesciences.
Single-lumen or double-lumen catheters are often insertedfor intermittent or continuous infusion of medication or fluid.They are applicable for the administration of a particular solution(i.e., chemotherapy, antibiotic, and/or nutritional therapies) inthe hospital or home setting. single-lumen catheters may lendthemselves to administration of total peripheral nutrition (TPN)through a dedicated line.
Multi-lumen catheters allow for multiple therapies to be performed through a single venous access site and are often seenin the critical care environment. These catheters, althoughdesigned for short-term access, generally see much use duringthis period.
Introducers are used to direct and place intravascularcatheters, especially pulmonary artery catheters (PAC), within adesignated blood vessel. They may be left in place to serve as acentral venous access after removal of the PAC.
Advanced Venous Access (AVA) devices combine the ability to insert PACs and to infuse multiple fluids in one multipurpose device.
Central Venous CathetersCatheter SpecificsPolyurethane (commonly used for catheter body)■ Tensile strength, which allows for thinner wall construction
and smaller external diameter■ High degree of biocompatibility, kink and thrombus resistance■ Ability to soften within the body
OV
ER
VIE
W
2

Central Venous CathetersCatheter Specifics (continued)
Nursing NoteAcetone and isopropyl alcohol should be avoided when
caring for these catheters.
Number of Lumens■ More than one lumen increases the functionality of a single
site (benefit)■ Multilumem catheters may be more prone to infection because
of increased trauma at the insertion site or because multipleports increase the frequency of manipulation
CDC Guideline (1996)Use a single-lumen central venous catheter, unless
multiple ports are essential for the management of thepatient.
Although one study showed that only a single port isoften used in one half of the triple lumens placed, triple-lumen CVCs appear to be the most commonly placed central line in ICU.
Practical PointCritically ill patients may need more IV access than
that obtained with a single multi-lumen CVC. Two triple-lumen CVCs or an introducer and a CVC may beplaced in the same vein or in two different veins. Thisprocedure is referred to as a double stick.
Flow Characteristics ■ Primarily determined by a catheter’s internal diameter and
length, not by the size of the blood vessel into which thecatheter is inserted
■ Is often incorrectly assumed to be proportional to the catheter’soutside dimensionFlow rates are usually calculated with normal saline at a head
height of 40" (101.6cm).
OV
ER
VIE
W
3

Central Venous CathetersCatheter Specifics (continued)
LengthVarious studies have shown that the average safe insertion
depth for central venous catheterization from the left or rightinternal jugular or subclavian vein is 16.5 cm for the majority ofadult patients.1 (This assumes correct tip placement above theright atrium.2)
CoatingsCatheter coatings may include the bonding of the catheter
surface with antimicrobial and/or antiseptic agents to decreasecatheter-related infection and thrombotic complications. Heparin-bonding process is one example; other agents reportedin the literature include antibiotics such as minocycline andrifampin, or antiseptic agents like chlorhexidine and silver sulfadiazine. Materials, in particular metals, that are antimicrobial in minute amounts are called oligodynamic. One of the most potent of these is silver, with the antimicrobialform being silver ions. The bactericidal action of silver ions iseffective against a broad spectrum of bacteria, including thecommon strains which cause infection and the more virulentantibiotic-resistant strains. Silver has been in medical use fordecades and was used in systemic drugs before the advent ofantibiotics. Today, silver is used routinely in antibacterial salves(silver sulfadiazine), to prevent infection and blindness in newborns (silver nitrate), and in medical devices and catheters.
Antibiotic- and antiseptic-coated catheters have demonstratedreduced rates of catheter colonization and associated bloodstream infection in some clinical trials, but it is important toremember that heparin-induced thrombocytopenia and/orallergy to the antibiotic used on a catheter could result inpatient morbidity. Additionally, there is always the possibilitythat antibiotic-resistant microorganisms may develop or that the catheter site becomes infected with other organisms, such as Candida.
OV
ER
VIE
W
4
Central Venous Catheters Catheter Specifics (continued)
Nursing NoteHeparin-induced thrombocytopenia is a reduction in
platelets caused by antiplatelet antibodies. It occurs inapproximately 0.4% of patients with heparin-coated catheters and has a high mortality and morbidity. Patientsso afflicted must not receive any more heparin, in anyform, until the heparin-associated antiplatelet antibodiesare no longer detectable.
Timely TipTwelve patients in Japan who had a silver sulfadiazine-
chlorhexidine catheter in situ developed anaphylacticshock. This was related to possible pre-exposure tochlorhexidine in skin creams.5
Other Considerations■ Soft tip to avoid injury or perforation■ Radiopaque■ Depth markings on all catheters and guidewires
Technical TipCatheter softness is a function not only of the material,
but also of the specific formulation of that material (oftenproprietary information). Triple lumen catheters need tobe stiffer because more septations and a firmer plastic areneeded to extrude a multi-lumen catheter.
OV
ER
VIE
W
5

CVC Port DesignationDISTAL (OR LARGEST GAUGE) MEDIAL PROXIMAL
Blood administration TPN or Medication Medications administration
High volume fluids Blood sampling
Colloid fluid administration Drug therapy
Drug therapy
CVP monitoring
These are suggestions only.
CVC Port Color DesignationPORT DOUBLE TRIPLE QUAD
Proximal white white white
Medial (1) blue blue blue
Medial (2) gray
Distal brown brown brown
Introducers as a Central LineSometimes an introducer is used for central venous access or
is left in place following the removal of a pulmonary arterycatheter. Components of the introducer system usually include:■ Flexible polyurethane sheath■ Guidewire and dilator■ Side port■ Hemostasis valve
After insertion, the guidewire and dilator are removed, leavingthe sheath in place. Fluids may be administered through theside port, while the hemostasis valve prevents bleedback and/orair embolization.
A single-lumen infusion catheter can be used with the introducer, placed through the hemostasis valve (after swabbingthe valve with Betadine), to convert to a double-lumen access.An obturator should be used to safely occlude the lumen aswell as to prevent air entry when the catheter is not in use.
OV
ER
VIE
W
6
OV
ER
VIE
W
7
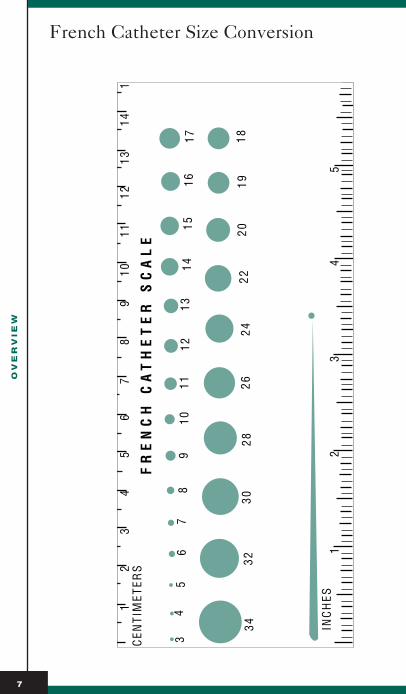
French Catheter Size Conversion

French Catheter Size Conversion (continued)
OV
ER
VIE
W
8
IN
SE
RT
IO
N A
ND
R
EM
OV
AL
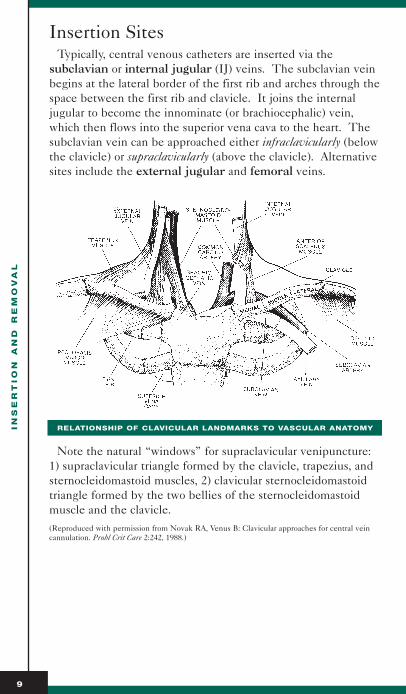
Insertion SitesTypically, central venous catheters are inserted via the
subclavian or internal jugular (IJ) veins. The subclavian veinbegins at the lateral border of the first rib and arches through thespace between the first rib and clavicle. It joins the internaljugular to become the innominate (or brachiocephalic) vein,which then flows into the superior vena cava to the heart. Thesubclavian vein can be approached either infraclavicularly (belowthe clavicle) or supraclavicularly (above the clavicle). Alternativesites include the external jugular and femoral veins.
RELATIONSHIP OF CLAVICULAR LANDMARKS TO VASCULAR ANATOMY
Note the natural “windows” for supraclavicular venipuncture:1) supraclavicular triangle formed by the clavicle, trapezius, andsternocleidomastoid muscles, 2) clavicular sternocleidomastoidtriangle formed by the two bellies of the sternocleidomastoidmuscle and the clavicle.(Reproduced with permission from Novak RA, Venus B: Clavicular approaches for central veincannulation. Probl Crit Care 2:242, 1988.)
9

Insertion Sites (continued)
ANATOMIC ILLUSTRATION OF SIDE PREFERENCE RATIONALE FOR CLAVICULAR APPROACHES
Right IJ, supraclavicular procedures and left infraclavicular pro-cedures are preferred. Note the close proximity of arterial andvenous structures. Venipunctures in the lateral region of theclavicle are more prone to arterial puncture, brachial plexusinjury, and pneumothorax. Note the prominent thoracic ductand higher apex of the lung on the left and the perpendicularentry of the left IJ into the left subclavian vein.(Reproduced with permission from Novak RA, Venus B: Clavicular approaches for central veincannulation. Probl Crit Care 2:242, 1988.)
Sites for Central Venous Catheterization:Advantages and DisadvantagesINTERNAL JUGULAR (58 - 99% SUCCESS RATE)
ADVANTAGES DISADVANTAGES
Relatively short and direct pathway Not ideal for prolonged to heart (right IJ) cannulation
High success rate Uncomfortable for patient
Easy access from head of bed Dressings difficult to maintain
Pneumothorax rare Left IJ increases risk of thoracicduct injury
Easier control of bleeding Poor landmarks in obese or edematous patients
IN
SE
RT
IO
N A
ND
R
EM
OV
AL
10

IN
SE
RT
IO
N A
ND
R
EM
OV
AL
11
Sites for Central Venous Catheterization:Advantages and Disadvantages (continued)
INTERNAL JUGULAR (58 - 99% SUCCESS RATE)
ADVANTAGES DISADVANTAGES
Continued chest compression Difficult access with during CPR possible tracheostomies
More prone to collapse with volume depletion or shock
Difficult access during emergencies when airway control is being established
Carotid artery puncture relatively frequent
Contraindications for patients with intracranial hypertension
INFRACLAVICULAR (85-99% SUCCESS RATE)
ADVANTAGES DISADVANTAGES
Easier to maintain dressings Higher risk of pneumothorax
More comfortable for patient Compression of bleeding site difficult
Better landmarks in obesity Long pass from skin to vein
Large vein less collapsible during hypovolemia
SUPRACLAVICULAR (85-99% SUCCESS RATE)
ADVANTAGES DISADVANTAGES
Low incidence of pneumothorax Control of bleeding difficult
High success rate Pneumothorax possible
Easier to pass catheter Uncomfortable for patient
Accessible from head of bed Not ideal for prolonged access
Good landmarks Dressing and catheter maintenance difficult
No interference with chest Thoracic duct puncture possiblecompression
Anatomic landmarks constant Not ideal approach when airwaycontrol is being established
Short path from skin to vein Not ideal for temporary hemodialysis
Sites for Central Venous Catheterization:Advantages and Disadvantages (continued)
EXTERNAL JUGULAR (60-90% SUCCESS RATE)
ADVANTAGES DISADVANTAGES
Part of surface anatomy High failure rate
Clotting abnormalities not prohibitive Not ideal for prolonged access
Pneumothorax avoided Uncomfortable for patient
Access from head of table Dressing maintenance difficult
Prominent in elderly Poor landmarks in obese and edematous patients
Unsuccessful in young patients
Difficult for threading central catheters
(Reproduced with permission from Novak RA, Venus B: Clavicular approaches for central veincannulation. Probl Crit Care 2:242, 1988.)
Practical PointCatheters inserted in the femoral vein and advanced into
the inferior vena cava may be utilized as a second alterna-tive to the superior vena cava, except for emergency IVfluid resuscitation or for superior vena cava injuries.Cannulation of this vein usually has a high success rate.This approach may, however, have the disadvantage ofrequiring longer catheters; the catheter tip should lie inthe inferior vena cava for infusions and should reach thelevel of the diaphragm for the purpose of central venouspressure monitoring.
Research RichesIn a study of anesthetized, mechanically ventilated
patients who were in a 10º head down position and receiving fluid loading, an inverse relationship between a large external jugular vein (as measured with an ultrasound imaging machine) and a small internal jugularvein was found. Mean IJV diameter was 17.4 mm(range 4-30 mm). There was no correlation betweenweight, height, or neck size and IJV diameter.A
IN
SE
RT
IO
N A
ND
R
EM
OV
AL
12

IN
SE
RT
IO
N A
ND
R
EM
OV
AL
13
Sites for Central Venous Catheterization:Advantages and Disadvantages (continued)
CDC Guideline (1996)■ Weigh the risk and benefits of placing a device at a
recommended site to reduce infectious complicationsagainst the risk of mechanical complications (e.g., pneumothorax, subclavian artery puncture, subclavianvein laceration, hemothorax, thrombosis, air embolism,catheter misplacement).
■ Use subclavian, rather than jugular or femoral, sites forcentral venous catheter placement unless medically contraindicated (e.g., coagulopathy, anatomic deformity).
Central Venous Catheterization via theSeldinger TechniqueONE
■ Enter vessel with 22gauge locating needleand attached 5ml syringe
■ Upon aspiration ofdark venous blood,remove needle and syringe
TWO
■ Attach 5ml syringe to18 gauge catheterover 20 gauge needle assembly
■ Insert needle and relocate vein previously entered
■ Upon aspiration ofvenous blood, removeneedle and syringe, leaving the 18 gauge catheter in place.
■ Insert guidewire into already placed 18 gauge catheter
wire in -needle out
Catheter overneedle inserted
together

Central Venous Catheterization via theSeldinger Technique (continued)
THREE
■ Remove catheter, leaving the guidewire in placeFOUR
■ Enlarge puncture site, if necessary with small scalpelFIVE
■ Further enlarge the insertion site and vessel by threadinga dilator over the guidewire
■ Leaving the guidewire in place, remove the dilatorSIX
■ Thread central venouscatheter over the guidewire.
■ Remove guidewireReproduced with permission from Darovic,GO: Hemodynamic Monitoring Invasiveand Non-invasive Clinical Application, 1987.
Patient PreparationCatheters can be inserted in a variety of settings under various
conditions. Recently, it has been shown that the setting ofcatheter placement may not be as critical a factor in minimizinginfection risk as the use of maximal barrier precautions. Two studies have shown the use of maximal barrier precautions(cap, mask, gown, gloves, and large drape) decrease the colonization of the catheter surface at the time of insertion,thereby decreasing the risk for catheter-related sepsis.
CDC Guideline (1996)Use sterile technique, including a sterile gown and
gloves, a mask, and a large sterile drape (i.e., maximal barrier precautions), for the insertion of central venous and arterial catheters. Use these precautions even if the catheter is inserted in the operating room.
IN
SE
RT
IO
N A
ND
R
EM
OV
AL
14
wire out
IN
SE
RT
IO
N A
ND
R
EM
OV
AL
15
Patient Preparation (continued)
The skin should be cleaned before insertion using an antiseptic agent to kill or inhibit growth of microorganisms.Popular antiseptics include:70% ALCOHOL
ADVANTAGES DISADVANTAGES
Fast kill Not effective against spores
Very effective against gram-negative Must rub the site vigorously forand gram-positive bacteria at least one minute
Effective fat solvent Drying nature of alcohol.
2% TINCTURE OF IODINE
ADVANTAGES DISADVANTAGES
Effective against the same May cause skin irritationorganisms as 70% alcohol
Prolonged contact may even kill Must be removed from skin certain fungi and spores before catheter is placed
10% POVIDONE-IODINE (IODINE SOLUTION)
ADVANTAGES DISADVANTAGES
Reduced toxicity Contact time of 2 minutes necessary for optimal microbial kill
Less skin irritation than Neutralized in presence of blood iodine tincture and pus
CHLORHEXIDINE
ADVANTAGES DISADVANTAGES
Active against gram-positive and Can be inactivated by compounds gram-negative organisms and viruses found in hard water and soap
Residual activity up to 6 hours Allergic reactions reported
Patient Position15 - 30 DEGREES TRENDELENBURG
■ Increases venous return by approximately 37%■ Increases intrathoracic pressure■ Helps prevent inadvertent air embolization■ Not always well tolerated by cardiac patients■ Not necessary when jugular venous distention (JVD) present
in supine position (right-sided failure)

IN
SE
RT
IO
N A
ND
R
EM
OV
AL
16
Patient Position (continued)
VALSALVA MANEUVER (FORCED EXPIRATION AGAINST CLOSED GLOTTIS)
■ Increases cross-sectional area of jugular vein by approximately 25%
■ May be accomplished in ventilated patients by causing aforced inflation via an Ambu bag
“BUMP” POSITION
Head turned to the contralateral side and a rolled towel placedin the back.
INFRACLAVICULAR APPROACH TO THE RIGHT SUBCLAVIAN VEIN
The patient is positioned with a rolled towel between thescapulae to increase the distance between the clavicle and thefirst rib.

IN
SE
RT
IO
N A
ND
R
EM
OV
AL
17
Catheter Tip PlacementTriple-lumen catheters should be inserted so that the tip
is approximately 2 cm proximal to the right atrium (forright-sided approaches) and similarly placed or well within theinnominate vein (for left-sided approaches), with the tip parallel with the vessel wall. A chest x-ray must be done post insertion, as it provides the only definitive evidence forcatheter tip location.
Probably the most important factor in the prevention of complications is the location of the catheter’s tip. The pericardium extends for some distance cephalad along theascending aorta and superior vena cava. In order to guarantee an extrapericardial location, the catheter’s tip should not beadvanced beyond the innominate vein or the initial segment ofthe superior vena cava. (It is important to note that a portionof the superior vena cava lies within the pericardium.)
Some practitioners may prefer a deep SVC placement (withinthe lower third of the SVC), but nearly half the length of theSVC is covered by pericardial reflection that slopes downwardtoward its lateral edge. To avoid the risk of arrhythmias andtamponade, the tip of a CVC should lie above this reflection andnot in the right atrium.
Clinical ConcernIt should be noted that even x-ray confirmation of the
catheter in a location above the pericardial reflection doesnot guarantee against possible tamponade. Cases of perforation with hydromediastinum and cardiac tampon-ade have been reported, with the site of extravasationbeing as distal as the subclavian vein. One concern withthe multi-lumen catheter is the necessity of advancing itsomewhat further than a normal catheter to ensure thatthe proximal opening is within a central vein.
Tips to assure catheter tip not extravascular or against a wallmight include:■ Syringe aspiration yields blood freely■ Venous pressure fluctuates with respiration■ Advancement of the catheter is unhindered
IN
SE
RT
IO
N A
ND
R
EM
OV
AL
18
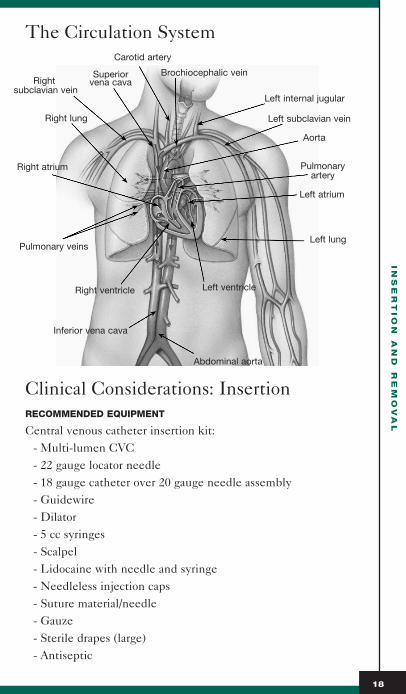
The Circulation System
Clinical Considerations: InsertionRECOMMENDED EQUIPMENT
Central venous catheter insertion kit:- Multi-lumen CVC- 22 gauge locator needle- 18 gauge catheter over 20 gauge needle assembly- Guidewire- Dilator- 5 cc syringes- Scalpel- Lidocaine with needle and syringe- Needleless injection caps- Suture material/needle- Gauze- Sterile drapes (large)- Antiseptic
Carotid artery
Brochiocephalic vein
Left internal jugular
Left subclavian vein
Superiorvena cavaRight
subclavian vein
Right lung
Right atrium
Pulmonary veins
Right ventricle
Inferior vena cava
Abdominal aorta
Aorta
Pulmonaryartery
Left atrium
Left lung
Left ventricle

IN
SE
RT
IO
N A
ND
R
EM
OV
AL
19
Clinical Considerations: Insertion (continued)
Additional items:- Sterile gloves, sterile gowns, masks and caps for everyone
in room - Dressing materials (dressing per hospital policy,
nonallergenic tape)- Heparin flush solution- Pressure monitoring setup for CVP determination, if
desired (flush solution, pressure bag, pressure tubing, trans-ducer and holder, stopcocks, monitor cable, leveling device)
CLINICAL RESPONSIBILITIES
■ Confirm orders■ Obtain informed consent from patient or designated power of
attorney■ Provide further information as requested by patient or family
members■ Check equipment to monitor patient (EKG, blood pressure,
pulse oximetry, etc)■ Assemble equipment and move into patient room■ Position the patient and provide privacy■ Assist with insertion of catheter under aseptic technique■ Monitor patient vital signs during insertion■ Assess patient comfort and intervene appropriately■ Protect the patient by:
- Assuring compliance with maximal barrier precautions- Calling in support personnel (i.e., respiratory therapy) as
necessary- Recording vital signs, rhythm strips or waveform traces, SaO2
values, etc.- Securing the catheter and dressing the site per hospital
protocol- Ordering chest x-ray post-insertion- Running fluids at TKO until chest x-ray results available- Contacting clinician to read chest x-ray or to inform of
abnormal findings- Documenting site, depth of insertion, and the patient’s
response to the procedure on progress/nursing notes

IN
SE
RT
IO
N A
ND
R
EM
OV
AL
20
Clinical Considerations: Insertion (continued)
CDC Guideline (1996)■ Wear non-latex or latex gloves when inserting an
intravascular device as required by the OccupationalSafety and Health Administration (OSHA) BloodbornePathogens Standard.
■ Do not routinely use cutdown procedures as a method to insert catheters.
■ Cleanse the skin site with an appropriate antiseptic,including 70% alcohol, 10% povidone-iodine, or 2% tincture of iodine, before catheter insertion. Allow the antiseptic to remain on the insertion site for anappropriate length of time before inserting the catheter.
■ When tincture of iodine is used for skin antisepsis beforecatheter insertion, it should be removed with alcohol.
■ Do not palpate the insertion site after the skin has beencleansed with the antiseptic (this does not apply to maximum barrier precautions during which the operatoris working in a sterile field).
■ Record the date and time of catheter insertion in anobvious location near the catheter insertion site (e.g., on the dressing or on the bed).
Insertion ComplicationsMechanical complication rates range from 1% to 10%,
although rates as high as 15% have been reported when theaccess is placed emergently. Complications related to insertioncan manifest themselves within minutes following insertion ormay not be obvious for several days.
Research RichesOne study shows, the strongest predictor of a complica-
tion is a failed catheterization attempt. Many cliniciansfeel that three attempts are enough,6 and then it is timeto ask another clinician to attempt catheterization fromanother site.

IN
SE
RT
IO
N A
ND
R
EM
OV
AL
21
Insertion Complications (continued)
Complications of Central Venous CatheterizationAir Embolism■ May be associated with insertion process
■ Patient positioning (Trendelenburg)
■ Often related to disconnection of tubing or at catheterremoval
■ Valsalva maneuver (forced exhalation)
■ Patients who are hypovolemic or snore are at highest risk
■ Can occur after removal, if subcutaneous tract made bycatheter has failed to close
■ Sudden onset tachycardia, pulmonary hyper-, or systemic hypo-tension
■ Neurologic deficit or potentially fatal position; aspirate air ifCVC still in place
■ Place patient in left lateral decubitus
Arterial Puncture■ Arterial and venous proximity
■ Local pressure may be enough to stop bleed
■ Variable venous anatomy
■ Appearance of bright red, pulsatile blood
■ Hematoma may resolve or evolve into false aneurysm or arteriovenous fistula
Clinical ConcernThe rare complication of tracheal puncture may also
occur with internal jugular cannulation attempts, especial-ly in patients with endotracheal tubes, since the inflatedcuff brings the tracheal wall closer to the adjacent veins.
IN
SE
RT
IO
N A
ND
R
EM
OV
AL
22
Insertion Complications (continued)
Arrhythmias■ Transient atrial/ventricular arrhythmias■ Usually related to over insertion of guidewire or catheter, with
impingement of the tips of these devices in the region of theright bundle branch
Cardiac Tamponade/Pericardial Effusion/Hydromediastinum■ Fluid in pericardial cavity due to perforation of structures
by catheter■ Cardiovascular collapse once critical volume reached■ Infusion of fluid through catheter prior to placement
confirmation■ Immediate pericardiocentesis
Pneumothorax/Hydrothorax■ Puncture of lung tissue■ Diminished breath sounds, tachypnea■ Atmospheric pressure causes air to enter and collapse portion
of lung■ Not clinically detectable if < 20%■ May heal itself or require chest tube
Malpositioned Catheters■ Arrhythmia, venous thrombosis■ Cardiac tamponade■ Falsely elevated pressure measurements■ Delivery of infusate into thoracic cavity■ Vascular erosion and perforation
Physiologic FactThe most common malposition occurs when a catheter
inserted via the infraclavicular route goes into the homolateral internal jugular vein with the tip of thecatheter facing oncoming blood flow. Other vessels inwhich a catheter might become malpositioned include the internal mammary, axillary, vertebral, and the greaterazygos veins.
IN
SE
RT
IO
N A
ND
R
EM
OV
AL
23
Insertion Complications (continued)
CARDIAC TAMPONADE
Pericardial tamponade caused by central venouscatheter perforation of the heart is a catastrophiccomplication that can be prevented by attention toproper positioning of the catheter tip proximal to thecardiac silhouette. In a recent study7 (1998), it wasdetermined that only 31% of the physicians studied whoinsert central venous catheters were aware that cardiactamponade is a potential complication, and only 10%recalled ever seeing or reading the package inserts that warned of cardiac tamponade. This is in spite of thefact that in 1993 the Food and Drug Administration (FDA)sent a three-volume video entitled “Central VenousCatheter Complications” to all hospitals where centralvenous catheters were inserted. This same study detailed25 previously unreported cases of cardiac tamponade afterplacement of central venous catheters in a nineteen-monthperiod. Eighty percent of the patients died and 12%remain in a persistent vegetative state. Post-insertionchest x-rays were available in 23 cases. All post-insertionchest x-rays showed the tip of the catheter to be with-in the pericardial silhouette.
Next, thirty local radiologists were interviewed. Ninety percent of them were not aware that the tip of thecentral venous catheter should be located outside of the pericardial silhouette on the radiograph. Noneof the inserting physicians believed that it was his or her responsibility to check the chest x-ray for catheterplacement.
Pulmonary symptoms were common, with 8 patients complaining of chest tightness, 12 of shortness of breath,and 15 were noted to have air hunger up to 6 hours prior to significant changes in vital signs occurring.Fourteen patients developed tachycardia and 8 were noted to be bradycardic. All patients developed significant, unexplained hypotension as a result of cardiactamponade. Many of these patients were intubated as partof their resuscitation. Seven patients developed EKGchanges consistent with inferior wall ischemia or injury.
IN
SE
RT
IO
N A
ND
R
EM
OV
AL
24
Insertion Complications (continued)
CARDIAC TAMPONADE (CONTINUED)
In all cases, the clinicians treated the patient for myocar-dial ischemia and did not suspect cardiac tamponade. Tenpatients developed new or different non-specific ST- andT-wave changes. Five developed worsening of theirhypotension when nitrates were administered.
This study is particularly discouraging, because the FDAand catheter companies have attempted to warn physiciansof the danger of cardiac tamponade through the use oftalks, posters, videos and package insets. However, thissurvey and surveys done previously have shown that aminority of physicians were aware of this potential complication. More importantly, few physicians are awarethat cardiac tamponade is preventable if the tip of the central venous catheter is outside the pericardial shadowon the chest radiograph. Any patient with a CVC in place who develops unexplained hypotension, chest tightness, or shortness of breath should have an emergency echocardiogram to rule out cardiactamponade.
Clinical Responsibilities■ Observe patient for any signs of cardiopulmonary distress■ Auscultate lungs every 2-4 hours; record findings on nursing
flow sheet/progress notes■ Observe daily chest x-ray and record interpretation as to
catheter position in the nursing notes/progress notes■ Include depth of catheter insertion daily in nursing
notes/progress notes■ Observe and record any change in neurological status.■ Report any change in patient condition to the clinician,
as appropriate■ Maintain emergency cart, including thoracentesis,
pericardiocentesis, and chest tube insertion trays

IN
SE
RT
IO
N A
ND
R
EM
OV
AL
25
Delayed ComplicationsThe most common delayed complications of vascular access
device insertion are thrombosis and infection. These two complications are somewhat related, as thrombotic complicationsare common in catheterized veins and are often associated withcatheter sepsis.
ThrombosisAll catheters are thrombogenic. Within seconds after
insertion, much of the catheter body is coated with body fluidsand proteins. Platelets adhere and thrombus forms.
Catheters can become encased within 5-7 days, forming a fibrin sheath. Some investigators state that a fibrin sleeve is found on 100% of subclavian catheters in postmortem examinations and in patients studied with cinefluoroscopy.
Clinical ConcernThree common organisms causing catheter-related
infections (S epidermidis, S aureus, C albicans) adhere wellto fibrin and fibronectin found in fibrin sheaths. Theseorganisms also produce a coagulase enzyme (slime) thatfurther enhances their adherence on the vascular catheteras well as protects them from the action of antibiotics.
Mural (wall) thrombi may form on the catheter and/or on the wall of the vessel. They may develop within 48 hours ofcannulation, and there have been many case reports of suchthrombi breaking off and resulting in pulmonary emboli. Some of these cases have resulted in mortality 4-5 days afterinsertion. Additionally, catheter removal may precipitate dislodgement of such thrombi.
Mangano found that the use of catheters with heparin-bondingoffers considerable protection from thrombosis for 24 hours orlonger.8 Thus the use of such catheters may be efficacious inminimizing the risks of embolism, infarction, and occlusivethrombosis over prolonged periods.
The use of prophylactic anticoagulants is variable. In arecent (1998) review of the literature, it was found that prophylac-tic use of heparin significantly decreases central venous catheter-related thrombosis, decreases bacterial colonization of thecatheter, and may decrease catheter-related bacteremia. Lowmolecular weight heparin seems to have lesspropensity for caus-ing heparin-induced thrombocytopenia and is 99% bioavailable.

Delayed Complications (continued)
Therapies may include:■ Mix heparin with TPN solution (3U/mL)■ Give heparin IV every 6 or 12 hours (5,000 U)■ Give low molecular weight heparin subcutaneously every day
(2,500 U)
Catheter OcclusionCatheter occlusion may be a result of fibrin sheath formation
and/or thrombus at the tip of the catheter but has also been associated with blood clots, lipid deposits or precipitateswithin the catheter lumen. Fibrin sheath formation is significantin that the sheath may eventually totally encase the catheter and affect the functional ability of the catheter. Withdrawalocclusion may occur if the fibrin sheath acts as a flap whichblocks the tip of the catheter when blood withdrawal is attempted, and then opens up with injection.
There is also evidence that partial occlusion is related to aresidue of blood products deposited within some accessdevices each time blood is aspirated or infused.
Other theories include drug precipitation. These occlusionsmay result from:■ Inadequate flushing between incompatible medications■ Simultaneous administration of incompatible medications■ Medications administered in a concentration exceeding that
required for stability Attempts to clear catheter occlusions include the use of
fibrinolytic agents. Catheter patency can often be restored if the solubility of the fluid components is changed by alteringthe pH through the use of 0.1 N hydrochloric acid and sodiumbicarbonate.
Clinical ConcernThe use of lipid-containing TPN, commonly referred
to as three-in-one, has been shown to be responsible for a unique type of catheter precipitate occlusion. Anaggregation that occurs with lipid/parenteral nutritionadmixtures causes the development of deposits thatresult in sludging in the catheter lumen and eventualocclusion. The use of an ethanol (70% ethyl alcohol) solution as a means of dissolving fat (the main componentof the occlusion) has been reported.
IN
SE
RT
IO
N A
ND
R
EM
OV
AL
26

IN
SE
RT
IO
N A
ND
R
EM
OV
AL
27
Delayed Complications (continued)
InfectionIt is estimated that 200,000 nosocomial (hospital-acquired)
bloodstream infections occur each year; most of these infections are related to the use of an intravascular device.These infections are associated with increased mortality andmorbidity, prolonged hospitalization and extended intensive careunit stays, and greater hospital costs. It has been estimated thateach bloodstream infection costs the hospital approximately$6,000- $40,000 and increases the length of stay by an additional 24 days per survivor.9
Catheter-related bloodstream infection – isolation of thesame organism by a semiquantitative technique from a removedcatheter associated in time with the recovery of the same organism from properly collected blood cultures (preferablydrawn from a peripheral vein) in a patient with accompanyingclinical symptoms and no other apparent source of infection.
Practical PointThere are rarely more than 50-100 colony-forming
units (CFU) at the site of insertion of a peripheral venouscatheter on the arm or wrist. On CVC sites located on the chest or neck, there are as many as 1000 to 10,000CFU/site, especially in long-term ICU patients.10
Research RichesAll other factors being equal, the general feeling is that
the longer the line stays in place, the more likely the pos-sibility of infection. However, more recent data suggestthat the daily risk of infection remains constant.11
Delayed Complications (continued)
Over the past two decades, there has been a marked change inthe distribution of pathogens reported to cause bloodstreaminfections (BSIs). Since the mid-1980s, an increasing portion ofnosocomial BSIs have been due to gram-positive, rather thangram-negative, species. The increase in nosocomial BSIs duringthe past decade is largely due to significant increases in fourpathogens: ■ Coagulase negative staphylococci (CoNS), including
Staphylococcus epidermidis■ Candida species■ Enterococci■ Staphylococcus aureus(N.B. Coagulase-negative organisms are gram-positiveorganisms.)
Prior to 1986, S aureus was the most frequently reportedpathogen causing nosocomial BSIs. Currently, coagulase negative staphylococci, particularly S. epidermidis, have become the most frequently isolated pathogens in catheter-related infections. The prevalence of these organismsalso shows that the hands of healthcare workers and the floraof patients’ skin are likely to be the predominant sources ofpathogens for most catheter-related infections.
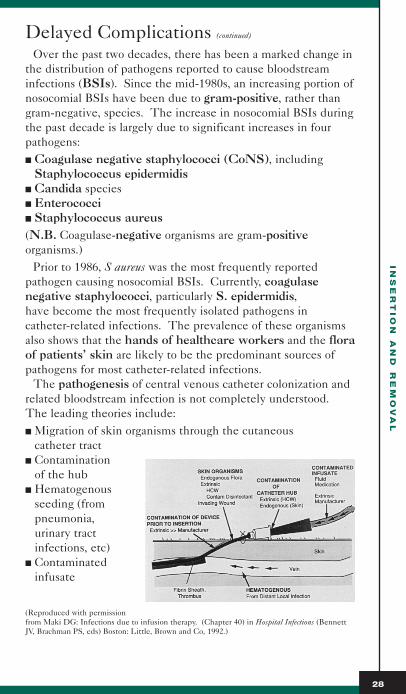
The pathogenesis of central venous catheter colonization andrelated bloodstream infection is not completely understood.The leading theories include:■ Migration of skin organisms through the cutaneous
catheter tract■ Contamination
of the hub■ Hematogenous
seeding (from pneumonia, urinary tract infections, etc)
■ Contaminatedinfusate
(Reproduced with permissionfrom Maki DG: Infections due to infusion therapy. (Chapter 40) in Hospital Infections (BennettJV, Brachman PS, eds) Boston: Little, Brown and Co, 1992.)
IN
SE
RT
IO
N A
ND
R
EM
OV
AL
28

IN
SE
RT
IO
N A
ND
R
EM
OV
AL
29
Delayed Complications (continued)
Research RichesRecent findings suggest that duration of catheteriza-
tion influences which of the mechanisms predominate.Hub contamination is the more likely mechanism forinfection for long-term catheters (i.e., in place > 30 days)while skin contamination is the most likely cause for short-term catheters (i.e., <10 days).12
Timely TipManipulations of the delivery system, especially the
administration set, appear to provide a highly effectivemeans for access of microorganisms to in-use infusate.This was illustrated by a spate of nosocomial outbreaksacross the US traced to in-use contamination of a newlyreleased intravenous anesthetic, propofol (Diprivan).The solution provides an almost uniquely rich medium for rapid microbial growth. (It is a lipid formulation, likeintralipids administered with TPN.)
Timely TipA recent (1998) editorial left this “take home” message.
“Antibiotic- and antiseptic-coated catheters have demonstratedreduced rates of catheter colonization and associated bloodstream infection. However, if all other measures are optimized,their value remains to be proven.” “...these devices may bestserve high-risk populations... patients undergoing change of acentral venous catheter over a guidewire and patients for whomthe consequence of infection is great... or when the duration ofCVC use is anticipated to exceed 5 days.” 13
CDC Guideline (1996)In adults, consider use of a silver-impregnated collagen
cuff or an antimicrobial- or antiseptic-impregnated centralvenous catheter if, after full adherence to other catheterinfection control measures (e.g., maximal barrier precau-tions), there is still an unacceptably high rate of infection.
DiagnosisThe best tests for venous access device infection are direct
specimens of the device itself and any attached material ororganisms, and these tests are possible only after thecatheter is removed. Otherwise, there is no identified goldstandard for diagnosing catheter-related infections.

Delayed Complications (continued)
DIAGNOSIS OF CATHETER-RELATED INFECTION
Semi-quantitative catheter culture (Maki)■ Catheter removed after skin is cleaned■ Most widely used, best studied■ At least 5 cm of tip and the catheter segment beginning 1-2 mm
inside the point of the skin-catheter junction are cultured■ Cutaneous segment may be better predictor than tip■ Only outside of catheter cultured■ Only determines catheter colonization■ Catheter segments are rolled on agar plate■ Catheter must be removed
Quantitative catheter culture■ Catheter segment flushed with broth■ Most sensitive■ Segment then immersed in broth■ Both luminal and external surfaces■ Sonicated to release organisms■ Catheter must be removed
Quantitative blood cultures■ Blood cultures simultaneously drawn from catheter and
peripheral IV sample■ Positive = catheter blood sample colonies > 5x peripheral ■ Compares concentration of organisms■ Does not require removing CVC
Catheter exchange■ Change catheter over wire■ Remove new catheter if positive culture obtained■ Culture catheter■ The critical step in the treatment of central line infections is to
remove the involved catheter. Antimicrobial therapy usually isgiven adjunctively, but is no substitute for catheter removal.
IN
SE
RT
IO
N A
ND
R
EM
OV
AL
30

IN
SE
RT
IO
N A
ND
R
EM
OV
AL
31
Delayed Complications (continued)
Clinical Responsibilities: Delayed Complications■ Monitor patient temperature frequently■ Monitor WBC levels (with differential) at least on a daily basis■ Administer medications, as ordered, to prevent thrombosis
and infection■ Collect blood or tip cultures as ordered, using
sterile technique■ Monitor coagulation parameters as ordered■ Report abnormal findings to the clinician
CDC Guideline (1996)Do not routinely perform surveillance cultures of
patients or of devices used for intravascular access.
Catheter ExchangeThere are a wide variety of practices concerning the changing
of short-term percutaneously-inserted CVCs. Policies run thegamut from routine changes every 3-4 days to leaving thecatheter in place until a complication develops or it is no longer needed.
Research RichesA recent controlled study showed that routine replace-
ment of CVCs every three days does not prevent infection. A prospective, randomized trial concluded that routine 72-hour catheter exchange does not confer an advantageover 7-day catheter exchange in the prediction of centralvenous infection in a critically ill patient requiring multi-ple lumen central venous access. 14
Central venous catheters can be exchanged for a variety of reasons. Replacement of these catheters can be achieved byusing de novo (in a new site) percutaneous placement or by usingthe Seldinger technique to change the catheter over a guide-wire in the same site. In general, exchanging catheters overa guidewire may be associated with fewer mechanical complications and no increased risk of infection, compared tonew-site venipuncture.
Catheter Exchange (continued)
However, these findings have not been consistently document-ed, and complications may relate to clinician experience.
Research RichesExchanging catheters over guidewires or at new sites
every three days is not beneficial in reducing infections,compared with catheter replacement on an as-neededbasis.15
CDC Guideline(1996)■ Do not routinely replace non-tunneled central venous
catheters as a method to prevent catheter-related infections.
■ Use guidewire assisted catheter exchange to replace a malfunctioning catheter or to convert an existingcatheter if there is no evidence of infection at thecatheter site.
■ If catheter-related infection is suspected, but there is no evidence of local catheter-related infection (e.g.,purulent drainage, erythema, tenderness), remove theexisting catheter and insert a new catheter over a guide-wire. Send the removed catheter for semiquantitative orquantitative culture. Leave the newly inserted catheterin place if the catheter culture result is negative. If thecatheter culture indicates colonization or infection,remove the newly-inserted catheter, and insert a newcatheter at a different site.
■ Do not use guidewire assisted catheter exchange whenever catheter-related infection is documented. If the patient requires continued vascular access, remove the implicated catheter and replace it withanother catheter at a different insertion site.
It has been a common practice to obtain a chest x-rayafter catheter exchanges over a guidewire.
IN
SE
RT
IO
N A
ND
R
EM
OV
AL
32

IN
SE
RT
IO
N A
ND
R
EM
OV
AL
33
Catheter Exchange (continued)
However, there has recently been controversy concern-ing this policy. Some clinicians now feel that chest x-raysare unwarranted after uncomplicated guidewire exchangesin hemodynamically stable, monitored patients. Rationaleincludes: ■ The results of several studies showing no complications■ The feeling that many complications would be picked
up by clinical signs■ Patients requiring CVC generally have routine chest
x-rays, usually within 48 hours of exchange
Clinical Responsibilities: Catheter Exchange■ Assist with catheter exchanges, as per insertion
responsibilities■ Assist with regloving and redraping the site between removal
and reinsertion
CVC RemovalCentral venous catheters may be removed for a variety of
reasons, including discontinuation of therapy and transfer toa subacute environment. Removal of the CVC generally isperformed by house staff or nurses. It should precede thepatient’s transfer, as this removal is ideally performed in a monitored situation.
Research RichesThe removal of a central venous catheter can be
complicated by a rare but potentially life-threatening neurocardiopulmonary distress, according to one recent(1998) study. The clinical courses of eight patients whohad CVCs removed were studied. The major complica-tions were: neurologic paresis or coma (4 patients), respiratoryfailure (4 patients), and shock (2 patients). One patientdied from pulmonary sepsis. The overall mortality ratewas 12.5%. The authors felt this syndrome to be an unappreciated complication of central venous catheterremoval. 16

CVC Removal (continued)
CDC Guideline (1996) ■ Remove any intravascular device as soon as its use is no
longer clinically indicated■ No recommendation for removal of central catheters
inserted under emergency conditions where breaks in aseptic technique are likely to have occurred
Clinical Considerations: RemovalRECOMMENDED EQUIPMENT
- Sterile gloves- Suture removal set- Sterile dressing material- Antibiotic/antiseptic ointment- Non-allergenic tape- Appropriate waste container- Culture container
CLINICIAN RESPONSIBILITIES
■ Confirm order■ Explain procedure to the patient and/or family members■ Remove existing dressing material and dispose of it in the
appropriate waste container. Clip any sutures■ Discontinue existing IV solutions running through CVC;
switch to alternate site■ Position the patient in a head-down position, if tolerated;
at least keep as flat as possible
Clinical ConcernThis is especially important if the patient is dehydrated,
as a low CVP may generate a sucking force of air into thesystemic circulation.
■ Observe careful aseptic technique as you remove the catheter.Change gloves
■ Slowly and continuously remove catheter while the patientholds his/her breath to prevent air embolization
IN
SE
RT
IO
N A
ND
R
EM
OV
AL
34

IN
SE
RT
IO
N A
ND
R
EM
OV
AL
35
CVC Removal (continued)
Clinical ConcernIf patient is intubated, have respiratory therapist provide
a forced inspiration via Ambu bag.Occlude catheter lumen or exit wound immediately,
again to prevent air entry. Be careful applying pressure to neck sites as this could:■ Dislodge arteriosclerotic plaques or thrombus in the
carotid artery, causing a stroke and/or■ Cause a vasovagal reflex, leading to acute onset
bradycardia and hypotensionApply antibiotic ointment to the exit wound to seal the
track opening.Apply air-tight occlusive dressing; leave in place for at
least 12 hours, preferably 24-72 hours.
Research RichesThe literature report cases of air embolization after line
removal due to a long-standing catheter track.17
Collect appropriate cultures. (This may require a second person to cut the tip while the first secures the site.)
Patient should remain lying flat in bed for 30 minutes after CVC removal.
Note: a suture may be needed to close a large and long-standing catheter track.
Chart patient’s response to the procedure, any untoward complications, and the type of culture sent.
Physiologic FactAny patient that has an opening between the right and
left sides of the heart is especially at risk if air enters thevenous system. Although the blood flow through an opening is usually left-to-right since pressures are higheron the left side, it is possible for the air to enter the leftside of the heart through a patent foramen ovale (thehole in the atrial septum that normally closes at birth) orthrough shunts in the pulmonary circulation. A verysmall amount of air is necessary to cause neurologic symptoms as the air enters the right carotid artery andgoes to the brain. This causes left-sided weakness. Theonly reason the right carotid is usually involved is that it is the first upward artery off the aortic arch.

Site CareCare of the catheter site is considered to be of primary
importance and is believed to play a critical role in decreasingthe risk for catheter-related sepsis. Universal standards for careof the catheter site have not been established. Unresolvedissues include use of ointments and antiseptic agents, dressingtype, and frequency of dressing changes.
Although exact protocols for site care vary from institution toinstitution, they all call for: ■ Removal of the old dressing■ Inspection of the site and surrounding area■ Cleansing of the site■ Covering the site with a sterile dressing
Sterile gloves and masks should be worn during dressingchanges.
CDC Guideline (1996)■ Wash hands before and after palpating, inserting,
replacing, or dressing any intravascular device■ Wear non-latex or latex gloves when changing the
dressings on intravascular devices■ No recommendation for the use of sterile versus
non-sterile clean gloves during dressing changes
Site InspectionAny signs or symptoms that might indicate an infection should
be reported at once. However, these signs are not always indicative of infection. Signs of infection may include rednessor exudate. However, many catheters exhibit slight erythemaat the site without necessarily being infected. Conversely, theimmunosuppressed patient may shown no signs of infectioneven when infection is present. Fever, however, in a patientwith a CVC is usually attributable to the catheter untilproven otherwise.
SIT
E M
AIN
TE
NA
NC
E
36

SIT
E M
AIN
TE
NA
NC
E
37
Site Inspection (continued)
CDC Guideline (1996)■ Palpate the catheter insertion site for tenderness daily
through the intact dressing■ Visually inspect the catheter site if the patient has
development of tenderness at the insertion site, feverwithout obvious source, or symptoms of local or bloodstream infection
■ In patients who have large, bulky dressings that prevent palpation or direct visualization of the catheter insertionsite, remove the dressing, visually inspect the cathetersite at least daily, and apply a new dressing
Site CleansingThe catheter exit site should be cleansed with an
appropriate antiseptic agent that includes 70% alcohol and 10% povidone-iodine. (Povidone-iodine has replaced iodine for use in the clinical setting.)
Cleansing with an appropriate antiseptic solution should proceed in a circular pattern, working outward from the insertion site. Typically, cleansing begins with the application of 70% isopropyl alcohol to remove skin oils and cells, exposingthe lower skin layers to the antimicrobial activity. Alcoholneeds to remain wet on the skin for at least 1 minute.Although alcohol provides the most rapid and greatest reductionin microbial counts on the skin, it does not have any residualantimicrobial activity.
Research RichesOne study by Maki found no significant antimicrobial
benefit for defatting the skin during dressing change.18
Technical TipAcetone, alcohol and ether have been shown to weaken
polyurethane and silicone materials.After the alcohol (if used), the insertion site is usually
prepped with povidone-iodine. This material mustremain in contact with the skin for at least 2-5 minutes before the procedure in order to achieve adequate microbial count reductions.

Site Cleansing (continued)
The sustained release of free iodine from povidone-iodinehas an antibacterial effect. The antimicrobial activity ofpovidone-iodine is significantly reduced by the presence of blood, mucous, and other organic matter.
CDC Guideline (1966)■ Wash hands before and after palpating, inserting,
replacing, or dressing any intravascular device■ Cleanse the skin site with an appropriate antiseptic,
including 70% alcohol, 10% povidone-iodine, or 2% tincture of iodine. Allow antiseptic to remain on the insertion site for an appropriate length of time
Chlorhexidine 0.5% in 70% isopropyl alcohol hasrecently been promoted for use as a skin disinfectant.Chlorhexidine leads to residual antibacterial activity thatpersists for hours after application, and it is not affected by protein.
Research RichesIn a prospective, randomized study by Maki, in which he
looked at the efficacy of several solutions, 2% chlorhexi-dine before insertion and for post-insertion site care sub-stantially decreased the incidence of catheter-relatedinfection.19
FDA Alert! Chlorhexidine allergy resulting in anaphylactic shock has been reported.
The use of ointments in the care of CVCs is controver-sial. Although it would appear that the use of an antimi-crobial ointment would be beneficial, clinical trials havenot conclusively confirmed the benefit of such ointments.Their use has been further complicated in that an increasein frequency of Candida infections has been shown. It hasbeen recommended that in patients who are considered tobe at increased risk, an antimicrobial agent such as povi-done-iodine ointment be used at the insertion site of cen-tral venous catheters placed for the administration of par-enteral nutrition. However, routine use of ointments isnot recommended.
CDC Guideline (1996) Do not routinely apply antimicrobial ointment to central
venous catheter insertion sites.
SIT
E M
AIN
TE
NA
NC
E
38

SIT
E M
AIN
TE
NA
NC
E
39
DressingsThe ideal frequency of dressing changes and the type
of dressing to use has not been established. Current recommendations by the Centers for Disease Control (1996) didnot include a recommendation as to the frequency of dressingchange. The types of dressings used for CVCs include gauzeand tape and transparent semi-permeable membrane (TSM)dressings. With all types of dressings, it is preferable to changethe dressing: ■ In conjunction with any tubing change■ When it becomes damp, loosened, or soiled
CDC Guideline (1996) ■ Replace catheter site dressings when the device is
replaced, when the dressing becomes damp, loosened, orsoiled, or when inspection of the site is necessary
■ No recommendation for the frequency of routinereplacement of dressings used on central catheter sites
The traditional gauze and tape dressings have been used foryears. Adhesive material should be applied over the entire gauzesurface to ensure that the dressing is closed and intact. Thesedressings may be preferred for a diaphoretic patients or thosewith fragile or inflamed skin. Unfortunately, there is no wayto observe the site without manipulating the dressing.
Transparent semi-permeable dressings are currently popularbecause they:■ Allow for continuous inspection of the site■ Adhere well to dry skin■ Provide protection against external moisture■ Are usually more comfortable■ May also assist in stabilizing and securing the catheter
The concern with these dressings is moisture retentionoccurring underneath the dressing. Moisture, of course, can leadto increased colonization of the site and increased risk ofcatheter-related infection.

SIT
E M
AIN
TE
NA
NC
E
40
Dressings (continued)
Research RichesAnother study by Maki found that, if the transparent
dressing was left on for up to 5-7 days, there was morethan a ten-fold increase in the density of cutaneous flora,which was then associated with a 50% increased risk ofcatheter-related infection.20
Newer dressing materials are available that allow for improvedvapor transmission rate. Opsite IV 3000, for instance, isreported to move 3-8 times more moisture away from the sitethan other transparent dressings.
Research RichesA recent study by Maki showed that, when this new
dressing was used, there was no difference in infection orcolonization rates when compared to gauze dressings.21
Other ConsiderationsStudies have shown that the use of special intravenous
therapy teams consisting of trained nurses or technicians hasbeen associated with substantially lower rates of catheter-relatedinfection. However, even without a dedicated team, institutionscan greatly reduce their rate of catheter-related sepsis by scrutinizing catheter care protocols and more intensively educating and training their clinicians.
Research RichesIn a study of cost effectiveness, Tomford and Hershey
reported that such a team reduced the costs of complica-tions of infusion therapy nearly ten-fold.22
Current trends in healthcare may also influence theinfection rate associated with CVCs. Downsizing canresult in inexperienced or insufficient personnel, and such trends maybe associated with increasing infectionrates. Conversely, education and experience with the insertion and use of CVCs may reduce or preventinfections.
SIT
E M
AIN
TE
NA
NC
E
41
Dressings (continued)
CDC Guideline (1966)Conduct ongoing education and training of health
care workers regarding indications for the use of and procedures for the insertion and maintenance of intravas-cular devices and appropriate infection control measures to prevent intravascular device-related infections.Audiovisuals can serve as a useful adjunct to standard educational effects.
Clinical Considerations: Dressing ChangeRECOMMENDED EQUIPMENT
- Sterile gloves- Mask- Sterile drape- Sterile gauze sponges and/or transparent dressings- Sterile applicators- Non-allergenic tape- Solutions, ointments
CLINICIAN RESPONSIBILITIES
■ Observe strict aseptic technique; change gloves betweenremoval of old dressing and application of new one
■ Position patient with head turned away from the dressing siteor have patient wear a mask
■ Remove old dressing and dispose of materials appropriately■ Inspect site for unusual warmth, erythema, edema, drainage,
tenderness or pain■ Drape catheter insertion site■ Cleanse area, working in a circular path from the catheter to
the periphery. Include the area under the hub■ Apply ointment, if appropriate. Check for patient allergies.■ Dress site with appropriate dressing material. Dressing
should be occlusive■ Indicate date, time, and initial the dressing■ Chart procedure, site inspection, and any complications in the
nursing/progress notes
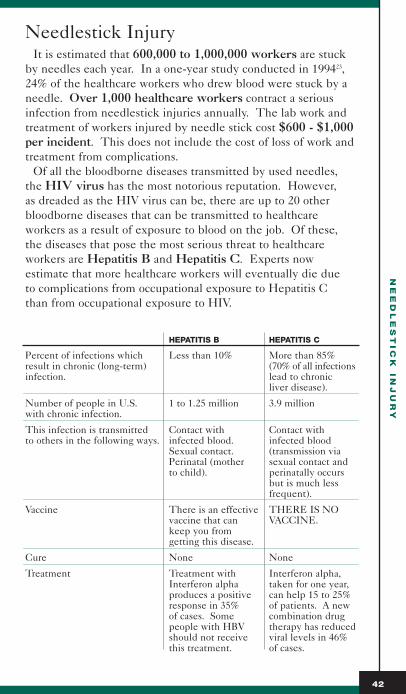
Needlestick InjuryIt is estimated that 600,000 to 1,000,000 workers are stuck
by needles each year. In a one-year study conducted in 199423,24% of the healthcare workers who drew blood were stuck by aneedle. Over 1,000 healthcare workers contract a seriousinfection from needlestick injuries annually. The lab work andtreatment of workers injured by needle stick cost $600 - $1,000per incident. This does not include the cost of loss of work andtreatment from complications.
Of all the bloodborne diseases transmitted by used needles,the HIV virus has the most notorious reputation. However, as dreaded as the HIV virus can be, there are up to 20 otherbloodborne diseases that can be transmitted to healthcare workers as a result of exposure to blood on the job. Of these,the diseases that pose the most serious threat to healthcare workers are Hepatitis B and Hepatitis C. Experts now estimate that more healthcare workers will eventually die due to complications from occupational exposure to Hepatitis C than from occupational exposure to HIV.
HEPATITIS B HEPATITIS C
Percent of infections which Less than 10% More than 85%result in chronic (long-term) (70% of all infectionsinfection. lead to chronic
liver disease).
Number of people in U.S. 1 to 1.25 million 3.9 millionwith chronic infection.
This infection is transmitted Contact with Contact with to others in the following ways. infected blood. infected blood
Sexual contact. (transmission via Perinatal (mother sexual contact and to child). perinatally occurs
but is much less frequent).
Vaccine There is an effective THERE IS NOvaccine that can VACCINE.keep you from getting this disease.
Cure None None
Treatment Treatment with Interferon alpha,Interferon alpha taken for one year,produces a positive can help 15 to 25%response in 35% of patients. A newof cases. Some combination drugpeople with HBV therapy has reducedshould not receive viral levels in 46%this treatment. of cases.
NE
ED
LE
ST
IC
K IN
JU
RY
42
NE
ED
LE
ST
IC
K IN
JU
RY
43
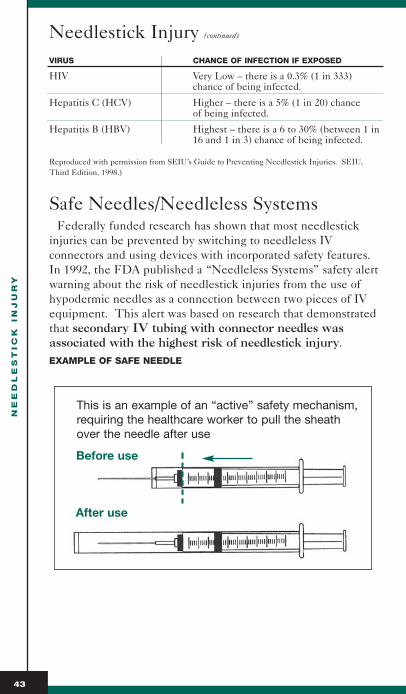
Needlestick Injury (continued)
VIRUS CHANCE OF INFECTION IF EXPOSED
HIV Very Low – there is a 0.3% (1 in 333) chance of being infected.
Hepatitis C (HCV) Higher – there is a 5% (1 in 20) chanceof being infected.
Hepatitis B (HBV) Highest – there is a 6 to 30% (between 1 in16 and 1 in 3) chance of being infected.
Reproduced with permission from SEIU’s Guide to Preventing Needlestick Injuries. SEIU,Third Edition, 1998.)
Safe Needles/Needleless SystemsFederally funded research has shown that most needlestick
injuries can be prevented by switching to needleless IV connectors and using devices with incorporated safety features.In 1992, the FDA published a “Needleless Systems” safety alertwarning about the risk of needlestick injuries from the use ofhypodermic needles as a connection between two pieces of IVequipment. This alert was based on research that demonstratedthat secondary IV tubing with connector needles was associated with the highest risk of needlestick injury.EXAMPLE OF SAFE NEEDLE
Before use
After use
This is an example of an “active” safety mechanism,requiring the healthcare worker to pull the sheathover the needle after use

Safe Needles/Needleless Systems (continued)
EXAMPLE OF NEEDLELESS SYSTEM
Timely TipSeveral states have mandated the use of safe needles and
needleless systems to reduce the risks of sharps injury and resultant transmission of blood borne diseases.
With the advent of needleless systems, it is now most commonfor each lumen to be capped off with an injection cap. Thesecaps need not be removed to allow the withdrawal of blood.This allows for a completely closed system, decreasing thechance of infection. Additionally, the use of stopcocks can also increase the risk of infection secondary to manipulation;however, the use of injection caps keeps the system closed. Theneedleless factor also contributes to patient and clinician safety.
Technical TipToday it is estimated by the FDA that more than 50% of
all hospitals use needleless IV connection systems.
NE
ED
LE
ST
IC
K IN
JU
RY
44

BL
OO
D S
AM
PL
IN
G
45
Blood SamplingBlood sampling for various laboratory tests can be
accomplished through central venous catheters. Generally, this procedure involves catheters with multiple lumens, butcould also apply to single-lumen devices. When using the triple-lumen CVC, blood withdrawal may be done via the designatedlumen, usually the proximal or distal lumen. The designation ofthese two lumens is arbitrary but is a result of the middle lumenusually being reserved for TPN administration. If the patient isnot receiving TPN, any lumen will suffice.
Any laboratory test that does not require arterial blood can usually be drawn through the CVC. These tests may include:■ Chemistries■ Hematolgy studies■ Blood levels of drugs■ Coagulation studies■ Blood culture■ Cardiac enzymes
Blood ConservationStudies have shown that patients in ICUs with an arterial line
in place had a mean blood volume of 944 mL withdrawn andwere phlebotomized a mean of 4 times daily during their ICUstay.24 This amount does not account for withdrawal and discard of flush solution mixed with blood; i.e., “clearing” volume. Additionally, this blood loss associated with diagnosticphlebotomy is superimposed on blood loss from other causes,such as gastrointestinal hemorrhage or surgery.
It is no wonder the terms iatrogenic or nosocomial anemiahave appeared. Blood loss from phlebotomy alone can make abig impact on ICU patients, especially critically ill pediatric andneonatal patients, and certain adult patients with chronic renalfailure, and those whose religious beliefs do not permit bloodtransfusions.
Draw MethodsThere are three methods to obtain blood from a central line;
direct, indirect or through a blood conservation device.Vacutainer devices can be connected directly to the injection
cap attached to the appropriate lumen of the CVC. The vacuumwithin the collection tube draws out precisely the amount ofblood needed for the specific laboratory test.
BL
OO
D S
AM
PL
IN
G
46
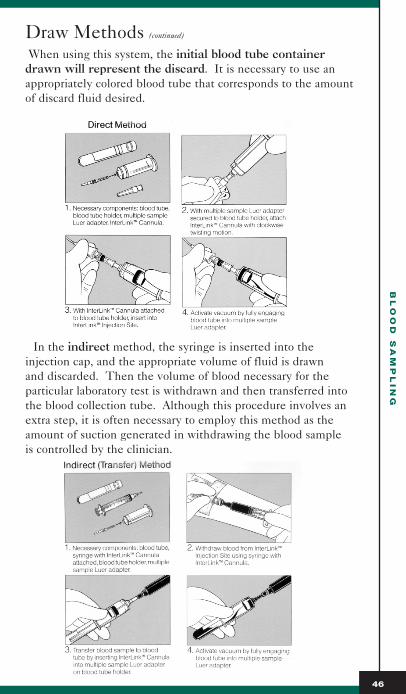
Draw Methods (continued)
When using this system, the initial blood tube containerdrawn will represent the discard. It is necessary to use anappropriately colored blood tube that corresponds to the amountof discard fluid desired.
In the indirect method, the syringe is inserted into the injection cap, and the appropriate volume of fluid is drawn and discarded. Then the volume of blood necessary for the particular laboratory test is withdrawn and then transferred intothe blood collection tube. Although this procedure involves anextra step, it is often necessary to employ this method as theamount of suction generated in withdrawing the blood sample is controlled by the clinician.

BL
OO
D S
AM
PL
IN
G
47
Blood Sampling (continued)
When using a blood conservation device, the discard amountis withdrawn into a closed system and then reinfused followingblood collection. (Although this line may attach directly througha luer lock to the central venous catheter, the system remainsclosed and is needleless.)
Research RichesStudies have shown that results do not differ as a
function of the method used to collect the sample if the samples are collected appropriately.25
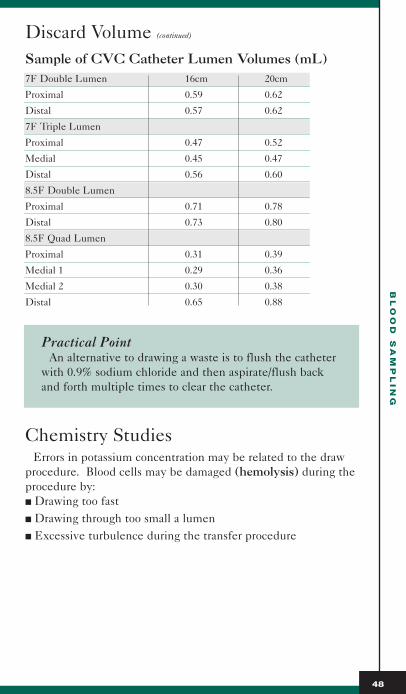
Discard VolumeA certain amount of blood is discarded prior to blood sampling
(the discard volume) to avoid contamination of laboratory samples with heparin or saline. The amount of blood drawnback to clear the line is dependent on several factors, including:■ Tubing size and length■ Amount of heparin in the line■ Line from which blood is to be drawn■ Type of study to be performed
This volume is often expressed as multiples of the dead spacewithin the catheter to be utilized for the blood draw. This is afunction of the volume contained in the catheter from the tip ofthe catheter to the port from which the sample is to be drawn.Anywhere from two to ten times the dead space have beenadvocated. Some clinicians merely recommend a discard volume of 5-10 mL with smaller waste volumes in neonatal and pediatric patients. However, hospital policies and procedures generally dictate the dead space specific to a particular institution.
BL
OO
D S
AM
PL
IN
G
48
Discard Volume (continued)
Sample of CVC Catheter Lumen Volumes (mL)7F Double Lumen 16cm 20cm
Proximal 0.59 0.62
Distal 0.57 0.62
7F Triple Lumen
Proximal 0.47 0.52
Medial 0.45 0.47
Distal 0.56 0.60
8.5F Double Lumen
Proximal 0.71 0.78
Distal 0.73 0.80
8.5F Quad Lumen
Proximal 0.31 0.39
Medial 1 0.29 0.36
Medial 2 0.30 0.38
Distal 0.65 0.88
Practical PointAn alternative to drawing a waste is to flush the catheter
with 0.9% sodium chloride and then aspirate/flush backand forth multiple times to clear the catheter.
Chemistry Studies Errors in potassium concentration may be related to the draw
procedure. Blood cells may be damaged (hemolysis) during theprocedure by: ■ Drawing too fast ■ Drawing through too small a lumen■ Excessive turbulence during the transfer procedure

BL
OO
D S
AM
PL
IN
G
49
Chemistry Studies (continued)
Practical PointAlways hold the blood sample level with the vacutainer
during transfer of blood, and never push blood into collection device.
Additionally, errors in potassium measurements havebeen identified in specimens obtained from newly inserted central catheters, secondary to the presence of benzalkonium salts and the sensitivity of certain analyzers to them.26
Accurate determination of sodium or glucoseconcentrations might be of concern, since 0.9% sodiumchloride is often used to flush catheters, and IV fluids usually contain glucose. However, studies have shownthat accurate results can be obtained if the dead space plustwo milliliters is withdrawn as the discard volume. 27
Practical PointIt is interesting to note that, in spite of CDC guidelines,
heparin mixed in dextrose solution is sometimes used tokeep intravascular lines patent. In this instance, specialcare would need to be exercised. Even venous blood samples drawn via venipuncture from an extremity infusedwith D5W are not reliable, even when they are drawnfrom below the site of entry or even from a site remotefrom the glucose infusion. 28
Hematology StudiesThese studies usually include determination of hemoglobin,
hematocrit and white blood cell count. If the laboratory specimen were to contain flush fluid, the hematocritdetermination could be falsely low due to the dilutional effect.The hemoglobin and white cell counts would be unaffected.
Blood CulturesBlood cultures can be drawn from central lines. There is
always the concern that any culture drawn from an indwellingintravascular catheter might show contamination that is relatedto the device rather than the patient. Of course, in some casesthat is precisely the point. Generally, however, blood culturesare ordered in a series, each drawn from separate sites.

Blood Cultures (continued)
Research RichesMost studies comparing the results of blood cultures
drawn from arterial and central venous lines versus directvenipuncture found no significant differences. One studyfound a 93.5% incidence of identical results in 92 bloodcultures simultaneously drawn from central venous pressure catheters and venipunctures. 29
CDC Guideline (1996)No recommendation for obtaining blood samples for
cultures through central venous or central arterial lines.
Coagulation StudiesPerhaps the one type of laboratory test that would be most
seriously affected by heparin flush fluid incorporated into thesample would be coagulation studies. Some hospitals mightrequire all coagulation studies to be done by venipuncture toeliminate such concern.
Research RichesHowever, studies have found no significant differences
between samples obtained from arterial catheters andthose obtained from venipuncture. Studies show reliableresults on activated clotting time (ACT), prothrombintime (PT), activated partial thromboplastin time (aPTT),and thrombin time (TT) after sufficient discard volumeshave been used. 30
Research RichesConfidence that six times the dead space volume is
adequate for discard in the nonsystemically heparinizedadult patient is supported in published literature. Resultsof two studies on heparinized patients indicated that thisdiscard volume may be adequate for this population aswell, but due to small sample size and exclusive use of thefemoral site in these studies, further research is indicated.These results should not be generalized to systematicallyheparinized patients, pediatric patients, or other types ofheparized lines such as pulmonary artery, central venous or Hickman catheters.31
BL
OO
D S
AM
PL
IN
G
50

BL
OO
D S
AM
PL
IN
G
51
Coagulation Studies (continued)
Practical PointA practical approach is to draw all other laboratory sam-
ples first, saving the coagulation studies for last.If laboratory values obtained from central venous
catheters are markedly different in a previously stablepatient, the test results should always be repeated beforetreating the patient.
There are not a lot of studies relating directly to drawingblood from central venous lines. Generally, the gold stan-dard is direct venipuncture. Many studies discussed hererelate to arterial lines as the source of blood that is com-pared to the venipuncture sample. However, centralvenous catheters have some similarities, especially interms of flush solution to keep the line patent. Therefore,the assumption is that, if it can be declared reliable witharterial line draws, then it can also be accurate with CVCdraws. Whenever possible, studies relating directly to cen-tral venous draws are discussed.
Clinical Considerations: Blood SamplingRECOMMENDED EQUIPMENT
- Syringes/Vacutainers- Heparin flush syringe with needleless cannula- Sterile gloves- Blood collection tubes- Antiseptic swabs
CLINICAL RESPONSIBILITIES
■ Review orders and check with the Laboratory if any concerns■ Inform patient of what procedure will entail and answer
questions■ Use aseptic technique and meticulous handwashing■ Avoid opening the system as much as possible■ Utilize safety precautions such as needleless access■ Utilize strategies to minimize blood loss

BL
OO
D S
AM
PL
IN
G
52
Coagulation Studies (continued)
■ Consider lumen choice based on drugs/fluids being infusedConsider turning off infusions for 2-3 minutes, if appropriate
■ Follow hospital policy and procedure as to appropriate discard volumes
■ Ascertain that correct volume of blood is placed in the appropriate lab collection container
Practical PointThe volume of blood cultured is critical to maximize
the yield of cultures. In adults, obtaining at least 20 mL,but ideally 30 mL, per drawing, with each specimen containing 10-15 mL, is recommended. 32
■ Flush lumen after sample withdrawn■ Appropriately label specimen and send to laboratory■ Evaluate laboratory results and communicate them to clinician■ Go to resource personnel in event of technique-related
questions

BL
OO
D S
AM
PL
IN
G
53
Coagulation Studies (continued)
Normal Reference Ranges for Laboratory Blood Tests
BLOOD CHEMISTRY STUDIES
Sodium (Na) 136-145 mEq/L
Potassium (K) 3.5-5.0 mEq/L
Chloride (Cl) 98-106 mEq/L
Carbon dioxide (CO2) 21-30 mEq/L
Glucose (BS) 75-115 mg/dL
Blood Urea Nitrogen (BUN) 10-20 mg/dL
Creatinine <1.5 mg/dL
Calcium (Ca) 8.5-10.5 mEq/L
Magnesium (Mg) 1.3-2.1 mEq/L
Osmolality 275-295 mOsm/kg
Bilirubin (direct) 0-0.3 mg/dl(indirect) 0.2-0.7 mg/dl(total) 0.2-1.0 mg/dl
Amalyse 25-125 U/L
Lipase 23-208 U/L
Anion Gap 8-16 mEq/L
Lactate 0.5-2.2 mEq/L
HEMATOLOGY STUDIES
Red Blood Cells (RBC) 4.25-5.5 x 10 6/µL (males)3.6-5.0 x 10 6/µL (females)
White Blood Cells (WBC) 5-10 x 10 3/µL
Hemoglobin (Hgb) 13.5-17.5 g/dL (males)12-16 g/dL (females)
Hematocrit (Hct) 40-54% (males)37-47% (female
COAGULATION STUDIES
Platelets 150-350 x 10 3/uµL
Prothrombin Time (PT) 10-14 sec
Plasma Thrombin Time (PTT) 30-45 sec
Activated Partial Thromboplastin 16-25 secTime (aPPT)
Activated Clotting Time (ACT) 92-128 sec
Normal value ranges depend upon specific laboratory determinations.
FL
US
HIN
G (I
NT
ER
MIT
TE
NT
)
54
Flushing (Intermittent)Although current practice mandates a flush procedure to
maintain patency and prevent complications, the type, concentration, and volume of the solution vary widely from institution to institution and sometimes from unit to unit withinthe same institution.
Positive Pressure FlushingRegardless of the amount and frequency of flush used,
it is important to use a positive pressure flushing technique. A proper positive pressure flushing technique creates positivepressure within the lumen of the catheter and is thought to minimize reflux of blood into the tip of the catheter, andthus prevent clotting. This flush can best be performed by clos-ing the catheter or extension clamp while flushing before thesyringe completely empties. Another way to accomplish thiswould be to maintain pressure on the syringe plunger whilewithdrawing the syringe from the injection cap.
Consideration must also be given to the syringe size used toflush. The smaller the syringe size, the greater the pressure generated. Catheters are designed to withstand various infusionpressures; however, infusion pressures should never exceed 25-40 pounds per square inch (psi). Smaller-sized syringes willgenerate pressures in excess of this amount and may cause damage to catheters, especially if an obstruction is present. A 10mL syringe is advocated by many for use with CVCs.
Saline vs. HeparinThe anticoagulant properties of heparin have led clinicians
to use heparin flushes to fill the lumens of central venouscatheters locked between uses in an attempt to prevent throm-bus formation and to prolong the duration of catheter patency. The efficacy of this practice is unproven.
There is a large amount of research indicating that peripheralintravenous catheters may be kept patent with intermittentsaline flushes. Can the same be said for central venous lines?Much of the literature on CVCs is hard to interpret, becausesome long-term CVCs have been maintained with weekly salineflushes. However, these catheters do not see anywhere near theuse involved in the care of critically ill patients.

FL
US
HIN
G (I
NT
ER
MIT
TE
NT
)
55
Saline vs. Heparin (continued)
There is some literature dealing with arterial and pulmonaryartery line patency. Most of the literature supports the use ofheparinized flush solutions delivered continuously (on average,3-5mL/hour) under 300 mmHg pressure. But what about thefrequent but intermittently utilized CVCs? So far there are noclear-cut answers.
Research RichesConclusions of the AACN Thunder Project are probably
applicable to CVCs: “....heparin does significantly affectpatency of arterial pressure lines over time. However,lines can be kept patent without heparin, and other factorsalso significantly affect patency of arterial monitoring lines. Furthermore, the flush solution does not guaranteepatency of the line.”33
Research RichesRecent in vitro studies suggest that the growth of CoNS
on catheters may be enhanced in the presence of heparin.34
ConcentrationVarious concentrations of heparinized saline from 5 to
1,000 USP units/ml are commonly used to flush CVCs. A questionnaire was distributed to a sample of persons attendingthe annual conference of the National Association of VascularAccess Networks in 1992. Heparin flushes were still used by97% to maintain patency. The most commonly used concentra-tion of heparin to maintain non-infusing CVCs was 100units/mL. The Intravenous Nursing Standards recommends thatthe lowest possible concentration of heparin be used.
Research RichesStern et al hypothesized that the daily amount of
heparinized saline solution injected via a heparin lock was 20 ml or approximately 2 ml of 1,000 U/ml heparinsodium – a total of 2,000 U/day.35

Saline vs. Heparin (continued)
Clinical ConcernAdministration of low-dose heparinized saline solution
has been associated with hypersensitivity reaction, transient increases in activated partial thromboplastintime, delayed fibrinolysis with platelet aggregation, and thrombocytopenia. Drug interactions occur withdiazepam, meperidine, promethazine, hydroxyzine, tetracylcine, penicillin G, methicillin, erythromycin gluceptate, gentamicin, and dacarbazine. At least one case of iatrogenic hemorrhage has resulted from the flushing of multiple catheters.36
Flush VolumeIt has been accepted that the volume of the heparinized saline
flush be equal to two times the volume capacity of the cannula.(See previous for catheter lumen volumes.) Typical flush volumes range from 1-5 mL.
Clinical Considerations: FlushingRECOMMENDED EQUIPMENT
- Antiseptic swabs- 10mL syringe with needleless cannula- Heparin flush solution (concentration per hospital policy)CLINICAL RESPONSIBILITIES
■ Cleanse injection site with approved antiseptic solution■ Use a 10 mL syringe■ Maintain positive pressure during flushing■ Monitor coagulation parameters
FL
US
HIN
G (I
NT
ER
MIT
TE
NT
)
56

IN
FU
SIO
N T
HE
RA
PY
57
Infusion TherapyOne of the major indications for the percutaneous placement of
a short-term polyurethane multi-lumen central venous catheteris to allow for the delivery of various therapies through a singlevenipuncture. Solutions that are infused through multi-lumencatheters in the critical care area may include maintenance orreplacement fluids, medications, blood products or totalparenteral nutrition (TPN).
Fluid AdministrationWith appropriate catheter tip placement within the central
circulation, large volumes of fluid can be administered and diluted rapidly. Most fluids can be administered safely.However, solutions/medications containing high concentrationsof alcohol should not be infused through polyurethane cathetersdue to alcohol’s weakening effect on the material.
CONCENTRATIONS IN FREQUENTLY USED INTRAVENOUS SOLUTIONS (MEQ/L)
FLUID GLUCOSE NA+ K+ CL- MOSM/L KCAL/L
D5W 50g 0 0 0 252 170
D10W 100g 0 0 0 505 340
D50W 500g 0 0 0 2520 1700
1/2 NS (0.45%NS) 0 77 0 77 154 0
NS (0.9% NS) 0 154 0 154 308 0
D51/4NS 50g 38 0 38 329 170
D5 1/2NS 50g 77 0 77 406 170
D5 NS 50g 154 0 154 560 170
LR 0 130 4 110 272 10
IV Delivery SystemMany policies have advocated routinely replacing the entire
infusion delivery system at certain intervals to reduce the risk ofsepsis from extrinsically contaminated fluid. If an infusion runscontinuously for an extended period, the cumulative risk of contamination increases, and there is increased risk that the con-taminants could grow to dangerously high concentrations, result-ing in septicemia.

IN
FU
SIO
N T
HE
RA
PY
58
IV Delivery System (continued)
However, contaminated infusion is not a common cause of mostcatheter-related bacteremias.
Contaminated infusate can result from intrinsic (introducedduring its manufacture) or extrinsic (introduced during itspreparation or administration in the hospital) contamination.Microorganisms can be introduced extrinsically into the fluidbeing infused from entry points into the administration set (during injections into the line or aspiration of blood specimensfrom the intravascular device through the line) or at the junctionbetween the administration set and the catheter hub. However,the majority of introduced contaminants are rapidly cleared fromrunning infusion by continuous flow.
Most studies indicate that intravenous delivery systems do notneed to be replaced more frequently than every 72 hours.
CDC Guideline (1996)■ Replace extension tubing when the vascular device
is replaced■ Replace IV tubing, including piggyback tubing and
stopcocks, no more frequently than at 72-hour intervals,unless clinically indicated
■ No recommendation for the hang time of IV fluids,including non-lipid containing parenteral nutrition fluids
In-Line FiltersThe use of filters continues to be advocated as a means of
reducing the hazard of contaminated infusate. However, filtersmust be changed at periodic intervals and can become blocked,leading to added manipulations of the system, and, paradoxically,greater potential for infection.
Additionally, the use of filters:■ May permit the passage of endotoxin ■ Are expensive ■ May not be justified as a control method for prevention of rare
sporadic septicemias deriving from extrinsic contamination ofinfusate

IN
FU
SIO
N T
HE
RA
PY
59
In-Line Filters (continued)
CDC Guideline (1996)Do not use filters routinely for infection control
purposes.
StopcocksStopcocks used for injection of medications, administration
of IV infusions, or collection of blood samples, may represent a source of entry for microorganisms. Although stopcock contamination is common (45-50%), the relative contribution of stopcock contamination to intravascular catheter or IV fluidcontamination is unclear. Few studies have been able todemonstrate that the organism colonizing the stopcock is thesame one responsible for catheter-related infection.
Even if stopcocks are used, injection caps may be placed oneach port to keep the system as closed as possible.
CDC Guideline (1996) ■ Clean injection ports with 70% alcohol or povidone-
iodine before accessing the system■ No recommendation for use, maintenance, or frequency
of replacement of needleless IV devices
Piggyback SystemsPiggyback systems may be used as an alternative to stopcocks.
They pose a risk for contamination of the intravascular fluid ifthe needleless cannula entering the injection port is partiallyexposed to air and/or subject to repeated connections and disconnections as might occur with intermittent administrationof antibiotics. The use of a closed piggyback system in whichthe piggyback line is never detached from the primary linewould seem to decrease the chance of infection.
Research RichesModified piggyback systems appear to prevent contami-
nation at these sites and reduce the incidence of catheter-related BSI six-fold when compared with conventionalstopcock and piggyback systems. 37
IN
FU
SIO
N T
HE
RA
PY
60
Piggyback Systems (continued)
Practical PointOne piggyback line can be used for multiple intermittent
infusions, even if the medications are incompatible, aslong as all medications to be piggybacked are compatiblewith the primary solution. When one medication is fin-ished, the line is back-flushed to fill the short line withprimary solution. Another partial-fill can then be spikedand administered.
CDC Guideline (1996)No recommendation for frequency of replacement IV
tubing used for intermittent infusions.
Medication AdministrationDrug administration is an important therapeutic intervention
in the care of the critically ill patient and is, therefore, a concernfor the critical care clinician. As a basic principle, only one drugshould be added to an infusion fluid, and no drugs shouldbe co-administered in the same line. Hence, the rationale for multi-lumen catheters in the critically ill population.
However, these patients often require several intravenous medications administered simultaneously, in excess of theamount of lumens available. This may be accomplished viathree-way stopcocks, multiple y-sites, or manifolds attachedto multi-lumen catheters. Therefore, more than one medicationmay be administered through a portion of a single line.
When using such devices, the clinician must be aware of several factors in order to safely administer drugs to the critically ill patient. Are the drugs compatible with each other?Compatible with the catheter material? Will the desired effectbe achieved? There are various charts available that attempt to delineated drug compatibilities/incompatibilities for the clinician; however, these are considered as guidelines only. It is always recommended that instructions provided byintravenous drug suppliers and/or device manufacturers be read carefully.

IN
FU
SIO
N T
HE
RA
PY
61
Medication Administration (continued)
Drug IncompatibilityA drug incompatibility is defined as failure of a drug or drug
mixture to combine with another drug, diluent, or infusion device system in an expected or desired manner. Drugs are assumed to be compatible when mixed if there is no sign of physical orchemical incompatibility.
Physical incompatibility – combination of two or more drugsresulting in a change in the appearance of the solution (precipitation, color change, or cloudiness)
Chemical incompatibility – significant drug degradation (usually a > 10% loss of potency) occurring with or without achange in the appearance of the solution
(Physical compatibility does not imply chemical compatibility)Due to the larger vessel size and flow velocity surrounding
the catheter lumen exit sites in the central venous system,simultaneous administration of incompatible medicationshas been practiced. However, few studies have evaluated thesafety and efficacy of this in clinical practice.
Grillo et al38 looked at the chemical compatibility of inotropic and vasoactive agents delivered via a multiple lineinfusion system. They studied three different triple-drug admixtures diluted with either 5% dextrose in water or 0.9%sodium chloride solution. The triple drug admixtures were combinations of dobutamine, dopamine, norepinephrine,nitroglycerin, and sodium nitroprusside. All triple-drugadmixtures were chemically stable when placed in single containers. Dobutamine, norepinephrine, and sodium nitroprusside showed chemical stability when delivered via a multiple-line infusion system. Therefore, these drugsshould be able to be administered through the same line in a multi-lumen central venous catheter.
Other ConsiderationsAlthough infusion of incompatible medications through various
lumens is possible through multi-lumen catheters, studies haveshown that blood volume and the configuration of the lumenexit sites at the distal end of the catheter may be important factors to consider. One recent study39 attempted to evaluate thesimultaneous administration of incompatible medications by using an in vitro venous flow model system designed tomimic an in vivo clinical situation.
IN
FU
SIO
N T
HE
RA
PY
62
Medication Administration (continued)
The study looked at the physiochemical phenomena that occurwhen two known incompatible drugs, phenytoin and TPN,were simultaneously administered through a multi-lumen CVC.
This study showed that the design of the catheter might havean impact on precipitate formation. Catheters designed withadjacent exit sites (ports) at the tip of the double-lumen catheterappeared to permit interaction of the two infusing incompatibledrugs. Staggered orifices (exit ports), on the other hand,reduced this interaction. This study concluded that the clinicalsignificance of this phenomenon has yet to be assessed.
Nitroglycerin AdministrationConsideration must be given to the effects that certain
medications have upon the catheter as well as on other simulta-neous infusions. The problem of the adsorption of nitroglycerinonto some catheter materials, namely polyvinyl chloride, hasbeen reported in the literature. Adsorption is the adhesion of a gas or liquid to the surface of a solid; i.e., the medication is“leached” out into the tubing or catheter material instead ofbeing delivered to the patient. Polyurethane, the material usedto make most central venous catheters, does not contribute toleaching of this drug.
This effect of adsorption is more prominent if agents areadministered in small quantities or at low concentrations andin the initial phase of administration. This is a particularlysignificant point to remember when starting a vasoactive drugthat will be titrated. After this initial phase, adsorption contin-ues, but at a lower rate. In consequence, the dose administered to the patient may increase with time, althoughthe infusion rate is kept constant. This may require adjustmentsin the rate of infusion.
The clinical significance of the adsorption is controversial, however, since the drug is often titrated to effect. Nitroglycerinis usually mixed in glass bottles to minimize the leaching effectof the container. Some institutions use non-PVC tubing whenadministering nitroglycerin; others do not. Some “saturate” thetubing initially by flushing it rapidly with the medication to beinfused. Follow the institution’s policy when it comes tonitroglycerin administration.

IN
FU
SIO
N T
HE
RA
PY
63
Medication Administration (continued)
Clinical ConsiderationLow dose dopamine (for renal perfusion, for instance)
may be administered through a peripheral line in somecases. However, titratable doses for vasoactive purposesneed to go through a central line for several reasons. Thedosages are greater and the action of the drug needs to becentral, rather than local. Also, local vasoconstriction fromhigher dosages of dopamine might limit the amount ofdrug that could get into the central circulation – as well aspotentially injure the surrounding tissues.
Blood AdministrationAnother indication for the placement of a central venous
catheter is for frequent administration of blood or blood products. According to the Core Curriculum for Critical CareNursing by the American Association of Critical-Care Nurses,peripheral IV sites may be used for this purpose as long as at least a 20 gauge access (to prevent hemolysis) is used.However, central venous catheters, with their larger lumens and more stable access, may be preferable.
CDC Guideline (1996)Replace tubing used to administer blood, blood
products, or lipid emulsions within 24 hours of initiatingthe infusion.
Administration of TPNAlthough enteral feeding is preferred, a substantial number
of critically ill patients receive parenteral nutrition. The riskof bloodstream infection remains one of the most important complications associated with TPN therapy. This is due to thefact that dextrose, amino acids, or lipid emulsions are more likelythan conventional IV fluids to support microbial growth.

IN
FU
SIO
N T
HE
RA
PY
64
Administration of TPN (continued)
Research RichesStudies randomizing trauma patients to TPN or enteral
feedings have continued to show increased infection ratesin the TPN groups.40
Special precautions need to be taken with TPN. Experiencedpharmacists use an aseptic technique when mixing solutionsunder a laminar flow hood. Total parenteral nutrition shouldideally be delivered in a dedicated line that should be leftunbroken in order to reduce the possibility of infection. No sec-ondary (or piggyback) tubings, except lipids, are permitted intothis line. Nearly all septicemias linked to contaminated infusatehave been gram-negative bacilli. However, microbial growth inmost parenteral solutions, with the exception of lipid emulsion,is actually very limited.
Lipid emulsions, however, are particularly suited for growth of specific bacteria and yeasts, including Candida species.Microbial growth occurs as early as 6 hours, with clinically significant levels being reached within 24 hours.
Nurses NotesCombined TPN solutions (3-in-1), which use glucose,
amino acids, lipid emulsion, and additives in one multi-liter bag, do not appear to support greater microbialgrowth than non-lipid containing TPN fluids.41
Clinical ConsiderationTPN may be administered peripherally as long as the
dextrose content is low enough not to irritate the vessel.However, peripheral TPN does not provide the nutritionalbenefit of central TPN solutions.
CDC Guideline (1996)■ Do not use single-lumen parenteral nutrition catheters
for purposes other than hyperalimentation (e.g., adminis-tration of fluids, blood, or blood products)
■ If a multi-lumen catheter is used to administer parenter-al nutrition, designate one port for hyperalimentation.Do not use the designated hyperalimentation port forother purposes (e.g., administration of fluids, blood, orblood products)

IN
FU
SIO
N T
HE
RA
PY
65
Administration of TPN (continued)
■ Complete infusions of lipid-containing parenteral nutrition fluids (e.g., 3-in-1 solutions) within 24 hours of hanging the fluid
■ When lipid emulsions are given alone, complete theinfusion within 12 hours of hanging the emulsion
Clinical Considerations: IV AdministrationRECOMMENDED EQUIPMENT
- Volumetric infusion pump- IV fluid and appropriate tubing
CLINICAL RESPONSIBILITIES
■ Review orders■ Identify patient■ Dedicate one lumen for TPN administration■ Do not infuse solutions with a high concentration of alcohol
through polyurethane catheters or tubing■ Flush after medication administration to deliver any residual
portion of the dosage to the patient■ Do not push IV medications through lumen containing
vasoactive drugs (since this may precipitate serious cardiovascular events)
■ Consult compatibility tables or pharmacist when administeringmore than one drug through a lumen
Practical PointIf in doubt as to compatibility of an intermittent push
medication, flush the intended line with a known compati-ble solution, follow push with similar flush.
■ Observe tubing and IV solution for precipitation or anyother signs of incompatibility
■ Follow specific guidelines for blood administration

IN
FU
SIO
N T
HE
RA
PY
66
Frequently Used Drugs in Critical Care
MECHANISMOF ACTION/
DRUG EFFECTS INDICATIONS DOSAGE PRECAUTIONS
Adenosine ↓ sinus rate. Conversion of Initial bolus = Side effects supraventricular 6 mg rapid IV but transient
Trade Name: ↓ conduction tachycardia to a bolus over 1-3 and usually Adenocard through AV node. regular sinus seconds followed resolve spon-
rhythm, including by a 20 ml saline taneouslyClass: Can interrupt PSVT associated flush. Wait 1-2 within 1-2Endogenous reentrant path- with accessory minutes. minutes – chemical, ways through bypass tracts that flushing, dyspnea,Antidysrhy- the AV node. involve the AV If no response chest pain.thmic node (as seen in observed, admin-
Has a direct WPW) that is ister 12 mg (may Consider ↑ doseeffect on refractory to vagal repeat the 12 mg in patients onsupraventricular maneuvers. dose once in the theophylline since tissue. 1-2 minutes). methylxanthines
Wide-complex prevent bindingHalf-life is less tachycardia of Due to extremely of adenosine atthan 5 seconds. uncertain type short half-life, receptor sites.
after lidocaine start IV line asadministration. proximal to the Consider ↓ dose
heart as possible, in patients onIf the dysrhythmia such as the dipyridamoleis not due to antecubital fossa. (Persantine)reentry involving because adenosinethe AV node or Onset: Seconds. potentiates itssinus node (atrial effects.fibrillation, atrial Peak: Seconds.flutter, atrial or Relatively highventricular Duration: 10-12 incidence oftachycardias), seconds. recurrence of theadenosine will tachycardia afternot terminate the 6 mg dose; 92%dysrhythmia but conversion to amay produce sinus rhythmtransient AV block after 12 mg bolus.that may clarifythe diagnosis.
Amrinone Potent inotropic Severe CHF that 0.75 mg/kg over ■ Incompatible effect. has not responded 2-3 minutes with furosemide.
Trade Name: to diuretics, followed by an ■ May exacerbateInocor ↑ cardiac function. vasodilators and infusion @ 5-15 myocardial
conventional µg/kg/min, titrated ischemia.Class: Induces inotropic agents. to effect. ■ May worsenNon- vasodilation. ventricularadrenergic, ectopy.non-ß-agonist ■ Should be
administered viaan infusion pump.■ Hemodynamicmonitoring issuggested foroptimal use.

IN
FU
SIO
N T
HE
RA
PY
67
Administration of TPN (continued)
MECHANISMOF ACTION/
DRUG EFFECTS INDICATIONS DOSAGE PRECAUTIONS
ß-Adrenegic ß-adrenergic ↓ incidence of Atenolol: 5 mg IV Should be Blockers blockade. VF in post-MI over 5 min, may avoided in:
patients who did repeat in 10 min. ■ bradycardia.Atenolol ↓ rate of discharge not receive ■ second or (Tenormin) of sinus node. thrombolytic Esmolo: 500 µ/kg third-degree
agents. over 1 minute AV block.Esmolol ↓ myocardial (loading dose) ■ hypotension.(Brevibloc) contractility. When used within followed by a main- ■ overt CHF.
4 hours after ad- tenance infusion ■ lung diseaseMetoprolol ↓ blood pressure. ministration of at 50 µ/kg/min associated with(Lopressor) thrombolytic over 4 minutes. bronchospasm.
↓ myocardial therapy, may ↓ ratePropranolo oxygen of nonfatal rein- Metoprolo: 5 mg(Inderal) consumption. farction and slow IV push at
recurrent ischemia. 5 min intervals tototal of 15 mg.
In thrombolytictreated patients, Propranolol: Totalmay ↓ mortality dose of 0.1 mg/kgand recurrent MI slow IV push if administered divided into 3 within 2 hours of equal doses at symptom onset. 2-3 intervals.
Bretylium Initial sympath- Not a first-line Refractory VF/ Postural Tosylate omimetic effects antidysrhythmic. pulseless VT: hypotension.
due to release of 5 mg/kg rapid IVTrade Name: norepinephrine: After defibrillation, bolus followed by Nausea/vomitingBretylol epinephrine and defibrillation. with rapid IV
■ ↑ heart rate. lidocaine have administration.Class: ■ ↑ peripheral failed to If VF persists, ↑ Ventricular vasoconstriction. convert VF. dose to 10 mg/kg Contraindicatedantidys- ■ ↑ blood pressure. and repeat every in digitalis rhythmic, ■ ↑ cardiac output. VF has recurred 5 min to maximum toxicity.Adrenegic despite epineph- dose 30-35 mg/kg.blocker Subsequent rine and lidocaine. Additive effects
sympatholytic If conversion with sympath-response after Lidocaine and occurs to a perfusing omimetics.15-20 minutes procainamide have rhythm after bolus(adrenergic block): failed to control therapy, initate a
VT associated continuous infusion■ ↓ blood pressure with a pulse. at 1-2 mg/min.■ Suppresses.ventricular ectopy. Lidocaine and To mix drip: ■ ↑ VF threshold. adenosine have 1 gram in 250 ml
failed to control or 2 grams in 500 ml.wide-complex Using a microdriptachycardias. (60 gtts/ml)
administration set: 1 mg/min = 15 gtts/min2 mg/min = 30 gtts/min
Persistently recurring VT (with a pulse): (IV infusion) 5-10 mg/kg dilutedin 50 ml and infusedover 8-10 min toavoid nausea/vomiting. If conver-sion occurs, initiate a continuos mg/min.infusion at 1-2

Administration of TPN (continued)
MECHANISMOF ACTION/
DRUG EFFECTS INDICATIONS DOSAGE PRECAUTIONS
Calcium ↑ myocardial Probably helpful 2-4 mg/kg (usually ■ BradycardiaChloride contractile (Class IIa) in: 500 mg – 1 gram) with rapid IV
function. ■ Hyperkalemia. of 10% calcium injection.■ Hypocalcemia. chloride solution ■ Use with ■ Calcium channel slow IV bolus caution in blocker toxicity. and repeated as digitalized
necessary at patients.May also be used 10 minute intervals. ■ Precipitatesto pretreat patients with bicarb.with PSVT priorto administrationof verapamil.
Diltiazem Slows conduction Multifocal atrial 0.25 mg/kg (20 mg) ■ Produces lessand increases tachycardia, atrial IV over 2 minutes myocardial refractoriness in fibrillation or atrial followed 15 minutes depression thanthe AV node. flutter with a later by 0.35 mg/kg verapamil.
rapid ventricular (25 mg) IV over ■ Avoid or useresponse. 2 minutes. with caution in
left ventricularIn atrial fibrillation dysfunction.with a rapid ■ Common sideventricular response, effects includediltiazem may be hypotensionused as a mainten- and flushing.ance infusion of ■ Avoid in 5-15 mg/hour. patients with
AV block, sinusnode dysfunctionor severe cardiacfailure.■ Do not admin-ister to patientswith WPW – may worsen dysrhythmia.■ Not effectivein VT.
Dobutamine ß-adrenergic Refractory 2-20 µg/kg/min ■ ↑ of heart rate stimulator. congestive heart (usual dose 2.5-10 of more than 10%
Trade Name: failure (systolic µg/kg/min). may induce or Dobutrex Potent inotropic BP > 100 mm Hg exacerbate
effect (↑ myocardial with normal To prepare infusion: myocardialClass: contractility → ↑ diastolic BP). Mix 250 mg in ischemia Sympathom- stroke volume → ↑ 250 ml (1000 µg/ml) (common at dosesimetic cardiac output). Cardiogenic shock. and titrated to > 20 µg/kg/min).
desired response. ■ Less likely Less chrono- to induce tropic effect tachycardia than(heart rate). isoproterenol or
dopamine.Stimulates ß-2 ■ Best admin-receptors at doses istered via an> 10 µg/kg/min → infusion pump.peripheral vasodila- ■ Do not mix tion → ↓ systemic with sodiumvascular resistance. bicarbonate –
inactivatesdobutamine.■ Correct hypo-volemia beforeadministration ofdobutamine.■ Do not discon-tinue abruptly –taper gradually.
IN
FU
SIO
N T
HE
RA
PY
68
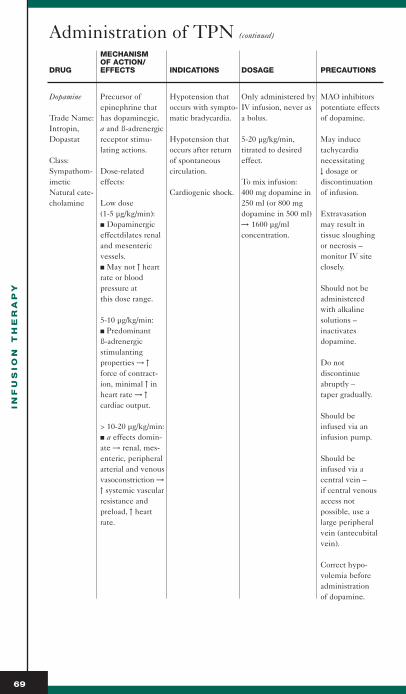
IN
FU
SIO
N T
HE
RA
PY
69
Administration of TPN (continued)
MECHANISMOF ACTION/
DRUG EFFECTS INDICATIONS DOSAGE PRECAUTIONS
Dopamine Precursor of Hypotension that Only administered by MAO inhibitorsepinephrine that occurs with sympto- IV infusion, never as potentiate effects
Trade Name: has dopaminegic, matic bradycardia. a bolus. of dopamine.Intropin, a and ß-adrenergicDopastat receptor stimu- Hypotension that 5-20 µg/kg/min, May induce
lating actions. occurs after return titrated to desired tachycardiaClass: of spontaneous effect. necessitatingSympathom- Dose-related circulation. ↓ dosage orimetic effects: To mix infusion: discontinuationNatural cate- Cardiogenic shock. 400 mg dopamine in of infusion.cholamine Low dose 250 ml (or 800 mg
(1-5 µg/kg/min): dopamine in 500 ml) Extravasation■ Dopaminergic → 1600 µg/ml may result in effectdilates renal concentration. tissue sloughingand mesenteric or necrosis – vessels. monitor IV site■ May not ↑ heart closely.rate or blood pressure at Should not bethis dose range. administered
with alkaline5-10 µg/kg/min: solutions –■ Predominant inactivates ß-adrenergic dopamine.stimulantingproperties → ↑ Do not force of contract- discontinueion, minimal ↑ in abruptly –heart rate → ↑ taper gradually.cardiac output.
Should be > 10-20 µg/kg/min: infused via an■ a effects domin- infusion pump.ate → renal, mes-enteric, peripheral Should be arterial and venous infused via avasoconstriction → central vein –↑ systemic vascular if central venousresistance and access not preload, ↑ heart possible, use arate. large peripheral
vein (antecubitalvein).
Correct hypo-volemia beforeadministrationof dopamine.
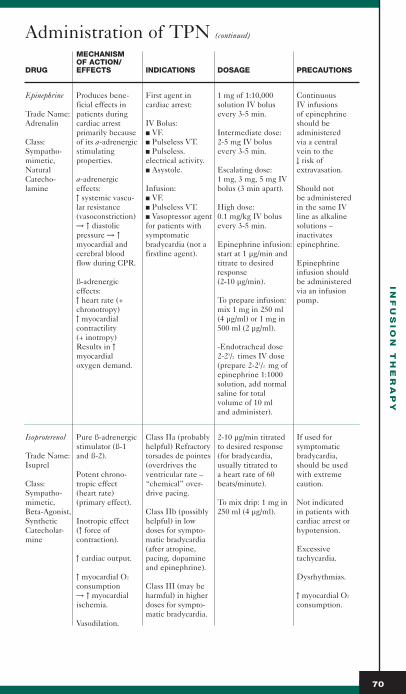
IN
FU
SIO
N T
HE
RA
PY
70
Administration of TPN (continued)
MECHANISMOF ACTION/
DRUG EFFECTS INDICATIONS DOSAGE PRECAUTIONS
Epinephrine Produces bene- First agent in 1 mg of 1:10,000 Continuous ficial effects in cardiac arrest: solution IV bolus IV infusions
Trade Name: patients during every 3-5 min. of epinephrineAdrenalin cardiac arrest IV Bolus: should be
primarily because ■ VF. Intermediate dose: administeredClass: of its a-adrenergic ■ Pulseless VT. 2-5 mg IV bolus via a centralSympatho- stimulating ■ Pulseless. every 3-5 min. vein to the mimetic, properties. electrical activity. ↓ risk of Natural ■ Asystole. Escalating dose: extravasation.Catecho- a-adrenergic 1 mg, 3 mg, 5 mg IVlamine effects: Infusion: bolus (3 min apart). Should not
↑ systemic vascu- ■ VF. be administered lar resistance ■ Pulseless VT. High dose: in the same IV (vasoconstriction) ■ Vasopressor agent 0.1 mg/kg IV bolus line as alkaline → ↑ diastolic for patients with every 3-5 min. solutions –pressure → ↑ symptomatic inactivatesmyocardial and bradycardia (not a Epinephrine infusion: epinephrine.cerebral blood firstline agent). start at 1 µg/min andflow during CPR. titrate to desired Epinephrine
response infusion shouldß-adrenergic (2-10 µg/min). be administeredeffects: via an infusion↑ heart rate (+ To prepare infusion: pump.chronotropy) mix 1 mg in 250 ml↑ myocardial (4 µg/ml) or 1 mg incontractility 500 ml (2 µg/ml).(+ inotropy)Results in ↑ -Endotracheal dosemyocardial 2-21/2 times IV dose oxygen demand. (prepare 2-21/2 mg of
epinephrine 1:1000 solution, add normal saline for total volume of 10 ml and administer).
Isoproterenol Pure ß-adrenergic Class IIa (probably 2-10 µg/min titrated If used forstimulator (ß-1 helpful) Refractory to desired response symptomatic
Trade Name: and ß-2). torsades de pointes (for bradycardia, bradycardia,Isuprel (overdrives the usually titrated to should be used
Potent chrono- ventricular rate – a heart rate of 60 with extremeClass: tropic effect “chemical” over- beats/minute). caution.Sympatho- (heart rate) drive pacing.mimetic, (primary effect). To mix drip: 1 mg in Not indicatedBeta-Agonist, Class IIb (possibly 250 ml (4 µg/ml). in patients withSynthetic Inotropic effect helpful) in low cardiac arrest orCatecholar- (↑ force of doses for sympto- hypotension.mine contraction). matic bradycardia
(after atropine, Excessive↑ cardiac output. pacing, dopamine tachycardia.
and epinephrine).↑ myocardial O2 Dysrhythmias.consumption Class III (may be→ ↑ myocardial harmful) in higher ↑ myocardial O2
ischemia. doses for sympto- consumption.matic bradycardia.
Vasodilation.
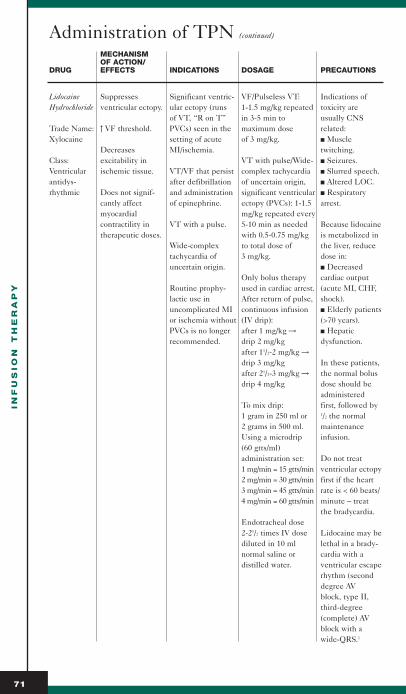
IN
FU
SIO
N T
HE
RA
PY
71
Administration of TPN (continued)
MECHANISMOF ACTION/
DRUG EFFECTS INDICATIONS DOSAGE PRECAUTIONS
Lidocaine Suppresses Significant ventric- VF/Pulseless VT: Indications ofHydrochloride ventricular ectopy. ular ectopy (runs 1-1.5 mg/kg repeated toxicity are
of VT, “R on T” in 3-5 min to usually CNSTrade Name: ↑ VF threshold. PVCs) seen in the maximum dose related:Xylocaine setting of acute of 3 mg/kg. ■ Muscle
Decreases MI/ischemia. twitching.Class: excitability in VT with pulse/Wide- ■ Seizures.Ventricular ischemic tissue. VT/VF that persist complex tachycardia ■ Slurred speech.antidys- after defibrillation of uncertain origin, ■ Altered LOC.rhythmic Does not signif- and administration significant ventricular ■ Respiratory
cantly affect of epinephrine. ectopy (PVCs): 1-1.5 arrest.myocardial mg/kg repeated everycontractility in VT with a pulse. 5-10 min as needed Because lidocainetherapeutic doses. with 0.5-0.75 mg/kg is metabolized in
Wide-complex to total dose of the liver, reducetachycardia of 3 mg/kg. dose in:uncertain origin. ■ Decreased
Only bolus therapy cardiac outputRoutine prophy- used in cardiac arrest. (acute MI, CHF,lactic use in After return of pulse, shock).uncomplicated MI continuous infusion ■ Elderly patientsor ischemia without (IV drip): (>70 years).PVCs is no longer after 1 mg/kg → ■ Hepaticrecommended. drip 2 mg/kg dysfunction.
after 11/2-2 mg/kg → drip 3 mg/kg In these patients,after 21/2-3 mg/kg → the normal bolusdrip 4 mg/kg dose should be
administeredTo mix drip: first, followed by1 gram in 250 ml or 1/2 the normal2 grams in 500 ml. maintenanceUsing a microdrip infusion.(60 gtts/ml)administration set: Do not treat1 mg/min = 15 gtts/min ventricular ectopy2 mg/min = 30 gtts/min first if the heart3 mg/min = 45 gtts/min rate is < 60 beats/4 mg/min = 60 gtts/min minute – treat
the bradycardia.Endotracheal dose2-21/2 times IV dose Lidocaine may bediluted in 10 ml lethal in a brady-normal saline or cardia with adistilled water. ventricular escape
rhythm (seconddegree AV block, type II, third-degree (complete) AVblock with awide-QRS.1

IN
FU
SIO
N T
HE
RA
PY
72
Administration of TPN (continued)
MECHANISMOF ACTION/
DRUG EFFECTS INDICATIONS DOSAGE PRECAUTIONS
Magnesium May ↓ early Torsades de Pulseless VT/VF: MagnesiumSulfate MI mortality. Pointes. 1-2 grams IV (2-4 ml deficiency is
of 50% solution) associated withMay ↓ incidence Pulseless VT/VF. diluted in 10 ml and cardiac dysrhyth-of dysrhythmias administered over mias, symptomsthat often occur Acute MI with 1-2 minutes. of cardiac insuf-in survivors of MI. known or ficiency and
suspected Acute MI, sudden cardiacMechanism hypomagnesemia. Hypomagnesemia. death.of action not Loading dose of 1-2completely grams mixed in Signs/symptomsunderstood. 50-100 ml of NS and of magnesium May ↓ administered over overdose includedue to: 5-60 minutes. ↓ respiratory rate,■ Systemic hypotension,vasodilation → ↓ Torsades de Pointes hyporeflexia.myocardial 1-2 grams IV (2-4 mloxygen demand. of 50% solution) Calcium chloride■ ↓ platelet diluted in 10 ml should be on aggregation. administered over hand for IV ■ Coronary 1-2 minutes followed administrationvasodilation. by the same amount if signs of ■ Improved (mixed in 50-100 ml magnesiummyocardial of NS) infused over overdose metabolism. 1 hour. develop.■ ↓ myocardialinfract size.■ Protectionagainst catechola-mine inducedmyocardial necrosis.
Norepine- Naturally occurring Cardiogenic shock. 0.5-30 µg/min Relativelyphrine potent vasocons- titrated to effect. contraindicated
trictor (a-receptor Severe in hypovolemicTrade Name: stimulating agent) hypotension To prepare infusion: patients.Levophed and inotropic (ß-1 (systolic BP < 70). Mix 4 mg in 250ml
receptor stimula- (16 µg/ml). Titrate Should not beClass: tor) agent. to desired effect. administeredSympatho- in the same IVmimetic, 90% a, 10% ß. line as alkalineNatural cate- solutions.cholamine a activity usually
dominant. Use with cautionin patients with
Usually causes ischemic heartrenal and disease as mesenteric myocardial O2
vasoconstriction. requirementsmay ↑.
Extravasationmay result intissue sloughingor necrosis.

IN
FU
SIO
N T
HE
RA
PY
73
Administration of TPN (continued)
MECHANISMOF ACTION/
DRUG EFFECTS INDICATIONS DOSAGE PRECAUTIONS
Procainamide Suppresses Recommended IV infusion of ↓ maintenanceventricular ectopy. when lidocaine is 100 mg over 5 min infusion in renal
Trade Name: contraindicated or (20 mg/min) until failure, CHF orPronestyl ↑ VF threshold. has failed to sup- one of the following liver dysfunction.
press ventricular occurs:Class: Shortens effective ectopy. ■ Dysrhythmia is Hypotension mayAntidys- refractory period suppressed. occur if injectedrhythmic of the AV node. Wide-complex ■ QRS widens by too rapidly –
tachycardias that 50% of its original use caution in Prolongs effective cannot be distin- width. patients withrefractory period guished from VT ■ Hypotension acute MI.and duration of (not a first-line develops.the action drug). ■ Total of 17 mg/kg Avoid in patientspotential in the has been adminis- with pre-existingHis-Purkinje Atrial fibrillation tered (1.2 gm for a QT prolongationsystem. with a rapid 70 kg patient). and torsades
ventricular de pointes.response (not a Note: Up to first-line drug). 30 mg/min may be Observe ECG
administered in for ↑ PR and Suppression of urgent situations. QT intervals, recurrent VT widening QRSthat cannot be To prepare infusion: and heart block.controlled with Mix 1 gram/250 mllidocain. or 2 grams/500 ml
(4 mg/ml).Refractorypulseless VT/VF. Maintenance infus-
ion is 1-4 mg/min.
Sodium Potent, rapid- Heart failure. Add 50 mg to 250 ml IV and tubingNitroprusside acting peripheral (200 µg/ml). should be
vasodilator Hypertension. wrapped inTrade Name: (arterial and 0.1-5.0 µg/kg/min aluminum foilNipride venous) → ↓ but higher doses (deteriorates
preload and (up to 10 µg/kg/min) when exposedafterload. may be needed. to light); use an
infusion pump.↑ cardiac output.
Nitroglycerin↓ myocardial. preferredoxygen vasodilator inconsumption. acute MI,
especially whencomplicated by CHF.
Primary -complicationis hypotension.
Other side effects:■ Headaches.■ Nausea/vomiting.■ Abdominal cramps.■ Palpitations.■ Dizziness.
Watch for thiocya-nate toxicity:■ Confusion.■ Hyperreflexia.■ Convulsions.■ Tinnitus.
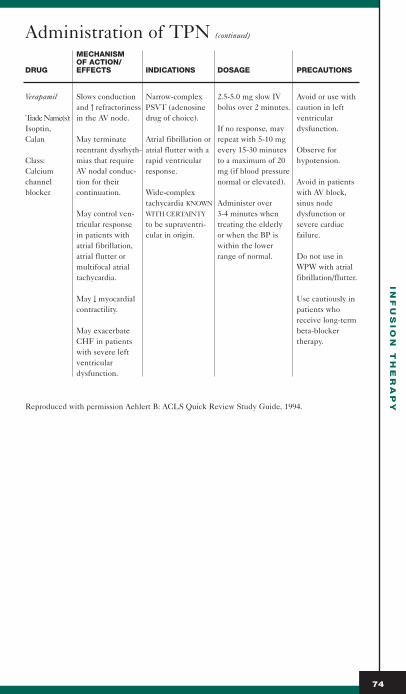
Administration of TPN (continued)
MECHANISMOF ACTION/
DRUG EFFECTS INDICATIONS DOSAGE PRECAUTIONS
Verapamil Slows conduction Narrow-complex 2.5-5.0 mg slow IV Avoid or use withand ↑ refractoriness PSVT (adenosine bolus over 2 minutes. caution in left
Trade Name(s): in the AV node. drug of choice). ventricularIsoptin, If no response, may dysfunction.Calan May terminate Atrial fibrillation or repeat with 5-10 mg
reentrant dysrhyth- atrial flutter with a every 15-30 minutes Observe for Class: mias that require rapid ventricular to a maximum of 20 hypotension.Calcium AV nodal conduc- response. mg (if blood pressurechannel tion for their normal or elevated). Avoid in patientsblocker continuation. Wide-complex with AV block,
tachycardia KNOWN Administer over sinus nodeMay control ven- WITH CERTAINTY 3-4 minutes when dysfunction ortricular response to be supraventri- treating the elderly severe cardiacin patients with cular in origin. or when the BP is failure.atrial fibrillation, within the loweratrial flutter or range of normal. Do not use inmultifocal atrial WPW with atrialtachycardia. fibrillation/flutter.
May ↓ myocardial Use cautiously incontractility. patients who
receive long-termMay exacerbate beta-blockerCHF in patients therapy.with severe leftventriculardysfunction.
Reproduced with permission Aehlert B: ACLS Quick Review Study Guide, 1994.
IN
FU
SIO
N T
HE
RA
PY
74

75
Monitoring Central Venous PressureCentral venous pressure (CVP) measurements are widely
used in both medical and surgical patients as a simple and easilyavailable guide to fluid therapy after hemorrhage, accidentaland surgical trauma, sepsis and emergency conditions associatedwith blood volume deficits.
Fluid Challenge Guideline Chart Baseline Values:
CHALLENGE VOLUMEPAWP* MMHG AMOUNT/10 MINUTES CVP* MMHG
< 12 mmHg 200 ml or 20 cc/minute < 8 mmHg
12 - 16 - 18 mmHg 100 ml or 10 cc/minute 8 - 13 mmHg
> 16 - 18 mmHg 50 ml or 5 cc/ minute > 13 mmHg
■ Re-profile at the end of 10 minutes or fluid challenge■ Discontinue challenge if PAWP increased > 7 mmHg or CVP
increased > 4 mmHg■ Repeat challenge if PAWP increased < 3 mmHg or CVP
increased < 2 mmHg■ Observe patient for 10 minutes and re-profile if PAWP
increased > 3 mmHg but < 7 mmHg or CVP increased > 2 mmHg or < 4 mmHg
■ Observe SVI and RVEDVI if RV volume values are available■ Discontinue challenge if: SVI fails to increase by at least 10 %
and RVEDVI increases by 25% or RVEDVI is > 140 ml/m2and PAWP increases > 7 mmHg
OPTIONAL BASELINE RVEDVI VALUE GUIDELINES:
■ If RVEDVI < 90 ml/m2 or mid range 90- 140 ml/m2, administer fluid challenge
■ If RVEDVI > 140 ml/m2, do not administer fluid
* References differ on PAWP and CVC ranges
MO
NIT
OR
IN
G C
EN
TR
AL
V
EN
OU
S P
RE
SS
UR
E

Physiologic RationaleCentral venous catheters are used to measure the pressure
under which the blood is returned to the right atrium and togive an assessment of the intravascular volume and rightheart function. The CVP is a useful monitor if the factorsaffecting it are recognized and its limitations are understood.Serial measurements are more useful than individual values, andthe response of the CVP to a volume infusion is a useful test ofright ventricular function. The CVP does not give any directindication of left heart filling but may be used as a crudeestimate of left-sided pressures in patients with good leftventricular function.
Research RichesMangano demonstrated that CVP could be used to
predict pulmonary artery wedge pressure in patients priorto, during, and after coronary artery surgery as long as thepatients had ejection fractions greater than 0.50 with noangiographically demonstrable ventricular dyssynergy preoperatively.42
Essentially, CVP measurements reflect events in the cardiac cycle and, in so doing, depict cardiac function. Duringventricular diastole, the AV valves are open, and each side ofthe heart is essentially unichambered. The pressure created byblood volume in the ventricles now extends back into the atriaso that pressure measured in the right atrium indirectly mirrorsthe volume status of the right ventricle. Preload, or the volumestatus of the heart, has been measured as CVP or PAWP, for theright and left ventricles, respectively.
MO
NIT
OR
IN
G C
EN
TR
AL
V
EN
OU
S P
RE
SS
UR
E
76
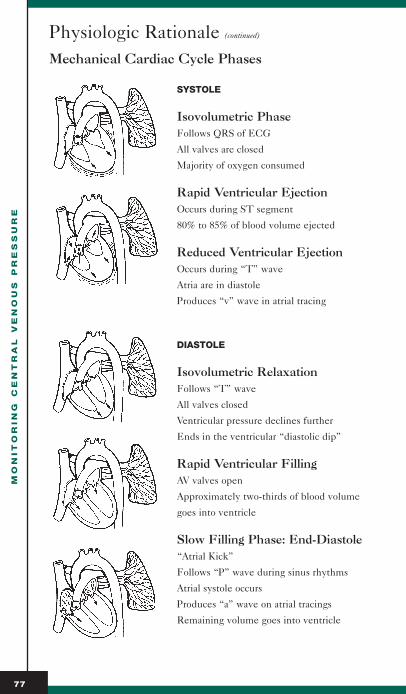
Physiologic Rationale (continued)
Mechanical Cardiac Cycle Phases
MO
NIT
OR
IN
G C
EN
TR
AL
V
EN
OU
S P
RE
SS
UR
E
77
SYSTOLE
Isovolumetric PhaseFollows QRS of ECG
All valves are closed
Majority of oxygen consumed
Rapid Ventricular EjectionOccurs during ST segment
80% to 85% of blood volume ejected
Reduced Ventricular EjectionOccurs during “T” wave
Atria are in diastole
Produces “v” wave in atrial tracing
DIASTOLE
Isovolumetric RelaxationFollows “T” wave
All valves closed
Ventricular pressure declines further
Ends in the ventricular “diastolic dip”
Rapid Ventricular FillingAV valves open
Approximately two-thirds of blood volume
goes into ventricle
Slow Filling Phase: End-Diastole“Atrial Kick”
Follows “P” wave during sinus rhythms
Atrial systole occurs
Produces “a” wave on atrial tracings
Remaining volume goes into ventricle

MO
NIT
OR
IN
G C
EN
TR
AL
V
EN
OU
S P
RE
SS
UR
E
78
Physiologic Rationale (continued)
Simplistically, by applying the principles expressed inStarling’s Law of the Heart, it can be deduced that if apatient’s CVP is low or normal, blood volume expanders may be given safely. This would serve to increase the presystolic (or end-diastolic) volume and therefore the ventricular musclefibers, resulting in increased cardiac output. Conversely, as the CVP rises to higher levels, cardiac reserve decreases, and further blood volume administration becomes progressively morehazardous and less effective in increasing the work of the heart.
However, despite the apparent relationship between CVP and blood volume, it is incorrect to assess blood volume status from CVP. There are many factors that influence CVP values, not the least of which are cardiac performance, blood volume and vascular tone, intrinsic venoustone, increased intraabdominal or intrathoracic pressures andvasopressor therapy.
Sheldon and Leonard43 showed that, contrary to what onemight expect clinically, arterial pressure and central venous pressure are relatively well maintained due to compensatorymechanisms until approximately 20-30% of the estimated bloodvolume has been extracted. Only then do these values begin tofall in a meaningful way.

MO
NIT
OR
IN
G C
EN
TR
AL
V
EN
OU
S P
RE
SS
UR
E
79
Physiologic Rationale (continued)
Upon resuscitation, CVP rises linearly but comes to baselinevalues prematurely. On the average, CVP returns to baseline after only 50% of the hemorrhage volume has been reinfused.
Clinical studies have shown that, in the presence of normalright heart function, severe deterioration of left ventricularfunction is not reflected in changes in CVP. Buchbinder,44 in1976, demonstrated a wide range of pulmonary wedge pressures(left ventricular preload) obtained from patients in the presenceof normal central venous pressure.
HEMODYNAMIC MONITORING: INVASIVE TECHNIQUES
Neil Buchbinder, M.D. and William Ganz, M.D.
Prompt recognition and accurateassessment of serious circulatorychanges in patients gravely ill or undergoing major surgical interventions is of critical importance.Although monitoring heart rate, arterial blood pressure, and centralvenous pressure has been a valuableguide, these values do not provide asufficient basis for accurate diagnosisand proper management.
PU
LMO
NA
RY
WE
DG
E P
RE
SS
UR
E (m
mH
g)
0
10
20
30
40
Figure 1. Data from 33 patients,showing the wide range of pulmonarycapillary wedge pressure valves measured in the presence of normalcentral venous pressure (1-5 mm Hg).

MO
NIT
OR
IN
G C
EN
TR
AL
V
EN
OU
S P
RE
SS
UR
E
80
Physiologic Rationale (continued)
The value of central venous pressure is limited by the fact that itbasically reflects the functional state of the right ventricle, whichfrequently does not parallel that of the left ventricle.Information about the function of the left heart is, however,often essential for proper evaluation. In recent years, techniquesthat allow easy monitoring and analysis of the function of bothventricles have become available. This paper describes thesetechniques and demonstrates how their use enables proper diag-nosis and therapy of commonly encountered clinical situations.
Monitoring TechniquesSystemic Arterial Blood Pressure
In most situations, the sphygmomanometer accurately deter-mines blood pressure. However, in some low-cardiac-outputstates,pulses may be poorly palpable, and Korotkoff sounds hardto hear while the intra-arterial pressure may be only moderatelyreduced. Monitoring of intra-arterial pressure is readily accomplished by percutaneous insertion of an 18- or 20-gaugesheath into a radial, brachial or femoral artery. With appropriatedisplay systems, continuous pressure monitoring is obtained.Long-term patency is facilitated by intermittent flushing with 2-5 ml of heparinized 5% dextrose in water.
Right Heart and Pulmonary Vascular PressuresWhile the right atrial (central venous) pressure can easily
be measured at the bedside, catheterization of the pulmonaryartery with semirigid catheters requires fluoroscopic guidanceand substantial skill. Even in experienced hands, a risk of serious complications exists when severely ill patients arecatheterized. These problems have been largely overcome by the introduction of balloon flotation catheters, which allow forrapid and relatively safe catheterization of the pulmonary arterywithout fluoroscopy.
Catheterization with Balloon Flotation CathetersCatheterization can be performed in any hospital location
where appropriate support devices are available for effectivedetection and therapy of arrhythmias and for recording hemody-namic data. Catheterization is performed during continuouselectrocardiographic monitoring. The basilic, brachial, femoral,subclavian and internal jugular veins are used as insertion sites,the latter two being particularly preferred by anesthesiologistsand surgeons.

MO
NIT
OR
IN
G C
EN
TR
AL
V
EN
OU
S P
RE
SS
UR
E
81
Physiologic Rationale (continued)
After entry into the selected vein, the catheter is advanced untilthe tip is in or near the right atrium. This usually occurs afteradvancement for approximately 15 cm when the jugular or sub-clavian vein is used, after 40 cm with use of a vein in the rightantecubital fossa, after 50 cm with use of a vein in the left ante-cubital fossa, and after about 30 cm when a femoral vein is used.Increase in respiratory fluctuation confirms that the catheter tipis in the thorax. At this time, the balloon is inflated to the rec-ommended volume and the catheter advanced further. Thecatheter tip pressure is continuously recorded as the catheterproceeds from the right atrium into the right ventricle, pul-monary artery, and finally into a “wedge” position. At this point, the diameter of the balloon (11 or 13 mm) slightlyexceeds that of the pulmonary artery. In the “wedge” positionthe tip senses the pressure transmitted with some delay anddamping from the left atrium retrograde through the pulmonaryveins and capillaries. With deflation of the balloon, pulmonaryarterial pressure will reappear. Reinflation will cause the balloonto float into “wedge” position again.
As the catheter material (polyvinylchloride) softens with time,the transcardiac catheter loop tends to diminish, and this mayresult in migration of the catheter tip into smaller branches andinto “wedge” position. Continuous or frequent (every 15 to 30minutes) monitoring of pulmonary arterial pressure is, therefore,recommended. Inflation of the balloon to full capacity when thecatheter tip is in a small branch of the pulmonary artery willresult in a spuriously high pulmonary wedge pressure reading,caused by compression of the catheter lumen. Reinflation of theballoon should, therefore, be performed slowly, adding incre-ments of 0.1 to 0.2 ml air until a change in pressure contour frompulmonary arterial to pulmonary wedge pressure is seen. If thepulmonary wedge pressure is obtained at a volume substantivelyless than the recommended inflation volume, the cathetershould be gradually withdrawn (several cm) until the volumerequired for wedging is equal or nearly equal to the full inflationvolume. When the balloon is deflated, the ideal catheter posi-tion is with the tip in one of the primary branches of the pul-monary artery.
One of the most important applications of the balloon flotationcatheter is in the recording of the pulmonary capillary wedgepressure obtained when the inflated balloon impacts into aslightly smaller branch of the pulmonary artery. The pulmonary

MO
NIT
OR
IN
G C
EN
TR
AL
V
EN
OU
S P
RE
SS
UR
E
82
Physiologic Rationale (continued)
capillary wedge pressure is of great significance in clinical practice in that it provides information about two importantdeterminants of cardiopulmonary function. First, the level ofthis pressure is a basic factor in pulmonary congestion and in theshift of fluid from the pulmonary capillaries into the interstitialtissue and alveoli. Second, the pulmonary capillary wedge pressure closely reflects left atrial pressure and can, therefore,serve as an index of left ventricular filling pressure.
The mean pulmonary capillary wedge and left atrial pressuresclosely approximate left ventricular end-diastolic pressure inpatients who have normal left ventricular and mitral valve func-tion. In left ventricular failure, the elevated left ventricular end-diastolic pressure may significantly exceed the mean left atrialand accordingly, pulmonary capillary wedge pressure.Nevertheless, in clinical practice the mean pulmonary capillarywedge pressure has proved to be a reliable and useful index ofleft ventricular filling, and as such provides highly relevant information on the function of the left ventricle.
Since the pulmonary vasculature is a low-resistance circuit, thepulmonary arterial end-diastolic pressure is normally only slightlyhigher (1 to 3 mm Hg) than the mean pulmonary capillary wedgepressure and can, therefore, be used as an index of left ventricu-lar filling, when the pulmonary capillary wedge pressure is notobtainable. However, in states associated with high pulmonaryvascular resistance, the pulmonary arterial end-diastolic pressuremay markedly exceed the mean pulmonary capillary wedge pressure.* Associate Director, Cardiac Catheterization Laboratory, Cedars-Sinai Medical Center; AssistantProfessor of Medicine, UCLA.
** Research Scientist, Cedars-Sinai Medical Center, Los Angeles, and the Department ofMedicine, UCLA School of Medicine, Los Angeles, California.
Address reprint requests to Dr. Ganz: Division of Cardiology, Cedars-Sinai Medical Center, 4833Fountain Ave., Los Angeles, California 90029.
(Reproduced with permission from Buchbinder N, Ganz W: Hemodynamic Monitoring: InvasiveTechniques. Anesth 45:2,1976.
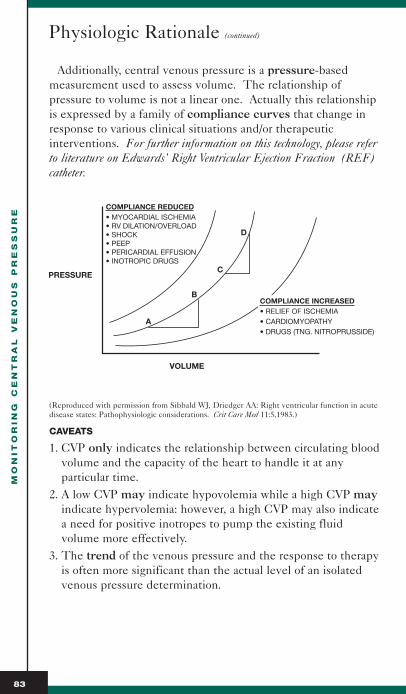
MO
NIT
OR
IN
G C
EN
TR
AL
V
EN
OU
S P
RE
SS
UR
E
83
Physiologic Rationale (continued)
Additionally, central venous pressure is a pressure-based measurement used to assess volume. The relationship of pressure to volume is not a linear one. Actually this relationshipis expressed by a family of compliance curves that change inresponse to various clinical situations and/or therapeutic interventions. For further information on this technology, please referto literature on Edwards’ Right Ventricular Ejection Fraction (REF)catheter.
(Reproduced with permission from Sibbald WJ, Driedger AA: Right ventricular function in acutedisease states: Pathophysiologic considerations. Crit Care Med 11:5,1983.)
CAVEATS
1. CVP only indicates the relationship between circulating bloodvolume and the capacity of the heart to handle it at any particular time.
2. A low CVP may indicate hypovolemia while a high CVP mayindicate hypervolemia: however, a high CVP may also indicatea need for positive inotropes to pump the existing fluid volume more effectively.
3. The trend of the venous pressure and the response to therapyis often more significant than the actual level of an isolatedvenous pressure determination.
D
C
B
A
VOLUME
PRESSURE
COMPLIANCE REDUCED• MYOCARDIAL ISCHEMIA• RV DILATION/OVERLOAD• SHOCK• PEEP• PERICARDIAL EFFUSION• INOTROPIC DRUGS
COMPLIANCE INCREASED• RELIEF OF ISCHEMIA• CARDIOMYOPATHY• DRUGS (TNG. NITROPRUSSIDE)

Physiologic Rationale (continued)
CVP Interpretation (CVP Range 2-6 mm Hg)
INCREASED CVP DECREASED CVP
Increased venous return from Decreased venous return conditions that cause hypervolemia and hypovolemia
Depressed cardiac function Loss of vascular tone caused by vasodilation (sepsis) which contributes to venous pooling and reduced blood return to the heart
Cardiac tamponade
Pulmonary hypertension
PEEP
Vasoconstriction
Clinical AssessmentVarious studies have documented that it is unreliable to assess
central venous pressure by clinical assessment alone. In 1983,Connors et al45 prospectively evaluated 62 right heart catheteriza-tions performed on critically ill patients with no evidence of arecent acute myocardial infarction to determine whether thehemodynamic measurements obtained could have been predict-ed by physical examination and review of the chest x-ray.Additionally, they looked at whether the procedure led tochanges in therapy. They found that estimates of the patient’shemodynamic status based on physical examination werefrequently in error and that catheterization often prompteda change in therapy.
Specifically, in each medical intensive care unit, a team ofphysicians consisting of an attending physician, a critical-carefellow, a third-year resident, an intern, and frequently afourth-year medical student determined the need for catheterization and the current therapy and formulated theoretical plans for therapy to be followed if catheterizationdata were not available. In 48.4% of all the cases studied,information obtained through catheterization prompted achange in therapy.
MO
NIT
OR
IN
G C
EN
TR
AL
V
EN
OU
S P
RE
SS
UR
E
84

MO
NIT
OR
IN
G C
EN
TR
AL
V
EN
OU
S P
RE
SS
UR
E
85
Clinical Assessment (continued)
(Reproduced with permission from Connors AF, McCaffree DR, Gray BA: Evaluation of Right-Heart Catheterization in the Critically Ill Patient without Myocardial Infarction. NE Jour Med 308:263-267,1983.)
Research RichesEisenberg et al examined 97 ICU patients to
determine the accuracy of clinical diagnosis compared to measurement by pulmonary artery catheterization.Clinical assessment correctly predicted right atrial pressureapproximately 50% of the time. Overall, planned therapywas altered by the information obtained from catheteriza-tion in 58% of all the cases. In 30%, a new (unanticipated)therapy was added after catheterization.46
Research RichesIn 1990, Cook examined 50 consecutive intensive care
patients with right internal jugular catheters. She alsofound considerable disagreement and inaccuracy in theclinical assessment of central venous pressure in criticallyill patients.47
Research RichesCook noted that the predictions of attending physicians
and critical care fellows were no more accurate than thoseof house staff and medical students. Cook also noted thatphysicians are better at identifying low CVP and moreaccurate when ventilated patients are excluded from the study.
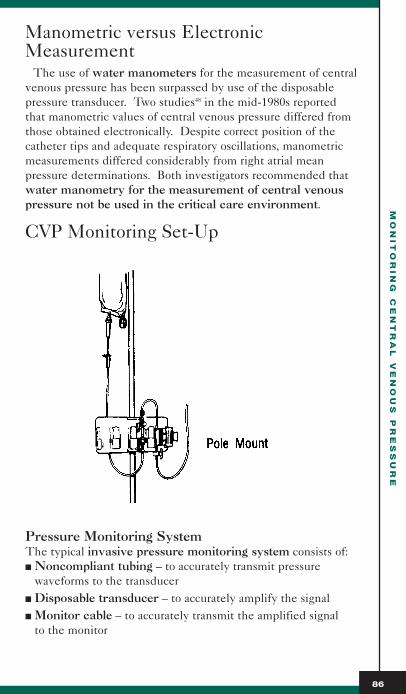
MO
NIT
OR
IN
G C
EN
TR
AL
V
EN
OU
S P
RE
SS
UR
E
86
Manometric versus ElectronicMeasurement
The use of water manometers for the measurement of centralvenous pressure has been surpassed by use of the disposablepressure transducer. Two studies48 in the mid-1980s reportedthat manometric values of central venous pressure differed fromthose obtained electronically. Despite correct position of thecatheter tips and adequate respiratory oscillations, manometricmeasurements differed considerably from right atrial mean pressure determinations. Both investigators recommended thatwater manometry for the measurement of central venouspressure not be used in the critical care environment.
CVP Monitoring Set-Up
Pressure Monitoring SystemThe typical invasive pressure monitoring system consists of:■ Noncompliant tubing – to accurately transmit pressure
waveforms to the transducer■ Disposable transducer – to accurately amplify the signal■ Monitor cable – to accurately transmit the amplified signal
to the monitor

CVP Monitoring Set-Up (continued)
Additional components include:■ Pressurized solution – pressurized to at least 300 mm Hg■ Integral flush device with a restrictor – to limit flow rate to
approximately 3 to 5mL/hr for adults■ Heparinized solution – 0.9% NS with Heparin 0.5-2 U/mL
CATHETER TUBING COMPONENT
This system, incorporating the catheter, tubing, and associated stopcocks, must be fluid-filled for the waveform tobe reproduced accurately. Fluid is essentially non-compressibleand allows the waveform signal to be transmitted across relatively long distances.
One factor likely to alter the waveform signal is the length of the tubing. The longer the tubing, the more likely thewaveform will be distorted. As a general rule, the tubingshould be kept as short as possible to obtain accurate waveforms.
The top trace represents a validarterial waveform.The bottom tracerepresents the samewaveform distortedby increased lengthof tubing.
Air bubbles arecompressible andwill, therefore, alsodistort the waveformsignal. Blood in thetubing will alsoabsorb more of thewaveform signalthan normal saline.
The top trace represents a validarterial waveform.The bottom tracerepresents the sametrace when distortedby an air bubble inthe line.
MO
NIT
OR
IN
G C
EN
TR
AL
V
EN
OU
S P
RE
SS
UR
E
87
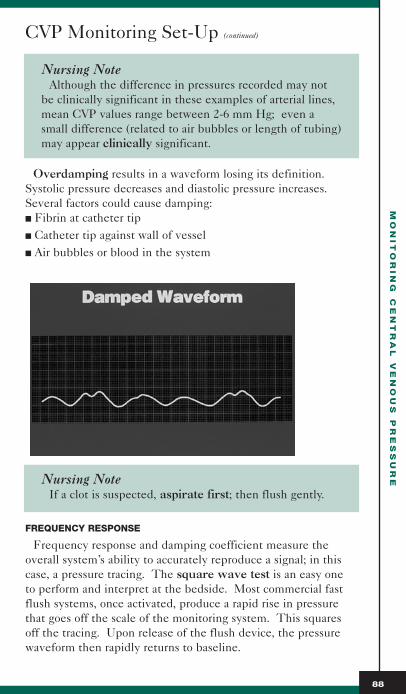
MO
NIT
OR
IN
G C
EN
TR
AL
V
EN
OU
S P
RE
SS
UR
E
88
CVP Monitoring Set-Up (continued)
Nursing NoteAlthough the difference in pressures recorded may not
be clinically significant in these examples of arterial lines,mean CVP values range between 2-6 mm Hg; even asmall difference (related to air bubbles or length of tubing)may appear clinically significant.
Overdamping results in a waveform losing its definition.Systolic pressure decreases and diastolic pressure increases.Several factors could cause damping:■ Fibrin at catheter tip■ Catheter tip against wall of vessel■ Air bubbles or blood in the system
Nursing NoteIf a clot is suspected, aspirate first; then flush gently.
FREQUENCY RESPONSE
Frequency response and damping coefficient measure theoverall system’s ability to accurately reproduce a signal; in thiscase, a pressure tracing. The square wave test is an easy one to perform and interpret at the bedside. Most commercial fastflush systems, once activated, produce a rapid rise in pressurethat goes off the scale of the monitoring system. This squaresoff the tracing. Upon release of the flush device, the pressurewaveform then rapidly returns to baseline.

MO
NIT
OR
IN
G C
EN
TR
AL
V
EN
OU
S P
RE
SS
UR
E
89
CVP Monitoring Set-Up (continued)
SQUARE WAVE TESTING
1. Activate snap or pull tab on flush device.2. Observe square wave generated on bedside monitor.3. Count oscillations after square wave. 4. Observe distance between the oscillations.
Optimally Damped: 1 - 2 oscillations before returning to tracing. Valuesobtained are accurate.
Underdamped: > 2 oscillations.Overestimated systolicpressure, diastolic pressuresmay be underestimated.
Overdamped: < 1 1/2 oscillations.Underestimation of systolicpressures, diastolic may notbe affected.
CALIBRATION
It is no longer important to calibrate the transducer, as the disposable transducer systems currently in use today have anaccuracy rate of 1-2%. If inaccuracy is suspected, the transducer is usually replaced after the monitoring cable hasbeen replaced and found not at fault.
ZERO REFERENCE
The accuracy of the CVP is determined, in part, by transducerplacement relative to an external reference point on the patient’sbody representing the location of the right atrium. Since itsidentification in 1945, the phlebostatic axis has been repeatedlyconfirmed as a valid external reference point for CVP, LAP andPAP measurements. It has been anatomically shown to be a trueexternal point for identifying the right atrium when the patientis supine.

MO
NIT
OR
IN
G C
EN
TR
AL
V
EN
OU
S P
RE
SS
UR
E
90
CVP Monitoring Set-Up (continued)
(Reproduced with permission from Woods SL, et. al.: CardiacNursing. J.B. Lippincott Co., Third Edition.)
The method tozero reference thepressure monitoringsystem requiresplacement of theair-fluid interfaceat the level of thephlebostatic axis.The stopcock located at the designated air-fluidinterface is thenopened to air, allowing for theinfluence of atmospheric
pressure to be eliminated. Usually, this stopcock is located atthe transducer but may be located anywhere within the lineitself. Once the leveling has been accomplished, the patientand transducer must remain in the same position. If thehead of the patient’s bed is elevated, then re-leveling needs tobe repeated in the new position.
(Reproduced with permission from Woods SL, et. al.: Cardiac Nursing. J.B. Lippincott Co., Third Edition.)

CVP Monitoring Set-Up (continued)
Practical PointThe only exception to re-zeroing with patient
movement is to mount the transducer on the patient.When patient-mounted, the transducer will not lose its relationship to the phlebostatic axis as long as themovement is in the same plane (i.e., the patient cannot be turned laterally).
Patient PositionThe literature suggest that accurate CVP measurements can
be obtained with the adult and pediatric patient in the supineposition in various degrees of backrest up to 30 degrees.Additionally, the effect of tilting on CVP measurement has been investigated and accuracy maintained with the use of thephlebostatic axis as the zero reference point.
Physiology FactActually, it is sometimes suggested that, in the assess-
ment of circulatory volume depletion, CVP should bemeasured with the patient at 45 degrees as measurementof CVP in the supine position may not detect or mayseverely underestimate circulatory volume depletion.49
The evidence supporting use of the phlebostatic axis to yieldaccurate CVP values in the lateral position is less clear. In the studies on pressure measurement in patients in the lateralposition, the phlebostatic axis yielded more reproducible valuesbetween the supine and lateral positions than other postulatedreference levels.
Potger and Elliott50 studied the lateral position when the trans-ducer was leveled at the supine phlebostatic axis and was not re-leveled when the patient was turned 30 degrees to the right orleft lateral position with the head of the bed elevated 20 degrees. Although there was no statistical significance, there were clinically significant changes. They suggested an alternative approach involving the identification of the transducer placement in the patient in the lateral position that yielded the same CVP reading as that obtained in thesupine position.
MO
NIT
OR
IN
G C
EN
TR
AL
V
EN
OU
S P
RE
SS
UR
E
91

MO
NIT
OR
IN
G C
EN
TR
AL
V
EN
OU
S P
RE
SS
UR
E
92
CVP Monitoring Set-Up (continued)
If there is any doubt about the CVP value obtained in the patient in the lateral position, the patient should bereturned to the supine position for re-measurement.
An interesting point to consider is the minimum stabilizationperiod after patient repositioning. Unfortunately, this has notbeen determined. However, it is prudent not to determine pressure measurements immediately after repositioning. Itshould also be remembered that, in elderly and critically illpatients, the change in position may have a greater contri-bution to variations in pressure than the position itself.
Port SiteMeasurement of CVP is usually performed through one of the
ports of a triple-lumen central venous catheter. In a study byScott et al,51 measurements of CVP in 48 adult intensive carepatients were obtained via each of the three ports of a triple-lumen CVC. Catheters were placed in either the right or leftsubclavian vein or the right or left internal jugular vein. Thedata showed significant differences across port sites. There were significant differences between the proximal and distalports and between the medial and distal ports. In some patients,the difference between CVP obtained from the distal port andpressure obtained from the proximal or the medial port couldhave been clinically significant. It would make sense toassure that CVP readings be standardized to a specific port to enhance validity of data and that the port utilized is documented in the clinical notes.
Respiratory InfluencesDuring spontaneous breathing, inspiration causes a decrease
in intrathoracic pressure that is transmitted in part to the rightatrium and produces a decline in CVP. The opposite is truewhen the patient is receiving mechanical ventilation. Most clinicians measure end-expiratory values for cardiac fillingpressures, because both pleural and pericardial pressuresapproach atmospheric pressure under these conditions, whetherthe patient is breathing spontaneously or receiving positive pressure mechanical ventilation. These pressure values can bedetermined by visual inspection of the CVP waveform on a calibrated monitor screen or digital printout.

MO
NIT
OR
IN
G C
EN
TR
AL
V
EN
OU
S P
RE
SS
UR
E
93
CVP Monitoring Set-Up (continued)
Physiology FactVentilatory support with positive pressure usually
elevates the central venous pressure only slightly (0-2 mm Hg). However, if more effective ventilation and oxygenation improve pump function, the CVP maydecrease as a result of the positive pressure ventilation.
PAP TO PAWP TRACING

MO
NIT
OR
IN
G C
EN
TR
AL
V
EN
OU
S P
RE
SS
UR
E
94
CVP Monitoring Set-Up (continued)
Infection Control for Pressure LinesIt is interesting to note that gram-negative microorganisms
account for the majority of catheter-related infections associatedwith the use of pressure monitoring systems. Apparently, such systems are considerably more vulnerable to becoming con-taminated during use. This may stem from the presence of astagnant column of fluid subjected to frequent manipulations.Studies suggest that if the infusion for hemodynamic monitoringis set up so that it flows continuously, it may not be necessary toroutinely change out at 24-48 hour intervals. With the use of dis-posable transducers, there appears to be no need to replacethe transducer and other components of the delivery systemmore frequently than every four days.
CDC Guideline (1996)■ Use disposable, rather than reusable, transducer
assemblies whenever possible.■ Replace disposable or reusable transducers at 96 hour
intervals. Replace other components of the system,including the tubing, continuous flush device, and flush solution, at the time the transducer is replaced.
■ Keep sterile all components of the pressure monitoringcircuit (including calibration devices and flush solution).
■ Minimize the number of manipulations and entries into the pressure monitoring system. Use a closed-flush (i.e., continuous flush), rather than an open system (i.e., onethan requires a syringe and stopcock), to maintain patency of the pressure monitoring catheters. If stopcocks are used, treat them as a sterile field, andcover them with a cap or syringe when not in use.
■ When the pressure monitoring system is accessedthrough a rubber diaphragm rather than a stopcock, wipethe diaphragm with appropriate antiseptic before access-ing the system.
■ Do not administer dextrose-containing solutions or parenteral nutrition fluids through the pressure monitoring circuit.
■ Do not routinely use pressure monitoring devices toobtain blood samples that do not require arterial blood.
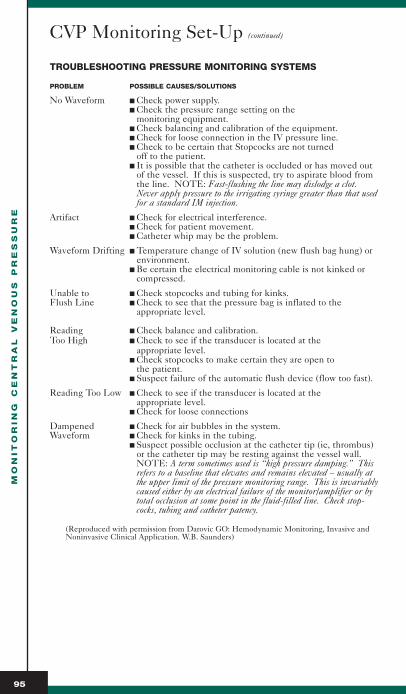
MO
NIT
OR
IN
G C
EN
TR
AL
V
EN
OU
S P
RE
SS
UR
E
95
CVP Monitoring Set-Up (continued)
TROUBLESHOOTING PRESSURE MONITORING SYSTEMS
PROBLEM POSSIBLE CAUSES/SOLUTIONS
No Waveform ■ Check power supply.■ Check the pressure range setting on the
monitoring equipment.■ Check balancing and calibration of the equipment.■ Check for loose connection in the IV pressure line.■ Check to be certain that Stopcocks are not turned
off to the patient.■ It is possible that the catheter is occluded or has moved out
of the vessel. If this is suspected, try to aspirate blood fromthe line. NOTE: Fast-flushing the line may dislodge a clot.Never apply pressure to the irrigating syringe greater than that usedfor a standard IM injection.
Artifact ■ Check for electrical interference.■ Check for patient movement.■ Catheter whip may be the problem.
Waveform Drifting ■ Temperature change of IV solution (new flush bag hung) orenvironment.
■ Be certain the electrical monitoring cable is not kinked orcompressed.
Unable to ■ Check stopcocks and tubing for kinks.Flush Line ■ Check to see that the pressure bag is inflated to the
appropriate level.
Reading ■ Check balance and calibration.Too High ■ Check to see if the transducer is located at the
appropriate level.■ Check stopcocks to make certain they are open to
the patient.■ Suspect failure of the automatic flush device (flow too fast).
Reading Too Low ■ Check to see if the transducer is located at the appropriate level.
■ Check for loose connections
Dampened ■ Check for air bubbles in the system.Waveform ■ Check for kinks in the tubing.
■ Suspect possible occlusion at the catheter tip (ie, thrombus)or the catheter tip may be resting against the vessel wall.NOTE: A term sometimes used is “high pressure damping.” Thisrefers to a baseline that elevates and remains elevated – usually atthe upper limit of the pressure monitoring range. This is invariablycaused either by an electrical failure of the monitor/amplifier or bytotal occlusion at some point in the fluid-filled line. Check stop-cocks, tubing and catheter patency.
(Reproduced with permission from Darovic GO: Hemodynamic Monitoring, Invasive andNoninvasive Clinical Application. W.B. Saunders)

Normal CVP WaveformWaveforms seen on the monitor merely reflect the intracardiac
events. The normal CVP waveform consists of three peaks (a, c and v waves) and two descents (x and y). The a waverepresents atrial contraction and follows the P wave on the EKGtrace. This is the atrial kick that loads the right ventricle justprior to contraction. As atrial pressure decreases, a c wave, resulting from closure of the tricuspid valve, may be seen. The x descent represents the continually decreasing atrial pressure. The v wave represents the atrial events during ventricular contraction – passive atrial filling – and follows the T wave on the EKG. When the atrial pressure is sufficient, the tricuspid valve opens, and the y descent occurs. Then thecycle repeats.
Accurate recognition of these waves requires that they bealigned with an EKG trace. As mechanical events follow electrical events, the waveforms can be identified by lining them up with the EKG events. Although the arterial pressure trace can be used for timing, this may be confusingdue to the time delay involved in transmitting the aortic pressure to the radial artery.
WA
VE
FO
RM
A
NA
LY
SIS
96
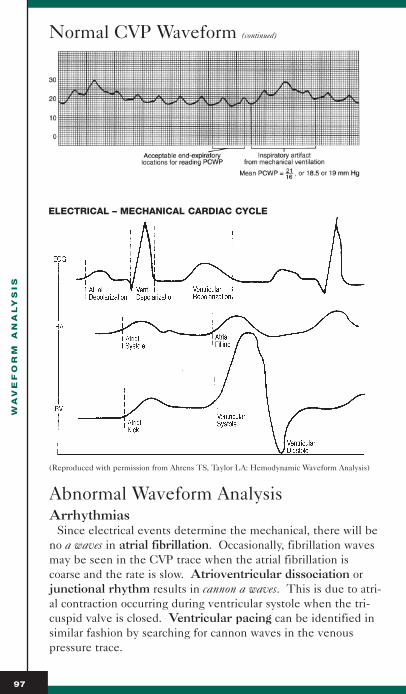
WA
VE
FO
RM
A
NA
LY
SIS
97
Normal CVP Waveform (continued)
(Reproduced with permission from Ahrens TS, Taylor LA: Hemodynamic Waveform Analysis)
Abnormal Waveform AnalysisArrhythmias
Since electrical events determine the mechanical, there will beno a waves in atrial fibrillation. Occasionally, fibrillation wavesmay be seen in the CVP trace when the atrial fibrillation iscoarse and the rate is slow. Atrioventricular dissociation orjunctional rhythm results in cannon a waves. This is due to atri-al contraction occurring during ventricular systole when the tri-cuspid valve is closed. Ventricular pacing can be identified insimilar fashion by searching for cannon waves in the venouspressure trace.
ELECTRICAL – MECHANICAL CARDIAC CYCLE
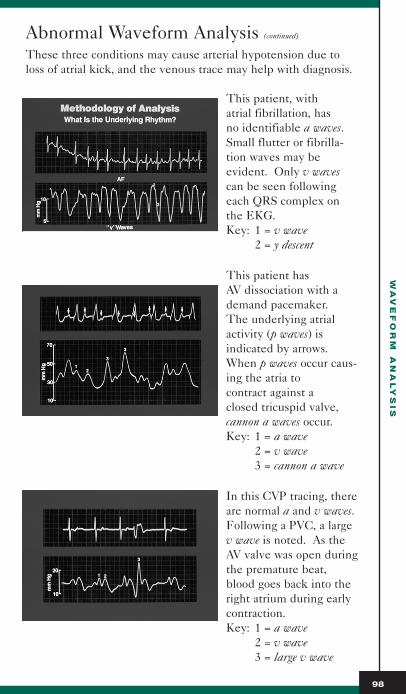
WA
VE
FO
RM
A
NA
LY
SIS
98
Abnormal Waveform Analysis (continued)
These three conditions may cause arterial hypotension due toloss of atrial kick, and the venous trace may help with diagnosis.
This patient, with atrial fibrillation, has no identifiable a waves.Small flutter or fibrilla-tion waves may be evident. Only v wavescan be seen followingeach QRS complex onthe EKG.Key: 1 = v wave
2 = y descent
This patient has AV dissociation with ademand pacemaker. The underlying atrialactivity (p waves) is indicated by arrows.When p waves occur caus-ing the atria to contract against a closed tricuspid valve,cannon a waves occur. Key: 1 = a wave
2 = v wave3 = cannon a wave
In this CVP tracing, thereare normal a and v waves.Following a PVC, a largev wave is noted. As theAV valve was open duringthe premature beat,blood goes back into theright atrium during earlycontraction.Key: 1 = a wave
2 = v wave3 = large v wave

WA
VE
FO
RM
A
NA
LY
SIS
99
Abnormal Waveform Analysis (continued)
Tricuspid Valve DiseaseTricuspid regurgitation produces giant v waves as abnormal
systolic filling of the right atrium through the incompetent valveoccurs during ventricular systole. Right ventricular end diastolicpressure is overestimated by the numeric readout on the bedsidemonitor that reports a single mean value for CVP. Reading thewaveform at the top of the a wave might prove a better indicatorof right ventricular filling.
In this CVP trace, botha and v waves are elevat-ed. However, the v waveis dominant and reflectstricuspid insufficiency. The elevated a wavedemonstrates a degree ofright ventricular failureas well.Key: 1 = a wave
2 = c wave3 = v wave
Tricuspid stenosis usually presents with an increased a wavethat represents the increased force of atrial contraction to pushblood across the stenotic valve. In this instance, CVP readingswill be falsely elevated. Right ventricular filling may actually bedecreased due to the valvular obstruction.
Right Ventricular InfarctionThis condition causes a disproportionate elevation of CVP
compared to PAWP. Often the CVP will exceed wedge pressureand display prominent a and v waves, the former suggesting atrial contraction into a stiff or incompletely relaxed right ventricle, and the latter suggesting tricuspid valve regurgitation,which is often associated with this condition.
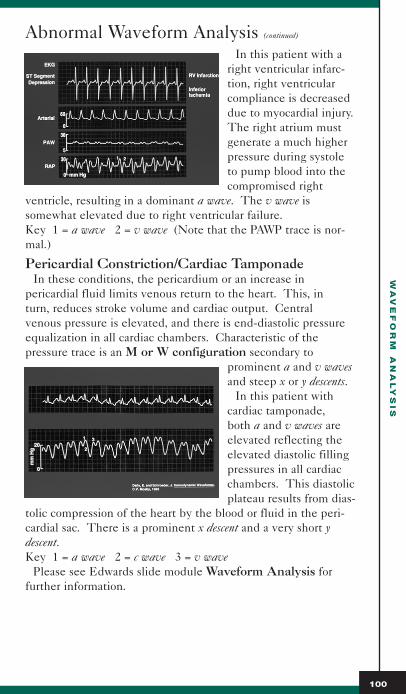
WA
VE
FO
RM
A
NA
LY
SIS
100
Abnormal Waveform Analysis (continued)
In this patient with aright ventricular infarc-tion, right ventricularcompliance is decreaseddue to myocardial injury.The right atrium mustgenerate a much higherpressure during systole to pump blood into thecompromised right
ventricle, resulting in a dominant a wave. The v wave is somewhat elevated due to right ventricular failure.Key 1 = a wave 2 = v wave (Note that the PAWP trace is nor-mal.)
Pericardial Constriction/Cardiac TamponadeIn these conditions, the pericardium or an increase in
pericardial fluid limits venous return to the heart. This, in turn, reduces stroke volume and cardiac output. Central venous pressure is elevated, and there is end-diastolic pressureequalization in all cardiac chambers. Characteristic of the pressure trace is an M or W configuration secondary to
prominent a and v wavesand steep x or y descents.
In this patient with cardiac tamponade, both a and v waves areelevated reflecting theelevated diastolic fillingpressures in all cardiacchambers. This diastolicplateau results from dias-
tolic compression of the heart by the blood or fluid in the peri-cardial sac. There is a prominent x descent and a very short ydescent.Key 1 = a wave 2 = c wave 3 = v wave
Please see Edwards slide module Waveform Analysis for further information.

Abnormal Waveform Analysis (continued)
Abnormal Waveform Chart
RIGHT ATRIAL WAVEFORMS
Decreased mean pressure- Hypovolemia- Transducer zero level too high
Elevated mean pressure- Fluid overload states- Right ventricular failure- Left ventricular failure causing right ventricular failure- Tricuspid stenosis or regurgitation- Pulmonic stenosis or regurgitation- Pulmonary hypertension
Elevated “a” wave: atrial systole, increased resistance to ventricular filling
- Tricuspid stenosis- Decreased right ventricular compliance- Right ventricular failure- Pulmonic stenosis- Pulmonary hypertension
Absent “a” wave- Atrial fibrillation- Atrial flutter- Junctional rhythms: cannon “a” waves
Elevated “v” wave: atrial filling, regurgitant flow- Tricuspid regurgitation- Functional regurgitation from right ventricular failure
Elevated “a” and “v” waves- Cardiac tamponade- Constrictive pericardial disease- Hypervolemia- Right ventricular failure
WA
VE
FO
RM
A
NA
LY
SIS
101

WA
VE
FO
RM
A
NA
LY
SIS
102
Abnormal Waveform Analysis (continued)
Abnormal Waveform Chart (continued)
RIGHT VENTRICULAR WAVEFORMS
Elevated systolic pressure- Pulmonary hypertension- Pulmonic valve stenosis- Factors that increase pulmonary vascular resistance
Decreased systolic pressure- Hypovolemia- Cardiogenic shock- Cardiac tamponade
Increased diastolic pressure- Hypervolemia- Congestive heart failure- Cardiac tamponade- Pericardial constriction
Decreased diastolic pressure- Hypovolemia
PULMONARY ARTERY WAVEFORMS
Elevated systolic pressure- Pulmonary disease- Increased pulmonary vascular resistance- Mitral stenosis or regurgitation- Left heart failure- Increased blood flow; left to right shunt
Reduced systolic pressure- Hypovolemia- Pulmonic stenosis- Tricuspid stenosis
WA
VE
FO
RM
A
NA
LY
SIS
103
Abnormal Waveform Analysis (continued)
CASE STUDY
Patient ProfileA 72-year-old male with a history of arteriosclerotic heart
disease and chronic obstructive lung disease was admitted to the intensive care unit following coronary artery bypass graftingof the left anterior descending and circumflex arteries. The following data are obtained four hours postoperatively:
B/P (S/D/M) 90/60/73 mm HgHR 100 bpmRAP/CVP 17 mm HgUrine Output 10 mL/hr
The patient is receiving Dopamine at 5 mcg/kg/min.
DiagnosisThe decreased blood pressure, elevated heart rate, and
decreased urinary output might point to pump failure. The high CVP seems to support this diagnosis. Remember the patient is already receiving inotropic support.
Does this patient have right heart failure secondary to hischronic lung disease and/or being on cardiopulmonary bypass?
AnalysisOne might think that the diagnosis of right heart failure is
justified based on these findings, and an increase in inotropicsupport might be indicated. However, what additional hemodynamic information can be gleaned from this patient?
The RAP/CVP waveform can be recorded and analyzed for any clues. The waveform is characterized by:■ Elevated mean pressure■ Prominent a and v waves■ Exaggerated x descent
This waveform is suggestive of cardiac tamponade – or a dryheart unable to fill secondary to compression.
If a pulmonary artery catheter were inserted, the followinghemodynamic data would be obtained:
CO 3.0 L/minCI 1.5 L/minPAWP 18 mm HgPAP 50/20 mm Hg

WA
VE
FO
RM
A
NA
LY
SIS
104
Abnormal Waveform Analysis (continued)
The elevated wedge pressure and decreased cardiac output areindicative of both heart failure (biventricular) and cardiac tam-ponade. However, whenever the PAWP and RAP equalize (dias-tolic plateau), cardiac tamponade should at least be suspected.
ResultsThe patient did indeed have cardiac tamponade and was
returned to the operating room for evacuation of a clot.
SummaryThe original treatment of increasing inotropic support would
not have been appropriate. The patient actually needed fluidadministration (contrary to what might be anticipated by theincreased CVP). Analysis of the right atrial waveform wouldhave provided increased impetus to obtain an echocardiogram for definitive diagnosis.
This is not an abstract scenario. Collier’s work on previouslyunrecognized cardiac tamponade secondary to central line placement should be reviewed. He stated that significant diagnostic clues might be:■ Worsening of hypotension after the administration of nitrates.
The nitrates reduce the venous return and worsen the physiology of cardiac tamponade; i.e., an already dry heart is now made drier.
■ Worsening of hypotension shortly after intubation. The negative intrathoracic pressure during normal respiration pullsblood back into the heart as a compensatory mechanism for thetamponade. Intubation converts this negative pressure to positive pressure. This dramatically reduces the venousreturn to the heart, and the cardiac output falls, usually leading to a precipitous drop in blood pressure.Waveform analysis to differentiate right ventricular
infarction, constrictive pericarditis and cardiac tamponadecan be very specific.

WA
VE
FO
RM
A
NA
LY
SIS
105
Abnormal Waveform Analysis (continued)
Additionally, the use of a right heart ejection fractioncatheter (RHEF) would have provided the following data:RVEF 50% normal range 30-40% contractility OKRVedv 60 mL normal range 100-160 mL hypovolemia
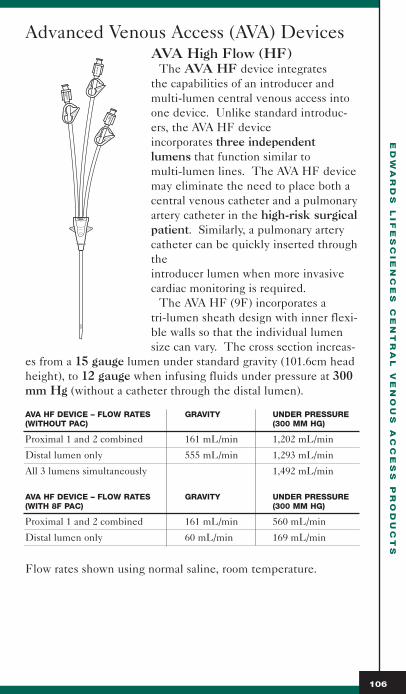
Advanced Venous Access (AVA) DevicesAVA High Flow (HF)
The AVA HF device integrates the capabilities of an introducer andmulti-lumen central venous access intoone device. Unlike standard introduc-ers, the AVA HF device incorporates three independentlumens that function similar to multi-lumen lines. The AVA HF devicemay eliminate the need to place both acentral venous catheter and a pulmonaryartery catheter in the high-risk surgicalpatient. Similarly, a pulmonary arterycatheter can be quickly inserted throughthe introducer lumen when more invasivecardiac monitoring is required.
The AVA HF (9F) incorporates a tri-lumen sheath design with inner flexi-ble walls so that the individual lumensize can vary. The cross section increas-
es from a 15 gauge lumen under standard gravity (101.6cm headheight), to 12 gauge when infusing fluids under pressure at 300mm Hg (without a catheter through the distal lumen).
AVA HF DEVICE – FLOW RATES GRAVITY UNDER PRESSURE(WITHOUT PAC) (300 MM HG)
Proximal 1 and 2 combined 161 mL/min 1,202 mL/min
Distal lumen only 555 mL/min 1,293 mL/min
All 3 lumens simultaneously 1,492 mL/min
AVA HF DEVICE – FLOW RATES GRAVITY UNDER PRESSURE(WITH 8F PAC) (300 MM HG)
Proximal 1 and 2 combined 161 mL/min 560 mL/min
Distal lumen only 60 mL/min 169 mL/min
Flow rates shown using normal saline, room temperature.
ED
WA
RD
S L
IF
ES
CIE
NC
ES
C
EN
TR
AL
V
EN
OU
S A
CC
ES
S P
RO
DU
CT
S
106
PR
OX
IMA
L1
15GA
PRO
XIMA
L215G
A
DIS
TA
L9F
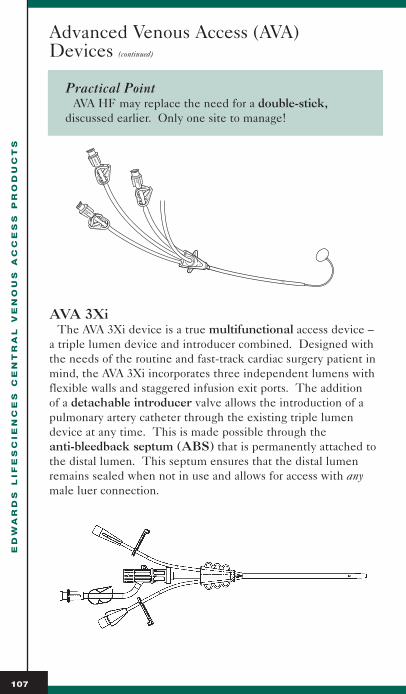
ED
WA
RD
S L
IF
ES
CIE
NC
ES
C
EN
TR
AL
V
EN
OU
S A
CC
ES
S P
RO
DU
CT
S
107
Advanced Venous Access (AVA) Devices (continued)
Practical PointAVA HF may replace the need for a double-stick,
discussed earlier. Only one site to manage!
AVA 3XiThe AVA 3Xi device is a true multifunctional access device –
a triple lumen device and introducer combined. Designed withthe needs of the routine and fast-track cardiac surgery patient inmind, the AVA 3Xi incorporates three independent lumens withflexible walls and staggered infusion exit ports. The addition of a detachable introducer valve allows the introduction of apulmonary artery catheter through the existing triple lumendevice at any time. This is made possible through the anti-bleedback septum (ABS) that is permanently attached tothe distal lumen. This septum ensures that the distal lumen remains sealed when not in use and allows for access with anymale luer connection.
ED
WA
RD
S L
IF
ES
CIE
NC
ES
C
EN
TR
AL
V
EN
OU
S A
CC
ES
S P
RO
DU
CT
S
108
Advanced Venous Access (AVA) Devices (continued)
FEATURE BENEFIT
Detachable introducer valve Provides flexibility for evolving central venous access requirements
Anti-bleedback septum Maintains hemostasis when not in use
Allows patient transfer to stepdown or telemetry unit when introducer isremoved
Compatible with any male luer connection (IV tubing, pressure tubing or syringe)
Locking contamination shield Secures PA catheter at both proximal and distal locations
Helpful HintsFlush all 3 lumens with heparinized saline pior to inser-
tion. Be sure that the introducer is attached to the anti-bleedback septum on the distal lumen beforeinserting dilator. (Do not insert dilator directly into anti-bleedback septum.)
To ensure proper attachment to introducer valve or anymale luer to the ABS, follow these steps.
1. Align desired male luer with ABS2. Push male luer into ABS (straight - not at an angle).3. Rotate male luer device clockwise to tighten.4. Ensure that connection is secure.
Insert the pulmonary artery catheter at least 25 cm beforeinflating the balloon to be sure that the PAC has exited thetip of the introducer sheath.
Do not pierce anti-bleedback septum with a needle. Usea luer syringe to attach directly to the anti-bleedback septum.
Draw blood samples from the distal lumen.
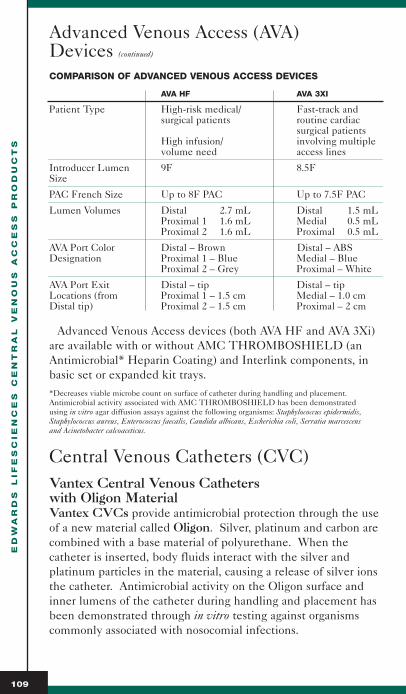
ED
WA
RD
S L
IF
ES
CIE
NC
ES
C
EN
TR
AL
V
EN
OU
S A
CC
ES
S P
RO
DU
CT
S
109
Advanced Venous Access (AVA) Devices (continued)
COMPARISON OF ADVANCED VENOUS ACCESS DEVICES
AVA HF AVA 3XI
Patient Type High-risk medical/ Fast-track and surgical patients routine cardiac
surgical patients High infusion/ involving multiple volume need access lines
Introducer Lumen 9F 8.5FSize
PAC French Size Up to 8F PAC Up to 7.5F PAC
Lumen Volumes Distal 2.7 mL Distal 1.5 mLProximal 1 1.6 mL Medial 0.5 mLProximal 2 1.6 mL Proximal 0.5 mL
AVA Port Color Distal – Brown Distal – ABSDesignation Proximal 1 – Blue Medial – Blue
Proximal 2 – Grey Proximal – White
AVA Port Exit Distal – tip Distal – tipLocations (from Proximal 1 – 1.5 cm Medial – 1.0 cmDistal tip) Proximal 2 – 1.5 cm Proximal – 2 cm
Advanced Venous Access devices (both AVA HF and AVA 3Xi)are available with or without AMC THROMBOSHIELD (anAntimicrobial* Heparin Coating) and Interlink components, inbasic set or expanded kit trays.*Decreases viable microbe count on surface of catheter during handling and placement.Antimicrobial activity associated with AMC THROMBOSHIELD has been demonstrated using in vitro agar diffusion assays against the following organisms: Staphylococcus epidermidis,Staphylococcus aureus, Enterococcus faecalis, Candida albicans, Escherichia coli, Serratia marcescens and Acinetobacter calcoaceticus.
Central Venous Catheters (CVC)Vantex Central Venous Catheters with Oligon MaterialVantex CVCs provide antimicrobial protection through the useof a new material called Oligon. Silver, platinum and carbon arecombined with a base material of polyurethane. When thecatheter is inserted, body fluids interact with the silver and platinum particles in the material, causing a release of silver ionsthe catheter. Antimicrobial activity on the Oligon surface andinner lumens of the catheter during handling and placement hasbeen demonstrated through in vitro testing against organismscommonly associated with nosocomial infections.

ED
WA
RD
S L
IF
ES
CIE
NC
ES
C
EN
TR
AL
V
EN
OU
S A
CC
ES
S P
RO
DU
CT
S
110
Central Venous Catheters (CVC) (continued)
The activity ofthe antimicrobial agents is localized at thecatheter surfaces and is not intended for treatment of systemicinfections.
In vitro testing demonstrated that the Oligon material provided broad spectrum effectiveness (≥ 3 log reduction frominitial concentration within 48 hours) against the organisms tested: Staphylococcus aureus, Staphylococcus epidermidis, Klebsiellapneumoniae, Enterococcus faecalis, Candida albicans, Escherichia coli,Serratia marcescens, Acinetobacter calcoaceticus, Corynebacteriumdiptheriae, Enterobacter aerogenes, GMRSa, and Pseudomonas aeruginosa. The impact of Oligon material on infection rates has not been demonstrated.
DOUBLE LUMENAvailable as catheter only, basic sets and expanded kit trays, with and without heparin coating, Interlink:
SIZE GAUGE LENGTH
7F 16/16 16 cm
7F 16/16 20 cm
8.5F 14/15 16 cm
8.5F 14/15 20 cm
TRIPLE LUMENAvailable as catheter only, basic sets and expanded kit trays, with and without heparin coating, Interlink:
SIZE GAUGE LENGTH
7F 18/18/16 16 cm
7F 18/18/16 20 cm
15

ED
WA
RD
S L
IF
ES
CIE
NC
ES
C
EN
TR
AL
V
EN
OU
S A
CC
ES
S P
RO
DU
CT
S
111
Central Venous Catheters (CVC) (continued)
QUAD LUMENAvailable as catheter only, basic sets and expanded kit trays, with and without heparin coating, Interlink:
SIZE GAUGE LENGTH
8.5F 15/18/18/18 16 cm
8.5F 15/18/18/18 20 cm
Commercial Comment Since Edwards’ Vantex CVC with Oligon material does
not contain chlorhexidine, the potential risk associatedwith chlorhexidine is avoided.
VANTEX CVC WITH OLIGON MATERIAL – AVERAGE FLOW RATES IN ML/HR
16CM LONG 20CM LONG GAUGE 7F DOUBLE LUMEN CATHETER CATHETER SIZE
Distal 3,781 3,481 16
Proximal 3,601 3,416 16
7F TRIPLE LUMEN
Distal 3,593 3,535 16
Medial 1,569 1,488 18
Proximal 1,754 1,628 18
8.5F DOUBLE LUMEN
Distal 6,190 5,900 14
Proximal 4,964 4,594 15
8.5F QUAD LUMEN
Distal 4,990 4,732 15
Medial 1 1,544 1,394 18
Medial 2 1,640 1,442 18
Proximal 1,784 1,566 18
Flow rates shown using normal saline, room temperature, at 40"(101.6cm) head height

Central Venous Catheters (CVC) (continued)
VANTEX CVC WITH OLIGON MATERIAL – AVERAGE LUMEN VOLUME (ML)
7F DOUBLE LUMEN 16CM 20CM
Distal 0.59 0.65
Proximal 0.61 0.66
7F TRIPLE LUMEN
Distal 0.52 0.63
Medial 0.45 0.52
Proximal 0.48 0.53
8.5F DOUBLE LUMEN
Distal 0.72 0.80
Proximal 0.71 0.78
8.5F QUAD LUMEN
Distal 0.64 0.71
Medial 1 0.28 0.30
Medial 2 0.29 0.31
Proximal 0.31 0.33
Multi-Med Central Venous Catheters
Multi-Med “High-Flow” Central Venous Catheters (CVCs) are constructed of soft polyurethane with a soft tip.Polyurethane material contributes to excellent handling, flexibility and kink-resistance. The Multi-Med CVC featuresoptimized lumen and backform design, providing optimal flowcharacteristics, up to 50% faster than standard CVCs. EdwardsCVCs are either 16cm or 20cm long to prevent the complicationsassociated with over-insertion of the catheter, (i.e., perforationand cardiac tamponade.)
ED
WA
RD
S L
IF
ES
CIE
NC
ES
C
EN
TR
AL
V
EN
OU
S A
CC
ES
S P
RO
DU
CT
S
112
EdwardsMULTI-MED
7F 20cm
15
MEDIAL/2cm
18 GA.
DASTAL 16 GA
PROXIMAL/5 CM 18 GA

ED
WA
RD
S L
IF
ES
CIE
NC
ES
C
EN
TR
AL
V
EN
OU
S A
CC
ES
S P
RO
DU
CT
S
113
Central Venous Catheters (CVC) (continued)
SINGLE-LUMENAvailable as catheter only, basic sets, and expanded kit trays, with and without AMC THROMBOSHIELD, Interlink:
SIZE GAUGE LENGTH
3F 20 13 cm
5F 16 20 cm
6F 14 20 cm
DOUBLE LUMENAvailable as catheter only, basic sets, and expanded kit trays, with and without AMC THROMBOSHIELD, Interlink:
SIZE GAUGE LENGTH
7F 16/16 16 cm
7F 16/16 20 cm
8.5F 14/15 16 cm
8.5F 14/15 20 cm
TRIPLE LUMENAvailable as catheter only, basic sets, and expanded kit trays, with and without AMC THROMBOSHIELD, Interlink:
SIZE GAUGE LENGTH
7F 16/18/18 16 cm
7F 16/18/18 20 cm
QUAD LUMENAvailable as catheter only, basic sets, and expanded kit trays, with and without AMC THROMBOSHIELD, Interlink:
SIZE GAUGE LENGTH
8.5F 15/18/18/18 16 cm
8.5F 15/18/18/18 20 cm

ED
WA
RD
S L
IF
ES
CIE
NC
ES
C
EN
TR
AL
V
EN
OU
S A
CC
ES
S P
RO
DU
CT
S
114
Central Venous Catheters (CVC) (continued)
AMC THROMBOSHIELD is a proprietary antimicrobialheparin coating that is coated on both the inner and outer surfaces of the catheter. Decreased antimicrobial activity associ-ated with AMC THROMBOSHIELD has been demonstratedusing in vitro agar diffusion assays against the following organ-isms: Staphylococcus epidermidis, Staphylococcus aureus, Enterococcus faecalis, Candida albicans, Escherichia coli, Serratia marcescens, andAcinetobacter calcoaceticus. AMC THROMBOSHIELD decreasesviable microbe count on surface of catheter during handling andplacement.
MULTI-MED CVC – AVERAGE FLOW RATES IN ML/HR
16CM LONG 20CM LONG GAUGE SIZESINGLE-LUMEN CATHETER CATHETER
1,362 20
3,483 16
6,210 14
7F DOUBLE LUMEN
Distal 3,608 3,292 16
Proximal 3,620 3,200 16
7F TRIPLE LUMEN
Distal 3,510 3,160 16
Medial 1,500 1,300 18
Proximal 1,670 1,420 18
8.5F DOUBLE LUMEN
Distal 6,126 5,886 14
Proximal 5,130 4,716 15
8.5F QUAD LUMEN
Distal 4,812 4,564 15
Medial 1 1,538 1,349 18
Medial 2 1,623 1,412 18
Proximal 1,741 1,471 18
Flow rates shown using normal saline, room temperature, at 40"(101.6cm) head height.

ED
WA
RD
S L
IF
ES
CIE
NC
ES
C
EN
TR
AL
V
EN
OU
S A
CC
ES
S P
RO
DU
CT
S
115
Central Venous Catheters (CVC) (continued)
MULTI-MED CVC – AVERAGE LUMEN VOLUMES (ML)
SINGLE-LUMEN 16CM 20CM
20ga — 0.41
16ga — 0.25
14ga — 0.09
7F DOUBLE LUMEN
Distal 0.57 0.62
Proximal 0.59 0.62
7F TRIPLE LUMEN
Distal 0.56 0.60
Medial 0.45 0.47
Proximal 0.47 0.52
8.5F DOUBLE LUMEN
Distal 0.73 0.80
Proximal 0.71 0.78
8.5F QUAD LUMEN
Distal 0.65 0.69
Medial 1 0.29 0.30
Medial 2 0.30 0.30
Proximal 0.31 0.32
Markings on the catheter body of Edwards Lifesciences’ CVCs (except for the single-lumen) are calibrated in 1cm intervals, starting at 10cm. The 15cm depth is clearlymarked. Guidewires are also marked at 10, 20 and 30cmdepths. These markings aid the clinician in correctly assessingthe amount of catheter or guidewire inserted. Catheter depthshould be routinely documented in the insertion and clinical notes.
PORT COLOR DESIGNATION
PORT DOUBLE TRIPLE QUAD AVA HF AVA 3XI
Proximal (1) white white white gray white
Proximal (2) blue
Medial (1) blue blue blue blue
Medial (2) gray
Distal brown brown brown brown brown

ED
WA
RD
S L
IF
ES
CIE
NC
ES
C
EN
TR
AL
V
EN
OU
S A
CC
ES
S P
RO
DU
CT
S
Central Venous Catheters (CVC) (continued)
Practical PointWith Edwards’ devices, the distal lumen is always the
largest. Look at the hub to see both catheter gauge anddistance of lumen from tip.
SUTURE LOOP/BOX CLAMP
If desired, the optional suture loop/box clamp can be placed onthe catheter and sutured to the skin.■ Place the optional suture loop onto the catheter by spreading
the suture loop wings and pressing onto the catheter. (See Figure 1)
■ Snap the box clamp over the optional suture loop to secureboth components to the catheter. (See Figure 2)
■ Suture the optional suture loop and box clamp together to thepatient to prevent catheter migration. (See Figure 3)Precaution: The box clamp must be removed from the
catheter before attempting guidewire passage prior tocatheter exchange.
116
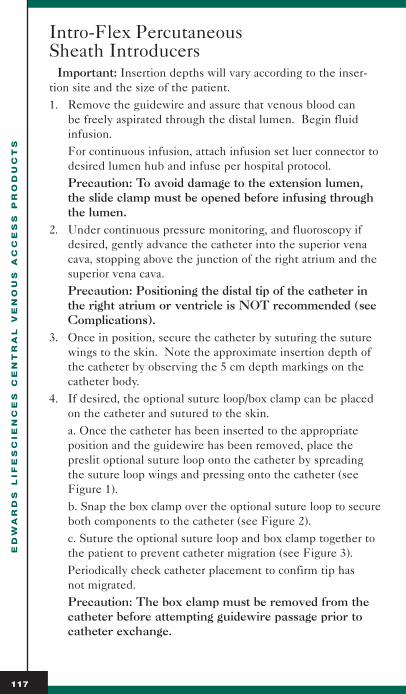
ED
WA
RD
S L
IF
ES
CIE
NC
ES
C
EN
TR
AL
V
EN
OU
S A
CC
ES
S P
RO
DU
CT
S
117
Intro-Flex Percutaneous Sheath Introducers
Important: Insertion depths will vary according to the inser-tion site and the size of the patient.1. Remove the guidewire and assure that venous blood can
be freely aspirated through the distal lumen. Begin fluid infusion.For continuous infusion, attach infusion set luer connector todesired lumen hub and infuse per hospital protocol.Precaution: To avoid damage to the extension lumen, the slide clamp must be opened before infusing throughthe lumen.
2. Under continuous pressure monitoring, and fluoroscopy ifdesired, gently advance the catheter into the superior venacava, stopping above the junction of the right atrium and thesuperior vena cava.Precaution: Positioning the distal tip of the catheter inthe right atrium or ventricle is NOT recommended (seeComplications).
3. Once in position, secure the catheter by suturing the suturewings to the skin. Note the approximate insertion depth ofthe catheter by observing the 5 cm depth markings on thecatheter body.
4. If desired, the optional suture loop/box clamp can be placedon the catheter and sutured to the skin.a. Once the catheter has been inserted to the appropriateposition and the guidewire has been removed, place thepreslit optional suture loop onto the catheter by spreadingthe suture loop wings and pressing onto the catheter (seeFigure 1).b. Snap the box clamp over the optional suture loop to secureboth components to the catheter (see Figure 2).c. Suture the optional suture loop and box clamp together tothe patient to prevent catheter migration (see Figure 3).Periodically check catheter placement to confirm tip has not migrated.Precaution: The box clamp must be removed from thecatheter before attempting guidewire passage prior tocatheter exchange.

ED
WA
RD
S L
IF
ES
CIE
NC
ES
C
EN
TR
AL
V
EN
OU
S A
CC
ES
S P
RO
DU
CT
S
118
Intro-Flex Percutaneous Sheath Introducers (continued)
5. Verify catheter tip position in the superior vena cava by chestX-ray film immediately after insertion.Note: The chest X-ray film should confirm that the cathetertip is in the superior vena cava, above the superior vena cavaand right atrial junction, with the catheter tip parallel to thevessel wall (Refs. 8, 11 & 16).
MAINTENANCE AND USE IN SITU
1. Adequate maintenance is required to avoid catheter occlu-sion. Keep pressure monitoring and infusion lumens patentby intermittent flush, continuous, slow infusion withheparinized saline solution, or use of a heparin lock using theprovided injection caps or Interlink injection sites in con-junction with heparinized saline solution (Ref. 20).
To use injection caps:a. Disinfect injection caps before entry with syringe needle(see Complications).b. Use a small bore needle (22 gauge or smaller) to punctureand inject through the injection caps.
To use Interlink injection sites:a. Ensure that the injection sites are securely connected tothe lumen hubs.b. Grasp finger flange to stabilize injection site (Figure 4).c. Swab septum with preferred antiseptic.d. Insert Interlink cannula, attach to an appropriate devicedirectly through the center of the septum.Precaution: If a conventional needle must be used,insert a small gauge needle into the perimeter of the sep-tum to avoid fluid leakage while the needle is in place.e. Engage locking features if applicable.
2. For blood sampling, attach blood sampling device to desiredlumen hub and draw blood sample per hospital protocol.

ED
WA
RD
S L
IF
ES
CIE
NC
ES
C
EN
TR
AL
V
EN
OU
S A
CC
ES
S P
RO
DU
CT
S
119
Intro-Flex Percutaneous Sheath Introducers (continued)
Intro-Flex Percutaneous Sheath Introducers feature the following design characteristics:
■ High infusion capability■ Tapered tip to dilator interface■ Choice of hemostasis valves■ V-shaped sidearm■ Optional infusion catheter with lock-in adapter■ Optional obturator - short or long versions■ Optional locking contamination shield
The Intro-Flex introducers are available with two valveoptions, either in an Automatic hemostasis valve, orAdjustable hemostasis valve that accommodates varyingcatheter sizes and helps prevent catheter migration. The v-shaped sidearm permits unobstructed path for fluid delivery,with or without a catheter in place. AMC THROMBOSHIELDcoating is available on selected models.
A single-lumen infusion catheter is available for use with theIntro-Flex introducers to be placed through the hemostasis valve(after swabbing the valve with Betadine) to convert to a doublelumen access. It has a lock-in adapter to safely secure the fitting between introducer and infusion catheter. The infusioncatheter extends beyond the sheath to allow unobstructed fluidflow. An obturator is available to safely occlude the lumen aswell as to prevent air entry when the catheter is not in use. The obturator is available in a short (cap) version or long 13cmoption.
INTRO-FLEX PERCUTANEOUS SHEATH INTRODUCERS
FRENCH SIZE CATHETER SIZEINTRODUCER (INFUSION CATHETER) PAC SIZE
5F 4F
6F 5F 5F
7F 5F 6F
8F 7F 7F
8.5F 7F 7F - 7.5F
9F 7F 7.5F - 8F

CD
C G
UID
EL
IN
E
120
CDC Guideline for the Prevention ofIntravascular Device-Related Infections(1996) Central Venous CathetersINSERTION
■ Use a single-lumen central venous catheter, unless multipleports are essential for the management of the patient.
■ In adults, consider use of a silver-impregnated collagen cuff or an antimicrobial- or antiseptic-impregnated central venouscatheter if, after full adherence to other catheter infection control measures (e.g., maximal barrier precautions), there isstill an unacceptably high rate of infection.
■ Weigh the risk and benefits of placing a device at a recommended site to reduce infectious complications against the risk of mechanical complications (e.g., pneumotho-rax, subclavian artery puncture, subclavian vein laceration, hemothorax, thrombosis, air embolism, catheter misplacement).
■ Use subclavian, rather than jugular or femoral, sites for centralvenous catheter placement unless medically contraindicated(e.g., coagulopathy, anatomic deformity).
■ Use sterile technique, including a sterile gown and gloves, a mask, and a large sterile drape (i.e., maximal barrier precautions), for the insertion of central venous and arterialcatheters. Use these precautions even if the catheter is inserted in the operating room.
■ Wear non-latex or latex gloves when inserting an intravasculardevice as required by the Occupational Safety and HealthAdministration (OSHA) Bloodborne Pathogens Standard.
■ Cleanse the skin site with an appropriate antiseptic, including70% alcohol, 10% povidone-iodine, or 2% tincture of iodine,before catheter insertion. Allow the antiseptic to remain onthe insertion site for an appropriate length of time beforeinserting the catheter.
■ When tincture of iodine is used for skin antisepsis beforecatheter insertion, it should be removed with alcohol.
■ Do not palpate the insertion site after the skin has beencleansed with antiseptic (this does not apply to maximum barrier precautions during which the operator is working in a sterile field).
CD
C G
UID
EL
IN
E
121
CDC Guideline for the Prevention ofIntravascular Device-Related Infections(1996) Central Venous Catheters (continued)
■ Do not routinely replace non-tunneled central venouscatheters as a method to prevent catheter-related infections.
■ Record the date and time of catheter insertion in an obviouslocation near the catheter-insertion site (e.g., on the dressing or on the bed).
GUIDEWIRE EXCHANGE
■ Use guidewire assisted catheter exchange to replace a malfunctioning catheter or to convert an existing catheter ifthere is no evidence of infection at the catheter site.
■ If catheter-related infection is suspected, but there is no evidence of local catheter-related infection (e.g., purulentdrainage, erythema, tenderness), remove the existing catheterand insert a new catheter over a guidewire. Send the removedcatheter for semiquantitative or quantitative culture. Leavethe newly inserted catheter in place if the catheter cultureresult is negative. If the catheter culture indicates colonizationor infection, remove the newly inserted catheter, and insert anew catheter at a different site.
■ Do not use guidewire assisted catheter exchange whenevercatheter-related infection is documented. If the patientrequires continued vascular access, remove the implicatedcatheter and replace it with another catheter at a differentinsertion site.
IV INFUSION
■ In general, administration sets include the area from the spikeof tubing entering the fluid container to the hub of the vascu-lar device. However, a short extension tube may be connected to the vascular device and may be considered a portion of the device to facilitate aseptic technique when changing administration sets. Replace extension tubing when the vascular device is replaced.
■ Wipe the catheter hub with an appropriate antiseptic beforeaccessing the system.
■ Replace extension tubing when the vascular device is replaced.■ Replace IV tubing, including piggyback tubing and stopcocks,
no more frequently than at 72-hour intervals, unless clinicallyindicated.

CDC Guideline for the Prevention ofIntravascular Device-Related Infections(1996) Central Venous Catheters (continued)
■ Replace tubing used to administer blood, blood products, orlipid emulsions within 24 hours of initiating the infusion.
■ Clean injection ports with 70% alcohol or povidone-iodinebefore accessing the system.
■ Do not use filters routinely for infection control purposes.
TPN
■ Do not use single-lumen parenteral nutrition catheters for purposes other than hyperalimentation (e.g., administration offluids, blood, or blood products).
■ If a multi-lumen catheter is used to administer parenteral nutrition, designate one port for hyperalimentation. Do notuse the designated hyperalimentation port for other purposes(e.g., administration of fluids, blood, or blood products).
■ Complete infusions of lipid-containing parenteral nutrition fluids (e.g., 3-in-1 solutions) within 24 hours of hanging the fluid.
■ When lipid emulsions are given alone, complete the infusionwithin 12 hours of hanging the emulsion.
SITE CARE
■ Wash hands before and after palpating, inserting, replacing, ordressing any intravascular device.
■ Wear non-latex or latex gloves when changing the dressings onintravascular devices.
■ Palpate the catheter insertion site for tenderness daily throughthe intact dressing.
■ Visually inspect the catheter site if the patient has develop-ment of tenderness at the insertion site, fever without obvioussource, or symptoms of local or bloodstream infection.
■ In patients who have large, bulky dressings that prevent palpation or direct visualization of the catheter insertion site,remove the dressing, visually inspect the catheter site at leastdaily, and apply a new dressing.
■ Use either a sterile gauze or transparent dressing to cover thecatheter site.
CD
C G
UID
EL
IN
E
122

CD
C G
UID
EL
IN
E
123
CDC Guideline for the Prevention ofIntravascular Device-Related Infections(1996) Central Venous Catheters (continued)
■ Replace catheter site dressings when the device is removed orreplaced, or when the dressing becomes damp, loosened, orsoiled. Change dressings more frequently in diaphoreticpatients.
■ Avoid touch contamination of the catheter insertion site whenthe dressing is replaced.
■ Do not routinely apply antimicrobial ointment to centralvenous catheter insertion sites.
■ Do not apply organic solvents (e.g., acetone or ether) to theskin before insertion of parenteral nutrition catheters.
■ Replace catheter site dressings when the device is replaced,when the dressing becomes damp, loosened, or soiled, or wheninspection of the site is necessary.
PRESSURE MONITORING SYSTEMS
■ Use disposable rather than reusable transducer assemblieswhenever possible.
■ Replace disposable or reusable transducers at 96-hour intervals. Replace other components of the system, includingthe tubing, continuous flush device, and flush solution, at thetime the transducer is replaced.
■ Keep sterile all components of the pressure monitoring circuit(including calibration devices and flush solution).
■ Minimize the number of manipulations and entries into the pressure monitoring system. Use a closed-flush (i.e., continuous flush), rather than an open system (i.e., one thanrequires a syringe and stopcock), to maintain patency of thepressure monitoring catheters. If stopcocks are used, treatthem as a sterile field, and cover them with a cap or syringewhen not in use.
■ When the pressure monitoring system is accessed through arubber diaphragm rather than a stopcock, wipe the diaphragmwith appropriate antiseptic before accessing the system.
■ Do not administer dextrose-containing solutions or parenteralnutrition fluids through the pressure monitoring circuit.
■ Do not routinely use pressure monitoring devices to obtainblood samples that do not require arterial blood.
CDC Guideline for the Prevention ofIntravascular Device-Related Infections(1996) Central Venous Catheters (continued)
MISCELLANEOUS
■ Conduct ongoing education and training of health care workersregarding indications for the use of and procedures for the insertion and maintenance of intravascular devices and appropriate infection control measures to prevent intravasculardevice-related infections. Audiovisuals can serve as a usefuladjunct to standard educational efforts.
■ Designate trained personnel for the insertion and maintenanceof intravascular devices.
NO RECOMMENDATION
■ For the use of sterile versus non-sterile clean gloves duringdressing changes.
■ For removal of central catheters inserted under emergency conditions, where breaks in aseptic technique are likely to have occurred.
■ For obtaining blood samples for culture through central venousor central arterial lines.
■ For the frequency of routine replacement of dressings used oncentral catheter sites.
■ For frequency of replacement IV tubing used for intermittentinfusions.
■ For the hang time of IV fluids, including non-lipid containingparenteral nutrition fluids.
■ For use, maintenance, or frequency of replacement of needleless IV devices.
These are selected guidelines only.
CD
C G
UID
EL
IN
E
124

CD
C G
UID
EL
IN
E
125
References1. McGee WT, Ackerman BL, Rouben LR, et al: Accurate placement of central
venous catheters: a prospective, randomized, multi-center trial. Crit Care Med21(8):1118-1123, 1993.
2. Collier PE, Blocker SH, Graff DM, et al: Cardiac tamponade from central venous catheters. Am J Surg 176:212-214, 1998.
3. Appelgren P, Ransjo U, Bindslev L, et al: Surface heparinization of central venous catheters reduces microbial colonization in vitro and in vivo: results from a prospective, randomized trial. Crit Care Med 24(9);1482-1489, 1996.
Tebbs SE, Elliott TSJ: A novel antimicrobial central venous catheter impregnated with benzalkonium chloride. Journal of Antimicrobial Chemotherapy31: 261-271, 1993.
4. Hall RE, Bender G, Marquis RE: Inhibitory and cidal antimicrobial actions ofelectrically generated silver ions. J Oral Maxillofac Surg 45(a):779-84, 1987.
Russell ED, Hugo WB: Antimicrobial activity and action of silver. Progress inMedicinal Chem 31:351-70, 1994.
5. Elliott TSJ, Tebbs SE: Prevention of central venous catheter-related infection. J Hosp Infect 40:193-201, 1998.
Stickle BR, McFarlane H: Prediction of a small internal jugular vein by external jugular vein diameter. Anesth 52:220-222, 1997.
6. Boyd R, Saxe A, Phillips E: Effect of patient position upon success in placingcentral venous catheters. Am J Surg 172(4):380-382, 1996.
Bernard RW, Stahl WM: Subclavian vein catheterization: a prospective study. I. Non-infective complications. Ann Surg 173(2):184-190,1971.
7. Collier PE, Blocker SH, Graff DM et al: Cardiac tamponade from centralvenous catheters. Am J Surg 176:212-214, 1998.
8. Mangano DT: Heparin bonding and long-term protection against thrombogenesis. N Engl J Med 307:894-895, 1982.
9. Hoppe B: Central venous catheter-related infections: pathogenesis, predictors,and prevention. Heart Lung 24(4):333-339, 1995.
Ross VM, Orr PA: Prevention of infections related to central venous catheters.Crit Care Nurs Q 20:79-88, 1997.
Civetta JM, Hudson-Civetta J, Ball S: Decreasing catheter-related infection and hospital costs by continuous quality improvement. Crit Care Med24(10):1660-1665, 1996.
10. Baranowski L: Central venous access devices: current technologies, uses, andmanagement strategies. J Intraven Nurs 16(3):167-194, 1993.
11. Ullman RF, Gurevich I, Schoch PE, et al: Colonization and bacteremia relatedto duration of triple-lumen intravascular catheter placement. Am J Infect Control18:201-207, 1990.
12. Raad I, Costerton W, Sabharwal U, et al: Ultrastructural analysis of indwellingvascular catheters; a quantitative relationship between luminal colonization andduration of placement. J Infect Dis 168:400-407, 1993.
References (continued)
13. Russell LM, Weinstein RA: Antimicrobial-coated central venous catheters – Icing on the cake or the staff of life? Crit Care Med26(2):195-196, 1998.
14. Bonawitz SC, Hammell EJ, Kirkpatrick JR: Prevention of central venouscatheter sepsis: a prospective randomized trial. Am Surg 57:618-623, 1991.
15. Cook D, Randolph A, Kernerman P, et al: Central venous catheter replacementstrategies: a systematic review of the literature. Crit Care Med25(8):1417-1424, 1997.
16. Kim DK, Gottesman MH, Forero A, et al: The CVC removal distress syndrome:an unappreciated complication of central venous catheter removal. Am Surg64:344-347, 1998.
17. Baranowski L: Central venous access devices. Current technologies, uses andmanagement strategies. J Intraven Nurs 16(3):167-194, 1993.
18. Maki DG, McCormack KN: Defatting catheter insertion sites in total parenteral nutrition is of no value as an infection control measure. Am J Med83:833-840, 1987.
19. Maki DG, Ringer M, Alvarado CJ: Prospective randomized trial of povidone-iodine, alcohol, and chlorhexidine for prevention of infection associated with central venous and arterial catheters. Lancet 338:339-343, 1991.
20. Maki DG, Will L: Colonization and infection associated with transparent dressings for central venous, arterial and Hickman catheters: a comparative trial.(Programs and Abstracts), 24th Interscience Conference on AntimicrobialAgents and Chemotherapy. Washington, DC, 1984,
21. Maki DG, Stolz W, Wheeler S: Prospective, randomized, three-way clinicalcomparison of a novel, highly permeable polyurethane dressing with 206 Swan-Ganz pulmonary artery catheters: Opsite IV 3000 vs. Tegaderm vs. gauzeand tape. Cutaneous colonization under the dressing, catheter-related infection. In: Maki DG (ed) Improving Catheter Site Care. New York: RoyalSociety of Medicine Services Ltd, 1991.
22. Tomford JW, Hershey CO: The IV therapy team. Impact on patient care andcosts of hospitalization. NITA 8(5):387-9, 1985.
23. SEIU’s Guide to Preventing Needlestick Injuries. Service EmployeesInternational Union, AFL-CIO, CLC, 1998.
24. Smoller BR, Kruskall MS: Phlebotomy for diagnostic laboratory tests in adults.N Engl J Med 314(19):1233-5, 1986.
25. Kacuba A, Adams-McLean A, Lutz RJ: Comparison of three methods of bloodwithdrawal from central venous catheters. NTI Poster Presentation, Anaheim,CA, May 1996.
Lea D, Kurzer S, Blaser C, et al: Accuracy of laboratory blood samples from afunctional intravenous catheter utilizing the Venous Arterial ManagementProtection System (VAMP). Anesth Analg 82:S267, 1996.
26. Johnston JB, Messina M: Erroneous laboratory values obtained from centralcatheters. J Intravenous Nurs 14(1):13-15, 1991.
27. Carlson KK, Synder ML, LeClair HW, et al: Obtaining reliable plasma sodiumand glucose determinations from pulmonary catheters. Heart Lung19:613-619, 1990.
RE
FE
RE
NC
ES
126

RE
FE
RE
NC
ES
127
References (continued)
28. Russo LT, Coombes DL, Underhill SL, et al: Reliable measurements of serumpotassium and glucose from radial artery lines. NTI Research Abstract. Heart Lung 13(3):310, 1984.
29. Tonnesen A, Peuler M, Lockwood WR: Cultures of blood drawn by cathetersvs. venipuncture. JAMA 235(17):1877, 1976.
Felices FJ, Hernandez JL, Ruiz J, et al: Use of the central venous catheter toobtain blood cultures. Crit Care Med 7(2):78-9,1979.
30. Rakowski AC, Tonneson AS, Goodnough SKC: Minimum discard volume from arterial catheters to obtain coagulation studies free of heparin effect.Heart Lung 16(6):699-705, 1987.
31. Rudisill P, Moore L: Relationship between arterial and venous activated partialthromboplastin time values in patients after percutaneous transluminal coronaryangioplasty. Heart Lung 18:514-519, 1989.
Templin K, Shively M, Riley J: Accuracy of drawing coagulation samples fromheparinized arterial lines. Am J Crit Care 2(1):88-95, 1993.
32. Maki DG: Infections due to infusion therapy. In Hospital Infections (Bennettand Brachman, Eds) Boston: Little, Brown and Company, 1992.
33. American Association of Critical-Care Nurses: Evaluation of the effects ofheparinized and non-heparinized flush solutions on the patency of arterial pressure monitoring lines: The AACN Thunder Project. Am J Crit Care2(1):3-14, 1993.
34. Pearson ML, Hospital Infection Control Practices Committee. Guideline forprevention of intravascular device-related infections. Infect Control HospEpidemiol 17:438-473, 1996.
35. Stern RC, Pittman S, Doershuk CF, et al: Use of a “heparin lock” in the intermittent administration of intravenous drugs: a technical advance in intravenous therapy. Clin Pediatr 11:521-523, 1972.
36. Passannante A, Macik BG: Case report: the heparin flush syndrome: a cause of iatrogenic hemorrhage. Am J Med Sci 296:71-73, 1988.
37. Inoue Y, Nezu R, Matsuda H, et al: Prevention of catheter-related sepsis duringparenteral nutrition: effect of a new connection device. J Parenter Enteral Nutr16:581-585, 1992.
38. Grillo JA, Gonzalez ER, Ramaiya A, et al: Chemical compatibility of inotropicand vasoactive agents delivered via a multiple line infusion system. Crit Care Med 23(6):1061-1066, 1995.
39. Collins JL, Lutz RJ: In vitro study of simultaneous infusion of incompatibledrugs in multi-lumen catheters. Heart Lung 20:271-277, 1991.
40. Moore FA, Moore EE, Jones T: Benefits of immediate jejunostomy feedingafter major abdominal trauma: a prospective randomized study. J Trauma26:874-881, 1986.
Moore FA, Moore EE: TEN vs. TPN following major abdominal trauma:reduced septic morbidity. J Trauma 29:916-923, 1989.
41. Goldman DA, Martin WT, Worthington JW: Growth of bacteria and fungi intotal parenteral nutrition solutions. Am J Surg 126:314-318, 1973.
D’Angio RG, Riechers KC, Gilsdorf RB, et al: Effect of the mode of lipidadministration on parenteral nutrition-related infections. Ann Pharmacother73:695-699, 1982.

References (continued)
42. Mangano DT: Monitoring pulmonary arterial pressure in coronary-artery disease. Anesthes 53(5):364-370, 1980.
43. Sheldon CA, Leonard AS: Continuous SVO2 and other new hemodynamicparameters as early indicators of hypovolemia. In Continuous Measurement ofBlood Oxygen Saturation in the High Risk Patient (ed. JF Schweiss) AbbottLaboratories, Inc, 1986.
44. Buchbinder N, Ganz W: Hemodynamic Monitoring: Invasive techniques.Anesthes 45(2):146-?, 1976.
45. Conners AF, McCaffree DR, Gray BA: Evaluation of right-heart catheterizationin the critically ill patient without acute myocardial infarction. N Engl J Med308:263-267, 1983.
46. Eisenberg Pr, Jaffe ASD, Schuster DP: Clinical evaluation compared to pulmonary artery catheterization in the hemodynamic assessment of critically illpatients. Crit Care Med 12(7):549-53, 1984.
47. Cook DH: Clinical assessment of central venous pressure in the critically ill.Am J Med Sci 299(3):175-178, 1990.
48. Verweij J, Kester A, Stroes W, et al: Comparison of three methods for measuringcentral venous pressure. Crit Care Med 14(4):288-90, 1986.
Mann RL, Carlton GC, Turnbull AD: Comparison of electronic and manometric central venous pressures. Influences of access route. Crit Care Med 9(2):98-100, 1981.
49. Amoroso P, Greenwood RN: Posture and central venous pressure in circulatoryvolume depletion. Lancet 2:555-556, 1989.
50. Potger KC, Elliott D: Reproducibility of central venous pressures in supine andlateral positions: a pilot evaluation of the phlebostatic axis in critically illpatients. Heart Lung 23(4):285-299, 1994.
51. Scott SS, Giuliano KK, Pysznik E, et al: Influence of port site on central venouspressure measurements from triple-lumen catheters in critically ill adults. Am J Crit Care 7(1):60-63, 1998.
RE
FE
RE
NC
ES
128

BIB
LIO
GR
AP
HY
129
BibliographyAIR EMBOLISMCoppa GF, Gouge TH, Hofstetter SR: Air embolism: a lethal but preventable complication of subclavian vein catheterization. J Parenter Enter Nutr5:166-168, 1981.
Gottiener JS, Papademetriou V, Notargiacomoa A, et al: Incidence and cardiaceffects of systemic venous air embolism. Arch Intern Med 148:795-800, 1988.
Kashuk JL, Penn I: Air embolism after central venous catheterization. Surg Gynecol Obstet 159:249-252, 1984.
Kuhn M, Firring JW, Leuenberger PH: Acute pulmonary edema caused by venousair embolism after removal of a subclavian catheter. Chest 92:364-365, 1987.
Marcus RH, Weinert L, Neumann A, et al: Venous air embolism: diagnosis by spontaneous right-sided contrast echocardiography. Chest 99:784-785, 1991.
Mennim P, Coyle CF, Taylor JD: Venous air embolism associated with removal ofcentral venous catheter. Br Med J 305:171-172, 1992.
Orebaugh SL: Venous air embolism: clinical and experimental considerations. Crit Care Med 20:1169-1177, 1992.
Phifer TJ, Bridges M, Conrad SA: The residual central venous catheter tract: an occult source of lethal air embolism. J Trauma 31:1558-1560, 1991.
Thielsen JB, Nyguist J: Subclavian catheter removal: Nursing implications to prevent air emboli. J Intravenous Nurs 14(2): 114-118, 1991.
Turnage WS, Hairer JV: Venous air embolism occurring after removal of a centralvenous catheter. Anesth Analg 72:559-560, 1991.
Sing RF, Steffe TJ, Branas CC: Fatal venous air embolism after removal of a centralvenous catheter. J Am Osteopath Assoc 96(3):204-205, 1995.
BLOOD DRAWSCarlson KK, Snyder ML, LeClair HW, et al: Obtaining reliable plasma sodium andglucose determinations from pulmonary artery catheters. Heart Lung19:613-619, 1990.
Chernow B, Salem M, Stacey J, et al: Blood conservation – a critical care imperative.Crit Care Med 19(3):313-314, 1991.
Cicala RS, Cannon K, Larson JS: E, et al: Evaluation of coagulation studies fromheparinized arterial lines with use of Lab-site high pressure tubing. Heart Lung17(6):662-666, 1988.
Crow S, Conrad SA, Chaney-Rowell K, et al: Microbial contamination of arterialinfusions used for hemodynamic monitoring: a randomized trial of contaminationwith sampling through conventional stopcocks versus a novel closed system. Infect Control Hosp Epidemiol 10(12):557-61, 1989.
Felices FJ, Hernandez JL, Ruiz J, et al: Use of the central venous pressure catheterto obtain blood cultures. Crit Care Med 7(2):78-79, 1979.
Gregersen RA, Underhill SL, Detter JC, et al: Accurate coagulation studies fromheparinized radial artery catheters. Heart Lung 16(6):686-686, 1987.
Johnson JB, Messina M: Erroneous laboratory values obtained from centralcatheters. J Intravenous Nurs 14(1): 13-15, 1991.
Kacuba A, Adams-McLean A: Comparison of three methods of blood withdrawalfrom central venous catheters. AACN NTI Poster Session, 1996.

Bibliography (continued)
Laxson CJ, Titler MG: Drawing coagulation studies from arterial lines: an integrative literature review. Am J Crit Care 3(1):16-22, 1994.
Lea D, Goodwin R, Kurzer S, et al: Accurate activated partial thromboplastin timesdrawn from arterial lines via the venous/arterial management protection device(VAMP™). Anesth Analg 82:S-266, 1996.
Peruzzi WT, Parker MA, Lichtenthal PR, et al: A clinical evaluation of a blood conservation device in medical intensive care unit patients. Crit Care Med21(4):501-506, 1993.
Pryor AC: A comparison of blood cultures withdrawn from the arterial line and byvenipuncture. Heart Lung 13(4):411-415, 1984.
Pryor AC: The intra-arterial line: a site for obtaining coagulation studies. Heart Lung 12(6):586-590, 1983.
Reinhardt AC, Tonneson AS, Goodnough SK: Minimum discard volume from arterial catheters to obtain coagulation studies free of heparin effect. Heart Lung 16(6):699-703, 1987.
Rudisill P, Moore L: Relationship between arterial and venous activated partialthromboplastin time values in patients after percutaneous transluminal coronaryangioplasty. Heart Lung 18:514-519, 1989.
Russo LT, Coombes DL. Underhill SL, et al: Reliable measurement of serum potassium and glucose from radial arterial lines. Heart Lung 13(3):310, 1984.
Silver MJ, Jubran H, Stein S, et al: Evaluation of a new blood-conserving arterialline system for patients in intensive care units. Crit Care Med 21(4):507-511, 1993.
Templin K, Shively M, Riley J: Accuracy of drawing coagulation samples fromheparinized arterial lines. Am J Crit Care 2(1):88-95, 1993.
CARDIAC TAMPONADEArbitman M, Kart BH: Hydromediastinum after aberrant central venous catheterplacement. Crit Care Med 7(1):27-29, 1979.
Brandt RL, Foley WJ, Fink GH, et al: Mechanism of perforation of the heart withproduction of hydropericardium by a central venous catheter and its prevention.Am J Surg 119:311-316, 1970.
Collier PE, Goodman GB: Cardiac tamponade caused by central venous catheterperforation of the heart: a preventable complication. J Am Coll Surg181(5):459-63, 1995.
Collier PE, Blocker SH, Graff DM, et al: Cardiac tamponade from central venouscatheters. Am J Surg 176:212-214, 1998.
Dosios TJ, Magovern GJ, Gay TC, et al: Cardiac tamponade complicating percutaneous catheterization of subclavian vein. Surg 78:261-263, 1975.
Edwards H, King T: Cardiac tamponade from central venous catheters. Arch Surg 117:965-967, 1982.
Eide J, Odegaard E: Cardiac tamponade as a result of infusion therapy. A potentially amenable complication of central venous catheters. Acta Anaesthesiol Scand 27:181-184, 1983.
Karnauchow PN: Cardiac tamponade from central venous catheterization. Can Med Assoc J 135:1145, 1986.
Maschke SP, Rogove HJ: Cardiac tamponade associated with a multi-lumen centralvenous catheter. Crit Care Med 12(7);611-613, 1984.
BIB
LIO
GR
AP
HY
130

BIB
LIO
GR
AP
HY
131
Bibliography (continued)
Sheep RE, Guiney WB: Fatal cardiac tamponade: occurrence with other complications after left internal jugular vein catheterization. JAMA248:1632-1635, 1982.
CATHETER EXCHANGE/REPLACEMENTCobb DK, High KP, Sawyer RG, et al: A controlled trial of scheduled replacementof central venous and pulmonary artery catheters. New Engl J Med327(15):1062-1068, 1992.
Gayo DS, Richey HM, Matthew JI: Safety and efficacy of guidewire exchangetechnique for central venous catheters in the ICU. Chest 92:101S, 1987.
Olson ME, Lam K, Bodey GP, et al: Evaluation of strategies for central venouscatheter replacement. Crit Care Med 20(6):797-804.
Powell C, et al: Effect of frequent guidewire changes on triple-lumen catheter sepsis. J Parent Enter Nutr 12(5):462-4, 1988.
Stuart RK, Shikora SA, Akerman P, et al: Incidence of arrhythmia with centralvenous catheter insertion and exchange. J Parent Enter Nutr 14:152-155, 1990.
CENTRAL VENOUS PRESSURE (GENERAL)Amoroso P, Greenwood RN: Posture and central venous pressure measurement incirculatory volume depletion. Lancet 2:258-260, 1989.
Ansley DM, Ramsay JG, Whalley DG, et al: The relationship between centralvenous pressure and pulmonary capillary wedge pressure during aortic surgery.Anesthiol 34(6):594-600, 1987.
Barrowsliffe MP: Spurious central venous pressure. Anaesth 42(3):293-295, 1987.
Buchbinder N, Ganz W: Hemodynamic monitoring: Invasive techniques.Anesthesiol 45(2):146-155, 1976.
Connors AF Jr, McCaffree DR, Gray BA: Evaluation of right heart catheterizationin the critically ill patient without acute myocardial infarction. N Engl J Med308:263-267, 1983.
Cook DJ: Clinical assessment of central venous pressure in the critically ill. Am J Med Sci 299(3):175-178, 1990.
Cotton DB, Gonik B, Dorman K, et al: Cardiovascular alterations in severe pregnancy-induced hypertension: relationship of central venous pressure to pulmonary capillary wedge pressure. Am J Obstet Gynec 151(6):762-764, 1985.
Eisenberg PR, Jaffe AS, Schuster DP: Clinical evaluation compared to pulmonaryartery catheterization in the hemodynamic assessment of critically ill patients. Crit Care Med 12:549-553, 1984.
Godje O, Peyerl M, Seebauer T, et al: Central venous pressure, pulmonary capillarywedge pressure and intrathoracic blood volumes as preload indicators in cardiacsurgery patients. Eur J Cardiothorac Surg 13(5):533-539, 1998.
Halck SE, Walther-Larsen S, Sanchez R: Measurement of central venous pressureafter open heart surgery and effect of positive end-expiratory pressure. Dan Med Bull 38(2):181-182, 1991.
Hardaway RM: Pulmonary artery pressure versus pulmonary capillary wedge pressure and central venous pressure in shock. Resusc 10(1):47-56, 1982.
Isaacson IJ, Lowdon JD, Berry AJ, et al: The value of pulmonary artery and centralvenous monitoring in patients undergoing abdominal aortic reconstructive surgery:a comparative study of two selected, randomized groups. J Vasc Surg12(6):754-760, 1990.

Bibliography (continued)
Jones RM, Moulton CE, Hardy KJ: Central venous pressure and its effect of bloodloss during liver resection. Brit J Surg 85(8):1058-1060, 1998.
Mangano DT: Monitoring pulmonary arterial pressure in coronary-artery disease.Anesthesiol 53(3):364-370, 1980.
Mark JB: Atlas of Cardiovascular Monitoring. New York: Churchill Livingston, 1998.
Mark JB: Central venous pressure monitoring: clinical insights beyond the numbers. J Cardiothorac Vasc Anesth 5:163-173, 1991.
Orlowski JP: The effects of central venous catheter location on waveform andresults. Cleve Clin J Med 55:171-174, 1988.
Rajacich N, Burchard KW, Hasan FM, et al: Central venous pressure and pulmonarycapillary wedge pressure as estimates of left atrial pressure: effects of positive end-expiratory pressure and catheter tip malposition. Crit Care Med17(1):7-11. 1989.
Shabetai R, Fowler NO, Guntheroth WG: The hemodynamics of cardiac tamponade and constrictive pericarditis. Am J Cardiol 26:480-489, 1970.
Sheldon CA, Leonard AS: Continuous SVO2 and other new hemodynamic parameters as early indicators of hypovolemia. In Continuous Measurement ofBlood Oxygen Saturation in the High Risk Patient (ed. JF Schweiss) AbbottLaboratories, Inc, 1986.
Wilson JN, Grow JB, Demong CV, et al: Central venous pressure in optimal bloodvolume maintenance. Arch Surg 85:563-578, 1962.
CENTRAL VENOUS PRESSURE (TECHNICAL)Bartz B, Maroun C, Underhill S: Differences in midanteroposterior level andmidaxillary level in patients with a range of chest configurations. Heart Lung17:308, 1988.
Callow LB, Pieper B: Effect of backrest on central venous pressure in pediatric cardiac surgery. Nurs Res 38(6):336-3338, 1989.
Cason CL, Lambert CW: Position and reference level for measuring right atrialpressure. Crit Care Nurs Q 12:77-86, 1990.
Chulay M, Miller T: The effect of backrest elevation on pulmonary artery and pulmonary capillary wedge pressure in patients after cardiac surgery. Heart Lung13:138-40, 1984.
Groom L, Frisch SR, Elliot M: Reproducibility and accuracy of pulmonary arterymeasurement in supine and lateral positions. Heart Lung 19:147-151, 1990.
Haywood GA, Joy MD, Camm AJ: Influence of posture and reference point on central venous pressure measurement. Brit Med J 303:626-627, 1991.
Kee LL, Simonson JS, Stotts NA, et al: Echocardiographic determination of validzero reference levels in supine and lateral positions. Am J Crit Care 2:72-80, 1993.
Laulive JL: Pulmonary artery pressures and position changes in the critically illadult. Dimen Crit Care Nurs 1(1):28-34, 1982.
Mann RL, Carlon GC, Turnbull AD: Comparison of electronic and manometriccentral venous pressures: influence of access route. Crit Care Med 9(2):98-100, 1981.
Paolella LP, Dorfman GS, Cronan JJ, et al: Topographic location of the left atriumby computed tomography: reducing pulmonary artery calculation error. Crit Care Med 16:1154-1156, 1988.
BIB
LIO
GR
AP
HY
132

BIB
LIO
GR
AP
HY
133
Bibliography (continued)
Potger KC, Elliott D: Reproducibility of central venous pressures in supine and lateral positions: a pilot evaluation of the phlebostatic axis in critically ill patients.Heart Lung 23(4):285-299, 1994.
Scott SS, Giuliano KK, Pysznik E, et al: Influence of port site on central venouspressure measurement from triple-lumen catheters in critically ill adults. Am J Crit Care 7(1):60-63, 1998.
Verweij J, Kester A, Stroes W, et al: Comparison of three methods for measuringcentral venous pressure. Crit Care Med 14(4):288-290, 1986.
Woods SL, Grose BL, Laurent-Bopp D: Effect of backrest position on pulmonaryartery pressures in critically ill patients. Cardiovasc Nurs 18:19-24, 1982.
Woods SL, Mansfield LW: Effect of body position upon pulmonary artery and pulmonary capillary wedge pressures in non-critically ill patients. Heart Lung6(5):83-90, 1976.
COATINGSAppelgren P, Ransjo U, Bindslev L, et al: Surface heparinization of central venouscatheters reduces microbial colonization in vitro and in vivo: results from a prospective, randomized trial. Crit Care Med 24(9):1482-1489, 1996.
Ciresi DL, Albrecht RM, Volkers PA, et al: Failure of antiseptic bonding to preventcentral venous catheter-related infection and sepsis. Am Surg 62(8):641-646, 1996.
Darouiche RO, Raad II, Heard SO, et al: A comparison of two antimicrobial-impregnated central venous catheters. Catheter Study Group. N Engl J Med 340(1):1-8, 1999.
Haxhe JJ, D’Hoore W: A meta-analysis dealing with the effectiveness of chlorhexidine and silver sulfadiazine impregnated central venous catheters. J Hosp Infect 40(2):166-168, 1998.
Heard SO, Wagle M, Vijayakumar E, et al: Influence of triple-lumen central venouscatheters coated with chlorhexidine and silver sulfadiazine on the incidence ofcatheter-related bacteremia. Arch Intern Med 158(1):81-87, 1998.
Laster J, Silver D: Heparin-coated catheters and heparin-induced thrombocytopenia. J Vasc Surg 7(5):667-672, 1988.
Maki DG, Stolz SM, Wheeler S, et al: Prevention of central venous catheter-relatedbloodstream infection by use of an antiseptic-impregnated catheter. A randomized,controlled trial. Ann Intern Med 127(4):257-266, 1997.
Mangano D: Heparin bonding and long-term protection against thrombogenesis. N Engl J Med 307:894-895, 1982.
Mermel L, Stolz S, Maki D: Surface antimicrobial activity of heparin-bonded andantiseptic-impregnated vascular catheters. J Infect Dis 167:920-924, 1993.
Pemberton LB, Ross V, Cuddy P, et al: No difference in catheter sepsis betweenstandard and antiseptic central venous catheters. A prospective randomized trial.Arch Surg 131(9):986-989, 1996.
Raad II: Vascular catheters impregnated with antimicrobial agents: present knowledge and future direction. Infect Control Hosp Epidemiol 18(4):227-9, 1997.
Raad II, Darouiche R, Dupuis J, et al: Central venous catheters coated withminocycline and rifampin for the prevention of catheter-related colonization andbloodstream infections. A randomized, double-blind trial. The Texas MedicalCenter Catheter Study Group. Ann Intern Med 127(4):267-274, 1997.
Bibliography (continued)
Raad II, Darouiche RO, Hachem R, et al: Antimicrobial durability and rare ultrastructural colonization of indwelling central catheters coated with minocyclineand rifampin. Crit Care Med 26(2):219-224, 1998.
Randolph AG, Cook DJ, Gonzales CA, et al: Benefit of heparin in central venousand pulmonary artery catheters: a meta analysis of randomized controlled trials.Chest 113(1):165-171, 1998.
Russell LM, Weinstein RA: Antimicrobial-coated central venous catheters – Icingon the cake or the staff of life? Crit Care Med 26(2):195-196, 1998
Tebbs SE, Elliott TS: A novel antimicrobial central venous catheter impregnatedwith benzalkonium chloride. J Antimicrob Chemother 31:261-271, 1993.
Veenstra DL, Saint S, Saha S, et al: Efficacy of antiseptic-impregnated centralvenous catheters in preventing catheter-related bloodstream infection: a meta-analysis. JAMA 281(3):261-267, 1999.
COMPLICATIONS (GENERAL)Bernard RW, Stahl WM: Subclavian vein catheterizations: a prospective study. I. Noninfectious complications. Ann Surg 173:184-190, 1971.
Eisenhauer ED, Derveloy RJ, Hastings PR: Prospective evaluation of centralvenous pressure (CVP) catheters in a large city-county hospital. Ann Surg196(5):560-564, 1982.
Feliciano DV, Mattox KL, Fraham JM, et al: Major complications of percutaneoussubclavian vein catheters. Am J Surg 138:869, 1978.
Kaye CG, Smith DR: Complications of central venous cannulation. Br Med J297:572-573, 1988.
Kim DK, Gottesman MH, Forero A, et al: The CVC removal distress syndrome: an unappreciated complication of central venous catheter removal. Am Surgeon64(4):344-347, 1998.
Mansfield PF, Hohn DC, Fornage BD, et al: Complications and failures of subclavian-vein catheterization. N Engl J Med 331:1735-8, 1994
Szmajder JI, Zweibel FR, Bitterman H, et al: Central vein catheterization: Failure and complication rates by three percutaneous approaches. Arch Intern Med146:259,1986.
Whitman ED: Complications associated with the use of central venous accessdevices. Curr Probl Surg 33:311, 1996.
DRESSINGSConly J, Grieves K, Peters B: A prospective, randomized study comparing transparent and dry gauze dressings for central venous catheters. J Infect Dis159:310-319, 1989.
Craven D, Lichtenberg D, Kunches M, et al: A randomized study comparing a transparent polyurethane dressing to a dry gauze dressing for peripheral intravenous catheter sites. Infect Control 6:361-366, 1985.
Hoffmann K, Weber D, Samsa G, et al: Transparent polyurethane film as an intravenous catheter dressing: a meta-analysis of the infection risks. JAMA267:2072-2076, 1992.
Katich M, Band J: Local infection of the intravenous-cannulae wound associatedwith transparent dressings. J Infect Dis 151:971-972, 1985.
BIB
LIO
GR
AP
HY
134
BIB
LIO
GR
AP
HY
135
Bibliography (continued)
Nelson DB, Kien CL, Mohr B, et al: Dressing changes by specialized personnelreduce infection rates in patients receiving central venous parenteral nutrition. J Parenter Enter Nutr 10(2):220-2, 1986.
Powell C, Regan C, Fabri P, et al: Evaluation of Opsite catheter dressings for parenteral nutrition: a prospective randomized study. J Parenter Enter Nutr6:43-46, 1982.
EMERGENCY DEPARTMENTEmerman CL, Bellon EM, Lukens TW, et al: A prospective study of femoral versussubclavian vein catheterization during cardiac arrest. Ann Emerg Med 19:26-30,1990.
Ferguson M, Max MH, Marshall W: Emergency department infraclavicular subclavian vein catheterization in patients with multiple injuries and burns. South Med J 81:433, 1988.
Rady MY: Triage and resuscitation of critically ill patients in the emergency department: Current concepts and practice. Eur J Emerg Med 1(4):175-89, 1994.
Schug CB, Culhane DE, Knoop RK: Subclavian vein catheterization in the emergency department: a comparison of guidewire and non-guidewire techniques.Ann Emerg Med 15:769, 1986.
FILTERSAdams SD, Killien M, Larson E: Inline filtration and infusion phlebitis. Heart Lung15(2):134-40, 1986.
Baumgartner TG, et al: Bacterial endotoxin retention by inline intravenous filter.Am J Hosp Pharm 43(3):681-4, 1986.
Falchuk KH, Peterson L, McNeil BJ: Microparticulate-induced phlebitis. Its prevention by in-line filtration. N Eng J Med 312(2):78-82, 1985.
Friedlland G: Infusion-related phlebitis – Is the in-line filter the solution? N Engl J Med 312(2):113-5, 1985.
Maddox RR, John JF, Brown LL, et al: Effect of inline filtration on post-infusionphlebitis. Clin Pharm 2(1):58-61, 1983.
FLUSHINGFry B: Intermittent flushing protocols: a standardization issue. J Intravenous Nurs15(3):160-163, 1992.
Goode CJ, Titler M, Rakel B, et al: A meta-analysis of effects of heparin flush andsaline flush: quality and cost implications. Nurs Res 324 40(6) 324-329.
HEMODYNAMIC MONITORINGAhrens TS, Taylor LA: Hemodynamic Waveform Analysis. Philadelphia: WB Saunders Company, 1992.
Daily EK, Schroeder JS: Techniques in Bedside Hemodynamic Monitoring. St Louis: CV Mosby Company, 1985.
Darovic GO: Hemodynamic Monitoring: Invasive and Noninvasive Clinical Application.Philadelphia: WB Saunders Company, 1987.
Mark JB: Atlas of Cardiovascular Monitoring. New York: Churchill Livingstone, 1998.

Bibliography (continued)
INFECTIONBrosnan KM, Parham AM, Rutledge B, et al: Stopcock contamination. Am J Nurs
Brun-Buisson C, Doyon F, Carlett J, et al: Bacteremia and severe sepsis in adults: a multi-center prospective survey in ICUs and wards of 24 hospitals. Am J Resp CritCare Med 154:617-624, 1996.
Civetta JM, Hudson-Civetta J, Ball S: Decreasing catheter-related infection and hospital costs by continuous quality improvement. Crit Care Med24(10):1660-1665, 1996.
Cooper B, Larsen E: Infection control issues for critical care units: An overview andchallenge – physician and nurse perspective. Heart Lung 21(4):317-319, 1992.
Cunha BA: Intravenous line infections. Crit Care Clin 14(2):339-346, 1998.
Dryden GE, Brickler J: Stopcock contamination. Anesth Analg 58(2):141-142,1979.
Garrison RN, Wilson MA: Intravenous and central catheter infections. Surg Clin North Am 74(3):557-570, 1994.
Hoppe B: Central venous catheter-related infections: pathogenesis, predictors, andprevention. Heart Lung 24(4):333-340, 1995.
Elliott TEJ: Intravascular-device infections. J Med Microbiol 27:161-167, 1988.
Elliott TS, Tebbs SE: Prevention of central venous catheter-related infection. J Hosp Infect 40(3):193-201, 1998.
Farkas J-C, Liu N, Bleriot J-P, et al: Single- versus triple-lumen central catheter-related sepsis: a prospective randomized study in a critically ill population. Am J Med 93:277-282, 1992.
Fridkin S, Pear S, Williamson T, et al: The role of understaffing in central venouscatheter-associated bloodstream infections. Infect Cont Hosp Epidem 150-158, 1996.
Goetz AM, Wagener MM, Miller JM, et al: Risk of infection due to central venous catheters: effect of site of placement and catheter type. Infect Control Hosp Epidemiol 19(11): 842-845, 1998.
Haslett T, Isenberg H, Hilton E, et al: Microbiology of indwelling central intravascular catheters. J Clin Microbiol 696-701, 1988.
Hilton E, Haslett TM, Borenstein MT, et al: Central catheter infections: single- versus triple-lumen catheters: influence of double-lumens on infection rateswhen used for replacement of catheters. Am J Med 84:667-672, 1988.
Kamal GD, Pfaller MA, Rempe LE, et al: Reduced intravascular catheter infectionby antibiotic bonding: a prospective, randomized, controlled trial. JAMA265(1):2364-2368, 1991.
Lee RB, Buckner M, Sharp K: Do multi-lumen catheters increase central venous catheter sepsis compared to single-lumen catheters? J Trauma28(10):1472-1475, 1988.
Maki DG, Brand JD: A comparative study of polyantibiotic and iodophor ointmentsin prevention of vascular catheter-related infection. Am J Med 70:739-744, 1981.
Maki DG, Ringer M, Alvarado CJ: Prospective randomized trial of povidone-iodine,alcohol, and chlorhexidine for prevention of infection associated with centralvenous and arterial catheters. Lancet 338:39-343, 1991.
Maki DG, Weise CE, Saratin HW: A semi-quantitative culture method for identifying intravenous catheter related infections. N Engl J Med298:1305-1308, 1977.
BIB
LIO
GR
AP
HY
136

BIB
LIO
GR
AP
HY
137
Bibliography (continued)
McLane C, Morris L, Holm K: A comparison of intravascular pressure monitoringsystem contamination and patient bacteremia with use of 48- and 72-hour systemchange intervals. Heart Lung 27(3):200-208, 1998.
Mimoz O, Pierone L, Lawrence C, et al: Prospective, randomized trial of two antiseptic solutions for prevention of central venous or arterial catheter colonizationand infection in intensive care unit patients. Crit Care Med 24(11):1818-1823, 1996.
Nafziger DA, Wenzel RP: Techniques for catheter removal and culture: diagnosing,and minimizing the risk of catheter-related sepsis. J Crit Ill 5(8):867-871, 1990.
Norwood S, Ruby A, Civetta J, et al: Catheter-related infections and associated septicemia. Chest 99:968-975, 1991.
Olson ME, Lam K, Bodey GP, et al: Evaluation of strategies for central venouscatheter replacement. Crit Care Med 20(6):797-804.
Pearson ML: Guideline for prevention of intravascular device-related infections.Infect Control Hosp Epidemiol 17:438, 1996.
Pittet D, Tarara D, Wenzel RP: Nosocomial bloodstream infection in critically illpatients: excess length of stay, extra costs, and attributable mortality. JAMA271(20):1598-1601, 1994.
Powell C, Fabri PJ, Kudsk KA: Risk of infection accompanying the use of single vs. double-lumen subclavian catheters: A prospective randomized study. J ParentEnter Nutr 12:127-129, 1988.
Raad II, Darouiche RO: Catheter-related septicemia: risk reduction. Infect Med13(9):807-823, 1996.
Raad II, Luna M, Khalil SM, et al: The relationship between the thrombotic andinfectious complications of central venous catheters. JAMA 271:1014-1016, 1994.
Raad II, Hohn DC, Gilbreath BJ, et al: Prevention of central venous catheter-related infections by using maximal sterile barrier precautions during insertion. Infect Cont Hosp Epidemiol 15(4):231-238, 1994.
Shapiro JM, Bond, EL, Garman JK: Use of a chlorhexidine dressing to reducemicrobial colonization of epidural catheters. Anesthesiol 73(4):625-631, 1990.
Sheikh W: Comparative antibacterial efficacy of Hibiclens and Betadine in thepresence of pus derived from human wounds. Curr Ther Res 40:1096-1102, 1986.
Sitges-Serra A, Linares J, Garau J: Catheter sepsis: The clue is the hub. Surg97(3):355-357, 1985.
Stillman R, Soliman F, Garcia L, et al: Etiology of catheter-associated sepsis. Arch Surg 112:1497-1499, 1977.
Ullman RF, Gurevich I, Schoch PE, et al: Colonization and bacteremia related toduration of triple-lumen intravascular catheter placement. Am J Infect Control18:201-207, 1990.
KNOTTINGGraff J, Gong R, Byron R, et al: Knotting and entanglement of multiple centralvenous catheters. J Parenter Enter Nutr 10(3): 319-321.
Kranz A, Mundigler G, Bankier H, et al: Knotting of two central venous catheters: a rare complication of pulmonary artery catheterization. Wein Klin Wochenschr18(13):404-406, 1996.

Bibliography (continued)
LINE CHANGEBand JD, Maki DG: Safety of changing intravenous delivery systems at longerthan 24-hour intervals. Ann Intern Med 91(2):173-8, 1979.
McLane C, Morris L, Holm K: A comparison of intravascular pressure monitoringsystem contamination and patient bacteremia with use of 48- and 72-hour systemchange intervals. Heart Lung 27(3):200-208, 1998.
Sitges-Serra A, Linares J, Perez JL, et al: A randomized trial on the effect of tubingchanges on hub contamination and catheter sepsis during parenteral nutrition. J Parenter Enter Nutr 9(3):322-5, 1985.
Snydman DR, Reidy MD, Perry LK, et al: Intravenous tubing containing burettescan be safely changed at 72 hour intervals. Infect Control 8(3):113-6, 1987.
MALPOSITIONED CATHETERSCarrasco CH, Ricchli WR, Charnsangavej C, et al: Technical note: repositioningmisplaced central venous catheters. Cardiovasc Intervent Radiol 10:234-236, 1987.
Hartnell GG, Roizental M: Percutaneous transfemoral repositioning of malpositioned central venous catheters. AJR 164:1003-1006, 1996.
Hawkins IF, Paige RM: Redirection of malpositioned central venous catheters. AJR140:393-394, 1983.
Kayal TJ, Salloum LJ, Synder AB, et al: A simple method of repositioning the wayward central venous catheter. J Parenter Enter Nutr 13(4):438-439, 1989.
Recht MP, Burke DR, Meranze SG, et al: Simple technique for redirecting malpositioned central venous catheters. AJR 154:183-184, 1990.
MEDICATION ADMINISTRATIONAltavela JL, Hass CE, Nowak DR: Clinical response to intravenous nitroglycerininfused through polyethylene or polyvinyl chloride tubing. Am J Hosp Pharm51:490-494, 1994.
Baaske DM, Amann AH, Wagenknecht DM, et al: Nitroglycerin compatibility withintravenous fluid filters, containers, and administration sets. Am J Hosp Pharm37:201-205, 1980.
Collins JL, Lutz RJ: In vitro study of simultaneous infusion of incompatible drugsin multi-lumen catheters. Heart Lung 20:271-277, 1991.
Cooke DA, Chase KA, Moody ML: Evaluation of the clinical significance of nitroglycerin adsorption. Am J Cardiol 55:1623-1626. 1985.
DeMonaco HJ: Intravenous drug compatibility. Crit Care Med 18(8):896, 1990.
Gonzalez ER: Titrating nitroglycerin. Am J Nurs 3:5, 1990.
Grillo JA, Gonzalez ER, Ramaiya A, et al: Chemical compatibility of inotropic andvasoactive agents delivered via a multiple line infusion system. Crit Care Med23(6):1061-1066, 1995.
Hola ET: Loss of nitroglycerin during micro infusion. Am J Hosp Pharm41:142-143, 1984.
Horrow JC, Digregario GJ, Barbieri EJ, et al: Intravenous infusions of nitroprusside,dobutamine, and nitroglycerin are compatible. Crit Care Med 18:858-861, 1990.
Nix DE, Tharpe WN, Francisco GE: Effects of presaturation on nitroglycerindelivery by polyvinyl chloride infusion sets. Am J Hosp Pharm 41:1835-1837, 1984.
BIB
LIO
GR
AP
HY
138

BIB
LIO
GR
AP
HY
139
Bibliography (continued)
MISCELLANEOUSAubaniac R: L’injection intraveineuse sous-claviculaire: advantages et technique.Presse Med 60: 1456, 1952.
Clemence MA, Walker D, Farr BM: Central venous catheter practices: results of asurvey. Am J Infect Control 23(1): 5-12, 1995.
Cook R, Kernerman A, Cupido C, et al: Central venous catheter replacement strategies: a systematic review of the literature. Crit Care Med25(8):1417-1427, 1997.
Donovan KD, Power BM, Hockings BE, et al: Usefulness of atrial electrogramsrecorded via central venous catheters in the diagnosis of complex atrial arrhythmias.Crit Care Med 21(4):532-537, 1993.
Feldman KW, Hickman RO: The central venous catheter as a source of medicalchaos in Munchausen by proxy. J Pediatr Surg 33(4):623-627, 1998.
Kalso E: A short history of central venous catheterization. Acta Anaesthsiol Scand81:7; 1985.
Koch T, Cook J: Benzalkonium interference with test methods for potassium andsodium. Clin Chem 36(5):807-808, 1990.
Stuart Rk, Shikora SA, Akerman P, et al: Incidence of arrhythmia with centralvenous catheter insertion and exchange. J Parenter Enter Nutr 14(2):152-155, 1990.
Wilson JN, Grow JB, Demong CV, et al: Central venous pressure in optimal bloodvolume maintenance. Arch Surg 85:563-578, 1962.
NEEDLELESS SYSTEMAdams KS, Zehrer CL, Thomas W: Comparison of a needleless system with conventional heparin locks. Am J Infect Control 21(5):263-9, 1993.
Larson EL, Cheng G, Choo JTE, et al: In vitro survival of skin flora in heparinlocks and needleless valve infusion devices. Heart Lung 22(5):459-62, 1993.
PATENCYAmerican Association of Critical-Care Nurses: Evaluation of the effects ofheparinized and non-heparinized flush solutions on the patency of arterial pressuremonitoring lines: The AACN Thunder Project. Am J Crit Care 2(1):3-15, 1993.
Butt W, Shann F, McDonnell G, et al: Effect of heparin concentration and infusionrate on the patency of arterial catheters. Crit Care Med 15(3):230-232, 1987.
Clifton GD, Branson P, Kelly HJ, et al: Comparison of normal saline and heparinsolutions for maintenance of arterial catheter patency. Heart Lung 20:115-118, 1991.
Epperson EL: Efficacy of 0.9% sodium chloride injection with and without heparinfor maintaining indwelling intermittent injection sites. Clin Pharm 3:626-629, 1984.
Garrelts JC, LaRocca J, Ast D, et al: Comparison of heparin and 0.9% sodium chloride injection in the maintenance of indwelling intermittent IV devices. Clin Pharm 8:34-39, 1989.
Hamilton RA, Plis JM, Clay C, et al: Heparin sodium versus 0.9% sodium chlorideinjection for maintaining patency of indwelling intermittent infusion devices. Clin Pharm 7:439-443, 1988.
Hook ML, Reuling J, Luettren ML, et al: Comparison of patency of arterial linesmaintained with heparinized and non-heparinized infusion. Heart Lung16(6):693-699, 1987.

Bibliography (continued)
Jowett NI, Stephens JM, Thompson DR, et al: Do indwelling cannulae on coronarycare units need a heparin flush? Intens Care Nurs 2:16-19, 1986.
Passannante A, Macik BG: Case report: the heparin flush syndrome: a cause ofiatrogenic hemorrhage. Am J Med Sci 296:71-73, 1988.
Peterson FY, Kirchhoff KT: Analysis of the research about heparinized versus non-heparinized intravascular lines. Heart Lung 20(6):631-640, 1991.
Pituk TL, DeYoung JL, Levin HJ: Volumes of selected central venous catheters:implications for heparin flush use. NITA 6:98-100, 1983.
Randolph AG, Cook DJ, Gonzales CA, et al: Benefit of heparin in central venousand pulmonary artery catheters: a meta-analysis of randomized controlled trials.Chest 113(1):165-171, 1998.
Shoad J, Oliver S: Efficacy of normal saline injection with and without heparin formaintaining intermittent intravenous site. Appl Nurs Res 5(1):9-12, 1992.
Stern RC, Pittman S, Doershuk CF, et al: Use of a “heparin lock” in the intermittent administration of intravenous drugs: a technical advance in intravenous therapy. Clin Pediatr 11:521-523, 1972.
Zevola DR, Dioso J, Moggio R: Comparison of heparinized and non-heparinizedsolutions for maintaining patency of arterial and pulmonary artery catheters. Am J Crit Care 6(1):52-55, 1997.
PERFORATIONGravenstein N, Blackshear R: In vitro evaluation of relative perforating potential ofcentral venous catheters: comparison of materials, selected models, number oflumens, and angles of incidence to simulated membrane. J Clin Monit7(1):1-6, 1991.
Mitchell M, Wood D, Naraghi M, et al: Fatal cardiac perforation caused by the dilator of a central venous catheterization kit. J Clin Monit 9(4):288-291, 1993.
Senderoff E, Lutchman G, Shevede K: Catheter-induced innominate vein perforation: anatomic considerations. J Cardiothoacic Anesth 1(1): 57-58, 1987.
PLACEMENTBoyd R, Saxe A, Phillips E: Effect of patient position upon success in placing central venous catheters. Am J Surg 172(4):380-382, 1996.
Hayashi Y, Maruyama K, Takaki O, et al: Optimal placement of CVP catheter inpaediatric cardiac patients. Can J Anesth 42(6):479-82, 1995.
McGee WT, Ackerman BL, Rouben LR, et al: Accurate placement of centralvenous catheters: a prospective, randomized, multi-center trial. Crit Care Med21(8): 1118-1123, 1993.
Muralidhar K, Acharva K, Dash P: Ideal position of central venous catheters: length to height of patient. Asian Cardiovasc Thorac Ann 2(2):87-89, 1994.
ROUTES/SITESBelani KG, Buckley JJ, Gordon JR, et al: Percutaneous cervical central venous lineplacement: a comparison of the internal and external jugular vein routes. Anesth Analg 59:40-44, 1980.
Eisenhauer ED, Derveloy RJ, Hastings PR: Prospective evaluation of centralvenous pressure (CVP) catheters in a large city-county hospital. Ann Surg196(5):560-564, 1982.
BIB
LIO
GR
AP
HY
140
BIB
LIO
GR
AP
HY
Bibliography (continued)
Emerman CL, Bellon EM, Lukens TW, et al: A prospective study of femoral versussubclavian vein catheterization during cardiac arrest. Ann Emerg Med19:26-30, 1990.
Ferguson M, Max MH, Marshall W: Emergency Department infraclavicular subclavian vein catheterization in patients with multiple injuries and burns. South Med J 81(4):433-435, 1988.
Kaiser CW, Koornick AR, Smith N, et al: Choice of route for central venous cannulation: Subclavian or internal jugular vein? A prospective randomized study.J Surg Oncol 17:345-354, 1981.
Mansfield PF, Hohn DC, Fornage BD, et al: Complications and failures of subclavian-vein catheterization. N Engl J Med 331:1735-8, 1994.
Nevarre DR, Domingo OH: Supraclavicular approach to subclavian catheterization:review of the literature and results of 178 attempts by the same operator. J Trauma42(2):305-309, 1997.
Stickle BR, McFarlane H: Prediction of a small internal jugular vein by externaljugular vein diameter. Anesthes 52:220-222, 1997.
Szmajder JI, Zweibel FR, Bitterman H, et al: Central vein catheterization: Failureand complication rates by three percutaneous approaches. Arch Intern Med146:259,1986.
STOPCOCK CONTAMINATIONAbbott N, et al: Infection related to physiologic monitoring: venous and arterialcatheters. Heart Lung 12:28:28-34, 1983.
Brosnan KM, Parham AM, Rutledge B, et al: Stopcock contamination. Am J Nurs88(3):320-4, 1988.
Dryden GE, Brickler J: Stopcock contamination. Anesth Anal 58:141-142, 1979.
McArthur BJ, et al: Stopcock contamination in an ICU. Am J Nurs 75:96-97, 1975.
Pinilla JC, et al: Study of the incidence of intravascular catheter infection and associated depticemia in critically-ill patients. Crit Care Med 11:21-25, 1983.
Shinozaki T, et al: Bacterial contamination of arterial lines: A prospective study.JAMA 249:223-225, 1983.
Walrath JM et al: Stopcock: bacterial contamination in invasive monitoring systems.Heart Lung 8:100-104, 1979.
SUMMARY ARTICLESAndris DA, Krzywda FA: Central venous access: clinical practice issues. Nurs Clin North Am 32(4): 719-740, 1997.
Baranowski L: Central venous access devices: current technologies, uses and management strategies. J Intravenous Nurs 16:167-194, 1993.
Hoelzer MF: Recent advances in intravenous therapy. Emerg Clin North Am4:487, 1986.
Lowell JA, Bothe A: Venous access: preoperative, operative and postoperativedilemmas. Surg Clin North Am 71(6):1231-1246, 1991.
Maki DG: Infections due to infusion therapy (Chapter 40) in Hospital Infections(Bennett JV and Brachman PS, eds) Boston: Little, Brown and Company, 1992.
Purdue GF, Hunt JL: Placement and complications of monitoring catheters. Surg Clin North Am 17(4): 723-731, 1991.
141
Bibliography (continued)
THROMBOGENICITY/THROMBOSISBorow M, Crowley JG: Evaluation of central venous catheter thrombogenicity. Acta Anaesth Scan 81:59-64, 1985.
Borrow M, Crowley JG: Prevention of thrombosis of central venous catheters. J Cardiovasc Surg 27(5):571-574, 1986.
Curelaru I, Gustavsson B, Hultman E, et al: Material thrombogenicity in centralvenous catheterization III. A comparison between soft polyvinylchloride and softpolyurethane elastomer, long antebrachial catheters. Acta Anesthesiol Scand28:204-208, 1984.
Hoar PF, Wilson RM, Mangano DT, et al: Heparin bonding reduces thrombogenicity for pulmonary artery catheters. N Engl J Med 305:993-995, 1981.
Pottecher T, Forrler M, Picardat P, et al: Thrombogenicity of central venouscatheters: prospective study of polyethylene, silicone, and polyurethane catheterswith phlebography or postmortem examination. Eur J Anesthesiol 1:361-265, 1984.
Raad II, Luna M, Khalil SM, et al: The relationship between the thrombotic andinfectious complications of central venous catheters. JAMA 271:1014-1016, 1994.
TOTAL PARENTERAL NUTRITIONArmstrong CS, et al: Clinical predictors of infection of central venous catheters usedfor total parenteral nutrition. Infect Control Hosp Epidemiol 11(2):71-8, 1990.
Bjornson H, Colley R, Bower R, et al: Association between microorganism growth atthe catheter insertion site and colonization of the catheter in patients receiving totalparenteral nutrition. Surg 92(4):720-727, 1982.
Clark-Christoff N, Watters VA, Sparks W, et al: Use of triple-lumen subclaviancatheters for administration of total parenteral nutrition. J Parenter Enter Nutr16(5): 403-407, 1992.
DiCicco M, Chiarandia V, Veronesi A, et al: Source and route of microbial colonisation of parenteral nutrition catheters. Lancet 2(8674):1258-61, 1989.
Dudrick SJ, Wilmore DW: Long-term parenteral feeding. Hosp Pract 3:65-78, 1968.
Dudrick SJ, Wilmore DW, Vars HM, et al: Long-term total parenteral nutrition withgrowth, development, and positive nitrogen balance. Surg 64:134-142, 1968.
Faubion WC, Wesley JR, Khaldi N, et al: Total parenteral nutrition catheter sepsis:Impact of the team approach. J Parenter Enter Nutr 10(6):642-5, 1986.
Friedman B, Kanter G, Titus D: Femoral venous catheters: a safe alternative fordelivering parenteral alimentation. Nutr Clin Pract 9(2):69-72, 1994.
Gianino MS, Brunt LM, Eisenberg PG: The impact of a nutritional support teamon the cost and management of multi-lumen central venous catheters. J Intraven Nurs 15(6):327-332, 1992.
Horowitz HW, Dworkin BM, Savino JA, et al: Central catheter-related infections:comparison of pulmonary artery catheters and triple-lumen catheters for the delivery of hyperalimentation in a critical care setting. J Parenter Enter Nutr14:588-592, 1990.
Maki DG, McCormack KN: Defatting catheter insertion sites in total parenteralnutrition is of no value as an infection control measure. Am J Med 83;833-840. 1987.
McCarthy MC, Shives JK, Robison RJ, et al: Prospective evaluation of single andtriple-lumen catheters in total parenteral nutrition. J Parenter Enter Nutr11(3):259-262, 1987.
BIB
LIO
GR
AP
HY
142

Bibliography (continued)
Murphy LM, Lipman TO: Central venous catheter care in parenteral nutrition: a review. J Parenter Enter Nutr 11(2):190-201, 1987.
Nelson DB, Kien CL, Mohr B, et al: Dressing changes by specialized personnelreduce infection rates in patients receiving central venous parenteral nutrition. J Parenter Enter Nutr 10:220-, 1986.
Savage AP, Picard M, Hopkins CC, et al: Complications and survival of multi-lumencentral venous catheters used for total parenteral nutrition. Br J Surg80(10): 1287-1290, 1993.
Sitges-Serra A, Linares J, Perez JL, et al: A randomized trial on the effect of tubingchanges on hub contamination and catheter sepsis during parenteral nutrition. J Parenter Enter Nutr 9(3):322-5, 1985.
Wolfe BM, Ryder MA, Nishikawa RA, et al: Complications of parenteral nutrition.Am J Surg 152(1):93-99, 1986.
143
144

Edwards Lifesciences, Edwards, the stylized E logo, Advanced VenousAccess (AVA), AVA 3Xi, AVA HF, AMC THROMBOSHIELD and Vantexare trademarks of Edwards Lifesciences Corporation. CCOmbo,Intro-Flex, Multi-Med, and Swan-Ganz are trademarks of EdwardsLifesciences Corporation and are registered in the US Patent andTrademark Office.
Interlink is a trademark of Baxter International Inc., registered in theU.S. Patent and Trademark Office. Oligon is a trademark ofImplemed, Inc.
© 2002 Edwards Lifesciences LLC. All rights reserved. 1098-6/99-CC
02 ED CVC Quick Guide CoverF 8/28/02 3:10 PM Page 2

QUICK GUIDE TO
Central VenousAccess
QU
ICK
GU
IDE
TO
Cen
tral Ven
ous A
ccess
Edwards Lifesciences LLC · One Edwards Way · Irvine, CA USA 92614Phone: 949.250.2500 · 800.424.3278 · Fax: 949.250.2275 · www.edwards.com
Edwards Lifesciences S.A. · Ch. du Glapin 6 · 1162 Saint-Prex · Switzerland Phone 41.21.823.4300
Edwards Lifesciences (Canada) Inc. · 1290 Central Pkwy West, Suite 300Mississauga, Ontario · Canada L5C 4R3 · Phone 905.566.4220 · 800.268.3993
Edwards Lifesciences Japan · 2-8 Rokubancho Chiyoda-ku, Tokyo 102-0085 · Japan · Phone 81.3.5213.5700
02 ED CVC Quick Guide CoverF 7/22/05 11:37 AM Page 1
Related Documents











