Quantitative Analysis of Mitral Valve Apparatus in Mitral Valve Prolapse Before and After Annuloplasty: A Three-Dimensional Intraoperative Transesophageal Study Francesco Maffessanti, MS, Nina A. Marsan, MD, Gloria Tamborini, MD, Lissa Sugeng, MD, Enrico G. Caiani, PhD, Paola Gripari, MD, Francesco Alamanni, MD, Valluvan Jeevanandam, MD, Roberto M. Lang, MD, and Mauro Pepi, MD, Milan, Italy; Chicago, Illinois Background: Intraoperative real-time three-dimensional transesophageal echocardiography has been shown useful in the evaluation of the mitral valve (MV) apparatus, and dedicated commercial software allows its quan- titative assessment. The aims of this study were to (1) quantify the effects induced by prolapse on MV anatomy in the presence of fibroelastic deficiency (FED) or Barlow’s disease (BD), (2) assess the effect of surgery on the MV apparatus, and (3) investigate the potential role of three-dimensional transesophageal echocardiography in surgical planning. Methods: Fifty-six patients (29 with FED, 27 with BD) undergoing MV repair and annuloplasty were studied immediately before and after surgery. Also, 18 age-matched patients with normal MV anatomy, undergoing coronary artery bypass, were included as a control group. Three-dimensional transesophageal echocardio- graphic data sets were acquired and analyzed to quantify several MV annulus and leaflet parameters using dedicated software. Results: MV prolapse and regurgitation were associated with a markedly enlarged annulus (area, 12.0 6 3.2 cm 2 in FED and 15.4 6 3.8 cm 2 in BD) and leaflets compared with controls (area, 7.5 6 2.1 cm 2 ), while annular height (4.5 6 1.3 mm in controls, 4.0 6 1.3 mm in FED, 5.3 6 1.6 mm in BD) and the mitral aortic angle (136 6 12 in controls, 141 6 12 in FED, 137 6 11 in BD) were similar. Patients with BD showed greater values than those with FED. MV repair and annuloplasty led to a significant undersizing of leaflet and annular areas (4.0 6 1.1 cm 2 in FED, 4.9 6 1.3 cm 2 in BD), diameters, and height (2.6 6 1.1 mm in FED, 3.4 6 1.4 mm in BD) compared with controls. Coaptation length remained in the normal range (30 6 5 mm in controls, 24 6 6 mm in FED, 28 6 6 mm in BD). Differences between BD and FED were reduced but still present after surgery. Conclusions: Intraoperative three-dimensional transesophageal echocardiography allows quantitative evalu- ation of the MV apparatus in the presence of FED or BD and could be useful for immediate assessment of the surgical procedure. (J Am Soc Echocardiogr 2011;24:405-13.) Keywords: Degenerative mitral valve prolapse, Mitral valve repair, Intraoperative real-time 3D echocardiography The mitral valve (MV) is a complex three-dimensional (3D) structure whose morphology is related to its function and may change as a con- sequence of altered physiologic conditions. Degenerative mitral re- gurgitation (MR), usually related to MV prolapse, is the most common cause of surgical MR in Western countries, representing the 60% to 70% of cases. 1 The two dominant etiologic subsets of this pathologic condition are Barlow’s disease (BD) and fibroelastic deficiency (FED). The preoperative differentiation between these two etiologies is a crucial aspect for referral, definition of the optimal surgical strategy, and postoperative outcome. In fact, in patients with BD, the prolapse is usually complex, and the best results are likely to be obtained via a full median sternotomy or lateral thoracotomy using several com- plex surgical techniques to restore valve competency, including leaflet sliding or resection, suture cleft, or annular plication. 2 In particular, leaflet sliding plasty aims to reduce posterior leaflet to the desired height by gathering up excess posterior leaflet tissue in the suture line. This procedure is often necessary in patients with BD to avoid postoperative systolic anterior motion with resultant left ventricular From the Department of Biomedical Engineering, Politecnico di Milano, Milan, Italy (F.M., E.G.C.); Centro Cardiologico Monzino IRCCS, Milan, Italy (N.A.M., G.T., P.G., F.A., M.P.); and the University of Chicago, Chicago, Illinois (L.S., V.J., R.M.L.). This study is part of the SurgAid project (http://www.surgaid.org), cofunded by the Italian Ministry of University and Research (Rome, Italy) (PRIN2007). Reprint requests: Francesco Maffessanti, MS, Department of Biomedical Engineering, Politecnico di Milano, Piazza L. da Vinci 32, 20133 Milan, Italy (E-mail: [email protected]). 0894-7317/$36.00 Copyright 2011 by the American Society of Echocardiography. doi:10.1016/j.echo.2011.01.012 405

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
From the Dep
(F.M., E.G.C.)
P.G., F.A., M
R.M.L.).
This study is p
Italian Ministry
Reprint requ
Engineering,
(E-mail: france
0894-7317/$3
Copyright 201
doi:10.1016/j.
Quantitative Analysis ofMitral Valve Apparatus inMitralValve Prolapse Before and After Annuloplasty:
A Three-Dimensional IntraoperativeTransesophageal Study
Francesco Maffessanti, MS, Nina A. Marsan, MD, Gloria Tamborini, MD, Lissa Sugeng, MD,Enrico G. Caiani, PhD, Paola Gripari, MD, Francesco Alamanni, MD, Valluvan Jeevanandam, MD,
Roberto M. Lang, MD, and Mauro Pepi, MD, Milan, Italy; Chicago, Illinois
Background: Intraoperative real-time three-dimensional transesophageal echocardiography has been shownuseful in the evaluation of themitral valve (MV) apparatus, and dedicated commercial software allows its quan-titative assessment. The aims of this study were to (1) quantify the effects induced by prolapse onMV anatomyin the presence of fibroelastic deficiency (FED) or Barlow’s disease (BD), (2) assess the effect of surgery on theMV apparatus, and (3) investigate the potential role of three-dimensional transesophageal echocardiographyin surgical planning.
Methods: Fifty-six patients (29 with FED, 27 with BD) undergoing MV repair and annuloplasty were studiedimmediately before and after surgery. Also, 18 age-matched patients with normal MV anatomy, undergoingcoronary artery bypass, were included as a control group. Three-dimensional transesophageal echocardio-graphic data sets were acquired and analyzed to quantify several MV annulus and leaflet parameters usingdedicated software.
Results: MV prolapse and regurgitation were associated with a markedly enlarged annulus (area, 12.0 63.2 cm2 in FED and 15.4 6 3.8 cm2 in BD) and leaflets compared with controls (area, 7.5 6 2.1 cm2), whileannular height (4.56 1.3 mm in controls, 4.06 1.3 mm in FED, 5.36 1.6 mm in BD) and the mitral aortic angle(136 6 12� in controls, 141 6 12� in FED, 137 6 11� in BD) were similar. Patients with BD showed greatervalues than those with FED. MV repair and annuloplasty led to a significant undersizing of leaflet and annularareas (4.06 1.1 cm2 in FED, 4.96 1.3 cm2 in BD), diameters, and height (2.66 1.1mm in FED, 3.46 1.4mm inBD) compared with controls. Coaptation length remained in the normal range (30 6 5 mm in controls, 24 66mm in FED, 286 6mm in BD). Differences between BD and FEDwere reduced but still present after surgery.
Conclusions: Intraoperative three-dimensional transesophageal echocardiography allows quantitative evalu-ation of the MV apparatus in the presence of FED or BD and could be useful for immediate assessment of thesurgical procedure. (J Am Soc Echocardiogr 2011;24:405-13.)
Keywords:Degenerativemitral valveprolapse,Mitral valve repair, Intraoperative real-time3Dechocardiography
The mitral valve (MV) is a complex three-dimensional (3D) structurewhose morphology is related to its function and may change as a con-sequence of altered physiologic conditions. Degenerative mitral re-
artment of Biomedical Engineering, Politecnico di Milano, Milan, Italy
; Centro Cardiologico Monzino IRCCS, Milan, Italy (N.A.M., G.T.,
.P.); and the University of Chicago, Chicago, Illinois (L.S., V.J.,
art of the SurgAid project (http://www.surgaid.org), cofunded by the
of University and Research (Rome, Italy) (PRIN2007).
ests: Francesco Maffessanti, MS, Department of Biomedical
Politecnico di Milano, Piazza L. da Vinci 32, 20133 Milan, Italy
6.00
1 by the American Society of Echocardiography.
echo.2011.01.012
gurgitation (MR), usually related to MV prolapse, is the mostcommon cause of surgical MR in Western countries, representingthe 60% to 70% of cases.1 The two dominant etiologic subsets ofthis pathologic condition are Barlow’s disease (BD) and fibroelasticdeficiency (FED).
The preoperative differentiation between these two etiologies isa crucial aspect for referral, definition of the optimal surgical strategy,and postoperative outcome. In fact, in patients with BD, the prolapseis usually complex, and the best results are likely to be obtained viaa full median sternotomy or lateral thoracotomy using several com-plex surgical techniques to restore valve competency, including leafletsliding or resection, suture cleft, or annular plication.2 In particular,leaflet sliding plasty aims to reduce posterior leaflet to the desiredheight by gathering up excess posterior leaflet tissue in the sutureline. This procedure is often necessary in patients with BD to avoidpostoperative systolic anterior motion with resultant left ventricular
405

Abbreviations
BD = Barlow’s disease
FED = Fibroelastic deficiency
LV = Left ventricular
MR = Mitral regurgitation
MV = Mitral valve
RT3D = Real-time three-
dimensional
TEE = Transesophageal
echocardiography
3D = Three-dimensional
2D = Two-dimensional
406 Maffessanti et al Journal of the American Society of EchocardiographyApril 2011
(LV) outflow tract obstruction.3
In contrast, FED lesions aremore localized and often causedby chordal rupture. For these rea-sons, patients with BD should beat times referred to a referenceMV repair surgical center, whileFED lesions can be frequently re-paired by experienced cardiacsurgeons through minimally in-vasive techniques.4
Although two-dimensional(2D) echocardiography is recog-nized as the reference techniquefor the preoperative assessmentof MV morphology, the accurateassessment of true MV shape has
been feasible only in animal models.5-10 In fact, in humans, in vivoevaluation has been based on an oversimplified description of MVmorphology using 2D main diameters together with a visualassessment of MV shape11,12 or using multiple 2D rotationalacquisitions, resulting in a time-consuming process followed by offline3D reconstruction.13-15 Real-time 3D (RT3D) transesophageal echo-cardiography (TEE) could overcome many of the above limitations.
Accordingly, our aim was threefold: (1) to quantitatively describethe morphology of the MV in degenerative MV disease, (2) to de-scribe the effects of MVrepair and annuloplasty on theMVapparatus,and (3) to investigate the potential role of RT3DTEE on surgical plan-ning and evaluation of MV repair.
METHODS
Patient Population
We studied 56 consecutive patients (44 men; mean age, 59 6 12years) with degenerative MV disease and severe MR with indicationsfor MV repair on the basis of complete 2D and RT3D transthoracicechocardiographic examinations. MR was defined as severe in thepresence of effective regurgitant orifice area $0.4 cm2 estimatedby the proximal isovelocity surface area technique or, alternatively,in the presence of vena contracta width >7 mm, according to recentrecommendations.16 Moreover, MR was considered severe in thepresence of chordal rupture associated with flail leaflets. Patientswith MV prolapse were retrospectively divided into two subgroupsaccording to the underlying pathology as established by surgical in-spection, those with FED (n = 29) and those with BD (n = 27), onthe basis of the classification of Carpentier et al.17 FED is characterizedby an impaired connective tissue production, leading to leaflet andchordal thinning, and chordal rupture, as the most common causeof regurgitation in these patients. Leaflet redundancy is limited withno billowing, and associated with slight annular dilation and an ab-sence of calcification. The prolapse usually involves a single scallop,frequently P2. In contrast, BD results in a myxomatous-appearingvalve, with thickened and redundant leaflets, a highly dilated annulus,and elongated chordae. Leaflet billowing and bileaflet multisegmentprolapse are common findings in BD.4
In addition, a control group of 18 age-matched patientswith normalMV anatomy undergoing coronary artery bypass was also studied.
Exclusion criteria were (1) associated MV stenosis, (2) tricuspid re-gurgitation greater than mild, (3) aortic valve disease, (4) contraindi-cations to TEE, (5) atrial fibrillation and cardiac arrhythmias, and (6)
myocarditis or pericardial or congenital heart disease. An additionalexclusion criterion for the control group was the presence of morethan mild MR.16
Study subjects were enrolled at Centro Cardiologico Monzino(Milan, Italy) or at the University of Chicago Hospitals (Chicago,IL). The protocol was approved by the respective institutional reviewboards, and informed consent was obtained from all participants.
Protocol
All patients underwent complete 2D transthoracic echocardiographicexaminations (S5 probe; Philips Medical Systems, Andover, MA) theday before surgery.
During surgery, standard 2D TEE was used to evaluate the mor-phology of the MV apparatus and to evaluate for MR, MV stenosis,and systolic anterior motion of theMV. In addition, after endotrachealintubation and before cardiopulmonary bypass, RT3D TEE was per-formed in all patients and repeated after the completion of MVrepair.All patients were examined under deep sedation and in sinus rhythm.
RT3D transesophageal echocardiographic images of the MV wereobtained in full-volume mode, in which electrocardiographically trig-gered wedge-shaped subvolumes were obtained over seven consecu-tive cardiac cycles, using an iE33 system equipped with a matrixprobe (X7-2t; Philips Medical Systems). The volumetric data setswere digitally stored and then transferred to a workstation for offlineanalysis.
The surgical approach for MV repair varied according to MV mor-phology and to the surgeon’s discretion. However, in both FED andBD groups, an annuloplasty ring was inserted to stabilize the annulusand the suture line. The surgical repair was considered successful inthe absence of significant residual MR (more than mild) and/or steno-sis (maximal mean gradient >6 mm Hg) and/or systolic anterior mo-tion of the anterior leaflet.
MV Quantification
Volumetric data sets were analyzed using MVQ software, part of theQLAB suite (Philips Medical Systems). After properly orienting the3D data set, the software automatically displays four quadrants:two 2D orthogonal-cut long-axis images of the mitral annulus, anMV en face image, and a panel with the rendered 3D data(Figure 1). In this visualization, the operator can separately optimizethe position of each of the three cut planes to improve the identifica-tion of MV structures. To ensure the best visualization of the prolapse,the late systolic frame, as the frame preceding aortic valve closure, wasselected for the analysis. Two couples of opposite reference annularpoints (anterolateral and posteromedial, anterior and posterior)were selected on the two orthogonal long-axis images. Additionally,the aortic root was manually labeled at the insertion of the posteriorcusp into the sinus of Valsalva.
The 3D model of the MV obtained from these initial referencepoints was subsequently further initialized by placing a couple of an-nular points in six additional rotational cross-sections of the volumet-ric data set, thus resulting in a total of 16 points to define the MVannulus.
After positioning the annular points, the leaflet profile was tracedand the coaptation points were marked on multiple cut planes or-thogonal to the anterolateral-posteromedial direction, with a distancebetween two subsequent planes equal to 0.25 cm. Finally, the oper-ator subdivided the anterior and posterior leaflets into the threescallops each (A1, A2, A3 and P1, P2, P3). The resulting 3D

Figure 1 Screenshot of the MVQ software showing the volume-rendered 3D data set (bottom right) as well as the three cut planesused to improve the visualization of the mitral valve. See text for details. A, Anterior; P, posterior.
Journal of the American Society of EchocardiographyVolume 24 Number 4
Maffessanti et al 407
representation was adjusted to visually match the anatomy as viewedin the 3D and 2D cut-plane views.
From this model, several parameters were calculated (Figure 2): (1)annular geometry: annular area, as the area of the minimal surfacespanning the annulus, anteroposterior diameter, anterolateral-posteromedial diameter, annular height, as the distance along theatrial-ventricular direction between the lowest and highest point ofthe annulus, and the planarity index, defined as the ratio of heightto anterolateral-posteromedial diameter, equal to zero for a flat MVand increasing when the MV’s saddle shape was more pronounced;2) leaflet size: exposed 3D area of the anterior or posterior leaflet,as well as the 3D total exposed leaflet area, as the sum of the twoprevious measurements; 3) coaptation geometry: the length of the co-aptation line projected to approximate leaflet surface, the area of theregion where the anterior and posterior leaflets overlap and the meanheight of the same region; and 4) the aortic-to-mitral plane angle.
Statistical Analysis
Continuous variables are expressed as mean 6 SD and categoricalvariables as absolute numbers or percentages.
A normal distribution of continuous variables was assessed usingthe Kolmogorov-Smirnov test. Preoperative and postoperative values
were compared using paired Student’s t tests or Wilcoxon’s signed-rank test as appropriate. Analysis of variance for independent mea-surements and Tukey’s honestly significantly different test for posthoc comparisons were used to assess the difference between theFED, BD, and control groups.
The association between the etiologic subgroups and the adoptionof a particular surgical approach was examined using Fisher’s exacttests.
Reproducibility of the 3Dmorphologic parameters was assessed ina randomly chosen subgroup of 15 patients. Intraobserver variabilitywas assessed using repeated measurements performed by the sameobserver a month later, while interobserver variability was evaluatedby repeating the analysis by a second independent observer, blindedto the results of all prior measurements. Variability was expressed interms of coefficients of variation between repeated measurementsas a percentage of their mean.
Significant determinants of leaflet sliding were evaluated by exam-ining their associations with several intraoperative variables by univar-iate analysis. Factors with significance on univariate analysis were usedas input in multivariate forward stepwise logistic regression to obtainthe independent determinants of leaflet sliding.
Statistical analyses were performed using SPSS version 17.0 (SPSS,Inc., Chicago, IL). P values < .05 were considered significant.
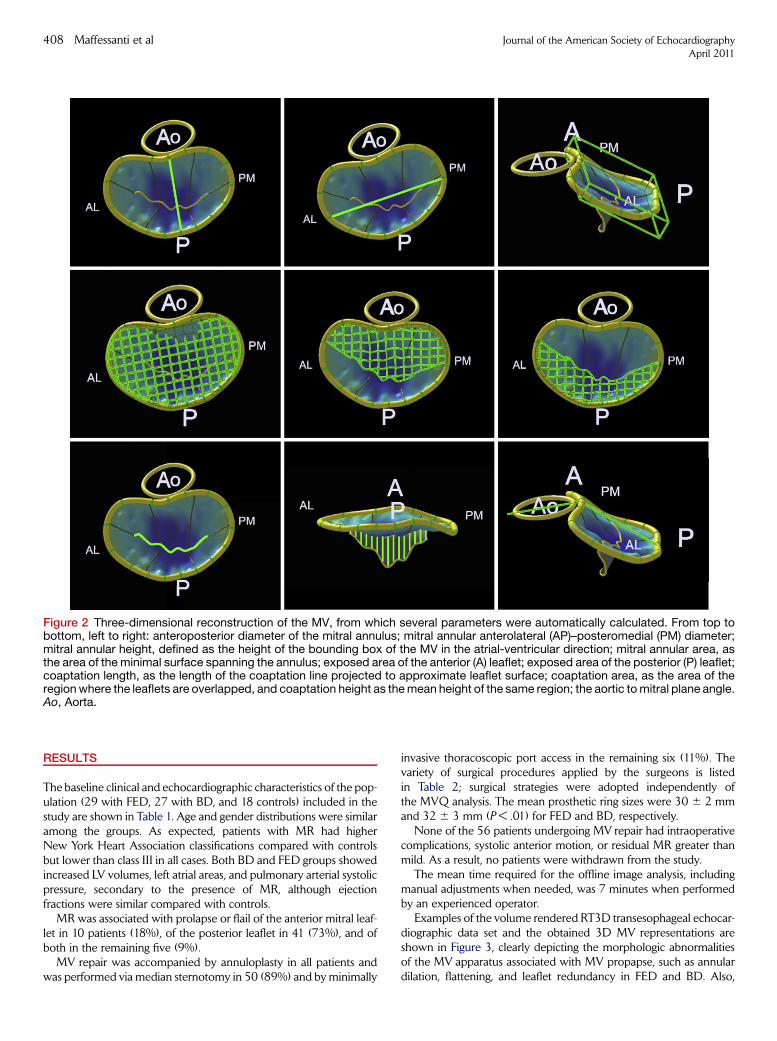
Figure 2 Three-dimensional reconstruction of the MV, from which several parameters were automatically calculated. From top tobottom, left to right: anteroposterior diameter of the mitral annulus; mitral annular anterolateral (AP)–posteromedial (PM) diameter;mitral annular height, defined as the height of the bounding box of the MV in the atrial-ventricular direction; mitral annular area, asthe area of the minimal surface spanning the annulus; exposed area of the anterior (A) leaflet; exposed area of the posterior (P) leaflet;coaptation length, as the length of the coaptation line projected to approximate leaflet surface; coaptation area, as the area of theregionwhere the leaflets are overlapped, and coaptation height as themean height of the same region; the aortic tomitral plane angle.Ao, Aorta.
408 Maffessanti et al Journal of the American Society of EchocardiographyApril 2011
RESULTS
The baseline clinical and echocardiographic characteristics of the pop-ulation (29 with FED, 27 with BD, and 18 controls) included in thestudy are shown in Table 1. Age and gender distributions were similaramong the groups. As expected, patients with MR had higherNew York Heart Association classifications compared with controlsbut lower than class III in all cases. Both BD and FED groups showedincreased LV volumes, left atrial areas, and pulmonary arterial systolicpressure, secondary to the presence of MR, although ejectionfractions were similar compared with controls.
MR was associated with prolapse or flail of the anterior mitral leaf-let in 10 patients (18%), of the posterior leaflet in 41 (73%), and ofboth in the remaining five (9%).
MV repair was accompanied by annuloplasty in all patients andwas performed via median sternotomy in 50 (89%) and by minimally
invasive thoracoscopic port access in the remaining six (11%). Thevariety of surgical procedures applied by the surgeons is listedin Table 2; surgical strategies were adopted independently ofthe MVQ analysis. The mean prosthetic ring sizes were 30 6 2 mmand 32 6 3 mm (P < .01) for FED and BD, respectively.
None of the 56 patients undergoing MV repair had intraoperativecomplications, systolic anterior motion, or residual MR greater thanmild. As a result, no patients were withdrawn from the study.
The mean time required for the offline image analysis, includingmanual adjustments when needed, was 7 minutes when performedby an experienced operator.
Examples of the volume rendered RT3D transesophageal echocar-diographic data set and the obtained 3D MV representations areshown in Figure 3, clearly depicting the morphologic abnormalitiesof the MV apparatus associated with MV propapse, such as annulardilation, flattening, and leaflet redundancy in FED and BD. Also,

Table 1 Clinical and echocardiographic characteristics incontrols and patients affected by FED or BD
Variable
Controls
(n = 18)
FED
(n = 29) P
BD
(n = 27) P
ClinicalAge (y) 57 6 4 64 6 12 .065 55 6 11 .477
Men 12 (67%) 23 (79%) .493 21 (78%) .499
BSA (m2) 1.8 6 0.2 1.9 6 0.3 .085 1.9 6 0.1 .108
NYHA class <.001 <.001
I 18 (100%) 12 (41%) 9 (33%)
II 0 (0%) 17 (59%) 18 (67%)III/IV 0 (0%) 0 (0%) 0 (0%)
EchocardiographicLVEDV (mL/m2) 54 6 8 82 6 25 <.001 79 6 22 <.001
LVESV (mL/m2) 20 6 7 32 6 14 <.001 27 6 10 <.001
LVEF (%) 62 6 8 61 6 10 .814 66 6 8 .078
LA area (cm2/m2) 12 6 4 17 6 5 .001 15 6 4 <.001
SPAP 27 6 5 42 6 16 <.001 34 6 8 <.001
Data are expressed as mean 6 SD or as number (percentage).
Unpaired t test or Fisher’s exact test versus controls.
BSA, Body surface area; LA, left atrial; LVEDV, LV end-diastolic
volume; LVEF, LV ejection fraction; LVESV, LV end-systolic volume;NYHA, New York Heart Association; SPAP, systolic pulmonary arte-
rial pressure.
Table 2 Characteristics of the surgical intervention,subdivided into two subgroups according to the underlyingpathology (FED or BD)
FED
(n = 29)
BD
(n = 27) P
Posterior leafletResection 13 (45%) 23 (85%) <.01
Sliding 8 (28%) 18 (67%) <.01Dreyfuss 2 (7%) 2 (7%) 1.00
Grossi 2 (7%) 6 (22%) .14
Gore-Tex neochord 4 (14%) 3 (11%) 1.00
Suture cleft 5 (17%) 1 (4%) .20
Chordal shortening 0 (0%) 1 (4%) .48
Anterior leafletResection 1 (3%) 0 (0%) 1.00
Gore-Tex neochord 3 (10%) 4 (15%) .70Dreyfuss 1 (3%) 0 (0%) 1.00
Chordal shortening 1 (3%) 0 (0%) 1.00
Edge to edge 1 (3%) 1 (4%) 1.00
Postoperative regurgitation .54
None 13 (45%) 16 (60%)
Trivial 15 (52%) 10 (37%)Mild 1 (3%) 1 (4%)
Journal of the American Society of EchocardiographyVolume 24 Number 4
Maffessanti et al 409
the RT3D transesophageal echocardiographic data sets relevant to thesame patients are illustrated in Videos 1 to 4 ( View video clipsonline).
The preoperative and postoperative values of annular diameter,height, and area for patients with FED, those with BD, and controlsubjects are shown in Figure 4. Similarly, Table 3 summarizes the re-sults obtained from the 3DMV quantification regarding leaflet, coap-tation, and annular flattening measurements, separately for eachstudy subgroup, immediately before and after MV repair, as well asthose relevant to the control group.
MV prolapse and MR were associated with markedly enlarged an-nulus and redundant leaflets. Both anteroposterior diameter andanterolateral-posteromedial diameter were found enlarged, leadingto a larger annular area compared with controls. Similarly, the ex-posed areas of both leaflets were greater in the presence of MV pro-lapse. Conversely, themitral aortic angle and themitral annular heightwere similar compared with controls, even if the planarity index wasreduced. Compared with patients with FED, those with BD werecharacterized by larger annuli with higher anteroposterior diametersand anterolateral-posteromedial diameters and higher mitral heightsin conjunction with increased annular and leaflets areas.
MV repair and annuloplasty led to significant decreases in all an-nular and leaflet parameters compared with preoperative values.Only the mitral aortic angle and the slight increase in the planarityindex, describing a more saddle-shaped annulus, did not reach sig-nificance.
As a consequence of MV repair, leaflet and annular areas, diame-ters, and heights were found to be undersized compared with con-trols. Similarly, coaptation length was shorter in patients with FEDthan in controls, whereas in patients with BD, this decrease was notsignificant. Differences between patients with BD and those withFED were reduced but still present after surgery: patients with BDhad larger annuli and leaflets, as evidenced by anterolateral-
posteromedial diameter, annular area, exposed 3D area, coaptationarea, and length.
Table 4 reports the results of the reproducibility analysis in the com-puted parameters. Intraoperator and interoperator analyses showedgood reproducibility in all parameters (<10%), except for MV height,characterized by the highest coefficients of variation (11.5% and17.2% for intraobserver and interobserver variability, respectively).
The relations between several preoperative parameters measuredfrom RT3D TEE and the sliding of the posterior leaflet performed bythe surgeon are described in Table 5. Univariate analysis showed thatonly two of the considered measurements, the area of the posteriorleaflet and the length of the P2 scallop, were significant factors asso-ciated with the choice to perform posterior leaflet sliding.
These significant factors were used as input for stepwise logisticregression analysis that resulted in only the length of the P2 scallopbeing a significant determinant of posterior leaflet sliding. The accu-racy of this parameter alone was equal to 72%, with positive and neg-ative predictive values of 74% and 71%, respectively.
DISCUSSION
The aim of this study was to characterize the 3D morphology of theMV using RT3D TEE in the presence of severe MR associated withFED or BD, immediately before and after MV repair, in comparisonwith a control group.
Annular Enlargement and Leaflet Redundancy
Quantitative 3D MV analysis on the basis of intraoperative data setswas feasible in all cases, and the time required for analysis was accept-able in a clinical setting. Intraobserver and interobserver variability ofannular diameters and leaflet area parameters wasminimal, thus dem-onstrating the good reproducibility of these measurements. Our

Figure 4 Bar graphs showing the results of annular measurements before and after MV repair in patients affected by FED (n = 29) orBD (n = 27). The shaded intervals in the background represent the reference range obtained in 18 age-matched normal subjects(mean 6 2 SDs). *P < .05 before versus after MV repair (paired t test); §P < .05 versus controls (unpaired t test).
Figure 3 Example of volume-renderedMV (top) as seen from the left atrium in patients withMV prolapse associatedwith FED (A,B) orBD (C,D). The 3D representations (bottom) clearly show themorphology of theMV and the region of prolapse in red scale: isolated P2scallop associated with FED and diffuse prolapse with redundant tissue in BD. The dynamic RT3D transesophageal echocardio-graphic data sets relevant to the same patients, are illustrated in Videos 1 to 4. Ao, Aorta.
410 Maffessanti et al Journal of the American Society of EchocardiographyApril 2011
findings demonstrated that severe MR is associated with a globalenlargement of the MV apparatus, including annular diameters andareas as well as leaflet surfaces. These changes were more pro-nounced in patients affected by BD compared with FED, consistent
with the characteristics of these two etiologic subsets as describedby Anyanwu and Adams.4 Indeed, the typical BDMV is characterizedby a more enlarged annulus, redundant leaflets, and multisegmentprolapse.
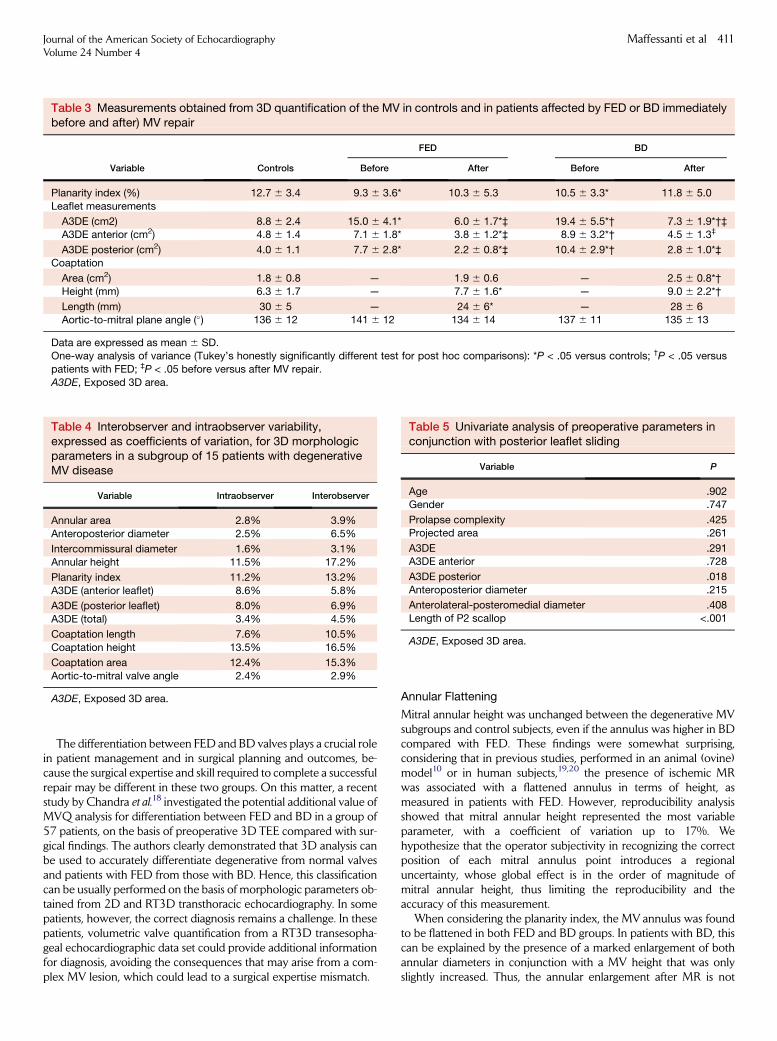
Table 3 Measurements obtained from 3D quantification of the MV in controls and in patients affected by FED or BD immediatelybefore and after) MV repair
Variable Controls
FED BD
Before After Before After
Planarity index (%) 12.7 6 3.4 9.3 6 3.6* 10.3 6 5.3 10.5 6 3.3* 11.8 6 5.0
Leaflet measurements
A3DE (cm2) 8.8 6 2.4 15.0 6 4.1* 6.0 6 1.7*‡ 19.4 6 5.5*† 7.3 6 1.9*†‡A3DE anterior (cm2) 4.8 6 1.4 7.1 6 1.8* 3.8 6 1.2*‡ 8.9 6 3.2*† 4.5 6 1.3‡
A3DE posterior (cm2) 4.0 6 1.1 7.7 6 2.8* 2.2 6 0.8*‡ 10.4 6 2.9*† 2.8 6 1.0*‡Coaptation
Area (cm2) 1.8 6 0.8 — 1.9 6 0.6 — 2.5 6 0.8*†Height (mm) 6.3 6 1.7 — 7.7 6 1.6* — 9.0 6 2.2*†
Length (mm) 30 6 5 — 24 6 6* — 28 6 6Aortic-to-mitral plane angle (�) 136 6 12 141 6 12 134 6 14 137 6 11 135 6 13
Data are expressed as mean 6 SD.One-way analysis of variance (Tukey’s honestly significantly different test for post hoc comparisons): *P < .05 versus controls; †P < .05 versus
patients with FED; ‡P < .05 before versus after MV repair.
A3DE, Exposed 3D area.
Table 4 Interobserver and intraobserver variability,expressed as coefficients of variation, for 3D morphologicparameters in a subgroup of 15 patients with degenerativeMV disease
Variable Intraobserver Interobserver
Annular area 2.8% 3.9%
Anteroposterior diameter 2.5% 6.5%
Intercommissural diameter 1.6% 3.1%
Annular height 11.5% 17.2%
Planarity index 11.2% 13.2%
A3DE (anterior leaflet) 8.6% 5.8%
A3DE (posterior leaflet) 8.0% 6.9%
A3DE (total) 3.4% 4.5%
Coaptation length 7.6% 10.5%
Coaptation height 13.5% 16.5%
Coaptation area 12.4% 15.3%
Aortic-to-mitral valve angle 2.4% 2.9%
A3DE, Exposed 3D area.
Table 5 Univariate analysis of preoperative parameters inconjunction with posterior leaflet sliding
Variable P
Age .902Gender .747
Prolapse complexity .425Projected area .261
A3DE .291A3DE anterior .728
A3DE posterior .018Anteroposterior diameter .215
Anterolateral-posteromedial diameter .408
Length of P2 scallop <.001
A3DE, Exposed 3D area.
Journal of the American Society of EchocardiographyVolume 24 Number 4
Maffessanti et al 411
The differentiation between FED and BD valves plays a crucial rolein patient management and in surgical planning and outcomes, be-cause the surgical expertise and skill required to complete a successfulrepair may be different in these two groups. On this matter, a recentstudy by Chandra et al.18 investigated the potential additional value ofMVQ analysis for differentiation between FED and BD in a group of57 patients, on the basis of preoperative 3D TEE compared with sur-gical findings. The authors clearly demonstrated that 3D analysis canbe used to accurately differentiate degenerative from normal valvesand patients with FED from those with BD. Hence, this classificationcan be usually performed on the basis of morphologic parameters ob-tained from 2D and RT3D transthoracic echocardiography. In somepatients, however, the correct diagnosis remains a challenge. In thesepatients, volumetric valve quantification from a RT3D transesopha-geal echocardiographic data set could provide additional informationfor diagnosis, avoiding the consequences that may arise from a com-plex MV lesion, which could lead to a surgical expertise mismatch.
Annular Flattening
Mitral annular height was unchanged between the degenerative MVsubgroups and control subjects, even if the annulus was higher in BDcompared with FED. These findings were somewhat surprising,considering that in previous studies, performed in an animal (ovine)model10 or in human subjects,19,20 the presence of ischemic MRwas associated with a flattened annulus in terms of height, asmeasured in patients with FED. However, reproducibility analysisshowed that mitral annular height represented the most variableparameter, with a coefficient of variation up to 17%. Wehypothesize that the operator subjectivity in recognizing the correctposition of each mitral annulus point introduces a regionaluncertainty, whose global effect is in the order of magnitude ofmitral annular height, thus limiting the reproducibility and theaccuracy of this measurement.
When considering the planarity index, the MV annulus was foundto be flattened in both FED and BD groups. In patients with BD, thiscan be explained by the presence of a marked enlargement of bothannular diameters in conjunction with a MV height that was onlyslightly increased. Thus, the annular enlargement after MR is not

412 Maffessanti et al Journal of the American Society of EchocardiographyApril 2011
isotropic, being more pronounced in the anteroposterior and inter-commissural directions rather than along the mitral height, resultingin flattening of theMV. The importance of the planarity index as a sur-rogate for the saddle shape of the annulus21 has been previously re-ported, both in an animal study22 and by computation analysis ofhuman data,8 and related to the minimization of leaflet stress.
We hypothesize that the LV volume overload due to MR, noted inboth FED and BD groups, plays a crucial role in mitral annulus flatten-ing. In fact, LV dilation, in particular at the basal level, could increasethe tension in the radial direction of the mitral annulus, explaining themore planar shape in the presence of MR and LV dilation, similar towhat was already demonstrated for leaflet stress by Salgo et al.8
Postoperative Morphologic Evaluation
The comparison between preoperative and postoperative measure-ments clearly depicts the effects of annuloplasty on MV morphology.Annular diameters and MV area were significantly smaller comparedwith preoperative values. The practice of undersizing the MVannulusafter annuloplasty in an attempt to improve reverse remodeling whilesimultaneously reducing the MR is well known and has been previ-ously described as an ‘‘annular solution to a LV problem.’’23 OnRT3D analysis, we were able to obtain a detailed collection of param-eters useful to quantify MVannular undersizing. Similar changes werefound in the exposed areas of both leaflets, even if the resection of theposterior leaflet was performed in 96% of the cases and only once forthe anterior leaflet. Moreover, the greater reduction in posterior leaf-let area in patients with BD compared with FED (Table 3) is in agree-ment with the higher rate of posterior leaflet resection and sliding(Table 2). The unexpected reduction of exposed area of the anteriorleaflet can be explained by the fact that undersizing themitral annulusled to an increase inMV coaptation height and area, thus reducing theexposed area of both leaflets.
Interestingly, after MV repair, the MV annulus was found to belarger in patients with BD than in those with FED, consistent withthe different mean sizes of the implanted prosthetic rings.Moreover, this result is in agreement with the conventional surgicalapproach that preferentially aims to place larger rings in patientswith BD to prevent systolic anterior motion of the MV.24
The ability to measuring coaptation height after MV repair, alwaysgreater than 7 mm, together with good prediction of posterior leafletresection on the basis of 3D measured leaflet length and area, furtherreinforces the clinical potentials of this technique.
Our findings, based on independently adopted surgical strategies,showed an association between preoperative posterior leaflet areaand height and sliding plasty. Because sliding plasty is considereda complex repair technique, requiring a highly skilled surgical team,the preoperative availability of these MVQ parameters could be use-ful in referring patients to reference centers at which this procedurecan be performed on the basis of the surgical decision after direct in-spection.
Advantages of RT3D TEE
The capability of 3D TEE to provide an exceptional overview of theMV apparatus and to improve the assessment of MV morphologyhas been demonstrated compared with standard 2D tech-niques.15,25-27 Compared with conventional 2D TEE, 3D TEEallows the computation of a larger set of measurements withoutbeing limited by individual cut planes, enabling complexmeasurements, such as area or planarity index. Our findingsconfirmed that 3D TEE allows an accurate and quantitative
description of the mitral apparatus that is helpful for both thediagnosis of degenerative MV disease and the potential surgicalplanning of the repair, as well as direct monitoring of the MVsurgical procedure.
Study Limitations
This study had several limitations, mainly related to the intraoperativedata acquisition. First, MV morphology was evaluated immediatelybefore and after cardiopulmonary bypass, with the patient being un-der deep sedation and intubated and thus in a nonphysiologic statethat could potentially introduce biases in the measurements.However, we tried to perform all acquisitions in similar hemodynamicconditions. Moreover, the entire 3D quantitative analysis was per-formed offline, and thus the objective potential benefit for surgicalplanning was limited in this study. Nevertheless, we suggest that iden-tical analysis could be easily performed during the preoperative as-sessment or on awake patients, thus enriching the knowledge ofMV morphology in patients undergoing MV repair and allowingcardiologists to assess the suitability for repair and predict surgicaloutcomes.12
Our study was focused on static behavior, thus ignoring the dy-namic changes in the MV apparatus that have been recently re-ported.19,28 However, because both annular control points andleaflet profiles must be trace manually, the analysis throughout thewhole cardiac cycle is time consuming, and its potential benefit ina surgical setting is unknown. For these reasons, we focused onlyon late systole, to be able to best visualize the MV prolapse.
Our study design included the involvement of two different med-ical centers, in Italy and the United States, with different surgicalschools, which could represent a potential source of bias in postoper-ative results. However, because our focus was on intraoperative post-repair and not on postoperative outcomes, this factor was considerednot a determinant. Moreover, statistical analysis applied to the twosubgroups separately for medical centers did not show any difference.
CONCLUSIONS
We applied a quantitative approach to study the morphology of theMV in the presence of severe MR. The preoperative assessmentshowed that this approach was able to characterize several character-istics of degenerative MV prolapse in terms of geometric changescompared with controls but also between the two most common eti-ologic subsets, FED and BD. Currently, this classification, based onmorphologic parameters obtained from 2D and 3D echocardiogra-phy, can be easily performed in most cases by an expert cardiologist,but in some patients, the correct diagnosis remains a challenge. In thissubset of patients, volumetric valve quantification from an RT3Dtransesophageal echocardiographic data set could play a crucial diag-nostic role, avoiding the consequences that may arise from a complexMV lesion, which could lead to a surgical expertise mismatch.Moreover, we showed that this tool is potentially adequate to assessMV morphology and the results of the surgical procedure also in theoperating room, thus providing the surgical team with additionalquantitative parameters for the evaluation of the immediate surgicaloutcome.
In conclusion, quantitative analysis of RT3D transesophageal echo-cardiographic data on the MV could have a clinical impact on diagno-sis, patient referral, and evaluation of the immediate surgical outcome.

Journal of the American Society of EchocardiographyVolume 24 Number 4
Maffessanti et al 413
REFERENCES
1. Enriquez-Sarano M, Akins CW, Vahanian A. Mitral regurgitation. Lancet2009;373:1382-94.
2. Adams DH, Anyanwu AC, Rahmanian PB, Filsoufi F. Current concepts inmitral valve repair for degenerative disease. Heart Fail Rev 2006;11:241-57.
3. Jebara VA, Mihaileanu S, Acar C, Brizard C, Grare P, Latremouille C, et al.Left ventricular outflow tract obstruction after mitral valve repair. Resultsof the sliding leaflet technique. Circulation 1993;88:II30-4.
4. Anyanwu AC, Adams DH. Etiologic classification of degenerative mitralvalve disease: Barlow’s disease and fibroelastic deficiency. Semin ThoracCardiovasc Surg 2007;19:90-6.
5. Eckert CE, Zubiate B, Vergnat M, Gorman JH III, Gorman RC, Sacks MS.In vivo dynamic deformation of themitral valve annulus. Ann Biomed Eng2009;37:1757-71.
6. Gorman JH III, Gupta KB, Streicher JT, Gorman RC, Jackson BM,Ratcliffe MB, et al. Dynamic three-dimensional imaging of the mitral valveand left ventricle by rapid sonomicrometry array localization. J ThoracCardiovasc Surg 1996;112:712-26.
7. Sacks MS, Enomoto Y, Graybill JR, Merryman WD, Zeeshan A,Yoganathan AP, et al. In-vivo dynamic deformation of the mitral valve an-terior leaflet. Ann Thorac Surg 2006;82:1369-77.
8. Salgo IS, Gorman JH III, Gorman RC, Jackson BM, Bowen FW, Plappert T,et al. Effect of annular shape on leaflet curvature in reducing mitral leafletstress. Circulation 2002;106:711-7.
9. Tsakiris AG, Von BG, Rastelli GC, Bourgeois MJ, Titus JL, Wood EH. Sizeand motion of the mitral valve annulus in anesthetized intact dogs. J ApplPhysiol 1971;30:611-8.
10. Ryan LP, Jackson BM, Parish LM, Plappert TJ, St. John-Sutton MG,Gorman JH III, et al. Regional and global patterns of annular remodelingin ischemic mitral regurgitation. Ann Thorac Surg 2007;84:553-9.
11. Caldarera I, Van Herwerden LA, Taams MA, Bos E, Roelandt JR. Multi-plane transoesophageal echocardiography and morphology of regurgitantmitral valves in surgical repair. Eur Heart J 1995;16:999-1006.
12. Omran AS, Woo A, David TE, Feindel CM, Rakowski H, Siu SC. Intra-operative transesophageal echocardiography accurately predicts mitralvalve anatomy and suitability for repair. J Am Soc Echocardiogr 2002;15:950-7.
13. Chen Q, Nosir YF, Vletter WB, Kint PP, Salustri A, Roelandt JR. Accurateassessment of mitral valve area in patients with mitral stenosis by three-dimensional echocardiography. J Am Soc Echocardiogr 1997;10:133-40.
14. Mahmood F, Subramaniam B, Gorman JH III, Levine RM, Gorman RC,Maslow A, et al. Three-dimensional echocardiographic assessment ofchanges in mitral valve geometry after valve repair. Ann Thorac Surg2009;88:1838-44.
15. Salustri A, Becker AE, van HL, Vletter WB, Ten Cate FJ, Roelandt JR.Three-dimensional echocardiography of normal and pathologic mitralvalve: a comparison with two-dimensional transesophageal echocardiog-raphy. J Am Coll Cardiol 1996;27:1502-10.
16. Zoghbi WA, Enriquez-Sarano M, Foster E, Grayburn PA, Kraft CD,Levine RA, et al. Recommendations for evaluation of the severity of nativevalvular regurgitation with two-dimensional and Doppler echocardiogra-phy. J Am Soc Echocardiogr 2003;16:777-802.
17. Carpentier A, Chauvaud S, Fabiani JN, Deloche A, Relland J, Lessana A,et al. Reconstructive surgery of mitral valve incompetence: ten-year ap-praisal. J Thorac Cardiovasc Surg 1980;79:338-48.
18. Chandra S, Salgo IS, Sugeng L, Weinert L, Tsang W, Takeuchi M, et al.Characterization of degenerative mitral valve disease using morphologicanalysis of real-time 3D echocardiographic images: objective insight intocomplexity and planning of mitral valve repair. Circ Cardiovasc Imaging2011;4:24-32.
19. Grewal J, Suri R, Mankad S, Tanaka A, Mahoney DW, Schaff HV, et al.Mitral annular dynamics in myxomatous valve disease: new insights withreal-time3-dimensional echocardiography.Circulation2010;121:1423-31.
20. Watanabe N, Ogasawara Y, Yamaura Y, Kawamoto T, Toyota E,Akasaka T, et al. Quantitation of mitral valve tenting in ischemic mitral re-gurgitation by transthoracic real-time three-dimensional echocardiogra-phy. J Am Coll Cardiol 2005;45:763-9.
21. Timek TA, Glasson JR, Lai DT, Liang D, Daughters GT, Ingels NB Jr., et al.Annular height-to-commissural width ratio of annulolasty rings in vivo.Circulation 2005;112(suppl):I423-8.
22. Padala M, Hutchison RA, Croft LR, Jimenez JH, Gorman RC,Gorman JH III, et al. Saddle shape of the mitral annulus reduces systolicstrains on the P2 segment of the posterior mitral leaflet. Ann ThoracSurg 2009;88:1499-504.
23. Cheng A, Nguyen TC, Malinowski M, Liang D, Daughters GT,Ingels NB Jr., et al. Effects of undersized mitral annuloplasty on regionaltransmural left ventricular wall strains and wall thickening mechanisms.Circulation 2006;114(suppl):I600-9.
24. Adams DH, Anyanwu AC, Rahmanian PB, Abascal V, Salzberg SP,Filsoufi F. Large annuloplasty rings facilitate mitral valve repair in Barlow’sdisease. Ann Thorac Surg 2006;82:2096-100.
25. Gripari P, Tamborini G, Barbier P, Maltagliati AC, Galli CA, Muratori M,et al. Real-time three-dimensional transoesophageal echocardiography:a new intraoperative feasible and useful technology in cardiac surgery.Int J Cardiovasc Imaging 2010;26:651-60.
26. Pepi M, Tamborini G, Maltagliati A, Galli CA, Sisillo E, Salvi L, et al. Head-to-head comparison of two- and three-dimensional transthoracic andtransesophageal echocardiography in the localization of mitral valve pro-lapse. J Am Coll Cardiol 2006;48:2524-30.
27. Sharma R, Mann J, Drummond L, Livesey SA, Simpson IA. The evaluationof real-time 3-dimensional transthoracic echocardiography for the preop-erative functional assessment of patients withmitral valve prolapse: a com-parison with 2-dimensional transesophageal echocardiography. J Am SocEchocardiogr 2007;20:934-40.
28. Veronesi F, Corsi C, Sugeng L, Caiani EG, Weinert L, Mor-Avi V, et al.Quantification of mitral apparatus dynamics in functional and ischemicmitral regurgitation using real-time 3-dimensional echocardiography.J Am Soc Echocardiogr 2008;21:347-54.
Related Documents











