I Quality Ratings and Patient Satisfaction with Norwegian GPs An Analysis of Municipal Capacity & Other Predictors of Overall GP Satisfaction & Waiting Time Satisfaction Evelyne Auer Master Thesis as part of the double-degree program European Master in Health Economics and Management UNIVERSITY OF OSLO Department of Health Management and Health Economics June 19, 2017

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

I
Quality Ratings and Patient Satisfaction with Norwegian GPs
An Analysis of Municipal Capacity & Other
Predictors of Overall GP Satisfaction & Waiting Time Satisfaction
Evelyne Auer
Master Thesis
as part of the double-degree program European Master in Health
Economics and Management
UNIVERSITY OF OSLO
Department of Health Management and Health Economics
June 19, 2017

II
“Today, patient satisfaction ratings are important indicators of the efficacy, quality, and
feasibility of healthcare services.” (Boquiren, Hack, Beaver, & Williamson, 2015)
© Evelyne Auer
2017
Quality Ratings and Patient Satisfaction of Norwegian GPs
Evelyne Auer
http://www.duo.uio.no/
Print: Reprosentralen, Universitetet i Oslo

III
Abstract
Background: Quality of care and patient satisfaction with health services and providers play
an ever increasing role and has been the focus of previous policy changes in Norwegian
healthcare. In light of the 2012 Coordination Reform and the 2013 GP Regulation that
introduced competition elements into primary care, the question arises whether patient
satisfaction measures are affected by municipal capacity and reflect previously observed quality
improvements.
Objective: The aim of this analysis is to investigate whether patient satisfaction ratings
obtained from the DIFI Citizen and GP User Surveys combined with data on municipal capacity
measures correspond to existing knowledge gained from previous research. More specifically,
we investigate users’ satisfaction levels in the survey periods 2010, 2012 and 2015, and examine
whether overall GP satisfaction and waiting time satisfaction are associated with socio-
demographic variables, self-assessed health, municipal capacity, and satisfaction measures.
Method: The study employs descriptive statistics, bivariate analysis and hierarchical binomial
logistic regression to investigate associations between various predictor variables with overall
GP satisfaction and waiting time satisfaction.
Results: We find that age, general life satisfaction and waiting time satisfaction are associated
with the odds of respondents’ Overall GP Satisfaction. In determining Waiting Time
Satisfaction, we detected a consistently significant positive association with age, municipal GP
supply satisfaction and general life satisfaction. Municipal capacity was negligible in its effect
on Overall GP Satisfaction and Waiting Time Satisfaction in 2010 but became increasingly
influential and significant in 2013 and 2015. Particularly in 2015, we find that high capacity
yields the highest odds of users to express high Overall GP Satisfaction and Waiting Time
Satisfaction.
Conclusion: The results of the present analysis are consistent with previous findings and add
to the theoretical framework of overall GP satisfaction and waiting time satisfaction. The results
suggest that municipal capacity has become increasingly important in determining patient
satisfaction and that high capacity and thus increased competition among primary care
physicians influences users’ satisfaction levels.

IV
Acknowledgements
Great gratitude I owe to my friends, who never stopped believing in my abilities and offered
mental support when the way towards the goal became rough. I am particularly thankful to
Karin Kraus for the countless encouraging and inspiring skype conversations and her
proofreading efforts.
Deep gratitude I owe to Paulius Olševskas for his understanding, his ceaseless encouragement
and infallible optimism, who supported me in so many ways during my time in Oslo. Without
him, a lot would not have been possible.
I am also grateful to my supervisor Tor Iversen for his academic expertise and productive
criticism. Special thanks I would like to express to Nils Mevenkamp for his expertise in
statistics and SPSS that were instrumental in my handling the data in a suitable, professional
way.
Last but not least, I would like to voice my deep gratitude to my family, who always
supported me in my decisions and next steps.
Evelyne Auer
Oslo, June 2017

V
Abbreviations
BLR Binomial Logistic Regression
DIFI Direktoratet for Forvaltning og IKT (Norwegian Agency for Public
Management and eGovernment)
GLM Generalized Linear Models
GP General Practitioner
HC Healthcare
LKU Norwegian Survey of Living Conditions (Levekårsundersøkelse)
OLS Ordinary Least Square
PS Patient Satisfaction
PE Patient Experience
TGPS Overall GP Satisfaction
WTS Waiting Time Satisfaction

VI
List of Tables
Table 1: Norwegian data sources assessing various dimensions of quality, patient
satisfaction & patient experience
Table 2: Variables before transformation
Table 3: Transformed variables
Table 4: Satisfaction variables for longitudinal view on satisfaction development
Table 5: Mann-Whitney U Test for group differences in TGPS and WTS 2015
Table 6: Model 1.1 TGPS_1 2015
Table 7: Significant variables & coefficients in TGPS_1 2015
Table 8: Model 1.2 TGPS_2 2015
Table 9: Model 1.3 TGPS_3 2015
Table 10: Model 2.1 WTA_1 2015
Table 11: Significant variables & coefficients in WTA_1 2015
Table 12: Model 2.2 WTA_2
Table 13: Model 2.3 WTA_3
Table 14: Mann-Whitney U Test for group differences in TGPS and WTS 2013
Table 15: Model 1.1 TGPS_1 2013
Table 16: Model 1.2 TGPS_2 2013
Table 17: Model 1.3 TGPS_3 2013
Table 18: Model 2.1 WTA_1 2013
Table 19: Model 2.2 WTA_2
Table 20: Model 2.3 WTA_3
Table 21: Mann-Whitney U Test for group differences in TGPS and WTS 2010
Table 22: Model 1.1 TGPS_1 2010
Table 23: Model 1.2 TGPS_2 2010

VII
Table 24: Model 1.3 TGPS_3 2010
Table 25: Model 2.1 WTA_1 2010
Table 26: Model 2.2 WTA_2 2010
Table 27: Model 2.3 WTA_3 2010
Table 28: Municipal capacity (absolute numbers)
Table 29: Mann-Whitney U Test on Satisfaction Variables 2015 – 2013
Table 30: Mean Ranks of Mann-Whitney U Test on Satisfaction Variables 2015 – 2013
Table 31: Mann-Whitney U Test on Satisfaction Variables 2013 – 2010
Table 32: Mean Ranks of Mann-Whitney U Test on Satisfaction Variables 2013 – 2010
Table 33: Mann-Whitney U Test on Satisfaction Variables 2015 – 2010
Table 34: Mean Ranks of Mann-Whitney U Test on Satisfaction Variables 2015 – 2010
Table 35: Mean Statistics for Satisfaction Variables 2015, 2013, 2010

VIII
List of Figures
Figure 1: Frequency Distribution of Satisfaction Variables 2015 (in %)
Figure 2: Frequency Distribution of Satisfaction Variables 2013 (in %)
Figure 3: Frequency Distribution of Satisfaction Variables 2010 (in %)
Figure 4: Overall GP Satisfaction 2015, 2013, 2010
Figure 5: Waiting Time Satisfaction 2015, 2013, 2010
Figure 6: Satisfaction with Referrals to Specialists 2015, 2013, 2010
Figure 7: Satisfaction with GP’s Medical Competence 2015, 2013, 2010
Figure 8: Satisfaction with Referrals to Other Services 2015 & 2013
Figure 9: Satisfaction with Time to Explain/Consultation Length 2015 & 2013
Figure 10: Level of Trust in the GP 2015 & 2013

IX
Table of Contents
1 INTRODUCTION ............................................................................................................ 3
1.1 Quality & Patient Satisfaction ................................................................................... 4
1.1.1 Quality ................................................................................................................ 4
1.1.2 Patient Satisfaction ............................................................................................. 5
1.2 The Norwegian Primary HC Setting ....................................................................... 11
1.2.1 Reforms in the Norwegian Primary HC System .............................................. 11
1.2.2 Financial Incentives & GP Payment Scheme ................................................... 13
1.2.3 Competition in the Norwegian Primary Healthcare Market ............................ 14
1.3 Relevant Research in Norway ................................................................................. 17
1.3.1 Measuring Quality & Patient Satisfaction in Norway ...................................... 17
1.3.2 Previous Research & Findings in Norway ....................................................... 19
1.4 Study Setting............................................................................................................ 20
1.5 Aim & Outline ......................................................................................................... 22
2 METHODOLOGY ......................................................................................................... 27
2.1 Data .......................................................................................................................... 27
2.1.1 Data Quality, Reliability & Validity ................................................................ 28
2.1.2 Data Limitation ................................................................................................ 29
2.1.3 Variables ........................................................................................................... 29
2.2 Analytical methods .................................................................................................. 33
2.2.1 Descriptive Statistics & Bivariate Analysis ..................................................... 33
2.2.2 Regression Analysis ......................................................................................... 34
3 RESULTS ....................................................................................................................... 43
3.1 2015 Analysis .......................................................................................................... 43
3.1.1 Descriptives 2015 ............................................................................................. 43
3.1.2 Bivariate Analysis 2015 ................................................................................... 44
3.1.3 Regression Analyses 2015 ............................................................................... 47
3.2 2013 Analysis .......................................................................................................... 59
3.2.1 Descriptives 2013 ............................................................................................. 59
3.2.2 Group Differences 2013 ................................................................................... 60

II
3.2.3 Regression Analysis 2013 ................................................................................ 63
3.3 2010 Analysis .......................................................................................................... 70
3.3.1 Descriptives 2010 ............................................................................................. 70
3.3.2 Group Differences 2010 ................................................................................... 71
3.3.3 Regression Analyses 2010 ............................................................................... 73
3.4 Longitudinal Analysis.............................................................................................. 79
3.4.1 Municipal Capacity Measures .......................................................................... 79
3.4.2 Overall GP Satisfaction .................................................................................... 79
3.4.3 Waiting Time Satisfaction ................................................................................ 80
3.4.4 Satisfaction w. Referrals to Specialists ............................................................ 81
3.4.5 Satisfaction w. GP’s Medical Competence ...................................................... 82
3.4.6 Satisfaction with Referrals to Other Services .................................................. 83
3.4.7 Satisfaction with Time to Explain/Consultation Length .................................. 84
3.4.8 Level of Trust in the GP ................................................................................... 85
3.4.9 Detecting Differences in Satisfaction Ratings ................................................. 86
4 DISCUSSION & CONCLUSION ................................................................................. 90
4.1 Summary of Findings .............................................................................................. 90
4.2 Main Results ............................................................................................................ 96
4.3 Limitations and Strengths ...................................................................................... 100
4.4 Policy Implications & Further Research ............................................................... 102
4.5 Conclusions ........................................................................................................... 105
References ............................................................................................................................ 106
Appendix .............................................................................................................................. 110

3
1 Introduction
Quality of care and patient satisfaction with health services and providers play an ever increasing
role in health care and have received particular attention since the dawn of the new millennium.
Norway reacted to this trend by adopting the continuous improvement of quality of care into
national law. After the introduction of the patient list system for GPs in 2001 and various other
laws on quality improvement in health care, the 2012 Coordination Reform (“Samhandlings-
reformen”) delegated more responsibility and governance to the municipal level in matters of
primary care. Targeting to strengthen primary care, competition elements were introduced that
incentivized quality of service provision. In addition, the 2013 GP Regulation (“Fastlegeforskrift
2013”) added another layer to improve primary care by increasing access through reducing waiting
time.
In the light of these policy changes, the question arises if the desired change can be measured in
terms of quality of, and patient satisfaction with, primary care services. To that end, multiple studies
have traced the development of quality and patient satisfaction over the past 15 years, basing the
studies on the two most widely used data sources, the Norwegian Survey of Living Conditions
(Levekårsundersøkelse) and the website Legelisten.no. While the first one provides important
insight into objective quality data such as actual waiting time and referrals to specialist care,
Legelisten is rather subjective, less specific on satisfaction measures, and self-sampled. Relatively
little is known regarding patients’ satisfaction with primary care physicians, particularly in relation
to previous policy changes that affected municipal capacity and competition in primary health care.
For this reason, the present study aims to depict the current status quo of patients’ perceived quality
of, and satisfaction with, GPs in relation to municipal capacity. The analysis is based on the DIFI
GP User Survey that includes extensive satisfaction measures, in combination with municipal
capacity data obtained from the Norwegian Directorate of Health (Helsedirektoratet). The main
focus will be on determining in how overall satisfaction with the GP and waiting time satisfaction
are influenced by potential predictors such as socio-demographic indicators, self-assessed health
status, other satisfaction measures and, most notably, municipal capacity. In tracing the
development of these measures before and after the introduction of the Coordination Reform
(utilizing the survey periods 2010, 2012, 2015), the study will examine to what extent patient

4
satisfaction measures and various related predictors reflect previous findings that were based on
different data sources. In this way, the analysis adds to the ongoing validation process and strives
to grant deeper insight into patients’ perception.
The present thesis is structured in the following way: The first part will provide an overview over
the current theory on quality and patient satisfaction, including determinants and limitations,
followed by an outline of the Norwegian primary healthcare setting and previous research related
to competition, quality and patient satisfaction with GPs in Norway, before stating the study aim.
The second part relates to the methodology and introduces the data and statistical tests that were
employed. In part three, we will present the results of the analysis. The fourth section will
summarize the results, discuss the main findings and implications and state further research options
as well as the final conclusion.
1.1 Quality & Patient Satisfaction
1.1.1 Quality
According to Donabedian (Donabedian & Bashshur, 2003), quality in health care results from “the
science and technology of health care” on the one hand, and “the application of that science and
technology”, on the other. Since it is impossible to guarantee quality itself, we can only strive for
an increase in probability of good or high-quality care, by taking actions “to establish, protect,
promote, and improve the quality of care”. George and Sanda (2007) define quality of health care
more concisely as “the degree to which health services for individual or populations increase the
likelihood of desired health outcomes and are consistent with current professional knowledge.”
In judging the quality as good or bad, improved or deteriorated, Donabedian (Donabedian &
Bashshur, 2003) identifies three information types of quality: structure, process and outcome.
These three types are interdependent as structure influences the process, and the process, in turn,
affects the outcome, which we judge as good or bad. Under structure, Donabedian (ibid) subsumes
“the conditions under which care is provided, including material resources, human resources and

5
organizational characteristics.” Process is defined by “the activities that constitute health care” as
carried out by professionals, patients and their families, such as diagnosis, treatment, rehabilitation,
and prevention. Outcome as the third information type of quality refers to “changes (desirable or
undesirable) in individuals and populations that can be attributed to health care” (ibid) including
changes in health status, changes in knowledge acquired by patients and family members, changes
in behavior of patients or family members that may influence future health, and the satisfaction of
patients and their family members with the care received and its outcomes.”
In Donabedian’s understanding of outcome, we find both an objectively measurable dimension in
the form of change in health status and change in a patient’s acquired knowledge or behavior, as
well as a subjective dimension through patient satisfaction. Accordingly, George and Sanda (2007)
distinguish between the patient perspective and the provider perspective with quality of care.
Patient-reported outcomes are consequently measured in terms of patient satisfaction.
1.1.2 Patient Satisfaction
Despite its widespread international use and its application in various healthcare contexts, the
concept of patient satisfaction has no clear, uniform definition nor a clear relation to the technical
quality of health services (Junewicz & Youngner, 2015). One of the most popular definitions is
Pascoe’s (1983), which establishes PS as “a health care recipient’s reaction to salient aspects of the
context, process, and result of their service experience.” And according to Boquiren et al. (2015),
PS measures the perceived quality of care, and as such forms the basis for evaluation and
improvement of health services, which shall serve as the preferred definition in the present thesis.
Satisfaction in particular reflects in how far expectations were met, as “it is influenced by varying
standards, different expectations, the patient’s disposition, time since care, and previous
experience” (Crow et al., 2002). Patients’ expectations indeed seem to play a vital role in the
subjective evaluation of health services. Apparently, high satisfaction ratings can be associated
with low or non-existent patient expectations (Junewicz & Youngner, 2015).
Returning to Donabedian, we adopt his view on PS as evaluative outcomes, i.e. “client opinions
about, and satisfaction with, various aspects of care, including accessibility, continuity,
thoroughness, humaneness, informativeness, effectiveness, and cost” that do not only reflect the

6
category of outcomes per se but links in with the structure and process as well (Donabedian &
Bashshur, 2003). Nowadays, PS measurement is largely seen in the light of the evolution of HC
service provision – as a driver for and consequence of patient engagement and focus – while also
adding to the ethical and legal obligations of institutions and providers, thus serving increased
accountability.
1.1.2.1 Determinants of Patient Satisfaction
PS is multi-dimensional as surveys investigate characteristics of both exogenous and endogenous
factors of the doctor-patient encounter, thus encompassing all the evaluative aspects summarized
by Donabedian (Donabedian & Bashshur, 2003); overall satisfaction, organization/structure and
accessibility/availability (relating to the facility), communication and interaction (between the HC
professional and the patient), technical skills and competence of the medical staff or HC personnel
as perceived by the patient or user. The following section shall provide a brief overview of the
various dimensions and their effect on PS.
Communication has proven to play a key role in achieving patient satisfaction. Specifically the
doctor’s ability to explain things in an understandable way, to listen effectively and to address
questions and concerns are vital elements for providing information to the patient, and thus for
creating a good doctor-patient relationship. For this reason, the majority of PS surveys include
questions or statements regarding the available time spent for asking questions, explaining, and
listening (Boquiren et al., 2015; Junewicz & Youngner, 2015).
In addition to communication, Boquiren et al. (2015) identified 4 more domains and key influencers
of PS. Relational conduct or humanistic characteristics, i.e. the doctor’s interpersonal skills,
respect, and shared decision-making together with the patient, form the second key domain.
Technical skills including expertise and competence are another major factor contributing to PS in
addition to personal qualities such as empathy, concern, kindness and friendliness. Lastly,
availability and accessibility are also important to patients. Consequently, high PS ratings correlate
with competent (as perceived), easily accessible doctors who listen carefully, spend efficient time
with the patient, treat the patient respectfully and explain well. Concurrently, the lowest PS ratings

7
were found for physicians of the high control type, while the highest ratings referred to person-
centered doctors (Flocke, Miller, & Crabtree, 2002).
PS is mainly but not exclusively defined by characteristics of the evaluated doctor or clinician.
Non-clinician related influencers of PS include organizational factors on a systemic or practice-
specific level such as staff interaction, difficulty of getting an appointment, waiting times,
equipment and accessibility, and also patient-related determinants such as socio-cultural beliefs,
socio-demographics, personality, and previous experience. All of these factors influence PS and
affect overall satisfaction ratings (Boquiren et al., 2015). Moreover, continuity of care is strongly
associated with higher PS, particularly in the context of primary care. Various studies show that
countries lacking continuity of care have generally lower satisfaction ratings than countries where
patients seek the same general practitioner over a long period of time (Fan, Burman, McDonell, &
Fihn, 2005).
On the individual level, a patient’s perception and evaluation is influenced by demographic factors,
socio-economic status, and self-assessed health status. Age has yielded the most consistent effect
on satisfaction ratings. Numerous studies found a positive correlation of age and satisfaction
(Carlin, Christianson, Keenan, & Finch, 2012; Hall & Dornan, 1990; Russell, Johnson, & White,
2015; Sitzia & Wood, 1997; Westaway, Rheeder, Van Zyl, & Seager, 2003), while there is some
counterevidence (Kahana, Lee, Kahana, & Yu, 2015). With regard to patients’ health status, studies
have been inconsistent in showing concrete one-sided associations with PS. Carlin et al.’s study
(2012), for instance, reports higher overall satisfaction ratings from patients with one or more
chronic conditions, while at the same time increased disease complexity combined with a good
understanding of the condition and treatment options as explained by the physician correlated with
lower overall satisfaction ratings. The influence of a patient’s health status on his/her satisfaction
level is relatively small. Fan et al. (2005) found that only 7% of the variance in PS can be explained
by the patient’s health status.
1.1.2.2 Measuring Patient Satisfaction
Conceivably because of its wide range of definitions and the influence of context, patient
satisfaction is measured with several tools. How patient satisfaction data are gathered not only
seems to depend on the use or underlying motive, the specific geographical context or the

8
healthcare system. Various satisfaction surveys have been developed based on different approaches
that are not always directly related to healthcare, such as defining the patient as user or customer
receiving a service. The particular challenge in creating standardized, reliable patient satisfaction
surveys lies in achieving comparability despite its multidimensional nature and in universal
applicability for all patients in a given setting, regardless of their disease and the resulting
differences in received care (George & Sanda, 2007).
1.1.2.3 Use of Patient Satisfaction Ratings
Measuring PS has multiple advantages. It can facilitate continuity of providers in that patients
remain with a “good” doctor through creating a long-term doctor-patient relationship. This, in turn,
increases the patient’s loyalty towards the doctor. PS ratings have also shown to correlate with
fewer malpractice suits, and a higher tendency to recommend one’s doctor (Boquiren et al., 2015).
It has also become increasingly common to link PS as an indicator of healthcare quality with
payment or reimbursement schemes to incentivize the quality improvement in healthcare provision
(Godager, Hennig-Schmidt, & Iversen, 2016; Junewicz & Youngner, 2015). In addition, PS ratings
are also used for marketing and quality assessment purposes and thus function as competitive
device, affecting patient volumes and thus also profits (Godager, Iversen, & Ma, 2015).
Performance standards and efficiency measures aid the patient in choosing, and potentially in
remaining with, a provider, which results in increased revenue and other financial benefits
(Boquiren et al., 2015; Junewicz & Youngner, 2015). Regarding its multifarious application, the
use of PS can be summarized as follows (Boquiren et al., 2015): “Today, patient satisfaction ratings
are important indicators of the efficacy, quality, and feasibility of healthcare services.” Although
it is essential to know how to achieve PS, particularly for GPs in markets with financial incentives,
there are also potential disadvantages stemming from an extensive focus on PS. Boquiren et al.
(2015) point out three elements necessary to satisfy a patient: 1) providing necessary care, thus
achieving positive outcomes; 2) granting the patient’s medically unnecessary wishes; and 3)
displaying good interpersonal skills, such as respect and communication skills.

9
In the Norwegian context, PS ratings are used to provide information about the perceived quality
of care (particularly by patients for patients) to facilitate the choice of a suitable GP (Biørn &
Godager, 2010; Godager et al., 2015). However, during the past 10 to 15 years, multiple reforms
in different countries linked quality measures to financial incentives in order to achieve improved
quality of care (Godager, Iversen, & Ma, 2009; Godager & Wiesen, 2013). More details on quality
ratings and PS with primary care in Norway will be given in section 1.3.
1.1.2.4 The Relation of Patient Satisfaction & Quality of Health Services
How is PS related to quality and does PS help improve the quality of care? Based on its use as
quality indicator, benchmarking tool for choice of provider, and incentive for quality improvement,
PS is often regarded a direct proxy for quality. However, the relationship between PS and quality
has not yet been completely clarified. Furthermore, the potential effect of PS on quality of care
improvement is not established (Junewicz & Youngner, 2015).
George & Sanda (2007) for instance, argue that PS reflects the care process (regarding waiting
time, provision of information, access, speed of treatment) but also correlates directly with outcome
of care. Junewicz & Youngner (2015), by contrast, warn against the conflation of PS and quality,
particularly with regard to the technical quality of care, due to patients’ lack of knowledge and the
prevalent information asymmetry in healthcare. Detsky & Shaul (2013) corroborate that PS does
not correlate with the technical quality of care since evidence-based standards are largely unknown
by patients. What seems to be agreed on in the literature is that PS is a prerequisite for patient
compliance. Only satisfied patients comply with the recommended treatment and follow physician
advice so that clinical outcomes improve. (Junewicz & Youngner, 2015)
1.1.2.5 Limitations & Criticism of PS
Boquiren et al. (2015) point to the contexts of PS as a potential caveat. For the adequate
interpretation of PS surveys, it is vital to know what the patient’s evaluation is referring to; whether
it concerns overall health care or specific services, one specific encounter or rather multiple
encounters during a given period of time, or a healthcare team instead of an individual clinician.

10
However, the prevailing main critical argument regarding PS is its subjectivity, which causes PS to
vary tremendously among individuals. In fact, in investigating variance of PS in primary care,
Salisbury et al. (2010) found that the vast majority of 95.4% of variance in PS ratings was caused
by individual differences of patients and random error, while only 4.6% resulted from differences
between practices. This was seemingly also true for patients who visited and rated the same GP or
practice. In satisfaction with waiting time, by contrast, less than 80% of the variance resulted from
individual differences between patients (Haggerty, 2010). From that we can conclude that overall
satisfaction is highly subjective and varies tremendously among individuals, while waiting time
satisfaction shows less variance and is therefore considered a more objective and reliable indicator.
Another aspect is the predominance of positive ratings and its compromising effect of sensitivity,
which lowers the precision of the measuring tool. One study has shown, for instance, that positive
ratings do not necessarily translate to high quality of care as positive ratings were also given after
negative experiences (Schneider & Palmer, 2002; Williams, Coyle, & Healy, 1998). These false
positives occurred when patients attributed the negative experience to other aspects that they
perceived to be beyond the physician’s control. In that way, insufficient consultation lengths were
interpreted by patients as organizational time constraints rather than the doctor’s lack of interest or
inability. It has been argued that negative ratings, by contrast, do not include false negatives and
therefore carry more weight with regard to reporting incidents such as medical errors or lack of
respect (Haggerty, 2010).
Considering its flaws and dangers of misinterpretation, one might question how much sense there
is in using PS surveys at all. A practical answer to that question is that in many settings and
countries, this is the best and sometimes only available option of assessing quality or how care is
perceived by patients or users. Haggerty (2010) and Junewicz & Youngner (2015) suggest in that
matter, that PS be used for assessing the interpersonal dimension of healthcare and the subjective
perceptions of soft skills that are difficult to measure objectively, while the patient’s subjective
view does not qualify for evaluating the technical quality of care. PS instruments are still useful for
benchmarking to recognize best practices and to highlight negative assessments. Nonetheless, these
need refinement “to maximize precision and minimize bias” (ibid).

11
It stands to reason that one should be very careful with the interpretation and particularly the
generalization of PS ratings. With regard to the concrete interpretation, Haggerty (2010) opines
that it would be “better to report the proportion of patients who are less than totally satisfied rather
than the average satisfaction” and concludes that “[h]igh satisfaction ratings indicate that care is
adequate not that it is of superior quality; low ratings indicate problems and should not be masked
by reporting average scores.”
1.2 The Norwegian Primary HC Setting
The Norwegian healthcare system is governed on three levels: the state, the four health regions and
the municipalities (an exception form dental services organized on the county level), which
organize the provision of sector-bound services. While hospitals are governed by the health
regions, primary care lies within the responsibility of the municipalities. GPs are the providers of
primary care in single practices, group practices and GP or emergency hospitals (“Legevakt” and
“Sykestue”). In the function of gatekeepers, they regulate the access to specialist care through
referrals. (Ringard, Sagan, Sperre Saunes, & Lindahl, 2013)
1.2.1 Reforms in the Norwegian Primary HC System
Since the beginning of the new millennium, the Norwegian healthcare system has undergone
several reforms that centered on patient empowerment and structural reorganization of health
service provision in order to improve the coordination of health care services between different
providers and to increase patient safety as well as quality of care (Ringard et al., 2013). The primary
care sector saw the first change in 2001 with the introduction of the patient list system. In order to
foster continuity of care, patients were registered with a regular GP and signed onto the GP’s patient
list. The length of the list ranges from a minimum of 500 to a maximum of 2500 patients per GP
and is agreed upon with municipalities. Since GPs can state their preferred list size, which may
deviate from the actual number of enlisted patients, lists can be open and accessible for new
patients, or closed, in which case the GP cannot take on any additional patients. Switching the GP
is possible but limited to GPs with open lists and restricted to two times per year. (Brekke &
Straume, 2017; Ringard et al., 2013)

12
The 2012 Coordination Reform (Samhandlingsreformen) was based on the identification of
particularly vulnerable patient groups that were prone to suffer from coordination problems, which
on a system level resulted in higher healthcare expenses. Consequently, the aim was to facilitate a
smoother transfer for the patient and improved coordination of services between the primary and
secondary sector in order to reduce unnecessary hospital admissions and pre-discharge waiting
times for subsequent services. The easier transition from hospitals to homes, for instance, arguably
enhances patient focus and simultaneously curbs healthcare expenditure. In addition, primary care
is strengthened through the increased focus on prevention on the municipality level (Ringard et al.,
2013)
The reform entered into force with the Municipality Health and Care Act and the Public Health
Act of 2011. These provide the legal framework for the coordination of public health work across
sectors and actors in healthcare, as well as between authorities at local, regional and national level.
This resulted in two major changes; Firstly, “municipalities were given full responsibility for
patients ready to be discharged from hospital treatment”, and secondly, municipalities are now co-
financing non-surgical healthcare services that are provided in specialist care (ibid). By means of
voluntary agreements between municipalities and hospitals and the strong financial disincentive to
treat patients in more costly specialist care facilities, the main goals of improved integration and
cost reduction were to be achieved. (ibid)
One original idea put forward as part of the reform was the increase in capacity in the form of
municipal GP density in order to strengthen service provision in primary care so that hospital
admissions would decline. An analysis by Seim (2010) prior to the introduction of the reform
concluded, however, that, contrary to expectations, an increased number of GPs in municipalities
would most likely increase hospital admissions. Only municipalities with so-called “GP hospitals”
(Sykestue) correlated with fewer hospital admissions. Nevertheless, a high density of primary care
institutions on the municipality level would decrease the elderly’s hospital admission rate. In the
light of multi-morbidity and disease complexity of this particular group, such reduced admissions
would translate to huge savings in healthcare costs. In the end, the proposal to increase GP density
in order to reduce the patient flow to specialist care was discarded, albeit the GP density still
increased steadily over the years (Godager & Iversen, 2016).

13
In 2013, a new GP regulation entered into force (Fastlegeforskrift 20131), which aimed particularly
at reducing waiting times and increasing access by listing the following demands:
- Patients shall receive appointments as soon as possible; usually within 5 work days.
- GPs are responsible for updating the patient’s “legemiddelliste” as soon as a change in
drug prescription has occurred.
- GPs shall offer more preventive measures.
- GPs shall offer home visits if necessary.
- 80% of phone calls to the GP shall be answered within 2 minutes.
- GPs shall be able to receive appointments electronically.
Investigating suitable data sources, what we would expect to observe as a consequence of the
successful adoption of the regulation is that 1) waiting time should have decreased from 2013 to
2015, which should coincide with higher waiting time satisfaction; 2) the number of home visits
should increase; and 3) access telephonically and electronically should improve, which should
translate to increased satisfaction in this domain.
1.2.2 Financial Incentives & GP Payment Scheme
In addition to the legal framework and various reforms addressing quality in primary healthcare,
the GP payment scheme provides financial incentives to balance self-motivated interests (income
generation) and patient wellbeing. A GPs’ income is subject to a mixed payment system consisting
of a lump sum and fees that is designed to balance over- and under-provision of medical services.
The basic practice income stems from the prospective capitation payment for each listed patient on
the GP’s list and constitutes one third of the income, which is paid by the municipality. The second
third is comprised of fee-for-service payments, which the GP receives from the national insurance
scheme as retrospective reimbursement for provided services. The last source of income is
composed of patients’ copayments for each visit. Both fee-for-service and copayments are fixed
across the country as negotiated on an annual basis, and no other financial arrangements exist.
(Iversen, 2005; Iversen & Lurås, 2000; Iversen & Ma, 2011)
1 http://www.ffo.no/Tema/Helse/Ny-fastlegeforskrift-innfort/

14
1.2.3 Competition in the Norwegian Primary Healthcare Market
Formerly, the Norwegian healthcare market was practically non-competitive due to the public
provision of services and the tax-based national insurance scheme covering costs. Previous
reforms, however, enhanced private provision of care and created financial incentives that
introduced some competition among providers in primary and secondary care.
The GP payment scheme combined with the patient list system introduced a competition element
in primary care. There is competition for patients among providers because patients are free to
enlist with their preferred GP. With fixed prices and financial incentives in place - capitation as
GPs’ base practice income and fee-for-service as an additional compensation for provided health
services -, doctors compete for patients due to their income-motivated self-interest (Brekke &
Straume, 2017; Godager et al., 2009).
Nonetheless, competition is limited due to the still largely public provision of services and strong
state regulation. Competition on price is very restricted since there are fixed prices for GP services
and caps on patients’ copayments, which renders demand highly price inelastic. As a consequence,
competition among providers relies heavily on non-price elements such as quality of care and
waiting time - the targets for improvement by previous primary care reforms. (Brekke & Straume,
2017)
Economic theory defines competition in terms of consumer choice. Thus, the number of providers
or producers in a specified market or geographical region are used to measure competition
(Bernstein & Gauthier, 1998). In the case of primary healthcare in Norway, we understand GP
services as the ‘supply’ market and define municipalities as the geographic entity in which GPs
operate. For this reason, one very intuitive way to measure competition in Norwegian primary
healthcare is to utilize municipal GP capacity, which has been used in previous studies (Iversen &
Ma, 2011), even though multiple other competition measures have been proposed and used
(Bernstein & Gauthier, 1998; Godager et al., 2015). Municipal capacity comprises of the total
number of registered GPs per municipality as well as related measures that are adjusted to
population density, such as GP density, i.e. registered GPs per 1000 inhabitants. Competition or
patient choice increases, the more GPs per municipality or per 1000 inhabitants are registered.
However, the number of registered GPs in a given municipality does not represent the real choice

15
patients have among GPs because real choice requires excess capacity (Brekke & Straume, 2017).
Only if there are sufficient accessible GPs, do patients have real opportunities to choose or switch
the GP. Therefore, it is much rather the number of GPs with open lists that serves as a proper
measure for competition intensity in the Norwegian GP market (Godager et al., 2015). In the
present study, we include the following municipality-specific capacity variables as theoretical and
real competition measures: free capacity (the number of available GPs with open lists), GP density,
available list places per 1000 inhabitants (LPPT), open lists per 1000 inhabitants (OLI), and open
list ratio (OLR).
The legal and financial framework (i.e. the Regular GP Scheme and list patient system) in
Norwegian PHC is steered from the municipality level. Municipalities regulate GP capacity (the
GP supply) by contracting a sufficient number of doctors and are responsible for doctors’ base
practice income that is defined by the number of listed patients on the GP’s patient list. In order to
secure their base practice income, GPs strive to keep their patients on their lists, thus ensuring not
only short-term quality of provided services but also continuity of care in the long run. On the
demand side, it was found that the quality of services (as perceived by the patients) is positively
associated with demand. The perceived quality of care and patient satisfaction with a GP do
influence the choice of GP, thus affecting demand. This renders quality and patient satisfaction a
competitive device in Norwegian primary healthcare (Biørn & Godager, 2010).
Another intriguing finding by Godager et al. (2015) is that additional competition in the form of
increased GP supply in a given municipality results in higher referral rates to specialized care.
Apparently, GPs also compete for patients by satisfying their requests for referrals in order to gain
and retain patients. This behavior, however, weakens the GP’s gatekeeping function and, in turn,
causes rising healthcare expenditures. This implies a positive association of patients’ overall
satisfaction with the GP and the number of referrals issued by the GP, or the corresponding
satisfaction with the GP’s referral policy. Simultaneously, structural indicators and competition
measures such as GP supply or available list places need to be balanced in order not to impose
counterproductive incentives that weaken other mechanisms such as the GP’s gatekeeping
function. (ibid)

16
Similarly to referrals, prescriptions can also function as a competitive device (Kann, Biorn, &
Luras, 2010; Schaumans, 2015) as indicated by the finding that GPs in Norwegian high-
competition municipalities (i.e. municipalities with a high GP density) issued 3% more reimbursed
and 2% more addictive drugs per patient. Under patient shortage (defined as more than 50 free list
places per GP), the prescription rates were even 5% and 6%, respectively, higher for reimbursed
and addictive drugs per patient. It was concluded that high competition can lead to a higher
inclination of GPs to achieve PS by following patients’ medically unnecessary demand for
prescriptions.
Another competitive device is waiting time. GPs can regulate their patients’ waiting time for an
appointment and in this way influence the frequency of consultations. Lower waiting time, for
instance, was found to translate to a higher number of consultations. Since GPs providing high
quality services are faced with excess demand, waiting time for an appointment increases. On the
other hand, GPs of lower popularity or patient shortage (due to patients’ perceived lower quality
of services) can offer shorter waiting times. This range of perceived quality and popularity of GPs
allows for the creation of multiple equilibria through the regulation of waiting time, where the least
popular providers offer the lowest waiting time to attract patients and the most popular providers
face persistent excess demand resulting in the longest waiting times. (Iversen & Lurås, 2002)
On investigating patient satisfaction and patient shortage, Lurås (2007) found that patients visiting
a GP with patient shortage (i.e. a considerably lower number of enlisted patients compared to the
potential maximum number of patients on a GP’s list) indeed expressed lower satisfaction with the
GP’s interpersonal skills, medical skills, referral practices and consultation length while being more
satisfied with waiting time. Godager and Iversen (2010) supported the finding that patient shortage
or low demand correlates with the GP’s personality, skills and behaviors in the doctor-patient
interaction.

17
1.3 Relevant Research in Norway
1.3.1 Measuring Quality & Patient Satisfaction in Norway
We currently find four independent instruments that measure quality, patient satisfaction or patient
experience to varying degrees with regard to primary care in Norway. These include the website
Legelisten.no, the Norwegian Survey of Living Conditions (“Levekårsundersøkelse” LKU), the
DIFI user report on GPs (Innbyggerundersøkelse – Brukerdel Fastlege), and the patient experience
questionnaire by the Norwegian Knowledge Centre for Health Services (Kunnskapssenteret).
The website legelisten.no, introduced in 2012, gives patients the possibility to rate their GPs with
a five-star rating system. Authenticated, yet anonymous patients can assign their GP up to five stars
in the satisfaction domains Overall satisfaction, satisfaction with Booking, Waiting, Consultation,
Listening, Insight and Advice. In addition, patients can formulate comments to give more detailed
information on why they rated their GP in a certain way or to state whatever else might seem
noteworthy. With its GP-specific content, the website presents an accessible, easy-to-use tool that
can guide patients’ decision-making regarding the choice of GP. Nonetheless, the scope of
satisfaction is so limited that it is not particularly suitable for evaluating quality of health care
services or for comparing geographical areas. Moreover, as the website is based on people’s own
initiative and thus self-selection, it does not count among the representative data sources, even
though the patterns of satisfaction have been shown to coincide with the ones found in other
representative studies (Sivertsen, 2014).
Kunnskapssenteret developed a method to measure patient experience with Norwegian GPs with
the specific goals: 1) to provide a standardized questionnaire for national and local surveys; and 2)
to test a data collection program that is usable for national surveys and recommendations for
conducting local surveys. As the name suggests, the questionnaire focuses on patients’ experience
with their GPs (Holmboe, Danielsen, & Iversen, 2015) rather than on patient satisfaction. Based
on 26 questions on the six dimensions of Patient Safety, Mastery, Coordination, Employees, GP,
and Availability, it combines some objective measures with the subjective patient experience and
thus allows for the comparison of patients’ expectations and the evaluation of their experience (e.g.
objective duration of waiting time and experienced length of waiting time). Judging from most

18
recent literature, this approach could well be considered the most advanced tool to measure the
perceived quality of care in Norway. However, it has some drawbacks as well. Due to its design
for single GP practices or primary care centers, it is comparatively narrow in the scope of questions
and of limited use for larger scale comparisons across regions or the country. In addition, it does
not include questions on complaints, referral behavior, and accessibility. As a relatively small
survey with only 2377 respondents of a non-randomized sample, it is also non-representative of
the Norwegian population. (ibid)
The LKU survey is part of the yearly EU SILC (EU Survey on Income and Living Conditions2).
With rotating focus topics each year, health & lifestyle are assessed every third year. The collected
data includes health status and lifestyle, diseases, effects of diseases, symptoms and disability of
the Norwegian population. It features predominantly objective measures (e.g. the number of visits,
or waiting time in days) with some very basic satisfaction questions regarding the use and attitude
towards health services. The GP-patient interaction is assessed by means of the following domains:
being taken seriously (“The GP takes me and my problems seriously”), trusting the GP (“I fully
trust the treatment I get from the GP”), time to talk (“The GP does not give me enough time”),
waiting time for an appointment (“It takes too much time to get an appointment with the GP”),
referrals (“The GP refers me to other services if I am in need of it”). These few basic questions on
patient satisfaction disregard the important domain of interaction and communication, and do not
provide a sufficient base for evaluating the patient’s perceived quality of services. Nonetheless, the
LKU survey provides a large, representative dataset, so that it has been used as the main source for
studying quality and patient satisfaction in the Norwegian setting.
Lastly, the DIFI survey on GP users3 has the most extensive and detailed questionnaire on patient
satisfaction with primary care, as it includes the satisfaction dimensions availability & accessibility
of facilities, waiting time, organization, the GP’s and employees’ competence and communication,
coordination of services with other providers & referral behavior, and complaints. These domains
are all subjective and evaluated by means of satisfaction ratings on a 7-item Likert scale. However,
it does not collect any objective data from the users apart from socio-demographic characteristics
2 https://www.ssb.no/innrapportering/personer-og-husholdning/lev 3 https://www.difi.no/rapporter-og-statistikk/undersokelser/innbyggerundersokelsen-2015/hva-mener-brukerne/fastlege

19
and broadly formulated health issues. One major weakness is therefore the lack of comparability
of subjective patient satisfaction to objective measures to establish an expectation baseline that
would aid the correct interpretation of data analysis. (Kjøllesdal Eide & Nonseid, 2015)
Legelisten.no Kunnskapssenteret Patient
experience with GPs
LKU Norwegian Survey
of Living Conditions
DIFI User Report on
GPs
Patient Satisfaction Patient Experience Patient Experience Patient Satisfaction
No objective data Limited objective data Extensive objective data
(waiting time, disease &
disability, use of services)
Little objective data
(socio-demographics)
Overall Satisfaction Overall Satisfaction --- Overall Satisfaction
Booking
Waiting
Availability
&
Waiting
Availability
Accessibility
Waiting
Consultation
Listening
Insight
Advice
GP (Competence &
Interaction);
Mastering patients’ health
Competence
Communication
Employees Employees
Coordination Coordination
Patient Safety
Self-assessed health Self-assessed health
Specifics on physician
(regular GP or other)
Public vs Private GP
Switching behavior
Complaints
Table 1: Norwegian data sources assessing various dimensions of quality, patient satisfaction & patient
experience
1.3.2 Previous Research & Findings in Norway
What determines patient satisfaction with the GP in Norway? Norwegian studies have shown that
the GP’s personal characteristics and interpersonal skills are most valued by patients, along with
technical competence. More specifically, characteristics such as respect, empathy, listening and
understanding the patient, taking time as well as the patient’s impression of being taken seriously
by the GP were the most prevalent determinants. (Folmo, 2014; Kilby, 2014)
Studies based on the LKU dataset such as “Brukernes erfaringer med fastlegeordningen 2001-
2015” (Godager & Iversen, 2016) give comparatively little insight into patient satisfaction,
particularly overall satisfaction with the GP. However, they provide crucial quantitative
information on the development of waiting time, consultation length, contact frequency and

20
referrals to specialists and allow for a comparison with waiting time satisfaction, satisfaction with
referrals to specialist care, and satisfaction with consultation length. The last study showed multiple
relevant developments in the context of the last policy change (Fastlegeforskrift 2013). Waiting
time decreased steadily from 1999 to 2005 before flattening out in 2008 and 2012, and then
dropping from 2012 to 2015. Overall there was a reduction of waiting time by 48% in the period
from 1999 to 2015. Median waiting time declined from 7 days in 1999 to 2 days in 2015. As both
median and average waiting time fell, waiting time satisfaction increased steadily from 2002 to
2012 (there are no available data on waiting time satisfaction in 2015). Respondents’ satisfaction
with referrals increased as well in 2015 compared to 2002 and 2012, and so did the public’s
satisfaction levels with consultation length. By contrast, the impression of being taken seriously by
the GP dropped in 2015 compared to 2002, although it increased slightly since 2012.
The DIFI GP User Report 2015 (Kjøllesdal Eide & Nonseid, 2015) points out that overall
satisfaction with the GP largely depends on the GP’s competence and communication with the
patient; two areas, with which the users are very satisfied. Of mediocre importance for overall GP
satisfaction is customization and user-focus, with which respondents expressed satisfaction. The
elements of minor influence include service (with high satisfaction), availability (satisfaction) and
providing important information (not significant). However, there is little information on the
determinants of waiting time satisfaction on the one hand, and other influencing factors of overall
GP and waiting time satisfaction such as socio-demographic or municipality-specific competition
indicators, which will be the main focus in the present analysis.
1.4 Study Setting
The present study is based on merged data from the DIFI Citizen Survey and GP User Survey
(“Innbyggerundersøkelse” and “Brukerdel Fastlege”) from the years 2010, 2013 and 2015. The
results of the DIFI surveys are published online and provide an overview of the current state and
development of user satisfaction with all available public services in Norway. All user reports
feature the same 7 key domains and ratings scales, which allows for a comparison and ranking of
all public services in Norway according to user satisfaction.

21
1) Total Satisfaction & Trust
2) Availability & Physical Conditions
3) Employee skills & User Customization
4) Employee Services
5) Digital Services
6) Information & Communication
7) Proceedings & Complaints
In comparing the various public services, the last user report (Kjøllesdal Eide & Nonseid, 2015)
showed that health and care services are located at the midpoint between public libraries with the
highest and government agencies with the lowest user satisfaction rates. Health services improved
continuously from 2010 to 2015, and, among these, particularly GPs received very good results in
terms of overall satisfaction. However, there is little change in waiting time satisfaction from 2010
to 2015. What determines overall satisfaction with any given public service are service provision
and user customization. Also overall GP satisfaction is largely determined by these two factors.
Taking a look at the results of the GP User Report 2015, we obtain an overview of the current state
of user satisfaction with GPs. Overall GP Satisfaction increased slightly, while overall
dissatisfaction remained stable compared to 2013 and 2010. Waiting time satisfaction (waiting time
for an appointment) improved lightly since more users expressed satisfaction and increased their
satisfaction rating, while simultaneously fewer respondents were dissatisfied. Only three percent
of users reported complaints in 2015, which corroborates the generally high satisfaction levels.
Further it was found that women generally rate more positively than men. More than two thirds of
users (67%) report having no health issues; 30% state physical conditions and 8% psychological
issues. This development corresponds to an increase in users with regular health issues over the
past five years. The most frequent contact reason in 2015 was follow-ups and prescription renewals.
The majority of users (58%) stated a contact frequency of two to five times per year, including
actual consultations as well as phone calls or accessing digital information. According to
respondents’ answers, 43% of users visited a public GP and 49% a private primary care physician.
This seems to be an unrealistic distribution given the fact that 95% of Norwegian GPs are self-
employed and only 5% count as public GPs (Brekke & Straume, 2017). Therefore, this variable is
treated cautiously in the analysis.

22
1.5 Aim & Outline
Previously, the fusions of LKU (Helse) with the GP database have been used as the main data
source to provide an overview over the development of various quality indicators and patient
satisfaction with primary and specialist care. The respective studies (Godager & Iversen, 2010,
2014, 2016) analyze quality and patient satisfaction both on the GP and municipality level. This
approach and the respective findings provide the main base of the present analysis. In this way, this
study serves as an additional source of information testing similar assumption based on DIFI data
and general municipality-specific GP data. Thus, it adds to the ongoing validation process of
scientific findings, which provides an opportunity to compare outcomes to draw wider conclusions.
By contrast to the by and large objective, quantitative data in the LKU studies, the present analysis
is limited to subjective satisfaction variables on various dimensions regarding GP services, which
were combined with quantitative municipality-specific capacity and competition measures. Thus,
patient satisfaction data was merged with indicators such as municipal GP density and free
capacity. In order to adjust for the difference in measurement level, the quantitative data was
transformed into categorical data of three groups, dividing the values into 33% percentiles.
The aim of this analysis is to investigate whether patient satisfaction ratings obtained from the DIFI
Citizen and GP User Surveys combined with data on municipality-specific capacity measures
correspond to existing knowledge gained from previous research, particularly the “User Experience
with the GP Scheme” (Godager & Iversen, 2016), by utilizing different data sources on quality
and patient satisfaction with Norwegian general practitioners (LKU and Legelisten). Moreover, the
analysis aims to trace the development of patient satisfaction before and after the introduction of
the coordination reform in 2012. The specific objective is to explore potential influencing factors
such as socio-demographic characteristics, health status, health care encounter variables and
municipal capacity in relation to Overall GP Satisfaction and waiting time satisfaction. While
previous studies investigated actual waiting times extensively and waiting time satisfaction to some
degree, Overall GP Satisfaction has hardly been studied in Norway since it is not part of LKU or
Legelisten data, the prime sources of satisfaction surveys. The relation of Waiting Time
Satisfaction and Overall GP Satisfaction with one another as with municipality-specific

23
competition indicators such as GP density and free capacity (GP’s with open lists) will also be
examined.
In light of undertaken healthcare reforms and previous study findings (particularly (Godager &
Iversen, 2010, 2014, 2016), the analysis shall answer the following research questions:
1) How did the perceived quality of GP services and patient satisfaction develop over
time, particularly in light of the 2012 Coordination Reform and the 2013 GP
Regulation?
2) More specifically, does municipality-specific capacity influence respondents’ ratings
of Overall GP Satisfaction and Waiting Time Satisfaction?
3) In how far do potential predictors such as socio-demographic variables, self-assessed
health status and other satisfaction ratings influence Overall GP Satisfaction and
Waiting Time Satisfaction?
In order to answer these questions, we will investigate exogenous and endogenous factors in
relation to Overall GP Satisfaction and Waiting Time Satisfaction, respectively. To do so, we
include in our analysis socio-demographic characteristics of the patient such as age, income and
level of education as exogenous factors, the GP type (private or public) as an endogenous factor,
self-assessed health status (exogenous), structural municipality-specific competition indicators
such as GP density and free capacity (exogenous) and the subjective determinants Waiting Time
Satisfaction, Life Satisfaction or overall happiness and Municipal GP Supply Satisfaction. Based
on the results of previous satisfaction studies relating to these predictors, the following hypotheses
were formulated:
H1: Overall GP Satisfaction is associated with the socio-demographic variables age, income,
and level of education. Numerous studies show internationally that higher age correlates with
higher satisfaction levels. Based on the findings Russel et al. (2015) and Zhang (2012), we expect
a positive association between overall GP satisfaction and age as well as a negative correlation
with income. In Norway, Zhang (2012) discovered more switching as an expression of
dissatisfaction with the GP among younger people and those with below-median income. We
further assume a negative correlation between overall GP satisfaction and education level based on
studies of Norwegian GP switching behavior due to overall dissatisfaction (Zhang, 2012).

24
H2: Both Overall GP Satisfaction and Waiting Time Satisfaction correlate with users’ self-
assessed health status. In the US, patients who assessed themselves as healthy were generally more
satisfied with their GP or the GP consultation compared to those who described their health as bad
(Badri, Attia, & Ustadi, 2009). On the other hand, patients with multiple chronic illnesses reported
higher overall satisfaction as well (Carlin et al., 2012). In Norway, Zhang (2012) showed that
worse health is associated with more frequent switching and thus lower satisfaction, while a better
health status correlates with higher satisfaction ratings (Jackson, Chamberlin, & Kroenke, 2001).
An analysis of LKU data showed that good health was also positively associated with waiting time
satisfaction (Grytten, Carlsen, & Skau, 2009).
H3: Waiting Time Satisfaction correlates with the socio-demographic variables age, income,
and level of education. Grytten et al. (2009) found that waiting time satisfaction is positively
associated with age in Norway. Based on the findings that Overall GP Satisfaction is negatively
correlated with income and education, a similar effect of these predictors is assumed for waiting
time satisfaction.
H4: We assume no correlation between Overall GP Satisfaction and type of GP (public or
private), while we expect a positive association of Waiting Time Satisfaction with private GPs.
Due to a lack of evidence, we can only assume to find higher waiting time satisfaction (due to its
inverse relation with actual waiting time) with private GPs since public GPs are likely to face higher
demand and therefore longer waiting times. Since the values of the variable do not correspond to
the Norwegian composition of public vas self-employed GPs, it will be regarded with caution and
interpreted in terms of users’ perception.
H5: There is a positive relation between Overall GP Satisfaction and Waiting Time
Satisfaction. While there are no Norwegian studies investigating the relation of overall GP
satisfaction and waiting time satisfaction so far, US studies found that both actual and perceived
waiting time influence patient satisfaction and perceived quality. (George & Sanda, 2007; Michael,
Schaffer, Egan, Little, & Pritchard, 2013; Russell et al., 2015; Vogus & McClelland, 2016).
H6: Life satisfaction is positively associated with both Overall GP Satisfaction and Waiting
Time Satisfaction. In the US context, George & Sanda (2007) found that life satisfaction and
general happiness or quality of life predict patients’ overall satisfaction with their GP. Based on

25
this finding, we assume to find the same relation in the Norwegian primary care setting and expect
a similar effect on patients’ ratings of waiting time satisfaction.
H7: Municipal GP Supply Satisfaction influences Waiting Time Satisfaction. We assume that
GP supply satisfaction presents a subjective measure of the available choice of GPs in a
municipality, reflecting users’ perceived GP density or free capacity in their municipality. Based
on the assumption that the actual municipal GP supply is positively associated with waiting time
satisfaction, we also suspect municipal GP supply satisfaction as ‘perceived GP supply’ to follow
the same positive relation. We expect that the more satisfied people are with the GP supply in their
municipality, the more satisfied they will be with waiting time. (However, a positive correlation
btw WTS and GPS could also be of a reversed direction; GP supply satisfaction could result from
waiting time satisfaction since people who perceive waiting time as satisfactory would probably
consider the municipal GP supply satisfactory as well, while dissatisfaction with waiting time could
correlate with decreased municipal GP supply satisfaction). This association has not been
investigated so far as it results from the merged DIFI dataset.
H8: Some municipality-specific capacity measures influence Overall GP Satisfaction and
Waiting Time Satisfaction. Previous studies found no relation between GP density and patient
satisfaction levels (Godager & Iversen, 2014, 2016; Wensing, Baker, Szecsenyi, Grol, & Group,
2004). Nonetheless, it is conceivable that a higher GP density would increase competition among
GPs and therefore raise quality, which, in turn, could result in higher overall satisfaction with the
GP. Waiting time satisfaction is presumably also positively related to GP density based on the
finding that higher GP capacity correlated with lower waiting time (Godager & Iversen, 2014).
Free capacity (the amount of GPs with open lists per municipality) correlates positively with the
switching behavior of Norwegian patients (Iversen & Lurås, 2008; Zhang, 2012) because more
choice appears to reduce patients’ satisfaction levels. For this reason, we assume that municipalities
with a high count of free capacity will coincide with lower levels of overall GP satisfaction but
higher levels of waiting time satisfaction based on good capacity correlating with shorter waiting
time (Godager & Iversen, 2010). Further, we do not expect any relation between overall GP
satisfaction and the competition measures open list ratio, open lists per 1000 inhabitants, and
available list places per 1000 inhabitants as they rather affect accessibility positively and therefore
influence waiting time satisfaction. Consequently, we expect to find positive relations between

26
waiting time satisfaction and GP density, free capacity, open lists per 1000 inhabitants based on
the finding of increased waiting time satisfaction in municipalities with patient-shortage (Grytten
et al., 2009) and available list places per 1000 inhabitants based on the outcome that more choice
increases competition and consequently reduces waiting time. Previous studies concluded that in
2008, GP capacity was associated with lower waiting time, while no such relation was found in
2012 (Godager & Iversen, 2010, 2014). Similarly, it was shown that more than 50 free list places
per 1000 inhabitants resulted in significantly shorter waiting time (Godager & Iversen, 2010). We
assume no relation between municipality size and Overall GP Satisfaction or Waiting Time
Satisfaction. Lastly, municipalities with patient shortage yielded significantly more waiting time
satisfaction (Grytten et al., 2009). Though patient shortage is a GP-specific indicator (reflecting
the desired GP list size compared to the actual number of listed patients), it is related to the number
of available GPs as well as the number of open lists per 1000 inhabitant.

27
2 Methodology
The present study aims to analyze patient satisfaction and the population’s quality ratings of
Norwegian GPs in relation to various specified variable groups, including, among others, socio-
economic and municipal supply-side data, to investigate potential developments since the 2012
coordination reform. The analysis therefore includes descriptive statistics on single variables,
bivariate analysis to investigate the relation of a pair of potentially associated variables, and
regression analysis for a deeper understanding of correlations among dependent and independent
variables. SPSS 24 and Excel were utilized as analytical tools.
2.1 Data
The empirical analysis is based on data retrieved from two different sources. DIFI (the Norwegian
Agency for Public Management and eGovernment) provided the datasets of
“Innbyggerundersøkelse” as well as “Fastlege Brukerdel”, each covering the years 2010, 2013 and
2015, which are publicly available online. These were combined with the municipality-specific
capacity data obtained from the Norwegian Directorate of Health (Helsedirektoratet) to gain insight
into potential relations of satisfaction and available doctors or list places.
The so-called “Innbyggerundersøkelse” (Norwegian Citizen Survey) is one of the biggest surveys
on Norwegian administration and public management, with the aim of assessing the population’s
satisfaction with various public services. It consists of a total of 23 surveys that address the various
national, regional and municipal public services. The “Fastlege Brukerdel” (henceforth ‘GP User
Survey’) is a special sub-survey targeting patients and recent “users” of GP services to collect data
specifically on patient satisfaction that is based on their previous experience (Kjøllesdal Eide &
Nonseid, 2015). The previous Norwegian Citizen Survey released in 2015 was conducted over a
time period from autumn 2014 until spring 2015 targeting the Norwegian population from the age
of 18 years onwards. The corresponding GP sub-survey on patient-satisfaction with primary care
physicians was sent to 6779 individuals that were identified as suitable respondents in the Citizen
Survey based on their stated experience, out of which 4324 replies were received
(Innbyggerundersøkelsen 2014/2015. Utvalg, respons og frafall, 2015).

28
2.1.1 Data Quality, Reliability & Validity
The DIFI data were collected and analyzed by the company Epinion who used the Norwegian
population register (“Folkeregisteret”) to randomly select 30 000 individuals for the main citizen
survey from pre-defined strata with regard to sex, age, and proportional distribution by population
size on a county level (‘fylke’). In order to adjust for any skewed population representation due to
the response rate, weights were employed (‘utvalgsvekt’ as selection weight and ‘populasjonsvekt’
as population weight). In assessing the potential selection bias, it was established that the
distribution of respondents does not differ significantly from the population distribution regarding
sex, age and geographical region. Thus, the stratified randomization combined with the included
weights adjusts for skewed selection in the dataset and thus reflects the demographic characteristics
of the Norwegian population, allowing for representative data analysis. (Innbyggerundersøkelsen
2014/2015. Utvalg, respons og frafall, 2015)
The question of data reliability and representativeness is, however, more complex with regard to
the GP User survey. Since the 23 User surveys (including the GP User survey) are based on self-
selection out of the pool of respondents answering the general Citizen Survey rather than on
drawing respondents from a known probability distribution of the various services, one cannot
easily generalize outcomes for all users of the respective services. It follows that each User survey
is not necessarily fully representative of Norwegian service users, which questions in part the
reliability of the GP survey. (ibid)
Despite the potentially skewed representation of population groups due this self-selection from the
respondent pool, the GP sub-survey can arguably still give a partially representative view since
these “users” of primary care services are part of the larger representative citizen survey and also
the respective weights have been employed in the analysis. In this way, it can cautiously be used
for an estimation of what a wide range of GP users think about various aspects of the primary care
services.

29
2.1.2 Data Limitation
For the present analysis, two unrelated and independently collected datasets were merged. Due to
the fact that the time frame of the DIFI surveys stretched over five months, more specifically from
19.09.2014 until 20.02.2015 (Innbyggerundersøkelsen 2014/2015. Utvalg, respons og frafall,
2015), a compromise with regard to the utilized time frame of capacity data had to be made that
allows for the complementary analysis of the two datasets. The respective time periods of both
overlap, but the municipal supply-side data specifically represent the distribution of GPs and
numbers of patients in any given municipality during the year 2014. Some respondents of the GP
User survey, however, sent their responses in early 2015. For this reason, the municipal competition
measures might not exactly reflect the situation with regard to patient list size at the point in time
of the respondent’s experience. Since this is the case for all three surveys of the years 2010, 2013
and 2015, it was decided to utilize the respective municipal supply datasets of the previous year,
i.e. 2009, 2012 and 2014, for merging and subsequent analysis.
An important point to consider is the original contrast in level of measurement between the
municipal supply-side and survey variables. While the survey variables are predominantly ordinal
based on a 7-item Likert scale representing people’s perceptions and opinions, the municipal
supply-side variables are continuous and very specific to each municipality. The general validity
and specificity of the continuous competition variables stand in some contrast to the ordinal-scaled
individual ratings of the survey respondents. Consequently, the continuous variables were
transformed into ordinal ones, thereby becoming less specific, in order to make the two variable
groups compatible for additional cohesion in the analysis and meaningful interpretation.
2.1.3 Variables
The present analysis is a longitudinal cross-sectional study, where variables were adopted from the
respective DIFI datasets. Except for the municipal capacity variables, all data have been planned
and developed by DIFI and Epinion, respectively, and were regarded reliable high-quality sources.
The analysis is limited to variables measured by the surveys and the municipal competition
measures. New variables have been computed as necessary based on the transformation of existing
variables. Table 2 below lists all variables used in the analysis, which were taken from the three
datasets.

30
Variable Group Code Variable Label
Satisfaction with
respondent’s GP S03q55
Overall GP Satisfaction:
Considering all the experiences you had with your GP, how
satisfied or dissatisfied are you with your GP overall?
Waiting Time
Satisfaction S03q13
Satisfaction with waiting time until appointment:
How satisfied or dissatisfied are you with the waiting time?
Socio-demographic
variables
AlderKat
Age group (5 categories):
Alder 1) 18 – 24 years; Alder 2) 25 – 34 years
Alder 3) 35 – 49 years; Alder 4) 50 – 66 years
Alder 5) 67 + years
q71
Income (yearly gross income per household, 8 categories):
1) Up to 150.000 NOK;
2) From 150.000 to 300.000 NOK
3) From 300.000 to 400.000 NOK
4) From 400.000 to 500.000 NOK
5) From 500.000 to 600.000 NOK
6) From 600.000 to 700.000 NOK
7) From 700.000 to 1 mio. NOK
8) More than 1 mio. NOK
q1 Education (highest level of education, 4 categories):
1) Primary school 2) Secondary School/High-school
3) Vocational school; 4) University or College
Respondent’s self-
assessed health
status
q68
Disabilities (6 categories): Do you have any physical or psychological impairment impacting
your daily life for over 6 months?
1) Yes, motoric impairment
2) Yes, visual or hearing impairment
3) Yes, psychological issues
4) Yes, learning difficulties
5) Yes, other
6) None
S03q5
Health issues: Do you have any health issues?
1) Mental issues or disorders
2) Substance addiction (alcohol etc.)
3) Physical disorders or issues
4) None of these
Municipality-
specific (supply-
side) variables
fkap Free capacity (available GPs with open lists)
GPD GP density (registered GPs per 1000 listed inhabitants)
LPPT Available list places per 1000 listed inhabitants
OLI Available GPs per 1000 listed inhabitants
OLR Open list ratio (ratio of available GPs and registered GPs)
S03q3 Public vs. private GP: Was your GP public or private?
Kommunestr
Municipality size (4 categories)
1) Below 5000 inhabitants
2) 5000 to 20.000 inhabitants
3) 20.000 to 110.000 inhabitants
4) More than 110.000 inhabitants
Other satisfaction
ratings
q13.35 Satisfaction with GP supply in respondent’s municipality: How
satisfied or dissatisfied are you with the GP supply in your
municipality?
q72 Overall happiness/life satisfaction: All in all, how satisfied or
dissatisfied are you with your existence?
Table 2: Variables before transformation

31
DEPENDENT VARIABLES
Variable Group Code Variable Label
Satisfaction with
respondent’s GP
TGPS_1
TGPS_2
TGPS_3
Dichotomized Overall GP Satisfaction: TGPS_1) 0 = dissatisfaction/neutral, 1 = satisfaction
TGPS_2) 0 = other, 1 = rather or highly satisfied
TGPS_3) 0 = other, 1 = highly satisfied
Waiting Time
Satisfaction
WTA_1
WTA_2
WTA_3
Dichotomized Waiting Time Satisfaction WTA_1) 0 = dissatisfaction/neutral, 1 = satisfaction
WTA_2) 0 = other, 1 = rather or highly satisfied
WTA_3) 0 = other, 1 = highly satisfied
INDEPENDENT VARIABLES
Socio-
demographic
variables
Age_cat
Age group (3 categories):
1) Young
2) Middle-aged
3) Old
bm_Income Below-median income
0) Above-median
1) Below-median
bhs_education
Education (highest level of education, 4 categories):
0) Primary education
1) Secondary or higher education
Respondent’s self-
assessed health
status
No_Disabilities 0) Some disability (any disability or impairment)
1) No disability
GoodHealth 0) No good health (having one or multiple issues)
1) Good health (having no health issues)
Municipality-
specific supply-
side variables
Fkap_cat Categorized free capacity (1= low, 2= medium, 3= high)
GPD_cat Categorized GP density (low, medium, high)
LPPT_cat Categorized LPPT (low, medium, high)
OLI_cat Categorized OLI (low, medium, high)
OLR_cat Categorized OLR (low, medium, high)
publicGP 0) Private GP
1) Public GP
Other satisfaction HappyLife Dichotomized life satisfaction
0) Dissatisfied with life
1) Satisfied with life
Utilization avg_contactfreq Average contact frequency
0) Non-average (below or above average)
1) Average (2-5 times per year)
Table 3: Transformed variables
Based on the aim of the analysis, two dependent variables were identified, i.e. Overall GP
Satisfaction and Waiting Time Satisfaction. These were dichotomized in order to facilitate the
interpretation of group differences that depict the immediate relationship with selected independent
variables, on the one hand, and serve the goal of predicting one category in the course of the logistic
regression models. All satisfaction variables initially consisted of 7 categories mirroring the 7-item
Likert scale ranging from -3 to +3, which were then aggregated and collapsed into meaningful

32
dichotomies. A similar procedure was employed to transform independent variables such as health
status, education, income, contact frequency as well as life satisfaction into compact dichotomies.
After computation and selection of the relevant municipality-specific capacity variables (including
free capacity, GP density, available list places per 1000 listed inhabitants, open list per 1000
inhabitants, and open list ratio), the originally continuous scale was transformed into categories by
defining two cut points on the 33% and 66% percentiles. These divide the cases into three
categories with roughly equal case count (low, middle and high). This grouping of cases is merely
a formal one and, as such, does not depend on the initial distribution of the variable. It enhances
the coherence of the analysis and brings these variables onto the same measurement scale as the
rest of the independent variables included in the regression analysis.
Further independent variables of interest are complaints (“Have you issued a complaint during the
past 12 months?”) and the utilization variables including contact frequency, contact type (home
visit or practice consultation), and contact reason (medical check-up, follow-up, prescription
renewal etc.). Due to the extremely low case count of complaints and the potentially disruptive
influence of demand-side effects (particularly in the regression analysis), the complaints and the
utilization variables were excluded from the main analysis. For the purpose of conducting a
longitudinal analysis to trace satisfaction development, the satisfaction variables listed in table 3
were used in a Mann-Whitney U Test.
Satisfaction related
to Customization
& Communication
S03q18 Satisfaction with time to explain/ consultation length: How satisfied or dissatisfied are you with the time you had
to explain your situation?
S03q21 Satisfaction with GP’s referral practice (specialist):
How satisfied or dissatisfied are you with the GP’s referral
practice to send you to a follow-up or a specialist?
S03q41 Satisfaction with the GP’s medical competence:
How satisfied or dissatisfied are you with the GP’s medical
competence to give you a good treatment?
S03q44 Satisfaction with GP referrals to other services:
How satisfied or dissatisfied are you with the GP’s practice
to refer you to other relevant services (psychologist etc.)?
S03q58 Level of trust in the GP:
How big or small is your level of trust in your GP?
Table 4: Satisfaction variables for longitudinal view on satisfaction development

33
2.2 Analytical methods
2.2.1 Descriptive Statistics & Bivariate Analysis
As an initial step, the relevant dependent and independent variables are investigated with regard to
their frequency and distribution. Bivariate analyses are conducted subsequently in order to provide
tables and figures that demonstrate an immediate picture of the relationship between the dependent
and independent variables. To that end, Mann-Whitney U Tests are run.
The Mann-Whitney U Test is a rank-based, nonparametric test that detects differences between
two groups on a continuous or ordinal dependent variable. It presents an alternative to the
independent-samples t-test when violating the assumptions of normal distribution of the dependent
variable and ordinal scale data (Huizingh, 2007). In the context of the present analysis, it is
particularly suitable for the longitudinal investigation of the two main variables TGPS and WTS
as it provides insight into whether satisfaction ratings differed significantly between 2010 and
2012, and between 2012 and 2015, for example.
The necessary assumptions of the test include a) one dependent variable of continuous or ordinal
scale (this criterion is met since both waiting time satisfaction and overall GP satisfaction are
ordinal variables measured on a 7-item Likert scale), 2) one independent variable with two
independent categorical groups (the multiple categories of ordinal independent variables such as
age, for instance, with young, middle-aged and old respondent groups where compared in pairs of
two at a time), 3) independent observations (the two groups are mutually exclusive), and 4) the
distribution shapes for both groups that are being compared need to be determined for correct
interpretation.
If p > .05 not significant Keep Null Hypothesis H0:
The median or mean ranks of the two groups are equal.
If p < .05 significant Reject Null Hypothesis H0 & adopt Alternate Hypothesis:
The median or mean ranks of the two groups differ.

34
The distribution shapes of the two groups determine the interpretation of the test result. If the
general distribution shapes are identical or very similar, the test result can be used to determine
differences in median. If, however, the distribution shapes of the two groups being compared differ,
then only the differences in mean ranks can be compared to identify higher (or lower) scores in one
group compared to the other. The null hypothesis assumes that the distribution of the two groups
is equal. Thus the median or mean rank of group A equals the median or mean rank of group B.
With differing medians or mean ranks, the alternative hypothesis is adopted. The relevant test
statistic for large case counts in SPSS is the ‘Asymptotic Significance’ value which yields the p-
value at a significance level of 0.05. ("Laerd Statistics: SPSS Statistics Tutorials and Statistical
Guides," 2015)
2.2.2 Regression Analysis
For the investigation of the ordinal dependent variables in relation to selected independent
variables, two analytical methods were identified, i.e. binomial logistic regression (BLR) and
ordinal regression (OR). The latter can be conducted in multiple ways, the most common of which
appears to be cumulative odds ordinal logistic regression. Cumulative odds ordinal logistic
regression is a more specialized type of binomial logistic regression. BLR consists, in fact, of
multiple binomial logistic regressions that treat the ordinal dependent variable as cumulatively split
into multiple dichotomous variables. This means that as part of the necessary assumption testing
process, BLR needs to be run on every dichotomous categorical variable created out of the original
ordinal variable in order to assess the assumption of proportional odds. However, we assume that
a violation of this assumption is very likely because independent variables do not necessarily show
equal influence on proportional splits of the dependent variable, particularly with a large number
of independent variables as in the present study. For this reason, binomial logistic regression was
chosen.
2.2.2.1 Binomial Logistic Regression
BLR is considered a special type of Generalized Linear Models (GLM) that are characterized by
one dependent variable and multiple independent variables. In GLM, which utilizes the ordinary
least squares (OLS) method for error prediction, the relationship between dependent and

35
independent variables is linear. In the special case of logistic regression, by contrast, the linear
relationship exists between the logit transformation of the dependent variable (the log odds) and
the independent variables. (Huizingh, 2007; "Laerd Statistics: SPSS Statistics Tutorials and
Statistical Guides," 2015)
Since BLR tests the probability of outcomes (the odds of one event occurring or not), aiming to
predict the odds of category A rather than category B, the main assumption and testing prerequisite
is the dichotomous nature of the dependent variable (ibid). Since the two main variables
(‘Satisfaction with Waiting Time until Appointment’ and ‘Overall GP Satisfaction’) are ordinal
with a 7-item Likert scale, these were transformed into meaningful binary categories prior to
analysis. Various cut-off points can be defined to achieve dichotomization depending on which
items are subsumed into the binary categories. Due to the nature of the 7-item Likert scale, it is
intuitive to subsume all negative and neutral items (ranging from -3 up to 0) into the first category
denoting dissatisfaction, and to integrate all positive items (from +1 to +3) into the second category
indicating satisfaction. This dichotomization yielded the two main regression models (1.1 and 2.1)
for the two dependent variables in each survey year.
In addition to the two main models (1.1 and 2.1), additional analyses were conducted based on
different cut-off points along the satisfaction scale. In doing so, we can circumvent the skewed
distributions of the main variables in favor of high satisfaction and achieve a more even distribution
of the frequencies in the dependent variables. Consequently, the models 1.2 and 2.2 range from -3
to +1 in the first category, and from +2 to +3 in the second category to distinguish between negative,
neutral or mildly positive ratings as opposed to rather or very positive ratings. A third cut-off point
was defined at item +2 facilitating the investigation of very high satisfaction (+3) compared to all
other items (from -3 to +2). As a consequence of adjusting cut-off points in the dichotomization,
the baseline correct prediction model changes and so the outcomes may be influenced regarding
significance levels of independent variables in the regression models. The change in outcome will
be traced and reflected on in the outcomes and discussion sections of this paper and add to the
robustness of results.

36
2.2.2.2 Hierarchical Structure & Model Versions
A hierarchical model structure was chosen since the goal of the analysis is to investigate a range
of different predictor variables and to trace the change in their significance and influence on the
dependent variable. This approach allows us to observe the interplay of predictor variables as the
model complexity increases through addition of variables in each step. Other studies have utilized
a similar multi-level approach (Godager et al., 2009; Godager & Wiesen, 2013; Iversen & Lurås,
2002), most notably (Grytten et al., 2009) to model patient satisfaction.
The model consists of 4 steps according to the 4 variable groups identified in the 2015 and 2013
data, and 3 steps for the 2010 data, in which the users’ self-assessed health status is not included.
Step one introduces the socio-demographic variables age, income and education. In step two,
respondents’ self-assessed health status is added to the model. The municipality-specific predictors
such as capacity variables (GP density, free capacity, LPPT, OLI), type of GP (public/private), and
municipality size are introduced to the model. In the final step, the respective satisfaction variables
were entered (life satisfaction and waiting time satisfaction to predict Overall GP Satisfaction, and
life satisfaction combined with Municipal GP Supply Satisfaction to predict Waiting Time
Satisfaction). These count as the most subjective and potentially unreliable variables, which might
produce the most noise in the model.
To reduce potential multicollinearity and uncontrolled interaction effects among predictor
variables, each model was created with two model versions that feature a different set of
capacity/competition variables. Consequently, the model versions differ in step 3 and 4 within the
2015 and 2013 dataset, and steps 2 and 3 within the 2010 dataset. Version one features free capacity
and LPPT, and version two includes GP density and OLI. The pairing of these variables resulted
from a correlation coefficient analysis of the categorized competition variables in all three datasets
(cf. Appendix table 1, 2, and 3) according to the lowest correlation among the paired variables.
2.2.2.3 The Empirical Model
The decision of which variables to include in the BLR analysis occurred according to theoretical
reasoning related to the study objective and empirical evidence. It is important to note that none of
the selected covariates constitute main explanatory variables for TGPS and WTS, respectively.

37
Since these are sufficiently explained (Kjøllesdal Eide & Nonseid, 2015) and not relevant for the
aim of the present analysis, they were excluded. To assess the potential contribution of included
independent variables to the model, we conducted correlation tests prior to fitting the regression
models. The results indicated significant correlations of every selected independent variable with
the two dependent satisfaction variables. In the course of the analysis, three measures served to
evaluate the quality of the model resulting from the added covariates. A decrease in -2Log
Likelihood (that tests significance of the model step against the initial Chi2 in the baseline model),
an increase in the explained variance R2, and a non-significant Hosmer & Lemeshow test value
indicate a meaningful, beneficial addition to the model (Huizingh, 2007).
In the form of a general linear regression model, the relationship between the dependent and
independent variables can be expressed in the following equation, whereby Y constitutes the
dependent variable (Overall GP Satisfaction or Waiting Time Satisfaction), β represents the
parameters (β0 as the constant and β1 as slope parameter of the first independent variable X1), X1
stands for the first of multiple independent variables, and ε refers to the error term.
Y = β0 + β1*X1 + β2*X2 + β3*X3 + ... +ε
Since BLR determines the impact of multiple independent variables to predict the occurrence of
one category of the dependent variable rather than the other (in this case expressing satisfaction
instead of dissatisfaction), the estimation process presumes a probabilistic, binomial distribution of
the two possible events ranging from 0 to 1, that are classified according to the maximum likelihood
method, i.e. predicting the event that is most likely to occur, (which matches OLS in linear
regression). Correspondingly, the coefficient B (β1 etc.) measures each independent variable’s
partial contribution to variations in the dependent variable. As we are predicting probabilities of an
event instead of discrete values, the BLR formula with the included independent variables looks as
follows:
Logit (TGPS) = β0 + β1*Sociodemographics (Patient) + β2*Health status + β3*Municipality-
specific predictors + β4*Satisfaction (Life, WTS) +ε
Logit (WTS) = β0 + β1*Sociodemographics (Patient) + β2*Health status + β3*Competition +
β4*Satisfaction (Life, Municipal GP Supply) +ε

38
The predicted outcome of the equation is the logit or natural log of the odds of the dependent
variable Y, which occurs with a probability py [0, 1]. Thus, logistic regression calculates changes
in the log odds of the dependent variable, which have to undergo transformation to represent actual
probabilities. As expressed in the equations below, the odds of one event occurring equal the
probability of this event occurring divided by the probability of this event not occurring. Odds
ratios consequently range from 0 to positive infinity (∞). (Huizingh, 2007)
Logit (py) = loge (py
1−py ) py =
𝑒β0+ β1∗X1+β2∗X2…
1+ 𝑒β0+β1∗X1+β2∗X2…
2.2.2.4 Assumptions
Logistic regression requires a number of different assumptions in order to yield valid results and
to allow for correct interpretation. Unlike GLM, logistic regression does not assume a linear
relationship between the dependent and the independent variables. The independent variables also
do not need to be continuous, normally distributed, nor of equal variance. The following section
provides an overview of the assumptions underlying BLR and information on in how far these are
met (Huizingh, 2007; "Laerd Statistics: SPSS Statistics Tutorials and Statistical Guides," 2015).
Assumption 1: The dependent variable is dichotomous. This assumption refers to the two
mutually exclusive categories of the dependent variable that are predicted by the regression model.
Due to the dichotomization of the ordinal dependent variable (as described above), the models
fulfill this assumption.
Assumption 2: We have one or multiple independent variables of continuous or nominal type.
The selected independent variables included in the regression models were ordinal or categorical,
thus conforming to the nominal type. Since ordinal variables cannot be entered as such in the
model, it is necessary to define them as either continuous or categorical variables. In the present
analysis, all ordinal independent variables are entered as covariates and so treated as categorical.
In the case of age groups, for instance, we have multiple categories representing different ranges
of respondents’ age. Despite the fact that we cannot translate an increase in age as a specific change
of odds in the dependent variable, the model still allows for a comparison of every age category
with a reference group upon specification. We therefore decided to define the highest category of
all categorical independent variables to function as the respective reference category. In this way,

39
we can observe a change of odds in the dependent variable based on the comparison of one category
with its reference group. Taking again «age» as an example, the significance levels and exponents
(yielding the odds ratio) of all age categories are each compared to the oldest age group so that we
can observe an increase or decline of odds of being satisfied in relation to the oldest respondent
group (cf. 2.2.2.5 for interpretation).
Assumption 3: BLR requires independence of observation. This means that cases can only be
assigned to one category, and all the categories of one variable need to be mutually exclusive and
exhaustive. We conclude this assumption to be met due to the independent, random collection of
cases and the careful process of defining and assigning categories.
Assumption 4: The sample size must be sufficient. Recommendations of the minimum sample
size vary from 15 up to a minimum of 50 cases per independent variable ("Laerd Statistics: SPSS
Statistics Tutorials and Statistical Guides," 2015). In this case, all categories of independent
variable count as single independent variables, so that we reach a maximum amount of 36
covariates in the most elaborate models. Adopting 50 cases as a minimum, this equals a minimum
sample size of 1500 included cases for each model. Examining the case counts of the models, we
find that the included cases exceed that threshold (the smallest sample amounts to 1881 cases in
the 2010 model of waiting time satisfaction).
Assumption 5: There must be a linear relationship between the continuous dependent
variable and the logit transformation of the dependent variable. This assumption is not
applicable in our case since the analysis does not include any continuous variables. The originally
continuous capacity variables were transformed into ordinal variables with three categories prior
to inclusion in the regression.
Assumption 6: There is no multicollinearity. Multicollinearity occurs when two independent
variables correlate highly with one another, which causes bias and distortions in the estimated
effect of single independent variables in the form of over- or underestimation. As a result, standard
errors can be inflated. The best way to test for multicollinearity is to investigate correlation
coefficients and the resulting Tolerance and VIF values (variance inflation factor). This entails
running numerous multiple regression analyses where each independent variable is modeled as a
dependent variable. Recommendations for the Tolerance statistics state that the VIF should not

40
exceed 2.5, and the correlation matrix depicting the relationships of all independent variables
should have no correlation coefficients exceeding 0.8 ("Laerd Statistics: SPSS Statistics Tutorials
and Statistical Guides," 2015). Since we know that many independent variables correlate to some
degree with each other (cf. Appendix tables 4 to 7), multicollinearity cannot be completely
discarded. However, with large sample sizes as in the present analysis, and low correlation
coefficients, multicollinearity is only a minor concern (Midi, Sarkar, & Rana, 2010). We made an
additional effort to avoid multicollinearity among competition variables (the most prone to that
effect in the present dataset) by creating two versions of each model (cf. section above). By
grouping capacity measures of lowest correlation into pairs of one version, and their high
correlating counterparts into the second version, we can avoid strong interaction effects. In any
case, the best way to deal with the remaining possibility of multicollinearity is to observe changes
in the influence of significant independent variables through a stepwise approach. This is done in
the present analysis, so that we can trace the change in significance levels of single variables based
on the addition of other variables in the model. (Huizingh, 2007)
Assumption 7: There are no significant outliers or unusual, highly influential points. This
assumption can be disregarded since there are no continuous variables in the regressions that could
cause outliers.
2.2.2.5 Interpretation of BLR Output and Results
This section provides a brief overview of the main SPSS output on BLR that facilitate meaningful
interpretation. Some caveats with regard to variable encoding and interpretation of the odds ratio
will be given.
To being with, the “Case Processing Summary” displays all included and excluded cases in the
regression model. Secondly, variable coding is crucial for correct understanding of the results. The
coding of the dichotomous dependent variable is shown in the “Dependent Variable Encoding”
table. In the present analysis, the predicted category of all models is “satisfaction” (either overall
GP satisfaction or waiting time satisfaction) rather than dissatisfaction. The covariates of the model
are listed in the table “Categorical Variables Coding”, which in the present analysis includes all
independent variables. Here it is paramount to check the parameters the model assigns to the
variable categories because the parameters may not be the same as the initial categorical coding of

41
the variable. In the case of the dichotomous variable “public vs private GP”, for instance, the initial
variable code 0 represents “private” and 1 denotes “public”, but the BLR parameter coding is
inversed (1 signifies “private” and 0 refers to “public”). In the “Variables in the Equation” table,
we find the included variable categories displayed according to the model’s parameter coding.
("Laerd Statistics: SPSS Statistics Tutorials and Statistical Guides," 2015)
The baseline analysis referred to as “Beginning Block” is created by means of the statistical
distribution of the dichotomous dependent variable and includes only the constant. Given the
skewed distribution in favor of satisfaction (lower frequency of dissatisfaction), the logical choice
for prediction is “satisfaction”. With all satisfied cases being correctly classified and consequently
all dissatisfied cases being misclassified, we obtain the baseline correct prediction rate displayed
as “Overall Percentage” in the “Classification Table”. This rate serves as baseline for the
comparison with subsequent model steps that include an increasing number of independent
variables. As variables are added to the model, we can observe a change (desirably an
improvement) in the prediction rate. While variables included in the model are displayed in the
“Variables in the Equation” table, excluded variables are listed in the “Variables not in the
Equation” table. (ibid)
In terms of model fit, the “Omnibus Test of Model Coefficients” table offers insight into the
statistical significance of the model or respective step. Reaching a significance level of p< 0.05,
we assume adequacy of the model. Alternatively, the “Hosmer and Lemeshow Test” refers to the
goodness of fit as long as the p-value does not reach a significant level. In this case, high values
approaching 1 in the significance column are desirable as they indicate a good fit. Conversely,
lower values approaching the significance level imply a bad fit. Lastly, the “Model Summary”
displays the explained variance in the dependent variable, offering both the Cox & Snell R2 as well
as the Nagelkerke R2 value. Through adding independent variables in each step, the explained
variance changes; through a meaningful addition of variables, the value of the explained variance
is expected to increase. Another model fit estimate is the -2Log Likelihood (-2LL), which decreases
with the stepwise addition of beneficial predictors. (ibid)

42
To identify significant independent variables, we examine the “Sig.” column in the “Variables in
the Equation” table. The table shows the contribution of each variable to the model by displaying
the B coefficient (the change in log odds for a one-unit change in the independent variable, ceteris
paribus), and more importantly, presents the odds ratios in the “Exp(B)” column and the respective
confidence intervals (95% CI). The interpretation of the odds ratios for a given variable or variable
category depends on its defined reference category as the odds ratio denotes a change in the
probability of occurrence of the predicted event that is achieved by one category compared to
another. In the present analysis, the highest category was defined as a default reference category
for each covariate. With the predictor age, for instance, the change in odds produced by the
youngest age group is relative to the oldest age group (e.g. “Young respondents were 0.5 times or
50% less likely to express satisfaction compared to the oldest respondent group.”). Thus, odds
ratios yield comparative statements with regard to the selected reference category. (ibid)

43
3 Results
The results section is divided into four main parts, one for each year of the DIFI survey followed
by a longitudinal comparison of these three points in time. We will therefore investigate the results
for each year separately, looking at the descriptive statistics, correlations and regression analyses,
before examining the longitudinal perspective to identify potential changes over time.
3.1 2015 Analysis
3.1.1 Descriptives 2015
Taking a look at the 8 selected satisfaction variables, we find that the respondents are generally
very satisfied. It is visible in the left-skewed distribution graphs below (table X) that few
respondents express dissatisfaction, and the relative amount of respondents increases with higher
satisfaction levels towards the right side of the graph. All selected satisfaction variables have very
similar distribution shapes and peak in the best possible rating (+3). Municipal GP Supply
Satisfaction and waiting time satisfaction are exceptions which have the mode in +2, the second
highest satisfaction rating, and therefore a fall in relative frequency in +3. We also see a relatively
higher amount of respondents being dissatisfied with waiting time compared to other satisfaction
indicators. While the graphs of all satisfaction variables are close together in the lower range of the
satisfaction scale (from -3 to -1), the difference in relative frequencies increases towards the
positive and more satisfied end of the satisfaction scale and peaks in the highest satisfaction
variable. Waiting Time Satisfaction and Municipal GP Supply Satisfaction show the lowest relative
frequencies of most satisfied respondents. By contrast, the level of trust, satisfaction with referrals
to specialists and the respondents’ satisfaction with the GP’s medical competence rank highest in
terms of relative frequencies in +3.
Comparing cumulative percentages of dissatisfaction and indifference (rating categories -3 to 0),
we see that Waiting Time Satisfaction has the highest proportion of dissatisfied/neutral respondents
(29.3%), while only 9.4% of respondents were dissatisfied or indifferent with Overall GP
Satisfaction. At the same time, Overall GP Satisfaction has the highest proportion of very satisfied

44
respondents rating +3 (48.7%), while Waiting Time Satisfaction has the lowest proportion of
respondents rating +3 (26.9%).
Figure 2: Frequency Distribution of Satisfaction Variables 2015 (in %)
Looking more closely at the dependent variables, we see that TGPS follows a steeper, steadier
incline than WTS. TGPS has its mode at +3, which means that the majority of respondents opted
for the highest TGPS satisfaction rating. WTS, by contrast, shows a flatter incline of distribution
shape towards the right end of the satisfaction scale. The mode is at +2 and the relative frequencies
of dissatisfied respondents are higher than the ones of TGPS.
3.1.2 Bivariate Analysis 2015
The bivariate analysis allows us to examine potential differences of sub-groups of independent
variables in the rating of the two dependent variables. By conducting a Mann-Whitney-U test, we
can identify significant group differences within the categorized independent variables based on
their effect on the satisfaction rating of the dependent variable. Thus we can answer the research
question whether for example young respondents rated significantly differently from old
respondents.
-3 -2 -1 0 1 2 3
Overall GP Satisfaction 0.8 1.6 2.6 4.4 12.4 29.5 48.7
Waiting Time Satisfaction 4.8 6.0 8.9 9.6 16.7 27.1 26.9
Referrals (specialist) 1.3 2.0 2.5 5.1 11.7 29.6 47.8
Referrals (other services) 2.0 2.1 3.5 7.5 13.2 29.0 42.6
Time to Explain 1.4 1.7 4.2 6.4 15.8 32.1 38.5
Trust in the GP 1.0 1.6 2.5 4.5 11.5 30.4 48.4
GP's Medical Competence 0.6 1.5 2.3 4.6 12.7 31.7 46.6
Municipal GP Supply 1.9 1.8 3.7 9.3 17.5 34.8 31.1
0
5
10
15
20
25
30
35
40
45
50

45
Table 5 below displays the results from the Mann-Whitney-U test for group differences in the
median of Overall GP Satisfaction and Waiting Time Satisfaction in 2015. For Overall GP
Satisfaction, we find significant results in almost all independent variables. There are no significant
differences for Overall GP Satisfaction ratings according to no_disabilities, free capacity, list
places per thousand inhabitants, open list ratio (low-high), and municipality size (2+3) at a p< 0.05
significance level. Open list ratio (low-high) and municipality size (3+4, and 1+4) yielded results
at a significance level of p< 0.10 (marked in italics).
Independent Variables Overall GP
Satisfaction*
Waiting Time
Satisfaction*
HappyLife (Life satisfaction) 0.000 0.000
Below-median Income 0.000 0.009
Below High-School Education 0.000 0.000
Average Contact Frequency 0.036 0.901
Public vs Private GP 0.000 0.000
GoodHealth 0.000 0.015
Having no disabilities 0.589 0.344
Age group: young - middle 0.851 0.813
Age group: young - old 0.000 0.000
Age group: middle - old 0.000 0.000
GP density: low - medium 0.009 0.100
GP density: medium - high 0.027 0.027
GP density: low - high 0.682 0.578
Free capacity/ free GPs: low - medium 0.410 0.001
Free capacity/ free GPs: medium - high 0.796 0.013
Free capacity/ free GPs: low - high 0.581 0.420
Open Lists per 1000 Inhabitants: low - medium 0.005 0.926
Open Lists per 1000 Inhabitants: medium - high 0.452 0.407
Open Lists per 1000 Inhabitants: low - high 0.040 0.461
List places per 1000 Inhabitants: low - medium 0.136 0.627
List places per 1000 Inhabitants: medium - high 0.219 0.483
List places per 1000 Inhabitants: low - high 0.828 0.278
Open List Ratio: low - medium 0.007 0.822
Open List Ratio: medium - high 0.418 0.879
Open list Ratio: low - high 0.058 0.934
Municipality size: 1+2 (below 5000 & 5000 - 20 000) 0.008 0.188
Municipality size: 2+3 (5000-20 000 & 20 000 - 110 000) 0.504 0.006
Municipality size: 3+4 (20 000 - 110 000 & more than 110 000) 0.072 0.013
Municipality size: 1+4 (below 5000 & more than 110 000) 0.068 0.169
* Asympt. Sig. (2-tailed); bold corresponds signify p< 0.05, italics represents p< 0.10.
Table 5: Mann-Whitney U Test for group differences in TGPS and WTS 2015

46
There is a significant difference in the Overall GP Satisfaction levels according to respondents’
satisfaction with life, income, level of education, contact frequency, perceived health status, and
age. Further independent variables of significant group difference include the type of GP (private
or public) and structural competition-related indicators such as municipal GP density, open lists
per 1000 inhabitants, open list ratio and municipality size. By contrast, we find no significant
difference in Overall GP Satisfaction according to respondents’ disabilities, municipal free
capacity, and available list places per 1000 inhabitants (LPPT).
More concretely, we observe significantly higher mean ranks (cf. Appendix Group difference
tables) in respondents that perceive themselves as generally satisfied with life compared to those
that describe themselves as dissatisfied (p< .001). People with below-median income were also
significantly more satisfied with their GP than those with above-median income (p<.001).
Respondents with primary education were significantly more satisfied with their GP than
respondents with high-school or higher education (p< .001). While there is no significant difference
in Overall GP Satisfaction levels of young and middle-aged respondents, we find significant
differences comparing the young and old (p< .001), and the middle-aged and old respondent groups
(p< .001), with the highest satisfaction levels in the oldest group. People with an average contact
frequency of two to five GP visits per year were significantly more satisfied with the GP than
respondents with more or less frequent GP visits (p=.036), as were respondents with a self-assessed
good health status compared to those with perceived bad health (p< .001). People with private GPs
were significantly more satisfied with their GP than those with a public GP (p< .001). With regard
to municipal competition indicators, we find that respondents from municipalities with medium
GP density were significantly more satisfied than respondents from either low or high GP density
areas (p< .009; p=.027). Also respondents from municipalities with a low count of open lists
(available doctors) per 1000 inhabitants (OLI) yielded a higher mean rank than those from medium
or high OLI municipalities (p=.005; p=.040). Similarly, respondents from municipalities with a
low-range open list ratio were significantly more satisfied than those from medium-range OLR
municipalities (p= .007) and also more satisfied than those from high-range OLR areas (p= .058).
Lastly, respondents were significantly less satisfied with the GP in the smallest compared to the
second smallest municipalities (p= .008), and were tendentially more satisfied in the second-
biggest rather than the biggest municipalities (p= .068).

47
Similarly to Overall GP Satisfaction, we encounter significant differences in Waiting Time
Satisfaction according to respondents’ life satisfaction, income, level of education, perceived
health status, and age group. Further significant variables include the type of GP (public vs private),
and the municipality-specific competition variables GP density, free capacity and municipality
size. By contrast, there were no significant differences according to respondents’ contact frequency
with the GP, disabilities, or the competition-related variables open lists per 1000 inhabitants,
available list places per 1000 inhabitants and the open list ratio.
Respondents with life satisfaction were significantly more satisfied with waiting time than
respondents dissatisfied with life (p< .001). Above-median income compared to below-median
income (p= .009), as well as high-school or higher education compared to primary education (p<
.001) yielded significantly lower levels of waiting time satisfaction. Respondents with a
subjectively good health status expressed significantly higher satisfaction with waiting time than
those with subjectively poor health (p= .015). Private GP users were also significantly more
satisfied with waiting time than users of public GPs, as were older respondents compared to young
or middle-aged ones (p< .001). In comparing medium and high-range municipal GP density, we
see that respondents are significantly more satisfied with waiting time in municipalities with
medium-range GP density (p= .027). Also medium-range free capacity yielded significantly higher
waiting time satisfaction levels in respondents than either low or high free capacity (p<=.001;
p=.013). And the comparison of municipality size produced significantly higher mean ranks of
respondents’ waiting time satisfaction in the second biggest and third biggest municipalities
compared to the biggest (p= .006) and second-biggest municipalities (p< .013), respectively.
3.1.3 Regression Analyses 2015
As mentioned in the methodology section, one main model was created for each dependent variable
as well as two additional models with different cut-off points to achieve a less skewed, more
symmetric distribution of Overall GP Satisfaction and Waiting Time Satisfaction, respectively.
Furthermore, each model features two versions differing in the set of added competition variables
in step and 4 of the regression (fkap & LPPT, and GPD & OLI) in order to avoid significant
interaction effects that could bias the regression outcome. For this reason, the two model versions
differ in step 3 and 4 in each model.

48
3.1.3.1 Overall GP Satisfaction 2015
The main model of TGPS (model 1.1) divides the dependent variable into category 1 for negative
or neutral rating (subsuming the lowest 4 rating categories) and category 2 for positive rating
(collapsing the highest 3 categories) provides the following results (see tables below). The model
including both versions is statistically significant (p< .01) and explains a variance (R2) of 9.8% to
20.9% (version 1) and 9.9% to 21.1% (version 2) in the dependent variable and correctly classified
90.6% of cases; the models are significantly different from the baseline model (p=0.001), and they
present an acceptable fit (H&L 0.189 and H&L .260). The predictions present a minor
improvement to the baseline model with 90.3% correct prediction based on the calculated constant.
Both model versions produce very similar results, differing only in the significant competition
variable in the final step. We find significant associations with age, free list places per thousand
inhabitants/open list places per inhabitants, waiting time satisfaction and life satisfaction. There is
no significant association of TGPS with below-median income, health status, public or private GP,
highest completed education, free capacity, GP density or municipality size.
BLOCK Prediction -2Log
Likelihood R2 H&L Significant variables categories
BLOCK 0 90.3% Constant
BLOCK 1 90.3% 1780 .016 - .033 .969 Age (1-5);
BLOCK 2 90.3% 1763 .021 - .045 .222 Age (1-5); GoodHealth; No_disabilities
BLOCK 3 90.3% 1750 .026 - .054 .004 Age (1-5); GoodHealth; No_disabilities;
publicGP;
BLOCK 4 90.6% 1527 .098 - .209 .486 Age (1-4); LPPT (2); Waiting time (1-7);
Life Satisfaction (1, 2, 4);
BLOCK 3’ 90.3% 1747 .027 - .056 .049 Age (1-5); GoodHealth; No_disabilities;
OLI (2); publicGP;
BLOCK 4’ 90.6% 1525 .099 - .211 .260 Age (1-4); OLI (2); Waiting time (1-7);
Life Satisfaction (1, 2, 4);
Table 6: Model 1.1 TGPS_1 2015 (category 1 = negative/indifferent rating; catg. 2 = positive rating);
N= 2991 (69.2%). Version 1: fkap & LPPT in step 3 & 4; Version 2: GPD & OLI in step 3’ & 4’.
In terms of the odds ratio (cf. Appendix table 8 and 9), old respondents were significantly more
likely to express general satisfaction with the GP compared to younger respondents. Thus, age
serves as a significant predictor of Overall GP Satisfaction as all but one age group show significant
results compared to the reference group. The oldest age group (67+) was most likely to rate
positively. By comparison, the 50-66 year olds were 38.3% (version 1) and 37.5% (version 2) less
likely to be somewhat, rather or very satisfied with their GP, and the 35 to 49 year old group has

49
reduced odds by 46.7% (version 1) and 46.8% (version 2), while the youngest display a reduced
likelihood by 59.8% (version 1) and 59% (version 2). We find the tendency that the younger the
respondents are, the less likely is the expression of overall satisfaction with their GP. In version 1,
medium LPPT reduced the respondents’ odds of rating TGPS positively by 31.8% compared to
high LPPT (the top third percentile of free list places per thousand inhabitants). Compared to a
high number of Open Lists per 1000 Inhabitants (OLI), medium OLI reduced the probability of
rating TGPS positively by 33.7% in version 2 compared to the top 33rd percentile. Since OLI and
LPPT are related measures indicating users’ actual choice among available GPs (GPs’ competition
for patients), the two model versions present a consistent picture of the positive impact of supply-
side measures on Overall GP Satisfaction. The effect of the respondents’ health status is cancelled
out in both versions by the effects of Waiting Time Satisfaction and Life Satisfaction, which are
both positively associated with Overall GP Satisfaction.

50
Table 7: Significant variables & coefficients in TGPS_1 2015; N= 2991 (69.2%); [italics p< .010; bold p< .005]
Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E.
Constant 2.235 0.063 3.018 0.217 3.265 0.227 3.309 0.307 5.043 0.428 3.442 0.347 5.082 0.458
Age (5) § § § § § § § § § § § §
Age (1) -1.243 0.329 -1.258 0.331 -1.185 0.334 -0.910 0.355 -1.156 0.334 -0.891 0.355
Age (2) -1.180 0.250 -1.218 0.251 -1.126 0.254 -0.558 0.269 -1.104 0.254 -0.539 0.269
Age (3) -1.171 0.230 -1.158 0.231 -1.106 0.233 -0.629 0.246 -1.114 0.232 -0.631 0.246
Age (4) -0.666 0.225 -0.629 0.226 -0.623 0.226 -0.483 0.236 -0.613 0.226 -0.470 0.236
Below-median
Income (1)0.011 0.140 -0.063 0.142 -0.094 0.143 -0.166 0.152 -0.095 0.143 -0.166 0.152
Education level (3) § § § § § § § § § § § §
Education level (1) 0.075 0.234 0.084 0.235 0.103 0.237 0.026 0.247 0.123 0.237 0.040 0.247
Education level (2) 0.025 0.140 0.021 0.141 0.037 0.144 0.098 0.153 0.026 0.144 0.089 0.154
GoodHealth (1) -0.369 0.137 -0.362 0.138 -0.270 0.148 -0.353 0.138 -0.261 0.148
No_disabilities (1) -0.338 0.166 -0.368 0.167 -0.197 0.180 -0.360 0.167 -0.187 0.180
free capacity (3) § § § §
free capacity (1) -0.093 0.368 -0.188 0.388
free capacity (2) 0.037 0.304 -0.088 0.323
free places per 1000
inhabitants (3)§ § § §
free places per 1000
inhabitants(1)-0.298 0.189 -0.264 0.199
free places per 1000
inhabitants (2)-0.341 0.186 -0.382 0.194
GP density (3) § § § §
GP density (1) -0.138 0.234 -0.125 0.246
GP density (2) 0.021 0.184 -0.003 0.198
open lists per 1000
inhabitants (3)§ § § §
open lists per 1000
inhabitants (1)-0.207 0.201 -0.119 0.210
open lists per 1000
inhabitants (2)-0.437 0.202 -0.412 0.210
Kommunestr (4) § § § § § § § §
Kommunestr (1) -0.152 0.432 -0.093 0.457 -0.465 0.306 -0.418 0.320
Kommunestr (2) 0.112 0.375 0.266 0.399 -0.134 0.237 -0.021 0.251
Kommunestr (3) 0.106 0.289 0.193 0.309 0.007 0.218 0.038 0.224
Public vs Private GP
(1)0.303 0.138 0.145 0.146 0.320 0.138 0.174 0.147
Waiting Time
Satsifaction (7)§ § § §
Waiting Time
Satsifaction (1)-3.247 0.334 -3.222 0.333
Waiting Time
Satsifaction (2)-2.723 0.332 -2.744 0.332
Waiting Time
Satsifaction (3)-2.030 0.328 -2.044 0.328
Waiting Time
Satsifaction (4)-2.275 0.322 -2.280 0.323
Waiting Time
Satsifaction (5)-1.599 0.319 -1.598 0.319
Waiting Time
Satsifaction (6)-0.862 0.326 -0.867 0.326
Life Satisfaction (4) § § § §
Life Satisfaction (1) -0.980 0.248 -0.989 0.249
Life Satisfaction (2) -0.633 0.219 -0.612 0.218
Life Satisfaction (3) -0.336 0.178 -0.334 0.178
Block 3' Block 4'Variables
Block 0 Block 1 Block 2 Block 3 Block 4
Regression Summary TGPS_1 2015 - N = 2991 (69.2%)

51
Additional Analyses of TGPS 2015:
Model 1.2 produces similar results as model 1.1. In both versions of model 1.2, we find that age,
Waiting Time Satisfaction and Overall Life Satisfaction show positive associations with the
respondents’ odds of rating the GP rather or very positively. In addition, having a private GP
increased respondents’ odds of rating the GP highly by 29.6% (in version 1) and 31.3% (version
2) compared to respondents with a public GP. In version 1, municipalities with a high amount (top
33rd percentile) of available List Places per 1000 Inhabitants were most likely to express high or
very high overall satisfaction with the GP. By comparison, respondents from municipalities in the
medium LPPT range had reduced odds of high or very high TGPS rating by more than a quarter
(26.2%). In version 2, the top 33% range of OLI (open lists per thousand inhabitants) has a
significance level of p= .052 and displays the highest probability for expressing high or very high
Overall GP Satisfaction.
BLOCK Prediction -2Log
Likelihood R2 H&L Significant variable categories
BLOCK 0 77.5% Constant
BLOCK 1 77.5% 2991 .025 - .038 .776 Age (1-5);
BLOCK 2 77.5% 2981 .028 - .043 .553 Age (1-5); No_disabilities;
BLOCK 3 77.5% 2955 .037 - .056 .139 Age (1-5); No_disabilities; LPPT (2);
BLOCK 4 78.7% 2575 .156 - .239 .844 Age (1-5); LPPT (2, 3); public GP;
Waiting Time Satisfaction; Life
Satisfaction (1-4);
BLOCK 3’ 77.5% 2953 .038 - .057 .236 Age (1-5); No_disabilities; publicGP;
BLOCK 4’ 79.3% 2574 .157 - .239 .144 Age (1, 3, 4, 5); OLI (3 at p= .052); public
GP; WTS (1-7); Life Satisfaction (1-4);
Table 8: Model 1.2 TGPS_2 2015 (category 1 = negative/indifferent/slightly positive rating; catg. 2 = rather & very positive
rating); N= 2991 (69.2%). Version 1: fkap & LPPT in step 3 & 4; Version 2: GPD & OLI in step 3’ & 4’.
Model 1.3 TGPS_3
In predicting very high Overall GP Satisfaction, all categories of age, Waiting Time Satisfaction
and Life Satisfaction are significantly positively associated with TGPS probability in both model
versions. We encounter the same tendency as in the two previous models. The odds ratios show a
downward trend in probability of rating TGPS very highly with decreasing age, declining Waiting
Time Satisfaction and dropping Life Satisfaction. In version 1, the competition variables free
capacity, free List Places per 1000 Inhabitants as well as municipality size have a significant,
positive correlation with the odds of very high Overall GP Satisfaction. High competition indicators

52
result in the highest probability of positive TGPS compared to their low-range counterparts. In
other words, the more free capacity or available List Places there are per 1000 Inhabitants in a
municipality, the higher is the probability of respondents expressing high TGPS. Similarly, the
bigger the municipality is (by number of inhabitants), the more likely were the respondents to rate
their Overall GP Satisfaction very highly. In version 2, by contrast, the competition variables do
not significantly correlate with the odds of very high TGPS. The smallest category of municipality
size (‘Kommunestr 1’ with below 5000 inhabitants) resulted in a significant outcome with
respondents’ reduced odds of high TGPS compared to the reference group comprising of
respondents from the biggest municipalities (with over 110.000 inhabitants).
BLOCK Prediction -2Log
Likelihood
R2 H&L Significant variable categories
BLOCK 0 52.5% Constant
BLOCK 1 57.4% 3887 .030 - .040 .889 Age (1-5);
BLOCK 2 57.4% 3882 .031 - .042 .695 Age (1-5);
BLOCK 3 58.7% 3857 .040 - .053 .868 Age (1-5); fkap (2, 3); publicGP;
BLOCK 4 69.5% 3329 .201 - .268 .791 Age (1-5); fkap (1, 2, 3); LPPT (2, 3);
Kommunestr (2, 3); WTS (1-7); Life
Satisfaction (1-4);
BLOCK 3’ 59.0% 3860 .039 - .052 .793 Age (1-5); Kommunestr (1); public GP;
BLOCK 4’ 69.4% 3335 .199 - .266 .967 Age (1-5); Kommunestr (1); public GP (at
p=.056); WTS (1-7); Life Satisfaction (1-
4);
Table 9: Model 1.3 TGPS_3 2015 (category 1 = all items except +3; catg. 2 = very positive rating); N= 2991 (69.2%).
Version 1: fkap & LPPT in step 3 & 4; Version 2: GPD & OLI in step 3’ & 4’.
Outcomes Summary of TGPS 2015 Models
In all three models, we find a consistently significant, positive influence of age, Waiting Time
Satisfaction, and Life Satisfaction on respondents’ likelihood to express overall satisfaction with
their GP. We observe that in determining high or very high Overall GP Satisfaction (as in models
2 and 3), the competition variables increased in significance, while respondents’ self-assessed
health status becomes more and more obsolete; in model 1.1, only 1 category of a single
competition variable is significant (medium LPPT and medium OLI, respectively), while in model
1.2 there are 2 significant variables (LPPT & private GP, OLI & private GP), and in model 1.3, we
find two or three competition variables with at least one significant category each. We also notice
a rather high goodness of fit in step 4 of model 1.2 and in both steps 3 and 4 of model 1.3, whereby
step 4 of model 1.3 with GDP and OLI as competitive variables present an almost perfect fit (H&L

53
= .967). Furthermore there is a decrease of Log2-Likelihood as well as an increase in the explained
variance (R2) with added variables in the models. In predicting higher TGPS satisfaction levels, R2
increases, indicating that the significant variables explain an increasing proportion of variation in
the dependent variable. While the significance of competition variables across the three models is
not fully consistent (with the exception of LPPT), we find a coherent effect of municipal
competition measures on Overall GP Satisfaction. There is no significant correlation with health
status, income (below or above median) or education level in any of the models when controlling
for all other factors.
3.1.3.2 Waiting Time Satisfaction 2015
The main model with Waiting Time Satisfaction as the dependent variable is based on the same
cut-off point as TGPS_1. Two versions of the model were created, both of which are statistically
significant, (p<.001). The final step including all variables explains 11.5% to 16.4% (version 1)
and 11.7% to 16.6% of variance (version 2) in the dependent variable. Version 1 correctly classified
73.7% and version 2 73.4% of cases, which is a considerable improvement to the baseline model
with 70.7% of correct predictions based on the calculated constant. The models are significantly
different from the baseline model (p=0.001) and present a good fit (H&L 0.416 and H&L .759).
Taking all variables into consideration, both versions show that Municipal GP Supply Satisfaction,
age (three out of five categories) as well as general Life Satisfaction (the lowest and highest
categories) display a significant, positive correlation with the odds of expressing satisfaction with
waiting time. Similarly to predicting Overall GP Satisfaction, age (p< .001) and the two highly
significant satisfaction variables point at a tendency of increased Waiting Time Satisfaction with
higher age, with rising Life Satisfaction (p< .01) and increasing Municipal GP Supply
Satisfaction (p< .001). In version 2, GP density presents an additional significant result; compared
to municipalities with a high GP density, low GP density municipalities decreased respondents’
probability of being satisfied with waiting time by almost a third (32%; p= .018). There is no
significant association of the odds of Waiting Time Satisfaction and respondents’ self-assessed
health status, the municipality size, competition variables, patient demographics or public/private
GPs. While a subjectively good health status is significant in early steps of the model, health status
loses its significance after adding GP Supply Satisfaction and Life Satisfaction in the final step.

54
BLOCK Prediction -2Log
Likelihood R2 H&L Significant variable categories
BLOCK 0 70.7% Constant
BLOCK 1 70.7% 3262 .039 - .056 .963 Age (2-5);
BLOCK 2 70.8% 3251 .043 - .061 .276 Age (2-5); GoodHealth;
BLOCK 3 71.5% 3232 .049 - .070 .849 Age (2-5); GoodHealth;
BLOCK 4 73.7% 3033 .115 - .164 .416 Age (2, 3, 5); GP Supply Sat. (1-7);
Overall Life Satisfaction (1, 4);
BLOCK 3’ 71.7% 3228 .051 - .072 .085 Age (2-5); GoodHealth; GPD (1);
Kommunestr (4, p=.055); public/private
GP (p=.053);
BLOCK 4’ 73.4% 3027 .117 - .166 .759 Age (2, 3, 5); GPD (1); GP Supply Sat.
(1-7); Overall Life Satisfaction (1, 4);
Table 10: Model 2.1 WTA_1 (category 1 = negative/neutral rating; catg. 2 = positive rating);
N= 2907 (67.2%). Version 1: fkap & LPPT in step 3 & 4; Version 2: GPD & OLI in step 3’ & 4’.
Examining the odds ratio (cf. Appendix table 12 and 13), we find that old respondents were
significantly more likely to express waiting time satisfaction compared to younger respondents.
Municipal GP Supply Satisfaction displays the same positive trend as it decreasing GPS
correlates with steadily decreasing odds of WTS. Compared to respondents stating that they were
highly satisfied with the municipality’s GP supply, the ones who were rather satisfied had reduced
odds of 39.7% (p< .001) to express WTS in both model versions. Similarly, respondents who
expressed the lowest life satisfaction (dissatisfaction) had reduced a probability of expressing
satisfaction with waiting time by 44.6% (p= .002) and 44.7% (p= .002), respectively, compared to
the ones rating their Life Satisfaction highest.

55
Table 11: Significant variables & coefficients in WTA_1 2015 - Model 2.1
N= 2907 (67.2%); [italics … p< .010; bold … p< .005]
Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E.
Constant 0.882 0.042 1.416 0.124 1.542 0.130 1.411 0.187 1.787 0.211 1.629 0.216 2.000 0.239
Age (5) § § § § § § § § § § § §
Age (1) -0.375 0.241 -0.378 0.241 -0.328 0.243 0.114 0.257 -0.331 0.244 0.106 0.257
Age (2) -1.165 0.153 -1.187 0.154 -1.155 0.157 -0.773 0.166 -1.157 0.157 -0.775 0.166
Age (3) -0.993 0.136 -0.984 0.137 -0.959 0.138 -0.606 0.146 -0.970 0.138 -0.615 0.146
Age (4) -0.357 0.130 -0.341 0.130 -0.337 0.131 -0.122 0.137 -0.339 0.131 -0.125 0.137
Below-median
Income (1)0.049 0.094 0.017 0.095 -0.004 0.096 -0.035 0.101 -0.004 0.096 -0.031 0.101
Education level (3) § § § § § § § § § § § §
Education level (1) 0.213 0.151 0.210 0.152 0.244 0.153 0.212 0.160 0.240 0.153 0.204 0.160
Education level (2) -0.039 0.094 -0.047 0.094 -0.010 0.097 0.014 0.101 -0.017 0.097 0.005 0.101
GoodHealth (1) -0.223 0.093 -0.225 0.094 -0.127 0.099 -0.222 0.094 -0.125 0.099
No_disabilities (1) -0.153 0.116 -0.154 0.116 -0.088 0.123 -0.157 0.116 -0.089 0.123
free capacity (3) § § § §
free capacity (1) -0.127 0.250 -0.023 0.261
free capacity (2) -0.131 0.209 -0.073 0.218
free places per 1000
inhabitants (3)§ § § §
free places per 1000
inhabitants(1)-0.107 0.120 -0.067 0.126
free places per 1000
inhabitants (2)0.017 0.120 0.066 0.125
GP density (3) § § § §
GP density (1) -0.344 0.156 -0.385 0.163
GP density (2) -0.073 0.120 -0.117 0.125
open lists per 1000
inhabitants (3)§ § § §
open lists per 1000
inhabitants (1)0.004 0.126 0.121 0.132
open lists per 1000
inhabitants (2)0.159 0.132 0.253 0.137
Kommunestr (4) § § § § § § § §
Kommunestr (1) 0.036 0.297 0.102 0.310 -0.316 0.206 -0.128 0.216
Kommunestr (2) 0.058 0.253 0.082 0.264 -0.290 0.157 -0.177 0.164
Kommunestr (3) 0.351 0.201 0.387 0.209 0.027 0.144 0.107 0.150
Public vs Private GP
(1)0.162 0.092 0.131 0.096 0.178 0.092 0.146 0.096
Municipal GP Supply
Satisfaction (7)§ § § §
Municipal GP Supply
Satisfaction (1)-2.178 0.336 -2.161 0.337
Municipal GP Supply
Satisfaction (2)-1.880 0.315 -1.892 0.315
Municipal GP Supply
Satisfaction (3)-1.649 0.233 -1.657 0.233
Municipal GP Supply
Satisfaction (4)-1.584 0.164 -1.594 0.164
Municipal GP Supply
Satisfaction (5)-0.977 0.141 -0.993 0.141
Municipal GP Supply
Satisfaction (6)-0.506 0.124 -0.506 0.124
Life Satisfaction (4) § § § §
Life Satisfaction (1) -0.590 0.189 -0.593 0.190
Life Satisfaction (2) -0.025 0.147 -0.019 0.147
Life Satisfaction (3) -0.001 0.107 -0.001 0.107
Block 3' Block 4'Variables
Block 0 Block 1 Block 2 Block 3 Block 4

56
Additional Analyses of WTS 2015:
Model 2.2 is similar to the main model, comprising of the significant variables age, private GP,
GP Supply Satisfaction and overall Life Satisfaction in both versions. Having visited a private GP
significantly increased the odds of expressing high or very high WTS by 40.9% in version 1 and
41.9% in version 2 compared to having consulted a public GP. In version 2, we additionally find
Open Lists per 1000 Inhabitants of significant influence. High OLI yielded the highest probability
of respondents expressing Waiting Time Satisfaction.
BLOCK Prediction -2Log
Likelihood R2 H&L Significant variable categories
BLOCK 0 78.1% Constant
BLOCK 1 78.1% 2945 .025 - .038 .902 Age (1-5);
BLOCK 2 78.1% 2937 .028 - .043 .720 Age (1-5);
BLOCK 3 78.1% 2914 .035 - .055 .404 Age (1-5); publicGP;
BLOCK 4 78.9% 2611 .132 - .203 .476 Age (3); private GP; GP Supply
Satisfaction (1-7); Life Sat. (1-4);
BLOCK 3’ 78.1% 2910 .037 - .056 .222 Age (1-5); publicGP; OLI (2, 3);
BLOCK 4’ 79.1% 2607 .133 - .205 .591 Age (3); OLI (3); private GP;
GP Supply Satisfaction (1-7);
Life Satisfaction (1-4);
Table 12: Model 2.2 WTA_2 (category 1 = negative/neutral/slightly positive rating; catg. 2 = rather or very positive
rating); N= 3029 (70.1%). Version 1: fkap & LPPT in step 3 & 4; Version 2: GPD & OLI in step 3’ & 4’.
Model 2.3 produces numerous significant results. As 4 out of 5 age groups showed significant
correlations, age did not lose its significant prediction effect for very high waiting time satisfaction
due to GP supply satisfaction and life satisfaction. We find a surprising correlation of education
with WTS; compared to respondents with a university or college degree, respondents with a high
school degree or vocational education were 21.8% (20.8% in version 2) more likely to rate WTS
very highly. On the municipality level, free capacity, municipality size and consulting a private GP
had significant effects on the odds of very high WTA. Compared to respondents living in
municipalities with high free capacity of GPs, people with medium-amount of free capacity were
33% less likely to opt for very high WTS compared to respondents living in high free capacity
municipalities. Patients consulting a private GP as opposed to a public one had increased odds of
stating very high WTS by 25% (25.6% in version 2). Compared to the largest municipality size
(over 110.000 inhabitants), inhabitants in municipalities of the second largest size increased the
probability of very high WTS by 47.5%. In version 2, the smallest municipality size compared to

57
the biggest one reduced the odds of respondents expressing very high WTS by a third (33.2%).
Lastly, GPS was highly significant in all categories. While there is a tendency of declining odds
for WTS as GPS diminishes, the lowest rating GPS respondents were not the least likely ones to
rate WTS very highly. In fact, the lowest odds were identified in the respondents who stated that
they were mildly dissatisfied with GPS. This mild dissatisfaction amounts to 85.7% (85.6% in
version 2) reduced odds for high or very high WTS compared to the highest rating GPS group).
BLOCK Prediction -2Log
Likelihood R2 H&L Significant variable categories
BLOCK 0 51.9% Constant
BLOCK 1 57.6% 3880 .034 - .045 .817 Age (1-5);
BLOCK 2 57.6% 3877 .035 - .046 .780 Age (1-5);
BLOCK 3 59.0% 3853 .043 - .057 .759 Age (1-5); Education (1); fkap (2, 3);
Kommunestr (3); publicGP;
BLOCK 4 67.3% 3545 .140 - .187 .140 Age (2-5); Education (2); fkap (2);
Kommunestr (3, 4); private GP;
GP Supply Satisfaction (1-7);
Life Satisfaction (1-4);
BLOCK 3’ 59.0% 3853 .043 - .057 .771 Age (1-5); Education (1); Kommunestr (1);
publicGP;
BLOCK 4’ 66.8% 3543 .140 - .187 .174 Age (1-5); Education (2); Kommunestr
(1); private GP; GP Supply Satisfaction
(1-7); Life Satisfaction (1-4);
Table 13: Model 2.3 WTA_3 (category 1 = negative to rather positive rating; catg. 2 = very positive rating);
N= 3029 (70.1%). Version 1: fkap & LPPT in step 3 & 4; Version 2: GPD & OLI in step 3’ & 4’.
Outcomes Summary of WTS 2015 Models
In all three models and all versions, age is the only consistent, significant socio-demographic
variable that resulted to be a positive predictor of WTS probability. All models corroborated the
trend and assumption that the oldest age group was most satisfied and that the youngest respondents
displayed a reduced probability of WTS. Since the same pattern was found in TGPS, it can be
concluded that age affects both types of satisfaction ratings significantly, even in the presence of
other significant variables. The satisfaction variables GPS and LS yielded consistent, significant
results in each model and version and show a trend of a positive correlation of GP Supply
Satisfaction and Life Satisfaction with the odds of WTS. These also increased the explained
variance in the dependent variables three- to fourfold in all models and versions compared to the
previous step. The respondents’ health status (both in the form of ‘GoodHealth’ and

58
‘No_disabilities’) was not significantly correlated with WTS in any model, version or step so that
we can conclude that health does apparently not affect WTS in the 2015 respondents.
Similarly to the three TGPS models, the three WTA models also show increasing significance of
competition variables as a higher cut-off point for WTS increases the probability to predict high
or very high satisfaction. Model 2.1 had no significant competition variable in version 1 and only
GP density in version 2, while model 2.3 produced the highest number of significant competition
variables in addition to two significant socio-demographic variables (age and education). The most
consistent municipality-specific supply-side variable of significance is private GP appearing in
models 2.2 and 2.3 (in all versions). Having a private rather than public GP is associated with
significantly increased odds of WTS by around 1.4 times in both models and versions. By contrast,
other competition variables were inconsistent across the three models. In version 2 of model 2.1,
GP density was significant (indicating that a low GP density correlated with low odds of WTS).
Model 2.2 yielded a significant outcome for OLI in that the highest odds for WTS were produced
by a high number of open lists per 1000 inhabitants, and model 2.3 showed a significant result
for free capacity (medium as opposed to high free capacity in a municipality reduced the odds of
respondents expressing very high waiting time satisfaction by a third).
There is no significant correlation with health status or below-median income in any of the
models. Education is only significant in determining very high WTS (model 3) and shows that the
respondents with high-school education or vocational training were significantly more likely to
express very high WTS compared to respondents with a university or college degree. With regard
to the development of R2, we observe that the explained variance in the dependent variable WTS
increases its minimum threshold when higher satisfaction ratings are predicted. However, the upper
R2 threshold is lower in model 3 than in model 2, despite integration of the same variables.

59
3.2 2013 Analysis
3.2.1 Descriptives 2013
In 2013, respondents were very satisfied in general. The main satisfaction variables show a left-
skewed distribution with the highest relative frequencies in the highest rating items. All satisfaction
variables peak in the highest rating item +3, the only exceptions being waiting time satisfaction
and satisfaction with the municipal GP supply with the mode in +2. In the graph below, we can
also see that the relative frequencies of waiting time satisfaction from item -3 to -1 (signifying
dissatisfaction) are the highest of all satisfaction variables. We can therefore conclude that
respondents were more dissatisfied with waiting time than with other measures, including trust in
the GP, the perceived medical competence of the GP, overall satisfaction with the GP, referral
satisfaction to specialists or to other services, and satisfaction with the available time to explain the
situation to the GP during a consultation.
Figure 2: Frequency Distribution of Satisfaction Variables 2013 (in %)
-3 -2 -1 0 1 2 3
Overall GP Satisfaction 1.1 1.7 2.4 5.5 11.9 30.6 46.8
Waiting Time Satisfaction 5.2 7.4 9.0 8.5 16.2 27.8 26.0
Referrals (specialist) 2.0 1.7 2.6 5.2 11.2 27.9 49.4
Referrals (other services) 2.0 1.8 3.6 8.8 12.0 30.3 41.4
Time to Explain 1.0 2.0 4.2 6.5 15.4 33.2 37.6
Trust in the GP 1.1 1.5 2.7 5.6 11.2 30.4 47.5
GP's Medical Competence 1.3 0.9 2.1 4.5 12.4 32.5 46.4
Municipal GP Supply 1.7 2.3 3.4 9.2 19.2 34.7 29.4
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
45.0
50.0

60
We find very similar results in the distributions for the 2013 satisfaction ratings as in 2015. Of all
satisfaction measures, WTS shows the lowest relative frequency of respondents expressing very
high satisfaction (26%) and the highest relative frequency of respondents being dissatisfied or
indifferent (30.1%). There is relatively little variation in the distributions of the lightly positive
(+1) and rather positive (+2) satisfaction ratings and very similar relative frequencies in all
variables. The biggest variations occur in the highest satisfaction rating (+3) and in the cumulative
relative frequencies of dissatisfaction/indifference (-3 to 0) across all variables. The comparison of
the two main satisfaction variables WTS and TGPS depict a picture similar to the 2015 data.
3.2.2 Group Differences 2013
The table below displays the results from the Mann-Whitney-U Test for group differences in the
median of Overall GP Satisfaction and Waiting Time Satisfaction in 2013. For Overall GP
Satisfaction, we find significant results according to respondents’ life satisfaction, income, level of
education, age and perceived health status. Further significant results were yielded by the type of
GP (public or private), free capacity, and municipality size. There are no significant differences in
respondents’ overall GP satisfaction ratings according to contact frequency, GP density, free
capacity, open lists per 1000 inhabitants, list places per thousand inhabitants, and open list ratio
(low-high).
Significantly higher Overall GP Satisfaction levels were yielded in respondents with general life
satisfaction (p<.001), with below-median income (p<.001), primary school education (p<.001),
subjective good health (p= .003), and increasing age (p= .019; p< .001) compared to dissatisfied
respondents, respondents with above-median income, higher education, subjectively bad health and
younger age. Respondents visiting a private GP were also significantly more satisfied with the GP
in general than respondents visiting public GPs. The comparison of municipality sizes produced a
significantly higher satisfaction level in respondents living in the second biggest municipalities
rather than the biggest ones (p= .002). Middle-range free capacity municipalities produced also
higher GP satisfaction levels in respondents compared to high free capacity areas (p= .055).

61
Concurrently with Overall GP Satisfaction, we find significant results for higher Waiting Time
Satisfaction in the same socio-demographic and patient-related independent variable groups.
Respondents who are generally satisfied with life (p<.001), have a below-median income (p<.001),
primary education (p<.001), subjectively good health, and higher age expressed significantly
higher satisfaction with waiting time. Users of private GPs rather than public GPs were also
significantly more satisfied with waiting time (p<.001), as were respondents living in
municipalities of medium-range free capacity compared to low capacity (p= .019). The same holds
true for respondents from geographic areas with medium count of available list places per 1000
inhabitants compared to low count areas (p= .037) and high count areas (p= .028). Also respondents
from the second biggest municipalities expressed more waiting time satisfaction compared to those
living in the next smallest municipal areas (p= .023).

62
Independent Variables Overall GP
Satisfaction*
Waiting Time
Satisfaction*
HappyLife (Life Satisfaction) 0.000 0.000
Below median Income 0.000 0.000
Below High-School Education 0.000 0.000
Average Contact Frequency 0.461 0.549
Public vs Private GP 0.000 0.000
GoodHealth 0.003 0.011
Age group: young - middle 0.019 0.048
Age group: young - old 0.000 0.000
Age group: middle - old 0.000 0.000
GP density: low - medium 0.494 0.692
GP density: medium - high 0.806 0.808
GP density: low - high 0.665 0.526
Free capacity/ free GPs: low - medium 0.194 0.019
Free capacity/ free GPs: medium - high 0.055 0.194
Free capacity/ free GPs: low - high 0.493 0.294
Open Lists per 1000 Inhabitants: low - medium 0.333 0.551
Open Lists per 1000 Inhabitants: medium - high 0.249 0.815
Open Lists per 1000 Inhabitants: low - high 0.872 0.731
List Places per 1000 Inhabitants: low - medium 0.101 0.037
List Places per 1000 Inhabitants: medium - high 0.124 0.749
List Places per 1000 Inhabitants: low - high 0.991 0.028
Open List Ratio: low - medium 0.349 0.559
Open List Ratio: medium - high 0.350 0.467
Open List Ratio: low - high 0.966 0.864
Municipality size: 1+2 (below 5000 & 5000 - 20 000) 0.213 0.900
Municipality size: 2+3 (5000-20 000 & 20 000 - 110 000) 0.490 0.023
Municipality size: 3+4 (20 000 - 110 000 & more than 110 000) 0.002 0.121
Municipality size: 1+4 (below 5000 & more than 110 000) 0.502 0.524
* Asympt. Sig. (2-tailed)
Table 14: Mann-Whitney U Test for group differences in TGPS and WTS 2013

63
3.2.3 Regression Analysis 2013
3.2.3.1 Overall GP Satisfaction 2013
Age, public GP, waiting time satisfaction and overall life satisfaction are significantly correlated
with the odds of TGPS. The oldest age group was most likely to rate TGPS positively. By
comparison, the age group 25-39 had reduced the odds of being generally satisfied with the GP by
52.8% and 53.8% (in version 2). People visiting private GPs were 46.9% (42.9% in version 2)
more likely to be generally satisfied with their GP compared to users of public GPs. WTS was
highly significant across all categories. The most satisfied respondents were most likely to express
overall satisfaction with their GP, and the odds of doing so decline steadily with every less satisfied
group. Compared to respondents expressing the highest level of WTS, participants expressing the
most dissatisfaction were 93.6% (93.7% in version 2) less likely to be satisfied with their GP. Also
being highly satisfied with life resulted in the highest probability of perceiving the GP as
satisfactory. By comparison, being only mildly satisfied with life reduced the odds of overall GP
satisfaction by 43.6% (43.3%), and being indifferent or dissatisfied with life reduced these odds by
57% (58.7%).
In version 1, we also find that there is a significant difference in the odds of positively rating TGPS
among municipalities with a low and high amount of free list places per 1000 inhabitants.
Respondents living in municipalities with high LPPT resulted in the highest probability of being
satisfied with their GP, while respondents from municipalities with low LPPT were 51.7% less
likely to do so. In version 2, GP density is significant in predicting Overall GP Satisfaction. We
find a reduced odds ratio by 75% for respondents in municipalities with low GP density compared
to respondents from high GP density municipalities. Municipality size is also a significant
predictor in this model version. The odds ratios show that there is a general tendency of participants
from smaller municipalities producing increasingly smaller probabilities of being satisfied with the
GP. However, the highest odds stem from respondents living in the smallest municipalities
(increased odds by 16.1% compared to the biggest municipality) and respondents from the biggest
municipalities display the second-highest likelihood of expressing TGPS.

64
BLOCK Prediction -2Log
Likelihood R2 H&L Significant variable categories
BLOCK 0 89.4% Constant
BLOCK 1 89.4% 1796 .020 - .042 .865 Age (2, 3, 5);
BLOCK 2 89.4% 1789 .023 - .047 .098 Age (2, 3, 5); GoodHealth;
BLOCK 3 89.4% 1767 .030 - .062 .077 Age (2, 3, 5); GoodHealth; publicGP;
BLOCK 4 89.6% 1572 .097 - .198 .735 Age (2, 5); LPPT (1, 3); private GP;
Waiting Time Satisfaction (1-5, 7);
Overall Life satisfaction (1-4);
BLOCK 3’ 89.4% 1766 .031 - .063 .595 Age (2, 3, 5); GoodHealth; publicGP;
BLOCK 4’ 89.5% 1572 .097 - .198 .709 Age (2, 5); GPD (1, 3 at p=.058);
Kommunestr (1-3; 4 at p=.058); private
GP; Waiting Time Satisfaction (1-5, 7;
6 at p=.059); Life Satisfaction (1, 2, 4; 3
at p=.051);
Table 15: Model 1.1 TGPS_1 2013 (category 1 = negative/neutral rating; catg. 2 = positive rating);
N= 2881 (74.2%). Version 1: fkap & LPPT in step 3 & 4; Version 2: GPD & OLI in step 3’ & 4’.
Additional Analyses TGPS 2013:
For Model 1.2, both versions yield very similar results. Version1, however, needs to be interpreted
with caution due to the near-significant H&L value of .067. The significant variables include the
socio-demographic predictors age and below-median income, private GP as a supply-side variable
and the two satisfaction variables WTS and LS. Age follows the expected pattern of highest odds
for expressing satisfaction with the GP in respondents of highest age and a steady decline of these
odds in younger age categories (the group 40-54 years had 36.2% less probability to be rather or
very satisfied with GP, and the 25-39 year old respondents had reduced odds of 56.3%). Above-
median income resulted in 21.4% reduced odds of TGPS compared to respondents with below-
median income. Private GP increased respondents’ probability of being rather or very satisfied
with the GP by 41.2% compared to users consulting a public GP. Both WTS and Life Satisfaction
show the familiar pattern of yielding the highest probability for high or very high Overall GP
Satisfaction in respondents with the highest satisfaction ratings. As respondents’ Life or Waiting
Time Satisfaction decreases, so do the odds of expressing high or very high satisfaction with the
GP.

65
BLOCK Prediction -2Log
Likelihood R2 H&L Significant variable categories
BLOCK 0 77.5% Constant
BLOCK 1 77.5% 2822 .038 - .058 .688 Age (1-5);
BLOCK 2 77.5% 2819 .039 - .059 .534 Age (1-5);
BLOCK 3 77.4% 2792 .048 - .074 .047 Age (1-5); publicGP;
BLOCK 4 78.5% 2490 .148 - .225 .067
(!)
Age (2, 3, 5); bm_Income; private GP;
Waiting Time Satisfaction (1-5, 7); Life
Satisfaction (1-4);
BLOCK 3’ 77.5% 2792 .048 - .074 .147 Age (1-5); publicGP;
BLOCK 4’ 78.2% 2492 .147 - .224 .898 Age (2, 3, 5); bm_Income; private GP;
Waiting Time Satisfaction (1-7); Life
Satisfaction (1-4);
Table 16: Model 1.2 TGPS_2 2013 (category 1 = negative/neutral/slightly positive rating; catg. 2 = rather or very positive
rating); N= 2881 (74.2%). Version 1: fkap & LPPT in step 3 & 4; Version 2: GPD & OLI in step 3’ & 4’.
Model 1.3 yields results corresponding to those encountered in the other models. Thus age, having
a private GP and expressing satisfaction with waiting time and life in general correlate positively
with the odds of being very satisfied with the GP. It is noteworthy in this model that having a
private GP increased respondents’ likelihood of expressing high TGPS by 19%, although this
result is not significant at the 5% level (p=.061). Moreover, above-median income compared to
below-median income reduced the odds of expressing very high overall satisfaction by 22.9% in
version 1, and by 23% in version 2. Also in version 2, education is a near-significant predictor
(p=.059) instead of having a private GP. Compared to respondents with a university or college
degree, high school or vocational training as highest completed education increased the odds of
expressing very high TGPS by 29.9%.
BLOCK Prediction -2Log
Likelihood R2 H&L Significant variable categories
BLOCK 0 53.6%
BLOCK 1 59.5% 3664 .044 - .059 .049 Age (1-5); Education (1);
BLOCK 2 59.8% 3662 .045 - .060 .057 Age (1-5); Education (1);
BLOCK 3 60.4% 3643 .051 - .069 .595 Age (1-5); bm_Income; Education (1);
private GP;
BLOCK 4 68.7% 3222 .186 - .249 .480 Age (2, 3, 5); bm_Income; Waiting Time
Satisfaction (1- 7); Life Satisfaction (1-
4); private GP (p=.061)
BLOCK 3’ 60.1% 3643 .052 - .069 .858 Age (1-5); bm_Income; Education (1);
private GP;
BLOCK 4’ 68.8% 3223 .186 - .248 .726 Age (2, 3, 5); bm_Income; Education (1 at
p=.059); Waiting Time Satisfaction (1-
7); Life Satisfaction (1-4);
Table 17: Model 1.3 TGPS_3 2013 (category 1 = negative to slightly positive rating; catg. 2 = rather or very positive
rating); N= 2881 (74.2%). Version 1: fkap & LPPT in step 3 & 4; Version 2: GPD & OLI in step 3’ & 4’.

66
Outcomes Summary of TGPS 2013 Models
All models provide coherent results with regard to significant main variables and their relation to
the dependent variable. Age, Waiting Time Satisfaction and general Life Satisfaction have a
consistent, significantly positive effect on the probability of Overall GP Satisfaction in all models.
Private GP is a significant predictor of TGPS probability in models 1 and 2 and yields a higher
probability of respondents’ Overall GP Satisfaction compared to respondents with public GPs.
Above-median income is significantly correlated with reduced odds of TGPS compared to below-
median income in the models 2 and 3, playing a significant role when predicting high overall GP
satisfaction.
There is no consistent significant effect of municipality-specific competition variables in the
three models. However, we find that LPPT and GPD are significant in the first model and observe
that both variables hint at a positive correlation with the odds of TGPS (both the highest LPPT and
the highest GPD resulted in the highest odds of TGPS compared to medium and low LPPT and
GPD, respectively). Municipality size is significant in model 1 (version 2) as well, and we observe
that the smallest municipality coincides with the highest odds of TGPS, while the second-smallest
to the biggest municipalities show continuously increasing odds of TGPS. With regard to the
development of the explained variance, we find that R2 increases with higher cut-off points
(towards predicting higher TGPS levels) in every model. Consequently, we find the highest
proportion of R2 in model 1.3 when predicting very high Overall GP Satisfaction.
3.2.3.2 Waiting Time Satisfaction 2013
In the main model, age is a significant, positively correlating predictor of the odds of WTS in both
model versions. Compared to the oldest age group, respondents between 40 and 54 years of age
were 48.3% (47.9%) less likely to express Waiting Time Satisfaction, people between 25 and 39
had reduced odds by 45.8% (46.2%), and the youngest age group from 18 to 24 resulted in a 50.5%
(48.9%) reduced probability for WTS. Having a private GP produced 40% (42.3%) higher odds
of being satisfied with waiting time (p=.001) compared to consulting a public GP. Also GP Supply
Satisfaction and overall Life Satisfaction have a highly significant effect in predicting the odds
of WTS (p=.000). We find steadily decreasing odds with diminishing Municipal GP Supply
Satisfaction. However, the two lowest GPS ratings (rather & very dissatisfied) do not yield the

67
lowest odds; in fact, the category of mild dissatisfaction produced the lowest odds (reduced odds
of 86.8% vs. 78.5%). Similarly, overall Life Satisfaction is also a significant positive predictor of
respondents’ likelihood of WTS as the highest life satisfaction correlated with the highest odds for
expressing WTS. For instance, respondents being mildly satisfied were 34.2% (33.5) less likely to
express WTS compared to the happiest respondents.
In model version 1, four municipality-specific variables showed significant results. High free
capacity (top third percentile) resulted in the highest odds of people expressing WTS. By
comparison, a middle range free capacity had reduced respondents’ odds by 51.7%, and low free
capacity decreased the probability by 97.6%. Available list places per thousand inhabitants was
significant in its highest category, which produced the highest odds for respondents’ WTS.
Municipality size has a significant positive effect on respondents’ probability to express WTS,
with the biggest municipality resulting in the highest odds. By comparison, living in the second
smallest municipalities (between 5.000 and 20.000 inhabitants) reduced respondents’ likelihood of
stating WTS by half (50.2%, p=.007), and the smallest municipalities decreased respondents’
probability by 55.9% (p=.009). In model version 2, GP density is positively correlated with WTS.
High-density municipalities produced the highest odds of respondents’ expressing WTS.
Compared to respondents living in high GP density municipalities, people from medium-density
municipalities were 28.7% less likely to be satisfied with WT.
BLOCK Prediction -2Log
Likelihood R2 H&L Significant variable categories
BLOCK 0 69.5%
BLOCK 1 69.5% 3081 .042 - .060 .988 Age (1-5);
BLOCK 2 69.5% 3074 .045 - .063 .115 Age (1-5); GoodHealth;
BLOCK 3 69.9% 3040 .057 - .081 .480 Age (1-5); Education (1); GoodHealth;
fkap (1); Kommunestr (1, 2, 4; 3 at
p=.064); publicGP;
BLOCK 4 71.2% 2834 .130 - 183 .603 Age (1-3, 5); fkap (1-3); LPPT (3);
Kommunestr (1, 2, 4); private GP; GP
Supply Satisfaction (1-7); Life
Satisfaction (2, 4);
BLOCK 3’ 69.2% 3041 .057 - .081 .764 Age (1-5); Education (1); GoodHealth;
GPD (2; 3 at p=.056); Kommunestr (1, 2,
4); publicGP;
BLOCK 4’ 71.6% 2838 .128 - .181 .210 Age (1-3, 5); GPD (2, 3); private GP; GP
Supply Satisfaction (1-7); Life
Satisfaction (2, 4);
Table 18: Model 2.1 WTA_1 2013 (category 1 = negative/neutral rating; catg. 2 = positive rating); N= 2736 (70.5%).
Version 1: fkap & LPPT in step 3 & 4; Version 2: GPD & OLI in step 3’ & 4’.

68
Additional Analysis of WTA 2013:
Model 2.2 yields similar significant results as the main model. Age, private GP, GP supply
satisfaction and life satisfaction are positively correlated with the odds of rating waiting time
satisfaction highly or very highly. In addition, education produces a near-significant prediction
effect (p=.059) version 1, showing that respondents with high-school or vocational training as
highest completed education increased the respondents’ odds of being rather or very satisfied with
WT by a fourth (25.4%) compared to those with a university or college degree. In version 2, we
find a negative correlation of open lists per 1000 inhabitants with the odds of high or very high
WTS. The municipalities in the top third percentile of OLI resulted in the lowest odds for WTS.
Moreover, municipalities with the second-lowest number of inhabitants (5.000 to 20.000) produced
increased odds of respondents expressing high or very high WTS by 47.7% (p=.050) compared to
the biggest municipalities with the most inhabitants.
BLOCK Prediction -2Log
Likelihood R2 H&L Significant variable categories
BLOCK 0 77.8%
BLOCK 1 77.8% 2673 .041 - .063 .579 Age (1-5);
BLOCK 2 77.8% 2670 .042 - .065 .377 Age (1-5);
BLOCK 3 77.8% 2646 .051 - .078 .045 Age (1-5); public GP;
BLOCK 4 80.4% 2287 .172 - .264 .301 Age (2, 3, 5); Education (2 at p=.059);
private GP; GP Supply Satsifaction (1-
7); Life Satisfaction (1-4);
BLOCK 3’ 77.9% 2646 .051 - .078 .295 Age (1-5); public GP;
BLOCK 4’ 80.9% 2285 .173 - .265 .092 Age (2, 3, 5); OLI (1-3); Kommunestr
(2); private GP; GP Supply Satsifaction
(1-7); Life Satisfaction (1-4);
Table 19: Model 2.2 WTA_2 2013; N= 2779 (71.6%). Version 1: fkap & LPPT in step 3 & 4; Version 2: GPD
& OLI in step 3’ & 4’.
In model 2.3, we find age and below-median income to be significant socio-demographic variables
in predicting very high waiting time satisfaction. Age shows the typical positive correlation with
WTS. Above-median income decreased the odds of respondents being very satisfied with WT by
almost a fifth (18.2% and 18.7%) compared to raters with below-median income. Respondents
having private GP were 1.3 times more likely to express very high WTS than respondents with a
public GP. Both GPS and LS are highly significant predictors indicating a positive correlation with
the odds of very high WTS. Compared to being very satisfied with the municipal GP supply,
respondents who were only rather satisfied were 68.9% less likely to express very high WTS
(p=.000).

69
In version 2, municipality size has a significant prediction effect, with the second-smallest
municipalities increasing the odds of respondents’ expression of very high WTS by 42.1%
compared to respondents living in the biggest municipalities and respondents from the second-
biggest municipalities having increased odds by 39.9%. This indicates a tendency towards a
negative correlation of municipality size and the probability of WTS (the smaller the municipality,
the higher the odds of WTS).
BLOCK Prediction -2Log likelih. R2 H&L Significant variables
BLOCK 0 52.9%
BLOCK 1 59.6% 3502 .050 - .066 .207 Age (1-5); Education (1; 3 at p=.051);
BLOCK 2 59.5% 3500 .050 - .067 .303 Age (1-5); Education (1);
BLOCK 3 60.4% 3486 .056 - .074 .827 Age (1-5); Education (1; 3); public GP;
BLOCK
4
68.8% 3099 .184 - .246 .697 Age (1-3; 5); bm_Income; private GP;
GP Supply Satsifaction (1-7); Life
Satisfaction (2-4);
BLOCK
3’
60.3% 3483 .056 - .075 .714 Age (1-5); Education (1; 3); publicGP;
BLOCK
4’
69.2% 3097 .185 - .247 .699 Age (1-3; 5); bm_Income; Kommunestr
(2, 3); private GP; GP Supply Satisfaction
(1-7); Life Satisfaction (2-4);
Table 20: Model 2.3 WTA_3 (category 1 = negative to rather positive rating; catg. 2 = very positive rating);
N= 2779 (71.6%). Version 1: fkap & LPPT in step 3 & 4; Version 2: GPD & OLI in step 3’ & 4’.
Outcomes Summary of WTA 2013 Models
Age is significantly positively correlated with the odds of WTS in all three models. Private GP is
the only consistently significant municipality-specific variable in all models (and versions) and
yielded higher odds of respondents’ WTS compared to the ones with a public GP. The
municipality size is significant in version 2 of models 2 and 3, and version 1 of model 1. In model
1, the biggest municipalities had the highest odds of respondents expressing WTS. In model 2, the
second-biggest municipalities yielded the highest odds for respondents’ WTS. And in determining
very high WTS (model 3), the odds rations indicate an inverse correlation of municipality size and
WTS as the smallest municipalities produced the highest odds of WTS. We find single significant
competition variables in single models: fkap, GPD and LPPT are significant in model 1 and yield
the highest odds for respondents’ WTS in their highest category. OLI is significant in model 2 and,
based on the odds ratios of each category, indicates a negative correlation with WTS (the category
of high OLI yielded the lowest probability of WTS). GP Supply Satisfaction and general Life

70
Satisfaction are both highly significant and correlate positively with the odds of WTS in all
models. There is no significant correlation with health status or education in any of the models.
Above-median income is significant in both versions of model 3 for predicting the highest
satisfaction with waiting time. Respondents with above-median income resulted in reduced odds
of very high WTS compared to below-median income by 18.2% in version 1 and 18.7% in version
2.
3.3 2010 Analysis
3.3.1 Descriptives 2010
Also in 2010, respondents appear rather satisfied in general. The main satisfaction variables show
a left-skewed distribution with the highest relative frequencies in the highest rating items. As in
the previous years, Overall GP Satisfaction, satisfaction with the GP’s Medical Competence and
satisfaction with the GP’s Referral Practice peak in the highest rating item +3. The only exceptions
are Waiting Time Satisfaction and satisfaction with Municipal GP Supply with the mode in +2. In
the graph below, we can see that the relative frequencies of Waiting Time Satisfaction from item -
3 to -1 (signifying dissatisfaction) are the highest of all satisfaction variables. We can therefore
conclude that respondents were more dissatisfied with waiting time than with other satisfaction
measures, including Trust in the GP, the perceived Medical Competence of the GP, Overall
Satisfaction with the GP, Satisfaction with Referrals to Specialists, and satisfaction with the
available time to explain the situation to the GP during a consultation.

71
Figure 3: Frequency Distribution of Satisfaction Variables 2010 (in %)
3.3.2 Group Differences 2010
The table below displays the results from the Mann-Whitney-U test for group differences in the
median of Overall GP Satisfaction and Waiting Time Satisfaction in 2010. For Overall GP
Satisfaction, we find significant results according to respondents’ life satisfaction, income, level
of education, and age group. Further significant results were yielded by available list places per
1000 inhabitants, and municipality size. There are no significant differences in respondents’ overall
GP satisfaction ratings according to GP density, free capacity, open lists per 1000 inhabitants, and
open list ratio (low-high).
We detect significantly higher Overall GP Satisfaction levels in respondents who are satisfied with
life compared to those who expressed overall dissatisfaction with life (p=.043). Being older rather
than young or middle-aged (p< .001), having below-median income (p< .001), and primary school
education rather than high-school or higher education (p< .001), produced significantly higher GP
satisfaction levels in respondents. Respondents living in municipalities with a medium count of
available list places per 1000 inhabitants were also significantly more satisfied than respondents
from either low or high count municipalities (p= .015). Similarly, respondents from the second
largest municipality areas expressed significantly higher overall GP satisfaction compared to those
from the largest municipalities (p= .022).
-3 -2 -1 0 1 2 3
Overall GP Satisfaction 1.1 1.7 2.8 5.3 12.7 29.1 47.3
Waiting Time Satisfaction 5.8 7.6 10.4 9.3 16.3 25.4 25.1
Referrals (specialist) 1.8 1.7 2.9 7.1 11.4 29.7 45.3
GP's Medical Competence 1.1 0.9 1.8 6.4 14.2 32.0 43.6
Municipal GP Supply 1.3 2.4 3.1 9.4 18.6 35.3 29.8
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
45.0
50.0

72
Further, we find the same significant group differences for life satisfaction, income, level of
education and age in Waiting Time Satisfaction as in Overall GP Satisfaction. Young people,
dissatisfied respondents, as well as those with above-median income and high-school or higher
education were significantly less satisfied than their counterparts with subjective life satisfaction
(p= .043), those of old age (p< .001), the ones with below-median income (p< .001), and primary
school education (p< .001). High free capacity areas produced significantly more satisfied
respondents than the low capacity counterparts (p= .007). By contrast, there are no significant
differences in waiting time satisfaction for open lists per 1000 inhabitants, municipality size or
open list ratio. However, we observe tendencies of higher waiting time satisfaction in respondents
Independent Variables Overall GP
Satisfaction*
Waiting Time
Satisfaction*
HappyLife (Life satisfaction) 0.000 0.043
Below median Income 0.000 0.000
Below High School Education 0.000 0.000
Age group: young - middle 0.029 0.026
Age group: young - old 0.000 0.000
Age group: middle - old 0.000 0.000
GP density: low - medium 0.916 0.098
GP density: medium - high 0.662 0.260
GP density: low - high 0.775 0.574
Free capacity/ free GPs: low - medium 0.849 0.195
Free capacity/ free GPs: medium - high 0.656 0.145
Free capacity/ free GPs: low - high 0.510 0.007
Open Lists per 1000 Inhabitants: low - medium 0.698 0.186
Open Lists per 1000 Inhabitants: medium - high 0.943 0.282
Open Lists per 1000 Inhabitants: low - high 0.725 0.779
List Places per 1000 Inhabitants: low - medium 0.015 0.107
List Places per 1000 Inhabitants: medium - high 0.015 0.409
List Places per 1000 Inhabitants: low - high 0.953 0.010
Open List Ratio: low - medium 0.345 0.428
Open List Ratio: medium - high 0.650 0.731
Open List Ratio: low - high 0.596 0.615
Municipality size: 1+2 (below 5000 & 5000 - 20 000) 0.300 0.972
Municipality size: 2+3 (5000-20 000 & 20 000 - 110 000) 0.244 0.347
Municipality size: 3+4 (20 000 - 110 000 & more than 110 000) 0.022 0.812
Municipality size: 1+4 (below 5000 & more than 110 000) 0.971 0.393
* Asympt. Sig. (2-tailed); significant values p<.05 marked in bold;
Table 21: Mann-Whitney U Test for group differences in TGPS and WTS 2010

73
from middle-range GP density municipalities compared to the ones from low GP density areas (p=
.098), and find that respondents from municipalities in the top 33% percentile of available list
places express higher waiting time satisfaction compared to those in the low 33% percentile (p=
.010).
3.3.3 Regression Analyses 2010
The hierarchical regression models feature three steps due to the lack of variables related to users’
self-assessed health status. Another missing variable constitutes the type of GP (public vs private),
that is also not part of the 2010 dataset.
3.3.3.1 Overall GP Satisfaction 2010
The model yields a high goodness-of-fit (H&L =.873 in version 1 and H&L =.741 in version 2) but
a diminished predictability of 88.7% and 88.6% compared to the 88.8% of the baseline model. This
fact should be kept in mind upon interpretation of the results. Both versions produce almost
identical outcomes with regard to the significant independent variables.
Contrary to the results found in the models for 2015 and 2013, we find age not to be a significant
predictor in the 2010 model of Overall GP Satisfaction at the 5% level. However, the youngest
respondents were 53.9% and 54% less likely to rate the GP satisfactory pared to the oldest age
group at a significance level of 10% (p=.057). There are no other significant socio-demographic or
municipality-specific variables correlating with general GP satisfaction. Both Waiting Time
Satisfaction and Life Satisfaction are highly significant predictors of TGPS, and the odds ratio
indicates a positive correlation trend. Thus, the more satisfied respondents were with waiting time,
the more likely they were to be satisfied with the GP in general. Compared to the happiest
respondents, the ones being dissatisfied or indifferent were only half as likely to be satisfied with
the GP, corresponding to reduced odds by 51.3% and 51.4%, respectively.

74
BLOCK Prediction -2Log
Likelihood R2 H&L Significant variable categories
BLOCK 0 88.8%
BLOCK 1 88.8% 1317 .014 - .028 .808 Age (1-3; 5);
BLOCK 2 88.8% 1309 .018 - .036 .215 Age (1-3; 5);
BLOCK 3 88.7% 1175 .085 - .168 .873 Age (1, p=.057); Waiting Time Satisfaction
(1-5; 7); Life Satisfaction (1, 3);
BLOCK 2’ 88.8% 1311 .017 - .034 .674 Age (1-3; 5);
BLOCK 3’ 88.6% 1178 .083 - .165 .741 Age (1, p=.057); Waiting Time Satisfaction
(1-5; 7); Life Satisfaction (1, 3);
Table 22: Model 1.1 TGPS_1 2010 (category 1 = negative/indifferent rating; catg. 2 = positive rating);
N= 1912 (83.9%). Version 1: fkap & LPPT in step 2 & 3; Version 2: GPD & OLI in step 2’ & 3’.
Additional Analyses of TGPS 2010
Both versions of Model 1.2 show a significant improvement in predictability compared to baseline
model amounting to 77.1% and 77%, respectively and an acceptable goodness-of-fit (H&L =.476;
H&L =.771). Age is only significant in the youngest age group at the 10% level (p=.059 and
p=.078). The youngest age category has 47% (44.7% in version 2) decreased odds of high or very
high GP satisfaction compared to the oldest respondents. Above-median income reduced
respondents’ probability to be rather or highly satisfied with the GP by 22.4% (and 21.9%, p= .051)
compared to below-median income GP users. Both waiting time satisfaction and life satisfaction
are highly significant and indicate a positive correlation with the likelihood of overall GP
satisfaction.
BLOCK Prediction -2Log
Likelihood R2 H&L Significant variable categories
BLOCK 0 75.8% Constant
BLOCK 1 75.8% 2067 .026 - .038 .608 Age (1-5);
BLOCK 2 75.8% 2060 .029 - .043 .994 Age (1-5);
BLOCK 3 77.1% 1814 .146 - .219 .476 Bm_Income; Age (1, p=.059);
Waiting Time Satisfaction (1-7);
Life Satisfaction (1-3);
BLOCK 2’ 75.8% 2062 .028 - .042 .388 Age (1-5);
BLOCK 3’ 77.0% 1814 .146 - .219 .771 Bm_Income (p= .051);
Waiting Time Satisfaction (1-7);
Life Satisfaction (1-3);
Table 23: Model 1.2 TGPS_2 2010 (category 1 = negative/indifferent/slightly positive rating; catg. 2 = rather & very
positive rating); N= 1912 (83.9%). Version 1: fkap & LPPT in step 2 & 3; Version 2: GPD & OLI in step 2’ & 3’.

75
In predicting very high satisfaction with the GP in Model 1.3, we find similar results as in previous
models. Age is significant at the 10% level (p= .087, p= .074) and results in reduced odds for young
respondents between age 25 and 34 to rate overall GP satisfaction highly compared to the oldest
respondents. Above-median income is significant and reduces the odds of the dependent variable
by 27.5% (26.7%) compared to respondents with below-median income. Both waiting time and
life satisfaction were highly significant and indicate a positive correlation with the likelihood of
high overall GP satisfaction. Neither municipality size nor GP density or free capacity have a
significant influence on very high overall GP satisfaction. In version 1, we also find 1 municipality-
specific variable of significant influence – free list places per thousand inhabitants. Compared to
municipalities with a high number of LPPT, the ones with medium LPPT had increased odds of
respondents expressing very high satisfaction with their GP by 42.2%. In version 2, education has
a significant effect. Respondents with less than a high-school education were 32.1% more likely to
rate their GP most positively compared to those with university or college education.
BLOCK Prediction -2Log
Likelihood R2 H&L Significant variable categories
BLOCK 0 53.3% Constant
BLOCK 1 57.7% 2582 .030 - .041 .594 Age (2, 3, 5); bm_Income; Education (1);
BLOCK 2 57.6% 2570 .037 - .049 .426 Age (2, 3, 5); bm_Income; Education (1);
LPPT (2, 3);
BLOCK 3 67.6% 2338 .147 - .196 .635 Age (2, p= .087), Bm_Income; LPPT (2,
3); Waiting Time Satisfaction (1-7);
Life Satisfaction (1-3);
BLOCK 2’ 58.6% 2575 .034 - .046 .471 Age (2,3,5); bm_Income; Education (1);
BLOCK 3’ 67.6% 2343 .144 - .193 .767 Age (2, p= .074), Bm_Income; Education
(1); Waiting Time Satisfaction (1-7);
Life Satisfaction (1-3);
Table 24: Model 1.3 TGPS_3 2010 (category 1 = all items except +3; catg. 2 = very positive rating); N= 1912 (83.9%).
Version 1: fkap & LPPT in step 2 & 3; Version 2: GPD & OLI in step 2’ & 3’.
Outcomes Summary of TGPS Model 2010
TGPS is most closely tied to Waiting Time Satisfaction and Life Satisfaction as the only
consistent predictors in all models. There is a positive correlation between these satisfaction
variables and the probability of TGPS. Age is not an influential significant predictor of TGPS
probability in the 2010 models, as there is only one significant age category at a 10% significance
level. Above-median income is significant in predicting high and very high TGPS (in models 2
and 3) and yields reduced odds for respondents’ overall GP satisfaction compared to below-median

76
income. There are no consistently significant municipality-specific competition variables in
the 2010 TGPS models. LPPT is the only exception that has a significant effect in 1 category in
determining very high TGPS in model 3. Compared to a high amount of available list places per
1000 inhabitants, a medium LPPT yielded a higher probability of respondents being very satisfied
with their GP. In terms of the explained variance in the dependent variable, we observe a
continuously increasing R2 value through adding predictors to the model. We find the highest
proportion of variation explained by significant variables in model 1.2 (predicting high or very
high TGPS).
3.3.3.2 Waiting Time Satisfaction 2010
Since step 3 of version 1 yields a significant H&L value (.041), so that the outcomes need to be
interpreted with caution and cannot be regarded reliable. In step 2 of version 1, all age categories
are significant in predicting waiting time satisfaction and the odds ratios suggest a tendency of a
positive correlation. Accordingly, the oldest age group was most likely to be satisfied with WT. By
comparison, the second-oldest respondent pool (55-66 years) was 27.8% less likely to express
WTS, the group from 40 to 54 years of age had reduced odds by 64.9%, and the category of 25 to
39 year olds had 80.1% less probability of being satisfied with waiting time. Above-median
income reduced the odds of WTS by 19.7% compared to respondents with below-median income
(p=.046). In step 3, we find that age is highly significant and following the same tendency as in
step 2. In addition, GP Supply Satisfaction and Life Satisfaction have a significant, effect on
respondents’ probability of expressing waiting time satisfaction. GP supply satisfaction was highly
significant in all categories and based on the odds ratios indicates a positive correlation. Lastly, life
satisfaction was significant in the category of dissatisfaction/indifference. Compared to high LS,
this category yielded a reduction of 30.1% (29.1%) in respondents’ likelihood of expressing WTS.
Version 2 yields additional significant results of competition variables. High GP density produced
the highest odds of respondents expressing WTS (p=.053). Compared to municipalities with high
GP density, low GP density reduced respondents’ probability of being satisfied with waiting time
by almost a third (32.9%). Similarly, the biggest municipality size resulted in the highest
probability of respondents’ WTS. By comparison, the second-largest municipalities reduced

77
respondents’ odds of WTS by 29.1%, and the next smaller municipality size yielded a 43.9%
reduced probability.
BLOCK Prediction -2Log
Likelihood R2 H&L Significant variable categories
BLOCK 0 66.2%
BLOCK 1 67.3% 2282 .054 - .075 .913 Age (1- 5); bm_Income;
BLOCK 2 67.6% 2265 .063 - .087 .250 Age (1- 5); bm_Income;
BLOCK 3 70.1% 2164 .112 - .155 .041 Age (1- 3; 5); GP Supply Satisfaction (1-
7); Life Satisfaction (1);
BLOCK 2’ 67.5% 2268 .061 - .085 .817 Age (1- 5); Kommunestr (2-4);
BLOCK 3’ 70.0% 2164 .112 - .155 .324 Age (1- 3; 5); GPD (1; 3 p=.053);
Kommunestr (2-4; 1 p=.053); GP Supply
Satisfaction (1-7); Life Satisfaction (1);
Table 25: Model 2.1 WTA_1 2010 (category 1 = negative/neutral rating; catg. 2 = positive rating); N= 1866 (81.8%).
Version 1: fkap & LPPT in step 2 & 3; Version 2: GPD & OLI in step 2’ & 3’.
Additional Analyses of WTA 2010:
In Model 2.2, age is a significant predictor for high or very high WTS in four categories. The oldest
group of respondents yielded the highest probability and the youngest age group the lowest chances
for WTS. We find that the odds decrease steadily with decreasing age of respondents. No
significant correlation was found with other socio-demographic or municipality-specific variables
but GP Supply Satisfaction and Life Satisfaction are again highly significant predictors of WTS
probability. Both variables are positively correlated with the probability of WTS. Additionally, GP
density is significantly correlated with WTS probability in version 2. Medium GP density reduced
respondents’ odds of opting for WTS by 29% compared to the high GP density municipalities.
BLOCK Prediction -2Log
Likelihood R2 H&L Significant variable categories
BLOCK 0 75.8%
BLOCK 1 75.8% 2022 .031 - .046 .329 Age (1- 5); bm_Income (p=.052);
BLOCK 2 75.8% 2016 .034 - .051 .975 Age (1- 5); bm_Income¸
BLOCK 3 76.7% 1854 .114 - .170 .388 Age (1- 3; 5); GP Supply Satisfaction (1-
7); Life Satisfaction (1-3);
BLOCK 2’ 75.8% 2017 .034 - .050 .759 Age (1- 5); bm_Income (p=.059);
BLOCK 3’ 76.3% 1851 .115 - .172 .348 Age (1- 3; 5); GPD (2); GP Supply
Satisfaction (1-7); Life Satisfaction (1-3);
Table 26: Model 2.2 WTA_2 2010 (category 1 = negative/neutral/slightly positive rating; catg. 2 = rather or very positive
rating); N= 1881 (82.5%). Version 1: fkap & LPPT in step 2 & 3; Version 2: GPD & OLI in step 2’ & 3’.

78
In predicting the probability of very high waiting time satisfaction (Model 2.3), age, income, GP
Supply Satisfaction as well as Life Satisfaction are significant. We encounter the familiar trends
of increasing probability for waiting time satisfaction with respondents’ increasing age and
increasing satisfaction levels with GP supply and life. Above-median income reduced
respondents’ odds of expressing very high WTS by 28% (26.8%) compared to people with below-
median income. Medium LPPT yielded significantly higher odds of WTS (by 31.9%) compared
to high LPPT.
BLOCK Prediction -2Log
Likelihood R2 H&L Significant variable categories
BLOCK 0 53.1% Constant
BLOCK 1 58.1% 2533 .035 - .047 .884 Age (2, 3, 5); bm_Income; Education (1 at
p= .051);
BLOCK 2 58.2% 2521 .041 - .055 .438 Age (2, 3, 5); bm_Income; Education (1);
LPPT (2, 3);
BLOCK 3 63.0% 2372 .114 - .152 .295 Age (2, 5); bm_Income; LPPT (2, 3); GP
Supply Satisfaction (1-7); Life
Satisfaction (1-3);
BLOCK 2’ 58.9% 2526 .039 - .051 .418 Age (2, 3, 5); bm_Income; Education (1);
BLOCK 3’ 63.4% 2380 .110 - .147 .438 Age (2, 5); bm_Income; GP Supply
Satisfaction (1-7); Life Satisfaction (1-3);
Table 27: Model 2.3 WTA_3 2010 (category 1 = negative to rather positive rating; catg. 2 = very positive rating);
N= 1881 (82.5%). Version 1: fkap & LPPT in step 2 & 3; Version 2: GPD & OLI in step 2’ & 3’.
Outcomes Summary of WTA Models 2010
Age is a significant predictor that correlates positively with the odds of Waiting Time Satisfaction
in all models. GP Supply Satisfaction and general Life Satisfaction are significantly, positively
associated with the odds of WTS as well. Above-median income is significant in predicting the
odds of WTS in both versions of model 3, resulting in reduced odds of WTS compared to below-
median income. There is no consistent significant association of any municipality-specific
variables in all three models. We find, however, single significant correlations of LPPT in model
3 (where medium LPPT yielded significantly higher odds of WTS compared to high LPPT), and
GP density in model 1 and 2 (where the highest GP density produced the highest odds of WTS).
Municipality size was significant in model (version 2) and correlated positively with WTS.

79
3.4 Longitudinal Analysis
This section investigates the main satisfaction variables across time by conducting Mann-Whitney
U tests to identify potential changes in respondents’ ratings and satisfaction levels. First, however,
we will take a look at the development of capacity variables over time before comparing the
outcomes of the regression models for the two main variables from a longitudinal perspective.
3.4.1 Municipal Capacity Measures
As we can see in the table below, total municipal capacity increased in the form of registered GPs,
free capacity (the number of physicians with open lists) and GP density. In this way, both the
general supply of GPs as well as the real choice of patients among GPs rose. At the same time, the
number of available list places per 1000 inhabitants went down steadily, and GPs with open lists
per 1000 inhabitants decreased from 2009 to 2012, before rising in 2014 again. Godager et al.
(2016) find in addition that the average number of available list places per 1000 inhabitants
decreased over time as well, thus limiting excess capacity and patient choice for switching the GP.
2009 2012 2014
Registered GPs 4064 4299 4531
Free Capacity (open lists) 1692 1726 1941
Free List Places 325763 290941 309514
GP Density* 477 491 497
LPPT* 72378 62898 62510
OLI* 317 312 325
* rounded numbers
Table 28: Collective municipal capacity in absolute numbers (whole Norway) based on data from
Helsedirektoratet
3.4.2 Overall GP Satisfaction
The variable shows a very similar, left-skewed distribution shape with steep incline in the shape of
an exponential curve in all three years. We can see the lowest relative frequencies of dissatisfied
or indifferent respondents in combination with the highest relative frequency of the most satisfied
respondents (rating +3) in 2015. Thus, respondents’ overall satisfaction with the GP seems to have
improved. This observation is supported by the outcome of the Mann-Whitney U test, which yields
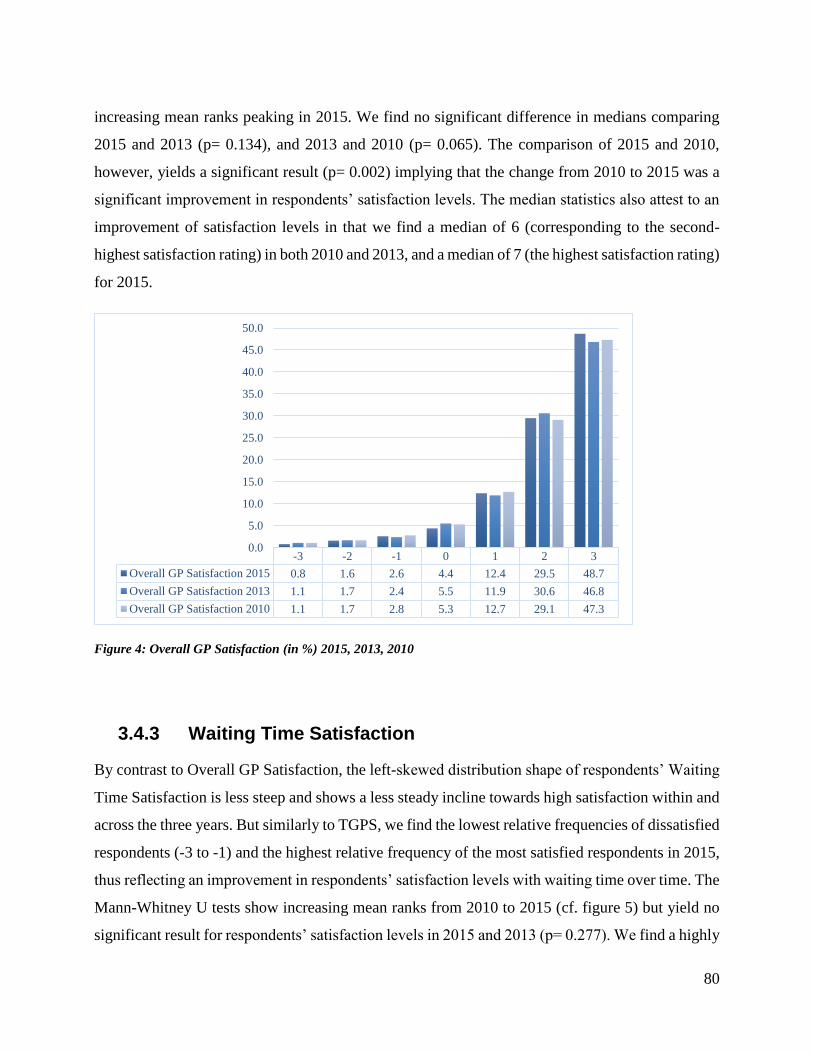
80
increasing mean ranks peaking in 2015. We find no significant difference in medians comparing
2015 and 2013 (p= 0.134), and 2013 and 2010 (p= 0.065). The comparison of 2015 and 2010,
however, yields a significant result (p= 0.002) implying that the change from 2010 to 2015 was a
significant improvement in respondents’ satisfaction levels. The median statistics also attest to an
improvement of satisfaction levels in that we find a median of 6 (corresponding to the second-
highest satisfaction rating) in both 2010 and 2013, and a median of 7 (the highest satisfaction rating)
for 2015.
Figure 4: Overall GP Satisfaction (in %) 2015, 2013, 2010
3.4.3 Waiting Time Satisfaction
By contrast to Overall GP Satisfaction, the left-skewed distribution shape of respondents’ Waiting
Time Satisfaction is less steep and shows a less steady incline towards high satisfaction within and
across the three years. But similarly to TGPS, we find the lowest relative frequencies of dissatisfied
respondents (-3 to -1) and the highest relative frequency of the most satisfied respondents in 2015,
thus reflecting an improvement in respondents’ satisfaction levels with waiting time over time. The
Mann-Whitney U tests show increasing mean ranks from 2010 to 2015 (cf. figure 5) but yield no
significant result for respondents’ satisfaction levels in 2015 and 2013 (p= 0.277). We find a highly
-3 -2 -1 0 1 2 3
Overall GP Satisfaction 2015 0.8 1.6 2.6 4.4 12.4 29.5 48.7
Overall GP Satisfaction 2013 1.1 1.7 2.4 5.5 11.9 30.6 46.8
Overall GP Satisfaction 2010 1.1 1.7 2.8 5.3 12.7 29.1 47.3
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
45.0
50.0

81
significant difference between 2013 and 2010 (p< 0.001) as well as between 2015 and 2010 (p<
0.001), even though the median remains constant at 6 (the second-highest satisfaction rating)
throughout all three years.
Figure 5: Waiting Time Satisfaction (in %) 2015, 2013, 2010
3.4.4 Satisfaction w. Referrals to Specialists
The distribution curve of respondents’ Satisfaction with Referrals to Specialists follows similar
patterns to the one of Overall GP Satisfaction, i.e. a steady and increasingly steep incline of relative
frequencies towards high satisfaction levels. While we encounter the highest relative frequency of
most satisfied respondents in 2013, the frequencies of mildly and rather satisfied respondents were
highest in 2015. Analogously, the lowest relative frequency of most dissatisfied respondents is
displayed in 2015, while moderately dissatisfied or indifferent respondents show very similar
relative frequencies in 2013 and 2015. The Mann-Whitney-U test yielded no significant result for
the comparison of 2015 and 2013 (p= 0.344), but highly significant results for the comparison
between 2013 and 2010 as well as 2015 and 2010 (p <0.001). Looking at the mean ranks, we see
an improvement of satisfaction with referrals to specialists from 2010 to 2013 and from 2010 to
2015 but overall respondents were most satisfied in 2013. This conclusion is corroborated by the
median statistics, which yield a median of 7 (corresponding to the highest satisfaction rating) in
2013 and a median of 6 (corresponding to +2 on the satisfaction scale) for both 2010 and 2015.
-3 -2 -1 0 1 2 3
Waiting Time Satisfaction 2015 4.8 6.0 8.9 9.6 16.7 27.1 26.9
Waiting Time Satisfaction 2013 5.2 7.4 9.0 8.5 16.2 27.8 26.0
Waiting Time Satisfaction 2010 5.8 7.6 10.4 9.3 16.3 25.4 25.1
0.0
5.0
10.0
15.0
20.0
25.0
30.0

82
Figure 6: Satisfaction with Referrals to Specialists (in %) 2015, 2013, 2010
3.4.5 Satisfaction w. GP’s Medical Competence
The left-skewed distribution follows a steady and steep incline in relative frequencies towards high
satisfaction in all three years. We observe the lowest relative frequency of respondents being very
dissatisfied in 2015, yet mild dissatisfaction (-2, -1) as well as the highest satisfaction (+3) show
the highest relative frequencies in 2015. We further find a stable median of 6 (corresponding to +2
on the satisfaction scale) for all three years. The Mann-Whitney U test yields no significant
difference for the comparison of 2015 and 2013 (p= 0.648) but highly significant results for the
comparison of 2013 and 2010 (p< 0.001) as well as 2015 and 2010 (p< 0.001) indicating an
improvement of satisfaction levels based on increasing mean ranks. Since the 2013 ratings
produced the highest mean ranks, we can conclude that satisfaction ratings were best in 2013 before
falling in 2015.
-3 -2 -1 0 1 2 3
Referrals (specialist) 2015 1.3 2.0 2.5 5.1 11.7 29.6 47.8
Referrals (specialist) 2013 2.0 1.7 2.6 5.2 11.2 27.9 49.4
Referrals (specialist) 2010 1.8 1.7 2.9 7.1 11.4 29.7 45.3
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
45.0
50.0

83
Figure 7: Satisfaction with GP’s Medical Competence (in %) 2015, 2013, 2010
3.4.6 Satisfaction with Referrals to Other Services
Since this variable was introduced in the 2013 dataset, we do not have available ratings for 2010,
thus limiting us to follow the development from 2013 to 2015. The relative frequencies follow the
familiar pattern of a left-skewed, increasingly steep distribution towards the right end of the
satisfaction scale in both years. We find the higher relative frequencies in +1 and +3 for 2015
respondents, while relative frequencies of dissatisfied respondents remain largely the same in 2013
and 2015. Based on the comparison of mean ranks, we detect an improvement of satisfaction ratings
in the 2015 respondents but this is not a significant difference (p=0.533), and also the median
remained stable at 6 (corresponding to +2 satisfaction rating). We can therefore conclude that
respondents were slightly but not significantly more satisfied with the referrals to other services in
2015.
-3 -2 -1 0 1 2 3
GP's Medical Competence 2015 0.6 1.5 2.3 4.6 12.7 31.7 46.6
GP's Medical Competence 2013 1.3 0.9 2.1 4.5 12.4 32.5 46.4
GP's Medical Competence 2010 1.1 0.9 1.8 6.4 14.2 32.0 43.6
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
45.0
50.0

84
Figure 8: Satisfaction with Referrals to Other Services (in %) 2015 & 2013
3.4.7 Satisfaction with Time to Explain/Consultation Length
This variable was not part of the 2010 survey and therefore only allows for comparison between
2015 and 2013 to track the development of satisfaction levels. Relative frequencies of high
dissatisfaction (-3) were slightly higher in 2015 than in 2013 and roughly equal for minor
dissatisfaction (-1) and indifference (0), while relative frequencies of the satisfaction levels of +1
and +3 were also higher in 2015. We find no change in median as it remained stable at 6 (second
highest satisfaction rating) and the Mann-Whitney U test yielded no significant difference in
respondents’ satisfaction levels (p= 0.904). Based on the mean ranks, we detect a minor
improvement in the satisfaction ratings of 2015 (cf. figure 9).
-3 -2 -1 0 1 2 3
Referrals (other
services) 20152.0 2.1 3.5 7.5 13.2 29.0 42.6
Referrals (other
services) 20132.0 1.8 3.6 8.8 12.0 30.3 41.4
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
45.0

85
3.4.8 Level of Trust in the GP
The respondents’ assessment of the level of trust towards the GP was entered into the survey in
2013. The graph below shows an increasing steep incline of relative frequencies towards the
positive end of the satisfaction scale. While the median was 6 (corresponding to +2 on the
satisfaction scale) in 2013, it was at the highest satisfaction level in 2015 indicating a generally
higher level of respondents’ satisfaction. We also find a higher mean rank score in 2015 but the
result of the Mann-Whitney U test yielded no significant difference between the 2013 and 2015
ratings (p= 0.411).
-3 -2 -1 0 1 2 3
Time to Explain 2015 1.4 1.7 4.2 6.4 15.8 32.1 38.5
Time to Explain 2013 1.0 2.0 4.2 6.5 15.4 33.2 37.6
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
Figure 9: Satisfaction with Time to Explain/Consultation Length (in %) 2015 & 2013
-3 -2 -1 0 1 2 3
Trust in the GP 2015 1.0 1.6 2.5 4.5 11.5 30.4 48.4
Trust in the GP 2013 1.1 1.5 2.7 5.6 11.2 30.4 47.5
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
45.0
50.0
Figure 10: Level of Trust in the GP (in %) 2015 & 2013

86
3.4.9 Detecting Differences in Satisfaction Ratings
To determine whether there is a significant difference in the satisfaction ratings of the main
satisfaction variables over time, Mann-Whitney U Tests were run. Visual inspection of the
distributions of each satisfaction variable across the three years showed very similar shapes
(skewed distributions in favor of high satisfaction ratings). The Mann-Whitney U Test can
therefore be used to interpret differences in medians.
3.4.8.1 Comparing 2015 & 2013
Comparing the satisfaction data from 2015 and 2013, we find no significant differences in any
satisfaction variables (cf. table 29). Satisfaction levels for both dependent variables (Overall GP
Satisfaction and Waiting Time Satisfaction) are not significantly different (p= 0.134; p= 0.277).
None of the median rating scores for the other satisfaction variables was significantly different in
2015 and 2013. Comparing the mean ranks between 2015 and 2013, we see only minor differences.
The mean ranks for the variables Overall GP Satisfaction, Waiting Time Satisfaction, Satisfaction
with Time to Explain/Consultation Length, Satisfaction with Referrals to Other Services and Level
of Trust show higher mean ranks in 2015 than in 2013. We can therefore conclude that respondents’
satisfaction increased in these domains in 2015. By contrast, Satisfaction with Referrals to
Specialists and Satisfaction with the GP’s Medical Competence show lower mean ranks in 2015
indicating a minor decrease in respondents’ satisfaction levels.
Table 29: Mann-Whitney U Test on Satisfaction Variables 2015 – 2013
2015 - 2013
Comparison
Overall GP
Satisfaction
Waiting Time
Satisfaction
Satisfaction with
Time to Explain
Satisfaction with
Referrals to
Specialists
Satisfaction with
GP's
Competence
Satisfaction with
Referrals to
Other Services
Level of Trust
Mann-Whitney U 7740854.500 7287944.500 7512359.500 5544238.000 7338767.500 2079094.500 7703255.000
Wilcoxon W 14826584.500 14101530.500 14392554.500 11646509.000 15441092.500 4270465.500 14710151.000
Z -1.497 -1.088 -0.121 -0.946 -0.457 -0.623 -0.822
Asymp. Sig. (2-tailed) 0.134 0.277 0.904 0.344 0.648 0.533 0.411

87
Year N Mean Rank Sum of
Ranks
Overall GP
Satisfaction
2013 3764 3939.05 14826584.50
2015 4188 4010.16 16794543.50
Waiting Time
Satisfaction
2013 3691 3820.52 14101530.50
2015 4005 3874.29 15516525.50
Satisfaction with
Time to Explain
2013 3709 3880.44 14392554.50
2015 4057 3886.30 15766706.50
Referral Satisfaction
(Specialists)
2013 3214 3375.47 10848769.00
2015 3493 3334.24 11646509.00
Satisfaction with
GP's Medical
Competence
2013 3667 3857.70 14146185.50
2015 4025 3836.30 15441092.50
Referral Satisfaction
(Other Services)
2013 2093 2040.36 4270465.50
2015 2008 2062.09 4140685.50
Level of Trust 2013 3743 3930.04 14710151.00
2015 4157 3968.92 16498799.00
Table 30: Mean Ranks of Mann-Whitney U Test on Satisfaction Variables 2015 – 2013
3.4.8.2 Comparing 2013 & 2010
Due to lack of comparative values in the 2010 dataset, the variables Satisfaction with the Time to
Explain, Satisfaction with Referrals to Other Services, and Level of Trust in the GP were not
included in the analysis of 2013 and 2010. In comparing respondents’ other satisfaction levels from
2013 and 2010, we discover significant results for Waiting Time Satisfaction (p< 0.001),
Satisfaction with Referrals to Specialists (p<0.001), and Satisfaction with the GP’s Medical
Competence (p< 0.001). By contrast, Overall GP Satisfaction is not significantly different in 2013
and 2010 (p= .065). The investigation of mean ranks reveals that the satisfaction levels for all
variables are higher in 2013 than in 2010. We can therefore conclude that satisfaction levels
increased from 2010 to 2013.

88
2013 - 2010
Comparison
Overall GP
Satisfaction
Waiting
Time
Satisfaction
Referral
Satisfaction
(Specialists)
Satisfaction
with GP's
Competence
Mann-Whitney U 4054625.500 3809167.500 2870107.000 3698215.500
Wilcoxon W 6504416.500 6210503.500 4700848.000 6012691.500
Z -1.847 -3.808 -4.299 -4.273
Asymp. Sig. (2-tailed) 0.065 0.000 0.000 0.000
Table 31: Mann-Whitney U Test on Satisfaction Variables 2013 – 2010
Year N Mean Rank
Sum of
Ranks
Overall GP
Satisfaction
2010 2213 2939.19 6504416.50
2013 3764 3018.29 11360836.50
Waiting Time
Satisfaction
2010 2191 2834.55 6210503.50
2013 3691 3004.98 11091399.50
Referral Satisfaction
(Specialists)
2010 1913 2457.32 4700848.00
2013 3214 2627.50 8444780.00
Satisfaction with
GP's Medical
Competence
2010 2151 2795.30 6012691.50
2013 3667 2976.49 10914779.50
Table 32: Mean Ranks of Mann-Whitney U Test on Satisfaction Variables 2013 – 2010
3.4.8.3 Comparing 2015 & 2010
The available satisfaction variables present in both datasets included Overall GP Satisfaction,
Waiting Time Satisfaction, Satisfaction with Referrals to Specialist, and Satisfaction with the GP’s
Medical Competence. We obtain significant results for all these variables (cf. Table 33).
Overall GP
Satisfaction
Waiting
Time
Satisfaction
Referral
Satisfaction
(Specialists)
Satisfaction
with GP's
Competence
Mann-Whitney U 4428823.500 4069883.500 3157349.000 4083923.500
Wilcoxon W 6878614.500 6471219.500 4988090.000 6398399.500
Z -3.161 -4.830 -3.606 -3.945
Asymp. Sig. (2-tailed) 0.002 0.000 0.000 0.000
Table 33: Mann-Whitney U Test on Satisfaction Variables 2015 – 2010

89
Year N Mean Rank
Sum of
Ranks
Overall GP
Satisfaction
2010 2213 3108.28 6878614.50
2015 4188 3250.00 13610986.50
Waiting Time
Satisfaction
2010 2191 2953.55 6471219.50
2015 4005 3177.80 12727086.50
Referral Satisfaction
(Specialists)
2010 1913 2607.47 4988090.00
2015 3493 2756.09 9627031.00
Satisfaction with
GP's Medical
Competence
2010 2151 2974.62 6398399.50
2015 4025 3149.36 12676176.50
Table 34: Mean Ranks of Mann-Whitney U Test on Satisfaction Variables 2015 – 2010
Table 35: Mean Statistics for Satisfaction Variables 2015, 2013, 2010
Overall GP
Satisfaction
Waiting Time
Satisfaction
Satisfaction
with Time to
Explain
Referral
Satisfaction
(Specialists)
GP's Medical
Competence
Referral
Satisfaction
(Other
Services)
Level of Trust
in the GP
Valid 2213 2191 0 1913 2151 0 0
Missing 67 89 2280 367 129 2280 2280
6,325 4,992 5,950 6,022
6,000 6,000 6,000 6,000
7,00 6,00 7,00 7,00
Valid 3764 3691 3709 3214 3667 2093 3743
Missing 118 191 173 668 215 1789 139
6,098 5,185 5,880 6,089 6,138 5,895 6,107
6,000 6,000 6,000 7,000 6,000 6,000 6,000
7,00 6,00 7,00 7,00 7,00 7,00 7,00
Valid 4188 4005 4057 3493 4025 2008 4157
Missing 136 319 267 831 299 2316 167
6,141 5,240 5,875 6,086 6,130 5,908 6,133
7,000 6,000 6,000 6,000 6,000 6,000 7,000
7,00 7,00 7,00 7,00 7,00 7,00 7,00
2015
N
Mean
Median
Mode
2010
N
Mean
Median
Mode
2013
N
Mean
Median
Mode
YEAR

90
4 Discussion & Conclusion
This section provides a summary of findings from a longitudinal perspective, points out the main
findings of the bivariate and regression analyses and discusses them in light of previous research
and literature, while considering the strengths and limitations of this analysis. Lastly, implications
will be inferred from the results and options for further research will be highlighted.
4.1 Summary of Findings
Satisfaction Levels
The very left-skewed frequency distributions of satisfaction levels over time indicate that
respondents are generally very satisfied; the majority of respondents expresses (high) satisfaction.
We find the mode in the highest rating item (+3) for Overall GP Satisfaction, Referrals to
Specialists, Referrals to Other Services, Time to Explain, Trust in the GP, and GP’s Medical
Competence. Only Waiting Time Satisfaction and GP Supply Satisfaction peak in +2 and display
a lower frequency of respondents expressing very high satisfaction. Moreover, we detect a higher
share of respondents expressing dissatisfaction with waiting time and municipal GP supply
compared to other satisfaction variables.
- Overall GP Satisfaction improved continuously from 2010 to 2015, peaking in 2015 with the
least amount of dissatisfied and the highest amount of highly satisfied respondents; Further, we
detect a significant improvement from 2010 to 2015.
- Waiting Time Satisfaction shows a similar development as Overall GP Satisfaction, and
significantly improved from 2010 to 2013. However, from 2013 to 2015 there was only a minor,
insignificant improvement in satisfaction with waiting time.
- Satisfaction with Referrals to Specialists significantly increased from 2010 to 2013.
Respondents were most satisfied in 2013 and satisfaction levels subsequently decline in 2015.

91
- We find a significant improvement in satisfaction with the GP’s Medical Competence from
2010 to 2013, followed by a mild, not significant decline in satisfaction levels from 2013 to
2015.
- The data indicate a minor, but not significant improvement in Satisfaction with Referrals to
Other Services from 2013 to 2015.
- Satisfaction with Time to Explain increased insignificantly from 2013 to 2015 as there is a
simultaneous increase in frequency of very dissatisfied and highly satisfied respondents.
- We observe a minor, yet insignificant increase in the level of Trust in the GP from 2013 to
2015.
- Overall municipal GP capacity increased over time in terms of GP density, registered GPs,
and free capacity (GPs with open lists), while the number of available list places decreased
steadily. We therefore observe a simultaneous increase and decrease in patients’ real choice of
GPs and competition among GPs.
Group Differences for Overall GP Satisfaction & Waiting Time Satisfaction
- Respondents who expressed general Life Satisfaction were significantly more satisfied with the
GP as well as waiting time in 2015, 2013, and 2010 compared to those who expressed
dissatisfaction with life.
- Respondents with below-median income were significantly more satisfied with the GP in
general as well as waiting time in 2015, 2013, 2010 compared to people with above-median
income.
- Respondents with primary education were significantly more satisfied with their GP and
waiting time than respondents with secondary or higher education in 2015, 2013 and 2010.
- Respondents with an average contact frequency of two to five GP visits per year were
significantly more satisfied with the GP in general in 2015 (but not in 2013) compared to those
with non-average (above or below) contact frequency. We find no significant difference in
waiting time satisfaction based on contact frequency in any year.

92
- Respondents with private GPs were significantly more satisfied with the GP as well as waiting
time in 2013 and 2015 (no data available for 2010). It has to be pointed out, though, that the
classification of public vs. private GP occurred on users’ judgment and does not correspond to
the actual distribution of 95% self-employed GPs in Norway. For this reason, we interpret the
variable as users’ subjective perception of GP type distinction, albeit we do not know the
distinguishing factor.
- Respondents with self-assessed “good health” were significantly more satisfied with their GP
as well as waiting time than those with perceived bad health in 2015 and 2013 (no data available
for 2010). By contrast, respondents with disabilities did not significantly differ in their
satisfaction levels with the GP or waiting time than respondents without disabilities in 2015 (no
data for 2013 or 2010).
- Age: We detect no significant difference in Overall GP Satisfaction or Waiting Time
Satisfaction levels comparing young and middle-aged respondents in 2015. However, these
groups differ significantly in both ratings in 2013 and 2010, with middle-aged respondents
expressing significantly higher satisfaction levels. Comparing the young with the old and the
middle-aged with the old, we find significant differences in Overall GP Satisfaction and Waiting
Time Satisfaction in every year indicating the old respondents are always more satisfied.
- GP density: In comparing low with medium-range and medium-range with high municipal GP
density, we encounter a significant difference in Overall GP Satisfaction levels in 2015, in that
respondents from municipalities with medium-range GP density were significantly more
satisfied with their GP than respondents from either low or high density areas. We detect no
such difference for TGPS or WTS in 2013 or 2010 but find also a significant difference between
low and medium-range density in respondents’ satisfaction levels with waiting time in 2015.
- Available GP’s with open lists per 1000 inhabitants (OLI): We find a significant difference
in users’ Overall GP Satisfaction levels in 2015 comparing municipalities with low and medium
as well as a low and high count of GPs with open lists per 1000 inhabitants indicating that areas
with low-count OLI yield significantly more satisfied users. We find no significant difference
for users’ Waiting Time Satisfaction in any year or for Overall GP Satisfaction in 2013 and
2010.

93
- Available List Places per 1000 Inhabitants (LPPT): There is a significant difference in users’
Overall GP Satisfaction in 2010 (but not in 2015 or 2013) comparing municipalities with a low
vs medium and a medium vs high-range of available list places per 1000 inhabitants, yielding
significantly higher satisfaction levels for respondents from medium-range rather than low or
high-count LPPT areas. We find no significant difference in TGPS comparing low and high-
count LPPT municipalities in any year. Waiting time satisfaction differed significantly in 2013
comparing low and medium-count LPPT as well as low and high-count LPPT areas (respondents
from middle-range LPPT areas were more satisfied with waiting time than those from low-range
areas, and people living in the top 33rd percentile LPPT areas also expressed significantly higher
satisfaction with waiting time than those from the bottom 33rd percentile). There is also no
difference in WTS levels comparing the middle with the top 33rd percentile of LPPT areas in
any year.
- Open List Ratio (OLR): No significant difference is detected for Waiting Time Satisfaction
according to respondents’ municipality-specific OLR range in any year. In Overall GP
Satisfaction, we do not detect significant differences comparing the middle and top 33rd
percentile. However, we find significantly more satisfied respondents in areas in the bottom
compared to the middle as well as the top (p= .058) 33rd percentile of OLR in 2015.
- Free Capacity: There is no difference in users’ Overall GP Satisfaction levels comparing
municipalities with low and medium range of free capacity as well as low and high-range free
capacity in any year. There is a near-significant result (p= .055) indicating higher Overall GP
Satisfaction levels in respondents living in the middle rather than the top third percentile of free
capacity municipalities in 2013. We find significant results in respondents’ Waiting Time
Satisfaction ratings based on range of free capacity in 2015, as respondents from the middle 33rd
percentile free capacity areas expressed more satisfaction compared to those from either the
bottom or top 33rd percentile areas. In 2010, we find that respondents from the top compared to
the bottom 33rd percentile were significantly more satisfied with waiting time.
- Municipality Size: In 2015, respondents from the second-smallest municipalities were
significantly more satisfied with their GP in general compared to those from the smallest
municipalities. Similarly, we find that in 2015, people living in the second-biggest rather than

94
the biggest municipalities tended to express higher Overall GP Satisfaction. By contrast, there
is no difference in Waiting Time Satisfaction levels between respondents from the smallest and
second-smallest or the biggest and smallest municipalities in any year. In 2015, Waiting Time
Satisfaction was significantly higher in respondents living in the second-biggest and third-
biggest municipalities compared to those from the biggest municipalities. We find a similar
significant result in 2013, in that respondents from the second-smallest municipalities were more
satisfied than those living in the smallest.
Regression Results for Overall GP Satisfaction & Waiting Time Satisfaction
In predicting Overall GP Satisfaction, the 2015 and 2013 models yield consistently significant,
positive correlation results for the independent variables age, Waiting Time Satisfaction and Life
Satisfaction. We encounter interesting outcomes in the 2015 and 2013 TGPS Models regarding
LPPT significance as there was no relation neither expected nor indicated in the bivariate analysis
with Overall GP Satisfaction. High LPPT compared to lower LPPT reflects increased patient choice
and thus a comparatively higher chance of being listed with the preferred GP of higher quality. A
similar finding is the significant correlation of OLI and TGPS in the 2015 models 1 and 2, as
anticipated in the Mann-Whitney U Test for TGPS. High OLI produced the highest likelihood of
expressing Overall GP Satisfaction compared to medium or low OLI. One possible reason for that
could be that the more GPs are available/have open lists, the higher is the probability of patients to
be able to pick the preferred GP, or the more choice there is for switching the GP. We also find
unexpected outcomes in predicting very high TGPS through free capacity and municipality size.
Contrary to assumptions based on previous findings, high free capacity resulted in the highest
probability of high Overall GP Satisfaction. The more available GPs we have in a municipality, the
higher is the likelihood that patients express Overall GP Satisfaction.
We obtain very similar results in modeling Waiting Time Satisfaction in 2015. Age, Municipal GP
Supply Satisfaction and Life Satisfaction are consistent, positive predictors. These outcomes are
consistent with the results from the Mann-Whitney U tests, which showed that old respondents and
the ones being satisfied with life yielded significantly higher satisfaction levels with waiting time.
Free capacity and GP density yielded significant results in that the middle 33rd percentile of both
variables yielded significantly higher waiting time satisfaction levels compared to low or high GP

95
density or free capacity areas. Similarly in the regression analyses, the competition measures GP
density and OLI yield the same relation to the odds of Waiting Time Satisfaction in 2015 as they
did in predicting Overall GP Satisfaction. Unlike expected from the bivariate analysis, it was high
instead of medium capacity areas that produced the highest odds of respondents expressing
satisfaction with waiting time. Moreover, municipal competition variables increasingly become
significant when we model high or very high satisfaction with the GP or waiting time in 2015.
Overall, these findings show that increased municipal capacity in the form of GP density, LPPT or
OLI augment satisfaction levels with both the GP and waiting time.
In a healthcare setting with restricted access, the municipal supply-side variables such as free
capacity, LPPT and OLI can be interpreted as measures of GP competition for users in a
municipality. As such, high capacity areas would simultaneously reflect intense competition among
GPs and enhanced accessibility for users. The results indicate that the higher the GP competition
is in a given municipality, the more high satisfaction users express. It is conceivable that people
are more satisfied, the more ‘real’ choice among available GPs exists (regardless of whether this
choice is utilized or not) rather than the amount of listed GPs that may in fact be inaccessible due
to full patient lists. This effect could mirror on a local level what has been observed on an
international level, namely that countries with free or increased access to medical services produce
higher scores of patient satisfaction compared to countries with a strong gatekeeping function and
restricted accessibility (Kroneman, Maarse, & van der Zee, 2006).
Similarly, the smallest municipalities coincided with a reduced probability of Overall GP
Satisfaction compared to big municipalities in 2015. The reason for that correlation could be that
bigger municipalities are potentially perceived as offering more choice to the users than smaller
municipalities even though the actual capacity per 1000 inhabitants (in the form of GP density,
LPPT or OLI) tends to be higher in smaller municipalities. In addition, smaller municipalities
produced higher odds of Waiting Time Satisfaction, except for the smallest municipalities which
significantly reduced satisfaction with waiting time. We assume that this is due to better access in
small municipal areas, which might coincide with lower actual waiting times. However, this
assumption would need further investigation.

96
Across all models and versions, satisfaction variables (Municipal GP Supply Satisfaction, Waiting
Time Satisfaction, Life Satisfaction) increased the explained variance in the dependent variable
tremendously (increasing it three- to fourfold), while also adding significantly to the models’
predictive accuracy. Municipal supply-side variables have a huge impact on the 2015 models of
Waiting Time Satisfaction and Overall GP Satisfaction, but this impact is diminished in 2013 and
not observable in 2010 altogether. Instead, socio-demographic variables become increasingly
influential, particularly as the cut-off points are adjusted to predict high or very high Overall GP
Satisfaction and Waiting Time Satisfaction. We therefore conclude that there seems to be a trend
of increasing influence of municipal supply-side/capacity measures and decreasing significance of
socio-demographic predictors other than age from 2010 to 2015.
4.2 Main Results
The main objective was to trace the development of satisfaction variables over time, most notably
Overall GP Satisfaction and Waiting Time Satisfaction, and to determine significant influencing
factors, particularly with regard to municipality-specific competition indicators. By means of
Mann-Whitney-U tests and multi-level binomial linear regression models, various associations
were analyzed between Overall GP Satisfaction and Waiting Time Satisfaction as dependent
variables and selected independent variables including socio-demographic predictors, self-assessed
health status, municipality-specific supply-side variables and relevant satisfaction measures. The
latter allowed to control for relevant predictors included in the model and yielded odds ratios that
were used to predict a change in the respondents’ probability to express satisfaction.
In the descriptive sections, we have seen that the majority of independent variables influence
Overall GP Satisfaction and Waiting Time Satisfaction. The BLR models on Waiting Time
Satisfaction and Overall GP Satisfaction shed additional light on the interplay of potential
determinants. While we find correlations of most independent variables with the two main
satisfaction variables conducting correlation tests, their effect is somewhat diminished through
mutual cancellation in the regression models. Below, we list each hypothesis and the respective
result that confirms or refutes it.

97
Hypothesis 1: Overall GP Satisfaction is associated with age, income and level of education. This
hypothesis was confirmed. Overall GP Satisfaction also correlates positively with age when
controlling for other predictors in the models of 2015 and 2013. In 2010, however, we do not find
a significant effect of age. Instead, below-median income as well as a low level of education
significantly increased the odds of high or very high Overall GP Satisfaction. The influence of
income and education level is inconsistent in its significance across models with different cut-off
points. In the instances where a significant association is detected (determining high or very high
satisfaction in 2013 and 2010), education and income correlate negatively with the odds of Overall
GP Satisfaction. The results confirm previous research findings (Russell et al., 2015; Zhang, 2012)
for the influence of age and education but stand in contrast to Zhang’s (2012) finding that below-
median income correlates with dissatisfaction.
Hypothesis 2: Overall GP Satisfaction and Waiting Time Satisfaction correlate positively with
health status. While the correlation and Mann-Whitney U tests revealed significant positive
associations of health with Overall GP Satisfaction and Waiting Time Satisfaction, we do not find
a significant effect in the presence of other independent variables when predicting the odds of
Waiting Time Satisfaction or Overall GP Satisfaction. This finding corroborates the results
provided by Zhang (2012) and Grytten et al. (2009).
Hypothesis 3: Waiting Time Satisfaction is associated with age, income and level of education.
Similarly to H1, this hypothesis was only partially confirmed. There is indeed a significant positive
correlation of age and Waiting Time Satisfaction in 2010, 2013 and 2015 even when controlling
for other predictors. Analogously to Overall GP Satisfaction, the predictive effect of income and
education level are of varying significance but display a negative association with Waiting Time
Satisfaction in the 2015 and 2013 models. Our findings therefore confirm previous ones (Grytten
et al., 2009) with regard to the influence of age. Additionally, they inform theory on the impact of
income and education on Waiting Time Satisfaction.
Hypothesis 4: Visiting a public or private GP does not influence the odds of Overall GP
Satisfaction while having a private GP will positively affect Waiting Time Satisfaction. This
assumption is partially refuted by the regression models in 2015 and 2013 because whenever we
detect a significant influence, we find that consulting a private GP in fact increases the odds of both
Waiting Time Satisfaction and Overall GP Satisfaction. This is a surprising result since there was

98
no indication in previous research that suggested higher overall satisfaction with private GPs.
Moreover, this result is contradictory to the fact that 95% of Norwegian GPs are self-employed and
therefore “private”. The question that is raised in this context is what the reason is for this
misperception of Norwegian GP users that categorizes GPs as public or private, or rather what the
characteristics are according to which users classify GPs as public or private. Due to the significant
relation of GP type with Overall GP Satisfaction and Waiting Time Satisfaction, it is conceivable
that users’ perception of having a ‘private’ GP increased satisfaction with waiting time and Overall
GP Satisfaction. Further research into this perception is needed to shed more light on the matter.
Hypothesis 5: Overall GP Satisfaction and Waiting Time Satisfaction are positively associated.
We found significant positive correlations in all models and all three years to confirm this
hypothesis. High levels of Waiting Time Satisfaction are a constant, significant predictor that
increased the odds of Overall GP Satisfaction in 2015, 2013 and 2010. This result confirms
previous findings from the US healthcare context (George & Sanda, 2007; Russell et al., 2015;
Vogus & McClelland, 2016) and provides the first such insight for the Norwegian primary
healthcare setting.
Hypothesis 6: Life Satisfaction correlates positively with Overall GP Satisfaction as well as with
Waiting Time Satisfaction. This hypothesis is confirmed since we detect a significant positive
correlation with the odds of Waiting Time Satisfaction and Overall GP Satisfaction in every
regression model in 2015, 2013, and 2010. We can therefore confirm the findings by George &
Sanda (2007) in the US and adopt them for the Norwegian primary care context.
We can confirm hypothesis 7 with every model of the three survey years and find that Municipal
GP Supply Satisfaction is positively associated with Waiting Time Satisfaction. Since the models
only tested Municipal GP Supply Satisfaction as an independent covariate to Waiting Time
Satisfaction, we cannot determine the direction of the correlation. It might therefore be the case
that Waiting Time Satisfaction is the actual independent variable predicting Municipal GP Supply
Satisfaction rather than vice versa as assumed in the models. We therefore suggest to conduct
further research on investigating Municipal GP Supply Satisfaction to find relevant influencing
factors and to better understand the relation with Waiting Time Satisfaction (as well as actual GP
supply).

99
Hypothesis 8 stated that various municipality-specific competition indicators influence Overall GP
Satisfaction and Waiting Time Satisfaction. Although no relation between available List Places
per 1000 Inhabitants (LPPT) and Overall GP Satisfaction was expected, we find significant
positive correlations in the 2015 and 2013 regression models suggesting that an increased
flexibility in patient lists seemingly contributes to Overall GP Satisfaction. This effect differs in
the 2010 model, however, where LPPT appears to be inversely related to Overall GP Satisfaction.
Contrary to expectations, GP density only had a significant positive effect on predicting Overall
GP Satisfaction in the 2013 model and free capacity actually increased rather than reduced the
odds of Overall GP Satisfaction in the 2015 model. We encounter little consistency in the effects
of competition indicators on Overall GP Satisfaction over time. In determining the odds of Waiting
Time Satisfaction, we observed a significant positive effect of high free capacity in the 2015 and
2013 models. Open Lists per 1000 Inhabitants served as a significant positive predictor for
Waiting Time Satisfaction in the 2015 but yielded a negative correlation in 2013. Available List
Places per 1000 Inhabitants correlated positively with the odds of Waiting Time Satisfaction in
2013 as well. In the 2010 models we detected a positive correlation of GP density and the odds of
Waiting Time Satisfaction and significantly reduced odds for high-range available List Places per
1000 Inhabitants. Consequently, we do not find a consistent influence of competition indicators on
modelling Waiting Time Satisfaction over time and suggest conducting further research to find
potential causes for this development.
To sum up, we find increased odds for respondents’ Overall GP Satisfaction in higher age, in
respondents consulting a ‘private’ GP, in users expressing high Waiting Time Satisfaction and high
Life Satisfaction. In determining Waiting Time Satisfaction, we detected a consistently significant
positive association with age, Municipal GP Supply Satisfaction and general Life Satisfaction, and
a not consistently significant influence of ‘private’ GPs. Adding satisfaction variables in the last
step of the hierarchical regression models increased the explained variance in the dependent
variable three- to fourfold. The significant effect of socio-demographic variables such as income
and education level as well as respondents’ self-assessed health status were largely cancelled out
by adding satisfaction variables in the final step of the regression models. Municipal capacity was
negligible in its effect on Overall GP Satisfaction and Waiting Time Satisfaction in 2010 but
became increasingly influential and significant in 2013 and 2015. Particularly in 2015, we find that
high capacity - in the form of GP density, available list places per 1000 inhabitants and open lists

100
per 1000 inhabitants - yields the highest probability of users to express high Overall GP Satisfaction
and Waiting Time Satisfaction.
4.3 Limitations and Strengths
Firstly, a few aspects need to be mentioned regarding the robustness and consistency of outcomes
of the bivariate and regression analyses. We find largely consistent results in both analytical types
and encountered no contradicting evidence in the regression analyses. This fact adds to the
robustness of results. We do find some minor differences with regard to the significance levels of
single variables when comparing the bivariate analysis with the additional regression models,
specifically in the capacity variables. The reason for that is the fact that the bivariate analysis is
based on the same intuitive cut-off point on the satisfaction scale of the dependent variable as the
main regression models (satisfaction vs dissatisfaction). Therefore, the results of the bivariate
analysis are best comparable to the outcomes of the main regression models rather than to the
results from the additional regression models. As we have seen, the higher cut-off points (to predict
high or very high satisfaction) yield more significant results for capacity and competition measures
and less significance for socio-demographic variables in the additional regression models that were
not indicated to that extent in the corresponding bivariate analysis. This is not surprising given the
fact that we expected the influence of predictor variables not to be equal across the ordinal scale of
the dependent variable (which was the reason for choosing BLR over ordinal logistic regression
with the proportional odds assumption). To investigate consistency and robustness of results more
deeply, further bivariate analyses could be conducted utilizing the same cut-off points that were
employed in the additional regression models. Another explanatory aspect for minor differences in
results is the methodological nature of the bivariate and regression analysis. In the bivariate
analysis, we investigate the significance of a single predictor on the dependent variable, while the
regression analysis investigates the interplay of multiple predictors that may influence each other
to some extent. In that regard, it is natural to find that not all significant variables found in the
bivariate analysis yield significant results in the regression analysis. The significant effect of some
variables, such as education or income, for instance, were cancelled out in the regression analysis
through the addition of other variables (predominantly through satisfaction measures) in the final
regression step.

101
In terms of general methodological limitations, we have to note three critical points. Although the
covariates included in the regression model were relevant to the study objective and created a broad
range of influencing factors, they are not exhaustive. Some variables of known high influence on
Overall GP Satisfaction were excluded from the analysis. Moreover, subjective patient satisfaction
data can be influenced by numerous factors so that it is difficult to consider all potential predictors.
Even with controlling for various determinants on the two main satisfaction variables, it is possible
that unobserved factors and latent variables could have influenced the outcome. Within the
category of socio-demographic variables, for instance, the gender of the patient or the visited GP
was not included in the analysis (not part of the available dataset) although previous studies have
found these factors to be significant (Godager, 2012; Sivertsen, 2014). By means of expanding the
regression models to include additional variables as well as by conducting a residual analysis, it
would be possible to investigate in how far Overall GP Satisfaction and Waiting Time Satisfaction
can be explained by other variables, which could be relevant for further studies. The second,
general methodological limitation is the relation of association and causation. Even though the
evidence shows an association, we cannot make causal inferences. Another methodological
drawback of BLR is the danger of over-fitting the model, i.e. overestimating the predictive power
as a result of sampling bias. While a certain combination of predictors might appear to predict a
category with «certainty», the actual accuracy of the prediction might be lower. (Huizingh, 2007)
The models’ goodness of fit was taken into consideration throughout the process of including
additional predictor variables by tracing the development of the explained variance in the
dependent variable, the -2Log Likelihood and the Hosmer & Lemeshow Test for goodness of
model fit. The strength of the present approach lies in the construction of multiple models based
on varying cut-off points in the dichotomized dependent variable. This process facilitated the
comparison of results from the main analyses and additional analyses. Since we obtained similar
results and observed coherent relationships between the predictors and dependent variables across
models and versions, we created additional robustness and assume reliability of results.
Lastly, a crucial question to address when analyzing patient satisfaction data is why such ratings
are skewed towards high satisfaction in general, and consequently, how useful such ratings are in
providing important, reliable information. Even though high satisfaction levels are not an
uncommon finding, neither in the international nor Norwegian context, one should consider

102
potential underlying reasons. Firstly, patients’ expectations might be low and therefore adjust the
experience accordingly. If, for instance, patients are fully aware of, and potentially even used to,
long waiting times, it is also likely that they expect and accept longer waiting times (Junewicz &
Youngner, 2015). The second reason relates to continuity of care, which has been associated with
generally higher PS reports. In Norway, continuity of care is prevalent due to the patient list system
and the relatively low rate of switching, i.e. 3% or patients (Iversen & Luras, 2011). Patients are
therefore more likely to remain with the same doctor. Thirdly, primary care has been observed to
yield generally higher PS levels than specialist care (Boquiren et al., 2015). The fourth reason could
be false positives. Patients may attribute problems to something else rather than to the GP’s
shortcomings in service quality. In particular waiting time satisfaction is higher since patients
realistically manage their expectations for the duration they have to wait (Williams et al., 1998).
Another possible cause of high ratings is long sampling time frames. GP visits that occurred longer
ago were shown to be remembered and rated more positively (Jackson et al., 2001). Lastly, it is of
course possible that patients’ satisfaction levels are that high in reality because users are genuinely
satisfied with the GP and the primary care services they receive.
4.4 Policy Implications & Further Research
The present analysis corroborates the general tendency of patient satisfaction surveys to yield very
positive outcomes indicating a generally high satisfaction of people with their GP in general
(Williams et al., 1998) as well as in the Norwegian primary healthcare setting in particular
(Godager & Iversen, 2016; Grytten et al., 2009; Zhang, 2012). The results concur with numerous
previous findings that were mainly based on two datasets (LKU and Legelisten) and add to the
ongoing validation process. Moreover, the thesis expands existing theory on patient satisfaction,
especially with regard to determinants of overall satisfaction with the GP and waiting time
satisfaction.
We observed a general trend of increasing capacity in terms of registered GPs, free capacity and
GP density, as well as in accessibility and satisfaction levels over time. By contrast, capacity
measures such as available list places per 1000 inhabitants and open lists per 1000 inhabitants were
less steady from a longitudinal perspective and even show a decline. While the increased capacity
facilitates access for patients and increases competition among GPs for patients, the decline in

103
actual accessibility through open lists and list places stands in a stark contrast. This development
creates a somewhat paradoxical situation that is reflected to some extent in the significance levels
of capacity measures in the various regression models. Nonetheless, we can conclude that real
choice and increased competition (affecting actual accessibility and switching options) have
significant effects on both users’ overall GP satisfaction and waiting time satisfaction. One possible
explanation of that is that the actual accessibility to GPs or real choice of available GPs indicates
a situation in which GPs compete for patients.
Another crucial aspect is that satisfaction measures have a large number of influencing factors. In
the context of previous reforms that sought to strengthen primary healthcare by increasing
accessibility and reducing waiting times, we might feel inclined to argue that the goals of these
reforms were achieved. We have to bear in mind, however, that firstly, we cannot make such causal
inferences, and secondly, other studies have also shown a tendency of improving quality and access
over time, even before the reforms. It is therefore possible that these improvements would have
occurred even without the 2012 Coordination reform and 2013 GP regulation. Moreover, we face
the question how users perceive or classify ‘private’ GPs, which yield significantly higher odds of
both waiting time satisfaction and overall GP satisfaction. As the underlying reasons for that
finding are not yet clarified, this leaves room for speculation. On the other hand, we find capacity
indicators to be most significant in the 2015 models, less so in 2013 and practically negligible in
2010, which coincides with the timing of previous reforms. For these reasons, it is difficult to
generalize the present findings in relation to the 2012 Coordination reform and 2013 GP regulation.
What we can argue, though, is that 1) the desired continuous improvement in Norwegian healthcare
is being achieved - not only in terms of objective quality but also as patient satisfaction - and that
2) structural improvements and capacity change and the introduction of competition elements in
primary care do affect user/patient satisfaction.
As meaningful insights were gained through the analysis of the DIFI and municipal capacity data,
we consider it a suitable dataset that builds on existing theory and knowledge and also offers a
wide range of further research opportunities to explore patient satisfaction and quality in primary
healthcare. One such opportunity is to investigate overall satisfaction with the GP in relation to
users’ referral satisfaction in order to better understand the scope of the relation. In tracing this
relationship over time, it would be possible to gain additional insight into changes that might be

104
related to previous healthcare reforms. Based on the findings related to waiting time satisfaction
and type of GP (public vs private), we suggest to conduct further research on users’ perception and
understanding of ‘public’ and ‘private’ GPs. This would yield important information about the
perception of the primary care sector and potential misconceptions regarding providers. A related
research topic would be to examine the relation of waiting time satisfaction and municipal GP
supply satisfaction to determine the direction of the relation and the underlying reasons for the
correlation. It would also be interesting to explore both municipal GP supply satisfaction and
referral satisfaction in relation to actual capacity measures and other determinants, possibly in a
similar way as conducted in the present thesis on waiting time satisfaction and overall GP
satisfaction. In doing so, we could gain a deeper understanding of the influencing factors for these
satisfaction measures and the relation of actual and perceived capacity. Yet another option is to
investigate primary care utilization in terms of contact frequency and contact reason, for instance,
in relation to waiting time satisfaction and overall GP satisfaction.
On a more general level, it would be desirable to develop and conduct standardized, nation-wide
surveys that are specifically designed for data collection on quality and patient satisfaction/
experience in primary care, as currently created by the Norwegian Knowledge Center for Health
Services (Kunnskapssenteret). Such an advanced analytical tool could generate a more complete
and specific picture of the quality of GPs and users’ satisfaction levels. On the other hand, DIFI
data could also be more widely used for research purposes on patient satisfaction because it is not
only based on a nationwide, standardized survey but also offers a much bigger set of satisfaction
variables than any other Norwegian dataset related to patient satisfaction in primary care. This
characteristic makes it a particular suitable complement to studies utilizing LKU data because it
allows to investigate whether objective quality improvement (for instance waiting time reduction
as observed in LKU) coincides with patients’ subjective perception (in the form of increased
waiting time satisfaction).

105
4.5 Conclusions
In the 2015 dataset, the consistent predictors of Overall GP Satisfaction include Age, Waiting Time
Satisfaction and Life Satisfaction, which are positively correlated. In predicting Waiting Time
Satisfaction, the variables Age, Municipal GP Supply Satisfaction and Life Satisfaction are
consistently significant and positively associated even when controlling for other influencing
factors. We detect a consistent pattern in which List Places per 1000 Inhabitants (in version 1) and
Open Lists per 1000 Inhabitants (in version 2) are positively associated with Overall GP
Satisfaction. As the highest range of competition measures (LPPT and OLI) produce the highest
probability of satisfied users, we conclude that the higher the competition for users is in a
municipality, the more satisfied users seem to be. Apparently, high capacity and thus increased
competition among primary care physicians for users does influence users’ Overall GP
Satisfaction.
Even though we find inconsistent significance levels of the various municipality-specific
competition variables in predicting Waiting Time Satisfaction, there is coherence in the positively
correlating relationships across model versions; the top percentile of competition variables (GP
density, Open Lists per 1000 Inhabitants, and free capacity) consistently yields the highest
probability of users expressing Waiting Time Satisfaction. In this way, we see that increased
capacity significantly increases the odds of Waiting Time Satisfaction. The underlying reason for
this observation could be that high municipal capacity facilitates accessibility to primary care
services and increases competition among GPs for users. This, in turn, creates an incentive for GPs
to lower waiting time and so translates to users’ high Waiting Time Satisfaction. Overall, we find
that municipality-specific competition variables become increasingly significant when predicting
high or very high levels of Overall GP Satisfaction or Waiting Time Satisfaction. These findings
are reflected to a diminished degree in the 2013 dataset and nonexistent in the 2010 models.

106
References
Badri, M. A., Attia, S., & Ustadi, A. M. (2009). Healthcare quality and moderators of patient
satisfaction: testing for causality. Int J Health Care Qual Assur, 22(4), 382-410.
doi:10.1108/09526860910964843
Bernstein, A. B., & Gauthier, A. K. (1998). Defining competition in markets: Why and how.
Health Services Research, 33(5), 1421-1438.
Biørn, E., & Godager, G. (2010). Does quality influence choice of general practitioner? An
analysis of matched doctor–patient panel data. Economic Modelling, 27(4), 842-853.
doi:10.1016/j.econmod.2009.10.016
Boquiren, V. M., Hack, T. F., Beaver, K., & Williamson, S. (2015). What do measures of patient
satisfaction with the doctor tell us? Patient Education and Counseling, 98(12), 1465-
1473. doi:10.1016/j.pec.2015.05.020
Brekke, K. R., & Straume, O. R. (2017). Competition policy for health care provision in Norway.
Health Policy, 121(2), 134-140. doi:https://doi.org/10.1016/j.healthpol.2016.11.013
Carlin, C. S., Christianson, J. B., Keenan, P., & Finch, M. (2012). Chronic illness and patient
satisfaction. Health Serv Res, 47(6), 2250-2272. doi:10.1111/j.1475-6773.2012.01412.x
Crow, R., Gage, H., Hampson, S., Hart, J., Kimber, A., Storey, L., & Thomas, H. (2002). The
measurement of satisfaction with healthcare: implications for practice from a systematic
review of the literature. Health Technol Assess, 6(32), 1-244.
Detsky, J., & Shaul, R. Z. (2013). Incentives to increase patient satisfaction: Are we doing more
harm than good? CMAJ : Canadian Medical Association Journal, 185(14), 1199-1200.
doi:10.1503/cmaj.130366
Donabedian, A., & Bashshur, R. (2003). An introduction to quality assurance in health care.
New York: Oxford University Press.
Fan, V. S., Burman, M., McDonell, M. B., & Fihn, S. D. (2005). Continuity of care and other
determinants of patient satisfaction with primary care. J Gen Intern Med, 20(3), 226-233.
doi:10.1111/j.1525-1497.2005.40135.x
Flocke, S. A., Miller, W. L., & Crabtree, B. F. (2002). Relationships between physician practice
style, patient satisfaction, and attributes of primary care. J Fam Pract, 51(10), 835-840.
Folmo, M. D. (2014). What Patients Want from their Doctors: An Analysis of Patients’ Online
Reviews and Ratings of their Regular General Practitioners. (Master Thesis).
George, A. K., & Sanda, M. G. (2007). Measuring Patient Satisfaction. In D. F. Penson & J. T.
Wei (Eds.), Clinical Research Methods for Surgeons (pp. 253-265). Totowa, NJ: Humana
Press.
Godager, G. (2012). Birds of a feather flock together: A study of doctor–patient matching.
Journal of Health Economics, 31(1), 296-305. doi:10.1016/j.jhealeco.2011.11.003
Godager, G., Hennig-Schmidt, H., & Iversen, T. (2016). Does performance disclosure influence
physicians’ medical decisions? An experimental study. Journal of Economic Behavior &
Organization, 131, 36-46. doi:http://dx.doi.org/10.1016/j.jebo.2015.10.005
Godager, G., & Iversen, T. (2010). Brukernes erfaringer med fastlegeordningen 2001 - 2008.
Trender i bruk, tilgjengelighet og fornøydhet. (2010: 1).
Godager, G., & Iversen, T. (2014). Brukernes erfaringer med fastlegeordningen 2001 – 2012.
Trender i bruk, tilgjengelighet og fornøydhet. (2014: 2).

107
Godager, G., & Iversen, T. (2016). Brukernes erfaringer med fastlegeordningen 2001 – 2015.
HERO, 2016(10).
Godager, G., Iversen, T., & Ma, C. T. (2009). Service motives and profit incentives among
physicians. Int J Health Care Finance Econ, 9(1), 39-57. doi:10.1007/s10754-008-9046-y
Godager, G., Iversen, T., & Ma, C. T. (2015). Competition, gatekeeping, and health care access. J
Health Econ, 39, 159-170. doi:10.1016/j.jhealeco.2014.11.005
Godager, G., & Wiesen, D. (2013). Profit or patients' health benefit? Exploring the heterogeneity
in physician altruism. J Health Econ, 32(6), 1105-1116.
doi:10.1016/j.jhealeco.2013.08.008
Grytten, J., Carlsen, F., & Skau, I. (2009). Services production and patient satisfaction in primary
care. Health Policy, 89(3), 312-321. doi:10.1016/j.healthpol.2008.06.006
Haggerty, J. L. (2010). Are measures of patient satisfaction hopelessly flawed? BMJ, 341, c4783.
doi:10.1136/bmj.c4783
Hall, J. A., & Dornan, M. C. (1990). Patient sociodemographic characteristics as predictors of
satisfaction with medical care: a meta-analysis. Soc Sci Med, 30(7), 811-818.
Holmboe, O., Danielsen, K., & Iversen, H. H. (2015). Utvikling av metode for måling av
pasienters erfaringer med fastleger. Retrieved from Oslo:
Huizingh, E. (2007). Applied Statistics with SPSS doi:http://dx.doi.org/10.4135/9781446249390
Innbyggerundersøkelsen 2014/2015. Utvalg, respons og frafall. (2015). Retrieved from Online:
Iversen, T. (2005) A study of income-motivated behavior among general practitioners in the
Norwegian list patient system. Working paper (Helseøkonomisk forskningsprogram :
online): Vol. 2005:8.
Iversen, T., & Luras, H. (2011). Patient switching in general practice. J Health Econ, 30(5), 894-
903. doi:10.1016/j.jhealeco.2011.07.008
Iversen, T., & Lurås, H. (2000). Economic motives and professional norms: the case of general
medical practice. Journal of Economic Behavior & Organization, 43(4), 447-470.
doi:http://dx.doi.org/10.1016/S0167-2681(00)00130-X
Iversen, T., & Lurås, H. (2002). Waiting Time as a Competitive Device: An Example from
General Medical Practice. International Journal of Health Care Finance and Economics.
Iversen, T., & Lurås, H. (2008). Bytte av lege i fastlegeordningen. Samfunnsøkonomen, 2008(3).
Iversen, T., & Ma, C.-t. A. (2011). Market conditions and general practitioners’ referrals.
International Journal of Health Care Finance and Economics, 11(4), 245.
doi:10.1007/s10754-011-9101-y
Jackson, J. L., Chamberlin, J., & Kroenke, K. (2001). Predictors of patient satisfaction. Social
Science & Medicine, 52(4), 609-620. doi:10.1016/S0277-9536(00)00164-7
Junewicz, A., & Youngner, S. J. (2015). Patient-satisfaction surveys on a scale of 0 to 10:
improving health care, or leading it astray? Hastings Cent Rep, 45(3), 43-51.
doi:10.1002/hast.453
Kahana, E., Lee, J., Kahana, B., & Yu, J. (2015). FACILITATORS OF PATIENT
SATISFACTION WITH HEALTH CARE: BOTH PATIENT AND DOCTOR
CHARACTERISTICS MATTER. The Gerontologist, 55(Suppl_2), 678-678.
doi:10.1093/geront/gnv348.02
Kann, I. C., Biorn, E., & Luras, H. (2010). Competition in general practice: prescriptions to the
elderly in a list patient system. J Health Econ, 29(5), 751-764.
doi:10.1016/j.jhealeco.2010.07.004

108
Kilby, G. (2014). A Qualitative Content Analysis of Online GP Reviews in Norway. (Master
thesis).
Kjøllesdal Eide, K., & Nonseid, J. (2015). Innbyggerundersøkelsen 2015 - Hva mener brukerne?
(2015:6). Retrieved from Oslo: https://www.difi.no/sites/difino/files/difi-
rapport_2015_6_innbyggerundersokelsen_2015_hva_mener_brukerne.pdf
Kroneman, M. W., Maarse, H., & van der Zee, J. (2006). Direct access in primary care and
patient satisfaction: a European study. Health Policy, 76(1), 72-79.
doi:10.1016/j.healthpol.2005.05.003
Laerd Statistics: SPSS Statistics Tutorials and Statistical Guides. (2015). Retrieved from
https://statistics.laerd.com/
Lurås, H. (2007). The association between patient shortage and patient satisfaction with general
practitioners. Scandinavian Journal of Primary Health Care, 25(3), 133-139.
doi:10.1080/02813430701286579
Michael, M., Schaffer, S. D., Egan, P. L., Little, B. B., & Pritchard, P. S. (2013). Improving Wait
Times and Patient Satisfaction in Primary Care. Journal for Healthcare Quality, 32(2).
Midi, H., Sarkar, S. K., & Rana, S. (2010). Collinearity diagnostics of binary logistic regression
model. Journal of Interdisciplinary Mathematics, 13(3), 253-267.
doi:10.1080/09720502.2010.10700699
Pascoe, G. C. (1983). Patient satisfaction in primary health care: a literature review and analysis.
Eval Program Plann, 6(3-4), 185-210.
Ringard, Å., Sagan, A., Sperre Saunes, I., & Lindahl, A. K. (2013). Norway Health System
Review. Health Systems in Transition, 15(8).
Russell, R. S., Johnson, D. M., & White, S. W. (2015). Patient perceptions of quality: analyzing
patient satisfaction surveys. International Journal of Operations & Production
Management, 35(8), 1158-1181. doi:doi:10.1108/IJOPM-02-2014-0074
Salisbury, C., Wallace, M., & Montgomery, A. A. (2010). Patients’ experience and satisfaction in
primary care: secondary analysis using multilevel modelling. BMJ, 341.
doi:10.1136/bmj.c5004
Schaumans, C. (2015). Prescribing behavior of general practitioners: competition matters. Health
Policy, 119(4), 456-463. doi:10.1016/j.healthpol.2014.12.018
Schneider, H., & Palmer, N. (2002). Getting to the truth? Researching user views of primary
health care. Health Policy Plan, 17(1), 32-41.
Seim, E. S. (2010). The Coordination Reform: Potential for substitution between primary- and
specialist health care in Norway.(Master thesis).
Sitzia, J., & Wood, N. (1997). Patient satisfaction: a review of issues and concepts. Soc Sci Med,
45(12), 1829-1843.
Sivertsen, C. T. (2014). Patient Satisfaction in General Medical Practice And The Association
With Patient Shortage.(Master thesis).
Vogus, T. J., & McClelland, L. E. (2016). When the customer is the patient: Lessons from
healthcare research on patient satisfaction and service quality ratings. Human Resource
Management Review, 26(1), 37-49. doi:10.1016/j.hrmr.2015.09.005
Wensing, M., Baker, R., Szecsenyi, J., Grol, R., & Group, E. (2004). Impact of national health
care systems on patient evaluations of general practice in Europe. Health Policy, 68(3),
353-357. doi:10.1016/j.healthpol.2003.10.010

109
Westaway, M. S., Rheeder, P., Van Zyl, D. G., & Seager, J. R. (2003). Interpersonal and
organizational dimensions of patient satisfaction: the moderating effects of health status.
Int J Qual Health Care, 15(4), 337-344.
Williams, B., Coyle, J., & Healy, D. (1998). The meaning of patient satisfaction: an explanation
of high reported levels. Soc Sci Med, 47(9), 1351-1359.
Zhang, Y. (2012). What characterizes Patients Who Switch General Practitioners?(Master
thesis).

110
Appendix
Appendix Table 1: Nonparametric Correlations of Categorized Capacity Variables 2015
GP density
free
capacity/
free GPs
open lists
per 1000
inhabitants
Open list
ratio
free places
per 1000
inhabitants
Correlation
Coefficient
1.000 -,591**
,372**
,247**
,159**
Sig. (2-tailed) 0.000 0.000 0.000 0.000
N 4465 4465 4465 4465 4465
Correlation
Coefficient-,591
** 1.000 -,058** -0.002 ,081
**
Sig. (2-tailed) 0.000 0.000 0.869 0.000
N 4465 4465 4465 4465 4465
Correlation
Coefficient,372
**-,058
** 1.000 ,915**
,561**
Sig. (2-tailed) 0.000 0.000 0.000 0.000
N 4465 4465 4465 4465 4465
Correlation
Coefficient,247
** -0.002 ,915** 1.000 ,557
**
Sig. (2-tailed) 0.000 0.869 0.000 0.000
N 4465 4465 4465 4465 4465
Correlation
Coefficient,159
**,081
**,561
**,557
** 1.000
Sig. (2-tailed) 0.000 0.000 0.000 0.000
N 4465 4465 4465 4465 4465
**. Correlation is significant at the 0.01 level (2-tailed).
Nonparametric Correlations of Categorized Capacity Variables 2015
Spearman's
rho
GP density
free
capacity/
free GPs
open lists
per 1000
inhabitants
Open list
ratio
free places
per 1000
inhabitants

111
Appendix Table 2: Nonparametric Correlations of Categorized Capacity Variables 2013
Appendix Table 3: Nonparametric Correlations of Categorized Capacity Variables 2010
GP density
free capacity
(open lists)
open lists
per 1000
inhabitants
open list
ratio
free places
per 1000
inhabitants
Correlation
Coefficient
1.000 -,581**
,193**
,038* 0.009
Sig. (2-tailed) 0.000 0.000 0.021 0.569
N 3683 3683 3683 3683 3683
Correlation
Coefficient-,581
** 1.000 0.019 ,106**
,184**
Sig. (2-tailed) 0.000 0.248 0.000 0.000
N 3683 3683 3683 3683 3683
Correlation
Coefficient,193
** 0.019 1.000 ,922**
,591**
Sig. (2-tailed) 0.000 0.248 0.000 0.000
N 3683 3683 3683 3683 3683
Correlation
Coefficient,038
*,106
**,922
** 1.000 ,621**
Sig. (2-tailed) 0.021 0.000 0.000 0.000
N 3683 3683 3683 3683 3683
Correlation
Coefficient
0.009 ,184**
,591**
,621** 1.000
Sig. (2-tailed) 0.569 0.000 0.000 0.000
N 3683 3683 3683 3683 3683
**. Correlation is significant at the 0.01 level (2-tailed).
*. Correlation is significant at the 0.05 level (2-tailed).
Nonparametric Correlations of Categorized Capacity Measures 2013
Spearman's
rho
GP density
free capacity
(open lists)
open lists
per 1000
inhabitants
open list
ratio
free places
per 1000
inhabitants
GP density free capacity
Open Lists
per
inhabitants)
Open List
Ratio
List Places
Per
Thousand
Inhabitants
Correlation
Coefficient
1.000 -,321**
,415**
,287**
,240**
Sig. (2-tailed) 0.000 0.000 0.000 0.000
N 2275 2275 2275 2275 2275
Correlation
Coefficient-,321
** 1.000 0.026 ,092**
,322**
Sig. (2-tailed) 0.000 0.208 0.000 0.000
N 2275 2275 2275 2275 2275
Correlation
Coefficient,415
** 0.026 1.000 ,925**
,556**
Sig. (2-tailed) 0.000 0.208 0.000 0.000
N 2275 2275 2275 2275 2275
Correlation
Coefficient,287
**,092
**,925
** 1.000 ,550**
Sig. (2-tailed) 0.000 0.000 0.000 0.000
N 2275 2275 2275 2275 2275
Correlation
Coefficient,240
**,322
**,556
**,550
** 1.000
Sig. (2-tailed) 0.000 0.000 0.000 0.000
N 2275 2275 2275 2275 2275
**. Correlation is significant at the 0.01 level (2-tailed).
Nonparametric Correlations of Categorized Capacity Variables 2010
Spearman's
rho
GP density
free capacity
Open Lists
per
inhabitants)
Open List
Ratio
List Places
Per
Thousand
Inhabitants

112
Appendix Table 4: Significant Correlations between TGPS + other variables 2015, 2013, 2010;
Correlating
Variables
Results 2015* Results 2013* Results 2010* Correlation
Strength
TGPS + WTA Kendall’s tau b= 0.389
Spearman’s rho= 0.456
Kendall’s tau b= 0.349;
Spearman’s rho= 0.411
Kendall’s tau b= 0.329;
Spearman’s rho= 0.391
Moderate - low
positive
correlation
TGPS + Age Kendall’s tau c = 0,135
Spearman’s rho = 0.189
Spearman’s rho= 0.238 Spearman’s rho= 0.391 Very low positive
correlation
TGPS +
Income Spearman’s rho =
-0.092
Spearman’s rho=
-0.111
Spearman’s rho= -0.114 Extremely weak
negative
correlation
TGPS +
Education Kendall’s tau c = -
0,069 Spearman’s rho =
- 0,089
Spearman’s rho=
-0.129
Spearman’s rho= -0.094 Extremely weak
negative
correlation
TGPS + GP
public/private Cramer’s V = 0,089
Gamma = 0,138
Cramer’s V= 0.112 Very low positive
correlation
TGPS +
Contact
frequency
Spearman’s rho = 0.074
Kendall’s tau b = 0.066
Kendall’s tau b= 0.079;
Spearman’s rho= 0.089
Very low positive
correlation
TGPS + Mun.
GP Supply
Satisf.
Spearman’s rho = 0.386
Kendall’s tau b = 0.337
Kendall’s tau b= 0.380;
Spearman’s rho= 0.435
Kendall’s tau b= 0.278
Spearman’s rho= 0.323
Moderate to low
positive
correlation
TGPS +
Satisfaction w.
Time to
Explanation
Kendall’s tau b = 0.598
Spearman’s rho = 0.661
Moderate positive
correlation
TGPS +
Satisfaction w.
Referrals
Kendall’s tau b = 0.586
Spearman’s rho = 0.645
Kendall’s tau b= 0.523;
Spearman’s rho= 0.587
Moderate positive
correlation
TGPS +
General
Happiness/
Life Satisf.
Kendall’s tau b = 0.198
Spearman’s rho = 0.224
Kendall’s tau b= 0.219;
Spearman’s rho= 0.250
Kendall’s tau b= 0.166;
Spearman’s rho= 0.189
Low positive
correlation
*nonparametric values

113
Appendix Table 5: Multicollinearity Testing of Regression-Relevant Variables 2015
Overall GP
Satisfaction Alder
Highest
completed
Education
Below
median
Income
Contact
frequency
Public vs
Private GP
Having
disabilities GoodHealth
Overall Life
Satisfaction
GP Supply
Satisfaction
Waiting time
for
appointment
Pearson
Correlation1 ,166
**-,082
**,063
** 0.030 -,080**
,033*
,074**
,173**
,403**
,421**
Sig. (2-tailed) 0.000 0.000 0.000 0.061 0.000 0.039 0.000 0.000 0.000 0.000
N 3941 3941 3914 3474 3912 3570 3800 3941 3873 3718 3707
Pearson
Correlation,166
** 1 -,221**
,232**
,044**
-,162**
-,108** 0.022 ,155
**,235
**,168
**
Sig. (2-tailed) 0.000 0.000 0.000 0.005 0.000 0.000 0.164 0.000 0.000 0.000
N 3941 4069 4040 3577 4031 3674 3925 4069 4001 3835 3813
Pearson
Correlation-,082
**-,221
** 1 -,338**
-,081**
-,065**
,123** -0.028 0.029 -,080
**-,062
**
Sig. (2-tailed) 0.000 0.000 0.000 0.000 0.000 0.000 0.075 0.071 0.000 0.000
N 3914 4040 4040 3557 4002 3647 3898 4040 3973 3806 3789
Pearson
Correlation,063
**,232
**-,338
** 1 ,109**
,072**
-,185** -0.027 -,104
**,080
**,051
**
Sig. (2-tailed) 0.000 0.000 0.000 0.000 0.000 0.000 0.113 0.000 0.000 0.003
N 3474 3577 3557 3577 3544 3250 3483 3577 3542 3382 3367
Pearson
Correlation0.030 ,044
**-,081
**,109
** 1 0.006 -,261**
-,268**
-,115** 0.031 ,049
**
Sig. (2-tailed) 0.061 0.005 0.000 0.000 0.708 0.000 0.000 0.000 0.056 0.003
N 3912 4031 4002 3544 4031 3659 3888 4031 3963 3798 3778
Pearson
Correlation-,080
**-,162
**-,065
**,072
** 0.006 1 0.019 0.021 -,047**
-,068**
-,099**
Sig. (2-tailed) 0.000 0.000 0.000 0.000 0.708 0.251 0.213 0.005 0.000 0.000
N 3570 3674 3647 3250 3659 3674 3542 3674 3611 3471 3450
Pearson
Correlation,033
*-,108
**,123
**-,185
**-,261
** 0.019 1 ,300**
,203** 0.022 0.016
Sig. (2-tailed) 0.039 0.000 0.000 0.000 0.000 0.251 0.000 0.000 0.178 0.333
N 3800 3925 3898 3483 3888 3542 3925 3925 3880 3702 3685
Pearson
Correlation,074
** 0.022 -0.028 -0.027 -,268** 0.021 ,300
** 1 ,223**
,076** 0.027
Sig. (2-tailed) 0.000 0.164 0.075 0.113 0.000 0.213 0.000 0.000 0.000 0.097
N 3941 4069 4040 3577 4031 3674 3925 4069 4001 3835 3813
Pearson
Correlation,173
**,155
** 0.029 -,104**
-,115**
-,047**
,203**
,223**
1**
,257**
,135**
Sig. (2-tailed) 0.000 0.000 0.071 0.000 0.000 0.005 0.000 0.000 0.000 0.000 0.000
N 3873 4001 3973 3542 3963 3611 3880 4001 4001 3777 3753
Pearson
Correlation,403
**,235
**-,080
**,080
** 0.031 -,068** 0.022 ,076
**,257
** 1 ,368**
Sig. (2-tailed) 0.000 0.000 0.000 0.000 0.056 0.000 0.178 0.000 0.000 0.000
N 3718 3835 3806 3382 3798 3471 3702 3835 3777 3835 3599
Pearson
Correlation,421
**,168
**-,062
**,051
**,049
**-,099
** 0.016 0.027 ,135**
,368** 1
Sig. (2-tailed) 0.000 0.000 0.000 0.003 0.003 0.000 0.333 0.097 0.000 0.000
N 3707 3813 3789 3367 3778 3450 3685 3813 3753 3599 3813
GP Supply
Satisfaction
Waiting time
for
appointment
**. Correlation is significant at the 0.01 level (2-tailed).
*. Correlation is significant at the 0.05 level (2-tailed).
Correlations of regression-relevant variables 2015
Overall GP
Satisfaction
Alder
Highest
completed
Education
Below
median
Income
Contact
frequency
Public vs
Private GP
Having
disabilities
GoodHealth
Overall Life
Satisfaction

114
Appendix Table 6: Multicollinearity Testing of Regression-Relevant Variables 2013
Overall GP
Satisfaction Age
Highest
completed
Education
Below
median
Income
contact
frequency
Public vs
Private GP GoodHealth
GP Supply
Satisfaction
Waiting time
Satisfaction
Overall Life
Satisfaction
Pearson
Correlation
1 ,205**
-,124**
,089**
,053**
-,099**
,056**
,434**
,370**
,206**
Sig. (2-tailed) 0.000 0.000 0.000 0.002 0.000 0.001 0.000 0.000 0.000
N 3569 3569 3518 3130 3548 3282 3569 3311 3457 3514
Pearson
Correlation,205
** 1 -,257**
,228**
,076**
-,158** -0.004 ,248
**,221
**,147
**
Sig. (2-tailed) 0.000 0.000 0.000 0.000 0.000 0.795 0.000 0.000 0.000
N 3569 3678 3623 3219 3618 3341 3678 3408 3509 3617
Pearson
Correlation-,124
**-,257
** 1 -,363**
-,085**
-,089** -0.030 -,125
**-,089
** -0.030
Sig. (2-tailed) 0.000 0.000 0.000 0.000 0.000 0.074 0.000 0.000 0.076
N 3518 3623 3623 3180 3564 3289 3623 3359 3464 3567
Pearson
Correlation,089
**,228
**-,363
** 1 ,100**
,082**
-,056**
,087**
,076**
-,080**
Sig. (2-tailed) 0.000 0.000 0.000 0.000 0.000 0.001 0.000 0.000 0.000
N 3130 3219 3180 3219 3169 2947 3219 2997 3086 3180
Pearson
Correlation,053
**,076
**-,085
**,100
** 1 0.018 -,211** 0.014 ,055
**-,091
**
Sig. (2-tailed) 0.002 0.000 0.000 0.000 0.297 0.000 0.425 0.001 0.000
N 3548 3618 3564 3169 3618 3328 3618 3355 3496 3559
Pearson
Correlation-,099
**-,158
**-,089
**,082
** 0.018 1 0.011 -,081**
-,133** -0.033
Sig. (2-tailed) 0.000 0.000 0.000 0.000 0.297 0.511 0.000 0.000 0.058
N 3282 3341 3289 2947 3328 3341 3341 3107 3231 3290
Pearson
Correlation,056
** -0.004 -0.030 -,056**
-,211** 0.011 1 ,063
**,050
**,182
**
Sig. (2-tailed) 0.001 0.795 0.074 0.001 0.000 0.511 0.000 0.003 0.000
N 3569 3678 3623 3219 3618 3341 3678 3408 3509 3617
Pearson
Correlation,434
**,248
**-,125
**,087
** 0.014 -,081**
,063** 1 ,371
**,244
**
Sig. (2-tailed) 0.000 0.000 0.000 0.000 0.425 0.000 0.000 0.000 0.000
N 3311 3408 3359 2997 3355 3107 3408 3408 3256 3357
Pearson
Correlation,370
**,221
**-,089
**,076
**,055
**-,133
**,050
**,371
** 1 ,153**
Sig. (2-tailed) 0.000 0.000 0.000 0.000 0.001 0.000 0.003 0.000 0.000
N 3457 3509 3464 3086 3496 3231 3509 3256 3509 3456
Pearson
Correlation,206
**,147
** -0.030 -,080**
-,091** -0.033 ,182
**,244
**,153
** 1
Sig. (2-tailed) 0.000 0.000 0.076 0.000 0.000 0.058 0.000 0.000 0.000
N 3514 3617 3567 3180 3559 3290 3617 3357 3456 3617
Waiting time
Satisfaction
Overall Life
Satisfaction
**. Correlation is significant at the 0.01 level (2-tailed).
Highest
completed
Education
Below
median
Income
contact
frequency
Public vs
Private GP
GoodHealth
GP Supply
Satisfaction
Correlations of regression-relevant variables 2013
Overall GP
Satisfaction
Age

115
Appendix Table 7: Multicollinearity Testing of Regression-Relevant Variables 2010
Overall GP
Satisfaction Age group
Highest
completed
Education
Below
median
Income
GP Supply
Satisfaction
Waiting
Time
Satisfaction
Life
Satisfaction
Pearson
Correlation
1 ,174**
-,079**
,071**
,311**
,367**
,166**
Sig. (2-tailed) 0.000 0.000 0.001 0.000 0.000 0.000
N 2213 2213 2193 2011 2111 2140 2151
Pearson
Correlation,174
** 1 -,246**
,228**
,199**
,236**
,128**
Sig. (2-tailed) 0.000 0.000 0.000 0.000 0.000 0.000
N 2213 2280 2256 2069 2176 2191 2213
Pearson
Correlation-,079
**-,246
** 1 -,285**
-,083**
-,087** 0.013
Sig. (2-tailed) 0.000 0.000 0.000 0.000 0.000 0.547
N 2193 2256 2256 2054 2152 2170 2191
Pearson
Correlation,071
**,228
**-,285
** 1 ,090**
,093**
-,051*
Sig. (2-tailed) 0.001 0.000 0.000 0.000 0.000 0.020
N 2011 2069 2054 2069 1974 1996 2044
Pearson
Correlation,311
**,199
**-,083
**,090
** 1 ,301**
,220**
Sig. (2-tailed) 0.000 0.000 0.000 0.000 0.000 0.000
N 2111 2176 2152 1974 2176 2091 2113
Pearson
Correlation,367
**,236
**-,087
**,093
**,301
** 1 ,114**
Sig. (2-tailed) 0.000 0.000 0.000 0.000 0.000 0.000
N 2140 2191 2170 1996 2091 2191 2128
Pearson
Correlation,166
**,128
** 0.013 -,051*
,220**
,114** 1
Sig. (2-tailed) 0.000 0.000 0.547 0.020 0.000 0.000
N 2151 2213 2191 2044 2113 2128 2213
*. Correlation is significant at the 0.05 level (2-tailed).
Correlations of regression-relevant variables 2010
Overall GP
Satisfaction
Age group
Highest
completed
Education
Below
median
Income
GP Supply
Satisfaction
Waiting
Time
Satisfaction
Life
Satisfaction
**. Correlation is significant at the 0.01 level (2-tailed).

116
Appendix Table 8: Significant Variables in TGPS_1 2015 Step 4 (Version 1)
Lower Upper
Age group (5) 8.878 4 0.064 1.000
Age group (1) -0.910 0.355 6.557 1 0.010 -0.598 0.402 0.200 0.808
Age group (2) -0.558 0.269 4.284 1 0.038 -0.427 0.573 0.338 0.971
Age group (3) -0.629 0.246 6.518 1 0.011 -0.467 0.533 0.329 0.864
Age group (4) -0.483 0.236 4.206 1 0.040 -0.383 0.617 0.389 0.979
Below median
Income (1)
-0.166 0.152 1.184 1 0.277 0.847 0.629 1.142
Education level (3) 0.416 2 0.812
Education level (1) 0.026 0.247 0.011 1 0.918 1.026 0.632 1.666
Education level (2) 0.098 0.153 0.404 1 0.525 1.102 0.816 1.489
GoodHealth (1) -0.270 0.148 3.336 1 0.068 0.763 0.571 1.020
Having no
disabilities
-0.197 0.180 1.194 1 0.275 0.821 0.577 1.169
free capacity (3) 0.262 2 0.877
free capacity (1) -0.188 0.388 0.236 1 0.627 0.828 0.387 1.773
free capacity (2) -0.088 0.323 0.074 1 0.785 0.916 0.486 1.725
free places per
1000 inhabitants (3)
3.948 2 0.139
free places per
1000 inhabitants (1)
-0.264 0.199 1.762 1 0.184 0.768 0.520 1.134
free places per
1000 inhabitants (2)
-0.382 0.194 3.897 1 0.048 -0.318 0.682 0.467 0.997
Kommunestr (4) 2.517 3 0.472
Kommunestr (1) -0.093 0.457 0.042 1 0.838 0.911 0.372 2.231
Kommunestr (2) 0.266 0.399 0.445 1 0.505 1.305 0.597 2.851
Kommunestr (3) 0.193 0.309 0.390 1 0.532 1.213 0.662 2.222
Public vs Private
GP (1)
0.145 0.146 0.981 1 0.322 1.156 0.868 1.539
Waiting Time
Satisfaction (7)
161.963 6 0.000 1.000
Waiting Time
Satisfaction (1)
-3.248 0.334 94.598 1 0.000 -0.961 0.039 0.020 0.075
Waiting Time
Satisfaction (2)
-2.723 0.332 67.105 1 0.000 -0.934 0.066 0.034 0.126
Waiting Time
Satisfaction (3)
-2.030 0.328 38.288 1 0.000 -0.869 0.131 0.069 0.250
Waiting Time
Satisfaction (4)
-2.275 0.322 49.769 1 0.000 -0.897 0.103 0.055 0.193
Waiting Time
Satisfaction (5)
-1.599 0.319 25.187 1 0.000 -0.798 0.202 0.108 0.377
Waiting Time
Satisfaction (6)
-0.862 0.326 6.995 1 0.008 -0.578 0.422 0.223 0.800
Life Satisfaction (4) 17.728 3 0.001 1.000
Life Satisfaction (1) -0.980 0.248 15.585 1 0.000 -0.625 0.375 0.231 0.611
Life Satisfaction (2) -0.633 0.219 8.391 1 0.004 -0.469 0.531 0.346 0.815
Life Satisfaction (3) -0.336 0.178 3.542 1 0.060 -0.285 0.715 0.504 1.014
Constant 5.043 0.428 138.568 1 0.000 154.970
Wald df Sig. Exp(B)
95% C.I.for EXP(B)
Odds
Model 1.1 TGPS 1_2015 - Version 1 (fkap & LPPT). N= 2991 (69.2%)
TGPS 1_2015 (Version 1) Step 4 - Variables in the Equation
B S.E.

117
Appendix Table 9: Significant Variables in TGPS_1 2015 Step 4 (Version 1)
Lower Upper
Age group (5) 8.723 4 0.068
Age group (1) -0.891 0.355 6.290 1 0.012 -0.590 0.410 0.205 0.823
Age group (2) -0.539 0.269 4.017 1 0.045 -0.417 0.583 0.344 0.988
Age group (3) -0.631 0.246 6.569 1 0.010 -0.468 0.532 0.328 0.862
Age group (4) -0.470 0.236 3.978 1 0.046 -0.375 0.625 0.394 0.992
Below median
Income (1)
-0.166 0.152 1.185 1 0.276 0.847 0.628 1.142
Education level (3) 0.337 2 0.845
Education level (1) 0.040 0.247 0.027 1 0.870 1.041 0.641 1.691
Education level (2) 0.089 0.154 0.337 1 0.562 1.093 0.809 1.478
GoodHealth (1) -0.261 0.148 3.113 1 0.078 0.770 0.576 1.029
Having no
disabilities (1)
-0.187 0.180 1.072 1 0.300 0.830 0.582 1.182
GP density (3) 0.336 2 0.845
GP density (1) -0.125 0.246 0.260 1 0.610 0.882 0.545 1.429
GP density (2) -0.003 0.198 0.000 1 0.989 0.997 0.676 1.470
open lists per 1000
inhabitants (3)
4.972 2 0.083
open lists per 1000
inhabitants (1)
-0.119 0.210 0.325 1 0.569 0.887 0.589 1.338
open lists per 1000
inhabitants (2)
-0.412 0.210 3.853 1 0.050 -0.337 0.663 0.439 0.999
Kommunestr (4) 2.969 3 0.396
Kommunestr (1) -0.418 0.320 1.714 1 0.191 0.658 0.352 1.231
Kommunestr (2) -0.021 0.251 0.007 1 0.934 0.980 0.599 1.601
Kommunestr (3) 0.038 0.224 0.029 1 0.866 1.039 0.669 1.611
Public vs Private
GP (1)
0.174 0.147 1.410 1 0.235 1.191 0.893 1.588
Waiting Time
Satisfaction (7)
160.884 6 0.000 1.000
Waiting Time
Satisfaction (1)
-3.222 0.333 93.580 1 0.000 -0.960 0.040 0.021 0.077
Waiting Time
Satisfaction (2)
-2.744 0.332 68.182 1 0.000 -0.936 0.064 0.034 0.123
Waiting Time
Satisfaction (3)
-2.044 0.328 38.798 1 0.000 -0.870 0.130 0.068 0.246
Waiting Time
Satisfaction (4)
-2.280 0.323 49.875 1 0.000 -0.898 0.102 0.054 0.193
Waiting Time
Satisfaction (5)
-1.598 0.319 25.158 1 0.000 -0.798 0.202 0.108 0.378
Waiting Time
Satisfaction (6)
-0.867 0.326 7.087 1 0.008 -0.580 0.420 0.222 0.796
Life Satisfaction (4) 17.638 3 0.001 1.000
Life Satisfaction (1) -0.989 0.249 15.781 1 0.000 -0.628 0.372 0.228 0.606
Life Satisfaction (2) -0.612 0.218 7.882 1 0.005 -0.458 0.542 0.353 0.831
Life Satisfaction (3) -0.334 0.178 3.512 1 0.061 0.716 0.505 1.015
Constant 5.082 0.458 122.893 1 0.000 161.135
95% C.I.for EXP(B)
Odds
TGPS 1_2015 (Version 2) Step 4' - Variables in the Equation
B S.E. Wald df Sig. Exp(B)

118
Appendix Table 10: Significant Variables in TGPS_2 2015
Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E.
Constant 1.236 0.045 1.800 0.138 1.931 0.145 1.824 0.204 3.443 0.273 1.877 0.234 3.425 0.298
Age (5) § § § § § § § § § § § §
Age (1) -1.078 0.234 -1.095 0.235 -1.000 0.237 -0.759 0.255 -0.986 0.238 -0.748 0.255
Age (2) -0.959 0.168 -0.987 0.169 -0.882 0.172 -0.379 0.186 -0.864 0.172 -0.354 0.186
Age (3) -0.931 0.152 -0.934 0.152 -0.881 0.153 -0.451 0.167 -0.889 0.153 -0.456 0.167
Age (4) -0.513 0.144 -0.498 0.145 -0.490 0.145 -0.337 0.155 -0.483 0.145 -0.327 0.155
Below-median
Income (1)-0.011 0.100 -0.055 0.101 -0.090 0.102 -0.193 0.110 -0.087 0.102 -0.192 0.110
Education level (3) § § § § § § § § § § § §
Education level (1) 0.217 0.163 0.225 0.164 0.250 0.166 0.221 0.176 0.260 0.166 0.228 0.176
Education level (2) 0.090 0.100 0.091 0.100 0.102 0.103 0.145 0.112 0.097 0.103 0.142 0.112
GoodHealth (1) -0.159 0.099 -0.158 0.100 -0.040 0.109 -0.148 0.100 -0.024 0.109
No_disabilities (1) -0.255 0.122 -0.272 0.123 -0.128 0.135 -0.274 0.123 -0.127 0.135
free capacity (3) § §
free capacity (1) -0.300 0.264 -0.340 0.284
free capacity (2) -0.266 0.220 -0.346 0.237
free places per 1000
inhabitants (3)§ § § §
free places per 1000
inhabitants(1)-0.022 0.132 -0.009 0.142
free places per 1000
inhabitants (2)-0.257 0.128 -0.304 0.137
GP density (3) § § § §
GP density (1) -0.113 0.167 -0.090 0.181
GP density (2) 0.050 0.129 0.054 0.140
open lists per 1000
inhabitants (3)§ § § §
open lists per 1000
inhabitants (1)-0.046 0.138 -0.004 0.149
open lists per 1000
inhabitants (2)-0.261 0.140 -0.275 0.151
Kommunestr (4) § § § § § § § §
Kommunestr (1) 0.176 0.314 0.207 0.338 -0.209 0.221 -0.161 0.237
Kommunestr (2) 0.290 0.268 0.365 0.290 -0.074 0.169 -0.006 0.183
Kommunestr (3) 0.306 0.211 0.349 0.228 0.037 0.154 0.048 0.165
Public vs Private
GP (1)0.374 0.098 0.259 0.106 0.380 0.098 0.272 0.106
Waiting Time
Satsifaction (7)§ § § §
Waiting Time
Satsifaction (1)-2.762 0.237 -2.707 0.236
Waiting Time
Satsifaction (2)-2.377 0.225 -2.376 0.224
Waiting Time
Satsifaction (3)-2.128 0.204 -2.138 0.204
Waiting Time
Satsifaction (4)-2.181 0.203 -2.184 0.203
Waiting Time
Satsifaction (5)-1.660 0.189 -1.644 0.188
Waiting Time
Satsifaction (6)-0.809 0.189 -0.803 0.189
Life Satisfaction (4) § § § §
Life Satisfaction (1) -0.800 0.199 -0.820 0.199
Life Satisfaction (2) -1.004 0.155 -1.012 0.155
Life Satisfaction (3) -0.383 0.124 -0.390 0.124
Block 3' Block 4'Variables
Block 0 Block 1 Block 2 Block 3 Block 4
Regression Summary TGPS_2 2015 - N= 2991 (69.2%)

119
Appendix Table 11: Significant Variables in TGPS_3 2015
Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E.
Constant -0.101 0.037 0.341 0.103 0.412 0.109 0.404 0.163 1.935 0.203 0.480 0.189 1.980 0.229
Age (5) § § § § § § § § § § § §
Age (1) -0.848 0.208 -0.854 0.208 -0.803 0.211 -0.498 0.228 -0.793 0.211 -0.481 0.228
Age (2) -0.978 0.140 -0.992 0.140 -0.931 0.143 -0.469 0.160 -0.912 0.143 -0.442 0.160
Age (3) -0.763 0.119 -0.762 0.119 -0.718 0.120 -0.334 0.135 -0.727 0.120 -0.342 0.134
Age (4) -0.471 0.107 -0.462 0.107 -0.452 0.107 -0.295 0.118 -0.449 0.107 -0.289 0.118
Below-median
Income (1)0.015 0.084 -0.008 0.085 -0.041 0.086 -0.132 0.096 -0.036 0.086 -0.129 0.096
Education level (3) § § § § § § § § § § § §
Education level (1) 0.182 0.126 0.182 0.127 0.223 0.128 0.251 0.141 0.219 0.128 0.245 0.141
Education level (2) 0.102 0.085 0.099 0.085 0.126 0.087 0.170 0.097 0.120 0.087 0.162 0.097
GoodHealth (1) -0.100 0.084 -0.101 0.085 0.028 0.094 -0.090 0.085 0.044 0.094
No_disabilities (1) -0.127 0.104 -0.129 0.104 -0.001 0.116 -0.137 0.104 -0.009 0.116
free capacity (3) § § § §
free capacity (1) -0.387 0.212 -0.523 0.233
free capacity (2) -0.442 0.174 -0.592 0.191
free places per 1000
inhabitants (3)§ § § §
free places per 1000
inhabitants(1)-0.003 0.108 0.031 0.120
free places per 1000
inhabitants (2)-0.195 0.106 -0.240 0.117
GP density (3) § § § §
GP density (1) -0.161 0.139 -0.149 0.155
GP density (2) -0.001 0.105 0.032 0.115
open lists per 1000
inhabitants (3)§ § § §
open lists per 1000
inhabitants (1)0.002 0.112 0.008 0.124
open lists per 1000
inhabitants (2)-0.156 0.116 -0.195 0.128
Kommunestr (4) § § § § § § § §
Kommunestr (1) 0.082 0.259 0.159 0.285 -0.394 0.189 -0.431 0.208
Kommunestr (2) 0.318 0.216 0.465 0.238 -0.166 0.142 -0.140 0.157
Kommunestr (3) 0.299 0.169 0.362 0.185 -0.117 0.129 -0.163 0.143
Public vs Private
GP (1)0.265 0.083 0.170 0.091 0.270 0.083 0.175 0.091
Waiting Time
Satsifaction (7)§ § § §
Waiting Time
Satsifaction (1)-2.496 0.234 -2.425 0.233
Waiting Time
Satsifaction (2)-2.502 0.217 -2.486 0.216
Waiting Time
Satsifaction (3)-2.113 0.169 -2.115 0.169
Waiting Time
Satsifaction (4)-2.210 0.172 -2.213 0.172
Waiting Time
Satsifaction (5)-1.644 0.133 -1.623 0.132
Waiting Time
Satsifaction (6)-1.163 0.116 -1.151 0.116
Life Satisfaction (4) § § § §
Life Satisfaction (1) -0.634 0.187 -0.649 0.188
Life Satisfaction (2) -1.122 0.143 -1.140 0.143
Life Satisfaction (3) -0.536 0.097 -0.538 0.097
Block 3' Block 4'Variables
Block 0 Block 1 Block 2 Block 3 Block 4
Regression Summary TGPS_3 2015 - N= 2991 (69.2%)

120
Appendix Table 12: WTS_1 2015 – Version 1 Step 4
Lower Upper
Age group (5) 41.149 4 0.000 1.000
Age group (1) 0.114 0.257 0.195 1 0.659 1.120 0.677 1.854
Age group (2) -0.773 0.166 21.658 1 0.000 -0.538 0.462 0.333 0.639
Age group (3) -0.606 0.146 17.169 1 0.000 -0.454 0.546 0.410 0.727
Age group (4) -0.122 0.137 0.796 1 0.372 0.885 0.677 1.157
Below median
Income (1)
-0.035 0.101 0.120 1 0.729 0.965 0.792 1.177
Education level (3) 1.892 2 0.388
Education level (1) 0.212 0.160 1.762 1 0.184 1.236 0.904 1.691
Education level (2) 0.014 0.101 0.020 1 0.888 1.014 0.832 1.236
GoodHealth (1) -0.127 0.099 1.647 1 0.199 0.881 0.725 1.069
Having no
disabilities
-0.088 0.123 0.507 1 0.476 0.916 0.720 1.166
free capacity (3) 0.205 2 0.902
free capacity (1) -0.023 0.261 0.008 1 0.931 0.978 0.586 1.629
free capacity (2) -0.073 0.218 0.113 1 0.736 0.929 0.606 1.425
free places per
1000 inhabitants (3)
1.231 2 0.540
free places per
1000 inhabitants (1)
-0.067 0.126 0.281 1 0.596 0.935 0.730 1.198
free places per
1000 inhabitants (2)
0.066 0.125 0.280 1 0.597 1.068 0.837 1.364
Kommunestr (4) 7.329 3 0.062
Kommunestr (1) 0.102 0.310 0.108 1 0.742 1.107 0.603 2.033
Kommunestr (2) 0.082 0.264 0.096 1 0.756 1.085 0.647 1.821
Kommunestr (3) 0.387 0.209 3.413 1 0.065 1.472 0.977 2.219
Public vs Private
GP (1)
0.131 0.096 1.875 1 0.171 1.140 0.945 1.376
GP Supply
Satisfaction (7)
158.873 6 0.000 1.000
GP Supply
Satisfaction (1)
-2.178 0.336 42.145 1 0.000 -0.887 0.113 0.059 0.219
GP Supply
Satisfaction (2)
-1.880 0.315 35.731 1 0.000 -0.847 0.153 0.082 0.283
GP Supply
Satisfaction (3)
-1.649 0.233 50.118 1 0.000 -0.808 0.192 0.122 0.304
GP Supply
Satisfaction (4)
-1.584 0.164 92.958 1 0.000 -0.795 0.205 0.149 0.283
GP Supply
Satisfaction (5)
-0.977 0.141 48.000 1 0.000 -0.624 0.376 0.286 0.496
GP Supply
Satisfaction (6)
-0.506 0.124 16.737 1 0.000 -0.397 0.603 0.473 0.768
Life Satisfaction (4) 11.623 3 0.009 1.000
Life Satisfaction (1) -0.590 0.189 9.706 1 0.002 -0.446 0.554 0.383 0.804
Life Satisfaction (2) -0.025 0.147 0.029 1 0.864 0.975 0.731 1.300
Life Satisfaction (3) -0.001 0.107 0.000 1 0.989 0.999 0.809 1.232
Constant 1.787 0.211 71.686 1 0.000 5.969
Model 2.1 WTS 1_2015 - Version 1 (fkap & LPPT). N= 2907 (67.2%)
Odds Exp(B)
95% C.I.for EXP(B)
WTA 1_2015 (Version 1) Step 4 - Variables in the Equation
Variables B S.E. Wald df Sig.

121
Appendix Table 13: WTS_1 2015 – Version 2 Step 4
Lower Upper
Age group (5) 41.555 4 0.000 1.000
Age group (1) 0.106 0.257 0.171 1 0.680 1.112 0.672 1.839
Age group (2) -0.775 0.166 21.710 1 0.000 -0.539 0.461 0.333 0.638
Age group (3) -0.615 0.146 17.672 1 0.000 -0.460 0.540 0.406 0.720
Age group (4) -0.125 0.137 0.835 1 0.361 0.883 0.675 1.154
Below median
Income (1)
-0.031 0.101 0.091 1 0.763 0.970 0.795 1.183
Education level (3) 1.821 2 0.402
Education level (1) 0.204 0.160 1.630 1 0.202 1.227 0.896 1.679
Education level (2) 0.005 0.101 0.002 1 0.963 1.005 0.824 1.225
GoodHealth (1) -0.125 0.099 1.580 1 0.209 0.883 0.727 1.072
Having no
disabilities
-0.089 0.123 0.518 1 0.472 0.915 0.719 1.165
GP density (3) 5.620 2 0.060
GP density (1) -0.385 0.163 5.567 1 0.018 -0.320 0.680 0.494 0.937
GP density (2) -0.117 0.125 0.869 1 0.351 0.890 0.696 1.138
open lists per 1000
inhabitants (3)
3.552 2 0.169
open lists per 1000
inhabitants (1)
0.121 0.132 0.842 1 0.359 1.128 0.872 1.460
open lists per 1000
inhabitants (2)
0.253 0.137 3.398 1 0.065 1.288 0.984 1.685
Kommunestr (4) 4.869 3 0.182
Kommunestr (1) -0.128 0.216 0.351 1 0.554 0.880 0.576 1.344
Kommunestr (2) -0.177 0.164 1.162 1 0.281 0.838 0.608 1.156
Kommunestr (3) 0.107 0.150 0.502 1 0.479 1.112 0.828 1.494
Public vs Private
GP (1)
0.146 0.096 2.295 1 0.130 1.157 0.958 1.396
GP Supply
Satisfaction (7)
159.542 6 0.000 1.000
GP Supply
Satisfaction (1)
-2.161 0.337 41.174 1 0.000 -0.885 0.115 0.060 0.223
GP Supply
Satisfaction (2)
-1.892 0.315 35.976 1 0.000 -0.849 0.151 0.081 0.280
GP Supply
Satisfaction (3)
-1.657 0.233 50.456 1 0.000 -0.809 0.191 0.121 0.301
GP Supply
Satisfaction (4)
-1.594 0.164 93.869 1 0.000 -0.797 0.203 0.147 0.280
GP Supply
Satisfaction (5)
-0.993 0.141 49.473 1 0.000 -0.630 0.370 0.281 0.488
GP Supply
Satisfaction (6)
-0.506 0.124 16.706 1 0.000 -0.397 0.603 0.473 0.768
Life Satisfaction (4) 11.756 3 0.008 1.000
Life Satisfaction (1) -0.593 0.190 9.784 1 0.002 -0.447 0.553 0.381 0.801
Life Satisfaction (2) -0.019 0.147 0.017 1 0.897 0.981 0.736 1.308
Life Satisfaction (3) -0.001 0.107 0.000 1 0.992 0.999 0.809 1.233
Constant 2.000 0.239 69.833 1 0.000 7.388
Model 2.1 WTS 1_2015 - Version 2 GPD & OLI). N= 2907 (67.2%)
Variables
95% C.I.for EXP(B)
WTA 1_2015 (Version 2) Step 4' - Variables in the Equation
S.E. Wald df Sig. Odds Exp(B)B

122
Appendix Table 14: Significant Variables in WTS_2 2015
Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E.
Constant 1.273 0.045 1.836 0.135 1.957 0.142 1.803 0.202 2.504 0.240 1.897 0.233 2.567 0.270
Age (5) § § § § § § § § § § § §
Age (1) -1.106 0.235 -1.121 0.236 -1.016 0.239 -0.462 0.257 -1.008 0.239 -0.460 0.257
Age (2) -0.978 0.168 -1.001 0.168 -0.908 0.171 -0.312 0.185 -0.891 0.171 -0.293 0.185
Age (3) -0.893 0.150 -0.891 0.151 -0.845 0.152 -0.353 0.164 -0.851 0.152 -0.355 0.164
Age (4) -0.505 0.141 -0.494 0.142 -0.491 0.142 -0.202 0.152 -0.487 0.142 -0.200 0.152
Below-median
Income (1)
-0.036 0.102 -0.072 0.103 -0.100 0.104 -0.158 0.112 -0.099 0.104 -0.156 0.112
Education level (3) § § § § § § § § § § § §
Education level (1) 0.180 0.160 0.187 0.160 0.215 0.162 0.166 0.172 0.225 0.162 0.174 0.172
Education level (2) 0.064 0.101 0.063 0.102 0.085 0.104 0.122 0.111 0.084 0.105 0.121 0.112
GoodHealth (1) -0.166 0.100 -0.168 0.101 -0.035 0.109 -0.160 0.101 -0.022 0.109
No_disabilities (1) -0.215 0.124 -0.225 0.125 -0.135 0.135 -0.231 0.125 -0.139 0.135
free capacity (3) § § § §
free capacity (1) -0.216 0.264 -0.062 0.281
free capacity (2) -0.155 0.219 -0.086 0.233
free places per 1000
inhabitants (3)§ § § §
free places per 1000
inhabitants(1)
0.019 0.133 0.043 0.142
free places per 1000
inhabitants (2)
-0.185 0.129 -0.163 0.137
GP density (3) § § § §
GP density (1) -0.052 0.170 -0.089 0.181
GP density (2) -0.021 0.130 -0.061 0.139
open lists per 1000
inhabitants (3)§ § § §
open lists per 1000
inhabitants (1)
-0.060 0.139 0.069 0.149
open lists per 1000
inhabitants (2)
-0.296 0.142 -0.222 0.152
Kommunestr (4) § § § § § § § §
Kommunestr (1) 0.065 0.314 0.086 0.335 -0.242 0.221 -0.032 0.238
Kommunestr (2) 0.208 0.268 0.237 0.286 -0.047 0.171 0.117 0.181
Kommunestr (3) 0.253 0.210 0.310 0.224 0.124 0.157 0.246 0.168
Public vs Private
GP (1)
0.348 0.099 0.343 0.106 0.353 0.099 0.350 0.106
Municipal GP Supply
Satisfaction (7)§ § § §
Municipal GP Supply
Satisfaction (1)
-2.434 0.324 -2.446 0.326
Municipal GP Supply
Satisfaction (2)
-2.440 0.320 -2.471 0.321
Municipal GP Supply
Satisfaction (3)
-2.108 0.245 -2.112 0.245
Municipal GP Supply
Satisfaction (4)
-1.868 0.179 -1.863 0.179
Municipal GP Supply
Satisfaction (5)
-1.410 0.160 -1.404 0.160
Municipal GP Supply
Satisfaction (6)
-0.520 0.151 -0.524 0.151
Life Satisfaction (4) § § § §
Life Satisfaction (1) -0.513 0.205 -0.530 0.206
Life Satisfaction (2) -0.702 0.156 -0.709 0.156
Life Satisfaction (3) -0.243 0.124 -0.242 0.124
Block 3' Block 4'Variables
Block 0 Block 1 Block 2 Block 3 Block 4
Regression Summary WTS_2 2015 - N= 3029 (70.1%)

123
Appendix Table 15: Significant Variables in WTS_3 2015
Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E.
Constant -0.077 0.037 0.354 0.100 0.417 0.106 0.378 0.161 1.098 0.182 0.536 0.187 1.257 0.209
Age (5) § § § § § § § § § § § §
Age (1) -0.925 0.212 -0.930 0.213 -0.871 0.215 -0.441 0.229 -0.873 0.215 -0.439 0.229
Age (2) -1.026 0.141 -1.037 0.142 -0.986 0.144 -0.521 0.155 -0.966 0.144 -0.499 0.155
Age (3) -0.735 0.118 -0.732 0.118 -0.692 0.119 -0.314 0.129 -0.704 0.119 -0.325 0.129
Age (4) -0.491 0.105 -0.485 0.105 -0.479 0.105 -0.257 0.112 -0.479 0.105 -0.257 0.112
Below-median Income
(1)
-0.014 0.085 -0.032 0.086 -0.060 0.087 -0.084 0.093 -0.055 0.087 -0.081 0.093
Education level (3) § § § § § § § § § § § §
Education level (1) 0.216 0.123 0.215 0.124 0.259 0.126 0.215 0.133 0.252 0.126 0.205 0.133
Education level (2) 0.128 0.085 0.125 0.086 0.157 0.088 0.198 0.093 0.151 0.088 0.189 0.093
GoodHealth (1) -0.099 0.084 -0.101 0.085 0.025 0.091 -0.090 0.085 0.041 0.091
No_disabilities (1) -0.105 0.104 -0.104 0.104 -0.017 0.111 -0.116 0.104 -0.029 0.111
free capacity (3) § § § §
free capacity (1) -0.400 0.212 -0.300 0.226
free capacity (2) -0.439 0.174 -0.401 0.185
free places per 1000
inhabitants (3)§ § § §
free places per 1000
inhabitants(1)
0.013 0.108 0.028 0.115
free places per 1000
inhabitants (2)
-0.143 0.106 -0.120 0.113
GP density (3) § § § §
GP density (1) -0.185 0.139 -0.211 0.148
GP density (2) -0.074 0.105 -0.089 0.111
open lists per 1000
inhabitants (3)§ § § §
open lists per 1000
inhabitants (1)
0.011 0.112 0.086 0.118
open lists per 1000
inhabitants (2)
-0.180 0.116 -0.136 0.123
Kommunestr (4) § § § § § § § §
Kommunestr (1) 0.081 0.259 0.037 0.275 -0.464 0.189 -0.403 0.200
Kommunestr (2) 0.353 0.216 0.387 0.229 -0.178 0.142 -0.070 0.151
Kommunestr (3) 0.340 0.169 0.388 0.179 -0.079 0.129 -0.007 0.137
Public vs Private GP (1) 0.232 0.083 0.223 0.088 0.240 0.083 0.228 0.088
Municipal GP Supply
Satisfaction (7)§ § § §
Municipal GP Supply
Satisfaction (1)
-1.836 0.362 -1.840 0.363
Municipal GP Supply
Satisfaction (2)
-1.756 0.355 -1.794 0.356
Municipal GP Supply
Satisfaction (3)
-1.947 0.276 -1.939 0.276
Municipal GP Supply
Satisfaction (4)
-1.671 0.166 -1.667 0.165
Municipal GP Supply
Satisfaction (5)
-1.199 0.125 -1.202 0.125
Municipal GP Supply
Satisfaction (6)
-0.717 0.099 -0.724 0.099
Life Satisfaction (4) § § § §
Life Satisfaction (1) -0.439 0.185 -0.453 0.186
Life Satisfaction (2) -0.883 0.139 -0.895 0.139
Life Satisfaction (3) -0.453 0.093 -0.450 0.093
Block 3' Block 4'Variables
Block 0 Block 1 Block 2 Block 3 Block 4
Regression Summary WTS_3 2015 - N= 3029 (70.1%)

124
Appendix Table 16: Significant Variables in TGPS_1 2013
Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E.
Constant 2.134 0.062 2.712 0.210 2.849 0.217 2.517 0.312 3.799 0.407 1.956 0.352 3.091 0.437
Age (5) § § § § § § § § § § § §
Age (1) -0.581 0.341 -0.582 0.341 -0.371 0.347 0.059 0.360 -0.386 0.347 -0.386 0.347
Age (2) -1.372 0.236 -1.368 0.236 -1.252 0.240 -0.750 0.254 -1.268 0.240 -1.268 0.240
Age (3) -0.817 0.225 -0.798 0.224 -0.726 0.226 -0.259 0.237 -0.724 0.226 -0.724 0.226
Age (4) -0.405 0.216 -0.374 0.216 -0.344 0.217 -0.145 0.226 -0.341 0.217 -0.341 0.217
Below-median Income
(1)-0.078 0.138 -0.117 0.139 -0.163 0.140 -0.213 0.149 -0.180 0.140 -0.180 0.140
Education level (3) § § § § § § § § § § § §
Education level (1) 0.173 0.225 0.146 0.225 0.227 0.228 0.137 0.239 0.212 0.228 0.212 0.228
Education level (2) 0.129 0.139 0.119 0.139 0.147 0.142 0.220 0.150 0.140 0.142 0.140 0.142
GoodHealth (1) -0.353 0.130 -0.360 0.131 -0.230 0.140 -0.352 0.131 -0.352 0.131
free capacity (3) § § § §
free capacity (1) -0.278 0.341 -0.471 0.357
free capacity (2) -0.197 0.286 -0.356 0.300
free places per 1000
inhabitants (3) § § § §
free places per 1000
inhabitants(1) 0.283 0.193 0.416 0.202
free places per 1000
inhabitants (2) -0.073 0.190 -0.062 0.200
GP density (3) § § § §
GP density (1) 0.399 0.224 0.560 0.236
GP density (2) 0.094 0.187 0.215 0.197
open lists per 1000
inhabitants (3)§ § § §
open lists per 1000
inhabitants (1)0.308 0.179 0.321 0.189
open lists per 1000
inhabitants (2)0.201 0.194 0.230 0.204
Kommunestr (4) § § § § § § § §
Kommunestr (1) 0.225 0.442 0.499 0.461 0.528 0.322 0.770 0.338
Kommunestr (2) 0.137 0.365 0.414 0.383 0.380 0.242 0.644 0.256
Kommunestr (3) 0.207 0.299 0.426 0.315 0.354 0.208 0.525 0.218
Public vs Private GP (1) 0.512 0.137 0.384 0.145 0.498 0.137 0.357 0.145
Waiting Time
Satsifaction (7)§ § § §
Waiting Time
Satsifaction (1)-2.749 0.306 -2.757 0.307
Waiting Time
Satsifaction (2)-2.138 0.297 -2.134 0.297
Waiting Time
Satsifaction (3)-2.105 0.290 -2.093 0.290
Waiting Time
Satsifaction (4)-2.056 0.297 -2.024 0.297
Waiting Time
Satsifaction (5)-1.157 0.293 -1.133 0.294
Waiting Time
Satsifaction (6)-0.546 0.295 -0.557 0.295
Life Satisfaction (4) § § § §
Life Satisfaction (1) -0.843 0.248 -0.884 0.249
Life Satisfaction (2) -0.573 0.212 -0.568 0.212
Life Satisfaction (3) -0.338 0.167 -0.325 0.167
Regression Summary TGPS_1 2013 - N= 2881 (74.2%)
Block 3' Block 4'Variables
Block 0 Block 1 Block 2 Block 3 Block 4

125
Appendix Table 17: Significant Variables in TGPS_2 2013
Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E.
Constant 1.234 0.046 1.863 0.149 1.925 0.154 1.621 0.228 2.828 0.283 1.418 0.258 2.541 0.309
Age (5) § § § § § § § § § § § §
Age (1) -0.791 0.237 -0.792 0.238 -0.621 0.242 -0.197 0.256 -0.628 0.242 -0.209 0.256
Age (2) -1.377 0.177 -1.375 0.177 -1.276 0.180 -0.808 0.192 -1.290 0.180 -0.827 0.193
Age (3) -0.937 0.160 -0.928 0.160 -0.865 0.161 -0.431 0.172 -0.876 0.161 -0.449 0.172
Age (4) -0.418 0.152 -0.404 0.152 -0.380 0.153 -0.200 0.162 -0.385 0.153 -0.212 0.162
Below-median Income
(1)-0.098 0.103 -0.115 0.104 -0.151 0.104 -0.234 0.113 -0.157 0.105 -0.240 0.113
Education level (3) § § § § § § § § § § § §
Education level (1) 0.110 0.160 0.096 0.161 0.185 0.163 0.139 0.174 0.168 0.163 0.120 0.174
Education level (2) 0.109 0.104 0.104 0.104 0.140 0.106 0.209 0.114 0.135 0.106 0.199 0.114
GoodHealth (1) -0.168 0.099 -0.168 0.100 0.000 0.108 -0.166 0.100 0.009 0.108
free capacity (3) § § § §
free capacity (1) -0.006 0.248 -0.176 0.265
free capacity (2) -0.162 0.205 -0.317 0.220
free places per 1000
inhabitants (3)§ § § §
free places per 1000
inhabitants(1)0.122 0.141 0.227 0.150
free places per 1000
inhabitants (2)-0.006 0.142 0.003 0.151
GP density (3) § § § §
GP density (1) 0.021 0.158 0.106 0.170
GP density (2) 0.020 0.138 0.126 0.149
open lists per 1000
inhabitants (3)§ § § §
open lists per 1000
inhabitants (1)0.228 0.131 0.226 0.140
open lists per 1000
inhabitants (2)0.210 0.144 0.238 0.153
Kommunestr (4) § § § § § § § §
Kommunestr (1) -0.033 0.325 0.167 0.346 0.168 0.239 0.294 0.254
Kommunestr (2) -0.010 0.266 0.197 0.284 0.082 0.176 0.223 0.189
Kommunestr (3) 0.135 0.217 0.304 0.232 0.117 0.154 0.202 0.163
Public vs Private GP (1) 0.457 0.101 0.355 0.108 0.456 0.101 0.345 0.109
Waiting Time
Satsifaction (7)§ § § §
Waiting Time
Satsifaction (1)-2.407 0.229 -2.395 0.229
Waiting Time
Satsifaction (2)-1.644 0.208 -1.642 0.209
Waiting Time
Satsifaction (3)-1.947 0.196 -1.930 0.196
Waiting Time
Satsifaction (4)-1.701 0.203 -1.689 0.203
Waiting Time
Satsifaction (5)-1.303 0.182 -1.293 0.182
Waiting Time
Satsifaction (6)-0.454 0.182 -0.457 0.182
Life Satisfaction (4) § § § §
Life Satisfaction (1) -1.026 0.195 -1.036 0.196
Life Satisfaction (2) -0.936 0.159 -0.937 0.159
Life Satisfaction (3) -0.451 0.123 -0.448 0.123
Block 3' Block 4'Variables
Block 0 Block 1 Block 2 Block 3 Block 4
Regression Summary TGPS_2 2013 - N= 2881 (74.2%)

126
Appendix Table 18: Significant Variables in TGPS_3 2013
Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E.
Constant -0.145 0.038 0.312 0.110 0.354 0.114 0.082 0.184 1.430 0.219 0.045 0.210 1.373 0.245
Age (5) § § § § § § § § § § § §
Age (1) -0.829 0.198 -0.830 0.198 -0.719 0.202 -0.332 0.218 -0.719 0.202 -0.343 0.218
Age (2) -1.031 0.153 -1.030 0.153 -0.969 0.155 -0.543 0.170 -0.967 0.156 -0.541 0.170
Age (3) -0.810 0.125 -0.804 0.125 -0.766 0.126 -0.407 0.138 -0.760 0.126 -0.403 0.138
Age (4) -0.300 0.110 -0.291 0.110 -0.279 0.111 -0.174 0.121 -0.276 0.111 -0.171 0.121
Below-median Income (1) -0.154 0.088 -0.164 0.088 -0.192 0.089 -0.260 0.097 -0.193 0.089 -0.261 0.097
Education level (3) § § § § § § § § § § § §
Education level (1) 0.254 0.125 0.245 0.126 0.292 0.128 0.258 0.138 0.296 0.128 0.261 0.138
Education level (2) 0.100 0.089 0.096 0.089 0.117 0.091 0.127 0.099 0.118 0.091 0.129 0.098
GoodHealth (1) -0.121 0.084 -0.121 0.085 0.016 0.093 -0.120 0.085 0.022 0.093
free capacity/ free GPs (3) § § § §
free capacity/ free GPs (1) -0.062 0.199 -0.198 0.219
free capacity/ free GPs (2) 0.032 0.164 -0.040 0.180
free places per 1000
inhabitants (3)§ § § §
free places per 1000
inhabitants(1)0.127 0.118 0.203 0.128
free places per 1000
inhabitants (2)0.053 0.119 0.052 0.129
GP density (3) § § § §
GP density (1) 0.150 0.131 0.194 0.143
GP density (2) 0.009 0.115 0.086 0.125
open lists per 1000
inhabitants (3)§ § § §
open lists per 1000
inhabitants (1)0.076 0.109 0.056 0.118
open lists per 1000
inhabitants (2)-0.042 0.120 -0.057 0.131
Kommunestr (4) § § § § § § § §
Kommunestr (1) -0.013 0.269 0.120 0.293 -0.009 0.203 0.023 0.220
Kommunestr (2) 0.030 0.217 0.174 0.238 0.075 0.148 0.149 0.161
Kommunestr (3) 0.112 0.175 0.199 0.192 0.157 0.128 0.187 0.139
Public vs Private GP (1) 0.274 0.085 0.174 0.093 0.267 0.086 0.161 0.093
Waiting Time Satsifaction
(7)§ § § §
Waiting Time Satsifaction
(1)-2.452 0.247 -2.447 0.247
Waiting Time Satsifaction
(2)-1.563 0.176 -1.553 0.176
Waiting Time Satsifaction
(3)-1.831 0.169 -1.827 0.169
Waiting Time Satsifaction
(4)-2.360 0.192 -2.348 0.192
Waiting Time Satsifaction
(5)-1.583 0.136 -1.571 0.136
Waiting Time Satsifaction
(6)-1.092 0.117 -1.091 0.117
Overall Life Satisfaction (4) § § § §
Overall Life Satisfaction (1) -0.637 0.177 -0.655 0.177
Overall Life Satisfaction (2) -0.868 0.145 -0.870 0.145
Overall Life Satisfaction (3) -0.500 0.097 -0.507 0.097
Block 3' Block 4'Variables
Block 0 Block 1 Block 2 Block 3 Block 4
Regression Summary TGPS_3 2013 - N= 2881 (74.2%)

127
Appendix Table 19: Significant Variables in WTS_1 2013
Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E.
Constant 0.823 0.043 1.427 0.134 1.514 0.138 1.507 0.213 2.166 0.243 1.697 0.240 2.277 0.269
Age (5) § § § § § § § § § § § §
Age (1) -1.009 0.216 -1.004 0.216 -0.933 0.221 -0.703 0.232 -0.902 0.221 -0.672 0.232
Age (2) -1.163 0.166 -1.157 0.166 -1.122 0.169 -0.612 0.180 -1.118 0.169 -0.620 0.180
Age (3) -1.068 0.145 -1.050 0.145 -1.037 0.147 -0.659 0.155 -1.022 0.147 -0.653 0.155
Age (4) -0.457 0.136 -0.435 0.136 -0.430 0.137 -0.267 0.143 -0.417 0.137 -0.254 0.143
Below-median
Income (1)0.033 0.096 0.010 0.097 -0.008 0.098 -0.046 0.104 -0.005 0.098 -0.042 0.104
Education level (3) § § § § § § § § § § § §
Education level (1) 0.230 0.149 0.211 0.150 0.303 0.152 0.196 0.159 0.310 0.152 0.196 0.159
Education level (2) -0.007 0.097 -0.014 0.097 0.042 0.100 0.048 0.105 0.043 0.100 0.050 0.105
GoodHealth (1) -0.245 0.092 -0.247 0.093 -0.155 0.099 -0.256 0.093 -0.168 0.099
free capacity (3) § § § §
free capacity (1) 0.488 0.228 0.681 0.239
free capacity (2) 0.321 0.186 0.417 0.195
free places per 1000
inhabitants (3) § § § §
free places per 1000
inhabitants(1) -0.204 0.132 -0.229 0.138
free places per 1000
inhabitants (2) 0.034 0.135 0.055 0.141
GP density (3) § § § §
GP density (1) -0.203 0.147 -0.221 0.154
GP density (2) -0.311 0.129 -0.339 0.136
open lists per 1000
inhabitants (3)§ § § §
open lists per 1000
inhabitants (1)0.081 0.123 0.152 0.129
open lists per 1000
inhabitants (2)-0.014 0.134 0.095 0.140
Kommunestr (4) § § § § § § § §
Kommunestr (1) -0.717 0.301 -0.819 0.315 -0.463 0.224 -0.319 0.235
Kommunestr (2) -0.685 0.246 -0.697 0.257 -0.477 0.164 -0.309 0.172
Kommunestr (3) -0.368 0.199 -0.387 0.207 -0.170 0.144 -0.078 0.150
Public vs Private GP
(1)0.333 0.095 0.336 0.100 0.352 0.095 0.352 0.100
Municipal GP Supply
Satisfaction (7)§ § § §
Municipal GP Supply
Satisfaction (1)-2.027 0.338 -1.996 0.339
Municipal GP Supply
Satisfaction (2)-1.517 0.289 -1.536 0.288
Municipal GP Supply
Satisfaction (3)-2.044 0.254 -2.024 0.254
Municipal GP Supply
Satisfaction (4)-1.686 0.174 -1.677 0.174
Municipal GP Supply
Satisfaction (5)-1.229 0.146 -1.231 0.146
Municipal GP Supply
Satisfaction (6)-0.571 0.135 -0.568 0.134
Life Satisfaction (4) § § § §
Life Satisfaction (1) -0.173 0.188 -0.125 0.188
Life Satisfaction (2) -0.419 0.150 -0.408 0.150
Life Satisfaction (3) -0.166 0.110 -0.149 0.110
Block 3' Block 4'Variables
Block 0 Block 1 Block 2 Block 3 Block 4
Regression Summary WTS_1 2013 - N= 2736 (70.5%)

128
Appendix Table 20: Significant Variables in WTS_2 2013
Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E.
Constant 1.254 0.047 1.889 0.153 1.946 0.157 1.743 0.234 2.738 0.288 1.484 0.265 2.298 0.317
Age (5) § § § § § § § § § § § §
Age (1) -0.781 0.248 -0.775 0.248 -0.618 0.252 -0.178 0.275 -0.616 0.252 -0.616 0.252
Age (2) -1.458 0.180 -1.452 0.180 -1.363 0.183 -0.664 0.203 -1.375 0.183 -1.375 0.183
Age (3) -1.031 0.164 -1.017 0.164 -0.965 0.165 -0.404 0.181 -0.974 0.165 -0.974 0.165
Age (4) -0.458 0.155 -0.441 0.156 -0.424 0.157 -0.189 0.169 -0.427 0.157 -0.427 0.157
Below-median Income
(1)-0.036 0.106 -0.053 0.106 -0.083 0.107 -0.155 0.118 -0.090 0.107 -0.090 0.107
Education level (3) § § § § § § § § § § § §
Education level (1) 0.113 0.164 0.101 0.165 0.183 0.167 0.049 0.181 0.167 0.167 0.167 0.167
Education level (2) 0.131 0.107 0.127 0.107 0.160 0.110 0.226 0.120 0.153 0.109 0.153 0.109
GoodHealth (1) -0.165 0.102 -0.162 0.102 0.033 0.114 -0.163 0.102 -0.163 0.102
free capacity (3) § § § §
free capacity (1) 0.009 0.258 0.321 0.281
free capacity (2) -0.150 0.214 -0.019 0.231
free places per 1000
inhabitants (3)§ § § §
free places per 1000
inhabitants(1)0.026 0.146 0.022 0.159
free places per 1000
inhabitants (2)-0.060 0.147 -0.056 0.160
GP density (3) § § § §
GP density (1) 0.029 0.163 0.051 0.178
GP density (2) 0.000 0.143 0.003 0.156
open lists per 1000
inhabitants (3)§ § § §
open lists per 1000
inhabitants (1)0.179 0.135 0.324 0.149
open lists per 1000
inhabitants (2)0.207 0.149 0.385 0.163
Kommunestr (4) § § § § § § § §
Kommunestr (1) -0.075 0.336 -0.232 0.365 0.172 0.248 0.482 0.273
Kommunestr (2) -0.062 0.276 -0.070 0.299 0.055 0.182 0.390 0.199
Kommunestr (3) 0.061 0.226 0.062 0.243 0.083 0.157 0.276 0.171
Public vs Private GP (1)0.453 0.104 0.488 0.114 0.456 0.104 0.482 0.114
Municipal GP Supply
Satisfaction (7)§ § § §
Municipal GP Supply
Satisfaction (1)-2.875 0.366 -2.852 0.366
Municipal GP Supply
Satisfaction (2)-2.567 0.311 -2.573 0.311
Municipal GP Supply
Satisfaction (3)-2.515 0.269 -2.519 0.269
Municipal GP Supply
Satisfaction (4)-2.378 0.201 -2.388 0.202
Municipal GP Supply
Satisfaction (5)-1.593 0.180 -1.613 0.180
Municipal GP Supply
Satisfaction (6)-0.626 0.177 -0.631 0.177
Life Satisfaction (4) § § § §
Life Satisfaction (1) -0.610 0.207 -0.594 0.207
Life Satisfaction (2) -0.857 0.168 -0.844 0.168
Life Satisfaction (3) -0.391 0.132 -0.376 0.132
Block 3' Block 4'Variables
Block 0 Block 1 Block 2 Block 3 Block 4
Regression Summary WTS_2 2013 - N= 2779 (71.6%)

129
Appendix Table 21: Significant Variables in WTS_3 2013
Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E.
Constant -0.116 0.039 0.338 0.112 0.383 0.116 0.153 0.188 1.171 0.217 0.079 0.214 0.978 0.244
Age (5) § § § § § § § § § § § §
Age (1) -0.902 0.204 -0.898 0.204 -0.803 0.208 -0.532 0.226 -0.795 0.208 -0.795 0.208
Age (2) -1.121 0.155 -1.117 0.155 -1.067 0.158 -0.491 0.173 -1.065 0.158 -1.065 0.158
Age (3) -0.882 0.127 -0.872 0.127 -0.841 0.128 -0.376 0.140 -0.833 0.128 -0.833 0.128
Age (4) -0.363 0.111 -0.350 0.112 -0.342 0.112 -0.160 0.122 -0.338 0.112 -0.338 0.112
Below-median
Income (1)-0.102 0.090 -0.114 0.090 -0.136 0.091 -0.201 0.099 -0.139 0.091 -0.139 0.091
Education level (3) § § § § § § § § § § § §
Education level (1) 0.304 0.128 0.294 0.128 0.331 0.130 0.202 0.141 0.335 0.130 0.335 0.130
Education level (2) 0.139 0.091 0.136 0.091 0.149 0.093 0.155 0.101 0.149 0.093 0.149 0.093
GoodHealth (1) -0.136 0.086 -0.137 0.087 -0.010 0.095 -0.137 0.087 -0.137 0.087
free capacity (3) § § § §
free capacity (1) -0.029 0.205 0.163 0.222
free capacity (2) 0.050 0.169 0.170 0.184
free places per 1000
inhabitants (3)§ § § §
free places per 1000
inhabitants(1)0.111 0.121 0.089 0.131
free places per 1000
inhabitants (2)0.035 0.122 0.042 0.132
GP density (3) § § § §
GP density (1) 0.192 0.134 0.224 0.144
GP density (2) -0.009 0.118 -0.019 0.128
open lists per 1000
inhabitants (3)§ § § §
open lists per 1000
inhabitants (1)0.072 0.112 0.155 0.121
open lists per 1000
inhabitants (2)-0.057 0.123 0.045 0.134
Kommunestr (4) § § § § § § § §
Kommunestr (1) -0.033 0.276 -0.123 0.298 0.037 0.208 0.238 0.226
Kommunestr (2) 0.002 0.224 0.028 0.242 0.100 0.152 0.351 0.164
Kommunestr (3) 0.087 0.181 0.093 0.195 0.180 0.131 0.336 0.142
Public/Private GP (1) 0.240 0.088 0.277 0.095 0.232 0.088 0.269 0.095
GP Supply Sat. (7) § § § §
GP Supply Sat. (1) -2.612 0.449 -2.607 0.449
GP Supply Sat. (2) -2.178 0.347 -2.178 0.347
GP Supply Sat. (3) -2.144 0.285 -2.154 0.285
GP Supply Sat. (4) -2.155 0.182 -2.160 0.183
GP Supply Sat. (5) -1.682 0.133 -1.692 0.134
GP Supply Sat. (6) -1.168 0.111 -1.171 0.111
Life Satisfaction (4) § § § §
Life Satisfaction (1) -0.331 0.185 -0.324 0.185
Life Satisfaction (2) -0.813 0.149 -0.806 0.150
Life Satisfaction (3) -0.365 0.099 -0.360 0.100
Block 3' Block 4'Variables
Block 0 Block 1 Block 2 Block 3 Block 4
Regression Summary WTS_3 2013 - N= 2779 (71.6%)

130
Appendix Table 22: Significant Variables in TGPS_1 2010
Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E.
Constant 2.066 0.072 2.659 0.227 2.409 0.265 3.648 0.387 2.526 0.360 3.756 0.466
Age (5) § § § § § § § § § §
Age (1) -1.245 0.381 -1.255 0.384 -0.775 0.408 -1.277 0.385 -0.777 0.408
Age (2) -0.912 0.303 -0.885 0.305 -0.256 0.325 -0.900 0.305 -0.271 0.324
Age (3) -0.802 0.243 -0.828 0.244 -0.382 0.257 -0.820 0.244 -0.368 0.257
Age (4) -0.274 0.222 -0.286 0.223 -0.121 0.234 -0.290 0.223 -0.112 0.234
Below-median Income
(1)-0.213 0.157 -0.225 0.158 -0.274 0.167 -0.222 0.157 -0.281 0.167
Education level (3) § § § § § § § § § §
Education level (1) -0.109 0.211 -0.147 0.215 -0.210 0.227 -0.145 0.214 -0.198 0.226
Education level (2) -0.050 0.171 -0.085 0.175 -0.116 0.184 -0.085 0.174 -0.109 0.183
free capacity (3) § § § §
free capacity (1) 0.020 0.319 0.071 0.335
free capacity (2) 0.183 0.237 0.199 0.249
free places per 1000
inhabitants (3)§ § § §
free places per 1000
inhabitants(1)0.232 0.210 0.333 0.222
free places per 1000
inhabitants (2)0.330 0.189 0.354 0.199
GP density (3) § § § §
GP density (1) -0.108 0.238 -0.023 0.252
GP density (2) -0.182 0.203 -0.147 0.213
open lists per 1000
inhabitants (3)§ § § §
open lists per 1000
inhabitants (1)0.280 0.226 0.260 0.237
open lists per 1000
inhabitants (2)0.130 0.210 0.088 0.222
Kommunestr (4) § § § § § § § §
Kommunestr (1) -0.070 0.374 -0.107 0.393 -0.047 0.333 -0.018 0.349
Kommunestr (2) 0.179 0.299 0.257 0.313 0.289 0.242 0.430 0.257
Kommunestr (3) 0.028 0.216 0.075 0.227 0.176 0.204 0.251 0.214
Waiting Time
Satsifaction (7)§ § § §
Waiting Time
Satsifaction (1)-2.816 0.349 -2.801 0.349
Waiting Time
Satsifaction (2)-2.013 0.347 -1.983 0.346
Waiting Time
Satsifaction (3)-1.916 0.331 -1.900 0.332
Waiting Time
Satsifaction (4)-1.833 0.342 -1.825 0.341
Waiting Time
Satsifaction (5)-1.281 0.331 -1.272 0.331
Waiting Time
Satsifaction (6)-0.591 0.339 -0.590 0.339
Life Satisfaction (1) § § § §
Life Satisfaction (2) -0.720 0.208 -0.722 0.208
Life Satisfaction (3) -0.023 0.192 -0.019 0.192
Block 2'Variables
Block 0 Block 1 Block 2 Block 3
Regression Summary TGPS_1 2010 - N= 1912 (83.9%)
Block 3'

131
Appendix Table 23: Significant Variables in TGPS_2 2010
Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E.
Constant 1.141 0.053 1.568 0.160 1.456 0.194 3.020 0.287 1.709 0.264 3.336 0.350
Age (5) § § § § § § § § § §
Age (1) -1.108 0.310 -1.094 0.312 -0.634 0.336 -1.084 0.313 -0.593 0.337
Age (2) -0.972 0.225 -0.949 0.227 -0.315 0.246 -0.944 0.226 -0.303 0.246
Age (3) -0.690 0.178 -0.686 0.179 -0.217 0.193 -0.676 0.178 -0.199 0.193
Age (4) -0.323 0.157 -0.322 0.158 -0.173 0.169 -0.330 0.158 -0.172 0.169
Below-median
Income (1)-0.210 0.116 -0.220 0.117 -0.253 0.127 -0.208 0.117 -0.248 0.127
Education level (3) § § § § § § § § § §
Education level (1) 0.181 0.155 0.170 0.157 0.153 0.170 0.180 0.157 0.169 0.170
Education level (2) 0.132 0.126 0.115 0.128 0.109 0.138 0.114 0.128 0.109 0.138
free capacity (3) § § § §
free capacity (1) 0.146 0.234 0.221 0.252
free capacity (2) 0.103 0.174 0.145 0.187
free places per 1000
inhabitants (3)§ § § §
free places per 1000
inhabitants(1)-0.204 0.154 -0.146 0.166
free places per 1000
inhabitants (2)0.094 0.142 0.122 0.153
GP density (3) § § § §
GP density (1) -0.145 0.172 -0.045 0.187
GP density (2) -0.137 0.150 -0.117 0.161
open lists per 1000
inhabitants (3)§ § § §
open lists per 1000
inhabitants (1)-0.116 0.164 -0.175 0.177
open lists per 1000
inhabitants (2)-0.138 0.157 -0.234 0.170
Kommunestr (4) § § § § § § § §
Kommunestr (1) -0.083 0.277 -0.074 0.298 -0.200 0.252 -0.148 0.271
Kommunestr (2) 0.086 0.214 0.195 0.230 0.038 0.177 0.211 0.193
Kommunestr (3) 0.169 0.160 0.229 0.173 0.158 0.152 0.246 0.164
Waiting Time
Satsifaction (7)§ § § §
Waiting Time
Satsifaction (1)-2.841 0.285 -2.851 0.286
Waiting Time
Satsifaction (2)-2.103 0.263 -2.116 0.263
Waiting Time
Satsifaction (3)-2.360 0.245 -2.373 0.246
Waiting Time
Satsifaction (4)-2.181 0.253 -2.194 0.253
Waiting Time
Satsifaction (5)-1.545 0.238 -1.553 0.238
Waiting Time
Satsifaction (6)-0.973 0.234 -0.986 0.234
Life Satisfaction (1) § § § §
Life Satisfaction (2) -0.876 0.166 -0.887 0.166
Life Satisfaction (3) -0.407 0.144 -0.413 0.144
Block 3'Variables
Block 0 Block 1 Block 2 Block 3 Block 2'
Regression Summary TGPS_2 2010 - N= 1912 (83.9%)

132
Appendix Table 24: Significant Variables in TGPS_3 2010
Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E.
Constant -0.134 0.046 0.091 0.128 0.021 0.162 1.163 0.202 -0.159 0.219 1.011 0.258
Age (5) § § § § § § § § § §
Age (1) -0.440 0.295 -0.447 0.297 -0.001 0.315 -0.433 0.297 0.020 0.316
Age (2) -0.927 0.218 -0.898 0.219 -0.400 0.234 -0.915 0.219 -0.416 0.233
Age (3) -0.407 0.148 -0.411 0.149 0.011 0.162 -0.420 0.149 0.004 0.161
Age (4) -0.055 0.122 -0.044 0.123 0.110 0.132 -0.052 0.123 0.103 0.131
Below-median
Income (1)-0.277 0.102 -0.299 0.102 -0.322 0.110 -0.288 0.102 -0.310 0.110
Education level (3) § § § § § § § § § §
Education level (1) 0.265 0.130 0.275 0.132 0.262 0.141 0.287 0.132 0.279 0.141
Education level (2) 0.051 0.111 0.056 0.113 0.026 0.121 0.065 0.113 0.036 0.120
free capacity (3) § § § §
free capacity (1) -0.015 0.197 0.003 0.210
free capacity (2) -0.064 0.148 -0.052 0.158
free places per 1000
inhabitants (3)§ § § §
free places per 1000
inhabitants(1)0.024 0.133 0.127 0.142
free places per 1000
inhabitants (2)0.277 0.120 0.352 0.129
GP density (3) § § § §
GP density (1) 0.154 0.145 0.213 0.155
GP density (2) 0.121 0.127 0.127 0.135
open lists per 1000
inhabitants (3)§ § § §
open lists per 1000
inhabitants (1)0.053 0.138 0.060 0.148
open lists per 1000
inhabitants (2)0.128 0.132 0.086 0.141
Kommunestr (4) § § § § § § § §
Kommunestr (1) -0.213 0.241 -0.144 0.258 -0.044 0.219 0.048 0.234
Kommunestr (2) 0.000 0.186 0.083 0.198 0.111 0.156 0.238 0.167
Kommunestr (3) 0.064 0.141 0.096 0.150 0.171 0.134 0.237 0.143
Waiting Time
Satsifaction (7)§ § § §
Waiting Time
Satsifaction (1)-1.872 0.253 -1.880 0.252
Waiting Time
Satsifaction (2)-1.893 0.219 -1.864 0.218
Waiting Time
Satsifaction (3)-1.739 0.191 -1.736 0.191
Waiting Time
Satsifaction (4)-1.631 0.198 -1.654 0.197
Waiting Time
Satsifaction (5)-1.379 0.160 -1.363 0.160
Waiting Time
Satsifaction (6)-0.918 0.142 -0.923 0.142
Life Satisfaction (1) § § § §
Life Satisfaction (2) -0.830 0.144 -0.825 0.144
Life Satisfaction (3) -0.436 0.114 -0.435 0.114
Block 3'Variables
Block 0 Block 1 Block 2 Block 3 Block 2'
Regression Summary TGPS_3 2010 - N= 1912 (83.9%)

133
Appendix Table 25: Significant Variables in WTS_1 2010
Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E.
Constant 0.674 0.049 1.374 0.147 1.662 0.186 2.221 0.219 1.718 0.245 2.399 0.281
Age (5) § § § § § § § § § §
Age (1) -1.124 0.305 -1.154 0.308 -1.047 0.317 -1.187 0.307 -1.080 0.317
Age (2) -1.540 0.215 -1.613 0.218 -1.345 0.227 -1.604 0.218 -1.325 0.226
Age (3) -1.026 0.163 -1.046 0.164 -0.872 0.170 -1.055 0.164 -0.869 0.170
Age (4) -0.336 0.142 -0.326 0.143 -0.257 0.147 -0.336 0.143 -0.262 0.147
Below-median
Income (1)-0.220 0.109 -0.219 0.110 -0.191 0.114 -0.205 0.109 -0.171 0.114
Education level (3) § § § § § § § § § §
Education level (1) -0.069 0.144 0.006 0.146 -0.011 0.151 -0.006 0.146 -0.020 0.151
Education level (2) -0.100 0.118 -0.029 0.121 -0.015 0.125 -0.030 0.121 -0.017 0.125
free capacity (3) § § § §
free capacity (1) -0.232 0.213 -0.110 0.220
free capacity (2) 0.004 0.163 0.122 0.168
free places per 1000
inhabitants (3)§ § § §
free places per 1000
inhabitants(1)-0.196 0.143 -0.201 0.147
free places per 1000
inhabitants (2)-0.002 0.132 0.024 0.136
GP density (3) § § § §
GP density (1) -0.263 0.159 -0.399 0.166
GP density (2) -0.092 0.137 -0.222 0.142
open lists per 1000
inhabitants (3)§ § § §
open lists per 1000
inhabitants (1)0.027 0.149 0.113 0.155
open lists per 1000
inhabitants (2)0.110 0.142 0.111 0.146
Kommunestr (4) § § § § § § § §
Kommunestr (1) -0.063 0.259 -0.173 0.268 -0.379 0.237 -0.473 0.245
Kommunestr (2) -0.280 0.203 -0.366 0.209 -0.532 0.171 -0.577 0.177
Kommunestr (3) -0.228 0.155 -0.293 0.160 -0.305 0.148 -0.345 0.153
Municipal GP Supply
Satisfaction (7)§ § § §
Municipal GP Supply
Satisfaction (1)-1.739 0.477 -1.750 0.476
Municipal GP Supply
Satisfaction (2)-1.750 0.347 -1.788 0.346
Municipal GP Supply
Satisfaction (3)-1.254 0.288 -1.275 0.288
Municipal GP Supply
Satisfaction (4)-1.382 0.195 -1.431 0.195
Municipal GP Supply
Satisfaction (5)-0.622 0.162 -0.646 0.162
Municipal GP Supply
Satisfaction (6)-0.398 0.141 -0.413 0.141
Life Satisfaction (3) § § § §
Life Satisfaction (1) -0.358 0.152 -0.344 0.152
Life Satisfaction (2) -0.183 0.125 -0.162 0.125
Regression Summary WTS_1 2010 - N= 1866 (81.8%)
Block 2' Block 3'Variables
Block 0 Block 1 Block 2 Block 3

134
Appendix Table 26: Significant Variables in WTS_2 2010
Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E.
Constant 1.142 0.054 1.630 0.162 1.517 0.195 2.511 0.249 1.795 0.268 2.988 0.322
Age (5) § § § § § § § § § §
Age (1) -1.177 0.318 -1.166 0.320 -0.973 0.338 -1.152 0.320 -0.957 0.339
Age (2) -1.068 0.228 -1.047 0.230 -0.637 0.245 -1.035 0.229 -0.617 0.245
Age (3) -0.792 0.180 -0.791 0.180 -0.529 0.190 -0.781 0.180 -0.508 0.190
Age (4) -0.383 0.159 -0.384 0.160 -0.267 0.167 -0.388 0.160 -0.269 0.167
Below-median
Income (1)-0.229 0.118 -0.236 0.118 -0.213 0.125 -0.223 0.118 -0.198 0.125
Education level (3) § § § § § § § § § §
Education level (1) 0.202 0.158 0.197 0.160 0.162 0.169 0.202 0.160 0.172 0.169
Education level (2) 0.134 0.127 0.123 0.129 0.136 0.136 0.120 0.129 0.133 0.136
free capacity (3) § § § §
free capacity (1) 0.125 0.237 0.310 0.251
free capacity (2) 0.093 0.177 0.242 0.186
free places per 1000
inhabitants (3)§ § § §
free places per 1000
inhabitants(1)-0.209 0.157 -0.206 0.165
free places per 1000
inhabitants (2)0.064 0.143 0.097 0.150
GP density (3) § § § §
GP density (1) -0.161 0.176 -0.335 0.188
GP density (2) -0.159 0.152 -0.343 0.160
open lists per 1000
inhabitants (3)§ § § §
open lists per 1000
inhabitants (1)-0.171 0.166 -0.074 0.176
open lists per 1000
inhabitants (2)-0.122 0.159 -0.140 0.167
Kommunestr (4) § § § § § § § §
Kommunestr (1) -0.036 0.280 -0.231 0.296 -0.198 0.256 -0.364 0.269
Kommunestr (2) 0.089 0.216 0.019 0.228 0.009 0.179 -0.005 0.189
Kommunestr (3) 0.205 0.161 0.169 0.170 0.175 0.153 0.169 0.161
Municipal GP Supply
Satisfaction (7)§ § § §
Municipal GP Supply
Satisfaction (1)-2.140 0.475 -2.213 0.476
Municipal GP Supply
Satisfaction (2)-1.826 0.339 -1.853 0.340
Municipal GP Supply
Satisfaction (3)-2.259 0.301 -2.295 0.303
Municipal GP Supply
Satisfaction (4)-1.803 0.216 -1.816 0.217
Municipal GP Supply
Satisfaction (5)-1.170 0.190 -1.190 0.190
Municipal GP Supply
Satisfaction (6)-0.746 0.176 -0.757 0.176
Life Satisfaction (3) § § § §
Life Satisfaction (1) -0.674 0.167 -0.684 0.167
Life Satisfaction (2) -0.303 0.143 -0.302 0.143
VariablesBlock 0 Block 1 Block 2 Block 3 Block 2' Block 3'
Regression Summary WTS_2 2010 - N= 1881 (82.5%)

135
Appendix Table 27: Significant Variables in WTS_3 2010
Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E. Coeff. S.E.
Constant -0.125 0.046 0.137 0.129 0.056 0.163 0.857 0.190 -0.024 0.221 0.879 0.250
Age (5) § § § § § § § § § §
Age (1) -0.538 0.304 -0.545 0.306 -0.299 0.317 -0.538 0.305 -0.303 0.317
Age (2) -1.047 0.224 -1.025 0.226 -0.698 0.237 -1.032 0.225 -0.708 0.236
Age (3) -0.421 0.149 -0.431 0.150 -0.177 0.158 -0.432 0.150 -0.176 0.157
Age (4) -0.079 0.122 -0.072 0.123 0.066 0.129 -0.078 0.123 0.057 0.129
Below-median
Income (1)-0.314 0.103 -0.329 0.104 -0.328 0.109 -0.319 0.103 -0.313 0.109
Education level (3) § § § § § § § § § §
Education level (1) 0.256 0.131 0.278 0.134 0.246 0.140 0.290 0.133 0.263 0.139
Education level (2) 0.055 0.112 0.070 0.115 0.071 0.119 0.082 0.114 0.084 0.119
free capacity (3) § § § §
free capacity (1) -0.027 0.200 0.048 0.208
free capacity (2) -0.022 0.151 0.040 0.157
free places per 1000
inhabitants (3)§ § § §
free places per 1000
inhabitants(1)0.012 0.135 0.045 0.141
free places per 1000
inhabitants (2)0.277 0.121 0.341 0.127
GP density (3) § § § §
GP density (1) 0.038 0.148 -0.075 0.156
GP density (2) 0.069 0.128 -0.042 0.134
open lists per 1000
inhabitants (3)§ § § §
open lists per 1000
inhabitants (1)0.026 0.140 0.106 0.146
open lists per 1000
inhabitants (2)0.122 0.132 0.117 0.138
Kommunestr (4) § § § § § § § §
Kommunestr (1) -0.169 0.243 -0.280 0.254 -0.102 0.221 -0.215 0.230
Kommunestr (2) -0.036 0.187 -0.075 0.195 0.019 0.158 -0.002 0.164
Kommunestr (3) 0.080 0.142 0.035 0.148 0.170 0.135 0.148 0.141
Municipal GP Supply
Satisfaction (7)§ § § §
Municipal GP Supply
Satisfaction (1)-1.402 0.505 -1.423 0.503
Municipal GP Supply
Satisfaction (2)-1.810 0.391 -1.784 0.391
Municipal GP Supply
Satisfaction (3)-1.589 0.317 -1.595 0.316
Municipal GP Supply
Satisfaction (4)-1.263 0.197 -1.259 0.196
Municipal GP Supply
Satisfaction (5)-1.098 0.150 -1.081 0.150
Municipal GP Supply
Satisfaction (6)-0.684 0.123 -0.674 0.123
Life Satisfaction (3) § § § §
Life Satisfaction (1) -0.658 0.145 -0.658 0.145
Life Satisfaction (2) -0.349 0.114 -0.345 0.113
Block 3'Variables
Block 0 Block 1 Block 2 Block 3 Block 2'
Regression Summary WTS_3 2010 - N= 1881 (82.5%)

136
GROUP DIFFERENCES 2015
Ranks
Being satisfied with Life N Mean Rank Sum of Ranks
Overall GP Satisfaction ,00 Dissatisfied 331 1791,62 593026,50
1,00 Satisfied 3927 2157,98 8474384,50
Total 4258
Ventetiden for å få time ,00 Dissatisfied 318 1688,68 536999,50
1,00 Satisfied 3768 2073,45 7812741,50
Total 4086
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 538080,500 486278,500
Wilcoxon W 593026,500 536999,500
Z -5,656 -5,726
Asymp. Sig. (2-tailed) ,000 ,000
a. Grouping Variable: Being satisfied with Life
Median Report
Being satisfied with Life
Overall GP
Satisfaction
Ventetiden for å
få time
,00 Dissatisfied 6,0000 5,0000
1,00 Satisfied 6,0000 6,0000
Total 6,0000 6,0000
Ranks
Below median Income N Mean Rank Sum of Ranks
Overall GP Satisfaction ,00 No 1832 1814,89 3324879,50
1,00 Yes 1969 1981,12 3900821,50
Total 3801
Ventetiden for å få time ,00 No 1807 1780,16 3216750,50
1,00 Yes 1842 1868,99 3442674,50
Total 3649

137
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 1645851,500 1583222,500
Wilcoxon W 3324879,500 3216750,500
Z -5,055 -2,610
Asymp. Sig. (2-tailed) ,000 ,009
a. Grouping Variable: Below median Income
Ranks
Below HS Education N Mean Rank Sum of Ranks
Overall GP Satisfaction ,00 Primary Education 781 2358,76 1842190,50
1,00 High School or higher
education
3521 2105,53 7413562,50
Total 4302
Ventetiden for å få time ,00 Primary Education 704 2222,71 1564787,00
1,00 High School or higher
education
3421 2030,13 6945088,00
Total 4125
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 1213081,500 1091757,000
Wilcoxon W 7413562,500 6945088,000
Z -5,601 -4,006
Asymp. Sig. (2-tailed) ,000 ,000
a. Grouping Variable: Below High School Education
Ranks
Avg. Contact Frequency N Mean Rank Sum of Ranks
Overall GP Satisfaction ,00 non-average 1817 2109,79 3833483,50
1,00 average (2-5 times) 2487 2183,71 5430876,50
Total 4304
Ventetiden for å få time ,00 non-average 1741 2061,12 3588402,00
1,00 average (2-5 times) 2375 2056,58 4884384,00
Total 4116

138
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 2181830,500 2062884,000
Wilcoxon W 3833483,500 4884384,000
Z -2,096 -,124
Asymp. Sig. (2-tailed) ,036 ,901
a. Grouping Variable: Average Contact Frequency
Ranks
Public vs Private GP N Mean Rank Sum of Ranks
Overall GP Satisfaction ,00 Private 2117 2061,13 4363405,50
1,00 Public 1836 1880,00 3451675,50
Total 3953
Ventetiden for å få time ,00 Private 2007 1999,55 4013092,50
1,00 Public 1776 1770,46 3144343,50
Total 3783
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 1765309,500 1566367,500
Wilcoxon W 3451675,500 3144343,500
Z -5,417 -6,605
Asymp. Sig. (2-tailed) ,000 ,000
a. Grouping Variable: Public vs Private GP
Ranks
GoodHealth N Mean Rank Sum of Ranks
Overall GP Satisfaction ,00 No 1489 2072,09 3085344,00
1,00 Yes 2847 2218,92 6317272,00
Total 4336
Ventetiden for å få time ,00 No 1442 2016,91 2908387,00
1,00 Yes 2712 2109,72 5721548,00
Total 4154

139
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 1976039,000 1867984,000
Wilcoxon W 3085344,000 2908387,000
Z -3,985 -2,435
Asymp. Sig. (2-tailed) ,000 ,015
a. Grouping Variable: GoodHealth
Ranks
Having no disabilities N Mean Rank Sum of Ranks
Overall GP Satisfaction ,00 Some Disability 892 2065,24 1842191,00
1,00 No Disability 3273 2087,84 6833504,00
Total 4165
Ventetiden for å få time ,00 Some Disability 839 1967,75 1650938,50
1,00 No Disability 3161 2009,19 6351061,50
Total 4000
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 1443913,000 1298558,500
Wilcoxon W 1842191,000 1650938,500
Z -,540 -,947
Asymp. Sig. (2-tailed) ,589 ,344
a. Grouping Variable: Having no disabilities
Ranks
Age group N Mean Rank Sum of Ranks
Overall GP Satisfaction 1,00 Young 755 766,54 578739,00
2,00 Middle-aged 773 762,51 589417,00
Total 1528
Ventetiden for å få time 1,00 Young 771 778,16 599960,00
2,00 Middle-aged 779 772,87 602065,00
Total 1550

140
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 290266,000 298255,000
Wilcoxon W 589417,000 602065,000
Z -,188 -,236
Asymp. Sig. (2-tailed) ,851 ,813
a. Grouping Variable: Age group: young - middle
Ranks
Age group N Mean Rank Sum of Ranks
Overall GP satisfaction 1,00 Young 755 1522,71 1149642,50
3,00 Old 2808 1851,72 5199623,50
Total 3563
Ventetiden for å få time 1,00 Young 771 1413,56 1089857,00
3,00 Old 2604 1769,26 4607143,00
Total 3375
Test Statisticsa
Overall GP
satisfaction
Ventetiden for å
få time
Mann-Whitney U 864252,500 792251,000
Wilcoxon W 1149642,500 1089857,000
Z -8,558 -9,157
Asymp. Sig. (2-tailed) ,000 ,000
a. Grouping Variable: Age group: young - old
Ranks
Age group N Mean Rank Sum of Ranks
Overall GP satisfaction 2,00 Middle-aged 773 1527,20 1180527,00
3,00 Old 2808 1863,62 5233044,00
Total 3581
Ventetiden for å få time 2,00 Middle-aged 779 1413,22 1100896,50
3,00 Old 2604 1775,40 4623139,50
Total 3383

141
Test Statisticsa
Overall GP
satisfaction
Ventetiden for å
få time
Mann-Whitney U 881376,000 797086,500
Wilcoxon W 1180527,000 1100896,500
Z -8,784 -9,335
Asymp. Sig. (2-tailed) ,000 ,000
a. Grouping Variable: Age group: middle - old
Ranks
GP density N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 1503 1407,08 2114842,00
2 Medium 1382 1482,06 2048213,00
Total 2885
Ventetiden for å få time 1 Low 1434 1353,75 1941275,00
2 Medium 1319 1402,28 1849606,00
Total 2753
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 984586,000 912380,000
Wilcoxon W 2114842,000 1941275,000
Z -2,630 -1,643
Asymp. Sig. (2-tailed) ,009 ,100
a. Grouping Variable: GP density: low - medium
Ranks
GP density N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 1503 1467,19 2205185,00
3 High 1442 1479,06 2132800,00
Total 2945
Ventetiden for å få time 1 Low 1434 1421,72 2038745,00
3 High 1392 1405,03 1955806,00
Total 2826

142
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 1074929,000 986278,000
Wilcoxon W 2205185,000 1955806,000
Z -,409 -,556
Asymp. Sig. (2-tailed) ,682 ,578
a. Grouping Variable: GP density: low - high
Ranks
GP density N Mean Rank Sum of Ranks
Overall GP Satisfaction 2 Medium 1382 1444,27 1995981,00
3 High 1442 1382,05 1992919,00
Total 2824
Ventetiden for å få time 2 Medium 1319 1389,39 1832601,00
3 High 1392 1324,36 1843515,00
Total 2711
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 952516,000 873987,000
Wilcoxon W 1992919,000 1843515,000
Z -2,210 -2,218
Asymp. Sig. (2-tailed) ,027 ,027
a. Grouping Variable: GP density: medium - high
Ranks
free capacity/ free GPs N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 1493 1445,96 2158815,00
2 Medium 1421 1469,63 2088340,00
Total 2914
Ventetiden for å få time 1 Low 1441 1349,59 1944763,00
2 Medium 1354 1449,52 1962647,00
Total 2795

143
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 1043544,000 905802,000
Wilcoxon W 2158815,000 1944763,000
Z -,824 -3,355
Asymp. Sig. (2-tailed) ,410 ,001
a. Grouping Variable: free capacity/ free GPs: low -
medium
Ranks
free capacity/ free GPs N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 1493 1445,81 2158589,00
3 High 1413 1461,63 2065282,00
Total 2906
Ventetiden for å få time 1 Low 1441 1384,37 1994882,50
3 High 1350 1408,41 1901353,50
Total 2791
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 1043318,000 955921,500
Wilcoxon W 2158589,000 1994882,500
Z -,552 -,806
Asymp. Sig. (2-tailed) ,581 ,420
a. Grouping Variable: free capacity/ free GPs: low - high
Ranks
free capacity/ free GPs N Mean Rank Sum of Ranks
Overall GP Satisfaction 2 Medium 1421 1421,14 2019434,00
3 High 1413 1413,84 1997761,00
Total 2834
Ventetiden for å få time 2 Medium 1354 1388,91 1880580,00
3 High 1350 1315,99 1776580,00
Total 2704

144
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 998770,000 864655,000
Wilcoxon W 1997761,000 1776580,000
Z -,258 -2,495
Asymp. Sig. (2-tailed) ,796 ,013
a. Grouping Variable: free capacity/ free GPs: medium -
high
Ranks
open lists per 1000
inhabitants N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 1430 1523,85 2179109,00
2 Middle 1532 1441,97 2209094,00
Total 2962
Ventetiden for å få time 1 Low 1362 1409,06 1919139,50
2 Middle 1458 1411,85 2058470,50
Total 2820
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 1034816,000 990936,500
Wilcoxon W 2209094,000 1919139,500
Z -2,834 -,093
Asymp. Sig. (2-tailed) ,005 ,926
a. Grouping Variable: open lists per 1000 inhabitants: low -
middle
Ranks
open lists per 1000
inhabitants N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 1430 1426,03 2039227,50
3 High 1365 1368,63 1868182,50
Total 2795
Ventetiden for å få time 1 Low 1362 1354,61 1844979,50
3 High 1325 1333,09 1766348,50
Total 2687

145
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 935887,500 887873,500
Wilcoxon W 1868182,500 1766348,500
Z -2,051 -,737
Asymp. Sig. (2-tailed) ,040 ,461
a. Grouping Variable: open lists per 1000 inh.: low - high
Ranks
open lists per 1000
inhabitants N Mean Rank Sum of Ranks
Overall GP Satisfaction 2 Middle 1532 1438,80 2204234,50
3 High 1365 1460,45 1993518,50
Total 2897
Ventetiden for å få time 2 Middle 1458 1403,73 2046642,00
3 High 1325 1379,09 1827294,00
Total 2783
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 1029956,500 948819,000
Wilcoxon W 2204234,500 1827294,000
Z -,752 -,828
Asymp. Sig. (2-tailed) ,452 ,407
a. Grouping Variable: open lists per 1000 inhabitants:
middle - high
Ranks
free places per 1000
inhabitants N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 1320 1582,30 2088636,50
2 Middle 1792 1537,50 2755191,50
Total 3112
Ventetiden for å få time 1 Low 1271 1481,83 1883405,00
2 Middle 1709 1496,95 2558285,00
Total 2980

146
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 1148663,500 1075049,000
Wilcoxon W 2755191,500 1883405,000
Z -1,493 -,486
Asymp. Sig. (2-tailed) ,136 ,627
a. Grouping Variable: free places per 1000 inhabitants: low - middle - middle
Ranks
free places per 1000
inhabitants N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 1320 1270,78 1677429,50
3 High 1215 1264,98 1536950,50
Total 2535
Ventetiden for å få time 1 Low 1271 1204,05 1530353,00
3 High 1165 1234,26 1437913,00
Total 2436
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 798230,500 721997,000
Wilcoxon W 1536950,500 1530353,000
Z -,217 -1,086
Asymp. Sig. (2-tailed) ,828 ,278
a. Grouping Variable: free places per 1000 inhabitants: low
- high
Ranks
free places per 1000
inhabitants N Mean Rank Sum of Ranks
Overall GP Satisfaction 2 Middle 1792 1489,22 2668676,00
3 High 1215 1525,80 1853852,00
Total 3007
Ventetiden for å få time 2 Middle 1709 1428,77 2441763,00
3 High 1165 1450,31 1689612,00
Total 2874

147
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 1062148,000 980568,000
Wilcoxon W 2668676,000 2441763,000
Z -1,230 -,701
Asymp. Sig. (2-tailed) ,219 ,483
a. Grouping Variable: free places per 1000 inhabitants:
middle - high
Ranks
Open list ratio N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 1431 1475,74 2111785,50
2 Middle 1443 1399,58 2019589,50
Total 2874
Ventetiden for å få time 1 Low 1359 1370,82 1862948,50
2 Middle 1375 1364,22 1875796,50
Total 2734
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 977743,500 929796,500
Wilcoxon W 2019589,500 1875796,500
Z -2,678 -,224
Asymp. Sig. (2-tailed) ,007 ,822
a. Grouping Variable: Open list ratio: low - middle
Ranks
Open list ratio N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 1431 1469,63 2103042,50
3 High 1453 1415,78 2057127,50
Total 2884
Ventetiden for å få time 1 Low 1359 1386,76 1884604,00
3 High 1411 1384,29 1953231,00
Total 2770

148
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 1000796,500 957065,000
Wilcoxon W 2057127,500 1953231,000
Z -1,894 -,083
Asymp. Sig. (2-tailed) ,058 ,934
a. Grouping Variable: Open list ratio: low - high
Ranks
Open list ratio N Mean Rank Sum of Ranks
Overall GP Satisfaction 2 Middle 1443 1436,83 2073348,00
3 High 1453 1460,09 2121508,00
Total 2896
Ventetiden for å få time 2 Middle 1375 1391,20 1912902,50
3 High 1411 1395,74 1969388,50
Total 2786
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 1031502,000 966902,500
Wilcoxon W 2073348,000 1912902,500
Z -,809 -,153
Asymp. Sig. (2-tailed) ,418 ,879
a. Grouping Variable: Open list ratio: middle - high
Ranks
Kommunestr N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Under 5 000 innbyggere 428 769,37 329289,50
2 5 000 - 20 000 innbyggere 1206 834,58 1006505,50
Total 1634
Ventetiden for å få time 1 Under 5 000 innbyggere 415 764,75 317373,00
2 5 000 - 20 000 innbyggere 1163 798,33 928458,00
Total 1578

149
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 237483,500 231053,000
Wilcoxon W 329289,500 317373,000
Z -2,659 -1,318
Asymp. Sig. (2-tailed) ,008 ,188
a. Grouping Variable: Kommunestr: under 5000 inh. – btw
5000 & 20 000 inh.
Ranks
Kommunestr N Mean Rank Sum of Ranks
Overall GP Satisfaction 2 5 000 - 20 000 innbyggere 1206 1379,87 1664128,00
3 20 000 - 110 000
innbyggere
1574 1398,64 2201462,00
Total 2780
Ventetiden for å få time 2 5 000 - 20 000 innbyggere 1163 1283,25 1492418,50
3 20 000 - 110 000
innbyggere
1492 1362,88 2033421,50
Total 2655
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 936307,000 815552,500
Wilcoxon W 1664128,000 1492418,500
Z -,668 -2,727
Asymp. Sig. (2-tailed) ,504 ,006
a. Grouping Variable: Kommunestr: (5000 – 20 000) vs. (20
000 – 100 000)

150
Ranks
Kommunestr N Mean Rank Sum of Ranks
Overall GP Satisfaction 3 20 000 - 110 000
innbyggere
1574 1372,52 2160345,00
4 110 000 innbyggere eller
fler
1128 1322,17 1491408,00
Total 2702
Ventetiden for å få time 3 20 000 - 110 000
innbyggere
1492 1318,80 1967643,50
4 110 000 innbyggere eller
fler
1084 1246,80 1351532,50
Total 2576
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 854652,000 763462,500
Wilcoxon W 1491408,000 1351532,500
Z -1,802 -2,492
Asymp. Sig. (2-tailed) ,072 ,013
a. Grouping Variable: Kommunestr: (20 000 – 110 000) vs
(110 000 +)
Ranks
Kommunestr N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Under 5 000 innbyggere 428 747,20 319803,50
4 110 000 innbyggere eller
fler
1128 790,37 891542,50
Total 1556
Ventetiden for å få time 1 Under 5 000 innbyggere 415 725,69 301162,50
4 110 000 innbyggere eller
fler
1084 759,31 823087,50
Total 1499

151
Test Statistic
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 227997,500 214842,500
Wilcoxon W 319803,500 301162,500
Z -1,822 -1,376
Asymp. Sig. (2-tailed) ,068 ,169
a. Grouping Variable: Kommunestr: under 5000 vs 110 000
or more
Median Report
Below High School
Education
Overall GP
Satisfaction
Ventetiden for å
få time
,00 Primary Education 7,0000 6,0000
1,00 High School or higher
education
6,0000 6,0000
Total 6,0000 6,0000
Median Report
Below median Income
Overall GP
Satisfaction
Ventetiden for å
få time
,00 No 6,0000 6,0000
1,00 Yes 7,0000 6,0000
Total 6,0000 6,0000
Median Report
Avg. Contact Frequency
Overall GP
Satisfaction
Ventetiden for å
få time
,00 non-average 6,0000 6,0000
1,00 average (2-5 times) 6,0000 6,0000
Total 6,0000 6,0000

152
Median Report
Public vs Private GP
Overall GP
Satisfaction
Ventetiden for å
få time
,00 Private 7,0000 6,0000
1,00 Public 6,0000 5,0000
Total 6,0000 6,0000
Median Report
GoodHealth
Overall GP
Satisfaction
Ventetiden for å
få time
,00 No 6,0000 6,0000
1,00 Yes 6,9159 6,0000
Total 6,0000 6,0000
Median Report
Having no disabilities
Overall GP
Satisfaction
Ventetiden for å
få time
,00 Some Disability 6,0000 6,0000
1,00 No Disability 6,0000 6,0000
Total 6,0000 6,0000
Median Report
Age group
Overall GP
Satisfaction
Ventetiden for å
få time
1,00 Young 6,0000 5,0000
2,00 Middle-aged 6,0000 5,0000
3,00 Old 7,0000 6,0000
Total 6,0000 6,0000

153
Median Report
GP density
Overall GP
Satisfaction
Ventetiden for å
få time
1 Low 6,0000 6,0000
2 Medium 7,0000 6,0000
3 High 6,0000 6,0000
Total 6,0000 6,0000
Median Report
free capacity/ free GPs
Overall GP
Satisfaction
Ventetiden for å
få time
1 Low 6,0000 6,0000
2 Medium 6,0000 6,0000
3 High 6,0000 6,0000
Total 6,0000 6,0000
Median Report
free places per 1000
inhabitants
Overall GP
Satisfaction
Ventetiden for å
få time
1 Low 7,0000 6,0000
2 Middle 6,0000 6,0000
3 High 6,0000 6,0000
Total 6,0000 6,0000
Median Report
open lists per 1000
inhabitants
Overall GP
Satisfaction
Ventetiden for å
få time
1 Low 7,0000 6,0000
2 Middle 6,0000 6,0000
3 High 6,0000 6,0000
Total 6,0000 6,0000

154
Median Report
Open list ratio
Overall GP
Satisfaction
Ventetiden for å
få time
1 Low 7,0000 6,0000
2 Middle 6,0000 6,0000
3 High 6,0000 6,0000
Total 6,0000 6,0000
Median Report
Kommunestr
Overall GP
Satisfaction
Ventetiden for å
få time
1 Under 5 000 innbyggere 6,0000 5,0000
2 5 000 - 20 000 innbyggere 6,0000 6,0000
3 20 000 - 110 000
innbyggere
7,0000 6,0000
4 110 000 innbyggere eller
fler
6,0000 6,0000
Total 6,0000 6,0000
GROUP DIFFERENCES 2013
Ranks
Being satisfied with Life N Mean Rank Sum of Ranks
Overall GP Satisfaction ,00 Dissatisfied 265 1410,98 373910,00
1,00 Satisfied 3278 1801,19 5904286,00
Total 3543
Ventetiden for å få time ,00 Dissatisfied 270 1495,04 403659,50
1,00 Satisfied 3203 1757,40 5628941,50
Total 3473

155
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 338665,000 367074,500
Wilcoxon W 373910,000 403659,500
Z -6,430 -4,228
Asymp. Sig. (2-tailed) ,000 ,000
a. Grouping Variable: Being satisfied with Life
Ranks
Below median Income N Mean Rank Sum of Ranks
Overall GP Satisfaction ,00 No 1458 1475,57 2151381,00
1,00 Yes 1685 1655,44 2789415,00
Total 3143
Ventetiden for å få time ,00 No 1437 1473,50 2117422,00
1,00 Yes 1652 1607,19 2655083,00
Total 3089
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 1087770,000 1084219,000
Wilcoxon W 2151381,000 2117422,000
Z -5,959 -4,254
Asymp. Sig. (2-tailed) ,000 ,000
b. Grouping Variable: Below median Income
Ranks
Below High School
Education N Mean Rank Sum of Ranks
Overall GP Satisfaction ,00 Primary Education 695 2021,34 1404833,00
1,00 High School or higher
education
2846 1709,87 4866278,00
Total 3541
Ventetiden for å få time ,00 Primary Education 677 1958,65 1326009,00
1,00 High School or higher
education
2798 1684,61 4713541,00
Total 3475

156
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 814997,000 797740,000
Wilcoxon W 4866278,000 4713541,000
Z -7,746 -6,531
Asymp. Sig. (2-tailed) ,000 ,000
a. Grouping Variable: Below High School Education
Ranks
Avg. Contact Frequency N Mean Rank Sum of Ranks
Overall GP Satisfaction ,00 non-average 1500 1774,59 2661888,00
1,00 average (2-5 times) 2076 1798,55 3733788,00
Total 3576
Ventetiden for å få time ,00 non-average 1467 1768,33 2594139,50
1,00 average (2-5 times) 2045 1748,01 3574688,50
Total 3512
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 1536138,000 1482653,500
Wilcoxon W 2661888,000 3574688,500
Z -,737 -,600
Asymp. Sig. (2-tailed) ,461 ,549
a. Grouping Variable: Average Contact Frequency
Ranks
Public vs Private GP N Mean Rank Sum of Ranks
Overall GP Satisfaction ,00 Private 1673 1743,64 2917118,00
1,00 Public 1636 1564,35 2559277,00
Total 3309
Ventetiden for å få time ,00 Private 1642 1742,30 2860857,50
1,00 Public 1607 1505,14 2418767,50
Total 3249

157
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 1220211,000 1126739,500
Wilcoxon W 2559277,000 2418767,500
Z -5,830 -7,379
Asymp. Sig. (2-tailed) ,000 ,000
a. Grouping Variable: Public vs Private GP
Ranks
GoodHealth N Mean Rank Sum of Ranks
Overall GP Satisfaction ,00 No 1169 1729,58 2021882,50
1,00 Yes 2429 1833,15 4452718,50
Total 3598
Ventetiden for å få time ,00 No 1156 1702,44 1968024,50
1,00 Yes 2370 1793,28 4250076,50
Total 3526
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 1338017,500 1299278,500
Wilcoxon W 2021882,500 1968024,500
Z -3,016 -2,547
Asymp. Sig. (2-tailed) ,003 ,011
a. Grouping Variable: GoodHealth
Ranks
Age group N Mean Rank Sum of Ranks
Overall GP Satisfaction 1,00 Young 682 673,27 459169,00
2,00 Middle-aged 713 721,66 514541,00
Total 1395
Ventetiden for å få time 1,00 Young 674 671,00 452256,50
2,00 Middle-aged 710 712,91 506163,50
Total 1384

158
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 226266,000 224781,500
Wilcoxon W 459169,000 452256,500
Z -2,347 -1,979
Asymp. Sig. (2-tailed) ,019 ,048
a. Grouping Variable: Age group: young - middle
Ranks
Age group N Mean Rank Sum of Ranks
Overall GP Satisfaction 1,00 Young 682 1142,05 778877,00
3,00 Old 2203 1536,17 3384178,00
Total 2885
Ventetiden for å få time 1,00 Young 674 1097,22 739525,00
3,00 Old 2142 1506,45 3226811,00
Total 2816
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 545974,000 512050,000
Wilcoxon W 778877,000 739525,000
Z -11,733 -11,703
Asymp. Sig. (2-tailed) ,000 ,000
a. Grouping Variable: Age group: young - old
Ranks
Age group N Mean Rank Sum of Ranks
Overall GP Satisfaction 2,00 Middle-aged 713 1227,98 875552,00
3,00 Old 2203 1533,11 3377434,00
Total 2916
Ventetiden for å få time 2,00 Middle-aged 710 1184,49 840986,50
3,00 Old 2142 1506,72 3227391,50
Total 2852

159
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 621011,000 588581,500
Wilcoxon W 875552,000 840986,500
Z -9,181 -9,291
Asymp. Sig. (2-tailed) ,000 ,000
a. Grouping Variable: Age group: middle-aged vs old
Ranks
GP density N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 1164 1171,97 1364168,50
2 Middle 1197 1189,78 1424172,50
Total 2361
Ventetiden for å få time 1 Low 1138 1164,47 1325172,50
2 Middle 1179 1153,72 1360230,50
Total 2317
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 686138,500 664620,500
Wilcoxon W 1364168,500 1360230,500
Z -,684 -,396
Asymp. Sig. (2-tailed) ,494 ,692
a. Grouping Variable: GP density: low – middle
Ranks
GP density N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 1164 1182,23 1376115,00
3 High 1211 1193,55 1445385,00
Total 2375
Ventetiden for å få time 1 Low 1138 1169,78 1331208,50
3 High 1183 1152,55 1363472,50
Total 2321

160
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 698085,000 663136,500
Wilcoxon W 1376115,000 1363472,500
Z -,432 -,634
Asymp. Sig. (2-tailed) ,665 ,526
a. Grouping Variable: GP density: low - high
Ranks
GP density N Mean Rank Sum of Ranks
Overall GP Satisfaction 2 Middle 1197 1207,75 1445678,50
3 High 1211 1201,29 1454757,50
Total 2408
Ventetiden for å få time 2 Middle 1179 1184,83 1396912,00
3 High 1183 1178,18 1393791,00
Total 2362
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 720891,500 693455,000
Wilcoxon W 1454757,500 1393791,000
Z -,246 -,243
Asymp. Sig. (2-tailed) ,806 ,808
a. Grouping Variable: GP density: middle - high
Ranks
free capacity (open lists) N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 1256 1196,50 1502806,00
2 Middle 1169 1230,73 1438719,00
Total 2425
Ventetiden for å få time 1 Low 1230 1156,41 1422383,50
2 Middle 1144 1220,93 1396741,50
Total 2374

161
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 713410,000 665318,500
Wilcoxon W 1502806,000 1422383,500
Z -1,298 -2,348
Asymp. Sig. (2-tailed) ,194 ,019
a. Grouping Variable: free capacity (open lists): low - middle
Ranks
free capacity (open lists) N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 1256 1210,64 1520563,50
3 High 1147 1192,54 1367842,50
Total 2403
Ventetiden for å få time 1 Low 1230 1164,74 1432632,00
3 High 1126 1193,53 1343914,00
Total 2356
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 709464,500 675567,000
Wilcoxon W 1367842,500 1432632,000
Z -,686 -1,049
Asymp. Sig. (2-tailed) ,493 ,294
a. Grouping Variable: free capacity (open lists): low - high
Ranks
free capacity (open lists) N Mean Rank Sum of Ranks
Overall GP Satisfaction 2 Middle 1169 1183,04 1382970,50
3 High 1147 1133,49 1300115,50
Total 2316
Ventetiden for å få time 2 Middle 1144 1152,79 1318793,00
3 High 1126 1117,93 1258792,00
Total 2270

162
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 641737,500 624291,000
Wilcoxon W 1300115,500 1258792,000
Z -1,921 -1,299
Asymp. Sig. (2-tailed) ,055 ,194
a. Grouping Variable: free capacity (open lists): middle - high
Ranks
open lists per 1000
inhabitants N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 1064 1206,14 1283337,50
2 Middle 1319 1180,59 1557198,50
Total 2383
Ventetiden for å få time 1 Low 1041 1172,50 1220573,00
2 Middle 1285 1156,21 1485728,00
Total 2326
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 686658,500 659473,000
Wilcoxon W 1557198,500 1485728,000
Z -,969 -,596
Asymp. Sig. (2-tailed) ,333 ,551
a. Grouping Variable: open lists per 1000 inhabitants
Ranks
open lists per 1000
inhabitants N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 1064 1124,83 1196821,00
3 High 1189 1128,94 1342310,00
Total 2253
Ventetiden for å få time 1 Low 1041 1112,85 1158476,50
3 High 1174 1103,70 1295743,50
Total 2215

163
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 630241,000 606018,500
Wilcoxon W 1196821,000 1295743,500
Z -,162 -,344
Asymp. Sig. (2-tailed) ,872 ,731
a. Grouping Variable: open lists per 1000 inhabitants
Ranks
open lists per 1000
inhabitants N Mean Rank Sum of Ranks
Overall GP Satisfaction 2 Middle 1319 1239,78 1635268,00
3 High 1189 1270,83 1511018,00
Total 2508
Ventetiden for å få time 2 Middle 1285 1226,87 1576527,50
3 High 1174 1233,43 1448042,50
Total 2459
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 764728,000 750272,500
Wilcoxon W 1635268,000 1576527,500
Z -1,154 -,234
Asymp. Sig. (2-tailed) ,249 ,815
a. Grouping Variable: open lists per 1000 inhabitants
Ranks
free places per 1000
inhabitants N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 1217 1327,01 1614975,00
2 Middle 1388 1281,95 1779340,00
Total 2605
Ventetiden for å få time 1 Low 1202 1247,00 1498889,50
2 Middle 1354 1306,47 1768956,50
Total 2556

164
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 815374,000 775886,500
Wilcoxon W 1779340,000 1498889,500
Z -1,641 -2,081
Asymp. Sig. (2-tailed) ,101 ,037
a. Grouping Variable: free places per 1000 inhabitants: low -
middle
Ranks
free places per 1000
inhabitants N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 1217 1092,38 1329422,00
3 High 967 1092,66 1056598,00
Total 2184
Ventetiden for å få time 1 Low 1202 1048,08 1259793,50
3 High 944 1105,87 1043937,50
Total 2146
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 588269,000 536790,500
Wilcoxon W 1329422,000 1259793,500
Z -,011 -2,194
Asymp. Sig. (2-tailed) ,991 ,028
a. Grouping Variable: free places per 1000 inhabitants: low -
high
Ranks
free places per 1000
inhabitants N Mean Rank Sum of Ranks
Overall GP Satisfaction 2 Middle 1388 1161,24 1611805,00
3 High 967 1202,05 1162385,00
Total 2355
Ventetiden for å få time 2 Middle 1354 1145,89 1551536,00
3 High 944 1154,68 1090015,00
Total 2298

165
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 647839,000 634201,000
Wilcoxon W 1611805,000 1551536,000
Z -1,540 -,320
Asymp. Sig. (2-tailed) ,124 ,749
a. Grouping Variable: free places per 1000 inhabitants:
middle - high
Ranks
open list ratio N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 1234 1272,37 1570098,50
2 middle 1284 1247,14 1601322,50
Total 2518
Ventetiden for å få time 1 Low 1202 1237,34 1487277,50
2 middle 1255 1221,02 1532375,50
Total 2457
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 776352,500 744235,500
Wilcoxon W 1601322,500 1532375,500
Z -,936 -,584
Asymp. Sig. (2-tailed) ,349 ,559
a. Grouping Variable: open list ratio
Ranks
open list ratio N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 1234 1144,00 1411691,50
3 High 1054 1145,09 1206924,50
Total 2288
Ventetiden for å få time 1 Low 1202 1120,86 1347278,50
3 High 1043 1125,46 1173856,50
Total 2245

166
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 649696,500 624275,500
Wilcoxon W 1411691,500 1347278,500
Z -,043 -,172
Asymp. Sig. (2-tailed) ,966 ,864
a. Grouping Variable: open list ratio
Ranks
open list ratio N Mean Rank Sum of Ranks
Overall GP Satisfaction 2 middle 1284 1158,52 1487536,50
3 High 1054 1182,88 1246754,50
Total 2338
Ventetiden for å få time 2 middle 1255 1140,54 1431374,50
3 High 1043 1160,28 1210176,50
Total 2298
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 662566,500 643234,500
Wilcoxon W 1487536,500 1431374,500
Z -,934 -,727
Asymp. Sig. (2-tailed) ,350 ,467
a. Grouping Variable: open list ratio
Ranks
Kommunestr_i N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Under 5 000 innbyggere 423 710,03 300341,50
2 5 000 - 20 000 innbyggere 1036 738,15 764728,50
Total 1459
Ventetiden for å få time 1 Under 5 000 innbyggere 416 713,89 296979,00
2 5 000 - 20 000 innbyggere 1015 716,86 727617,00
Total 1431

167
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 210665,500 210243,000
Wilcoxon W 300341,500 296979,000
Z -1,246 -,126
Asymp. Sig. (2-tailed) ,213 ,900
a. Grouping Variable: Kommunestr_i
Ranks
Kommunestr_i N Mean Rank Sum of Ranks
Overall GP Satisfaction 2 5 000 - 20 000 innbyggere 1036 1155,59 1197190,50
3 20 000 - 110 000
innbyggere
1294 1173,43 1518424,50
Total 2330
Ventetiden for å få time 2 5 000 - 20 000 innbyggere 1015 1107,75 1124367,50
3 20 000 - 110 000
innbyggere
1268 1169,42 1482818,50
Total 2283
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 660024,500 608747,500
Wilcoxon W 1197190,500 1124367,500
Z -,690 -2,278
Asymp. Sig. (2-tailed) ,490 ,023
a. Grouping Variable: Kommunestr_i

168
Ranks
Kommunestr_i N Mean Rank Sum of Ranks
Overall GP Satisfaction 3 20 000 - 110 000
innbyggere
1294 1101,73 1425643,00
4 110 000 innbyggere eller
fler
845 1021,40 863087,00
Total 2139
Ventetiden for å få time 3 20 000 - 110 000
innbyggere
1268 1064,12 1349303,50
4 110 000 innbyggere eller
fler
827 1023,28 846256,50
Total 2095
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 505652,000 503878,500
Wilcoxon W 863087,000 846256,500
Z -3,166 -1,549
Asymp. Sig. (2-tailed) ,002 ,121
a. Grouping Variable: Kommunestr_i
Ranks
Kommunestr_i N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Under 5 000 innbyggere 423 643,65 272263,50
4 110 000 innbyggere eller
fler
845 629,92 532282,50
Total 1268
Ventetiden for å få time 1 Under 5 000 innbyggere 416 613,06 255031,50
4 110 000 innbyggere eller
fler
827 626,50 518114,50
Total 1243

169
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 174847,500 168295,500
Wilcoxon W 532282,500 255031,500
Z -,671 -,637
Asymp. Sig. (2-tailed) ,502 ,524
a. Grouping Variable: Kommunestr_i
Median Report
Being satisfied with Life
Overall GP
Satisfaction
Ventetiden for å
få time
,00 Dissatisfied 6,0000 5,0000
1,00 Satisfied 6,0000 6,0000
Total 6,0000 6,0000
Median Report
Below High School
Education
Overall GP
Satisfaction
Ventetiden for å
få time
,00 Primary Education 7,0000 6,0000
1,00 High School or higher
education
6,0000 6,0000
Total 6,0000 6,0000
Median Report
Below median Income
Overall GP
Satisfaction
Ventetiden for å
få time
,00 No 6,0000 5,0000
1,00 Yes 7,0000 6,0000
Total 6,0000 6,0000

170
Median Report
Average Contact
Frequency
Overall GP
Satisfaction
Ventetiden for å
få time
,00 non-average 6,0000 6,0000
1,00 average (2-5 times) 6,0000 6,0000
Total 6,0000 6,0000
Median Report
Public vs Private GP
Overall GP
Satisfaction
Ventetiden for å
få time
,00 Private 7,0000 6,0000
1,00 Public 6,0000 5,0000
Total 6,0000 6,0000
Median Report
GoodHealth
Overall GP
Satisfaction
Ventetiden for å
få time
,00 No 6,0000 6,0000
1,00 Yes 6,0000 6,0000
Total 6,0000 6,0000
Median Report
Age group
Overall GP
Satisfaction
Ventetiden for å
få time
1,00 Young 6,0000 5,0000
2,00 Middle-aged 6,0000 5,0000
3,00 Old 7,0000 6,0000
Total 6,0000 6,0000
Median Report
GP density
Overall GP
Satisfaction
Ventetiden for å
få time
1 Low 6,0000 6,0000
2 Middle 6,0000 6,0000
3 High 6,0000 6,0000
Total 6,0000 6,0000

171
Median Report
free capacity (open lists)
Overall GP
Satisfaction
Ventetiden for å
få time
1 Low 6,0000 6,0000
2 Middle 6,0000 6,0000
3 High 6,0000 6,0000
Total 6,0000 6,0000
Median Report
free places per 1000
inhabitants
Overall GP
Satisfaction
Ventetiden for å
få time
1 Low 6,0000 6,0000
2 Middle 6,0000 6,0000
3 High 6,0000 6,0000
Total 6,0000 6,0000
Median Report
open lists per 1000
inhabitants
Overall GP
Satisfaction
Ventetiden for å
få time
1 Low 6,0000 6,0000
2 Middle 6,0000 6,0000
3 High 6,0000 6,0000
Total 6,0000 6,0000
Median Report
open list ratio
Overall GP
Satisfaction
Ventetiden for å
få time
1 Low 6,0000 6,0000
2 middle 6,0000 6,0000
3 High 6,0000 6,0000
Total 6,0000 6,0000

172
Median Report
Kommunestr_i
Overall GP
Satisfaction
Ventetiden for å
få time
1 Under 5 000 innbyggere 6,0000 6,0000
2 5 000 - 20 000 innbyggere 6,0000 6,0000
3 20 000 - 110 000
innbyggere
6,0000 6,0000
4 110 000 innbyggere eller
fler
6,0000 6,0000
Total 6,0000 6,0000
GROUP DIFFERENCES 2010
Ranks
Being satisfied with Life N Mean Rank Sum of Ranks
Overall GP Satisfaction ,00 Dissatisfied 134 890,19 119286,00
1,00 Satisfied 2017 1088,34 2195190,00
Total 2151
Ventetiden for å få time ,00 Dissatisfied 138 963,93 133022,50
1,00 Satisfied 1990 1071,47 2132233,50
Total 2128
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 110241,000 123431,500
Wilcoxon W 119286,000 133022,500
Z -3,839 -2,028
Asymp. Sig. (2-tailed) ,000 ,043
a. Grouping Variable: Being satisfied with Life

173
Median Report
Being satisfied with Life
Overall GP
Satisfaction
Ventetiden for å
få time
,00 Dissatisfied 6,0000 5,0000
1,00 Satisfied 6,0000 6,0000
Total 6,0000 6,0000
Ranks
Below median Income N Mean Rank Sum of Ranks
Overall GP Satisfaction ,00 No 941 946,67 890817,50
1,00 Yes 1070 1058,18 1132248,50
Total 2011
Ventetiden for å få time ,00 No 939 939,21 881922,50
1,00 Yes 1057 1051,17 1111083,50
Total 1996
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 447606,500 440592,500
Wilcoxon W 890817,500 881922,500
Z -4,610 -4,416
Asymp. Sig. (2-tailed) ,000 ,000
a. Grouping Variable: Below median Income
Median Report
Below median Income
Overall GP
Satisfaction
Ventetiden for å
få time
,00 No 6,0000 5,0000
1,00 Yes 7,0000 6,0000
Total 6,0000 5,0000

174
Ranks
Below High School
Education N Mean Rank Sum of Ranks
Overall GP Satisfaction ,00 Primary Education 592 1202,23 711722,00
1,00 High School or higher
education
1601 1058,09 1693999,00
Total 2193
Ventetiden for å få time ,00 Primary Education 582 1193,12 694394,00
1,00 High School or higher
education
1588 1046,06 1661141,00
Total 2170
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 411598,000 399475,000
Wilcoxon W 1693999,000 1661141,000
Z -5,079 -4,941
Asymp. Sig. (2-tailed) ,000 ,000
a. Grouping Variable: Below High School Education
Median Report
Below High School
Education
Overall GP
Satisfaction
Ventetiden for å
få time
,00 Primary Education 7,0000 6,0000
1,00 High School or higher
education
6,0000 5,0000
Total 6,0000 6,0000
Ranks
Age group N Mean Rank Sum of Ranks
Overall GP Satisfaction 1,00 Young 239 307,55 73503,50
2,00 Middle-aged 416 339,75 141336,50
Total 655
Ventetiden for å få time 1,00 Young 241 305,26 73567,50
2,00 Middle-aged 411 338,95 139310,50
Total 652

175
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 44823,500 44406,500
Wilcoxon W 73503,500 73567,500
Z -2,189 -2,231
Asymp. Sig. (2-tailed) ,029 ,026
a. Grouping Variable: Age group: young – middle-aged
Median Report
Age group
Overall GP
Satisfaction
Ventetiden for å
få time
1,00 Young 6,0000 4,0000
2,00 Middle-aged 6,0000 5,0000
3,00 Old 7,0000 6,0000
Total 6,0000 6,0000
Ranks
Age group N Mean Rank Sum of Ranks
Overall GP Satisfaction 1,00 Young 239 701,62 167686,50
3,00 Old 1558 929,28 1447816,50
Total 1797
Ventetiden for å få time 1,00 Young 241 623,98 150379,50
3,00 Old 1539 932,24 1434710,50
Total 1780
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 139006,500 121218,500
Wilcoxon W 167686,500 150379,500
Z -6,827 -8,860
Asymp. Sig. (2-tailed) ,000 ,000
a. Grouping Variable: Age group: young – old

176
Ranks
Age group N Mean Rank Sum of Ranks
Overall GP Satisfaction 2,00 Middle-aged 416 868,29 361207,00
3,00 Old 1558 1019,33 1588118,00
Total 1974
Ventetiden for å få time 2,00 Middle-aged 411 778,40 319923,00
3,00 Old 1539 1028,14 1582302,00
Total 1950
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 274471,000 235257,000
Wilcoxon W 361207,000 319923,000
Z -5,193 -8,170
Asymp. Sig. (2-tailed) ,000 ,000
a. Grouping Variable: Age group: middle-aged vs old
Ranks
GP density N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 634 740,73 469623,00
2 Middle 849 742,95 630763,00
Total 1483
Ventetiden for å få time 1 Low 621 708,72 440114,50
2 Middle 837 744,92 623496,50
Total 1458
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 268328,000 246983,500
Wilcoxon W 469623,000 440114,500
Z -,106 -1,656
Asymp. Sig. (2-tailed) ,916 ,098
a. Grouping Variable: GP density: low vs middle

177
Median Report
GP density
Overall GP
Satisfaction
Ventetiden for å
få time
1 Low 6,0000 5,0000
2 Middle 6,0000 6,0000
3 High 6,0000 6,0000
Total 6,0000 6,0000
Ranks
GP density N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 634 684,04 433682,00
3 High 727 678,35 493159,00
Total 1361
Ventetiden for å få time 1 Low 621 669,16 415550,50
3 High 729 680,90 496374,50
Total 1350
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 228531,000 222419,500
Wilcoxon W 493159,000 415550,500
Z -,286 -,562
Asymp. Sig. (2-tailed) ,775 ,574
a. Grouping Variable: GP density: low vs high
Ranks
GP density N Mean Rank Sum of Ranks
Overall GP Satisfaction 2 Middle 849 792,82 673101,00
3 High 727 783,46 569575,00
Total 1576
Ventetiden for å få time 2 Middle 837 795,27 665637,50
3 High 729 769,99 561323,50
Total 1566

178
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 304947,000 295238,500
Wilcoxon W 569575,000 561323,500
Z -,437 -1,126
Asymp. Sig. (2-tailed) ,662 ,260
a. Grouping Variable: GP density: middle vs high
Ranks
free capacity N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 793 752,61 596818,00
2 Middle 715 756,60 540968,00
Total 1508
Ventetiden for å få time 1 Low 796 736,62 586353,00
2 Middle 703 765,15 537897,00
Total 1499
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 281997,000 269147,000
Wilcoxon W 596818,000 586353,000
Z -,191 -1,297
Asymp. Sig. (2-tailed) ,849 ,195
a. Grouping Variable: free capacity: low vs middle
Median Report
free capacity
Overall GP
Satisfaction
Ventetiden for å
få time
1 Low 6,0000 5,0000
2 Middle 6,0000 6,0000
3 High 6,0000 6,0000
Total 6,0000 6,0000

179
Ranks
free capacity N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 793 741,56 588054,50
3 High 702 755,28 530205,50
Total 1495
Ventetiden for å få time 1 Low 796 715,00 569139,00
3 High 688 774,32 532731,00
Total 1484
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 273233,500 251933,000
Wilcoxon W 588054,500 569139,000
Z -,659 -2,712
Asymp. Sig. (2-tailed) ,510 ,007
a. Grouping Variable: free capacity: low vs high
Ranks
free capacity N Mean Rank Sum of Ranks
Overall GP Satisfaction 2 Middle 715 704,54 503747,50
3 High 702 713,54 500905,50
Total 1417
Ventetiden for å få time 2 Middle 703 680,81 478608,00
3 High 688 711,52 489528,00
Total 1391
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 247777,500 231152,000
Wilcoxon W 503747,500 478608,000
Z -,445 -1,457
Asymp. Sig. (2-tailed) ,656 ,145
a. Grouping Variable: free capacity: middle vs high

180
Ranks
Open Lists per inhabitants N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 720 742,83 534835,00
2 Medium 773 750,89 580436,00
Total 1493
Ventetiden for å få time 1 Low 705 719,57 507293,50
2 Medium 763 748,30 570952,50
Total 1468
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 275275,000 258428,500
Wilcoxon W 534835,000 507293,500
Z -,388 -1,324
Asymp. Sig. (2-tailed) ,698 ,186
a. Grouping Variable: Open Lists per inhabitants: low vs
middle
Median Report
List Places Per Thousand
Inhabitants
Overall GP
Satisfaction
Ventetiden for å
få time
1 Low 6,0000 5,0000
2 Medium 7,0000 6,0000
3 High 6,0000 6,0000
Total 6,0000 6,0000
Ranks
Open Lists per inhabitants N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 720 715,42 515103,00
3 High 717 722,59 518100,00
Total 1437
Ventetiden for å få time 1 Low 705 709,47 500175,50
3 High 719 715,47 514424,50
Total 1424

181
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 255543,000 251310,500
Wilcoxon W 515103,000 500175,500
Z -,352 -,281
Asymp. Sig. (2-tailed) ,725 ,779
a. Grouping Variable: Open Lists per inhabitants: low vs
high
Ranks
Open Lists per inhabitants N Mean Rank Sum of Ranks
Overall GP Satisfaction 2 Medium 773 746,21 576821,00
3 High 717 744,73 533974,00
Total 1490
Ventetiden for å få time 2 Medium 763 752,88 574444,50
3 High 719 729,43 524458,50
Total 1482
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 276571,000 265618,500
Wilcoxon W 533974,000 524458,500
Z -,071 -1,076
Asymp. Sig. (2-tailed) ,943 ,282
a. Grouping Variable: Open Lists per inhabitants: medium
– high
Median Report
Open Lists per inhabitants
Overall GP
Satisfaction
Ventetiden for å
få time
1 Low 6,0000 5,0000
2 Medium 6,0000 6,0000
3 High 6,0000 6,0000
Total 6,0000 6,0000

182
Ranks
List Places Per Thousand
Inhabitants N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 731 688,12 503012,50
2 Medium 692 737,23 510163,50
Total 1423
Ventetiden for å få time 1 Low 723 687,32 496933,00
2 Medium 684 721,63 493595,00
Total 1407
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 235466,500 235207,000
Wilcoxon W 503012,500 496933,000
Z -2,429 -1,613
Asymp. Sig. (2-tailed) ,015 ,107
a. Grouping Variable: List Places Per 1000 Inhabitants:
low vs medium

183
Ranks
List Places Per Thousand
Inhabitants N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 731 758,85 554719,00
3 High 787 760,10 598202,00
Total 1518
Ventetiden for å få time 1 Low 723 722,70 522512,50
3 High 780 779,16 607743,50
Total 1503
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 287173,000 260786,500
Wilcoxon W 554719,000 522512,500
Z -,059 -2,570
Asymp. Sig. (2-tailed) ,953 ,010
a. Grouping Variable: List Places Per Thousand
Inhabitants: low – high
Ranks
List Places Per Thousand
Inhabitants N Mean Rank Sum of Ranks
Overall GP Satisfaction 2 Medium 692 766,73 530575,50
3 High 787 716,50 563884,50
Total 1479
Ventetiden for å få time 2 Medium 684 722,96 494502,00
3 High 780 740,87 577878,00
Total 1464

184
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 253806,500 260232,000
Wilcoxon W 563884,500 494502,000
Z -2,432 -,826
Asymp. Sig. (2-tailed) ,015 ,409
a. Grouping Variable: List Places Per Thousand
Inhabitants: medium – high
Ranks
List Places Per Thousand
Inhabitants N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 731 758,85 554719,00
3 High 787 760,10 598202,00
Total 1518
Ventetiden for å få time 1 Low 723 722,70 522512,50
3 High 780 779,16 607743,50
Total 1503
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 287173,000 260786,500
Wilcoxon W 554719,000 522512,500
Z -,059 -2,570
Asymp. Sig. (2-tailed) ,953 ,010
a. Grouping Variable: List Places Per Thousand
Inhabitants: low – high
Ranks
Open List Ratio N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 757 729,48 552215,00
2 Medium 720 749,01 539288,00
Total 1477
Ventetiden for å få time 1 Low 741 720,09 533584,00
2 Medium 715 737,22 527112,00
Total 1456

185
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 265312,000 258673,000
Wilcoxon W 552215,000 533584,000
Z -,945 -,793
Asymp. Sig. (2-tailed) ,345 ,428
a. Grouping Variable: Open List Ratio: low vs medium
Ranks
Open List Ratio N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Low 757 740,07 560233,50
3 High 733 751,11 550561,50
Total 1490
Ventetiden for å få time 1 Low 741 731,08 541731,00
3 High 731 741,99 542397,00
Total 1472
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 273330,500 266820,000
Wilcoxon W 560233,500 541731,000
Z -,530 -,502
Asymp. Sig. (2-tailed) ,596 ,615
a. Grouping Variable: Open List Ratio: low vs high
Median Report
Open List Ratio
Overall GP
Satisfaction
Ventetiden for å
få time
1 Low 6,0000 5,0000
2 Medium 6,0000 6,0000
3 High 6,0000 6,0000
Total 6,0000 6,0000

186
Ranks
Open List Ratio N Mean Rank Sum of Ranks
Overall GP Satisfaction 2 Medium 720 731,68 526810,00
3 High 733 722,40 529521,00
Total 1453
Ventetiden for å få time 2 Medium 715 727,24 519976,50
3 High 731 719,84 526204,50
Total 1446
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 260510,000 258658,500
Wilcoxon W 529521,000 526204,500
Z -,454 -,344
Asymp. Sig. (2-tailed) ,650 ,731
a. Grouping Variable: Open List Ratio: medium vs high
Ranks
Kommunestr_i N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Under 5 000 innbyggere 261 448,95 117175,00
2 5 000 - 20 000 innbyggere 663 467,84 310175,00
Total 924
Ventetiden for å få time 1 Under 5 000 innbyggere 273 463,46 126524,50
2 5 000 - 20 000 innbyggere 652 462,81 301750,50
Total 925
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 82984,000 88872,500
Wilcoxon W 117175,000 301750,500
Z -1,037 -,034
Asymp. Sig. (2-tailed) ,300 ,972
a. Grouping Variable: Kommunestr_i (size 1 & 2)

187
Ranks
Kommunestr_i N Mean Rank Sum of Ranks
Overall GP Satisfaction 2 5 000 - 20 000 innbyggere 663 721,34 478250,50
3 20 000 - 110 000
innbyggere
805 745,34 599995,50
Total 1468
Ventetiden for å få time 2 5 000 - 20 000 innbyggere 652 710,87 463484,00
3 20 000 - 110 000
innbyggere
791 731,18 578362,00
Total 1443
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 258134,500 250606,000
Wilcoxon W 478250,500 463484,000
Z -1,166 -,940
Asymp. Sig. (2-tailed) ,244 ,347
a. Grouping Variable: Kommunestr_i (size 2 & 3)
Median Report
Kommunestr_i
Overall GP
Satisfaction
Ventetiden for å
få time
1 Under 5 000 innbyggere 6,0000 6,0000
2 5 000 - 20 000 innbyggere 6,0000 5,0000
3 20 000 - 110 000
innbyggere
7,0000 6,0000
4 110 000 innbyggere eller
fler
6,0000 6,0000
Total 6,0000 6,0000

188
Ranks
Kommunestr_i N Mean Rank Sum of Ranks
Overall GP Satisfaction 3 20 000 - 110 000
innbyggere
805 662,16 533042,50
4 110 000 innbyggere eller
fler
484 616,45 298362,50
Total 1289
Ventetiden for å få time 3 20 000 - 110 000
innbyggere
791 631,65 499634,00
4 110 000 innbyggere eller
fler
475 636,58 302377,00
Total 1266
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 180992,500 186398,000
Wilcoxon W 298362,500 499634,000
Z -2,298 -,237
Asymp. Sig. (2-tailed) ,022 ,812
a. Grouping Variable: Kommunestr_i (size 3 & 4)
Ranks
Kommunestr_i N Mean Rank Sum of Ranks
Overall GP Satisfaction 1 Under 5 000 innbyggere 261 372,63 97257,00
4 110 000 innbyggere eller
fler
484 373,20 180628,00
Total 745
Ventetiden for å få time 1 Under 5 000 innbyggere 273 365,79 99860,50
4 110 000 innbyggere eller
fler
475 379,51 180265,50
Total 748

189
Test Statisticsa
Overall GP
Satisfaction
Ventetiden for å
få time
Mann-Whitney U 63066,000 62459,500
Wilcoxon W 97257,000 99860,500
Z -,036 -,854
Asymp. Sig. (2-tailed) ,971 ,393
a. Grouping Variable: Kommunestr_i (size 1 & 4)
Related Documents











![Hunter Highlights - Volume 154 - Hunter Engineering ...0].pdfSales Representatives who achieve the highest sales performance and customer satisfaction ratings join Hunter’s prestigious](https://static.cupdf.com/doc/110x72/5f443501ac6dcd013d3f60ee/hunter-highlights-volume-154-hunter-engineering-0pdf-sales-representatives.jpg)