Complementary Therapies in Medicine (2008) 16, 155—162 available at www.sciencedirect.com journal homepage: www.elsevierhealth.com/journals/ctim Quality of STIs and HIV/AIDS care as perceived by biomedical and traditional health care providers in Zambia: Are there common grounds for collaboration? Berthollet Bwira Kaboru a,∗ , Maureen Muchimba b , Torkel Falkenberg c,d , Bengt H¨ ojer e , Elisabeth Faxelid a,f , The Bridging Gaps Research Team 1 a Division of International Health (IHCAR), Department of Public Health Sciences, Karolinska Institutet, Stockholm, Sweden b Institute of Economic and Social Research (INESOR), University of Zambia, Lusaka, Zambia c Centre for Studies of Complementary Medicine, Division of International Health (IHCAR), Department of Public Health Sciences, Stockholm, Sweden d Division of Nursing, Department of Neurobiology, Caring Sciences and Society, Karolinska Institutet, Stockholm, Sweden e Dalarna University College, Falun, Sweden f Division of Reproductive and Perinatal Care, Department of Women and Child Health, Karolinska Institutet, Stockholm, Sweden Available online 8 April 2008 KEYWORDS Quality of care; STIs; HIV/AIDS; Traditional healers; Health workers; Collaboration; Integrative medicine; Zambia Summary Objective: To explore biomedical and traditional health care providers’ (BHPs and THPs, respec- tively) perceptions of good quality of care and opinions on weaknesses in the services they provide to patients with STIs and HIV/AIDS. Methods: Using data from a cross-sectional survey, we post-coded two open-ended questions related to THPs’ and BHPs’ perceptions on good quality of care and on provided care. The post-coding was done following Donabedian’s framework of assessment of quality of care, and allowed transformation of qualitative data into quantitative. The analysis is based on comparison of frequencies, proportions and subsequent chi-square tests and odds ratios. Setting: Ndola and Kabwe, Zambia Main measures: Proportions of responses from 152 BHPs and 144 THPs. Results: Substantial proportions of providers from both sectors perceived drugs availability (63% of BHPs and 70% of THPs) and welcoming attitude (73% of BHPs and 64% of THPs) as important components of good quality care. BHPs were more likely than THPs to mention proper examination, medical management (provider’s technical ability) and explanation of causes and Funding source: This study was performed as part of a project supported by the European Commission (EC). ∗ Corresponding author. Tel.: +46 8 524 833 36/70 275 20 89; fax: +46 8 31 15 90. E-mail address: [email protected] (B.B. Kaboru). 1 See Acknowledgements section. 0965-2299/$ — see front matter © 2008 Elsevier Ltd. All rights reserved. doi:10.1016/j.ctim.2008.02.005

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Complementary Therapies in Medicine (2008) 16, 155—162
avai lab le at www.sc iencedi rec t .com
journa l homepage: www.e lsev ierhea l th .com/ journa ls /c t im
Quality of STIs and HIV/AIDS care as perceived bybiomedical and traditional health care providers inZambia: Are there common grounds forcollaboration?�
Berthollet Bwira Kaborua,∗, Maureen Muchimbab, Torkel Falkenbergc,d,Bengt Hojere, Elisabeth Faxelida,f,
The Bridging Gaps Research Team1
a Division of International Health (IHCAR), Department of Public Health Sciences, Karolinska Institutet, Stockholm, Swedenb Institute of Economic and Social Research (INESOR), University of Zambia, Lusaka, Zambiac Centre for Studies of Complementary Medicine, Division of International Health (IHCAR),Department of Public Health Sciences, Stockholm, Swedend Division of Nursing, Department of Neurobiology, Caring Sciences and Society, Karolinska Institutet, Stockholm, Swedene Dalarna University College, Falun, Swedenf Division of Reproductive and Perinatal Care, Department of Women and Child Health, Karolinska Institutet, Stockholm, SwedenAvailable online 8 April 2008
KEYWORDSQuality of care;STIs;HIV/AIDS;Traditional healers;Health workers;Collaboration;Integrative medicine;
SummaryObjective: To explore biomedical and traditional health care providers’ (BHPs and THPs, respec-tively) perceptions of good quality of care and opinions on weaknesses in the services theyprovide to patients with STIs and HIV/AIDS.Methods: Using data from a cross-sectional survey, we post-coded two open-ended questionsrelated to THPs’ and BHPs’ perceptions on good quality of care and on provided care. Thepost-coding was done following Donabedian’s framework of assessment of quality of care,and allowed transformation of qualitative data into quantitative. The analysis is based on
proportions and subsequent chi-square tests and odds ratios.
Zambia comparison of frequencies, Setting: Ndola and Kabwe, Zambia Main measures: Proportions of responses from 152 BHPs and144 THPs.Results: Substantial proportions of providers from both sectors perceived drugs availability(63% of BHPs and 70% of THPs) and welcoming attitude (73% of BHPs and 64% of THPs) asimportant components of good quality care. BHPs were more likely than THPs to mention properexamination, medical management (provider’s technical ability) and explanation of causes and� Funding source: This study was performed as part of a project supported by the European Commission (EC).∗ Corresponding author. Tel.: +46 8 524 833 36/70 275 20 89; fax: +46 8 31 15 90.
E-mail address: [email protected] (B.B. Kaboru).1 See Acknowledgements section.
0965-2299/$ — see front matter © 2008 Elsevier Ltd. All rights reserved.doi:10.1016/j.ctim.2008.02.005

156 B.B. Kaboru et al.
prognosis of the disease as important. More THPs than BHPs cited short waiting time and cost ofcare. A majority of BHPs (87%) and of THPs (80%) reported deficiencies in their STIs and HIV/AIDS-related services. Both groups regarded training of providers and nutritional support and healtheducation to patients as lacking. None of the THPs alluded to voluntary counselling and testing(VCT) or supportive/home-based care as aspects needing improvement.Conclusion: Drugs availability and welcoming attitude were two aspects of quality highly valuedby THPs and BHPs. Future collaborative interventions need to respond to aspects of joint concernincluding training of providers, nutritional support and health education to patients. Further,there is an imperative of expanding and adapting VCT, home-based care and palliative care to
and Hs res
I
TtstptemtHe
tmprrvFoaashuwawag
Acmpfciofa
awwa
nadie(aii
tgciteitis
Tas
M
S
TKnmib
twcpthe availability of or proximity to a centre with voluntarycounselling and testing (VCT) services. Six centres in north-ern part of Kabwe and seven in southern part of Ndola were
THPs for better care of STIs© 2008 Elsevier Ltd. All right
ntroduction
he burden of caring for patients with HIV/AIDS is expectedo increase for the foreseeable future while health careystems in most affected settings remain poorly preparedo face the needs implied by the increasing number ofeople living with HIV/AIDS.1 The World Health Organiza-ion (WHO), in its attempts to design a response to thepidemic, has suggested integration of prevention, treat-ent and care with the conviction that increased access
o good quality sexually transmitted infections (STIs) andIV/AIDS care would simultaneously strengthen preventionfforts.2
In the same vision of setting up an appropriate response,he importance of involving practitioners of traditionaledicine (referred to here as traditional health careroviders (THPs)), in the efforts to scale up AIDS care hasecently been re-emphasized.3,4 However, fears have beenaised that involvement of THPs in formal health care pro-ision would result in deteriorations of quality of care.5
urthermore, alarming voices have warned against the riskf HIV transmission among patients at THPs’ shrines as
result of poor quality of care due to risky practicesnd use of non-sterilized tools.6 The risk of HIV transmis-ion among patients at biomedical health care facilitiesas also been mentioned, particularly in relation to these of injections.7 Quality and safety are critical issuesith respect to possible collaboration between traditionalnd biomedical health care providers,8 just as they areith respect to the integration of complementary andlternative medicine in conventional clinical practice ineneral.9
With the increasing access to anti-retroviral therapies,IDS is becoming a chronic disease.10,11 Care for chroniconditions require a broader approach beyond the mereedication regimens, including aspects such as social sup-ort, palliative care, psychosocial care and an increasedocus on self-management by patients.12 This trend towardshronicity of HIV/AIDS-related illnesses suggests that anntegrative care approach to care would lead to beneficialutcomes for AIDS patients.13 Such an approach to care callsor continuity over time and coordination across settings andcross types of providers.14
In Zambia, sexually transmitted infections and HIV/AIDSre major public health problems. Fifty percent of peopleith a history of sexually transmitted infections are infectedith HIV.15 Nearly one of about eleven million inhabitantsre estimated to be living with HIV/AIDS in Zambia and the
sipoi
IV/AIDS.erved.
eeds in terms of care and support to the infected personsre substantial.16,17 Like in most African countries, the bur-en of sexually transmitted infections and HIV/AIDS caren Zambia is shared by the Western medicine practition-rs, also called biomedically trained health practitionersBHPs) employed in the public health sectors, the THPsnd the communities. Collaboration between BHPs and THPss therefore key for better control of sexually transmittednfections and HIV/AIDS.
However, considering the gaps in perspectives and prac-ices between THPs and BHPs, the exploration of whatood quality care is for the concerned providers is criti-al in the collaborative endeavour. Even more importants the understanding of deficient aspects of quality inhe actual service as seen by the respective practition-rs themselves. This understanding can be useful in thedentification of areas where collaboration might best con-ribute to quality enhancement in sexually transmittednfections and HIV/AIDS care and to expansion of coverage ofervices.
The aim of this study was therefore to explore BHPs’ andHPs’ perceptions of good sexually transmitted infectionsnd HIV/AIDS care and their opinions on weaknesses in theervices they provide to patients with these conditions.
aterials and methods
etting and participants
his study was conducted in two cities in Zambia: Ndola andabwe. The study population consisted of BHPs includingurses, midwives, physicians, and laboratory and environ-ental health technicians on the one hand; and THPs,
ncluding herbalists, spiritualists, diviners and traditionalirth attendants (TBAs), on the other.
Twenty research assistants (RAs) were selected andrained as data collectors (10 in each town). Half of themere THPs and the other half were BHPs. Health centresonstituted the departing point in the selection of the studyarticipants. The selection criteria for health centres were
elected. We attempted to interview all BHPs at these facil-ties. Interviews with BHPs were conducted individually inrivacy at their respective workplace. Workers on leave orff-duty were followed up and interviewed at home. Thenterviews with BHPs were conducted in English. Out of 172

gfiwartucPccpqotc
fCpitaccuv
co
R
Quality of STIs and HIV/AIDS care in Zambia
BHPs eligible, 152 (80 in Kabwe and 72 in Ndola) were inter-viewed while 20 (12%) were not accessible.
As for THPs, district branches of Traditional Health Prac-titioners Association of Zambia (THPAZ) provided lists ofall THPs operating within the residential areas surroundingthe selected health centres and from which the centres gettheir clients. The compiled information included names andaddresses of THPs who, according to their own statement,attended to patients with sexually transmitted infectionsand HIV/AIDS. All identified THPs consented to participatein the study. They were interviewed in Bemba, the local lan-guage used in Kabwe and Ndola, at their workplaces. Thetotal number of THPs interviewed was 144 (81 in Kabweand 63 in Ndola). In the analysis, we excluded one BHP andthree THPs for non-response or for irrelevant response tothe questions of interest.
Coding and analysis of the data
The present study was based on the health care providers’responses to the following two specific questions: (1) whenyou go to a health unit, what would be good care? and (2)are there some parts of the care you provide to patients withsexually transmitted infections and HIV/AIDS that you coulddo better? If yes, what are these aspects of service?
In order to reduce the data and to facilitate its analy-sis, we opted for a process of transforming the responsesfrom qualitative, open-ended questions into quantitativedata by post-coding the responses. In order to be done sys-tematically, this post-coding of qualitative responses to thetwo open-ended questions (the first on perceptions of goodquality care and the second on opinions on weaknesses inprovided services) was performed following a guide adapted
from the framework of quality of care assessment first devel-oped by Donabedian18—20 that highlights three dimensions:structure, process and outcome (Table 1). This frameworkhas been used elsewhere to deal with issues regarding inte-gration of biomedical and alternative medicine.21,22P
Tv
Table 1 Analytical framework used as post-coding guide
Dimensions of quality of care
Structure: The organizational framework of the activities
Process: The activities themselves, i.e. how the service is organisedelivered and used
Outcome: The impact/effectiveness of the activities on patients
Adapted from Donabedian20, Bell et al.20 and Duffy and Hoskins22.
157
In order to ensure reliability of the post-coding, the cate-orisation of the responses required consensus between therst and the second author. This means that each responseas read by both authors, its meaning was discussed andny difference in interpretation was cleared and consensuseached before coding. The quantitative data resulting fromhe post-coding of the qualitative responses were analysedsing STATA 8 (Stata Corporation, Texas, USA). Frequen-ies of responses were calculated. For binary responses, theearson chi-square test (�2) was applied to test the statisti-al difference between proportions. Odds ratios (OR) werealculated to see the extent to which the two groups ofroviders were equally likely or not to mention differentuality aspects as pertinent to their perception of qualityf care or self-evaluation of care provided. Fisher’s exactest was used when at least one of the frequencies beingompared was low (<3).
This study was part of a broader survey within theramework of a 40 months long (2002—2006) Europeanommission-funded project called ‘‘Bridging gaps betweenublic and traditional health sectors: testing a model tomprove quality and uptake of sexually transmitted infec-ions and HIV/AIDS in sub-Saharan Africa’’. The generalim of this broad project was to improve dialogue andollaboration between traditional and biomedical healthare providers in order to improve quality of care andptake of sexually transmitted infections and HIV/AIDS ser-ices.
Ethical clearance: The study was approved by the Ethicsommittees at Karolinska Institutet (Sweden) and Universityf Zambia (Zambia).
esults
erceptions of good quality care
he respondents were asked about the aspects they wouldalue if they were to seek care themselves as patients.
Aspects within dimensions of quality of care
EquipmentClean environmentStaffing (and their distribution in terms oftraining)Medicine availability (not only prescriptions)
d, Opening hoursWaiting timeWelcoming attitude/respect/friendlinessProper examinationExplanation of the causes and prognosis of thedisease/reassurancePrivacy/confidentiality
Cost of careCure/recoveryRecommendation for review/follow-up
158 B.B. Kaboru et al.
Table 2 Comparison of providers’ perceptions of good quality care
Aspects of quality Frequencies (%) [BHPs n = 151,THPs n = 141]
OR (95% CI) p-Value
StructureClean environment BHPs: 6 (3.97) 1.90 (0.47 − 7.60) 0.503a
THPs: 3 (2.14) 1.00
Medicines’ availability BHPs: 96 (63.57) 0.76 (0.46 − 1.24) 0.283THPs: 98 (69.50) 1.00
ProcessWaiting time BHPs: 33 (21.85) 0.55 (0.33 − 0.93) 0.028
THPs: 47 (33.33) 1.00
Welcomingattitude
BHPs: 111 (73.50) 1.57 (0.95 − 2.58) 0.074THPs: 90 (63.82) 1.00
Properexamination
BHPs: 51 (33.77) 6.02 (3.14 − 11.54) <0.001THPs: 11 (7.80) 1.00
Good medical management BHPs: 15 (9.93) 5.07 (1.60 − 16.03) 0.006a
THPs: 3 (2.12) 1.00
Explanation of the disease BHPs: 43 (28.47) 4.72 (2.36 − 9.43) <0.001THPs: 10 (7.09) 1.00
Privacy BHPs: 13 (8.60) 13.18 (2.65 − 65.57) 0.001a
THPs: 1 (0.70) 1.00
OutcomeCost BHPs: 2 (1.32) 0.14 (0.03 − 0.54) 0.004a
THPs: 12 (8.51) 1.00
Review/follow-up BHPs: 11 (7.28) 5.46 (1.38 − 21.53) 0.020a
THPs: 2 (1.41) 1.00
Cure/recovery THPs: 2 (1.41) 0.93 (0.12 − 6.73) 1 a
OR = odds ratios and n = number of respondents with valid responses.
VapaavvoctnmnwavdmwdgT
A
Av(ftad(odiocop
a Fisher’s exact test.
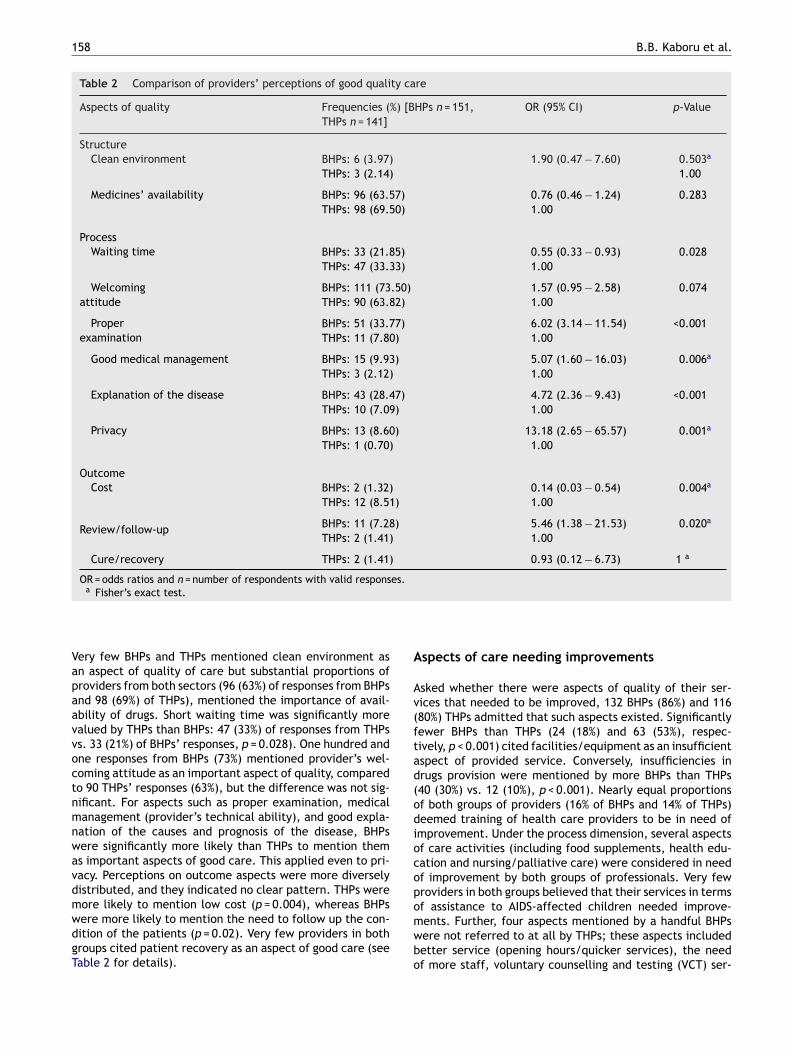
ery few BHPs and THPs mentioned clean environment asn aspect of quality of care but substantial proportions ofroviders from both sectors (96 (63%) of responses from BHPsnd 98 (69%) of THPs), mentioned the importance of avail-bility of drugs. Short waiting time was significantly morealued by THPs than BHPs: 47 (33%) of responses from THPss. 33 (21%) of BHPs’ responses, p = 0.028). One hundred andne responses from BHPs (73%) mentioned provider’s wel-oming attitude as an important aspect of quality, comparedo 90 THPs’ responses (63%), but the difference was not sig-ificant. For aspects such as proper examination, medicalanagement (provider’s technical ability), and good expla-
ation of the causes and prognosis of the disease, BHPsere significantly more likely than THPs to mention thems important aspects of good care. This applied even to pri-acy. Perceptions on outcome aspects were more diverselyistributed, and they indicated no clear pattern. THPs were
ore likely to mention low cost (p = 0.004), whereas BHPsere more likely to mention the need to follow up the con-ition of the patients (p = 0.02). Very few providers in bothroups cited patient recovery as an aspect of good care (seeable 2 for details).omwbo
spects of care needing improvements
sked whether there were aspects of quality of their ser-ices that needed to be improved, 132 BHPs (86%) and 11680%) THPs admitted that such aspects existed. Significantlyewer BHPs than THPs (24 (18%) and 63 (53%), respec-ively, p < 0.001) cited facilities/equipment as an insufficientspect of provided service. Conversely, insufficiencies inrugs provision were mentioned by more BHPs than THPs40 (30%) vs. 12 (10%), p < 0.001). Nearly equal proportionsf both groups of providers (16% of BHPs and 14% of THPs)eemed training of health care providers to be in need ofmprovement. Under the process dimension, several aspectsf care activities (including food supplements, health edu-ation and nursing/palliative care) were considered in needf improvement by both groups of professionals. Very fewroviders in both groups believed that their services in terms
f assistance to AIDS-affected children needed improve-ents. Further, four aspects mentioned by a handful BHPsere not referred to at all by THPs; these aspects includedetter service (opening hours/quicker services), the needf more staff, voluntary counselling and testing (VCT) ser-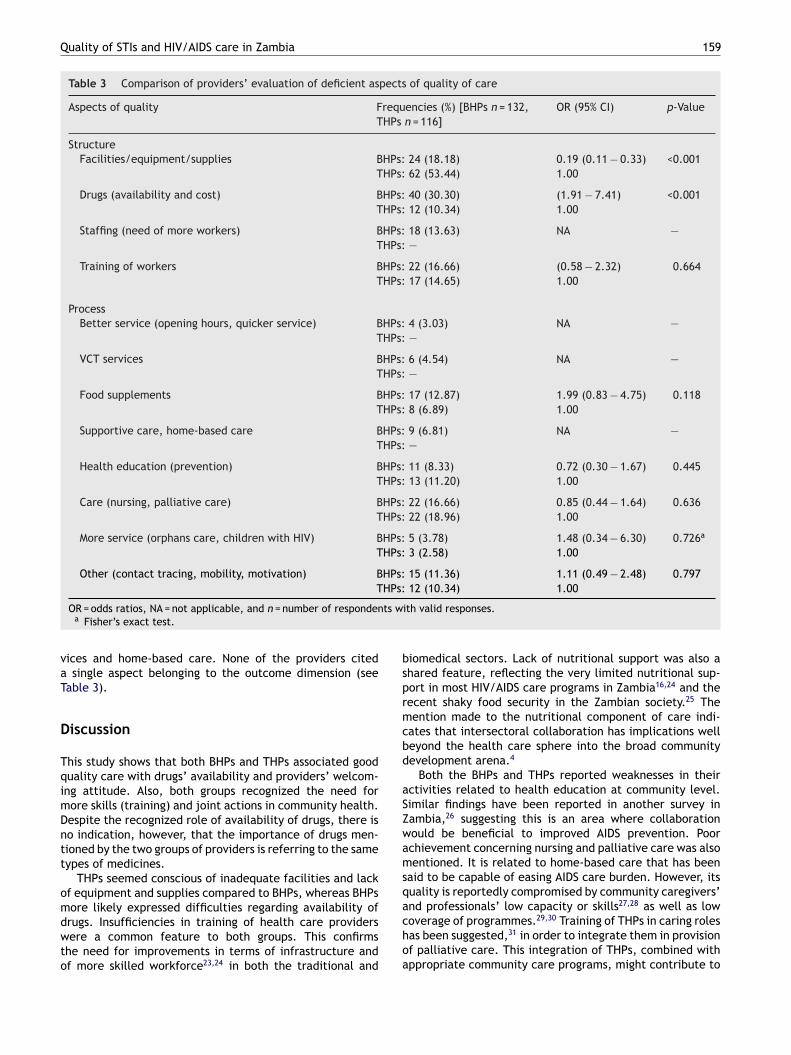
Quality of STIs and HIV/AIDS care in Zambia 159
Table 3 Comparison of providers’ evaluation of deficient aspects of quality of care
Aspects of quality Frequencies (%) [BHPs n = 132,THPs n = 116]
OR (95% CI) p-Value
StructureFacilities/equipment/supplies BHPs: 24 (18.18) 0.19 (0.11 − 0.33) <0.001
THPs: 62 (53.44) 1.00
Drugs (availability and cost) BHPs: 40 (30.30) (1.91 − 7.41) <0.001THPs: 12 (10.34) 1.00
Staffing (need of more workers) BHPs: 18 (13.63) NA —THPs: —
Training of workers BHPs: 22 (16.66) (0.58 − 2.32) 0.664THPs: 17 (14.65) 1.00
ProcessBetter service (opening hours, quicker service) BHPs: 4 (3.03) NA —
THPs: —
VCT services BHPs: 6 (4.54) NA —THPs: —
Food supplements BHPs: 17 (12.87) 1.99 (0.83 − 4.75) 0.118THPs: 8 (6.89) 1.00
Supportive care, home-based care BHPs: 9 (6.81) NA —THPs: —
Health education (prevention) BHPs: 11 (8.33) 0.72 (0.30 − 1.67) 0.445THPs: 13 (11.20) 1.00
Care (nursing, palliative care) BHPs: 22 (16.66) 0.85 (0.44 − 1.64) 0.636THPs: 22 (18.96) 1.00
More service (orphans care, children with HIV) BHPs: 5 (3.78) 1.48 (0.34 − 6.30) 0.726a
THPs: 3 (2.58) 1.00
Other (contact tracing, mobility, motivation) BHPs: 15 (11.36) 1.11 (0.49 − 2.48) 0.797HPs:
ts w
bsprmcbd
aSZwamsq
T
OR = odds ratios, NA = not applicable, and n = number of respondena Fisher’s exact test.
vices and home-based care. None of the providers citeda single aspect belonging to the outcome dimension (seeTable 3).
Discussion
This study shows that both BHPs and THPs associated goodquality care with drugs’ availability and providers’ welcom-ing attitude. Also, both groups recognized the need formore skills (training) and joint actions in community health.Despite the recognized role of availability of drugs, there isno indication, however, that the importance of drugs men-tioned by the two groups of providers is referring to the sametypes of medicines.
THPs seemed conscious of inadequate facilities and lackof equipment and supplies compared to BHPs, whereas BHPs
more likely expressed difficulties regarding availability ofdrugs. Insufficiencies in training of health care providerswere a common feature to both groups. This confirmsthe need for improvements in terms of infrastructure andof more skilled workforce23,24 in both the traditional andachoa
12 (10.34) 1.00
ith valid responses.
iomedical sectors. Lack of nutritional support was also ahared feature, reflecting the very limited nutritional sup-ort in most HIV/AIDS care programs in Zambia16,24 and theecent shaky food security in the Zambian society.25 Theention made to the nutritional component of care indi-
ates that intersectoral collaboration has implications welleyond the health care sphere into the broad communityevelopment arena.4
Both the BHPs and THPs reported weaknesses in theirctivities related to health education at community level.imilar findings have been reported in another survey inambia,26 suggesting this is an area where collaborationould be beneficial to improved AIDS prevention. Poorchievement concerning nursing and palliative care was alsoentioned. It is related to home-based care that has been
aid to be capable of easing AIDS care burden. However, itsuality is reportedly compromised by community caregivers’
27,28
nd professionals’ low capacity or skills as well as lowoverage of programmes.29,30 Training of THPs in caring rolesas been suggested,31 in order to integrate them in provisionf palliative care. This integration of THPs, combined withppropriate community care programs, might contribute to
1
dot
ipffivtbbtat
Tsiatcstfv9ictVwiaaepTptt
oitr
cwantCntbbisaa
loilql
so(taaateTc
qamlmiCwhwrsrmoic
caetiinpscip
C
TBcm
60
ecrease readmissions of terminally ill patients who oftenverburden hospitals.27 Such integration, however, remainso be tried and tested.
Surprisingly, few providers in both sectors referred to thessue known as ‘‘the palliative total care’’,30 i.e. the com-lexity of palliative AIDS care in African contexts where careor orphans, income generation and payment of school feesor patients, children, etc., need to be taken into accountn care interventions. This is a societal challenge very rele-ant to practitioners in the medical or caring field. Indeed,he implementation of palliative total care calls for contri-ution from several agencies and providers. Collaborationetween THPs and BHPs would fit into this kind of initia-ives. A recent study from Tanzania has showed that THPsre providing psychosocial support to children orphaned dueo AIDS.32
Some aspects did not render any responses from THPs.his can be interpreted either that THPs considered theirervices to be of optimal quality (i.e. staffing, open-ng hours, quick service); or that the concerned aspectsre totally absent from their worldviews, their concep-ual framework of activities or perceived roles. Voluntaryounselling and testing (VCT) has so far been limited to coun-elling patients before and after undergoing HIV test. It isherefore not surprising that only providers with HIV testingacilities (BHPs) can evaluate it. Evidently, THPs do conductoluntary counselling but not linked to testing. Given that5% of people in Africa have no access to HIV testing,23
ntegration of VCT in other programs such as antenatalare or family planning has been called for in the perspec-ive of comprehensive HIV care.33 However, extending theCT concept (at least the counselling component) to THPsorkplaces has not been suggested to date. We argue that
nterprofessional collaboration could broaden the notionnd coverage of VCT, expanding it beyond pre—post HIV testnd health facility. With adequate referral systems, suchxpanded VCT services would simultaneously strengthenrevention and uptake of HIV/AIDS treatment programs.HPs would for example continue to provide counselling toatients with HIV diagnosis, even long after the HIV testing,o encourage sustainable behavioural change, among otherhings.
Despite the identified convergent views among providersn aspects of care that needed improvement, other equallymportant issues have not appeared in our findings, includinghe need for guidelines or care protocols as well as effectiveeferral and information systems.30,33
The findings in this study might have important impli-ations on efforts to improve quality of care of patientsith sexually transmitted infections and HIV/AIDS as wells to open arenas of joint health actions in the commu-ity by THPs and BHPs. It is fundamental to keep in mindhat HIV/AIDS care should be regarded as a continuum.1,34
are is more than just drugs. It also encompasses termi-al, palliative, spiritual and psychosocial care as well asreatment of opportunistic infections.12,35 Studies in Zam-ia and other sub-Saharan countries have shown that the
urden of sexually transmitted infections and HIV/AIDS cares shared between three main arenas: the patients them-elves (and their families and communities), the modernnd the traditional health care providers.28,36,37 Sustain-ble quality enhancement of AIDS care requires more oriwcca
B.B. Kaboru et al.
ess simultaneous improvements at all arenas and in mostf the concerned aspects. More research is needed todentify ways of integrating all these dimensions in col-aborative frameworks without jeopardizing efficiency anduality of services but maximizing outcomes at patients’evel.
This study has its strengths and weaknesses. The maintrength is the novelty in the approach. No previous studyn THPs and BHPs has tried to explore aspects of careperceived or actual) through exposing both groups tohe same questions at once. These providers have usu-lly been researched separately as if they never sharednything related to quality of care—–perceived or actu-lly provided. Our approach, we believe, clarifies aspectshat need further attention by clinicians and policymak-rs in the perspective of increased collaboration betweenHPs and BHPs with focus on improvement of quality ofare.
This study has methodological limitations. The low fre-uencies of responses related to some quality aspects (suchs clean environment, VCT services, cure/recovery, etc.)ight be due to the nature of the questions rather than to
ack of interest by respondents. As described earlier, the twoain questions that this study builds upon were open-ended,
.e. prompted and broadly asked, rather than closed-ended.losed-ended questions would have provided respondentsith a directive response set and might have resulted intoigher frequencies of responses. Consequently, the resultsould have been different from what we found. In this
espect, the strength of this study is that we did not con-train respondents into a given response set. The providedesponses should therefore be regarded as aspects seen asost critical by the respondents. From this point of view,
ur findings can be said to be related to the fundamentalssues in quality improvement from the perspective of theoncerned providers.
Unanswered questions that need further research con-ern the cost of care for patients who use both THPsnd BHPs services simultaneously during the same diseasepisode, or in multiple episodes from a chronic care perspec-ive, for instance for patients with HIV/AIDS. To date, theres no data on the cost of care provided by THPs, although its believed that THPs are often more expensive than BHPs. Ifot well structured within the framework of a clear policy,arallel use of BHPs and THPs services might be too expen-ive to patients. Another area requiring further researchoncerns patients’ experiences of parallel use of biomed-cal and traditional health care, in terms of satisfaction anderceived quality of care.
onclusion
his study shows that despite differences between THPs andHPs, issues perceived by both groups as being of signifi-ance to quality of care or issues in need of improvementight serve starting point for collaboration for better qual-
ty of care. Such issues are for instance availability of drugs,elcoming attitudes and training of providers. Interventionsalled for collaboratively address these aspects of joint con-ern as well as to expand and adapt VCT, home-based carend palliative total care to THPs. Nevertheless, more opera-
Quality of STIs and HIV/AIDS care in Zambia
tional research is needed on ways of safeguarding processes,quality as well as outcomes at patients’ level.
Acknowledgements
The authors are grateful to their colleagues members ofthe Bridging Gaps Project’s Research Group affiliated withthe following collaborating institutions: the Karolinska Insti-tutet, Department of Public Health Sciences, Division ofInternational Health (IHCAR), Stockholm, Sweden; the Lon-don School of Hygiene and Tropical Medicine (LSHTM),London, UK; the University of Zambia, Institute of Eco-nomic and Social Research (INESOR), Lusaka, Zambia; theMakerere University, Institute of Public Health (IPH), Kam-pala, Uganda; Traditional and Modern Health PractitionersTogether Against AIDS (THETA), Kampala, Uganda; and Tra-ditional Health Practitioners Association of Zambia (THPAZ),Lusaka, Zambia. These persons are: Oke T and Pharris-CiurejA from IHCAR; Mayaud P, Oliff M and Todd J from LSHTM;Muchimba M, Mwambazi C, Ndulo J and Zulu R from INESOR;Atuyambe L, Nalwadda C, Zimbe I and Zirabamuzaale C fromIPH; Balaba D, King R, Kyeyune P, Munobwa J and NsubugaC from THETA and Mwale W, Nyambo R and Solo K fromTHPAZ.
The authors would also like to thank the PostgraduateSchool of Health Care Sciences, Karolinska Institutet forfinancially supporting the first author of this article. Thanksto all traditional and biomedical providers who took theirtime and answered the questionnaire.
This study was funded by the European Commission (Con-tract Number ICA4-CT-2002-10031).
References
1. Gilks CF. HIV care in non-industrialised countries. Brit Med Bull2001;58:171—86.
2. World Health Organization (WHO). The world health report2003—–shaping the future. Geneva: WHO; 2003.
3. Homsy J, King R, Balaba D, Kabatesi D. Traditional health prac-titioners are key to scaling up comprehensive care for HIV/AIDSin sub-Saharan Africa. AIDS 2004;18:1723—5.
4. Kaboru BB, Falkenberg T, Ndulo J, Muchimba M, Solo K,Faxelid E. Communities’ views on prerequisites for collab-oration between modern and traditional health sectors inrelation to STI/HIV/AIDS care in Zambia, Health Policy 2006;78:330—9.
5. van der Geest S. Is there a role for traditional medicine in basichealth services in Africa? A plea for a community perspective.Trop Med Int Health 1997;2:903—11.
6. Peters EJ, Immananagha KK, Essien OE, Ekott JU. Traditionalhealers’ practice and the spread of HIV/AIDS in South EasternNigeria. Trop Doct 2004;34:79—82.
7. Hutin YJF, Hauri AM, Armstrong GL. Use of injections in healthcare settings worldwide 2000. Literature review and regionalestimates. BMJ 2003;327:1075—80.
8. Homsy J, King R, Tenywa J, Kyeyune P, Opio A, Balaba D. Defin-ing minimum standards of practice for incorporating Africantraditional medicine into HIV/AIDS prevention, care, and sup-
port: a regional initiative in Eastern and Southern Africa. JAltern Complem Med 2004;10:905—10.9. Wayne JB. Alternative medicine—–learning from the past,examining the present, advancing to the future. JAMA1998;280:1616—8.
161
10. Livingston J. AIDS as a chronic illness: epidemiological transi-tion and health care in south-eastern Botswana. Afr J AIDS Res2004;3:15—22.
11. Halloran J. Increasing survival with HIV: impact on nursing.AACN Clin Issues 2006;17:8—17.
12. Selwyn PA, Forstein M. Overcoming the false dichotomy of cura-tive vs palliative care for late-stage HIV/AIDS: let me live theway I want to live, until I can’t. JAMA 2003;290:806—14.
13. Foote-Ardah CE. The meaning of complementary and alterna-tive medicine practices among people with HIV in the UnitedStates: strategies for managing everyday life. Sociol Health Illn2003;25:481—500.
14. Pruitt SD, Epping-Jordan JE. Preparing the 21st century globalhealthcare workforce. BMJ 2005;330:637—9.
15. MoH [Zambia]. National HIV/AIDS/STI/TB policy. Lusaka; Min-istry of Health, Government of Zambia; 2005.
16. Nsutebu EF, Walley JD, Mataka E, Fikansa Simon C. Scaling-up HIV/AIDS and TB home-based care: lessons from Zambia.Health Policy Plann 2001;16:240—7.
17. WHO [Zambia]. Summary country profile for HIV/AIDS treat-ment: 3 by 5. Geneva: World Health Organisation; 2004.
18. Donabedian A. Exploration in quality assessment and monitor-ing. Vol. 1. The definition of quality and approaches to itsassessment. Ann Arbor, Michigan: Health Administration Press;1980.
19. Handler A, Issel M, Turnock B. A conceptual framework to mea-sure performance of the public health system. Am J PublicHealth 2001;91:1235—9.
20. Donabedian A. Evaluating the quality of medical care. MilbankQ 2005;83:691—729.
21. Bell IR, Caspi O, Schwartz GER, et al. Integrative medicineand systemic outcome research: issues in the emergenceof a new model for primary health care. Arch Intern Med2002;162:133—40.
22. Duffy JR, Hoskins LM. The quality-caring model: blending dualparadigms. Adv Nurs Sci 2003;26:77—88.
23. Mukherjee JS, Farmer PE, Niyizonkiza D, et al. Tackling HIV inresource poor countries. BMJ 2003;2003:1104—6.
24. Kombe G, Galaty D, Mtonga V, Banda P. Resource crisis in theZambian health system: A call for urgent action. Bethesta, MD:The Partners Health Reformplus; 2005.
25. USAID. Southern Africa—–food insecurity. Available at http://www.usaid.gov/our work/humanitarian assistance/disasterassistance/countries/southern africa/fy2006/southern africafi sr01 02-03-2006.pdf. Accessed May 2, 2006.
26. CSO, MoH [Zambia]. MEASURE evaluation: Zambia sexualbehaviour survey. Lusaka: Central Statistical Office, Ministryof Health [Zambia] and MEASURE Evaluation; 2004.
27. Ndaba-Mbata RD, Seloilwe ES. Home-based care of the termi-nally ill in Botswana: knowledge and perceptions. Int Nurs Rev2000;47:218—23.
28. Orner P. Psychological impacts on caregivers of people withAIDS. AIDS Care 2006;18:236—40.
29. Uys LR. The practice of community caregivers in a home-basedHIV/AIDS project in South Africa. J Clin Nurs 2002:99—108.
30. Harding R, Higginson IJ. Palliative care in sub-Saharan Africa.Lancet 2005;365:1971—7.
31. Harding R, Stewart K, Marconi K, O’Neill J, Higginson I. CurrentHIV/AIDS end-of-life care in sub-Saharan Africa: a survey ofmodels, services, challenges and priorities. BMC Public Health2003;3:33.
32. Kayombo EJ, Mbwambo ZH, Massila M. Role of traditionalhealers in psychosocial support in caring for the orphans: a
case of Dar-es-Salaam City, Tanzania. J Ethnobiol Ethnomed2005:1.33. Kitahata MM, Tegger MK, Wagner EH, Holmes KK. Comprehen-sive health care for people infected with HIV in developingcountries. BMJ 2002;2002:954—7.

1
among lay persons in rural and urban Zambia. Sex Transm Dis
62
34. UNAIDS. Report on the global HIV/AIDS epidemic 2002. World
Health Organization; 2002.35. Uys LR. Aspects of the care of people with HIV/AIDS in SouthAfrica. Public Health Nurs 2003;20:271—80.
36. Ndulo J, Faxelid E, Tishelman C, Krantz I. ‘‘Shopping’’ for sex-ually transmitted diseases treatment: focus group discussions
B.B. Kaboru et al.
2000;27:496—503.37. Hatchett LA, Kaponda CPN, Chihana CN, et al. Health-
seeking patterns for AIDS in Malawi. AIDS Care 2004;16:827—33.
Related Documents











