Quality Management System: 90-day innovation cycle Second literature review Supporting better quality health and social care for everyone in Scotland

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Quality Management System: 90-day innovation cycle Second literature review
Supporting better quality health and
social care for everyone in Scotland

© Healthcare Improvement Scotland 2018
Published May 2018
This document is licensed under the Creative Commons Attribution-
Noncommercial-NoDerivatives 4.0 International Licence. This allows for the copy
and redistribution of this document as long as Healthcare Improvement Scotland
is fully acknowledged and given credit. The material must not be remixed,
transformed or built upon in any way. To view a copy of this licence, visit
https://creativecommons.org/licenses/by-nc-nd/4.0/
www.healthcareimprovementscotland.org

3
Contents
Questions informing the second literature review ................................................................................. 4
Key findings ............................................................................................................................................. 4
Developments in quality management principles/components ............................................................. 5
Theoretical principles from Juran and Deming ................................................................................... 5
The relationship between quality control and quality improvement ................................................. 6
High performance management systems ........................................................................................... 7
Key challenges when implementing quality management systems........................................................ 9
Leadership ......................................................................................................................................... 10
Structure and function ...................................................................................................................... 11
Customer focus and person-centred care ......................................................................................... 11
References ............................................................................................................................................. 10
4
Questions informing the second literature review
What can be learned from quality management models and frameworks in the published literature
about an effective and coordinated approach to quality management?
How do theoretical principles from Juran and Deming inform how to achieve an effective quality
management approach?
What can be learned from high performance management systems?
Key findings
The Institute for Healthcare Improvement’s (IHI’s) white paper, Sustaining Improvement, outlines an
integrated framework for achieving quality management which is grounded in Juran and Deming’s
principles and informed by the attributes of high performing systems.
IHI’s framework for high-performance management systems requires a focus on developing
standard work and using quality control to monitor and adjust the system as needed. Without
quality control, IHI argue that even the best quality improvement is likely to fall short. However,
quality control is distinguished from activities relating to quality assurance or inspection.
Quality control is seen as acting as a mechanism embedded within operations for monitoring and
adjusting what should be standard for quality. When problems arise that are beyond the scope of
the local team at the front line (such as fundamental changes in clinical protocols or problems
requiring interdepartmental coordination) this is escalated to quality improvement.
Any framework for quality management requires to be translated to a specific context or situation if
it is to be implemented successfully. IHI outlines a range of factors needed to implement and
maintain a high-performance management system specific to healthcare that relate to structure,
process and culture.
Leadership and structure are key considerations for overcoming obstacles to quality management in
health and social care. The application of hard factors of quality management without addressing
structural issues and soft factors is a common cause of implementation failure.
Juran recognised the leadership challenge in healthcare organisations and how their traditional
structure is likely to feature divided leadership. The learning from high performance systems is that
flattened structures are required to reduce boundaries between units and ensure cross-function
collaboration.
In health and social care there are multiple customers with different needs, and subsequently
variable ways of defining quality. Therefore, quality planning is key for being able to identify and
addressgaps in the delivery of services to meet customer needs.

5
Developments in quality management principles/components
Theoretical principles from Juran and Deming
The Juran trilogy1 is used to explain the interrelationship of three quality functions that bring about quality
management for performance: quality planning, quality control, and quality improvement. Together these
functions constitute an integrated system for coordinated and integrated attention to customers’ (that is
patients’) needs, the design and delivery of services consistent with the best technical specifications to
consistently meet those needs, and the ongoing management of the systems of delivering these services.
These processes are described in Juran’s Quality Handbook as being universal to quality management in any
context and also as being interrelated in order to achieve continuous improvement. The initial activities in
the series that relate to quality planning are described as involving planners determining who the customers
are and what their needs are1. From there, the planners then develop process designs to respond to those
needs as part of quality control which is finally handed over to operations to produce the planned design
features as part of quality improvement. IHI’s white paper, Sustaining Improvement2, describes how the
trilogy principles should work in healthcare:
Quality planning: requires an understanding of customer needs which in healthcare is
conceptualised in relation to the Triple Aim. Quality planning also includes the design and
operation of quality management systems including the principles of high performance
management.
Quality control: focuses on monitoring operations in terms of whether process remains stable in
relation to performance. When gaps in performance are identified then quality improvement
should be implemented to address these at the front line of operations.
Quality improvement: involves designated teams of managers and staff with expertise and
technical support from quality improvement specialists carrying out initiatives to develop, test
and implement changes to improve performance using a variety of tools and, if needed, carrying
out redesign. Quality control is then used to monitor the redesigned process as a result of quality
improvement to ensure it performs at a new level (with new upper and lower control limits).
Deming also shared the view that quality control was key for continuous improvement and described how
management should be responsible for establishing and maintaining quality management systems as a set
of interdependent components relating to structures, people and processes. While Juran focused
considerations of control in relation to sporadic vs chronic waste and the cost of poor quality related to
processes and systems as creating the opportunity for continuous improvement, Deming focused on causes
of variation from set standards. Both agreed that management must be responsible for implementing
necessary actions in constantly improving the quality due to common causes.
To achieve standardisation through continuous learning and improvement, the Deming Cycle, also known as
the Shewhart Cycle, was developed as a model for incremental and continuous improvement through
creating a balance between ‘planning’, ‘studying’, ‘doing’, and ‘acting’. For Deming, the cycle was how
quality management should be planned and a programme for quality control should be achieved. At a
roundtable discussion on product quality at the US Government Accounting Office, Deming is described as
having said that ‘The Deming circle is a quality control program. It is a plan for management. Four steps:
Design it, make it, sell it, then test it in service. Repeat the four steps, over and over, redesign it, make it,
etc’3. In 1991, Moen, Nolan and Provost developed Deming’s cycle to require the use of prediction and
associated theory. This enhanced the study step to compare observed data to the prediction that was made
and therefore provided the deductive-inductive process necessary for learning.

6
The relationship between quality control and quality improvement
Juran’s quality control is described by IHI as being an integral component of everyday work and
management required for quality3. It involves the routine enactment of standard tasks and monitoring
performance. Juran distinguished quality control from quality assurance or inspection in the Quality
Handbook: ‘Quality control and quality assurance have much in common. Each evaluates performance. Each
compares performance to goals. Each acts on difference. However they also differ from each other. Quality
control has its primary purpose to maintain control. Performance is evaluated during operations, and
performance is compared to goals during operations. The resulting information is received and used by the
operating forces. Quality assurance’s main purpose is to verify that control is maintained. Performance is
evaluated after operations, and the resulting information is provided to both the operating forces’. 1 (p4.3)
Figure 1 from IHI’s white paper, Sustaining Improvement3, shows how quality control and quality
improvement components of quality management can be seen as interlocking cycles. Quality control acts as
a mechanism for monitoring and adjusting according to what should be standard. The ‘Adjust’ step in this
cycle is seen to involve frontline application of the Model for Improvement, with its own nested Plan-Do-
Study-Act, or PDSA, cycles to test and refine changes that will lead to improvement. When problems arise
that are beyond the scope of the local team at the front line (such as when a new protocol is introduced
that fundamentally changes processes of care or patient expectations, or when the problem requires
interdepartmental coordination), this is escalated to a higher-level quality improvement initiative to
redesign the process as part of quality improvement.
Figure 1. Quality control and quality improvement relationship from IHI (Scoville et al, 2016, p.8)3

7
High performance management systems
The characteristics of high performing organisations and systems are consistent with the Juran Trilogy.
There are number of frameworks describing the characteristics of high performing systems in the literature.
A review by MacIntosh-Murray et al (2006) identified nine key attributes of high-performing organisations
and their component elements which are summarised in Table 1. For an organisation or system to achieve
high performance then they would be expected to be fulfilling the majority of these.
Table 1: Attributes of high performing systems (MacIntosh-Murray et al 2006)4
Attribute Description
Culture Organization/leaders support and expect learning and innovation.
Organization/leaders value staff and empower all members to participate.
Organization/leaders focus on customers/patients.
Organization/leaders value collaboration and teamwork.
Organization/leaders are flexible.
Leadership Strong administrative leadership that provides role models for organizational
values.
Leadership celebrates and even participates in improvement initiatives.
Emphasis on developing, fostering and inclusion in decision-making for clinical
leadership and champions.
Board support: Board sets expectations by asking for reports on improvement
initiatives and results.
Board provides continuity of expectations if administrative leadership changes.
Strategy and
policy
Leaders set clear priorities for improvement.
Improvement plans are integrated in the overall strategic plan as the means to
achieve key strategic goals.
Leaders demonstrate both constancy of purpose and flexibility.
Operational policies and procedures, including human resources policies, provide
incentives, rewards and recognition.
Incentives, rewards and recognition are aligned to support improvement work.
Structure Roles and responsibilities for improvement are clearly articulated.
Steering/oversight committees provide direction. Teams and teamwork are part of
structure.
8
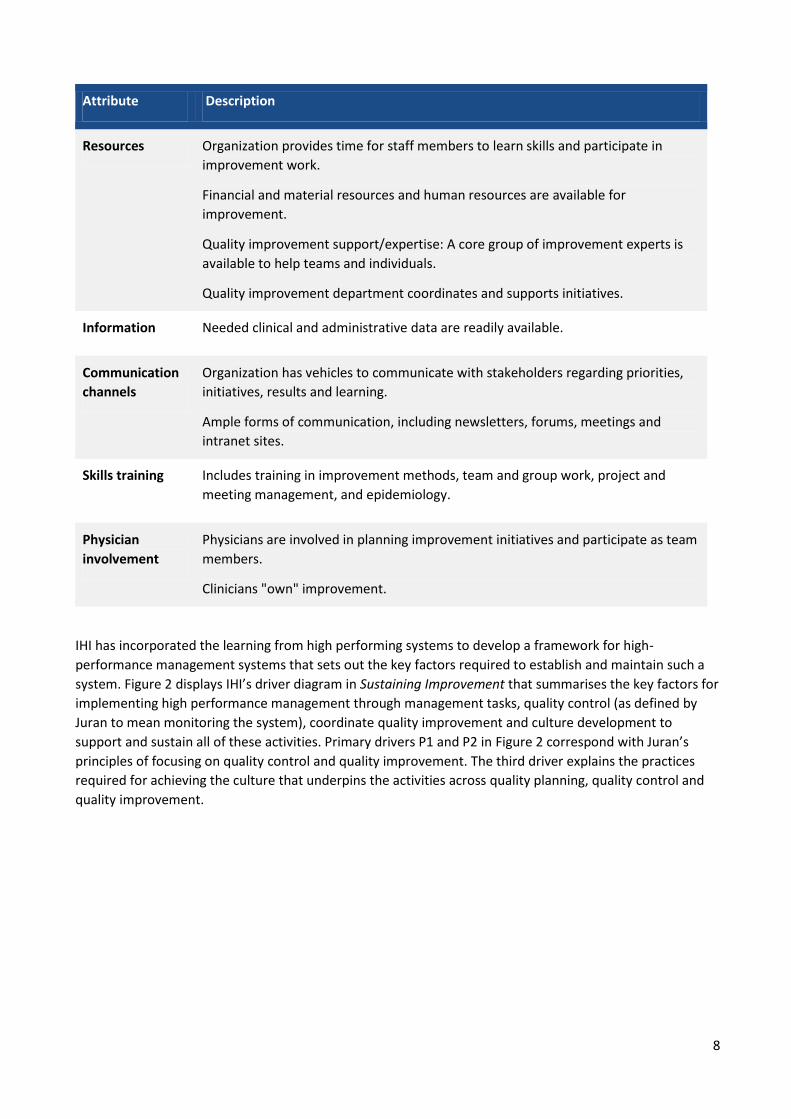
Attribute Description
Resources Organization provides time for staff members to learn skills and participate in
improvement work.
Financial and material resources and human resources are available for
improvement.
Quality improvement support/expertise: A core group of improvement experts is
available to help teams and individuals.
Quality improvement department coordinates and supports initiatives.
Information Needed clinical and administrative data are readily available.
Communication
channels
Organization has vehicles to communicate with stakeholders regarding priorities,
initiatives, results and learning.
Ample forms of communication, including newsletters, forums, meetings and
intranet sites.
Skills training Includes training in improvement methods, team and group work, project and
meeting management, and epidemiology.
Physician
involvement
Physicians are involved in planning improvement initiatives and participate as team
members.
Clinicians "own" improvement.
IHI has incorporated the learning from high performing systems to develop a framework for high-
performance management systems that sets out the key factors required to establish and maintain such a
system. Figure 2 displays IHI’s driver diagram in Sustaining Improvement that summarises the key factors for
implementing high performance management through management tasks, quality control (as defined by
Juran to mean monitoring the system), coordinate quality improvement and culture development to
support and sustain all of these activities. Primary drivers P1 and P2 in Figure 2 correspond with Juran’s
principles of focusing on quality control and quality improvement. The third driver explains the practices
required for achieving the culture that underpins the activities across quality planning, quality control and
quality improvement.

9
Figure 2: Key factors for implementing high performing quality management systems (Scoville et al, 2016,
p.8)3
Key challenges when implementing quality management systems
Successful quality management implementation in healthcare has tended to be limited to individual
organisations or departments or in a specific area of organisational performance. Øvretveit (2000)5 analysed
all European TQM implementations in the healthcare sector concluding that only few small-scale efforts
have had great success. In a comprehensive literature review, Mosadeghrad (2013)6 identified different
categories of failures to explain why quality management has limited success in healthcare. These failures
correspond with the attributes known to be important for high performance in organisations such as
leadership and structure. Table 2 summarises the key obstacles explained in the review in relation to each
of the nine attributes required for high performance4. Juran also considered the challenges for quality
management in healthcare and how those leading quality management might respond to these.
10
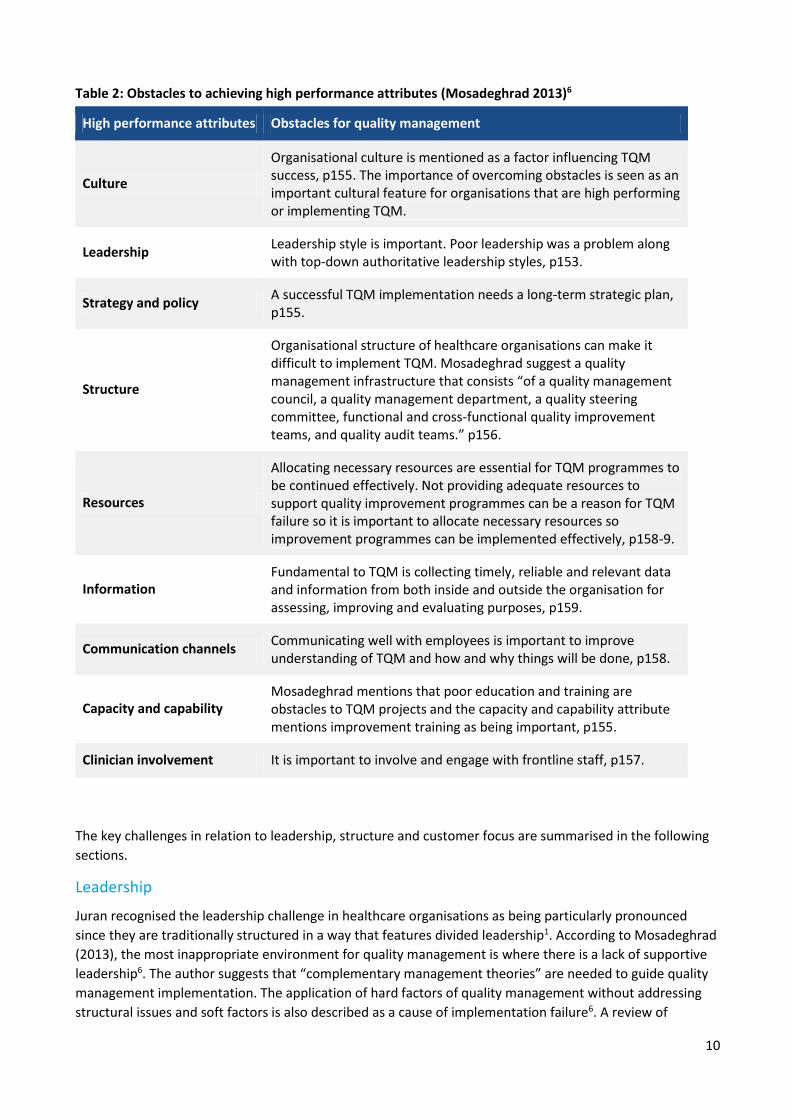
Table 2: Obstacles to achieving high performance attributes (Mosadeghrad 2013)6
The key challenges in relation to leadership, structure and customer focus are summarised in the following
sections.
Leadership
Juran recognised the leadership challenge in healthcare organisations as being particularly pronounced
since they are traditionally structured in a way that features divided leadership1. According to Mosadeghrad
(2013), the most inappropriate environment for quality management is where there is a lack of supportive
leadership6. The author suggests that “complementary management theories” are needed to guide quality
management implementation. The application of hard factors of quality management without addressing
structural issues and soft factors is also described as a cause of implementation failure6. A review of
High performance attributes Obstacles for quality management
Culture
Organisational culture is mentioned as a factor influencing TQM success, p155. The importance of overcoming obstacles is seen as an important cultural feature for organisations that are high performing or implementing TQM.
Leadership Leadership style is important. Poor leadership was a problem along with top-down authoritative leadership styles, p153.
Strategy and policy A successful TQM implementation needs a long-term strategic plan, p155.
Structure
Organisational structure of healthcare organisations can make it difficult to implement TQM. Mosadeghrad suggest a quality management infrastructure that consists “of a quality management council, a quality management department, a quality steering committee, functional and cross-functional quality improvement teams, and quality audit teams.” p156.
Resources
Allocating necessary resources are essential for TQM programmes to be continued effectively. Not providing adequate resources to support quality improvement programmes can be a reason for TQM failure so it is important to allocate necessary resources so improvement programmes can be implemented effectively, p158-9.
Information Fundamental to TQM is collecting timely, reliable and relevant data and information from both inside and outside the organisation for assessing, improving and evaluating purposes, p159.
Communication channels Communicating well with employees is important to improve understanding of TQM and how and why things will be done, p158.
Capacity and capability Mosadeghrad mentions that poor education and training are obstacles to TQM projects and the capacity and capability attribute mentions improvement training as being important, p155.
Clinician involvement It is important to involve and engage with frontline staff, p157.

11
leadership difficulties in relation to implementing quality management in healthcare suggests that quality
management implementation needs “monolithic” visionary leadership, as described by Deming7. One
recognised category of leadership failure is a lack of senior management involvement and commitment. The
authors propose two other categories as being important, namely “combined leadership” and “political
leadership”. The former is described as being typical of large healthcare organisations with many
departments and senior managers who need to be aligned. The second category is the effect of political
influence which is particular to public healthcare which can hinder the leadership quality required for
successful implementation.
Structure and function
The complexity of the healthcare systems and their bureaucratic and departmentalised structure is
suggested to be one of the most significant challenges to achieving quality management for high
performance6. The autonomy of action that features in this structure makes resistance to change more
likely, while the multiple layers of authority inherent can impede the empowerment of employees for
ensuring quality at the front line. The traditional structure of how healthcare is delivered can therefore
make it difficult to ensure that there is coordination and integration of improvement efforts in the system
which is necessary for effective quality management. Juran considered the problem of structure for crucial
aspects of quality management. Breaking down these barriers across functions and professional autonomies
is necessary for the system change required in quality management which requires quality control and
improvement of the system of care as a whole. The characteristics of high performing organisations are how
they effectively use flattened structures with reduced boundaries between units and cross-function
collaboration4.
Customer focus and person-centred care
Quality management requires that customers are identifiable and that they can recognise and define
quality1. However, in health and social care, it is challenging to identify the range of customers and their
needs. Furthermore, the patient is not necessarily the ultimate customer because of the influence of
external stakeholders. The lack of ability of customers to judge the technical aspects of healthcare services
and variability of needs is a further challenge for having customer focus. There is the view that healthcare
organisations can tend to focus on internal quality requirements rather than actual customer needs1. Juran
considered how customer focus can be achieved in healthcare and highlighted the importance of taking a
person-centred approach in order to have ‘health care that continually views itself from the patient’s
perspective and adjusts processes to meet needs’1. Leaders in quality management are explained by Juran
as needing to understand that there are multiple ‘customers’, including patients, families, communities, and
referring institutions, and that each defines quality differently. He also describes how high performance
requires communities’ participation in collaborative health improvement and coordinated services,
especially for the elderly and people with multiple problems.

12
References
1. Juran JM, Godfrey AB (eds). Juran's Quality Handbook. 5th ed. New York: McGraw Hill; 1999.
2. Moen R, Norman C. Circling back: clearing up the myths about the Deming cycle and seeing how it keeps
evolving. Qual Progress 2010;42:23–8.
3. Scoville R, Little K, Rakover J, Luther K, Mate K. Sustaining Improvement. IHI White Paper. Cambridge,
Massachusetts: Institute for Healthcare Improvement; 2016.
4. MacIntosh-Murray et al, 2006 in Baker GR, MacIntosh-Murray A, Porcellato C, Dionne L, Stelmacovich K
and Born K. High Performing Healthcare Systems: Delivery Quality By Design. Toronto: Longwoods
Publishing. 2008.
5. John Øvretveit. Total quality management in European healthcare. International Journal of Health Care
Quality Assurance, 2000;13(2):74-80.
6. Mosadeghrad AM. Obstacles to TQM success in health care systems. International journal of health care
quality assurance. 2013;26(2):147-73.
7. Andrea Chiarini, Emidia Vagnoni. TQM implementation for the healthcare sector: The relevance of
leadership and possible causes of lack of leadership, Leadership in Health Services, 2017; 30 (3):210-216.
You can read and download this document from our website.
We are happy to consider requests for other languages or formats.
Please contact our Equality and Diversity Advisor on 0141 225 6999
or email [email protected]
Healthcare Improvement Scotland
Edinburgh Office Gyle Square 1 South Gyle Crescent Edinburgh EH12 9EB
0131 623 4300
Glasgow Office Delta House 50 West Nile Street Glasgow G1 2NP
0141 225 6999
www.healthcareimprovementscotland.org
Related Documents











