Radiotherapy and Oncology, 7 (1986) 269-279 Elsevier RTO 00267A 269 Quality assurance control in the EORTC cooperative group of radiotherapy. 2. Dosimetric intercomparison K.-A. Johansson 1, J. C. Horiot 2, J. Van Dam 3, D. Lepinoy 2, I. Sentenac 2 and G. Sernbo 1 1Department of Radiation Physics, University of G6teborg, Sahlgren Hospital, S-413 45 G6teborg, Sweden, 2Department of Radiotherapy, Centre G.F. Leelerc, Dijon, France and aDepartment of Radiotherapy, University Hospital, Sint Rafael, Leuven, Belgium (Received 29 november 1985, accepted 10 June 1986) Key words: Quality assurance control in radiotherapy; Dosimetric intercomparison; Dosimetric uncertainty Summary The European Organization for Research on Treatment of Cancer (EORTC) has performed site reviews at 17 institutions participating in clinical trials organized by the Cooperative Group of Radiotherapy. In this paper the dosimetric part of the quality assurance control programme is presented. In a previous paper (part 1) the medical profile of the participating centres was presented. In part 3 an integrated clinical and dosi- metric investigation in an anatomical phantom will be presented. The deviations between the absorbed dose values, for specific points along the beam axis in a water phantom, determined by us and reported by the hospitals were within an acceptable level of variation (about + 3%) for 85, 70 and 71% of the 0~ gamma, X-ray and electron beams, respectively. In some scanning electron beams, too large deviations were found. The flatness and symmetry of the beams were measured. 73% of the X-ray and 60% of the electron beams were within the acceptable levels of variations. Dosimetric recommendations for institutions participating in EORTC clinical trials are presented. Introduction The EORTC (European Organization for Research on Treatment of Cancer) Cooperative Group on Radiotherapy decided to undertake an extensive quality control study, and two teams were elected to draw up and carry out a quality assurance pro- gramme. One team, consisting of radiation oncol- ogists, evaluated medical aspects of the treatment and the second team, consisting of physicists, re- viewed the dosimetry at the different institutions. The objectives of the quality assurance pro- gramme were as follows: (1) To compare the medi- cal profile of the participating centres (human en- vironment and equipment) and to check the con- tents and reliability of the clinical data and of the treatment parameters of the patients entered in EORTC clinical trials. This is covered in part I of this report ~11]. (2) To review the dosimetric pro- cedures applied in all centres to all high-energy beam machines treating patients entered in EORTC trials (part II of this report). (3) To integrate clinical 0167-8140/86/$03.50 1986 Elsevier Science Publishers B.V. (Biomedical Division)

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Radiotherapy and Oncology, 7 (1986) 269-279 Elsevier
RTO 00267A
269
Quality assurance control in the EORTC cooperative group of radiotherapy. 2. Dosimetric intercomparison
K.-A. Johansson 1, J. C. Horiot 2, J. Van Dam 3, D. Lepinoy 2, I. Sentenac 2 and G. Sernbo 1
1Department of Radiation Physics, University of G6teborg, Sahlgren Hospital, S-413 45 G6teborg, Sweden, 2Department of Radiotherapy, Centre G.F. Leelerc, Dijon, France and aDepartment of Radiotherapy, University Hospital, Sint Rafael, Leuven, Belgium
(Received 29 november 1985, accepted 10 June 1986)
Key words: Quality assurance control in radiotherapy; Dosimetric intercomparison; Dosimetric uncertainty
Summary
The European Organization for Research on Treatment of Cancer (EORTC) has performed site reviews at 17 institutions participating in clinical trials organized by the Cooperative Group of Radiotherapy. In this paper the dosimetric part of the quality assurance control programme is presented. In a previous paper (part 1) the medical profile of the participating centres was presented. In part 3 an integrated clinical and dosi- metric investigation in an anatomical phantom will be presented. The deviations between the absorbed dose values, for specific points along the beam axis in a water phantom, determined by us and reported by the hospitals were within an acceptable level of variation (about + 3%) for 85, 70 and 71% of the 0~ gamma, X-ray and electron beams, respectively. In some scanning electron beams, too large deviations were found. The flatness and symmetry of the beams were measured. 73% of the X-ray and 60% of the electron beams were within the acceptable levels of variations. Dosimetric recommendations for institutions participating in EORTC clinical trials are presented.
Introduction
The EORTC (European Organization for Research on Treatment of Cancer) Cooperative Group on Radiotherapy decided to undertake an extensive quality control study, and two teams were elected to draw up and carry out a quality assurance pro- gramme. One team, consisting of radiation oncol- ogists, evaluated medical aspects of the treatment and the second team, consisting of physicists, re- viewed the dosimetry at the different institutions.
The objectives of the quality assurance pro- gramme were as follows: (1) To compare the medi- cal profile of the participating centres (human en- vironment and equipment) and to check the con- tents and reliability of the clinical data and of the treatment parameters of the patients entered in EORTC clinical trials. This is covered in part I of this report ~11]. (2) To review the dosimetric pro- cedures applied in all centres to all high-energy beam machines treating patients entered in EORTC trials (part II of this report). (3) To integrate clinical
0167-8140/86/$03.50 �9 1986 Elsevier Science Publishers B.V. (Biomedical Division)
270
and dosimetric data of a simulated case with an anatomical (Alderson) phantom. These results will be presented in part III of this report.
This paper, part II of the report, presents the method used and the results obtained in the basic physics and dosimetric intercomparison which has been going on for the past 3 years. The dosimetric review comprises determination of the absorbed dose in water for certain points and measurements of the absorbed dose distribution at one depth per- pendicular to the beam axis.
Acceptable levels of variations for physical parameters that affect the absorbed dose distribu- tion in the patient have been stated by various or- ganizations [1,14]. It has been concluded by the Radiological Physics Center (RPC) in the USA that the goal of quality control review is to ensure that the absorbed dose in reference points in water is equal within t 3 % for all beams and the tumor dose prescription is equal within + 5 % [10]. The reason for requiring such a high level of accuracy in the absorbed dose determination is that most tu- mours and mammalian normal tissues have steep, sigmoid-shaped dose-response curves with little separation between the two curves. Criteria for the acceptable levels of variations for the flatness and symmetry in the beam at different depths in a phan- tom have been proposed by the IEC [16], and should comply with values specified by the IEC.
Materials and methods
The dosimetry team has no full-time staff, but con- sists of voluntary hospital physicists from different countries. However, the coordinator and the meas- uring equipment come from the University of Gothenburg, Sweden. This equipment was brought to all centres by two physicists. Seventeen of 30 European institutions participating actively in the EORTC Cooperative Group on Radiotherapy were visited, and 45 therapy machines were reviewed. See Table I in part I [11].
Absorbed dose in specific points
Ionization chambers and measuring procedures recommended by the NACP [21,22] were used for the absorbed dose determination in a water phan- tom. A Farmer-type chamber with graphite wall and a NACP flat chamber [19] were used for mea- surements in photon and electron beams, respec- tively. The ionization chambers were calibrated at the Swedish National Institute of Radiation Pro- tection and the constancy of response was checked prior to each set of measurements.
At each machine, the EORTC team measured the absorbed dose for several combinations of field siz- es (square and rectangular), depths along the beam axis, and with different beam modifiers such as wedge filters and shadow trays (see Table I). The institutions used their own method to calibrate the machines [6,13,21,22]. The institutions had to state at the depth of measurement the absorbed dose per unit of the timer (for 6~ or the monitor (for ac- celerators) used for the absorbed dose calculations for patient treatments on the day of our review. Furthermore, the institution had to carry out a check measurement for its reference field size and depth with its own dosimetry equipment just before or after our measurement. These check measure-
TABLE I
Combinations of field sizes, depths along the beam axis and beam modifiers reviewed.
Beam Field size Depth Modifiers quality (cm • cm) (cm)
Photons 6 • 6 5 - 10 • 10 5 20 x 20 5 10 • 10 5 Wedge filter 10 • 10 5 Shadow tray 12 x 20 8
Electrons 10 • 10 Dmax 20 • 20 Dmax
ments were used to compare with the stated ab- sorbed dose values.
A principal goal of this quality control is to en- sure by review that the absorbed dose in specific points for all beams are within + 3% of that stated by the institutions. This value is the maximum ac- ceptable level of variation for all beam qualities. It has been shown by many independen t reviews (cf Refs. 10,18) that the frequency distributions of the ratios determined to stated absorbed dose are nor- mal distributed. The total variations in these dis- tributions are caused by variations in the stated ab- sorbed dose values and also by the experimental uncertainties introduced by the reviewer. A review- er who has a large experimental uncertainty will in- crease the spread of the frequency distribution, and vice versa. These two types of uncertainties are as- sumed to be normally distributed and can then be individually analyzed by statistical rules. We have taken into account our experimental uncertainty for determination of the acceptable level o f varia- tion. The acceptable level of variation, given in Table II, is therefore the root of the square sum of the goal, + 3%, and the relative experimental un- certainty for the different qualities.
The random errors in our measuring equipment and in the set-up of the measuring equipment used for the intercomparison were determined at one 6~ gamma source with many independent checks. The random variation of the readings was 4-0.6% (1 S.D.). Johansson [17] has shown that the total overall uncertainty in absorbed dose deter-
271
minations in water with ionization chambers is be- tween 3 and 5% (95% confidence level), depending on the quality of the beam. All of the errors con- tributing to the total overall uncertainty are not of interest for estimation of the variation in absorbed dose values between different beams, since some of the uncertainties contributing to the total overall uncertainties are similar for all beams when iono- metric methods were used by all centres and also used by us. However, uncertainties depending on the quality of the beam which have influence on the interaction coefficients must be included in the es- timations of the relative uncertainties in the deter- minations carried out by the EORTC. When the random uncertainties, expressed as 1 S.D., and sys- tematic uncertainties of interest for the intercom- parison are combined in quadrature [5] the relative uncertainty, expressed as 1 S.D., is 4-0.8, 4- 1.0 and + 1.6% for 6~ gamma-ray, X-ray and electron beams, respectively. For swept/scanned electron beams, the uncertainty may be somewhat higher, depending on the uncertainties in the factor used for correction for loss of ions due to recombinat ion [25].
A major deviation is defined as being greater than twice the acceptable level of variation f rom the ref- erence value and a minor deviation is between these two levels. A similar definition has been used to distinguish appropriate from inappropriate treat- ments by Glicksman et al. [9].
At most of the machines, an independent ab- sorbed dose intercomparison was made for one
TABLE II
Acceptable levels of variations of the absorbed dose determined by the EORTC team from the reference value for different quality of the beam.
Quality Acceptable level of variation
Deviation from the reference value
Minor Major
Photon, 6~ 0.969 1.031 > 4-3.1% > 4- 6.2% Photon, 4-25 MV 0.981-1.045" > 4- 3.2% > 4- 6.4% Electron, 4-25 MeV 0.966-1.034 > 4- 3.4% > 4- 6.8%
These values include the experimental uncertainties. * The average ratio is adopted as the reference value.
272
<
s
O
O
O
o
�9 L~
E o
N 0
N
~.~
O~
O
O
< ~
O
O
8 ~
~.-.q A
o
A
"I.
A A
A
4
.g
'-d
E
s
O 8
E
O
(,- ;>
field size using thermoluminescence dosimeters in a polystyrene phantom. These measurements were made in order to find large errors in our ionization chamber dosimetry, and for future investigations.
Absorbed dose distribution
A film irradiated perpendicular to the beam axis in a polystyrene phantom was used to evaluate the absorbed dose distribution at one depth for a 20 x 20 cm field size. The measuring depths were 5
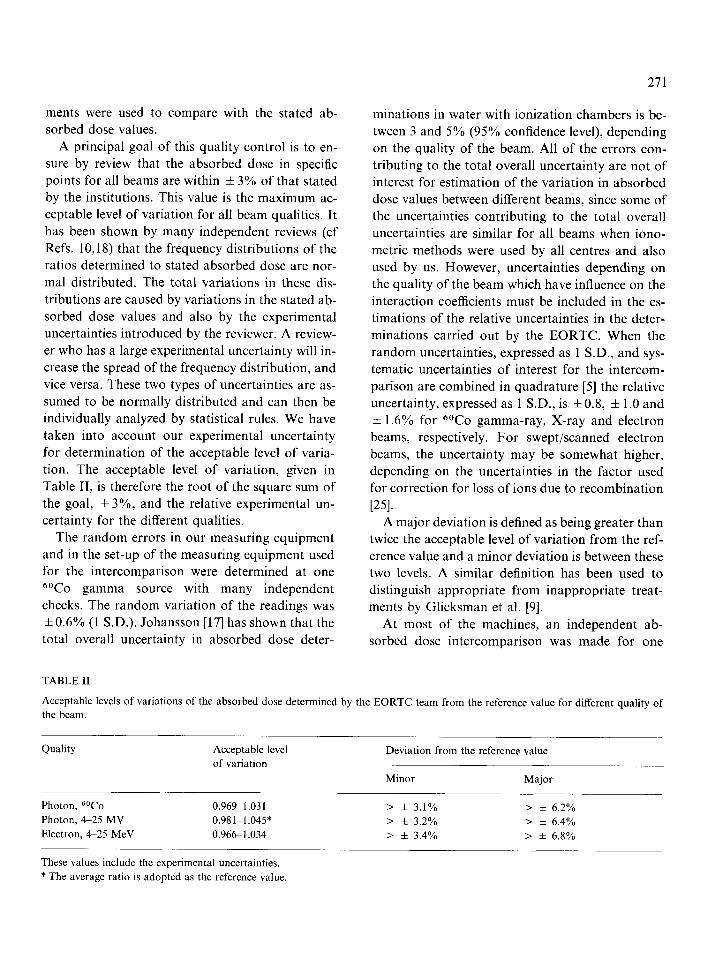
cm for photon beams and the depth of dose maxi- mum for electron beams. The film density was mea- sured and flatness and symmetry in the beam were determined according to the IEC method [16]. The symmetry in the beam for photon and electron beams is defined as the ratio of the absorbed dose at points symmetrical with respect to the beam axis. For photon beams the flatness is defined as the ratio along the major axes of the maximum absorbed dose to the minimum absorbed dose within the flat- tened area. However, for electron beams according to IEC [16] the flatness is defined by a combination of two parts: (1) the distance along the major axes between the 90% isodose contour and the 50% is- odose contour in the penumbra region, and (2) the absorbed dose at any point shall be less than 103% of the absorbed dose on the beam axis. Johansson [17] has demonstrated good agreement between film density distribution and absorbed dose distri- bution in electron beams. However, in photon beams the agreement is not so good, particularly in 6~ gamma, 4 and 5 MV X-ray beams. The de- viation between film density and absorbed dose is about 3% in 6~ gamma beams and about 1% in 10 MV beams, and varies somewhat depending on the field size. The acceptable levels of variation for the measured absorbed dose distribution from the uniform distribution have been defined in a similar way as for the absorbed dose determination (Table II). The values recommended by IEC for flatness and symmetry and the relative experimental uncer- tainties, added in square and the root of the sum, give the acceptable levels of variations. Table III gives the acceptable levels of variations, the minor deviations and the major deviations.
273
Results and discussion
Absorbed dose in specific points
The distribution of the ratios of the absorbed dose to water determined by the EORTC team to the absorbed dose stated for patient treatments by the institutions for all checked combinations and for all units are shown in Figs. 1, 2 and 4 for 6~ gamma, X-ray and electron beams from accelerators, re: spectively. In the figures are given the number of measuring points, n, the mean value, 2, the value of 1 S.D., a, and the difference between the highest and lowest ratios, A.
6~ gamma beams For the 6~ gamma beams, the mean value of the ratio is close to unity and the standard deviation is + 2.0% (Fig. 1). Of all 6~ beams, 85% are within the acceptable level of variation, + 3.1% from unity. No major deviation was found. The spread is somewhat larger for beams with beam modifiers than for open square field sizes. The larg- est deviation of the ratio from unity was 5.5% and was obtained in a wedge filter beam.
At one institution the local ionization chamber calibration factor had an error of about 3%, caus- ing an error in the absorbed dose calibration of one 6~ gamma unit. Another institution had an error of several millimeters in the definition of the iso- centre, causing an error in the absorbed dose de- termination. Large deviations were also found for small field sizes (6 x 6 cm). This is in agreement with Engler and Jones [7], showing that large errors may be introduced in the absorbed dose measure- ments for small field sizes when common commer- cial ionization chambers are used.
The agreement between the absorbed dose values determined by us and the absorbed dose values re- ported by the institutions was acceptable for most of the 6~ gamma beams. However, simple pre- cautions such as re-calibration and constancy con- trol of the local reference ionization chamber, more accurate determination of wedge filter and shadow tray factors, and uniformity in the method of de- termination of absorbed dose can reduce the spread

274
2 5 -
2O >-
z i
15 O I i i
r r I I I
10 I ,
I i
5
, , r , , , I , , , v ,
0.92 0.96 1.00 1.04 1.08
ABS. DOSE DETERMINED/ABS. DOSE STATED
Fig. 1. The distr ibution of the ratio of determined to stated ab-
sorbed dose for ~~ 7-beams for different field sizes, beam mod-
ifiers and depths for 20 machines. Lined bars represent square
field s izesn = 5 9 , 2 = 1.001, a = 0.019, A = 0.10, and open
bars beams with modifiers and rectangular field sizes n = 51, 2
= 0.999, a = 0.021, A = 0.10. The vertical lines indicate the
acceptable level of variation.
25
2O
z uJ
15 o UJ rr LL
lO
i r i , ,
0.92 096 1.00
g_ 1.04 1.08 1.12
A B S . DOSE DETERMINED/ABS. DOSE STATED
Fig. 2. Distr ibut ion of the ratio of determined to stated absorbed
dose for photon beams with qualities between 4 and 25 MV
X-rays for different field sizes, beam modifiers and depths for 24
accelerators. Lined bars represent accelerators with sealed mon-
itor chambers n = 62, )~ = 1.025, cr = 0.029, A = 0.13, and
open bars unsealed monitor chambers n = 78, 2 = 1.003, cr
= 0.035, A = 0.12. The vertical lines indicate the acceptable
level of variation.
further. Precautions have already been taken by several of the institutions to reduce the dosimetric deviations in 6~ gamma beams.
4-25 M V X-ray beams For photon beams with the qualities between 4 and 25 MV from 26 accelerators, we have on average found the absorbed dose to be 1.3% higher than the value stated by the institutions (see Fig. 2). One standard deviation of the ratios is 4- 3.2%. Of all photon beams, 70% are within the acceptable level of variation 4- 3.2% from the average value and 5% of the beams have major deviations. The largest deviation of the ratio from the average ratio was 9%.
The main reason for the significant deviation of the mean ratio from unity in Fig. 2 is that the ICRU procedure [13] for absorbed dose determination with an ionization chamber used by most of the
institutions underestimates the absorbed dose by 2-3% [2]. However, the NACP procedure used by us has taken into account recently published new knowledge about ionization chamber dosimetry. It has been shown by Mattsson [20] that the consist- ency in the NACP procedure for absorbed dose de- termination in different beam qualities is very good. Other national dosimetry protocols [6] and local methods have also been used, causing the spread in Fig. 2 to increase to + 3.2% compared to 4-2.0% for cobalt beams. Another reason for this increased spread is that some centres with the dose-monitors of the accelerators sensitive to air pressure and tem- perature do not correct for changes of pressure and temperature. These unsealed monitor chambers can cause an error in the dosimetry of up to 5% [12,23].
A correction was determined by the local physi- cist by check measurement of a reference field be- fore or after our review. The results of the inter-
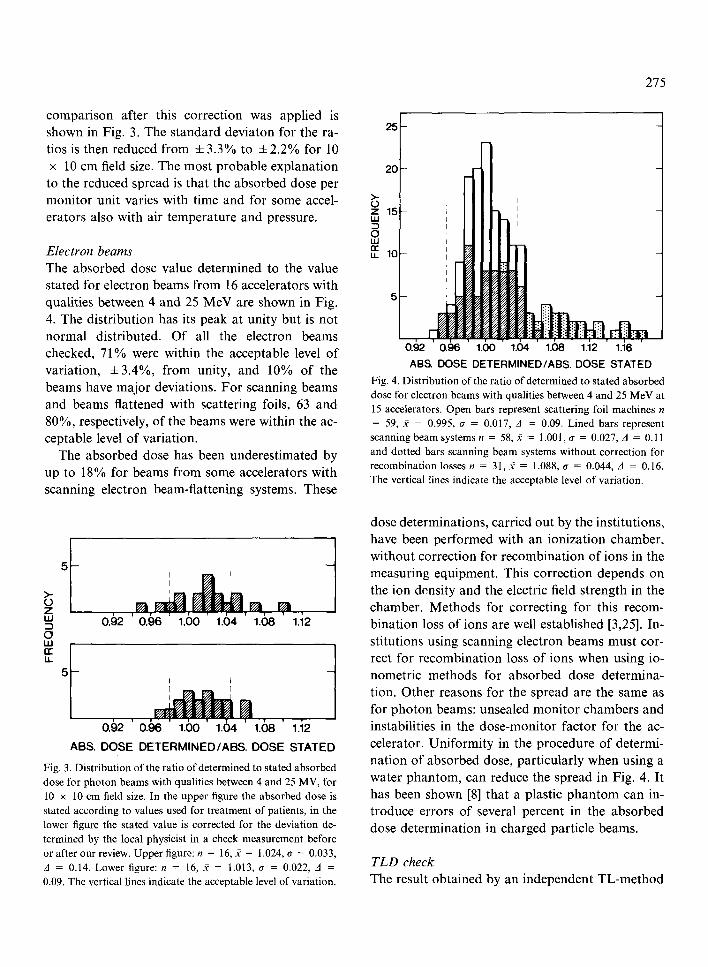
comparison after this correction was applied is shown in Fig. 3. The standard deviaton for the ra- tios is then reduced from • to 4-2.2% for 10 x 10 cm field size. The most probable explanation to the reduced spread is that the absorbed dose per monitor unit varies with time and for some accel- erators also with air temperature and pressure.
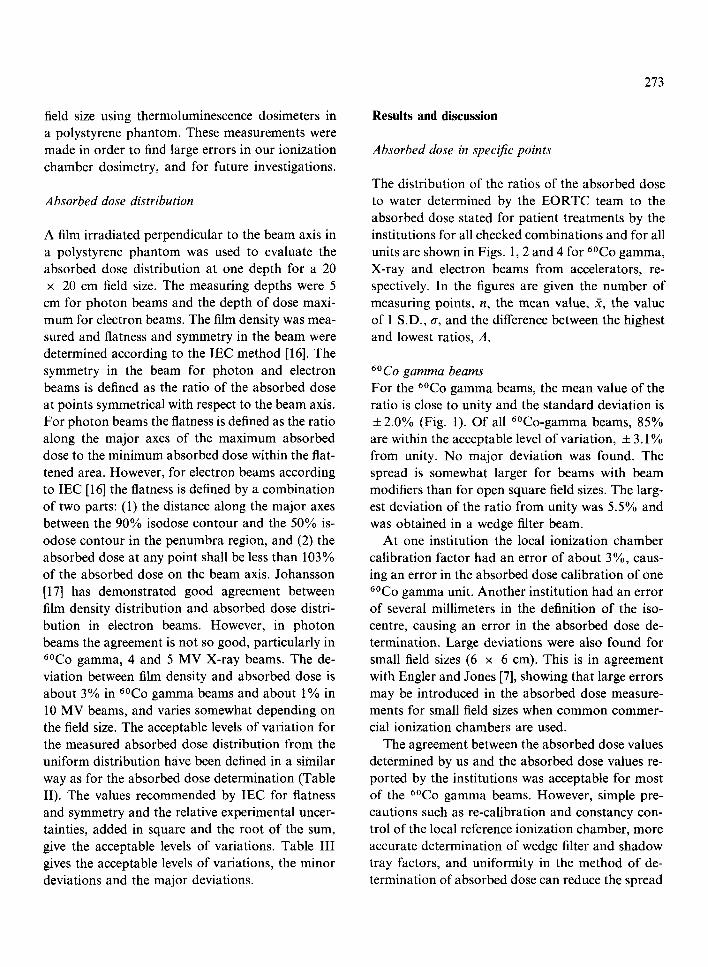
Electron beams The absorbed dose value determined to the value stated for electron beams from 16 accelerators with qualities between 4 and 25 MeV are shown in Fig. 4. The distribution has its peak at unity but is not normal distributed. Of all the electron beams checked, 71% were within the acceptable level of variation, +3.4%, from unity, and 10% of the beams have major deviations. For scanning beams and beams flattened with scattering foils, 63 and 80%, respectively, of the beams were within the ac- ceptable level of variation.
The absorbed dose has been underestimated by up to 18% for beams from some accelerators with scanning electron beam-flattening systems. These
. . . . . . . 6 8 ' i 0. 2 0.96 1.00 1.04 1. 1. 2
>- 0 Z I,LI
0 I,LI n"
0.~)2 ' 0 . 9 6 ' 1 .60 ' 1.()4 ' 1.(~)8' 1.'12
ABS. DOSE DETERMINED/ABS. DOSE STATED
Fig. 3. Distribution of the ratio of determined to stated absorbed dose for p h o t o n b e a m s wi th qua l i t ies be tween 4 and 25 MV, for
10 • 10 cm field size. In the uppe r figure the a b s o r b e d dose is
s ta ted accord ing to values used for t r e a t m e n t of pa t ients , in the
lower figure the s ta ted va lue is cor rec ted for the dev i a t i on de-
t e rmined by the local phys ic i s t in a check m e a s u r e m e n t before
or af ter our review. U p p e r figure: n = 16, 2 = 1.024, a = 0.033,
A = 0.14. Lower f i g u r e : n = 1 6 , ~ = 1.013, a = 0.022, A =
0.09. The ver t ical l ines ind ica te the accep tab le level o f va r ia t ion .
275
25
2 0 -
>- O i z 1 5 - I - UJ
0 LU
1 0 -
5 -
0.92 0.96 1.00 1.04 1.08 1.12 1.16
ABS. DOSE DETERMINED/ABS. DOSE STATED
Fig. 4. Distribution of the ratio of determined to stated absorbed dose for e lec t ron beams wi th qual i t ies be tween 4 and 25 M e V at
15 accelera tors . O p e n bars represent sca t t e r ing foil m a c h i n e s n
= 59, ff = 0.995, ~ = 0.017, A = 0.09. L ined bars represent
s cann ing b e a m sys tems n = 58, ff = 1.001, a = 0.027, A = 0.11
and do t t ed bars s cann ing b e a m sys tems w i t h o u t co r rec t ion for
r e c o m b i n a t i o n losses n = 31, 92 = 1.088, a = 0.044, A = 0.16.
The ver t ica l l ines ind ica te the accep tab le level o f va r i a t ion .
dose determinations, carried out by the institutions, have been performed with an ionization chamber, without correction for recombination of ions in the measuring equipment. This correction depends on the ion density and the electric field strength in the chamber. Methods for correcting for this recom- bination loss of ions are well established [3,25]. In- stitutions using scanning electron beams must cor- rect for recombination loss of ions when using io- nometric methods for absorbed dose determina- tion. Other reasons for the spread are the same as for photon beams: unsealed monitor chambers and instabilities in the dose-monitor factor for the ac- celerator. Uniformity in the procedure of determi- nation of absorbed dose, particularly when using a water phantom, can reduce the spread in Fig. 4. It has been shown [8] that a plastic phantom can in- troduce errors of several percent in the absorbed dose determination in charged particle beams.
TLD check The result obtained by an independent TL-method
276
used by us agrees with results obtained by our ion- ization chamber measurements. The spread, given as one standard deviation, for the absorbed dose ratios obtained between our TL method and our ionometric method is +1.6% for all types of beams, including scanning electron beams. The maximum deviation between these two methods was 3.5%.
Absorbed dose distribution
The symmetry of the absorbed dose distribution in 6~ gamma beams at 5 cm depth in the plastic phantom was good, and none of the beams had an asymmetry larger than 3%.
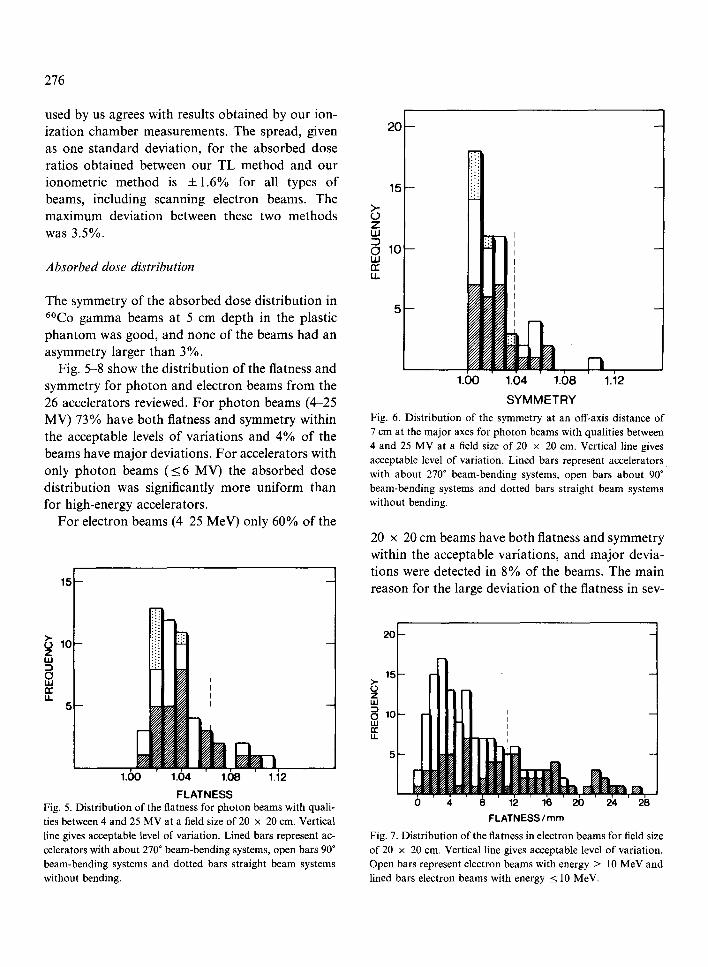
Fig. 5-8 show the distribution of the flatness and symmetry for photon and electron beams from the 26 accelerators reviewed. For photon beams (4-25 MV) 73% have both flatness and symmetry within the acceptable levels of variations and 4% of the beams have major deviations. For accelerators with only photon beams (<6 MV) the absorbed dose distribution was significantly more uniform than for high-energy accelerators.
For electron beams (4-25 MeV) only 60% of the
15
2 0 - -
15- -
>- l O -
z I l l
0 UJ I = ', u.
1.60 1.64 1.08 1.i2
FLATNESS Fig. 5. Distribution of the flatness for photon beams with quali- ties between 4 and 25 MV at a field size of 20 x 20 cm. Vertical line gives acceptable level of variation. Lined bars represent ac- celerators with about 270* beam-bending systems, open bars 90* beam-bending systems and dotted bars straight beam systems without bending.
>-
Z ILl
LL
WO 10
1.60 1.04 ' 1.08
S Y M M E T R Y
n i
1.12
Fig. 6. Distribution of the symmetry at an off-axis distance of 7 cm at the major axes for photon beams with qualities between 4 and 25 MV at a field size of 20 x 20 cm. Vertical line gives acceptable level of variation. Lined bars represent accelerators with about 270" beam-bending systems, open bars about 90" beam-bending systems and dotted bars straight beam systems without bending.
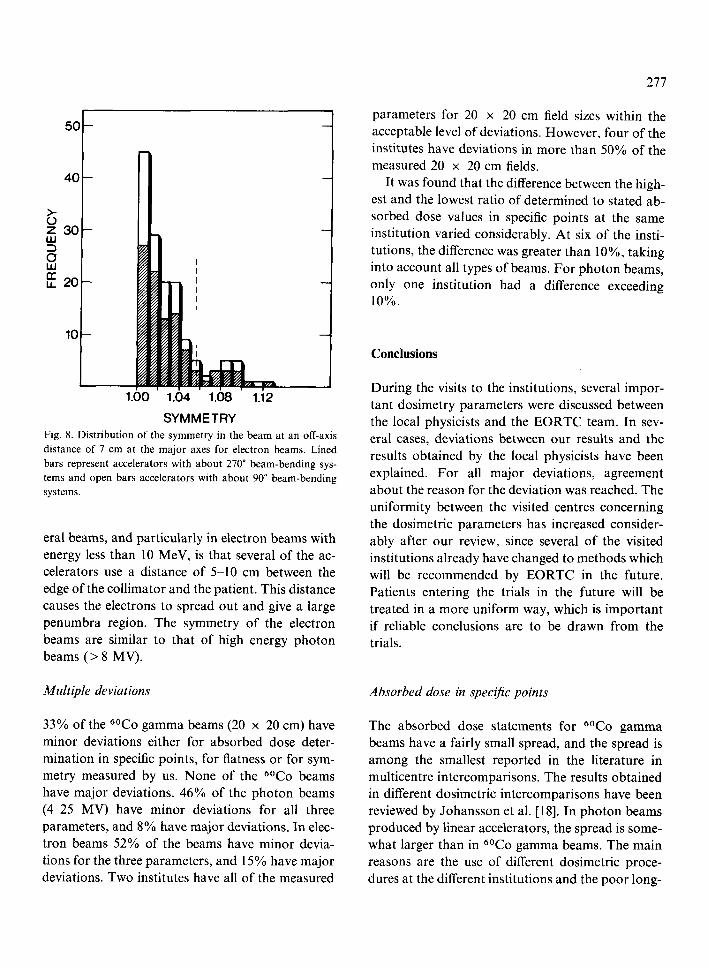
20 x 20 cm beams have both flatness and symmetry within the acceptable variations, and major devia- tions were detected in 8% of the beams. The main reason for the large deviation of the flatness in sev-
20
1 5 >,. o z LU
~ lO r r
0 4 8 12 16 20 2'4 2i3 FLATNESS / mm
Fig. 7. Distribution of the flatness in electron beams for field size of 20 x 20 cm. Vertical line gives acceptable level of variation. Open bars represent electron beams with energy > 10 MeV and lined bars electron beams with energy < 10 MeV.
5 0 -
4 0 -
>- ~9
30--
?, tl
,~ I I i | i i
1.00 1.04 1.08 1.12
SYMMETRY Fig. 8. Distribution of the symmetry in the beam at an off-axis
distance of 7 cm at the major axes for electron beams. Lined
bars represent accelerators with about 270 ~ beam-bending sys-
tems and open bars accelerators with about 90 ~ beam-bending
systems.
eral beams, and particularly in electron beams with energy less than 10 MeV, is that several of the ac- celerators use a distance of 5-10 cm between the edge of the collimator and the patient. This distance causes the electrons to spread out and give a large penumbra region. The symmetry of the electron beams are similar to that of high energy photon beams (> 8 MV).
Multiple deviations
33% of the 6~ gamma beams (20 • 20 cm) have minor deviations either for absorbed dose deter- mination in specific points, for flatness or for sym- metry measured by us. None of the 6~ beams have major deviations. 46% of the photon beams (4 25 MV) have minor deviations for all three parameters, and 8% have major deviations. In elec- tron beams 52% of the beams have minor devia- tions for the three parameters, and 15% have major deviations. Two institutes have all of the measured
277
parameters for 20 x 20 cm field sizes within the acceptable level of deviations. However, four of the institutes have deviations in more than 50% of the measured 20 x 20 cm fields.
It was found that the difference between the high- est and the lowest ratio of determined to stated ab- sorbed dose values in specific points at the same institution varied considerably. At six of the insti- tutions, the difference was greater than 10%o, taking into account all types of beams. For photon beams, only one institution had a difference exceeding 10%.
Conclusions
During the visits to the institutions, several impor- tant dosimetry parameters were discussed between the local physicists and the EORTC team. In sev- eral cases, deviations between our results and the results obtained by the local physicists have been explained. For all major deviations, agreement about the reason for the deviation was reached. The uniformity between the visited centres concerning the dosimetric parameters has increased consider- ably after our review, since several of the visited institutions already have changed to methods which will be recommended by EORTC in the future. Patients entering the trials in the future will be treated in a more uniform way, which is important if reliable conclusions are to be drawn from the trials.
Absorbed dose in specific points
The absorbed dose statements for 6~ gamma beams have a fairly small spread, and the spread is among the smallest reported in the literature in multicentre intercomparisons. The results obtained in different dosimetric intercomparisons have been reviewed by Johansson et al. [18]. In photon beams produced by linear accelerators, the spread is some- what larger than in 6~ gamma beams. The main reasons are the use of different dosimetric proce- dures at the different institutions and the poor long-

278
term stability of the dose-monitor in the accelera- tors. In electron beams, even larger deviations were found, some of them being unacceptable. The main reason for these very large deviations is absence of correction for ion recombination in the measuring ionization chamber, but different dosimetry proto- cols and phantom materials also contribute to the spread. All of the institutions using scanning elec- tron beams have introduced the correction for loss of ions in the dosimetry after our review. The sys- tematic difference in the absorbed dose values in X-ray beams caused by different dosimetric recom- mendations [13,21] in use gives an average ratio of determined to stated absorbed dose of 1.013. This value has been adopted as the reference value for the acceptable level of variation (see Table II). For all other qualities the ratio 1.000 is adopted as the reference value, even if the average value differs from unity.
Absorbed dose distribution
The flatness and symmetry in the beam was found to be acceptable for most of the beams. Particularly in accelerators without beam-bending systems, the flatness and symmetry at the reference depth were very good for the checked depth and field size.
However, in electron beams with an energy below 10 MeV with a large distance between the colli- mator and the patient, an unacceptably large pen- umbra was measured.
Recommendations for the future
The EORTC Radiotherapy Group recommends that all participating centres entering patients in the clinical trials of the group be required to follow the following guidelines:
The Nordic [21,22], French [4], Spanish [24] or ICRU Report 35 [15] dosimetric protocol should be used for absorbed dose determinations. It has been shown by Mattsson [20] that the differences be- tween these new protocols can cause errors of less than 1%, which must be considered acceptable.
Correction for the recombination loss of ions in the ionization chamber should be made according to the methods described by Boag [3] or by Van Dam et al. [25], when measured in scanning beams. The electrometer should therefore at least have two levels of polarizing voltage in order to determine the correction.
The measurements should be carried out in water for all beams. Particularly for electron beams, the uncertainties increase when measurements are made in plastic. The institute should have both a cylindrical and a plane parallel ionization chamber for measurements in photon and electron beams, respectively, in order to fullfil the requirements giv- en in the recommended dosimetric protocols.
Other important precauses that can further in- crease the accuracy in the physical part of radio- therapy are regular check measurements of the cal- ibration factor and absorbed dose distribution, par- ticularly for accelerators. Daily correction for air temperature and pressure for accelerators with un- sealed dose monitors is advisable.
This dosimetric part of the EORTC quality as- surance programme will continue. The programme will be modified slightly and the dosimetric team will be split up into some dosimetric reference centres geographically distributed in Europe. The reference centres will cooperate and internally com- pare methods and results. Such a comprehensive quality assurance programme will ensure that the radiation equipment with accessories accurately and uniformly can deliver the prescribed absorbed dose.
Acknowledgements
This investigation was supported by grants from the EORTC organization and the Jubilee Clinic Foundation for Cancer Research in G/Steborg and Stockholm. All visited institutions are thanked for their kind assistance with the working procedures, and friendly reception.

References
I AAPM (American Association of Physicists in Medicine). Physical aspects of quality assurance in radiation therapy. Report. 1984,
2 Almond, P. R. and Svensson, H. Ionization chamber dosi- metry for photon and electron beams. Acta Radiol. Ther. Phys. Biol. 16: 177-186, 1977.
3 Boag, J. W. The recombination correction for an ionization chamber exposed to pulsed radiation in a "swept beam" technique. I Theory. Phys. Med. Biol. 27:201-211, 1982.
4 CFMRI (Comit6 Fran~ais Measure des Rayonnements Ion- isants) Recommendations pour la d6termination de la dose absorb~e en radioth6rapie dans les faisceaux de photons et d'~lectrons d'bnergie comprise entre 1 MeV et 50 MeV. Re- port CFMRI No. 2, 1984.
5 CIPM (Comit~ International des Poids et Mesures). Assign- ment of experimental uncertainties, Recommendation 1 (CI-1981).
6 DIN (Deutsches Institut ffir Normung). Dosismessverfah- ren in der radiologischen Technik: Ionisationsdosimetrie. Manuskript DIN 6800 Teil 2, 1980.
7 Engler, M. J. and Jones, G. L. Small-beam calibration by 0.6- and 0.2-cm 3 ionization chambers. Med. Phys. 11: 822- 826, 1984.
8 Galbraith, D. M., Rawlinson, J. A. and Munro, P. Dose errors due to charge storage in electron irradiated plastic phantoms. Med. Phys. 11: 253-261, 1984.
9 Glicksman, A. S., Reinstein, L. E., McShan, D. and Laurie, F. Radiotherapy quality assurance program in a cooper- ative group. Int. J. Radiation Oncol. Biol. Phys. 7: 1561- 1568, 1981.
10 Golden, R., Cundiff, J. H., Grant, W. H. and Shalek, R. J. A review of the activities of the AAPM radiological physics center in interinstitutional trials involving radiation therapy. Cancer 29: 1468-1472, 1972.
11 Horiot, J. C., Johansson, K.-A., Gonzalez, van der Schueren, E., Van den Bogaert, W. and Notter, G. Quality assurance control in the EORTC cooperative group of radiotherapy. I. Assessment of radiotherapy staff and equipment. Radioth- er. Oncol. 6: 275-284.
12 Hrejsa, A. F., Soen, J. and Jankowiak, P. Temperature-pres- sure compensation for a linear accelerator electron beam dosimeter. Med. Phys. 12: 260-261, 1985.
13 ICRU Report 14. Radiation Dosimetry: X-rays and gamma rays with maximum photon energies between 0.6 and 50 MeV. International Commission on Radiation Units and Measurements, Washington D.C., U.S.A., 1969.
279
14 ICRU Report 24. Determination of Absorbed Dose in Patient Irradiated by Beams of X or Gamma Rays in Radio therapy Procedures. International Commission on Radia tion Units and Measurements, Washington D.C., U.S.A.
1976. 15 ICRU Report 35. Radiation Dosimetry: Electron beam:
with energies between I and 50 MeV. International Corn mission on Radiation Units and Measurements, Bethesda MD, U.S.A., 1984,
16 IEC (International Electrotechnical Commission). Medica electron accelerators in the range 1-50 MeV. Performance tolerance. Sub Committee 62C-18, 1981.
17 Johansson, K.-A. Studies of different methods of absorbec dose determination and a dosimetric intercomparison at the Nordic Radiotherapy Centres. Thesis, G6teborg, Sweden, 1982.
18 Johansson, K.-A., Mattsson, L. O. and Svensson, H. Do simetric intercomparison at the Scandinavian radiation ther- apy centres. I. Absorbed dose intercomparison. Acta Radiol. Oncol. 21: 1-10, 1982.
19 Mattsson, L. O., Johansson, K.-A. and Svensson, H. Cali- bration and use of plane-parallel ionization chambers for the determination of absorbed dose in electron beams. Acta Ra- diol. Oncol. 20: 385-399, 1981.
20 Mattsson, O. Comparison of different protocols for the do- simetry of high-energy photon and electron beams. Radioth- er. Oncol. 4: 313-318. 1985.
2l NACP (Nordic Association of Clinical Physics). Procedures in external radiation therapy dosimetry with electron and photon beams with maximum energies between 1 and 50 MeV. Acta Radio/. Oncol. 19: 55~79, 1980.
22 NACP (Nordic Association of Clinical Physics). Electron beams with mean energies at the phantom surface below 15 MeV. Acta Radiol. Oncol. 20: 402-415, 1981.
23 Sharma, S. C., Wilson, D. L. and Jose, B. Variation of out- put with atmospheric pressure and ambient temperature for Therac-20 linear accelerator. Med. Phys. 10: 712, 1983.
24 SEFM (Sociedad Espanola de Fisica medica) Procedimien- tos recomendados para la dosimetria de fotones y electrones de energias comprendidas entre 1 MeV y 50 MeV en radio- terapia de haces externos. SEFM No. 1, 1984.
25 Van Dam, J., Rijnders, A., Ang, K. K., Mellaerts, M. and Grobet, P. Determination of ionization chamber collection efficiency in a swept electron beam by means of thermolu- minescent detectors and the "two-voltage" method. Ra- diother. Oncol. 3: 363-370, 1985.
Related Documents











