Quality Assessment Lecture 2

Quality Assessment
Jan 02, 2016
Quality Assessment. Lecture 2. Laboratory Analysis. The goal of laboratory analysis is to provide the reliable laboratory data to the health-care provider in order to assist in clinical decision-making. - PowerPoint PPT Presentation
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Quality Assessment
Lecture 2

Laboratory Analysis
The goal of laboratory analysis is to provide the reliable
laboratory data to the health-care provider in order to assist
in clinical decision-making.
M. Zaharna Clin. Chem. 2009

Modern medicine relies on the provision of accurate analytical results from the laboratory both to confirm diagnosis and to monitor therapy.
If laboratory results are to play a proper role in diagnoses and treatment then they must be trustworthy
Experience has shown that all analytical results are subject to errors arising from a variety of causes
It is essential that these errors be kept to a minimum.
M. Zaharna Clin. Chem. 2009
Laboratory Analysis
QA in Laboratories The assurance of high-quality laboratory results relies
on a commitment to all aspects of the testing system, including attention to:
1. Preanalytical factors are those factors that affect the laboratory results due to handling of the specimen sample prior to analysis.
2. The analytical phase includes verification of instrument linearity, precision, accuracy, and overall reliability through the use of standard materials, quality control (QC) samples, procedures, and QC rules.
3. Postanalytical factors include timely and accurate laboratory result reporting and other aspects that occur after the analysis phase.
M. Zaharna Clin. Chem. 2009

M. Zaharna Clin. Chem. 2009
Quality assurance has been defined by WHO as: The total process whereby the quality of the laboratory
reports can be guaranteed. It has been summarized as the: Right result, at the Right time, on the Right specimen, from the Right patient, With the result interpretation based on,
Correct reference data, and at the Right price.
WHO Definition
M. Zaharna Clin. Chem. 2009
Quality Assessment
DefinitionQuality assessment or quality
assurance (QA) is a complete system of creating and following procedures and policies to aim for providing the most reliable patient laboratory results and to minimize errors in the preanalytical, analytical, and postanalytical phases.
M. Zaharna Clin. Chem. 2009
Sources of Error
Erroneous results are at best a nuisance; at worst, they have potential for causing considerable harm.
Errors can be minimized by careful adherence to robust, agreed protocols at every stage of the testing process: this means a lot more than ensuring that the analysis is performed correctly.
Errors can occur at various stages in the process: pre-analytical, occurring outside the laboratory, analytical, occurring within the laboratory, post-analytical, whereby a correct result is generated
but is incorrectly recorded in the patient's record,
M. Zaharna Clin. Chem. 2009

PROCESS POTENTIAL ERRORS
Test ordering
• Inappropriate test• Handwriting not legible• Wrong patients ID• Special requirements not specified
Specimen acquisition
• Incorrect tube or container• Incorrect patient ID• Inadequate volume• Invalid specimen (hemolysed or diluted)• Collected at wrong time• Improper transport conditions
Preanalytical errors
M. Zaharna Clin. Chem. 2009
Specimen collection and handling
A test result is no better than the quality of the specimen received in the laboratory.
Specimen collection and handling procedures must be explained to all parties involved in the processing of specimens ( nursing personnel, physician assistants, and health-care professionals)
Laboratory personnel are responsible for for training other personnel involved in specimen
collection and transport and for communicating effectively in order to maintain optimal quality of specimens for laboratory testing.
minimizing preanalytical errors based on acceptance or rejection of the received specimens.
Since preanalytical errors seem to make up the majority of most laboratory test problems, proper training is an important area to address.
M. Zaharna Clin. Chem. 2009

Hemolysis
Hemolysis is generally a preanalytical problem that can be avoided.
It is graded based on visible presence of hemoglobin, when greater than 20 mg/dL, and it is often graded as mild, moderate, or gross hemolysis.
Gross hemolysis will often impact on almost every test method due to release of intracellular constituents into the serum
(potassium, phosphates, LDH, and AST) and colorimetric interference due to pigments.
Grossly hemolyzed specimens should always be rejected.
M. Zaharna Clin. Chem. 2009

Specimen Contamination
The type of blood specimen contamination resulting from IV fluids would vary with the type of fluid being infused. A dextrose solution (sugar) IV infusion would yield
extremely high glucose results in venous specimens collected above or near the infusion area.
Total parenteral nutrition (TPN) fluid contains most of the required daily nutrients for a person who can’t ingest food.
TPN fluid contamination in a specimen creates gross turbidity along with elevated lipid and glucose values and potassium levels too high to be compatible with life.
In specimens from a patient receiving a saline IV infusion, Sodium and chloride results will be falsely elevated due to
contamination from saline IV fluid.
M. Zaharna Clin. Chem. 2009

Specimen Transport
Many chemical compounds are stable within plasma or serum in vitro for only a short time.
Levels of potassium, ammonia, lactate, bilirubin, glucose, CO2 , sodium, urea, and alkaline phosphatase, for example, are particularly affected by contact with blood cells, which can continue to undergo cellular metabolic processes after blood has been removed from the body. E.g. Glucose will decrease as much as 12% per
hour if not separated from blood cells or preserved.
M. Zaharna Clin. Chem. 2009

Specimen Transport
M. Zaharna Clin. Chem. 2009
Additives to Blood
Using the wrong additives or the wrong amount of additive can cause adverse effects on blood specimens. Sodium oxalate, sodium fluoride, or sodium heparin cannot
be used for samples needed for sodium analysis because they increase the level of sodium.
Ammonium heparin should not be used for specimens intended for plasma ammonia or urea testing
because it adds to the chemical being measured. Sodium fluoride cannot be used for enzyme analysis
samples because fluoride acts as an inhibitor to most enzyme activity.
Ethylenediaminetetra-acetic acid (EDTA), sodium citrate, and sodium oxalate cannot be used in samples that will be used for mineral analysis
because they remove calcium and magnesium.
M. Zaharna Clin. Chem. 2009
Sample Preparation
Sample preparation involves processing of the sample prior to and in preparation for analysis.
Processing involves centrifugation, and making an aliquot of the specimen
in a test tube or sample cup Keep in mind that clotted or whole blood cells
can affect chemicals in the sample over a period of time, such that additional chemicals arise or some chemicals are consumed
M. Zaharna Clin. Chem. 2009
It is very difficult to establish effective methods for monitoring and controlling preanalytical variables because many of the variables are outside the laboratory areas.
Requires the coordinated effort of many individuals and hospital departments Patient Identification
The highest frequency of errors occurs with the use of handwritten labels and request forms. The use of bar code technology has significantly reduced ID problems.
How To Control Preanalytical Errors
M. Zaharna Clin. Chem. 2009
How To Control Preanalytical Errors
Training of personnel for proper collection and handling of samples, including adherence to specific steps and maintaining turnaround time involving sample receiving and processing.
Use of well-written procedures and policies can help to minimize preanalytical errors (specimen collection manual)
M. Zaharna Clin. Chem. 2009

Analytical Measurement
• Instrument not calibrated
Correctly
• Specimens mix – up
• Incorrect volume of specimen
• Interfering substances present
• Instrument precision problem
Analytical errors
M. Zaharna Clin. Chem. 2009

Test interpretation
• Previous values not available for comparison
Test reporting
• Wrong patient ID
• Report not legible
• Report delayed
• Transcription error
Post Analytical errors
M. Zaharna Clin. Chem. 2009
Analytical variables and Quality Control
The ideal analytical method is accurate, precise, sensitive and specific. Accurate: It gives a correct result Precise: that is the same if repeated Sensitive: It measures low concentrations of the
analyte Specific: is not subject to interference by other
substances In addition, it should preferably be cheap, simple and
quick to perform.
M. Zaharna Clin. Chem. 2009
There are many analytical variables that must be carefully controlled:
Water quality Calibration of analytical balances Calibration of volumetric glassware and pipettes Stability of electrical power Stability of temperature of heating baths,
refrigerators, freezers and centrifuges
Control of analytical variables
M. Zaharna Clin. Chem. 2009
These are also referred to as laboratory bench manual
Important features of SOP’s Applicable and available in the laboratory
where they will be used Clearly written and easy to understand and
follow Kept up to date using appropriate
technologies
Standard operating procedures
M. Zaharna Clin. Chem. 2009

The Standard operating Procedure should contain the following:
Procedure name Clinical significance Principle of method Specimen of choice Reagents and equipments Procedure Reference values Comments References
The Standard operating Procedure
M. Zaharna Clin. Chem. 2009

Method Validation
Method validation should be performed before a test procedure is placed into routine use.
Validation may be accomplished by thoroughly testing reference materials or by comparison of results of tests performed by an alternative method.
M. Zaharna Clin. Chem. 2009

Method Validation
Method validation should provide evidence of the following:
Accuracy Precision Sensitivity Specificity Linearity
M. Zaharna Clin. Chem. 2009

M. Zaharna Clin. Chem. 2009

Accuracy - the closeness of the estimated value to the true mean- can be checked by the use of reference materials which
have been assayed by independent methods of known precision
Precision - reproducibility of a results, whether accurate or inaccurate
within a define frame time ( eg: within the same day, from week to week etc )
- can be controlled by replicate tests, check tests on previously measured specimens and statistical evaluation of results
Accuracy & Precision
M. Zaharna Clin. Chem. 2009
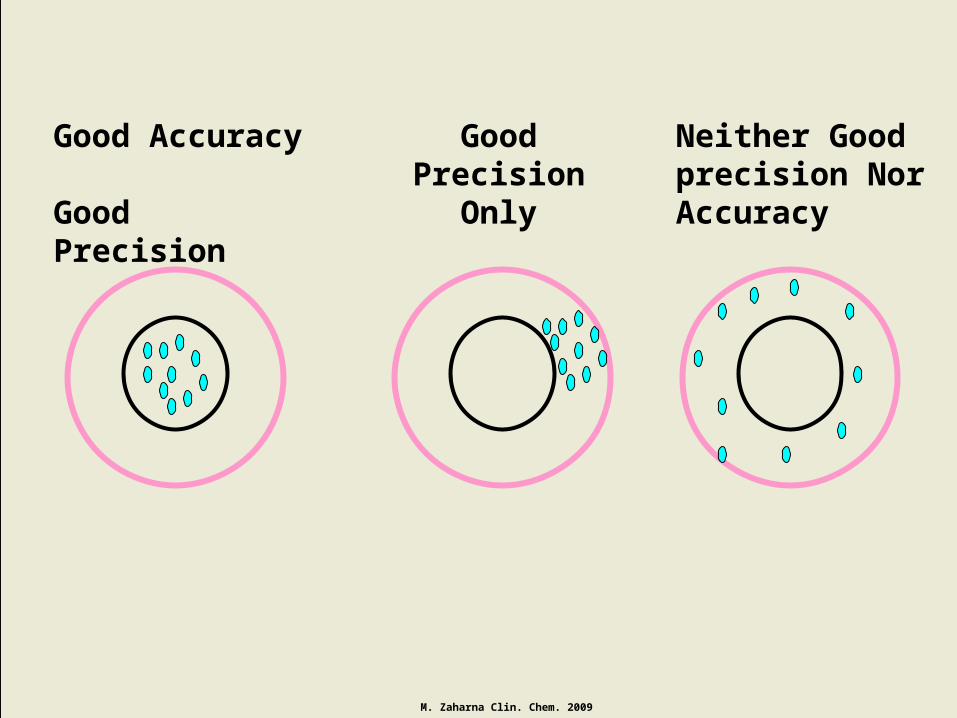
Good Accuracy Good Precision
Good Precision
Only
Neither Good precision Nor Accuracy
M. Zaharna Clin. Chem. 2009
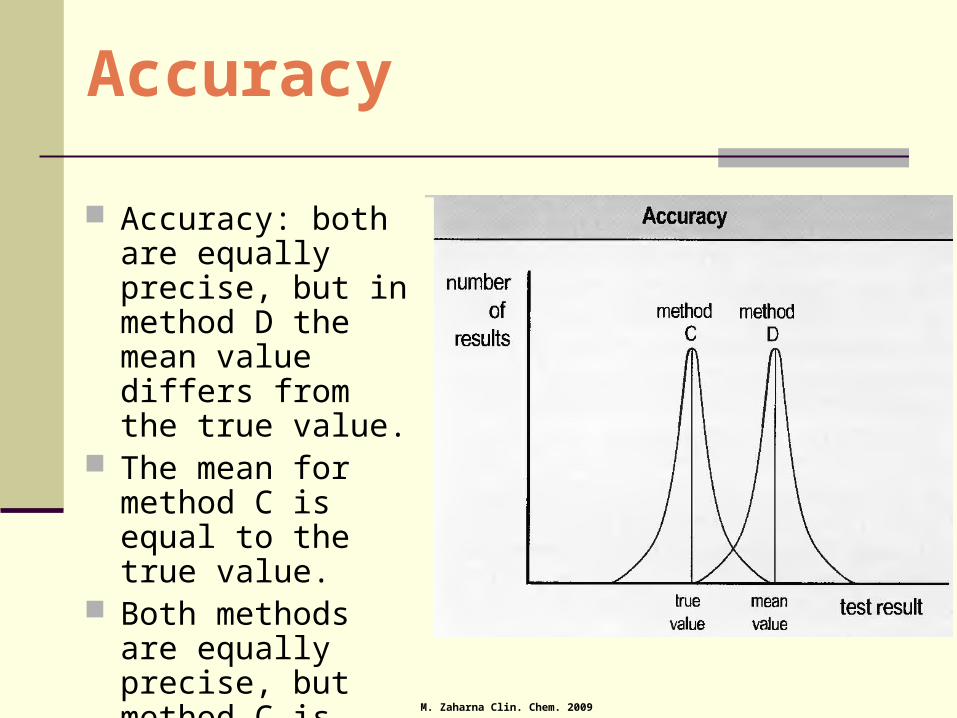
Accuracy: both are equally precise, but in method D the mean value differs from the true value.
The mean for method C is equal to the true value.
Both methods are equally precise, but method C is more accurate.
M. Zaharna Clin. Chem. 2009
Accuracy

The graph shows the distribution of results for repeated analysis of the same sample by different methods.
Precision: the mean value is the same in each case, but the scatter about the mean is less in method A than in method B.
Method A is, therefore, more precise.
M. Zaharna Clin. Chem. 2009
Precision
Sensitivity(Ability to exclude false negatives) Sensitivity is a measure of the incidence of
positive results in patients known to have a condition, that is 'true positive' (TP).
A sensitivity of 90% implies that only 90% of people known to have the disease would be diagnosed as having it on the basis of that test alone: 10% would be 'false negatives' (FN).
M. Zaharna Clin. Chem. 2009

Specificity(Ability to exclude false positives)
The specificity of a test is a measure of the incidence of negative results in persons known to be free of a disease, that is 'true negative' (TN).
A specificity of 90% implies that 10% of disease-free people would be classified as having the disease on the basis of the test result: they would have a 'false positive' (FP) result.
M. Zaharna Clin. Chem. 2009
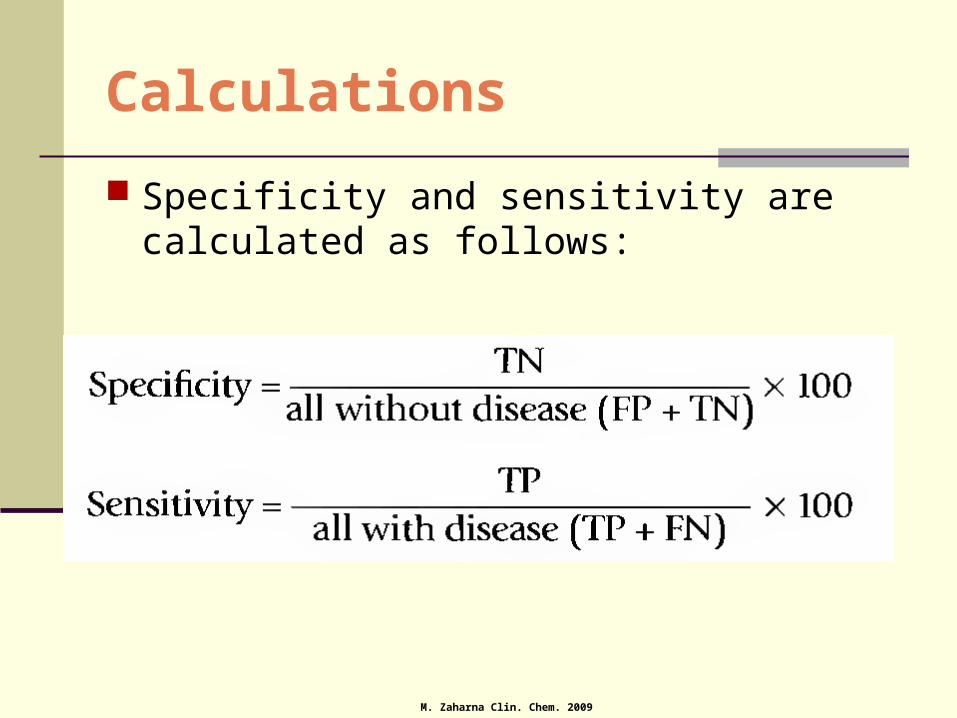
Calculations
Specificity and sensitivity are calculated as follows:
M. Zaharna Clin. Chem. 2009

Sensitivity
Ability to correctly identify individuals with disease 1000 people tested
875 positive tests (275 false positive) 125 negative tests (25 false negative)
TP/(TP + FN) – may be expressed as a percent Sensitivity = 600/600 +25 = 0.96 (96%)
M. Zaharna Clin. Chem. 2009

Specificity
Ability to correctly identify individuals without disease 1000 people tested
875 positive tests (275 false positive) 125 negative tests (25 false negative)
TN /(TN + FP) Specificity = 100/(100+275) = 0.27 or 27%
M. Zaharna Clin. Chem. 2009

High Sensitivity desired when
Disease is serious and should not be missed Disease is treatable False positives do not lead to serious
psychological or emotional trauma
M. Zaharna Clin. Chem. 2009
High Specificity desired when
Disease is serious but is not treatable or curable
Knowledge that disease is absent has physiological or public health value
False-positive results can lead to serious psychological or economic trauma
M. Zaharna Clin. Chem. 2009

Ideal Test
An ideal diagnostic test would be: 100% sensitive,
giving positive results in all diseased subjects, and also 100% specific,
giving negative results in all subjects free of disease.
Individual tests do not achieve such high standards. Factors that increase the specificity of a test tend to
decrease the sensitivity and vice versa.
M. Zaharna Clin. Chem. 2009
If it were decided to diagnose thyrotoxicosis only if the plasma free thyroxine concentration were at least 32 pmol/L (the upper limit of the reference range is 26 pmol/L), the test would have 100% specificity; positive results
(greater than 32 pmol/L) would only be seen in thyrotoxicosis.
On the other hand, the test would have a low sensitivity in that many patients with mild thyrotoxicosis would be misdiagnosed.
If a concentration of 20 pmol/L were used, the test would be very sensitive (all those with
thyrotoxicosis would be correctly assigned) but have low specificity,
because many normal people would also be diagnosed as having thyrotoxicosis.
M. Zaharna Clin. Chem. 2009

Linearity
The linear range is the concentration range over which the measured concentration is equal to the actual concentration without modification of the method.
The wider the linear rang, the less frequent will be specimen dilution

Linearity
A quantitative analytical method is said to be linear when: the measured value from a series of sample
solutions is linearly proportional to the actual concentration or content of the analyte (true value) in the sample solutions.
The points at the upper and lower limits of the analytic measurement range that acceptably fit a straight line determine the linear range.
Related Documents











