
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript


Page 1
QUALITY ACCOUNT PART 1, CHAPTER 1 – INTRODUCTION
Welcome to our 2019/20 Quality Account, which describes how we performed against our main patient
safety, outcome and experience standards during the year. Our Annual Report and Accounts is a separate
document which provides detailed information about how we performed across the full spectrum of
standards, including financial performance and waiting times.
Over the last year, despite the challenges of the global pandemic, we have maintained our focus on
strengthening the quality and safety of care that we are privileged to provide to our patients. We have made
excellent progress against our quality priorities, achieving 10 so far.
We’ve used digital advances to improve the care we offer, Nervecentre assists us in screening all adult
inpatients for sepsis, and we’ve successfully implemented our electronic assessment tool, NEWS2, to support
the identification and care of acutely unwell patients.
We’ve listened to our patients and, in response to their feedback, we’ve developed sleep guides to support
them. Four of our teams were also finalists at the 2019 National Patient Experience Awards (PENNA).
We are committed to ensuring our patients receive consistently high quality, safe care, with outstanding
outcomes and experience. A Medical Examiner Team was implemented to support the review and learning
from deaths. And we’ve maintained our mortality position (SHMI) in line with the expected national position.
We consistently achieved the national CQUIN (quality improvement) targets for the first three quarters –
with the fourth quarter being disrupted by the Covid-19 pandemic. We have also continued to perform well
with national audit outcomes, including benchmarking against peers.
We continue to prioritise the areas highlighted in our Care Quality Commission (CQC) inspection of
2018/2019 with our ambition to be outstanding at the next inspection. In particular we have focused on the
improvement of Do Not Attempt Resuscitation (DNACPR) documentation and end of life care. End of life care
has been further improved in our organisation, with the ongoing implementation of the SWAN initiative and
our work across the care community.
We also vaccinated 80% of staff against flu over the winter.
One of our continued challenges is providing timely emergency care. Our clinical teams appreciated the
opportunity, from May 2019, to take part in the national field testing programme for new clinical standards
in urgent and emergency care. This enabled them to both test and challenge assumptions around this area.
Our focus during this process remained the delivery of safe, timely care, as well as providing a positive overall
experience for our emergency patients. This was, however, challenged during the winter with increased
numbers of patients needing our services. We were pleased to receive funding to redesign our acute urgent
and emergency care services, enabling us to increase the number of beds, particularly in our admission areas.
In mid-January we were delighted to open our brand new Acute Medical Unit at the Queen’s Medical Centre.
This unit has a very large assessment and treatment area for patients with medical problems that require a
stay in hospital of less than 48 hours. It is a mixture of new and old estate and provides us with 91 acute

Page 2
beds. It also helps us care for our older patients with dementia and we incorporated some dementia friendly
designs into the new build. Whilst this important work has delivered what it set out to, we still struggle to
admit patients in a timely way due to a shortage of beds, particularly in our medical wards at the Queen’s
Medical Centre. This therefore remains a key priority during 2020/21.
We recognise other challenges in our furtherance of improving the quality and safety of care we provide, not
least responding to the current pandemic and seeking to restore activity as far as possible.
Our 2020/2021 quality priorities, described in this report, set out our programme of work for the year to
come, showing our commitment to further improve the safety and quality of care we provide for our patients
and their families. These are summarised below:
Priority 1 - Improve Patient Experience
WHAT HOW ASSOCIATED MEASURES
Improve patient, family and carer experience of loved ones with dementia
Implement the Trust’s Dementia Strategy
Implement year one objectives.
Improve the quality of complaint investigations and responses
Implement the Complaints Quality Improvement Plan
Reopened complaints (% of total closed complaints) will be ≥15%.
By the end of 2020/21, 100% of all nominated complaint investigators will be trained.
By the end of 2020/21, 25 complaint case Peer Reviews will have been completed.
A pilot will be evaluated to achieve ≥10% improvement in meeting agreed complain response timescales within 30 working days.
Provide timely and useful patient information
Information leaflets will be accessible and in a format that meets patient, carer and family needs
By the end of 2020/21, 100% of all patient leaflets will be updated within review dates.
A review of the Patient Information Service will have been undertaken and a Trust-wide Strategy and Policy developed.
Priority 2 - Improve Patient Safety
WHAT HOW ASSOCIATED MEASURES
Page 3
Escalate and respond to deteriorating patients in a timely manner
The national NEWS2 CQUIN will be used as a lever to support improvements in care of the acutely unwell patient (with an ambition to reduce unplanned ward transfers to Critical Care)
By the end of 2020/21, 70% of patients who have triggered for medical review will be seen within agreed (NEWS2 policy) timescales.
Escalate and respond to deteriorating patients in a timely manner (continued)
A focus on A-E patient assessment (and standardised management planning) will form part of high quality reviews of acutely unwell patients
A Trust, Division and Speciality QLik app will be developed to make visible key measures of care of the acutely unwell patient to measure and monitor for improvement
Investment in the City Hospital campus medical specialities through SPR level twilight cover will be implemented
NUH will scope the feasibility of implementing an electronic fluid balance system via Nervecentre
A-E patient assessment will form part of mandatory training for all Registered Nurses.
Fluid balance electronic monitoring for all adult inpatient areas with the exception of critical care/ theatres.
Reduce the incidence of grade 3 and 4 pressure ulcers
The Trust’s pressure ulcer prevention strategy will be reviewed, updated and implemented to positively impact the care of patients who are at risk of developing pressure ulcers.
Establish baseline and set target reduction at the end of Q1.
Optimise information flow by implementing a standardised handover process
A standardised handover process will be defined and implemented to improve transfer of critical information within and across teams.
Initial work will focus on a daily clinical handover at the end of the day on city based medical admission areas.
Standardised process (such as SBAR) to be implemented for use in adult emergency admission areas and at internal transfer of patients.
Priority 3 - Improve Clinical Effectiveness
WHAT HOW ASSOCIATED MEASURES

Page 4
Improve the way we plan and respond at the end of life with patients and families
Focus on improving conversations and documentation of Do Not Attempt Resuscitation (DNACPR) decisions
100% of patient demographics will be completed fully on the DNACPR forms by June 2020.
A date to review the decision will be documented on 100% of forms by December 2020.
100% of forms will have a valid clinical reason for DNACPR decision documented by June 2020.
Improve the way we plan and respond at the end of life with patients and families (continued)
100% of patients requiring a Mental Capacity Assessment (MCA) will have this completed by September 2020.
Conversations will occur with the patient and family and these conversations will be documented in 100% of instances by June 2020 (the achievement date for this measure will be extended due work stream delays during the COVID-19 pandemic).
90% of patients and/or their family will receive a DNACPR leaflet by December 2020.
Improved Local Surveys Programme
Develop and enhance our Local Surveys Programme to identify actions for improvement
Establish a tool and benchmark to define improvement target during Q1.
Identification of a defined number of projects (≤5).
Implementation of agreed improvement goals in line with Trust objectives during Q2-Q4.
Align improvement resources to support delivery of Trust objectives
Develop a programme of Trust-wide Quality Improvement projects aligned to Trust objectives
Scope current projects and map to objectives in Q1.
Identify priority projects and implementation plan during Q2.
Implementation of agreed priority projects during Q3 to Q4.
DECLARATION OF ACCURACY
I confirm, on behalf of all Executive Directors at NUH, that to the best of my knowledge the information
provided in our Quality Account is accurate.
Tracy Taylor
Chief Executive

Page 5
QUALITY ACCOUNT PART 2:
2.1 Priorities for Improvement - a review of 2019/20 achievements
Ensuring our patients receive consistently high quality, safe care, with outstanding health outcomes and
experience, is at the centre of all we do. NUH has six strategic objectives (called our 6 Promises - or 6 ‘Ps’ for
short). These are:
Our patients: We will ensure our patients receive consistently high quality, safe care, with outstanding
outcomes and experience
Our people: We will build on our position as an employer of choice; with an engaged, developed and
empowered team that puts patient care at the heart of everything it does
Our places: We will invest in our estate, equipment and digital infrastructure, to support the delivery of
high quality patient care
Our performance: We will consistently achieve our performance standards and make the best use of
resources that contribute to an affordable healthcare system
Our partners: We will support the improvement of the health of the communities we serve through
strong system leadership and innovative partnerships to deliver integrated models of care
Our potential: We will deliver world-class research and education and transform health through
innovation
Under the promise to our patients we identified a number of quality priorities for 2019/20, outlined below
along with an overview of achievements against delivery.
Quality Aim Priority How will we know that we
have done it? Progress
Improve Patient Experience
Make it easier for patients to stay in touch with relatives and friends.
Introduce charging points in all admission and discharge areas and across ED and outpatient areas.
Mobile charging point in place in the ED. Plans for patient areas and main entrances awaiting approval.
Keeping patients active to aid their recovery.
Developing staff and patient/carer information. Get patients up, dressed and moving as early as possible.
Patient Participation Group led Placemat Project and the first draft of placemat produced.
Improve the night time experience of patients by reducing unnecessary light sources and the level of noise from staff.
Develop and implement a Trust-wide ‘better sleep’ strategy. 85% of patients will respond negatively to the question ‘were you bothered by noise at night from staff’.
Produced Sleep Guide for staff and made information available to patients. Continuing to review feedback and to identify areas for further improvement.

Page 6
Enhance Patient Safety
Focus on timely escalation and response to the deteriorating patient.
Integrate NEWS 2 into practice. Evaluate the NEWS2 programme including impact on number of escalations. Reduce avoidable harm and death associated with missed opportunities to detect and manage the deteriorating patient. Rate of unplanned in-patient transfers to Critical Care (baseline by Q2 followed by identification of improvement interventions).
NEWS2 was successfully implemented electronically using Nervecentre across NUH and evaluated. Whilst escalations increased, the model is more sensitive and supports earlier identification of the acutely unwell patient. Incident data, including serious incidents, does not support a significant reduction in avoidable harm associated with the acutely unwell patient (risk remains 20). During 2019/20, our rate of unplanned ward transfers to Critical Care remained with expected levels of variation.
Increased involvement of families when something goes wrong.
Implement and evaluate revised Duty of Candour process. Involve patients in incident investigation through co-design. Implement Patient and Family Liaison Officer role. Roll out the Complaints with Compassion programme.
Duty of Candour processes revised and published, including Trust Policy (see page 29 for detail). Patient and Family Liaison Officer role introduced. Review of complaints processes completed locally. Quality assurance checks introduced. Letter Writing workshops delivered, which focus on compassionate complaints handling.
Improve support for patients and staff involved in incidents.
Establish a rapid incident support team to respond to serious incidents.
Trialled and work continues to resource ability to establish team.
Develop an evaluation tool for families and staff involved in incidents.
Evaluation tool drafted and clinical academic recruited to support formal evaluation.
Increase the rate of incident reporting.
Rate of incident reporting increased from 38.2 incidents per 1,000 occupied bed days in 2018/19 to 48.6 incidents per occupied bed days in 2019/20.
Improve Clinical Effectiveness
Increase our learning from deaths to improve outcomes.
Implement Medical Examiner Role by September 2019.
Medical Examiner Team implemented.
Page 7
Maintain SHMI within confidence intervals.
SHMI remains within national mean and confidence intervals (see page 57).
Improve outcomes for patients using audit and benchmarking.
Take part in all relevant National audits and quality standard reviews. Benchmark against peer organisations. Screen for sepsis within one hour of admission for all patients.
NUH participated in all but one eligible national audits (see page 31). NUH has established a clinical audit outcomes bi-annual report to compare outcomes against peers. All adult and paediatric patients admitted to NUH are screened for sepsis. In 2019/20 100% of adult (non-maternity) and paediatric patients admitted to NUH were screened for sepsis on every set of observations taken and entered electronically. 84.4% of obstetric patients unwell with infection were screened for sepsis during 2019/20.
Increase improvement capability across the organisation to enable greater learning from incidents and feedback.
Roll out QSIR1 programme across teams and services. Develop data base of Quality Improvement projects and outcomes.
QSIR has been rolled out across NUH. QSIR Practitioner training delivered to staff across the Integrated Care System (101 were NUH staff). QSIR Fundamentals training delivered to 286 NUH staff.
NUH has made good progress across the quality priorities with 10 achieved and two partially achieved. An
update on the work underway to achieve outstanding priorities is described in the quality account along with
a summary of work NUH has implemented to improve the quality of care through 2019/20.
1 Quality, Service Improvement and Redesign (QSIR) programmes are delivered using improvement tools to increase
quality improvement capability within organisations and across the healthcare system.

Page 8
Patient Safety - making care safer
Safety thermometer
The safety thermometer is a national measurement tool for improvement that focuses on commonly
occurring harms in healthcare: Pressure ulcers, falls, urinary tract infection (UTI) in-patients with a catheter
and venous-thromboembolism (VTE, or blood clots). Data is collected through a point of care survey on a
single day each month on 100% of adult and neonatal inpatients on that date. This enables wards, teams and
the organisation to understand the burden of particular harms, measure improvement over time and
connect frontline teams to the issues of harm, enabling immediate improvements to patient care.
NUH has consistently performed well against the safety thermometer, with a consistent harm-free care rate
of greater than 97% since April 2017.
The proportion of patients with harm free care (new harms only) April 2018 to March 2020
Pressure Ulcers
NUH achieved its aim of reducing pressure ulcers by 50% over three years from the 2012/14 baseline.
Subsequently, NUH aimed to further reduce avoidable pressure ulcers by 10% year-on-year concluding in
2019/20. This is however unlikely to be achieved and following recent NHSI guidance, we no longer record
avoidable harm.
Category 2 pressure ulcers
Between 01 April 2019 and 29 February 2020, there was an increase in category 2 pressure ulcer incidents of
33% from 491 (during 2018/19) to 655. This increase may be due to a change in process where Tissue
Viability Nurses no longer validate all the pressure ulcer incidents reported.
Page 9
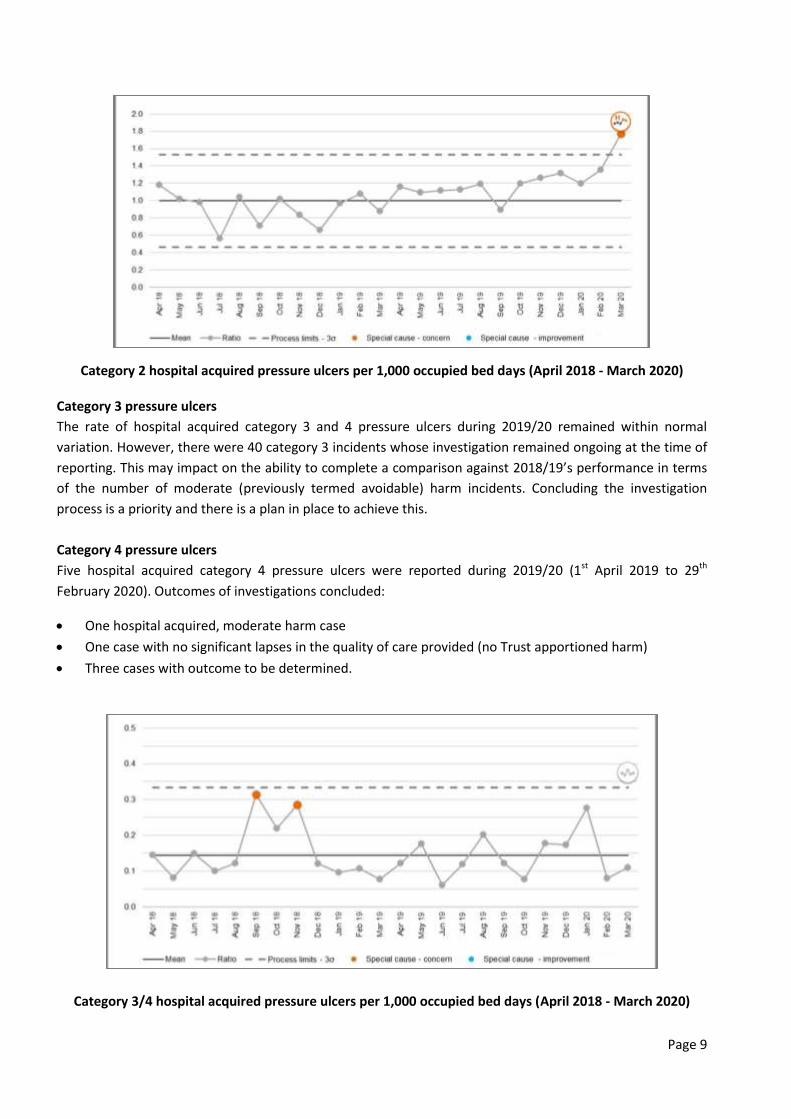
Category 2 hospital acquired pressure ulcers per 1,000 occupied bed days (April 2018 - March 2020)
Category 3 pressure ulcers
The rate of hospital acquired category 3 and 4 pressure ulcers during 2019/20 remained within normal
variation. However, there were 40 category 3 incidents whose investigation remained ongoing at the time of
reporting. This may impact on the ability to complete a comparison against 2018/19’s performance in terms
of the number of moderate (previously termed avoidable) harm incidents. Concluding the investigation
process is a priority and there is a plan in place to achieve this.
Category 4 pressure ulcers
Five hospital acquired category 4 pressure ulcers were reported during 2019/20 (1st April 2019 to 29th
February 2020). Outcomes of investigations concluded:
One hospital acquired, moderate harm case
One case with no significant lapses in the quality of care provided (no Trust apportioned harm)
Three cases with outcome to be determined.
Category 3/4 hospital acquired pressure ulcers per 1,000 occupied bed days (April 2018 - March 2020)
Page 10
Themes/learning from investigations:
Delayed and ineffective repositioning
Inaccurate skin assessments
Lack of effective continence care
Substandard management of non-compliance
Lack of individualised care
Omissions in documentation
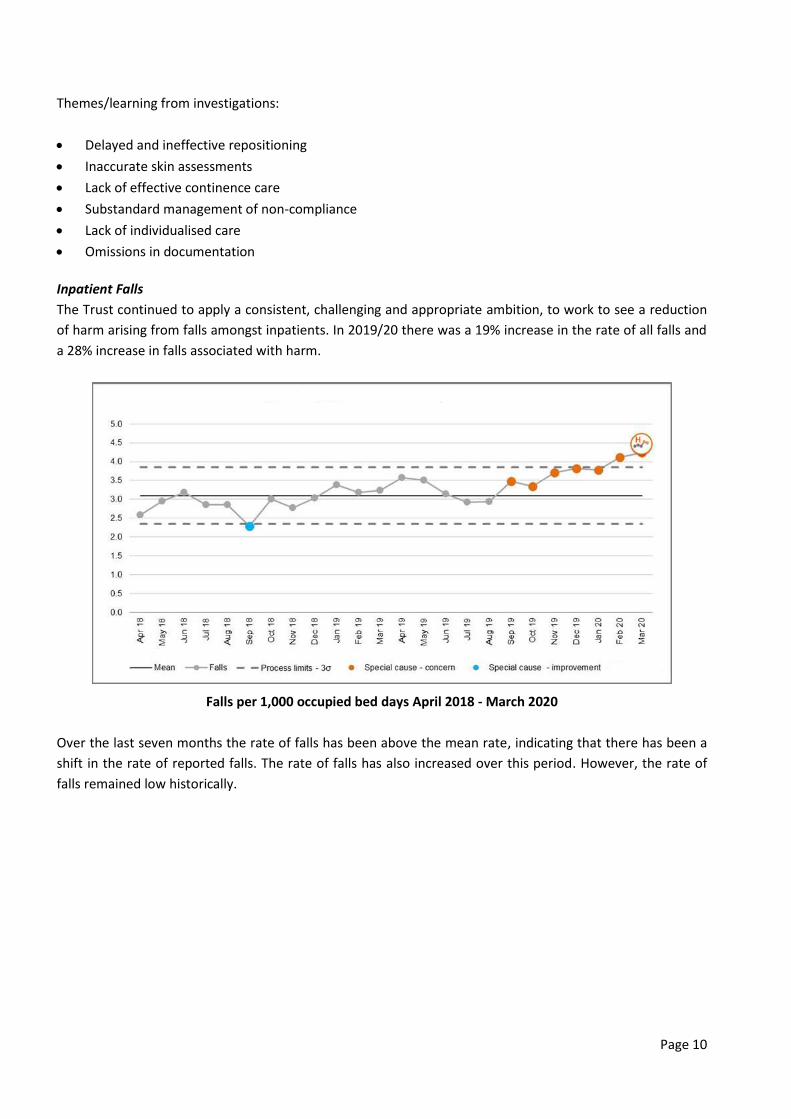
Inpatient Falls
The Trust continued to apply a consistent, challenging and appropriate ambition, to work to see a reduction
of harm arising from falls amongst inpatients. In 2019/20 there was a 19% increase in the rate of all falls and
a 28% increase in falls associated with harm.
Falls per 1,000 occupied bed days April 2018 - March 2020
Over the last seven months the rate of falls has been above the mean rate, indicating that there has been a
shift in the rate of reported falls. The rate of falls has also increased over this period. However, the rate of
falls remained low historically.

Page 11
Harmful Falls per 1,000 occupied bed days April 2018 - March 2020
Over the last seven months the rate of harmful falls has been above the mean rate indicating that there has
been a shift in the rate of reported harmful falls. There was also an aberration in October 2019 where the
rate was above expected levels. This was linked to staffing issues and performance immediately returned
within the control limits.
The Falls Learning Group recognises the increase in falls and harmful falls and continues to work with
frontline clinicians to further understand the drivers and apply appropriate safety control measures.
Ratio of falls to fallers April 2018 - March 2020
There were no concerns as the rate remains within the control limits.
Learning from inpatient fall investigations
Inadequate patient supervision due to:
o No change to the planned care despite a change in the patient’s condition

Page 12
o Staffing levels
o Inappropriate patient placement to a clinical area
Lack of effective patient continence assessment and individualised care; urinary and faecal urgency a
particular issue
Missed opportunities to assess patient for orthostatic hypotension. Inconsistent assessment of lying and
standing blood pressure
Catheter-acquired and new urinary tract infection (CAUTI)
Training in the basics of effective continence promotion, urinary catheter and basic bowel care has been
available since September 2019 and up to the end of February 2020, 22 sessions had been delivered.
Gillies Ward had been piloting the use of the PureWick external female catheter device since February 2020.
The aim is to reduce the duration of post-operative urinary catheters. This is due for evaluation by 30th April
2020.
Mar
-19
Ap
r-1
9
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
t-1
9
Oct
-19
No
v-1
9
De
c-1
9
Jan
-20
Feb
-20
Mar
-20
% of Catheter
and New UTI
Harm
0.00% 0.22% 0.00% 0.00% 0.36% 0.15% 0.22% 0.08% 0.14% 0.00% 0.22% 0.00% 0.00%
Number of actual
patients 0 3 0 0 5 2 3 1 2 0 3 0 0
Venous thrombo-embolism (VTE)
Our VTE programme aims to reduce preventable harm to our patients, by promoting timely and accurate VTE
risk assessment and ensuring thromboprophylaxis is prescribed accurately and administered effectively when
required.
NUH’s overall VTE risk assessment compliance for 2019/20 was 94.7% (against a target of 95%).
VTE Risk Assessment Compliance April 2018-March 2020

Page 13
NUH recognises that its compliance level is below target in 2019/20 but has shown improvement since
2018/19. In-depth analysis of performance within the Divisions has been undertaken to identify areas where
focussed action is needed and strategy developed. Advanced Nurse Practitioners and prescribing pharmacists
are now trained to complete the VTE Risk Assessments to provide support to the medical teams. A new IT
system is prepared for rollout in 2020/21 which will improve usability of the assessment tool, making it more
accessible to medical teams. Hospital Associated Thrombosis (HAT) route cause analysis compliance is 100%
and the rate of preventable HAT remains low. The Trust is committed to investigating and sharing knowledge
in cases where an element of preventability has been found to drive improvement and has a clear
governance structure to facilitate this.
VTE risk assessment by provider (peer group) April to December 2019
Harms associated with infection, prevention and control
C. Difficile & MRSA
There were 152 cases of C. difficile at NUH against a control total of no more than 120 cases.
We had two cases of hospital acquired MRSA bacteraemia against a zero tolerance target. We continue to
do all we can to prevent and reduce healthcare-associated infections and remain committed to improving
and sustaining high levels of environmental cleanliness and total room decontamination by the investment in
developed hydrogen peroxide technology against C. difficile spores.
NUH has well developed and effective programmes of surveillance and audit and continues to effectively
investigate manage sometimes complex outbreaks of infection. NUH promotes the optimum use of
antibiotics as a patient safety priority to prevent and reduce the risk from multi-resistant organisms, e.g. CRE.
In 2019/20 emphasis has been placed on the continued development of a safe and sustainable organisation
wide approach in order to embed:
• Getting the diagnosis of infection right first time and every time
• Ensuring appropriate antibiotic use and review.
94
.4%
71
.8%
10
0.0
%
England ave.
0%
20%
40%
60%
80%
100%
Bri
sto
l
Sou
tham
pto
n
Live
rpo
ol
No
ttin
gham
Leed
s
Shef
fie
ld
Man
ches
ter
Cam
bri
dge
Lan
cash
ire
Ne
wca
stle
Leic
este
r
Oxf
ord
Bir
min
gham
Engl
and
Low
est
Engl
and
Hig
hes
t

Page 14
Rate of C. Difficile infections per 100,000 occupied bed days for April 2019 - December 2019, compared
with peer group
19
.72
England ave.
0
10
20
30
40
50
60
70
Sou
tham
pto
n
Leic
este
r
Live
rpo
ol
Oxf
ord
Bri
sto
l
Man
ches
ter
Bir
min
gham
Shef
fie
ld
Leed
s
Ne
wca
stle
No
ttin
gham
Cam
bri
dge
Lan
cash
ire
Engl
and
Lo
wes
t
Engl
and
Hig
hes
t
Rat
e p
er
10
0,0
00
OB
D
0
5
10
15
20
25
Ap
r-1
8
May
-18
Jun
-18
Jul-
18
Au
g-1
8
Sep
-18
Oct
-18
No
v-1
8
Dec
-18
Jan
-19
Feb
-19
Mar
-19
Ap
r-1
9
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Cas
es
Cases Healthcare Assoc. Control total

Page 15
NUH acquired C. difficile cases
Cumulative NUH acquired C. difficile cases (2019/20)
Reducing the impact of serious infections (Antimicrobial Stewardship and Sepsis)
Antimicrobial Stewardship (AMS)
AMS is a programme of ensuring appropriate antibiotics are prescribed and administered to our patients.
This programme of work will improve the safety and quality of patient care and reduce the development and
spread of antibiotic resistance. The following initiatives have been undertaken by the AMS team:
Trust-wide roll-out of diagnostic stewardship quality improvements:
o ‘Skip the dip’, to reduce the over diagnosis and inappropriate treatment of urinary tract infections
(UTI)
o Launch of an interprofessional staff training resource ‘getting infection right first time.’
Creation of a diagnostic stewardship group, bringing together hospital and community teams
Creation of an antifungal dashboard to improve the accessibility of antifungal consumption data to all
staff
Joint pharmacy and microbiology led AMS ward rounds, enabling timely interventions
0
20
40
60
80
100
120
140
160
Apr-19 May-19 Jun-19 Jul-19 Aug-19 Sep-19 Oct-19 Nov-19 Dec-19 Jan-20 Feb-20 Mar-20
Cas
es
Total 19/20 Control total
UCL
CL
0
50
100
150
200
250
300
350
400
450
14
/04
/14
06
/09
/14
19
/12
/14
21
/02
/15
07
/07
/15
13
/07
/15
07
/10
/15
28
/10
/15
29
/10
/15
18
/12
/15
02
/05
/16
11
/05
/16
23
/05
/16
02
/12
/16
29
/01
/17
26
/06
/17
03
/02
/18
19
/04
/18
07
/02
/19
20
/04
/19
05
/11
/19
31
/03
/20
Day
s b
etw
ee
n c
ase
s
MRSA Case
Days between MRSA cases Days since last MRSA case

Page 16
Revision of the AMS work plan to reflect the Department of Health five year plan
Response to the COVID-19 pandemic with team emphasis on Infection Prevention and Control
o Contribution to NICE COVID -19 guidance consultations, alongside the development of local
guidance
o Staff mask fit testing, Personal Protective Equipment (PPE) advice and training, diagnostic testing
and front line staff support.
2019/20 achievements
CQUINs
Q1 Q2 Q3 Q4
Lower Urinary Tract Infections in Older People
Diagnosis based on signs
and symptoms
Baseline 9/19
(47%) 38/52 (73%)
Q2 and Q3
73/102 (71.5%)
Q2, Q3 and Q4
108/153 (71%)
Dipstick not used to justify
diagnosis 14/19 (74%) 39/52 (75%)
Q2 and Q3
75/102 (73.5%)
Q2, Q3 and Q4
119/153 (78%)
Antibiotics in-line with
guidance 12/19 (63%) 42/52 (81%)
Q2, Q3 and Q4
81/102 (79%)
Q2, Q3 and Q4
123/153 (80%)
Urine sent for culture 11/19 (58%) 41/52 (79%) Q2, Q3 and Q4
82/102 (80%)
Q2, Q3 and Q4
120/153 (78%)
Antibiotic prophylaxis in
Colorectal Surgery 91.6% 92.4% 97.6% 99.0%
Anti-Fungal Stewardship Achieved Achieved Achieved Achieved
Antibiotic consumption
The current target is to reduce our total antibiotic consumption by 1% from 2018 calendar year baseline. Our
performance was 5.5% higher than baseline.
Data has continued to be produced during the COVID -19 pandemic with March 2020 seeing the highest
antibiotic consumption levels across the Trust in the last five years.
Due to the lack of an e-prescribing system, there is no real-time measure of antibiotic consumption and
figures are based on stock issues. Therefore this data does not take into account whether it is appropriate
antibiotic use.
The impact of the UTI quality improvement work
NUH has greatly improved the way it diagnoses and treats UTIs in older people. This reflects the large
amount of quality improvement work that has been done in this area and the uptake of the ‘skip the dip’
training by Trust staff.
High level priorities and ambitions for 2020/21
To engage the public on antimicrobial resistance, with attendance at the NUH Patient Partnership Group
to discuss this
Page 17
To continue the great progress being made to including AMS within Trust mandatory training for all staff
groups
In the absence of e-prescribing, to review patient level antibiotic consumption data from high
consumption areas
To continue to embed diagnostic stewardship principles within the Trust to improve the way we
diagnose and manage infection.
Recognise and Rescue (R&R) the Deteriorating Patient
R&R aims to improve the care of the deteriorating patient by reducing and preventing avoidable harm from
clinical deterioration. This is achieved through early recognition and reducing avoidable delays in escalation
of unwell patients, reducing critical care admissions and reducing cardiac arrest. NUH has employed a
Matron from September 2019 to lead the R&R programme of work with oversight from the Associate
Medical Director for Patient Safety. The R&R education committee was reinstated January 2020. The R&R
committee has agreed priorities for 2020/21, which include delivery of improved outcomes associated with
Community Acquired Pneumonia, implementation of the NEWS2 deteriorating patient CQUIN, maintaining
our excellent Sepsis care and introducing standardised handovers in clinical practice.
2019/20 Safety Priorities and deliverables:
Timely escalation and response to deteriorating patients
Roll-out of the new National Early Warning Score (NEWS) 2 system
NEWS2 was successfully rolled out across the Trust on 25th June 2019 following mandate from NHS England
and Royal College Physicians. NEWS2 has been found to be more sensitive than the historic scoring system
and a review of our electronic observations system data (Nervecentre) indicates that there has been a 4%
increase in the total number of e-Observations taken and a 31% increase in the total number of escalations.
NUH has shown the achievement of over 72% of all clinical observations performed on-time across the Trust
during 2019/20, which has fallen slightly since introduction of NEWS2. Consistently NUH’s principle acute
admission areas continue to show over 80% of clinical observations were taken on-time during 2019/20.
In-depth clinical evaluation has been carried out to ascertain compliance with NEWS2 policy with varying
results. National compliance targets with escalation in response to NEWS2 do not exist due to insufficient
data nationally, leading to a challenge with benchmarking. However, the compliance rate at NUH is similar
and in several instances is higher than one other comparable trust that has completed similar in-depth
evaluation. The NEWS2 evaluation reported that 83% (n=256/309) of patients were rated as receiving good
or excellent care, 13% as adequate, 3.6% poor care and 0.3% (n=1) as very poor care (the latter was
confirmed as already under investigation). We will work on setting interim local targets for improving timely
response to acute deterioration and implement the deteriorating patient CQUIN for 2020/21.
Reducing avoidable harm and death associated with missed opportunities to identify and respond to
deteriorating patients
The risk associated with failure to rescue remains high (20), which is in keeping with trends across other NHS
Trusts and is recognised nationally as a safety priority. NUH rate of cardiac arrests is lower than the national

Page 18
median and comparing the same three month period pre and post roll-out of NEWS2, cardiac arrest rates
suggest a slight downward trend.
Improved outcomes for patients
All patients screened for sepsis within 1 hour of admission
92% of all patients diagnosed with high risk sepsis receive antibiotics within 1 hour of confirmed
diagnosis
During 2019/20, NUH continued to maintain good management of patients with High Risk Sepsis as outlined
in the NHS Standard Contract. Introduction of a “Sepsis screening and bundle toolkit” in Midwifery services in
May 2019 further strengthened the already high rate of screening.
Antibiotic compliance <1hour as per Standard Contract requirement 2019/20
NUH has consistently achieved greater than 90% of patients being screened for high risk Sepsis electronically,
and on average 91.5% of patients audited receive antibiotics within one hour of diagnosis with High Risk
Sepsis (see graph above for Antibiotic compliance <1hour as per Standard Contract requirement 2019/20).
Adherence with general Sepsis management as per the Quality Standard (NICE QS161) continues to be
monitored and well adhered to (see average times for each key stage of the sepsis bundle).
In addition, 92% of patients had timely blood cultures taken in Q4 which provides valuable opportunity for
good antimicrobial stewardship, with timely diagnostics to enable targeted antibiotic therapy.
Ensuring that NUH identifies and manages Septic patients appropriately is key to reducing mortality and
morbidity. The key actions undertaken during 2019/20 to support this have been:
Maintenance audit as outlined in the NHS Standard Contract
Bimonthly delivery of Sepsis Survivor Support groups sponsored by the UK Sepsis Trust
70%
75%
80%
85%
90%
95%
100%
Apr 19 May 19 Jun 19 Jul 19 Aug 19 Sep 19 Oct 19 Nov 19 Dec 19 Jan 20 Feb 20 Mar 20
Compliance with IVAb <1hr as per NHS Standard Contract and CQUIN Definition Target

Page 19
Strengthening of Sepsis Link Staff across all clinical areas
Continued Sepsis education to all clinical staff
Intensive work focussed on the Emergency Department in support of prompt identification of Sepsis.
This included sending two sets of blood cultures [which is gold standard] in a timely manner. The
national requirement is one set (between 60-80% of NUH ED patients have 2 sets sent) and
administration of antibiotics, with encouraging results (see graph below)
An electronic Sepsis bundle has been designed and tested and is due to be rolled out in April 2020.
Do Not Attempt CPR (DNACPR)
NUH’s DNACPR Quality Improvement project is a response to the CQC ‘must do’ action that “the Trust must
ensure that DNACPR forms are fully completed and conversations with patients and relatives are
documented in the patient’s medical records”.
Progress to date includes collaborative working across all Divisions through the DNACPR Steering group,
which aims to enhance the experience of patients and their families in relation to the DNACPR decision and
support implementation of the actions required to meet the CQC recommendations for the Trust.
Key interventions in 2019/20:
Identification of improvements to the DNACPR form and dissemination of a new form throughout NUH
Identification and definition of trajectories to work towards attainment of required standards
Attending ward rounds on an acute medical admissions ward, reviewing current DNACPR decisions and
engaging with medical and nursing teams
Flow mapping the DNACPR process to identify barriers
Engagement with Patient Partnership representation in identifying required improvements from the
patient’s perspective
Identification of clinical areas in which to focus improvements.
Initial improvements have been identified in small sample areas following key interventions.
Focus for 2020/21:
Roll out of ward-round clinician review of the DNACPR decision, to ensure all elements are completed
and that the decision is supported by the patients’ consultant
Observation of the DNACPR pathway in the Emergency Department to guide future improvement
programmes
Review current educational strategies and develop platforms for further support in ‘having difficult
conversations’, Mental Capacity Assessments’ and ‘DNACPR decision making’
Introduce a standardised audit process to measure the impact of improvement strategies and allow
comparison of results through Qliksense
Commencement of individual clinician feedback reports
Implement an electronic fluid management system
A standardised handover process will be defined and implemented to improve transfer of critical
information within and across teams.

Page 20
Medication optimisation
There has been a Trust-wide focus on Medication Optimisation in 2019/20 including:
The review and update of the Trust’s vitamin K antagonist prescription chart with the supporting policy
and quick reference guide to support all staff with the safe prescribing, supply and administration of all
vitamin K antagonists
Trust-wide audit of omitted doses of critical medication resulting in:
o Further improvement and audit work around the documentation of omitted critical medicines
o Launch of the critical medicines poster on the Trust clinical guidelines intranet and app
Successful implementation of an electronic referral mechanism to community Pharmacy at the point of
discharge to reduce medication related harm across interfaces of care
Implementing further actions to ensure safe storage, supply and administration of potassium
permanganate to reduce the risk of severe harm or death from ingesting potassium permanganate
Review of the resources, procedures required for the safe prescribing, administration and monitoring of
gentamicin for in-patients
Resources to support the safe prescribing and administration of insulin doses (short and long acting)
The introduction of regular five minute medicines safety messages for all junior medical staff
Progression of quality improvement projects to support the management of key medicines priorities
Successes include:
o The introduction of an acute pain guideline for adults to support better pain management and
strong opioid prescribing
o Collaborative working with primary care to reduce risk of readmission with harm events due to
interactions with anticoagulants
o Pilot of a Pharmacist led medication review targeting patients identified as high risk for falls.
Digital solutions are being designed to support the scalability of the intervention
o Development of a digital tool, supported by an enhanced clinical pharmacy model in ED to target
medicines reconciliation at the point of entry to NUH
We have fully implemented the recommendations of national alerts including:
Risk of death and severe harm from ingesting supra-absorbent polymer gel granules.
The medicines optimisation priorities for 2020/21 include:
Improving the safety and quality of prescribing and administration of anticoagulants, opioids and
insulins
Reducing unintentional missed doses of medication
Further digitalisation of medicines systems within the Trust
Patient Experience
NUH is committed to providing services to patients which value people and act in their best interests.
Patients and their families will be treated with respect, compassion and understanding. We have measured
this through our real-time local patient survey with the following results (on average, 1,000 inpatients per
month complete this survey):
During the year 97.3% of our patients reported that they were treated with dignity and respect whilst in
hospital
92.4% of our patients reported that they were involved in decisions about care and treatment
87.1% of our patients were aware of who the nurse looking after them was on any given day

Page 21
80% of our patients were given information on how to provide feedback on the quality of their care.
In 2019/20 there has been a significant focus on Dementia Carers and their feedback about our services:
97.4% of Carers of Dementia patients recommended the support the ward gave them
75.8% of Carers of Dementia patients had been asked before if they were a carers
86.9% of Carers of Dementia patients have been involved in care and worked with patients as a carer
76.3% of Carers of Dementia patients have been given information about the support they could get as a
carer
Development of SWAN occasion boxes to facilitate weddings or for example an early Christmas. These
have been funded by the Nottingham Hospitals Charity
Development of cultural, spiritual and religious resources for a range of faiths that wards can access
through the Chaplaincy to meet these needs at end of life
We have seen a number of ward developments and an increase in staff resourcefulness to meet patients
and family’s needs, which is the very essence of SWAN, which offers compassionate support to patients
in their last days of life and to their families into bereavement.
Patient Priorities for 2020/21 include:
Implementing the year two milestones of the Trust-wide Dementia Strategy 2019-22
Improving the identificationand support of carers
Improving and standardising customer care across the organisation.
Reduce patient waiting times in the Emergency Department
Our ambition to reduce unnecessary delays in the Urgent and Emergency Care pathway remains a significant
challenge for NUH.We have worked relentlessly to improve systems and processes within our Emergency
Department, across the hospital and wider system to improve flow and reduce discharge delays during
2019/20. The transformation of urgent and emergency care at NUH is a highly ambitious project to ensure
that our patients receive high quality, timely care, in the right environment. We are disappointed that too
many of our patients waited too long in ED and we continue efforts to improve this situation.
Last summer the Prime Minister asked the NHS to undertake a clinical review of current emergency access
targets. NUH was selected as one of the field testing sites (one of 14 Trusts across the country) and has been
reporting against new standards since May 2019. Due to our participation in the national pilot, we are not
able to publically share performance information. Our duty to our patients and focus remains unchanged
whereby we aim to improve the timeliness of emergency patient care and overall patient experience.
The first phase of testing focussed on the total time in the Emergency Department (ED) with indicators
relating to mean time in the department and number of 12-hour waits from time of arrival. Following the
first phase of testing, an initial ‘target’ mean time in the department was set as 200 minutes or less. The
second phase of testing commenced at the end of July 2019 and included additional measures, including
mean time to initial assessment and mental health metrics. This includes the time it takes to get a
psychological assessment and how long it takes for patients to be transferred to mental health beds.
Page 22
From October we have also been asked to measure the time that patients spend in ED from the time that
they are fit to transfer to an inpatient ward (which we call the “fit for ward time”).
From the start of October we have also been reporting on measures associated with “Critical Hour Standards
(CHORUS)”. These are submitted monthly and include measures of our response to abnormal patient
observations within ED, as well as our hospital’s response to heart attacks and strokes.
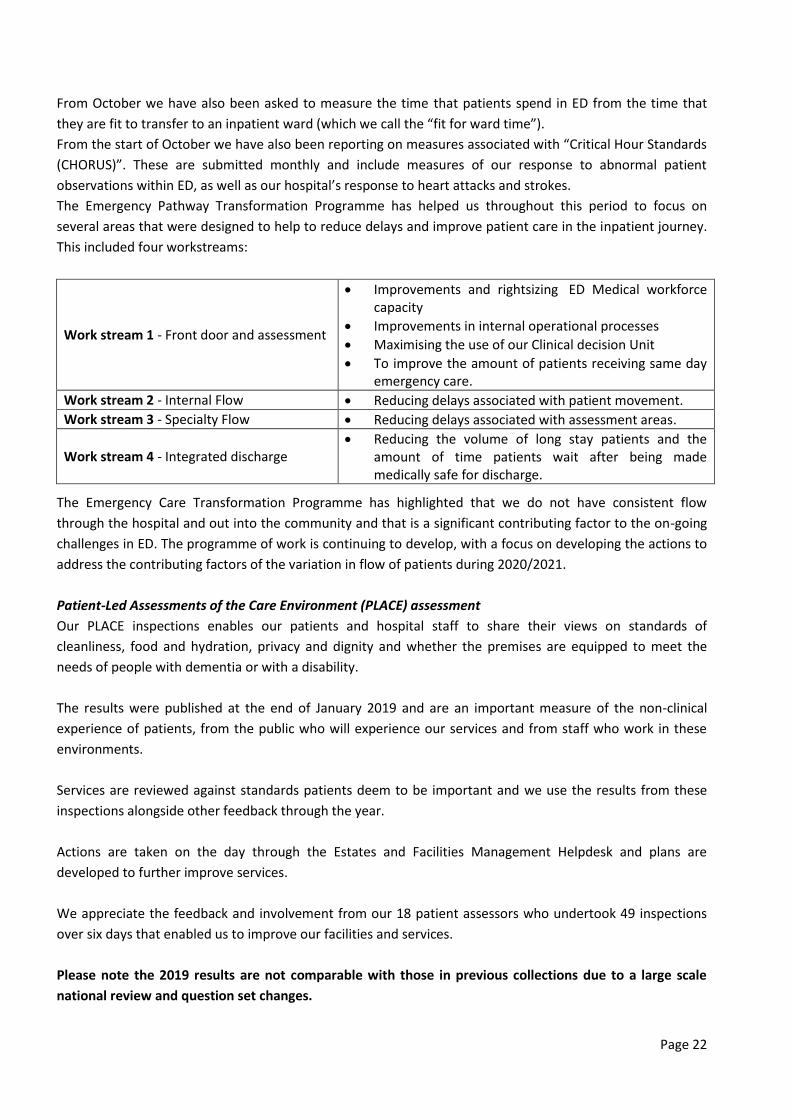
The Emergency Pathway Transformation Programme has helped us throughout this period to focus on
several areas that were designed to help to reduce delays and improve patient care in the inpatient journey.
This included four workstreams:
Work stream 1 - Front door and assessment
Improvements and rightsizing ED Medical workforce capacity
Improvements in internal operational processes
Maximising the use of our Clinical decision Unit
To improve the amount of patients receiving same day emergency care.
Work stream 2 - Internal Flow Reducing delays associated with patient movement.
Work stream 3 - Specialty Flow Reducing delays associated with assessment areas.
Work stream 4 - Integrated discharge Reducing the volume of long stay patients and the
amount of time patients wait after being made medically safe for discharge.
The Emergency Care Transformation Programme has highlighted that we do not have consistent flow
through the hospital and out into the community and that is a significant contributing factor to the on-going
challenges in ED. The programme of work is continuing to develop, with a focus on developing the actions to
address the contributing factors of the variation in flow of patients during 2020/2021.
Patient-Led Assessments of the Care Environment (PLACE) assessment
Our PLACE inspections enables our patients and hospital staff to share their views on standards of
cleanliness, food and hydration, privacy and dignity and whether the premises are equipped to meet the
needs of people with dementia or with a disability.
The results were published at the end of January 2019 and are an important measure of the non-clinical
experience of patients, from the public who will experience our services and from staff who work in these
environments.
Services are reviewed against standards patients deem to be important and we use the results from these
inspections alongside other feedback through the year.
Actions are taken on the day through the Estates and Facilities Management Helpdesk and plans are
developed to further improve services.
We appreciate the feedback and involvement from our 18 patient assessors who undertook 49 inspections
over six days that enabled us to improve our facilities and services.
Please note the 2019 results are not comparable with those in previous collections due to a large scale
national review and question set changes.

Page 23
The Estates and Facilities Management Team review the results alongside the feedback received throughout
the year, much of which gives more real-time feedback about what patients think of the environment and
related standards at our hospitals. This includes monthly cleaning audits, results from the annual patient
surveys, friends and family test results, as well as online and social media feedback e.g. NHS Website, Care
Opinion, Twitter and Facebook.
2019 NUH % scores: QMC campus City Hospital
campus Ropewalk
House Treatment
Centre
Cleanliness 96.56 98.76 100 97.92
Food 90.52 91.69 N/A N/A
Food organisational 100 100 N/A N/A
Ward food 89.18 90.61 N/A N/A
Privacy, dignity and well being 81.82 82.89 85.19 83.87
Condition and appearance and maintenance
93.37 96.44 94.37 93.04
Dementia 62.76 70.39 69.57 57.97
Disability 69.46 74.16 64.29 62.26
QUALITY ACCOUNT PART 2:
2.2 Statements of Assurance from the Board
During 19/20, NUH provided 157 NHS services as identified in Schedule 2A of the contract between the Trust
and its principal Commissioners and NHS England. NUH has reviewed all the data available to them on the
quality of care in all of these relevant health services.
The income generated by the relevant health services reviewed in 2019/20 represents 100% of the total
income generated from the provision of NHS services by NUH for 2019/20. The Trust’s review of quality of
care data for all contracted services is carried out via coding audit, a monthly confirm and challenge process
with commissioners, reviews by Divisions for accuracy and improvements in manual data processes.
The table below provides a summary of the income generated through the commissioned health services for
2019/20:
NHS England services: Total contract income £385,013,337
Acute Services £280,089,052
Cancer Services £90,127,734
Diagnostic screening and/or Pathology £4,223,585
Radiotherapy Services £10,572,966
Clinical Commissioning Groups: Total Contract Income £508,032,502
Accident & Emergency (A&E) £31,549,827
Acute Services £386,157,768
Cancer Services £74,782,528
Diagnostic, Screening and/or Pathology £15,542,379

Page 24
Cancer Drugs Fund, NHS England (national) £7,841,911
Review of Clinical Strategies/Trust Strategy
Ensuring our patients receive consistently high quality, safe care, with outstanding health outcomes and
experience is at the centre of all we do. Following the launch of our revised Trust strategy (2018-2028), we
have defined clear ambitions for our patients in order to think differently about how we deliver safe, high
quality and effective care.
We have six strategic objectives (called our 6 Promises, or 6 ‘Ps’ for short). These are:
Our patients: We will ensure our patients receive consistently high quality, safe care with outstanding
outcomes and experience
Our people: We will build on our position as an employer of choice; with an engaged, developed and
empowered team that puts patient care at the heart of everything it does
Our places: We will invest in our estate, equipment and digital infrastructure to support the delivery of
high quality patient care
Our performance: We will consistently achieve our performance standards and make the best use of
resources that contribute to an affordable healthcare system
Our partners: We will support the improvement of the health of the communities we serve through
strong system leadership and innovative partnerships to deliver integrated models of care
Our potential: We will deliver world-class research and education and education and transform health
through innovation
Underpinning each promise, we have described key milestones for years one, two and three so that we can
closely monitor our progress, which we publish quarterly. Each year, detailed actions are created for the
current year milestones which form the basis of the Trust’s Annual Plan. This ensures specific plans are in
place for each area and service, which enables appropriate resources to be directed, to ensure achievement
of the vision and our promises. We are developing our priorities and milestones for 2020/21 as we respond
to Covid-19 and will publish these later in the year.
Our NUH Clinical Service Strategy provides a foundation to achieve our vision of being “outstanding in health
outcomes and patient and staff experience”. The underpinning drive is a paradigm shift towards focusing on
population health outcomes and holistic patient-centred care (Our Patients promise). We are not able to
deliver the required paradigm shift in isolation of our partners (Our Partners promise). As an organisation we
will also need to change the way we work and focus on new priorities that will have the biggest positive
impact on our population.
To respond to our population health challenges, we have established five planning principles for our services
to adopt as they transform over the next 5-10 years in order to support the Trust’s vision.
• Planning principle one: Person-centred care and how we manage multiple health conditions

Page 25
• Planning principle two: Focussed clinical priority conditions on the most pressing areas of health need
to improve our overall population health outcomes (Clinical areas include: Cardiovascular diseases
(CVD), Diabetes (Endocrine), Cancer, Respiratory diseases, Musculoskeletal disease, Healthcare of Older
People (including Frailty/Dementia) and Gastroenterology. We also know that we will continue to
deliver core services that our population will need such as: Accident and emergency, major trauma,
maternity and neonatal services and diagnostic services
• Planning principle three: Embedding Health promotion, prevention and holistic care
• Planning principle four: Developing Partnerships to deliver high-quality specialised services
• Planning principle five: Driving clinical innovation and emerging technologies.
We are embedding our five planning principles at all levels in the organisation to influence how we do
business and create the right focus to improve population health outcomes. We use our five planning
principles to:
1. Inform our clinical approach: The principles provide a reference point to ask ‘does what we’re doing
support the Clinical Service Strategy?’ (For example we will now ask this question as part of our annual
planning process)
2. Agree priorities: The principles provide clear criteria to inform our future investment e.g. infrastructure,
staffing and transformation projects
3. Transform our clinical decision-making: The principles and priorities provide a strong steer and underpin
our future approach to planning and decision-making, organisational structures and support
mechanisms at all levels including service/specialty level.
Our enablers to making it happen
Our staff engagement highlighted a number of barriers to delivering our Clinical Service Strategy ambitions
that span all five principles. From this we have identified five enablers that provide the building blocks to
making this happen, and suggest how we will take this forward.
• The ICS Long-term plan will promote better integration of care and sharing of information and will
identify key priorities for delivery in both the short and long-term
• Aligning our planning process to our Clinical Service Strategy (e.g. investment, capacity planning, and
infrastructure). We will review our processes and develop new ‘quick’ approaches to facilitate rapid
investment and focus on areas of transformation, aligned to agreed priorities e.g. create a health
promotion and prevention fund
• Getting the basics right with our ICT systems. Review of systems to streamline, prioritisation of areas for
investment. Common systems across the ICS to share information; all electronic patient records,
including prescribing. Standardisation of data to improve transferability
• Involving patients in developing our plans for services to gain their perspectives and insights,
understanding the wider non-health issues (e.g. accommodation, access to ICT). Improved links with key
patient groups to gain feedback and perspectives to inform decision-making
• Leadership and leadership development will promote a culture change to embed our five planning
principles. Through leadership we will transform our approach to focus on our population heath needs
and ‘system’ ways of working within the ICS.

Page 26
Divisional performance management
NUH has six clinical Divisions: Medicine, Surgery, Cancer and Associated Specialties, Ambulatory Care, Family
Health and Clinical Support.
Each Division is led by a Divisional Leadership Team comprising a Divisional Director, Divisional General
Manager and Divisional Nurse/Midwife.
Each month our Divisional Leadership Teams are held to account for their performance against the Trust’s
agreed quality and performance targets, and with compliance against expected standards in each of their
clinical services. This accountability has been enhanced with the establishment of an Operational Quality,
Risk and Safety Committee, chaired by either the Medical Director or Chief Nurse. Through the scheduled
reporting to this committee, Divisions are held to account for performance in the domains of safety,
effectiveness, patient experience and risk management. Additionally, during 19/20 Divisions have provided a
quality account to the Board committee, the Quality Assurance Committee, twice a year against the same
domains.
In 2020/21 a sixth Division will be formed incorporating a number of specialities with a focus on ambulatory
care. The Treatment Centre will form part of this Division.
Developing our quality priorities with patients, families and carers
Our quality improvement priorities are based on feedback from our patients, carers and staff, and on
national standards and developments. We have engaged and worked with our patients, public and carers
from the communities we serve and with staff through a range of meetings and events, including:
NUH Patient Partnership Group
NUH Patient and Public Involvement Steering Group (PPISG)
NUH Divisional Patient and Carer Groups
Healthwatch (Nottingham City and Nottinghamshire)
NUH Public Members
Page 27
Health Scrutiny Committees (County and City)
External Visits, Audits and Peer Reviews
Patient safety conversations between Board members and ward/department teams
We also collect regular feedback through the year from: National and local surveys, the ‘Friends and Family’
Test, complaints, concerns, comments and compliments, social media and online feedback. This helps us to
identify areas where patients say they wish to see improvements.
In 2019/20, we held 479 patient and public involvement events with 10,195 participants. PPI Events included
the Daisy Awards, Bowel Cancer Awareness Events, Memory Menu Tasting, BAME Networks, Patient Safety
Leaflet Review, Local Community Engagement Events, Team NUH Awards and Carers Drop in Sessions. PPI
Groups also supported our Neonatal Unit achieving the Bliss Baby Charter Accreditation Award which
recognises high quality family-centred care delivered against seven core principles.
Our quality priorities for 2020/21 have been developed from PPI and Engagement Events, consultation and
feedback with our local communities. The priorities reflect the things that our people and patients have told
us are important to them. They will be monitored through our Quality Governance Committees with regular
updates from the priority leads.
Our quality priorities for 2020/21
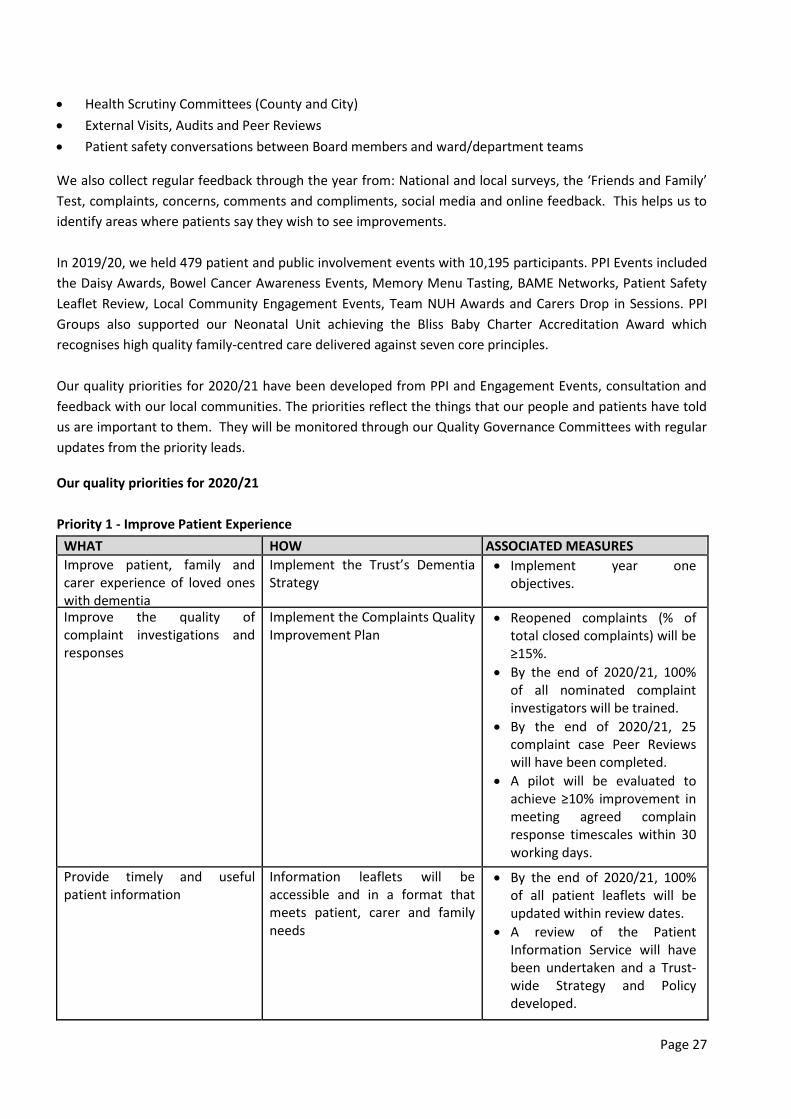
Priority 1 - Improve Patient Experience
WHAT HOW ASSOCIATED MEASURES
Improve patient, family and carer experience of loved ones with dementia
Implement the Trust’s Dementia Strategy
Implement year one objectives.
Improve the quality of complaint investigations and responses
Implement the Complaints Quality Improvement Plan
Reopened complaints (% of total closed complaints) will be ≥15%.
By the end of 2020/21, 100% of all nominated complaint investigators will be trained.
By the end of 2020/21, 25 complaint case Peer Reviews will have been completed.
A pilot will be evaluated to achieve ≥10% improvement in meeting agreed complain response timescales within 30 working days.
Provide timely and useful patient information
Information leaflets will be accessible and in a format that meets patient, carer and family needs
By the end of 2020/21, 100% of all patient leaflets will be updated within review dates.
A review of the Patient Information Service will have been undertaken and a Trust-wide Strategy and Policy developed.
Page 28
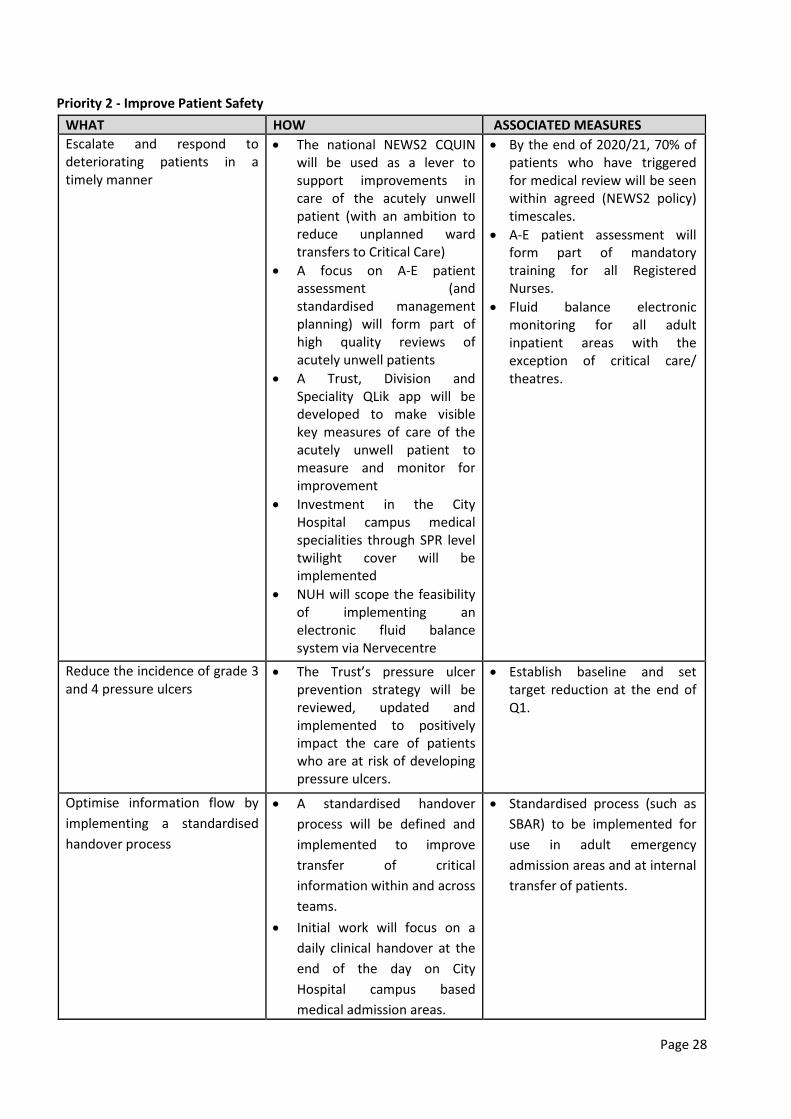
Priority 2 - Improve Patient Safety
WHAT HOW ASSOCIATED MEASURES
Escalate and respond to deteriorating patients in a timely manner
The national NEWS2 CQUIN will be used as a lever to support improvements in care of the acutely unwell patient (with an ambition to reduce unplanned ward transfers to Critical Care)
A focus on A-E patient assessment (and standardised management planning) will form part of high quality reviews of acutely unwell patients
A Trust, Division and Speciality QLik app will be developed to make visible key measures of care of the acutely unwell patient to measure and monitor for improvement
Investment in the City Hospital campus medical specialities through SPR level twilight cover will be implemented
NUH will scope the feasibility of implementing an electronic fluid balance system via Nervecentre
By the end of 2020/21, 70% of patients who have triggered for medical review will be seen within agreed (NEWS2 policy) timescales.
A-E patient assessment will form part of mandatory training for all Registered Nurses.
Fluid balance electronic monitoring for all adult inpatient areas with the exception of critical care/ theatres.
Reduce the incidence of grade 3 and 4 pressure ulcers
The Trust’s pressure ulcer prevention strategy will be reviewed, updated and implemented to positively impact the care of patients who are at risk of developing pressure ulcers.
Establish baseline and set target reduction at the end of Q1.
Optimise information flow by
implementing a standardised
handover process
A standardised handover
process will be defined and
implemented to improve
transfer of critical
information within and across
teams.
Initial work will focus on a
daily clinical handover at the
end of the day on City
Hospital campus based
medical admission areas.
Standardised process (such as
SBAR) to be implemented for
use in adult emergency
admission areas and at internal
transfer of patients.
Page 29
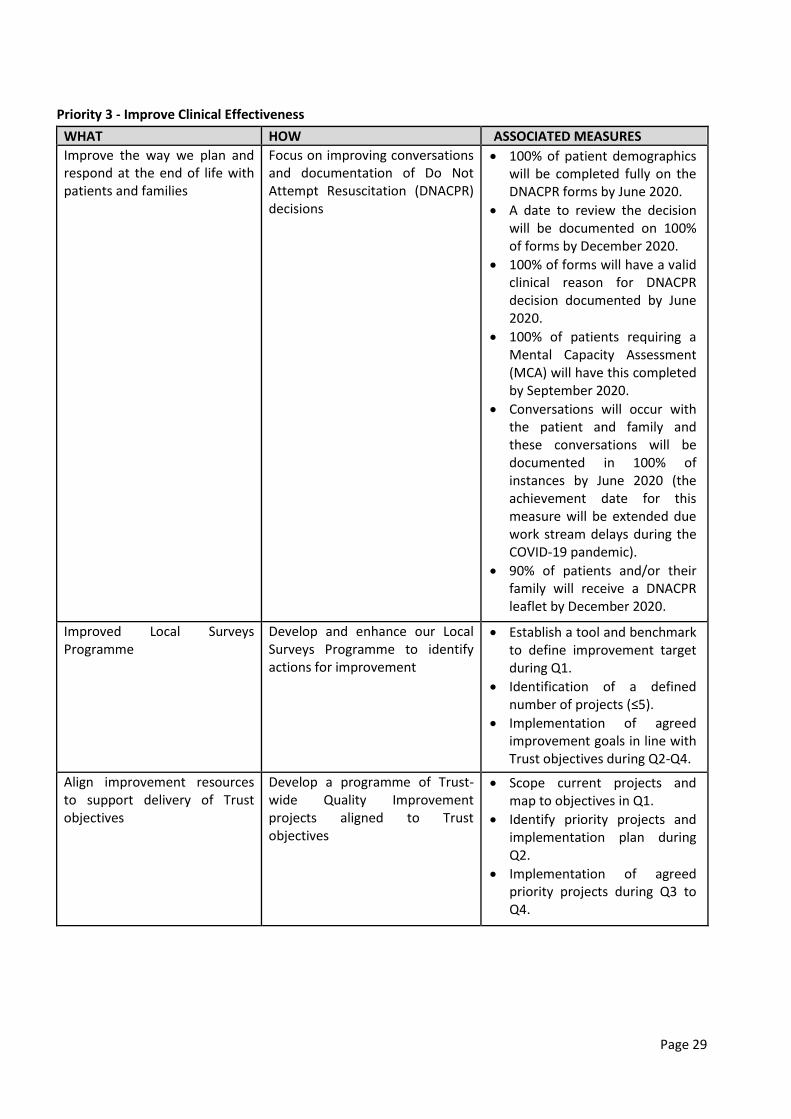
Priority 3 - Improve Clinical Effectiveness
WHAT HOW ASSOCIATED MEASURES
Improve the way we plan and respond at the end of life with patients and families
Focus on improving conversations and documentation of Do Not Attempt Resuscitation (DNACPR) decisions
100% of patient demographics will be completed fully on the DNACPR forms by June 2020.
A date to review the decision will be documented on 100% of forms by December 2020.
100% of forms will have a valid clinical reason for DNACPR decision documented by June 2020.
100% of patients requiring a Mental Capacity Assessment (MCA) will have this completed by September 2020.
Conversations will occur with the patient and family and these conversations will be documented in 100% of instances by June 2020 (the achievement date for this measure will be extended due work stream delays during the COVID-19 pandemic).
90% of patients and/or their family will receive a DNACPR leaflet by December 2020.
Improved Local Surveys Programme
Develop and enhance our Local Surveys Programme to identify actions for improvement
Establish a tool and benchmark to define improvement target during Q1.
Identification of a defined number of projects (≤5).
Implementation of agreed improvement goals in line with Trust objectives during Q2-Q4.
Align improvement resources to support delivery of Trust objectives
Develop a programme of Trust-wide Quality Improvement projects aligned to Trust objectives
Scope current projects and map to objectives in Q1.
Identify priority projects and implementation plan during Q2.
Implementation of agreed priority projects during Q3 to Q4.
Page 30
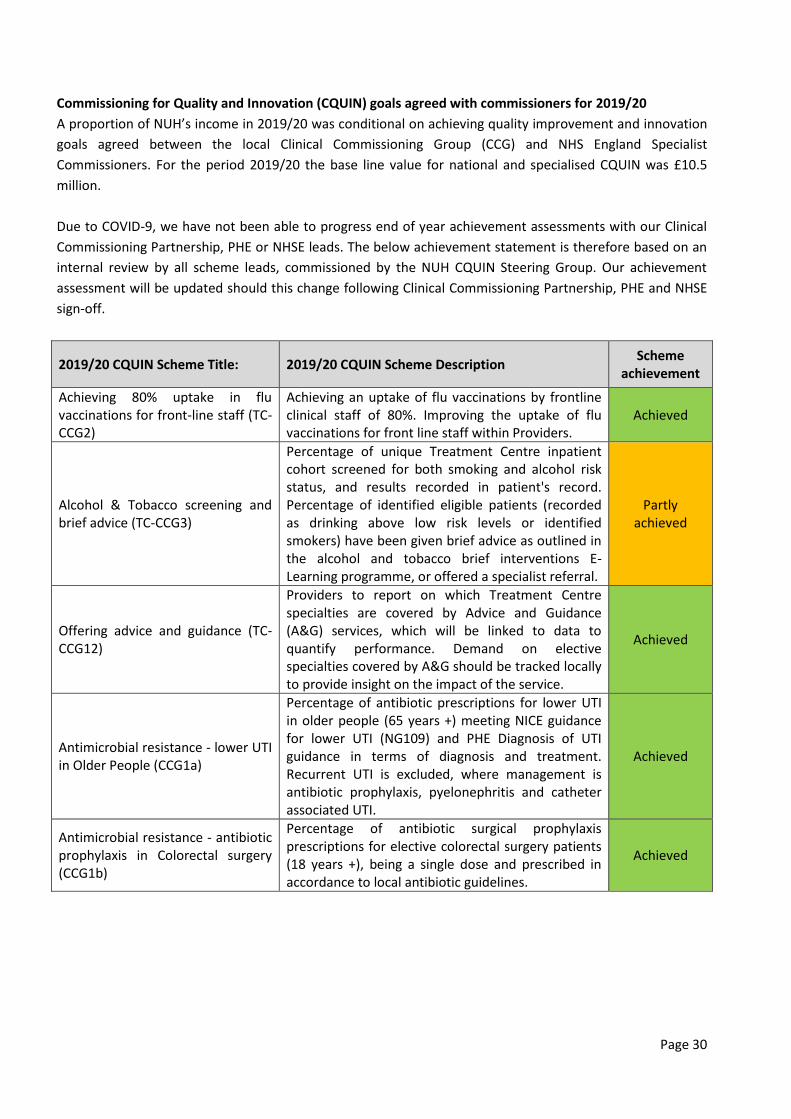
Commissioning for Quality and Innovation (CQUIN) goals agreed with commissioners for 2019/20
A proportion of NUH’s income in 2019/20 was conditional on achieving quality improvement and innovation
goals agreed between the local Clinical Commissioning Group (CCG) and NHS England Specialist
Commissioners. For the period 2019/20 the base line value for national and specialised CQUIN was £10.5
million.
Due to COVID-9, we have not been able to progress end of year achievement assessments with our Clinical
Commissioning Partnership, PHE or NHSE leads. The below achievement statement is therefore based on an
internal review by all scheme leads, commissioned by the NUH CQUIN Steering Group. Our achievement
assessment will be updated should this change following Clinical Commissioning Partnership, PHE and NHSE
sign-off.
2019/20 CQUIN Scheme Title: 2019/20 CQUIN Scheme Description Scheme
achievement
Achieving 80% uptake in flu vaccinations for front-line staff (TC-CCG2)
Achieving an uptake of flu vaccinations by frontline clinical staff of 80%. Improving the uptake of flu vaccinations for front line staff within Providers.
Achieved
Alcohol & Tobacco screening and brief advice (TC-CCG3)
Percentage of unique Treatment Centre inpatient cohort screened for both smoking and alcohol risk status, and results recorded in patient's record. Percentage of identified eligible patients (recorded as drinking above low risk levels or identified smokers) have been given brief advice as outlined in the alcohol and tobacco brief interventions E-Learning programme, or offered a specialist referral.
Partly achieved
Offering advice and guidance (TC-CCG12)
Providers to report on which Treatment Centre specialties are covered by Advice and Guidance (A&G) services, which will be linked to data to quantify performance. Demand on elective specialties covered by A&G should be tracked locally to provide insight on the impact of the service.
Achieved
Antimicrobial resistance - lower UTI in Older People (CCG1a)
Percentage of antibiotic prescriptions for lower UTI in older people (65 years +) meeting NICE guidance for lower UTI (NG109) and PHE Diagnosis of UTI guidance in terms of diagnosis and treatment. Recurrent UTI is excluded, where management is antibiotic prophylaxis, pyelonephritis and catheter associated UTI.
Achieved
Antimicrobial resistance - antibiotic prophylaxis in Colorectal surgery (CCG1b)
Percentage of antibiotic surgical prophylaxis prescriptions for elective colorectal surgery patients (18 years +), being a single dose and prescribed in accordance to local antibiotic guidelines.
Achieved

Page 31
Efforts for Reducing Smoking at the Time of Delivery (CCG3)
To localise the National CQUIN for reducing smoking at the time of delivery (SaToD), and work collaboratively with all partners across the local health system with providers being challenged to be the system leaders, be innovative with service improvements, provide services, skill staff and educate and support future mothers to quit smoking.
Achieved
2019/20 CQUIN Scheme Title: 2019/20 CQUIN Scheme Description Scheme
achievement
Same day Emergency care (CCG11)
Percentage of patients with confirmed pulmonary embolism (PE), atrial fibrillation (AF) and community-acquired pneumonia (CAP) being managed in a same day setting where clinically appropriate (total number of patients attending ED, aged 18 years + who are discharged to usual place of residence on the same day as attendance/admission). Clinical exclusion criteria applied.
Partly achieved
Medicines Optimisation and Stewardship (PSS1)
To support the procedural and cultural changes required to optimise use of medicines commissioned by specialised services through a series of procedural and cultural changes.
Achieved
Supporting Hepatitis C Virus (HCV) Elimination (PSS2)
To respond to the WHO strategy for elimination by 2030 and NHS England’s ambition to accelerate this to 2025, with increased focus on improving treatment of diagnosed patients and increasing rates of testing and diagnosis. Whilst the wider health and social care system has a role to play, ODNs, as expressed in the service specification, have a leadership role to play in supporting these actions.
Achieved
Cystic fibrosis; supporting self-care (PSS3)
To support changes in clinician and patient behaviour that will transform Cystic Fibrosis (CF) care from an emphasis on clinician led reactive hospital based rescue, to patient led community based prevention.
Achieved
Severe asthma specialised care review (PSS8)
To promote a networked model of care as a vehicle for delivering an optimal pathway and maximising patient outcomes and experience.
Achieved
Cirrhosis Care bundle (PSS14)
Improve patient care and reduced care costs through a network model to ensure adoption of nationally developed clinical guidelines and policies regarding management of patients with decompensated cirrhosis. The network should be rolled out and developed over three years. First stage implementation to be rolled out.
Achieved

Page 32
Neonatal Outreach (PSS Local)
To improve community support and to take other steps to expedite discharge, pre-empt re-admissions, and otherwise improve capacity within the neonatal unit for those babies requiring a higher level of care and reducing out of Network transfers due to a lack of capacity.
Achieved
Identify and reduce local inequalities in Abdominal Aortic Aneurysm Screening (PHE1)
Continue to implement, monitor and evaluate a health inequalities action plan for the Abdominal Aortic Aneurysm screening programme (2-year CQUIN with two stages).
Achieved
Identify and reduce local inequalities in Breast Cancer Screening Programme (PHE2)
Develop, implement and evaluate a health inequalities action plan for the Breast Screening service (2-year CQUIN with two stages).
Achieved
Identify and reduce local inequalities in Diabetic Eye Screening Programme (PHE3)
Develop, implement and evaluate a health inequalities action plan for the Diabetic Eye Screening programme (2-year CQUIN with two stages).
Achieved
Care Quality Commission (CQC)
NUH has been registered with the CQC since its inception in 2010 and has maintained its registration without
conditions or enforcement action ever since, including 2019/20.
The Trust is registered by the CQC to provide the following regulated activities:
Assessment of medical treatment for persons detained under the Mental Health Act 1983
Diagnostic and screening procedures
Surgical procedures
Treatment of disease, disorder or injury
Maternity and midwifery
Termination of pregnancy
Family planning
The last comprehensive inspection of NUH (QMC and City Hospital campuses) took place between
20thNovember 2018 and 10th January 2019, when a total of seven core services provided by the Trust across
two locations were inspected. NUH was rated ‘good’ overall with the following individual ratings:

Page 33
In November 2019 the CQC undertook a standalone inspection of the children’s Sexual Assault Referral
Centre (SARC) and issued its inspection report in February 2020. These inspection findings do not impact on
the Trust’s ratings. The outcome of the inspection was as follows:
SAFE
CQC found that the service was providing safe care in accordance with the relevant regulations
EFFECTIVE
CQC found that the service was providing effective care in accordance with the relevant regulations
CARING
CQC found that the service was providing care in accordance with the relevant regulations
RESPONSIVE
CQC found that the service was providing responsive care in accordance with the relevant regulations
WELL LED
CQC found that this service was not providing well-led care in accordance with the relevant regulations,
specifically that “governance arrangements and board assurance on the safe and effective operation of the
SARC were underdeveloped”. The CQC issued four compliance actions in relation to this finding, all of which
are being actioned and monitored as part of the established CQC oversight arrangements.
It should be noted that the CQC explicitly stated that the impact of their concerns, in terms of the safety of
clinical care, were regarded as minor and that once the shortcomings had been put right the likelihood of
them occurring in the future was low.
Progress with the action plan from both inspections continues to be closely monitored by the Quality and
Safety Committee, with quarterly reports to both Management Board and the Trust Board’s Quality
Assurance Committee, augmented by regular quality visits by commissioners and NHS Improvement.
The action plan oversight arrangements were reviewed by internal audit who awarded a significant
assurance opinion in November 2019.
Page 34
As part of its engagement strategy, the CQC meets regularly with the Trust, undertakes visits to clinical areas,
holds focus groups with staff, and attends Trust Board meetings a minimum of twice a year.
Duty of Candour
Duty of Candour (DoC), Regulation 20 of the Health and Social Care Act 2008, is a statutory requirement for
all providers registered with the CQC. It covers any patient safety incident that appears to have caused, or
has the potential to cause, significant harm and requires the provider to undertake:
Initial disclosure of the incident
Provision of a written account
Completion of an investigation and sharing of investigation findings to include a formal apology.
At NUH, the Being Open Policy clearly outlines the requirements for the Trust to comply with Regulation 20
and the key responsibilities for staff are regularly shared and updated through mandatory training and
newsletters. Divisions are responsible for ensuring Duty of Candour occurs in those incidents that meet the
threshold and the Corporate Patient Safety Team ensures Duty of Candour occurs for any Serious Incidents
that occur.
During 2019/20, NUH undertook an audit of its compliance with Regulation 20 for all incidents of moderate
or above avoidable harm. The audit showed:
90% compliance with initial disclosure
73% compliance with written notification
61% compliance with follow-up.
NUH has explored its compliance and these results are influenced by the availability of information
evidencing Duty of Candour. NUH has an open and transparent culture which has been recognised.
Improvements during 2019/20:
NUH continues to be open and honest after patient safety incidents
Being Open and Duty of Candour have been truly embedded in Serious Incident processes
In August 2019 the Corporate Patient Safety Team employed a Patient and Family Liaison Officer. This
role is new to the Trust and has evidenced early benefits in supporting patients, families and SI
investigation panel members
In May 2019- the Trust having undertaken significant engagement and re-design work- launched its
revised Duty of Candour guidance in the Trust, including bespoke patient/family letters co-designed with
patient involvement.
Areas for future improvement 2020/21:
Utilise local audit results and independent 360 assurance review findings to strengthen sharing of local
investigations where statutory candour is indicated
Formally evaluate the impact of the Patient and Family Liaison Officer role in conjunction with a Patient
Safety Academic.
Safeguarding Patients

Page 35
Safeguarding the health and wellbeing of all our patients remains a high priority for the Trust. The Trust is
committed to safeguarding all children, young people and adults at risk of abuse. We believe that everyone
has an equal right to protection from abuse, regardless of their age, race, religion, gender, ability,
background or sexual identity.
NUH continues to work to enhance safeguarding practice and standards across the whole organisation to
safeguard our most vulnerable patients and to continue to develop and embed a culture that puts
safeguarding at the centre of care delivery.
The Safeguarding Team continues to raise the profile of safeguarding across the Trust, the aim being for the
Safeguarding Team and the process to be integrated into the work of NUH. The team are visible and staff feel
informed and confident in accessing safeguarding advice.
NUH is recognised as a key multi-agency partner on, and a valuable contributor to, local adult safeguarding
boards and children’s partnerships.
Key achievements in 2019/20:
The safeguarding team has been strengthened to meet the increasing demand
During 2019/20, the mandatory training theme for training was ‘Back To Basics’ which was delivered as
part of our three year cycle of training with a different area of focus in each of the three years
Launch of a new IT system for the safeguarding team, enabling better information sharing with the
clinical teams and improving the collection of data
Representation by the Safeguarding Team on a number of serious case reviews, rapid reviews,
safeguarding adult reviews and domestic homicide reviews. The Trust continues to play a full part in
safeguarding across the region. Partnerships with our multi-agency partners continue to be
strengthened year on year.
Priorities for 2020/21:
Implementation of the Liberty Protection Safeguards.
Participation in National Clinical Audits 2019/20
The NUH 2019/20 Clinical Audit Programme consisted of 356 registered projects, 183 (51%) of which were
registered on the database as “National Clinical Audits”.
A total of 116 (63%) of these ‘registered’ National Clinical Audits were described in the NHS
England/Healthcare Quality Improvement Partnership (HQIP) Quality Account Schedule for 2019/20 (as
either National Clinical Audits or National Confidential Enquiries).
There were seven National Clinical Audits/Audit programmes which were deemed as not applicable to NUH
(i.e. we do not provide that particular type of service or participation was not required by the organising
bodies) and so were excluded from the 2019/20 Clinical Audit programme. These are as follows:
2019/20:
Specialty Audits that NUH has not participated in:
Respiratory Medicine National Audit of Pulmonary Hypertension
Upper GI Surgery National Bariatric Surgery Registry (NBSR)

Page 36
Rheumatology National Clinical Audit for Rheumatoid and Early Inflammatory Arthritis
(NCAREIA)
Trust-wide National Clinical Audit of Psychosis
Surgery Prescribing Observatory for Mental Health (POMH-UK).
Trust-wide National Clinical Audit of Anxiety and Depression (re-confirmed with Royal
College of Psychiatrists 01/03/19).
Children & Young People National Child Mortality Database (NCMD)
Of the 116 National Clinical Audits and National Confidential Enquiries registered on the Trust Clinical Audit
Database that NUH were expected to participate in from the NHS England/HQIP Quality Account schedule,
we participated in 115 (99%).
The National Audit that was registered on the Trust Database that NUH is understood to provide the service
for but for 2019/20 did not participate in were:
“Society of Acute Medicine Benchmarking Audit” (SAMBA) - it was felt that there was little return in
terms of learning for the specialty, due to the very small sample size after the specialty underwent
operational redesign. The National Lead was made aware and agreed for 19/20 exemption.
In addition to the 116 National Audits ‘registered’ on the Audit Database, there was one National Audit, that
NUH did not participate in, this was the National Audit of Seizure Management in Hospitals (NASH3)
2019/20.
The table below shows the number and percentage of cases submitted into each of the National
Audits/Confidential Enquiries: (Please note some audits may ‘appear’ to be duplicates, but they were either
carried over from the previous year’s audit plan (awaiting publication of the National Report) or, if the audit is
“continual data collection”, then a new audit ID will have been generated in order to enable NUH to comment
on that reports recommendations.
Specialty Audit Title Expected
Sample Size
Number
Submitted
Percentage of
participation
compliance
Audit
completed or
action plan
received National Audits carried over from 2018/19 and completed with action plan
Ophthalmology National Ophthalmology Database (NOD) Audit 2018 report
1198 1198 100% Yes
Renal Medicine Renal replacement therapy (Renal Registry)
1238 1238 100% Yes
Urology National Prostate Cancer Audit (2018/19)
655 655 100% Yes
Urology BAUS Urology Audit - Female Stress Urinary Incontinence (2018/19)
104 104 100% Yes
Neonatal Unit National Neonatal Audit Programme (NNAP) 2017 Report
1741 1741 100% Yes
PICU Paediatric Intensive Care Audit (PICAnet) (2017)
1723 1723 100% Yes
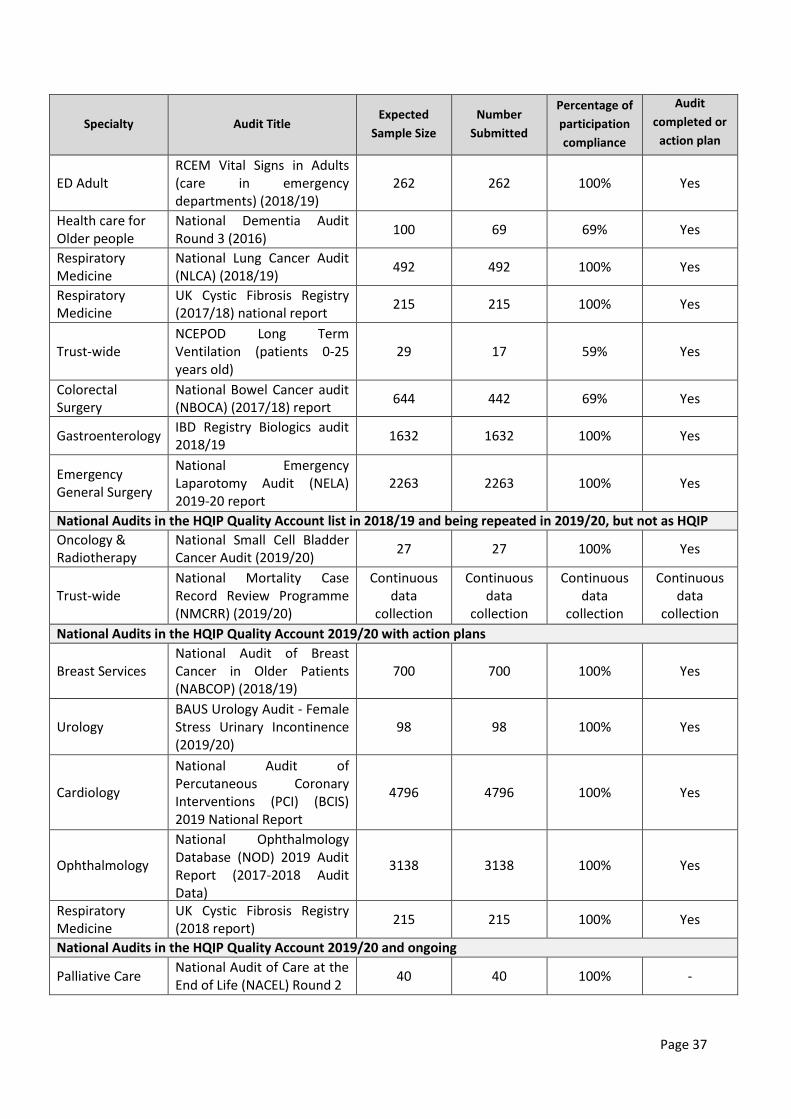
Page 37
Specialty Audit Title Expected
Sample Size
Number
Submitted
Percentage of
participation
compliance
Audit
completed or
action plan
received
ED Adult RCEM Vital Signs in Adults (care in emergency departments) (2018/19)
262 262 100% Yes
Health care for Older people
National Dementia Audit Round 3 (2016)
100 69 69% Yes
Respiratory Medicine
National Lung Cancer Audit (NLCA) (2018/19)
492 492 100% Yes
Respiratory Medicine
UK Cystic Fibrosis Registry (2017/18) national report
215 215 100% Yes
Trust-wide NCEPOD Long Term Ventilation (patients 0-25 years old)
29 17 59% Yes
Colorectal Surgery
National Bowel Cancer audit (NBOCA) (2017/18) report
644 442 69% Yes
Gastroenterology IBD Registry Biologics audit 2018/19
1632 1632 100% Yes
Emergency General Surgery
National Emergency Laparotomy Audit (NELA) 2019-20 report
2263 2263 100% Yes
National Audits in the HQIP Quality Account list in 2018/19 and being repeated in 2019/20, but not as HQIP Quality Account Audits Oncology & Radiotherapy
National Small Cell Bladder Cancer Audit (2019/20)
27 27 100% Yes
Trust-wide National Mortality Case Record Review Programme (NMCRR) (2019/20)
Continuous data
collection
Continuous data
collection
Continuous data
collection
Continuous data
collection
National Audits in the HQIP Quality Account 2019/20 with action plans
Breast Services National Audit of Breast Cancer in Older Patients (NABCOP) (2018/19)
700 700 100% Yes
Urology BAUS Urology Audit - Female Stress Urinary Incontinence (2019/20)
98 98 100% Yes
Cardiology
National Audit of Percutaneous Coronary Interventions (PCI) (BCIS) 2019 National Report
4796 4796 100% Yes
Ophthalmology
National Ophthalmology Database (NOD) 2019 Audit Report (2017-2018 Audit Data)
3138 3138 100% Yes
Respiratory Medicine
UK Cystic Fibrosis Registry (2018 report)
215 215 100% Yes
National Audits in the HQIP Quality Account 2019/20 and ongoing
Palliative Care National Audit of Care at the End of Life (NACEL) Round 2
40 40 100% -

Page 38
Specialty Audit Title Expected
Sample Size
Number
Submitted
Percentage of
participation
compliance
Audit
completed or
action plan
received Palliative Care
National Audit of Care at the End of Life (NACEL)
81 81 100% -
Urology BAUS Urology Audit - Cystectomy
64 8 12% -
Urology BAUS Urology Audit - Nephrectomy
332 133 40% -
Urology BAUS Urology Audit - Percutaneous Nephrolithotomy (PCNL) (2019/20)
189 187 90% -
Urology BAUS Urology Audit - Radical Prostatectomy
316 221 70% -
Urology National Prostate Cancer Audit (2019/20)
595 595 100% -
Critical Care Case Mix Programme (CMP) - ICNARC
897 897 100% -
Children & Young People
National Clinical Audit of Seizures and Epilepsies in Children and Young People (Organisation Report 2018).
1 1 100% -
Children & Young People
Paediatric Intensive Care Audit (PICANET)
3451 3451 100% -
Children & Young People
National Paediatric Diabetes Audit (NPDA) 2019/20
376 376 100% -
Children & Young People
Child Health Clinical Outcome Review Programme 2019/20 (NCEPOD)
29 17 58.6% -
Maternity
Maternal, Newborn and Infant Clinical Outcome Review Programme - MBRRACE - UK
See individual studies in
this document
See individual studies in
this document
100%
See individual
studies in this document
Maternity
National Maternity and Perinatal Audit (NMPA) UK Perinatal Deaths for Births from January to December 2017
8407 8407 100% -
Neonatal Unit
Intensive and special care: Neonatal (inc. National Neonatal Audit programme - NNAP) (2019/20)
1504 1504 100% -
Acute Medicine Society for Acute Medicine's Benchmarking Audit (SAMBA)
NUH did not participate
NUH did not participate
NUH did not participate
Divisional Governance
aware
Cardiology National Audit of Cardiac Rehabilitation
685 685 100% -

Page 39
Specialty Audit Title Expected
Sample Size
Number
Submitted
Percentage of
participation
compliance
Audit
completed or
action plan
received
Diabetes & Endocrinology
National Diabetes Inpatient Audit 2019
Figures not expected until May
2020
Figures not expected until May
2020
Figures not expected until May
2020
ED Adult RCEM Mental Health - Care in Emergency Departments 2019
42 42 100% -
ED Adult
RCEM Assessing Cognitive Impairment in Older People /Care in Emergency Departments
132 132 100% -
ED Paediatrics RCEM Care of Children in Emergency Departments
292 292 100% -
Respiratory Medicine
National Asthma Audit (NACAP) Adults
273 273 100% -
Respiratory Medicine
BTS National Smoking Cessation Audit
216 216 100% -
Respiratory Medicine
Cancer: Lung (NLCA) 2019/20
Continuous data
collection, awaiting
collation of report
Continuous data
collection, awaiting
collation of report
Continuous data
collection, awaiting
collation of report
Data still being
collected
Stroke National Audit of Dementia Round 4 (2018)
148 148 100% -
Stroke Stroke: Sentinel stroke national audit programme (SSNAP) (2018/19 report)
1213 1213 100% -
Trust-wide UK Parkinson’s National Audit
40 40 100% -
Elective Orthopaedics
Elective Surgery (National PROMs Programme) 2019/20
1798 1798 100% -
Elective Orthopaedics
Elective Surgery (National PROMS programme) (2018/19)
1715 1715 100% -
Elective Orthopaedics
Joint replacement surgery: the National Joint Registry (NJR) 2019/20
1798 1798 100% -
Emergency General Surgery
National Emergency Laparotomy Audit (NELA) 2018/19 REPORT
363 363 100% -
Endocrine Surgery
Endocrine and Thyroid National Audit 2019/20
218 218 100% -
ENT Cancer: Head and neck cancer audit (HANA) 2019/20
GT reports Rishi
Srivastava to report back
asap
Awaiting
data
Gastroenterology National Gastro-intestinal Cancer Programme
GT reports Lindsay
Stevens is getting info
asap
Awaiting
data
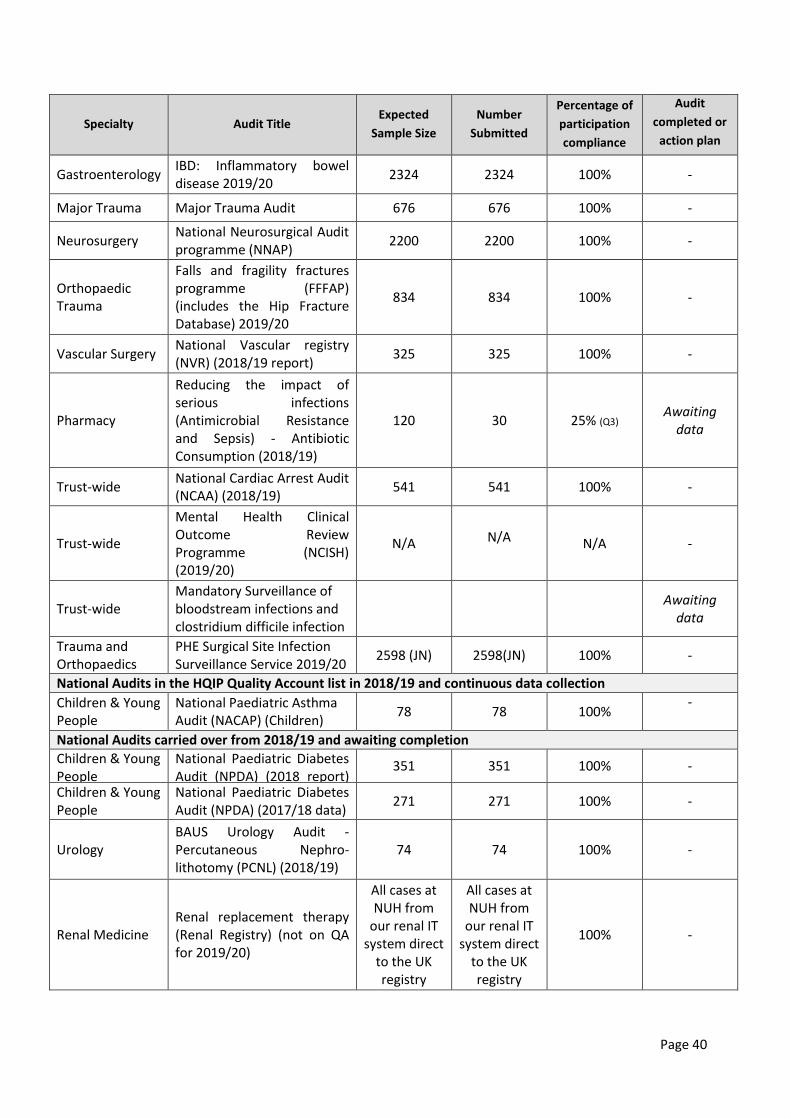
Page 40
Specialty Audit Title Expected
Sample Size
Number
Submitted
Percentage of
participation
compliance
Audit
completed or
action plan
received Gastroenterology
IBD: Inflammatory bowel disease 2019/20
2324 2324 100% -
Major Trauma Major Trauma Audit 676 676 100% -
Neurosurgery National Neurosurgical Audit programme (NNAP)
2200 2200 100% -
Orthopaedic Trauma
Falls and fragility fractures programme (FFFAP) (includes the Hip Fracture Database) 2019/20
834 834 100% -
Vascular Surgery National Vascular registry (NVR) (2018/19 report)
325 325 100% -
Pharmacy
Reducing the impact of serious infections (Antimicrobial Resistance and Sepsis) - Antibiotic Consumption (2018/19)
120 30 25% (Q3) Awaiting
data
Trust-wide National Cardiac Arrest Audit (NCAA) (2018/19)
541 541 100% -
Trust-wide
Mental Health Clinical Outcome Review Programme (NCISH) (2019/20)
N/A N/A N/A -
Trust-wide Mandatory Surveillance of bloodstream infections and clostridium difficile infection
Awaiting
data
Trauma and Orthopaedics
PHE Surgical Site Infection Surveillance Service 2019/20
2598 (JN) 2598(JN) 100% -
National Audits in the HQIP Quality Account list in 2018/19 and continuous data collection
Children & Young People
National Paediatric Asthma Audit (NACAP) (Children)
78 78 100% - National Audits carried over from 2018/19 and awaiting completion
Children & Young People
National Paediatric Diabetes Audit (NPDA) (2018 report) (2016/17 data)
351 351 100% -
Children & Young People
National Paediatric Diabetes Audit (NPDA) (2017/18 data)
271 271 100% -
Urology BAUS Urology Audit - Percutaneous Nephro-lithotomy (PCNL) (2018/19)
74 74 100% -
Renal Medicine Renal replacement therapy (Renal Registry) (not on QA for 2019/20)
All cases at NUH from
our renal IT system direct
to the UK registry
All cases at NUH from
our renal IT system direct
to the UK registry
100% -
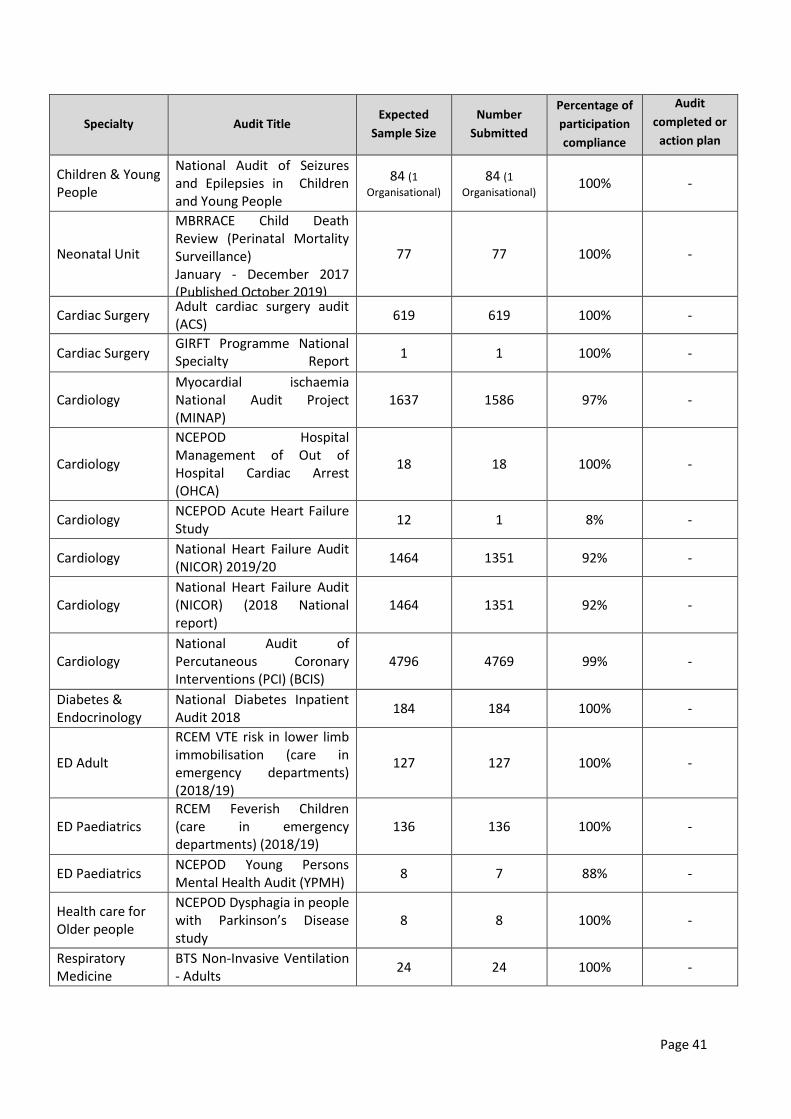
Page 41
Specialty Audit Title Expected
Sample Size
Number
Submitted
Percentage of
participation
compliance
Audit
completed or
action plan
received Children & Young People
National Audit of Seizures and Epilepsies in Children and Young People
84 (1
Organisational) 84 (1
Organisational) 100% -
Neonatal Unit
MBRRACE Child Death Review (Perinatal Mortality Surveillance) January - December 2017 (Published October 2019)
77 77 100% -
Cardiac Surgery Adult cardiac surgery audit (ACS)
619 619 100% -
Cardiac Surgery GIRFT Programme National Specialty Report (Cardiothoracic Surgery)
1 1 100% -
Cardiology Myocardial ischaemia National Audit Project (MINAP)
1637 1586 97% -
Cardiology
NCEPOD Hospital Management of Out of Hospital Cardiac Arrest (OHCA)
18 18 100% -
Cardiology NCEPOD Acute Heart Failure Study
12 1 8% -
Cardiology National Heart Failure Audit (NICOR) 2019/20
1464 1351 92% -
Cardiology National Heart Failure Audit (NICOR) (2018 National report)
1464 1351 92% -
Cardiology National Audit of Percutaneous Coronary Interventions (PCI) (BCIS)
4796 4769 999%9 -
Diabetes & Endocrinology
National Diabetes Inpatient Audit 2018
184 184 100% -
ED Adult
RCEM VTE risk in lower limb immobilisation (care in emergency departments) (2018/19)
127 127 100% -
ED Paediatrics RCEM Feverish Children (care in emergency departments) (2018/19)
136 136 100% -
ED Paediatrics NCEPOD Young Persons Mental Health Audit (YPMH)
8 7 88% -
Health care for Older people
NCEPOD Dysphagia in people with Parkinson’s Disease study
8 8 100% -
Respiratory Medicine
BTS Non-Invasive Ventilation - Adults
24 24 100% -

Page 42
Specialty Audit Title Expected
Sample Size
Number
Submitted
Percentage of
participation
compliance
Audit
completed or
action plan
received Respiratory Medicine
BTS Adult Community Acquired Pneumonia (2018/19)
152 152 100% -
Respiratory Medicine
National Asthma and Chronic Obstructive Pulmonary Disease Audit Programme (NACAP) COPD clinical audit (for patients from 2017/18)
273 273 100% -
Respiratory Medicine
UK Cystic Fibrosis Registry 208 208 100% -
Trust-wide NCEPOD Non-Invasive Ventilation Study
5 11 45% -
Trust-wide NCEPOD Pulmonary Embolism
10 8 80% -
Colorectal Surgery
National Bowel Cancer audit (NBOCA) (2018/19)
189 189 100% -
Emergency General Surgery
NCEPOD acute bowel obstruction study
17 11 65% -
Major Trauma Trauma and Audit Network (TARN) (2018/19)
1942 1942 100% -
Neurosurgery GIRFT Programme National Specialty Report (Cranial Neurosurgery)
1 1 100% -
Ophthalmology GIRFT Ophthalmology - Surgical Site Infection 2019
N/A Awaiting
data
Ophthalmology National Audit for Cataract Surgery
1198 1198 100% -
Orthopaedic Trauma
Falls and Fragility Fracture audit programme (FFFAP) (Annual Report 2018)
806 806 100% -
Upper GI Surgery
National Oesophago-Gastric Cancer Audit report 2018 (NOGC) (version 2, March 2019)
273 273 100% -
Upper GI Surgery National Oesophago-gastric cancer audit (NOGCA) (2017 report)
334 334 100% -
Vascular Surgery National Vascular Registry (2016/17)
75 75 100% -
Respiratory Medicine
National Asthma and COPD Audit Programme (2017/18 National Report)
190 190 100% -
Trust-wide Learning Disability Mortality Review Programme (LeDeR) 2019/20
27 27 100% -
Audits that have been registered as “National Audits”, but not part of the HQIP Quality Account list

Page 43
Specialty Audit Title Expected
Sample Size Number
Submitted Percentage
Blood Transfusion
National Comparative Audit of The Use of Fresh Frozen Plasma, Cryoprecipitate and other Blood Components in Neonates and Children
20 15 75%
Blood Transfusion National Comparative Audit 2018 Massive Haemorrhage Audit
10 6 60%
Blood Transfusion 2019 National Comparative re-audit of the medical use of red cells
80 0 0%
Breast Services Mastitis And Mammary Abscess Management Audit (MAMMA STUDY)
80 Not yet started
Not yet started
Breast Services Breast Angiosarcoma Surveillance Study 15 15 100%
Breast Services Neoadjuvant systemic therapy in breast cancer (previously under ID 17-316C)
13 13 100%
Breast Services GIRFT Breast Surgery N/A 22 100%
Breast Services
The iBRA-2 Study - A National prospective multi-centre audit of the impact of immediate breast reconstruction on the delivery of adjuvant therapy (see project ID 16-938C)
86 86 100%
Children & Young People
NCEPOD Chronic Neurodisability Study 8 6 75%
Specialty Audit Title Expected
Sample Size Number
Submitted Percentage
Children & Young People
National Audit of Paediatric Stoma patient outcomes
25 25 100%
Children & Young People
NCEPOD Cancer in Children, Teens and Young Adults
12 10 83%
Children & Young People
Phototherapy Service Audit 20 20 100%
Clinical Pathology GIRFT Thrombosis Survey 2019 120 120 100%
Colorectal Surgery
Postoperative ileus and provision of management after colorectal surgery (IMAGINE)
32 32 100%
Colorectal Surgery
International, prospective snapshot collaborative audit of acute diverticulitis (DAMASCUS)
4000 Postponed
Diabetes & Endocrinology
NCEPOD Peri-operative management of surgical patients with diabetes
18 8 44%
Elective Orthopaedics
GIRFT Programme National Specialty Report (Orthopaedic Trauma)
1 1 100%
Elective Orthopaedics
GIRFT Orthopaedic Surgery - Surgical Site Infection 2019
N/A 860 100%
ENT GIRFT Programme National Specialty Report (ENT)
1 1 100%
ENT Head and Neck Cancer Surveillance Audit 2018 (BAHNO)
190 190 100%
ENT National Epistaxis Audit 1826 1826 100%

Page 44
ENT GIRFT ENT Surgery - Surgical Site Infection 2019
N/A Awaiting data
Gastroenterology RICOCHET audit 56 56 100%
General Surgery GIRFT General Surgery - Surgical Site Infection 2019
N/A Awaiting data
General Surgery Trauma Emergency Laparotomy Audit (TELA)
26 26 100%
General Surgery GIRFT Programme National Specialty Report (General surgery)
1 1 100%
Genetics National Von Hippel-Lindau Syndrome (VHL) screening audit: Genetics - 2018
48 48 100%
Major Trauma Liver and Pancreatic Trauma Audit (LiPTA) 100 0 0%
Maxillofacial Surgery
GIRFT Dentistry - Oral and Maxillofacial Surgery - Surgical Site Infection 2019
N/A Awaiting data
Neurosurgery GIRFT Neurosurgery, Surgical Site Infection 2019
1 1 100%
Neurosurgery Multi-disciplinary team management of cerebral metastases in the UK
101 101 100%
Obstetrics Antenatal Screening Programmes 2017-2018
200 201 100%
Obstetrics National Comparative Audit of the Management of Maternal Anaemia (2018)
10 10 100%
Obstetrics GIRFT Obstetrics and Gynaecology - Surgical Site Infection 2019
N/A Awaiting data
Specialty Audit Title Expected
Sample Size Number
Submitted Percentage
Obstetrics Each Baby Counts (2018/19) 27 27 100%
Oncology & Radiotherapy
UK National Radium-223 audit project 19 19 100%
Ophthalmology GIRFT Programme National Specialty Report (Ophthalmology)
1 1 100%
Paediatric Surgery Audit of Outcomes in Major Burns (> 25% TBSA)
N/A 10 100%
Paediatric Surgery GIRFT Paediatric General Surgery - Surgical Site Infection 2019
N/A Awaiting data
Pain Management
National audit of inpatient complex and chronic pain (CHIPS)
41 41 100%
Pharmacy Antimicrobial NHS Improvement / CQUIN - Colorectal
400 95 24%
Pharmacy Antimicrobial NHS Improvement / CQUIN - Urinary Tract Infection
400 0 0%
Pharmacy Antimicrobial NHS Improvement / CQUIN - Antifungal
20 20 100%
Physiotherapy The EU-PARK-PICU Study: European Prevalence of Acute Rehab for Kids in the PICU
16 16 100%
Plastic Surgery & Burns
National Quality Outcome Measures: Quality dashboard for specialised burn care
63 63 100%

Page 45
Radiology RCR National Audit Evaluating Radiological Reporting of Fragility Fractures
50 50 100%
Radiology RCR National Audit of Seven Day Care Radiology.
1 1 100%
Sexual Health BHIVA national clinical audit 2018: monitoring of adults with HIV aged 50 or over
39 39 100%
Spinal A Multi-centre Retrospective Audit of Native Vertebral Osteomyelitis Cases (NITCAR)
11 8 73%
Spinal GIRFT Spinal Surgery - Surgical Site Infection 2019
N/A Awaiting data
Stroke National Audit of Dementia / Delirium (NAD) - Spotlight Audit
20 20 100%
Thoracic Surgery GIRFT Cardiothoracic Surgery - Surgical Site Infection 2019
N/A 2 100%
Trust-wide (GIRFT) Surgical Site Infection audit "Umbrella" Registration
2512 2512 100%
Trust-wide Community Acquired Pneumonia CQUIN 2019
600 600 100%
Trust-wide NCEPOD Provision of Mental Health Care in Acute Hospitals
9 8 89%
Trust-wide Pulmonary Embolus CQUIN 2019 600 600 100%
Trust-wide Tachycardia with Atrial Fibrillations CQUIN 2019
400 200
(data collection ongoing)
50% (data collection
ongoing)
Specialty Audit Title Expected
Sample Size Number
Submitted Percentage
Trust-wide GlobalSurg: Quality and outcomes in global cancer surgery: a prospective, international cohort study
120 120 100%
Upper GI Surgery Oesophago-gastric Anastomosis Audit (OGAA)
21 21 100%
Urology GIRFT Urology - Surgical Site Infection 2019 No expected sample size
Awaiting data
Vascular Surgery GIRFT Programme National Specialty Report (Vascular Surgery)
1 1 100%
Vascular Surgery GIRFT Vascular Surgery - Surgical Site Infection 2019
No expected sample size
Awaiting data
Vascular Surgery Groin wound Infection after Vascular Exposure Audit (VERN)
NUH not participated.
NUH not participated.
Awaiting response
*Denotes audits where data collection is either still underway or there was no actual minimum expected sample size
specified (hence the figure represents the number of submissions to date)
Participation in National Confidential Enquiries 2019/20
During 2019/20 NUH participated in all relevant enquiries set by the National Confidential Enquiry into
Patient Outcome and Death (NCEPOD) and by the Maternal Infant and Newborn Programme (MBRRACE-UK).
NCEPOD projects improve standards by identifying common poor practice. NUH participated in the NCEPOD
studies outlined below.
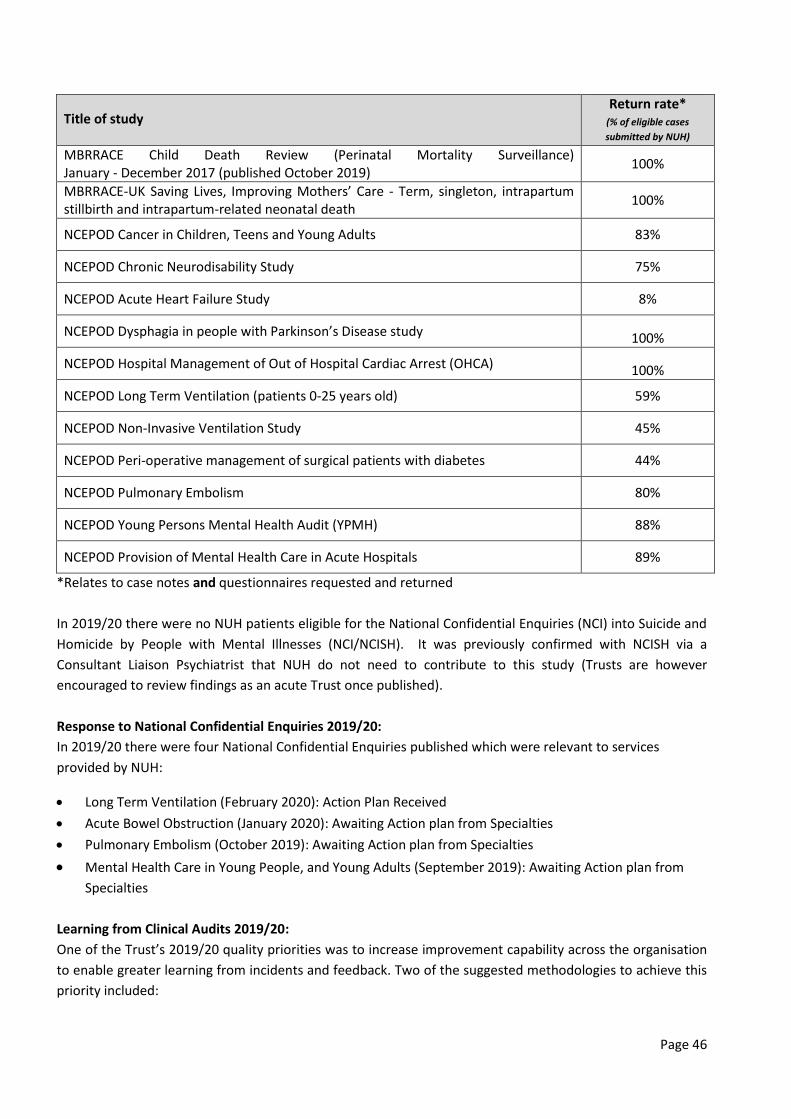
Page 46
Title of study Return rate*
(% of eligible cases
submitted by NUH)
MBRRACE Child Death Review (Perinatal Mortality Surveillance) January - December 2017 (published October 2019)
100%
MBRRACE-UK Saving Lives, Improving Mothers’ Care - Term, singleton, intrapartum stillbirth and intrapartum-related neonatal death
100%
NCEPOD Cancer in Children, Teens and Young Adults 83%
NCEPOD Chronic Neurodisability Study 75%
NCEPOD Acute Heart Failure Study 8%
NCEPOD Dysphagia in people with Parkinson’s Disease study 100%
NCEPOD Hospital Management of Out of Hospital Cardiac Arrest (OHCA) 100%
NCEPOD Long Term Ventilation (patients 0-25 years old) 59%
NCEPOD Non-Invasive Ventilation Study 45%
NCEPOD Peri-operative management of surgical patients with diabetes 44%
NCEPOD Pulmonary Embolism 80%
NCEPOD Young Persons Mental Health Audit (YPMH) 88%
NCEPOD Provision of Mental Health Care in Acute Hospitals 89%
*Relates to case notes and questionnaires requested and returned
In 2019/20 there were no NUH patients eligible for the National Confidential Enquiries (NCI) into Suicide and
Homicide by People with Mental Illnesses (NCI/NCISH). It was previously confirmed with NCISH via a
Consultant Liaison Psychiatrist that NUH do not need to contribute to this study (Trusts are however
encouraged to review findings as an acute Trust once published).
Response to National Confidential Enquiries 2019/20:
In 2019/20 there were four National Confidential Enquiries published which were relevant to services
provided by NUH:
Long Term Ventilation (February 2020): Action Plan Received
Acute Bowel Obstruction (January 2020): Awaiting Action plan from Specialties
Pulmonary Embolism (October 2019): Awaiting Action plan from Specialties
Mental Health Care in Young People, and Young Adults (September 2019): Awaiting Action plan from
Specialties
Learning from Clinical Audits 2019/20:
One of the Trust’s 2019/20 quality priorities was to increase improvement capability across the organisation
to enable greater learning from incidents and feedback. Two of the suggested methodologies to achieve this
priority included:

Page 47
Rolling out the Quality, Service, Improvement and Redesign (QSIR) Fundamentals Programme across
teams and services
Developing a database of Quality Improvement (QI) projects and outcomes
Four of the five members of the Trust-wide Clinical Effectiveness team are QSIR trained. A robust audit
database including QI projects are captured regularly and a live report of this database is now available to
NUH staff through the Clinical Effectiveness Qlik App.
In addition, a bi-annual National Clinical Audits benchmarking report is generated to describe NUH’s
outcomes in national clinical audits against other Trusts and peers across the country. Each NUH Division,
and the Quality and Safety Committee, receives reports on a quarterly basis from the Clinical Effectiveness
team which include national and local audit outcomes.
The Clinical Audit Programme/database comprised of 356 ‘registered’ audits
Some of these were new additions to the plan, whilst others were audits that were carried over from
the previous year’s plan because they were still at data collection/analysis stage or were awaiting the
return of a completed audit review/action plan
183 (51%) of these 356 were “national audits” (Either NHSE / HQIP QA or any other “national”)
116 (63%) of these 183 registered on the Trust database were national audits on the NHSE / HQIP
Quality Account list for 2019/20. The remaining 67 (37%) were non-HQIP national audits.
Partially Supported Audit Registrations
A total of 579 Partially Supported Audits were registered in 2019/20, which is similar to the previous year
(589 for 2018/19). A breakdown of these partially supported audits is in the table below:
Examples of improvements in, or assurance of the quality of care for NUH patients as a result of National
or local Clinical Audit
The reports of 26 National Clinical Audits were reviewed by the provider in 2019/20 and NUH intends to take
the following actions to improve the quality of healthcare provided/can celebrate the following excellence in
care provided.
National Audit / Quality Improvement Programmes
The National Audit of Percutaneous Coronary Interventions (PCI) (BCIS) 2019 (Cardiology):

Page 48
Service is compiling a list of re-interventions at one year and pneumothorax/haemothorax post
procedure (by cross-referencing ICD code from discharge letters obtained from coding and pacing
procedures)
Most current operators are (at least for complex devices) compliant with data completeness
Lead Clinician has provided more reinforcement regarding this to operators following March 2019
NICOR validation exercise.
Respiratory Medicine National Lung Cancer Audit (NLCA) (2018/19):
Overall 91.6% of patients had performance status recorded which is an improvement on 2018/19 (84%).
This is higher than the England average (81.6%) and higher than the East Midlands (84.1%)
97.9% had a stage recorded which again is an improvement from the 2018/19 report (94.7%). This is
higher than the England figure of 96.1%
Pathological confirmation rate in stage I/II was 89.3% which is in line with the England average of 88.9%
Chemotherapy in SCLC is 81.8% which is good practice
Recruitment to a lung cancer administrative staff is currently underway to enhance and improve the
data collection
A business case for a sixththoracic surgeon is underway which will increase capacity. Robotic thoracic
surgery has also commenced which allows more extensive surgery in borderline patients.
The National Ophthalmology Database (NOD) 2019 Audit Report: (2017-2018 Audit Data):
PCR rate is better than the national average
A cataract pathway day has been arranged to facilitate maximising the recording of both pre-operative
and post-operative data for every operation as per national recommendations
Medisoft has the facility and is being completed to enhance Patient Reported Outcome Measures
(PROMs) before and after surgery to quantify and validate patient benefit from surgery, as advised in
the NOD recommendations and 2019 NICE Quality Standard for serious eye disorders (QS180).
BHIVA Sexual Health National Clinical Audit: monitoring of adults with HIV aged 50 or over:
National recommendation is to use proformas where feasible as prompts and to set up electronic
reminder systems with appointments for annual review, which for older patients should focus especially
on:
o CVD and bone risk assessment
o Review of mood, memory and cognition
o Poly-pharmacy and potential for drug-drug interactions
Use of a new electronic system has enabled staff to see parameters and timescales more easily. Pop-up
reminders are also set up.
Local Audit/Quality Improvement Programmes
The Trust intends to take the following actions to improve patient care and experience and/or notes the
following improvements and excellence in outcomes as a result of local Clinical Audit:
Obesity Prevention in Children and Young People (NICE QS 94):
Obesity Guideline updated and available through intranet. URL links to patient leaflets are part of the
guideline. Updated guideline submitted for peer review
Leaflet printed and offered in Childrens Outpatient clinics.

Page 49
Reviewing Sodium levels in postnatal women (Maternity):
30 sets of maternal notes were reviewed during the course of this audit. Of these 30 sets, two babies
had low sodium levels. The two babies had their sodium levels escalated appropriately and received
appropriate intervention as per NUH guidelines.
A Cellular Pathology audit of biopsy reporting for NSCLC:
100% compliance with the standards (1. Biopsy classified according to recommended terminology 100.
2. Percentage of non-resected cases classified as NSCLC-NOS100)
100% compliance with RCPath recommended terminology
100% compliance with acceptable percentage of non-resected cases classified as NSCLC-NOS.
Antimicrobial use in ENT:
100% of patients had a clear documented decision to start all antibiotics in the medical notes
100% had antibiotics prescribed in-line with guidelines/microbiology
Consultant reviews increased to 80%.
PATIENT FEEDBACK
4Cs (Compliments, Complaints, Concerns and Comments)
2019/2020 is the ninth year that NUH has been using the 4C (complaints, concerns, compliments and
comments) approach to capture feedback from patients, carers and families. Patient Experience Quarterly
Reports on complaint themes and examples of learning are received by the Quality Assurance Committee.
The charts below describe the number of complaints received, the number referred to the Parliamentary
Health Service Ombudsman (PHSO), the number of compliments and the five most common complaint
themes for each year 2016/17 to 2019/20.
Number of local complaints and PHSO referrals:
2016/17 2017/18 2018/19 2019/20
Complaints 656 637 683 735
Complaints Upheld 122 fully 177 partially
87 fully 129 partially
104 fully 199 partially
80 fully 198 partially
PHSO Contacts 76 75 70 53*
Investigations taken up by the PHSO
16 15 6 6*
Upheld PHSO referrals (in year)
0 fully 12 partially
0 fully 3 partially
0 fully 5 partially
0 fully* 1 partially*
*National PHSO annual data only available up to 30/11/2019.
Most frequent complaint themes:
2016/17 2017/18 2018/19 2019/20
Standards of care (treatment)
Standards of care (treatment)
Standards of care (diagnosis)
Standards of care (treatment)

Page 50
Standards of care (diagnosis)
Standards of care (assessment)
Standards of care (treatment)
Standards of care (diagnosis)
Complications during/after surgery
Standards of care (diagnosis)
Verbal Communication Complications
during/after surgery
Lack of communications regarding discharge
Complications during/after surgery
Complications during/after surgery
Standards of care (assessment)
Standards of care (assessment)
Verbal Communication Lack of communication
regarding discharge Verbal communication
Total Compliments:
2016/17 2017/18 2018/19 2019/20
5892 6415 5703 5463
Reopened Complaints:
Reopened complaints are reported monthly in the Integrated Performance Report.
Divisions are informed of all reopened complaints on a monthly basis so they can review these and identify
whether the complaint could have been handled differently in order to resolve this at the first response.
Q1 2019/20 Q2 2019/20
Q3 2019/20 Q4 2019/20
Total complaints 159
237 193 146
Reopened 17
23 26 14
% resolved at first response
90% 91% 87% 91%
Examples of learning from complaints taken from most frequent complaint themes:
Reason for
Complaint Quality Objective Action taken
Standards of care (treatment)
Improve clinical effectiveness
Clinical Educator changed practice to work directly with staff involved as a result of a complaint.
Patient experience shared with staff for reflection and learning.
All learning points from complaints are collated into a learning document. This is shared with the staff involved and wider team for continuous learning and improved good practice.

Page 51
Standards of care (diagnosis)
Improve clinical effectiveness
A review of capacity and demand work was completed in the outpatient specialty. This resulted in a workforce change that led to virtual clinics.
New equipment purchased to aid in the identification of cleft palate.
Process implemented to improve timeliness of triage and to ensure that patients have a wristband issued within one hour of attendance.
Complications during/after surgery
Improve clinical effectiveness
Audit findings have shown that surgical team have improved their compliance of the use of the internal transfer document. The actions and recommendations from the audit have also been implemented.
Ward Sister has discussed with staff the use of anti-embolism stockings. Further checks have been implemented to ensure this is reviewed on handover. A full review of the nursing handover has also been completed.
Standards of care (assessment)
Improve clinical effectiveness
A complaint regarding standards of assessment was shared at the specialty governance forum for reflection and learning by the wider team.
Staff have been updated on the Traffic Light Assessment Process and Resource Box to assist in providing care.
Verbal communication
Improve patient experience
Patient and relatives experience anonymously shared with staff and added to induction program for awareness.
Surgical ward have reviewed their processes on how they communicate discharge plans with their patients and relatives. This includes implementing afternoon leadership rounds to ensure that the discharge coordinator or nurse in charge makes contact with relatives and carers early on in the process.
HCOP Liaison Service reviewed their DNAR systems and conversations. The service has liaised with surgical colleagues to agree who will undertake these discussions to improve standards of communication.
Improving complaint handling:
In 2019/20:
NUH has continued to participate in the Peer Review process on a bi-monthly basis. This involves
reviewing the complaint process and peer assessment of complaints handling. This year we have met
our annual goal of reviewing 25 complaint files. Recommendations and learning from the Peer Review
process have been implemented by the Complaints Team to improve local systems and processes.
Patient stories, taken from complaints which have demonstrated learning within the organisation are
presented monthly at Trust Board. Patients and relatives have attended Trust Board this year in person
to share their story.

Page 52
The Complaints Team is actively engaged with the weekly Incident Review Meetings, led by the Patient
Safety Team, to identify cases for escalation or joint investigation. The meetings also provide an
opportunity for information sharing and triangulation of intelligence relating to complaints, incidents
and claims
We have introduced new quality standards for checking all complaints letters before they are approved
within the current signing off process
An internal review of complaints handling systems and processes has been undertaken resulting in the
development of the Complaints Quality Improvement Plan 2020/21. The plan outlines quality initiatives
aimed at improving the overall quality of complaint investigations, timeliness of responses as well as
improving shared learning
In partnership with our Patient Participation Group and Clinical Psychology Team, we have developed
and delivered a Letter Writing Workshop which focusses on compassionate complaints handling.
Patient Surveys
During 2019, the results of the National Urgent and Emergency Care Survey 2018 and Children & Young
People’s Survey 2018 were published by the Care Quality Commission (CQC). A summary of our results is
given below.
Urgent and Emergency Care 2018 Survey, published by the CQC in October 2019
Our response rate to the survey improved from the previous year. Overall, our patients felt listened to and
confident in their care. We did significantly better than most Trusts in providing privacy and dignity to
patients when discussing their conditions. The Medicine Division participated in a shared learning workshop
and developed a plan for improving patient experiences in response to the survey feedback.
Children and Young People’s 2018 Survey, published by the CQC in November 2019
Children and young people feel they are well looked after in our services. We have seen a number of
improvements since the last survey in 2016. The survey feedback identified the following areas where we are
doing well:
• Speaking to children about their worries
• Children liking the hospital food
• Parent being able to prepare food and hot drinks using the available facilities
• Parents feeling there are enough activities for their child to do during their stay in hospital
• Children feeling wards are suitable for their age group
• Staff communicating information clearly about a child’s condition or treatment.
We also participated in the following national patient surveys during the year:
Maternity Services Survey 2019, published by the CQC in January 2020
The CQC results show our performance compared to 125 other acute Trusts. All sections scores in the
antenatal, labour and birth and postnatal reports were in the expected range compared to other Trusts. We
have seen an improvement in a total of nine questions when compared to the previous survey. The survey
feedback identified the following areas where we are doing well:
• Partners being supported to stay as long as they wanted

Page 53
• Women being given enough information about their physical recovery and information about changes
to mental health
• Midwives giving active support and encouragement about feeding
• Women being able to see their midwife as much as they wanted
• Midwives being aware of a woman’s medical history
• Women being offered a choice of where they have their baby
• Women feeling their concerns are taken seriously.
The Family Health Division participated in a shared learning workshop and developed a plan for improving
patient experiences in response to the survey feedback.
Adult In-patient Survey 2019
The Trust is awaiting the publication of the national results of this survey by the CQC.
Patient Friends and family test (FFT)
Patients are invited to give feedback on their care and experience by answering one simple question – ‘How
likely is it that you would recommend this service to friends and family if they needed similar treatment?’ A
total of 44,044 inpatient and day case patient FFT responses were received in 19/20 with an overall
recommend rate of 96.7%. We also received 14,588 emergency department FFT responses with an overall
recommend rate of 89.4%.
FFT Survey Total Responses % Recommended
Emergency Department 14,588 89.4%
Inpatient & Daycase 44,044 96.7%
Outpatients 61,385 96.2%
Maternity (Antenatal) 1,070 99.3%
Maternity (Labour Ward/ Birthing Unit) 607 96.4%
Maternity (Postnatal Ward) 1,526 96.1%
Maternity (Postnatal Community Service) 1,948 99.6%
Learning from real-time feedback:
Here are some of the actions we have taken to improve patient experience in direct response to the FFT
survey as well as our local surveys.
Communication
The #hellomynameis campaign is being promoted and is now included on all new ID badges
We have developed a new information video for patients Preparing For Surgery - Live Brief - YouTube
Patients and carers continue to be involved and contribute to our culture and values work across the
Trust and offer advice on a range of projects and leaflets.
Food
We have improved our food including special diet menus and the availability of drinks and snacks. Our
Memory Menu has been developed, implemented and promoted

Page 54
We have focussed our efforts on improving nutrition. Our Critical Care team have menus on display for
easy access and to help promote better patient choice
In response to feedback around requirements to have more assistance for patients at mealtimes, we
have developed training through the Teams Helping Teams staff volunteering initiative. Support for
mealtime assistance is available for wards who have requested this.
Sleep
We have focussed on identifying what helps patients sleep well at home and replicating this in hospital
where possible e.g. music, drinks, pillow, blankets etc
In response to feedback about noise at night and patients experiencing difficulties in sleeping we have
produced ‘Top Tips for Patients and Staff’: https://www.nuh.nhs.uk/sleep-guidance-for-patients
Pain
A number of education and support sessions for staff have been held and the development of a pain
application is underway to enable staff to review, monitor and action pain care more easily.
Carers
We have improved support for carers through working in partnership with the Carers Trust. We have
set up new monthly carers support sessions at both QMC and City sites
We have introduced an Excellence in Dementia Discharge information ID Wallet Card for staff.
Other
In response to patient feedback around inactivity and having limited things to do during their
hospital stay, we have introduced fitness fiends and boredom busters
Pet Therapy visits help us reduce stress, anxiety, isolation, boredom and improve the patient and
staff experience.
% recommended provider Trust (peer group) comparison April 2018-December 2019
STAFF FEEDBACK
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Bri
sto
l
Sou
tham
pto
n
New
cast
le
No
ttin
gham
Leic
este
r
Leed
s
Cam
bri
dge
Oxf
ord
Man
ches
ter
Shef
fiel
d
Bir
min
gham
Lan
cash
ire
Live
rpo
ol
Eng
Ave
.
Eng
Hig
h
Eng
Low
Inpatients A & E Attendances

Page 55
Staff ‘Friends and Family’ Test (FFT)
Staff are invited to provide feedback on the quality of care and the likelihood of recommending NUH as a
place to work through the Staff Friends and Family Test (FFT) , the results of which are shown below.
Factor Q1 Q2* Q4
% of respondents would be extremely likely or likely to recommend NUH services to friends and family if they needed care or treatment
83% 83%* 87%
% of respondents would be extremely likely or likely to recommend NUH as a place to work.
54% 80%* 62%
*These values reflect only new starters within the organisation as a sample group was chosen in Q2 to
undertake the Staff FFT.
National Staff Survey 2019
A total of 38% (5,899) of staff responded to the national staff survey. The median national response rate was
47%.
Highlights from our national survey results across 11 themes include:
• The Trust is above average for four themes of which two (Safe Environment - Bullying and Harassment
and Safe Environment – Violence) are within the best 20% of benchmarked Trusts in the country)
• The Trust is average for three themes (Immediate managers, Morale and Staff engagement)
The Trust is below average for four themes of which three (Quality of Appraisals, Quality of Care and Team
Working) are in the lowest 20% of benchmarked Trusts.
The focus for improvements in 2020/21 will be:
• Review of car parking provision and transport to work
• Looking after staff health and well-being at work, including working flexibly and making reasonable
adjustments for staff who need them
• Making sure everyone has the same opportunity to progress their career
• Making sure that everyone is treated fairly
• Making sure staff have the resources to do their job
• Making sure staff feel they can influence decisions and make improvements in their role
• Improving the skill set of managers, including communication and visibility and ensuring that staff are
supported in challenging times and recognised for their efforts.
Social media and online feedback
During the 2019/20 period, we gained 2,421 new followers to our main Twitter account, taking our total
followers to 18,748. Nearly six million people have seen our Tweets over the past year.
NUH received on average, 1,500 Twitter mentions per month during the 2019/20 period. Of these mentions
over the year, 514 related directly to patient feedback; 316 (62%) were positive, 155 were negative (30%)
and 43 were neutral (8%).

Page 56
The most common themes were care standards (52%), staff attitudes and behaviours (43%), the Emergency
Department (10%), parking (6%) and phone communication (6%). The vast majority of these particular
Tweets were positive with the exception of Tweets about parking and phone communication.
94% of parking Tweets were concerns. The majority of the parking concern Tweets were received Q1 and
Q2, and amounted to 21 tweets. This is a reduction of 39 from Q3 and Q4 of 2018/19 but is a carry-over of
the announcement in the third quarter 2018/19 that the Trust would no longer be offering free parking to
drivers who held blue disabled parking badges, and the implementation of this policy in Q4. Parking is still an
area of concern for many people due to the lack of available spaces and the cost of parking for certain
groups.
97% of all Tweets relating to phone communication were negative, however, there is no emerging theme for
why this is other than known operational pressures within services.
NUH received 233 pieces of feedback from patients/relatives on the Care Opinion and NHS (formerly NHS
Choices) websites. Of these, 58% were compliments and 36% were concerns, with 6% neutral. Consistent
with social media subject of concerns, the comments received related to care standards (67%), and staff
attitudes and behaviours (66%). Feedback posted online has reduced slightly overall since 2018/19 when we
received 288 comments.
We have continued to share feedback from Care Opinion and the NHS website on Twitter. A selection of
patient and relative comments (including compliments and concerns and complaints) are shared weekly with
all staff as part of the Trust Briefing sent by the Communications Team. NUH continues to receive praise
nationally for our commitment to openness and transparency, including regularly sharing both positive and
negative feedback and our learning from such feedback.
Improving patient information
We continually build on our commitment to providing high quality patient information. We provide all
necessary guidance, templates and other information for authors of patient information leaflets, to enable
them to produce good quality information in line with the Trust Patient Information Policy and national best
practice guidance.
Overall, we have a total of 745 leaflets in use across the Trust. A total of 63 new leaflets were produced in
2019/20.
Our 2020/21 Quality Priority is to undertake a full review of our current Patient Information Policy and
Processes and to improve information leaflets to be more accessible and in a format that meets patient,
carer and family needs. We will also be considering quality improvements within the wider aspects of Patient
Information.
Data quality management and assurance
The Trust submitted records during 2019/20 to the Secondary Uses Service (SUS) for inclusion in the Hospital
Episode Statistics (HES), which are included in the latest published data.
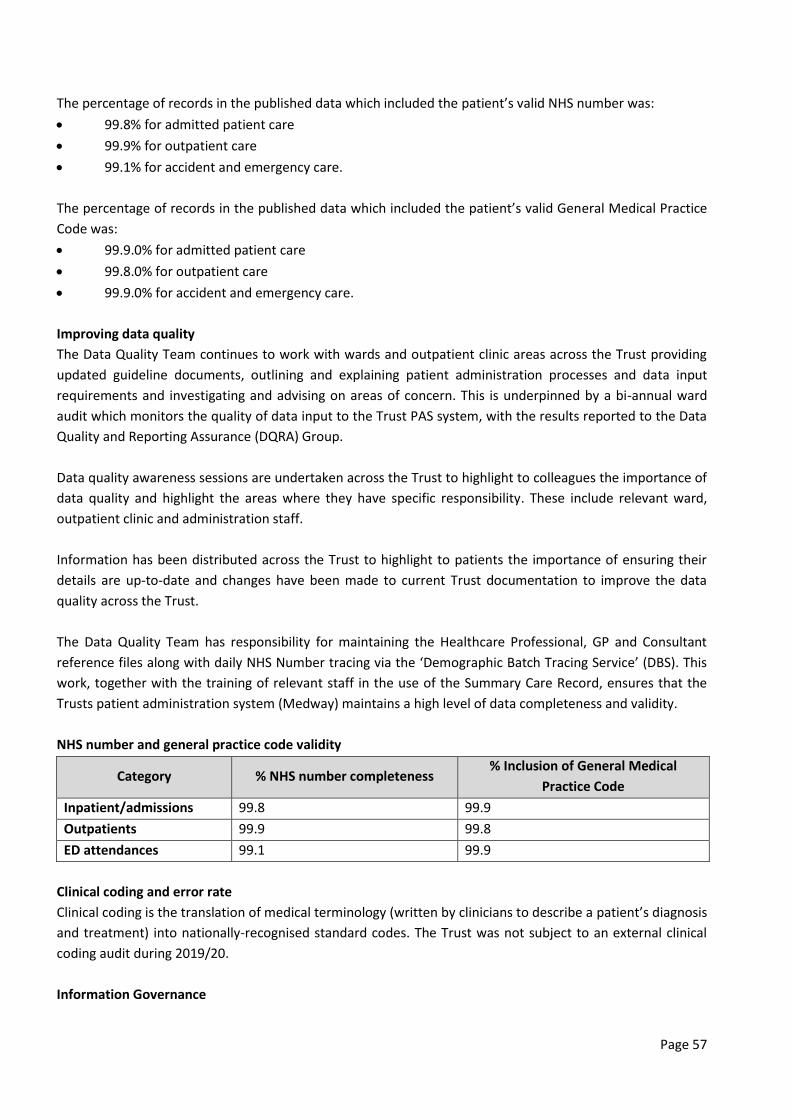
Page 57
The percentage of records in the published data which included the patient’s valid NHS number was:
99.8% for admitted patient care
99.9% for outpatient care
99.1% for accident and emergency care.
The percentage of records in the published data which included the patient’s valid General Medical Practice
Code was:
99.9.0% for admitted patient care
99.8.0% for outpatient care
99.9.0% for accident and emergency care.
Improving data quality
The Data Quality Team continues to work with wards and outpatient clinic areas across the Trust providing
updated guideline documents, outlining and explaining patient administration processes and data input
requirements and investigating and advising on areas of concern. This is underpinned by a bi-annual ward
audit which monitors the quality of data input to the Trust PAS system, with the results reported to the Data
Quality and Reporting Assurance (DQRA) Group.
Data quality awareness sessions are undertaken across the Trust to highlight to colleagues the importance of
data quality and highlight the areas where they have specific responsibility. These include relevant ward,
outpatient clinic and administration staff.
Information has been distributed across the Trust to highlight to patients the importance of ensuring their
details are up-to-date and changes have been made to current Trust documentation to improve the data
quality across the Trust.
The Data Quality Team has responsibility for maintaining the Healthcare Professional, GP and Consultant
reference files along with daily NHS Number tracing via the ‘Demographic Batch Tracing Service’ (DBS). This
work, together with the training of relevant staff in the use of the Summary Care Record, ensures that the
Trusts patient administration system (Medway) maintains a high level of data completeness and validity.
NHS number and general practice code validity
Category % NHS number completeness % Inclusion of General Medical
Practice Code
Inpatient/admissions 99.8 99.9
Outpatients 99.9 99.8
ED attendances 99.1 99.9
Clinical coding and error rate
Clinical coding is the translation of medical terminology (written by clinicians to describe a patient’s diagnosis
and treatment) into nationally-recognised standard codes. The Trust was not subject to an external clinical
coding audit during 2019/20.
Information Governance

Page 58
Information Governance (IG) provides a framework for effective handling of information, particularly the
personal and sensitive information of patients and employees, to ensure that information is processed
legally, securely and confidentially. The Data Security and Protection Toolkit mandates NHS organisations to
self-assess their compliance with current legislation and national guidance. The Trust has yet to submit its
final submission for 2019/20 as NHSD postponed the final submission to the end of September 2020 due to
the Covid-19 pandemic.
The Trust is continuing to undertake work in preparation for the submission of the Data Security and
Protection Toolkit, looking to: Make improvements wherever it can do so, work to deliver national initiatives
such as the National Data Opt Out, alongside ensuring Information Governance and Security practices
remains robust during the current Covid-19 pandemic and the new and changing ways of working this has
resulted in.
Information Commissioner’s Office Reported Incidents
Seven IG incidents were reported to the Information Commissioner’s Office (ICO) and/or Department of
Health and Social Care (DHSC) in 2019/20.
All reported IG incidents are assessed for severity according to national guidance. Where it is considered the
incident needs to be reported to the ICO, they are escalated to the Trust’s Caldicott Guardian and Data
Protection Officer who confirm the scoring, ensure appropriate action has been taken and authorise
reporting to the ICO or DHSC, via the Data Security and Protection Toolkit.
The Trust has recently made changes to its incident management process to ensure that all reported
incidents receive a level of follow-up relevant to the nature of the incident, regardless of severity. The Trust
believes this is important to ensure there is a strong culture of IG awareness in the organisation.
Quality Impact Assessments (QIA)
The Trust has a Quality Impact Assessment process which is described in the QIA policy. All projects that sit
within the Trusts Quality and Efficiency programme have to be assessed to evaluate whether there is a
possibility of a negative impact of an financial saving on Patient Safety, Clinical Outcomes or Patient
Experience.
Performance against national quality standards and targets
Emergency access standard
In 2019/20 there has been a Trust-wide focus and determination to improve the experience of our
emergency patients and flow in and through our Emergency Department (ED) and out of our hospitals. In
May 2019 we started reporting against new clinical standards for Urgent and Emergency Care as part of the
national field testing programme. Reporting against the four-hour standard paused for 2019/20 for the pilot
Trusts to avoid contaminating the study design.
Cancelled operations
There were 67 instances where NUH breached the 28-day readmission guarantee in 2019/20 but no urgent
operations were cancelled more than once.

Page 59
Number of breaches of the 28-day cancelled operations guarantee by provider (peer Trusts) April 2019-
December 2019 (due to COVID-19, this data publication was paused nationally and therefore data is
only available to December 2019).
Referral to treatment (RTT) - 18-week wait
The 18-week RTT performance was 86.5% (against >92% national target) at end of March 2020 with 13
specialties reporting under performance. For full details of our broader performance, including waiting times,
please see our Annual Report.
Waiting lists have grown and for the first time since June 2012 we under-performed against the 18-week RTT
standard in October 2019, with performance remaining below standard for the remainder of the year. Our
ability to recover elective activity has been compromised by the national pension’s issue that has resulted in
a reduction in the number of clinicians undertaking additional sessions. The decision in mid-March by NHS
England to cease all routine elective work to create capacity for Covid-19 patients has and will continue to
impact heavily on the Trust’s RTT performance and associated elective pathway metrics.
Performance over time against the RTT is outlined below:
Performance over time (RTT)
2011/12 90.5%
2012/13 95.6%
2013/14 96.6%
2014/15 98.2%
2015/16 97.5%
2016/17 96.1%
2017/18 92.9%
2018/19 93.2%
2019/Feb20 93.2%
2.3 Reporting against Core Indicators
51
0
50
100
150
200
250Sh
effi
eld
Cam
bri
dge
Live
rpo
ol
Ne
wca
stle
Oxf
ord
No
ttin
gham
Man
ches
ter
Bri
sto
l
Bir
min
gham
Sou
tham
pto
n
Leed
s
Lan
cash
ire
Leic
este
r

Page 60
We aim to deliver safe, caring and person centred care for our patients throughout Nottingham and the East
Midlands. Our patients will have health outcomes that achieve or exceed those required in the NHS
Outcomes Framework and by NICE Quality Standards. We aim to do this in a way which is recognisable,
measurable and meaningful to everyone in the community we serve.
We seek assurance that we are delivering on these expectations through regularly monitoring the quality and
outcome of our services by a number of Board Committees. In particular:
The monthly Quality Assurance Committee (of the Trust Board) monitors the quality of our services and
the risks associated with the delivery of care
The Audit Committee of the Board monitors the quality of our risk management systems and assurance
processes
Management Board is responsible for leading ensuring delivery of the required quality of care and for
driving forward sustainable improvement to the quality of the services we provide.
These committees are supported by a Trust Quality Management structure as shown below.
Organogram to be inserted
PERFORMANCE AGAINST NHS OUTCOMES DOMAINS (HEADING)
In this section we report our performance in the five domains/areas of the NHS national outcomes
framework and compare it with last year and with other hospitals.
Domains 1 and 2 - preventing people from dying prematurely
Mortality indices
The Summary Hospital-level Mortality Indicator (SHMI) reports on mortality at Trust level across the NHS in
England. The SHMI is the ratio between the actual number of patients who die following hospitalisation at
the Trust and the number that would be expected to die on the basis of average England figures, given the
characteristics of the patients treated there. It covers patients admitted to hospitals in England who died
either while in hospital or within 30 days of discharge.
SHMI values for each Trust are published along with bandings indicating whether a Trust's SHMI is '1 - higher
than expected', '2 - as expected' or '3 - lower than expected'. For any given number of expected deaths, a
range of observed deaths is considered to be 'as expected'. If the observed number of deaths falls outside of
this range, the Trust in question is considered to have a higher or lower SHMI than expected.
The SHMI for NUH is 1.05 with a banding of 'as expected' for the period November 2018 - October 2019
(source: NHS Digital; published 12 March 2020). The England average SHMI is 1.0 by definition, and this
corresponds to a SHMI banding of 'as expected'. For the SHMI, a comparison should not be made with the
highest and lowest Trust level SHMIs because the SHMI cannot be used to directly compare mortality
outcomes between Trusts and, in particular, it is inappropriate to rank Trusts according to their SHMI.
The SHMI methodology does not make any adjustment for patients who are recorded as receiving palliative
care. This is because there is considerable variation between Trusts in the coding of palliative care. However,
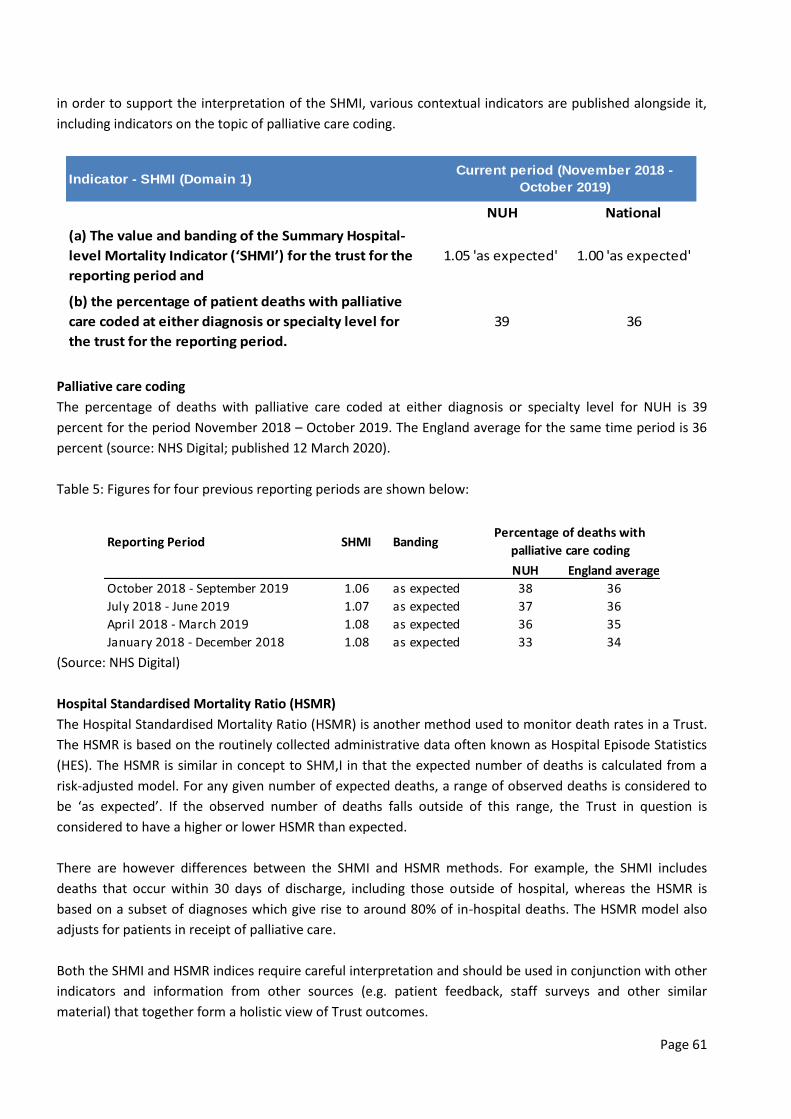
Page 61
in order to support the interpretation of the SHMI, various contextual indicators are published alongside it,
including indicators on the topic of palliative care coding.
Palliative care coding
The percentage of deaths with palliative care coded at either diagnosis or specialty level for NUH is 39
percent for the period November 2018 – October 2019. The England average for the same time period is 36
percent (source: NHS Digital; published 12 March 2020).
Table 5: Figures for four previous reporting periods are shown below:
(Source: NHS Digital)
Hospital Standardised Mortality Ratio (HSMR)
The Hospital Standardised Mortality Ratio (HSMR) is another method used to monitor death rates in a Trust.
The HSMR is based on the routinely collected administrative data often known as Hospital Episode Statistics
(HES). The HSMR is similar in concept to SHM,I in that the expected number of deaths is calculated from a
risk-adjusted model. For any given number of expected deaths, a range of observed deaths is considered to
be ‘as expected’. If the observed number of deaths falls outside of this range, the Trust in question is
considered to have a higher or lower HSMR than expected.
There are however differences between the SHMI and HSMR methods. For example, the SHMI includes
deaths that occur within 30 days of discharge, including those outside of hospital, whereas the HSMR is
based on a subset of diagnoses which give rise to around 80% of in-hospital deaths. The HSMR model also
adjusts for patients in receipt of palliative care.
Both the SHMI and HSMR indices require careful interpretation and should be used in conjunction with other
indicators and information from other sources (e.g. patient feedback, staff surveys and other similar
material) that together form a holistic view of Trust outcomes.
Indicator - SHMI (Domain 1)
NUH National
(a) The value and banding of the Summary Hospital-
level Mortality Indicator (‘SHMI’) for the trust for the
reporting period and
1.05 'as expected' 1.00 'as expected'
(b) the percentage of patient deaths with palliative
care coded at either diagnosis or specialty level for
the trust for the reporting period.
39 36
Current period (November 2018 -
October 2019)
Reporting Period SHMI Banding
NUH England average
October 2018 - September 2019 1.06 as expected 38 36
July 2018 - June 2019 1.07 as expected 37 36
April 2018 - March 2019 1.08 as expected 36 35
January 2018 - December 2018 1.08 as expected 33 34
Percentage of deaths with
palliative care coding

Page 62
The HSMR for NUH is ‘higher than expected’ [HSMR 111.7, 95% confidence interval: 107.6 to 115.9]. The
England average for the HSMR is 100, which corresponds to a banding of 'as expected'. (Source: Hospital
Evaluation Data [HED] portal; HSMR discharges in the period December 2018 - November 2019; as published
on 26 February 2020.)
LEARNING FROM DEATHS
NUH considers that this data is as described for the following reasons. NUH is fully engaged in the national
mortality surveillance programme. NUH has built and implemented an e-coroner and mortality screening
tool which supports an initial high-level screening of all adult inpatient deaths and provides clinical teams
with intelligence of cases that may warrant a more in-depth review. The Trusts Mortality and End of Life
Care Group, Quality Assurance Committee and Board receives a quarterly Learning from Deaths report.
These are available on our public web site at: Board Papers
Total number of deaths (2019/20
In 2019/20:
90% (3,081) of adult inpatient deaths were verified using Nervecentre
99% (3,397) of adult inpatient deaths were screened in Nervecentre (mortality and coroner screening)
54% (1,849) of adult inpatient deaths were referred to HM Coroner of which 18% [339] of the cases
were taken by HM coroner for review.
The total number of deaths per quarter based on age groups are outlined in the table below.
Quarterly (and total) deaths 2019/20 (as at 6 April 2020)

Page 63
Number of deaths subject to a Structured Judgement Case Review (SJCR)
As of 19th March 2020, 218 colleagues have been trained to undertake SJCRs at Nottingham University
Hospitals.
A total of 135 (with a further 32 in progress as at 6 April 2020) Structured Judgement Case Reviews (SJCR)
and 15 Serious Incident investigations have been commissioned in relation to 3,527 patients that died while
an inpatient during 2019/20 (excluding Still Births). In one case a death was subjected to both a SJCR and a
Serious Incident investigation (converted from SJCR to SI).
During 2019/20 there were three Serious Incidents commissioned where the outcome was death where the
investigation was completed during 2019/20 (excluding Still Births). The outcome of death does not mean
that the death was avoidable.
The number of deaths in each quarter during 2019/20 for which a SJCR or a Serious Incident investigation
was commissioned are outlined in table 1.
Table 1: SJCRS and Serious Incidents undertaken per quarter in relation to deaths in 19/20 (as at 6 April
2020).
2019/20 Q1 Q2 Q3 Q4 Total
SJCR completed 52 48 29 6 135
Serious Incident Commissioned 1 0 3 2 6

Page 64
where outcome was death
Serious Incident investigation
completed where outcome was
death associated with above cases
1 0 2
(1 in
progress)
0
(2 in
progress)
3
(3 in
progress)
All infant, children and young people and neonatal inpatient deaths are reviewed under the Child Death
Review Process (CDRP). All still births in 2019/20 were reviewed under the perinatal mortality review
process. Of the total still births in 2019/20, four were investigated under the national Serious Incident
framework.
Deaths in patients with a Learning Disability
All learning disability (LD) deaths should be reviewed using the Learning Disabilities Mortality (LeDeR)
methodology. In 2019/20 50 adult patients who died while an inpatient, were assessed following initial
screening as having a learning disability. These cases are reviewed by the Learning Disability Team along with
the Trust’s LFD lead. A total of 32 deaths have been considered for SJCR to date and a SJCR was undertaken
in 21 cases, with a further two in progress. Two of the reviews identified potentially poor care and both have
had a second stage review.
Thematically, there were frequent examples of excellent communication between clinicians, patients and
families alongside good interdisciplinary working. End of Life Care and communication in general in those
cases reviewed were positive with greater involvement of Learning Disabilities Specialist Nurses over the last
12 months in particular. Issues of capacity and consent noted previously have become less evident but
inaccuracies and errors in the completion of DNACPR forms remains problematic, on occasion. The results of
SJCR in these cases are fed back directly to the Specialty M&M meeting. All NUH learning disability deaths
are reported to the LeDeR Programme by the Adult LD Nurse Specialists.
Judgement and Care Quality Scores (refer to Serious Incident section)
Of the 135 SJCR cases completed in 2019/20 a judgement score was made in three cases as to a death being
“more likely than not” associated with problems in care/service delivery (table 3). Of the total (135)
completed SJCRs three deaths were deemed more likely than not to be due to care of service deficiencies.
Table 3: SJCR judgement of care/service delivery contributing to death (as at 6 April 2020).
2019 Q1 Q2 Q3 Q4 Total
Total deaths 825 820 924 958 3,527
SJCR completed 52 48 29 6 135
Number of cases where it is thought ‘more likely than not’ that problems in care/service delivery contributed to the death.
1 2 0 0 3
Overall care judgements of the 135 SJCRs completed for 2019/20 deaths were assessed as poor in 1 (1%)
case, adequate in 32 (24%) cases and as good or excellent in the remaining 102 (75%) of cases, table 4.
Table 4: Overall quality of care ratings for 135 SJCR cases completed in 19/20.

Page 65
Themes, issues and learning identified through review and investigation (including examples of good
practice)
The purpose of the SJCR process is to identify areas for improvement in care/services and to highlight
good/excellent practice. A summary is provided in table below.
Table 4: Thematic analysis of learning from SJCRs (2018/19 and 2019/20).

Page 66
In addition to reviewing SJCR themes, consideration has been given to learning from review of Serious
Incidents and a sample of speciality based Morbidity and Mortality meeting minutes. This learning is
summarised below:
1. Clinically urgent amendments to results and reports (such as radiology/laboratory results) should be
rung through to the relevant team, rather than relying on electronic solutions alone
2. Internal capacity and flow can impact on tertiary transfer times significantly. Processes must be in place
to escalate tertiary referrals or waits based on clinical need to reduce the clinical risk associated with
delays to treatment
3. Appropriate communication of Fast Track discharge plans to receiving “home” and primary care is
required to prevent inappropriate re-admission/ED attendance
4. There is evidence from SJCRs of exemplary documentation of family discussions by medical staff
associated with end of life care
5. Changes to end of life care management were highlighted as having been managed sensitively by teams,
with excellent examples of good multi-professional care demonstrated in many palliative care cases.
NUH considers that the data is as described for the following reason: The data is reviewed and discussed at
the NUH Mortality and End of Life Care Group and interrogated in line with the Key lines of enquiry identified
by that group.
Page 67
NUH is taking the following actions to improve this indicator and so the quality of its services by:
1. The establishment of the Medical Examiner Team, which comprises of eight Medical Examiners to date.
The service has reviewed over 400 deaths with the vast majority of families very appreciative of the care
at NUH (following telephone consultations)
2. A newly appointed Patient and Family Liaison Officer commenced in post in August 2019. This post
supports patients, families and carers in relation to their involvement and support in investigations (SI
and SJCR). The post holder has engaged early on with multiple internal and external stakeholders to help
identify priorities. They have met with families either involved in historical SI and inquest cases or in
support of current investigations. A family member and PPI representative are supporting the co-design
of this important role
3. The SJCR process has led to increased cross speciality case reviews and learning. A number of specialities
are starting to align their Morbidity & Mortality reviews through utilising the SJCR format
4. The function of the Mortality Surveillance Group (MSG) has been reviewed, along with the terms of
reference. The group from January 2020 is chaired by the Medical Director and is focusing further on
end of life care and DNACPR improvement work
5. The ReSPECT tool designed to support the healthcare system to understand an individual patient’s
wishes and preferences around end of life, DNACPR and ceilings of treatment is being trialled in
Hayward House. This will support learning and conversations around possible wider adoption
6. A prevention of future deaths SOP and log has been developed. Learning from inquests is being shared
via the legal services team at the Learning and Review Group (LRG) and with the Mortality and End of
Life Care Group.
7. Audit and clinical observation of the pneumonia pathway across both campuses in response to our
mortality position has commenced
8. Work developing a shared understanding across the ME service and Patient Safety Team in regard to the
review and investigation of deaths continues with HM Coroner and assistants. Two learning events have
been held
9. QLik Sense LFD portal has been modified to track completion of SJCRs aligned to the national SI
timescale of 60 working days (no mandated timescales have been set nationally, rather this is an
internal process measure).
Priorities 2019/20:
1. Establish weekend and out of hours cover via the Medical Examiner Team
2. Ongoing delivery of the DNACPR project to further support improvements in the management and
documentation of DNACPR decisions
3. Evaluate the Patient and Family Liaison Officer role in support of helping patients and families following
an incident or a loved one’s death
4. Formalise links within the context of the Integrated Care System in support of cross boundary learning
5. Finalise analysis of pneumonia work, identifying recommendations to be shared with relevant fora,
aligning the national Community Acquired Pneumonia (CAP) CQUIN requirements to this work.

Page 68
Domain 3 - Helping people to recover from episodes of ill-health or following injury
Indicator 1 - Patient Reported Outcome Measures (PROMS)
PROMS describe the health gains after four operations using pre and post-operative surveys. NUH
undertakes two2 of these four operations and the date is provided below. NUH is one of the largest
providers of hip and knee replacement surgery in the country and performs a large proportion of complex
cases. The functional outcome of the operation is measures independently and nationally for all providers.
The results are expressed in terms of an improvement in function expressed by the patient as a result of the
surgery and labelled as patient reported outcome measures (PROMS). The improvement for hip function is
expressed as the improvement in the Oxford hip score and for the knee function, the Oxford knee score.
An adjustment is made to the figures to account for any co-existing conditions that may influence the
outcome.
The table shows the mean (average) improvement for patient who had orthopaedic surgery at NUH during
2018/19 (finalised) and April to September 2019 (the latest provisional data available), and the national
average.
2018/19 April 2019 to September 2019 (Provisional)
Indicator detail
NUH National Lowest/Highest NUH National Lowest/Highest
Hip replacement surgery
22.7 22.3 18.6 - 24.4 21.9 22.5 18.7 – 25.5
Knee replacement surgery
17.8 17.2 13.5 –19.9 18 17.6 14.4 – 21.3
NUH considers that this data is as described for the following reasons. NUH continues to perform in line with
expectations. The data is reviewed regularly by the service management team. NUH intends to take the
following actions to improve this indicator and so the quality of its services by ensuring that the results are
regularly reviewed by the Divisional Governance Forum in order to inform and support multi-professional
team working.
Indicator 2 – Emergency Readmissions within 30 days
Our readmission rate for the 12 months to November 2019 was 14.5%. This is a rise from the previous 12
month period of 14.0%. Table below shows the NUH monthly readmit rate – December 2017- November
2019.
2 NUH does not provide routine hernia and varicose vein surgery [provided by external provider to the Trust]

Page 69
NUH considers the data to be as described, which is regularly reviewed as part of the Trust internal
performance management process. NUH continues to take action to improve this indicator and the quality of
its services by monitoring the readmit rate with monthly Trust Board oversight through defined Performance
management reporting.
Domain 4 - ensuring people have a positive experience of care
Indicator 1 - The Trust’s responsiveness to the personal needs of its patients during the reporting period
(most current data at the time of writing, May 2020).
Indicator 4.2 Responsiveness to inpatients' personal needs (most current data at the time of writing, May
2020).
69.4
65.5
66.6
65.3 65.9
66.4
67.4
69
67.7
70.8
69.2
67.1 67.4
62
63
64
65
66
67
68
69
70
71
72
20
06
-07
20
07
-08
20
08
-09
20
09
-10
20
10
-11
20
11
-12
20
12
-13
20
13
-14
20
14
-15
20
15
-16
20
16
-17
20
17
-18
20
18
-19

Page 70
NUH considers that this data is as described, having participated fully in the National Patient Survey
Programme. NUH is taking the following action to improve this composite score and so the quality of its
services:
A detailed action plan is in development to respond to the findings and drive improvement in patient
experience.
Indicator 2 - Staff ‘Friends and Family’ test (FFT)
The percentage of staff employed by, or under contract to the Trust during the reporting period who would
recommend the Trust as a provider of care to their family or friends, is shown in the table below. We use our
staff Friends and Family Test (FFT) results as another method of monitoring the experience of our staff and
the results for 19/20 are shown below (the Quarter 3 FFT is replaced by the national survey)
Factor Q1 Q2 Q4
% of respondents would be extremely likely or likely to recommend
NUH services to friends and family if they needed care or treatment
83 83* 87%
% of respondents would be extremely likely or likely to recommend
NUH as a place to work.
54 80* 62%
*These values reflect only New Starters within the organisation as a sample group was chosen in Q2 to undertake the
Staff FFT
NUH considers that the data is as described for the following reasons. Within the National Staff Survey
Results (Quarter 3) NUH is above the NHS average for Acute Trusts in recommend for care and average for
recommend to work and is comparable to other large university teaching hospitals.

Page 71
Trust I would recommend my
organisation as a place to work
If a friend or relative needed treatment I would be happy
with the standard if care provided by this organisation
NUH 62.5% 75.3%
Leeds Teaching Hospitals 69.9% 79.3%
Oxford University Hospitals NHS Foundation Trust
64.2% 78.1%
University Hospitals Birmingham NHS Foundation Trust
58.9% 69.2%
University Hospitals of Coventry and Warwickshire NHS Trust
65.3% 73.7%
University Hospitals of Derby & Burton NHS Foundation Trust
67.5% 78.7%
University Hospital of Leicester NHS Trust
62.5% 67.0%
University Hospitals of North Midlands 60.4% 73.9%
Acute Trust Average 62.5% 70.5%
NUH is taking the following action to improve the overall survey scores and so the quality of its services by:
Launch of Culture and Leadership Strategy April 2020
Implementation of Improvement programme
Embedding values and behaviours
Review of the Health and Wellbeing Policy
Work around Just Culture and Civility Saves Lives
Support to existing/launch of specific task and finish groups to address specific areas of need identified
through NSS focus groups (February/March 2020).
Indicator 3 - Patient ‘Friends and Family’ test (FFT)
The Trust considers both in-patient and emergency department Friends and Family Test scores are an
authentic representation of our performance during 2019/20.
96
.92
%
0%10%20%30%40%50%60%70%80%90%
100%

Page 72
FFT Inpatients would recommend the Trust to their family or friends by provider (peer group) April 2019-
December 2019
FFT ED Attendances would recommend the Trust to their family or friends by provider (peer group) April
2019-December 2019.
NUH considers that this data is as described because it is regularly reviewed and discussed by Divisional and
Trust-wide patient experience forum.
NUH is taking action to improve these scores, and so the quality of its services. The scores, including analysis
and actions to improve are discussed by: Specialties and Divisions as part of their quality governance
arrangements and also at the quality, risk and safety and Board quality assurance committees. NUH’s
recommend rates are among the best in the country.
Domain 5 - Treating and caring for people in a safe environment and protecting them from avoidable harm
Indicator 1 - Venous Thromboembolism (VTE)
Venous Thromboembolism (VTE) is a significant risk to hospitalised patients. Our VTE programme aims to
reduce preventable harm to our patients by promoting timely and accurate VTE risk assessment and ensuring
thromboprophylaxis is prescribed accurately and administered effectively when required.
NUH’s overall VTE risk assessment compliance for 2019/20 was 94.4% (against a target of 95%).
NUH recognises that its compliance level is below target in 2019/20 but has shown improvement since
2018/19. In-depth analysis of performance within the Divisions has been undertaken to identify areas where
focussed action is needed and strategy developed. Advanced Nurse Practitioners and prescribing pharmacists
are now trained to complete the VTE Risk Assessments to provide support to the medical teams.
The graph below shows our performance against peers and the national average for England; this gives us an
accurate representation of NUH data.
96
.92
%
0%10%20%30%40%50%60%70%80%90%
100%

Page 73
VTE risk assessment by provider (peer group) April - December 2019
NUH is taking the following action to further improve this indicator and so the quality of its services:
Rollout of new IT system which will improve usability of the assessment tool, making it more accessible
to medical teams
Maintain Hospital Associated Thrombosis (HAT) route cause analysis compliance at 100%, where current
rate of preventable HAT remains low. The Trust is committed to investigating and sharing knowledge in
cases where an element of preventability has been found to drive improvement and has a clear
governance structure to facilitate this.
Indicator 2 - C. Difficile and MRSA infections
Rate per 100,000 bed days of cases of C. Difficile infection in the Trust amongst patients aged two or over
during the reporting period are described in table 1 (appendicies). Please see table 1 (appendices) for how
we do compared with our peers for C. Difficile and MRSA. We publish our infection rates for C. Difficile and
MRSA monthly on our website and on TV screens inside our hospitals.
NUH considers this to be an accurate representation of the data and is taking the following actions to
improve this indicator and so the quality of its services:
Continued strong emphasis on environmental cleaning and high level disinfection against C. Difficile
spores using our hydrogen peroxide systems
Regularly reviewing antibiotic prescribing and monitoring and feeding back on cases where
inappropriate prescribing is a possible contributory factor
Publication of outcome data
NUH supports the publication of outcomes of operations by our surgeons. This information enables patients
to make decisions and helps us provide better services. Clinical outcome data at Trust and consultant level in
the following specialties are available publically via online national audit registries including:
Cardiac surgery
Vascular
Bariatric
Interventional cardiology
Orthopaedics
94
.4%
71
.8%
10
0.0
%
England ave.
0%
20%
40%
60%
80%
100%
Bri
sto
l
Sou
tham
pto
n
Live
rpo
ol
No
ttin
gham
Leed
s
Shef
fie
ld
Man
ches
ter
Cam
bri
dge
Lan
cash
ire
Ne
wca
stle
Leic
este
r
Oxf
ord
Bir
min
gham
Engl
and
Low
est
Engl
and
Hig
hes
t
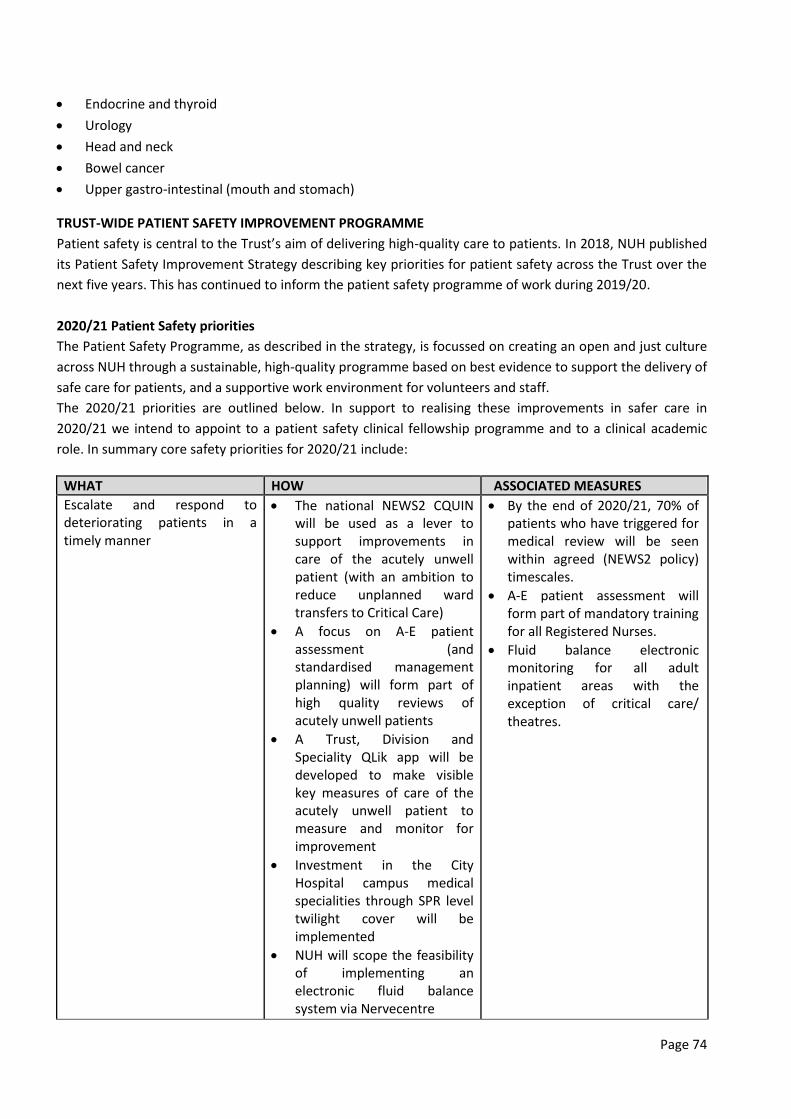
Page 74
Endocrine and thyroid
Urology
Head and neck
Bowel cancer
Upper gastro-intestinal (mouth and stomach)
TRUST-WIDE PATIENT SAFETY IMPROVEMENT PROGRAMME
Patient safety is central to the Trust’s aim of delivering high-quality care to patients. In 2018, NUH published
its Patient Safety Improvement Strategy describing key priorities for patient safety across the Trust over the
next five years. This has continued to inform the patient safety programme of work during 2019/20.
2020/21 Patient Safety priorities
The Patient Safety Programme, as described in the strategy, is focussed on creating an open and just culture
across NUH through a sustainable, high-quality programme based on best evidence to support the delivery of
safe care for patients, and a supportive work environment for volunteers and staff.
The 2020/21 priorities are outlined below. In support to realising these improvements in safer care in
2020/21 we intend to appoint to a patient safety clinical fellowship programme and to a clinical academic
role. In summary core safety priorities for 2020/21 include:
WHAT HOW ASSOCIATED MEASURES
Escalate and respond to deteriorating patients in a timely manner
The national NEWS2 CQUIN will be used as a lever to support improvements in care of the acutely unwell patient (with an ambition to reduce unplanned ward transfers to Critical Care)
A focus on A-E patient assessment (and standardised management planning) will form part of high quality reviews of acutely unwell patients
A Trust, Division and Speciality QLik app will be developed to make visible key measures of care of the acutely unwell patient to measure and monitor for improvement
Investment in the City Hospital campus medical specialities through SPR level twilight cover will be implemented
NUH will scope the feasibility of implementing an electronic fluid balance system via Nervecentre
By the end of 2020/21, 70% of patients who have triggered for medical review will be seen within agreed (NEWS2 policy) timescales.
A-E patient assessment will form part of mandatory training for all Registered Nurses.
Fluid balance electronic monitoring for all adult inpatient areas with the exception of critical care/ theatres.
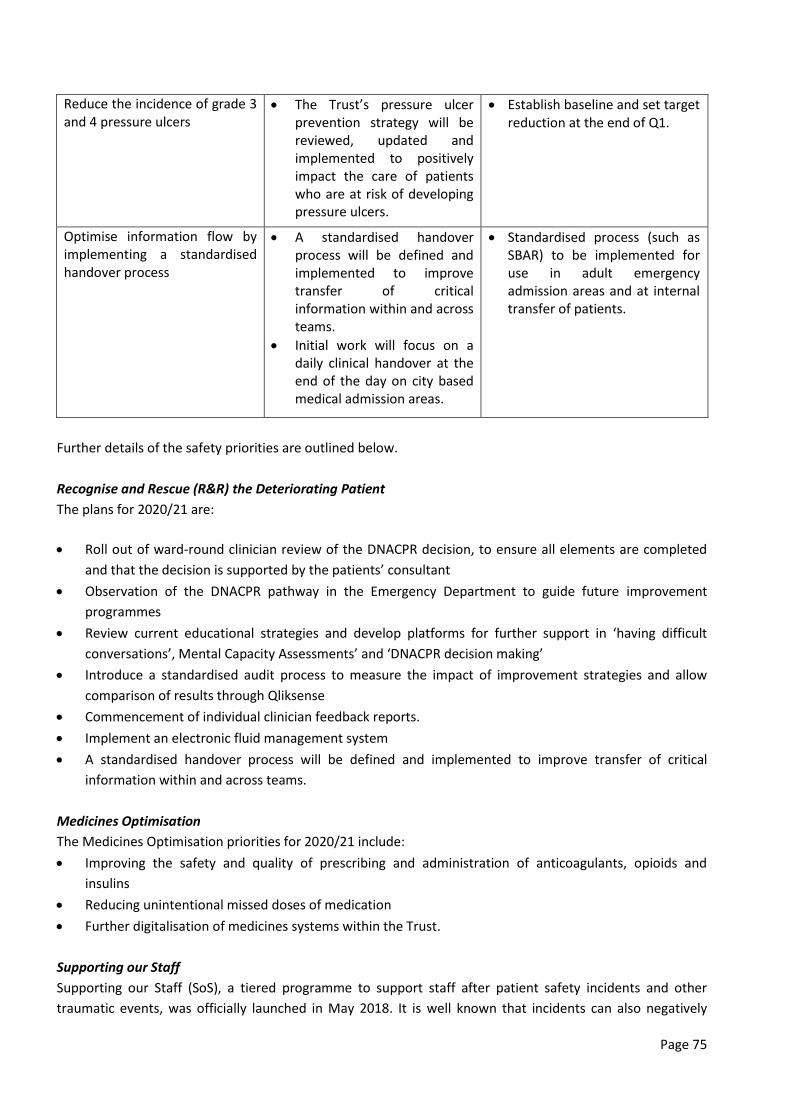
Page 75
Reduce the incidence of grade 3 and 4 pressure ulcers
The Trust’s pressure ulcer prevention strategy will be reviewed, updated and implemented to positively impact the care of patients who are at risk of developing pressure ulcers.
Establish baseline and set target reduction at the end of Q1.
Optimise information flow by implementing a standardised handover process
A standardised handover process will be defined and implemented to improve transfer of critical information within and across teams.
Initial work will focus on a daily clinical handover at the end of the day on city based medical admission areas.
Standardised process (such as SBAR) to be implemented for use in adult emergency admission areas and at internal transfer of patients.
Further details of the safety priorities are outlined below.
Recognise and Rescue (R&R) the Deteriorating Patient
The plans for 2020/21 are:
Roll out of ward-round clinician review of the DNACPR decision, to ensure all elements are completed
and that the decision is supported by the patients’ consultant
Observation of the DNACPR pathway in the Emergency Department to guide future improvement
programmes
Review current educational strategies and develop platforms for further support in ‘having difficult
conversations’, Mental Capacity Assessments’ and ‘DNACPR decision making’
Introduce a standardised audit process to measure the impact of improvement strategies and allow
comparison of results through Qliksense
Commencement of individual clinician feedback reports.
Implement an electronic fluid management system
A standardised handover process will be defined and implemented to improve transfer of critical
information within and across teams.
Medicines Optimisation
The Medicines Optimisation priorities for 2020/21 include:
Improving the safety and quality of prescribing and administration of anticoagulants, opioids and
insulins
Reducing unintentional missed doses of medication
Further digitalisation of medicines systems within the Trust.
Supporting our Staff
Supporting our Staff (SoS), a tiered programme to support staff after patient safety incidents and other
traumatic events, was officially launched in May 2018. It is well known that incidents can also negatively

Page 76
affect staff involved and this work stream has focussed on supporting staff to normalise their reactions and
look after themselves. This also creates support to maintain effective working. Work in 2019/20 has included:
Supporting our Staff (SoS) peer support network has now 60 trained members of staff to independently
assist where needed. This has resulted in 15 peer support conversations held across the Trust during
2019/20. This does not include those held locally by Specialties/Divisions
Whilst formal evaluation is planned, both managers and individuals accessing SoS have expressed how
much they value the support through the tiered programme.
During 2020/21, the SoS work stream will continue to be developed with plans to develop staff with expert
debriefing skills after major traumatic events.
Safety Spaces
Safety Spaces were developed by the Patient Safety Team as an opportunity for staff members to talk with
members of the safety team. Similar to those launched by the national Sign up to Safety team where they
encourage ‘kitchen table conversations’. Four Safety Spaces were held during 2019/20 and themes
highlighted included: Staffing, equipment and environmental challenges. Two of these conversations formed
part of a wider quality review.
Whilst we acknowledge the multiple competing demands, NUH must continue to prioritise these
conversations as they are a valuable opportunity for frontline staff to have an open and honest dialogue with
the Patient Safety Team and to develop a supportive focused culture at NUH.
Safety Spaces will continue into 2020/21 with plans to re-launch Patient Safety Conversations. These
conversations take place across the Trust within clinical workplaces and are usually attended by an Executive
and Non-Executive Director, with a member of the Patient Safety Team.
Freedom to Speak Up
Freedom to Speak Up (FTSU) guardians were introduced following Sir Robert Francis’s Freedom to Speak Up
Review in 2015. Their role is to work with leadership teams to create a culture where people can speak-up to
protect patient safety.
NUH is committed to creating a culture where staff feel able to speak up about any concerns they may have.
NUH appointed its first Freedom to Speak Up Guardian in 2016 as a stand-alone role to provide independent
and impartial advice and support to colleagues.
Handling of cases
The Trust’s Speak Up policy makes it clear that all cases will be handled with the strictest of confidence and
outlines the types of concerns the Guardian can support staff with.
The total number of cases reported to the Freedom to Speak up Guardian in 2019/20 was 51, an 8% increase
from the previous year. Key themes emerging within the 51 cases raised with the Guardian include culture,
leadership and quality of care.
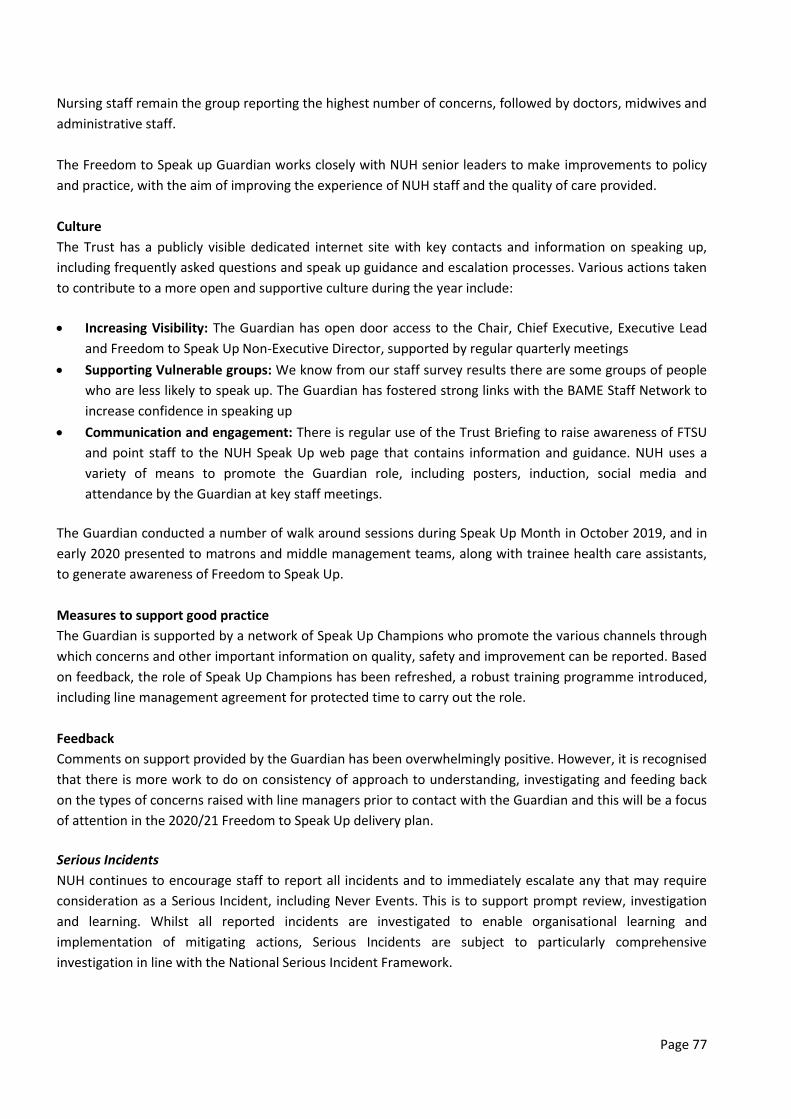
Page 77
Nursing staff remain the group reporting the highest number of concerns, followed by doctors, midwives and
administrative staff.
The Freedom to Speak up Guardian works closely with NUH senior leaders to make improvements to policy
and practice, with the aim of improving the experience of NUH staff and the quality of care provided.
Culture
The Trust has a publicly visible dedicated internet site with key contacts and information on speaking up,
including frequently asked questions and speak up guidance and escalation processes. Various actions taken
to contribute to a more open and supportive culture during the year include:
Increasing Visibility: The Guardian has open door access to the Chair, Chief Executive, Executive Lead
and Freedom to Speak Up Non-Executive Director, supported by regular quarterly meetings
Supporting Vulnerable groups: We know from our staff survey results there are some groups of people
who are less likely to speak up. The Guardian has fostered strong links with the BAME Staff Network to
increase confidence in speaking up
Communication and engagement: There is regular use of the Trust Briefing to raise awareness of FTSU
and point staff to the NUH Speak Up web page that contains information and guidance. NUH uses a
variety of means to promote the Guardian role, including posters, induction, social media and
attendance by the Guardian at key staff meetings.
The Guardian conducted a number of walk around sessions during Speak Up Month in October 2019, and in
early 2020 presented to matrons and middle management teams, along with trainee health care assistants,
to generate awareness of Freedom to Speak Up.
Measures to support good practice
The Guardian is supported by a network of Speak Up Champions who promote the various channels through
which concerns and other important information on quality, safety and improvement can be reported. Based
on feedback, the role of Speak Up Champions has been refreshed, a robust training programme introduced,
including line management agreement for protected time to carry out the role.
Feedback
Comments on support provided by the Guardian has been overwhelmingly positive. However, it is recognised
that there is more work to do on consistency of approach to understanding, investigating and feeding back
on the types of concerns raised with line managers prior to contact with the Guardian and this will be a focus
of attention in the 2020/21 Freedom to Speak Up delivery plan.
Serious Incidents
NUH continues to encourage staff to report all incidents and to immediately escalate any that may require
consideration as a Serious Incident, including Never Events. This is to support prompt review, investigation
and learning. Whilst all reported incidents are investigated to enable organisational learning and
implementation of mitigating actions, Serious Incidents are subject to particularly comprehensive
investigation in line with the National Serious Incident Framework.

Page 78
Patients, relatives or carers are invited to meet with Serious Incident investigation panels in order to
contribute their experiences and questions as part of the investigation process. The Trust Learning and
Review Group ensures wide dissemination of the learning from Serious Incidents across the organisation, and
monitors implementation of recommendations to completion. Patient safety incident data is uploaded
regularly to NHS England via the National Reporting and Learning System (NRLS).
In 2019/20, NUH reported 38 Serious Incidents (excluding Level 1 harm free care serious incidents). Two of
these incidents were Never Events.
SERIOUS INCIDENTS 2019/20
(Excluding Harm Free care Level 1 SIs) NEVER EVENT TOTAL
Failure to rescue (Clinical Deterioration) 11
Delay / failure to treatment or procedure 11
Maternity triggers 1 7
Communication failure 2
Medication 2
Diagnosis, Scans and Tests 2
Other (Patient-Safety) 1 1
Nutrition 1
Contact with / Exposure to Harmful Agent, Substance or Object 1
Total 2 38
LEVEL 1 SERIOUS INCIDENTS (SI) CLASSIFICATIONS 2016/17 2017/18 2018/19 2019/20
Patient Fall 3 7 4 2
Infection Prevention and Control 20 10 10 6
Pressure Ulcer (stage 3)* 52 42 54 38
Total 75 59 68 46
*Pressure ulcer data is subject to validation. A lag of 45 days means incidents reported in March 20 could be
subject to removal or amendment.
Never Events
Never Events are a subset of Serious Incidents and are defined as ‘Serious Incidents that are wholly
preventable because guidance or safety recommendations that provide strong systemic protective barriers
are available at a national level and should have been implemented by all healthcare providers’ (NHS
Improvement January 18). They are infrequent events as outlined below (days between never events).
Page 79
NUH reported two Never Events during 2019/20:
1) A patient was found to have a retained vaginal swab post-delivery
2) A patient had the wrong strength lens implanted post cataract surgery.
Incident Reporting (via Datix)
Incident reporting is essential for NUH to learn about unintended or unanticipated occurrences in patient
care. NUH staff appreciate the importance of incident reporting and this is regularly updated through
mandatory training. Recognising and reporting an incident (or near-miss), no matter the level of harm, is the
first step in learning to reduce the risk of future occurrence.
Crude data from Datix (incident reporting system) shows that the majority of our patient safety incidents
continue to cause no harm (74.11%) or low harm (24.80%) (see table), with a total of 28,604 patient safety
incidents with an incident date in 2019/20 (25,851 incidents in 2018/19).
The number and rate of patient safety incidents reported within the Trust during the reporting period, and
the number and percentage of such patient safety incidents that resulted in severe harm or death are shown
in the table below.
Table: degree of harm for patient safety incidents reported in 2019/20 based on crude Datix reports.
CL
UCL
0
50
100
150
200
250
300
350
400
450
16
/03
/11
28
/03
/11
18
/04
/11
09
/05
/11
25
/05
/11
26
/09
/11
27
/09
/11
30
/04
/12
09
/11
/12
21
/12
/12
17
/01
/13
22
/12
/13
17
/06
/14
21
/08
/14
09
/12
/14
19
/08
/15
08
/09
/15
04
/11
/15
09
/11
/15
06
/02
/16
12
/03
/16
29
/04
/16
20
/06
/16
16
/07
/16
16
/09
/16
24
/09
/16
07
/02
/17
08
/02
/17
28
/12
/17
15
/02
/19
25
/02
/19
30
/05
/19
01
/08
/19
31
/03
/20
Day
s b
etw
ee
n c
ase
s
Degree of Harm n %
None 21197 74.11
Low 7095 24.80
Moderate 260 0.91
Severe 44 0.15
Catastrophic (e.g. death caused by the incident) 8 0.03
Total 28604 100
Days between Never Events Days since last Never Event

Page 80
Figure xx: patient safety incidents per 1000 bed days from April 2018 to the end of March 2020.
Examples of learning from Serious Incidents
NUH is committed to learning from its Serious Incident investigations. During 2019/20 we have continued to
code Serious Incidents against a human factors analysis framework to extract the learning. These emerging
themes over time can be compared with organisations known risks and shortfalls escalated. The learning
from these incidents are shared via “Safety Snippets”; short communications to be read out at all handovers
and ward rounds for seven days after release. They are duplicated in the Patient Safety Newsletter.
Examples of learning from Serious Incidents:
Communication:
o Ensure that patients/families and colleagues are fully appraised and updated regarding the
management of care and treatment plans; use all available sources
o Contemporaneous documentation must be easily accessible to all staff involved to include
conversations with patient/family
o Regular communication across specialties should be considered good clinical practice.
o Ensure instructions are clear, with designated roles and responsibilities. Ensure what has been
said has been heard and understood.
Process:
o Processes must be clear, written-down and communicated to those who use it; avoid ambiguity
o Ensure staff are aware of the guidelines that are relevant to the care they deliver
o Ensure all necessary staff can access emergency equipment and facilities when they need it
o Staff must be fully aware of whose responsibility it is to request further investigations
o New staff, either on a substantive or temporary basis must be clear of local process for arranging
follow up tests and investigations.
Checking and distractions:
o Let checking become a habit. We should trust colleagues, but also recognise that humans make
errors. Independent checks allow us to safely work as a team
o Avoid distracting colleagues when undertaking critical tasks. Remove distractors from areas of
critical work processes

Page 81
o Be familiar with equipment before using it. Ensure equipment is included in in local induction and
that support is always available.
Wider learning:
o Vitamin K Antagonist Prescription Chart revised to minimise the risk of further errors, positively
identify the patient and ensure that an identification band is applied as soon as possible on
admission
o Complex contact and referral processes. Specialties should review their availability to the clinical
areas they cover and other clinical teams. Any rota changes should be communicated clearly to
both switchboard and relevant clinical areas.
Serious Incident Learning Events
Serious Incident Learning Events were developed by the Patient Safety Team during 2019. The aim of these
events are through a shared learning and development workshop, develop an aspirational improvement plan
with agreed priorities and approaches to achieve it. A number of appreciative inquiry methods are used to
support conversations around learning themes.
During 2019/20 the Patient Safety Team have facilitated five learning events in a variety of specialties.
Serious Incident Investigation Faculty
NUH launched its Serious Incident Investigation Faculty. This group of medical and non-medical staff are
responsible for undertaking high-quality Serious Incident investigations in line with the Trust’s and external
expectations. These investigators ensure in-depth analysis is undertaken, staff support is provided and the
patient/family is involved. Training is delivered in line with national expectations. Significant improvements
have been made internally to the quality of SI training, investigation and reports.
2020/21 priorities
The Patient Safety Team has the following priorities for improvement:
Developing the Serious Incident Investigation Faculty so that investigators have protected time to
ensure high-quality reports completed, with clear learning identified as a result of changes in
response to investigation
Ensure Duty of Candour processes are strengthened to meet the expectations of Regulation 20
Evaluate the impact of the Patient and Family Liaison Officer role to support patients and families
through investigations
Implement a rapid incident response team to support patients, families and staff early on following
adverse events
Respond to the new national Patient Safety Incident Response Framework as guided by NHS E/I.
PEOPLE METRICS
Mandatory training attendance
A total of 77% of staff attended their mandatory training refresher in 2019/20 (against a target of 90%).
There have been some challenges around access and recording of staff as the Trust moved on to bookings via
Employee Self-Serve (ESS) accessed through the 'NHS ESR Login' application. Improvements in compliance
have been noted within the last quarter as new systems and processes become embedded, to include
changes to the content and delivery of Mandatory Training.

Page 82
Appraisal rate (medical and non-medical)
84% of non-medical and dental staff had an annual appraisal during 2019/20 (against a target of 90%). A
simplified new appraisal process was introduced Trust-wide in November 2018 and is supported by using
quality conversation between appraiser and appraisee. It has been well received, with operational pressures
noted as the main challenge to achieving target.
Medical and dental appraisal consistently performs well with 98.3% of medical and dental staff (excluding
Junior Doctors) having had an appraisal within the last 12 months. Appraisal of medical and dental
practitioners is linked to revalidation.
Turnover
The Trust performance for turnover is currently 11.27%, (against a target of 10.8%) improvements have
continued in 2019/20 for Registered Nursing (RN) staff and Healthcare Assistants as part of the work with
NHS Improvement.
It should be noted that a level of turnover should be expected and encouraged within the Trust. The leavers
survey (launched in 2018), which continues to provide additional detail as to why people leave the
organisation, is shared with recruitment and retention groups across the Trust to enable the Trust to respond
accordingly.
Sickness absence
Rolling sickness absence rate of 4.33% for 2019/2020 (against a target of 3.8%) and whilst an increase on last
year is still one of the lowest in the East Midlands. The continued operational pressures of the Trust have
impacted on the absence of staff on occasions.
Job Planning
85% of our consultants have job plans which have either been submitted for approval, or have been
approved-an increase of 6% on the previous year.
Time to Hire
Our time to hire is at 47 days against the 45 day target for 2019/2020.
STAFF ENGAGEMENT
Staff Friends and Family Test (FFT)
The last Staff FFT was undertaken in March 2020. The Staff FFT is a quarterly measure of the satisfaction rate
of the staff within the Trust. It asks two key questions:
Would you recommend NUH as a place to receive care or treatment?
Would you recommend NUH as a place to work?
Factor Quarter 1 Quarter 2 Quarter 4
% of respondents would be extremely likely or likely to recommend NUH services to friends and family if they needed care or treatment
83% 83%* 87%
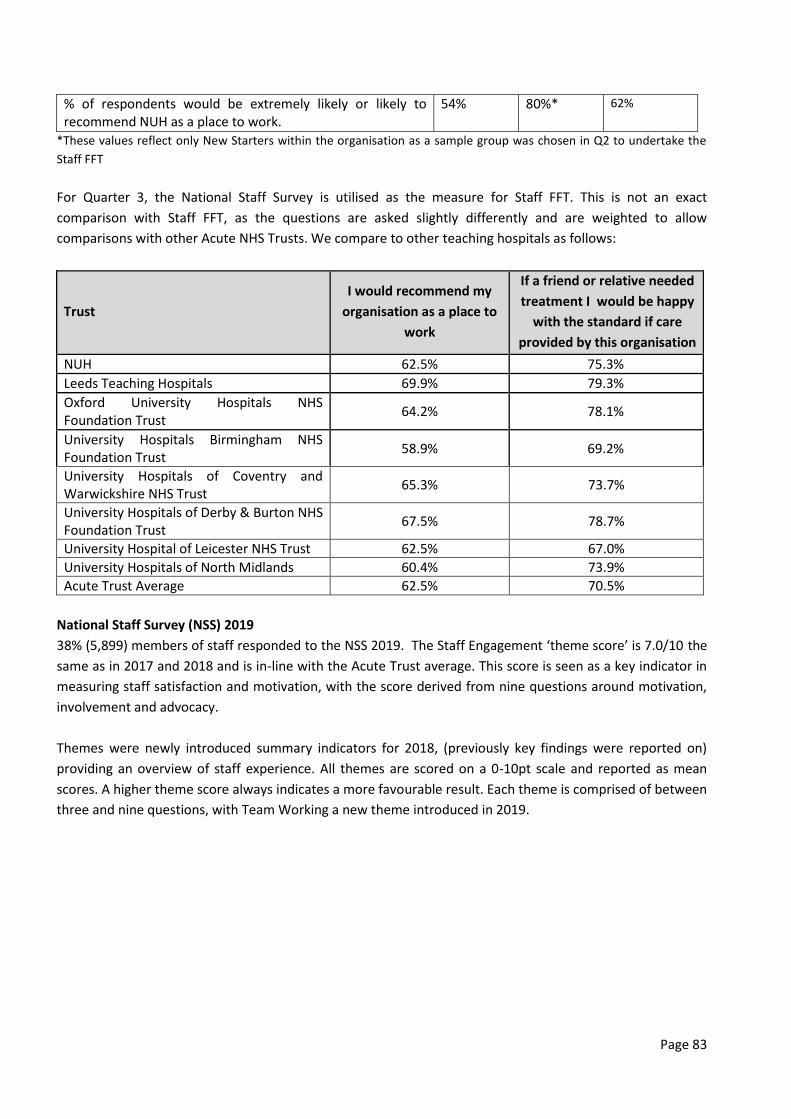
Page 83
% of respondents would be extremely likely or likely to recommend NUH as a place to work.
54% 80%* 62%
*These values reflect only New Starters within the organisation as a sample group was chosen in Q2 to undertake the
Staff FFT
For Quarter 3, the National Staff Survey is utilised as the measure for Staff FFT. This is not an exact
comparison with Staff FFT, as the questions are asked slightly differently and are weighted to allow
comparisons with other Acute NHS Trusts. We compare to other teaching hospitals as follows:
Trust
I would recommend my
organisation as a place to
work
If a friend or relative needed
treatment I would be happy
with the standard if care
provided by this organisation
NUH 62.5% 75.3%
Leeds Teaching Hospitals 69.9% 79.3%
Oxford University Hospitals NHS Foundation Trust
64.2% 78.1%
University Hospitals Birmingham NHS Foundation Trust
58.9% 69.2%
University Hospitals of Coventry and Warwickshire NHS Trust
65.3% 73.7%
University Hospitals of Derby & Burton NHS Foundation Trust
67.5% 78.7%
University Hospital of Leicester NHS Trust 62.5% 67.0%
University Hospitals of North Midlands 60.4% 73.9%
Acute Trust Average 62.5% 70.5%
National Staff Survey (NSS) 2019
38% (5,899) members of staff responded to the NSS 2019. The Staff Engagement ‘theme score’ is 7.0/10 the
same as in 2017 and 2018 and is in-line with the Acute Trust average. This score is seen as a key indicator in
measuring staff satisfaction and motivation, with the score derived from nine questions around motivation,
involvement and advocacy.
Themes were newly introduced summary indicators for 2018, (previously key findings were reported on)
providing an overview of staff experience. All themes are scored on a 0-10pt scale and reported as mean
scores. A higher theme score always indicates a more favourable result. Each theme is comprised of between
three and nine questions, with Team Working a new theme introduced in 2019.

Page 84
Of the 11 reported themes:
Four themes are better than average: Equality, diversity & inclusion, Safe environment – Bullying &
harassment, Safe environment – Violence and Safety culture, (of which 2 are within the best 20% of
benchmarked Trusts)
Three themes are average:Immediate managers, Morale and Staff engagement
Four themes are worse than average: Health and Wellbeing, Quality of appraisals, Quality of care and
Team working (of which 3 are in the lowest 20% of benchmarked Trusts).
When comparing with NSS 2018 results, a statistical significant change (decrease) for Trust results is
suggested for two themes, as detailed in the table below.

Page 85
N.B. Theme score remains at 7.0 for Staff Engagement in both 2018/2019. On checking with SCC the score
was 7.03 in 2018 and 6.96 in 2019, so the figure in 2018 has rounded down to 7.0 and the figure in 2019 has
rounded up to 7.0. Rounding is one factor that will impact why results that look different to one decimal
point aren’t significantly different, yet those that look similar to one decimal point can be significantly
different. Other factors can affect determination of statistical significance, such as differences in the sample
sizes at different questions (for instance due to non-response data).
The Trust has analysed the quantitative results and qualitative comments, sharing with divisions and
corporate departments to enable development of Trust-wide and local actions which will be delivered and
monitored through Divisional People Committees and People Experience Group.
Seven day services
The seven day service standards were founded on published evidence and on the position of the Academy of
Medical Royal Colleges (AoMRC) on Consultant-delivered acute care. Ten standards were agreed. With the
support of the AoMRC, four were identified as priority clinical standards on the basis of their potential to
positively affect patient outcomes. NUH has a seven day service project group and has undertaken and a
number of self-assessments adopting the NHS Improvement Board Assurance Framework tool. The self-
assessments along with operational plans have been reviewed by Trust Board and submitted to NHS
England/Improvement. Key outcomes are summarised below:
An audit of emergency patients’ admissions from 1st to 7th September 2019 was used to inform our self-
assessment against delivery of the priority standards, detailed below.
Standard 2 - 54% (weekday 55%, weekend 53%) - non compliant
Standard 5 - compliant
Page 86
Standard 6 - compliant
Standard 8 - compliant
NUH has self-assessed as compliant against nine of the ten 2019 standards, the exception being:
Priority standard 2 (All emergency admissions must be seen and have a thorough clinical assessment by
a suitable consultant as soon as possible but at the latest within 14 hours from the time of admission to
hospital).
Priorities 2020/21
Develop business cases to support increased consultant cover in key admission areas
Review current risk rating/assessment.
Research and Innovation
The Research and Innovation department at NUH is responsible for leading, managing and developing clinical
research in every part of our hospitals.
In 2019/20 NUH continued to be at the forefront of clinical research development in the country based on
National Institute for Health Research (NIHR) data. We carried out a total of 472 clinical trials involving
14,415 adults and children. NUH is now the third most active research hospital in England.
Clinical research is part of everything we do as a teaching hospital, bringing the skills of front-line NHS staff in
every profession together with scientists, academics, data analysts and industry partners to ensure that NUH
patients can benefit from the latest advances in clinical care.
In 2019/20 we were particularly pleased to see the contributions of nurses in our research workforce
recognised with three national awards.
NUH was one of the most successful hospital Trusts in the country in the National Institute for Health
Research (NIHR) 70@70 programme which was set up to mark the 70th anniversary of the NHS. The
programme selected 70 nurses and midwives from across the country with the aim of enabling more
professionals to get involved in clinical research.
Currently over 400 nurses, midwives, doctors and health professionals are directly involved in helping to
deliver research trials at NUH each year. The 70@70 programme is designed to open up new opportunities to
support the world-class research taking place in Nottingham.
One of those selected for the programme, Dr Sarah Brand, Senior Research Nurse for the NUH Renal and
Transplant Unit, is using her 70@70 role to explore how clinical research can be more integrated within
frontline nursing practice, sharing research skills with all nursing staff and making research part of “business
as usual”. Sarah, who is based at Nottingham City Hospital, said: “I am delighted to have been awarded a
prestigious NIHR 70@70 Nurse Research Leader role. This gives me the chance to influence the development
and embedding of a culture of research within nursing at NUH - a culture which is the foundation of
evidence-based nursing practice and excellent patient care.”

Page 87
Awards were also given to Aquiline Chivinge, Ambulatory Care Pathway Matron, and chair of the NUH BAME
(Black, Asian and Minority Ethnic) Shared Governance Council, and Dr Louise Bramley, Clinical Lead for
Research and Innovation at the NUH Institute of Nursing and Midwifery Care Excellence.
In 2019/20 our key performance achievements were:
2019/20
Target Actual
Minimum % of patients offered the opportunity to participate in research 20% 30%
Number of patients recruited in NIHR studies 14,000 14,115
Total Research and Innovation Income £26m £25.9M
Research Following Patient Need
Our research portfolio and activity prioritises diseases which have a high prevalence in our region. A total of
2,685 cancer patients helped deliver 106 different research studies. The NIHR Nottingham Biomedical
Research Centre is strategically aligned to the clinical needs of the Nottingham and Nottinghamshire
population. More than 15,000 patients suffering from respiratory, gastrointestinal, hearing loss and
musculoskeletal disorders benefited from access to innovative therapies.
NIHR Nottingham Biomedical Research Centre (BRC)
The Nottingham Biomedical Research Centre is our centre of excellence which was set up in 2017 to fast-
track scientific developments from the research laboratory to patient care.
In the last 12 months our research has produced breakthrough results for understanding why some patients
develop a fatal respiratory illness, Idiopathic Pulmonary Fibrosis (IPF); in our understanding of Tinnitus, a
hearing condition for which there is no cure; a genetic link between the health of our guts and hardening of
the arteries which can lead to heart disease; and the impact of some cancer drugs on hearing loss.
During 2019/20 the Nottingham BRC carried out 406 translational research projects, supported 197 early
researchers in their careers and published 437 research articles available to all researchers which will help to
develop new treatments for patients.
NIHR Nottingham Clinical Research Facility (CRF)
Our Clinical Research Facility provides the equipment, skilled staff and dedicated facilities to enable us to
carry out experimental medicine research.
It is part of a network of facilities across the country who have been selected by the National Institute for
Health Research (NIHR) to increase our capabilities in complex research into new drugs and therapies.
Nottingham hosted the national conference for all Clinical Research Facilities across the UK and Ireland. The
conference heard from scientists and researchers at the cutting edge of new medicine and from Nottingham,
the 400 delegates learned about our work with young people in developing a new treatment for childhood
constipation. The volunteer group swallowed harmless mini-capsules that show up on MRI scans to track
their digestion. One in ten children and young people suffers from constipation at some point and the
problem becomes chronic in a third of them, with 27,500 per year needing hospital treatment in England
alone.
Page 88
Up to now, there has been no completely safe and efficient way of tracking the movement of food through
the gut, so possible reasons for constipation have been hard to diagnose.
The ‘MAGIC’ (MAGnetic resonance Imaging in paediatric Constipation) programme has been designed by
experts at the birthplace of MRI in Nottingham. The study involved gastroenterology experts from NUH, the
University of Nottingham and the Nottingham BRC.
The ‘Magic Bean’ mini-capsules are made of a medical-grade plastic shell and are smaller than Tic Tacs to
make them easy for children and young people to swallow. They do not dissolve in the gut, and are filled
with a MRI-visible liquid that stands out clearly in the scan pictures of the gut.
In 2019/20, the Nottingham CRF delivered 503 projects, a 22% year on year increase in Nottingham’s
experimental medicine activity with the largest growth in therapeutic areas outside the BRC such as cancer,
neurology and renal diseases.
Links with the Life Sciences Industry
NUH recruited 316 patients in 76 contract commercial studies in 2019/20. The new business development
team made significant progress in leveraging strategic partnerships at local, national and international level
to drive innovation and financial growth.
Priorities for 2020/21
NUH is a research hospital, with clinical research taking place in each of the Clinical Divisions as well as in our
centres of research excellence.
In 2019/20 we set out four key priorities to ensure that local patients continue to benefit from better
healthcare, treatments and technology which our research provides. These included aligning clinical research
with the needs of the wider health system in Nottingham.
For 2020/21 our ambitions include supporting the development and delivery of novel Covid-19 treatments,
launching the Nottingham Health Science Partners as a vehicle for greater joint working and alignment with
our local partners in research, increasing our partnerships with industry to ensure that we provide new
treatments and better evidence to improve the health of our local communities and increasing the number
of members of Team NUH who are research active through our Research Futures School, which supports
research careers for all professional groups.
Highlights
Hat-trick of national research awards for NUH doctors
Consultant neurologists Doctors Akram Hosseini and Radu Tanasescu, and Consultant Respiratory physician
Dr Sherif Gonem, are among a select group of doctors who have been awarded grants by the Medical
Research Council (MRC). The Clinical Academic Research Partnerships (CARP) is a new initiative which aims to
support more NHS clinicians to take part in clinical research.

Page 89
For her research project, Dr Akram Hosseini, Consultant Neurologist, will be harnessing powerful Magnetic
Resonance Imaging (MRI) – an area in which Nottingham leads the world – to study the build-up of iron in
patients’ brains, a factor which contributes to the development of Alzheimer’s disease.
There are 850,000 people in the UK living with dementia – many of whom have Alzheimer’s disease – a
devastating condition that causes gradual decline in memory, thinking and reasoning skills and therefore
disruption to their daily lives.
Dr Hosseini said: “It is a golden opportunity to draw on the physics expertise at the Nottingham Sir Peter
Mansfield Imaging Centre, for clinical studies and biomedical sciences. Professor Richard Bowtell and I will be
working together to apply new MRI sequences to investigate dementia.
“I’m grateful to work at a leading medical centre and be able to conduct clinical research using high
resolution MRI in a study that is meaningful to patients.”
Dr Radu Tanasescu and his study team will be using MRI and clinical data routinely collected from people
with Multiple Sclerosis (MS) and apply AI (Artificial Intelligence) techniques to identify models that predict
MS outcomes. AI will be used to extract hidden-information from MRI scans.
Where patients have given consent for their data to be used, the researchers will analyse information about
the patients' clinical condition, their demographics and MRI scans, using AI.
The study team’s IT specialists will train a computer to use mathematical models to predict whether a
person's MS will mean greater disability or cognitive impairment over the long-term.
The AIMS study will take advantage of a collaborative environment which includes the Nottingham MS clinic
and research programme and its international exposure and networking, the NIHR Nottingham Biomedical
Research Centre and the University of Nottingham.
Dr Tanasescu said: “I feel very honoured to be the recipient of this award. The CARP award involves
collaborative high-quality research partnerships with established leading biomedical researchers.
“We intend to harness more valuable information from routine MRI scans and existing NHS clinical data with
our study, which makes the research cost-efficient. I am aware of the complexity and challenge the clinical
application of AI entails, but through collaboration and support from AI experts and a robust plan of external
validation, we aim to make a breakthrough. This can provide a tool for informed decision-making and
personalised treatment in MS.”
Dr Tanasescu added: “We hope this study will have in the end a direct benefit for patients – it is not science
for the sake of it. And we aim to expand our knowledge of Multiple Sclerosis using real-world clinical data.”
Respiratory Consultant Dr Sherif Gonem is based at Nottingham City Hospital.
The CARP award is enabling him to work with respiratory medicine Professor Dominick Shaw on a
retrospective study to improve the early warning system used to monitor patients on respiratory (lung
disease) wards.

Page 90
Drawing on five years of existing patient data to predict potentially life-threatening events occurring during a
hospital stay, the study also aims to reduce the rate of false alarms. As a result, doctors and nurses should be
able to better manage their workloads.
Sherif’s study will draw on the expertise of computer scientists and use AI and machine learning - where
computer programmes access data and use it learn for themselves - to analyse anonymised data generated
by the existing NUH Nerve Centre clinical system.
He said: “I’m very pleased to be one of the three recipients of CARP at NUH. It’s a great opportunity and I
hope my research project will have a positive impact on patients with lung disease both in Nottingham and
further afield.”
Professor Stephen Ryder, Clinical Director of Research & Innovation said: “It is a fantastic achievement for
our colleagues at NUH to have been successful in this new area of research funding. NUH is already one of
the most research-active hospitals in the country, and the quality of our research is recognised nationally and
internationally.
“We know the importance of supporting clinicians at every stage of their careers to take part in research, and
the CARP funding is an excellent opportunity for front-line staff to bring their skills and knowledge to clinical
research.”
Nottingham joins national research programme for asthma and COPD
Patients in Nottingham and across the East Midlands with respiratory illnesses including asthma and COPD
are benefitting from a pioneering new research programme.
Researchers in Leicester and Nottingham are part of the UK’s first dedicated data hub for respiratory illnesses
that is enabling cutting-edge research for health discoveries to give patients across the UK faster access to
pioneering new treatments.
The BREATHE Health Data Research Hub for Respiratory Health is one of seven data hubs set up to improve
the lives of people with debilitating conditions by linking up different types of health data to make it more
easily accessible and user-friendly for research. Researchers from centres of excellence based at NUH and in
Leicester are joining with partners from across the UK, including the NHS, academia and charities to develop
the new Hub.
Professor Ian Hall, COPD lead for the BREATHE Hub and Director of the NIHR Nottingham Biomedical
Research Centre said: “I am delighted that researchers in Leicester and Nottingham will be playing a major
role in helping the national Hub deliver its objectives. This builds on a decade of close collaboration between
the NIHR Nottingham and Leicester Biomedical Research Centres, and on the extensive links we have already
put in place across the UK. Ultimately our aim is to accelerate access to relevant health data to facilitate
research into lung diseases and to improve patient care.”
Patients, researchers and clinicians are working together to explore the safe and ethical use of health data
for research into specific diseases including cancer, Crohn's disease and asthma. They will also enable access

Page 91
to data for trialling new treatments and support improvements in clinical care. Patients will be involved in
decisions about how their data is used to ensure the benefits are returned to the NHS and the wider UK
community, and existing rules for accessing data safely and securely will continue to apply.
The Health Data Research Hubs are part of a four-year £37million investment from the UK Government
Industrial Strategy Challenge Fund (ISCF) announced in November 2017 led by UK Research and Innovation,
to create a UK-wide system for the safe and responsible use of health-related data on a large scale. The hubs
will also stimulate further economic growth through greater research activity.
Each hub was selected following an open competition by an independent panel involving patient and public
representatives. They were assessed against criteria that included the potential for impact, the innovative
uses of data, plans for involving patients and the public, and the value for public funding.
We took our research to the zoo this year
Our orthopaedic surgeons swapped their operating theatres and clinics for a day out at the zoo in the hope
of encouraging young people and their families from across the East Midlands to take part in the
international CORE-Kids research trial.
Their research is funded by the National Institute for Health Research (NIHR) and involves children from
around the world, looking at how broken bones (fractures) are treated in children aged 5-15. Overall,
researchers are hoping to speak to over 300 children and families over the next year.
Ben Marson, Orthopaedic Surgery registrar at Nottingham Children’s Hospital and NIHR Doctoral Fellow
explains: “Children and young people who suffer a fracture may be living in pain and may miss out on doing
activities they enjoy such as playing sports and generally being active.
“These kinds of injuries may mean that children experience disrupted sleep, they may need to take time off
school, and their general happiness can be affected. And 10 per cent of children who suffer from a fracture
won’t make a full recovery a year after their injury.”
Ben added: “With CORE-Kids, which is an international study, we will be finding out which outcomes - or
results - are the most important ones to measure.
“This will mean that we will shape all future research trials on children’s fractures. This should lead to better
care and management of these children through better evidence-based medicine.”
The CORE-Kids trial will also help to provide more consistent standards of treatment and follow-up after a
fracture.
Twycross Zoo was chosen as a popular location to help raise awareness of this research trial among parents
and children affected by fractures.

Page 92
QUALITY ACCOUNT PART 3
The tables below show the Trust’s latest performance for 2019/20 and the last three financial years against a
range of indicators for patient safety, clinical effectiveness and patient experience. The Board of Directors
have chosen to include the same set of indicators included in the 2017/19 Quality Account to enable patients
and the public to understand performance over time. The latest data available for 19/20 is shown below and
has been subject to data quality checks by the NUH Informatics team in line with NUH processes.
Table 1. Overview of Quality of Care Indicators provided over 2019/20
201920 QA Appendices.xlsx
Table 2. Performance against indicators in the Standard Operating Framework
Table 3 Performance against core indicators
201920 Quality Accounts Prescribed Content.xlsx

Page 93
Appendix A - Peer hospitals
University Hospitals of Leicester NHS Trust
Leeds Teaching Hospitals NHS Trust
Sheffield Teaching Hospitals NHS Foundation Trust
University of Southampton NHS Foundation Trust
Newcastle Hospitals NHS Foundation Trust
Cambridge University Hospitals NHS Foundation Trust
University Hospitals Birmingham NHS Foundation Trust
Manchester University NHS Foundation Trust
University Hospitals Bristol NHS Foundation Trust.

Page 94
Appendix B - Statistical Process Control Charts
Statistical Process Control (SPC) is an analytical technique that plots data over time. It helps us understand
variation and in so, doing guides us to take the most appropriate action. SPC is widely used in the NHS to
understand whether change results in improvement. We have used the NHS Improvement SPC tool to
produce the SPC charts in this report. Below is a key to the icons used in these charts.

Page 95
Annex 1 - Statements of assurance from:
Nottingham University Hospitals NHS Trust - Statement of Assurance from NHS Nottingham
and Nottinghamshire Clinical Commissioning Group
NHS Nottingham and Nottinghamshire Clinical Commissioning Groups (NNCCG) (formally consisting of
Greater Nottingham Clinical Commissioning Partnership, Mansfield and Ashfield CCG and Newark and
Sherwood CCG) collaboratively commission services from Nottingham University Hospital NHS Trust (NUH).
Since July 2019 NUH has held the contract to deliver services in the Nottingham Treatment Centre. There
was a period of mobilisation and transformation followed by a short number of months of ‘normal’ delivery,
followed by the impact of Covid-19. The months of normal delivery showed significant transformation of the
delivery of services however, performance reporting was impacted by mobilisation and therefore it is
difficult to comment on the national performance indicators. NNCCG acts as the co-ordinating commissioner
and leads on the contract on behalf of the other CCGs in gaining assurance on patient safety and quality of
care delivered by NUH.
The quality assurance framework that Commissioners use consists of reviewing information on safety,
patient experience, outcomes and performance, in-line with the quality schedule and national and local
contractual requirements. Intelligence is gained in various formats, including local and national reported
data, this is complemented by quality visits to clinical areas, which enables commissioners to experience the
clinical environment and gain first hand experiences from patients and front-line staff, including the clinical
environment.
NUH has continued to provide the CCG with high level reporting in line with their 2019/20 contract. The CCG
has measured and reviewed reporting via Quality and Performance Scrutiny Group meetings. The CCG has
also undertaken quality and insight visits to various wards and departments with the Trust, to gain additional
assurance around: Safety, effectiveness of services and patient experience. The Quality Account provides
information which is consistent with the information received by the CCG during the year.
In 2019/20, NUH has continued to ensure that patients receive consistent high quality, safe care, with good
health outcomes and experience. The Trust has performed well against the safety thermometer, with a
consistent harm-free care rate. NUH has achieved its aim of reducing pressure ulcers by 50% over three
years. It is noted that there was an increase in the rate of all falls, and falls associated with harm, but the
rate of falls remained low historically. The Falls Learning Group continues to work with frontline clinicians to
understand the drivers and apply appropriate safety control measures. Commissioners are part of the core
membership to the Falls Learning Group and Pressure Ulcer Learning Group.
NUH reported 38 Serious Incidents (SI) in 2019/20 (excluding level 1 harm free care serious incidents).
Serious incidents are events in health care where the potential for learning is so great, or the consequences
to patients, families and carers, staff or organisations are so significant, that they warrant using additional
resources to mount a comprehensive response. Serious incidents can extend beyond incidents which affect
patients directly and include incidents which may indirectly impact patient safety or an organisation’s ability
to deliver on-going healthcare. There is not an exhaustive list which details what events would be included.

Page 96
Two of the incidents were Never Events. Never Events are defined as Serious Incidents that are wholly
preventable because guidance or safety recommendations that provide strong systemic protective barriers
are available at a national level and should have been implemented by all healthcare providers.
The Trust encourages staff to report all incidents and to immediately escalate any that may require
consideration as a SI, including Never Events. NUH has internal processes in place for reporting SIs on the
Strategic Executive Information System (StEIS) and to Commissioners. Commissioners review all SIs regularly
and work closely with NUH on obtaining further assurance when needed and then final closure of incidents.
NUH confirms in the Quality Account that the Trust is committed to learning from its SI investigations.
The Quality Account demonstrates examples of good work and achievement undertaken by NUH over the
past year around: Do Not Attempt CPR and medication optimisation, antibiotic consumption, impact of UTI
quality improvement, recognise and rescue the deteriorating patient, roll-out of the new NEWS 2 system,
reducing avoidable harm and death associated with missed opportunities to identify. and respond to
deteriorating patients.
Commissioners note that the CQC undertook a standalone inspection of the children’s sexual assault referral
centre in November 2019 and the only area for concern was within the ‘Well Led’ domain. The CQC is
monitoring actions and has oversight arrangements in place. However, it is to be noted that the inspection
findings do not impact on the Trust’s ratings.
NUH has achieved a majority of the Commissioning for Quality and Innovation (CQUIN) goals in 2019/20.
Commissioners recognise that NUH has been working relentlessly to improve systems and processes within
the Emergency Department. NUH was selected as one of the field testing sites for new metrics and has been
reporting against these since May 2019. Patients waited too long in ED which is a significant issue for NUH
and there is need for urgent improvements. . The number of patients waiting on a trolley in ED for 12 hours
or more continues to be monitored by Commissioners.
NUH participated in 99% of National Clinical Audits with learning and actions identified, from which the Trust
intends to improve the quality of healthcare provided. Results from the most of the Patient Surveys
published by CQC highlighted that patients felt listened to, confident in the provision of care and well looked
after. To strengthen this, plans and actions have been taken to improve patient experience in response to
the Maternity Services and Patient Friends and Family Test (FFT) Surveys. Improvement plans are also in
place for 2020/21 in response to the National Staff Survey.
NUH has demonstrated good progress around safety and quality in 2019/20 but some challenges still remain
for the Trust. For the first time since June 2012, NUH underperformed against the 18 week RTT standard.
This is largely due to increase in waiting lists and reduction in number of clinicians undertaking additional
sessions as a result of issues relating to the NHS Pension Scheme. The decision to cease all routine elective
work to create capacity for COVID-19 patients will continue to impact on the Trust’s RTT performance.
NUH’s overall VTE risk assessment compliance was still below target in 2019/20 but has seen an
improvement over 2018/19. Training on completing VTE Risk Assessments and a new IT system in 2020/21
will improve usability of the assessment tool. C.Difficile and MRSA at NUH were above trajectory for 2019/20
but the Trust has developed effective programmes of surveillance and remains committed to improving and
sustaining high levels of environmental cleanliness.
Page 97
The Quality Account highlights that NUH had challenges achieving its target for mandatory training
attendance due to access issues and recording while staff were moved on to different systems. Appraisal
rates for non-medical and dental staff were below target but a new simplified appraisal process has been
introduced. Medical and dental appraisal consistently performs well at NUH.
Commissioners acknowledge the commendable work by the Research and Innovation Department at NUH
and extend their praise to the doctors on their national research awards. Commissioners also recognise
NUH’s journey to MAGNET® to be nationally and internationally recognised for excellence in care. Magnet
recognition will build upon the 'Outstanding for Caring' rating from the Care Quality Commission providing a
roadmap to nursing excellence, which benefits the whole of an organisation.
Commissioners recognise that NUH is working actively with system partners as a member of the
Nottinghamshire Integrated Care System, to transform the Trust’s approach to focus on population health
needs and ‘system’ ways of working.
The Trust-wide patient safety improvement programmes for 2020/21 explained in detail in the Quality
Account are innovative and ambitious which Commissioners are supportive of.
As Commissioners we have worked closely and built close relationships with NUH over the course of 2019/20
to review the Trust’s progress. We hope to continue to build good relationships as we move into 2020/21.
Commissioners support the quality priorities set by NUH for 2020/21 and look forward to working with NUH
over the coming year as they continue to look for opportunities to make improvements to safer care and to
the quality of care provided to patients and families.
Nottingham County Council Health Scrutiny Committee
The Health Scrutiny Committee for Nottinghamshire welcomes this opportunity to comment on Nottingham
University Hospital’s draft Quality Account.
The committee is pleased to see a strong focus on reducing the incidence of Grade 3 & 4 pressure sores
within the Trust’s quality priorities. It is, however, unfortunate that the 10% year on year improvement
target is unlikely to be met.
The move to improve the quality of patients’ sleep by reducing unnecessary light sources and noise from
staff is to be particularly welcomed.
The development of the Trust’s Duty of Candour processes, and the involvement of families when things go
wrong, is something that the committee would like to hear about in more detail in due course.
It is unfortunate that cases of C.Difficile remain stubbornly high. It would be interesting to know what further
innovative measures could be deployed by the Trust to reduce the number of cases.
The committee commends the crucial work undertaken by the Trust in the appropriate management of
sepsis patients, particularly, the delivery of the bi-monthly sepsis survivors support group.
The Trust is to be congratulated on the high uptake of flu vaccination amongst frontline staff (80%) as well as
the generally high level of achievement of CQUIN targets.

Page 98
The Committee also congratulates the Trust on achieving a rating of ‘Good’ overall at its last CQC inspection.
We hope that the Trust will make all possible efforts to make the improvements necessary to achieve a
higher rating in the safety domain next time.
The Health Scrutiny Committee would also like to take this opportunity to thank the staff of NUH for all of
the work they have undertaken during the particularly challenging time of the COVID-19 pandemic.
Councillor Keith Girling
Chairman of the Health Scrutiny Committee
Nottinghamshire County Council
July 2020
In the context of COVID-19 statements of assurance were not recived from Healthwatch Nottingham and
Nottinghamshire and Nottingham City Health Scrutiny Committee.

Page 99
Annex 2 - Statement of Directors responsibilities in respect to the quality account
The directors are required under the Health Act 2009, National Health Service (Quality Accounts) Regulations
2010 and National Health Service (Quality Account) Amendment Regulation 2011 to prepare Quality
Accounts for each financial year. The Department of Health and Social Care has issued guidance on the form
and content of annual Quality Accounts which incorporate these legal requirements.
In preparing the Quality Account, Directors are required to take steps to satisfy themselves that:
The Quality Account presents a balanced picture of the Trust’s performance over the period covered;
The performance information reported in the Quality Account is reliable and accurate;
There are proper internal controls over the collection and reporting of the measures of performance
included in the Quality Account, and these controls are subject to review to confirm that they are
working effectively in practice;
The data underpinning the measures of performance reported in the Quality Account is robust and
reliable, conforms to specified data quality standards and prescribed definitions and subject to
appropriate scrutiny and review; and
The Quality Account has been prepared in accordance with Department of Health and Social Care
guidance.
The directors confirm to the best of their knowledge and belief that they have complied with the above
requirements in preparing the Quality Account.
Eric Morton Tracy Taylor
Chair Chief Executive
Insert date Insert date
Page 100
Related Documents








![UNIVERSITY HOSPITALS OF NORTH MIDLANDS NHS TRUST … Quality... · [University Hospitals of North Midlands NHS Trust Quality Account] 2017/2018 2 Part A: Statement on Quality OVERVIEW](https://static.cupdf.com/doc/110x72/5e735a6359ff9f4bf9401b4a/university-hospitals-of-north-midlands-nhs-trust-quality-university-hospitals.jpg)


