Punjab Academy of Forensic Medicine & Toxicology JOURNAL OF Volume: 21, Number: 01 January to June Publication: Half Yearly ISSN: 0972-5687 2021 A Peer Reviewed Journal on Forensic Medicine, Toxicology, Analytical Toxicology, Forensic Science, Environmental Pollution, Forensic Pathology, Clinical Forensic Medicine, Identiication, Legal Medicine, State Medicine, Medical Jurisprudence, Medical Ethics, Forensic Nursing, Forensic Odontology, Forensic Anthropology, Forensic Psychiatry and other Allied branches of Medicine and Science dedicated to administration of Justice. • Indexed with Index Copernicus (Poland), Scopus (Elsevier Products), IndMed (ICMR New Delhi), Safetylit, Worldcat Library & WHO Hinari • Available online at Indian Journals.com, pafmat.org and pafmat.com • UGC Approved (as per UGC care list) Place of Publication: Bathinda (Punjab) India • JPAFMAT is also having PubMed/NLM catalogue number (NLM Unique ID: 101232466). Editor-in-Chief Dr. Parmod Kumar Goyal

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Punjab Academy of Forensic Medicine & Toxicology
JOURNAL OF
Volume:21,Number:01JanuarytoJunePublication:HalfYearly
ISSN:0972-5687
2021
APeerReviewedJournalon
ForensicMedicine,Toxicology,AnalyticalToxicology,ForensicScience,EnvironmentalPollution,
ForensicPathology,ClinicalForensicMedicine,Identi�ication,LegalMedicine,StateMedicine,
MedicalJurisprudence,MedicalEthics,ForensicNursing,ForensicOdontology,ForensicAnthropology,
ForensicPsychiatryandotherAlliedbranchesofMedicineandScience
dedicatedtoadministrationofJustice.
• Indexed with Index Copernicus (Poland), Scopus (Elsevier Products), IndMed (ICMR New Delhi), Safetylit, Worldcat Library & WHO Hinari
• Available online at Indian Journals.com, pafmat.org and pafmat.com• UGC Approved (as per UGC care list)
Place of Publication: Bathinda (Punjab) India
• JPAFMAT is also having PubMed/NLM catalogue number (NLM Unique ID: 101232466).
Editor-in-ChiefDr.ParmodKumarGoyal

PUNJAB ACADEMY OF FORENSIC MEDICINE AND TOXICOLOGY
(Registration No. 139 / 1998-99, Chandigarh)
HO: Department of Forensic Medicine, Govt. Medical College Patiala (Punjab) 147001
PresidentDr. D. S. Bhullar
Vice PresidentDr. Rajiv Joshi
General SecretaryDr. Akashdeep Aggarwal
Editor-in-ChiefDr. Parmod Kumar Goyal
Finance SecretaryDr. Shilekh Mittal
Joint EditorDr. Amandeep Singh
Dr. Ashok Chanana
Dr. Ishwar Tayal
Dr. Dasari Harish
Dr. Preetinder S. Chahal
Dr. Puneet Khurana
Dr. Ajay Kumar
Dr. Amit Singla
Dr. Ashwani Kumar
Dr. Deep Rattan Mittal
Dr. O.P. Aggarwal
Dr. S.S. Oberoi
Dr. Balbir Kaur
Dr. Gurmanjit Singh
Dr. K.K. Aggarwal
Dr. R.K. Sharma
Dr. R.K. Gorea
Dr. Vijaypal Khanagwal
Executive Members
Advisors
GOVERNING COUNCIL (2019 - 2021)
Patron
Dr Jagdish Gargi
Advisors
Dr J. S. Dalal
Dr Harish Tuli
Dr Maj. Gen (Rtd.) Ajit Singh
President
Dr. R. K. Gorea
Vice President
Dr. D. S. Bhullar
Secretary
Dr. Sat Pal Garg
Treasurer
Dr. Nirmal Dass
Executive Members
Dr A S Thind,
Dr Jagjiv Sharma,
Dr Kuldeep Kumar,
Dr I. S. Bagga,
Dr Baljit Singh
FOUNDER GOVERNING COUNCIL OF PAFMAT
Special Invitee
Dr. Adish Goyal Dr. Mukul Chopra
Joint SecretaryDr. Didar Singh Walia
J Punjab Acad Forensic Med Toxicol 2021;21 (1) ISSN : 0972-5687
From the Desk of Editor-in-Chief
I am pleased to present the first issue of the year 2021 of Journal of Punjab Academy of Forensic Medicine & Toxicology. First of all
I apologize for delay release of this issue due to covid pandemic. I am thankful to the authors and contributors for the scientific
articles and research papers which are being published in this issue. I am also thankful to the editorial team and the members of the
Academy for supporting me in its publication and my special thanks to Joint Editor Dr Amandeep Singh.
The Journal publishes original research papers, review articles, case reports and review of books on Forensic Medicine and
Toxicology. The Journal highlights the achievements of the academy and its members. This journal is meant for achieving the aims
and goals of the academy to expand the academic activities, spread the knowledge and latest research in the field of Forensic
Medicine and Toxicology.
Any suggestions and advice for further improving the standards and quality of the journal will be highly appreciated and may be sent
to me through email or my whattsapp no. 9876005211.
J Punjab Acad Forensic Med Toxicol 2021;21 (1) ISSN : 0972-5687
ISSN Numbers:
ISSN-L: 0972-5687, p-ISSN: 0972-5687, e-ISSN: 0974-083X.
Indexed with:
IndexCopernicushttp://journals.indexcopernicus.com/karta.php?id=4715
Scopus (SCI):
http://www.scimagojr.com/journalsearch.php?q=19900194914&ip=sid&clean=0
Volume of Distribution:
300 copies.
Funding Bodies: Punjab Academy of Forensic Medicine & Toxicology, Donations from Philanthropists and manuscript handling charges
Address for submission of articles Online (Soft Copy):
[email protected], indianjournals.com
Copyright:
No part of this publication may be reprinted or republished without the prior permission of Editor-in-Chief of Journal of Punjab Academy of Forensic Medicine & Toxicology. Submission of all papers to the journal is understood to imply that it is not being considered for publication elsewhere. Submission of multi-authored paper implies that the consent of each author has been taken and there is no dispute among the
sequence of authorship. Researchers/Authors should adhere to publication requirements that submitted work is original, not plagiarized, ethical and has not been published elsewhere.
As per new CPA 2019 Act. confidentiality of the participants shall be maintained.
To expedite the review process, video conferencing with the authors for clarification and verification of the data was done.
All the articles had passed through the plagiarism software.
Every effort has been made not to publish any inaccurate or misleading information. However, the Editor-in-Chief, the Joint Editor or any member of the editorial committee accept no liability in consequences of any such publications. For any further information/query please contact with Editor-in-Chief.
Dr Parmod Kumar GoyalProfessor & Head (Forensic Medicine)
Member Secretary, Ethics Committee,Adesh UniversityController of Examinations, Adesh University, Bathinda
Convener, BOS(PG) Adesh University, BathindaCoordinator, Body Donation Programme
FAIMER 2013, ACME 2015Editor in Chief, Journal of Punjab Academy of Forensic
Medicine and Toxicology (JPAFMAT) Adesh Institute of Medical Sciences & Research, Bathinda
1

*From the Desk of Editor-in-Chief 1
*Contents 2-5
*Editorial :
Guidelines for Cremation/Burial of COVID19 - Need of the Hour 6-9
Kamal Singla, Yatiraj Singi
*Original Research Papers
1. Medical Students Perception on Ethics and Communication Module: 10-13
What It Means to be a Patient
Vikram Palimar, Chandni Gupta
2. Anthropometric Correlation between Stature and Measurements of Hand & Finger Length 14-21
Jaspinder Pratap Singh, Ashok Chanana, Kuldip Kumar, Jatinder Pal Singh, Manpreet Kaul
3. A Clinical Forensic Medicine Study of Mechanical Injuries in Assault Cases 22-28
Aashish Sharma, Kuldip Kumar, Ashok Chanana, Didar Singh Walia,
Jatinderpal Singh, Manpreet Kaul
4. Multifactorial Analysis of Deaths Due To Hanging 29-33
Prasenjit Das, Amandeep Singh, Dasari Harish
5. Age Estimation of Dead Foetus from Anthropology, Radiology of Femur & Humerus Bone 34-38 Piyush Sandhu, Amandeep Singh, Dasari Harish, Mahesh Sharma
6. Perception of relatives towards Medico-legal autopsy 39-43
in a tertiary care centre of Northeast India
Daunipaia Slong, AD Ropmay, Aelifeter R Marak, Anamika Nath,
Rangme B Y Marbaniang, AJ Patowary
7. Evaluation of Morphological Changes in Natural Tooth Exposed to 44-46
Organophosphorous Compounds
Mithra S, Abirami Arthanari, Pratibha Ramani
8. Pattern of Injuries and manner of Death in Alleged Railway Accident Deaths : 47-57
An Autopsy Study
Amarjit Singh, Guriqbal Singh
9. Estimation of Sexual Dimorphism by Osteometric Analysis of Patella 58-67
Kamal Singla, Yatiraj Singi, Rajiv Kumar Sinha, S K Dhattarwal
10. A Retrospective Autopsy Study of Deaths due to Compression of Neck 68-71
Munish Kumar, Kanika Kohli, Harpreet Singh
11. Impact of Covid-19 Pandemic on Suicidal and Homicidal Deaths in Jabalpur, 72-74
Madhya Pradesh, India
Nidhi Sachdeva, Divyam Singh Modi, Mukesh Rai, Vivek Shrivastava
12. Cypermethrin-induced liver toxicity in Balb/c mice 75-82
Dolly Mahna, Sanjeev Puri, Shweta Sharma
13. Estimation of Formaldehyde Contamination In Selected Sea Fish Species Sold 83-90
In Ernakulam District of Kerala State
Nirmal Kumar V, Pillay VV, Ramakrishnan UK, Arathy SL, Renjitha Bhaskaran
Punjab Academy of Forensic Medicine & Toxicology
JOURNAL OF
ISSN:0972-5687
Volume:21,Number:01JanuarytoJunePublication:HalfYearly
Contents
2

Punjab Academy of Forensic Medicine & Toxicology
JOURNAL OF
ISSN:0972-5687
Contents 14. Ameloglyphics : An Adjuvant in Individual Identification 91-96
Aneeta Sajan, Priya Thomas
15. A Comparative Study of Digital Forensic Tools for 97-104
Data Extraction From Electronic Devices
Harshita Tara, Amarnath Mishra
16. Introduction And Evaluation of Effective Image Based Interactive Teaching Learning 105-108
Method In Forensic Medicine Amongst Second MBBS Students
Rohit Zariwala, Krunal Pipaliya, Dimple Patel
17. Epidemiological Profile of Fatal Snakebite Cases in a Tertiary Care Centre in South India 109-113
Sathish.K, Kusa Kumar Shaha, Ambika Prasad Patra, J. Sree Rekha
18. Forensic Examination of Forensic expert's Disguise Handwritings 114-117
Shalvi Upadhyay, Lalit P. Chandravanshi
19. Students' Perception of Emergency Remote Teaching during COVID -19 Pandemic 118-123
Smitha Rani, Vinay J, Aravind GB, Arun M, Chandrakanth HV
20. Association of alcohol and psychoactive substances use with Mental Health Symptoms, 124-128
crime and violence
Gurmeet Kaur Brar, Vineet Jalota
21. Forensic Identification of Mifepristone and Misoprostol by TLC and FT-IR Methods 129-135
Bhuvnesh Yadav, Meena Jha, Lingaraj Sahoo, Sonu Kumar Maurya
22. Profile of Paraquat Poisoning in Bellary District- A Retrospective Study 136-138 Gururaj Biradar, Pavanchand Shetty H, Haneil Larson Dsouza, B Suresh Kumar Shetty,
Prateek Rastogi, Charan Kishor Shetty, V Yogiraj
23. Assessment of Knowledge and Awareness towards Medical Negligence among 139-142
Consultants in a Tertiary Care Teaching Hospital in North India
Siddhartha Taneja, Jaswinder Singh, K.K. Bairagi, Tarun K. Singh
24. Estimation of stature from Percutaneous Length of Tibia in Living Subjects in 143-148
Jhalawar region of Rajasthan
Mukesh Kumar Meena, Sanjaya Kumar Jain, Ramakant Varma
25. Pattern of fatal Injuries in Road Traffic Accidents in & around Jammu region: 149-152
An Autopsy Based Study
Preet Mohinder Singh, Kirandeep Kour Raina, Sandya Arora
26. Comparative Study of Forged Urdu Signatures Done By Persons Not Familiar To 153-155
Language Belongs To Region of Sikkim And Kashmir
Syed Ahmar Ali Hashmi, Shalvi Upadhyay, Rajeev Kumar
27. Forensic Characteristic Identification of Forged Urdu Signature Written By 156-158
Population of Delhi Who Are Stranger To The Language.
Syed Ahmar Ali Hashmi, Shalvi Upadhyay, Rajeev Kumar
28. Clickers in Medical Education – Boon or Bane? 159-164
Latif Rajesh Johnson, Ranjit Immanuel James
3
Volume:21,Number:01JanuarytoJunePublication:HalfYearly

Punjab Academy of Forensic Medicine & Toxicology
JOURNAL OF
ISSN:0972-5687
Contents 29. Correlation of Stature With Finger- Length of Native Haryana Population 165-167
Sabina Bashir, Rajender Kumar Saini, Yatiraj Singi
30. Pattern of Thoraco-abdominal Injuries Sustained In Road Traffic Accidents: 168-172
An Autopsy Based Observational Study
B Rupesh Kumar Naik, Siddhartha Das, Kusa Kumar Shaha
31. Reliability of age estimation using periodontal ligament visibility in South Indian Population 173-178
Ayan Bhadra Ray, Kushaggr Rastogi, Srikant N, Shweta Yellapurkar,
Nidhin Philip Jose, Ceena Denny
32. 179-186An Approach Towards Integrated Teaching: Case-Based Learning (CBL) in Physiology
Ashwani Ummat, Sonia Kochhar
33. Study of the Profile of Verbal and Non- verbal Clues of Deception among People of 187-191
South Indian descent.
Vijay Kautilya D, Shruti Prabhat Hegde, Pramika Rajashekaran
34. Knowledge and practice of smart phones and medical related applications in 192-196
learning by medical undergraduates.
Sakshi Singh Chauhan, Arti Ajay Kasulkar
35. Validation of University of Texas (UT) Age Estimation Software in Indian Population 197-202
Abirami Arthanari, Nagabhushana Doggalli, Vidhya A, Karthikeya Patil,
Sushma Rudra Swamy, Sowmya Srinivas
36. A Time Interval Based Forensic Study on Estimation of ABO Blood Group & 203-207
Rh Typing From Dental Pulp: An Aid in Personal Identification
Abirami Arthanari, Usha Hegde, Nagabhushana Doggalli, Priyanka Nithin
*Case Reports
1. Dressler's Syndrome – A Case Report. 208-211
Varun Krishna B, Nirmal Krishnan M, Deepak Nayak M, Vinod C Nayak
2. Decomposition in Drowning Obscures Cause and Manner of Death 212-215
Vivek K. Chouksey, Atul S. Keche, Daideepya C. Bhargava, S. Mahaluxmi
3. Papillary Renal Cell Carcinoma - an Incidental Finding at Autopsy 216-219
Niranjan P. Khadilkar, K.R. Nagesh
4. Development of an analytical method for detection of Imidacloprid Insecticide from 220-225
Biological Matrix using LC-MS/MS
Majji. Sai Sudha Rani, Chintan Singh, Amarnath Mishra
*Review Article
1. Covid-19 Vaccination Hesitancy: Causes, Legislation And Ethics 226-230
Anvita Ahuja, Jasmeen Kaur, Prateek Rastogi
2. Review on Bioremediation of Carbofuran & Different Factors Influencing the Process 231-237
Suryapratap Ray, Shikha Choudhary
3. Switching Gears of DNA Extraction: From Destructive to Non- Destructive 238-244 Ghuge Arun, Verma Pratibha, Sangle Sandeep, Gaiki Shweta, Paikrao Hariprasad
4
Volume:21,Number:01JanuarytoJunePublication:HalfYearly
Punjab Academy of Forensic Medicine & Toxicology
JOURNAL OF
ISSN:0972-5687
Contents
5
Volume:21,Number:01JanuarytoJunePublication:HalfYearly
4. Cadaveric Transplantation- The legal and Ethical issues 245-248
J.S.R.G. Saran, Jagadish Rao Padubidri
5. Developing and building high performance teams to achieve Accreditation 249-253
through different Leadership styles
Vijay Pratap Singh, Bidita Khandelwal, Parmod Kumar Goyal
*Commentary/Scientific Correspondence
1. Estimation of Zinc Concentration in Yamuna River (Delhi) Water Due to Climatic Changes 254-257
Mahipal Singh Sankhla, Rajeev Kumar, Lalit Prasad
2. Differences between Graduate Medical Education Regulations 1997 (GMER 1997) and 258-262
Graduate Medical Education Regulations 2019 (GMER 2019) in respect to teaching and
assessment of subject of Forensic Medicine and Toxicology
Parmod Kumar Goyal, Monika Gupta
*Instructions to Authors 263
*Life Members PAFMAT 264-265
Editorial
Corresponding Author :
Dr. Yatiraj Singi,
Associate Professor,
Department of Forensic Medicine & Toxicology, AIIMS Bilaspur
Contact : +91 99728-28903
Email: [email protected]
KEYWORDS : COVID-19, Cremation, Burial
Article History:Received: 8 June 2020Received in revised form: 8 December 2020Accepted on: 8 December 2020Available online: 31 August 2021
INTRODUCTION:
Coronavirus disease (COVID-19) is an infectious disease
caused by a newly discovered coronavirus.Most people
infected with the COVID-19 virus will experience mild to
moderate respiratory illness and recover without requiring
special treatment. Older people, and those with underlying
medical problems like cardiovascular disease, diabetes,
chronic respiratory disease, and cancer are more likely to 1develop serious illness . Infection can be transmitted from
droplets of different sizes or contact routes or by airborne
transmission in special cirumstances i.e. endotracheal
intubation, b r o n c h o s c o p y, o p e n s u c t i o n i n g ,
administration of nebulized treatment, manual ventilation
before intubation, turning the patient to the prone position,
disconnecting the patient from the ventilator, non-invasive
posi t ive-pressure vent i la t ion, t racheostomy, and 2cardiopulmonary resuscitation . There is some evidence that
COVID-19 infection may lead to intestinal infection and be
present in faeces. However, to date only one study has cultured 3the COVID-19 virus from a single stool specimen .
Indian Stand:
Being a new disease there is knowledge gap on how to dispose
of dead body of a suspect or confirmed case of COVID-19.
The main driver of transmission of COVID-19 is through
droplets. There is unlikely to be an increased risk of COVID
infection from a dead body to health workers or family
members who follow standard precautions while handling 4body . However MOHFW, India issued guidelines on
4management of COVID-19 dead bodies .4As per the MOHFW, India guidelines , the crematorium/
burial ground staff should be sensitized that COVID 19 does
not pose additional risk.The staff will practice standard
precautions of hand hygiene, use of masks and gloves.
Viewing of the dead body by unzipping the face end of the
body bag (by the staff using standard precautions) may be
allowed, for the relatives to see the body for one last time.
ABSTRACT:
Coronavirus disease (COVID-19) is an infectious disease caused by a newly discovered coronavirus.Most people infected with the
COVID-19 virus will experience mild to moderate respiratory illness and recover without requiring special treatment. People in
extremes of age and those having pre-existing disease are more prone to the infection. Transmission is by droplet/contact route or by
airborne transmission in special circumstances i.e endotracheal intubation, bronchoscopy, tracheostomy, cardiopulmonary
resuscitation etc.
Not only the treatment of living infected subjects, handling of COVID-19 dead bodies is also having utmost importance to prevent
the transmission of deadly virus to the body handlers (hospital staff/cremation staff/family members) in the hospital or at the
cremation/burial site. Here in this review paper, we have discussed about the pros and cons of the cremation and burial of the body
keeping in mind that no further spread of the virus could occur to the community. However for eg China and Sri Lankan authorities
made cremation compulsory by official order while WHO, India and many other did not objected to either of them. In our opinion,
cremation should be preferred for complete elimination of chances of infection. However keeping in mind the religious views
of the family, if the burial of the body is requested, then it should be assured that the body is buried in a thick, air tight coffin and
placed at normal depth of about 2 meter. It is recommended that the area above and adjacent to the grave should be cemented
immediately as an additional precautionary to avoid scavenging by animal.
1. Kamal Singla, Assistant Professor, Department of Forensic Medicine & Toxicology, Faculty of Medicine & Health Sciences,
SGT University, Gurugram, Haryana 122505
2. Yatiraj Singi, Associate Professor, Department of Forensic Medicine & Toxicology, AIIMS Bilaspur
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00001.7
Guidelines for Cremation/Burial of COVID19 - Need of the Hour
6

Religious rituals such as reading from religious scripts,
sprinkling holy water and any other last rites that does not
require touching of the body can be allowed. Bathing, kissing,
hugging, etc. of the dead body should not be allowed. The
funeral/ burial staff and family members should perform hand
hygiene after cremation/ burial. The ash does not pose any risk
and can be collected to perform the last rites. Large gathering at
the crematorium/ burial ground should be avoided as a social
distancing measure as it is possible that close family contacts
may be symptomatic and/ or shedding the virus.5As per the protocol of dignified management of the COVID-
19 dead bodies released by Dept of Forensic Medicine &
Toxicology, AIIMS, New Delhi, cremation should be
preferred for complete elimination of chances of infection in
either electric or gas crematorium in situ in zipped body bag.
However keeping in mind the religious views of the family, if
the burial of the body is requested, then it should be assured
that the body is buried in a thick, air tight coffin and placed at
normal depth of burial (4 to 6 feet). It is recommended that the
area above and adjacent to the grave should be cemented
immediately as an additional precautionary measure and the
space should be marked and required precautions should be
taken to avoid scavenging by animals. As a precautionary
measure large gathering at the crematorium/ burial ground
should be avoided to maintain a healthy distancing. The
remains of the last rites like ashes do not pose any risk of
infection and can be collected for religious immersion.
Remove personal protective equipment after handling of the
dead body. Then, perform hand hygiene immediately.
WHO Stand:
Transmission of COVID-19 pathogen is through droplets,
fomites and close contact, with possible spread through faeces. 2It is not airborne .
Except in cases of hemorrhagic fevers (such as Ebola,
Marburg) and cholera, dead bodies are generally not
infectious. Only the lungs of patients with pandemic influenza,
if handled improperly during an autopsy, can be infectious.
Otherwise, cadavers do not transmit disease. It is a common
myth that persons who have died of a communicable disease
should be cremated, but this is not true. Cremation is a matter
of cultural choice and available resources. To date there is no
evidence of persons having become infected from exposure to
the bodies of persons who died from COVID-19. The dignity
of the dead, their cultural and religious traditions, and their
families should be respected and protected throughout. Hasty
disposal of a dead from COVID-19 should be avoided.
Authorities should manage each situation on a case-by-case
basis, balancing the rights of the family, the need to investigate 6the cause of death, and the risks of exposure to infection .
People who have died from COVID-19 can be buried or
cremated. Confirm national and local requirements that may
dictate the handling and disposition of the remains. Family and
friends may view the body after it has been prepared for burial,
in accordance with customs. They should not touch or kiss the
body and should wash hands thoroughly with soap and water
after the viewing; Those tasked with placing the body in the
grave, on the funeral pyre, etc., should wear gloves and wash
hands with soap and water after removal of the gloves once the 6burial is complete .
6Burial by family members or for deaths at home : In contexts
where mortuary services are not standard or reliably available,
or where it is usual for ill people to die at home, families and
traditional burial attendants can be equipped and educated to
bury people under supervision. Any person (e.g. family
member, religious leader) preparing the deceased (e.g.
washing, cleaning or dressing body, dying hair, trimming nails
or shaving) in a community setting should wear gloves for any
contact with the body. For any activity that may involve
splashing of bodily fluids, eye and mouth protection (face
shield or goggles and medical mask) should be worn. Clothing
worn to prepare the body should be immediately removed and
washed after the procedure or an apron or gown should be
worn. The person preparing the body should not kiss the
deceased. Anyone who has assisted in preparing the body
should thoroughly wash their hands with soap and water when
finished. Apply principles of cultural sensitivity and ensure
that family members reduce their exposure as much as
possible. Children, older people (>60 years old), and anyone
with underlying illnesses (such as respiratory illness, heart
disease, diabetes, or compromised immune systems) should
not be involved in preparing the body. A minimum number of
people should be involved in preparations. Others may observe
without touching the body at a minimum distance of 1 meter.
Family and friends may view the body after it has been
prepared for burial, in accordance with customs. They should
not touch or kiss the body and should wash their hands
thoroughly with soap and water following the viewing.
Physical distancing measures should be strictly applied (at
least 1 meter between people). People with respiratory
symptoms should not participate in the viewing or at least wear
a medical mask to prevent contamination of the place and
further transmission of the disease to others. Those tasked with
placing the body in the grave, on the funeral pyre, etc. should
wear gloves and wash hands with soap and water once the
burial is complete.
Cleaning of reusable PPE should be conducted in accordance
with manufacturer's instructions for all cleaning and
disinfection products (e.g. concentration, application method
7
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00001.7

paper we will discusss about the pros and cons of various
practices of last rites in current scenario of COVID-19
pandemic irrespective of his/her religion faith keeping in mind
that no further spread of the virus could occur to the
community.
In the case of COVID-19, the pathogen is highly infectious
and transmits from one person to another through droplets or
contact. This means it requires body fluid to keep finding new
victims. So theoretically, novel coronavirus can be transmitted
during preparing the body for burial to body handlers. 10Secondly, body inside the earth usually takes 8x times to
decompose in comparision if body is in the open air posing risk
of animal scavanging and tranmission. However, cementing
the grave immediately can be done as an additional
precautionary measure to prevent animal scavanging.11 While cremation invloves 1400 to 1800 degree fahrenheits of
temperature to cremate the body. At this high temperature,
chances of infection from viable virus particles in the ashes is
not questionable. However transmission can occur while
preparing the body for cremation from bodiely secretions as
while preparing for burial. In addition, there will no danger for
animal scavanging activity after cremation.
Suggestions:
We propose to suggest following measures, in addition to the
COVID-19 guidelines on dead body management4, published
by the MOHFW, GOI.
1) Instead of handing over the body (confirmed/suspected
COVID-19) to the relatives in cases of hospital deaths, we
suggest the body should be transferred directly to the place
of cremation/burial by the designated health worker
person who is involved primarily in packing of the body to
ensure minimal exposure to others including family
members.
2) In case of death at home with suspicion of having
COVID-19, it should be mandatory to inform the local
authorities which will ensure transportation and packing
of the body to the cremation/ burial site as per the
guidelines. This will also help the local authorities in
contact tracing.
3) Personell from the local authorities and staff of
cremation/burial site should be well trained in infection
prevention control practices.
4) Cremation/burial staff should be duty bound to complete
the last rite process (cremation/burial) without involving
family members or relatives.
5) Proper treatment and handling instructions of the
belongings and clothing of the deceased should be given
to the family members by the staff involved in packing of
and contact time, etc.). Children, adults > 60 years, and
immunosuppressed persons should not directly interact with
the body. Although burials should take place in a timely
manner, in accordance with local practices, funeral ceremonies
not involving the burial should be postponed, as much as
possible, until the end of the epidemic. If a ceremony is held,
the number of participants should be limited. Participants
should observe physical distancing at all times, plus
respiratory etiquette and hand hygiene.
The belongings of the deceased person do not need to be
burned or otherwise disposed of. However, they should be
handled with gloves and cleaned with a detergent followed by
disinfection with a solution of at least 70% ethanol or 0.1%
(1000 ppm) bleach. Clothing and other fabric belonging to the
deceased should be machine washed with warm water at
60−90°C (140−194°F) and laundry detergent. If machine
washing is not possible, linens can be soaked in hot water and
soap in a large drum using a stick to stir and being careful to
avoid splashing. The drum should then be emptied, and the
linens soaked in 0.05% chlorine for approximately 30 minutes.
Finally, the laundry should be rinsed with clean water and the 7linens allowed to dry fully in sunlight
Global Stand:
China, where novel Coronavirus outbreak took place first in
December, decided to cremate the bodies. In many cases,
bodies of COVID-19 were cremated immediately after the
death and even in the absence of family members without
giving any consideration if the religious belief of the
coronavirus victim and released a formal order directing the
local authorities to immediately cremate bodies of COVID-19 8victims and laid out procedure on how to do it .
In neighbouring Sri Lanka too, the government made
cremation of body mandatary if the deceased is a COVID-19
patient or suspected to have novel coronavirus infection. The
order has been resented by Muslims in Sri Lanka. But the
government has cited the highly infectious nature of novel 9coronavirus to dismiss the objections on account of health .
Pros and Cons in relation to Burial/Cremation:
As of today (19/05/2020), total confirmed cases of COVID are 12 134618821 worldwide and 97975 in India & the number of
12 13deaths are 311847 worldwide and 3163 in India . There is
currently a disproportionate focus on the living instead of the
dead. India is the largest democracy in the world and having
about 1.4 billion population and accomodating people of
almost all religions with different cultural practices while
performing the last rites of the individual/family member.
Hindu practices cremation while Christians and Muslims
perform burial as per religious belief and practices. In this
8
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00001.7
Management of COVID-19 Dead bodies available at
https://aiims.edu/images/pdf/notice/CoVID%2019.pdf
accessed on 20/04/2020.
6. WHO International: Infection Prevention and Control for
the safe management of a dead body in the context of
COVID-19 - Interim guidance Published on 24/03/2020
available at :
h t t p s : / / a p p s . w h o . i n t / i r i s / b i t s t r e a m / h a n d l e
/10665/331538/WHO-COVID-19-lPC_DBMgmt-
2020.1-eng.pdf accessed on 30/03/2020.
7. World Health Organization. (2020). Water, sanitation,
hygiene, and waste management for the COVID-19 virus.
I n t e r i m g u i d a n c e : 1 9 M a r c h 2 0 2 0 .
https://apps.who.int/iris/bitstream/handle/10665/33
1499 / W H O -2019-nCoV- I P C _ WA S H -2020 .2 -
eng.pdf?sequence=1&isAllowed=y (Accessed March 22,
2020).
8. National Health Commission, Ministry of Civil Affairs,
PRC, Notice regarding the issuance of guildlines for the
managment of the remains of pneumonia patients infected
with new coronavirus (for trial implementation) published
on 1/2/2020 available at :
h t t p : / /www.nhc .gov. cn /yzyg j / s7659 /202002 /
163c26a24057489dbf64dba359c59a5f.shtml accessed on
20/04/2020.
9. Prabash K Dutta, Burial or Cremation: What is a safer
funeral if someone dies of Covid-19?, Published on
1 8 / 0 4 / 2 0 2 0 I n d i a To d a y a v a i l a b l e f r o m
https://www.indiatoday.in/india/story/burial-or-
cremation-what-is-a-safer-funeral-if-someone-dies-of-
covid19-1668257-2020-04-18 accessed on 20/04/2020.
10. KSN Reddy & OP Murthy, Essentials of Forensic
Medicine & Toxicology, 34th Edn, Jaypee Brothers, Pg.
161.
11. https://www.cremationresource.org/cremation/how-is-a-
body-cremated.html accessed on 21/04/2020.
12. WHO International: Situation Report - 119 Published on
18/05/2020 available at :
https://www.who.int/emergencies/ diseases/novel-
coronavirus-2019/situation-reports accessed on
19/05/2020.
13. MOHFW, GOI: COVID-19 DATA, published
19/05/2020 available at https://www.mohfw.gov.in/
accessed on 19/05/2020.
body, if willing to take these items with them.
6) Mandatory presence of police and a health care
worker/worker from local authorities to be present at the
time of cremation/burial to ensure proper adherence to the
guidelines. This will ensure smooth implementation of the
guidelines without any delay, deviation or any violence at
the cremation or burial site.
7) Specify the number of mourners permitted to be present at
the crematorium/burial ground instead of mentioning the
word “Large gathering should be avoided”. We suggest
the number to be limited to maximum 10.
Opinion:
In our opinion, cremation should be preferred for complete
elimination of chances of infection. However keeping in mind
the religious views of the family, if the burial of the body is
requested, then it should be assured that the body is buried in a
thick, air tight coffin and placed at normal depth of burial
(about 2 meter). It is recommended that the area above and
adjacent to the grave should be cemented immediately as an
additional precautionary measure to avoid scavenging by
animals. As a precautionary measure large gathering at the
crematorium/ burial ground should be avoided to maintain a
healthy distancing. The remains of the last rites like ashes do
not pose any risk of infection and can be collected for religious
immersion. The number of mourners should be limited as less
as possible subject to maximum of 10.
REFERENCES:
1. https:// www.who.in / health-topics / coronavirus # tab =
tab_1 accessed on 20/04/2020.
2. WHO International: Modes of transmission of virus
causing COVID-19: implications for IPC precaution
Recommendations-Scientific brief, Published 29/03/2020
a v a i l a b l e a t h t t p s : / / w w w. w h o . i n t / n e w s -
room/commentaries/detail/modes-of-transmission-of-
virus-causing-covid-19-implications-for -ipc-precaution-
recommendations accessed on 20/04/2020.
3. Zhang Y, Chen C, Zhu S et al. [Isolation of 2019-nCoV
from a stool specimen of a laboratory-confirmed case of
the coronavirus disease 2019 (COVID-19)]. China CDC
Weekly. 2020;2(8):123–4. (In Chinese).
4. MOHFW, GOI: COVID-19: GUIDELINES ON
DEAD BODY MANAGEMENT, published 15/03/2020
available at :
https://www.mohfw.gov.in/pdf/1584423700568_COVI
D19GuidelinesonDeadbodymanagement.pdf accessed
on 18/03/2020.
5. Deptt. of FMT, AIIMS, Delhi: Protocol on Dignified
9
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00001.7
10
Original Research Paper
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2021.00002.9
1. Vikram Palimar, Professor & Head, Department of Forensic Medicine, Kasturba Medical College, Manipal, Manipal
Academy of Higher Education, Manipal, India, 576104
2. Chandni Gupta, Additional Professor, Department of Anatomy, Kasturba Medical College, Manipal, Manipal Academy of
Higher Education, Manipal, India, 576104
Key words: Patient care, Empathy, Curriculum, Students.
Corresponding Author:
Dr. Chandni Gupta,
Additional Professor,
Department of Anatomy, Kasturba Medical College, Manipal,
Manipal Academy of Higher Education, Manipal, India,
Contact : +91 98867-38555
Email :[email protected]
Article History :
Received : 18 August 2020
Received in revised form : 18 September 2020
Accepted on : 7 November 2020
Available online : 15 August 2021
INTRODUCTION :
Ethics is the study of morality careful and systematic scrutiny
of moral judgments and behaviors and practicing those
decisions. Medical ethics emphasizes mainly on problems [1]arising out of the practice of medicine.
Till now, medical program and training courses were designed
around specific educational or learning objectives which were roamingaround three main territories: Cognitive, psychomotor
and affective. And medical education in India mainly deals
with the head, sparsely with the hand, and almost they have
neglected the heart, consequently they fail to produce a
clinician who would realize and deliver complete care which
should include preventive, promotive, curative and palliative [2, 3]care with empathy.
Nowadays, there is an increased level of mistrust of the general
population on medical specialists due to carelessness,
misbehavior, and immoral practices that have led to violence
and legal problems. These all point to the fact that there is a
terrible requirement for modification of the current medical [4-6]curriculum.
Because of all these reasons MCI (Medical Council of India)
has taken a step forward in this connection and they have
proposed a new organized longitudinal program on attitude,
ethics and communication which is known as the AETCOM. It
Medical Students Perception on Ethics and Communication Module: What It Means to be a Patient
ABSTRACT :
Introduction: Student insights about their importance towards the patient begin to play an important role as their clinical
experiences advance. Doctors should provide health care which should be tailored for each patient, care which is given to the
patient should be coordinated, family and friends on whom the patient trusts should be involved, and care should deliver physical stwell-being and emotional support. So, in our college, we conducted the module what it means to be a patient for our 1 -year medical
undergraduate students and took their views regarding the module.
Material and Methods: A study was conducted on 198 undergraduate students from Kasturba Medical College, Manipal. They
were told to fill the questionnaire containing six questions regarding the module after the module was over. The survey was made
on Google form and the link was sent on their e-mail ids. Later the results were analyzed.
Results: 77.2% of students mentioned that the module had a positive impact on them. 89.9% of students feel that empathy and
compassion are required for the doctor while dealing with patients. 76.2% of students think that this module helps them to become
better doctors. 76.3% of the student feel this module should be taught to students. 82.8% feel that role play is the best method to
teach this module.
Conclusion: From our study, it is clear the even students feel that this module is essential in their profession. So, it is vital to
implement these types of modules in their regular curriculum.
11
has an outline of competency-based learning in the attitude,
ethics and communication domains that a medical professional
should have at the time of graduation so that they should
successfully fulfill the criteria of Indian medical graduate as an
excellent clinician, a perfect leader and an efficient member of
health-care team and system. They will also become an
excellent communicator, a lifelong learner, and a well-[7]developed professional.
Student insights about their importance towards the patient
begin to play an important role as their clinical experiences
advance. Doctors should provide health care which should be
tailored for each patient, care which is given to the patient
should be coordinated, family and friends on whom the patient
trusts should be involved, and care should deliver physical
well-being and emotional support.
So, keeping that in mind we also have incorporated a structured
program on ethics and communication consisting of 26
modules in our medical college. One such module was what it stmeans to be a patient which was done for our 1 -year
undergraduate medical students and we took their views
regarding the module. The objective of our study was to know
the student's views regarding the module.
MATERIAL AND METHODS:
The study was conducted on 198 undergraduate students from
Kasturba Medical College, Manipal who attended the module.
The study was exempt from review by the institutional ethics
committee as per the ICMR (Indian Council of Medical
Research) guidelines.
It was a qualitative study. Students were told to fill the
questionnaire containing six questions regarding the module
after the module was over which was based on the likert scale.
The questionnaire was made on Google form and the link was
sent on their e-mail ids.
Later the results were analyzed in percentage based on the
student's responses.
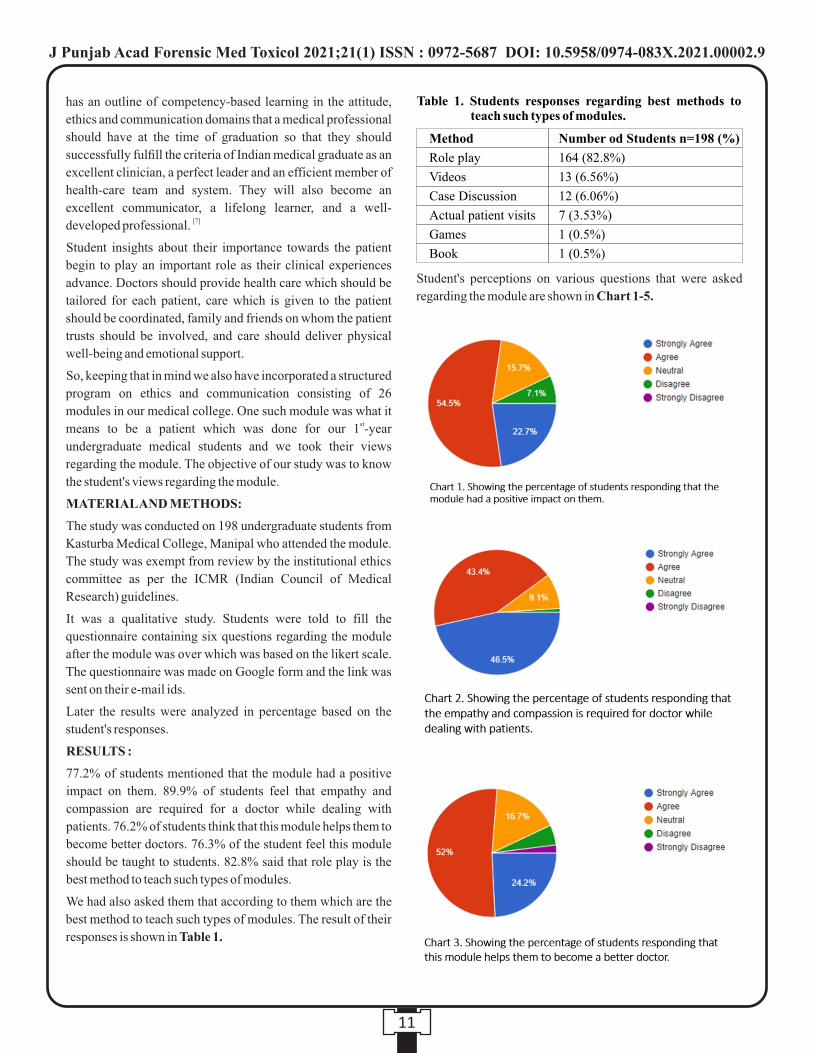
RESULTS :
77.2% of students mentioned that the module had a positive
impact on them. 89.9% of students feel that empathy and
compassion are required for a doctor while dealing with
patients. 76.2% of students think that this module helps them to
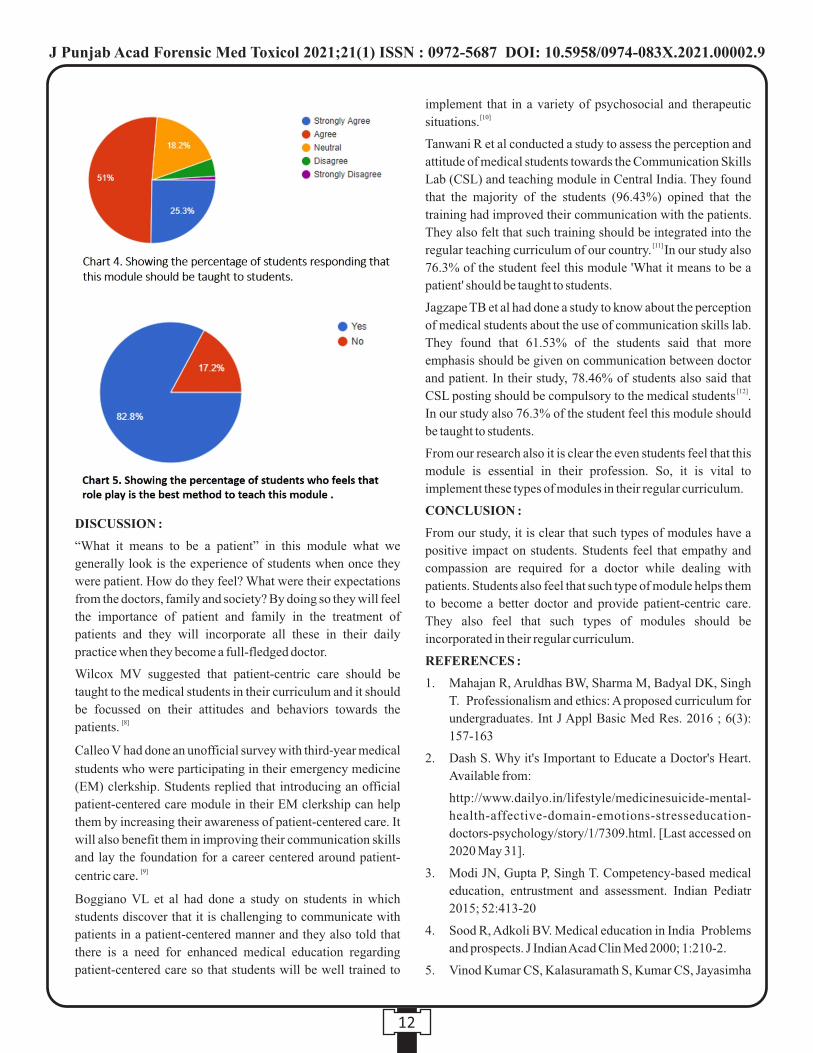
become better doctors. 76.3% of the student feel this module
should be taught to students. 82.8% said that role play is the
best method to teach such types of modules.
We had also asked them that according to them which are the
best method to teach such types of modules. The result of their
responses is shown in Table 1.
Student's perceptions on various questions that were asked
regarding the module are shown in Chart 1-5.
Table 1. Students responses regarding best methods to teach such types of modules.
Method
Role play
Videos
Case Discussion
Actual patient visits
Games
Book
Number od Students n=198 (%)
164 (82.8%)
13 (6.56%)
12 (6.06%)
7 (3.53%)
1 (0.5%)
1 (0.5%)
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2021.00002.9
12
DISCUSSION :
“What it means to be a patient” in this module what we
generally look is the experience of students when once they
were patient. How do they feel? What were their expectations
from the doctors, family and society? By doing so they will feel
the importance of patient and family in the treatment of
patients and they will incorporate all these in their daily
practice when they become a full-fledged doctor.
Wilcox MV suggested that patient-centric care should be
taught to the medical students in their curriculum and it should
be focussed on their attitudes and behaviors towards the [8]patients.
Calleo V had done an unofficial survey with third-year medical
students who were participating in their emergency medicine
(EM) clerkship. Students replied that introducing an official
patient-centered care module in their EM clerkship can help
them by increasing their awareness of patient-centered care. It
will also benefit them in improving their communication skills
and lay the foundation for a career centered around patient- [9]centric care.
Boggiano VL et al had done a study on students in which
students discover that it is challenging to communicate with
patients in a patient-centered manner and they also told that
there is a need for enhanced medical education regarding
patient-centered care so that students will be well trained to
implement that in a variety of psychosocial and therapeutic [10]situations.
Tanwani R et al conducted a study to assess the perception and
attitude of medical students towards the Communication Skills
Lab (CSL) and teaching module in Central India. They found
that the majority of the students (96.43%) opined that the
training had improved their communication with the patients.
They also felt that such training should be integrated into the [11] regular teaching curriculum of our country. In our study also
76.3% of the student feel this module 'What it means to be a
patient' should be taught to students.
Jagzape TB et al had done a study to know about the perception
of medical students about the use of communication skills lab.
They found that 61.53% of the students said that more
emphasis should be given on communication between doctor
and patient. In their study, 78.46% of students also said that [12]CSL posting should be compulsory to the medical students .
In our study also 76.3% of the student feel this module should
be taught to students.
From our research also it is clear the even students feel that this
module is essential in their profession. So, it is vital to
implement these types of modules in their regular curriculum.
CONCLUSION :
From our study, it is clear that such types of modules have a
positive impact on students. Students feel that empathy and
compassion are required for a doctor while dealing with
patients. Students also feel that such type of module helps them
to become a better doctor and provide patient-centric care.
They also feel that such types of modules should be
incorporated in their regular curriculum.
REFERENCES :
1. Mahajan R, Aruldhas BW, Sharma M, Badyal DK, Singh
T. Professionalism and ethics: A proposed curriculum for
undergraduates. Int J Appl Basic Med Res. 2016 ; 6(3):
157-163
2. Dash S. Why it's Important to Educate a Doctor's Heart.
Available from:
http://www.dailyo.in/lifestyle/medicinesuicide-mental-
health-affective-domain-emotions-stresseducation-
doctors-psychology/story/1/7309.html. [Last accessed on
2020 May 31].
3. Modi JN, Gupta P, Singh T. Competency-based medical
education, entrustment and assessment. Indian Pediatr
2015; 52:413-20
4. Sood R, Adkoli BV. Medical education in India Problems
and prospects. J Indian Acad Clin Med 2000; 1:210-2.
5. Vinod Kumar CS, Kalasuramath S, Kumar CS, Jayasimha
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2021.00002.9

13
VL, Shashikala P. The need of attitude and
communication competencies in medical education in
India. J Educ Res Med Teacher 2015; 3:1-4.
6. Kumar R. Medical education in India: An introspection.
Indian J Public Adm 2014; 60:146-54.
7. Attitude and Communication (AT-COM) Competencies
for the Indian Medical Graduate. Reconciliation Board.
Academic Committee of Medical Council of India. July
2015. Available from: www.mciindia.org.
8. Wilcox MV, Orlando MS, Rand CS, Record J, Christmas
C, Ziegelstein RC, and Hanyok LA. Medical students'
perceptions of the patient-centredness of the learning
environment. Perspect Med Educ. 2017; 6(1): 44-50.
9. Calleo V. The Patient Experience: Increasing Medical
Student Awareness of Patient-Centered Care. Annals of
Emergency Medicine. 2017; 70 (4): S148.
10. Boggiano VL, Yufan W, Janine B, Sylvia B, Erika S.
Patient-Centered Care Challenges and Surprises: Through
the Clerkship Students' Eyes. Family Medicine. 2017; 49:
57-61.
11. Tanwani R, Chandki R, Joshi A, Arora VK, Nyati P, Sutay
S. Perception and Attitude of Medical Students towards
Communication Skills Lab and Teaching Module. J Clin
Diagn Res. 2017 Jun; 11(6): JC12-JC14.
12. Jagzape TB, Jagzape AT, Vagha JD, Chalak A, Meshram
RJ. Perception of medical students about Communication
Skills Laboratory (CSL) in a rural medical college of
central India. Journal of Clinical and Diagnostic
Research. 2015; 9(12):JC01-JC04.
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2021.00002.9
Original Research Paper
INTRODUCTION :
Human stature estimation is one of the essential aspects of
forensic anthropological investigation which is defined as the
maximum height a t ta ined during one 's l i fespan.
Anthropometry is a science that deals with methods and
techniques of measurement of living and skeletons of 1individuals.
The scope of forensic anthropology is to identify the human 2skeleton remains. With the increasing frequency of mass
disasters, it is essential to find out correlations between stature,
age, and sex of an individual with variable information
collected from different systems, organs, or its part, which is of 3immense importance. The condition is worsened when only
mutilated and fragmentary remains are available for the
examination, which is not uncommon in today's world due to
mass disasters both natural and human-made, e.g.,
earthquakes, cyclones, tsunamis, floods, terror attacks, bomb
blasts, rail accidents, wars, and plane crashes, etc. Estimating a
person's stature from such fragmented remains forms an 4essential tool of identification in such circumstances. Stature
estimation occupies a relatively central position both in
anthropological research and in identification necessitated by 5medical jurisprudence or medico-legal experts.
The hand may be available for the analysis and also that part
may not be having sufficient ridge characteristic to establish
identity. Many time impressions of any of the phalanges or
only outline of the palm may available. In these cases, only
possibility to use that information is to measure the available
path to determine the stature estimation to identify the missing 6person.
Corresponding Author :
Dr Kuldip Kumar,
Associate Professor,
Department of Forensic Medicine and Toxicology, Government
Medical College, Amritsar.
Contact : +91 98146-39916
Email : [email protected]
KEYWORDS : Anthropometry, Hand length, Finger length, Stature Estimation
Article History:Received: 5 December 2020Received in revised form: 13 December 2020Accepted on: 13 December 2020Available online: 15 August 2021
rd1. Jaspinder Pratap Singh, Junior Resident 3 year*2. Ashok Chanana, Professor and Head*3. Kuldip Kumar, Associate Professor*4. Jatinder Pal Singh, Assistant Professor*5. Manpreet Kaul, Lecturer* *Department of Forensic Medicine and Toxicology, Government Medical College, Amritsar.
Anthropometric Correlation between Stature and Measurements of
Hand & Finger Length
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2021.00003.0
14
ABSTRACT :
Introduction: Stature is defined as the maximum height attained during one's lifespan. Human stature estimation is one of the
essential aspects of Forensic anthropological investigation which helps in the identification of a person or a body in different civil
and criminal matters.
Material and Method:The present prospective cross-sectional study was carried out in the Department of Forensic Medicine and
Toxicology, Government Medical College, Amritsar on 200 healthy undergraduate Punjabi students (100 males and 100 females)
to find out the bilateral and bisexual variations from the percutaneous measurement of length and breadth of hand and fingers except
thumb to reconstruct the stature for identification purposes.
Results: The mean height in males was 174.3690±6.18 cm, in females were 159.50±6.22 cm and in all the subject (N=200), the
mean height calculated was 166.94±9.68 cm. coefficient, 't' test and ANOVA test and regression equation for height is formulated.
The regression equation for all the subjects (n=200) is Y = 36.734 + (4.994 * LHL) + (2.683 * RHW) + (5.023 * RMFL) – (3.489 *
LRFL).
Conclusion: Stature is observed significantly related to hand length, width and length of fingers. Linear regression equations for
estimation of stature would be of immense value for medical professionals and can be used for identification of a person from stature
for civil and criminal purpose wherever required.
MATERIAL AND METHOD
The present prospective cross-sectional study was carried out
in the Department of Forensic Medicine and Toxicology,
Government Medical College, Amritsar to find out the bilateral
and bisexual variations from the percutaneous measurement of
length and breadth of hand and fingers except thumb to
reconstruct the stature for identification purposes.
INCLUSION CRITERIA: 200 healthy undergraduate
students (100 males and 100 females) were taken up for the
study with age group 18 years to 25 years with valid age proof
(Birth certificate/High school Certificate/Ration card/Bank
passbook/Voter ID/ Driving license). Before the procedure,
written informed consent was obtained from the students.
EXCLUSION CRITERIA: Cases with any pathology,
congenital anomaly/amputation (surgical or accidental) of the
hand or any finger are excluded from the study.
MATERIALS AND METHODS :
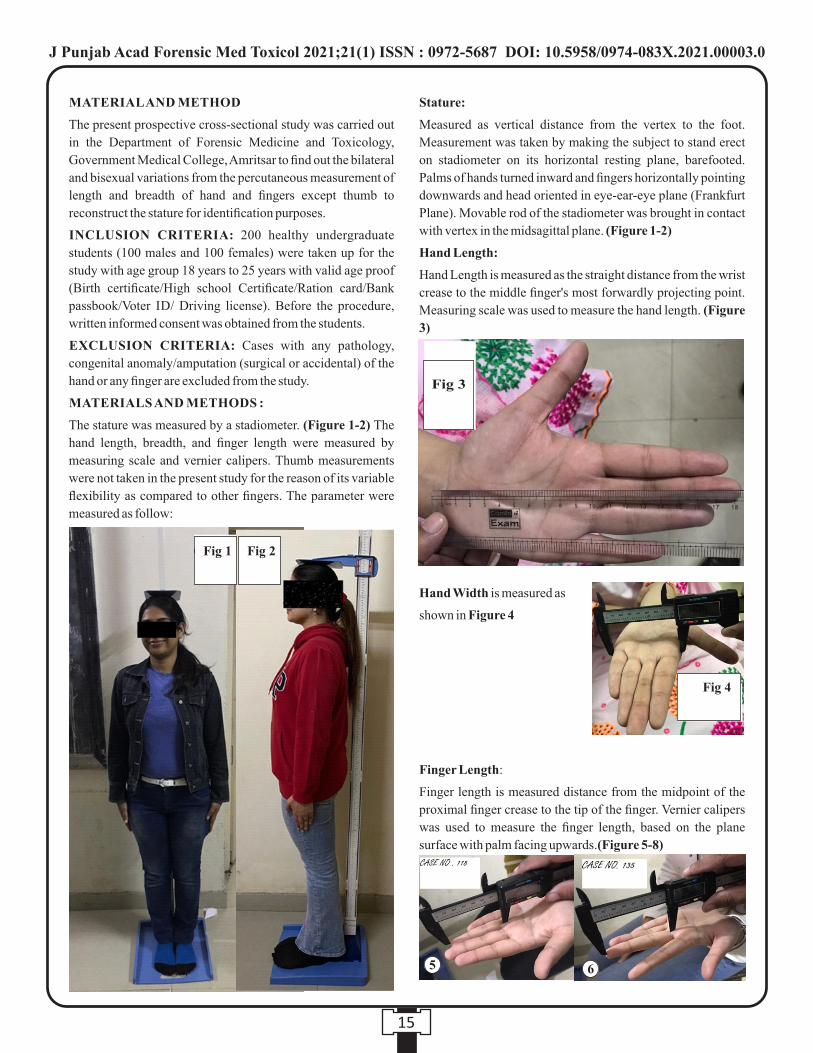
The stature was measured by a stadiometer. (Figure 1-2) The
hand length, breadth, and finger length were measured by
measuring scale and vernier calipers. Thumb measurements
were not taken in the present study for the reason of its variable
flexibility as compared to other fingers. The parameter were
measured as follow:
Stature:
Measured as vertical distance from the vertex to the foot.
Measurement was taken by making the subject to stand erect
on stadiometer on its horizontal resting plane, barefooted.
Palms of hands turned inward and fingers horizontally pointing
downwards and head oriented in eye-ear-eye plane (Frankfurt
Plane). Movable rod of the stadiometer was brought in contact
with vertex in the midsagittal plane. (Figure 1-2)
Hand Length:
Hand Length is measured as the straight distance from the wrist
crease to the middle finger's most forwardly projecting point.
Measuring scale was used to measure the hand length. (Figure
3)
Hand Width is measured as
shown in Figure 4
Finger Length:
Finger length is measured distance from the midpoint of the
proximal finger crease to the tip of the finger. Vernier calipers
was used to measure the finger length, based on the plane
surface with palm facing upwards.(Figure 5-8)
15
Fig 1 Fig 2
Fig 4
Fig 3
5 6
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2021.00003.0

RESULTS :
The mean height in males was 174.3690±6.18 cm and females
were 159.50±6.22 cm while, in all the subject (N=200) the
mean height was calculated as 166.94±9.68 cm. (Table 1)
The mean value of right hand length in males was 19.74±0.87
cm while in females, it was 17.92±0.84 cm and in total number
of subjects was 18.83±1.25 cm. The mean width of the right
hand in males was 8.84±0.77 cm and females were 7.69±0.44
cm, while the total number of subjects was 8.26±0.85 cm. The
mean length of right index finger length in males was
7.50±0.45 cm and females were 7.05±0.48 cm, while the total
number of subjects was 7.28±0.52 cm. The mean length of
right middle finger length in males was 8.32±0.45 cm and
females were 7.81±0.50 cm, while the total number of subjects
was 8.07±0.54 cm. The mean length of right ring finger length
in males was 7.77±0.46 cm and females were 7.32±0.48 cm,
while the total number of subjects was 7.54±0.52 cm. The
mean length of right little finger length in males was 6.38±0.43
cm and females were 6.04±0.53 cm, while the total number of
subjects was 6.21±0.51 cm. (Table 2)
The mean value of left hand length in males was 19.65±0.83
cm while in females, it was 17.83±0.88 cm and in total number
of subjects was 18.74±1.25 cm. The mean width of left hand in
males was 8.66±0.74 cm and females were 7.58±0.44 cm,
while the total number of subjects was 8.12±0.82 cm. The
mean length of left index finger length in males was 7.51±0.49
cm and females were 7.06±0.46 cm, while the total number of
subjects was 7.29±0.52 cm. The mean length of left middle
finger length in males was 8.28±0.49 cm and females were
7.80±0.46 cm, while the total number of subjects was
8.04±0.53 cm. The mean length of left ring finger length in
males was 7.73±0.47 cm and females were 7.22±0.48 cm,
while the total number of subjects was 7.47±0.54 cm. The
mean length of left little finger length in males were 6.27±0.52
cm and females were 5.93±0.44 cm, while the total number of
subjects was 6.10±0.51 cm. (Table 3)
16
7
8
Male
Female
Total
Male
Female
Total
Male
Female
Total
Male
Female
Total
Male
Female
Total
Male
Female
Total
Table 2 : Bisexual Variation of Right Hand Length, Width And Finger Lengths
Lengths N
100
100
200
100
100
200
100
100
200
100
100
200
100
100
200
100
100
200
Mean±S.D. (in cm)
19.74±0.87
17.92±0.84
18.83±1.25
8.84±0.77
7.69±0.44
8.26±0.85
7.50±0.45
7.05±0.48
7.28±0.52
8.32±0.45
7.81±0.50
8.07±0.54
7.77±0.46
7.32±0.48
7.54±0.52
6.38±0.43
6.04±0.53
6.21±0.51
Std. Error
0.09
0.08
0.09
0.08
0.04
0.06
0.05
0.05
0.04
0.05
0.05
0.04
0.05
0.05
0.04
0.04
0.05
0.04
Right Hand Length
Right Hand Width
Right Index Finger Length
Right Middle Finger Length
Right Ring Finger Length
Right Little Finger Length
Male
Female
Total
Mean±S.D.(in cms)
174.37±6.18
159.50±6.22
166.94±9.68
N
100
100
200
Std. Error
0.62
0.62
0.68
p<0.001 (Highly Significant)
Table 1 : Bisexual Variation of Height of All Subjects
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2021.00003.0

In the paired sample test, the mean value of right hand length
and left hand length was 0.09±0.36 with standard error of mean
was 0.04. The mean width of the right hand and the left hand of
males was 0.18±0.28 with a standard error of mean of 0.03.
The mean value of index finger length of left hand and right
hand of males was 0.00±0.23 cm with standard error of mean
was 0.02. The mean value of middle finger length of right hand
and left hand of males was 0.04±0.26 cm with standard error of
mean was 0.26. The mean value of ring finger length of right
hand and left hand of males was 0.03±0.22 cm with standard
error of mean was 0.02. The mean value of little finger length of
right hand and left hand of males was 0.11±0.32 cm with
standard error of mean was 0.03. (Table 4)
In the paired sample test, the mean value of right hand length
and left hand length of females was 0.09±0.35 cm with
standard error of mean was 0.04. The mean width of right hand
and left hand of females was 0. 0.11±0.20 cm with standard
error of mean was 0.02. The mean value of index finger length
of left hand and right hand of females was -0.02±0.22 cm with
17
Paired Differences
0.09±0.36
0.18±0.28
0.00±0.23
0.04±0.26
0.03±0.22
0.11±0.32
0.04
0.03
0.02
0.26
0.02
0.03
2.49
6.27
-0.21
1.65
1.58
3.62
0.14
0.00
-0.84
0.10
0.12
0.00
Mean±S.D (in cms) Std Error Mean
Table 4: Paired Sample Test Right Hand Versus Left Hand Among Males
Lengths in Male
Right Hand Length-Left Hand Length
Right Hand Width-Left Hand Width
't' test 'p' value
Right Index Finger Length-Left Index Finger Length
Right Middle Finger Length-Left Middle Finger Length
Right Ring Finger Length-Left Middle Finger Length
Right Little Finger Length-Left Middle Finger Length
Mean±S,D.(in cms)
19.65±0.83
17.83±0.88
18.74±1.25
8.66±0.74
7.58±0.44
8.12±0.82
7.51±0.49
7.06±0.46
7.29±0.52
8.28±0.49
7.80±0.46
8.04±0.53
7.73±0.47
7.22±0.48
7.47±0.54
6.27±0.52
5.93±0.44
6.10±0.51
Male
Female
Total
Male
Female
Total
Male
Female
Total
Male
Female
Total
Male
Female
Total
Male
Female
Total
Table 3 : Bisexual Variation of Left Hand Length, Width And Finger Lengths
Lengths N
100
100
200
100
100
200
100
100
200
100
100
200
100
100
200
100
100
200
Std. Error
0.08
0.09
0.09
0.07
0.04
0.06
0.05
0.05
0.04
0.05
0.05
0.04
0.05
0.05
0.04
0.05
0.04
0.04
Left Hand Length
Left Hand Width
Left Index Finger Length
Left Middle Finger Length
Left Ring Finger Length
Left Little Finger Length
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2021.00003.0
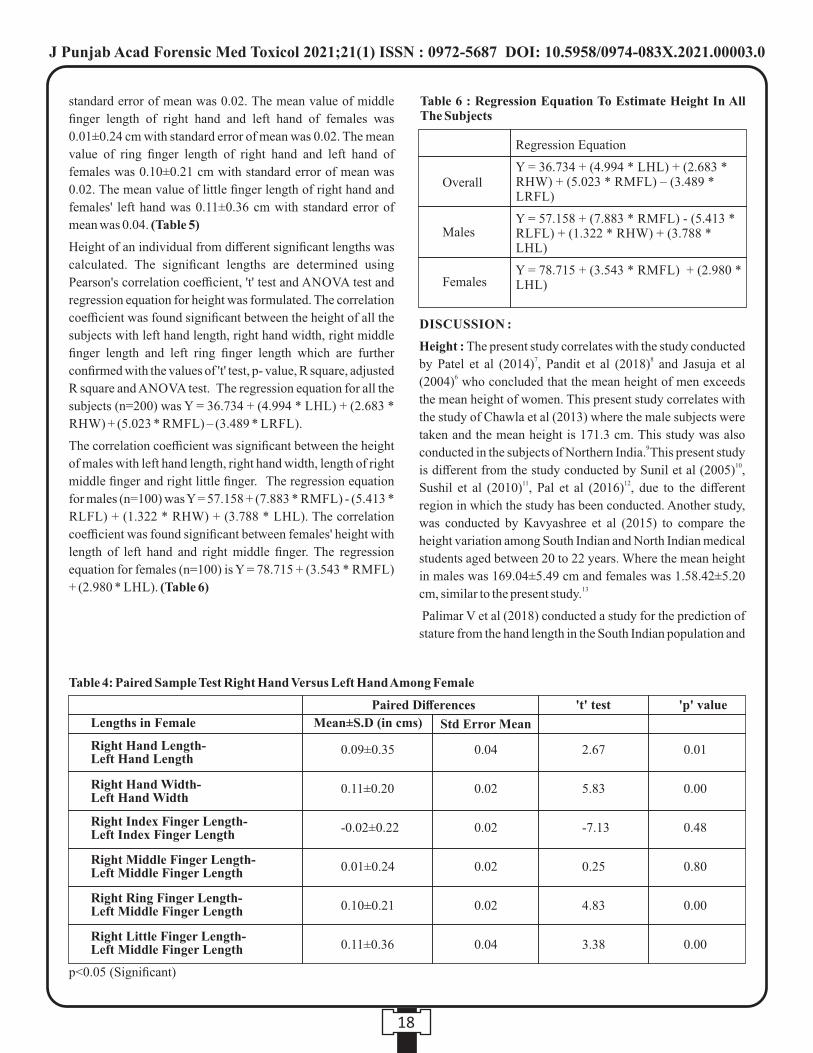
standard error of mean was 0.02. The mean value of middle
finger length of right hand and left hand of females was
0.01±0.24 cm with standard error of mean was 0.02. The mean
value of ring finger length of right hand and left hand of
females was 0.10±0.21 cm with standard error of mean was
0.02. The mean value of little finger length of right hand and
females' left hand was 0.11±0.36 cm with standard error of
mean was 0.04. (Table 5)
Height of an individual from different significant lengths was
calculated. The significant lengths are determined using
Pearson's correlation coefficient, 't' test and ANOVA test and
regression equation for height was formulated. The correlation
coefficient was found significant between the height of all the
subjects with left hand length, right hand width, right middle
finger length and left ring finger length which are further
confirmed with the values of 't' test, p- value, R square, adjusted
R square and ANOVA test. The regression equation for all the
subjects (n=200) was Y = 36.734 + (4.994 * LHL) + (2.683 *
RHW) + (5.023 * RMFL) – (3.489 * LRFL).
The correlation coefficient was significant between the height
of males with left hand length, right hand width, length of right
middle finger and right little finger. The regression equation
for males (n=100) was Y = 57.158 + (7.883 * RMFL) - (5.413 *
RLFL) + (1.322 * RHW) + (3.788 * LHL). The correlation
coefficient was found significant between females' height with
length of left hand and right middle finger. The regression
equation for females (n=100) is Y = 78.715 + (3.543 * RMFL)
+ (2.980 * LHL). (Table 6)
DISCUSSION :
Height : The present study correlates with the study conducted 7 8by Patel et al (2014) , Pandit et al (2018) and Jasuja et al
6(2004) who concluded that the mean height of men exceeds
the mean height of women. This present study correlates with
the study of Chawla et al (2013) where the male subjects were
taken and the mean height is 171.3 cm. This study was also 9 conducted in the subjects of Northern India. This present study
10is different from the study conducted by Sunil et al (2005) , 11 12Sushil et al (2010) , Pal et al (2016) , due to the different
region in which the study has been conducted. Another study,
was conducted by Kavyashree et al (2015) to compare the
height variation among South Indian and North Indian medical
students aged between 20 to 22 years. Where the mean height
in males was 169.04±5.49 cm and females was 1.58.42±5.20 13cm, similar to the present study.
Palimar V et al (2018) conducted a study for the prediction of
stature from the hand length in the South Indian population and
18
Regression Equation
Y = 36.734 + (4.994 * LHL) + (2.683 * RHW) + (5.023 * RMFL) – (3.489 * LRFL)
Y = 57.158 + (7.883 * RMFL) - (5.413 * RLFL) + (1.322 * RHW) + (3.788 * LHL)
Y = 78.715 + (3.543 * RMFL) + (2.980 * LHL)
Overall
Males
Females
Table 6 : Regression Equation To Estimate Height In All The Subjects
Paired Differences
0.09±0.35
0.11±0.20
-0.02±0.22
0.01±0.24
0.10±0.21
0.11±0.36
0.04
0.02
0.02
0.02
0.02
0.04
2.67
5.83
-7.13
0.25
4.83
3.38
0.01
0.00
0.48
0.80
0.00
0.00
Mean±S.D (in cms) Std Error Mean
Table 4: Paired Sample Test Right Hand Versus Left Hand Among Female
Lengths in Female
Right Hand Length-Left Hand Length
Right Hand Width-Left Hand Width
't' test 'p' value
Right Index Finger Length-Left Index Finger Length
Right Middle Finger Length-Left Middle Finger Length
Right Ring Finger Length-Left Middle Finger Length
Right Little Finger Length-Left Middle Finger Length
p<0.05 (Significant)
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2021.00003.0
mean height was 165.67±6.46cm in males and 157.97±6.5 cm 14in females. In Another study by Pournima et al (2019) where
the mean height was 162cm, which is less as compared to the
subjects of the present study as the region of study is different.
The studies conducted in South Indian population indicated
that the mean height in both males and females is less as 15compared to the mean height in the North Indian population.
Hand Length : The present study correlates with the study of 3Tandon et al (2016) which investigated the association of hand
length with height. The present study correlates with the study 16of Rastogi et al (2009) where the mean height in right hand of
males is 18.89 cm and in females was 17.01 cm while in left
hand of males is 18.87 and in females is 17.01 cm and it was
observed that mean hand length in females was less as compared to the present study. Jasuja et al (2004) in his study
concluded that the mean hand length in males is 19.8 on right
side while 19.79cm in left hand while in females is 17.51 cm of
right hand and 17.47 cm of left hand. Similarity of results was 6observed because the study was conducted in the same region.
Another study, was conducted by Kavyashree et al (2015) to
compare the hand length variation among south Indian and
North Indian medical students aged between 20 to 22 years.
Where the mean hand length in males was 18.70±2.13 cm in
males and 17.31±1.05 cm in females, the mean hand width was
found 8.10±0.33 cm in males which was found similar to the
present study where the mean hand width in males was 138.84±0.77 cm.
This present study differs from the studies carried out by
Krishan et al(2014) conducted in North India between the age
group of 17 years to 20 years where the mean hand length was
found 16.80±0.80 cm in females. The mean hand width was
7.30±0.40 cm which is less as compared to the present study.
Probable reason is the age group was different as compared to 17the present study.
Another study conducted by Pal et al (2016) conducted in
Bengalee population, West Bengal was different from the
present study perhaps due to the different region in which the
study has been conducted as the mean hand length in Bengalee
population was found out to be 16.30±0.86 cm. The mean hand
length in Bengalee population is found less as compared to the
mean hand length in the present study conducted in Punjabi 12population.
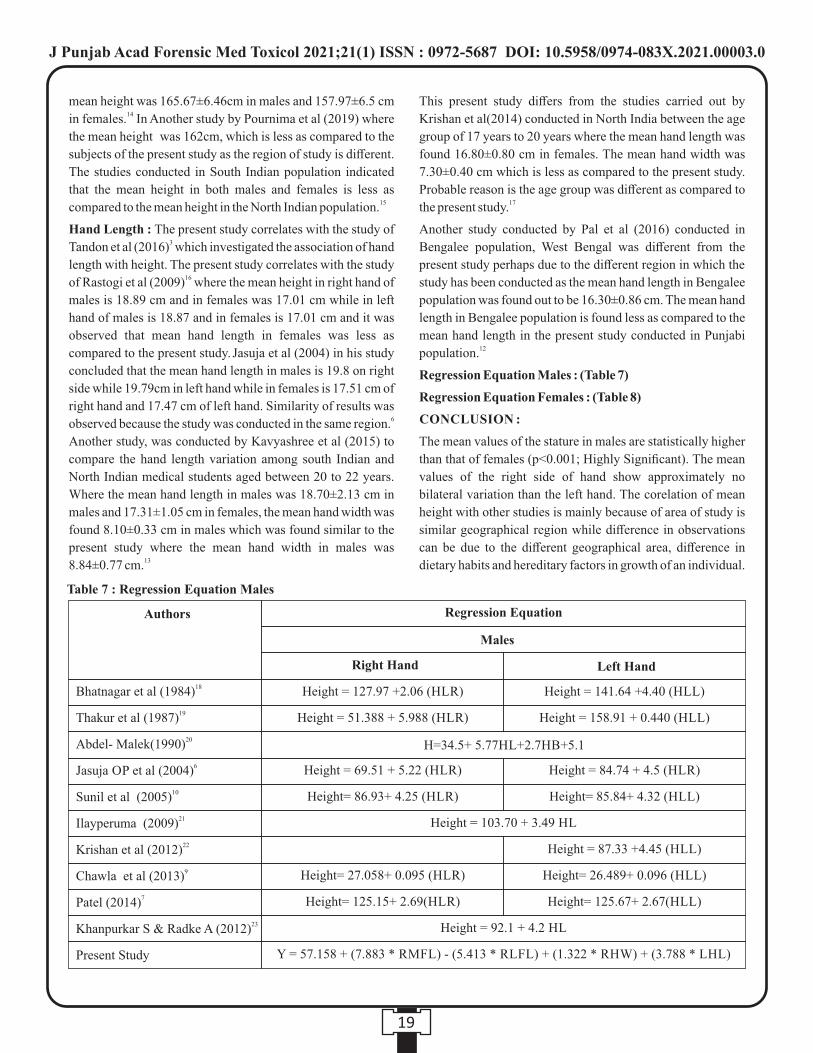
Regression Equation Males : (Table 7)
Regression Equation Females : (Table 8)
CONCLUSION :
The mean values of the stature in males are statistically higher
than that of females (p<0.001; Highly Significant). The mean
values of the right side of hand show approximately no
bilateral variation than the left hand. The corelation of mean
height with other studies is mainly because of area of study is
similar geographical region while difference in observations
can be due to the different geographical area, difference in
dietary habits and hereditary factors in growth of an individual.
19
Authors Regression Equation
Males
Right Hand Left Hand
Height = 127.97 +2.06 (HLR) Height = 141.64 +4.40 (HLL)18Bhatnagar et al (1984)
19Thakur et al (1987)
20Abdel- Malek(1990)
6Jasuja OP et al (2004)
10Sunil et al (2005)
21Ilayperuma (2009)
22Krishan et al (2012)
9Chawla et al (2013)
7Patel (2014)
23Khanpurkar S & Radke A (2012)
Present Study
Height = 51.388 + 5.988 (HLR) Height = 158.91 + 0.440 (HLL)
H=34.5+ 5.77HL+2.7HB+5.1
Height = 69.51 + 5.22 (HLR) Height = 84.74 + 4.5 (HLR)
Height= 86.93+ 4.25 (HLR) Height= 85.84+ 4.32 (HLL)
Height = 103.70 + 3.49 HL
Height = 87.33 +4.45 (HLL)
Height= 27.058+ 0.095 (HLR) Height= 26.489+ 0.096 (HLL)
Height= 125.15+ 2.69(HLR) Height= 125.67+ 2.67(HLL)
Height = 92.1 + 4.2 HL
Y = 57.158 + (7.883 * RMFL) - (5.413 * RLFL) + (1.322 * RHW) + (3.788 * LHL)
Table 7 : Regression Equation Males
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2021.00003.0
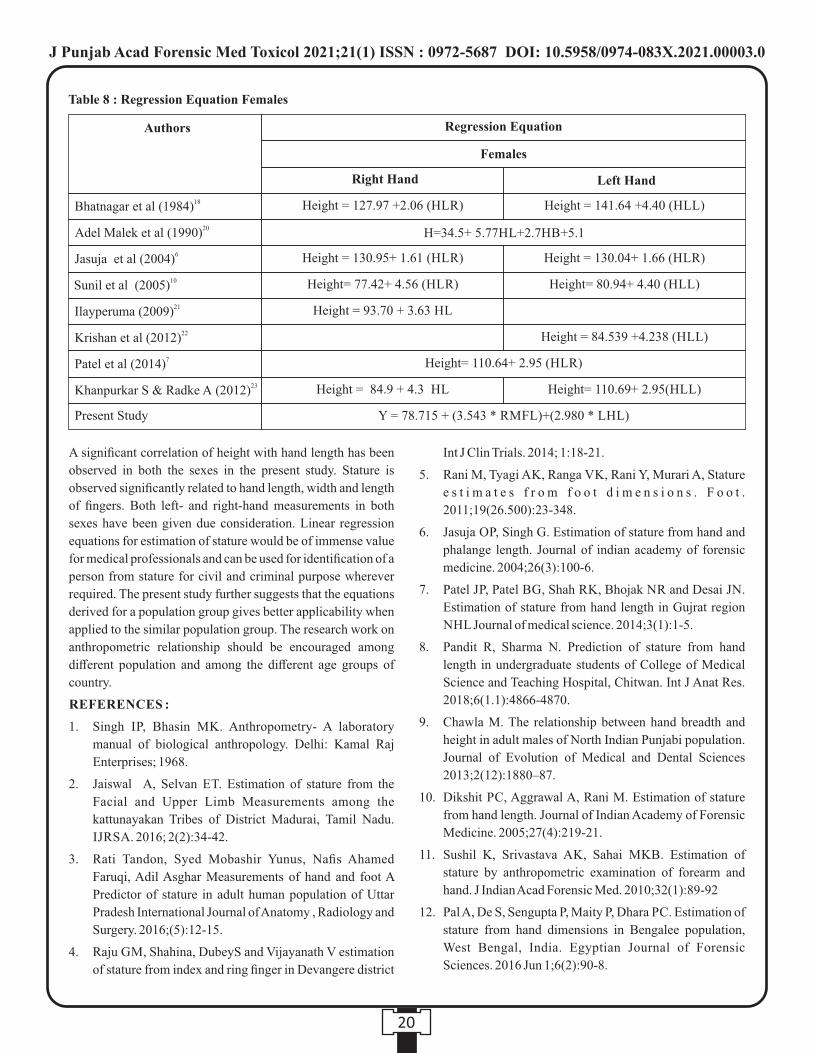
A significant correlation of height with hand length has been
observed in both the sexes in the present study. Stature is
observed significantly related to hand length, width and length
of fingers. Both left- and right-hand measurements in both
sexes have been given due consideration. Linear regression
equations for estimation of stature would be of immense value
for medical professionals and can be used for identification of a
person from stature for civil and criminal purpose wherever
required. The present study further suggests that the equations
derived for a population group gives better applicability when
applied to the similar population group. The research work on
anthropometric relationship should be encouraged among
different population and among the different age groups of
country.
REFERENCES :
1. Singh IP, Bhasin MK. Anthropometry- A laboratory
manual of biological anthropology. Delhi: Kamal Raj
Enterprises; 1968.
2. Jaiswal A, Selvan ET. Estimation of stature from the
Facial and Upper Limb Measurements among the
kattunayakan Tribes of District Madurai, Tamil Nadu.
IJRSA. 2016; 2(2):34-42.
3. Rati Tandon, Syed Mobashir Yunus, Nafis Ahamed
Faruqi, Adil Asghar Measurements of hand and foot A
Predictor of stature in adult human population of Uttar
Pradesh International Journal of Anatomy , Radiology and
Surgery. 2016;(5):12-15.
4. Raju GM, Shahina, DubeyS and Vijayanath V estimation
of stature from index and ring finger in Devangere district
Int J Clin Trials. 2014; 1:18-21.
5. Rani M, Tyagi AK, Ranga VK, Rani Y, Murari A, Stature
e s t i m a t e s f r o m f o o t d i m e n s i o n s . F o o t .
2011;19(26.500):23-348.
6. Jasuja OP, Singh G. Estimation of stature from hand and
phalange length. Journal of indian academy of forensic
medicine. 2004;26(3):100-6.
7. Patel JP, Patel BG, Shah RK, Bhojak NR and Desai JN.
Estimation of stature from hand length in Gujrat region
NHL Journal of medical science. 2014;3(1):1-5.
8. Pandit R, Sharma N. Prediction of stature from hand
length in undergraduate students of College of Medical
Science and Teaching Hospital, Chitwan. Int J Anat Res.
2018;6(1.1):4866-4870.
9. Chawla M. The relationship between hand breadth and
height in adult males of North Indian Punjabi population.
Journal of Evolution of Medical and Dental Sciences
2013;2(12):1880–87.
10. Dikshit PC, Aggrawal A, Rani M. Estimation of stature
from hand length. Journal of Indian Academy of Forensic
Medicine. 2005;27(4):219-21.
11. Sushil K, Srivastava AK, Sahai MKB. Estimation of
stature by anthropometric examination of forearm and
hand. J Indian Acad Forensic Med. 2010;32(1):89-92
12. Pal A, De S, Sengupta P, Maity P, Dhara PC. Estimation of
stature from hand dimensions in Bengalee population,
West Bengal, India. Egyptian Journal of Forensic
Sciences. 2016 Jun 1;6(2):90-8.
20
Authors
18Bhatnagar et al (1984)
20Adel Malek et al (1990)
6Jasuja et al (2004)
10Sunil et al (2005)
21Ilayperuma (2009)
22Krishan et al (2012)
7Patel et al (2014)
23Khanpurkar S & Radke A (2012)
Present Study
Regression Equation
Females
Right Hand Left Hand
Height = 127.97 +2.06 (HLR) Height = 141.64 +4.40 (HLL)
H=34.5+ 5.77HL+2.7HB+5.1
Height = 130.95+ 1.61 (HLR) Height = 130.04+ 1.66 (HLR)
Height= 77.42+ 4.56 (HLR) Height= 80.94+ 4.40 (HLL)
Height = 93.70 + 3.63 HL
Height = 84.539 +4.238 (HLL)
Height= 110.64+ 2.95 (HLR)
Height = 84.9 + 4.3 HL Height= 110.69+ 2.95(HLL)
Y = 78.715 + (3.543 * RMFL)+(2.980 * LHL)
Table 8 : Regression Equation Females
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2021.00003.0

13. K a v y a s h r e e A N , B i n d u r a n i M K , A s h a K R .
Determination of stature from hand dimensions in Indian
population, Journal of International Medicine and
Dentistry. 2015;2(3):209-214.
14. Palimar V, Gupta C, Guru P. Prediction of stature from the
hand length of an individual in South Indian population.
Journal of Punjab Academy of Forensic Medicine &
Toxicology. 2018;18(2):12-4.
15. Pournima, Rajesh JJ, Kumar KM, Reddy BS, Feula A.
Stature estimation from length of fingers in South Indian
population – A cross sectional study, J Indian Acad
Forensic Med. 2019 Oct-Dec; 41(4): 226-228.
16. Rastogi P, Kanchan T, Menezes RG, Yoganarasimha.
Middle finger length- a predictor of stature in the Indian
population. Med Sci Law. 2009;49(2):123-126.
17. Krishan K. Determination of stature from foot and its seg-
ments in a north Indian population. Am J Forensic Med
Pathol. 2008;29(4):297–303.
18. Bhatnagar DP, Thapar SP, Batish MK. Identification of
personal height from somatometery of hands in the
Punjabi males, Forensic science international.
1984;24:137-141.
19. Thakur SD, Rai KS. Determination of Stature from hand
measurement. Medicine Science and Law. 1987;78:25-8.
20. Abdul-Malek AK, Ahmed AM, EL-Sharkawi SA and EL-
Hamid N A. Predic t ion of s ta ture f rom hand
measurements. Forensic Science International.
1990;46:181–7.
21. Ilayperuma I, Nanayakkara G, Palahepitiya N. Prediction
of personal stature based on the hand length. Galle Med J.
2009;14 (1):15–8.
22. Krishan K. Determination of stature from foot and its seg-
ments in a north Indian population. Am J Forensic Med
Pathol. 2008;29(4):297–303.
23. Khanpurkar S, Radke A. Estimation of stature from foot
length, hand length and head length in Maharashtra
region. Indian Journal of Basic and applied Medical
Research 2012;1(2):77-85
21
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2021.00003.0

Original Research Paper
INTRODUCTION :
Medicolegal cases are imperative part of medical practice and
is an important constituent of emergencies of tertiary care
center . Violence in any form is a social and health problem for
all who experience and witness it. Intentional injury, including
interpersonal violence and self-harm is found to be one of the
leading causes of preventable injury in the world. Clinically an
injury or wound means disruption of the anatomical or natural 1continuity of any of the tissues of the body. As per Sec. 44,
IPC – An injury is defined as any harm whatsoever illegally 2caused to any person in body, mind, reputation or property.
According to Sec. 351, IPC 'assault' is defined as every attack
or threat or attempt to apply force on the body of another in a 3 hostile manner. The incidence of assaults are rising up
significantly with most probable factors contributing to this
hike are unemployment, illiteracy, low wages, decreased
capacity to cope up with prevailing situation and stress, drug
addiction, prevalent economic, social and political
environment, easy availability of weapon and long delays in
the delivery of justice to the victims. Assessment and
interpretation of injury depends upon a good medicolegal
history, an appropriate physical examination and recording the
findings clearly, accurately and unambiguously. Such
documentation in the form of medicolegal reports etc. may be
reviewed by other doctors, legal advisors and in the court of
law as an important documentary evidence.
MATERIAL AND METHODS:
Present prospective study of 500 medico-legal assault cases,
Corresponding Author :
Dr Kuldip Kumar,
Associate Professor,
Department of Forensic Medicine and Toxicology, Government
Medical College, Amritsar.
Contact : +91 98146-39916
Email : [email protected]
KEYWORDS : Medicolegal Cases, Assault, Mechanical Injuries, Fracture .
Article History:Received: 8 December 2020Received in revised form: 30 May 2021Accepted on: 30 May 2021Available online: 15 August 2021
1. Aashish Sharma, Junior Resident 3rd year*2. Kuldip Kumar, Associate Professor*3. Ashok Chanana, Professor & Head*4. Didar Singh Walia, Associate Professor* 5. Jatinderpal Singh, Assistant Professor*6. Manpreet Kaul, Lecturer* *Department of Forensic Medicine & Toxicology , Government Medical College, Amritsar
A Clinical Forensic Medicine Study of Mechanical Injuries in Assault Cases
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2021.00004.2
22
ABSTRACT :
Introduction: Medicolegal cases are imperative part of medical practice and is an important constituent of emergencies of tertiary
care centers and the doctor on duty prepares medicolegal reports of such cases. The pattern of mechanical injuries due to assault
differ between countries and communities due to their specific traditional , cultural and social factors prevalent in their areas. The
major chunk of these medicolegal cases are of injuries caused as result of violence in this part of India.
Materials & Methods: The present study of 500 medicolegal cases of mechanical injuries of assault was conducted of those
patients, who were admitted to Emergency department of Guru Nanak Dev Hospital attached to Government Medical College,
Amritsar noting down their demographic details and injury details both clinically as well as radiologically.
Results: In this study it was observed that majority of medicolegal cases were seen among males (89%) of age group of 21-40
years (61%). Majority of the cases belonged to rural background (77%) and most commonly involved occupational group was the
labourers (35.4%) . Also, the majority of injuries were simple in nature(79.8%) and were predominantly inflicted by blunt
weapon(67.6%) however the reverse trend was seen in injuries with grievous nature where the most common weapon was sharp
edged weapon(55.1%) .
Conclusions: Since the assault related injury cases were higher among males, in young age group and in a rural population so for
prevention of assault related activities, the main focus should be on encouraging the young age group, the concept of tolerance and
rationalism.

for mechanical injuries, who attended the emergency &
causality department of Guru Nanak Dev Hospital attached to
Government Medical College, Amritsar was conducted with
effect from 01/11/2018 to 18/04/2020. All the details related to
patient and detailed history of violence were mentioned in the
attached pre designed proforma. The detailed examination of
assault cases was done after taking written informed consent
from the patient and of one witness mostly his or her relative or
friend. The injuries were examined and documented in detail
with respect to its location, size, nature, causative factor,
probable weapon and it was correlated with the history with
specific attention to its age, nature of injury. Radiological
findings and hospital record findings were incorporated for
proper evaluation of injuries. The data collected from this
study had been organized by presenting it in the form of
appropriate tables and graphs, which is statistically analysed
for percentage and inferences.
RESULTS:
Gender wise distribution of cases
In the present study it was observed that majority of the cases
i.e. 445 (89%) of the victims were males & only 55 (11%) were
females out of total 500 medico-legal cases.
Age & gender wise distribution of medicolegal cases
Majority of male victims were in the age group of 21 to 30
years with 178 cases (35.6%) and in females, maximum
number of cases were found in the age group of 31 to 40 years
with 21 cases (4.2%). Least number of cases in males were
found in age group of 0 to 10 years i.e. 3 cases (0.6%).
However, no female cases were reported in age group of 0 to10
years. This study also showed that in both males and females
21 to 40 years of age group were most commonly involved in
scuffle. (Table1)
Occupation wise distribution of cases
As far as occupation wise distribution of medicolegal cases
was concerned labourers were more commonly involved
occupational group with 177 cases (35.4%) followed by
victims engaged in private jobs with 132 cases (26.4%) and
farmers with 103 medicolegal cases (20.6%). Least number of
medcolegal cases were found in student group with 38(7.6%).
(Table 2)
Religion wise distribution of cases
In the present study majority of assault cases 408(81.6%); were
from Sikh community while Hindu community constituted
only 64 cases (12.8%) further followed by Christians with 23
(4.6%) medicolegal cases. Least number of cases 5(1%) were
reported in Muslim community with mechanical injuries
Distribution of cases according to type of mechanical
injury
In the present study the most common type of mechanical
injuries recorded among medicolegal cases were Incised
wound in 243 cases (48.6%) followed by Lacerated wound in
157 cases (31.4%), Bruises in 82 cases (16.4%) and Abrasions
in 16 cases(3.2%). Only 2 cases of Stab wound injury were
recorded in this study. Out of 243 cases of Incised wounds,
92.5% males had suffered from Incised wounds as compared to
only 7.5% females. For 157 cases of Lacerated wounds, 90.4%
cases were of males and only 9.6% are of females. Of 82 cases
of Bruises, 72.6% cases were of males and 24.4% were of
females. For 16 cases of Abrasions, 87.5% were of males and
12.5% were of females. Stab wounds were present only in
males. This study clearly depicted that the most common type
of injury inflicted among males were Incised wounds whereas
in case of females predominance of Bruises were seen. Incised
wounds (7.5%) being the least common type of mechanical
injury recorded among females. Moreover no case of Stab
wound injury was noticed in females. (Table 3)
Area wise distribution of cases
Majority of medicolegal cases in the present study were from
rural background with 385 (77%) cases as compared to urban
areas which constituted only 115 (23%) of the total cases.
23
Table 2 : Occupation wise distribution of cases
Occupation
Labour
Private job
Farmer
Unemployed
Student
Total
No.
177
132
103
50
38
500
%
35.4
26.4
20.6
10
7.6
100
Table 1 : Age & gender wise distribution of cases
Age Range
(Years)
0-10
11-20
21-30
31-40
41-50
51-60
61-70
>70
TOTAL
No
3
43
178
98
62
28
24
9
445
No
0
3
8
21
10
2
9
2
55
No
3
46
186
119
72
30
33
11
500
%
0.6
8.6
35.6
19.6
12.4
5.6
4.8
1.8
89
%
0
0.6
1.6
4.2
2
0.4
1.8
0.4
11
%
0.6
9.2
37.2
23.8
1434
6
6.6
2.2
100
Male Female Total
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2021.00004.2

Type of mechanical injury in relation to total no of injuries
in victims
Out of the total 1362 mechanical injuries inflicted to 500
patients the most common type of mechanical injuries were
Incised wounds in 480 (35.2%) injuries followed by Bruises
with 423 (31.1%) injuries further followed by Lacerated
wound with 286 (20.9%) injuries, Abrasion with 170 (12.5%)
injuries and Stab wound with only 3 (0.2%) injuries.
Gender wise distribution of mechanical injuries according
to the anatomical sites of the body
The most common site of infliction of injuries in case of males
as well females was head and neck region with 289 (57.8%)
cases for males as compared to only 29 (5.8%) cases for
females followed by upper limbs with 106 (21.2%) cases for
males and 11(2.2%) cases for females and in lower limbs with
26 (5.2%) cases for males and 9 (1.8%) cases for female. Least
number of cases in males was seen over chest i.e. 5 (1%) cases
followed by abdomen 3 (0.6%) cases. However least number
of cases in females was seen over abdomen with 2 (0.4%) and
back with only 1 (0.2%) case with no injury over the chest was
noted.
Relationship between body part involved & type of
mechanical injury
The most commonly encountered injury over the head and
neck region of the body in the present study were Incised
wounds with 217 (36.5%) injuries, Lacerated wounds with 202
(33.8%) injuries followed by Bruises with 132 (22.2%)
injuries. Abrasions (7.5%) were least common type of
mechanical injury present over the head and neck region. The
commonest type of injury in upper limb region was similar to
that found in head and neck area which were incised wounds
with 197(47.8%) injuries. However, the second most
commonly encountered injury in upper limb area were Bruises
with 116 (28.1%) injuries followed by Lacerated wound and
Abrasions with 50(12.8%) and 49(11.8%) injuries
respectively. A different scenario was seen in lower limb area
with respect to type of injury inflicted with predominance of
Bruises i.e. 57(33.3%) injuries followed by Abrasions with
43(25.1%) injuries, Incised wound with 41(23.9%) injuries
and least number of injuries over lower limb area were of
Lacerated wound i.e. 30(17.5%) injuries.
Trunk region was least commonly involved anatomical site in
relation to infliction of Incised and Lacerated wounds.
However Bruises were inflicted more commonly over head &
neck region, upper limbs followed by trunk region in contrast
to findings observed in case of other mechanical injuries in this
study.
Duration of mechanical injuries
In maximum number of injuries 1135 (83.1%); the time
interval between the incidence of assault and medicolegal
cases was less than 6 hours. In this study, 95.9% of the injuries
were examined within 24 hours of the occurrence of the scuffle
and only 1.1% of the injuries were examined after 48 hours.
Direction of mechanical injuries
Most of the victims of the assault in the present study sustained
injuries in oblique direction 686 (83.9%) injuries followed by
vertical direction in 102 (12.4%) injuries. Horizontal cuts were
least commonly sustained over the body with only 88 (10.7%)
injuries.
Weapon of offence in mechanical injuries
The most commonly used weapon of offence for infliction of
injuries were blunt inflicting 846 (63.4%) injuries followed by
sharp edged weapons inflicting 480 (35.2%) injuries. Least
number of injuries 18 (1.3%) were inflicted by sharp pointed
weapon.
Kind of weapon used in relation to body parts affected
The most commonly used weapon of offence over the head and
neck region of the body was blunt weapon inflicting 376
(63.9%) injuries, as compared to sharp edged weapons
inflicting 211 (35.9%) injuries. Only a single injury was caused
by sharp pointed weapon over the head and neck region. The
commonest type of weapon used in upper limb region was
similar to that found in head and neck area which was blunt
weapon inflicting 208(50.5%) injuries closely followed by
sharp edged weapons inflicting 199 (48.3%) injuries. Sharp
pointed weapon resulted in 5 (1.2%) injuries over the upper
limb region. Similarly in case of lower limbs predominance of
blunt weapon inflicted injuries i.e. 135 (77.1%) was seen
followed by sharp edged weapons inflicting 40 (22.9%)
injuries. However no injury by sharp pointed weapon was
inflicted over the lower limbs. On the abdomen, 10 (52.6%)
injuries were inflicted by blunt weapon, followed by only 8
(42.2%) injuries which were caused by sharp edged weapon
and least number of injuries were inflicted by sharp pointed
weapon amounting to 1 (5.2%) injury.
24
Table 3 : Distribution of cases according to type of injury
Type of Injury
Incised Wound
Lacerated Wound
Bruise
Abrasion
Stab wound
Total
No.of
Cases
225
142
62
14
2
445
No.of
Cases
18
15
20
2
0
55
%
92.5
90.4
75.6
87.5
1.00
89
%
7.5
9.6
24.4
12.5
0
11
243
157
82
16
2
500
Male FemaleTotal
Victims
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2021.00004.2

Nature of mechanical injuries
In majority of cases i.e. 346 cases with 1088 (79.8%) injuries
were declared as simple in nature followed by 135 cases with
234 (17.1%) injuries were declared as grievous in nature which
also included fabricated or self-inflicted injuries. Only 1 case
(0.07%) was declared dangerous to life in this study. Out of
total 500 medicolegal cases examined for mechanical injuries
in only 63 (12.6 %) cases with 94 injuries were declared as
fabricated or self inflicted injuries while 87.4 % injuries were
genuine injuries .The nature of 39 injuries of 18 cases was not
declared either because of the noncompliance of patient for
getting medicolegal X-ray done or because of unavailability of
circumstantial evidences as asked from the investigating
officer.
Gender wise distribution of nature of mechanical injuries
The incidence of simple injuries in males were 301 (70.5%)
cases of the total male victims whereas in case of females
simple injuries were 45 (81.9%) in number. Incidence of
injuries declared grievous in nature in case of males was found
in 125 (29.3%) cases out of total male cases while in case of
females only 10 (18.1%) cases were reported with grievous
nature injuries. Only a single (0.2%) case of injury with
dangerous to life was noted in male victim. In this study no
injury with dangerous to life was found in female victims.
Kind of weapon used and relationship with nature of
injuries
This study showed that majority of injuries with simple nature
were predominantly inflicted by blunt weapon i.e 736 (67.6%)
out of total 1088 simple injuries followed by those inflicted
with sharp edged weapons with 336 (30.9%) injuries. However
on the other hand reverse trend was seen in injuries with
grievous nature where the most common weapon of offence for
inflicting injuries with grievous nature was sharp edged
weapon with 129 (55.1%) injuries followed by injuries
inflicted with blunt weapon with 105 (44.9%) injuries out of
total 234 grievous injuries. In this study no injury with
grievous nature was inflicted by sharp pointed weapon. This
study also showed that the single injury with dangerous to life
was inflicted by a sharp pointed weapon.
Relationship between mechanical injuries & grievous hurt
The present study depicted that out of total 234 injuries
declared as grievous in nature, majority were incised wounds
with 130 (55.5%) injuries, followed by bruises with 55
(23.5%) injuries, lacerated wounds with 41 (17.6%) injuries
and abrasions with only 8 (3.4%) injuries. This study showed
that sharp edged weapons are most commonly used as
compared to blunt weapons in inflicting injuries with grievous
nature.
Relationship of injuries with grievous nature and site of
infliction
The present study showed that the most common anatomical
site for injury with grievous nature was upper limb with 108
(46.1%) injuries and head & neck region with 89 (38.1%)
injuries. The other anatomical site for injuries with grievous
nature included lower limb with 28 (12.1%) injuries. This
study observed that the limbs (58.2%) were the commonest site
for injuries with grievous hurt followed by head & neck region
(38.1%). The least commonly involved body parts in this study
were chest, back and shoulder region with 3 (1.2%) injuries
each. No injury with grievous nature was found over the
abdominal region.
Radiological & hospital findings in association with
grievous injuries
The present study showed a mixed pattern of radiological and
hospital findings in association with grievous injuries. In
general; majority of fractures i.e 46.2% were seen in upper
limb bones followed by 33.4% of fracture are inflicted over
skull bones. Incidence of fractures were also seen in lower
limbs bones accounting for 16.6% of the total grievous
injuries. Only 1.4% fracture were observed in case of ribs. This
study showed that maximum number of injuries 98.4% with
grievous nature were covered under the clause 7 of Sec. 320
IPC involving mostly fracture of limb bones & skull bones.
Least number of injuries declared as grievous in nature were
either due to amputation of finger (0.8%), fracture tooth
(0.8%), permanent scar leading to disfiguration of face (0.4%)
and tendon injury (0.4%) leading to loss of power of member or
joint.
DISCUSSION :
In the present study it was observed that majority of cases, 89%
(445) of the victims were males and only 11% (55) were
females. Results of present study are more or less similar to the 4 studies conducted by Zargar et al (2004) , Tajammul et al
5, 6.(2005) Thube et al (2015) However, in contrast to present
study increase in trend in relation to occurrence of assault in
female victims is observed in the studies conducted by Hofner 7 8 9et al (2009) , Ranney et al (2009) , Kruise et al (2010) ,
10 11Kjaeruff et al (1989) , Fothergill and Hashemi (1990) , 12 13Chalmers et al (1995) , Wright and Kariya (1997) and Howe
14and Crilly (2002) . This can be explained by the reason that
the pattern of assault is different in developing countries like
India as compared to the western countries where the above
said studies were conducted with different cultural and
socioeconomic factors. Mostly Indian women are housewives
and more often involved at home leading to less involvement in
assault cases. It is also inferenced from the studies conducted
by above mentioned authors that male patients, in general,
25
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2021.00004.2

admitted as a result of assault related injuries were more
frequent than female suggesting that being a male is a strong
demographic risk factor. These findings can be explained by
the fact that males are, in general, more violent by nature as
compared to females and are more prone to get involved in
violence
As far as most common age group is concerned in the present
study out of total medicolegal 500 cases, young age people of
21-40 years (61%) were the most common group involved in
assault cases in this study. The cases of assault were least
common in the age group of 0-10 years with only 3 cases
(0.6%) followed by the age group of more than 70 years with 15 511 cases (2.2%). Mittal et al (2005) , Tajammul et al (2005) ,
16 17Bhullar and Aggarwal (2007) , Akdur et al (2008) , Oberoi et 18 19 20al (2012) , Rao (2014) , Trangadia et al (2014) , Thube et
6 21al(2015) and Sharma et al (2020) have observed that
maximum number of victims involved in assault are of young
age group of 21-30 years which is more or less similar with the
findings observed in the present study. This could be attributed
to the fact that young age group is the most active phase of
one's life which is more commonly involved in outdoor
activities. This phase is also characterized by aggressive and
short tempered behavior which leads to increase incidence of
assault among this age group. Another finding observed in the
study is that extremes of age group were less commonly
involved in the scuffle which is similar to the findings of most
of the authors. The possible reason for this finding could be
explained by the fact that the age group of 0-10 years is tender
and age of innocence while people of older age group are senile
and prone to chronic diseases.
As far as area wise distribution is concerned rural area
predominance with 385 cases (77%) was seen in this study as
compared to urban areas which constitutes only 115 (23%) of
the total cases. This is more or less comparable to the study 21conducted by Sharma et al (2020) .However in the study
18conducted by Oberoi et al (2012) , though rural predominance
was again seen with 57% cases and urban cases amounting to
only 43% of the total, the values of rural area predominance is
comparatively lower than the present study. The population of
Majha region were more frequently involved in assault related 26crimes as compared to Malwa region. The disparity in the
incidence of assault cases in urban and rural area can be due to
the fact that majority of population in Punjab is residing in rural
areas.
In the present study, majority of medicolegal assault cases 408
(81.6%) were from Sikh community while Hindu community
constituted only 64 cases (12.8%) further followed by
Christians with 23 (4.6%) medicolegal cases. Least number of
cases, 5 (1%) were reported from Muslim community with
20mechanical injuries. However, Trangadia et al (2014) , in
their study reported that Hindus constituted 79.6% of the total
medicolegal cases followed by Muslims who constituted, 19%
of the total. The least involved religion in this study was of
Sikhs with 0.3% of total cases. The only reason for higher
incidence of occurrence of assault among Sikhs in the present
study is due to the fact that Punjab is a Sikh majority state.
In the present study, labourers were more commonly involved
occupational group with 177 cases (35.4%) followed by
victims engaged in private jobs with 132 cases (26.4%) and
farmers with 103 medicolegal cases (20.6%). Least number of
medicolegal cases were found in student group with 38 (7.6%) 18cases only. In study conducted by Oberoi et al (2012) , same
trend was observed. The rising trend in the incidence of assault
in labourers as compared to farmers can be explained by the
fact that in recent times there has been increased employment
of migrant labourers on daily wages by the Zamindars for
farming on their lands.
In Maximum 27% (137)cases in this study were reported with
only single injury over the body and 24.8% (124) cases
reported with two injuries, closely followed by 21.4% (107)
cases who were having three injuries over the body out of the
total medicolegal cases. This is in concurrence with study 22conducted by Subba et al (2010) .
The most common type of mechanical injuries recorded
among medicolegal cases were Incised wound in 48.6% (243)
cases followed by lacerated wound in 31.4% (157) cases,
bruise in 16.4% (82) cases and abrasion in 3.2% (16) cases.
Only 0.4% (2) cases of stab wound injury were recorded in this
study. However individually, the most common type of
mechanical injury among females were bruise (24.4%) in
contrast to males where incised wound (92.5%) was the
commonly encountered injuries sustained on the body. The
present study is in contrast to the findings observed by 11Fothergill and Hashemi (1990) . Another study conducted by
23Shephard et al (1990) noted that men suffer more laceration
(45.01%) than women who on other hand had suffer more
contusions (53.3%).These findings are alike of the current 13study. Wright and Kariya (1997) in contrast to our study
reported that bruise and abrasion were the most frequently
recorded mechanical injury sustained. Another study 4conducted by Zargar et al (2004) was inconsistent with the
present study where the most common type of mechanical
injury frequently suffered by men were the penetrating trauma 22with 57.8% of total cases. Subba et al (2010) in their study
interpreted that contusion (28.7%) was the most commonest
type of injury inflicted followed by incised wound (25.7%)
which is inconsistent with the findings of present study. The
reason for incidence of this parameter could be that other
26
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2021.00004.2

studies were conducted in different geographical regions.
The present study showed that the most common site of
infliction of mechanical injuries was head and neck region of
the body with 43.7% injuries. Least number of cases were
found in chest and abdomen area with 2.5% & 1.3% injuries
respectively. These findings are more or less consistent with 24the findings of study conducted by Raj et al (2018) and
25 Chalya and Gilyoma (2012) . The proportion of head and
neck injuries in the studies conducted by Kjaeruff et al 10 12 13(1989) , Chalmers et al(1995) , Wright and Kariya (1997) ,
17 18Akdur et al (2008) and Oberoi et al (2012) was higher as
compared to the present study. The reason for higher incidence
of involvement of head in above mentioned studies including
the present study could be the head being the presenting part of
the body is more prone to violence as assailant knows that it is
the most vital part of human system which could cause severe
damage to his enemy. Upper limb involvement is higher in the 16studies conducted by Bhullar and Aggarwal (2007) , Chalya
25 19and Gilyoma (2012) and Rao (2014) in contrast to the
present study with only 30.2% injuries on the upper limbs. The
possible reason for this variation could be due to difference in
the socio-demographic profile
As far as weapon of offence for inflicting mechanical injury is
concerned, the most common weapon used was blunt,
inflicting 63.4% injuries followed by sharp edged weapons
inflicting 35.2% injuries. In this study, least number of injuries
1.3% were inflicted by sharp pointed weapon. These findings
are more or less comparable with the study conducted by 18Oberoi et al (2012) These values were more or less raised in
14the studies conducted by Howe and Crilly (2002) , Zargar et 4 15 19al (2004) , Mittal et al (2005) , Rao (2014) , Thube HR et al
6(2015) , which are more or less comparable with the present
study. The most probable reason for the use of blunt weapon in
infliction of injuries is due to easy availability of the weapon.
As far as nature of mechanical injuries is concerned in majority
of cases, 79.8% injuries were declared as simple in nature
followed by 17.1% injuries, which were declared as grievous
in nature. Only one injury was declared dangerous to life in this
study. The present study also showed that majority of simple in
nature injuries were predominantly inflicted by blunt weapon
with 67.6% simple injuries followed by those inflicted with
sharp edged weapons with 30.9% injuries out of total 1088
injuries. However on the other hand reverse trend was seen in
injuries with grievous nature where the most common weapon
of offence for inflicting injuries with grievous hurt was sharp
edged weapon with 55.5% injuries followed by injuries
inflicted with blunt weapon with 44.5% injuries out of total 234
grievous injuries in 135 victims. These findings are in line with 16the studies conducted by Bhullar and Aggarwal (2007) .
However in this study the incidence of injury being declared as
Dangerous to life was on higher trend contributing to 3% of the 6total injuries. Another study conducted by Thube et al (2015)
was in concurrence with the present study where the 73%
injuries were declared as simple in nature and 24.7% injuries
were declared as Grievous in nature and no injury was declared
Dangerous to life. This trend in regard to grievous hurt was on
higher side as compared to the present study. The findings of 21the study of Sharma et al (2020) were in slight variance with
the present study In this study also no injury was declared
dangerous to life. This variation could be because of difference
in regional conditions that is political, social as well as other
law and order problems.
Out of the total fractures encountered in the present study,
46.2% fractures were of upper limb bones followed by fracture
of skull bones and lower limb bones which were 33.4% and
16.6% respectively. These findings were more or less similar to 6the study conducted by Thube et al (2015) . This could be
explained by the fact that the limbs are the most common site of
defense injuries during a scuffle.
CONCLUSION :
The present study was conducted with the aim to evaluate socio
demographic distribution of mechanical injuries in assault
cases. Since the assault related injury cases were higher among
males, in the young age group and in a rural population so for
prevention of assault related activities the main focus should be
on encouraging the young age group the concept of tolerance
and rationalism. The casualty & emergency department of any
hospital not only caters to the needs of the patients who reports
in emergencies but also carry out important legal
responsibilities to examine, document and certify medico legal
cases, which puts a lot of burden on casualty department. Also
the doctors who are involved in handling medico legal cases
need to be more trained regarding various aspects of
mechanical injuries. Due to increase in violence Law should be
suitably amended to punish those involved in self-harm against
the spirit of the constitution.
Funding : None
Ethical clearance : From the institutional ethical committee ,
Govt. Medical College , Amritsar
Conflict of interest : None
REFERENCES :
1. Reddy NK, Murty OP. Mechanical Injuries. The
Essentials of Forensic Medicine and Toxicology. 34th
edition. Jaypee Brothers Medical Publishers; 2014, pp.
170-97.
2. Law Publishers (India) Pvt. Ltd. The Indian Penal
Code,1860 (Act no. 45 OF 1860); 2005, pp.11.
27
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2021.00004.2
3. Law Publishers (India) Pvt. Ltd. The Indian Penal
Code,1860 (Act no. 45 OF 1860); 2005, pp.199.
4. Zargar M, Karbakhsh M, Zareei M, Moez AK. Patterns of
assault: experience from an urban hospital-based study in
a developing country. Mjih. 2004;6(2):50–4.
5. Tajammul N, Chaudhry TH, Hanif S, Bhatti MA. Profile
of Medicolegal Cases At Jinnah Hospital Lahore. Annals
Kemu 2005;11(3):1-5.
6. Thube HR, Chikhalkar BG, Nanandkar SD. A
Prospective Study Of Injury Pattern In Victim Of Assault
Attended In South Mumbai Government Hospital. J
Indian Acad Forensic Med. 2015;37(1):37-40.
7. Hofner MC, Burquier R, Huissoud T, Romain N, Graz B,
Mangin P. Characteristics Of Victims Of Violence
Admitted To A Specialized Medico-Legal Unit In
Switzerland. Journal Of Forensic And Legal Medicine.
2009;16(5):269–72.
8. Ranney ML, Odero W, Mello MJ, Waxman M, Fife RS.
Injuries From Interpersonal Violence Presenting To A
Rural Health Center In Western Kenya: Characteristics
And Correlates. Inj Prev. 2009;15(1):36–40.
9. Kruse M, Sørensen J, Brønnum-Hansen H, Helweg-
Larsen K. Identifying Victims of Violence Using Register-
Based Data. Scandinavian Journal of Public Health.
2010;38:611–7.
10. Kjaerulff H, Jacobsen J, Aalund O, Albrektsen SB,
Breiting VB, Danielsen L, Helweg-Larsen K, Staugaard
H, Thomsen Jl. Injuries Due To Deliberate Violence In
Areas Of Denmark. Iii. Lesions. The Copenhagen Study
Group. Forensic Sci Int. 1989;41(1-2):169-80.
11. Fothergill NJ, Hashemi K. A Prospective Study of Assault
Victims Attending A Suburban A & E Department. Arch
Emerg Med. 1990;7(3):172–7.
12. Chalmers DJ, Fanslow JL, Langley JD. Injury From
Assault In New Zealand: An Increasing Public Health
Problem. Aust J Public Health. 1995;19(2):149–54.
13. Wright J, Kariya A. Assault Patients Attending A Scottish
Accident And Emergency Department. J R Soc Med.
1997;90(6):322–6.
14. Howe A, Crilly M. Identification and Characteristics of
Victims of Violence Identified by Emergency Physicians,
Triage Nurses, and The Police. Inj Prev. 2002;8(4):321–3.
15. Mittal S, Chanana A, Rai H, Dalal JS. Medicolegal study
of mechanical injuries in culpable homicides (excluding
deaths due to rash and negligent act). Journal of Indian
Academy of Forensic Medicine. 2005;27(4):226-30.
16. Bhullar DS, Aggarwal KK. Medico Legal Diagnosis &
Pattern of injuries with sharp weapons. Journal of Indian
Academy of Forensic Medicine. 2007;29(4):112-4.
17. Akdur O, Durukan P, Ozkan S, Avsarogullari L, Salt O,
Ikizceli I. Interpersonal Violence Related Injuries In
Central Anatolia, Turkey. The Internet Journal Of
Emergency Medicine 2008;6(1):1-3.
18. Oberoi SS, Aggarwal KK, Bhullar DS, Aggarwal A,
Walia DS, Singh S. Profile Of Assault Cases In Patiala.
Journal Of Punjab Academy Of Forensic Medicine And
Toxicology. 2012;12:17–21.
19. Rao D. A study of pattern of non fatal injuries due to
assault. Journal of Punjab Academy of Forensic Medicine
& Toxicology. 2014;14(2):82-5.
20. Trangadia M, Mehta R, Rada N, Gupta B. Profile Of
Medico-Legal Cases In Tertiary Care Hospital In
Jamnagar, Gujarat: Retrospective Study Of One Year. J
Res Med Den Sci. 2014;2(4):57–62.
21. Sharma A, Tellewar S, Gupta B, Singh V, Singh G. A One
Year Epidemiological Study of Mechanical Injury Cases
Brought To Sims Hospital, Western Uttar Pradesh. Indian
Journal of Forensic Medicine & Toxicology. 2020 Jan
16;14(1):1–4.
22. Subba SH, Binu VS, Menezes RG, Kumar V, Rana MS.
Physical Assault Related Injuries In Western Nepal – A
Hospital Based Retrospective Study.Journal of Forensic
And Legal Medicine. 2010 May 1;17(4):203–8.
23. Shepherd JP, Shapland M, Pearce NX, Scully C. Pattern,
Severity And Aetiology Of Injuries In Victims Of
Assault. J R Soc Med. 1990;83(2):75–8.
24. Raj D, Kumar V, Venkatesha V, Pawar G, Maddileti B.
Pattern Of Injuries In Homicidal Victims In South
Bangalore. Journal Of Indian Academy Of Forensic
Medicine. 2018;40:392.
25. Chalya Pl, vGilyoma Jm. The Burden of Intentional
Injuries In Mwanza City, North-Western Tanzania: A
Tertiary Hospital Survey. Tanzan J Health Res.
2012;14(3):204–11.
26. Crime Statistics of Punjab. 2013. Available from:
http://www.neighbourhoodinfo.co.in/crime/Punjab
28
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2021.00004.2

Original Research Paper
Corresponding Author :
Dr. Amandeep Singh,
Professor,
Department of Forensic Medicine & Toxicology, Government
Medical College & Hospital, Chandigarh Karnataka – 570015
Contact : +91 96461-21610
Email: [email protected]
KEYWORDS : Hanging, Ligature material, Ligature mark, Complete hanging, Hyoid bone.
Article History:Received: 23 September 2020Received in revised form: 23 December 2020Accepted on: 23 March 2021Available online: 15 August 2021
INTRODUCTION:
Suicide is the deliberate act of taking one's own life. It is the
result of the complex interaction of biological, genetic, 1psychological, sociological and environmental factors. In
India, deaths because of hanging is one of the common ways of
committing suicide in conjunction with poisoning, burning 2and drowning. Among the asphyxia death encountered in day
to day practice by forensic expert hanging is one of the 3commonest. Hanging is a form of ligature strangulation in
which the force applied to the neck is derived from the 4gravitational drag of the weight of the body or part of the body.
Almost all hanging deaths are suicidal, accidental hangings are
uncommon and homicidal hanging is rare. In homicidal cases
it is seen that a victim is killed and after that dead body is
suspended to avert the suspicion. While giving the final
opinion regarding the antemortem hanging, it is necessary to
give special attention to the details of the place of incidence,
the posture of the body and the manner in which the clothes are disarranged, etc. in addition to routine finding.Although most
of the cases are suicidal, they always cause suspicion among
relatives and the investigating officers, as well as at times, to
5the autopsy surgeon.
The term typical hanging means when the point of suspension
is placed centrally over the occiput i.e. the knot is at the nape of
neck on the back. The term atypical hanging is often applied if
the point of suspension is at any other position. Complete
hanging means when the feet do not touch the ground or any
other material so that the body is completely suspended; the
constricting force here is the weight of the entire body.
Whereas if any part of the body touches the ground or any other
material the term used is incomplete or partial hanging e.g.
hanging in a sitting, kneeling or even lying position. Here only 6a part of the body weight acts as the constricting force. The
ligature mark is usually situated above the thyroid cartilage
and going obliquely upwards following the line of mandible
and it may be interrupted due to presence of knot. In some
cases, like partial hanging the ligature mark may be present at
the thyroid cartilage or below it. The ligature mark is like a
groove, its base is pale, hard, and leathery and parchment like.
The ligature mark is deepest at the place opposite to the knot
and the colour of the ligature mark is usually reddish brown .7
In this study we analyzed death due to hanging occurring in
ABSTRACT:
Objective: The objective of this study was to analyze hanging deaths occurring in Punjab, Haryana, Chandigarh in relation to
several factors associated with such deaths.
Materials and Methods: This study was performed on 50 cases of hanging deaths brought for an autopsy to the mortuary of
Government Medical College, Chandigarh. Factors associated with these deaths and post-mortem findings were recorded and
statistically analyzed.
Results: It was observed that the most vulnerable age group was 20 - 29 years. Among all the victims, 54% were married; 70% of the
victims were from urban area. In 30% cases motive of hanging was not known. 92% of suicides by hanging occurred indoors and
most of the incidence occurred at evening time, in 56% cases. Complete hanging was found in 68% cases and partial hanging in 32%
cases. The commonly used ligature materials were means which were easily available to the victim viz. dupatta, nylon rope, saree
etc. and in 68% cases ligature mark were above the level of thyroid cartilage. Fracture of Hyoid bone was found in 6% cases.
Conclusion: The findings of the present study will help in highlighting the prevailing scenario of hanging deaths in this region.
1. Prasenjit Das, PG JR 3years*
2. Amandeep Singh, Professor*
3. Dasari Harish, Professor & Head*
*Department of Forensic Medicine & Toxicology, Government Medical College & Hospital, Chandigarh
Multifactorial Analysis of Deaths Due To Hanging
29
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00005.4
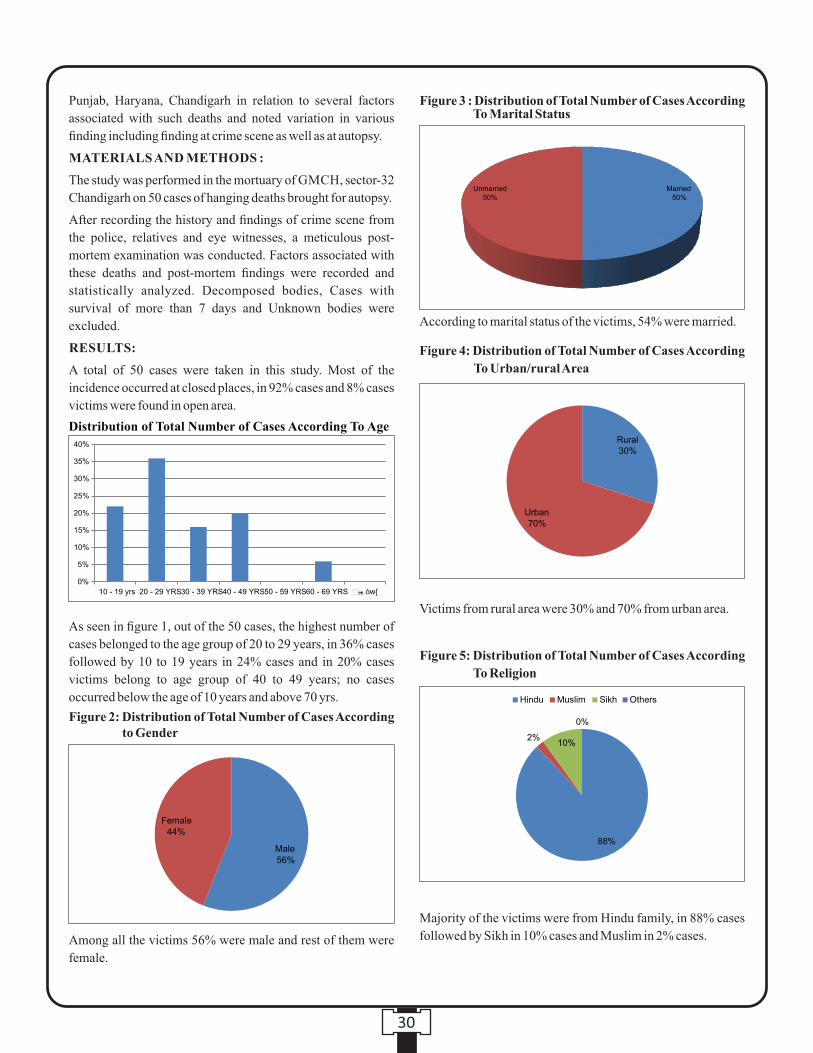
Punjab, Haryana, Chandigarh in relation to several factors
associated with such deaths and noted variation in various
finding including finding at crime scene as well as at autopsy.
MATERIALS AND METHODS :
The study was performed in the mortuary of GMCH, sector-32
Chandigarh on 50 cases of hanging deaths brought for autopsy.
After recording the history and findings of crime scene from
the police, relatives and eye witnesses, a meticulous post-
mortem examination was conducted. Factors associated with
these deaths and post-mortem findings were recorded and
statistically analyzed. Decomposed bodies, Cases with
survival of more than 7 days and Unknown bodies were
excluded.
RESULTS:
A total of 50 cases were taken in this study. Most of the
incidence occurred at closed places, in 92% cases and 8% cases
victims were found in open area.
As seen in figure 1, out of the 50 cases, the highest number of
cases belonged to the age group of 20 to 29 years, in 36% cases
followed by 10 to 19 years in 24% cases and in 20% cases
victims belong to age group of 40 to 49 years; no cases
occurred below the age of 10 years and above 70 yrs.
Among all the victims 56% were male and rest of them were
female.
According to marital status of the victims, 54% were married.
Victims from rural area were 30% and 70% from urban area.
Majority of the victims were from Hindu family, in 88% cases
followed by Sikh in 10% cases and Muslim in 2% cases.
30
Distribution of Total Number of Cases According To Age
Figure 2: Distribution of Total Number of Cases According to Gender
Figure 4: Distribution of Total Number of Cases According
To Urban/rural Area
Figure 5: Distribution of Total Number of Cases According
To Religion
Figure 3 : Distribution of Total Number of Cases According To Marital Status

Figure 7 : Occupation Wise Distribution of Total Number of Cases
Figure 6 : Distribution of Cases According To Type of Family
Most of the time cause was not known, among the known
causes 26% cases mental illness is one of the leading cause
followed by marital disharmony in 20% cases, love failure in
10% cases and in 4% cases exam failure.
Dupatta was the commonest ligature material used by the
victims in 58% cases followed by nylon rope in 12% cases, in
22% cases others soft material like dhoti, saree were used. In
2% cases belt and in another 2% cases electric wire were used
among others hard ligature materials.
As per the placement of ligature mark, in 68% cases ligature
mark was present above the level of thyroid cartilage followed
by overriding the thyroid cartilage in 28% cases and in 4%
cases it was present below the level of thyroid cartilage.
In 58% cases victims were from joint family and 42% cases
victims were the member of nuclear family.
Among the victims 24% were housewives followed by 16%
were self employed, 14% were student and 12% were laborers.
Most of the incidence occcur during evening time (12 PM to 8
PM), in 56% cases followed by morning (4 AM to 12 AM) in
30% cases and in 14% cases were recorded during night(8 PM
to 4 AM) time.
31
Figure 8 : Distribution of Total Number of Cases According To Time of Incidence
Figure 9 : Motive of Hanging
Figure 10: Distribution of Total Number of Cases
According To Type of Ligature Material
Figure 11: Distribution of Total Number of Cases
According To Placement of Ligature Mark
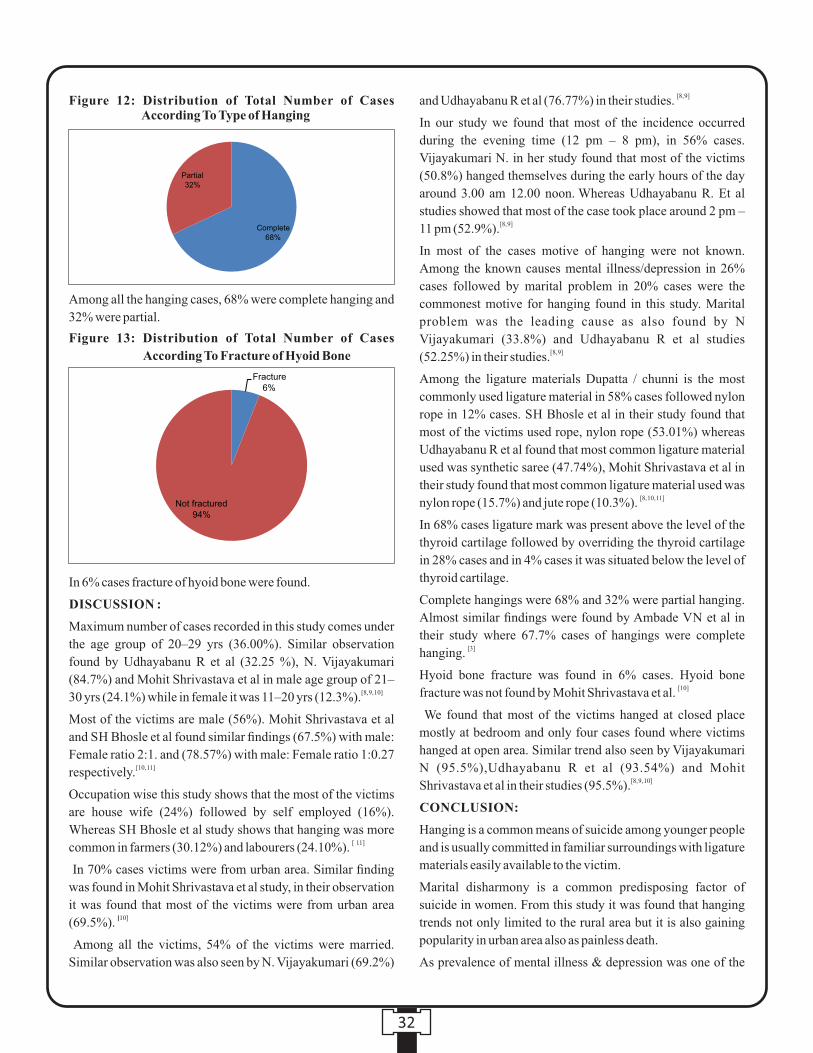
[8, 9]and Udhayabanu R et al (76.77%) in their studies.
In our study we found that most of the incidence occurred
during the evening time (12 pm – 8 pm), in 56% cases.
Vijayakumari N. in her study found that most of the victims
(50.8%) hanged themselves during the early hours of the day around 3.00 am 12.00 noon. Whereas Udhayabanu R. Et al
studies showed that most of the case took place around 2 pm – [8, 9]11 pm (52.9%).
In most of the cases motive of hanging were not known.
Among the known causes mental illness/depression in 26%
cases followed by marital problem in 20% cases were the
commonest motive for hanging found in this study. Marital
problem was the leading cause as also found by N
Vijayakumari (33.8%) and Udhayabanu R et al studies [8, 9](52.25%) in their studies.
Among the ligature materials Dupatta / chunni is the most
commonly used ligature material in 58% cases followed nylon
rope in 12% cases. SH Bhosle et al in their study found that
most of the victims used rope, nylon rope (53.01%) whereas
Udhayabanu R et al found that most common ligature material
used was synthetic saree (47.74%), Mohit Shrivastava et al in
their study found that most common ligature material used was [8, 10, 11]nylon rope (15.7%) and jute rope (10.3%).
In 68% cases ligature mark was present above the level of the
thyroid cartilage followed by overriding the thyroid cartilage
in 28% cases and in 4% cases it was situated below the level of
thyroid cartilage.
Complete hangings were 68% and 32% were partial hanging.
Almost similar findings were found by Ambade VN et al in
their study where 67.7% cases of hangings were complete [3]hanging.
Hyoid bone fracture was found in 6% cases. Hyoid bone [10]fracture was not found by Mohit Shrivastava et al.
We found that most of the victims hanged at closed place
mostly at bedroom and only four cases found where victims
hanged at open area. Similar trend also seen by Vijayakumari
N (95.5%),Udhayabanu R et al (93.54%) and Mohit [8, 9, 10]Shrivastava et al in their studies (95.5%).
CONCLUSION:
Hanging is a common means of suicide among younger people
and is usually committed in familiar surroundings with ligature
materials easily available to the victim.
Marital disharmony is a common predisposing factor of
suicide in women. From this study it was found that hanging
trends not only limited to the rural area but it is also gaining
popularity in urban area also as painless death.
As prevalence of mental illness & depression was one of the
Among all the hanging cases, 68% were complete hanging and
32% were partial.
In 6% cases fracture of hyoid bone were found.
DISCUSSION :
Maximum number of cases recorded in this study comes under
the age group of 20–29 yrs (36.00%). Similar observation
found by Udhayabanu R et al (32.25 %), N. Vijayakumari
(84.7%) and Mohit Shrivastava et al in male age group of 21– [8, 9, 10]30 yrs (24.1%) while in female it was 11–20 yrs (12.3%).
Most of the victims are male (56%). Mohit Shrivastava et al
and SH Bhosle et al found similar findings (67.5%) with male:
Female ratio 2:1. and (78.57%) with male: Female ratio 1:0.27 [10, 11]respectively.
Occupation wise this study shows that the most of the victims
are house wife (24%) followed by self employed (16%).
Whereas SH Bhosle et al study shows that hanging was more [ 11]common in farmers (30.12%) and labourers (24.10%).
In 70% cases victims were from urban area. Similar finding
was found in Mohit Shrivastava et al study, in their observation
it was found that most of the victims were from urban area [10](69.5%).
Among all the victims, 54% of the victims were married.
Similar observation was also seen by N. Vijayakumari (69.2%)
32
Figure 12: Distribution of Total Number of Cases According To Type of Hanging
Figure 13: Distribution of Total Number of Cases
According To Fracture of Hyoid Bone

common factors seen in such cases, proper counseling and
timely treatment of vulnerable populations with such risk
factors for suicide is one of the important ways of prevention of
such incidents.
Mostly preferable places chosen by the victims were closed
places especially at their home, thus patients having suicidal
tendencies should not be left alone unattended even at their
home.
REFERENCES :
1. Rane A, Nadkarni A. Suicide in India: a systemic
review. Shanghai Arch Psychiatry. 2014; 26(2):69-80.
2. Ambade VN, Keoliya AN, Wankhede AG. Availability
of means of suicides. Int J Med Toxicol Leg Med. 2012;
14(3):83-89.
3. Ambade VN, Tumran N, Meshram S, Borkar J. Ligature
material in hanging deaths: The neglected area in forensic
examination. Egypt J Forensic Sci. 2015; 5(3):109-113.
4. Saukko P and Knight B. Knight's forensic pathology. 3rd
ed. London: Edward Arnold, 2004: pp 319-331
5. Dimaio VJ, Dimaio D. Forensic pathology. 2nd ed. Boca
Raton: CRC Press; 2001: p 258-75.
6. Krishan V. Textbook of Forensic Medicine and thToxicology. 5 edition. Gurgaon. Elsevier; 2011:p120-9.
7. Sharma RK. Concise Textbook of Forensic medicine and r d Toxicology. 3 Edn. Noida. Global Education
Consultants; 2011:p55-6.
8. Udhayabanu R, Senti Toshi, Baskar R. Study of hanging
cases in Pondicherry Region. IOSR Journal of Dental and
Medical Sciences (IOSR-JDMS). 2015; 4(7):41-44
9. Vijayakumari N. Suicidal hanging: a prospective study. J
Indian Acad Forensic Med. 2011; 33(4):353- 355
10. Mohit Shrivastava, P.S. Thakur, Devesh Pateria, B.K.
Singh, Sunil K. Soni. Autopsy based on one year
prospective study of deaths due to hanging. Indian Journal
of Forensic and Community Medicine. 2018;5(4):240-
244
11. Dr. SH Bhosle, Dr. AK Batra, Dr. SV Kuchewar. Violent
asphyxia deaths due to hanging: A prospective study. J
Forensic Med Sci Law. 2014; 23(1):1-8
33

Original Research Paper
Corresponding Author :
Dr. Amandeep Singh,
Professor,
Department of Forensic Medicine & Toxicology, Government
Medical College & Hospital, Chandigarh Karnataka – 570015
Contact : +91 96461-21610
Email: [email protected]
KEYWORDS : Fetus, Age Estimation, Gestational Age, Anthropology, Radiology
Article History:Received: 16 April 2021Received in revised form: 16 May 2021 Accepted on: 18 May 2021Available online: 15 August 2021
INTRODUCTION :
Identification is the determination of the individuality or
personality of a person based on certain physical 1characteristics . Various components in combination help in
identifying individual dead or alive; of which age forms an
important component. Age can be determined from teeth,
ossification of bones, secondary sex characters and general
development, in case of children. Accurate age estimation of
dead fetuses can be very important to medicolegal authorities,
particularly to determine if it is a full-term neonate or a pre-
term fetus. It is often the only means of identification for
fetuses and neonates since they do not usually have any other 2,3type of identification with them. Determination of fetal age,
specifically if the fetus reached full-term, can have legal 4importance in forensic cases, particularly whether the baby
5was liveborn or stillborn is significant . In cases of criminal
abortion or infanticide, the age of the fetus is integral to the
prosecution. Fetal age estimation is still a difficult task as the
soft tissue of fetal remains are often so deteriorated that
accurate estimations of size and age can only be made after 6they are processed into clean, dry bones.
Foetal age estimation can be done by foetal biometry which is
measurement of several parts of foetal anatomy and their
growth. Foetal measurements include biparietal diameter,
crown -rump length, crown-heel length, foot length, hand
length ,abdominal circumference, chest circumference, head
circumference, intercanthal distance, outer canthal distance,
philtrum, arm length, thigh length etc. The two main criteria
used for fetal age estimation are dental mineralization and
skeletal data, such as long bone diaphyseal length. Although
dental age is more reliable than skeletal age, in many forensic
instances, the human remains do not include dentition thus
diaphyseal length evaluation becomes important for the 7purpose of age evaluation.
A study on use of radial diaphyseal length in estimating fetal
body length showed that measurements from the radius
ABSTRACT :
Introduction: The estimation of gestational age (GA) of fetal remains can be an important forensic issue. Forensic specialists
usually use reference tables and regression equations derived from reference collections, which are quite rare, when fetuses are
concerned. There is a strong correlation between the longitudinal length of studied bones and GA.
Aims and objectives: This study is aimed at estimation of the age of the dead fetuses in Indian population on the basis of diaphyseal
bone length measurements (femur and humerus) of 25 fetuses of known GA, measured ultrasonographically, using radiographs
along with measurements done anthropologically, after dissection of foetal long bones.
Methods: The regression equation for the humerus and the femur bone were GA = MX + C. Here, GA is the gestational Age, X is
the length of the long bone in mm, M is the regression curve and C is the constant.
Results: The anthropological/ radiological GA coincided with ultrasonographic GA in 11 cases (44%) and with an error of ±
1week. GA of all the 25 cases lay within 95% confidence interval limit by both radiological and anthropological methods.
Conclusion: It was concluded on analysis that radiological measurements are less significant as compared to anthropological
measurements of both humerus and femur bones.
1. Piyush Sandhu, PG JR III*
2. Amandeep Singh, Professor*
3. Dasari Harish, Profesor & Head, Department of Forensic Medicine & Toxicology*
4. Mahesh Sharma, Professor, Department of Anatomy*
*Government Medical College & Hospital, Chandigarh
Age Estimation of Dead Foetus from Anthropology, Radiology of Femur & Humerus Bone
34
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00006.6
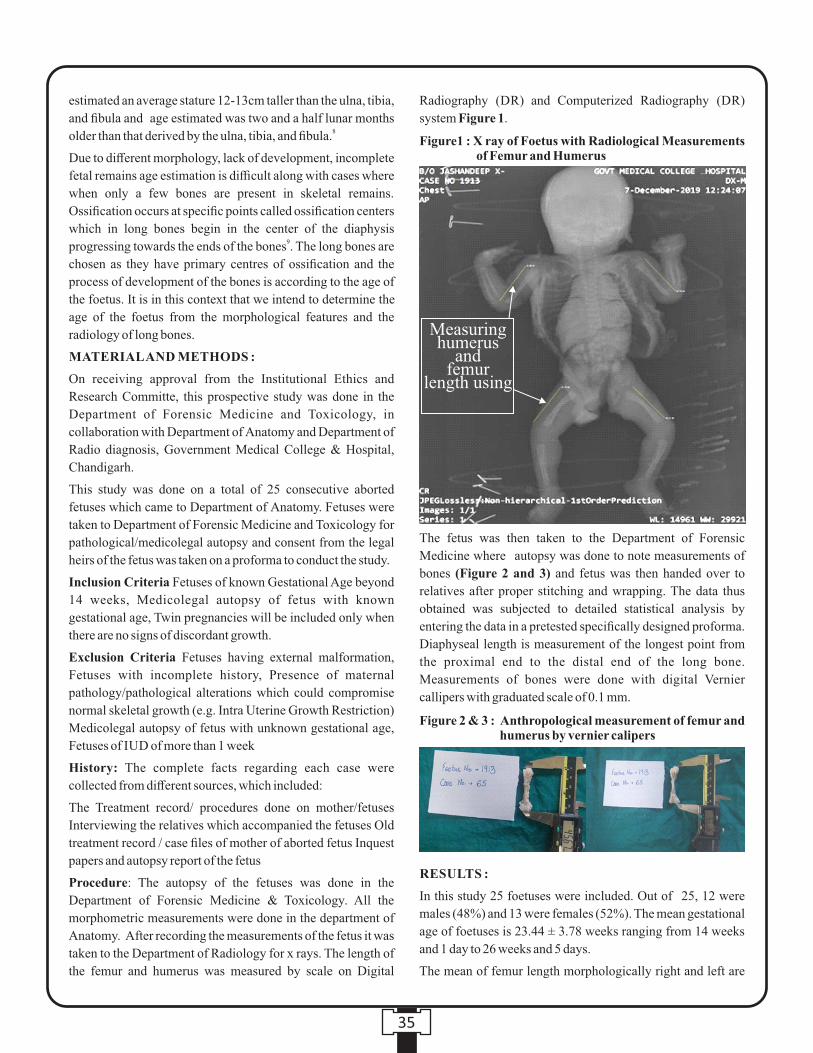
estimated an average stature 12-13cm taller than the ulna, tibia,
and fibula and age estimated was two and a half lunar months 8older than that derived by the ulna, tibia, and fibula.
Due to different morphology, lack of development, incomplete
fetal remains age estimation is difficult along with cases where
when only a few bones are present in skeletal remains.
Ossification occurs at specific points called ossification centers
which in long bones begin in the center of the diaphysis 9progressing towards the ends of the bones . The long bones are
chosen as they have primary centres of ossification and the
process of development of the bones is according to the age of
the foetus. It is in this context that we intend to determine the
age of the foetus from the morphological features and the
radiology of long bones.
MATERIAL AND METHODS :
On receiving approval from the Institutional Ethics and
Research Committe, this prospective study was done in the
Department of Forensic Medicine and Toxicology, in
collaboration with Department of Anatomy and Department of
Radio diagnosis, Government Medical College & Hospital,
Chandigarh.
This study was done on a total of 25 consecutive aborted
fetuses which came to Department of Anatomy. Fetuses were
taken to Department of Forensic Medicine and Toxicology for
pathological/medicolegal autopsy and consent from the legal
heirs of the fetus was taken on a proforma to conduct the study.
Inclusion Criteria Fetuses of known Gestational Age beyond
14 weeks, Medicolegal autopsy of fetus with known
gestational age, Twin pregnancies will be included only when
there are no signs of discordant growth.
Exclusion Criteria Fetuses having external malformation,
Fetuses with incomplete history, Presence of maternal
pathology/pathological alterations which could compromise
normal skeletal growth (e.g. Intra Uterine Growth Restriction)
Medicolegal autopsy of fetus with unknown gestational age,
Fetuses of IUD of more than 1 week
History: The complete facts regarding each case were
collected from different sources, which included:
The Treatment record/ procedures done on mother/fetuses
Interviewing the relatives which accompanied the fetuses Old
treatment record / case files of mother of aborted fetus Inquest
papers and autopsy report of the fetus
Procedure: The autopsy of the fetuses was done in the
Department of Forensic Medicine & Toxicology. All the
morphometric measurements were done in the department of
Anatomy. After recording the measurements of the fetus it was
taken to the Department of Radiology for x rays. The length of
the femur and humerus was measured by scale on Digital
Radiography (DR) and Computerized Radiography (DR)
system Figure 1.
The fetus was then taken to the Department of Forensic
Medicine where autopsy was done to note measurements of
bones (Figure 2 and 3) and fetus was then handed over to
relatives after proper stitching and wrapping. The data thus
obtained was subjected to detailed statistical analysis by
entering the data in a pretested specifically designed proforma.
Diaphyseal length is measurement of the longest point from
the proximal end to the distal end of the long bone.
Measurements of bones were done with digital Vernier
callipers with graduated scale of 0.1 mm.
RESULTS :
In this study 25 foetuses were included. Out of 25, 12 were
males (48%) and 13 were females (52%). The mean gestational
age of foetuses is 23.44 ± 3.78 weeks ranging from 14 weeks
and 1 day to 26 weeks and 5 days.
The mean of femur length morphologically right and left are
35
Figure1 : X ray of Foetus with Radiological Measurements of Femur and Humerus
Measuring humerus
andfemur
length using
Figure 2 & 3 : Anthropological measurement of femur and humerus by vernier calipers

of ± 4 weeks in 1 cases (4 %), difference of >± 4 weeks in 4 case
(16 %).
Formula was applied to each of the cases and it was observed
that predicted gestational age was comparable with known
gestational age in 11 cases with difference of ± 1 week (44 %
cases), difference of ±2 weeks was observed in 8 cases (32%),
and difference of ±3 weeks was seen in 1 case (4 %), difference
of ± 4 weeks in 1 cases (4 %), difference of >± 4 weeks in 4
case (16 %)
DISCUSSION :
In our study, the sample size was 25 (Table 1). In some studies
like by Trotter M et al, Mehta L et al and Scheuer JL et al, the 10,13,14sample size was less than 100, while in other studies like
by that by Quinlan RW et al, Goldstein RB et al, and others, it 15-19was more than 100.
25The study by Carneiro et al on Portuguese population
involved greater number of cases (100) as our study (25), while
also recruiting nearly larger number of male and female
foetuses, (55 male,45 females in comparison to 12 male,13
female in our study) as our study. The foetal osteometry by
radiography yielded performed by them yielded comparable
results to our study i.e. femur length as a reliable indicator of
gestational age, besides involving same inclusion and
exclusion criteria as our study. The mean age at death is 23.44
weeks (SD = 3.78) in Portuguese study in comparison to 21.42
± 3.77 weeks in our study. (Table 1)
In our study, the gestational age of samples ranged from 14
weeks and 1 day to 26 weeks and 5 days, while studies by
Goldstein et al, Jeanty et al, Hadlock et al and Bareggi et al
included fetuses of gestational age ranging from 14 to 36
weeks, 12 to 40 weeks, 14 to 22 weeks and 4 lunar months to 16-19,23newborns, respectively. (Table 1)
In consonance with our methodology, studies by Scheuer JL et
43.65 ± 14.5 mm (21-63.49) and 43.51 ± 14.60 mm (21-63.5)
respectively. The mean of femur length radiologically right
and left are 25.50 ± 10.90 (2.2-42.7) and 25.86 ± 10.98mm (2-
43) respectively as shown in Table1.
The mean of humerus length morphologically right and left are
39.26±12.44 (20-56.70) and 39.39±12.42 (20-56.71)
respectively. The mean of humerus length radiologically right
and left are 26.33±12.33 (3.4-44.9) and 26.60±12.19 (3.4-
44.9) respectively as shown in Table 2.
Anthropological gestational age for male and female fetuses
showed significant positive correlation with gestational age (p
value less than 0.05), as depicted in Table 3.
All regression formulae for radiological and anthropological
lengths of bones were derived in terms of y=mx + c where y is
derived gestational age, m is slope or gradient, m is variable or
bone length and c is constant. Value of m and c for regression
formulae based on anthropological and radiological lengths of
femur and humerus are shown in Table 4.
Formula was applied to each of the cases and it was observed
that predicted gestational age was comparable with known
gestational age in 11 cases with difference of ± 1 week (44 %
cases), difference of ±2 weeks was observed in 8 cases (32%),
and difference of ±3 weeks was seen in 1 case (4 %), difference
36
Pearson CoeffP Value
.530
.042.541.037
.536
.040.553.033
.701
.004.685.005
.676
.006.689.004
Table 3: Correlation analysis
Femur Length Humerus Length Femur Length Humerus Length
Radiological Radiological Morphological Morphological
Femur Length Morphological Right
Femur Length Morphological Left
Femur Length Radiological Right
Femur Length Radiological Left
Humerus Length Morphological Right
Humerus Length Morphological Left
Humerus Length Radiological Right
Humerus Length Radiological Left
.183
.177
.184
.187
.205
.210
.164
.172
13.459
13.718
16.746
16.616
13.375
13.167
17.113
16.877
Table 4: Regression formulae
Table 1: Statistical mean, standard deviation, range of anthropological and radiological parameters of femur
Mean
SD
Min
Max
Weeks
23.4381
3.78214
14.14
26.71
Right
43.6520
14.4958
21.00
63.49
Left
43.506
14.6066
21.0
63.5
Right
25.494
10.8927
2.2
42.7
Left
25.86
10.977
2
43
Morphological Radiological
Mean
SD
Min
Max
Right
39.258
12.4432
20.0
56.7
Left
39.3893
12.41549
20.00
56.71
Right
26.325
12.3339
3.4
44.9
Left
26.594
12.1899
3.4
44.9
Morphological Radiological
Table 2: Statistical mean, standard deviation, range of anthropological and radiological parameters of humerus
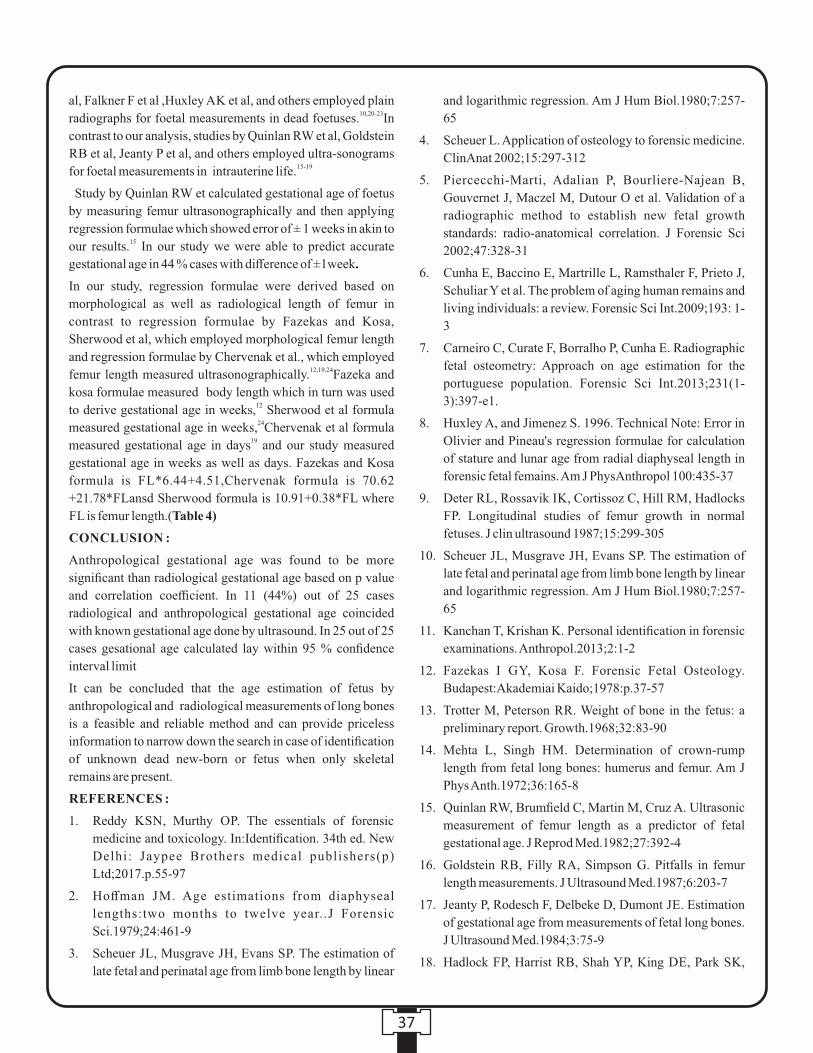
and logarithmic regression. Am J Hum Biol.1980;7:257-
65
4. Scheuer L. Application of osteology to forensic medicine.
ClinAnat 2002;15:297-312
5. Piercecchi-Marti, Adalian P, Bourliere-Najean B,
Gouvernet J, Maczel M, Dutour O et al. Validation of a
radiographic method to establish new fetal growth
standards: radio-anatomical correlation. J Forensic Sci
2002;47:328-31
6. Cunha E, Baccino E, Martrille L, Ramsthaler F, Prieto J,
Schuliar Y et al. The problem of aging human remains and
living individuals: a review. Forensic Sci Int.2009;193: 1-
3
7. Carneiro C, Curate F, Borralho P, Cunha E. Radiographic
fetal osteometry: Approach on age estimation for the
portuguese population. Forensic Sci Int.2013;231(1-
3):397-e1.
8. Huxley A, and Jimenez S. 1996. Technical Note: Error in
Olivier and Pineau's regression formulae for calculation
of stature and lunar age from radial diaphyseal length in
forensic fetal femains. Am J PhysAnthropol 100:435-37
9. Deter RL, Rossavik IK, Cortissoz C, Hill RM, Hadlocks
FP. Longitudinal studies of femur growth in normal
fetuses. J clin ultrasound 1987;15:299-305
10. Scheuer JL, Musgrave JH, Evans SP. The estimation of
late fetal and perinatal age from limb bone length by linear
and logarithmic regression. Am J Hum Biol.1980;7:257-
65
11. Kanchan T, Krishan K. Personal identification in forensic
examinations. Anthropol.2013;2:1-2
12. Fazekas I GY, Kosa F. Forensic Fetal Osteology.
Budapest:Akademiai Kaido;1978:p.37-57
13. Trotter M, Peterson RR. Weight of bone in the fetus: a
preliminary report. Growth.1968;32:83-90
14. Mehta L, Singh HM. Determination of crown-rump
length from fetal long bones: humerus and femur. Am J
Phys Anth.1972;36:165-8
15. Quinlan RW, Brumfield C, Martin M, Cruz A. Ultrasonic
measurement of femur length as a predictor of fetal
gestational age. J Reprod Med.1982;27:392-4
16. Goldstein RB, Filly RA, Simpson G. Pitfalls in femur
length measurements. J Ultrasound Med.1987;6:203-7
17. Jeanty P, Rodesch F, Delbeke D, Dumont JE. Estimation
of gestational age from measurements of fetal long bones.
J Ultrasound Med.1984;3:75-9
18. Hadlock FP, Harrist RB, Shah YP, King DE, Park SK,
al, Falkner F et al ,Huxley AK et al, and others employed plain 10,20-23radiographs for foetal measurements in dead foetuses. In
contrast to our analysis, studies by Quinlan RW et al, Goldstein
RB et al, Jeanty P et al, and others employed ultra-sonograms 15-19for foetal measurements in intrauterine life.
Study by Quinlan RW et calculated gestational age of foetus
by measuring femur ultrasonographically and then applying
regression formulae which showed error of ± 1 weeks in akin to 15our results. In our study we were able to predict accurate
gestational age in 44 % cases with difference of ±1week.
In our study, regression formulae were derived based on
morphological as well as radiological length of femur in
contrast to regression formulae by Fazekas and Kosa,
Sherwood et al, which employed morphological femur length
and regression formulae by Chervenak et al., which employed 12,19,24femur length measured ultrasonographically. Fazeka and
kosa formulae measured body length which in turn was used 12to derive gestational age in weeks, Sherwood et al formula 24measured gestational age in weeks, Chervenak et al formula
19measured gestational age in days and our study measured
gestational age in weeks as well as days. Fazekas and Kosa
formula is FL*6.44+4.51,Chervenak formula is 70.62
+21.78*FLansd Sherwood formula is 10.91+0.38*FL where
FL is femur length.(Table 4)
CONCLUSION :
Anthropological gestational age was found to be more
significant than radiological gestational age based on p value
and correlation coefficient. In 11 (44%) out of 25 cases
radiological and anthropological gestational age coincided
with known gestational age done by ultrasound. In 25 out of 25
cases gesational age calculated lay within 95 % confidence
interval limit
It can be concluded that the age estimation of fetus by
anthropological and radiological measurements of long bones
is a feasible and reliable method and can provide priceless
information to narrow down the search in case of identification
of unknown dead new-born or fetus when only skeletal
remains are present.
REFERENCES :
1. Reddy KSN, Murthy OP. The essentials of forensic
medicine and toxicology. In:Identification. 34th ed. New
Delhi: Jaypee Brothers medical publishers(p)
Ltd;2017.p.55-97
2. Hoffman JM. Age estimations from diaphyseal
lengths:two months to twelve year..J Forensic
Sci.1979;24:461-9
3. Scheuer JL, Musgrave JH, Evans SP. The estimation of
late fetal and perinatal age from limb bone length by linear
37
Sharman RS. Estimating fetal age using multiple
parameters: a prospective evaluation in a racially mixed
population. Am J Obstet Gynecol.1987;156:955-7
19. Chervenak FA, Skupski DW, Romero R, Myers MK,
Smith-Levitin M, Rosenwaks Z, Thaler H. How accurate
is fetal biometry in the assessment of fetal age? Am J
Obstet Gynecol.1998;178:678-87
20. Falkner F, Roche AF. Relationship of femoral length to
recumbent length and stature in fetal, neonatal, and early
childhood growth. Hum Biol.1987;59:769-73
21. Huxley AK. Comparability of gestational age values
derived from diaphyseal length and foot length from
known forensic foetal remains. Med Sci Law.1998;38:42-
51
22. Warren MW. Radiographic determination of development
age in fetuses and stillborns. J For Sci.1999;44:708-12
23. Bareggi R, Grill V, Zweyer M, Sandrucci MA, Narducci P,
Forabosco A. The growth of long bones in human
embryological and fetal upper limbs and its relationship to
other developmental pat terns. Anat Embryol .
1994;189:19-24
24. Sherwood R, Meindl RS, Robinson HB, May RL. Fetal
age: Methods of estimation and effects of pathology. Am J
Phys Anthropol.2000;113:305-15
25. Carneiro C, Curate F, Borralho P, Cunha E. Radiographic
fetal osteometry: Approach on age estimation for the
portuguese population. Forensic Sci Int.2013; 231:397-e1
38
Original Research Paper
INTRODUCTION :
Autopsy is mainly of two types – clinical autopsy and medico-
legal autopsy. The former is carried out with the consent of the
relatives, mainly to find the cause of natural deaths where the
disease condition responsible for the death could not be [1]ascertained during life. It not only helps in determining the
cause of death but also plays an important role for the [2]betterment and advancement of medical science. Yet, over
the years there have been a gradual decline in the number of
clinical autopsy attributed to various factors including [3-5]relatives of the deceased not consenting for the same.
Medico-legal autopsy on the other hand is a statutory
requirement that need to be fulfilled for any unnatural, sudden
and suspicious death in order to ascertain the cause and manner
of death. In such situations, the medico-legal autopsy
conducted is carried out without the consent of the next of kin [6, 7]of the deceased. However, studies conducted on the general
population have shown that many do not wish medico-legal
autopsies to be conducted on their relatives.
There is not much literature on this important aspect,
highlighting the relative's perception towards medico-legal
autopsy in India and to the best of our knowledge no such study
has been previously reported from the North-eastern region of
the country. Therefore, this study aimed at determining the
perception of the relatives of the deceased to medico-legal
autopsy and the reasons for their positive and negative
responses.
MATERIALS AND METHODS :
This cross-sectional questionnaire based study was conducted
in the Department of Forensic Medicine, NEIGRIHMS, st stShillong over a period of one year from 1 January 2018 to 31
December 2018. The relative (above 18 yrs of age and related
to the deceased by a social bond) of the deceased of
consecutive medico-legal cases brought to the mortuary for
medico-legal autopsy were approached to participate in this
study. All cases of unidentified and unclaimed dead bodies,
Corresponding Author :
Dr AJ Patowary,
Professor and Head
Department of Forensic Medicine
North Eastern Indira Gandhi Regional Institute of Health and
Medical Sciences (NEIGRIHMS) Mawdiangdiang, Shillong
Meghalaya - 793018
Contact : +91 70020-63345
Email : [email protected]
KEYWORDS : Medico-legal autopsy, relatives, perception
Article History:Received: 15 July 2020Received in revised form: 21 August 2020Accepted on: 21 August 2020Available online: 15 August 2021
ABSTRACT :
Introduction : Unlike clinical autopsy, medico-legal autopsy is conducted irrespective of the relative's consent. However, many of
these autopsies are done against their wishes.
Materials and Methods :This one year cross sectional questionnaire based study includes 179 relatives of the deceased person out
of the 195 medico-legal cases brought to the mortuary for medico-legal autopsy.
Results : Out of the 179 cases included in this study, 113 (63.1%) participants had negative attitude towards medico-legal autopsy
and 66 (36.9%) participants had positive attitude. The main reasons for the negative attitude towards the autopsy were fear of
mutilation of the body, delay funeral and the relatives not interested in knowing the cause of death.
Conclusion : Many had a negative perception towards medico-legal autopsy mainly due to fear of mutilation of the body and delay
in funeral.
1. Daunipaia Slong, Assistant Professor*2. AD Ropmay, Associate Professor*3. Aelifeter R Marak, Senior Resident*4. Anamika Nath, Senior Resident*5. Rangme B Y Marbaniang, Technical Assistant*6. AJ Patowary, Professor & Head* *Department of Forensic Medicine, NEIGRIHMS, Shillong
Perception of relatives towards Medico-legal autopsy in a tertiary care centre of Northeast India
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00007.8
39
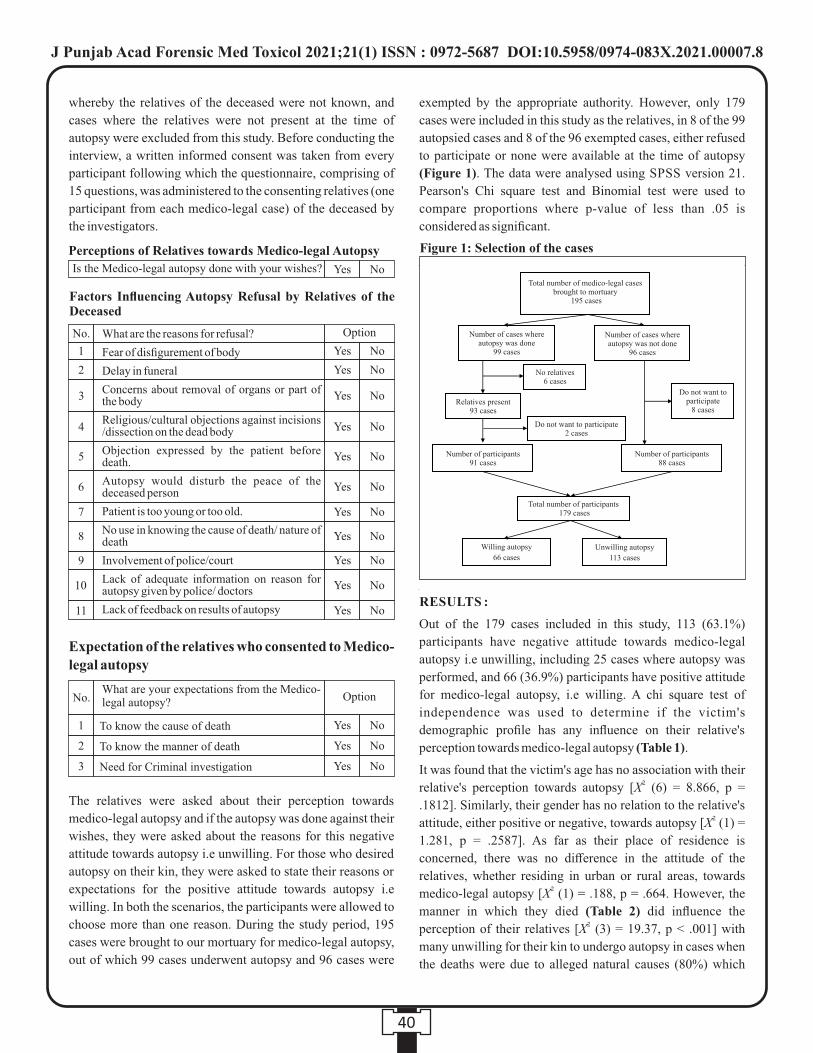
whereby the relatives of the deceased were not known, and
cases where the relatives were not present at the time of
autopsy were excluded from this study. Before conducting the
interview, a written informed consent was taken from every
participant following which the questionnaire, comprising of
15 questions, was administered to the consenting relatives (one
participant from each medico-legal case) of the deceased by
the investigators.
The relatives were asked about their perception towards
medico-legal autopsy and if the autopsy was done against their
wishes, they were asked about the reasons for this negative
attitude towards autopsy i.e unwilling. For those who desired
autopsy on their kin, they were asked to state their reasons or
expectations for the positive attitude towards autopsy i.e
willing. In both the scenarios, the participants were allowed to
choose more than one reason. During the study period, 195
cases were brought to our mortuary for medico-legal autopsy,
out of which 99 cases underwent autopsy and 96 cases were
exempted by the appropriate authority. However, only 179
cases were included in this study as the relatives, in 8 of the 99
autopsied cases and 8 of the 96 exempted cases, either refused
to participate or none were available at the time of autopsy
(Figure 1). The data were analysed using SPSS version 21.
Pearson's Chi square test and Binomial test were used to
compare proportions where p-value of less than .05 is
considered as significant.
RESULTS :
Out of the 179 cases included in this study, 113 (63.1%)
participants have negative attitude towards medico-legal
autopsy i.e unwilling, including 25 cases where autopsy was
performed, and 66 (36.9%) participants have positive attitude
for medico-legal autopsy, i.e willing. A chi square test of
independence was used to determine if the victim's
demographic profile has any influence on their relative's
perception towards medico-legal autopsy (Table 1).
It was found that the victim's age has no association with their 2relative's perception towards autopsy [X (6) = 8.866, p =
.1812]. Similarly, their gender has no relation to the relative's 2attitude, either positive or negative, towards autopsy [X (1) =
1.281, p = .2587]. As far as their place of residence is
concerned, there was no difference in the attitude of the
relatives, whether residing in urban or rural areas, towards 2medico-legal autopsy [X (1) = .188, p = .664. However, the
manner in which they died (Table 2) did influence the 2perception of their relatives [X (3) = 19.37, p < .001] with
many unwilling for their kin to undergo autopsy in cases when
the deaths were due to alleged natural causes (80%) which
40
Figure 1: Selection of the cases
Total number of medico-legal cases brought to mortuary
195 cases
Number of cases where autopsy was done
99 cases
Number of cases where autopsy was not done
96 cases
No relatives 6 cases
Relatives present 93 cases
Do not want to participate 2 cases
Do not want to participate
8 cases
Number of participants 91 cases
Number of participants 88 cases
Total number of participants 179 cases
Willing autopsy
66 cases
Unwilling autopsy
113 cases
Perceptions of Relatives towards Medico-legal Autopsy
Is the Medico-legal autopsy done with your wishes? Yes
Option
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
No.
6
7
8
9
10
11
No
No
No
No
No
No
No
No
No
No
No
No
Factors Influencing Autopsy Refusal by Relatives of the Deceased
What are the reasons for refusal?
Fear of disfigurement of body
Delay in funeral
Concerns about removal of organs or part of the body
Religious/cultural objections against incisions /dissection on the dead body
Objection expressed by the patient before death.
Autopsy would disturb the peace of the deceased person
Patient is too young or too old.
No use in knowing the cause of death/ nature of death
Involvement of police/court
Lack of adequate information on reason for autopsy given by police/ doctors
Lack of feedback on results of autopsy
1
2
3
4
5
Option
Yes
Yes
Yes
No.
No
No
No
What are your expectations from the Medico-legal autopsy?
1
2
3
Expectation of the relatives who consented to Medico-
legal autopsy
To know the cause of death
To know the manner of death
Need for Criminal investigation
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00007.8

were brought dead to the Institute and accidental deaths
(61.82%).
Among the cases included in this study, 113 (63.1%) relatives
of the deceased person expressed their undesirability for their
kin to undergo medico-legal autopsy. A binomial test (two
tailed) on the reasons for their negative attitude towards
autopsy (Table 3) indicated that the number of relatives who
felt that autopsy will lead to disfigurement of the dead body
(92.04%, p < .001), delay in funeral (72.57%, p < .001) and
there is no use in knowing the cause of death (70.80%, p <
.001) are proportionally higher than expected. However, for
the other reasons which cause the negative attitude towards
autopsy, each showed lesser proportion than expected (p <
001) except for organ removal which the relatives responded
as expected (59%, p = .707).
Out of the 179 cases, 66 (36.9%) relatives had a positive
attitude towards medico-legal autopsy. A binomial test (two
tailed) on the reasons for their positive attitude towards
autopsy (Table 4) indicated that the number of relatives who
wants to know the cause of death (92.42%, p < .001) is
proportionally higher than expected. While the number of
relatives who wants to know the manner of death (30.30%, p =
.002), for their positive attitude, is proportionally lesser than
expected; the proportion of those who want to initiate criminal
investigation (40.91%, p = .176) did not differ from what is
expected.
DISCUSSION :
Medico-legal autopsy is conducted in all medico-legal cases
compulsorily, irrespective of the relative's wishes. However,
88 of the 179 medico-legal cases included in this study are
exempted from autopsy, on the request of the relatives,
41
To know the cause of death
To know the manner of death
Table 4: Reasons for Willingness to Medico-legal autopsy
SlNo.
Reasons for Unwillingness Yes N (%) No N (%)
61 (92.42)
20 (30.30)1
2
05 (7.58)
112 (99.12)
Table 1: Demographic profile of victim and relative's perception towards Medico-legal autopsy
Relative's perception
66 (36.87)
57 (38.78)
09 (28.12)
03 (27.27)
07 (33.33)
15 (34.88)
19 (46.34)
15 (51.72)
04 (22.22)
03 (18.75)
34 (35.40)
32 (38.60)
113 (63.13)
90 (61.22)
23 (71.88)
08 (72.73)
14 (66.67)
28 (65.12)
22 (53.66)
14 (48.28)
14 (77.78)
13 (81.25)
62 (64.60)
51 (61.40)
179
147
32
11
21
43
41
29
18
16
96
83
Gender
Male
Female
Age (Yr.)
0-10
10-20
20-30
30-40
40-50
50-60
>60
Address
Urban
Rural
Victim's
profile
Total
NWilling autopsy
N (%)
Not willing autopsy
N (%)
Table 2: Manner of death and relative's perception towards Medico-legal autopsy
Relative's perception
10 (20.00)
42 (38.18)
11 (84.62)
03 (50.00)
40 (80.00)
68 (61.82)
02 (15.38)
03 (50.00)
50
110
13
6
Natural
Accidental
Homicidal
Suicidal
Manner
of
death
Total
NWilling autopsy
N (%)
Not willing autopsy
N (%)
Table 3: Reasons for Unwillingness to Medico-legal autopsy
SlNo.
Reasons for Unwillingness Yes N (%) No N (%)
Fear of disfigurement of body
Delay in funeral
Concerns about removal of organs or part of the body
R e l i g i o u s / c u l t u r a l objections against incisions / dissection on the dead body
Objection expressed by the patient before death.
Autopsy would disturb the peace of the deceased person
Patient is too young or too old.
No use in knowing the cause of death/ nature of death
Involvement of police/ court
L a c k o f a d e q u a t e information on reason for autopsy given by police/ doctors
Lack of feedback on results of autopsy
104 (92.04)1
2
3
4
5
6
7
8
9
10
11
82 (72.57)
59 (52.21)
03 (2.65)
01 (0.88)
00 (0.00)
16 (14.16)
80 (70.80)
03 (2.65)
00 (0.00)
01 (0.88)
09 (7.96)
31 (27.43)
54 (47.79)
110 (97.35)
112 (99.12)
113 (100)
97 (85.84)
33 (29.20)
110 (97.35)
113 (100)
112 (99.12)
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00007.8

following an order from the appropriate authority; although it
may be noted that majority of these cases are brought dead to
the emergency department with history of chronic illness (38/
88) and alleged Road Traffic Accident (34/88). Altogether,
113 (63.1%) respondents are unwilling for their next of kin to
undergo medico-legal autopsy, a finding similar to Goel S et al [8](69.70%). The main reasons for such negative response
towards autopsy, whether autopsy is done or not, are fear of
disfigurement of the dead body, delay in funeral and no use in
knowing the cause of death; age, gender and place of residence
(Urban or Rural) of the deceased person does not affect the
perception of relatives towards medico-legal autopsy. This
fear of disfigurement of the dead body, which is a concern also [6,8]shared among relatives of the other study population, can be
addressed by proper counseling of the relatives explaining to
them the purposes and procedures for conducting an autopsy
including reconstruction of the body post autopsy. This view is [9,10]supported by earlier studies which demonstrated that prior
explanation of the autopsy procedures will not only bring
about a better understanding of medico-legal autopsy but also
improve its acceptability by the relatives as many people had [11]misconception about medico-legal autopsy. Previous
[6,8]studies, including ours, observed that most of the relatives
felt autopsy will delay funeral. Therefore, efforts should be
made by both the investigating agencies, which have an
unenviable job, and the autopsy surgeons to ensure that
autopsy be conducted as early as possible so that the dead body
can be handed over to the relatives at the earliest. Another
important factor expressed by the relatives as a reason for the
negative perception towards autopsy is their disinterest to
know the cause of death because they believed there is no foul
play involving the death of their kin and that the cause of death
was already known to them. Such responses are given mostly
by relatives whose dear ones died following alleged RTA,
natural death and fall from height. Interestingly, two cases of
alleged homicide also stated that they do not want to know the
cause of death with both being victims of mob violence. This
unwillingness to know the cause of death is also reported by [8]Goel S et al as one of the major reasons expressed by
respondents who give a negative response towards autopsy.
Apart from the above mentioned reasons for the negative [6,8]attitude towards medico-legal autopsy, previous studies
have shown that religious objections, autopsy disturb the peace
of the deceased, the patient is too young or old, objection
expressed by the deceased before death, involvement of the
police or court and lack of information on the reasons and
feedback on the results of autopsy play important roles; even
though this is not the case in our study. [10]A majority of the respondents seen in a study from Japan,
including those in this study, asserted that the main reason for
their consenting to autopsy was to determine the cause of
death. Knowing the cause of death may help the relatives to [8]cope better with the loss of their beloved or help to settle
claims. Another common response among the consenting [10]relatives, seen not only in our study but in Ito T et al as well,
is that autopsy will help initiate criminal investigation into the
death of their kin. This is not at all surprising considering the
fact that a majority of these deaths, where the relatives give this
response, are due to alleged homicide and autopsy findings is
an important factor that may lead to a logical conclusion of the
investigation.
Looking at the various responses given by the relatives in this
study, it may be suggested that virtual autopsy is something
which can be explored in the future in order to address most of
the concerns expressed by them. In virtopsy, the relatives
neither needs to fear of disfigurement of the body as it is not
dissected nor would there be any delay in funeral as the
procedure is less time consuming and moreover it can be done
at any time of day. This will increase the acceptance of medico
legal autopsy among the relatives thereby avoiding
miscarriage of justice which may arise out of exemption to
autopsy.
CONCLUSION :
Even though consent of the relatives is not required for
conducting medico-legal autopsy, many had a negative
perception towards medico-legal autopsy which may
ultimately result in exemption of autopsy. The main reasons are
fear of disfigurement of the dead body, delay in funeral and no
use in knowing the cause of death. Therefore, effort should be
made to address the various issues expressed by the relatives of
the deceased not only to ease their apprehension towards
autopsy but also to deliver justice.
REFERENCES :
1. Aggrawal A. Forensic Medicine and Toxicology for
MBBS. 1st Edition. New Delhi: Avichal Publishing
Company; 2016. p. 93-108.
2. Randall BB, Fierro MF, Froede RC. Practice guideline for
forensic pathology. Archives of Pathology & Laboratory
Medicine. 1998 Dec; 122(12):1056-64.
3. Wood MJ, Guha AK. Declining clinical autopsy rates
versus increasing medicolegal autopsy rates in Halifax,
Nova Scotia: why the difference? A historical perspective.
Archives of Pathology & Laboratory Medicine. 2001 Jul;
125(7):924-30.
4. Blokker BM, Weustink AC, Hunink MM, Oosterhuis JW.
Autopsy rates in the Netherlands: 35 years of decline.
PLoS One. 2017 Jun 15; 12(6):e0178200. [internet].
42
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00007.8

[ c i t e d 2 0 2 0 J u n e 2 9 ] ; A v a i l a b l e f r o m :
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC547226
6/.
5. Park JP, Kim SH, Lee S, Yoo SH. Changes in Clinical and
Legal Autopsy Rates in Korea from 2001 to 2015. Journal
of Korean Medical Science. 2019 Nov 5; 34(47): e301.
[internet]. [cited 2020 June 29]; Available from:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC690041
0/
6. Parmar P, Rathod GB. Study of knowledge, attitude and
perception regarding medico-legal autopsy in general
population. International Journal of Medical and
Pharmaceutical Sciences. 2013; 3(6):1-6.
7. Chandran M, Vijayakumari N. Knowledge and Attitude of
General Public in Sub-Urban Chennai to Autopsy.
Medico-Legal Update. 2015 Jul; 15(2):35-39.
8. Goel S, Chikkara P, Chhoker VK, Singh A, Bhardwaj A,
Rajesh DR, Singh NK. Perceptions of Relatives' towards
Medico-Legal Investigation and Forensic Autopsy: A
Survey from Rural Haryana. Journal of Indian Academy
of Forensic Medicine. 2014; 36(4):371-3.
9. Plattner T, Scheurer E, Zollinger U. The response of
relatives to medicolegal investigations and forensic
autopsy. The American journal of forensic medicine and
pathology. 2002 Dec; 23(4):345-8.
10. Ito T, Nobutomo K, Fujimiya T, Yoshida KI. Importance
of explanation before and after forensic autopsy to the
bereaved family: lessons from a questionnaire study.
Journal of medical ethics. 2010 Feb; 36(2):103-5.
11. Pawar MN, Suryawanshi DM, Kumar JP. Myths and
misconceptions about medico-legal autopsies among the
people of Tamil Nadu, India. Journal of forensic and legal
medicine. 2015 Aug; 34:159-63.
43
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00007.8
44
Original Research Paper
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00008.X
1. Mithra. S, *
2. Abirami Arthanari, Senior Lecturer, Department of Forensic Odontology*
3. Pratibha Ramani, Professor and Head, Department of Oral Pathology & Microbiology*
*Saveetha Dental College and Hospitals,Saveetha Institute of Medical and Technical Sciences (SIMATS), Saveetha
University, Chennai-77, Tamilnadu.
Key words: Tooth morphology, Forensic odontology, Toxicology, Organophosphorous, compound, OP compounds
Corresponding Author:
Dr. Abirami Arthanari,
Senior Lecturer,
Department of Forensic Odontology,
Saveetha Dental College and Hospitals, Saveetha Institute of
Medical and Technical Sciences (SIMATS), Saveetha
University, Chennai-77,Tamilnadu.
Contact : +91 63668-11772
Email :[email protected]
Article History :
Received : 16 May 2021
Received in revised from : 16 June 2021
Accepted on : 17 June 2021
Available online : 31 August 2021
INTRODUCTION:
Organophosphorus compounds (OPs) are a wide group of
chemicals which are highly toxic for natural ecosystem. OPs
are mainly a derivative of phosphoric acid or phosphonic acid.
The phosphonic acid derivatives are usually more reactive and (1)more toxic than the phosphoric acid derivatives . OPs are
highly utilized for manufacturing effective pesticides and
insecticides. The chemical pressure on natural environments
has been increased by the industrialization of the agricultural (2)sector . However, their side effects can be a significant
environmental health risk factor due to their documented
potential to cause a large number of negative health and (2)environmental effects . These OPs causes several toxic effects
to human life but in general post organophosphorous exposure,
Salivation, Lacrimation, Urination, Defecation, Gastric
cramps, Emesis (SLUDGE) symptoms occurs acutely within
minutes to hours. Most symptoms occur within minutes or (3)hours following acute exposure . However apart from all
these, due to personal grievances, people themselves have used
OPs as poisons to end their lives (suicide) or to cause harm to
other fellow beings (homicide). In such cases forensic team,
examines the dead body to identify the causative for death. The
Evaluation of Morphological Changes in Natural Tooth Exposed to Organophosphorous Compounds
ABSTRACT :
Introduction: Pesticide poisoning has indeed been recognized as a significant global health problem, and it is the most common
cause of morbidity and mortality. Organophosphorus compounds (OP) are extensively used in agriculture, omestic pest control,
and biological agents. Each year, an estimated 25 million farmers in developing countries are poisoned by pesticides, commonly
OP, which is known to cause serious health ill effects.
Aims & Objectives: To assess the histomorphological alterations in natural tooth due to exposure to different organophosphorus
compounds.
Materials & Methods: This research was carried out with organophosphorus compound - purchased PHOSKILL, insecticide,
from local commercial market. The natural tooth were immersed in the respective solution for an hour and assessed for
morphological & histological alterations through ground sections (200 m). μ
Results: Visually, mild colour changes were noted on the tooth external surface, especially on the root surface. This yellow orange
tint noted of the tooth surface could be because of the concentration of the dye added to the OP compound. The structure and the
morphology of the tooth remain undisturbed. Morphologically, the incremental lines of retzius are brownish bands found due to the
successive apposition of layers of enamel during formation. There are also few hypocalcified structures evident. The dentinal
tubules and interglobular dentin are more prominent in this current ground section and the pulpal tissue was completely lost in OP
compound exposed tooth.
Conclusion: The OP compounds did not prove to show any morphological or histological alterations to natural tooth.

45
natural teeth are most resistant to destruction and they can
persist for long after other skeletal structures have been
destroyed by physical agents. The identification of dental (4)remains is of prime importance when the deceased person .
Also foreign materials subsequently placed inside oral cavity
by dental practitioners, such as fillings, dentures, crowns,
bridges and implants are used as a medium of individual
identification. With passage of time, the role of teeth has
increased and very often teeth and dental restorations are the (5)only means of identification . This study utilizes the teeth as a
newer approach to assess the morphological alterations in
dentin of natural tooth exposed to OP compounds.
Previous literatures reported changes to tooth structures
exposed to different acids in different concentrations. Jadhav (4)K, et al. used hydrochloric acid, nitric acid and sulphuric acid
and identified positive changes in the teeth depending upon the (5)duration of exposure. Seethapathy, et al. analyzed the
morphological changes in the teeth exposed to hydrochloric
acid (HCl) and nitric acid (HNO3) by 48 hrs and 20 hours. No
other studies have been performed to estimate the dentin
changes in natural tooth exposed to different OPs. The aim of
the current study is to assess the morphological alterations in
dentin of natural tooth exposed to OP compounds.
MATERIALS AND METHODS:
10 freshly extracted human natural teeth (free of any defects,
preferably orthodontic tooth extraction and impacted tooth)
used for the study were obtained as per the protocol approved
by the institutional ethics committee of department of Oral
pathology & Microbiology from Saveetha dental college &
hospitals, Chennai. The randomly selected tooth samples were
initially immersed in an organophosphorous compound
purchased from local commercial market [PHOSKILL,
insecticide, Gujarat]. The exposed teeth were retrieved after a
time span of 1 hour and washed with distilled water, dried,
photographed and 200μm ground sections were made using a
hard tissue microtome. The alterations in the dentin of the tooth
exposed were assessed using light microscopy for
morphological alterations. Carious teeth, teeth with pulpal,
periapical or periodontal diseases, teeth with physiological
wear, developmental defects were excluded from the study.
RESULTS:
Visual changes:
After 1-hour, mild color changes were noted on the tooth
external surface, especially on the root surface. The structure
and the morphology of the tooth remain undisturbed. Figure 1
shows mild yellowish-orange tint, especially in the root
surface.
Morphological changes in Enamel:
The incremental lines of retzius are brownish bands found due
to the successive apposition of layers of enamel during
formation. There are also few hypocalcified structures evident.
Figure 2 (10X magnification) shows prominent hypocalcified
enamel structures and prominent incremental lines of retzius.
Figure 3 (40X magnification) shows dentinal tubules and
interglobular dentin are more prominent in ground section .
Pulp: The pulp was completely lost in OP compound exposed
tooth and hence couldn't be assessed.
DISCUSSION:
In developing countries, poisoning is the commonest suicidal
technique with 10.3% - 20.6% suicidal cases reported in India
due to organophosphorous poisoning. Pesticides containing
organophosphorous compounds are among the most (6)commonly used poisons . These OP compounds are proven to
cause SLUDGE (salivation, lacrimation, urination, defecation, (7)gastric cramps and emesis) symptoms . There might be
differences in signs and symptoms observed with each of the
cases but then as observed, cumulatively the most common
oral cavity manifestations are swelling of the lips, thickening
of the oral mucous membranes with mild yellow to whitish
discoloration and moderate to intense white discoloration with
the attached gingival and tongue also displayed yellowish (8)white patches which indicates that the signs and symptoms
are observed in the soft tissue component of the oral cavity. The
precise compound, amount, route of exposure, and rate of
metabolic degradation all influence when and how (9)organophosphate symptoms appear . People may come into
contact with OP through a variety of methods, including (9)ingestion, eating, drinking, inhalation, and dermal contact .
Most OP compounds are highly lipid soluble compounds and
absorbed better through skin, oral mucous membranes, and (9)conjunctiva . This research is an attempt to evaluate any
alterations in the hard tissue component, teeth; exposed to OP
compounds.
The visual changes noticed in the tooth immersed in OP
composed are the change in colour of the tooth. After 1-hour,
mild colour changes were noted on the tooth external surface,
especially on the root surface. This yellow-orange tint noted of
the tooth surface could be because of the concentration of the
dye added to the OP compound. The structure and the
morphology of the tooth remain undisturbed. There are no
much evidences about the dyes used in the OP compounds.
1 2 3
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00008.X

46
There was noticeable increase in the number of hypocalcified
structures, especially the enamel lamellae in tooth immersed in
OP compounds that the tooth not exposed to OP compounds.
The enamel lamellae were more than the enamel tufts and
spindles. The enamel lamellae were proven to be a permeable
pathway that allows caries-causing bacteria to reach the
dentine-enamel junction. Caries may thus grow inside the
tooth without leaving noticeable signs on the surface due to the
presence of lamellae. These are formed when there are
disturbances during enamel formation, also when the external
forces are more at stage of life these lamellae propagates to a (10-11)crack . This OP compound must have induced the lamellae
to crack. There were prominent also prominent incremental
lines of retzius noted. The incremental lines of retzius are
brownish bands found due to the successive apposition of
layers of enamel during formation but not any external force
involved.The dentin showed prominent interglobular dentin.
This is not regressive change due to OP compound. They are (12)the poorly mineralized area during the formation stages . The
outermost structure of tooth is enamel which showed very mild
alterations when exposed to OP compounds, so the
possibilities of alterations in dentin not possible.
There is no evidence of pulp in the ground sections. This could
be the dissolution of the soft tissue, pulp through the apical
foramen or the other possibility could be wear off during
ground sectioning but the procedural error cannot be evident in
all the samples evaluated. There are no literature evidences to
prove this dissolution of pulp due to OP compounds.
Unfortunately, these structures are normal to be anticipated in a
ground section of a natural tooth. No alterations are evident to
conclude positively that OP compounds influenced changes in
natural tooth.
REFERENCES:
1. Inch TD. The biological importance of organophosphorus
compounds containing a carbon- phosphorus bond. Ciba
Found Symp. 1977 Sep 13-15;(57):135-53.
2. Nicolopoulou-Stamati P, Maipas S, Kotampasi C,
Stamatis P, Hens L. Chemical Pesticides and Human
Health: The Urgent Need for a New Concept in
Agriculture. Front Public Health. 2016;4:148.
3. Peter JV, Sudarsan TI, Moran JL. Clinical features of
organophosphate poisoning: A review of different
classification systems and approaches. Indian J Crit Care
Med. 2014; 18(11):735-45.
4. Jadhav K, Nidhi Gupta, et al. Effect of acids on the teeth
and its relevance in postmortem identification. Indian
Journal of Dental Research. 2009; 1(2): 93-8.
5. Thanuja Seethapathy. Effect of Acids on Teeth and
Restorative Materials: An Aid in Forensic Odontology.
J.Hard Tissue Biology 2019;28(1): 21-30.
6. Kar N. Lethality of suicidal organophosphorus poisoning
in an Indian population: exploring preventability. Ann
Gen Psychiatry. 2006;5:17. Published 2006 Nov 21.
7. Peter JV, Sudarsan TI, Moran JL. Clinical features of
organophosphate poisoning: A review of different
classification systems and approaches. Indian J Crit Care
Med. 2014;18(11):735-745. doi:10.4103/0972-
5229.144017
8. Sneha Sethi, et al. Oral Cavity: An insight to forensic
diagnosis. Asian Pac. J. Health Sci., 2015; 2(2): 142-147
9. Abirami Arthanari1, et al. Oral Manifestations of Poisons
in View of Forensic Odontology-A Review. Medico-legal
Update, October-December 2020, Vol. 20, No. 4.
10. B N Walker , O F Makinson, M C Peters, et al. Enamel
cracks. The role of enamel lamellae in caries initiation.
Aust Dent J. 1998 Apr;43(2):110-6
11. C F BODECKER. Enamel lamellae and their origin. J
Dent Res. 1953 Apr;32(2):239-45.
12. Chantha Jayawardena, et al. Regional distribution of
interglobular dentine in human teeth. Arch Oral Biol. 2009
Nov;54(11):1016-21.
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00008.X

Original Research Paper
Corresponding Author :
Dr. Guriqbal Singh,
Assistant Professor,
Department of Forensic Medicine, Punjab Institute of Medical
Sciences, Jalandhar
Contact : +91 9915044296
Email : [email protected]
KEYWORDS :
Article History:Received: 11 July 2019Received in revised form: 11 August 2019Accepted on: 11 March 2021Available online: 31 August 2021
INTRODUCTION :
Deaths due to railway track injuries remain more or less
constant every year. Incidence of death due to railway injuries
constitute a significant group of transportation related
mortalities. Abrasions and lacerations are characteristics of
railway accident injuries. Primary impact injuries are mainly
caused as a result of striking of the body with the protruding
parts of engine/train and are most commonly present on head
and/or both upper and lower extremities. Whereas secondary
impact injuries i.e. abrasions mainly are present on the trunk as
a result of subsequent fall on the ground. However the type of
injury depends upon the position of the person at the time of
impact and speed of the approaching train. Criteria for
differentiating suicide, homicide and accident was as under :
Suicide : Where history & inquest report favoured suicidal
intent and on autopsy, decapitation and transverse severing of
the trunk without any associated fatal injuries/suicide note was
detected.
Homicide: Included cases of injuries caused by particular type
of weapon on the body, fatal poisoning (excluding cases of
suicides) or passengers who were thrown from trains after
assault on trains or at stations.
Accident: Included bizarre type of injuries which are not [1-5]coinciding the injuries of suicide and homicide.
MATERIAL AND METHODS :
Present study was carried out on 196 cases at Mortuary wing of
Forensic Medicine Department, Govt. Medical College, st stAmritsar with effect from 1 January 2000 to 31 December
2001 on alleged railway accidental deaths. History of
incidence was taken from the relatives, friends, eyewitnesses
and investigating agency. Detailed examination of the body
and injuries were done to endorse/corroborate or rule out the
alleged manner of death. Railway related deaths were defined
as all deaths that occurred as result of commuting (including
assaults on trains) or occurred on or close to a railway line or
station. All bodies were subjected to a full autopsy
examination. In all those cases of suicides where the history of
alcohol was positive or alcohol consumption (just before
death) by the deceased was mentioned in the inquest report,
viscera was preserved for the detection of intoxicants.
RESULTS :
Incidence of deaths due to railway injuries was 9.66%.
Number of deaths due to railway injuries remained almost
constant each year in the two year study i. e. 9.98% and 9.36%
respectively for the year 2000 & 2001. (Table 1)
Abrasions and lacerated wounds observed in maximum
number (73.97%) of deaths due to railway injuries which
constituted (49.48%) of deaths due to railway accidents and
ABSTRACT :
Introduction : Railway related deaths were defined as all deaths that occurred as result of commuting (including assaults on trains)
or occurred on or close to a railway line or station.
Materials and Methods: Study was carried out at Mortuary wing of Forensic Medicine Department, Govt. Medical College, st stAmritsar with effect from 1 January 2000 to 31 December 2001 on alleged railway accidental deaths.
Results : Most common age group involved in suicidal deaths was 21-30yrs and 41-50 yrs age group. Clothes/body were showing
evidence of grease in 87.76% of cases. Maximum (46.42%) number of cases dying due to railway injuries were unknown followed
by those belonging to urban and rural areas.
1. Amarjit Singh, Medical Officer, Punjab Health System Corporation2. Guriqbal Singh, Assistant Professor, Department of Forensic Medicine, Punjab Institute of Medical Sciences, Jalandhar.
Pattern of Injuries and manner of Death in Alleged Railway Accident Deaths : An Autopsy Study
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00009.1
47
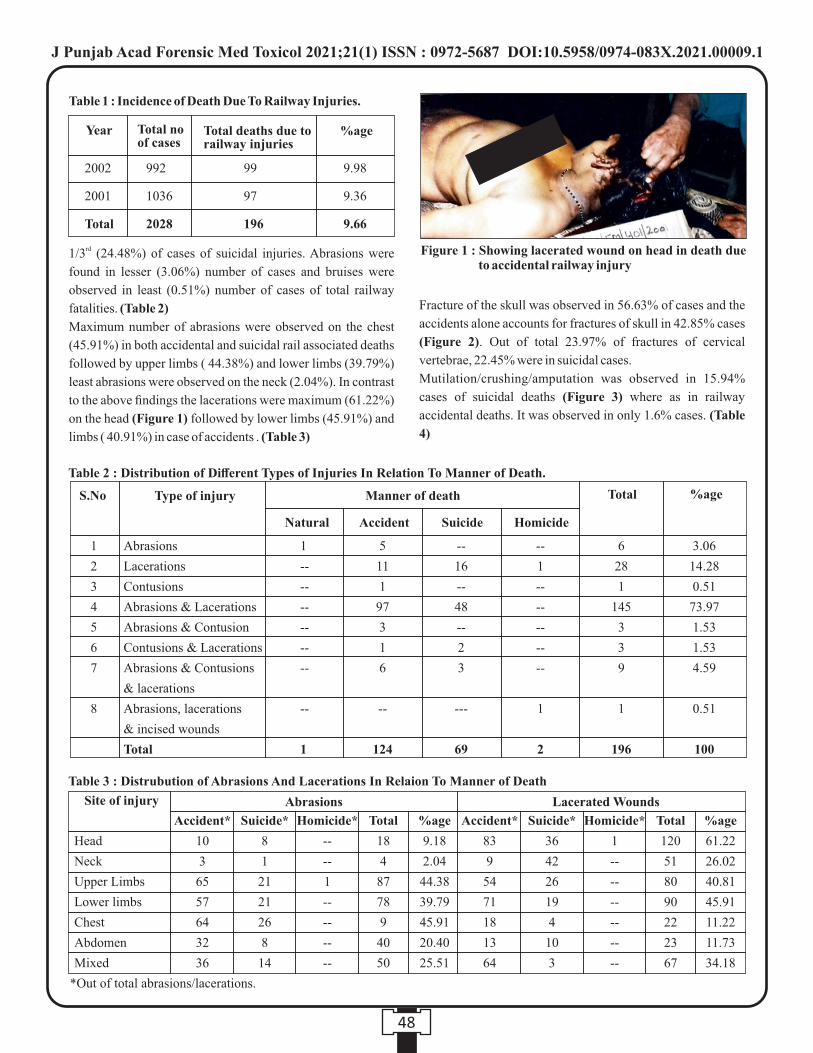
rd1/3 (24.48%) of cases of suicidal injuries. Abrasions were
found in lesser (3.06%) number of cases and bruises were
observed in least (0.51%) number of cases of total railway
fatalities. (Table 2)
Maximum number of abrasions were observed on the chest
(45.91%) in both accidental and suicidal rail associated deaths
followed by upper limbs ( 44.38%) and lower limbs (39.79%)
least abrasions were observed on the neck (2.04%). In contrast
to the above findings the lacerations were maximum (61.22%)
on the head (Figure 1) followed by lower limbs (45.91%) and
limbs ( 40.91%) in case of accidents . (Table 3)
Fracture of the skull was observed in 56.63% of cases and the
accidents alone accounts for fractures of skull in 42.85% cases
(Figure 2). Out of total 23.97% of fractures of cervical
vertebrae, 22.45% were in suicidal cases.
Mutilation/crushing/amputation was observed in 15.94%
cases of suicidal deaths (Figure 3) where as in railway
accidental deaths. It was observed in only 1.6% cases. (Table
4)
48
Table 1 : Incidence of Death Due To Railway Injuries.
Year Total no of cases
Total deaths due to railway injuries
%age
2002
2001
Total
992
1036
2028
99
97
196
9.98
9.36
9.66
Table 2 : Distribution of Different Types of Injuries In Relation To Manner of Death.
S.No Type of injury Manner of death Total %age
Natural Accident Suicide Homicide
Abrasions
Lacerations
Contusions
Abrasions & Lacerations
Abrasions & Contusion
Contusions & Lacerations
Abrasions & Contusions
& lacerations
Abrasions, lacerations
& incised wounds
Total
1
--
--
--
--
--
--
--
1
1
2
3
4
5
6
7
8
5
11
1
97
3
1
6
--
124
--
16
--
48
--
2
3
---
69
--
1
--
--
--
--
--
1
2
6
28
1
145
3
3
9
1
196
3.06
14.28
0.51
73.97
1.53
1.53
4.59
0.51
100
Table 3 : Distrubution of Abrasions And Lacerations In Relaion To Manner of Death
Site of injury
*Out of total abrasions/lacerations.
Abrasions Lacerated Wounds
Head
Neck
Upper Limbs
Lower limbs
Chest
Abdomen
Mixed
Accident*
10
3
65
57
64
32
36
Accident*
83
9
54
71
18
13
64
Suicide*
8
1
21
21
26
8
14
Suicide*
36
42
26
19
4
10
3
Homicide*
--
--
1
--
--
--
--
Homicide*
1
--
--
--
--
--
--
%age
9.18
2.04
44.38
39.79
45.91
20.40
25.51
%age
61.22
26.02
40.81
45.91
11.22
11.73
34.18
Total
120
51
80
90
22
23
67
Total
18
4
87
78
9
40
50
Figure 1 : Showing lacerated wound on head in death due to accidental railway injury
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00009.1
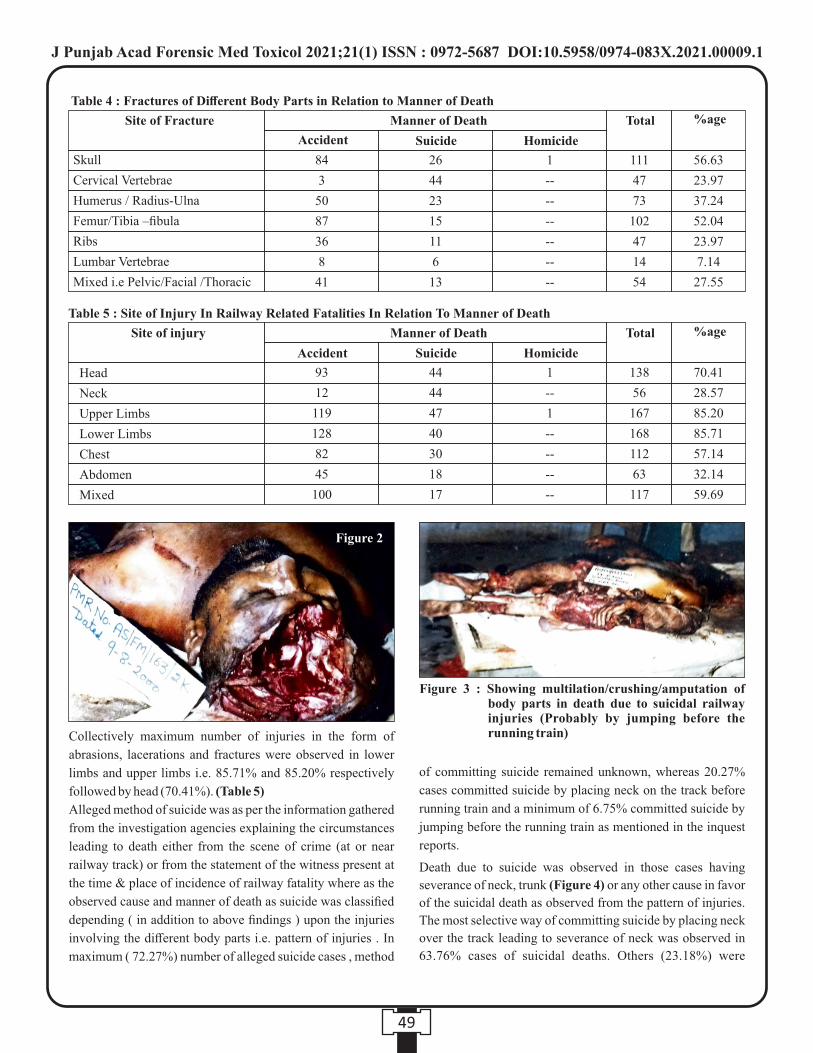
Collectively maximum number of injuries in the form of
abrasions, lacerations and fractures were observed in lower
limbs and upper limbs i.e. 85.71% and 85.20% respectively
followed by head (70.41%). (Table 5)
Alleged method of suicide was as per the information gathered
from the investigation agencies explaining the circumstances
leading to death either from the scene of crime (at or near
railway track) or from the statement of the witness present at
the time & place of incidence of railway fatality where as the
observed cause and manner of death as suicide was classified
depending ( in addition to above findings ) upon the injuries
involving the different body parts i.e. pattern of injuries . In
maximum ( 72.27%) number of alleged suicide cases , method
of committing suicide remained unknown, whereas 20.27%
cases committed suicide by placing neck on the track before
running train and a minimum of 6.75% committed suicide by
jumping before the running train as mentioned in the inquest
reports.
Death due to suicide was observed in those cases having
severance of neck, trunk (Figure 4) or any other cause in favor
of the suicidal death as observed from the pattern of injuries.
The most selective way of committing suicide by placing neck
over the track leading to severance of neck was observed in
63.76% cases of suicidal deaths. Others (23.18%) were
49
Table 5 : Site of Injury In Railway Related Fatalities In Relation To Manner of Death
93
12
119
128
82
45
100
44
44
47
40
30
18
17
138
56
167
168
112
63
117
70.41
28.57
85.20
85.71
57.14
32.14
59.69
1
--
1
--
--
--
--
Site of injury Total %ageManner of Death
Accident Suicide Homicide
Head
Neck
Upper Limbs
Lower Limbs
Chest
Abdomen
Mixed
Table 4 : Fractures of Different Body Parts in Relation to Manner of Death
84
3
50
87
36
8
41
26
44
23
15
11
6
13
111
47
73
102
47
14
54
56.63
23.97
37.24
52.04
23.97
7.14
27.55
1
--
--
--
--
--
--
Site of Fracture Total %age
Skull
Cervical Vertebrae
Humerus / Radius-Ulna
Femur/Tibia –fibula
Ribs
Lumbar Vertebrae
Mixed i.e Pelvic/Facial /Thoracic
Manner of Death
Suicide Homicide
Figure 3 : Showing multilation/crushing/amputation of body parts in death due to suicidal railway injuries (Probably by jumping before the running train)
Accident
Figure 2
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00009.1
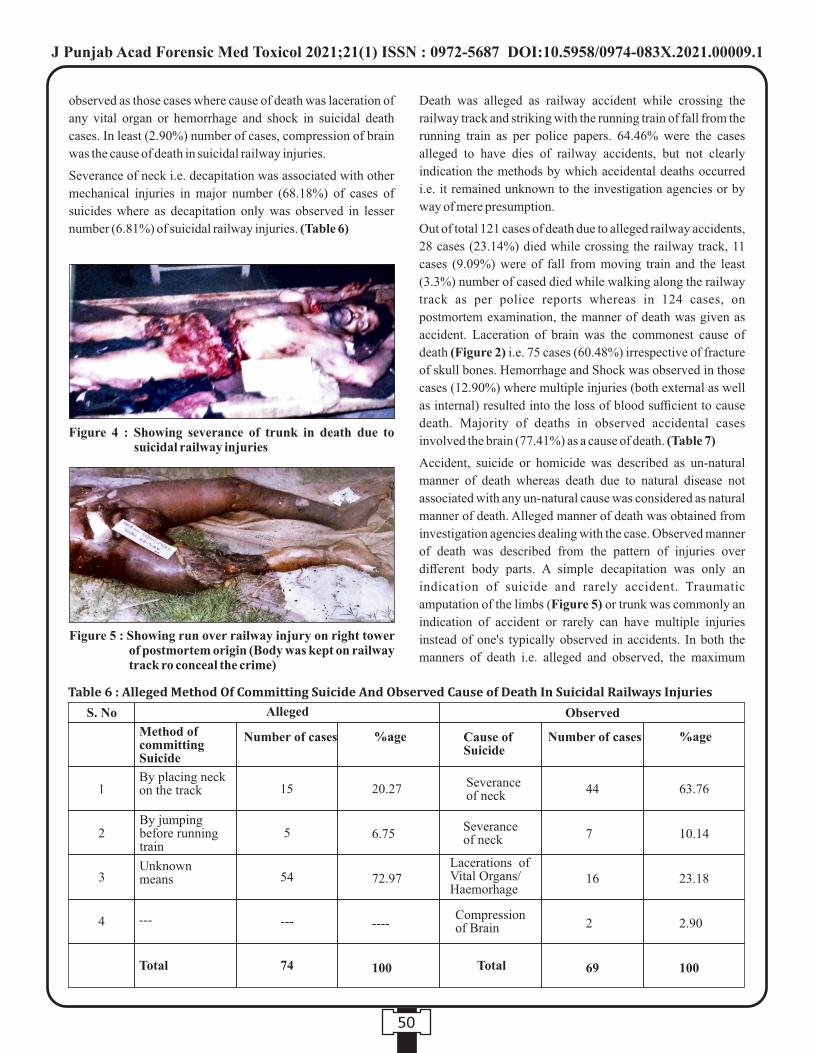
Figure 4 : Showing severance of trunk in death due to suicidal railway injuries
observed as those cases where cause of death was laceration of
any vital organ or hemorrhage and shock in suicidal death
cases. In least (2.90%) number of cases, compression of brain
was the cause of death in suicidal railway injuries.
Severance of neck i.e. decapitation was associated with other
mechanical injuries in major number (68.18%) of cases of
suicides where as decapitation only was observed in lesser
number (6.81%) of suicidal railway injuries. (Table 6)
Death was alleged as railway accident while crossing the
railway track and striking with the running train of fall from the
running train as per police papers. 64.46% were the cases
alleged to have dies of railway accidents, but not clearly
indication the methods by which accidental deaths occurred
i.e. it remained unknown to the investigation agencies or by
way of mere presumption.
Out of total 121 cases of death due to alleged railway accidents,
28 cases (23.14%) died while crossing the railway track, 11
cases (9.09%) were of fall from moving train and the least
(3.3%) number of cased died while walking along the railway
track as per police reports whereas in 124 cases, on
postmortem examination, the manner of death was given as
accident. Laceration of brain was the commonest cause of
death (Figure 2) i.e. 75 cases (60.48%) irrespective of fracture
of skull bones. Hemorrhage and Shock was observed in those
cases (12.90%) where multiple injuries (both external as well
as internal) resulted into the loss of blood sufficient to cause
death. Majority of deaths in observed accidental cases
involved the brain (77.41%) as a cause of death. (Table 7)
Accident, suicide or homicide was described as un-natural
manner of death whereas death due to natural disease not
associated with any un-natural cause was considered as natural
manner of death. Alleged manner of death was obtained from
investigation agencies dealing with the case. Observed manner
of death was described from the pattern of injuries over
different body parts. A simple decapitation was only an
indication of suicide and rarely accident. Traumatic
amputation of the limbs (Figure 5) or trunk was commonly an
indication of accident or rarely can have multiple injuries
instead of one's typically observed in accidents. In both the
manners of death i.e. alleged and observed, the maximum
50
Figure 5 : Showing run over railway injury on right tower of postmortem origin (Body was kept on railway track ro conceal the crime)
Table6:AllegedMethodOfCommittingSuicideAndObservedCauseofDeathInSuicidalRailwaysInjuries
S. No Alleged Observed
Method of committing Suicide
Cause ofSuicide
Severance of neck
Severance of neck
Lacerations ofVital Organs/Haemorhage
Compressionof Brain
Number of cases Number of cases %age %age
15 20.27
6.75
72.97
----
100
44
7
16
2
69
63.76
10.14
23.18
2.90
100
5
54
74
---
By placing neck on the track 1
2
3
4
By jumping before running train
Unknown means
---
Total Total
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00009.1
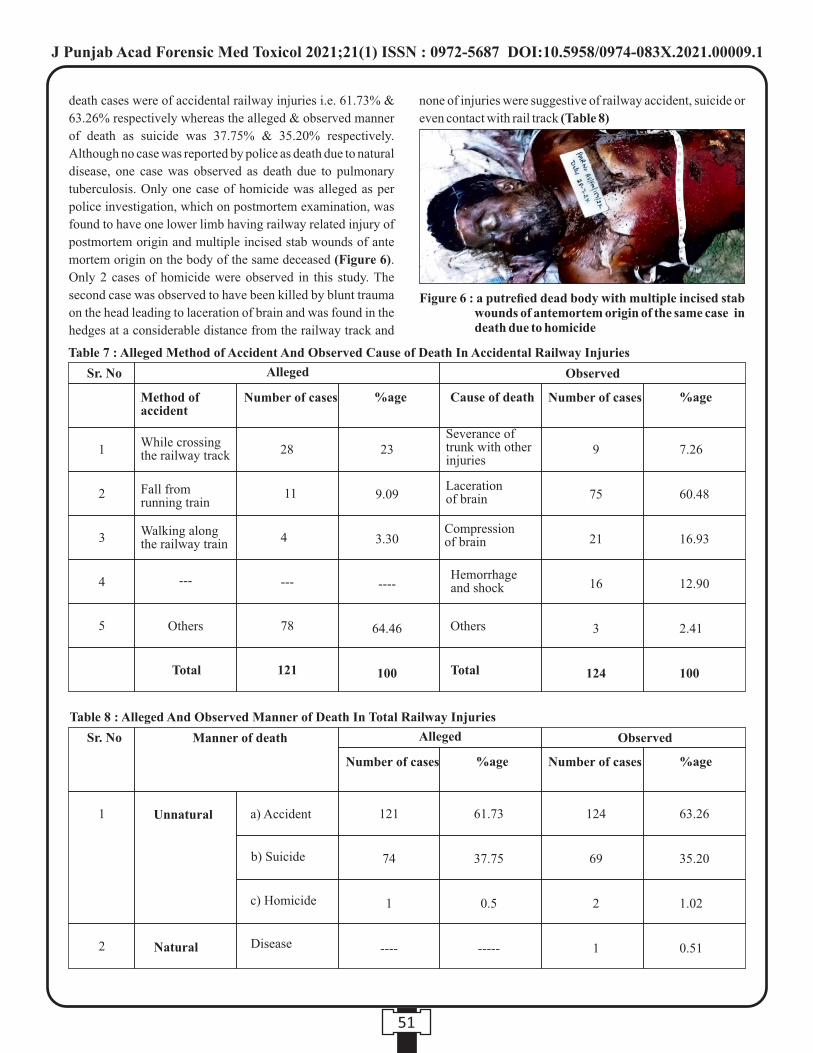
Figure 6 : a putrefied dead body with multiple incised stab wounds of antemortem origin of the same case in death due to homicide
death cases were of accidental railway injuries i.e. 61.73% &
63.26% respectively whereas the alleged & observed manner
of death as suicide was 37.75% & 35.20% respectively.
Although no case was reported by police as death due to natural
disease, one case was observed as death due to pulmonary
tuberculosis. Only one case of homicide was alleged as per
police investigation, which on postmortem examination, was
found to have one lower limb having railway related injury of
postmortem origin and multiple incised stab wounds of ante
mortem origin on the body of the same deceased (Figure 6).
Only 2 cases of homicide were observed in this study. The
second case was observed to have been killed by blunt trauma
on the head leading to laceration of brain and was found in the
hedges at a considerable distance from the railway track and
none of injuries were suggestive of railway accident, suicide or
even contact with rail track (Table 8)
51
Table 7 : Alleged Method of Accident And Observed Cause of Death In Accidental Railway Injuries
Sr. No Alleged Observed
Number of cases Number of cases %age %age
28 23
9.09
3.30
----
64.46
100
9
75
21
16
3
124
7.26
60.48
16.93
12.90
2.41
100
11
4
78
121
---
1
2
3
4
5
---
Total Total
Method of accident
While crossing the railway track
Fall from running train
Walking along the railway train
Others
Cause of death
Severance of trunk with other injuries
Laceration of brain
Compression of brain
Hemorrhage and shock
Others
Table 8 : Alleged And Observed Manner of Death In Total Railway Injuries
Sr. No Observed
Number of cases %age
124
69
2
1
63.26
35.20
1.02
0.51
1
2
Alleged
Number of cases %age
61.73
37.75
0.5
-----
121
74
1
----
Manner of death
a) Accident
b) Suicide
c) Homicide
Unnatural
Natural Disease
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00009.1

In maximum number (42.34%) of cases, the cause of death was
laceration of brain followed by severance of neck (22.44%)
and compression of brain (11.73%). Both head and neck
involvement lead to death in 76.4% of cases. Severance of
trunk was observed in 8.16% of cases. (Table 9)
Maximum number of male to female ration was reported in the
age group of 31-40 years both in death due to accidents and
suicides i.e. in railway accidents, male to female ratio was 27:1
and in suicidal deaths, male to female ratio was 11:1. Minimum
number of male to female ratio was observed in 21-30 year age
group both in death due to railway accidents (male to female
ratio 2.6:1) and death due to suicides (male to female ratio
3.9:1). The largest percentage of male death was from suicides
(87.95%) out of total 69 cases of suicides. In the present study
109 cases (87.90%) of males died due to accident where as
females died only in 15(12.09%) cases of accidental injuries.
Similar is the pattern in suicide cases where 60 (86.95%) males
and 9 (13.04%) females committed suicide. Homicidal deaths
on railway tracks were reported in males only.
Non vulnerable age for railway injury was below 10yrs. 41-50
yr age group was involved in majority of cases of deaths
(27.04%) out of total railway fatalities followed by 21-30yr
age group (21.42%) and 31-40yr age group (20.91%). Least
number of cases were observed in extremities of age i.e. 10.2%
in age group 11-20yrs and 9.18% in age group above 60yrs.
There was remarkable difference in the ratio of two sexes i.e.
7.1:1. (Table 10)
Condition of the clothes/body in respect to the presence of
black soot (carbon from the rail tracks) was in one way
conclusive to the extent that the body came in contact with the
railway track, which was observed in cases of accidents and
suicides, but absence of these findings on the clothing's or body
of the deceased may raise a reasonable suspicion of homicide.
Soiling of clothes or body with grease were resulted from the
primary impacts only. In maximum number of cases (87.75%)
of deaths due to railway injuries, soiling of clothes/body with
grease was observed irrespective of manner of death (Table
11)
Area wise distribution was detected as rural (21.42%) or urban
(32.14%) depending upon the residential belongings of the
deceased dies as a result of railway fatalities. Unknown cases
(46.42%) were those whose identity including the residence
was not known to the investigation agencies till the conduction
of the post- mortem examination. (Table 12)
Month wise incidence of railway related deaths was divided
into first four months, middle four months and last four months
to know whether there was any effect of fog, overcrowding or
various other activities on railway fatalities due to any seasonal
52
Sr.No
1
2
3
4
5
6
7
Cause of death
Laceration of brain
Severance of neck
Compression of brain
Severance of trunk
Hemorrhage and shock
Laceration of other
vital organs
Disease
Total
No. of cases
83
44
23
16
17
11
1
196
%age
42.34
22.44
11.73
8.16
8.67
5.61
0.51
100
Table 9 : Distributions of cases as per Causes of Death In Total Railway Injuries
Manner of Death Age groups (yrs) Natural
Male Male Male MaleFemale Female Female Female
Accident Sucide Homicide
Total %age Male/Female
ratio
Table 10 : Age And Sex wise Distribution of Cases in Relation to Manner of Death.
11-20
21-30
31-40
41-50
51-60
>60
Total
---
---
---
---
1
---
1
---
---
---
---
---
---
---
9
16
27
31
13
13
109
3
6
1
3
---
---
15
7
15
11
16
8
---
60
1
4
1
3
---
---
9
---
1
1
---
---
---
2
---
---
---
---
---
---
---
20
42
41
53
22
18
198
10.20
21.42
20.19
27.04
11.22
9.18
100
4:1
3.2:1
19.5:1
7.8:1
----
8:1
7.1:1
Sr. No
1
2
3
4
5
6
Table 12 : Area Wise Distribution of Death Due To Railway Injuries
Sr. No
1
2
3
Area
Rural
Urban
Unknown
Total
No of Cases
42
63
91
196
Percentage
21.42
32.16
46.42
100
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00009.1

variations. The number of deaths during the last four months of
the year was maximum (35.71%) followed by middle four
months (34.69%) and least in first four months (29.59%) of the
year. (Table 13)
96.42% victims died with in few hours of sustaining injuries on
the rail tracks which included instantaneous deaths (29.59%)
and immediate (32.65%) deaths i.e. deaths within 3-5 minutes
of sustaining railway injuries. The deceased as survived 1-2
days or more than that were hospital admitted cases which
were accidentally injured. Only case was of suicide amongst
the person seeking admission. (Table 14)
53
Manner of Death
Natural Accident Sucide HomicideTotal %age
109
15
63
9
---
2
---
1
172
196
87.75
100
Table 11 : Incidence of Soiling of Clothes/body With Grease In Relation To Manner of Death.
Sr. No
1
2
Soiling of cloths
With grease
Without greases
January
February
March
April
May
June
July
August
September
October
November
December
Total
Manner of Death
NaturalAccident Sucide Homicide
Total noof deaths
%age
8
9
9
11
10
14
9
12
10
10
6
16
124
5
5
4
6
8
4
4
6
5
7
11
4
69
---
---
---
---
---
---
1
---
---
1
---
---
2
1
---
---
---
---
---
---
---
---
---
---
---
1
14
14
13
17
18
18
14
18
15
18
17
20
196
7.14
7.14
6.63
8.67
9.18
9.18
7.14
9.18
7.65
9.18
8.67
10.20
100
Table 13 : MonthWiseIncidenceofRailwayTrackDeathCasesInRelationToMannerofDeath
Sr. No
1
2
3
4
5
6
7
8
9
10
11
12
Month
Manner of Death
Natural Accident Suicide HomicideTotal %age
---
---
---
---
---
1
1
9
53
56
1
4
---
123
49
11
9
1
---
---
70
---
---
2
---
---
---
2
58
64
67
2
4
1
196
29.59
32.65
34.18
1.02
2.04
0.51
100
Table 14 : Details of case as per time between injury and death in relation to manner of death.
Sr. No
1
2
3
4
5
6
Time between injury and death
Instantaneous
Immediate
With in few minutes
to few hours
About 1-2 days
More than 2 days
Not determined
Total
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00009.1

DISCUSSION :
The incidence of death due to railway injuries Table-1 in the
present study is 9.66% which is higher than 5.41% as reported [7]in the study conducted by Gargi et al (1990) , perhaps the
increase in railway injuries is because of addition of more
trains on the rail tracks, increasing population of the cities,
unmanned crossings. Increasing intolerance in the society
gives rise to more suicides adding to the problems of railway
injuries. In the present study, there was no major accident and
all the cases were as a result of individual mishap similar to the
study conducted by Gargi et al (1990). All the other studies
published so far includes, in majority head on collisions and [8] [9]derailments (Tedeschi, 1977 and Huq, 1982 ) Out of total
transportation related mortalities (38.26%), railway injury
deaths in the present study is 25.25% (i.e. more than 1/4” of
transport related fatalities). Whereas in the study conducted by [10]Lerer et al 1997 in the Cape Town, South Africa, railway
fatalities constituted 14% of transport related mortalities. The
reason for this variation of the study might be due to the fact
that as compared to the Cape Town of South Africa, here at
Amritsar, commuters run across the track more so to board
incoming trains in addition to trespassing and unmanned
crossings. Although trespassing is an offence under section
147 of Indian Railway Act punishable with a fine of Rs.1,000/-
or imprisonment for six months.
In the study conducted by Gargi et al (1990), abrasions bruises
and lacerations were the commonest injuries as were expected
in blunt trauma and combination of abrasions and lacerations
formed a single largest group (45.57%) where as in the present
study, although pattern of distribution of of abrasions injuries
(Table 2) is the same but the proportion and lacerations is
higher (73.97%), which is highly suggestive of characteristics
of accidents similar to above mentioned study.
Irrespective of the manner of death the maximum (45.91%)
number of abrasion were found on the chest (Table-3)
followed by upper limbs (44.38%) and lower limbs (39.79%).
Minimal (9.18%) abrasions were found on the head where as
maximum (61.22%) lacerations were found on head followed
by lower limbs (45.91%) Upper and minimal (11.22%)
lacerations were found on the chest. Similarly (Table - 4)
maximum (56 63%) fractures were of the skull followed by
fractures of femur/ tibia-fibula (52 04%) of both sides and
humerus/radius and ulna (37.24%) of both sides. Maximum
number of lacerations over the head and both upper and lower
limbs are due to the fact that the result of primary impact
injuries is mostly on those parts of the body which comes first
in contact with the protruding parts of the approaching train
whereas maximum number of abrasions over the chest and
both upper and lower limbs in all probabilities are due to the
secondary impact injuries which are not directly in contact
with the moving train. Since no such comparative data about
the type of injuries i.e. abrasions, lacerations and fractures in
relation to manner of death due to railway injuries is reported
till date to the best of our knowledge, so no comparison can be
drawn.
In the inquest reports of present study, in maximum (72.97%)
number of cases, the alleged method of suicide was not known
(Table -6) and in 20.27% cases, the eye witness/circumstantial
evidence' favored/stated that the deceased died by placing neck
on the track. 6.75% cases died by jumping before the running
train. Autopsy examination in the present study revealed
severance of neck and trunk in 67.76% and 10.14% cases
which is more or less similar to the study conducted Gargi et al
(1990) where 60% and 12% committed suicide by placing
neck and trunk on the track respectively. In the present study,
2.90% cases tried to commit suicide were rescued and
hospitalized who later on succumbed to their injuries and were
declared to have died as a result of compression of brain. No
such comparison of alleged method of suicide with observed
cause of death is reported by any author. The findings of
decapitation and rarely severance of trunk not associated with
other injuries, goes highly in favour of suicidal railway deaths.
Very rarely the victims who jump in front of the moving trains
have pattern of injuries which is similar to that of accidental [11-13]injuries. In the study conducted by Gargi et al ( 1 9 9 0 ) ,
mutilation/crushing/amputation was observed in 72.15%
cases where as in the present study these features were
observed in 17%cases only . This single feature of
mutilation/crushing/amputation is rather diagnostic of railway
injuries when taken in combination' with finding of [14]grease/blackish material on the body or clothes. This finding
of grease/blackish material on the body or clothes was seen in
73.41% cases in the study conducted by Gargi et al (1990),
whereas in the present study, 87.76% cases show evidence of
soiling of clothes/body with grease.
Though in the present study, alleged method of accident and
observed cause of death in the accidental deaths due to railway
injuries are more or less similar (Table-7) but the alleged
accidental deaths remained unwitnessed in maximum
(64.46%) number of cases and in the inquest reports these were
reported as deaths due to railway accidents. Whereas in
observed railway accidental deaths, laceration of brain was the
cause of death in 60.48% of cases. No similar study is available
for comparison and it was observed that a person while
walking along the side of the track may be struck by the
protruding parts of the passing train on the side of the body
usually on the head leading to laceration of brain due to
primary impact injuries or both upper and/or lower extremities
54
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00009.1

may be struck. A person hit while crossing the line receives
primary impact injuries on the side of the approaching train
and secondary impact injuries as a result of subsequent fall on
the ground. Amputation of different body parts while walking
along or crossing the track also go in favour of railway
accidental injuriés and rarely gross mutilation of the body parts
may occur while crossing the track and hit by moving train
causing bizarre type of injuries in favour of accidental
fatalities. Any incised wound on the body which is not usually
as a result of railway injuries or any postmortem injury present
over the body to conceal the crime or simulate it as a case of [15]accident goes in favour of homicide.
In the study conducted by Gargi et al (1990), 25.32% cases of
alleged accidents were actually suicides and homicides
otherwise which would have passed of as accidents. However
in the present study, (Table 8) observed manner of death is
more or less similar to the alleged manner in respect of railway
accidental injuries and suicidal injuries. However homicide
was observed in 2 cases as against one case alleged to have died
with criminal motive. In the study conduct by Sahoo & Kar [16]1998 , maximum number of - cases of railway fatalities were
from accidents (55%)followed by suicides (43. 3%) and
Homicides (1.3%). Similarly in the study conducted by Gargi
et al (1990) maximum number of cases of railway fatalities
were from accidents (64.55%) followed by suicides (32.91%)
and homicides (2.53%).
In the present study similar pattern has been observed i.e.
accidents (63.26%), suicides(35.20%) and homicides (1.02%)
clearly showing that deaths due to railway injuries are mostly
accidental though suicidal injuries are also not uncommon.
Infrequently homicidal cases have also been reported in
railway injuries and low incidence of homicide is in
consonance with above mentioned studies. One case was
alleged to have died due to injuries by sharp edged weapon and
later on the dead body was put on railway track to simulate the
cases of railway accident i.e to conceal the crime. Multiple
incised stab wounds were inflicted on abdomen, front and back
of chest to conceal the crime which clearly indicated the
criminal motive of the assailant. In the study conducted by
Lerer et al (1997), 80.21% of railway injuries were reported as
accidental, 11.34% of cases were homicides and 8.44% of
cases were from suicides whereas in the present study least
(1.02%) number of cases were from homicides. The reason for
high percentage of homicide in the Cape Town, South Africa as
reported by Lerer et al in comparison to this study was the high
prevalence of criminal violence in Cape Town and strict law
enforcement in our country prohibits such concealment of
crime making it difficult to dispose off the body on railway
tracks. In 0.51% (1 case) the manner of death was natural in
which the case was an unidentified body found at railway track
alleged to have died due to railway accident. However on
postmortem examination, no demonstrable injury was found
on the body and on opening the chest, Pulmonary Tuberculosis
was evident in favour of the natural death.
In maximum (42.34%) number of cases, the cause of death was
laceration of brain and in another 11.73% of the cases, it was
compression of brain which, together constituted 54. 07%
followed by severance of neck in 22 44% of cases (Table-9).
Head, the most vulnerable part of body to accidental injuries is
responsible for maximum number of involvement of brain- a [17] vital organ leading to death of deceased. No such parallel
study which may show the incidence of different causes of
death due to railway fatalities has been found.
In the study conducted by Gargi et al (1990), the most common
age group involved in railway fatalities was 21-30yrs (46.83%)
which was also the most common age group (42.14%) in study
conducted by Sahoo & Kar (1998). In the present study (Table
- 10), the most common age group involved in railway
fatalities was 41-50yrs (27.04%) followed by 21-30yrs age
group (21.42%). The reason for the shift of age group from 21-
30yrs in the study conducted by Gargi et (1990) and Sahoo &
Kar (1998) to 41-50yrs age group in this study might be the
daily activities and the factors like responsibilities with
complexities of mind in the age group of 41-50yrs. The
remarkable feature is that no child below age of 10 year was
involved in any mishap in our study and the study conducted by
Gargi et al (1990) and Sahoo and Kar (1998) as the children are
considered gifts of God in India and they are better cared as
compared to the Western Countries eg in Great Britain in which
considerable number of children were killed in railway injuries
during 1969 -71 (Tadeschi, 1997).
In our Study 87.24% of victims were male which is more or
less similar to the study conducted by Sahoo & Kar (1998)
where 82.22% of the victims were males. In the study
conducted by Lerer et al (1997) the deceased were also
predominantly men (85%). The male to female ratio (Table-
10) in all the different age groups is more on account of outdoor
activities among males, that is the reason of its preponderance.
In this study, clothes/body were showing evidence of grease,
(Table-11) in 87.75% of cases. In study conducted by Gargi et
al, blackish material/grease was present over clothes and body
in 73.41% of cases. Evidence of grease highly goes in favour of
both accidental and suicidal railway injuries whereas absence
of grease was more evidently in favour of homicidal cases or
presence of blackish material/grease in cases of homicide is
possible if the body has been disposed of after killing on the rail
track. This evidential material is suggestive of contact of the
body with rail track but in no way conclusive of manner of
55
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00009.1
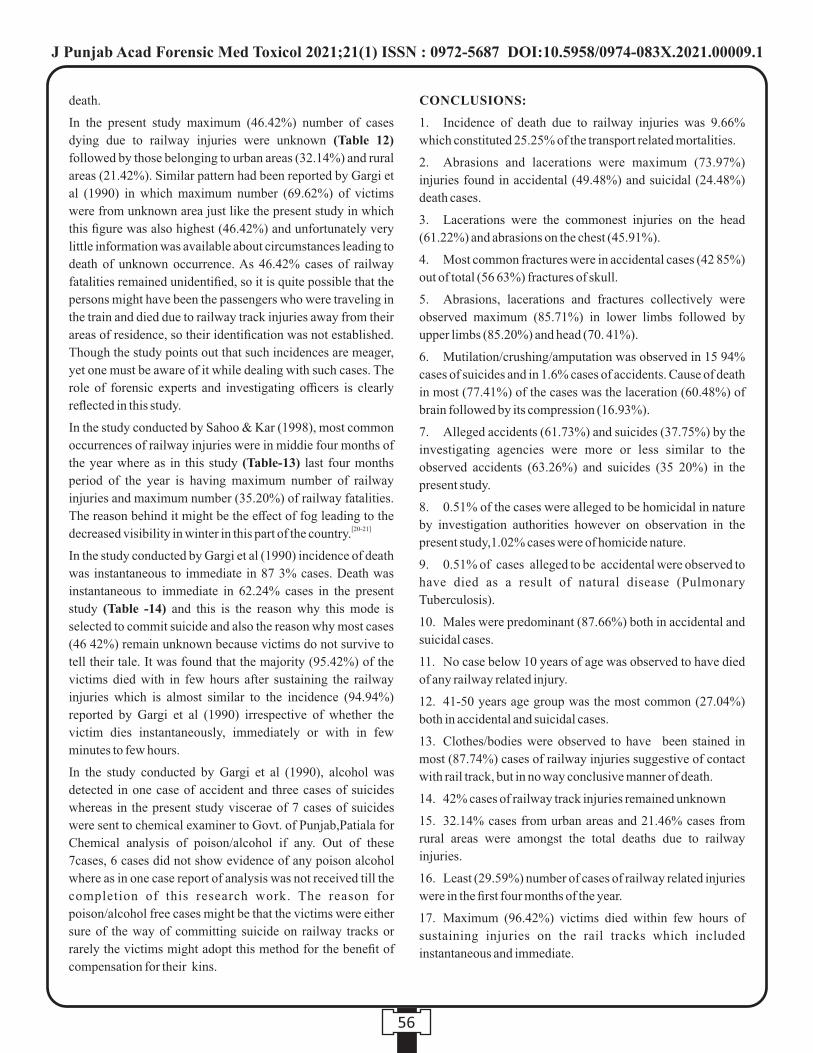
death.
In the present study maximum (46.42%) number of cases
dying due to railway injuries were unknown (Table 12)
followed by those belonging to urban areas (32.14%) and rural
areas (21.42%). Similar pattern had been reported by Gargi et
al (1990) in which maximum number (69.62%) of victims
were from unknown area just like the present study in which
this figure was also highest (46.42%) and unfortunately very
little information was available about circumstances leading to
death of unknown occurrence. As 46.42% cases of railway
fatalities remained unidentified, so it is quite possible that the
persons might have been the passengers who were traveling in
the train and died due to railway track injuries away from their
areas of residence, so their identification was not established.
Though the study points out that such incidences are meager,
yet one must be aware of it while dealing with such cases. The
role of forensic experts and investigating officers is clearly
reflected in this study.
In the study conducted by Sahoo & Kar (1998), most common
occurrences of railway injuries were in middie four months of
the year where as in this study (Table-13) last four months
period of the year is having maximum number of railway
injuries and maximum number (35.20%) of railway fatalities.
The reason behind it might be the effect of fog leading to the [20-21]decreased visibility in winter in this part of the country.
In the study conducted by Gargi et al (1990) incidence of death
was instantaneous to immediate in 87 3% cases. Death was
instantaneous to immediate in 62.24% cases in the present
study (Table -14) and this is the reason why this mode is
selected to commit suicide and also the reason why most cases
(46 42%) remain unknown because victims do not survive to
tell their tale. It was found that the majority (95.42%) of the
victims died with in few hours after sustaining the railway
injuries which is almost similar to the incidence (94.94%)
reported by Gargi et al (1990) irrespective of whether the
victim dies instantaneously, immediately or with in few
minutes to few hours.
In the study conducted by Gargi et al (1990), alcohol was
detected in one case of accident and three cases of suicides
whereas in the present study viscerae of 7 cases of suicides
were sent to chemical examiner to Govt. of Punjab,Patiala for
Chemical analysis of poison/alcohol if any. Out of these
7cases, 6 cases did not show evidence of any poison alcohol
where as in one case report of analysis was not received till the
completion of this research work. The reason for
poison/alcohol free cases might be that the victims were either
sure of the way of committing suicide on railway tracks or
rarely the victims might adopt this method for the benefit of
compensation for their kins.
CONCLUSIONS:
1. Incidence of death due to railway injuries was 9.66%
which constituted 25.25% of the transport related mortalities.
2. Abrasions and lacerations were maximum (73.97%)
injuries found in accidental (49.48%) and suicidal (24.48%)
death cases.
3. Lacerations were the commonest injuries on the head
(61.22%) and abrasions on the chest (45.91%).
4. Most common fractures were in accidental cases (42 85%)
out of total (56 63%) fractures of skull.
5. Abrasions, lacerations and fractures collectively were
observed maximum (85.71%) in lower limbs followed by
upper limbs (85.20%) and head (70. 41%).
6. Mutilation/crushing/amputation was observed in 15 94%
cases of suicides and in 1.6% cases of accidents. Cause of death
in most (77.41%) of the cases was the laceration (60.48%) of
brain followed by its compression (16.93%).
7. Alleged accidents (61.73%) and suicides (37.75%) by the
investigating agencies were more or less similar to the
observed accidents (63.26%) and suicides (35 20%) in the
present study.
8. 0.51% of the cases were alleged to be homicidal in nature
by investigation authorities however on observation in the
present study,1.02% cases were of homicide nature.
9. 0.51% of cases alleged to be accidental were observed to
have died as a result of natural disease (Pulmonary
Tuberculosis).
10. Males were predominant (87.66%) both in accidental and
suicidal cases.
11. No case below 10 years of age was observed to have died
of any railway related injury.
12. 41-50 years age group was the most common (27.04%)
both in accidental and suicidal cases.
13. Clothes/bodies were observed to have been stained in
most (87.74%) cases of railway injuries suggestive of contact
with rail track, but in no way conclusive manner of death.
14. 42% cases of railway track injuries remained unknown
15. 32.14% cases from urban areas and 21.46% cases from
rural areas were amongst the total deaths due to railway
injuries.
16. Least (29.59%) number of cases of railway related injuries
were in the first four months of the year.
17. Maximum (96.42%) victims died within few hours of
sustaining injuries on the rail tracks which included
instantaneous and immediate.
56
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00009.1
REFERENCES :
1. Burgess AW, Sekula LK, Carretta CM. Homicide-suicide
and duty to warn. Psychodyn Psychiatry. 2015
Mar;43(1):67–90
2. Richards TN, Gillespie LK, Givens EM. Reporting
femicide-suicide in the news: the current utilization of
suicide reporting guidelines and recommendations for the
future. J Fam Violence. 2014;29:453–63.
3. Chaudhary P: Social Welfare, Vol. 32 No. 1, Central
Welfare Board, New Delhi, 1985 pp 29
4. Bardon C., Mishara B.L. Systematic review of the impact
of suicides and other critical incidents on railway
personnel. Suicide Life-Threat. Behav. 2015;45:720–731
5. Cina SJ, Koelpin JL, Nichols CA & Conradi SE: A decade
of train pedestrian fatalities: the Charleston experience. J.
Forensic. Sci. 1994. 39. 668-73.
6. Bardon C, Mishara BL. Systematic Review of the Impact
of Suicides and Other Critical Incidents on Railway
Personnel . Suic ide Li fe Threa t Behav. 2015
Dec;45(6):720-31
7. Gargi J Gorea RK & Chanana Ashok : Death due to
railway injuries, a five year study JFMT ,VOL. VII, No 1
& 2 jan-june 1990 pp71 75
8. Huq Muzahuerul M: Injury patterns in railway accident
observation in 3'4 Indo Pacific Congress Bangladesh, rd congress hand book of 3 Indo Pacific Congress on legal
Medicine and Forensic Sciences, 1982, .pp- 201
9. Tedeschi CJ, Eckert WG & Tedeschi LG: Forensic
Medicine, A Study of Trauma and Environmental hazards
Vol 3, Part Ill WB Saunders Company Philadelphia,
London, Toronto, 1° Edition 1977 pp 1186-1 1911
10. Lerer LB & Matzopoulos RG : Fatal railway injuries in
Cape Town, South Africa. American J Forensic Med
Pathol 1997:18:144-7.Clarke M: Railway suicide in
England and Wales, 1850- 1949. Soc. Sci. Med. 1994,
38.401-8.
11. Andriessen K, Krysinska K. Railway suicide in Belgium
1998–2009: incidence and prevention. Crisis.
2012;33:39–45.
12. Dinis-Oliveira RJ, Carvalho F, Duarte JA,et al. Collection
of biological samples in forensic toxicology. Toxicol
Mech Methods. 2010;20:363–414.
13. Gorrie CA, Brown J, Waite PM. Crash characteristics of
older pedestrian fatalities: dementia pathology may be
related to “at risk” traffic situations. Accid Anal Prev.
2008;40:912–919.
14. Chau N, Gauchard GC, Dehaene D, Benamghar L, Touron
C, Perrin PP, Mur JM. Contributions of occupational
hazards and human factors in occupational injuries and
their associations with job, age and type of injuries in
railway workers. Int Arch Occup Environ Health. 2007
May;80(6):517-25
15. Vadysinghe AN, Thambirajah B. Bizarre use of log
splitter: a case of decapitation. Forensic Sci Med Pathol.
2019 Dec;15(4):607-611
16. Sahoo PC & KarSM: Pattern of injuries in railway deaths :
A retrospective study in MDCG Medical College,
Behrampur. Journal of Indian Academy of Forensic
Medicine, vol. 2, No. 3, 1998, pp 67-68
17. Shao X, Wang Q, Shen J, Liu J, Chen S, Jiang X.
Treatment of Traumatic Depressed Compound Skull
Fractures. J Craniofac Surg. 2019 Oct;30(7):2239-2244.
18. Bommer C, Heesemann E, Sagalova V, Manne-Goehler J,
Atun R, Bärnighausen T, Vollmer S. The global economic
burden of diabetes in adults aged 20-79 years: a cost-of-
illness study. Lancet Diabetes Endocrinol. 2017
Jun;5(6):423-430.
19. Tang X, Lou L, Xu Y, Jin K, Cao J, Shao J, Gao Z, Yao K.
Socioeconomic inequality in the global burden of
refraction disorders: results from the Global Burden of
Diseases Study 2017. Acta Ophthalmol. 2020
20. Chang X, Li H, Qin L, Rong J, Lu Y, Chen X. Evaluation
of cooperative systems on driver behavior in heavy fog
condition based on a driving simulator. Accid Anal Prev.
2019 Jul;128:197-205.
21. Kampczyk A. An Innovative Approach to Surveying the
Geometry of Visibility Triangles at Railway Level
Crossings. Sensors (Basel). 2020 Nov 19;20(22):6623.
57
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00009.1
Original Research Paper
Corresponding Author :
Dr. Kamal Singla,
Assistant Professor
Department of Forensic Medicine & Toxicology, Faculty of
Medicine & Health Sciences, SGT University, Gurugram,
Haryana, India.
Contact : +91 9991995200, 9718127000
Email: [email protected]
KEYWORDS : Sexual Dimorphism, Patella, India, Haryana, Osteometric Analysis, Anthropology
Article History:Received: 17 April 2020Received in revised form: 5 May 2020Accepted on: 5 May 2020Available online: 31 August 2021
INTRODUCTION:
Identification is the act of establishing the identity. The ethical
and humanitarian need to know about the identification from
anatomical and medical features especially needed for the
information which comprises few major aspects- surviving
relatives to establish the fact of death in respect of that
individual, for official, statistical and legal purposes; to record
the identity for administrative and ceremonial purposes in
respect of burial or cremation; to discharge legal claims and
obligations in relation to property, estate and debts; to prove
claims for life insurance contracts, and other financial matters;
and to allow legal investigations into overtly criminal or
suspicious deaths, as the identity of the deceased person is a 1vital factor in initiating investigations.
The establishment of identity may be required upon in cases of:
intact fresh corpses, decomposed corpses, mutilated &
1 dismembered corpses and skeletonised material. Mutilation of
the dead body is either done by criminal to destroy all traces of 2identity and thus facilitate the disposal of the dead, or it may be
caused by scavengers.
There are four basic categories associated with biological
identity: sex, age-at-death, stature and ethnic origin. Each of
these, taken either in isolation or collectively, allow a
preliminary picture to be built regarding the possible identity
of the deceased and permits targeting of specific aspects of a 3missing persons register. It has been well established within
osteological and paleoanthropological research that sexual
dimorphism has been present throughout human evolution as 4well as in modern populations.
Determination of sex in non-skeletonised bodies is usually
obvious and rarely presents problems. In general, the external
genitalia remain recognizable until a late stage of putrefaction.
ABSTRACT:
Introduction: Identification is the act of establishing the identity. The pelvic bone and skull are the first choices for morphological
sexing if not recovered in fragmentary states and if recovered in a fragmentary state, other bones such as the patella can be used for
sex determination from osteometric analysis.
Materials and Methods: Patella from 400 subjects including male (199) and female (201) from both sides and studied nine
dimentions which showed that there were definite sexual osteometric differences between male and female patella bones from the
population of Haryana.
Results: For both sides, weight had the maximum AUC (0.979 for right and 0.982 for left side), thus indicating it can be used for
differentiation between males and females. For right and left sides, the projected sensitivity of weight was 96.5% and 97%
respectively and value of patella parameters can be used for differentiation in gender. Using these techniques, projected specificity
for right and left side of weight was 89.6% and 91% respectively.
Conclusions:These findings implied that, the determination of sex can be accomplished by comparing the dimension of unknown
patella bone with the cut off value given. The present study produced standard for sex determination from patella and will be useful
for forensic anthropologists.
1. ,Kamal Singla Assistant Professor*
2 Yatiraj Singi, Associate Professor, Department of Forensic Medicine & Toxicology, AIIMS Bilaspur, Himachal Pradesh
3. Rajiv Kumar Sinha, Assistant Professor*
4. S K Dhattarwal, Professor & HOD, Department of Forensic Medicine & Toxicology, Pt BD Sharma, PGIMS, Rohtak, Haryana
*Department of Forensic Medicine & Toxicology, Faculty of Medicine & Health Sciences, SGT University, Gurugram,
Haryana, India.
Estimation of Sexual Dimorphism by Osteometric Analysis of Patella
58
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00010.8
In addition, breasts and general body shape, as well as the
pattern of pubic hair, reveal the sex. Where putrefaction is
advanced, examination of the internal pelvic organs may still
reveal unequivocal evidence of sex. The uterus is the organ in
the body most resistant to decomposition, though the prostate 5is also quite persistent.
It is not easy to determine sex in cases of mutilated or
skeletonised remains. This problem also arises in sexual
crimes where genital mutilation is common phenomenon and
also in cases where dead body is destroyed by scavenging activities.
Obvious sex differences do not become apparent until after
puberty usually in the 15-18-year period, though specialized
measurements on the pelvis can indicate the sex even in foetal 1material. Krogman (1962) comments that he scored 100 per
cent accuracy using the whole skeleton, 95 % on pelvis, 92 %
on skull, 98 % on pelvis plus skull, 80 % on long bones and 98
% on long bones plus pelvis.
In general, adult female skeletal measurements are about 94 %
that of the male of the same race, but different measurements
may vary from 91 to 98 %. The criteria set out above exclude
pre-pubertal and senile persons, and are less valid for those 6outside the 20-55 age groups.
There are two methodological approaches to sexing human
remains: morphological and osteometric. Morphologic
techniques focus on the shape of the bony configurations that
are macroscopically visible and differ between males and 8females. Osteometric analysis, based on bone dimensions, is
the method of choice for skeletal parts like long bones that do
not exhibit clearly definable shape variants. The major
problem with this technique is that standards are temporarily
sensitive and population specific Most of the older studies of 9.
sex differences in the skeleton (skull and pelvis mainly)
centred on morphological traits in a descriptive manner. The
newer studies focus on metric analysis in a largely quantitative 7and statistical sense.
The techniques used in sex determination have been primarily
focused on the pelvis where reproductive difference is best
seen. The pelvis affords the best results and is considered as the
principal bone with most reliable and pronounced
characteristics for distinguishing sex which provides the most 10-12marked and typical sexual differences. Skull is the second
major bone after the pelvic bones by which one can determine
the sex of an individual with high degrees of accuracy. Some
past studies showed that the skull alone can accurately 13-15determine the sex in more than 80% of the individuals.
Recently, long bones became the most actively studied part of
the skeleton. To these, one would add the ribs, vertebrae, 16-23clavicle, and bones of the hand and foot. Determination of
sex, while well established for many populations, is a 24population specific phenomenon. Studies have been done on
establishing the sex from femur, sternum, clavicle, radius, 25-30ulna, scapula and others.
Morphological and metrical features of some bones that 31display sexual differences have been described. These
32 33 34include the pelvis , the cranium , bones of the upper and 35lower limbs . Recently, there has been an increased interest in
the use of metrical methods in sex assignment. The most
commonly used metrical method is discriminant function 35analysis . Nearly every bone has been subjected to
35discriminant function analysis but not much literature has
been found on the usefulness of measurements of the patella in
the determination of sex using this method. If body recovered
in fragmentary or mutilated condition, patella bone can be used 38,40for sex determination by metric analysis.
MATERIALS AND METHODS :
The present study was undertaken in the Department of
Forensic Medicine & Toxicology, Pt. B D Sharma, PGIMS,
Rohtak, Haryana. A total of 400 subjects including both sexes
were chosen during postmortem examination for retrieving the
sample. Only intact patellae from known sex subjects were
chosen for the study and patellae showing any signs of
pathology and any kind of abnormality (congenital as well as
acquired) were excluded from the study.
MEASUREMENTS :
The following measurements of each patella were taken to
know the sexual dimorphism:-
1. Maximum height (MAXH)—the greatest distance
between the base and apex.
2. Maximum breadth (MAXB)—the greatest distance
between the medial and lateral sides.
3. Maximum thickness (MAXT)—the greatest distance
between the anterior and posterior surface
4. Height of articular facet (HAF)—maximum height of the
articular facet on the posterior aspect of the patella.
5. Medial articular facet breadth (MAFB)—distance
between the medial edge of the patella and the median
ridge of the articular facet.
6. Lateral articular facet breadth (LAFB)—distance
between the lateral edge of the patella and the median
ridge of the articular facet.
7. Weight of patella (Wt)
8. Volume of patella (Vol)
9. Specific gravity of patella (SG) = Density of bone/Density oof water (4 C)
59
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00010.8
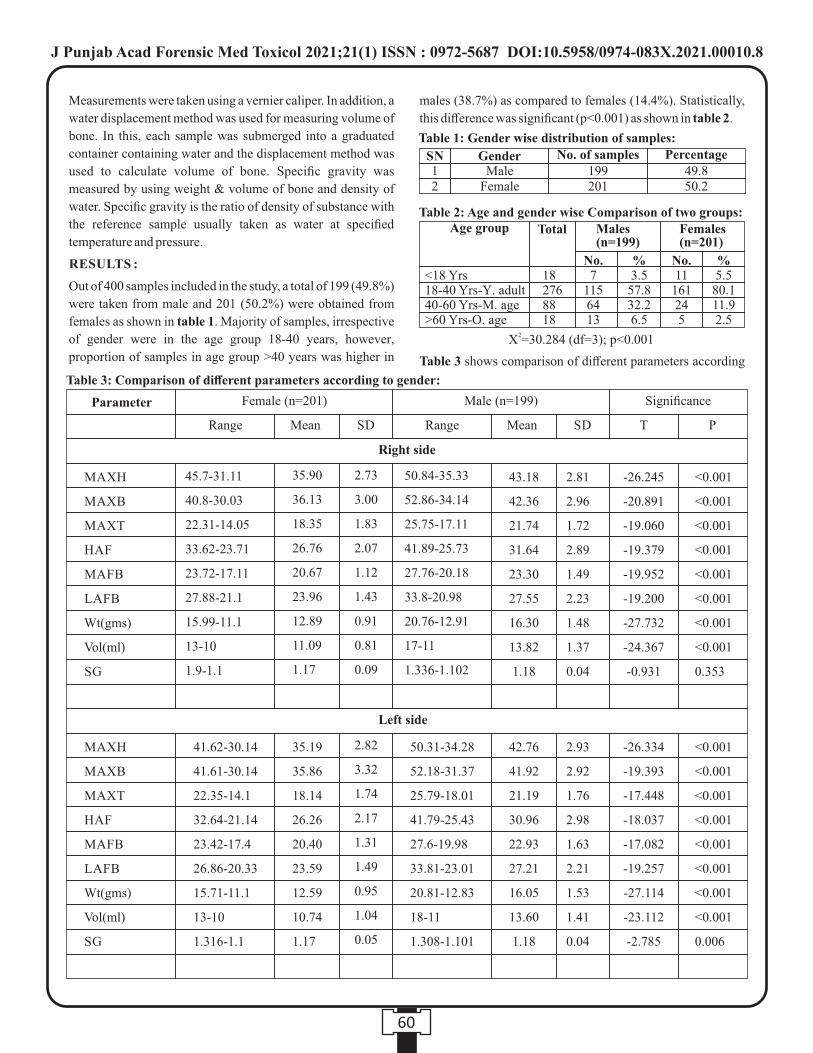
males (38.7%) as compared to females (14.4%). Statistically,
this difference was significant (p<0.001) as shown in table 2.
Table 3 shows comparison of different parameters according
Measurements were taken using a vernier caliper. In addition, a
water displacement method was used for measuring volume of
bone. In this, each sample was submerged into a graduated
container containing water and the displacement method was
used to calculate volume of bone. Specific gravity was
measured by using weight & volume of bone and density of
water. Specific gravity is the ratio of density of substance with
the reference sample usually taken as water at specified
temperature and pressure.
RESULTS :
Out of 400 samples included in the study, a total of 199 (49.8%)
were taken from male and 201 (50.2%) were obtained from
females as shown in table 1. Majority of samples, irrespective
of gender were in the age group 18-40 years, however,
proportion of samples in age group >40 years was higher in
60
Table 1: Gender wise distribution of samples:
SN12
MaleFemale
199201
49.850.2
Gender No. of samples Percentage
Parameter Female (n=201)
Range RangeMean MeanSD SD T P
Male (n=199) Significance
-26.245
-20.891
-19.060
-19.379
-19.952
-19.200
-27.732
-24.367
-0.931
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001
0.353
Right side
MAXH
MAXB
MAXT
HAF
MAFB
LAFB
Wt(gms)
Vol(ml)
SG
45.7-31.11
40.8-30.03
22.31-14.05
33.62-23.71
23.72-17.11
27.88-21.1
15.99-11.1
13-10
1.9-1.1
35.90
36.13
18.35
26.76
20.67
23.96
12.89
11.09
1.17
2.73
3.00
1.83
2.07
1.12
1.43
0.91
0.81
0.09
50.84-35.33
52.86-34.14
25.75-17.11
41.89-25.73
27.76-20.18
33.8-20.98
20.76-12.91
17-11
1.336-1.102
43.18
42.36
21.74
31.64
23.30
27.55
16.30
13.82
1.18
2.81
2.96
1.72
2.89
1.49
2.23
1.48
1.37
0.04
-26.334
-19.393
-17.448
-18.037
-17.082
-19.257
-27.114
-23.112
-2.785
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001
0.006
Left side
MAXH
MAXB
MAXT
HAF
MAFB
LAFB
Wt(gms)
Vol(ml)
SG
2.82
3.32
1.74
2.17
1.31
1.49
0.95
1.04
0.05
42.76
41.92
21.19
30.96
22.93
27.21
16.05
13.60
1.18
2.93
2.92
1.76
2.98
1.63
2.21
1.53
1.41
0.04
41.62-30.14
41.61-30.14
22.35-14.1
32.64-21.14
23.42-17.4
26.86-20.33
15.71-11.1
13-10
1.316-1.1
35.19
35.86
18.14
26.26
20.40
23.59
12.59
10.74
1.17
50.31-34.28
52.18-31.37
25.79-18.01
41.79-25.43
27.6-19.98
33.81-23.01
20.81-12.83
18-11
1.308-1.101
Table 3: Comparison of different parameters according to gender:
Table 2: Age and gender wise Comparison of two groups:Age group
<18 Yrs18-40 Yrs-Y. adult40-60 Yrs-M. age>60 Yrs-O. age
182768818
Total Males (n=199)
No.7
1156413
No.11
161245
%3.557.832.26.5
%5.5
80.111.92.5
Females (n=201)
2X =30.284 (df=3); p<0.001
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00010.8
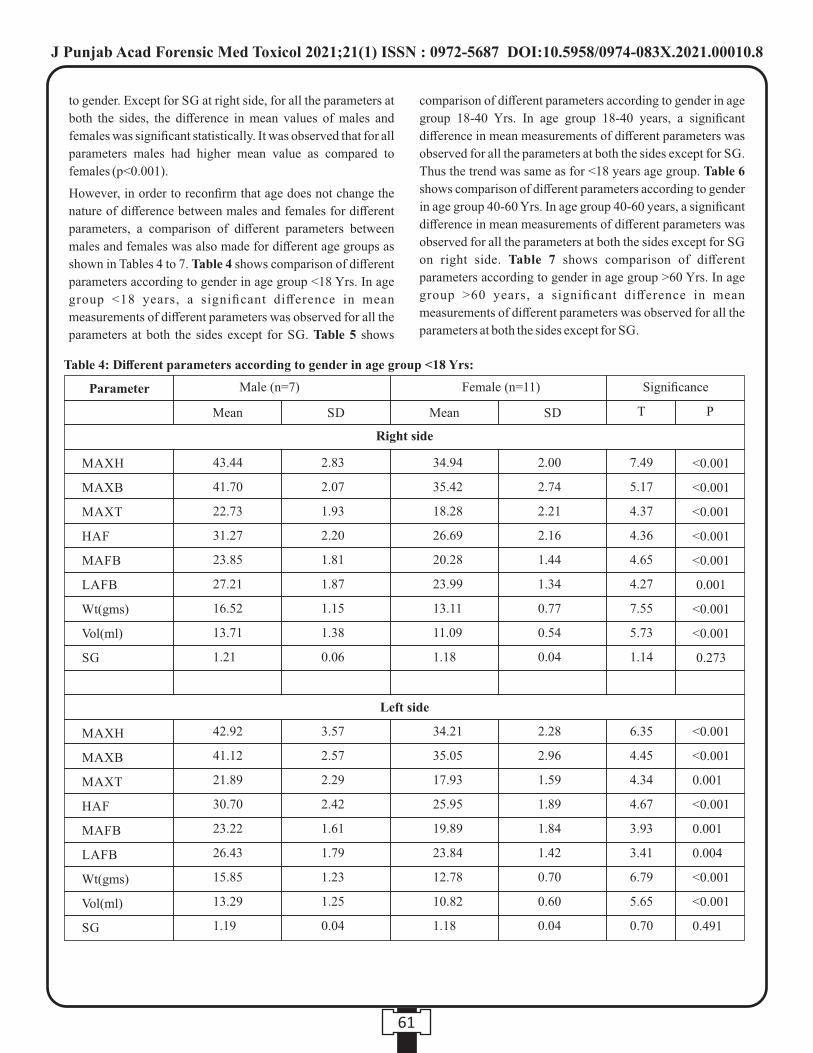
comparison of different parameters according to gender in age
group 18-40 Yrs. In age group 18-40 years, a significant
difference in mean measurements of different parameters was
observed for all the parameters at both the sides except for SG.
Thus the trend was same as for <18 years age group. Table 6
shows comparison of different parameters according to gender
in age group 40-60 Yrs. In age group 40-60 years, a significant
difference in mean measurements of different parameters was
observed for all the parameters at both the sides except for SG
on right side. Table 7 shows comparison of different
parameters according to gender in age group >60 Yrs. In age
group >60 years, a significant difference in mean
measurements of different parameters was observed for all the
parameters at both the sides except for SG.
to gender. Except for SG at right side, for all the parameters at
both the sides, the difference in mean values of males and
females was significant statistically. It was observed that for all
parameters males had higher mean value as compared to
females (p<0.001).
However, in order to reconfirm that age does not change the
nature of difference between males and females for different
parameters, a comparison of different parameters between
males and females was also made for different age groups as
shown in Tables 4 to 7. Table 4 shows comparison of different
parameters according to gender in age group <18 Yrs. In age
group <18 years, a significant difference in mean
measurements of different parameters was observed for all the
parameters at both the sides except for SG. Table 5 shows
61
<0.001
<0.001
0.001
<0.001
0.001
0.004
<0.001
<0.001
0.491
Parameter Male (n=7)
Mean MeanSD SD T P
Female (n=11) Significance
Right side
MAXH
MAXB
MAXT
HAF
MAFB
LAFB
Wt(gms)
Vol(ml)
SG
Left side
MAXH
MAXB
MAXT
HAF
MAFB
LAFB
Wt(gms)
Vol(ml)
SG
Table 4: Different parameters according to gender in age group <18 Yrs:
43.44
41.70
22.73
31.27
23.85
27.21
16.52
13.71
1.21
2.83
2.07
1.93
2.20
1.81
1.87
1.15
1.38
0.06
34.94
35.42
18.28
26.69
20.28
23.99
13.11
11.09
1.18
2.00
2.74
2.21
2.16
1.44
1.34
0.77
0.54
0.04
7.49
5.17
4.37
4.36
4.65
4.27
7.55
5.73
1.14
<0.001
<0.001
<0.001
<0.001
<0.001
0.001
<0.001
<0.001
0.273
42.92
41.12
21.89
30.70
23.22
26.43
15.85
13.29
1.19
3.57
2.57
2.29
2.42
1.61
1.79
1.23
1.25
0.04
34.21
35.05
17.93
25.95
19.89
23.84
12.78
10.82
1.18
2.28
2.96
1.59
1.89
1.84
1.42
0.70
0.60
0.04
6.35
4.45
4.34
4.67
3.93
3.41
6.79
5.65
0.70
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00010.8
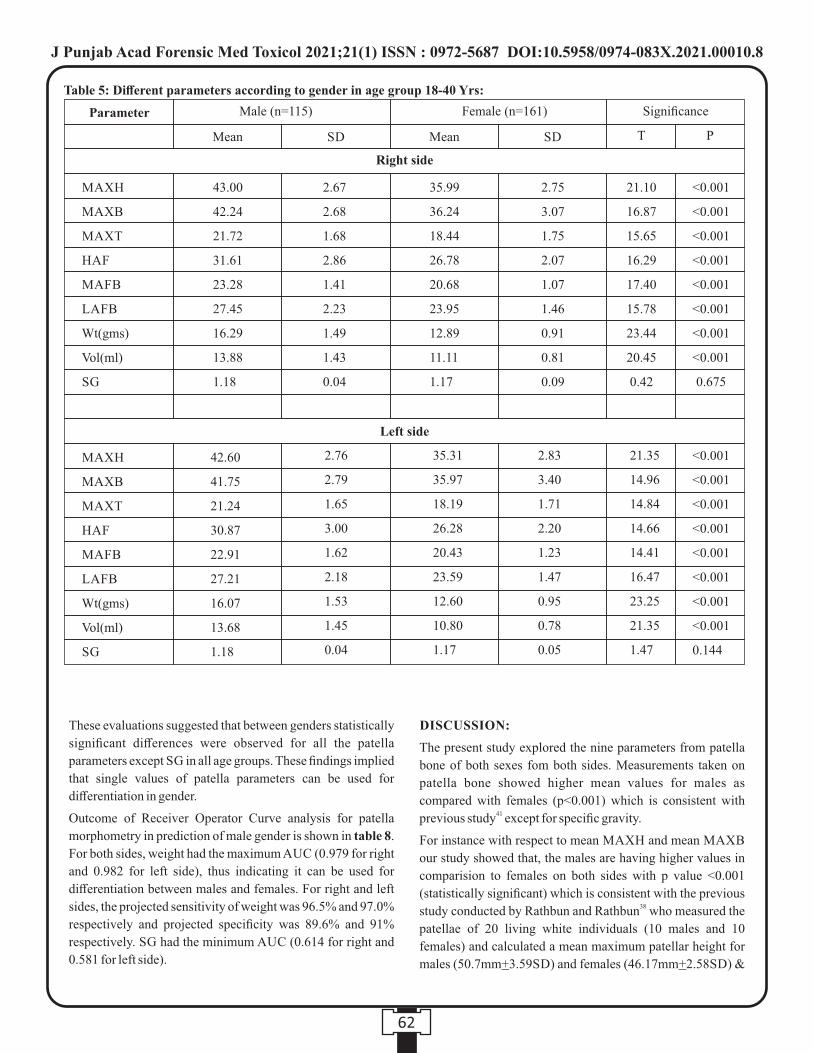
DISCUSSION:
The present study explored the nine parameters from patella
bone of both sexes fom both sides. Measurements taken on
patella bone showed higher mean values for males as
compared with females (p<0.001) which is consistent with 41previous study except for specific gravity.
For instance with respect to mean MAXH and mean MAXB
our study showed that, the males are having higher values in
comparision to females on both sides with p value <0.001
(statistically significant) which is consistent with the previous 38study conducted by Rathbun and Rathbun who measured the
patellae of 20 living white individuals (10 males and 10
females) and calculated a mean maximum patellar height for
males (50.7mm+3.59SD) and females (46.17mm+2.58SD) &
These evaluations suggested that between genders statistically
significant differences were observed for all the patella
parameters except SG in all age groups. These findings implied
that single values of patella parameters can be used for
differentiation in gender.
Outcome of Receiver Operator Curve analysis for patella
morphometry in prediction of male gender is shown in table 8.
For both sides, weight had the maximum AUC (0.979 for right
and 0.982 for left side), thus indicating it can be used for
differentiation between males and females. For right and left
sides, the projected sensitivity of weight was 96.5% and 97.0%
respectively and projected specificity was 89.6% and 91%
respectively. SG had the minimum AUC (0.614 for right and
0.581 for left side).
62
35.99
36.24
18.44
26.78
20.68
23.95
12.89
11.11
1.17
2.75
3.07
1.75
2.07
1.07
1.46
0.91
0.81
0.09
21.10
16.87
15.65
16.29
17.40
15.78
23.44
20.45
0.42
42.60
41.75
21.24
30.87
22.91
27.21
16.07
13.68
1.18
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001
0.144
Parameter Male (n=115)
Mean MeanSD SD T P
Female (n=161) Significance
Right side
MAXH
MAXB
MAXT
HAF
MAFB
LAFB
Wt(gms)
Vol(ml)
SG
Left side
MAXH
MAXB
MAXT
HAF
MAFB
LAFB
Wt(gms)
Vol(ml)
SG
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001
0.675
2.76
2.79
1.65
3.00
1.62
2.18
1.53
1.45
0.04
35.31
35.97
18.19
26.28
20.43
23.59
12.60
10.80
1.17
2.83
3.40
1.71
2.20
1.23
1.47
0.95
0.78
0.05
21.35
14.96
14.84
14.66
14.41
16.47
23.25
21.35
1.47
Table 5: Different parameters according to gender in age group 18-40 Yrs:
43.00
42.24
21.72
31.61
23.28
27.45
16.29
13.88
1.18
2.67
2.68
1.68
2.86
1.41
2.23
1.49
1.43
0.04
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00010.8
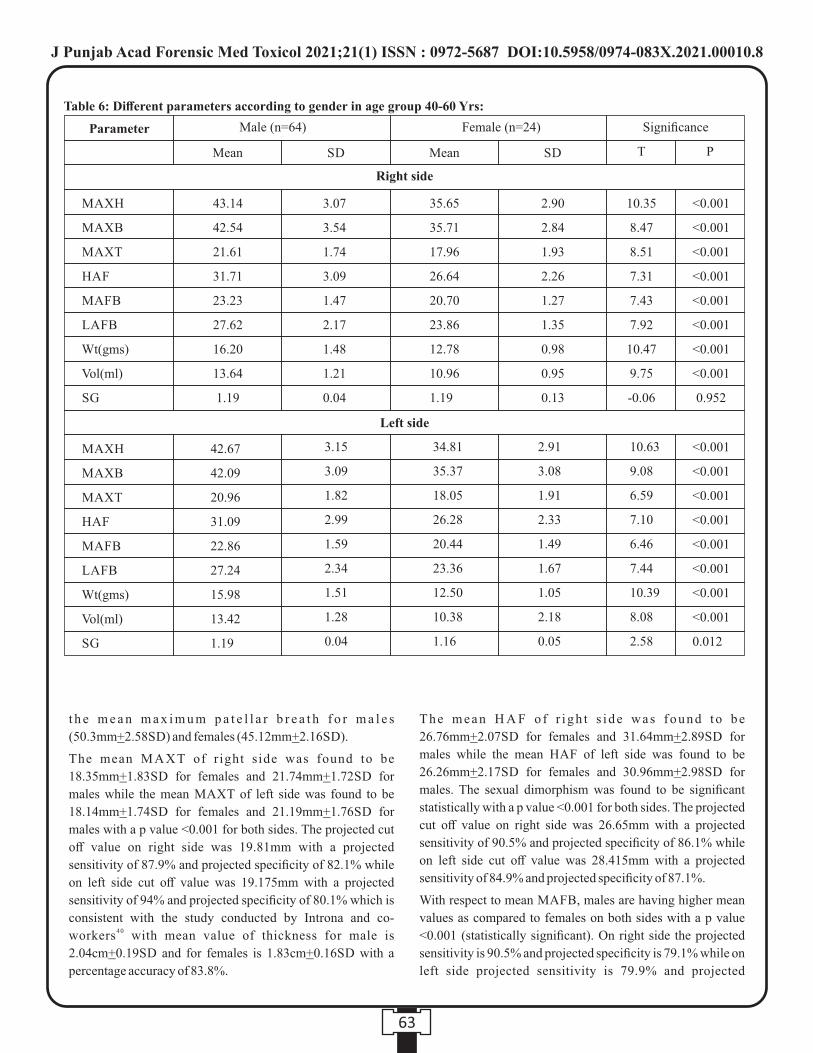
The mean H A F o f r i gh t s i de was found t o be
26.76mm+2.07SD for females and 31.64mm+2.89SD for
males while the mean HAF of left side was found to be
26.26mm+2.17SD for females and 30.96mm+2.98SD for
males. The sexual dimorphism was found to be significant
statistically with a p value <0.001 for both sides. The projected
cut off value on right side was 26.65mm with a projected
sensitivity of 90.5% and projected specificity of 86.1% while
on left side cut off value was 28.415mm with a projected
sensitivity of 84.9% and projected specificity of 87.1%.
With respect to mean MAFB, males are having higher mean
values as compared to females on both sides with a p value
<0.001 (statistically significant). On right side the projected
sensitivity is 90.5% and projected specificity is 79.1% while on
left side projected sensitivity is 79.9% and projected
t h e m e a n m a x i m u m p a t e l l a r b r e a t h f o r m a l e s
(50.3mm+2.58SD) and females (45.12mm+2.16SD).
The mean M A X T of r ight side was found to be
18.35mm+1.83SD for females and 21.74mm+1.72SD for
males while the mean MAXT of left side was found to be
18.14mm+1.74SD for females and 21.19mm+1.76SD for
males with a p value <0.001 for both sides. The projected cut
off value on right side was 19.81mm with a projected
sensitivity of 87.9% and projected specificity of 82.1% while
on left side cut off value was 19.175mm with a projected
sensitivity of 94% and projected specificity of 80.1% which is
consistent with the study conducted by Introna and co-40workers with mean value of thickness for male is
2.04cm+0.19SD and for females is 1.83cm+0.16SD with a
percentage accuracy of 83.8%.
63
35.65
35.71
17.96
26.64
20.70
23.86
12.78
10.96
1.19
2.90
2.84
1.93
2.26
1.27
1.35
0.98
0.95
0.13
10.35
8.47
8.51
7.31
7.43
7.92
10.47
9.75
-0.06
Parameter Male (n=64)
Mean MeanSD SD T P
Female (n=24) Significance
Right side
MAXH
MAXB
MAXT
HAF
MAFB
LAFB
Wt(gms)
Vol(ml)
SG
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001
0.952
Table 6: Different parameters according to gender in age group 40-60 Yrs:
3.07
3.54
1.74
3.09
1.47
2.17
1.48
1.21
0.04
42.67
42.09
20.96
31.09
22.86
27.24
15.98
13.42
1.19
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001
0.012
Left side
MAXH
MAXB
MAXT
HAF
MAFB
LAFB
Wt(gms)
Vol(ml)
SG
3.15
3.09
1.82
2.99
1.59
2.34
1.51
1.28
0.04
34.81
35.37
18.05
26.28
20.44
23.36
12.50
10.38
1.16
2.91
3.08
1.91
2.33
1.49
1.67
1.05
2.18
0.05
10.63
9.08
6.59
7.10
6.46
7.44
10.39
8.08
2.58
43.14
42.54
21.61
31.71
23.23
27.62
16.20
13.64
1.19
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00010.8
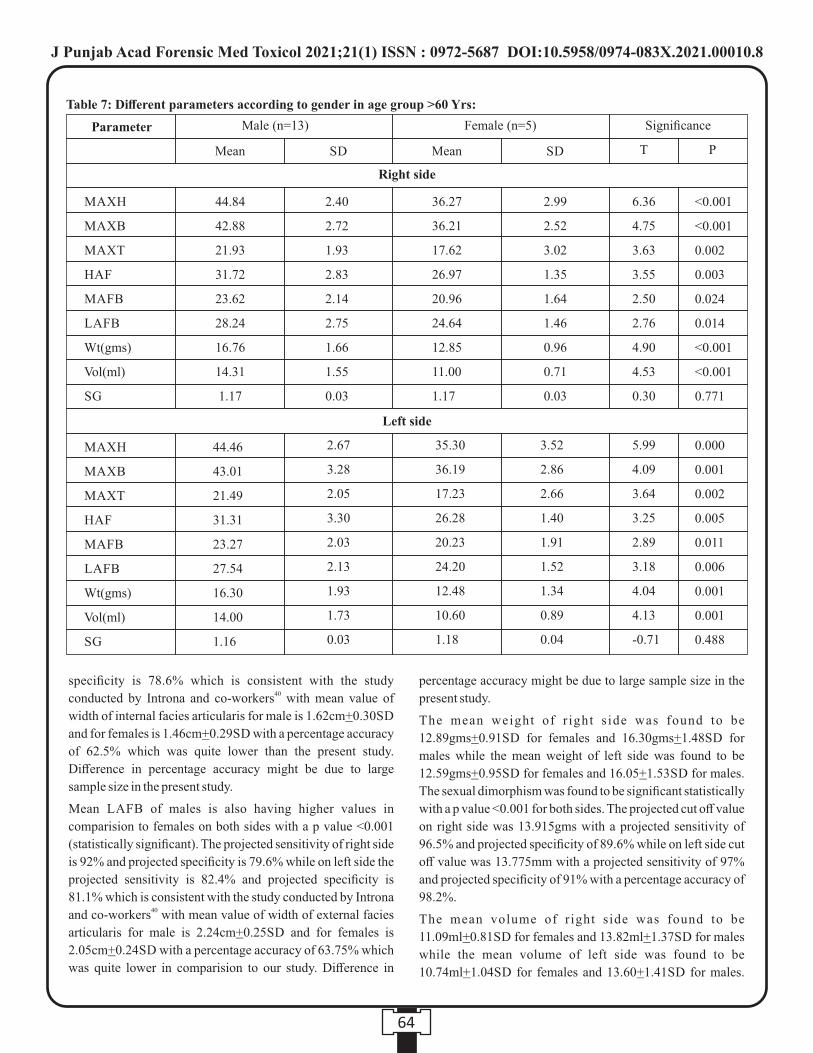
64
<0.001
<0.001
0.002
0.003
0.024
0.014
<0.001
<0.001
0.771
36.27
36.21
17.62
26.97
20.96
24.64
12.85
11.00
1.17
2.99
2.52
3.02
1.35
1.64
1.46
0.96
0.71
0.03
6.36
4.75
3.63
3.55
2.50
2.76
4.90
4.53
0.30
Parameter Male (n=13)
Mean MeanSD SD T P
Female (n=5) Significance
Right side
MAXH
MAXB
MAXT
HAF
MAFB
LAFB
Wt(gms)
Vol(ml)
SG
Table 7: Different parameters according to gender in age group >60 Yrs:
2.40
2.72
1.93
2.83
2.14
2.75
1.66
1.55
0.03
44.46
43.01
21.49
31.31
23.27
27.54
16.30
14.00
1.16
0.000
0.001
0.002
0.005
0.011
0.006
0.001
0.001
0.488
Left side
MAXH
MAXB
MAXT
HAF
MAFB
LAFB
Wt(gms)
Vol(ml)
SG
2.67
3.28
2.05
3.30
2.03
2.13
1.93
1.73
0.03
35.30
36.19
17.23
26.28
20.23
24.20
12.48
10.60
1.18
3.52
2.86
2.66
1.40
1.91
1.52
1.34
0.89
0.04
5.99
4.09
3.64
3.25
2.89
3.18
4.04
4.13
-0.71
44.84
42.88
21.93
31.72
23.62
28.24
16.76
14.31
1.17
percentage accuracy might be due to large sample size in the
present study.
The mean weight of r ight s ide was found to be
12.89gms+0.91SD for females and 16.30gms+1.48SD for
males while the mean weight of left side was found to be
12.59gms+0.95SD for females and 16.05+1.53SD for males.
The sexual dimorphism was found to be significant statistically
with a p value <0.001 for both sides. The projected cut off value
on right side was 13.915gms with a projected sensitivity of
96.5% and projected specificity of 89.6% while on left side cut
off value was 13.775mm with a projected sensitivity of 97%
and projected specificity of 91% with a percentage accuracy of
98.2%.
The mean volume of right side was found to be
11.09ml+0.81SD for females and 13.82ml+1.37SD for males
while the mean volume of left side was found to be
10.74ml+1.04SD for females and 13.60+1.41SD for males.
specificity is 78.6% which is consistent with the study 40conducted by Introna and co-workers with mean value of
width of internal facies articularis for male is 1.62cm+0.30SD
and for females is 1.46cm+0.29SD with a percentage accuracy
of 62.5% which was quite lower than the present study.
Difference in percentage accuracy might be due to large
sample size in the present study.
Mean LAFB of males is also having higher values in
comparision to females on both sides with a p value <0.001
(statistically significant). The projected sensitivity of right side
is 92% and projected specificity is 79.6% while on left side the
projected sensitivity is 82.4% and projected specificity is
81.1% which is consistent with the study conducted by Introna 40and co-workers with mean value of width of external facies
articularis for male is 2.24cm+0.25SD and for females is
2.05cm+0.24SD with a percentage accuracy of 63.75% which
was quite lower in comparision to our study. Difference in
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00010.8
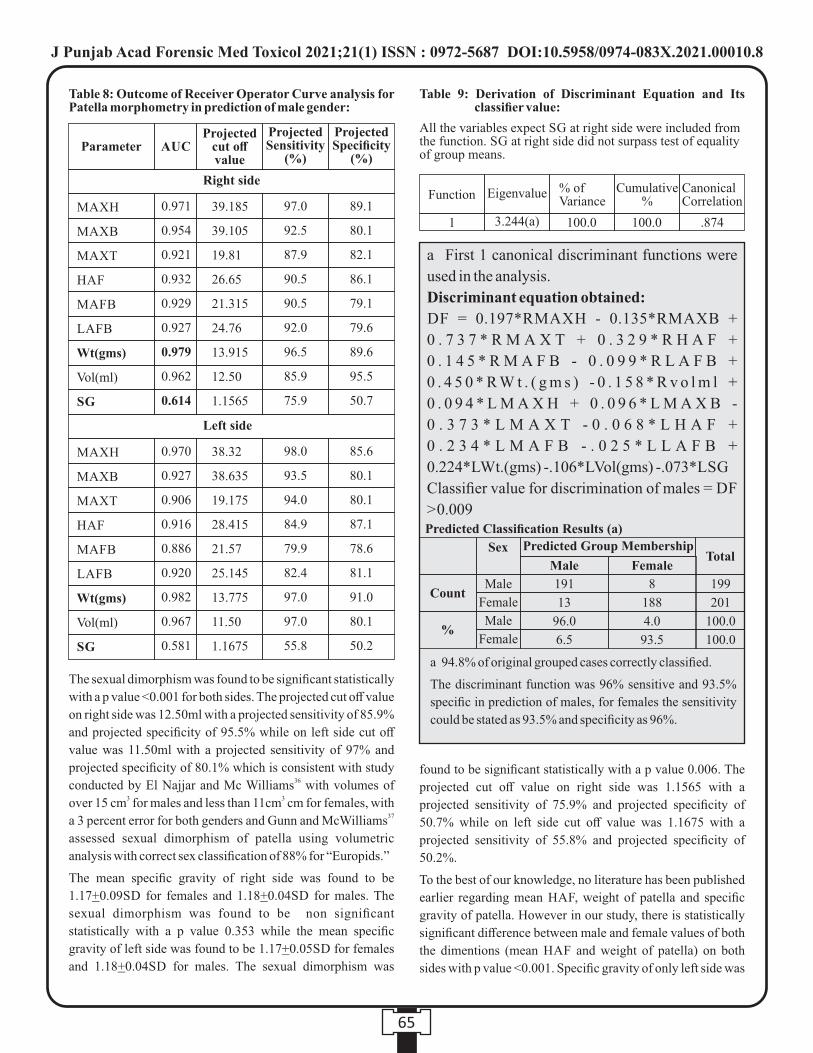
65
MAXH
MAXB
MAXT
HAF
MAFB
LAFB
Wt(gms)
Vol(ml)
SG
39.185
39.105
19.81
26.65
21.315
24.76
13.915
12.50
1.1565
0.971
0.954
0.921
0.932
0.929
0.927
0.979
0.962
0.614
97.0
92.5
87.9
90.5
90.5
92.0
96.5
85.9
75.9
89.1
80.1
82.1
86.1
79.1
79.6
89.6
95.5
50.7
MAXH
MAXB
MAXT
HAF
MAFB
LAFB
Wt(gms)
Vol(ml)
SG
38.32
38.635
19.175
28.415
21.57
25.145
13.775
11.50
1.1675
0.970
0.927
0.906
0.916
0.886
0.920
0.982
0.967
0.581
98.0
93.5
94.0
84.9
79.9
82.4
97.0
97.0
55.8
85.6
80.1
80.1
87.1
78.6
81.1
91.0
80.1
50.2
Parameter AUCProjected Sensitivity
(%)
Projected Specificity
(%)
Projected cut off value
Right side
Left side
Table 8: Outcome of Receiver Operator Curve analysis for Patella morphometry in prediction of male gender:
Table 9: Derivation of Discriminant Equation and Its classifier value:
All the variables expect SG at right side were included from the function. SG at right side did not surpass test of equality of group means.
Function Eigenvalue % of Variance
Cumulative %
Canonical Correlation
1 3.244(a) 100.0 100.0 .874
a First 1 canonical discriminant functions were
used in the analysis.
Discriminant equation obtained:
DF = 0.197*RMAXH - 0.135*RMAXB +
0 . 7 3 7 * R M A X T + 0 . 3 2 9 * R H A F +
0 . 1 4 5 * R M A F B - 0 . 0 9 9 * R L A F B +
0 . 4 5 0 * R W t . ( g m s ) - 0 . 1 5 8 * R v o l m l +
0 . 0 9 4 * L M A X H + 0 . 0 9 6 * L M A X B -
0 . 3 7 3 * L M A X T - 0 . 0 6 8 * L H A F +
0 . 2 3 4 * L M A F B - . 0 2 5 * L L A F B +
0.224*LWt.(gms) -.106*LVol(gms) -.073*LSG
Classifier value for discrimination of males = DF
> 0.009
Sex
Count
%
Predicted Group MembershipTotal
Male
Male 191
13
96.0
6.5
8
188
4.0
93.5
199
201
100.0
100.0
Male
Female
Female
Female
Predicted Classification Results (a)
a 94.8% of original grouped cases correctly classified.
The discriminant function was 96% sensitive and 93.5%
specific in prediction of males, for females the sensitivity
could be stated as 93.5% and specificity as 96%.
found to be significant statistically with a p value 0.006. The
projected cut off value on right side was 1.1565 with a
projected sensitivity of 75.9% and projected specificity of
50.7% while on left side cut off value was 1.1675 with a
projected sensitivity of 55.8% and projected specificity of
50.2%.
To the best of our knowledge, no literature has been published
earlier regarding mean HAF, weight of patella and specific
gravity of patella. However in our study, there is statistically
significant difference between male and female values of both
the dimentions (mean HAF and weight of patella) on both
sides with p value <0.001. Specific gravity of only left side was
The sexual dimorphism was found to be significant statistically
with a p value <0.001 for both sides. The projected cut off value
on right side was 12.50ml with a projected sensitivity of 85.9%
and projected specificity of 95.5% while on left side cut off
value was 11.50ml with a projected sensitivity of 97% and
projected specificity of 80.1% which is consistent with study 36conducted by El Najjar and Mc Williams with volumes of
3 3over 15 cm for males and less than 11cm cm for females, with 37a 3 percent error for both genders and Gunn and McWilliams
assessed sexual dimorphism of patella using volumetric
analysis with correct sex classification of 88% for “Europids.”
The mean specific gravity of right side was found to be
1.17+0.09SD for females and 1.18+0.04SD for males. The
sexual dimorphism was found to be non significant
statistically with a p value 0.353 while the mean specific
gravity of left side was found to be 1.17+0.05SD for females
and 1.18+0.04SD for males. The sexual dimorphism was
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00010.8
officers or physician (who perform autopsy) for determination
of sex; it can be used for the teaching of medical students at the
medical college or hospital level.
CONCLUSION:
To conclude, the present study showed that there are definite
sexual osteometric differences between male and female
patella bones from the population of Haryana and produced
standard for sex determination from patella that will be useful
for forensic experts.
REFERENCES:rd1. Saukko P, Knight B. Knight's Forensic Pathology. 3 ed.
London: A Hodder Arnold Publication; 2004. p. 98-131.
2. Stewart T.D. Identification by skeletal structures. Grahdwohl's ndLegal Medicine. 2 ed. In Camps F.E. (Ed.); 1968. p. 123-54.
3. Dix J, Graham M. Time of death, decomposition and
identification – an atlas. Boca Raton: CRC Press; 2000. p. 81-7.
4. Frayer DW, Wolpoff MH. Sexual dimorphism. Ann Rev
Anthropol. 1985;14:429-73.
5. Mathiharan K, Patnaik AK, editors. Modi's medical
jurisprudence and toxicology. 23rd ed. New Delhi: Lexis Nexis
Butterworths Wadhwa; 2006. p. 264-5.
6. Giles E, Elliot O. Sex determination by discriminant functional
analysis of Crania. Am J Phys Anthropol. 1960;21:53-8.
7. Krogman WM, Iscan MY. The human skeleton in forensic rdmedicine. 3 ed. Springfield: CC Thoma; 1986. p. 112-50, 189-
90.
8. Iscan MY, Loth SR, King CA, Shihai D, Yoshino M. Sexual
dimorphism in the humerus: a comparative analysis of Chinese,
Japanese and Thais. Forensic Sci Int. 1998;98:17-29.
9. Scheur L. Application of osteology in forensic medicine. Clin
Anat; 2002. p. 297-312.
10. Kimura K. Sex difference of the hip bone among several
Japanese populations. Okajima's Folia Anat Jpn. 1982;5:266-73.
11. Wu X, Shao X, Heng W. Sex differences and sex determination
of the innominate bone of modern Han nationality. Acta
Anthropal Sinica. 1982;1:118-31.
12. Singh S, Potturi BR. Greater sciatic notch in sex determination. J
Anat. 1978;5(3):619-24.
13. Wang L. A study of recent human skull from Hongkong
assessment of sex and of regional population. Acta Anthropal
Sinica. 1989;8:222-30.
14. Li C. A study on sex difference of adult skull of the northeast
China by fourier transform. Acta Anthropal Sinica.
1992;11:312.
15. Tanaka T, Hanihara K, Koizumu K. Sex determination of the
modern Japanese skull by means of discriminant function.
Sappora Med J. 1979;48:583-93.
16. Acsadi G, Nemeskeri J, Kiado A. History of human life span and
mortality. Budapest: Springer; 1970.
found to be statistically significant with p value <0.006.
In all (n=400) cases, a significant difference in mean
measurements of different parameters was observed for all the
parameters at both the sides except for SG on right side. In age
group <18 years, 18-40 and >60yrs, a significant difference in
mean measurements of different parameters was observed for
all the parameters at both the sides except for SG. However, in
age group 40-60 years, a significant difference in mean
measurements of different parameters was observed for all the
parameters at both the sides except for SG on right side.
These evaluations suggested that between genders,
statistically significant differences were observed for all the
patella parameters except SG. These findings implied that
single values of patella parameters can be used for
differentiation in gender.
For both sides, weight had the maximum AUC (0.979 for right
and 0.982 for left side) with projected sensitivity of 96.5% and
97.0% for right and left side respectively and projected
specificity of 89.6% and 91% for right and left side
respectively. SG had the minimum AUC (0.614 for right and
0.581 for left side). The discriminant function was 96%
sensitive and 93.5% specific in prediction of males, for females
the sensitivity could be stated as 93.5% and specificity as 96%.
The present study showed that, there are definite sexual
osteometric differences between male and female patella
bones from the population of Haryana. The determination of
sex can be accomplished by comparing the dimension of
unknown patella bone with the cut off value given. The study
produced standard for the population of Haryana for sex
determination and will be useful for forensic experts.
STRENGTHS AND LIMITATIONS:
To best of our knowledge, our study is the first of its kind in the
Indian subcontinent where all the nine dimensions of the
patella bone have been studied. Earlier, studies have either
explored one or two dimensions of the patella bone. We have
also explored specific gravity and volume of the patella bone
along with the physical dimensions like length, breath,
thickness etc. Second, our study was done on a larger sample
of 400 subjects while the earlier studies have been done on
much smaller samples. Third, we have studied the dimensions
of both the left and right patellar bones of same individual
(total 800 patella bones) and thus provided an extensive insight
on the dimensions on both sides while previous studies have
not explored this aspect. The present study does not include
prepubertal subjects which is one of the limitation of the study.
Not including the prepubertal subjects is due to growing age of
the individual which might interfere with the results.
Result of the study can be used by the forensic experts, medical
66
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00010.8
Specificity of Discriminant Function Equations for Sex
Determination Using the Talus of South African Blacks. J.
forensic Sci. 2004;49(6):1-6.
36. El Najjar MY, McWilliams KR. Forensic Anthropology. Charles
C Thomas, Springfield, IL; 1978. p. 89.
37. Gunn MC, McWilliams KR. A Method for estimating Sex of the
Human Skeleton from the Volume of the Patella, Talus, or
Calcaneus. HOMO. 1980;31:189–98.
38. Rathbun TA, Rathbun BC. Human remains recovered from a
shark's stomach in South Carolina. J. Forensic Sci. 1984;29:269-
76.
39. O'Connor WG. The dimorphic sesamoid: differentiating the
patella of females and males by height, width and thickness
measurements. Master's thesis of Arts in the Department of
Anthropology-University of South Carolina; 1996.
40. Introna Jr F, Di Vella G, Campobasso CP. Sex Determination by
Discriminant Function Analysis of Patella Measurements.
Forensic Sci. Int. 1998;95(1):39–45.
41. Dayal MR, Bidmos MA. Discriminating Sex in South African
Blacks Using Patella Dimensions. J. Forensic Sci. 2005;50(6):1-
4.
Units of Measurement:
1. Maximum height (MAXH), Maximum breadth
(MAXB), Maximum thickness (MAXT), Height of
articular facet (HAF), Medial articular facet breadth
(MAFB), Lateral articular facet breadth (LAFB) are
measured in millimetre (mm).
2. Weight of patella (Wt) is measured in gram (gm).
3. Volume of patella (Vol) is measured in millilitre (ml).
Abbreviations:
HAF : Height of articular facet - maximum height of the
articular facet on the posterior aspect of the patella.
LAFB : Lateral articular facet breath - distance between the
lateral edge of the patella and the median ridge of the articular
facet.
MAFB : Medial articular facet breath - distance between the
medial edge of the patella and the median ridge of the articular
facet.
MAXB : Maximum breath - the greatest distance between the
medial and lateral sides.
MAXH: Maximum height - the greatest distance between the
base and apex.
MAXT : Maximum thickness - the greatest distance between
the anterior and posterior surface
SD : Standard Deviation SG: Specific Gravity
Vol: Volume Wt: Weight
17. Steyn M, Iscan MY. Sex determination from the femur and tibia
in South African whites. Forensic Sci Int. 1997:111–9.
18. Iscan MY, Loth SR, King CA, Ding S, Yoshino M. Sexual
dimorphism in the humerus: a comparative analysis of Chinese,
Japanese and Thais. Forensic Sci Int. 1998:17–29.
19. Iscan MY. Osteometric analysis of sexual dimorphism in the
sternal end of the rib. J Forensic Sci. 1985;30:1090–9.
20. Wiredu EK, Kumoji R, Seshadri R, Biritwum RB. Osteometric
analysis of sexual dimorphism in the sternal end of the rib in a
West African population. J Forensic Sci. 1999;44:921–5.
21. MacLaughlin SM, Oldale KL. Vertebral body diameters and sex
prediction. Ann Hum Biol. 1992;19:285–92.
22. McCormick FW, Stewart JH, Greene H. Sexing of human
clavicles using length and circumference measurements. Am J
Forensic Med Pathol. 1991;12:175–81.
23. Smith SL. Attribution of foot bones to sex and population
groups. J Forensic Sci. 1997;42:186–95.
24. Macho GA. Is sexual dimorphism in the femur a ''population
specific'' phenomenon. Zeitschrift fu¨r Morphologie und
Anthropologie. 1990;78:229–42.
25. Srivastava R, Saini V, Rai RK, Pandey S, Tripathi SK. A study of
sexual dimorphism in the femur among North Indians. J
Forensic Sci. 2012 Jan;57(1):19-23.
26. Singh J, Pathak RK. Sex and age related non-metric variation of
the human sternum in a Northwest Indian post-mortem sample:
A pilot study. Forensic Sci Int. 2013 May 10;228(1-3):181.e1-
e12.
27. Akhlaghi M, Moradi B, Hajibeygi M. Sex determination using
anthropometric dimensions of the clavicle in Iranian population.
J Forensic Leg Med. 2012 Oct;19(7):381-5.
28. Akhlaghi M, Sheikhazadi A, Ebrahimnia A, Hedayati M,
Nazparvar B, Saberi Anary SH. The value of radius bone in
prediction of sex and height in the Iranian population. J Forensic
Leg Med. 2012 May;19(4):219-22.
29. Purkait R. Measurements of ulna--a new method for
determination of sex. J Forensic Sci. 2001 Jul;46(4):924-7.
30. Dabbs G. Sex determination using the scapula in New Kingdom
skeletons from Tell El-Amarna. Homo. 2010 Dec;61(6):413-20.
31. Galdames ICS, Matamala DAZ, Smith RL. Blind Test of
Mandibular Morphology with Sex Indicator in Subadult
Mandibles. Int. J. Morphol. 2008;26(4):845-8.
32. Albanese J. A Metric Method for Sex Determination Using the
Hipbone and the Femur. J Forensic Sci. 2003;48(2):1-11.
33. Sangvichien S, Boonkaew K, Chuncharunee A, Komoltri C,
Udom C, Chande T. Accuracy of Cranial and Mandible
Morphological Traits for Sex Determination in Thais. Siriraj
Med J. 2008;60:240-3.
34. Patil G, Kolagi S, Ramadurg U. Sexual Dimorphism in the
Humerus: A Study on South Indians. Journal of Clinical and
Diagnostic Research. 2011;50(3):538-41.
35. Bidmos MA, Dayal MR. Further Evidence to Show Population
67
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00010.8
68
Original Research Paper
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00011.X
1. Munish Kumar, Additional Senior Medical Officer, Civil Hospital, Ambala Cantt.
2. Kanika Kohli, Associate Professor, Department of Forensic Medicine and Toxicology, M.M. Institute of Medical Sciences
and Research, Mullana, Ambala
3. Harpreet Singh, Professor, Department of Forensic Medicine and Toxicology, Adesh Medical College & Hospital, Mohri,
Shahbad (M), Distt. Kurukshetra
Key words: Hanging, Ligature mark, Mechanical asphyxia, Strangulation, , Throttling.
Corresponding Author:
Dr. Kanika Kohli,
Associate Professor,
Department of Forensic Medicine and toxicology, M.M.
Institute of Medical Sciences and Research, Mullana, Ambala
Contact : +91 9728405109
Email : [email protected]
Article History :
Received : 2 July 2020
Received in revised form : 7 September 2020
Accepted on : 7 September 2020
Available online : 31 August 2021
INTRODUCTION:
Asphyxia is a condition caused by interference with respiration
due to lack of oxygen in the respired air that results in
deprivation of O in organs & peripheral tissues resulting in 2
loss of consciousness or death.
Violent asphyxia deaths have significant contribution to
unnatural deaths such as suicides, homicides, and accidental
deaths. Among various violent asphyxia deaths like hanging,
strangulation, smothering, throttling, traumatic asphyxia,
choking and drowning. Hanging is one of the leading manner
of suicide in which there is suspension of the body by a ligature
material compressing the neck externally, the constricting 1 force being the weight of the body. Hanging is always
considered suicidal except accidental hanging in sexual
perverts, homicidal hanging in lynching and justifiable judicial
hanging.
Strangulation is another form of asphyxia death in which there
is compression of neck structures by a constricting force other
than the body's own weight. Strangulation is always presumed
to be homicidal unless proved otherwise. The constricting
mark is usually found at the lower level on the neck and 2 frequently the direct pressure is exerted upon the neck.
There are different psychosocial and psychological factors.
Mental illness is important in young for act of suicide and
homicide, whereas physical illness is main cause of suicide
among old persons.
In many cases of hanging and strangulation ligature mark
creates doubt. So proper assessment of various postmortem
findings is necessary under such circumstances. Therefore
attempt to study external as well as internal features in the neck
in cases of neck compression mainly hanging and 3 strangulation is required.
Transmission of vital structures like major blood vessels,
nerves, oesophagus and wind pipe from head to other parts of
the body is through neck. Ligature and manual strangulation is
A Retrospective Autopsy Study of Deaths due to Compression of Neck
ABSTRACT :
Background: The study was conducted in the Department of Forensic Medicine, MMIMSR, Mullana to analyse the various
demographic variables of the subjects who died due to hanging, manual strangulation, ligature strangulation and had undergone
postmortem examination.
Methods: Out of 363 medico-legal deaths autopsied at MMIMSR, Mullana, details were collected from those medico-legal deaths
identified to be due to compression of neck.
Results: Out of 363 medico-legal autopsies, 77 cases were of death due to neck compression. Combined injuries of all neck
structures were seen in 8.7% cases of strangulation and 4.3% of throttling . Study comprised of 74.1% males & 25.9% females
with maximum deaths in age group of 20-30 years in hanging and 73.9% males and 26.1% females in strangulation. Rope was
ligature material of choice in hanging and strangulation. Frequency of hyoid bone fracture was maximum in strangulation.

4 most commonly responsible for mechanical asphyxia. The
purpose of the study was to see the pattern of injuries in
hanging and strangulation and weather antemortem or
postmortem in nature as majority of the cases coming for the
autopsies are due to violent asphyxia deaths out of which some
are suicidal, some are homicidal and some due to accidental
nature.
MATERIALS AND METHODS :
Present retrospective study was conducted on cases of death
due to compression of neck irrespective of age and sex in the
department of Forensic Medicine and Toxicology MMIMSR,
Mullana, Ambala. For this study data of postmortem reports of
hanging and strangulation was collected regarding name, age,
sex, alleged cause of death by investigating officer and
external and internal findings. Decomposed bodies were
excluded.
RESULTS:
Maximum number of deaths due to hanging was seen in the age
group of 21-30 years. Out of 54 cases 40 males (74.1%) and 14
females (25.9%) died due to hanging. (Table 1)
Table No. 2 depicts that the maximum 13 cases of
strangulation were seen in the age group of 21-30 years. Out of
23 cases 17 (73.9%) males and 06 (26.1%) females died due to
strangulation.
Table No. 3 depicts total 54 cases of hanging out of which 34
(63%) males and 14 (25.9%) females were from rural area,
whereas 6 (11.1%) males and no females were from urban area.
So 88.9 % were from rural and 11.1% were from urban origin.
Table No. 4 depicts that total 23 cases of strangulation out of
which 14 (60.9%) males and 4 (17.4%) females were from
rural area, whereas 3 (13%) males and 2 (8.7%) females were
from urban area. So 78.3 % were from rural and 21.7% were
from urban origin.
Table No. 5 shows rope was used as a ligature material in
maximum 26 (48.1%) cases of hanging followed by chunni 8
(14.8 %) and cloth 8 (14.8 %) cases. Whereas in strangulation 7
(30.5%) cases were of manual strangulation where ligature
material was not used and then maximum 4 (17.4%) cases
where ligature material used was chunni followed by muffler
in minimum number. Out of 77 cases of hanging and
strangulation rope was used as a ligature material in maximum
number of cases i.e. 29 (37.7%)
69
Age group
0-10
11-20
21-30
31-40
41-50
51-60
>60
Total
Female
0
4
9
1
0
0
0
14
Male
0
7
17
8
6
2
0
40
Total
0
11
26
9
6
2
0
54
%
0
7.4
16.7
1.8
0
0
0
25.9
%
0
13
31.5
14.8
11.1
3.7
0
74.1
%
0
20.4
48.1
16.7
11.1
3.7
0
100
Table No. 1: Age & sex wise distribution of Hanging cases
Table 2: Age wise & sex wise distribution of Strangulation cases
Age group
0-10
11-20
21-30
31-40
41-50
51-60
>60
Total
Male
1
1
4
0
0
0
0
6
Female
0
2
9
5
0
0
1
17
Total
1
3
13
5
0
0
1
23
%
4.3
4.3
17.4
0
0
0
0
26.1
%
0
8.7
39.1
21.8
0
0
4.3
73.9
%
4.3
13.1
56.5
21.8
0
0
4.3
100
Rural/Urban
Rural
Urban
Total
Hanging
Male
No.
34
6
40
No.
14
0
14
No.
48
6
54
%
63
11.1
74.1
%
25.9
0
25.9
%
88.9
11.1
100
Female
Total
Table 3: Sex & area wise distribution of hanging cases
Rural/Urban
Rural
Urban
Total
Hanging
Male
No.
14
3
17
No.
4
2
6
No.
18
5
23
%
60.9
13
73.9
%
17.4
8.7
26.1
%
78.3
21.7
100
Female
Total
Table 4: Sex & area wise distribution of strangulation cases
Total
Type of ligature
material
Rope
Chunni
Parna
Cloth
Shirt
Woolen muffler
Wire
Not Known
Other
No.
26
8
3
8
0
1
4
4
0
No.
3
4
3
0
2
1
0
3
7
No.
29
12
6
8
2
2
4
7
7
%
48.1
14.8
5.6
14.8
0
1.9
7.4
7.4
0
%
13
17.4
13
0
8.7
4.4
0
13
30.5
%
37.7
15.6
7.8
10.3
2.6
2.6
5.2
9.1
9.1
Type of asphyxial death
Hanging Strangulation
Table 5: Type of ligature material in hanging & strangulation cases
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00011.X

Table No. 6 shows out of 54 cases of hanging no case in both
sexes had injuries together to larynx, trachea, hyoid bone and
thyroid cartilage.
Out of 23 cases of strangulation cases, 2 (8.7%) male cases had
combined injuries to larynx, trachea, hyoid bone and thyroid
cartilage in ligature strangulation but no female case had
injuries together to larynx, trachea, hyoid bone and thyroid
cartilage in ligature strangulation.
1 (4.3%) male case had combined injuries to larynx, trachea,
hyoid bone and thyroid cartilage in manual strangulation but
no female case had injuries together to larynx, trachea, hyoid
bone and thyroid cartilage in manual strangulation
DISCUSSION :
The extent of passing because of hanging and strangulation in 5our examination period was seen as very like Momin SG et all .
Hanging cases number is 2.4 occasions that of strangulation
cases which is very like 2.9 occasions as saw in the 6examination by Sheik et all . A lower frequency was accounted
7 8for by Singh RK et al (8.04%), Tirmizi et al (7.08%) and Bhim 9Singh et al (8.83%). In our current investigation the most
extreme number of cases for example 50.6% was noted in age
bunch between 21 to 30 years (Table 1 and 2) Sheik et al 6announced 42.42% cases in 21 to 30 years old group. Joshi R
et al additionally revealed 44.18% cases in 21 to 30 years old 10group. Momin SG et al likewise detailed 40.2% cases in 21 to
530 years old group.
In the hanging cases 74.1% male and 25.9% female cases were
seen in present examination. Sheik et al detailed 71.2% males 6and 28.8% females in hanging cases which is very
comparative with the current investigation Joshi R et al 10detailed 64% males and 36% females in hanging cases
Out of strangulation cases, 73.9% males and 26.1% females
were seen in present investigation which is in dissimilarity to
the examination by Sheik et al who announced no female 6instance of strangulation.
In present investigation 84.2% male were of provincial
inception and 15.8% had a place with urban area.
Correspondingly 90% females were of provincial beginning
and 10% were of urban district (Table 3 and 4). Joshi R females 10had a place with urban areas.
In present examination 88.9% hanging cases were from
country region and 11.1% were from urban region which is
very like Pal SK et al concentrate in which 90.16% hanging
cases were from rustic starting point and 9.83% had a place 11with urban region. In present investigation strangulation
cases female survivor of provincial territory were more 17.4%
Joshi R et al likewise revealed in strangulation cases female 10casualty of urban region were more 38.9%.
In present investigation rope was utilized as a ligature material
in 37.7% cases. Joshi R et al additionally watched rope as 10commonest strategy for ligature material in 32.5% cases.
12David and Marshall likewise noted rope in 51.4% cases.
CONCLUSION :
A retrospective study on deaths due to neck compression
concludes that majority of victims were in the age group of 21
to 30 years and were from rural areas. The most commonly
used ligature material was rope. More injuries to neck
structures were found in case of ligature strangulation.
REFERENCES :
1) Reddy KSN, The Synopsis of Forensic Medicine & thToxicology, 29 Ed, 2017, Jaypee Brothers Medical
Publishers (P) Ltd, New Delhi, Pg. 171
2) Glaister J. Medical jurisprudence and toxicology,
hanging, strangulation. Edinberg, living stone 1962 :165-
84.
3) Shaikh MMM, Chotaliya HJ, Modi AD, Parmar AP,
Kalele SD. A study of gross postmortem findings in cases
of hanging and ligature strangulation. JIAFM 2013; 35
(1):63-5
4) Nadar S, Iqbal M, Raja KS, Rana PA, Khokhar JI. Position
of knot in hanging and strangulation in asphyxia deaths in
medicolegal autopsies in Lahore. Medical Forum 2014;
25(9):32-5.
5) Momin SG, Mangal HM, Kyada HC, Vijapura MT, Bhuva
SD. Pattern of ligature mark in cases of compressed neck
in Rajkot region: A prospective study. JIAFM 2012;
34(1):40-3
6) Sheikh MI, Agarwal SS. Medico-legal implication of
hyoid bone fracture: A study 1999. JIAFM 2000-2001;
26(1-6): 61-3
7) Singh RK, Sonatomba Devi M, Femate L., Analysis of
changing pattern of unnatural deaths in Manipur during
1991-1995. J Forensic Med Toxicol,1997;26: 23-25
70
Total
Type of
Asphyxia
Hanging
Ligature
strangulation
Manual
strangulation
No.
0
2
1
No.
0
0
0
No.
0
2
1
%
0
8.7
4.3
%
0
0
0
%
0
8.7
4.3
Type of asphyxial death
Hanging Strangulation
Table No. 6: Distribution of injuries of larynx, trachea, hyoid bone and thyroid cartilage in hanging and strangulation
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00011.X
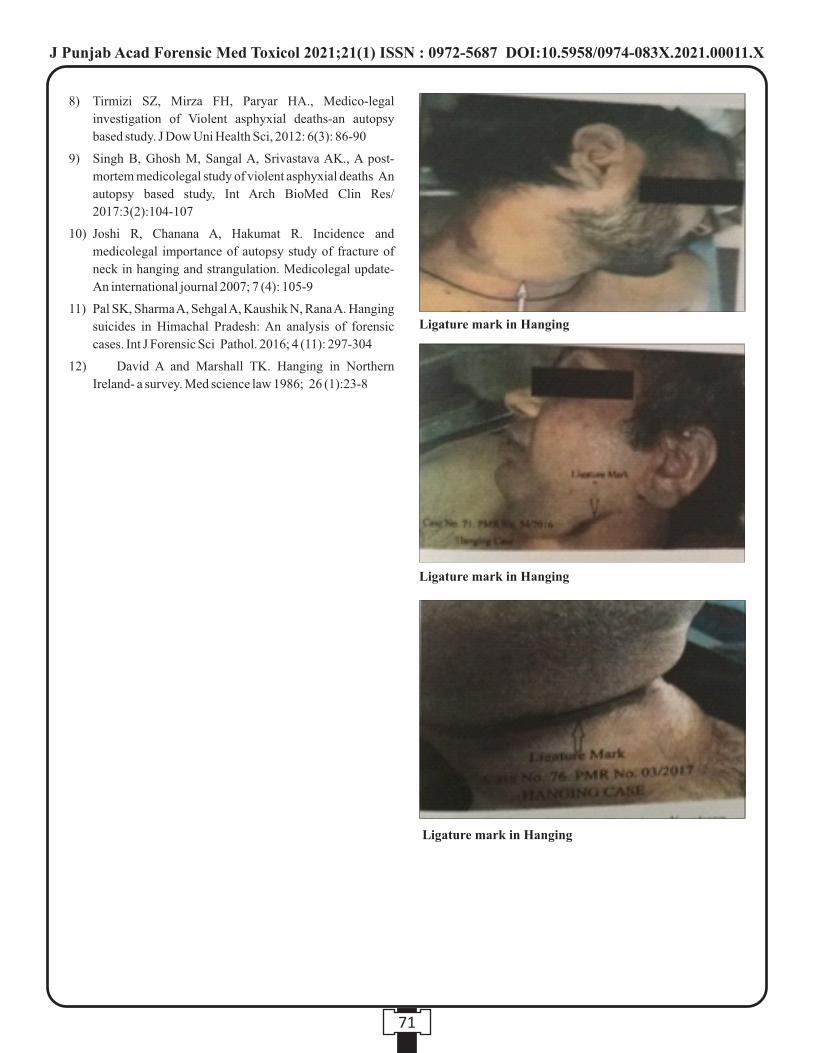
8) Tirmizi SZ, Mirza FH, Paryar HA., Medico-legal
investigation of Violent asphyxial deaths-an autopsy
based study. J Dow Uni Health Sci, 2012: 6(3): 86-90
9) Singh B, Ghosh M, Sangal A, Srivastava AK., A post-
mortem medicolegal study of violent asphyxial deaths An
autopsy based study, Int Arch BioMed Clin Res/
2017:3(2):104-107
10) Joshi R, Chanana A, Hakumat R. Incidence and
medicolegal importance of autopsy study of fracture of
neck in hanging and strangulation. Medicolegal update-
An international journal 2007; 7 (4): 105-9
11) Pal SK, Sharma A, Sehgal A, Kaushik N, Rana A. Hanging
suicides in Himachal Pradesh: An analysis of forensic
cases. Int J Forensic Sci Pathol. 2016; 4 (11): 297-304
12) David A and Marshall TK. Hanging in Northern
Ireland- a survey. Med science law 1986; 26 (1):23-8
71
Ligature mark in Hanging
Ligature mark in Hanging
Ligature mark in Hanging
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00011.X

72
Original Research Paper
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00012.1
1. Nidhi Sachdeva, Associate Professor, Deptartment of Forensic Medicine And Toxicology,N.S.C.B. Jabalpur
2. Divyam Singh Modi, Junior Resident, Deptartment of Forensic Medicine And Toxicology,N.S.C.B. Jabalpur
3. Mukesh Rai, Assistant Professor, Deptartment of Forensic Medicine And Toxicology,N.S.C.B. Jabalpur
4. Vivek Shrivastava, Professor and Head, Department of Forensic Medicine and Toxicology, N.S.C.B. Jabalpur
Key words: Hanging, Ligature mark, Mechanical asphyxia, Strangulation, , Throttling.
Corresponding Author:
Dr. Vivek Shrivastava,
Professor and Head,
Department of Forensic Medicine and Toxicology, N.S.C.B.
Jabalpur
Contact : +91 88713-38541
Email : [email protected]
Article History :
Received : 11 December 2020
Received in revised form : 7 January 2021
Accepted on : 7 January 2021
Available online : 15 August 2021
INTRODUCTION:
The novel coronavirus-2019 (COVID-19) pandemic has
impacted significantly on many sectors globally, and has also (1) impacted mental health of many individuals and in greater
numbers than those who are actually infected with the disease (2) The World Health Organization declared the virus outbreak
as a pandemic in March 2020. Current lockdown scenarios
have led to different behavioural consequences which lead to (3)increase in homicidal cases and suicidal behaviours
At present, various measures such as isolation, social
distancing, quarantine of infected individuals, and lockdown (4)have been implemented worldwide , which has affected the
normal day to day life of people across the world leading to
increase in mental health problems such as depression, anxiety, (5)phobias etc. . India being a developing country with limited
human resources in the field of mental health care, a lot of
psychological problems related to mental health go unnoticed.
A study of data from past pandemics such as influenza and
Severe Acute Respiratory Syndrome (SARS) have showed
that these outbreaks were followed by significant increases in (6)suicidal deaths . It is of interest that suicidal deaths related to
COVID-19 have already been reported in the Asian Journal of (7)Psychiatry
Main aim of our study here is to create and raise awareness
about the importance of mental health to health providers and
general public and how COVID-19 pandemic has contributed
to an increase in suicide and homicides.
MATERIALS AND METHOD:
Our study sample comprised all medico legal cases examined
from March to July, 2019 (1260 cases) and from March to July
2020 (979 cases), in the Department of Forensic Medicine and
Toxicology, Netaji Subhash Chandra Bose Medical College,
Jabalpur in total. Only the confirmed cases of suicidal and
Impact of Covid-19 Pandemic on Suicidal and Homicidal Deaths in Jabalpur, Madhya Pradesh, India
ABSTRACT :
Introduction: The novel coronavirus-2019 (COVID-19) pandemic has impacted significantly on many sectors globally, and has
also impacted mental health of many individuals. actually infected with the disease. The World Health Organization declared the
virus outbreak as a pandemic in March 2020. Current lockdown scenarios have led to different behavioural consequences which
lead to increase in homicidal cases and suicidal behaviours.
Aim: To study the effect of COVID-19 pandemic on suicidal and homicidal deaths in Jabalpur district between months' March to
July 2020, to cause awareness among health care professionals about impact of COVID-19 on mental health.
Materials and Methods: Present study was conducted in the department of forensic medicine and toxicology, Netaji Subhash
Chandra Bose Medical College, Jabalpur. Only confirmed cases of suicide and homicide were included in the study based on post
mortem reports and police inquest.
Result: COVID-19 pandemic caused an expected rise in the number of suicide and homicidal cases in the year 2020 in Jabalpur,
when compared with the year 2019.
Conclusion: A need for adequate mental health programs to combat the increase in mental health problems by initiatives along
with tele-mental health care, where mental health providers are expected to play a vital role in promoting psychological and
emotional well-being, strengthening problem-solving and health-promoting habits in service recipients.
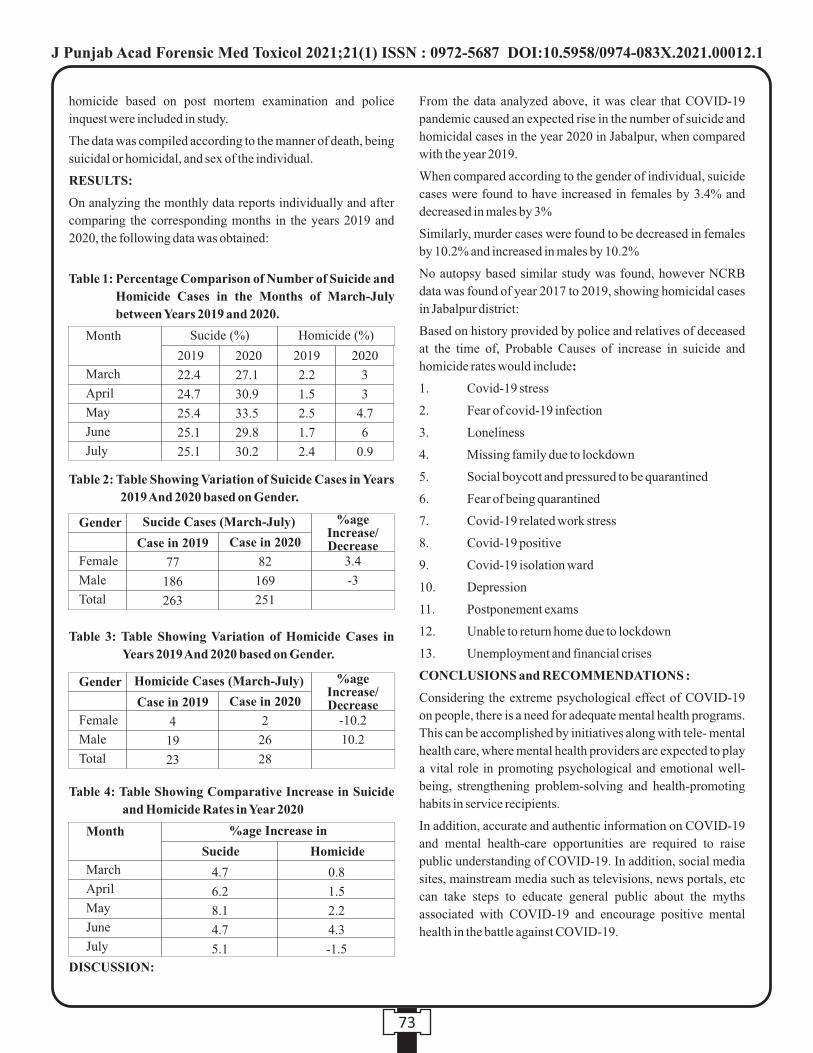
homicide based on post mortem examination and police
inquest were included in study.
The data was compiled according to the manner of death, being
suicidal or homicidal, and sex of the individual.
RESULTS:
On analyzing the monthly data reports individually and after
comparing the corresponding months in the years 2019 and
2020, the following data was obtained:
DISCUSSION:
From the data analyzed above, it was clear that COVID-19
pandemic caused an expected rise in the number of suicide and
homicidal cases in the year 2020 in Jabalpur, when compared
with the year 2019.
When compared according to the gender of individual, suicide
cases were found to have increased in females by 3.4% and
decreased in males by 3%
Similarly, murder cases were found to be decreased in females
by 10.2% and increased in males by 10.2%
No autopsy based similar study was found, however NCRB
data was found of year 2017 to 2019, showing homicidal cases
in Jabalpur district:
Based on history provided by police and relatives of deceased
at the time of, Probable Causes of increase in suicide and
homicide rates would include:
1. Covid-19 stress
2. Fear of covid-19 infection
3. Loneliness
4. Missing family due to lockdown
5. Social boycott and pressured to be quarantined
6. Fear of being quarantined
7. Covid-19 related work stress
8. Covid-19 positive
9. Covid-19 isolation ward
10. Depression
11. Postponement exams
12. Unable to return home due to lockdown
13. Unemployment and financial crises
CONCLUSIONS and RECOMMENDATIONS :
Considering the extreme psychological effect of COVID-19
on people, there is a need for adequate mental health programs.
This can be accomplished by initiatives along with tele- mental
health care, where mental health providers are expected to play
a vital role in promoting psychological and emotional well-
being, strengthening problem-solving and health-promoting
habits in service recipients.
In addition, accurate and authentic information on COVID-19
and mental health-care opportunities are required to raise
public understanding of COVID-19. In addition, social media
sites, mainstream media such as televisions, news portals, etc
can take steps to educate general public about the myths
associated with COVID-19 and encourage positive mental
health in the battle against COVID-19.
73
Table 2: Table Showing Variation of Suicide Cases in Years
2019 And 2020 based on Gender.
Gender
Female
Male
Total
Sucide Cases (March-July)
Case in 2019
77
186
263
Case in 2020
82
169
251
3.4
-3
%ageIncrease/Decrease
Table 3: Table Showing Variation of Homicide Cases in
Years 2019 And 2020 based on Gender.
Gender
Female
Male
Total
Homicide Cases (March-July)
Case in 2019
4
19
23
Case in 2020
2
26
28
-10.2
10.2
%ageIncrease/Decrease
Table 1: Percentage Comparison of Number of Suicide and
Homicide Cases in the Months of March-July
between Years 2019 and 2020.
Month
March
April
May
June
July
Sucide (%)
2019
22.4
24.7
25.4
25.1
25.1
2019
2.2
1.5
2.5
1.7
2.4
2020
27.1
30.9
33.5
29.8
30.2
2020
3
3
4.7
6
0.9
Homicide (%)
Table 4: Table Showing Comparative Increase in Suicide
and Homicide Rates in Year 2020
%age Increase inMonth
March
April
May
June
July
Sucide
4.7
6.2
8.1
4.7
5.1
0.8
1.5
2.2
4.3
-1.5
Homicide
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00012.1

REFERENCES:
1. Ahorsu DK, Lin , Imani V, Safari M, Griffiths MD, Amir
H, Pakpour. The fear of COVID-19 scale: Development
and Initial Validation. Int. J. Ment Health Addict. 2020
Mar 27;1-9.
2. Ornell F, Schuch JB, Sordi AO , Kessler FH. Pandemic
fear and COVID-19: Mental Health Burden and
strategies. Braz-J. Psychiatry. 2020;42(3):232-23
3. Ahmed et al. First confirmed detection of SARS-Cov-2 in
untreated wastewater in Australia: A proof of concept for
the wastewater surveillance of COVID-19 in the
community. Science of the total environment. 2020 Aug
1;728:138764.
4. Bodrud-Doza et al. Exploring COVID-19 stress and its
factors in Bangladesh: A perception-based study. Heliyon.
2020 Jul 10;6(7):e04399
5. Brooks et al., the psychological impact of quarantine and
how to reduce it: rapid review of the evidence. The Lancet.
2020 Mar 14;395(10227):912-920
6. Wasserman IM. Impact of Epidemic, War, Prohibition and
media on Suicide: United States ,1910- 1920.Suicide and
life threatening behavior.1992;22(2):240-54.
7. Mamun and Griffiths. COVID-19 Suicidal behavior
among couples and suicide pacts: case study evidence
from press reports. Psychiatry Res.2020 Jul;289:113105.
8. Sahoo et al. Self harm and COVID-19 Pandemic: an
emerging concern- A report of 2 cases from India. Asian J
psychiatr. 2020 Jun;51:102104.
74
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00012.1
Original Research Paper
INTRODUCTION :
The use of insecticides in the modern times has evidently
improved the socio-economic well- being of people in
developing nations. Whilst, the use of insecticides has
increased food production and has effectively put a check on
vector-borne diseases, on the other side there is an increasing
concern over the possible adverse effects of insecticides on the (1)environment along with human and animal health . The
current scenario of pesticide market is also changing
worldwide. With the introduction of strict rules in many
developed countries, organophosphates and carbamates are
being replaced by their less toxic counterparts such as
pyrethroids. The main reason for the increasing popularity of
pyrethroids over organophosphate and organochlorine (2)pesticides is that they are biodegradable , more effective
(3) (4)against target species and less toxic to mammals . Although,
initially considered as safe pesticides and used all over the
world, pyrethroids are capable of inducing many toxic effects
such as apoptosis, oxidative stress, neurotoxicity and (5-8)hepatotoxicity .
Cypermethrin (CYP), [(RS)-a-cyano-3-phenoxybenzyl
( 1 R S ) - c i s - t r a n s - 3 - ( 2 , 2 - d i c h l o r o - 6 0 v i n y l ) - 2 , 2 -
dimethylcyclopropanecarboxylate], a pyrethroid insecticide,
is commonly used as a pest control. It is a type II pyrethroid
containing an alpha-cyano group which tends to accumulate in (9)organs and tissues due to its lipophilic properties . Owing to
its lipophilic nature, CYP tends to get deposited in body fat and
destroys various organs like liver, kidneys, skin, ovaries and (10)brain .It is a synthetic pyrethroid, classified as a weak
category C-oncogene, considered as relatively less toxic to
mammals making it a preferred insecticide to be used for
domestic, agricultural and veterinary purposes but there are
studies where CYP has resulted in DNA damage and cell (11-12)damage in the target as well as non-target species. Various
studies on cell lines and animal models have shown that CYP
is capable of inducing other toxic effects including oxidative
Corresponding Author :
Dr. Shweta Sharma,
Assistant Professor (Chemistry),
Institute of Forensic Science & Criminology,
Punjab University, Chandigarh, INDIA 160 014
Contact : +91-172-2534121(O) +91-9872688577 (M)
Email : [email protected]
KEYWORDS : Cypermethrin, pyrethroid toxicity, domestic exposure, liver damage, forensic cases, liver enzyme activity
Article History:Received: 15 December 2020Received in revised form: 11 February 2021Accepted on: 11 February 2021 Available online: 15 August 2021
ABSTRACT :
Introduction :Hepatotoxicity of cypermethrin (CYP) has been widely studied. However, the adverse outcomes of sub-chronic
exposure have not been adequately estimated. This study was performed on Balb/c mice to investigate the changes in liver function
enzymes and liver structure after exposure to low dose CYP in mice.
Materials and Methods: Male Balb/c mice were segregated into two groups with Group I serving as the normal control. Group II
mice were given 2.5 mg/kg CYP dose orally once in a week for 56 days. Liver damage was assessed by performing liver function
tests i.e. AST, ALT and ALP along with histological analysis of liver by H&E staining followed by visualization under the
microscope.
Results : The changes in liver enzyme activities and histo-architecture of liver cells show that exposure to CYP leads to time-
dependent changes in the liver. The study reveals that low exposure to cypermethrin for longer periods of time results in liver injury
damaging the normal organization of the tissue. It also induces noteworthy elevation in hepatic markers enzymes viz. ALT, AST,
ALP along with necrosis, extensive vacuolar degeneration and decrease in number of hepatocytes. We found that CYP was able to
generate elevation in the expression of p53 (0.036) and p21 (0.0076) and decrease in CDK4 (p=0.0224) CDK2 (p=0.0458) thus
suggesting a role of cell cycle regulatory genes in the CYP caused liver toxicity.
Conclusions: These findings yield the evidence of sub-chronic CYP-induced toxicity in liver cells by showing changes in liver
enzyme activity, histology and cell cycle regulatory genes in the liver of Balb/c mice.
1. Dolly Mahna, PhD Research Scholar, Institute of Forensic Science & Criminology, Panjab University, Chandigarh2. Sanjeev Puri, Professor, Biotechnology, University Institute of Engineering & Technology, Panjab University, Chandigarh ,
India 160 014 3. Shweta Sharma, Assistant Professor , Institute of Forensic Science & Criminology, Panjab University, Chandigarh
Cypermethrin-induced liver toxicity in Balb/c mice
75
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00013.3

(13-14)stress, apoptosis and developmental neurotoxicity . It can
persist for a long time in air, walls and 71 furniture after any
household treatment which increases the possibility of (15)exposure . It is widely used in developing countries as an
insect-controlling agent. CYP is easily available in the market
which makes it quite accessible to people making way for
accidental, homicidal as well as suicidal acts. In this study, we
have examined p53, CDKN1A, CDK4 and cdk2 as liver
toxicity markers because these genes are known for their roles
in cell cycle regulation. The estimation of adverse effects due
to sub-chronic intoxication which may develop due to CYP
exposure is quite difficult. In addition to this, the information
available on the possible adverse effects due to sub-chronic
exposure of CYP on liver remains limited. To explore the sub-
chronic 80 effects of cypermethrin, we exposed mice to
2.5mg/kg dose for 56 days and to look for its effects on liver
enzymes, liver histopathological structure and cell cycle
perturbation.
MATERIALS AND METHODS :
Chemicals
Commercially available formulation of cypermethrin
(Cypermethrin 25% EC), ―Cyperbullǁ purchased from local
market of Assandh, Haryana produced by Bharati Minerals
Limited was used. Adequate dilutions were prepared in corn
oil to obtain the required test concentration. The test
concentrations were calculated based upon the percentage of
active ingredient of CYP in the commercially available
formulation. Fresh solutions were made every time before
dosing.
Animal Experiment and treatment
Male Balb/C mice in the weight range of 25-30 g were
purchased from the Central Animal House of Panjab
University, Chandigarh. The animals had free reach to pellet
diet as well as water. All the protocols followed in the study had
a valid approval by the Institutional Animal Ethics Committee
of Panjab University (PU/IAEC/S/15/113). The animals were
segregated into two groups consisting of 6 mice each.
Whereas, the test group received oral dose with an oral feeding
canula for 8 weeks, the control group received corn oil with no
pesticide exposure. The rats were indiscriminately segregated
into two groups namely-Normal control and CYP Group,
where each group had 6 animals each.
Group I animals served as normal control and were given corn
oil weekly.
Group II received 2.5 mg/kg CYP dose orally once in a week
for 56 days.
1/10 LD50 dose of CYP was chosen which was decided by (16)keeping in reference the LD50 of CYP in mice . This dose
doesn't cause immediate death or toxicity symptoms in the test
animals.
Collection of Serum and Tissue sample
Blood was taken out from the orbital sinus of mice under the
effect of mild ether anaesthesia. An approximate volume of 1
mL of blood was saved in test tube and for 30 minutes it was
kept undisturbed at room temperature. It was centrifuged at
2000 g for 10 min to obtain serum. After the collection of
blood, the scarification of animals was done by cervical
dislocation. It was followed by the dissection of liver which
was then rinsed in ice cold isotonic saline. Liver were stored at
-80°C for further investigation. One part of liver was kept for
histological analysis and saved in neutral buffered saline at
room temperature. Every possible effort was done to cut down
animal suffering in each experiment.
Liver Function Tests
The activity assessment of ALT i.e. alanine amino transferase ,
AST i.e. Aspartate amino transferase and ALP i.e. Alkaline
Phosphatase was done by kinetic method utilizing the kits
available commercially.
Histopathological Examination
For histology analysis, liver tissues were kept in 10% buffered
formalin for subsequent processing and histopathological
studies. Washing of formalin-fixed tissues was done
thoroughly in running tap water followed by dehydration in
ascending grades of alcohol.the tissues were cleared in
benzene, and then embedded in paraffin at the temperature of
58°C. Hematoxylin and eosin (H and E) method was employed (17)to stain the 5 μ-thick sections of paraffin-embedded tissues . It
was done under the supervision of expert pathologist at
Medicos centre Sector-22, Chandigarh.
Gene Regulatory Studies
RNA isolation from liver tissue of control as well as test
animals was carried out by Trizol isolation method. The quality
of isolated RNA was assessed by Nanodrop through which
RNA samples with a ratio of 1.8-2.0 at 260/280 nm were
employed for the study. 300 ng of total RNA for each sample
was converted to double-stranded cDNA by using RevertAid
Reverse Transcriptase from Thermo Scientific. KAPA SYBR
FAST qPCR Master Mix (2X) was utilized for carrying out
real time PCR supplied by KAPA BIOSYSTEMS (KK4603).
A 10 μl reaction mixture was made in thin walled PCR tubes
which had 4 μl of 2X SYBR GREEN reaction mixture,1 μM of
each forward and reverse primers, 1 μl of cDNA template and 3
μl of nuclease free water. PCR was carried out in a 20 μL total o omixture volume for 35 cycles at 95 C for 1 minute, 55 C for 1
ominute, 72 C for 1 minute. The reaction was run on the AB
Biosystems Step One Plus Real-Time PCR System (Thermo
76
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00013.3
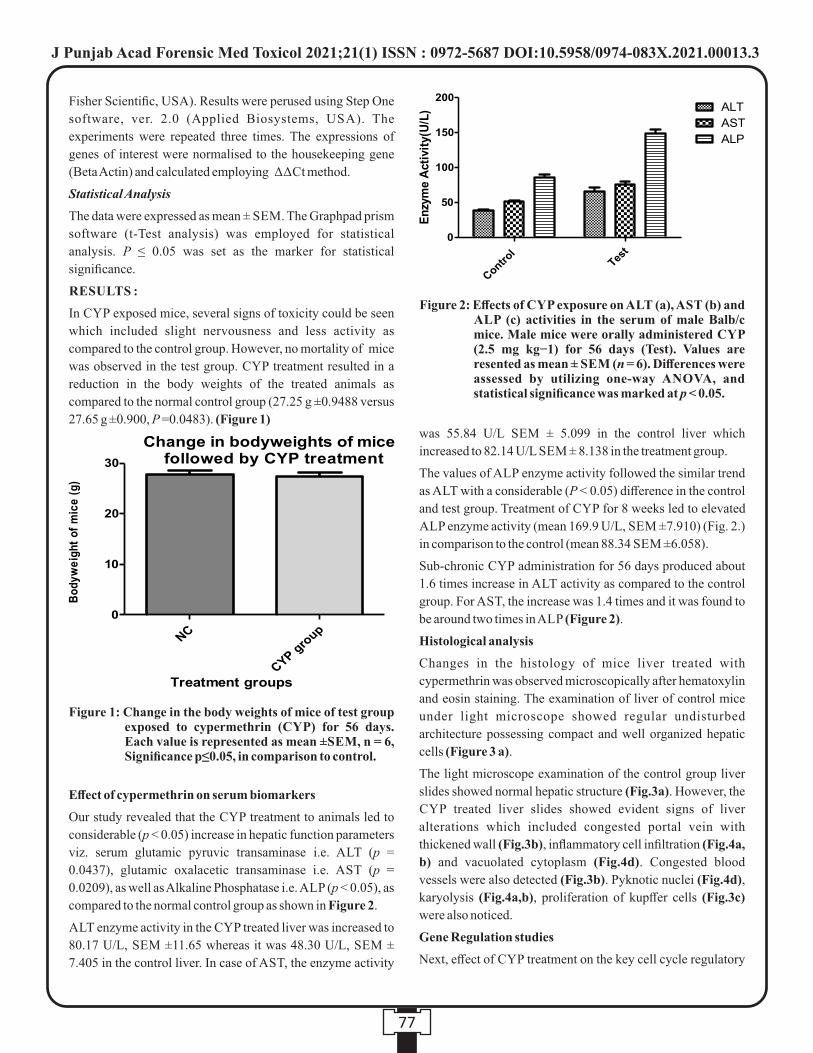
Fisher Scientific, USA). Results were perused using Step One
software, ver. 2.0 (Applied Biosystems, USA). The
experiments were repeated three times. The expressions of
genes of interest were normalised to the housekeeping gene
(Beta Actin) and calculated employing ΔΔCt method.
Statistical Analysis
The data were expressed as mean ± SEM. The Graphpad prism
software (t-Test analysis) was employed for statistical
analysis. P ≤ 0.05 was set as the marker for statistical
significance.
RESULTS :
In CYP exposed mice, several signs of toxicity could be seen
which included slight nervousness and less activity as
compared to the control group. However, no mortality of mice
was observed in the test group. CYP treatment resulted in a
reduction in the body weights of the treated animals as
compared to the normal control group (27.25 g ±0.9488 versus
27.65 g ±0.900, P =0.0483). (Figure 1)
Effect of cypermethrin on serum biomarkers
Our study revealed that the CYP treatment to animals led to
considerable (p < 0.05) increase in hepatic function parameters
viz. serum glutamic pyruvic transaminase i.e. ALT (p =
0.0437), glutamic oxalacetic transaminase i.e. AST (p =
0.0209), as well as Alkaline Phosphatase i.e. ALP (p < 0.05), as
compared to the normal control group as shown in Figure 2.
ALT enzyme activity in the CYP treated liver was increased to
80.17 U/L, SEM ±11.65 whereas it was 48.30 U/L, SEM ±
7.405 in the control liver. In case of AST, the enzyme activity
was 55.84 U/L SEM ± 5.099 in the control liver which
increased to 82.14 U/L SEM ± 8.138 in the treatment group.
The values of ALP enzyme activity followed the similar trend
as ALT with a considerable (P < 0.05) difference in the control
and test group. Treatment of CYP for 8 weeks led to elevated
ALP enzyme activity (mean 169.9 U/L, SEM ±7.910) (Fig. 2.)
in comparison to the control (mean 88.34 SEM ±6.058).
Sub-chronic CYP administration for 56 days produced about
1.6 times increase in ALT activity as compared to the control
group. For AST, the increase was 1.4 times and it was found to
be around two times in ALP (Figure 2).
Histological analysis
Changes in the histology of mice liver treated with
cypermethrin was observed microscopically after hematoxylin
and eosin staining. The examination of liver of control mice
under light microscope showed regular undisturbed
architecture possessing compact and well organized hepatic
cells (Figure 3 a).
The light microscope examination of the control group liver
slides showed normal hepatic structure (Fig.3a). However, the
CYP treated liver slides showed evident signs of liver
alterations which included congested portal vein with
thickened wall (Fig.3b), inflammatory cell infiltration (Fig.4a,
b) and vacuolated cytoplasm (Fig.4d). Congested blood
vessels were also detected (Fig.3b). Pyknotic nuclei (Fig.4d),
karyolysis (Fig.4a,b), proliferation of kupffer cells (Fig.3c)
were also noticed.
Gene Regulation studies
Next, effect of CYP treatment on the key cell cycle regulatory
77
Figure 1: Change in the body weights of mice of test group exposed to cypermethrin (CYP) for 56 days. Each value is represented as mean ±SEM, n = 6, Significance p≤0.05, in comparison to control.
Figure 2: Effects of CYP exposure on ALT (a), AST (b) and ALP (c) activities in the serum of male Balb/c mice. Male mice were orally administered CYP (2.5 mg kg−1) for 56 days (Test). Values are resented as mean ± SEM (n = 6). Differences were assessed by utilizing one-way ANOVA, and statistical significance was marked at p < 0.05.
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00013.3
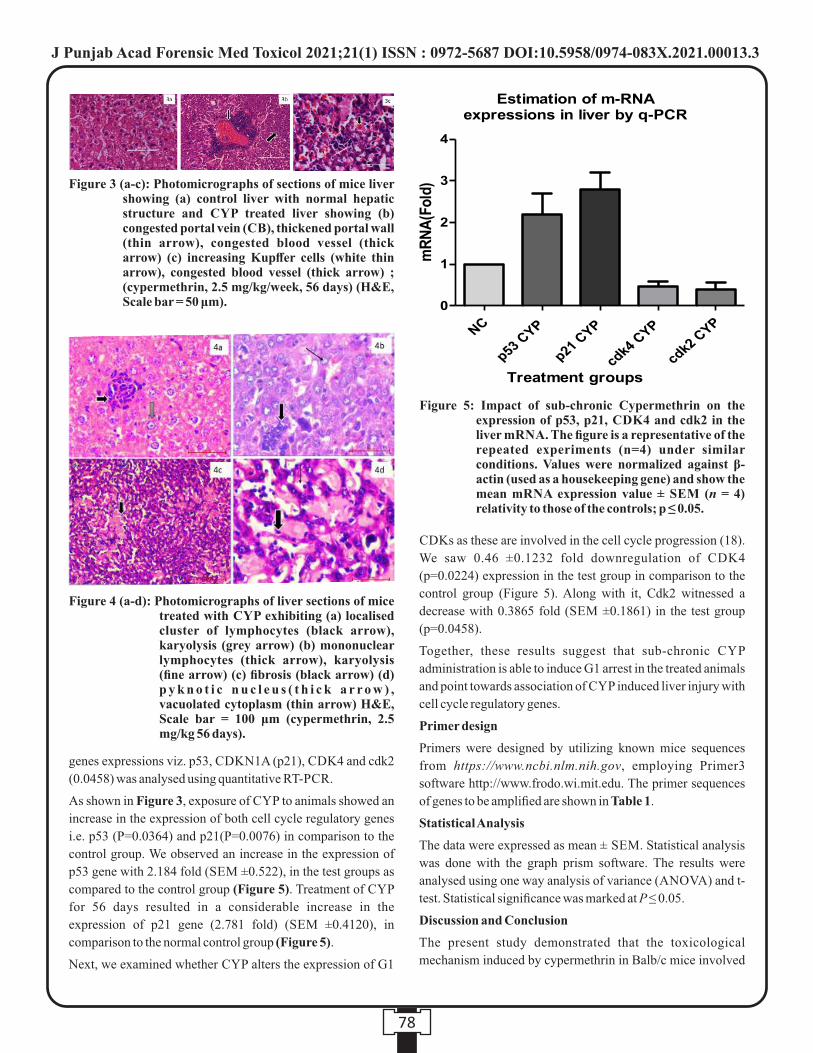
genes expressions viz. p53, CDKN1A (p21), CDK4 and cdk2
(0.0458) was analysed using quantitative RT-PCR.
As shown in Figure 3, exposure of CYP to animals showed an
increase in the expression of both cell cycle regulatory genes
i.e. p53 (P=0.0364) and p21(P=0.0076) in comparison to the
control group. We observed an increase in the expression of
p53 gene with 2.184 fold (SEM ±0.522), in the test groups as
compared to the control group (Figure 5). Treatment of CYP
for 56 days resulted in a considerable increase in the
expression of p21 gene (2.781 fold) (SEM ±0.4120), in
comparison to the normal control group (Figure 5).
Next, we examined whether CYP alters the expression of G1
CDKs as these are involved in the cell cycle progression (18).
We saw 0.46 ±0.1232 fold downregulation of CDK4
(p=0.0224) expression in the test group in comparison to the
control group (Figure 5). Along with it, Cdk2 witnessed a
decrease with 0.3865 fold (SEM ±0.1861) in the test group
(p=0.0458).
Together, these results suggest that sub-chronic CYP
administration is able to induce G1 arrest in the treated animals
and point towards association of CYP induced liver injury with
cell cycle regulatory genes.
Primer design
Primers were designed by utilizing known mice sequences
from https://www.ncbi.nlm.nih.gov, employing Primer3
software http://www.frodo.wi.mit.edu. The primer sequences
of genes to be amplified are shown in Table 1.
Statistical Analysis
The data were expressed as mean ± SEM. Statistical analysis
was done with the graph prism software. The results were
analysed using one way analysis of variance (ANOVA) and t-
test. Statistical significance was marked at P ≤ 0.05.
Discussion and Conclusion
The present study demonstrated that the toxicological
mechanism induced by cypermethrin in Balb/c mice involved
78
Figure 3 (a-c): Photomicrographs of sections of mice liver showing (a) control liver with normal hepatic structure and CYP treated liver showing (b) congested portal vein (CB), thickened portal wall (thin arrow), congested blood vessel (thick arrow) (c) increasing Kupffer cells (white thin arrow), congested blood vessel (thick arrow) ; (cypermethrin, 2.5 mg/kg/week, 56 days) (H&E, Scale bar = 50 μm).
Figure 4 (a-d): Photomicrographs of liver sections of mice treated with CYP exhibiting (a) localised cluster of lymphocytes (black arrow), karyolysis (grey arrow) (b) mononuclear lymphocytes (thick arrow), karyolysis (fine arrow) (c) fibrosis (black arrow) (d) p y k n o t i c n u c l e u s ( t h i c k a r r o w ) , vacuolated cytoplasm (thin arrow) H&E, Scale bar = 100 μm (cypermethrin, 2.5 mg/kg 56 days).
Figure 5: Impact of sub-chronic Cypermethrin on the expression of p53, p21, CDK4 and cdk2 in the liver mRNA. The figure is a representative of the repeated experiments (n=4) under similar conditions. Values were normalized against β-actin (used as a housekeeping gene) and show the mean mRNA expression value ± SEM (n = 4) relativity to those of the controls; p ≤ 0.05.
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00013.3

cell cycle regulatory genes. In addition, cypermethrin induced
histological alterations as well as disturbed liver function
enzyme levels. The foreign substances entering the body are
known to cause the most harm to liver as it is the first organ to (19)face the xenobiotics carried through portal circulation . M.J.
Derelanko has earlier reported that a significant decrease in
antioxidant defences of liver occur in case of liver damage by (20)exogenous substances . Our study also portrays that a
significant decrease in body weight in mice exposed to CYP at
the end of the experiment. Change in the body weights of CYP
exposed mice is considered to be an important indicator of
pesticide induced damage. This might be a result of direct
toxicity of CYP and due to the effect of insecticide on
gastrointestinal tract causing reduced appetite and nutrient (21)absorption from gut . Other studies on CYP-induced liver
damage have also reported change in body weight of CYP (22) (23)treated rats and rabbits .
The elevated ALT and AST levels in the test groups definitely
point towards CYP-driven hepatic damage leading to
depletion of cell integrity. These observations are in
accordance with the previous CYP toxicity findings in rabbits (24) (25) (26) (27) and rats . Increase in the activities of these enzymes in
cypermethrin treated mice may be attributed to liver
dysfunction and perturbation in the biosynthesis of these (28)enzymes along with change in the liver permeability . Serum
ALT and AST are considered to be among the most sensitive (29)markers utilized in the diagnosis of hepatotoxicity . Pesticide
exposure induced liver damage causes leakage of cytosolic
enzymes from hepatocytes and various other body organs into (28)blood which causes their elevated levels . Elevation of liver
enzymes may also be caused by hiked gene expression due to (30)long term need of detoxification of pesticides in the body .
The induction of liver damage and elevation of liver function
enzyme activities as observed in our study is in accordance
with the observation of Abdul-Hamid et al in liver cells of
albino rats in response to CYP dose of 30 mg/kg/day for 30 (31)days .
The CYP treatment group showed several histopathological
alterations such as vacuolated cytoplasm, congested blood
vessels, inflammatory cell infilteration and distorted
architecture of hepatocytes in the liver tissue as compared to
the control. Several other degenerative changes such as
Pyknotic nuclei and karyolysis were seen pointing towards
cypermethrin induced liver injury. Sub chronic cypermethrin
administration was able to induce noticeable changes in the
hepatic structure which may be due to the inhibitory effect of
CYP on the adenine triphosphate activity in the liver leading to
disorganization of Na+ , K+ and Ca2+ ions thus causing (32)hepatic injury . The current histological findings are in
accordance with sundry earlier studies which have already
shown that CYP leads to rigorous histological turbulence in a (33) (24)variety of experimental animals namely fish , rabbit ,
(34) (35) (36)broiler chicks , mice and rats . The reported hepatic
histopathological findings in this study are also concurrent (37)with the previous studies by Abdou et al. and Soliman et al.
(38) where the researchers observed degenerative alterations in
the liver such as necrosis, vacuolation, lymphocytic infiltration
and congestion due to CYP dose of 12 mg/kg b.w. for 30 days.
CYP administration for 56 days caused major degeneration in
the liver histological structure including the presence of
inflammatory cells which is again in synchronization with the
study by Bhushan et al. in which liver damage was observed in (39)wistar rats following sub-acute cypermethrin poisoning and
another study where wistar rats were exposed to CYP mixed (15)with their food for 28 days .
The present study suggests the involvement of cell cycle
regulatory genes as contributors of CYP induced liver toxicity
and here we have investigated p53, CDKN1A, CDK4 and 286
cdk2 as hepatotoxicity markers owing to their roles in cell
cycle regulation. Disruption of cell cycle seems to be a major
event involved in the liver damage caused by cypermethrin.
The p53 tumor suppressor protein is significantly involved in a
majority of events such as cell cycle modulations and apoptosis (40). It also shows alterations in its activity in response to several
stress stimuli such as xenobiotics and pesticides. Due to its
activation because of various posttranslational modifications,
79
Gene Name (Mus musculus)
CDKN1A(p21)
p53
CDK4
CDK2
Beta Actin
Primers
Forward: 5'-AAGTGGGATTCCCTGGTCTT-3' Reverse: 5'-GCTTTGACACCCACGGTATT-3'
Forward: 5'-GATGACTGCCATGGAGT 3' Reverse: 5'-CTCGGGTGGCTCATAAGGTA-3'
Forward: 5'-TAAGATCCCCTGCTTCGAGA 3' Reverse: 5'- GGAGGTGCTTTGTCCAGGTA -3'
Forward: 5'- TCTCTCAGGGATACACAACCC-3' Reverse: 5'- GGCGGCAACATTGTTTCAAG-3'
Forward: 5'-AAATCGTGCGTGACATCAAA-3' Reverse : 5'-ACATCTGCTGGAAGGTGGAC-3' 58
Annealingtempera-ture
58°C
58°C
58°C
58°C
58°C
Table 1: List of primers employed in RT-PCR analysis.
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00013.3

it holds potential to influence several other genes which
collectively brings about cell cycle arrest in response to
cellular damage by pesticides. Under stress conditions
activation of p53 takes place affecting several other (41) (40)downstream genes necessitated in cell cycle regulation .
These are known to be well-established events in xenobiotic (42)induced liver damage situations . Our study demonstrated
that CYP induced liver injury occurs via activation of
p53/p21pathway. Several other research studies have
stipulated that xenobiotic caused hepatic toxicity is related to
the activation of p53 gene expression which is important in the (43)liver injury pathogenesis . Further, p53 seems to be an
important regulator of p21 (Cdkn1a) transcription in relation to (44)the toxicogenomic response to liver injury . At the
concentration of 2.5 mg/kg, CYP led to a noteworthy increase
in the CDKN1A [CDK (cyclin-dependent-kinase) inhibitor,
p21] expression, a gene associated to G1/S phase of cell cycle
arrest along with an upregulation of p53 in the test group. The
p53/p21 is involved in the cell cycle regulation and p53 is
swiftly activated in case the cells encounter severe DNA (45)damage .
Contrarily, down-regulation of CDK4 which is a cell cycle
promoting gene is accounting to the opposing roles of p21 and
CDK4 in G1 phase cell cycle progression regulation. The
kinase activity of CDK2 in the normal cell cycle is elevated
particularly at the G0/G1-phase transition and the activity of (46)CDK4 is required during the G1 /S and G2 /M transitions .
Various studies have already reported the involvement of
cyclin-dependent kinase 2 (CDK2) in the G1- phase of cell
cycle and the present PCR data showed that CYP exposure led
to decrease in its expression.
The PCR data showed that CYP promoted the expressions of
p53 and p21 while inhibiting CDK2 and CDK4 expressions
which may be a reason for toxicity caused by G0/G1 arrest in
the cell cycle. The modulation of above mentioned cell cycle
regulatory genes as observed in our study is in line with the (47) (18)previously published reports .
Our findings give a collective evidence of changes in gene
expression of the mentioned genes in CYP-induced liver
damage. Taken together, modulation of cell cycle regulatory
gene activities at implicate the role of above mentioned genes
in the toxicological outcomes of CYP thus suggesting the
utilization of the genes in utilized as biomarkers of CYP
induced toxicity. Additionally, the toxicity and amount of
pesticides must be thoroughly investigated before these are
used in daily use items such as pet shampoos, household
cleaners and residential pest control sprays. Along with acute
toxicity, the potential of sub-chronic toxicity of pesticides
including CYP has to be identified and serious efforts towards
elimination of pesticide residues from the daily lives of human
beings and other non-target organisms have to be made to
improve the overall health and living conditions. The
biochemical as well as histological markers can be utilized in
forensic cases to establishing the cause of death in CYP
mediated toxicity.
Acknowledgements
The authors are grateful to DST, Govt. of India, for providing
financial assistance to IFSC and Centre for SCTE through the
PURSE grant. Financial aid from UGC in the form of JRF
Ref. No.: 5008/ (NET-JUNE 2012) is highly acknowledged.
Conflict of interest
The authors declare no conflicts of interest.
REFERENCES :
1. Kanbur M, Sili Y. The Acute and Chronic Toxic Effect of
Cypermethrin, Propetamphos , and Their Combinations in
Rats. (April 2015):1415–29.
2. Kingdom U. Metabolism and environmental degradation
of pyrethroid insecticides produce compounds with
endocrine activities. 2000;19(4):801–9.
3. Patel S, Pandey AK, Bajpayee M, Parmar D, Dhawan A.
Cypermethrin-induced DNA damage in organs and
tissues of the mouse: Evidence from the comet assay.
Mutat Res Toxicol Environ Mutagen. 2006;607 (2) :
176–83.
4. Caglayan A, Kocer-Gumusel B, Erkekoglu P, Hincal F.
The effects of fenvalerate on hepatic and cerebral
xenobiotic metabolizing enzymes in selenium and/or
iodine deficient rats. Iran J Basic Med Sci. 2016
Oct;19(10):1040–8.
5. Alkahtane AA, Alarifi S, Al-qahtani AA, Ali D, Alomar
SY, Aleissia MS, et al. Cytotoxicity and Genotoxicity of
Cypermethrin in Hepatocarcinoma Cells : A Dose-and
Time-Dependent Study. 2018;(June):1–9.
6. Alavanja MCR. Introduction: pesticides use and exposure
e x t e n s i v e w o r l d w i d e . R e v E n v i r o n H e a l t h .
2009;24(4):303–9.
7. Lidova J, Stara A, Kouba A, Velisek J. The effects of
cypermethrin on oxidative stress 16 and antioxidant
biomarkers in marbled crayfish (Procambarus fallax f.
v i r g i n a l i s ) . N e u r o E n d o c r i n o l L e t t . 2 0 1 6
Dec;37(Suppl1):53–9.
8. El-Tawil OS, Abdel-Rahman MS. The role of enzyme
induction and inhibition on cypermethrin hepatotoxicity.
Pharmacol Res. 2001 Jul;44(1):33–40.
9. Aggarwal P, Jamshed N, Ekka M, Imran A. Suicidal
poisoning with cypermethrin: A clinical dilemma in the
80
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00013.3
emergency department. J Emerg Trauma Shock [Internet].
3 5 8 2 0 1 5 ; 8 ( 2 ) : 1 2 3 – 5 . A v a i l a b l e f r o m :
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4411577
10. Mahna D, Puri S, Sharma S. Cypermethrin Induced Liver
Toxici ty: Altered Gene Expression and D N A
Methylation. FASEB J. 2019 Apr;33 (1_supplement):
621.9-621.9.
11. Mahna D, Puri S, Sharma S. DNA methylation signatures:
Biomarkers of drug and alcohol abuse. Mutation
Research/Reviews in Mutation Research. 2018.
12. Shukla Y, Yadav A, Arora A. Carcinogenic and
cocarcinogenic potential of cypermethrin on mouse skin.
2002;182:33–41.
13. Kusano C, Ferrari B. Free radicals , lipid peroxidation and
antioxidants in apoptosis : implications in cancer ,
cardiovascular and neurological diseases Free radicals ,
lipid peroxidation and antioxidants in apoptosis :
implications in cancer, cardiovascular and neurological
diseases. 2015;(December 2000).
14. Huang F, Liu Q, Xie S, Xu J, Huang B, Wu Y, et al.
Cypermethrin Induces Macrophages Death through Cell
Cycle Arrest and Oxidative Stress-Mediated JNK / ERK
Signaling Regulated Apoptosis. 2016;
15. Yavasoglu A, Sayım F, Uyanıkgil Y, Turgut M, Ülkü
Karabay-Yavasoglu N. The 17 Pyrethroid Cypermethrin-
Induced Biochemical and Histological Alterations in Rat
Liver. J Heal Sci. 2006;52(6):774–80.
16. Macbean EC. The Pesticide Manual.
17. Bancroft JD, Gamble M. Theory and Practice of
Histological Techniques. Churchill Livingstone; 2008.
(ClinicalKey 2012).
18. Huang F, Liu Q, Xie S, Xu J, Huang B, Wu Y, et al.
Cypermethrin Induces 381 Macrophages Death through
Cell Cycle Arrest and Oxidative Stress-Mediated 382
JNK/ERK Signaling Regulated Apoptosis. Int J Mol Sci.
2016 Jun;17(6):885.
19. Mossa A-TH, Swelam ES, Mohafrash SMM. Sub-
chronic exposure to fipronil induced oxidative stress,
biochemical and histopathological changes in the liver
and kidney of male albino rats. Toxicol reports.
2015;2:775–84.
20. Derelanko MJ, Ph D. toxicologist ' s POCKET
HANDBOOK. 2000.
21. Venkateshwarlu P, Sharma BJR, Kalakumar B, Reddy
KS, Ravikumar P. Comparative evaluation of toxicity of
carbaryl, cypermethrin and malathion of testis in mice.
Indian J Toxicol. 1997;4(1):33–7.
22. Sangha GK, Kaur K, Khera KS, Singh B. Toxicological
effects of cypermethrin on female albino rats. Toxicol Int.
2011 Jan;18(1):5—8.
23. Mossa A-TH, Heikal TM, Belaiba M, Raoelison EG,
Ferhout H, Bouajila J. Antioxidant activity and
hepatoprotective potential of Cedrelopsis grevei on
cypermethrin induced oxidative stress and liver damage in
male mice. BMC Complement Altern Med. 2015
Jul;15:251.
24. Yousef MI, El-Demerdash FM, Kamel KI, Al-Salhen KS.
Changes in some hematological and biochemical indices
of rabbits induced by isoflavones and 18 cypermethrin.
Toxicology. 2003;189(3):223–34.
25. Sankar P, Telang AG, Manimaran A. Protective effect of
curcumin on cypermethrin-induced oxidative stress in
Wistar rats. Exp Toxicol Pathol. 2012;64(5):487–93.
26. Hussain S, Khan MZ, Khan A, Javed I, Asi MR. Toxicon
Toxico-pathological effects in rats induced by concurrent
exposure to aflatoxin and cypermethrin. Toxicon.
2009;53(1):33–41.
27. Thapa BR, Walia A. Liver Function Tests and their
Interpretation. 2007;74:67–75.
28. Ikpeme E V, Okonko LE, Udensi OU. Detrimental Effects
of Chlorpyrifos and Reproductive Physiology of Male
Albino Rats Cypermethrin on. Res J Environ Toxicol.
2016;10(1):68–74.
29. Kullak-Ublick GA, Andrade RJ, Merz M, End P, Benesic
A, Gerbes AL, et al. Drug-induced liver injury: recent
advances in diagnosis and risk assessment. Gut. 2017
Jun;66(6):1154 LP – 1164.
30. Roberts JR, Karr CJ, HEALTH CONE. Pesticide
E x p o s u r e i n C h i l d r e n . P e d i a t r i c s . 2 0 1 2
Dec;130(6):e1765–88.
31. Abdul-Hamid M, Moustafa N, Abd Alla Asran AEM,
Mowafy L. Cypermethrin-induced histopathological,
ultrastructural and biochemical changes in liver of albino
rats: The protective role of propolis and curcumin. Beni-
Suef Univ J Basic Appl Sci. 2017;6(2):160–73.
32. Khan A, Faridi HAM, Ali M, Khan MZ, Siddique M,
Hussain I, et al. Effects of cypermethrin on some clinico-
hemato-biochemical and pathological parameters in male
dwarf goats (Capra hircus). Exp Toxicol Pathol.
2009;61(2):151–60.
33. Velmurugan B, Mathews T, Cengiz EI. Histopathological
effects of cypermethrin on 19 gill, liver and kidney of fresh
water fish Clarias gariepinus (Burchell, 1822), and
recovery after exposure. Environ Technol. 2009
81
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00013.3

Dec;30(13):1453–60.
34. Kammon AM, Brar RS, Sodhi S, Banga HS, Singh J,
Nagra NS. Chlorpyrifos chronic toxicity in broilers and
effect of vitamin C. Open Vet J. 2011/02/25.
2011;1(1):21–7.
35. Grewal KK, Sandhu GS, Kaur R, Brar RS, Sandhu HS.
Toxic impacts of cypermethrin on behavior and histology
of certain tissues of albino rats. Toxicol Int.
2010;17(2):94–8.
36. Raj J, Mohineesh, Ray R, Dogra TD, Raina A. Acute oral
toxicity and histopathological study of combination of
endosulfan and cypermethrin in wistar rats. Toxicol Int.
2013;20(1):61–7.
37. Abdou HM, Hussien HM, Yousef MI. Deleterious effects
of cypermethrin on rat liver and kidney: protective role of
sesame oil. J Environ Sci Health B. 2012;47(4):306–14.
38. Soliman MM, Attia HF, El-Ella GAA. Genetic and
histopathological alterations induced by cypermethrin in
rat kidney and liver: Protection by sesame oil. Int J
Immunopathol Pharmacol. 2015;28(4):508–20.
39. Bhushan B, N Saxena P, Saxena N. Biochemical and
Histological Changes in Rat Liver Caused by
Cypermethrin and Beta-Cyfluthrin. Vol. 64, Arhiv za
higijenu rada i toksikologiju. 2013. 57–67 p.
40. Kruiswijk F, Labuschagne CF, Vousden KH. p53 in
survival, death and metabolic health: a lifeguard with a
licence to kill . Nat Rev Mol Cell Biol. 2015
Jul;16(7):393–405.
41. Riley T, Sontag E, Chen P, Levine A. Transcriptional
control of human p53-regulated genes. Nat Rev Mol Cell
Biol. 2008 May;9(5):402–12.
42. Viswanathan P, Sharma Y, Gupta P, Gupta S. Replicative
stress and alterations in cell cycle checkpoint controls
following acetaminophen hepatotoxicity restrict liver
r egenera t ion . Ce l l P ro l i f . 2018/03 /05 . 2018
Jun;51(3):e12445–e12445.
43. Yan M, Huo Y, Yin S, Hu H. Mechanisms of
acetaminophen-induced liver injury and its implications
for therapeutic interventions. Redox Biol. 2018
Apr;17:274–83.
44. Stamper BD, Garcia ML, Nguyen DQ, Beyer RP,
Bammler TK, Farin FM, et al. p53 Contributes to
Differentiating Gene Expression Following Exposure to
Acetaminophen and Its Less Hepatotoxic Regioisomer
Both In Vitro and In Vivo. Gene Regul Syst Bio. 2015
Jun;9:1–14.
45. Antony ML, Kim S-H, Singh S V. Critical role of p53
upregulated modulator of apoptosis in benzyl
isothiocyanate-induced apoptotic cell death. PLoS One.
455 2012;7(2):e32267.
46. Baker SJ, Reddy EP. CDK4 : A Key Player in the Cell
Cycle , Development , and Cancer. 2013;3:658–69.
47. Kavvalakis MP, Tzatzarakis MN, Alegakis AK, Vynias D,
Tsakalof AK, Tsatsakis AM. Development and
application of GC-MS method for monitoring of long-
term exposure to the pesticide cypermethrin. Drug Test
Anal. 2014 Jun;6 Suppl 1:9–16.
82
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00013.3
83
Original Research Paper
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00014.5
1. Nirmal Kumar V, Forensic Medicine Resident, Department of Forensic Medicine and Toxicology, Amrita School of
Medicine, AIMS, Kochi, Kerala
2. Pillay VV, Professor & Head, Department of Forensic Medicine and Toxicology, AIMS, Kochi, Kerala
3. Ramakrishnan UK, Associate Professor, Department of Forensic Medicine and Toxicology, AIMS, Kochi, Kerala
4. Arathy SL, Senior Research Officer, Analytical Toxicology, Poison Control Centre, AIMS, Kochi, Kerala
5. Renjitha Bhaskaran, Lecturer & In-charge, Department of Biostatistics, AIMS, Kochi, Kerala
Key words: Formaldehyde, Formalin, High Performance Liquid Chromatography, Sea Fish
Corresponding Author:
Dr. Ramakrishnan UK,
Associate Professor,
Department of Forensic Medicine and Toxicology, AIMS,
Kochi, Kerala
Contact : +91 97457-31022
Email :[email protected]
Article History :
Received : 3 December 2020
Received in revised form : 13 December 2020
Accepted on : 13 December 2020
Available online : 15 August 2021
INTRODUCTION :
Fish is an important source of food rich in protein all over the
world. Aquaculture and Indian fisheries play an important role
in production of food, providing nutritional security and
engaging around fourteen million people in various activities.
In agricultural exports of India, fish products have become one
of the biggest groups, with Rs. 33,442 crores in value and 10.51 rdlakh tonnes in terms of quantity. India stands 3 in Fisheries
nd 1and 2 in Aquaculture globally.
In terms of fisher folk population, Kerala stands second among
the coastal states in India. In almost every household in Kerala,
there is a minimum of one meal with fish each day and the
consumption of fish is higher in rural areas when compared to 2the urban areas. The consumption of fish in Kerala is four
3times the national average. With an average per capita fish
consumption of 27-30 kg, Kerala is the highest fish consuming 4state in India.
Fish serves as an important source of animal proteins, omega-3
polyunsaturated fatty acids (PUFAs), and micronutrients.
Estimation of Formaldehyde Contamination In Selected Sea Fish Species Sold In Ernakulam District of Kerala State
ABSTRACT :
Introduction: Fish is an important source of food rich in protein. Fish consumption pattern has seen an upward trend in recent
times owing to wide publicity of health benefits of fish consumption. However, there appears to be rampant adulteration of fresh
fish using unapproved chemicals and additives which are being highlighted in both print and electronic media. Among the added
contaminants, volatile toxic aldehydes such as formaldehyde are quite commonly used, which are classified as Group 1
carcinogenic agents to humans by the International Agency for Research on Cancer (IARC).
Materials and Methods: The present study was undertaken in the Department of Forensic Medicine and Toxicology, Amrita
Institute of Medical Sciences and Research Centre, Kerala state. This is a cross sectional study of commonly consumed sea fish
species sold in Ernakulam district of Kerala State. The selected sea fish samples were collected and qualitatively screened for
contamination with formaldehyde, using a formaldehyde detection kit. Quantitative estimation of formaldehyde was done in those
samples that tested positive during qualitative screening using High Performance Liquid Chromatography (HPLC) and the values
were compared with the standard tolerable level for humans.
Results: Out of 65 fish samples qualitatively screened for formaldehyde, 16 samples tested positive with a percentage prevalence
of 24.62%. The values of formaldehyde concentrations obtained from the quantitative estimation of those samples that tested
positive during qualitative screening were within a range of 1.162-17.341 mg/kg and were found to be within the tolerable levels
for humans
Conclusions: From this study we conclude that even though the formaldehyde values were within the tolerable level for humans,
the issue of adulteration of fish with formaldehyde still exists, though the Food Safety and Standards Authority of India (FSSAI)
completely prohibits its use.

84
Also, fish is a good source of proteins, calcium, selenium, 5phosphorus and vitamin D.
Fish contains water, free amino acids and fat as composition,
which are prone to spoilage by microbial and biochemical
reactions during post-mortem changes. Thus, fish and seafood
are highly perishable and can only be kept fresh in ice for 8 to
14 days depending on the species. Fishermen and fish vendors
tend to use unapproved chemicals as preservative agents in 6 order to preserve the freshness. Among such added
contaminants, volatile toxic aldehydes such as formaldehyde
are commonly used. Formaldehyde is classified as a Group 1
carcinogenic agent to humans by the International Agency for 7Research on Cancer (IARC). As per Food Safety and
Standards Regulation, 2011, the use of formaldehyde in food is
not permitted in India. The situation has been made more
complex because fish itself can contain some amount of
endogenous formaldehyde and it is difficult to assess whether the formaldehyde present has been exogenously added to it.
Trimethylamine oxide (TMAO) constitutes a characteristic
and important part of non-protein nitrogen fraction in marine
fish species which is responsible for osmoregulation and is
found in all marine fish species in quantities from 1% to 5% of
the muscle tissue. Dimethylamine (DMA) and formaldehyde
(FA) originate from some species of fish from the breakdown 8of TMAO. According to studies, the FA production is greatest
9at high frozen storage temperatures.
There have been studies conducted to estimate the presence
and levels of formaldehyde in various food products especially
sea fish, by a variety of methods including Formaldehyde
Detection Kit for fish, Spectrophotometry, Digital Image
Colorimetry, High Performance Liquid Chromatography
(HPLC), and Solid Phase Micro Extraction (SPME)-Gas
Chromatography-Mass Spectrometry (GC-MS). Both HPLC
and GC-MS methodologies have been adopted by researchers
for quantification of formaldehyde with highest degree of 10specificity and precision.
According to the Italian Ministry of Health (1985), the
standard tolerable limit of formaldehyde for humans in fish is 1160 mg/kg. The World Health Organization (WHO) and the
United States Environmental Protection Agency (USEPA)
have fixed a maximum daily reference dose (RfD) of 0.15 and
0.2 mg/kg body weight per day for formaldehyde 12,13respectively. Intake of levels above the permitted values
may cause serious adverse effects on human health. European
Food Safety Authority (EFSA) recommends an oral exposure
to formaldehyde as 100 mg formaldehyde per day, -1corresponding to 1.7 and 1.4 mg kg bw per day for 60 kg and
1470 kg respectively in humans. According to the Malaysian
Food Act (1985) and Malaysian Food Regulations (1985), the
maximum permissible limit of formaldehyde concentration in 15processed fish and fish products is 5 mg/kg. The estimated
-1average dietary exposure is about 11 mg kg per person per day
as per Agence Francaise de Securite Sanitaire des Aliments
(AFSSA). As per Yasuhara & Shibamoto, formaldehyde in the -1rage of 10-20 mg kg in fish cannot be considered as palatable
14for humans.
The Food Safety and Standards Authority of India (FSSAI)
was established under Food Safety and Standards in 2006 in
India. FSSAI has been created for laying down science based
standards for articles of food and to regulate their manufacture,
storage, distribution, sale and import to ensure availability of
safe and wholesome food for human consumption. FSSAI has
not set a fixed limit for formaldehyde in fish in India.
Considering the above, it was felt that estimating the levels of
formaldehyde in some commonly consumed sea fish species
and checking whether they are within the tolerable limit for
human consumption would be of great health importance and
benefit to the common public. Such studies have not been
commonly undertaken in the state of Kerala where fish
consumption is high. Further, this study will be utilizing High
Performance Liquid Chromatography (HPLC) which is a more
sophisticated method for quantitative estimation, than
methods which have been used in some other studies which are
not as accurate.
MATERIALS AND METHODS :
The present study was undertaken in the Department of
Forensic Medicine and Toxicology, Amrita Institute of
Medical Sciences and Research Centre, Kerala state. This is a
cross sectional study of commonly consumed sea fish species
sold in Ernakulam district of Kerala. The dissertation review
committee of this institute had given scientific, ethical and
financial clearance to conduct the study.
Selection and Description of Participants: As there were no
previous studies on estimation of formaldehyde in sea fish
species using the prevalence of adulterated formaldehyde in
fish, we tested 50 samples for the presence of added
formaldehyde, out of which 30 turned out to be positive for
formaldehyde. Thus the prevalence of fish adulterated with
formaldehyde was found to be 60%. Using this prevalence and
with relative precision of 20% and 95% confidence level, the
calculated sample size worked out to 65. Samples of three
commonly consumed sea fish species were collected from
different wet markets and local vendors in Ernakulam district
of Kerala state at different time points. The selected sea fish
species included Indian oil sardine (Sardinella longiceps),
Indian mackerel (Rastrelliger kanagurta), and Spotted seer fish
(Scomberomorus guttatus). The exclusion criteria included all
other sea fish species. The fish samples were immediately
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00014.5

85
transferred to the laboratory for qualitative screening and kept
under refrigerated storage for further analysis.
Technical Information: The primary objective of the study
was to qualitatively screen some selected sea fish species for
contamination by formaldehyde. Secondary objectives were to
quantitatively estimate the formaldehyde in those samples that
tested positive during qualitative screening, and to check
whether the formaldehyde concentration is within the tolerable
levels for human consumption. Qualitative screening test of
the samples was done using Formaldehyde Detection Kit
developed by Central Institute of Fisheries Technology
(CIFT), Kochi. Positive tests show a colour change of greenish
blue to blue within 1 to 2 minutes, whereas no such colour
change is noticed in negative tests. The quantitative estimation
of formaldehyde in those samples that tested positive in
qualitative screening was done using High Performance
Liquid Chromatography (HPLC) which is a sophisticated
method for quantitative estimation of formaldehyde with high
degree of precision and specificity.
The chemicals used for sample extraction were HPLC grade
methanol, acetonitrile and phosphoric acid, formaldehyde
certified reference material (formaldehyde CRM) and 2,4-
dinitrophenylhydrazine (DNPH) procured from Sigma, and
Millipore water. The HPLC machine specifications are as
follows: Shimadzu prominence i LC2030, Photodiode array
detector. 150 mg of re-crystallized DNPH crystals were
weighed and dissolved in 49.5 ml of acetonitrile and mixed
with 0.5 ml 85% phosphoric acid to prepare the 2,4-
Dinitrophenylhydrazine reagent. The formaldehyde CRM
standard was considered as first stock solution. CRM has a
concentration of 4815 mg /litre, and from that the second stock
solution of reference standard was prepared by diluting 2.6 ml
of first stock solution in 25 ml, and from that, solutions of
subsequent concentrations of working standards were
prepared by progressively diluting. All working standards
were prepared using Millipore water. Stock solutions were
stored at -20°C until analysis, and protected from light.
About 5 g fish samples were taken, and blank and spiked
formalin was added. 5 ml of acetonitrile was added to this and
vortexed. The samples were then sonicated for 30 min at room 0temperature (25-30 C). The samples were shaken for 30 min in
a shaking water bath at room temperature at 150 rpm and then 0centrifuged for 5 min in 6000 rpm at 22 C. The samples were
then filtered through Whatman filter paper (90 mm). The upper
layer of the extract of approximately 5 mL was carefully taken
and 2.5 mL working DNPH solution was added and vortexed 0well. This was then derivatised by shaking at 150 rpm, at 40 C
for 1 hour in a shaking water bath. After incubation the
supernatant was filtered and collected using a syringe micro
filter (0.45 µm).
The sample derivatives were analysed by HPLC and compared
with the standard formaldehyde retention time for qualitative
detection. The peak area of the sample solution was substituted
in the calibration equation of the standard curve to calculate the
formaldehyde concentration.
Indian oil sardine (Sardinella longiceps)
Indian mackerel (Rastrelliger kanagurta)
Spotted seer fish (Scomberomorus guttatus)
High Performance Liquid Chromatography (HPLC)
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00014.5
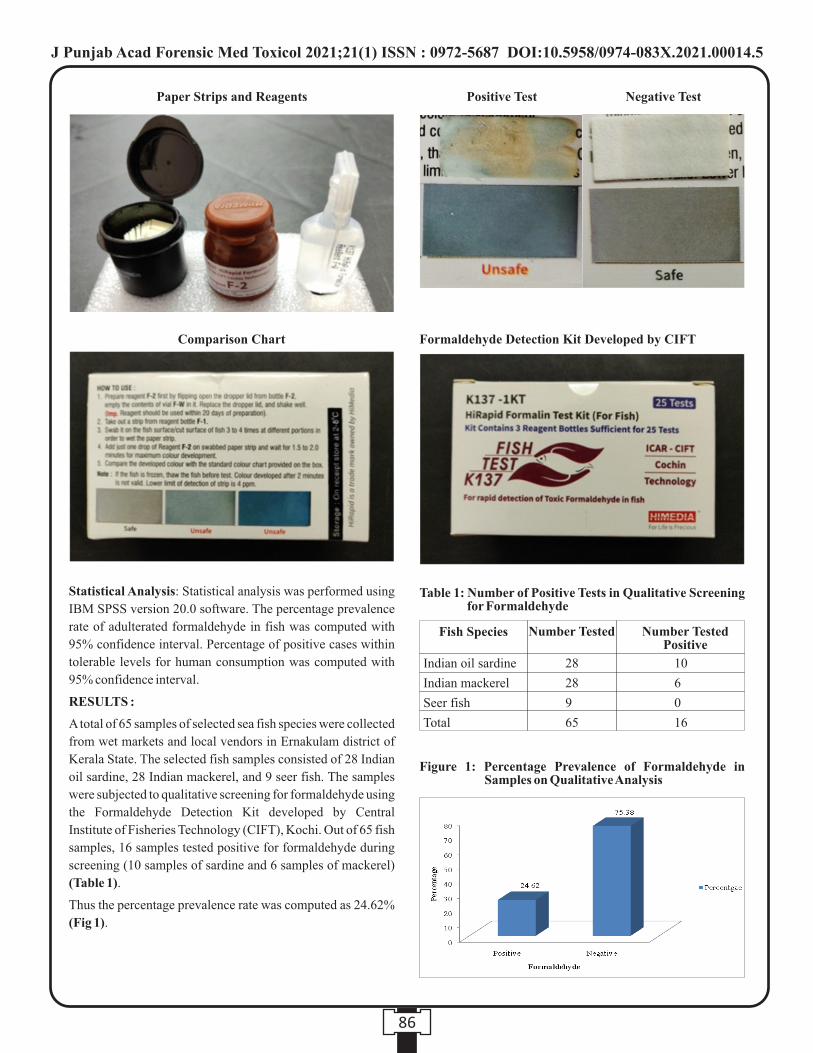
86
Statistical Analysis: Statistical analysis was performed using
IBM SPSS version 20.0 software. The percentage prevalence
rate of adulterated formaldehyde in fish was computed with
95% confidence interval. Percentage of positive cases within
tolerable levels for human consumption was computed with
95% confidence interval.
RESULTS :
A total of 65 samples of selected sea fish species were collected
from wet markets and local vendors in Ernakulam district of
Kerala State. The selected fish samples consisted of 28 Indian
oil sardine, 28 Indian mackerel, and 9 seer fish. The samples
were subjected to qualitative screening for formaldehyde using
the Formaldehyde Detection Kit developed by Central
Institute of Fisheries Technology (CIFT), Kochi. Out of 65 fish
samples, 16 samples tested positive for formaldehyde during
screening (10 samples of sardine and 6 samples of mackerel)
(Table 1).
Thus the percentage prevalence rate was computed as 24.62%
(Fig 1).
Positive Test Negative Test
Formaldehyde Detection Kit Developed by CIFT
Paper Strips and Reagents
Comparison Chart
Table 1: Number of Positive Tests in Qualitative Screening for Formaldehyde
Fish Species
Indian oil sardine
Indian mackerel
Seer fish
Total
28
28
9
65
10
6
0
16
Number Tested Number Tested Positive
Figure 1: Percentage Prevalence of Formaldehyde in Samples on Qualitative Analysis
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00014.5

87
Those samples that tested positive for formaldehyde during
qualitative screening were subjected to quantitative analysis
using High Performance Liquid Chromatography (HPLC).
HPLC was done for a total of 16 samples including 10 samples
of sardine and 6 samples of mackerel. Formaldehyde values
ranging from 1.162 to 7.92 mg/kg and 1.343 to 17.341 mg/kg
were obtained for sardine and mackerel respectively (Table 2).
These values were compared with the standard tolerable level
of formaldehyde in fish for humans, that is 60 mg/kg fixed by
the Italian Ministry of Health (1985). It was found that all the
16 values of formaldehyde concentration were within the
tolerable level for humans (Table 3). The percentage of
positive cases within the tolerable levels for human
consumption was computed as 100%.
DISCUSSION :
In the present study, formaldehyde tested positive during
qualitative screening in 16 samples out of 65 samples. The
percentage prevalence rate of adulterated formaldehyde in fish
was computed as 24.62%. Formaldehyde tested positive in 10
samples of Indian oil sardine and 6 samples of Indian
mackerel. However all the samples of spotted seer fish tested
negative for formaldehyde during qualitative screening using
the formaldehyde kit. Formaldehyde concentrations obtained
from the positively tested samples were in the range of 1.162 -
17.341 mg/kg. In Indian oil sardine, the formaldehyde
concentration was in the range of 1.162 - 7.92 mg/kg. In Indian
mackerel, the formaldehyde concentration was in the range of
1.343 - 17.341 mg/kg. The highest value of formaldehyde was
seen in Indian mackerel, i.e., 17.341 mg/kg, which is one of the
highest values noted when comparing with other similar
studies on formaldehyde concentration in Indian mackerel. As
per the Italian Ministry of Health (1985), the standard tolerable
level of formaldehyde in fish for humans is 60 mg/kg. Similar
tolerable level has not been specified by the Indian Ministry of
Health. All formaldehyde concentrations in the present study
were found to be within the tolerable level as specified by the
Italian Ministry of Health.16Haque et al (2009) conducted a study in consumable fish in
Dhaka city of Bangladesh to determine the intensity of
formaldehyde contamination, using a Formaldehyde
Detection Kit developed by Bangladesh Council of Scientific
and Industrial Research (BCSIR). They found that a total of 50
formalin treated fish were found among 800 species, which
works out to almost 5% of total consumable fish of Dhaka city 17fish market. Yeasmi et al (2010) conducted a study to detect
the formaldehyde adulteration in local and imported fish sold
in different markets in Bangladesh using the same
Formaldehyde Detection Kit. Their study showed that
formalin was not detected in locally produced fish, but was
detected in 0.5% to 1% of imported ones. The shelf life of the
locally produced fish was much longer than those of imported
fish.18Uddin et al (2011) made an attempt to detect the presence of
formalin on different fish species using the Formalin Detection
Kit developed by BCSIR. They found that 50% of fish samples
tested positive for formaldehyde. This is by far the highest
prevalence of formaldehyde adulteration in fish. Rahman et al 19(2012) conducted a study to determine the quality
characteristics and presence of formaldehyde in fish from wet
markets in Sylhet City of Bangladesh. Detection of formalin
was conducted using the Formalin Detection Kit. They
concluded that 6% to 26% fish were formalin treated. Islam et 20al (2015) conducted a study using a similar kit and found that
22.68% of total samples were directly contaminated with
formalin. It was also clear that the formalin contamination and
the organoleptic characteristics of the imported fish were
greatly different than the local fish.21Paul et al (2014) conducted a study in consumable fish
species in markets of Bangladesh to investigate the intensity of
formaldehyde misuse using the Formalin Detection Kit. They
found presence of formalin in 4.2 % of total sampled fish. The
misuse of formalin was more in marine fish. They also
observed that the fish sellers who handled these formalin
treated fish regularly were affected by various skin diseases,
Table 3: Percentage of Positive Cases within the Tolerable Levels for Humans
Tolerable Limit
<60mg/kg
>60mg/kg
Total
Frequency
16
0
16
Percentage
100
0
100
Table 2: Formaldehyde Concentration in Positively Tested Samples
1
2
3
4
5
6
7
8
9
10
2.934
3.280
1.162
3.281
4.660
3.972
7.920
7.013
1.984
1.984
17.341
3.811
1.960
4.285
1.343
3.365
Formaldehyde Concentration (mg/kg)
Sardine
Sl No. Mackerel
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00014.5

88
inhalation problems, and eye irritation. They concluded that
the consumers are exposed to varying degree of formalin
through consumption of fish which is alarming both for
retailers and consumers.22Saba et al (2015) conducted a qualitative study in Ghana on
32 samples including both imported and local fish using a
ChemSee Formaldehyde and Formalin Detection Kit and
found that there was no presence of formaldehyde in both.
Mackerel was one of the imported species involved in the
study.23Jawahar et al (2017) conducted a study in Kerala, India, on
Indian mackerel (Rastrelliger kanagurta) dip-treated with
different concentrations of formaldehyde (0.2, 0.5 and 1 %)
and stored in ice along with undertreated control fish. The
method used was UV spectrophotometry. They concluded that
marketed fish with fresh appearance having lower microbial
load, higher values of total volatile base nitrogen, and a higher
formaldehyde residue can be considered as clear indications of
formaldehyde treatment.24Chandralekha et al (1992) conducted a study on different fish
species in Sri Lanka. They found that no formaldehyde content
was detected in Indian oil sardine and Indian mackerel, but
detected formaldehyde values ranging from 0.001 to 17.6
mg/kg in other species. The analytical method used for the
formaldehyde analysis in this study was a colorimetric method. 11Bianchi et al (2007) conducted a study on 12 different species
of fish in Italy and detected formaldehyde values ranging from
2.6±0.4 to 24.9±5.4 mg/kg and <1 to 5.93±0.5 mg/kg in
mackerel and sardine respectively. This is the highest value of
formaldehyde reported in mackerel. The overall formaldehyde
concentration in 12 species ranged between 6.4±1.2 mg/kg to
293±26 mg/kg. 14 samples were above the tolerable level of
60mg/kg. The analytical method used in this study was Solid
Phase Micro Extraction coupled with Gas Chromatography
Mass Spectrometry.6Noordiana et al (2011) conducted a study on fish and sea food.
They found formaldehyde level of 1.37 mg/kg in mackerel.
Overall formaldehyde level was in the rage of 0.38 to 15.75
mg/kg. The analytical method used in this study was UV 25Spectrophotometry. Siti et al (2013) conducted a study on
formaldehyde contamination of different fish species. They
found formaldehyde levels of 2.557 mg/kg and 2.946 mg/kg in
mackerel and sardine respectively. Overall formaldehyde was
in the range of 2.38 to 2.95 mg/kg. The analytical method used
in this study was UV Spectrophotometry.26Laly et al (2016) conducted a study in Kerala, India on Indian
mackerel. They found that the formaldehyde concentration
was 1.24±0.02 mg/kg. This value was low compared to the
values obtained in the present study for Indian mackerel. The
analytical method used in their study was UV 27Spectrophotometry. Nayana et al (2018) conducted a study on
seer fish in Kerala, and found that the formaldehyde
concentration was in the range of 0.7±0.03 5.83±1.37 mg/kg.
In the present study seer fish samples tested negative during
qualitative screening for formaldehyde. 8Chung et al (2009) conducted a study on chub mackerel in
Hong Kong, China. They detected formaldehyde
concentration of < 1 mg/kg. The analytical method used in this 28study was UV Spectrophotometry. Bechmann et al (1996)
conducted a study on Alaska pollock in Denmark. They found
out formaldehyde values in the range of 6.7 to 7 mg/kg. The
analytical method used was Flow Injection Analysis.29Wahed et al (2016) conducted a study on different food items
in Bangladesh. They found that the average formaldehyde
concentration in fish was 26.6 mg/kg. The analytical method
used in this study was High Performance Liquid 30Chromatography. Bhowmik et al (2016) conducted a study to
determine the formaldehyde content in marketed fish in Dhaka
city, Bangladesh. They found that the formaldehyde values
were in the range of 9.42±2.68 to 19.23±4.32 mg/kg in fresh
fish. They also observed notable seasonal variation of
formaldehyde in fish. They concluded that the formaldehyde
values were within the tolerable levels. The analytical method
used in this study was UV Spectrophotometry. Bhowmik et al 31(2017) conducted a study on marine finfish species in Dhaka
city, Bangladesh. They found that the formaldehyde
concentrations were within the range of 10.8±1.72 39.68±7.87
mg/kg. The analytical method used in this study was High
Performance Liquid Chromatography.32Sanyal et al (2017) conducted a study on fish samples in
Kolkata and found that formaldehyde concentration was
12.19±0.814 mg/kg for formaldehyde treated samples and
8.10±0.068 mg/kg for treated samples stored in ice. The
analytical method used in this study was Spectrophotometry. 33Putri et al (2018) conducted a study on opa fish. They found
that the formaldehyde concentration was in the range of 4.62
58.1 mg/kg. The analytical method used in this study was UV
Spectrometry.34Donkor et al (2018) conducted a study to determine the
formaldehyde exposure to the Ghanaian population of the
Kumasi Metropolis through the consumable fish. They found
that formaldehyde found in different fish species ranged from
0.174 to 3.710 mg/kg. They concluded that the formaldehyde
levels in the fish were within the tolerable limit for human
consumption. The analytical method used in this study was
Spectrophotometry.35Bhowmik et al (2019) conducted a study on wet fish in
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00014.5
89
Bangladesh. They found that the formaldehyde values were in
the range of 9.39±39 32.57±11.23 mg/kg. The analytical
method used in this study was UV Spectrophotometry.
Strength and Limitations: The quantitative estimation of
formaldehyde in the fish samples that tested positive during
qualitative screening was performed by High Performance
Liquid Chromatography which is a more sophisticated method
for quantitative estimation of formaldehyde with high degree
of precision and specificity. Qualitative and quantitative
studies of formaldehyde contamination of fish were done on a
relatively small sample size of fish in this study, due to cost
constraints. Effects of storing, cooking, and seasonal variation
on formaldehyde contamination of fish have to be determined.
The level of distribution chain at which the formaldehyde
contamination occurs has to be identified clearly.
Conclusions: Out of 65 fish samples qualitatively screened for
formaldehyde, 16 samples tested positive with a percentage
prevalence rate of 24.62%. Formaldehyde adulteration was
only noticed in Indian oil sardine and Indian mackerel, but not
in Spotted seer fish. The values of formaldehyde concentration
obtained from quantitative estimation were found to be within
the tolerable level for humans as per the Italian Ministry of
Health (1985). The percentage of positive cases within the
tolerable level for humans was 100%. Tolerable level for
humans has not been specified by the Indian Ministry of
Health. The highest value of formaldehyde was seen in Indian
mackerel which is one of the highest values noted when
comparing with other similar studies on formaldehyde
concentration in Indian mackerel. Even though the values of
formaldehyde concentration were within the tolerable level for
humans, the issue of adulteration of fish with formaldehyde
still exists when the FSSAI clearly states the complete
prohibition of its use. The government and other agencies need
to take necessary steps to prevent such type of activities by the
fish traders in order to safeguard public health, and proper
washing and cooking techniques to be adopted while preparing
dishes with fish, must be highlighted.
Acknowledgement
I express my sincere gratitude and thanks to Dr Prem Nair,
Medical Director, Dr (Col.) Vishal Marwaha, Principal, Amrita
School of Medicine, Dr Sanjeev K Singh, Medical
Superintendent, Dr D M Vasudevan, Chairman, Dissertation
Review committee for their support and guidance.
REFERENCES :
1. National Fisheries Development Board. About Indian
F i sher ies [ In te rne t ] . Ava i lab le f rom: URL
http://nfdb.gov.in/about-indian-fisheries.htm (Accessed
on 2018 Sep 22).
2. Salim SS. Consumer's willingness to pay more for
shrimps in suburban Mumbai. Agricultural Economics
Research Association. 2012; 25(2): 347-350.
3. Salim SS. Demand and supply paradigms for fish food
security in India. Seafood Export Journal 2013; 43(5): 34-
40.
4. Salim SS, Athira NR, Ratnakaran AP, Safeena PK,
Ramees RM, Fernandez R, et al. Assessing demand
drivers in augmenting fish consumption in Ernakulam.
Indian J Econ Dev 2019; 7(5): 1-8.
5. Tilami SK, Sampels S. Nutritional value of fish: lipids,
proteins, vitamins, and minerals. Rev Fisheries Sci
Aquaculture 2018; 26(2): 243-253.
6. Noordiana N, Fatimah AB, Farhana YC. Formaldehyde
content and quality characteristics of selected fish and
seafood from wet markers. Int Food Res J 2011; 18: 123-
136.
7. International Agency for Research on Cancer (IARC).
Monographs on the evaluation of carcinogenic risks to
humans. Vol 88. Lyon, France. 2004.
8. Chung SW, Chan BT. Trimethylamine oxide,
dimethylamine, trimethylamine and formaldehyde levels
in main traded fish species in Hong Kong. Food Addit
Contam 2009; 2(1): 44-51.
9. Rehbein H, Schubring R, Havemeister W, Sotelo CG,
Nielsen MK, Jorgensen B et al. Relation between TMAO
activity and content of formaldehyde in fillet minces and
bellyflap minces from gadoid fishes. Inf Fischwirtsch
1997; 44(3): 114-118.
10. Mohanty BP, Mohanty A, Parida PK, Parija SC, Das BK.
Formaldehyde adulteration in fish as a public health
concern and need for mass awareness. JIFSI. 2018; 50(1):
71-74.
11. Bianchi F, Careri M, Musci M, Mangia A. Fish and food
safety: determination of formaldehyde in 12 fish species
by SPME extraction and GC-MS analysis. Food Chem
2007; 100: 1049-1053.
12. Zhang X, Hui Y, Cai Y, Huang D. The research progress of
endogenous formaldehyde in aquatic products. World J
Eng Technol 2015; 3(3). 272276.
13. Asare-Donkor NK, Adaagoam RA, Voegborlo RB,
Adimado A. Risk assessment of Kumasi metropolis
population in Ghana through consumption of fish
contaminated with formaldehyde. J Toxicol 2018; 1: 1-7.
14. Laly SJ, Priya ER, Panda SK, Zynudheen AA.
Formaldehyde in seafood: a review. Fish Technol 2018;
55: 87-93.
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00014.5
90
15. Zailina H, Fatimah A. Health risk assessment of adults
consuming commercial fish contaminated with
formaldehyde. Food Public Health 2013; 3 (1): 5258.
16. Haque E, Mohsin ABM. Intensity of formalin use for
consumable fish preservation in Dhaka City, Bangladesh.
J Fish Int 2009; 4(3): 51-53.
17. Yeasmin T, Reza MS, Khan MN, Shikha FH, Kamal M.
Present status of marketing of formaldehyde treated fishes
in domestic markets at Mymensigh District in
Bangladesh. Int J BioRes 2010; 1(4): 21-24.
18. Uddin R, Wahid MI, Jesmeen T, Huda HN, Sutradhar KB.
Detection of formalin in fish samples collected from
Dhaka City, Bangladesh. S J Pharm Sci 2011; 4(1): 49-52.
19. Rahman MM, Ahmed S, Hosen MM, Talukder AK.
Detection of formalin and quality characteristics of
selected fish from wet markets at Sylhet City in
Bangladesh. Bangladesh Res Pub J 2012; 7(2): 161-169.
20. Islam R, Mahmud S, Aziz A, Sarker A, Nasreen M. A
comparative study of present status of marketing of
formalin treated fishes in six districts of Bangladesh. Food
Nutr Sci 2015; 6: 124-134.
21. Paul L, Mondal DK, Paul M, Riar MG, Ali A. Intensity of
formalin misuse for fish preservation in five markets of
Jessore District, Bangladesh. Int J Nat Soc Sci 2014; 1: 77-
81.
22. Saba CK, Atayure SI, Adzitey F. Assessment of
formaldehyde levels in local and imported fresh fish in
Ghana: A case study in the Tamale Metropolis of Ghana. J
Food Prot 2015; 78(3): 624-627.
23. Jawahar LS, John C, Shafeekh M, Anupama TK, Sankar
TV. Retention of residual formaldehyde in treated Indian
Mackerel (Rastrelliger kanagurta) under iced storage and
related food safety concerns. Indian J Fish 2017; 64(4):
87-93.
24. Chandralekha AP, Baranage C. Formaldehyde levels in
fish from the Kandy Market. J National Sci Council Sri
Lanka. 1992; 20(1): 115-121.
25. Siti A, Zalina H, Fatima AB. Health risk assessment of
adults consuming fish contaminated with formaldehyde.
Food Public Health 2013; 3(1): 52-58.
26. Laly SJ, John C, Shafeekh M, Anupama TK, Sankar TV.
Quality and Safety Concerns of Formaldehyde Treated
Indian Mackerel. Fish Tech Rep. 2016; 2(1): 1-2.
27. Nayana A, Sabu S. Incidence of formaldehyde residues in
fresh seer fish (Scomberomorus guttatus) collected from
Ernakulam Fish Market. Indian J Sci Res 2018; 19(2): 56-
61.
28. Bechmann IE. Determination of formaldehyde in frozen
fish with formaldehyde dehydrogene using a flow
injection system with an incorporated gel-filtration
chromatography column. Analytica Chimica Acta 1996;
320: 155-164.
29. Wahed P, Razzaq A, Dharmapuri S, Corrales M.
Determination of formaldehyde in food and feed by an in-
house validated HPLC method. Food Chem 2016;
202:476-483.
30. Bhowmik S, Begum M, Alam AK. Seasonal variation of
formaldehyde and risk assessment of marketed fish
contaminated with formaldehyde: fish and food safety
issue. Asian Food Safety Food Security Assoc 2016; 1: 50-
54.
31. Bowmik S et al. Determination of formaldehyde in wet
marketed fish by HPLC analysis: a negligible concern for
fish and food safety in Bangladesh. 2017. 43(3): 245-248.
32. Sanyal S, Sinha K, Saha S, Banerjee S. Formalin in fish
trading: an inefficient practice for sustaining fish quality.
Arch Pol Fish 31 2017; 25: 43-50.
33. Putri AK, Anissha U, Ariyani F, Wibowo. Probabilistic
health risk assessment due to normal formaldehyde intake
through Opah fish (Lampris guttatus) consumption in
Indonesia. Squalen Bull Mar Fish Postharvest Biotech
2018; 13(2): 69-78.
34. Donkor NK, Adaagoam RA, Voegborlo RB, Adimado
AA. Risk assessment of Kumasi Metropolis population in
Ghana through consumption of fish contaminated with
formaldehyde. J Toxicol 1 2018; 1: 1-7.
35. Bhowmik S, Begum M, Alam AK. Formaldehyde
associated risk assessment of fish sold in local markets of
Bangladesh. Agric Rec 2019; 9(1): 102-108.
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00014.5
91
Original Research Paper
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00015.7
1. Aneeta Sajan, B.D.S Student*
2. Priya Thomas, M.D.S, PG Dip in Bioethics, Associate Professor*
*Department of Oral Pathology & Microbiology, Annoor Dental College & Hospital, Muvattupuzha
Key words: Ameloglyphics, enamel rod end, tooth prints, forensic odontology, Verifinger, Mass disaster
Corresponding Author:
Dr. Priya Thomas,
Associate Professor,
Department of Oral Pathology & Microbiology, Annoor
Dental College & Hospital, Muvattupuzha, Kerala-686673
Contact : +91 9544186644
Email :[email protected]
Article History :
Received : 27 July 2020
Received in revised form : 17 May 2021
Accepted on : 17 May 2021
Available online : 15 August 2021
INTRODUCTION:
Personal identity stands out as an important aspect in a human's
life. Many characteristic features exist in a human being,
unique to an individual, like finger print, retinal scan, facial
recognition, birth marks etc. that are used for personal
identification.
Forensic odontology involves a variety of methods for
identification, utilizing soft and hard tissues of the oral cavity.
Currently employed methods include dental age estimation
using teeth, enamel rod patterns, DNA analysis from dental
pulp, palatoscopy, cheiloscopy, bite mark analysis, ante (1)mortem dental charts comparison etc .
The use of hard tissues overrides the use of oral soft tissues as
the former can preserve information or features better, (2)compared to the latter . Teeth or enamel being the hardest
substance in the body, resist decomposition and can withstand
extreme temperatures. The use of dental evidence stands out as
the method of choice in forensic, to establish identity from
extremely traumatized, decomposed, burnt, skeletonized
remains, for those working in hazardous occupations like fire
Ameloglyphics : An Adjuvant in Individual Identification
ABSTRACT :
Introduction : In today's world, with increasing homicides and mass disasters, advanced identification methods are the need of the
hour. Human identification is easily possible with skeletal remains, especially teeth, when soft tissue analysis is not reliable. The
human tooth is considered as the most reliable evidence in a decomposed body. Enamel formation is a dynamic process. Enamel rods/prisms are deposited in an undulating, intertwining path.These rods reflect as
rod ends on the outer surface of enamel and hence form a specific pattern. These patterns are referred to as rod end patterns or
“Tooth Prints” and the study of enamel rod end patterns as “Ameloglyphics “. These patterns are unique to an individual tooth of
same individual and different individuals and an analogy to fingerprint.
Aims and Objectives: To study and analyze the tooth print patterns of different individuals and to determine if there is any
difference in the rod end patterns in males and females.stMaterials and Methods: 30 maxillary 1 premolars extracted for the purpose of orthodontic treatment were used for the study. A
representative area on the labial aspect was etched using 37% orthophosphoric acid etchant for 1min. A transparent cellophane
tape was applied to the etched site for 20 mins, gently removed and placed on a glass slide. The glass slide was then observed under
microscope and photographed. The images obtained were compared in Verifinger Standard SDK version 6.5 software.
Results: Most predominant pattern observed among the study population was observed to be loop pattern. Among the other
patterns observed were wavy branched and whorl open. 43 % of the population depicted a mixture of two viz: loop and wavy
branched/ whorl open. The tooth prints of males showed a tendency towards loop pattern. The verification with software revealed
that no two patterns were identical.
Conclusions : Tooth being the hardest substance in the body, will be preserved during mass disasters. Enamel rod end patterns are
unique for each tooth in an individual and may be used as an adjunct with other methods for personal identification. This technique
is simple, inexpensive and rapid and can be considered as adjunct ante-mortem dental records in the identification of mass disasters
victims.

92
(3,4)fighters, soldiers, jet pilots, divers etc .
Ameloglyphics is the study of enamel rod end patterns (amelo
meaning enamel and glyphics meaning carvings) and the rod (5)end patterns are termed as “Tooth prints” . These patterns
have been found to be unique to intra-individual (of the same (6)individual) and inter-individual/ different individual's teeth
and this uniqueness of the tooth patterns can be used as a (4)valuable tool in personal identification .
Enamel rod\ prisms form the basic structural unit of enamel.
Deposition of enamel is a highly organized process, in an
incremental manner. The ameloblasts lay down the enamel
rods in an undulated and inter-twining path. This is reflected on
the outer surface of the enamel as patterns of the enamel rods (5,7)ends . Groups of enamel rods run in an unique direction,
differ from adjacent group of enamel rods that result in the
formation of different patterns of enamel rod endings on the (8)tooth surface . The rod patterns are different in different
individuals but not many studies have been conducted to
analyze which patterns prevail or predominates amongst the
genders.
Biometric identification is being commonly used with
fingerprint and iris verification. These identification methods
have limitations and may not be effective during extreme (9)disasters where the soft tissues get destroyed . Automated
biometrics has been useful in reproducing complete and
accurate enamel rod end patterns. Verifinger software readily
matches the enamel rod end patterns with specific (2,7)identification number .
Considering the above factors, the current study has been
conducted to identify the enamel rod patterns of different
individuals and to analyze the difference in the rod pattern
between gender.
MATERIALS AND METHODS :
The present analytical observational study was done following
Institutional Human Ethical Committee approval (IHEC No.
019-B/04) over a period of two months (July -August 2019).
The study was conducted on 30 premolars (extracted for the
purpose of orthodontic treatment). Teeth with decay, attrition,
abrasion, erosion, hypoplasia, fracture and with restoration
were excluded from the study. Extracted premolar teeth were
collected in two separate bottles based on gender. The teeth
extracted were cleansed with hydrogen peroxide and stored in
the designated bottles. The tooth used for analysis was labeled
as F1-15 and M1-15 respectively indicative of males and
females.
Each tooth was cleaned thoroughly and dried. The labial
surface of the tooth was selected, debris removed from the
surface and then etched with 37% orthophosphoric acid
(Dental Etch etching gel) for 1min, washed with water and
dried with the three-way syringe. A thin strip of cellophane
tape was applied immediately over the etched surface of the
tooth without any finger pressure for 20 minutes [Figure 1].
The tape was then gently peeled, placed on the slide and
observed under the light microscope. A photomicrograph of
the peel was obtained at x400 magnification [Figure 1F].
Images were captured using Digiscope (Amscope 3.7 digital
camera MU500).
The photographs obtained were converted to 1500 * 2000
pixels with adobe photoshop and then subjected to the
automated biometrics (Verifinger standard SDK version 5.0-
NEUROtechnology) software for enamel rod pattern
evaluation. The software works on certain points called
minutiae for identification of each pattern. These points are
used by the software to compare the similarity/variability of
two patterns. Images are processed and patterns are
categorized manually.
RESULTS:
Among the patterns assessed were loop and two sub patterns
(wavy branched & whorl open). Loop pattern was found to be
the most predominant pattern (56.7%) among all the prints
(Fig 2, Table 1). The remaining 43.3% showed a combination
of all the three patterns. Only 3.3% of the teeth had whorl open
pattern and thus it can be considered to be rare. All the 30 prints
obtained were dissimilar and varied from each other. Inter-
individuality was retained. Between genders, the loop pattern
was found to be predominant but with no statistical
Figure : 1A: Marking of tooth surface 1B: Acid etching of labial surface 1C:Adhesion of cellophane tape to tooth print
imprint 1D: Tooth print imprint of the cellophane tape 1E: Print transferred to the slide 1F: Photomicrograph of tooth pattern
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00015.7
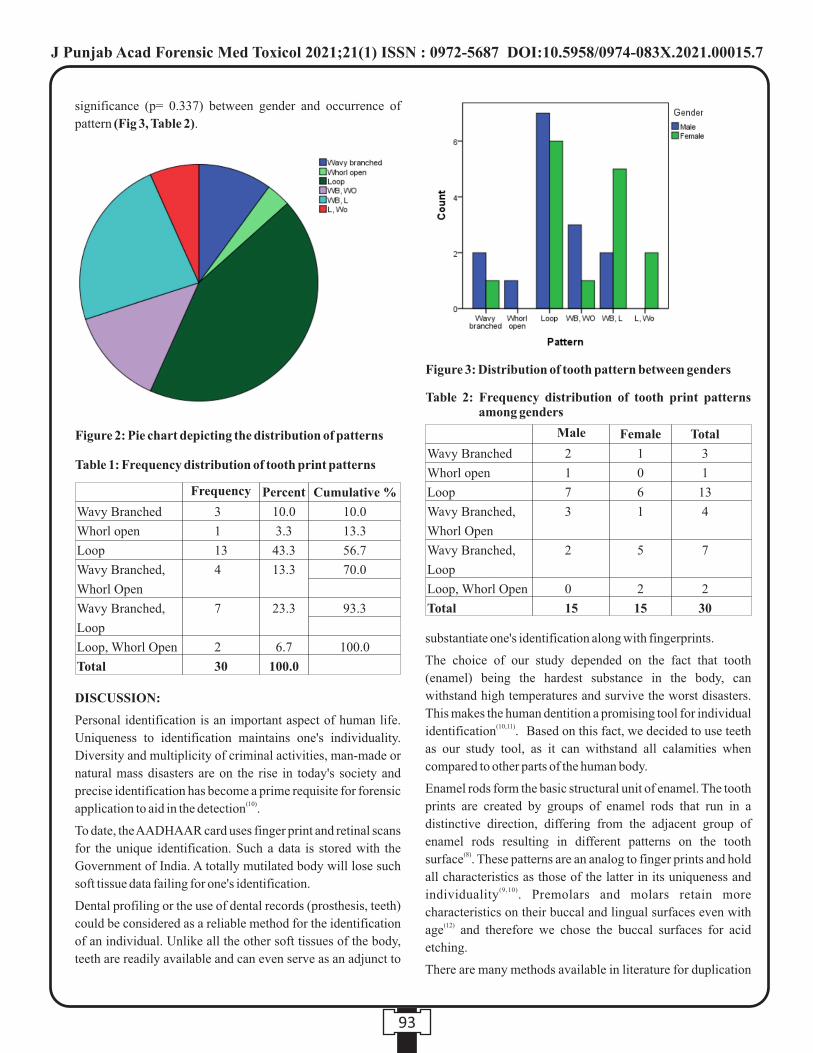
93
significance (p= 0.337) between gender and occurrence of
pattern (Fig 3, Table 2).
DISCUSSION:
Personal identification is an important aspect of human life.
Uniqueness to identification maintains one's individuality.
Diversity and multiplicity of criminal activities, man-made or
natural mass disasters are on the rise in today's society and
precise identification has become a prime requisite for forensic (10)application to aid in the detection .
To date, the AADHAAR card uses finger print and retinal scans
for the unique identification. Such a data is stored with the
Government of India. A totally mutilated body will lose such
soft tissue data failing for one's identification.
Dental profiling or the use of dental records (prosthesis, teeth)
could be considered as a reliable method for the identification
of an individual. Unlike all the other soft tissues of the body,
teeth are readily available and can even serve as an adjunct to
substantiate one's identification along with fingerprints.
The choice of our study depended on the fact that tooth
(enamel) being the hardest substance in the body, can
withstand high temperatures and survive the worst disasters.
This makes the human dentition a promising tool for individual (10,11)identification . Based on this fact, we decided to use teeth
as our study tool, as it can withstand all calamities when
compared to other parts of the human body.
Enamel rods form the basic structural unit of enamel. The tooth
prints are created by groups of enamel rods that run in a
distinctive direction, differing from the adjacent group of
enamel rods resulting in different patterns on the tooth (8)surface . These patterns are an analog to finger prints and hold
all characteristics as those of the latter in its uniqueness and (9,10)individuality . Premolars and molars retain more
characteristics on their buccal and lingual surfaces even with (12)age and therefore we chose the buccal surfaces for acid
etching.
There are many methods available in literature for duplication
Figure 2: Pie chart depicting the distribution of patterns
Table 1: Frequency distribution of tooth print patterns
Wavy Branched
Whorl open
Loop
Wavy Branched,
Whorl Open
Wavy Branched,
Loop
Loop, Whorl Open
Total
3
1
13
4
7
2
30
10.0
3.3
43.3
13.3
23.3
6.7
100.0
10.0
13.3
56.7
70.0
93.3
100.0
Frequency Percent Cumulative %
Figure 3: Distribution of tooth pattern between genders
Table 2: Frequency distribution of tooth print patterns among genders
Wavy Branched
Whorl open
Loop
Wavy Branched,
Whorl Open
Wavy Branched,
Loop
Loop, Whorl Open
Total
2
1
7
3
2
0
15
1
0
6
1
5
2
15
3
1
13
4
7
2
30
Male Female Total
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00015.7
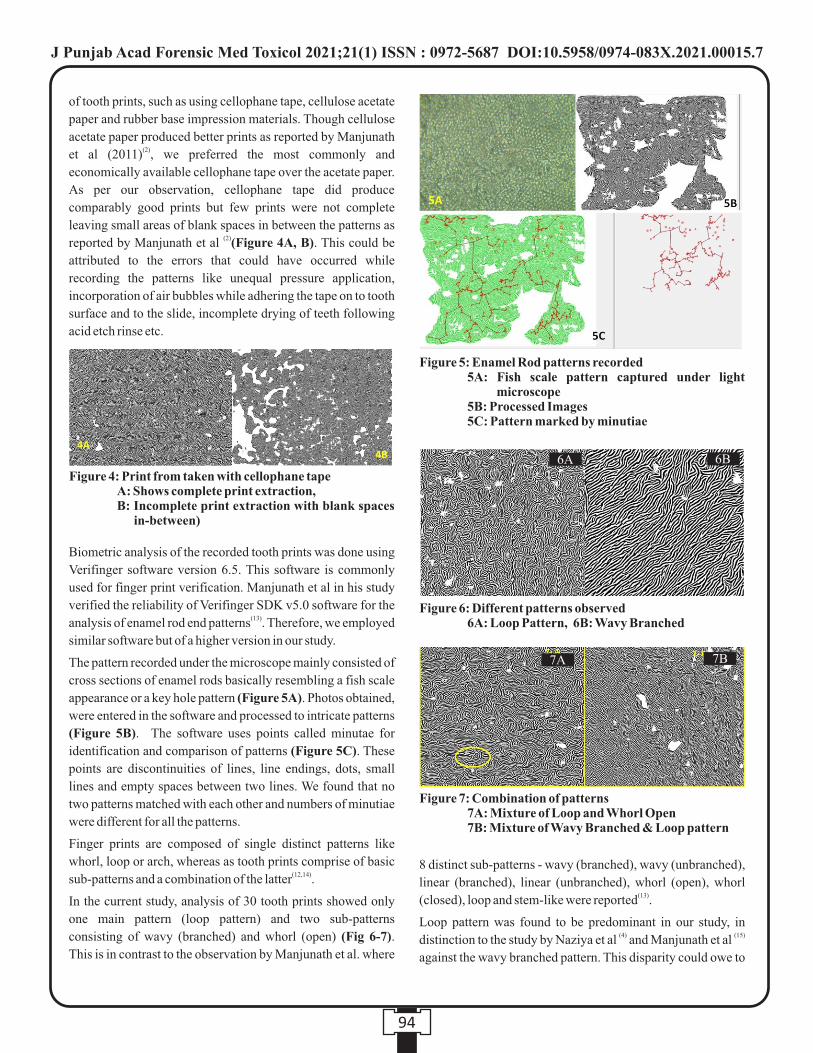
94
of tooth prints, such as using cellophane tape, cellulose acetate
paper and rubber base impression materials. Though cellulose
acetate paper produced better prints as reported by Manjunath (2)et al (2011) , we preferred the most commonly and
economically available cellophane tape over the acetate paper.
As per our observation, cellophane tape did produce
comparably good prints but few prints were not complete
leaving small areas of blank spaces in between the patterns as (2)reported by Manjunath et al (Figure 4A, B). This could be
attributed to the errors that could have occurred while
recording the patterns like unequal pressure application,
incorporation of air bubbles while adhering the tape on to tooth
surface and to the slide, incomplete drying of teeth following
acid etch rinse etc.
Biometric analysis of the recorded tooth prints was done using
Verifinger software version 6.5. This software is commonly
used for finger print verification. Manjunath et al in his study
verified the reliability of Verifinger SDK v5.0 software for the (13)analysis of enamel rod end patterns . Therefore, we employed
similar software but of a higher version in our study.
The pattern recorded under the microscope mainly consisted of
cross sections of enamel rods basically resembling a fish scale
appearance or a key hole pattern (Figure 5A). Photos obtained,
were entered in the software and processed to intricate patterns
(Figure 5B). The software uses points called minutae for
identification and comparison of patterns (Figure 5C). These
points are discontinuities of lines, line endings, dots, small
lines and empty spaces between two lines. We found that no
two patterns matched with each other and numbers of minutiae
were different for all the patterns.
Finger prints are composed of single distinct patterns like
whorl, loop or arch, whereas as tooth prints comprise of basic (12,14)sub-patterns and a combination of the latter .
In the current study, analysis of 30 tooth prints showed only
one main pattern (loop pattern) and two sub-patterns
consisting of wavy (branched) and whorl (open) (Fig 6-7).
This is in contrast to the observation by Manjunath et al. where
8 distinct sub-patterns - wavy (branched), wavy (unbranched),
linear (branched), linear (unbranched), whorl (open), whorl (13)(closed), loop and stem-like were reported .
Loop pattern was found to be predominant in our study, in (4) (15)distinction to the study by Naziya et al and Manjunath et al
against the wavy branched pattern. This disparity could owe to
Figure 4: Print from taken with cellophane tape A: Shows complete print extraction, B: Incomplete print extraction with blank spaces
in-between)
Figure 5: Enamel Rod patterns recorded 5A: Fish scale pattern captured under light
microscope 5B: Processed Images 5C: Pattern marked by minutiae
Figure 6: Different patterns observed 6A: Loop Pattern, 6B: Wavy Branched
6A 6B
Figure 7: Combination of patterns 7A: Mixture of Loop and Whorl Open 7B: Mixture of Wavy Branched & Loop pattern
7A 7B
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00015.7
95
the fact of a larger sample size being included in the other
studies or associated with the change in the direction of
movement of ameloblast, influenced by environmental (12)conditions or even genetic factors .
Loop pattern was also found to be predominant between both (4)the genders, in contrast to the study by Naziya et al . However
no statistical significant difference in tooth prints were
observed between the genders and this was in accordance with (14) (4)the studies conducted by Raju et al and Naziya et al . On the
whole, none of prints were similar to each other and this study
was concurrent with the many studies reported in (4,15,16)literature
Though enamel is the hardest substance in the body, it is always
subjected to wear and tear. The permanency of tooth patterns
with depth or with wear has to be still corroborated though (17)Manjunath et al has cited that the pattern has to be recorded
every 4 years for its application.
This study further verifies and produces a stronger evidence for
the use of tooth prints as an analog to finger prints or in
association with finger prints as an adjunct.
Limitations:
From the current study, we propose that further studies, with
larger sample size are required to analyze the variations in
patterns, distribution of patterns on the various surfaces of a
single tooth and also the need to focus its variability on a single
tooth surface (comparison between two microscopic fields/
two different photographs taken on a single surface). The
stability of such patterns has to be validated against the
permanency of finger prints as enamel can be subjected to wear
and tear.
CONCLUSION:
The study has proven that no individual has the same tooth
print as another individual and stands out by itself inimitable as
possible, making it a reliable tool for identification,
maintaining its uniqueness in equivalence to finger prints.
Such a tool can be used in adjunct with fingerprints for an
individual's identification. Ameloglyphics is a simple,
economical, rapid and reliable technique that can be used as an
additional aid for personal identification. We thereby propose
that such data can be also added to one's unique identification
as an adjunct.
ACKNOWLEDGMENTS:
We acknowledge and wholeheartedly thank Indian Council of
Medical Research (ICMR) for the approval and financial
assistance given towards the Studentship Project (ICMR STS
no.08685 project of 2019).
REFERENCES:
1. Bharanidharan R, Karthik R, Rameshkumar A, Rajashree
P, Rajkumar K. Ameloglyphics: An adjunctive aid in
individual identification. SRM J Res Dent Sci.
2014;5(4):264-68.
2. Manjunath K, Sivapathasundharam B, Saraswathi TR.
Efficacy of various materials in recording enamel rod
endings on tooth surface for personal identification. J
Forensic Dent Sci. 2011;3(2):71-6.
3. Sansare K. Forensic odontology, historical perspective.
Indian J Dent Res 1995;6: 55-7.
4. Naziya J, Sunil S, Jayanthi P, Rathy R, Harish RK.
Analysis of enamel rod end pattern for personal
identification. J Oral Maxillofac Pathol. 2019;23(1):165-
76.
5. Sha SK, Rao BV, Rao MS, Kumari KH, Chinna SK, Sahu
D. Are tooth prints a hard tissue equivalence of finger print
in mass disaster: A rationalized review. J Pharm Bioallied
Sci. 2017;9(Suppl 1):29-33.
6. Girish HC, Murgod S, Ravath CM, Hegde RB.
Ameloglyphics and predilection of dental caries. J Oral
Maxillofac Pathol. 2013;17(2):181-4.
7. Joshi PS, Bhosale SS. Study of Enamel Rod End Patterns
Using Acetate Peel Technique and Automated Biometrics
for Personal Identification. Int J Dent Med Res
2014;1(4):47-50.
8. Boyde A. Amelogenesis and the structure of enamel. In:
Cohen B, Kramer IR, editors. Scientific Foundations of
Dentistry. London: William Heinemann Medical Books
Ltd.; 1976. p. 341-43.
9. Rakesh N, Sujatha S, Pavan Kumar T, Yashoda Devi BK,
Gupta D, Harish BN. Reliability of Ameloglyphics for
Person Identification Following Adverse Conditions. J
Dent Orofac Res. 2018;14(1):26.
10. Patidar KA, Parwani R, Wanjari S. Effects of high
temperature on different restorations in forensic
identification: Dental samples and mandible. J Forens
Dent Sci. 2010; 2: 3743.
11. Lake AW, James H, Berketa JW. Disaster victim
identification: quality management from an odontology
perspective. Forensic Sci Med Pathol. 2012;8(2):15763.
12. M a n j u n a t h K , S r i r a m G , S a r a s w a t h i T R ,
Sivapathasundharam B. Enamel rod end patterns: a
preliminary study using acetate peel technique and
automated biometrics. J Forensic Odontol 2008 1: 33-6.
13. M a n j u n a t h K , S a r a s w a t h i T R , S r i r a m G ,
Sivapathasundharam B, Porchelvam S. Reliability of
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00015.7
96
automated biometrics in the analysis of enamel rod end
patterns. J Forensic Dent Sci. 2009;1(1):32-6.
14. Raju S, Rao TM, Nandan SRK, Kulkarni PG, Reddy SP,
Keerthi M. Ameloglyphics Can it aid in forensic
identification. Indian J Dent Adv. 2014; 6:166973.
15. Manjunath K, Sivapathasundharam B, Saraswathi TR.
Analysis of enamel rod end patterns on tooth surface for
personal identificationameloglyphics. J Forensic Sci.
2012;57(3):78993.
16. Juneja M, Juneja S, Rakesh N, Kantharaj YDB.
Ameloglyphics: A possible forensic tool for person
identification following high temperature and acid
exposure. J Forensic Dent Sci. 2016;8(1):28-31.
17. Manjunath K, Sivapathasundharam B. Analysis of enamel
rod end pattern at different levels of enamel and its
significance in ameloglyphics. J Forensic Res.
2014;5(4):13.
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00015.7

97
Original Research Paper
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00016.9
1. Harshita Tara, M.Sc. Forensic Science Student*
2. Amarnath Mishra, Assistant Professor and Program Leader*
*Amity Institute of Forensic Sciences, Amity University, Sector-125, Noida-201313 (Uttar Pradesh), India
Key words: Digital forensics, Data extraction tools, Data acquisition, Data Analysis, FTK Imager.
Corresponding Author:
Dr. Amarnath Mishra
(M.Sc., M.Phil., Ph.D. Forensic Sc.)
Amity Institute of Forensic Sciences, Amity University,
Sector-125, Noida-201313 (Uttar Pradesh), India
Contact : +91 91-9818978527
Email: [email protected], [email protected]
Article History :
Received : 20 May 2020
Received in revised form : 24 June 2020
Accepted on : 24 June 2020
Available online : 31 August 2021
INTRODUCTION
Digital forensics is one of the branch of forensic science which
play an extremely significant role in the society due to the
prevalence of various digital devices. The main aim of this is to
acquire the courtroom evidences which are extracted from
various digital devices (such as servers, desktops, laptops,
netbooks and mobile devices) that are used by perpetrators in
various cybercrimes (such as phishing, unauthorized access
into the system and intellectual property theft in corporate
espionage etc.) and also physical crimes (such as drug [1]trafficking etc.) .Conventional crimes leave behind the
various clues such as fingerprints, DNA, footprints, and
witnesses for the investigators to examine and investigate.
Similarly, any kind of digital activity on electronic devices
leaves a trail of data for cyber investigators to investigate and
inspect the particular type of crimes to find the perpetrators. In
all the cybercrime cases it is very crucial to acquire the digital
evidences and they should be handled properly so that they can [2]be further admissible in the court of law . This is the one and
only way of acquiring the information from digital devices
which act as digital evidences and then they can be further used
to support the allegations against the perpetrator or defend an
innocent from false accusations.
Digital forensics tools
These tools have been developed by the programmers and the
various software companies which help the investigators and
digital forensic analysts to collect the digital evidences from
the electronic devices at the crime scene. Digital devices can be
desktops, laptops, USB drives, tablets, mobile phones,
CCTVs, many more. These tools can be both hardware and
software. These can be the commercial ones that can be bought
or these are available online which can be used free of cost.
There are pros and cons to every tool. Not all tools can perform
every digital forensic process whether it is acquisition,
extraction or analysis. So it's a good technique to have various
different tools available to perform the multiple tasks from
basic to advanced level.
A Comparative Study of Digital Forensic Tools for Data Extraction From Electronic Devices
ABSTRACT :
Background - Today, a wide range of digital forensic tools are available, produced by a number of software businesses for digital
forensics investigations. In a court of law, selecting and employing the right instrument might be a deciding factor. As a result,
proper rating and comparison of diverse forensic tools is required. This article discusses the various hardware and software forensic
techniques available for analysing digital evidence.
Method- Different digital forensic tools such as FTK Imager, Encase, Paladin suite, Cellebrite, Oxygen forensic tool and Tableau
hardware have been analysed using computer system and USB drive. Imaging of USB have been performed for retrieve the
information that have been performed.
Result - The acquisition and verification times were measured using the FTK imager and EnCase forensic imager tools. Physical
acquisition on the FTK imager took about 22 minutes, while physical acquisition on the EnCase forensic imager took about 1 hour
1 minute. Physical image verification took 13 minutes with the FTK imager and 50 minutes with the EnCase forensic imager.
Conclusion - When compared to EnCase imager, FTK imager is simpler, faster, and easier to use because EnCase takes longer to
acquire the image than FTK. The capabilities of Cellebrite UFED and Oxygen detective forensic instruments are nearly same,
although UFED is preferable when it comes to ease of use.
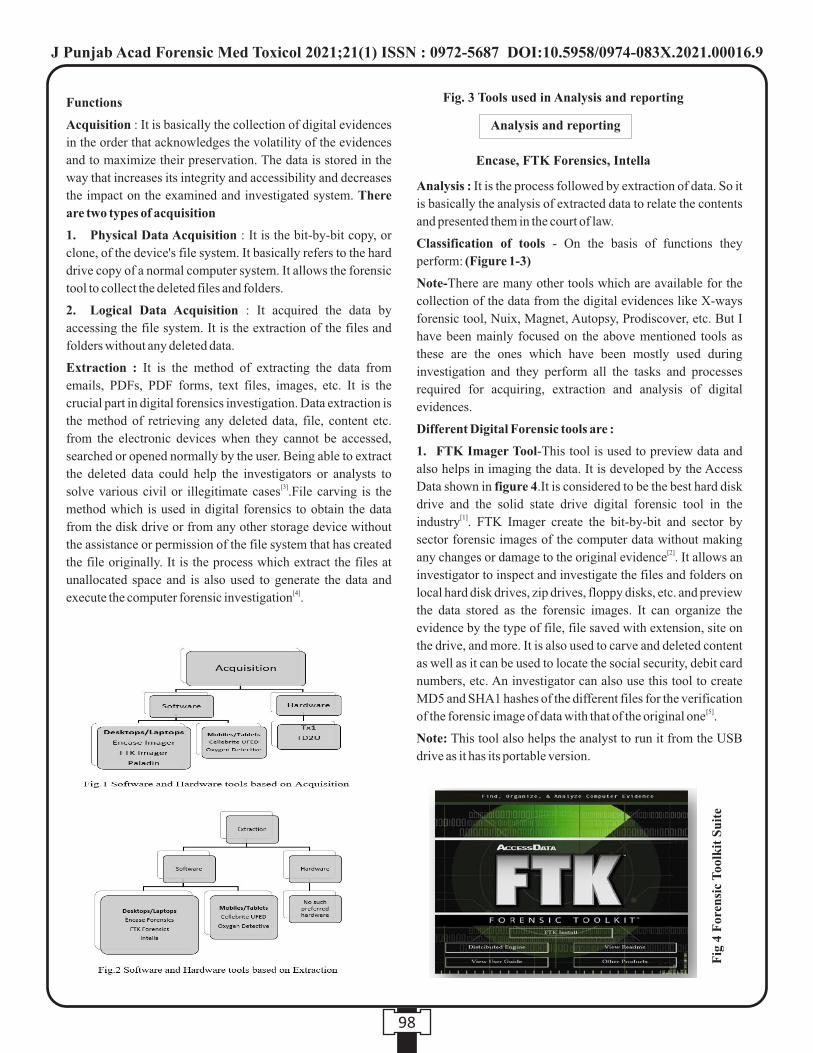
98
Functions
Acquisition : It is basically the collection of digital evidences
in the order that acknowledges the volatility of the evidences
and to maximize their preservation. The data is stored in the
way that increases its integrity and accessibility and decreases
the impact on the examined and investigated system. There
are two types of acquisition
1. Physical Data Acquisition : It is the bit-by-bit copy, or
clone, of the device's file system. It basically refers to the hard
drive copy of a normal computer system. It allows the forensic
tool to collect the deleted files and folders.
2. Logical Data Acquisition : It acquired the data by
accessing the file system. It is the extraction of the files and
folders without any deleted data.
Extraction : It is the method of extracting the data from
emails, PDFs, PDF forms, text files, images, etc. It is the
crucial part in digital forensics investigation. Data extraction is
the method of retrieving any deleted data, file, content etc.
from the electronic devices when they cannot be accessed,
searched or opened normally by the user. Being able to extract
the deleted data could help the investigators or analysts to [3]solve various civil or illegitimate cases .File carving is the
method which is used in digital forensics to obtain the data
from the disk drive or from any other storage device without
the assistance or permission of the file system that has created
the file originally. It is the process which extract the files at
unallocated space and is also used to generate the data and [4]execute the computer forensic investigation .
Analysis : It is the process followed by extraction of data. So it
is basically the analysis of extracted data to relate the contents
and presented them in the court of law.
Classification of tools - On the basis of functions they
perform: (Figure 1-3)
Note-There are many other tools which are available for the
collection of the data from the digital evidences like X-ways
forensic tool, Nuix, Magnet, Autopsy, Prodiscover, etc. But I
have been mainly focused on the above mentioned tools as
these are the ones which have been mostly used during
investigation and they perform all the tasks and processes
required for acquiring, extraction and analysis of digital
evidences.
Different Digital Forensic tools are :
1. FTK Imager Tool-This tool is used to preview data and
also helps in imaging the data. It is developed by the Access
Data shown in figure 4.It is considered to be the best hard disk
drive and the solid state drive digital forensic tool in the [1]industry . FTK Imager create the bit-by-bit and sector by
sector forensic images of the computer data without making [2]any changes or damage to the original evidence . It allows an
investigator to inspect and investigate the files and folders on
local hard disk drives, zip drives, floppy disks, etc. and preview
the data stored as the forensic images. It can organize the
evidence by the type of file, file saved with extension, site on
the drive, and more. It is also used to carve and deleted content
as well as it can be used to locate the social security, debit card
numbers, etc. An investigator can also use this tool to create
MD5 and SHA1 hashes of the different files for the verification [5]of the forensic image of data with that of the original one .
Note: This tool also helps the analyst to run it from the USB
drive as it has its portable version.
Fig. 3 Tools used in Analysis and reporting
Fig
4 F
oren
sic
Too
lkit
Su
ite
Analysis and reporting
Encase, FTK Forensics, Intella
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00016.9

99
2. EnCase Forensic Imager tool- EnCase version7.12.01.18
is the tool which is distributed and maintained by Guidance
Software shown in figure 5. It is the tool which offers the
functionality and the flexibility. Investigators have the
flexibility to complete the investigation efficiently and quickly
with this tool.
It provides the flexibility for any investigator to acquire data
from the wide variety of digital devices and it also includes 25
types of mobile devices such as smart phones, tablets, iOS etc.
It helps an investigator to complete the investigation in the
forensically defined manner.
It produces the extensive reports of the whole investigation and [5]also maintain the integrity of the evidence .
It is used to transfer evidence files directly either to law [6]enforcement or to the legal representatives .
It creates the exact duplicate files of original data which is
further verified by hash and Cyclic Redundancy Check (CRC)
values.
3. Paladin Forensic Suite :
It is a Live “Linux” distribution which is created based on
Ubuntu that simplifies various tasks and processes in a
forensically sound manner via this toolbox. It is available in
64-bit and 32-bit versions. It is used by thousands of digital
analysts or forensic examiners such as law enforcers, military,
federal, state and corporate agencies. With the Paladin toolbox,
user can easily triage- search – image and more. It includes
more than 80 tools which are simplified into 25 groups such as
Imaging Tools, Social Media Analysis, etc.
Characteristics :
• It helps in complete visibility into your network.
• It also helps in acquiring the volatile data including
internet history and RAM and then it stores that content
in the pen drive or any other storage drive.
• It also works efficiently in apple windows, android
windows, and Linux. (Figure 6)
4. Cellebrite UFED - Cellebrite has developed the series of
products called 'Universal Forensic Extraction Device' i.e.
(UFED) for computer forensics examination. Basically this
system i.e. Universal Forensic Extraction Device is a portable
device with optional personal computer software, data cables, [7]chargers etc.
UFED 4PC- Cellebrite presents UFED 4PC (Figure 7) which
is the cost-effective, flexible and the most convenient
application suite for any investigative personnel requiring a
specialized mobile forensic tool kit on their existing desktops
or laptops. UFED 4PC provides digital analysts with advanced
capabilities to perform tasks like data extraction, decoding and
analysis on the same platform from the widest range of mobile
devices.
Key Features :
—Physical abstraction and decrypting while bypassing the
pattern lock / security password / postal index number from
android or iOS gadgets.
—It contains the unique and enough set of analysis
characteristics that includes timeline, malware detection, etc.
—It also helps in logical eradication of contents i.e.
Applications data, passwords, instant messaging, contacts, [8]emails, pictures, audios, videos, call logs, phone details etc.
—It also performs the cloning of Subscriber Identity Module
(SIM) ID which is used to quarantine the phone from network
activity during the investigation.
—It has the many software updates that occur frequently to
ensure its compatibility with the newly introduced phones in
the market.
—It generates the reports that are easy to read in the different
forms using the UFED Physical Analyzer Tool.
UFED Physical Analyzer- UFED PA is available with the
UFED Touch Ultimate. It offers the advanced analysis,
decrypting and reporting features in the mobile forensics. It
also helps in malware detection, advanced decoding and
reporting features, transferring data capabilities etc.
Fig
5. E
nC
ase
For
ensi
c Im
ager
Fig
6. P
alad
in T
ool
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00016.9
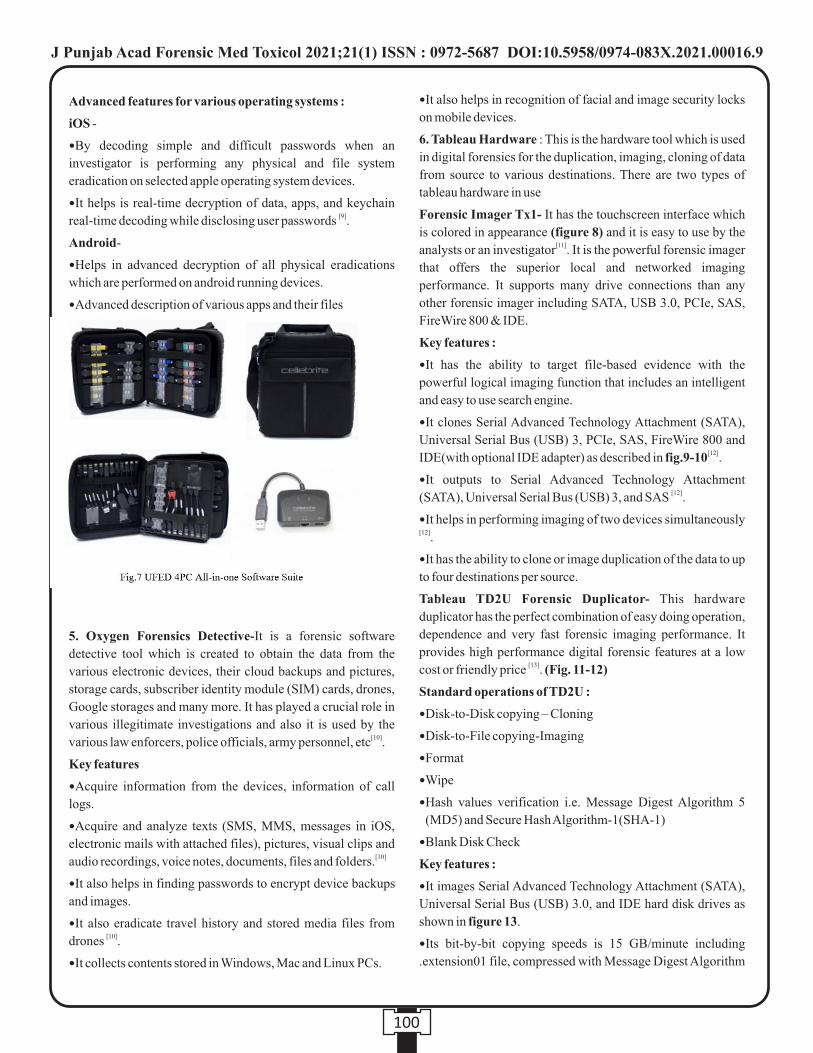
100
Advanced features for various operating systems :
iOS -
—By decoding simple and difficult passwords when an
investigator is performing any physical and file system
eradication on selected apple operating system devices.
—It helps is real-time decryption of data, apps, and keychain [9]real-time decoding while disclosing user passwords .
Android-
—Helps in advanced decryption of all physical eradications
which are performed on android running devices.
—Advanced description of various apps and their files
5. Oxygen Forensics Detective-It is a forensic software
detective tool which is created to obtain the data from the
various electronic devices, their cloud backups and pictures,
storage cards, subscriber identity module (SIM) cards, drones,
Google storages and many more. It has played a crucial role in
various illegitimate investigations and also it is used by the [10]various law enforcers, police officials, army personnel, etc .
Key features
—Acquire information from the devices, information of call
logs.
—Acquire and analyze texts (SMS, MMS, messages in iOS,
electronic mails with attached files), pictures, visual clips and [10]audio recordings, voice notes, documents, files and folders.
—It also helps in finding passwords to encrypt device backups
and images.
—It also eradicate travel history and stored media files from [10]drones .
—It collects contents stored in Windows, Mac and Linux PCs.
—It also helps in recognition of facial and image security locks
on mobile devices.
6. Tableau Hardware : This is the hardware tool which is used
in digital forensics for the duplication, imaging, cloning of data
from source to various destinations. There are two types of
tableau hardware in use
Forensic Imager Tx1- It has the touchscreen interface which
is colored in appearance (figure 8) and it is easy to use by the [11]analysts or an investigator . It is the powerful forensic imager
that offers the superior local and networked imaging
performance. It supports many drive connections than any
other forensic imager including SATA, USB 3.0, PCIe, SAS,
FireWire 800 & IDE.
Key features :
—It has the ability to target file-based evidence with the
powerful logical imaging function that includes an intelligent
and easy to use search engine.
—It clones Serial Advanced Technology Attachment (SATA),
Universal Serial Bus (USB) 3, PCIe, SAS, FireWire 800 and [12]IDE(with optional IDE adapter) as described in fig.9-10 .
—It outputs to Serial Advanced Technology Attachment [12](SATA), Universal Serial Bus (USB) 3, and SAS .
—It helps in performing imaging of two devices simultaneously [12].
—It has the ability to clone or image duplication of the data to up
to four destinations per source.
Tableau TD2U Forensic Duplicator- This hardware
duplicator has the perfect combination of easy doing operation,
dependence and very fast forensic imaging performance. It
provides high performance digital forensic features at a low [13]cost or friendly price . (Fig. 11-12)
Standard operations of TD2U :
—Disk-to-Disk copying – Cloning
—Disk-to-File copying-Imaging
—Format
—Wipe
—Hash values verification i.e. Message Digest Algorithm 5
(MD5) and Secure Hash Algorithm-1(SHA-1)
—Blank Disk Check
Key features :
—It images Serial Advanced Technology Attachment (SATA),
Universal Serial Bus (USB) 3.0, and IDE hard disk drives as
shown in figure 13.
—Its bit-by-bit copying speeds is 15 GB/minute including
.extension01 file, compressed with Message Digest Algorithm
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00016.9

101
5 (MD5) and Secure Hash Algorithm-1 (SHA-1) hash values [14].
—It is capable of creating 1:1, 1:2, and 1:3 forensically-sound
copies of the digital evidences.
—It outputs to raw demand draft, .extension01, .ex01, or .dmg
file formats.
—Its data wiping speed is 25 GB/minute.
—It supports whole disk coding of the destination disk drives.
MATERIALS AND METHODS :
Intel core i3-4005U CPU, 4 GB of RAM (with Microsoft
Windows 10 Pro operating system), USB Drive of 32 GB (It
contained the data of 12.1 GB). This USB Drive was used for
the comparison between the FTK imager and EnCase based on
the acquisition and verification.
ANALYSIS :
Digital Forensic software such as Encase forensic imager,
version 7 have acquired the image of the USB drive (digital
evidence) and tested how long it would take to acquire (both
physical and logical acquisition) the information and the
verification time of the image.
Next tool used was FTK Imager 4.3.0.1.8, a simpler imaging
program and same USB drive was imaged to retrieve the
information and then compared the acquisition as well as
verification time of both EnCase forensic imager and FTK
imager with same compression level.
RESULTS AND DISCUSSIONS :
Table 1-3 Showing the results of completion time of
acquisition and verification by FTK imager and EnCase
forensic imager tools
The initial tool used was FTK imager. First test was the
simple acquisition.
—FTK imager took approximately 22 minutes for physical
Fig. 11 Tableau
TD2U Duplicator
Fig
. 12
Upp
er P
art
of T
D2U
Fig
. 13
Low
er P
art
of T
D2U
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00016.9
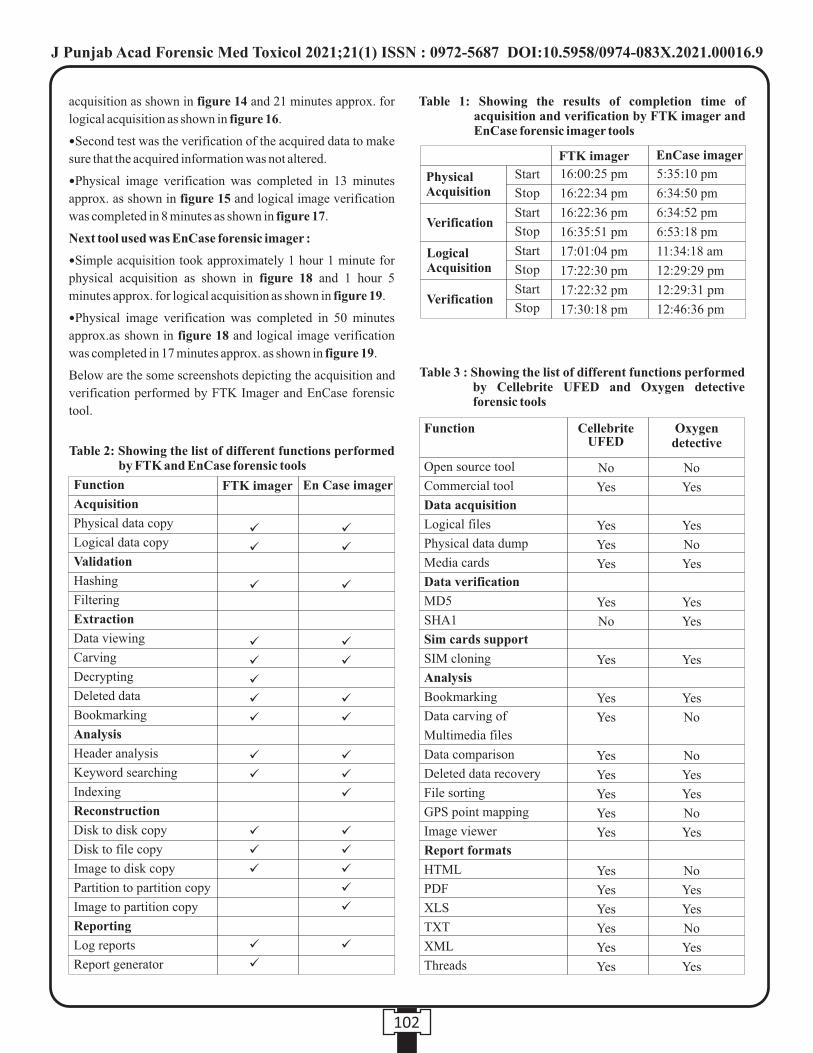
102
acquisition as shown in figure 14 and 21 minutes approx. for
logical acquisition as shown in figure 16.
—Second test was the verification of the acquired data to make
sure that the acquired information was not altered.
—Physical image verification was completed in 13 minutes
approx. as shown in figure 15 and logical image verification
was completed in 8 minutes as shown in figure 17.
Next tool used was EnCase forensic imager :
—Simple acquisition took approximately 1 hour 1 minute for
physical acquisition as shown in figure 18 and 1 hour 5
minutes approx. for logical acquisition as shown in figure 19.
—Physical image verification was completed in 50 minutes
approx.as shown in figure 18 and logical image verification
was completed in 17 minutes approx. as shown in figure 19.
Below are the some screenshots depicting the acquisition and
verification performed by FTK Imager and EnCase forensic
tool.
Physical Acquisition
Verification
Logical Acquisition
Verification
Start
Stop
Start
Stop
Start
Stop
Start
Stop
16:00:25 pm
16:22:34 pm
16:22:36 pm
16:35:51 pm
17:01:04 pm
17:22:30 pm
17:22:32 pm
17:30:18 pm
5:35:10 pm
6:34:50 pm
6:34:52 pm
6:53:18 pm
11:34:18 am
12:29:29 pm
12:29:31 pm
12:46:36 pm
FTK imager EnCase imager
Table 1: Showing the results of completion time of acquisition and verification by FTK imager and EnCase forensic imager tools
Table 2: Showing the list of different functions performed by FTK and EnCase forensic tools
Function
Acquisition
Physical data copy
Logical data copy
Validation
Hashing
Filtering
Extraction
Data viewing
Carving
Decrypting
Deleted data
Bookmarking
Analysis
Header analysis
Keyword searching
Indexing
Reconstruction
Disk to disk copy
Disk to file copy
Image to disk copy
Partition to partition copy
Image to partition copy
Reporting
Log reports
Report generator
ü
ü
ü
ü
ü
ü
ü
ü
ü
ü
ü
ü
ü
ü
ü
ü
ü
ü
ü
ü
ü
ü
ü
ü
ü
ü
ü
ü
ü
ü
ü
FTK imager En Case imager
Table 3 : Showing the list of different functions performed by Cellebrite UFED and Oxygen detective forensic tools
Function
Open source tool
Commercial tool
Data acquisition
Logical files
Physical data dump
Media cards
Data verification
MD5
SHA1
Sim cards support
SIM cloning
Analysis
Bookmarking
Data carving of
Multimedia files
Data comparison
Deleted data recovery
File sorting
GPS point mapping
Image viewer
Report formats
HTML
XLS
TXT
XML
Threads
Cellebrite UFED
No
Yes
Yes
Yes
Yes
Yes
No
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
No
Yes
Yes
No
Yes
Yes
Yes
Yes
Yes
No
No
Yes
Yes
No
Yes
No
Yes
Yes
No
Yes
Yes
Oxygen detective
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00016.9
103
CONCLUSION :
For EnCase V7.04.01, we have recorded that it took 1hour
1minute to acquire the physical image 12.1 GB data from the
32 GB USB drive and another 50 minutes to verify that the data
acquired was indeed the same as on the USB drive while it took
1 hour 5 minutes to acquire the logical image and another 17
minutes for its verification.
For FTK Imager 4.3.0.1.8, the physical imaging of the USB
drive was completed in 22 minutes and another 13 minutes for
the verification while it took approximately 21 minutes to
acquire logical image and another 8 minutes for its
verification.
Based on the above results of acquiring the image and
verification, FTK imager is simpler, faster, and easier as
compared to EnCase imager as EnCase took longer time for
acquiring the image than FTK.
Although Cellebrite UFED and Oxygen detective forensic
tools have more or less similar functions but among two UFED
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00016.9

104
is more preferred when it comes to easy to use. Also it supports
maximum number of devices such as iOS devices including
all iPhone models (iPhone 4S to iPhone XS/XR), iPad, iPad
mini, iPad Pro and iPod touch, running iOS 5 to iOS 12 ,
Samsung devices including Galaxy S6/S7/S7+/S8/
S8+/S9/S10, A5/A7/A8, J1/J2/J3\/J6/J7, Note 5/Note 7/Note
8/Note 9 , Huawei including P8Litem, P10Lite, P20Lite,
Honor Note 10, Mate 9, Mate 10, Y7, Nova 2, Nova 3, Honor
Magic 2, Enjoy 8 Plus , LG including G5, Nexus 5X, V20, V33
Qua, M327, G6 , Other androids including Alcatel, Motorola,
ZTE, HTC, Nexus, Xiao MI and more.
REFERENCES :
1. Powell A, Haynes C. Social media data in digital forensics
investigations. In Digital Forensic Education 2020 (pp.
281-303). Springer, Cham.
2. Hassan NA. Digital Forensics Basics: A Practical Guide
Using Windows OS. A press; 2019 Feb 25.
3. Surviving with Android.
Available at https://www.survivingwithandroid.com /,
accessed 2020
4. InfoSec Resources 2020.
Available at https://resources.infosecinstitute.com/.
5. Tabona O, Blyth A. A forensic cloud environment to
address the big data challenge in digital forensics. In2016
SAI computing conference (SAI) 2016 Jul 13 (pp. 579-
584). IEEE.
6. UFL Research Repository.
Available at https://repository.uel.ac.uk/,accessed 2019.
7. Pyramid Cyber Security.
Available at https://pyramidcyber.com/ ,accessed 2018.
8. Military Systems and Tecchnology.Available at
https://www.militarysystems-tech.com/,accessed 2020.
9. Myspace International.
Available at http://myspaceintl.com/index.html,accessed
2019.
10. Oxygen forensics. Available at https://www.oxygen-
forensic.com/en/.
11. Digital Intelligence.
Available at https://digitalintelligence.com/,accessed
2016-20.
12. Digital forensics.
Available at https://shop.avatu.co.uk/,accessed 2020.
13. Fulcrum management.
Available at https://fulcrum.net.au/,accessed 2012.
14. Siva Kumar P. Effectual web content mining using noise
removal from web pages. Wireless Personal
Communications. 2015 Sep 1;84(1):99-121.
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00016.9
105
Original Research Paper
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00017.0
1. Rohit Zariwala, Professor & Head, Department of Forensic Medicine, Gujarat Adani Institute of Medical Sciences, Bhuj
2. Krunal Pipaliya, Associate Professor, Department of Forensic Medicine, Banas Medical College, Palanpur, Gujarat.
3. Dimple Patel, Professor & Head, Department of Anatomy, AMC MET Medical College, Maninagar, Ahmedabad.
Key words: Image based, Non image based, Teaching learning methods(TLM), Forensic medicine & Toxicology (FMT)
Corresponding Author:
Dr. Rohit Zariwala,
Professor & Head,
Department of Forensic Medicine, Gujarat Adani Institute of
Medical Sciences, Bhuj - 370001.
Contact : +91 99250-30322
Email: [email protected]
Article History :
Received : 10 July 2020
Received in revised form : 26 July 2020
Accepted on : 26 July 2020
Available online : 31 August 2021
INTRODUCTION :
Images are frequently used as 'icebreakers' at the start of a
presentation to motivate an audience to listen and pay
attention. The image is chosen to promote the relevance of the
lecture content 'perhaps it might happen to me', which is [1] [2]important in adult learning. Cosgrov described the use of
images of a toy train-set to illustrate oxygen delivery to tissues.
Physiotherapy students in the study group obtained higher
marks in MCQ papers following the lecture, compared with a
control group. This suggests the imagery significantly
increased understanding of the topic and possibly memory
retention as well.
Careful structured use of images improves attention, [3]cognition, reflection and possibly memory retention .
4Memory for pictures may be better than for words and this fits
with the dual code theory that images are stored via a different [4]pathway to auditory information in the brain
MATERIAL AND METHODS :
After taking ethical approval from institutional ethics
committee, GAIMS, Bhuj and written informed consent from
participants, Present study was conducted at Forensic thMedicine Department, GAIMS, Bhuj from 15 October 2018
thto 15 Mach 2019 on 146 students of 2nd year MBBS (2017-
18) to evaluate effectiveness of image based interactive
teaching learning method on academic performance by taking
their feedback.
The study group was divided in two groups (Group A and
Group B) consisting 73 students in each group. Randomization
Introduction And Evaluation of Effective Image Based Interactive Teaching Learning Method In Forensic Medicine Amongst Second MBBS Students
ABSTRACT :
Introduction: Use of carefully structured image improves attention, cognitionand reflection.
Aim: To facilitate learning in FMT by image based interactive teaching.
Objectives: To obtain student's perception after introduce and evaluation of effectiveness of image based interactive teaching
learning method.
Materials and Methods: Prospective, interventional and cross over study was conductedover 6 months period on 144 second
MBBS students of GAIMS. Pre Sensitization of session of one hour was conducted. Participants were randomized into two groups
- A (n = 73) and B (n = 71). Two topics were taught by image based and none imaged based TLM with Crossover. Assessment was
done by pre validated 10 MCQs test after each topic. Data were statically analysed. Participant feedback was taken in Google form
by using questioners based on Liker's scale.
Result: Mean ± SD of imaged based TLM was higher (7.53 ± 1.35) than nonimage based TLM (5.94 ± 1.80) on Abrasion. Mean ±
SD of imaged based TLM was higher (6.15 ± 1.80) than non image based TLM (4.77 ± 1.70) on Contusion. P value was statically
highly significant on image based TLM. Student's feedback most of the students agreed with imaged based TLM.
Conclusion Image based TLM is found to be useful learning tool for FMT. Ithastens understanding of complex components of
FMT in shorter period of time than non-image based teaching.

106
of students was done. Absent participants on day of teaching
were excluded. Faculty and Students were sensitized regarding
the project prior to study.
Topics included in the project were Abrasion and Contusion
which is decided after discussion with the faculties of
Department of Forensic Medicine and students. MCQs were
validated by two experts from the Department of Forensic
Medicine.
Topic I (Abrasion): GROUP A: Teaching with use of image
based & GROUP B: Teaching with use of non-image based.
Topic II (Contusion): GROUP A: Teaching with use of non-
image based & GROUP B: Teaching with use of image based.
Both topics were taken by same teacher. The impact of
teaching-learning methods was analyzed by assessing
performance of students in printed copies of the MCQ based
test consisting of 10 MCQs (10 marks) on respective topic
taught. Time for the test was ten minutes.
The entire process was part of the teaching methodology and it
was completed in the class time. No sensitive questions were
asked as part of the feedback and anonymity was maintained.
The students was asked to fill the pre validated structured
questionnaire about their views and perception of two
teaching-learning methods. Feedback given by students was
evaluated on a five point Likert scale (i.e., strongly agree,
agree, agree/disagree, disagree and strongly disagree)
Collection of Data: Collected data of questionnaires and
MCQ tests was recorded in Microsoft excel worksheet.
Statistical analysis: It was done by two tailed independent t
test after consulting to the statistician
Evaluation: The data was collected, tabulated, and
statistically analyzed by an appropriate statistical tool (e.g.
Prism software trial version)
RESULTS :
Table 1 show that Means ± SD for the topic Abrasion in image
based teaching was 7.53 ± 1.35 as compared to the non-image
based traditional teaching i.e. 5.94±1.80. And for the topic
Contusion Means±SD in image based teaching was 6.15 ± 1.80
as compared to the non image based traditional teaching i.e.
4.77 ±1.70.
P value for the 2 tailed independent t test in Abrasion and
Contusion is <0.001 respectively which is highly significant.
Figure 1, 2 and 3 Vertical Bar - Diagram shows average
percentage scored by students from image and non image
based TL method. It is clearly evident that percentage scored
by students in topics taught by image based teaching is higher
than the topic taught by non-image based teaching.
Figure 4 shows the students feedback for the image based
teaching on 5 point Likert scale.
DISCUSSION :
FM is a visually oriented subject. Investigation of MLC cases
in FM primarily depends on the inspection findings in most
cases. Hence, the images can serve as a valuable teaching
material. Further, the interpretation of MLC cases in the native
skin color poses challenges to a beginner who is baffled by the
variations in presentation. Repeated exposure to images is [5]expected to increase the diagnostic skills, as well.
Table 1 : Comparative performance of students with image based teaching and non image based teaching ( mean±SD)
TL METHOD
COUNT (n)
Mean±SD
P VALUE IMAGEV/S NON IMAGETEACHING
IMAGES IMAGES
73
7.53±1.35*
*<0.001*p<0.001, Highlysignificant
*<0.001*p<0.001, Highlysignificant
NON IMAGE NON IMAGE
71
5.94±1.80
68
6.15±1.80**
70
4.77±1.70
TOPIC ABRASION CONTUSION
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00017.0

107
Advantages for image based teaching :
1. Repeated exposure to image facilitates active learning and
retention of knowledge.
2. It will be an effective supplement in a set up where clinical
teaching material is limited.
3. Ti will be a time saving method of teaching.
4. D/D of particular condition can be discussed easily with
image alone.
5. It provides long lasting visual memory of subtle
diagnostic clue for students.
6. Unlimited number of image of different patients can be
used which will be as effective as clinical cases.
7. Creation of an image bank ensures uniformity in exposure
to the teaching material used.
We also could perceive a change in the learning behavior of the
students who showed constant enthusiasm in learning
throughout this method of teaching.
Teaching students in a clinical setup give them the opportunity
to handle the clinical problem in a reality wherein all
components described in Millers pyramid of assessment can be 6addressed . This setup also addresses the affective domain of
learning among students.7Aubrey et al. used interactive teaching mechanisms such as
didactic lectures, preceptor-led live patient sessions, poster
exhibit, and CD-ROM program composed of digital
reproduction of Kodachrome slide images presented in
lectures, to teach “Introduction of Dermatology” to 2nd year
medical students. They found that among the teaching
mechanisms, live patient session program, CD-ROM and
poster exhibits (in decreasing order) generated highest ratings.
In the feedback given by students, there had been a
considerable number of requests for even greater access to 6virtual images of skin diseases.
CONCLUSION :
Image based interactive teaching is found to be a useful
learning tool for Forensic Medicine & Toxicology. It hastens
understanding of complex components of Forensic Medicine
& Toxicology in a shorter period of time than non image based
teaching. It is recommended that the technique may be
explored for the core area learning in FMT on regular basis in
class room teaching.
RECOMMENDATION :
It is recommended to further evaluate effectiveness of image
based interactive teaching learning method in other subjects.
LIMITATIONS :
•Image based Interactive teaching requires greater preparation
& planning.
•Inter topic variability may exist depending on availability of
images and levels of difficulties.
•Participants were not followed-up to assess the long-term
retention of knowledge acquired during the FM posting.
•Faculty feedback was not available as study was not be
planned for these objectives.
ACKNOWLEDGEMENTS
We are thankful to Dr Gurudas Khilnani, Dean, Dr Tejas
Khakhkhar, Associate Professor, Pharmacology and Ms.
Maitri Hathi, Statistician, of GAIMS.
REFERENCES :
1. Knowles MS, Holton EF, Swanson RA.Emerging issues
in the practice of University Learning and Teaching.
Publisher AISHE, Eire. 2005:
http://www.aishe.org/readings/2005-1/toc.html (last
accessed 1 March 2010) the Adult Learner 6th Edition.
Elsevier, London, 1998
2. Cosgrove JF, Fordy K, Nesbitt IDl. Thomas the tank
engine and friends improve the understanding of oxygen
delivery and the pathophysiology of hypoxaemia.
Anaesthesia: 2006;61:106974 [PubMed]
3. Elizabeth M Norris. Journal of the Royal Society of
Medicine : “TheConstructive use of Images in medical
teaching: a literature review”, 2012 May; 3(5):33.
4. Sadoski, M , and Paivio, A. 'Imagery and Text a dual
coding theory of reading and writing', Erlbaum Assoc,
New Jersey 2001 Google Scholar
5. Fawcett RS, Widmaier EJ, Cavanaugh SH. Digital
Figure 4 : Students feedback
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00017.0
108
technology enhances Dermatology teaching in a family
medicine residency. Fam Med. 2004; 36:89-91.
6. Wass V, Van der Vleuten C, Shatzer J, Jones R.
Assessment of clinical competence. Lancet. 2001;
357:9459. Hartmann AC, Cruz PD., Jr Interactive
mechanisms for teaching dermatology to medical
students. Arch Dermatol. 1998; 134:72-58.
7. Hartmann AC, Cruz PD., Jr Interactive mechanisms for
teaching dermatology to medical students. Arch Dematol.
1998; 134:725-8 (PubMed) (Google Scholar)
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00017.0

109
Original Research Paper
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00018.2
1. Sathish.K, Assistant Professor, Department of Forensic Medicine and Toxicology, Shri Sathya Sai Medical College and
Research Institute, Ammapettai, Nellikuppam, Chengalpet, Tamilnadu, India, 603108.
2. Kusa Kumar Shaha, Professor, Department of Forensic Medicine and Toxicology*
3. Ambika Prasad Patra, Associate Professor, Department of Forensic Medicine and Toxicology*
4. J. Sree Rekha, Associate Professor, Department of Pathology*
*Jawaharlal Institute of Postgraduate Medical Education & Research, Puducherry, India, 605006.
ABSTRACT :
Introduction : Snake bite is considered as an occupational hazard, especially in rural and semi-urban regions where agriculture is
the major source of occupation. According to the National Crime Records Bureau, there were 8,660 deaths due to snake bite
reported in the year 2015, but this does not reflect the actual data because of the traditional methods and healers opt by the people.
Materials and Methods: An autopsy based prospective study was conducted on fatal cases of snakebite reported at the Mortuary
of JIPMER, Puducherry over 2 years from January 2017 to December 2018. Epidemiological and demographic data were collected
and analysed.
Results: The cases studied about 2.7% (38) of the total 1407 medico-legal autopsies conducted during the study period. Most of the
cases were male with the age group of 41-60 (36.9%) was affected the most. Most of the incidents occur in the agricultural fields
(52.6%) and the people working there become more vulnerable to the bite. There was a marked increase in the number of cases in
the summer season (50%). Snakes were unidentified in 25 cases (65.8%) and among the identified cases the most common culprit
was Viper amounting to 12 (31.6%) cases. The lower extremity was the most frequently involved site of the bite (81.6%). Majority
victims (78.9%) had been applied a tourniquet or native traditional methods before hospitalization.
Conclusions: These results urge in educating the rural population about the preventive measures of snakebite and the importance
of early hospitalization to save the golden period engulfed by the traditional healers.
Key words: Snake bite, Epidemiology, Autopsy, South India, Occupational Hazard
Corresponding Author:
Dr. Sathish.K, Assistant Professor, Department of Forensic
Medicine and Toxicology, Shri Sathya Sai Medical College
and Research Institute, Ammapettai, Nellikuppam,
Chengalpet, Tamilnadu, India, 603108.
Contact : +91 9789672020
Email : [email protected]
Article History :
Received : 26 October 2020
Received in revised form : 15 December 2020
Accepted on :15 December 2020
Available online : 15 August 2021
INTRODUCTION:
Snakes are enthralling and also an essential constituent of
fauna are the objects of wonder and curiosity since the origin of
civilization. Snake venom is one of the oldest known poisons
to the human being and has been described in ancient epics,
myths and medical writings. It has appeared in various
traditions, either as a demon or as divine. In Greek mythology,
it represented Goddess Hygeia and was worshipped, along
with Asclepius the God of Health. The tradition is carried over
to the modern time and the snake has found a place in the 1universal symbol of the medical profession. Snakebite is one
of the common causes of unnatural death ever since the
evolution of mankind. The prevalence of snake bites is
common in tropical countries such as Africa, South and
Southeast Asia, and Latin America. There are about 3500
species of snakes known to the world out of which only around
350 are poisonous. In India snakes of around 330 species are
found of which 70 are poisonous. These include 40 species of 2land snakes and 30 species of sea snakes. Snake bite is one of
the neglected tropical diseases that the World Health
Organization (WHO) aims to exterminate, which constitutes a
major public health problem in the tropical areas of the world.
WHO states that around 5.4 million snake bites occur each
year, causing in 1.8 to 2.7 million cases of envenoming. It is
estimated these effect in the deaths of 81000-138000 people a 3year and leaves added 400000 with permanent disabilities.
India, being a tropical country where farming is a major source
of employment, snake bite has become a common medical
emergency and an occupational hazard with the highest
snakebite mortality in the world, about 45,000 deaths per
Epidemiological Profile of Fatal Snake bite Cases in a Tertiary Care Centre in South
India
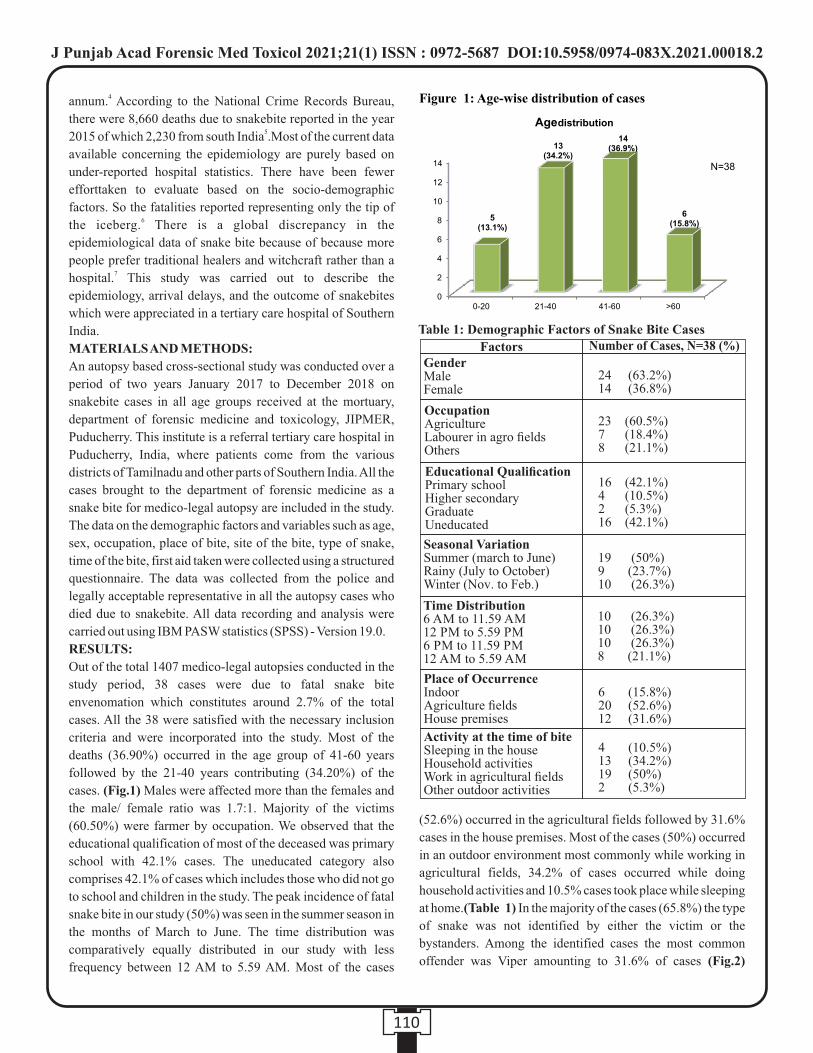
4annum. According to the National Crime Records Bureau,
there were 8,660 deaths due to snakebite reported in the year 52015 of which 2,230 from south India .Most of the current data
available concerning the epidemiology are purely based on
under-reported hospital statistics. There have been fewer
efforttaken to evaluate based on the socio-demographic
factors. So the fatalities reported representing only the tip of 6the iceberg. There is a global discrepancy in the
epidemiological data of snake bite because of because more
people prefer traditional healers and witchcraft rather than a 7hospital. This study was carried out to describe the
epidemiology, arrival delays, and the outcome of snakebites
which were appreciated in a tertiary care hospital of Southern
India.
MATERIALS AND METHODS:
An autopsy based cross-sectional study was conducted over a
period of two years January 2017 to December 2018 on
snakebite cases in all age groups received at the mortuary,
department of forensic medicine and toxicology, JIPMER,
Puducherry. This institute is a referral tertiary care hospital in
Puducherry, India, where patients come from the various
districts of Tamilnadu and other parts of Southern India. All the
cases brought to the department of forensic medicine as a
snake bite for medico-legal autopsy are included in the study.
The data on the demographic factors and variables such as age,
sex, occupation, place of bite, site of the bite, type of snake,
time of the bite, first aid taken were collected using a structured
questionnaire. The data was collected from the police and
legally acceptable representative in all the autopsy cases who
died due to snakebite. All data recording and analysis were
carried out using IBM PASW statistics (SPSS) - Version 19.0.
RESULTS:
Out of the total 1407 medico-legal autopsies conducted in the
study period, 38 cases were due to fatal snake bite
envenomation which constitutes around 2.7% of the total
cases. All the 38 were satisfied with the necessary inclusion
criteria and were incorporated into the study. Most of the
deaths (36.90%) occurred in the age group of 41-60 years
followed by the 21-40 years contributing (34.20%) of the
cases. (Fig.1) Males were affected more than the females and
the male/ female ratio was 1.7:1. Majority of the victims
(60.50%) were farmer by occupation. We observed that the
educational qualification of most of the deceased was primary
school with 42.1% cases. The uneducated category also
comprises 42.1% of cases which includes those who did not go
to school and children in the study. The peak incidence of fatal
snake bite in our study (50%) was seen in the summer season in
the months of March to June. The time distribution was
comparatively equally distributed in our study with less
frequency between 12 AM to 5.59 AM. Most of the cases
(52.6%) occurred in the agricultural fields followed by 31.6%
cases in the house premises. Most of the cases (50%) occurred
in an outdoor environment most commonly while working in
agricultural fields, 34.2% of cases occurred while doing
household activities and 10.5% cases took place while sleeping
at home.(Table 1) In the majority of the cases (65.8%) the type
of snake was not identified by either the victim or the
bystanders. Among the identified cases the most common
offender was Viper amounting to 31.6% of cases (Fig.2)
110
FactorsGenderMaleFemale
Number of Cases, N=38 (%)
24 (63.2%)14 (36.8%)
23 (60.5%)7 (18.4%)8 (21.1%)
16 (42.1%)4 (10.5%)2 (5.3%)16 (42.1%)
19 (50%)9 (23.7%)10 (26.3%)
10 (26.3%)10 (26.3%)10 (26.3%)8 (21.1%)
6 (15.8%)20 (52.6%)12 (31.6%)
4 (10.5%)13 (34.2%)19 (50%)2 (5.3%)
Figure 1: Age-wise distribution of cases
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00018.2
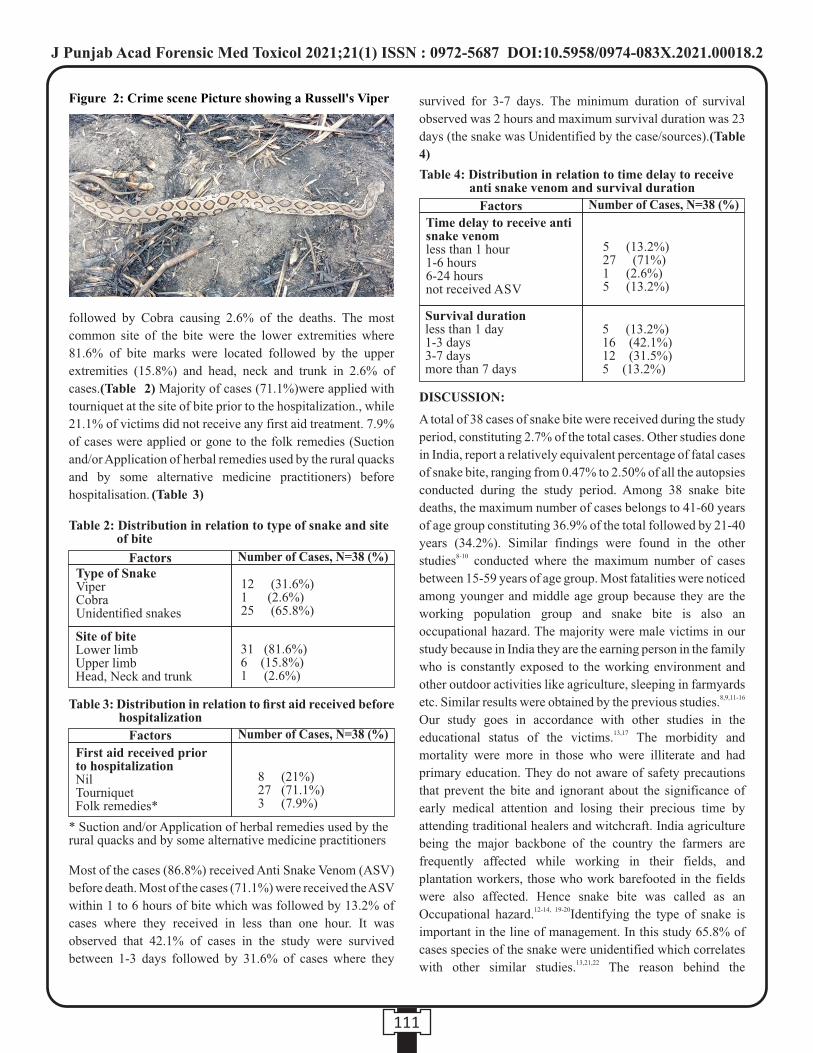
followed by Cobra causing 2.6% of the deaths. The most
common site of the bite were the lower extremities where
81.6% of bite marks were located followed by the upper
extremities (15.8%) and head, neck and trunk in 2.6% of
cases.(Table 2) Majority of cases (71.1%)were applied with
tourniquet at the site of bite prior to the hospitalization., while
21.1% of victims did not receive any first aid treatment. 7.9%
of cases were applied or gone to the folk remedies (Suction
and/or Application of herbal remedies used by the rural quacks
and by some alternative medicine practitioners) before
hospitalisation. (Table 3)
Most of the cases (86.8%) received Anti Snake Venom (ASV)
before death. Most of the cases (71.1%) were received the ASV
within 1 to 6 hours of bite which was followed by 13.2% of
cases where they received in less than one hour. It was
observed that 42.1% of cases in the study were survived
between 1-3 days followed by 31.6% of cases where they
survived for 3-7 days. The minimum duration of survival
observed was 2 hours and maximum survival duration was 23
days (the snake was Unidentified by the case/sources).(Table
4)
DISCUSSION:
A total of 38 cases of snake bite were received during the study
period, constituting 2.7% of the total cases. Other studies done
in India, report a relatively equivalent percentage of fatal cases
of snake bite, ranging from 0.47% to 2.50% of all the autopsies
conducted during the study period. Among 38 snake bite
deaths, the maximum number of cases belongs to 41-60 years
of age group constituting 36.9% of the total followed by 21-40
years (34.2%). Similar findings were found in the other 8-10studies conducted where the maximum number of cases
between 15-59 years of age group. Most fatalities were noticed
among younger and middle age group because they are the
working population group and snake bite is also an
occupational hazard. The majority were male victims in our
study because in India they are the earning person in the family
who is constantly exposed to the working environment and
other outdoor activities like agriculture, sleeping in farmyards 8,9,11-16etc. Similar results were obtained by the previous studies.
Our study goes in accordance with other studies in the 13,17educational status of the victims. The morbidity and
mortality were more in those who were illiterate and had
primary education. They do not aware of safety precautions
that prevent the bite and ignorant about the significance of
early medical attention and losing their precious time by
attending traditional healers and witchcraft. India agriculture
being the major backbone of the country the farmers are
frequently affected while working in their fields, and
plantation workers, those who work barefooted in the fields
were also affected. Hence snake bite was called as an 12-14, 19-20Occupational hazard. Identifying the type of snake is
important in the line of management. In this study 65.8% of
cases species of the snake were unidentified which correlates 13,21,22with other similar studies. The reason behind the
111
Factors Number of Cases, N=38 (%)
Site of biteLower limbUpper limbHead, Neck and trunk
12 (31.6%)1 (2.6%)25 (65.8%)
31 (81.6%)6 (15.8%)1 (2.6%)
Factors Number of Cases, N=38 (%)
Survival durationless than 1 day1-3 days3-7 daysmore than 7 days
5 (13.2%)16 (42.1%)12 (31.5%)5 (13.2%)
5 (13.2%)27 (71%)1 (2.6%)5 (13.2%)
Factors Number of Cases, N=38 (%)
First aid received prior to hospitalizationNilTourniquetFolk remedies*
8 (21%)27 (71.1%)3 (7.9%)
Figure 2: Crime scene Picture showing a Russell's Viper
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00018.2

unidentified snake species could be due to that the victims
could not see and recollect when the incident happened
because of the dark environment and when the snake rushed off
suddenly. The time distribution between the cases was
comparatively equally distributed with less incidence between
12 to 6AM. Other studies showed greater incidence both in day 13-18,20,21,23and night time. Our results were similar to the other
previous studies where the incidence happened in the outdoors 13,18,24,25mostly in the agricultural fields. Increased incidence of
cases during the summertime attributes in this study may be
due to the more number of harvest and new plantation occur
during this time in the regions of study, and thereby more
encounter to the snake in the agricultural fields. This is similar 26to the other results reported by Jayahrishnanet al. The site of
the bite was lower limb in 81.6% of cases in this study followed
by upper limb in 15.8% cases. Since most of the victims work
barefooted in the agricultural fields they get bitten by the
snake. Some people might accidentally step into the snake
during walking. These results are comparable to other studies
where lower extremity was the most common site 8,9,12,13,18,22-26involved. We observed that 71.1% of cases were
applied with tourniquet above the site of bite when arrived at
the hospital. This was similar to the other studies where most of
the victims where they go for native first aid methods in which 13,18,21,24,26,27,30tourniquet application was more common. The
custom of tourniquets, which increases the local complications
by cumulative the tissue anoxia and by producing severe
systemic envenoming right after their removal, has currently
been strongly discouraged. Most of the victims (71.1%)
received the ASVbetween 1 to 6 hours after the bite followed
by 13.2% of cases within 1 hour of the bite. Other studies also 13, 24,26,28,29showed comparable results. In the present study 42.1%
of cases were survived between 1 to 3 days. As our study was
conducted in the tertiary care centre the duration of treatment
and the services attributed to the increased survival duration.
These results were analogous to other studies where mean
hospital stay in snake bite victims was 6 days with ranges from 1,13,18,241 to 26 days.
CONCLUSION:
Snakebite remains a significant cause of accidental deaths in
this modern era and its occurrence is usually underestimated. It
is considered an occupational hazard and it can be easily
prevented by simple health education among the high-risk
population especially those working in agricultural fields,
plantations and other outdoor activities. It can also be termed
as a disease of poverty endemic to the geographical
distribution of farming and its related activities. The present
study highlights the various facets of demographic data on the
fatal cases of snakebite. It shows that snake bites were more
common in rural areas and among people who were engaged in
agricultural fields. Males were affected the most and lower
limbs were bitten in the majority of cases. Most of the
traditional methods for the first aid treatment of snakebite have
been found to affect more harm than good. The immobilization
and the quick transport of the victims to the hospital, along with
the early administration of ASV will reduce the morbidity and
the mortality in near future.
Conflict of interest: None
Funding: None
Ethical approval: Obtained from Institutional Ethics
Committee.
REFERENCES:
1. Anjum A, Husain M, Hanif SA, Ali SM, Beg M, Sardha M.
Epidemiological profile of snake bite at tertiary care
hospital, north India. J Forensic Res. 2012;3(4):201-5.
2. Organic Irritant Poisons. In: Pillay VV. Modern medical
toxicology. 4th ed. New Delhi: Jaypee Brothers Medical
Publishers; 2013; p. 145-56.
3. World Health Assembly. Addressing the burden of
snakebite envenoming [Internet]. Geneva: 2018 [updated
24th May 2018;cited 06th August 2018]. Available from
http://www.who.int/neglected_diseases/news/Snakebite-
envenoming-mandate-global-action/en/
4. Mohapatra B, Warrell DA, Suraweera W, Bhatia P,
Dhingra N, Jotkar RM, et al. Snakebite mortality in India:
a nationally representative mortality survey. PLoSNegl
Trop Dis. 2011;5(4):e1018.
5. National Crime Records Bureau Ministry of Home
Affairs. Accidental deaths and suicides in India 2015
[Internet]. [Cited 2018 Feb 21]. Available from:
http://ncrb.gov.in/StatPublications/ADSI/ADSI2015/cha
pter-1%20accidents.pdf
6. Rao CP, Shivappa P, Mothi VR. Fatal snake
bitessociodemography,latency pattern of injuries. J Occup
Med Toxicol.2013 Mar 25;8(1):1.
7. Snow RW. The prevalence and morbidity of snake bite and
treatment-seeking behaviour among a rural Kenyan
population. Ann Trop Med Parasitol 1994;88:665-71.
8. LeiteRde S, Targino IT, Lopes YA, Barros RM, Vieira AA.
Epidemiology of snakebite accidents in the municipalities
of the state of Paraíba, Brazil. CienSaude Colet. 2013;
18(5):1463-71.
9. Lal P, Dutta S, Rotti SB, Danabalan M, Kumar A.
Epidemiological profile of snakebite cases admitted in
JIPMER hospital. Indian J Community Med. 2001;
26(1):36-8.
112
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00018.2
10. VenkataRaghava S, Sumangala C N. Study of deaths due
to snake bite. J SIMLA. 2017; 9(1):48-50.
11. Bhargava S, Kaur R, Singh R, Epidemiological profile of
snake-bite cases from Haryana: A five year (20112015)
retrospective study. J Forensic Leg Med. 2018; 54:0913.
12. Majumder D, Sinha A, Bhattacharya SK, Ram R,
Dasgupta U, Ram A. Epidemiological profile of snake bite
in South 24 Parganas district of West Bengal with focus on
underreporting of snake bite deaths. Indian J Public
Health 2014; 58:17-21.
13. Halesha BR., Harshavardhan L, Lokesh A,
Channaveerappa P, Venkatesh K. A study on the clinico-
epidemiological profile and the outcome of snake bite
victims in a tertiary care centre in Southern India. J
ClinDiagn Res. 2013; 7(1):1226.
14. Bayapa Reddy N, Magesh B, Singh RK, Pallavi M,
Nagarjuna Reddy. Factors affecting the snake bite and
health seeking behavior of snake bitten individuals of
Madurai district, Tamilnadu. Nat J Res Com Med.
2012;1(2).
15. Manigandan G, Selvaraj T, Epidemiological Profile of
deaths due to snake bite at Tertiary care Hospital, South
India. Indian Journal of Forensic Medicine & Toxicology.
2016; 10(2):155-8.
16. Vijay Kautilya D, Shruti P Hegde , Guru Raghavendra.
Study of Snake Bite and Factors Influencing Snake bite
among the rural population of Kancheepuram District. J
Punjab Acad Forensic Med Toxicol 2019;19 (2).
17. Navinkumar M. Varma&P.R.Kulkarni: Postmortem study
of snake bite cases. Int J Current Med Applied Sci. 2017;
16(2):110-16
18. Farooqui JM, Mukherjee BB, Manjhi SN, Farooqui AA,
Datir S. Incidence of fatal snake bite in Loni, Maharashtra:
An autopsy based retrospective study (20042014). J
Forensic Leg Med. 2016; 39:61-4.
19. Sharma R, Dogra V, Sharma G, Chauhan V. Mass
awareness regarding snake bite induced early morning
neuroparalysis can prevent many deaths in North India.
Int J CritIllnInj Sci. 2016; 6:1158.
20. Srivastava A, Gupta A, Singh KS. Epidemiological profile
of snake bite at tertiary care hospital, East India. Int J Adv
Med. 2017; 4(5):1422-8.
21. Logaraj M, Thirumavalavan R, Gopalakrishnan S.
Epidemiology of snakebite reported in a Medical College
Hospital in Tamil Nadu. Int J Health Allied Sci. 2013;
2:53-5.
22. Paudel KM, Poudyal VP, Rayamajhi RB, Budhathoki SS.
Clinico-epidemiological profile and outcome of
poisonous snake bites in children using the WHO
treatment protocol in western Nepal. J Nobel Medical
College. 2016; 4(1):21-5.
23. Kularatne SA. Epidemiology and clinical picture of the
Russell's viper (Daboiarusseliirusselii) bite in
Anuradhapura, Sri Lanka: a prospective study of 336
patients. Southeast Asian J Trop Med Public Health. 2003;
34(4):855-62.
24. Mohankumar P, Sivagurunathan C, Umadevi R. Study on
the clinico-epidemiological profile and the outcome of
snake bite victims in a rural health centre in
Kancheepuram district, Tamilnadu. Int J Pharm Bio Sci.
2015; 6(2):544-50.
25. Thapar R, Darshan BB, Unnikrishnan B, Mithra P, Kumar
N, Kulkarni V, et al. Clinico-epidemiological profile of
snakebite cases admitted in a tertiary care centre in South
India: A 5 years study. Toxicol Int. 2015; 22:66-70.
26. Jayakrishnan MP, Geeta MG, Krishnakumar P, Rajesh TV,
George B. Snake bite mortality in children: beyond bite to
needle time. Arch Dis Child. 2016; 102:445-9.
27. Suchithra N, Pappachan J M, Sujathan P. Snakebite
envenoming in Kerala, South India: clinical profile and
factors involved in adverse outcomes. Emerg Med J.
2008; 25:20004.
28. Ahmed SM, Nadeem A, Islam MS, Agarwal S, Singh L.
Retrospective analysis of snake victims in Northern India
a d m i t t e d i n a t e r t i a r y l e v e l i n s t i t u t e . J
AnaesthesiolClinPharmacol. 2012; 28(1):45-50.
29. Sarkhel S, Ghosh R, Mana K, Gantait K. A hospital based
epidemiological study of snakebite in PaschimMedinipur
district, West Bengal, India. Toxicology Rep. 2017; 4:415-
90.
30. Mishra A, MohantySN ,Rastogi P. A Study on Snake Bite
Poisoning in a Tertiary Care Hospital in Rural Odisha,
India. J Punjab Acad Forensic Med Toxicol 2019;19(1).
113
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00018.2
114
Original Research Paper
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00019.4
1. Shalvi Upadhyay, Ph.D. Scholar, Galgotias University, Greater Noida and Assistant Professor & Course Coordinator
(Forensic Science), Sharda University, Greater Noida, India
2. Lalit P. Chandravanshi, Ex. Assistant Professor, Galgotias University, Greater Noida, India
Key words: Forensic Science, Disguise Handwriting, Handwriting Characteristics, Forensic Experts, Occupations
Corresponding Author:
Shalvi Upadhyay,
Ph.D. Scholar,
Galgotias University, Greater Noida and Assistant Professor
& Course Coordinator (Forensic Science), Sharda University,
Greater Noida, India
Contact : +91 98188-10892
Email : [email protected]
Article History :
Received : 15 July 2020
Received in revised form : 25 July 2020
Accepted on : 25 July 2020
Available online : 31August 2021
INTRODUCTION:
Disguise handwriting is deliberate change of ones handwriting
from its normal handwriting, which is used for some criminal
act or to hides its own identity while doing any wrongful act. It
is activity in which persons needs to supress the habit of (1)writing . When we talk about disguise then we generally look
for the formation of letters which most of the people try to
changes but they focus less on the characteristics like
alignment, pen-pressure, slant, speed etc. which is not very
easy to disguise. Forensic document examiners also mainly
give their opinion in form of simulation or disguised instead of (2)giving their opinion on authorship . One of the studies shows
that if a person is writing its genuine signature, disguised
signature and forged signature then there will be significant
change in velocity, size and pen pressure also said on
comparison of genuine signature with any one of the other
category of signature at least one parameter shows
(3)differences . In another study it is also been shown that
Structural features of handwriting extracted from three
character 'd', 'y', 'f' and grapheme 'th' and the study shows more
discrimination were found in grapheme 'th' then other single
characters i.e the differences in handwriting depends on the (4)adjacent characters also .
In the present study the disguised samples of forensic experts
were analysed with the help of different instruments like (5) (6)DocuCentre Nirvis (PIA 7000) , Docubox HD(PIA 7000)
and it is done to know that the knowledge related to disguise
and their occupation will affect the persons act of disguise or
whether it will show some kind of similarity in the particular
occupation when they disguise their handwriting.
MATERIAL & METHODS :
Handwriting samples were collected by 100 Forensic experts
by taking their original writing of London letter paragraph and
again at same time told them to disguise their writing on the
Forensic Examination of Forensic Expert's Disguise Handwritings
ABSTRACT :
Introduction: Disguise handwriting is change of handwriting for hiding the identity of writer. This is only done for some mean
purpose. In present study disguise handwriting of forensic experts were analysed and seen the similarities in particular occupation
while disguising their writing and also their occupational impact on the act of disguise handwriting.
Material and methods: In this study 100 original and 100 disguise handwriting samples were taken from the forensic experts and
analysed on the basis of different handwriting characteristics & also with the help of different instruments like Docubox HD,
Docucenter Nirvis etc.
Result: After comparison and analysis, it is found that mostly the experts emphasised on disguise of skill and letter formation i.e.
73% and 79% of experts which shows the impact of their occupation as being a forensic expert they know these two characteristics
are having much values in examination. Whereas, there are very few who are able to disguised their alignment and slant i.e. 28%
and 16%.
Conclusion: This study shows that instead of having a knowledge of disguise writing no one is able to fully change their writing as
their sub-conscious habit cannot be supressed fully also due to high number of people emphasized in changing their skill and
formation of letters shows impact of their occupation while disguising their handwriting.
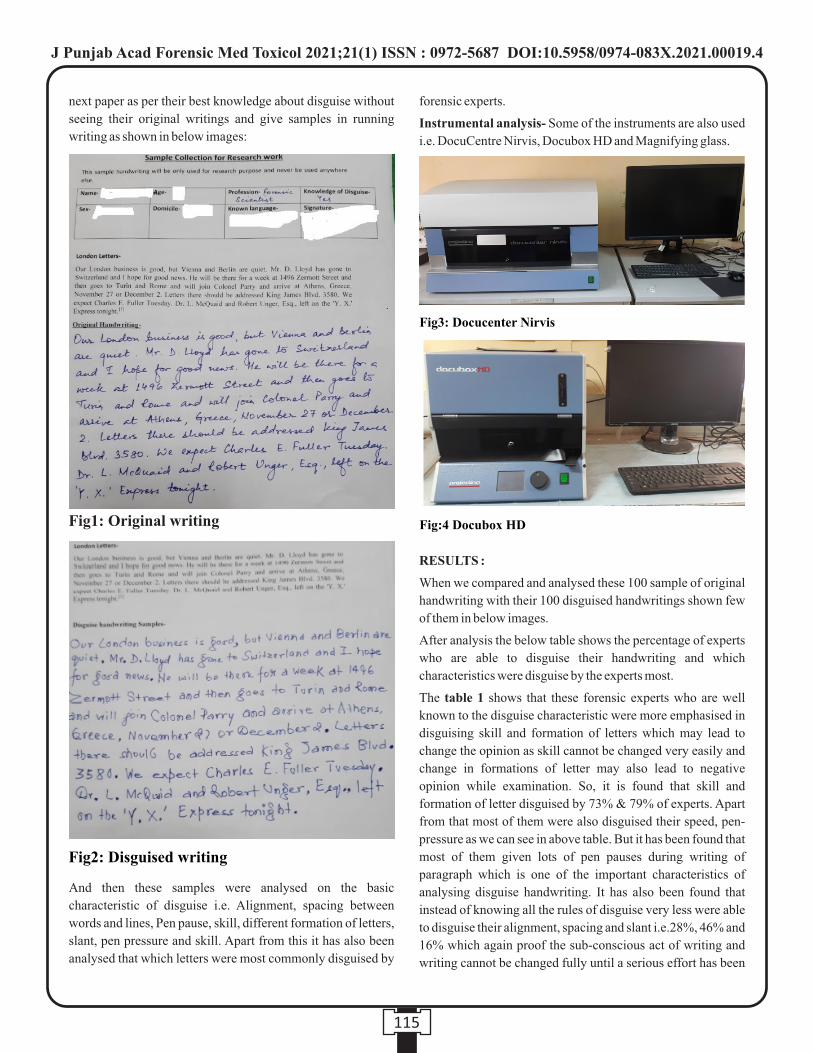
next paper as per their best knowledge about disguise without
seeing their original writings and give samples in running
writing as shown in below images:
And then these samples were analysed on the basic
characteristic of disguise i.e. Alignment, spacing between
words and lines, Pen pause, skill, different formation of letters,
slant, pen pressure and skill. Apart from this it has also been
analysed that which letters were most commonly disguised by
forensic experts.
Instrumental analysis- Some of the instruments are also used
i.e. DocuCentre Nirvis, Docubox HD and Magnifying glass.
RESULTS :
When we compared and analysed these 100 sample of original
handwriting with their 100 disguised handwritings shown few
of them in below images.
After analysis the below table shows the percentage of experts
who are able to disguise their handwriting and which
characteristics were disguise by the experts most.
The table 1 shows that these forensic experts who are well
known to the disguise characteristic were more emphasised in
disguising skill and formation of letters which may lead to
change the opinion as skill cannot be changed very easily and
change in formations of letter may also lead to negative
opinion while examination. So, it is found that skill and
formation of letter disguised by 73% & 79% of experts. Apart
from that most of them were also disguised their speed, pen-
pressure as we can see in above table. But it has been found that
most of them given lots of pen pauses during writing of
paragraph which is one of the important characteristics of
analysing disguise handwriting. It has also been found that
instead of knowing all the rules of disguise very less were able
to disguise their alignment, spacing and slant i.e.28%, 46% and
16% which again proof the sub-conscious act of writing and
writing cannot be changed fully until a serious effort has been
115
Fig1: Original writing
Fig2: Disguised writing
Fig3: Docucenter Nirvis
Fig:4 Docubox HD
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00019.4

done. When we see the letters which the experts were focussed
to change are mostly 's', 'D', 'B', 'H', 'a', 'g', 'f', 'w', 'N', 'q', 'L', 'R',
'J', 't', 'm', 'n' and very few were able to change the letter 'o'
which is having very less scope to change in formation.
DISCUSSION :
Handwriting is something which at one focus shows the exact (7)personality and nature of person . It is something which tells
us the mental ability of person and also states of mind. When
we see for the disguise of handwriting a study has been done in
which it is shown that if a person is using secondary hand for
disguising their handwriting many letters show similar (8)formation due to subconscious act of handwriting . In other
study on the basis of statistical method 'Pearson chi square'
estimated the common characteristic of handwriting which can
be changed during the process of disguise and it concluded that
all the class characteristic can be changed except the spacing (9)between the words which shows consistency . But one of the
study also claim that if expert pen men penmen can produce
very skill stimulated writing of model then a normal layman
and even it can be difficult for Forensic handwriting examiner (10)to identify . In this study it is found that some of the experts
disguised their writing so well that it is difficult to give opinion
on them at one look but when we see it in context of each
characteristic of handwriting which were considered for
analysis then none of the expert able to fully disguise their
writing but due to their knowledge about disguise and
handwriting examination they disguised mostly to the
characteristic which plays most important part at the time of
examination and framing a report. So, this shows the impact of
their profession at the time of act of disguise.
CONCLUSION :
In this study disguise handwriting has been taken from the
Forensic experts who are well known to all rules of hiding their
handwritings and after analysis it has been found that they used
the most important characteristic to disguise which they
analyse first at the time of giving opinion and also which can
change opinion i.e. skill and formation of letters. Apart from
that most of them were disguised their speed, pen-pressure etc,
but instead of knowing every point of disguise writing they are
unable to change their alignment and slants which shows that
the sub-consciousness overlaps on consciousness and they
unable to hide their writing perfectly. Hence, after analysis of
samples of forensic expert's disguise handwriting it is found
that in their samples impact of their occupations are also found
and except the two characteristic which we have considered for
analysis they are able to disguised each of them very easily.
Also, some of the letters which are mentioned above they all
used that common letters only to change the formation.
Conflict of Interest: No potential conflict of interest reported
by the authors.
Source of funding : NIL
REFERENCES :
1. Kelly J, Lindblom B. What is forensic document
examination? Scientific Examination of Questioned
Documents: Boca Raton, FL, CRC/Taylor & Francis;
2006. p. 65.
2. Bird C, Found B, Ballantyne K, Rogers D. Forensic
handwriting examiners' opinions on the process of
production of disguised and simulated signatures.
Forensic Science International. 2010;195(1-3):103-7.
116
Alignment
Speed
Pen pressure
Pen Pause
Skill
Difference in formation of letter
Spacing
Slant
28%
67%
61%
61%
73%
79%
46%
16%
Percentage of Forensic
Expert disguised
Characteristic of handwriting
Table 1
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00019.4

3. Mohammed LA, Found B, Caligiuri M, Rogers D. The
dynamic character of disguise behavior for text‐based,
mixed, and stylized signatures. Journal of forensic
sciences. 2011;56:S136-S41.
4. Pervouchine V, Leedham G. Extraction and analysis of
forensic document examiner features used for writer
identification. Pattern Recognition. 2007;40(3):1004-13.
5. Projectina. Docucenter Nirvis 2020 [cited 2020 07].
Av a i l a b l e f r o m : h t t p s : / / w w w. a s s i n g . i t / w p -
content/uploads/2017/04/dc_nirvis.pdf.
6. Ultra. Docubox Hd 2020 [cited 2020 07]. Available from:
https://www.ultra-forensictechnology.com/en/our-
products/document-examination/docubox-hd.
7. Osborn AS, Osborn AD. Questioned document problems,
the discovery and proof of the facts. 2d ed. Albany, N.Y.,:
Boyd printing company; 1946. xxx, 2, 569 p. incl. front.,
illus. (incl. facsims.) ports. p. 240.
8. Zhen-yi S. Distinguishment and Identification of the
Character of Chinese Handwriting Disguised by Left
Hand. Chinese Journal of Forensic Sciences. 2015(2):11.
9. Mohameda R, Hazira NM, Yongb WK, Ahmada UK,
Mohamadc I. Statistical Examination of Common
Characteristics for Disguised Handwriting amongst
Malaysian. Malaysian Journal of Forensic Sciences.
2011;2:8-15.
10. Dewhurst T, Found B, Rogers D. Are expert penmen better
than lay people at producing simulations of a model
s igna tu re? Fo rens i c s c i ence in t e rna t iona l .
2008;180(1):50-3.
117
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00019.4
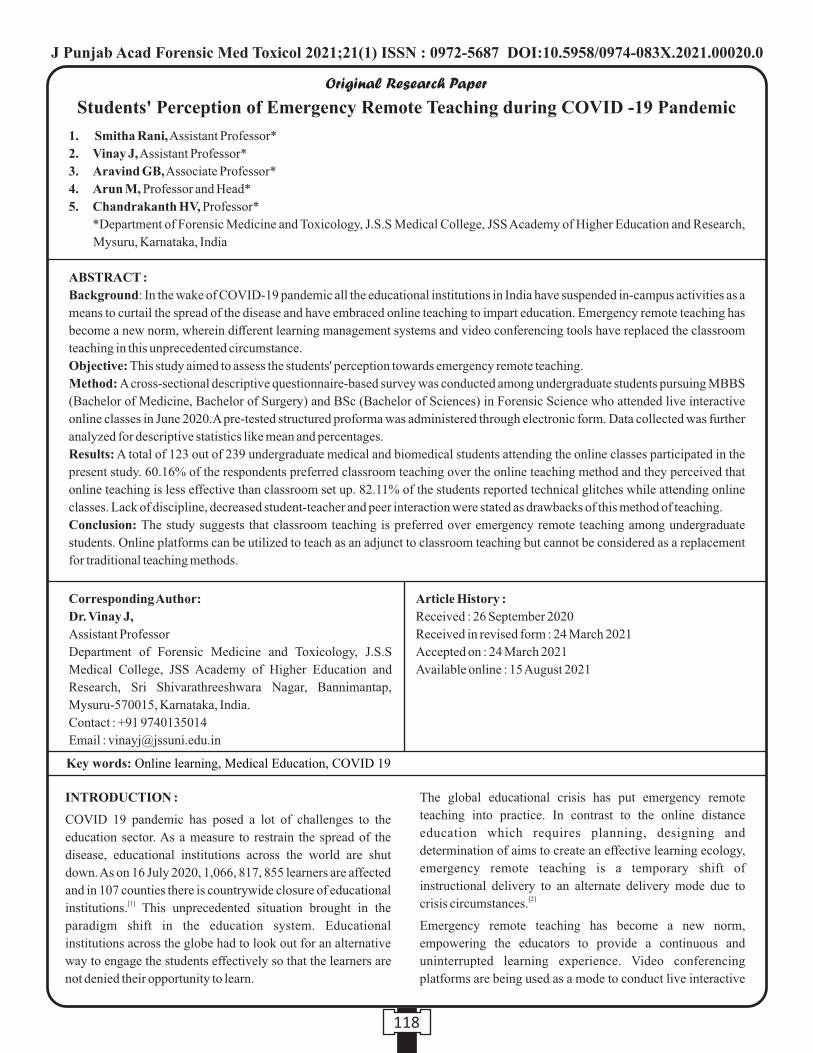
118
Original Research Paper
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00020.0
1. Smitha Rani, Assistant Professor*
2. Vinay J, Assistant Professor*
3. Aravind GB, Associate Professor*
4. Arun M, Professor and Head*
5. Chandrakanth HV, Professor*
*Department of Forensic Medicine and Toxicology, J.S.S Medical College, JSS Academy of Higher Education and Research,
Mysuru, Karnataka, India
Key words: Online learning, Medical Education, COVID 19
Corresponding Author:
Dr. Vinay J,
Assistant Professor
Department of Forensic Medicine and Toxicology, J.S.S
Medical College, JSS Academy of Higher Education and
Research, Sri Shivarathreeshwara Nagar, Bannimantap,
Mysuru-570015, Karnataka, India.
Contact : +91 9740135014
Email : [email protected]
Article History :
Received : 26 September 2020
Received in revised form : 24 March 2021
Accepted on : 24 March 2021
Available online : 15 August 2021
INTRODUCTION :
COVID 19 pandemic has posed a lot of challenges to the
education sector. As a measure to restrain the spread of the
disease, educational institutions across the world are shut
down. As on 16 July 2020, 1,066, 817, 855 learners are affected
and in 107 counties there is countrywide closure of educational [1]institutions. This unprecedented situation brought in the
paradigm shift in the education system. Educational
institutions across the globe had to look out for an alternative
way to engage the students effectively so that the learners are
not denied their opportunity to learn.
The global educational crisis has put emergency remote
teaching into practice. In contrast to the online distance
education which requires planning, designing and
determination of aims to create an effective learning ecology,
emergency remote teaching is a temporary shift of
instructional delivery to an alternate delivery mode due to [2]crisis circumstances.
Emergency remote teaching has become a new norm,
empowering the educators to provide a continuous and
uninterrupted learning experience. Video conferencing
platforms are being used as a mode to conduct live interactive
Students' Perception of Emergency Remote Teaching during COVID -19 Pandemic
ABSTRACT :
Background: In the wake of COVID-19 pandemic all the educational institutions in India have suspended in-campus activities as a
means to curtail the spread of the disease and have embraced online teaching to impart education. Emergency remote teaching has
become a new norm, wherein different learning management systems and video conferencing tools have replaced the classroom
teaching in this unprecedented circumstance.
Objective: This study aimed to assess the students' perception towards emergency remote teaching.
Method: A cross-sectional descriptive questionnaire-based survey was conducted among undergraduate students pursuing MBBS
(Bachelor of Medicine, Bachelor of Surgery) and BSc (Bachelor of Sciences) in Forensic Science who attended live interactive
online classes in June 2020.A pre-tested structured proforma was administered through electronic form. Data collected was further
analyzed for descriptive statistics like mean and percentages.
Results: A total of 123 out of 239 undergraduate medical and biomedical students attending the online classes participated in the
present study. 60.16% of the respondents preferred classroom teaching over the online teaching method and they perceived that
online teaching is less effective than classroom set up. 82.11% of the students reported technical glitches while attending online
classes. Lack of discipline, decreased student-teacher and peer interaction were stated as drawbacks of this method of teaching.
Conclusion: The study suggests that classroom teaching is preferred over emergency remote teaching among undergraduate
students. Online platforms can be utilized to teach as an adjunct to classroom teaching but cannot be considered as a replacement
for traditional teaching methods.
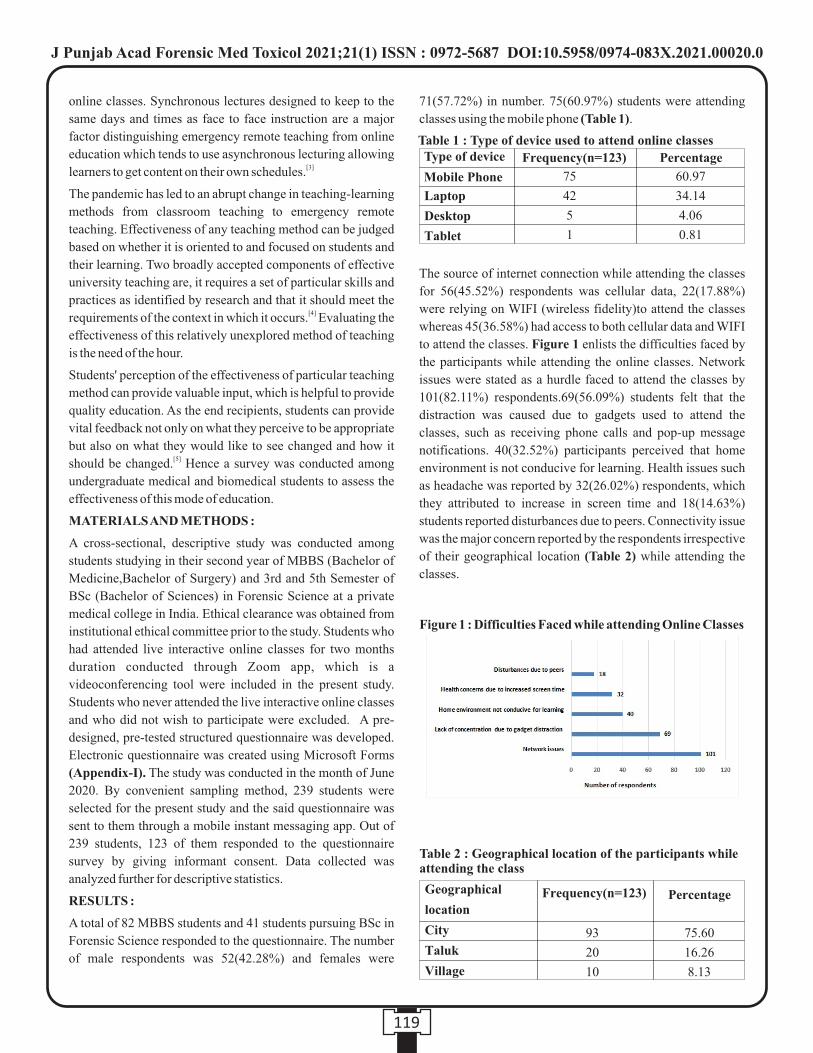
online classes. Synchronous lectures designed to keep to the
same days and times as face to face instruction are a major
factor distinguishing emergency remote teaching from online
education which tends to use asynchronous lecturing allowing [3]learners to get content on their own schedules.
The pandemic has led to an abrupt change in teaching-learning
methods from classroom teaching to emergency remote
teaching. Effectiveness of any teaching method can be judged
based on whether it is oriented to and focused on students and
their learning. Two broadly accepted components of effective
university teaching are, it requires a set of particular skills and
practices as identified by research and that it should meet the [4]requirements of the context in which it occurs. Evaluating the
effectiveness of this relatively unexplored method of teaching
is the need of the hour.
Students' perception of the effectiveness of particular teaching
method can provide valuable input, which is helpful to provide
quality education. As the end recipients, students can provide
vital feedback not only on what they perceive to be appropriate
but also on what they would like to see changed and how it [5]should be changed. Hence a survey was conducted among
undergraduate medical and biomedical students to assess the
effectiveness of this mode of education.
MATERIALS AND METHODS :
A cross-sectional, descriptive study was conducted among
students studying in their second year of MBBS (Bachelor of
Medicine,Bachelor of Surgery) and 3rd and 5th Semester of
BSc (Bachelor of Sciences) in Forensic Science at a private
medical college in India. Ethical clearance was obtained from
institutional ethical committee prior to the study. Students who
had attended live interactive online classes for two months
duration conducted through Zoom app, which is a
videoconferencing tool were included in the present study.
Students who never attended the live interactive online classes
and who did not wish to participate were excluded. A pre-
designed, pre-tested structured questionnaire was developed.
Electronic questionnaire was created using Microsoft Forms
(Appendix-I). The study was conducted in the month of June
2020. By convenient sampling method, 239 students were
selected for the present study and the said questionnaire was
sent to them through a mobile instant messaging app. Out of
239 students, 123 of them responded to the questionnaire
survey by giving informant consent. Data collected was
analyzed further for descriptive statistics.
RESULTS :
A total of 82 MBBS students and 41 students pursuing BSc in
Forensic Science responded to the questionnaire. The number
of male respondents was 52(42.28%) and females were
71(57.72%) in number. 75(60.97%) students were attending
classes using the mobile phone (Table 1).
The source of internet connection while attending the classes
for 56(45.52%) respondents was cellular data, 22(17.88%)
were relying on WIFI (wireless fidelity)to attend the classes
whereas 45(36.58%) had access to both cellular data and WIFI
to attend the classes. Figure 1 enlists the difficulties faced by
the participants while attending the online classes. Network
issues were stated as a hurdle faced to attend the classes by
101(82.11%) respondents.69(56.09%) students felt that the
distraction was caused due to gadgets used to attend the
classes, such as receiving phone calls and pop-up message
notifications. 40(32.52%) participants perceived that home
environment is not conducive for learning. Health issues such
as headache was reported by 32(26.02%) respondents, which
they attributed to increase in screen time and 18(14.63%)
students reported disturbances due to peers. Connectivity issue
was the major concern reported by the respondents irrespective
of their geographical location (Table 2) while attending the
classes.
119
Table 1 : Type of device used to attend online classes
75
42
5
1
93
20
10
75.60
16.26
8.13
60.97
34.14
4.06
0.81
Type of device
Mobile Phone
Table 2 : Geographical location of the participants while attending the class
Figure 1 : Difficulties Faced while attending Online Classes
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00020.0
Only six participants answered that they did not face any
difficulties while attending online classes. Table 3 indicates
the drawback of online teaching as perceived by the
participants.27(21.95%) students thought that there were no
drawbacks.
74(60.16%) students preferred classroom teaching over live
interactive online classes and 43 (34.95%) respondents
preferred both methods of teaching equally. 41(33.33%)
participants believed that both methods are equally effective.
74(60.16%) of them felt that classroom teaching is more
effective than online teaching (Figure2).
76(61.78%) participants felt that practical classes cannot be
conducted in online mode, 39(31.70%) responded that it might
be possible whereas 8(6.50%) felt that it is possible.
62(50.40%) respondents answered that they would not prefer
to attend the online classes once the pandemic ceases,
23(18.69%) said that they would like to attend such classes
whereas the response of 38(30.89%) was equivocal.
DISCUSSION :
The COVID-19 pandemic has resulted in an unprecedented
change in the method of imparting education. Medical
educators are also adopting to currently available technologies [6]in medical education. Emergency remote teaching methods
are widely used to impact education in medical colleges. Use
of technology in medical education is not devoid of challenges
which need to be addressed to obtain the desired outcome and [7]impact. Students' perception of a particular teaching method
is useful in determining its impact. Hence, we carried out this
survey to learn the students' preferences, determine the
difficulties faced by them and drawbacks if any in this method
of teaching.
Out of 123 respondents in the present study, 75 of them used
mobile phones to attend the live interactive online classes
followed by a laptop which was used by 34.14% of the study
population. Findings of the present study are in concurrence
with results of a Pakistani study who found 75.7% of the
students of the medical and dental stream used mobile phones
for their e-learning followed by a laptop which was used by [8] 21.2% of the students. Our findings were in contrast to the
study conducted by Murphy A et al on Australian student
population, who found that the dominant technology used to
support learning was a laptop which was used by 85% of the [9]respondents. In research conducted at Lancaster Medical
School, the authors concluded that their students seldom used [10] smart phones for learning. The disparity of findings between
our study and those conducted in the western world could be
because most of the medical universities in the United States
and the United Kingdom provide their medical students with
laptop/ tablet as an institutional policy to support their [11-12]studies.
In a study conducted on students' perception on the practice of
long-distance learning, the researchers noted that 40% of the
study population used a combination of cellular data and WIFI
to connect to the internet during long-distance learning, 31.9%
relied on cellular data only and 28.1% of them had access to [13]only WIFI. Participants using only WIFI to connect to the
classes was the least in our study, which is comparable to the
former study however we found that most of our students
(45.52%) relied on cellular data to attend the classes. Hence the
chance of losing network connectivity is higher in the absence
of an alternate source of internet. The success of e-learning is
dependent upon internet connectivity. Lower speed or [14] interruptions lead to sub-optimal use of this modality.
Although the majority of the study subjects (75.60%) hailed
from different cities across India, the unstable network was
reported as a hindrance for attending the online classes by
82.11% of the participants. A similar report was given by QS
I·GAUGE student survey involving 7594 Indian students,
which revealed that connectivity and signal issues are the most
prevailing problem while attending online classes. As per the
said survey, the infrastructure in terms of technology in India
has not achieved a state of quality to ensure sound delivery of
online classes to students across the country. Technology
enablers and telecom companies need to scale up their services
120
Table 3 : Drawback of online teaching as perceived by the participants
Teacher-studentinteraction is less
Frequency* (n=123)
*Multiple Responses
Lack of discipline
Lack of peerinteraction
55
55
51
44.7
44.7
41.5
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00020.0

[15]for effective online learning.
Lack of concentration due to gadget distraction had been
reported by 56.09% of respondents. Attia NA et al have
reported that the pop-up messages in laptops have been found
to reduce students' performance and increase the number of
errors. Even with the use of mobile phones students get easily
distracted by the text messages and feel the urge to reply [16] instantly. In a study conducted at Chile to assess the strengths
and weaknesses of digital education in orthopaedic programs,
the challenge noted by the researchers was the necessity to
obtain a conducive learning environment at home, avoiding
the distractions that usually are not present in the classroom set [17] up. Absence of a favourable learning environment at home
has been expressed by 32.52% of the participants in the present
study.
In a study conducted to investigate the association of excessive
screen time exposure and headache in young adults, the
authors reported that high levels of screen time exposure are
associated with migraine in young adults. No significant 18association was found with the non-migraine headache. In the
present study, 26.01% of the students reported health concerns
such as headache as a difficulty faced while attending the
online classes. Since the live interactive online classes
conducted in our setup lasts for the maximum of 3 hours per
day and some days it is even lesser, the headache cannot be
attributed to the classes alone because we do not have the
information regarding their overall screen exposure per day.
Distraction due to peers is reported to be the least, which was
expressed by 14.63% of the students. Unlike classroom
teaching, this could be very well addressed in live interactive
online classes conducted through videoconferencing tools
such as Zoom application. The host of the meeting, which is
usually the faculty engaging the classes, has the control to mute
the participants and restrict the chat between them. Hence the
distractions due to peers can be reduced to the bare minimum.
Interaction is one of the most important components of
teaching and learning experiences. In a study conducted at
Indonesia Open University, Taiwan branch, face to face
learning was perceived to have a more social presence, social
interaction, and satisfaction in comparison to online [19] learning. Lack of interaction between the teacher and
students was reported to be the drawback of emergency remote
learning by 44.71% of respondents and 41.46% opined that
there is lack of peer interaction. Although in live interactive
online classes, the interaction between the teacher and students
and amongst the peers is possible utilizing chats and face to
face interaction, it becomes difficult if a larger group of
students are to be catered for.
Lack of discipline has been perceived as a drawback of remote
learning by 44.71% of the students in the present study. Self-
discipline is considered to be a key indicator to improve
learning outcomes in an e-learning environment. Course
instructors should take initiatives to motivate the students and
is also dependent on the ability of the teacher to maintain the [20]discipline in the most democratic form.
60.16% of the participants in the present study preferred
classroom teaching and found it more effective than
emergency remote teaching. Similar findings were expressed [8,19] by certain other researchers. If the shortcomings of this
method of teaching are adequately addressed and when both
teacher and students become more experienced in this mode of
instruction, the perception towards it might change.
76(61.78%) participants felt that practical classes cannot be
conducted in online mode. Despite the undoubted advantage of
IT and simulation-based education, in the current situation,
there are distinct disadvantages. The foremost is the fact that all
these tools can be supplemental to clinical teaching but not a
replacement. Clinical teachings are best-learnt bedside with a
"live" patient. Not only does the medical student get a first-
hand experience of patient's clinical findings but also learns
about the dynamics of patient interaction, psychology and [21]counselling.
50.40% of the respondents in our study answered that they
would not prefer to attend the online classes once the pandemic
ceases. This is in accord with the findings of the study 17conducted at Chile. These findings infer that classroom
teaching is still perceived to be an irreplaceable component of
medical education.
Limitations of the study:
The present study was conducted on small sample size and the
study population was drawn from a single medical institution
hence the perceptions expressed may not be reflective of the
entire student population.
CONCLUSION :
Although emergency remote learning is helping the educators
and learners to tide over the present pandemic situation, the
results of the present study suggest that undergraduate medical
and biomedical students still value classroom teaching as a
means of learning. Hence, we conclude that online platforms
can be utilized to teach as an adjunct to classroom teaching but
cannot be considered as a replacement for traditional skill
imparting teaching methods.
REFERENCES :
1. UNESCO. COVID-19 Impact on Education. Available
from: https://en.unesco.org/covid19/educationresponse.
(Accessed 17 July 2020).
121
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00020.0
devices in the clinical setting and the influence of patients.
BMC Med Educ 2019, 19:376.
13. Daroedono E et al. The impact of COVID-19 on medical
education: our students perceptionon the practice of long
distance learning. Int J Community Med Public Health.
2020 Jul;7(7):2790-2796.
14. Dhir SK, Verma D, Batta M, Mishra D. E-learning in
medical education in India. Indian Pediatr 2017; 54:871-7.
15. QS. I GAUGE.COVID-19: A wake-up call for Indian
I n t e r n e t S e r v i c e P r o v i d e r s . Av a i l a b l e
from:https://www.igauge.in/news/2020/4/covid-19-a-
wake-up-call-for-indian-internet-service-providers.
(Accessed 24 July 2020).
16. Attia NA, Baig L, Marzouk YI, Khan A. The potential
effect of technology and distractions on undergraduate
students' concentration. Pak J Med Sci. 2017;33(4):860-
865. https://doi.org/10.12669/pjms.334.12560.
17. Figueroa F, Figueroa D, Calvo-Mena R, Narvaez F,
Medina N, Prieto J. Orthopedic surgery residents'
perception of online educationin their programs during the
COVID-19 pandemic: should it be maintained after the
c r i s i s ? A c t a O r t h o p a e d i c a 2 0 2 0 ; D O I :
10.1080/17453674.2020.1776461.
18. Montagni I, Guichard E, Carpenet C, Tzourio C, Kuth T.
Screen time exposure and reporting of headaches in young
adults: A cross-sectional study.Cephalalgia. 2016; 36
(11):1020 1027.
19. Bali S, Liu MC.Students' perceptions toward online
learning and face-to-facelearning courses.J. Phys.: Conf.
Ser 2018;1108 012094. doi :10.1088/1742-
6596/1108/1/012094.
20. Gorbunovs A, Kapenieks A, Cakula S.Self-discipline as a
key indicator to improve learning outcomes in elearning
environment. Procedia - Social and Behavioral Sciences
2016; 231:256- 262.
21. Sahi PK, Mishra D, Singh T. Medical education amid the
COVID-19 pandemic . Ind ian Ped ia t r.2020;
https://www.indianpediatrics.net/COVID29.03.2020/SA
-00181.pdf.
2. Hodges C, Moore S, Lockee B, Trust T, Bond A. The
Difference Between Emergency Remote Teaching and
O n l i n e L e a r n i n g . A v a i l a b l e f r o m :
https://er.educause.edu/articles/2020/3/the-difference-
between-emergency-remote-teaching-and-online-
learning . (Accessed 19 July 2020).
3. Gurung RAR. Pandemic Pedagogy: Will Remote
Te a c h i n g I m p r o v e E d u c a t i o n ? Av a i l a b l e
from:https://www.psychologytoday.com/us/blog/the-
psychological-pundit/202004/pandemic-pedagogy-will-
remote-teaching-improve-education. (Accessed 19 July
2020)
4. Devlin M, Samarawickrema G. The criteria of effective
teaching in a changing higher education context. Higher
Education Research & Development 2010;29(2): 111-
124. https://doi.org/10.1080/07294360903244398.
5. Govender SM. Students' perceptions of teaching methods
used at South African higher education institutions. South
African Journal of Higher Education 2015; 29 (3) :23-41.
6. Goh P, Sandars J. A vision of the use of technology in
medical education after the COVID-19 pandemic. Med
Ed Publish 2020; 9:49.
7. Saiyad S, Virk A, Mahajan R, Singh T. Online teaching in
medical training: Establishing good online teaching
practices from cumulative experience. Int J App Basic
Med Res 2020; 10:149-55.
8. Abbasi S, Ayoob T, Malik A, Memon SI. Perceptions of
students regarding E learning during COVID 19 at a
private medical college. Pak J Med Sci. 2020 May; 36
(COVID19- S4): S57- S61.
9. Murphy A, Farley H, Lane M, Hafeez-Baig A, Carter B.
Mobile learning anytime, anywhere: What are our
students doing? Australasian J Inf Syst. 2014;18(3)
doi:10.3127/ajis.v18i3.1098.
10. Curtis F, Cranmer S. “Laptops are better”: Medical
students' perceptions of laptops versus tablets and
smartphones to support their learning. In: Bayne S, Jones
C, de Laat M, Ryberg T, Sinclair C., (Eds.) Proceedings of
the 9th International Conference on Networked Learning.
2014:6775.
11. Mathis J.Yale gives iPads to med school students.
Available from:
https://www.macworld.com/article/1162076/yale_gives_
ipads_to_med_school_students.html. (Accessed 23 July
2020).
12. Clarke, E., Burns, J., Bruen, C. et al. The 'connectaholic'
behind the curtain: medical student use of computer
122
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00020.0

123
Appendix-I (Questionnaire)
1. Please specify your gender.
2. Your geographical location while attending online classes
(Please specify the name of the village, taluk, district and
state wherever applicable)
3. What gadget do you use to attend the online classes?
· Desktop · Laptop
· Mobile phone · Table
4. What is your source to connect to the internet?
· Cellular data only
· WiFi only
· Both
5. Which method of teaching do you prefer?
· Classroom teaching · Online Teaching
· Equally prefer classroom and online teaching.
6. How do you rate the effectiveness of online teaching in
comparison with classroom teaching?
· Equally · Less · More
7. What difficulties do you face with this form of education?
(A multiple response question)
· Health concerns due to increased screen time (Please
specify the health issue)
· Lack of concentration due to gadget/ home
distraction
· Network issues
· Home environment is not conducive for learning
· Disturbance due to peers
· None of the above
8. What according to you are the drawbacks of online
classes? (A multiple response question)
· Lack of peer interaction
· leads to lack of discipline
· Teacher - student interaction is less
· No drawbacks.
9. Do you believe practical classes can be conducted in
online mode?
· Yes · No · Maybe
10. After the pandemic is over, would you prefer to attend the
online classes?
· Yes · No · Maybe
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00020.0
124
Original Research Paper
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00021.2
1. Gurmeet Kaur Brar, Associate Professor*
2. Vineet Jalota, Senior Resident*
*Department of Psychiatry, Adesh Institute of Medical Sciences and Research ,Bathinda
Key words: Externalizing symptoms, Internalizing symptoms, Drug abuse violence
Corresponding Author:
Dr. Vineet Jalota,
Senior Resident
Department of Psychiatry, Adesh Institute of Medical
Sciences and Research ,Bathinda
Contact : +91 7986509403
Email :[email protected]
Article History :
Received : 3 May 2021
Received in revised form : 4 June 2021
Accepted on : 4 June 2021
Available online : 15 August 2021
INTRODUCTION :
Harmful use of psychoactive substances acts as a leading risk
factor for population worldwide and causes impact on health
related targets of sustainable development goals(SDGs)
including those for non communicable diseases, maternal and
child health, injuries, poisonings and mental health. The
effects of alcohol consumption on mortality are greater than
those of tuberculosis (2.3%), HIV/AIDS (1.8%), diabetes (1)(2.8%), road injuries (2.5%) and violence (0.8%). Alcohol
and other psychoactive substances when abused affect the
personal, social, economic, and occupational domains
significantly, with many suffering from psychotic disorders,
mood disorders, and a few among committing deliberate self-(2)harm. These substances affect cognition and perception
profoundly, impairing their ability to exercise control over (3) substance taking behaviour. Recent studies have
demonstrated a significant portion of Disability Adjusted Life (4)Years(DALYs) and years lived with disability. Drugs of
abuse can range from stimulants causing psychomotor
agitation, euphoria to benzodiazepines causing disinhibition
leading to recreational ,self medication misuse. Crimes
committed by substance abusers usually focus on stealing,
burglary, shoplifting ,matters related to finance substance (5,6)use. Symbolically crime and violence have become major
cause of mortality and morbidity in patients with injectable (7)drug use. Specially for intimate partner violence(IPV)
psychoactive substance abuse has been seen as an considerable (8)risk factor. Violence has been found to influence
neurobiological pathways related to threat perception,
potentially altering the response not only in the presence but in (9)the absence of the threat on daily basis. Externalizing and
internalizing symptoms both pose an independent risk factor
for substance use as they confer risk of likelihood of alienation
from institutions like school ,prosocial peers and increased
tendency to self medicate which is enhanced by negative (10,11)reinforcement of pharmacological use. Alcohol weakens
cognitive controls and allows for dominant cues and dominant (8)response options to have a stronger influence on behavior.
Relationship of mental illness and violence has a significant (12,13)impact on mental health policy in guiding allocation of
(14-16)limited resources and imposing mandatory treatment to
recognize and protect public health safety at the expense of (17-20)patient's liberty. Previously quantitative correlation have
been studied, keeping in the view paucity of published
Association of alcohol and psychoactive substances use with Mental Health Symptoms, crime and violence
ABSTRACT :
Introduction: Harmful use of psychoactive substances acts as a leading risk factor for population worldwide. Violence has been
found to influence neurobiological pathways related to threat perception, potentially altering the response. Externalizing and
internalizing symptoms both pose an independent risk factor for substance use as they confer risk of likelihood of alienation from
institutions like school ,prosocial peers and increased tendency to self medicate
Materials and Methods: A cross sectional study on 82 consenting patients between 19-65 years of age was undertaken for 3
months at a tertiary care centre. The aim of the study was to assess association between mental health symptoms, alcohol and
psychoactive substance abuse and crime and violence.
Results and Conclusions: Variables externalizing symptoms and crime and violence were positively correlated to psychoactive
substance abuse.
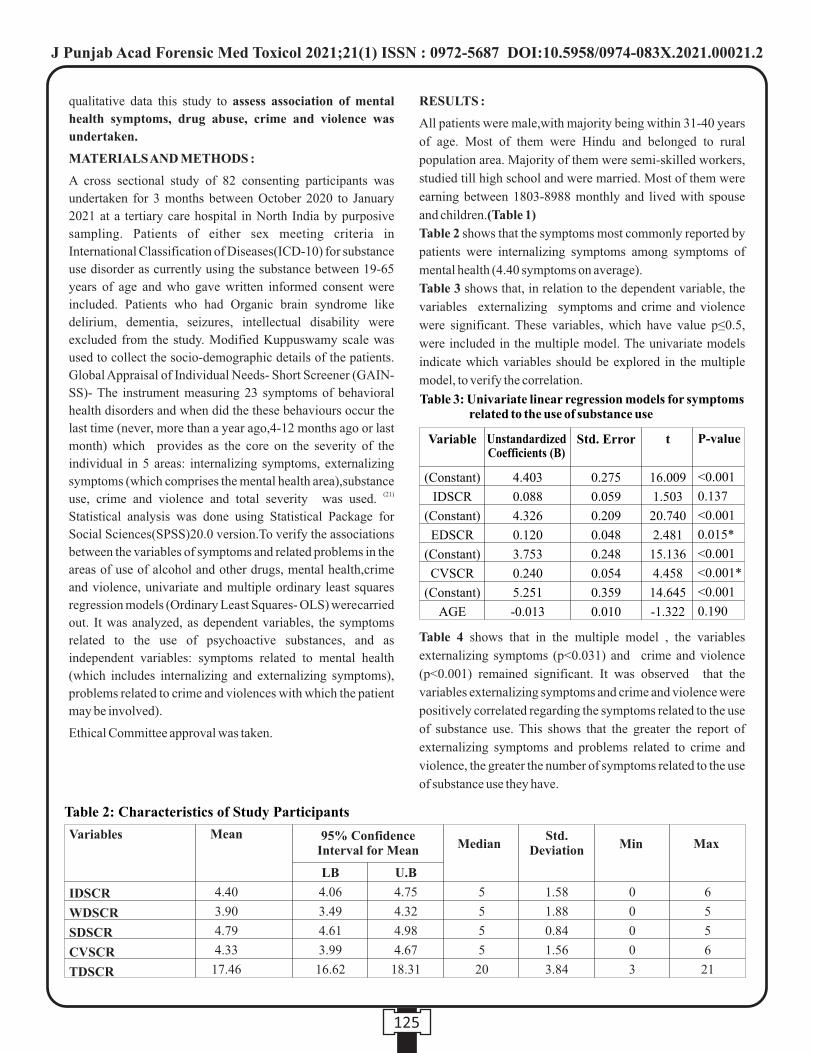
qualitative data this study to assess association of mental
health symptoms, drug abuse, crime and violence was
undertaken.
MATERIALS AND METHODS :
A cross sectional study of 82 consenting participants was
undertaken for 3 months between October 2020 to January
2021 at a tertiary care hospital in North India by purposive
sampling. Patients of either sex meeting criteria in
International Classification of Diseases(ICD-10) for substance
use disorder as currently using the substance between 19-65
years of age and who gave written informed consent were
included. Patients who had Organic brain syndrome like
delirium, dementia, seizures, intellectual disability were
excluded from the study. Modified Kuppuswamy scale was
used to collect the socio-demographic details of the patients.
Global Appraisal of Individual Needs- Short Screener (GAIN-
SS)- The instrument measuring 23 symptoms of behavioral
health disorders and when did the these behaviours occur the
last time (never, more than a year ago,4-12 months ago or last
month) which provides as the core on the severity of the
individual in 5 areas: internalizing symptoms, externalizing
symptoms (which comprises the mental health area),substance (21)use, crime and violence and total severity was used.
Statistical analysis was done using Statistical Package for
Social Sciences(SPSS)20.0 version.To verify the associations
between the variables of symptoms and related problems in the
areas of use of alcohol and other drugs, mental health,crime
and violence, univariate and multiple ordinary least squares regression models (Ordinary Least Squares- OLS) werecarried
out. It was analyzed, as dependent variables, the symptoms
related to the use of psychoactive substances, and as
independent variables: symptoms related to mental health
(which includes internalizing and externalizing symptoms),
problems related to crime and violences with which the patient
may be involved).
Ethical Committee approval was taken.
RESULTS :
All patients were male,with majority being within 31-40 years
of age. Most of them were Hindu and belonged to rural
population area. Majority of them were semi-skilled workers,
studied till high school and were married. Most of them were
earning between 1803-8988 monthly and lived with spouse
and children.(Table 1)
Table 2 shows that the symptoms most commonly reported by
patients were internalizing symptoms among symptoms of
mental health (4.40 symptoms on average).
Table 3 shows that, in relation to the dependent variable, the
variables externalizing symptoms and crime and violence
were significant. These variables, which have value p≤0.5,
were included in the multiple model. The univariate models
indicate which variables should be explored in the multiple
model, to verify the correlation.
Table 4 shows that in the multiple model , the variables
externalizing symptoms (p<0.031) and crime and violence
(p<0.001) remained significant. It was observed that the
variables externalizing symptoms and crime and violence were
positively correlated regarding the symptoms related to the use
of substance use. This shows that the greater the report of
externalizing symptoms and problems related to crime and
violence, the greater the number of symptoms related to the use
of substance use they have.
125
Table 2: Characteristics of Study Participants
Variables
IDSCR
WDSCR
SDSCR
CVSCR
TDSCR
Mean
4.40
3.90
4.79
4.33
17.46
LB
4.06
3.49
4.61
3.99
16.62
U.B
4.75
4.32
4.98
4.67
18.31
5
5
5
5
20
1.58
1.88
0.84
1.56
3.84
0
0
0
0
3
6
5
5
6
21
MedianStd.
Deviation Min Max95% Confidence
Interval for Mean
Table 3: Univariate linear regression models for symptoms related to the use of substance use
P-value
<0.001
0.137
<0.001
0.015*
<0.001
<0.001*
<0.001
0.190
t
16.009
1.503
20.740
2.481
15.136
4.458
14.645
-1.322
Std. Error
0.275
0.059
0.209
0.048
0.248
0.054
0.359
0.010
4.403
0.088
4.326
0.120
3.753
0.240
5.251
-0.013
Variable
(Constant)
IDSCR
(Constant)
EDSCR
(Constant)
CVSCR
(Constant)
AGE
Unstandardized Coefficients (B)
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00021.2
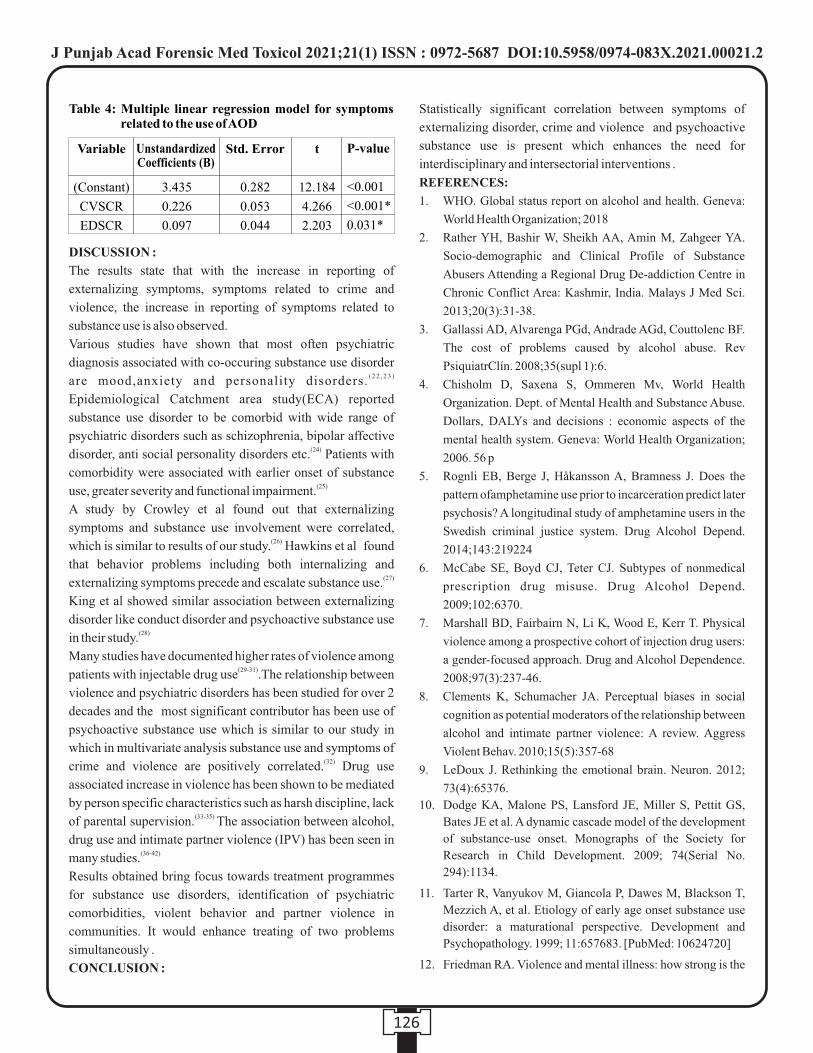
126
DISCUSSION :
The results state that with the increase in reporting of
externalizing symptoms, symptoms related to crime and
violence, the increase in reporting of symptoms related to
substance use is also observed.
Various studies have shown that most often psychiatric
diagnosis associated with co-occuring substance use disorder ( 2 2 , 2 3 )are mood,anxiety and personality disorders.
Epidemiological Catchment area study(ECA) reported
substance use disorder to be comorbid with wide range of
psychiatric disorders such as schizophrenia, bipolar affective (24)disorder, anti social personality disorders etc. Patients with
comorbidity were associated with earlier onset of substance (25)use, greater severity and functional impairment.
A study by Crowley et al found out that externalizing
symptoms and substance use involvement were correlated, (26)which is similar to results of our study. Hawkins et al found
that behavior problems including both internalizing and (27)externalizing symptoms precede and escalate substance use.
King et al showed similar association between externalizing
disorder like conduct disorder and psychoactive substance use (28)in their study.
Many studies have documented higher rates of violence among (29-31)patients with injectable drug use .The relationship between
violence and psychiatric disorders has been studied for over 2
decades and the most significant contributor has been use of
psychoactive substance use which is similar to our study in
which in multivariate analysis substance use and symptoms of (32)crime and violence are positively correlated. Drug use
associated increase in violence has been shown to be mediated
by person specific characteristics such as harsh discipline, lack (33-35) of parental supervision. The association between alcohol,
drug use and intimate partner violence (IPV) has been seen in (36-42)many studies.
Results obtained bring focus towards treatment programmes
for substance use disorders, identification of psychiatric
comorbidities, violent behavior and partner violence in
communities. It would enhance treating of two problems
simultaneously .
CONCLUSION :
Statistically significant correlation between symptoms of
externalizing disorder, crime and violence and psychoactive
substance use is present which enhances the need for
interdisciplinary and intersectorial interventions .
REFERENCES:
1. WHO. Global status report on alcohol and health. Geneva:
World Health Organization; 2018
2. Rather YH, Bashir W, Sheikh AA, Amin M, Zahgeer YA.
Socio-demographic and Clinical Profile of Substance
Abusers Attending a Regional Drug De-addiction Centre in
Chronic Conflict Area: Kashmir, India. Malays J Med Sci.
2013;20(3):31-38.
3. Gallassi AD, Alvarenga PGd, Andrade AGd, Couttolenc BF.
The cost of problems caused by alcohol abuse. Rev
PsiquiatrClín. 2008;35(supl 1):6.
4. Chisholm D, Saxena S, Ommeren Mv, World Health
Organization. Dept. of Mental Health and Substance Abuse.
Dollars, DALYs and decisions : economic aspects of the
mental health system. Geneva: World Health Organization;
2006. 56 p
5. Rognli EB, Berge J, Håkansson A, Bramness J. Does the
pattern ofamphetamine use prior to incarceration predict later
psychosis? A longitudinal study of amphetamine users in the
Swedish criminal justice system. Drug Alcohol Depend.
2014;143:219224
6. McCabe SE, Boyd CJ, Teter CJ. Subtypes of nonmedical
prescription drug misuse. Drug Alcohol Depend.
2009;102:6370.
7. Marshall BD, Fairbairn N, Li K, Wood E, Kerr T. Physical
violence among a prospective cohort of injection drug users:
a gender-focused approach. Drug and Alcohol Dependence.
2008;97(3):237-46.
8. Clements K, Schumacher JA. Perceptual biases in social
cognition as potential moderators of the relationship between
alcohol and intimate partner violence: A review. Aggress
Violent Behav. 2010;15(5):357-68
9. LeDoux J. Rethinking the emotional brain. Neuron. 2012;
73(4):65376.
10. Dodge KA, Malone PS, Lansford JE, Miller S, Pettit GS,
Bates JE et al. A dynamic cascade model of the development
of substance-use onset. Monographs of the Society for
Research in Child Development. 2009; 74(Serial No.
294):1134.
11. Tarter R, Vanyukov M, Giancola P, Dawes M, Blackson T,
Mezzich A, et al. Etiology of early age onset substance use
disorder: a maturational perspective. Development and
Psychopathology. 1999; 11:657683. [PubMed: 10624720]
12. Friedman RA. Violence and mental illness: how strong is the
Table 4: Multiple linear regression model for symptoms related to the use of AOD
P-value
<0.001
<0.001*
0.031*
t
12.184
4.266
2.203
Std. Error
0.282
0.053
0.044
3.435
0.226
0.097
Variable
(Constant)
CVSCR
EDSCR
Unstandardized Coefficients (B)
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00021.2
127
link?. N Engl J Med. 2006;355(20):2064-2066.
13. Appelbaum PS. Violence and mental disorders: data and
public policy. Am J Psychiatry. 2006;163(8):1319-1321.
14. Cole TB, Glass RM. Mental illness and violent death: major
issues for public health. JAMA. 2005;294(5):623-624.
15. Skeem JL, Monahan J, Mulvey EP. Psychopathy, treatment
involvement, and subsequent violence among civil
psychiatric patients. Law Hum Behav. 2002;26 (6):577-603
16. Monahan J, Bonnie RJ, Appelbaum PS, Hyde PS, Steadman
HJ, Swartz MS. Mandated community treatment beyond
outpatient commitment. Psychiatr Serv.2001;52(9):1198-
1205.
17. Erstling SS. Police and mental health collaborative outreach.
Psychiatr Serv. 2006;57(3):417-418.
18. Cerulli C, Conner KR, Weisman R. Bridging healthcare,
police, and court responses to intimate partner violence
perpetrated by individuals with severe and persistent mental
illness. Psychiatr Q. 2004;75(2):139-150.
19. McNiel DE, Binder RL. Effectiveness of a mental health court
in reducing criminal recidivism and violence. Am J
Psychiatry. 2007;164(9):1395-1403.
20. Swanson JW, Van Dorn RA, Monahan J, Swartz MS. Violence
and leveraged community treatment for persons with mental
disorders. Am J Psychiatry. 2006;163(8):1404-1411.
21. Dennis M, Chan Y, Funk R. Development and validation of the
GAIN Short Screener (GSS) for internalizing, externalizing
and substance use disorders and crime/violence problems
among adolescents and adults. Am J Addict. 2006;15 Suppl
1:80-91.
22. Jane-Llopis, E., & Matytsina, I. (2006). Mental health and
alcohol, drugs and tobacco: A review of the comorbidity
between mental disorders and the use of alcohol, tobacco and
illicit drugs. Drug and Alcohol Review,25, 515536.
23. Langas, A. M., Malt, U. F., & Opjordsmoen, S. Substance use
disorders and comorbid mental disorders in first-time
admitted patients from a catchment Area. European
Addiction Research.2012; 18, 625.
24. Regier DA, Farmer ME, Rae DS, Locke BZ, Keith SJ, Judd
LL et al. Comorbidity of mental disorders with alcohol and
other drug abuse. Results from the Epidemiologic Catchment
Area (ECA) Study. Jama. 264(19):2511-2518
25. Johnson JG, Spitzer RL, Williams JB, Kroenke K, Linzer M,
Brody D et al. Psychiatric comorbidity, health status, and
functional impairment associated with alcohol abuse and
dependence in primary care patients: findings of the PRIME
MD-1000 study. Journal of consulting and clinical
psychology. 63(1):133-140.
26. Crowley TJ, Mikulich SK, Macdonald M, Young SE, Zerbe
GO. Substance-dependent, conduct disorder edadolescent
males: Severity of diagnosis predicts 2-year outcome. Drug
and Alcohol Dependence 1998;49:225-237. [PubMed:
9571387]
27. Hawkins JD, Catalano RF, Miller JY. Risk and protective
factors for alcohol and other drug problems in adolescence
and early adulthood: Implications for substance abuse
prevention. PsychologicalBulletin. 1992; 112(1):64-105.
[PubMed: 1529040]
28. King SM, Iacono WG, McGue M. Childhood externalizing
and internalizing psychopathology in the prediction of early
substance use. Addiction. 2004; 99(12):15481559. [PubMed:
15585046]
29. Chermack ST, Blow FC. Violence among individuals in
substance abuse treatment: The role of alcohol and cocaine
consumption. Drug Alcohol Depend 2002;66:2937.
[PubMed: 11850133]
30. Farris CA, Fenaughty AM. Social isolation and domestic
violence among female drug users. Am J Drug Alcohol Abuse
2002;28:339351. [PubMed: 12014819]
31. Vlahov D, Wientge D, Moore J, Flynn C, Schuman P,
Schoenbaum EE, Zierler S. Violence among women with or
at risk for HIV infection. AIDS Behav 1998;2:53-60.
32. Parker RN, Auerhahn K. Alcohol, drugs, and violence. Annu
Rev Sociol 1998;24:291-311.
33. Chermack ST, Giancola PR. The relation between alcohol
and aggression: An integrated biopsychosocial
conceptualization. Clinical Psychology Review
1997;17(6):621-649. [PubMed:9336688]
34. Roth, JA. Psychoactive substance and violence. National
Institute of Justice, Office of Justice Programs; Washington,
DC: 1994.
35. Giancola PR. Irritability, acute alcohol consumption and
aggressive behavior in men and women. Drug and Alcohol
Dependence 2002;68(3):263-274. [PubMed: 12393221
36. Coker AL. Frequency and correlates of intimate partner
violence by type: Physical, sexual, and psychological
battering. American Journal of Public Health
2000;90(4):553-559. [PubMed:10754969]
37. Cunradi CB, Caetano R, Schafer J. Alcohol-Related
Problems, Drug Use, and Male Intimate Partner Violence
Severity Among US Couples. Alcoholism: Clinical &
Experimental Research 2002;26(4):493-500.
38. Jewkes R. Intimate partner violence: causes and prevention.
The Lancet 2002;359:1423-1429.
39. Silverman JG. Dating violence against adolescent girls and
Associated substance use, unhealthy weight control, sexual
risk behavior, pregnancy, and suicidality. Journal of
theAmerican Medical Association 2001;286 (5):572579.
[PubMed: 11476659]
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00021.2

128
40. McCauley J. The “Battering Syndrome”: Prevalence and
clinical characteristics of domestic violence in primary care
internal medicine practices. Annals of Internal Medicine
1995;123(10):737746. [PubMed: 7574191]
41. Leonard E, K. Senchak M. Prospective prediction of husband
marital aggression within newlywedcouples. Journal of
Abnormal Psychology 1996;105:369380. [PubMed:
8772007]
42. Moore TM. Drug abuse and aggression between intimate
partners: A meta-analytic review.Clinical Psychology
Review 2008;28(2):247274. [PubMed: 17604891]
Table 1: Socio-demographic Characteristics of Study Participants
Category
<=30
31-40
41-50
>50
Mean ±SD
Male
Hindu
Sikh
Rural
Urban
Single
Married
Divorced
Widowed
Separated
Illiterate
Primary School
Middle School
High School
High School Diploma
Graduate/Post Graduate
Unemployed
Unskilled Worker
Semi-Skilled Worker
Skilled Worker
Clerical
Semi Profession
<1802
1803-5386
5387-8988
8989-13494
13495-17999
18000-36016
>36017
Parents
Alone
Spouse and Children
Frequency
29
31
13
9
36.17±9.73
82
47
35
50
32
24
49
3
4
2
5
7
20
32
15
3
9
19
37
12
4
1
15
21
21
18
5
1
1
23
13
46
Percentage
35.4
37.8
15.9
11.0
100.0
57.3
42.7
61.0
39.0
29.3
59.8
3.7
4.9
2.4
6.1
8.5
24.4
39.0
18.3
3.7
11.0
23.2
45.1
14.6
4.9
1.2
18.3
25.6
25.6
22.0
6.1
1.2
1.2
28.0
15.9
56.1
VARIABLES
AGE
GENDER
RELIGION
ADDRESS
MATRIAL STATUS
EDUCATION
EMPLOYMENT
STATUS
TOTAL MONTHLY
INCOME
LIVING WITH
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00021.2

Original Research Paper
Forensic Identification of Mifepristone and Misoprostol by TLC and FT-IR Methods
1. Bhuvnesh Yadav, PhD, Assistant Professor II, Dept. of Chemistry, Biochemistry and Forensic Science, Amity School of
Applied Sciences, Amity University, Gurugram, Haryana, India.
2. Meena Jha, M.Sc., Sr. Scientific Assistant, Toxicology division, Forensic Science Laboratory, Madhuban, Haryana, India.
3. Lingaraj Sahoo, PhD, Senior Scientific officer, Forensic Science Laboratory, Rohini, New Delhi, India.
4. Sonu Kumar Maurya, M.Sc., Sr. Scientific Assistant, Forensic Science Laboratory, Rohini, New Delhi, India.
ABSTRACT :
Introduction: Medical abortion while a necessity is a social taboo depending upon the situations. Since ancient times, numerous
methodologies have been employed for carrying out abortions. Developments in medical sciences have made the procedure easy
by use of some abortive drugs like Mifepristone and Misoprostol. However, these drugs have been misused with impunity for
forced abortions, especially for female foeticide. The study was conducted to standardize the method for identification of these
drugs in forensic cases related to illegal abortions. Thin Layer Chromatography (TLC) and Fourier Transform – Infrared
Spectroscopy (FTIR) technologies were employed for the same.
Results: Various combinations of solvents were employed and it was observed that Mifepristone was best separated in
Chloroform-Acetone (9:1) and Toluene-Ethyl acetate (7:3) solvent systems. A unique inverted foetus shaped spot of Mifepristone
can be visualized with Dragondorff's reagent, Zwikker reagent and Iodine fumes. However, visualization of Misoprostol was
difficult by Thin Layer Chromatography method with these developers. Fourier Transform – Infrared Spectroscopy analysis gave
the positive results in both the drugs.
Conclusion: The standardization of Thin Layer Chromatography for forensic identification of abortive drug (Mifepristone) was
done in this study. FTIR can be concluded as the method of choice in the identification of Misoprostol in forensic cases.
Key words : Drug Analysis, Misoprostol, Mifepristone, Thin Layer Chromatography, Fourier Transform – Infrared Spectroscopy.
Corresponding Author:
Dr. Bhuvnesh Yadav, PhD,
Assistant Professor II,
Department of Chemistry, Biochemistry and Forensic
Science, Amity School of Applied Sciences, Amity
University, Gurugram, Haryana, India.
Contact : +91 98994-02613
Email : [email protected]
Article History :
Received : 18 May 2020
Received in revised form : 2 September 2020
Accepted on : 2 September 2020
Available online : 15 August 2021
INTRODUCTION:
Unsafe abortions are the major cause of female fatality across
the world, as non-surgical strategies involved lead to sepsis,
uterine perforation, cervical laceration, incomplete
evacuation, haemorrhage, miscarriage, future sterility and [1]finally death . As per WHO, 19 million women had unsafe
abortions worldwide every year; of which 18.5 million have [2]taken place in the developing countries . In developing
countries, of the 28 million pregnancies that take place each
year, 36% end in abortion. Serious efforts are being made to
reduce the number of unsafe procedures, by replacing them
with safer choices for pregnancy termination. A number of
drugs have since been introduced in the markets that are meant
for early termination of pregnancy and combination of two
medicines (Mifepristone and Misoprostol) was introduced as a
successive regimen for early medical abortion in the fourteenth
[3-4]WHO essential drug list .
Mifepristone, commonly called "The Abortion Pill ", or RU-
486, is hostile to progestin that hinders the activity of
progesterone, which is important to build and keep the
placenta and embryo attached. Because of its antiprogesterone
action, it was suggested that mifepristone be utilized in the [5]early end human pregnancy up to gestational age of 49 days .
Misoprostol, when used orally or vaginally, empowers uterine
constrictions that remove the developing life and placental [6]tissue .
The main concern, however, is their extensive use as a self-
medication and pharmaceutical has also supported their
endorsement in different nations, predominantly in countries
like India where foetus removal is viewed as unlawful. In
2000, the Food and Drug Administration (FDA), US has
endorsed Mifepristone, in combination with Misoprostol for
129
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00022.4
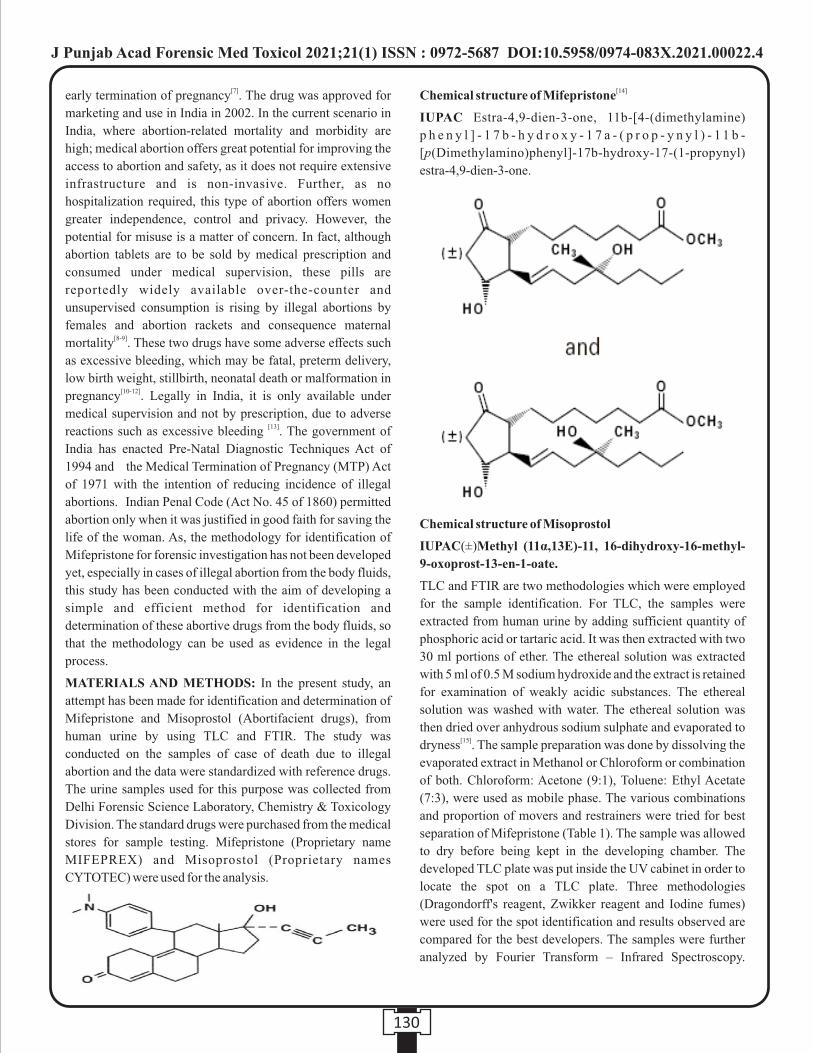
[7]early termination of pregnancy . The drug was approved for
marketing and use in India in 2002. In the current scenario in
India, where abortion-related mortality and morbidity are
high; medical abortion offers great potential for improving the
access to abortion and safety, as it does not require extensive
infrastructure and is non-invasive. Further, as no
hospitalization required, this type of abortion offers women
greater independence, control and privacy. However, the
potential for misuse is a matter of concern. In fact, although
abortion tablets are to be sold by medical prescription and
consumed under medical supervision, these pills are
reportedly widely available over-the-counter and
unsupervised consumption is rising by illegal abortions by
females and abortion rackets and consequence maternal [8-9]mortality . These two drugs have some adverse effects such
as excessive bleeding, which may be fatal, preterm delivery,
low birth weight, stillbirth, neonatal death or malformation in [10-12]pregnancy . Legally in India, it is only available under
medical supervision and not by prescription, due to adverse [13]reactions such as excessive bleeding . The government of
India has enacted Pre-Natal Diagnostic Techniques Act of
1994 and the Medical Termination of Pregnancy (MTP) Act
of 1971 with the intention of reducing incidence of illegal
abortions. Indian Penal Code (Act No. 45 of 1860) permitted
abortion only when it was justified in good faith for saving the
life of the woman. As, the methodology for identification of
Mifepristone for forensic investigation has not been developed
yet, especially in cases of illegal abortion from the body fluids,
this study has been conducted with the aim of developing a
simple and efficient method for identification and
determination of these abortive drugs from the body fluids, so
that the methodology can be used as evidence in the legal
process.
MATERIALS AND METHODS: In the present study, an
attempt has been made for identification and determination of
Mifepristone and Misoprostol (Abortifacient drugs), from
human urine by using TLC and FTIR. The study was
conducted on the samples of case of death due to illegal
abortion and the data were standardized with reference drugs.
The urine samples used for this purpose was collected from
Delhi Forensic Science Laboratory, Chemistry & Toxicology
Division. The standard drugs were purchased from the medical
stores for sample testing. Mifepristone (Proprietary name
MIFEPREX) and Misoprostol (Proprietary names
CYTOTEC) were used for the analysis.
[14]Chemical structure of Mifepristone
IUPAC Estra-4,9-dien-3-one, 11b-[4-(dimethylamine)
p h e n y l ] - 1 7 b - h y d r o x y - 1 7 a - ( p r o p - y n y l ) - 1 1 b -
[p(Dimethylamino)phenyl]-17b-hydroxy-17-(1-propynyl)
estra-4,9-dien-3-one.
Chemical structure of Misoprostol
IUPAC(±)Methyl (11α,13E)-11, 16-dihydroxy-16-methyl-
9-oxoprost-13-en-1-oate.
TLC and FTIR are two methodologies which were employed
for the sample identification. For TLC, the samples were
extracted from human urine by adding sufficient quantity of
phosphoric acid or tartaric acid. It was then extracted with two
30 ml portions of ether. The ethereal solution was extracted
with 5 ml of 0.5 M sodium hydroxide and the extract is retained
for examination of weakly acidic substances. The ethereal
solution was washed with water. The ethereal solution was
then dried over anhydrous sodium sulphate and evaporated to [15]dryness . The sample preparation was done by dissolving the
evaporated extract in Methanol or Chloroform or combination
of both. Chloroform: Acetone (9:1), Toluene: Ethyl Acetate
(7:3), were used as mobile phase. The various combinations
and proportion of movers and restrainers were tried for best
separation of Mifepristone (Table 1). The sample was allowed
to dry before being kept in the developing chamber. The
developed TLC plate was put inside the UV cabinet in order to
locate the spot on a TLC plate. Three methodologies
(Dragondorff's reagent, Zwikker reagent and Iodine fumes)
were used for the spot identification and results observed are
compared for the best developers. The samples were further
analyzed by Fourier Transform – Infrared Spectroscopy.
130
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00022.4

Tablets purchased from pharmacy were taken for assay, finely
powdered and homogenized. An accurately weighed quantity
of powder was dissolved in 5 ml phosphate buffer pH 6.0
followed by 20 ml of methanol. The solution is maintained
under stirring for 5 min and was centrifuged in order to
separate excipients. The analysis was done by mounting the
drugs in the form of thin film on KBr plate. The plate was
placed into specimen holder and then spectrum was generated.
The spectrum was analysed and compared with previously
available data. The statistical accuracy was determined by
adding known amount of Mefipristone and misoprostol as
reference standard to the sample.
RESULTS:
It has already been reported that Misoprostol is widely
retained, and experiences fast de-esterification to its free
carboxylic group, which is in charge of its clinical action, and
unlike to the parent compound, is noticeable in plasma and
urine. TLC has been used as a broad-spectrum screening test
for detection of various drugs of abuse.
In the comparative analysis of different solvents and the
developing agents, it was observed that in TLC, Mifepristone
was best separated in Chloroform-Acetone (9:1) and Toluene-
Ethyl acetate (7:3), solvent systems as compared to the other
solvent systems (Table 1). It was observed that the TLC were
significantly good with all the three reagents for Mifepristone
and all the developing techniques gave a peculiar inverted
foetus shaped spot for Mifepristone in standard (Figure 1) and
the test sample (Figure 2).
Similar results were observed with Iodine fuming also,
however, the spots faded with time after preservation in case of
iodine fuming (Figure 3).
131
Figure 1: TLC plate analysis with UV Illumination for
Mifepristone Standard
Figure 2: TLC plate analysis with UV Illumination for
Mifepristone test sample
Figure 3: Mifepristone Sample spot analysis by Iodine
Fuming
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00022.4
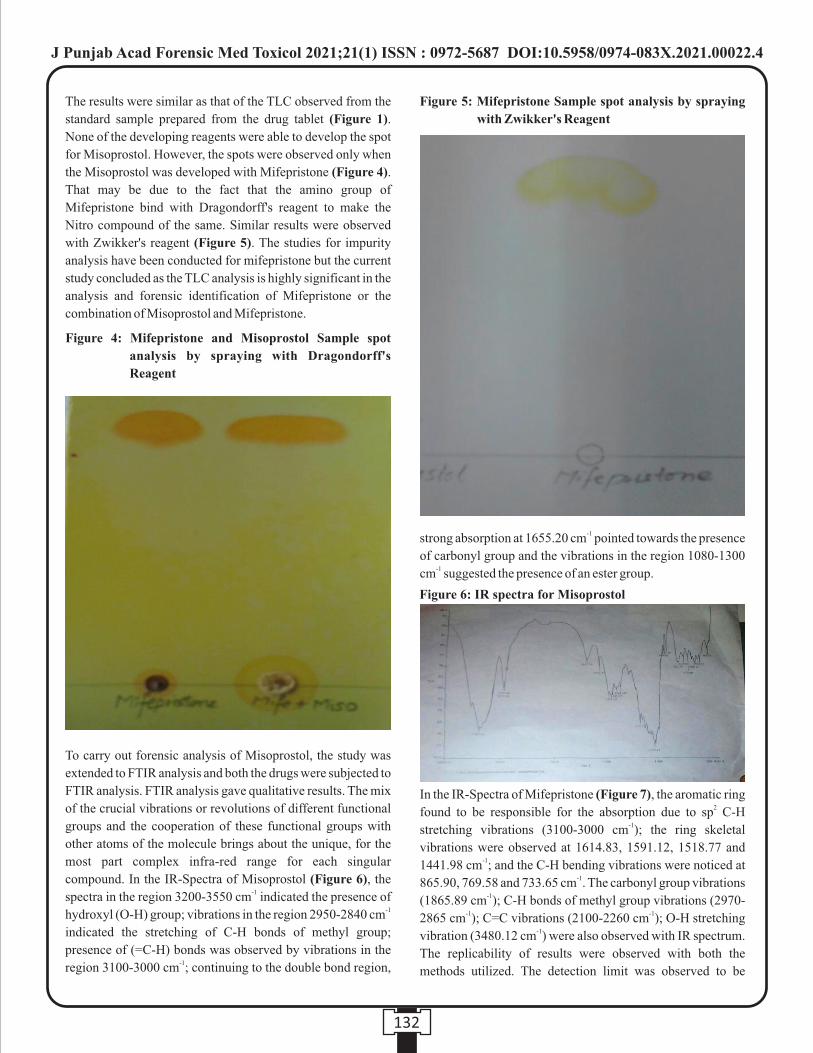
Figure 4: Mifepristone and Misoprostol Sample spot
analysis by spraying with Dragondorff's
Reagent
The results were similar as that of the TLC observed from the
standard sample prepared from the drug tablet (Figure 1).
None of the developing reagents were able to develop the spot
for Misoprostol. However, the spots were observed only when
the Misoprostol was developed with Mifepristone (Figure 4).
That may be due to the fact that the amino group of
Mifepristone bind with Dragondorff's reagent to make the
Nitro compound of the same. Similar results were observed
with Zwikker's reagent (Figure 5). The studies for impurity
analysis have been conducted for mifepristone but the current
study concluded as the TLC analysis is highly significant in the
analysis and forensic identification of Mifepristone or the
combination of Misoprostol and Mifepristone.
To carry out forensic analysis of Misoprostol, the study was
extended to FTIR analysis and both the drugs were subjected to
FTIR analysis. FTIR analysis gave qualitative results. The mix
of the crucial vibrations or revolutions of different functional
groups and the cooperation of these functional groups with
other atoms of the molecule brings about the unique, for the
most part complex infra-red range for each singular
compound. In the IR-Spectra of Misoprostol (Figure 6), the -1spectra in the region 3200-3550 cm indicated the presence of
-1hydroxyl (O-H) group; vibrations in the region 2950-2840 cm
indicated the stretching of C-H bonds of methyl group;
presence of (=C-H) bonds was observed by vibrations in the -1region 3100-3000 cm ; continuing to the double bond region,
-1strong absorption at 1655.20 cm pointed towards the presence
of carbonyl group and the vibrations in the region 1080-1300 -1cm suggested the presence of an ester group.
In the IR-Spectra of Mifepristone (Figure 7), the aromatic ring 2found to be responsible for the absorption due to sp C-H
-1stretching vibrations (3100-3000 cm ); the ring skeletal
vibrations were observed at 1614.83, 1591.12, 1518.77 and -11441.98 cm ; and the C-H bending vibrations were noticed at
-1865.90, 769.58 and 733.65 cm . The carbonyl group vibrations -1(1865.89 cm ); C-H bonds of methyl group vibrations (2970-
-1 -12865 cm ); C=C vibrations (2100-2260 cm ); O-H stretching -1vibration (3480.12 cm ) were also observed with IR spectrum.
The replicability of results were observed with both the
methods utilized. The detection limit was observed to be
132
Figure 5: Mifepristone Sample spot analysis by spraying
with Zwikker's Reagent
Figure 6: IR spectra for Misoprostol
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00022.4

1ng/ml. This technique extends the use of a standard IR
spectrophotometer, typically used for forensic identification
purpose.
DISCUSSION:
The validation of TLC technique for the detection of these
abortive drugs from forensic samples has not been done yet,
but the utility of mass spectroscopy has been reported in
forensic samples for detection of Misoprostol and its urinary [16]metabolites . With the analysis of FTIR graphs of
Misoprostol and Mifepristone, the functional groups of both
the drugs were identified that can be compared with standard [14, 17]graphs and can be used for the forensic analysis and
identification of these abortive drugs from the various
biological samples. The identification methods will help in the
forensic cases of toxic shocks or death due to these abortive [18, 19]drugs . These techniques will be helpful in correlating the
[20]congenital abnormalities with misoprostol misuse . The
combination of diclofenac and misoprostol has been identified
by liquid and gas chromatographic/tandem mass spectrometric [16]methods . The sensitivity and limit of detection (LOD) was
1ng/ml for FTIR, however, the sensitivities was previously
reported from HPLC method was 10 ng/ml for mifepristone [21] [22]after 120 h and 20.4 ng/ml after 96 hr . For the forensic
utility, thin layer chromatography and FTIR can be used as the
test of choice for the determination of Mifepristone and
Misoprostol in the body fluids.
CONCLUSION:
The study can be concluded with the development of novel
approach for the determination of the Mifepristone and
Misoprostol. TLC can be the earmarking and cheap techniques
for determination of the Mifepristone from body fluids. FTIR
can be utilized as the confirmative test for Mifepristone and
Misoprostol and will be highly helpful in criminal cases like
illegal abortions and female feticides.
List of abbreviations:
TLC - Thin Layer Chromatography
FTIR- Fourier Transform Infrared Spectroscopy
HPLC - High Performance Liquid Chromatography
LOD - Limit of Detection
MTP - Medical Termination of Pregnancy
GFMER-Geneva Foundation for Medical Education and
Research
WHO- World Health Organization
REFERENCES:
1. Grimes DA, Creinin MD. Induced abortion: An overview
for internists. Ann Intern Med. 2004;140:620-626.
2. World Health Organization, Department of Reproductive
Health and Research. Safe Abortion: Technical and Policy
Guidance for Health Systems. 2012. SBN:
9789241548434
3. WHO Model List of Essential Medicines. World Health
Organization, April 2015. Archived (PDF) from the
original on 13 December 2016. Retrieved 8 December
2016.
4. Geneva Foundation for Medical Education and Research
(GFMER). Application for inclusion of mifepristone
combined with misoprostol for first trimester (until 9
weeks) medical abortion in the WHO Model List of
Essential Medicines.
5. Kshirsagar SC, Wankhede UN. Combination of
mifepristone and misoprostol: An effective method of
medical abortion upto gestational age of 49 days. Int J
Reprod Contracept Obstet Gynecol. 2017;6(7):2923-
2925.
6. Thong KJ, Baird DT. Induction of abortion with
mifepristone and misoprostol in early pregnancy. Br J
Obstet Gynaecol. 1992; 99:1004-1007.
7. Corey EJ. Molecules and Medicine. John Wiley & Sons.
2007. ISBN 9781118361733
8. Coêlho HL, Teixeira AC, Santos AP, Forte EB, Morais
SM, La Vecchia C, Tognoni G, Herxheimer A.
Misoprostol and illegal abortion in Fortaleza, Brazil.
Lancet. 1993;341(8855):1261-1263. 9. Daisley H Jr. Maternal mortality following the use of
misoprostol. Med Sci Law. 2000;40(1):78-82.
10. Chen A, Yuan W, Meirik O, Wang X, Wu S, Zhou L, et al.
Mifepristone-induced early abortion and outcome of
subsequent wanted pregnancy. Am J Epidemiol.
2004;160:110–117.
11. Virk J, Zhang J, Olsen J. Medical abortion and the risk of
subsequent adverse pregnancy outcomes. N Engl J Med.
2007;357:648–653.
12. Elul B, Ellertson C, Winikoff B, Coyaji K. Side effects of
133
Figure 7: IR Spectra of Mifepristone
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00022.4
mifepristone-misoprostol abortion versus surgical
abortion. Data from a trial in China, Cuba, and India.
Contraception. 1999; 59(2):107-14.
13. Baird DT. Medical abortion in the first trimester. Best
Pract Res Clin Obstet Gynaecol. 2002;16:221-236.
14. Gallagher P, Young AH. Mifepristone (RU-486) treatment
for depression and psychosis: a review of the therapeutic
implications. Neuropsychiatr Dis Treat. 2006;2(1):33-42.
15. Clarke's Analysis of Drugs and Poisons in rdpharmaceuticals, body fluids and postmortem material. 3
edition, edited by Anthony C Moffat, M David Osselton &
Brian Widdop. Publisher: Pharmaceutical Press:London.
2004;2:1176. ISBN: 0-853-69473-7.
16. Watzer B, Lusthof KJ, Schweer H. Abortion after
deliberate Arthrotec® addition to food. Mass
spectrometric detection of diclofenac, misoprostol acid,
and their urinary metabolites. Int J Legal Med.
2015;129(4):759-69. doi: 10.1007/s00414-014-1136-4.
17. Verma K, Sharma PK, Dudhe R, Patro SK. Formulation,
design and development of mifepristone immediate
release tablet. Int J Pharma Sci and Res. 2017;5(11):760-
769.
18. Cittadini F, Loyola G, Caradonna L, Minelli N, Rossi R. A
case of toxic shock due to clandestine abortion by
misoprostol self-administration. J Forensic Sci.
2014;59(6):1662-1664.
19. Murray S, Wooltorton E. Septic shock after medical
abortions with mifepristone (Mifeprex, RU 486) and
misoprostol. Canadian Medical Asso J. 2005;173(5):485.
doi:10.1503/cmaj.05098.
20. Gonzalez CH, Marques-Dias MJ, Kim CA, Sugayama
SM, Da Paz JA, Huson SM, Holmes LB. Congenital
abnormalities in Brazilian children associated with
misoprostol misuse in first trimester of pregnancy. Lancet.
1998;351(9116):1624-1627.
21. Guo Z, Chu C, Yin G, He M, Fu K, Wu J. An HPLC
method for the determination of ng mifepristone in human
plasma. J Chromatography B. 2006;832:181-184.
22. Wei Y, Zhang M, Wang G, Zhao Z and Shao Q.
Pharmacokinetics of mifepristone after low oral dose in
healthy Chinese women. Chinese J Clin Pharm.
2003;19:430-433.
134
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00022.4

135
Table 1: Comparative result analysis of different solvent systens and developers for the identification of the Mifepristone
and Misoprostol
No. Sample Solvent system Mobile Phase Developer Result
Mifepristone
Mifepristone
Mifepristone
Mifepristone+
Mifepristone
Mifepristone
Mifepristone
Mifepristone
Mifepristone
Mifepristone
Mifepristone
Mifepristone
Mifepristone
Mifepristone
Mifepristone
Mifepristone
Mifepristone
Mifepristone
Mifepristone
Misoprostol
Misoprostol
Misoprostol
Misoprostol
Misoprostol
Misoprostol
Misoprostol
Misoprostol
Misoprostol
Misoprostol
Misoprostol
Misoprostol
Misoprostol
Misoprostol
Misoprostol
Misoprostol
Misoprostol
Misoprostol
Misoprostol
Chloroform-Acetone (9:1)
Chloroform-Acetone (9:1)
Chloroform-Acetone (9:1)
Chloroform-Acetone (9:1)
Chloroform-Acetone (9:1)
Chloroform-Acetone (9:1)
Chloroform-Acetone (9:1)
Chloroform-Acetone (9:1)
Chloroform-Acetone (9:1)
Toluene-Ethyl acetate(7:3)
Toluene-Ethyl acetate(7:3)
Toluene-Ethyl acetate(7:3)
Toluene-Ethyl acetate(7:3)
Toluene-Ethyl acetate(7:3)
Toluene-Ethyl acetate(7:3)
Toluene-Ethyl acetate(7:3)
Toluene-Ethyl acetate(7:3)
Toluene-Ethyl acetate(7:3)
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
Methanol
Chloroform
Methnol +Chloroform
Methanol
Chloroform
Methnol+Chloroform
Methanol
Chloroform
Methnol+Chloroform
Methanol
Chloroform
Methnol+Chloroform
Methanol
Chloroform
Methnol+Chloroform
Methanol
Chloroform
Methnol+Chloroform
Dragondorf's reagent
Dragondorf's reagent
Dragondorf's reagent
Zwikker reagent
Zwikker reagent
Zwikker reagent
Iodine fumes
Iodine fumes
Iodine fumes
Dragondorf's reagent
Dragondorf's reagent
Dragondorf's reagent
Zwikker reagent
Zwikker reagent
Zwikker reagent
Iodine fumes
Iodine fumes
Iodine fumes
Positive
Positive
Positive
Positive
Positive
Positive
Positive
Positive
Positive
Positive
Positive
Positive
Positive
Positive
Positive
Positive
Positive
Positive
Positive
Negative
Negative
Negative
Negative
Negative
Negative
Negative
Negative
Negative
Negative
Negative
Negative
Negative
Negative
Negative
Negative
Negative
Negative
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00022.4

Original Research Paper
INTRODUCTION :
India has one of the largest agrarian societies in the world with
the majority of the population dependent on agriculture both
for income and survival. Agriculture as an occupation has seen
a lot of technological advancements along with an increased
use of chemicals for better agricultural returns. This
inadvertent overuse to chemicals has led to human morbidity
and its complications. Poisoning is considered to be one of the 1. most common methods of committing suicide The most
common reasons for poisoning are because of the common use 2.of chemicals and pesticides for better agricultural output
Among these agricultural poisons, paraquat is found to be one 3of the chemicals causing deaths among agriculturists .
Paraquat (PQ) is N, N'-dimethyl-4, 4′-bipyridinium
dichloride, a synthetic quaternary nitrogenous organic 4compound . There are various reasons for the lethality of this
chemicals one among them is the lack of specific treatment. In
fact, paraquat has been banned in many of the developed
countries because of its severe toxic effects, and even if
available, they are subject to strict regulatory licensing and
oversight. In developing countries, it is still available because
of lack of strict enforcing of laws, its inexpensive nature of and
Corresponding Author :
Dr. Pavanchand Shetty H
Associate Professor,
Department of Forensic Medicine,
Kasturba Medical College Mangalore, Manipal Academy of
Higher Education, Manipal, India
Contact : +91 95917-02214
Email : [email protected]
KEYWORDS : Paraquat poisoning, Autopsy, Agriculture
Article History:Received: 31 May 2021Received in revised form: 30 June 2021 Accepted on: 30 June 2021Available online: 15 August 2021
ABSTRACT :
Introduction: India has one of the largest agrarian societies in the world with the majority of the population dependent on
agriculture both for income and survival. Agriculture as an occupation has seen a lot of technological advancements along with an
increased use of chemicals for better agricultural returns. This inadvertent overexposure to chemicals has led to human morbidities
and its complications. Among agricultural poisons, paraquat is found to be one of the common chemicals causing deaths among
agriculturists.
Materials and Methods: This study was conducted in VIMS Bellary, Karnataka, India with the data collected from the
postmortem report of the bodies brought in for autopsy with confirmation of poison involved based on chemical analysis reports
issued by the forensic science laboratories. The study was a retrospective one done on 235 deaths due to paraquat poisoning.
Results: In this study it was found out that male mortality was higher in comparison to females. The vulnerable or susceptible age
group was found to be individuals aged between 41-50 years among the studied sample and those involved in the agricultural
profession.
Conclusion: The study gives us an understanding about the population and the occupation of the population in the region studied
with respect to the chemical paraquat. It brings into focus the young and middle-aged productive group exposed to paraquat and
hopefully can give directions for various preventive steps to be taken in future.
1. Gururaj Biradar, Assistant Professor, Department of Forensic Medicine, VIMS Bellary2. Pavanchand Shetty H, Associate Professor*
3. Haneil Larson Dsouza, Associate Professor*4. B Suresh Kumar Shetty, Professor*5. Prateek Rastogi, Professor and Head*6. Charan Kishor Shetty, Assistant Professor and Unit Head, Department of Forensic Medicine, University Sultan Zainal
Abidin (UniSZA) Malaysia 7. V Yogiraj, Professor and Head, Department of Forensic Medicine, VIMS Bellary
*Department of Forensic Medicine, Kasturba Medical College Mangalore, Manipal Academy of Higher Education, Manipal, India
Profile of Paraquat Poisoning in Bellary District- A Retrospective Study
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00023.6
136
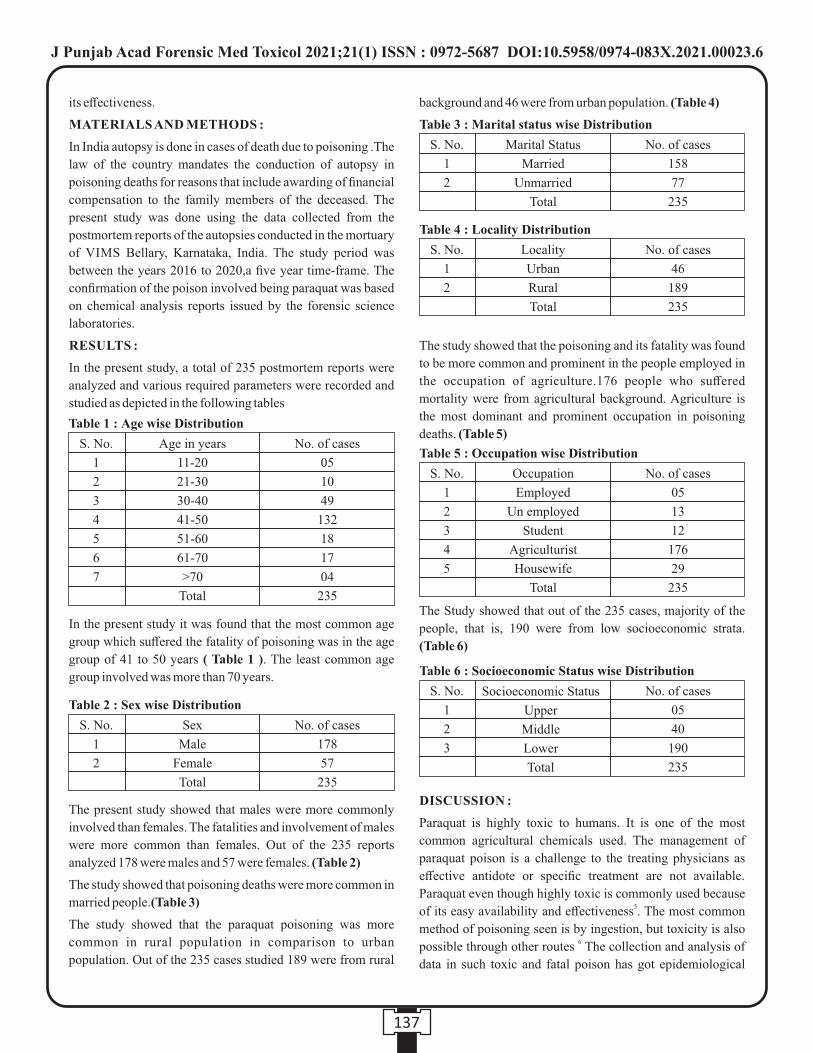
its effectiveness.
MATERIALS AND METHODS :
In India autopsy is done in cases of death due to poisoning .The
law of the country mandates the conduction of autopsy in
poisoning deaths for reasons that include awarding of financial
compensation to the family members of the deceased. The
present study was done using the data collected from the
postmortem reports of the autopsies conducted in the mortuary
of VIMS Bellary, Karnataka, India. The study period was
between the years 2016 to 2020,a five year time-frame. The
confirmation of the poison involved being paraquat was based
on chemical analysis reports issued by the forensic science
laboratories.
RESULTS :
In the present study, a total of 235 postmortem reports were
analyzed and various required parameters were recorded and
studied as depicted in the following tables
In the present study it was found that the most common age
group which suffered the fatality of poisoning was in the age
group of 41 to 50 years ( Table 1 ). The least common age
group involved was more than 70 years.
The present study showed that males were more commonly
involved than females. The fatalities and involvement of males
were more common than females. Out of the 235 reports
analyzed 178 were males and 57 were females. (Table 2)
The study showed that poisoning deaths were more common in
married people.(Table 3)
The study showed that the paraquat poisoning was more
common in rural population in comparison to urban
population. Out of the 235 cases studied 189 were from rural
background and 46 were from urban population. (Table 4)
The study showed that the poisoning and its fatality was found
to be more common and prominent in the people employed in
the occupation of agriculture.176 people who suffered
mortality were from agricultural background. Agriculture is
the most dominant and prominent occupation in poisoning
deaths. (Table 5)
The Study showed that out of the 235 cases, majority of the
people, that is, 190 were from low socioeconomic strata.
(Table 6)
DISCUSSION :
Paraquat is highly toxic to humans. It is one of the most
common agricultural chemicals used. The management of
paraquat poison is a challenge to the treating physicians as
effective antidote or specific treatment are not available.
Paraquat even though highly toxic is commonly used because 5of its easy availability and effectiveness . The most common
method of poisoning seen is by ingestion, but toxicity is also 6possible through other routes The collection and analysis of
data in such toxic and fatal poison has got epidemiological
137
Table 1 : Age wise Distribution
S. No.
1
2
3
4
5
6
7
Age in years
11-20
21-30
30-40
41-50
51-60
61-70
>70
Total
No. of cases
05
10
49
132
18
17
04
235
Table 2 : Sex wise Distribution
S. No.
1
2
Sex
Male
Female
Total
No. of cases
178
57
235
Table 3 : Marital status wise Distribution
S. No.
1
2
Marital Status
Married
Unmarried
Total
No. of cases
158
77
235
Table 4 : Locality Distribution
S. No.
1
2
Locality
Urban
Rural
Total
No. of cases
46
189
235
Table 5 : Occupation wise Distribution
S. No.
1
2
3
4
5
Occupation
Employed
Un employed
Student
Agriculturist
Housewife
Total
No. of cases
05
13
12
176
29
235
Table 6 : Socioeconomic Status wise Distribution
S. No.
1
2
3
No. of cases
05
40
190
235
Socioeconomic Status
Upper
Middle
Lower
Total
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00023.6

benefits. The present article examines the most vulnerable age
group, socio economic status and the gender of the victims of
poisoning. The results in the present study show that the
middle age group, and gender-wise, males are the most prone
for death due to poisoning. This may be due to the fact that the
particular age group and gender are the ones who are actively
involved in the agricultural profession. Hopefully, this data can
be used to get some reforms in the administrative and health
sectors. The present study was possible due to the information
collected from the postmortem reports, thus further
emphasizing the importance of data collection during the
process of postmortem examination. The present study has
concentrated on a particular region wherein the rural
population were found to be more involved . The study also
focused on the availability of the poisons in the particular
occupation which can give a guidance to restrict the use of
paraquat or regulate it to prevent further casualty.
CONCLUSION :
The study gives us an understanding about the population and
the occupation they are engaged in and the accessibility of the
chemical to this population in the region studied. It brings into
focus that young and middle aged productive group are more
exposed to the poison paraquat and hopefully can give
directions for various preventive steps to be taken in future.
Research Funding-None
Conflict of Interest-None
Ethical Clearance-Taken from VIMS, Bellary
REFERENCES :
1. Kanchan T, Menon A, Menezes RG. Methods of choice in
completed suicides: Gender differences and review of
literature. J Forensic Sci. 2009;54:938–42.
2. Bumbrah GS, Krishan K, Kanchan T, Sharma M, Sodhi
GS. Phosphide poisoning: A review of literature. Forensic
Sci Int. 2012;214:1–6.
3. Ram P, Kanchan T, Unnikrishnan B. Pattern of acute
poisonings in children below 15 years - A study from
Mangalore, South India. J Forensic Leg Med.
2014;25:26–9
4. D M Roberts L S Herbicides ; Nelson N A Lewin M A
Howland R S Hoffman L R Goldfrank Goldfrank's
Toxicologic Emergencies9th editionMcGraw HillNew
York201115026
5. MA Janeela A Oommen AK Misra I Ramya Paraquat
poisoning: Case report of a survivorJ Fam Med Prim
Care201763672310.4103/2249-4863.222042
6. Wesseling C, van Wendel de Joode B, Ruepert C, Leon C,
Monge P, Hermosillo H, et al. Paraquat in developing
countries. Int J Occup Environ Health. 2001;7:275–86.
138
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00023.6
Original Research Paper
INTRODUCTION :
It is a well-established fact that a good doctor is a boon while a
negligent one, a curse.
Professional negligence is defined as the omission to do
something (act of omission) which a reasonable person would
do or doing something (act of commission) which a reasonable [1]person would not do.
Criminal negligence - Section 304-A of the Indian Penal
Code,1860 states that whoever causes the death of a person by
a rash or negligent act not amounting to culpable homicide
shall be punished with imprisonment for a term of two years, or
with a fine, or with both.
A negligent person is one who inadvertently commits an act of
omission and violates a positive duty. A person who is rash
knows the consequences but foolishly thinks that they will not
occur as a result of his/ her act. A reckless person knows the
consequences but does not care whether or not they result from
his/ her act. Any conduct falling short of recklessness and
deliberate wrongdoing should not be the subject of criminal
liability. Thus, a doctor cannot be held criminally responsible
for a patient's death unless it is shown that he/ she was
negligent or incompetent, with such disregard for the life and
safety of his patient that it amounted to a crime against the [2] State.
Mistakes can be fatal and negligence in the field of medicine
can have drastic consequences for both the doctor and the
patient. An increase in the knowledge and awareness among
general populations about their rights and medical negligence
has led to a rise in suits against doctors for medical
malpractice.
A report published in Hindustan Time on August 30, 2017
states that Complaints of negligence rise by 30-40% over the
past 5 years, but less than 10% of doctors are held accountable.
This study is being carried out with the intention of assessing
the knowledge and awareness among consultants and their
Corresponding Author :
Dr. Jaswinder Singh,
Professor,
Shri Ram Murti Smarak Institute of Medical Sciences,
(SRMS-IMS), Bareilly.
Contact : +91 90458-60105
Email : [email protected]
KEYWORDS : Medical Malpractice; Medical Negligence; Medical Malpraxis
Article History:Received: 17 July 2020Received in revised form: 18 June 2020Accepted on: 18 June 2020Available online: 31August 2021
ABSTRACT :
Introduction: Medical malpractice is prevalent and alleged cases of negligence widespread. Most cases are to tarnish image of the
doctor and to gain monetary benefit.
Materials and Methods: Present study was undertaken with aim to assess knowledge and awareness of consultants towards
medical negligence at SRMS-IMS, Bareilly. Participants were subjected to a questionnaire of 10 questions with responses based on
LIKERT scale varied from strongly agree to strongly disagree.
Results: Out of 80 participants, 75% agreed that professional negligence in any form should be considered a violation of
Hippocratic oath, 82.5% agreed that refusing to attend a patient in emergency is negligence. 36.3% agreed that imprisonment as a
punishment for criminal negligence by law is appropriate.
Conclusions: Present study reflected that the consultants of SRMS-IMS, Bareilly have profound knowledge and are aware about
medical negligence.
1. Siddhartha Taneja, MBBS Student* 2. Jaswinder Singh, Professor*3. K.K.Bairagi, Professor*4. Tarun K. Singh, Assistant Professor* *Department of Forensic Medicine, Shri Ram Murti Smarak Institute of Medical Sciences (SRMS-IMS), Bareilly.
Assessment of Knowledge and Awareness towards Medical Negligence among Consultants in a Tertiary Care Teaching Hospital in North India
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00024.8
139
views towards medical negligence.
MATERIALS AND METHODS :
This study is being undertaken with the aim to assess the
knowledge and awareness among consultants towards medical
negligence in a tertiary care teaching hospital of SRMS-IMS,
Bareilly.
Total 80 consultants from departments of medicine, surgery,
obstetrics and gynaecology, paediatrics, otorhinolaryngology,
ophthalmology, orthopaedics, radiodiagnosis, oncology,
anaesthesia, dermatology, respiratory medicine are subjected
to a questionnaire containing 10 questions related to medical
negligence with responses based on LIKERT scale which vary
from strongly agree to strongly disagree. (Table 1)
Consultants are chosen as the sample population for the
research as they are the pivot around which the issue of
negligence rotates, they are not only responsible for their
actions but also their juniors and the staff as under contributory
negligence. Institutional ethical approval was obtained prior to
commencement of the study.
RESULTS :
Out of the 80 participants, 45% strongly agreed, 30% agreed
upon that professional negligence in any form be considered a
violation of Hippocratic oath, 13.8% were neutral while 2.5%
strongly disagreed and 8.8% disagreed with the same.
45% consultants strongly agreed while 37.5% agreed that
refusing to attend a patient in emergency is negligence only
7.5% disagreed and 2.5% strongly disagreed with the same
while 7.5% remain neutral.
35% consultants stayed neutral on the question that is
performing or helping for euthanasia a negligence,17.5%
agreed and 6.3% strongly agreed upon it while 26.3%
disagreed and 15% strongly disagreed with it.
Out of 80 participants, 36.3% agreed that imprisonment as a
punishment for criminal negligence by law is appropriate,
12.5% strongly agreed, 16.3% disagreed, 16.3% strongly
disagreed and 18.8% stayed neutral.
47.5% consultants disagreed, 27.5% strongly disagreed and
10% stayed neutral about toxic result of drug administration in
a patient should be considered negligence, 11.3% agreed while
3.8% strongly agreed it.
50% consultants agreed while 26.3% strongly agreed, 13.8%
remain neutral, 6.3% disagreed and 3.8% strongly disagreed
that failure to give proper post-operative care be considered
negligence.
37.5% consultants agreed and 2.5% strongly agreed that
concealing negligence of another doctor is negligence, 16.3%
disagreed, 8.8% strongly disagreed and 35% stayed neutral.
31.3% consultants agreed, 6.3% strongly agreed that treating a
patient without his consent even for his own good is
negligence, 30% disagreed and 10% strongly disagreed and
140
No.
1
2
3
4
5
6
7
8
9
10
SA
45%
45%
6.3%
12.5%
3.8%
26.3%
2.5%
6.3%
10%
41.3%
Table 1: Knowledge and Awareness of Consultants towards Medical Negligence.
A
30%
37.5%
17.5%
36.3%
11.3%
50%
37.5%
31.3%
45%
52.5%
N
13.8%
7.5%
35%
18.8%
10%
13.8%
35%
22.5%
23.8%
3.8%
D
8.8%
7.5%
26.3%
16.3%
47.5%
6.3%
16.3%
30%
18.8%
1.3%
SD
2.5%
2.5%
15%
16.3%
27.5%
3.8%
8.8%
10%
2.5%
1.3%
QUESTIONS
Should professional negligence in any form be considered a violation of Hippocratic oath?
Refusing to attend patient in emergency is negligence?
Is performing or helping for euthanasia a negligence?
Imprisonment as a punishment for criminal negligence, appropriate by law?
Should toxic result of drug administration in a patient be considered negligence?
Failure to give proper post-operative care be considered negligence?
Should concealing negligence of another doctor be considered negligence?
Is treating a patient without his consent negligence, even if it is for his own good?
Inability to produce required medical records upon requirement, by a consultant considered negligence?
Should a death review committee be set up in hospitals to counter negligence?
SA: Strongly Agree A: Agree N: Neutral D: Disagree SD: Strongly Disagree
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00024.8

22.5% remain neutral.
45% consultants agreed,10% strongly agreed that inability to
produce required medical records upon requirement, by a
consultant considered negligence,18.8% disagreed, 2.5%
strongly disagreed while 23.8% stayed neutral.
52.5% consultants agreed, 41.3% strongly agreed on setting up
a death review committee in hospitals to counter negligence,
1.3% disagreed, 1.3% strongly disagreed and 3.8% stayed
neutral.
DISCUSSION :
Medical malpractice is prevalent and alleged cases of
negligence widespread. Most of the suits made are to tarnish
the image of the doctor and to gain monetary benefit.
According to a study conducted by Pragnesh Parmar and
Gunvanti Rathod on Knowledge and Awareness among
general population towards medical negligence, showed that
general population has quite a good knowledge regarding
medical negligence which may increase gradually over a [3]period of time.
Due to this increasing knowledge often, the public is
confounded in the actual scenario of the doctor patient
relationship and deviation in their slightest of expectations
leads them to believe that the doctor is negligent. The present
study resolved on the fact that the consultants have a good
knowledge and are aware about medical negligence.
While answering the questionnaire, majority (75%) said that
professional negligence in any form violates the Hippocratic
oath.
Again majority (82.5%) agreed that refusing to attend a patient
in emergency due to any reason is negligence. As per the law,
any doctor who provides first aid in an emergency case will not
be held liable or negligent in case any mishap occurs after that [4]patient leaves his care.
While in another judgement, it was held that the amount of
care, skill and caution expected of a reasonable and prudent
medical practitioner in normal times and during an emergency [5]may not be the same.
Being asked upon performing or helping for Euthanasia is a
negligence or not, majority (35%) stayed neutral while next
majority (26.3%) disagreed to it. Euthanasia is a widely
debated topic but as per law today, only passive euthanasia is
legal in India. In a study conducted by Dr. Shreemanta Kumar
Dash in Kallinga institute of medical sciences, on the question
Do you favour euthanasia? 85% of consultants said NO, while [6]5% said Don't Know.
Majority (48.8%) agreed that it is appropriate by law, to
imprison a medical practitioner as punishment if found guilty
of criminal negligence.
75% disagreed that toxic result of drug administration should
be considered negligence by a doctor. Upon discussion
majority supported spontaneous monitoring but ultimately
resolved on the fact that adverse reaction is unpredictable if
otherwise caused by a negligent act.
There was a strong agreement (76.3%) that failure of a
consultant to give proper post-operative care is in fact
negligence and worsening of the condition of patient due to any
deficiency in post-operative care makes the doctor guilty.
Majority (40%) agreed that it will be in fact considered
negligence to hide the faults of another doctor who is guilty,
resulting in any sort of harm to the patient. While 35% stayed
neutral and 25.1% disagreed the same.
Majority (40%) disagreed that treating a patient without
consent even for his own good should be considered
negligence. While almost 37.6% agreed that it would be an act
of negligence to treat a patient without his consent. Although
law withholds any medical practitioner to start any treatment or
procedure without taking appropriate consent however, if a
doctor feels that providing information to a patient who is
anxious or disturbed would not be processed rationally by him
and is likely to psychologically harm him, the information can [7]be withheld from him as a therapeutic privilege.
Majority agreed (55%) that it is negligence on part of a doctor
to not produce required medical records when needed.
Provisions of the Limitation Act 1963 and section 24A of the
consumer protection Act 1986, lays down time within which a
complaint can be filed; it is advisable to maintain records for 2
years for outpatient records and 3 years for inpatient and
surgical cases. The records that are subject to medicolegal
cases should be maintained until the final disposal of the case [8]even though only a complaint or notice is received.
Strong majority (93.8%) agreed that a death review committee
should be set up in hospitals to counter negligence and aid in
justice if any. The committee would not only serve as a
valuable check to the actions of consultants but also document
all the sensitive facts in case of any death appearing to be due to
alleged negligent act. This would also contribute to education
of medical, paramedical and nursing staff to decrease death [9]rate due to a preventable cause.
CONCLUSION :
Present study reflected that the consultants of SRMS-IMS,
Bareilly have profound knowledge and are aware about
medical negligence. Their interaction with their patients, on a
daily basis incorporates all the aspects of medical ethics which
begins right from the out-patient department, treatment,
operation theatre and post-operative.
141
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00024.8

CONFLICT OF INTEREST: Nil
SOURCE OF FUNDING: Self-Funded
REFERENCES :
1. Parikh C. K., Parikh's textbook of medical jurisprudence,
forensic medicine and toxicology. New Delhi: CBS
Publishers & Distributors; 6th edition 2007: 1.42-1.43.
2. House of Lords decision in R vs Adomako (1994).
Available from:
https://www.casemine.com/judgement/uk/5a8ff8c960d0
3e7f57ecd71e. Accessed on 24th April 2021.
3. Parmar P, Rathod GB. Knowledge and awareness among
general population towards medical negligence. IAIM,
2016; 3(7): 250-254.
4. In Amir Ali Shakir v. St John's Medical College Hospital,
Bangalore, 1996(1) CPJ 169; 1995(3) CPR 174
( K A R N ATA K A S C D R C ) . Av a i l a b l e f r o m :
https://kscdrc.kar.nic.in . Accessed on 24th April 2021.
5. In New India Assurance Co. Ltd. V Dr Kriti Kumar S sheth
And Anr. 1997 ACJ 1103, Para 13. Available from:
https://indiankanoon.org/doc/1711277/ . Accessed on
24th April 2021.
6. Dash, Shreemanta. (2010). Original research paper
Medical Ethics, Duties & Medical Negligence Awareness
among the Practitioners in a Teaching Medical College
Hospital - A Survey. JIAFM, 2010; 32(2): 153-156.
7. Kannan JK, Mathiharan K. Legal and ethical aspects of
medical practice. In: Modi A, editor. Textbook of Medical
Jurisprudence and Toxicology. 24th edition Nagpur: Lexis
Nexis Butterworths Wadhwa; 2012. P. 61-118.
8. Thomas J. Medical records and issues in negligence.
Indian J Urol 2009;25(3):384-388.
9. Vargas-Rosendo R, Alemán-Velázquez P, Jasso-Gutiérrez
L. The Mortality Committee: a hospital need. Bol Med
Hosp Infant Mex. 1992 Oct;49(10):683-8.
142
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00024.8
Estimation of stature from Percutaneous Length of Tibia in Living Subjects in Jhalawar region of Rajasthan
1. Mukesh Kumar Meena, PG 2nd Year*
2. Sanjaya Kumar Jain, Senior Professor*
3. Ramakant Varma, Associate Professor*
*Department of Forensic Medicine & Toxicology, Jhalawar Medical College, Jhalawar, Rajasthan
ABSTRACT :
Background: As said “to identify the individuality of human being and to reconstruct stature from different body part is his birth
right” and also the stature of a person is considered as an inherent character by the anthropologists. So, for establishment of the
identity of a person, measurement of stature is considered as the most valuable parameter in forensic anthropology.
AIM: The present study made an attempt to establish the statistical correlation between stature and pre-cutaneous tibial length
(PCTL) BY formulating a simple regression equation and multiplication factor (M.F.) for the people of Jhalawar region.
Material and methods: between the Present study was carried out on 200 subjects (100 male and 100 female) among the people of
Jhalawar region. Between the age group of 18-24 years were chosen. PCTL of right and left tibia was measured with the help of
spreading caliper. The stature was estimated from percutaneous tibial length was measured and the data was analyzed statistically
and the regression equation was derived.
Result: The linear regression equation derived from percutaneous tibial length for the measurement of height t showed statistically
significant relationship (p < 0.05) in both the sexes.
Conclusion: It was concluded that the stature in Jhalawar region. present study revealed that there is a positive correlation exists
between the stature and percutaneous tibial length. Hence, this study is very much useful for forensic expert as well as for the
anthropologist.
Key words: Anthropometry, Percutaneous tibial length, Stature.
Corresponding Author:
Dr. Ramakant Varma,
Associate Professor,
Department of Forensic Medicine & Toxicology,
Jhalawar Medical College, Jhalawar, Rajasthan
Contact : +91 94609-62020
Email : [email protected]
Article History :
Received : 19 October 2020
Received in revised from : 13 December 2020
Accepted on : 13 December 2020
Available online : 15 August 2021
INTRODUCTION :
Anthropometry is a systematic study of measurement on man
and it involves scientific techniques for taking various
measurements and somatic observation on the living subjects.
Stature estimation is an important part of the identification in
human skeletal remains or body parts, especially long bones of 1,2,3,4the limbs. The estimation of stature from femur and tibia,
5are more accurate than the humerus and ulna, especially the
tibia and the femur as these have a direct correlation to the 6height of an individual. Forensic's While dealing with skeletal
remains use of anatomical method for stature reconstruction
has limited role due to non-availability of the complete 7skeleton from a scene of crime in most of the cases.
The mathematical method can be used in these cases where 8 9-10only a part of the body or part of the bone are available for
determination of the stature.
Anthropology is the branch of science which deals with the
comparative study of human being, their origin, physical and 11-13.cultural development and biological characteristics . It also
gives us knowledge about the evolutionary history of human
being, the variation in social and cultural behavior among the
different race of people, the structural development and
variation in physical status of different group of human 14population and it also proved itself as a boon for researchers .
The term anthropology comes from the Greek word
“Anthropos” meaning “human being” and “logia” meaning
“study”. Deals with the study of human being, their working
style and the culture in the society and the variation among
them is also included.
Physical Anthropology: Subdivision of anthropology:
Anthropology can be subdivided into the following two parts:
Social Anthropology: it is the branch which deals with the
Original Research Paper
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00025.X
143

study of human being, their working style and the culture in the
society and the variation among them is also included. It deals
with the long-term development of human being and the study 25of biological behavior of humans .
In the field of forensic anthropology determination of identity
of an individual is considered as the most important character,
specifically when a damaged body or mutilated bodies are
found and also if bones are available after the death of 26individual at the site of crime or any other place .
As we know that various part of the body like head, trunk and
length of upper and lower limbs are in close relation with the
height of a person. So, for anatomist, anthropologist, and
forensic medicine experts, height estimation has become a
matter of interest by measuring the different parts of the 21,27,28body .
Stature and percutaneous tibial length: Stature is the body
height of an individual subjects in standing position. It
represents the distance between the top of the head(the vertex)
and the bottom of the feet. The legs should be kept parallel to
each other with both feet joined together and the great toe
should face forward. The person should be stand bare footed
and should maintain the anatomical position of the body with 19the head adjusted in Frankfurt plane . Percutaneous tibial
length is the total length of tibia significantly presenting the
distance between the medial most superficial point on the
upper border of the medial condyle to the superficial lower
most point (tip) of medial malleolus of tibia, and the person
should maintain the angle between flexor surface of leg and 1thigh at 90° .
The standing height is in great contribution with the lower limb
length; hence the most predictive equation is based on the 20bones of lower extremity length like tibia, femur and fibula .
21Tibia holds about 22% of the total human body length . The
height of the new generation is increasing with improved
socioeconomic condition of the world. Hence the relationship
between height and length of long bones is changing day by 22day, therefore fresh formula is needed for each generation. It
is also useful for medicolegal experts and anthropological 23,24studies.
MATERIALS AND METHODS:
The study was conducted on 200 subjects (100 male and 100
female) between the age group of 18-24 year among the
population of Jhalawar region. The stature and per cutaneous
tibial length were measured. The stature was measured with
the help of stadiometer and percutaneous tibial length was
measured by spreading caliper.
Technique for measurement of stature: The person was
asked to stand erect, eyes forward and both arm by the side of
the body, palm faces forward and both the leg parallel to each
other, both feet are joined together and the great toe faces
forward, and the head were adjusted in the frankfurt¼s plane.
All the measurement was taken by bringing the sliding
horizontal bar up to the vertex. All the measurement was taken
in centimeter. (Figure 1)
Technique of measuring percutaneous tibial length: For
measuring the percutaneous length of tibia the person was
asked to sit on a stool so that the thigh should be placed in a
straight line, and the leg and thigh should be placed right angle
to each other (maintain the angle of 90°with each other ), foot
was rotated laterally, so that the bony projection were
prominently seen. Then proximal and distal points of tibia
were marked by marker pencil. Then the two points (proximal
and distal) were measured by spreading caliper. To determine
the length of tibia spreading caliper was used. The length of
tibia was measured in centimeter. (Figure 2)
Proximal point: The superficial superior most point of upper
border of the medial tibial condyle was considered as the
proximal point of measurement of the tibia.
Distal point: superficial inferior most point which is the tip of
medial malleolus of tibia was considered as the distal point in
measuring the tibia.
Statistical analysis: The data was statistically evaluated by
calculating the mean, the standard deviation (SD) as well as the
standard error (SE). Pearson's correlation coefficient was used
to correlate between stature and percutaneous tibial length.
The regression formula was derived by calculating the stature
as well as the PCTL of left as well as right side of both the
sexes. The regression formula used was Y = a + b (x) Where,
144
Figure 1 Figure 2
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00025.X
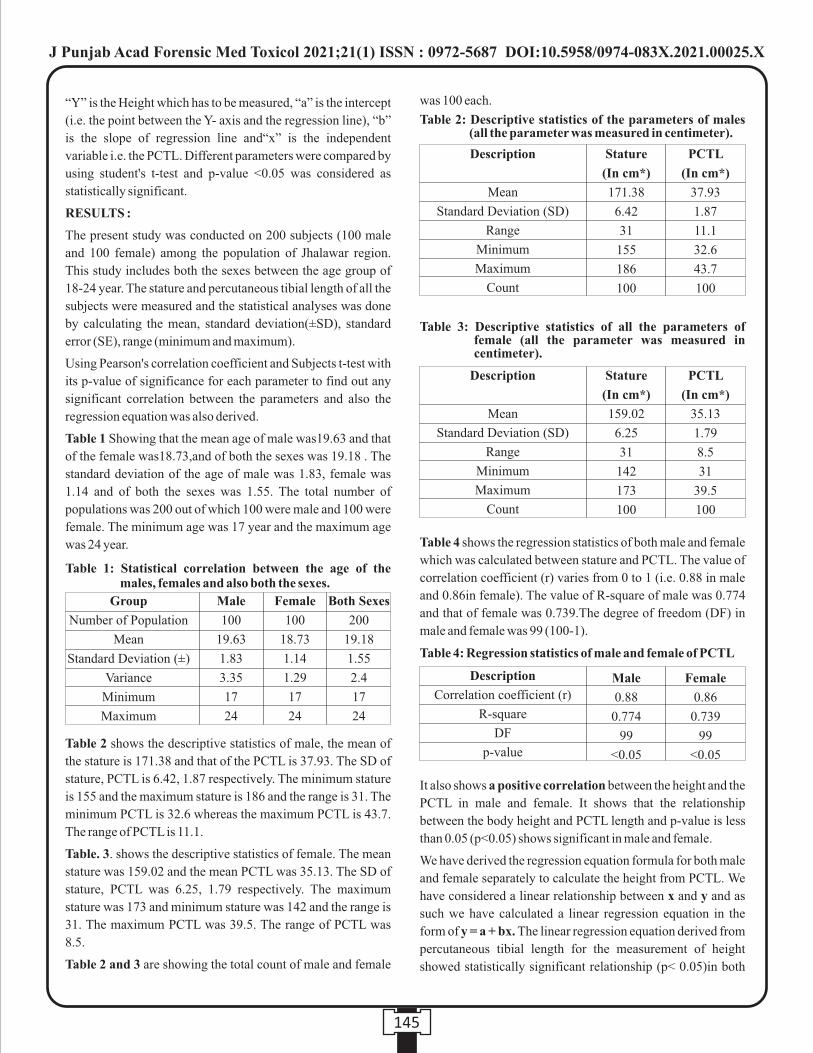
“Y” is the Height which has to be measured, “a” is the intercept
(i.e. the point between the Y- axis and the regression line), “b”
is the slope of regression line and“x” is the independent
variable i.e. the PCTL. Different parameters were compared by
using student's t-test and p-value <0.05 was considered as
statistically significant.
RESULTS :
The present study was conducted on 200 subjects (100 male
and 100 female) among the population of Jhalawar region.
This study includes both the sexes between the age group of
18-24 year. The stature and percutaneous tibial length of all the
subjects were measured and the statistical analyses was done
by calculating the mean, standard deviation(±SD), standard
error (SE), range (minimum and maximum).
Using Pearson's correlation coefficient and Subjects t-test with
its p-value of significance for each parameter to find out any
significant correlation between the parameters and also the
regression equation was also derived.
Table 1 Showing that the mean age of male was19.63 and that
of the female was18.73,and of both the sexes was 19.18 . The
standard deviation of the age of male was 1.83, female was
1.14 and of both the sexes was 1.55. The total number of
populations was 200 out of which 100 were male and 100 were
female. The minimum age was 17 year and the maximum age
was 24 year.
Table 2 shows the descriptive statistics of male, the mean of
the stature is 171.38 and that of the PCTL is 37.93. The SD of
stature, PCTL is 6.42, 1.87 respectively. The minimum stature
is 155 and the maximum stature is 186 and the range is 31. The
minimum PCTL is 32.6 whereas the maximum PCTL is 43.7.
The range of PCTL is 11.1.
Table. 3. shows the descriptive statistics of female. The mean
stature was 159.02 and the mean PCTL was 35.13. The SD of
stature, PCTL was 6.25, 1.79 respectively. The maximum
stature was 173 and minimum stature was 142 and the range is
31. The maximum PCTL was 39.5. The range of PCTL was
8.5.
Table 2 and 3 are showing the total count of male and female
was 100 each.
Table 4 shows the regression statistics of both male and female
which was calculated between stature and PCTL. The value of
correlation coefficient (r) varies from 0 to 1 (i.e. 0.88 in male
and 0.86in female). The value of R-square of male was 0.774
and that of female was 0.739.The degree of freedom (DF) in
male and female was 99 (100-1).
It also shows a positive correlation between the height and the
PCTL in male and female. It shows that the relationship
between the body height and PCTL length and p-value is less
than 0.05 (p<0.05) shows significant in male and female.
We have derived the regression equation formula for both male
and female separately to calculate the height from PCTL. We
have considered a linear relationship between x and y and as
such we have calculated a linear regression equation in the
form of y = a + bx. The linear regression equation derived from
percutaneous tibial length for the measurement of height
showed statistically significant relationship (p< 0.05)in both
145
Table 1: Statistical correlation between the age of the males, females and also both the sexes.
Group
Number of Population
Mean
Standard Deviation (±)
Variance
Minimum
Maximum
Male
100
19.63
1.83
3.35
17
24
Female
100
18.73
1.14
1.29
17
24
Both Sexes
200
19.18
1.55
2.4
17
24
Table 2: Descriptive statistics of the parameters of males (all the parameter was measured in centimeter).
Description
Mean
Standard Deviation (SD)
Range
Minimum
Maximum
Count
Stature
(In cm*)
171.38
6.42
31
155
186
100
PCTL
(In cm*)
37.93
1.87
11.1
32.6
43.7
100
Table 3: Descriptive statistics of all the parameters of female (all the parameter was measured in centimeter).
Description
Mean
Standard Deviation (SD)
Range
Minimum
Maximum
Count
Stature
(In cm*)
159.02
6.25
31
142
173
100
PCTL
(In cm*)
35.13
1.79
8.5
31
39.5
100
Table 4: Regression statistics of male and female of PCTL
Description
Correlation coefficient (r)
R-square
DF
p-value
Male
0.88
0.774
99
<0.05
Female
0.86
0.739
99
<0.05
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00025.X
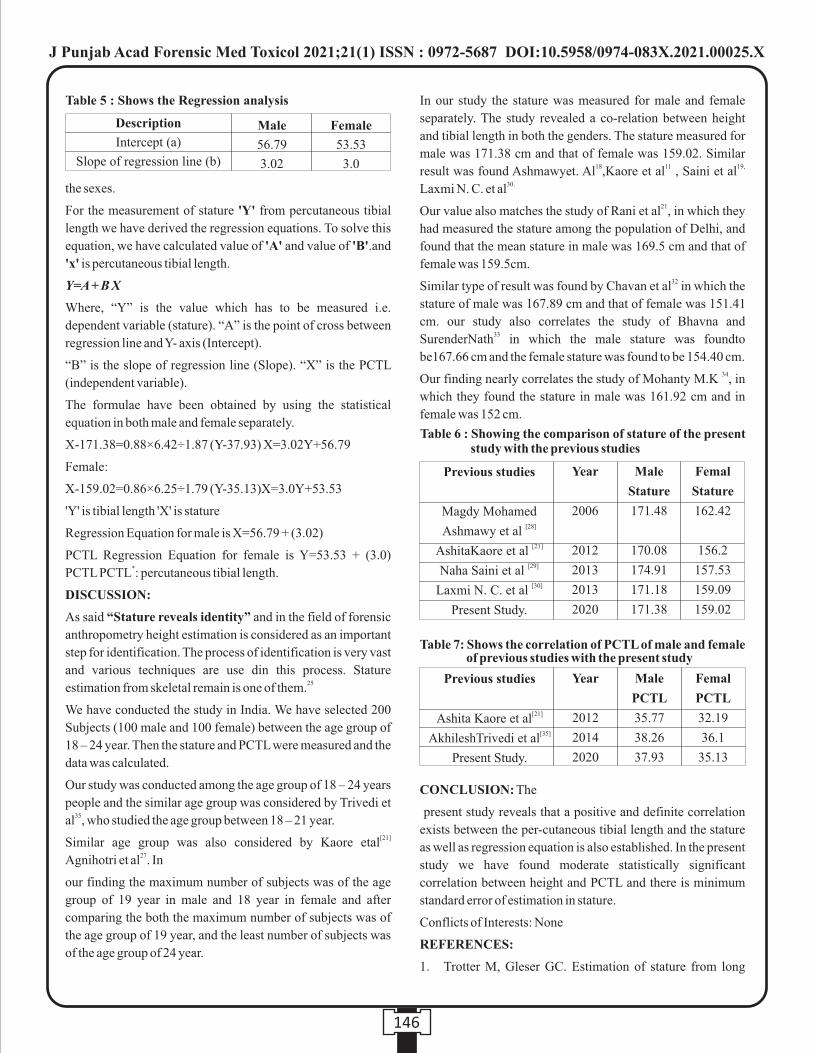
the sexes.
For the measurement of stature 'Y' from percutaneous tibial
length we have derived the regression equations. To solve this
equation, we have calculated value of 'A' and value of 'B'.and
'x' is percutaneous tibial length.
Y=A + B X
Where, “Y” is the value which has to be measured i.e.
dependent variable (stature). “A” is the point of cross between
regression line and Y- axis (Intercept).
“B” is the slope of regression line (Slope). “X” is the PCTL
(independent variable).
The formulae have been obtained by using the statistical
equation in both male and female separately.
X-171.38=0.88×6.42÷1.87 (Y-37.93) X=3.02Y+56.79
Female:
X-159.02=0.86×6.25÷1.79 (Y-35.13)X=3.0Y+53.53
'Y' is tibial length 'X' is stature
Regression Equation for male is X=56.79 + (3.02)
PCTL Regression Equation for female is Y=53.53 + (3.0) *PCTL PCTL : percutaneous tibial length.
DISCUSSION:
As said “Stature reveals identity” and in the field of forensic
anthropometry height estimation is considered as an important
step for identification. The process of identification is very vast
and various techniques are use din this process. Stature 25estimation from skeletal remain is one of them.
We have conducted the study in India. We have selected 200
Subjects (100 male and 100 female) between the age group of
18 – 24 year. Then the stature and PCTL were measured and the
data was calculated.
Our study was conducted among the age group of 18 – 24 years
people and the similar age group was considered by Trivedi et 35al , who studied the age group between 18 – 21 year.
[21]Similar age group was also considered by Kaore etal 27Agnihotri et al . In
our finding the maximum number of subjects was of the age
group of 19 year in male and 18 year in female and after
comparing the both the maximum number of subjects was of
the age group of 19 year, and the least number of subjects was
of the age group of 24 year.
In our study the stature was measured for male and female
separately. The study revealed a co-relation between height
and tibial length in both the genders. The stature measured for
male was 171.38 cm and that of female was 159.02. Similar 18 11 19,result was found Ashmawyet. Al ,Kaore et al , Saini et al
30.Laxmi N. C. et al21Our value also matches the study of Rani et al , in which they
had measured the stature among the population of Delhi, and
found that the mean stature in male was 169.5 cm and that of
female was 159.5cm.32Similar type of result was found by Chavan et al in which the
stature of male was 167.89 cm and that of female was 151.41
cm. our study also correlates the study of Bhavna and 33SurenderNath in which the male stature was foundto
be167.66 cm and the female stature was found to be 154.40 cm.34Our finding nearly correlates the study of Mohanty M.K , in
which they found the stature in male was 161.92 cm and in
female was 152 cm.
CONCLUSION: The
present study reveals that a positive and definite correlation
exists between the per-cutaneous tibial length and the stature
as well as regression equation is also established. In the present
study we have found moderate statistically significant
correlation between height and PCTL and there is minimum
standard error of estimation in stature.
Conflicts of Interests: None
REFERENCES:
1. Trotter M, Gleser GC. Estimation of stature from long
146
Table 5 : Shows the Regression analysis
Description
Intercept (a)
Slope of regression line (b)
Male
56.79
3.02
Female
53.53
3.0
Previous studies
Magdy Mohamed [28]Ashmawy et al
[21]AshitaKaore et al [29]Naha Saini et al
[30]Laxmi N. C. et al
Present Study.
Table 6 : Showing the comparison of stature of the present study with the previous studies
Year
2006
2012
2013
2013
2020
Male
Stature
171.48
170.08
174.91
171.18
171.38
Femal
Stature
162.42
156.2
157.53
159.09
159.02
Previous studies
[21]Ashita Kaore et al[35]AkhileshTrivedi et al
Present Study.
Table 7: Shows the correlation of PCTL of male and female of previous studies with the present study
Year
2012
2014
2020
Male
PCTL
35.77
38.26
37.93
Femal
PCTL
32.19
36.1
35.13
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00025.X
bones of Americanwhites and negroes. Am J Phys
Anthropol 1952;10:463-514.
2. Mall G, Hubig M, Büttner A, Kuznik J, Penning R, Graw
M. Gender determination and estimation of stature from
the long bones of the arm. Forensic Sci Int 2001;117: 23-
30.
3. Duyar I, Pelin C. Body height estimation based on tibia
length in different stature groups. Am J Phys Anthropol
2003;122:23-7.
4. Petrovečki V, Mayer D, Šlaus M, Strinović D, Škavić J.
Prediction of stature based on radiographic measurements
of cadaver long bones: a study of the Croatian population.
Journal of Forensic Sciences. 2007; 52 (3):547-52.
5. Lundy JK, Feldesman MR. Revised equations for
estimating living stature from long of the South African
Negro. S Afr J Sci 1987; 83: 54-55.
6. Brothwell D, Zakrzewski. Metric and non-metric studies
of archaeological human bone. In: Brickley M, McKinley
JI, editors. Stature estimation. Guidelines to the Standards
for recording Human Remains. South ampton/Reading:
BABAO/ Institute of Field Archeologists; 2004
7. Allbrook D. The estimation of stature in British and East
African males based on tibial and ulnar bone lengths. J.
For. Med.1961; 8: 15-28.
8. Ozaslan A, Iscan MY, Ozaslan I, Tugcu H, Koc S.
Estimation of stature from body parts. Forensic Sci Int
2003;132:40-5.
9. Badkur P, Nath S. Use of regression analysis in
reconstruction of maximum bone length and living stature
from fragmentary measures of the ulna. Forensic Sci Int
1990;45:15-25.
10. Holland TD. Estimation of adult stature from fragmentary
tibias. J Forensic Sci 1992;37:1223-9.
11. Pan N, lengths of long bones and their proportions to body
height in Hindus. Journal Anatomy; 1924;58:374-8.
12. Abdul Malik AK, Ahmed AM, EL Sharwaki SA, Hamid
NA. Prediction of stature from hand measurement.
Forensic Sci Int., 1990;46(2):181-87.
13. Das BM, outlines of anthropology. Allahabad kitab mahal,
2008;26ed :1.
14. Singh A, Kumar A, Chavli KH, Dasari H, Use of arm span
and foot length for estimation of height of the person. J
Punjab Academy of Forensic Med Toxicology,
2010;12(2):87-91.
15. Singh IP, Bhasin MK, Anthropometry – a laboratory
manual or biological anthropology. Delhi Kamla Raj
Enterprises, 1968;18(39):3-7.
16. Choi BY, Chae YM, Chung IH, Kang HS, Correlation
between the postmortem stature and dried limb bone
length of Korean adult's male. Yonsei medical journal,
1997;38:79-85.
17. Chavan SK, Chavan KD, Mumbre SS, Makhani CS.
Stature andpercutaneous tibial length- a study in
Maharashtrian population. Indian journal of forensic
medicine and pathology; 2009:2(3):109-111
18. Joshi NB, Patel MP and Dongre AV,Regression equation
of height on Ulnar length. Ind. J. Med. Res.
1964;52(2):1088-91.
19. Bogin D, Silva MIV, Leg length, body proportion and
health:a review with a note on beauty. Int J environ Res
Public Health, 2010;7:1047-1075.
20. Bokariya P, Sontakke B, Waghmare JE, TarnekarAditya,
Tripure BH, Shende MR, The anthropometric
measurement of tibia. J Indian Accad Forensic Med,
2012;34(4):223- 234.
21. Kaore A, Kaore BP, Kamdi A, Kaore A. Stature estimation
from tibial length. NJIRM; 2012;3(2).
22. Lal CS, Lala JK. Estimation of height from tibial and ulnar
length in North Bihar. Journal of Indian Medical
Association, 1972;58(4):120-121.
23. Mondal MK, Jana TK, Das J, Biswas S. Use of length of
ulna for estimation of stature in living adult male in
Burdwan district and adjacent area of west Bengal.
Journal of the Anatomical Society of India,
2009;58(1):121- 23.
24. Joshi NB, Patel MP, Dongre AV. Regression equation of
height on ulnar length. Ind. J. Med. Res. 1964;52(2):1088-
1091.
25. Ilayperuma I, Nanayakkara G, Palahepitiya N. A model
for the estimation of personal stature from the length of
forearm. Int. J. Morphol, 2010;28(4):1081-86.
26. Vercelloti G. Stature estimation in an early medieval (xi-
xii) polish population: Am J. Physical Anthropol
2009;16(42):140-135.
27. Agnihotri AK, Kachhwaha S, Vandna J, Pratap S.
Estimation of stature from percutaneous length of tibia
and ulna in Indo-Mauritian population. Forensic Science
International, 2009;187:109-113.
28. Ashmawy MM, Ayman Abdel –hamid Nagy. Prediction of
height from percutaneous tibial length among Egyptians.
Sebha Medical Journal2006;5(2):223- 229.
29. Saini N, Chauhan S, Katara P, Parashar R. A correlational
147
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00025.X
study between stature and PCTL in adult males and
females of Rajasthan. Indian Journal of Basic and Applied
Medical Research, 2013;3(1):21-26.
30. Chandravadiya LN, Patel SM, Goda JB, Patel SV.
International journal of biological and medical research,
2010;66-85.
31. Mukta R, Tyagi AK, Verma SK, Kohli A. Estimation of
stature from percutaneous measurements of legs. Journal
of forensic medicine and toxicology, 2004;21(1):12- 14.
32. Chavan SK, Chavan KD, Mumbre SS, Makhani CS.
Stature andpercutaneous tibial length- a study in
Maharastrian population. Indian journal of forensic
medicine and pathology; 2009:2(3):109-11.
33. Bhavna S, Surinder Nath. Use of lower limb measurement
in reconstructing stature among Shia Muslims. The
international journal of biological anthropology;
2009:2(2).
34. Mohanty NK, Prediction of height from percutaneous
tibial length amongst Oriya population. Forensic Sci Int.,
1998;98(3):137-41.
35. Trivedi A, Saxena S, Morya R, Jehan M. Stature
estimation using percutaneous tibial length in people of
Gwalior Region:JOSR- JDMS,2014;13(5):65-70.
36. Pearson K, Length of long bones and their proportion to
body height in Hindus. J. Anat. 1899; 192:169- 244.
37. Trotter M, Glasser GC, Trends in stature of American
Whites and Negroes born between 1840 – 1924. Am. J.
Phys. Anthropol. 1951;9:103-117.
148
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00025.X
Original Research Paper
INTRODUCTION :
Fatal road traffic accidents (RTA) are a major cause of death all
over the world. It is considered as one of the most significant
but preventable cause of death. Approximately 1.35 million
people die as a result of RTA worldwide. That account for
almost 3700 deaths per day due to road traffic accidents. As per
World Health Organization the RTA can rise upto 2.4 million rdby 2020 and will make it the 3 most common killer in the
nd [1]World and 2 most common in the developing countries. As
per history it was 1896 when the First automobile accident
occurred when a car hit a bicycle rider whereas in 1899 was the
year when first fatal accident occurred in the city of London. In
same year in the New York City a pedestrian died after he was
hit by a car. The factors that decide the outcome of injuries
sustained in an RTA but are not limited to: the type of vehicle
involved in the accident, the condition of road, the location and
time of accident, etc. The significant factors that lead to
accident vary from driver fatigue, over speeding, fault in the
vehicle, error in human assessment, drunken driving, poor [2]road conditions, traffic rules violations etc. It is the only
problem in the society where decision makers still can't refuse
[3]mortality and morbidity among young people on high scale.
It was highest among the people between 15-44 years age
group and predominantly in males with greater the 1.8 lakh [4]death under the age of 15 years. The aim of present study was
to assess the pattern of road traffic injuries.
MATERIAL AND METHODS :
The present study was based on the autopsy findings of 87 fatal
cases due to road traffic accident conducted in the Department
of Forensic Medicine & Toxicology, Govt. Medical College &
Hospital, Jammu. The duration of the study was from August
2017 to August 2019.The cases included in this study were
from various police stations in and around Jammu.
RESULTS :
During the study period out of the total number of cases of
medico-legal autopsies 87 cases were of fatal road traffic
accident. Age group between 31-40 years (31.03%) was
among the most frequent age group seen that was followed by
21-30yrs (20..68%). (Table 1). Road traffic accident victims
aged above 61 years and lesser then 10 years were least [5-6]involved with 5.74% and 3.4% respectively.
Corresponding Author : Dr. Preet Mohinder Singh,
Assistant Professor,
Department of Forensic Medicine & Toxicology, Govt.
Medical College, Kathua
Contact : +91 78897-85106
Email : [email protected]
KEYWORDS : Road traffic accidents, RTA, Injuries, fatal road traffic accident, Jammu
Article History:Received: 25 January 2020Received in revised form: 30 April 2020Accepted on: 30 April 2020Available online: 31 August 2021
ABSTRACT :
Introduction: Fatal road traffic accidents (RTA) are considered as a major cause of death all over the world. Approximately 1.35
million people die as a result of RTA worldwide. That account for almost 3700 deaths per day due to road traffic accidents. The aim
of this study was to know the injury pattern from fatal road traffic accidents either found dead on arrival or died during treatment and
presented in the mortuary of Govt. Medical college & hospital, Jammu. During the study period out of total 181 cases of medico-
legal autopsies 87 cases were of fatal road traffic accident.
Results: Among the age group 31–40 years, highest number (31.03%) of road traffic fatalities occurred. Males predominated over
the female by almost four and a half times. Most common external injuries were seen in Head, Neck & face (34.82%) followed by
lower extremities (17.58%) with abrasion dominated (57.24%) follower by laceration (23.1%).Abdomen and Pelvis were least
involved among other injuries (11.03%). Fracture of the skull was the most frequently fractured bone (28.96%) whereas the pelvis
and the spine were the least fractured bones with 3.44% & 1.37% respectively. Brain was the most commonly injured internal organ
seen on autopsy(34.69%).
1. Preet Mohinder Singh, Assistant Professor, Department of Forensic Medicine & Toxicology, Govt. Medical College, Kathua.2. Kirandeep Kour Raina, Medical Officer, PHC Mansar.
3. Sandya Arora, Associate Professor, Department of Forensic Medicine & Toxicology, Govt. Medical College, Jammu.
Pattern of fatal Injuries in Road Traffic Accidents in & around Jammu region: An Autopsy Based Study
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00027.3
149
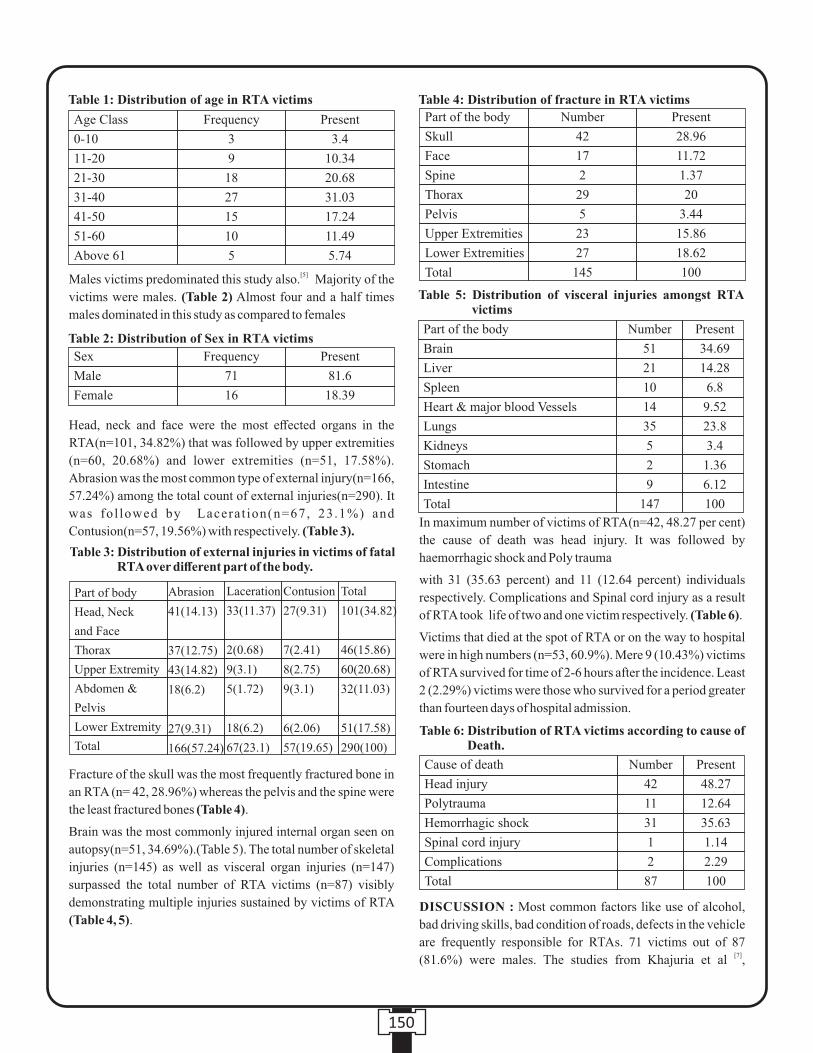
Part of the body
Brain
Liver
Spleen
Heart & major blood Vessels
Lungs
Kidneys
Stomach
Intestine
Total
Number
51
21
10
14
35
5
2
9
147
Present
34.69
14.28
6.8
9.52
23.8
3.4
1.36
6.12
100
Table 5: Distribution of visceral injuries amongst RTA victims
[5]Males victims predominated this study also. Majority of the
victims were males. (Table 2) Almost four and a half times
males dominated in this study as compared to females
Head, neck and face were the most effected organs in the
RTA(n=101, 34.82%) that was followed by upper extremities
(n=60, 20.68%) and lower extremities (n=51, 17.58%).
Abrasion was the most common type of external injury(n=166,
57.24%) among the total count of external injuries(n=290). It
was fol lowed by Lacerat ion(n=67, 23.1%) and
Contusion(n=57, 19.56%) with respectively. (Table 3).
Fracture of the skull was the most frequently fractured bone in
an RTA (n= 42, 28.96%) whereas the pelvis and the spine were
the least fractured bones (Table 4).
Brain was the most commonly injured internal organ seen on
autopsy(n=51, 34.69%).(Table 5). The total number of skeletal
injuries (n=145) as well as visceral organ injuries (n=147)
surpassed the total number of RTA victims (n=87) visibly
demonstrating multiple injuries sustained by victims of RTA
(Table 4, 5).
In maximum number of victims of RTA(n=42, 48.27 per cent)
the cause of death was head injury. It was followed by
haemorrhagic shock and Poly trauma
with 31 (35.63 percent) and 11 (12.64 percent) individuals
respectively. Complications and Spinal cord injury as a result
of RTA took life of two and one victim respectively. (Table 6).
Victims that died at the spot of RTA or on the way to hospital
were in high numbers (n=53, 60.9%). Mere 9 (10.43%) victims
of RTA survived for time of 2-6 hours after the incidence. Least
2 (2.29%) victims were those who survived for a period greater
than fourteen days of hospital admission.
DISCUSSION : Most common factors like use of alcohol,
bad driving skills, bad condition of roads, defects in the vehicle
are frequently responsible for RTAs. 71 victims out of 87 [7](81.6%) were males. The studies from Khajuria et al ,
150
Table 1: Distribution of age in RTA victims
Age Class
0-10
11-20
21-30
31-40
41-50
51-60
Above 61
Frequency
3
9
18
27
15
10
5
Present
3.4
10.34
20.68
31.03
17.24
11.49
5.74
Sex
Male
Female
Frequency
71
16
Present
81.6
18.39
Table 2: Distribution of Sex in RTA victims
Table 3: Distribution of external injuries in victims of fatal RTA over different part of the body.
Abrasion
41(14.13)
37(12.75)
43(14.82)
18(6.2)
27(9.31)
166(57.24)
Part of body
Head, Neck
and Face
Thorax
Upper Extremity
Abdomen &
Pelvis
Lower Extremity
Total
Laceration
33(11.37)
2(0.68)
9(3.1)
5(1.72)
18(6.2)
67(23.1)
Contusion
27(9.31)
7(2.41)
8(2.75)
9(3.1)
6(2.06)
57(19.65)
Total
101(34.82)
46(15.86)
60(20.68)
32(11.03)
51(17.58)
290(100)
Part of the body
Skull
Face
Spine
Thorax
Pelvis
Upper Extremities
Lower Extremities
Total
Number
42
17
2
29
5
23
27
145
Present
28.96
11.72
1.37
20
3.44
15.86
18.62
100
Table 4: Distribution of fracture in RTA victims
Table 6: Distribution of RTA victims according to cause of Death.
Cause of death
Head injury
Polytrauma
Hemorrhagic shock
Spinal cord injury
Complications
Total
Number
42
11
31
1
2
87
Present
48.27
12.64
35.63
1.14
2.29
100

[8] [9] [10] Ganveer and Tiwari , Kochar et al. , Azmani et al.[11] [12]Moharamzad et al. , Jha G et al. also reported similar results
in their respective studies.
In the present study victims between 21-30 years of age were [7]the most commonly effected. As per Khajuria et al. 53.01%
victims suffered in RTA belong to the age group between 20-40 [6] [8] years. , Ganveer and Tiwari observed most of the victims,
about 75% were in the age group of 18-37 years. The capability
for negligence in the use of safety features like seatbelt,
helmets, restraints etc and ignorance of traffic rules &
regulations of 20-40 years of age group can explain the this
scenario. It forces us to think about the grave loss of economy
to the community due to the involvement of this highly
productive age group in RTA. These are similar with [13-16]authors.
The dominance of males in this study coincides with reporting [9,10,12,17-20]from other research studies . As per the traditional
ways more males work outside homes and are more exposed to
RTA, this could be the reason behind the gender bias. This
could lead to very adverse impact on economy of the family as [21]most of them were the sole bread winners of their families.
In this study the injuries to musculoskeletal with regards to
pattern of injuries in RTA was mostly seen on limbs when
counted together that was followed by head(neck and face), [22]thorax and abdomen. In their study Singh et al. reported
extremity injuries when taken together were present in
78.5%,followed by head, thorax and abdomen with 77.6%, [12]44% and 31.8% respectively . These are similar with other
[23,24]studies.
The most common injury site in victims of RTA was Brain, it [12]was followed by lungs as second most common. Jha et al. in
his research study reported one-third of victims had head
injuries, that was followed by lower limb injuries and face.
Most of the victims of RTA (60.9%) either died on spot or on
the way to hospital. The similar finding were observed by other 11,18,19,20research studies . It can be explained due shortage of pre-
24 hospital teams shortage In case of cranial injury the survival
time of the victim depends upon the degree of injury and also
services in health care that were given to the victim. This is [23,24]consistent with studies made by other researchers.
The commonest type of external injury seen in victims were
Abrasions. The total number of injuries(external)that were
sustained by 87 cases of RTA were 290.This shows occurrence
of multiple injuries in the victims of RTA. If calculated the
total external injuries sustained were 3.33 per victim. [25] Chaudhary et al observation showed 1.66 external injuries
per victim. Skull has maximum number (28.96%) of fractures. [21,25] Other studies also report a similar nature of fracture.
CONCLUSION :
Deaths because of Road traffic accidents is an alarming
problem in the society. Due to the death or disability of the
affected person their families, friends, colleagues get effected
financially, emotionally and otherwise too. There is loss of
resources which ultimately decreases the economic growth of
the society. It asks for the necessity of establishing a decent and
prompt trauma services at the site and excellent pre hospital
care for the victims of RTA. The most common and life-
threatening injury suffered in RTA remains Head injuries. A
good neurosurgical care is the demand for such patients Apart
from that hospitals near to such sites should be equipped with
well experienced surgery, orthopaedic & anaesthetic teams
with advanced facilities like CT scans, USG and blood banks
can decrease the motility in case of RTA victims. It also
stresses upon the enhancement of the roads with the
upgradation of surfaces, increasing the visibility and
appropriate placement of road signs n traffic lights, removal of
unnecessary obstacles placed in the roads and extending the
width of roads at the narrow sections.
Source of Funding: None.
Conflict of Interest: None.
REFERENCES :
1. WHO Global status report on road safety 2018, Available
from:
https://www.who.int/violence_injury_prevention/road_s
fety status/2018/GSRRS2018_Summary_EN.pdf
7.12.19
2. Kaul A, Sinha U.S, Pathak Y.K, Singh A, Kapoor A.K,
Sharma S, Singh S.Fatal Road Traffic Accidents, Study of
Distribution, Nature and Type of Injury. JIAFM.2005;
27(2):71-75.
3. Mohan D. Road traffic injuries-a neglected pandemic.
Bulletin World Health Organisation 2003; 81(9):684-5.
4. Health Action Road Safety, a collective responsibility
April 2004.
5. Singh B, Palimar V, Arun M, Mohanty MK.Profile of
Trauma related Mortality at Manipal. KUMJ 2008;
6(23):393-398.
6. Sindhu DS, Sodi GS, Banerjee AK.Mortality Profile in
Trauma Victims. J Indian Med Assoc. 1993; 91(1):16-8.
7. Khajuria B, Sharma R, Verma A. A profile of the autopsies
of road accident victims in Jammu. J Clin Diag Res
2008;2:639- 42.
8. Ganveer GB and Tiwari RR. Injury pattern among non-
fatal road traffic accidents: A cross-sectional study in
151

central India; Indian J Med Sci 2005;59:9-12.
9. Kochar A, Sharma GK, Mutari A, Rehan HS. Road traffic
accidents and alcohol: A prospective study. International
Journal of Medical Toxicology & Legal Medicine.
2002;5:22–4.
10. Azmani W, Rusli MA, Ismail AA, Hashim M. Factors and
road accidents during festive seasons in Kelantan. NCD
Malaysia. 2005;4:24–7.
11. Moharamzad Y, Taghipour H, Firoozabad NH.
Mortality pattern according to autopsy findings
among traffic accident victims in Yazd, Iran. Chinese
J Traumatol 2008;11:329-34.
12. Jha N, Srinivasa DK, Roy G. Injury pattern among
road traffic accident cases: A study from South India.
Indian J Comm Med. 2003;28:85-90.
13. Rajesh DR, Kaur B, Singh A, Venkateshan M,
Aggarwal OP. Pattern of Injuries due to Fatal Road
Tr a ffi c A c c i d e n t s i n R u r a l H a r y a n a : A n
Epidemiological Survey. JIAFM 2012;34(3):229-
32.
14. Rajesh DR, Kaur B, Singh A, Venkateshan M,
Aggarwal OP. Pattern of Injuries due to Fatal Road
Tr a ffi c A c c i d e n t s i n R u r a l H a r y a n a : A n
Epidemiological Survey. JIAFM 2012;34(3):229-
32.
15. Kaul A, Sinha U.S, Pathak Y.K, Singh A, Kapoor AK,
Sharma Set al. Fatal Road Traffic Accidents , Study of
Distribution, Nature Type of Injury. JIAFM
2005;27(2):71-5.
16. Singh B, Palimar V, Arun M, Mohanty MK. Profile of
Trauma related Mortality at Manipal KUMJ
2008;6(23):393-8.
17. Menon A, Pai VK, Rajeeev A. Pattern of fatal head
injuries due to vehicular accidents in Mangalore.
Journal Forensic & Legal Medicine. 2008;15:75–7.
18. Bansal YS, Dikshit PC. Pattern of chest injuries in
fatal vehicular accidents in central Delhi.
International Journal of Medical Toxicology & Legal
Medicine. 2001;4:21–6.
19. Henriksson E, Ostrom M, Erikson A. Preventability
of vehicle-related fatalities. Accident Analysis
Prevention. 2001;33:467–75.
20. Toro K, Hubay M, Sotonyi P, Keller E. Fatal traffic
injuries among pedestrians, bicyclist and motor
vehicle occupants. Forensic Science International.
2005;151:151–6.
21. Salgado MSL, Colombage SM. Analysis of fatalities
in road accidents. Forensic Science International.
1988;36:91–6.
22. Singh H, Dhattarwal S, Mittal S. A review of
pedestrian traffic fatalities. J Indian Acad Forensic
Med 2007;29(4):55-8.
23. Gopal B K, Ahamed A, Ahamed F, Tonse S.B. Pattern
of Skull Fractures due to Blunt Force. JKAMLS
2015;24(2):27-31.
24. Singh YN, Bairagi KK, Das KC. An Epidemiological
Study of Road Traffic Accident Victims in Medico
Legal Autopsies. JIAFM 2005;27(3):166-9.
25. Chaudhary BL, Singh D, Tirpude BH, Sharma RK,
Veena M. Profile of road traffic accident cases in
Kasturba Hospital of M.G.I.M.S., Sevagram,
Wardha, Maharashtra. Medico-Legal Update.
2005;5:127–33.
152

Original Research Paper
INTRODUCTION :
Forgery is been practised since long back in all countries
where writing and papers were used for the financial purpose.
Forgery is fraudulent of genuine writing or alteration of
documents. In this case forgery can be done of full (1)documents/paper or only of writing/ signatures . But when we
talk about writing it is skill which is been acquired by ones in (2)his/her life-time. It is also a neuro-muscular task , so, copying
of one's character is bit impossible because copying of
anyone's minute detail of writing or living of own special
writing feature is work of lot practise. In forgery we consider
many characteristics of handwriting to identify its
genuineness. Some of the characters taken are:
•Unnatural appearance •Line quality
• Absence of rhythm
•Patching, Retouching & overwriting(3)• Emphasis on letter formation
In the present study we are comparing the Forged Urdu
signatures of two region peoples those who are not familiar to
Urdu language. The area covered in this study are Sikkim and
Kashmir. This study is useful for the forensic documents
examiners as when they examine the cases to link with the area
and person. Other study shows that when person do forgery
then their strokes are clumsy and tremorous. Also, they have
careful connection to hide the pen-lift while writing,
retouching looks like pen painting than original or genuine (4)writing . The study shows that Speed, wrinkleless and
acceleration of writing is more helpful while differentiation (5)between the genuine and forged writing . In one of the study it
is shown that when we examine single letter there is less
difference from original letter formation but in combination of
letters there is always more differences found, which shows (6)forgery also depend on letter connection and combinations . A
study was also done dependent on local base-line and primary (7)base-line to analyse different style of Arabic language . In one
of the studies it is found 12% of forged signature shown less
pen lift than the original and 22% shown the more pen lift than
the original. So, on the basis of this study it was concluded that
alone one of the characters i.e. pen-lift cannot form any definite (8)opinion in case of fixing the authorship .
MATERIAL S AND METHODS :
For this study 100 samples were collected out of which 50
Corresponding Author :
Dr. Rajeev Kumar,
Associate Professor,
Galgotias University, Greater Noida, India.
Contact : +91-9411923188
Email : [email protected]
KEYWORDS : Forensic Science, Handwriting, Forgery, Urdu handwriting, Docubox HD, Docucenter Nirvis.
Article History:Received: 29 November 2020Received in revised form: 13 December 2020Accepted on: 13 December 2020Available online: 15 August 2021
ABSTRACT :
Introduction: Forgery is an act of copying someone else signature or writing and while copying the act we have to keep in mind that
we imitate the characteristic of the real signatory in our forged writing and hide our own real characteristics of handwriting.
Material and Methods: In this study we have studied and analysed the forged Urdu signatures of Kashmir & Sikkim population
and target only to those people who are not familiar with the Urdu language.
Result: While analysing their sample we found that the Kashmir population have done forgery with less caution as they are not very
much emphasised on letter formation and re-touching and overwriting is found very less. While in Sikkim population its opposite as
their writing shows much stress on letter formation which automatically caused slower speed, retouching, overwriting in their
writing.
Conclusion: So, this study shows that knowledge of language is not only show impact while forgery but also the region cause
impact but both regions have different line-quality which is found common.
1. Syed Ahmar Ali Hashmi, Ph.D. Scholar, Galgotias University, Greater Noida & Junior Forensic/Assistant Chemical Examiner (Documents), Forensic Science Laboratory, Govt. of NCT of Delhi, India.
2. Shalvi Upadhyay, Assistant Professor & Coordinator, Forensic Science Department, Sharda University, Greater Noida, India.3. Rajeev Kumar, Associate Professor, Galgotias University, Greater Noida, India.
Comparative Study of Forged Urdu Signatures Done By Persons Not Familiar To
Language Belongs To Region of Sikkim And Kashmir
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00028.5
153
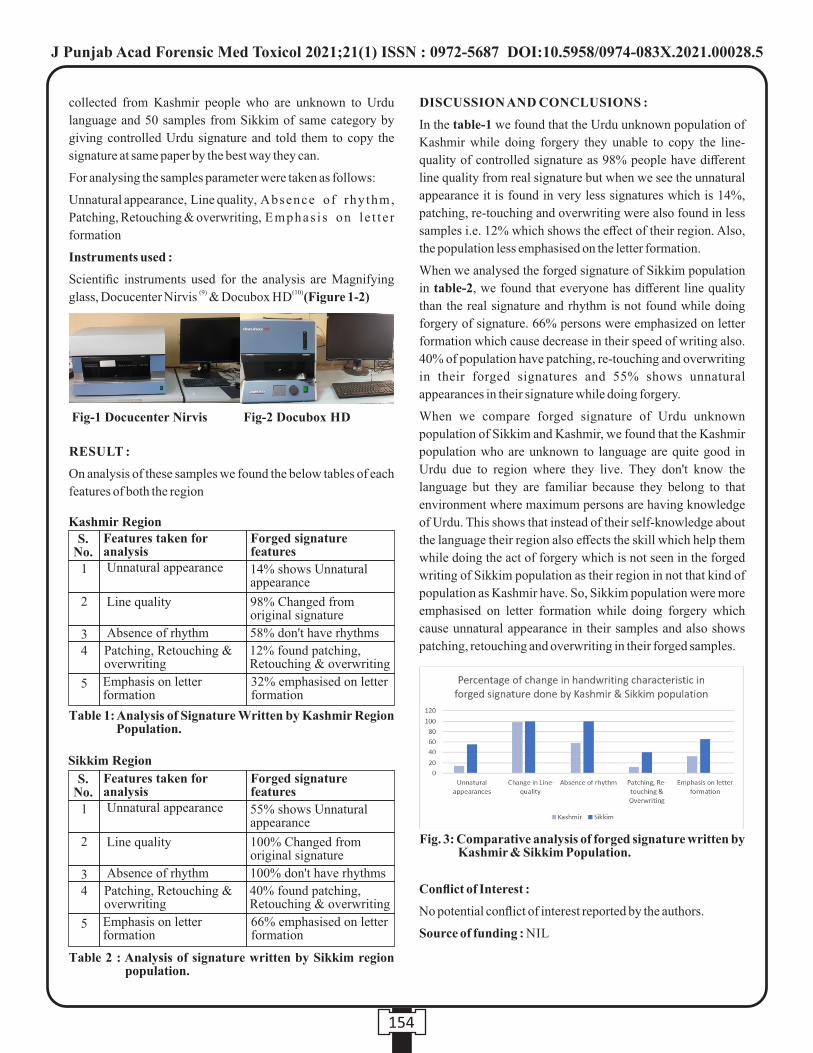
collected from Kashmir people who are unknown to Urdu
language and 50 samples from Sikkim of same category by
giving controlled Urdu signature and told them to copy the
signature at same paper by the best way they can.
For analysing the samples parameter were taken as follows:
Unnatural appearance, Line quality, Absence of rhythm,
Patching, Retouching & overwriting, Emphas i s on l e t t e r
formation
Instruments used :
Scientific instruments used for the analysis are Magnifying (9) (10) glass, Docucenter Nirvis & Docubox HD (Figure 1-2)
RESULT :
On analysis of these samples we found the below tables of each
features of both the region
DISCUSSION AND CONCLUSIONS :
In the table-1 we found that the Urdu unknown population of
Kashmir while doing forgery they unable to copy the line-
quality of controlled signature as 98% people have different
line quality from real signature but when we see the unnatural
appearance it is found in very less signatures which is 14%,
patching, re-touching and overwriting were also found in less
samples i.e. 12% which shows the effect of their region. Also,
the population less emphasised on the letter formation.
When we analysed the forged signature of Sikkim population
in table-2, we found that everyone has different line quality
than the real signature and rhythm is not found while doing
forgery of signature. 66% persons were emphasized on letter
formation which cause decrease in their speed of writing also.
40% of population have patching, re-touching and overwriting
in their forged signatures and 55% shows unnatural
appearances in their signature while doing forgery.
When we compare forged signature of Urdu unknown
population of Sikkim and Kashmir, we found that the Kashmir
population who are unknown to language are quite good in
Urdu due to region where they live. They don't know the
language but they are familiar because they belong to that
environment where maximum persons are having knowledge
of Urdu. This shows that instead of their self-knowledge about
the language their region also effects the skill which help them
while doing the act of forgery which is not seen in the forged
writing of Sikkim population as their region in not that kind of
population as Kashmir have. So, Sikkim population were more
emphasised on letter formation while doing forgery which
cause unnatural appearance in their samples and also shows
patching, retouching and overwriting in their forged samples.
Conflict of Interest :
No potential conflict of interest reported by the authors.
Source of funding : NIL
154
Fig. 3: Comparative analysis of forged signature written by Kashmir & Sikkim Population.
Fig-1 Docucenter Nirvis Fig-2 Docubox HD
Kashmir RegionFeatures taken for analysis
S.No.
Unnatural appearance
Line quality
Absence of rhythm
Patching, Retouching & overwriting
Emphasis on letter formation
1
2
34
5
Forged signature features
14% shows Unnatural appearance
98% Changed from original signature
58% don't have rhythms
12% found patching, Retouching & overwriting
32% emphasised on letter formation
Table 1: Analysis of Signature Written by Kashmir Region Population.
Features taken for analysis
S.No.
Unnatural appearance
Line quality
Absence of rhythm
Patching, Retouching & overwriting
Emphasis on letter formation
1
2
34
5
Forged signature features
55% shows Unnatural appearance
100% Changed from original signature
100% don't have rhythms
40% found patching, Retouching & overwriting
66% emphasised on letter formation
Table 2 : Analysis of signature written by Sikkim region population.
Sikkim Region
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00028.5

REFERENCES :
1. Koppenhaver KM. Forensic document examination:
principles and practice: Springer Science & Business
Media; 2007.
2. Huber RA, Headrick AM. Handwriting identification:
facts and fundamentals: CRC press; 1999.
3. Sharma B. Handwriting forensic2018. 341-59 p.
4. Puri D. Study of a copied forgery. Journal of Security
Administration. 1980;3(2):79-87.
5. Chen H-C. Forged Handwriting Detection,”. Proceedings
of Student Research Day, CSIS, Pace University.
2003:9.1-9.6.
6. Pervouchine V, Leedham G. Extraction and analysis of
forensic document examiner features used for writer
identification. Pattern Recognition. 2007;40(3):1004-13.
7. Razzak MI, Sher M, Hussain S. Locally baseline
detection for online Arabic script based languages
character recognition. International Journal of Physical
Sciences. 2010;5(7):955-9.
8. Dewhurst TN, Ballantyne, K. N., & Found, B. Exploring
the significance of pen lifts as predictors of signature
simulation behaviour. . Journal of the American Society of
Questioned Document Examiners. 2015;18(2):3–16.
9. Projectina. Docucenter Nirvis 2020. Available from:
https://www.assing.it/wp-content/ uploads/ 2017/ 04/
dc_nirvis.pdf.
10. U l t r a . D o c u b o x H D 2 0 2 0 . Av a i l a b l e f r o m :
https://www.ultra-forensictechnology.com/en/our-
products/document-examination/docubox-hd.
155
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00028.5

Original Research Paper
INTRODUCTION :
The Urdu language is originated in north India in 12th century.
It is influenced by four different languages i.e. Persian, Arabic,
Turkish and Hindi. Due to similarity in grammar with Hindi
language, Urdu language is referred as sister language of
Hindi. During 14th century the Urdu language used for official
work & literature. After partition of India & Pakistan in 1947 (1)Urdu language was chosen as official language in India . In
present, there are almost 26Lakh people in Delhi who have a
knowledge of Urdu language which is around 14% of the total (2)population of Delhi . When we take under consideration of
forgery of Urdu language then still maximum population are
unknown about the script and rules of writing to this language.
So, when we study the writing habit of unknown Urdu writer
which we generally got in case of forgery which is done for
some mean purpose, then many of the characteristic been
found which shows their knowledge of Urdu script. Apart from (3)the characteristic of forgery which is commonly found in any
forgery case of any language some new characteristic are
found like many of them don't focus on the starting point of
letters and some knows that Urdu is written from right to left so
they start from right to left point but at the time of formation of
letters in the middle of any signature of sentence they only
focus on pictorial effect and forget to focus on initial or
commencement of letters. In the below study we focused on
the characteristic of forgery and also some of the new criteria
which can be only found in forgery of Urdu language and
which also establish the fact that forgery of Urdu signature or
writing done by any population also shows the knowledge of
that population in language. Pervouchine & Leedham shows in
their studies that when we take single character its shows less
discr iminat ion but in the combinat ion of le t ters
discriminations are more which shows writing in forgery also (4)effected by the adjacent letters and combination of letters .
Razzak & Hussain also studied different style of Arabic
language with the help of local base-line and primary base-(5)line .
KEYWORDS : Forensic Science, Urdu script, Forgery, Tremors, Docucenter Nirvis, Docubox HD, handwriting characteristics.
ABSTRACT :
Introduction: Urdu is considered as one of the official languages of Delhi and used in almost all official old documents.
Materials and Methods: In this study we find out the common characteristics features of forged Urdu signature written by Urdu
Unknown Population of Delhi. The considered population is a group of people who are graduate by educational qualification and
know at least Hindi & English language. For better & conclusive result 100 sample of forged Urdu writings/signatures were taken
from the group of people by showing them sample Urdu signature. Tremors, Movement, Strokes, Speed, Connectivity of letters and
Alignment are the parameters which were consider for examination, also some of the instruments like Docucenter Nirvis works on
software PIA 7000, Docubox HD works on software PIA 7000, Different Magnifying Glasses etc were used.
Results :The analysis revels that the unknown writer of Urdu script initiated the formation of letters in a mixed movement which
shows in some letter's writers started from left to right and some letters they started from right to left. Whereas, Urdu is always
written from right to Left. Also, pen pressure is extremely high, the width of stroke is comparatively thick. This identification is
based upon basic characteristic of forgery and Urdu letter formation.
Forensic Characteristic Identification of Forged Urdu Signature Written By
Population of Delhi Who Are Stranger To The Language.
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00029.7
156
1. Syed Ahmar Ali Hashmi, Ph.D. Scholar, Galgotias University, Greater Noida & Junior Forensic/Assistant Chemical Examiner (Documents), Forensic Science Laboratory, Govt. of NCT of Delhi, India.
2. Shalvi Upadhyay, Assistant Professor & Coordinator, Forensic Science Department, Sharda University, Greater Noida, India.3. Rajeev Kumar, Associate Professor, Galgotias University, Greater Noida, India.
Corresponding Author:
Dr. Rajeev Kumar,
Associate Professor,
Galgotias University, Greater Noida, India
Contact : +91 94119-23188
Email : [email protected]
Article History :
Received : 15 July 2020
Received in revised form : 25 July 2020
Accepted on : 25 July 2020
Available online : 31August 2021
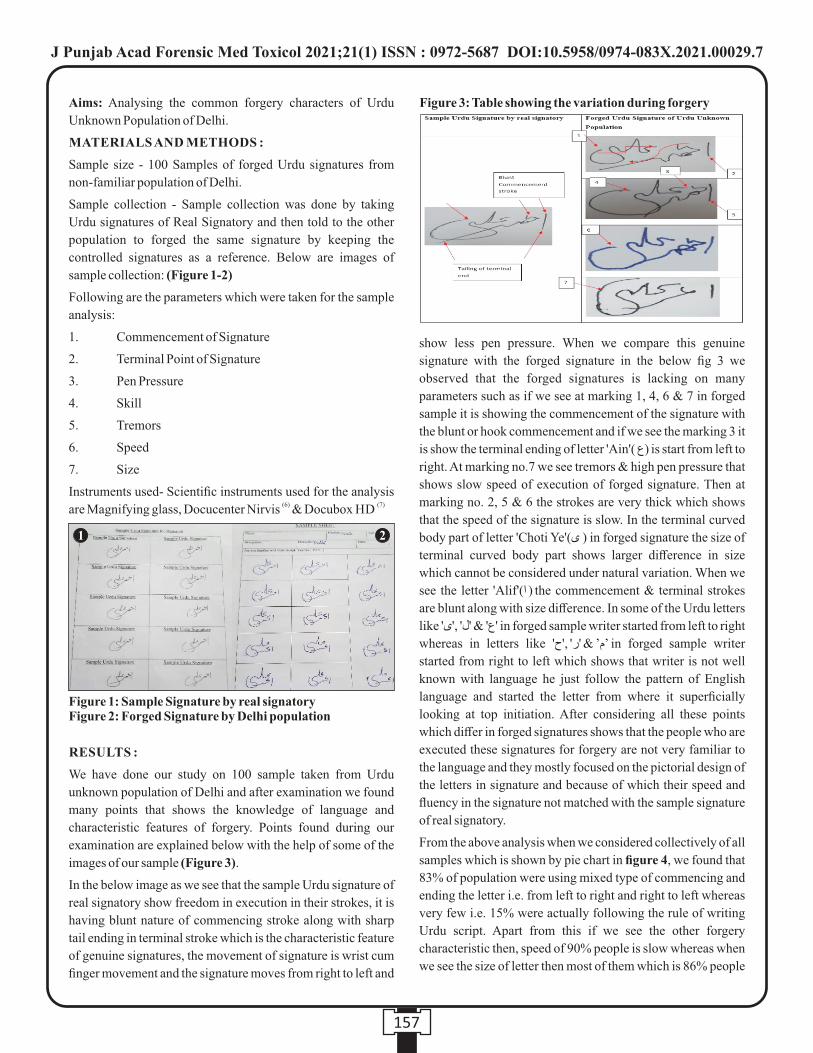
Aims: Analysing the common forgery characters of Urdu
Unknown Population of Delhi.
MATERIALS AND METHODS :
Sample size - 100 Samples of forged Urdu signatures from
non-familiar population of Delhi.
Sample collection - Sample collection was done by taking
Urdu signatures of Real Signatory and then told to the other
population to forged the same signature by keeping the
controlled signatures as a reference. Below are images of
sample collection: (Figure 1-2)
Following are the parameters which were taken for the sample
analysis:
1. Commencement of Signature
2. Terminal Point of Signature
3. Pen Pressure
4. Skill
5. Tremors
6. Speed
7. Size
Instruments used- Scientific instruments used for the analysis (6) (7)are Magnifying glass, Docucenter Nirvis & Docubox HD
RESULTS :
We have done our study on 100 sample taken from Urdu
unknown population of Delhi and after examination we found
many points that shows the knowledge of language and
characteristic features of forgery. Points found during our
examination are explained below with the help of some of the
images of our sample (Figure 3).
In the below image as we see that the sample Urdu signature of
real signatory show freedom in execution in their strokes, it is
having blunt nature of commencing stroke along with sharp
tail ending in terminal stroke which is the characteristic feature
of genuine signatures, the movement of signature is wrist cum
finger movement and the signature moves from right to left and
show less pen pressure. When we compare this genuine
signature with the forged signature in the below fig 3 we
observed that the forged signatures is lacking on many
parameters such as if we see at marking 1, 4, 6 & 7 in forged
sample it is showing the commencement of the signature with
the blunt or hook commencement and if we see the marking 3 it
is show the terminal ending of letter 'Ain'( ع) is start from left to
right. At marking no.7 we see tremors & high pen pressure that
shows slow speed of execution of forged signature. Then at
marking no. 2, 5 & 6 the strokes are very thick which shows
that the speed of the signature is slow. In the terminal curved
body part of letter 'Choti Ye'(ى ) in forged signature the size of
terminal curved body part shows larger difference in size
which cannot be considered under natural variation. When we
see the letter 'Alif'(ا ) the commencement & terminal strokes
are blunt along with size difference. In some of the Urdu letters
like 'ع' & 'ل' ,'ى' in forged sample writer started from left to right
whereas in letters like 'م’ & 'ر' ,'ح’ in forged sample writer
started from right to left which shows that writer is not well
known with language he just follow the pattern of English
language and started the letter from where it superficially
looking at top initiation. After considering all these points
which differ in forged signatures shows that the people who are
executed these signatures for forgery are not very familiar to
the language and they mostly focused on the pictorial design of
the letters in signature and because of which their speed and
fluency in the signature not matched with the sample signature
of real signatory.
From the above analysis when we considered collectively of all
samples which is shown by pie chart in figure 4, we found that
83% of population were using mixed type of commencing and
ending the letter i.e. from left to right and right to left whereas
very few i.e. 15% were actually following the rule of writing
Urdu script. Apart from this if we see the other forgery
characteristic then, speed of 90% people is slow whereas when
we see the size of letter then most of them which is 86% people
157
Figure 1: Sample Signature by real signatory Figure 2: Forged Signature by Delhi population
1 2
Figure 3: Table showing the variation during forgery
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00029.7
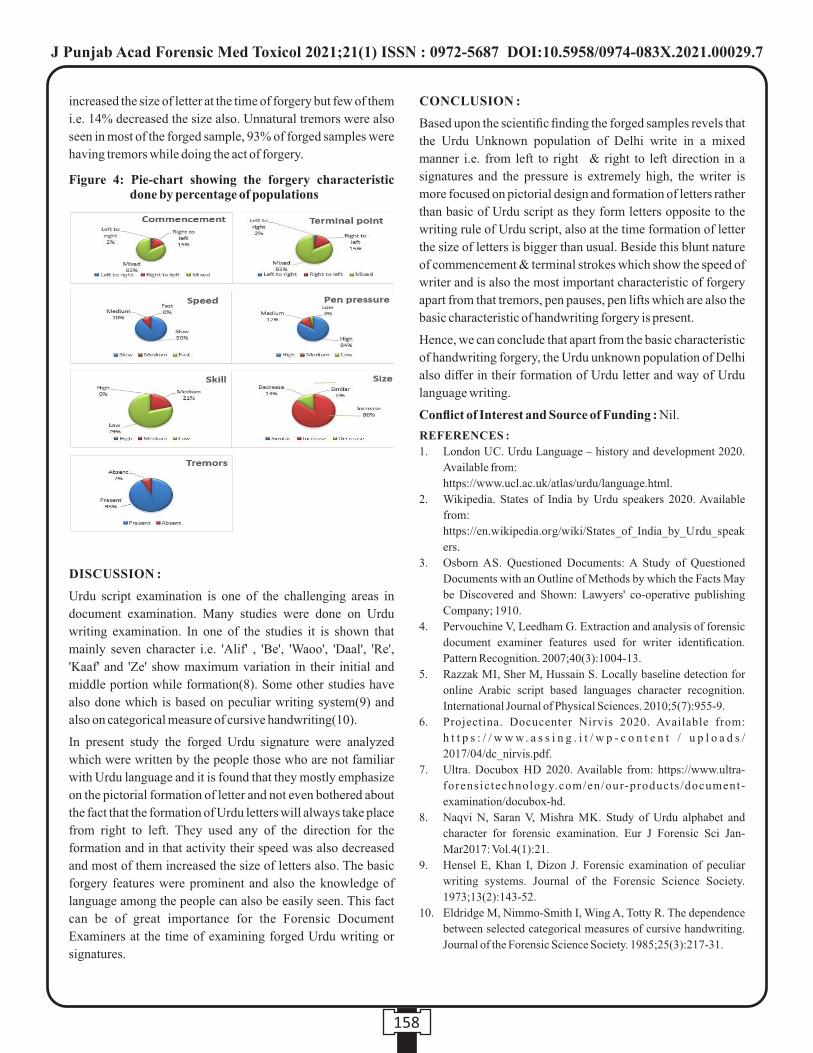
increased the size of letter at the time of forgery but few of them
i.e. 14% decreased the size also. Unnatural tremors were also
seen in most of the forged sample, 93% of forged samples were
having tremors while doing the act of forgery.
DISCUSSION :
Urdu script examination is one of the challenging areas in
document examination. Many studies were done on Urdu
writing examination. In one of the studies it is shown that
mainly seven character i.e. 'Alif' , 'Be', 'Waoo', 'Daal', 'Re',
'Kaaf' and 'Ze' show maximum variation in their initial and
middle portion while formation(8). Some other studies have
also done which is based on peculiar writing system(9) and
also on categorical measure of cursive handwriting(10).
In present study the forged Urdu signature were analyzed
which were written by the people those who are not familiar
with Urdu language and it is found that they mostly emphasize
on the pictorial formation of letter and not even bothered about
the fact that the formation of Urdu letters will always take place
from right to left. They used any of the direction for the
formation and in that activity their speed was also decreased
and most of them increased the size of letters also. The basic
forgery features were prominent and also the knowledge of
language among the people can also be easily seen. This fact
can be of great importance for the Forensic Document
Examiners at the time of examining forged Urdu writing or
signatures.
CONCLUSION :
Based upon the scientific finding the forged samples revels that
the Urdu Unknown population of Delhi write in a mixed
manner i.e. from left to right & right to left direction in a
signatures and the pressure is extremely high, the writer is
more focused on pictorial design and formation of letters rather
than basic of Urdu script as they form letters opposite to the
writing rule of Urdu script, also at the time formation of letter
the size of letters is bigger than usual. Beside this blunt nature
of commencement & terminal strokes which show the speed of
writer and is also the most important characteristic of forgery
apart from that tremors, pen pauses, pen lifts which are also the
basic characteristic of handwriting forgery is present.
Hence, we can conclude that apart from the basic characteristic
of handwriting forgery, the Urdu unknown population of Delhi
also differ in their formation of Urdu letter and way of Urdu
language writing.
Conflict of Interest and Source of Funding : Nil.
REFERENCES :
1. London UC. Urdu Language – history and development 2020.
Available from:
https://www.ucl.ac.uk/atlas/urdu/language.html.
2. Wikipedia. States of India by Urdu speakers 2020. Available
from:
https://en.wikipedia.org/wiki/States_of_India_by_Urdu_speak
ers.
3. Osborn AS. Questioned Documents: A Study of Questioned
Documents with an Outline of Methods by which the Facts May
be Discovered and Shown: Lawyers' co-operative publishing
Company; 1910.
4. Pervouchine V, Leedham G. Extraction and analysis of forensic
document examiner features used for writer identification.
Pattern Recognition. 2007;40(3):1004-13.
5. Razzak MI, Sher M, Hussain S. Locally baseline detection for
online Arabic script based languages character recognition.
International Journal of Physical Sciences. 2010;5(7):955-9.
6. Projectina. Docucenter Nirvis 2020. Available from:
h t t p s : / / w w w. a s s i n g . i t / w p - c o n t e n t / u p l o a d s /
2017/04/dc_nirvis.pdf.
7. Ultra. Docubox HD 2020. Available from: https://www.ultra-
forensictechnology.com/en/our-products/document-
examination/docubox-hd.
8. Naqvi N, Saran V, Mishra MK. Study of Urdu alphabet and
character for forensic examination. Eur J Forensic Sci Jan-
Mar2017: Vol.4(1):21.
9. Hensel E, Khan I, Dizon J. Forensic examination of peculiar
writing systems. Journal of the Forensic Science Society.
1973;13(2):143-52.
10. Eldridge M, Nimmo-Smith I, Wing A, Totty R. The dependence
between selected categorical measures of cursive handwriting.
Journal of the Forensic Science Society. 1985;25(3):217-31.
158
Figure 4: Pie-chart showing the forgery characteristic done by percentage of populations
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00029.7

159
Original Research Paper
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00030.3
1. Latif Rajesh Johnson, Assistant Professor*
2. Ranjit Immanuel James, Assistant Professor*
*Department of Forensic Medicine & Toxicology, Christian Medical College Vellore, Tamil Nadu
Key words: Assessment, Classroom response system, Clickers, Didactic lecture, Medical education
Corresponding Author:
Dr. Ranjit Immanuel James,
Assistant Professor,
Department of Forensic Medicine & Toxicology, Christian
Medical College Vellore, Tamil Nadu
Contact : +91 81056-94947
Email: [email protected]
Article History :
Received : 4 November 2020
Received in revised form : 16 April 2021
Accepted on : 16 April 2021
Available online : 31August 2021
INTRODUCTION :
Since time immemorial, knowledge has been passed from one
generation to the next. Like all other professions, healers and
physicians have also imparted their knowledge and skills to
students or apprentices. Many different techniques have been
developed and used by teachers over centuries to help teach
their students. Similarly, many techniques have also been
developed to assess if the student has learnt or acquired
knowledge and skill.
The traditional, didactic lecture is the most common teaching
tool in medical education. Didactic lecture is a time efficient
and economical way to teach concepts in medicine to large
groups of students. However, they have their drawbacks.
Medical students may find them very unidirectional, passive
and even monotonous. Despite the best efforts of the teacher 1,2
to encourage students to focus and understand the core
concepts, the lecture may not always suit the learning needs of
all students.3
Modern day medical education has evolved to demand a lot
from both the student and the teacher. The medical teacher has
to not only take a class but also keep the class fresh, relevant
and interesting for the students. Medical students are
increasingly comfortable with technology and interactive
content. They often find it challenging to maintain
concentration during a class. Engaging a class during a lecture
is an even bigger challenge when the number of students is
very high, often 200 to 250 students in a batch. Encouraging
active learning and making teaching sessions engaging is now
of great interest to educators.4-7
Teachers often use basic methods of instant evaluation like a
simple show of hands as an agree or disagree response to a
question. Others have used colour coded flashcards with each
colour corresponding to a particular option in a multiple-
choice question (MCQ). The use of “clickers”, which are small
hand-held devices that students can use to respond to
questions, posed during a teaching session is fast gaining wide
popularity.
Clickers in Medical Education – Boon or Bane?
ABSTRACT :
Introduction: Modern-day medical education has evolved to demand a lot from both the student and the educator. The medical
teacher has to not only take a class but also keep the class fresh, relevant and interesting for the students. Despite the best efforts of
the teacher to engage the students, the traditional didactic lecture may fall short in holding their attention. Classroom response
system (CRS) like “clickers” provide an accessible means of assessing students and also provide immediate feedback.
Methodology: The authors used the clickers during theory classes in the form of pre- and post-lecture tests, and as monthly exams
of Forensic Medicine & Toxicology. Towards the end of their Forensic Medicine & Toxicology curriculum, the students were asked
to give their feedback anonymously in the form of a 5 point Likert scale. Ninety-four students submitted the feedback, which was
then analysed.
Results: Although 77.7% of students agreed that the clicker-based tests were far less stressful than conventional written tests, only
49.9% felt that clicker-based tests were more convenient. 56.4% thought that the clicker-based tests removed variability between
the examiners. 45.7% felt that adequate assessments were conducted over the duration of their course and 73.3% felt they had
sufficient preparation time. From a technical standpoint, 69.2% students faced a glitch at least once during the clicker-based tests.
Conclusion: Clickers can be a useful teaching tool, especially when used to review performance and give immediate feedback
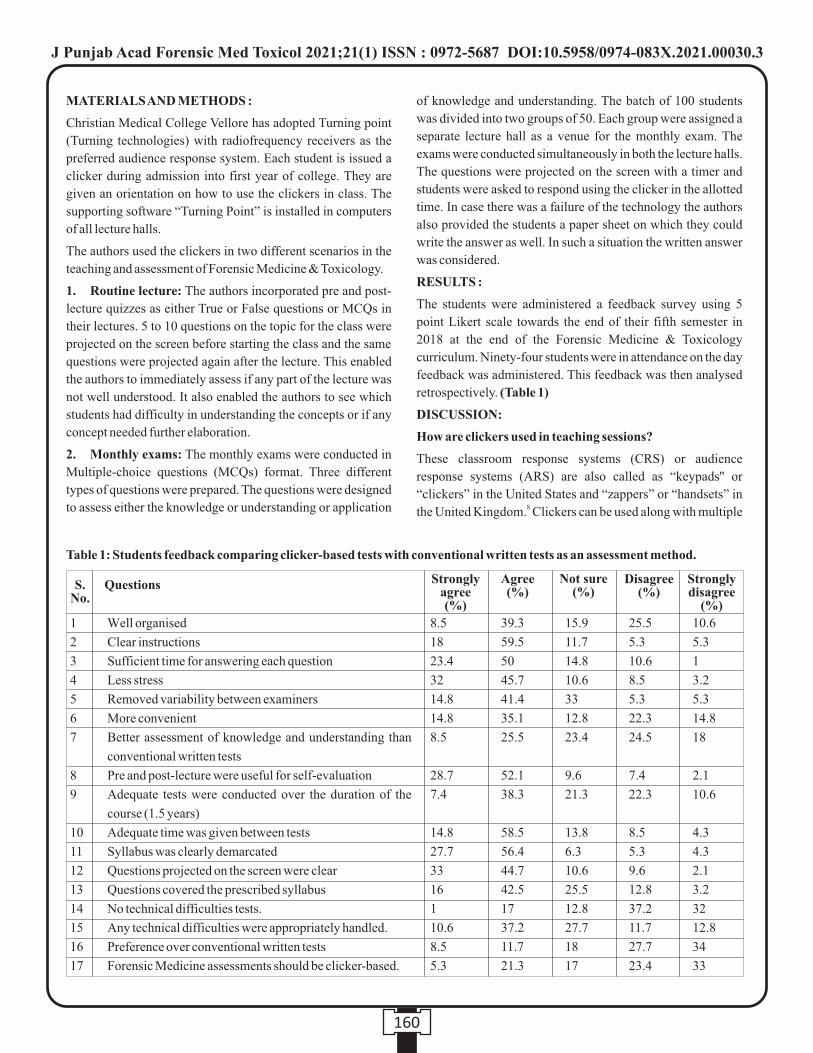
160
MATERIALS AND METHODS :
Christian Medical College Vellore has adopted Turning point
(Turning technologies) with radiofrequency receivers as the
preferred audience response system. Each student is issued a
clicker during admission into first year of college. They are
given an orientation on how to use the clickers in class. The
supporting software “Turning Point” is installed in computers
of all lecture halls.
The authors used the clickers in two different scenarios in the
teaching and assessment of Forensic Medicine & Toxicology.
1. Routine lecture: The authors incorporated pre and post-
lecture quizzes as either True or False questions or MCQs in
their lectures. 5 to 10 questions on the topic for the class were
projected on the screen before starting the class and the same
questions were projected again after the lecture. This enabled
the authors to immediately assess if any part of the lecture was
not well understood. It also enabled the authors to see which
students had difficulty in understanding the concepts or if any
concept needed further elaboration.
2. Monthly exams: The monthly exams were conducted in
Multiple-choice questions (MCQs) format. Three different
types of questions were prepared. The questions were designed
to assess either the knowledge or understanding or application
of knowledge and understanding. The batch of 100 students
was divided into two groups of 50. Each group were assigned a
separate lecture hall as a venue for the monthly exam. The
exams were conducted simultaneously in both the lecture halls.
The questions were projected on the screen with a timer and
students were asked to respond using the clicker in the allotted
time. In case there was a failure of the technology the authors
also provided the students a paper sheet on which they could
write the answer as well. In such a situation the written answer
was considered.
RESULTS :
The students were administered a feedback survey using 5
point Likert scale towards the end of their fifth semester in
2018 at the end of the Forensic Medicine & Toxicology
curriculum. Ninety-four students were in attendance on the day
feedback was administered. This feedback was then analysed
retrospectively. (Table 1)
DISCUSSION:
How are clickers used in teaching sessions?
These classroom response systems (CRS) or audience
response systems (ARS) are also called as “keypads'' or
“clickers” in the United States and “zappers” or “handsets” in
the United Kingdom. Clickers can be used along with multiple 8
Well organised
Clear instructions
Sufficient time for answering each question
Less stress
Removed variability between examiners
More convenient
Better assessment of knowledge and understanding than
conventional written tests
Pre and post-lecture were useful for self-evaluation
Adequate tests were conducted over the duration of the
course (1.5 years)
Adequate time was given between tests
Syllabus was clearly demarcated
Questions projected on the screen were clear
Questions covered the prescribed syllabus
No technical difficulties tests.
Any technical difficulties were appropriately handled.
Preference over conventional written tests
Forensic Medicine assessments should be clicker-based.
8.5
18
23.4
32
14.8
14.8
8.5
28.7
7.4
14.8
27.7
33
16
1
10.6
8.5
5.3
39.3
59.5
50
45.7
41.4
35.1
25.5
52.1
38.3
58.5
56.4
44.7
42.5
17
37.2
11.7
21.3
15.9
11.7
14.8
10.6
33
12.8
23.4
9.6
21.3
13.8
6.3
10.6
25.5
12.8
27.7
18
17
25.5
5.3
10.6
8.5
5.3
22.3
24.5
7.4
22.3
8.5
5.3
9.6
12.8
37.2
11.7
27.7
23.4
10.6
5.3
1
3.2
5.3
14.8
18
2.1
10.6
4.3
4.3
2.1
3.2
32
12.8
34
33
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
Questions S.No.
Strongly agree (%)
Agree (%)
Not sure (%)
Disagree (%)
Strongly disagree
(%)
Table 1: Students feedback comparing clicker-based tests with conventional written tests as an assessment method.
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00030.3

161
choice questions (MCQ) to independently assess students
understanding in real-time during a class. The responses can
be recorded in real time and the results can be displayed if
needed, making the class more engaging. This method of
assessment encourages the student to commit to an answer,
thus promoting engagement in both the assessment process
and subsequent feedback. Such an assessment provides the 9-12
teacher with a chance to identify students who are struggling
with understanding concepts, allowing an opportunity for
clarifications. The electronic classroom response systems 13
have other advantages such as anonymity of respondents and
storage of data for future reference. Towards this end, the
authors have used CRS during lectures in the form of pre-test
and post- tests and to conduct monthly examinations.
A student responds to a question projected on a screen using the
clicker which transmits the information to a receiver connected
to a computer. The software on the computer records the results
and collates the data, allowing the teacher to get real-time
information. The first-generation clicker only had a single
button for response. The latest versions of the clickers have a 14
10-digit alpha-numeric keypad, screen, accessory functions
keys, power button, and channel button which permit text
entries. The earliest generations of clickers were connected by
wires to the computer but the latest versions are wireless and
they transmit their response either by radiofrequency (RF)
signals or infrared (IR). The radiofrequency signals require a
single receiver, don't interfere with other IR emitting devices
and don't need a direct line of sight between the receiver and
the student.
Each student is assigned a clicker with a unique ID, thus the
response from each student can recorded and identified
accurately by using the clicker ID. Once the polling or time to
respond to the questions is over, the teacher can choose to
display the correct response and the percentage of various
responses on the screen in the form of a bar diagram or other
such representations. Some software offer more sophisticated
analysis of the responses, and most setups are easy to use with 15
intermediate computer skills.
Are clickers necessary for interactive teaching sessions?
There is increasing use of technology in classes and it is
worthwhile using technology in the classroom when it
addresses a specific instructional requirement. This is 16
certainly relevant when simple technology can be used to
overcome difficulties and maximize the potential of traditional
delivery. Many institutions have adopted the use of clickers
with hoping to address the lofty attrition rates of didactic
lectures.17
Studies show that students recall the initial five minutes of a
lecture the most. We can use clickers to leverage this time and 18
attempt to engage the students and emphasize the important
concept. This activity during the initial period, can make the
students attentive for the rest of the session. Studies have 19
shown that the use of clickers have enhanced the engagements
of the students in the classroom. 20-23
The anonymity granted to students by using clickers is
probably another benefit. Even a student who is shy and does
not normally engage with the teacher in the class, can use the
clicker to participate in the class and can also assess where they
are in comparison to the rest of the class. This helps them gain
confidence. Clickers give students the opportunity to
independently assess their understanding of core concepts in a
non-threatening manner. According to a study conducted by
Caldwell, students were twice as likely to respond to a question
if the mode of submitting answers is through clickers. Some 12
studies suggest that higher order of learning is due to classroom
participation and interaction, as peer discussions also
encourage peer learning. However, many studies have 24,25
shown that the use of clickers may potentially decrease the
time available for the lecture. Their application in clinical 26
teaching is also becoming common and studies have shown
their use to be beneficial due to their ability to increase student
interaction and to promote knowledge retention.27-30
What can clickers be used for?
1. To initiate or increase interaction with students: The
teacher can use questions which focus on or start
discussions, or questions which require peer 31-33interactions. The teacher can also use open ended
questions to get feedback on a particular question
2. To evaluate the preparedness of the student and ensure
accountability: The teacher can give homework or self-
directed learning assignment to the students. A quick quiz
or poll can be conducted before the next class to assess the
students on that topic. This will ensure that the student is 32accountable for completing the assignment.
3. To assess the students' knowledge
i. Conduct a Pre-test to assess the pre-existing
knowledge on the topic.
ii. Conduct a Post-test after the class to assess the change
in knowledge.
iii. Higher order questions can be designed and
administered using clicker.
iv. Open ended questions requiring short answers can be
asked.
4. For quiz programs: Clickers can be used to conduct
quizzes among students. Depending on the question it can
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00030.3
162
determine the active thinking process or reasoning skills of the 33 students. Analysis of the student feedback shows that a
majority of the students felt that the clicker-based tests were
well organised. The students also agree they were given clear
instructions regarding the use of clickers and the nature of the
assessments. 73.4% of the students also concurred that they
were given sufficient time to answer questions during the
clicker-based tests.
A better part of the class, (77.7%) agreed that the clicker-based
tests were far less stressful than written tests. Surprisingly, only
half the students (49.9%) felt that clicker-based tests were
more convenient than conventional written tests. Although
more than half the students (56.4%) thought that the clicker-
based tests removed variability between the examiners, almost
a third of them were not sure. Less than half the students
(45.7%) felt that adequate assessments were conducted over
the duration of their course and nearly three-fourth of them
(73.3%) felt they had sufficient preparation time.
Studies suggest that using clickers in a lecture can transform a
didactic lecture into a discussion-style session, with the 11responses via clicker facilitating deeper discussions.
Unfortunately, the time taken for discussion may not leave
sufficient time for covering all the topics unless the class is
planned meticulously. Now, contrary to the other studies,
almost two-third of the students did not have a positive
response regarding understanding of the topic being covered.
In fact, 42.5% of the students felt that knowledge retention and
understanding were better during conventional written tests.
Although an overwhelming majority of them (80.8%) agree
that clicker-based tests were the ideal tools for self-evaluation.
From a technical standpoint, 69.2% students faced a glitch at
least once during the clicker-based tests, although, most of
them agreed that they were promptly assisted by the teaching
faculty. A concern raised by the students was that the
University examinations are in the conventional written
format, so they would rather familiarize themselves with that
pattern of assessment. These factors probably are a reason why
two-third of the students (61.7%) preferred conventional
written tests.
Advantages of using clickers:
a. Real time and instant evaluation are possible
b. Active participation from students
c. Detailed statistical analysis possible
d. No need for attendance as their clicker IDs can be matched
with their names
e. Multiple options are available:
i. First response only (if a student once responds he/she
cannot change their answer)
ii. Timer function for every question (polling will stop
as soon as the timer ends)
iii. Colour coding or highlighting the correct answers
iv. Hiding the response results in histogram
f. Manual evaluation is not needed
g. Data can be analysed in many ways. For example:
question to question based (comparative results will show
whether students correct their mistakes after the lecture),
question to student based, etc.
h. While taking a poll in the class, the anonymous nature of
responses encourages shy students to participate.
i. Instant feedback can be given based on the responses
recorded.
j. It saves a lot of time since the evaluation and analysis of
the result is automatic.
k. The data can be exported into excel for documentation
Disadvantages of using clickers:
a. The students or the college have to purchase the clickers
and the receivers
b. Some basic computer knowledge is needed by the teacher
to use the software
c. Despite your best effort technical errors may still happen
d. The battery in the clicker can run out and hence the student
should check the clicker prior to every exam.
e. It is possible that one receiver may receive responses from
another hall if both the halls are using the same channel
number. The authors have faced such difficulties during
one of the examinations.
f. Clicker-based tests is not congruent with current
University examinations, which is based on conventional
written tests.
Alternative to using clickers: The ongoing pandemic has put
a fresh emphasis on technological assistance for taking classes.
One of the developments that has come to the fore is the use of
online polling software like poll everywhere which is available
from www.pollev.com. The poll everywhere can be
downloaded as a plugin to Microsoft PowerPoint. During an
online class using PowerPoint all participants can log onto
www.pollev.com and enter responses. These responses can be
seen live on the screen in real time or can be saved for analysis
and review later.
CONCLUSION :
Several studies have questioned the effectiveness of a didactic
lecture as a teaching tool. It is often said that lectures are more
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00030.3
163
teacher-centric and that they do not promote problem solving.
It has also been said that lectures lack interaction and are not
engaging enough for students to foster their critical skills. The
Competency Based Medical Education guidelines has
significantly reduced the time allotted for didactic lectures and
is actively encouraging other forms of teaching and learning.
For the students, the sessions when clickers were used were
more enjoyable and engaging and the majority perceived the
devices to have a positive impact on their self-evaluation.
Various studies have shown, the positive effects of clicker
usage surpass their disadvantages. Though there are technical
aspects to consider for the usage of clickers on a regular basis,
it is evident that clickers positively influence the student
response rates and drastically minimizes the time required for
assessment. Furthermore, the anonymity offered to students
by clickers encourage inclusion and engagement. In
conclusion, clickers can be a useful teaching tool, especially
when used to review performance and give immediate
feedback.
Acknowledgement: The authors would like to thank Dr.
Daniel Manoj for his critical inputs and valuable insights.
Ethical Committee Clearance: Approved by Institutional
Review Board
Funding: None
Conflict of interest: None
REFERENCES :
1. Mascolo MF. Beyond student-Centered and teacher-
Centered pedagogy:teaching and learning as guided
participation. Pedagogy Human Sci.2009;1(1):3–37.
2. Young MS, Robinson S, Alberts P. Students pay attention!
Act Learn High Educ. 2009;10(1):41–55.
3. Mattick K, Crocker G, Bligh J. Medical student
attendance at noncompulsory lectures. Adv Health Sci
Educ Theory Pract. 2007;12(2):201–10.
4. Courtier J, Webb EM, Phelps AS, Naeger DM. Assessing
the learning potential of an interactive digital game versus
an interactive-style didactic lecture: the continued
importance of didactic teaching in medical student
education. Pediatr Radiol. 2016;46(13):1787–96.
5. Duggan PM, Palmer E, Devitt P. Electronic voting to
encourage interactive lectures: a randomised trial. BMC
Med Edu. 2007;7:25.
6. Palocaren J, Pillai LS, Celine TM. Medical biochemistry:
is it time to change the teaching style? Natl Med J India.
2016;29(4):222–4.
7. Dhaliwal HK, Allen M, Kang J, Bates C, Hodge T. The
effect of using an audience response system on learning,
motivation and information retention in the orthodontic
teaching of undergraduate dental students: a cross-over
trial. J Orthod. 2015;42(2):123–35.
8. D'Inverno R. Using a personal response system for
promoting student interaction. Teach Math Appl Int J
IMA. 2003;22(4):163–9.
9. Wit E. Who wants to be… The Use of a Personal Response
System in Statistics Teaching. MSOR connect.
2003;3(2):14–20.
10. Beatty ID. Transforming student learning with classroom
communication systems [Internet]. arXiv [physics.ed-
ph]. 2005. Available from:
http://arxiv.org/abs/physics/0508129
11. Beatty ID, Gerace WJ, Leonard WJ, Dufresne RJ.
Designing effective questions for classroom response
system teaching. Am J Phys. 2006;74(1):31–9
12. Caldwell JE. Clickers in the large classroom: current
research and best-practice tips. CBE Life Sci Educ. 2007
Spring;6(1):9–20.
13. Lang J. Metacognition and Student Learning [Internet].
The Chronicle of Higher Education. 2012 [cited 29
October 2020]. Available from:
https://www.chronicle.com/article/metacognition-and-
student-learning/
14. Poulis J, Massen C, Robens E, Gilbert M. Physics
lecturing with audience paced feedback. Am. J. Phys.
1998;66(5):439-441.
15. Roschelle J, Penuel WR, Abrahamson L. The networked
classroom. Educ. Leadership. 2004;61(5):50-54.
16. Draper S. Niche-based success in CAL. Comput. Educ.
1998;30(1):5-8.
17. Burnstein RA, Lederman LM. Using wireless keypads in
lecture classes. Phys Teach. 2001;39(1):8–11.
18. Burns RA. (1985). Information Impact and Factors
Affecting Recall. Presented at Annual National
Conference on Teaching Excellence and Conference of
Administrators, Austin, TX, May 22–25, 1985. Available
from: https://eric.ed.gov/?id=ED258639
19. Elliott C. Using a personal response system in economics
teaching. Int Rev Econ Educ. 2003;1(1):80–6.
20. MacGeorge E, Homan SR, Dunning JB, Elmore D, Bodie
GD, Evans D, Lichti S. The influence of learning
characteristics on evaluation of audience response
technology. Journal of Computing in Higher Education.
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00030.3
164
2008;19(2):25-46.
21. Boatright-Horowitz SL. Useful pedagogies or financial
hardships? Interactive response technology (clickers) in
the large college classroom. International Journal of
Teaching and Learning in Higher Education.
2009;21(3):295-298.
22. Hoffman C, Goodwin S. A clicker for your thoughts:
technology for active learning. New Libr World.
2006;107(9/10):422–33.
23. Greer L, Heaney PJ. Real-time analysis of student
comprehension: An assessment of electronic student
response technology in an introductory earth science
cour se . Jou rna l o f Geosc ience Educa t ion .
2004;52(4):345-351.
24. McKeachie W. Research on college teaching: The
historical background. Journal of Educational
Psychology. 1990;82(2):189-200.
25. Smith D. College classroom interactions and critical
thinking. Journal of Educational Psychology.
1977;69(2):180-190.
26. Simpson V, Oliver M. Electronic voting systems for
lectures then and now: A comparison of research and
practice. Australas J Educ Technol [Internet]. 2007;23(2).
Available from: http://dx.doi.org/10.14742/ajet.1264
27. Pradhan A, Sparano D, Ananth CV. The influence of an
audience response system on knowledge retention: an
application to resident education. Am J Obstetr Gynecol.
2005;193(5):1827–30.
28. Schackow TE, Chavez M, Loya L, Friedman M. Audience
response system: effect on learning in family medicine
residents. Fam Med. 2004;36(7):496–504.
29. Latessa R, Mouw D. Use of an audience response system
to augment interactive learning. Fam Med.
2005;37(1):12–4.
30. Mains TE, Cofrancesco Jr J, Milner SM, Shah NG,
Goldberg H. Do questions help? The impact of audience
response systems on medical student learning: a
randomised controlled trial. Postgrad Med J.
2015;91(1077):361–7.
31. Trees AR, Jackson MH. The learning environment in
clicker classrooms: student processes of learning and
involvement in large university‐level courses using
student response systems. Learn Media Technol.
2007;32(1):21–40.
32. Knight JK, Wood WB. Teaching more by lecturing less.
Cell Biol. Educ. 2005;4(1):298–310.
33. Draper S, Cargill J, Cutts Q. Electronically enhanced
classroom interaction. Aust. J. Educ. Technol.
2002;18(1):13–23.
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00030.3

Original Research Paper
Corresponding Author :
Dr. Rajinder Saini,
Post Graduates,
Department of Forensic Medicine, MMIMSR, Mullana Distt. Ambala
Contact : +91 9138149887
Email: [email protected]
KEYWORDS : Stature, Index finger, Length
Article History:Received: 30 November 2019Received in revised form: 20 December 2019Accepted on: 20 December 2019Available online: 31 August 2021
INTRODUCTION :
Identification of deceased especially in a dismembered body is
a herculean task for forensic expert and estimation of stature
helps in such cases. There is an established relationship
between stature and different parts of the body. Every body
part has a more or less constant relationship with stature. This
relationship between different body parts can help a forensic
expert to calculate stature from mutilated and dismembered
body parts in forensic examinations.
Various studies in past have utilized various body parts such as
upper and lower extremities including hand and foot 1-2dimensions for estimation of stature. Studies were also
3-conducted to estimate stature from hand and phalange lengths4 however only recently studies were conducted using finger
5-12lengths.
The formula for stature estimation has to be population
specific and there is paucity of studies on such parameters.
Thus in view of above said reasons & importance of estimation
of stature from the different body parts, the present study was
undertaken.
MATERIALS AND METHODS :
The present study was undertaken with aim of measuring the
stature from the length of right index finger on 31 male & 33
female normal healthy MBBS students of MMIMSR,
Mullana who are natives of State of Haryana (3 generations &
above).
Individuals with any musculo-skeletal deformity like
kyphosis, scoliosis, poliomyelitis, trauma, amputation
(surgical or accidental) and Individuals with nails extending
over the fingers were excluded.
Measurements: The measurements were taken at a fixed time
between 2.00 to 4.00 PM to eliminate diurnal variation and by
the same person to avoid personal error in methodology.
a) Stature (Using Stadiometer) It was measured as vertical
distance from the vertex to the foot by making the subject
to stand erect on a horizontal resting plane on the
stadiometer bare footed. Palms of hand turned inwards
and fingers horizontally pointing downwards and head
oriented in eye-ear-eye plane (Frankfurt Plane). The
movable rod of the stadiometer is brought in contact with
ABSTRACT:
Introduction: Stature is an important and useful anthropometric parameter to establish partial identity of an individual. There is an
established relationship between stature and different parts of the body which can help a forensic expert to calculate stature from
mutilated and dismembered body parts in forensic examinations.
Materials and Methods: Relationship between percutaneous length of right index finger and stature was carried out on 31 males
and 33 females students.
Results: Significant correlation exists between stature and finger length. Pearson correlation between finger length and stature was
higher among females than males.
Conclusions: These findings suggest that index finger length can be used as predictive tool for stature calculation of an individual
by Anthropologists and Forensic Medicine experts.
1. Sabina Bashir, Senior Resident, Department of Forensic Medicine & Toxicology, SKIMS Medical College and Hospital,
Bemina, Srinagar
2. Rajender Kumar Saini, Post Graduates, Department of Forensic Medicine, MMIMSR, Mullana Distt. Ambala 3. Yatiraj Singi, Associate Professor, Department of Forensic Medicine & Toxicology, SKIMS Medical College and Hospital,
AIIMS, Bilaspur (HP)
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00031.5
Correlation of Stature With Finger- Length of Native Haryana Population
165
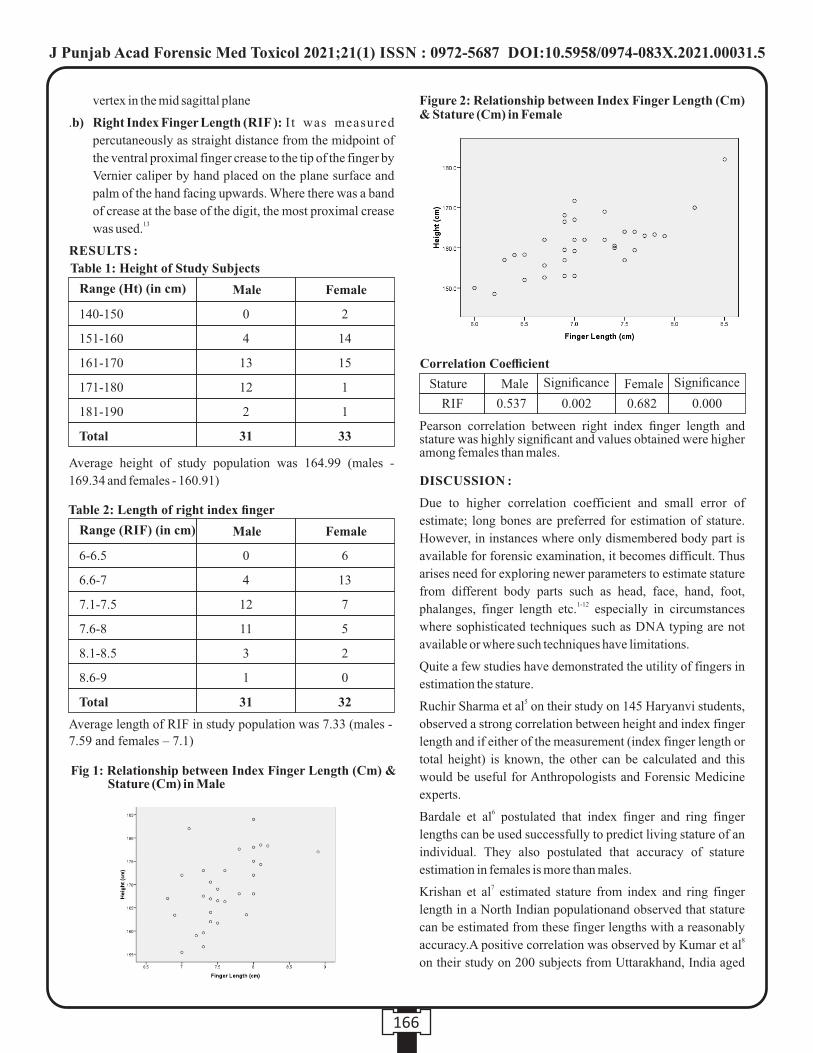
vertex in the mid sagittal plane
.b) Right Index Finger Length (RIF ): I t was measured
percutaneously as straight distance from the midpoint of
the ventral proximal finger crease to the tip of the finger by
Vernier caliper by hand placed on the plane surface and
palm of the hand facing upwards. Where there was a band
of crease at the base of the digit, the most proximal crease 13was used.
RESULTS :
DISCUSSION :
Due to higher correlation coefficient and small error of
estimate; long bones are preferred for estimation of stature.
However, in instances where only dismembered body part is
available for forensic examination, it becomes difficult. Thus
arises need for exploring newer parameters to estimate stature
from different body parts such as head, face, hand, foot, 1-12phalanges, finger length etc. especially in circumstances
where sophisticated techniques such as DNA typing are not
available or where such techniques have limitations.
Quite a few studies have demonstrated the utility of fingers in
estimation the stature.5Ruchir Sharma et al on their study on 145 Haryanvi students,
observed a strong correlation between height and index finger
length and if either of the measurement (index finger length or
total height) is known, the other can be calculated and this
would be useful for Anthropologists and Forensic Medicine
experts.6Bardale et al postulated that index finger and ring finger
lengths can be used successfully to predict living stature of an
individual. They also postulated that accuracy of stature
estimation in females is more than males.7Krishan et al estimated stature from index and ring finger
length in a North Indian populationand observed that stature
can be estimated from these finger lengths with a reasonably 8accuracy.A positive correlation was observed by Kumar et al
on their study on 200 subjects from Uttarakhand, India aged
Table 1: Height of Study Subjects
Average height of study population was 164.99 (males -
169.34 and females - 160.91)
Range (Ht) (in cm) Male
140-150
151-160
161-170
171-180
181-190
Total
0
4
13
12
2
31
2
14
15
1
1
33
Female
Range (RIF) (in cm) Male
6-6.5
6.6-7
7.1-7.5
7.6-8
8.1-8.5
8.6-9
Total
0
4
12
11
3
1
31
6
13
7
5
2
0
32
Female
Table 2: Length of right index finger
Average length of RIF in study population was 7.33 (males -
7.59 and females – 7.1)
Fig 1: Relationship between Index Finger Length (Cm) & Stature (Cm) in Male
Figure 2: Relationship between Index Finger Length (Cm) & Stature (Cm) in Female
Correlation Coefficient
Pearson correlation between right index finger length and stature was highly significant and values obtained were higher among females than males.
Stature Male Significance Female Significance
RIF 0.537 0.002 0.682 0.000
166
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00031.5

phalanges lengths of Egyptians. J Forensic Leg Med
2010;17:156-60
5. Sharma R, Dhattarwal SK; Estimation of Stature by using
Linear Regression Equation from Length of Index Finger
in Haryana Region, Int J Basic Appl Biol 2015 2(6), 430-
32
6. Bardale RV, Dahodwala TM, Sonar VD, Estimation of
Stature from Index and Ring Finger Length, JIAFM,
2013, 35(4), 353-7
7. Krishan K, Kanchan T, Asha N. Estimation of stature from
index and ring finger length in a north Indian adolescent
population. J Forensic Leg Med 2012; 19:285-90
8. Kumar L, Jain SK, Mishra P. Study of correlation between
length of thumb and stature in Uttarakhand population.
JIAFM 2012; 34:203-5
9. Shivakumar AH, Vijaynath V, Raju GM. Estimation of
correlation between middle finger length and stature of
females in Southern Indian population. Indian J Forensic
Med Toxicol. 2011; 5:75-6
10. Verghese AJ, Balraj BM, Kumar PN. A study of
estimation of stature from length of fingers in Mysore.
Indian J Forensic Med Toxicol. 2010; 4: 12-3
11. Rastogi P, Kanchan T, Menezes RG, Yoganarasimha K.
Middle finger length a predictor of stature in the Indian
population. Med Sci Law 2009; 49:123-6
12. Tyagi AK, Kohli A, Verma SK, Aggarwal BB. Correlation
between stature and finger length, Int J Medical Toxicol
Legal Med 1999; 1:20-22
13. Fink, BJ. Manning T, Neave N, Tan U; Second to fourth
digit ratio and hand skill in Austrian children. Biol.
Psychol., 67(3): 375-84
between 21 years to 30 years for correlation between length of 9thumb and stature.Shivakumar et al while studying south
Indian female students found correlation coefficient of 0.53
between middle finger length and stature.
Best finger to predict the height was proposed by Varghese et 10al who suggested that ideal finger to estimate stature in case of
males was left thumb and in females it was right thumb.Study
conducted on both north and south Indian population by 11Rastogi et al to estimate stature from middle finger,
researchers noted a positive correlation from 0.504 to 0.696 12between middle finger length and stature.Tyagi et al observed
a positive correlation between stature and finger lengths and
have suggested that index finger was best for the prediction of
stature in both males and females in Delhi population.
Results of our study are encouraging. Statistically significant
correlation was noted between length of right index finger and
stature. In female (r=0.682) the correlation was higher
compared to males (r=0.537) In other words the accuracy of
stature estimation in females is more than males.
Findings of our study are in consistency with study by Bardale 6et al who also observed higher correlation coefficient for
females than males in Maharastrian population. However, 5Ruchir et al observed exactly the opposite in Haryanvi
11population. Whereas Rastogi et al noted that statistically no
significant difference existed between the mean stature and
middle finger length of south Indian and north Indian
populations.
Thus similar studies should be encouraged in this and other
geographical areas and with different sets of populations
across various age groups so as to evaluate existence of any
population and geographical difference or not.
CONCLUSION :
Stature calculation is important mode of partial identification
and importance of stature estimation from different body part
cannot be undermined. The results of this study suggest that
(right) index finger length can be used to assess stature of an
individual.
REFERENCES :
1. Ozaslan A, Iscan MY, Ozaslan I, Tugcu H, Koc S.
Estimation of stature from body parts. Forensic Sci. Int.
2003; 132:40-5.
2. Krishan K, Sharma A. Estimation of stature from
dimensions of hand and feet in a north Indian population. J
Forensic Leg Med 2007; 14:327-32
3. Jasuja OP, Singh G. Estimation of stature from hand and
phalange length. JIAFM 2004; 26:100-6
4. Habib SR, Kamal NN. Stature estimation from hand and
167
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00031.5
Original Research Paper
INTRODUCTION :
It was reported that annually 1.24 million people die globally,
which comes to around 3400 deaths in a day due to RTI. Nearly
90% of the total road traffic mortalities occur in low- and (1) middle-income countries.
According to National Transportation Planning and Research
centre (NTPRC) of New Delhi in India for every four minutes,
a person is injured or succumbed in road accident. Around 45
percent of the accidents occur due to the negligence of the (2) drivers. There occurs an accident for every two minutes and a
(3)suicide for every five minutes in India. According to the
Indian government the estimated rate of deaths per 1000
vehicles is 1.3. In India among the total accidental deaths Road
traffic accidents comprises 37.2 % and Railway accidents -(4)7.7%. In this study the Thoraco-abdominal (TA) injuries
were compared according to age, sex, place, time, pattern of
injury, occupation, period of survival etc., after sustaining
injury. In future this information will play a significant role in
reducing morbidity and mortality and help to improve
strategies for prevention of TA injuries.
Corresponding Author :
Dr. Siddhartha Das,
Additional Professor and Head,
Jawaharlal Institute of Post Graduate Medical Education and
Research, Puducherry
Contact : +91 9445803019
Email : [email protected]
KEYWORDS : Fatal thoraco-abdominal injuries, Road traffic accidents
Article History:Received: 30 November 2019Received in revised form: 3 March 2020Accepted on: 3 March 2020Available online: 15 August 2021
ABSTRACT :
Introduction : The increase in the number of RTA is caused by the increase in the number of different types of vehicles used on
various types of roads. In India we see the transportation system is very weak because of which people started using their own
vehicles in cities as well as rural areas by which people's health has been affected.
Aims and Objectives : To describe the Pattern of TA Injuries in RTA 2. To identify the association between type of vehicle and TA
injuries.
Materials and Methods : This was a prospective descriptive study done for all the cases of RTA attending to the mortuary with TA
injuries for a period of 18 months and were either found dead on arrival or died during treatment. All the victims were autopsied at
the post-mortem centre of jipmer puducherry.
Results : In the present study there were 200 road traffic accidents with TA injury in a period of 18 months. Males outnumbered
females (81.5 % vs 18.5%) with a ratio of 4.4:1. RTAs are more commonly seen in 30-40 years age group followed by 20-30 years
and the least in 0-10 years. In the present study the un-employed n=95 (47.5%), were commonly injured with RTAs subsequently to
students (n=50, 25%).Majority of the accidents were occurred during summer season (n=73, 36.5%). In our study most of the
accidents occurred in the evening hours 13.00-18.00 (n=62, 31%) followed by 19.00-24.00 hours (n=59, 29.5%). The most
common type of vehicle involved is two wheeler vehicle (n=102, 51%).followed by light motor vehicles (n=58, 29.0%). Of all the
external injuries abrasion were most common n=176, followed by laceration n=150, contusion n=34
Conclusion : Our study displays that RTAs are a foremost concern to human life. Major thing to avoid accidents is the prevention.
In order to prevent these RTAs some interventions like restriction of speed, strict implement of helmets, graduate licensing etc.
There is a need for government to involve and strictly plan accordingly in a systematic way to reduce the problem in India.
1. B Rupesh Kumar Naik, Assistant Professor, Sri Venkateshwara Institute of Medical Sciences-SPMCW Tirupathi, Andhra
Pradesh.
2. Siddhartha Das, Additional Professor and Head*
3. Kusa Kumar Shaha, Professor*
*Jawaharlal Institute of Post Graduate Medical Education and Research, Puducherry
Pattern of Thoraco-abdominal Injuries Sustained in Road Traffic Accidents:
An Autopsy Based Observational Study
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00032.7
168
AIMS AND OBJECTIVES :
1. To describe the Pattern of TA Injuries in RTA
2. To identify the association between type of vehicle and TA
injuries.
MATERIALS AND METHODS :
Place of study : Mortuary attached to Department of Forensic
Medicine, JIPMER hospital, Pondicherry a tertiary level
health care centre.
Study design : It was a prospective descriptive study.
Study duration :18 months
(i) INCLUSION CRITERIA :
Autopsies with an alleged history of RTA with TA
injuries are included in the study.
(ii) EXCLUSION CRITERIA:
1. Autopsies with a history of RTA but having only
a) Head injuries.
b) Injuries to the extremities.
2. Fall from height.
3. Assault cases.
4. Autopsies that have no history of RTA like Burns, poisoning,
hanging, etc.
STUDY DESIGN AND ANALYSIS :
The study was conducted for a period of 18 months. After
receiving the inquest report given by the investigating officer,
the history of the case is obtained from the police personnel.
The hospital records regarding the case have gone through.
History of the case from the relatives are also recorded.
Identification of the body is done for the name, age and
identification mark present in the documents of the
investigating officer and by the relatives. A detailed external
examination was carried out with special reference to the
wounds regarding its type, dimension, direction, and site of the
wound.
An I-shaped incision is given to expose the ribs and examine
for any fractures. The thorax is first opened by disarticulating
both sternoclavicular joints and the other ribs by cutting along
the cartilaginous part of the joint lateral to costochondral
junction. The whole sternal plate is lifted and examined for any
fractures. Individually each organ is retrieved carefully and
noting any contusions, lacerations, etc. Any associated injuries
in the head, spine, pelvis, fractures of limbs are also examined.
Details regarding age, sex, date, time and the circumstances of
the incident were analysed. Concerning TA injuries, in
particular, details like fracture of the ribs, Laceration of lung,
heart, liver, kidney, etc. with gross findings were studied. A
Proforma was specially designed for this study and used for
collection of data. After collection of data analysis is done by
using SPSS-20.
RESULTS :
During the study period a total of 200 cases were analysed. A
detailed post mortem examination was conducted in these
cases at department of forensic medicine and toxicology,
JIPMER subject to inclusion and exclusion criteria.
Distribution of RTA with respect to age and gender :
In all the age group males are more commonly involved.
(Table.1) Among females > 50 age group was more commonly
affected and the least was in the 0-10 age group
Occupation of the victims
The Unemployed persons were the highest n=95 (47.5%) in
number among the 200 victims. The students were the next
highest (n=50, 25%). Labourers were 25 (12.5%), employee in
service 16 victims (8%), house wife 12 (6%).
Distribution of cases with respect to season
In this study cases are categorized into season wise as winter
(January to February), Summer (March to May), Rainy (June
to September), Post monsoon (October- December).
Maximum number of deaths were seen in the summer season
(n=73 cases, 36.5%) followed by Post monsoon (n=49 cases,
29.5%), rainy (n=46 cases, 23.0%) and the least in winter
(n=32 cases, 16%).
Distribution of cases with respect to place of death
In this study most of the victims died in hospital (n=141,
70.5%), followed by spot dead n=56, 28.0% and least (n=3,
1.5%) during transport.
Distribution of cases with respect to roads
In our study the roads have been categorized as national
highways, State highways, City roads and Village roads. It is
observed that most of the accidents occur in the state highways
(n= 82, 41.0%) followed by city roads (n=68, 34.0%), national
highways (n=32, 16.0%) and village roads (n=18, 9.0%).
169
Table 1: Distribution of RTA victims based on age and sex
Age (years)
0-10
11-20
21-30
31-40
41-50
> 50
Total
Male (%)
2 (1.2)
16 (9.8)
39 (23.9)
38 (23.3)
30 (18.4)
38 (23.3)
163
Female (%)
2 (5.4)
3 (8.1)
3 (8.1)
8 (21.6)
6 (16.2)
15 (40.5)
37
Total no of
cases (%)
4 (2)
19 (8.5)
42 (21)
46 (23)
36 (18)
56 (28)
200
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00032.7
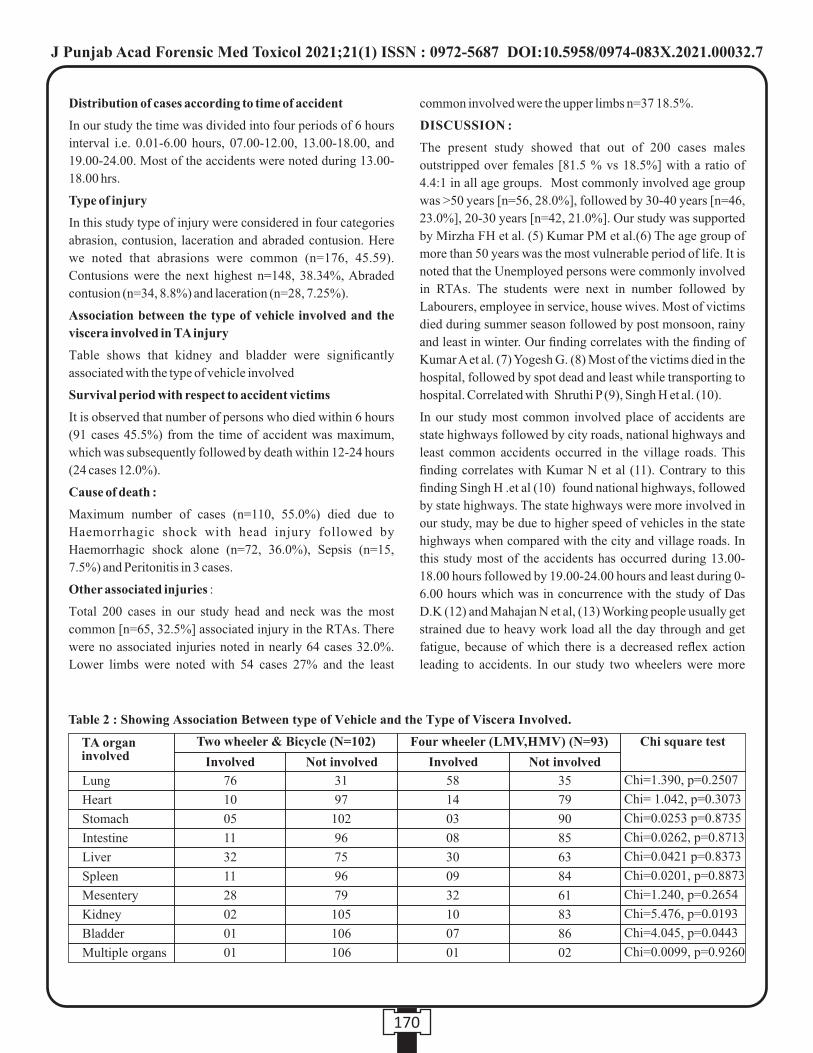
Distribution of cases according to time of accident
In our study the time was divided into four periods of 6 hours
interval i.e. 0.01-6.00 hours, 07.00-12.00, 13.00-18.00, and
19.00-24.00. Most of the accidents were noted during 13.00-
18.00 hrs.
Type of injury
In this study type of injury were considered in four categories
abrasion, contusion, laceration and abraded contusion. Here
we noted that abrasions were common (n=176, 45.59).
Contusions were the next highest n=148, 38.34%, Abraded
contusion (n=34, 8.8%) and laceration (n=28, 7.25%).
Association between the type of vehicle involved and the
viscera involved in TA injury
Table shows that kidney and bladder were significantly
associated with the type of vehicle involved
Survival period with respect to accident victims
It is observed that number of persons who died within 6 hours
(91 cases 45.5%) from the time of accident was maximum,
which was subsequently followed by death within 12-24 hours
(24 cases 12.0%).
Cause of death :
Maximum number of cases (n=110, 55.0%) died due to
Haemorrhagic shock with head injury followed by
Haemorrhagic shock alone (n=72, 36.0%), Sepsis (n=15,
7.5%) and Peritonitis in 3 cases.
Other associated injuries :
Total 200 cases in our study head and neck was the most
common [n=65, 32.5%] associated injury in the RTAs. There
were no associated injuries noted in nearly 64 cases 32.0%.
Lower limbs were noted with 54 cases 27% and the least
common involved were the upper limbs n=37 18.5%.
DISCUSSION :
The present study showed that out of 200 cases males
outstripped over females [81.5 % vs 18.5%] with a ratio of
4.4:1 in all age groups. Most commonly involved age group
was >50 years [n=56, 28.0%], followed by 30-40 years [n=46,
23.0%], 20-30 years [n=42, 21.0%]. Our study was supported
by Mirzha FH et al. (5) Kumar PM et al.(6) The age group of
more than 50 years was the most vulnerable period of life. It is
noted that the Unemployed persons were commonly involved
in RTAs. The students were next in number followed by
Labourers, employee in service, house wives. Most of victims
died during summer season followed by post monsoon, rainy
and least in winter. Our finding correlates with the finding of
Kumar A et al. (7) Yogesh G. (8) Most of the victims died in the
hospital, followed by spot dead and least while transporting to
hospital. Correlated with Shruthi P (9), Singh H et al. (10).
In our study most common involved place of accidents are
state highways followed by city roads, national highways and
least common accidents occurred in the village roads. This
finding correlates with Kumar N et al (11). Contrary to this
finding Singh H .et al (10) found national highways, followed
by state highways. The state highways were more involved in
our study, may be due to higher speed of vehicles in the state
highways when compared with the city and village roads. In
this study most of the accidents has occurred during 13.00-
18.00 hours followed by 19.00-24.00 hours and least during 0-
6.00 hours which was in concurrence with the study of Das
D.K (12) and Mahajan N et al, (13) Working people usually get
strained due to heavy work load all the day through and get
fatigue, because of which there is a decreased reflex action
leading to accidents. In our study two wheelers were more
170
Lung
Heart
Stomach
Intestine
Liver
Spleen
Mesentery
Kidney
Bladder
Multiple organs
76
10
05
11
32
11
28
02
01
01
31
97
102
96
75
96
79
105
106
106
58
14
03
08
30
09
32
10
07
01
35
79
90
85
63
84
61
83
86
02
Table 2 : Showing Association Between type of Vehicle and the Type of Viscera Involved.
TA organ involved
Two wheeler & Bicycle (N=102) Four wheeler (LMV,HMV) (N=93) Chi square test
Involved InvolvedNot involved Not involved
Chi=1.390, p=0.2507
Chi= 1.042, p=0.3073
Chi=0.0253 p=0.8735
Chi=0.0262, p=0.8713
Chi=0.0421 p=0.8373
Chi=0.0201, p=0.8873
Chi=1.240, p=0.2654
Chi=5.476, p=0.0193
Chi=4.045, p=0.0443
Chi=0.0099, p=0.9260
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00032.7

commonly involved in accidents followed by light motor
vehicles, heavy motor vehicles and least common involved
were cycles. Our study correlates with study of Kumar N et al
(11), Kumar PM et al (6) Jha N et al (14). The increasing trend
in the young generation to drive fast may be the reason behind
this. It is noted that there is a significant association for kidney
and bladder with type of vehicle involved. In our study
abrasions were more common followed by contusion, abraded
contusion and laceration. Yogesh G. (8) was noted with same
finding. Abrasions were more common. This may be due to
decreased level of resistance for the body. Most common
injured viscera is lung followed by liver, mesentery, heart,
spleen and least in bladder. This finding is similar with studies
done by Hanumantha et al (15), Further it is noted that multiple
organ injury was the commonest. Uterus involvement was
very rare. Bladder involvement was seen in cases with pubic
symphysis fracture. With regard to time maximum number of
person died within 0-6.00 hours followed by 12.00-24.00
hours and 3- 7 days. Our study correlates with study of Numan
H et al.(16) Our study found that accidents are more common
in the evening hours 13.00-18.00 hours. This may be attributed
to high over load of vehicles and not following traffic rules.
In our study the most common cause of death is haemorrhagic
shock with head injury followed by haemorrhagic shock alone,
sepsis and peritonitis. Our study co-relates with Singh H et al
(10) Kumar PM et al. (6) This can be explained, as the majority
of the vital organs are located in the TA region of the body,
injury to this region causes contusion and laceration of vital
organs which leads to haemorrhagic shock. Most common
associated injury was with the head and neck, followed by nil,
lower limbs and in the upper limbs. Chaudhary et al (25)
supports our findings.
CONCLUSIONS :
The present study is based on the observation of 200 cases of
road traffic accidents with TA injuries. To meet the objectives
of the study listed in the earlier sections, epidemiological and
scientific analysis of the cases are done.Our study displays that
RTAs are at foremost concern to human life. In order to prevent
these RTAs some interventions like restriction of speed, strict
implement of helmets, graduate licensing etc. It needs a
holistic approach to coordinate and monitor the problem.
There is a need for government to involve and strictly plan
accordingly in a systematic way to reduce the problem in India.
Our study explains the significance protecting and preventing
the TA region by wearing seat belt; like the head region where
there is use of helmet to protect vital organ. This study helps us
to make strategies and various policies in reduction of
mortality and morbidity from TA injuries. Meanwhile this
improves the knowledge of clinicians in the treatment of
trauma victims and various medico legal specialists to deposit
their evidence in the court of law.
Conflict of Interest – None
REFERENCES :
1. World Health Organization (WHO) 1957. Technical
Report Serial No. 118.
2. Mathiharan K, Patnaik AK. Modi's medical jurisprudence
and toxicology. 23rd edition; Lexis Nexis publication:
Railway injuries: pp - 783.
3. Verma PK, Tewari KN. Epidemiology of Road Traffic
Injuries in Delhi: Result of a Survey; Regional Health
Forum WHO South-East Asia Region 2004; 8(1).
4. National Crime Records Bureau, Ministry of Home
Affairs, Govt. of India. Accidental Deaths & Suicides in
India - 2010 Available at: http://ncrb.nic.in. Accessed Oct
24, 2015.
.5. Mirza FH, Hassan Q, Jajja N. An autopsy-based study of
death due to road traffic accidents in metropolis of
Karachi. J Pak Med Assoc.2013; 63 (2):156-160.
6. Kumar PM, Ziya A, Prashant A. Fatality due to chest
injury in road traffic accident victims of Varanasi and
adjoining Districts, U.P. Medico-Legal Update. 2006;
6(3): 65-70.
7. Kumar A, Pandey SK. Epidemiological Study of Road
Traffic Fatalities: 5 Years Retrospective Autopsied Cases
Study in Varanasi, Uttar Pradesh, India. International
Journal of Science and Research. 2014; 8 (3): 502-506.
8 . Yogesh G. Pattern of Injuries in Fatal Road Traffic
Accidents: Autopsy Based Study. Journal of Evidence
based Medicine and Healthcare.2015; 2 (4): 321-327.
9. Shruthi P, Venkatesh VT, Viswakanth B, Ramesh C,
Sujatha PL , Dominic IR. Analysis of Fatal Road Traffic
Accidents in a Metropolitan City of South India. J Indian
Acad Forensic Med. 2013; 35 (4): 317-320.
10. Singh H, Dhattarwal SK, MD. Mittal S, Aggarwal A,
Sharma G, MD. Chawla R. A Review of Pedestrian Traffic
Fatalities. J Indian Acad Forensic Med. 2007; 29(4): 55-8.
11. Kumar N, Kumar M. Medicolegal Study of Fatal Road
Traffic Accidents in Varanasi Region. International
Journal of Science and Research. 2015; 4 (1):1492- 96.
12. Das DK. Study of Road Traffic Accidental Deaths in and
around Barpeta District: An Autopsy Based Study. Journal
of Evidence based Medicine and Healthcare. 2015; 2 (22):
3329-3337.
13. Mahajan N, Aggarwal M, Raina S, Verma LR, Mazta SR,
Gupta BP. Pattern of non-fatal injuries in road traffic
171
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00032.7
crashes in a hilly area: A study from Shimla, North India.
Int J Crit Illn Inj Sci 2013; 3: 190-4.
14. Jha N, Srinivasa DK, Roy G, Jagdish S. Injury pattern
among road traffic accident cases: a study from South
India. Indian J Community Med. 2003; 28(2):84 90.
15. Hanumantha A, Reddy BN, Pallavi M, Reddy NN,
Radhakrishna L, Reddy SN. An epidemiological study on
pattern of thoraco-abdominal injuries sustained in fatal
road traffic accidents of Bangalore: Autopsy Based Study.
Narayana Medical Journal. 2012; 1(2):19-27.
16. Numan H, Chavan KD, Bangal RS, Singh B. Pattern of
Thoraco-abdominal Injuries in Rural Region. Indian
Journal of Forensic Medicine and Pathology. 2009; 2 (3):
97-103.
17. Chaudhary B L, Deepak S, Tirpude B H, Sharma R K,
Veena M. Profile of Road Traffic Accident Cases in
Kasturba Hospital of M.G.I.M.S., Sevagram, Wardha,
Maharashtra. Medico-Legal Update. (2005-10-2005-12)
5 (4). www.indmedica.com-accessed on 20-11-2015.
172
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00032.7
Original Research Paper
INTRODUCTION :
Forensic Odontology is that branch of dentistry which in the
interest of justice deals with proper handling and examination
of dental evidence and with the proper evaluation and
presentation of dental findings. Establishing one's identity is [1]an important aspect in any forensic investigation . Age
Estimation is a vital component of forensic odontology in
human identification. In this regard teeth are apposite tissue
structures as they can survive for several decades or even
thousands of years due to their hardness and resistance to
corrosion and can estimate the age of an individual right from
the individual's journey from cradle to the grave.
In India, birth certificates may not be readily available from a
few people from rural or tribal background. This becomes a
hassle for the justice system where age is a requisite for
criminal/civil proceedings. Age estimation practices using
sexual and somatic maturity can be coupled with dental age
estimation in these situations. This is possible owing to the
continuous and progressive change a tooth undergoes with
age.
Gustafson's technique of age estimation (1950) uses factors
like attrition, secondary dentin deposition, apical migration of
periodontal attachment, cementum deposition at the root apex, [2]root resorption at the apex and root dentin translucency .
Later, investigators explored individual variables for their
efficiency to estimate age. However, there are factors like race,
diet, gender and masticatory forces which affect the
development and maintenance of teeth, which may alter the
Corresponding Author :
Dr. Shweta Yellapurkar,
Assistant Professor,
Department of Oral Pathology and Microbiology,
Manipal College of Dental Sciences, Mangalore.
Manipal Academy of Higher Education, Manipal.
Contact : +91 95919-55590
Email : [email protected]
KEYWORDS : Age estimation, Odontology periodontal ligament, Radiographic visibility
Article History:Received: 4 May 2021Received in revised form: 6 June 2021Accepted on: 6 June 2021Available online: 31 August 2021
ABSTRACT :
Introduction: Teeth are apposite tissue structures as they can survive for several decades or even thousands of years due to their
hardness and resistance to corrosion and can indicate the age of an individual. Not only the hard tissue changes but also, the visibility
of the dental soft tissues, periodontal ligament can be used for age estimation.
Material and methods : The study sample consisted of 330 OPGs of patients [aged between 14 and 76 (mean age of 32.82±12.75
years)]. Visibility of the periodontal ligament in lower third molars was done in accordance with the method followed by Guo et al
(2020) and was graded in 4 stages. The regression equations were derived using simple linear regression analysis to estimate the
efficiency of prediction of the age in total as well as stratified by gender.
Results :
Our study results showed a significant trend (p<0.001) of increasing age with higher grades of periodontal ligament score in males
and females as well as in total.
Conclusion :
Periodontal ligament visibility scores can be used as an adjunct to other age estimation techniques for confirming the age of living
individuals as well as deceased.
1. Ayan Bhadra Ray, Intern*2. Kushaggr Rastogi, Intern*3. Srikant N, Professor and Head, Department of Oral Pathology and Microbiology and Coordinator, Centre of Forensic
Odontology*4. Shweta Yellapurkar, Assistant Professor, Department of Oral Pathology and Microbiology*5. Nidhin Philip Jose, Associate Professor, Department of Orthodontics and Dentofacial Orthopaedics*6. Ceena Denny, Associate Professor, Department of Oral Medicine and Radiology* *Manipal College of Dental Sciences, Mangalore. Manipal Academy of Higher Education, Manipal, Karnataka, India
Reliability of age estimation using periodontal ligament visibility in South Indian
Population
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00033.9
173
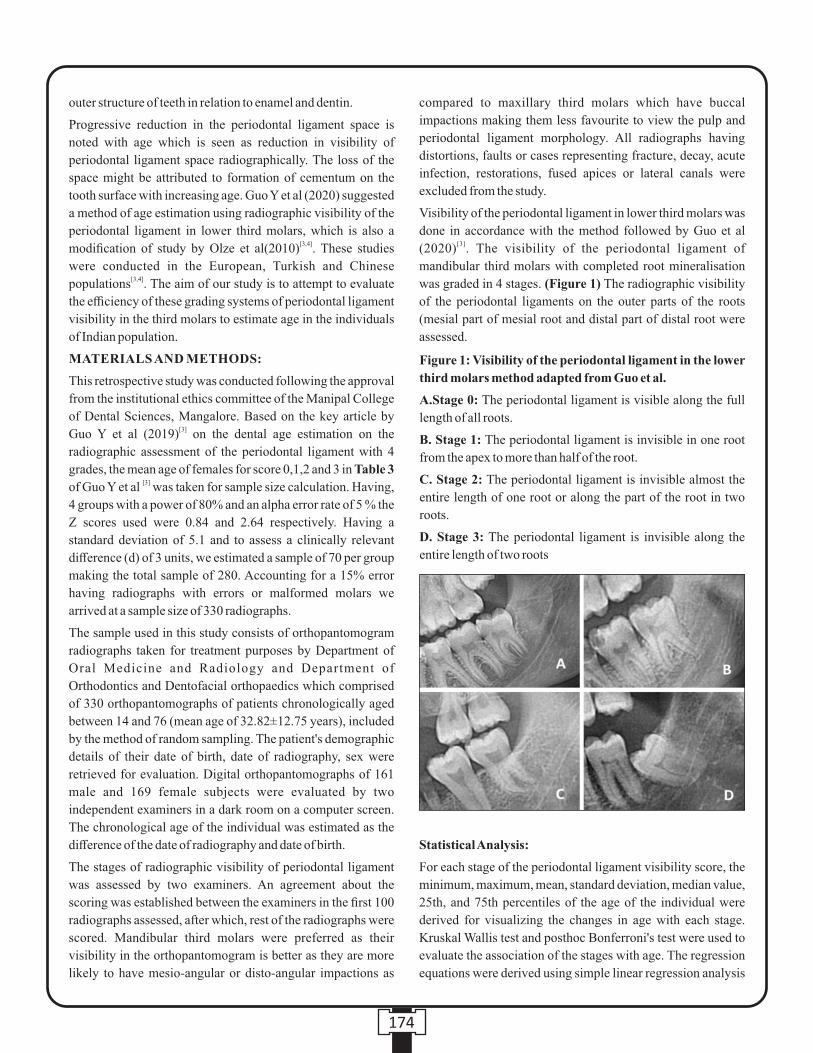
Figure 1: Visibility of the periodontal ligament in the lower
third molars method adapted from Guo et al.
A.Stage 0: The periodontal ligament is visible along the full
length of all roots.
B. Stage 1: The periodontal ligament is invisible in one root
from the apex to more than half of the root.
C. Stage 2: The periodontal ligament is invisible almost the
entire length of one root or along the part of the root in two
roots.
D. Stage 3: The periodontal ligament is invisible along the
entire length of two roots
outer structure of teeth in relation to enamel and dentin.
Progressive reduction in the periodontal ligament space is
noted with age which is seen as reduction in visibility of
periodontal ligament space radiographically. The loss of the
space might be attributed to formation of cementum on the
tooth surface with increasing age. Guo Y et al (2020) suggested
a method of age estimation using radiographic visibility of the
periodontal ligament in lower third molars, which is also a [3,4]modification of study by Olze et al(2010) . These studies
were conducted in the European, Turkish and Chinese [3,4]populations . The aim of our study is to attempt to evaluate
the efficiency of these grading systems of periodontal ligament
visibility in the third molars to estimate age in the individuals
of Indian population.
MATERIALS AND METHODS:
This retrospective study was conducted following the approval
from the institutional ethics committee of the Manipal College
of Dental Sciences, Mangalore. Based on the key article by [3]Guo Y et al (2019) on the dental age estimation on the
radiographic assessment of the periodontal ligament with 4
grades, the mean age of females for score 0,1,2 and 3 in Table 3 [3]of Guo Y et al was taken for sample size calculation. Having,
4 groups with a power of 80% and an alpha error rate of 5 % the
Z scores used were 0.84 and 2.64 respectively. Having a
standard deviation of 5.1 and to assess a clinically relevant
difference (d) of 3 units, we estimated a sample of 70 per group
making the total sample of 280. Accounting for a 15% error
having radiographs with errors or malformed molars we
arrived at a sample size of 330 radiographs.
The sample used in this study consists of orthopantomogram
radiographs taken for treatment purposes by Department of
Oral Medicine and Radiology and Department of
Orthodontics and Dentofacial orthopaedics which comprised
of 330 orthopantomographs of patients chronologically aged
between 14 and 76 (mean age of 32.82±12.75 years), included
by the method of random sampling. The patient's demographic
details of their date of birth, date of radiography, sex were
retrieved for evaluation. Digital orthopantomographs of 161
male and 169 female subjects were evaluated by two
independent examiners in a dark room on a computer screen.
The chronological age of the individual was estimated as the
difference of the date of radiography and date of birth.
The stages of radiographic visibility of periodontal ligament
was assessed by two examiners. An agreement about the
scoring was established between the examiners in the first 100
radiographs assessed, after which, rest of the radiographs were
scored. Mandibular third molars were preferred as their
visibility in the orthopantomogram is better as they are more
likely to have mesio-angular or disto-angular impactions as
compared to maxillary third molars which have buccal
impactions making them less favourite to view the pulp and
periodontal ligament morphology. All radiographs having
distortions, faults or cases representing fracture, decay, acute
infection, restorations, fused apices or lateral canals were
excluded from the study.
Visibility of the periodontal ligament in lower third molars was
done in accordance with the method followed by Guo et al [3](2020) . The visibility of the periodontal ligament of
mandibular third molars with completed root mineralisation
was graded in 4 stages. (Figure 1) The radiographic visibility
of the periodontal ligaments on the outer parts of the roots
(mesial part of mesial root and distal part of distal root were
assessed.
Statistical Analysis:
For each stage of the periodontal ligament visibility score, the
minimum, maximum, mean, standard deviation, median value,
25th, and 75th percentiles of the age of the individual were
derived for visualizing the changes in age with each stage.
Kruskal Wallis test and posthoc Bonferroni's test were used to
evaluate the association of the stages with age. The regression
equations were derived using simple linear regression analysis
174
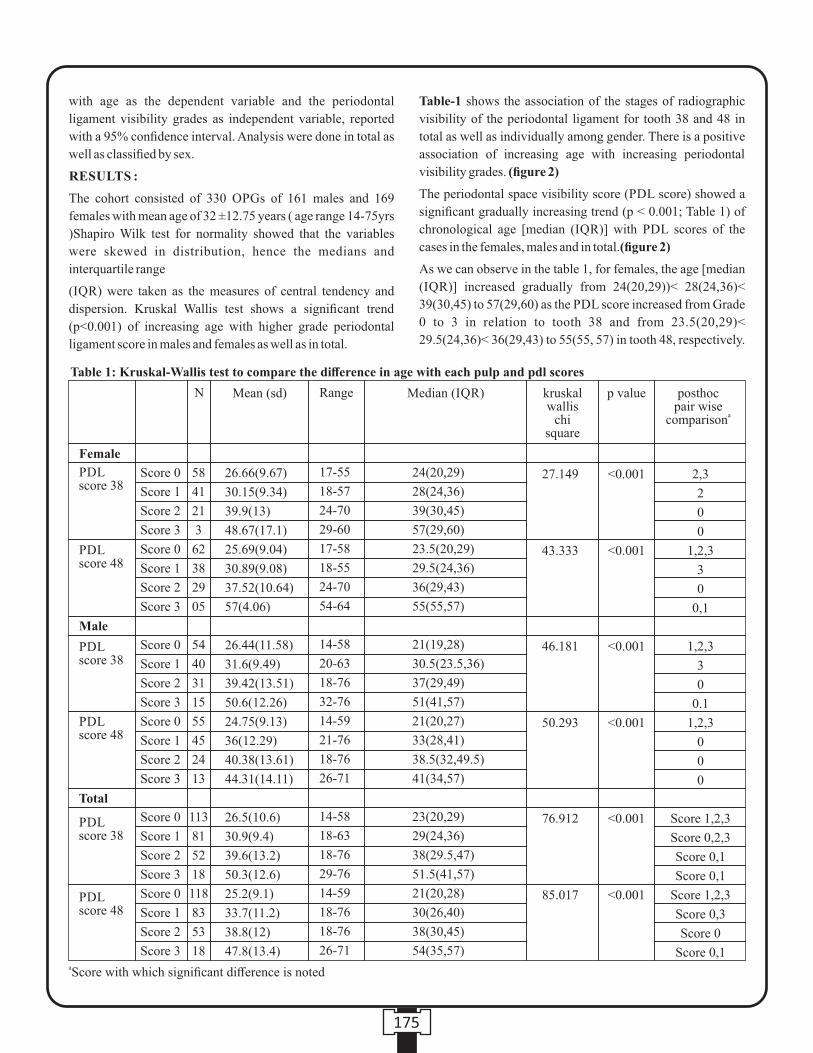
with age as the dependent variable and the periodontal
ligament visibility grades as independent variable, reported
with a 95% confidence interval. Analysis were done in total as
well as classified by sex.
RESULTS :
The cohort consisted of 330 OPGs of 161 males and 169
females with mean age of 32 ±12.75 years ( age range 14-75yrs
)Shapiro Wilk test for normality showed that the variables
were skewed in distribution, hence the medians and
interquartile range
(IQR) were taken as the measures of central tendency and
dispersion. Kruskal Wallis test shows a significant trend
(p<0.001) of increasing age with higher grade periodontal
ligament score in males and females as well as in total.
Table-1 shows the association of the stages of radiographic
visibility of the periodontal ligament for tooth 38 and 48 in
total as well as individually among gender. There is a positive
association of increasing age with increasing periodontal
visibility grades. (figure 2)
The periodontal space visibility score (PDL score) showed a
significant gradually increasing trend (p < 0.001; Table 1) of
chronological age [median (IQR)] with PDL scores of the
cases in the females, males and in total.(figure 2)
As we can observe in the table 1, for females, the age [median
(IQR)] increased gradually from 24(20,29))< 28(24,36)<
39(30,45) to 57(29,60) as the PDL score increased from Grade
0 to 3 in relation to tooth 38 and from 23.5(20,29)<
29.5(24,36)< 36(29,43) to 55(55, 57) in tooth 48, respectively.
175
aScore with which significant difference is noted
Female
PDL score 38
PDL score 38
PDL score 38
PDLscore 48
PDLscore 48
PDLscore 48
Male
Total
N Mean (sd) Range Median (IQR) kruskal wallis
chi square
p value posthoc pair wise
acomparison
Score 0
Score 1
Score 2
Score 3
Score 0
Score 1
Score 2
Score 3
Score 0
Score 1
Score 2
Score 3
Score 0
Score 1
Score 2
Score 3
Score 0
Score 1
Score 2
Score 3
Score 0
Score 1
Score 2
Score 3
58
41
21
3
62
38
29
05
54
40
31
15
55
45
24
13
113
81
52
18
118
83
53
18
Table 1: Kruskal-Wallis test to compare the difference in age with each pulp and pdl scores
26.66(9.67)
30.15(9.34)
39.9(13)
48.67(17.1)
25.69(9.04)
30.89(9.08)
37.52(10.64)
57(4.06)
26.44(11.58)
31.6(9.49)
39.42(13.51)
50.6(12.26)
24.75(9.13)
36(12.29)
40.38(13.61)
44.31(14.11)
26.5(10.6)
30.9(9.4)
39.6(13.2)
50.3(12.6)
25.2(9.1)
33.7(11.2)
38.8(12)
47.8(13.4)
17-55
18-57
24-70
29-60
17-58
18-55
24-70
54-64
14-58
20-63
18-76
32-76
14-59
21-76
18-76
26-71
14-58
18-63
18-76
29-76
14-59
18-76
18-76
26-71
24(20,29)
28(24,36)
39(30,45)
57(29,60)
23.5(20,29)
29.5(24,36)
36(29,43)
55(55,57)
21(19,28)
30.5(23.5,36)
37(29,49)
51(41,57)
21(20,27)
33(28,41)
38.5(32,49.5)
41(34,57)
23(20,29)
29(24,36)
38(29.5,47)
51.5(41,57)
21(20,28)
30(26,40)
38(30,45)
54(35,57)
27.149
43.333
46.181
50.293
76.912
85.017
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001
2,3
2
0
0
1,2,3
3
0
0,1
1,2,3
3
0
0.1
1,2,3
0
0
0
Score 1,2,3
Score 0,2,3
Score 0,1
Score 0,1
Score 1,2,3
Score 0,3
Score 0
Score 0,1
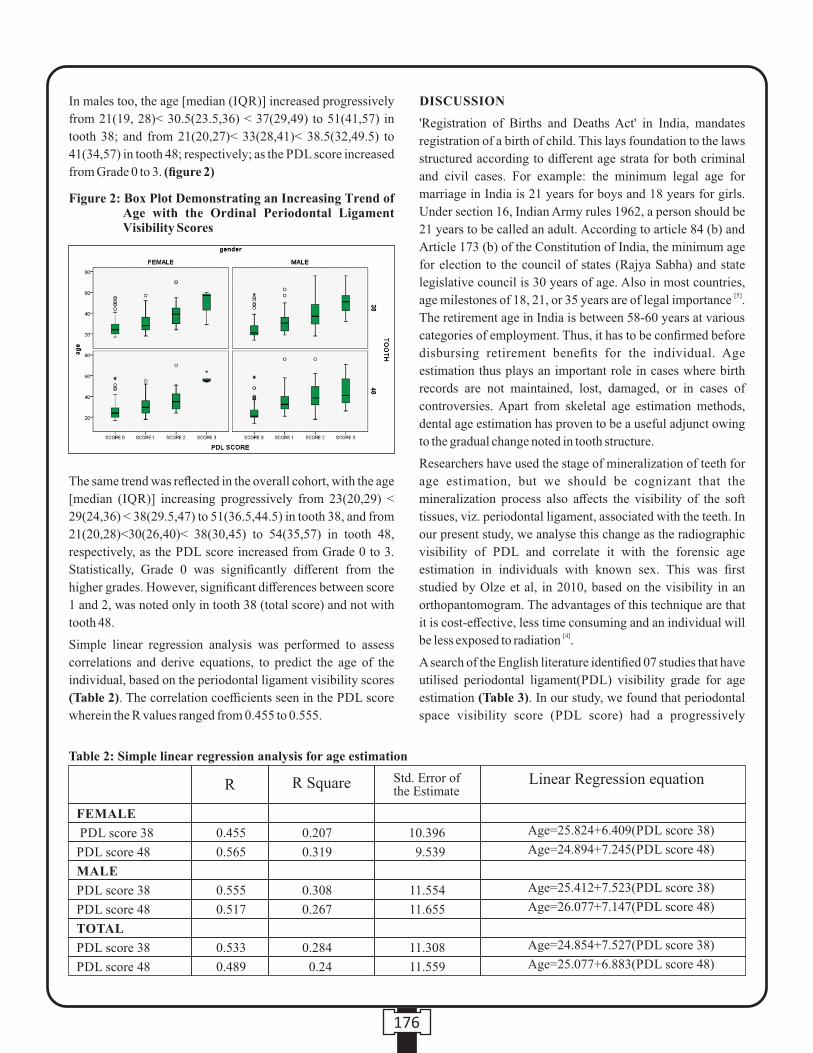
In males too, the age [median (IQR)] increased progressively
from 21(19, 28)< 30.5(23.5,36) < 37(29,49) to 51(41,57) in
tooth 38; and from 21(20,27)< 33(28,41)< 38.5(32,49.5) to
41(34,57) in tooth 48; respectively; as the PDL score increased
from Grade 0 to 3. (figure 2)
The same trend was reflected in the overall cohort, with the age
[median (IQR)] increasing progressively from 23(20,29) <
29(24,36) < 38(29.5,47) to 51(36.5,44.5) in tooth 38, and from
21(20,28)<30(26,40)< 38(30,45) to 54(35,57) in tooth 48,
respectively, as the PDL score increased from Grade 0 to 3.
Statistically, Grade 0 was significantly different from the
higher grades. However, significant differences between score
1 and 2, was noted only in tooth 38 (total score) and not with
tooth 48.
Simple linear regression analysis was performed to assess
correlations and derive equations, to predict the age of the
individual, based on the periodontal ligament visibility scores
(Table 2). The correlation coefficients seen in the PDL score
wherein the R values ranged from 0.455 to 0.555.
DISCUSSION
'Registration of Births and Deaths Act' in India, mandates
registration of a birth of child. This lays foundation to the laws
structured according to different age strata for both criminal
and civil cases. For example: the minimum legal age for
marriage in India is 21 years for boys and 18 years for girls.
Under section 16, Indian Army rules 1962, a person should be
21 years to be called an adult. According to article 84 (b) and
Article 173 (b) of the Constitution of India, the minimum age
for election to the council of states (Rajya Sabha) and state
legislative council is 30 years of age. Also in most countries, [5]age milestones of 18, 21, or 35 years are of legal importance .
The retirement age in India is between 58-60 years at various
categories of employment. Thus, it has to be confirmed before
disbursing retirement benefits for the individual. Age
estimation thus plays an important role in cases where birth
records are not maintained, lost, damaged, or in cases of
controversies. Apart from skeletal age estimation methods,
dental age estimation has proven to be a useful adjunct owing
to the gradual change noted in tooth structure.
Researchers have used the stage of mineralization of teeth for
age estimation, but we should be cognizant that the
mineralization process also affects the visibility of the soft
tissues, viz. periodontal ligament, associated with the teeth. In
our present study, we analyse this change as the radiographic
visibility of PDL and correlate it with the forensic age
estimation in individuals with known sex. This was first
studied by Olze et al, in 2010, based on the visibility in an
orthopantomogram. The advantages of this technique are that
it is cost-effective, less time consuming and an individual will [4]be less exposed to radiation .
A search of the English literature identified 07 studies that have
utilised periodontal ligament(PDL) visibility grade for age
estimation (Table 3). In our study, we found that periodontal
space visibility score (PDL score) had a progressively
176
Figure 2: Box Plot Demonstrating an Increasing Trend of Age with the Ordinal Periodontal Ligament Visibility Scores
Table 2: Simple linear regression analysis for age estimation
FEMALE
PDL score 38
PDL score 48
MALE
PDL score 38
PDL score 48
TOTAL
PDL score 38
PDL score 48
0.455
0.565
0.555
0.517
0.533
0.489
0.207
0.319
0.308
0.267
0.284
0.24
10.396
9.539
11.554
11.655
11.308
11.559
Age=25.824+6.409(PDL score 38)
Age=24.894+7.245(PDL score 48)
Age=25.412+7.523(PDL score 38)
Age=26.077+7.147(PDL score 48)
Age=24.854+7.527(PDL score 38)
Age=25.077+6.883(PDL score 48)
R R Square Std. Error of the Estimate
Linear Regression equation
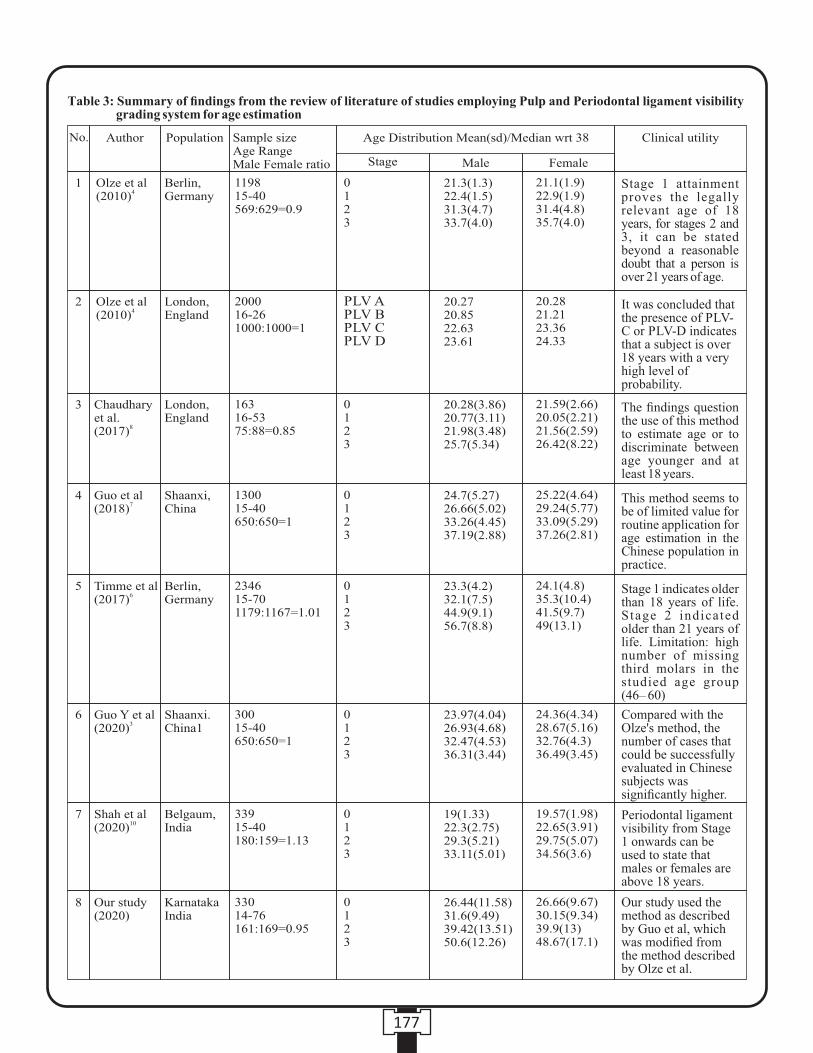
177
Table 3: Summary of findings from the review of literature of studies employing Pulp and Periodontal ligament visibility grading system for age estimation
No. Author Population Sample size Age Range Male Female ratio
Age Distribution Mean(sd)/Median wrt 38 Clinical utility
Stage Male Female
0123
Olze et al4
(2010)1 Berlin,
Germany119815-40569:629=0.9
21.3(1.3)22.4(1.5)31.3(4.7)33.7(4.0)
21.1(1.9)22.9(1.9)31.4(4.8)35.7(4.0)
Stage 1 attainment proves the legally relevant age of 18 years, for stages 2 and 3, it can be stated beyond a reasonable doubt that a person is over 21 years of age.
It was concluded that the presence of PLV-C or PLV-D indicates that a subject is over 18 years with a very high level of probability.
PLV APLV BPLV CPLV D
Olze et al4
(2010)2 London,
England200016-261000:1000=1
20.2720.8522.6323.61
20.2821.2123.3624.33
The findings question the use of this method to estimate age or to discriminate between age younger and at least 18 years.
This method seems to be of limited value for routine application for age estimation in the Chinese population in practice.
Stage 1 indicates older than 18 years of life. Stage 2 indicated older than 21 years of life. Limitation: high number of missing third molars in the studied age group (46– 60)
Compared with the Olze's method, the number of cases that could be successfully evaluated in Chinese subjects was significantly higher.
Periodontal ligament visibility from Stage 1 onwards can be used to state that males or females are above 18 years.
Our study used the method as described by Guo et al, which was modified from the method described by Olze et al.
0123
0123
0123
0123
0123
0123
Chaudhary et al.
8(2017)
Guo et al7
(2018)
Timme et al 6
(2017)
Guo Y et al 3
(2020)
Shah et al10
(2020)
Our study (2020)
3
4
5
6
7
8
London, England
Shaanxi, China
Berlin, Germany
Shaanxi. China1
Belgaum, India
KarnatakaIndia
16316-5375:88=0.85
130015-40650:650=1
234615-701179:1167=1.01
30015-40650:650=1
33915-40180:159=1.13
33014-76161:169=0.95
20.28(3.86)20.77(3.11)21.98(3.48)25.7(5.34)
24.7(5.27)26.66(5.02)33.26(4.45)37.19(2.88)
23.3(4.2)32.1(7.5)44.9(9.1)56.7(8.8)
23.97(4.04)26.93(4.68)32.47(4.53)36.31(3.44)
19(1.33)22.3(2.75)29.3(5.21)33.11(5.01)
26.44(11.58)31.6(9.49)39.42(13.51)50.6(12.26)
21.59(2.66)20.05(2.21)21.56(2.59)26.42(8.22)
25.22(4.64)29.24(5.77)33.09(5.29)37.26(2.81)
24.1(4.8)35.3(10.4)41.5(9.7)49(13.1)
24.36(4.34)28.67(5.16)32.76(4.3)36.49(3.45)
19.57(1.98)22.65(3.91)29.75(5.07)34.56(3.6)
26.66(9.67)30.15(9.34)39.9(13)48.67(17.1)

increasing age from score 0 to score 3 (p < 0.001; Table 1). The
age ranged from 26 to 50 yrs [median (IQR)] as scores noted
were 0 to 3, in the females, males as well as in total. This trend
is similar to the study done by Timme et al.
who demonstrated an age range of 23-56 years. Other studies [3,7] [4,6] [10]in Chinese , British[8,9], German and one Indian study
shows a narrower age range with stage 0 in range of 19-25
years and stage 3 in range of 23-37 years. The biological
explanation for the disappearance of the periodontal ligament,
according to a few authors may be that, as age advances, the
membrane becomes so narrow that it can't be seen on
radiographs. This could be attributed to the continuous
deposition of cementum to adapt to the changes in the
occlusion and attrition. Furthermore, the tooth root surface
might become rougher as time elapses and also the alveolar
bone adjacent to it making the visualization indistinct. It is
also, observed that the radiographic image of the periodontal
ligament disappears sometime after the age of 20 years. These [11]findings were true in our scenario . Moreover, periodontal
ligament attachment level is subjected to the action of various
physical and chemical changes such as occlusal trauma, pulp-
periapical pathoses, and conditions like osteomyelitis. [12]However, these criteria were excluded from our study . Our
[6]results mirror the findings of Timme et al and we concur that
stage 1 indicates an individual to be ≥18 years and stage 2 to be
≥21 years.
The advantage of our present study is that the cohort had
samples well distributed across the age groups with sufficient
representation across strata of age. The variation noted in the
review of literature across the population could be attributed to
the multitude of physical and chemical changes associated
with teeth, like trauma from occlusion, pulp and periapical
diseases, habits like bruxism, tobacco, etc. and weather
conditions. Another drawback of the study could be the lack of
delineation of impacted and non-impacted third molars.
Erupted 3rd molars may be influenced by oral changes which
may stimulate PDL changes as compared to impacted ones.
Further, we must be aware of the prevalence of missing third
molars, which may render the technique for age estimation
invalid.
CONCLUSION :
The present study demonstrates the positive trend shown by
periodontal ligament visibility grading system with age. These
techniques can be used as an adjunct to other age estimation
techniques for confirming the age of living individuals as well
as deceased. Additionally, the review of the literature showed
the efficiency of the technique across the populations, with
possible variations owing to the differences in the habits,
weather and cultural influences.
Institutional Ethics Committee Approval : Ref no:20020.
Conflicts of interest/Funding/ : NoneInformed consent
REFERENCES:
1. Divakar KP.Forensic Odontology: The New Dimension in
Dental Analysis. Int J Biomed Sci. 2017;13(1):1-5.
2. G. Gustafson.“Age determination on teeth,” The Journal of
American Dental Association.1950; 41:45–54.
3. Guo Y., Wang Y., Olze A., Schmidt S., Schulz R., Pfeiffer H.,
Chen T. and Schmeling A.Dental age estimation based on the
radiographic visibility of the periodontal ligament in the lower
third molars: application of a new stage classification.
International Journal of Legal Medicine. 2020;134(1):369-
374.
4. Olze A., Solheim T., Schulz R., Kupfer M., Pfeiffer H.,
Schmeling A. Assessment of the radiographic visibility of the
periodontal ligament in the lower third molars for the purpose
o f fo rens ic age . In te rna t iona l Journa l o f Lega l
Medicine.2010;124;445-448 .
5. Aggrawal A.Age estimation in the living - Some Medicolegal
Considerations. Anil Aggrawal's Internet Journal of Forensic
Medicine and Toxicology [serial online] 2002; 1:2.
6. Timme M, Timme WH, Olze A, Ottow C, Ribbecke S, Pfeiffer
H, Dettmeyer R, Schmeling A.The chronology of the
radiographic visibility of the periodontal ligament and the root
pulp in the lower third molars. Sci Justice. 2017; 57(4):257-
261.
7. Guo YC, Li MJ, Olze A, Schmidt S, Schulz R, Ottow C,
Pfeiffer H, Chen T, Schmeling A.Studies on the radiographic
visibility of the periodontal ligament in lower third molars: can
t h e O l z e m e t h o d b e u s e d i n t h e C h i n e s e
population?.2018;132(2):617-622.
8. Chaudhary MA, Liversidge HM .A radiographic study
estimating age of mandibular third molars by periodontal
ligament visibility. J Forensic Odontostomatol.2017;
35(2):79-89.
9. Lucas VS, McDonald F, Andiappan M, Roberts G. Dental age
estimation: periodontal ligament visibility (PLV)-pattern
recognition of a conclusive mandibular maturity marker
related to the lower left third molahr at the 18-year threshold.
Int J Legal Med. 2017;131(3):797-801.
10. Shah R & Angadi PV.Radiographic assessment of periodontal
ligament visibility in mandibular third molars as a tool for
defining the 18 year threshold among Indians. Australian
J o u r n a l o f F o r e n s i c S c i e n c e s . 2 0 2 0 ; D O I :
10.1080/00450618.2019.1711179
11. Ozle et al, Sequeira CD, Teixeira A, Caldas IM, Afonso A,
Pérez-Mongiovi D.Age estimation using the radiographic
visibility of the periodontal ligament in lower third molars in a
Por tuguese popula t ion . J Cl in Exp Dent . 2014;
6(5):e546–e550.
12. Narayan V K, Varsha V K, Girish H C, Murgod S.
Stereomicroscopic study on unsectioned extracted teeth. J
Forensic Dent Sci. 2017; 9(3):157–164.
178
Original Research Paper
INTRODUCTION :
Physiology is one of the foundation sciences in medical
curriculum, which has immense importance in understanding
the future clinical sciences. Traditionally teaching in
Physiology has always been through didactic lectures,
practical and tutorials. There is no single method of teaching
that ensures thorough understanding of a topic among
students. So, there has always been a need for an alternative to
the traditional didactic format of lectures in medical education.
The medical curriculum is vast and students are expected to
learn many subjects at the same time. The teachers are also
involved in a number of activities apart from teaching like
research, administrative, updating their knowledge etc. In
doing so, teaching undergraduate medical students frequently
remains a separate academic department without integration to
interrelate or unify subjects. Therefore, Medical Council of
India desires the incorporation of integration in the medical
curriculum in order to provide the students with a holistic [1]rather than fragmented learning perspectives.
The term integration in education means coordination in
the teaching learning activities to ensure harmonious [2]functioning of the educational processes. It is defined as
organization of teaching matter to interrelate or unify
subjects frequently taught in separate academic courses or [3]departments. Integrated teaching aims to provide knowledge
to the students in a complete organized and wholesome
manner thereby enabling the students to have a more
Corresponding Author :
Dr. Sonia Kochhar,
Associate Professor and Head (Oficiating),
Department of Physiology, All India Institute of Medical
Sciences, Bathinda.
Contact : +91 98966-72381
Email : [email protected]
KEYWORDS : Case based learning, Self directed learning, Reasoning skills, Integrated Teaching, Physiology
Article History:Received: 8 August 2020Received in revised form: 18 February 2021Accepted on: 18 February 2021Available online: 15 August 2021
ABSTRACT :
Objectives: Small group teaching in the form of Case Based Learning (CBL) –a guided inquiry approach was used to teach
Endocrine Physiology. The aim was to assess the effectiveness of case-based learning in the first year MBBS students. The
objectives were to promote self directed learning, to enhance reasoning skills in the students & to motivate faculty to adopt new
integrated teaching methodology.
Methods: The study was conducted in the department of Physiology. The study group of 150 students (n=150), was divided into 2
groups A & B based on their roll numbers. Group A students experienced CBL & Group B students experienced Didactic lectures.
Both groups were examined by MCQs, pretest & posttest respectively. The scores of the two tests were compared for student's
comprehension. Students & faculty feedback was evaluated for the teaching method using Likert scale. Appropriate parametric &
non-parametric tests were used to analyze the data.
Results: The student's performance in MCQ tests was statistically significantly better after CBL (Mean±SD, 10.0±1.96)) as compared to after traditional teaching (Mean±SD, 7.7±2.17) (Paired t test, p- value of 0.004). In student's feedback 86% agreed that CBL encouraged active learning & improved problem solving ability. 76.8% considered it to be more informative & helpful in relating & retaining knowledge. 80.2% students acknowledged that it helped to develop communication skills & 72.6% agreed that it improved group dynamics. More than 90% of the students felt that CBL would promote a better teacher-student relationship. Faculty feedback stated CBL useful for developing interest, improving understanding & clinical reasoning of the students. They also showed their willingness to participate in such sessions in future & acknowledged Case Based Learning as a better method of teaching. Conclusions: Students performance & strong preference for CBL inferred more modules of CBL should be implemented in medical education.
1. Ashwani Ummat, Professor & Unit Head, Department of Orthopaedics, Adesh Institute of Medical Sciences & Research, Bathinda.
2. Sonia Kochhar, Associate Professor and Head (Oficiating), Department of Physiology, All India Institute of Medical Sciences, Bathinda.
An Approach Towards Integrated Teaching: Case-Based Learning (CBL) in Physiology
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00034.0
179

clear view of the topic, while on the other hand it takes a toll [4]on the students themselves. To put it simply, instead of
imparting knowledge on a topic in disintegrated manner, a
particular topic can be taken by two or more departments
by forming a co-ordinated integrated teaching program [5](correlation level).
Current drift in medical education is a shift from teacher
centered submissive learning environment to student centered [6]energetic, positive learning. The Medical council of India has
framed the learning process for graduate medical education
which incorporates case studies and problem-oriented
approach as well as introduction of horizontal and vertical [7]integration throughout the UG curriculum.
Medical Council of India also uplifts learner centric attitudes.
Various methods are used by many institutes to reinforce
lectures in teaching medical education for undergraduate
students. These are case based learning, problem based [8,9]learning and patient centered learning. One of such
approach is CBL (case-based learning) where the students
learn with the help of case scenarios and are actively engaged
to solve a problem to attain the learning objectives. CBL is
known to transmit analytical skills and ability to solve real [10,11]medical problems in the students. CBL is the method of
learning not perceptibly different from PBL (problem based
learning) but without patient exposure & in a protected [12]environment. Since CBL motivates students toward self-
directed learning and to develop analytic and problem solving
skills; thus, CBL could be beneficial for students entry into
clinical departments and finally, in managing patients.
CBL is one method where students are motivated to learn on
their own and integrate knowledge from different subjects to
solve problems. It is a small-group method in which both
students and faculty members contribute to discussion,
learning issues are preidentified, and preparatory readings are
assigned while student discussion and guided inquiry around [13] clinical problems are still promoted.
Hence we thought of incorporating innovative teaching
methods to make the learning process student centered. In our
study the teaching learning intervention in the form of CBL
was conducted in the Department of Physiology to compare
the academic performance of undergraduate medical students
by using traditional methods and innovative methods (CBL).
It was an attempt towards making students responsible for their
own learning and narrow down the gaps between students and
teachers.
AIMS & OBJECTIVES:
1. To compare the academic performance by using traditional
methods (Didactic lecture) and innovative methods (CBL).
2. To promote self-learning among students & to encourage
application of theory based knowledge to solve problems by
integrating basic science subjects with clinical scenarios.
3. To motivate the peer group to adopt a new teaching learning
methodology & make process of learning interesting &
enjoyable.
MATERIALS AND METHODS :stThis study was conducted on 150 students of 1 Year MBBS
(Bachelor of Medicine, Bachelor of Surgery) in MMIMSR,
Mullana during the academic year 2018-2019. Permission was
obtained from the Institutional Ethics Committee of our
institute. The study population was the undergraduate students
of first year MBBS. All first year MBBS students who
voluntarily gave the informed consent were included for the
evaluation of performance difference.
After the ethical committee clearance for the CBL
intervention, 7 topics were selected, cases were constructed,
and faculty of Physiology was trained. MCQ's and feedback
questionnaire for students and the faculty were designed, they
were prevalidated and validated. A facilitator training program
was undertaken in the department under the guidance of Chief
(Head) of the Medical Education Unit of the institute. The
“facilitators” were physiologists and physicians. Before
intervention counseling of the students was done. Informed
written consent was obtained from first MBBS students who
were willing to participate in the study. The study group
(n=150), was divided into 2 groups A & B based on their roll
numbers. For each topic, all the students were given MCQ
pre-test in order to elicit their base line knowledge about the
given topic. Group A consisted of students with Odd Roll
Numbers & Group B of students with Even Roll Numbers.
Group A students experienced CBL & Group B students
experienced Didactic lectures. The Interventional group was
divided into small groups of 15 with one facilitator for each
group. CBL session was conducted wherein they were
presented with a case scenario. (Appendix A) The case
scenario included the clearly written symptoms and signs
related to the topic. Adequate time was given for case
discussion and for solving the Specific Learning Objectives by
the students. The facilitator during the phase, motivated and
guided the students. Then afterwards, the case was discussed
under the guidance of facilitator properly & systematically.
Relevant questions were asked by the facilitator, so as to
streamline the thought process. Students were also encouraged
to ask questions to the facilitator during the session. This was
followed by MCQ post-test. The faculty from other
departments also attended the CBL session as observers.
A five-point Likert scale was used ranging from strongly
disagree to strongly agree to determine the overall rating of the
180
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00034.0
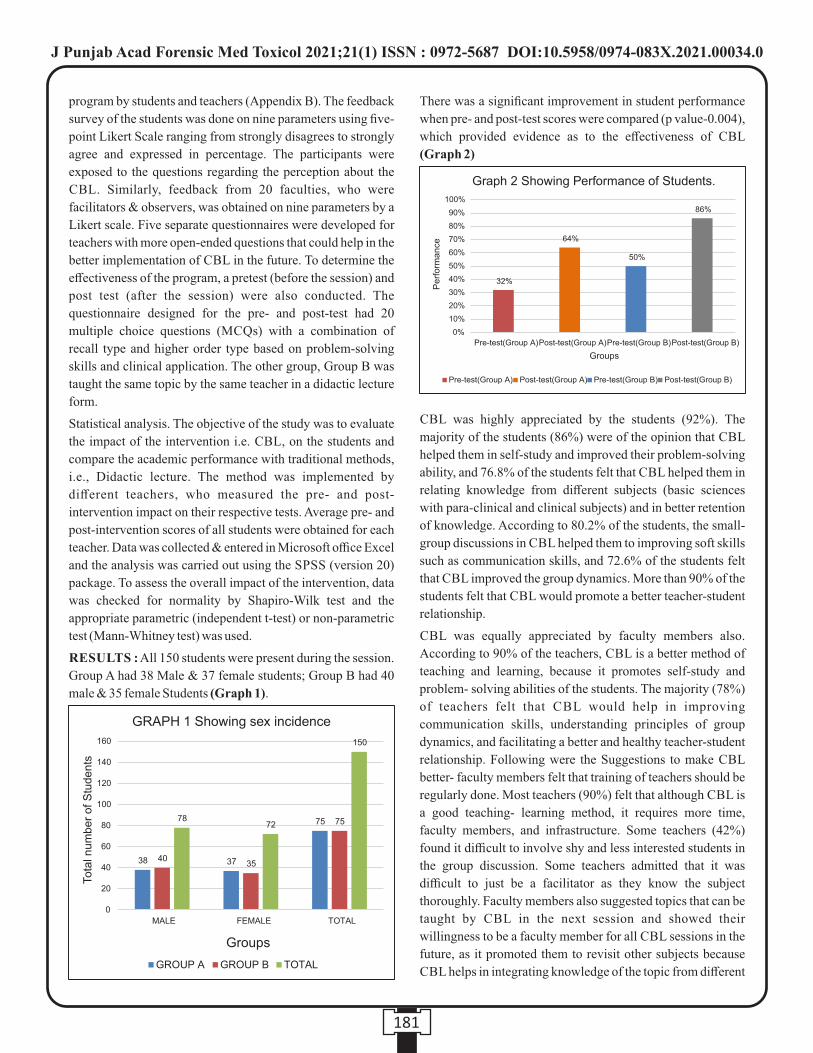
program by students and teachers (Appendix B). The feedback
survey of the students was done on nine parameters using five-
point Likert Scale ranging from strongly disagrees to strongly
agree and expressed in percentage. The participants were
exposed to the questions regarding the perception about the
CBL. Similarly, feedback from 20 faculties, who were
facilitators & observers, was obtained on nine parameters by a
Likert scale. Five separate questionnaires were developed for
teachers with more open-ended questions that could help in the
better implementation of CBL in the future. To determine the
effectiveness of the program, a pretest (before the session) and
post test (after the session) were also conducted. The
questionnaire designed for the pre- and post-test had 20
multiple choice questions (MCQs) with a combination of
recall type and higher order type based on problem-solving
skills and clinical application. The other group, Group B was
taught the same topic by the same teacher in a didactic lecture
form.
Statistical analysis. The objective of the study was to evaluate
the impact of the intervention i.e. CBL, on the students and
compare the academic performance with traditional methods,
i.e., Didactic lecture. The method was implemented by
different teachers, who measured the pre- and post-
intervention impact on their respective tests. Average pre- and
post-intervention scores of all students were obtained for each
teacher. Data was collected & entered in Microsoft office Excel
and the analysis was carried out using the SPSS (version 20)
package. To assess the overall impact of the intervention, data
was checked for normality by Shapiro-Wilk test and the
appropriate parametric (independent t-test) or non-parametric
test (Mann-Whitney test) was used.
RESULTS : All 150 students were present during the session.
Group A had 38 Male & 37 female students; Group B had 40
male & 35 female Students (Graph 1).
There was a significant improvement in student performance
when pre- and post-test scores were compared (p value-0.004),
which provided evidence as to the effectiveness of CBL
(Graph 2)
CBL was highly appreciated by the students (92%). The
majority of the students (86%) were of the opinion that CBL
helped them in self-study and improved their problem-solving
ability, and 76.8% of the students felt that CBL helped them in
relating knowledge from different subjects (basic sciences
with para-clinical and clinical subjects) and in better retention
of knowledge. According to 80.2% of the students, the small-
group discussions in CBL helped them to improving soft skills
such as communication skills, and 72.6% of the students felt
that CBL improved the group dynamics. More than 90% of the
students felt that CBL would promote a better teacher-student
relationship.
CBL was equally appreciated by faculty members also.
According to 90% of the teachers, CBL is a better method of
teaching and learning, because it promotes self-study and
problem- solving abilities of the students. The majority (78%)
of teachers felt that CBL would help in improving
communication skills, understanding principles of group
dynamics, and facilitating a better and healthy teacher-student
relationship. Following were the Suggestions to make CBL
better- faculty members felt that training of teachers should be
regularly done. Most teachers (90%) felt that although CBL is
a good teaching- learning method, it requires more time,
faculty members, and infrastructure. Some teachers (42%)
found it difficult to involve shy and less interested students in
the group discussion. Some teachers admitted that it was
difficult to just be a facilitator as they know the subject
thoroughly. Faculty members also suggested topics that can be
taught by CBL in the next session and showed their
willingness to be a faculty member for all CBL sessions in the
future, as it promoted them to revisit other subjects because
CBL helps in integrating knowledge of the topic from different
181
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00034.0

subjects.
DISCUSSION :
Teaching in Physiology has traditionally been through didactic
lectures, practicals, and tutorials. There is no single method of
teaching that ensures thorough understanding of a topic among
students. Lectures are definitely a powerful method of
delivering information to a large number of students quickly.
However, there are many limitations, such as lectures are a
passive method of learning by students and too much
information is given without application or a problem-solving
approach.
There has always been a need for an alternative to the [14,15]traditional didactic format of lectures in medical education.
Thus, we thought of adopting a combination of didactic
lectures and CBL sessions as a new innovative method in our
institute so as to retain the lectures and supplement them with a
new teaching learning methodology, which will give a
problem-solving approach. As medical teachers, we provide
students a large amount of information, but, at same time, it is
necessary to ensure that it should be used to establish and
optimize students' understanding.
In Case Based Learning by discussing a clinical case related to
the topic taught, students evaluated their own understanding of
the concept using a high order of cognition. This process
encourages active learning and produces a more productive [16,17]outcome. In our study CBL was incorporated with the
[18]following purpose :
1. To provide students with a relevant opportunity to see theory
in practice.
2. To require students to analyze data to reach a conclusion.
3. To develop analytic, communicative, and collaborative
skills along with the content knowledge.
4. To provide an opportunity for students to put themselves as
the decision maker's.
The results of our study prove that the learning of students is
significantly improved with the new learning methodology
(CBL) as students were able to answer application-based
questions as well. The result of the study also proves that the
assimilation of the knowledge was also improved because
discussing a case after the didactic lecture was helpful in
reinforcing the key elements of the topic. The retention of
knowledge was also better because students were required to
study the same topic from all subjects simultaneously so as to
integrate the knowledge to solve the given problem.
In some medical colleges in India, similar types of studies have [1,19]been introduced and the results have been encouraging An
early clinical exposure program consisting of CBL in
Endocrine Physiology in a medical college in India also
demonstrated that the majority of students (96.4%) gave an
overall rating of the program as good to excellent on a five-[20]point Likert Scale.
[21]According to study by VariRC et al. teaching endocrine
physiology in a patient-centered learning curriculum, students
are better equipped to analyze clinical problems, find and apply
appropriate basic science knowledge, and present their
patients compared with students from a traditional curriculum. [13]In a comparative study by Srinivasan M et al. between
problem-based learning and CBL, both students and faculty
members preferred the CBL method, as it offers more
opportunities for problem- solving skills within a session. In a [22]similar study carried out in India by Setia S et al. , the
majority of students reported CBL as a more suitable way of
learning compared with problem-based learning and that CBL
helped to improve their diagnostic skills and lateral thinking.
The teachers who were facilitators & observers in the CBL
project admitted that with this exposure to a new teaching-
learning process, their knowledge about the new teaching-
learning method has increased, Also they observed an
improvement in Student teacher relationship and so they were
ready to experiment with new methods of teaching (theory or
practical), assessment, and evaluation. Hence, we suggest the
incorporation of this new learning method in physiology,
which can be implemented in other departments also.
CONCLUSION :
Physiology forms the backbone of medicine and a lot of
medicinal subjects rely mainly on the normal physiology for
its understanding. So what a student learns and imbibes in the
first year of MBBS curriculum forms the base of future
education. From this study we conclude that the newer
concept of integrated teaching is a better and more
effective. CBL motivates students toward self-directed
learning and to develop analytic and problem-solving skills.
Hence, it will be desirable for students' entry into clinical
departments and ultimately in managing patients successfully.
ACKNOWLEDGEMENT :
The authors acknowledge the guidance and the support
provided by the dean of the institute and faculty members of
the department. We would like to specially thank the students stof 1 year MBBS for their continuous engagement with this
research.
Funding- No funding resources.
Conflict of Interest- None declared.
REFERENCES :
1. Arun V. Jamkar, Vishwnath L Yemul and Gurpreet Singh:
182
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00034.0
Integrated teaching program with student centered case
base learning for undergraduates at B J Medical College
Pune.
www.faimer.org/education/fellows/abstracts/04jamkar.p
df
2. Irby D, Wilkerson L. Educational innovations in academic
medicine and environmental trends. J Gen Intern Med
2003; 18: 370-376.
3. Muller JH, Jain S, Loeser H, Teby DM. Lesson
learned about integrating a medical school curriculum:
perceptions of students, faculty and curriculum leaders.
Med Edu. 2008; 42: 778-785.
4. Sameer M. Khan. “Integrated Teaching: A New
Approach in Medical Teaching”. Journal of Evolution of
Medical and Dental Sciences 2014; Vol. 3, Issue 57,
October 30;12939-45.
5. Atwa HS, Gouda EM (2014) Curriculum Integration in
Medical Education: A Theoretical Review. Intel Prop
Rights 2: 113. doi:10.4172/ 2375-4516.1000113
6. Naheed Bano, Farhat Arshad, Sadia Khan, C. Aqeel
Safdar; Case Based Learning and Traditional Teaching
Strategies: Where Lies The Future. Pak Armed Forces
Med J 2015;65(1): 118-24
7. Srabani N. Bhattacharya, Aniruddha A. Malgaonkar,
Sundaram Kartikeyan: Effect of case-based learning in
reproductive physiology on cognitive domain scores of
first year medical students in Western India; International
journal of Reproduction, contraception, Obstetrics and
Gynecology; 2017; Jun;6(6):2559-564.
8. Monika Bansal, Manoj Goyal: To introduce and measure
the effectiveness of case-based learning in physiology;
Internat ional journal of Research in medical
students;2017, Feb; 5(2); 437-445.
9. Vision 2015; Medical Council of India.
10. Nair SP, Seth S, Pandit N, Shah GCV: Case Based
Learning: A Method for Better Understanding of
Biochemistry in medical Students; Journal of clinical
Diagnosis Research; 2013,7 (8):1576-8.
11. Majjed F: Effectiveness of case-based teaching of
physiology for nursing students; Journal of Taibah
University Medical Sciences, 2014;9 (4): 289-292.
12. Tabassum Naveed, Naveed Mazhar Bhatti, Romana
Malik: Perception of Medical students regarding Case
Based Learning; Journal of Rawalpindi Medical College;
2017;21 (3); 303-305.
13. Srinivasan M, Wilkes M, Stevenson F, Nguye T, Slavin S.
Comparing problem-based learning with case-based
learning: effects of a major curricular shift at two
institutions. Acad Med 82: 74–82, 2007.
14. Ghosh S. Combination of didactic lectures and case based
problem solving tutorials toward better learning:
perception of students from a conventional medical
curriculum. Adv Physiol Educ 31: 193–197, 2007.
15. Lujan HL, DiCarlo SE. Too much teaching, not enough
learning: what is the solution? Adv Physiol Educ 30:
17–22, 2006.
16. Lake DA. Student performance and perception of a
lecture-based course compared with the same course
utilizing group discussion. Phys Ther 81:896–902, 2001.
17. Modell HI. Preparing students to participate in an active
learning environment. Adv Physiol Educ 270: 69–77,
1996.
18. Centre for Teaching and Learning, Queen's University.
W h a t I s C a s e - B a s e d l e a r n i n g ? ( o n l i n e ) .
www.queensu.ca/ctl/resources/topicspe - cific/casebased.
html [7 January 2012].
19. Vyas R, Jacob M, Faith M, Isaac B, Rabi S, Sathishkumar
S, Selva- kumar D, Ganesh A. An effective integrated
learning program in the first year of the medical course.
Natl Med J India 21: 21–26, 2008.
20. Sathishkumar S, Thomas N, Tharion E, Neelakantan N,
Vyas R. Attitude of medical students towards early clinical
exposure in learning endocrine physiology. BMC Med
Educ 7: 30, 2007.
21. Vari RC, Borg KE, McCleary VL, McCormack JT, Ruit
KG, Sukalski KA, Olson LM. Endocrine physiology in a
patient centered learning curriculum. Adv Physiol Educ
25: 241–248, 2001.
22. Setia S, Bobby Z, Ananthnarayanan P, Radhika M,
Kavitha M, Prashanth T. Case-based learning versus
problem-based learning: a direct comparison from first-
year medical students perspective. Webmedcentral Med
Educ 2: WMCOO1976, 2011.
183
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00034.0

Case 1: A 21-year-old noncompliant male with a history of type
I (insulin-dependent) diabetes mellitus was found in a coma. His
blood glucose was high, as well as his urine glucose, urine
ketones, and serum ketones. His serum bicarbonate was <12
mEq/L. His respiration was exaggerated and his breath had an
acetone odor. His blood pressure was 90/60 and his pulse weak
and rapid (120).
Case 2: A 45-year-old male presented with the following
symptoms during February: weakness, fatigue, orthostatic
hypotension, weight loss, dehydration, and decreased cold
tolerance.
His blood chemistry values follow: Serum sodium:128 mEq/L,
Serum potassium:6.3 mEq/L, Fasting blood glucose:65 mg/dL,
BUN:4.5 mg/dL and Serum creatinine:0.5 mg/dL
Hematology tests resulted in the following values:
Hematocrit:50%, Leukocytes:5000/cu mm
He also noticed increased pigmentation (tanning) of both
exposed and non exposed portions of the body and back. A
plasma cortisol determination indicated a low cortisol level.
Following administration of ACTH, plasma cortisol did not rise
significantly after sixty and ninety minutes. Endogenous
circulating levels of ACTH were later determined to be
significantly elevated.
Case 3: A 28-year-old male complained of abrupt polydipsia
and polyuria.
Blood and urine analyses provided the following results:
Fasting blood glucose:93 mg/dL, Serum sodium:145 mEq/L,
Serum potassium:2.8 mEq/L, Urine specific gravity<1.005,
Urine osmolality<200 mOsm/L, Urine volume:15 L/day, Urine
glucose:Nil
Water deprivation and hypertonic saline infusion do not cause a
significant reduction in the polyuria and concentration of urine.
Complete water-deprivation results in the following: Urine
specific gravity:1.009, Urine osmolality:225 mOsm/L
However, there is a significant concentration of the urine and a
decrease in urinary output following administration of ADH.
Case 4: A 50-year-old male had a total thyroidectomy followed
by thyroid hormone-replacement therapy. Thirty-six hours later
he developed laryngeal spasms, a mild tetany, and cramps in the
muscles of the hands and arms.
The following tests were performed: Urine calcium 20 mg/dL,
Urine phosphorus 0.1 g/day, Plasma calcium 7.0 mg/dL, Plasma
phosphorus 5.0 mg/dL.
Calcium gluconate and vitamin D (calcitriol) were given orally
each day and the tetany and laryngeal spasms were alleviated
Case 5: A 20-yr-old woman, visited the Medical Outpatient
Department with a history of swelling in the front of the neck
since the last 6 month. Recently, she also developed complaints
of palpitation, excessive sweating, and tremors. There is a
significant history of weight loss in last 3 month, but with no loss
of appetite. She does not have any hoarseness of voice or
difficulty in swallowing or breathing. On examination, she was
told that she is suffering from goiter and advised to seek further
investigations. It was further found that there were no signs of
exophthalmoses.
In next session: After 1 wk, she returned to the doctor with her
reports. Upon investigation, it was found that her thyroxine
levels were raised and thyroid-stimulating hormone levels were
less than normal. A thyroid scan confirmed the diagnosis of
multinodular goiter. She was prescribed anti-thyroid drugs and
β-blockers and advised to consult a surgeon.
Case 6: A mother came with a 24-month old girl child who has
failure to thrive and an unusual gait. She has bowed legs, thick
wrists and dental caries. Her weight (8Kg) and height (72.5cm) rdare below the 3 percentiles for her age. Her diet consists
predominantly of breastfeeding 5 times daily. The mother's
antenatal, delivery and post-natal history are unremarkable.
Case 7: A 63 year old women presents with history of acute low
back pain. She had menopause at 44 years of age, but never
received postmenopausal HRT. Reported a history of a Colles'
fracture at the age of 60 years.
Lumbar spine X-ray reveals veretrbrae fracture (L1). DXA of
the hip shows a BMD T-score of -1.8SD, and of -2.7 at LS (L2-
L4).
184
APPENDIX A: Case Scenarios
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00034.0
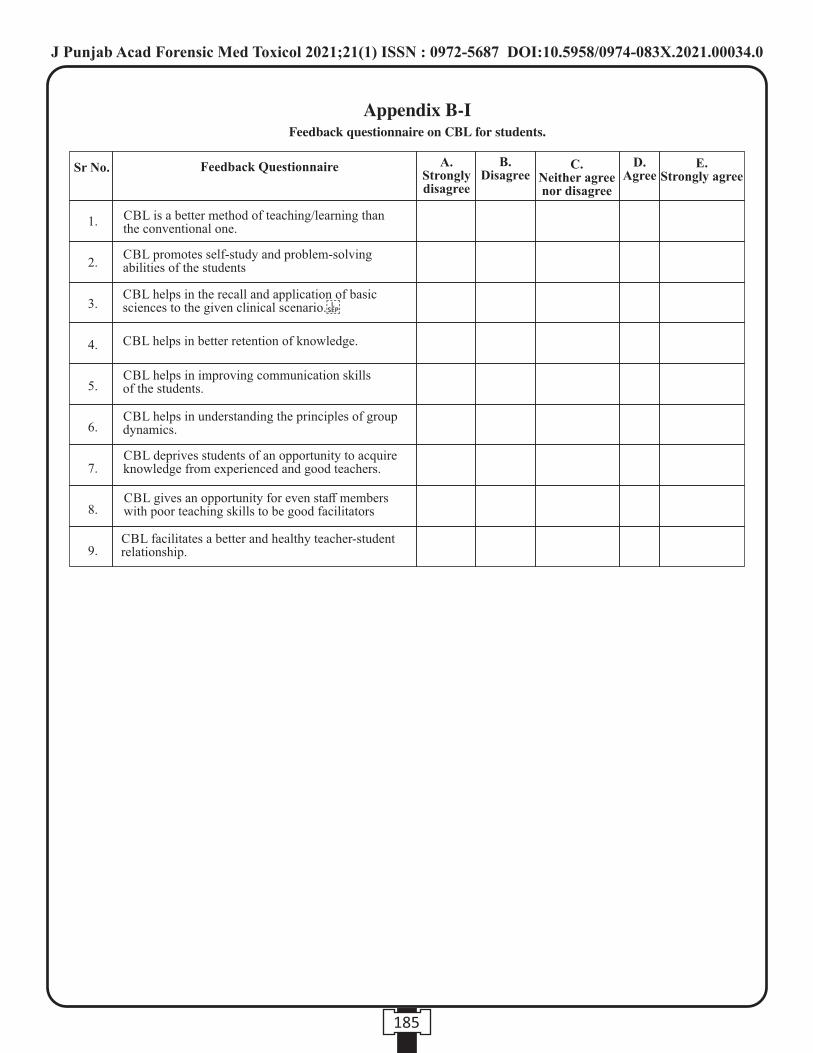
185
Feedback questionnaire on CBL for students.
Sr No.
1.
2.
3.
4.
5.
6.
7.
8.
9.
Feedback Questionnaire A.Strongly disagree
B.Disagree
C.Neither agree nor disagree
D. Agree
E.Strongly agree
CBL is a better method of teaching/learning than the conventional one.
CBL promotes self-study and problem-solving abilities of the students
CBL helps in the recall and application of basic sciences to the given clinical scenario.
CBL helps in better retention of knowledge.
CBL helps in improving communication skills of the students.
CBL helps in understanding the principles of group dynamics.
CBL deprives students of an opportunity to acquire knowledge from experienced and good teachers.
CBL gives an opportunity for even staff members with poor teaching skills to be good facilitators
CBL facilitates a better and healthy teacher-student relationship.
Appendix B-I
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00034.0
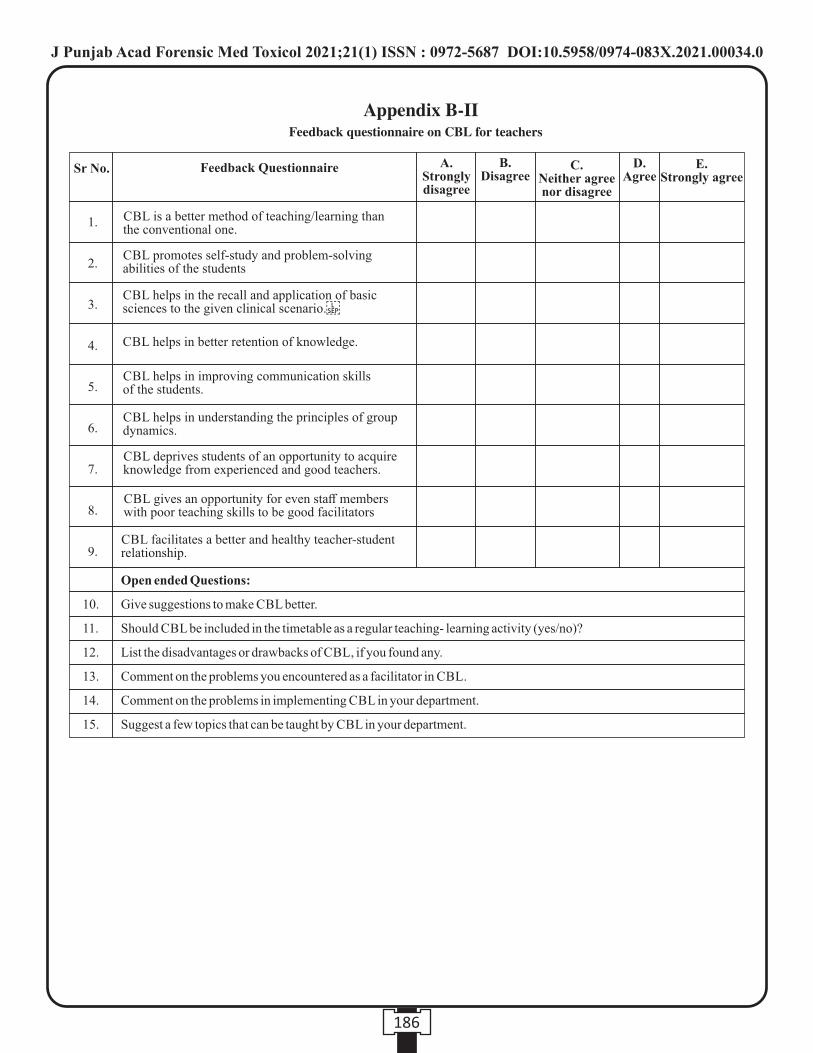
Open ended Questions:
10. Give suggestions to make CBL better.
11. Should CBL be included in the timetable as a regular teaching- learning activity (yes/no)?
12. List the disadvantages or drawbacks of CBL, if you found any.
13. Comment on the problems you encountered as a facilitator in CBL.
14. Comment on the problems in implementing CBL in your department.
15. Suggest a few topics that can be taught by CBL in your department.
Sr No.
1.
2.
3.
4.
5.
6.
7.
8.
9.
Feedback Questionnaire A.Strongly disagree
B.Disagree
C.Neither agree nor disagree
D. Agree
E.Strongly agree
CBL is a better method of teaching/learning than the conventional one.
CBL promotes self-study and problem-solving abilities of the students
CBL helps in the recall and application of basic sciences to the given clinical scenario.
CBL helps in better retention of knowledge.
CBL helps in improving communication skills of the students.
CBL helps in understanding the principles of group dynamics.
CBL deprives students of an opportunity to acquire knowledge from experienced and good teachers.
CBL gives an opportunity for even staff members with poor teaching skills to be good facilitators
CBL facilitates a better and healthy teacher-student relationship.
186
Feedback questionnaire on CBL for teachers
Appendix B-II
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00034.0
Original Research Paper
INTRODUCTION :
Lying has been an integral part of human society since its
beginning. We may not want to admit this or not be aware of it,
but lying has become a part of our everyday lives. A study of
social interactions reported that on an average, college
students told two lies per day, and community members told
one lie per day. Undergrads reported lying in about one third of
their social interactions, while people from the community lied 1in one fifth . Most of these lies have low stakes though.
Lying is described as the deliberate act of deviating from the
truth. A person is said to lie when he intends to mislead another 2without having been explicitly asked to do so by the victim .
Newer techniques, other than polygraph, like use of verbal
clues, linguistic analysis, voice analysis, micro expression
analysis and f-MRI for detecting memory and encoding
related multifaceted electroencephalographic response 2(MERMER) have shown promising results.
Darwin was of the belief that emotions are universal, evolved 3and cannot be controlled easily . In this emotional approach to
lying, it is emphasized that deceiving causes physiological,
psychological and emotional responses due to the arousal. The
arousal is the result of the guilt and fear of being caught. Part of
these emotions can be controlled but most of the times this
conscious approach to control emotions leads to leaks that give 4away a lie . Non-Verbal communication is perhaps the most
important communicative tool that one can learn to use,
observe and interpret. Mehrabian formulated that,
transmission of emotional messages in a brief interaction
between strangers more on facial expressions (55%), than
vocals (38%) and verbal's (7%). These non-verbal and vocal
clues are thought to be subconscious leaks of one's inner 5emotional states and can deceive a person's lie . It is by far
concluded from many previous studies that there is no single
Pinochio response that can give away a lie. When these facial
behaviors are studied in context of the lie, they can be an effective means to detect a lie.
As behavior, emotion and expression are strongly influenced 6by cultural factors , there is a strong need for studying micro
expressions in Indian settings. The intention of this study was
to observe the behavior of participants when lying or telling the
Corresponding Author :
Dr. Vijay Kautilya D,
Professor,
Department of Forensic Medicine & Toxicology, Manipal
TATA Medical College, Jamshedpur.
Contact : +91 94486-51848, 90949-43338
Email : [email protected]
KEYWORDS : Lie detection, Micro expressions, verbal cues, Non-verbal cues
Article History:Received: 13 April 2021Received in revised form: 9 July 2021Accepted on: 9 July 2021Available online: 31 August 2021
ABSTRACT :
Background: Use of verbal and nonverbal clues for deception have been analyzed recently and have shown promising results.
This study attempts to cataloged the various verbal and nonverbal cues of deception and analyze their significance.
Methodology: - The study was conducted among 50 subjects of south Indian origin who participated in an experiment which
required them to generate true statements and statements of deceit. The recordings of these statements were analyzed for verbal and
nonverbal clues and the results tabulated.
Results: - In the study it was found that the rate of occurrence of various nonverbal responses increased in a deceit statement. Blink
rate and rate of shift of posture showed statistically significant increase in deceit statements. Asymmetric and false smiles were
associated with deceit statements.
Conclusion: From the findings of the study, it can be concluded that there is no single response that can detect deceit statement.
These cues of deception have to be viewed in comparison to the persons own baseline and cannot be generalized.
1. Vijay Kautilya D, Professor, Department of Forensic Medicine & Toxicology, Manipal TATA Medical College, Jamshedpur*
2. Shruti Prabhat Hegde, Professor, Department of Ophthalmology, Manipal TATA Medical College, Jamshedpur*
3. Pramika Rajashekaran, MBBS student, Shri Sathya Sai Medical College & Research Institute.
*Manipal Academy of Higher Education, Manipal
Study of the Profile of Verbal and Non- verbal Clues of Deception among People of South Indian descent.
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00035.2
187

truth. In our study we have attempted to catalogue and
establish a profile of various verbal and Non-verbal clues of
deception in South Indians and also attempt to determine their
significance in detecting a lie individually and in the context of
the statement analysis annotations. The results of this study
will be of benefit to police interrogators, psychotherapists,
lawyers, judges, teachers, personal managers and voters in
detecting deception.
MATERIALS AND METHODS:
The study was conducted in Shri Sathya Sai Medical College
and Research center, Ammapettai, Chennai over a period of
two months. After obtaining Institutional Ethics Committee
Clearance an advertisement was put up in the college campus
asking for volunteers willing to participate in the study. The
subjects above 18yr of age (n=50, 24male & 26 female) were
selected from faculty, office staff and students on first come
first serve basis. Mother tongue (Telugu, Tamil, Kannada, and
Malayalam) was noted to select subjects from south of India.
Subjects resisting emotions in public sphere, subjects wearing
glasses and subjects unwilling to tell a lie were excluded from
the study. The participants were informed of the procedure and
purpose of the study and informed consent was obtained in
writing from all the participants.
Procedure of collection of data:
The study was designed in line with the study done by Biland et 7 5al and “20 Dollars for a Lie test” by Paul Ekman . In our
experiment, two subjects were to face each other and play a
game where one had to either tell the truth or lie to the other.
One player would try to discover if the other was lying. Care
was taken to pair male with another male subject and female
with another female subject in order to avoid gender
interaction effects and to balance the belief that women are
more skilled at observing and detecting nonverbal cues (NVC) 5based on evolutionary principals .
The Participants of the study performed the following
exercises as part of the game.
a) Exercise :- The participants had to write down six
statements describing incidences in their personal life which
they feel have an emotional value. Three of the statements need
to be true and the other three deceptive. The participant then
was asked to describe the statement convincingly to another
participant who judges if the statement is a lie or truth. For
every successful deceptive statement which the partner could
not identify the participant would get rupees 100. The reward
was given to provide motivation for lying so as to create high
stakes environment.
Data Analysis: -
The video recordings in the exercises were meticulously
analyzed for Verbal and Non-Verbal clues for deception using
video (kinovea 0.08.15) and audio (audacity 1.3 beta) analysis
software. Various nonverbal modulators of deception like
blinking, eye contact, gaze aversion, head movement, smile,
hand movement, posture shift, self-manipulation (scratch etc.)
and verbal modulators like voice, verbal style, verbal
statement, speech latency, repeated phrases or words studied in
the previous studies were analyzed for their frequency of
occurrence.
The data was statistically analyzed using SPSS (Statistical
Package for Social Sciences) computer software. As the
response variables are clustered within the participants with
each response being measured twice for the same participant
especially in exercise one repeated measure or paired sample
analysis was used. Frequency of occurrence of each parameter
in relation to the lie or truth with its statistical significance
waste calculated.
RESULTS:
The study sample consisted of 50(26 female & 24 Male)
subjects from Shri Sathya Sai Medical College & Research
Institute between the age group of 18 to 35 years with the
average age being 22.52yrs. As the study group consisted of
medical students (n=40) and medical teachers (n=10). All the
participants were already acquainted to their partners with an
average period of acquaintance being 3.5 yrs (Min-1yr, Max
10yrs).
Verbal and non-verbal cue analysis:
In the process of participation, each participant recorded three
true ad three false statements which were analyzed for the
average occurrence of each of the verbal and nonverbal cues of
deception described in earlier studies (Table no 1). The
variables were measured in an objective manner to ensure
reproducibility.
188
25 (50%)
0 (0%)
25 (50%)
25 (50%)
0 (0%)
25 (50%)
10 (20%)
15 (30%)
25 (50%)
35 (70%)
0 (0%)
15 (30%)
15 (30%)
5 (10%)
20 (40%)
0 (0%)
30 (60%)
20 (40%)
Smile congruence with motion of the statement
Smile symmetry
True smile
True statement
(n=50)
Factor analyzed False statement
(n=50)
Congruent smile
Incongruent smile
Smile absent
Symmetric
Asymmetric
Absent
Involves upper face
Lower face only
Absent smile
Table 1: Frequency of occurrence of various verbal andnonverbal clues of deception in truth and deceit statement.
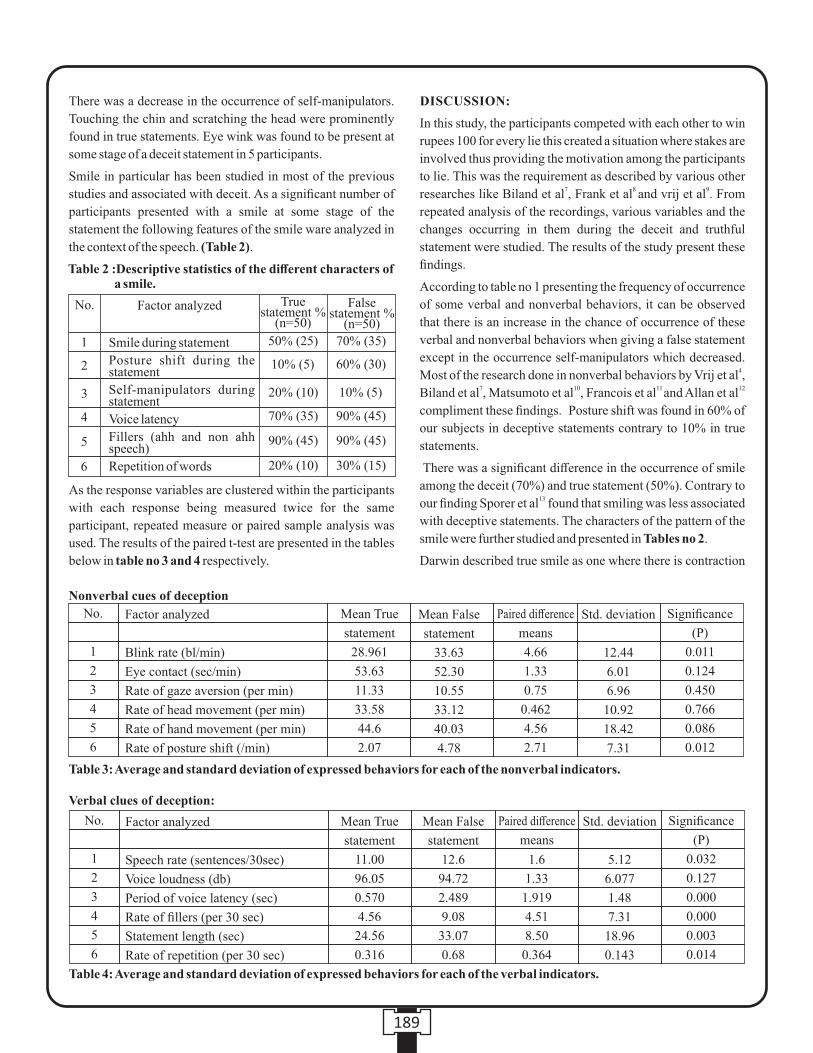
There was a decrease in the occurrence of self-manipulators.
Touching the chin and scratching the head were prominently
found in true statements. Eye wink was found to be present at
some stage of a deceit statement in 5 participants.
Smile in particular has been studied in most of the previous
studies and associated with deceit. As a significant number of
participants presented with a smile at some stage of the
statement the following features of the smile ware analyzed in
the context of the speech. (Table 2).
As the response variables are clustered within the participants
with each response being measured twice for the same
participant, repeated measure or paired sample analysis was
used. The results of the paired t-test are presented in the tables
below in table no 3 and 4 respectively.
DISCUSSION:
In this study, the participants competed with each other to win
rupees 100 for every lie this created a situation where stakes are
involved thus providing the motivation among the participants
to lie. This was the requirement as described by various other 7 8 9researches like Biland et al , Frank et al and vrij et al . From
repeated analysis of the recordings, various variables and the
changes occurring in them during the deceit and truthful
statement were studied. The results of the study present these
findings.
According to table no 1 presenting the frequency of occurrence
of some verbal and nonverbal behaviors, it can be observed
that there is an increase in the chance of occurrence of these
verbal and nonverbal behaviors when giving a false statement
except in the occurrence self-manipulators which decreased. 4Most of the research done in nonverbal behaviors by Vrij et al ,
7 10 11 12 Biland et al , Matsumoto et al , Francois et al and Allan et al
compliment these findings. Posture shift was found in 60% of
our subjects in deceptive statements contrary to 10% in true
statements.
There was a significant difference in the occurrence of smile
among the deceit (70%) and true statement (50%). Contrary to 13our finding Sporer et al found that smiling was less associated
with deceptive statements. The characters of the pattern of the
smile were further studied and presented in Tables no 2.
Darwin described true smile as one where there is contraction
189
No.
1
2
3
4
5
6
Smile during statement
Posture shift during the statement
Self-manipulators during statement
Voice latency
Fillers (ahh and non ahh speech)
Repetition of words
True statement %
(n=50)
50% (25)
10% (5)
20% (10)
70% (35)
90% (45)
20% (10)
Factor analyzed False statement %
(n=50)
70% (35)
60% (30)
10% (5)
90% (45)
90% (45)
30% (15)
Table 2 :Descriptive statistics of the different characters of a smile.
Table 4: Average and standard deviation of expressed behaviors for each of the verbal indicators.
Factor analyzed
Speech rate (sentences/30sec)
Voice loudness (db)
Period of voice latency (sec)
Rate of fillers (per 30 sec)
Statement length (sec)
Rate of repetition (per 30 sec)
Mean True
statement
11.00
96.05
0.570
4.56
24.56
0.316
Mean False
statement
12.6
94.72
2.489
9.08
33.07
0.68
1.6
1.33
1.919
4.51
8.50
0.364
No.
1
2
3
4
5
6
Paired difference
means
Std. deviation
5.12
6.077
1.48
7.31
18.96
0.143
Significance
(P)
0.032
0.127
0.000
0.000
0.003
0.014
Verbal clues of deception:
Table 3: Average and standard deviation of expressed behaviors for each of the nonverbal indicators.
Nonverbal cues of deception
Factor analyzed
Blink rate (bl/min)
Eye contact (sec/min)
Rate of gaze aversion (per min)
Rate of head movement (per min)
Rate of hand movement (per min)
Rate of posture shift (/min)
No.
1
2
3
4
5
6
Mean True
statement
28.961
53.63
11.33
33.58
44.6
2.07
Mean False
statement
33.63
52.30
10.55
33.12
40.03
4.78
Paired difference
means
4.66
1.33
0.75
0.462
4.56
2.71
Std. deviation
12.44
6.01
6.96
10.92
18.42
7.31
Significance
(P)
0.011
0.124
0.450
0.766
0.086
0.012

of both the muscles of the upper and lower part of the face. 7False smiles involve the lower part of the face only .Congruent
smile is considered when it is appropriate to the content of the
statement made. A symmetrical smile is one which presents
with contraction of the required muscles bilaterally.
Though the smiles in most of the situations were symmetrical,
asymmetrical smiles were only found in deceit statement (5%). 7These findings are in line with other finding by Biland et al ,
12 14Allen et al and Gamson et al .
Further as the verbal and nonverbal variables were measured
objectively for the true and false statement given by the same
person. The average difference of the means was measured and
paired sample analysis was performed to check for the
significance of the difference in the findings.
From the table no 3 it can be clearly seen that all the variables
studied show difference in the means for the true and false
statement. However statistically significant difference at P<
0.05 is found only with blink rate and rate of shift of posture per
minute. Blink rate showed an increase among the deceit
statements (about 4.66) compared to true statements. This was
statistically found to be significant at p<0.05. Blink rate has
been found to be one of the most reliable factors to differentiate
a true from a false statement by most of the resent studies by 3 2 12 14Vrij et al , Dhar et al , Allan et al Gamson et al & Porter et
(15,16)al . This increase in the motor responses during the deceit
statements is expected to be because of the arousal response
experienced by the subject during the deceit statements. Some 9researchers like Vrij et al have also shown decrease in the
motor responses during the deceit due to a conscious attempt
made by the participant to control his response.13Sporer et al in his study found that the period of eye contact
decreases during the deceit statement and there was an increase
in the frequency of gaze aversion however the results have not
been found to be significant statistically. Rate of sift of posture
has been found to be significantly increased during the deceit 11statements. This is similar to the findings of Francois et al .
Other differences found were statistically insignificant.
From the table no 4 showing paired sample analysis for verbal
cues of deception, it is clear that period of voice latency, rate of
fillers (ahh, other irrelevant sounds) and repetition of words 17showed the best statistical significance. Conellac et al
described similar linguistic clues in his study. The findings
were very significant at p<0.001. The rate of fillers, repetition
of words, and period of latency in the speech showed a
significant increase in deceit statement. However, speech rate
and loudness of voice decreased in deception statements. 9 11These finding are also described by Frank et al , Francois et al ,
17 18Conellae et al & Matsumoto et al .
CONCLUSION:
From the study of the verbal and nonverbal cues of deception in
this study it can be concluded that there is no single response
that can differentiate a lie from the truth. Deceptive statements
are associated with an increase in the rate of occurrence of
motor responses and incongruent false smiles. Blink rate and
postural shift are significantly important in deception analysis.
Gaze aversion, eye contact, head movement and self-
manipulation are not significant in identifying deceptive
statement. Vocal clues like voice latency, rate of fillers and
repetition are significant indicators of deception. All these
findings are relevant only when compared with the persons
baseline behavior and cannot absolute or generalized.
Acknowledgement: The study was accepted as an ICMR-
STS project and has been presented as a paper in IMALE-
2014 conference.
REFERENCES:
1. Dyer, Rebecca. Are You Lying to Me?: Using Nonverbal
Cues to Detect Deception. Diss. Haverford College,
Department of Psychology. 2007: P4-5. Available from :
URL: http://hdl.handle.net/10066/995
2. Dhar A , Shriharsh V. The theoretical study of lying and
micro-expressions. Astitva Int J of Commerce
Management and Social Sci. Dec 2012; 1(1): P39.
3. Ursula H, Thibault P. Darwin and emotion expression.
American Psychologist. 2009; 64(2): p 120. DOI:
10.1037/a0013386
4. Vrij A, Semin G. R. Lie experts' beliefs about nonverbal
indicators of deception. J of Nonverbal Behaviour. 1996;
20: p 65-80.
5. Lang Erick. Lie to me: video Analysis of Non-Verbal
Communication Between female Students in a Game of
Deceit. Diss. Dept of social psychology. London School
of Economics and Political Science. P 6-7. Available
from: url:
http://www.lse.ac.uk/socialPsychology/research_activiti
es/Lang_Erik160809.pdf
6. Matsumoto D. Culture and emotional expression.
Problems and solutions in cross cultural theory, research
and application. New York: Psychology press; 2009;
p263
7. Biland , Allione J, Demarchi S, Abric J. The effect of lying
on intentional versus unintentional facial expressions.
Revue européenne de psychologie appliqué. 2008; 58:
p65–73.
8. Frank MG, Menasco AM, O'Sullivan M. Human behavior
and deception Detection. Handbook of Science and
190
Technology for Homeland Security. newyork: John Wiley
& Sons; 2008;p4-5.
9. Vrij A, Edward K, Robert P K, Bull R. Detecting deceit via
analysis of verbal and nonverbal behavior. Journal of
Nonverbal Behavior. 2000; 24(4): p-236- 263.
10. Matsumoto D, Hwang HS, Skinner L, Frank M.
Evaluating Truthfulness and Detecting Deception. FBI
law enforcement Bulletin. June 2011;80(6): p1-8.
Available from: URL: http://www.fbi.gov/stats-
s e r v i c e s / p u b l i c a t i o n s / l a w - e n f o r c e m e n t -
bulletin/june_2011/school_violence
11. Francois P, Gracia E. Studying Liars: Tips for Detecting
Deception. Third Degree Communications, Inc. March
2007; Available from: URL:
http://www.tdcorg.com/download/StudyingLiars-03-24-
07.pdf
12. Allan Peace, Barbra Peace. Evaluation and Deceit signals.
The definitive book of body language. Ed1; Australia
,Peace International: 2004; p 142-192
13. Sporer LS, Schwandt B. Moderators of nonverbal
indicators of deception-a meta-analytic synthesis.
Psychology, Public Policy, and Law. 2007; 13(1): p34.
DOI: 10.1037/1076-8971.13.1.1
14. Gamson, Rachel, Gottesman J, Milan N, Weerasuriya S.
Cues to Catching Deception in Interviews. National
Consortium for the Study of Terrorism and Responses to
Terrorist START. 2012; p2-9.
15. Porter S, Brinke L. Reading between the Lies Identifying
Concealed and Falsified Emotions in Universal Facial
Expressions. Psychological science. 19(5): p508-514.
16. Porter S, Brinke L, Wallace B. Secrets and Lies:
Involuntary Leakage in Deceptive Facial Expressions as a
Function of Emotional Intensity. J Nonverbal Behav.
2012; 36: p23–37. DOI 10.1007/s10919-011-0120-7
17. Connell AC. Linguistic Cues to Deception. Diss. Virginia
Polytechnic Institute and State University. 2012; p6-
Available from: Url:
http://scholar.lib.vt.edu/theses/available/etd-05092012-
160131/unrestricted/ Connell_CA_T_2012.pdf
18. Matsumoto D, Hwang HS, Skinner L, Frank M.
Evaluating Truthfulness and Detecting Deception- New
Tools to Aid Investigators. FBI law enforcement Bulletin.
2011; P1-9. Available from: Url:
http://davidmatsumoto.com/content/Evaluating%20
Truthfulness%20and%20Detecting%20Deception.pdf
191

Original Research Paper
INTRODUCTION:
Education and technology have been inextricably linked in
recent decades, as education is the bedrock of academic fields.
As a result, scientists have coined the terms "information age," 1"computer age," and "digital age" to define the new period .
The constant evolution of medical science in general, and in
particular of medical services, has created the need for
advances and improvements in medical education. Graduate
medical education has traditionally been lecture-based, and
students rely heavily on textbooks and clinical training for
learning purposes. Clinical training plays an important role in
the growth of medical skills and in the training of individuals
and students are able to apply learned principles in practice.
Research results suggest that deficiencies, such as lack of
coordination between theoretical learning and clinical
services, lack of proper training facilities and equipment,
diversity in the role of trainers and lack of training time, have
made the standard of clinical training not satisfactory, as well
as ensuring the safety and satisfaction of patients facing 2-4challenges . Medical students, on the other hand, rely heavily
on medical books and tools and need timely access to
information such as algorithms and clinical recommendations,
drug reference, statistical statistics, demographic information,
and also the latest scientific evidence at the point of care from 3-6anywhere at any time . Therefore to meet such information
needs in clinical training, it is must for students to have
knowledge about the latest technology and also use them in
practice.
The emergence of new technology, such as smartphones, is not
limited to clinical practice, but has also made its way into
medical training.Smartphones have been identified as mobile
telecommunications devices with advanced features such as
medical applications, word processing, internet access and 7other computing capabilities . The ability to access medical
knowledge through a smartphone often expands its use beyond
Corresponding Author :
Dr. Arti Ajay Kasulkar,
Associate Professor,
Department of Forensic Medicine & Toxicology, NKP Salve
Institute of Medical Sciences & Research Center and Lata
Mangeshkar Hospital, Digdoh Hills, Hingana Road, Nagpur-
440019.
Contact : +91 9881907277
Email : [email protected]
KEYWORDS : Smart phones, Medical related applications, Learning, Medical undergraduates, Questionnaire.
Article History:Received: 9 June 2021Received in revised form: 9 July 2021Accepted on: 9 July 2021Available online: 31 July 2021
ABSTRACT :
Introduction: Smart phones are becoming a more relevant forum for delivering health information and medical interventions. The
majority of newer generation smart phones are increasingly being seen as portable computers.
Material and Method: A cross-sectional questionnaire-based online survey was conducted among medical students to assess their
knowledge regarding use of smart phones and medical related applications and to identify barriers if any in its usage.
Result: 197 (98.5%) students owned a smart phone, android 173(86.5%) being the preferred operating system. Marrow (49.6%),
Prepladder (34.1%), and Medscape (22.9%) were the top one medical application they preferred to use. 145(72.5%) students used
Medical information education programming for learning purpose and found useful and reliable for learning.
Conclusion: Rapid introduction of modern technology has altered many facets of our communication and has the ability to alter
how we educate, read, and practice medicine. Smartphone technology is transforming how medicine is learned and practiced, with
medical students increasingly preferring to access convenient, frequently updated web-based literature over hard copies of books or
journals.
1. Sakshi Singh Chauhan, MBBS Student, NKP Salve Institute of Medical Sciences & Research Centre and Lata Mangeshkar Hospital, Nagpur.
2. Arti Ajay Kasulkar, Associate Professor, Department of Forensic Medicine & Toxicology, NKP Salve Institute of Medical Sciences & Research Centre and Lata Mangeshkar Hospital, Nagpur.
Knowledge and practice of smart phones and medical related applications in learning by medical undergraduates.
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00036.4
192

simple communication devices. Recently, there has been a
meteoric rise in the popularity of smartphones and
subsequently the use of medical applications (commonly 8referred to as "apps") . There are currently more than 10,000
9apps in the category medical, health and fitness on app store .
Smartphone apps are self-contained software programs that 10can be downloaded and run from these smartphones . The
emerging trend in smartphone-related medical apps is also
providing medical students with groundbreaking means of
education. Some of the most common and useful smartphone
apps on the Android market are Medscape, Medicogram, Fast
LabRef, Marrow, Prepladder, and medscape, offer case-based
knowledge to students. In addition, students are also given the
opportunity to learn about rare medical conditions that are not
available in general clinical rotation. From this point of view,
researching the use of apps among medical students varies
considerably across other subjects.It is therefore crucial to
understand all facets of medical students' devices, smart
phones and academic life. The goal is to explore the use of
smartphones as an m-learning tool among medical students.
Mobile learning, or m-learning,is broadly defined as the
provision of learning material using mobile technology that
can be accessed at the convenience of a student from any 11location .
Although there are many benefits to using these smartphones
and medical-related apps, there are some challenges that
students face when implementing these applications. Some of
them could be expensive smartphones to buy, network
connectivity issues as some applications need a good internet
connection to work, privacy issues, usability of the battery, and
time consuming. With the emergence of new technology, it is
important to determine whether students have access to and
attitudes about new technology before it is incorporated in the
medical curriculum. With this in mind, the present study was
carried out to know about the use of smart phones and related
medical applications by medical graduates and to identify
barriers (if present) in its use.
MATERIALS AND METHODS:
After obtaining permission from the Institutional Ethics
Committee, a cross-sectional questionnaire-based online
survey was conducted among medical students of N.K.P. Salve
Institute of Medical Sciences & Research Centre and Lata
Mangeshkar Hospital, Nagpur from August 2020 to September
2020. The online validated questionnaire was developed with a
consent form attached to it.
The questionnaire covered demographic details, questions
assessing the knowledge of students regarding use of
smartphones and medical related applications, sources from
which they got to know about these applications and their
frequency of usage of these applications. The questionnaire
also focused towards understanding the barriers that prevent
the accessibility of this application for learning in medical
students. The questions elicit responses of students of all
academic year ranges regarding knowledge, usefulness and
reliability on these medical applications in learning.
The link of the questionnaire was sent to medical students
through E-mails and WhatsApp. On receiving and clicking the
link, the participants got auto directed to the information about
the study and informed consent.
Inclusion criteria: The students who were willing to
participate and consent were included.
Exclusion criteria: The students who were unwilling to
participate were not included in the study.
The online responses were tabulated and analyzed for
frequencies and percentage.
RESULTS :
The online survey was conducted among 200 medical
undergraduate students of all batches [Males = 107 (53.5%)
and Females = 93 (46.5%)]. The cohort comprised of first year
(n=47), second year (n=78), third year (n=47) and fourth year
(n=28) students. Year of study and gender wise distribution is
depicted in Table 1.
We observed that 197 (98.5%) medical undergraduate students
owned a smart phone (Fig. 1) and android 173(86.5%) was the
preferred operating system in their phones (Fig. 2).
Marrow (49.6%), Prepladder (34.1%), and Medscape(22.9%)
were the top one medical applications they preferred to use.
E m e d i c o z ( 1 8 . 6 % ) M e d i c a l e n c y c l o p e d i a ( 1 3 % ) ,
Pubmed(10.5%), Medicogram(3.1%) were the other popular
ones. In open ended question students also mentioned about
Dr. Najeeb, Osmosis, Histogram/Plexus, Prognosis,
auscultation, Medical pneumonic, GRG, General anatomy
app, Ankidroid, Clinical scenario, etc. (Fig. 3). Most of the
students 145(72.5%) used Medical information education
programming for learning purpose and found useful and
reliable for learning (Fig. 4).
It was also observed that 165(82.5%) students used social
media applications also for medical learning purpose with
Google and YouTube being the two topmost priorities of
students in all the MBBS professional years (Fig. 5).
As shown in Table 2, majority of the students 185(92.5%) were
aware about various medical related online available
applications, of which 161(80.5%) owned those applications.
Maximum participants 117(58.5%) had 1 to 2 applications in
their smart phones. When inquired about the source of
information regarding the medical applications, it was
193
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00036.4

predominantly through their friends followed by internet.
Medical applications were being used for educational
124(62%) as well as clinical learning 37(18.5%) several times
a day approximately spending 45 minutes a day.
A multiple-choice question with more than one answer correct
addressed barriers to using mobile devices for study and
practice. “No wireless access in the college or hospital” was
reported as the main barrier to using mobile devices for
information seeking, with 48.4%of students recognizing it as
being a problem (Fig. 6). Wireless access was broadly
recognized as a problem among all groups. As the college also
has some dead spots in cellular network coverage, the situation
even worsens. “Technical problems” (31%) and “Lack of
knowledge about the availability” are the other most
commonly reported barriers to access. Also, 22.3% students
faced no barriers at all.
DISCUSSION:
Smart phones and their incorporation with information
technology in health care facilities have the potential to change
the way health care is provided in the future due to rapid rise in
usage of medical applications and its users for efficient
learning. To our knowledge, very few studies of such kind have
been carried out. The collected data could be a useful
component to form smartphone ownership and usage 12landscape. Previous research by Chatzipavlou, Ioannis et al
finds Smartphone ownership equal to 96.6% but in our study,
98.5% ownership was observed. The slight increase shows the
increased popularity of smart phones among students. The 13result of the research conducted by Sefdari R et al shows that
in terms of prioritizing, the varieties of medical applications
are Up to date, Skyscape and Pubsearch. But the results of this
study show Marrow, Prepladder and Medscape are the first
three priorities.14The results of researches conducted by Vinay KV et al
indicates that Smart phones and their increasing integration
with information technology in colleges and hospitals can
change the way inwhich healthcare is delivered in the future.
When asked about if the students will recommend these
medical applications to their fellow students and juniors,
152(94.4%) students answered in yes. Almost 100% students thof 4 MBBS answered in yes. Such application by medical
college will help in compilation of all the presentations at one
place which in turn can be a great help for the students to learn.
CONCLUSION:
Today, technology is changing the way medicine is taught and
practiced. In particular, there is a rapid rise in medical
applications worldwide and an increase in people around the
world using these medical applications and other resources
available on smart phones for efficient learning. With the
widespread availability of downloadable medical applications
related to medical education, the level of smart phone use by
medical students and professionals is growing day by day. It is
therefore necessary to assess the current knowledge of Indian
universities' medical undergraduates regarding the use of
smartphones and medical applications for learning, so that
students can compete globally with other medical
undergraduates.
A thorough use of the resources available on smartphones for
learning purposes can expose students to recent medical
developments and keep them up-to-date. It is therefore very
important for us to know how medical graduates use these
applications and what the barriers that prevent them from
doing so are.
Acknowledgement:
We are grateful to the participants of the present study, without
their cooperation this study could not have been carried out.
Financial support and sponsorship: Nil.
Conflicts of interest: There are no conflicts of interest.
REFERENCES:
1. Abu-Faraj ZO, Barakat SS, Chaleby MH, Zaklit JD. A
S I M c a r d - b a s e d u b i q u i t o u s m e d i c a l r e c o r d
bracelet/pendant system — A pilot study. 4th International
Conference on Biomedical Engineering and Informatics
(BMEI); 2011: 1931-35.
2. Harati R. Collaboration teaching and its role on education
performance and student's achievement. European
Journal of Experimental Biology 2012; 2 (6):2182-2187.
3. Hoffman KG, Donaldson JF. Contextual tensions of the
clinical environment and their influence on teaching and
learning. Med Educ. 2004;38(4):448–54.
4. León SA, Fontelo P, Green L, Ackerman M, Liu F.
Evidence-based medicine among internal medicine
residents in a community hospital program using smart
phones.BMC Medical Informatics and Decision
Making2007; 7: 5.
5. Rahnema B, Rahnema F, Noure Elahi MH. An empirical
probe into integration of communication information
technology on psychological management of students and
staff at science and research branch, Islamic Azad
University, Tehran. European Journal of Experimental
Biology 2013; 3(5):46-60.
6. Davies BS, Rafique J, Vincent TR, Fairclough J, Packer
MH, Vincent R, et al. Mobile Medical Education
(MoMEd) - how mobile information resources contribute
to learning for undergraduate clinical students - a mixed
194
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00036.4
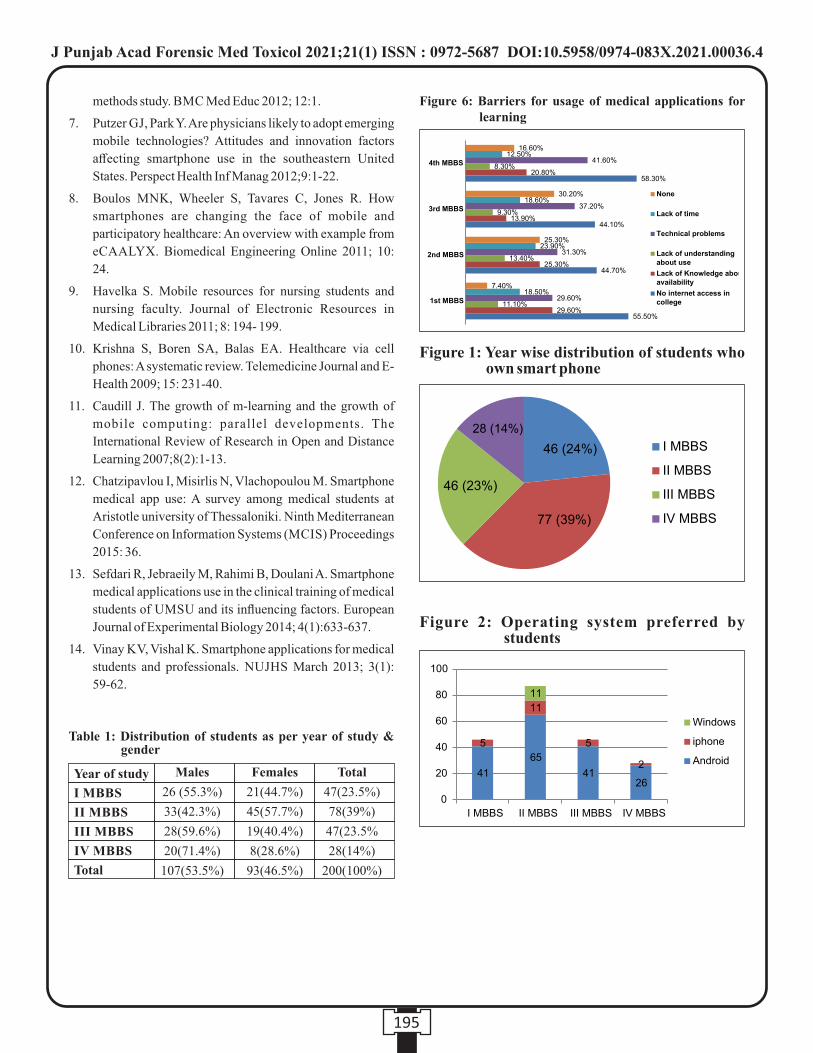
methods study. BMC Med Educ 2012; 12:1.
7. Putzer GJ, Park Y. Are physicians likely to adopt emerging
mobile technologies? Attitudes and innovation factors
affecting smartphone use in the southeastern United
States. Perspect Health Inf Manag 2012;9:1-22.
8. Boulos MNK, Wheeler S, Tavares C, Jones R. How
smartphones are changing the face of mobile and
participatory healthcare: An overview with example from
eCAALYX. Biomedical Engineering Online 2011; 10:
24.
9. Havelka S. Mobile resources for nursing students and
nursing faculty. Journal of Electronic Resources in
Medical Libraries 2011; 8: 194- 199.
10. Krishna S, Boren SA, Balas EA. Healthcare via cell
phones: A systematic review. Telemedicine Journal and E-
Health 2009; 15: 231-40.
11. Caudill J. The growth of m-learning and the growth of
mobile computing: parallel developments. The
International Review of Research in Open and Distance
Learning 2007;8(2):1-13.
12. Chatzipavlou I, Misirlis N, Vlachopoulou M. Smartphone
medical app use: A survey among medical students at
Aristotle university of Thessaloniki. Ninth Mediterranean
Conference on Information Systems (MCIS) Proceedings
2015: 36.
13. Sefdari R, Jebraeily M, Rahimi B, Doulani A. Smartphone
medical applications use in the clinical training of medical
students of UMSU and its influencing factors. European
Journal of Experimental Biology 2014; 4(1):633-637.
14. Vinay KV, Vishal K. Smartphone applications for medical
students and professionals. NUJHS March 2013; 3(1):
59-62.
195
Table 1: Distribution of students as per year of study & gender
Year of study
I MBBS
II MBBS
III MBBS
IV MBBS
Total
Males
26 (55.3%)
33(42.3%)
28(59.6%)
20(71.4%)
107(53.5%)
Females
21(44.7%)
45(57.7%)
19(40.4%)
8(28.6%)
93(46.5%)
Total
47(23.5%)
78(39%)
47(23.5%
28(14%)
200(100%)
Figure 6: Barriers for usage of medical applications for learning
Figure 1: Year wise distribution of students who own smart phone
Figure 2: Operating system preferred by students
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00036.4
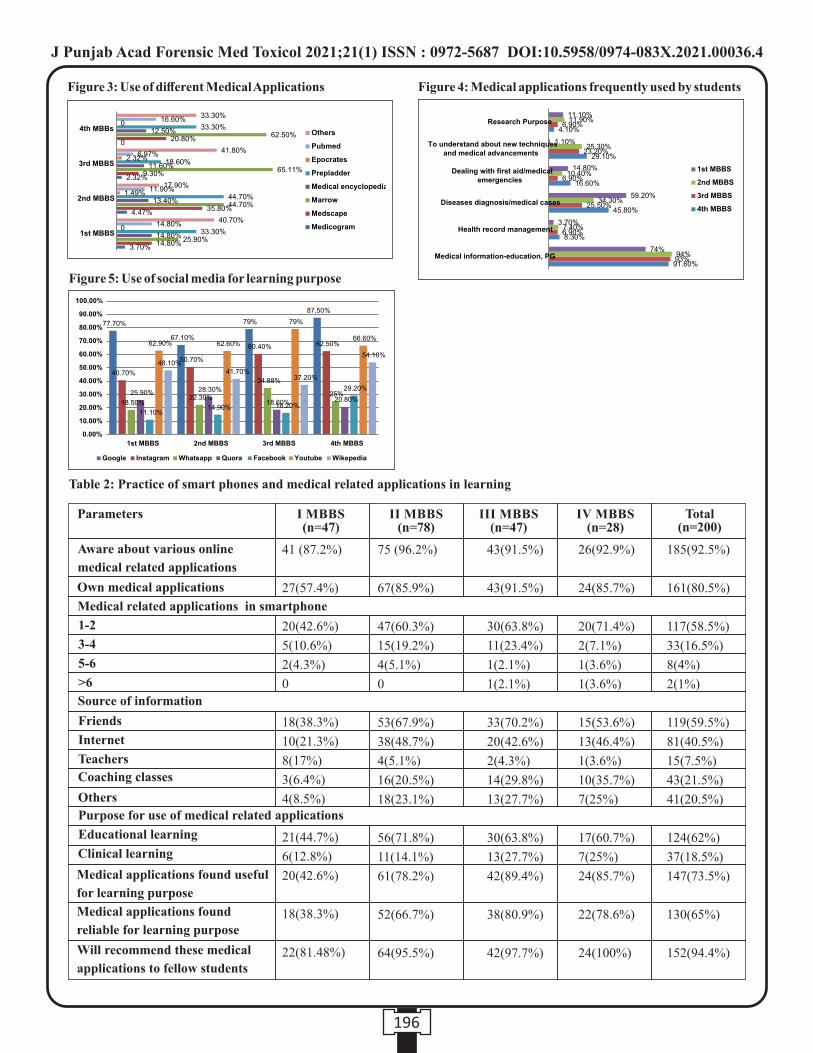
196
Figure 3: Use of different Medical Applications Figure 4: Medical applications frequently used by students
26(92.9%)
24(85.7%)
20(71.4%)
2(7.1%)
1(3.6%)
1(3.6%)
15(53.6%)
13(46.4%)
1(3.6%)
10(35.7%)
7(25%)
17(60.7%)
7(25%)
24(85.7%)
22(78.6%)
24(100%)
185(92.5%)
161(80.5%)
117(58.5%)
33(16.5%)
8(4%)
2(1%)
119(59.5%)
81(40.5%)
15(7.5%)
43(21.5%)
41(20.5%)
124(62%)
37(18.5%)
147(73.5%)
130(65%)
152(94.4%)
Table 2: Practice of smart phones and medical related applications in learning
Parameters
Aware about various online
medical related applications
Own medical applications
Medical related applications in smartphone
1-2
3-4
5-6
>6
Source of information
Friends
Internet
Teachers
Coaching classes
Others
Purpose for use of medical related applications
Educational learning
Clinical learning
Medical applications found useful
for learning purpose
Medical applications found
reliable for learning purpose
Will recommend these medical
applications to fellow students
I MBBS (n=47)
II MBBS (n=78)
III MBBS(n=47)
IV MBBS (n=28)
Total (n=200)
41 (87.2%)
27(57.4%)
20(42.6%)
5(10.6%)
2(4.3%)
0
18(38.3%)
10(21.3%)
8(17%)
3(6.4%)
4(8.5%)
21(44.7%)
6(12.8%)
20(42.6%)
18(38.3%)
22(81.48%)
75 (96.2%)
67(85.9%)
47(60.3%)
15(19.2%)
4(5.1%)
0
53(67.9%)
38(48.7%)
4(5.1%)
16(20.5%)
18(23.1%)
56(71.8%)
11(14.1%)
61(78.2%)
52(66.7%)
64(95.5%)
43(91.5%)
43(91.5%)
30(63.8%)
11(23.4%)
1(2.1%)
1(2.1%)
33(70.2%)
20(42.6%)
2(4.3%)
14(29.8%)
13(27.7%)
30(63.8%)
13(27.7%)
42(89.4%)
38(80.9%)
42(97.7%)
Figure 5: Use of social media for learning purpose
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00036.4

197
Original Research Paper
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00037.6
1. Abirami Arthanari, BDS, PG (MSc Forensic Odontology)*
2. Nagabhushana Doggalli, Reader, Department of Forensic Odontology*
3. Vidhya A, BDS, PG (MSc Forensic Odontology)*
4. Karthikeya Patil, Professor and Head, Department of Oral Medicine and Radiology*
5. Sushma Rudra Swamy, Senior Lecturer, Department of Public Health Dentistry*
6. Sowmya Srinivas, Senior Lecturer, Department of Prosthodontics*
* JSS Dental College & Hospital, Mysuru, Karnataka- 570015
Key words: Forensic Odontology, Dental Age Estimation, UT Age Estimation software, Blankenship method, Kasper method
Corresponding Author:
Dr. Nagabhushana Doggalli,
Reader,
Department of Forensic Odontology,
JSS Dental College & Hospital, Mysuru, Karnataka- 570015
Contact : +91 9844413396
Email :[email protected]
Article History :
Received : 4 August 2020
Received in revised form : 19 August 2020
Accepted on : 19 August 2020
Available online : 31 August 2021
INTRODUCTION:
Forensic age estimation has been beneficial in assisting
authorities in narrowing the search possibilities of unknown
victims, estimating the age at death, differentiation of cluster
victims, determining eligibility for social benefits, and aiding
immigration services in the processing of undocumented
immigrants. Numerous studies have demonstrated the
reliability of using the human dentition as an estimator of
chronologic age. Dental techniques that use progressive
morphologic changes have proven to be the most accurate
methods for estimating the ages of infants, children and (1-2)adolescents . Toward the end of human skeletal growth and
development only a few age-dependent features can be
evaluated by morphological methods. The third molar is the
latest tooth to initiate and complete development and therefore (3-6)is the last available dental morphologic predicator of age .
MATERIALS AND METHODS:
The study was carried out from March 2019 to May 2019 on
samples consisted of 210 OPG's (105 males and 105 females)
of age ranging from 14.0 to 20.9 years with known date of
birth. Samples were divided into seven age groups (Table 1).
All the collected OPG's were taken with PROMAX digital
Planmeca Machine, archived in the Department of Oral
Medicine and Radiology, Mysore, Karnataka, India.
The validation of UT Age Estimation Software was done in the
versions 2.0.22 (Application Developed by: James M. Lewis,
David R. Senn, Jeff Silvaggi, UT Age Estimation Manual 2008
Database)
Installation of the Software was done as follow :
1. Access the Center for Education and Research in Forensics
website: www.utforensic.org
2. Left click on the “Age Estimation” tab.
3. Left click on the UT-Age 2008 Estimation Database
program installation tab.
4. Follow the directions on screen for installation. It is
Validation of University of Texas (UT) Age Estimation Software in Indian Population
ABSTRACT :
Introduction : The present study is to check the validity of Chronological age and Estimated age by using the University of Texas
(UT) age estimation software in Indian Population.
Materials and Methods : The study was conducted to assess the dental age utilizing third molar eruption using UT Age estimation
software of age group from 14.0 to 20.9 years of 210 samples (105 Males, 105 Females) in south Indian population. All four third
molars were included in this study. Statistical analysis was done to obtain Mean Absolute Error (MAE).
Results: Out of 5 methods least mean absolute error of 0.4 years for males in Blankenship method (D3) and MAE 0.7 years for
females in Unknown method (D5) and overall MAE irrespective of sex showed 0.6 years in Unknown method (D5). This proved
that Unknown method (D5) provides best result when compared to others.
Conclusions: Thus this method can be used to estimate age from developing third molar in Indian population by using this
software.

198
recommended to allow the program to be installed in the (11)default directory. Shown in figure 1
OPERATING THE PROGRAM:
After installation of the UT Age Estimation Software, the
window page appears. There are total Four Icons available in
the database like FILE, EDIT, WINDOW, and HELP. Then the (11)New Case entering procedure will begin as follows
Entering New Case Details:
Case data is entered on the Case Information page. Highlight
and left-click “File” then left-click “New Case” (File > New (11) Case) to activate the Case Information page. (Figure 2)
In this Software there are seven required data fields are specific
to each individual case. Those are the DATE, CASE #, FIRST
AND LAST NAME, SEX, ANCESTRY AND 3RD MOLAR
STAGING. If an entry is not made into any one of these fields,
the program will not allow the case information to be saved or
the age estimation to be calculated. The first data field to be
entered is the date.
The current date is always given as a default date but may be
changed. The date should be entered in the (mm/dd/yy) or
(mm-dd-yy) format. After entering the correct date, move to
the next field by pressing the TAB key. Continue entering data
into the appropriate fields and using the TAB key to move to
the next field. Fields that have a downward arrow to their right
are dropdown-box fields that can be populated with previously (11)saved and commonly used entries.
rdHere 3 molar staging scores (Demirjian's Stage 1973) were rdentered to each tooth in appropriate manner, if the 3 molar is
not available in any of the quadrant, that field should be left
blank.
Panoramic Radiographs Entering Procedure:
After entering the case details, Note the small rectangular
button to the upper right of the “Panoramic Radiograph field”.
Left clicking on this button will transform the “Panoramic
Radiograph” field into four fields, labelled “Quadrant PA's) for
the option to enter four periapical radiographs images. It is
possible to enter both a panoramic image and any or all of the
individual periapical images. To the right of the radiograph
image box is a box labelled “Print” with two circles and the
words “Panoramic” and “Quadrant PA's” within it. By default,
the panoramic radiograph image will be printed in the report as
indicated by the blue dot. If you desire to have the PA's as the
default radiograph printed in the report, left click on the empty
circle beside “Quadrant PA's”. If only a panoramic or PA
radiographs are entered, then the application will print that
image by default.
Once at last all the case information entered and panoramic
radiographs entered there is one button “APPLY” click on the
button to save the case information into the UT Age Estimation
Database. The “Cancel” button will clear the form of any (11)unsaved information. (figure 3)
A Demirjian staging chart showing the development of 3rd
molars according to Kasper is available for consultation by
clicking Help>Demirjian Staging. The chart can be enlarged
by maximizing the window screen accomplished by clicking (11)the rectangle in the upper right corner of the window (figure
4)
Table 1: Sample Distribution
Group
1
2
3
4
5
6
7
Total
Age (years)
14-14.9
15-15.9
16-16.9
17-17.9
18-18.9
19-19.9
20-20.9
Male
15
15
15
15
15
15
15
105
Female
15
15
15
15
15
15
15
105
(11)Figure 1: UT Age Estimation 2008 Software
(11)Figure 2: Showing the Case information details
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00037.6
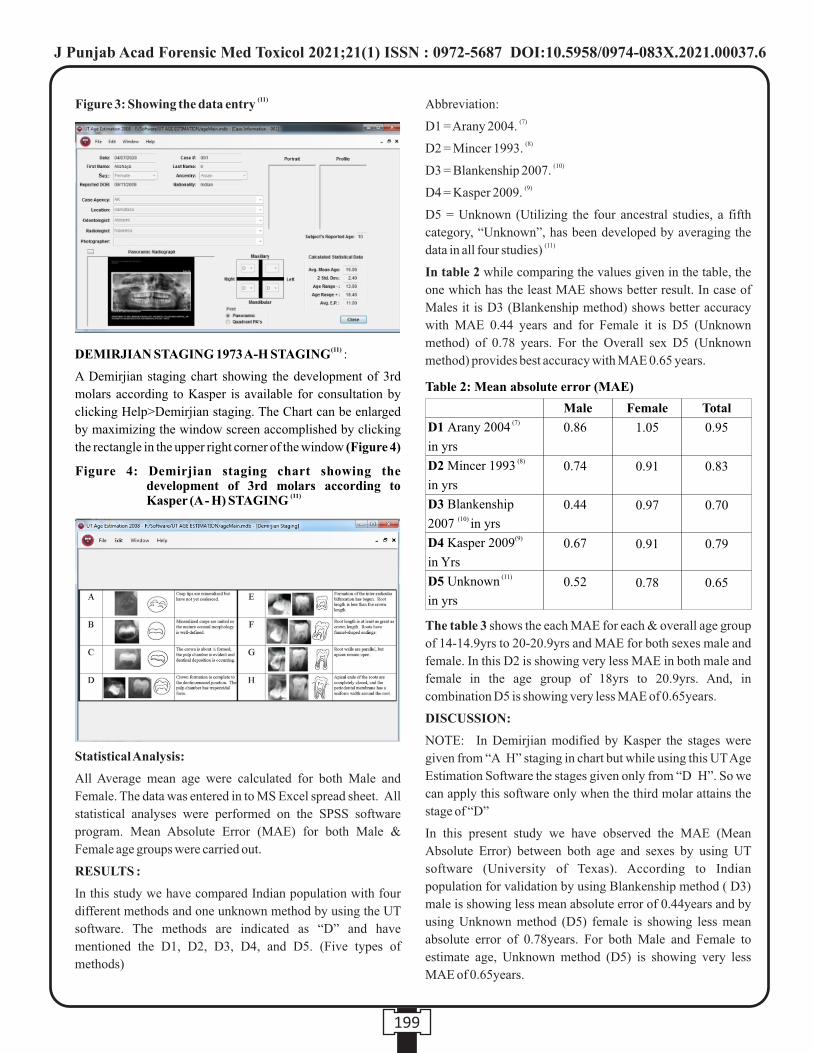
199
(11)DEMIRJIAN STAGING 1973 A-H STAGING :
A Demirjian staging chart showing the development of 3rd
molars according to Kasper is available for consultation by
clicking Help>Demirjian staging. The Chart can be enlarged
by maximizing the window screen accomplished by clicking
the rectangle in the upper right corner of the window (Figure 4)
Statistical Analysis:
All Average mean age were calculated for both Male and
Female. The data was entered in to MS Excel spread sheet. All
statistical analyses were performed on the SPSS software
program. Mean Absolute Error (MAE) for both Male &
Female age groups were carried out.
RESULTS :
In this study we have compared Indian population with four
different methods and one unknown method by using the UT
software. The methods are indicated as “D” and have
mentioned the D1, D2, D3, D4, and D5. (Five types of
methods)
Abbreviation:(7)D1 = Arany 2004.
(8)D2 = Mincer 1993. (10)D3 = Blankenship 2007.
(9)D4 = Kasper 2009.
D5 = Unknown (Utilizing the four ancestral studies, a fifth
category, “Unknown”, has been developed by averaging the (11)data in all four studies)
In table 2 while comparing the values given in the table, the
one which has the least MAE shows better result. In case of
Males it is D3 (Blankenship method) shows better accuracy
with MAE 0.44 years and for Female it is D5 (Unknown
method) of 0.78 years. For the Overall sex D5 (Unknown
method) provides best accuracy with MAE 0.65 years.
The table 3 shows the each MAE for each & overall age group
of 14-14.9yrs to 20-20.9yrs and MAE for both sexes male and
female. In this D2 is showing very less MAE in both male and
female in the age group of 18yrs to 20.9yrs. And, in
combination D5 is showing very less MAE of 0.65years.
DISCUSSION:
NOTE: In Demirjian modified by Kasper the stages were
given from “A H” staging in chart but while using this UT Age
Estimation Software the stages given only from “D H”. So we
can apply this software only when the third molar attains the
stage of “D”
In this present study we have observed the MAE (Mean
Absolute Error) between both age and sexes by using UT
software (University of Texas). According to Indian
population for validation by using Blankenship method ( D3)
male is showing less mean absolute error of 0.44years and by
using Unknown method (D5) female is showing less mean
absolute error of 0.78years. For both Male and Female to
estimate age, Unknown method (D5) is showing very less
MAE of 0.65years.
(11)Figure 3: Showing the data entry
Figure 4: Demirjian staging chart showing the development of 3rd molars according to
(11)Kasper (A - H) STAGING
Table 2: Mean absolute error (MAE)
Male
0.86
0.74
0.44
0.67
0.52
Female
1.05
0.91
0.97
0.91
0.78
Total
0.95
0.83
0.70
0.79
0.65
(7)D1 Arany 2004
in yrs (8) D2 Mincer 1993
in yrs
D3 Blankenship (10) 2007 in yrs
(9)D4 Kasper 2009
in Yrs (11) D5 Unknown
in yrs
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00037.6
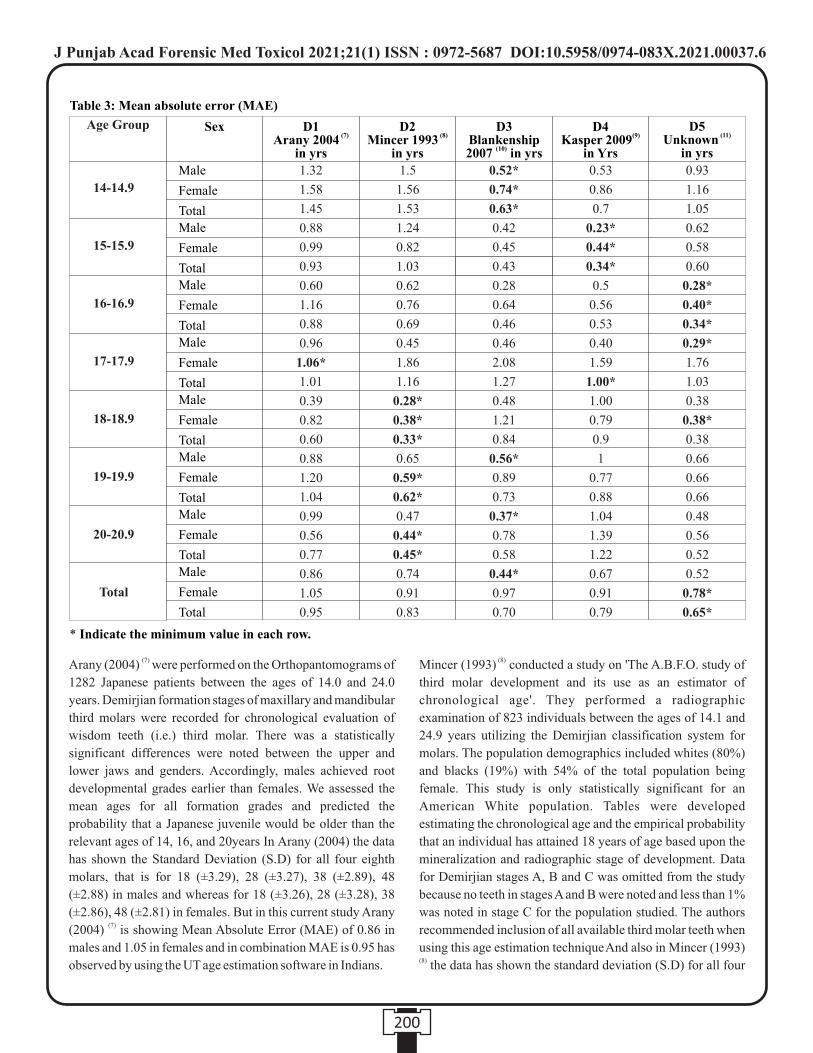
200
(7)Arany (2004) were performed on the Orthopantomograms of
1282 Japanese patients between the ages of 14.0 and 24.0
years. Demirjian formation stages of maxillary and mandibular
third molars were recorded for chronological evaluation of
wisdom teeth (i.e.) third molar. There was a statistically
significant differences were noted between the upper and
lower jaws and genders. Accordingly, males achieved root
developmental grades earlier than females. We assessed the
mean ages for all formation grades and predicted the
probability that a Japanese juvenile would be older than the
relevant ages of 14, 16, and 20years In Arany (2004) the data
has shown the Standard Deviation (S.D) for all four eighth
molars, that is for 18 (±3.29), 28 (±3.27), 38 (±2.89), 48
(±2.88) in males and whereas for 18 (±3.26), 28 (±3.28), 38
(±2.86), 48 (±2.81) in females. But in this current study Arany (7)(2004) is showing Mean Absolute Error (MAE) of 0.86 in
males and 1.05 in females and in combination MAE is 0.95 has
observed by using the UT age estimation software in Indians.
(8)Mincer (1993) conducted a study on 'The A.B.F.O. study of
third molar development and its use as an estimator of
chronological age'. They performed a radiographic
examination of 823 individuals between the ages of 14.1 and
24.9 years utilizing the Demirjian classification system for
molars. The population demographics included whites (80%)
and blacks (19%) with 54% of the total population being
female. This study is only statistically significant for an
American White population. Tables were developed
estimating the chronological age and the empirical probability
that an individual has attained 18 years of age based upon the
mineralization and radiographic stage of development. Data
for Demirjian stages A, B and C was omitted from the study
because no teeth in stages A and B were noted and less than 1%
was noted in stage C for the population studied. The authors
recommended inclusion of all available third molar teeth when using this age estimation techniqueAnd also in Mincer (1993)
(8) the data has shown the standard deviation (S.D) for all four
Age Group
Table 3: Mean absolute error (MAE)
Male
Female
Total
1.32
1.58
1.45
0.88
0.99
0.93
0.60
1.16
0.88
0.96
1.06*
1.01
0.39
0.82
0.60
0.88
1.20
1.04
0.99
0.56
0.77
0.86
1.05
0.95
1.5
1.56
1.53
1.24
0.82
1.03
0.62
0.76
0.69
0.45
1.86
1.16
0.28*
0.38*
0.33*
0.65
0.59*
0.62*
0.47
0.44*
0.45*
0.74
0.91
0.83
0.52*
0.74*
0.63*
0.42
0.45
0.43
0.28
0.64
0.46
0.46
2.08
1.27
0.48
1.21
0.84
0.56*
0.89
0.73
0.37*
0.78
0.58
0.44*
0.97
0.70
0.53
0.86
0.7
0.23*
0.44*
0.34*
0.5
0.56
0.53
0.40
1.59
1.00*
1.00
0.79
0.9
1
0.77
0.88
1.04
1.39
1.22
0.67
0.91
0.79
0.93
1.16
1.05
0.62
0.58
0.60
0.28*
0.40*
0.34*
0.29*
1.76
1.03
0.38
0.38*
0.38
0.66
0.66
0.66
0.48
0.56
0.52
0.52
0.78*
0.65*
Male
Female
Total
Male
Female
Total
Male
Female
Total
Male
Female
Total
Male
Female
Total
Male
Female
Total
Male
Female
Total
D1 (7) Arany 2004
in yrs
Sex D2 (8) Mincer 1993
in yrs
D3 Blankenship
(10) 2007 in yrs
D4 (9)Kasper 2009
in Yrs
D5 (11) Unknown
in yrs
14-14.9
15-15.9
16-16.9
17-17.9
18-18.9
19-19.9
20-20.9
Total
* Indicate the minimum value in each row.
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00037.6

201
eighth molar by using Univariate and multivariate regression
analysis. By using Univariate regression analysis standard
deviation for 18 (±1.25), 28 (±1.22) 38 (±1.13), 48 (±1.19) and
by using Multivariate regression analysis standard deviation is
±1.10 respectively. While, in this current study the Mean
Absolute Error is 0.74 for male, 0.91 for female and in
combination MAE is 0.83 has observed by using the UT age
estimation software. (9)Kasper (2009) conducted a study on 'Reliability of third
molar development for age estimation in a Texas Hispanic
population'. They evaluated third molar development from a
Texas Hispanic population of 950 individuals ranging in age
from 12 to 22 years with 56% of the studied population being
female. Slightly more than half of the individuals (55%) were
examined in North Texas (Dallas) and the remainder primarily
from colonies in Cameron County in Deep South Texas. This
study utilized the Demirjian classification system as modified
by Kasper. From the resulting data, the estimated age at each
stage and the probability of the individual reaching age 18 was
calculated for males and females sub-grouped by maxillary
and mandibular third molars. While, in this current study the
Mean Absolute Error is 0.69 in male, 0.91 in female and in
combination MAE is 0.79 has observed by using the UT age
estimation software. (10)Blankenship (2007) Third molar (M3) development
determined from dental radiographs in American blacks
(African Americans; n = 637) aged 1424 years was contrasted
against American whites (n = 563) from a previous study using
the method of Demirjian et al. Differences were assessed using
descriptive statistics and the parametric proportional hazards
model. For each developmental stage, the probability of an
individual being at least 18 years old was evaluated. As in other
M3 studies, there were highly significant modal differences,
but the age ranges at each stage overlapped considerably.
Blackwhite differences were highly significant with
developmental stages occurring in blacks a year or so earlier.
Gender differences also varied significantly, both with
increasing age and between races. The empirical likelihood
that an African American male with fully developed M3's is at
least 18 years old is 93% and that for African American female
is 84%. Corresponding risks for whites are 90% and 93%.
While, in this current study the Mean Absolute Error is 0.44 for
male, 0.97 for female and in combination MAE is 0.70 has
observed by using the UT age estimation software.
In this current study, Mean Absolute Error (MAE) has been
observed to obtain the accuracy. Thus this method can be used
to estimate age from developing third molar in Indian
population by using this software.
Comparing our results with a previous results done by Arany
(7) (8) (9)(2004) , Mincer (1993) , Kasper (2009) and Blankenship (10)(2007) we have got a Mean Absolute Error (MAE) of within
few months. Compared to others (Overall error) total of
0.65years. And other studies are like population specific study
and it is useful for population specific variation too. This
present study is completely for Indian population with good
MAE results.
CONCLUSION:
In this study third molar root development is reliably used to
validate the chronological age and estimated age by using four
known method and one unknown method with the help of UT
software (University of Texas). Hence, irrespectively
Unknown method has given the very less Mean Absolute Error
(MAE) of 0.65years for both Male and Female groups.
Estimation of age in living and dead individuals utilizes growth
and developmental indicators that can be active until, the early
fourth decade in the human beings. Data regarding the
development of the third molar compliments of the skeletal
data available to estimate the age of unknown juveniles and
young adults, third molar development is most significant for
age estimation of individuals from mid teens to early twenties.
Acknowledgement:
Mr. Mahadevayya Muddapur, Biostatistician, for his
contribution in biostatistics report.
Contact: [email protected]
Dr. Roshan K. Chaudhary, BDS, MSc (Forensic Odontology)
for his contribution in this study.
REFERENCES:
1. Senn. R. David., P.G. Stimson, Forensic Dentistry, 2nd
edition, Taylor & Francis, Boca Raton, 2010. 263 - 270
2. Demirjian, H. Goldstein, J.M. Tanner, A new system of
dental age assessment, Ann. Hum. Biol. 45 (2) (1973)
211227.
3. Gleiser, E.E. Hunt Jr., The permanent mandibular first
molar: its calcification, eruption and decay, Am. J. Phys.
Anthropol. 13 (2) (1955) 253283.
4. G. Gustafson, G. Koch, Age estimation up to 16 years of
age based on dental development, Odontol. Rev. 25 (3)
(1974) 297306.
5. M.J. Harris, C.J. Nortje, The mesial root of the third
mandibular molar. A possible indicator of age, J. Forensic
Odontostomatol. 2 (2) (1984) 3943.
6. L. Kullman, G. Johanson, L. Akesson, Root development
of the lower third molar and its relation to chronological
age, Swed. Dent. J. 16 (4) (1992) 161167.
7. A. Szilvia, L. Mitsuyoshi, Y. Naofumi, Radiographic
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00037.6
202
Survey of Third Molar Development in Relation to
Chronological Age Among Japanese Juveniles, J Forensic
Sci, May 2004, Vol. 49, No. 3. 2 4.
8. H.H. Mincer, E.F. Harris, H.E. Berryman, The A.B.F.O.
study of third molar development and its use as an
estimator of chronological age, J. Forensic Sci. 38 (2)
(1993) 379390.
9. K.A. Kasper, et al., Reliability of third molar development
for age estimation in a Texas Hispanic population: a
comparison study, J. Forensic Sci. 54 (3) (2009) 651657.
10. J.A. Blankenship, H.H. Mincer, K.M. Anderson, M.A.
Woods, B. L. Eddie Third molar development in the
estimation of chronologic age in American blacks as
compared with whites, J. Forensic Sci. 52 (2) (2007)
428433.
11.Lewis James. M, Senn David. R, Silvaggi. J, UT- Age
Estimation Database Version 2008 2.0.22 Manual. (2008)
4 12.
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00037.6
203
Original Research Paper
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00038.8
1. Abirami Arthanari, BDS, PG (MSc Forensic Odontology)*
2. Usha Hegde, Professor & Head, Department of Oral Pathology & Microbiology*
3. Nagabhushana Doggalli, Reader, Department of Forensic Odontology*
4. Priyanka Nithin, Assistant Professor, Department of Oral Pathology & Microbiology*
*JSS Dental College & Hospital, Mysuru, Karnataka- 570015
Key words: Forensic Odontology, Dental Age Estimation, UT Age Estimation software, Blankenship method, Kasper method
Corresponding Author:
Dr. Usha Hegde
Professor & Head,
Department of Oral Pathology & Microbiology,
JSS Dental College & Hospital, Mysuru, Karnataka- 570015
Contact : +91 98444-53444
Email :[email protected]
Article History :
Received : 29 May 2020
Received in revised form : 24 June 2020
Accepted on : 24 June 2020
Available online : 15 August 2021
INTRODUCTION:
Teeth play a crucial role in personal identification since they
are the hardest and biologically most stable material in the
human body. Teeth have the ability to resist adverse
environmental conditions and the pulpal tissue is well
protected, thus ensuring that it can be used to retrieve
information and aid in forensic investigations. Forensic
identification by its nature is a multidisciplinary approach
relying on positive identification methodology as well as 1presumptive or exclusionary methodologies.
Blood grouping has been one of the corner stone in
identification of biological material. The term blood group is
applied to the presence of inherited antigens on the red cell 2surface by specific antibodies.
A person's ABO type depends upon the presence of two genes
the A and B genes and these genes are encoded on chromosome
9 (in band 9q34.1). They determine part of the configuration on
the red blood cell surface. A person can be A, B, AB, or O blood 3 group based on the expression of the genes. Based on the Rh
blood group system each of the ABO blood groups can be 4either Rh+ or Rh-. Pulp tissue is enclosed within the dental
hard tissues, where post-mortem changes are seen very late.
Since tooth pulp is highly vascular, blood group antigens are
most certainly bound to be present. The possible distribution of
A Time Interval Based Forensic Study on Estimation of ABO Blood Group & Rh Typing From Dental Pulp: An Aid in Personal Identification
ABSTRACT :
Aims & Objectives: To assess the viability of pulp tissue in identifying the ABO blood group of an individual at various time
intervals (same day, after one week and six months of extraction) and assess its reliability by comparing with the routine capillary
agglutination method.
Materials and Methods: The study was conducted on 75 patients. The capillary blood samples were obtained by finger prick
method, the blood grouping and rhesus typing was done by slide agglutination method for each of the 75 patients and considered as
controls. The pulp obtained from the extracted teeth of the same 75 patients was considered as case. The cases were divided into 3
groups based on the time interval of pulp extirpation and examination for blood grouping & rhesus typing after extraction. Group I
(pulp extirpation on day of extraction), Group II (pulp extirpation after one week of extraction) and Group III (pulp extirpation after
six months of extraction). Blood grouping, Rhesus typing for extirpated dental pulp was done by modified absorption elution
method. The results of the cases were compared with the respective controls to arrive at conclusions.
Results: In Group I (n = 25) and Group III (n = 25), the results of blood group estimation by both the methods matched completely
and showed 100% sensitivity. In Group II (n = 25), 24 teeth samples showed consistent results with only one case being non
confirmatory and hence a sensitivity of 96%.
Conclusion: Teeth are hard structures and resist adverse environmental conditions. The pulp tissue within the tooth is well
protected and remains stable retaining the viability of the blood group antigen for at least up to 6 months. Thus, it could be
concluded from the present study that the dental pulp tissue can be used with good reliability in person identification.

204
ABO substances from the pulp cavity wall to the dentin edge
and to the enamel gradually decreases because of fewer
possibilities of diffusion of antigens from both blood and 5saliva.
6Absorption elution (AE) technique was devised by Siracusa 7and modified by Kind. Various modifications have taken place
since then to improve the sensitivity. This technique has been
used acceptably to determine blood group from dried stains,
tissues, secretions, and teeth in various forensic laboratories.
This method is sensitive, highly specific, and least interfered 8with the nature of the substrata.
MATERIALS AND METHODS:
The present study was conducted in JSS Dental College and
Hospital, Mysore for 6 months on Intact extracted teeth
collected from patients who underwent dental extraction
procedure for orthodontic or periodontal conditions. Decayed
and filled teeth were not included in the study.
The extracted teeth were the study samples and were divided
into three groups with each group having 25 teeth. Group 1:
Same day of extraction, Group 2: One week after extraction
and Group 3: Six months after extraction. All teeth samples
were decoded and labeled appropriately for an unbiased
evaluation.
Following aseptic protocol, the index finger was pricked with a
sterile needle and three separate drops of blood were placed on
a glass slide. To each drop, a drop of antiserum A, antiserum B
and antiserum D were added respectively. Based on the
agglutination occurring with the specific antiserum, the blood
grouping was established as either A (agglutination with
antiserum A), B (agglutination with antiserum B), O (no
agglutination with either antiserum A or antiserum B) and AB
(agglutination with both antiserum A and antiserum B). If
agglutination occurred with Antiserum D, it was Rh+,
otherwise Rh-. The obtained results were recorded and kept as
gold standard.
The extracted tooth was split vertically with carborundum disc
and the dental pulp was scooped out with a spoon excavator.
Tooth pulp was divided into three equal parts and put into
sterile labeled test tubes. To each of the test tube, 3 drops of one
antiserum, either A, B or D were added. It was made sure that
the test samples were sufficiently soaked in antiserum and left
at room temperature for 2 ½ hours to allow the antibodies to
combine with their specific antigens. The antiserum was
removed and each sample was washed three times with cold
saline solution. The samples were agitated by adding two to
three drops of saline, and then centrifuged for 5 min at 4,000
rpm. The supernatant was discarded using a Pasteur pipette and
the excess saline was removed. Two drops of fresh saline was
added to the sample and the test tubes were heated in a water
bath at 56°C for 10 min to elute the antibodies. A drop of 0.5%
A or B group red cell suspension was immediately placed into
each respective test tube to combine the eluted antibodies with
known red blood cells, resulting in agglutination of the
respective antibodies with the antigen present on the cell
surface of red cells. This was incubated at 37°C for 30 min to
enhance agglutination, followed by centrifugation at
1500-2000 rpm for 1 min for flocculants formation. By mildly
shaking of the test tube the presence or absence of red cell
agglutination was ascertained. This sample was used to make a
smear on the slide and a drop of Leishman Stain was added to it
to confirm the coagulation under microscope at magnification
of 100x. The above mentioned procedure was done for all the
samples of Group I. Similar procedure was carried out after
one week for group II samples and six months after the
extraction for group III samples. All the results were recorded.
The results were cross verified with the blood groups which
were already noted by slide agglutination method.
Preparation of A or B Cell Suspension:
Step 1: Withdraw 1ml of blood from a patient of known A/B
blood group.
Step 2: Store in a sterile test tube.
Step 3: Add 10ml of Normal Saline to the collected blood in the
test tube.
Step 4: Mix both collected blood and normal saline well. Then
the preparation of A/B cell suspension is ready.
NOTE: The prepared A/B cell suspension can be stored for 4 to
7 days at -4°c (in a refrigerator).
Statistical Method:
The data was entered into MS excel followed by the analysis
using SPSS version 23 (Statistical Package for the Social
Sciences 23). The demographic characters such as age, gender
etc were represented using arithmetic mean, standard deviation
and proportions. The estimation of the blood groups was done
in percentages and the same were followed at day of extraction,
after one week and after six months using Chi square test/
Fishers exact test. The p value of <0.05 was considered as
statistically significant.
RESULTS:
The results were given with the total number of samples and
ties being equal. When blood grouping from the pulp
correlated with blood group of the person, the result was
recorded as positive and if they did not match, the result was
recorded as negative.
The results were analyzed for the 75 test samples, distributed in
3 groups: Group 1 (blood grouping done on the day of
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00038.8
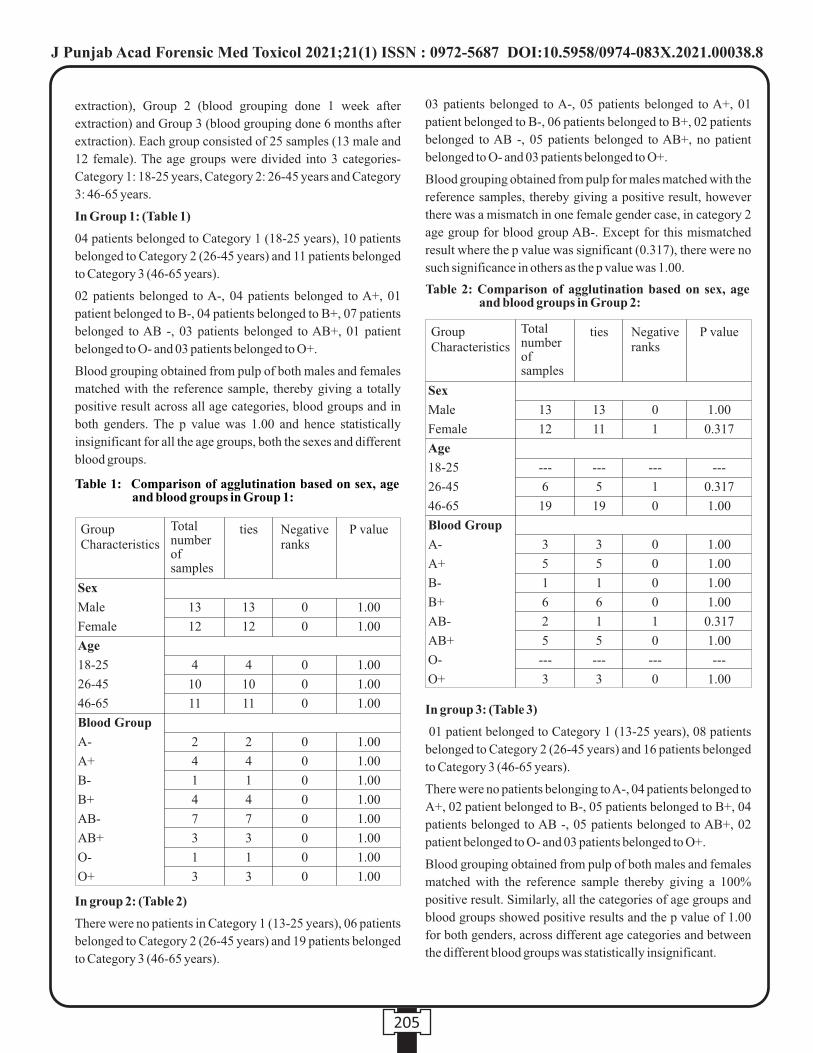
205
extraction), Group 2 (blood grouping done 1 week after
extraction) and Group 3 (blood grouping done 6 months after
extraction). Each group consisted of 25 samples (13 male and
12 female). The age groups were divided into 3 categories-
Category 1: 18-25 years, Category 2: 26-45 years and Category
3: 46-65 years.
In Group 1: (Table 1)
04 patients belonged to Category 1 (18-25 years), 10 patients
belonged to Category 2 (26-45 years) and 11 patients belonged
to Category 3 (46-65 years).
02 patients belonged to A-, 04 patients belonged to A+, 01
patient belonged to B-, 04 patients belonged to B+, 07 patients
belonged to AB -, 03 patients belonged to AB+, 01 patient
belonged to O- and 03 patients belonged to O+.
Blood grouping obtained from pulp of both males and females
matched with the reference sample, thereby giving a totally
positive result across all age categories, blood groups and in
both genders. The p value was 1.00 and hence statistically
insignificant for all the age groups, both the sexes and different
blood groups.
In group 2: (Table 2)
There were no patients in Category 1 (13-25 years), 06 patients
belonged to Category 2 (26-45 years) and 19 patients belonged
to Category 3 (46-65 years).
03 patients belonged to A-, 05 patients belonged to A+, 01
patient belonged to B-, 06 patients belonged to B+, 02 patients
belonged to AB -, 05 patients belonged to AB+, no patient
belonged to O- and 03 patients belonged to O+.
Blood grouping obtained from pulp for males matched with the
reference samples, thereby giving a positive result, however
there was a mismatch in one female gender case, in category 2
age group for blood group AB-. Except for this mismatched
result where the p value was significant (0.317), there were no
such significance in others as the p value was 1.00.
In group 3: (Table 3)
01 patient belonged to Category 1 (13-25 years), 08 patients
belonged to Category 2 (26-45 years) and 16 patients belonged
to Category 3 (46-65 years).
There were no patients belonging to A-, 04 patients belonged to
A+, 02 patient belonged to B-, 05 patients belonged to B+, 04
patients belonged to AB -, 05 patients belonged to AB+, 02
patient belonged to O- and 03 patients belonged to O+.
Blood grouping obtained from pulp of both males and females
matched with the reference sample thereby giving a 100%
positive result. Similarly, all the categories of age groups and
blood groups showed positive results and the p value of 1.00
for both genders, across different age categories and between
the different blood groups was statistically insignificant.
Table 1: Comparison of agglutination based on sex, age and blood groups in Group 1:
Group Characteristics
Sex
Male
Female
Age
18-25
26-45
46-65
Blood Group
A-
A+
B-
B+
AB-
AB+
O-
O+
13
12
4
10
11
2
4
1
4
7
3
1
3
13
12
4
10
11
2
4
1
4
7
3
1
3
0
0
0
0
0
0
0
0
0
0
0
0
0
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
ties Negative ranks
P valueTotal number of samples
Table 2: Comparison of agglutination based on sex, age and blood groups in Group 2:
Group Characteristics
Sex
Male
Female
Age
18-25
26-45
46-65
Blood Group
A-
A+
B-
B+
AB-
AB+
O-
O+
13
12
---
6
19
3
5
1
6
2
5
---
3
13
11
---
5
19
3
5
1
6
1
5
---
3
0
1
---
1
0
0
0
0
0
1
0
---
0
1.00
0.317
---
0.317
1.00
1.00
1.00
1.00
1.00
0.317
1.00
---
1.00
ties Negative ranks
P valueTotal number of samples
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00038.8
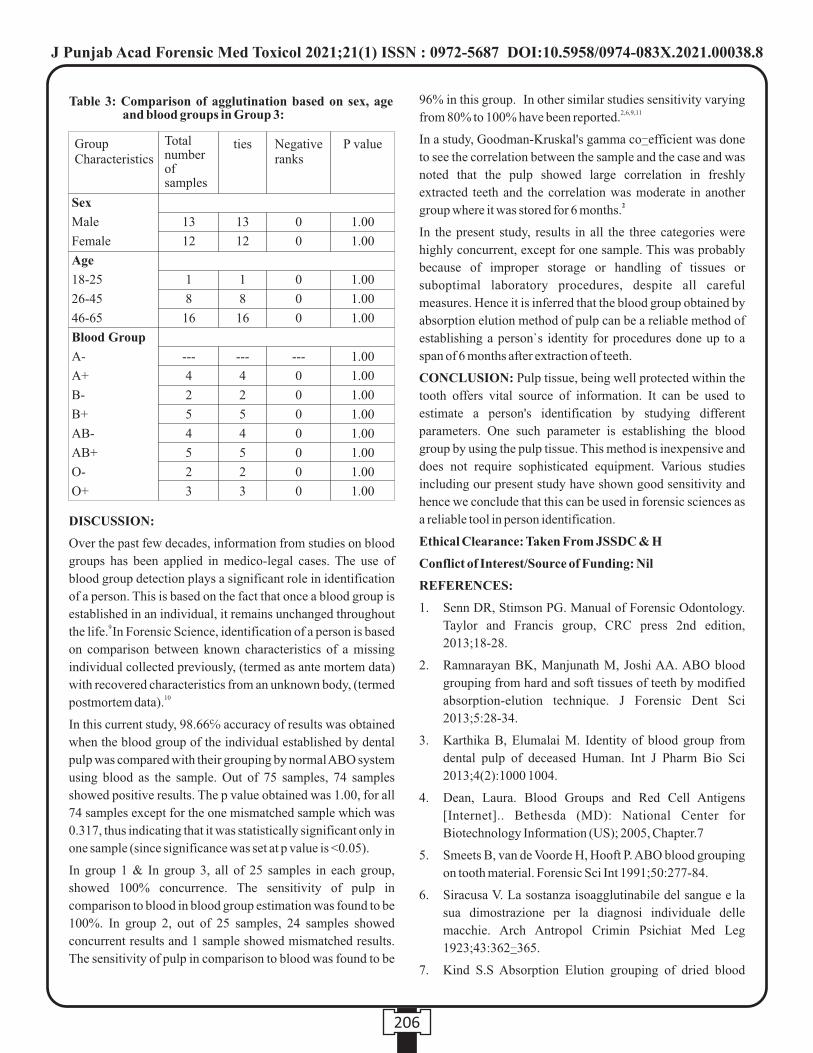
206
DISCUSSION:
Over the past few decades, information from studies on blood
groups has been applied in medico-legal cases. The use of
blood group detection plays a significant role in identification
of a person. This is based on the fact that once a blood group is
established in an individual, it remains unchanged throughout 9 the life. In Forensic Science, identification of a person is based
on comparison between known characteristics of a missing
individual collected previously, (termed as ante mortem data)
with recovered characteristics from an unknown body, (termed 10postmortem data).
In this current study, 98.66℅ accuracy of results was obtained
when the blood group of the individual established by dental
pulp was compared with their grouping by normal ABO system
using blood as the sample. Out of 75 samples, 74 samples
showed positive results. The p value obtained was 1.00, for all
74 samples except for the one mismatched sample which was
0.317, thus indicating that it was statistically significant only in
one sample (since significance was set at p value is <0.05).
In group 1 & In group 3, all of 25 samples in each group,
showed 100% concurrence. The sensitivity of pulp in
comparison to blood in blood group estimation was found to be
100%. In group 2, out of 25 samples, 24 samples showed
concurrent results and 1 sample showed mismatched results.
The sensitivity of pulp in comparison to blood was found to be
96% in this group. In other similar studies sensitivity varying 2,6,9,11from 80% to 100% have been reported.
In a study, Goodman-Kruskal's gamma co-efficient was done
to see the correlation between the sample and the case and was
noted that the pulp showed large correlation in freshly
extracted teeth and the correlation was moderate in another 2group where it was stored for 6 months.
In the present study, results in all the three categories were
highly concurrent, except for one sample. This was probably
because of improper storage or handling of tissues or
suboptimal laboratory procedures, despite all careful
measures. Hence it is inferred that the blood group obtained by
absorption elution method of pulp can be a reliable method of
establishing a person`s identity for procedures done up to a
span of 6 months after extraction of teeth.
CONCLUSION: Pulp tissue, being well protected within the
tooth offers vital source of information. It can be used to
estimate a person's identification by studying different
parameters. One such parameter is establishing the blood
group by using the pulp tissue. This method is inexpensive and
does not require sophisticated equipment. Various studies
including our present study have shown good sensitivity and
hence we conclude that this can be used in forensic sciences as
a reliable tool in person identification.
Ethical Clearance: Taken From JSSDC & H
Conflict of Interest/Source of Funding: Nil
REFERENCES:
1. Senn DR, Stimson PG. Manual of Forensic Odontology.
Taylor and Francis group, CRC press 2nd edition,
2013;18-28.
2. Ramnarayan BK, Manjunath M, Joshi AA. ABO blood
grouping from hard and soft tissues of teeth by modified
absorption-elution technique. J Forensic Dent Sci
2013;5:28-34.
3. Karthika B, Elumalai M. Identity of blood group from
dental pulp of deceased Human. Int J Pharm Bio Sci
2013;4(2):1000 1004.
4. Dean, Laura. Blood Groups and Red Cell Antigens
[Internet].. Bethesda (MD): National Center for
Biotechnology Information (US); 2005, Chapter.7
5. Smeets B, van de Voorde H, Hooft P. ABO blood grouping
on tooth material. Forensic Sci Int 1991;50:277-84.
6. Siracusa V. La sostanza isoagglutinabile del sangue e la
sua dimostrazione per la diagnosi individuale delle
macchie. Arch Antropol Crimin Psichiat Med Leg
1923;43:362-365.
7. Kind S.S Absorption Elution grouping of dried blood
Table 3: Comparison of agglutination based on sex, age and blood groups in Group 3:
Group Characteristics
Sex
Male
Female
Age
18-25
26-45
46-65
Blood Group
A-
A+
B-
B+
AB-
AB+
O-
O+
13
12
1
8
16
---
4
2
5
4
5
2
3
13
12
1
8
16
---
4
2
5
4
5
2
3
0
0
0
0
0
---
0
0
0
0
0
0
0
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
ties Negative ranks
P valueTotal number of samples
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00038.8

207
smears. Nature 1960;185;397.
8. Landsteiner, K.; Weiner, A. (1940). "An Agglutinable
Factor in Human Blood Recognized by Immune Sera for
Rhesus Blood". Exp Biol Med. 43 (1): 223.
9. Pramod JB, Marya A, Sharma V. Role of forensic
odontologist in post mortem person identification. Dent
Res J 2012;9:522-30.
10. Neiders ME, Standish SM. Blood group determinations in
forensic dentistry. Dent Clin North Am 1977;21:99-111.
11. Vrinda Saxena, Manish Jain, Ravikant Shah. The
credibility of dental pulp in human blood group
identification. Journal Forensic Dent Sci 2017;9(1):6-9.
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00038.8

Case Report
INTRODUCTION :
Ischemic heart diseases (IHDs) are one of the common cause
of sudden death. According to the World Health Organization
(WHO), sudden death is defined as death had taken place [1]within 24 hours of the onset of symptoms and signs of illness .
IHD occurs due to coronary insufficiency resulting from the
atherosclerotic plaque deposition in the coronary vessels
which supplies nutrition to the heart muscles. This plaque
formation results in ischemia of the cardiac muscles resulting
in reduced functionality and the condition are collectively
called Ischemic Heart Diseases. The mean age is 53 years for [2]the prevalence of myocardial infarction in India . Ischemic
heart disease results in complications like cardiomyopathies,
pericarditis, arrhythmias, myocardial rupture, valvular heart [2] disease . The infarctions of the myocardium can be resulting
in weakening and rupture of the myocardium leading to
cardiac tamponade which is a complication observed among
10 % of the population. The weakened myocardium may be
due to the immune- inflammatory disease which occurs at the
infarction site resulting in the necrosis of cardiac myocytes and
is called Dressler's syndrome. This occurs as a late
complication of myocardial infarction or post-traumatic
pericarditis[3]. We herein report one such unique case
Case Report:
A 59 year old man, driver by occupation, had epigastric pain
for 4 weeks before death, for which he had been taking
medication bought from a nearby pharmacy. He was a known
smoker and alcoholic for 30 years. Otherwise, his medical
history did not reveal any significant disease or past
hospitalization. In his house, he went for a bath and was found
lying unconscious inside the bathroom. The patient was found
by his daughter and was immediately brought to the hospital by
his family members. After examination by the casualty
doctors, he was declared brought dead to the hospital. The
autopsy was conducted 14 hours after death, to find the cause
of death.
Autopsy findings:
Internal examination: Both the pleura was adherent over the
apex on the anterolateral aspect of the lungs. The pericardial
sac showed a bluish hue
and appeared full. The
e x p l o r a t i o n o f t h e
pericardial sac revealed
258 grams of reddish
blood clot adhered to the
heart muscle, along with
some serous fluid. The
clot was rubbery and
retained the shape even
after removal (suggestive
of an antemortem clot). (Figure 1)
Corresponding Author :
Dr. Nirmal Krishnan M,
Assistant Professor
Department of Forensic Medicine and Toxicology, Kasturba
Medical College, Manipal, India.
Contact : +91 81293-29510
Email : [email protected]
KEYWORDS : Dressler syndrome, Myocardial infarction, Sudden death, Cardiac tamponade.
Article History:Received: 18 January 2021Received in revised form: 19 February 2021Accepted on: 19 February 2021Available online: 31August 2021
ABSTRACT :
Dressler's syndrome is pericarditis which develops 2-10 weeks after myocardial infarction or due to a traumatic etiology. Dressler's
syndrome is an immune system response that damages the heart tissues or pericardium secondary to events like myocardial
infarction, heart surgery, or traumatic injury with incidence of 3-4 %. This is usually diagnosed in autopsy due to the narrow
treatment window which makes clinical diagnosis difficult. This case highlights the rare condition called Dressler's syndrome.
1. Varun Krishna B, Post Graduate Resident*
2. Nirmal Krishnan M, Assistant Professor*
3. Deepak Nayak M, Associate Professor, Department of Pathology, Kasturba Medical College, Manipal, India.
4. Vinod C Nayak, Professor & Head*
*Department of Forensic Medicine and Toxicology, Kasturba Medical College, Manipal, India.
Dressler's Syndrome – A Case Report.
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00039.X
208
Figure 1: Hemopericardium (Yellow arrow).

Heart: Weighed 321 grams, measured 12.5 x 9.5 x 7.5 cm.
heart walls had a muscular defect, measuring 4 x 0.5 cm x
ventricular cavity deep, which was present over the posterior
lateral aspect of the left ventricular surface situated at a point 5
cm above the apex. (Figure 2)
The right and left coronary artery showed near-total occlusion.
Both coronaries had narrowing of lumen it was hard and gritty
on cut section. The left anterior descending artery showed 80
% lumen occlusion with atheromatous plaques throughout its
course.
On cut section through the ruptured ventricular wall showed a
yellow tan area, measuring 4 x 2 cm, which was present over
the posterolateral aspect of the left ventricle with the center
area showing features of softening of the tissues suggestive of
coagulative necrosis. One of the papillary muscle was ruptured
with the blood clots present over the exposed region of the
myocardium.
The blood investigations suggested severe myocardial
infarction Creatine phosphokinase (CPK) 15406 U/L,
Troponin T 2.810 ng/ml, Creatine Kinase MB (CK MB) 128
ng/ml, N- Terminal B- type Natriuretic peptide 745 pg/ml.
Cardiac tissues were then subjected to Triphenyl
tetrazolium staining:
In the year 1960, triphenyl tetrazolium chloride test, a
histochemical staining method was introduced as
identification of early myocardial infarction. Tetrazolium
chloride is a redox indicator widely used to distinguish
metabolically active and inactive tissues, especially in [4 ]biochemical experiments . Coagulative necrosis of
myocardial tissue occurs at the stage of ischemic injury,
resulting in a marked decrease in the level of enzymes such as
dehydrogenase, diaphorase and coenzymes. The infarction
areas of the above enzymes would be depleted. Non-infarcted
myocardial tissues act with dehydrogenase enzyme and give [5][11]brick red color remains a stained area . The staining
technique helps the identification of early myocardial
infarction in sectioning of gross heart in the morgue with
easier, simpler equipments and it helps the general pathologist
to mount the infarcted area and visualize histopathologically
and correlate the MI features.
Cardiac tissues sent for histopathological examination
after the Triphenyl tetrazolium chloride (TTC) staining:
Microscopy features:
Left ventricular wall defect showed extensively infarcted zone
of myocytes necrosis, neutrophilic infiltrates, and hemorrhage
seen extending to the pericardial cavity, suggestive of a
myocardial rupture. The pericardial adipose tissue showed
inflammatory cells and hemorrhage. Left coronary artery
shows an intimal atheromatos plaque with luminal narrowing.
(Figure 3-4)
209
Figure 2: Left ventricular wall free rupture (Yellow arrow)
Figure 3: An infarct with necrotic myocytes and a neutrophil rich inflammatory infiltrate (H&E; 400x)
Figure 4: Picture showing a transverse section of the heart after triphenyl tetrazolium chloride (TTC) staining. Old infarct (White arrow) and transmural infarction (Black circle).
Figure 4

DISCUSSION:
Myocardial infarction is the most common ischemic heart
disease due to imbalance supply and demand of oxygenated [6]blood leads to the death of myocytes as a result of ischemia . It
is the leading cause of death in developing countries. About
45% of individuals are affected under 65 years when
associated with hypertension as a stronger risk factor than [1]hypercholesterolemia . Myocardial infarction involving 40%
of ventricular mass leads to sudden death and females above 60
years of age with preexisting hypertension are more prone. The
risk of developing deep vein thrombosis and the likelihood of
pu lmonary embol i sm i s t r iggered by pro longed [8]immobilization in MI patients . Post-myocardial infarction
syndrome is sometimes called Dressler syndrome. William
Dressler first identified it in 1956. In post-myocardial [1]syndrome, the prevalence of Dressler's syndrome is 3-4% .
Most commonly associated with disease of the pericardium
causes pericarditis. It is an immunoinflammatory syndrome
that activates an inflammatory response due to heart injury
(traumatic or non-traumatic pericarditis) and is associated with [9]myocardial infarction . Pericarditis is inflammation of the
pericardium with or without pericardial effusion (pericardial [10]exudate or cardiac tamponade) . The pericardium is the fibro-
elastic sac covering the heart it comprises of a visceral and
parietal layer which are separated by each other and forms a
potential sac. The pericardial sac can hold about 200 ml of
blood in acute condition and a rapid increase in the pericardial
sac leads to sudden accumulation of blood up to 2000 ml it is
called cardiac tamponade or hemopericardium which can [14].cause sudden death Our patient had 1040 ml of blood
containing 258 grams of a reddish blood clot in the
pericardium. The time observed for immune reaction is 2 to 3
weeks after myocardial infarction to onset of Dressler [7]syndrome . Coronary re-perfusion or fibrinolysis reduces the
risk of Dressler syndrome in post-myocardial infarction [9].patients The syndrome is ranging from early to late
pericarditis to more complicated cases representing cardiac
tamponade. The symptoms usually start anywhere from 3-4
days to 2-6 weeks after post-cardiac injury when post-cardiac
syndrome is detected. The actin and myosin antibodies are
more elevated in those patients who had undergone cardiac
intervention and these groups of people are more prone to the
post-cardiac syndrome.
The pericardial layer can respond to an event such as an acute
mycocardial infarction either by inciting a pericardial effusion [12]or more lethally, a pericarditis . In the context of a
pericarditis, it is essential to differentiate an early post-infarct
pericarditis from an actual Dressler syndrome. Transmural
infarctions with accompanying necrosis with inflammatory
cells can infiltrate the adjacent visceral and parietal
pericardium, simulating a Dressler syndrome. This condition [13]has been referred to as 'pericarditis epistenocardica' (PEC) .
This disorder, which typically occurs within the first three days
of an acute MI, initially presents with pain and a pericardial
rub. The differentiating characteristics are: In order to damage
the visceral pericardium, PEC requires a transmural infarction,
but Dressler syndrome is independent of this. In Dressler
syndrome I, PEC is more symptomatic with symptoms such as [14]fever, malaise, and chest pain . It has been hypothesised that a
combination of events result in pericarditis seen in a Dressler [15]syndrome . The first trigger is the blood entering the
pericardial space as a result of an transmural infarct. Secondly,
the suffusion of blood additionally inflicts damage to the lining
mesothelial cells, thus creating a pro-inflammation friendly
microenvironment. Thirdly, the necrosed myocytes reveal
neo-antigens (hitherto sequestered within the myocytes),
resulting in a breach of immunologic tolerance, thus activating
the immune system. The net effect is an increase in
antimyocardial antibody titers and an expansion of CD4 T
cells unique to the heart; more inflammatory cells are recruited [16][17]into the insult area .
CONCLUSION:
We strongly believe that our patient had Dressler Syndrome
because of various reasons:
1) Based on the history given by the patient relatives prior to
autopsy as mentioned above earlier.
2) The previous episode of chest pain with compatible late
pericarditis causing scaring of the pericardial layer.
3) Appearances of a yellow-tan area in a cross-section of
heart suggestive minimum of 7- 10 days old myocardial
infarction.
4) Microscopic feature of pericarditis.
5) Old infarct appearing in TTC staining of heart suggestive
of old MI.
6) Unstained area of left ventricle suggesting transmural
infarction in TTC staining of heart with posterior
papillary muscle rupture leading to cardiac tamponade
(Figure 4).
Conflict of Interest : None declared.
Funding : None declared.
Ethical Approval :None declared.
REFERENCES :
1) Thiago Andrade Macedo, Roberto Nery Dantas Junior,
Pedro Gabriel Melo de Barros e Silva,1 and Marcio
Campos Sampaio, Dressler Syndrome: A Case Report.
Google Search [Internet]. [cited 2020 Dec 17].
210
2) Yash Lokhandwala, Gopi Krishna Panicker, Shantanu
Deshpande, Sudden cardiac death-an Indian perspective.
Google Search [Internet]. [cited 2020 Dec 17].
3) Rao D, Sood D, Pathak P, Dongre SD. A cause of Sudden
Cardiac Deaths on Autopsy Findings; a Four-Year Report.
Emerg (Tehran). 2014;2(1):12–7.
4) Kundal R, Bhullar DS, Kaur M. The autopsy diagnosis of
early myocardial infarction (MI) by triphenyltetrazolium
chloride (TTC) or nitrobluetetrazolium (NBT) dye test. J
Punjab Acad Forensic Med Toxicol. 2012 Jan 1;12:60–1.
5) Fishbein MC, Meerbaum S, Rit J, Lando U, Kanmatsuse
K, Mercier JC, et al. Early phase acute myocardial infarct
size quantification: Validation of the triphenyl tetrazolium
chloride tissue enzyme staining technique. Am Heart J.
1981 May 1;101(5):593–600.
6) Kloner RA, Darsee JR, DeBoer LW, Carlson N. Early
pathologic detection of acute myocardial infarction. Arch
Pathol Lab Med. 1981 Aug;105(8):403–6.
7) Jennings RB, Wartman WB. Reactions of the
Myocardium to Obstruction of the Coronary Arteries.
Medical Clinics of North America. 1957 Jan
1;41(1):3–15.
8) Varga M, Zsonda L. A simple method for postmortem
detection of acute myocardial infarction. Forensic Sci Int.
1988 Jun;37(4):259–63.
9) Dressler W. A Post myocardial- infarction syndrome:
Preliminary report of a complication resembling
idiopathic, recurrent benign pericarditis. Journal of the
American Medical association. 1956 Apr 21;160 (16):
1379–83.
10) Chiabrando JG, Bonaventura A, Vecchié A, Wohlford GF,
Mauro AG, Jordan JH, et al. Management of Acute and
Recurrent Pericarditis. Journalmof the American College
of Cardiology. 2020 Jan;75(1):76–92.
11) P Shenoy R, Bakkannavar S, Monappa V, Nb D, Bhat A,
Kumar M, et al. JPBMS Journal of Pharmaceutical and
biomedical sciences. Identification of Myocardial
Infarction in Human Autopsy Population Using TTC.
2011 Jan 1;09.
12) P. Vaideeswar, J. P. Chaudhari, and J. Butany,
“Mechanical complications of myocardial infarction,”
Diagnostic Histopathology, vol. 19, no. 1, pp. 13–19,
2013.
13) D. L. Mann, D. P. Zipes, P. Libby, R. O. Bonow, and E.
Braunwald, Braunwald's Heart Disease: A Textbook of
Cardiovascular Medicine, Elsevier Saunders ,
Philadelphia, Pa, USA, 2015.
14) D.H. Spodick, “Decreased recognition of the
postmyocardial infarction (Dressler) syndrome in the
postinfarct setting: does it masquerade as 'idiopathic
pericarditis' following silent infarcts?” Chest, vol. 126,
no. 5, pp. 1410–1411, 2004.
15) Imazio M, Hoit BD. Post-cardiac injury syndromes. An
emerging cause of pericardial diseases. Int J Cardiol. 2013
Sep 30;168(2):648-52.
16) Scheerder I, De, Buyzere M, De, Robbrecht J, De Lange
M, Delanghe J, Bogaert AM, Clement D. Postoperative
immunological response against contractile proteins after
coronary bypass surgery. Br Heart J. 1986 Nov;56(5):440-
4.
17) Nomura Y, Yoshinaga M, Haraguchi T, Oku S, Noda T,
Miyata K, Umebayashi Y, Taira A. Relationship between
the degree of injury at operation and the change in
antimyosin antibody titer in the postpericardiotomy
syndrome. Pediatr Cardiol. 1994 May-Jun;15(3):116-20.
211

212
Case Report
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00040.6
1. Vivek K. Chouksey, Senior Resident, Department of Forensic Medicine and Toxicology, AIIMS, Bhopal
2. Atul S. Keche, Associate Professor, Department of Forensic Medicine and Toxicology, AIIMS, Bhopal.
3. Daideepya C. Bhargava, Post Graduate student, Department of Forensic Medicine and Toxicology, AIIMS, Bhopal.
4. S. Mahaluxmi, Post Graduate student, Department of Forensic Medicine and Toxicology, AIIMS, Bhopal.
Key words: Drowning, Decomposition, Suspicious, Meticulous autopsy, Alcohol intoxication.
Corresponding Author:
Dr.Atul S. Keche,
Associate Professor,
Department of Forensic Medicine and Toxicology, AIIMS,
Bhopal
Contact : +91 82080-72886
Email :[email protected]
Article History :
Received : 25 May 2021
Received in revised from : 26 June 2021
Accepted on : 26 June 2021
Available online : 15 August 2021
INTRODUCTION :
The definition adopted by the World Congress on drowning
that convened in Amsterdam in 2002 and endorsed by the
WHO defines drowning as “the process of experiencing
respiratory impairment from submersion/immersion in
liquid”. Drowning, which typically involves a watery
environment, remains a serious public health concern claiming
an estimated 362,000 lives per year worldwide across all
socioeconomic classifications. A significant number of water-
related deaths are attributed to accidental drowning. These
deaths are often prematurely, and at times subconsciously,
labelled as accidental drowning. Presumption that a body
recovered from within or near a body of water is an accidental
drowning can hinder timely recognition of indicators of foul (1)play. A thorough scene investigation must be undertaken to
determine if the location of the death and that of the body
recovery are the same. Once a body is removed from the water,
putrefaction will be accelerated. Post-mortem predation if
there should be interpreted with care. Establishing cause and
manner of death for bodies recovered from water, is
challenging enough with the interpretation of post-mortem
changes. Characteristic changes that occur to a body after
death follow a somewhat predictable timetable. The death
scene investigation and witness accounts, as available helps
the investigator to estimate time of death. On the other hand,
post-mortem changes alter the appearance of the body, making
wounds and other evidence of the body's interaction with the (2)environment more difficult to interpret or even recognize.
Mechanisms for death from drowning are complex. Major
factors seem to be osmotic and perhaps also hydrostatic effects
of the inhaled fluid once it reaches alveolar spaces and gains
access to semipermeable alveolar membranes where water and
electrolyte exchanges take place. This is influenced by the
tonicity of the inhaled fluid, fresh or salt water. Thus
hemodynamic and electrolyte changes develop very rapidly (3)over a few minutes in fresh water drowning.
CASE DETAILS:
A body of 35 years old male was retrieved from a shallow drain
(Nala) in early decomposed condition with partially
distinguishable facial features (Figure 1) on 08/06/2020 and
was brought for autopsy. According to the relatives, the person
was missing since 7/6/2020 afternoon. The autopsy was
conducted on 09/06/2020. Body had a scarf (gamchha) around
the neck in situ which was tightened due to bloating (Figure 2).
The surrounding circumstances like his footwear and empty
liquor bottle near the bank of the drain raised suspicion
Decomposition in Drowning bscures Cause and Manner of DeathO
ABSTRACT :
Establishing cause and manner of death for bodies recovered from water, is challenging enough with the interpretation of post-
mortem changes.Decomposition alters the appearance of the body, making wounds and other evidence of the body's interaction
with the environment more difficult to interpret or even recognize and vice versa. We report a case of drowning and decomposition,
a 35 years male whose body was retrieved from a shallow drain with suspicious surroundings. His footwear and empty liquor bottle
was found on the bank with a scarf tied around his neck tightened by bloating of the body due to decomposition. History and
meticulous autopsy revealed the facts.
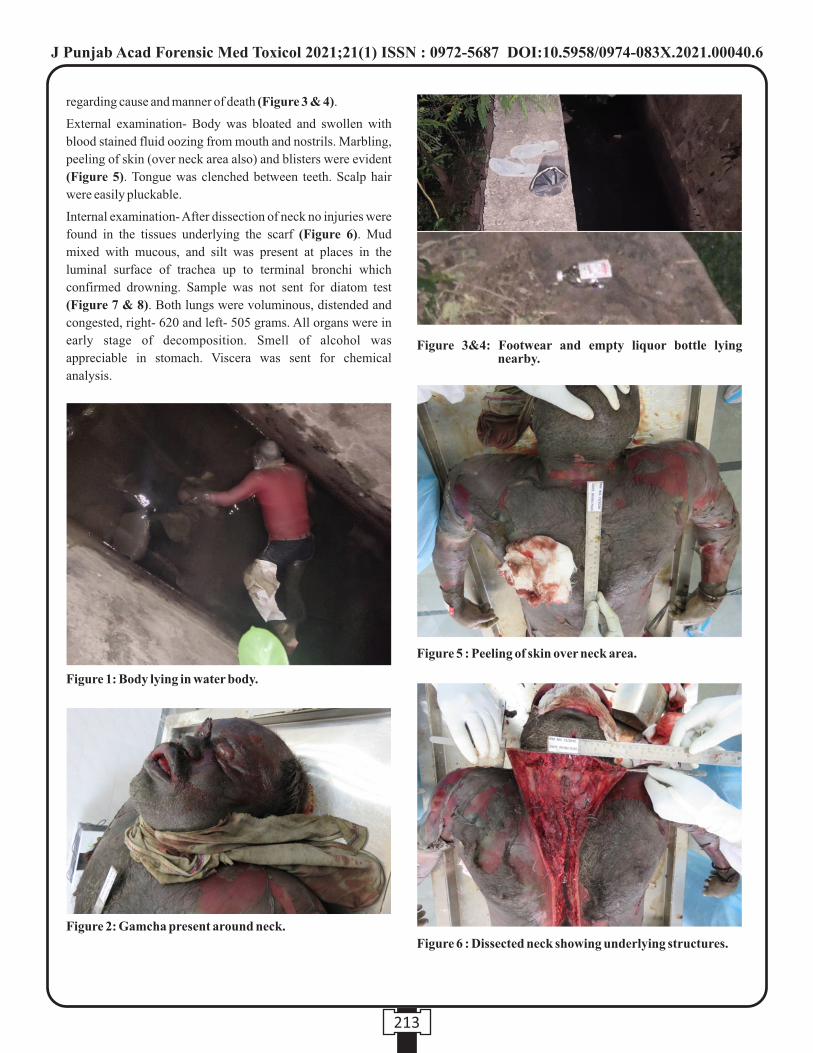
213
regarding cause and manner of death (Figure 3 & 4).
External examination- Body was bloated and swollen with
blood stained fluid oozing from mouth and nostrils. Marbling,
peeling of skin (over neck area also) and blisters were evident
(Figure 5). Tongue was clenched between teeth. Scalp hair
were easily pluckable.
Internal examination- After dissection of neck no injuries were
found in the tissues underlying the scarf (Figure 6). Mud
mixed with mucous, and silt was present at places in the
luminal surface of trachea up to terminal bronchi which
confirmed drowning. Sample was not sent for diatom test
(Figure 7 & 8). Both lungs were voluminous, distended and
congested, right- 620 and left- 505 grams. All organs were in
early stage of decomposition. Smell of alcohol was
appreciable in stomach. Viscera was sent for chemical
analysis.
Figure 1: Body lying in water body.
Figure 2: Gamcha present around neck.
Figure 3&4: Footwear and empty liquor bottle lying nearby.
Figure 5 : Peeling of skin over neck area.
Figure 6 : Dissected neck showing underlying structures.
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00040.6
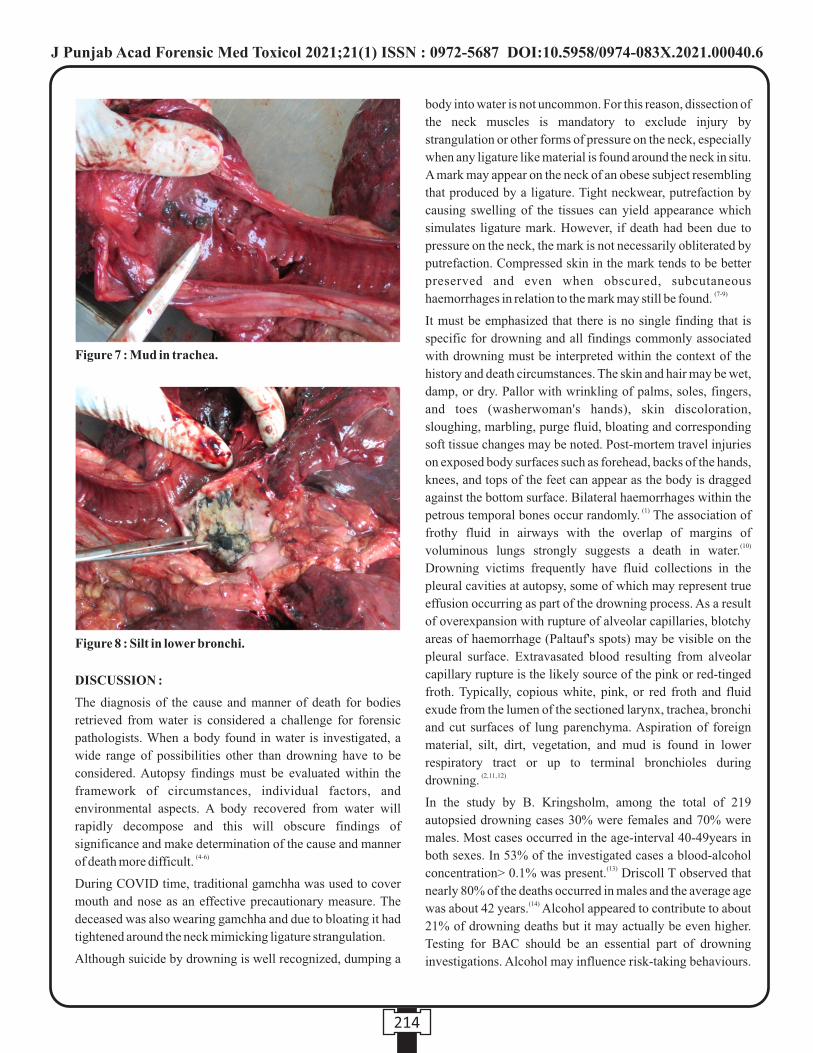
214
DISCUSSION :
The diagnosis of the cause and manner of death for bodies
retrieved from water is considered a challenge for forensic
pathologists. When a body found in water is investigated, a
wide range of possibilities other than drowning have to be
considered. Autopsy findings must be evaluated within the
framework of circumstances, individual factors, and
environmental aspects. A body recovered from water will
rapidly decompose and this will obscure findings of
significance and make determination of the cause and manner (4-6)of death more difficult.
During COVID time, traditional gamchha was used to cover
mouth and nose as an effective precautionary measure. The
deceased was also wearing gamchha and due to bloating it had
tightened around the neck mimicking ligature strangulation.
Although suicide by drowning is well recognized, dumping a
body into water is not uncommon. For this reason, dissection of
the neck muscles is mandatory to exclude injury by
strangulation or other forms of pressure on the neck, especially
when any ligature like material is found around the neck in situ.
A mark may appear on the neck of an obese subject resembling
that produced by a ligature. Tight neckwear, putrefaction by
causing swelling of the tissues can yield appearance which
simulates ligature mark. However, if death had been due to
pressure on the neck, the mark is not necessarily obliterated by
putrefaction. Compressed skin in the mark tends to be better
preserved and even when obscured, subcutaneous (7-9)haemorrhages in relation to the mark may still be found.
It must be emphasized that there is no single finding that is
specific for drowning and all findings commonly associated
with drowning must be interpreted within the context of the
history and death circumstances. The skin and hair may be wet,
damp, or dry. Pallor with wrinkling of palms, soles, fingers,
and toes (washerwoman's hands), skin discoloration,
sloughing, marbling, purge fluid, bloating and corresponding
soft tissue changes may be noted. Post-mortem travel injuries
on exposed body surfaces such as forehead, backs of the hands,
knees, and tops of the feet can appear as the body is dragged
against the bottom surface. Bilateral haemorrhages within the (1)petrous temporal bones occur randomly. The association of
frothy fluid in airways with the overlap of margins of (10)voluminous lungs strongly suggests a death in water.
Drowning victims frequently have fluid collections in the
pleural cavities at autopsy, some of which may represent true
effusion occurring as part of the drowning process. As a result
of overexpansion with rupture of alveolar capillaries, blotchy
areas of haemorrhage (Paltauf's spots) may be visible on the
pleural surface. Extravasated blood resulting from alveolar
capillary rupture is the likely source of the pink or red-tinged
froth. Typically, copious white, pink, or red froth and fluid
exude from the lumen of the sectioned larynx, trachea, bronchi
and cut surfaces of lung parenchyma. Aspiration of foreign
material, silt, dirt, vegetation, and mud is found in lower
respiratory tract or up to terminal bronchioles during (2, 11, 12)drowning.
In the study by B. Kringsholm, among the total of 219
autopsied drowning cases 30% were females and 70% were
males. Most cases occurred in the age-interval 40-49years in
both sexes. In 53% of the investigated cases a blood-alcohol (13)concentration> 0.1% was present. Driscoll T observed that
nearly 80% of the deaths occurred in males and the average age (14)was about 42 years. Alcohol appeared to contribute to about
21% of drowning deaths but it may actually be even higher.
Testing for BAC should be an essential part of drowning
investigations. Alcohol may influence risk-taking behaviours.
Figure 7 : Mud in trachea.
Figure 8 : Silt in lower bronchi.
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00040.6
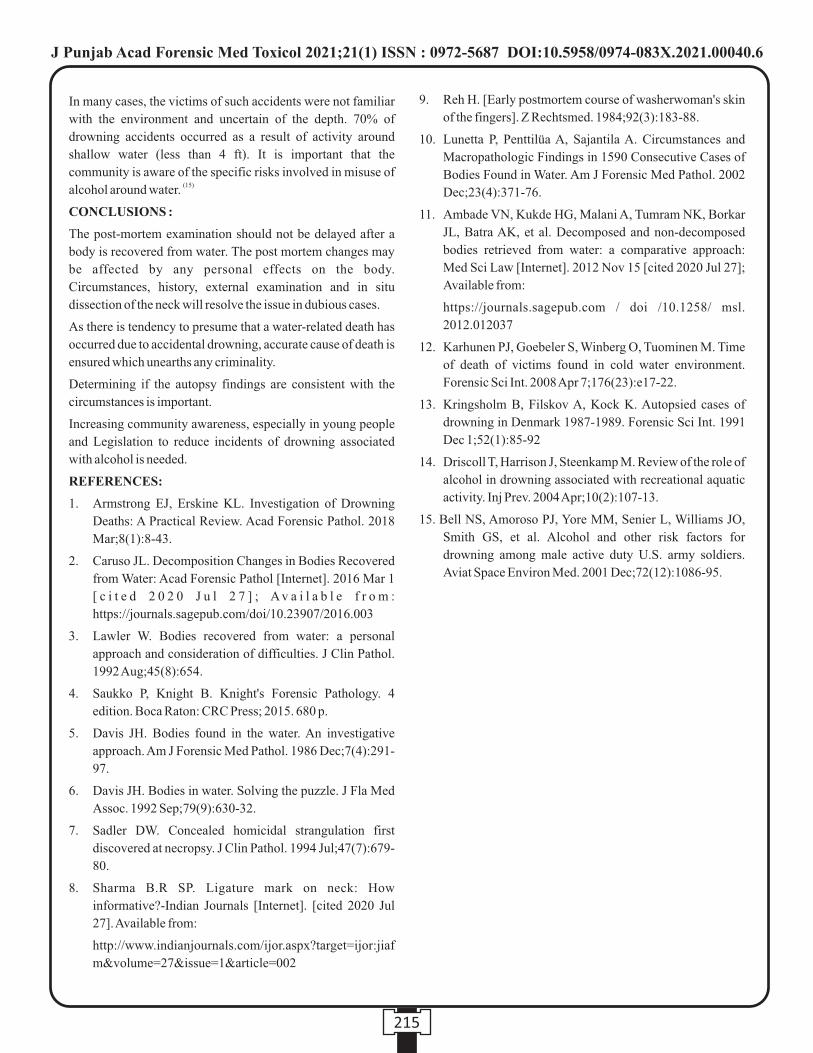
215
In many cases, the victims of such accidents were not familiar
with the environment and uncertain of the depth. 70% of
drowning accidents occurred as a result of activity around
shallow water (less than 4 ft). It is important that the
community is aware of the specific risks involved in misuse of (15)alcohol around water.
CONCLUSIONS :
The post-mortem examination should not be delayed after a
body is recovered from water. The post mortem changes may
be affected by any personal effects on the body.
Circumstances, history, external examination and in situ
dissection of the neck will resolve the issue in dubious cases.
As there is tendency to presume that a water-related death has
occurred due to accidental drowning, accurate cause of death is
ensured which unearths any criminality.
Determining if the autopsy findings are consistent with the
circumstances is important.
Increasing community awareness, especially in young people
and Legislation to reduce incidents of drowning associated
with alcohol is needed.
REFERENCES:
1. Armstrong EJ, Erskine KL. Investigation of Drowning
Deaths: A Practical Review. Acad Forensic Pathol. 2018
Mar;8(1):8-43.
2. Caruso JL. Decomposition Changes in Bodies Recovered
from Water: Acad Forensic Pathol [Internet]. 2016 Mar 1
[ c i t e d 2 0 2 0 J u l 2 7 ] ; Av a i l a b l e f r o m :
https://journals.sagepub.com/doi/10.23907/2016.003
3. Lawler W. Bodies recovered from water: a personal
approach and consideration of difficulties. J Clin Pathol.
1992 Aug;45(8):654.
4. Saukko P, Knight B. Knight's Forensic Pathology. 4
edition. Boca Raton: CRC Press; 2015. 680 p.
5. Davis JH. Bodies found in the water. An investigative
approach. Am J Forensic Med Pathol. 1986 Dec;7(4):291-
97.
6. Davis JH. Bodies in water. Solving the puzzle. J Fla Med
Assoc. 1992 Sep;79(9):630-32.
7. Sadler DW. Concealed homicidal strangulation first
discovered at necropsy. J Clin Pathol. 1994 Jul;47(7):679-
80.
8. Sharma B.R SP. Ligature mark on neck: How
informative?-Indian Journals [Internet]. [cited 2020 Jul
27]. Available from:
http://www.indianjournals.com/ijor.aspx?target=ijor:jiaf
m&volume=27&issue=1&article=002
9. Reh H. [Early postmortem course of washerwoman's skin
of the fingers]. Z Rechtsmed. 1984;92(3):183-88.
10. Lunetta P, Penttilüa A, Sajantila A. Circumstances and
Macropathologic Findings in 1590 Consecutive Cases of
Bodies Found in Water. Am J Forensic Med Pathol. 2002
Dec;23(4):371-76.
11. Ambade VN, Kukde HG, Malani A, Tumram NK, Borkar
JL, Batra AK, et al. Decomposed and non-decomposed
bodies retrieved from water: a comparative approach:
Med Sci Law [Internet]. 2012 Nov 15 [cited 2020 Jul 27];
Available from:
https://journals.sagepub.com / doi /10.1258/ msl.
2012.012037
12. Karhunen PJ, Goebeler S, Winberg O, Tuominen M. Time
of death of victims found in cold water environment.
Forensic Sci Int. 2008 Apr 7;176(23):e17-22.
13. Kringsholm B, Filskov A, Kock K. Autopsied cases of
drowning in Denmark 1987-1989. Forensic Sci Int. 1991
Dec 1;52(1):85-92
14. Driscoll T, Harrison J, Steenkamp M. Review of the role of
alcohol in drowning associated with recreational aquatic
activity. Inj Prev. 2004 Apr;10(2):107-13.
15. Bell NS, Amoroso PJ, Yore MM, Senier L, Williams JO,
Smith GS, et al. Alcohol and other risk factors for
drowning among male active duty U.S. army soldiers.
Aviat Space Environ Med. 2001 Dec;72(12):1086-95.
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00040.6

Case Report
INTRODUCTION:th thRenal cancer is the 9 most common cancer in males and 14
[1]most common cancer in females. Renal cell carcinoma th th(RCC) is most commonly seen in 5 and 6 decade of life in
[2-3] India, with male:female ratio 3.5:1. Smoking, hypertension
and obesity are associated with increased incidence of renal [4]cancer.
The use of histopathology and molecular diagnosis helped in
identifying more than ten types and subtypes of renal
carcinoma. Among these, clear cell renal carcinoma is the
commonest type followed by non-clear cell carcinoma,
papillary renal cell carcinoma, chromophobe cell carcinoma [2,5]etc.
Classically, renal cancer presents with symptoms of hematuria, [3]abdominal mass and flank pain. Rarely, there may be upper
GI bleeding due to invasion of the tumor to the second part of [6] duodenum. Majority of the renal cancers are diagnosed at a
later stage of disease where the patient experiences symptoms
of pressure effect on surrounding organs or with metastases to [3] distant organs. Lung is the most common site of metastasis
7 followed by lymph nodes, bones and liver. Rarely, it may
metastasize to pancreas and cause portal vein thrombosis and [8]portal hypertension.
It is a common practice in developing countries where the
patient ignores some of early symptoms of renal carcinoma
and consults the doctor at a late stage. Sometimes it may be
detected incidentally in the surgical and medico-legal [9] specimens. Hereby, we report an incidental case of renal cell
carcinoma detected during a medico-legal autopsy.
CASE REPORT:
A 61-year-old man was hit by a rashly driven scooter while
walking on a pavement and was admitted to a hospital with
injuries. Patient was brought to hospital in an unconscious
state. On examination, patient's Glasgow Coma Scale was 5/15
with non-reacting pupils, bleeding from nose, mouth and right
ear. CT scan head showed diffuse cerebral oedema with
traumatic subarachnoid haemorrhage and multiple
haemorrhagic contusions in frontal and temporal lobes on both
sides. Patient was treated conservatively with ventilator
support. As there was no improvement of patient's condition,
ventilator support was removed and declared dead. The total
survival period was 54 hours. As per the protocol, the body was
subjected to a medicolegal autopsy.
At autopsy, the external examination showed contusion
measuring 6x5 cm over anterior surface of the chest, contusion
measuring 8x4 cm over medial surface of the left leg, abrasion
measuring 4x3 cm over the left shoulder, and abrasion
measuring 10x2 cm over anterior surface of the left arm. The
occipital region was diffusely swollen with an abrasion
measuring 2x2 cm in the midline, 8 cm above the external
occipital protruberance. The internal examination showed
diffuse contusion of the brain in the left parietotemporal
region, occipital region, and bases of the right frontal and both
temporal lobes. Brain weighed 1350 gm and edematous.
Subarachnoid hemorrhage was present over the both cerebral
hemispheres and the cerebellum. Multiple petechial
haemohages were present in the pons. Both lungs and the heart
Corresponding Author :
Dr. K.R. Nagesh,
Professor and Head,
Department of Forensic Medicine, Father Muller Medical
College, Mangalore, India.
Contact : +91 9845775907
Email : [email protected]
KEYWORDS : Sudden natural death, Renal Cancer, Renal carcinoma, Renal neoplasm.
Article History:Received: 30 July 2020Received in revised form: 23 December 2020 Accepted on: 23 December 2020Available online: 30 August 2021
ABSTRACT :
Papillary renal cell carcinoma (PRCC) is the second most common type of renal cell carcinoma. It accounts for about 10-15% of all
renal epithelial neoplasms. It has characteristic gross and histologic features that distinguish it from other types of renal cell
carcinoma. We report a case of PRCC which was detected as an incidental finding during autopsy of a patient who was involved in a
road traffic accident. PRCC may be considered as one of the rare causes of death in a medicolegal autopsy of sudden natural death.
1. Niranjan P. Khadilkar, Associate Professor, Department of Pathology, Kanachur Institute of Medical Sciences, Mangalore, India.
2. K.R. Nagesh, Professor and Head, Department of Forensic Medicine, Father Muller Medical College, Mangalore, India.
Papillary Renal Cell Carcinoma - an Incidental Finding at Autopsy
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00041.8
216
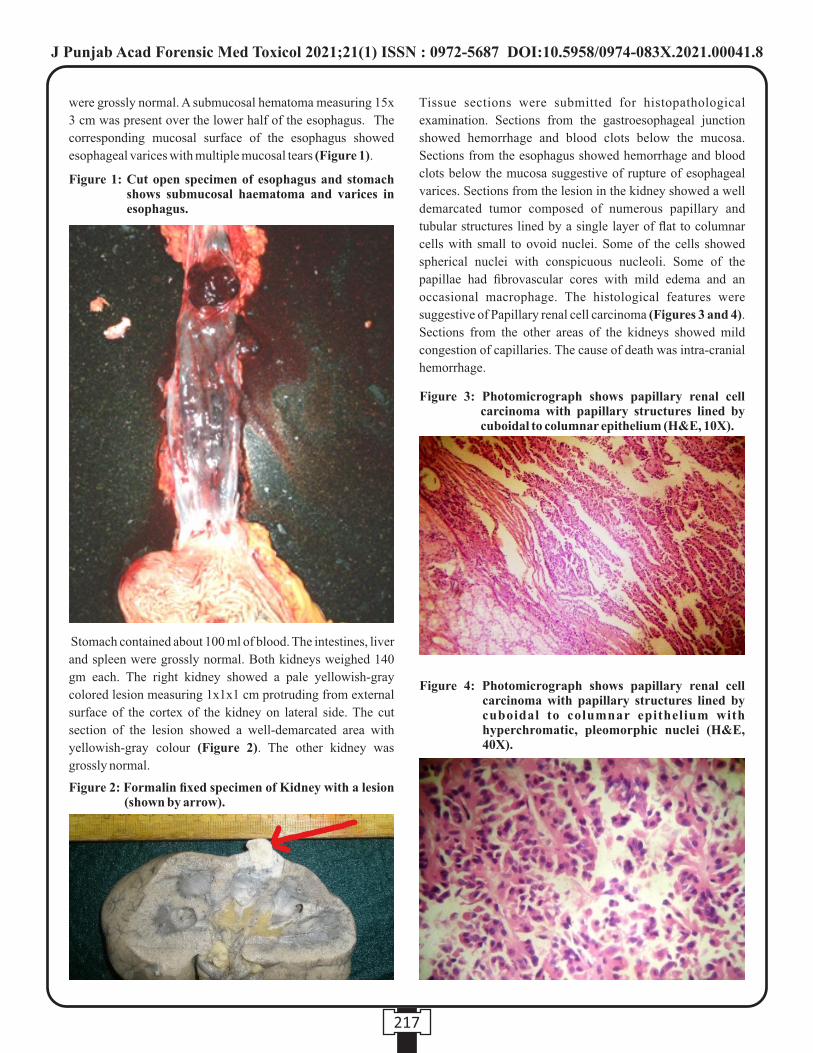
were grossly normal. A submucosal hematoma measuring 15x
3 cm was present over the lower half of the esophagus. The
corresponding mucosal surface of the esophagus showed
esophageal varices with multiple mucosal tears (Figure 1).
Stomach contained about 100 ml of blood. The intestines, liver
and spleen were grossly normal. Both kidneys weighed 140
gm each. The right kidney showed a pale yellowish-gray
colored lesion measuring 1x1x1 cm protruding from external
surface of the cortex of the kidney on lateral side. The cut
section of the lesion showed a well-demarcated area with
yellowish-gray colour (Figure 2). The other kidney was
grossly normal.
Tissue sections were submitted for histopathological
examination. Sections from the gastroesophageal junction
showed hemorrhage and blood clots below the mucosa.
Sections from the esophagus showed hemorrhage and blood
clots below the mucosa suggestive of rupture of esophageal
varices. Sections from the lesion in the kidney showed a well
demarcated tumor composed of numerous papillary and
tubular structures lined by a single layer of flat to columnar
cells with small to ovoid nuclei. Some of the cells showed
spherical nuclei with conspicuous nucleoli. Some of the
papillae had fibrovascular cores with mild edema and an
occasional macrophage. The histological features were
suggestive of Papillary renal cell carcinoma (Figures 3 and 4).
Sections from the other areas of the kidneys showed mild
congestion of capillaries. The cause of death was intra-cranial
hemorrhage.
217
Figure 1: Cut open specimen of esophagus and stomach shows submucosal haematoma and varices in esophagus.
Figure 2: Formalin fixed specimen of Kidney with a lesion (shown by arrow).
Figure 4: Photomicrograph shows papillary renal cell carcinoma with papillary structures lined by cuboidal to columnar epithelium with hyperchromatic, pleomorphic nuclei (H&E, 40X).
Figure 3: Photomicrograph shows papillary renal cell carcinoma with papillary structures lined by cuboidal to columnar epithelium (H&E, 10X).
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00041.8

DISCUSSION:
According to the current WHO classification of kidney
tumors, the papillary renal cell carcinoma (PRCC)is a
malignant renal parenchymal tumor with papillary or
tubulopapillary architecture. They comprise approximately [10,11] 10% of all the renal cell carcinomas. The age and sex
distribution of PRCC is quite similar to the clear cell
carcinoma with mean age ranges from 52-66 years and [10,12-14] male:female incidence ranges from 1.8:1 to 3.8:1. Our
reported case is that of a 61 year old male.
The clinical presentation of PRCC is similar to clear cell 14 carcinoma. Majority of these cancers clinically presents in an
advanced stage and classically it presents as haematuria, 3abdominal mass and flank pain. Radiological investigations
are non-specific though renal angiography shows relative [11] hypovascularity for PRCC. In the present case, it was an
incidental finding at postmortem examination and relatives
revealed that the deceased did not complain of any of these
symptoms during his life time.
P R C C i s a w e l l - c i r c u m s c r i b e d t u m o r w i t h a [12,14] pseudocapsule. Two morphological types of PRCC are
described. Type I tumors are usually multifocal and have
papillae covered by small cells with scanty cytoplasm,
arranged in a single layer of the papillary basement membrane.
Type II tumor cells are often of a higher nuclear grade with
eosinophilic cytoplasm and pseudostratified nuclei on
papillary cores. Sarcomatoid dedifferentiation is seen in
approximately 5% of PRCC and has been associated with both [15]type I and type II tumors.
Microscopic examination of PRCC shows malignant
epithelial cells forming varying proportions of tubules and
papillae. Tumor lined cysts with papillary excrescences may [11,14,15] be seen. Tumor papillae contain a delicate fibrovascular
core and aggregates of foamy macrophages and cholesterol
crystals may be present. Occasionally papillary cores are [10,15]expanded by edema or hyalinized connective tissue.
Necrosis and hemorrhage is frequently seen along with [14] calcified concretions. In the present case, lesion in the kidney
showed flat to columnar cells with small to ovoid nuclei,
spherical nuclei with conspicuous nucleoli, fibrovascular cores
and macrophage. However, there was no evidence of
sarcomatous dedifferentiation. These features were suggestive
of type II PRCC.
The fatality depends on the factors such as tumor size, nuclear
grade, and stage in the assessment of prognosis of renal [16] carcinoma. The prognosis is good in cases of organ confined
tumors. And the prognosis is bad in cases of metastases to [2] lymph node or distant organs. In an Indian study, the 5-year
survival with renal carcinoma in stages 1, 2, 3, and 4 was found
[3]to be 92.7%, 72.9%, 54.6%, and 11.5%, respectively. In the
present case, there was no evidence of metastases to distant
organs and so has not affected the overall prognosis.
Incidental renal carcinoma in surgical and medicolegal
specimens is not uncommon. Careful observation during gross
examination with high index of suspicion may help in 9detecting such conditions in histopathological diagnosis. In
the present case, a small nodular lesion over the renal surface
was found during a medicolegal autopsy which was confirmed
to be renal papillary carcinoma in the histopathological
examination. In a medicolegal case involving sudden natural
death, renal cell carcinoma should be considered in the
differential diagnosis in the absence of other significant causes
of death.
In the present case, there is no relationship between trauma and
tumor as the subject developed a head injury and died of
intracranial hemorrhage. Esophageal varices or trauma could
not have contributed to the cause of death as the amount of
blood found in the stomach was only about 100 ml which will
not lead to hypovolemic shock. Also, renal cell carcinoma was
found to be restricted to only the kidney without any significant
metastases so might have not been the main cause of death but
only an incidental finding.
CONCLUSION:
Determining the cause of death is one of the important
objectives of any medicolegal autopsy. In a case of sudden
natural death that was brought dead to hospital, a meticulous
autopsy including investigations such as chemical analysis,
histopathology and microbiology examinations may give a
clue about the cause of death. In the present case, we report an
incidental detection of papillary renal cell carcinoma (PRCC).
PRCC with increased tumor size and/or distant metastasis can
be fatal. Hence, the PRCC should be considered as one of the
differential diagnosis of sudden natural deaths.
REFERENCES:
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA,
Jemal A. Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36
cancers in 185 countries. C A Cancer J Clin.
2018;68(6):394-424. Erratum in: CA Cancer J Clin.
2020;70(4):313.
2. Ray RP, Mahapatra RS, Khullar S, Pal DK, Kundu AK.
Clinical characteristics of renal cell carcinoma: Five years
review from a tertiary hospital in Eastern India. Indian J
Cancer. 2016;53(1):114-117.
3. Tiwari P, Kumar L, Singh G, Seth A, Thulkar S. Renal cell
cancer: Clinicopathological profile and survival
outcomes. Indian J Med Paediatr Oncol. 2018;39(1):23-
218
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00041.8
27.
4. Capitanio U, Bensalah K, Bex A, Boorjian SA, Bray F,
Coleman J et al.Epidemiology of Renal Cell Carcinoma.
Eur Urol. 2019;75(1):74-84.
5. Hsieh JJ, Purdue MP, Signoretti S, Swanton C, Albiges L,
Schmidinger M et al. Renal cell carcinoma. Nat Rev Dis
Primers. 2017;3:17009.
6. Soin S, Verkhovsky E. Locally advanced renal cell
carcinoma: cause of upper gastrointestinal bleeding. BMJ
Case Rep. 2019; 12(4): e229992.
7. Sadler GJ, Anderson MR, Moss MS, Wilson PG.
Metastases from renal cell carcinoma presenting as
gastrointestinal bleeding: two case reports and a review of
the literature. BMC Gastroenterol. 2007; 7(1):4-8.
8. Shrikhande SV, Büchler P, Esposito I, Loos M, Büchler
MW, Friess H. Splenic and portal vein thrombosis in
pancreatic metastasis from Renal cell carcinoma. World J
Surg Oncol. 2006; 4(1):25-27.
9. Lavekar A, Chandran S, Ram D, Sadar A, Manjari KS.
Awareness about Irritable Bowel Syndrome among
Interns of Medical College. J Med Sci Health. 2018; 4(3):
13-19.
10. del Vecchio MT, Lazzi S, Bruni A, Mangiavacchi P,
Cevenini G, Luzi P. DNA ploidy pattern in papillary renal
cell carcinoma. Correlation with clinicopathological
pa rame te r s and su rv iva l . Pa tho l Res P rac t .
1998;194(5):325-33.
11. Mydlo JH, Bard RH. Analysis of papillary renal
adenocarcinoma. Urology. 1987;30(6):529-34.
12. Amin MB, Corless CL, Renshaw AA, Tickoo SK, Kubus
J, Schultz DS. Papillary (chromophil) renal cell
carcinoma: histomorphologic characteristics and
evaluation of conventional pathologic prognostic
pa rame te r s i n 62 ca se s . Am J Su rg Pa tho l .
1997;21(6):621-35.
13. Delahunt B, Eble JN, McCredie MR, Bethwaite PB,
Stewart JH, Bilous AM. Morphologic typing of papillary
renal cell carcinoma: comparison of growth kinetics and
patient survival in 66 cases. Hum Pathol. 2001;32(6):590-
5.
14. Mancilla-Jimenez R, Stanley RJ, Blath RA. Papillary
renal cell carcinoma: a clinical, radiologic, and pathologic
study of 34 cases. Cancer. 1976;38(6):2469-80.
15. Delahunt B, Eble JN. Papillary renal cell carcinoma: a
clinicopathologic and immunohistochemical study of 105
tumors. Mod Pathol. 1997;10(6):537-44.
16. Abraham GP, Cherian T, Mahadevan P, Avinash TS,
George D, Manuel E. Detailed study of survival of
patients with renal cell carcinoma in India. Indian J
Cancer. 2016;53(4):572-4.
219
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00041.8
220
Case Report
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00042.X
1. Majji. Sai Sudha Rani, M.Sc. Forensic Science Student*
2. Chintan Singh, M.Sc. Forensic Science Student*
3. Amarnath Mishra, Assistant Professor & Program Leader*
* Amity Institute of Forensic Sciences, Amity University, Noida (U.P), India.
Key words: Forensictoxicology,Imidacloprid,biological sample, dispersive solid phase extraction method, LC-MS/MS.
Corresponding Author:
Dr.Amarnath Mishra,
Assistant Professor & Program Leader,
Amity Institute of Forensic Sciences, Amity University, Noida
(U.P), India.
Contact : +91 9818978527
Email : [email protected], [email protected]
Article History :
Received : 29 April 2020
Received in revised from : 14 July 2020
Accepted on : 14 July 2020
Available online : 31 August 2021
INTRODUCTION :
In forensic toxicology the dispersive solid phase extraction
(DSPE) method has wide use due to the increase in cases
reported on intake of pesticides by accidental or homicidal or
suicidal to the forensic laboratories, the drastic use of
pesticides to increase the yield of crop became one of the major
problem in causing severe health issues in human. To decrease
the deaths caused by pesticides, new compounds are developed
with low toxicity and high effect. Imidacloprid comes under [1]this group which is newly developed with least toxicity .
Imidacloprid comes under the class of neonicotinoids that acts [2]on the vertebrate . But in recent years this insecticide also
shows severe health effects in mammals I.e., human and birds
and also nervous system of insects. These chemicals mainly
block the neuronal pathway and also interferes in the stimuli
transmission in insect's nervous system. This results in
preventing the impulses transmission by acetylcholine that [3]leads to paralysis . Imidacloprid (1-(6-chloro- 3-
pyridylmethyl)-N- nitroimadozolidin- 2 ylideneamine) is a
chloro-nicitnyl in figure 1 which is a neonicotinoid which have
reversibility towards intoxication and have safety in mammals
and human. Birds which eat the grains or seeds that are
obtained from these insecticides sprayed plants or crops shows
severe health problems like kidney damage and the
malfunction of reproductive system. These insecticide [4]residues are detected from the liver and kidney of birds . In
Development of an analytical method for detection of Imidacloprid Insecticide from Biological Matrix using LC-MS/MS
ABSTRACT :
Introduction : The aim of this paper is to develop an accurate and rapid method to extract neonicotinoid insecticide from
biological matrices. There is increase in number of cases reported in forensic laboratories due to the intake of insecticides by
accidental or homicidal or suicidal manner. In these cases, dispersive solid-phase extraction method helps to give accurate and
rapid results. In forensic toxicology, there will be wide use of this method to extract insecticides from the viscera samples.
Imidacloprid is a neonicotinoid insecticide used in agriculture to kill insects and mites etc. In humans, it is moderately toxic. This
insecticide mainly acts on the central nervous system of insects but, it does not show effects in mammals. Some studies reported
that Imidacloprid causes severe gastrointestinal problems along with respiratory distress and neuropsychiatric issues when it is
ingested or inhaled.
The chickenmeatwastakenas biologicalsampleinwhich20ppbconcentrationof Imidacloprid insecticide is spiked. The dispersive
solid-phase extraction method is used to extract the insecticide from the biological matrix, and further this is analyzed in the LC-
MS/MS for the detection and quantification of insecticide. For the detection, standard temperature, flow rate, suitable solvent
system and pressure are maintained. Graphs are obtained, and the concentration of Imidacloprid insecticide obtained from chicken
meat sample is 19.206ppb andthe retentiontimeis5.018 . Itshowsthattheextraction process used gave the better recovery of 99. max
88% and is between LOD I.e., 70-120%. it proves all the validation parameters I.e., Limit of quantification, recovery, precision,
and selectivity. Hence it is proved that dispersive solid-phase extraction method used gave the good recovery in extraction of
Imidacloprid insecticide from biological matrix.

221
some studies, it is also shown that this insecticide also causes
gastrointestinal problems, respiratory problems and also [5]causes neuropsychiatric issues in human when it is inhaled .
Imidacloprid shows different level of toxicity based on its
toxicity when it is through dermal exposure it shows less [6]toxicity when it is ingested it shows moderate toxicity. If it is
[7]in the form of aerosol it is highly toxic it also causes vomiting, [8-9]drowsy and dizzy feeling .
The DSPE method is mainly used for the better recovery of the
pesticide samples. Imidacloprid is a polar pesticide which
causes difficulty in detection and extraction of it and it also
causes more difficulty due to interference of compounds i.e.,
fats etc., in meat samples in this case, DSPE method helps in
better extraction which is further detected by using LC-[10]MS/MS . DSPE method is used as the pretreatment method
analysis of compounds. This method mainly involves the steps
like the dispersion of a solid sorbent in liquid samples in the
extraction, isolation and cleanup of different analytes which
are of complex or biological matrices. The samples are injected
into the liquid chromatography and further these samples are
analyzed by using mass spectrometer detector. LC-MS/MS is
also used for the fractionation and analysis of the samples.
Quantitative precision is achieved with the help of triple
quadrupole system which breaks sensitivity and size barriers
of analytes in LC-MS/MS. LC-MS/MS is used to detect the
compounds like organic and inorganic compounds, drugs,
pesticides analysis in food samples, veterinary drugs analysis.
LC-MS/MS is better than GC-MS because it can detect polar
compounds also it is mainly used for better recovery and better
detection
MATERIALS AND METHODS :
CHEMICALS AND REAGENTS USED: Chemicals and
reagents used in extraction and diluents used to dilute the
Imidacloprid are 10ml of milli Q water, 10ml of acetonitrile
acts as diluent for Imidacloprid and salts like sodium chloride
and sodium Sulphate of 2g weight.
Reagents and chemicals used in cleanup process are 250mg of
primary and secondary amine is used to break the bonds
between compounds, 150mg of C is used to extract non polar 18
or neutral compounds from biological matrices, 600 mg of
magnesium sulphate is used to remove moisture and water
molecules from the meat sample.
For mobile phase in LC-MS/MS chemicals and reagents used
are 1 milli molar ammonium formate, 0.1% formic acid in
water.
For mobile phase B 0.1% formic acid in acetonitrile is used.
For the sample vial preparation solvent system used is 0.1%
formic acid in acetonitrile and water in the ratio of 20:80.
Imidacloprid standard is taken from the sima laboratory.
individual stock standard solution and working standard
solution were prepared with acetonitrile and is freshly
prepared.
INSTRUMENTATION: LC-MS/MS is the instrument from
the Agilent series mass spectrometer that analyses and detects
the compounds contain the electron spray interface operating
in positive mode was used. The vials that are kept in instrument
from which samples are taken by the injector and then it is
injected into the column. The column contains the c18 coating
and also contains silica beads that is in hydrophobic in nature
helps in movement of sample. Column is 5cm long and the
inner diameter of column is 2.1mm and silica bead size is
1.9μm due to the small bead size high pressure is required and
also contain less gaps between silica beads. Mobile phase A of
1mM ammonium formate and 0.1%formic acid in water is run
with the flow rate of 0.5ml/min. and mobile phase B that is
0.1% formic acid in acetonitrile is used to run in the column.
The volume of injection is 5μl. Mass spectrometer-mass
spectrometer which is mainly worked on the principle of mass
by charge ratio and it contains triple quadrupole and a detector.
The mass spectrometric analysis of sample is done with the
electron spray in the positive ionization form. The mass
spectrometer should contain the following parameters i.e., the
oven temperature is 550°c. Nitrogen gas is used as the
nebulizer and collision gas. The pressure of nitrogen as [11]nebulizer is of 550psi . After analyzed in the LC the
molecules move to mass spectrometer through a column it
contains oven and ionization is done and in this positive mode
is present that repel positive ions electron spray ionizer sprays
these ions and moves through a filter and then these ions are
further fragmented based on mass by charge ratio of ions these
ions are called precursor ions and further the ions are again
fragmented based on mass by charge ratio and gives the
product ions this occurs in the triple quadrupole that are
detected by the detector of MS-MS and it contains the software
that have library that helps in detecting the ions present in the
sample and gives a result as graph that is shown on system.
LOQ -limit of quantification is the lowest amount of analyte in
a sample that can be quantitatively determined with suitable
precision and accuracy. The LOQ of spiked Imidacloprid
sample is 5μg/l
VALIDATION: validation is required to prove whether the
sample gave better result or better recovery or not. To prove
validation three main parameters are most important i.e.,
recovery and precision, LOQ, selectivity. These parameters
help to know the used process is good or not to get better
recovery of the analyte in the meat sample. Matrix also shows
effect by interfering in the detection of analyte these all are
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00042.X

222
seen and then conclusion should be given whether the better [12]recovery is obtained or not .
SAMPLE PREPARATION: chicken sample is taken and it is
homogenized by grinding it in mixer and then sample is
weighed. 5g of meat sample is weighed by using measuring
balance. Two portions of two 5g samples is weighed one is
used as spiked sample and one is used as bank sample.
Standard Imidacloprid of 20ppb (parts per billion) volume is
spiked into the 5g meat sample. The meat sample is mixed
thoroughly by using vortex shaker and keep it overnight under
sterilized conditions. For the extraction, In the spiked meat
sample add 10ml of water for uniform mixing and 10 ml of
acetonitrile is added as diluent to dilute the pesticide in meat
sample and it is mixed with the help of vortex shaker for 2min
as vortex shaker helps to mix the sample uniformly.
Acetonitrile acts as a diluent for the Imidacloprid insecticide.
And then it is kept in wrist action shaker for 10mins to
homogenize the meat sample. 2g of NaCl is weighed by using
measuring balance and add it in the sample mixture. 2mins
sample is mixed by using vortex shaker and then for 10 mins
sample is mixed by using wrist action shaker. This sample
mixture is centrifuged with the help of refrigerated centrifuge
of 5000 rpm for 5mins. The supernatant layer is taken from the
centrifuge because supernatant layer contains insecticide
residues that is diluted in the acetonitrile and in this add 250mg
of PSA, 150mg of C18 and 600 mg of MgSo4 is weighed in this
supernatant layer is added and mixed for 2mins in vortex
shaker this step is called cleanup. Keep this tube in wrist action
shaker for 10mins. Centrifuge the sample mixture by keeping it
in refrigerated centrifuge for 5000rpm for 5mins. 2ml of
supernatant layer is taken and is kept in nitrogen concentrator
at 45°c until the sample is dried. Allow it for dryness. This step
helps to get only pesticide residue in the test tube by removing
all the water and diluents from the sample. Reconstitute the
sample by adding 1ml of solvent system in the ratio of 80:20 of
water and 0.1%formic acid in acetonitrile. Now the sample is
prepared and the vials are prepared for detection of meat
sample in LC/MS-MS.
SAMPLE VIAL PREPARATION: Three vials are prepared
one for the standard sample which is used for comparison and
checking and another is the spiked chicken meat sample with
known concentration of 20ppb of Imidacloprid and last vial is
of blank chicken meat sample to know whether it contain any
amount of insecticides. Sample vials are prepared by adding
1ml of reconstitute in the vial and 1ml of solvent system i.e.,
80:20 ratio of water and 0.1%formic acid in acetonitrile. These
sample vial are mixed by using vortex shaker for 2mins this
helps in uniform mixing. Now the samples are ready to keep for
the detection.
CASE REPORT:
Chicken sample is taken as biological sample and these
samples are kept in the vials which are kept in the vial case and
these are taken by the injector and is injected into the column
and column do not contain the oven. The analyte runs through
the column and is analyzed in the LC. The analyzed analytes
are sent to the MS-MS through the column which contains
oven the total run time of the sample is 16 minutes and
retention time is calculated. Linearity is plotted at 5, 10, 20, 30,
40, 50 etc., Three graphs are obtained one graph is of standard
insecticide sample another graph is of spiked chicken meat
sample and last graph is of blank chicken meat sample in which
matrix interference is seen.
In figure 1 linearity is plotted by taking the sample at 5, 10, 20,
50, 100, etc., by taking the standard Imidacloprid sample. This
helps in the comparison of the graphs of spiked and blank
samples. Linearity plot of standard sample is very important
for the validation of the analytes in the chicken meat sample.
In figure 2 the graph showed the Imidacloprid peak of spiked
chicken meat sample. The graph is obtained at 5.018 of
retention time. The graph also shows the quantity of
Imidacloprid obtained from the chicken meat sample. The
concentration of Imidacloprid sample obtained is 19.206ppb
which means a good recovery.
In figure 3 the graph shows the noise peaks that is the peaks are
obtained due to the matrix interference of the chicken meat
sample. The blank meat sample is analyzed to know whether
the blank sample contains pesticides or not and this also helps
to study the spiked sample clearly. The blank meat sample also
shows a peaks these are mainly due to matrix effects in sample.
These peaks don't match with the peak of the Imidacloprid ions
hence these peaks are noise peaks that are due to matrix
interface of meat sample. MATRIX EFFECT: the matrix effect
values are acceptable for the Imidacloprid insecticide.it shows
only minimal values and low matrix effect on the sample. so
this matrix effect is acceptable. Hence the matrix matched
process is preferred for the quantification of Imidacloprid
insecticide.
LOQ- limit of quantification is set at 5μl and peak of
Imidacloprid contain the S/N which is greater than 10.
SELECTIVITY: In the spiked meat sample the interference
peaks are observed which is less than 1/3 area of the peak
which is compared with the Imidacloprid insecticide due to the
cleanup process in extraction process helps to reduce
interference peaks.
RECOVERY AND PRECISION: Recovery of the
Imidacloprid insecticide is observed and the tested sample is
seen. The analyte is recovered for 19.206 and the limit of
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00042.X

223
detection should be between 70-120% hence the total sample
detected and recovered is 99.88%. this value is between the
limit of detection hence the precision and recovery is good for
the Imidacloprid insecticide in meat sample. So the extraction
process used for the extraction gave the accurate result and
better recovery of insecticides. These parameters help in
validating the extraction process of insecticide in the spiked
meat sample. Validation helps to know whether the process
gave better recovery or not. In this paper, Imidacloprid spiked
meat sample meets all the characteristics of validation process
hence it confirms that the sample process gave the better
recovery i.e., of 99.8%. and this value is also between 70-120%
of limit of detection.
DISCUSSION:
In the chemical examiner laboratories, the extraction methods
that are used generally are liquid-liquid extraction method [13](LLE), solid phase extraction method (SPE) , solid phase
micro extraction method (SPME), and in some laboratories
supercritical fluid extraction (SFE) method is also used. The
SPE, SPME and LLE methods are the conventional methods
which are having several limitations as these require additional
pretreatments and also have the filtration and precipitation [14]steps which are removed in DSPE method . The SPE method
has limitations like less accuracy and low reliability. The SFE
method has several limitations. it is costly due to the usage of
carbondioxide as solvent due to this it is limited in dissolving [15]mainly for polar compounds like Imidacloprid. In
comparison with conventional and modern methods, DSPE
method gives better recovery, accuracy and low cost due to less [16]intake of solvents and also gives ample limit of detection .
thus it can be used in forensic and various chemical examiner
laboratories.This extraction method gives better recovery for
high polarity compounds i.e., Imidacloprid and it gives
accurate results and better recovery when it is detected under [17]LC-MS/MS when compared with GC-MS .
CONCLUSION:
In this paper, it concludes that the dispersive solid phase
extraction method gave the better recovery of the analyte
i.e.,99.8% and also gave better results in both qualitatively and
quantitatively. This analyte recovered also meets the LOD and
LOQ which proves that it gives better results when it is
detected under LC/MS-MS. This method acts effectively in
extraction, isolation and cleanup. This paper mainly concludes
that the DSPE method used for extraction of insecticides is an
accurate process and also gives the better recovery of the
analyte i.e., Imidacloprid. Hence, this extraction method has
wide use in forensic laboratories for the extraction of pesticides
from the viscera samples as this method also costs very low.
This method helps to give accurate and rapid results from the
viscera samples. This concludes that this extraction method
and the detection of analytes using LC/MS-MS has wide use in
forensic medicine and forensic toxicology.
REFERENCES :
1. EPA U. Pesticide fact sheet: imidacloprid. Washington,
DC. 1994.
2. Matsuda K, Buckingham SD, Kleier D, Rauh JJ, Grauso
M, Sattelle DB. Neonicotinoids: insecticides acting on
insect nicotinic acetylcholine receptors. Trends in
pharmacological sciences. 2001 Nov 1;22(11):573-80.
3. Tomizawa M, Casida JE. Neonicotinoid insecticide
toxicology: mechanisms of selective action. Annu. Rev.
Pharmacol. Toxicol.. 2005 Feb 10;45:247-68.
4. Berny PJ, Buronfosse F, Videmann B, Buronfosse T.
Evaluation of the toxicity of imidacloprid in wild birds. A
new high performance thin layer chromatography
(HPTLC) method for the analysis of liver and crop
samples in suspected poisoning cases. Journal of liquid
chromatography & related technologies. 1999 Jan
1;22(10):1547-59.
5. Kumar A, Verma A, Kumar A. Accidental human
poisoning with a neonicotinoid insecticide, imidacloprid:
A rare case report from rural India with a brief review of
literature. Egyptian Journal of Forensic Sciences. 2013
Dec 1;3(4):123-6.
6. Bais SS. An Overview on Imidacloprid Pesticide
Inducing Oxidative Stress.
7. Reigart JR, Roberts JR. Recognition and management of
pesticide poisonings. US Environmental Protection
Agency; 1999.
8. Wu IW, Lin JL, Cheng ET. Acute poisoning with the
neonicotinoid insecticide imidacloprid in N-methyl
pyrrolidone. Journal of Toxicology: Clinical Toxicology.
2001 Jan 1;39(6):617-21.
9. Shadnia, S., & Moghaddam, H. H. (2008). Fatal
intoxication with imidacloprid insecticide. The American
journal of emergency medicine, 26(5), 634-e1.
10. Matsuoka, T, Akiyama Y, Mitsuhashi T. Validation of
multi-residue method for determination of pesticides in
meat products using official guideline of analytical
methods in Japan. Journal of Pesticide Science.
2010:1011050169.
11. Ferrer C, Martínez-Bueno MJ, Lozano A, Fernández-
Alba AR. Pesticide residue analysis of fruit juices by
LC–MS/MS direct injection. One year pilot survey.
Talanta. 2011 Feb 15;83(5):1552-61.
12. European Food Safety Authority. Use of the EFSA
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00042.X

224
Standard Sample Description for the reporting of data on
the control of pesticide residues in food and feed
according to Regulation (EC) No 396/2005 (revision 1).
EFSA Journal. 2013 Jan;11(1):3076.
13. Singh C, Rani MS, Mishra A. Development of analytical
method for detection of monocrotophos insecticide from
biological matrix using lc-ms/ms. International Journal of
Medical Toxicology & Legal Medicine. 2020;23
(1and2):210-9.
14. Malone EM, Elliott CT, Kennedy DG, Regan L. Rapid
confirmatory method for the determination of sixteen
synthetic growth promoters and bisphenol A in bovine
milk using dispersive solid-phase extraction and
liquid chromatography–tandem mass spectrometry.
Journal of Chromatography B. 2010 May 1;878(15-
16):1077-84.
15. Friedrich JP, Pryde EH. Supercritical CO2 extraction of
lipid‐bearing materials and characterization of the
products. Journal of the American Oil Chemists' Society.
1984 Feb;61(2):223-8.
16. Diez C, Traag WA, Zommer P, Marinero P, Atienza J.
Comparison of an acetonitrile extraction/partitioning and
“dispersive solid-phase extraction” method with
classical multi-residue methods for the extraction of
herbicide residues in barley samples. Journal of
Chromatography A. 2006 Oct 27;1131(1-2):11-23.
17. Pang GF, Cao YZ, Zhang JJ, Fan CL, Liu YM, Li XM, Jia
GQ, Li ZY, Shi YQ, Wu YP, Guo TT. Validation
study on 660 pesticide residues in animal tissues by gel
permeat ion chromatography c leanup/gas
chromatography–mass spectrometry and liquid
chromatography–tandem mass spectrometry. Journal
of Chromatography A. 2006 Aug 25;1125(1):1-30.
Figure 1 : Linearity graph of Standard Imida cloprid Insecticide Sample
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00042.X

225
Figure 2: Chromatogram of Imidacloprid peak in Spiked Chicken Meat Sample
Figure 3: Chromatogram showing matrix interference in Blank Meat Sample
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00042.X

226
Review Article
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00043.1
1. Anvita Ahuja, MBBS Student*
2. Jasmeen Kaur, MBBS Student*
3. Prateek Rastogi, Professor and Head, Department of Forensic Medicine and Toxicology*
*Kasturba Medical College Mangalore, Manipal Academy of Higher Education Manipal, India
Key words: Keywords: Covid-19, Vaccine Hesitancy, Vaccine Refusal
Corresponding Author:
Dr. Prateek Rastogi,
Professor and Head, Dept. of Forensic Medicine and
Toxicology, Kasturba Medical College Mangalore, Manipal
Academy of Higher Education Manipal, India
Contact : +91 9448501376
Email :[email protected]
Article History :
Received : 27 April 2021
Received in revised from : 28 May 2021
Accepted on : 28 May 2021
Available online : 15 August 2021
INTRODUCTION:
As we continue to battle with a staggering death toll and
innumerable covid-19 cases, there emerges at long last a ray of
hope for humanity. Based on the most fundamental and basic
principles of immunology, a vaccine is a simple yet
tremendously efficacious tool employed for controlling the
spread of communicable diseases. To say that it was a
Herculean task to concoct vaccines for a novel virus
threatening the entire world- at such a short notice; would
admittedly be a gross understatement. Nevertheless, with an
army of highly competent researchers, billions of dollars of
funding and clinical trials; numerous contenders have arrived
in the market now:Johnson & Johnson's Janssen Covid-19 1 1Vaccine , Pfizer-BioNTech's vaccine , The Moderna 1 2 2Vaccine, Oxford's AstraZeneca , Bharat BioTech' Covaxin
and so on.All the aforementioned vaccines of-course must
have been subjected to stringent trials and scientific standards
and the findings must have been reassuring. But despite such
promising outcomes, there is little a vaccine can achieve if the
vial is never opened. It is now a widely held belief that
containment and barrier measures may stop the disease from
spreading but eradication would necessitate the use of a
vaccine.
This paper will explore not the therapeutic parameters and/or
the results/effects of these vaccines, but rather the public
initiative and willingness to get vaccinated; along with
relevant precedents, the need for appropriate legislature and
ethical concerns.
Problem Statement:
With a mountain of conspiracy theories and misinformation
floating around the internet, more and more people are opting
out of vaccination- a phenomenon known as “vaccine refusal”.
This reluctance to take the shot is not newfound and is certainly
not limited to the Covid vaccines. WHO listed “vaccine
hesitancy”- the unwillingness to get vaccinated despite
sufficient availability of vaccines- as one of the 10 global 3health threats in 2019 . This vaccine hesitancy and/or the
vaccine refusal, in the instant case of Covid-19 vaccine may be
a game changer, losing a surely winnable game or at least
delaying the much sought after win. An individual's choice (of
hesitancy or refusal) may cost, in unfathomable proportions,
the entire society, nation or even the world. The question is
how to and whether to surmount this problem with or without
the force of legislation?
Covid-19 Vaccination Hesitancy: Causes, Legislation And Ethics
ABSTRACT :
Covid-19 vaccines have now been around for quite some time and inoculation is in progress all around the world. However, some
apprehensions with regards to efficacy do seem to be existing for some founded/unfounded reasons, and at the same time, a
substantial reluctance (“Vaccine Hesitancy”) and/or non-acceptance (“Vaccine Refusal”) of the vaccine basedlargely on personal
choice seems to be emerging as a major cause of concern. This matter of individual choice apparently has the potential of
compromising success of the entire vaccination drive both qualitatively as well as quantitatively, that is; not only the desired results
of near total success evade us but the expected outcome may get inordinately delayed as well. This article, while looking into
historical as well as recent impediments to Vaccination (Hesitancy and Refusal), is an effort to analyze the reasons for the same and
bring out some remedial measures.

227
The Historical Scenario and now:
Any vaccine is bound to fail in achieving the desired outcome
if the uptake is below the threshold required to usher-in herd 4immunity . In a study by Jerome NyhalahDinga,
LeontineKouemouSinda, and Vincent P. K. Titanji on the
assessment of vaccine hesitancy to a covid-19 vaccine in
Cameroonian adults, the prevalence of Vaccine Hesitancy was
found to be 84.6% and their research states that for the vaccines
to achieve their intended goal, this figure has to brought down 5to around 30-25%.
Most of us are familiar with the phrase “prevention is better
than cure”. While we do not (and realistically, may not, in the
near future) have the cure for covid-19, we have been fortunate
enough to survive the pandemic long enough to see the birth of
vaccines against it. Reluctance to get vaccinated endangers the
progress made in combating diseases that are vaccine
preventable. A vaccine does not only confer individual
immunity, but also disrupts the transmission of disease as the
number of susceptible hosts are decreased. This promotes herd
immunity. In some cases- such as the Oral Polio Vaccine- the
mutant vaccine virus multiplying in the gut of the vaccinee is
shed into feces and is transmitted to other people of the same
community via feco-oral route, thus imparting immunity to 6them . It is clear as crystal that although the decision to get
vaccinated is personal, the consequences of the said decision
are community wide or nation-wide or even the world-wide.
In a paper on the society's response to the risks of vaccine
rejection, the author has compared vaccine refusal as
equivalent to drunk driving, smoking in closed spaces and
having unprotected intercourse with others despite being 7diagnosed with a venereal disease , as in all these situations,
people are making conscious choices which are also putting
other members of the community in danger.From an ethical
point of view, it is important to note that some-if not all- of
these are choices that they, as individuals, do reserve the right
to make, however risky and/or unsocial those may be. This 8warrants mention of John Stuart Mill's Harm Principle which
states “people should be free to act however they wish unless
their actions cause harm to somebody else” or, more crassly,
“your freedom to swing your fists ends where my nose begins”.
In the same article, the consequences of declining vaccination
have been briefly described; namely, spread of vaccine-
preventable diseases not only among the ones refusing
vaccination, but also among those in whom the vaccine has
differing degrees of effectiveness, the immunocompromised
and the ones who are too young to be vaccinated. Besides, the
authors make a good point that vaccine denial costs billions of
dollars of taxpayer's money- both in direct and an indirect
fashion. Direct expenditure would be the healthcare costs that
would accrue from spread of the disease (Which, note, would
otherwise have been controlled by the vaccine) public health
care facilities including infrastructure, material costs for PPEs,
masks, hospital tools and equipment, disinfectants, sterilizers,
ventilators, beds and so on. The indirect costs would include
money spent on research and development and production of
the vaccines. Finally, yet importantly, due to subjective and
largely irrational risk perception, vaccine anxiety remains 7immune to all the evidences of vaccine safety.
What causes vaccine hesitancy/refusal?
There has existed a community of myriads of people who do
not believe in and have emphatically rejected vaccines- since
before the pandemic- and they call themselves as
“antivaxxers.”When questioned as to why anyone would reject
vaccines, different answers come to light:religious sentiments,
misguided information, anti-vaccination propaganda as well
as the abundance of conspiracy theorists and universal
antagonistics. Few other contributing factors might be lack of 9confidence and complacent behavior . Tremillia Hobbs- a
nursing staffer feels overwhelmed by how quickly the vaccines
were brought into being and fears long term complications and 10possible driving political agendas. In general, vaccine
opponents have not been found to hold any single common
unifying notion.
Reeling back in, let's have a look at 2 stories that changed
the course of vaccination drastically:
1. 1998; Lancet publishes a paper by a British
gastroenterologist Andrew Wakefield who became fixated
on the prospect of a potential association between the 11measles virus and autism. While studying inflammatory
bowel disease, he hypothesizes a “leaky gut” that lets the
measles virus molecule from the MMR vaccines escape
digestion and reach the brain causing autism.Wakefield
used the media to his own advantage- garnering publicity
after airing his flawed views; while also covering up
possible conflicts of interests that he had. The publication 12was later retracted.
2. July 9, 1999; American Academy of Pediatrics and the
Centers for Disease Control and Prevention (CDC) release
a joint statement on the removal of vaccines containing a
mercury based preservative 'thimerosal'; despite no hard
evidence of any real damage induced by it, but rather
based only on speculations of mercury based compounds
causing autism and concerns raised by the Environmental
Protection Agency regarding the deleterious effects of 13mercury.
Such events later influenced environment lawyer Robert F. 12Kennedy , thereby creatinga most outspoken proponent of the
modern anti-vaccination movement.
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00043.1

228
Fueling the anti-vaccine drive, in 2005, a grief ridden parent
'Sarah Bridges' goes over to Kennedy's house with piles of
paper containing theories of links between autism and
thimerosal containing vaccines- right after her son gets
diagnosed with autism. Kennedy gets alarmed and wages a
proverbial war against the vaccines and vaccine advocates. He
starts a column called “deadly immunity”- in print and on
digital platforms- it was rife with inaccuracies and misquotes.
Kennedy went on to earn a reputation as he facilitated the
making of and produced several anti-vaccination
“documentaries”.He became rather notorious and is said to
have wrongly quoted expert opinions and even recruited fake
experts on purpose. He managed to steer the issue away from
that of public health, morphing itinto a typical political
squabble- he wasn't beneath dragging race in between,
launching the concept of “medical racism” through his movie
“Medical Racism: The New Apartheid” which showcased a
combination of very real and saddening manifestations of
racism encountered in healthcare (which, in the authors'
opinion, warrants a discussion by itself) along with anti-
vaccination myths to impose the agenda on a vulnerable 12population.
This becomes concerning when one takes into consideration
the fact that there exists already a feeling of discomfort and
mistrust amongst the marginalized community of people of
color regarding the government, science and research; all
rooted in the abuse, some of them may have had to face in the
name of research: for instance, the Tuskegee Syphilis Study,
Henrietta Lacks' cells being used for research without proper 14consent and compensation , and in a later case where blood
samples from Havasupai Tribe members were inappropriately 15used for testing. The combination of this valid skepticism and
animosity- that has been germinating in the minds of black
people-with the influence exerted by Robert Kennedy, has
resulted in most black people now believing that the vaccine is
more of a threat to them than covid-19. One person even
compared the vaccination drive to the Tuskegee tragedy and 12exclaimed that he won't be anyone's guinea pig. According to
new CDC data, 5.4 percent of those who have had at least the
first dose of a vaccine are Black, compared to 60.4 percent who 16are white.
How to overcome vaccine rejection/ increase vaccine
uptake:
Given the dire and cascading effects of poor vaccine uptake, it
appears reasonable to opine that some effort is required to
ensure adequate uptake. We may also opine that, given the
deep roots of vaccine apprehension, some strong steps may be
needed to improve vaccine acceptance.
A Reddit user going by the name of “mishyfishy25” writes
“Vaccines need a rebrand. From now on, let's just start calling
them gluten-free, all natural nucleotides, specifically 17formulated to bolster immunity” the humorous implication
being people are more inclined to embrace a fad (even if it is
not backed by science) than they are to accept a well-
researched commodity in which billions of dollars have been
invested, lots of efforts put-in and a myriad of checks and
controls performed. Although it is not as simple as
mishyfishy25 proposes, it seems to be a viable suggestion.
Vaccines can be endorsed by celebrities and influencers just
like they would any other commodity. And it has also been
done; with polio. “do boondzindagigi” ads endorsing the
“Pulse Polio Program” used to blare on the media all day
long,seeking to keep India polio-free.
Other measures that may help improving vaccine uptake
includea positive attitude on the part of the physician,
educative seminars, honesty about the risks and benefits as
well as patient counselling. A doctor, for example, may say “I
have taken the vaccine and I think you should too”- as a result,
obtaining the patient's confidence by demonstrating that they-
as a doctor believe in the vaccine, and so the patient should as
well. These measures- though effective at an individual level,
are only practicable in a clinical setting where the physician
has direct access to the patient. Hence, at a large scale, the
results of this approach may remain limited.
Another initiative which may gather more willing vaccine
recipients is the incentivization of vaccines. This can be done
in a number of ways- offering certain financial incentives or
perks like discounts and health insurance related offers and so
on. While incentivization will bring about an air of positivity
around the topic, it may backfire as well on ethical grounds.
Over-incentivisation may be seen as “undue inducement”-
where a reward is so high, that it may be unduly enticing,
leading to someone disregarding risks.
On the contrary, under-incentivisation may be seen as
exploitative- where people in a vulnerable situation can agree
to get vaccinated because they believe they have little other
choice, and even a small reward would provide a great deal of
relief. This way, offering the incentive may get projected as 18taking advantage of a person who is in a tough spot.
Another option that one might consider is to deincentivise
vaccine rejection. This approach too has been in practice since
long. One cannot enter certain countries in Africa without 19appropriate yellow fever shots school admissions are difficult
for unvaccinated children in various states of the USA. The
immunization laws varyby state.Some state senates have
removed exemptions based on religious beliefs (example: New
York Senate Bill 2994) etc. Virginia House Bill 1090 states that
The Immunization Schedule created and reported by the
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00043.1

229
Centers for Disease Control and Prevention, the Advisory
Committee on Immunization Practices, the American
Academy of Pediatrics, and the American Academy of Family
Physicians is to be followed by the Board of Health's 20Regulations for the Immunization of School Children.
A rather drastic measure which may be taken subject to
rigorous ethical examinations and considerations- is to
mandate the vaccine by law. The mandate could be of 2 stages.
One where defaulters are subjected to mild punishment;
probably some sort of fine, and another where vaccine refusal
leads to more serious consequences like imprisonment. There
has been a historical precedent, although not without a
resounding ethical backlash. To stop Smallpox outbreak, the
British Government in India passed the Vaccination Act in
1880, followed by the Compulsory Vaccination Act in 1892.
Non-vaccination without justification resulted in
incarceration. Some of these legislations were overturned as 19recently as in 2001. The authors of this paper acknowledge
that attempts to make vaccination mandatory could be an
ethical miscarriage of justice in view of laws and legislations
of a country,and further clarify that mandatory vaccination
may not at all be required particularly wherever there is
sufficient voluntary vaccination or improvement in vaccine
acceptance is achievable by other, far less drastic methods.
This paper is merely an effort at exploring some of the options
one might like to choose from.
In favor of mandating vaccination by law, Jason Brennan, in
his paper describes how the state can coercively enforce at
least some-if not all- moral duties on its citizens. He makes his
case by giving various analogies, one of which is; that whilst
the state might not be able to prevent him from writing a book
promoting genocide, it can coerce him into refraining from
carrying it out. It is not clear why some morals are coercively 21enforceable and some are not. How this applies in the real
world; Jason Brennan implies; is that the state can use force
and/or intimidation to prevent an individual from actively
spreading an infection.Besides, there might be a compelling
argument to make any vaccine mandatory if the following four 22conditions are met :
— The public's welfare is in great danger: (the larger the
probability and/or extent of harm, the more it favors 18mandatory vaccination .
— The vaccine has been shown to be both safe and reliable.
— When compared to other options, mandatory vaccine has a
better cost-benefit profile.
— The amount of coercion is appropriate
— Each condition merits appropriate value and the state may
choose to act as considered appropriate in the larger interest of
the humanity.
—CONCLUSION:
Any Vaccination program is founded in painstaking research
with the expense of large quantum of vital resources. One of
the most critical aspect taken care of, during the development
phase of any vaccine is, eliminating possibilities of any harm to
the recipients, while ensuring the sought after protection/
benefits. This, to our opinion, hardly leaves any reason for an
individual to go in the denial mode. Still, individual's choice
may be an issue worth overlooking and permissible, as long as
it doesn't infringe upon essential protection- (like the law does
against unsocial/criminal elements)- and benefits of the state
sponsored programs that the residents of the state are entitled
to. In a situation where such an infringement has occurred,
should the state use force of law, or use the stick and carrot
policy or any other inclusion/exclusion policy, to ensure that
larger section of the society does not suffer and/or lose benefits
due to non-cooperation by a few- is the opinion point this
article leaves you at.
REFERENCES:
1. Centers for Disease Control and Prevention. Different
COVID-19 Vaccines. [Online]. Available from:
h t t p s : / / w w w . c d c . g o v / c o r o n a v i r u s / 2 0 1 9 -
ncov/vaccines/different-vaccines.html [Accessed 23
April 2021].
2. Times of India. Coronavirus vaccines in India: Here's a list
of all the COVID-19 vaccines being made in India.
[Online]. Available from:
https://timesofindia.indiatimes.com/life-style/health-
fitness/health-news/coronavirus-vaccines-in-india-heres-
a-l is t-of-al l-covid-19-vaccines-made-in-india/
photostory/79463339.cms [Accessed 23 April 2021].
3. World health organization. Ten threats to global health in
2019. [Online]. Available from:
https://www.who.int/news-room/spotlight/ten-threats-to-
global-health-in-2019 [Accessed 23 April 2021].
4. Mayo clinic. Herd immunity and COVID-19
(coronavirus): What you need to know. [Online].
Available from: https://www.mayoclinic.org/diseases-
conditions/coronavirus/in-depth/herd-immunity-and-
coronavirus/art-20486808 [Accessed 23 April 2021].
5. Dinga JN, Sinda LK, Titanji VPK. Assessment of vaccine
hesitancy to a COVID-19 vaccine in Cameroonian adults
and its global implication. Vaccines. 2021;9(2):175
6. Holubar, M., Troy, S., Nathoo, K., Stranix-Chibanda, L.,
Musingwini, G., Srinivas, N., Huang, C., Junn, A.,
Halpern, M. and Maldonado, Y., 2016. Shedding of Oral
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00043.1
230
Poliovirus Vaccine (OPV) by HIV-Infected and -
Uninfected Mothers of OPV-Vaccinated Zimbabwean
Infants. Journal of the Pediatric Infectious Diseases
Society, 6(1), pp.105-108.
7. Ropeik D. How society should respond to the risk of
vaccine rejection. Human Vaccines & Immun other
apeutics. 2013;9(8):1815-1818.
8. What is The Harm Principle? Ethics Explainer by The
Ethics Centre [Internet]. THE ETHICS CENTRE. 2016
[cited 23 April 2021]. Available from:
https://ethics.org.au/ethics-explainer-the-harm-principle/
9. Alvira X. Vaccine hesitancy is a global public health
threat. Are we doing enough about it? [Internet]. Elsevier
Connect. 2019 [cited 23 April 2021]. Available from:
https://www.elsevier.com/connect/vaccine-hesitancy-is-
a-global-public-health-threat-are-we-doing-enough-
about-it
10. Pattani A. Vaccine Hesitancy vs. Vaccine Refusal:
Nursing Home Staffers Say There's a Difference
[Internet]. Kaiser Health News. 2021 [cited 23 April
2021]. Available from:
https://khn.org/news/article/vaccine-hesitancy-vs-
vaccine-refusal-nursing-home-staffers-say-theres-a-
difference/
11. Larson H.J, Mnookin S. Chapter 27 - Trust and
Confidence in Vaccines: Tales of Three Vaccines, Lessons
for Others. In: Bloom, B.R, Lambert, P.H (eds.) The
Vaccine Book. : Academic Press; 2016. p. 529-540.
12. Jarry, J. The Anti-Vaccine Propaganda of Robert F
Kennedy, Jr Or how an environmental lawyer led a
crusade against vaccines and spread lies to marginalized
c o m m u n i t i e s . [ O n l i n e ] . Av a i l a b l e f r o m :
https://www.mcgill.ca/oss/article/covid-19-health-
pseudoscience/anti-vaccine-propaganda-robert-f-
kennedy-jr [Accessed 23 April 2021]
13. Baker J. Mercury, Vaccines, and Autism. American
Journal of Public Health. 2008;98(2):244-253
14. Young S. Black Vaccine Hesitancy Rooted in Mistrust,
Doubts [Internet]. WebMD. 2021 [cited 23 April 2021].
Available from:
h t tp s : / /www.webmd.com/vacc ines / cov id -19 -
vaccine/news/20210202/black-vaccine-hesitancy-
rooted-in-mistrust-doubts
15. Quinn S, Andrasik M. Addressing Vaccine Hesitancy in
BIPOC Communities Toward Trustworthiness,
Partnership, and Reciprocity | NEJM [Internet]. New
England Journal of Medicine. 2021 [cited 23 April 2021].
Available from:
https://www.nejm.org/doi/full/10.1056/NEJMp2103104
?query=infectious-disease
16. Painter EM, Ussery EN, Patel A, et al. Demographic
Characteristics of Persons Vaccinated During the First
Month of the COVID-19 Vaccination Program United
States, December 14, 2020January 14, 2021. MMWR
Morbidity and Mortality Weekly Report2021;70:174177.
17. RandomThoughts [Internet]. Reddit.com. 2021 [cited 23
April 2021]. Available from:
https://www.reddit.com/r/RandomThoughts/comments/
mpxohr/vaccines_need_a_rebrand_from_now_on_lets_j
ust/
18. Savulescu J, Giubilini A, Danchin M. Global Ethical
Considerations Regarding Mandatory Vaccination in
Children. The Journal of Pediatrics. 2021;231:10-16.
19. Dubey R. State activism: Should COVID-19 vaccination
be compulsory? [Internet]. Bar and Bench - Indian Legal
news. 2021 [cited 23 April 2021]. Available from:
https://www.barandbench.com/columns/state-activism-
should-covid-19-vaccination-be-compulsory
20. States With Religious and Philosophical Exemptions
From School Immunization Requirements [Internet].
Ncsl.org. 2021 [cited 23 April 2021]. Available from:
h t tps : / /www.ncs l .o rg / research /hea l th / school -
immunization-exemption-state-laws.aspx
21. Brennan JA libertarian case for mandatory vaccination.
Journal of Medical Ethics.2018;44:37-43.
22. Savulescu J. Good reasons to vaccinate: mandatory or
payment for risk? Journal of Medical Ethics.2021;47:78-
85
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00043.1

231
Review Article
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00044.3
Review on Bioremediation of Carbofuran & Different Factors Influencing the Process
1. Suryapratap Ray, M Sc Forensic Sciences Lovely Professional University, Jalandhar, Punjab India (144411)
2. Shikha Choudhary, Assistant Professor, Department of Forensic Science, Lovely Professional University, Jalandhar
ABSTRACT :
Carbofuran is a carbamate pesticide, which is used widely in agriculture production. We can consider carbofuran as one of the most
toxic carbamate pesticides. Usually we can encounter this pesticide in market as FURADAN (FMC corporation), CURATERR 10
GR (Bayer). The degradation of carbofuran is very important as it is toxic to environment which ultimately affects the living
organisms. It is extremely lethal because of its anticholinesterase activity, which inhibits acetylcholinesterase and
butyrylcholinesterse activity. Apart from carbofuran other carbamates such as Carbaryl, Aldicarb, Methomyl, Carbofuran, and
Propoxur etc are also needs to be degraded. Several conventional technologies are used for the removal of carbofuran
includingphysicochemical processing like photo-catalysis, ozonation/UV- irradiation, membrane filtration, adsorption and Fenton
degradation. However, none of these technologies is feasible and cost effective for complete mineralization of carbofuran pollution
from the environment. In such case, microbial degradation found to be the most effective, feasible and eco-friendly method. The
degradation process also relies on various other ecological factors such as hydrolysis, oxidation etc along with naturally occurring
microbes. This review point outs various microbes that can be helpful in degradation of carbamates, their metabolism and other
ecological factors involved in this process.
Key words: Carbofuran, Carbamate pesticide, Carbofuran degradation, Carbamate degradation, CURATERR 10 GR, Metabolic
pathway, Microbial degradation.
Corresponding Author:
Dr. Shikha Choudhary,
Assistant Professor,
Department of Forensic Science, Lovely Professional
University, Jalandhar
Contact : +91
Email : [email protected]
Article History :
Received : 20 November 2020
Received in revised form : 6 December 2020
Accepted on :6 December 2020
Available online : 15 August 2021
INTRODUCTION :
Pesticide in simple terms refers to the substance or chemical
formulation that helps in controlling pests by preventing and
destroying them. We can consider weeds, birds, insects,
microorganisms or mammals as pests, as they interfere or
destroy valuable things. We can categorize pesticides into
Inorganic Pesticide, Synthetic Pesticide and biological
pesticide based on their chemical structure, physical form and
their target species. Various types of pesticide that are being
used now a days very commonly includes- organophosphate,
pyrethroid, organochlorine and carbamate pesticides.This is
further classified by various researchers. That is rodenticides,
weedicides, fungicide, herbicide, and insecticide. Carbamate
insecticides are basically derivative of carbamic acids. The
first carbamate insecticide is Carbazyl. It was introduced in
1956. They inhibit the AChE (Acetylcholinesterase) enzyme
and cause over stimulation of nervous system. Considering
their chemical structures and biological actions carbamate
pesticides are basically categorized into two parts. One is N-
methyl-carbamate insecticides and the other one is N-allyl-[1]carbamate herbicides . Carbamates are highly toxic to plants
and animals as well. It is useful when we consider its
insecticide properties. But various non-targeted living
organisms are suffering due to its high toxicity nature. So, it is
very much necessary to degrade this pesticide after getting the
targeted work done.Various technologies are introduced for
the removal of carbofuran including physicochemical
processing like photo-catalysis, ozonation/UV- irradiation,
membrane filtration, adsorption and Fenton degradation. But
none of those technologies are feasible and price effective for
complete degradation of carbofuran pollution from the
environment in a eco-friendly manner. Carbamate pesticides
are converted to various products applying various chemical
processes, such as oxidation, biotransformation, hydrolysis,
bio-augmentation, photolysis, biodegradationand metabolic [2]reactions in living organisms (microbial degradation) .
Biodegradation of various pesticides by bacterial activity
under certain physiological condition have already been
observed by various researchers. Even in many cases it is

observed that, various soil microbes which are frequently
getting exposed to such pesticides developed new capabilities
in order to survive in that hazardous condition. They can
actually degrade these toxic pesticides. There are some soil
microbes that can degrade carbamates. Some microbes that are
found in soil got the ability to use carbofuran as the only source
of carbon dioxide and energy. So, they can easily adapt to that
condition. However, carbamates pesticide and their [3]metabolites can affect the micro flora and soil productivity .
Degradation of Carbamate pesticide using microbes can be
considered as a conventional technique. Microbial degradation
found to be the most effective, feasible and eco-friendly
method.
Structure and properties of carbofuran
Carbofuran is marketed under the trade name FURADAN
(FMC corporation), CURATERR 10 GR (Bayer),
FURACARB. The IUPAC name is- 2,2-dimethyl-2,3-
dihydro-1-benzofuran-7-yl methylcarbamate. The chemical
formula can be written as C H NO . It appears as white 12 15 3
-1crystalline solid with molar mass 221.256 g.mol . It is soluble
in water with solubility 320mg/L and highly soluble in N-
methyl-2-pyrrolidone, Dimethylformamide, Acetone,
Acetonitrile etc. The structure (Figure 1 Structure of
Carbofuran) is given below:
Carbofuran pesticide is banned in Canada and European
Union. The main concern is obviously the toxicity to mammals
and environment. It is having LD of 8-14 mg/kg body weight 50
(as observed in dog). Carbofuran, which possesses high acute
toxic effect retain itself in the soil in the form of organic
compounds. So, the process of metabolism or breakdown may [4]take weeks or more duration . Carbamates are basically
insecticides, herbicides, and fungicides that act similarly as
organophosphates pesticides. It acts by inhibiting AChE
(Acetylcholinesterase) enzyme, exception is that the action is
reversible. The toxicity generally varies from different
derivates, wherein aldicarb is very toxic. Carbamate pesticide
plays a vital role in agriculture because of its broad-spectrum
nature and varied degree of compounds which are degradable [5]in soil . We generally consider carbofuran as a plant systemic
pesticide.It acts through phloem sap against piercing-sucking
pests of rice crop like Nephotettixvirescens(green
leafhoppers), Nilaparvatalugens(brown plant hopper), stem [6]borers and whorl maggots . This pesticide is also applied on
potatoes, strawberries, grapes, wheat, corn, soybeans and alfa-
alfa for controlling corn rootworm, wireworms, aphids, white
grubs etc. When we use this pesticide in form of liquid or
powder, it generally gets absorbed by the plant and
translocated to different plant parts. Although carbofuran
pesticide was used in liquid and granular form but USEPA and
European Union completely banned its use in both the forms [7]because of its toxicity on the birds . The granular form of
carbofuran usually looksimilar to the seeds and mistakenly
eaten by birds as grit or food that causes toxicity leading to
death. However, liquid formulations of carbofuran are still
used in various countries including India, Kenya, China, [8]Thailand, Pakistan and Sri Lanka
Sources of toxicity
Direct applications in agricultural fields and industries or
indirectly through drifting andvolatilization from the treated
fields can be the main source of carbofuran contamination to
environmentcontaminating air, soil and water eco system, [8]nontarget plants, animals as well .The exact quantity of any
kind of pesticide that is applied on to any agriculture fields,
never ever completely reaches to the targeted organisms and
most of its amount is dispersed into the environment. This
amount of unused pesticide cause aircontamination, along with
soil and water ecosystems. Evert in 2000 and Donovan2012
studied the environmental fate, chemistry and detection of
carbofuran insoil and water in a very good manner, which
explains this particular thing in details.
Mechanism of toxicity[3,9]The toxicities related to carbofuran is documented . It is
highly toxic to non-targeted organisms such as birds, rodents,
honeybees, fishes and other water organisms through direct
inhalation, ingestionor dermal absorption. Although it is not
considered as carcinogen but can cause genotoxic, mutagenic,
carcinogenic and teratogenic effects (according to
WHO,2009). Carbofuran causes acute and chronic toxicities
byinhibiting acetylcholinesterase in synapses of central
nervous system (CNS) that is the main toxicological property
of this pesticide (FAO/WHO, 2009). Carbofuran also causes
severe developmental and reproductive issues in maternal-
placental-fetal unit by crossing placental barrier. Various
s tud ies conc luded tha t , th i s pes t i c ide causes
significantdecrease in isoenzyme-I and isoenzyme-II in [9]mother and foetus . Research on the same concluded the toxic
concentration of carbofuran in biological tissues. This is found
to be ranging from 0.4-18μg/mL inblood, in bile it is 0.4-60
232
Structure of carbofuran
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00044.3

μ/mL, in liver 2.2 μg/gand 0.3-300 μ/g in stomach [10]contents/stomachin a homicidal case .Carbofuran toxicity
mechanism is based on reversible competitive inhibition of
acetylcholinesterase enzyme (AChE) in the central and
pe r iphera l ne rvous sys tems (PNS) .Carbofuran
affectscarbamylation or modification of serine residue active
site withincarboxylesterase and butyrylcholinesterases [9]enzymes . The inhibition of AChEase enzymes causes
successive accumulation of acetylcholine (Ach) insynapses
thatbreaks into choline and acetate residues leading to clinical.
Considering the stimulation Ach receptor, there are two types
of acuteclinical manifestations occurs. Namely Nicotinic and
Muscarinic. Nicotinic effects result in muscleweakness and
tremors whereas muscarinic effects can damage cardiac,
gastrointestinal andrespiratory systems resulting in
defecation, increased salivation, gastroenteritis, bradycardia [3]andobstruction of airways .
Effect of carbofuran on aquatic ecosystem
Water bodies such as river, ponds etc are highly prone to
carbofuran toxicity as indicated by its groundwaterubiquity
score (GUS) index of 4.5, showing a relatively high risk of
being transported from the targeted site to adjacent water
bodies after raining or by any other method. Carbofuran can
cause acute and chronic toxicities to aquatic organisms by
interrupting in hematological, biochemical and enzymatic
activities. Detrimental effect of this pesticide carbofuran has
been reported in several algal species, such as
Chlorellavulgarius, and Raphidocelissubcapitataand rotifers
(Philodina roseola). Among Pocecilia reticulate, Daphina
Magna and Rhapidocelissubcapitata(green alga), Daphnia
magna is considered to be the most sensitive towards [10]carbofuran acutetoxicity with EC50= 0.187 mg/L after 48 h .
Carbofuran acts as a neuro-toxicant and Acetylcholinesterase
inhibitor in brain, liver and muscles of fish especially.
Cyprinicarpioand Oreochromis niloticusare fresh water fishes
helpful in toxicity model organisms and play animportant role
to observe and moniter the toxicity profile of aquatic
environments. Carbofuran exposure also leads to functional
abnormalities in fish such as change in body colour, balance
loss, in some cases they fail to feed, growth rate reduction and
reduction in swimming performance. These studies reveals
that fish are the most appropriate and feasible biomarker to
study and moniter acute effects of the carbofuran in aquatic [11]environments .
Effect of carbofuran on soil and plant
Commercial formulations of carbofuran residues can easily
contaminate soil ecosystems and plants through direct
spraying, surface-runoff, flooding or accidental
exposure.Considerable experiments had been carried out
about the efficacy of carbofuran against pests, insectsand soil
nematodes. Carbofuran uses result in life-threatening soil
contamination that can harshly affect soil fertility, respiration,
microbial biomass and diversity, nitrogen and phosphate
mineralization capacity, and enzymatic activities of plants and [12]microbes . Itactually inhibits dehydrogenases.This represent
[13]soil microbial activity . Due to the barrier in microbial
growth, dehydrogenase and alkaline phosphatase activity in
fertilized soil is significantly decreasing with increasing
carbofuran doses (0.02-1.0 kg/ha to 5.0 kg/ha) in comparison
to controls. Contamination of soil and water due to carbofuran
pesticide.He found high environmental contamination of
carbofuran and its two toxic metabolites 3-ketocarbofuran and
3-hydrocarbofuran in dry surface soil (0.010-1.009 mg/kg) and
watersamples that was taken (0.005-0.495 mg/L). High
concentrations of carbofuran pesticide and metabolites
ranging 0.04-1.328 mg/kg of dry Maize plant tissues have been
reported as well. The experiment demonstratedlocal exposure
and impact of carbofuran by domestic applications. Hence, the
extensive use of carbamatepesticides in agricultural soils
results in serious ecological consequences.
Effect of carbofuran on humans and other animals
Carbofuran is found to have very high mammalian toxicity,
oral LD50 8-11 mg/kg in rats and is dangerously lethal to [14]invertebrates, birds as well . Environmental Protection
Agency (EPA) considered it in “Toxicity Category I'', that is the
most toxic category based on hazardous effects via oral and
inhalation exposures. Carbofuran basically causes acute
toxicities and fatalities in humans through accidental exposure
whereas continuous exposures result in chronic toxicities.
According to Environmental Protection Agency, California,
drinking water which is carbofuran contaminated can produce
detrimental effects on reproductive function in humans, as
reported in “Public Health Goals for Chemicals in Drinking [15]Water” . Long-term carbofuran pesticide exposures to
farmers, industrial workers and animals results in chronic
toxicity. It includes dermal, endocrine, cytotoxic, mutagenic,
reproductive, neurotoxic, genotoxic, disrupting, embryo-toxic [16]and dermal-skin problems . basically, it is not considered as
carcinogen but Bonner in 2005 indicated that carbofuran
pesticide exposure is positively associated with increased
cancer risk in lungs. It basically enters human and animal body [15]by inhalation, ingestion and dermal absorption . Wherein
dermal exposure is less toxic with respect to direct inhalation
or ingestion of carbofuran. High concentration or volume of
carbofuran exposures to humans primarily cause weakness in
muscles, dizziness, sweating and body discomfort and
headache, salivation, nausea, vomiting, abdominal pain,
diarrhoea. Dilated pupils and blurred vision, incoordination,
233
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00044.3

and muscle twitching and slurred speech have also been [16]studied after short-term carbofuran exposure . Carbofuran
intoxication extensively causes significant decrease in
haemoglobin content, total red blood cells (RBC) count,
platelets, erythrocyte sedimentation rate (ESR) and
haematocrit value in body.
Metabolism of carbamate pesticide
In mammals, insects, and plants the metabolic product of
carbamates pesticide is generally very similar. This pesticide is
absorbed in the body by respiratory tract, dermal contact and
mucous membrane. Usually, carbamate metabolites after
degradation are less toxic as compared to their parent
compounds. In some circumstances, the metabolites of
degraded carbamate or any other pesticide found to be more [16]toxic than the original compound . Hydrolysis is the primary
phase of metabolic degradation of carbamate pesticide in soil.
This process ultimately leads to formation of the carbamic
acid. Again, the breakdown process will form the carbon [17]dioxide and similar amines . N-methyl carbamate and N-
dimethyl derivatives both are having different hydrolysis
mechanism. The N-methyl carbamates pass through an
isocyanatemetabolite. Wherein the hydrolysis of Ndimethyl
carbamates, a product containing hydroxyl ion is formed. This
ultimately results in alcohol and N-dimethyl replaced acid [18]formation . Keeping aside hydrolysis, oxidation also happen.
Thisinvolves hydroxylation of the aromatic ring, N-
dealkylation, oxidation of aliphatic side chains, O-[19]dealkylation, N-methyl hydroxylation, and sulfoxidation .
Degradation studies in soil contaminated with the
insecticidecarbofuran and its metabolites (3-ketocarbofuran
and 3-hydroxycarbofuran) were performed using laboratory
systems with controlled conditions (temperature, water
content, light). Bacterial abundance and the concentration of
the different chemicals were assessed by adding the
insecticides to soil samples and subsamples of the soil were
analysed at different times. The epifluorescence direct count
method was applied here to the samples to point out
microorganism numbers (N=g soil). Evaluation of the effects
of the application of the insecticides on microbial abundance
done by using the untreated samples of soil as control sample.
Subsamples treated with the pesticides then analysed using
HPLC and the DT50s or the half-life of the different
compounds studied were analysed.
Carbofuran and its microbial degradation
2,3-Dihydro-2,2-dimethylbenzofuran-7-yl methylcarbamate
is the chemical name of carbofuran and it is a broad-spectrum
insecticide commonly used in agriculture sector. Carbofuran is
basically soluble in water and highly mobile in soil. This is the [16]reason of ground water contamination in different regions .
The table presented as TABLE-1 shows the microbes that can
be helpful in degradation of Carbofuran.
Degradation of any pesticide implicating microbes is not at all
a newly introduced method. Micro-organisms usually supply
the energy required for the chemical reactions that needs to be
take place in order to carry out their metabolism as well as the [17]biodegradation . A number of factors are involved in
pesticide biodegradation using microbes or microbial activity.
Microbial strain consortia that metabolize the carbofuran and
other carbamates and helps in degradation process has been [20]studied . The pesticide is commonly used for over decades.
This caused the tolerance in some microbes to that particular
pesticide, wherein in some other cases some microbes started
to develop mechanism, enzymatic pathways to degrade the
pesticide. In 1973 the bacteria that degrades organophosphate
was first isolated in Philippines in a paddy field area.
Frequently afterwards many different microbes were isolated
by different researchers which can degrade different pesticides [21]as per report . Pesticides are directly implicated tom the soil
for the protection of plants from pests. After the application of
such pesticides they usually undergo various processes. Some
process such as volatilization, degradation, sorption, or surface [22]transport are studied . Various researches conducted on these
topics explains that the soil of those agriculture fields which
have a history of pesticide application is found to be have less
half-life as compare to the soil which is not having any such [23]pesticide application history . Other microbial sources apart
from soilincludes; pesticide industry, drainage water, activated
sludge, sewage, even surface waters and their sediments can be
considered, area which is close proximity to pesticide
industries. We can categorise microbes based on their growth [24]and ability to degrade pesticides . There are various microbe
species which are involved in pesticide degradation. Such as
234
Pesticide
Carbofuran
Microbes
Consortia
Pseudomonas sp.
Pseudomonas and
Alcaligenes
Mucor
Ramannianus
Novosphin-gobium sp
Aspergillus sp.
Environ-mentaction
References
Tien et al. (2017)
Devi et al. (2017)
Omolo et al. (2012)
Fareed et al. (2017)
Seo et al. (2007)
Fareed et al. (2017) Seo et al. (2007)
Fareed et al. (2017) Seo et al. (2007)
Soi
lD
egra
dati
on
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00044.3
Pseudomonas, Flavobacterium, Achromobacterium sp.,
Sphingomonas sp., Arthrobacter and Bacillus speciesas
mentioned in the table-1. Thesehave been isolated and
characterized in various reserches. This helped researchers to
get knowledge regarding pesticide degradation mechanism.
Carbofuran phenol and subsequently degraded to 2-hydroxy-
3- (3-methylpropan-2-ol) phenol by Sphingomonassp. and [25]Arthrobacter sp. strains in the degradation of Carbofuran.
Carbofuran phenol formation is the first step in the
degradation. The table-1 contains various microbes that are
useful in degradation of carbamate pesticides. It is very much
essential to understand the biochemical bases involved in
micro-organisms inorder to develop various degradation [26]capabilities in them . Enzyme based degradation is mostly
recommended in the bio remediation over the traditional [27]method . Various enzymes thatactually hydrolyse carbamate
compounds are either esterase or amidases in most of the cases.
The chemical structure of the side chains and substrate [28]influence the hydrolysis of carbamate pesticides .
Detoxification of the original carbamates takes place by
hydrolysis reaction. This process of hydrolysis results in the
formation of an alcohol and methylamine along with carbon-[28]dioxide gas . There are many enzymes that are involved in
degradation and formation of carboxylesterases are already [29]reported .
GMOs in biodegradation of carbofuran
GMO stands for genetically modified organisms. In various
cases we can use genetically engineered microbes for
bioremediation. This is economically feasible alternate for the [27]removal of contaminants in soil . The recombinant DNA and
RNA technology helped in constructing various types of
genetically modified microbes, which are actually found to be
result oriented when it comes to degradation of pollutants in [30]various polluted sites . Here, the technique that is used is to
change or modify certain regions in DNA to produce desired
enzyme which will degrade the carbofuran. We can also
modify the specificity of the catabolic genes that was present
earlier. The genes of microbes always try to modify the
metabolic pathway, so as to increase the degradation ability.
Genetically modified microorganisms can be a best suitable
tool for biodegradation of any pesticide because of the unique
features of their metabolic pathways. Various research studies
found the way to create a genetically modified organism
(GMO) with a better metabolic pathway for the degradation of
organic compounds such as carbamates which includes [31]carbofuran and many others .
CONCLUSION :
After considering all the methods that can be implicated for
degradation process of pesticide, we can clearly consider the
microbial bio-remediation as a feasible and eco-friendly
method. Various microbes can be used for this purpose. Some
are mentioned above. Apart from this we can genetically
modify organisms so as to get a desirable GMO which can be
helpful in degrading various pesticides. In certain case we can
observe the metabolites of microbial degradation found to be
even more toxic due to various factors. Although various
researches done on this area but still research needs to be done
for such metabolites and development of GMOs.
REFERENCES :
1. Mohamed A Abo-El-Seoud AE-MMRA. Stimulating of
biodegradation of oxamyl pesticide by low dose gamma
irradiated fungi. J Plant PatholMicrobiol [Internet].
2013;04(09).
2. Alvarez A, Saez JM, Davila Costa JS, Colin VL, Fuentes
MS, Cuozzo SA, et al. Actinobacteria: Current research
and perspectives for bioremediation of pesticides and
heavy metals. Chemosphere. 2017;166:4162.
3. Anguiano OL, Vacca M, Rodriguez Araujo ME,
Montagna M, Venturino A, Ferrari A. Acute toxicity and
esterase response to carbaryl exposure in two different
populations of amphipods Hyalellacurvispina.
AquatToxicol. 2017;188:729.
4. Berman T T, Göen T, Novack L, Beacher L, Grinshpan L,
Segev D, et al. Corrigendum to Urinary concentrations of
organophosphate and carbamate pesticides in residents of
a vegetarian community [Environment International
volume 96 (2016) 34-40]. Environ Int. 2017;106:267.
5. Cai Z, Wang J, Ma J, Zhu X, Cai J, Yang G. Anaerobic
degradation pathway of the novel chiral insecticide
Paichongding and its impact on bacterial communities in
soils. J Agric Food Chem. 2015;63(32):715160.
6. Chan-Cupul W, Heredia-Abarca G, Rodríguez-Vázquez
R. Atrazine degradation by fungal co-culture enzyme
extracts under different soil conditions. J Environ Sci
Health B. 2016;51(5):298308.
7. Chanika E, Georgiadou D, Soueref E, Karas P, Karanasios
E, Tsiropoulos NG, et al. Isolation of soil bacteria able to
hydrolyze both organophosphate and carbamate
pesticides. Bioresour Technol. 2011;102(3):318492.
8. Chapalamadugu S, Chaudhry GR. Microbiological and
biotechnological aspects of metabolism of carbamates
and organophosphates. Crit Rev Biotechnol.
1992;12(56):35789.
9. Doddamani HP, Ninnekar HZ. Biodegradation of carbaryl
by a Micrococcus spec ies . CurrMicrobio l .
2001;43(1):6973.
235
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00044.3
10. Fang H, Wang Y, Gao C, Yan H, Dong B, Yu Y. Isolation
and characterization of Pseudomonas sp. CBW capable of
d e g r a d i n g c a r b e n d a z i m . B i o d e g r a d a t i o n .
2010;21(6):93946.
11. Fareed A, Zaffar H, Rashid A, Maroof Shah M, Naqvi TA.
Biodegradation of N-methylated carbamates by free and
immobilized cells of newly isolated strain Enterobacter
c l o a c a e s t r a i n T A 7 . B i o r e m e d i a t J .
2017;21(34):11927.
12. Felsot A, Maddox JV, Bruce W. Enhanced microbial
degradation of carbofuran in soils with histories of
Furadan® use. Bull Environ ContamToxicol.
1981;26(1):7818.
13. Gupta RC. Carbofuran toxicity. J Toxicol Environ Health.
1994;43(4):383418.
14. Gupta M, Mathur S, Sharma TK, Rana M, Gairola A,
Navani NK, et al. A study on metabolic prowess of
Pseudomonas sp. RPT 52 to degrade imidacloprid,
endosulfan and coragen. J Hazard Mater. 2016;301:2508.
15. Head IM, Cain RB, Suett DL. Characterization of a
carbofuran-degrading bacterium and investigation of the
role of plasmids in catabolism of the insecticide
carbofuran. Arch Microbiol. 1992;158(4):3028.
16. Jury WA, Focht DD, Farmer WJ. Evaluation of pesticide
groundwater pollution potential from standard indices of
soil-chemical adsorption and biodegradation. J Environ
Qual. 1987;16(4):4228.
17. Lalah JO, Wandiga SO, Dauterman WC. Mineralization,
volatilization, and degradation of carbofuran in soil
samples from Kenya. Bull Environ ContamToxicol.
1996;56(1):3741.
18. Han X, Balakrishnan VK, Buncel E. Alkaline degradation
of the organophosphorus pesticide fenitrothion as
mediated by cationic C12, C14, C16, and C18 surfactants.
Langmuir. 2007;23(12):651925.
19. Kazumi J, Capone DG. Microbial aldicarb transformation
in aquifer, lake, and salt marsh sediments. Appl Environ
Microbiol. 1995;61(8):28209.
20. Moorman TB. Adaptation of microorganisms in
subsurface environments: Significance to pesticide
degradation. In: ACS Symposium Series. Washington,
DC: American Chemical Society; 1990. p. 16780.
21. Moye HA, Miles CJ. Aldicarb contamination of
g roundwater. Rev Envi ron ContamToxico l .
1988;105:99146.
22. Bano N, Musarrat J. Characterization of a novel
carbofuran degrading Pseudomonas sp. with collateral
biocontrol and plant growth promoting potential. FEMS
Microbiol Lett. 2004;231(1):137.
23. Ou L-T, Rao PSC, Edvardsson KSV, Jessup RE, Hornsby
AG, Jones RL. Aldicarb degradation in sandy soils from
different depths. Pestic Sci. 1988;23(1):112.
24. Onunga DO, Kowino IO, Ngigi AN, Osogo A, Orata F,
Getenga ZM, et al. Biodegradation of carbofuran in soils
within Nzoia River Basin, Kenya. J Environ Sci Health B.
2015;50(6):38797.
25. Otieno PO, Lalah JO, Virani M, Jondiko IO, Schramm K-
W. Carbofuran and its toxic metabolites provide forensic
evidence for furadan exposure in vultures (Gyps
africanus) in Kenya. Bull Environ ContamToxicol.
2010;84(5):53644.
26. Öztürk B, Ghequire M, Nguyen TPO, De Mot R, Wattiez
R, Springael D. Expanded insecticide catabolic activity
gained by a single nucleotide substitution in a bacterial
carbamate hydrolase gene. Environ Microbiol.
2016;18(12):487887.
27. Pandey G, Dorrian SJ, Russell RJ, Brearley C, Kotsonis S,
Oakeshott JG. Cloning and biochemical characterization
of a novel carbendazim (methyl-1H-benzimidazol-2-
ylcarbamate)-hydrolyzing esterase from the newly
isolated Nocardioides sp. strain SG-4G and its potential
for use in enzymatic bioremediation. Appl Environ
Microbiol. 2010;76(9):29405.
28. Parks P, Lipman J, Eidelman J. Carbamate toxicity. A case
report. S Afr Med J. 1987;72(3):222.
29. Plangklang P, Reungsang A. Bioaugmentation of
carbofuran residues in soil using Burkholderiacepacia
PCL3 adsorbed on agricultural residues. Int Biodeterior
Biodegradation. 2009;63(4):51522.
30. Plangklang P, Reungsang A. Effects of rhizosphere
remediation and bioaugmentation on carbofuran removal
f r o m s o i l . Wo r l d J M i c r o b i o l B i o t e c h n o l .
2008;24(7):9839.
31. Chaudhry GR, Ali AN. Bacterial metabolism of
carbofuran. Appl Environ Microbiol. 1988;54(6):14149.
32. Trotter DM PhD, Kent RA BSc, Wong MP MSc. Aquatic
fate and effect of Carbofuran. Crit Rev Environ Contr.
1991;21(2):13776.
33. Liu Z, Hong Q, Xu J-H, Jun W, Li S-P. Construction of a
genetically engineered microorganism for degrading
organophosphate and carbamate pesticides. Int
Biodeterior Biodegradation. 2006;58(2):659.
34. Mahboob S, Al-Ghanim KA, Al-Misned F, Ahmed Z.
Determination of pesticide residues in muscle
236
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00044.3
ofCyprinuscarpiofrom River Ravi. Toxicol Environ
Chem. 2014;96(5):799807.
35. Li X, Li Y, Zhang X, Zhao X, Sun Y, Weng L, et al. Long-
term effect of biochar amendment on the biodegradation
of petroleum hydrocarbons in soil microbial fuel cells. Sci
Total Environ. 2018;651(Pt 1):796806.
36. Sakunthala Tennakoon DAS, Karunarathna WDV,
Udugampala USS. Carbofuran concentrations in blood,
bile and tissues in fatal cases of homicide and suicide.
Forensic Sci Int. 2013;227(13):10610.
37. Hesselsoe M, Boysen S, Iversen N, Jørgensen L, Murrell
JC, McDonald I, et al. Degradation of organic pollutants
by methane grown microbial consortia. Biodegradation.
2005;16(5):43548.
38. Cycoń M, Mrozik A, Pio t rowska-Seget Z.
Bioaugmentation as a strategy for the remediation of
pesticide-polluted soil: A review. Chemosphere.
2017;172:5271.
39. Hsu C-A, Wen T-N, Su Y-C, Jiang Z-B, Chen C-W, Shyur
L-F. Biological degradation of anthroquinone and azo
dyes by a novel laccase from Lentinus sp. Environ Sci
Technol. 2012;46(9):510917.
40. Beklová M, Dobšiková R, Pikula J. 642 Toxicity of
carbofuran for aquatic and terrestrial organisms. Toxicol
Lett. 2003;144:s172.
41. Ghazala, Mahboob S, Ahmad L, Sultana S, Alghanim K,
Al-Misned F, et al. Fish cholinesterases as biomarkers of
sublethal effects of organophosphorus and carbamates in
tissues of Labeorohita: Cholinergic biomarkers for
pesticides. J Biochem Mol Toxicol. 2014;28(3):13742.
42. Mohd-Nor D, Ramli N, Sharuddin SS, Hassan MA,
Mustapha NA, Ariffin H, et al. Dynamics of microbial
populations responsible for biodegradation during the
full-scale treatment of palm oil mill effluent. Microbes
Environ. 2019;34(2):1218.
43. Kalam A, Mukherjee AK. Influence of hexaconazole,
carbofuran and ethion on soil microflora and
dehydrogenase activities in soil and intact cell. Indian J
Exp Biol. 2001;39(1):904.
44. Sharma P, Dube D, Sinha M, Mishra B, Dey S, Mal G, et
al. Multiligand specificity of pathogen-associated
molecular pattern-binding site in peptidoglycan
recognition protein. J Biol Chem. 2011;286(36):3172330.
45. Lado-Abeal J, Hickox JR, Cheung TL, Veldhuis JD,
Hardy DM, Norman RL. Neuroendocrine consequences
of fasting in adult male macaques: effects of recombinant
rhesus macaque leptin infusion. Neuroendocrinology.
2000;71(3):196208.
46. Hudson A. Reviews. Notes Queries. 1984;31(3):4112.
47. Rosman Y, Makarovsky I, Bentur Y, Shrot S, Dushnistky
T, Krivoy A. Carbamate poisoning: treatment
recommendations in the setting of a mass casualties event.
Am J Emerg Med. 2009;27(9):111724.
48. Bedada SK, Boga PK. Influence of diosmin on the
metabolism and disposition of carbamazepine in healthy
subjects. Xenobiotica. 2017;47(10):87984.
49. Gong T, Liu R, Che Y, Xu X, Zhao F, Yu H, et al.
Engineer ingPseudomonas put idaKT2440 for
simultaneous degradation of carbofuran and chlorpyrifos.
MicrobBiotechnol. 2016;9(6):792800.
50. Ishag AESA, Abdelbagi AO, Hammad AMA, Elsheikh
EAE, Elsaid OE, Hur J-H, et al. Biodegradation of
chlorpyrifos, malathion, and dimethoate by three strains
of bacteria isolated from pesticide-polluted soils in Sudan.
J Agric Food Chem. 2016;64(45):84918.
51. Choudhary MI, Musharraf SG, Mukhmoor T, Shaheen F,
Ali S, Rahman A-U. Isolation of Bioactive Compounds
from Aspergillus terreus. Z Naturforsch B J Chem Sci.
2004;59(3):3248.
52. Sogorb MA, Vilanova E. Enzymes involved in the
detoxification of organophosphorus, carbamate and
pyrethroid insecticides through hydrolysis. Toxicol Lett.
2002;128(13):21528.
53. Nguyen TPO, Helbling DE, Bers K, Fida TT, Wattiez R,
Kohler H-PE, et al. Genetic and metabolic analysis of the
carbofuran catabolic pathway in Novosphingobium sp.
K N 6 5 . 2 . A p p l M i c r o b i o l B i o t e c h n o l .
2014;98(19):823552.
54. Li Z, Qu S, Cui L, Zhang S. Detection of carbofuran
pesticide in seawater by using an enzyme biosensor. J
Coast Res. 2017;80:15.
55. Ufarté L, Laville E, Duquesne S, Morgavi D, Robe P,
Klopp C, et al. Discovery of carbamate degrading
enzymes by functional metagenomics. PLoS One.
2017;12(12):e0189201.
56. Yang T, Lin C, Fu H, Jiang Y, Zhao Y. Copper-catalyzed
synthesis of medium- and large-sized nitrogen
heterocycles via N-arylation of phosphoramidates and
carbamates. Org Lett. 2005;7(21):47814.
237
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00044.3

Review Article
INTRODUCTION:
Skin, hair and blood are conventional sources of DNA in
forensic analysis; however in multiple cases, identification of
deceased individuals is difficult due to accidents, explosions,
plane crash, mass disasters, brutal murders, decaying body,
war crimes, terrorist attacks, etc. The chances of cross
contamination and decomposition are high and this makes the
conventional sources a poor choice for DNA extraction.
Owing to their high protective structure in such cases, bones
and teeth are the only available sources of DNA. (Hervella et
al. 2015; Jakubowska et al. 2012; Malaver et al 2003;
Gaytmenn et al.2003 ). DNA analysis of evidence samples
such as teeth and bones from cadavers have major role in
identification of dead body which is devoid of any other
potential source of DNA (Ferreira et al. 2013). In criminal
cases it is used for identification of culprit, victim and suspect.
Bones and teeth are considered as the most significant
evidences for DNA analysis owing to their ability in sustaining
harsh environmental conditions. The degradation of soft
tissues (i.e., blood samples and muscle tissue) carried out by
bacteria is relatively faster as compared to tooth and bone
tissues (Kitayama et al. 2010). In spite of several methods
being available for DNA extraction from bones and teeth,
these are not widely used as a standard protocols, since they are
time consuming, expensive and equally complex (Anderung et
al. 2008). Working with such ancient samples for DNA
extraction remains a delicate and challenging task.
An anthropological study proposes the use of bones and teeth
in determination of sex, age and identification of cadaver from
previous/historical medical records. DNA extraction from
ancient human skeletal remains can provide vital information
of prehistoric human civilization. Curators and museum
authorities are highly concerned about the integrity of skeletal
remains to reconstruct the life history of an individual; forensic
Corresponding Author : Dr Arun D Ghuge, M.Sc., M. Phil.
Assistant Professor and Head ,
Department of Forensic Biology, Government Institute of
Forensic Science, Government of Maharashtra, Nipat Niranjan
Nagar, Caves road, Aurangabad 431004, India
Contact : +91 82752-19852
Email : [email protected]/[email protected]
KEYWORDS : Non-destructive; Destructive; Bones; Teeth; Enamel; Pulp.
Article History:Received: 21 November 2019Received in revised form: 15 May 2020Accepted on: 15 May 2020Available online: 31 August 2021
1. Ghuge Arun, M.Sc., M. Phil. Assistant Professor & Head*2. Verma Pratibha, M.Sc. Research Scholar, Gamete Immunobiology Division, National Institute for Research in Reproductive
Health, ICMR, Mumbai 400012, India 3. Sangle Sandeep, M.Sc. Assistant Professor*,
4. Gaiki Shweta, M.Sc. Assistant Chemical Analyzer, Regional Forensic Science Laboratory, Government of Maharashtra, Nagpur
5. Paikrao Hariprasad, M.Sc., Ph.D. Assistant Professor* *Department of Forensic Biology, Government Institute of Forensic Science, Government of Maharashtra, Nipat Niranjan
Nagar, Caves road, Aurangabad 431004, India
Switching Gears of DNA Extraction: From Destructive to Non- Destructive
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00045.5
238
ABSTRACT :
In many cases where samples such as historical remains, museum samples, missing person and criminal sample needs to be
preserved for years; DNA extraction by destructive methods is not feasible due to loss of precious samples. Hard tissue and
mineralised body parts like bones and teeth are only accessible sources of DNA in mass disasters like earthquakes, floods,
tornadoes, aircraft crashes, train wreck, derailments, and building fires with disfigured and decomposed bodies. The protective
composition of teeth and bones provides an extra protection over soft tissue and thus its high resistance to the action of physical and
chemical agents makes them the only choice for DNA extraction. This review summarises the previous and current methods of
DNA extraction from tooth and bone, emphasizing its effect on DNA yield, efficiency to yield amplifiable amount of mitochondrial
DNA and nuclear DNA, PCR amplification, PCR inhibition and its morphology. The likelihood to recover DNA from ancient teeth
and bones in short time, with little contamination is the need of the hour and future thrust area of forensic biology. It will not only
benefit forensic field but will be equally insightful in solving, archaeological and medical questions.
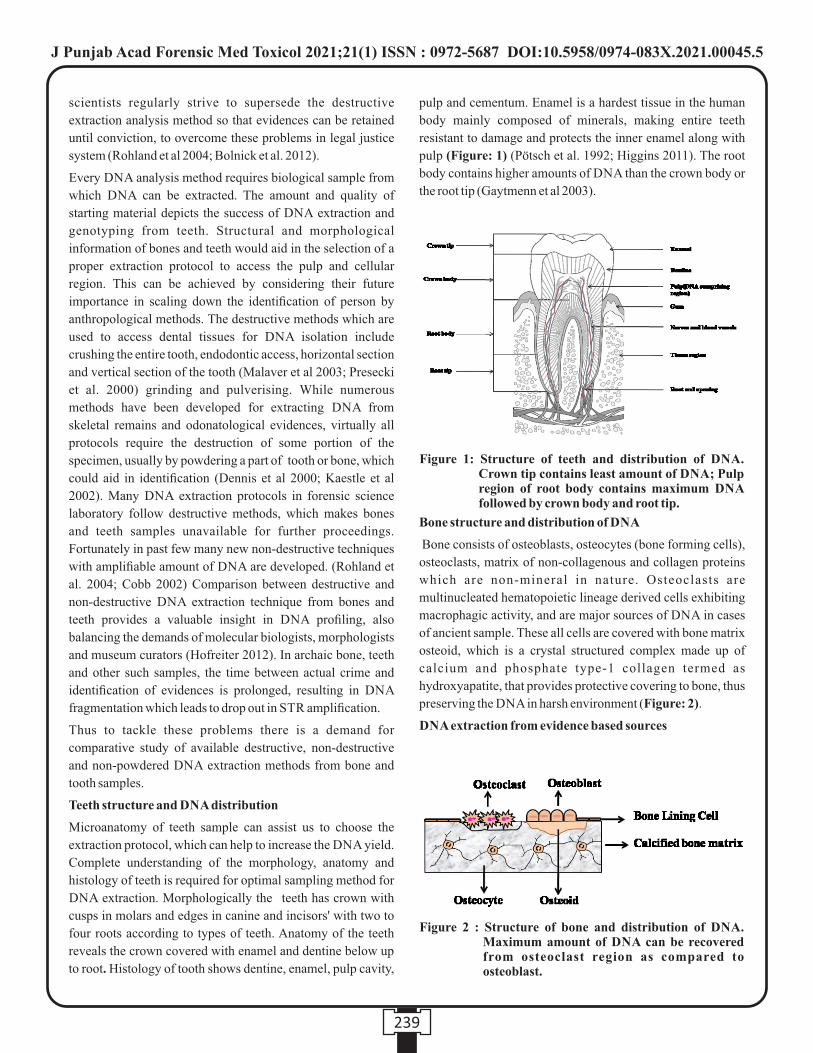
scientists regularly strive to supersede the destructive
extraction analysis method so that evidences can be retained
until conviction, to overcome these problems in legal justice
system (Rohland et al 2004; Bolnick et al. 2012).
Every DNA analysis method requires biological sample from
which DNA can be extracted. The amount and quality of
starting material depicts the success of DNA extraction and
genotyping from teeth. Structural and morphological
information of bones and teeth would aid in the selection of a
proper extraction protocol to access the pulp and cellular
region. This can be achieved by considering their future
importance in scaling down the identification of person by
anthropological methods. The destructive methods which are
used to access dental tissues for DNA isolation include
crushing the entire tooth, endodontic access, horizontal section
and vertical section of the tooth (Malaver et al 2003; Presecki
et al. 2000) grinding and pulverising. While numerous
methods have been developed for extracting DNA from
skeletal remains and odonatological evidences, virtually all
protocols require the destruction of some portion of the
specimen, usually by powdering a part of tooth or bone, which
could aid in identification (Dennis et al 2000; Kaestle et al
2002). Many DNA extraction protocols in forensic science
laboratory follow destructive methods, which makes bones
and teeth samples unavailable for further proceedings.
Fortunately in past few many new non-destructive techniques
with amplifiable amount of DNA are developed. (Rohland et
al. 2004; Cobb 2002) Comparison between destructive and
non-destructive DNA extraction technique from bones and
teeth provides a valuable insight in DNA profiling, also
balancing the demands of molecular biologists, morphologists
and museum curators (Hofreiter 2012). In archaic bone, teeth
and other such samples, the time between actual crime and
identification of evidences is prolonged, resulting in DNA
fragmentation which leads to drop out in STR amplification.
Thus to tackle these problems there is a demand for
comparative study of available destructive, non-destructive
and non-powdered DNA extraction methods from bone and
tooth samples.
Teeth structure and DNA distribution
Microanatomy of teeth sample can assist us to choose the
extraction protocol, which can help to increase the DNA yield.
Complete understanding of the morphology, anatomy and
histology of teeth is required for optimal sampling method for
DNA extraction. Morphologically the teeth has crown with
cusps in molars and edges in canine and incisors' with two to
four roots according to types of teeth. Anatomy of the teeth
reveals the crown covered with enamel and dentine below up
to root. Histology of tooth shows dentine, enamel, pulp cavity,
pulp and cementum. Enamel is a hardest tissue in the human
body mainly composed of minerals, making entire teeth
resistant to damage and protects the inner enamel along with
pulp (Figure: 1) (Pötsch et al. 1992; Higgins 2011). The root
body contains higher amounts of DNA than the crown body or
the root tip (Gaytmenn et al 2003).
Bone structure and distribution of DNA
Bone consists of osteoblasts, osteocytes (bone forming cells),
osteoclasts, matrix of non-collagenous and collagen proteins
which are non-mineral in nature. Osteoclasts are
multinucleated hematopoietic lineage derived cells exhibiting
macrophagic activity, and are major sources of DNA in cases
of ancient sample. These all cells are covered with bone matrix
osteoid, which is a crystal structured complex made up of
calcium and phosphate type-1 collagen termed as
hydroxyapatite, that provides protective covering to bone, thus
preserving the DNA in harsh environment (Figure: 2).
DNA extraction from evidence based sources
239
Figure 1: Structure of teeth and distribution of DNA. Crown tip contains least amount of DNA; Pulp region of root body contains maximum DNA followed by crown body and root tip.
Figure 2 : Structure of bone and distribution of DNA. Maximum amount of DNA can be recovered from osteoclast region as compared to osteoblast.
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00045.5

To gain a better understanding of different DNA extraction
methods one needs to acquire the in-depth knowledge of
evidences used. The main problem of DNA extraction from
bones is DNA degradation due to environmental factors and
soil-derived inhibitors (Davoren et al. 2007). While new
methods are still being searched for and improvised, till date
there is no such universal method reported for DNA extraction
from materials of degraded samples with good quality DNA.
One of the new methods of DNA extraction from aggregates
(EA), which assumes extraction of DNA, fixed in bone
crystals aggregates (Jakubowska et al. 2012). Intergrown
crystal aggregates can preserve DNA within fossil bones that
cannot be disaggregated by oxidation with sodium
hypochlorite (NaOCl), even though bone is grinded into a fine
powder (Weiner and Price 1986; Salamon et al. 2005).
Salamon reported that NaOCl-treated aggregates enhance the
ability to differentiate between contaminant DNA, highly
damaged DNA, and better preserved DNA.
Pusch used collagenase and dispase as proteases in addition
muramidase to isolate good quality DNA from small quantities
of bone meal (Pusch and Scholz 1997). Extensive
mineralization within the bone and teeth result in a physical
barrier to the extraction reagents, thus preventing the release of
DNA molecules (Loreille et al 2007). Lyavoo described DNA
extraction from bone samples using silica-based extraction kit ChargeSwitch gDNA Plant Kit (Life Technologies), DNA
IQTM system kit (Promega), DNeasy blood and tissue kit (Qiagen) and PrepFilerBTA forensic DNA extraction kit (Life
Technologies) along with conventional phenol-chloroform
method. The comparative study showed that the phenol-
chloroform extraction method (PCI) yields more DNA than
the silica-based extraction methods (Iyavoo et al 2013).
Excluding yield, PCI method is laborious, time consuming,
with direct chemical exposure and can only be done if either
abundant or ample amount of sample is available (Manjunath
et al 2011).
Protocols used for sampling and extraction of tooth tissues
predominantly shows those which are used for bone even
though the two tissues are morphologically and biochemically
different. Hence no standard protocol has explained the proper
handling, sampling and DNA extraction from teeth. For
example the protocols for teeth used by the International
Commission of Missing Persons (ICMP) are identical to those
used for bone with the exception of pre-treatment to the outer
surface of bone (Davoren et al. 2007). The DNA extraction
practice, which involves grinding of entire teeth, does not take
into consideration the tooth morphology or the relative
distribution of mineral, protein and DNA in teeth.
Furthermore, grinding of whole teeth (Alonso et al. 2005;
Marjanović et al. 2015) does not consider that these tissues
may be useful to other disciplines involved in the identification
process. Grinding of whole teeth also inordinately adds excess
mineral into the extraction process necessitating the use of
large volume of reagents. Tooth tissues contain large quantities
of calcium (especially enamel) and collagen, which if co-
extracted with the DNA can be problematic for DNA
amplification via polymerase chain reaction (PCR). Thus tooth
extraction and sampling protocols should aim to target DNA
rich tissues, minimal sampling of high-mineral/ low-DNA
tissue and reduction in co-extraction of inhibitory substances
with the DNA (Rohland and Hofreiter 2007).
Conventional sampling of teeth for DNA analysis generally
follows one of the two pathways, either targeted sampling of
the pulp (the DNA-rich soft tissue component of the tooth) by
splitting or by drilling through the crown or non-targeted
sampling of the entire tooth (root). Grinding of the entire tooth
provides access to the largest amount of DNA but also contains
a large amount of mineral (cementum is 45%, dentine 70% and
enamel 97% composed of mineral) that must be removed prior
to downstream analysis (Higgins et al 2013). Most of the
current DNA extraction protocols for bones and teeth are based
on the incubation of powdered material in extraction buffer
containing ethylene diamine tetracetic acid (EDTA). EDTA is
generally accepted as the most effective chelating agent in
endodontic technique (Loreille et al. 2007) and when coupled
with proteinase-K digestion, EDTA maximises the efficiency
of DNA extraction (Caputo et al. 2013; Hossain et al. 2014). It
is used to enlarge root canal and expose dentin (Tabatabaei et
al. 2016). The phenol-chloroform method works on an initial
digestion to break down the minerals, proteins, and lipids
present in the sample mixture (Barnett and Larson 2012).
Further processing detaches the DNA portion from other
protein components by solvent extraction into aqueous and
hydrophobic phases respectively. Finally filtration through
membrane filter concentrates DNA in the sample.
Methods of DNA extraction1. DNAzol Method (Betancor et al. 2011)
2. PrepFiler BTAMethod (Betancor et al. 2011)3. Bolnick DNA extraction (Non-destructive) (Bolnick et
al. 2012)4. GuSCN based Non-destructive extraction protocol
(Rohland et al. 2004)5. New experimental kit DNA extraction (Kitayama et al.
2010)6. Grinding-free method for DNA extraction from teeth
(Hughes-Stamm et al. 2016)7. Silica-based DNA extraction (Davoren et al. 2007)8. Phenol-Chloroform DNA extraction (Davoren et al.
2007)9. DNA extraction from aggregates [EA] (Salamon et al.
2005)
240
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00045.5
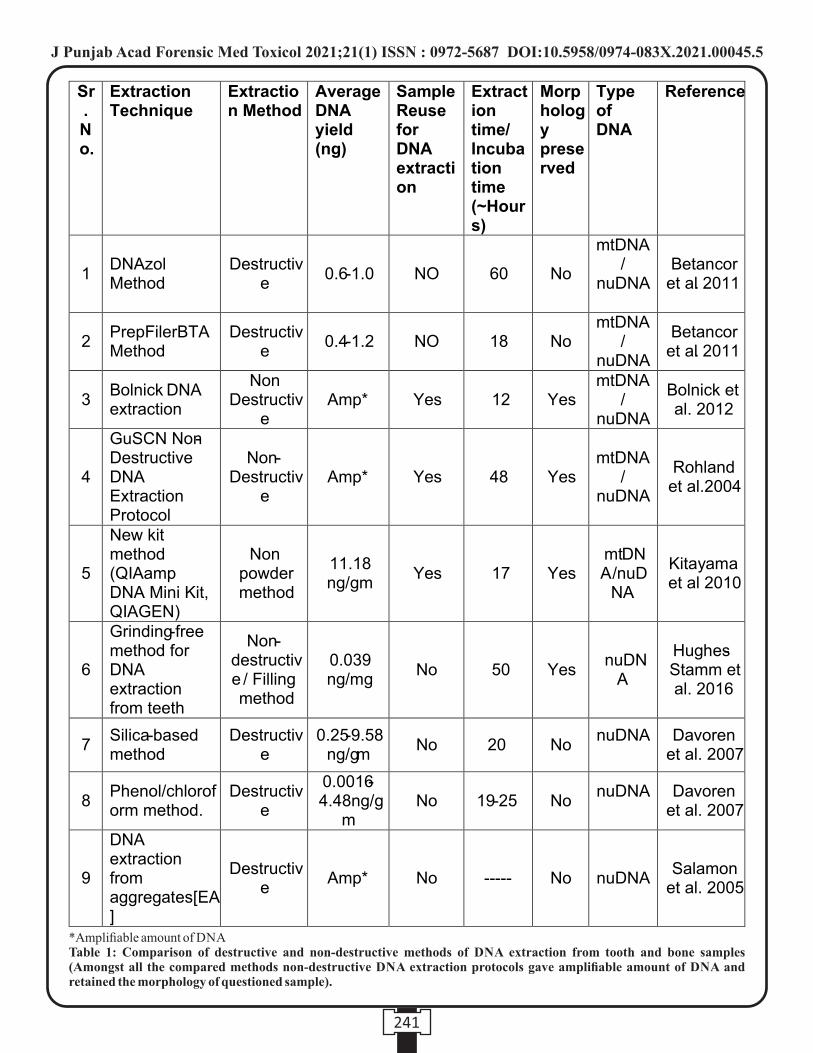
241
*Amplifiable amount of DNATable 1: Comparison of destructive and non-destructive methods of DNA extraction from tooth and bone samples (Amongst all the compared methods non-destructive DNA extraction protocols gave amplifiable amount of DNA and retained the morphology of questioned sample).
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00045.5

Silica-based method has yielded maximum DNA in
destructive extraction protocol category which ranges 0.25-
9.58ng/gm. surpassing both DNAzol and Prep Filer BTA
Method. In non-destructive category new kit method has yield
of 11.18ng/mg, Considering above studies non-destructive
DNA extraction is best for tooth and bone samples which are
intact and has further study prospective for forensic analysis.
It is very evident from recent studies that mechanism of DNA
extraction from crushed teeth has been well established. But
mechanism explained till date regarding the DNA extraction
from teeth sample by non-destructive method is still unclear.
As per Rohland and Hofreiter's Protocol GuSCN extraction
buffer has EDTA which de-mineralises the teeth/bone
samples, giving accessibility to nucleated cells of o
pulp/Osteoid. GuSCN is a strong protein-denaturing agent
and, when used in combination with a reducing agent like DTT
has also been shown to bring cross-linked proteins back into
solution (Rohland et al.2004). It is possible that GuSCN as a
chemical agent is more efficient in denaturing proteins if these
are bound to the hydroxyapatite matrix of the bone than
proteinase K. Moreover, GuSCN may break certain chemical
cross-links even in the absence of reducing agents; Triton X-
100 has similar but more efficient anionic surfactant than SDS,
which breaks the cell wall of cells present in pulp of teeth and
hydroxyapatite matrix of bone, last in the list EDTA which
demineralise the enamel, dentin and hydroxyapatite matrix to
elute cells and DNA from samples (Steadman et al.2012).
Challenges in DNA amplification
Working with DNA extracted from degraded teeth and bone
samples from crime scene requires more comprehensive
knowledge and precaution to carry out successful PCR
amplification.While damaged DNA is repaired in living cells
but not in dead, this result in very few intact copy of DNA in
sample While due to hydroxyapatite matrix teeth and bones .
can sustain for long time, which makes analyst easy to work on
it for STR profiling. Though some external environmental
factors affect DNA and cause damage, to avoid this tooth and
bone samples as recovered must be decontaminated and stored
in cold condition to minimize further damage.
PCR amplification of extracted DNA from mass disaster or
burning cases samples always poses a major problem due to
co-extracted products which inhibits reaction. Extracting
DNA from samples also co-extract some proteins and enzymes
like humic acid, fulvic acid, hematin, collagen type-1 which
are termed as Maillard products. It does not inactivate
polymerase, but they can be considered as inhibitors because
the DNA trapped in these sugar derived condensation products
is inaccessible to polymerase. Number of approaches has been
developed to remove the co-extracted Maillard products such
as: Manipulating PCR reaction component or by removing it
during DNA extraction procedure. Manipulation of PCR
reaction component involves dilution of template DNA, so
inhibitors get diluted to an extent that results in inability to
inhibit reaction. Some inhibitors block Taq polymerase, to
counter-balance it. Taq-polymerase unit can be increased and
also the inhibitors can be blocked by adding BSA enhancing
the polymerase activity. Using different chemicals during
extraction of DNA removes these inhibitors leading to 2+successful reaction. Ca is commonly found in bone and teeth
2+and is known to interfere with Mg concentration, which in
turn may affect the activity of Taq polymerase during PCR
amplifications.
Several chemicals have been used during DNA extraction to
remove PCR inhibitors, for example Cetyl Trimethyl
Ammonium Bromide (CTAB) to increase the yield of DNA
extracted from burned bones (Ye et al. 2004).
In case of DNA extraction based on size, DNA is extracted
from agarose blocks leading to co-extraction of inhibitors
along with it. This has been overcome by washing it with lysis
buffer followed by TE buffer which readily diffuses out small
size inhibitors compared to DNA. DNA precipitation with
isopropanol shows less inhibition compared to precipitation
c a r r i e d o u t u s i n g e t h a n o l . T h e a d d i t i o n o f N -
phenacylthiazolium bromide (PTB) during DNA extraction
process cleaves Maillard products. Several studies have shown
successful extraction of both nuclear and mitochondrial DNA
using PTB from 20,000 years old samples.
Non-destructive methods of DNA extraction: Driving force
to future forensic studies
DNA analysis for individuals has a major role in forensic
investigation, mass disaster cases etc. In the present review
nine different extraction protocols were compared for best
DNA yield, quality and sustained sample integrity. The five
destructive extraction protocols are as follows: DNAzol
Method, PrepFiler BTA method, Silica-based method,
Phenol/chloroform method and DNA extraction from
aggregates [EA]. The rest four non-destructive protocols are as
follows: New experimental kit DNA extraction, Grinding-free
method for DNA extraction, new kit method and GuSCN non-
destructive DNA extraction protocol used by Rohland and
Hofreiter's.
In destructive protocol, samples are pulverized. In case of teeth
and bone a part or complete sample is crushed to be used in
extraction buffer. Grinding of entire teeth for extraction
process requires extensive demineralisation steps and these are
difficult to automate thus increasing the chance of
contamination. Since tooth and bone samples are available in
small quantities this can lead to sample integrity issues.
242
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00045.5

Destruction of such precise samples increases waste products
and also affects amplification of DNA, also limiting the
analysis only up to DNA profiling (Hervella et al. 2015). In
case of deceased unidentified dead body it is hard to get
reference sample for comparison. This problem can be solved
by using non- destructive DNA extraction protocol which
makes sample available for further anthropological analysis,
after using it for extraction with no visible and morphological
damage to sample, thus helping in individualization.
But most of the present DNA extraction protocols are
destructive in nature which limits studies only to DNA
profiling. This is considered as major drawback in cases where
no reference DNA sample is available due to unavailability of
any commanding clue required for individual identification.
In such cases non-destructive extraction method makes it
possible to analyse the sample for further anthropological
studies which aids in narrowing down the individual from
mass sample that can be reused for consecutive extraction
many times. Especially In cases where reference DNA sample
is available from relatives or belongings or individual STR
profile. In non-destructive methods the morphology remains
intact for prehistoric studies and no effect of demineralisation
on PCR amplifications is seen.
CONCLUSION:
The battle between destructive and non-destructive methods of
DNA extraction from bone and teeth samples continues,
researchers would probably come up with refinement of
protocol for non-destructive method due sample preservations
of forensically important samples like teeth and bones for
individual identification covering all possible obstacles and
solutions to aid in forensic analysis.
Abbreviations:
NaOCl: Sodium Hypochlorite
PCI: Phenol-Chloroform Extraction Method
ICMP: International Commission of Missing Persons
EDTA: Ethylene Diamine Tetracetic Acid
GuSCN: Guanidinium Thiocyanate
CTAB: CetylTrimethylAmmonium Bromide
PTB: N-Phenacylthiazolium Bromide
REFERENCES:
1. Anderung C, Persson P, Bouwman A (2008) Fishing for
ancient DNA. J. Forensic Sci. Int. Genet 2:104–107.
doi:10.1016/j.fsigen.2007.09.004.
2. Alonso A, Martin P, Albarrán C, Garcia P, Fernandez de
Simon L, Jesús Iturralde M, Fernández-Rodriguez A,
Atienza I, Capilla J, García-Hirschfeld J, Martinez P,
Vallejo G, García O, García E, Real P, Alvarez D, León A,
Sancho M (2005) Challenges of DNA profiling in mass
disaster investigations. Croat. Med. J. 46:540–548.
3. Barnett R, Larson G (2012) A phenol-chloroform
protocol for extracting DNA from ancient samples,
Methods Mol Biol.840:13-9. doi: 10.1007/978-1-61779-
516-9_2
4. Betancor E, et al., (2011) An Efficient Method of
Extracting DNA from Bone Remains from the Spanish
Civil War—A Comparative Study of Two Methods:
PrepFiler BTA™ and DNAzol® Methods. Forensic
News January; [Internet]
5. Bolnick DA, Bonine HM, Mata-Míguez J, Kemp BM,
Snow MH, Leblanc SA (2012) Nondestructive sampling
of human skeletal remains yields ancient nuclear and
mitochondrial D N A. Am. J. Phys. Anthropol.
147:293–300. doi:10.1002/ajpa.21647.
6. Caputo M, Irisarri M, Alechine E, Corach D (2013) A
DNA extraction method of small quantities of bone for
high-quality genotyping. Forensic Sci. Int. Genet.
7:488–493. doi:10.1016/j.fsigen.2013.05.002.
7. Cobb JC (2002) Ancient DNA Recovered by a Non-
destructive Method., Anc. Biomol. 4:169-172.
doi:10.1080/1358612021000028461.
8. Davoren J, Vanek D, Konjhodzić R, Crews J, Parsons
TJ (2007) Highly Effective DNA Extraction Method for
Nuclear Short Tandem Repeat Testing of Skeletal
Remains from Mass Graves.Croat Med J. 48(4):478–485.
9. Dennis H. O'Rourke M. Geoffrey Hayes and Shawn W.
Carlyle (2000) Ancient DNA studies in physical
anthropology, Annual Review of Anthropology 29(1):
217-42. DOI: 10.1146/annurev.anthro.29.1.217
10. Ferreira S.TG, Paula KA, Maia FA, Moraes AV, (2013) A
comparative study between two protocols for DNA
extraction from bones, Forensic Sci. Int. Genet. Suppl.
Ser. 4:374–375. doi:10.1016/j.fsigss.2013.10.190.
11. Gaytmenn R, Sweet D, (2003) Quantification of Forensic
DNA from Various Regions of Human Teeth,J Forensic
Sci 48:1–4.Paper ID JFS2002372_483.
12. Hervella M, Iñiguez MG, Izagirre N, Anta A, De-la-Rúa
C (2015) Nondestructive Methods for Recovery of
Biological Material from Human Teeth for DNA
E x t r a c t i o n . J . F o r e n s i c S c i . 6 0 : 1 3 6 – 1 4 1 .
doi:10.1111/1556-4029.12568.
13. Higgins D, Kaidonis J, Townsend G, Hughes T, Austin JJ
(2013) Targeted sampling of cementum for recovery of
nuclear DNA from human teeth and the impact of
243
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00045.5
common decontamination measures. Investig. Genet.
4:18. doi:10.1186/2041-2223-4-18.
14. Higgins D, Kaidonis J, Austin J, Townsend G, James H,
Hughes T (2011) Dentine and cementum as sources of
nuclear DNA for use in human identification, Aust. J.
F o r e n s i c S c i . 4 3 : 2 8 7 – 2 9 5 .
doi:10.1080/00450618.2011.583278.
15. Hofreiter M (2012) Special issue ancient DNA, Ann.
Anat. 194:1–2. doi: 10.1016/.2011.04.011.
16. Hossain HM, Kumar T, Majumder A, Momtaz P, Sharmin
T, Sufian A, Akhteruzzamani S (2014) National Forensic
DNA Profiling Laboratory, Dhaka Medical College
Campus, Dhaka ‐ 1000. Bangladesh Key words:,
23:101–107.
17. Hughes-Stamm S, Warnke F, van Daal (2016) A An
a l t e r n a t e m e t h o d f o r e x t r a c t i n g D N A f r o m
environmentally challenged teeth for improved DNA
a n a l y s i s . L e g . M e d . 1 8 : 3 1 – 3 6 .
doi:10.1016/j.legalmed.2015.11.008.
18. Iyavoo S, Hadi S, Goodwin W (2013) Evaluation of five
DNA extraction systems for recovery of DNA from bone.
Forensic Sci. Int. Genet. Suppl. Ser. 4:e174–e175.
doi:10.1016/j.fsigss.2013.10.090.
19. Jakubowska J, Maciejewska A, Pawłowski R (2012)
Comparison of three methods of DNA extraction from
human bones with different degrees of degradation, Int. J.
Legal Med. 126:173–178. doi:10.1007/s00414-011-
0590-5.
20. Kaestle FA, Horsburgh KA (2002) Ancient DNA in
anthropology: Methods, applications, and ethics, Yearb.
Phys. Anthropol. 45: 92–130. doi:10.1002/ajpa.10179.
21. Kitayama T, Ogawa Y, Fujii K, Nakahara H, Mizuno N,
Sekiguchi K, Kasai K, Yurino N, Yokoi T, Fukuma Y,
Yamamoto K, Oki T, Asamura H, Fukushima H, (2010)
Evaluation of a new experimental kit for the extraction of
DNA from bones and teeth using a non-powder method,
L e g .
Med.12:84–89.doi:10.1016/j.legalmed.2009.12.004.
22. Loreille OM, Diegoli TM, Irwin JA, Coble MD,
Parsons TJ (2007) High efficiency DNA extraction from
bone by total demineralization, Forensic Sci. Int. Genet.
1:191–195. doi:10.1016/j.fsigen.2007.02.006.
23. Malaver P, Yunis J (2003) Different dental tissues as
source of DNA for human identification in forensic cases.,
Croat. Med. J. 44:306–309.
24. Manjunath BC, Chandrashekar BR, Mahesh M, Vatchala
Rani RM (2011) DNA profiling and forensic dentistry - A
review of the recent concepts and trends. J. Forensic Leg.
Med. 18:191–197. doi:10.1016/j.jflm.2011.02.005.
25. Marjanović D, Hadžić Metjahić N, Čakar J, Džehverović
M, Dogan S, Ferić E, Džijan S, Škaro V, Projić P, Madžar
T, Rod E, Primorac D, Iyavoo S, Hadi S, Goodwin W
(2015) Identification of human remains from the Second
World War mass graves uncovered in Bosnia and
Herzegovina. Croat . Med. J . 56:257–62. doi:
10.3325/cmj.2015.56.257
26. Pötsch L, Meyer U, Rothschild S, Schneider PM,
Rittner C (1992) Application of DNA techniques for
identification using human dental pulp as a source of
D N A . I n t J L e g . M e d . 1 0 5 : 1 3 9 – 1 4 3 .
http://www.ncbi.nlm.nih.gov/pubmed/1419874.
27. Presecki Z, Brkic H, Primorac D, Drmic I (2000)
Methods of Preparing the Tooth for DNA Isolation. Acta
Stomatol Croat. 34:21–24.
28. Pusch C, Scholz M (1997) DNA extraction from ancient
human bones via enzymatic treatment. Tech. Tips Online.
2:160–163. doi:10.1016/S1366-2120(08)70072-2
29. Rohland N, Hofreiter M (2007) Ancient DNA extraction
from bones and teeth, Nat. Protoc. 2 :1756–1762.
doi:10.1038/nprot.2007.247.
30. Rohland N, Siedel H, Hofreiter M. (2004)
Nondes t ruc t ive D N A ex t rac t ion me thod fo r
mitochondrial DNA analyses of museum specimens.
Biotechniques. 36(5):814-818
31. Salamon M, Tuross N, Arensburg B, Weiner S (2005)
Relatively well preserved DNA is present in the crystal
aggregates of fossil bones. Proc Natl Acad Sci USA
102:13783–13788.
32. Steadman DW, Pack FL, Algee-hewitt B.FB, Hulsey BI,
Cabana GS (2012) Validation of a Non-Destructive DNA
Recovery Method in Forensic-Age Samples.
33. Tabatabaei FS, Tatari S, Samadi R, Moharamzadeh K
(2016) Different methods of dentin processing for
application in bone tissue engineering: A systematic
review, Journal of Biomedical Material Research
doi.org/10.1002/jbm.a.35790.
34. Weiner S, Price P (1986) Disaggregation of Bone Into
C r y s t a l s . C a l c i f . T i s s u e I n t . 3 9 : 3 6 5 – 3 7 5 .
https://doi.org/10.1007/BF02555173.
35. Ye J, Ji A, Parra EJ, Zheng X, Jiang C, Zhao X, Hu L, Tu Z
(2004) A Simple and Efficient Method for Extracting
DNA From Old and Burned Bone. J. Forensic Sci. 49:1–6.
doi:10.1520/JFS2003275
244
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00045.5

Review article
INTRODUCTION :
A person being useful even after their demise is an emerging
notion amongst people. Even though many people have used
dead bodies for understanding the human body since time
immemorial, instead of appreciation, they faced blasphemy,
were called heretics and were shunned by priests and other
holy men. In literal sense, if no cadavers were ever taken for
study and research, we would not have known our basic body
structure at all. Previously, a dead body was considered as non-
viable, but now, with further research, we are able to harvest
organs from such bodies, within a stipulated time after
declared dead. This advent has helped many patients suffering
from end stage organ failures as they had to wait to get an organ
transplant from a donor, who inevitably had to be brain dead or
a living person and finding these donors was not very common,
which led to people dying whilst waiting for a donor. Even
though this procedure is being practiced extensively in the
western world, not many cases are seen in India where only 8transplantation from living donors is being done. It is due to
many prejudiced people who do not accept the concept of
getting an organ from a dead patient into a living person, but
awareness has to be created.
Transplantation and its types
Transplantation is a procedure where a living viable organ,
tissues or a group of cells are removed from its original site or
donor site and surgically placed at a new specified site or 1recipient site for the benefit of the recipient. It can be an
autograft, allograft or a xenograft. In an autograft, the donor
and recipient is the same individual, used in skin, bone and
nerve grafting commonly. An allograft is where the donor and
recipient are two different individuals but of the same species,
which is used in all hollow viscous organ transplants.
Xenograft is where the donor and recipient are of two different
species, where the use of heart valves of pigs for human heart is
the most common.
The donors and recipients
Generally, the recipients are the patients who suffer from end
stage organ failure and are in need for a new organ whereas the
donor either can be a healthy living person or a deceased
person. The former includes living related donors, spousal 7donors and other than living related donors. The latter
Corresponding Author :
Dr Jagadish Rao Padubidri,
Associate Professor, Department of Forensic Medicine,
Kasturba Medical College, Mangalore,
Manipal Academy of Higher Education, Manipal, India
Contact : +91-9900405085
Email : [email protected], [email protected]
KEYWORDS : Cadaver, Transplantation, Irreversible brain damage, donor, recipient, Ethical, Legal
Article History:Received: 29 November 2020Received in revised form: 13 December 2020Accepted on: 13 December 2020Available online: 31 August 2021
ABSTRACT :
Using parts of a cadaver to treat the living has been a topic of interest amongst emerging medical professionals to treat irreversible
organ damage. Transplantation is an approach where living tissues or organs are taken from their original site or donor site and 1 placed surgically at a new specified site or recipient site for the benefit of the recipient. It is of three types which are autograft,
allograft and xenograft. The recipient is the one who is the victim of end stage organ failure and the donor is the one who either be
living or dead, who will provide the organ. Since this procedure has been introduced for treatment, there was a lot of demand to
procure organs with limited supply, which in turn gave stimulus to research the cadaveric transplantation. Hence, there have been
studies and research being done to meet the demand and reduce complications as this procedure is a boon to patients suffering from
end stage organ failure. There are complications with the procedure which include graft rejection and ischemia-reperfusion injury.
This article focuses on legal procedure for procurement of organs after a person has been declared brain dead or cardiac dead by
THOTA in India and various Ethical issues related to consent, myths, religious reasons and notions related with cadaveric
transplantation have been discussed.
1. J.S.R.G. Saran, Undergraduate Medical Trainee, Kasturba Medical College, Mangalore, Manipal Academy of Higher
Education, Manipal, India
2. Jagadish Rao Padubidri, District Medicolegal Consultant & Associate Professor, Department of Forensic Medicine,
Kasturba Medical College, Mangalore, Manipal Academy of Higher Education, Manipal, India
Cadaveric Transplantation-The legal and Ethical issues
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00046.7
245

7includes brain dead individuals and cardiac dead individuals.
There are very limited organs that can be procured from a
living person, which most commonly include one kidney, one
lung, piece of liver, pancreas or intestine. Most of the other
organs like the heart, both the kidneys, both the lungs, liver,
pancreas and other organs require a brain dead person.
Recently, hand and face transplantation, which come under
vascularized composite allograft (VCA) have been added to 10the donor list. But in case of a cardiac dead person, bone, skin,
heart valves and corneas can be harvested within 24 hours of
death.
The need for cadaveric transplant
Initially, the age of transplantation started with the advent of
kidney transplant between identical twins by Joseph Murray in 41954. Then, other organ transplants were experimented on
with live individuals and only limited organs could be
transplanted. With the advent of heart and liver transplantation
procedures which were transplanted from vegetative patients,
along with use of combination of immunosuppressive drug
therapy to prevent rejection, there was an increased demand for 4organs but limited supply. This created a paradox. Hence,
more and more research on cadaveric transplantation is being
done to meet the demand.
Legal importance and procedure
In India, before the laws for human organ transplantation were
not present, as early as 1962, even though it was being done, 7they were unregulated and organ trafficking was quite high.
Later, the Transplantation of Human Organs Act, 1994
(THOA) came into place which states that the donor can be a
deceased donor, who can be a brain dead or a cardiac dead 7 person, who can serve as a source for organ donation. This was
brought about by a few collective sates initially and later was
adopted to all the states with the exception of Andhra Pradesh
and Jammu and Kashmir. The law also states that the donor
should be a near relative, which is being used a s a loophole by
many doctors to illegally do transplantations from the poor to
the rich. There was a case back in 2004, where a doctor, a
nephrologist, who would procure the kidneys to the patients
through agents, who in turn go to the poor, fabricate documents
that the donors were far relatives or friends to the recipient and
would receive large amounts of money for it but the recipients
get charged triple or quadruple times the initial amount, 13making illegal profits, was later arrested and found guilty.
Many similar incidents kept happening everywhere, which led
to the exposure of the loopholes in the laws and due to the
insufficiencies in the effectiveness, applicability and effects of
the act , an amendment was proposed in 2009 by the states of
Goa, Himachal Pradesh and West Bengal, which was legally
amended in 2011 and the rules made clear in 2014, which is
now called the Transplantation of Human Organs and Tissues 7Act, 2014 (THOTA). In case of a brain stem death, it is
certified by a panel of medical experts comprising of four
members, namely a medical superintendent of the hospital, a
specialist appointed by him belonging to the same hospital, a
neurology specialist and the doctor who was in charge of the 5 patient. Then, confirmatory tests should be done with 6 hour
14interlude and later declared as brain dead. After the
declaration of brain stem death, the transplant coordinator asks
the deceased individuals' immediate related family members
for consent of organ transplantation. If they agree, then they are
made to sign a form documenting which organs they will be 6donating. Even if the deceased had committed to donate his or
her organs, a consent from their near relative has to be taken for 7lawful documentation. Organ extraction from expired donors
require a lot of hospitals and transplant teams should make sure
that the donated organs are as close a match to the recipient as
possible. In case of a MLC (Medico-Legal Case), a post-
mortem will be necessary and will require the police as well as 14 a Forensic expert. In case a person suffers severe brain injuries
but not brain dead, he or she can also consider to be an organ
donor if the family agrees to removal of life support system. In
this case, they wait for 2 to 5 minutes and when there is no more
circulation of blood, then he or she is pronounced dead and 5viable organs will be harvested. Just before removing the
organs from the donor, each one is cleared of blood by flushing
them with a specially prepared ice-cold preservation solution.
The organs are then placed in sterile containers, packed in wet
ice, and are transported to the recipients' transplant centre.
Different organs have different time ranges for preservation 6 before they become non-viable. Heart must be transplanted by
4 to 6 hours of retrieval from the donor, lung between 4 to 8
hours, liver between 12 to 15 hours, pancreas between 12 to 24
hours, intestines between 6 to 10 hours and lastly kidneys can 14be stored between 1 to 2 days. Now, the central government
has introduced network which keeps a check on the organ and
tissue removal and its storage throughout the country, known
as National Organ and Tissue Transplant Organisation
(NOTTO), which is further subdivided into 5 regional
networks, i.e. Regional Organ and Tissue Transplant
Organisations (ROTTO) and each region further comprising
of state networks, i.e. State Organ and Tissue Transplant
Organisations (SOTTO) to which every hospital in the state is
linked . NOTTO functions by maintaining national registries,
which include the organ transplantation registry, organ
donation registry, tissue registry and organ donor pledge
registry by which they keep a check on all the transplant
procedures occurring within the country and prevent any form 14of malpractice.
246
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00046.7

Complications
The most common complication is graft rejection by the
recipient body. This is due to incompatibility of the HLA
haplotypes of the donor tissue with that of recipient body. It can 9be host vs. graft or graft vs. host reaction. In host vs. graft ,
there can be hyper acute, acute or chronic. In hyper acute, the
rejection occurs within first 24 hours due to preexisting
antibodies against the donor antigens. In acute, it usually
occurs within the initial few weeks, where it is a cell mediated
immunological destruction of the donor tissue. In chronic, it 9occurs over many years. In graft vs. host type, antibodies
present on donor tissue proliferate and attack recipient body,
leading to clinical manifestations like rash, diarrhoea and 9jaundice, commonly seen in bone marrow transplants.
Another complication known to arise is ischaemia-reperfusion
injury. This happens due to reperfusion of an organ, which has
accumulated metabloites, which cause oxidative injury to
recipient tissues.
Ethical issues
There have been many issues regarding the concept of
presumed consent where, when a patient is brain dead,
irrespective of his family wishes, he becomes a candidate for
donating organs. It can only be opposed by that person when he
was in his usual healthy self before the unforetold incident.
This was being done in several countries in Asia and Europe, 8mainly in Spain and Singapore. There were no oppositions
from the factions of Christianity, Judaism and Islam. But there
were some people against it as they wanted an intact body
burial due to social, cultural and religious norms and beliefs 8and also considered this rule as a means for body snatching.
Also, in China, organs were being harvested from people who 8were issued a death warrant immediately after execution. The
next issue came with allocation of organs to people. In the
Unites States of America, they followed a criteria by the name
United Network of Organ Sharing (UNOS) which is based on
geographical area of the donor with respect to recipient, blood
group compatibility and a point system for the waiting list
candidates in which time of waiting, immunological
compatibility, age of recipient and medical urgency are 8compared. Generally, paediatric patients less than 11 years are
given most priority. Similarly, use of organs from foetuses, as
in cases from anencephaly also caused major ethical 8problems. Also due to the increasing demand for organs and
the supply not able to meet the needs, black market for organ
selling has become a very big business where the dealers
procure organs from unknown sources, mostly by illegal
means and malpractices in exchange for high monetary
benefit.
In India, organ donation rate is 0.36 per million, which is a very
11low value. This is due to lack of awareness regarding donation
of organs and transplantation, a major reason being associated
with various myths, which include; brain dead person is not
dead but still alive, diagnosis of brain death is very complex
and exorbitant, donation of organs after the same is not legal,
religious reasons, notions that if they donate an organ, they
might be born without the same organ when they are reborn in
another life and so on, which just proves on to say that very
little knowledge and awareness has been created regarding this 12 process.
CONCLUSION :
Cadaveric transplantation is still being researched for
shortening the gap between demand and harvest. Research is
being done to reduce the potential complications like using
combination therapy of immunosuppressants decreases the
chances for graft rejection. A recent study showed that the
solution to ischaemia-reperfusion injury is preconditioning of
the organ before surgery.2 Also, in recent study done in Japan,
in case where the waiting time for renal transplant patients is
more, extended hours hemodialysis in long term renal
transplant patients may improve transplant outcomes. Hence,
many techniques to improve procedure outcomes are being
done. People should be encouraged to donate organs for saving
the lives of others who very much require them.
REFERENCES:
1. Department of Health & Human Services. Organ and
tissue transplantation [Internet]. Better Health Channel.
Department of Health & Human Services; 2015 [cited
2021May16]. Available from:
https://www.betterhealth.vic.gov.au/health/ConditionsA
ndTreatments/organ-and-tissue-transplantation
2. Tavares-da-Silva E, Figueiredo A. Renal Procurement:
Techniques for Optimizing the Quality of the Graft in the
Cadaveric Setting [Internet]. Current urology reports.
U.S. National Library of Medicine; 2020 [cited
2021May16]. Available from:
https://www.ncbi.nlm.nih.gov/pubmed/32166407
3. Yamazaki T, Shirai H, Yashima J, Tojimbara T. Successful
cadaveric kidney transplantation in an extended-hours
hemodialysis patient with long-term hemodialysis vintage
for 297 months [Internet]. Urology case reports. Elsevier;
2 0 2 0 [ c i t e d 2 0 2 1 M a y 1 6 ] . Av a i l a b l e f r o m :
https://www.ncbi.nlm.nih.gov/pubmed/32140420
4. Sade RM. Brain death, cardiac death, and the dead donor
rule [Internet]. Journal of the South Carolina Medical
Association (1975). U.S. National Library of Medicine;
2 0 11 [ c i t e d 2 0 2 1 M a y 1 6 ] . Av a i l a b l e f r o m :
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC337291
2/
247
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00046.7
5. Saran J, Padubidri JR. Brain stem death - an overview
[Internet]. The Medico-legal journal. U.S. National
Library of Medicine; 2019 [cited 2021May16]. Available
from: https://www.ncbi.nlm.nih.gov/pubmed/30785835
6. Cadaver Organ Donation: The Biru Kumars Of India
[Internet]. Organ Donation India. 2015 [cited
2 0 2 1 M a y 1 6 ] . A v a i l a b l e f r o m :
h t t p s : / / w w w . o r g a n i n d i a . o r g / O R G A N -
DONATION/cadaver-organ-donation-the-biru-kumars-
of-india/
7. Sahay M. Transplantation of human organs and tissues
Act-“Simplified.” Indian Journal of Transplantation.
2018;12(2):84.
8. Abouna GM. Ethical issues in organ transplantation
[Internet]. Medical principles and practice : international
journal of the Kuwait University, Health Science Centre.
U.S. National Library of Medicine; 2003 [cited
2021May16]. Available from:
https://www.ncbi.nlm.nih.gov/pubmed/12566971
9. Kloc M, Ghobrial RM. Chronic allograft rejection: A
significant hurdle to transplant success [Internet]. Burns
& trauma. BioMed Central; 2014 [cited 2021May16].
Available from:
h t t p s : / / w w w. n c b i . n l m . n i h . g o v / p m c / a r t i c l e s /
PMC4994504/
10. What Can Be Donated [Internet]. Organ Donor. 2020
[cited 2021May16]. Available from:
https://www.organdonor.gov/about/what.html
11. Palaniswamy V, Sadashivam S, Selvakumaran C, Jayabal
P, Ananth SR. Organ donation after brain death in India: A
trained intensivist is the key to success. Indian J Crit Care
Med. 2016;20(10):593-6.
12. Singh K. Expert blog: Myths associated with brain death
and organ donation in India [Internet]. Ndtv.com. 2017
[cited 2021 May 16]. Available from:
https://sites.ndtv.com/moretogive/expert-blog-myths-
associated-with-brain-death-and-organ-donation-in-
india-2072/
13. Mudur G. Kidney trade arrest exposes loopholes in India's
transplant laws. BMJ. 2004;328(7434):246.
14. FAQs: NOTTO [Internet]. Gov.in. [cited 2021 May 16].
Available from: https://notto.gov.in/faqs.htm
248
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00046.7

Review Article
INTRODUCTION :
Accreditation is the formal approval for a stated period of an
institution and its program by a recognised body after self-
review and external evaluation and based on predetermined (1)standards. Accreditation is not same as Regulation.
Regulation is a system of controlling institutions by rules, laws
or restrictions often made by government or its elected people
who get their power from the laws. In India MCI is a
regulatory body for medical profession which ensures entry
level standard of students, quality of education being
imparted, curriculum and its impact on society.
Accreditation has got its own objectives. Institutions know
about their strengths and weaknesses through an informed
review process. It understands the collegiality on the campus
and provides information to allocated resources in deficient
areas as well as to know areas of strength so that research and
development can be strengthened. It provides feedback upon
innovative pedagogy. It provides opportunity for institution to
work upon inter-university collaboration in research and
training inside country and outside both. It also provides a
platform for society which wants to know comparisons among
institutions available; reliable information on quality
education. It also informs employer about reliable institutions
about prospective campus recruitment as per their
(2)requirement. It also provides adequate information to
funding agencies for prospective collaborations having known
required availability of structure in organization. Accreditation
also provides characteristic of institution e.g. Tuberculosis
research centre of India. It clearly tells inside medical
circumference, it's a special institution for tuberculosis
research and care.
Many countries have established bodies responsible for
regulating the medical and other healthcare professions.
Examples include the General Medical Council, UK, the (3)Australian Medical Council & the Medical Council of India.
WHO and WFME strongly recommend accreditation of
medical education. But, there is no uniformity across the
countries. Some countries have regulation and accreditation
both while others have one of the two or none. Some countries
have well regulation for private institutions while others have
not.
This study mainly focuses at Indian context. NAAC is one of
the accrediting bodies and its accreditation gives many benefits
to institution or university. There are more than 400 medical (4)colleges in India and 950 universities. Accreditation is
something being newly adapted by universities. But there are
many organizations who don't know how to initiate the process
Corresponding Author :
Dr. Vijay Pratap Singh,
Associate Professor,
Department of Physiotherapy, Kasturba Medical College,
Mangalore, Manipal Academy of Higher Education, Manipal
Contact : +91 89670-35789
Email : [email protected]
KEYWORDS : Accreditation, Education, University, Health
Article History:Received: 14 May 2021Received in revised form: 15 June 2021Accepted on: 15 June 2021Available online: 31 August 2021
ABSTRACT :
Accreditation of institutions and universities are important for visibility and showcase of quality. In India NAAC is one of the
accrediting agency which institutions aspire for. With diverse geography and limited resources all organizations are not aware of
how to make a roadmap to achieve accreditation. Institutional leaders have also different leadership styles. This study puts forward a
roadmap to initiate accreditation, team building and galvanize among a common goal even if institution heads or Deans adapt
different leadership styles.
1. Vijay Pratap Singh, Associate Professor, Department of Physiotherapy, Kasturba Medical College, Mangalore, Manipal Academy of Higher Education, Manipal
2. Bidita Khandelwal, Professor and Ex-Head, Associate Dean-Research, Department of Medicine, Sikkim Manipal Institute of Medical Sciences, Sikkim Manipal University, 5 Mile, Tadong,Gangtok-737102
3. Parmod Kumar Goyal, Professor and Head, Department of Forensic Medicine, Adesh Institute of Medical Sciences & Research Bathinda
Developing and building high performance teams to achieve Accreditation through different Leadership styles
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00047.9
249

and how such mammoth work can be accomplished. Faculties
in institution have reported that their Dean or leaders are of
different work style and its difficult to understand how leaders
of different styles can achieve it through team work, self-
review and external review. This study elaborates a step-by-
step process of achieving accreditation to enable institutions
and universities to achieve accreditation by simple steps of
team work even if Institution heads have different leadership
styles.
Approaches of Two Deans with different Leadership styles
:
Imagine a scenario where there are two medical universities
with two different styles of leaders. Dean A wants to assert a
personal management style and lead from front in achieving
NAAC accreditation. But he wants to keep a group of senior
faculties who would have an opportunity to galvanize along a
strong leader. Senior team will have freedom to work, put
forward their views but in line with Dean's goals. Non working
and ingratiated faculties of the group may be replaced.
Dean B wants to go by Laissez-faire style of leadership where
senior team takes over and works together to manage the
project and deliver the strategy. The team would report to the
Dean, but would bring all their creativity to the task and
execute it in their way. It was suggested that there would be
benefits to the team in terms of their own development, which
would aid the later delivery of the plan.
Dean A leadership style appears to be assertive leadership.
Assertive leaders are those who are convinced by their goal
setting and they stand for themselves and people around them
without being aggressive or passively accepting wrong.
Townend A. (2007) reported Assertive leaders are confident,
validate other's feelings, good listeners, problem-solving, and
know-how to manage others' feelings to persuade them to (5)understand the organizational goal. A recent study reported
that assertive leaders must also exercise some caution.
Assertive leaders are perceived as honest and integrated but (6)they are also perceived as aggressive.
Assertive leaders have to be very intelligent in the
communication. Dean must manage to give honest feedback.
Feedbacks can build a broken castle or destroy the strongest (7)castle. Sensitivity and privacy in giving feedback help both
classes of employees. Decision making is another crucial
thing. Here dean wants to galvanize senior members. In this
style members get a chance to criticize, and voice their
concerns to make better decisions emerge and at the same time
members feel accountable and empowered. Therefore.
Assertive leaders use this as an opportunity while making
decisions, they go by facts, analysis, and trends, and
consultations to reach a decision.
Dean B seemingly relates to Laissez-faire style of leadership.
This type of leadership is the opposite of authoritarian
leadership and autocratic style. Laissez-faire is a French word
that means 'let it be' or 'leave alone'. This style is delegative
kind of leadership. Here the leader believes in building a highly
capable team that often puts up the goal in front of the team but
leaves the team with their own devices. Leaders who subscribe
to such style do it based on trust and leader has always read that
the team is highly experienced, skilled, and motivated. The
leader intervenes minimum and allows members with freedom
of choice. There is a controversy that a leader does not
intervene and is absent from the work scene until the result is (8)achieved but it can sometimes lead to a mess.
After all, its individual choice and a consultant can only advise.
Other popular styles of leadership Dean may like are derived
from Goleman(2000) study; autocratic, authoritative,
pacesetting, democratic, coaching and affiliative. The
autocratic style is 'do as I say' and is a command and control
approach with almost no scope for followers to opine.
Authoritative leadership is visionary and 'follow me' style.
Unlike autocratic, the leader here explains its vision and keeps
followers energized and engaged. Pacesetting style is 'do as I
do'. Here leader leads by example but followers may get
fatigued. Democratic style depends on what do you think? It
consults and reaches to a shared objective. The coaching style
is mainly unlocking people's potential where they have low
confidence despite having talent or they need someone to show
some light. Whereas affiliative leadership is premised on
'people come first' approach. The success of this style depends
on attention and support to members by forming a meaningful (9)collaborative relationship.
For them to do this, pioneers inside associations need to have a
solid feeling of what their identity is, and what driving with
uprightness intends to them. This requires bringing their "best
selves" to their initiative, monitoring the effect of their conduct
on others inside and remotely to the association. This not only
helps to achieve the goal but prepares a future leader inside the
organization. Next time, organization need not hire a leader (10)from outside instead it can rely on its own pool of leaders.
The concerns are both leadership as well as management. It's a
blend of issues. There are two types of issues that have surfaced
after internal and external reviews. Dean has classified them
under two headings. One set of issues are infrastructural,
logistic, information technology (IT), and clerical. Whereas
other sets of issues are motivation among faculty members,
lack of awareness about accreditation, resistance to moving out
of comfort zone, overshooting time frame or non-compliance,
and inability to bring junior faculties in a loop. Dean realizes
that the first set of issues are management task and second is
250

(11)leadership demands. He thinks of bringing a competent
human resource manager (HR) for managerial tasks while
leadership issues he wishes to carry on his own with the help of
senior faculties who have galvanized around him and are ready
to take the vision forward.
Dean has voiced his concern that unless both the works go
parallel and in tandem, goals can not be achieved. There were a
lot of publications made by faculties but it could not be brought
in to one data set when it was sent to the external review. When
Dean went into depth of such an issue he found trivial things
and could have been solved. It was clerical support, issues of
printers and cartridges supply, formatting, and IT support.
DISCUSSION :
Dean after suggestions from other senior faculties of college
decided to handle the second set of issues by themselves. He
believed that those were leadership issues and can be solved by
persuasion and gaining the confidence of non-contributors.
When Dean enquired from junior faculties as to why they are
not cooperating with some Heads of departments. Various
comments came out which were seemingly true on further
triangulation. Some junior faculties of a department pointed
out that their HOD delegates all surgeries and operation
theatre (OT) works to them while HOD never takes up any
surgery. He is not available on the days of his call-duty and
absconds during important works. There is no encouragement
from HOD for any work or publication by juniors while he
keeps nit-picking faults and is trivial. Juniors of the ENT
department felt that they are primarily physicians and research
is not their primary work. They looked very supportive to their
HOD and their track record revealed that even HOD has got no
publication on record and gives the least important to research
while he is a good clinician. Juniors of one more department
from clinical subjects revealed that teaching of students is not
required and students are supposed to learn on their own and
from clinical experiences of ward posting. One pre-clinical
department reported that they are underestimated by clinical
departments and they wanted to implement horizontal and
vertical integration of teaching but got no support from allied
departments. Dean found that this department has got the best
track records of teaching and is eager to take up teaching
challenges. Department of community medicine reflected that
researches and publications are the only ways to showcase the
brand visibility of colleges. Nobody bothers how teaching is
happening but a good paper makes them visible at the
international level. Some inquiries revealed that teaching in
the community medicine department is most lackadaisical and
students are overloaded with research. Often they are
intimidated if they do not carry out research responsibilities
and are judged based on publications only. After such feedback
Dean concluded that faculty development programs are
important where thrust will be to make faculties understand
teaching, research and clinics are three wheels of the same cart
which must move together at the same speed. Accelerating one
by decelerating others will fail institutional vision. Dean also
figured out external experts for FDP and briefed them
problems of different departments, where they felt self
internalization tasks to be given during workshops and groups
will be mixed of each thinking. One who thinks research is
important, others who think teaching is important, and the who
thinks clinical work is only work of a doctor should
intermingle and sit in one group and reflect. It may have some
argument initially but Dean decided to preside personally such
meetings as 'Guide on the side' to moderate and boil down to
the vision of the institution and work together and give equal (2,12)importance to each important work.
Change involves humans and their reactions. People just don't
accept change without a strong purpose. Things involved in
managing change would range from decision making,
problem-solving, handling disputes, consultations, hierarchy,
and mutual respect to resource allocation. In this context, there (13)are several levels of change. Strategic changes are to bring
change in organizational vision, mission, and objectives by
making senior faculties and all levels to understand the
importance of accreditation and working as a group. Structural
changes like pending promotions and bringing a change of
some head of departments who are in place for a very long time
as per the policy and have brought no change but second-in-
line is more driving, capable, and enthusiast. Change in the
process of delivering the outcome of work at the right time and
showing compliance to reviews. Bringing personnel and
technological changes with the inclusion of skilled
information technologists who can handle data and solve
problems of departments with newer methods of technology.
Having an app in the place where all data can be entered and
generated centrally at any point in time rather than floating
notices each time when data is required.
But, Dean must approach it with reactions of people in mind.
The leader here dean is responsible to get the vision across for
change and change for good. The need for change must be
realized across all levels of stakeholders. Dean can have a
before-hand preparation with some tools available for
managing the change. It will require the first attitudes and
behaviors of different people at all levels and in each area.
Dean may take the help of some trusted people but not many as
the thought may leak and resistances may start developing
before time. These tools are 'People chart' and Force field (14)analysis. These tools have a grid where analysis can be jotted
down for clarity.
251
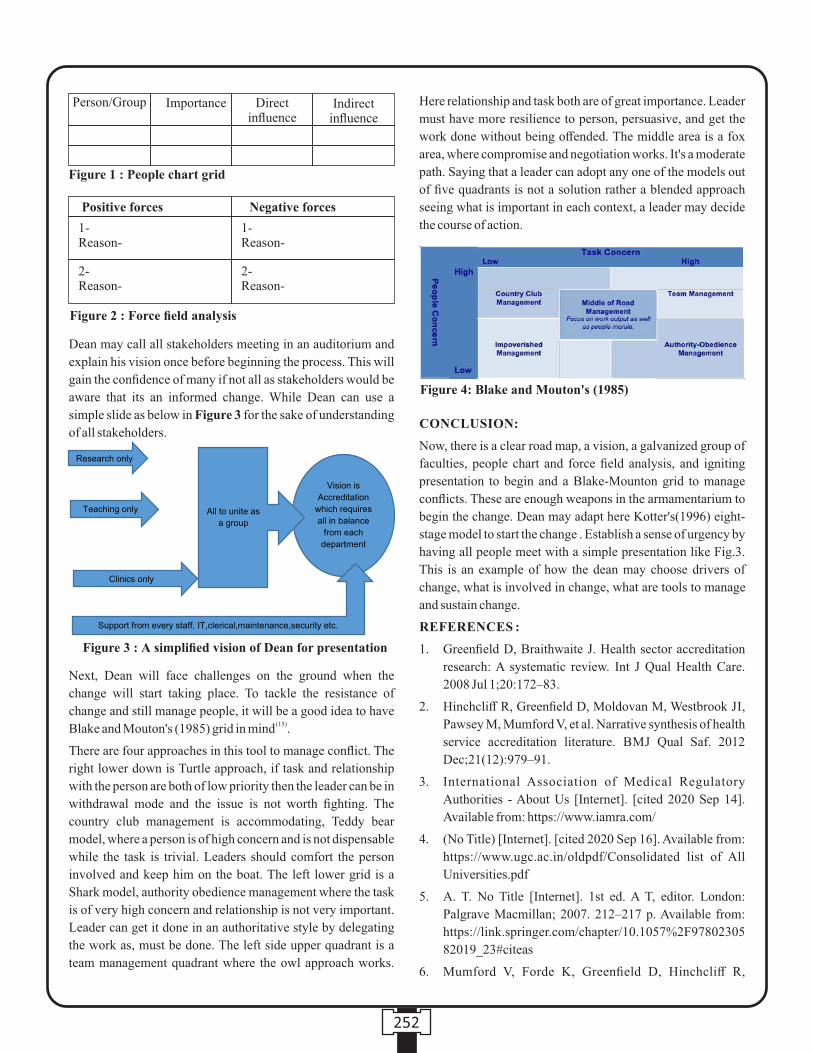
Dean may call all stakeholders meeting in an auditorium and
explain his vision once before beginning the process. This will
gain the confidence of many if not all as stakeholders would be
aware that its an informed change. While Dean can use a
simple slide as below in Figure 3 for the sake of understanding
of all stakeholders.
Next, Dean will face challenges on the ground when the
change will start taking place. To tackle the resistance of
change and still manage people, it will be a good idea to have ( 15)Blake and Mouton's (1985) grid in mind .
There are four approaches in this tool to manage conflict. The
right lower down is Turtle approach, if task and relationship
with the person are both of low priority then the leader can be in
withdrawal mode and the issue is not worth fighting. The
country club management is accommodating, Teddy bear
model, where a person is of high concern and is not dispensable
while the task is trivial. Leaders should comfort the person
involved and keep him on the boat. The left lower grid is a
Shark model, authority obedience management where the task
is of very high concern and relationship is not very important.
Leader can get it done in an authoritative style by delegating
the work as, must be done. The left side upper quadrant is a
team management quadrant where the owl approach works.
Here relationship and task both are of great importance. Leader
must have more resilience to person, persuasive, and get the
work done without being offended. The middle area is a fox
area, where compromise and negotiation works. It's a moderate
path. Saying that a leader can adopt any one of the models out
of five quadrants is not a solution rather a blended approach
seeing what is important in each context, a leader may decide
the course of action.
CONCLUSION:
Now, there is a clear road map, a vision, a galvanized group of
faculties, people chart and force field analysis, and igniting
presentation to begin and a Blake-Mounton grid to manage
conflicts. These are enough weapons in the armamentarium to
begin the change. Dean may adapt here Kotter's(1996) eight-
stage model to start the change . Establish a sense of urgency by
having all people meet with a simple presentation like Fig.3.
This is an example of how the dean may choose drivers of
change, what is involved in change, what are tools to manage
and sustain change.
REFERENCES :
1. Greenfield D, Braithwaite J. Health sector accreditation
research: A systematic review. Int J Qual Health Care.
2008 Jul 1;20:172–83.
2. Hinchcliff R, Greenfield D, Moldovan M, Westbrook JI,
Pawsey M, Mumford V, et al. Narrative synthesis of health
service accreditation literature. BMJ Qual Saf. 2012
Dec;21(12):979–91.
3. International Association of Medical Regulatory
Authorities - About Us [Internet]. [cited 2020 Sep 14].
Available from: https://www.iamra.com/
4. (No Title) [Internet]. [cited 2020 Sep 16]. Available from:
https://www.ugc.ac.in/oldpdf/Consolidated list of All
Universities.pdf
5. A. T. No Title [Internet]. 1st ed. A T, editor. London:
Palgrave Macmillan; 2007. 212–217 p. Available from:
https://link.springer.com/chapter/10.1057%2F97802305
82019_23#citeas
6. Mumford V, Forde K, Greenfield D, Hinchcliff R,
252
Person/Group
Figure 1 : People chart grid
Importance Direct influence
Indirect influence
Positive forces
1-Reason-
1-Reason-
2-Reason-
2-Reason-
Negative forces
Figure 2 : Force field analysis
Figure 3 : A simplified vision of Dean for presentation
Figure 4: Blake and Mouton's (1985)
Braithwaite J. Health services accreditation: what is the
evidence that the benefits justify the costs? Int J Qual
H e a l c a r e J I n t S o c Q u a l H e a l C a r e . 2 0 1 3
Oct;25(5):606–20.
7. Carman AL, Scutchfield FD, McGladrey ML, Vorbeck J.
Pursuing Public Health Accreditation: A Focus on HOW.
J Public Health Manag Pract. 2019;25(5):431–9.
8. The 7 Most Common Leadership Styles (and How to Find
Your Own) [Internet]. [cited 2020 Aug 18]. Available
f rom: h t tps : / /www.amer icanexpress . com/en-
us/business/trends-and-insights/articles/the-7-most-
common-leadership-styles-and-how-to-find-your-own/
9. Goleman D, Boyatzis R. Social intelligence and the
biology of leadership. Harv Bus Rev. 2008 Sep;86(9):74-
81,136.
10. Greenfield D, Debono D, Hogden A, Hinchcliff R,
Mumford V, Pawsey M, et al. Examining challenges to
reliability of health service accreditation during a period
of healthcare reform in Australia. J Health Organ Manag.
2015;29(7):912–24.
11. Toor S-R, Ofori G. Leadership versus Management: How
They Are Different, and Why. Leadersh Manag Eng. 2008
Apr 1;8.
12. Greenfield D, Lawrence SA, Kellner A, Townsend K,
Wilkinson A. Health service accreditation stimulating
change in clinical care and human resource management
processes: A study of 311 Australian hospitals. Health
Policy. 2019 Jul;123(7):661–5.
13. Frich JC, Brewster AL, Cherlin EJ, Bradley EH.
Leadership development programs for physicians: a
sys temat ic rev iew. J Gen In te rn Med. 2015
May;30(5):656–74.
14. Bozak MG. Using Lewin's force field analysis in
implementing a nursing information system. Comput
Inform Nurs. 2003;21(2):80–7.
15. The Blake Mouton Manager ia l Gr id - From
MindTools.com [Internet]. [cited 2020 Aug 21]. Available
from:
https://www.mindtools.com/pages/article/newLDR_73.
htm
253

254
Scientific Correspondence
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00048.0
1. Mahipal Singh Sankhla, Research Scholar, Department of Forensic Science, School of Basic and Applied Sciences,
Galgotias University, Greater Noida, U.P. India.
2. Rajeev Kumar, Associate Professor, Department of Forensic Science, School of Basic and Applied Sciences, Galgotias
University, Greater Noida, U.P. India.
3. Lalit Prasad, Associate Professor, Department of Chemistry, School of Basic and Applied Sciences, Galgotais University,
Greater Noida, U.P. India.
Key words: Key-Words: - Zinc, Yamuna River, Water, Toxicity, Human, etc.
Corresponding Author:
Dr. Rajeev Kumar,
Associate Professor,
Department of Forensic Science, School of Basic and Applied
Sciences, Galgotias University, Greater Noida.
Contact : +91 9411923188
Email : [email protected]
Article History :
Received : 19 July 2020
Received in revised form : 24 July 2020
Accepted on : 24 July 2020
Available online : 15 August 2021
INTRODUCTION :
Water is vital for human existence. There's no life without
water. To survive man has to go to several extents to search for
water. Water can be obtained from oceans, rain, streams, lakes, [1]glacier, or underground . Water is essential for life and life
without it, as we know it would have not been possible. Though
its precious it brings disease and disabilities to the public.
Water already contains minerals and organisms that may cause
harm to humans as well as animals because of their [2]concentration and contents . Rivers are a vital source for
human civilizations as they meet water demand for rivers are
important resources for human various uses apart from
supporting flora and fauna, improving aesthetic and landscape
quality, moderating climate and providing resources for
[3]hydropower .
The river Yamuna passes through a distance of about 1370 km
in the basic from Saharanpur district of Uttar Pradesh to the
flowing together with river Ganga at Prayagraj. The major
streams of the river are Tons, Betwa, Chambal, Ken, and
Sindh, and these altogether contribute 70.9% of the catchment
area and sense of balance 29.1% is the direct drainage of main
River and smaller streams. Based on the area, the catchment
basin of Yamuna volumes to 40.2% of the Ganga Basin and [4]10.7% of the nation . The Yamuna river is one of the most
polluted rivers in India. The capital of the nation, Delhi is the
major contributor to pollution in the Yamuna River, followed [5]by Agra and Mathura .
Zinc is found in the physical background on earth's crust and
Estimation of Zinc Concentration in Yamuna River (Delhi) Water Due to Climatic Changes
ABSTRACT :
Introduction: Water is increasingly becoming an unusual resource, both in the relation to quantity and quality. Yamuna river water
may become contaminated by the accumulation of Zinc through emissions from the rapidly expanding industrial areas, disposal of
high element wastes, fertilizers, animal manures, sewage sludge, pesticides, and wastewater irrigation.
Material and Methods: Samples of water were collected from the five different sampling sites. Samples collected in the duration
of 8 months from January to August with the gap of 20-25 days keeping the climatic change as a major parameter. The
concentration of Zinc (Zn) in water from River Yamuna, Delhi was determined by Inductively Coupled Plasma Mass Spectrometry
(ICP-MS).
Result and Discussion: It was found that the concentration of zinc (Zn) is higher than the permissible limits of WHO and lower
than permissible limits only in the month of August. This can be established that the concentration increases with rising
temperature and reducing humidity.
Conclusions: It is universally-known that zinc is majorly toxic in nature and humans & animals. Exposure of zinc through water
may produce chronic toxicity that could be quite harmful to human life.

255
can consequently enter water sources through natural
procedures and the example of sometimes heavy rains and [6]water can leach zinc out of natural sources . Zinc
insufficiently has been recognized by several experts as an
important public health issue, especially in developing
countries. The prevalence and clinical consequences of zinc
deficiency on growth delay, diarrhea, pneumonia, disturbed
neuropsychological performance, and abnormalities of fetal [7]development .
Zinc has naturally originated either from geological and
chemical variance or tailings site. Zinc indicates an
anthropogenic source due to the sulfide minerals oxidation in
mine waste disposal sites. Over the past year's environmental
principles have developed more stringent, necessitating an
enhanced better quality of removing toxic waste for treatment
and zinc material to the defense of the environment, human [8]health, and aquatic life . The zinc (Zn) enters the environment
through aquatic life systems and plants and animals [9]surrounding the river . Zinc is a very communal pollutant in
the environment; its occurrence may be impeding the water's
ecological environment. Consequently, much study effort has
been directed toward the spreading of Zn in the water
environment. Anthropogenic actions counting municipal
wastewater releases, coal-burning power plants; industrial
methods involving metals; and the atmospheric outcome are [10]the main source of Zn contamination . Extreme discharge of
zinc contaminates the surface water and subsurface
environment and contribute to groundwater pollution.
Groundwater is often extremely polluted near mines of sulfide [11]minerals .
In natural waters, zinc can be found in some chemical methods,
such as hydrated ions, metal-inorganic complexes, or metal-
organic complexes. Hydrated zinc cations may be hydrolyzed
to form zinc hydroxide or zinc oxide. In anaerobic [12]environments, Zinc sulfide may be formed .
The environmental contaminations by the toxic substances are
increasing which is causing a major threat to the local users. A
wide range of pollutants are endlessly introduced into the
aquatic environment mainly due to enlarged industrialization,
technological growth, increasing human populace and misuse
of agricultural, natural resources, and domestic wastes run-off.
Among these pollutants, heavy metals constitute one of the
most unsafe groups because of their persistent toxicity, nature,
and tendency to gather in organisms and undergo food chain [13]amplification, and more still, they are non-degradable .
Polluted water of Yamuna River is a matter of concern as the
population of Delhi is dependent on the water of Yamuna. The
hazard of biomagnification and bioaccumulation of the Zn [14]causes extreme harm to human health and welfare . Citizens
might experience during disease on drinking water with a high
concentration of heavy metals. They might contain
physiological effect as on kidney, digestive system, circulatory
system, nervous system, etc. different additional organs and [15]diverse systems of the body .
This research study noted that dissolved zinc concentration
was more in the rise in environmental temperature and
humidity. Zinc toxicity has established to be a major risk and
there are several health threats related to humans and animals.
The toxic effects of zinc, even though they do not have any
organic role, persist current in approximately or the other form
damaging for the people's body and its suitable working.
Consequently, the present study aimed to measure the
concentration of zinc from the Yamuna River climate changes
to appreciate the change in dissolved zinc concentrations.
MATERIALS AND METHODS :
Samples Collection :The water samples were collected from
the five different Sites of Yamuna River in Delhi, India.
Site 1: Okhala Bird Sanctuary
Site 2: Kalindi Kunj Ghat
Site 3: Okhala Barrage
Site 4: Yamuna Bridge
Site 5: Yamuna Bank
All sampling sites were used for farming and drinking purpose.
Water samples were collected for analysis from each Site. All
samples were collected in 1.5 liters of sterile polyethylene
bottles, which were pre-washed with 10% nitric acid and de-
ionized water. Before sampling, the bottles were rinsed at least
three times with water from the sampling site. The bottles were
immersed to about 20 cm below the water surface to prevent
contamination of trace elements from the air also collected for
analysis from each site.
All water samples were immediately brought to the laboratory
where they filtered through Whatman No.41 (0.45 μm pore
size) filter paper. The samples were acidified with 2 ml
concentrated Nitric acid to prevent precipitation of Zinc,
reduce adsorption of the analyses onto the walls of containers
and to avoid microbial activity, then water samples were stored [16]at 4°C until the analysis .
The concentration of Zinc (Zn) in water collected in every 20-
25 days during four months from January to August 2019 from
Yamuna river, Delhi were Zinc (Zn) measured and compared
with the permissible limits as set by the World Health
Organization (WHO).
Instrumentation
The concentrations of heavy metals were determined in all
samples by Inductively Coupled Plasma Mass Spectrometry
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00048.0

256
(ICP-MS). It is a standard laboratory analytical tool for metal
analysis.
RESULTS & DISCUSSION :
The concentration of Zinc in Water samples :
In the month of January, the concentration of zinc (Zn) in water
samples was 5.4 ppm followed by a slight decrease in February
concentration was 5.7 ppm whereas there was an increase in
the March 6.0 and increases in the month of April 6.2 ppm and
further it increases in the month of May, the concentration of
zinc in water was 7.0 ppm and decrease in the month of June
5.3 ppm and July 5.0 ppm or month of august 4.5 ppm
According to the WHO guidelines, the maximum permissible
limit of zinc is 5.00ppm. We found that the concentration of
zinc is very high as compared to the permissible limit, and
almost 1.4 times higher than the WHO limit in the month of
May and month of August concertation is lower than WHO
Permissible Limit. There were significant differences between
the concentration of WHO limit and Zn levels measured during
these months. On comparison of the concentration of Zn
among the different months, we found significant differences
in concentration of Zn with temperature and humidity result
shows that in the month of April or May can be established that
the concentration increases with rising temperature and
reducing humidity (Figure 1)
CONCLUSION :
The concentrations of zinc (Zn) have already crossed or are at
the borderline of the permissible limit as declared by the World
Health Organization in most river bodies. Although some
previous data suggests that somewhere the elemental
concentrations are still below the permissible limit. Human
health is directly affected by the consumption of polluted
water, sediment, fishes, fruits, vegetables, plants, etc. Studies
show that Industrial wastes, Sewage, Natural source,
anthropogenic source, and Agricultural actions that have
contaminated dangerous and toxic constituents in the Yamuna
River water thereby, led to pollution of drinking water in near
areas. Diseases like Neurotoxicity, Carcinogenicity related to
contamination of Zinc in water in such areas. The practice of
trace element detection should be continued to lower the
possible consumption of contaminated eatables. People should
be aware of the hazardous effects of the consumption of
polluted water and eatables. On account of the research of the
drinking water samples, contain Heavy metal concentration
more than the admissible and desirable levels (WHO). Most of
the water samples were highly contaminated, which are not
possible to use for drinking purposes.
REFERENCES :
1. Chege MW, Hashim NO, Merenga AS, Tschiersch J. Lead
contamination of traditional hand-dug wells in parts of
Kwale County, Kenya. International Journal of Physical
Sciences. 2013 May 9;8(17):835-9.
2. Fagoyinbo CV, Dairo VA. Groundwater Contamination
and Effective Ways of Rectification. International Journal
of Information Research and Review. 2016;3:1749-56.
3. Sharma MP, Singal SK, Patra S. Water quality profile of
Yamuna river, India. Hydro Nepal: Journal of Water,
Energy and Environment. 2008;3:19-24.
4. Central Water Commission, Yamuna Basin Organization,
New Delhi, (2007); 1-127.
5. Misra AK. A river about to die: Yamuna. Journal of water
resource and protection. (2010);1, 2(5):489.
6. Sankhla MS, Kumari M, Nandan M, Kumar R, Agrawal P.
Heavy metals contamination in water and their hazardous
effect on human health-a review. Int. J. Curr. Microbiol.
App. Sci (2016). 22;5(10):759-66. Bhowmik D, Chiranjib
KP, Kumar S. A potential medicinal importance of zinc in
human health and chronic. Int J Pharm. (2010);1(1):05-11.
8. Sankhla MS, Kumar R, Prasad L. Zinc Impurity in
Drinking Water and Its Toxic Effect on Human Health.
Indian Internet Journal of Forensic Medicine &
Toxicology. 2019;17(4):84-7.
9. Malik D, Singh S, Thakur J, Singh RK, Kaur A, Nijhawan
S. Heavy metal pollution of the Yamuna River: An
introspection. Int. J. Curr. Microbiol. App. Sci.
2014;3(10):856-63.
10. Toli K, Misailidis P, Godelitsas A. Distribution of heavy
metals in the aquatic environment of the Kerkini lake (N.
Greece): An exploratory study. Fresenius Environmental
Bulletin. (1997);6:605-10.
11. Ghadimi F, Ghomi M, Hajati A. Identification of
groundwater contamination sources of Lakan lead and
zinc mine, Khomain, Iran. Journal of Mining and
Figure 1: Climatic changes and Concertation of Zinc in water.
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00048.0

257
Environment. 2012;3(2):121-34.
12. Callahan MA. Water-related environmental fate of 129
priority pollutants. Office of Water Planning and
Standards, Office of Water and Waste Management, US
Environmental Protection Agency; (1979); (1).
13. USGAO, Health Effect of lead in drinking water. U.S.
General Accounting Office reports (2000); (1).
14. Sankhla MS, Kumari M, Sharma K, Kushwah RS, Kumar
R. Heavy metal pollution of Holy River Ganga: A review.
Int. J. Res. 2018 Jan;5(1):421-36.
15. Parihar K, Sankhla MS, Kumar R. Water Quality Status of
Yamuna River and its Toxic Effects on Humans. (2019); 6
(1):597-601.
16. Sankhla MS, Kumar R, Biswas A. Dynamic nature of
heavy metal toxicity in water and sediments of Ayad River
with climatic change. Int J Hydro. 2019;3(5):339-43.
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00048.0
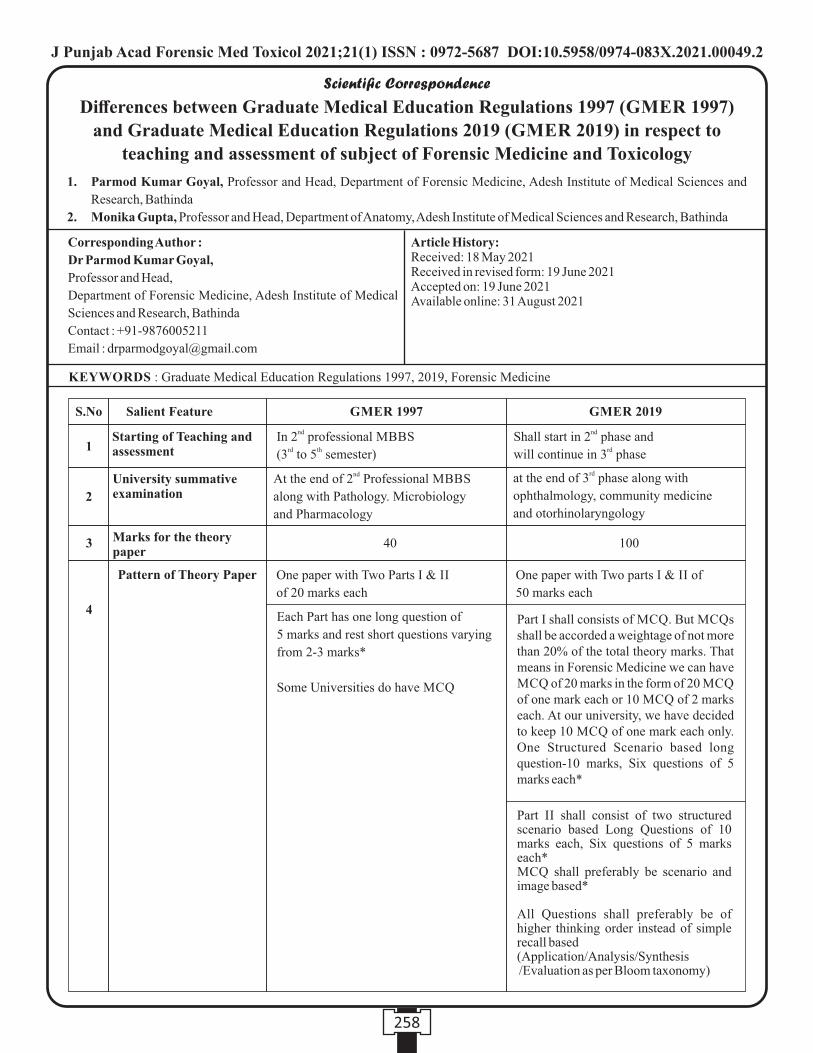
Scientific Correspondence
Corresponding Author :
Dr Parmod Kumar Goyal,
Professor and Head,
Department of Forensic Medicine, Adesh Institute of Medical
Sciences and Research, Bathinda
Contact : +91-9876005211
Email : [email protected]
KEYWORDS : Graduate Medical Education Regulations 1997, 2019, Forensic Medicine
Article History:Received: 18 May 2021Received in revised form: 19 June 2021Accepted on: 19 June 2021Available online: 31 August 2021
1. Parmod Kumar Goyal, Professor and Head, Department of Forensic Medicine, Adesh Institute of Medical Sciences and
Research, Bathinda
2. Monika Gupta, Professor and Head, Department of Anatomy, Adesh Institute of Medical Sciences and Research, Bathinda
Differences between Graduate Medical Education Regulations 1997 (GMER 1997)
and Graduate Medical Education Regulations 2019 (GMER 2019) in respect to
teaching and assessment of subject of Forensic Medicine and Toxicology
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00049.2
258
S.No
1
2
3
4
40 100
Salient Feature GMER 1997 GMER 2019
Starting of Teaching and assessment
University summative examination
Marks for the theory paper
Pattern of Theory Paper
ndIn 2 professional MBBS rd th(3 to 5 semester)
ndShall start in 2 phase and rdwill continue in 3 phase
ndAt the end of 2 Professional MBBS
along with Pathology. Microbiology
and Pharmacology
rdat the end of 3 phase along with
ophthalmology, community medicine
and otorhinolaryngology
One paper with Two Parts I & II
of 20 marks each
One paper with Two parts I & II of
50 marks each
Each Part has one long question of
5 marks and rest short questions varying
from 2-3 marks*
Some Universities do have MCQ
Part I shall consists of MCQ. But MCQs shall be accorded a weightage of not more than 20% of the total theory marks. That means in Forensic Medicine we can have MCQ of 20 marks in the form of 20 MCQ of one mark each or 10 MCQ of 2 marks each. At our university, we have decided to keep 10 MCQ of one mark each only.One Structured Scenario based long question-10 marks, Six questions of 5 marks each*
Part II shall consist of two structured scenario based Long Questions of 10 marks each, Six questions of 5 marks each*MCQ shall preferably be scenario and image based*
All Questions shall preferably be of higher thinking order instead of simple recall based (Application/Analysis/Synthesis /Evaluation as per Bloom taxonomy)
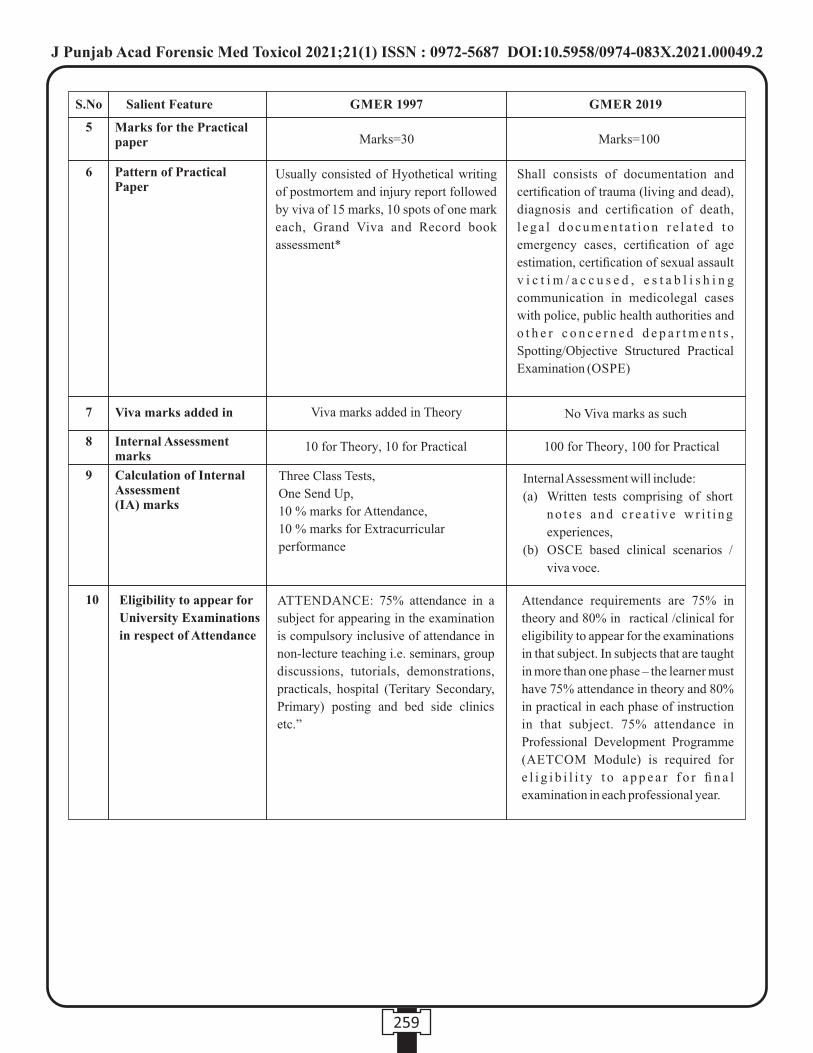
259
Usually consisted of Hyothetical writing
of postmortem and injury report followed
by viva of 15 marks, 10 spots of one mark
each, Grand Viva and Record book
assessment*
Shall consists of documentation and
certification of trauma (living and dead),
diagnosis and certification of death,
l e g a l d o c u m e n t a t i o n r e l a t e d t o
emergency cases, certification of age
estimation, certification of sexual assault
v i c t i m / a c c u s e d , e s t a b l i s h i n g
communication in medicolegal cases
with police, public health authorities and
o t h e r c o n c e r n e d d e p a r t m e n t s ,
Spotting/Objective Structured Practical
Examination (OSPE)
Viva marks added in Theory No Viva marks as such
10 for Theory, 10 for Practical 100 for Theory, 100 for Practical
Three Class Tests,
One Send Up,
10 % marks for Attendance,
10 % marks for Extracurricular
performance
Internal Assessment will include:
(a) Written tests comprising of short
n o t e s a n d c r e a t i v e w r i t i n g
experiences,
(b) OSCE based clinical scenarios /
viva voce.
Eligibility to appear for
University Examinations
in respect of Attendance
ATTENDANCE: 75% attendance in a
subject for appearing in the examination
is compulsory inclusive of attendance in
non-lecture teaching i.e. seminars, group
discussions, tutorials, demonstrations,
practicals, hospital (Teritary Secondary,
Primary) posting and bed side clinics
etc.”
Attendance requirements are 75% in
theory and 80% in ractical /clinical for
eligibility to appear for the examinations
in that subject. In subjects that are taught
in more than one phase – the learner must
have 75% attendance in theory and 80%
in practical in each phase of instruction
in that subject. 75% attendance in
Professional Development Programme
(AETCOM Module) is required for
e l i g i b i l i t y t o a p p e a r f o r fi n a l
examination in each professional year.
Marks for the Practical paper
Pattern of Practical Paper
Viva marks added in
Internal Assessment marks
Calculation of Internal Assessment (IA) marks
S.No
5
6
7
8
9
10
Salient Feature GMER 1997 GMER 2019
Marks=30 Marks=100
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00049.2
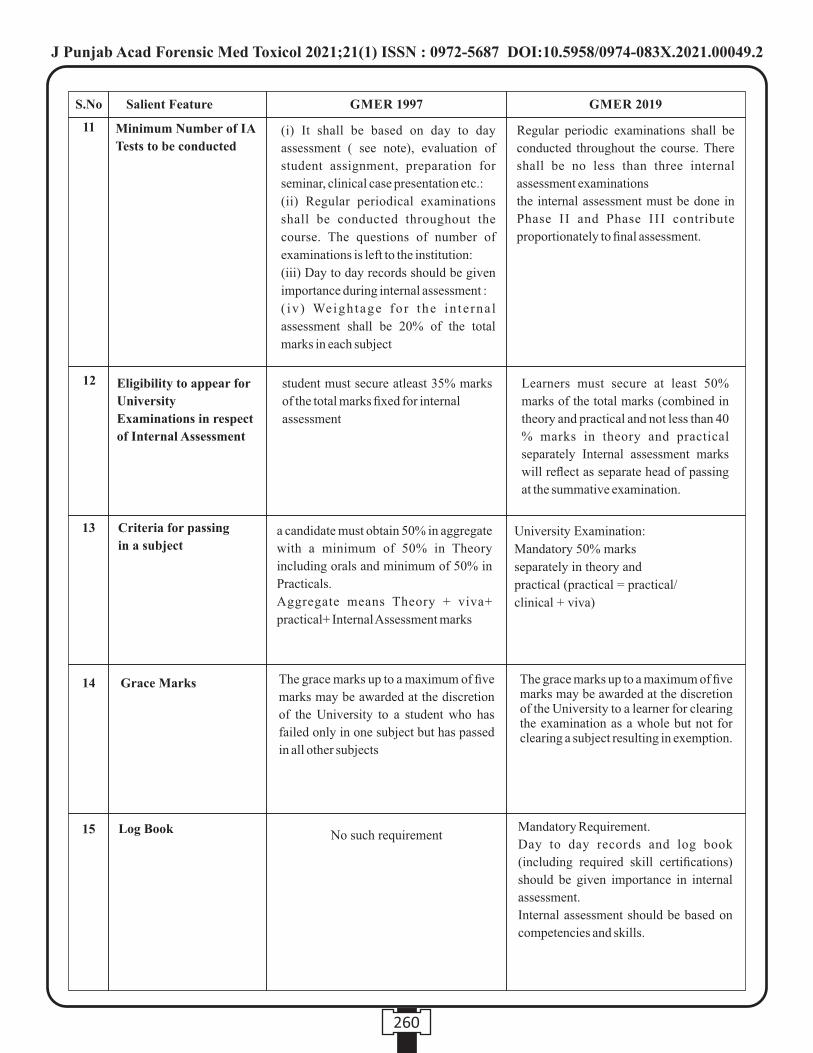
260
Minimum Number of IA
Tests to be conducted(i) It shall be based on day to day
assessment ( see note), evaluation of
student assignment, preparation for
seminar, clinical case presentation etc.:
(ii) Regular periodical examinations
shall be conducted throughout the
course. The questions of number of
examinations is left to the institution:
(iii) Day to day records should be given
importance during internal assessment :
( iv ) Weigh tage fo r the in te rna l
assessment shall be 20% of the total
marks in each subject
Regular periodic examinations shall be
conducted throughout the course. There
shall be no less than three internal
assessment examinations
the internal assessment must be done in
Phase II and Phase III contribute
proportionately to final assessment.
Eligibility to appear for
University
Examinations in respect
of Internal Assessment
student must secure atleast 35% marks
of the total marks fixed for internal
assessment
Learners must secure at least 50%
marks of the total marks (combined in
theory and practical and not less than 40
% marks in theory and practical
separately Internal assessment marks
will reflect as separate head of passing
at the summative examination.
Criteria for passing
in a subjecta candidate must obtain 50% in aggregate
with a minimum of 50% in Theory
including orals and minimum of 50% in
Practicals.
Aggregate means Theory + viva+
practical+ Internal Assessment marks
University Examination:
Mandatory 50% marks
separately in theory and
practical (practical = practical/
clinical + viva)
Grace Marks The grace marks up to a maximum of five
marks may be awarded at the discretion
of the University to a student who has
failed only in one subject but has passed
in all other subjects
The grace marks up to a maximum of five marks may be awarded at the discretion of the University to a learner for clearing the examination as a whole but not for clearing a subject resulting in exemption.
Log Book No such requirementMandatory Requirement.
Day to day records and log book
(including required skill certifications)
should be given importance in internal
assessment.
Internal assessment should be based on
competencies and skills.
S.No
11
12
13
14
15
Salient Feature GMER 1997 GMER 2019
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00049.2
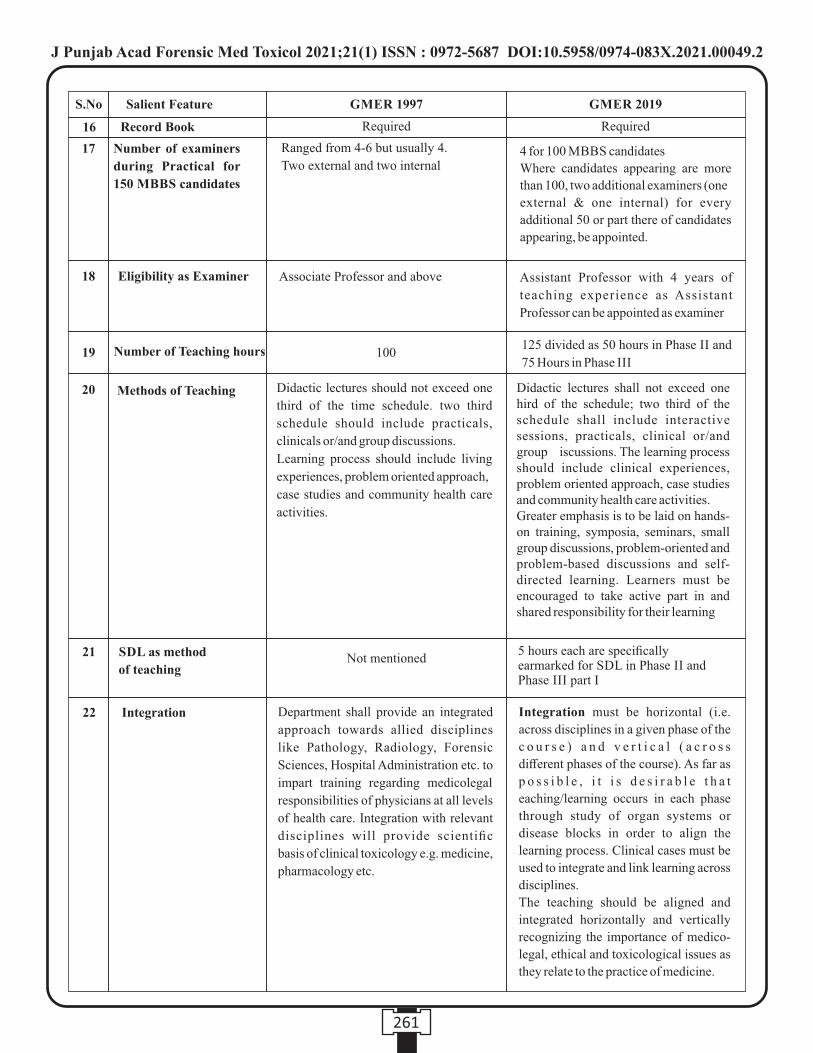
19
20
Number of Teaching hours 100125 divided as 50 hours in Phase II and
75 Hours in Phase III
Methods of Teaching Didactic lectures should not exceed one
third of the time schedule. two third
schedule should include practicals,
clinicals or/and group discussions.
Learning process should include living
experiences, problem oriented approach,
case studies and community health care
activities.
Didactic lectures shall not exceed one hird of the schedule; two third of the schedule shall include interactive sessions, practicals, clinical or/and group iscussions. The learning process should include clinical experiences, problem oriented approach, case studies and community health care activities. Greater emphasis is to be laid on hands-on training, symposia, seminars, small group discussions, problem-oriented and problem-based discussions and self-directed learning. Learners must be encouraged to take active part in and shared responsibility for their learning
21 SDL as method
of teachingNot mentioned
5 hours each are specifically earmarked for SDL in Phase II and Phase III part I
22 Integration Department shall provide an integrated
approach towards allied disciplines
like Pathology, Radiology, Forensic
Sciences, Hospital Administration etc. to
impart training regarding medicolegal
responsibilities of physicians at all levels
of health care. Integration with relevant
disciplines will provide scientific
basis of clinical toxicology e.g. medicine,
pharmacology etc.
Integration must be horizontal (i.e.
across disciplines in a given phase of the
c o u r s e ) a n d v e r t i c a l ( a c r o s s
different phases of the course). As far as
p o s s i b l e , i t i s d e s i r a b l e t h a t
eaching/learning occurs in each phase
through study of organ systems or
disease blocks in order to align the
learning process. Clinical cases must be
used to integrate and link learning across
disciplines.
The teaching should be aligned and
integrated horizontally and vertically
recognizing the importance of medico-
legal, ethical and toxicological issues as
they relate to the practice of medicine.
S.No
16
17
18
Salient Feature GMER 1997 GMER 2019
Record Book Required Required
Number of examiners
during Practical for
150 MBBS candidates
Ranged from 4-6 but usually 4.
Two external and two internal4 for 100 MBBS candidates
Where candidates appearing are more
than 100, two additional examiners (one
external & one internal) for every
additional 50 or part there of candidates
appearing, be appointed.
Eligibility as Examiner Associate Professor and above Assistant Professor with 4 years of
teaching experience as Assistant
Professor can be appointed as examiner
261
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00049.2

262
S.No
23
24
25
Salient Feature GMER 1997 GMER 2019
Attitude, Ethics and Communication (Aetcom) Module
No formal Teaching At least one question in each paper of the
c l in ica l spec ia l t i es should tes t
knowledge - competencies acquired
during the professional development
programme (AETCOM module); Skills
competencies acquired during the
Professional Development programme
(AETCOM module) must be tested
during clinical, practical and viva.**
Limit of Teaching
Foundation Course
Observation of Autopsy cases
ndTo 2 Professional MBBS and optional postings in Internship
Not there
Not specifically mentioned
With Aetcom, we can start teaching from Phase I till internship.
One month foundation course has specific skill component 2 F as “Documentation”
FM 14.15 specifically mentions that Conduct & prepare post-mortem examination report of varied etiologies (at least 15) in a simulated/ supervised environment
*Distribution of marks may vary slightly from University to University
** Aetcom Module is a good opportunity for the faculty of forensic medicine as many topics directly relate to our branch so we
must grab this opportunity and own it. It will definitely increase the importance of the subject of forensic medicine. Following
Modules can be taught by faculty of forensic medicine :
Module 2.7 : Case studies on autonomy and decision making
Module 3.4 : Case studies in bioethics-confidentiality
Module 4.2: Case studies in medico-legal and ethical Situations
Module 4.3: Case studies in medico-legal and ethical Situations
Module 4.9: Medical Negligence
REFERENCES:
1. Medical Council of India (MCI). Competency Based Undergraduate Curriculum for the Indian Medical Graduate. Vol. 1.
MCI; Medical Council of India (MCI); 2018. p. 28-258. Available from:
https://www.nmc.org.in/wp-content/uploads/2020/01/UG-Curriculum-Vol-I-III.pdf. [Last accessed on 2021 August 30].
2. Medical Council of India (MCI). Aetcom Booklet Available from:
https://www.nmc.org.in/information-desk/for-colleges/ug-curriculum/[Last accessed on 2021 August 30].
3. Medical Council of India (MCI). Skill Training Module Booklet Available from:
https://www.nmc.org.in/information-desk/for-colleges/ug-curriculum/[Last accessed on 2021 August 30]
4. Regulations on Graduate Medical Education (Amendment) 2019. Available from:
https://egazette.nic.in/WriteReadData/2019/213805.pdf[Last accessed on 2021 August 30]
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687 DOI:10.5958/0974-083X.2021.00049.2
INSTRUCTIONS TO AUTHORS
•Unpublished, Ethical, Un-Plagiarised original manuscript written in English should be sent to: Dr. Parmod Kumar Goyal,
Editor-in-Chief, Journal of Punjab Academy of Forensic Medicine and Toxicology by email at:
•Images (Good quality) should be sent separately in JPEG format.
•References should be in Vancouver Style only.
The Publication Particulars
The JPAFMAT is the official publication of the Punjab Academy of Forensic Medicine & Toxicology, published since 2001.
The Contents of the Journal
The journal accepts a range of articles of interest, under several feature sections as follows:
Original Papers: Includes conventional observational and experimental research.
Commentary: Intended for Reviews, Case Reports, Preliminary Report and Scientific Correspondences.
Letter to the Editor
Designed to be an avenue for dialogue between the authors of the papers published in the journal and the readers restricted to the
options expressing reviews, criticisms etc. It could also publish letters on behalf of the current affairs in the field of Forensic
Medicine in the country.
Editorial
Intended as a platform, for the Editor-in-Chief and for others with a keen interest in forensic medicine that wished to comment on the
current affairs.
Special Features
In the History of Indian Forensic Medicine, Book Review, Abstracts, Announcement etc, which appear frequently,
but not necessarily in every issue.
News and Notes
Intended for providing information of members and activities of the Academy and other such other organizations affiliated to the
Academy may appear frequently and not in every issue.
General Principles
The text of observational and experimental articles is usually (but not necessarily) divided into the following sections: Introduction,
Methods, Results, and Discussion. This so-called “IMRAD” structure is not an arbitrary publication format but rather a direct
reflection of the process of scientific discovery. Long articles may need subheadings within some sections (especially Results and
Discussion) to clarify their content. Other types of articles, such as case reports, reviews, and editorials, probably need to be
formatted differently. Electronic formats have created opportunities for adding details or whole sections, layering information,
cross linking or extracting portions of articles, and the like only in the electronic version. Double spacing all portions of the
manuscript— including the title page, abstract, text, acknowledgments, references, individual tables, and legends—and generous
margins make it possible for editors and reviewers to edit the text line by line and add comments and queries directly on the paper
copy. If manuscripts are submitted electronically, the files should be double-spaced to facilitate printing for reviewing and editing.
Authors should number all of the pages of the manuscript consecutively, beginning with the title page, to facilitate the editorial
process.
International Uniform Requirements
Please visit http://www.icmje.org/ for detailed instructions for manuscript submission.
Note : Manuscript handling charges Rs. 1500/- to be paid after acceptance for Indian Authors.
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687
263
1 Dr. R.K. Gorea
2 Late Dr. Sat Pal Garg
3 Dr. D.S. Bhullar
4 Late Dr. A.S. Thind
5 Dr. Hakumat Rai
6 Dr. K.K. Aggarwal
7 Dr. Jaswinder Singh
8 Dr. Karamjit Singh
9 Dr. Harjinder Singh
10 Dr. Virender Pal Singh
11 Dr. Ashok Chanana
12 Dr. J.S. Dalal
13 Dr. Jagdish Gargi
14 Dr. R.S. Parsad
15 Late Dr. Ajit Singh
16 Dr. Harish Tuli
17 Dr. S.K. Bal
18 Dr. S.S. Sandhu
19 Dr. Akashdeep Aggarwal
20 Dr. Kuldeep Singh
21 Dr. Vishal Garg
22 Dr. S.S. Oberoi
23 Late Dr. Ram Lubhaya
24 Dr. Amandeep Singh
25 Dr. Harkirat Singh
26 Dr. I.S. Bagga
27 Dr. Harpreet Singh
28 Dr. Parminder Singh
29 Dr. Anil Garg
30 Dr. O.P. Aggarwal
31 Dr. Gaurav Sharma
32 Late Dr. Madhur Tayal
33 Dr. Gurmanjit Rai Mann
34 Dr. Didar Singh
35 Dr. Kuldeep Singh
36 Dr. Pankaj Gupta
37 Dr. Karam Singh
38 Dr. Baljit Singh
39 Dr. Puneet Khurana
40 Dr. Puneet Arora
41 Dr. Prabhsharan Singh
42 Dr. Dildar Singh
43 Dr. Mian Abdur Rashid
44 Dr. Shilekh Mittal
45 Dr. B.R. Sharma
46 Dr. D.Harish
47 Dr. Krishna D. Chavali
48 Dr. Ashwani Kumar
49 Dr. Vikram Bains
50 Late Dr. Kirpal Singh
51 Dr. Gurbachan Singh
52 Dr. Sangeet Dhillon
53 Dr. Sukhbir Singh Chauhan
54 Dr. Parminder Singh Bhatti
55 Dr. Rakesh Kumar
56 Dr. Jagbir Singh
57 Dr. Karnveer Singh
58 Dr. Rajiv K. Chowdhary
59 Dr. Parmod Kumar Goyal
60 Dr. Ajay Kumar
61 Dr RK Sharma
62 Dr Brij M. Gupta
63 Dr Sunil Gambhi
64 Dr Vijal Pal Khangwal
65 Dr Rajiv Joshi
66 Dr Manpreet Kaul
67 Dr Sheikh AnayatUllah
68 Dr Satinder Pal Singh
69 Dr Preetinder Singh Chahal
70 Dr Kulbhushan Garg
71 Dr Imran Sabri
72 Dr Bindu Aggarwal
73 Dr Adish Goyal
74 Dr Charak Sangwan
75 Dr Pardeep Singh
76 Dr Ishwer Tayal
77 Dr Ripan Chanana
78 Dr Gurvinder Singh Kakkar
79 Dr Ravdeep Singh
80 Dr Rohit Kumar Singal
81 Dr Prabhdeep Singh
82 Dr Jasbir Singh
83 Dr Jatinder Pal Singh
84 Dr Alok Kandpal
No. Name No. Name85 Dr Iram Khan
86 Dr Charanpreet K. Pawar
87 Dr Mukul Chopra
88 Dr Mohit Gupta
89 Dr Rahul Chawla
90 Dr Maneel Grover
91 Dr Y.S. Bansal
92 Dr C.S. Gautam
93 Dr S.P. Mandal
94 Dr Murli . G
95 Dr Anil Kumar Mittal
96 Dr G.A. Sunil Kumar Sharma
97 Dr Abhishek Yadav
98 Dr Jagdev Kullar
99 Dr Gurpreet Kaur Randhawa
100 Dr Gursirat Singh Khokhar
101 Dr Saginder Samara
102 Dr Saginder Samaraj
103 Dr Neha Sharma
104 Dr Sunil Mahajan
105 Dr Harshdeep Kashyap
106 Dr Kiran Kumar
107 Dr Swati Tyagi
108 Dr Mini
109 Dr Mandeep Kaur
110 Dr Gurinder Singh
111 Dr Minal
112 Dr Kanchan Jyoti Heera
113 Dr Manpinder Kaur Bhullar
114 Dr Arashdeep Singh
115 Dr Chamandeep Singh Bains
116 Dr Maninder Singh
117 Dr Akhilesh Agarwal
118 Dr Guneet
119 Dr Hitesh Bhatia
120 Dr. Deep Rattan Mittal
121 Dr. Arun Kumar Maria
122 Dr. S Valliappan
123 Dr. Preet Inder Singh
124 Dr. Harvinder Singh Chhabra
125 Dr. Bhoj Kumar Sahu
126 Dr. Amarnath Mishra
No. Name
264
Life Members (PAFMAT)
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687

127 Dr. Shekhar Chumber
128 Dr. Navroz Goyal
129 Dr. Gurjeet Singh
130 Dr. Deepika Kanwar
131 Dr. Mohd. Amjad Bhatt
132 Dr. Nikhil Mehta
133 Dr. Charan Kamal
134 Dr. Amit Singla
135 Dr. Sukhdeep Singh
136 Dr. Munish Kumar
137 Dr. Arindam Chatterjee
138 Dr. Ranjodh Jeet Singh
139 Dr. Kanika Kohli
140 Dr. Vinka Maini
141 Dr. Ravi Tejpal
142 Dr. Preet Mohinder Singh
143 Dr. Satbir Singh
144 Dr. Kamaljit Singh
145 Dr. Mrinal Kanti Jha
146 Dr. Vijay Arora
147 Dr. Vivek Srivastava
148 Dr. Pankaj Chhikara
149 Dr. Lalit Kumar
150 Dr. Prem Chandra
Srivastava
151 Dr. Niraj Kumar
152 Dr. Om Parkash Saini
153 Dr. Rajesh Kumar Verma
154 Dr. Shailender Kumar
155 Dr. B.L. Chaudhary
156 Dr. Parmod Kumar Saini
157 Dr. Rajendra Singh Kulhari
158 Dr. Nidhi Sachdeva
Agarwal
159 Dr. Rajeev Varma
160 Dr. Pragnesh Bharatkumar
Parmar
161 Dr. Yatiraj Singi
162 Dr. Navpreet Kaur
163 Dr. Kunal Khanna
164 Dr. Smitha Rani Shetty
165 Dr. Vivekanshu Verma
166 Dr. B.V. Naga Mohan Rao
167 Dr. Anju Gupta
168 Dr. Guriqbal Singh
169 Dr. Prashanthi Krishna Dharma
170 Dr. Amarjit Singh
171 Dr. Keshav Soni
172 Dr. Faisal Nasim Gilani
173 Dr. Ashok Sagar
174 Dr. Suresh Chand
175 Dr. Jaswinder Singh
176 Dr. Prateek Rastogi
177 Dr. Varun Garg
178 Dr. Hitesh Chawla
179 Dr. Sanjeev Buri
180 Dr. Sunil M Doshi
181 Dr. Sanjay Kumar
182 Dr. Akhilesh Pathak
183 Dr. Raghvendra Kumar Vidua
184 Dr. Jitendra Kumar Gupta
185 Dr. Manoj Kumar Pathak
186 Dr. Surendra Kumar Pandey
187 Dr. Mayank Gupta
188 Dr. Amandeep Kaur
189 Dr. Mukesh Kumar Meena
190 Dr. Jitender Kumar Jakhar
191 Dr. Kamal Singla
192 Dr. Rajender Kumar Saini
193 Dr. Chandra Pal
194 Dr. Rattan Singh
195 Dr. Jyoti Barwa
196 Dr. Chaitanya Mittal
197 Dr. Atul Shankarrao Keche
198 Dr. Niranjan Sahoo
199 Dr. Vanshikha
200 Dr. Pulkit Girdhar
201 Dr. Alwin Varghese
202 Dr. Karan Pramod
203 Dr. Balbir Kaur
204 Dr. Malvika Lal
205 Dr. Shashank Shekhar Jha
No. Name No. Name
Life Members (PAFMAT)
265
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687
Punjab Academy of Forensic Medicine & Toxicology
Undertaking format for organizing PAFMATCON/Any Other CME/Workshop
under the banner of PAFMAT
To
The President / General Secretary
Punjab Academy of Forensic Medicine & Toxicology
Subject : Consent for Holding the Conference.
Dear Sir
As discussed and decided in the general / executive body meeting of the academy dated ……………………….at
……..……………………………………(name the venue), I give my consent to hold the ………………annual conference of
Punjab Academy of Forensic Medicine & Toxicology on ..……………………...................……(Tentative date) in
……………………………………… (Name of the medical college / venue)
Subject to the following:-
a. The conference and / or the CME programme shall be under the auspices of Punjab Academy of Forensic Medicine &
Toxicology. The banner showing the same will be displayed at a suitable area on the main venue.
b. The President and the General Secretary of the Academy will be suitably seated on the dais during the inaugural
programme. The President will address the gathering about the policies, programs or other relevant aspects of the
Academy. The General Secretary will read out the annual report.
c. The registration of the President, General Secretary, Secretary Finance and the Editor-in-Chief of the Academy will be
complimentary.
d. The conference will get accredited with at least 4 CME Credit hours from Punjab Medical Council.
e. The President and / or General Secretary of the Academy along with one member of Punjab Medical Council will be the
signatory to the certificate issued to delegate attending the conference / CME / workshop.
f. The organizing committee will send formal invitation to all the office bearers of the academy.
g. The Journal of the Academy will be released during the inaugural programme. The Editor-in-Chief and the Joint Editor
will be invited to the dais for the release ceremony.
h. The Organizing Secretary of the programme will hand over the list of the delegates to the General Secretary of the
Academy at the end of the conference.
i. The Organizing Committee will collect Rs. 100/- ( Rupees one hundred only) per delegate of the programme and will
deposit the collected amount in the account of the Journal of PAFMAT / hand over the Cheque for the collected amount
favoring Journal of Pb. Aca. Of Forensic Med. & Toxicology to the Editor-in-Chief after the conference.
Sd/-
Organizing Chairman / Secretary
Name:
PAFMATCON :
266
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687
Format of Application for Subscription of Journal
To
The Editor-in-Chief
Journal of Punjab Academy of Forensic Medicine & Toxicology (JPAFMAT)
Dear Sir,
I wish to Subscribe the Journal of Punjab Academy of Forensic Medicine & Toxicology. I am furnishing the required
particulars below with a request to subscribe the Journal. The fee for Journal of Punjab Academy of Forensic Medicine is enclosed.
PARTICULARS
1. Full Name ( in block letters )
2. Father's / Husband's name
3. Date of Birth
4. Qualification ( with name of university & date of passing )
5. Official Designation & Place of Posting
6. Permanent Address
7. Address for Correspondence ( subsequent change of address to be intimated)
8. Phone No. & Email
9. Photo
10. Copy of Medical Council Registration Certificate
Place Yours Sincerely
Date
(Signature)
Note : 1. Payment can be made through online transfer in the Journal Account. For any query related to subscription of the
Journal, feel free to talk/whattsapp on mobile no. 98760-05211
2. The above information can be sent by email to editor-in-chief
3. Subscribers of the Journal are entitled for Five (5) CME credit hours per year as per CME Accredition Guidelines
issued by Punjab Medical Council.
267
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687

268
J Punjab Acad Forensic Med Toxicol 2021;21(1) ISSN : 0972-5687
Glimpse of PAFMATCON-2021
J Punjab Acad Forensic Med Toxicol 2021;21 (1) ISSN : 0972-5687
Editorial Board
NationalAdvisoryBoardDr T.D. DograDr J.S. DalalDr R.K. GoreaDr O P AggarwalDr K K AggarwalDr Balbir KaurDr K. VijDr Dalbir SinghDr Sanjoy DassDr E.J. RodrigeusDr Gurudatta PawarDr D.S. BadkurDr Jagadeesh. N.Dr Pramod KumarDr C.B. JaniDr. Vijal Pal Khanagwal
EditorialCommittee:Dr S. S. OberoiDr Sangeet DhillonDr Ishwar TayalDr Kuldeep SinghDr Harjinder SinghDr Harpreet SinghDr Parul KherDr Antara DebBarmanDr Gurpreet S. SandhuDr S K DhattarwalDr Jaskaran SinghDr Manoj PathakDr Jaswinder SinghDr PC SrivastavaDr Om Parkash SainiDr OP MurtiDr V. V. PillayDr. Ranjit Immanuel JamesDr Shiv KochharDr Mukesh Yadav
Dr R.K. SharmaDr N K AggarwalDr Amitabh ShrivastvaDr Shankar M. BakkannavarDr. Samita SinhaDr. Manjot KaurMrs. Ritika Gupta, FSL BathindaDr. Nidhi SachdevaDr. Sindhu Sudha SahooDr. Virendar Pal SinghDr. Shilekh MittalDr. Puneet KhuranaDr. Manpreet KaulDr. Rajvinder SinghDr. Priyamvada KurvetiDr. Amarnath MishraDr. Anupama RainaDr. Balbir KaurDr. ShruthiDr. Vijay Kautilaya
SubscriptionratesforYear2021
Personal: Rs. 1,000/- Institutions: Rs. 5,000/-
PostalChargesExtra
l Subscription request be sent on email to [email protected]
l Payments be made in Bank Account of Journal of Punjab Academy of Forensic Medicine (A/c No. 65075504236, State Bank of India, Branch Rajindra Hospital Patiala, IFS Code SBIN0050263
Printed&Publishedby:Dr Parmod Kumar Goyal
Professor & Head,Department of Forensic Medicine & ToxicologyAdesh Institute of Medical Sciences & Research,
Bathinda (Pb.) India M. 9876005211, 0164-5055073E-mail: [email protected]
Printedat:Subhash Mittal Printing Press
Hospital Bazar, BathindaM. 99880-11022
e-mail: [email protected]
Editor-in-ChiefDr Parmod Kumar Goyal
Joint EditorDr Amandeep Singh
Dr. Vivek SrivastavaDr. Pardeep SinghDr. Monika GuptaDr. Tanvir Kaur SidhuDr. Sandeep KaurDr. Priti ChaudharyDr. Vijay SuriDr. Saranpal SinghDr. Tanuj KanchanDr. Raghuvendra K. ViduaDr. Vivek Kumar (Siliguri)Dr. Pragnesh ParmarDr. Imran SabriDr. Meenakshi AggarwalDr. Anupama RainaDr. Chaitanya MittalDr. Krishan Dutt ChavaliDr. Rajendra SinghDr. Yatriraj SingiDr. Vikram Palimar
ManuscriptReviewCommittee
J Punjab Acad Forensic Med Toxicol 2021;21 (1) ISSN : 0972-5687
Related Documents











