1| Wong Pumping the Brakes on Continuous Infusion: Prevention of Peptic Ulcer Rebleeding Dana Wong, Pharm.D. PGY2 Internal Medicine Pharmacy Resident South Texas Veterans Health Care System, San Antonio, TX Division of Pharmacotherapy, The University of Texas at Austin College of Pharmacy Pharmacotherapy Education and Research Center, University of Texas Health Science Center at San Antonio October 23, 2015 Learning Objectives 1. Describe the etiology, risk factors, and classification of peptic ulcers 2. Evaluate current literature comparing continuous infusion and intermittent dosing of proton pump inhibitors (PPIs) for prevention of peptic ulcer rebleeding 3. Recommend appropriate dosing strategies for PPIs for prevention of peptic ulcer rebleeding

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1| Wong
Pumping the Brakes on Continuous Infusion:
Prevention of Peptic Ulcer Rebleeding
Dana Wong, Pharm.D.
PGY2 Internal Medicine Pharmacy Resident
South Texas Veterans Health Care System, San Antonio, TX
Division of Pharmacotherapy, The University of Texas at Austin College of Pharmacy
Pharmacotherapy Education and Research Center,
University of Texas Health Science Center at San Antonio
October 23, 2015
Learning Objectives
1. Describe the etiology, risk factors, and classification of peptic ulcers
2. Evaluate current literature comparing continuous infusion and intermittent dosing of proton pump
inhibitors (PPIs) for prevention of peptic ulcer rebleeding
3. Recommend appropriate dosing strategies for PPIs for prevention of peptic ulcer rebleeding

2| Wong
I. Upper Gastrointestinal (GI) Bleeding and Peptic Ulcers
A. Upper GI bleeding1-3
1. Diagnosed in 50-150 per 100,000 individuals per year
2. 300,000 hospitalizations per year
3. Mortality rate of 6-10% annually
4. Hospitalization costs >$2.5 billion per year
B. Causes of acute upper GI bleeding4
1. Peptic ulcer disease (PUD)— 40-79%
2. Gastritis/duodenitis—5-30%
3. Esophageal varices—6-21%
4. Mallory-Weiss tear—3-15%
5. Esophagitis—2-8%
6. Gastric cancer—2-3%
C. Symptoms of bleed4
1. Anemia, hemodynamic instability
2. Vomiting fresh blood, “coffee ground” emesis, melena, hematochezia, abdominal pain
D. Peptic ulcer disease
1. Three common forms5
a. Nonsteroidal anti-inflammatory drug (NSAID)-induced (~30%)
b. Helicobacter pylori (H. pylori) positive (~20%)
c. Stress-related mucosal damage (75-100%)
2. Risk factors for peptic ulcers1: smoking, alcohol, corticosteroids, oral anticoagulants
3. Pathophysiology6:
Figure 1. http://www.hopkinsmedicine.org
4. Forrest classification7-8
Stigmata of
hemorrhage
Forrest
classification
Prevalence Rebleeding
rate
Mortality
Active spurting
bleeding
IA
12% 55% 11%
Active oozing
bleeding
IB
Non-bleeding visible
vessel
IIA 8% 43% 11%
Adherent clot IIB 8% 22% 7%
Flat spot IIC 16% 10% 3%
Clean base III 55% 5% 2%
Table 1.
3| Wong
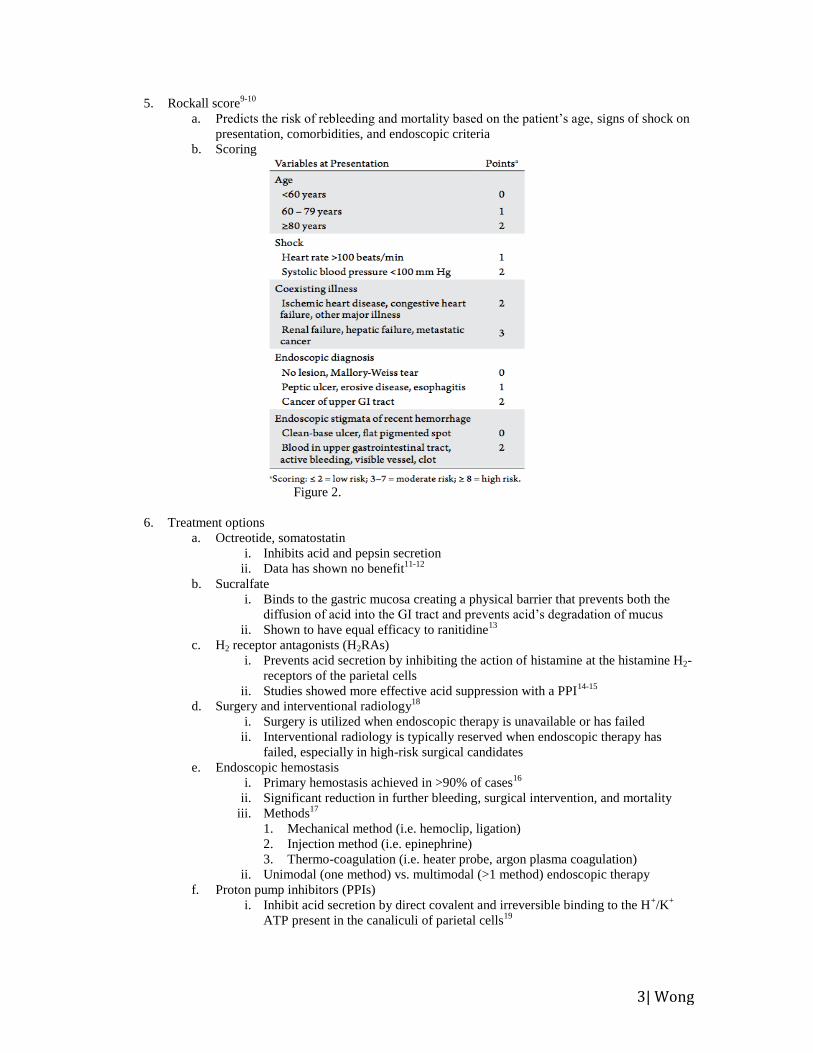
5. Rockall score9-10
a. Predicts the risk of rebleeding and mortality based on the patient’s age, signs of shock on
presentation, comorbidities, and endoscopic criteria
b. Scoring
Figure 2.
6. Treatment options
a. Octreotide, somatostatin
i. Inhibits acid and pepsin secretion
ii. Data has shown no benefit11-12
b. Sucralfate
i. Binds to the gastric mucosa creating a physical barrier that prevents both the
diffusion of acid into the GI tract and prevents acid’s degradation of mucus
ii. Shown to have equal efficacy to ranitidine13
c. H2 receptor antagonists (H2RAs)
i. Prevents acid secretion by inhibiting the action of histamine at the histamine H2-
receptors of the parietal cells
ii. Studies showed more effective acid suppression with a PPI14-15
d. Surgery and interventional radiology18
i. Surgery is utilized when endoscopic therapy is unavailable or has failed
ii. Interventional radiology is typically reserved when endoscopic therapy has
failed, especially in high-risk surgical candidates
e. Endoscopic hemostasis
i. Primary hemostasis achieved in >90% of cases16
ii. Significant reduction in further bleeding, surgical intervention, and mortality
iii. Methods17
1. Mechanical method (i.e. hemoclip, ligation)
2. Injection method (i.e. epinephrine)
3. Thermo-coagulation (i.e. heater probe, argon plasma coagulation)
ii. Unimodal (one method) vs. multimodal (>1 method) endoscopic therapy
f. Proton pump inhibitors (PPIs)
i. Inhibit acid secretion by direct covalent and irreversible binding to the H+/K
+
ATP present in the canaliculi of parietal cells19
4| Wong
ii. Following endoscopic therapy, rebleeding within 72 hours is still prevalent (up
to 20%) and is associated with high mortality rate9
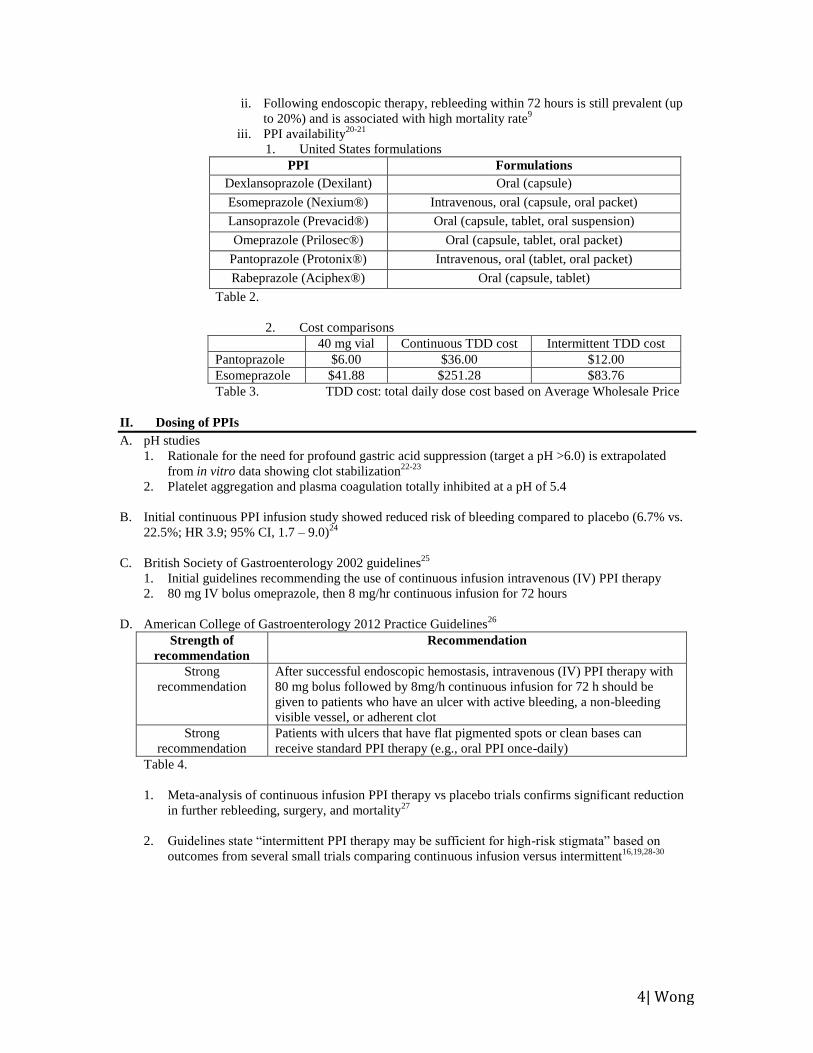
iii. PPI availability20-21
1. United States formulations
PPI Formulations
Dexlansoprazole (Dexilant) Oral (capsule)
Esomeprazole (Nexium®) Intravenous, oral (capsule, oral packet)
Lansoprazole (Prevacid®) Oral (capsule, tablet, oral suspension)
Omeprazole (Prilosec®) Oral (capsule, tablet, oral packet)
Pantoprazole (Protonix®) Intravenous, oral (tablet, oral packet)
Rabeprazole (Aciphex®) Oral (capsule, tablet)
Table 2.
2. Cost comparisons
40 mg vial Continuous TDD cost Intermittent TDD cost
Pantoprazole $6.00 $36.00 $12.00
Esomeprazole $41.88 $251.28 $83.76
Table 3. TDD cost: total daily dose cost based on Average Wholesale Price
II. Dosing of PPIs
A. pH studies
1. Rationale for the need for profound gastric acid suppression (target a pH >6.0) is extrapolated
from in vitro data showing clot stabilization22-23
2. Platelet aggregation and plasma coagulation totally inhibited at a pH of 5.4
B. Initial continuous PPI infusion study showed reduced risk of bleeding compared to placebo (6.7% vs.
22.5%; HR 3.9; 95% CI, 1.7 – 9.0)24
C. British Society of Gastroenterology 2002 guidelines25
1. Initial guidelines recommending the use of continuous infusion intravenous (IV) PPI therapy
2. 80 mg IV bolus omeprazole, then 8 mg/hr continuous infusion for 72 hours
D. American College of Gastroenterology 2012 Practice Guidelines26
Strength of
recommendation
Recommendation
Strong
recommendation
After successful endoscopic hemostasis, intravenous (IV) PPI therapy with
80 mg bolus followed by 8mg/h continuous infusion for 72 h should be
given to patients who have an ulcer with active bleeding, a non-bleeding
visible vessel, or adherent clot
Strong
recommendation
Patients with ulcers that have flat pigmented spots or clean bases can
receive standard PPI therapy (e.g., oral PPI once-daily)
Table 4.
1. Meta-analysis of continuous infusion PPI therapy vs placebo trials confirms significant reduction
in further rebleeding, surgery, and mortality27
2. Guidelines state “intermittent PPI therapy may be sufficient for high-risk stigmata” based on
outcomes from several small trials comparing continuous infusion versus intermittent16,19,28-30
5| Wong
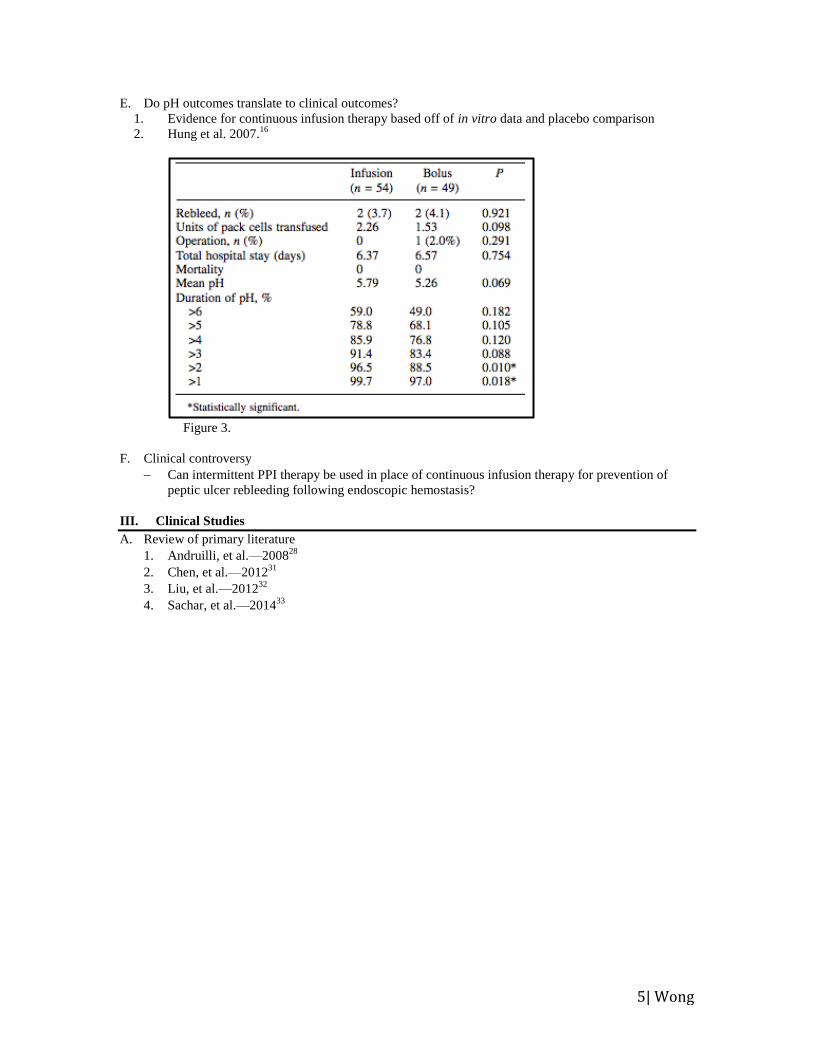
E. Do pH outcomes translate to clinical outcomes?
1. Evidence for continuous infusion therapy based off of in vitro data and placebo comparison
2. Hung et al. 2007.16
Figure 3.
F. Clinical controversy
Can intermittent PPI therapy be used in place of continuous infusion therapy for prevention of
peptic ulcer rebleeding following endoscopic hemostasis?
III. Clinical Studies
A. Review of primary literature
1. Andruilli, et al.—200828
2. Chen, et al.—201231
3. Liu, et al.—201232
4. Sachar, et al.—201433
6| Wong
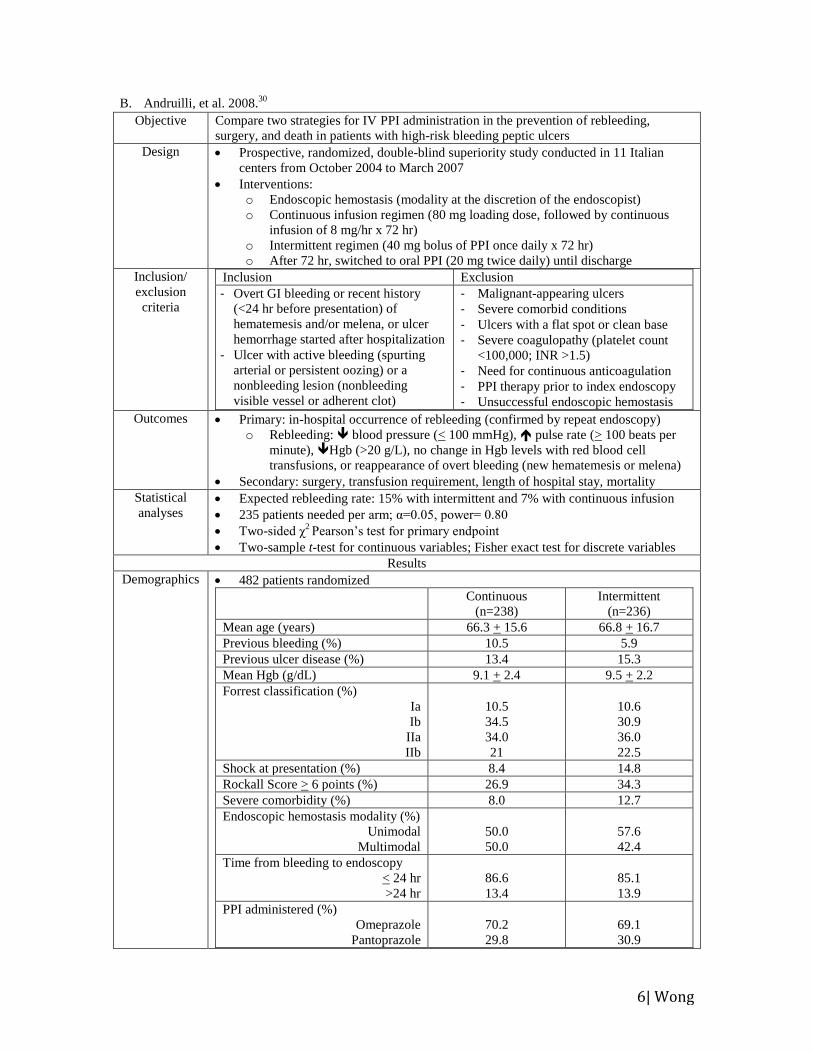
B. Andruilli, et al. 2008.30
Objective Compare two strategies for IV PPI administration in the prevention of rebleeding,
surgery, and death in patients with high-risk bleeding peptic ulcers
Design Prospective, randomized, double-blind superiority study conducted in 11 Italian
centers from October 2004 to March 2007
Interventions:
o Endoscopic hemostasis (modality at the discretion of the endoscopist)
o Continuous infusion regimen (80 mg loading dose, followed by continuous
infusion of 8 mg/hr x 72 hr)
o Intermittent regimen (40 mg bolus of PPI once daily x 72 hr)
o After 72 hr, switched to oral PPI (20 mg twice daily) until discharge
Inclusion/
exclusion
criteria
Inclusion Exclusion
- Overt GI bleeding or recent history
(<24 hr before presentation) of
hematemesis and/or melena, or ulcer
hemorrhage started after hospitalization
- Ulcer with active bleeding (spurting
arterial or persistent oozing) or a
nonbleeding lesion (nonbleeding
visible vessel or adherent clot)
- Malignant-appearing ulcers
- Severe comorbid conditions
- Ulcers with a flat spot or clean base
- Severe coagulopathy (platelet count
<100,000; INR >1.5)
- Need for continuous anticoagulation
- PPI therapy prior to index endoscopy
- Unsuccessful endoscopic hemostasis
Outcomes Primary: in-hospital occurrence of rebleeding (confirmed by repeat endoscopy)
o Rebleeding: blood pressure (< 100 mmHg), pulse rate (> 100 beats per
minute), Hgb (>20 g/L), no change in Hgb levels with red blood cell
transfusions, or reappearance of overt bleeding (new hematemesis or melena)
Secondary: surgery, transfusion requirement, length of hospital stay, mortality
Statistical
analyses Expected rebleeding rate: 15% with intermittent and 7% with continuous infusion
235 patients needed per arm; α=0.05, power= 0.80
Two-sided χ2 Pearson’s test for primary endpoint
Two-sample t-test for continuous variables; Fisher exact test for discrete variables
Results
Demographics 482 patients randomized
Continuous
(n=238)
Intermittent
(n=236)
Mean age (years) 66.3 + 15.6 66.8 + 16.7
Previous bleeding (%) 10.5 5.9
Previous ulcer disease (%) 13.4 15.3
Mean Hgb (g/dL) 9.1 + 2.4 9.5 + 2.2
Forrest classification (%)
Ia
Ib
IIa
IIb
10.5
34.5
34.0
21
10.6
30.9
36.0
22.5
Shock at presentation (%) 8.4 14.8
Rockall Score > 6 points (%) 26.9 34.3
Severe comorbidity (%) 8.0 12.7
Endoscopic hemostasis modality (%)
Unimodal
Multimodal
50.0
50.0
57.6
42.4
Time from bleeding to endoscopy
< 24 hr
>24 hr
86.6
13.4
85.1
13.9
PPI administered (%)
Omeprazole
Pantoprazole
70.2
29.8
69.1
30.9
7| Wong
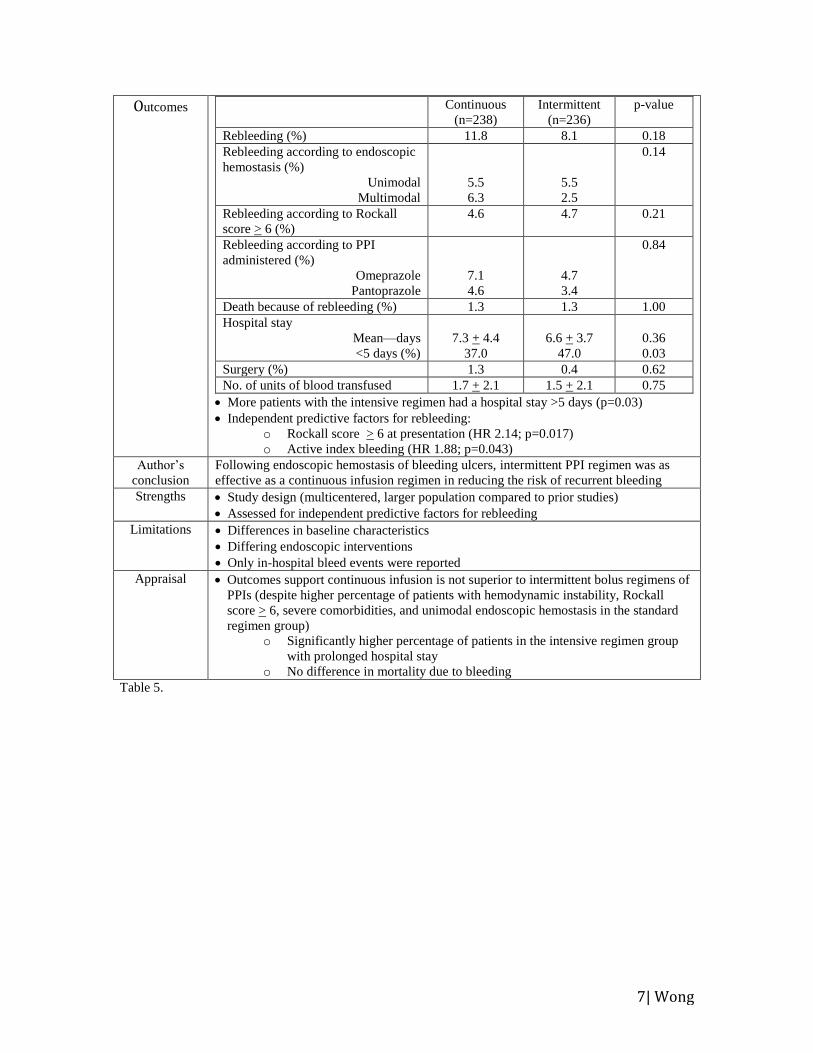
Outcomes Continuous
(n=238)
Intermittent
(n=236)
p-value
Rebleeding (%) 11.8 8.1 0.18
Rebleeding according to endoscopic
hemostasis (%)
Unimodal
Multimodal
5.5
6.3
5.5
2.5
0.14
Rebleeding according to Rockall
score > 6 (%)
4.6 4.7 0.21
Rebleeding according to PPI
administered (%)
Omeprazole
Pantoprazole
7.1
4.6
4.7
3.4
0.84
Death because of rebleeding (%) 1.3 1.3 1.00
Hospital stay
Mean—days
<5 days (%)
7.3 + 4.4
37.0
6.6 + 3.7
47.0
0.36
0.03
Surgery (%) 1.3 0.4 0.62
No. of units of blood transfused 1.7 + 2.1 1.5 + 2.1 0.75
More patients with the intensive regimen had a hospital stay >5 days (p=0.03)
Independent predictive factors for rebleeding:
o Rockall score > 6 at presentation (HR 2.14; p=0.017)
o Active index bleeding (HR 1.88; p=0.043)
Author’s
conclusion
Following endoscopic hemostasis of bleeding ulcers, intermittent PPI regimen was as
effective as a continuous infusion regimen in reducing the risk of recurrent bleeding
Strengths Study design (multicentered, larger population compared to prior studies)
Assessed for independent predictive factors for rebleeding
Limitations Differences in baseline characteristics
Differing endoscopic interventions
Only in-hospital bleed events were reported
Appraisal Outcomes support continuous infusion is not superior to intermittent bolus regimens of
PPIs (despite higher percentage of patients with hemodynamic instability, Rockall
score > 6, severe comorbidities, and unimodal endoscopic hemostasis in the standard
regimen group)
o Significantly higher percentage of patients in the intensive regimen group
with prolonged hospital stay
o No difference in mortality due to bleeding
Table 5.
8| Wong
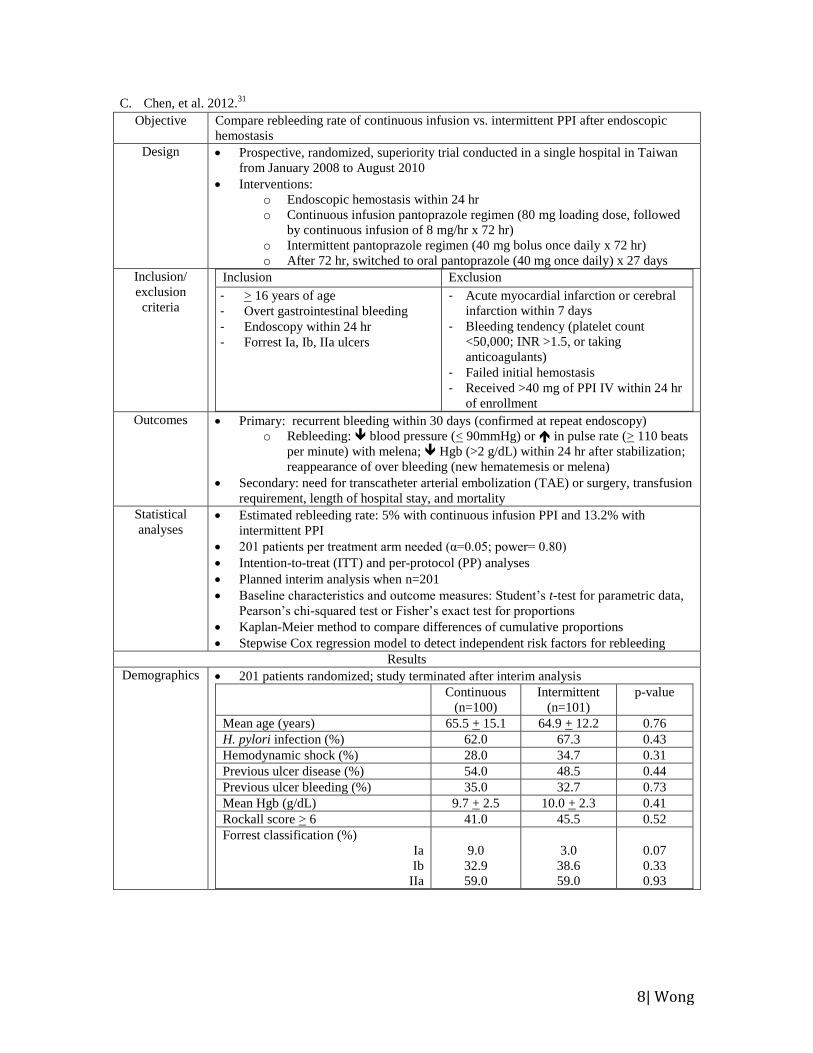
C. Chen, et al. 2012.31
Objective Compare rebleeding rate of continuous infusion vs. intermittent PPI after endoscopic
hemostasis
Design Prospective, randomized, superiority trial conducted in a single hospital in Taiwan
from January 2008 to August 2010
Interventions:
o Endoscopic hemostasis within 24 hr
o Continuous infusion pantoprazole regimen (80 mg loading dose, followed
by continuous infusion of 8 mg/hr x 72 hr)
o Intermittent pantoprazole regimen (40 mg bolus once daily x 72 hr)
o After 72 hr, switched to oral pantoprazole (40 mg once daily) x 27 days
Inclusion/
exclusion
criteria
Inclusion Exclusion
- > 16 years of age
- Overt gastrointestinal bleeding
- Endoscopy within 24 hr
- Forrest Ia, Ib, IIa ulcers
- Acute myocardial infarction or cerebral
infarction within 7 days
- Bleeding tendency (platelet count
<50,000; INR >1.5, or taking
anticoagulants)
- Failed initial hemostasis
- Received >40 mg of PPI IV within 24 hr
of enrollment
Outcomes Primary: recurrent bleeding within 30 days (confirmed at repeat endoscopy)
o Rebleeding: blood pressure (< 90mmHg) or in pulse rate (> 110 beats
per minute) with melena; Hgb (>2 g/dL) within 24 hr after stabilization;
reappearance of over bleeding (new hematemesis or melena)
Secondary: need for transcatheter arterial embolization (TAE) or surgery, transfusion
requirement, length of hospital stay, and mortality
Statistical
analyses Estimated rebleeding rate: 5% with continuous infusion PPI and 13.2% with
intermittent PPI
201 patients per treatment arm needed (α=0.05; power= 0.80)
Intention-to-treat (ITT) and per-protocol (PP) analyses
Planned interim analysis when n=201
Baseline characteristics and outcome measures: Student’s t-test for parametric data,
Pearson’s chi-squared test or Fisher’s exact test for proportions
Kaplan-Meier method to compare differences of cumulative proportions
Stepwise Cox regression model to detect independent risk factors for rebleeding
Results
Demographics 201 patients randomized; study terminated after interim analysis
Continuous
(n=100)
Intermittent
(n=101)
p-value
Mean age (years) 65.5 + 15.1 64.9 + 12.2 0.76
H. pylori infection (%) 62.0 67.3 0.43
Hemodynamic shock (%) 28.0 34.7 0.31
Previous ulcer disease (%) 54.0 48.5 0.44
Previous ulcer bleeding (%) 35.0 32.7 0.73
Mean Hgb (g/dL) 9.7 + 2.5 10.0 + 2.3 0.41
Rockall score > 6 41.0 45.5 0.52
Forrest classification (%)
Ia
Ib
IIa
9.0
32.9
59.0
3.0
38.6
59.0
0.07
0.33
0.93
9| Wong
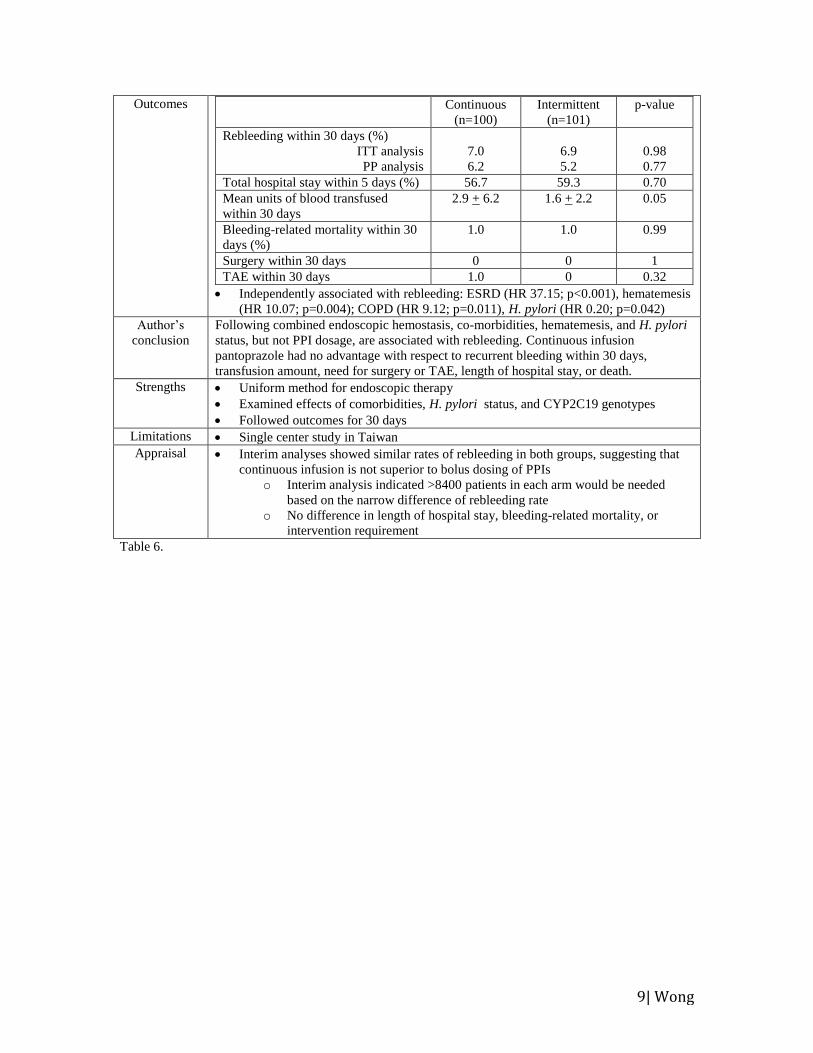
Outcomes Continuous
(n=100)
Intermittent
(n=101)
p-value
Rebleeding within 30 days (%)
ITT analysis
PP analysis
7.0
6.2
6.9
5.2
0.98
0.77
Total hospital stay within 5 days (%) 56.7 59.3 0.70
Mean units of blood transfused
within 30 days
2.9 + 6.2 1.6 + 2.2 0.05
Bleeding-related mortality within 30
days (%)
1.0 1.0 0.99
Surgery within 30 days 0 0 1
TAE within 30 days 1.0 0 0.32
Independently associated with rebleeding: ESRD (HR 37.15; p<0.001), hematemesis
(HR 10.07; p=0.004); COPD (HR 9.12; p=0.011), H. pylori (HR 0.20; p=0.042)
Author’s
conclusion
Following combined endoscopic hemostasis, co-morbidities, hematemesis, and H. pylori
status, but not PPI dosage, are associated with rebleeding. Continuous infusion
pantoprazole had no advantage with respect to recurrent bleeding within 30 days,
transfusion amount, need for surgery or TAE, length of hospital stay, or death.
Strengths Uniform method for endoscopic therapy
Examined effects of comorbidities, H. pylori status, and CYP2C19 genotypes
Followed outcomes for 30 days
Limitations Single center study in Taiwan
Appraisal Interim analyses showed similar rates of rebleeding in both groups, suggesting that
continuous infusion is not superior to bolus dosing of PPIs
o Interim analysis indicated >8400 patients in each arm would be needed
based on the narrow difference of rebleeding rate
o No difference in length of hospital stay, bleeding-related mortality, or
intervention requirement
Table 6.
10| Wong
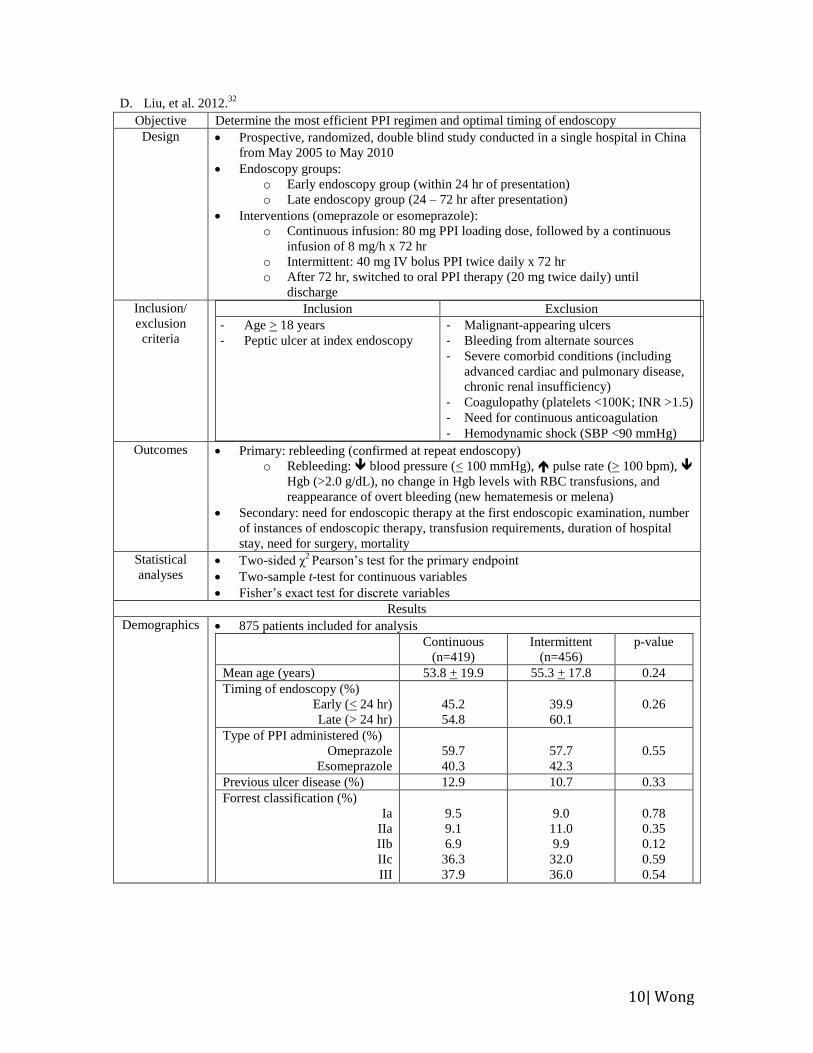
D. Liu, et al. 2012.32
Objective Determine the most efficient PPI regimen and optimal timing of endoscopy
Design Prospective, randomized, double blind study conducted in a single hospital in China
from May 2005 to May 2010
Endoscopy groups:
o Early endoscopy group (within 24 hr of presentation)
o Late endoscopy group (24 – 72 hr after presentation)
Interventions (omeprazole or esomeprazole):
o Continuous infusion: 80 mg PPI loading dose, followed by a continuous
infusion of 8 mg/h x 72 hr
o Intermittent: 40 mg IV bolus PPI twice daily x 72 hr
o After 72 hr, switched to oral PPI therapy (20 mg twice daily) until
discharge
Inclusion/
exclusion
criteria
Inclusion Exclusion
- Age > 18 years
- Peptic ulcer at index endoscopy
- Malignant-appearing ulcers
- Bleeding from alternate sources
- Severe comorbid conditions (including
advanced cardiac and pulmonary disease,
chronic renal insufficiency)
- Coagulopathy (platelets <100K; INR >1.5)
- Need for continuous anticoagulation
- Hemodynamic shock (SBP <90 mmHg)
Outcomes Primary: rebleeding (confirmed at repeat endoscopy)
o Rebleeding: blood pressure (< 100 mmHg), pulse rate (> 100 bpm),
Hgb (>2.0 g/dL), no change in Hgb levels with RBC transfusions, and
reappearance of overt bleeding (new hematemesis or melena)
Secondary: need for endoscopic therapy at the first endoscopic examination, number
of instances of endoscopic therapy, transfusion requirements, duration of hospital
stay, need for surgery, mortality
Statistical
analyses Two-sided χ
2 Pearson’s test for the primary endpoint
Two-sample t-test for continuous variables
Fisher’s exact test for discrete variables
Results
Demographics 875 patients included for analysis
Continuous
(n=419)
Intermittent
(n=456)
p-value
Mean age (years) 53.8 + 19.9 55.3 + 17.8 0.24
Timing of endoscopy (%)
Early (< 24 hr)
Late (> 24 hr)
45.2
54.8
39.9
60.1
0.26
Type of PPI administered (%)
Omeprazole
Esomeprazole
59.7
40.3
57.7
42.3
0.55
Previous ulcer disease (%) 12.9 10.7 0.33
Forrest classification (%)
Ia
IIa
IIb
IIc
III
9.5
9.1
6.9
36.3
37.9
9.0
11.0
9.9
32.0
36.0
0.78
0.35
0.12
0.59
0.54

11| Wong
Outcomes Continuous
(n=419)
Intermittent
(n=456)
p-value
Endoscopic therapy (%)
Early therapy
Late therapy
25.5
15.9
10.0
29.8
16.7
13.2
0.20
0.64
0.50
Rebleeding (%)
Early endoscopy
Late endoscopy
6.4
2.4
4.0
11.0
3.5
7.5
0.02
0.32
0.03
Rebleeding after endoscopic
therapy (%)
Early therapy
Late therapy
7.5
4.7
2.8
16.2
8.8
7.4
0.04
0.31
0.20
Number of endoscopic
therapies (%)
1
> 2
23.6
1.9
25.0
4.8
0.64
0.02
No. of units of blood transfused
Early endoscopy
Late endoscopy
1.23 + 2.13
0.65 + 1.64
1.81 + 2.62
1.93 + 2.12
1.15 + 1.89
2.71 + 2.35
<0.001
0.007
<0.001
Hospital stay (days)
Early endoscopy
Late endoscopy
6.2 + 4.6
5.2 + 4.0
7.2 + 5.2
9.4 + 5.7
8.5 + 5.1
10.3 + 6.3
<0.001
<0.001
<0.001
Surgery (%) 3.1 4.2 0.40
Death within 180 days (%) 0.2 1.3 0.16
Blood transfusion (0.90 + 1.76 units vs. 2.26 + 2.48 units; p<0.001) was significantly
lower and hospital stay (6.8 + 4.6 days vs. 8.8 + 5.8 days; p<0.001) was significantly
shorter in the early endoscopy group vs. late endoscopy group
Author’s
conclusion
Continuous infusion PPI is more efficacious in reducing rebleeding rate, blood
transfusion requirements, and hospital stay. The difference in rebleeding was restricted to
patients in the late endoscopy group, suggesting the special role of continuous infusion
when endoscopy is delayed >24 hours. Early endoscopy is safe and more effective than
late endoscopy.
Strengths Large sample size
Patients followed for 180 days after randomization
Limitations Single center
Excluded patients with severe comorbidities or hemodynamic shock
Method of endoscopic therapy was at the discretion of the treating endoscopist
Difficulty separating effects of timing of endoscopy from effects of PPI regimen
Unclear statistics
Appraisal Results show increased rebleeding with intermittent therapy; however, study may be
limited by several confounding factors and methodological limitations (i.e.,
exclusion criteria, and unclear statistics)
Table 7.
12| Wong
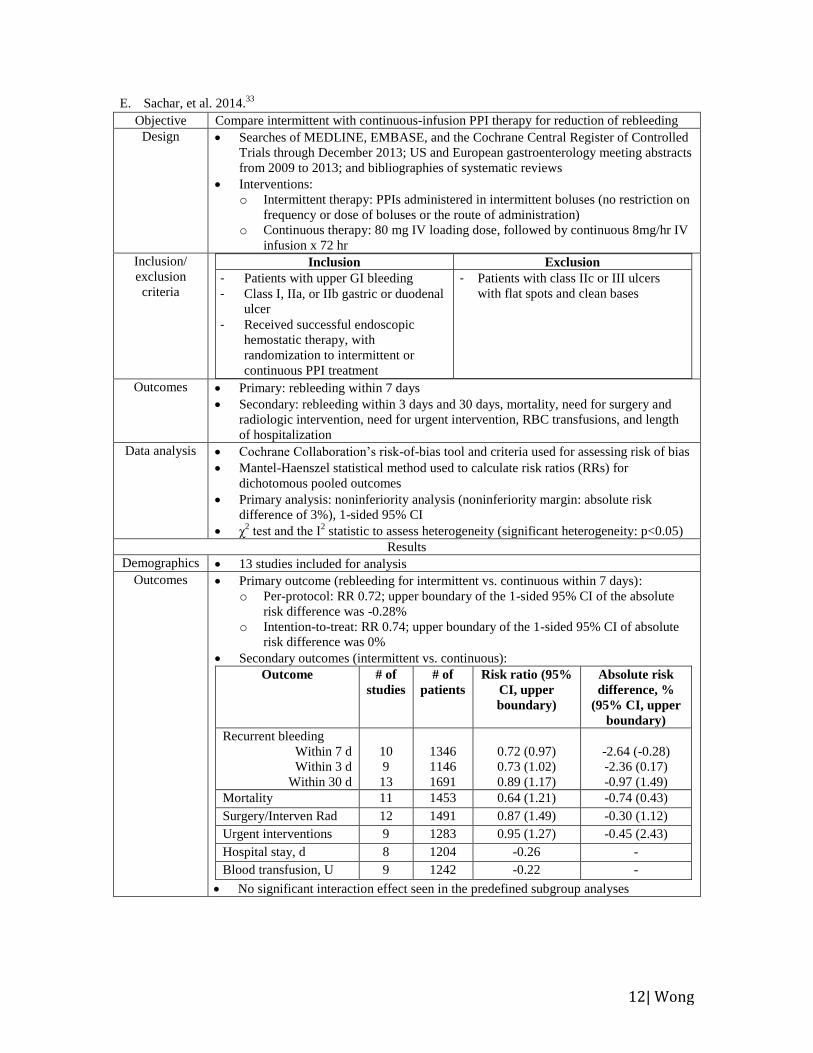
E. Sachar, et al. 2014.33
Objective Compare intermittent with continuous-infusion PPI therapy for reduction of rebleeding
Design Searches of MEDLINE, EMBASE, and the Cochrane Central Register of Controlled
Trials through December 2013; US and European gastroenterology meeting abstracts
from 2009 to 2013; and bibliographies of systematic reviews
Interventions:
o Intermittent therapy: PPIs administered in intermittent boluses (no restriction on
frequency or dose of boluses or the route of administration)
o Continuous therapy: 80 mg IV loading dose, followed by continuous 8mg/hr IV
infusion x 72 hr
Inclusion/
exclusion
criteria
Inclusion Exclusion
- Patients with upper GI bleeding
- Class I, IIa, or IIb gastric or duodenal
ulcer
- Received successful endoscopic
hemostatic therapy, with
randomization to intermittent or
continuous PPI treatment
- Patients with class IIc or III ulcers
with flat spots and clean bases
Outcomes Primary: rebleeding within 7 days
Secondary: rebleeding within 3 days and 30 days, mortality, need for surgery and
radiologic intervention, need for urgent intervention, RBC transfusions, and length
of hospitalization
Data analysis Cochrane Collaboration’s risk-of-bias tool and criteria used for assessing risk of bias
Mantel-Haenszel statistical method used to calculate risk ratios (RRs) for
dichotomous pooled outcomes
Primary analysis: noninferiority analysis (noninferiority margin: absolute risk
difference of 3%), 1-sided 95% CI
χ2 test and the Ι
2 statistic to assess heterogeneity (significant heterogeneity: p<0.05)
Results
Demographics 13 studies included for analysis
Outcomes Primary outcome (rebleeding for intermittent vs. continuous within 7 days):
o Per-protocol: RR 0.72; upper boundary of the 1-sided 95% CI of the absolute
risk difference was -0.28%
o Intention-to-treat: RR 0.74; upper boundary of the 1-sided 95% CI of absolute
risk difference was 0%
Secondary outcomes (intermittent vs. continuous):
Outcome # of
studies
# of
patients
Risk ratio (95%
CI, upper
boundary)
Absolute risk
difference, %
(95% CI, upper
boundary)
Recurrent bleeding
Within 7 d
Within 3 d
Within 30 d
10
9
13
1346
1146
1691
0.72 (0.97)
0.73 (1.02)
0.89 (1.17)
-2.64 (-0.28)
-2.36 (0.17)
-0.97 (1.49)
Mortality 11 1453 0.64 (1.21) -0.74 (0.43)
Surgery/Interven Rad 12 1491 0.87 (1.49) -0.30 (1.12)
Urgent interventions 9 1283 0.95 (1.27) -0.45 (2.43)
Hospital stay, d 8 1204 -0.26 -
Blood transfusion, U 9 1242 -0.22 -
No significant interaction effect seen in the predefined subgroup analyses
13| Wong
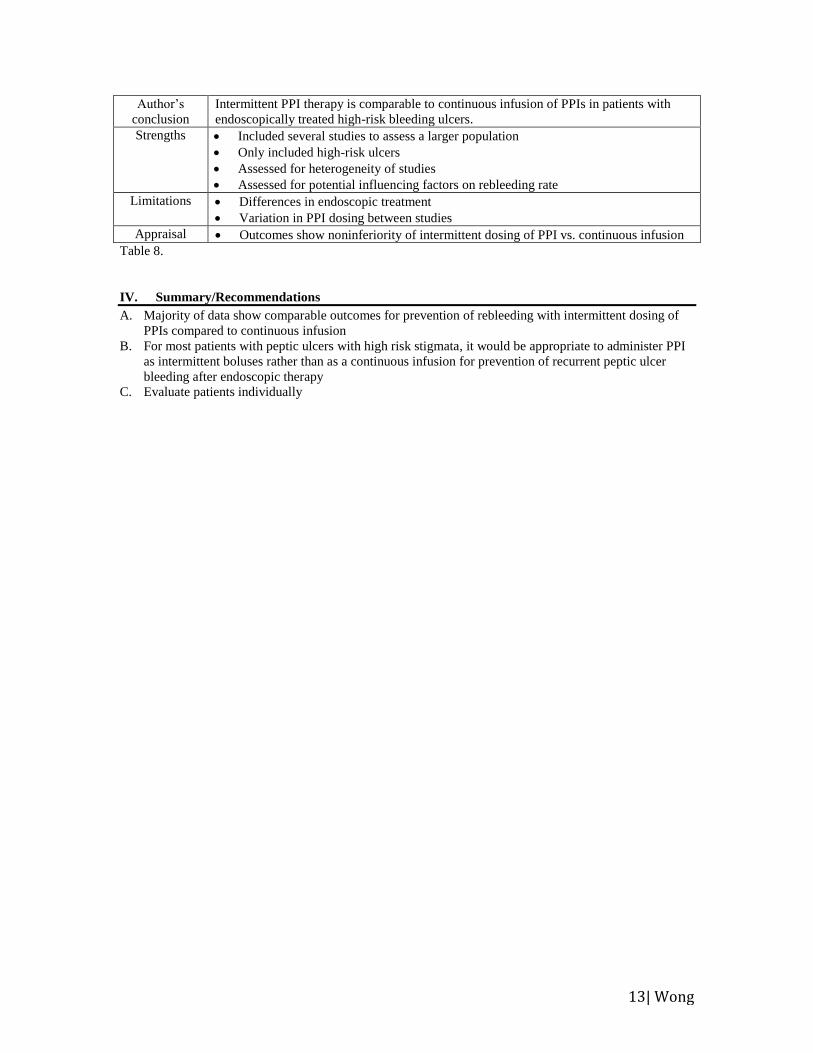
Author’s
conclusion
Intermittent PPI therapy is comparable to continuous infusion of PPIs in patients with
endoscopically treated high-risk bleeding ulcers.
Strengths Included several studies to assess a larger population
Only included high-risk ulcers
Assessed for heterogeneity of studies
Assessed for potential influencing factors on rebleeding rate
Limitations Differences in endoscopic treatment
Variation in PPI dosing between studies
Appraisal Outcomes show noninferiority of intermittent dosing of PPI vs. continuous infusion
Table 8.
IV. Summary/Recommendations
A. Majority of data show comparable outcomes for prevention of rebleeding with intermittent dosing of
PPIs compared to continuous infusion
B. For most patients with peptic ulcers with high risk stigmata, it would be appropriate to administer PPI
as intermittent boluses rather than as a continuous infusion for prevention of recurrent peptic ulcer
bleeding after endoscopic therapy
C. Evaluate patients individually
14| Wong
V. References
1. British Society of Gastroenterology Endoscopy Committee. Non-variceal upper gastrointestinal
hemorrhage: guidelines. Gut. 2002; 51(Suppl IV):iv1-iv6.
2. Erstad BL. Proton-pump inhibitors for acute peptic ulcer bleeding. Ann Pharmacother. 2001; 35:730-
40.
3. Fallah MA, Prakash C, Edmundowicz S. Acute Gastrointestinal Bleeding. Med Clin North Am. 2000;
84(5):1183-1208.
4. Manning-Dimmitt LL, Dimmitt SG, Wilson GR. Diagnosis of Gastrointestinal Bleeding in Adults. Am
Fam Physician. 2005; 71(7):1339-1346. Accessed 9/13/15. http://www.aafp.org/afp/2005/0401/p1339.
html.
5. Love BL, Thomas MN. Chapter 20. Peptic Ulcer Disease. In: DiPiro JT, Talbert RL, Yee GC, Matzke
GR, Wells BG, Posey L. eds. Pharmacotherapy: A Pathophysiologic Approach, 9e. New York, NY:
McGraw-Hill; 2014. Accessed September 27, 2015. http://accesspharmacy.mhmedical.com.ezproxy.
lib.utexas.edu/content.aspx?bookid=689&Sectionid=48811467.
6. Peptic Ulcer Disease: Introduction. Johns Hopkins Medicine. Accessed 9/17/15. http://www.hopkins
medicine.org/gastroenterology_hepatology/_pdfs/esophagus_stomach/peptic_ulcer_disease.pdf
7. Laine L, Jensen D. Management of Patients with Ulcer Bleeding. Am J Gastroenterol. 2012; 107:345-
360.
8. Bruno J. Intravenous Pantoprazole(Protonix®). Pharmacotherapy Update. 2003;6(5). Cleveland Clinic.
Accessed 9/15/15. http://www.clevelandclinicmeded.com/medicalpubs/pharmacy/septoct2003/
pantoprazole.html.
9. Rockall TA, Logan RF, Devlin HB, et al. Risk assessment after acute upper gastrointestinal
haemorrhage. Gut. 1996;38:316-321.
10. Kim J. Management and Prevention of Upper GI Bleeding. PSAP-VII: Gastroenterology and Nutrition.
Accessed 08/27/15. https://www.accp.com/docs/bookstore/psap/p7b11sample01.pdf.
11. Morgan DG, Hunt RH. Medical management of gastrointestinal bleeding. Eur J
GastroHepato. 1990;2:73–78.
12. Barkun AN, Cockeram AW, Plourde V, et al. Review article: acid suppression in non-variceal acute
upper gastrointestinal bleeding. Aliment Pharmacol Ther. 1999; 13(12):1565-84.
13. Blum AL, Bethge H, Bode JC, et al. Sucralfate in the Treatment and Prevention of Gastric Ulcer:
Multicentre Double Blind Placebo Controlled Study. Gut. 1990; 31(7):825-30.
14. Netzer P, Gaia C, Sandoz M, et al. Effect of repeated injection and continuous infusion of omeprazole
and ranitidine on intragastric pH over 72 hours. Am J Gastroenterol. 1999; 94(2):351-7.
15. Labenz J, Peitz U, Leusing C, et al. Efficacy of primed infusions with high dose ranitidine and
omeprazole to maintain high intragastric pH in patients with peptic ulcer bleeding: a prospective
randomised controlled study. Gut. 1997; 40(1):36-41.
16. Hung WK , Li VK , Chung CK et al. Randomized trial comparing pantoprazole infusion, bolus and no
treatment on gastric pH and recurrent bleeding in peptic ulcers . ANZ J Surg. 2007; 77:677 – 81.
17. Anjiki H, Kamisawa T, Sanaka M, et al. Endoscopic hemostasis techniques for upper gastrointestinal
hemorrhage: A review. World J Gastrointest Endosc. 2010; 2(2);54-60.
18. Gralnek IM, Barkun AN, Bardou M. Management of Acute Bleeding from a Peptic Ulcer. N Engl J
Med. 2008; 359:928-37.
19. Yuksel I, Ataseven H, Seyfettin Koklu, et al. Intermittent versus Continuous Pantoprazole Infusion in
Peptic Ulcer Bleeding: A Prospective Randomized Study. Digestion. 2008; 78:39-43.
20. Esomeprazole. Lexicomp Online®. Lexi-Drugs®. Hudson, OH: Lexi-Comp, Inc. Accessed 09/23/15.
21. Pantoprazole. Lexicomp Online®. Lexi-Drugs®. Hudson, OH: Lexi-Comp, Inc. Accessed 09/23/15.
22. Green FW, Jr, Kaplan MM, Curtis LE, et al. Effect of acid and pepsin on blood coagulation and
platelet aggregation. Gastroenterology. 1978; 74:38-43.
23. Patchett SE, Enright H, Afdhal N, et al. Clot lysis by gastric juice: an in vitro study. Gut. 1989;
30:1704-7.
24. Lau YW, Sung JY, Lee KC, et al. Effect of intravenous omeprazole on recurrent bleeding after
endoscopic treatment of bleeding peptic ulcers. N Engl J Med. 2000; 343:310-316.
25. Palmer KR. Non-variceal upper gastrointestinal haemorrhage: guidelines. British Society of
Gastroenterology Endoscopy Committee. Gut. 2002; 51 Suppl 4:1-6.
26. Laine L, Jensen DM. American College of Gastroenterology: Management of Patients with Ulcer
Bleeding. Am J Gastroenterol. 2012; 107:345-360.
15| Wong
27. Laine L, McQuaid KR. Endoscopic therapy for bleeding ulcers: an evidence-based approach based on
meta-analyses of randomized controlled trials. Clin Gastroenterol Hepatol. 2009; 7:33–47.
28. Choi KD, Kim N, Jang IJ, et al. Optimal dose of intravenous pantoprazole in patients with peptic ulcer
bleeding requiring endoscopic hemostasis in Korea. J Gastroenterol Hepatol. 2009; 24:1617–24.
29. Javid G, Zargar SA, U-Saif R, et al. Comparison of p.o. or i.v. proton pump inhibitors on 72-h
intragastric pH in bleeding peptic ulcer . J Gastroenterol Hepatol. 2009; 24:1236–43.
30. Andriulli A, Loperfido S, Focareta R, et al. High vs. low-dose proton pump inhibitors after endoscopic
hemostasis in patients with peptic ulcer bleeding: a multicentre, randomized study. Am J
Gastroenterol. 2008; 103:3011-8.
31. Chen CC, Lee JY, Fang YJ, et al. Randomised clinical trial: high-dose vs. standard-dose proton pump
inhibitors for the prevention of recurrent haemorrhage after combined endoscopic haemostasis of
bleeding peptic ulcers. Aliment Pharmacol Ther. 2012; 35:894-903.
32. Liu N, Liu L, Zhang H, et al. Effect of intravenous proton pump inhibitor regimens and timing of
endoscopy on clinical outcomes of peptic ulcer bleeding. J Gastroenterol Hepatol. 2012; 27(9):1473-9.
33. Sachar H, Vaidya K, Laine L. Intermittent vs Continuous Proton Pump Inhibitor Therapy for High-
Risk Bleeding Ulcers: A Systematic Review and Meta-analysis. JAMA Intern Med. 2014;
174(11):1755-1762.
Related Documents











