Pumping at camp What do we need to know Summer 2008 Kris Tiernan RN, MSN, CPNP, ARNP, CDE

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Pumping at camp
What do we need to know
Summer 2008
Kris Tiernan RN, MSN, CPNP, ARNP, CDE

Many thanks to our friends at Camp Hertko Hollow for providing this presentation.
Camp Hertko Hollow101 Locust St.Des Moines, IA 50309 Ann Wolf, Executive [email protected] Vivian Murray, Camp Director352-750-6759 or 888-437-8652 (Toll free)[email protected]
This presentation is intended to be a general guide that will help you create a thorough staff training tool for your camp. It is not intended to be a comprehensive resource or to fully cover the topic. We hope you will take this presentation and adapt it so that it fits your camp’s specific needs and meets the guidelines established for the safe and effective operation of your program.
Each diabetes camp operates under detailed policies and procedures that follow Board of Health and national accreditation standards that ensure the health and safety of children with diabetes. It is essential that camp staff be trained according to your camp’s policies and procedures. Staff should be encouraged to carefully review materials before arriving at camp, participate fully in pre-camp training, ask questions and use good judgment as they provide diabetes management supervision and educate youth with diabetes at camp.
While doing so, it is equally important that camp staff not lose focus – camp is a place for youth to have fun with peers – to feel supported and understood, and to feel part of a passionate community. Good luck!
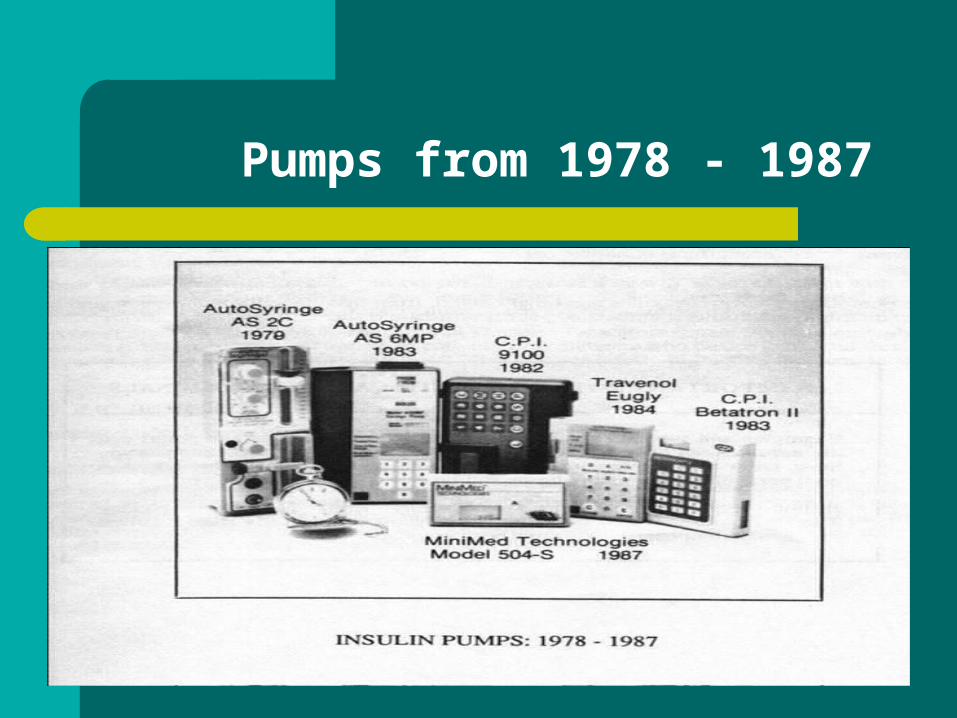
Pumps from 1978 - 1987
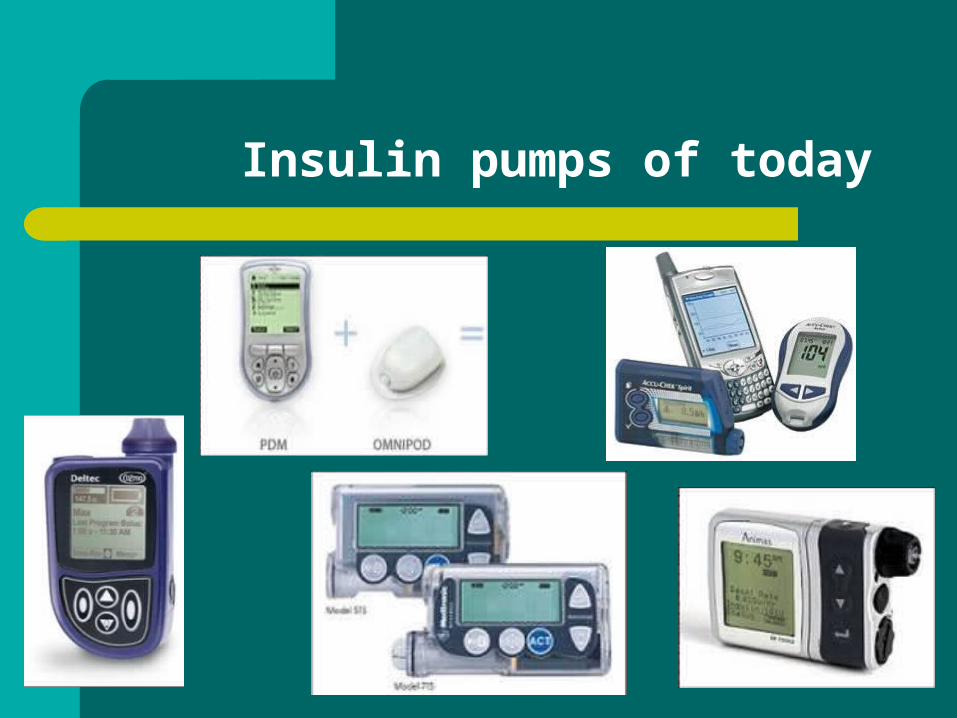
Insulin pumps of today

Pumps simulate insulin delivery of the pancreas: 24/7 rapid – acting insulin
External glucose testing and response Basal rate
– Immediate manipulation vs. pooled insulin– Even absorption vs. interrupted absorption
Bolus– Easier to give– Easier to forget?
What is an Insulin Pump?
A pump is a delivery system for insulin A pump replaces insulin injections A pump delivers insulin through a small
catheter under the skin A pump can more closely mimic the
pancreas A pump uses only short acting insulin to
deliver both the bolus and basal insulin A pump is a computer that is programmed to
specific criteria individualized to the person
Blood Sugar Terms
Hypoglycemia: low blood sugar Nocturnal hypoglycemia: low blood sugar just
before awakening Dawn phenomenon: rise in blood sugar just
before awakening Hyperglycemia: high blood sugar Ketoacidosis: usually high blood sugar plus
ketones Ketones: fat breakdown when not enough
insulin is present

Pump terms
Basal insulin: insulin that is given continuously or the long term insulin given by injection
Meal bolus: insulin given to cover food intake determined by counting carbohydrates
Insulin sensitivity: indicates how much your blood glucose is reduced by 1 unit of insulin
Correction bolus: amount of insulin needed to return a high blood sugar back to a target range
Blood sugar target: predetermined blood sugar range Active insulin time: number of hours that the insulin
remains active in the body
Insulin Pump: Advantages
Increased precision in insulin dosing with rapid acting insulin
Increased flexibility in lifestyle by matching doses to eating, sleeping, and activity
No need for multiple injections Nighttime stability increased Math by computer decreases error in dosing Potential for decreased hypoglycemia Potential for improved blood sugar control
Insulin Pump: Advantages (cont.)
Easier to have frequent meals or snacks Can give insulin over a longer period of time
or split doses which comes closer to pancreas function
One type of insulin, no mix up Short acting insulin is more accurate than
long acting insulin, 3% error vs. 60% Can tailor the basal rate to meet individual
needs with up to 48 different rates
Does the pump have a brain? NO
Human needs to initiate doses and make the appropriate dose changes
Human still needs to carry the correct supplies
A person still needs to review the data and assess the quality of life
Even with a bolus calculator there is still the need for a human to determine whether the dose is correct or not
What a Pump is Not
It is not a cure to diabetes It does not have a brain It does not eliminate the need for blood sugar
monitoring It is not the perfect treatment for diabetes It does not require surgical placement
Insulin Pump: Disadvantages
Potential for inflammation and infection at infusion site
Susceptibility to ketoacidosis Potential for catheter occlusion Initial purchase expensive 24 hour attachment Potential to forget to bolus
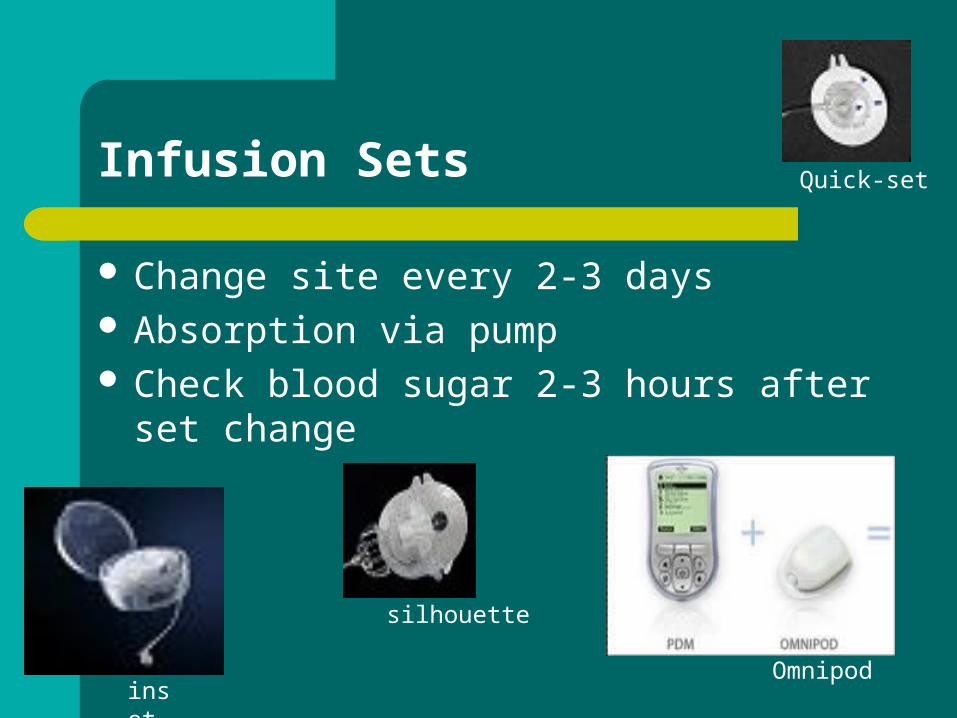
Infusion Sets
Change site every 2-3 days Absorption via pump Check blood sugar 2-3 hours after set
change
inset
silhouette
Quick-set
Omnipod
Important to remember…
Pumps deliver a continuous SQ delivery of rapid acting insulin
What works quickly will also wear off quickly
Your pump will not necessarily tell you if the supply of insulin has been interrupted

Diabetes at Camp:Times are changing
A few years ago only a handful of kids at camp were on pumps
Today, many camps have 40-70% of their kids on pumps

Insulin pumps are changing camp
More technology More supplies and equipment Different terms (bolus, basal, Bolus Wizard, etc.) Different management Pump removal Pump malfunction Kids may or may not know how to use their pump
BIG DIFFERENCES BETWEEN PUMP AND INJECTIONS
PUMPS USE ONLY SHORT-ACTING INSULIN: NEED TO WATCH FOR HIGHS
SOME ARE WATERPROOF, SOME ARE NOT
SITE CHANGES EVERY 2-3 DAYS THERE ARE SEVERAL TYPES OF PUMPS ALWAYS USE CARB COUNTING WITH
PUMPS

INFORMATION PRIOR TO CAMP
1 WEEKS WORTH OF BLOOD SUGARS INCLUDING CARBS, INSULIN RATIO AND CORRECTIONS
ALL PUMP SETTINGS, INCLUDING TEMORARY SETTINGS AND WHEN USED
ACTIVITY LEVEL PRIOR TO CAMP LENGTH OF TIME ON PUMP CHILD’S LEVEL OF UNDERSTANDING AND
PARTICIPATION IN PUMP CARE
INFORMATION PRIOR TO CAMP
USUAL ROUTINE FOR SET CHANGES (HOW OFTEN, DOES CHILD SIT OR LIE DOWN, IV PREP, EMLA CREAM, INSERTER, ETC.)
HAS ANYONE BUT MOM OR DAD CHANGED THE SITE
PREVIOUS PROBLEMS WITH DIABETES CARES (FORGETTING BOLUSES, HIGH BLOOD SUGARS, ETC.)
WHAT DO YOU WANT YOUR CHILD TO LEARN AT CAMP
MOST IMPORTANT
WITH A PUMP HYPERGLYCEMIA IS INCREASED IF PUMP SITE IS BAD
CANNOT TELL BY LOOKING AT THE PUMP OR THE SITE IF IT IS BAD
PUMP DOES NOT ALARM IF INSULIN ISN’T GOING IN
MUST GO BY BLOOD SUGARS AND URINE KETONES TO KNOW IF PUMP IS WORKING
CAN GET SICK QUICK!
SITE CHANGES
MANY KIDS WITH MANY ROUTINES MANY PUMPS WITH MANY SETS IMPORTANT TO HAVE A CAMP ROUTINE SUGGESTION FROM CWD IS TO CHANGE SITES
EVERY OTHER DAY: GIRLS ONE DAY AND BOYS THE NEXT
SOME CHILDREN HAVE NEVER HAD ANYONE BUT THEIR PARENTS CHANGE THEIR SITES (WOULD BE NICE TO KNOW AHEAD OF TIME SO THAT PARENT CAN PREPARE THEM)
SITE CHANGES (CONT.)
LOOK AT CHILD’S OLD SITES SUGGEST NEW SITES IF OLD SITES ARE
PUFFY AND/OR RED BEST TO PLACE SITES IN ABDOMEN OR
HIPS/BUTTOCKS ARM AND LEG SITES CAN CAUSE LOWS PLACE SITES NEXT TO EACH OTHER,
NOT ALTERNATING SIDES
HOW DO WE HELP THEM AT CAMP?
IF BLOOD SUGARS ARE ALWAYS HIGH PRIOR TO CAMP MAY NOT NEED TO DECREASE BASALS
CHANGE ALL SITES EVERY 2 DAYS NO MATTER WHAT THEIR USUAL ROUTINE
DECREASE BASAL BY 20-50% IF THEY ARE LESS ACTIVE AT HOME
MAY NEED TO INCREASE BASAL IF MORE ACTIVE AT HOME
WHAT TO DO FOR HIGH BLOOD SUGARS
IF BLOOD SUGAR IS >250 GIVE CORRECTION BY PUMP AND CHECK IN 1 HOUR AND CHECK FOR KETONES
IF STILL >250 GIVE CORRECTION ACCORDING TO PUMP BUT BY SYRINGE AND CHANGE PUMP SITE
FOR KETONES, DO AS ABOVE AND ENCOURAGE FLUIDS
AVOID PUMP SITE CHANGES BEFORE BED WHENEVER POSSIBLE
SWIMMING AND PUMPING
CHECK BLOOD SUGAR BEFORE SWIMMING (MUST BE ABOVE 100 TO ENTER POOL AREA)
MAKE SURE ALL THE KIDS HAVE THEIR NAMES WRITTEN ON THEIR PUMPS
REMOVE PUMP FOR SWIMMING IF IT IS NOT WATERPROOF AND PLACE IN A SAFE, DRY PLACE AWAY FROM WATER
CHECK BLOOD SUGARS BEFORE SWIMMING AND EVERY 1 HOUR AND AS NEEDED WHILE SWIMMING
GIVE INSULIN AND/OR SNACK AS NEEDED FOR BLOOD SUGAR
KEEP HYDRATED WHILE SWIMMING

PHYSICAL ACTIVITY
MAY WANT TO DECREASE BASAL RATE FOR PHYSICAL ACTIVITY (TO 50% OR GREATER)
MAY WANT TO DECREASE BASAL AFTER ACTIVITY
MAY NEED TO TAKE PUMP OFF FOR CERTAIN ACTIVITIES (IE. CANOEING)
Staff training
Make sure to find out the type of pump campers are using at least a month before camp, longer if possible
Have all staff complete the online training for all pumps that will be used at camp (we plan to have a test with this online to be completed before camp)
Have at least 2 people at camp who are trained in each of the pumps and to help with site changes
Make sure that all staff are aware of the significance of high blood sugars with pumps

Staff training
Ideally a counselor in the cabin would have the same pump as the campers or know how to use it
At least one staff in cabin should have a basic understand of pump therapy
WHAT WE NEED TO DO
NEED TO STAY CURRENT ON THE LATEST TECHNOLOGY
KNOW WELL AHEAD OF TIME WHAT EQUIPMENT THE CAMPERS ARE USING SO THAT STAFF CAN BE TRAINED
HAVE COPIES OF ALL THE MANUALS AND EXTRA SETS FOR ALL EQUIPMENT BEING USED
Continuous Glucose Monitoring
Device that checks blood sugars on a continuous basis
Provides up to 288 glucose readings in 24 hours
Some have predictive arrows Potential for greatly improved blood
sugars (staying between the lines) Step closer to artificial pancreas SQ site like the insulin pump
NEW CHALLENGES FOR CAMP
NEW PUMPS CONTINUOUS GLUCOSE MONITORS FUTURE TECHNOLOGIES WE NEED TO CONTINUE TO MOVE
FORWARD WITH THE CHANGES
WE MUST CONTINUE TO MOVE FORWARD AND BE FLEXIBLE TO BE THE BEST WE CAN BE
Related Documents











