i 495 0361-803X/95/1 646-1495 © American Roentgen Ray Society Pulse-Spray Pharmacomechanical Thrombolysis of Thrombosed Hemodialysis Access Grafts: Long-Term Experience and Comparison of Original and Current Techniques .. ..-. ? . ..... .. :. . -,. . 4 Karim Vabji1’2 Joseph J. Bookstein1’2 Anne C. Roberts1’2 Steven B. 2 Christopher tt’2 Michael P. O’Neill1’2 Received November 4, 1 994: accepted after re- vision January 11 , 1995. 1 Department of Radiology, 8756, University of California, San Diego, Medical Center, 200 W. Ar- bor Dr., San Diego, CA 92103. Address correspon- dence to K. Valji. 2Veterans Affairs Medical Center, La Jolla, CA 92161. OBJECTIVE. Pulse-spray pharmacomechanical thrombolysis is an evolving method for the treatment of vascular occlusions in which a highly concentrated fibrin- olytic agent is injected as a high-pressure spray directly into thrombus. The purpose of this retrospective study was to analyze our long-term experience with this tech- nique for the treatment of clotted hemodialysis grafts and to compare the efficacy and safety of the original and current methods. SUBJECTS AND METHODS. Over 6 years, 284 cases of dialysis graft thrombosis were considered suitable for treatment with pulse-spray thrombolysis. The original technique involved the injection of highly concentrated urokinase directly into a clot through two crisscross catheters with multiple side holes. The current technique includes early frag- mentation of residual clot with a balloon catheter, intrathrombic injection of heparin, mechanical treatment of a bysis-resistant clot at the arterial anastomosis, and routine administration of aspirin. After thrombolysis, underlying obstructions were treated with balloon angioplasty, atherectomy, or stents. The technical success, immediate clinical success, and frequency of complications for the entire population were analyzed. In addition, the results for 36 cases treated with the original technique were compared with the results for 37 recent cases treated with the current technique. RESULTS. Of 284 cases considered suitable for treatment, thrombolysis was not done in eight cases because the venous anastomosis could not be crossed. Throm- bolysis was discontinued in two cases because of extravasation of contrast material. The technical success for all grafts considered for treatment was 96%; 92% of treated grafts remained patent for at least 24 hr. Major complications occurred in 1% of cases, and minor complications occurred in 9% of cases. The clinical efficacies of the original and current techniques were 86% and 92%, respectively. The mean throm- bolytic agent infusion time was reduced from 44 ± 20 mm to 23 ± 13 mm (p < .001). The overall procedure time for the recently treated subgroup was 67 ± 26 mm. There was no significant difference in the frequencies of major and minor complications between the treatment subgroups. CONCLUSION. Pulse-spray pharmacomechanical thrombolysis is a reliable, rapid, and safe method for recanabization of occluded dialysis grafts. The current technique has been proven as safe and effective as the original technique but offers the advantage of a significant reduction in the time required for the infusion of thrombolytic agent. AJR 1995;164:1495-1500 Because of the recent development of methods for rapid pharmacologic and mechanical clot dissolution, percutaneous treatment of clotted hemodialysis grafts has become a practical alternative to surgical repair. In i 989, we described the original technique of pulse-spray pharmacomechanical thrombolysis (PSPMT) for the treatment of dialysis graft, arterial, and bypass graft occlusions [i]. Our initial report indicated that this method enabled reliable, rapid, and safe treatment of thrombosed dialysis grafts, with long-term patency comparable to that achieved with operative techniques [2]. On the basis of developing concepts in the experi- mental and clinical arenas, the pulse-spray technique has evolved substantially since its introduction [3-5]. Although we have documented the benefit of the origi-

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
i 495
0361-803X/95/1 646-1495© American Roentgen Ray Society
Pulse-Spray PharmacomechanicalThrombolysis of ThrombosedHemodialysis Access Grafts:Long-Term Experience and Comparison ofOriginal and Current Techniques
..� � ..-. �? . ....�...� :. � . �
-,.
� .� 4
Karim Vabji1’2
Joseph J. Bookstein1’2
Anne C. Roberts1’2Steven B. � 2
Christopher tt’2Michael P. O’Neill1’2
Received November 4, 1 994: accepted after re-vision January 11,1995.
1 Department of Radiology, 8756, University of
California, San Diego, Medical Center, 200 W. Ar-bor Dr., San Diego, CA 92103. Address correspon-dence to K. Valji.
2Veterans Affairs Medical Center, La Jolla, CA92161.
OBJECTIVE. Pulse-spray pharmacomechanical thrombolysis is an evolvingmethod for the treatment of vascular occlusions in which a highly concentrated fibrin-olytic agent is injected as a high-pressure spray directly into thrombus. The purposeof this retrospective study was to analyze our long-term experience with this tech-nique for the treatment of clotted hemodialysis grafts and to compare the efficacy andsafety of the original and current methods.
SUBJECTS AND METHODS. Over 6 years, 284 cases of dialysis graft thrombosis wereconsidered suitable for treatment with pulse-spray thrombolysis. The original techniqueinvolved the injection of highly concentrated urokinase directly into a clot through twocrisscross catheters with multiple side holes. The current technique includes early frag-mentation of residual clot with a balloon catheter, intrathrombic injection of heparin,mechanical treatment of a bysis-resistant clot at the arterial anastomosis, and routineadministration of aspirin. After thrombolysis, underlying obstructions were treated withballoon angioplasty, atherectomy, or stents. The technical success, immediate clinicalsuccess, and frequency of complications for the entire population were analyzed. Inaddition, the results for 36 cases treated with the original technique were compared withthe results for 37 recent cases treated with the current technique.
RESULTS. Of 284 cases considered suitable for treatment, thrombolysis was notdone in eight cases because the venous anastomosis could not be crossed. Throm-bolysis was discontinued in two cases because of extravasation of contrast material.The technical success for all grafts considered for treatment was 96%; 92% of treatedgrafts remained patent for at least 24 hr. Major complications occurred in 1% ofcases, and minor complications occurred in 9% of cases. The clinical efficacies of theoriginal and current techniques were 86% and 92%, respectively. The mean throm-bolytic agent infusion time was reduced from 44 ± 20 mm to 23 ± 13 mm (p < .001). Theoverall procedure time for the recently treated subgroup was 67 ± 26 mm. There wasno significant difference in the frequencies of major and minor complicationsbetween the treatment subgroups.
CONCLUSION. Pulse-spray pharmacomechanical thrombolysis is a reliable, rapid,and safe method for recanabization of occluded dialysis grafts. The current techniquehas been proven as safe and effective as the original technique but offers the advantageof a significant reduction in the time required for the infusion of thrombolytic agent.
AJR 1995;164:1495-1500
Because of the recent development of methods for rapid pharmacologic andmechanical clot dissolution, percutaneous treatment of clotted hemodialysis graftshas become a practical alternative to surgical repair. In i 989, we described theoriginal technique of pulse-spray pharmacomechanical thrombolysis (PSPMT) forthe treatment of dialysis graft, arterial, and bypass graft occlusions [i]. Our initialreport indicated that this method enabled reliable, rapid, and safe treatment ofthrombosed dialysis grafts, with long-term patency comparable to that achievedwith operative techniques [2]. On the basis of developing concepts in the experi-mental and clinical arenas, the pulse-spray technique has evolved substantiallysince its introduction [3-5]. Although we have documented the benefit of the origi-

i 496 VALJI ET AL. AJR:164, June 1995
nab PSPMT technique, we have not evaluated the efficacy ofthe technique currently used in practice. In this retrospectivestudy, we analyzed our 6-year experience with PSPMT ofclotted hemodialysis grafts and compared the efficacy andsafety of the initial and current techniques.
Subjects and Methods
Study Groups
Between January 1988 and December 1993, 284 episodes of hemo-dialysis access graft thrombosis in 122 patients were considered suit-able for transcatheter treatment. Exclusion criteria included (1) recentgraft placement or surgical revision (<2 weeks), (2) the presence of arisk factor for bleeding from anticoagulation or fibrinolytic therapy, or (3)suspected graft infection. All grafts were constructed of expanded poly-tetrafluoroethylene, with the exception of one for a patient with a radio-cephalic arteriovenous fistula. Angiographic reports and dialysisrecords were retrospectively analyzed for technical details of the proce-dure, angiographic findings, complications, and graft patency at i dayafter treatment. Two subgroups of patients for whom complete datawere available were identified; 36 treatments were performed from1988-1989 with the original PSPMT technique, and 37 patients weretreated in 1993 with the refined PSPMT technique. The characteristicsofthe two subgroups are outlined in Table 1.
Original Technique
The original PSPMT technique has been described in detail [1 , 2]. Inbrief, graft access was obtained by puncture at two sites in the midpor-tion of the graft. 5-French dilators were inserted in a crisscross fashion.Pulse-spray catheter systems were made for each case with straight 5-French polyethylene catheters. Side holes were placed in the cathetersat 8- to 10-cm intervals in a spiral pattern with a 27-gauge needle. Thecatheters were placed into the graft in a crisscross fashion, with thecatheter tips situated at the edge of the thrombus. The catheter endholes were occluded with 0.032-inch (-0.081-cm) beaded wires (Cook,Bloomington, IN). The catheters were fitted with hemostatic valves, andthe injection systems were flushed with heparinized saline. The throm-bolytic solution was prepared by dissolving 250,000 IU of urokinase(Abbokinase; Abbott Laboratories, North Chicago, IL) in 10 ml of sterilewater. About 150,000 IU was injected in 0.2-mI increments at twopulses per catheter per minute. The remaining 100,000 IU was given atone pulse per catheter per minute. Patients were given 5000 U of hep-arm iv at the onset of thrombolytic agent injections. Additional heparin(500-1500 U/hr) was given during the course of the procedure.
After treatment with 250,000 IU of urokinase, contrast injectionswere made through the catheters. When other than small (2- to 3-mm) clot fragments remained, additional urokinase was adminis-tered at 25,000 lU/mI at one pulse per catheter per minute. Serialangiograms were obtained to identify areas of stenosis or residual
TABLE 1 : Characteristics of Study Subgroups
Parameter Initial Technique Current Technique
No. of grafts 36 37
No. of patients 24 24No. of males/females i 1/i 3 13/1 iMean age in yr (range) 50 (12-76) 43 (16-76)
No. of grafts at:
Forearm 28 20Upperarm 5 16Thigh 3 1
thrombus. Underlying stenoses were treated by balloon angioplastywith 6- or 7-mm balloon catheters. A lysis-resistant thrombus on the
graft side of the arterial anastomosis usually was treated by macera-tion with a balloon dilatation catheter. After thrombolysis and angio-plasty, the catheters were removed and hemostasis was achieved.
Interim Techniques
Two important alterations in technique were used during the mid-dIe of the study period (i 990-1991). Tissue-type plasminogen acti-vator (tPA) (Alteplase; Genentec, South San Francisco, CA) wasused in place of urokinase for 23 patients. The concentration of tPAwas 0.5 mg/mI. For 29 patients, a prototype mechanical pump (E-Z-Em, Glens Falls, NY) was used to deliver pulses at a pump pressureof 20 or 40 PSI (-14 or -28 kPa). Neither ofthese technical featureswas included in the current method.
Current Technique
Patients were given aspirin at 325 mg before the procedure. Thegraft was punctured about one third of the distance away from the arte-rial anastomosis with a single-wall needle. A 5-French dilator or straightcatheter was inserted, and a guidewire was advanced toward thevenous anastomosis. If the anastomosis could not be crossed, the pro-cedure was abandoned. The catheter was advanced into the venousoutflow tract and then withdrawn while small amounts of contrast mate-rial were injected to identify the upper extent of thrombosis. A secondcatheter was inserted through a puncture made about one third of thedistance away from the venous anastomosis and was directed towardthe arterial anastomosis. The dilators were replaced with 5-Frenchpulse-spray catheters (Angiodynamics Division, E-Z-Em; or Cook). Theactive catheter length (length of catheter with side holes) was selectedon the basis ofthe length of the clotted graft to be treated. Tip-occludingwires were inserted to obstruct the end holes, and the catheters werefitted with hemostatic V-shaped adapters to allow injections to be madearound the wires. The system was purged of air with heparinized saline.Heparin (2000-3000 U) then was given IV.
Avial of 250,000 IU of urokinase (Abbokinase) was reconstituted with
9 ml of degassed sterile water, which was used to avoid the formation ofbubbles in solution during pulse injections. Sterile water was degassedin a 60-mi syringe by repeated aspiration and shaking of saline against aclosed stopcock, with subsequent expulsion of released gas. One millili-ter of heparin (5000 U/mI) then was added tothe urokinase solution. The10-mI mixture was divided between the two catheters. One milliliter ofsolution was slowly injected to prime each catheter. Pulse injections thenwere applied to each catheter by manual injection of 0.2- to 0.3-mI ali-quots about every 30 sec with a tuberculin syringe. Forceful and rapidinjections were essential to maximize fluid penetration into the thrombus.Care was taken to keep air bubbles out of the system. When the activecatheter length was shorter than the length of the clotted graft to betreated, the catheter was partially withdrawn into the untreated segmentafter half of the mixture had been injected. After 5 ml had been injectedinto each catheter, the thrombolytic solution remaining in the catheterwas delivered to the clot as 0.2-mI injections of 1 ml of heparinizedsaline. In this way, the entire dose of urokinase was given in about 15-
20 mm. The activated clotting time (ACT) (Hemotec, Englewood, CO)was measured to ensure that adequate anticoagulation had beenachieved. Additional heparin was given IV to achieve an ACT of 250-300 sec (normal range, i20-160 sec).
The tip-occluding wires were removed, and small injections of con-trast material were used to assess the degree of clot lysis and to evalu-ate the venous anastomosis. For establishment of outflow from thegraft, venous anastomotic stenoses were dilated with a 6- or 7-mm 5.8-French high-pressure balloon catheter (Medi-tech, Watertown, MA).
Insubstantial clot lysis after about 15 mm of therapy usually is attrib-utable to incomplete delivery of the fibrinolytic agent to the entire graft,inadequate anticoagulation, a hypercoagulable state, or the presence
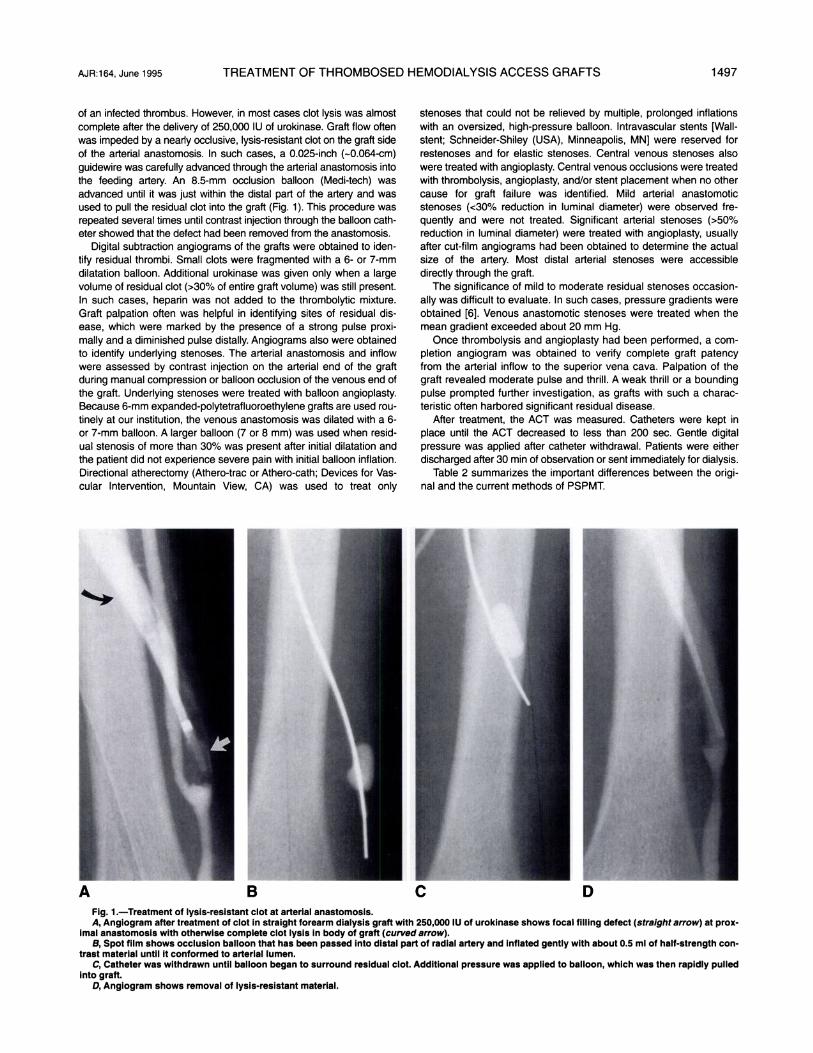
A B C DFig. 1 .-Treatment of lysis-resistant clot at arterial anastomosis.A, Angiogram after treatment of clot in straight forearm dialysis graft with 250,000 IU of urokinase shows focal filling defect (straight arrow) at prox-
imal anastomosis with otherwise complete clot lysis in body of graft (curved arrow).B, Spot film shows occlusion balloon that has been passed into distal part of radial artery and inflated gently with about 0.5 ml of half-strength con-
trast material until it conformed to arterial lumen.C, Catheter was withdrawn until balloon began to surround residual clot. Additional pressure was applied to balloon, which was then rapidly pulled
into graft.D, Angiogram shows removal of lysis-resistant material.
AJR:164, June 1995 TREATMENT OF THROMBOSED HEMODIALYSIS ACCESS GRAFTS i 497
of an infected thrombus. However, in most cases clot lysis was almostcomplete after the delivery of 250,000 IU of urokinase. Graft flow oftenwas impeded by a nearly occlusive, lysis-resistant clot on the graft sideof the arterial anastomosis. In such cases, a 0.025-inch (-0.064-cm)
guidewire was carefully advanced through the arterial anastomosis into
the feeding artery. An 8.5-mm occlusion balloon (Medi-tech) was
advanced until it was just within the distal part of the artery and was
used to pull the residual clot into the graft (Fig. 1). This procedure was
repeated several times until contrast injection through the balloon cath-
eter showed that the defect had been removed from the anastomosis.
Digital subtraction angiograms of the grafts were obtained to den-
tify residual thrombi. Small clots were fragmented with a 6- or 7-mm
dilatation balloon. Additional urokinase was given only when a large
volume of residual clot (>30% of entire graft volume) was still present.
In such cases, heparin was not added to the thrombolytic mixture.
Graft palpation often was helpful in identifying sites of residual dis-
ease, which were marked by the presence of a strong pulse proxi-
mally and a diminished pulse distally. Angiograms also were obtained
to identify underlying stenoses. The arterial anastomosis and inflow
were assessed by contrast injection on the arterial end of the graft
during manual compression or balloon occlusion of the venous end of
the graft. Underlying stenoses were treated with balloon angioplasty.Because 6-mm expanded-polytetrafluoroethylene grafts are used rou-tinely at our institution, the venous anastomosis was dilated with a 6-
or 7-mm balloon. A larger balloon (7 or 8 mm) was used when resid-
ual stenosis of more than 30% was present after initial dilatation and
the patient did not experience severe pain with initial balloon inflation.Directional atherectomy (Athero-trac or Athero-cath; Devices for Vas-
cular Intervention, Mountain View, CA) was used to treat only
stenoses that could not be relieved by multiple, prolonged inflationswith an oversized, high-pressure balloon. Intravascular stents [Wall-
stent; Schneider-Shiley (USA), Minneapolis, MN] were reserved forrestenoses and for elastic stenoses. Central venous stenoses alsowere treated with angioplasty. Central venous occlusions were treatedwith thrombolysis, angioplasty, and/or stent placement when no other
cause for graft failure was identified. Mild arterial anastomoticstenoses (<30% reduction in luminal diameter) were observed fre-quently and were not treated. Significant arterial stenoses (>50%
reduction in luminal diameter) were treated with angioplasty, usually
after cut-film angiograms had been obtained to determine the actualsize of the artery. Most distal arterial stenoses were accessibledirectly through the graft.
The significance of mild to moderate residual stenoses occasion-ally was difficult to evaluate. In such cases, pressure gradients were
obtained [6]. Venous anastomotic stenoses were treated when themean gradient exceeded about 20 mm Hg.
Once thrombolysis and angioplasty had been performed, a corn-pletion angiogram was obtained to verify complete graft patency
from the arterial inflow to the superior vena cava. Palpation of thegraft revealed moderate pulse and thrill. A weak thrill or a bounding
pulse prompted further investigation, as grafts with such a charac-teristic often harbored significant residual disease.
After treatment, the ACT was measured. Catheters were kept in
place until the ACT decreased to less than 200 sec. Gentle digitalpressure was applied after catheter withdrawal. Patients were eitherdischarged after 30 mm of observation or sent immediately for dialysis.
Table 2 summarizes the important differences between the origi-nal and the current methods of PSPMT.

TABLE 3: Comparative Results of Pulse-SprayThrombolysis for Occluded Dialysis Grafts
ap< .001.bN,A = data not available.
i 498 VALJI ET AL. AJR:164, June 1995
TABLE 2: Comparison of Pulse-Spray Thrombolysis Techniques for Treatment ofOccluded Dialysis Grafts
Variable Original Technique Current Technique
Antiplatelet agent None AspirinAntithrombin agent IV heparin lntrathrombic and IV heparin
Assessment of coagulation statusEndpointfor thrombolytic
NoneMinimal residual clotsa
Activated clotting timeModerate residual clotsb
agent infusionTreatment of residual clot Pharmacologic lysis Mechanical fragmentationTreatment of lysis-resistant clot Additional fibrinolysis and Balloon displacement
at arterial anastomosis balloon fragmentation and fragmentationAssessment of significance None Pressure gradients
of stenoses
Treatment of residual or recurrent Surgical revision Atherectorny and/or stentsvenous stenoses
aScaftered 2- to 3-mm thrombi.
bLess than 30% residual clot by volume.
Data Analysis
Thrombolytic agent infusion time was defined as the interval duringwhich urokinase injections were made. Procedure time was defined
as the interval from the start of thrombolytic agent injections to thecompletion of the final angiograrn; procedure time was not docu-mented for patients treated with the original technique. Technical suc-
cess was defined as complete graft recanalization with a palpablethrill after treatment. Clinical success was defined as graft patency
sufficient to allow successful dialysis within 24 hr of treatment. Calcu-
lations of technical and clinical successes for the study groups were
based on all patients considered suitable for treatment (all patientsreferred for treatment less those meeting exclusion criteria). Compli-cations were considered major when they necessitated blood transf u-sion, operative intervention, or hospital admission. Complicationswere considered minor when they were self-limited or were treateddirectly during the transcatheter procedure.
Results are expressed as mean ± standard deviation. Mean inf u-sion times for the two subgroups were compared with the unpairedtest. Technical and clinical successes for the two subgroups werecompared by use of chi-square analysis.
ResultsGraft access was obtained in every case. For the 284
patients in whom the procedure was started, thrombolysiswas not done in eight patients because of an inability totraverse the venous anastomosis. Thrombolysis was startedfor 276 patients but was discontinued before completion of afull course of therapy in two patients because of extravasa-tion from the graft. For the 274 patients who underwent acomplete course of thrombolysis, graft recanalization wasaccomplished in all but two, resulting in a technical successrate of 96% for all grafts considered suitable for treatment.For 259 patients, grafts were functional at dialysis within 24hr of the procedure, resulting in an overall clinical successrate of 92% for grafts considered suitable for treatment.
For the 23 patients treated with tPA, the mean dose of tPAwas 7.i ± 3.6 mg and the mean lytic agent infusion time was32 ± 16 mm. For the 29 patients in whom a mechanical pumpwas used to deliver the thrombolytic agent, the mean lyticagent infusion time was 32 ± i6 mm.
Results for the subgroups treated with the original and cur-
rent techniques are compared in Table 3. The thrombolytic
i’n�rm�cnmecnanicai
Parameter Initial Technique Current Technique
No. of cases 36 37Urokinase dose (IU) 324,000 ± 124,000 31 9,000 ± 122,000Lytic agent infusion time (mm) 44 ± 20a 23 ± 13a
Proceduretime(min) N/Ab 67±26
Technical success rate (%) 100 100Clinical success rate (%) 86 92Complications (%)
Minor 3 5
Major 0 0
agent infusion time was reduced from 44 ± 20 mm to 23 ± i 3mm (p < .OOi). The clinical success rate increased from 86%to 92%. Complication rates were not significantly different forthe two treatment subgroups; no major complicationsoccurred in either treatment subgroup.
A lysis-resistant clot at the arterial anastomosis was identi-fied on angiograms or noted in the radiographic reports for59% of all treated cases. Such thrombi were noted for 18 of36 patients (50%) in the original technique group and for 27of 37 patients (73%) in the currenttechnique group. Mobiliza-tion of the clot with an occlusion balloon and/or fragmenta-tion with a dilatation balloon were successful in removing thismaterial in all but two patients. For these patients, atherec-tomy was successful in removing residual material. Angio-plasty was done to fragment the residual clot in the body ofthe graft and to treat underlying obstructions responsible forgraft failure (Table 4). For two patients, atherectomy was suc-cessfully used to weaken stenoses that were initially resis-tant to balloon angioplasty. Intravascular stents were placedat the venous anastomosis in five patients and in the axillaryor subclavian veins in three patients.
Minor complications occurred in 9% of cases, and major
complications occurred in i%. The one significant hemorrhagiccomplication occurred in a patient who underwent graft throm-bolysis with tPA and then lysis of a subclavian vein occlusion

AJR:164, June 1995 TREATMENT OF THROMBOSED HEMODIALYSIS ACCESS GRAFTS i499
TABLE 4: Anatomic Causes for Dialysis Graft Thrombosis in272 Cases with Complete Recanalization
Source No. (%) of Cases
Venous anastornotic stenosis 216 (79)Venous outflow stenosis and/or occlusion 55 (20)Arterial anastornotic stenosis 28 (10)Intragraft stenosis 15 (6)Arterial inflow stenosis 9 (3)Graft pseudoaneurysm 2 (1)
No anatomic source identified 7 (3)
Note-Percentages total more than 100 because of multiple causes ofgraftfailurein some cases.
with tPA. Ten hours later, while the patient was undergoing hep-arm infusion, a large retroperitoneal hematoma requiring bloodtransfusion developed. Thrombolytic agent infusions were
stopped because of the development of a large perigrafthematoma in one patient and extravasation from the graft in
another patient. Symptomatic clot embolization into the efferentarterial bed occurred in five patients. One patient required notreatment, one patient underwent successful treatment with anadditional urokinase infusion, two patients underwent transcath-etertherapy that involved pulling the embolus back into the graftwith an inflated occlusion balloon, and one patient required
operative removal. Additional minor complications includedsmall perigraft hematomas (n = 9); extravasation of contrastmaterial from the graft (n = 3); vein rupture or dissection from
balloon angioplasty (n = 4); shearing of a catheter by an accessneedle, with subsequent percutaneous retrieval of the fragment(n = i); and adverse reaction to contrast material (n = 2). Two
patients noted transient focal chest wall discomfort that couldhave represented a pulmonary embolus; both ofthese incidentsoccurred in the first 2 years of the study. No other patients hadsymptoms or signs suggestive of pulmonary embolism. Sincei99i , some patients have experienced rigor within 30 mm afterthe initiation of urokinase injections; however, the exact fre-quency of this reaction has not been tabulated.
Discussion
The results ofthis study indicate that recanalization of clotteddialysis grafts can be performed reliably, rapidly, and safely withthe current, modified PSPMT technique. Technical success canbe achieved in virtually all cases. Refinements in the techniquehave not significantly improved its technical efficacy. However,early treatment of residual clots by balloon fragmentation ratherthan further thrombobytic agent infusion has reduced the lyticagent infusion time substantially. Given that graft access cangenerally be obtained in about is mm, the current total proce-
dure time usually is less than 2 hr.The safety of the PSPMT method has now been established
after experience with almost 300 cases. The frequencies ofminor and major complications have not changed with varia-
tions in the technique designed to shorten the treatment time.Minor perigraft bleeding was unusual and self-limited in ourexperience. Only one major hemorrhagic complication occurredin the 6-year study period, in a patient treated with tPA for bothdialysis graft and subclavian vein thromboses.
We have adopted a more aggressive approach to clot dis-solution in our current technique. Pulse-spray injections ofurokinase and heparin are administered at about twice therate described in our initial report. In addition, moderate num-bers of residual clots are fragmented with a balloon catheterrather than being subjected to further pharmacologic lysis.These alterations in technique have not been associated withmore frequent symptomatic arterial embobization or pulmonaryembolism. Only two patients experienced symptoms that weresuggestive of pulmonary embolism, and these two casesoccurred early in our study, before the more aggressiveapproach to mechanical clot maceration was instituted. None-theless, we believe that the injection of pulse volumes largerthan 0.3 ml per pulse is not advisable, as large-volume injec-tions could increase the risk of distal arterial or pulmonaryemboli. Although mechanical thrombobysis without fibrinolyticagents has been used by some investigators [7, 8], we andothers [9] suspect that the risk of significant pulmonary embo-lism is reduced by initial pharmacologic lysis.
The response of clot within an occluded hemodialysis graftto fibrinolytic agents is not uniform. Typically, rapid lysis willoccur within the midportion and distal portion of the graft.However, a lysis-resistant clot (“plug”) often remains at thearterial anastomosis. The exact composition of this material isnot known. Experience has shown that such a lysis-resistantthrombus does not respond readily to further treatment withurokinase, although lysis may occur with prolonged local infu-sion. Most plugs can be successfully treated by fragmentationwith a dilatation balloon. We preferto delay fragmentation untilthe plug is pulled from the arterial anastomosis into the bodyof the graft with an occlusion balloon. This maneuver avoidspotential damage to the efferent artery from a 6- or 7-mmangioplasty balloon. In addition, embolization of clot fragmentsinto the efferent artery may be avoided by fragmentation withinthe body of the graft rather than directly at the anastomosis.For all five patients in our series who developed arterialembobi, embolization occurred after treatment of the residualclot directly at the anastomosis or after vigorous injection ofcontrast material into the clot at the arterial anastomosis.When embolization did occur, operative removal was onlyrequired for one patient.
Venous anastomotic stenoses were by far the most com-mon cause for graft thrombosis. However, significant venousoutflow obstructions were found in 20% of cases. This figureis higher than the 9% frequency noted in our original report[2]. The apparent increase in the detection of venous outflowobstructions is probably related to more complete angio-graphic evaluation after graft thrombolysis and the increaseduse of temporary venous access devices for hemodialysis.For this reason, thorough evaluation of graft inflow and out-flow is important for identifying and correcting underlyingstenoses to prevent early graft reocclusion.
Thrombolytic therapy incites ongoing thrombosis by theactivation of platelets, the release of clot-bound thrombin,and the effects of plasminogen activator inhibitors [iO, ii].Recent work has suggested that concurrent rethrombosis isa major factor limiting the speed ofthrombolytic therapy [i2].We previously showed that intrathrombic but not IV injectionof heparin enhances clot dissolution during PSPMT with tPAin a rabbit thrombus model [i3]. On the basis of the collected

i500 VALJI ET AL. AJR:i64, June 1995
experimental evidence, we now administer oral aspirin andintrathrombic heparin along with IV heparin during PSPMTtreatment of all vascular occlusions. However, any potentialbenefit of these adjunctive agents in the reduction of lysistime may not be realized in the treatment of clotted dialysisgrafts because of the aggressive approach to mechanicalclot fragmentation now being used.
REFERENCES
1. Bookstein JJ, Fellmeth B, Roberts A, Valji K, Davis G, Machado T. Pulsed-
spray pharmacomechanical thrombolysis: preliminary clinical results. AJR1989:152:1097-1100
2. Valji K, Bookstein JJ, Roberts AC, Davis GB. Pharmacomechanicalthrombolysis and angioplasty in the management of clotted hemodialysisgrafts: early and late clinical results. Radiology 1991:178:243-247
3. Bookstein JJ, Valji K. Pulse spray pharmacomechanical thrombolysis:updated clinical and laboratory observations. Semin intervent Radiol
1992:9:174-182
4. Valji K, Roberts AC, Bookstein JJ. Thrombosed hemodialysis grafts: man-
agement with pulse-spray thrombolysis and balloon angioplasty. In:
Strandness DE, van Breda A, eds. Vascular diseases: surgical and inter-ventionaltherapy. New York: Churchill Livingstone, 1994:1087-1095
5. Roberts AC, Valji K, Bookstein JJ, Hye RJ. Pulse spray pharmacome-
chanical thrombolysis for treatment of thrombosed dialysis access grafts.Am J Surg 1993:16:221-226
6. Sullivan KL, Besarab A, Bonn J, Shapiro MJ, Gardiner GA, Moritz MJ.Hemodynamics offailing dialysis grafts. Radiology 1993;186:867-872
7. Trerotola SO, Lund GB, Scheel PJ, Savader SJ, Venbrux AC, Osterman
FA. Thrombosed dialysis access grafts: percutaneous mechanical declot-ting without urokinase. Radiology 1994:191:721-726
8. Vorwerk D, Sohn M, Schurmann K, Hoogeveen Y, Gladziwa U, GuentherRW. Hydrodynamic thrombectomy of hemodialysis fistulas: first clinicalresults. J VasclntervRadioll994:5:813-82i
9. Dolmatch BL, Gray RJ, Horton KM. Will iatrogenic pulmonary emboliza-tion be our pulmonary embarrassment? Radiologyl994:191:615-617
10. Penny WF, Ware JA. Platelet activation and subsequent inhibition by plasmin
and recombinanttissue-type plasminogen activator. Blood 1992:79:91-9811 . Seitz A, Blanke H, Praetorius G, et al. Increased thrombin activity during
thrombolysis. Thromb Haemost 1988;59:54i-54212. Fitzgerald DJ, FitzGerald GA. Antiplatelet and antithrombin therapy during
coronary thrombolysis. Trends Cardiovasc Med 1991:1:29-3513. Valji K, Bookstein JJ. Efficacy of adjunctive intrathrombic heparin with
pulse spray thrombolysis in rabbit inferior vena cava thrombosis. investRadiol 1992:27:912-917
The reader’s attention is directed to the commentary on this article, which appears on the following pages.
Related Documents











