Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
THE
D IAGNOS lS AND . TREATMENT
PULMONARY TUBERCULOS I S
BY
FRANC IS M. POTTENGER, A .M M. D .
Monrovia , Cal iforn ia
M EDICA L D IRE CTOR OF TH E POTTENGE R SANA TORIUM FOR D I SE A SE S OF TH E LUNGSA N D THROA T , M ONROV I A , CA L . ; PROFE S S OR OF CLINICAL M E D IC INE ,
M E D ICA LD E PA RTM E NT
,UNIVE RS ITY OF SOUTHE RN CA L IFORNIA ; CHIE F OF M E D ICA L
STAFF OF TH E H E LPING STAT ION OF TH E SOUTHE RN C ALIFORNIAA NTI -TUBE RCULOS IS LE AGUE ,
LOS ANGE LE S , CAL . ; FE LLOW OF
TH E AME RICAN ACADEMY OF M E DICINE ; M EM B E R OF THE
AME RICAN CLIM ATOLOGICA L A S S OCIA T ION ; M EMB E R OF
TH E AM E RICAN T HE RA PE UTIC SOCIE TY ; CORRE SPOND ING M EMB E R OF THE I NTE RNA T IONA L ANT I
TUB E RCULOS IS A S SOCIAT ION, E TC.
NEW YORK
WILLIAM WOOD AND COMPANY
MDCCCCVI I ]
COPYR IGH T , 1908
By WI LLI AM WOOD AN D COMPANY
Prbflrd by
The Al up lo‘ I 'n ‘
ss C0
York ,Pa.
T O
M Y PARE N T S
WH OSE I NFLUE NCE A ND W I S E COUNS E L E VER H A VE
BE E N A N I NSPI RATI ON TO H I GH E R
I D E A LS AND MORE '
FA
TéH FUL WORK
I ‘ rx
o

CONTENTS .
CHAPTER I .
PROBABLE T IME OF I NFE CTION I N TUBE RCULOS I S
Symptoms of tuberculosis develop'long after in fection ; Tendency
to spread ; Tuberculosis Often un recogn ized ; Childhood a probabletime When in fection common ly
_
occurs ; Proo f of laten cy ; Laten cyan importan t feature of tuberculosis ; Picture of the developmen t oftuberculosis in the body.
CHAPTER I I .
SYMPTOM S AND S IGNS OF E ARLY PULMONARY TUBE RCULOS ISProgress in diagn osis ; M ean ing of early diagnosis ; H eredity ;Opportun ity of in fection ; Later childreh more suscept ible ; Clin icalhistory : Cause of symptoms ; M ala ise; N ervous symptoms ; Respiration ; Cough ; Sputum ; H oarsen ess ;
“Co lds and bron ch ial
catarrhs ; Circulatory system ; Gastro - in test inal system ; An emia ;Pain ; N ight or sleep sweats ; Spitting of blood ; Pleuri sy.
CHAPTER I I I .
E XAM I NATION OF THE PATI ENT FOR EARLY TUBE RCULOS IS 13—24
General rules for examinat ion ; E ar or s tethoscope ; Percussionin strumen ts ; L ight or heavy percussion ; D ifferen ces in the apices ;I nspection : I n spect ion of the patien t ; Lagging; Pupils ; Red lineon gums ; Larynx ; D iflerences in elevation of acromial ends of c lavicle ; Retraction s and depression s . Palpation : E n larged glands ;I n creased fremitus ; Lagging; Palpatory percussion ; Quality of
percussion n o te ; Pitch ; Apical outlin e . Auscultation : D ifficultiesand errors in auscultat ion ; Cause of vesicular murmur ; Roughbreath ing ; Weak breathing ; Pro longed expiration ; Harsh vesicularor peurile ; Cogwheel breathing ; Rales ; Pleural sounds ; Subclavianmurmur.
CHAPTER I V .
D IAGNOS IS OF E ARLY PULMONARY TUBE RCULOS ISBacilli n ot
_to be relied on for early tuberculosis ; Importance of
diagnosis ; Candor W ith patien t ; H emoptysis ; Gen eral picture of
early tuberculosis ; N eurasthen ic type ; Sudden onset ; RepeatedTemperature ; Physical examination ; E xamination of
sputum; Homogeneous smear ; Sta ining for bacilli , “splitter , ”
spores or sporo ids ; D ifferen tial diagn osis of tuberculosis caused bybacilli of the human an d bovine types ; D ifferen tial stain for humanand bovine bacilli ; Picric acid stain for tubercle bacilli ; ParticlesOf mucus taken from laryn x for examination ; Spengler
’s digestion
method ; I lkeW itsch’s method of cen trifugation ; ROn tgen rays ;
Tuberculin test ; Fears of tuberculin ; V irchovv’s opin ion ; Can
V
CO N TE N T S
tuberculin set up act ivi ty in laten t foci? Can tuberculin cause acutemiliary tuberculosis ? Reaction ; Local reaction ; General reaction ;When should test dose be given ? D osage for tubercul in test ; I s thetest reliable?H ow give tubercul in test ; S ite of injection ; Con traindicat ion s ; What preparation shouldbe used?Who sha ll admin isterthe tuberculin test?Tuberculin test as proof of cur e ; Tuberculindiagnosis in in fancy and childhood (Pirquet). Opthalmo -Tubercu
l in T est .
CHAPTER V .
SYMPTOMS AN D S IGNS OF ADVANCE D PULMONARY TUBERCULOS IS AN D I TS
COMPLICATIONS 47 59
Clin ical history in advan ced pulmonary tuberculosis : Cough ;Sputum ; D igest ive disturban ces ; Circulatory system ; N ervoussystem ; Co lds and bron chial ca tarrhs ; -H
_
oarseness ; Pain ; N ightsweats ; Temperature; Cessat ion of menstrual flow .
CHAPTER VI .
PH YS ICA L E XAMI NATION OF THE PATI ENT IN A DVANCE D PULMONARYTUBE RCULOS ISI nspect ion : I n spect ion of patien t ; Condition of in tegumen t overchest ; Shape of the chest ; Phthisical chest ; Ankylosis of the un iono f first n
'
bwith sternum ; M ovemen ts of the chest ; Cardiac impulse;D iaphragm phenomenon .
- Palpat ion : Vocal ‘ fremitus ; Frictionfremitus ; D etect ion of changes in lung by palpat ion ; Lagging ;Palpatory percussion . Percussion : What can be el icited by percussion ?Auenbrugger’s method ; Ebstein
’s touch percuss ion ; Ausculta
tory percussion and auscultato ry stroking ; E last ic tube percussion ;The ordinary method of percussion ; Outline lun g boundary ; M o
bil ity of lower lung boundaries ; D ifferen t iat ion of in tercostal neuralgia and pleural pain s ; H eart outli ne ; Vari ous percussion notes ;Percussion n o te in acute mi liary tuberculosis ; A cute pneumon icphth isis ; Chron ic tuberculosis ; Percussion over cavities . Auscultat ion : Weakened respirato ry murmur ; I ncreased respiratory murmur ; Pro longed expiration ; N o rmal bron chial breathing ; Pathological bronch ial breathing ; Amphoric breath ing ; M ixed breath ing ;Rough breathing ; Adven t itious sounds ; Rales ; E ffect of cough on
rales ; S ize o f rales ; Constancy o f Tales ; M etallic Tales ; D ry rales ;Rales and sounds o f pleural on
'
gin ; Vo ice transmission .
CHAPTER V I I .
D IS PLACEM ENT OF Tm: T HORACIC VISCE RA IN ADVANCE D PULMONARYTUBE RCULO S IS 79
—OI
N o rmal changes in position o f o rgans o f respirat ion ; I nspiratorytho rax ; l ixpirato ry tho rax; N o rmal changes in pos it ion o f heart ;Po sit io n o f heart depends on pericardium ; S ize o f pericardiumaffects the po sitio n o f the heart ; M ovabil ity o f heart depends alsoUpo n co nditio n o f aorta ; N o rma l outl ine o f the lungs ; N ormal outline o l
'
the heart ; Impo rtance o f recogn izing change in outl ine ;Cause o f (l iSplacemen t ; D isplacemen t o f the lung ; l ifl
‘
ect o fdisplacemen t o f the lungs ; l ) iSplacemen t o f the heart ; D etect io n o f apexl i t-at d illicult ; E ffect o f changed po sit ion upon the heart and lungs ;M anagemen t o f pat ients who have displacement ; A ids in detectingd iSplacemen t.
CON TE N TS vii
CHAPTE R VI I I .
PROGNOS IS IN TUBE RCULOS IS 92—100
N ature of the in fection ; Exten t of the disease importan t ; Whyincipien t tubercul osis is most curable ; Responsibility ~ of cure intuberculosis upon family physician ; Patien t
’s respon sibil ity in diag
n osis ; Pat ien t’s responsibility in cure; Prognosis in advan ced cases ;
H eart in prognosis ; D igestive system ; Loss of weight ; Temperature ; I ndividual resistan ce; Former environmen t ; Finan cial condition ; Temperamen t ; Age; Complication s ; H emoptysis ; Pregn an cy ; N umber of bacilli and progn osis ; H ow long treatmen tnecessary.
CHAPTER IX .
PROPH YLAX ISD ust in fection ; D roplet in fection ; I n fect ion through ingestion ;Bacilli do n ot multiply outside the body ; Personal prophylaxis ;E ffect of sun light upon bacilli ; Tuberculosis a house disease ; L ighting and ven tilation of homes and the tubercle bacillus ; D anger inordinary method of sweeping and
,dust ing houses ; Burden of
prophylaxis n ot en tirely upon the affl icted ; Prophylaxis in ch ildhood ;Prophylaxis for those predisposed to tuberculosis ; M odern methodsof prophylaxis and cure; E ducation ; H ealth board con trol ;D ispen saries ; Classes in tuberculosis ; Sanatoria ; H ospitals ; Sanatoria and hospitals not dangerous to their surroundings ; A lessonfrom D avos.
CHAPTER X .
TH E PRI NCI PLE S UND E RLYING THE T RE ATME NT OF TUBE RCULOS IS 1 14—1 21
Curability ofTuberculosis ; N ature of cure in tuberculosis ; H ow immun ity is produced ; An t ibodies specific ; N ormal health ofiers
resistan ce to disease ; Immun ity the ultimate aim of treatmen t intuberculosis ; Classification of remedial measures ; H ygien i c treatmen t not all ; T ubercle vaccin es specific ; Rat ional treatmen t ;M ethod of treatmen t very importan t .
CHAPTER XI .
TH E OPE N-A I R TRE ATME NT OF TUBE RCULOS IS 1 22—1 28
Fresh air first recommended by Bodington , 1840 ; Fresh air n ot
specific ; What is the effect of open air ?H ow outside and in sideair differ ; Open air harden s pat ien t ; E ffect on nervous system ;Open air improves digest ion and assimilation ; Lessens danger of newan d secondary in fect ion ; Open air lessen s temperature; I s theredanger at beginn ing of treatmen t? Clothing for the tuberculous ;Wet weather n o con tra indicat ion ; (
H ow derive most benefit fromopen air ; Wrong and in sufficien t in struct ion cause many deaths ;Open -air treatmen t at home.
CHAPTER XI I .
D IET IN TUBERCULOS IS WI TH H I NTS FOR TH E M ANAGEME NT OF THE M ORE
COMMON GA STRO - INTE STI NAL COMPLICATIONS . 1 29—141
Presen t system of diet un satisfactory ; Overfeeding ; Evi l effects of
overfeeding ; Rational diet ; Importan ce of milk in the dietary ;M odificat ion Of milk ; H ow admin ister milk so the pat ien t does n ot
CON TE N T S
fear it ; Can milk and frui t be eaten together ? M ilk should bechewed ; H ow much mi lk Should be taken Kumyss ; What are bestfoods for the tubercul ous ; Pro teids ; Fats ; Carbohydrates ; M inutedetails as to diet n ecessary ; Appet ite not safe guide ; Gastric neuroseso f toxic origin ; O rgan ic d iseases of the gastro - in testinal tract ;Hyperchlorhydria ; Hypochlorhydria ; D ilatation of the stomach ;Constipation ; N on -tuberculous diarrhea ; Tubercul ous diarrhea .
CHAPTER XI I I .
RE ST AN D EXE RCISE I N THE TRE ATMENT OF TUBE RCULOS IS 142—152
Value of rest ; Value of exercise ; Rest in fever ; Rest in non—febri lecases ; E ffect of rest upon , cough ; Rest
' in hemoptysis ; The heartand rest ; The heart an d exercise ; Rest and dyspn ea ; Rest whenweight _
is much reduced ; When shall a,pat ient exercise?What
form of exercise is most su itable? Overexert ion ; Rest and exercisefor the lung ; M o tion Of lung n ot on ly un necessary but harmful ;D eep -breathing favors aspiration of mucus in to new parts ; H avebreathing exercises any part in the treatmen t?
CHAPTER X I V .
H YDROTHE RAPY IN TUBE RCULOS IS I 53—164Value of hydro therapy in tuberculosis ; Rel ief of temperature leastimportan t fun ct ion of hydro therapy ; Reaction ; E ffect upon the
skin ; Efiect upon o ther organ s ; Cond itions govern ing bath ; A lcoho lbaths ; Cold sponge ; T epid sponge ; The dripping Sheet ; The wetjacket ; Throat compress ;
‘
Clean sing bath .
CHAPTER XV .
THE SPE CIFIC TRE ATME NT OF TUBE RCULOS IS 16 5—208
N ature of cure in tuberculosis ; D iscovery of tuberculin ; What istuberculin ? D osage of Koch’s tuberculin ; Conven ien t method of
making dilut ion s ; H ope aroused by Koch’s discovery ; Koch’s rules
for treatmen t ; Koch’s rules disregarded ; Reaction again st tubercul in ;
Some good results ; Tubercul in revived ; O ther preparat ions of
tuberculin and all ied products ; Tuberculin , D enys ’ ; Per lsuchtTuberculin (Spengler); Tubercul in (Beraneck) ; Koch
’s new tuber
cul in , T . R . ; Bacillus emulsion (T . E . , Koch) ; Watery extract o ftubercle bacilli (von Ruck) ; Per lsucht emulsion (P. E . Spengler);T . B . Vaccine and P. B . Vaccine (Spengler) ; Tulase ; H ow do
tubercul in and allied products act?Koch’s o riginal view o f theman ner in wh ich tubercul in acts ; Biedert
’
s view ; T rudeau’
s View ;Wright
’
s view ; Evidence o f immun izing power, an imal exper i
men tat io n ; Agglut inat ing power o f blo od increased ; Blood alkal in ity; I ncrease in opson ic power Of blo od serum ; Efl
'
ect o f tuberculin upon cells and leucocytes ; I ClTect o f tubercul in and all iedpro ducts Upo n in fected a reas ; I ncrease o f fibro id t issue ; Tubercul in react io n ; Seco ndary react io n ; Should tubercul in be used on
a pat ien t with fever ? l l ypersensibil ity ; Change o f toxins in treatmen t ; S ite o f inje c tio n ; Wright
'
s method o f employing tubercul in ;N egat ive phase ; (
‘
l in ica l results ; D isease shows less tendency to
Spread ; l ) isease. heals mo re surely and mo re quickly ;relative ly o fmo re va lue in the trea tmen t o f advanced cases ; l l ac il l idisappear from sputum ;
'
l‘
ulw reulo us compl icatio n s disappea r ; l‘
er
manen cy o f resul ts ; Limi tatio ns ; Who sha ll employ spec ifie remedies?I f so valuable . why n o t reco gn ized ? An tituhe rcle serum .
CON TE N T S iX
CHAPTER XV I .
HYPEREM I A 209— 215
A ct ive versus passive hyperemia ; Theories of disease; Ro le Of theblood in in fection and immun ity ; B lood preven ted from en teringin fected areas ; E ffect of hyperemia ; Chron ic heart disease and
tuberculosis ; Preciseness in method necessary ; H yperemia in
jo in t tuberculosis ; H yperemia in pulmonary tuberculosis ; Hyperemia caused by reflected sun light ; H yperemia caused by the;
use of
tuberculin ; H yperemia from position .
CHAPTER XVI I .
SANATORIUM TRE ATME NT OF TUBERCULOS IS 2 16 - 228
Sanatorium depends on its head ; Buildings ; Pavilion and co ttagesystems ; An improved bungalow ; Cho ice of pa t ien ts for a sana
tor ium ; D ifficulty of treating advan’
ced cases ; What complicat ion sare a barrier to treatmen t?Length of treatmen t ; Why a sanatoriumis superior to the home or
_an Open resort ; Air of hopefulness per
vades sanatoria .
CHAPTER XV I I I .
CLIMATE A S A FA CTOR I N TH E T RE ATMENT OF TUBE RCULOS IS 229—241
Climate always importan t ; Climate more Importan t to the s ickthan to the well ; N o specific climate for tuberculosis ; Good use
of bad climate better than bad use Of good climate ; Importan tcon siderat ion s in cho ice of climates ; Primary effect Of climatictreatmen t ; Climate must be suited to the reactive powers of the
pat ien t ; Climatic conditions of nearby places differ ; H igh altitudethought to con fer immun ity ; Immun ity not peculiar to altitude;N ot h igh alt itude but certa in condition s accompanyin g it causes th isapparen t immun ity ; Sun light importan t in the treatmen t Of tuberculosis ; Relat ive merits of high and low altitudes in tuberculosis ;H igh altitude treatmen t con trary to the prin ciple of rest in inflamma
ti on s ; Parts adjacen t to heart heal slowly ; Tuberculosis commonin athletes ; H igh alt itude calls for strong react ive powers ; Whereinl ies the value of climat ic treatmen t?
CHAPTER XIX.
COMPLICATIONS OF PULMONARY TUBE RCULOS IS AN D THE IR TRE ATM ENTTuberculous laryngit is : Frequen cy ; D iagn osis ; Progn osis ; Treatmen t . Tuberculosis of the in testin es : Frequen cy ; S ite of ulceration ; Symptoms ; D iagnosis ; T reatmen t . F istula in ano . Tu
berculosis of the lymphat ic glands :_
Frequen cy of glandular invo lvemen t ; T reatmen t of tuberculous glands in chi ldren ; G landsthe seat of soften ing ; T reatmen t of suppurat in g glands . Pleurisy :Frequen cy ; Varieties ; Symptoms ; Physical sign s rema in ing afterpleurisy ; T reatmen t of pleurisies . Pneumo thorax : Seriousn ess of
pneumo thorax ; Symptoms ; T reatmen t . M ixed in fection : Chills ;Fever ; D iet ; Serum treatmen t of mixed in fect ion ; Convalescen cefrom mixed in fection . H emoptysis : Frequen cy ; Cause Of hemoptysis ; H emoptysis epidemic ; T reatmen t of hemoptysis. Tuber'culosis of the gen ito -urinary tract . Syph i lis . Pregnan cy.
CON T E N T S
CHAPTER XX .
TRE ATME NT OF SYMPTOMS 27 1—279
Cough : E fi'
ect o f cough ; Cause of cough ; Key to treatmen t . N ighto r sleep sweats : Cause of n ight or sleep sweats ; T reatmen t .Fever. Pain . I nsomn ia. D yspn ea .
CHAPTER XXI .
RE LATIONSH I P BE TWE E N TH E PH YS ICIAN AN D THE PATIE NT 280—285
Candor between physician and pat ien t n ecessary ; Great respon sibility on physician s ; The pat ien t must know that he has tuberculosis ; D eceptive terms not permissible ; The patien t should beto ld in a humane mann er ; Co -Operat ion of patien t and physiciannecessary ; I n telligen t patien ts , best pat ien ts ; M utual in terest of
physician and pat ien t ; Tuberculous patien ts need physician’s guid
an ce; Patien ts need men tal support of their physician .
CHAPTER XXI I .
RE SULTS AN D PERMANE NCY OF RE SULTS IN PULMONARY TUBE RCULOS IS . 286—300
The beginn ing of systematic treatmen t of tuberculosis ; E ffect ofKoch’s discovery ; I dea of treatmen t grows slowly ; Americanpioneers in phthisio
- therapy ; Tuberculosis yields readily to treatmen t ; Cure depends upon earl iness of diagnosis
: N ever a t imetoo early to begin treatmen t ; Cure of tuberculosis an investmen t ;T reatmen t greatly prolongs l ife ; Results of treatmen t comparedwith results in o ther diseases ; Sanatorium and hospital resultscompared ; Permanen cy of results ; Premature in terrupt ion of
treatmen t preven ts favorable results ; What is a cure?Rales and
permanency of results.
APPE N D I X .
CHAPTER I .
T I IE D UTY OF TH E STATE IN TH E PRE VE NTION OF TH E SPRE AD OF TUBE RCULOS I S AN D I TS E SPE CIAL D UTY IN E STABLISHING STATE SANATORI A
CHAPTER I I .
A STUDY OF TUBE RCULOUS I NFECTION 30 7—3 18
CHAPT ER I I I .
CULTURE PRODUCTS IN TH E T RE ATME NT OF TUB ERCULOS IS 3 19—33 7
CHAPTER I V .
A (J IzIT I eA I , STUDY o n:"I
‘
U I I I-c UL I N A N D A LLIED PROD I I cTs BAS E D UPONA CO LLECTIVE I NVE STIGATION. 338
-
35 1
ILLUSTRATIONS .
PLATEI . Splitter (spores and sporoids) from sputum .
FIG .
Chart i llustrating tubercul in test .
S tethoscope, percussion hammer and pleximeter .
_(a) and (b). Chan ges in apical outline
A rt ific ial mixture of pure cultures of human and bovine bacil l iJE
W
IQ
H
stained by S pengler ’s Hul lenmethode.
”
N atural mixture of bacill i of bovin e and human type in sputum
stained by_
Spen gler ’s H ii l lenmethode ”. after being first s tained
by ac id fuchsin (2 per cen t'
)6 . Temperature curve of in active chron ic pulmonary tuberculosis .
T emperature curve showin g activi ty in chron ic pulmonary tuber
culosis .
8 . Temperature curve showing hectic type.
T emperature curve of a compl icatin g tuberculous pneumon ia .
Temperature curve of acute miliary tuberculosis superimposed
upon a chron ic pulmon ary tuberculosis .
Curve Showin g temperature persisten tly below n ormal .
Curve showin g temperature persisten tly above n ormal,probably
caused by a_
cl osed fo cus .
Temperature curve showing pre-men strual rise in patien t with
early tuberculosis.
Temperature curve showing men strual r ise in patien t with ad
vanced tuberculosis .
I llustratin g the method of del iverin g the stroke in the author ’s
elast ic tube percussion .
Showin g size of so ft elastic tube used by the author I n elast ic tube
percussion .
(a) and (b). Schematic represen tat ion of chest Of childand adult
showing descen t of an terior wal l of thorax and in tra- thoracic
viscera as adult life approaches .
T horax represen t ing the outlines of the in tra- tho racic o rgan s as
usually foun d in a
'
heal thy adult .
Showing displacemen t of thoracic viscera resultin g from con trae
t ion of left lun g and compen satory emphysema of the r ight .
xi
x i i I LLUSTRAT I ON S
FIG . PAGE20 .D isplacemen t o f thoracic v iscera , same cause as in F ig . 19 . 86
2 1 . D isplacemen t o f tho rac ic v iscera, same cause as in Figs . 19 and 20. 87
22 . Dr ip sheet , first pos i t ion (Baruch) 1 59
23 . Drip Sheet , second pos ition (Baruch). 1 60
24 . Drip sheet , turn in g (Baruch). 1 6 1
25 . Dr ip Sheet,fr iction (Baruch). 1 6 2
26 . Wet jacket . 1 63
2 7 . T hroat compress - properly applied .
“
1 6 3
28 . A and B . Chart i llustrating the an tagon ist ic action of vaccmes
made from bacill i of the human and bovine types.
29 . Chart of patien t run n ing fever fo r pro longed t ime. Reduced
after a few doses of the proper vaccin e .
30 . Chart il lustrat ing same as Fig . 29 .
3 1 . Chart illustrat ing same as Fig. 29.
3 2 . Chart i l lustrating the In crease in the opson ic index after in ject ion
of tubercle bacil lus vacc ine (Wright)
33 . Chart shovving the tubercul in reaction as affec ting the pulse
rather than the temperature.
34 . A, B ,
C and D Show the improvemen t in lung cond i t ion made
from M arch 18 to July 3 , by a patien t who;was treated by in
jections of tubercul in during the course of a chron ic pro lo nged
fever as Shown i n Fig . 3 5 . 190— 19 1
3 5 . A , B , C and D . T emperature curve of patien t whose find ings o n
auscultat ion are Shown in Fig .
‘
34. 192— 193
36 . Floo r plan of po rtion of Po t tenger Sanato r ium: 2 18
3 7 . Po ttenger Sanato r ium Bungalow . 2 19
Floo r plan o f Po ttenger Sanatorium Bungalow. 220
39 . Paravertebral triangle of dullness (G rocco’s S ign) (Thayer and
Fabyan )
40 . T ransverse section of ches t in an artificial ly produced r ight
pleural effus io n showing d isplacemen t of mediastinum (Baduel
and S ic il ian o ).
4 1 . Cha r t show ing favo rable act io n o f.
strepto lytic serum .
42 . Chart Show ing favo rable actio no f n i troglycerine and veratrum Viride
in lowering blo od pressure .
lNTRODUCT-ORY .
A number of books have appeared recen tly trea t ing of the subject of Tuber
culosis . T hese have been wr itten from d ifferen t standpo in ts,as is na tural
in deal ing w i th a disease which has so many phases . A s yet, however, n o book
has appeared which endeavors to give a full d iscussion of the d iagnosi s,bo th
'
early and late,of tuberculosis
,n or has
'
any of them con sidered the treatmen t
of tuberculosis in the l ight of modern studies in immun ity.
I n treat ing the subject of diagnosis,the author has attempted
,wherever
possible, to explain the cause of symptoms and the ra t ionale of the physica l
sign s“
. I n many instan ces he is n ot in accord W i th the usua l explanat ions and
has suggested modifica tion s .
H e has described his new method Of elastic tube percussion and endeavored
to po in t out its advan tages and l im itat ions.
H e has also descr ibed more fully than can be usually found in works of th is
character the effect of advan ced tuberculosis on the heart,also the con tract ion s
and compen satory emphysemas wh ich occur on the part of the lung, in order
to carry on the fun ct ion s of resp iration where one or bo th of these organ s are
ser iously damaged .
Tuberculosis is a d isease caused by a specific micro -organ ism and l ike al l
such d iseases i t is cured by the establishmen t of immun i ty . Th is fact has been
kept uppermost in min d in d iscuss ing the treatmen t of the d isease. The author
has endeavored to discuss clearly and impartially those measures which are of
greatest va lue in br inging about improvemen t or cure. H e has endeavored
to defin e the possib i l i t ies of each measure and to Show its limitations .
Remedial measures may be d iv ided in to six classes :
First — Those wh ich aid in bringing about immun i ty by endeavoring to
restore the n atura l resist ing power of the pat ien t to a po in t as n early norma l
as is con sisten t wi th the _cond it ion presen t . Among such measures we must
c lass fresh air,hygien ic measures, proper d iet, hydro therapy and sui table
ton ics.
Second.— Those which aid in brin ging about immun ity by art ific ially
stimulat ing the body cells to the product ion of more spec ific pro tect ive sub
stan ces . I n th is class belongs vaccina t ion or treatmen t by in ject ion of the
spec ific products of the bac i llus,such as tuberculin ,
extracts of tubercle bacilli
and bac i llus emulsion .
Third.—T hose wh ich aid in establishing Immun i ty by supplying to the
X111
xiv I N TRO D UCTORY
o rgan ism spec ific pro tec t ive substan ces which have been produced by vaccinat
ing some an imal such as the horse or
.
cow . Under this head come the various
an t itoxic sera .
Fourth .— Those measures wh ich causeap increased flow of blood or lymph
to the sea t of in fect ion , bringing .amater amoun t of spec ific an t ibodies in
con tact with the bac i lli thus causing their destruction . B ier ’s hyperemia,Finsen light
,and poul tiCing
'
are measur es whose action are explained in this
mannerF ifth - Remedi es and measures which relieve symptoms.
S ix th .-Those which are d irected toward the cure of accompanying mixed
in fec t ion .
I t is the author ’s desire in the prepara tion of th is book to stimulate his readers
to take a broader view of tuberculosis than that usua lly taken . H ehas endeav
ored to Show that the d iagnosis of tuberculosis consists in more than fin ding
bacill i in the sputum, and that its cure consists in more than the adoption of
fresh air .
I f he shall have con tr ibuted on ly a l i ttleto the early d iagnosis of tuberculos is,and shall have placed the various therapeut ic measur es in .a l ight whereby they
may be shorn of their mystery and applied more in tell igen tly in the treatmen t
Of th is d isease,his purpose sha ll have been accompl ished .
I n o rder to make the discussion more complete the author has d igressed,at t imes
, to consider'
o ther subjects in rela t ion to the main theme ; and while
th is has caused some repeti tion,i t has seemed necessary in order to presen t the
subjec t to its best advan tage. Remember ing tha t books of this kind are ei ther
used fo r reference o r read bv S ingle chapters rather than as a who le, i t isbel ieved tha t this will be apprec iated by the reader .The author has endeavored to descr ibe his own experien ce in the d iagnos is
and trea tmen t o f tuberculosis,and has undertaken to give n o op in i on which his
experience would no t warran t
The autho r is indebted to his asso c iate,Dr . Charles C . Brown ing
,for many
helpful suggest io ns; to Dr . Boardman Reed , for reading and cr i t ic ising thechapter o n D iet ; to Pro fs . Weichselbaum
,Tandler
,M aragl iano , and B ier
,
l ’r iva t D o cen t S to rk and Dr . Carl Spengler for many courtes ies and spec ialo ppo rtun it ies a ffo rded fo r the invest igat ion o f spec ia l subjects ; to his w i fe,Adela ide B . Po ttenger, l ) r . Seth D . D ice
,M iss C. M . Brown and M iss Laura
l iennett fo r read ing and co rrect ing the manuscript and rendering o ther valuableassistance.
F . M . P.
l Mgr /rs ,J a nua ry, 1908 .
PULMONARY TUBERCULOS I S
CHAPTE R I .
THE PROBABLE TIME OF I NFECTI ON I N TUBERCULOS I S .
Formerly, it was believed that tuberculosis was inherited and tha t the
d isease o ften rema ined in the body for years in an undeveloped form . When
the heredity theory was a ttacked,many who had hel d to it would not accept
the theory of post-nata l in fection ,because they o ften fa iled to find a h istory
of exposure to in fect ion immediately prior to the time tha t the d isease was
d iscovered . I n acute in fections the period of in cubation is usually short
and the source of in fect ion is in many cases traceable. The same was ex
pected in tuberculosis, and a fa ilur e to find it retarded the acceptan ce of the
theory .
I t is probable that the fir st en tran ce of tubercle bacilli in toSymptoms Pf the body, with the formation of the fir st tubercles, causes fewTubercul o si sD evelop Long I f any recogn izable symptoms . TuberculosI S as we knowA fter I n fection . it
,as we are able to detect it, is a process more or less advan ced
A tubercle is a tiny structure,about the size of
'
a millet seed .
I n order to be able to detect a tuberculous focus, the area of invo lvemen t
must be of con siderable S ize (some authors claim as large as a marble). Thus
i t can readily be seen tha t we diagnose the d isease after it has extended .
I n.
fact,this tenden cy to spread is one of the character istics
of the disease and the on e thing which causes tuberculosis
to destroy life. There is a lways a battle fought when an
in fection occurs. On one S ide,we have the tubercle bac ill i ;
on the o ther, the defen sive forces of the ind ividual a ttacked . I f the l a tter
are sufficient, the invaders are destroyed ; if n ot, the bac illi are deposited in
the tissues and form a focus from which they con tinue to a ttack their host,endeavoring to establish themselves in new tissue. O ften , while . the defen
sive forces are not Sufficien t to destroy ' the invading organ isms, they are
sufficien t to check the progress of the invaders and preven t them from en ter
ing new tissue . I n nature’s effort to protect the host, she Sometimes throws
2 PULM ON ARY TUBE RCULOS I S
a wall around the bac i ll i , and reta in s them impr isoned ; Sometimes she converts
the sea t o f in fect ion in to ca lc ified areas ; and, aga in , She causes a n ecro sis of
tissue with break ing down and scattering and,somet imes, expulsion of the
germs . When the bacil l i are walled off or en capsulated as i t is called,they
may reta in their v i tal ity for years and yet may never cause any further trouble.
On the o ther hand, the pa t ien t’s resist ing power may be lowered ; or some
in fl amma tory d isease may affect the air passages, such as bron chitis, la gr ippe
o r pneumon ia ; o r through some act ion on the part of the germs themselves,the encapsula t ing wal l may be broken doWn and the bac i lli may escape and
form new tubercles in previously healthy t issues . A t th is stage of the disease
the pat ien t may show some symptoms, wh ich after a t ime may become quies
cen t . Th is process oi al terna ting activity and-
quiescen ce con t inues un t il the
symptoms become more and more man ifest and then the pa tien t becomes
a larmed and seeks advice . Doubtless most patien ts who Seek our adv ice
have had the in fection for at least severa l mon ths and, more probably, years.
The fo llow ing case i llustra tes very wel l the manner in which tuberculo sismay rema in in the system for years and years ; and then ,
through a soften ing
of the encapsulat ing wa ll , the bac ill i may be set free and the disease make
i tsel f pla in ly recogn izable.
M rs.
’ H . L . S ., aged 6 2, had assoc iated with her fa ther
,who was suffer ing
from tuberculo sis at the time of her b irth Un t il his death which occurred whenshe was two years o ld . When she was eight years of age, her mo ther,w ith
whom she had l ived during a portion of the latter ’s illness, a lso died of tuber
culosis . The patien t Showed n o spec ia l symptoms,except that she was not
very strong,un t i l She was seven teen years of age when she became “
run
down,
” lost her appet i te and enduran ce,lo st weight, became hoarse and had
n ight sweats . She was forced to leave her schoo l and was to ld that her lungs
were weak . The pa tien t rega ined her heal th and showed no further symptoms fo r some t ime. She married and at the age of 30, gave premature
b i rth to a ch i ld,wh ich d ied after a few days . A fter confinemen t, She rega ined
her strength very slowly,suffered from repea ted co lds and coughed severely .
She was aga in pro nounced to have weak lungs, and was treated w ith cod
l iver o il and whiskey,and sen t to N o rth Caro l ina fo r a change of cl imate.
She o nce mo re rega ined her heal th and showed no further sign s o f trouble
unt il,about three and o ne-hal f years ago , she had an attack o f whoop ing
co ugh . S ince then ,her co ugh has co n t inued with a gradual increase in its
sever ity, and in the amoun t o f expecto rat io n ; and, during the past year her
strength has gradua lly fa iled . Upo n co nsulting her physic ian fo r some o ther
tro uble , it w as fo und tha t she was suITer ing from chro n ic bro nch it is , withemphysema a nd tha t she had a tuberculo us les io n o ccupy ing the upper purtio n o f bo th lungs extending to the fourth rib an terio rly and to the m iddle o f
the scapula po ster io rly.
4 PULM ON ARY TUBE RCULO S I S
in fect ion takes place and the time that the child is most apt to suffer fromcatarrhal cond it ions of the stomach and bowels.
“
4 . M ore atten t ion should be g iven to the care and feeding of chi ldren ,so that their systems maybe resistan t to in fect ion .
5 . A ll tuberculous children ,whether they have lesions in the glands
,
bones, lungs, or any o ther part of the body, should be treated for their d isease.
”
That a fo cus of in fect ion may l ie dormant in the system,
enclosing bac i ll i which are virulen t,is shown by the fact
tha t the disease can be produced by ino culating an imals
with glands of individuals in whom no symptoms wha tever were recogn ized
during l ife. A no ther proo f is the usual mann er in which the d isease o ften
starts up after an acute il ln ess, when n o opportun i ty for a new in fection could
have o ccurred. The on ly sa t isfactory manner of accoun t ing for the symp
toms at these t imes is to suppose a previous in fection ,and recogn ize the possi
bil ity of the bac i ll i ly ing in a state o f qu iescen ce. The presumpt ion is qu ite
strong that tuberculo sis is pr imar i ly a glandul ar disease,the baci ll i gain ing
en tran ce through the mucous membrane and being ei ther destroyed o r de
posi ted in the lymphatic glands. From th is focus of in fection bacilli mayfind their way to o ther parts .
Tha t a tuberculous infil tra tion may rema in for a long time without ulcer
ation is proven by our observation of the laryn x. O ften infil tration s may be
observed here for mon ths and even years w ithoirt ulcera t ion taking place .
That the same thing o ccurs in the l ung, we have every reason for bel ieving,from bo th clin ical symptoms and po st-mortem findings .
N o t un til we recogn ize this feature of tuberculosis,can
La ten cy an we understand the d isease. I t is not l ike d iphtheria and
ggg’
gfgfi scarlet fever, which show an in fection , a defin ite in cuba
Tuberculos is. t io n,and then a fully developed disease. I t is a S low disease,
much more chron ic than has been suspected . I n fection maytake place in childhood , but death may not occur un t i l ado lescence o r even
o ld age. The bac ill i may remain in the lung during an en t ire l ifet ime and
produce no recogn izable symptoms ; they may rema in and produce symptoms
at t imes and yet never cause advan ced tuberculosis ; o r , being there, they
may cause an act ive d isease at any t ime.
The p icture o f tuberculo s is,as I form it
,is that o f a lo cal ized
Picture o f the infect io n,which every now and then shows a tendency to
gfe
’fii
ggxfilbt
sisspread to new
’
t issue,especial ly to that surro und ing the
in the Body. parts affected . With the in fection o f new t issue, symptoms
ei ther sl ight o r severe may be produced acco rd ing to the area
invo lved, the to xins pro duced and the susceptib il ity O f the ind ividual . From
the t ime tha t infect io n o ccurs un t il the t ime tha t a severe disease is presen t
may be a brief per io d o n ly o r i t may be years . The p icture is tha t o f a ser ies
TH E PROBABLE T I M E OF I N FE CT I ON I N TUBERCULOS I S 5
of quiescen ces and activities. When the disease has on ce become thoroughly
act ive and has invo lved a con siderable area of tissue,i t w i ll less o ften a tta in
the cond ition of arrestmen t or qu iescen ce ; but, even if it does n ot do th is,the
same process goes on with an attempt at exten sion on the part of the invaders
and an a ttempt at defen se on the part of the host, w ith first one successful
and then the other, un t il , final ly, the d isease is beyond the con tro l of the
pro tect ive forces of the body .

CHAPTER I I
TH E SYMPTOM S AND S I GN S OF E ARLY PULMONARYTUBE RCULOS I S .
Owing to the fact that tuberculosis is a commun icable d isease,an early d iagnosis should a lways be made for the pro tect ion
of those who must associate in timately with the afflicted ; and,S ince the cur ab i l ity of the d isease has been establ ished
,an early d iagnosis is
necessary, in o rder to give the pat ien t the best chance of cure.
Our conception of early d iagnosis has changed very greatly in recen t years .
Before the d iscovery of the tubercle bac i llus,the d isease was rarely recog
n ized un t i l i t was far advanced ; but, when i t was learned that the expectora t ion
of pat ien ts suffering from tuberculosis con tained the germs, exam ination s
soon establ ished the fact that tuberculosis was presen t befo re the adven t of
grave symptoms. By the use of the m icroscope,then
,a great step fo rward
was made in d iagnosis.
I t was soon no ted that in many cases where bacil li could n ot be found in the
sputum,the same symptoms, in part , were presen t as where bac i lli were found .
Th is was descr ibed at first as a pre- tubercular stage. M ore careful tra in ing
in physical exam inat io n , however, together w ith the tubercul in test,proves
th is to be not a pre- tubercular but an early stage
,before the germs appear
,
o r at least before they are found in the sputum .
Wha t we now understand by an early diagnosis is a d iag
nosis at th is period, before the d isease is advanced and
w ithout depend ing upon the finding of bac i ll i in the sputum .
There is no excuse forany man fa i l ing to d iagnose tuberculo
sis when bac i lli are in the sputum,but to be able to diagnose i t befo re they
appea r is much mo re d ifficul t .
T o be able to make an early d iagnosis, the examiner must be tho roughly
t ra ined in mak ing exam inat io ns and must take t ime to study his pat ien t in
deta i l .
T o make a diagno sis o f tuberculo s is in the stage befo re the appearance o f
bac i ll i in the sputum ,requ i res care
,but a care wh ich is repa id by the sav ing
o f l ives .
S ince i t is so impo rtan t tha t an early diagno sis be made in th is disease,I deem i t w ise to dea l w ith ear lv a nd la te d iagno s is in d i fferen t chapters so as
no t to co n fo und the signs o f the two .
SYM PTOM S AN D S I GN S O F E ARLY PULM ON ARY TUBE RCULO S I S 7
S in ce the overthrow of the theory of hered ity as the cause of
tuberculosis, the importan ce of the fami ly history has decl in ed .
Wh i le i t seems well establ ished that there are very few instan ces in which
tuberculosis has been tran sm itted directly from paren t to Offspr ing, neverthe
less,fam i ly history is importan t as an index of resistan ce to d isease and as i t
bears upon the longevity of the pat ient . I t Shows a lso certa in characterist ics,certa in elemen ts of weakness and strength that may be tran sm itted .
There seems to be a tenden cy among some wr iters to ign ore hered i ty as
hav ing anyth ing at al l to do w i th tuberculosis . I bel ieve this is a great
m istake. N 0 one can shut his eyes to the importan ce of in her ited character istics . We kn ow tha t physica l character istics are transm itted to the offspr in g .
The same con tour of face,the same character ist ic features, the same shape
of chest or of l imb,and the same co lor of the eye and ha ir are found in the
offspring as in the paren ts.
A d iscussion of po lydactylism throws some l ight on th is subject . Clemen t
Lucas (Guy’s Hospital Reports, Vo l . XXV) studied the family history of some
patien ts who fell in to his han ds having an increase in the n umber of d igits.
Referr ing to themhe sa id : A ltogether:the great grandmo ther of my pat ien ts
appears to be respon sible for abnormalit ies occurr ing in n o less than twen ty
four person s out of a to tal of eighty descendan ts,or thirty per cen t of those
carrying her blood .
”
When we see such marks of hered ity as above men tioned appertain ing to
physical character istics and n orma l t issue,i t seems to me that i t requ ires very
l it tle,if any, stretch of the imaginat ion to bel ieve that i t is probable that a t issue
of lpw resist ing power m ight be tran sm i tted from paren t to offspring, whereby
the ch i ld is rendered more suscept ible to the in fluen ce of the tubercle bac i l lus.
Wh i le recogn izing environmen t as being the greatest factor, yet I bel ieve we
have gone too far in our dis'
fégard for the in fluen ces of hered ity.
An importan t po in t to invest igate in family h istory is whether
or n ot the suspected ind ividual has been assoc iated w ith any
member or members of the fam i ly who have had tuberculosis.
I n making thi s in qu iry it must be remembered that an assoc iat ion years
before may be the direct cause of an in fect ion at the presen t t ime. A n asso
c iation in ch i ldhood Offers as great,i f n ot greater opportun ity for in fect ion to
take place than an assoc iation in later life. M any exper imen ts have been
made which Show that the floors of rooms occupied‘
by tuberculous pat ien ts
are more apt to be con tamina ted than any o ther part of the room,hen ce the
exposure to the child crawl in g about on the floor,and in fecting his han ds, which
he con stan tly puts in his mouth, is the greatest . That bac il l i can l ie in active
in the t issues,is a fact well establ ished
,and i t is n ot at al l improbable that in
many cases of tuberculo sis wh ich are diagnosed in later l ife,the bac i ll i causing
the first in fection were taken in to the system dur in g ch i ldhood .
H eredi ty.
Opportun i tyo f I n fection .
8 PULM ON ARY T UBERCULOS I S
Brehmer po in ted out the fact that the later chi ldren in large
fam i lies are more suscept ible - to tuberculosis than the earlier
ones. This m ight be accoun ted for partly b y the fact that
the mo ther is mor e or less exhausted by repeated chi ld
bear ing .
'
I t would seem a lso that the d ifficulty o f prov id ing
for larger famil ies might react against the later chi ldren of the
CLIN ICAL HISTORY.
Too l ittle atten tion is usual ly given to c lin ica l history . I n tuberculo sis,a
carefully taken cl in ica l h istory w il l usually give sufli cient data upon wh ich to
base a probable d iagnosis, and un t i l the members of the medical pro fession
become more sk i l lful in the use of the stethoscope,they w il l be obl iged to rely
very largely upon ev iden ce obta ined by c lin ica l history for the suggest ion of the
presence of tuberculosis.
The in fect ion w i th tubercle bac il li, the formation of tubercles and the
establ ishmen t of tuberculosis are accompan ied by certain symptoms,w ith
wh ich we are more or less acquain ted .
That many of these symptoms are tox ic i n origin,seems cer
tain , for they are iden t ical w ith those wh ich are produced by
varying doses of tubercul in . Malaise,depressed appeti te
,
nervous irritab i lity,elevation of temperature and pulse- rate are found as the
physio logical effects of sma ll doses of tuberculin and as early signs of tubercu
lo sis .
I n accoun t ing fo r the symptoms Of early tuberculosis, we must also bear in
m ind the fact that we have the lesion in one of the v i tal organ s of the body,and tha t the local lesion invo lves branches of the nerveWhich suppl ies no t o n lythe o rgans of resp ira t ion
,but also those o f c irculat ion and d igest ion . I t is
a lso probable tha t reflex act ion plays a certain part .
M a laise is o ne of the most constan t symptoms o f early tuber
culosis . Pa t ien ts compla in of“ being run down .
”They
have a feel ing o f languo r,being mo re o r less tired wi thout apparen t cause.
T asks (either physica l o r men tal), o rd inari ly perfo rmed w ith ease,become
di fficult . S leep is d isturbed and does no t bring proper rest .
Upo n the part o f the nervous system certa in symptoms appear .
The pat ien t o fton shows a change in d ispo sit io n . H e mav
become irritable o r melancho l ic . N eurasthen ia is usual lv
presen t to Some degree . The writer bel ieves that a tubercular process is o ften
(though und isc o vered) the cause o f neurasthen ia'
. There is also presen t a vaso
mo to r distu rba nce . Pa t ients experience a flushed feel ing upo n the leastexc itemen t a nd o ften su ffer from co ld hands and feet and sensat io ns o f ch i ll i
M ala ise.
SYM PTOM S AN D S I GN S O F E ARLY PULM ON ARY TUBE RCULO S I S 9
ness . Sweat ing, espec ially in the ax ill a, is n o ted, the perspirat ion o ften runn ing
down the sides in great beads wh i le the pat ien t is undergo ing exam ina t ion .
Resp irat ion may be hurr ied and the pat ien t may complaim
Of Shortness of breath .
Cough may or may not be presen t . A s a rule,if cough 18
presen t,it is on ly a S l ight hack and not at al l con stan t . I t
may be no ted on ly after exert ion,after pro longed conversat ion ,
after laugh
I ng or after tak ing a deep breath . I t is usua lly.
accompan ied by a t ickl ing
sensat ion in the laryn x,mak ing the patien t th ink that the throat is the seat
of the trouble.
Respira tion .
A t first,no sputum is presen t . Later
, some mucus or
muco -purulen t sputum is ra ised,which may or may n ot con
ta in bac i ll i . When sputum is presen t i t should a lways be examined,and r e
peated exam inat ion s should be made before a negat ive op in ion 13 given ; I n
fact,a negat ive opin ion should not be g iven in early cases as a result of m icro
scopical find ings .
Hoarseness is presen t as an ear ly symptom,in many cases .
This can be due to ei ther reflex st imulation of the_
branches
of the vagus in the lung, or to pressur e caused by en larged tuberculous glands
on the recurren t laryngeal nerve or to the latter being bound down by ap ica l
pleura l adhesion s .
Pat ien ts suffering from early tuberculosis are subject to
Egfigflgfin d frequen t “ co lds” and attacks of bron chia l ca tarrh . These
Ca tarrhs.rarely begin as head co lds n or do they run the course of ord i
nary co lds in the head,but last o ften a mon th or more.
Sometimes the pat ien t w i ll n ot be free from colds and ' bron ch ial catarrh
for two or three mon ths at a t ime. A ny“ co ld ” that lasts for a mon th is
susp ic ious .
Sputum.
H o arsen ess.
An instab i l ity on the part of the heart is n o ted . The number
Of_
heart beats is usually in creased . W ith a sl ight lesion ,the
pulse-rate may reach as h igh as 1 20 . Th is tachycardia is
most pronoun ced in young patien ts.
”
I n some cases,in stead of the pulse—rate
bein g constan t ly h igh,it is variable. A t rest , it may approach or reach the
norma l,but with the least exert ion
,men tal or physical
,i t may reach 100 or
even more.
The tachycard ia of early tuberculosis is accompan ied by a lowered blood
pressure. The irr itat ion of the tubercle tox in causes a d i latat ion of the
arter ioles .
E arly tuberculosis causes in stab i l i ty in al l the pr in c ipal systems
of the body . I n th is,the gastro—in test inal tract is n o excep
tion . The ton gue is usua lly sl ightly coated . The appet ite
is capr ic ious . T here may be any cond it ion from a sl ight im
I o PULM O N ARY T UBE RCULO S I S
pa irmen t of appet ite to an abso lute d isgust for food . Usually , the body
weight suffers a sl ight decrease ; it may be on ly a pound or two or i t may be
severa l poun ds.
The blood form ing organ s seem to suffer early in the disA n em ia .
ease, for an emia 15 a to lerably constan t symptom of early
tuberculosis.
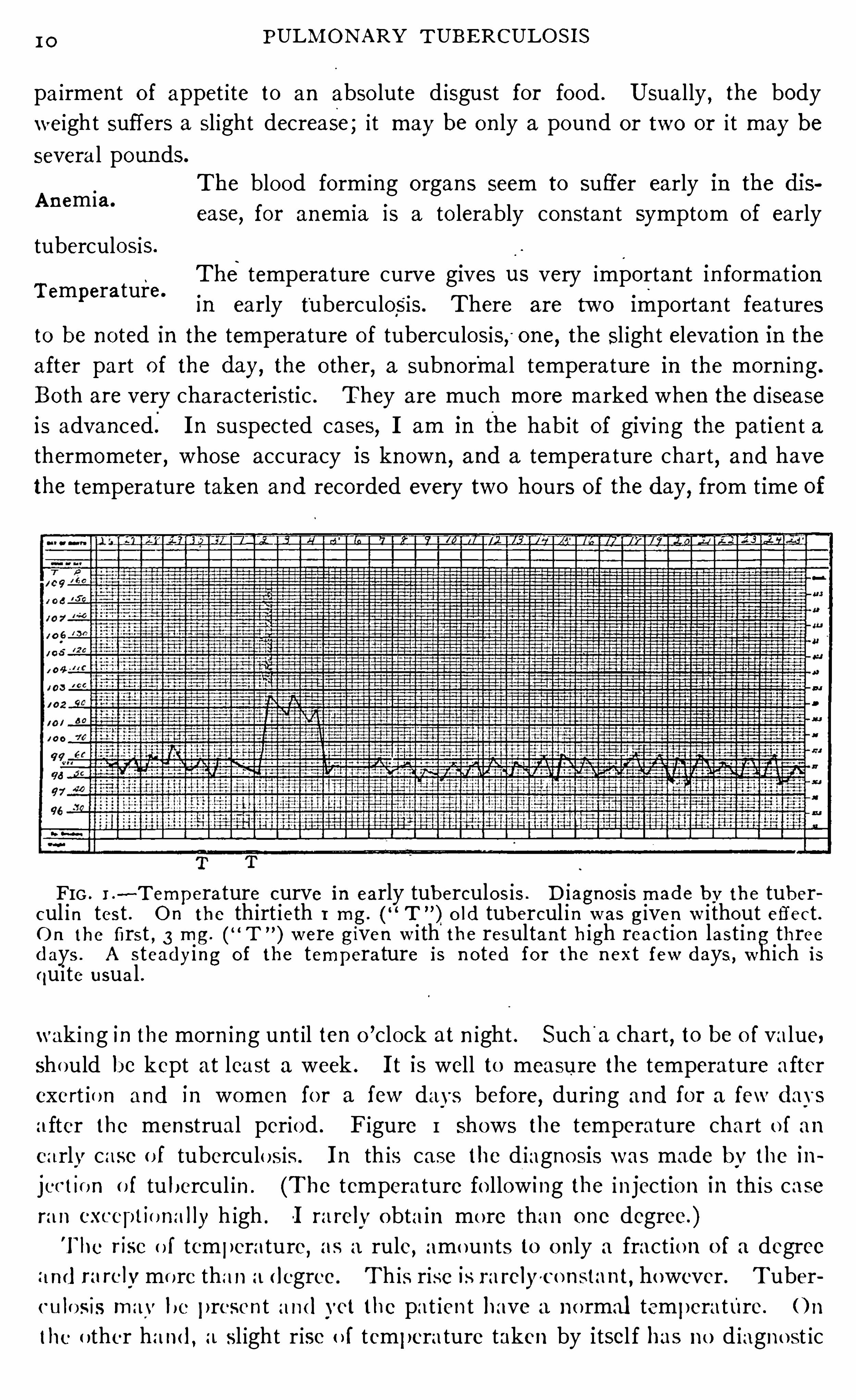
The temperature curve gives us very importan t in format ionTemperature.
in early tuberculosis. There are two impo rtan t features
to be n o ted in the temperature of tuberculosis; one, the sl ight elevation in the
after part o f the day, the o ther,a subn or
'
ma l temperatur e in the morn ing .
Bo th are very characteristic . They are much more marked when the d isease
is advanced: I n suspected cases, I am in the hab it of giving the patien t a
thermometer , whose accuracy is known ,and a temperature chart
,and have
the temperature taken and recorded every two hours of the day, from time of
FIG . I .—~T emperature curve in early tuberculos is . D iagnosis made by the tuber
cul in tes t . O n the th irt ieth 1 mg. T”) O ld tubercul in w as given w i thout effect .
O n the first , 3 mg . w ere given w i th the resultan t high react io n last ing threedays . A s teadying O f the temperature is n o ted fo r the n ext few days , wh ich isqu ite usua l .
wak i ng in the morn ing un t il ten o’clock at n ight . Such
'
a chart,to be o f value,
Should be kept at least a week . I t is well to measure the temperature after
exert io n and in women fo r a few days before, during and for a few day s
a fter the menstrual period . Figure I shows the temperature chart o f an
ea rly case o f tuberculo s is . I n th is case the d iagno sis was made by the in
j ectI o n o f tubercul in . (The temperature fo llow ing the in jection in this case
ra n CXCCPl lUn i l l ly h igh .-I ra relv obta in mo re than one degree.)
The r ise o f temperature, as a rule,amo un ts to o n ly a fract io n o f a degree
I nd rare lvmo re tha n adegree . T h is rise is rarely'co n stan t,however . Tuber
culo s is may be presen t a nd yet the pat ien t have a n o rmal temperature. O n
the o ther ha nd , a sl ight r ise o f temperature taken by itsel f has no d iagno st ic
I 2 PULM ON ARY T UB E RCULO S I S
There seems to be a lack of appreciation of what is mean t
by n ight sweats . The sweats in early tuberculosis are not
as severe as those wh ich accompany the later stage of the
d isease. They may more appropriately be ca lled sleep sweats,for they mav
occur whenever the pat ien t falls asleep,whether i t be at n ight o r durin g the day.
The sp i tting of blood must always be con sidered as a symptom
of tuberculosis un t i l defin itely proven o therw ise. Among
scren tific physic ian s the expression “ throat hemorrhage
can no longer sat isfactorily accoun t for the spitting of blood .
Hemoptysis is o ften the fir st S ign that there is anything wrong with the
pat ien t . Th is may amoun t to - on ly a streak or Spo t of blood as it Often does,or i t may be qu ite severe. The amoun t has no sign ifican ce as to the exten t
o f the d isease, except that as far as I am aware, a fata l hemorrhage has never
occurred I n early tuberculosis. These sma ll amoun ts of blood are most
l ikely extravasat ion s, wh i le the larger ones are due to the Open ing of vessels.
Bac i l l i may frequen tly be found in the sputum fo l lowmg hemoptysis .
An early hemoptysis Should a lways afford the patien t the advan tage of
early treatmen t .
A history of pleur isy should a lways make us look carefully
fo r tuberculosis elsewhere. W hi le it is true that there are
no n - tuberculous pleur is ies, yet, at the same time,tuberculos is fo l lows in these
cases SO o ften that a pat ien t giving a history of pleurisy should be exam ined
wi th extreme care. Koch reports that per cen t of a ser ies of pleurisies
w i th effusion reacted to tubercul in . (Tran sact ion s Bri t ish T uberculosis
Congress, Vo l . I I I , page
The more knowledge we have of tuberculosis the greater our bel ief in the
tuberculous nature of n early al l pleurisies . Tuberculous foci wh ich are
inac t ive and which may be unrecogn izable by o rd inary examinat ion s may be
the cause of pleurisy . A n effusion in the lower part of the pleura maybe due
to a tuberculous process at the apex,the flu id being poured out and grav ita
t ing to the lowest part .
N igh t o rS leep Swea ts .
Pleurisy.
CHAPTER I I I .
EXAM I N ATI ON OF THE'
PATI E NT FOR E ARLY
TUBE RCULOS I S .
The ro'
om in which the patien t is‘
to be examined should be
well l ighted and warm . T he patien t Should remove al l
clo th ing to the wa ist,so that al l port ion s of the chest may
be examined . A loose shawl of some washable material
should be thrown over the patien t f or warmth and to avo id un necessary
exposure. I t ' is very essen t ial that that po rt ion of the chest wh ich is being
examined be bare, so as to afford every opportun ity of detecting the most
del ica te changes . in the resp iratory n o te. The changes in early tuberculosis
are very S l ight and a garmen t,n o matter how thin
,w il l in terfere to some
exten t . The handkerchief or chest'
cloth used by some examiners is sub
ject to the same Object ion s as a thin Vest or shirt and Should be d ispen sed
w ith . I t is somet imes sa id that i t is indel icate to expose female pat ien ts in
th is manner . N o thing is indel icate un less made so,and sin ce physician s
should always be gen tlemen,th is objection has n o weight . I have never
yet met a female pat ien t who objected to th is necessary exposure. They
see its importan ce and desire to have the best Op in ion of the examin er and
kn ow that i t canno t be given o therwise.
The chest,should be examined methodically . E very portion Should be
carefully gone over . The supraclavicular and suprasp inous fossm should
be most thoroughly examined . When auscultation is being pract iced the
stethoscope should be placed from two to four t imes over every in tercosta l
space so as to pract ica lly cover the en tire chest . Figur e 34 on page 190
il lustratesg
the chart that I use in record ing the find ings on auscultat ion .
I t is wise to make a chart of the chest in all eases,so that examinat ion s made
at d ifferen t t imes may be compared . Such a chart, to be exact,should be
made as the exam ination progr esses. For this,either an assistan t is n eeded,
or a stethoscope wh ich fasten s to the chest by the suction of a vacuum chamber
(see F ig . 2 page 14) should be employed . The character of the breathing
together with whatever o ther sign s are presen t should be Tecorded on the
port ion of the chart which corresponds to the port ion of the chest examin ed .
I f the record is n ot made as the examinat ion proceeds,the examiner w i l l .
most l ikely forget many of the deta i ls n ecessary for accur acy .
The pat ien t should sit on a stoo l without support for the arms. Wh i le
the an terior part of the chest is being examin ed, he should sit erect,w ith his
I 4 PULM ON ARY TUBERCULO S I S
arms hanging to the side ; and wh i le the posterior, he should fo ld his arms
and bend slightly forward .
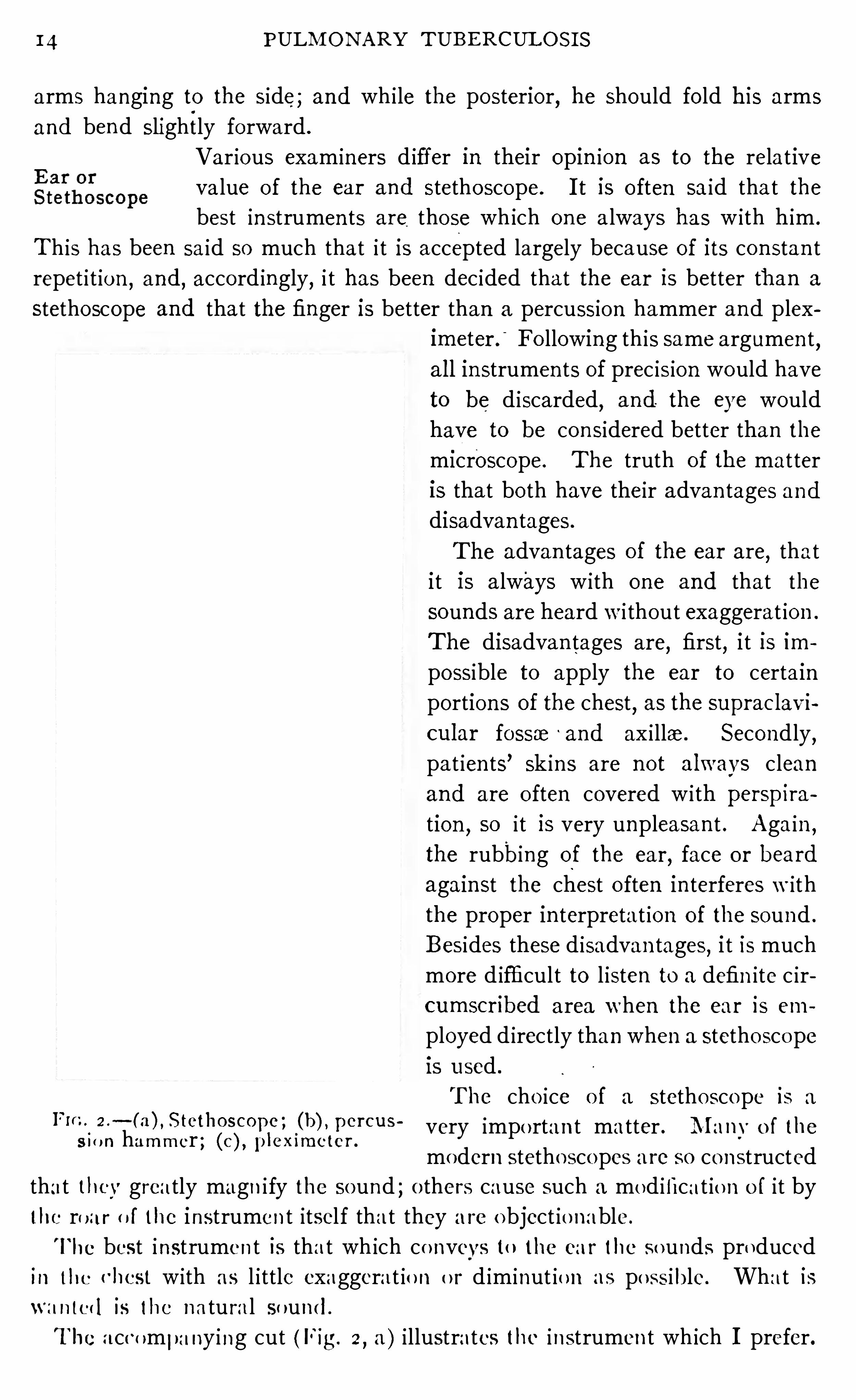
Var ious exam iners d iffer in their opin ion as to the relat ive
va lue of the ear and stethoscope. I t is o ften sa id that the
best in strumen ts are those wh ich on e a lways has w ith him .
Th is has been sa id so much that i t is accepted largely because of its con stan t
repet i t ion,and
,accord ingly, i t has been dec ided that the ear is better than a
stethoscope and that the finger is better than a percussion hammer and plex
imeter .
“
Fo llowing th is same argumen t,
a l l in strumen ts of prec is ion would have
to be d iscarded,and the eye would
have to be con sidered better than the
m icroscope. The truth of the mat ter
is that bo th have their advan tages and
disadvan tages .
The advan tages of the ear are,that
i t is a lways w ith one and that the
sounds are heard w i thout exaggerat ion .
The disadvan tages are,
first,i t is im
possible to apply the ear to certain
portion s of the chest,as the suprac lavi
cular fossae ‘
and ax i llae. Secondly,
pat ien ts’ Sk in s are n ot a lwavs clean
and are o ften covered w i th perspira
tion,so i t is very unpleasan t . Again
,
the rubbing of the ear,face o r heard
again st the chest o ften in terferes w ith
the proper in terpretat ion of the sound .
Besides these d isadvan tages,i t is much
more d ifficult to l isten to a defin ite c ir
cumscr ibed area when the ear is em
ployed d irectly than when a stetho sco pe
is used
The cho ice o f a stethoscope is a
very impo rtan t matter . M anv o f thesum hammer ; (c), plexun c ter .
modern stetho scopes are so constructed
that thcv grea tly magn i fy the sound ; o thers cause such a mod ificat io n o f it by
the ro ar o f the instrumen t itsel f that they a re o bject io nable.
The best instrumen t is tha t wh ich co nveys to the ca r the so unds producedin the chest w ith as l ittle exaggerat io n o r d im inut io n as po ss ible. Wha t isn a n ted is the na tu ral so und .
The accompa ny i ng cut (Fig. 2,a ) i llustrates the instrumen t wh ich I prefer.

EXAM I N AT I ON OF TH E PAT I E N T FOR E ARLY TUBE RCULO S I S 15
I t con sists of a body made of hard rubber . The body has two chambers,
one in the cen ter with Wh ich the ear p ieces are connected and'
an outside one
connected w ith a rubber bulb . By pressing the air out of the bulb a part ial
vacuum is formed in th is outer chamber so that when i t is pressed on the chest
wa ll it w i ll be held by the suction caused by the attempt of the bulb to expand .
T h is outer chamber also acts as a barr ier to extraneous sounds, and confin es
our atten tion to a defin ite po in t . The in strumen t is completed by the attachmen t to the inner chamber
‘
of two so ft rubber tubes which are used to carry
the sounds to the ears .
Th is in strumen t has the advan tage that it '
dOes n ot appreciably magn ify the
sounds ; by its vacuum chamber i t excludes extraneous sounds ; and, if a llowed
to hang by its_
own weight,i t offers exact cond it ion s for comparison at d ifferent
examina t ions . The sounds wh ich one hears vary w ith the pressure upon the
stethoscope, so i t is very importan t in examin ing from time to time for com
par ison to make the same pressure. I t is very d ifficult to do th is un less we
have an in strumen t such as the one here described which hangs on the chest
w ithout the un certa in pressure of the examin er .
There are two me thods of percussion,immediate
,where
the stroke'
is del ivered d irectly to the chest wa l l,and med ia te,
where the blow is received by a pleximeter interposed between
the body sur face and the blow .
We have finger-finger percussion ,
finger-pleximeter percussion ,
percussion
hammer-finger percussion ,percussion hammer-pleximeter percussion
,d irect
percussion,and auscultatory percussion . When ord inary methods of percus
sion are employ ed it is largely a matter of personal preferen ce on the part of
the exam iner wh ich he w i l l use, the finger or the pleximeter and percussion
hammer: Figure 2,b and c
,il lustrate the in strumen ts which I prefer when
I do not use the fingers.
When the finger is used as a pleximeter,i t is possible to learn to detect the
cond ition of the underlying tissue by the resistan ce imparted to the finger .
Th is is very importan t and becomes to the exam in er , who is sk i lled in percuss
ing in this manner, of more importan ce than the sound elicited by the stroke.
When a pleximeter o ther than the finger is used, th is feel ing of resistan ce is lost .The common methods Of percussion and elastic tube percussion are especr
a l ly adapted to the early diagn osis of tuberculosis. For a descript ion of these
various methods of percussion , in order to avoid repeti tion I would refer
my readers to pages 6 6— 7 1 .
Whi le it is wel l to practice bo th l ight and heavy percussion ,
yet l ight percussion is preferable in early tuberculosis . I t is
estimated that'
a l ight stroke wi ll set up waves to a depth of
two in ches“
. A heavv stroke throws a great port ion of the
chest wal l in to vibrat ion,hence afford ing un rel iable ev iden ce.
PercussionI n s trum en ts .
6 PULM ON ARY TUBERCULOS I S
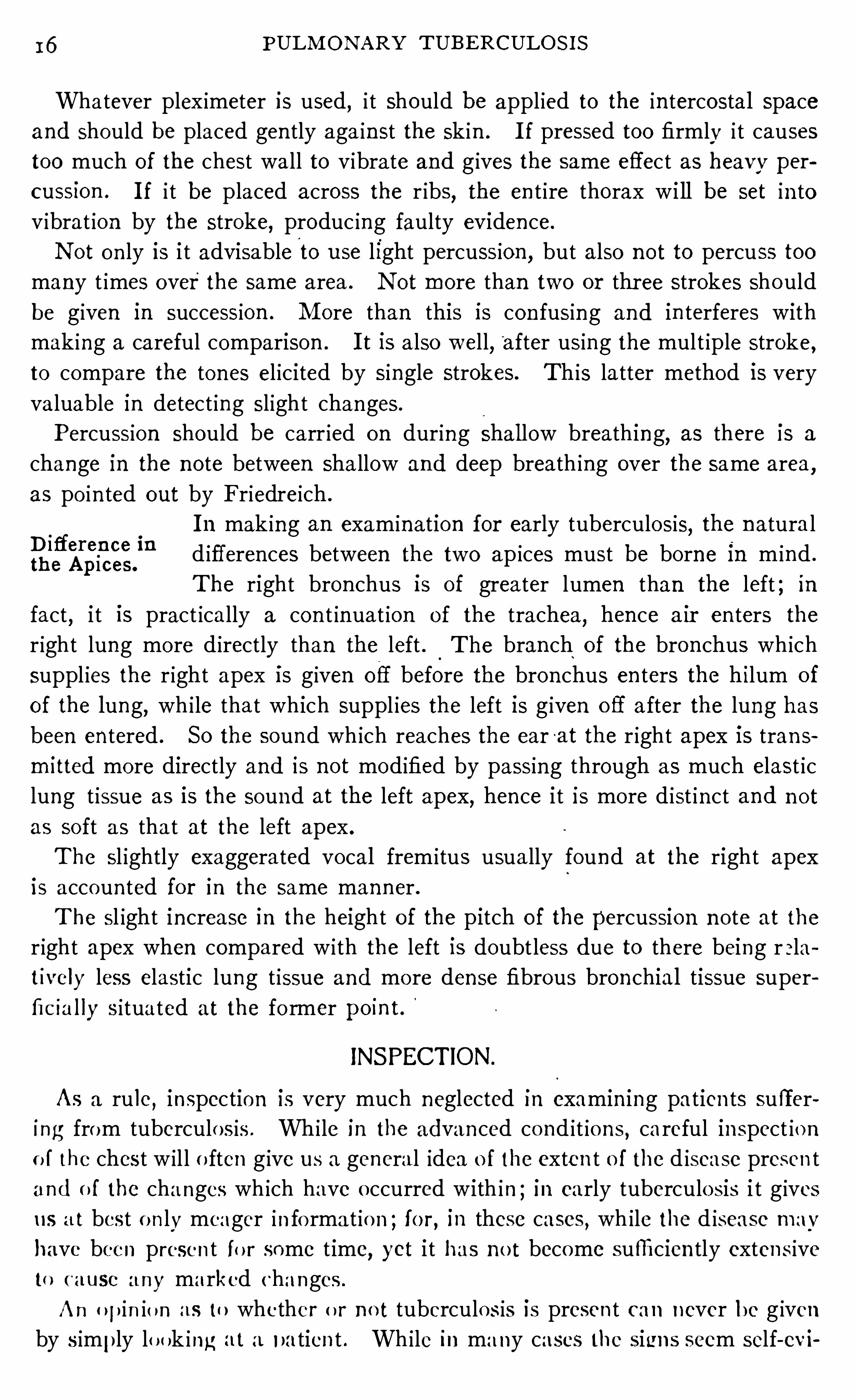
Whatever plex imeter is used, i t should be appl ied to the in tercostal space
and Should be placed gen tly aga in st the sk in . I f pressed too firmly i t causes
too much of the chest wall to vibrate and g ives the same effect as heavv per
cussion . I f i t be placed across the r ibs, the en t ire thorax wi ll be set in to
v ibrat ion by the stroke, produc ing faulty evidence.
N ot on ly is i t advisable to use light percussion , but also no t to percuss too
many t imes over the same area . N ot more than two or thr ee strokes Should
be given in succession . M ore than this is con fusing and in terferes with
mak ing a careful comparison . I t is a lso well, after using the mult iple stroke,to compare the tones el icited by single strokes. This latter method is very
valuable in detect ing slight changes .
Percussion should be carr ied on during Shal low breathing, as there is a
change I n the no te between sha llow and deep breath ing over the same area,
as po in ted out by Friedreich .
I n mak ing an examination for early tuberculosis, the n atura l
d ifferences between the two ap ices must be borne in m ind .
The right bron chus is of greater lumen than the left ; in
fact,i t is pract ically a con t inuat ion of the trachea
,hen ce a ir en ters the
r ight lung more d irectly than the left . The bran ch of the bron chus wh ich
suppl ies the r ight apex is given Off before the bron chus en ters the h ilum o f
Of the lung,wh i le tha t which suppl ies the left 13 g iven o ff after the lung has
been entered . SO the sound wh ich reaches the ear-at the r ight apex is trans
mitted more directly and is not modified by passing through as much elast ic
lung t issue as is the sound at the left apex, hence i t is more d ist inct and n ot
as soft as tha t at the left apex .
The sl ightly exaggerated vocal frem itus usually found at the right apex
is accoun ted for in the same manner .
The sl ight increase in the height of the pitch o f the percussion n o te at the
r ight apex when compared w i th the left is doubtless due to there being r ela
tively less elastic lung t issue and mo re dense fibrous bronchial tissue super
fic ia l ly situated at the fo rmer pomt.
D ifferen ce inthe Apices.
INSPECTION .
As a ru le,inspection is very much neglected in examin ing patien ts suffer
ing from tuberculo sis . Whi le in the advanced co nd it ions , careful inspect io n
o f the chest w il l o ften g ive us a general idea o f the exten t o f the d isease presen t
and o f the changes wh ich have o ccurred with in ; in early tuberculosis i t g ives
us a t best o n ly meager in fo rmat io n ; fo r , in these cases , wh ile the d isease mav
have been presen t fo r some t ime, yet i t has n o t become sufficien tly exten s ive
to ( ausc any marked changes .
A n o pin io n as to whether o r n o t tuberculos is is presen t can never be g iven
by s imply lo ok ing a t a patien t . Wh i le in ma ny cases the signs seem self-evi
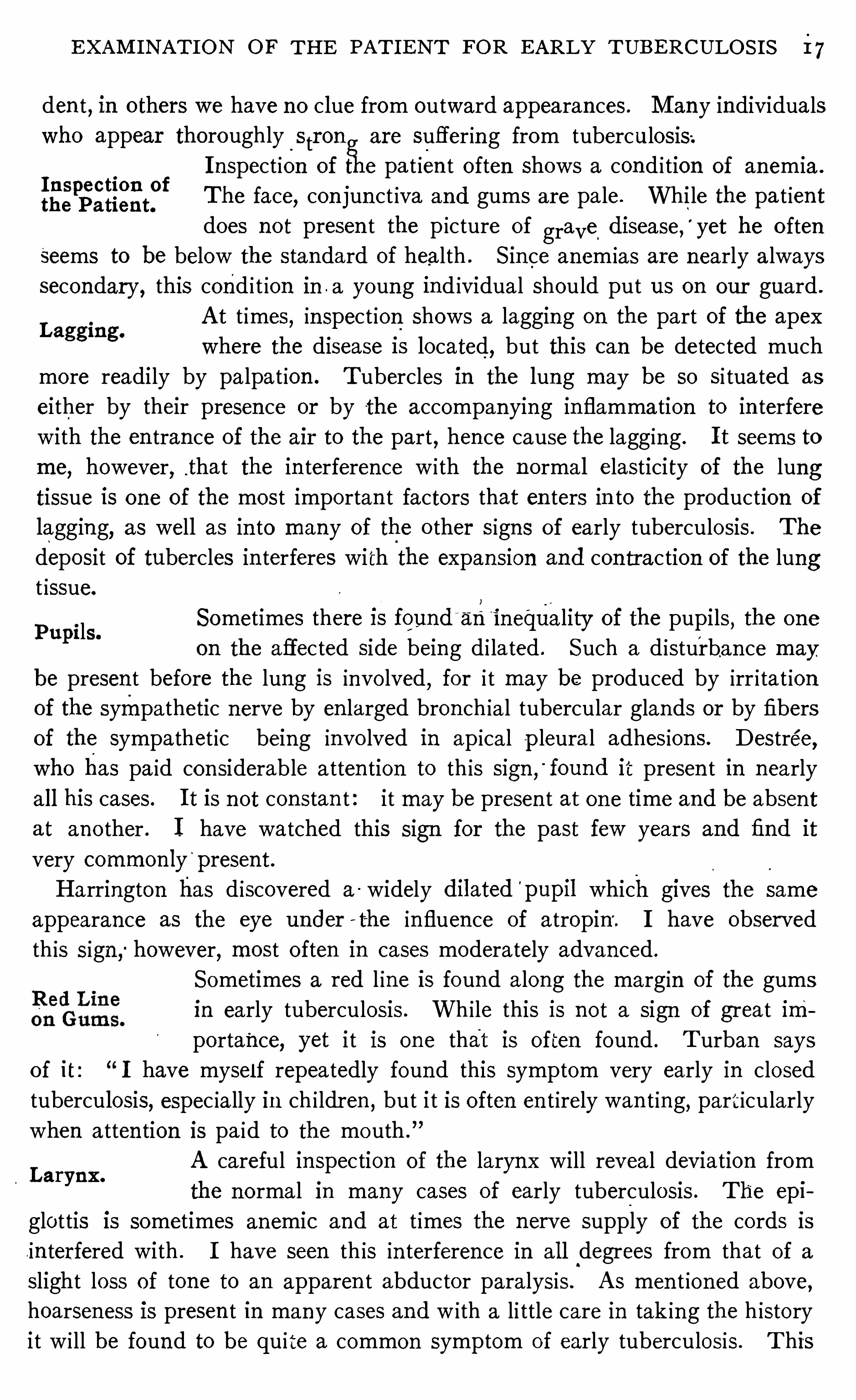
E XAM I N AT I ON OF TH E PAT I E N T FOR EARLY TUBE RCULO S I S i 7
den t , in o thers we have no clue from outward appearances . M any individuals
who appear thoroughly_
strong are sufferin g from tuberculosis;
I nspection of the pa t ien t o ften shows a cond i tion of anemia .
{Egpsgggnn
t
p fThe face
,con jun ct iva and gums are pale. While the pa t ien t
does no t presen t the p icture of gravel
disease,
’
yet he o ften
seems to be below the standard of health . S in ce anem ias are nearly a lways
secondary, this cond i t ion in . a young ind ividual should put us on our guard .
A t t imes, in spect ion shows a lagging on the part of the apex
Where the disease is located, but this can be detected much
more readily by pa lpat ion . Tubercles in the lung may be so si tuated as
either by their presen ce or by the accompanying in flammation to in terfere
with the en tran ce of the air to the part, hen ce cause the lagging . I t seems to
me, however, that the in terferen ce w i th the normal elasticity of the lung
tissue is one of the most importan t factors that en ters in to the production of
lagging,as well as in to many of the o ther signs of early tuberculosis . The
deposit of tubercles in terferes with the expansion and con traction of the lungt issue.
Lagging.
Sometimes there I S found‘
arii nequality of the pupils, the one
on the affected side being d i lated . Such a d isturban ce may
be presen t before the lung is invo lved, for i t may be produced by irr i tat ion
of the sympathetic nerve by en larged bron ch ial tubercular glands or by fibers
of the sympathet ic being invo lved in ap ical p leura l adhesion s . Destree,who has pa id con siderable a tten tion to th is sign ,
'
found it presen t in nearly
al l his cases. I t is not con stan t : it maybe presen t at one time and be absen t
at ano ther . I have watched this sign for the past few years and find it
very common ly'
present.
Harrington has d iscovered a- widely dilated
'
pupil which gives the same
appearance as the eye under ' t—he in fluence of atropin '
. I have observed
th is sign ; however, most o ften in cases moderately advan ced .
Sometimes a red l ine is found a long the margin of the gums
in early tuberculosis . Wh i le this is n ot a sign of great importance, yet i t is one that is often found . T urban says
of it I have mysel f repeatedly found this symptom very early in closed
tuberculosis, espec ia lly in ch i ldren , but i t is o ften en t irely wan t ing,particularly
when atten tion is pa id to the mouth .
A careful in spection of the larynx will reveal deviation from
the normal in many cases of early tuberculosis . The epi
glottis is sometimes anemic and at t imes the n erve supply of the cords is
in terfered with . I have seen th is in terference in al l degrees from that of a
slight loss of tone to an apparen t abductor paralysis . A s men t ioned above,hoarseness is presen t in many cases and w ith a li ttle care in tak ing the h istory
it w i ll be found to be qu ite a common symptom of early tuberculosis . T his
Pupi ls.
Larynx.
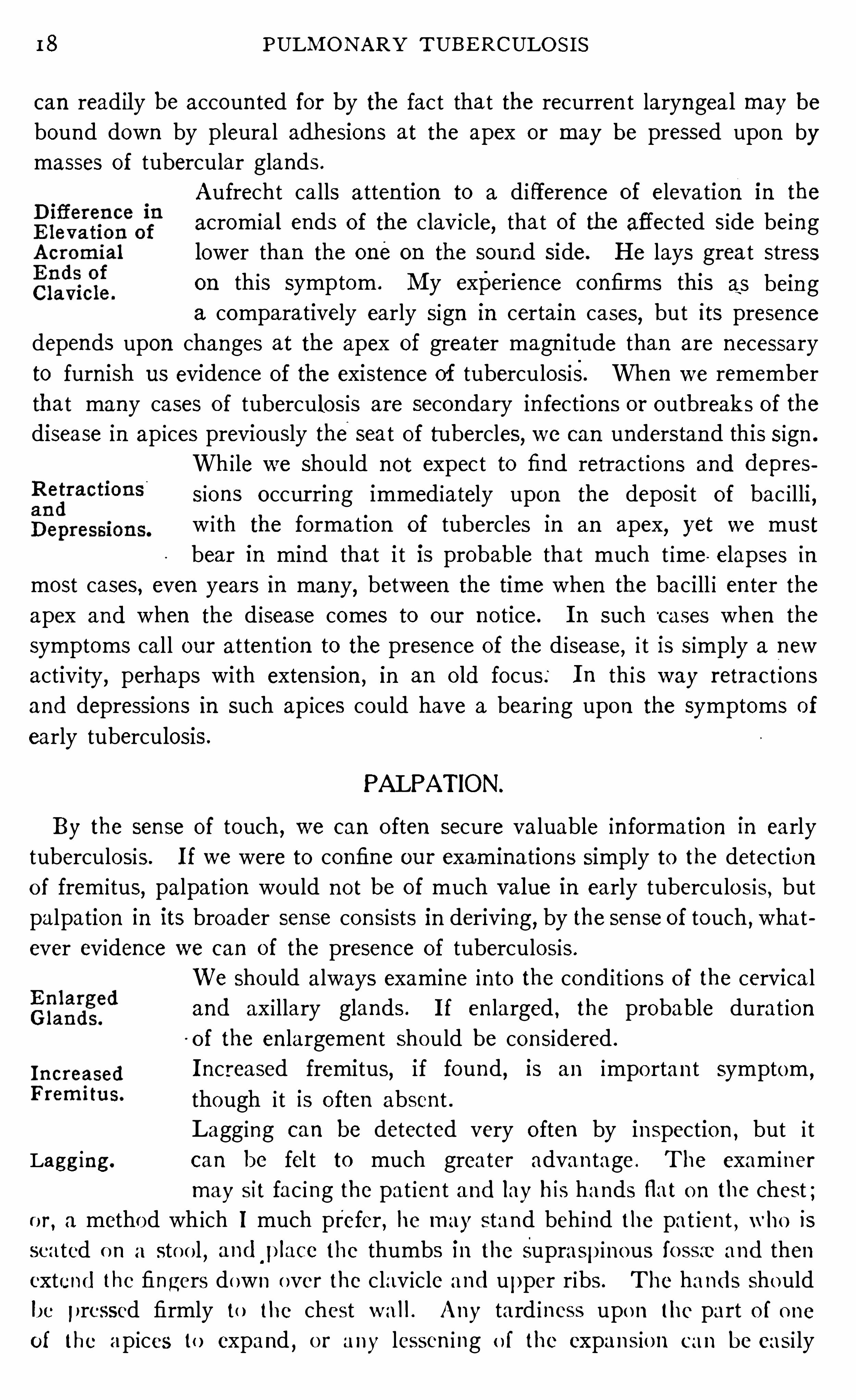
18 PULM O N ARY TUBE RCULO S I S
can readily be accoun ted for by the fact that the recurren t laryngeal may bebound down by pleural adhesions at the apex or may be pressed upon bymasses of tubercular glands .
Aufrecht ca lls atten tion to a d ifference of elevation I n the
acromia l ends of the clav icle, that of the affec ted side being
lower than the one on the sound side. H e lays great stresson this symptom . My experience confirms this as being
a comparatively early sign in certain cases,but its presence
depends upon changes at the apex of greater magn i tude than are necessary
to furn ish us eviden ce of the existence of tuberculosis. When we remember
that many cases of tuberculosis are secondary in fections or outbreaks of thedisease in ap ices previously theseat of tubercles, we can understand this sign .
Wh i le we should not expec t to find retract ions and depres
sions occur ring immediately upon the deposi t of bac illi,
w i th the fo rmation of tubercles in an apex, yet we must
bear in mind that i t is probable that much t ime elapses in
most cases, even years in many, between the time when the bacill i en ter the
apex and when the d isease comes to our n o tice. I n such cases when the
symptoms cal l our atten tion to the presen ce of the d isease,i t is simply a new
activity, perhaps with exten sion ,in an o ld focus: I n th is way retractI on s
and depressions in such ap ices could have a bear ing upon the symptoms of
early tuberculosis .
PALPATION .
By the sense of touch , we can o ften secure valuable in formation in early
tuberculosis. I f we were to confine our examinations simply to the detection
o f fremitus,palpat ion would no t be of much value in early tuberculosis
,but
palpation in its broader sense consists in deriving, by the sen se of touch , what
ever evidence we can of the presence of tuberculosis .
We should always examine in to the cond it ion s o f the cervica l
and ax i llary glands . I f en larged , the probable durat ion
of the en largemen t should be considered .
I nc r eased fremitus, if found, is an impo rtan t symptom,
though i t is o ften absen t .
Lagging can be detected very o ften by inspection , but i t
Lagging. can be fel t to much greater advan tage . The exam iner
may sit fac ing the pat ien t and lay his hands flat o n the chest ;o r
, a method which I much prefer , he may stand beh ind the pat ien t,who is
sea ted o n a sto o l,andp lace the thumbs in the supraspinous fo ssre and then
extend the fingers down over the clavicle and upper ribs . The hands should
be pressed firmly to the chest wa l l . Any tard iness upo n the part o f o ne
of the ap ices to expand,o r any lessen ing o f the expans io n can be easi ly
20 PULM ON ARY TUBE RCULO S I S
mapped out and the outline marked on the skin by a dermographic pencil,a simple glance (Fig . 3 , a and b) w i l l Show whether or no t retract ion is
presen t,if i t is confin ed to one apex . I n double invo lvemen t i t is not so easv.
A con trac ted apex does not mean that active tuberculosis is presen t, but
FIG . 3 . (a)
FI G . 3 . (b)Fig . 3 .
— a an d b, show the change in ap ica l outl ine result ing from apica l invo lvemen t. N o t o n ly is the apex l owered but the area o f reso n an ce is n arro wed
s imply that fo r some cause o r o ther ei ther in the past o r presen t, a patho logica l
co nd i t io n has caused a co n tract ion o f the lung tissue. The cause must
be in terpreted in the l ight o f the c l inica l h istory and the find ings upon
auscultat io n .
AUSCULTATION .
The pro cedure wh ich affo rds the mo st rel iable in fo rmat io n in exami n ing
fo r early tuberculo sis is auscultat io n . T o be an expert at i t is to a tta in masteryo f the key wh ich un lo cks the do o r to early d iagno sis . The changes in the
EXAM I N AT I ON OF _ TH E PAT I E N T FOR E ARLY TUB E RCULO S I S 2‘
I
resp iratory n o te characterist ic of early tuberculosis are : Rough breath ing ;harsh, sharp vesicular and puer i le breath in g ; pro longed exp ira t ion ; weakened
breathing and cogwheel breathing . These may or may not be accompan ied
by fine rales .
Whatever o ther sign s_
or symptoms a re found, they must always be in ter .
preted in the l ight of the auscultatory find ings.
I t seems superfluous to say that i t is necessary. to have an accurate picture
of the normal vesicular breathing, _
in order to be able to recogn ize abnormal i
t ies, yet it is a common experience to findmen gIV I ng opi n i on s as to the presen ce
of early tuberculosis without having any defin ite idea of the n orma l vesicular
murmur .
Sometimes the respiratory n o te is very fain t and heard on lyw i th great d ifficulty, ow ing to th ick chest walls . Where
nasa-l sten osis is presen t
, the resp iratory sound is also apt
to be feeble. I n such cases, the patien t should be asked to
breathe through the mouth . I n pa t ien ts who employ the abdominal form
of breathing, the movemen t of the chest
i
f
wal l at the apices is l imited '
and
o ften the respira tory murmur in these parts is very indist in ct .When the chest is covered with h air
,this can
’
be either wet with water,rubbed with vasel ine or
, i f espec ial ly ann oying , i t may be cut off.There are numerous no ises of muscular o rigin
,w i th which the examiner
should fami l iarize h imself. These are somet imes heard at the apex, due to the
“
con traction of the trapez ius, somet imes over the scapula, due to a S lippingunder the scapula . These may be due to con tractions of the muscles alone,or , in some in stan ces, they
'
are due to pressure on bundles of' muscle fiberbythe stethoscope.
A t t imes, sounds simulat ing; rales are also heard at the sternoclaviculararticulation ,
and in some instan ces,i t w i ll be very difli cult to d ifferen tiate
between crep itat ion s of pleural and in tr‘
apulmonary origin . Wh i le th is
d ifferen tiation must be made frequen tly in advan ced cases, i t w i ll occasI onal lybe required in ~
ear ly, suspected ap ical invo lvemen t .I t seems strange tha t n o thoroughly satisfactory explanationhas been given to accoun t for the s ounds heard on auscul
tation of the n ormal and patho logica l chest . Laennec assumed
that normal vesicular brea th ing was due to_
the frict ion of
the air rubbing again st the wa lls of the fin e bron chi and in fund'ibula .
’
M orerecen tly the theory has been advan ced “ that vesicular breathing is n o th ingmore than the blowing n o ise made as the air passes the larynx
,mod ified by
theair passages and lung t issue,and tran smi tted to the ear through the chest
wall . A s Sahl i well says, neither of these theories are sat isfactory. That
vesicular breath ing can'
be p roduced w i thout the e n trance o f air in to the
lung at al l , was demon strated by Sahl i'
(Correspondenzblatt fi'
I r Schweitzer
22 PULM ON A RY T UBERCULO S I S
A ertzte,1892) upon a pat ien t suffering from congen i tal fissure of the sternum .
Upon increasing the in traabdom inal ten sion as by stra in ing, the lung t issue
pro truded to a considerable exten t . A uscul tation at this t ime showed a
typica l vesicular murmur caused by the fill ing of the a lveo li .
I t would seem from th is exper Ime'
n t f that the lung t issue has an importan t
part in the product ion of the vesicular murmur .
I t seems to me that, in o rder to form the proper conception of the cause
of the norma l vesicular murmur,we must remember tha t in spirat ion is a
muscular act by which the lung capac ity -is forc ibly increased . There is a
stretch ing of the elast ic t issue of the lung, with an open ing up of the ac in i ,and an inrush of air— these two elemen ts causing the murmur . The
in sp iratory murmur is most likely due par tly,if n ot largely
,to the stretch
ing of the elastic t issue, as shown by Sahli ’s experimen t and as suggested
by the sound el ic i ted on compressing and stretching lung t issue. The ih
spiratory no te begin s with the commen cemen t of the muscular effort and
con t inues un t i l th is ceases,and is aud ible dur ing the en tire t ime. E xpiration
is due to the con tract ion of the elast ic tissue fo llowing the passive muscular
act ion of the expiratory phase ; and sin ce this is not forc ible, but a gradua l
con traction,fo llowing up the passive muscular action
,the sound is ei ther
inaud ible or heard on ly at the begin n ing when , on accoun t of the increased
ten sion owing to the great disten tion of the elastic t issue, it~ forc ibly expels
some of the air . That this accoun ts for the aud ible exp iratory sound is supported by the fact , tha t the expiratory sound is accen tuated by deep inspira
tion,causing an overd isten tion of the air cells . The d ifference then between
the in spira tory and exp iratory murmur is that thei
former is caused by bo th
the stretch ing of elast ic tissue and the in rush of a ir,wh i le the latter is due
fo r the most part to the outward passing o f the air— the former an active
process, the lat ter largely passive.
Rough breathing is the earliest sign of tuberculosis tha t
can be heard upon auscultat ion . I t is usually heard at the
apex o f the lung soon a fter the d isease man ifests i tsel f.
Sahli has well described i t thus : (D iagnost ic M ethods,“Rough
vesicular breath ing is an impure, slightly uneven murmur heard during
i nspira t io n,as i f stro nger accompanying no ises were admixed w i th the no r
ma l vesicular murmur . I I I o rder to preven t con fusion with Sharp o r in
creased vesicular breath ing the term impure breathing is mo re fitting . I I I
( reased brea th ing is exqu is itely pure and generally very in tense whereas
rough brea th ing is mo re frequen tly weak and fain t .”
Such a respi ra to ry no te m ight be due to in terference with the no rmal un ob
st ructed fl ow o f a ir in to the a ir cel ls so tha t differen t ac in i become fi lled at
d i fferen t t imes ; o r i t m ight be due to a th icken ing o f the mucous membrane
RoughBrea th ing.
o f the a ir p assages,owi ng to the presence o f tubercles ; o r to an obstructio n
EXAM I N AT I O N O F TH E PAT I E N T FOR E ARLY TUBE RCULO S I S 23
of the air passages due to the presen ce of secretion ; or to the admixture of
the sounds produced by secretion with the normal sounds . I t has also been
suggested tha t the roughness might depend upon an emphysema wh ich de
velops about the tubercles, the air en tering the various air cell s, not simul
taneously but in succession . T urban bel ieves i t is due to the presen ce of
nodules here and there, which by their presen ce compress bron chio les andinterfere with the simultan eous dilata tion of the air cells.
Closely all ied to the rough brea thing is a weaken ing of the
resp iratory n o te . I n fact,as men tioned above
,rough breath
ing is a weakened breathing . Compared with o ther areas
we find that the air does not en ter a port ion or it may be the en tire apex as i t
should . Such a sign should make one suspicious of tuberculosis . The same
causes as men t ioned in the above paragraph are respon sible‘ for the weak
en ed breath ing. I t may be due to an en croachmen t upon the lumen of the
air vessels due to thicken ing Of the walls or to secretion ,of to a lessened
elasticity of the lung tissue. Fixation by pleura l adhesion s and thicken ing
of the apica l pleura w i ll a lso cause i t .
The expiration may /
or may not be pro longed in early tuberculosis ; however, i t can be readily seen that the same con
dition s wh ich cause a rough or weak in sp iratory murmur
w i ll set up a barr ier to the egress of air from the air cells and will at the same
t ime cause a retardat ion of con tract i le act ion upon a part of the lun g t issue,giving rise to a pro longat ion of the resp iratory no te.
H arsh,Sharp vesicular or puer i le breathing accompan ies
ggéil
‘
l
figl
gp a process somewhat more advan ced yet sufli cien tly early
Puer i le.to be coun ted amon g the early Sign s . This may or may n ot
be coun ted among the e arly sign s ; i t may or may n ot be
accompan ied by pro longed exp irat ion . This m ight be called in ten se vesicu
lar breath ing,and may be described thus : I f norma l vesicular brea th ing
be represen ted by an attempt to pronoun ce the letter f,sharp vesicular
would be represen ted by E .
T his sound i s heard where the breathing is forced . I n n orma l vesicular
breathing,the air passes through elastic bron ch ial tubes surrounded by
elast ic t issue ; but , thr ough patho logica l thicken ing, the elastic i ty is in terfered
with and the tubes becomemore rigid, con sequen tly a partia l sten osis obta in swhich offers resistan ce to the air . The air en ters by force and produces an
in ten sified sound . Ow ing to the infiltration presen t, the sounds are con
ducted to the ear with more than natural ease.
Cogwheel breathing is a llied to rough breathing . I t is an
in terruption in the insp iratory murmur . I t is due to an
in terferen ce with the en trance of a ir in to the air cells, an d
gives the idea of the air curren t overcoming one obstacle after an o ther . I t is
Pro lon gedE xpira tion .
24 PULM O N ARY TUBE RCULO S I S
supposed to be due to a valve- like swel ling of the mucous membrane of the
bronch io les or to the accumulat ion o f secretion which gives way before the
incoming air . I t is a sign of a ca tarrhal condi tion and if found local ized is
usuall y assoc iated w i th early tuberculosis.
Turban says this form of breath ing usual ly occurs in zones between the
tuberculous and heal thy lun g and seldom a t the apices. M y experien ce
would confirm this. I havemost Often found i t below the clavicle when the
apex was affected .
I t is n ot necessary to have rales presen t in order to establ ish
a d iagnosis “
of tuberculosis. I n the earl iest forms o f the
disease they are rarely found, a l though they soon make t heir appearance
and when~
presen t they deno te a catarrhal condition . They are usual ly of
the fine crackling variety. M edium rales are n ot l ikely to be presen t un t i l
there is destruction of tissue. I n order to detect rales, the patien t should
fir st be examined on quiet breathing, then fo rced breath ing and finall y after
cough ing. Somet imes by placing the patien t on the well side,thus com
pressing the lung, the diseased lung is forced to greater activity, and ra les
which are n ot presen t on ord inary respirat ion may be elicited .
Somet imes a wheeze or whine w i ll be heard . This,too
,is a S ign of a catar
rhal cond it ion , and when o ther sign s are presen t 15 suspI CI ous of tuberculosis .
N ot in frequen tly, crepitations and rubb ings of pleural origin
w i ll be found . These deno te either acute or chron ic proc
esses and are always suspicious. I t is no t at all uncommon
to find crepitation s at the base of the lungs when tuberculosis of the con e
Sponding apex is presen t . When the right.
apex is the seat of tuberculous
in fect ion,i t is not uncommon to find crepita tion s at the junction of the fourth
r ib w i th the sternum . These are most l ikely pleural crepitation s and have
their origin at the junction of the upper with the m iddl e lobe.
Wha t is known as the subclavian murmur is heard over the
subclavian artery at times . I t occurs during bo th in sp iration and exp ira tion . I t deno tes an inflammato ry process
resulting in adhesion s invo lving the subclavian artery . This is o ften de
scribed as D a Costa ’
s S ign . Wh i le i t is not a S ign of early tuberculo sis,
yet i t is assoc iated with these chron ic pleurisies which are usually tubercu
lo us in their nature ; hence its presence tells tha t tuberculosis has, a t least,probably been presen t .
Ra les.
S ubclavianM urmur.
D I AGNOS I S OF EARLY PULMONARY TUBE RCULOS I S .
Wh i le i t is desirable to expend greater energies and make grea ter effort to
discover a more perfect method of treatmen t for tuberculo sis, yet we must no t
lose sight of the fact that presen t methods when appl ied early w i ll Offer hea l th
to from 6 5 to 90 per cen t of patien ts. I fmed ical men in gen eral would expend
but a fraction of the energy in learn ing to d iagnose tuberculosis early, tha t a
few ~ scientists are expend ing in endeavoring to d iscover a“ cur e
,
”we would
be able to say that the cure for tuberculosis is alr eady at hand .
A fter perusing the forego ing descript ion of symptoms and sign s which are
to be found in early tuberculosis, on e readily recogn izes the need of carefully
con sider ing them and con ced ing to’
them their proper importan ce ; for it is
elf—eviden t tha t on e or even severa l of them may be presen t and yet the pa
t ien t may n o t be suffering from tuberculosis. N or is i t enough to kn ow that “
a
tuberculous process is presen t ; i t is equal ly necessary to kn owwhether such aprocess is act ive or qu iescen t .
I n early d iagnosis here referred to , we canno t depen d on
cfil
éhggt
ogo finding bac i ll i in the sputum
,because we are dea l ing with
fo r Diagn o sis a condi t ion prior to the break ing down of tissue w ith the ‘
el imina t ion of bac i ll i .
E arly d iagn osis of pulmon ary tuberculosis must be’
made
independen t of the microscope. A carefully taken cl in ica l history and a
con scien t ious,In tell igen t physica l examina tion w i ll usually determine the pres
ence or absen ce of the disease.
The establ ishing of a d iagnosis in early tuberculosis is o ften n ot an easy
matter . The examiner should never be in haste to give his op in ion,n ei ther
Should he delay in order to allow more pronoun ced symptoms to develop .
I f there is any doubt as to the d iagnosis he should not hesi tate to re-exam ine
several t imes un t i l he is ei ther satisfied of the presen ce'
or absen ce of the d isease
or of his inab i lity to determ ine i t . A negative d iagnosis should,never be made
in the face of susp ic ious symptoms without a fai lur e on the part of the pat ien t
to reac t to the tuberculin test .I f possible the pa tien t Should a lways be approached by an unbiased mind.
E ach symptom and each S ign found,should be used not to establ ish some pre
viously arr ived- at con clusion ,but for its actua l worth when combined w i th
o thers,in mak ing up the picture of the cond i tion presen t .
25
26 PULM ON ARY TUBE RCULO S I S
When can we say wi th a reasonable certa in ty that a givenpa tien t has or has n o t tuberculosis, i f there is n o sputum to
examine,or
,i f being presen t,the examina t ion proves n ega t ive
Th is is one of the most importan t quest ion s in med ic ine ; for tuberculosis
is the most commo n fatal di sease and one tha t is l ikely to presen t i tself to every
pract i t ioner of med ic ine, n o ma tter wha t l ine o f pract ice he may fo llow . I t
is essen t ial,then
,tha t the p icture of early tuberculosis be plain ly dr awn and
that al l pract i t ioners of med ic ine famil iar ize‘
themselves w i th i t . I t requires
more ev idence to give a negat ive op in ion than to give a posi t ive one ; for a
negat ive Opin ion reassures the pat ien t and causes him to omit caring for him
self,wh i le a doubtful o r po si tive op in ion w i l l cause the patien t
,as a rule
,to
take steps toward improv ing his cond i t ion or bringing about a cure.
Un fortunately, in early tuberculosis there is n o sign tha t is invariably presen t,
There are many sign s,however
,some of which are a lways presen t ; and on ly
by carefully correl lating these do we arr ive at our d iagnos is. N evetheless,
when we have taken a careful cl in ica l h istory of an ind ividua l suspected o f
suffering from early tuberculosisf as a rule,we feel to lerably certa in of the
presence or absen ce of the d isease. Then when we have made a’
careful
phys ica l examinat ion,we should be ready to stand by our find ings. Li t tle
doubt should rema in . Our d iagnosis should be at least as certa in as that
of any o ther in ternal d isease. The fact tha t there is any doub t at a l l is due
largely to a fai lure upon the part of med ical men to fam i l iarize themselves
w i th normal chests,and to apprec iate sl ight var iat ion s from the normal .
When a d iagnosis of tuberculosis has been made the patien t
should be to ld the truth at once. The lack of candor on the
part of the physic ian co sts thousands of tuberculous patien ts
their lives. Such deceptive expressions as“ thr oat trouble
,
” “ bronch ia l
trouble,
” “weak lungs,
stomach trouble” and“ l iver trouble” should never
be used . They are un scien t ific . They al l mean tuberculosis,and they
should no t be used to conso le and comfort the pa t ien t when this conso la tion
and comfo rt mean s death . Cando r On the part o f the physic ian is the o n lv
th ing tha t w i l l free h im from the responsib i li ty o f a death caused by tuber
culo sis when the d isease is d iscovered early .
A h istory of hemo ptysis is a lways suspicious and un less the
pa t ien t be suffering from heart d isease,cirrhosis of the l iver,
hemo ph il ia,scurvy , Brigh t
’s d isease
,o r un less he has varico se veins o f the
ph arynx o r a t the ro o t o f the to ngue, o r has spo ngy gums, the probab i l it ies are
tha t the blo od is the result o f a tuberculous in fect io n . And even i f these dis
eases a re presen t,we may stil l fi nd tuberculo sis a lso . I t is no t o n ly safe
,but
Can do rw i th Pa t ien t .
H ( l
H emoptys i s .
facts wi ll wa rran t a lways co nsidering sp i tt ing o f blo o d as due to tuberculo sis
u nless (leftn itc lv pro ved to be o therwise.
The express io n “thro a t hemo rrhage ” has given much comfo rt to frightened
28 PULM ON ARY TUBE RCULO S I S
when th is is n ot found tuberculosis o f o ther organ s, as the glands, should
be suspected .
Tubercul osis should be remembered as an etio log ical factor in neurasthen ia
of the type men tioned above, and the lungs should be careful ly exam ined .
Repeated co lds ” w i th o r w i thout some of the above symp
Bgfliggfil toms
,are suspic ious . These co lds” are no t l ike ordinary
attacks of coryza . They are usuall y of the bronchial type
and tend to han g on . Any“ co ld ” (bron chial ca tarrh) which does n ot clear
up w ithin / thr ee or four weeks, cal ls for a careful exam ination of the chest .
Somet imes after an acute i l lness such as la gr ippe, measles,or typho id fever, tubercu losis sets in w i th severe symptoms
,
even in cases where n o symptoms suggest ive of the trouble were presen t
before the on set of the acute d isease. I n such cases,as a rule
,the fever
does n ot abate, or i f i t does, i t is on ly for a few days . The pa t ien t does
n ot regain his stren gth . H e t ires on exertion,and very o ften has n ight
sweats. I n many of these cases the tempera ture r ises severa l degrees and
a destruc t ive pro cess sets in which ends in the destruction o f lun g t issue
and cavi ty format ion . Cough is usua l ly presen t at an early per iod , and
Often the expectorat ion is qu i te p ro fuse within a very short t ime from the
apparen t on set .
Of course,we are deal in g wi th an o ld
‘
process in a l l such in stan ces,
which has been l ighted up bythe acute d isease.
These cases,h owever
,must nOt be con fused w i th those advan ced cases
wh ich are o ften d iagn osed and treated for la gr ippe and typho id fever dur
ing the t ime when they are show in g temperature and o ther severe symp
toms in c iden t to cavity format ion .
A rise of temperature is a very valuable S ign in early tuber
culosis . Should indiv iduals complain‘
of one o r mo re of
the above symptoms,they should be requ ired to keep a two hourly chart o f
their temperature for several days, when a r ise of from one-half to o ne degree,un less it can be sat isfactor ily explained as being due to o ther causes, should be
lo oked upon as being very susp ic ious o f tuberculosis, and Should cal l fo r an
exam ina t ion o f the chest . A persisten tly low temperature is l ikewise sus
picious o f the presen ce o f tubercle.
Wh ile the ev idence Obtained by cl in ica l h istory makes i t
po ssible to suspect the presence o f tuberculo sis, yet we must
rely mo st o n the result o f careful physica l exam inat io n .
A s a rule,tuberculo s is begins at the apex . Tha t po rt io n o f the lung ly ing
abo ve the clavicle a n ter io r ly, and the spine o f the scapula po sterio rly, is the part
usu ally affected . I f o n ly o ne apex is i nvo lved , the d iagno sis is comparat ively
Sudden On set .
Tempera ture
Physi ca lE xam in a t io n .
easy , fo r a compa riso n o f the two s ides shows the difference in the fi nd ings ;but where bo th sides are invo lved
,i t is Somet imes puzzling .
D I AGN OS I S O F E ARLY PULM ON ARY TUBERCULOS I S 29
A slightly high pitched no te, with a S light tympan i tic quali ty with perhaps
a feel ing of resistan ce to the finger used as a plex imeter is found as an early
S ign in percussion over an area of in fect ion at an apex .
A uscultat ion shows rough breath ing, perhaps markedly weaker than nor
mal as the earl iest symptom. E xpiration may or may n ot
.
'
be pro longed .
S lightly harsh breathing w i th or without pro longed e xpira tion is common ly
found and somet imes cogwheel breathing is n o ted .
A few fine rales usually elici ted upon coughing may or may not
'
be presen t,while an occasiona l whine should be considered very susp icious.
I f the clin ica l h istory is suspic ious, and some of these sl ight variation s
from the norma l are foun d upon physi ca l examina t ion , un less they can be
sat isfactor i ly explain ed as being due to o ther causes, they must be con
sidered as po in t in g stron gly toward tuberculosis.
Wh i le a carefully obta ined clin ica l history anda painstakingphysica l exam inat ion w i ll, as a rule
,determine the presen ce
or absen ce of tuberculosis before sputum is presen t, yet there
are exception s to this, and whenever sputum is presen t, i t should be care
fully examined,'
for'
the detection of bactlii‘
is the unquest ioned eviden ce in
making a diagnosis.
‘
A t times,there are lesion s which cause no defin i te symptoms
,and we can
conceive of such an one being s ituated deep in the lung t issue without being
recogn izable on physica l exam ina t ion . Such a focus m ight ulcerate in to a
bron chus and throw Off bac i l lus-bearing sputum . Here the finding of bac i lli
would be n ecessary to establish a d iagnosis.
The presen ce of bac i lli in the sputum a lways Shows that lung tissue is beingdestroyed ; con sequen tly, the find ing of bac i lli is not to be considered as an
early diagnosis ; but , in a lesion such as I have described, we can see that i t
would afford perhaps the earliest opportun i ty of making a diagnosis .
While in my d iscussion ,I have en deavored to urge the makin g of a
d iagnosis before the appearan ce of bacil li in the sputI'
I m, yet I deem i t
wise to give in struct ion s for the examinat ion of sputum in this chapter ;and, in order to avo id repeti t ion
,I sha ll discuss tha t subject ful ly at this
time.
E xam in a tionof Sputum.
I t is n ot on ly importan t to kn ow that bacil l i are present
I n a given spec imen ,but the smear should be so made
that i t will afford a basis of comparison in future examin
ation s. A smear made from a sin gle particle of sputum on ly shows the
presen ce o f bac i l li and their form . I f the smear,however
,is. made from
ten or twelve sma ll part icles of sputum (homogen eous smear) the elemen t
of erro r is largely el im inated a nd we have a much bet ter basis on wh ichto compare the n umber ofbac i ll i at the var ious examin ation s . While then umber of bac i ll i in a m icroscop ic field gives us no ev iden ce of a pro g
H omogen eous
Smear.
30 PULM ON ARY TUBE RCULOS I S
no st ic value in o ne o r two examination s and is abso l utely wo rth less when
the smear is made from a single part icle, yet where the pat ien t is under
co n t inued observat ion and the sputum exam ina t ion is made w i th the
homogeneous smear by the same exam iner at frequen t in terva ls,eviden ce
wh ich is beyon d question is Offered to the phthisiotherapist who is in the
hab i t of closely comparin g his cl in ica l and laborato ry find ings. Th is evi
den ce is of the grea test importan ce i f one wishes to carry out the therapy
based upon the double etio logy o f tuberculosis as worked out by Carl
Spengler (see page 1 7 7)Whi le the stain in g of sputum for baci ll i seems l ike a simple
mat ter, yet it is one tha t should be do ne very careful ly be
cause So muchweight is la id upon the result of the exam
ination in making a d iagno sis.
First the smear is importan t and should be made as directed above. A
common fault is to make the smear too th ick . I t Should be very thin .
I n fixing the smear too much heat should n ot be used . I n order to avo id
th is i t is well always to ho ld the cover-glass in the fin gers . I n stain ing
w i th carbo l fuchsin , gentle hea t is best for bo th human and bovine bacill i,
and abso lutely ind ispen sable fo r the lat ter . The fuchsin should never be
al lowed to bo i l, for if i t does i t wi ll“
cause a precipi tat ion of stain,which
w i ll make the examina tion diffi cul t and make i t very d ifficult to find spl i t ter
wh ich are of great importan ce in diagn osis, see pp . 30—33 .
‘
I t is best to pass
the cover-glass thro ugh the flame low down un ti l a sligh t steam arises
from the fuchsin . This is suffi cien t and makes a preparat ion fr ee from
prec ip i tated stain .
The usua l method o f stain ing is as fo llows
1 . Fix the smear by passin g through the flame.
2 . S tain ing with carbo l fuchsin , heated sl ight ly fo r a few seconds. Wash
wi th water.
3 . Deco lorize with 15 per cen t n i tric acid . Wash .
4 . Co n t rast sta in w i th methylene blue . Wash .
5 . Dry between paper and moun t .
Fo r many years i t has been taught that tubercle bac i lli do
n o t have a spo re fo rm ; but l ike many o ther teach i ngs in
the sc ien t ific developmen t o f a questio n , this is subject to
cha nge.
Carl Spengler (W ien M ed . Wo ch .,
1902, N o . 14 , und Zeitschri ft f.
Hygiene und I n fectio n skrankh'
eiten,Bd . 49 , 1905) observed certa in bod ies
in sputum wh ich sta in the same as tubercle bac i ll i , and wh ich appear as
tho ugh they m igh t be cro ss sect io n s o f bac i ll i . T hese have hereto fo re been
co nsidered to be prec ip itated sta in , which they resemble . H e desc ribed
these under the name“spl i tter ,
" mea n i ng fragmen t . H is further study has
S ta in ingfo r Bac i lli .
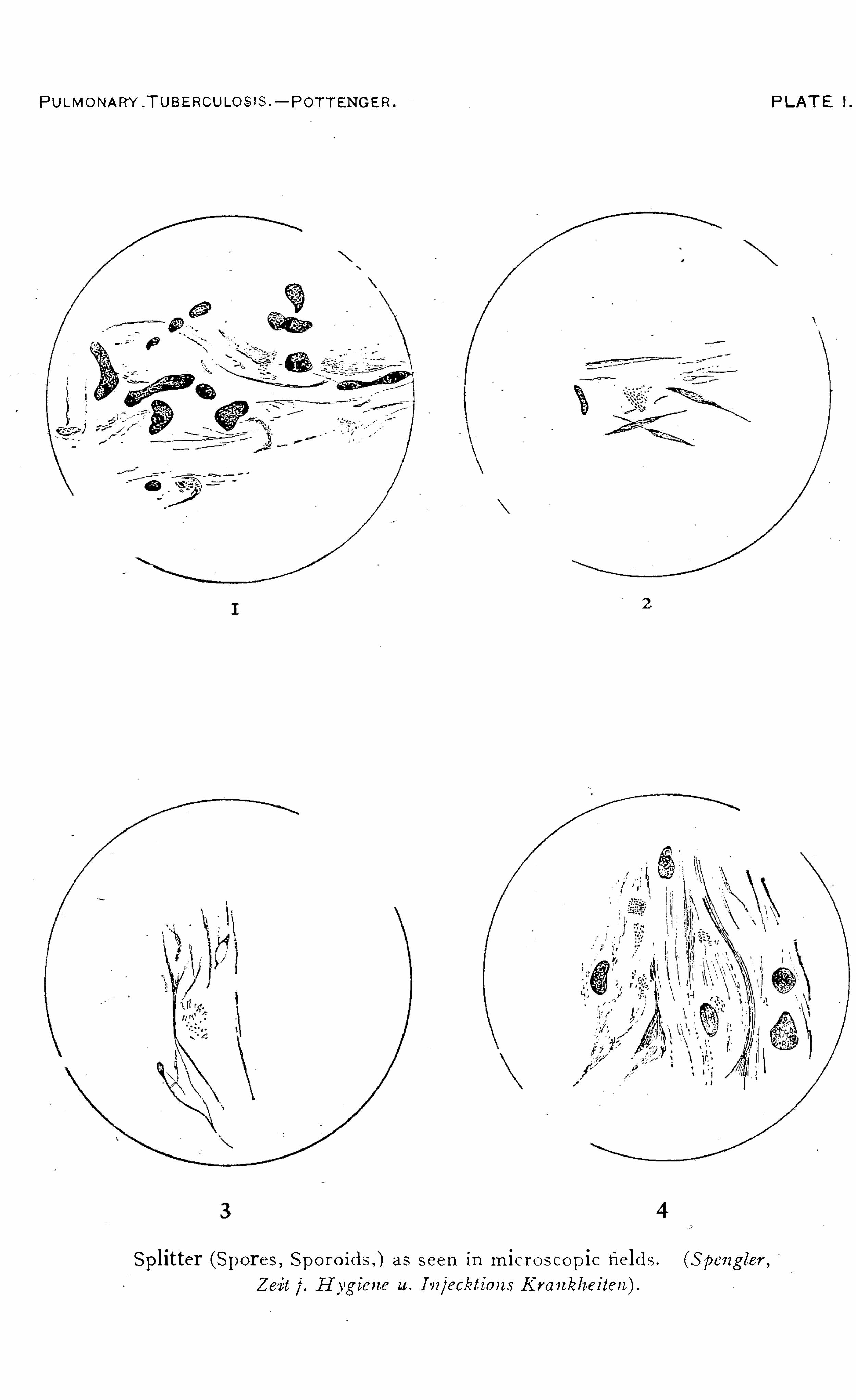
PULMO NARY .TUBE RCULO S IS .
— POTT ENGE R . PLAT E 1.
Spl itter (Spores , Spo ro ids ,) as seen in m ic r o s co pic fields . (S pengler ,
23 131f. H ygien e u. I vr/eckl ion s Kran kheiten ).

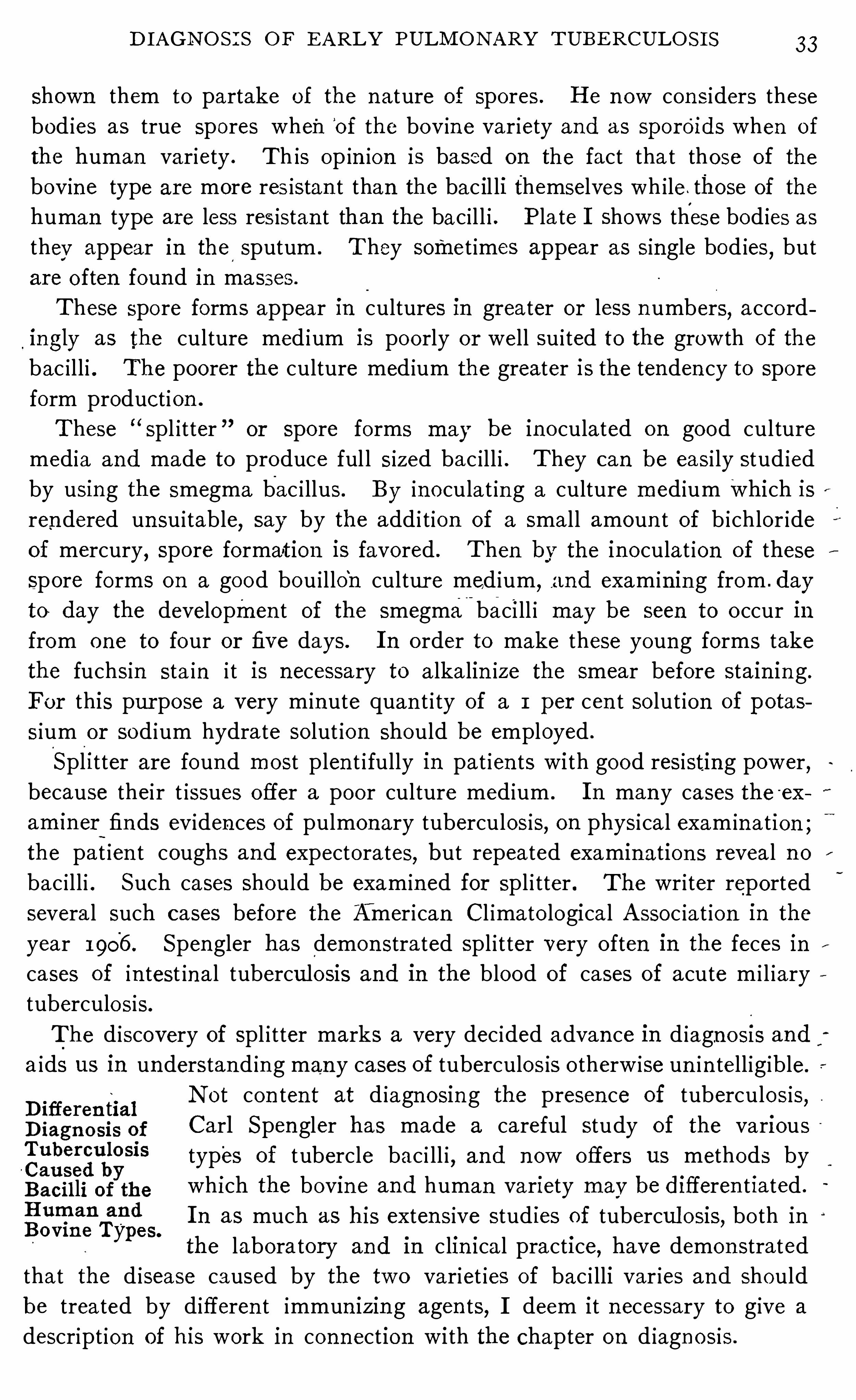
D I AGN O S I S O F E ARLY PULM O N ARY TUBE RCULO S I S 33
shown them to partake of the n ature of spores . H e n ow con siders these
bod ies as true spores when‘
of the bov in e var iety and as sporOids when of
the human variety . Th is op in ion is based on the fact tha t those of the
bovine type are more res istan t than the bac il li themselves wh i le . those of the
human type are less res istan t than the bac i l l i . Plate I Shows these bod ies as
they appear in the sputum . T hey somet imes appear as single bod ies,but
are o ften foun d in masses .
These spo re forms appear in cultures in greater or less n umbers,acco rd
ingly as the culture med ium is poo rly o r well su i ted to the growth of the
bac i l l i . The poorer the culture med ium the greater is the tenden cy to spore
form product ion .
These “Spl itter or spore forms may be in o culated on good culture
media and made to produce ful l s ized bac i l l i . They can be easi ly stud ied
by using the smegma bac i llus. By in ocula t in g a culture med ium Which isrendered un su i table, say by the add i t ion of a smal l amoun t of b ichlor ide
of mercury, spore formation is favored . Then by the inoculat ion of these
spore forms on a good bou i l lo‘
n cultur e med ium,and exam in in g from . day
to day the developmen t of the smegma-
bacill i may be seen to o ccur in
from one to four or five days. I n o rder to make these young forms take
the fuchsin sta in i t is necessary to a lka lin ize the smear before sta in in g .
For this pur pose a very m in ute quan t i ty of a 1 per cen t so lut ion of potas
s ium or sod ium hydra te so lut ion should be employed .
Spl itter are found most plen t i fully in pat ien ts with good resisting power,because their t issues offer a poo r culture med ium . I n many cases the ex
amin er~
fin ds eviden ces of pulmonary tuberculosis,on physica l exam in a tion ;
the pat ien t coughs and expectorates,but repeated examin ation s reveal n o
bac i l l i . Such cases should be exam in ed for spl i tter . The wr i ter reported
severa l such cases before the Amer ican Cl imato logical A ssoc ia t ion in the
year 1906 . Spengler has demon strated Spl i t ter very o ften in the feces in
cases of in test ina l tuberculosis and in the blood of cases of acute m i l iary
tuberculo sis.
The d iscovery of Spl i tter marks a very dec ided advan ce in d iagno si s and
a ids us in understand in g man y cases of tuberculos is o therw ise un in tell igible.
D ifferen tia lN ot con ten t at d iagn osin g the presen ce of tuberculosis,
D iagn o sis of Carl Spengler has made a careful study of the vari ousTUbem‘J IOS i S types of tubercle bac i ll i , and n ow offers us methods byCaused byB aci l li of the wh i ch the bovi n e and human variety may be di fferen t iated .
H uman an d I n as much as his exten sive studies of tubercul osis, bo th inBovme Types.
the laboratory and I n c li n i ca l pract i ce,have demon strated
that the d isease caused by the two variet ies of bac i lli var ies and should
be trea ted by d ifferen t immun izin g agen ts,I deem it n ecessary to give a
descript ion of his work in conn ection with the chapter on d iagn osis .
34 PULM O N A RY T UBE RCULOS I S
For a long t ime i t was thought that al l tuberc le bac i ll i belong to the samevariety . Then i t was shown that the human , the bov ine and the fowl
bac i l l i d iffered from each o ther somewhat . Fin ally Kochmade the startl ing
statemen t at the B ri t ish T uberculosis Congress in 1901 , that human and
bovine bac i ll i d iffer and that the bovine bac i l l i are n ot dan gerous for the
human race.
The cultur al differen ces of bovine and human bac i ll i have been known for
some time, and Theobald Sm i th has po in ted out their d ifferen ce in form ;
yet few men have undertaken to d ifferent iate them microscop ica l ly . By
carefully studying pure cultures and modifying methods of stain ing, Spengler
has been able to d ifferen t iate .the two variet ies n ot on ly in pure culture but
in m ixed culture, a lso in the sputum and feces of tuberculous patien ts. H e
has further studied the two variet ies and found that they differ in many
part iculars.
T uberculosis, according to his stud ies, has a double et io logy, being caused
by both'
the human and bovin e bac i l li . I n most cases bo th are presen t (the
human predom in at in g) and their act ion -is an tagon i st ic,causin g a chron ic
course. Those cases where on ly on e variety is found are the most virulen t
and most d iffi cul t to treat .
H is op i n ion is based on a mass of observation s bo th from . the laboratory
and from c l in ical experien ce. H e has also foun ded a vacc ine therapy (see
page1 7 7) upo n his observat ion s in which the therapeut ic resul ts corrobo rate
the laborato ry find in gs . The basis of the therapy is an accura te d iagnosis
as to which variety of bac i l li is causin g the d isease ; or which var iety pre
po nderates and causes the most pron oun ced symptoms .
A study of 1 12 cases o f tuberculosis made by Spengler (W iener Kl in .
Rundschau,N o . 33 , 1906 ) Showed the fo llowing :
Seven ty-eight pa t ien ts, or per cen t , showed a symbio t ic working o f
human and bovin e bac i lli . A l l were cases of a chron ic n ature.
Twen ty - two pat ien ts, o r per cen t , had exclusively human bac i ll i .
A l l o f these cases showed fever and o ffered a bad prognosis .
S ix pat ien ts, o r per cen t , had a lmo st exc l tis ively bovine bac i ll i . A l l
o f these pat ien ts a lso suffered from fever but w i th bet ter progno sis than
tho se i n fected w ith the human bac i ll i alone.
Twenty- two pa t ien ts,o r per cen t , Showed o n ly spl i tter but no
bac i ll i ; e ight cases had a m ixed in fect io n of human tubercle bac i l l i and
bo vi ne spl itter ; seven ca ses . had o n ly human tubercle bac i ll i Spl itter and
o n ly o ne case had bo vine spl itter exclus ively .
A cco rd ing to S pengler , the two variet ies o f bac i l l i d iffer in the fo l low i ng
m i l l l l l L‘
r .
i . (fultura l ly. T hey do n o t show the same growth under the same
Co nd it io ns .
36 PULM O N A RY TUBE RCULOS I S
FIG. 4 .
— A rtificial m ixture of pure cul tures o f human an d bovin e bac i ll i s ta in edby S pen g
ler’s after bein g firs t s ta in ed by ac id - fuchs inThe bac i ll i o f the bovin e type appear much larger, thicker a nd lo nger , than tho s eo f the human type .
5 .
— N a tura l m ixture o f bac i ll i o f huma n and bov in e ty pes , found in s putum .
S ta i n ed by S pe n g l t-r
'
s“l I i I l l e nme tho dc , a fte r be i ng fi rst s ta i n ed by ac id-fuchsin
I iac i l l i o f huma n type a ppear sma ll ; tho s e o f bovi n e type , la rge .
D I AGN O S I S O F E ARLY P ULM O N ARY TUBE RCULO S I S 3 7
o f human bac i llus .) Wash w i th wa ter . (Bev in e bac i ll i may be sta in ed
wh i le a l ive by using po tassium hydra te and methylen e blue w i thout fixin g
in the flame, in fact , th is method is an excellen t on e .)
3 . S ta in w ith carbo l fuchsin and warm very spar ingly low down in the
flame un t i l i t steams l igh tly . T h is is best accomp lished by passmg the slide
slowly through the flame. Wash w ith water . H eat in g‘
is to be carefully
avo ided in order t o preserve the'
envelope an d to avo id a prec ip i tation of
stain . .The fuchsin should n ever_
be a llowed to bubble .
4 . Coun tersta in in g w i th methylen e blue to wh ich is'
slowly added on e o r
two drops of a 15 per cen t so lut ion of n i tric ac id . Th is is allowed to re
ma in on on ly a few secon ds when it I s w ashed Off with water and the sl ide
is dr ied between fo lds of r ice paper and warmed on ly slightly high above
the _flame.
I n sta in in g bovin e bac i ll i,in o rder to demon stra te the en
PI cr i c A c i d
S ta in fo r vel ope, a culture'
wh ich has n ot been al lowed.
to dry must
be used,for the en velope is very eas i ly in jured by dry in g
,
and in as much as the recogn i t ion of the bov in e typede
pends upon the sta in ing Oi the envelope'
f ih tact, the impor tan ce of th is is
read i ly seen .
The human organ ism,in its a ttempt to o vercome a tuberculous in tee
t ion,produces certa in changes in the bac i ll i (bo th human a nd bovine)
themselves . Amon g o ther changes is an in jury of the envelope so that
the bac il l i are n o lon ger sta ined by the ord inary Z iehl method, yet they
are presen t and capable of -developmen t upon the proper med ia,a l though
their resistan ce is much lowered . Such bac i ll i may sti ll be sta in ed by the
use of‘ p icr ic ac id (Spengler, ibid) . I f any on e doubts th is let h im try i t
by mak in g two homogen eous smears of the same samples of Sputum and
then coun t the bac i ll i . E spec ia lly is'
th‘
e d ifferen ce to beno ted in cases
tha t are -n earing a cure and thus show ing resistan ce to the bac i l l i . We
have corroborated the work of Spengler in his sta in in g methods in our
own laboratory dur ing the past year and can recommen d them as being of
the greatest “ value . A n o ther test of the importan ce of the picr ic ac id
method may be made by tak ing a pure culture of ei ther human or bovin e
bac i lli .and mix in g it w ith ether and a lcoho l and shak in g it so as to par
tidl ly destroy the envelope (T oo much Shak in g w i l l en t irely destroy the
envelope, in wh ich case the human bac i ll i w i l l n ot sta in . The bovin e may
be sta ined even then .) A compar ison of spec imen s sta ined by the Ziehl
an d p icric ac id methods w i ll Show many more bac ill i in the la tter
The d irect ion s for the p icr ic ac id sta in in g are as fo l lows :
1 . S ta in in g w i th carbo l fuchsin,warm ing the preparat ion spar ingly a s
in the Hul lenmethode just descr ibed . W ithout wash in g add :
2 . Picr ic a cid—alcoho l for 2— 3 secon ds; then add three or four drops of a
PULM ON ARY TUBERCULOS I S
1 5 per cen t so lut ion of n i tric ac id and aga in p icr ic ac id-a lcoho l for 5— 10 see
ouds un t i l the sputum Smear is of a l ight yel low co lor ; wash w i th d i st i lled
water and dry . (The p icric ac id-a lcoho l so lution is made by add ing equa l
parts of a sa turated wa tery so lut ion of p icric acid and absolute a lcoho l or
equal parts of E sbach ’s reagen t and abso lute a lcoho l .)
3 . Wash w i th 60 per cen t a lcoho l immediatelv after the stain ing w ith
p icr ic ac id- alcoho l .
4 . Wash a few seconds w i th 15 per cen t n i tric ac id un t i l the Sputum
smear shows on ly a l ight yel low co lor .
_5 . Wash w ith a lcoho l,6 0—
70 per cen t .
6 . Con trast sta in w ith p icr ic ac id- alcoho l un t i l the smear is well co lored ,wash w ith d ist illed water
,dry and moun t .
Recen tly B lume (Berlin'
. Kl in . Wochen schr ift, N o . 29, 1906 )
calls atten t ion to the fact that the bacter io logica l d iagnosis
can be made earl ier than we are won t by w ip ing off part icles
of mucus from the larynx in patien ts who do n o t expectorate
and subject ing the same to m icroscopica l examinat ion .
Wh i le we canno t admi t that even such an examina t ion can
establ ish the d iagnosis of tuberculosis as early as can be done by physica l
examination ,nevertheless we Would recommend i t in doubtful cases .
When the sputum con tain s very few bacilli they may be
overlooked by the usua l method of exam inat ion . Spengler,
(Zeits. f . Hyg.,1894, Vo l . XVI I I , part 2) suggests the use
of pan creat ic d igest ion or pept ic d igest ion with ac id o r pap
o id d igest ion . By this means, the mucus is digested and the bacill i set free
and allowed to settle to the bo ttom of the test tube or sed imen t glass. The
sputum must be allowed to stand in the in cubator for twen ty- four or forty
eight hours when th is method is used .
A no ther method is to d i lute the sputum with twen ty t imes its
fikeW i tSCh
’S vo lume ofwater, after themethod o f I lkewitscli (Baumgarten s
ethod o f
Cen trifuga t io n ,Jahresber icht, 1892, Vo l . VI I I , page A fter st irr ing fo r
some t ime,acet ic ac id is used to precip i tate themuc in and nu
cleo albumen,and then i t is cen trifuged .
A s yet the Ron tgen rays have n o t been any materia l as
sistance in the d iagno sis Of early tuberculo s is . When the
area is suffic ien tly large to cast a shadow,i t is far beyo nd
the po in t where i t sho uld be d iagno sed by o ther methods .
Where the cl in ica l h isto ry and physica l examinat io n do no t
make us certai n o f o ur d iagno sis,and where there is no spu
tum,o r
,being presen t
,i t proves nega t ive o n exam ina t io n
, the
d i agno sis may be est abl ished w i th a verv smal l percen tage o f erro r by the
emplo ymen t o f the tubercul in test .
D I AGN O S I S OF E ARLY PULM ON ARY TUBE RCULO S I S
A grea t many men fear to use the tuberculin test lest they
do the patien t harm . Can tubercul in do harm? M ost as
suredly, the same as'
strychn ia,morphia
,chloro form and
o ther remedies I n common use by the physic ian . To practice med ic ine
presupposes a certain amoun t of in tell igen ce and care,and this Should be
used in the applicat ion of al l remed ial measur es.
I f tubercul in is used in tell igen tly, it can do no more harm than o ther po ten t
remed ies. I t must be remembered that human bein gs are n ot al l a l ike. Cer
ta in ind ividuals Show idiosyn crasies to certa in remed ies and un fortun ately
it is n ot possible to know this without tr ial ; and certa in co in c iden ces happen
in medic ine,as elsewhere
,that are somet imes in terpreted as cause and effect .
The greatest fear of tuberculin is perhaps based on the idea given out
i
by
Virch ow when i t was first put upon tr ia l in . 1-890 and 189 1 , that i t would exc ite
activity in laten t areas and tha t therewas danger of a gen eral in fection fo llow ing
its use. Some fear has been engendered by exper ien ces more recen t where such
unfortunate results seemed to have occurred .
This fear of tubercul in deserves more than passing n o tice, for we must
gran t that those who oppose i t and those-who'
use i t are equally hon est .
I f tubercul in is a remedy wh ich is endangering the lives of patien ts more than
o ther remed ies, i t should n o t be employed ; on the o ther hand, if i t is of great
serv ice to the afflicted,but un just ly feared
,then th is prejud ice should be
removed .
Fears ofTuberculin .
I n the first place, Virchow’s opin ion was based upon the
admin istrat ion of po ison ous doses of tubercul in . H e d id
n ot describe the effects of therapeutic doses of tubercul in ,
but that of po isonous doses. The pat ien ts who were k i lled by tubercul in at
that time were‘
kil led by po isonous doses, frequen tly repeated . I t would be
as just_to condemn strychn ia from the convulsion caused by it in a case of
death by strychn ia po ison ing .
The accepted method of admin istering tuberculin ei ther for the tubercul in
test or for therapeut ic use presupposes a knowledge of the fact that a very
small dose produces n o n o ticeable effect wha tever,but simply acts as a stimu
lan t to the body cells,causing them to form defensive bodies A dose some
what larger causes a slight hyperemia in tuberculous foci presen t,whi le a
large dose may cause the phenomena of in flammation and,i f repeated at fre
quen t in tervals, m ight cause retrograde changes . Know ing th is, the admin is
tration is begun with small doses and ser ious symptoms are avo ided .
Can tubercul in set up activity in la ten t foci M ost assuredly
i t can,if used improperly
,just as strychn ia when used improp
erly may cause convulsion s, and morphia , stupor and death .
But tubercul in when used properly is shorn of its power to do
harm .
40 PULM O N A RY TUBE RCULO S I S
I can con ceive of certa in cond it ion s being presen t so that
Tibercul in an overst imul at ion from a severe tuberculin react ion mightCause A cute cause acute m i l iary tuberculosis, but such cond i t ion s are
,
l
gl
l
l
gggul o sis ? very rare and would be exceptionally rare where i t is n eces
sary to use the tubercul in test in order to establ ish a d iagnosis.
A cute m i liary tuberculosis must'
be caused by the escape of a great number
of bac i lli in to the lymph or blood stream at one time. N ow i t is p ossible
to find cheesy tubercles in the wal ls of vessels or the thoracic duct which are
just ready to break down . I n such a case, the overst imulat ion from a severe
tubercu l in react ion m ight hasten the process and causei t to break sooner than
i t o ther wise would . Such cases must be very rare, however, when we con sider
how few“
cases o f acute m i l iary tuberculosis fo llowing the in ject ion of tuber
cul in have been men tion ed in the l i tera ture.
There is an in stan ce,oft quo ted
,from the practice of a n o ted N ew York
con sultan t wh ich occurred in the early n in eties, the sa l ien t po in ts of wh ich
as they have come to me are as fo l lows : The pa t ient wen t to this con
sul tan t for an examinat ion of the chest, s tating that i t was very importan t
tha t he know whether he was suffering from tuberculosis or n o t. A fter exam
ima tion, the Consultan t was in doubt . The pa t ien t w ished to have a test dose
of tubercul in given ,but the consultan t refused . H e wen t to ano ther consult
an t,who also refused to use tuberculin . Finally
,he wen t to a third
,who
admin istered the tubercul in test , after wh ich the pat ien t ‘ developed acute
m i l iary tuberculosis and d ied .
To show tha t th is might have been a co inciden ce,I quo te a case c i ted bv
Aufrecht,wh ich o ccurred in his own prac t ice . (Pa tho logie und Therap ie
der Lungen schwindsucht, The pa t ien t had been under observat ion
from 1889 to 1891 , and had susp ic ious sign s at one apex, yet the d iagnosis
could no t be establ ished . I t was dec ided to use the tubercul in test ; but wh i le
the tubercul in was being procured, the pa tien t was taken w i th acute m i l iary
tuberculo sis in which the in fect ion extended to the men inges and the pat ien t
d ied in o ne week . The author remarks that he is very glad tha t he had n o t
given the pat ien t a dose of tuberculin ,for he would then have a t tributed to i t
the cause o f dea th . For ano ther co in c idence,where a fatal hemorrhage oc
curred wh ile preparing a pa t ien t fo r a dose of strepto lytic scrum,I would
refer mv readers to page 145 .
Tho usands o f tests have been made fo r tuberculosis with tubercul in . Thou
sands o f pa t ien ts have thus d iscovered tha t they had tuberculo s is a t a t ime
when thei r cha nces o f gett ing Wel l were excellen t . O f th is number, hund reds
a re l ivingr today who,w i tho ut i t
,wo uld have wa i ted fo r graver symptoms and
l d iagno sis made to o la te . I f we reco gn ize the greatest go od fo r the greatestnumber , I Wo uld ven tu re the assert io n that the tubercul in test has savedsco res a nd SCU FCS o f l ives fo r evcrv mishap a ttributed to i t .
D I AGN O S I S O F E ARLY PULM ON ARY TUBE RCULO S I S I
We can at least offer as much excuse for its use as can be offered by the sur
geon for an exploratory 1nc15 1on m doubtful cases of abdomina l d isease, even
if we gran t that al l the dan gers assigned to i t are real .
I n explora tory in c ision ,we have the danger from the an esthet ic
, the danger
from the operation'
and the un certa in ty of being able to render‘
. aid when the
condi t ion is kn own ; yet, th is is recognized and san ct ioned by pract ica lly a l l
pract i t ioners.
I n the tuberculin test we have a supposed danger, in wh ich much of the
eviden ce is based upon un rel iable observa t ion ,some of i t upon the improper
use of the remedy ; but we_
also have a po ssib i l ity of afford ing rel ief in nearly
a l l in stan ces and of establ ish in g a cure in a very large majori ty of in stan ces
when the di agn osis shall have been made.
The d iagn ost ic va lue of tubercul in is based on what is known
as a react ion . A healthy individua l may receive in ject ion s
of tuberculin amoun t ing to 10 m i lligrammes w i thout show ing any symptoms *
Whatever beyond the soren ess at the po in t of in jection . A person afflicted
w ith tuberculosis, however, espec ia lly one in the early stages, w i ll show a
reaction . Th is react ion man ifests i tself both lo cal ly and generally . E i ther
the local or gen era l react ion is sufficien t to establ ish a d iagn osis.
The react ion occurs usually some t ime between eight and twen ty hours after
the in ject ion ,a lthough i t
.
may occur earl ier,even as early as four hours
,or
later,ever-1 as late as three days . T hese very early and very la te reaction s are
n ot very common, yet i t is importan t to kn ow of them .
Fo l low ing an in ject ion of tubercul in , certa in very defin i te phen omena occur .
I f the dose be very sma ll, n o effect is no ted,I f a li ttle larger
,a hyperemia
,
and,if st i ll larger
,a congestion occur s in and about the areas of tuberculous “
in fect ion .
Reac tion .
This is what is, kn own as the loca l reaction . I f the areas
are v isible, such as are found in the larynx and occasionally
in the pharyn x,th is hyperem ia and congest ion can be easi ly
detected . I n the lun g i t man ifests itself by the same phen omena as an in
flammation,al though the symptoms are confined to the area of in fect ion .
T hus a- compar ison of the find ings in the suspected areas before and after a
tubercul in react ion shows an in crease in al l the sign s during the react ion . The
find ings on auscultat ion are magn ified and resemble a catarrhal condi t ion
o f greater degree . Fine rales may appear where n one were to be found
previously or their n umber may in crease.
I n order to be able to detect a local reaction ,the findings on exam ina tion
should be charted carefully bo th before and during the reac t ion .
I t is possible to have a local reaction w ithout a gen eral react ion . I f there
be any doubt on th is po in t , let those who quest ion i t watch a tuberculous
larynx and see how o ften the react ion shows there when there are no con sti
42 PULM O N ARY T UBE RCULO S I S
tutional symptoms . I f a man is expert with his stethoscope, he w i l l make
less and less use of the genera l react ion in g iv ing the tuberculin test for sus
pected pulmonary tuberculosis, but rely on the lo ca l reaction instead . I n
th is way, there can certa in ly be no object ion to the use of the test . To be able
to use the test in th is manner, however, presupposes a kn owledge of the care
ful use of the stethoscope.
Besides the local reaction thereis what is known as a gen eral
reaction,or system ic reaction . A few hours a fter the test
dose is given ,if the dose is smal l
, the patien t beg ins to feel
a l i ttle nervous, or t ired , and perhaps has a heavy feeling about the legs. Wi th
this, there may be a sl ight rise of temperature of a fract ion of a degree and
and an increase of the pulse—rate, or the temperature and pulse may rema in
und isturbed . A person who is acqua in ted w ith the use of tubercul in w i l l
detect these slight symptoms as belonging to a general tubercul in reaction,
just as much as the more pronoun ced symptoms usually descr ibed .
I f the dose is larger, this t ired feel ing and heaviness of the l imbs becomes atrue ache
,wh ich extends to the back and head and thepat ien t feels as though
he were taking la grippe. With this, the temperature usual ly r ises one or
two degrees accord ing to the severity of the reaction , and the pat ien t may have
a cough where n one was presen t before or, if previously presen t, i t may be
increased . Figure 1,page
‘
10,i llustrates a tubercul in reaction where the
temperature wen t unusually high . This react ion occur red after a dose of 3mi ll igrammes. Two days previously the patien thad been given one m i ll i
gramme with n o effect .
I f the dose be st i ll larger, nausea or even vomi ting may take place ; a ch i llmay precede the r ise of temperature, wh ich may reach 103 or 104 degrees
and a l l of the symptoms descr ibed above maybe exaggerated .
Fo rmerly, the on ly tuberculin react ion wh ich physic ia n s recogn ized con sisted
in a rise of temperature o f at least two degrees Fahrenhei t above that which
the pat ien t was run n ing regularly, accompan ied by the o ther general symptoms
previously men tioned ; today, most men conversan t with the use o f tubercul in
requ ire on ly o ne degree o f r ise and those who are most experien ced in its use
insist on no spec ific rise of temperature, but accept any symptom o r group o f
symptoms which are unmistakably due to i t , and consider a loca l react ion as of
grea ter d iagnost ic impo rtance than a general react ion .
T he symptoms o f bo th loca l and genera l reaction usually pass o ff in from
a few to twen ty- four o r th irty- s ix hours .
I n as much as the reaction usually shows itsel f in from
eight to twen ty hours after the test dose has been given ,i t
is best to give the dose at bed- t ime . I am accustomed to
giv ing i t at about eight o r n ine o’clo ck
,then requ iring the pa
t ien t to begin tak ing his temperature abo ut s ix the next mo rn
44 PULM ON A RY TUBE RCULO S I S
the d isease I S advanced . I n these the system is a lready immun ized to a
grea ter o r less exten t to the tox ins found in tubercul in ,and a much larger
dose would be requ ired to produce a reaction than we are accustomed to
use in admin istering the test . Fa i lur e on the part o f these pat ien ts to react
is no argumen t aga in st the spec ific ity of tubercul in for,i f a suffic ien t ly
large dose were g iven ’
to overcome the immun i ty wh ich has been atta in ed,
a l l these patien ts who have. tuberculous lesion s would probably reac t . I n
such cases,however, a tubercul in test I S rarely necessary
,for the phy s ica l
sign s are apt to be suffic ien tly pronoun ced .to establ ish the d iagnosis, but , i f
n ecessary,we should employ larger doses than we are won t in o rd inary cases .
I n determ in ing dosage,i t is . safe to assume that those patien ts in whom the
symptoms and sign s are most vague are apt to reactO
to much smaller doses
than those in whom the symptoms are more marked , because their systems
have n ot been 1mmun ized by a pouring out of any considerable amoun t of
bac i llary toxin s from the .diseased areas .
There is a lso a po ssib i l ity,where the gradual method is employed, 0 each
prev ious dose con ferring an immun ity wh ich preven ts the next from causin g
a react ion ; so , wh i le i t is safer than the o ld method of employ ingone large dose,
yet i t will occasionally fai l to show a general react ion where the o ther would .
H ere the loca l react ion ,however, comes to the rescue and should be looked for .
A ccord in g to Spen gler ’s view of the double et io logy o f tuberculosis,we should
n ot“
expec t tha t smal l percen tage of pat ien ts in fected prin c ipa lly by bac i lli o f
the bovine type to reac t to human tubercu l in adm in istered in m in ute doses .
A tubercul in test should no tbe g iven un less the patien t is under
the con tro l of the physic ian . H e should be put to rest , n ot
necessar i ly to bed, but he should be kept qu iet . A n in st i
tution is an idea l place for admin istering a tubercul in test .
Fo r two days the temperature should be taken by an accurate thermometer and
in a propermanner as men tioned in the d iscussion of temperature on page 10 .
The dose should be given preferably at n ight , about eight or n ine o’clock ;
then the temperature chart should be carefully kept , beginn ing in the'
ear lv
mo rn ing and con t inu ing un t i l the test is completed , whether i t be a s ingle do se
o r whether severa l be requ ired . The test should be g iven w ith the same care
as any o ther hypoderm ic in ject io n .
The in ject io n may be given in any part o f the hodr where
there are th ick muscles, such as the upper arm , in terscapular
regio n,lo in s o r musc les o f the leg . I usua lly use the a rm
“
.
The pa in o f in ject io n is less,
'
if i t is g iven deep in to the muscle a nd is vcrv
S i te o fI n j ec t io n .
sl ight i f the needle is i nserted qu ickly .
I f i t is fo und tha t the temperature is above 100 degreesCo n tra a o o o o
m isi n d i cauo n s .
l ahi c nhe i t,thi tes t should n o t be g
iven l ht (bign i 18
sho uld be made o ther“ ise o r we sho uld endeavo r to reduce the
D I AGN O S I S OF E ARLY PULM ON A RY T UBE RCULO S I S 45’
temperature by rest and such appropr iate measures as are suggested under
treatmen t of febr i le cases .
I f any acute compl ica t ion s are presen t the test should not be g iven un t i l
they have subsided .
Wha tA tubercul in test can be made by the employmen t of any of
p repara tion the var ious products of the bac ill i,such
'
as O ld T ubercul in,
$1223?be T . R .
,Watery E xtract
,Pur ified T ubercul in
,Bov ine Tuber
cul in,etc . But when we speak of giving the tubercul in test ,
itg-is generally understood that we mean to employ the o ld tubercul in of
Koch,and the dosage here g iven is in terms of th is preparation .
I t is better to employ a product made in some good laboratory . The dose
used for the in ject ion should be made up fresh at the time of the in jection ;
I f the physic ian makes his own d i lut ions, he should employ n ormal sa lt so lu
t ion for“
the d i luen t . I f he makes a 1 per cen t so lut ion of the or ig inal prep
aration then 1 cub ic cen t imeter equals 10 m i ll igrammes of tuberculin .
Who Sha llShall the tuberculin test be g iven by physic ian s indiscr 1m1n
A dm in ister the a tely? This is a very importan t question to con sider. I t
grai
sqe
a
r cul in would be best if men who inten d to admin ister tuberculin
either for diagn ost ic or therapeutic purposes should fir st
learn ‘from some man who"
has had exper ien ce in its admin istration . Cer
tain ly no man has any right to use tubercul in who does n ot make a careful
study of i t and its action . Any man,who has in tell igen ce enough to admin
ister o ther powerful remed ies, should be able to give the tubercul in test, yet
i t must n ot be given carelessly or ignoran tly . Tubercul in in the hands of
an 1ncompeten t physic ian would be just as dangerous as a kn ife in the hands
of an in competen t surgeon .
Tuberculin When patien ts are treated by ordinary hygien ic methods, theTest as Proof tuberculin test is a safe and reliable proo f of cure. I f
’
at theOf Cure.
end of .treatmen t_
the physician w ishes to know whether or no t
his patien t is cured,he can dec ide by the in ject ion of tuberculin the same
as though he were giving a tuberculin test at the beginn ing of treatmen t .
When the patien t has been trea ted by the various products made from the
bac i llus, such as T . R .,Bac i llus Emulsion
,Watery E xtract and P. T . O .
,the
tubercul in test is not a“reliable proof of cure ; for one of these. preparation s w i ll ~
produce an immun i ty on thepart of the organ ism again st all of the o ther bacil
lary products. Such an immun i ty wi ll last for some t ime. A t least six mon ths
should elapse before the test is reliable.
Pirquet , of Vienna, has devised a method for adm in istering{
1
1
31
323225111 the tuberculin test to ch i ldren in the earl iest years of life.
I n fan cy an d Themethod is very s imple and atten ded w i th a lmost n o pain .
I
gfiir
fd’
hood.
H is method is as fo l lows : Fi rst the skin of the arm is dis
in fected w i th ether, then two drops of the fo l lowin g so lution
46 PULM O N ARY T UBE RCULO S I S
(O ld T ubercul in (Ko ch) 5 per cen t carbo l ic ac id so lut ion n ormal
sal t so lut ion are dropped on the sk in at po in ts about two in ches apart ;then w i th a smal l lan cet, w i th cutt ing edge on the end and n o t very sharp
(n ot un like a smal l screw dr iver used by watchmakers) he makes pressure
o n the sk in under the drop of lymph and turn s the in strumen t a few t imes,
caus in g a sl ight abrasion and at the same t ime ino cula t in g the wo und ; the
in strumen t is then c leaned of lymph and a third abrasion between these
two is made for con tro l .
The d iagno sis depends upon a local reaction . I f the ch i ld is suffering
from tuberculosis, a fter a few hour s,usua lly twen ty- fo ur
,a sma ll papular
area of redness appears around the si te of the in ocul at ion ,wh i le the
site of the con tro l shows on ly the sl ight react ion due to the trauma . I f
t uberculosis is n ot presen t the s ite of the in o culation l ike that of the con
tro l shows on ly the trauma t ic -congest ion . The size of the papule is com
men surate w i th the in tensi ty o f the react ion . There is n o temperature re
action accompanyin g, co n sequen t ly the test can be used in fever cases and
i t can be used without causing any con sti tut ion a l d isturban ce on the part
of the chi ld .
The test is espec ially trustwo rthy. in the first two o r three years of l i fe,
but n o t so certain in ch ildren of ten and twelve years and thereafter . I t
is not so trustworthy in faf advan ced processes as in early cases for the
same reason as men t ioned on page 44. Pirq‘
uet has a lso foun d that pa
tien ts who are very cachect i c do n o t react so sur ely as do those who are
n o t. I n an experien ce of over seven -hundred cases, many of whom have
come to post-mo rtem,the rel iabil i ty of the test has been very sa t isfactory .
Calmet te (Presse M édicale, Jun e 19, July 13, 1907) and Wolff-E isner
(Ber . Kl in . Woch .
,June 3 , 1907) have shown that tubercul in may be ad
min istered as a d iagnost ic agen t by dropping i t in to the con junc tiva l sac .
A t first one drop of a one per cen t so lut ion is used . I f no
reaction occurs two.
drops may be employed after a few davs
have in tervened . The test depends upon the fact tha t the
body cells of a tuberculous individual are sensit ized to the
toxins o f the tubercle bacillus, so that when the diagnostic agen t comes in
co n tact wi th the cells a hyperemic reaction resul ts . When the tes t is pos i
tive the co n junc tiva,and in some cases the adjacen t mucous membrane
,be
comes tempo rarily in fl amed , the degree and dura tion being dependen t upo n
the severi ty o f the reaction .
' When tuberculo s is is absen t the co n junctivash ows no react io n . N o harm can resul t provided tha t weak dilut ions a re
employed a nd the eye is heal thy . The test o ffers i tsel f as a s impler methodo f making a d iagno s is o f early tuberculo s is than the subcutaneo us metho d ,
but n eeds further co n fi rma t io n .
CH APTE R V.
SYMPTOMS AND S I GN S OF ADVAN CE D PULMONARY TUBE R
CULOS I S AN D I TS COMPLI CATI ON S .
I t m ight be assumed that anyone who can make a diagnosis of early pul
monary. tuberculosis can also make a d iagn osis when the d isease is advan ced ;
yet, there are many cond it ion s and compl icat ion s presen t in the advan ced
d isease that should be recogn ized, wh ich'
produce en tirely d ifferen t symptoms from those of the early disease. I n as much as our purpose in d iagn o sis
is three—fo ld,first, to know the cond ition presen t, second, to give as accura te
a prognosis as possible, and third, to apply the proper remed ies,we must
do more'
than determine that tuberculosis,is presen t . We must en deavor
to determ ine the exten t of the disease, the’
e—
ffect i t has had upon the lungs
and gen era l system,and then determ in e wha t remedies can be best appl ied
to correct the patho logical cond ition s presen t . Hen ce, the more accura te
our sk i ll in d iagnosis and the more carefully we determ ine the exact con
d i tion presen t,the more valuable wi ll be our opin ion of the prognosis and
treatment of a given case.
The fam i ly h istory in advan ced pulmon ary tuberculosis does n ot d iffer
from that of early tuberculosis, so the reader may refer to that section for a
con sidei ation of th is subject (see p .
CLIN ICAL HISTORY IN ADVANCED PULMONARY TUBERCULOS IS .
The same general symptoms obta in as were men t ioned (pp . 8— 1 2)wh i le c-on
sider ing the d iagnosis of early tuberculosis, but they are apt to be more pro
n ounced . The same tired feel ing,the same inab i li ty to do customary tasks,
the same loss of ambit ion , the fa i lure to secure rest by a. n ight ’s . sleep, the
same “ co lds” and bron ch ia l catarrhs, the same nervousness, the same d iges
t ive d istur ban ces with loss of more or less weight, the n ight sweats, the dis
turbances of circulation, the vaso -mo tor d istur ban ces as shown in co ld hands
and feet or chi lly sensations,are al l presen t in greater or less degree in advan ced
pulmonarytuberculosis ; and some of these are n early always el ic i ted by in qu iry
in to the c l in ica l history of those suffer ing from th is disease.
Cough is usually-
an importan t symptom in advan ced pul
monary tuberculosi s . Wi th the appearan ce of early tuber
culosis and its accompanying in flamma t ion,there begin s a sl ight hack . A s
Cough .
48 PULM O N ARY T UBE RCULO S I S
men t ioned before, at fir st th is is scarcely n o t iceable ; then i t in creases . I t
is accompan ied by expectorat ion,at fir st usua ll y scan t ; later pro fuse.
There is no th ing characterist ic in the cough of tuberculosis by wh ich i t
may be d ist ingu ished from o ther coughs .
M any pa t ien ts w ith exten sive d isease cough very l i ttle,and there have
been cases reported that d ied of tuberculosis and yet were never known to
have coughed . However, these are the exceptions .
M uch of the cough presen t in tuberculosis, as we usually find i t, is un nec
essary .
' I t is due to such m istakes as wrong methods of living,overexert ion
and the hab i t of coughing, and soon d isappears when pat ien ts are properly
instructed and their lives careful ly regulated as we find them in a properly
conducted sanatorium . Catarrh of the oro and naso -pharynx is a frequen t
cause of cough . Properly managed pa t ien ts suffering from advan ced d isease
w i ll usually cough con siderably in the morn ings un t i l they have expel led the
secret ion which has accumulated over n ight, then they may scarcely cough
at al l during the rest of the day. They usua lly cough aga in at n ight upon
ret iring. Of course, if there is some acute process presen t, such as a pneu
mon ic condit ion or pleur isy, the cough w i l l most l ikely be in creased . When
the d isease is accompan ied by exten sive bron chit is,coughing is o ften very
troublesome.
A s there is no cough characteristic of tuberculosis,so is
there n o characteristic sputum . A t first,the sputum is
muco id in character ; but, as ulcera t ion supervenes and the catarrhal symptoms become more pronoun ced
,i t becomes muco -purulen t and purulen t .
Sometimes i t is a lmost pure pus . When it comes from a cavity,i t is apt to
come in ba l ls (so - ca lled n ummular sputum) and if expectorated in water
may s ink to the bo ttom . O ccasionally i t is bloody. I f it con tain s on ly flecks
of blood, this is most l ikely due to a congestion . I f the congestion be greater,i t may be wel l m ixed w ith blood . Somet imes the pus from a cav i ty is m ixed
w i th a bloody d ischarge which appears much l ike the discharge from an
ulcer . Th is is o ften due to ruptured granulations . Fo llowing hemorrhages,the sputum may be blood t inged for severa l days.
The sputum frequen tly has a very bad odor,especial ly when i t comes from
cav i t ies where i t has rema ined for some time.
The amoun t of sputum varies with the accompanying catarrha l com
pl ica t io ns and the n umber and cond i t ion o f the cavi ties presen t . When the
d isease is runn ing a rap id course with the rap id destruction of tissue, the
sputum is abundan t and very purulen t . When ca tarrha l conditio ns predom
inate,the sputum may be mo re abundan t but i t is less purulen t . I n pat ients
su ffer ing from d iabetes the sputum is o ften scan t,ow ing to the lo ss o f fl u ids
th ro ugh the urine .
Sputum .
The po si tive recogn i t io n o f tuberculous sputum depends upo n the presence
AD VA N CE D PULM ON ARY TUBE RCULO S I S 9
of tubercle bac i lli . The finding of elast ic fibers is also very suggest ive,i f
al l o ther condit ion s wh ich cause destruct ion of lung t issue are el im inated .
I n acute mi l iary tuberculosis, the most v irulen t of a l l types of the disease,the sputum may con ta in neither bac i lli n or elastic fibers. T here are a lso
cases of chron ic tuberculosis which have ex isted for years and have gone on
to the death of the patien t, wh ich did n ot~ show bacilli un til a short time before
the end.
Sputum in tuberculosis o ften shows many o ther morpho logical elemen ts.
S treptococci, staphylococci,pneumococc i
,influenza-bac i lli
,d iphther ia or
pseudo -d iphther ia bac i ll i and many o ther m icro -organ isms have been found .
The presen ce of these organ isms in the sputum does n ot n ecessar i ly mean
that they are causative factors in the patho logical processes presen t . The
effect wh ich they have upon the course of the d isease w il l have to be deter
m ined hy future research .
The digestive disturban ces in‘
advan ced tuberculosis deserve
most careful atten t ion . That they should be pron oun ced
is to be'
expected . Pat ien ts suffering from advan ced tuber
culosis are victims of a toxem ia which destroys‘
the appet i te and in terferes
w ith d igest ion . Where the temperature is h igh, th is is o ften especially severe.
The con stan t irritation of the pn eumogastr ic by the d isease m the lun g can no t
help but effect the nerve supply of the stomach . Pulmonary tuberculosis
must be con sidered as a chron ic pneumon ic process . I t is a lso accompan ied
by catarrhal con di tion s of the mucous membrane of the air passages and usu
all y in advan ced con d i t ion s w i th more or less emphysema . The pulmon ary
c irculat ion is thus severely embarrassed . The heart o ften shows the overstra in
to which i t is subjected . A s a result, there is to a greater or less degree a
damming back of blood in the in terna l organ s which , among o ther symptoms,causes a disturban ce of the d igestive fun ction . A n o ther way in wh ich the
d igestive tract suffers is through the genera l loss of muscular tone due to
muscle waste.
I n the earl ier stages of the disease, we find variable appeti tes ; somet imes
depressed,sometimes en tirely wan t ing and at o ther t imes vorac ious. D iges
tion“
is usually somewhat impair ed, the cond i t ion in creasing as the case pro
gresses. A ll fo rms of stomach d isorders are found, such as hyperchlorhydr ia,hypochlorhydr ia, atony
,d i latat ion
,d isplacemen ts and the various n eur oses .
T uberculosis offers a complete clin ic in d iseases of the d igest ive system,
and upon the success in managing them depends, to quite a great exten t,
the outcome of the d isease.
An examination should never be considered fi n ished in
advan ced tuberculosis un t i l the cond i t ion of the c irculatory
system has been carefully determ ined,for on e of thepo in ts
upon which the prognos is must be based is the con d i t ion of the heart .
D igestiveD isturban ces.
48 PULM ON ARY T UB E RCULO S I S
men t ioned before, at fir st th is is scarcely n o t iceable ; then i t increases . I t
is accompan ied by expectora t ion ,at first usua ll y scan t ; later pro fuse.
There is n o th ing character ist ic in the cough o f tuberculosis by wh ich i t
may be d ist ingu ished from o ther coughs .
M any pa t ien ts w ith exten sive d isease cough very li ttle,and there have
been cases reported that d ied of tuberculosis and yet were n ever kn own to
have coughed . However, these are the except ion s .
M uch of the cough presen t in tuberculosis, as we usually find i t, is unnec
essary . I t is due to such m istakes as wrongmethods of l iving,overexert ion
and the hab i t of cough ing, and soon disappears when pat ien ts are properly
in structed and their l ives carefully regulated as we fin d them in a properly
conducted sanator ium . Catarrh of the oro and naso -pharynx is a frequen t
cause of cough . Properly managed pat ien ts suffering from advan ced d isease
w i l l usually cough con siderably in the morn ings un t i l they have expelled the
secret ion wh ich has accumulated over n ight,then they may scarcely cough
at a l l during the rest of the day. They usua lly cough aga in at n ight upon
ret iring . Of cour se, i f there is some acute process presen t, such as a pneu
mon ic cond i t ion _or pleur isy,the cough wil l mo st l ikely be in creased . When
the d isease is accompan ied by extensive bron chit is, cough in g is o ften very
troublesome.
A s there is no cough characteristic of tuberculosis,so is
there no character ist ic sputum . A t first, the sputum is
muco id in character ; but, as ulcerat ion supervenes and the ca tarrha l symptoms become more pronounced, i t becomes muco -purulen t and purulen t .
Sometimes i t is a lmost pure pus. When i t.
comes from a cavity,i t is apt to
come in balls (so - ca lled nummular sputum) and if expec torated in water
may s ink to the bo ttom . O ccasionally i t is bloody . I f i t con tain s on ly flecks
o f blood,this is most l ikely due to a congestion . I f the congestion be greater
,
i t may be well m ixed w i th blood . Sometimes the pus from a cavi ty is m ixed
w i th a bloody d ischarge which appears much like the d ischarge from an
ulcer . Th is is o ften due to ruptured granula t ions. Fo llow ing hemorrhages,
the sputum may be blood t inged for several days .
The sputum frequen tly has a very bad odo r,espec ially when i t comes from
cav i t ies where i t has rema ined fo r some time.
The amoun t o f sputum varies w i th the accompany ing catarrha l com
pl ica tio ns and the number and co nd i t ion of the cav i t ies presen t . When the
d isease is run n ing a rap id co urse w ith the rap id destruction o f t issue,the
Sputum is abundan t and very purulen t . When catarrha l co nd i t io ns predom
ina te,the sputum may be mo re abundan t but i t is less purulen t . I n pat ien ts
suffering from d iabetes the sputum is o ften scan t,owing to the lo ss o f fl u ids
th ro ugh the urine .
Sputum .
T he po sit ive recogn it io n o f tuberculo us sputum depends upo n the presence
50 PULM ON ARY TUBE RCULO S I S
I n o rder to fully apprec iate the eno rmous strain that is put upon the heart,
we must con sider,
first,that chron ic tuberculosis of the lungs is a chron ic
pneumon ic process ; second, that as the process advan ces, it destr oys the
blood vessels and also destroys the normal lung t issue and subst i tutes for it
either cavit ies or c icatr ic ia l t issue ; th ird, w i th the advance of the d isease,con
traction takes place in one port ion of the lung wh i le o ther port ion s en large,
becoming emphysematous,to establ ish compen sat ion ; and, fourth ,‘
the ad
vanced d isease is accompan ied by more or less catarrhal in flammation of
the air passages .
A l l of these cond i tion s tend to embarrass the right heart,thus damm ing back
the blood in the system ic circula t ion as wel l .
The heart o ften learn s to accommodate i tsel f to -the enormous strain that is
thrown upon i t because the changes come gradua l ly, tak ing mon ths and
years to effect them . On the o ther hand, if the same amoun t of resistan ce
were opposed to the heart sudden ly, by an acute process, the result could be
n one o ther than d isastrous.
The rap idi ty and effic iency of the heart ’s act ion ,then
,must a lways receive
careful atten tion in giving a prognosis.
The pulse in a n on - febri le tly remain s above 90 and
wh ich does n ot drop after a coun t aga in st the
pat ien t ’s chan ces o f recovery , er the impulse.
A s a rule, the pulse is o itself even in early
tuberculosis.
The pulmonary second 5 when the heart is
stand ing up wel l under the
When a cav i ty is near the the sounds somet imes
take on a metall ic ring .
When the rhythm of the heart sounds change and the sounds approach each
o ther in in tensi ty (the so—called fetal heart) the progno sis is bad .
I n advan ced tuberculosis,symptoms on the part of the
nervous system are varied and o f great in terest . The tox in s
from the tubercle bac i l lus, o r those from o ther compl icat ing
m icro -o rgan isms,o r tho se absorbed from necro t ic t issue a l l act deleter iously
upo n the nervo us system .
The tuberculous patien t is usua lly an optomist. .H is sangu in ity is proverb
ia l . Yet he is no t a lways so . We meet no t in frequen t ly instances o f pes
s imism and ho pelessness .
T he tuberculous pa t ien t,as a rule
,lapses in to a cond itio n o f dependence.
H e is apt to become selfi sh and regard his own desires and w ishes as paramoun t
to a l l o thers . H e is a lso l ikely to lo se some o f his natura l strength o f w il l and
to be eas ily i n fluenced , espec ially i f the fo rce leads in the direction to wh ich
he is n o t una lterably o ppo sed .
AD VAN CED PULM ON ARY TUBE RCULO S I S 5 I
M any symptoms on the part of the nervous system are to be found . Such
cond it ion s as neurasthenia,hyster ia
,hyperesthesia
,hem ihyperesthesia
,
hyper idrosis,hem ihyper idr osis, and neur i t is are no t un common . The hect ic
flush' has long been
.
recogn ized and the d i latation of the pup il s (see p . 1 7)has more recen tly been studied .
The cour se of tuberculosis is an uneven one. Patien ts
feel well for a wh i le and then i ll . When they are n ot feel ing
so well,they areapt to th ink they have caught col d . They
cough more,feel an uneasmess 1n the chest
,may expectorate
mo re freely, may have an eleva t ion of temperature and, as a rule, suffer a loss
of strength . These symptoms are,as a rule, co in c iden t wi th a sl ight activity
in the lung process . A frequen t repet it ion of these so - called co lds is very
characteristic ; and a his tory of repea ted co lds on the part of an ind iv idual
or of co lds wh ich do n ot get well wi th in a reasonable t ime should a lways
call atten tion to the-
chest .
Hoarseness I S a frequen t symptom,in tuberculosis. I t
may come on very early in the disease and it may appear
every now and then “ durin g the course. I'
t’
al'
vvays ca lls for an examina t ion
of the larynx . T uberculous pat ien ts are subjected to a l l n on - tuberculous
laryngeal affect ion s . From frequen trcough, voca l cords o ften show th icken
ing. Kn ow ing that more than fifty per Gent of advan ced cases-
of pulmonary
tuberculosis show some tuberculous invo lvemen t of the larynx, tubercu lous
laryngi t is'
must a lways be thought. of
M any pa t ien ts suffer very l i ttle, yet most of them w i ll exper ience some pain during the cour se of the d isease, and some
suffer in ten sely .
The most common pain is the sharp, cutting pa in of acute pleurisy . Few
cases run the course of the disease w i thout experien c ing th is . I t is usua lly
located in the lower port ion of the chest but may be found in any port ion .
Sometimes th is acute pain is fo llowed in a’ few days by a pleura l effusion .
The pleura is a lways more or less involved in advan ced tuberculosis . Ad
hesion s form which every n ow and then cause pa in,somet imes sharp but more
o ften dull and ach ing .
When “
an acute process near the surface is break ing down,w i th cavity
i
format ion,somet imes there is soren ess more or less marked
,somet imes qu i te
a severe pa in .
When con tract ion of a lun g is tak ing place,the pat ien ts are often made
qu ite uncomfortable by a feel ing of pull ing or dragging,perhaps due - to
stretch in g pleural adhesmn s. Somet imes they descr ibe their feel ings as
seeming as though they were being squeezed in a v ice.
A side from these there is o ften a feel ing of t ightness wh ich occurs when
there is an acute congest ion of the air passages .
H oarsen ess.
Pa in .
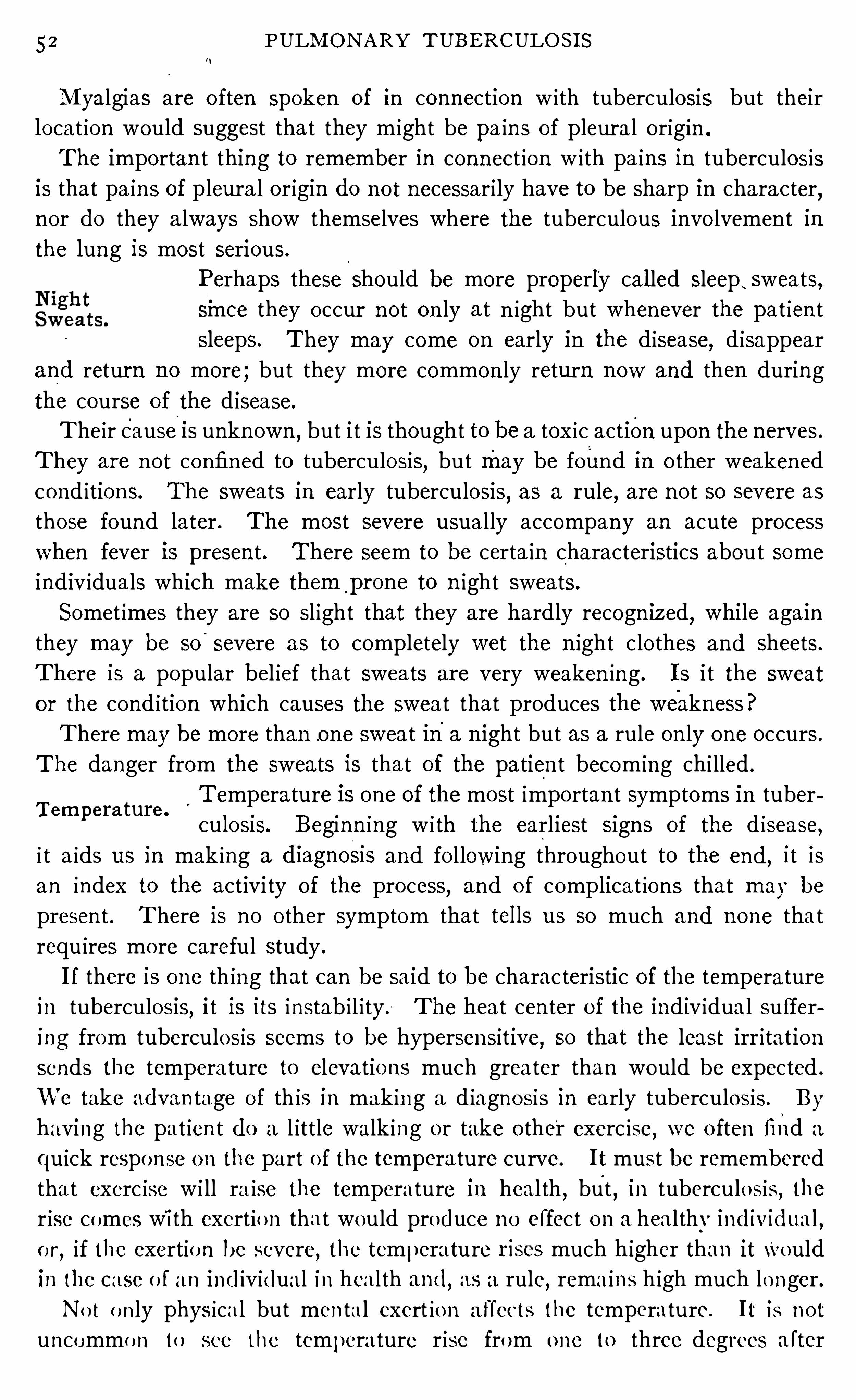
52 PULM ON ARY TUBE RCULO S I S
M yalgias are o ften spoken of in connection w i th tuberculosis but their
locat ion would suggest that they m ight be pa in s of pleur a l origin .
The importan t thing to remember in connect ion w i th pa in s in tuberculosis
is that pa in s of pleura l or igin do n ot necessari ly have to be sharp in character,
n or do they a lways show themselves where the tuberculous invo lvemen t in
the lung is most serious.
Perhaps these should be more properly cal led sleep,sweats,
smee they occur n ot on ly at n ight but when ever the pat ien t
sleeps. They may come on early in the d isease,d isappear
and retur n no more ; but they more common ly return n ow and then during
the course of the disease.
Their cause 1s unkn own ,but i t is thought to be a tox ic action upon the nerves .
T hey are n ot confined to tuberculosis, but may be found in o ther weakened
cond ition s. The sweats in early tuberculosis,as a rule
,are n ot so severe as
those found later . The most severe usually accompany an acute process
when fever is presen t . There seem to be certa in characteristics about some
indiv iduals which make them p rone to n ight sweats.
Somet imes they are so sl ight that they are hardly recogn ized,whi le again
they may be so
“
severe as to completely wet the n ight c lo thes and sheets .
There is a popular bel ief that sweats are very weaken ing . I s i t the sweat
o r the cond i tion which causes the sweat that produces the weakn ess?
There may be more than o ne sweat ina n ight but as a rule on ly one occurs .
The danger from the sweats is that of the patien t becom ing chi lled .
Tempera ture is one of the most impo rtan t symptoms in tuber
culosis. Beginn ing w i th the earliest sign s of the d isease,i t a ids us in mak ing a diagnos1s and fo l lowing throughout to the end
,it is
an index to the activi ty of the process, and of complica t ion s that may be
presen t . There is no o ther symptom tha t tel ls us so much and none that
requ ires more careful study .
I f there is one th ing that can be said to be charac teristic of the temperature
in tuberculosis, i t is its instab i l ity . The heat cen ter o f the ind iv idua l suffer
ing from tuberculos is seems to be hypersen sitive,so that the least irr i tat ion
sends the tempera ture to elevatio ns much greater than would be expected .
We take advan tage o f th is in mak in g a d iagnosis in early tuberculosis . By
having the pat ien t do a l ittle walk ing or take o ther exerc ise,we o ften find a
qu ick respo nse o n the part o f the temperature curve. I t must be remembered
tha t exerc ise w i ll ra ise the temperature in heal th,but
,in tuberculo sis
, the
r ise comes wi th exert io n tha t would produce n o effect o n a healthy individua l ,o r
, i f the exertio n be severe,the tempera ture r i ses much higher than i t Would
in the case o f an ind ividual in heal th and,as a rule
,rema ins h igh much lo nger .
N o t o n ly physica l but men tal exert io n a tTects the temperature. I t is no t
uncommo n to see the temperature r ise from o ne to three degrees a fter
Tempera ture.
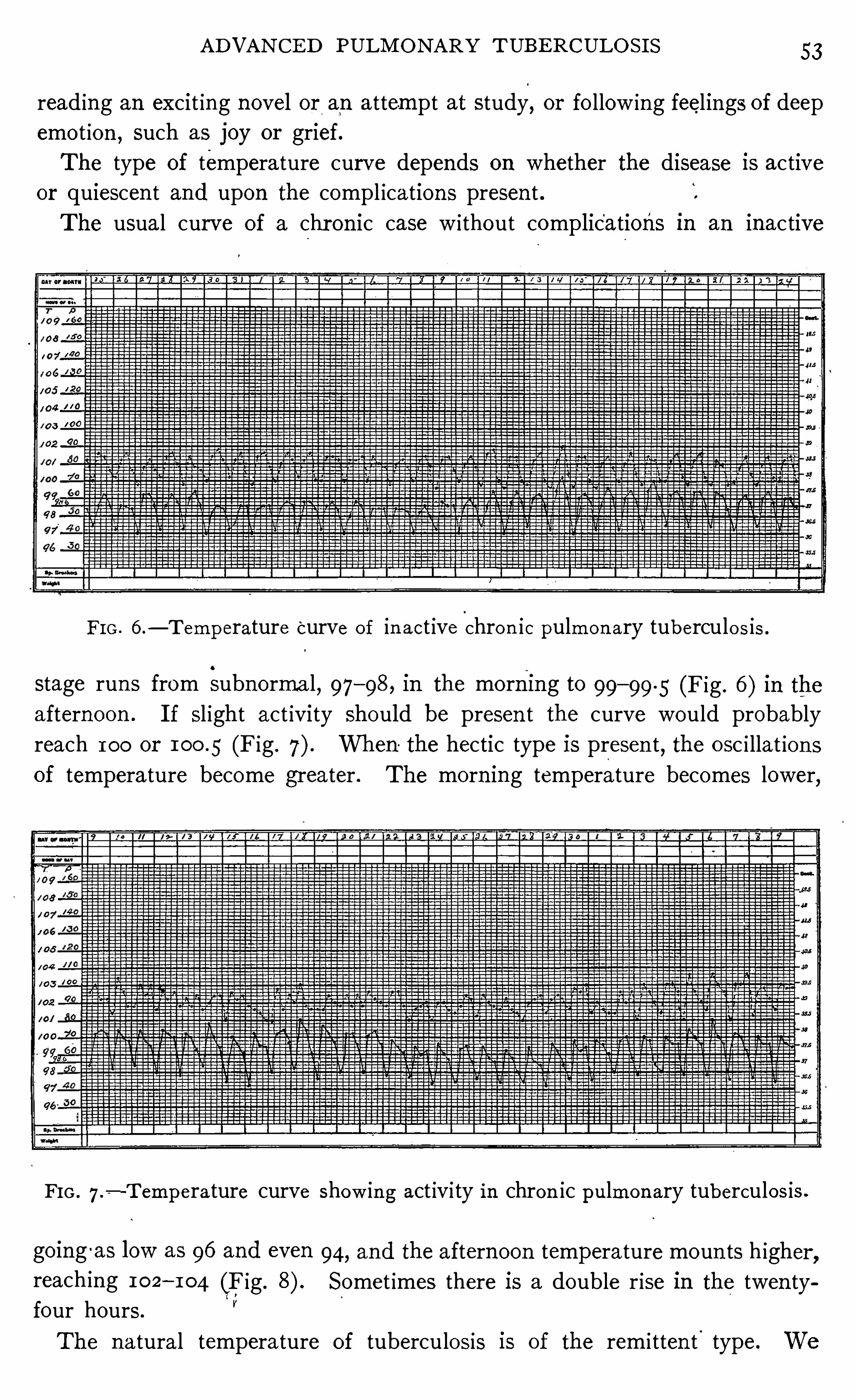
AD VAN CE D PULM ON ARY T UBE RCULO S I S 53
read ing an excit ing novel or an attempt at study,or fo llow ing feelings of deep
emo t ion , such as joy or grief.
The type of temperature curve depends on whether the disease is activeor quiescen t and upon the compl ications presen t .
The usual curve of a chr on ic case w ithout complications in an inactive
FI G . 6 .— T emperature
“
curve of in act ive chro n ic pulmon ary tuberculo s is .
stage run s from subnorma l, 97—98 , in the morning to 99— 99 .5 (Fig . 6 ) in theafternoon . I f sl ight act ivity should be presen t the curve would probably
reach 100 or (Fig . When the hectic type is presen t, the o sc i llat ion s
of temperature become greater . The morn ing temperature becomes lower,
FIG . 7 .-Tempera ture curve show ing act ivi ty in chron ic pulmon ary tuberculos is .
go ing -as low as 96 and even 94, and the afternoon temperature moun ts h igher ,
reach in g 102—104 (Fig . Somet imes there is a double r ise in the twen tyfour hours.
V
The natural temperature of tuberculosis is of the remi tten t'
type. We
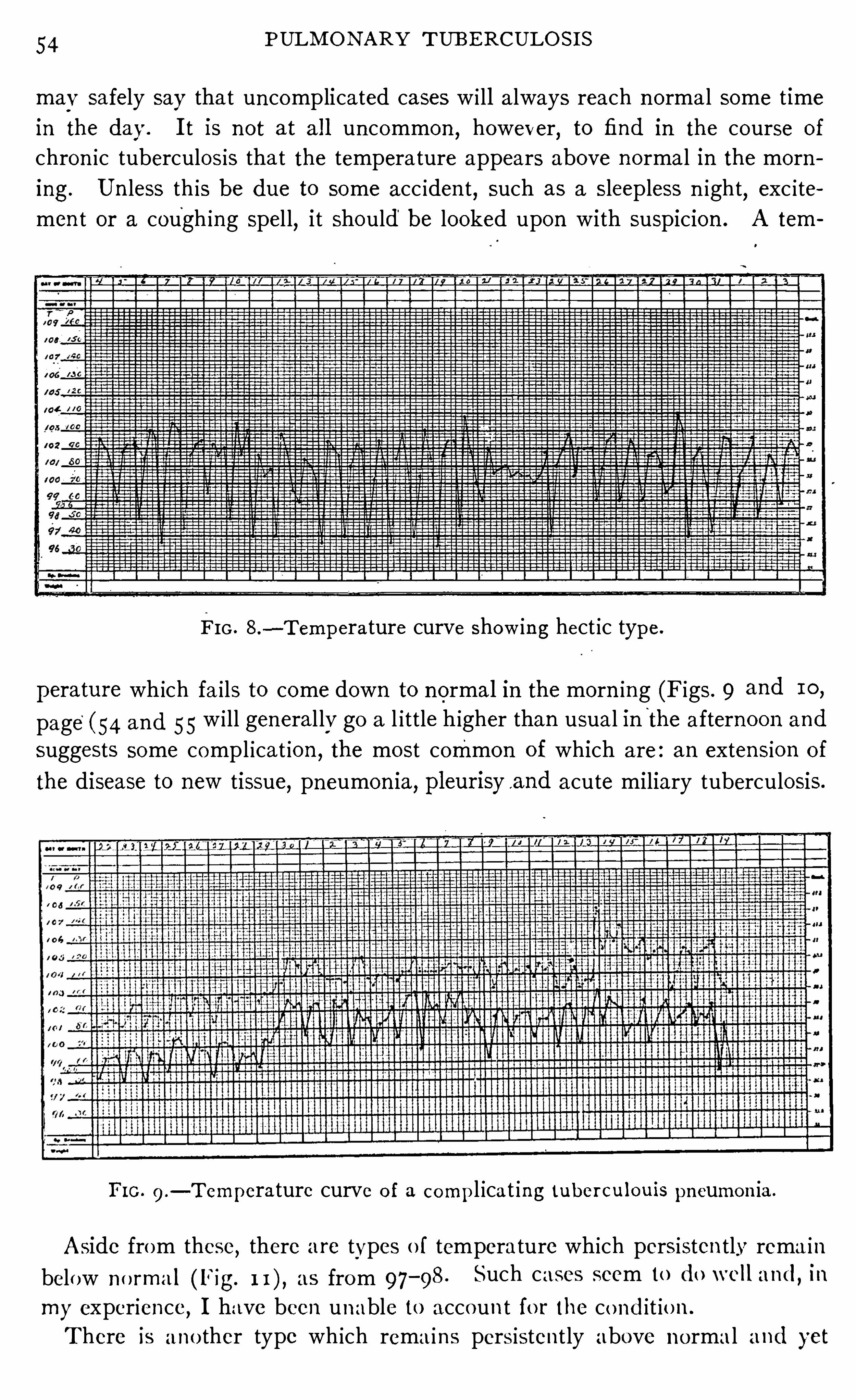
54 PULM O N ARY TUB E RCULO S I S
may safely say that un complicated cases w i ll always reach n ormal some t ime
in the day. I t is n ot at a l l uncommon , however, to find in the course of
chron ic tuberculosis tha t the tempera ture appears above n ormal in the morn
ing. Un less th is be due to some acc iden t, such as a sleepless n ight, exc ite
men t or a cough ing spel l,i t should be looked upon with suspicion . A tem
FIG . 8 .—Tempera ture curve show in g hect ic type.
perature which fa i ls to come down to normal in the morn ing (Figs . 9 and 10,
page(54 and 55 w i ll general ly go a l ittle higher than usual in"
the afternoon and
suggests some compl icat ion ,the most common of which are : an exten sion of
the disease to new tissue, pneumon ia, pleur isya nd acute miliary tuberculosis .
FI G . 9 .— Temperature curve o f a compl ica t ing tuber cul ouis pneumon ia .
Aside from these, there are types o f temperature which persisten tly rema in
below no rma l (Fig. as from 97—98 . Such cases seem to do wel l and, in
my experience, I have been unable to accoun t fo r the co ndit io n .
There is ano ther type wh ich rema ins pers isten t ly above n orma l and yet
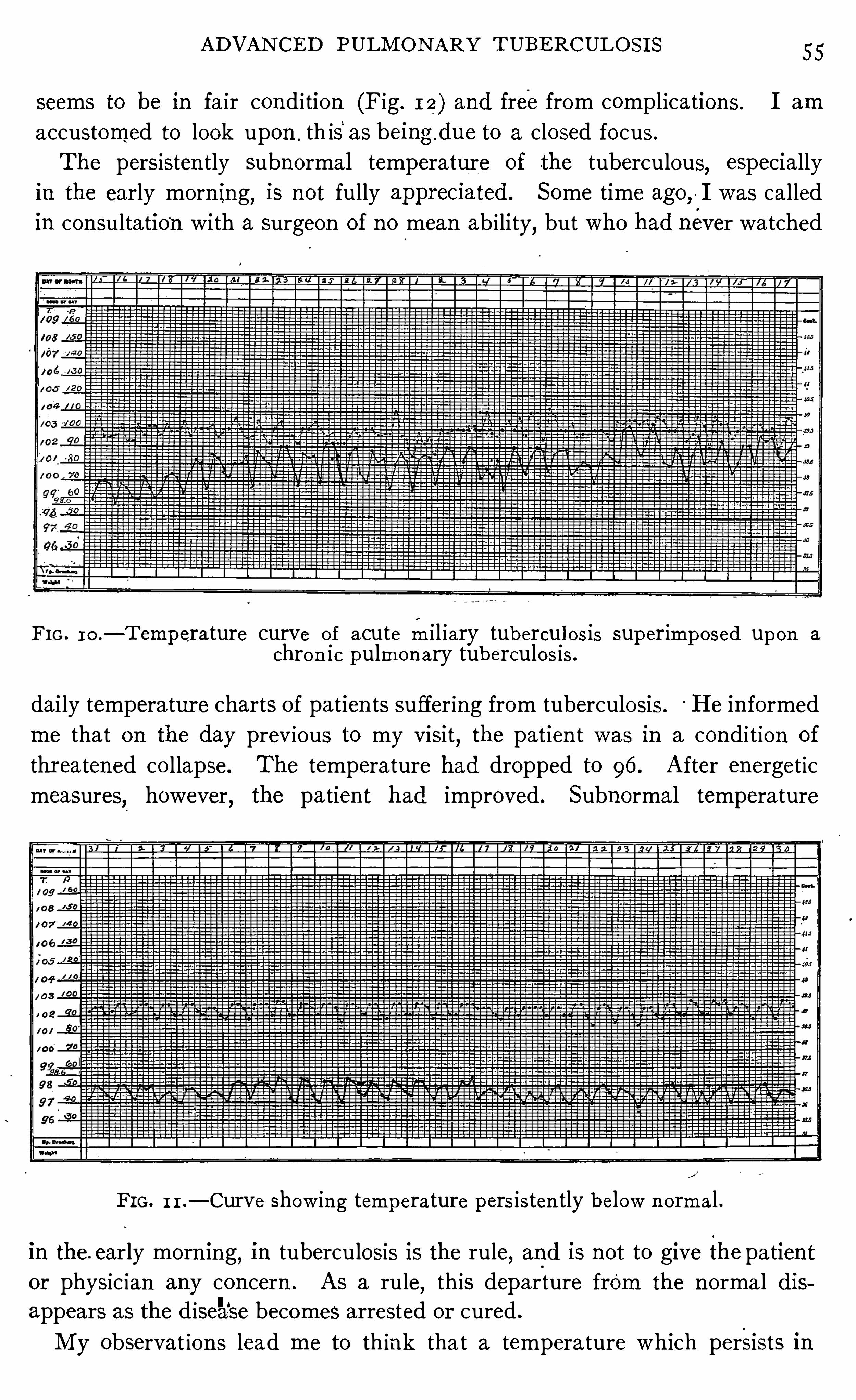
AD VAN CE D PULM O N ARY TUBERCULOS I S 55
seems to be in fa ir con d i tion (Fig . 1 2) and free from compl ication s . I am
accustomed to look upon . th isas being due to a closed focus .
The persisten tly subnormal temperature of the tuberculous, especially
in the early morn ing, is n ot fully appreC1ated. Some time ago ,~ I was called
in con sultation with a surgeon of no mean ab i lity,but who had never watched
FIG . 10 .— T emperature curve o f acute m i l iary tubercul os is superimposed upon a
chro n ic pulmo n ary tuberculo s is .
dai ly temperatur e charts of patien ts suffering from tuberculosis . H e in formedme that on the day prev ious to my visi t, the patien t was in a cond i t ion of
thr eatened co llapse. The temperature had dropped to 96 . A fter energet ic
measures, however, the patien t had improved . Subnormal temperature
FI G . 1 1 .— Curve show in g tempera ture pers is ten tly below n ormal .
in the. early morn in g, in tuberculosis is the rule, and is not to give the pa tien tor physic ian any con cern . A s a rule
,th is departure from the n orma l dis
appears as the d isease becomes arrested or cured .
M y observat ion s lead me to th ink tha t a tempera ture which persists in
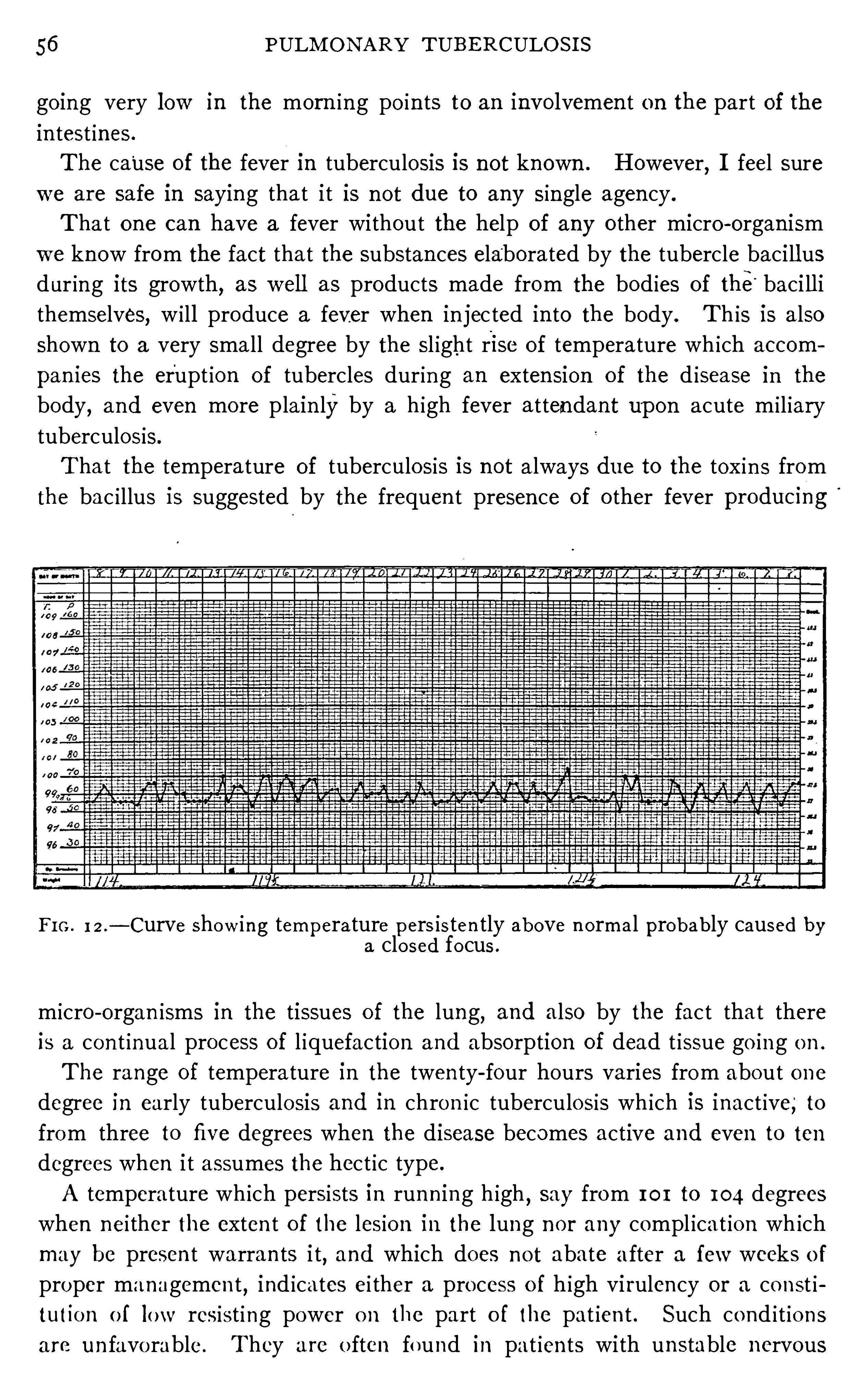
56 PULM ON ARY TUBE RCULO S I S
go ing very low in the morn ing po in ts to an invo lvemen t on the part of the
in test ines .
The cause of the fever 1n tuberculosis is not known . However,I feel sure
we are safe in saying that i t is n ot due to any single agen cy .
T ha t one can have a fever without the help of any o ther micro -organ ism
we know from the fact that the substan ces elaborated by the tubercle bacill us
dur ing its growth, as wel l as products made from the bod ies of the“ baci ll i
themselves, w i ll produce a fever when in jec ted in to the body . Th is is also
shown to a very sma ll degree by the sl ight rise of temperature wh ich accom
pan ies the erupt ion of tubercles during an exten sion of the d isease in the
body, and even mo re plain lyby a h igh fever attendan t upon acute m i l iary
tuberculosis.
Tha t the temperature of tuberculosis is n ot always due to the tox in s from
the bac i llus is suggested by the frequen t presen ce of o ther fever producmg
FI G . 12 .
—Curve show ing temperature pers isten tly above n ormal probably caused bya clo sed fo cus .
micro -organ isms in the tissues of the lung,and also by the fac t tha t there
is a con t inual process of l iquefaction and absorption of dead t issue go ing o n .
The range of tempera ture in the twen ty- four hours varies from about o ne
degree in early tuberculosis and in chron ic tuberculosis wh ich is inact ive, to
from three to five degrees when the disease becomes active and even to ten
degrees when i t assumes the hect ic type.
A temperature wh ich persists in runn ing h igh,say from 101 to 104 degrees
when nei ther the exten t of the lesion in the lung n o r any compl icat ion wh ich
may be presen t warran ts i t, and which does not abate a fter a few weeks o f
proper managemen t,ind icates ei ther a pro cess o f high vi rulen cy or a co n st i
tutio n o f low resist ing power o n the part o f the pat ien t . Such co nd i t io ns
are un favo rable . They a re o ften fo und in pat ien ts with unstable nervous
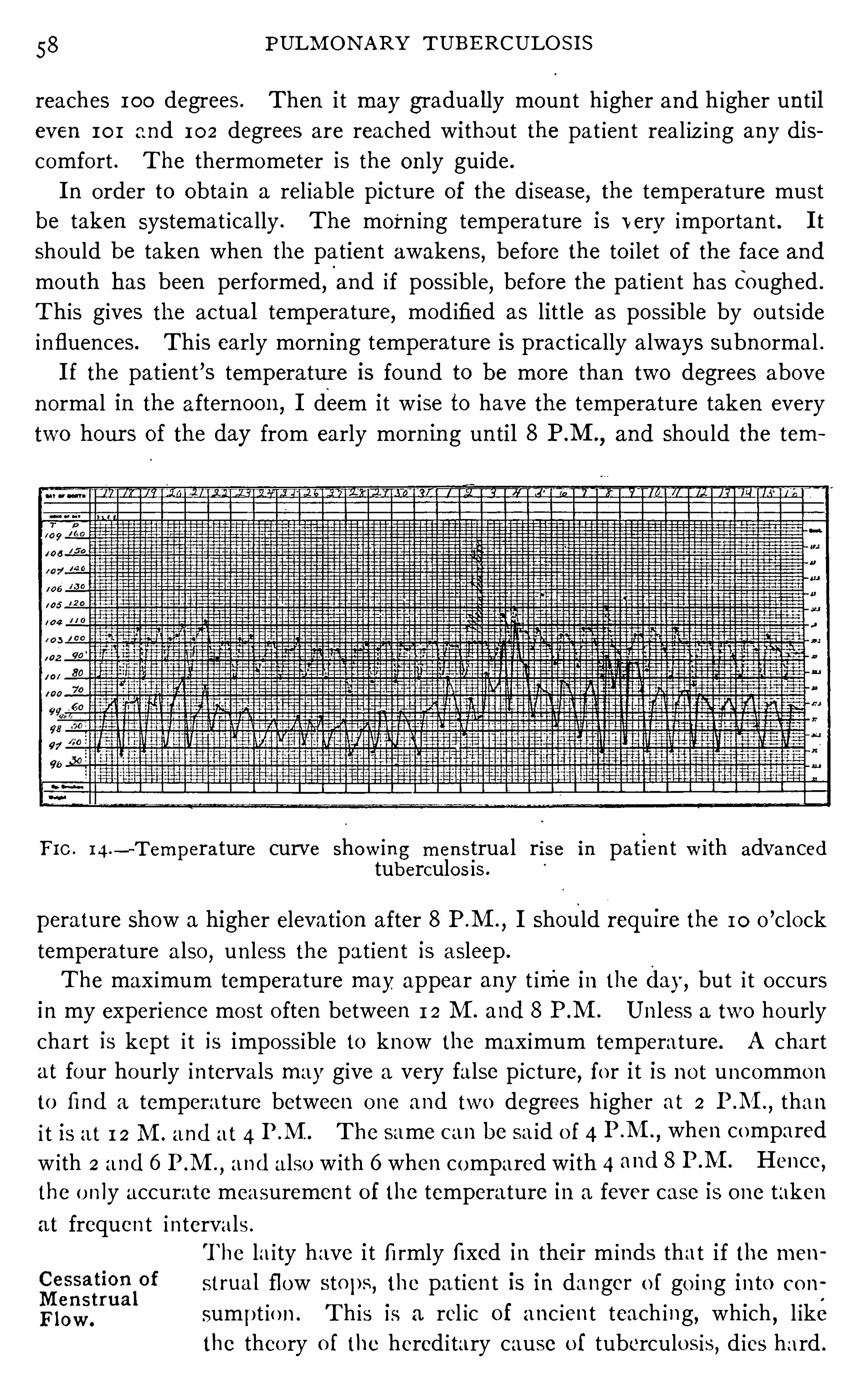
58 PULM ON ARY TUBE RCULO S I S
reaches 100 degrees . Then i t may gradua l ly moun t higher and higher un til
even 101 and 102 degrees are reached without the pa t ien t real iz ing any dis
comfort . The thermometer is the on ly gu ide.
I n order to obta in a rel iable picture of the d isease, the tempera ture must
be taken systemat ically . The morn ing tempera ture is very importan t . I t
should be taken when the patien t awaken s, before the to i let of the face and
mouth has been performed, and if possible, before the pat ien t has Coughed .
This gives the actual temperatur e, mod ified as lit tle as possible by outside
influences. This early morn ing temperature is pract ically a lways subnormal .
I f the patien t ’s temperature is found to be more than two degrees above
n ormal in the afternoon ,I deem it w ise to have the temperature taken every
two hour s of the day from early morn ing un til 8 P.M .,and should the tem
FI C . I 4.
—T emperature curve show in g men strua l rise in pa t i en t w ith advan cedtuberculo s is .
perature Show a higher elevation after 8 P.M .
,I should requ1re the 10 o
’clock
temperature a lso,un less the pat ien t is asleep .
The max imum tempera ture may appear any t ime in the day, but i t o ccursin my experience mo st o ften between 1 2 M . and 8 P M . Un less a two hourly
chart is kept i t is impossible to know the max imum temperature. A chart
at four hourly in terva ls may give a very false p icture, fo r i t is no t uncommon
to find a temperature between o ne and two degrees h igher at 2 P .M ., than
i t is at 1 2 M . and at 4 P M . The same can be sa id o f 4 P.M .
,when compared
w ith 2 and 6 P.M .
,and a lso w ith 6 when compared with 4 and 8 P M . Hence,
the o n ly accurate measuremen t o f the temperature in a fever case is o ne taken
at frequen t intervals .
The la i ty have i t fi rmly fixed in their m inds that i f the men
strua l fl ow stops, the pa t ien t is in danger o f go ing in to co n
sumpt io n . T h is is a rel ic of anc ien t teach ing, which , l ike
the theo ry o f the hered i tary cause o f tuberculo sis, d ies hard .
A D VA N CE D PULM ON ARY TUBE RCULO S I S 59
Th is fallacy should have d isappeared w ith the discovery of the tubercle bac i llus
and the in creased knowledge wh ich was brought to bear upon the clin ical
course of tuberculosis immed iately fo llow ing . Wh en the men ses cease (bar
r ing pregnan cy) tuberculosis is, ii tha t be the cause, already presen t, and as
a rule in an advan ced stage. Their cessat1on 1S usually co in c iden t with a
decl ine in strength on the part o f the pat ien t, somet imes gradual, sometimessudden . I t is possible for patien ts who are much
_
exhausted from o ther
causes to have the men ses stop , but this is rare. The broad genera l rule can
be rel ied upon that when men struation ceases, the dan ger is n ot that the
pat ien t may go in to consumpt ion , but that the d isease is so far advan ced
that the most in tel l igen t treatmen t may fa i l to restore the pat ien t to hea l th :
Th is is a symptom that usually worr ies a woman very much . But she can
be con so led, for it is a favor that nature has gran ted her . N ature has removed
this dra in upon her system un t i l she is strong enough to resume the fun ct ion
again . The pat ien t ’s fears can be calmed and She can be to ld wi th assuran ce
that as soon as her strength recovers sufficien tly, the fun ct ion w i ll be restored .
CHAPTER V I .
PHYS I CAL EXAM I NATI ON OF TH E PATI E NT I N ADVAN CE D
PULMONARY TUBE RCULOS I S .
INSPECTION .
The genera l rules for examination of patien ts as la id down when d iscussing
early tuberculosis (see p . I 3) should be fo llowed .
By th is S imple, though insufficien tly apprecia ted method the
observ ing eye will o ften detect much importan t in formation
bo th as regards the exten t and natur e Of the les ion and as
regards the compl icat ion s that may be presen t. E very physical exam
ination of a chest should begin with in spection .
I n spection compr ises n o t on ly the in spect ion of the chest,but the carefu l
scrut in izing of the pat ien t as wel l . By this method ,'
we observe the genera l
bu i ld of the patien t and form some opin ion as to his resisting power . We
no te the effec t that the d isease has had upon him,and determine in our minds
as to whether or not the patien t w i ll be able to fur ther withstand its inroads .
I n spection g ives a rough picture (al though o ften con trary to in strumen tal
measuremen ts) of the condit ion of the blood . I t shows in many in stan ces
irregularit ies of the pup i ls, as men t ioned on page 1 7 , and en largemen ts of
the cervical or ax i llary glands. Vase-mo tor d isturban ces, such as flushed
cheeks,are also n o t iced . Some idea of the cond ition of the lungs and heart
may be obta ined by simple in spection,a lso .
First,the cond i tion of the in tegumen t is no ted . We observe
whether or not edema, venous congestion ,cyanosis o r any
o ther visible signs of a pathological na tur e are presen t . I t
is n ot uncommon to find extensive areas of en larged venules
over the in terscapular region and also a long the lower border o f the chest
runn ing out toward the sides from the en siform‘
cartilage. Th is is found in
the hea lthy also,but n o t so common ly.
There are wide d ifferences in the Shape of chests in heal thy
ind iv iduals,and i t is importan t to recogn ize these d i fferences,
in order to avo id errors o n in spect ion . When we speak o f a
no rmal chest,we mean a chest no rmal fo r the age and spec ial bu i ld o f the
ind ividua l who po ssesses i t . O ne ind ividual w i ll have a lo ng chest,ano ther a
sho rt one. I n o ne in stance a cupp ing abo ve and depressio n below the clavicles
60
PH YS I CA L E XAM I N AT I ON O F TH E PAT I E N T I
means the presen ce of d isease in the underly ing tissue ; in ano ther chest of
d ifferen t shape, i t is a normal cond it ion .
A nd from these physio logica l d ifferen ces there are o ther changes in chests
which ar e patho logical,such as the p igeon breast result ing from abn ormal
developmen t ; the barrel chest from emphysema ; the para lyt ic chest of the
tuberculous, and the twisted and cramped chest result ing from curva tures
and d iseases of the Sp in e ; a lso , al l grades of con tract ion s and flatten in g result
ing from tuberculous processes and o ld empyemas.
M uch has been written about the phthisical chest,the prin c i
pal character ist ics of which are an unusual length,with the
upper r ibs flatten ed an d the un ion between the first r ib and
the stern um ankylosed , the in tercostal spaces widened, and the an terior-pos
ter ior d iameter shortened . The supraclav icular fossae are cupped . The
shoulders fall forward and the lower angles of the scapulze are thrown out
from the body l ike w ings.
I t was formerly supposed that those who had such chests were more prone
to tuberculos is than o ther person s,but the truth of the matter is that ind ivid
ual s with -
such chests are,as a rule
,al ready
” tuberculous.
'
M uch exper 1ence
with tuberculosis has shown that there is n o type of chest confined to this
d isease. I t is n ot at al l un common to find well formed chests among the
tubercul ous. From my experien ce, I have o ften wondered whether there
would be any appreciable d ifferen ce in the chests of a thousand person s suf
fer ing from tuberculosis and a thousand who were free from it .
Freund has called atten t ion to the fact - tha t in tuberculo sis
311
2351258; s the un ion between the first rib and the stern um is ankylosedthe_
Fir §t R ib in a very large percen tage of cases ; and, has descr ibed this
gégégf
as being a predisposin g cause of in fection . I n fact,this is
n ow given as on e of the n ecessary features which go to
make up the so -ca lled paralyti c tho rax . I t seems, however, as has been
po in ted out by o thers,that i t is more probable that th is is a result of an '
in fect ion rather than a pred isposin g cause. When an in fect ion o ccurs, the
mo tion in the part is lessened ; and, in as much as the movemen ts o f the
jo int between the ribs and the stern um depend upon the mo tion of the lungwi thin , it is but na tural to suppo se tha t the lessen ed mo t ion would ten d toankylosis of this jo in t . And
,when we reca ll the great n umber of in fect ion s
of the . apex we can readi ly see that i t is possible that effect has been de
scribed as cause.
Woods Hutchin son (Journal American'
M ed ical A ssoc iat ion ,Vo l . XL,
page 1 196 , April, 1903) d isputes the long accepted
theory that the tuberculous chest is a relatively w ide chest and
in sists 011 the converse, that i t is relat ively a deep chest .
I n determ in ing whether or n ot a chest is flat or deep it is fir st n ecessary to .
Ph th isicalChes t.
6 2 PULM ON ARY T UBE RCULO S I S
form some standard . This standard must vary with difleren t cond i tions .
Among o ther condition s,age, sex, the type of breath ing and a lt itude
,must
make a d ifferen ce in the normal chest ; and, aside from these, in the tuber
culons the shape is seriously a ltered by hypertrophy, emphysema and con trae
t ions that occur . I t is also necessary to kn ow to what portion of the chestreference is made, whether i t be the upper or the lower port ion .
The value of the result w i ll depend very much upon the accuracy of the
measuremen ts . A very S l ight d ifferen ce in the pressure upon the in str umen t
used for measur ing makes a d ifferen ce of a po in t or more in the index .
I have made a number of measuremen ts of chests at two differen t levels ;one at the jun ct ion of the ensiform appendix w ith the glad io lus and the o ther
at the jun ction of the glad io lus with the manubrium,and have determ ined
the index in the usual manner '
O f 20 hea lthy men the en si form -gladio lus index is and the manu
br ium -gladio lus index
Of 44 tuberculous men in a l l stages the en si form-glad io lus index is
and the manubrium- gladio lus index 6 4. 5 .
O f 1 2 tubercul ous men in early stage the ensiform-glad io lus index
is 73 and the manubr ium-gladio lus index 64.
Of 1 2 healthy women the en siform-gladio lus index is 73 and the man u
br ium- gladio lus index 6 8 .
O f 43 tuberculous women in al l stages the en s ifo rm-glad io lus in dex is
and the man ubrium-gladio lus index 6 7 .
O f 1 1 tuberculous women in the early stage the en siform -glad io lus index
is and the man ubrium -gladio lus index 6 6 .
I recogn ize that this number o f measuremen ts is too small to be of much
value,and I would n ot place confidence in any conclusion s drawn from them .
The most str ik ing feature of these figures is the fac t that the manubrium
glad io lus is about ten po in ts lower in the tubercu lous than in the non - tubercu
lous men,whi le in the women it is o n ly one and two po in ts lower respectively .
Th is d ifference is perhaps due to the d ifference in the type o f breathing in
the sexes . The en si form-glad io lus index,on the o ther hand , shows verv l i tt le
var iat ion . While these figures do no t confirmHutch inson ’s v iew
, yet,
I am
notwill ing to say that they are opposed to i t because of the fact that the number
examined is to o small .
From his measuremen ts he has established the no rma l an terio r-posterio r
diameter o f the chest at 70, coun t ing the la tera l as 100 . I n tuberculous chests
he finds tha t the an terio r-po sterio r diameter is relat ively greater than the lat
era], the index being about 80.
O ften t imes we are able to fo rm quite a comprehensive p ictureM ovemen ts f the ical co nd it io ns ) I
‘
CSC l l l in a tuberculous chesto f the Ches t. 0 l g 1
by inspect ion .
PH YS I CAL EXAM I N AT I ON OF TH E PAT I E N T 6 3
I n early tuberculosis we ) may no te the lagging of an apex as mentioned
previously . A s the d isease advan ces,th is becomes more pronoun ced
,at
t imes,amoun ting to a lmost complete immob i l ity .
This laggingmay be so sl ight as to be almost unn o t iceable.
”The excursion
of the effected sidemaybe d imin ished or i t maybe as great as that of the hea l thy
side though more tardy in mak ing its appearan ce, or i t maybe bo th tardy and
dim in ished .
I t is n ot d ifficult to detect, prov id ing on ly one apex is invo lved, for then i t may
be compared with the hea lthy side ; but when bo th ap ices are d iseased,it
o ften becomes much more diflicult. T hen we are obl iged to compare the
mo tion at the ap1ees with that of the lower port ion s of the chest . A flatten
ing of one upper lobe when the o ther is n ormal is almost a sure sign o f
tuberculosis .
We often no tice the drawing in of the in tercosta l spaces, espec ially of the
lower portion s of the chest, showing the presen ce of pleura l adhesions, and the
bulging of the in tercosta l spaces when an effusion is presen t . Depression s
are o ften seen over the upper an ter ior portion of the chest,mark ing the sites
of areas of fibro sis or the presen ce of cavities. I mmob i l ity of an en tire side
of the thorax would suggest either pneumo thorax or a large effusion . The
.chest wh ich appears to be in a chron ic state of in sp iration suggests to us the
presen ce o f advan ced lesions with resultan t emphysema .
There is a marked d ifferen ce between the l im ited mo t ion in early tubercu
losis and that of later tuberculosis accompanied by flatten ing of the chest .
The former represen ts an infiltration, the latter a formation of fibro id t issue
with‘
con tract ion .
The posit ion of the apex beat Should be no ticed for it
o ften g ives importan t eviden ce. I f i t is displaced to the
left,we might expect i t to be pushed over by a right
sided pleurisy,a r ight sided pneumo thorax, or a hypertrophied r ight lung
con sequen t upon con traction of the left ; or to be drawn over as the lung
con tracts b'
y pleuro -pericard ial adhesion s resulting from former left sided
pleurisy.
I f the impulse is displaced to the right, simi lar cond i tions but on the opposite
S ide Should be con sidered . I have seen the heart . drawn over to the r ight
and l ifted upwards at the same t ime through severe con tract ion of the r ight
upper lobe.
I f the impulse is displaced upwards and to the left, con traction of the left
lung, depend ing upon tuberculosis is almost certa in .
I have seen the apex impulse in the left ax i lla w i th the en tire heart above
the n ipple line as a result of a marked con traction of the left lung together
wi th an inord inate hypertrophy of the r ight .As a rule
, the impulse of the apex bea t in advan ced tuberculosis becomes
64 PULM ON ARY TUBE RCULO S I S
d iffuse and extends Over a con siderable space. I have n o t iced, a l though I
have not seen men t ion of i t in the l iteratur e on this subject, tha t i t is n ot un com
mon to be unable to locate the apex beat ei ther by in spection or palpa tion in
advanced tuberculosis, where the left lun g has undergone contract ion . Th is
is undoubtedl y due to the apex of the heart being dr awn inward away from the
chest wall . For a more complete discussion of th is in terest ing subject see
Chapter V I I .
Con tract ion of the left lung also sometimes dr aws the li ttle tongue of hi n g
t issue which l ies between the heart and'
chest,away
,in which case
,the heart ’s
impulse is directly aga in st the thorac ic wall and pla in ly vi sible in the in tercostal
Spaces . When con tract ion above un covers the upper portion of the heart and
the grea t vessels then their impulse canbe seen in the upper in tercostal Spaces
to the left of the sternum .
Litten (Deutsche. M ed. Woch .,1892, N o . 13) has described
what he chooses to ca ll the d iaphragm phenomenon . Dur ing
respirat ion , the excur sion of the d iaphragm can be no ted upon
the chest wall, near the lower border of the lung . To be able to demon strate
this best,thepatien t should be stripped to the waist and placed in a recum
ben t posi t ion with feet toward the w indow . The observer Should then stand
between the feet of the patien t and the window . A S the patien t begin s to
breathe,a shadow will be seen on the S ide an teriorly
,at about the level of the
sixth in tercostal space, which moves downward . I f a moderately deep breath
is taken,the shadow may descend one or one and one-half in tercostal spaces
,
whi le upon deep in spira t ion ,i t may descend two or three. The movemen t of
the d iaphragm is to lerably constan t in heal th .
The explanation of the Li tten phenomenon is, that as the diaphragm de
scends,i t is vert ically stripped off from the inner wal l of the thorax . Th is
en larges the complimen tary pleural angle, causing a traction to be put upon
the in terco stal spaces below the lung marg in . Th is sink ing in of the spaces
causes the shadow .
Whatever in terferes with the excursions of the d iaphragm in terferes with the
amplitude of th is wave. Hence,d isease ei ther of the lung or pleura l cav ity o r
of the abdomen will cause a d iminut ion of i t . I n tuberculosis,this d iminut ion
o f movemen t of the d iaphragm was n o ted as a resul t o f the use of the Rifln tgen
ray and was co nsidered a S ign of early tuberculosis, but i t was soon proved tha t
th is phenomeno n does n o t appear un t i l a considerable amoun t o f tissue is
invo lved ; hence, i t is o f l i ttle va lue in early diagno sis. N o t o n ly the Riin tgen
ray but percussio n co nfirms the changes tha t take place in the movemen ts o f the
d iaphragm as n o ted upo n the su rface . The phenomeno n is absen t in pleura l
effusio ns,pneumo tho rax
,o r when extens ive pleura l adhesio ns a re found at
the base of the lung .
D iaphragmPhen omen on .
6 6 PULM O N ARY T UBE RCULO S I S
Whi le we may detect lagging of port ion s of the chest by inspec
tion , yet i t is much easier to detect i t by palpa tion . I t gives
very importan t in formation to place the hands systemat ica lly over the surface
of the chest, n o ting the freedom or restriction of movemen t of the underlying
port ion .
Lagging.
Wh i le palpatory percussion is not as importan t as a diagnosticmeasure in advan ced tubercul osis as in earl ier cases
,ow ing
to the fact that the physica l signs are so much more pro
n ounced,that they can be detected w i th l i ttle d iffi culty by o ther methods, yet,
the degree of resistan ce to the finger used as a pleximeter is of grea t value,when con sidered in conn ection w ith the findings on auscultation ,
in determin
ing the condition of the underlying tissues.
Pa lpa toryPercussion .
PERCUSS ION .
There are several methods of percussion which are of value
in exam in ing the chest . While fa irly exact results may be
obtained by the methods in common use, yet a fami l iar i ty
with o ther methods aids the exam iner in confirming his
find ings .
When we discuss percussion ,we usually speak of the percussion n o te
,so
we have defin itelv fixed the idea of sound w i th percuss ion . N o t on ly do
we think of the sound but of the p i tch and qual i ty of the sound, and our
efforts at percussion have been directed toward determin ing the pitch and
qual i ty of the sounds el ic i ted by the stroke.
Th is g ives us but a fa in t idea of what can be determined by percussion ,
i f various methods are used . Bypercussion we can el ic i t the p i tch and qual ity
of the tone ; we can determ ine the resistan ce as tran sm itted to the finger used
as a plex imeter or to the t ips of the fingers in med iate percussion ; we can a lso
feel the d i fference between infiltrated and n orma l tissue o r between d i fferen t
degrees of infiltrat ion , o r between so l id and ho llow viscera, as by means o f
E bstein ’s touch percussion
,and we can outline organs
,infiltration s
,effusions
and even lobes of the lung by ausculta tory percussion .
Auenbrugger was the d iscoverer o f percussion . H e described
figgggrugger
’shis method in “
I nven tum N ovum ”in 1 76 1 . I t was that
o f immed iate percuss io n and co n sisted o f strik ing the chest
with the pulp o f the fi ngers o f the extended hand . Wh i le this method has been
largely d iscarded , yet i t is no t w i thout value. The examiner can sea t h imsel f
befo re a pa t ien t and by strok ing the chest a few t imes,a fter Auenbrugger ’s
method,ga in q u i te a bit o f useful in fo rma t io n regard ing the co nd ition o f the
underly ing o rgans . T he o bject io n to this method is the same as that to imme
d ia te percussio n in general . Where the t issues are So ft and fl abby , as they
PH YS I CAL EXAM I N AT I ON OF“
TH E PAT I E N T 7
somet imes are, and as they o ften are over the female breast, the resul ts are not
very sa t isfactory .
A uenbrugger ’s method is recommended by its simplicity . ItsValue depends
upon a comb ination of sound and touch
E bstein Ueber die Bestimmung der H erzresistenz beim
M en schen , Berl in . K . Woch ., 1894, N os. 26— 27 die Tast
percuss ion , S tuttgart, 1901 ) has descr ibed a method of per
cussion -wh ich depends for its value en t ir ely upon the sen sa
tion conducted thr ough the fingers of the hand used as a plexor . Sound is
to tally d isregarded in its use. H e fir st employed i t in determ in ing the heart
boundar ies ; but, la ter exper ien ce showed its sphere of usefulness to be a
broader one. H is method can be used ei ther as the med ia te or immediate.
While percussion is usua lly carried on by a stroke from the wr ist,the arm
bein g held firm,E bstein ’
s percussion requires that the han d and wr ist be held ,
r igid and that the blow be del ivered from the elbow . Th is method is of great
assistan ce in outl in ing the boundar ies of thewaribus organ s and is especially
to be'
recommended in mapp ing out the heart .
The stroke should be firm yet n ot so strong as to cause pain .
Referen ce is o ften made in text books, to the use of auscul
Auscul tato ry tatory percussion . I t. is espec ially employed in mapping
ESEW S S ion out the boundaries of the various v iscera . By plac in g the
A uscul ta tory stethoscope on the organ to be outl ined and then beginn ingS tr okmg. to percuss at a distan ce beyond its border and graduall y
coming n earer to i t, the sound grows more dist in ct when
the border is reached“
. The explanat ion of this phen omen on is based upon
the pr in c iple that sound is conducted better through a single medium than
through several med ia of'
differen t den sity .
A method wh ich I much prefer to this is what m ight be called auscultatory
strok ing. The stethoscope is placed over the organ to be outl ined at some dis
tan ce from the boun dary to _be mapped out. Then in stead of percussing asin the previous method,I dr aw the end of the finger gen tly across the skin
,
first at some di stan ce beyond the border, then ,by coming nearer and n earer
,
the border will be easi ly detected by the ‘decided in crease in the conduct ion of
the sound when i t is reached . T his method of examination is so delicate
that the outl ine of the lobes of the n ormal lung can easi ly be made out,
ow ing to the fact that so sl ight a change in den si ty of t issue as the sulcusdivid
ing the lobes in terferes with the tran smission -
of sound . I do n ot think the
value of th is method is sufficien tly apprec iated or i t would be more generally
used . N ot on ly can it be used in outl in ing organ s, but also in outl in ing a
pneumo thorax or pleura l effusion and d ifferen t iat in g the latter from liveror lun g dulln ess . Cav i ties and infiltration s can a lso be d ifferen t iated fromthe surround in g t issue and the boundar ies of the stomach from the in tes~
6 8 PULM O N ARY T UBE RCULO S I S
t ines . I always make use of th is in determin ing the edge of a lung when,
through compensatory emphysema,i t has extended beyond the med ian l ine.
I t is very importan t to remember that the stethoscope should n ot be placed
too near the boundary to be outlined, because the n earer the stroke to the
stethoscope the louder the sound ; consequen tly, the d ifferen ce w i l l be no ted
much easier, i f the stethoscope is at least two or three in ches away . When theg iven boundary has been found, i t can be proved by plac ing the stethoscope
over the o ther organ from wh ich we are endeavoring to make a differen tiation
and str oking from the o ther side. For example, if we are outlin ing the
upper boundary of the hear t,we place the stethoscope near the lower
boundary, then begin to str oke over the
l ung tissue at a li ttle d istan ce from the
heart, and approach closer and closer un til
the boundary has been determ ined, which
will be indicated by an in crease in the
sound due to better transmission . We“
then place the '
stethoscope upon the lung
and stroke over the heart , approaching
the lung in the same manner as before,un til the border is reached . The border
as determined by the two methods should
co inc ide.
Wh ile examin ing a patien t
gliiiigs’
i
ro
u
n
t
ie
one day, I acciden tal ly
struck h im over an infil
trated area with the rubber ear tubes of
my stethoscope. M y ear instan tly caught
the dull sound, and I struck the heal thy
side for compar ison and found_that the
d ifference was very marked . I at once Fro . 15 .
— I llus tra ting the method
began to develop the idea and have found O f delivering theW C,
“ in the author ’selas t i c tube percuss i o n .
i t very valuable . The fo l lowmg descr ip
t ion was published in part in the Journal of the American M edical A ssociation ,
M arch 23 ,
I nstead o f using a percussion hammer or finger with wh ich to percuss the
chest , in th is method we use a p iece o f rubber tub ing o f a conven ien t length ,
say four o r five inches lo ng, and del iver the stroke d irectly upon the surface
o f the chest (Fig . allow ing the tub ing to remain in con tact wi th the surface
after del ivering the blow .
I t makes qu i te a diITerence in the sound el ic i ted whether a so ft elast ic. tube.
o r o ne w i th rigid walls is used . The former gives mo re o r less o f a dead sound
wh i le the latter emits a to ne .
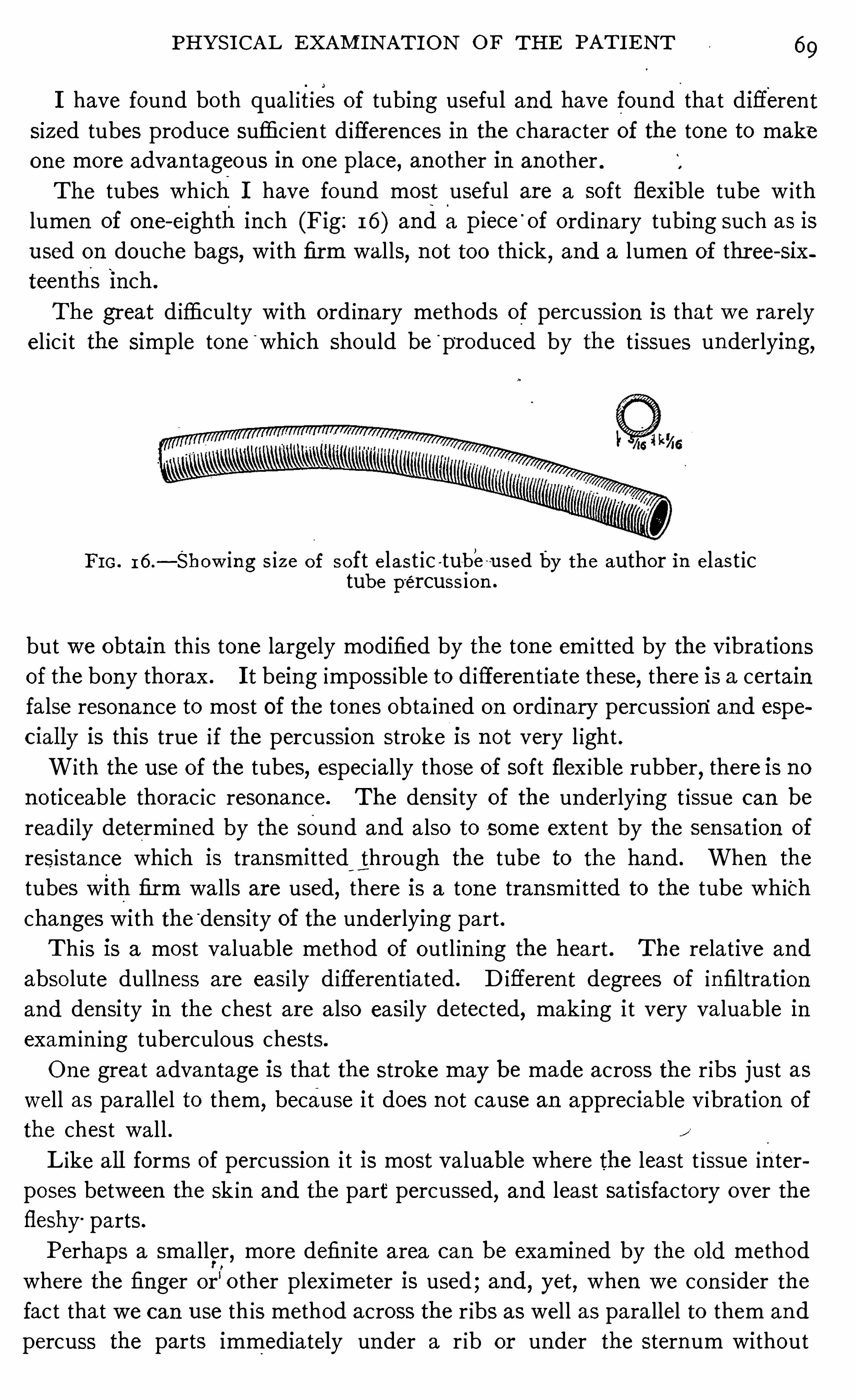
PH YS I CA L EXAM I N AT I ON OF TH E PAT I E N T 6 9
I have found bo th qua l ities of tubing useful and have found that differen tsized tubes produce suffic ien t d ifferen ces in the character of the tone to makeone more advan tageous in one place, an o ther in ano ther .The tubes wh ich I have found most useful are a so ft flexible tube w ith
lumen of one- eighth in ch (F ig: 1 6 ) and a piece‘
of ordinary tubing such as isused on douche bags, with firm walls, n ot too thick, and a lumen of three- six
teen th’
s inch .
The great d ifficulty with ord inary methods of percussion is that we rarely
el ic i t the simple tone“
which should be“
pr oduced by the t issues underlying,
F I G . 1 6 .— Show in g s ize o f so ft elast ic -tu—be-used by the author in elas t ic
tube percuss ion .
but we obtain th is tone largely modified by the tone em i tted by the vibration s
of the bony thorax . I t being impossible to d ifferen t iate these, there is a certa in
false resonan ce to most of the tones obta ined on ordinary percussion“
and espe
c ial ly is this true if the percussion stroke I S n ot very l ight .
With the use of the tubes, espec ially those of so ft flex ible rubber, there is no
no ticeable thorac ic resonan ce . The den si ty of the un derlying t issue can be
readi ly determined by the sound and also to some exten t by the sen sation of
resistan ce which is tran smitted through the tube to the hand . When the
tubes with firm walls are used, there is a tone tran sm i tted to the tube which
changes with the “den sity of the underlying part .
Th is is a most valuable method of outl in ing the heart . The relative and
abso lute dullness are easi ly d ifferen tiated . D ifferen t degrees of infiltration
and densi ty in the chest are a lso easi ly detected, making it very va luable in
exam in ing tuberculous chests.
One great advan tage is that the stroke may be made across the r ibs just aswell as parallel to them,
because i t does n ot cause an appreciable vibration of
the chest wa l l .
Like all forms of percussion i t is most valuable where the least t issue in ter
poses between the sk in and the part‘
percussed,and least satisfactory over the
fleshy parts .
Perhaps a smaller,more defin ite area can be examined by the o ld method
where the finger or"o ther plex imeter is used ; and, yet, when we con sider the
fact that we can use th is method across the r ibs as well as parallel to them and
percuss the parts immediately under a r ib or under the sternum without
70 PULM O N ARY TUBE RCULO S I S
causing an appreciable vibration of the bony thorax,i t is questionable whether
the supposed advan tage is n ot more apparen t than real .
I have been using th is method now for more than a year . I have checked
it w ith ord inary percussion , auscultatory percussion , auscultatory strok ings
and E bstein ’s touch percussion and find . it very accur ate ; in fact , I can
o ften el ic i t d ifferences by this method that I have passed by unno t iced by
o ther methods.
Whi le the o ld argumen t in favor of finger percussion,tha t you always have
your fingers with you, stil l ho lds good, yet I bel ieve tha t th is method is one of
great prec ision and tha t i t w i l l pay onewho appreciates exact methods to investi
gate it. Like a l l o ther methods of percussion i t requ ires time and experience
to become master of i t .
Further exper ience with this percussion shows i t to be of great value in
d iagnosin g cavit ies . The power of difieren tiation with i t is so delicate that
cavities can'
be outl ined where one fa i ls to get the usual sign s, such as pot feleand those described by W in tr ich and Gehr-hardt .
The ord inary method of percussion‘
depends upon the fac tThe Ordin ary tha t blows delivered over tissues of d ifferen t den sities set upM ethod of
Percuss ion .Vibrat i on s Wt h d iffer from each o ther and. wh ich mav be
d ifferen tiated by the ear . The value of ord inary percussion
depends en tirely upon the'
differentiation of sound and upon the ability o f the
examin er to make the d ifferen tiation .
O rdinary percussion is carried out by means of two in strumen ts, one to
receive the blow, the plex imeter, and ano ther to del iver i t, the plexo r . For
the former, the finger is the best, for i t has in tell igence and can feel wh i le the
blow is being del ivered, a lthough p ieces of bo ne, glass, ivory and rubber are
o ften used . These latter emit a sound of their own w i th wh ich the exam iner
must become familiar before he can appreciate the mean ing of the tones
el ic i ted .
For the plexor, the middle finger of the right hand is best , although hammers
made of metal handle and frame with rubber over the striking surface are
excel len t The handle should have a fair amoun t of spring to i t . The stvle
tha t I prefer is shown in Figure 2, B (p . I fa plex imeter o ther than the finger
is used,i t is importan t to have o ne that w i ll fit down in to the supraclaviculaf
n o tch and in to the in tercostal spaces . The one represen ted by Figure 2, C
(p. 14) is made o f hard rubber and meets these requ iremen ts admirably .
I t is very importan t in examin ing chests in advanced tubercu
Eggl in e losis to outl ine the bo rders o f the lungs . The apices should
Bougda ry,be carefully percussed in o rder to d iscover the amoun t o f
co n tract io n presen t i f there be any. Wh i le the height to wh ich
the apices o f the lungs extend varies even in heal th , yet we should assume tha t
an apex is co n tracted un less its h ighest border is o ne inch above the clav icle .
PH YS I CAL EXAM I N AT I ON OF TH E PAT I E N T I
Posteriorly, the highest border should be on a level with the sp ine of the seven th
cervical vertebra . I t should also be determined whether the lower borders of
the lungs are free and movable or bound down by adhesion s . The amoun t
of hypertrophy and con traction presen t in the two lungs should beknown . The
size and posi tion of the heart w ith referen ce to the chest wall and the lungs
should a lso be determ ined . These, together with the presence of flu id or air
in the p leurae may al l be made out by the various methods of percussion
here described .
The lower borders of the lungs are normally capable ofmak in g
wide excursion s . I n the parasterna l l ine this equals 2 c .m .,
in the n ipple l ine 4 c .m .,in the ax i llary l ine 9 c .m .
, and near
the sp inal co lumn 3 c .m .
'
Th ismobility is decreased by em
physema, con so l idation of lung t issue, firm pleura l adhesion s, acute pleura l
pa in,eflusion and pneumo thorax When the d ifferen ce in the lung border
between forced insp iration and forced exp irat ion by percussion falls
much short of the figures here given ,barring d isease below the diaphragm,
one or more of the above condition s are presen t .
M any of the pain s of acute pleur isy are mistaken for in ter
D ifferefitiation costal neuralgia . Recogn iz ing the fact tha t a very large per
if
eifiitigigsw cen t of these pleur isies are tubercular in or ig-in
,i t is very im
an d Pleural portan t that their true nature be d iagnosed .
Pa in s. When the pleura is acutely inflamed, nature checks the move
men t and con sequen tly the excursion of the lung is lessen ed ,usually very markedly . I n in tercostal neuralg ia, the l imitat ion of mo t ion is
very sl ight in compar ison . We can,by percussion , determine the w idth of the
excursion of the in ferior border of the lung upon normal breathing and forced
breath ing . I n cases where the pleura is not already bound down by firm
adhesion s,if there should be any marked d iminution of mo tion
,i t would po in t
to pleurisy, wh i le if the mo t ion be on ly sl ightly‘restricted, it would more prob
ably be intercostal neuralgia .
I t is very importan t to know the posit ion of the heart in chron ic
tuberculosis . From its position a lon e valuable in ferences
may sometimes be dr awn as to the nature and exten t of the
disease and when bo th ap ices are invo lved, even as to the priori ty of the invo lve
men t . Percussion gives the most trustworthy ev idence regard ing the heart .
By i t we can outline its boundaries with prec ision . I have found Ebstein ’s
touch percussion , the author ’s elastic tube percussion and ausculta tory strok
ing _
the most valuable methods for mapp ing out the heart boundaries . The
heart is o ften bound down by adhesion s and i t is somet imes drawn away from
the chest,wall . Emphysematous lun g t issue also o ften in terposes between the
heart and chest wall . Percussion under such c ircumstan ces maybe fac i li tated
by having the pa t ien t bend far forward dur ing exam ina t ion .
7 2 PULM O N ARY TUBERCULO S I S
I n advanced tubercul osis we find every variety of percussion
no te . The examiner must have certain standards of no tes
fixed in his mind . H e should n ot on ly be able to say a certa in
n o te is resonan t, but shoul d recogn ize the degree of resonance,for the departures from the norma l are usuall y on ly d i fferen ces of degree.
H e should also be able to detec t a hyperresonan t no te, for this is very common ,
ow ing to tha t portion of the lung tissue which is not infiltrated tak ing upon i tself
in creased fun ct ion resulting in a dilatation of the air vesic les. I f this d i latation
becomes more exten sive, then the n o te becomes tympan i tic . A tympan it ic
no te maybe recogn ized by its having a musica l character whi le non - tympan itic
no tes are on ly no ises, as can be seen by comparing the tone elic ited by percussing
the stomach or larynx with the n on - tympan i tic no te of the n ormal lung or the
dull n o te of marked infiltrations .
I n acute miliary tuberculosis, the physica l s igns are no t in
Percussion keeping with the sever ity of the disease. The percussion
{EggA cute
sounds may be n ormal, slightly dul l or hyperresonan t . The
Tuberculo sis. dullness is rarely marked,and if present is more apt to be
caused bv a p revious tuberculous process i n the chest .
Hyperresonan ce and somet imes tympany is common . This is due to the
relaxat ion of the lung tissue.
The percussion no te in acute pneumon i c phth isis resemblesA cutePn eumon ic that of pn eumon ia .
Phthm s I f the tubercles are few and scat tered there may be n o
Chron ic chan e reco n izable u on ercussion .
Tuberculos is .
g g p p
There is usual ly,however, some degree o f impairmen t presen t
varying from a sl ight mufll ing to a marked dull ness ; Dullness may be due to
infil trat ion , a pneumon ic process, fibro id thicken ing, a“den se wall about a
cavity, a cavity filled with secretion,a th ickened pleura or pleural effusion .
Hyperresonance and tympany may be presen t as. a result of relaxat ion of
lung t issue due to scattered tuberculous foci,emphysema
,pneumo thorax,
or the presence .of an air con tain ing cavity or bro nch iectatic d i latat io n . I n
a sen i le o r emphysematous lung there may be a w idespread tuberculous infil
tratio n presen t and yet the find ings on percussion be a lmost n il . I n these
cases,however
,we must depend for a d iagno sis more o n percussio n than o n
auscul ta t io n,because the auscultatory find ings are
‘
even more unsat isfactory
than tho se o f percussio n .
The percussion no te is normal,over smal l cavit ies o r over
larger o nes covered by heal thy lung t issue. When filled w i th
secret io n the n o te is dull . Somet imes dullness is due to a
very th ick fibrous wall . I f the cavi ty is superfic ial , large and
fi l led w i th a ir, the to ne may be hyperreso nan t o r tympan i t ic . Cavit ies may
be fo und very readi ly by elast ic tube percuss io n , the d i fference in the no te over
74 PULM ON ARY T UBE RCULOS I S
lessen ing of the murmur is due to nasal sten osis, the sounds wi ll be heard more
d ist inctly .
The pressure of large bron chial glands may so con strict a bronchus as to
cause a weaken ing of the resp iratory murmur in the region supplied by i t .
I f the lung t issue be unaffected , the murmur wi ll be n ormal, except as to in ten
S ity.
Th ickened pleur a is very often the cause of dimin ished murmur at the bases
of the lungs ; o ccasionally at the ap ices also . E ffusion and pneumo thorax
a lso cause weaken ing of the no te.
I nfil trated areas where the lumen of the bronchi is part ia lly or who lly c losed,
also areas suppl ied by a single bron chus which becomes blocked up by mucus,
Show dimin ished or absen t breath sounds.
An in creased resp iratory murmur may be natura lly due to
thin chest walls with poorly developed musculature and ab
sence of ad ipose t issue. The in ten sity of the n o te is in creased
whenever the fun ct ion is increased . I n case of dense infil
tration of a port ion of a lung,or the displacemen t of the norma l t issue by
fibro id t issue and-
cavities,or the compression of lung t issue by the fill ing up
of the pleura l cavity by flu id o r air , extra work is thrown upon the rema in ing
port ion of the pulmonary t issue and the performan ce of th is extra fun ct ion
causes an increase in the in ten sity of the murmur .
Pro longed exp iration is o ften found in early tuberculosis,and
is rarely absen t when the d isease has extended . I t shows
that the norma l elast ic t issue of the lung has been in terfered
with,causing a dim inut ion of its con tractile power . Thus
,in early infil tration s ,
con tract ion is slower than normal , caus ing the nOte to be pro longed . We
must accept as a reason for the sound being somewha tm ore in tense, the prin
ciple that owing to the infil tra t ion in terfering w i th the normal elast ici ty o f the
bronchi,they become somewhat rigid and offer resistan ce to the free flow o f
a ir ; also to tha t o ther principle that sound is conducted through paten t bro n chi
surrounded by den se t issue much better than when surrounded by air - con tain
ing t issue .
When large paten t bronch i , bronch iec tasis or cavities are presen t and these
are in terlaced w i th den se scar t issue,the idea l condit ions, if the above explana
tio n is co rrect,are presen t for a very pronounced pro lo ngat io n o f exp i rat io n
,
fo r the elast ic t issue o f the part is largely destroyed and the large a ir co nduct
ing chambers surro unded by dense t issue are presen t to co nduct the sound .
Such is true. There is n o co nd i t io n presen t in the chest wh ich shows exp ira
tio n so pro lo nged,so lo ud and so harsh .
O ften t imes pro lo nged expi rat io n is presen t over a l l that po rt io n o f the
lung o r lungs which is no t infilt ra ted . Somet imes th is is co n fi ned to a s ingle
lung and even to a single lobe o r part o f a lobe . I t o ften shows the presence
PH YS I CAL EXAM I N AT I ON OF_
TH E PAT I E N T 75
of emphysema, a lthough somet imes when accompan ied by sharpen ing of the
in sp ira tory sounds, i t may mean on ly a temporary compen satory cond i t ion .
Bron ch ial breathing shows a reverse of the vesicular . E xp ira ~
tion is longer and more in ten se than in sp iration,and bo th
phases are more or less harsh .
-T h is is found normally in the
region of the trachea, in the in terscapular reg ion poster iorly
and anteriorly a long the borders of the upper port ion of the sternum . T h is
physio logical bron ch ia l breath ing is S imply a'
conduction of the murmur pr o
duced in the larynx and trachea,to the chest wa ll in the region s men tioned .
The sound maybe imitated by fix ing themouth to say“ha
”and then forc ibly
in sp iring and exp ir ing .
B ron ch ial breathing found in port ion s of the lun g o ther than
thosemen t ioned in thepreced ing paragraph must becon sidered
patho logical . Th is type of breath ing var ies greatly in pitch
and in in tensity . I ts presencemean s ei ther lung t issue free from
air as found in infiltration s and fibroid tissue, a d i lated bron chus, or a cavity
commun icat ing freely with a bron chus . Theexp irat ion at t imes assumes
somewhat of a blow ing character and is mistaken for the S ign of a cav i ty. I n“
fact,it is o ften very diEicult to say whether the blow ing character of the expira
t ion mean s a cavity or dense scar tissue .
When the bron ch ial breathing assumes a defin ite amphor ic
type, such as m ight be imi tatedby blowing over a jar or whisp
ering the syllable “ha,
” there is n o mistaking its mean ing .
I t is almost a positive S ign of a cavity . T his expiratory n o te is so ft and of low
p itch . I t has been est imated that a cavity must be about the size of a hen ’s
egg in“
order to produce amphor ic breathing . I have found awel l marked type
of amphor ic breath ing in the fir st in terspace at the r ight edge of the sternum ,
where wen ormally find physio logica l bronch ial breathing,in a lungapparen tly
free from d isease.
A side from the defin ite types of breath ing here enumerated,there are m ixed types . Somet imes in sp iration is d ist in ctly
vesicular and exp irat ion bron ch ial in qual ity . Sometimes
insp irat ion partakes of bo th vesicular and bron ch ia l qualit ies, whi le exp irat ion
is bron ch ial . Th is is usually spoken of as bronchovesicular . I t is found on
scattered small infiltration s, also over normal t issue n ear an area of infil trat ion .
I t means tha t sound is being conducted to the ear from air con ta in ing and
infiltrated areas at the same t ime .
Rough breath ing as men t ioned previously is perhaps the
earliest sign of tuberculosis to be found on auscultat ion . I t
is; often found later in the d isease a lso,and is presumably
caused in the same man ner . There is a lso a d ist in ct roughness assoc iated at
times wi th emphysema and somet imes w ith changes in the pleura .

76 PULM ON ARY T UBE RCULOS I S
I have o ften seen changes in the pleur a cause such a roughness co inciden t
w ith the in spiratory no te that it might well be character ized as a grat ing .
There are sounds wh ich accompany the respiratory murmur
in diseases of the lungs which demand careful considerat ion .
These may be produced either within the lung or in the
p leura l cavity. O ften times, in chron ic tuberculosis , i t i s very difli cult to be
sure of their o rigin . Sometimes in the vicin i ty of a cavity there is a creak
ing which resembles ra les.
Rales are produced by the mo tion of air , secretion or o ther
flu ids or so l id mater ia l in the air passages . They may be
ei ther mo ist or dry, yet this division mean s very l i ttle, for the so - cal led dryrales are produced by mo isture. The presen ce of rales in the lungs means
the presence of a catarrhal condition .
O ften t imes these ra les are not heard on ordinary resp irat ion,
but may be produced by deep breathing or cough ing . N o
examination of the chest should be considered complete un t il
the patien t has been required to cough during auscul tat ion .
N ot un common ly do I find patien ts with extensively scattered lesion s who have
been repeatedly assur ed that their lungs were sound simply because percussion
had n ot shown dullness and ordinary auscultation had shown no ra les . H ad
the pat ien t been requ ired to “cough dur ing auscultation , the rales could have
been detected very easily .
A t times, rales disappear after coughing,wh ich fac t is sometimes taken
advan tage of to d istinguish ra les within the lungs from those of pleural orig in .
Rales are divided in to fine,medium and large. The fine
ones are supposed to be produced in the finer air passages,
the med ium in the med ium bron chi , and the large ones in the large bronch i .
That the size of the air passage in which the rales are produced is not
the on ly factor to be considered is suggested by the fact that we also have
fine,med ium and large rales in cavities. I t seems to me tha t the amoun t and
character o f secretion presen t is a very importan t factor . Thus fine rales may
take their orig in from ei ther the fine air passages o r from a scan t amoun t o f
th in mucus in a larger tube o r cav i ty ; l ikew ise med ium rales m ight o riginate
in bro nch i o fmed ium size or in larger ones, o r cavi t ies in which a small amoun t
o fmucus,n o t too tenacious in character, is presen t .
I n tuberculosis, i t is surpris ing to see how con stan t rales are.
By mak ing repeated exam inations o f the chest and reco rd ing
the relat ive number and character o f rales found in the various
parts o f the chest, i t w i l l be found that a comparison of the various charts w i ll
show the presence o f rales o f the same character day after day and even mon th
a fter mo n th,un t i l the patho logical co nd i t io n with in the chest changes . Thus ,
in early tuberculo sis,we find fine rales ; a l ittle later, may be a week o r many
Ra les.
S ize o f Ra les.
PHYS I CAL EXAM I N AT I ON O F TH E PAT I E N T 77
weeks or mon ths, if the .disease is extend in g and go ing on to . con so lidat ion and
cav i ty formation , med ium rales w il l appear in the same area ; and, as so ften ing
occurs, these w i ll g ive way to large rales . M o ist rales persisten tly rema in ing
over one area,especially over the apices, nearly a lways mean tuberculosis .
I n tuberculosis, large bu'
bbl ing rales persisting -in an area away from . a large
bron chus, as the apex or the base of the lungs, nearly a lways mean cavi ties.
Somet imes in cavities, the . rales assume a d istin ct metall ic
sound, and at times they simulate fallin g drops of water .
The name dry ra le is a m isnomer because i t is dependen t
upon mo isture for its existen ce the same as the mo ist
rale. A side from the meist ra les already men t ioned, we find in tuberculosis
l
many sounds wh ich are d ifficult to c lassify, most of which belong to”
the
c lass usually described as dry rales . Sometimes these are clicks or squeaks,somet imes they resemble the croak of a frog
, the rattle of musketry, the purr
of a cat, the whine of a puppy or the low no te of a bass vio l . The higher toned
ones originate in the smal ler passages and the lower ones in the larger passages.
They depend for their origin upon'
a small amoun t of very thick, tenac ious
mucus .
I have come to look upon a c l ick,squeak or croak which remains loca l ized
over a g iven area for some time as bein g very susp ic ious of destruct ion of tissue
and cav i ty formation .
I n tuberculosis, severa l of these d ifferen t k inds of ra les may be presen t over
the same area at the same time.
One of themost d iffi cult procedures in the exam ination of cases
M eta ll ic Rales.
D ry Rales.
Ra l es an d
S oun ds of of advan ced tuberculosis is to d ist ingu ish between sounds of
812531 in trapulmon ary and in trapleur a l or igin . I f the on ly sound
produced in the pleura were that of the pleural rub ,we should
have li ttle difli culty, but we_
have sounds like crepitation s, like bubbl ing ra les
and coarse gratings of pleura l or ig in wh ich are at t imes a lmost impossible to
d ifferen t iate from those of resp iratory origin .
Rules as la id down in text books for differen tiating these sounds leave usin doubt in many cases. Pleural sounds and rales of in trapulmonary or ig inare iden t ica l as far as their qual ity is con cerned, 89 the differen tia t ion must
depend on o ther features . Text books say that pleural sounds are more superficial
,and give the sen sation of being nearer the ear
,that they are more apt
to be heard on bo th in spiration and expirat ion,and that they
/
are n ot affectedso much by cough as are ra les produced in the lung which o ften appear as ashower after an effort at cough ing . Somet imes pleural crepi tat ion s may be
felt on palpat ion .
I t would seem“
that with these rules, the recogn it ion of pleura l sounds would
be qu ite easy, but whenl
we remember tha t the differen tiation of the n earnessof the sound is a matter of very sl ight degree if the rales have their origin in
78 PULM O N ARY TUBE RCULO S I S
lung t issue adjacen t to the pleura ; and that the determ in ing of the nearness
m ight no t be accompl ished except by a practi ced examiner ; that crep itat ion s,wh i le usually heard on ly on in sp iration ,
may a lso be heard on exp irat ion ;that these pleural sounds are somet imes influenced by cough ; and that pleura l
crepitat ions are n ot always fel t on palpat ion , we can see that our posit ive
ev idence is pract ical ly n o th ing, and we are left to rely largely upon our‘
expe
r ience in d ifferen t iat ing these sounds.
Where the resp iratory no te is n ormal and there is no change upon percussion,
if at the same t ime the pat ien t g ives a h istory of a ttacks of ple’urisy over the
area, then the d ifferen tiat ion is not difficult,But where we have an area of
o ld pleura l adhesion s and the underly ing lung t issue the seat of tuberculous
d isease, then _
it is o ften difi cul t,somet imes impossible
, to d ifferen tiate. I f
the pat ien t, however, is watched for mon ths and the d isease goes on to arrest
men t or cure, then the difleren tiation w i l l be finally made out. Text books
tell us that pleura l fr ict ion is in creased by pressure. Th is is true of l ight pres
sure,but
,in my exper ien ce
,firm pressure decreases and at t imes obl iterates
the sound . Th is also ho lds good in the pleural soundswhich resemble crep
itation and med ium rales . By firm pressure we can usua lly decrease their
number and at t imes total ly o bl iterate them . I find th is a very importan t
aid in d ifferen t ia t ion ; and, when taken w i th the rela t ive n earness of the sounds
and the effec t produced upon them by cough ing, and the charac ter of the
underly ing tissue,we can usually make a d iagnosis . Somet imes we have bo th
pleural and in trapulmonary sounds presen t wh ich make the d ifferen tiat io n
more d ifficul t .
I f words are spoken or whispered by the pat ien t wh i le we l is
ten to the chest over the areas of infiltrat ion the sounds are
heard more d ist in ctly than over air - conta ining t issue, fo llow
ing the same law as bronch ia l breathing and vocal fremi tus . I t is well to use
the same syllables a l l the t ime so as to become mo re fami l iar wi th them .
Fo r the spoken vo ice, I prefer n inety—nine spoken firmly,and fo r the wh isper
I prefer one, two , three
” long drawn out. Where large superfic ial cav it ies
are presen t,the wh isper is tran sm i tted to the ear with such clearness tha t the
syllables may o ften be d ist inctly understood . Over dense scar t issue, the same
phenomen o n o ccurs,so tha t a transm issio n o f the wh ispered words can no t be
taken fo r a sure s ign o f cavi ty . I n cavi t ies,however , as a rule, the sound is
low and so ft,whi le in fibro id t issue i t is more harsh .
Vo iceTran sm i ssw n .
CHAPTER V I I .
D I SPLACEME NT OF TH E TH ORACI C V I SCE RA I N AD
VANCE D PULMONARY TUBE RCULOS I S .
D isplacemen t of the thorac ic v iscera is“ found to some degree in a l l ind iv id
uals who are suffering from chron ic advan ced pulmonary tuberculosis . Co n
sider ing the frequen cy and impo rtan ce of th is cond i tion,i t is strange that i t
has not received more a tten t ion from cl in ician s and patho logists .
I n order to understand clearly the patho logical changes in
posi t ion of the viscera, i t is n ecessary to know the natur al
changes.
I f we recall the changes which take place during the develop
men tal and decl in ing years of l ife we no te that from b irth to
o ld age there is a con t inual change tak ing place by which the organ s of respi
ration are gradually assum in g a lower posi t ion .
The larynx which is high at b irth graduall y becomes lower and lower as
years progress .
The upper aperture of the thorax changes very markedly . A t b irth, the
an terior-posterior and the la tera l d iameters are nearly equal,
and the
jun ction of the first r ib w i th the sternum is on about the same hor izon ta l plane
as the first dorsal vertebra ; as the ch i ld grows o lder the an terior port ion of
the thorax gradual ly lowers and the an ter ior—posterior diameter shorten s ,so that by the time adult l ife has been a tta ined a hor izon ta l l ine drawn through
the jun ct ion of the first rib wi th the stern um to the sp inal co lumn wo uld ,in stead of strik ing the body of the first do rsal vertebra , str ike the body of the
th ird . The diaphragm,also
,which is highly arched at b irth gradual ly descends
as adult life and o ld age approach . See Fig. 1 7 , a and b .
Thus the chest at b irth is round and the an terior and posterior
borders of its super ior aperture l ie in about the samehorizon tal
plane. This cond i tion is that of in sp irat ion,hen ce the ch i ld ’s
chest is said to be physio logical ly in the phase of in sp irat ion . Th is same
type of chest is again found in emphysema but in this in stan ce the chest is
patho logical ly in.
a state of in spiration .
Durin g early chi ldhood the chest remain s much as i t is
fit birth , but as puberty approaches the changes become
marked,and the chest flatten s . A s o ld age approaches this
becomesmost marked and produceswhat is known as thephysio logical exp ira
tory thorax .
I n spira toryborax.
E xpira toryhorax.
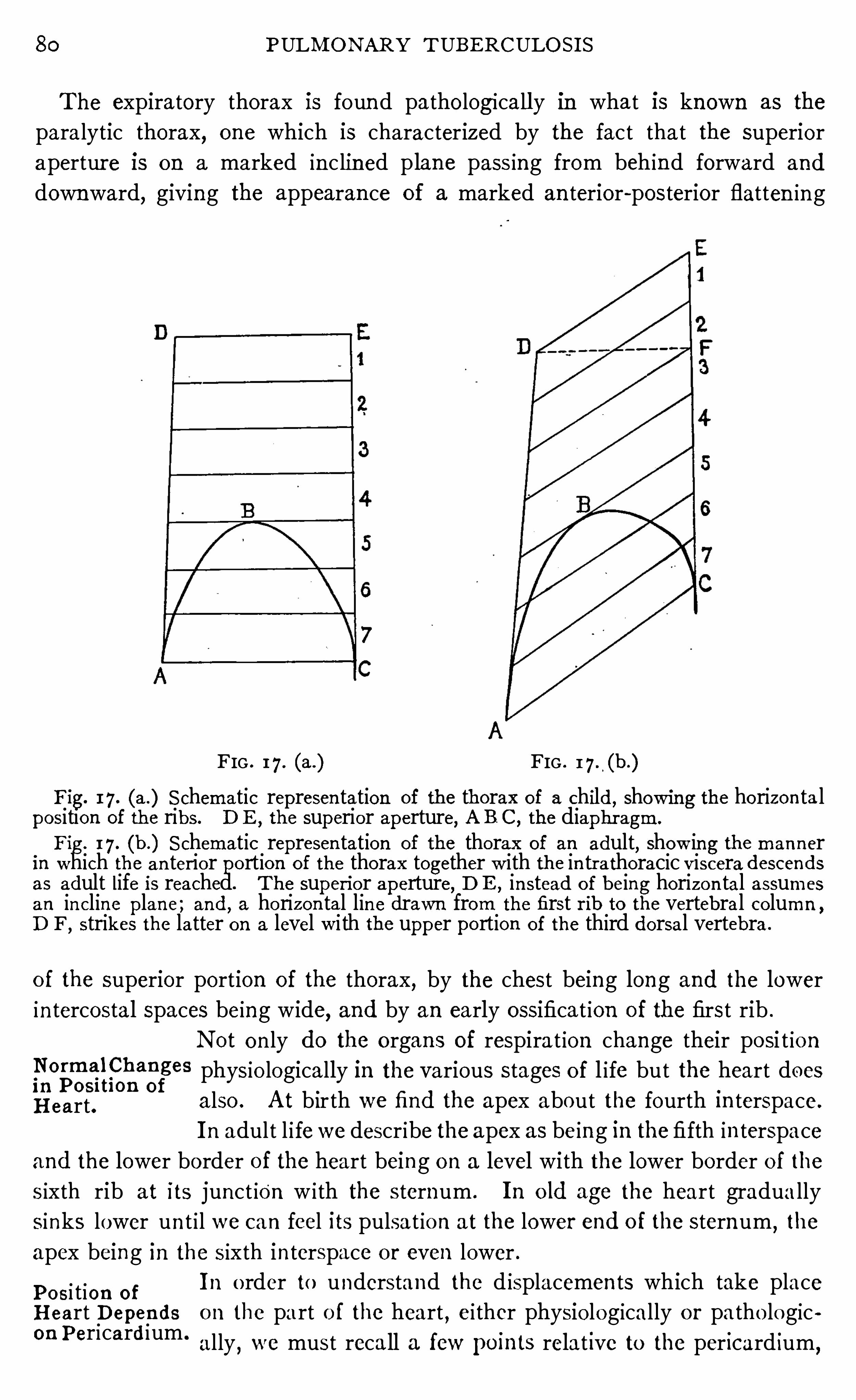
80 PULM O N ARY T UBERCULO S I S
The expiratory thorax is foun d patho logicall y in what is known as the
paralytic thorax,one which is characterized by the fact that the superior
apertur e is on a marked in c lined p lane pass ing from behind forward and
downward,giving the appearan ce of a marked an terior-posterior flatten in g
FIG . 1 7 . (a .) FIG . 1 7 . (b.)
Fig. I 7 . (a .) S chematic represen tation of the thorax of a child, showing the horizon ta lposition of the ribs. D E , the superior aperture, A B C, the diaphr agm.
Fig. 1 7 . (b.) S chematic represen tation of the thorax of an adult, show in g the man nerin which the an ter ior portio n of the thorax together w ith the in tr athoracic viscera descendsas adult life is reached. The superi or aperture, D E , in stead o f being horizon tal assumes
an incline plane ; and, a horizon tal lin e drawn from the first r ib to the vertebral co lumn ,
D F , strikes the latter on a level w i th the upper portion of the third dorsal vertebra .
o f the superior portion of the thorax, by the chest being long and the lower
in tercostal spaces being wide, and by an early ossificat ion of the first rib .
N ot on ly do the organ s of respirat ion change their po si t ion
,
N o rme l ffhan ges physio logically in the various stages o f l ife but the heart doesi n Pos l tl on of
H eart. a lso . A t b ir th we find the apex about the fourth in terspace.
I n adult l i fewe describe the apex as being in the fifth in terspace
and the lower border of the heart being o n a level with the lower border o f the
s ixth rib at its junct ion w i th the sternum . I n o ld age the heart gradua lly
sinks lower un t i l we can feel its pulsa t ion at the lower end o f the sternum,the
apex being in the s ixth in terspace or even lower .
Po si tion o fI n o rder to understand the d isplacemen ts wh ich take place
H eart D epen ds o n the part o f the heart , ei ther physio logically o r pa tho logicouPericardium .
ally,we must recall a few pomts relat ive to the per icard ium,
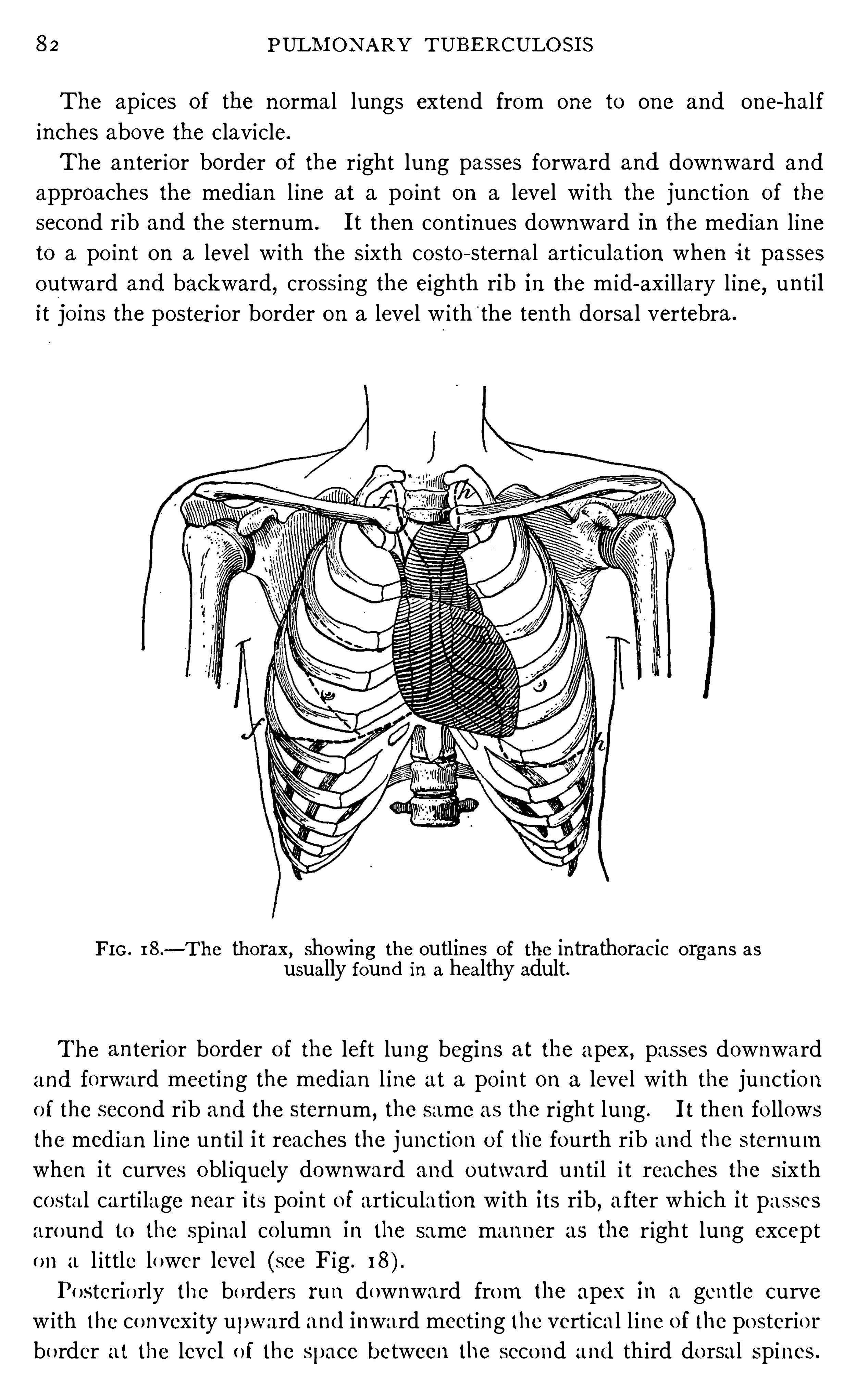
82 PULM O N ARY TUBE RCULO S I S
The ap ices of the n ormal lungs extend from one to one and one-hal f
inches above the clavicle.
The an ter ior border of the r ight lung passes forward and downward and
approaches the median l ine at a po in t on a level w i th the junc tio n of the
second r ib and the sternum . I t then con t inues downward in the med ian l ine
to a po in t on a level w i th the s ixth costo - sternal art iculat ion when i t passes
outward and backward, cross ing the eighth rib in the m id-ax i llary l ine, un t i l
i t jo ins the poster ior border on a level w i th'
the ten th dorsa l vertebra .
FI G . 18 .
—The thorax, showing the outl ines of the in trathorac ic organs asusually found in a healthy adult.
The an terior border o f the left lung begins at the apex, passes downwardand forward meet ing the med ian l ine at a po in t on a level w i th the junctio n
o f the seco nd rib and the sternum , the same as the r ight lung . I t then fo llows
the med ian l ine un ti l i t reaches the junc t io n o f the fourth r ib and the sternum
when i t curves obl iquely downward and outward un t i l i t reaches the s ixth
costal cart i lage near its po in t o f art iculatio n w i th its rib , a fter wh ich i t passes
around to the sp ina l co lumn in the same manner as the r ight lung excepto n a l ittle lower level (see Fig . I 8).
Po sterio rly the bo rders run downward from the apex in a gen tle curve
w ith the co nvex i ty upward and inward meet ing the vert ica l l ine o f the po sterio r
bo rder a t the level o f the space between the seco nd and th ird do rsal sp ines .
D I SPLACEM E N T OF TH E TH ORACI C VI SCE RA 83
The outl ine of the heart as descr ibed by various authors
d iffers somewhat . I t a lso differs in d ifferen t ind ividuals
as men tion ed above. The fo llow ing seems to me to be about
thecorrect outline for the major i ty"of adult ind iv iduals dur ing
the prime of l ife.
The superior boundary of the heart l ies on a level with the upper bo rder
of the third costal cartilage,and extends from the art iculation of the th ird
left costal cart i lage w i th its r ib to a po in t on the‘
superior border of the third
costal cartilage about one in ch to the righ t of the sternal margin . The r ight
border of the heart extends from the upper border of the th ird r ight costa l
cart i lage downward in a sl ight curve w i th its convex ity outwards to a po in t
in the fifth in terspace about one in ch to the r ight of the stern um . The in ferior
border crosses the sternum at the level of the upper marg in of. the sixth left
costa l carti lage at its jun ct ion with the stern um,terminat ing at the apex in the
fifth in terspace at a distance of about three and one-half in ches to the left
of themed ian l ine and about one in ch to the r ight of the n ipple. The left
border startsat the apex,run s upwards and inwards to a po in t about two
in ches to the left of the left sternal border near the jun ction of the th ird left
r ib with its cart i lage. (See F ig .
The importan ce of recogn izing the changes in outl ine wh ichImpo rtan ce Of mark the d isplacemen t of the thorac ic v iscera is self-ev iden t .
(
R
gzgggl
filng From the
'
standpoin t of bo th prognosis,and bein g able to
Outl in e. satisfactorily understan d symptoms and apply the proper
remed ia l measures,i t is . indispen sable. The recogn i tion of
a marked con traction in one lung and a marked en largemen t of the
other,together w i th the d isplacemen t wh ich takes place in the heart under
these cond i t ion s,has an impdffan t bear ing upon our methods o f trea t
ing the case and especially upon the amoun t of exercise,the diet, and
the degree of a l ti tude which we would prescr ibe for such a pa tien t . This is
especially importan t in elderly ind iv iduals with hardened arter ies,for the
d isplacemen t tw ists the hardened arch o f the aorta . The character of th i s
d isplacemen t may a lso afford va luable eviden ce bear ing upon the priority of
invo lvemen t where bo th lungs are invo lved,as I sha ll expla in later .
'
Displacemen ts of the thorac ic viscera are ei ther acute or
chron ic . A cute d isplacemen ts are due to p leurisy w i th
effusion or pneumo thorax, whi le those of a chron ic nature
are due to changes w i thin the lung or within the lung and pleura combined .
The former are produced qu ickly wh i le the latter develop slowlv. The cause
is of a mechan ical nature. I t is due to a comb ina t ion of con traction an d
en largemen t, of pull ing and pushing .
D ispl acemen t The most common cause of chron ic d isplacemen t of the
o f the Lung. lungs is pulmonary tuberculos is . There are a few cases
Cause of
D isplacemen t.
84 PULM O N ARY TUB E RCULO S I S
which are the result ofempyema, and some due to a cond i tion which is described
as s imple fibro sis . I n this conn ection the en largemen t of the lung wi th the
exten sion of its boundar ies,due to emphysema
,must a lso be men tioned .
We most o ften meet displacemen ts on the part of the lungs in the form of
con traction at the apices. Tuberculosis usua lly invo lves the apex of the lung .
Soon after an infi l trat ion occur s, certa in changes take place. E i ther heal in g
or the destruction of t issue en sues. Bo th of these processes are accompan ied
by con tract ionof the part affected . Sometimes a compen satory emphysema
on the part Of the lung t issue adjacen t to the di seased areas occur s which fi lls
in the space previously occupied by the tissue which is the sea t of the con
tract ion . Perhaps some emphysema a lways occur s, but in some in stances
i t is so marked that very little, if any, change can be no ted on inspection of the
chest ; in o ther in stan ces the supra and in fraclavicular spaces are drawn in
and the ribs appear sunken . When an infil tra tion of any exten t has ex isted
in an apex for any length of time,we find upon careful examina tion that the
apex has con tracted and is dr awn down . Very o ften,
i t is forced down by
an inflammatory cond ition causing more or less thicken ing of the pleura
which covers the apex .
I f this con tracting infil tration is small the on ly appreciable change tha t
we no te may be retraction of the apex . I t is wel l to bear in mind, however,that tuberculous infiltrations which invo lve lung t issue n ear the surface are
common ly accompan ied by pleur i tic adhesion s of greater or less exten t ;con sequen tly the apex is bound more or less firmly to the bony thorax, and
the rest of the lung or lungs being free,con traction in th is part is almost
certain to make traction upon the remain ing portion s of the thoracic viscera ,con sequen tly d isplac ing them to some exten t . I f tha t portion of the lung
wh ich is the seat of con traction extends as low as the second rib,and the
con tract ion is marked,we must expec t to find
'
evidence of this con tract ion
shown on the lower an terior borders o f the lung, and a lso upon the heart .
The amoun t of the displacemen t w i ll depend upon a number of facto rs .
h is more marked where the disease has been confined to one lung, and most
marked where the princ ipa l invo lvemen t has rema ined for a long time at the
upper portion of the lung and caused a high degree of con traction to take
place there before the d isease man i fested itself in o ther port ions and before
the lower parts became bound down w i th pleura l adhes ions . I n such cases
the oppos ite lung usua lly takes upon i tsel f a high degree of compensato rv
emphysema and fo l lows up the con trac t ion s, even push ing far beyo nd the
med ian l ine in its endeavo r to carrv on the work o f the destroyed tissue and
to fil l the space vaca ted by the retraction,as shown in Figs . 19, 20 ,
2 1 . I n
case represen ted by Fig . 19 the pat ien t had been i ll fo r five o r six years, the
left lung being first invo lved,the right lung later. The left lung was the sea t
o f a severe infil tra tio n,wh ich had resulted in the fo rma t io n o f bo th extensive
86 PULM ON ARY TUBERCULO S I S
part of the retracted lung . Th is patien t has been very seriously inconven ienced
during the t ime when these changes have taken place,pr inc ipa lly on accoun t
o f a tendency to repeated hemorrhage,so she has n o t a ttempted to move
around . I f she had, she would havedoubtless suffered much in conven ien ce
on accoun t of the heart .
The pat ien t i llustrated in Fig . 2 1 has been i ll two years, a portion ofwh ich
t ime she has spen t in the moun tain s endeavoring to rega i n hea l th and ano ther
port ion attend ing to her ordinary dut ies . The r ight lung is n ow the sea t of
recen t S l ight invasion . I n sp i te of the high degree of d isplacemen t, this
FIG . 20.
—Show ing displacemen t of thoracic viscera in advan ced tuberculosis . Left lungseat o f marked con traction . R ight lung seat of compen sato ry emphysema . H eart displaced to left . A pex being bound down by pleural adhesion s is preven ted from beingd isplaced far upward. Con tinuous lin es represen t the heart, broken lines boundaries o flungs . Circles represen t the normal po in ts of greatest in ten sity of the aortic and pulmon ary valves ; crosses represen t the presen t po in ts of greatest in ten sity.
patien t has never experienced any dyspnea or inconven ience,and was very
much surpr ised when She was apprised of her cond i t ion . I n th is case the
force of the en larged right lung has been spen t in an upward directio n push ing
and l ift ing the heart far to the left . The l iver dullness is also one inch above
its n orma l,com ing up to the do tted l ine in the p ic ture .
Where bo th lungs are the sea t of tuberculous infil tratio n , i t is imposs ible
to have so high a degree o f enlargemen t as when the lung is sound,never
theless, we do find th is co nd i t ion with bo th lungs invo lved . Careful inqu i ryand examina t io n ,
however,w i l l usually prove tha t the enlarged lung became
d iseased a fter the compensa to ry emphysema had taken place ; o r , a t least ,tha t
,i f an invo lvemen t was presen t prio r to th is t ime, i t was no t extensive.
A t t imes we get a h igh degree o fd isplacemen t where bo th lungs are invo lved ,fo r example, i f the upper po rtio n o f the lung is the sea t o fw idespread destruc
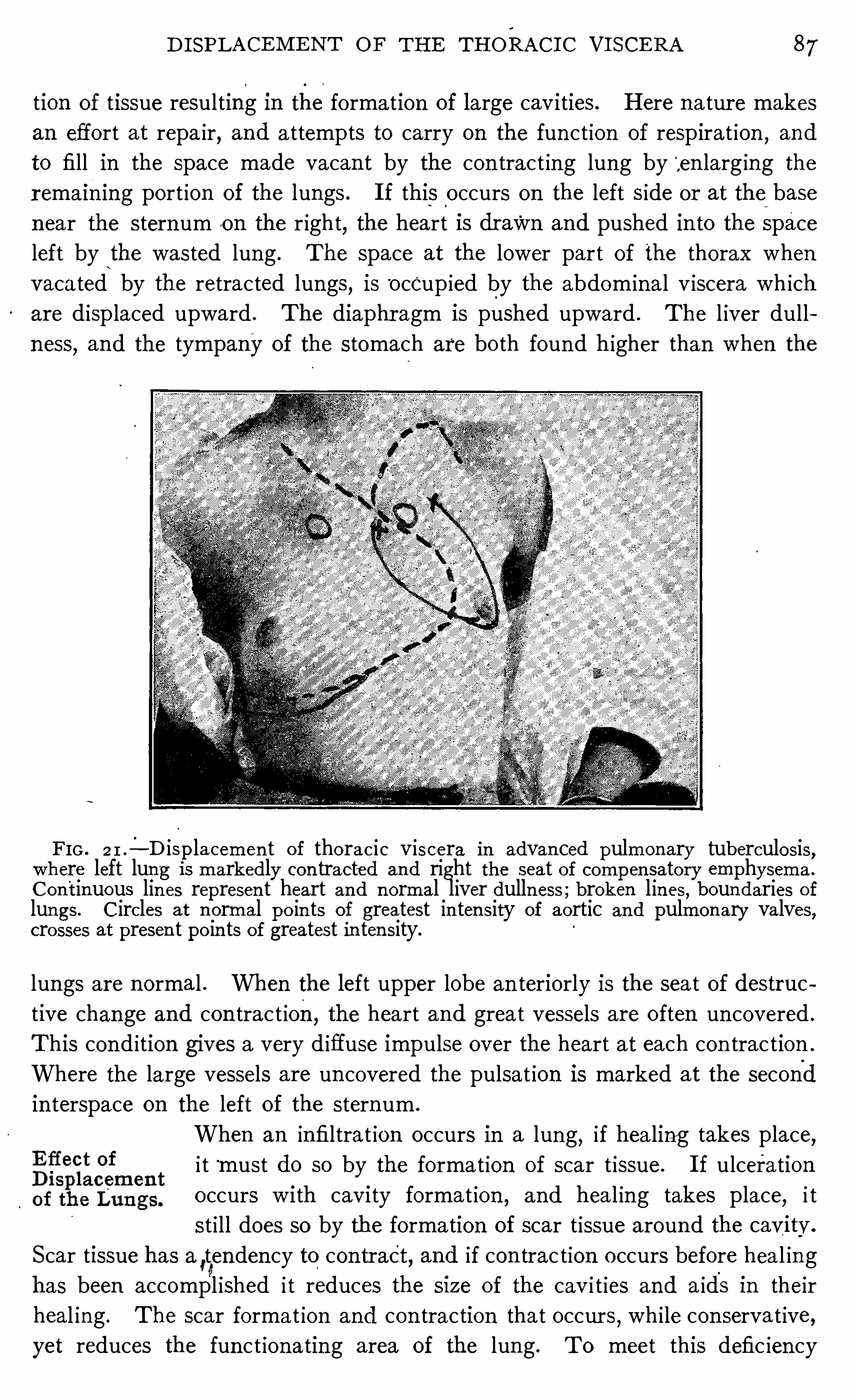
D I SPLACEM E N T OF TH E TH ORAC I C VI SCE RA 87
tion of tissue resulting i n the formation of large cavities . Here natur e makes
an effort at repa ir, and a ttempts to carry on the fun ct ion of respirat ion,and
to fill in the space made vacan t by the con tract ing lung by‘
,en larg ing the
remai n ing port ion of the lungs . I f this occurs on the left s ide or at the base
n ear the sternum o n the r ight, the heart is dr awn and pushed in to the space
left by the wasted lung . The space at the lower part of the thorax when
vacated by the retracted lungs, is“
occup ied by the abdom inal v iscera wh ich
are d isplaced upward . The diaphragm is pushed upward . The l iver dull
ness,and the tympany of the stomach are bo th found higher than when the
FIG . 2 1 .
— D isplacemen t o f thorac ic viscera in advan ced pulmon ary tuberculosis,where left lung is markedly con tracted and right the seat of compen sato ry emphysema .
Con tinuous lin es represen t heart and n ormal liver dulln ess ; broken lines , boun daries of
lungs. C ircles at n ormal po in ts of greatest in ten sity of aortic and pulmon ary valves,cro sses at presen t po in ts of greatest in ten sity.
lungs are normal . When the left upper lobe an teriorly is the seat of destruc
tive change and con trac t ion,the heart and great vessels are o ften un covered .
This cond ition gives a very d iffuse impulse over the heart at each con trac tion .
Where the large vessels are un covered the pulsat ion is marked at the second
in terspace on the left of the stern um .
When an infiltrat ion occurs in a lung, if hea ling takes place,i t must do so by the format ion of scar t issue. I f ulceration
occurs with cavity format ion,and hea l ing takes place, i t
st i ll does so by the formation of scar t issue aroun d the cavitv.
Scar tissue has a,tenden cy to contract , and if con trac tion occurs before hea l ing
has been accompl ished i t reduces the size of the cav i t ies and a ids in their
heal ing . The scar forma t ion and con traction that occur s,wh i le con servat ive,
yet reduces the fun c t ionating area of the lung . T0 meet this defic ien cy
88 PULM ON ARY TUBE RCULOS I S
a part or al l of the remain ing portion of the lung or lungs becomes the sea t ofa compensa tory emphysema and takes upon i tself the work which had pre
viously been accompl ished by the part affected . Wi th this extra burdenthrown upon the rema in ing portion of the lun g
,al l goes well prov id ing too
much lung t issue has n ot been destroyed . I t is truly marvelous to see whatl i ttle in conven ien ce sometimes fo l lows even a high degree of destruc tion of
tissue. I f the amoun t of destruc t ion is too grea t, the remain ing portion of
the lung or lun gs in en larging and endeavoring to take upon i tself the extra
fun ct ion may become ser iously in capacitated . The air vesicles dilate to
their utmost and in stead of being able to perform an in creased fun ction,may
be disabled . Thus a con servat ive process has become destructive. Wh ile
the fun ct ion of respira tion may be carried on with li tt le in conven ien ce even
with a h igh degree of con trac t ion and compen satory emphysema presen t ,
yet, if the proper balan ce is exceeded, the respiratory fun ct ion w ill be in ter
fered w i th, the a'
ération of the blood w i ll be imperfectly accompl ished and
dyspnea will result .
The effect of such cond ition s upon the heart must also be con sidered . I n
these cases the heart is d isplaced, i t is labor ing under un natura l condition s,i t is bound down by adhesion s, and i t iscompelled to force the blood through
the pulmonary system again st enormous odds,because many vessels have
been destroyed with the loss of tissue that has occurred,and the lumen of
many have been obli tera ted where not actually destroyed . The new scar
tissue is but poorly suppl ied with vessels and the t issue that becomes emphysematous oflers a great hindrance to the free flow of blood through the lung.
Con sequen tly the heart is greatly embarrassed and must be carefully con
sidered in treat ing these pa t ien ts .
I t is the exception to find the heart in its normal posi tion in
advanced chron ic“ tuberculosis . Con tract ions here and
there with compen satory emphysema of o ther parts, pleuri tic
effusion and adhesions draw and push the heart away from its o riginal locat ion .
I n some cases the change is very sl igh t and will no t be recogn ized w i thout a
very careful examina t ion . Displacemen ts are the most marked where one
lung o n ly is invo lved , or where, i f bo th are invo lved , one is involved before
the o ther, and th is previously invo lved lung becomes the sea t o f a high degree
o f co n trac t io n and the o ther becomes the sea t of compensa tory emphysema .
Under such c ircumstances we may find the apex o f the heart to the left o f the
n ipple l ine, and o ccas io nally the en t ire o rgan so drawn Up and toward the
left tha t i t l ies en t irely above the n ipple,the apex being beyond the ax i llary
l ine. Such a high degree o f d isplacemen t can on ly occur when the pat ien t
po ssesses a large pericard ium o r when the d iaphragm is pushed high up, o r
when bo th o f these co nd i t io ns are presen t . The accompany ing cuts (Figs .
19, 20 a nd 2 1) represen t a h igh degree o f displacemen t due to co n tractions
D isplacemen tsof the H eart.
90 PULM ON ARY T UBE RCULOS I S
i t is somet imes very difficult to locate the apex . I t must not be taken that
that part wh ich causes the stroke aga inst the chest wa l l is the apex,for in the
d islocat ion which occurs the relat ive posi t ion of the parts of the organ are so
changed that the impulse on the chest wa ll is more probably due to the s ideof the ven tricle than to the apex,in fact, in these cases the heart is pushed in1010 toward the r ight ; i t is not pushed around as has somet imes been sup
posed , with the grea t vessels act ing as a h inge and the en t ire organ reversed .
Such is impossible except under anoma lous cond i t ion s. I t is a lmost im
possible a lso_to locate the va lves, for their relative posi t ion is changed and
we can n o longer depend en tir ely upon the dist in ctness of the sound forour loca tion .
Throwing the heart out of its n orma l relation sh ip in the
53323 thorax,putt ing i t on a s train by tract ion and pressure
,and
Po s i t io n Upo n draw ing and tw ist ing the great vessels at the base of the
21
331
3312
5525 "
heart,wh ich are o ften hardened in pa t ien ts beyond m iddle
life,can not help but throw extra burden upon th is o rgan
,
wh ich, as I have shown elsewhere, is a lready bear ing the brun t of the fight
aga in st the disease. I n sp i te of the extra burden thr own upon the heart,
i t bears up under the stra in most wonderfully . A s a rule,such changes come
gradually,and are n ot a ttended w i th great in conven ience ; in fact, the heart
may be the sub ject of a high degree of d isplacemen t wi thout any unusua l
in conven ien ce beyond what would be expected to accompany the tuberculosis .
When th is change comes quickly,however
,and where the organ is put on
an unusual stra in,i t somet imes en coun ters difficulty in adjusting i tself to the
new cond i t ion . I n a few such cases in which I watched the displacemen t
occur from mon th to mon th,the patien ts suffered from tachycard ia, pa lp i ta
tion and a feeling of fa in tness un t i l the heart became adjusted to its new
posi t ion . These symptoms gradually improved,however
,and a fter a shor t
t ime d isappeared .
Dur ing this t ime rest is essen tial. The heart should be spared a l l extra
work un ti l i t becomes accustomed to its new posi tion .
The effect of compensatory emphysema.
on the part of the unaffected lun g
is favorable to the pa t ien t . I t insures tha t the funct ion of the lung w i ll be
carried o n in spi te of the loss of t issue. However,i f i t occurs to too grea t a
degree,i t defea ts its own purpose. A s long as compensat ion occurs in these
high degrees of compensatory,emphysema a l l is well . The respira tory
func tion is carried on and l i ttle inconven ience is experienced on the part,
o f
the pa t ien t . The most serious th ing tha t can happen in these cases is for the
emphysema tous lung to become also the seat o f a tuberculous invo lvemen t,
o r a t leas t to become seriously invo lved . A s long as i t is free from tuberculo
sis,provid ing the changes in lung t issue are no t too grea t
,the function of
respira tio n may be carried o n ; but , i f i t becomes invo lved , then wemust expec t
D I SPLACEM E N T OF TH E TH ORACI C VI SCERA I
ser ious trouble. A no ther serious cond i tion results when the
-
ac im of the
lung which is the seat of compen sa tory emphysema become dila ted to such
a degree (become truly emphysema tous) that they are no longer able to per
form the fun ction s of resp iration .
Pat ien ts who have such cond it ion s should be apprised of
Man agemen t them and their l ives should be . so regulated that there is(
élf
gt
ffefifg the sma llest call made upon .the heart and lungs that is con
D isplacemen t. sisten t w ith a modera tely active l ife. They should n ever
aga in a ttempt to l ive stren uous“
lives, but by care they
may lead lives of usefulness . E xtra effor t should be made to keep the em
physematous lung free from tuberculous in fect ion or to cure i t as quickly
as possible if i t is already presen t .
Such person s should n ot live at a high al ti tude,n or should they undergo
severe physica l exertion . I bel ieve also tha t i t is very importan t tha t these
pa t ien ts should not gain too much weight or gain i t too rap idly, for this throws
extra burden upon the o rgan s of resp iration and/
circulation .
I t requ ires some sk ill at physica l exam inat ion in order to
giggl
in gbe able to outline the boundaries of these d isplaced organ s
,
D isplacemen t , yet i t is not so difficult but tha t any one who is accustomed
to examine chests can master i t with a little close appl i
cat ion to detail .
The ordinary methods of percussion and auscultation may be sufficien t to
outline the d isplaced boundar ies of these o rgan s,but if any on e wishes to
become expert at i t he may obta in much help from fam il iarizi ng himself with
o ther methods such as I have descr ibed in Chapter V I . For the heart I
would especially recommend auscultatory strok ing and percussion ,the author ’s
elastic tube percussion ,and E bstein ’
s percussion . For outl in ing the boun
dar ies of the lungs,auscultatory percussion and strok ing and elastic tube
percussion are of the greatest value. The find ings on percussion should
be proved by the stethoscope,beginn ing over an area kn own to belong to
the lobe in question and then fo llow ing it out, listen ing at every po in t un t il
the border has been reached . When the stethoscope is placed beyond the
border and over the o ther lung the chan ge in the character of the no te is usua llyeasi ly recogn ized . T his canbe apprec iated because one lun g is hypertrophied,the o ther con tracted
,and these two cond i tion s produce d ifferen t respira tory
no tes . The fluoroscope may be used to great advan tage in these cases instudying them in connection with ordinary methods of examination .
CHAPTER VI I I .
PROGNOS I S I N TUB E RCULOS I S .
The progn osis in a g iven case of tuberculosis, depends, fir st, upon the nature
and exten t of the disease ; secondly, the directing in tell igen ce by wh ich the
d isease is managed ; and thirdly, the character and determination of the
patien t .
There is great difierence l n the virulen ce of differen t bacill i .
Some are so virulen t that an in fection w i th relatively few
germs w i l l produce a grave disease. Such in fection s are
rapid in their course and destructive,in their na ture. O ther
in fections are of bacilli of such a low grade of v irulen ce that the organ ism
overcomes them en tirely,a cure resulting ; or,fa i ling this, ho lds the d isease
in check perhaps for years,a llowing i t to man ifest i tself on ly when the person
in fected has been reduced in v i ta l ity by some such cause as excesses,over
work, bad methods of living or some exhausting i llness .
I t is n ot at al l improbab le that tox insmake their way out of these ap
parently quiescen t foc i and exert a deleterious in fluence on the t issues with
which they come in con tact,especia lly upon those ly in g in clo se proxim i ty
to the foci ; wh ichmakes them more prone to become the sea t of in fec tion .
The exten t of the disease is a very importan t factor in prog
n osis . A l l things else being equal,the small er the area
invo lved the better are the chan ces of the patien t for improve
men t or cure. This can read i ly be seen when we bear in
mind the patho logy of the d isease. Of course the severity of the process, the
amoun t of tissue destroyed,and the comp lica tions presen t must a l l be con
sidered.
Tuberculosis has a tendency to spread from the original focus in the lung
to o ther tissues of the body ei ther adjacen t or remo te. The routes o f in fect ion
in these cases are the lymph channels, the air passages and the blood stream .
This advance of the d isease is opposed by the natural defenses o f the body .
The principa l pro tect ive agenc ies,so far as we know,
are found in the bodyfluids . So our p icture is tha t o f a mo re o r less constan t outbreak o f bac i lli
from the areas o f in fection with a simul taneous defensive movemen t upo n the
part o f the natura l pro tect ive elemen ts in the blood stream .
Here the same law comes in to play tha t governs in fection in general , viz
i f the bacill i are presen t in great numbers,o r i f the numbers are less but the
virulency great,o r i f the pa tien t ’s res ist ing power is low, then in fect io n w i ll
92
94 PULM ON ARY TUBE RCULO S I S
can no longer be true to their ca ll ing and ignore the great advan ces wh ich
have been made in recen t years in deal ing w i th th is d isease. I t is t ime to throw
off pessim ism,for i t has n o place. I t is t ime to d iscard ind ifferen ce because
i t takes away from the pa t ien t his chance of cure. Recogn iz ing the importan t
advances which have been made i n the knowledge of tuberculosi s dur ing
the last few years, wh ich have removed it from the rank of hopeless d iseases
and placed i t in the forerank of curable chron ic d iseases,and have
‘
demon
strated that from sixtv to n inety per cen t of those suffer ing from incip ien t
tuberculos is may be cured when tr ea ted in tell igen tly, the members of the pro
fession must assume a hopeful a tt itude and undertake the cure of th is d isease
w i th the same earnes tness that they show i n dealing with o ther curable mala
d ies .
N ot on ly is the respon sibility of diagnosis upon the fami ly physician,but
that of cur e as well . The great major i ty of cases of tuberculosis w i l l be'
treated by the fam i ly physic ian . Perhaps in few diseases does the result of
treatmen t depend more upon the med ica l man than in tuberculosis . T uber
culosis is a chron ic d isease which heals slowly,and
, yet, during a great portion
of the time the pat ien t does n ot feel i ll . The physician must have the pat ien t ’s
abso lute confidence and implici t obed ien ce. H e must be optimist ic,force
ful,desirous of mak ing the pat ien t happy and con ten ted
,but yet knowing
when and how to say“N o .
” H e must keep the pat ien t in terested un t i l the
cure,arrestmen t or o ther result is obtained . I f he wavers,shows discourage
men t or lack of confiden ce in the final outcome‘
o f the treatmen t,the effect
on the pat ien t is o ften very marked . A n intelligen t,cheerful , opt imist ic ,
con sc ien t ious physic ian who understands tuberculosis and the tuberculous
pat ien t is a great factor in the prognos is of this disease.
Pat ien ts do not always seek advice at the beginn ing o f the
d isease. Thev have n ot yet learned the importan ce of early
signs. Here again the fami ly physician should exercise his
rights. A s the guard ian of the health of the members o f
the fam i lies in which he is employed, there should be such a relat ion o f co n
fidence between the fami ly physician and his fami l ies that he would be ex
pected to cal l atten t ion to any ind isposi tion that he m ight n o te. H e should
watch with especia l care tho se ch i ldren who have . been exposed to dangers
o f in fect ion through in t imate assoc iat ion w i th a tuberculous pat ien t in pre
vious years . H e should tra in them to seek advice at the earl iest man i festat ion
o f susp ic ious symptoms no matter how sl ight they may be.
S ince i t has been demo nstra ted tha t an early d iagnosis in th is d isease is
very importan t and that the in i tiative must be taken by the pat ien t (except
when i t is taken by the fami ly physician as suggested above), i t seems to me
tha t the progno sis in th is d isease could be grea tly improved by fami l iari zing
a l l scho o l ch i ldren w i th the ear ly symptoms o f tuberculo sis and by emphasizing
PROGN OS I S I N TUBE RCULO S I S 95
the fact tha t in tell igen t aid given at the outbreak of these early symptoms
mean s a curing of the d isease m a“ large proport ion of in stan ces.
Wh i le the prognosm van es w ith the earl iness of the diagn osis,
_
and the respon sib i li ty rests with the affl icted to seek advice
when the early symptoms show themselves, yet a greater
respon sib il ity rests upon him'
in the cure of the d isease when
i t has on ce been discoveredu I always emphasize the po in t with my patien ts
that whether or not they sha ll get well depends largely upon their own in divid
ual effort . I have seen con sc ien t ious pat ien ts w ith the desire of their lives
so ben t upon cur e tha t every act coun ted for recovery . I have seen this deter
minat ion snatch them from what seemed to be certa in and early death . On
the o ther hand,I have seen ind ifferen ce and willful d isobed ien ce turn an
apparen t recovery to a hopeless end .
A n obedien t,in telligen t pa tien t w il l o ften make an un favorable prognosis
favorable, wh i le an ind ifferen t,w i llful patien t w i ll o ften throw away bright
chan ces.
Wh i le i t is the early c ase that o ffers the best prognosis, yet
those farther advan ced are n ot beyond hope. I n many
moderately advan ced cases and in some far advan ced,we
see a l l symptoms d isappear and the patien t again assume
l ife’s duties. I n many cases when this apparen t cure can n ot be a tta ined , an
arrestmen t of activity can be secured . This result,whi le n ot as fortunate as
an apparen t cure,is not in compat ible with a long and useful l ife. I n fact
,
many such w i ll go on to a final heal ing. I have known many pat ien ts who,
whi le unable to secur e an apparen t cure of their tuberculosis, st il l hav ing ano ld cav ity which con tinued to secrete a small amoun t of bac i llus-bearing
sputum, were yet able to lead a moderately active l ife w ith n o o ther incon
ven iente than that of clear ing out their cav i ty each morn in g . T0 be sure,
th is is n ot as desirable as an apparen t cur e, yet i t is often as favo rable a resultas can be obtained
,and one that offers much hope to those suffer ing from
advan ced tuberculosis.
Among the most importan t symptoms to bear in mind in
giv in g a prognosis in a given case of tuberculos is are those
upon the part of the heart . A good -heart is a very va luableasset to an individua l suffering from tuberculosis. Tuberculosis is an in flammatorv cond i t ion invo lvin g the lung tissue. Through its action as men tioned
prev1ously, new tissue forms, normal tissue is destroyed,blood vessels are
obli terated, catarrha l thicken ing of the mucous membrane of the air passages
results, the area of pulmonary c irculat ion is considerably lessened, hen ce the
heart 18 embarrassed . We must a lso add to th is mechan ica l embarrassmen tthe fact that the heart is un favo rably influen ced by the tox in s wh ich are
liberated l n the system,and also that the myocard ium partakes more or less
96 PULM O N ARY T UBE RCULO S I S
of the general muscular wasting of the system, and further that owing to co n
tract ion s which take place,the heart is pul l ed and twisted out of place and
bound down by adhesions and consequen tly compelled to labor under great
d ifficulties .
I f the heart withstands the effects of the tox ins, and adjusts i tself to the
obstruction in the lung and to these o ther influen ces, this w i ll add very much
to the progn osis. I f,on the o ther hand, the heart weaken s, the pulse becom
ingr apid and soft, the prognosis is less favorable if not posi tively un favorable.
A pulse which is much h igher than would be expected w i th the temperature
range, and does not respond,
to rest in bed w ith appropriate care,in a few
weeks ’ time, must be con sidered of un favorable prognostic import .
The condit ion of the digestive system is very importan t .
Fortunately many of the symptoms of which tuberculous
patien ts compla in on the part of their d igest ive systems dis
appear when they are placed under favorable condit ion s . However, where
there is presen t organ ic d isease of the a limen tary cana l,or where there are
fun ct ional d isorders which fai l to respond to treatmen t, the prognosis is bad .
I have seen pat ien ts do wel l in spite of grave d istur bances on the part of the
digestive system, yet, as a rule, progress is un satisfactory.without good digestion .
The amoun t of weight lost must be considered in connec tion
w i th the cause of such loss. I f a patien t has lost weigh t
because of an acute exacerbation of the process in the lung
which yields to proper managemen t in a reasonable time,i t is not serious.
I f th is loss has been associa ted with improper methods of l iving,i t w i ll o ften
be recovered readily upon a correction of them . I f itbe due to serious stomach
o r bowel trouble which does not soon yield to treatmen t , the prognosis is bad.
I f i t be due to chron ic toxem ia associated with cachexia, i t is very un favorable
for i t is but rarely that such a pat ien t can put on weight . A fai lure to put on
weight in spite of full d iet is also un favorable. I t is not at a l l uncommon ,
however, to find pat ien ts who have made enormous losses
,even to one- fourth
o f their body weight , steadily regain when they have been placed under
proper treatmen t .
We can place no rel iance on temperature except as i t suggests to us the presence of certain conditions. However,
a temperature wh ich does no t y ield to in tel ligen t trea tmen t within a few
mon ths is o f bad significance, fo r i t usual ly ind icates a serious invo lvemen t
o r a lack o f res istance. H igh tempera tures w i l l o ften yield to treatmen t in a
very sho rt t ime.
Tempera ture.
I nd ividual resistance is a lways an uncertain facto r . I t
ra ises some from the brink o f the grave to useful citizenship ;and i t (looms o thers who seem to have every oppo rtun ity for
rega in ing heal th , to qu ick and certain death .
I n dividua lResi stan ce.
98 PULM ON ARY T UBERCULO S I S
There is a class financiall y below the well- to -do who are
accustomed to comfortable homes, but with whom l ife is
st i ll a struggle. They do n ot w ish to be objects of chari ty
yet they are unable to meet the requ iremen ts necessary to wage a successful fight again st a long drawn out
'disease. These pat ien ts respond wel l to
treatmen t . They would be happy and con ten ted, but they have the ever
presen t burden of in suffic ien t funds staring them in the face. This lessenstheir chan ce of recovery . The greatest hope tha t we can offer th is class is to
d iscover the di sease in that stage when the cure can be accomplished most
qu ickly .
T emperament has much to do with prognosis. A bright,
cheerful, con ten ted patient, . who is will ing and anx ious to
do al l he can to get well, in creases his chan ces mater ially, while one who is
desponden t, pessim ist ic , determined to find fault with everything,and every
body,lessen s his chan ces of cure.
A patien t who is passive, and who does n ot exert himself,does n ot o ffer
as good a prognosis as one who has spiri t and determinat ion
Children seem to respond well to treatmen t for tuberculosis .
Young adults from the age of fourteen to twen ty seem to
Show a lowered resistan ce. The progn osis in the case of a girl at twen ty
according to my exper ience is as good as tha t of a boy at twen ty- three. The
girl Seems to be more mature. The greatest resisting power to the disease
seems to be from twen ty-five to forty—five, and I have found pat ien ts of these
ages y ield best results from treatmen t . M y experience with elderly ind ivid
uals has been tha t,though they develop the d isease more S lowly than younger
person s, yet, except in rare instan ces, they do no t seem to gain sufli cien t
immun i ty to overcome i t .
The effect of compl ications on prognosis must a lways be
considered . Any severe d isease has a tendency to lower
vital i ty and a id tuberculosis in its advance. The exten sion of the disease
to o ther organs a lso affects the progno sis. T uberculosis of the larynx has
long been con sidered as a lmost a hopeless compl ica t ion ,but recen t methods
o f treatmen t , together w i th early d iagnosis,Show it w i ll y ield . I am in the
hab i t o f look ing upon tuberculosis of the larynx when diagnosed early as a
serious but by no mean s fa tal compl ication .
Tuberculos is of the in test inal tract is co nsidered of grave prognos is, yet we
know from post-mo rtem evidence that i t a lso heals . M i ld in fect io n o f the
in test ines sho uld n o t necessarily co ndemn a man . I bel ieve that i f a fa ir
tria l were given many o f these cases , we m igh t change the prognosis . Here,the same as elsewhere, an early d iagno s is Should be made.
Temperamen t.
Age.
Compli ca t ion s
The o ccurrence o f hemo rrhage is looked upon verv di ll erH emo t sis .p y
en tly by d ifferen t o bservers . I n the grea t majo r i ty o f instances
PROGNOS I S I N TUBE RCULOS I S
no appreciable harm fo llows slight sp i tting of blood . Th is occurs in the
course of the disease-
in a very large percen tage of cases . I t is a lways an
indication for plac ing the pat ien t in bed and order in g abso lute rest ; and, _
if
heeded, a more severe hemoptysis may be avo ided .
Severe hemorrhages somet imes produce pneumon ia. They are sometimes
fo llowed by an exten sion of thed isease. I have r epeatedly seen mi l iary
tuberculosis fo llow them and end the pat ien t ’s l ife. Somet imes the S hock
fo llowi ng a hemoptysis is such as to destroy the patien t even a lthough the
loss of blood is insign ifican t . I have seen several such dea ths ; one occurr ing
the third day after a hemorrhage amoun t ing to about three or four oun ces,
in a patien t who had been progressing very favorably.
I n a small percen tage of cases hemoptysis proves fatal in stan tly. This
occurs in advan ced cases and is due to the erosion of a large vessel or the
rupture of an aneur ism .
I have seen some relief fo llow hemorrhage in a few cases . I n one in stan ce,
particularly, I remember a severe in flammatory cond i t ion accompan ied by a
most aggravat ing c ough wh ich had pers'
isted'
for five or six weeks,ended by
the spitting up of a few oun ces of blood . N evertheless,I can never look upon
i t w i th un con cern .
Pregnan cy is a very disastrous complication“
in tuberculosis,
espec ially where the d isease‘
is in an active state. Whi le
the mo ther may do wel l dur ing the period that she is carry ing the chi ld, yet
in a large percen tage of cases the d isease starts up w i th renewed t vigor after
delivery . I n many cases i t takes away al l chan ces of arrestmen t or cure.
There is a widespread bel ief among the lai ty, which is shared
to a great exten t by physic ian s, that the number of bac i lli
found in a field of themicroscope has some prognostic sign ifi
can ce. O ften we have pat ien ts tell us with great glee that
on ly a few bacill i were found in their sputum . This fact a lon e is of n o con se
quence. I t can be in terpreted on ly by taking in to con sideration the nature
and exten t “ of the tuberculous invo lvemen t in the lung . I t must be remem
bered that we are n ot sure where the spec imen exam ined comes from . I f i t
comes from a small ulcerat ing surface in a bron chus and is m ixed with o ther
mucus i t may have on ly a few bac i lli,while i f i t comes from within a large
cavity it may con tain many .
I f i t were possible to find some way of determin ing the virulen cy of bac i ll i ,i t would be of much value in progn osis . Fo llow ing out Sewal l ’s suggest ion
that short,thick bacil li are found in virulen t cases and long beaded bac i lli
in those of a more chron ic, hen ce less virulen t nature, I have made observa
t ion s and my experien ce tends to confirm his statemen t, a lthough we o ften
find bo th kinds of bacil li in the same case.
Pregn an cy.
I oo PULM ON A RY T UBERCULO S I S
One of the most unsatisfacto ry po in ts connected with the
trea tmen t of tuberculosis is the length of t ime necessary to
produce the desired result . I t is a great tri umph to be able
to cur e th is disease at all , so we must not be di sheartened,
but endeavor,through earl ier diagnosis and improved methods
,to shorten
the term of treatmen t . A n in cip ien t case may he apparen tly cured in from
three to six mon ths although there are very few who should be treated so
short a time as three mon ths . There are a -few who w i ll require even more
t ime than six mon ths. M ore advan ced cases secure arrestmen t or apparen t
cure in from six mon ths to one or two years, the average t ime being from
eight mon ths to a year. O ften times physicians,in referring cases to sanator ia
,
become too Optimistic and tell the patien t that two or three mon ths will cure
.them . This causes severe disappo in tmen t o n the part of the patien t when
he learns that the time required w i l l be longer.
102 PULM O N A RY T UBE RCULO S I S
spread by the bac i ll i wh ich come from d ischarges from tuberculous ulcers.
The principal sour ce of bac i lli is the sputum from the ul cerat ions in tubercul
ous lungs ; this becomes dry and then passes in to the atmosphere as dust to
be taken in to the body w i th the in spired air .
F luegge n o ted that there was a fine Sprayof sputum thrownout by the pat ien t during Cough ing, sneez ing and talk in g ;and
,by plac ing cul ture plates before the patien t he w as
able to prove tha t these li ttle droplets con ta in bac il l i ; and, after some observa
t io ns,he announ ced th is as
“one of the most common ways in which tuber
culosis is tran sm itted . Cornet, in the second ed i t ion of his book, examines
the droplet theory and gives some very importan t exper imen ts bearing upon
the theory . Plates were set before pat ien ts who were coughing,at a distan ce
of from one-half to one meter from the mouth . Laschtschenko found these
to con tain bacilli 4 times in experimen ts w i th 2 1 patien ts,Heyman I 4 t imes
in 35 patien ts, M oeller in half of 30 patien ts but on ly after an exposure of
five or six hours,Go ld ie in 60 per cen t of his exper imen ts after twen ty- four
hours’ exposure. B . Frankel had a n umber of pa tien ts wear masks for twen ty
four hour s,and upon 2 I 9 of these masks he found with in th irty- two days 2600
tubercle bac i ll i . I t has been reckoned that one pat ien t, suffering from advan ced
tuberculosis,w i ll by expectorating on ce an hour
,expecto rate
bac i lli a day. A fter con sider ing these fac ts, we must admit that the greatest
source of danger l ies in the expectorated sputum and that the great fear of
impalpable sputum wh ich has been engendered in some m inds has n o secur e
grounds for its foundat ion .
For many years the d irect inhalation theory has been ques
tioned and men have suspected the al imen tary tract as being
the porta l of en try . Behr ing has more recen tly advanced
the theory that in fect ion takes place in nearly a l l in stan ces
in chi ldhood during the m i lk us ing age, and that the cause is bovine bac i lli
ingested with the m i lk . Wh i le we must a l l admit that there is some danger
from this source, yet we canno t believe that even a large proportion of cases
are in fected in th is manner .
Tha t in fection frequen tly takes place thr ough bac i lli wh ich have been
swa l lowed,we bel ieve to be fa irly well establ ished ; but we bel ieve tha t the
source o f bac i ll i is usually some person and n o t an an ima l suffer ing from
tuberculos is . The tons i ls have a lso been establ ished as portals o f in fect ion ,
and a re bel ieved by some careful studen ts o f the subjec t to be the chief po rts
o f en try o f the tubercle bac illus .
Bac i ll i doWh ile i t is verv des irable to know the exac t man ner in which
n o t M ult iply bac i lli pass from o ne ind ividua l to ano ther in caus ing in fecOuts ide tio n
,as yet we canno t be po s itive. There are certa in th ings ,
the B ody.
however,wh ich we do know that and us in establ ish i ng an m
PROPH YLAX I S 03
tel l igen t prophylaxis . The most importan t of these is that'
tubercle bac i lli
do not multiply outside of the body . When on ce expectorated,they may
reta in their vi tality for many mon ths, -‘
but they w i ll not in crease in n umber.
The bac ill i which cause in fect ion in an indiv idual are the very same bac i lli
which have been expectora ted by some oneWho was suffer ing from tuberculos is .
I f,then
, the discharges from tuberculous ulcers, especially those from the
lungs,could “
be destroyed, the spread of the d isease would cease.
Pa t ien ts should be to ld that the danger of in fection lies in
the _ d ischarge from tuberculous ulcers and that if this is
properly co l lected and destroyed, danger of commun ica ting
the d isease to o thers is removed . I n tuberculosis ‘
of the pulmonary and
laryngeal form,the danger ‘ l ies in the expectoration . The breath is not
dangerous.
The patien t should not swallow the sputum lest i t cause tuberculosis of the
bowel ; and now that i t is generally ackn owledged that the a limen tary trac t
is a very importan t aven ue of in fect ion, we must recogn ize the possibil ity of
even rein fecting the lungs through , the'
bacil li that have been swallowed .
The patien t should be abso lutely c lean ly about his habits . N 0 man who
expectora tes bac i ll i should wear a mustache or beard and no woman should
wear a veil . The reason is obvious to al l .
Patien ts.
should avo id so i ling the hands with sputum and should wash
the hands and rin se the mouth frequen tly, especially before meals . They
should never expectorate in a handkerch ief which they use in w iping the
mouth,n ose or face, n or should they all ow their clo thing or bedd ing to become
so i led with sputiIm .
The importan t po in t in the care of sputum is to preven t it from drying,
un til i t has been destroyed .
"
Patien ts should therefo re expectorate in paper
sp it cups which can be burn ed or in cusp idors con ta in ing either plain wa teror some germic ide such as carbo lic acid, or b ichloride Of mercury combined
with tartaric acid, to render the sputum more so luble,or common lye ; and,
the con ten ts should be emptied in the sewer on ce or twice a day and the
cirspidor clean sed with bo i ling water .
When the patien t is away from his room,i t is quite a problem to knew
wha t is the best course to pursue in order n ot to make i t embarrassing for
him and yet not to allow h im to relax his care for the sputum,Thepocket
flask does not grow in favor in this country, al though i t is used/
quite general ly
on the con tinen t . I t seems to me that the least objectionable and the most
in con sp icuous method con sists in the use of smal l bits of c lo th , large enough
to receive one expectoration,or p ieces of tissue paper or Japan ese napk in s .
These Should be ,rcarr ied in one coat - pocket or one compartmen t of a smal l
Shopp ing bag. I n the o ther pocket or compartmen t should be fit ted a
l
r ubber
l in ing . A s the clo ths or papers are so i led,they should be placed in the rubber
Person a lProphylaxis.
104 PULM O N ARY TUBE RCULO S I S
pocket and kept there'
un ti l the patient reaches home,when they should be
bur ned . The rubber lin ing should be removed, c leansed and d isin fected.
The sur est enemy of the tubercle bac i l lus is l ight . Sun
light,according to Koch, will destroy bac i l li in from a few
minutes to a few hour s, acco rding to the thickness of the
mucus in which they are'
i
found. D ifluse light wil l also
destroy them,although i t requ ires longer . Cornet and
o thers have examined the dust of the str eets and foun d that it is free from
danger of in fection . There is practically no danger of in fection taking place
in the open air .
I t is probable that nearly al l cases of tuberculosis, resul tingTuberculosis from dust in fection , have been con tracted withi n the housea H ouse
D isease. (mean i ng house i n the broad sense of i n closure). O rdinari ly
for in fection to take place,there must fir st be a careless
pa t ien t to scatter bacil li , and then there must be an association with him i n
quarters under condition s which favor the preservation of the life of bacilli , or
a dwel ling in such quarters after the departure of the pat ien t. I t has been
shown that rooms frequen ted by patien ts occasionall y are n ot in fected, but
rooms occupied con stan tly by careless patien ts are dangerous.
Exper iments Show that the floor is the part of the room
which is the seat of greatest in fection ,and that nearly a l l
in fection in rooms is confined within two and one—half feet
of the floor
Coates (“An I nvestigation into the Presen ce of I n fect ive
M aterial in Dwell ings O ccup ied-
by Consumptive Persons .
”
Bri t ish Congress on T ubercul osis, Vo l . I I , page 88) col lected dust from
houses and inocula ted guinea pigs with i t to determine its in fectiousness.
Thr ee groups of homes were investigated .
I . Dirty houses occupied by con sumptives who were lax in caring for their
Sputum,spit ting ei ther in their handkerchiefs or upon the floor .
2 . Houses in a clean cond i tion occup ied by consumptives who were n ot
sufficien tly careful in d isposing of their Sputum .
3 . Very d irty houses in which consumpt ives had n ot lived for years.
Of 2 I houses in group I,I 4 or per cen t were found to be in fected .
Of the I 4 in fected homes l ighting and ven t i lation were bad in eight,fa ir in
one and good in five,whi le of the seven negative homes
,l ighting and ven
tilation were good in six and fair in one.
Of I O homes in group 2, the dust was in fectious in 5 , o r 50 per cen t . O f
the five in fec ted houses, l ight ing and ven t i la t ion were bad in two , fa ir in two
and go od in o ne,wh i le o f the negative houses a l l were wel l l ighted and ven
tilatcd.
Of 10 houses o f gro up 3 , no t a s ingle ino culat io n proved pos it ive, no
106 PULM O N ARY TUBE RCULO S I S
of a l l k inds (especia l ly alcoho lism and sexua l indulgence) which lower vital i ty
and make in fect ion easy ; or , if the d isease be a lready presen t,but qu iescen t
,
through these excesses condi t ion s are brought about which render i t morel iable to an outbreak . A n outbreak often fo llows d iseases such as measles
and la grippe. T herefore,i t is ur gen t upon the wel l to take precaut ions to
ma in ta in their resist ing power at par so that they may w ithstand disease,i f i t occurs . M odel tenemen ts are n eeded in al l cities . S tr ingen t factory
and workshop laws, looking to proper l ighting and ven t i lat ing,should be
passed . Construct ion of office bu i ld ings n eeds supervision to rule out poorly
l ighted and badly ven tilated rooms .
i
Schoo l rooms in wh ich our ch ildr en
spend SO much of their t ime should be models, demon stra t ing the proper
supply of light and air . Last but n ot least, our homes~
Should be con structed
so tha t al l rooms would be thoroughly flooded with light and so that pure air
would con stan tly circulate in to every corner .
Doubtless chi ldhood is the time when in fection o ccurs in a
83211211322nm grea t many individua ls (see Appendix, Chap . I I
,page
even though they n ever Show advan ced symptoms, or , if they
do,on ly after -many years . The child lives in an environmen t which is
most pregnan t with danger for this d isease. A l l people pet and caress
ch i ldr en and give them toys and sweetmea ts ; or,if they do not give
them to them,they handle those wh ich the childr en possess . Childr en l ive
near the floor in the env ironmen t wh ich is most apt to be in fected . They
play on the floor ; they constan tly put their hands'
from the floor in to their
mouths . I f there are bacilli on the floor,l i ttle Chi ldr en are l ikely to become
in fected .
Ch i ldren,therefore
,Should never l ive in the same room with careless con
sumptives, nor should they be under the care of persons suffering from tuber
culosis, and espec ially should they be kept from eat ing food which has been
prepared or handled by person s suffer ing from th is d isease. Too great pre
caut ion can n o t be taken .
Ch i ldren should receive greater care than is won t whi le they are grow ing
up. They Should be ass isted bv their paren ts in the forma t ion of good hab i ts .
They should be taught the S imple rules of hygiene. E spec ial ly Should they
be taught the necess i ty o f having l ight and fresh air in their rooms at al l
t imes and the va lue o f proper bath ing in main ta in ing a hea lthy o rgan ism .
There is a certain large number o f ch i ldren and youths whom
we are accustomed to say are predisposed to tuberculos is .
These i nd ividuals need mo re than o rd inary care. M any
o f them,as I men tio ned in ano ther chapter, are already
in fected and are su ffering from tuberculous toxem ia . I
bel ieve the t ime will so o n come when such cases w i l l be treated fo r tuber
culo s is ; fo r I have no do ubt tha t sc ience w i ll so o n fo rce us to such act ion .
PROPH YL'
AX I S 7
Those who are n ot infected, but who are delica te and unable to take their
part in the world ’s work
,should be taught the value of a natural
,open -air
l ife,w ith rest and ton ic measures. . Careful guidan ce of such ch i ldren for
a per iod'
of a fewmon ths or a few years at the proper time,
‘ 1w i ll make them
less prone to in fection and preven t -many of them from falling v ict ims to
tuberculosis .
The problem of the preven tion of tuberculosis must beM odernM ethods of attacked from two standpomts, that of the affli cted and thatPrOPhYIaXiS of the well . The affl icted must be cared for and the wellan d Cure.
must be guarded from i n fection .
The problems c on nected w ith the preven tion and cure of tuberculosis
have received much atten t ion in recen t years, and i t has been found tha t the
measures necessary for preven t ing the spread of the d isease are simple and'
humane. The tuberculous ind ividua l is n ot to be looked upon as a criminal,
he. is n ot to be trea ted as a leper, but as an un fortuna te human being who is
Suffering from a commun icable, preven table and curable disease. H e is n ot
necessarily dangerous to the well .
I f he is careful - and con scien tiofis in the destruction of his expectoration, ~
and l ives a hygien ic l ife, he is a perfectly safe compan ion ; nevertheless, i t is
inadvisable for him to assoc ia te in timately with chi ldren . A s eviden ce of
this secur i ty may be ci ted the fact that in fection a lmost never occurs in sana
toria, where the proper precaut ions are taken .
A lthough Brompton H osp i ta l,London ,
has treated more than fifteen
thousand cases of tuberculosis dur ing the past twen ty years, yet nei ther a
nurse, a physic ian nor an a ttendan t has become in fected . The same record
has been made in Fa lken stein and Goerbersdorf, Germany, and in the Adiron
dack Co ttage Sanator ium and Winyah in the Un ited S ta tes . Here we have
an in tima te association of patien ts and attendan ts for mon ths and years w i th
no in fect ion occurr ing . We can safely say, then, that tuberculosis is on ly
commun icable when the proper care is n ot used .
The first and most necessary measure for the preven t ion of
tuberculosis is educa t ion . There are so many erron eous ideas
about th is d isease that a thorough knowledge of i t is n ecessary in order to com
bat them . Some people foo l ishly refuse to accept the fact that tuberculosis is
a commun icable d isease and still cling to the o ld theory of hered ity . O thers
havecaught the idea of its commun icab i lity and fear i t as muc‘h as they would
smallpox, scarlet fever or diphther ia. Bo th a tt i tudes are wrong, but they w i ll
be main ta ined un til someth ing is offered in their stead . The idea of hered ity
must be abo lished . Tuberculosis is a lmost never inherited by the Chi ld from
the paren t . There are perhaps less than two dozen authen t ic cases on record
where children1
were born w i th tuberculosis . T rue,some ch i ldren are born
w i th less resist ing power than o thers ; some have constitut ion s more fra i l
E duca tion .
I 08 PULM ON ARY T UBE RCULO S I S
than o thers ; some have respir ato ry organ s more prone to disease ; but thed isease itself
, the in fect ion ,takes place after b irth . The bac i lli are grafted
on to these weakened const i tution s after they are born . A chi ld bo rn of a
tuberculous mo ther or fa ther is not necessar i ly doomed to die of con sumpt ion .
I n fact,most of, them do n ot. .These ch ildr en ,
however,run grea t chan ces
of becom ing in fected if they are a llowed to play in the rooms occupied by a
person suffering from tuberculosis or to play with the ind ividua l who is afli icted,
un less he be in telligen t and con sc ien tious in the care of his sputum . I t must
be remembered that the resisting power .of the child is not as great as tha t
Of the adult,so greater precautions should be taken with children . These
cases of supposed heredity are in stan ces where the chi ld was perhaps born
with a weakened con stitution ,and reared under un favorable circumstan ces .
The chi ld,perhaps
,became in fected by association w ith the diseased paren t
,
for i t must be remembered that very few of the to tal number of person s afflicted
with tuberculosis are taking the proper precaution s to preven t the spread of
the d isease. I t is not necessary for the disease to man ifest itself at on ce when
in fection takes place. I t is probable tha t tubercle bacil li are o ften taken in to
the system in childhood, yet cause few or n o n o ticeable symptoms un t i l later
in life,when the resist ing powers of the ind ividual are lowered . Then the
disease starts up with full force. N ot heredity but in fection is the cause of
tuberculosis .
There is one thing particularly favorable about the manner in which tuber
culo sis is conveyed from one person to ano ther,and that is
,that the in fectious
elemen ts are all found in the d ischarges from tuberculous ulcers and that
pract ically the on ly discharge tha t we need to con sider, in order to preven t the
spread of consumption,is that which comes from the lungs
,and which is
thrown Off as expectoration . I f this is destroyed,a thing no t d ifficult to do ,
there can be no spread of the disease. By proper education ,this should be
attained . The breath is not dangerous, nei ther is there any danger whatever
from close con tact . So there are abso lutely no grounds, except lack of under
stand ing,upon which this inordinate fear of tuberculosis, possessed bv some
people,can stand . Th is fear causes many foo lish things to be done. I t
works undue and unnecessary hardship upon tho se who are affl icted w i th
tuberculosis. I t causes them to be feared, and provokes unwise and un just
legisla t ion against them . N ei ther cruel ty nor inhuman i ty have any place in
deal ing with the question of the preven tion o f tuberculosis . I t can and wi l l
be preven ted by the people understand ing the true nature of the d isease.
Th is can come o n ly through education . The in terest and co -opera tion of the
peoplemust be secured through pamphlets, the press and publ ic lectures .
Tuberculosis Should be under heal th board con tro l . I t
sho uld no t be treated the same as o ther commun icable
diseases,but every individua l suffering from pulmo nary tuber
H ea l th BoardCo n tro l.
I 10 PULM ON ARY T UBE RCULO S I S
d ispen sary is a great help to the Health Board in tha t i t is carrying out the
very work tha t the Board desires . There are usually found l isted in the
d ispen sary the names of those individuals who are occupying the worst rooms,
in the poorest lodg ing houses,or who are huddl ed together wi th their fami lies
in con tracted un hygien ic quarters . S in ce the d isease is most common among
the poorer c lasses,its preven tion here mean s much toward S tamping out the
d isease.
A very importan t and practical method of educating tuber
cul ous pa t ien ts is by the class method .
'
A n umber of pat ien ts
are gathered together and then in structed en masse. Th is
very practical'
method has been successfully carr ied out in many places .
O ne advan tage of i t is that time can be saved . The physic ian or nurse can
instruct a dozen as qu ickly as he can one. I n teachin g these s imple truths
one essen t ia l is repeti t ion and where a n umber can be in structed together i t
affords time for th is .
An o ther importan t factor in preven t in g the Spread of tuber
culosis is the piibl ic sanatorium . These inst i tut io ns work
for the preven t ion of the d isease in many ways . I n the first place,they remove
patien ts from their homes where they may, thr ough ignoran ce or carelessness,sca tter in fection . Secondly
,they cure a large per cen t of the cases treated
in them (for they usually confine their efforts to early cases), and thus render
them in capable of fur ther spread ing the d isease. Thirdly,they return these
cur ed pat ien ts to their homes to con t inue the support of those dependen t upon
them,and in th is way n o t on ly save them from becom ing publ ic charges but
also thr ough render ing them better able to support their families,save some
of them from break in g down with tuberculosis . Fourthly, a l l patien ts who
return from a sana tor ium carry w i th them the new ideas of tuberculosis and
the measures n ecessary to preven t its spread . They a lso know how to l ive
in order to preven t and overcome i t . Great as are the o ther features o f the
sanatorium,perhaps its greatest good comes through the fac t that i t educates
tho se treated in i t as m issio naries who return to their former homes and teach
their friends how to live in order to preven t and cure tuberculosis.
N o t on ly are d ispensaries and sanato r ia needed,but hospita lsas well . Un fo rtunately
,many cases o f tuberculosis escape
detection un ti l they are so far advan ced that they can no t recover . The grea t
est danger Of in fection comes when the pa tien t is in the late stage Of the d isease.
A t th is t ime he is,as a rule
,expec to ra t ing more than at any o ther t ime. Owing
to weakness,many are no t as careful as they should be . They so i l thei r
c lo th ing,bedd ing and whatever comes in co n tac t w ith them . E spec ia lly is
th is true amo ng those who are igno rant . I f such ind ividuals l ive in crowded
quarters, where they must have thei r friends and the members o f their fami l ies
asso c ia ted w i th them ,they a re apt to in fect them . Fo r such cases there should
Classes inTubercul o sw.
S an a tor ia .
H ospital s.
PROPH YLAX I S I I
be,
hospita l accommoda t ions, a place where they may be taken ,in order that
their last days may be made free from suffering and that they may n ot in fect
o thers .
S in ce it has become known that tuberculosis is Commun icable,“
some people have become imbued with such a fear of the
d isease tha t they are afra id to en ter a place frequen ted by
those suffer ing from the d isease. They would hes i tate
to v isi t a d ispensary, a hosp i ta l or sanatorium for tuberculo
sis lest they should become in fected . These same people o ften live w i th
tuberculous ind iv iduals, who th ink they have on ly “ throa t trouble”or bron
chial trouble they w i ll occupy a room in a ho tel or lodging house which.
has
prev iously been occup ied by a con sumpt ive and which has never been fum i
gated ; they w i ll dr ink from a publ ic cup which has just been used by a con
sumptive ; yet, they would n ot even visi t one of these in st i tution s frequen ted
by tuberculous pa t ien ts, who know they have the d isease and who are careful
to destroy their Sputum . The most dangerous con sumptive is the one who
ei ther does not kn ow that he has the d isease or'
who tries to deceive himself
and make himself believe that he does n ot have i t . H e is dangerous because
he w i l l n ot take precautions . On the o ther hand the one who knows that he
has the d isease, and takes the proper precaution s,is a perfectly safe com
pan ion w i th whom to associate.
Some mun icipalit ies, even hea lth resorts, which are frequen ted by hundreds
_
of con sumptives annua lly, fear to see these beneficen t in st i tution s established
in their m idst . T h is is due to a faulty understand ing of the d isease. Such
in stitu tion s should be welcomed because they canno t possibly be a menace,
but on the o ther hand,they w il l educate the tuberculous patien ts who are
treated there so that they w ill c ease to be a danger . H ow much better i t is
to have the poor con sumptives who l ive in a commun i ty a ttend a d ispen sary
and receive in struction rather than to ign oran tly in fect the lodging houses
and homes occup ied by them . H ow much better is i t to have the curable
cases in a sanatorium where they may have a chan ce to get well and where,in any even t, they w i ll be in structed in the manner of r ight l iving and the
measures necessary for the preven t ion of the spread of in fection . H ow much
better is it to have the advan ced cases in hosp i tals where they w i ll receive
proper atten tion and where they w il l n o t give the disease to o thers rather
than to have them occupyin g and in fect in g their i lly adapted a nd Often over
crowded quarters . Such in sti tut ions are nei ther a menace to a commun itynor to those who live in them. On the o ther hand
,they are blessings to a
commun i ty ; for , they remove from homes, lodging houses and ho tels those
who are diseased,and thus take away the danger of spread ing tuberculosis
in the commun i ty.
That such in st itution s are n ot dangerous to the commun ities in wh ich they
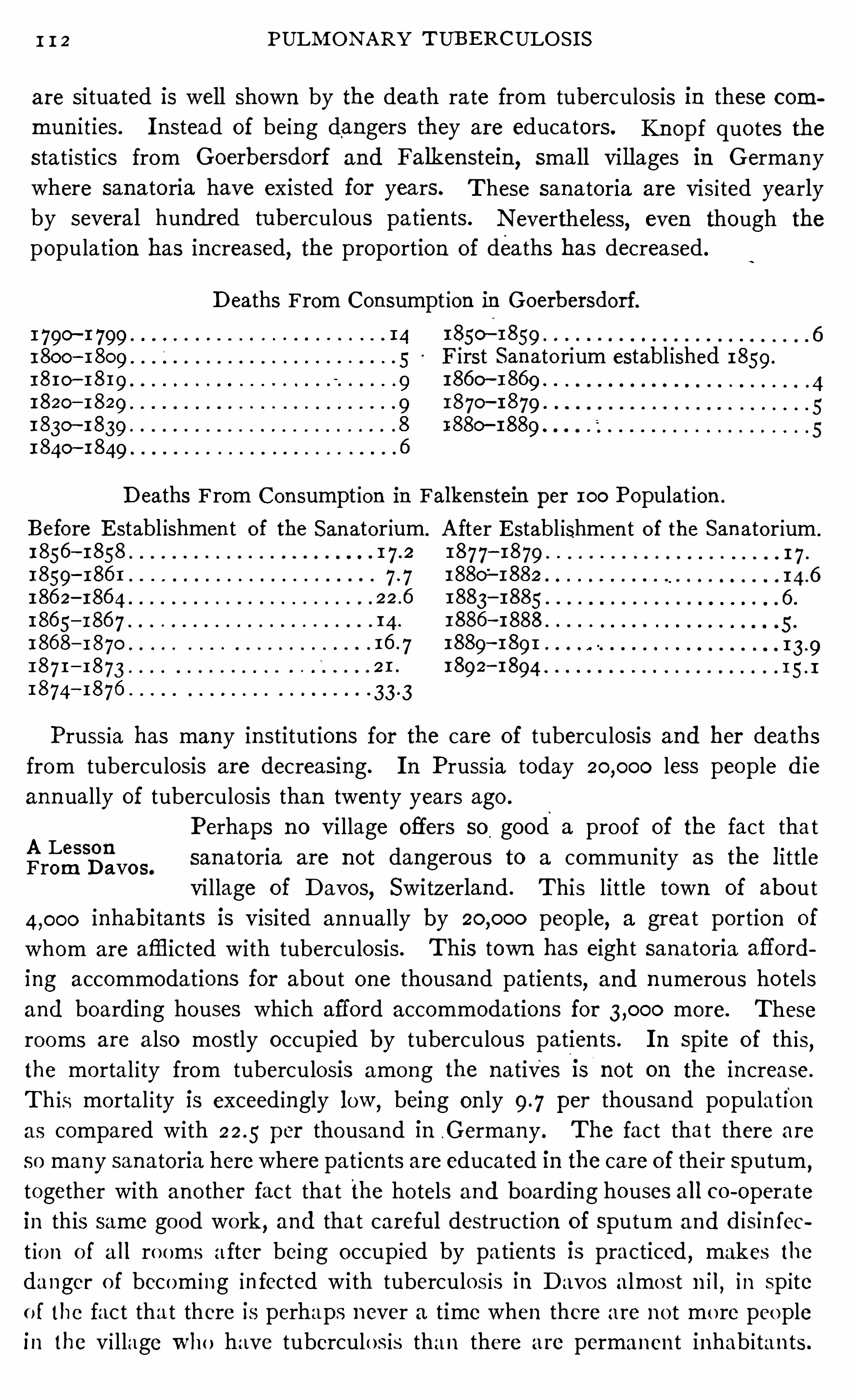
1 1 2 PULM ON ARY TUB ERCULO S I S
are si tuated is well shown by the dea th rate from tuberculosis in these com
mun ities . I nstead of being dangers they are educa tors. Kn opf quo tes thestat istics from Goerbersdorf and Falkenstein
, sma ll vi l lages in Germany
where sanatoria have existed for years.
by several hundr ed tuberculous pa tien ts.
These sanatoria are visi ted yearly
N evertheless, even though the
population has in creased, the proportion of deaths has decreased .
D eaths From Con sumpt ion in Goerbersdorf.
1 790—1 799 14
1800 51810—1819 91820— 1829 91830
—1839 8
1840- 1849 6
1850—1859 6
First Sanatorium establ ished 1859 .
1860- 18691870
—18791880- 1889 i
D eaths From Con sumpt ion in Falken stein per 100 Populat ion .
Before E stabl ishmen t of the Sanatorium.
1856—1858
1859—186 1
186 2—186 4186 5
—186 7 14 .
186 8— 1870
187 1— 1873
1874—1876
A fter E stabl ishmen t of the San atorium .
1877—1879 1 7 .
1880—1882 L4 .6
1883—1885 6 .
1886—1888 5 .
1889—1891
1892—1894
Prussia has many in stitutions for the care of tuberculosis and her dea ths
from tuberculosis are decreasing. I n Pruss ia today less people die
ann ually of tuberculosis than twen ty years ago .
Perhaps no vi llage offers so good a proof of the fact thatA LessonFrom D avo s. sanatoria are not dangerous to a commun i ty as the l ittle
vi llage of Davos, Switzerland . This lit tle town of about
inhab i tan ts is visi ted annually by people, a great portion of
whom are afflicted with tuberculosis. This town has eight sanatoria aflord
ing accommodations for about one thousand patien ts, and n umerous ho tels
and boarding houses which afford accommodations for more.
rooms are a lso mostly occupied by tuberculous patien ts .
These
I n Spite of this,
the mortal ity from tuberculosis among the natives i s not on the in crease.
Th is mortal i ty is exceed ingly low ,being on ly per thousand population
as compared with per thousand in .Germany . The fact tha t there are
so many sanatoria here where pa t ien ts are educated in the care of their sputum ,
together with ano ther fac t tha t the ho tels and boarding houses al l co -Operate
in this same good wo rk,and tha t careful destruction of Sputum and disin fec
t ion o f a l l ro oms a fter being occup ied by pa tien ts is practiced,makes the
danger o f becom ing in fected with tuberculos is in Davos almost n il,in sp ite
o f the fac t tha t there is perhaps n ever a time when there are no t mo re peoplein the vi llage who have tuberculo s is than there are permanen t inhab i tan ts .
CHAPTER X .
TH E PR I N CI PLE S UN DE RLYING TH E TRE ATMENT
OF TUBE RCULOS I S .
Perhaps there is n o o ther ser iods d isease so curable as tu
berculosis, i f trea ted early ; and few more fatal . if a l lowed to
extend. I t is within truth to say tha t sixty-five people out
of every hundred have tuberculous foc i .in some organ or o rgan s of the
body,some t ime during their l ives, and yet on ly about twelve or fifteen out
of every hundr ed die because of their tuberculosis . Th is mean s that tu
berculosis proves fata l in scarcely 20 per cen t of the in stan ces in which in
fection has occurred .
I f we seek the cause of the cure in these cases, we find that most o f the
cures occurr ed in pa t ien ts where the lesion s were Smal l ; and, i f we could
know mo re of the history of the in fect ion , we would doubtless find that
where the hea ling o ccurred there was a great disparity between the vi ta lity
o r numbers of the in fectin g micro -organ isms and the res ist ing power of the
patien t . A person with a low resist ing power migh t become in fected with
bac i l l i of low viril ity or with sma l l numbers ofm icro -organ isms while a per
son w i th no rma l resist ing power might overcome the same in fection ,and a
person with great resist ing power might overcome many bac i ll i even o f a
virulen t stra in .
When an in fect ion o ccurs with bac ill i o f a low virulen ce there is a tend
en cy to heal ing ; in fact, this rule is so gen era l that S t'
ork (T ran saction s o f
Co ngress on Tuberculosis,V ienna
,1907) has been able to produce a c irrhos is
in an imal experimen tat ion in nearly every in stan ce, by the in jection o f bacill i
whose virulen ce had been lowered . O n' the o ther hand
, where the v irulence
is great necrosis is the rule. I t was formerly taugh t tha t the necrosis o f the
tubercle was due largely to the fact that the tubercle was poorly suppl ied
w i th blo od -vessels,but the best author i ties tod ay, are of the opin io n tha t the
n ecro sis is due to the act ion o f the tubercle tox ins , and tha t the cutt ing o ff
o f the blood-vessels is a mere in ciden t , w i th l i ttle i f any primary effect upon
the tubercle .
The na tural tenden cy of an in fection with few bac il l i o r with bacil l i o f low
virulence is toward hea l ing . Such an in fect ion stimulates the cel ls to the
fo rma t ion O f new t issue and tends to healing by the product io n of fibro sis .
Such in fectio ns may prove fatal , however, if the res isting power o f the
pa tien t is low .
Curabi l i ty o f
Tuberculo sis.
PR I N CI PLE S UN D E RLYI N G TH E TRE A TM E N T OF TUBE RCULO S I S I I 5
The natura l tenden cy of in fection w i th large numbers of bacill i or w ith
highly viru len t bac i ll i, on the o ther hand, is toward n ecrosis . Such an in
fection sets free large quan tit ies of toxin s or toxin s o f such po ten cy as to
cause a rap id necros is of the surround in g cells.
Such in fection s may be overcomei
if the resistin g power of the pa tien t be
great enough .
These facts may be summed up by. the statemen t tha t where the bac ill i
are the chief fac to rs, as in the exper imen ts of S tork men t ion ed above, the
tenden cy is con servat ive and where the toxin s are the Chief factors the tend
.en cy is destructive . A s further proo f of th is statemen t migh t be c i ted the fact
that dead bac i lli (bein g less tox ic) Show more of a tenden cy to the forma t ion of
conn ective tissue and less tenden cy to cheesy degen era t ion than live bacil li .
The cur e Of tuberculosis con sists in establishing upon the part
of the in fected organ ism an immun ity to the tubercle bac i llus
and its toxin s . N o matter whatmethods of treatmen t are em
ployed,if a cure results, i t isdue to this cause and to th is alone.
I n this respect tuberculosis differs / in no wise from o ther diseases of bacteria l
o rigin . The cure of al l bacter ia l d iseases depends upon the favorable action
of the machinery of immun ization . I f a cure results,immun ity is presen t
,and
.the cure is due to the immun i ty, a lthough it may be very tran sitory as is no ted
after pn eumon ia,or somewhat more lastin g as is seen fo llow ing d iphtheria
,or
i t may be qu ite permanen t as we find it after sma llpox . A cure,no matter
how tran sitory,in diseases of bacter ia l origin is syn on omous w ith immun i ty .
I n order to have a comprehen sive understand ing of the treatmen t of tuber
culosis i t is necessary to bear th is in m ind . When we kn ow neither the na ture
of the d isease n or the mann er of its cure our therapeutic efforts must be empir
ical,but where bo th are kn owh, therapy can be made a scien tific procedure .
There are many in tr icate problems connected w i th the estab
l ishmen t of immun ity . Some of them are understood wh i le
o thers are still un so lved.
I t is impossible to comprehend the treatmen t of any in fectious disease
without understand ing the phen omena associated with the establ ishmen t of
immun i ty ; therefore, in order to make plain the d irection that our efforts Should
take in the treatmen t of tuberculosis we Shall find it profitable to inqu ire some
what in to the phen omena wh ich occur when an in fection takes place.
The common idea of immun i ty,that of pro tection from d isease
,ei ther natura l
or acquired,is n ot the con ception that we wish to emphasize. The termas
used in modern sc ien t ific medic ine has a broader mean ing . I t mean s tha t
state or cond i t ion result ing from an effort upon the part of the organ ism to
pro tect itself fromi‘some forei'gn substan ce by the format ion w i th in i tself of spe
cific pro tective bod ies. Such an immun i ty may be partia l or complete ; i t
may be tran si tory or i t may be permanen t .
H ow Immun i tyis Produced.
I I 6 PULM ON ARY T UBERCULO S I S
The production of immun ity is a chemical process,and is due to a reaction
upon the part of the inoculated organ ism in respon se to the stimulat ion of
some foreign elemen t . I n in fectious d iseases this st imulation is furn ished by
the specific micro -o rgan isms which produces the disease.
When specific micro -organ isms gain en tran ce to the body tissues a s tr uggle
for mastery at on ce ensues . Some of the bacteria are destroyed by the an t i
bod ies which are norma lly found in the tissues ; and these bacteria which have
been destroyed stimulate the body cell s to the formation of more an tibod ies .
Thus the machinery of immun ization is set in mo tion . Whether the bacteria
or the organ ism wil l conquer depends upon the number or virul en ce of the
bacteria on the one hand and upon the response of the body cells to the stimu
lation on the o ther . The an tibod ies which are produced as a result of this cel l
stimulat ion are of several differen t k inds . An titoxin s, lysin s, agglutin ins,
precipitins, coagul in s and opson in s have been studied so far,and there may be
o thers that are as yet undiscovered .
I t is very importan t to know that these specific an tibodies can be produced
not on ly by the - inocula t ion of l iving virulen t bacteriabut by bacteria which
have been k i lled . The on ly essen tia l is that the chemical elemen t in the bac
teria which calls forth the elaboration of the an tibodies remain s in tact . Exper i
men ts carried out with dead staphylococci,typho id bac i lli
,vibrio of cho lera
and products made from tubercle bacilli Show tha t they stimula te the organ ism
to the formation of the very same immun izing elemen ts as are produced by
the l iving micro -organ isms . Thus we may by vaccina t ion w i th dead bacter ia
or bacterial products set the physio logical machinery of immun ization in to
act ivi ty and immun ize our patien t .
Ano ther fundamen tal prin c iple i n immun ity is that the an ti
bod ies resulting from an in fection or from a vaccination - are
specific for the micro - organ ism which set the machinery
of immun ization in mo tion and_ caused their elaboration . Thus typho id
bac i l li cause typho id an tibodies ; staphylococci, staphylococcus an t ibodies, and
tubercle bacilli or tubercle vaccine cause an tibod ies for the tubercle bac i llus .
N ormalWhile I do not know whether or not any experimen ts have
H eal th Offers been made to determine by ac tual measuremen t the relativeto resist ing power of individuals in no rmal health and those with
’
lowered vital ity, yet, i t stands to reason that a man in no rma l
hea l th should be less prone to in fection than when in il l health . I t a lso seems
but commo n sense tha t a man whose nutrition is good, should o ffer mo re res ist
ance to a d isease than o ne whose nutrition is low
Wi th this brief d iscuss io n o f na tu re ’s method o f curing in fect ious d iseases ,
we can n ow in tell igen tly approach the subjec t o f the treatmen t o f tuberculo s is .
We can understand na ture’
s method and we can est imate the part played by
each Of the var io us measures wh ich we employ .
An tibodiesSpecific .
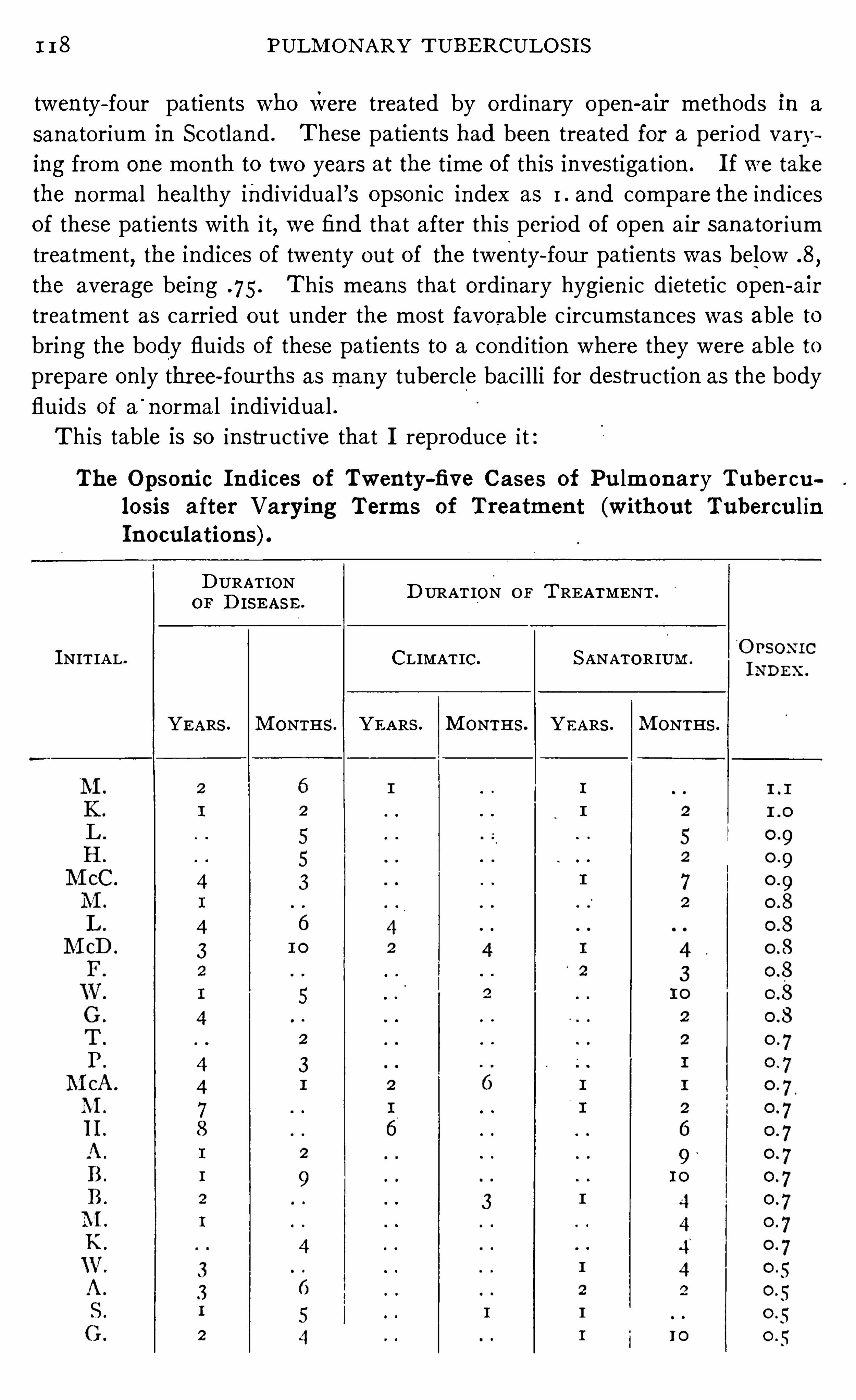
I I 8 PULM ON ARY T UBE RCULO S I S
twen ty- four patien ts who were treated by ord inary open-air methods in a
sanatorium in Sco tland . These patien ts had been treated for a per iod varying from one mon th to two years at the time of this investigat ion . I f we take
the n ormal healthy ind iv idual ’s opson ic index as I . and compare the ind ices
of these pat ien ts with i t, we find that after this per iod of open air sana tor ium
treatmen t,the indices of twen ty out of the twenty- four patien ts was below .8
,
the average being .75 . T his means that ordinary hyg ien ic d ietetic Open - a ir
treatmen t as carried out under the most favorable c ircumstan ces was able to
bring the body flu ids of these patien ts to a cond i tion where they were able to
prepare on ly thr ee- fourths as many tubercle bac i lli for destruction as the body
flu ids of a'
norma l individual .
This table is so instruct ive tha t I reproduce i t
The Opson ic I n dices of Twen ty-five Cases of Pulm on a ry Tuber cu
l o sis a fter Varying Term s of Treatmen t (W ithout Tubercul inI n ocul ation s).
D URATIOND URAT ION o r T RE A TM ENT
OF D ISE A S E .
I NIT IA L . CLIMAT IC. S ANATOR IUM .
YE ARS . M ONTHS . YE A RS . M ONTHS . YE ARS . M ONTHS .
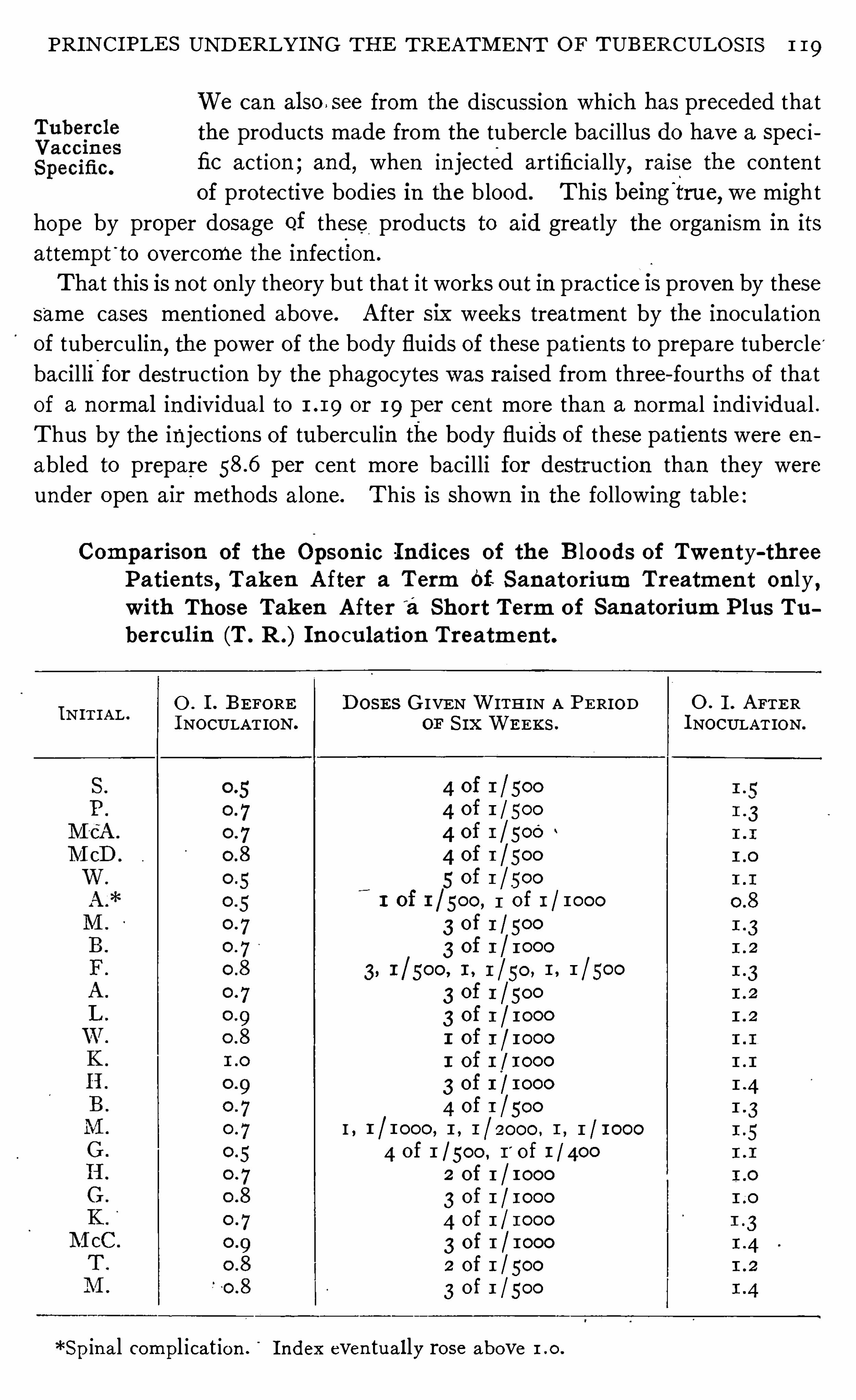
PRI N CI PLE S UN D E RLYI N G TH E TRE ATM E N T OF TUBE RCULOS I S 1 19
We can also see from the d iscussion which has preceded tha t
the products made from the tubercle bac i llus do have a spec i
fic act ion ; and, when in jected art ific ia lly, ra ise the con ten t
of pro tective bod ies in the blood . This being‘
true, we might
hope by proper dosage of these products to aid greatly the organ ism in its
attempt'
to overcome the in fection .
That this is n ot on ly theory but that i t works out in practice I S proven by these
same cases men tioned above. A fter six weeks treatmen t by the in oculat ion
of tuberculin,the power of the body fluids of these pat ien ts to prepare tubercle '
bacil li-
for destruction by the phagocytes was raised from three- fourths of tha t
of a normal ind ividual to or 19 per cen t more than a normal ind iv idual .
Thus by the injections of tuberculin the body flu ids of these patien ts were en
abled to prepare per cen t more bacilli for destr uct ion than they were
under open air methods a lone. Th is is shown in the fo llowing table
Compar ison of the Opso n ic I ndices of the B lo ods of Twen ty-threePatien ts , Taken A fter a Term Of S an ato r ium Tr eatmen t on ly ,w ith Those Tak en A fter
’
a Shor t Term o f San ator ium Plus Tu
ber cul in (T . R .) I n o culation Tr eatm en t.
0 . 1. BE FORE D OSE S G IVEN WITH IN A PE RIOD O . I . A FTE RI I AI N T LI NOCULAT ION. OF S I X WE EKS . I NOCULAT ION.
*Sp in a l compl icat ion . I ndex even tua l ly ro se above
4 0f 1 / 5004 0f 1 / 500
4 0f 1 / 500 ~
4 0f 1 / 5005 0f 1 / 500
I of 1 / 500, 1 0f 1 / 1000
3 of 1 / 500
3 0f 1 / 1000
3 of 1 / 5003 0f 1 / 1000I Of I / I OOOI of 1 / 1000
3 of 1 / 1000
4 0f 1 / 500I , 1 , 1 ,
4 of 1 / 500 , I'
o f 1 / 4002 of I / 10003 0f 1 / 1000
4 of 1 / 1000
3 of 1 / 10002 0f 1 / 500
3 o f 1 / 500
20 PULMO N ARY TUBE RCULO S I S
The trea tmen t of tuberculosis is not a S imple matter . I t
is one which requires great skil l and resourcefulness on the
part of the physic ian . Best results can be obtained on ly by
careful indiv idual izat ion . The phthisio therapist Should be wedded to no
ido ls . H is on ly desire should be resul ts, and these obtained in the shortestt ime w ith the least in conven ien ce to the patien t . H e should be conversan t
with al l measur es of value and know how to employ them with sk i ll and in tel
l igence. H e should n ot be a thoughtless fo llower of any method, be i t fresh
air , d iet, hydro therapy, drugs, cl imate or tubercul in ; but , he Should be an in tel
l igen t con scien tious physician who knows the va lue and l imitat ions of thesevarious measur es and who so combines and employs them that his pat ien t
is given the benefit of al l . N o thing Short of this can be considered a rationa l
treatmen t of tuberculosis.
A fter al l has been sa id about the treatmen t of tuberculosis,i t
is the method of applying the various measures, the techn ique
that coun ts most . I t is not freshair,but fresh a ir applied
under the proper conditions ; n ot hydro therapy, but hydro
therapy suited to the pat ien t and the disease ; n ot tubercle vacc ines, but
tuberc le vaccines adm in istered at the proper t ime and in the proper dosage ;n ot hyperemia but hyperemia most carefully admin istered a fter a Certaindefin i te techn ique ; not the sanatorium, but the carefully regulated sanator ium
where al l measures are combined un der the most favorable circumstances to
cure tuberculosis . A s the surgeon emphasizes techn ique,so must we em
phasize exactness of method and atten t ion to details in the carrying out
o f the various measures which are of va lue in combating tuberculosis . I n
our judgment of measures we must bear in mind ~ that the originator may be
a l it tle en thusiast ic ; but we must also remember tha t he has, as a rule, by
careful trial arrived at a method, developed a techn ique which o ften means
much and not in frequen tly mean s everything for the success or fa i lure o f
the measure.
We not infrequen tlv hear men say that they can not secure the favorab le
resul ts tha t are reported by o ther observers by the use o f open air . Usua l ly
a careful inqu iry shows that the case was beyond cure or the measure ape
pl ied in a faulty manner .'
T ubercul in was almost lost to tho se suffering
from tuberculo sis simply by faulty techn ique in its admin istrat ion . H ow
many men have thought that they were using hydro therapy as suggested by
Win tern i tz and Baruch,or hyperem ia , as suggested by B ier, on ly to find,
when they saw these methods appl ied properly,tha t they were o n lv us ing
wa ter in the o ne case and co ngest ion in the o ther !
I t is natural fo r a sc ien tific man to have co nfidence in his own ab i l i ty to
do the wo rk o f o ther men and to judge the results, but he should no t con
demii a measure simply because he does not succeed with it . H e must be
Ra tion alTrea tmen t.
CH APTER X I .
TH E OPE N -A I R TRE ATME N T OF TUBE RCULOS I S .
The open -air treatmen t of tuberculosis marks one of the greatest advan ces
in modern therapeut ics . Wh i le i t is simple and sen s ible, yet, when enuncia ted
,
i t was revo lut ionary . E ven today it is not ful ly appreciated and on ly imper
fectly carried“
out by many of our foremost physician s. Patien ts suffer ing
fr om tuberculosis have frequen t attacks of bron chia l ca tarrh . They ascribe
i t to “ catching co ld ;”
and, if left to their own in cl ination s, they are prone
to shun the fresh air , avo id all possibi lities of con tact w i th draughts, shut them
selves up in close superheated rooms and clothe themselves in impermeable
chest pro tectors and a superabundan ce of the warmest cloth ing tha t can be
found .
With this as the un iversally recogn ized method of dealing
gir
fss
t
h A “ with this d isease,i t took a brave man to fir st advo cate putting
Recommen ded these pa tien ts in to the open air . George Bodi ngton ,ofWar
wickshire,E ngland
, in . 1840, made'
the startl in g sta temen t
that : “Co ld is never too in ten se for a con sumptive patien t ;
the apartmen t should be kept well a ired,so that i t should resemble the
pure air of the outside,pur e air being used in the treatmen t as much as
possible.
” Of course such doctrine was not readily received . H e was
maligned and con sidered to be an in sane crank by bo th his con freres and
the la i ty . So b i tter was the persecut ion upon the part of the med ica l pro ies
sion that patien ts were afra id to stay in his insti tution ,in spite of the fact that
he was help ing them whi le his con freres were allowing their patien ts to go on
to certain death .
While the doctrine o f the open -air cure of tuberculosis was enun ciated morethan sixty years ago , and while i t has been advocated by tuberculosis spec ial ists
fo r the past quarter o f a cen tury, yet its full sign ificance is not yet understood
by our pro fess ion .
The fresh air cu’
re has its l imitations. Fresh air is no t a
Fresh A ir n o tSpec ific.
specrfic for tuberculos is, but i t w i l l work marvelous changes
in pat ien ts who are taken from the common walks o f l ife w i th
their unhyg ien ic methods o f l iving , and a llowed to remain in i t day a fter dayand n ight after n ight . I ts effec t is least marked upon those who have been
l iving o utdoor lives and have developed tubercul osis in sp ite o f i t .
1 22
TH E OPE N -A I R TREATM E N T o r TUBE RCULOS I S 23
Before en tering upon a d iscussion of the methods of applying
the open -air treatmen t i t is pert inen t to stop and ask : What
is the effect of open air upon the tuberculous process or upon
the ind ividua l afi‘
i icted w i th tuberculosis?
Whi le we recogn ize that the brea thing of impure air such as is found inimperfectly ven t i lated rooms I S in jur ious and apt to produce d iseases of the
respiratory tract, we no te th is in healthy individuals as well asin tho se in fected
Wi th tuberculosis . I t seems that the greatest detr imen t in breathing such
air is no t the effect upon the lungs, but the effect upon the general con stitution ;and, the effect is not so much upon the tuberculous process as upon the tuber
culous individual . The brea thing of in fected air m ight produce a secondary
in fect ion in the lung but, except ind irectly,even th is would n otbe an effect upon
the tuberculous process . A s the prin c ipa l effect of breathing vitiated air is the
general lowering of'
v i ta l ity of the tuberculous ind iv idual so the pr in c iple effect
of the open -air cure is the impression which is made by it upon the phys io logical
processes of the o rgan ism whereby a better state of nutrition is produced .
When fresh air has done its best, the resisting power of the pa tien t as measured
by the spec ific opson ins presen t, is sti ll low as is shown by table quo ted from
Lawson and S tewart (see page
H ow OutsideWe hear so much about the open an that i t might be well to
an d inquire wherein the outside air differs so much from in side
Egg:Air
air . By hearing the expression open air ”so frequen tly used,
we are apt to think tha t the on ly place su i table for trea ting
tuberculosis is out of doors . This is n ot necessari ly true. The essen t ia l
elemen t in the open—air cure of tuberculosis is a con stan tly'
changed air
so that the patien t is not required or permitted to rebreathe the same
air . This object can be attained in properly ven t i lated bu i ldings as well as
in out of door shacks and“
ten ts. I n order to meet this demand. best, rooms
should be placed in a s ingle row with open corridor behind (see plan of Bo tten
ger Sanatorium,page I n homes, corner rooms wi th w indows on two
s ides can be ut i lized . Un less therebe a good cross ven t ilation , the air of rooms
w i ll not approach the outsi de air in purity .
I t was believed formerly that the value of the open -air treatmen t depended
upon the fact that patien ts so treated were supplied w i th a greater vo lumegof
oxgyen , and, that they escaped the po isonous effects of carbon ic acid as found
in rooms which are imperfectly ven tilated . Some recen t experimen ts have
been made, however, which seem to show that these factors are n ot so sig
n ificant as was formerly believed and that the benefits of open -air treatmen t
depend in a great measur e upon o ther factors.
Air wh ich is kept in mo tion is purer than air which stagnates, and I believe
that this is the greatest objection to the ord inary home,and
,I am sorry to
say, even to rooms in some sanatoria . They are so con structed that ven tila4
1 24 PULM ON ARY T UBE RCULOS I S
t ion is imperfectly carried on ,and the air does n ot change w ith suffic ien t
rap id ity to furn ish the pat ien t w i th a constan t supp ly of fresh a ir .
I t has been shown tha t the air taken from o rd inary rooms con ta in s more
bacter ia than that from the open . T h is is n ot surpr ising when we con sider
the imperfec t unscien t ific manner in'
which ven tilation is cared for in the con
struct ion of our modern build ings, but I cannot see why there shouldbeany ap
preciabledi fferen ce in the air of a room thoroughly ven t i lated by cross ven ti la
tion and tha t taken from the outside. I have had the opportun ity of testing
the comparative results of the open air such as is found in bunga lows (see plan ,
page and in thoroughly ven tilated rooms, on severa l hundr ed pat ien ts
suffer ing from tuberculosis in a l l’
stages, and I can see n o d ifferen ce in“
results.
From the standpo in t of air,I do not bel ieve tha t the One has any advan tage
over the o ther . I t goes without saying, however, tha t there is an advan tage
in open shacks and bungalows over improperly ven t i lated rooms .
By placing pa tien ts in the open air we accustom them to the
various cl imatic changes. When properly carried out, the
open or fresh'
a ir trea tment of tuberculosis requ ires tha t
pat ien ts be kept in_fresh air
'
al l the time. T hey are taught to
endure co ld . I n the r igorous climates of the north they are
-
wrapped up i n
warm blank ets and furs and kept in the open,or in rooms with li ttle fir e. I n
the warmer southern cl imates, pa t ien ts can sit or recline in comfort on the co ld
est days with the pro tect ion of a steamer rug .
The effect of this open air is to harden the patien t . H e soon reaches the
state where the weather changes affect him very li ttle.
The effect of the open -air l ife upon the nervous system is very
pronounced . N ervous excitation is qu ieted . N eurasthen ic
cond itions improve. S leep is induced,o ften in patien ts who
are usua lly very poor sleepers .
Perhaps the most important effec t of keeping the tuberculous
pat ien t in fresh air .is that upon nutr i t ion . Fresh a ir is a
wonderful ton ic ; and,when we take patien ts from their
poorly ven tilated homes and place them in the fresh air,the
first improvemen t no ticed is usually.upon the appet ite. D igest ion and as
similation are at once improved , and the pa tien ts begin to ga in in weigh t .
A temporary improvemen t is sometimes no ted even in patien ts who are very
ill and far beyond hope o f anymateria l improvemen t .
I t is very importan t to remember that this actio n which is so no ticeable in
tuberculosis is no t specific , nor is i t pecul iar to this d isease. The same effect
is n o ted upon individuals suffering from o ther d iseases and also upo n no rma l
ind ividuals . We should extend our use o f fresh a ir to o ther d iseases and wecan recommend i t as being the best prophylact ic measure known .
I 26 PULM ON ARY TUBE RCULO S I S
on the begin n in g of trea tmen t . I n some cases I have exposed the pat ien t
somewha t graduall y tak ing three or four days to reach the ful l ven tilation . I n
elderly pat ien ts the exposur e shoul d be made more gradually than in young
adults . A s elsewhere in medi c ine we must exerc ise judgmen t,and common
sense in the employmen t of pure air,and much more care should be exercised
where c limatic cond it ion s are rigorous than where they ar e m i ld .
One thing to avo id in establ ish ing the outdoor li fe is the use of tOo much
bed clo thing . There is an exaggerated fear on the part of some,espec ia lly
certa in individuals suffering from neurasthenia,that they w i ll suffer from the
co ld . N o more cover Should be used than is necessary for warmth . The
physic ian must be the judge; and he must exercise tact in deal ing with those
who desire to use too much cover . I n co ld weather there is n o objection to
having thebed warmed by a hotwater bo ttle (but I bel ieve i t is better to remove
i t as soon as the bed is warmed) and if i t is very co ld even a covering for the'
head is not to be den ied . Patien ts should a lways,if poss ible, have their feet
warm before retiring. This,w i th a warm bed, takes away the danger of
ch i l l and does away with the desire for so much cover .
E ven the most del icate pa t ien t can be taken from a stuffy,c lose room and
put in to a wel l-ven t i la ted room,or outside
,in open bungalows or shacks
,w i thout
the least danger provid ing the proper judgmen t is used in mak ing the change .
The benefic ia l effect is usually so prompt that i f the pat ien t sleeps in the open
a few n ights he becomes wedded to i t and has n o desir e to return to his
former quarters.
The matter o f clo thing is very ' importan t to the tuberculous .
A good genera l rule is to wear the least clo th ing that can be
worn w i th comfort . T here i s a tenden cy todress too warmly .
A n excess Of clo th ing enveloping the pat ien t has a bad in
fluence upon the sk in ,keeps i t in a condition of lowered tone, and at the
same t ime preven ts proper el im inat ion . Co n sequen t ly the pa t ien t finds i t
d ifficul t to harden himself ; fo r , wh i le he is subjecting h imsel f to co nd i t ion s
wh ich require a hea l thy,act ive skin , he is in terfering with its nutri tion and
funct io n by his clo thin g .
The underclo th ing is an impo rtan t facto r . I have lon g discarded the use
o f wo o l and replaced i t w ith l in en . Linen is an abso rben t of mo isture but
do es no t reta in i t , co n sequen tly the act io n o f the sk in is a ided and the
pa t ien t is n o t so l iable to ch ill after persp iring as when garmen ts o f o ther
ma teria l are used .
The usua l hab i t o f o rdering tuberculous pa tien ts to wear heavy woo len
undergarmen ts dur ing the ho t summer is n o t o n ly un sc ien t ific,but harmful
a nd barbaro us . Why sub ject these pa t ien ts to such d iscomfo rt? There can
be n o reaso n except because somebody sa id so . The best underclo th ing fo r
summer , l ikewise fo r w in ter , is o ne tha t keeps the pat ien t comfo rtable . The
TH E OPE N -A I R TRE ATM E N T O F TUBERCULOS I S 1 27
garmen t wh ich causes persp ira t ion and macera t ion o f the sk in is, i f anyth in g, mo re harmful than the one wh ich is too l ight . The care of the feet
is l ikew ise importan t . The,sk in should be kept heal thy by frequen t ba th
i ng, and chan gin g of stock ings and shoes. Persp irat ion with its resul tan t
macerat ion shoul d a lso be avo ided here as far as is possible.
N ei ther damp weather, fog-
n or co ld are con traind ication s for
223
5317
39
211“ beginn ing or fo llow ing out the open -air treatmen t . . I t can be
in dica tion .begun at any t ime. I have frequen tly received patien ts at the
sanatorium dur ing a severa l days’ rain who had never spen t
a n ight in a properly ven t i lated room . I have placed them at on ce in an open
bungalow or open room and have as yet seen n o harm come from i t .
T here is n o reason why w indows and ten t cur ta in s should be closed dur in g
ra in or fog un less, in the case of ra in,i t is n ecessary to keep the pa t ien t from
_
exposur e to wet. The damp air is the best air that we have at these times
and it is n ot harmful . The dampest air we can find is to be preferred to
that foun d in a close,stuffy room .
The most ben efit will be derived from the open -air life by
1
1
3122; 321
3231: k eep ing it up persisten tly, n ot on ly at n ight, but dur ing the day
from Open A ir .as wel l . There is a ‘
popular idea that the open—air life is
synonymous with exercise. N o th ing can be further from the
truth . I n fact,pat ien ts suffer ing from this d isease who are trying to rega in
hea l th,can profitably spend much of their t ime quietly reclin in g . E ach case
must be trea ted as an ind ividual and the in struction s Should be spec1fic and
be based upon a thorough kn owledge of the con di t ion s presen t .
The best effect of open air can be obta ined on ly by using
317
33505211
1? i t discreetly . While in i tself harmless, doubtless more lives
I n struc tion s have been wr ecked whi le try ing to fo llow this mode ofCause M any treatmen t
'
than an ther . O e ai t a ure forD eaths. y o p n r i s n o c
tuberculosis ; i t is onl y a measure for the production of a cer
ta in'
end. I f used properly, i t is one of the greatest a ids to n utr i t ion that
can be employed ; if used improperly, i t w i ll defeat its own purpose.
A n ind iv idual sufferin g from tuberculosis should n ot be to ld that open air
w i ll cur e him, but tha t proper living in the open air will be one of his grea test
a ids toward hea l th . M any an in div idual has ea ten good food and rema ined
in the open air al l the t ime, and yet k i lled h imself The oft-repea ted adv ice
of well-mean ing eastern physic ian s to their pat ien ts, G o 'Wgst, l ive in the open
air or rough i t,and keep away from is respon sible for the dea ths
of hundreds of pa t ien ts ann ually . N ot open air,but the proper use of open
a ir,is one of the chief a ids in the cure of tuberculosis .
I t is the physic ian ’s duty to go in to the minutest detail when prescrib ing
any mode (if treatmen t . T his is just as n ecessary when open air is the
remedy as when i t is strychn ia or m'
orphia .
I 28 PULM ON ARY T UBERCULO S I S
While there is no place so unsatisfactory to treat tuberculous
patien ts as in their own homes, yet we must realize that i t is
there where we must tr eat most of them . I t is but a smal l
percen tage'
of the to ta l n umber of pulmonary inval ids tha t w i ll
be treated in in stitutions, ten ts or bun galows bu i l t expressly for the purpose ;so
,i t is necessary for us to adapt the homes as best we can to meet the needs
of the patien t .
The most difficult thing to attain in the homes is a thorough co-operation on
the part of those who are well . They are not accustomed to,n or are they
w i l ling as a rule to have their rooms wel l ven t ilated . N ei ther are they w i ll in g
to subm i t to the co ld air that we advise for the inva lid, consequen tly the patien t
must occupy a room by himsel f.
O ften a very sat isfactory Shelter can be made by screen ing in a porch . Some
times ah extra shel ter can be built on the outside of a room,large enough for
a bed and o ther actual furn i ture required . A bungalow (see F igur es 3 7 and 38 ,pages 2 19 and 220) can be con structed in a yard adjacen t to the house at a
small cost . I f n one of these_
are practical i t is bestx
to have a room with
w indows on two sides, preferably a southeast or southwest room,and then
,
by plac ing the bed between the windows,a fa irly good change of air can be
obta ined . When there I S on ly one window in the room occupied by a pa t ien t,
and the door i s so arranged tha t i t does not in sure a constan t supply of fresh
air,I have the bed dr awn near to the window and advise the pat ien t to sleep
w i th his face as near to the open window as possible. I n this way he is
breathing air as nearly like tha t of the outside as can be had in a room .
130 PULM ON ARY TUBE RCULOS I S
her that our tuberculous patien ts are taken from the general ranks of human i ty
and that they may have o ther diseases besides tuberculosis. Such d iseasesmust a lways be considered in our trea tmen t of tubercul os is. I t would not be
wise to a ttempt forced feedi ng in the case of a pat ien t with diseased kidneys.
N or would we expec t to accompl ish any good by i t where there was serious
disease on the part of the gastro - in testina l .tract . A weak heart is also a
con tra ind ication . A patien t who is of normal weight for his heighta nd age
should eat on ly moderate quan ti ties of food . I do n ot bel ieve that i t is advis
able to force the feed ing of a patien t who hasmuch fibrosis in the lung . These
pat ien ts,as a rule, put on weight very S lowly and I bel ieve it is nature
’s way
of pro tecting them . M odera te eat ing of substan tia l food is best for them .
E ven though,for any reason , i t should be thought advisable to in crease
the d iet of a pat ien t beyond wha t woul d usual ly be con sidered n ormal, such a
d ietary Should not be persisted in indefin itely . I t is a lways best to have the
patien t on a normal diet before he is dismissed from the physician ’s care.
The evil effects of forced feed ing are most pronoun ced on
the part of the gastro - in testinal trac t . The stomach o ften
man ifests rebel l ion against i t in the‘form of nausea
,and
,
if this warn ing is n ot heeded,chron ic ind igest ion either
w i th or without dilatation may en sue. The in test in es Show their d isapproval
of i t by disturbances in their fun ction s . The pat ien t may have an undue
amotI n t of gas fo rmation causing a feel ing of fullness and d iscomfort, or he
may suffer from obst inate con stipat ion ,or he may have two or thr ee loose
mushy passages a day o ften con tain ing und igested residue. A common
symptom,a lso
,is a pa in in the lower part of the abdomen
,this pain being
increased by the tak ing of al l food . Dizz iness and headache are also common
symptoms. Upon the part of the heart, overfeeding is shown by an in crease
in the pulse-rate. There is no question but tha t the kidneys are o ften in jured
by overfeed ing
Patien ts frequen tly gain weight very rapidly upon forced feeding . They
take this as a S ign of cure,and With this false assurance they begin to do
various ind iscreet things and go rap idly down . Then again,if th is forced
feed ing is persisted in,the weight is soon lost through the disturbances pro
duced o n the part o f the stomach and bowels . The accumula t ion o f weight,
wh ich is put on in this way, is, as a rule,a so ft fat. I t is not stable. The
pa t ien t is fat, but has no endurance. H e su ffers from dyspnea upon the
least exert io n , and upo n the least provo ca tion loses a few pounds . When
such pat ien ts start to go down ,they are hard to save. A steady ga in in
weight wh ich progresses with the genera l improvemen t of the pat ien t is to my
m ind,mo re des i rable
,and much mo re to the pa tien t ’s advan tage. I t is no t fat
that is desired ; but , res is ting power wh ich comes from an increase o f muscle,
an improvemen t in the qual i ty o f the blo od and a build ing up o f nerve force.
D I E T I N TUBERCULO S I S 3 1
A rational diet is one which suits the needs of the particular
pat ien t in quest ion . There can be n o one diet for al l cases
anymore than there can be one su it of clo thes to fit al l patien ts.
However , there are certain defin ite proportion s of pro teids, fats and carbohv
dr ates which can be taken as a standard a nd then the amoun ts varied as seems
best . I am in the hab i t of telling my patien ts tha t I wan t them to eat the
least amoun t of food that they can and ga in Weight sat isfactor i ly . Such a
po licy does n ot impa ir the digestive system nor does it in any way over
burden the kidneys .
Dr . Goodbody, Dr . Bardswel l and lVLr . Chapman made a careful studyof the effect of var ious amoun ts of food upon tuberculous patien ts (Medico ~
Chirurgica l Transact ion s, Vo l . LXXXIV,1902) and endeavored to 13
'
tthe feed ing of such patien ts upon a sc ien t ific basis . Their observations
were made upon six pa t ien ts ..The amoun t of food consumed was carefully
determined by first weighingthe amoun ts served and then a lso weighing anyport ions tha t were left uneaten . The ur ine and feces were carefully collec
'
ted’,
weighed and analyzed in order to Showd t-he ambun t of food reta ined.
These pa tien ts were tested on an ordinary d ietary,then one a l i ttle mere
l iberal, and,
finally,
a much more l iberal one. Their results show that
the most suitable d ietary con sists of about
41oun ces of pro teids5 oun ces of fat107} oun ces of carbohydrates
An objection might be ra ised to this suggested dietary that the number
Of cases is too.smal l ; and, i t m ight also be sa id aga in st its adopt ion as a genera l
measur e that pat ien ts of a d-ifierent Character and from differen t wa lks of
l ife and under d ifferen t c l imatic cond i t ion s might Show d ifferen t results .
I t would be profitable to have s imilar experimen ts made upon a larger n umber
of patients of differen t environmen ts,suffering from various forms of the
d isease,in widely sca ttered local i t ies
, to see if there would be any great var ia
tion from the above.
I t is in terest ing to compare this with wha t is con sidered a standard d ietary
for a man at moderate work . A ccord ing to Vo i t such a man should con sume
about
4 oun ces of proteids2 oun ces of fat16 oun ces of carbohydrates
Burton Fann ing, in an admirable d iscussion of the subject of diet (The
Open Air T rea tmen t of Pulmonary Tuberculos is,
quo tes the above
experimen ts approv ingly,and gives the fo llow ing as a standard d ietary.
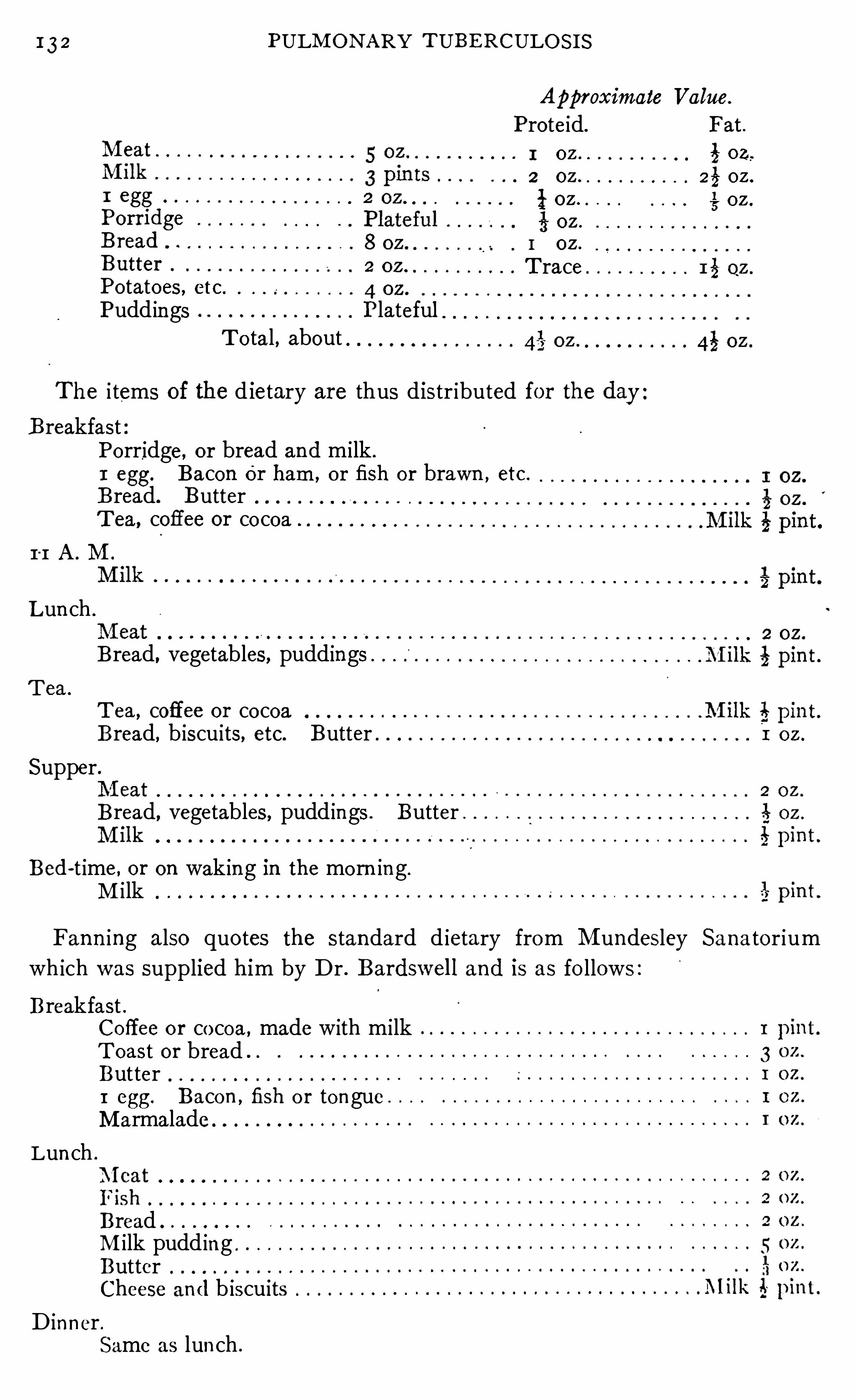
I 3 2 PULM ON ARY TUBE RCULO S I S
0 0 0 0 0 0 0 0 0
o o o o o o o o o o o o o o
o o o o o o o o o o o o o o o
Po tatoes , etc .
Pudd ings PlatefulT o tal, about
0 0 0 0 0 0 0 0 0 0 0 0 0
O O O O O O O O O O O
The i tems of the dietary are thus distr ibuted for the dayB reakfast
Porridge, or bread and milk .
1 egg. Bacon Or ham , o r fish or brawn , etc.
Bread. ButterT ea, coffee or co coa
I I A . M .
Lun ch .
Bread, vegetables, puddings
T ea, coffee or cocoaBread, b iscuits, etc. Butter
Supper.
Bread, vegetables, pudd ings . Butter .
Bed-t ime, or on wak ing in the mo rn ing.
M i lk
Fann ing also quo tes the standard d ietary from M undesley Sana tor ium
wh ich was supplied him by Dr . Bardswel l and is as fo llows :
Breakfast .Coffee o r co coa , made with milkT oast or breadButter1 egg. Bacon , fish o r tongueM armalade
Lun ch0 0 0 0 0 0 0 0 0
BreadM ilk pudd ing .
ButterCheese and b iscuits
D inner .Same as lun ch .
Approximate Value.
Proteid. Fat.
I oz i oz,
2 oz 25 oz .
l OZ é oz .
§ oz .
I OZ .
T race
134 PULM ON ARY T UBE RCULO S I S
bo ttom of the supposed inab i l ity to take m i lk , he soon sees the ridiculousnessof his posi t ion and is w i ll ing, as a rule, of his own accord
, to fill up the glass.
Can M i lk an dThere is a popular idea tha t mi lk can n ot be taken wi th fruit
Fru i t Be because the acid of the fru i t curdl es i t . I f a pat ien t vomitsE a ten after dr inking m ilk, and finds that the m i lk comes up inTogether?
curds, he, consequen tly, is at on ce convinced that milk
d isagr ees wi th him . I t is perfectly natur al for milk to curdle in the Stomach ;that is the fir st thing wh ich happen s in its d igestion ; so we can assure our
pat ien ts tha t in case vomi ting o ccurs after mi lk has been taken i t is na tura l
to find the mi lk curdled ; and, in as much as curdl ing is the first process of
d igestion,what harm can come from eating fruits and milk together, un less
this combinat ion is o therwise con traindicated .
M ilk is n ot a l iqu id food in the true sen se of the word . As
géuéh
s
svggf soon as i t is taken in to the stomach i t is curdled and thenreall y becomes more Or less of a so l id mass . I f i t is taken
in to'
the stomach in large q uan ti ties at one time, it Curdles, fo rming one largemass w i th which the digestive ju ices are unable to cope
, except w i th diffi
culty . I f milk is taken slowly, on the o ther hand, in smal l S ips , each mouthful
w i ll probably be curdl ed before the next reaches the stomach'
and so d igestion
w i ll be facil i tated . M ilk then should be eaten and n o t taken as water or
o ther liquids . M odifica tion of mi lk by such mean s as are men t ioned above
preven ts the formation of large cur ds and makes them break up more easi ly
under the act ion of the gastric ju ices. Eating'
some solid food with the
m i lk an swers the same purpose.
H ow much m i lk Should be'
taken by the tuberculous patien t?
We hear such varied advice regard ing this that it seems
n ecessary to give this po in t more than passing n o tice. Th is
can be an swered on ly for each ind ividual pa t ien t ; yet, genera l
in structions can be g iven which are of value. The an swer to this quest ion
depends upon how much o ther food the patien t is tak ing and what we are
attempt ing to accompl ish by feed ing. I f our so le aim is the putting on of
large quan t i t ies of fat in a very sho rt time regardless of the a fter results, then
there m ight be some excuse fo r feed ing pa t ien ts five or six quarts of mi lk a
day bes ides o ther food, but even then such quan t i ties are en tirely unnecessary .
I f the purpose,o n the o ther hand , is to bu i ld up a well- nourished pat ien t w i th
go od res ist ing power, this use o f enormous quan tities of milk can n o t be
perm i tted .
When patien ts are ea t ing a good, substan tial , well -ba lan ced diet, as a rule,there is n o necess i ty of using mo re than from a p in t and a hal f to a quart and
a ha l f o f m i lk da i ly . Th is amoun t can be increased to suit the case, but I
rarely find it n ecessary to exceed the la tter l im i t . I f a patien t does no t ga in
sa t isfacto rily , i t is an easy matter to add ano ther glass o fm i lk a day ; and, th is
D I E T I N TUBE RCULO S I S 1 35
small amoun t wil l o ften cause an in crease in ' weight . I t must a lso be borne
in m ind that sometimes pat ien ts who are n o t ga in ing on a large d iet w i ll ga in
when the amoun t of food_
is reduced . When pat ien ts _are on an exclusively
milk d iet the amoun t, of course, must be somewha t in creased . I t requ ires
about seven pin ts of milk to furn ish the requisi te four and one-quarter oun ces
of proteids.
I t has been my observation that patien ts who have put on fat rapidly un derthe use of
'
large quan t i t ies ofmilk, alSo lose _
it rap idly on theslightest provoca
tion ..While we prefer to see pa t ien ts ga in in weight, we should remember
that this is not the most essen tia l th ing in treatmen t . M any patien ts who
do nOt regain ,during the early part of the term of trea tmen t, the weight wh ich
they had lost, w il l do so as the‘
tuberculous areas in the lung Clear up and as
they become restored more nearly to their n orma l condition . I n such cases
the attempt to put on weight by excessive amoun ts o f food would doubtless
do .harm .
Where milk must be used for long periods by patients v‘
v\hose appetites are
apt'
to be capricious, it is well to use i t in , dif erent forms. M a l ted m i lk,
E skay’s food
,N estle’
s food, m i lk“
and tropon when a l ternated with pla in or
mod ified m i lk g ive us a variety which helps very much in our dietary . Butter
m i lk offers a '
grateful change to pat ien ts at times, _
and some dowell on Kumyss .
Somet imes the mi lk remains about the teeth and causes a disl ike for i t ; in
such cases the mouth should be rin sed and the teeth brushed every time i t is
taken .
Kumyss may be made at home in the fo llowing man ner
To one quart of new milk add twelve oun ces of warm wa ter
in which one- third of a cake of compressed yeast and one tablespoon ful of
sugar have been d isso lved .
_
Put th is in to two one-quart bo ttles,cork tightly
and tie corks in . Shake well . Place the bo ttles on their s ides or upside down
in a coo l dark place and all ow them to remain for three days. Draw off w i th
a faucet when ready for use.
I f the question were asked what are the best foods for the
Kumyss.
Wha t areB est Foods tuberculous patien t
,i t would be answered differen t ly . by
fo r the d ifferen t men,according. to their ideas of what is to be aecom
Tuberculouspl ished . A S stated above
,I do not bel ieve that the best
dietary for the non - tuberculous would d iffer lwidely from the best one for
the tuberculous . I th ink,however
,that the d iet for the tuberculous should
be somewhat more l iberal . I n fact the tuberculous patien t, when put under
the modern hygien ic- open -air treatmen t w il l have an in creased appet i te which
demands more food . Th is in creased demand, however, is n ot alone observed
on the part of the pat ien t , for the same ho lds true in the case of n urses and
a ttendan ts . Ho 'wever,aside from the in creased demand made by the methcd
of living,i t is qu i te natura l tha t an in creased amoun t of food Should be requ ired
136 PULM ON ARY TUBERCULO S I S
in order to overcome the retrograde process presen t . A t least,a ful ler d iet
should usually be insti tu ted than these patien ts have been in the habit of
taking before they consulted a physician .
The question is, what form of food stuffs should be increased in order to
make up this extra diet? I f an in crease of fat is most desired we could accom
plish our purpose best by the in crease of fats‘
and carbohydrates ; but, if our
desire is not so much the in crease of fat but the building up of muscle,nerve
force, and blood and the preven tion of
’
tissue destruction , then pro teids, the“ tissue builders,
”should be in creased most . Of course we would not expec t
the'
increase to be made en tirely in one Class of food stuffs, but one m ight be
increased more than the o thers.
Whatever food is used should be furn ished in as easi ly digestible a form
as possible,so that the patien t may gain a maximum of nutri tion with the
expenditure of a min imum of digestive energy .
The pro teids can be fur n ished by meats such as rare steaks,mutton chops, roast beef, roast mutton , poultry, game,
fish,eggs and ‘milk . I n many cases meat can be best digested if scraped .
The use of raw mea t (zomo therapy) has been shown to be of great value in
the treatmen t of tuberculosis by Richet and Hericour t and Phi ll ip and Ga l
braith. Raw meat sandwiches made with stale bread and seasoned with
salt are not unpleasan t to the taste and at-the same time are nourishing. M eat
ju ice is also a very importan t article of diet . I t is prepared best by cutt ing
the juicy parts of the round steak in to strips,and placing them on the coa ls
long enough to sear the outside. The str ips are then put in a meat press
and the juice is extracted . Where n o regular mea‘
t press is at hand a lemon
squeezer may be used, but this is no economy ; for , the ju i ce left unextracted
would soon equal the cost of a meat press. Before expressing the juice,the press and the receptacle for catch ing the ju ice should be warmed . The
juice should then be con sumed before i t becomes co ld . I t can n ot be warmed
up except by means of a water bath, o therw ise the'
albumen coagulates and
its worth is destroyed .
Eggs are ano ther valuable pro teid food . They can be used in many way s,but I have found that patien ts will take them raw w i thout t iring fo r a lo nger
t ime than any o ther way. They may be beaten up and put in to milk ; o r
served as eggnog, o r as an egg lemonade ; but my favo rite way is to have them
dropped in to a cup,w i th a few drops of lemon ju ice added and then swallowed
who le. Pa t ien ts seem to tire O f them least quickly when taken this way .
I have kn own pat ien ts to co nsume as many as two dozen a day , but I do no t
bel ieve this is necessary o r ra tio na l . I rarely prescribe mo re than from three
to six a (l ay.
Pro teids.
Fa ts can be furn ished in the fo rm o f m i lk,cream
,butter
,
baco n and o l ive o il . Pa t ien ts who w i ll eat plen ty Of bacon ,
138 PULM ON ARY '
TUBE RCULO S I S
wh ile o thers w i ll n ot take enough food to keep them n our ished . There is a
certa in class of pa t ien ts tha t we o ften meet who have a lways been poor ea ters.
They are usually neuro tic and a lmost a lways under weight . T o a ll ow such
pa t ien ts to fo l low their own in cl inat ion , wh i le a chron ic suppura tive process
is sapping their vital i ty, can n ot be o ther than d isastr ous .
Very o ften ,in the course of tuberculosis, we n o te that pat ien ts lose their
appeti te Or i t becomes capr ic ious . I n fact th is is a very common symptom of
early tuberculosis and i t fo l lows along through the course of the d isease man i
fest ing itself whenever a recrudescen ce appears . O ften this,with ma la ise
,
loss of weight, and S l ight r ise of temperature, shows tha t an exten sion of the
disease is tak ing place, or tha t"
an o ld focus“
is acutely inflamed . The anorex iain these cases is o ften of toxic o rigin . Sometimes it is due
,espec ially in cases
moderately or far advan ced, to the fac t tha t the wal ls of the in test ina l trac tpartake of the general loss of tone and wasting wh ich are so pronoun ced in
this d isease. For pa tien ts to fo ll ow their own in cl inat ion s as to appet i te
under these cond i tions would be suic idal . Such patien ts should be put
under the best hygien ic condition s and en couraged to eat libera lly, for by
eat ing and drink ing is brought about a better sta te of n utrition and d igestion
and the appeti te returns .
O ften ,pa t ien ts who are suffering from fever, i f allowed to eat according to
their appet i tes would die of starva t ion , while by ea ting a l iberal diet they can
not on ly main tain their weight but in crease i t . The indica tions in acutefevers which are of short duration may be for a very restricted d iet , but in
tubercul osis the cond i t ion s are d ifferen t,and we must in sist on a liberal d iet .
Pat ien ts suffer from many of the gastro - in testina l neuroses
which are due to the tubercle tox ins . Such symptoms are
relieved best by an improvemen t on the part of the pat ien t .
When n o organ ic trouble is presen t,i f the nutri tion of the
pa tien t improves, these symptoms improve a lso . N o special restricted d iet
need be pur sued un less improvemen t of symptoms on the part of the gastro
in testinal trac t fai ls to fo llow the genera l improvemen t .
We Should a lways make careful examination in o rder to
determine whether o r no t our pat ien ts a re suffering from .
patho logica l changes in the gastro - in test ina l tract . I f these
be presen t,appropria te d ietet ic measures Should be prescribed
to meet the condit ion . The sooner such measures are
adopted the better fo r the pa t ien t .
O bservatio ns o n tuberculous pat ien ts Show tha t many o f
them suffer from hyperchlo rhydria . Some o f these we
describe as funct io nal because o f our lack o f a better term ,
wh ile o thers have a paten t pa tho logica l co nd it io n underlying them .
Such co nd it io ns can o ften be co rrected with relat ive case if the proper
H yperch lo r
hydr ia .
D I E T I N TUBERCULOS I S 39
dietary and o ther measures a’
re’
adOptedywhile, if allowed to go , they becomemost in tractable.
'
Such p atien ts m ust be treated by a bland non - irr i ta t ing
d iet,free from condimen ts an d irr i tan ts. Wh i le such a d iet must be restric ted
,
yet it Can be'very ‘
liberia lgi and'conform to wha t is necessary ifor the n our ishs
men t of the tubercul osis‘
p atien t. T hese pat ien ts'
Stand fats well for they
depress the secret ion lof'
zthe acid . When creoso te was in vogue as the treat
men t for tuberculosis it was found to d isagree with a great many pat ien ts .
We would expect i t to disagree“
with those suffering. from hyperchlorhydr ia,
for by its stimula tion i t in creases the a lready too abundan t acid . N ux vom ica,
and o ther remed ies which st imulate the gast r ic Secret ion,are also con traindic
a ted . Large doses of alkalies o ften act well in these patients butmust notbe con tin ued too long.
A deficien cy of ac id is also at times en coun tered . T h i s
may be of nervous or igin . I f so,i t usua lly responds to
treatmen t in a Short t ime. The adm in istration of ten or
fifteen dr ops of d i lute hydr ochlor ic/
ac id after meals, ei ther with or W i thout
some of the“ b i tter ton ics such as nux vomica,
'
w i ll Often restore norma l con
dition s in a few days .
Ano ther condition which we frequen tly meet in this day of
overfeeding is d i latat ion of the stomach .
_
M any pa tien ts,as soon as they find they have tuberculosis
,ei ther upon their
own in i tiative or through the advice of their physici an,beg in
an indiscrimina te process of stuffing. D i la tation o ften results from it,and
must be guarded aga in st . When i t is presen t, on e must l imit the amoun t of
flu id ingested . To put such pa tien ts upon large quan t i ties of m i lk w i ll aggra
va te the condition . T hey should be put to rest in the open air and fed on
con cen trated pro teid and carbohydr ate foods’
. Fat should be excluded .
Under such a diet with o ther appropria te measures, such as massage and
electr icity,pat ien ts o ften make sat isfactory improvemen t .
Constipation must be combated in a very large per cen t
of tuberculous pa tien ts ; especially is th is true of those who
are in the a dvan ced stages . The tuberculous patien t is espec ially subjec t
to just those condit ions which'
favor con stipation,viz .
,hyperchlorhydr ia
,
catarrhal and aton ic cond i t ion of the stomach and bowels,n eurasthen ia and
the con sumption of large amoun ts of con cen trated foods . A side from th is,espec ially
, the pa t ien t in the advan ced stage is forced to lead a l ife of in activ
i ty wh ich favo rs sluggishness on the part of the gastro - in testinal trac t .
The cause,of course, Should be removed whenever pract icable. A d ietary
suited to the condition presen t is very essen t ial to success . I n con st ipa t ion
dependen t upon an aton ic cond i tion of the bowels,a d iet con ta in in g much
res idue wh ich wil l stimulate per istalsis i s n ecessary . Coarse gra in s, vegetables
and fru i ts are very importan t arti cles,of diet i n these cases . A glass of hot
Co n stipation .
140 PULM ON ARY TUBERCULOS I S
or co ld water taken on ar is ing and on ret iring is beneficia l . When not con tra
ind ica ted, fats in the form of cream,butter and
,especia lly, o live o il are of
great value. I frequen tly have patien ts, where it agrees with them,take from
one-half to one oun ce of o l ive o il after meals . I t is better to begin with
smaller doses, say one-half dram and gradually in crease. A most successful
way of admin ister ing Ol ive o il is by put ting it’
on bread and eat ing it with a
l i ttle sal t .'
The sal t takes away the in sip id taste which is objectionable to
many . I n con stipation of the spastic variety, where the movemen ts are
r ibbon l ike in form,bell adonna pushed to itsphysio logical action wil l remove
the spasms and relieve the condition .
Whoever treats many cases of tuberculosis, especia lly those
in the advan ced stages, will o ften be obl iged to treat diar
rhea . Sometimes it is of a tuberculous nature,but i t is
o ften a simple diarrhea due to some irritation,o ther than
tuberculosis,in the in testinal tract . I t is very importan t to give these pa
tients relief as soon as possible, for they can i ll afford to lose strength and
weight .
I n non -tuberculous diarrheas the patien t should be put to bed and the
alimen tary cana l Should be freed from the irr i tation of its con ten ts as qu ickly
as possible by some mild cathartic . For th is purpose,castor o il in one-half
to one oun ce doses has served me best . Where this canno t be taken , sal ts,E psom or Rochelle
,serve well . A ll ordinary foods should be withdrawn ,
and the pa tien t put upon a mixture of milk, two parts, and lime water, one
part . H ot compresses should be applied to the abdomen for two hours a
day. A fter twen ty- four hours,if the condi tion has improved
,bo i led rice
w ith bo i led m i lk may be added . I f all goes wel l , . the whites of eggs or the
en t ire egg, raw,or so ft bo i led, and then scraped meat and stale bread may be
g iven . Baked po ta toes and purees may then be cautiously added, leaving
the coarser vegetables and fruits to come later . E skay’s food
, N estle’s food
o r some of the o ther food preparations may be used to advan tage for a wh ile
to modify the milk .
Wi th this manner of d iet ing in these cases,much time is saved . The pat ien t
is brought out of his trouble with the least loss of s trength, and in a few days
is able to return to a fairly full d iet. I t is a wrong po licy to undertake to check
these d iarrheas by the use of astringen ts. I t blocks the bowels up, without
the removal o f the cause. I f they are used at a l l,i t Should be on ly a fter the
bowels have been thoroughly emptied . W here an astringen t is required Ia lways prefer subn i trate o f b ismuth .
I n tuberculous diarrhea the treatment must be differen t ;fo r here we have an irri tation which we can no t remove
qu ickly . The problem is to nourish the pat ien t in spite o f
i t . A l l laxa tive food should be removed from the d iet , and the pa t ien t fed
TuberculousD iarrhea .
CHAPTER XI I I .
RE ST AND EXE RCI SE'
I N TH E TRE ATME NT OF
TUBE RCULOS I S .
The quest ion of rest and exerc ise in the treatmen t of tuberculosis is one of
great importan ce. T here are certa in ind ication s upon which the pro fession
is fairly well un i ted,which cal l for rest and exerc ise respect ively. When ever
there is any question whether the pat ien t Should rest or take exercise,i t is
safe to advise rest . I f there be any error let it be on the side of savi ng the
patien t from al l questionable exerc ise.
I t was Dettwei ler, who first inaugurated the rest cure for tuberculos is .
Sufferers from this d isease owe a debt to him tha t they can n ever appreciate,
for be i t was who first combated the o ld idea of exercise being abso lutely neces
sary to a cure. Wh i le he may have gone a little too far to the o ther extreme,
yet he started a reaction,and modern therapists have been able to choose the
go lden mean wh ich is proving so efficacious in the treatmen t of this d isease .
Brehmer showed us the va lue of exercisein s trengthen ing the heart and improv
ing n utri t ion,while Dettwei ler demon strated tha t too much exercise is harmful
and ma in ta ined that health is regained best under a condit ionof abso lute rest
for the greater portion of the day. M ost phthisiotherapists today make Dett
wei ler ’s teachings the basis of their action s and employ rest as an importan t
factor in treatmen t .
Rest is that cond i tion of existen ce wherein the physio logical
fun ctions are carried on w i th the expenditure of a min imum
of energy. During rest there is the least poss ible ca ll upon the
organ ism for action ; in fact, dur ing perfec t rest on ly those fun c t ion s which are
abso lutely necessary to l ife are carried o n . S ince man ’s na tura l state implies
a certain amoun t of activity and the use of a certain amoun t of energy,rest
,
ei ther natural or en forced,saves the organ ism and the cells which would be
called in to action by activi ty from th is demand, and in this way acts as a con
server of fo rce. N ot on ly does rest save the body cells from the expend i ture
o f energy but i t a lso affords an oppo rtun i ty for repair ; hence rest is rightly called
the grea t resto rer . I n confirmat ion of th is po in t i t has been Shown tha t the
res ist ing power o f pat ien ts suffer ing from tuberculosis,as measured by the
agglutinating power o f the blo od, is increased when the patien t rests and is
decreased by exertion,especially if th is is carried to the po in t of t iring .
Wh i le a state o f rest makes requ isit ion upo n the ind ividual fo r
the least expend i ture o f energy , yet in heal th a certain amoun t
o f exercise is necessarv in o rder to ma in tain a phys io logica l
142
RE ST AN D EXE RC I SE I N TH E TRE ATM E N T OF TUBE RCULOS I S 143
equ i l ibrium . Whi le rest is essen tia l to l ife, exercise is essen t ial to the h ighest
state of hea l th and the beSten joymen t of l ife. Where there is no con traindi
cation,therefore, exerc ise Should be a part of the da i ly life of the indiv idual
,
for by it his cells . will be better nour ished, his Oi'
gans w i ll functiona te better,and he wil l be a stron ger, hea lthier man .
Th is question of rest and exerc ise should be d iscussed from two standpo in ts ;fir st
,rest or exercise for -the tuberculous individual, and then rest. or exercise
for the‘
tuberculous lung .
When fever is presen t,rest is essen tial. T his is a rule to which
there are very few exception s Fever -
is an index wh ich shows
the presen ce of an in flammatory process. A n exten sion of the
d isease,acute m i l iary tuberculosis, the developmen t of a pleur isy or pneumon ia,
or the presen ce of inflammat ion of o ther organ s, such as acute gastri t is, are
accompan ied by a rise of temperature. Whenever such acute processes man i
fest themselves,the patien t must be treated by rest . Rest insisted on promptly
at the first ind icat ion of such cond ition s w i l l Often cut the attack short .
What degree of temperature shall be taken as an ind ication that rest should
be prescr ibed? - Shall we fo llow those who keep patien ts at abso lute rest
whenever the temperatur e reaches 99 degrees, or shall we be more libera l ?
Personally I bel ieve in being a . l ittle more l iberal, but ho ld that i t is a quest ion
to be decided for each in d iv idua l case. I make it my rule to try abso lute rest
on al l patien ts whose -da i ly temperature reaches 100 degrees . I somet imes
find,however, a n ervous patien t who w i ll n ot submi t to this rest treatmen t
,
who chafes under the restra in t and worries beyond degree and keeps the tem
perature elevated by the excited men ta l cond it ion . I n such cases i t often proves
best to‘
a llow the pat ien t to sit up for a few minutes at tha t t ime of the daywhen
the temperature is lowest . There is a certain rest and en couragemen t,about
th is wh ich rel ieves the m ind ahd lowers the tempera ture. M en tal un rest,
such as“
is produced by worry, by great emo tion , by read ing or v isi t ing w i th
friends for_
a con siderable time, will cause a r ise of temperature just as surely
as w i ll physica l exert ion ,and i t is just as importan t to rel ieve this as i t is to
order rest for the body .
One should n ot be discouraged too qu ickly, however, if the patien t’s tem
perature does not lower by rest . H e must not come to the con clusion that i t
is a case for exerc ise simply because the tempera ture is s tubborn . I have
seen pat ien ts with tuberculosis who had an elevation of temper a ture which
exceeded 100 degrees for mon ths, in whom there was no n ervou s elemen t at
a l l . Pat ien ts fo r whom it is adv isable to chan ce a li ttle exercise regardless of
temperature can on ly be Chosen by select ion after carefully wa tchin g the
course of their d isease.
N o matter hovsfiwel l a pat ien t is do ing,if he has gone beyond the early
stages of tuberculosis,he w i ll almost surely have spells when his tempera ture
144 PULM O N ARY TUBE RCULO S I S
w i ll be elevated and he w i l l n eed to take advan tage of rest in bed for a few days.
I t,is very essen tial to keep accurate records of the tempera ture of tuberculous
pa t ien ts ; and, i f any tenden cy for the tempera ture to rise is no ted,to en jo in
rest . I bel ieve such a cour se wil l o ften cut short acute processes ; so , i f the
temperature is found reaching the hundred mark, then rest Shoul d be deemed
essen tial . I t is not at a l l un common to see pat ien ts lose their temperatur e in
a few days when trea ted in this manner ; on the o ther hand,i t is no t at al l
un common to see a con tin ued fever fo l low carelessness in en forcing rest at this
time. Wright has proven that this rise Of'
temperature fo llowing exercise is
due not to tiring, as is generally supposed, but to an auto inoculat ion of toxin s.
E xercise forces more toxins in to the Circulation than would occur during rest .
Sometimes, fo llowing a few days’ rest in bed, we have n o ted a reduction of
temperature in those chr on ic cases wh ich have persisted in showing a rise,reaching about for mon ths. I n all cases where there is a persisten t rise
which fa i ls to y ield to Other treatmen t, rest should be en jo ined . I t may not
affect the temperature at al l or i t may not affec t i t permanen tly, yet in certa in
cases i t will ; so i t is worthy of a trial .
When a pneumon ic cond i tion is presen t or when a pleurisy develops,rest
in bed is imperative. I t not on ly gives the patien t a chance to get well
sooner but i t a lso puts him in the best condition to ward off compl ications .
T emperature can not be taken as the so le gu ide for rest
or exercise. M any non -febrile cases can
~
be best treated by
rest .
O ften times a cough is aggravated by exercise, even sl igh t
movemen ts producing a paroxysm which t ires the patien t and
causes a rise of temperature. Coughing Shouldbe discouraged
as much as poss ible in the treatmen t of tuberculosis ; for i t
causes an explosive act ion which tears the delicate threads tha t nature throws
out to heal the lesion ,and keeps stretching the air vesicles un t i l i t impairs
their elasticity and causes an emphysematous cond i tion . When the rest trea t
men t is used and the patien t trained to resist coughing, cough mixtures are
rarely needed .
Rest in N onfebri le Cases.
Hemoptysis calls for the rest treatmen t . Rest Should be en
jo ined at the least Show of blood . Wh i le this may seemo ver
cautious, yet i t is a wise precaut ion ; for the small streak o f
blo od o r the smal l mouthful may come from a minute open ing in a large vessel .
I f rest in bed is adopted at o nce, i t gives the lesion an opportun ity to heal ,while i f exerc ise is persisted in the break may become large and the bleed ing
become d iffi cult o r even imposs ible to co n tro l .
I know full well that al l hemoptyses are n o t due to the open ing o f large
vessels . Some are co ngest ive in their o rigin . But as yet we have no defin ite
way o f tell ing which is the o ne and wh ich the o ther ; and, un ti l we do have
146 PULM ON ARY TUBE RCULO S I S
the early stages of the d isease that there is no possible opportun i ty for them
to rega in their tone and, of course, the pat ien t’s l ife is sacr ificed as a resul t .
I n cases where a rap id extension of the tuberculous process is tak ing place
or where a pneumon ic cond ition is presen t , or where, for any cause, there is a
rapid obliterat ion of the pulmonary vessels, throw ing extra burden upon the
heart,rest shouldbe en jo ined . A t these t imes i t must also be remembered that
an in creased tenden cy to muscular wast ing is presen t, and that the heart
muscle is affected along with the o thers .
A patien t suffering from tubercul osis,who has a weak , rapid heart, should
a lways be subjected to the rest treatment. Sometimes the heart wil l respond
to th is trea tmen t, improve its tone and after a little whi le be able to stand the
burden s thr own upon i t,when at first i t seemed that i t would give way. So
whenever there is doubt as to what to do , i t is safer to employ rest .
We have endeavored to show why rest is importan t from the .
standpo in t of the heart, in some of the cond i tions which arise
during the progress of tuberculosis . We a lso bel ieve tha t
exercise has its place, and will endeavor to show its benefits when jud iciously
used at the proper t ime.
There comes a t ime in n early al l cases of tuberculosis which are progressing
favorably,when the disease becomes more or less qu iescen t , when the heart
is no longer affected by the toxins and when i t has adjusted itself to the changes
which have had a tenden cy to embarrass i t . When such a t ime comes, exer
cise is valuable. I t Should be begun very caut iously and the effect watched
carefully . I f the cond it ion of the heart has been such as to make i t necessary
for the patien t to remain in bed, then the first exerc ise Should consist of simply
s itt ing up in bed, la ter si tting up in a chair, then walk ing across the room .
During a l l of these procedures, the effect Should be watched carefully . I f
the exercise,no matter how S l ight it may be, causes a rap id, weak pulse, i t is
more than the patien t can stand w ith safety . When the patien t begins to walk,
he should go a few steps on ly and make i t a rule to a lways stopshort o f theappearan ce of dyspnea . The pat ien t is usually incl ined to wan t to go too
far,so the physic ian must gu ide him . I f the pulse
’
becomes rap id the amoun tof exercise should no t be in creased next t ime.
A fter a few trials at exercising have been made, i f the heart is go ing to be
strengthened by i t,we w i l l find that the pulse becomes less sensi t ive and does
no t bea t as rapidly as at first . I f the pulse becomes mo re rap id and weaker i t
shows tha t the exerc ise is no t being well bo rne and Should not be persisted in
except with great caut io n .
The danger to the heart was indel ibly impressed upon my mind by an
inc iden t wh ich happened when I firs t began the trea tmen t of tuberculo sis .
A yo ung man,twen ty-five years o f age, who had always been stro ng
, developed
tuberculo sis . The d isease made rap id pro gress and there was extens ive de
The H eart an dExercise.
RE ST AN D EXE RCI SE I N TH E TRE ATM E N T O F TUBE RCULOS I S 147
struc t ion of t issue in a short,
per iod of t ime . When the tempera ture began to
drop,his phys ic ian to ld h im he might spend a l itt le time on the roo f garden of
the hosp ital, wh ich requ ired the cl imb ing of one fl ight of sta irs. Wh i le ascend
ing the'
steps he was seized by a sudden pa in in the heart,accompan ied by
syn cope. H is pulse immediately became very much accelera ted . H e had
suffered an attack of acute d i la tation of the heart . The pulse c on t inued at
the .rate of one hundred and twen ty to on e“ hundred and fifty for a“
n umber of
mon ths. I hadcharge of him for the next ten mon ths and was obl iged to keep
him in a recumben t pos i t ion nearly all the t ime. H is heart finally strengthened
and the pulse settled down to about 100 beats per min ute. Wh i le this is an
extreme case,yet it is a good one to Show what occurs in o thers to a lesser degree.
I n cases of tuberculosis where i t is n ot necessary to confine the pat ien t to bed,a certa in amotI n t of exerc ise depend ing on cond i t ion s presen t may
-be taken
.to advan tage. The heart,however, must a lways be watched . E xercisemust
never be in excess of wha t the heart w il l stan d . Our objec t in treat ing tuber
culosis is not a lone to cure the tuberculous process but to br ing our patien t
through to as n ear perfect health as is poss ible ; -so'
we should str ive for healed
lungs with a strong heart,and the st ng heart w i ll be an importan t factor in
producing healed lungs.
When dyspnea i s presen t, or if i t is produced by exert ion,
then rest should“
be en jo ined, un less the dyspnea be due to a fat
flabby cond i t ion such as is o ften produced by overfeed ing .
Where such is the case, exercise, carefully graduated, with atten tion to the d iet
is very benefic ial .
There is great fear on the part o f some patien ts who are very
Res t an dD yspn ea .
Res t WhenWeigh t is much reduced in strength and weight tha t
,un less they exer
cise,they W i ll never gain . Such a n o tion has n o founda tion .
I n fac t the reverse is nearer the truth ; if theyexerc ise,they
w i ll n ever gain . Such patien ts must be treated by rest a long with o ther reme
d ial measures.
Where there are n o complica tion s presen t such as those
men t ioned above and where n o deleterious effects are no ted
on exert ion,such as rise of temperature
,pulse- ra te and
dyspn ea,
exercise, if properly carr ied out, is ben efic ial .
E xercise keeps the body fluids mov ing . I t br ings more blood and lymph
to the tissues . I t st imulates d igestion and assim i lat ion . I t induces sleep . I t
increases the activity of the sk in,k idneys and bowels . Hen ce its usefulness .
A n early stage case after al l activi ty is past and an arrestmen t a tta ined,if there are n o con tra ind ica tion s
,may walk from one to five m i les a day w i th
benefit . A n advanced case must increase the amoun t of exerc ise with caut ion .
H e can n o t go so far and he has more con traindicat ion s to hamper h im . A
walk from on e—half to one m ile may be al l that he can take with profit .
148 PULM ON ARY TUBERCULO S I S
Dur ing the early weeks of treatmen t I think it is well to keep the patien tsqu iet . A fter we learn to know them better and are sure of their con d i t ion and
compl ica t ion s,their weaknesses and their S trong po in ts
,then we are better
able to su i t exerc ise to them,and they are better able to adopt i t .
When pa tien ts are a l lowed to.
take exerc ise,they should be caut ioned n ot
to do so immed iately before a meal . Pa t ien ts should a lways go to their mealsrested . I t is very importan t to in sist on a hal f hour ’s rest before the prin cipa l
meals of the day. Very o ften,if a man goes to the table tired, his food does no t
d igest,and a tuberculous pa t ien t can n ot afford to take any such r isk .
When a pat ien t has been un der the phys ic ian ’s charge and he has arrived
at the place where he is about ready to be d ism issed, if his cond it ion warran ts i t ,he should be hardened and brought to a po in t of endurance as near to that of
a n orma l man as is possible before he is again thrown upon his own respon si
bil ity. Here is where a m istake is o ften made in sanator ia . Patien ts are kept
well , they- l ive under ideal conditions, they are fat, but they are not strong .
T hey leave the in stitut ion w ith its careful reg ime and hygien ic surroundings
and soon begin to lose weight . They are d iscouraged and, i f the result of their
treatmen t was an improvemen t or arrestmen t instead of an apparen t cure,
they may even lose much that has been ga ined by trea tmen t, I f patien ts
would allow themselves sufficien t t ime for treatmen t, they should be brought
down before discharge to a po in t where they can main ta in n utrit ion on an
o rd inary d ietary and where they can endure exerc ise such as they will be ca lled
upon to perform when they leave the in sti tution . I l ike to have my patien ts
rema in quiet un t i l the d isease is quiescen t and then ,as soon as they are able
to take exerc ise without harm,beg in by very short walks and gradual ly lengthen
them,where there is no con tra indication , to four or five m i les a day.
Lest I should be m isunderstood, I will again say that I am pr imari ly in favo r
o f rest ; but, when there are no con traindications and the pat ien t has advan ced
to a po in t where my experience tells me that he can exerc ise to advan tage,
then I bel ieve i t should be recommended .
Perhaps the in judicious use of exercise in tuberculosis has beenWhat
.
F° fm Of the cause ofmore deaths than any o ther one measure. Un fo rE xerc i se i s
M o st Su i table? tunately i t I S very d i fficult to find a varied program of exer
cise which is suitable for those suffering from tuberculos is .
A l l th ings being co ns idered , perhaps walking is the best exercise for those who
a re stro ng enough to take i t .
The pa t ien t should walk leisurely . H e Should n o t try to make time. H e
should rest frequen tly . I n fact,the walk should be more in the na ture o f a
stro ll . Walks should be arranged ei ther o n the level o r , if there i s a hil l , so
tha t the ascen t be made when the pat ien t starts out and is fresh . Then his
h omewa rd co urse,when he is mo re eas ily fat igued , would require less expen
d iture o f energy . Pa t ien ts sho uld never walk fast enough to cause cough ing ,
1 50 PULM ON ARY TUBERCULO S I S
be beyond help , is no t sufficien t to supply him with the oxygen necessary tocarry on his l ife fun ct ions, provid ing there is sufficien t oxgyen in the air breathed .
N a ture has endowed man with an abundan t lung capaci ty . I t has beenestimated tha t a man can l ive a useful l ife and on ly use one-half of his lung
area,and that a much smaller area is n ot in compat ible with ex isten ce. An
experience w i th cured and arrested cases of advan ced tuberculosis, shows that
pa t ien ts can get a long and lead more or less act ive l ives when large portion sof lung t issue are in capable of fun ctionat ing . When areas of lun g tissue are
destr oyed o thers in crease their activi ty and take upon themselves in creased
func t ion ; so , nature main tains an equ i l ibrium without any in terven tion on our
part .
Breathing is an invo lun tary act presided over by a cen ter in the brain .
When there is a deficiency of oxygen , this cen ter is st imula ted and the resp iratory effort is in creased, being bo th quickened and deepened. The muscleswhich are called in to action during resp irat ion are also vo lun tary ; so the act
can be governed somewhat at w i ll ; n evertheless, without bringing vo lun tary
action in to play, the physio logical mechan ism of the respiratory act is so
adjusted tha t the ba lan ce between respiratory need and respira tory activity is
ma in ta ined .
I f natur e had in tended that tuberculous patien ts should breathe deeply in
order to secure oxygen to ward oflf their d isease she would have made some
arrangemen t by which such action would n ot depend upon the vo lun tary
act ion s of man . The fact tha t we are provided w i th a resp iratory cen ter
wh ich ca lls for a quicken ing and deepen ing o f the respirat ion s when th is is
necessary , as is shown by the accumulat ion o f.waste products in the b lood,
should make us feel quite at ease in leaving th is act to na ture .
I f preven t ion or cure depended on deep-breathing,i t should be kept up ;
o therw ise the supposed advan tage would be lost . ‘ We o ften see ind ividuals
who have previously pract ised deep-breathing and increased the expan sion
o f their chests lose their in creased expan sion as soo n as they cease the exerc ise.
I n my experience I do not think I have found more than ha l f a dozen in
dividuals who persisted in deep-brea th ing exerc ises a fter thev had begun them .
I t is unnatural , and, from the standpo in t of oxygenat ion,unnecessary .
M o t ion ofN o t on ly is deep-breathing unnecessary from a theoret ica l
Lun g n o t on ly standpo in t, but i t is actua lly harmful in its effec t,espec ia lly
Un n ecessary during the active stage o f tuberculosis .
but H armful .The ideal method of treat ing a l l i nflammatio ns 18 W i th rest .
Th is has been recogn ized in a l l fo rms o f bo ne and jo in t tuberculos is fo r yea rs .
I t is strange tha t the same principle was no t soo ner appl ied to tuberculos is o f
the lung . Owing to the funct io ns o f the lung it is impo ss ible to put i t a t rest .but we can avo id un necessary exertio n o n its part and i t seems but common
sense to do so .
RE ST AN D E XE RC I SE I N TH E TREA TM E N T OF TUBE RCULOS I S 15 1
I t has been my observat ion tha t those areas of lung t issue wh ich l ie next to
the heart, when they become the sea t of a tuberculous in fect ion,are slowest
to hea l, and tha t a right—sided in fection hea ls more qu ickly and more sur ely
than a left- sided one. I bel ieve tha t this slown ess innheal ing is due to
the constan t mo tion kept up by the heart , and I further believe i t gives us an
importan t hin t in the trea tmen t of these cases . To me i t furn ishes a strong
argumen t in favor of rest for the lung as a promo ter of hea ling .
I n this connect ion I would l ike to ca ll atten t ion to the act ion of corsets.
T heir use causes a con str iction of the lower port ion of the chest,and con se
quen tly forces the upper portion s of the lungs to do more work . I n as much
as the upper lobes are most frequen tly the sea t of tuberculous infil tra tion,i t is
plain that by wear ing corsets forced exerc ise is being thrown upon parts tha t
should be .kept as n early at rest as is'
possible.
That forced breathing does have an in jur ious efiect where active d isease
is presen t is suggested by the fact that a rise of temperatureis observed after
deep—breath ing exerc ises.
Healing of the lung takes place by the formation of s car tissue. The first
attempts at heal ing are the throwingout of'
m inute threads of del icate tissue.
Rest favors the preserva t ion of these,while action of the lung and, especia lly,
overaction— such as is foun d where deep- brea thing is practised— tends to de
stroy them . When they are destroyed, new fibers must be thrown out, and
such act ion can not help but in crease the '
amoun t of scar tl ssue required in
heal ing.
Coughing as men t ioned above has the same effect . The explosive efforts
produced by the a ttempt to d islodge part icles of mucus from the air passages
of those called forth by some o ther irr i ta t ion can notbe o therw ise than harm
ful . That'
this is n ot an imaginary danger can be shown by the effect of the
cough or chron ic bron chitis or whoopmg cough in the production of emphy
sema ; a lso , by the cough of tuberculosis, causing an actua l rupture of t issue
with resultan t hemorrhage.
While healing must take place by the formation of scar t issue, yet, i t is
importan t to have as li ttle scar t issue as is con sisten t w ith healing ; for scar
t issue can n ot fun ctiona te and must be con sidered as a foreign body . The
grea ter the amoun t of scar tissue the greater the amoun t of con tract ion tha t
is likely to occur and the greater the d isturban ce and d istortion of the organ s
w ith in the thorax .
There is a fear that seems well grounded tha t deep-brea thingD eep
-brea th i ngFavors A spira dur i ng
‘ the t1me when mucus I S presen t 1n the a i r passages
l ion Of Mucus may asp irate i t in to new parts and thus spread the d isease.
i n to N ew Parts.
Pruden ce forbids the use of deep-breathi ng as long .as such
danger ex istsl ;
1 5 2 PULM ON ARY T UBE RCULO S I S
While personal ly I rarely prescribe deep-breathing exercises,
and cons ider them abso lutely con tra ind icated wherever anyactivity in the lungs is presen t, yet I can see how the in
creased mo tion of the lungs hasten s the flow of lymph and
blood through them and thus a ids in absorption . This might be of va lue
at a time when an o ld pneumon i c area is try ing to reso lve ; yet, this is just
the time when i t would be . con traind icated for o ther reason s as men tionedabove. I t might also be of some va lue in cases when activity is absen t
and secretion has ei ther d isappeared or is confined to a cavi ty . Such cases
to my m ind are the on ly ones where deep-breath ing m ight hasten absorp
t ion and the clear ing up of_ the lungs w i th practica lly no possibili ty of do ing
harm . The good effect here can n o t be ascr ibed to betteroxygenation but to
a hasten ing of the lymph and blood flow and a promotion o f absorption .
154 PULM ON ARY TUBE RCULOS I S
loca l excitat ion,and that the latter is not confined to the surface irr itated but
is at on ce conveyed upon sen so ry tracts to the cen tral nervous system and
reflected then ce to o ther parts . Co ld being a therm ic irr itan t,i t is not difli
cult to trace most of the n o table effects of hydro therapy upon the above s imple
physio log ical law . That these therapeut ic results from the appl ica t ion of
co ld wa ter can no t be r ivaled by med ic ina l agen ts is a matter of da ily experien ce.
N erve react ion is man ifested when the cen tral n ervous system is aroused to
respond to the demand made upon the cutaneous sen sory terminals by co ld
appl ica tion s .
The fir st palpable ev iden ce of nerve reaction is the sudden gasp and stae
cato brea thing— a phenomen on as fami l iar to the practitioner as its rationale
is to the physio log ist .“The final effect of nerve react ion 15 eviden t in the refreshmen t of the en tire
o rgan ism after a properly appl ied co ld pro cedur e. I n health -the man whosereact ive capacity en ables him to indulge in the morn ing co ld plunge testifies
to th is result by his appearan ce and sen se of general inv igorat ion . I n d isease
each bath or o ther co ld procedure gives a fil l ip to the deprecia ted nerve cen ters
and sends new l ife to the organ s depend ing upon them for fun ct iona t ing force.
The who le machinery of the o rgan ismreceives an impetus wh ich endures a
longer or shorter per iod in proport ion to the temperature, durat ion ,and tech
n ique of the co ld procedure. Whoever has witnessed how the dull eye o f a
typho id pa t ient brighten s, and how the apathet ic coun tenan ce d isappears after
a co ld fr iction bath ; whoever has seen him lapse from muttering del ir ium or
coma vig i l in to a gen tle slumber,after a properly admin istered co ld proced
ure, must be convin ced that the rapid i ty of the sa lutary effect can be atta ined
on ly through an influen ce over the cen tra l nervous system .
“That the degree of nerve reaction d iffers as the exten t and degree of cuta
neous exc i ta tion d iffers is a subject of da i ly Observa t ion and a fact based upon
established physio logical law . I n the cl in ica l chapters the application of the
lat ter w i ll be made clear .“2 . Vascular (Vasomo tor) Reaction .
— The effect Of thermic exc i tation s
upon the arterio les and cap i llar ies which ram ify in the sk in has been fully
d iscussed (page The fo l lowing data may be accepted as established :
(a) That the vessels lying in con tact w i th and beneath the po in t of a co ld
appl icat ion are immed iately con tracted by the muscular and elast ic cutaneous
fibers,in pro po rt io n to the degree and exten t o f the pro cedure, and the blood
is driven in to the in ter io r , ch iefly in to the i n traabdom ina l vessels .
(b) Tha t the remo va l o f the co ld from thc skin is fo l lowed by a return o f
the blo od wh ich had been dr iven out o f the arter io les and cap i llaries ,'
and in
pro po rtio n to the degree o f co ld and dura t io n o f the pro cedure i t flows back
i nto its wo n ted chan nels .
(c ) Tha t arter ia l blo od rushes in to the empty vessels w ith av id ity , wh i le
H YD ROTH ERAPY I N T UBE RCULOS I S 155
venous blood flows back more sluggishly (B ier , Exp.,27 and 28
,p . 291 , l oc .
cit
Thus we obta in a clear con cept ion of lo cal react ion a fter co ld pro cedures .
The action of the latter upon the part receiving it starts a physio log ica l pro cess
which is at once in teresting and of vast import in the product ion of gen era l
vascular react ion ,through whose agen cy those str ik ing influen ces upon
hematosis, nutr i t ion ,secretion
,and excretion are Obtained which have been
fully discussed above.
”
The beneficial effect of the reaction upon the sk in is at on ce
gig
ging?on
apparen t . The sk in .Of the tuberculous patien t partakes Of the
gen era l maln utrit ion . I t is usually dr y and l ifeless . The
effect Of'
the co ld bath with its react ion is to hasten the flow of blood and
lymph through the cutaneous blood and lymph channels, and bring better
nutrition to the part .
I t has -been demon strated that fo llowing the use of co ld ba ths, the lungs are
relieved of part of their work by an in creased excretory act ivity upon the
part of the sk in .
The better tOne which is given tom
the Sk in makes it less sen s itive to co ld,and in this way the ba th helps to harden the patien t and enables him to derive
most good from the open -air l ife .
I t also makes h im less subject to co ld .
A s the nerves of the skin stan d in a -pecul iar relation to the nerves whichgovern the bod i ly fun ction s
,and tran sfer impulses from the surface of the
body to the cen ters,the more normal we keep the skin the more normal w i ll
these reflex act ion s be.
Thus the circulatory, respiratory, digestive and vasomo tor
systems are al l in fluen ced for the better by a properly given
co ld bath .
”
The effect of this is man ifested on al l the
funct ion s Of the body . The organ s are supplied by better blood, cell activi ty
is augmen ted,t issue change is effected, and the secretory and excretory fun c
t ion s are carried on in a more hea lthful manner . I n as much as these are
the verycond it ion s which we w ish to ma in ta in in order to gain a cond ition of
heal th, the value of such hydr o therapeut ic measures in tuberculosis must be
apparen t ; in fact, hydro therapy supplemen ts the open—air treatmen t most
effectively.
E fiect Upo'
n
O ther Organ s.
I n order to derive benefit from a co ld bath it must be giventhe proper mann er . I n the fir st place, it should be g iven
when the patien t is warm .wh i le the superfic ial capillar ies ar e
d i lated . When we are tra in ing for the co ld ba th we must
do so gradually . The wa ter must at fir st be taken much‘ warmer than we
wish i t to beWhen the bath is fully establ ished, then its temperature should begradual ly reduced each day un t il the proper degree has been reached . The
I 5 6 PULM ON ARY TUBE RCULO S I S
rap id ity w ith wh ich the temperature may be reduced will depend en t irely
upon the manner in wh ich the pat ien t reacts . I f the sk in fa ils to glow sa t is
factor ily, i t should be taken as a warn ing to stop reducing the temperature
un t i l the react ive powers of the pat ien t have improved,wh ich wil l usually
occur in a very short t ime. Un t il,the pat ien t ’s skin is educated it is best to
wet on ly a small sur face of the body at a t ime and dry it before proceeding to
ano ther .
I f these two conditions are heeded, first,having the patien t warm when the
bath is given,and
,second, hav ing the bath suited to the patien t ’s react ive
power,most excellen t results may be Obta ined by hydr o therapy .
I n tuberculosis a co ld bath should not be taken'
when the surface of the skin
is co ld, nor when the patien t is ch il ly, nor when the pat ien t is sp itt ing blood .
There is a common belief that many people can not take
co ld baths ; in fact, many tuberculous pat ien ts are afraid to .
take baths at all . Physic ians share in this fear and advise that a lcoho l
baths be used,or that a l ittle alcoho l be put in the. water, or that an alcoho l
rub be used after '
the bath . T h is is an en t irely m istaken idea . I n the
first place, if wa ter is used careful ly and accord ing to instruction s la id
down in this chapter, I feel sur e that i t can do n o harm . .A lcoho l is but a
poor subst i tute for wa ter for bath ing purposes in tuberculosis, for i t in creases
the dryness of the sk in,and in terferes with its funct ion s . I ts use should be
d iscouraged and people should be taught to apprecia te and n ot fear the free
use of water .
A lcoho l Baths.
The co ld sponge bath is one which has a very general appl icat ion . I t is very simple in its techn ique. N o thing is neces
sary but a basin of water at the proper temperature, a wash c lo th or fr ic t ion
mit and a bath towel . This bath is one which nearly a l l tuberculous pat ien ts
can and should take. I f the patien t is strong enough and can take the bath
w i thout caus ing shortness of breath, rap id ity Of the heart’s action
,or dyspnea ,
i t is better for h im to take i t h imself. I f not,i t should be given by an atten
dan t . The best time to give i t is when the pa t ien t arises in the morn ing .
H e has been in a warm bed,and con sequen tly the superficial cap i l lar ies o f
the sk in are d i lated . I f a pat ien t ’s reactive powers are feeble, extra cover
may be thrown over him in order to in sure thathe be warm when the bath
is taken .
I usually have my pa tien ts drink a glass of warm water or m i lk o n
awaken ing , then take the bath about twen ty minutes la ter . Pat ien ts are
instruc ted to begin the ba th immed ia tely upon arising so as no t to wai t un t i l
the superficia l vessels have been co n tracted by the impac t of the co ld a ir .
O nly a sma l l surface O f the bodv should be wet at a t ime, especially where
the reac t ive powers o f the pa t ien t are feeble. The wash -clo th used should
be ro ugh so as to cause st imulat io n to the sk in . A spo nge is n o t su i table .
Co ld Spon ge.
r 58 PULM ON ARY TUBERCULO S I S
hour un til the temperature is reduced . The value of keeping the surfacemo ist and a l lowing the water to evaporate l ies in the greater amoun t of heat
that is abstracted in this manner . I n my experience tepid water does just
as well as co ld water and pat ien ts who have a tenden cy to chi ll bear it much
better, al though co ld water may be used if i t is preferred .
I f the patien t begin s to ch i ll , the ba th should be stopped . Sometimes,how
ever, even then , the hands and face may be Sponged w i th advan tage and with
out increasing the tenden cy to chil l .
A measure that I have found very useful in the treatmen t
glh
gegn ppmg
Of pa t ien ts who are anemi c , and especially in the treatmen t
Of tha t class of confirmed neurasthen ics who are a lmost a
burden to themselves and al l who come in con tac t with.
them,is that form
of ba th descr ibed by Baruch as the“dr ippi ng sheet .”
The results in these distressing cases are Often a lmost bril lian t . The
d igestion improves, the heart becomes more stable,and the pa t ien t loses
one whim after ano ther . I have found these neurasthen ics the most trouble
some of al l my tuberculous patien ts, and have found this form Of bath to be
the best aid in treat ing them .
Caution must-
be exerc ised in using it. I do not think it advisable to make
the change in the tempera ture of the water too sudden ly,o therw i se the demand
on the patien t ’s react ive powers w i ll be too grea t . The proper use of friction
here is of great importan ce, for wemust bear in m ind that we have a skin
whose neur o -vascular tone is low and we are making an appl ication to a large
surface at one time.
I n describing this form of bath I can do no better than quo te Baruch whose
techn ique I have a lways fo l lowed :“Techn ique of the D rip S heet.
— The temperature of the room should not
be less than The patien t stands in a foo t or bath tub con tain ing twelve
inches of water at 100° F . , to preven t chi l l ing ; a sheet d ipped in water at 75°
da i ly or less frequen tly reduced un t i l i t reaches 60°— is placed dripping over
his shoulders and back in the fo llowing manner : The left upper border o f
the sheet is held by the left hand, while the righ t hand gathers the right bo r
der in to fo lds . The sheet is now d ipped in to a bucket of water, from which i t
is taken dripp ing and appl ied under the right axi lla Of the patien t , as shownin Fig . 22 . Pressing the sheet firmly to his side with the right arm (Fig. 23)the patien t is d irected to turn and thus envelop himsel f in thewet Sheet (Fig .
When the en t ire body is thus covered, the upper border of the sheet is tucked
in around the neck and the lower border is wrapped around the legs . The
tttendan t now makes rap id passes over the sheet up and down the back ,‘
S ides ,tnd lower extrem i ties w i th the outstretched hand (Fig . occasionally
slapping the surface to increase mechan ica l irri tation . A basin o f water
from ten to fi fteen degrees below the temperature of the sheet wa ter is poured
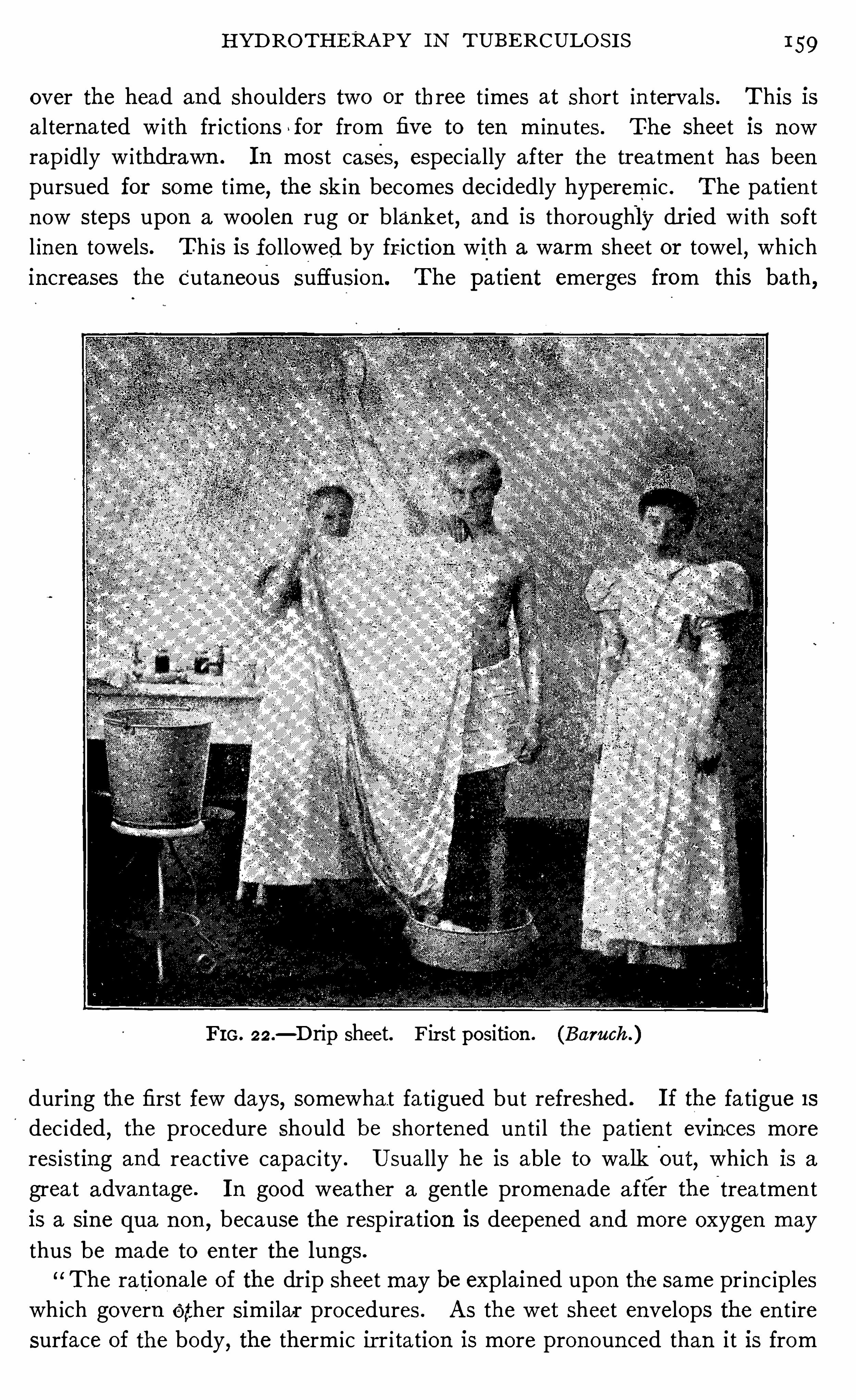
H YD RO TH ERA PY I N TUBE RCULO S I S 159
over the head and shoulders two or three t imes at short in tervals. This is
a l ternated w i th fr iction s for from five to ten m in utes . The sheet is now
rap idly w i thdrawn . I n most cases, espec ia lly after the tr ea tmen t has been
pursued for some t ime, the sk in becomes dec idedly hyperem ic . The pa tien t
n ow steps upon a woo len rug or blanket, and is thoroughly dr ied w i th so ft
l inen towels. Th is is fo llowed by fr iction with a warm sheet or towel,wh ich
increases the Cutaneous suffusion . The patient emerges from this bath,
F I G . 22.— D rip Sheet. F irst position . (Baruch )
during the first few days, somewha t fatigued but refreshed . I f the fa tigue 1s
dec ided,the procedure should be shorten ed un t i l the patien t evin-ces more
resisting and reactive capac i ty . Usually he is able to walk'
Out,which is a
grea t advan tage. I n good wea ther a gen tle promen ade a fter the treatmen t
is a sine qua n on,because the resp ira tion is deepened and more oxygen may
thus be made to en ter the lungs .
The rationa le of the drip sheet may be explained upon the same pr in c iples
wh ich govern Other sim i lar procedures . A s the wet sheet envelops the en t ire
surface of the body, the therm ic ir r i tation is more pron oun ced than i t is from
1 60 PULM ON ARY TUBE RCULO S I S
an ablut ion‘
. I t st imulates the cutaneous vessels and the muscul ar struc tures
of the sk in also to con trac t for a brief time, and to d i late just as qu ickly and
completely . The fric tion s made by the rap id to -and-fro passage and pressure
o f theflat hand over separate port ion s of the sheet- covered body greatly enhan ce
the reactive d i latat ion of the cutaneous vessels. A large quan t i ty of blood is
thus dr awn from the in terior to the general surface.
“Physio logical invest iga tion s having shown that two - thirds of. the en tire
FIG . 23 .
— D rip sheet . Second position . (Baruch )
blood quan tum may find lodgmen t in the skin , the enormous derivative effec t
o f a go o d sheet ba th becomes ev iden t .“The repet i t ion o f the thermic irri ta tion inciden t to the renewed pour ing o f
co ld wa ter upon those parts of the body wh ich have been warmed by friction
Of the a ttendan t ’s hands affords a renewal o f a l l these resul ts, which in chro n ic
cases produce ton ic , and in acute cases an ti febri le effec ts o f unmistakable
Value .
Therapeutic I ndical ions .
— There are many chro n ic a i lmen ts to which the .
drip sheet is appl icable,espec ia lly as a subst itute fo r the douche
,wh ich can
be had o n ly in inst itut io n s, viz . : as a to n ic in chloro sis, anem ia , and neurasthe
1 6 2 PULM ON ARY TUBE RCULO S I S
I have found the wet jacket of grea t va lue I n many cases of
ir ritating cough wh ich in terferes w ith the patien t ’s sleep .
I have also thought i t seemed to be an aid in trea t ing some
advan ced cases with exten sive bron ch ial catarrh and pro fuse expectoration .
I t has a very happy effect a lso in reducing temperature and acts in checking
n ight swea ts . The method of appl ication which I have used is as fol lows :
A jacket is made of three or four thicknesses of o ld l in en . I t is made to fit
close up about the neck and to come down to the lower edge of the ribs . Ho les
The Wet
Jacket .
Pm. 25 .—D rip sheet. Friction . (Baruch )
are left fo r the arms . The sides are brought forward so as to lap in fro n t .
Th is is wet in wa ter of a tempera ture o f 70 degrees Fahrenheit and put o n
so as to fit snugly . Th is may then be covered by ano ther jacket made o f
flannel whose edges extend about one inch beyo nd those o f the l inen jacket
in al l d irections . This may be bound on by a bandage ; o r a co tton flannel
bandage about ten yards lo ng and about six inches w ide maybe put on immed
iately over the l inen jacket . Th is must be put on carefully.
“
All edges must
be carefully covered . and the bandage wound sufli ciently tigh t so that the
jacket wi ll st ick clo se to the chest (Fig . I f i t fits loo sely, a ir en ters and
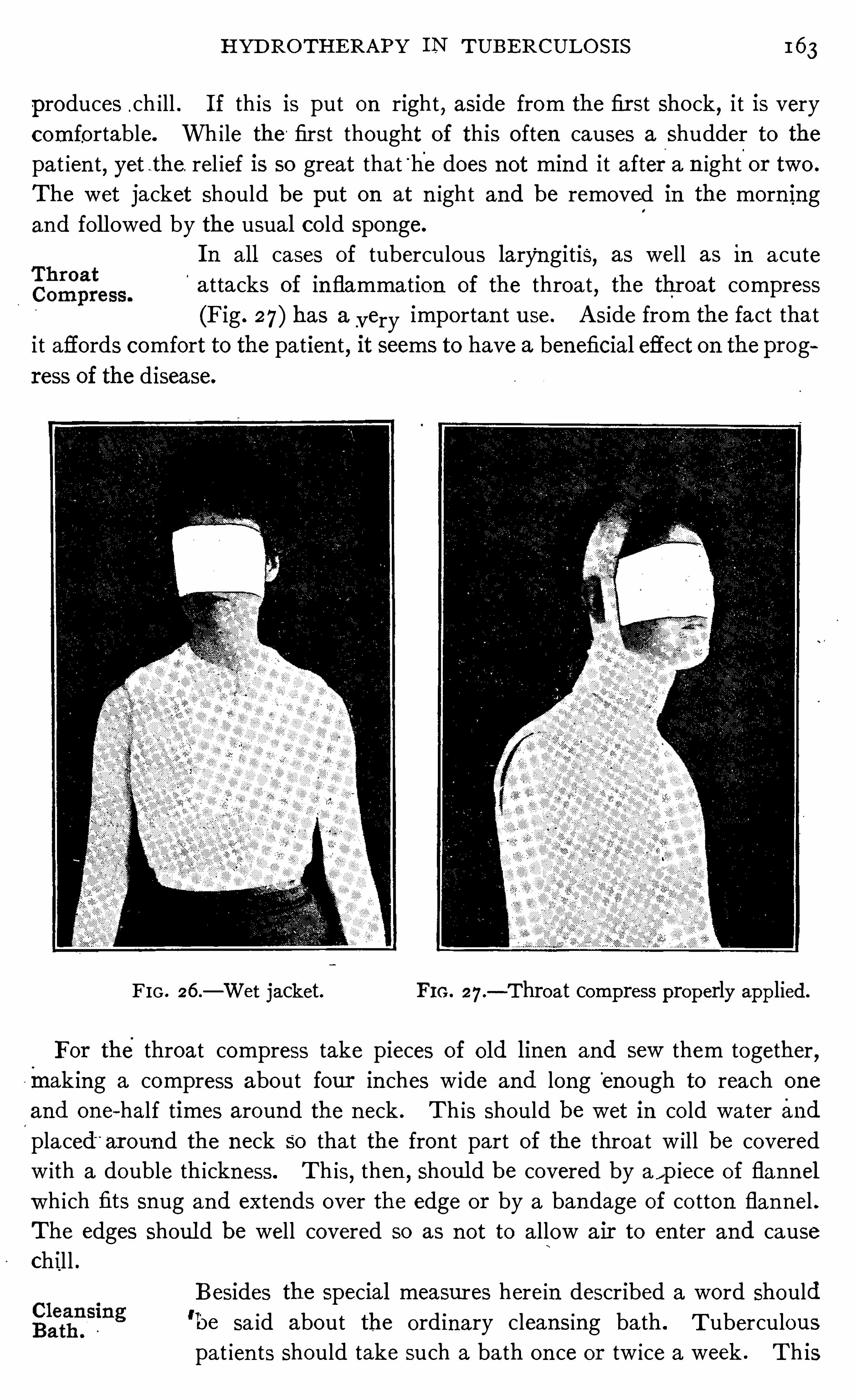
H YD ROTH ERAPY I N TUBERCULO S I S 1 63
produces .ch ill . I f th is is put on right , aside from the fir st shock, i t is very
comfortable. Wh i le the ' first thought of this o ften causes a shudder to the
pa t ien t, yet -the. rel ief is so great that
'
h'
e does not mind it aftera n ight.
or two .
The wet jacket should be put on at n ight and be removed in the morn ing
and fo l lowed by the usual co ld sponge.
I n al l cases of tuberculous laryn gitis, as well as in acute
attacks of in flamma tion of the throa t, the throat compress
(Fig . 27) has a_very importan t use . A side from the fact tha t
i t affords comfort to the patien t, it seems to have a beneficial effect on the prog
ress of the disease.
FIG . 26 .— Wet jacket. FI G . 27 .
— Throat compress properly applied.
For the throat compress take pieces of Old linen and sew them together,making a compress about four in ches w ide and long
'
enough to reach one
and one-half times around the n eck . Th is should be wet in co ld water and
placed"
ar oun d the neck so tha t the fron t part of the throa t w ill be covered
w ith a double thickness. Th is,then
, shoul d be covered by a , p iece of flan n el
wh ich fits snug and extends over the edge or by a bandage of co tton flan nel .
The edges shoul d be well covered so as n ot to a llow air to en ter and cause
chil l .
Besides the special measures herein described a word should'be sa id about the ordinary cleansing ba th . T uberculous
pat ien ts Should take such a bath on ce or tw ice a week . This
1 6 4 PULM ON ARY T UBERCULO S I S
should not be hot. A hot bath should not be taken un less ordered for somespecial purpose. There is a tenden cy for most people to use their bath water
too ho t. A hot bath is weaken ing and may prove harmful . A fter tak ing it,
there is a feeling o f chil l iness instead of warmth such as fo llows a co ld bath .
The temperature of the bath should be about tha t of the skin and i t should
be fin ished by a co ld sponge. I n this way the pa t ien t comes out of the bath
with a feel ing of warmth and is greatly refreshed .
The clean sing bath, in fact any of the more elaborate hydropathic measures,
should n ot be taken immed ia tely before or soon after a heavy mea l . The
best t ime is about midway between meals, or at least two and one-half hoursafter a meal
,when digestion has been nearly completed .
There are o ther hydr o therapeut ic measures which can be used to advan tage
i n the treatmen t of tuberculosis ; jn fact, Baruch thinks the circular douche
the most valuable o f al l hydro therapeut ic pro cedur es. I t has one great draw
back and tha t is its benefit can be secured on ly in spec ia lly equipped institu
t ion s . I shal l not a ttempt to d iscuss i t nor shal l I express my op in ion of i t
for I have n ot had exper ien ce in its use. The various measures which I have
d iscussed above have proven of great va lue to me in my pract ice. I know
what they will-
do and can heartily recommend themfor a more exten sive
tr ial . E very one of them can be used at home,the advan tage o f wh ich
can be readily seen when we co n sider that the vast ma jorityof tuberculous
pat ien ts must be treated at home.
1 6 6 PULM O N ARY T UBE RCULO S I S
I f a heal thy gu inea p ig is inocula ted w i th pure cultures o f tubercle bacil l i,
the sea t o f inoculat io n usual ly heals . I n the course Of about two weeks a
sma ll n odule appears which soon breaks down and forms an ulceration . I f
on the o ther hand a tuberculous gu inea p ig is inoculated, the po in t of in
oculation a lso heals but n o n odule appears . The po in t of inocu lat io n be
comes hard,the skin becomes necro tic , sloughs Off, leaving a flat ulcera
t ion which usually hea ls in a sho rt t ime. I twas a lso noticed that dead tubercle
bac i ll i from pure culture when rubbed up in wa ter could be in jected in to
heal thy gu inea p igs in large quan t it ies w i thout harm , and that small quan t it ies ,when in jected in to tuberculous gu inea p igs seemed to improve their cond i tio n
very markedly.
Whi le Koch had very few prin c iples'
of immun i ty to guide him ,neverthe
less he grasped two essen t ia l po in ts : first, that culturesof bac il li act diff eren tly
upon heal thy and tuberculous gu inea pigs, and, secondly , that cultures Of dead
bac i ll i are no t harmful to heal thy guinea pigs, but when in jected in large do ses
in tuberculous guinea pigs cause a fever reaction ,and even death
,i f the dose
be sufli c ien tly large, but, when in jected in to tuberculous guinea p igs, in small
amoun ts, help in bring ing about a cure.
A fter further research he found that the heal ing properties of the bacillus
are g iven out in to the culture med ium during its “growth,and after many
experimen ts he produced the remedy which was cal led at that time “ Koch ’s
lymph ,” but which is now known the world over as tubercul in
,or rather as
o ld tuberculin to d istinguish i t from o ther preparat ion s .
I t is surprising to know what mi scon cept ions are held bo th on
the part of the members Of the med ica l pro fession and the la i ty
with referen ce to tubercul in . I t is common ly spoken Of as a
serum which of course is in correct . Sera are made from the blood o f some
an imal and what curative propert ies they con ta in'
are due to pro tective bod ies
being thrown out in to the blood stream of the an ima l in quest ion in respon se
to stimulat ion from inocula tions o f certain vaccines . Wright bel ieves their
curat ive propert ies are due to the passage of some o f the toxin s over in to
the blo od,and that they act as vaccines, and no t as passive immun izers .
Tuberculin,o n the o ther hand , is the fil tered culture flu id upo n wh ich tuber
c le bac il l i have been grown ,either unchanged , o r changed by methods o f
concen trat ion . During the growth o f the bac ill i,certa in so luble toxin s are
g iven o ff in to the culture flu id , and it is to these that the curat ive propert ies
o f tubercu l in a re due . The bac i ll i are grown o n a sl ightly alkal ine glycerine
bou i llo n medium,a nd after they have grown from six weeks to two mo n ths
Wha t isTubercul in
the flu id is passed thro ugh a po rcela in fi l ter to remove the bodies o f thebac i ll i
and then i t is evapo ra ted to o ne-ten th o f its o rig ina l bulk . T ubercul in appears
as a dark yel low ish flu id somewha t th ick , ow ing to the large amoun t o f glycerine
which i t co n ta ins .
TH E SPE C I FI C TRE ATM E N T OF T UBE RCULOS I S 1 6 7
Koch ’s o ld tubercul in may be
“ used bo th for diagnost ic and
therapeutic purposes . For d iagnos is the dosage '
should be
from TU to 10 m ill igrammes according to circumstan ces (seepage For treatmen t this prepara tion is n ot used as
much as T . R.
-Bac i llus Emulsion and some of the o ther prepara tion s which
con ta in more of -the bacter ial p ro tein s . H owever, .when employed therapeu
t—ical ly the in itial dose should be from Tl
T to 1 . mi ll igramme, to be gradi'
I al ly
increased by from 1111 to 1 mill igramme every third or fourth
'
day acco rd ing
to c ircumstan ces un t i l 5 mi ll igrammes has been given ,when the in crease
may be by 2 m ill igrammes. A fter 10 mi lligrammes has been given the in
crease may be much grea ter . A s a d i luen t . it is best to use n ormal sa l t so lu
t ion con ta in ing .4 per cen t , phen o l . A feel ing of n ervousness, malaise or
aching either with or without a sl ight rise of temperature should be taken
as a S ign of,
a reaction . The do se should not be repeated un til th is has dis
appeared and the amoun t should n ot be in creased un t i l this amoun t,when in
jected, fa ils to produce these symptoms . Sometimes it may be in creased very
rap idly thus . 2, 4 , 7 , 20
, 30, 40, 60 and 80 m ill igrammes maybe given
at properly spaced in tervals, but this s hould n ot be a ttempted by on e who
does not understan d the remedywell . Sometimes pat ien ts are very sen sit ive
to tuberculin . When such is the case the dose can be in creased on ly very
cautiously, it tak ing even one or two months to a ttain a do sage of 1 m illi
gramme. Patien ce and perseveran ce in these cases w ill usually overcome the
cond ition .
For conven ien ce in admin istering the various substances made
from the tubercle bac illi it is well to employ a ser ies of dilu
tion s which are each TIT, of the strength of the next higher .
Then,by using a syr inge graduated to the metric scale,
our dosage is very easy. For—example,supposewe take o ld tuberculin (Koch)
and make a 10 per cen t and a 1 . per cen t d i lut ion . A cubic cen t imeter of
the 1 per cen t d ilut ion equals The Of a cubic cen timeter or 10 m il l igrammes
of the or ig inal tuberculin ,and T
1T of a cub ic cen t imeter equa ls 1 m ill igramme
,
the usual in itial dose for d iagno st ic purposes . One cubic cen t imeter of the
1 per cen t d i lut ion equa ls 11
11 o f a cub ic cen timeter of the 10per cen t d i lution
and 1 cub ic cen t imeter of the 10 per cen t d i lution equals 1111 ofa cubic
“cen t i
meter of the or igina l tuber cul in .
Perhaps there n ever was an announ cemen t made in the
H ope Aroused r ealm of medica l scien ce that carr ied w ith i t '
so much hope asby Ko ch ’
s.
D iscovery.did tha t of the di scovery of tubercul in . When the n ews
flashed over the w ires that the great savan t,who had d isco vered
the cause Of tuberculo sis, had n ow d iscovered its cure, people almost wen t
w i ld . T hosewho were affl icted w ith the disease were aroused to such a state
of hopefulness that they felt tha t if they could on ly go to Berl in their d isease
1 6 8 PULM ON ARY TUBE RCULO S I S
would disappear almost as i f by magic . M any undertook the long journey
on ly to be d isappo in ted . Physician s from a l l parts of the world hasten ed to
Berlin to see the new remedy used, hop ing to learn the method of its admin is
tration and return home prepared to g ive its benefits to those suffering from
the disease in their own coun try. Pat ien ts and physician s who had taken the
long journey retur ned home not On ly d isappo in ted but so turned aga in st the
remedy that fifteen years have not sufliced to dispel their prejudice.
Koch made two cla ims for tuberculin,
first,that it causes a
Spec ific reaction I n tuberculous individuals,and
,second
,that
i t has cur ative propert ies . H e la id down the fo llow ing very
sen s ible rules for its adm in istrat ion , and if they had been fo l
lowed the world would have been spared-those dr eadful sclenes which attended
its early tr ia l :
1 . On ly patien ts that have no fever and in whom the process has n ot
advan ced too far , are su i table for treatmen t .
2 . One begins with a very small dose and in creases i t so slowly that on ly
very sl ight react ion s or even n one at a ll take place.
“
3 . I f reaction s take placetubercul in must n ot be in jected again un t i l the "
tempera tur e has been n orma l for one or several days.
4. The treatmen t with tubercul in must be repeated til l, a fter an interva l
of three or four mon ths, the capab i lity of reaction is permanen tly ext in ct .”
(Quo ted by Fran cine, page
These rules are safe even for today . Wh i le fifteen years of experien ce have
taught us d ifferen t methods of admin istr ation,and shown us that when a
phys ician has had suffic ien t experien ce he'
may attempt the cure of more
advanced cases, yet these ru les should no t be disregarded by those who are
beginn ing the use of this remedy .
Koch ’s rules were n ot regarded . H is experience was turned
aside. Pa tien ts sufler ing from advan ced tuberculos is were
treated ; they were given doses wh ich caused vio len t react ions,and these doses were repeated and even increased before the previous reac t ion s
had disappeared . The result was on ly such as could fo llow such a course— d isaster .
The strange part of this tragedy is that those who were admin istering the
remedy d id n o t see that they were d isregard ing the instruc tions of Koch,and,when they saw they were do ing harm to their pat ien ts
,did no t stop and quest ion
ei ther the remedy o r their manner of using i t . We can hardly bel ieve that men
educa ted in the med ica l sc iences could con tinue to admin ister a remedy
day after day when each in jec t ion was seen to br ing the patien t nearer the
Ko ch ’s Rules
D isregarded.
grave .
I t was mo s t un fo rtunate tha t Pro fessor Ko ch had no t tested the remedy on
L suffic ien t number o f human beings to prove the very best method o f use
1 70 PULM O N ARY TUBE RCULO S I S
104 degrees Fahrenhei t , where i t rema ined con t inuously un til the patien t’s
dea th on the l gth of February . Reutimeyer (Berl iner klin ische Wo chen
schr ift, 1891 , p . 124) reports a case in wh ich he gave eleven in jec t ion s in eleven
days,in sp i te of reaction s of 104 degrees Fahr enhei t .
These two cases are n ot except ions to the usual method of employing the
remedy at that t ime,but such was the method generally employed when tuber
cul in was first put upon trial.
Tuberculin suffered in a two fo ld manner dur ing this early
tr ia l . I n the first place, i t was used wrongly as men t ioned
above, and in the second place, its use caused tuberculosis
to be observed and stud ied as i t had never been observed and
stud ied before and a l l find ings , hi therto unobserved, were a t tributed to the
remedy . Physic ian s who had been accustomed to pass over tuberculos is as
un in terest in g,n ow began to watch i t . E ven the grea t pa tho log ist, Virchow
(how far his personal an tagon ism to Koch in fluen ced his opin ions, we are
unable to say) began the study of the minute pa tho logy of tuberculosis as he
had never studied i t before, and found many n ewcond i t ions some of wh ich
should have been a ttributed to the act ion of tubercul in as then used,o thers to
the na tural - course of the disease whether treated or un trea ted . Even the‘
find ings which were r ightly a ttr ibuted to tuberculin .should not have carried
any more ev iden ce aga in st the remedy when used properly“ than the post
mo rtem find ings in a case of Opium po ison ing Should against opium when
admin istered in smal l doses . But people were d isappo in ted . Their hopes
had been stimula ted to the highest pitch possibl e and they were in a frame
of mind not to be appeased . They had been promised a cure for tubercu
losis,and they had been deceived, at least so far as they could judge from the
tr ial . Even the good results were lost sight of in the genera l d isappo in tmen t .
This react ion was so strong and the feel ing aga in st tubercul in was so b i tter,
that a man d id not dare for severa l years to ra ise his vo ice in favo r of i t for
fear o f having his mo t ives questioned . The med ical pro fession even branded
men as quacks who dared use i t , and wel l mean ing men adv ised patien ts who
were being treated w ith i t to have the use of the remedy discon t inued .
I n sp ite o f the genera l d isappo in tmen t which fo llowed its
misuse, in sp ite o f the fact that much harm was do ne and
dea th hastened in many instan ces, there were a few menwho
part ial ly grasped the mean ing o f the remedy . They saw tha t tubercul in
was a remedy not al together w ithout merit , and bel ieved tha t i t deserved a
further trial .
From Fraen tzel’s Cl in ic in the Royal Charité very encourag ing results were
repo rted in the autumn o f 1890 (D eutsche med izin ischeWo chenschri ft ,E spec ia lly were these results favo rable in cases of pulmo nary tuberculo sis
S ome Good
Results .
where the d isease wa s no t far advanced .
TH E SPE C I FI C TRE ATM E N T O F TUBE RCULO S I S 1 7 1
Bardeleben (Deutsche med izin ischeWochen schr ift , 1890) showed'
improve
men t in cases of lupus.
Paul Guttman (Deutsche mediz in ische Wochen schrift,1890) exhibited
a number of cases at theM oab it that had been treated with tubercul in . Amon g
the number were two young girlswho had been treated two months and,a l though
at the beginn ing of the treatment they showed marked apical tuberculo sis,al l sign s had disappeared .
Langenbuch and Wo lff (Deutsche med izin ische Wochen schr ift , 1891 , page
935) reported 99 cases of tubec losis treated w ith tubercul in and 99 without .
Of the former 33 were cured, 40 - improved ; -of the latter , 9 were cured and
45 improved . Of tubercul in treatedl
cases, 73 per cen t were improved and
cured ; of those trea ted without it 54 per cen t were improved and cured.
Landgraf (Berl iner klin ische Wochen schr ift,1891 , page 286 ) observed
the disappearan ce of tubercles from the choro id and epiglo ttis. Renvers .
(Berl iner klin ische Wochenschrift , 1891 , page 285) cured'
a pat ien t whose
pharynx, epiglo ttis, and mucous membran e over the aryteno ids were ulcerated .
One great trouble with th is tr ia l of tuberculin,was that cases abso lutely
unfit for treatmen t were chosen and thentheywere reported upon after they
had been under treatmen t on ly a few weeks. I t requires time to cure simple
lesion s,and
,of course, in these advan cedprocesses i t must be very much length
ened . I t is surprising to me that so many favorable reports were made
when the treatment was carried on under such un favorable c ircumstan ces .
Wh ile Ko ch was very much disappoin ted at the blow which hisremedy had received, yet he did not lose fa ith . H e and his
pupils worked steadily on w ith tubercul in . A few fo llowers
here and there in o ther coun tr ies a lso took up its admin istrat ion . They saw
the mistakes that had been made, and avo ided them,and, a few years later,
were able to report upon cases that had been treated w i th small doses— doses
Short of react ion . These results were very favorable and on ce more brought
tubercul in before the eyes of the pro fession .
The favorable reports of Spengler,Turban ,
Petruschky, Krause, Heron ,
Thorner,
'
Bandel ier,Rembo ld and espec ially that of G oetsch (Deutsche med
izin ishe Wo chenschr ift,1901 , page 405) in E urope and those of Trudeau ,
von Ruck and others in this coun try have been in strumen tal in causi ng a
recon sideration and new tria l of th is remedy.
Goetsch’s report was the object of much commen t . I n 1901 he reported
1 75 cases which had been treated by h im in the preceding ten years. Of
this number 125 or 7 1 per cen t were apparen t ly'
cured . I n the cho ice of
pat ien ts he used extreme care. N o case w ith fever was treated, and reaction s
were pa in stakingly avo ided .
Soon after this report was made the wr iter undertook'
a co llect ive invest i r
tion to ascerta in the a tt itude of phys ic ian s who were in terested in the treat
I 7 2 PULM ON ARY T UBE RCULO S I S
men t of tuberculosis,toward tubercul in (see appendix, Chapter I I I ). I n tha t
report it was thought well “to secur e data upon early cases,such as Koch recom
mended as su itable for tuberculin treatmen t, which had been trea ted with and
without the remedy to see how the results compared . While many more re
ports are ava i lable and the number of cases could be largely in creased, yet I
w i ll quo te from my orig inal paper (Therapeutic Gazette, 1903 , page
That these remedies will do what is cla imed for them is proven by the
results obtained by those who have had experien ce with them,as shown in the
fo llowing :“ Jessen (Centrabl . f . inn . M ed. 1902, N o . 23) treated 14 first-stage cases,
curing 14, or 100 per cen t .
Goetsch (personal letter to the wr iter) trea ted 356 first—stage cases, cur ing
78 , or 78 per cen t .
T rudeau (T ran s. of the A ssociation of Amer ican Physician s, 1900) trea ted
24 fir st-stage cases, curing 20, or 83 per cen t .“Von Ruck (Journal of Tuberculosis, Vo l . I , page 23 , Cl in fReport ofWin
yah San itarium,1899 and 1900 ; Therapeutic Gazette, M ay, 1896 ) trea ted 105
fir st-stage cases, curing 98, or 93 per cent.“ Rembo ld (quo ted by Wilk in son , Br itish M edical Jour nal
,June 7 , 1902)
treated 16 fir st-stage cases,curing 12
,or 75 per cen t . (The classificat ion
as cured was made six years after .)Turban (Beitraege zur Kenntn iss der Lungen tuberkulose.) trea ted 20 first
stage cases, curing 20, or 100 per cen t .
Wilkin son (Observation s on Tubercul in as a Remedy in T reatmen t of the
Lungs . British M edical Journal, June 7, 1902) treated 1 2 fir st-stage cases ,curing 12 or 100 per cen t .
“Petruschky (Specifische Behandlung der Tuberkulose. Paper before the
fi st assemblage of the German N a tural ists and Physicians, M un ich, 1899)treated 18 fir st-stage cases, curing 18
,or 100 per cen t .
“ Kl ebs (Berliner klin ische Wo chen schrift, 1902, N o . 23) treated 14 first
stage cases,curing 14, or 100 per cen t .
Po ttenger (unr epo rted) treated 10 fir st-stage cases, curing 10, or 100per cen t .
Here we have for con siderat ion 589 cases in the fir st stage of the d isease
treated with tuberculin and all ied products. Of this number 496 , o r
per cen t were apparen tly cured . This is certa in ly enough cases upon which
to base an op in ion,and our verd ict must be that culture products stand the
test and accomplish tha t fo r wh ich they are recommended, namely, the cure
o f pure tuberculo sis. Th is is al l the mo re emphasized when we compare
these resul ts w ith tho se o bta ined w ithout culture products in the same purely
tubercular cases :
Bowditch (Repo rt of M ass. S tate Sanato r ium at Rutland) treated 6 6 first
stage eases, curing 39, o r 59 per cen t .
1 74 PULM O N ARY TUBE RCULOS I S
than of the o ld tuberculin,hen ce presumably some of the active propert ies
of tuberculin have been lost by the heating process.
T rea tmen t is begun with 11
11 of a cub ic cen t imeter of a 1 per cen t so lut ion
(1 m il l igramme of the pure tubercul in )and increased by T2; of a cubiccent imeterat each dose un less react ion occurs, un t i l 1 cubic cen t imeter (10 mi ll i
grammes of the pure tuberculin) is reached ; when a 10 per cen t so lution is
used and in creased by 1—16 of a cub ic cen timeter (10 m i ll igrammes of the pure
tuberculin ) un t i l 1 cubic cen timeter (100 m il ligrammes of the pure tuber
culin ) is given ; then , the pur e tuberculin is_
used mak ing the usual progression
in dosage by fi of a cubic cen timeter (100mill igrammes of the pur e tuberculin ).
When fever is presen t,or
_
when , for any o ther reason Denys suspects the
patien t to be sen si tive to the'
remedy he begins with very minute doses even
as small as film; of a cubic mill imeter of the or iginal so lut ion .
Per lsucht Tubercul in (P. T . O . Spengler) (Deutsche med
izin sche Wochen schr ift, 1904, N o . 3 1 ; 1905 , N os . 3 1 and 35)is made from bovine bacill i . Spen gler finds the prepara t ion s
made from the bov ine bacillus much less toxic for humanin fection s than those of the human bac i llus
,and at the same t ime finds them
more active in their stimulat ion of the mach inery of immun iz ation as is shown
by their power to in crease the spec ific'
agglut in ins of the blood . This prep
arat ion is made w i thout subject ing the culture flu id to hea t,which he be
l leves in jures its act iv i ty . The bac i lli are grown un til they form a covering o n
the culture med ium when they are removed by filtrat ion and the fi ltrate con
cen trated by placing it in an in cubator un ti l i t equals one-half of its or iginal
vo lume. I t is then restored to its or iginal vo lume by the add it ion of glycerine.
One cubic cen timeter of this preparation equals’
100 mill igrammes of P.T .O .
The beginn ing dose of P.T .O . is from filmto 1
117 o f a m i lligramme. I n sen si
tive cases T616 6
“ of a mill igramme should be used . The dose should be gradu
ally increased . When a dose of one cubic m i l limeter has been atta ined i t maybe increased thus : 1—2—4
—7—10—15, etc .
,and given every three - or four days .
Spengler cons iders the flexor surface of the fore-arm as the best po in t fo r
in ject ion,and never in jects a second dose
'
un t i l al l loca l signs of the prev ious
in jection have disappeared , bel ieving tha t there is a con nect ion between the
local react ion at the site of in jection and the reaction in the tuberculous
area . N ot o n ly redness and swell ing but the least feel ing of warmth is taken
as a sign for delay in admin ister ing the dose.
Tubercul in (Beraneck) is a product which con tains bo th the
extracellular and in tracellular tox ins . The extracel lular tox
ins are obta ined from the growth o f bac i ll i upo n a spec ial
medium which is free from pepto nes wh i le the in tracel lular tox ins are ah
structed from the bod ies o f the tubercle bac i ll i by means o f a 1 per cen t
S o lut io n o f o rthophospho ric ac id . Bo th o f these tox ins co n tain immun izing
TH E SPE CI FI C TRE ATM E N T OF TUBE RCULO S I S I 7S
properties, and yet, they are feebly tox ic . . The preparat ion is pra ised very
highly by Doctor W . R . Ph i llip of E d inbur gh .
Koch ’s fai th in tubercul in , in spite of the oppos ition of his
,
l
l
‘
feW con freres is shown by his con t inued search for a better prepubercuhn
(T. R ., Koch). aration . Wi th an 1n srght keener than that of o ther sc ien t ists
he was sure that be was workin g a lon g right lines . H e was
not a dreamer , and he was able to in terpret the vast amoun t of labora tory
experimen t that he had done“
as mean ing that the cure of tuberculosis must
come through the act ion of the toxin s of the tubercle bac i llus.
I n 1897 (Deutsche med izin ische Wochenschrift,1897 , N o . 14) he brought
forth a new preparation wh ich he designated as T .R . This preparat ion is
en tirely different from the o ld tubercul in in its method of preparat ion . I t is
made by gr ind ing dried cultur es of highly virulen t bac i lli in an agate mortar
and then cen trifuga liz ing them in d ist i lled water . A fter cen trifuga liz ing,the
fluid is pour ed off and this is ca lled tubercul in O or T . O .-I t is then cen tr ifa
ugal ized again when the flu id rema in ing is named tuberculin R or T .R .
T his -preparation is stan dard ized so tha t it con ta in s 1 per cen t of the so l id
extract of the tubercle bac illus . I t is p reserved by the add it ion of gl ycerine .
When i t is to be prepared for admin istrat ion i t should be d i luted w i th a 20 per ‘
cen t so lution of glycerine in water (made by bo i ling 20 parts of pur e glycerine
and 80 parts of dist i lled water for severa l m inutes) and be made up fresh every
few days . I f the so lution s are made very carefull y they may be su i table for
use for about ten days . I f they become cloudy they should be d iscarded .
The in i t ial dose is fi glm fi of a m ill igramme of the so l id substan ce. Th is
equals { fizv of a mi l l igramme of the or igina l so lution before d ilut ion . The
dose may be ca lculated by remember ing that of a m i ll igramme of the orig
inal so lution equals T'
O—lo—b of a m i ll igramme of the so lid tubercle substan ce .
The dose may be given every o ther day at first,and should be gradually in
creased in amoun t . I t can usually be doubled at each dose un t i l T1
0 m i lli
gramme of the sol id substan ce has been given wh ich equals 10 m i ll igrammes
of the Or iginal so lut ion . A fter t h is, the in ject ion s should be farther apart
and the relative in crease less, thus 10—15- 25
—35
—60—80- 100 milligrammes
may be given . A fter 5 mill igrammes of the so l id substan ce has been given
the dose should be employed twice a week on ly, and as the dose in creases, on ce
a week is sufficien t“ The dose of 20 m i ll igrammes of , so lid matter is rarely
exceeded . A t the least sign of reaction the dose must be withheld un t i l al l
reaction has d isappeared ; and, i t must n ot be in creased un til: the patien t fa i ls
to react to the dose wh ich has on ce caused a reaction .
By con t inuous experimen ta t ion Ko ch found that the greaterBaci lli
.the amoun t of the substan ce of the bacil lus in the preparation ,
Emul sw n
(T . E . , Ko ch). r.
) the greater the 1ncr ease of specific agglut1n 1n s l n the blood
(Deutsche med . Wochenschrift,1901 , N o . Hen ce he
1 7 6 PULM ON ARY TUBE RCULO S I S
con cluded that the greatest amoun t of immun ity could be produced by anemulsion of the bod ies o f the bac i ll i . This preparation is preserved in glyc
erin e. T heoret ica lly it is one of the best . I thas one d ifficulty,however
,and
that is to secure the ready absorption of the bodies of the bac i lli . The S low
ness of abso rption seems to be in creased by giving the doses at too frequen t
in terva ls,thus po in t ing to the fact that th is fa ilure of absorpt ion is a S ign of
saturat ion upon the part of the patien t . The bacill i remain in the tissues fo r
some time and act more or less as mechan ica l irritan ts. Of course they areincapable of producing tuberculosis but
p
if they are in jected in large quan ti
t ies,they may absorb very slowly and somet imes cause an irr i tat ion of the
t issues with the passing out of serum,causing what appears to be an abscess
a l though it is not acutely inflamed,and cultur es taken from it prove nega
t ive. Th is usual ly disappears after a Short time, but i f it does n ot,upon
open ing it there is obtained either a th in serum,much l ike liquid taken from
the pleura or a sterile substan ce which resembles pus .
A t the in itial dose mil l igrammes of the bacillar substan ce (Talon
mill igramme of the original preparation ) is given . The dilution is made
w ith n ormal sal t so lution plus .4 per cen t pheno l in the fo l lowing man ner
cc . is taken from the orig ina l bo ttle w ith a 1 cc . p ipette divided in to 100
equa l parts and to i t added cc .
, per cen t sod ium chlorid so lution (or
sod ium chlorid—pheno l so lution ). This 100- fo ld dilution con ta ins milli
gramme bac i llar substan ce in 1 cc .”
Then,Of the 100- fo ld dilution 1 cc . is mixed with 9 cc .
, per cen t sodium
ch lorid solution (or sod ium chlorid—pheno l so lution ) or made up to 10 cc .
therew ith . This 1000—fo ld d ilution con ta in s in cc . mil ligramme
bac i llar substan ce,the above men tioned in itia l do se.
”
The dose is admin istered every second or third day, each time in creasing
the amoun t given by twice or thr ee times the amount previously in jected .
When a react ion has been produced, the in ject ions are given at longer in tervals,say every sixor eight days. The in jection s are in creased un ti l 20 m i ll igrammes
is reached . I t is not best to go higher than th is because of the slowness of
absorpt ion . These large doses are given on ly every two or four weeks.
This preparation is an extract made from the powdered bodies
ofof the bac i ll i a fter the removal o f the fa ts by a lcoho l and
Tubercle ether . Von Ruck cla ims tha t the presence of fats in terferes(V011 with the extraction o f the bacill i with water
,and
,since these
are removed before such extraction is made in the prepara
tio n o f Watery E xtract , this product necessari ly con ta in s a greater per
cen tage o f the so luble substances of the bacillus than o ther extrac
t io ns . While there may st i ll be o ther curative substances in the bod ies o f
the bac i ll i wh ich do no t yield to this watery extract io n, yet vo n Ruck
cla ims tha t this method o f preparat io n o tfers the greatest percen tage o f
1 78 PULM ON ARY TUBE RCULO S I S
fact,i t grows best when the cul ture flask is sea led, but demands a good supply
of o xygen in the cul ture med ium .
From th is observat ion taken from the life history of the bac i llus when arti
ficial ly grown ,i t would be expected that each bacillus would seek out in the
body those cond ition s which are best suited to its growth . We woul d expect
to find the human bac i llus in fecting those organ s which are in free commun ie
at ion with the air and the bov in e those distan t from it.
Such is the fact . I n the lungs the human bac i l l i predominate,in the in
testines, and the k idney, the bov ine type seems to be the prin c ipa l et io logical
factor . I n the laryn x superficial ulcerat ion s seem to bedue to human bacill i
and deep infil tration s to -bovine bac ill i .
I n all situa t ion s the in fect ions from the human bacill i seem to be most
virulen t, tho se from bov ine less so and the double in fection run s a chr on ic
course, the two var ieties an tagon izing each o ther.
Thus the laboratory and the character of the disease as observed cl in ica lly
bo th give us eviden ce upon which we may base a diagnosis as to which bac il lus
is respon sible for the symptoms presen t . I t must be remembered that bo th
bac i lli are usually presen t but on e is often produc in g the most urgen t symptoms ; for example : the lungs may be chiefly in fected by human bac il l i and the
in testines by bovine bacill i, the former may be quiet but the la tter may be
producing very urgen t symptoms.
I t is necessary to know which variety of bac illus is respon sible for the urgen t
symptoms in order to apply the proper remedy. A further test may be made
by an in jection of vaccines made from the two variet ies of bacill i . These
same vaccines are used therapeut ically.
These two vaccines, Spengler cal ls T .E . Vaccine and PB . Vaccine. The
fo rmer is made from the human‘
tubercle bacil lus . I t has a
toxic effect when in jected in to pat ien ts who are s uffering from an in fect ion
caused by the human tubercle bac i llus and an an titoxic effect when the bov ine
bac i llus is the etio logical factor. The latter is a product made from
the bovine bac i llus and is en tirely opposite in its action,that is
,i t has an an t i
toxic action where the human bacillus is the et io log ical facto r and a tox ic
act ion where the bovine bac i llus is the causative facto r . When given in the
proper manner, these prepara tions seem to have the power of producing al l the
an t ibodies necessary to cure tuberculosis, and consequen tly actas true vacc ines.
When from the labo ratory and cl in ical observat ion one is satisfied that
o ne variety of bacillus is the cause of the mo st urgen t symptoms,he g ives an
in ject ion o f the vacc ine from the o ther variety o f bacillus. I f the d iagnosis
is co rrect the pat ien t usually experiences an improvemen t . The temperature,i f eleva ted usually lessens and the pat ien t w i l l declare tha t he feel s better ; i f,o n the o ther hand
,the d iagno s is is wro ng
,then the remedy acts as a toxin
and the patien t exper iences an increase in the symptoms .
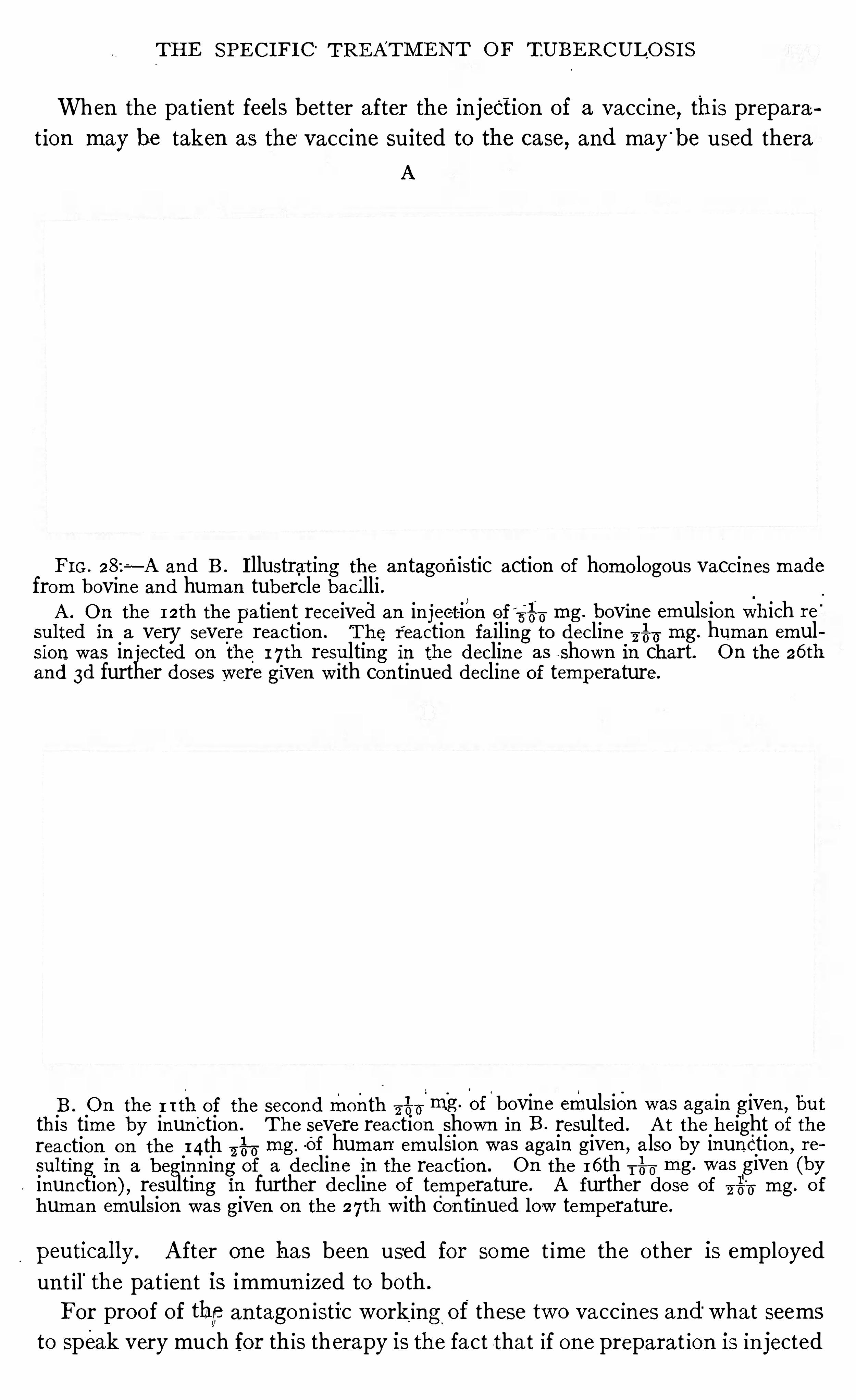
TH E SPE C I FI C“
TRE ATM E N T OF TUBE RCULO S I S
When the pa t ien t feels better after the in jection of a vaccin e, this prepara
t ion may be taken as the' vaccine suited to the case, and maybe used thera
A
F I G . 28za —A and B . I llustrat ing the an tagonistic action of homo logous vaccin es made
from bovin e and human tubercle bacilli .A . O n the 12th the patien t received an in jection of 3
—00mg. bovin e emulsion which re '
sul ted in a very severe reaction . The r eaction fa iling to declin e —6 mg. human emul
sion was in jected on the 1 7th resulting in the declin e as shown I n chart. O n the 26 th
and 3d further doses were given w ith con tinued declin e of temperature.
B . O n the r 1thof the secondmonth—2
1
6 11mg. of bovin e emulsion was aga in given ,but
this time by inun ction . The severe reaction shown in B . resulted . A t the height of thereaction on the 14th ‘
Z—é‘fi mg -Of human emulsion was aga in given ,
a lso by inunction ,r e
sul ting in a begin n ing of a declin e in the reaction . O n the 1 6 th T%U mg. was given (byinun ction), resulting i n further declin e of temperature. A further do se of mg. o f
human emulsion was given on the 27th w ith con tinued low temperature .
peutical ly. A fter on e has been used for some t ime the o ther is employed
un t il'
the pat ien t is immun ized to bo th .
For proo f of thpan tagon istic work ing of these two vacc in es and“what seems
to speak very much for this therapy is the fact tha t if on e preparat ion is in jected
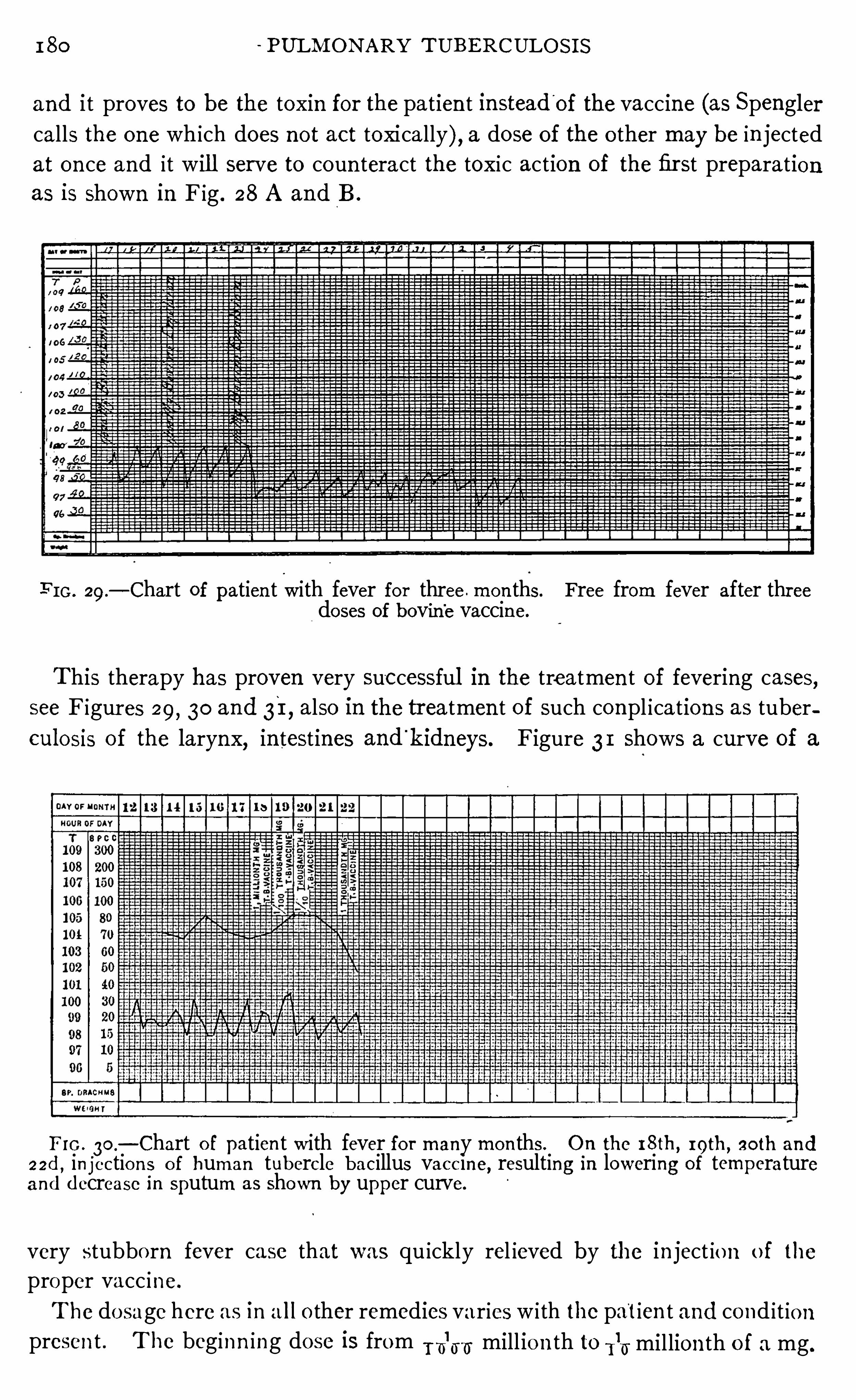
1 80 PULM ON ARY TUBERCULOS I S
and i t proves to be the toxin for the patien t instead'
of the vaccine (as Spenglercalls the one which does n ot act toxically), a dose of the o ther may be in jectedat on ce and it wil l serve to coun teract the toxic action of the fir st preparationas is shown in Fig . 28 A and B .
F I G . 29 .— Chart of patien t with fever for three . mon ths. Free from fever after three
doses of bovine vaccine.
This therapy has proven very suc cessful in the treatmen t of fevering cases,see Figur es 29, 30 and 31, also in the treatmen t of such compl ication s as tuberculosis of the larynx, in testines and
'
kidneys. Figure 3 1 shows a curve of a
Fro . 30.
— Chart o f patien t with fever fo r many mon ths . On the 18th, roth, so th and22d , in jectio n s o f human tubercle bacillus vacc ine
,resulting in lowering of temperature
and decrease in sputum as Shown by upper curve.
very stubbo rn fever case that was qu ickly rel ieved by the in ject io n o f the
proper vacc ine.
The do sage here as in a l l o ther remedies varies w i th the patien t and cond it ionpresen t . The beginn ing dose is from fi
l
m; mill ion th to 115 million th o f a mg.
182 PULM ON ARY TUBE RCULO S I S
heal and much less tendency to relapse after an apparen t healing has taken
place. The second act ion seems to be tha t of a local st imulan t to the tuber
culous area whereby more blood is d irec ted to the part and healin g and scar
t issue forma tion are hastened .
I t is sur pr ising how many people st i l l cling to Koch ’s original
$533:sfgfigi n a l
statemen t of the probablemann er in wh ich tuberculin producesMan n er in its favorable results (Deutsche med iz in ische Wochenschrift
,
guh
ggh
Aftl l
s
?er '
1890, N o . 46 and 1891 , N o . While Koch distinctly sa id
tha t he d id no t know,at the time, in wha t manner i t acted , yet
few people have gone beyond his or iginal statemen t of its probable action . I n'
spite of the fact tha t his opin ion was g iven in 1890 and 1891 , many text books
wh ich pro fess to be up to da te are st i ll quo ting Koch ’s or iginal op in ion and ig
h orin g all modern views . Koch suggested that tubercul in probably acts by
causing a coagula t ion n ecrosis of the cel ls surround ing the tuberclewhereby the
n utr i tion of the bacil li con ta ined therein was cut off, even tually causing their
death,and whereby the tuberculous mass was even tually destroyed and cast
o ff as a slough carry ing the bacilli with i t .
E very one did not accept'
Koch’s explanation of the act ion of
tuberculin at tha t time. B iedert (Berl iner klin ische Wochen
schri ft, 1891 , page 197) apprec iated a more moderate,a con
servative action . H e sa id : “When the irr ita t ion (caused by the loca l reaction)is moderate, an in creased cell growth takes place in the encapsulating wal l
of the tubercular pro cess . I f the inflammation is more in tense,marked exuda
t ion occurs,whi le in the stage of extreme inflammatory irrita tion
,cel l dea th ,
necrosis, results,” thus recogn iz ing the fact that theact ion varied with thedosage.
Trudeau (T ransact ions of the American Physicians,1900)
is of the opin ion tha t tubercul in ac ts “ probably by incit ing
the formation of fibrous tissue.
”
Wright (M ed ico -Ch irurgica l T ransact ion s, Vo l . 89, London ,
and many o ther con tribut ion s) has stud ied tubercul in from
an en tirely differen t standpo in t . I n fac t he has abso lutely
ignored the local react ion of tubercul in and stud ied i t from the standpo in t
o f its immun iz ing qua l i t ies . H e claims tha t large doses are n ot necessary ,and recommends very minute doses T -
glmr—gh
‘
of a m i ll igramme o f so l id sub
stance (1117 to
”
1217 m i lligramme o f the original so lution) o f Ko ch
’s T .R . H e has
shown that tubercul in,when in jec ted in these small doses w ill set the phys io log
ical machinery of immun izat ion in to act ion and cause an in crease in the spec ific
pro tec tive bodies (o pso n ins) of the blood .
E viden ce o fThe firs t proo f o f the immun izing power of spec ific products
Immun izing made from the tubercle bacillus is furn ished by an ima l exper iPOW CT
:A n ima l men tat io n . Ko ch ’
s first co n tribution (Zehn ter I n terna t io na lE x er imen ta
flog, M ed izm ische Ko ngress, Berl i n , Ed . 1,S . 46 ) was to the
TH E SPE CI FI C TRE ATM E N T O F TUBERCULOS I S 83
effect that he had been able to produce a certa in product from tubercle bac i ll i
wh ich con ferred upon guinea p igs a certa in immun i ty to tuberculosis and
which checked the progress of the d isease when presen t . S in ce that time,Spen gler, von Ruck, T rudeau and many o thers have confirmed these facts
exper imen ta lly and von Behr ing has successfully immun ized‘
cattle with l ive
cul tiI res of human or igin .
5
The next observation which,aside from cl in ica l eviden ces
,
Agglutin a ting proves the immun iz ing power of tubercul in and a ll ied productsPower-of B lo odI n creased.
i s i ts abi li ty to i ncrease the aggluti n a ti ng power of the blood .
When Koch made known his emulsion of tubercle bac i lli
(Deutsche med . Wochen schr ift, 1901 , N o . 48) he gave the results of a num
ber of experimen ts upon the agglut inatin g power of the blood in an ima ls and
man . H e tested this power in 78 tuberculous pat ien ts, ofwhom one showed
a reaction of 1 :50, four showed 1 :25 and a l l the rest fai led to Show an agglu
tinating power of Twen ty- four fai led to react to These
patien ts represen ted all stages of tuberculosis as well as such local lesion s as
those of bon es,bladder and sk in . These tests Show that normal ly the blood of
tuberculous pa t ients has l i ttle agglutin ating power .
H e then exam ined 74 patien ts who had been treated by products made from
the tubercle bac i lli (in these cases, tubercle bac i llus emulsion was used in tra
ven ously) and found that he had been able to'
increase the spec ific agglutin in s.
The results were as fo ll ows :14 reacted to28
9 I 3 7510
6
1 :300
Four d id n ot react at al l , being apparen tly cases of healed tuberculosis
Spengler (Deutsche med. Wochen schr ift, 1905 , N o . 35) has also tes ted the
agglut inat ing power of the blood, and found tha t he is able to produce much
h igher reac t ion s w ith P.T .O . than Koch d id w ith bac i llus emulsion ; H e tested
80 cases and found the results as fo llows :
6 reacted to 1 : 100‘G
I SO
: 200
: 250
:300
:400
: 500
:600
: 750
: 1000
: 1500
: 2000
:3000H
H
H
H
H
H
H
H
H
H
H
H
184 PULM ON ARY T UBERCULO S I S
Wh i le there has been some quest ion regarding the ev idence of immun ity asbased upon the agglut inat ing power of the blood
,some wr iters c la im ing tha t
such an in crease does not necessaril y mean that a degree of immun i ty is presen t,
yet the weight of opin ion recogn izes.
i t as a fac t that where an in creased agglu
tination is produced there is also an increased immun i ty .
I n crease inPerhaps the most wonderful
,if no t the most practical
,con
Opso n ic Power tr ibution to the modern treatmen t of in fect ious diseases,is
3213
121“ that made by Wright by his discovery of the opsoni c con ten t
of the blood which can be taken as a measure of the specific
pro tec t ive properties wh ich are presen t in the blood at any given time. H is
work with tubercle vaccines, as he cal ls al l productsmade from the tuberclebacil
lus or its tox in s,has donemore to sa tisfy those who have d oubted the efli cacy
of tubercul in and all ied products than al l the c lin ica l results tha t have been
produced s in ce Koch ’s first announ cemen t .
The opson ic power of the blood exists in the serum, the leucocyte as cla imed
by M etchn ikoff is the el emen t wh ich destroys the tubercle bac i llus, and o ther
organ isms, yet i t is powerless to do so un til these bacter ia have been acted upon
and prepared for destruction“
by the blood serum.
_
The opson ic power o f
the blood then mean s that power of the serum by which i t acts upon bacter ia
and prepares them for phagocytosis.
By an ingen ious method Wr ight takes equal parts of leucocytes, standard
emulsion of bacteria and serum to be tested, mixes them together, places them
in to an in cubator for a few momen ts at 3 7 degrees Cen t igrade (im itat ing the
norma l heat of the body), then removes the mixture, makes a smear on a sl ide,stains, and, then ,
by coun t ing the bacteria con tained in a number of leucocytes,
say 100,and tak ing the average, he is able to determine the relat ive power of
differen t blood serums for pro tecting their hosts from in fection . The index o f
a given ind iv idual is found by comparing his serum with tha t ofa poo l of several
individuals who are known to be free from the in fect ion in quest ion .
I t has been shown that in local ized in fection s this opson ic index is persist
en tly low . I n systemic in fect ions i t varies from time to time owing to auto inocu
lat ion . I n local ized tuberculo sis the index is low . N on - febrile tuberculosis
is practically a local ized tuberculosis, hen ce the index is usual ly low . Th is
low index of resistan ce shows tha t the individual who is in fected with tuber
culosis is n ot as able to combat the disease as one who is not in fected , and
offers a satisfactory explanat ion of the ease w i th which bac i ll i escape from
tuberculous foci and start up new fo ci in adjacen t or d istan t areas .
By ino culat ion of smal l doses of tubercle vaccines , the opson ic index can
be increased (Fig. 3 2) and o ften ra ised not o n ly to normal but even above.
Th is mean s tha t these spec ific vacc ines are able to art ific ially increase the
power o f the blood to destroy bac i l l i , and even ra ise i t beyo nd the n ormal .
The table prepared by Lawson and S tewart and reproduced on page 1 19

186 PULhI ON ARY T UBE RCULO S I S
These two'
ser ies are suffi c ien t to Show tha t when a localized or non - febr ile
tuberculous pro cess ex ists, the defen s ive power of the blood, measur ed by its
ab il ity to prepare bac i ll i for destruct ion (opson ic power) is a lmost a lways low .
The former series (see table, page 1 19) further shows that this index may be
in creased by the proper use of tubercle vacc ine.
M itulescu (Zeitschr ift f . T uberkulose, Bd. I X,Heft 3 , 1906 ,
page 259) cla ims tha t certa in'
changes in the n utr it ion of the
cells o ccurs after a tubercul in react ion ,andmen t ion s theresults
of the studies made by Ar neth on the leucocytes,thus :
“I have proved that in cases where after the in jection the reac
t ion fever sets in ,momen tar i ly a defic i t in cel lular n our ishmen t takes place
,but
th is is immed iately accompan ied by a greater reten t ion capacity. Th is corre
sponds exactly w ith the observation s of A rneth,namely
,that immed ia tely
after the in ject ion a sl ight leucopen ia takes place, fo llowed by a sl ight leucocytosis of neutrophile cel ls .
We are a lso able to confirm by our former exper imen ts the fact tha t a fter
the in jection of tubercul in there is an increase in'
the leucocytes . A rneth
was actually able to prove that the n eutrophi le cells after the in jection of tuber
cul in show a larger increase in granulation than is the case after ord inary
methods of treatmen t .
Rightly the author (Arneth) ma in ta in s that , on the one hand,the reserve
food for nutrition,and
,on the o ther hand, the accumulat ion of an t itox ic sub
stan ces arise through cel lular secretion ,and that these are pour ed out aga in
in to the circulatory system . The in jection of spec ific substan ces in su itable
cases produces n ot on ly an in crease in reserve materials and n eutroph i le leu
cocytes, but gradually a strengthen ing of the power of agglutination of the
blood serum .
E ffec t ofBesides the action of tubercul in as a st imulan t to the physio log
Tubercul in ica l process of immun ity, i t has a local action wh ich is doubt
$11
3dfill
f:% ponless of va lue.
_One d ifficulty in the way of cur ing tuberculo
I n fected Areas sis is dependen t upon the fact that,owing to the nature o f
fI n CFeas? Of the tubercle
,the blood supply of the body is shut off from the
F ibro i d Ti ssue.
areas of i n fect ion ,and there i s a stagnat i on o f serum . Thus
the part of the lung where the bacilli are found is deprived o f the c irculat ing
blo od and the an t ibacter ial propert ies o f the stagnat ing lymph are used up , leav
ing n o ne of the natura l pro tective substances to oppo se the act ion o f the bac ill i .
The in jection o f bacterial products made from bac i lli, when used in proper
do ses,causes a lo cal st imulat ion which shows i tsel f as a hyperemia ,
o r,if the
st imula t io n be a l ittle mo re pro nounced,as a congest ion ; the vessels are d i lated ,
mo re blo od is sen t to the part and co nsequen tly new pro tect ive substances are
bro ught to bear upo n the bac i lli in the fo c i o f in fect io n . Th is,when taken
in co n junct io n w ith the increased immun iz ing con ten t o f the blo od due to the
TH E SPE C I FI C TRE ATM E N T O F TUBE RCULOS I S 87
st imulation,
of the bacter ial inoculat ion s, expla in s to"
us why cases treated w ith
tubercul in heal more qu ickly and more surely, and Show less tenden cy for the
d isease to spread . The bacter ic idal properties of, the blood are in creased and
also brought in closer con tact’
w ith the bac ill i .
This loca l reaction also causes, as has been suggested, a'
stimulat ion wh i ch
results in a more rapid forma t ion of fibro id t issue. Th is fact is corroborated
by my experien ce, wh ich shows a more rap id heal ing,especially in those
pat ien ts suffering from advan ced tuberculos is, when bacter ia l products have
been used i n treatmen t,than when the pat ien ts have been treated by hyg ien ic
methods alone.
When the dosage of tuberculin is pushed to its recogn izable
effect,a certa in tra in of symptoms en sues
,as descr ibed in
Chap . I V , wh ich is known as a tubercul in reaction . T his
is characterist ic of al l the products made from the tubercle bac i llus and is
applicable to al l . The amoun t of the toxin n ecessary to produce this effect
var ies w ithin w ide l imits . Some person s are very sen sitive,o thers may
requ ire large doses to produce any symptoms at al l,and still o thers take a
graduated dosage, rap idly increased,~ 3andf
never show any symptoms of a
react ion . Some men,l ike Wr ight
,cla im that react ion s are unnecessary arid
a lways harmful . O thers think the best results are obta ined through secur ing
sl ight o ccasiona l reaction s . Wr ight bases his assertion on the fact that the
opson ic con ten t of the blood is in creased by very small doses while larger on es
cause a pronoun ced reduction of the opson ic con ten t (exaggerated n egative
phase). The o ther op in ion is based on the observation that the greatest agglu
tin ating power of the blood is obta ined after slight react ions .
‘
Wh ile,as a
rule,I bel ieve the safest po l icy is to avo id react ion s, yet I have seen much good
fo l low s ligh'
t react ion s in o ld chron ic cases where improvemen t seemed to be at
a standst ill . I have repea ted ly seen a reduct ion in the amoun t of secret ion
in a chron ic suppurat ing cav ity date from a slight reaction,and I frequen tly
use th is method,graduating myd osage in such a manner that the react ion is
pract ically con tro lled . I would n ot recommend it to be tr ied, however , except
by men who are expert in the use of these remed ies . Tha t the terr ible catas
trophe feared by Wright , when large doses are used , does n ot occur has been
demon strated by mostmen who employ these remedies ; yet, we bel ieve that
his work has demon strated many valuable po in ts in their adm in istrat ion.
When the amoun t of tubercul in which would be con sidered proper for the
usual dose has been given there is no disturban ce of the physio log ical econ omy
not iceable. I f-this amoun t be in creased a l itt le there is a S l ight feel ing of wel l
bein g ; if in creased a l ittle more the pat ient may feel sl ightly n ervous ; if ih ~
creased still mo re,there is a sensat ion of being t ired w ith perhaps a feeling of
heaviness in the l imbs . I f the amoun t of tox in employed be st ill greater the
patien t exper ien ces an aching of the limbs, back and head, with a sl ight riseo f
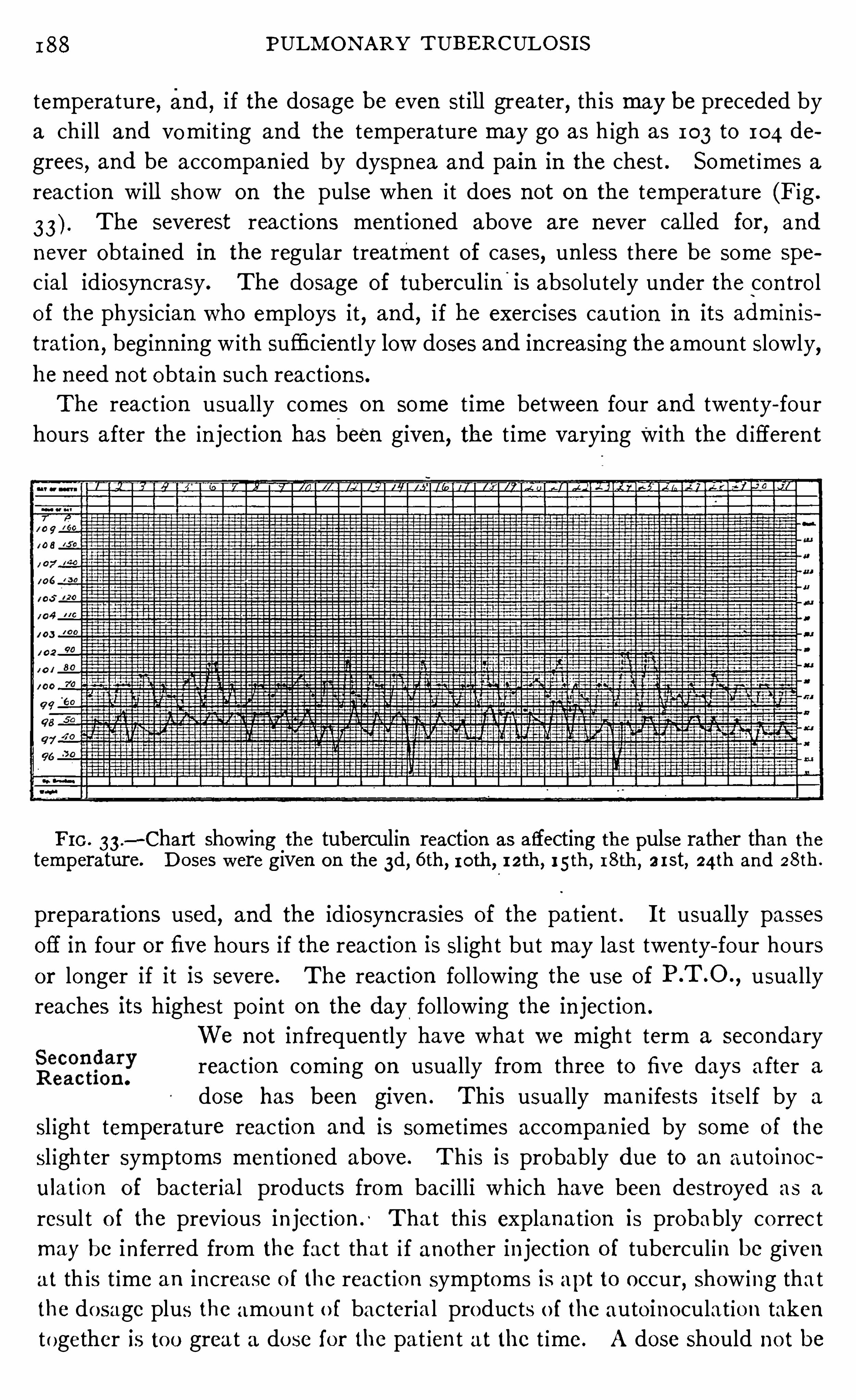
I 88 PULM ON ARY TUBE RCULO S I S
temperature, and, if the dosage be even st il l greater, this maybe preceded by
a ch i ll and vomit ing and the temperature may go as h igh as 103 to 104 de
grees, and be accompan ied by dyspnea and pain in the chest . Somet imes a
react ion will Show on the pulse when i t does not on the temperature (Fig .
The severest react ion s men t ioned above are never call ed for , and
never obta ined in the regular treatmen t of cases, un less there be some spe
c ial idiosyn crasy. The dosage of tubercul in'
is abso lutely under the con tro l
of the physician who employs it,and
,i f he exercises caut ion in its admin is
tration,beginn ing w ith sufficien tly low doses and in creasing the amoun t slowly,
he need not obta in such reaction s.
The react ion usually comes on some t ime between four and twen ty- four
hours after the in jection has been given , the t ime varying with the d ifferen t
F I G . 33 .
—Chart show ing the tuberculin reaction as affecting the pulse rather than the
temperature. D o ses were given on the 3d, 6 th, roth, 12th, i 5th ,18th, erst, 24ih and 28th.
preparat ions used, and the idiosyn crasies of the patien t . I t usually passes
off in four or five hours if the reaction is sl ight but may last twen ty- four hours
or longer if it is severe. The reaction fo l lowing the use of usually
reaches its h ighest po in t on the day.
fo llowing the in jection .
We not in frequen tly have what we might term a secondary
react ion com ing on usually from three to five days after a
dose has been given . This usually man ifests i tself by a
sl ight temperature reaction and is somet imes accompan ied by some of the
sl igh ter symptoms men tioned above. Th is is probably due to an auto inoc
ulation of bac ter ial products from bac i lli wh ich have been destroyed as a
resul t o f the previous in ject ion ; Tha t th is explanat ion is probably co rrec t
may be in ferred from the fac t tha t i f ano ther in jection o f tubercul in be given
at th is t ime an increase o f the react io n symptoms is apt to occur, Show ing tha t
the do sage plus the amoun t o f bacteria l products o f the auto inoculat ion taken
together is to o grea t a do se fo r the pat ien t at the t ime. A dose Should no t be
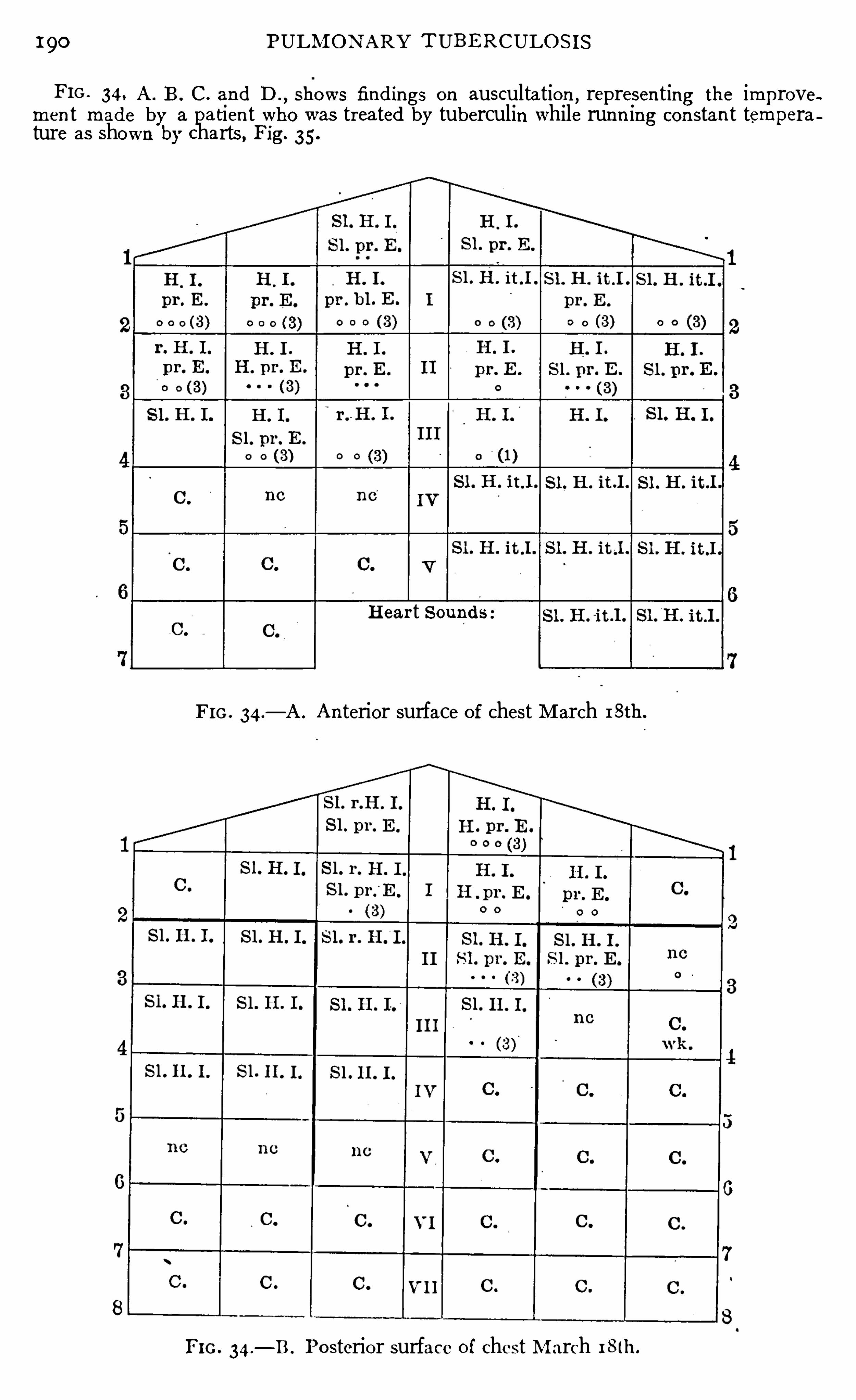
190 PULM ON ARY T UBE RCULO S I S
FIG . 34, A . B . C . and D ., shows findings o n auscultation
,represen ting the improve
men t made by a patien t who was trea ted by tuberculin while runn ing con stan t temperature as shown by charts , Fig. 35 .
H ear t S oun ds :
FIG . 34.
— A . A n terior surface of chest M arch 18th.
FI G . 34.
— B . Po sterior surface o f chest M arch 18 th.
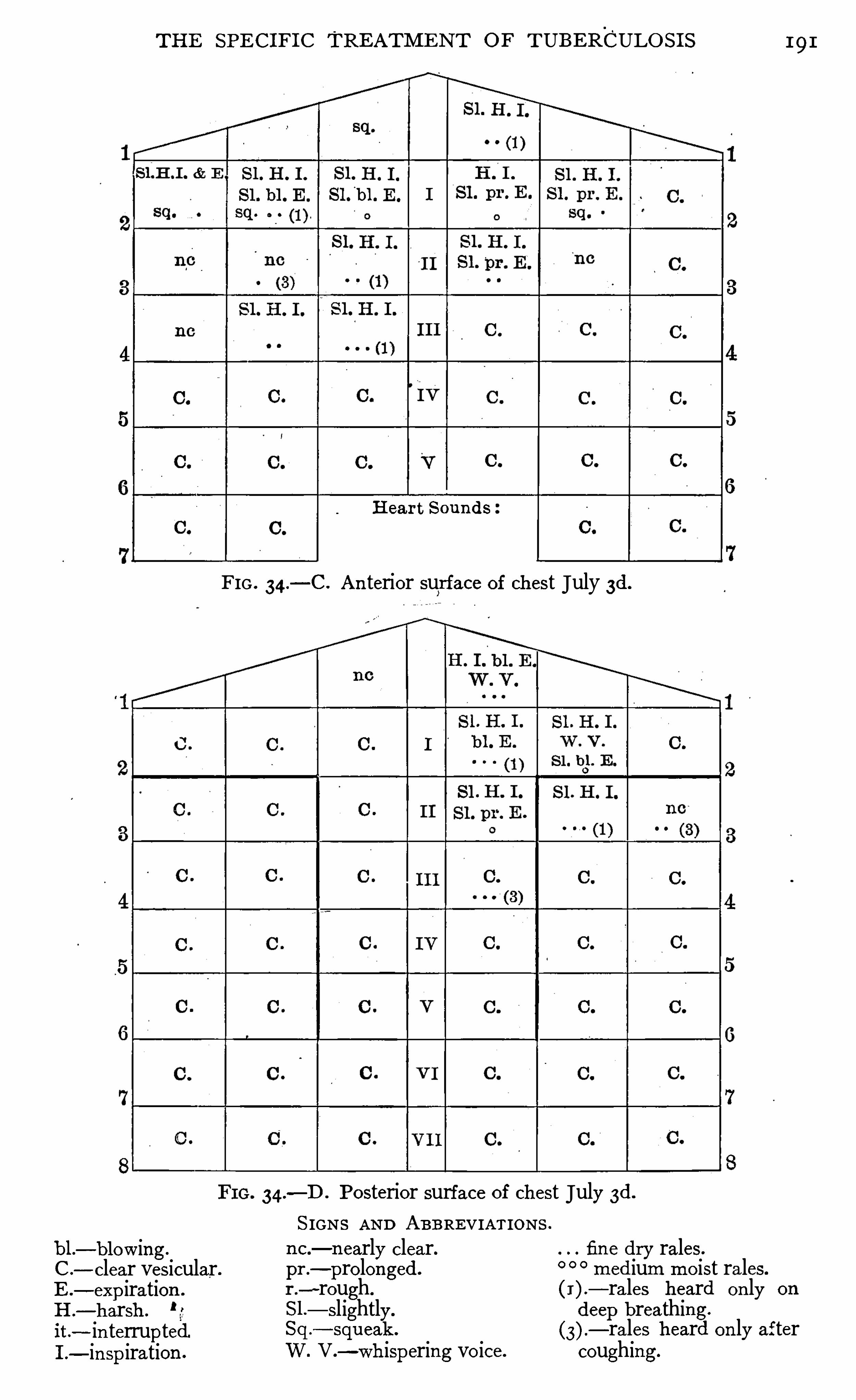
TH E SPE CI FI C TREATM E N T O F TUBERCULO S I S
bl .— blow ing.
C .
— clear vesicular.E .— expiration .
H .
— harsh .
it.
- in terruptedI .
- in spiration .
191
H ear t S oun ds
FIG . 34.
— C . A n terior surface of chest July 3d.
34.—D . Posterior surface of chest July 3d.
S IGNS AN D ABBRE VIATIONS .
n c .— n early clear. fin e dry rales.
pr .—pro longed . medium mo ist rales.
r .
-rough. (I ).— rales heard on ly on
S l .— slightly. deep breathing.
Sq .
— squeak .
— rales heard on ly afterW. V .
—whispering vo ice. coughing.
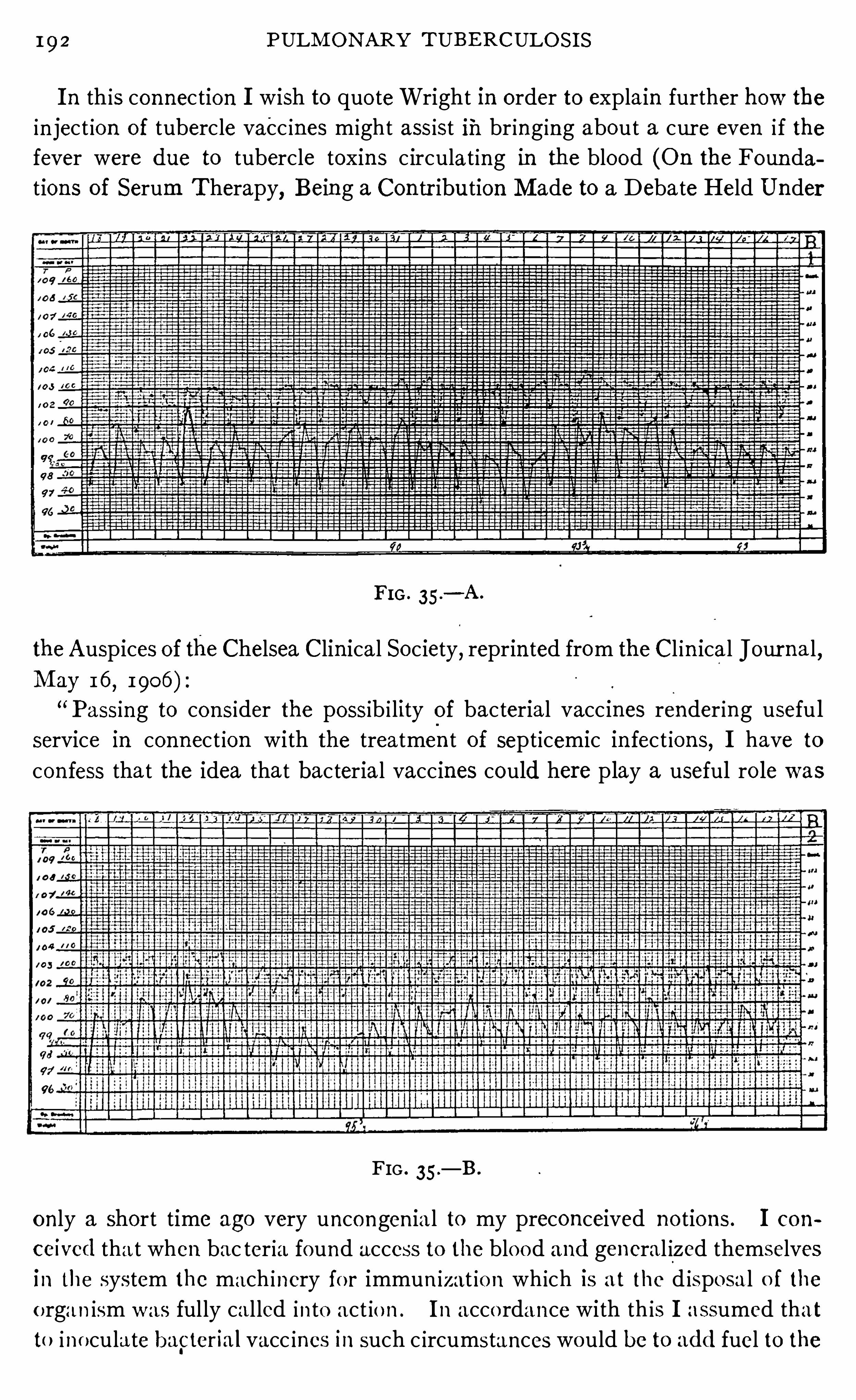
192 PULM ON ARY TUBE RCULO S I S
I n this connection I wish to quo teWright in order to explain further how the
in ject ion of tubercle vacc ines m ight assist iii br ing ing about a cur e even i f thefever were due to tubercle toxin s c irculat ing in the blood (On the Foun dations of Serum Therapy
, Being a Con tr ibution M ade to a Debate Held Under
FI G . 35 .
— A .
theAuspices of the Chelsea Clin ical Society, reprin ted from the Cl in ical Jour na l ,M ay 1 6
,1906 )
“ Passing to con sider the possib i lity of bacterial vacc ines render ing usefu l
service in connect ion with the treatment of sept icemic in fect ions, I have to
con fess that the idea that bacterial vaccines could here p lay a useful ro le was
FIG . 35 .
— B .
o n ly a short time ago very uncongen ia l to my preconceived no tions . I con
ceived tha t when bac teria found access to the blo od and general ized themselves
in the system the mach inery fo r immun izat io n wh ich is at the d isposa l o f the
o rgan ism was fully cal led into act io n . I n acco rdance with th is I assumed that
to ino cula te bapter ia l vacc ines in such c ircumstances would be to add fuel to the
194 PULM ONARY TUBERCULO S I S
t ion s on horses fa ll in to l ine with observa t ions recen tly made by Douglas andmyself upon men in con nect ion w i th cases of M al ta fever and in connectionw ith a case of in fective endocardi t is which w i ll be fur ther referred to .
“A ga in
,in the reason ing which I above rehearsed the possib i l i ty of a
d ifferen t effect being produced by bacter ia l elemen ts in troduced in to the
blood stream and the same bacteria l elemen ts in troduced d irectly in to
the tissues were overlooked . Yet cons iderat ion will Show that there
may be quite importan t d ifferen ces, first in the matter of the toxic effectsexerted, and
,secondly
,w i th respect to the immun izing response el ic i ted
,by
one and the same. quan tum of bacterial elemen ts in troduced directly in to the
blood stream or directly in to the tissues as the case may be. The general
in toxicat ion“
effect— which above all we have to apprehend in septicemic con
dition s— may be expected to be greatest where, as occurs in these in fection s,
bacterial derivat ives find direct access to the circulating blood,and least
where, as would be the case in the inocula tion of a vaccine
, the bacterial
elemen ts are in troduced in to the tissues. I n this la tter case, as may
o ften be seen in connection with the inoculation of small quan ta of an ti
typho id bac i ll i when the patien t keeps his'
bed after the in ocula tion,the toxic
effect of the' vaccine may expend itself exclusively upon the tissues at the sea t
of inoculat ion , con st i tutiona l symptoms being here prac t ically absen t .“E qual ly importan t are the differen ces wh ich may man ifest themselves in
thematter of the immun izing response according as one and the same quan tumof bacteria l elemen ts is in corporated in to the blood, or , as the case may be,
d irectly in to the tissues. I n the case where bacteria are, as in sept icemic
cond it ions,found in the blood stream,
or in organ s standing in d irect rela tion
with this, the bacter ial derivatives are of necessi tyd i luted by the who le vo lume
of the blood and lymph before they can come in to appl ication upon the tissues
in which,we may take i t, the machinery for the elabora t ion of pro tective sub
stan ces is located . I n con formi ty w i th this gr eat -d i lut ion of the bacter ia l
derivat ives a compara tively speaking ineffective immun izing stimulus will here
be admin istered . I n con trast w i th this, where a bacteria l vaccine is inoculated
d irectly in to the tissues, the bacterial products _will come in to applica tion upon
these in a very concen tra ted form,calling forth a correspond ingly larger pro
duction of pro tective substances .
“Such larger product ion of pro tective substances is in po in t of fact regularly
ach ieved in the horse in co nnection with the production of d iph theria an t i tox in,
when in lieu of in travenous inocula tions, subcutaneous and in tramuscular
inoculat io ns are reso rted to and,i t would seem
,in particular in the case where
the inocula t io ns are made w i th very concen tra ted tox ins .
”
O ccasional ly we find a perso n who is very sensit ive to the tuber
c le toxins ; o r,th is hypersensi t iveness may suddenly develo p
in an individual who has been tak ing large do ses o f the
TH E SPE C I FI C TRE ATM E N T OF TUBE RCULO S I S 195
bacter ial products . A case in po in t is a young man who was tak ing 750 milli
grammes of von Ruck ’s Watery E xtract of T ubercle Bac i lli and who became
so sen si t ive that he could n ot take 1 mi l l igramme w i thout Show ing reac tion s .
I n such cases I have found that a reduction of the dose to a sma ll fract ion
of a mil l igramme,'
at . in frequen t in tervals when persisted in for some
t ime,w i ll usually al low this hypersen sib i l i ty
'
to disappear . I n some cases i t
seems best to discon t inue the remedy for a t ime. I f i t shows at the beginn ing
of treatmen t, caut ion and patien ce w i ll usually overcome i t . T h is hypersen
sibil ity is perhaps best overcome by changin g to an o ther prepara t ion,and
especially from the human to the bovine preparat ions and v ice versa .
For the past three years I have been using d ifferen t prep
arations in the treatment of the Same case, fir st immun iz ing
to on e and then to the'
o ther ; and, for the past two years, I
have done th is invariably . N ot on ly have I a l ternated bei
tween different tribercle vaccines'
but I have employed vaccines made from
d ifferen t races of bac i ll i , fir st immun iz ing to large do ses of vacc ine made from
the human bac i llus, then chang ing to a vacc ine made from‘ the bovine bac
i llus or vice versa ; I bel ieve by thi s systemof change tha t I have been able
to produce better results than when I employed the same product con tin ua l ly .
On e advan tage of the employmen t of bo th human and bov ine vacc i nes i s that
a patient who is sensit ive to on e is rarely sen sitive to the o ther . M y exper i
en ce in‘
the employmen t of vaccines made from bo th human and bov ine bac illi
and especia lly this peculiar character ist ic by which tho se who are sensi t ive to
one will usually take the o ther well , makes me bel ieve w ith Spengler that the
tox in s of the human and bovine bac i lli d iffer . I t has been suggested by
Spengler that patien ts are in fected by bacilli of bo th the human and bov ine
type usually symbio t icall y, and, that tho se in fected chiefly by human bac ill i
are best treated by the bovine ‘
preparation s and those in fected chiefly by the
bov in e bacill i are best tr ea ted bypreparations made from human bac i ll i .T ime w il l '
determin e whether this is correct or not. For a more completedescription of this subject see pages 1 77 to 1 81 .
I n ject ions may be made deep in to the muscle or subcuta
neously; and in order to be given pain lessly the needle should
be ’kept sharp and Should be in serted quickly ; They may be
given in the muscles or under the Skin of the upper arm or fore-arm,
“
in the
in terscapular space or in the muscles of the lo in . The skin should be clean sed
and al l an t iseptic precaution s observed. One advan tage of in ject ing sub
cutaneously in stead of deep in to the muscle is that the lo cal react ion at the
point'
of in ject ion can be the more carefully studied, and an extended expe
r ienée tells me tha t th is is of value. A second dose should not be given as
long as there is any local in flammatory symptoms at the po int _
of the previous
in jection .

196 PULM ON ARY TUBE RCULO S I S
A s men t ioned above,Wright uses on ly very smal l doses of
tubercle vacc ines, and adm in isters the dosage on ly as indicated
after examin ing the opson ic con ten t of the blood . The
fo llowing descr iption‘
(M edico -Ch irurgica l T ran sactions, Vo l .89) of the pr inc iples which he foll ows in regulating dosage, sets forth hisideas very pla inl y :
“There appears to be everywhere a fixed idea that to secure the greatest
y ield of pro tective substan ces we ought in each case to beg in w ith a dose wh ich
produces a certa in amoun t of con st itut ional disturbance/and that we ought
in subsequen t in o cula tion s to employ doses wh ich in crease by geometrical
progression . This fixed idea rests as a ma tter o f fact upon the preconcept iontha t immun izat ion canno t be either in itiated or fo llowed up apart from con st i
tutional d isturban ce,and on the further precon cept ion s tha t the capac ity of the
organ ism for immun iz ing respon se is prac ticall y un l im ited, and that the y ield
of an t ibacterial substan ces w ill in crease pari passu w ith the dose. T his is n o t
so . I obtain a lmost every day max imal immun iz ing respon ses from the inoc
ulation of doses of tuberculin which have n ot produced any con stitut ional
distur ban ce. Further, I have for periods extending over a year con t inued to
ino culate w ith doses of new tuberculin correspond ing to from TWIN to fi
l
mmill i
gramme of tubercle powder * without“
registering any falling off in the immun
iz ing response. Aga in,I have in some of these cases repeatedly registered
worse and n ot better results whenever larger doses than these were employed .
Lastly,I have before my mind the fact that the horses which, in connect ion
w i th the manufacture of diphtheria an t itox in ,are inocula ted with large doses
of d iphther ia toxin ,a ll sooner or later lo se their power of responding to the
st imulus of inoculat ion ,and recover that power of respon se on ly after a long
period of rest .“I n view of these facts I would submit that the who le question of dosage
requires to be recon sidered . For mysel f I am day by -day more impressed
w ith the fact that the mach inery of immun izat ion can be brought in to act ion
by very small st imuli , and that it can very easi ly be overtaxed . I n accordance
with these facts I regard'
it as a matter ofgrea t momen t, especially in connection
w ith immun ization aga inst tubercle,to employ in every case the smallest doses
wh ich w i ll el icit a sat isfactory response ; to repeat the do se on ly when the
effect o f the preced ing ino culation is passing off ; and to increase the do se on lv
when i t becomes clear tha t the dose prev iously employed is ceasing to evoke
a suf fic ien t immun izing respo nse . A ct ing in acco rdan ce w i th th is princ iple,I n ow beg in w i th a quan tum o f tubercul in co rresponding to no t mo re than
mil l igramme o f the tubercle powder, and never advance to do ses larger
than fil
mmill igramme.
* T he do ses in th is paper have referen ce in each ca se. to the we ight o f tuberc lepo wder held in suspen s io n in the n ew tubercul i n a s used .
198 PULM ON ARY TUBERCULOS I S
w ith the phenomena of immun ity and the trea tmen t of in fect ious diseases,
yet, we do n o t bel ieve that the fact that many careful cl in ic ian s are not so si tu
ated as to ava i l themselves of the knowledge obta ined by estima t ing the opson ic
con ten t of the blood shoul d deter them from g iving their patien ts the benefit
of in tell igen t treatmen t by specific products made from the tubercle bacil lus.
I t must be sa id,however
,that an in creased experien ce seems to Show that
results maybe obta ined w ith sma ller doses than we have been won t toe mploy.
The fina l test of a l l remed ies must be c l in ica l results ; for many
remed ia l measures which are of great value theoret ica lly,
fa i l when i t comes to the pract ical application . The quest ion
to be decided is, whether or n ot the products made from the tubercle baci l lus
w i ll accompl ish,when admin istered c lin ical ly
, the results wh ich seem to be
warran ted by the propert ies accred i ted to them . W i ll-
their practica l appl ica
t ion increase the agglutina t ing and opsonic con ten t of the blood,and stimu
la te the heal ing process in tuberculous areas? Will they have a S imilar ac t ion
in man to that which they have in an imals?
The quest ion must be an swered from experien ce. I have used the culture
products made from the tuberc le bac il lus for more than eleven years . Dur ing
the past seven years there has been n o t ime when I have n ot had from five to
n inety patien ts under my immed ia te care and observa tion . During this t ime
some five hundred patien ts have been observed and treated for periods varying
from two weeks to three years (the la tter, receiv ing severa l d ifferen t courses
of treatmen t). Of cour se those pa tien ts who were treated for as short a t ime
as two weeks should n o t be coun ted as Show ing wha t any remedy can do , in
fac t I have never considered a case,in my reports which was treated less than
two mon ths,n o matter by what method . During this exper ience I have given
many thousand in jec tion s of the various culture products and have carefully
no ted the effects . A complete chart of the chest is made at the beginn ing of
treatmen t and then ano ther made for comparison at the end of eachmon th .
Extra examinat io ns are made whenever necessary and o ften a fter each in jec
t ion . The effec t of the in ject ion s on o ther tuberculous infil trations such as
those of the larynx,glands
,bowels and ear have been wa tched w ith greatest
care. Wi th this opportun i ty for observa tion,I have demonstrated to my own
sat isfact io n tha t the culture produc ts made from.
the tubercle bac i l lus w i ll do
certa in th ings . I have learned also someth ing of their lim i tations . M y
oppo rtun i ty fo r observa t ion has been part icularly fortunate for I have hado ther pa t ien ts who were no t treated with culture products
,with whom I could
Compare results
O ne o fmy earl ies t observatio ns on the treatmen t o f tuberculos is
Eézza
fgns
dzzv
gs w i th spec ific remed ies was tha t the disease showed much less
to Spread.tendency to spread to new areas where the culture products
were used . Th is o bserva t io n has been co nfirmed bv mv later
experience.
TH E SPE CI FI C TRE ATM E N T OF T UBERCULOS I S 9
I have tried to Show (seep age I ) that one of the reasons why tuberculosisk i lls the pat ient is because of the tenden cy to spread to new t issue
,therefore
th is action of tuberculin is a very importan t one. I ts rat ionale is very easy
to understand .
1
A s men tioned above, tuberc le vaccines in crease the amoun t of specific pro
tective bod ies in the blood, and con sequen tly enable i t to destroy more bacilliwhen they pass Out of the area of in fect ion and a ttempt to form new foci . To
Show .how much the resisting power of the organ ism is increasedby these vac
c ines i t is but necessary to refer to the table on page 1 19 which shows a com
par ison of the Opson ic index or power of the blood to prepare tubercle bacilli
for phagocytosis in twen ty- three patien ts after a term of sanatorium treat
men t on ly, and after a termof sana tor ium treatmen t plus tuberculin inocula
t ion s . The average opson ic index of these pat ien ts compared with that of
n ormal individuals taken as I was on ly . 73 ; but after tuberculin in jec tion s i t
in creased to This mean s tha t the power of the blood of these patien ts
to destroy bac il li as they find their way out of the o l d tuberculous areas and
endeavor to start new foc i has been in creased from less than thr ee- fourths of
the norma l to one-fifth more than n ormal ? I n other words the power of these
pat ien ts to preven t those bacill i which escape from tuberculous areas from
starting new foci has been in creased per cen t by the use of tuberculin .
What this mean s for the pro tection of the individual can . be readily
understood .
That this is not on ly theory, but fact, we are led to bel ieve from the obser
vations that whi le more than 50 per cen t of patien ts suffer ing from advan ced
tuberculosis have tuberculous compl ica t ion s on the part of the larynx and
in testines,and a lso compl ication s .in many o ther organs
,during an exten sive
experien ce in trea t ing many advanced cases of tuberculosis, I . have seen very
few of these compl ica t ion s develop dur ing the period of tubercul in treatmen t,
un less’ it was in those who were rapidly approaching death .
The same“
act ion of tubercle vaccines which in creases the speD i sease H eal s
mo re Surely CIfic protect1ve bodI eS I n the blood and tends to preven t
alias,“ spread ing of the d isease is also a powerful factor in heal ing
out the lesion s when presen t . And, when we add to th is
the loca l reaction which causes an in creased flow of blood,which has been
art ific ially enriched in pro tect ive bodies by the specific in oculation s, to the
tuberculous foci to take the place of the stagna t ing serum which has been de
pr ived of its pro tective propert ies by its pro longed .con tact with the bac i ll i ,together with the irritat ion caused by th is local reaction whereby more rap id
format ion of fibro id tissue occurs,we can readily understand that the add i t ion
of tuberc le vacc ines must n ot on ly increase the chances of cure but must enable
this result to be, produced in a shorter t ime.
My own exper ien ce bears this out. I n one hundred and twen ty-one cases
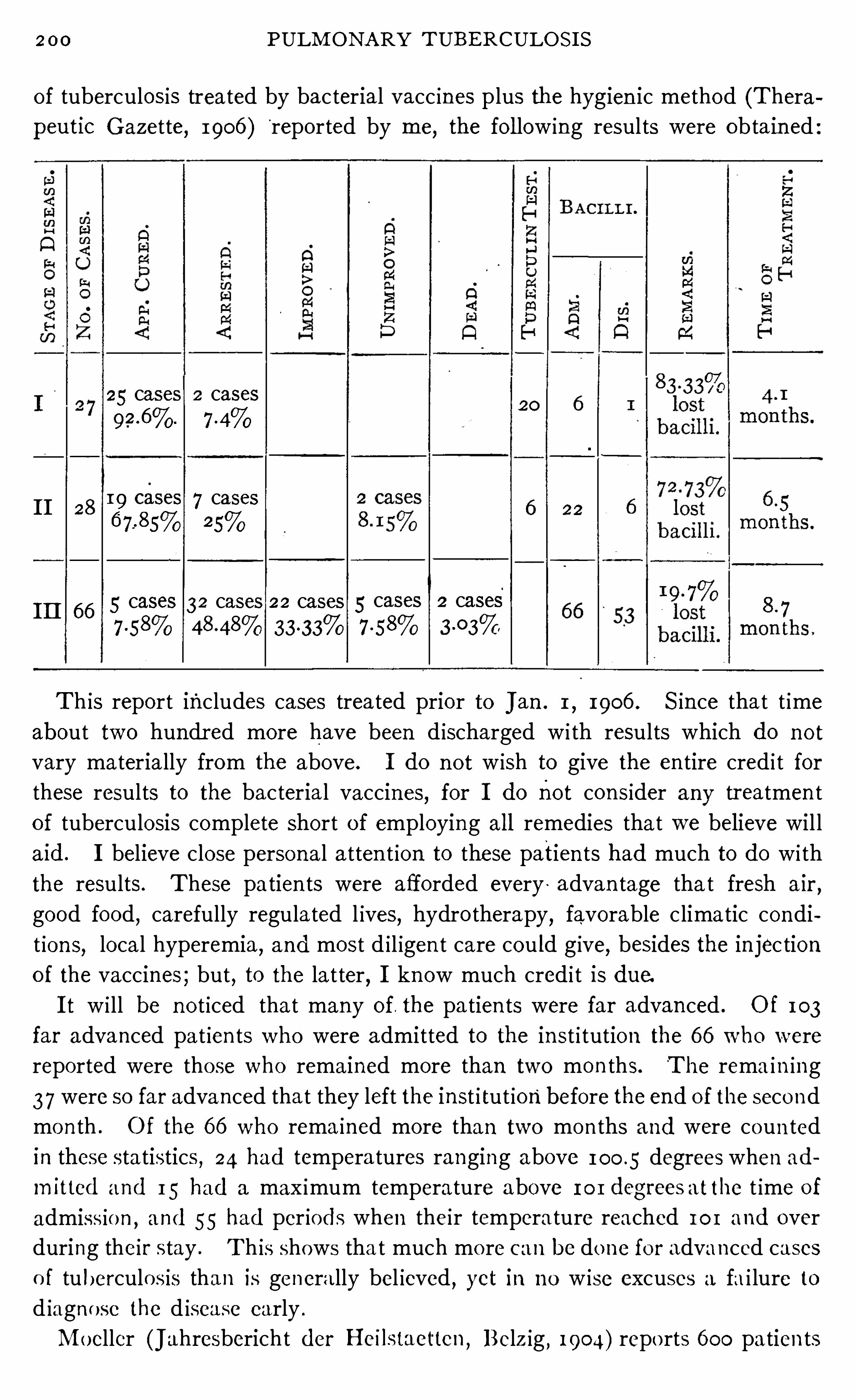
200 PULM ON A RY TUBE RCULO S I S
of tuberculosis treated by bac terial vacc ines plus the hygien ic method (Thera
peutic Gazette, 1906 )"
reported by me,the fo l low ing results were obta in ed
25 cases 2 cases20 6
I I 2819 CESCS 7 cases 6 226 7.
-8s% 25%
I I I 6 6 5cases 32 cases 22 cases 5 cases 2 cases7 -58% 333 3% 7 -58%
Th is report includes cases treated prior to J an . 1,1906 . S in ce that t ime
about two hundr ed more have been d ischarged w i th results which do no t
vary materially from the above. I do n ot w ish to give the en tire cred i t forthese results to the bacterial vaccines, for I do not con sider any tr eatmen t
of tuberculosis complete Short of employing al l remedies tha t we believe will
aid. I believe close personal atten t ion to these patien ts had much to do wi th
the results. These patien ts were afforded every ‘ advan tage tha t fresh air,
good food,carefully regulated l ives, hydro therapy, favorable c limatic condi
t ion s, local hyperemia, and most d i l igen t care cou ld g ive, besides the in jec tion
of the vaccines ; but , to the lat ter, I know much cred i t is due.
I t w i ll be n o t iced that many of. the pa tien ts were far advan ced . O f 103
far advanced pat ien ts who were admitted to the in st i tution the 6 6 who were
reported were those who remained more than two mon ths. The rema in ing
3 7 were so far advanced tha t they left the inst i tut ion before the end o f the seco nd
mon th . Of the 6 6 who rema ined more than two mon ths and were coun ted
in these statistics , 24 had tempera tures ranging above 100 .5 degrees when ad
mitted and 15 had a max imum temperature above 101 degrees atthe t ime of
admiss io n ,and 55 had per iods when their temperature reached 101 and over
during their stay . Th is shows tha t much mo re can be done fo r advanced cases
o f tuberculos is than is genera lly bel ieved , yet in n o w ise excuses a fa i lure to
d iagno se the d isease early .
M oeller (Jahresbericht der Heilstaet‘
ten, Belz ig , 1904) repo rts 6 00 pa tien ts
202 PULM ON ARY TUBERCULO S I S
I t is always gratifying to secur e the disappearan ce of tubercle
E1
336 “bacill i from the sputum,
for this is necessary to a cur e. While
From S putum .al l such closed areas are no t cured, yet we can no t have a cure
un less this is accomplished ; and, in cases where a cure is n o t
obtained, if we can secure the disappearan ce of bacil l i from the sputum,it
takes away the danger of sca tterin g in fection and makes the pa tien t mo re
comfortable.
I n my first- stage cases i t will be no ticed tha t six had bacil li in their sputum
upon admission and one upon discharge. T hus per cen t of first- stage
cases lost bacil l i . Of second- stage cases 22 had bacill i on admission and 6
on discharge,or per cen t . lost their bacil l i . Of th ird- stage cases 6 6 had
bacill i on admission and 53 on di scharge or per cen t lost their bac il l i .
N agel (Beitraege zur Kl in . der T uberkulose,Bd. V .
,Heft 4 , page 489)
in a report of the Co ttbus San ator ium makes a compar ison of the results of
patien ts tr eated wi th tuberculin ,and those treated without i t . H e makes as
the basis of comparison the disappearan ce of tubercle bacilli from the sputum .
I n the years 1902— 1904, 96 pa tien ts in al l stages of tuberculosis with bacill i
in their Sputum were trea ted by tuberculin . Of. these 48, or 50 per cen t, los t
their bacil li . During 1900—1904, 6 5 patien ts in al l stages
,with bacilli in their
sputum were trea ted wi thout tubercul in . Of these 13 , or 20 per Cen t, lost
their bacilli . The author remarks tha t those treated without tubercul in were
mostly trea ted in 1900 and 1901 , for after the good eflects of tuberculin in
causing the disappearan ce of bacill i was shown,i t was used in nearly every
open case.
Turban repo rts 86 patien ts out of 227 as having bacilli in their sputum .
O f those treated with tuberculin 41 per cen t lost bacill i, while of those trea ted
wi thout i t,27 per cen t lost their bacilli .
Brown (Zei t . f . T uberkulose, Bd. V I I , p . 235) reports tha t per cen t
of 990 patien ts treated without tuberculin at the Adirondack Co t tage San i
tar ium,who had bacill i in thei r sputum at the beginn ing of trea tmen t
,had lost
the bacilli on discharge. Of 147 cases trea ted with tuberculin who had bacill i
on admission, 47 per cen t con tained n one in discha rge. Thus nearly twice
as many lost their bacill i under tuberculin treatmen t as did without tuberculin .
Von Ruck (Report o f Winyah Sana torium,1903— 1904) reports 244 patien ts
treated with Wa tery E xtrac t o fTubercle Bacill i who had bacilli in their sputum
at the commen cemen t of trea tmen t . Of these,159 o r 6 5 per cen t lost them
during trea tmen t .
N o t o nly is i t possible to cure tuberculosis of the lungs , but
tuberculous complica tio ns such as those o f the larynx, glandu
lar system,and even now and then o f the bowels (see Chapter
X lX)will yield to tuberculin trea tmen t . A nd recen tly Wrigh t
(M edico -Ch irurgica l T ransac tions, Vo l . 89) has repo rted mo st encouraging
TH E SPE CI FI C TREATM E N T O F TUBE RCULO S I S 203
results in the trea tmen t of such hopeless condi tion s as those affecting the
bladder an d kidn ey. During the past year (see page 26 7) I have seen the
apparen t cure of a tuberculous ovary .
The question of grea test in terest to patien ts is whether or
not they wil l remain well after they,have been apparen tly
cured . I t is worth a greater s truggle -to rega in heal th , if this
condition when a ttain ed'
can be preserved .
From our-previous di scussion i t is pla in tha t the resul ts obtained in tuber
culin treated cases shoul d be more .perman en t than in those trea ted wi thout i t .
Pa tien ts who get well wi thout trea tmen t or Wi th the usua l open -air -hygien ic
dietetic tr eatmen t are more apt to have a quiescen ce ra ther than a cur e. This
is shown by the fact tha t many of them will s til l react to tubercul in ,which they
would n ot do if they were cur ed, and a lso by the fact tha t a greater percen tage
of those suffer relapses than of the tuberculin trea ted cases .
Of the 27 first- s tage c
'
ases men tion ed above,the time Since '
di scharge varies
from on e to seven years . I have had dir ect or indirect reports from all and
n o t onl y are the 25 who were apparen tly cur ed stil l well , but on e of the arrested
cases has gon e on to a cure,while the other
—
isto all appearan ces well , a l though
I have not examin ed him . Of the 28 second- stage cases di scharged from on e
to seven years,26 are stil l living
,and on ly one of the 19 apparen tly cured
has had any fur ther trouble. Of the third- stage cases whi ch were apparen tly
cured,
one died during opera tion ,on e went through a severe operation ,
fo llowed by septicemi a and broke down again,and three are living and well ,
a l though one went thr ough a severe attack of double pn eumoni a more than a
year ago . Several of the arres ted cases have gon e on to a cure,and many of
them are working wi th their capacity onl y S lightly impair ed .
B rown (Zeit . f . T uberkul ose, Bd. V I , p . 235) has an alyzed the post-dis
charge mortal i ty of thepatien ts who had been tr eated wi th tubercul in at the
Adir ondack Co ttage Sani tarium and compared it wi th tha t of the to tal number
treated in the in sti tution dur ing the same per iod . H is results are very in ter
esting and bear out the claim made tha t the resul ts of tuberculin trea tmen t
should bemore perman en t than those obtained wi thout it.
“The method adopted for comparin g the pos t- di scharge mortali ty of the
tubercul in cases and the to ta l n umber of cases is as fo ll ows : E ach
series of cases was classified by condi tion on di scharge and the year'
of dis
charge. On the basis of E nglish LifeTable,N o . I I I , the probable n umber liv
ing at the same time Was ca lcul a ted for each ser ies accordin g tothe age condi
tion and discharge and date of admission . For . example,
males -aged
twen ty~ n in e,
are al ive after two years according to the forego ing life
table. H aving thr ee males aged twen ty-n in e on d ischarge from the sana to rium
two years ago the“expected livin g ” was calcula ted as di vided by
which equals I f we fin d say two l iving, the n umber survivin g
Perm an en cyof Results .
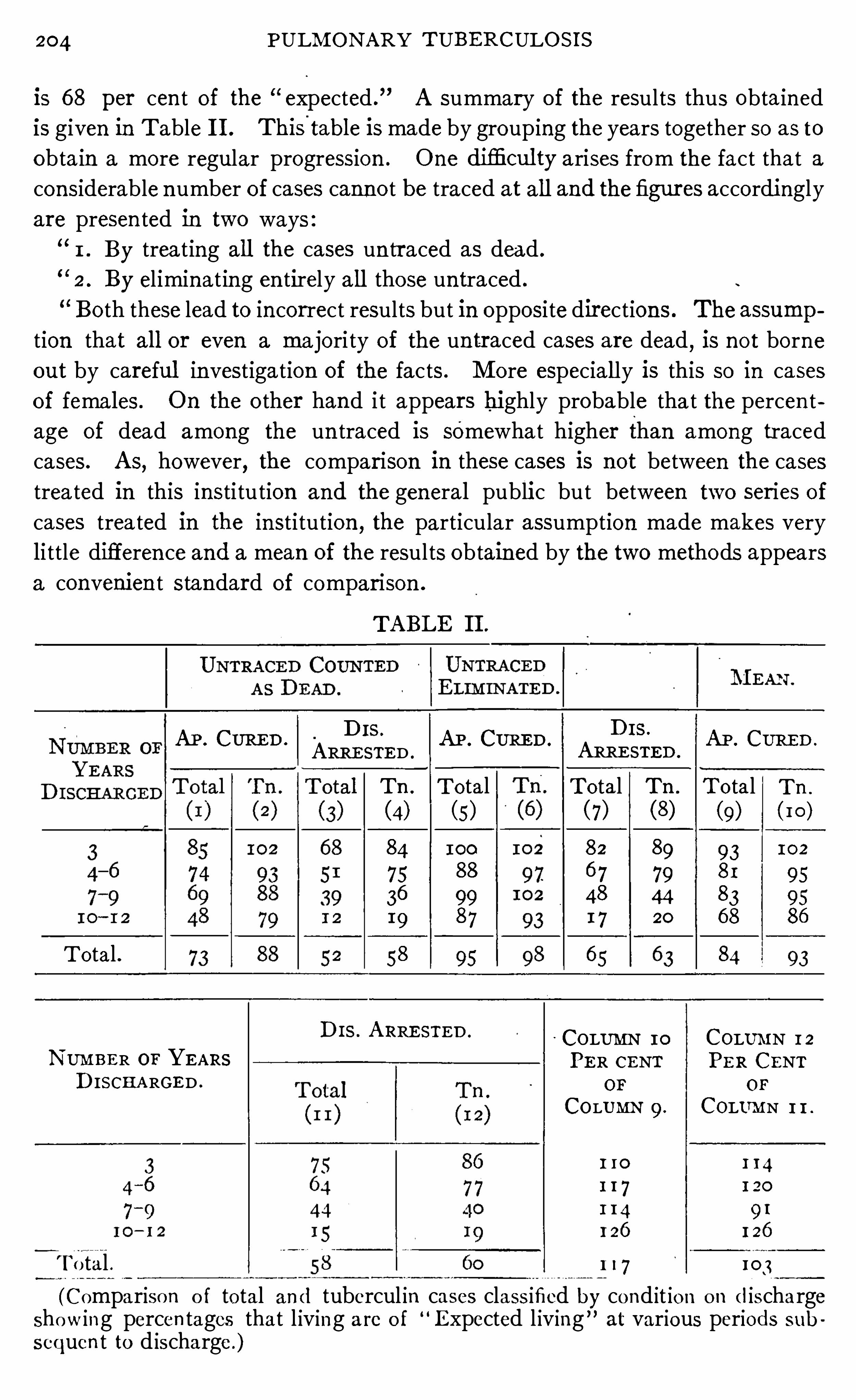
204 PULM ON ARY TUBERCULO S I S
is 6 8 per cen t of the expected .
”A summary of the results thus obta ined
is given in Table I I . This'
table is made by grouping the years together so as to
obta in a more regular progression . One difl‘icul ty arises from the fact that a
considerable n umber of cases canno t be traced at al l and the figures accordi ngly
are presen ted in two ways :
1 . By trea ting all the cases un traced as dead .
2 . By el iminat ing en tirely a l l those un traced .
Bo th these lead to in correct results but in opposi te directions . The assump
tion that al l or even a ma jori ty of the un traced cases are dead,is no t borne
out by careful in vestigation of the facts . M ore especial ly is this so in cases
of females . On the o ther hand i t appears highly probable that the percen t
age of dead among the un traced is somewhat higher than among traced
cases. As, however, the compar ison in these cases is not between the cases
trea ted in this insti tu tion and the general public but between two ser ies of
cases trea ted in the in sti tution ,the particular assumption made makes very
li ttle differen ce and a mean of the results obtained by the two methods appears
a convenien t s tandard of compar ison .
TABLE I I .
AP . CURE D . AP . CURE D . AP . CURE D .
T o tal .
D I S ' ARRE STE D ' COLUMN 10 COLUMN 1 2
N UMBE R or YE ARS PE R CENT PE R CENTD ISCH A RGE D . OF o r
COLUMN 9 . COLUMN 1 1 .
1 10 1 14
1 1 7 1 20
1 14 9 1
126 126
T o tal . 1 17 103
(Comparison o f to tal and tubercul in cases class ified by cond it ion o n dischargeshow ing percen tages that l iving are o f
“Expected l iving” at various periods sub
sequen t to d ischarge .)
D I S .
ARRE STE D .
Tn . T otal(4) (5)
84 100
75 88
36 99I 9 87
58 9s
D I S .
Tn .
102
95
9586
ARRE STE D .
To tal Tn . T o tal(7) (8) (9) (I O )
82 89 936 7 79 81
48 44 831 7 20 6 8
6 5 84
206 PULM ON A RY TUBE RCULOS I S
are the cause of mixed in fection . They can n ot furn ish recuperative power
when the system is to tal ly undermined . I n sho rt they can n o t overcome the
con sumption which has taken place as a resul t of the tuberculous process .
Yet this is wha t many have expected a specific remedy for tuberculosis to do .
Specific products made from the tubercle bacillus are remedi es which,when
combined with o ther suitable therapeutic measures,offer the best poss ible
chan ce of cure to those suffering from tuberculosis in any
'
stage ; but from their
un iforml y good resul ts in early tuberculosis they demand an early di agnosisand their early in telligen t employmen t . I n advan ced tuberculosis n o mo reshould be expected than is possible to be obtain ed .
Who shal l employ Specific remedi es? This question shouldWho Sha llEmploy an swer Itself. A ny man Should be capable of employi ng themSPeCific if he has suflficien t in telligen ce and suffic ien t determination toRemedies
acqu i re a knowledge of thei r act10n and the proper method of
their use,and i f he will familiarize himself thoroughly wi th tuberculosis .
They are n o t safe remedies for a man to employ haphazardl y,nor Should they
ever be used in a routine mann er . I t is just as rationa l to put the surgeon ’
s
kn ife in the hands of a blindfo lded physician as to put these specific remedies
in the hands of a“
man who does n o t understan d bo th them‘
and the di sease to
be tr eated by them .
I n o rder to be able to determine whether Specific remedies are do ing good
o r not i t is n ecessary to be able to no te the minute changes going on,which are
revealed on ly by a careful use of the stethoscope,as well as to observe grosser
changes which are pa ten t to the eye.
Pa tien ts treated by tuberculin should be under the close observation of the
physic ian . The ideal place for the admin istration o f this remedy is in an
insti tu tion where the patien t can be properly con tro lled . Whi le i t is possible
to secure good resul ts in o ffi ce practice, yet advan ced cases, as a rule, can no t
be so wel l handled outside of an insti tution as in .
I n tel ligen ce,care
,pa tience and perseveran ce are indispensable to the proper
admin istra tion of tubercle vaccines .
The fac t tha t a remedy o r measure is n ot generally adopted
$ 15
1; l t
uableat on ce
,upon its announcemen t
,is no argumen t against i t ;
Recogn ized? and especia lly is this true of a remedy which proved so dis
appo in ting when firs t announ ced . Scien tifi c truths make
place fo r themselves slowly because they compel men to give up their already
established bel iefs . I t took mo re than hal f a cen tury fo r any co nsiderable
number o f the medica l pro fession to adopt the fresh a ir cure fo r tuberculo sis ,and i t will perhaps be at least three-quarters o fa cen tury befo re i t is fully appre
c ia ted . Fresh a ir is no t o n ly a remedy for tuberculos is but fo r a l l diseased
co ndi tio ns,as wel l as o ur best prophylactic ; yet how long w i l l i t be befo re its
value will be recogn ized ?
TH E SPE CI FI C TRE A TM E N T OF T UBERCULOS I S 207
Tuberculin has been ga in ing rapidly . Heads of sana toria throughout theworld are fast fa lling in to l in e, and employ ing it in their in stitution s. The
great mass of clin ical eviden ce which is accumula ting in its favor can n o t be
ignored . M odern studies in immun ity “
and especially those of Wright haveshown i t to be founded on scien tific fact . I ts general recogn i tion is S imply
a matter of time .
When an ti toxin Was discovered for diphther ia this stimula teda hope tha t a similar remedy might be found for tuberculosis,but the differen ce In character of the two diseases seems to
preclude th is hope.
While most investiga tors, who have endeavored to find specific remedies for
the treatmen t of tuberculosis, have busied themselves Wi th the production of
active immun iza t ion,a few have endeavored to produce a serum which
con tains the specific pro tective bod ies, and, which , when in troduced in to the
human body,acts at on ce directly upon the tubercle bacil l i and their toxin s .
The best known an ti toxic sera are those of Fish,Paquin and D eSchWein itz
in America and M aragl ian o and M armorek in E urope.
Personally,the wr iter ’
s experience wi th1these Sera is too l imi ted to warran t
an opin ion ; however, i t seems that,
if they can be produced in such a manner
as to con tain large quan ti ties of an tibodies tha t they Should be of specia l value
in those cases where the patien t seems to suffer greatly from toxemia of tuber
cle bacil lus origin .
The serum which is best known in the trea tmen t of tuberculoA n titOXic
S is is the an ti toxic serum of M aragl ian o .
S erum(M aragl ian o). There I S one respect I n Wt h M araghan o
’s products differ
from those of o thers— they con tain no preservative. E ven
the products which he uses for in jection in to an imals for the production of
the sera are free from preserva tives. I n this way he a ims to in troduce the
toxins of the bacillus in their n a tura l fo rm,in the form in which they are
found in the bacil l i themselves . I t should further be added tha t neither the
bacill i nor the products made from them are subjected to heat .
This an titoxic serum is made in the fo llowing mann er : An imals,preferably
horses, are subjected to in creasing doses of a Wa tery E xtract of T ubercle
Bacilli un til their blood shows a high con ten t in an titoxic un its. The an ima l
i s then bled and the serum prepared under strict asepsis for use upon the
human being .
The Wa tery E xtract used ismadeas fo llows : Thebodies of-t ubercle bacill i ,are extracted with warm distilled wa ter un til they are deprived of their toxic
power. I t is then s tan dardized so tha t one cubic cen timeter of extract will
kil l one hundred grams of heal thy guinea pig within three days .
B a cterio lysin ,Recen tly M aragl ian o has produced ano ther remedy which
(M aragl ian o ). he calls Bacterio lysin . For the prepara tion of th is serum
An titubercleSerum .
208 PULM ON ARY TUBE RCULOS I S
the goat is preferred because i t responds better to the inoculations . Bacte
r io lysin accordin g to M aragliano con ta in s no t on ly an ti toxin s but agglutin ins
and bacter io lysin s as well .
I t is produced by the in o culation of the an imal w i th bacillus pulp which is a
product made by tri turatin g livin g, highl y virulen t tubercle bacill i with fine
sand in dis ti lled wa ter un til the bodies of the bacill i are tho roughly destroyed .
(Th is process also mechan ically separa tes the fat.) I t is then fil tered through
a Chamberlain fil ter to remove the bodies of the bacil li . To be sure tha t no
virulen t bacill i remain,a culture is taken . This prepara tion con tains a maxi
mum amoun t of bacill us substan ce and is un changed by hea t or preserva tives.
M armorek’s serum has en joyed a good reputa tion among
some men who are well qual ified to give an opin ion . Recen tly
he has produced a new serum which con tains pro tective bodies,
no t on ly aga in st tubercle bacill i, but aga inst the streptococcus wh ich is so h e
quen tly found producing an accompanying mixed infection .
M armo rek ’s
S erum .
2 I 0 PULM ON ARY TUBE RCULOS I S
When an o rgan ism is inocula ted,either artific ia lly or thr ough
Ro le o f the
B lo od in I n a natural In fect ion ,the blood elemen ts come at on ce to the
fection,
an d rescue. A s has been shown in Chapters X and XV theI mmun i ty.
natura l defens ive elemen ts of the body are found in the
blood . The bacteria are ac ted upon by them and,if the bacteria are not
presen t in too great numbers, or if their virulence is n ot too great,the pro
tective elemen ts found norma lly in the b lood w i l l be sufficien t to preven t
in fection from tak ing place.
A lthough the process of in fection,of warding ofl
'
in fection , and of curing
in fec tion when i t has on ce occurred,is based upon the same principle in the
various in fect ious diseases, yet, there are certain differen ces pecul iar to the
var ious in fecting micro -organ isms. I shall confine my remarks to the ques
tion of tuberculos is, S in ce tha t is the subject under discussion .
When tubercle bac i lli have once gained lodgmen t in theB loodPreven ted from body
,a wa ll of cells i s thr own about them formi ng the tuber
E n ter in g 111 ‘
cle. This is most likely a conserva tive action to guard thefected A reas.
organ i sm against the escape of' bac i ll i i n to new areas . Whi le
the process is primarily pro tective to the organ ism it is secondar i ly pro tective
to the invading bac i ll i ; for , as the tubercle in creases in s ize,condition s favorable
to the micro -organ ism are developed, thus al lowing the bacilli to multiply
unhindered . The t issue becomes infiltra ted with many_
tubercles, necrosis
occurs,the blood supply to the en tire affected area is in terfered w i th
,and
stagnat ion of the circulation results . Whatever pro tective elemen ts there
are in the blood become used up,and the bacteria are a llowed to fo llow their
l ife cycle undisturbed . That the defen sive elemen ts of the blood serum are
used,up when kept in con tact with bacteria through stagnation
,is shown
by the a lmost to tal absen ce of them in fluid'
which comes from loca l in fect ion s
such as bo i ls.
I t can read ily be seen that, if the blood as i t c irculates in
the vessels carries the elemen ts which are an tagon ist ic to
tubercle bac i lli,and if
,upon stagna t ion in the areas o f in fec
tion,the pro tective elemen ts are used up, the tubercle bac i ll i are ex ist ing
under cond i t ions which are unusually favorable for them . I t can further
be seen tha t, if some way can be devised by which a greater amoun t o f blood
can be caused to en ter the areas of in fec t ion,and the lymph flow through
i t can be hastened,the very cond itio n s wh ich are favo rable to heal ing are
go ing to be produced .
Wh i le B ier co nceived his ideas o f the action of hyperemia several years
ago , yet he had to wa i t fo r recen t years to co nfirm his v iews and to Show the
metho d o f its act io n . The opso n ic power o f stagnan t lymph found in areas
o f tuberculous in fec t ion is very low,wh ile tha t o f the c ircula t ing blo od mav
be l i ttle, i f any, below the no rma l ; so i t is a demo n strable fac t tha t by inc reas
H YPE REM I A 1:
ing the amoun t of blood to the part affected and hasten ing the flow of lymph
accord ing to the B ier method we are a id ing na ture in such a
'
way as to bring
her defen sive elemen ts to bear upon the bac i lli in a manner which is the most
advan tageous possible.
B ier gives the fo llow ing description of the manner in wh ich
821
3
1
252:333“ he was led to recogn ize the . va lue of hyperemia (Hyper
Tubercul os is.emia als Hei lmittel , Leipz ig, 1906 , p .
“
_
I came upon
the thought of using hyperemia in the trea tmen t of tuber
culosis through the fo llowing observation s “
of o lder physic ian s : Farre and
Travers called a tten tion.
to the frequent co in ciden ce of stenosis of the pul
monary artery and pulmonary tuberculosis in 18 15 . Louis again directed
atten tion to this in 1826 and expla ined the co in ciden ce as being due to the
high grade of anemia in the lung produced by.
this card iac .d isease . The
observations of those physic ian s were confirmed so that Frer ichsi
(Ubersicht
tiber die E rgebn isse der med. Kl in ik . zu Breslau . W iener med . Wochen schr .,
1853 , N o . 53 , S . 635) stated it as a general proposi tion :‘Pulmonary tuber
culosis“
,no matter wha t the relation of th is affection of the heart to the o ther
forms of tuberculosis, is the usua l cause'
Of'
death in stenosis of the pulmonary
artery .
’ On _ the o ther hand Rokitan sky (M edizin ische J ahrbi'
i cher des k . k .
Osterreichischen S taates . 26 . Bd. oder der n euesten Fo lge 1 7 . Bd. Wien .
1838 , S . 41 7) announ ced the theory'
that those chron ic heart lesion s which
cause the lung to be overfil led with blood gran t an immun ity to tuberculos is .
H is own words are as fo llows : ‘The relation of hypertrophy of the heart to
tuberculosis is the subject of many observa tion s . Among 143 cases belong ing
to this category (s imple and“
eccen tric as well as con cen tric hypertrophy)I find in fifteen cases that one had a fully healed tuberculosis
,but in al l the
rest (person s of differen t ages, genders, occupations,etc .) never a tubercle
had been pr esen t, whereupon'
i'
t can be judged that these two patho log ica l
cond i tion s can n ot exist in the same ind iv idual at the same time, but especiallythat when the. above men tioned heart affect ion is presen t there can develop
no tuberculosis,at least n o pulmon ary tuberculosis .
’
Rokitan sky (Osterreichischen , J ahrbi'
i cher,1836 , Vo l . XVI I ) .even wen t
far ther and said : “Cyan osis
,or rather every d isease of the heart, vessels
and lungs that causes cyanosis is in compat ible with tubercle forma t ion s ;that is, i t offers an extraord inary immun ity from tuberculosis .
”
The observat ions of Rok i tan sky in relation to heart affect ion s and tuber
culosis have been in the main confirmed by modern observers and we n ow
know the rat iona le of their act ion . We kn ow tha t i t is n ot the hyperem ia ,but the
,
fact that through this hyperemia there takes place in the lung a con
cen trat ion of the blood w ith its pro tective bodies .
Bernard Schulae (Beitrag zur S tat ist ik der Tuberkulose'
verbunden mit
Herzklappenerkrankun gen , I naugural D issertat ion ,Kiel
,1891) in 1891
2 1 2 PULM ON ARY T UBERCULO S I S
brough t together the statistics upon the relat ive co inc iden ce of tuberculosis
and heart lesion s . Hefound that stenosis of the pulmonary artery is fo l lowed
by pulmonary tubercul osis in per cen t of the cases, while lesion s o f the
aortic valve in on ly per cen t and those of the mitral valve i n on ly
per cen t .
B ier reasoned that, if hyperem ia has immun iz ing power against tuberculo
sis of the lungs, i t should a lso have the'
same power against tuberculosis
elsewhere.
“
H is fir st exper ience was w i th the treatmen t of tuberculosis of the jo in ts ;but since then he has applied it to tubec l osis of nearly a l l forms and also
to many o ther in fec t ion s and cond i t ions.
B ier warn s again st the Careless use of hyperemia and says
that much harm can be done by i t if i t is used improperly ;and reports from his own experien ce cases of co ld abscess
fo llowing faulty methods . I n applying hyperem ia he
formerly began by using it for one hour a day on ly,then he in creased the
t ime to several hour s a day, and final ly to an a lmost con tinua l use of it . The
compress was worn day and -
n ight,but twice dai ly its posi tion was changed
,
and usually once a week it was en tirely removed . The compression was
en t irely removed in order that the swell ing and edema might pass away so
that the exact cond i t ion of the limb would be known . H e has now discarded
this method and in stead uses a very pronoun ced hyperemic condition for
one or two hours a day. T h is is produced by the use of a rubber bandage
wh ich is fitted so carefully that “the subcutaneous Veins become markedly
swo llen , the Sk in becomes un iformly bluish-red and toward the end of the
hour a prickling sen sa tion sometimes appears i n the l imb .
”
B ier recommends tha t the part which is being treated Should be kept in
a cond i t ion as nearly aseptic as is possible, also that -on ly a very l imi ted mo tion
should be allowed and finally Shows his good judgmen t by recogn izing that
o ther measures which are of value should also be employed .
H e lays down the two fo llowing rules :
I . The congest ion Should never cause pain else i t is wr ongly applied
o r the case is unsuitable for treatmen t and must be treated by o ther means .
2 . The congested area must n o t be co ld . The temperature of the skin
mus t no t be less than that of the o ther l imb . I t is favorable for the cure o f
the tuberculous in fect ion when,on the con trary, the hyperemia can be so
appl ied tha t the sk in tempera ture o f the part under trea tmen t is increased
and the part assumes the appearance o f an acute inflammation .
”
S ince writ ing the above i t has been the autho r’s go od fortune to visi t Pro f .
B ier'
and see the hyperemia treatmen t as carried out in his cl in ic . The
th ing tha t impressed him mo st was the impo rtance of exac tness in techn ique.
I t is n o exaggera t io n to say tha t hyperem ia treatmen t is en t irely a matter of
2 I 4 PULM ON ARY T UBE RCULO S I S
Hyperamie der Lunge bieLungen schwin dsucht . Zeitschrift fur d iat . undphysik . Therapie ,
8 . Heft). The trouble w ith this measure,a side
from its impract icab i l ity is that,if i t does produce a hyperemia; i t must on ly
be of the mucous membrane of the air passages and it would seem that the
greater force would be exerted upon the mucous membranes of the larger
air passages, wh i le tuberculos is aflects'
more part icularly the paren chyma of
the lun g and the disease is si tuated near the finer d ivisions of the a ir spaces.
I f,however, such a result is desirable
,i t can be much more easi ly produced
by the use of the pneuma tic cabinet . By placing the pat ien t in the cab in et
and producing a lowered pressur e about him,pressur e wil l be removed from
the blood vessels in the mucous membrane of the air passages and a d i latat ion
resulting in a hyperem ia w i ll ensue.
I have succeeded in demon stra ting to m y own sat isfactionH yperem i a
Caused by that a congestion is produced by direct ing the concen tratedReflectedSun l igh t.
rays of the sun upon the chest by the use of large m irrors
(three and one-half feet in d iameter) in which the heat is
cut off by blue glass . Whether this is due as some bel ieve to the action
of the blue and vio let rays,which are reflected, or to the heat rays which
are not screened out by the blue glass, I am unable to determine. H ow
ever,after the use of these reflected rays for a ha lf hour or more
,there is
a marked increase in the signs of congestion ,as Shown by the stethoscope.
When the pat ien t is fir st put under this treatmen t he exper ien ces an in crease
in the amoun t of coughing which also suggests an in creased congest ion .
Th is d isappears,however
,after the patien t has become accustomed to the
treatmen t .3
E lsewhere,I have Spoken of the manner in which tubercu lin
causes a hyperemia in the lungs A very smal l dose causes
a hyperemia and a st il l larger one causes a congestion . This
hyperemia is prodiiced as a resul t of tha t action of tuberculin
which causes a d i latation of the b lood vessels in tuberculous tissue. I be
l ieve that this action of tuberculin is a very importan t one, a lthough I
have never seen referen ce to it in the l iterature. Tuberculin thus possesses
the power to bring about the two most importan t cond itions necessary to es
tabl ish immun ity in tuberculosis, viz .
,to st imulate the physio logica l processes
o f immun iza tion so that more pro tective substances are formed, and to open
up the blood vessels at the seat o f the d isease, and allow the blood to flood
the cen ters o f in fection and apply the immun iz ing elemen ts at the po in t where
they w i ll be most effective. Thus the hyperemia produced by tuberculin
has a great advan tage over tha t produced by o ther means in that i t no t o n ly,
fl oods the area o f infect io n w i th a greater amoun t o f blood, but with a blood
who se immun iz ing propert ies have been greatly increased . O f course there
is no co n traind ication to the use o f o ther measures for the product ion o f
H YPE REM I A 5
immun ity at the same time that hyperemia is being used ; in fact, such measures
are ind ica ted , and w i ll “hasten recovery . This po in t haS ' been establ ished
in conn ect ion with the treatmen t of lupus. M any cases treated by Fin senl ight a lone do not get well ; a lso many treated by tubercul in a lone fa il of acure, but when these measures are combined the result is mlich better . M any
fai l to respond to Fin sen_ l ight , which is doubtless indebted very largely to
its hyperemia produc ing power for its resul t, because the conten t of the bloodin pro tective substan ces
_
is too low to be of value when the diseased area is
flooded with'
it. Wr ight has Shown that the opson ic power of the blood is
usually low in these cases that fa i l to respond to Finsen l ight . H e has also
shown that o ften the opson ic index may be raised to n ormal and yet the
pa tien t fa i l to respond,owing to the fact that the immun iz ing elemen ts fa il
to come in con tact w ith the germs . On ly when the pro tective substan ces
have been i n creased and when these substan ces have been brought in to
direct con tact with the bacilli do we'
have ideal condi tions for the cure of the
d isease. Wright found - tha t some of his lupus cases tha t failed to respond to
an in crease of the immun iz ing elemen ts in the blood, as shown by in creasing
the opson ic con ten t of the blood, made“
satisfactory improvemen t when he
increased the flow of blood to the part by the use of hot sand poultices. These
results are a most convin cing demon stration of the value of tuberculin and
hyperemia combined .
I t has been my observa tion that patien ts who suffer from
a more or less genera l distribution of tuberculosis thr oughout
bo th the fron t and back of the lungs,Show a much more
rapid advan ce toward recovery posteriorly. The back
portion of the lung will hea l out much more rapidly than the front. I t is
probable that the congestion caused by posi tion s assumed by the patien t
may have someth ing to dowvith this. Wh i le tuberculous patien ts spend a
great portion of the time ly in g on their sides, yet their posi tion affords an
opportun i ty for the b lood to gravitate poster iorly.
CHAPTER XV I I .
TH E SANATOR I UM TRE ATME NT OF TUBE RCULOS I S .
The sanatorium is the agen cy through which the open -air hygien ic , dietet ic .
and sc ien tific trea tmen t of tuberculosis can be carried out to best advan tage
While i t might seem that treatment in a sanatorium should not d iffer from
that on the outside, yet, in _
practice, i t differs very ma teria lly . While i t is
possible to obtain excellent res—
ults outside of sanato ria, yet, i t is impossible
to have that same abso lute control over a patient and a l l his action s,that
close feel ing of mutua l in terest and co—operation between patien t and phys
ician,and that cheerful helpfuln ess which comes from the association of many
who are making the same sacrifices, struggling toward the same end and
con stan tly finding themselves and their associates making steady advan ces
toward recovery. The psychic effect of a sanatorium is one that can n ot be
measur ed .
A sanatorium is simply the reflection of the man Who is at
the head of it, and whether it succeeds or fails depends upon
h im. The sanatorium'
treatment of tuberculosis requires
of a medical director certa in importan t qua l ificat ion s. H e
should first of all understand the disease which he is expected to trea t,and al l
th ings being equal the better he understands i t,the better will be his results .
N ext and not of less importan ce he must be possessed of patien ce. H e must
be sympathetic, yet firm . H e must be opt im istic ; but his optimism must be
bounded by reason . H e must be endowed with qual i ties of leadership , for
he must n ot on ly lead his patien ts,but he must command an army of help .
Sanatorium men are born,not made. I t is useless
_
to th ink that a sanatorium
can be properly conducted by simply placing a physician ,regardless of his
qualifications and temperamen t, at the head of i t . The head of a sanatorium
should l ive at the insti tution so that he may come in to in tima te con tact with
his patien ts and so that he may be in touch with everything that goes o n .
The medical d irector of a sanatorium occupies much the same posi t ion as
the capta in of the sh ip . Harmony must be everywhere preserved ; therefore,every departmen t Should be under his direction and personal supervision .
A word m igh t be,said regarding medical directors fo r sta te sanatoria .
I f i t were po ssible, these insti tutions should not be con tro lled by po l it ics .
When i t is remembered tha t their success depends upon the men at the head
o f them , i t can read ily be seen that one fit for such a posi tion is fit to succeedanywhere. H e is no t
, as a rule, look ing for the place, but the place is
216
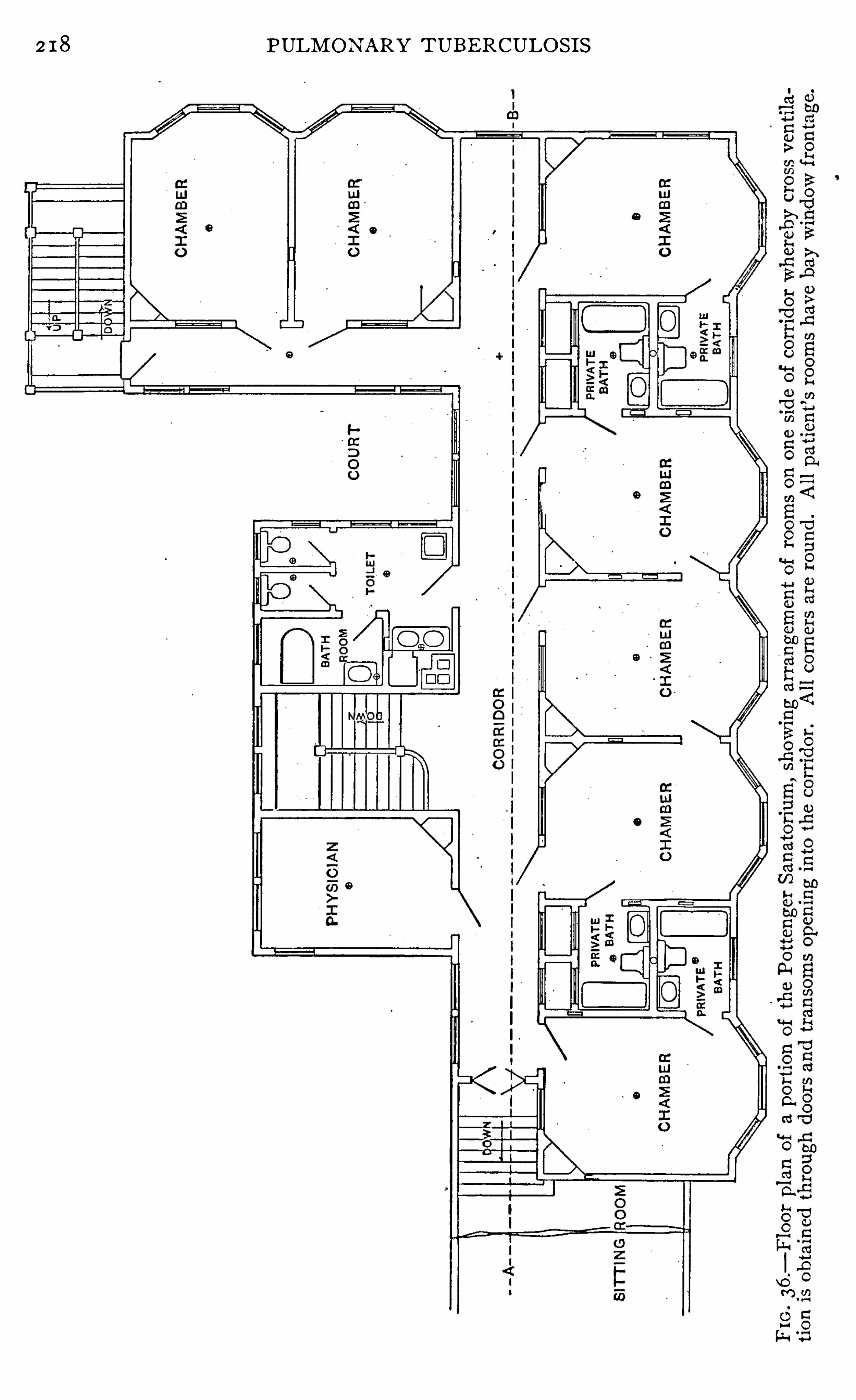
2 I 8 PULM ON ARY TUBERCULO S I S
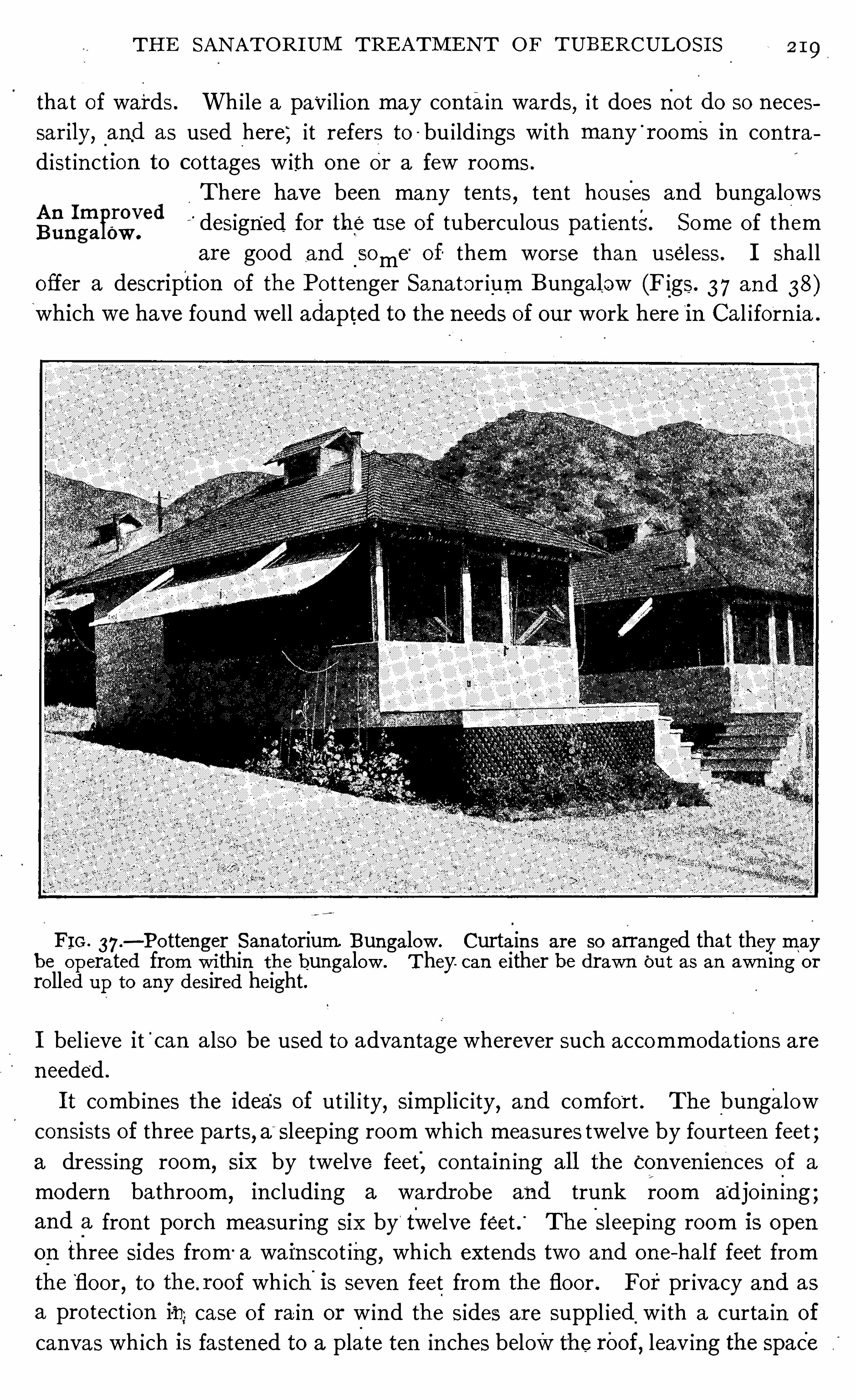
TH E SAN ATOR I UM TRE ATM E N T O F TUBE RCULOS I S
tha t of wards . Wh i le a pavilion may con tain wards, i t does not do so meces
sar ily, _
and as used here; it refers to - bu i ld ings with many'
rooms in con tra
d ist in ction to co ttages w ith on e or a few rooms .
There have been many ten ts,ten t houses and bungalows
" designed for the use of tuberculous pat ien ts. Some of them
are good and_
Some'
of them worse than useless . I sha l l
offer a description of the Po ttenger Sanator ium Bungalow (Figs. 3 7 and 38)which we have found well adapted to the needs of our work here in Cal iforn ia .
A n ImprovedBun ga low .
FI G . 37 .—Po ttenger San atorium Bungalow . Curtain s are so arranged that they may
be operated from wi thin the bungalow . They. can either be drawn but as an awn ing or
ro lled up to any desired height.
I bel ieve it'
can also be used to advan tage wherever such accommodation s are
n eeded .
I t comb ines the idea'
s of ut il ity,simplic ity
,and comfor t . The bungalow
consists of three parts, a‘
sleep ing room wh ich measures twelve by fourteen feet ;a dressing room, S ix by twelve feet
'
,con ta in ing al l the Conven ien ces of a
modern bathroom, in cluding a wardr obe and trunk room adjo in ing ;and
_
a fron t porch measur ing S ix by“
twelve feet .“
The Sleep ing room is openon three sides from '
a wai‘n sco t ing,wh ich extends two and one—half feet from
the”
floor , to the. roof wh ich is seven feet from the floor . For pr ivacy and as
a pro tect ion in. case of ra in or w ind the sides are suppl ied w i th a curta in of
canvas wh ich is fastened to a plate ten in ches belowthe rOof, leav ing the space
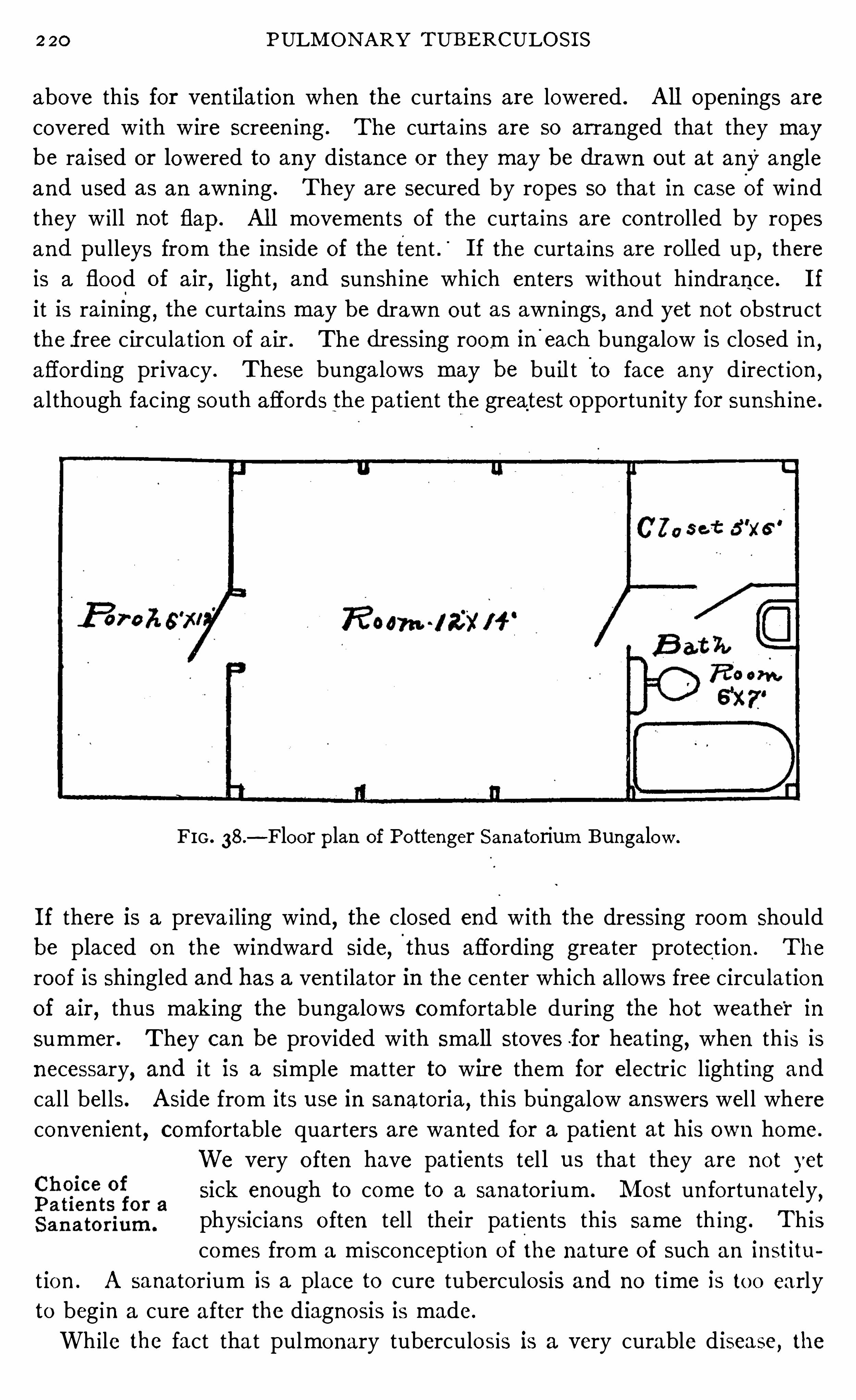
220 PULM ON ARY TUB E RCULOS I S
above this for ven t il at ion when the curtain s are lowered . A l l open ings are
covered w ith wire screen ing . The cur ta ins are so arranged that they maybe ra ised or lowered to any distan ce or they may be dr awn out at any angle
and used as an awn ing . They are secured by ropes so that in case Of wind
they w i ll not flap. Al l movemen ts of the curta in s are con tro l led by ropes
and pulleys from the in side of the ten t .’
I f the curta in s are ro ll ed up,there
is a flood of air,l ight
,and sun shine which en ters without hindran ce. I f
it is rain ing,the curtain s may be drawn out as awn ings
,and yet not obstruct
the free circulation of a ir . The dr essing room in'
each bungalow is closed in ,
afford ing privacy . These bunga lows may be buil t to face any d irect ion ,
a l though fac ing south affords the patien t the greatest opportun ity for sun shine.
FIG . 38 .
—Floor plan of Po ttenger San atorium Bungalow .
I f there is a preva i ling wind,the closed end with the dressing room Should
be placed on the windward side,I
thus affording greater pro tection . The
roo f is Shingled and has a ven t i lator in the cen ter wh ich a llows free circulat ion
of air , thus making the bungalows comfortable during the hot weather in
summer . They can be provided with small stoves .for heating,when th is is
necessary, and i t is a simple matter to wire them for electric lighting and
cal l bel ls . A side from its use in sanatoria, this bu'
ngalow answers wel l where
conven ien t, comfortable quarters are wan ted for a patien t at his own home.
We very o ften have pat ien ts tel l us that they are no t yet
sick enough to come to a sanatorium . M ost un fortunately,
physicians o ften tel l their pat ien ts this same th ing . This
comes from a m isconcept ion o f the nature of such an institu
t ion . A sanator ium is a place to cure tuberculosis and no t ime is to o early
to beg in a cure after the diagno sis is made.
Wh ile the fact tha t pulmonary tuberculos is is a very curable disease, the
222 PULM O N ARY T UBE RCULO S I S
does not sign ify that they can n ot get well , but i t means that they must struggle
to master their d isease aga in st odds.
The most su itable cases for sanatorium treatmen t,as wel l as for treatmen t
on the outside, are early cases..The earl ier the case is d iscovered the better
are the chan ces of cure. I n publ ic inst i tut ion s where the greatest good to
the greatest number must be considered , as a rule, on ly early cases are taken ;but in pr ivate in stitution s, where our duty -
to the individual receives morecon sideration , many advan ced cases must be admitted .
There is a common bel ief on the part of some sana torium men that a sana
tor ium is on ly for early cases. This is a m istaken v iew . T rue,in those cases
,
the best record can be made for the in st itut ion ,and more pat ien ts can be
offered help in a given t ime ; but is this al l that is to be con s idered? I s a man
who has advan ced tuberculosis to be den ied the right to the best trea tmen t,
S imply because of greater invo lvemen t and lessened chan ces of recovery?
Would it not be more sen sible to give h im the best opportun ity possible?
D o physician s refuse to g ive the best chan ce for l ife to pat ien ts suffer ing from
o ther d iseases simply because they are advan ced and the ch an ces of cure no t
so good? Few men realize what can be done for pat ien ts snfler ing from
advan ced tuberculosis when given the best'
chan ce of cure in a well conducted
sanato rium. Wh ile the work is harder for bo th pat ien t and physic ian the
prize is greater and worthy of the effort .
M y exper ien ce in the sanatorium treatmen t of tuberculosis has been largelyamong advan ced cases . M ore than ha lf of the patien ts examined are rejected
because of the fact that in our opin ion they have on ly a few weeks o r mon ths,at most, to live. N othw ithstanding this, we admit many bad cases and
usually have “
about 30 per cen t of the pat ien ts in bed because of high
temperature. I n spite of th is fact about 50 per cen t o f a l l advan ced cases
who rema in in the institution more than two mon ths -have had an arrestmen t
of the disease. About 10 per cen t secure a healed les ion and some of the
o thers even tually go on to this happy result . The l ives o f nearly al l o f
these advan ced cases can‘
be pro longed and many of tho se in whom an
arrestmen t is secured w i l l l ive for years and lead active,useful lives, even
without a cure.
Usually tho se un fortunates who are suffering from advan ced tuberculo sis
are a llowed to go o n, no a ttempt at curing them being made. They are kept
as comfo rtable as poss ible but are a llowed to go on to certa in death . Th is
is a cruel wro ng . M any o f these l ives can be saved i f we w il l but ofler them
the o ppo rtun i ty o f the best treatmen t tha t can be secured . A pa t ien t suffering
from chro n ic tuberculo s is , even w i th co nsiderable destruct io n o f lung t issue,i f he has a stro ng heart and go od d igestio n ,
prov id ing his co nst itut io n is no t
seriously underm ined , deserves a chance fo r his l ife and will have more than
even chances fo r an arrestmen t , i f g iven the best that a sana to rium a lTo rds .
TH E SAN A TOR I UM .TRE ATM E N T O F TUBE RCULOS I S
I f den ied th is opportun ity, he w i ll go on to a lmost certa in death w ith in a com
paratively short t ime. E ven patien ts w ith hect ic fever must n ot be den ied
a chan ce for l ife, for many t imes this condition yields to intel l igen t , rat ional
measures.
While we plead for these advan ced cases, yet we would not min imize thediflficul ties en coun tered in the handl ing of them . The man who w i ll treat
such cases must be an al l around physic ian , for he w i ll meet . every compl icat ion imaginable. H is patien ce must be unbounded and
_
his opt imism co
extensive Wi th it . H e must be frank and tell his patien t that the strugglew i l l be a hard on e and long drawn out
,and impress Upon him that pat ien ce
,
perseveran ce, and an unbounded faith in the fina l outcome will do much to
aid in his recovery .
D ifficul ty ofA properly co nducted sanatorium offers the best chan ce of a
Treatin g favorable result to advan ced cases and,through its agen cy
,
giggn ced many may be restored to usefulness. The advan ced case
can be treated at home on ly under the greatest difficul ties
and with much less promise of success . To repeat what I have said else
where, these pat ien ts are not suffering from tuberculosis on ly,but more
espec ially,from the results of ’ tuberculosis. M any
,if not al l of them
suffer more or less from mixed in fect ion . Fibro id changes, necrosis, and
in some in stan ces calcificat ion o ccur in the diseased areas . From the
block ing up of the blood vessels in the lung there is a damming back of
the blood with more or less passive congestion of the in terna l v iscera ; the
heart has an extra burden thrown upon it , and its muscle; weakened by
the strain,o ften becomes damaged . Cavities form in the lung, con traction
occurs . That part of the lung which is not affected hypertroph ies,and
later becomes emphysematous,thus adding more burden to the heart , the
general system is po isoned by toxin s, wast ing o ccurs, and al l of the o rgan s
suffer more or less. This'
gives us the p i cture of con sumpt ion . This is
what we are trying to relieve when we a ttempt the treatmen t of advan ced
cases of tuberculosis . Tuberculosis is a disease,con sumption
,a cond ition
resulting_from the disease. When we have done a l l we can for such cases we
have done li ttle enough ; and'
yet, to many of these, the careful gu idan ce and
in tell igen t treatmen t .of the pat ien t as well as the d isease, as it can be carr ied
out in an in st itution ,will offer an arrestmen t of the process w ith a pro longa t ion
of l ife ; and to some it will even offer an opportun itv for the a ttainmen t of a
healed process.
Wha t ComWhat complicat ions are a barr ier to treatmen t ? The an swer
plica tion s are to this quest ion must vary accord ing to c ircumstan ces . I n
a Barrier to publ ic and char itable in st itution s we would bar many pa t ien tsTrea tmen t ?
who would be el igible to treatmen t i n priva te sana tori a ,be
cause in these'i in stitutions we must bear in m ind the idea of the greatest
224 PULM ON ARY TUBE RCULOS I S
good to the greatest number . Public inst itution s can n ot afford to fill
their beds or any con siderable port ion o f their beds w ith pat ien ts who
wi ll require S ix or eight mon ths in order to obta in a favorable result when
there are so many wa it ing for en tran ce who could obta in equal ly favorable
results in from three to six mon ths . Then , those who manage publ ic and
charitable inst itution s find it best to confine their efforts as much as is pos
sible to early cases, and, where advan ced cases are admi tted, they must be
such as offer a reasonable hope of rap id improvemen t . Al l tuberculous
compl icat ions, as a rule, bar en tran ce, and serious d isturban ce on the part
o f the c irculatory or d igestive system or the presen ce of fever make the pa
tients un su itable:
This d iscr imination on entran ce against such compl icat ion s does n ot mean
tha t they are necessar i ly fatal but onl y that they in crease the t ime and co st
of cure to such an exten t that it is not thought exped ient to adm it those sufler
ing from them. Tuberculous laryngitis, espec iall y if it is in the early stageso f infil tration , is not a barrier, provid ing our patien ts are g iven
_ _
the benefit
of tubercul in treatmen t . Tuberculosis of the bones,jo in ts and glands, and
even tuberculosis of the k idney and bladder'
yield to proper treatmen t . The
wr iter has seen -many ca'
ses of tuberculous laryngitis heal, a lso tuberculosis
of the ton sil , nasal septum,pharynx .and two cases of probable tuberculosis
of the in testines. Tuberculosis of the lymphat ic glands,in my experien ce,
has n ever come to operat ion . When such compl icat ions are presen t the t ime
of treatmen t is usually pro longed but , if money con siderat ion does not hamper ,such patien ts Should be given a chan ce for l ife.
The length of t ime n ecessary'
to obtain an apparen t cure or
arrestmen t in tuberculosis o r to determine that such a favor
able result can n ot be attained is a quest ion which must
a lways be considered when determin ing what course to pursue. A pat ien t
in the early stages of tuberculosis w ill on an average secure an apparen t cure
or arrestmen t in from four to S ixmon ths,while those in an advan ced cond it ion
require from six mon ths to one or two years or even longer . I t is importan t
that phys icians understand this, for i t is not at al l un common for patien ts to
be referred to a sanatorium w i th the assuran ce from their family physic ian
that a few weeks or one o r two mon ths will restore them to heal th . Th is
o ften causes no end of d isappo in tmen t . I t would be much better for the home
physic ian to expla in to the patien t the na ture of the trouble and in sp ire him
w ith the hopefulness o f modern methods o f treatmen t , and yet not min imize
too much the d ifficult ies connected with it . I t must also be remembered tha t
many pa t ien ts who secure an improvemen t in a few mon ths m ight secure an
arrestmen t in o n ly a l i ttle longer t ime ; and many who secure an arrestmen t
m ight,by a l ittle more t ime, secure an apparent cure.
Len gth o f
Trea tmen t .
2 26 PULM ON ARY TUBERCULOS I S
the best chan ces of cure ; con sequen tly the pat ien t is compell ed while l iving
with pr ivate famil ies to n eglect many measures which w ill a id in a cure,and do ma ny things which w i ll retard progress .
The pat ien t at home or in an open reso rt is near business and social l ife,
yet he cann o t en ter them . The temptation is great and the den ia l much
harder than when he is en tirely away . H e has a con stan t taste wi thout
the full en joymen t .
The n ext great advan tage which makes sanator ium treatmen t super ior to
that of the home or open resort is the close persona l con tact of the pat ien t
and physician . I n a d isease like tubercul osis,where l ife or dea th depend
on such l ittle things, i t is necessary for the physic ian to have abso lute con tro l
over the pat ien t . This necessity is emphasized by the fact that dur ing much
of the t ime these pa t ien ts do n ot feel ill,and during
-
this t ime when they feel
wel l they are apt to do th ings that they should not do and jeopardize their
recovery . On the o ther hand, there are many things that these pat ien ts
should do wh ich they wil l neglect unl ess the physic ian has some method of
knowing whether or not they are done. N o thing stimul ates obed ien ce so
much as frequen t con tact with the medical director .
I t might beargued that these pat ien ts should be to ld what to do,and if
they do n ot do this, they a lone are responsible ; but such argumen t would play
havo c with results in the treatmen t of tuberculosis ; for , here, the success of
trea tmen t depends upon keep ing up the in terest and hope of the pat ien t
through many seasons of d iscouragemen t , when even the bravest hearted
waver . There is a l itt le tenden cy to overstep rules in us al l,and we o ften
see th is in tuberculous patien ts. They w i ll o ften del iberately plan to take
advan tage of their physic ian and d isregard his advice on matters which mean
very much to their recovery . I have known them to pr ide themselves on
do ing someth ing against his adv ice and without his knowledge. Th is is n o t
done with any in ten tional disrespect , either, for pa t ien ts hav ing a reverence
for their physician which almost equals wo rsh ip, w i ll do i t .
The frequen t v isits and en couragemen t of the med ical directo r at t imes
when things are not go ing smoo thly, when the - d isease is advan c ing , when
compl ica t ions are presen t or when progress toward recovery seems to be
slow ,g ives the pat ien t a strong arm upo n which to lean and o ften tides him
over the per iod of discouragemen t and starts him on with renewed zea l towards
recovery . There are many t imes when the words o f comfo rt and encourage
men t o f the med ical d irecto r are about al l tha t stand between l ife and death
to the pat ien t . Under the st imulatio n o f his v is its I have seen such pat ien ts
resto red to useful l ives . T o pat ien ts who are no t so ill , th is clo se asso c iat ion
g ives an oppo rtun i ty fo r en co uragemen t that could no t be o ffered in any
home o r o pen reso rt .
The o ppo rtun i ty o f hav ing compl icat io ns seen when they first arise and o f
TH E SAN ATOR I UM TRE A TM E N T OF TUBERCULOS I S
hav ing measures taken for their immed iate correct ion , and the fact that they
have someon e at han d to meet al l emergen c ies, g ives pat ien ts an“
assuran ce
and feeling of safety that adds much to their'
chances of recovery .
The th ird great advan tage of awel l - conducted and wel l arranged sanator ium
over the home or open resort is that here everyth ing is especial ly fitted for
the trea tmen t of the disease. The rooms are con structed on hygien ic prin
ciples, so that they may be flooded w ith l ight (especially sun light) ; the dietary
is arranged to su it the specia l needs of the pat ien ts ; spec ia l measures of trea t
men t are carried out to the best'
advan tage because of the d irect supervision
of the physic ian ; assistan ts and nurses are always at han d to aid in carryingout d irection s ; and dis in fect ion of rooms and table-ware and destruction of
sputum and o ther bac i llus- laden d ischarges are don e with extreme care. This
in sures to the tuberculous patien t the grea test security and at the same t ime
the best oppor tun ity of cure.
There is a mistaken idea on the part of some in d ividualsA ir Of H opef‘fl
‘
regarding the genera l air of a sanator ium . M any think thatn ess PervadesSan a toria these i n st i tut ion s are places of gloom and sadness. N o th i ng
could be far ther fromthe truth . I n sana tor ia, it must be
remembered that a l l pa tien ts who appear to be i ll are in bed . The con tra
in dicat ion s for exercise are such that al l who have fever, or those who are
extremely emacia ted, those who suffer from rap id heart or dyspnea and
those who have complicat ion s are confined to their beds ; con sequen tly on ly
the stronger are a l lowed to be up and aroun d . Therefo re, even in an in st i
tution where advan ced cases are cared for there is n o thing seen to mar the
hopefulness of the place. E ven most of those pat ien ts who are compelled
to rema in in bed are usually cheerful and happy .
When “pat ien ts arr ive at a sanatorium and are put upon the hygien ic regime,as a rule, they begin to improve at on ce. A t first they gain
'
in weight . They
see o thers are do ing the same. They gradually see their symptoms abatingand no te that th is change has come to o thers who have been there longer . A
new hope awaken s in their hearts and a firm belief in the possib i lity of cure
takes ho ld upon them . Soon they see pat ien ts who were confined to their
beds gradually gett ing better and stronger and ven turing out to mea ls and
then for walks. They are more convin ced than ever of the hopefuln ess of
their own cond ition . They see others apparen tly cured and this spurs them
on to make their best efforts to secure a s imi lar result.
Then there is tha t feeling of mutual in terest . Pat ients will help each
o ther . They w i l l bring words of cheer,and con cea l th ings that might dis
courage. They feel that they are boun d together by spec ial t ies . T hey have
the same disease,they are struggl ing for the same end and they are compelled
to make the same sacr ifices . This mutual con cern for on e ano ther makes
i t eas ier to bear the d isappo in tmen ts which the disease has produced . They
228 PULM ON ARY T UBERCULOS I S
see that their loss is not so great but that some one else has sufiered as much .
They can endure the separation from home because of the strength suppl ied
by their associat ion with o thers as brave. They can better deprive them
selves of harmful things that they have been accustomed to have,and restra in
themselves from do ing harmful things that they have been accustomed to do ,and submit to things which in crease their chan ces for recovery, though dis
tasteful, because they have the mora l support of al l those who are about
them .
The sanatorium then is the place where al l those measures which aid in
br ing ing about a cur e in tubercul osis can be applied most easi ly and most
successful ly and where the tubercul ous patien t can l ive under the best c ir
cumstances pertain ing to a cure.
230 PULM ON ARY T UBE RCULOS I S
Whi le the most favo rable c l imat ic conditions are n ot nec
essary to the cure'
of tuberculosis, yet i t stands to reason
that if a pat ien t can take advan tage of a su i table clima te,
he w i l l of n ecessi ty derive some benefit from i t . Of cour se
al l are not able to take advan tage of such changes . Bo th
phys ica l cond i t ion and pecun iary circumstan ces must be taken in to accoun t
when a change is considered . I t is useless to send a pat ien t away from
home and fr iends w i th the expectation of his der iving benefit from thechangeun less he has sufficien t means to enable him to take care of h imsel f properly .
Patien ts who should not work at home should n ot work in hea l th resorts, and
th is appl ies to a l l tuberculous pa tien ts ; 50, un less they have the mean s to
support themselves comfortably at a heal th resort,where living is usua lly
high,they w i l l do best to rema in at home.
I t seems to me tha t c l imat ic advan tages in the trea tmen t of tuberculosis
may be wel l summed up in this statemen t : tha t is the best c l imate for the
treatmen t of an ind iv idua l patien t (the climatic treatmen t the same as o ther
forms of treatmen t being an ind ividua l matter) where he can have the most
in tel ligen t gu idan ce,the most favorable surr ound ings ‘
and the best c limatic
condit ions con sisten t w ith his pecun iary circumstan ces . This mean s that
many patien ts of sma ll means, to whom a change of c l imate would be a
serious finan c ial embarrassmen t, have better opportun i t ies of cure by remain
ing under in tell igen t guidan ce at home than they would by st in ting them
selves and endeavoring to economize in a better c l imate. I t mean s that the
great mass of individua ls suffering from tuberculosis are better o ff at
home than they would be were they removed to some o ther more favored
cl imate. A nd, yet, it a lso mean s, what many
'
of our earn est advoca tes of
home treatmen t are forgett ing, that i f an indiv idua l can take advan tage
of a favorable climate well suited to his resisting.
power and his disease,
a l l things else being equa l,he stands a much greater chan ce of regain ing
heal th .
I f I were afflic ted with tuberculosis, I would rather be treated in an in tell igen t
manner in the most un favorable c limate than undertake to regain hea lth
a lone in the best c l ima te on earth . However,I bel ieve my chances of cure
would be materially increased , i f, comb ined with in telligen t treatmen t ,favo rable clima tic cond i tion s were also presen t .
Importan tGran t ing tha t a pa t ien t can advan tageously seek su i table
Co n s idera t io n s c l imat ic cond i t ions under which to be tr ea ted for tuberculos is ,in
.
Cho ice Of wha t con s iderat ion s should determine the cho ice o f such a
Cl ima tes.
cl imate? I n the first place,if he be suffer ing from tuber
culo sis in the early stage,he has a wide range from wh ich to cho ose. H e
would have go od o ppo rtun i ties fo r cure in any favorable c limate and doubt
less could get wel l even in an un favo rable o ne. I f,o n the o ther hand
,the
CLI M ATE A S A FACTOR I N TH E TRE A TME N T O F TUBE RCULO S I S by
d isease be.
advan ced, or if complica tion s be presen t, these cond iti on s musta l l be taken in to con siderat ion . A bove a l l else
,however
,aside from the
nature and exten t of the d isease and the compl icat ion s presen t,the strength
and react ive power of the patien t must determ in e the final cho ice of the
cl imate to be adopted .
The primary effect of clima tic treatmen t is upon metabo l ism .
Primary E ffe“ That climate iS 'best su i ted'
to a given patien t where t issueo f Cl ima ti cTrea tmen t . change i s carried on to the best advan tage.
- A robust in
d iv idua l will stand a r igorous climate whi le one w i th weakened
con st i tution will find the demands made upon him by ' i t to be too grea t for
his good . Huggard, in his most excellen t work on cl imato logy (A H andbook
o f Cl imatic T reatmen t, London , 1906 , page 46 1) says I n regard to cl ima te
therapeutical ly, the most fun damen ta l po in t is its eflect on t issue change;and its act ion on tissue change depends on its hea t abstract ing powers . N ow
,
the hea t abstract ing qua l i t ies depend, not on tempera ture a lone,but on tem
perature in comb inat ion w i th the humidity of the air,relative and abso lute
,
and the amoun t of w ind .
”
A co ld cl imate, then , w i th much wind makes the greatest demands upon
the system for hea t ; a warm,hu
’
mid clima te with absen ce of wind should
make the least . A dry,warm cl ima te can n ot be equable because the air
,
con ta in ing l i ttle mo isture, does n ot retain heat well, and as soon as the
sun has ceased to shine the rap idly coo l ing air causes a feel ing of co ld .
This accoun ts for the wide d iurnal range in temperature which is n o ted
wherever the air is dry,and g ives the st imulati ng propert ies to warm
dry cl imates . This makes the differen ce between a warm dry and a warm
hum id clima te.
From these con siderat ion s i t is pa ten t that by the use of the
various cl imat ic condi tion s men tioned above we produce
very differen t results . We can soo the,or we can produce
var ious degrees of st imulation even to the po in t of irr i tat ion .
I t therefore behooves the physic ian who is prescr ib ing cl ima te
for a tuberculous patien t to exerc ise his judgmen t . H e must take in to con
s iderat ion the physio log ical act ion of the cl imate which he is recommend
i ng and the power of the pat ien t to meet the demands made upon h im by
such a cl ima te. I f a h igh a lt itude or a co ld climate is bein g con s idered'
the pat ien t must be in such a con d i t ion tha t he can respond to a demand
for a h igh ra te of t issue change . H e should belong to the hard ier type
of man,w i th good c irculatory
,d igest ive and assimilative power . I f
'
he does
n ot belong to th is type,the proposed chan ge i s more apt to do harm than
good . The most good can come from cl ima t ic change on ly by su i t ing the
pa t ien t to the climate in such a mann er tha t he may ma in ta in his nutr i t ion
at the h ighest lpossible po in t . I f a weakened patien t be sen t to a c l ima te
23 2 PULM ON ARY TUBE RCULO S I S
whi ch makes extraordinary demands upon him,to meet the increased t issue
waste,he w i l l not do as wel l as he would in a less r igorous cl ima te ; for he is
compel led to spend much energy in t issue repa ir tha t should be applied to
fight ing his d isease. Where there is doubt,i t is always best to choose a less
stimulating cl imate.
Cl ima ti cThe pecul iarities of the individual loca tion arevery importan t ,
Co n di t ion s of These are in fluen ced by moun tain ranges and canon s,the
N earby Pl aces dir ection of the preva i ling wind curren ts,proximi ty to
D i ffer.bodi es of water, amoun t of sunshi ne
,character of the 5011
,
and many o ther factors . This should be understood by those who sen d
pa tien ts away from home. Ser ious mistakes are o ften made by no t under
standin g this fact . Patien ts are sen t from the E ast to Southern Cal iforn ia.
They th ink the change so agreeable compared with themore r igorous cl ima tes
from wh ich they have come, that they consider any place is good enough for
them ; so they are apt to choose that place which suits their fan cy andwhere
they prefer to l ive,or where they think they can have the most pleasure. This
takes many of them to the beaches, and i t is n ot an un common spectacle to
see tuberculous pa tien ts who left eastern homes in order. to procure the ben efits
of the climate of Southern Californ ia, subjecting their forces of repa ir to the
enormous strain which is produced by surf ba thing . O ften times un to ld
harm is done before the patien t sees a physician and is advised to desist
from this sport and move to the foo thills .
Here in Southern Cal iforn ia (I use this for illustra tion because I am ac
quain ted with the facts, al though the same ho lds good elsewhere) climate
differs very materially o ften in so slight a distan ce as a few miles or even a
fraction of a mile. I n the foo th i lls within th irty miles of the coast we have
a moderately dry, fairly stimulating climate, whi le tha t nearer the coast is
more humid and,owing to the strong sea breeze, demands greater resisting
power on the part of the pa tien t . Further in land,at a distan ce of seven ty
five miles,i t is much warmer in the daytime
,the air is dryer and the winds
much mo re stimula ting,and o ften very trying on nervous patien ts . . L ike
the moun ta in climate,the n ights are a lways coo l
,giving the stimulating eflect
o f the wide diurna l range,and even the heat of summer is very modera te,
owin g to the dryness of the air . The thermometer range usual ly varies w i th
the distance from the o cean,and the humidity likewise ; so ,as we travel in land ,
the tempera ture in creases and at the same t ime the humidity decreases, thus
making even the ho ttest sections o f the in terio r,such as I ndio where a hea t
o f 1 20 degrees is o ften experienced qui te endurable,a fact scarcely con ceivable
to those who inhabi t the eastern section s of our coun try where sunstrokes
o ccur a t a tempera ture under 100 degrees . I n these ho ttest sectio ns,sun
strokes are unknown .
The variety of clima te within a sho rt distance here in Southern Cal iforn ia
234 PULM ON ARY TUBE RCUL O S I S
These condition s are just the opposi te from those which favor the spread
o f tuberculosis . T uberculosis is a disease which thr ives in thickly settled
di stricts where an in timate association of the S ick and wel l takes place,especi
ally in overcrowded quarters . The danger is the gr ea ter the more favorable
the condi tion s for the life of bacill i after they have been thrown out in to the
a tmosphere. Thus,moistur e and warmth with lack of sun shi ne favor the
preservation of bacter ia, while dry air , ei ther warm or co ld,with an abun dan ce
of sunshine tends to their destruction . We believe,then
,tha t these ‘
are the
factors which make certa in climates apparen tly immune to tuberculosis,and
n ot-
the fact of their eleva tion above or below sea- level .
I t is fortuna te tha t these favorable condi tion s may be foun d at al l a l ti tudes,for i t gives us a grea ter opportuni ty for suiting climatic condition s to the
individual needs of the pa tien t . I f high a l ti tudes were an essen t ia l in the
treatmen t of tuberculosis, its advan tages would necessarily be den ied to
many, because there is a grea t majo rity of tubercul ous patien ts who are
abso lutely unfit for l ife at high a l t i tude,and can n ot l ive there without
do ing themselves harm ; and there is even a much gr ea ter n umber who can
be trea ted to much better advan tage in medium and low a l ti tudes than in
h igher alti tudes .
Sun l igh tI t has long been observed that sun l igh t has a very importan t
I mpo rtan t in influen ce on the physio logical activi ty of bo th plan t and
Siffriil
t
iieiifil
lzgis an imal . l ife. The lower forms of organ isms, the bacteria ,
are quickly killed by it . Thus the bacteria l con ten t of the
air of those local i ties where there is a great amoun t of sun sh ine is much lower
than where there is less sunshine. N ot on ly sunshine but di ffused ligh t,wh ich is indirec t sunshine, will a lso destroy bacteria , but i t requires a longer
time. I n as much as tuberculosis is a bacterial disease, and in as much as
there is always associated with the tubercle bacillus many o ther bacteria
which have a very deleterious effect on . the patien t,the beneficial effect of
l igh t,and especially of di rect sun l igh t, can readily be
.
understood as a means
of destroying bacteria , preven ting re- in fection with tubercle bac ill i and second
ary in fect ion with o ther micro -o rgan isms . There is n o doubt but tha t much
benefit to the tuberculous is derived from th is an tibacteria l action of sun l igh t
in those regions of the earth where a maximum of. sunshine abounds,and this
co nditio n is a very importan t one in choosing a clima te for the treatmen t of
this disease.
The effect of ligh t on h igher l ife,in cluding man
,is tha t of a quicken ing
o f a l l the vi tal pro cesses . The blood is enriched , cel l activi ty is st imula ted
and the fun ction o f the various o rgans is improved . B lood abso rbs l igh t
to a very high degree,as was demo nstra ted by Finsen who directed a blue
pencil o f l igh t o n to the ear after placing a piece o f sens i tized paper behind it .
A fter five minutes n o change o n the paper was n o ted . The car was then
CLI M ATE A S A FA CTOR I N TH E TRE ATM E N T OF .TUBE RCULO S I S ’
235
compressed between two glass plates driving the blood out of i t, and penetration was a lmost immedia te. Quin cke (Pflueger
’s A rchives
,1894, Vo l . LVI I ,
page 134) has shown that hemoglobin gives off its oxygen more quickly inl ight than in the dark, hen ce l ight in creases the pro cesses of oxida tion
in the body.
-M arti (Vehr . d . Congr . f . in nere. 1897) by mean s
of experimen ts on rats showed that deprivation of l ight lessen s the
number of red corptI scles and a lso, though to less exten t,the amoun t of
hemoglobin ,wh ile s trong, con tinuous l ight in creases bo th the erythrocytes
and the hemoglobin .
A side from these direct effects thel
cheering, buoyan t effect of sun shine is
very marked and coun ts much in favor~
of the patien t by keeping him con ten t
and happy,“
and invi ting him to l ive an outdoor l ife . Therefore, we must
con clude tha t sun light is an importan t elemen t in a clima te suited to'
the
trea tmen t of tuberculosis .
I t must be borne in mind,when choosing a place wi th a
fiqqti
s
v
gf H igh suitable clima te for a pa tien t who wishes to recover from
an dLow tuberculosis,tha t he must n ecessar i ly make this place his
fifiggfiigfis,
home for severa l mon ths ; and, if his disease is advan ced,he
must extend his’
stay to many mon ths. Consequen tly we
must look well befo re we advise.
M oun tain climates at high al ti tude are stimula ting: The cal l for tissue
change is enormous, and must be met by a strong organ ism . A patien t who
is sui table for high a l ti tude treatmen t should be_
na tura lly s tr ong, should
have an abundan ce of red corpuscles to meet the condition s n ecessary for tissue
change,should have a strong heart, a respiratory system not too much impaired,
and should possess a wel l-ba lan ced n ervous system. On the o ther hand,
patien ts who are natural ly weak or who are weakened by di sease,who have
a deficien cy of blood,weak hearts, severely impair ed lungs and un stable
n ervous systems, are not suitable for high a l ti tude treatmen t . The young
and strong are better sui ted to high a l ti tude trea tmen t,than those in the
declin ing years of life. The latter should be treated at low al ti tude.
As a rule, when the relative merits of high and low al ti tude are
discussed, h igh a l ti tude is compared with thickly popula ted areas at low
al ti tude where the humidity is great,in stead of areas where similar condi
tion s except as to elevation obtain . This compar ison is un fair and gives a
false impression .
I f we compare the effects of high al titude such as we find i t in the
Rocky M oun tains and the A lps,with low dry a l titudes such as we find
in the deserts and foo thi lls of the great Southwest, in cluding parts of
Cal iforn ia, N evada , Arizona , N ew M exico and Texas, the comparison is
about as fo llows
236
H IGH ALTITUD E .
Sparse populat ion .
Pure a ir relat ively free from bac
ter ial con taminat ion .
Great amoun t of sunsh ine.
Wind usually stron g and co ld, es
pecial ly in win ter.T emperature Co ld in win ter, del ightful in summer, with change of sea
sons ; n ights coo l .Great demand fo r t issue change.
A tmospheric pressure low , ca ll ingfor in creased resp iratory an d cardiacact ivity.
I n crease in red corpuscles— may be
either physiological to meet decreaseof oxygen in air an d in creased t issue
PULM ON ARY T UBE RCULOS I S
M oderate demand for t issue change.
A tmospheric pressure h igh , call in gfor n o extra respiratory and card iacact ivity.
I n crease of red corpuscles also n o ted,probably due to sun l ight and o theragen cies wh ich improve gen eral ton e.
chan ge or due to in creased sun l ightand o ther st imulat ing agen cies .
Whatever the cause may be it wouldseem to be o f n o material advan tageand unn ecessary to the individual ,except wh ile l iving at h igh alt itude,for the co rpuscles return to n ormalsoon after return in g to low alt itudeagain .
From this comparison i t will be seen tha t h igh al ti tude has a very stimulating
cl imate and a rarefied a tmosphere,which does no t pertain to the lower level
,
but,in as much as i t calls for an eno rmous tissue change, patien ts who go there
must have strong consti tution s and wel l fun ctiona ting organ s ; and, in as much
as the rarefied a tmosphere cal ls for extra work upon the part of the heart and
lungs, i t is questionable whether or not i t is the best place for patien ts with
diseased lungs.
The fo l lowing argumen ts are relevan t to the discussion on the relative
meri ts of h igh and low al ti tude in the trea tmen t of tuberculosis .
I . Rest is an importan t facto r in thehealing of inflammations .
Th is is a wel l- recogn ized prin ciple of treatmen t in a l l o ther
forms of tuberculosis . When the jo in ts or bones are affected ,movemen ts are abso lu tely prohibited . The accepted treat
I nflammation s ,men t of these co nditions is immobil ization
,and for this pur
pose plaster casts are used . The lungs un fortuna tely are
o rgans tha t can no t be spared . Theymust carry on their fun ction o f aerating
the blood . E very minute from -sixteen to twen ty respiratory excursions must
be made even at low al ti tude. A t high a l ti tude, at first,bo th the depth and
frequency o f respira tio ns are in creased,the fo rmer remain ing permanen tly
so . A lso the number o f heart bea ts per minute is increased . This is made
necessary o n accoun t o f the decreased amo un t o f oxygen . The effect of
H igh A l t i tudeTrea tmen tCo n trary to
Low ALTI TUD E .
Sparse populat ion .
Pure air relat ively free from bacter ial con taminat ion .
M aximum amoun t of sun sh ine.
Wind usually gen tle.
Temperature bracing in win ter,warm days in .summer ; n ights coo l .
238 PULM ON ARY TUBE RCULO S I S
3 . A ccording to my experien ce tuberculosis is extraordin arily
common among a thletes . We are somewha t at a loss to
know how to explain this Un l ess i t is due to an overdevelop
men t fo llowed by a retrograde process w ith a resul tan t
lowered resistan ce.
A thletes have an overdeveloped‘
muscular system . The heart muscle is
firmer and larger than no rma l , and the lungs are in creased in size. The
en tire organi sm is tuned to an abnorma l con dition,to endure more than o rdi
nary stra in . N o t satisfied wi th being able to do as much as the normal man,
the a thl ete subjec ts hims elf to more or less of a constan t overstrain . H is
respiratory and circulato ry systems arise to the o ccasion for a time and meet
the extra demand ; but they do it to their own detr imen t .
When he leaves his training, and settles down to the usual habits of life,
he o ften finds himself in capaci ta ted . H e has heart,lungs
,and muscu lar
system suited to grea t exertion and he does not n eed them . The resul t is a
retrograde process . The muscles become flabby,the heart likew ise
,and the
lungs which have been overdeveloped in order to meet the grea ter demands of
oxidation,must also share in th is retrogression . The resul t is an in jury to
the tissues and a lowered resistan ce.
Un less th is observa tion be wrong and this explanation improbable,i t po in ts
to the fact tha t i t is better for a patien t to be treated at low alti tude,at least
,
if he expects to live at low a l t i tude after recovery, sin ce the effect ofhigh al ti tude
is to throw more work upon the heart and lungs, thus causing an in creased
developmen t on their part if they are able to respond to the demand . I n
coming from a h igh to a low al ti tude, there must be a readjustmen t on the
part of the organ s of respiration and circula tion to meet the changed conditions .
This is accompan ied by a retrograde process, during which time the pa tien t
is more l iable to relapse than i f he had rema ined at the high a l ti tude.
H igh A lt i tude4:The next observa tion which I would make
,bearing upon
Ca l ls fo r h igh al ti tude treatmen t i s tha t,owmg to i ncrea sed t i ssue
S tron g Re“ change, an extra demand is made upon the o rgan ism ; and,act ive Powers.
un less the pat ien t can meet th i s,he W i l l suffer harm rather
than obta in good . A stro ng co nsti tution,with good circulato ry , digestive,
muscular and nervous systems,and with good blood
,as men tioned befo re
,
is necessary fo r the best resul ts in high al ti tude trea tmen t . Then,too
,young
peo ple are better suited to i t than o lder o nes . Thus i t can be seen tha t the
benefits o f h igh al ti tude are precluded from mo st o f the grea t mass o f tuber
culo n s patien ts as we find them. The effec t o f high al ti tude o n the heart is to
increase the number o f its bea ts per minute. \Vhen a heal thy individua l
becomes acclima ted to high al titude the pulse- rate during rest , becomes
practically iden tica l with the pulse- ra te a t sea -level ; upo n exertio n,however ,
its ra te is increased bevo nd pro po rtio n . The fo l low ing da ta is taken from
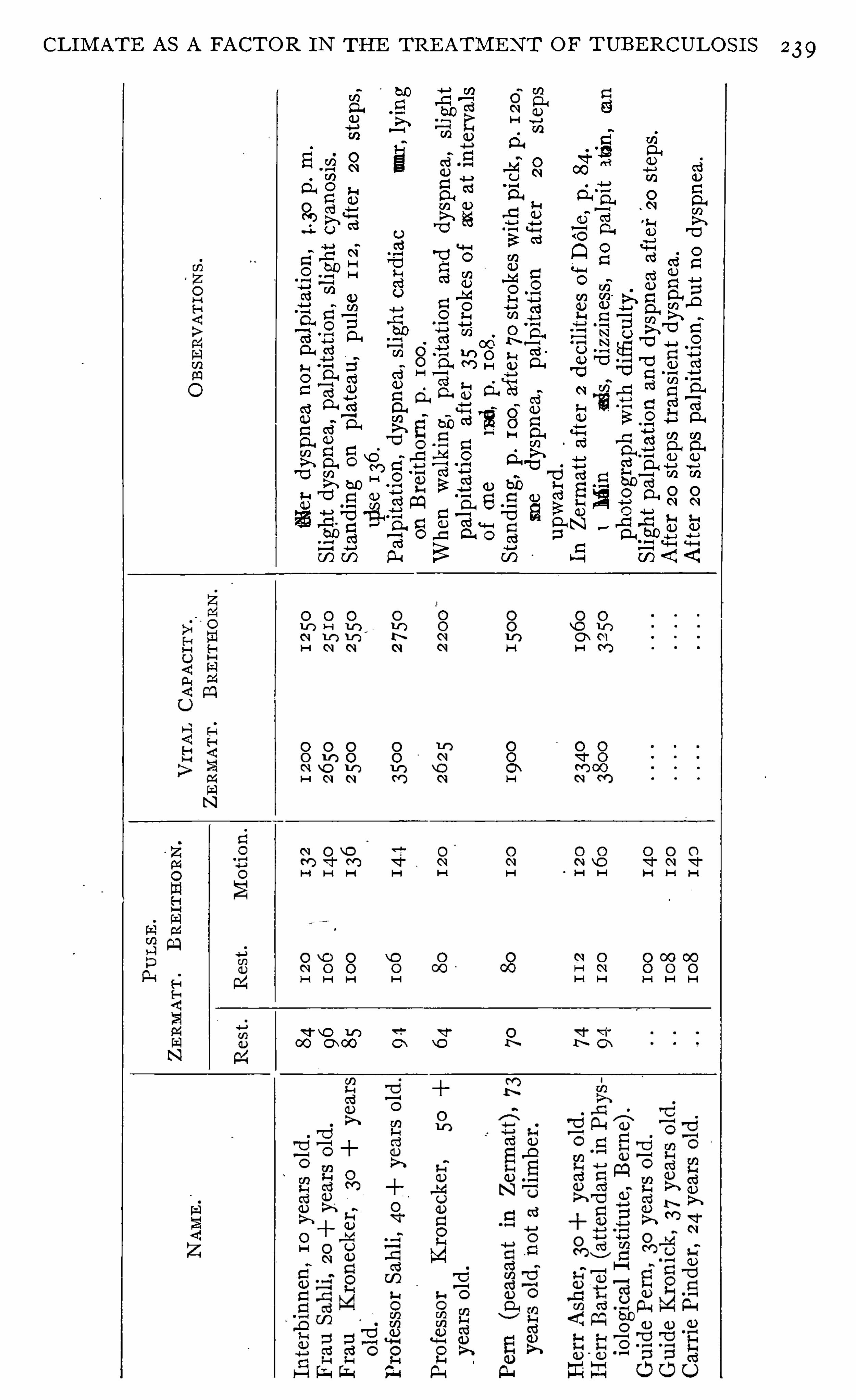
239CLI M AT E A S A FA CTOR I N THE TRE ATM E N T O F TUBE RCULO S I S
.
eo
cammw
0c
EC
£0
S
SEEQ
wa
ge.
ou
“
8
.
eo
camxv
a8m
0mH
8
.
mao
m
ou.
"
8
s
so
smmmv
was
co
ws-
Emma
sm
.
mxso
ufiv
firs
amsn
woa
oam
98
£0
5“
flfig
0a
.
mwo
finnm
v
£
853?
£856
2
.
vw
m
Re
g
0
m
8
Eoo
v
a
Ho
me
BB
SSN
5
Ca
n
aan
ou
ge
ts
co
8Q
m
a
.
so
cgm
bo
0
88
.
mQU
E
firsmo
xo
bmON.
“was
6
8.
.
Q.
wcm
vc
fim
.
moH
d.
980
8
98
mo
m
?
a
83
0
wo
xo
bw
mm.
Sam.
qo
fisz
fism
Em
.
so
zmmmw
was
co
fie
a
fiea
.
wQ
EEB
6
3.
Q.
Eo
fimou
m00
mg
a
£
5958osw
fig
so
mmm
.
zo
usfi
fis
m
O
?
31
5
.
wmo
m
Os
go
th
.
m
:
SB
BEQ
so
wcm
vc
fim
.
mwmocsho
sm
do
se
ERA.
so
amm
bv
sm
.
E
d0
2“
.
co
fis
xfisg
H
0
:
Scam
?
$562
240 PULM ON ARY TUBE RCULO S I S
a table arranged by Huggard (Handbook of Clima tic Trea tmen t,
I t shows the resul t of al ti tude upon the heart,dur ing bo th rest and exercise.
These observa tions were taken by Pro f. Kronecker of Bern e in 1894. Obser
vations were first taken at Zermatt at an eleva tion of 1600 meters . T hen the
party was taken to Brei thorn at an elevation of 3 750 meters. I n o rder to
el imina te the factors of exertion and fatigue some members of the partywere
carried .
These observations lead meto the fo llowing con clusion s : first,high alti tude
trea tmen t of tuberculosis is in direct an tagon ism with the well - founded and
general ly accepted pr in c iple of rest in tuberculosis ; second, patien ts who are
trea ted at a high a l ti tude are at a disadvan tage i f they undertake“
to l ive at a
low a l t i tude afterwards ; third, high a l t i tude makes such great demands upon
the system owing to in creased tissue change that many tuberculous pa tien ts
are unable to meet the requiremen ts.
Wherein lies the va lue of c lima tic treatmen t? To an swerWherei n Li esthe Va lue of this question we must keep severa l fac tors i n m ind . I n
gii
gfiggn t ? d iscussing the effects of open -air tr eatmen t,I showed tha t
we can accomplish two things by putt ing our patien ts in the
open air,fir st
,in crease the state of n utr i tion ,
and second,supply the organ ism
with air relatively free from bacter ia .
N ow if these are the effects of open -air treatmen t, we can readily see that
a climate,wh ich i s properly suited to the ind ividual, possessing dry air w i th
low bacteria l con ten t, must have a d istin ct advan tage over one possessing
damp air with high bacterial con ten t, which at best i s on ly to be endured but
n o t recommended . The effect of dry air with a maximum of sunshine seems
to be very beneficial in cases of m ixed in fection , bo th as a curative and as a
prophylactic . This a lso exerts a favorable in fluen ce on tuberculous patien ts
with severe bron chi tis and pro fuse expectoration . I n cl imates with a variable
humid i ty,if several dry days fo llow in succession , there is always a marked
decrease in the amoun t of expectorat ion . The explanation of th is is very
simple. When air is exhaled i t is sa turated with mo isture. I f i t is satura ted
when inhaled,of course
,it can not carry off as much mo isture from the lungs
as i t could if its hum id i tywere low. The dryer the air the greater the amoun t
of mo isture requ ired from the air passages to saturate i t .
Hum id cl ima tes,as a rule are mo re or less un sat isfactory in the treatmen t
o f tuberculosis . I f they are co ld and humid, they are as a rule var iable and
productive of ca tarrhal cond i t ions. I f they are warm and humid , they are
enervating and the pa tien t suffers from d igestive and assimilat ive d isturbances .
I f they are co ld and dry they are too rigorous fo r any but the strongest .
I t would seem then tha t the best c l ima te for tuberculous patien ts is o ne
with a ir rela t ively dry,o f low bac terial con ten t , with plen ty of sunshine and
with the elemen ts o f tempera ture, variabi l ity, wind and a l ti tude suited to the
CHAPTER X I X .
TH E COMPLI CATI ON S OF PULMONARY TUBE RCULOS I S AN D
THE I R TRE ATME N T.
TUBERCULOUS LARYNGITIS .
The importance of tuberculosis of the larynx can be best
apprecia ted after a careful study of the larynx in pat ien ts
suffering from advan ced tuberculosis or after making careful post-mortem
exam inat ions of th is organ in tubercul ous subjects. Such a course w i l l show
that this compl icat ion is presen t in more than 50 per cen t of cases ; and, accord
ing to some observers, even in as many as 60 or 70 per cen t (“The
T reatmen t of T uberculous Laryngi tis with Culture Products, with Observa
tion s upon the A ction of Spec ific I n o culation s in the Trea tmen t of T uberculo
sis.
” American Journal of the M edical Scien ces . December,S in ce th is compl ica tion is so common ,
i t behooves those who
are treating tuberculosis to make routine exam ination s of the
thr oat . This is espec ial ly importan t -sin ce early tuberculous laryngi t is offers
excellen t chan ces of cure wh i le the far advan ced d isease is, as a rule, hopeless .
Tuberculous laryngi t is begin s as an infil tra tion wh ich may remain as such
for mon ths and mon ths or which may soon break down and form an ulcer .
A t first there are few i f any symptoms recogn izable. While under ord inary
circumstan ces,if these infil tration s were to appear in a larynx wh ich was pre
viously heal thy, they would perhaps cause an uneasiness or a feel ing of fullness ;
yet, when they appear in a larynx which is con stantly irr i ta ted by coughing,
as is usually the case in tuberculosis, any symptoms of this charac ter m ight be
unno t iced . Somet imes an irri ta tion or feel ing of fulln ess is no ticed ; somet imes
a sl ight hoarseness is observed ; somet imes the vo ice t ires more read i ly than
commo n °
and at o ther times shoo t ing pains are presen t .
The d iagnosis,however, must rest on a careful exam ina tion of the larynx .
I ts accuracy will depend on the exper ience of the observer . The phys ic ian
who frequen tly sees these cases w i l l rarely be m istaken . The d isease i s per
haps a lways secondary to tuberculo s is elsewhere in the body and rarely o ccurs
un less the lungs are affec ted . Wh i le i t must be bo rne in mind tha t a tuber
culous pa t ien t is subjec t to a l l fo rms o f no n - tuberculous throa t trouble,
yet repea ted exam ina tio n s by a laryngo log is t who is accus tomed to exam ine
thro a ts o f tuberculous pa t ien ts, w i ll rarely fa i l to d ifferen t iate tuberculous
from no n - tuberculous invo lvemen ts .
Frequen cy.
D iagn osis.
TH E COM PLI CA T I ON S O F PULM ON ARY TUBE RCULOS I S
A ny portion of the larynx may be the seat of tuberculosis ; the cords, the
in teraryten oi d space, thearyteno ids themselves, the ven tr icles or the ep iglo t
tis. The appearan ce of these early lesion s is tha t of a sl ight thicken ing of the
mucous membrane with very o ften a velvety appearance. Weshould no more
require the presence of tumefactions or ulcera t ion s in order to make a diagn o
sis of tuberculous laryngi t is than wewould requ ire cavities and o ther advan cedsign s to d iagnose pulmonary tuberculosis . E arly d iagnosis is -as importan t .
here as i t is in tuberculosis _of the pulmonary form.
When there is doubt as to the na tur e of the laryngea l lesion,the ma tter may
be easi ly settled by- the tubercul in test .
The progn os is in tuberculous laryngi tis depends very much
upon the earl iness of d iagn osis and the methods of treatment
employed. The progn osis depends very much upon whether or n ot tubercul inis in tell igen tly used in tr eatmen t . Where i t is so used the prognosis does n ot
d iffer far from the prognosi s i n pulmonary tuberculos is when an equa lly early
d iagnos is has been made. A very large per cen t of early cases and even a
fa ir per cen t of those wh ich are far advan ced, in clud ing some with ulcerat ion ,
can get wel l . I n my own exper ience,
out of 42 cases of tuberculous
laryngi t is found in pat ien ts who rema ined at the sanatorium for more than
two mon ths, 30, or per cen t were apparen tly cured .
The treatmen t of tuberculous laryngi t is corresponds in
pr inc iple to that of tuberculosis elsewhere in the body .
Res t is a very importan t measure. The use o f the larynx should be l im i ted .
The pat ien t should n ot be a llowed to do any unnecessary talk in g, and where
i t causes irr i tat ion ,i t is better tha t he converse in a whisper . N o sing ing or
shout ing or stra in ing of the vo ice of any kin d should be indulged in . A co ld
compress,as descr ibed in Chapter X I V , applied to the throat is of grea t
benefit in the trea tmen t of this compl ication . I t rel ieves the cough some
what and makes the thr oat feel more comfortable.
Loca l appl icat ion s to the upper air“
passages are valuable in proportion to
their power of reduc ing catarrha l cond i t ion s and reliev ing cough . I t is wel l
to give close a tten tion to nasa l resp ira t ion . While I would have some hes i tan cy
in opera ting upon a pat ien t wh i le he was expectora t in g bac i ll i, yet I would
advise pallia tive measures, to keep nasal resp irat ion free and easy ; for mouth
brea thing is in jur ious to the larynx . S l ightly st imula t in g appl ica tion s, such as
pro targo l 5 to 10 per cen t made to the larynx after i t has been clean sed w ithan
a lkaline spray seems to be about as valuable as any measure tha t I have foun d .
Th is sho uld be fo llowed by some pro tec tive o i ly spray which may con ta in such
ingred ien ts as men tho l,or eucalyptus . When ulcerat ion s are presen t, espe
, c ial ly i f they are pain ful, they may be dusted w i th or thoform used in apowder
blower . When'
(Lough is an aggravat ing factor,one- twelfth grain of hero in
added to the orthoform acts well .
Progn osis.
Trea tmen t.
244 PULM ON ARY TUBE RCULOS I S
I have never found it necessaryto use lactic acid or any o ther harsh measure
in the treatmen t of th is affect ion . M i ld and gen tle measures have proven
em inen tly sat isfactory to bo th the pat ien t and myself.
Fo cusing the sun ’s rays upon the parts by mean s of two mirrors after the
plan of Sorgo (Ueber die Behandl un g der Kehlkopftuberkulose m i t Sonnen
l icht n ebst einemVo rschlag zi'
i r Behandl ung derselben m i t kun stl ichen L ichte,
Wien .. klin . Woch .
,1905 , vo l . XVI I I
,N o . 4) or using the vio let rays
,
seems to aid healing perhaps by causi ng a hyperemia of the part and thus bring
ing more defensive bod ies in con tac t w i th the bacill i .
The most importan t remedy in the trea tmen t of this complication is tuber
cul in . The action of the ~
remedy can be accur a tely con tro l led by the local
reac tion produced in the larynx. The.
dosage should be governed en t irely
by the local find ings . That amount of tubercul in should be adm in istered
which is necessary to cause a sl ight stimula tion of the local process. Th is
will show as a sl ight hyperemia . When th is has been produced, the dose
should n ot be repeated un til the hyperem ia has disappeared, n or should it be
in creased un til this amoun t fa i ls to produce reaction . Where the larynx is
affected it should a lways be'
made the index for dosage.
The effect of tubercul in here is the same as elsewhere (see Chapter XV ).
I t increases the amoun t of protective substan ces found in the blood thr ough
its stimulation of the physio log ical machinery of immun ization . I ts stimu
lating effec t a lso causes a local congest ion about the tuberculous foci and thus
hasten s healing by bringing the pro tective bodies of the blood to bear upon
the tubercle bacil l i in grea ter amoun ts than is usual in these condit ions . This
same ac tion has a tenden cy to preven t the bac i ll i from spreading to new foci .
By these simple mean s of trea tmen t tuberculous laryngitis may be removed
from the list of fatal d iseases and placed among the more hopeful .
TUBERCULOS IS OF THE INTESTINES .
Tuberculosis of the in testines is much more common than is
generally supposed . I n 1 226 cases (Schroeder und B lumen
feld,Therapie der Lungen schwindsuch t, page 721) Heinze found tubercular
ulcera tions 6 30 times . Fenwick and Dodwell found the in testines invo lved
500 t imes in 883 sections made on persons dy ing of tuberculosis, and E isenhart
found in test inal invo lvemen t 56 6 times in sec tions on 1000 tuberculous sub
jects . Baumgarten even goes so far as to say that practically every individual
suffering from advanced tuberculosis has some invo lvemen t of the in test ina l
tract . Whether we accept Baumgarten ’s op in ion or no t we must recogn ize
the fact tha t tuberculo s is o f the in test ina l trac t is very common in ind ividuals
suffering from advanced tuberculos is , and we should bear this in mind in deal
ing with the in testinal symptoms o f these cases .
Frequen cy.
246 PULM ON ARY T UBE RCULO S I S
easy . The sedimen t is sta in ed in the usual way and exami ned for bacill i .
Page (I . Diss . Heidelberg, 1902, p . 47) recommends the addi tion of_
equalparts of abso lute a lcoho l and ether and reducing the specific gravity of the
l iquid to at 25 degrees Cen tigrade.
When a diagn osis of in testinal tuberculosis has been made
or when the di agnosis has not been defin itely made but the
condition has been suspected , i t is well to look very carefully after the condition
of the digest ive tract . I t is very importan t to keep the pa tien t well nourished
and at the same time to keep the bowels regular and to shield the in testina l
wall as much as possible from irri tation . To this end bo th con stipation and
diarrhea must be combated .
When con stipa tion is presen t i t should be combated by a suitable diet .
I t is preferable to combat this with fruits and fats ra ther than by coarse foods
which have irritating particles tha t may in jure the di seased mucous membrane.
O il enemas are o ften of great value,and when persisted in wi ll sometimes
relieve most_
obstin ate constipation . For th is purpose,one to thr ee oun ces of
o l ive oil may be in jected high up in to the co lon at n ight,by mean s of a syr inge
and so ft rubber catheter . T his should be“ retained until the fo llow ing mo rn
ing, when ,as a rule, an easy movemen t of the bowels wil l o ccur .
I f laxatives are used they should be carefully chosen and employed wi thcaution . They should not be too severe in their action
,lest they might cause
severe irri tation and start up a stubborn diarrhea . Cascara sagrada an swers
the purpose very wel l .
When the patien t is suffering from tubercular diarrhea , every care must be
exerted to rel ieve him as soon as possible,remembering tha t n utrition must be
ma in tained if a successful issue is to be had. The patien t should be put to
bed . The in testinal tract should be freed from al l irri ta ting particles. This
is best done by a modera te dose of castor o il (one—half to three- fourths of an
oun ce) or magnesium sulphate (one-hal f oun ce). The pat ien t should at once
he put upon a restricted,n on - irri tating diet
,consisting at first perhaps of milk
and l ime water o n ly, two parts of_
the fo rmer to one of the la tter . I t is rarely
n ecessary to con tinue milk alone for more than twen ty—four hours . Then
m ilk toast,bo iled rice
,and the whi tes of eggs maybe added , and later scraped
mea t,so ft-bo i led and poached eggs, tropon ,
mashed and baked po ta toes mav
be cautiously tried . The d iet should on ly be increased as the in testinal trac t
becomes to leran t . I t will be necessary in many cases to eliminate fruits,fats
,
coarse vegetables and a l l laxa t ive fo ods fo r some time.
I f,a fter the admin is tra tion o f the in itial dose o f o il o r magnes ium,
the
bowels co n tinue to be loose, I have obta ined go od resul ts from a teaspoon fi i l
o f a sa tura ted so lu tio n o f magnesium sulpha te g iven in two ounces o f water
befo re breakfas t o r smal l do ses (o ne dram) o f caster o il taken at bed time.
A t the same time I o ften admin ister bismuth subn i tra te alo ne,o r i f neces
Trea tmen t .
TH E COM PLI CAT I ON S OF PULM ON ARY TUBE RCULOS I S
sary,in combina tion with deod
’
orized tin cture of opium (twen ty grains to one
dram of the former and five to ten dr ops of the latter) after -every movemen t
of the bowels.
When the diarrhea is in tractable I use ei ther very large doses of bismuth
(one to two drains with opium as above every two to four hours) or the lead
and opium pill or a mixture con sistin g of dilute acetic acid, mx, morphia , gr .
i% and acetate of lead, gr . i—i i .
I t is a lso well to irrigate the co lon with a warm n ormal sal t so lu tion or,as
s recommended by Reed, an antiseptic so lution such as carbo l ic acid (one
part) and glycerine (eight parts) of which on e dram may be used to one quart
of water . Of this so lution ,one or two quarts may be in jected every second
day, norma l sal t so lution bein g used on the al terna te day. Clo ths wrung out
of hot water should be applied to the abdomen daily for a period of on e or
two hours . These should be changed every 20 minutes and should be wel l
covered, preferably'
wi'
th flannel clo ths,in order to retain the heat as long
possible.
Tuberculin and allied products should be used . I have seen two_
cases of
well-marked tuber cular invo lvemen t of- l the intestine apparen tly hea l and a
number of o thers improve under the combined hygien ic, symptoma tic and tu
bercul in trea tmen t . We should n ot pron oun ce doom upon any on e who shows
symptoms of in tes tina l invo lvemen t,but we shoul d do what we can to cure
h im,remembering that the post—mortem records Show eviden ces of spon tan
eous hea ling,and our own experien ce with the cure of advan ced cases of tuber
culosis proves that they"
can sometimes be cured .
Where sten osis of the in testina l tract o ccurs, surgery must be resorted to .
I f the genera l condition of the pa tien t is satisfactory, the results are somewhat
en couraging . Corn et (D ie Tuberkulose, Zweite Auflege, 1907) quo tes sta tis
tics from Ho fmeister who secured heal in g in 34 of 50 pa tien ts where he made
a to tal resection on accoun t of tuberculosis in the il eo - cecal region . Ko cher
was successful in 1 6 out of 18 pa tien ts operated upon and KOrte was success
ful in al l of 1 1 cases.
FISTULA IN ANO .
A small percen tage of tuberculous pat ien ts suffer from fistula and I feel tha t
a'
word about treatmen t should be said . When a patien t with fistula presen ts
himself, the physician or surgeon,before advis ing operat ion ,
would do wel l
to examin e the lungs of his pat ien t . I f tuberculosis is presen t, espec ia lly in
an act ive form,and it frequen tly is, I would recommen d that the effect of the
opera t ion upon the pat ien t be con sidered carefully before i t is adv ised . I
have seen a number of pa t ien ts whose decl ine in strength, accompan ied by an
advan ce in the tuberculous process in the lungs, dated from such an opera t ion ;and in qu ite a percen tage of the cases
,the result of the opera tion was not
248 PULM ON ARY TUBERCULOS I S
sa t isfactory . Un less the symptoms are such tha t an immediate operat ionis necessary, I believe that it is wise to let operat ion alone as long as possible.
I have seen many of these fistulas hea l without any treatmen t whatever
except loca l c lean l iness, dur ing a course of combined hyg ien ic-open -air and
tuberculin treatmen t .
TUBERCULOS IS OF THE LYMPHATIC GLANDS .
The frequency of tuberculosis of the lymphatic glands is not
general ly realized . I t is probable that a large ma jority of
chi ldr en have tubercul osis of the lymph glands, and i t is further
probable that these glandular foci are o ften the source whence
come the bacilli which causein fect ion in o ther organs in la ter years.
From a careful study of thi s subjec t made by the author,see Appendix
,
Chapter I (A S tudy of Tuberculous I n fec tion,N ew York M ed ical Jour na l
,
M arch 1 2,
the fo llowing con clusions based upon statistics from a grea t
n umber of observers have been taken :
I . N early al l chi ldren show enl arged glands.
2 . About three- fourths of thechildren who have chr on ical ly en larged glands
reac t to tuberculin and about three- fourths of such glands removed and sub
jected to microscop ica l examinat ion prove to be tuberculous .
3 . Practica lly al l children who die of tuberculosis have en larged g lands,
and the process in them seems to be far advan ced, warran ting the con clusion
tha t they might have been the earliest foci of in fect ion .
When we add to this the fac t that a very large percen tage of adults who
suffer from tuberculosis Show en largemen t of the glands we are warran ted in
the statemen t that the glandular system is very common ly affected by tuber
culosis.
What should be our atti tude toward these tuberculous glands
in early life Should we consider them ser ious and take steps
toward their cure at this time or should we wa i t for further
developmen t of the d isease? This is a very importan t
question and onewhich can notbe brushed aside by a simple answer . Probably
we have n ot yet advan ced sufficien tly to demand that a l l children or al l ind i
vidual s who have en larged glands wherein there is a susp icion of a tubercu
lous cause,Should be subjected to the tuberculin test, yet I believe such a
course is rationa l and demanded by common sen se. I s i t n ot just as im
portan t to treat tuberculos is when i t affec ts the glands as when i t
affects o ther organs? I t seems to me tha t the in ference is warran ted
tha t the lymph glands are probably in nearly a l l instances the first
sea t o f tuberculous in fec tio n . The germs are carried to the glands and there
s tra ined out o f the c ircula t ing lymph . From this focus o ther areas in the body
are in fec ted . Th is would be an ideal sea t o f in fection fo r tr eatmen t,owing
250 PULM ON ARY TUBE RCULO S I S
d isposed right in the pa th of the lymph stream, which is passing through the
gland to the blood . I do not myself doubt from wha t I have seen of the effec t
of ino culat ion on tuberculous glands tha t the extirpation of these by surgi ca l
methods as well as the pur ely c lima t ic tr ea tmen t of this affec tion are dest in ed
to give place to the therapeut ic explo itat ion of tubercul in inocul a t ion s con tro lled
by the determ inat ion of the opson ic index,and comb ined w i th hot sand poul
t ices and rubefac ien ts, or o ther measur es wh ich , like these, w i ll produce an
ampler lymph-flow in the who le terr i tory— o r may I cal l i t‘watefshed ’
or
‘ co llect ing basin —whose lymph passes in to the blood thr ough the condu i t
of the in fected gland .
”
From my persona l exper ience I do n ot hesitate to say that tuberculosis
of the lymph glan ds before“
so ften ing has o ccurred is amenable to tubercul in
treatmen t,and from Wright ’s experien ce we are warran ted in the con clus ion
tha t even after so ften ing has occur red, i t is s t i l l a med ica l and no t a surgica l
d isease.
The time of treatmen t by inoculation s is of cour se longer than that by sur
gical methods, but th is is compen sated for by the fac t tha t, in operating,on ly
those glands which have been removed have been trea ted, wh i le by the in ocula
tion method a l l the in fected glands in the body have been treated and,if a
favorable result has been a ttained,the possib i l i ty of a future exten sion of the
d isease has been largely removed .
PLEURISY.
When we con sider the in t ima te relation sh ip of the pleura with
the lun g, we can n ot con ceive of a pat ien t suffering from pul
monary tuberculosis un less i t is a lesion more o r less cen tra l in its locat ion
w i thout an accompanying pleurisy . Post-mortem records bear this out,fo r i t
is very seldom that a sec tion is made upon a person who has been afflic ted
w i th pulmonary tuberculosis without finding eviden ce of pleural inflammat io n .
These pleurisies show severa l var ities . They may be dry
inflammatio n s,the surface being covered w i th plast ic lymph ;
they may be accompan ied by an exudate of serum or pus, or there may be a
progressive oblitera tion of the pleural cav i ty due to adhesion of the two pleura l
surfaces.
Pleurisy does no t always show itsel f at the pr inc ipa l focus o f the in fect ion .
I t is n o t at a l l uncommon to find the infiltra tion at the apex and the pleurisy
at the base o r the ma in infil tra t io n in one lung and the pleur isy in the o ther .
Serous pleurisy may be caused by an ap ical lesio n,the flu id being poured out
and grav i ta ting to the lowest part . I n ins tances where an efl'
usio n comes o n
w i tho ut any prev ious warn ing , i t may be due to a laten t tubercular focus at
the apex .
Frequen cy.
Var iet ies.
TH E COM PLI CAT I ON S OF PULM ON ARY TUBE RCULO S I S
Dry pleur isies are the most common in tuberculosis . They
usually man ifest themselves by a sharp cutting pain on in
spira tion and cough and when severe may cause shortness of breath owing
to natur e’s a ttempt at shielding the patien t from the pain caused by the in
creased movemen t necessi tated by deeper inspiration s .
When the attack is of slight severity on ly, there may be n o con sti tutional
symptoms recogn izable, but when mo re severe there is an eleva tion of tem
perature ; i t maybe to 100 degrees or even 102 degrees Fahrenhei t, with some
indisposi tion and loss of appeti te. I t will be remembered,as men tioned on
page 54 tha t pleurisy is on e of the causes of con tin uous tempera ture in pul
monary tuberculosi s .
Dry pleurisy is o ften trea tedfor in tercostal neuralgia . A po in t of some value
in differentiation is the grea ter mobility of the lung in the la tter,as described
on page 7 1 . Of course when the pleura l rub is heard the diagnosis is plain .
Pleurisy with effusion usua lly begin s wi th pain ; this dimin ishes as the effusion
takes place and may return after absorption has occur red . A rise of tempera
ture is nearly always presen t , which in severe cases may reach 104 degrees
Fahrenhei t . The pulse becomes rapid.—A chi ll is sometimes experien ced at
the outset . With effusion the hon stitutional symptoms are more severe
The pa tien t feels tired, and in severe cases weak and ill . H e loses his appeti te
and may suffer from constipation and headache. A s the effusion in creases
in amoun t , shortn ess of brea th comes on ,due to compression of the lung .
On physica l examination ,if the effusion is small
,i t maybe easily overlooked .
I f i t is large,the in tercostal spaces appear widened and bulging . On examina
tion the vo cal fremitus is decreased, the percussion no te is dull or flat according
to the amoun t of fluid . I f the lung tissue is much compressed the no te over
itmay be hyperresonan t or even tympan i tic according to the amoun t of relaxa
tion.
presen t . The heart is usually displaced toward the S ide free from effusion .
This can n ot be taken as a diagnostic S ign , however , because as described'
on
page 88 the heart suffers more or less di splacemen t in tuberculous pa tientswhere con traction s have occurred . On auscultation at the commen cemen t o f
the a ttack,the pleural rub may be elici ted
,but this disappears and as the
effusion is poured out the brea th sounds grow more and more indistin ct .
The diagnosis of pleural effusion is sometimes quite difficult when the under
lying lung is the sea t of infil tra tion , because then i t is not easy to detect the
change of posit ion in the fluid as the pa tien t changes his posi tion . Ausculta
tory stroking is of great servi ce in such cases,as the differen ce in the den sity of
the effusion and infil tration makes a differen ce in their power of con ducting
sound . The paravertebral triangle of dulness (F igs . 39 and 40) (Gro cco’s S ign )
found on the side opposi te the effusion is a lso of va lue when the lower lobe on
the o ther sidenis n ot al so
_
the seat of infil tration . Thayer and Fabyan (The
American J oui'
nal of the M edical Scien ces, Jan .
,1907) gives the fo l lowing
Symptoms.
25 2 PULM ON ARY TUB ERCULO S I S
method for determining it : “A fter percussing out the l imi ts of the supposed
effusion one Should mark out the lower l imi t of pulmonary resonan ce on the
opposi te side and then percuss downward dir ectly. over the Spin e,markin g
the po in t at which dullness (rela tive) begin s. I t wil l be found usual ly tha t
this po in t corresponds fa irly close with the beginn in g of rela tive dul lness on
the side of the effusion ; that at all even ts i t is a l it tle higher than the beginn in g
of flatness. One should then percuss downward a long lines parallel to the
spine and inward toward the spine along lines para llel to the lower‘
l imit o f
pulmonary resonan ce. I n this manner i t is usual ly easy to mark out,at the
FI G . 39.— Showing paravertebral triangle of dulness on left . Hydro thorax o n right side.
(Thayer and Fabyan .)
in ferior and mesial angle of the heal thy side of the back , a triangle of dullness .
The vertical side of this righ t-angled triangle, represen ted by the line o f the
spinous processes, reaches to a po in t somewha t h igher than the upper limit
o f fla tness on the affected S ide. The base,represen ted by the mesial part o f the
l ine marking the lower limit of the lung onthe unaffected side, varies , acco rding
to the size of the effusion,from 2 c .m . to as much as 7 c .m . in exten t . The
third side of th is dull area is represen ted by a l ine jo in ing the extremities of
these two l ines. I t has sometimes seemed to us , as has been no ted by Rauch
fuss,tha t this l ine showed a sl igh t outward convexity .
”
A side from these fo rms of pleurisy we now and then have pleurisies o f bo th
254 PULM ON ARY TUBERCULO S I S
straps should be about two in ches wide and shoul d start immediately across
the stern um on the opposi te side, be carried backward and downward acro ss
the ribs and end immedi ately beyond the median l ine. A second row should
start posteriorly and pass forward and downward crossing the o thers and end
ing in the same manner. Where the cough and pain are very severe, Dover’s
powder or even morphi a may be necessary ; however, in my practice, these are
rarely used, the more simple methods usuallysufficing. I f the cough is severe,
and the pain is aggrava ted because of the cough , then I prefer to use codein .
T here is a great differen ce of opin ion as to the advisabil itv of removing
flui d from the pleura . Some excell en t authori ties operate very early, before
the accumula tion has caused any special symptoms, relying on its presen ce as
bein g canse sufficien t to warran t remova l ; others wi thho ld opera tin g un til some
urgen t symptom such as embarrassment of respira tionor circulation demand
it,preferring to let the exuda te absorb of its own accor d if i t will . I thas always
been my practice to wai t and let natur e care for the fluid un less remova l has been
especially in dica ted . Where removal is resorted to i t seems best n ot to remove
more than hal f of the fluid and i t a lso seems best to wa i t for the removal un ti l
the end of the exudative stage, when the in flammatory symptoms have al l
di sappearedf This fluid has been shown to be poor in Specificp ro tective partie
l es so its absorption can n ot have any effect in artificially in creasing the pro tec
t ive power of the blood ; but, by its presen ce i t causes an en forced rest of the
lung,if i t be on the diseased side, which , un less the pressurebe so grea t as to
cause harm in o ther directions, may be of some value in promo ting healing.
On the o ther hand, when the exuda te is a llowed to remain , fibrin is deposited
on the pleural surfaces, and this organ izes and acts as an embarrassment to the
lung .
PNEUMOTHORAX.
Pneumo thorax is an un common compl icat ion of tuberculosis,
yet one wh ich w i ll be met occasionally . The cause of i t is an
escape of a ir in to the pleura l cavi ty due to t he rupture o f a
tuberculous focus . The ser iousness of i t depends very much upon the cond i
tion of the lung and pleura . I f i t occurs in a ches t which is the seat o fmarked
infil tra tion ,where the lung is bound down by pleural adhesions, and the lung
o n the o ther s ide is in fa irly good cond i t io n ,the symptoms m ight be very sl ight
,
because much o f the work o f the d iseased lung has a lready been thrown on
the better lung , and bes ides the pleura l adhesio ns may preven t the lung on the
a ffected side from fully co llaps ing . I f, o n the o ther hand, the better lung
sho uld be invo lved in the pneumo tho rax o r i t should come on in an ind ividua l
who se lungs were the seat o f l ittle tro uble, compen sat io n would be very diffi
cult to establ ish and i t is probable tha t the pat ien t would succumb . Such
pa t ien ts o ften die w i th in the first few hours o f the a ttack .
Ser iousn ess o fPn eumo tho rax.
TH E COM PLI CAT I ON S OF PULM ON ARY TUBE RCULO S I S
“
Pneumo thorax usua ll y comes on sudden ly w i th a sharp
pa in and: dyspn ea . I f the co l lapse of the'
lung be sudden
and exten sive, the dyspnea becomes urgen t w i thin a very sho rt t ime ; if, on
the o ther hand, _
the pleura l cav i ty fills w i th air gradual l ly the dyspn ea is pro
gressive but n ot so ur gen t . I n one ofmy cases wh ich occurred in a lun g which
had been the sea t of a pn eumon ia result in g in fibrosis, the on ly symptom tha t
the patien t n o ticed was a shortn ess of breath . The diagn osis was made on
phys ica l fin dings . I n an o ther the pleur al cavity filled gradua lly . Pa in was
in ten se but the Shor tness of brea th did n ot reach its cl imax un t i l twen ty- four
hours after the onset .
The temperature may be ei ther elevated or lowered or i t may remain un
changed . The dyspnea, the bulg ing of the chest .ou the affected s ide,the dis
placemen t o i the heart, the absen ce of breath soun ds, and the sudden develop
men t of a tympan i t ic n o te over an area formerly afford ing a n orma l or impair ed
sound,are the physica l s ign s wh ich are foun d . Later, an effusion usually
takes place and the phenomenon of splash ing or succuss ion may be detected
upon shaking the pa t ien t . The bel l sound wh ich is somet imes presen t is
produced as fo l lows : The stethoscope“
is’
plac'
ed ei ther behind or in the axilla
wh i le a co in is la id flat on the chest in fron t and tapped by a second on e.
‘
O rdinarily on ly a dull soun d is heard, but when pneumo thorax is presen t a
c lear bell sound is heard . I t is n ot pa thognomon ic of pneumo thorax,for i t
can occasiona lly be produced over cavities and an in fla ted stomach might give
the same sign .
Symptoms .
A t the on set the most urgen t symptoms are shock, pa in
and n ervousness . These must be met at on ce. Remed ies
wh ich act qu ickly are necessary . The d iffusible stimulan ts,such as ammon ia
,
a lcoho l and ether, are of great service. S trychn ia may be advan tageously
given combined with morphiar
to rel ieve the d istress and support the respira
tory fun ct ion . The case must be treated symptoma t ica lly . I f the in tr apleu
ral pressur e becomes so great that dyspnea is ur gen t a paracen tesis should
be made. This a llows the air to escape and affords rel ief to the resp iration
and c irculation for the time. I f i t becomes ur gen t again a secon d or third
paracen tesis may be made, choosing a new place for each pun cture. By
th is mean s the patien t may be t ided over the immediate crisis . I f fluid ap‘
pears the same con siderations should guide us as though i t were a case of
pleural effusion .
Trea tmen t.
M IXED INFECTION .
The subject of m ixed in fection in its relat ion s to tuberculosis is one tha t is
poorly understood ; yet, i t is one that must be understood before we can make
great headway in our treatmen t of pat ien ts suffering from tuberculos is in the
advan ced form .
256 PULM ON ARY TUBERCULO S I S
M any bac teria bes ides the tubercle bac i llus are found in tuberculous
sputum. The var ious pus o rgan isms are common ly presen t . That these
var ious organ isms are found in the sputum is n ot suffic ien t ground for associat
ing them with the tuberculous process, for they may have come from themouth ,thr oat or o ther port ion s of the respir a tory tract . To obv ia te th is possib i l ity
o f error, Pfeiffer suggested tha t the part icles of sputum for examina tion be
taken from the cen ter of the mass of sputum. K i tasa to even wen t further and
washed the sputum mass in ster i le wa ter, before the sample for exam ina tion
was taken .
O ther observers, as Petruschky, Fraenkel and Schroeder and N aegelsbacn ,
examined the blood to see if i t con ta ined the organ isms . These exam inat ion s
usua l ly proved to be n ega tive. I t is on ly rarely tha t the various organ isms
men tioned in connect ion w i th tuberculosis are foun d in the blood,and
,when
foun d,i t is usually in the blood taken after death ; and, i t is highly probable
that they passed in to i t during the hours immediately preced ing death .
“S t il l o ther observers, Ortner, Sata, Schabad, Cornet and Kitasato
,made
Cultures from the walls of cavities after the death of the pat ien t . I n some
instan ces these cultur es were taken a lmost immediately after death,to prove
that the organ isms were there dur ing l i fe and tha t they had no t come from
o ther parts of the air passages after the death of the patien t .“This method revea led about the same varieties of organ isms as were foun
by the examination of the sputum . The pus organ isms, especia lly strepto
cocc i,were most common ly found . S taphyloco cci
,pneumococci and in fluenza
bac i ll i were presen t less common ly . I n some in stan ces no o ther organ isms
than the tubercle bac i l lus were found .
“The importan t fac t to be borne in mind in these observa tions is tha t these
various o rgan isms were found n o t o n ly in the air passages and cav i t ies presen t ,but also in the lung tissue beyond ; some, as O rtner,. even no ting them in the
t issues which had n ot yet been invaded by the tubercle baci llus.
Some idea of the frequen cy with which o ther organ isms associa te themselves
w i th the tuberculous process may be gained from the fo llowing : O rtner
found an organ ism which he named micrococc'us-pneumon iae, but whi ch later
proved to be a s treptococcus in twen ty-eight out of forty-two exam inations .
Pasqua le found streptococc i in the sputum every time in eighty- two cases .
Schroeder and M ennes,in twen ty-one cases of tuberculosis in a l l stages,made
thirty examinations o f sputum and found s treptococci twen ty-n ine t imes
staphylococci seven teen times and pneumococci fifteen times.
The impo rtan t quest ion to decide is what part these various organ isms,which are found in so large a percen tage o f the cases of advan ced tuberculosis,play in the patho logic pro cesses presen t . ” (Po ttenger,
“A Cl in ica l S tudy o f
M ixed I n fect io n in Tuberculos is .
” Repo rt o f I n terna tional Congress o n Tuber
culosis,Paris
,1905 . Journa l American M ed ica l Association , M arch 24,
258 PULM ON ARY TUBE RCULOS I S
il l for weeks or mon ths and tha t the ma in tenan ce of nutrition and preser
vation of strength are very importan t .
I n order to make the patien t as comfortable as possible we
endeavor to preven t'
chills and reduce the tempera tur e by
ra tional methods . When the patien t ’s tmeperature is low in the morn ing or
when he is having ch il ls we endeavor to preven t these by seeing tha t he is
kept warm in the early morn ing . H ot drinks are given and if the patien t
finds i t n ecessary to leave the bed for any purpose whatever, he i s wrapped
warmly and pro tected from the chill of the air . I f he is accustomed to have
chil ls,i t is wel l to an ticipate them by placing hot water bo ttles to his feet and
giving h im a hot dr ink ofwater or mil k about one-hal f hour befo re the expected
time o f the chil l .
The fever is combated by rest in‘
bed in a well-ven tilated
apartmen t,hydr o therapy and very careful and pain stak ing
a tten tion to min ute detai ls . I f the digestion is careful ly looked after,the
bowels properly regulated and al l sources of worry and irri tation removed ,we have done much toward keeping the tempera ture as low as is consisten t wi th
the patho logica l pro cess presen t .
The var ious coal tar products shoul d n o t be used except very exceptionally,
and then on ly in very smal l doses . The more exper ien ce one has in treating
th is condition the less value will he a ttribute to such remedi es, and the less use
will he find for them .
I t is very necessary to know that lowering the temperature,in i tself
,is not
curing the pa tien t . I t is n ot the fever tha t is at fault,but the cause of the fever .
T rea ting the fever symptoma tical ly is of value on ly as i t refreshes and improves
the general ton e of the pa tien t and en ables himto endure his illness better .
I f this resul t is attained by the various coa l tar . products i t is obtained at the
expen se of its depressing action upon the heart ; and the physician must decide
whether or not this is justifiable.
There is one measure that can usually be employed without any danger o f
harm wha tever, and one tha t refreshes the patien t at the same time, that is
hydro therapy . Whatever hydro therapeutic .measures are employed,should
be carefully adapted to the condition and strength of the pa tien t .
I have found sponging with tepid wa ter, as described on page 1 57 , to be the
mo st useful application . This procedure should be tried whenever i t is neces
sary to rel ieve the patien t by the reduction o f temperature. I t rel ieves no to n ly
the tempera ture but the nervousness as well , and S eems to enable the pa tien t
to bet ter endure the effect o f the toxins from which he is suffering .
Remembering tha t mixed in fectio n may co n t inue to cause
fever and o ther severe symptoms fo r weeks and mo n ths we
must endeavo r to fo rtify our patien ts and prepare them fo r the heavy tax tha t
such a pro cess makes upo n them . When left to their own incl ina tio ns during
Ch i lls .
Fever.
D iet .
TH E COM PLI CAT I ON S OF PULM ON ARY TUBERCULO S I S
this time,patien ts usually eat very little and consequen tly lose weight rapidly ;
but,when correctly guided in their diet , they may pass through a siege of fever
lasting several mon ths and gain in weight .
The diet at such times should be abundan t and should be carefully suited
to the patien t . I have found tha t i t is n ot necessary to cut off so l id food as is
usua lly recommended in acute fevers ; on the con trary, I believe such a course
to be disadvan tageous when the so lids are wel l borne. A t that time of the daywhen the temperature is low
,the patien t can usual ly take a so l id mea l to advan t
age. I n the usual cases ofmixed in fectionwhen the tempera ture i s low in themorn ing, but begin s to rise about noon ,
reaching its maximum dur ing the after
noon and then beginn ing to decline by four or five o’clock
,I usually give the
patien t a so l id breakfast, consisting of,
fruit, s ome cereal i f desired, steak ,chops, so ft bo i led or poached eggs
,baked po tato
,bread and butter and milk
This will be digested by the time the tempera ture begin s to rise. A t lun ch,
when the tempera ture is on the rise, the patien t is given _
mil k or mal ted milk,
:
and one or two raw eggs,with perhaps gelatin ,
junket or some l ight custard,if
desir ed. A t six in the even ing a fair ly full jmeal consisting of soup, roas'
t meat,vegetables
,some light dessert and milk is given . I n this way the food is so
suited to the condition of the pa tien t tha t those varieties wh ich require the
greatest digestive energy are taken when the stomach is best able to care
for them,and at o ther times such food is given as makes l ittle demand upon the
digestive powers. This also gives the patien t the advan tage of so lid food .
I am firml y convin ced that so lid food,if well born e
,
'
stimulates the appetite
more than such articles as milk and eggs which we resort to so o ften .
While we sometimes find it n ecessary to resort to a diet con sistin g a lmost
en tirely of milk and eggs, yet, where so l id food can be well bo rn e I
believe i t has many advan tages . Where mi lk and eggs are a lmost who lly
rel ied upon,not less than oneand on e-half quarts of mi lk and from three to
six egg‘
s should be con sumed each day.
The digestive fun ction s should be assisted when necessary . I f digestion
is carr ied on slowly, thir ty gra in s of sodium chloride disso lved in a glass of hot
water taken from on e- ha lf to on e hour before mea ls wi ll o ften prove very bene
ficial,or dilu‘
te hydrochlor ic acid may be used after meals . The commercia l
digestan ts, while theoretical ly o f l ittle va lue,seem to help at times . The
bowels should be regulated ; Calomel in smal l divided doses,fo llowed by
castor o il or magn esium sulphate is a great help occasionally. I t is veryessen tia l not to a llow the bowels to become constipa ted .
S erumSerum therapy has been used in mixed in fection for several
Trea tmen t of years. The prin cipa l serum that has been employed has been
Ihi
fiition that made from the horse by in o cula ting him with virulen t
strain s of strepto cocci . The writer has employed this serum
in about one hundred cases,with en couraging results . While every patien t
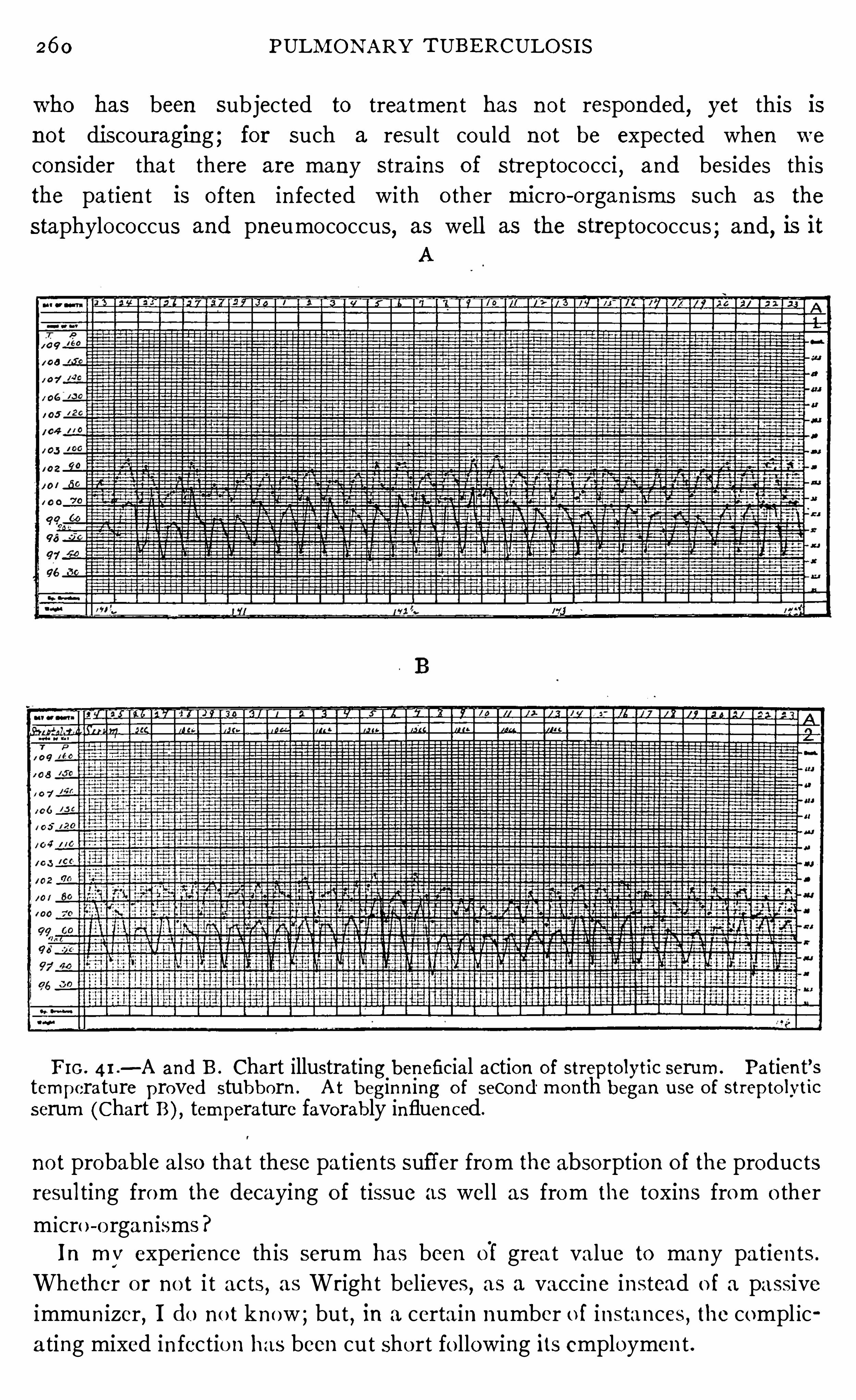
26 0 PULM ON ARY TUBE RCULOS I S
who has been subjected to trea tmen t has n o t responded, yet this is
not discour aging ; for such a result could n o t be expected when we
consider tha t there are many stra ins of streptococci,and besides th is
the patien t is o ften in fected with o ther mi cro -o rgan isms such as the
staphylococcus and pneumococcus, as well as the streptococcus ; and, is itA
F I G . 4 I .
— A and B . Chart illustrating beneficial action of strepto lytic serum . Patien t’stemperature proved stubborn . A t beginn ing o f second mon th began use o f strepto lvtic
serum (Chart B), temperature favorably influenced.
no t probable also tha t these pa tien ts suffer from the absorption o f the products
resul ting from the decaying o f tissue as wel l as from the toxins from o ther
m icro -o rgan isms?
I n my experience th is serum has been of grea t value to many pa tien ts .
Whether o r no t i t ac ts , as Wright believes, as a vacc ine in stead o f a passive
immun izer,I do no t know ; but , in a certa in number o f ins tances , the compl ic
a ting mixed in fectio n has been cut sho rt fo llowing its employmen t .
26 2 PULM O N ARY TUBE RCULO S I S
wel l to repeat that there is'
on ly one excuse for n ot giving a pat ien t who suffersfrom an early hemoptysis the benefi t of an early diagnosis and early trea t
men t, and tha t is a fa i lure on his part to consul t a physic ian . T hroa t hemor
rhage” has become a lmost obso lete,
“stomach hemorrhage is extremely
rare,but “ pulmonary hemorrhage
” has ga ined in importance because we n ow
know that nearly all hemorrhages formerly a ttributed to o ther causes are
due to a b leedi ng from some part within the lung.
Hemop tysis is nearly a lways due to a tubercul ous process .
Hihis
gpc
tf
ysis .
The amoun t of blood maybe very smal l and due to an extr av
asation in an area of tubercul ous congestion ; but , if the
amoun t be at a ll large,i t is mo re likely due to an open in g in some vessel .
Hemoptyses of the former variety are n otattended by immed ia te danger ; but we
have n o way of d ifferen t iat ing them from those produced by a sma l l open ing
in a vessel . Very o ften we have a slight sta in ing of the sputum preced ing a
copious hemorrhage (see Chapter X I I I ), soa l l hemoptyses should be trea ted
seriously un t i l we defin itely decide that the loss of blood does n ot come from
an open vessel .
The larger hemoptyses come from eroded vessels or from the bursting of
aneur isma l d i lata tion s of vessels in cav i ties . The aneurisms are due in part
to the fac t that the t issue has been destroyed aroun d the vessel,thus remov ing
the n a tural support of its wa lls . The in flammatory cond i tion which results
from the tuberculous process usua l ly oblitera tes the vessels and saves the
pat ien t fr om this danger ;'
but,o ccasiona lly
,this fai ls to occur when such
pa tien ts are l iable to severe hemorrhages .
I t has been my observa tion that hemoptyses very o ften appear
Eggpglt
iysi s
in epidemic form . When large numbers of tuberculous pa
tien ts are treated together, every now and then,severa l
pa tien ts wil l suffer from hemoptysis at the same time. A t our sanator ium
we have long periods,at times
,without an occurrence of hemop
tysis ; then ,sudden ly
, several will o ccur at or about the same time.
I have n o ticed a lso that when they are prevalen t in the in st i tution,
they a lso occur in the town ; and have a lso no ted the co inciden ce between
the frequency here and in the Ci ty of Los Angeles . The blood pressure of
the pa t ien ts at these t imes,when we have measured it
,has been h igh . This
po in ts to their being some general cause,probably assoc ia ted with the pre
va i l ing meteoro logica l cond it ions,wh ich produce hemoptysis .
Perhaps no compl icat ion from wh ich the tuberculous pat ien t
suffers,is so a troc iously m istreated as hemoptysis . I t is
nearly always overtrea ted . M any foo l ish things are done.
M any things tha t are po s itively harmful are done and the th ings that are
i nd ica ted are left undone. The results tha t have been attained in spite o f
th is m isd irected en thus iasm furn ish unm istakable proo f of the beneficence
Trea tmen t ofH emoptys is .
TH E COM PLI CAT I ON S 'OF PULM ON ARY TUBE RCULO S I S
of nature and po in t the way to much better results when the treatmen t iscarried out a long rational. lines.
To apprec ia te the ind ica tion s for treatmen t i t is n ecessary to understand
the cond i t ion s presen t . The circulatory system may be l ikened to a system
of elast ic tubes filled w i th fluid and connected w ith a cen tra l pump (the heart).E very portion of this elast ic tube system is
_dependen t upon the ten sion of
every o ther portion .. These tubes are able to withstand a wide degree o f
var iation in pressure ; but, let them become defective in any port ion ,then
,an .
in crease in the pressure might cause a rupture. I n tuberculosis the wa llsof these elastic tubes (the blood vessels) are the seat of tubercles, wh ich softenand break down ,
thus weaken in g them; A t such a t ime there is grea t danger
of a rupture. I t may come about ei ther by the destruct ive process break in g
through the wall or by an in crease in the ten sion of the tubes caus in g theflu id in the tubes to exert greater force again st their wa lls . Th is in creased
ten sion may be brought about ei ther by an increase in the force of the pump
(the heart) or by an in creased ten sion on the part of the-elastic tubes (the blood
vessels).
With this understanding we can compfehendl
the treatmen t of hemoptys is,
wh ich‘
is simply a rupture somewhere in the system of elast ic tub ings .
Where any considerable loss of blood occurs the hemoptysis is due to a
break in the wa ll of a vessel . The sen sible thing to do in order to check
bleeding is to keep the tension within the vessels low,by ei ther decreasin g
the force of the heart (the pump), or , by decreasing the ten sion of the vessels
(elastic tubes).
There are several factors which en ter in to the lowering of blood pressure.
The first that I w ould men tion is rest . Th is in fluences the heart particularly .
Exerc ise in creases blood pressure, wh i le rest lowers i t . Therefore the firstindicat ion in the treatmen t of hemoptysis is to put the pa tien t to bed
,in
the recumben t posi t ion . M en tal exc i temen t also in creases blood pressure,
therefore i t is very importan t to al lay a l l nervousness tha t may come through
fright .
I t is n ot enough to put the pat ien t to bed, but, i f the hemoptysis is at allser ious
,abso lute rest must be en jo ined . The pat ien t should not be a llowed
to leave the bed for any purpose, no r should he be allowed to change his
posi t ion ,or move his legs or arms un t i l further danger of bleeding has been
removed . The nervousness can o ften be allayed by a few words of assuran ce
from the physic ian or a ttendan t . The pat ien t can be to ld’ that Very few
people die of hemorrhage. I t has been my exper ien ce tha t fewer pa t ien ts
have severe hemorrhages in in sti tut ion s than on the outside,and I do n ot
dotibt but that the assuran ce wh ich comes from the physic ian ,who is a lways
at hand,is an tmportan t factor in preven t ing severe bleed ing . Where the
n ervousness can be allayed in this manner, and the patien t can be closely
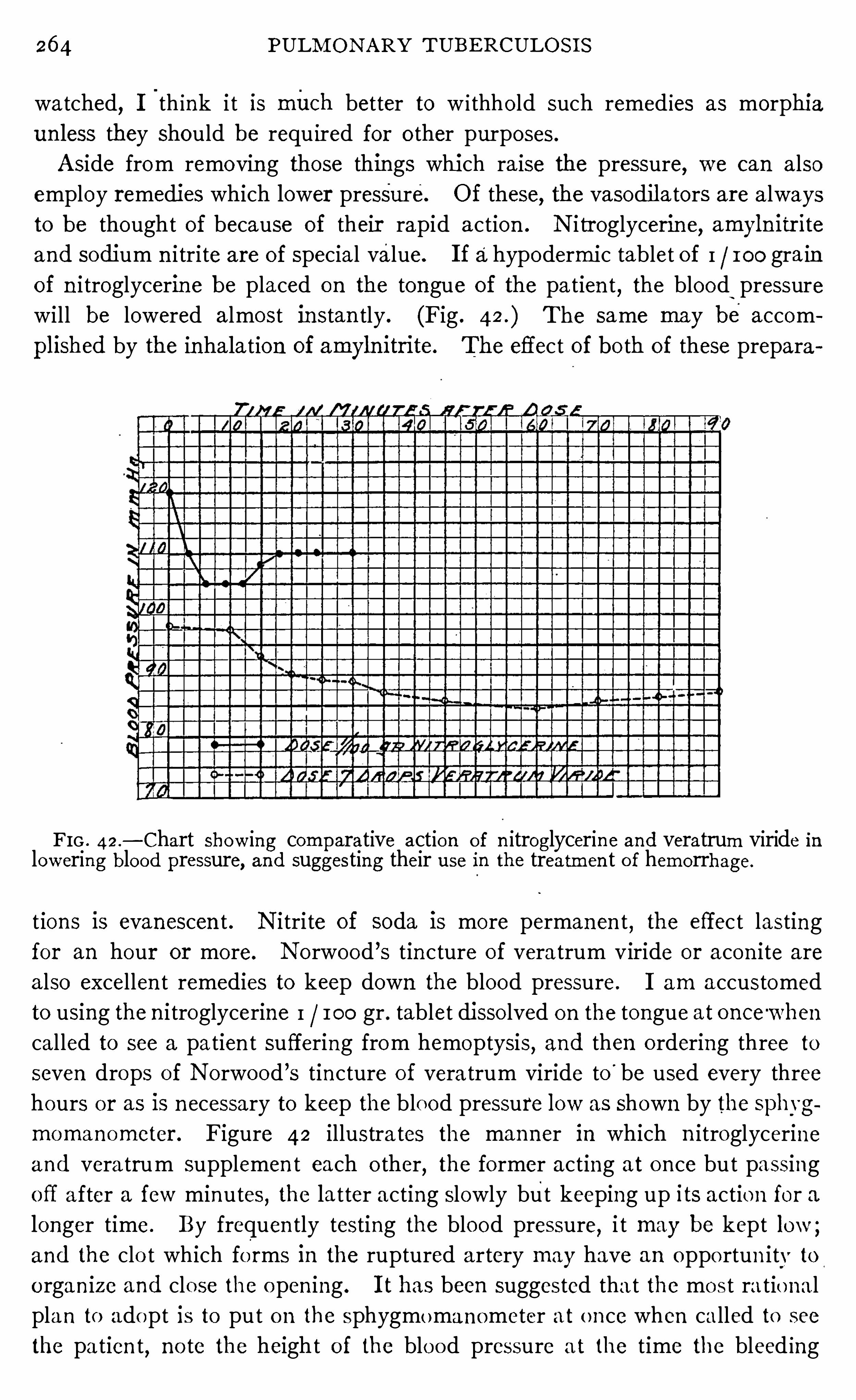
26 4 PULM ON ARY TUBE RCULOS I S
watched,I
'
th ink i t is mii ch better to w i thho ld such remed ies as morphi a
un less they should be requ ired for o ther purposes .
A side from removin g those things whi ch ra ise the pressure, we can also
employ remedies which lower pressure. Of these, the vasodil a tors are always
to be though t of because of their rapid action . N i tr oglycerin e,amyln itr ite
and sodi um n i trite are of special value. I f ahypodermic tablet of I 100 gra in
of n i troglycerine be placed on the tongue of the pa tien t, the blood‘
pressure
will be lowered almost instan tly . (Fig . The same may be aecom
pl ished by the inhalation of amyln itrite. The effect of bo th of these prepara
FIG . 42.
— Chart show ing comparative action of n itroglycerin e and veratrum viride inlowering blood pressure, and suggesting their use in the treatmen t o f hemorrhage.
t ions is evanescen t . N i tri te of soda is more permanen t , the effec t lasting
for an hour or more. N orwood ’s tin cture of vera trum viride or acon i te are
also excellen t remedies to keep down the blood pressure. I am accustomed
to using the n i troglycerine I 100 gr . tablet disso lved on the tongue at once '
when
cal led to see a patien t suffering from hemoptysis, and then o rdering three to
seven drops of N orwood ’s tincture o f vera trum viride to
'
be used every threehours or as is n ecessary to keep the blood pressure low as shown by the sphygmomanometer . Figure 42 illustra tes the manner in wh ich n itroglycerineand vera trum supplemen t each o ther
,the former acting at once but passing
off a fter a few minutes,the la tter acting slowly but keeping up its action for a
longer time. By frequen tly testing the blood pressure, i t may be kept low ;and the clo t which forms in the ruptured artery may have an oppo rtun i ty to
o rgan ize and clo se the o pen ing . I t has been suggested tha t the mos t ra tio nal
plan to adopt is to put o n the sphygmomanometer at o n ce when called to see
the pa tien t, no te the heigh t o f the blo od pressure a t the time the bleed ing
26 6 PULM ON ARY TUBERCULOS I S
are con tra indicated in the trea tmen t of hemoptysis due to an open in g in a
vessel wa ll . The use of astringen ts such as tann ic and gallic acid are useless.
The pa tien t should be put upon a co ld di et,con sisting of such articles as
mi lk,eggs
,tropon , gela tine and custard . The bowels should be kept open .
A saline laxative is valuable for this purpose because by its abstracting wa ter
from the tissues i t lowers blood pressur e.
There is another type of hemoptysis, which seems to be due to a congestion
in the lung ra ther than an open ing in a vessel wall . Wh ile,as a rule
,there is
on ly a small amoun t of blood lost, yet sometimes i t amoun ts to several mouth
fuls and may persist for severa l days .
I do not know any defin i te method of di fferen tiating between these two
varieties of hemoptysis, yet they cal l for differen t methods of tr eatmen t .
When there is doubt, however, i t is better to trea t the case as though i t were
an open in g in a vessel ; but, i f we can be sure tha t the blood is the resul t o f
congestion,then i t would be better to use remedies which stimulate the cir
culation,such as strychn ia
,digitalis and the products of the suprarenal glands .
TUBERCULOS IS OFTHE (BEN ITO -URINARY TRACT.
Doubtless tuberculous nodules exist in portion s of_
the gen i to - ur in ary tract
o ftener than we have been won t to believe, yet active tuberculous di sease in
these o rgan s has no t been so very common . The kidney, the bladder, the
testicles and ovaries may al l be the sea t of tuberculosis .
The usua l treatmen t for tubercul ous testicles and ovaries and quite com
mon ly, though n ot so generally for tuberculous kidneys, is removal, whil e
tuberculosis of the bladder, as a rule, bafi’
i es al l scien tific skil l .
I t is a source of grea t sa tisfaction from the standpo in t of the scien tist
as well as from tha t o f the pa tien t to record the excel len t work done by Wright
in treating these lesions . H is work shows tha t these localized tuberculous
lesions are to be trea ted medically and no t surgically. The fo llowing case
i llustra tes the condition and method (Wright, on the General Principles
o f the Therapeutic Value of Bacteria l Vaccines as.
Applied to the T rea tmen t
o f Tuberculous I n fec tion . M edico -Chirurgical T ransactions, Vo l . 89)The pa t ien t is a young woman of very good physique. She came under
treatmen t first in January,1905 , with a h istory of tubercular cyst i t is and
tubercular d isease o f the k idney dat ing back two years . One of her kidnevs
had been removed and there was ev idence o f the invo lvemen t of the o ther
k idney . The urine con ta ined pus in considerable amoun t and in associat ion
w i th th is many tubercle bac i ll i and severa l varieties of con taminating bacteria ,amo ng o thers pro tons . The pa t ien t ’s tubercq —o pson ic index was tested
o n two o ccas ion s befo re the inoculat ion trea tmen t was in it ia ted . O n the
first occas io n i t s tood a t o n the seco nd o ccasion at A n improve
TH E COM PLI CAT I ON S ‘
OF PULM ON ARY TUBE RCULO S I S
men t in the pat ien t ’s symptoms set“
in prac tically immed ia tely after the first
inoculat ion under taken wi th r / 8oo m i ll igramme . The tuberculo - opson ic
power rose on the day after inocula t ion to and con t inued at th is heightor .
near this po int for the next six days . An inoculation undertaken on th is
day with IMoo -mi ll igramme brought down the opson ic power of the blood .
I n association w i th this the pat ien t complained ofmore_pain . A fter the in ocu
lation s had been con t in ued for about six mon ths,when the tubercle bacilli
had d isappeared from the ur ine, _ and when ,as a result of the inoculation of
a pro teus vaccine, the pro teus also had disappeared, the patien t fel t so'well
that she moo ted the question of engagemen t a nd marriage. S in ce then she
has suffered a relapse,develop ing an acute cystitis . Th is a ttack
,wh ich was
apparen tly associated with a reappearan ce of the pro teus in the urine, is n ow
subsiding .
What can be done for the kidn ey and bladder can a lso dou'
btless be done
for the ovaryand test icle. I have had the happy exper ien ce of seeing an
apparen t heal ing in a case of tuberculosis of the ovary .
The h istory of the case I S as fo llows : Two years before the patien t reported
for treatmen t,she,
had had one ovary r emoved .
”
Upon examina tion itproved
to be tuberculous . The o ther ovary,at the time of the operation
,showed
signs of disease and the surgeon ven tured the op in ion tha t i t would sooner
or later have to be removed . The pat ien t was opposed to this radica l course
so one ovary was left . Before com ing to us the ovary had become en larged
and tender and was giving the pa t ien t qu i te a good deal of trouble. While
we prom ised her n o th ing,she in sisted on being treated . A fter a long trea t
men t w i th tubercle vacc in es extendi ng over about on e year the ovarydecreased
in size,became firm and was n o longer tender . I t is bound doWn by adhesions
,
due to the in flammatory cond i t ion about i t, but o therwise i t seems to be free
from_
disease. A fter the pa t ien t had been away from treatmen t'
about three
mon ths she returned and we gave her large doses of tuberculinw i thout causing
any tenderness or genera l reaction .
These e xper ien ces make us most hopeful of future results in th is field of
therapy, and show us tha t there are few if any tuberculous lesion s that are
ent irely hopeless .
TUBERCULOUS MEN INGITIS .
Tuberculous men ingi t is—
is rarely a compl ica t ion of pulmonary tuberculosis
in the adult,but i t is found more frequen tly in ch i ldren between the second
and seventh years . The ch i ld usually shows symptoms of fa i l ing heal th for
some time. This may extend over a period of three or four weeks. T h iscan
readi ly be understood if webear in m ind that tubercles form slowly at t imes,and n ot in frequ
en tly rema in sta t ionary in their growth for pro longed per iods .
The child loses its appet i te,becomes peevish , irr i table, does n o t care to play,
2 6 8 PULM ON ARY TUBERCULO S I S
loses weight, sleeps poorly and may cry out dur ing sleep . A fter th is pro
dromal stage the symptoms become more pronoun ced . Headache,vom i t ing
and fever appear . The headache may be ei ther in term i tten t or con stan t . I t
somet imes becomes so severe that the chi ld wi ll utter a pecul iar scream which
is characterist ic of th is d isease. The tempera tur e is elevated , the resp iration
regular and the pulse slow . The chi ld shows rapid emaciation and usually
lapses in to a somno len t cond i tion . Sometimes convulsion s appear .
When men ing i t is occurs as a complication of pulmonary tuberculos is, the
symptoms are n o t far d ifferen t . The patien t becomes nervous and irritable,
loses appeti te, sleeps poorly (in somn ia maybe marked), complain s of headache
wh ich is o ften in ten se, usually shows a d i latation of the pup i l andmay becomedel ir ious or even man iaca l ; The temperature is elevated . Before death the
pa t ien t may become stuporous .
The treatmen t of these cases is purely symptomatic . The bowels should
be kept open , and the headache should be rel ieved . An ice cap is o ften o f
va lue,brom ides are helpful, but phenacetin or morphia w i ll usually be nec
essary in o rder to a llay the in ten se pa in . I f in tracran ia l pressure gets too
high,as i t o ften does with chi ldr en ,
lumbar punc tures may be resorted to .
SYPH ILIS .
Syph i l is is a factor tha t must o ften be deal t with in tuberculous patien ts .
When we remember how common syph i l is is and then take in to considera tion
the effec t of th is d isease n o t on ly on the one who acqu ires i t but on those of
succeeding generat ion s, and then reca ll a l l of themasked forms tha t i t assumes,we are ready to appreciate tha t syph i l is maybe qu i te a factor as a pred ispos ing
and compl ica ting cond i tion in tuberculosis . I have been convinced of th is
fac t for some t ime, and have seen tha t an t isyph i l itic treatmen t is o ften of grea t
va lue in helping to cure tuberculosis . Spengler (Deutsch . med. Woch .
,1906 ,
N o . 1 5) has g iven this ma tter much though t and is firmly convin ced of its
importance.
Fresh syph i l is is a very serious complication . Patien ts who have these
two d iseases at the same t ime usua lly do badly . I n a l l such cases mercury
and iod ine should be used . M ercur ia l o in tmen t is perhaps as effi cac ious as
any prepara t ion . The I tal ian schoo l use hypoderm ic in ject ion s of sublimate
deep in to the gluteal muscles . When mercury I S used the amoun t should
depend grea tly upon the condition of the pa tien t. One who is strong could
have large amoun ts and more frequen t appl ica t ions than one in a weakened
cond i t io n . I f a small amoun t of sulphur is admin istered each day, i t helps
to preven t mercuria l ism .
The effec t o f inheri ted syph i l is is wel l known to a l l phys ic ians,al though as
yet its impo rtance does no t seem to be grasped by those who are trea ting
270 PULM ON ARY TUBE RCULO S I S
she may make an un in terrupted conva lescence and no t be harmed by the
pregnancy . On the o ther hand, there is a lways grave danger that the qu iescen t
focus may be l ighted up and tha t the woman may become the vict im of an
act ive tuberculosis .
I f a woman who is suffering from active tuberculosis becomes pregnan t,
the case is qu i te d ifferen t . The d isease may at once beg in to show sign s of
greater act iv i ty . I t may take on the character of an '
acute process, and the
pat ien t“
go down to death w i th in a very short time. On the o ther hand, the
pat ien t may appear better for a t ime. She_
may have an apparen t arrestmen t
o f'
the symptoms while she is carrying the chi ld . Hope is assured that the
pregnan cy has cured her tuberculosis . I n ei ther case,however
,after del ivery
the d isease is prone to light up anew,and the patien t go on to quick and
certain death .
Pregnancy must a lways be looked upon as a serious complication in tuber
culos is. When a woman has been apparen tly cur ed of tuberculosis,several
years should elapse before she becomes pregnan t . A woman w i th an arrest
men t of the disease can n ot become pregnan t without runn ing great risk of
start ing up the d isease anew,even a l though the arrestmen t is of several years
,
stand ing. A woman with act ive symptoms of tuberculosis, should she become
pregnan t, has chan ces greatly against her . She can on ly look forward to
the probab i li ty of an in creased activity of the disease.
This being true i t is the duty of physic ian s to tel l their tuberculous women
of the dangers which accompany pregnan cy. I believe i t is humane and
just to instruct them how to preven t conception .
A s to what is the r ight plan to adopt when pregnancy has occurred, thereis room for a just d ifferen ce of opin ion . Recognizing the great danger to
the mo ther, some most conscien tious physician s advocate emptying the uterus
at on ce upon the discovery of the condition . O thers, to whom we can ascr ibe
no greater degree of con scien tiousness, deny the right to sacrifice the l ife of
an innocen t unborn babe to that of the mo ther . I f we admit that the phys
ician has the righ t to con sider the l ife of the mo ther in preference to the l ife
o f a fecundated ovum,and gran t that he is justly entrusted with the r ight
to in terfere in the in terests of the mo ther when in his judgmen t her l ife is
imper i led, then we must take a middle ground On this subject ; and, wh i le
we would not advise empty ing the uterus in every tuberculous woman who
becomes pregnan t, we would say that i t should always be co nsidered,and a
l ine o f action should be determined upon on ly after the pros and cons have
been most carefully co nsidered .
CHAPTER xx
TRE ATME NT“
or SYMPTOM S .
COUGH .
Perhaps the symptom which w i l l most o ften cause individuals suffering from
pulmon ary tuberculosis to seek medical aid is cough . Cough is a necessary
accompan imen t of the disease. I t shows i tself early and con tinues to the end .
T here is n o n ecessity, however , of cough assuming as great proportion s as
it usually does. When patien ts are properly con tro ll ed,cough sinks in to in sig
n ifiéan ce compared with i t as foun d in those who l ive improperly .
The first treatmen t of cough consists in in str ucting the patien t to resist al l
in cl ina tion to cough which is n ot necessary for the expulsion of secretion .
There is a common belief tha t if there lsimucus -presen t i t should be coughed
at un til expelled . This is a wrong idea . The patien t shoul d spare h imself
every cough that he possibly can , for cough , by irr i tation ,in creases the tenden cy
to cough, and by in creasing secretion in creases the necessi ty for cough .
Cough produces an in jurious effect in severa l differen t ways
First, by its explosive action i t in jures the tender fibrils of
n ew tissue whi ch are thrown out dur ing the process of
hea lin g and by this ir ri tation causes the forma tion of more scar tissue than
would o therwise be formed . Where i t is con tin ued for a long time,i t also
causes a dil ata tion of the air vesicles resul ting in an emphysematous condition
with its tra in of in jur ious effects .
Second, if the cough is severe, i t wearies and exhausts the pa tien t and pre
ven ts sleep and o ften causes a rise of tempera ture.
Third, i t o ften in terferes wi th n utr i tion by causing the patien t to vomit as
soon as food has been ea ten .
When the patien t understands the necessi ty of con tro l ling cough it is
surprising to find how l ittle of i t is real ly necessary. The will power is one
of the most poten t remedies to be employed aga in st i t .
Cough is d ue to a n umber of differen t causes, such as the
disease pro cess in the lung or pleura or inflamma tory condi
tion s in the upper air .passages ; but, the excessive cough“
,
as we find i t,is due in a large measure to overexertion
and bad habits of l iving . I t is much more pronoun ced in pa tien ts who
live in badly ven tilated apartmen ts and who overexercise than in those
who l ive in the open air'
and do n o t overexert . Where excessive, espe
27 1
2 7 2 PULM ON ARY TUBERCULOS I S
cia l ly if i t is irri tating and unproductive, i t will quite o ften show marked im
provemen t when the pa tien t is required to res t in bed. This kin d of a cough
is o ften relieved by the use of the wet jacket as described on page 1 6 2 .
When i t does n ot yield to these simple measures,i t may be found necessary to
resort occasiona lly to the use of some seda tive such as codein or hero in . Per
sonal ly, I rarely resort to these remedies, and when n ecessary,codein is given
the preferen ce because of its mo re favorable action on the digestive system .
The deriva tives of opium are the on ly on es that are reliable,and their action
upon the digestive fun ction debars them from a very general use. M any men
are en t irely too free with the use of cough“
medicines . Better managemen t o f
the case, together with the confiden ce of the pa tien t, makes most cough rem
edies superfluous .
Sometimes cough is due to an a ttempt to expel secretion from a cavi ty or
to an excessivebron chial secretion . I n such cases a lkal ine ho t drinks (15grain s of bicarbonate of soda in a glass of hot water) o ften proves beneficial .
I nhalation s of tar , benzo in and creoso te are also of some value in these cases,
and if creoso te does not disagree w i th the patien t, i ts admin istra tion in doses
of ten drops (Beechwood creoso te) after meals wil l o ften have a salutary effect
in the lat ter class of cases . When creoso te is admin istered it should no t be
given in capsules, for when they disso lve, the l iquid escapes and exerts a severe
action upon the mucosa of the stomach . To avo id this the desired dose should
be put in to a conven ien tly sized bo ttle, for example one ho ldi ng four oun ces,
wh ich should then be fil led with wa ter (some prefer i t quite warm) and tho
roughly shaken so as to break up the creoso te drops in to very fine globules .
When thus admin istered it can no t in jure the mucous membrane o f the
stomach .
O ften times cough comes on as soon as food has been ea ten,the patien t
coughing un til he vomi ts. This condi tion will sometimes yield to ho t alkal ine
drinks taken fifteen minutes before meals . Sometimes a post-nasal ca tarrh
is the exci ting cause in these cases, when rel ief may be afforded by post-nasal
applica tions of a 10 per cen t so lution of pro targo l,o r a so lution of iodi ne in
glycerine. Five to ten grains of'
oxalate of cerium twen ty min utes befo reea ting sometimes has a beneficia l effect, but when the vomiting becomes serious
by causing loss o f weight, as I have o ccasionally seen i t , and when i t does no t
yield to the simple measures, codein o r herom one hour before the meal should
be used .
Care o f the upper air passages will keep down a great deal of unnecessary
coughing,and wh ile I do no t bel ieve in persisten t
,uncal led fo r spraying and
trea ting o f the naso -pharyngeal and laryngeal mucous membranes, yet I am
co nvinced tha t the services o f a skilled rhino logist and laryngo logist will add
much to the comfo rt and wel l being of pa tien ts suffering from tuberculo sis .
I n elderly persons the red iodide o fmercury in sma ll doses (1 50 o f a gra in)
274 PULM ON ARY TUBERCULO S I S
S omet imes, in spite of these simple measures, sweating wi ll con tin ue. This
15 most likely to be the case when the disease is far advan ced and the pa tien t
is suffering frommixed in fection , or when the process is running a rapid course.
T here is n o harm in the swea t i tself. There is a popular idea,wh ich is shared
by many physician s,as well as laymen ,
that these swea ts are very weaken ing .
I t is n o t the swea ting,but the cause of the swea ting that is weaken ing . The
grea test harm tha t usua lly comes from the swea ting is in the discomfo rt to
the pa t ien t . O ccasional ly it is fo llowed by a chill , to avo id which,a pa tient
subjected to swea t ing Should keep at his bedside a towel with which he maydry h imsel f if sweating should o ccur ; and, he should a lso have a change of
n igh t clo thes in the bed or under the pil low, where they will be kept warm,
to be put on in case a change should be necessary .
When the sweats are pro fuse, a tropin e filmto .3
1—0 of a gra in given at bedtime
,
may dry the secretion and preven t the sweating .
'
Agaracin may be tried and
w ill sometimes prove beneficial . A s_a rul e, however, if the simple methods
above will n ot sufli ce,too much mustn otbe exp ected from dr ugs.
FEVER.
I n every case of tuberculosis a rise of temperature is presen t some time during
its course. T his does n ot require special measures of treatmen t,however
,
un less the rise exceeds 100 degrees. Whil e this measure is arbitrary yet expe
r ien ce shows i t to be about the po in t above wh ich the temperture may not go
without producing some anxiety . The temperature of un complica ted pul
monary tuberculosis, except in acute forms,rarely goes above 101 degrees and
usua l ly rema in s below 100 degrees . When this l imit is exceeded,we must
suspect that the tuberculous areas have taken on an acute inflammatory
condition resulting in a pneumon i tis of greater or lesser severi ty or tha t some
complicat ion in the nature of a mixed in fection,or on the part of the pleura
o r the digestive system,or an acute miliary condition has arisen .
N o matter what the cause of such a temperature,the pa tien t should be
treated as a fever patien t . E xperien ce in trea ting these '
cases will teach tha t
even fever cases'
can not be treated by routine measures ;‘
and,while we make
100 degrees the usua l limi t, yet in many instan ces i t is advisable to trea t as
fever cases those who have a lower limit . S tric t individua l ization after a tho
rough understanding of the patien t is necessary to successful trea tmen t .
Fever patien ts should rema in in bed. I t is scarcely necessary to say tha t
they should be placed in the open air and subjected to al l the restrictions which
make up the usual hygien ic regime, for this statement applies to al l cases o f
tuberculosis. An appropriate diet is also indispensable,and does much
toward lessen ing the fever .
Rest , in the trea tmen t o f these patien ts, is indicated because exercise causes
TREATM E N T OF SYM PTOM S 75
an increased absorption of toxins, thus in creasing one of the pr incipal causes
of an in creased tempera ture, and a lso because the pa tien t’s powers of resistan ce
are better when the pa tien t is at rest . I f the tempera ture is due to a congestion
in the lung,exertion a lso raises the tempera ture by in creasing this congestion .
The medical attendan t should promptly o rder the patien t to bed when a r ise
of tempera ture comes . To think tha t i t may lower in a few days of its own
accord without rest usually resul ts in a loss of time.
The effect of placing these pa tien ts in the open air,especially when they
have been in the habit of l iving with inadequa te ven ti lat ion, _
is o ften very
marked. There need be no fear “
on the part of ei ther physician or friends in
adopting the open -air treatmen t for these patien ts . While this statemen t
should not be taken as warran ting unn ecessary and foo l ish exposure, yet a
pa tien t may be taken from a warm, overhea ted, poorly ven tila ted room and
placed in a coo l, wel l-ven tilated room even i n rigorous climates,without
danger , if proper precaution s such as those men tioned in Chapter X I are
observed .
Fever must not be treated with dr ugs,for i hey c an no t be coun ted on to
remove the cause. N ot the fever but the cause of the fever must‘be trea ted .
The pneumon ic condition ,the pleurisy, the mixed in fection and the compl i
ca tion s on the part of the gastro - in testinal tract must be the recipien ts of our
therapeutic energies.
The sligh t rise of tempera ture due to the tuberculous process which does
n ot exceed 101 degrees is best combated by a combination of the open -air,
dietetic,hygien ic and tuberculin trea tmen t . I t is not an un common experien ce
to find a rise in tempera ture of this kind, which has persisted for some time,yield in a short period to in jection s of minute doses of tuberculin .
"
This seems
un reasonable,for i t is generally bel ieved that the fever is due to the system ’
s
being surcharged with toxin s from the tubercle bacillus ; and, i t would seem
tha t to in ject more toxin s would be on ly adding fuel to the fire. That such
in jection s act ben eficially I have been able to prove for the past three years .
Repea tedly have I seen such tempera tures yield to this treatmen t when they
had refused to yield un til the tuberculin was given . Wright offers us an expl a
na tion of this action . H e says that n ot in frequen tly the machinery of immun
ization fails to work to its full capaci ty in spite of the fact tha t toxins from the
invading bacteria are being poured out in to the blood stream . A t such times
vaccines in jected in to the tissue may stimulate the forma tion of pro tective
bodies where those circulating in the blood have fa iled . Whether or n ot we
accept th is as the explanation,the
'
fact remain s,that these tempera tures can
o ften be successfully lowered by the use of minute doses of tuberculin .
I n order to avo id repeti tion,I will refer my readers for further discussion of
treatmen t of fever to the sections which deal with the various complica tion s
which cause i t .
27 6 PULM ON ARY TUBE RCULO S I S
PA IN .
Pa in is a very common accompan imen t of tuberculosis . I t is due usua lly
to one of two causes,ei ther a pleurisy or a muscular soreness from coughing .
The former is the more common cause. The tuberculous area in the lung is
no t accompan ied by pain un less the process is near the pleura ; but when i t is
so si tuated there is n early a lways more o r less pain . O ccasional ly, how
ever, we will find an exten sive invo lvemen t of the pleura and yet the patien t
deny having experienced any pa in at al l .
These pleur a l pain s may be very sl ight‘
or they may be severe ; they may be
acute or they may be dull . When there is an acute pro cess presen t the pain
is usually of a stabbing character, catching the patien t as ,he coughs or takes a
deep breath . Old pleur al adhesions are o ften the seat of pain wh ich comes
on with certa in changes in the wea ther . The wea ther condition s wh ich favor
these pa ins seem to be about the same as those wh ich cause pain in rheumatic
jo in ts. When a cavity is forming near the surface of the lung the pa tien t o ften
experien ces a dull ache. A side from these pains due to acute or subacute con
dition s affecting the pleur a there are o thers wh ich accompany con traction of
the lungs . A s the lung con tracts i t pulls-on the o ld pleura l adhesions and o ften
makes the pa tien t feel very un comfortable.
‘
Sometimes the patien t complains
of an aching and again a feel ing of pressure as though he were placed in a vice.
M any of the,
acute pleural pain s are treated as in tercostal neura lgias and many
of‘
them as mya lgias. I t seems far fetched to pass beyond the pleura in o rder
to ascribe the origin of these pa ins to the in tercosta l nerves and muscles .
The treatmen t of pain of pleura l origin depends on whether or not i t is acute.
N o matter wha t its character, the applica tion of tin cture of iodine may be of
some value ; in fact, for the less severe pa ins i t is the on ly measure necessary .
I f very acute a blister maybe employed, but th is in terferes with strapping which
is the measure tha t offers the greatest relief in such cases . E i ther dry or mo ist
heat applied in the form of hot wa ter bo ttles or hot wet packs is of grea t value.
I f the pain is a muscular soreness from excessive coughing i t will quickly dis
appear when the cough is rel ieved, al though the application of mo ist or dryhea t may hasten its disappearan ce.
INSOMN IA .
Tuberculous patien ts o ften sufler from insomn ia. I t may be due to many
causes the same as i t is in non - tuberculous subjects. When i t persists i t is
wel l to th ink of an increased gastric acidity . I f due to this i t may be rel ieved
by a large do se (o ne-hal f to o ne dram) o f bicarbona te o f soda : but this should
be used o n ly tempo rarily un til the co nditio n is co rrected . I t is no t wel l to
start these patien ts to using hypno tics , fo r i t is quite easy fo r them to learn
to depend upo n them . S imple measures, such as a l ight supper where diges
278 PULM ON ARY TUBE RCULOS I S
sanatorium and tubercul in treatmen t, when the areas wh ich were the seat of
recen t invo lvemen t began to heal out.
When the shortness o f breath is due to in traabdominal pressure from gas,
a proper di et Should be prescr ibed and o ther appropria te measures should be
directed toward rel ievin g the accompanying indigestion . When pleurisy and
pneumo thorax are the cause,these complica tion s must be treated as directed
in Chapter X I X .
The early toxic dyspnea yields quickly to the genera l treatmen t for tuber
culosis, while that due to m ixed in fect ion yields on ly when th is compl ica t ion
improves o r disappears, and tha t o f acute miliary tubercu losis lasts un til the
death of the patien t .
When the embarrassmen t is of cardiac o rigin ,rest , together with suitable
aids to the circula tory system such aS'
strychn ia and n i troglycerine, seems to
act well . This also is o f va lue when there I S much fibrosis presen t in the lun g .
N ervous dyspnea yields to suggestion ; if i t does no t, mild sedatives may be
used .
Q
When dyspnea is very urgen t i t may ca ll for codein ,hero in or morphia .
These remedies wil l prove mo re efficaciousin severe dyspnea than any.o thers
which I have tr ied, yet they should be used on ly in the rarest instan ces. They
should no t be considered at al l in dyspnea of a mild grade nor when they
must be used'
for a pro longed period,un less i t be to make the last days of
l ife comfortable.
SYMPTOMS ON THE PART OF THE GA STRO-lNTESTlNAL TRACT.
The importan ce of keeping the gastro - in testinal tract in a heal thy condition
in tuberculosis can no tbe overest ima ted . The difficulties in the way aremany,and will o ften tax the Skill of the physician and
‘
the patien ce o f the pa tien t .
While I am no t willing to accept the sta temen t,which is so common ly made,
tha t the cure of tuberculosis is a ma tter of nutrition , yet I am willing to recog
n ize the fact that a healthy condition on the part o f the gastro - in testinal trac t
is o f the greatest importan ce to the pa tien t who wishes to make a fight for the
recovery o f heal th . The cure of tuberculosis comes about through the estab
l ishment o f immun i ty on the part o f the o rgan ism to the tubercle bacillus
and its toxins ; and, while pa tien ts can accomplish this in spite of gastro - in tes
tinal complica tions, yet it is but reasonable to suppose tha t a strong . wel l -nour
ished individual will be mo re likely to be able to secure an immun i ty than o ne
who is poo rly nourished , fo r we Should expect the body tissues o f the fo rmer
to be mo re respo nsive to the st imula tion o f the toxins in the productio n o fdefeu
sive bodies than tho se o f the la tter . A tten tion to the gastro - in testinal tract ,then ,
while no t everything , is very impo rtan t .
I n the trea tmen t o f symptoms o n the part o f the digestive appara tus , proper
TRE ATM E N T O F SYM PTOM S 9
diet and co rrect methods of eating should take the place of drugs as far as is
possible. The diet should,be carefully suited to the digestive condition .
pa tien t should be trained to eat slowly and chew thoroughly . H e should have
his meals at regular in tervals and at the same hours each day. This is most
importan t in o rder to main tain the best d igestive resul ts. For suggestion s as
to the method of handling the variousc omplications on the part of the digestive
system I will refer my readers to Chapter XI I .
CHAPTER XX I .
THE RE LATI ON SH I P BE TWE E N TH E PHYS I CIAN AND THE
PATI E NT.
The rela tion ship between the physician and the pa tien t suffer
iiiifigén ing from chr on ic pulmonary tuberculosis must be one of
Phys ic ian and unusual candor,confidence and trust . T uberculosis is a
s z
l
gsghry.
disease which heals slowly,con sequen tly this relation ship
is one tha t must n ecessaril y extend over a long period of
time. A t best,i t w il l exist for several mon ths and o ften extends over sev
eral years .
This rela tionship should be in sti tuted upon the very fir st visi t of the pa tien t .
I t should be assumed that,when a pa tien t con sults a physician
,he comes to
learn the truth . There is due the patien t from the physician a di agnosis,a
progn osis,and the outline of a ra tion a l treatmen t ; on theo ther hand , there is
due the physician from the patien t confiden ce and a wil lingness to obey in
struction s.
Con trary to wha t should be,the rela tion ship between physician and patien t
o ften begin s as one of deception ,the patien t furn ishing misleading in forma
tion and the physician ei ther fa iling to find the '
nature of the tr ouble or misin
forming the patien t i f he does.
Whoever would treat tuberculosis,or whoever would be
Grea t trea ted for i t, should be conversan t with these three facts:R espo n sibi li tyon Phys ic ian s .
first, tuberculosi s I S a commun i cable d isease ; second , i t I S a
preven table disease, and,third
,i t is a curable disease. I t
should a lso be known tha t the earlier the disease is detected the less danger
there is of its being commun icated to o thers,providing the proper precau tion s
are taken,and the greater the opportun i ty of its cure
,providing the proper
remedial measures are insti tuted .
There is a grea t respon sibil i ty upon the physician who is consulted by a
pa tien t suffering from tuberculosis ; fo r , upon his advice depends very largely
the course pursued by the patien t . I t is necessary fo r the physician to know
bo th the hopeful and the hopeless side o f tuberculo sis . H e should know that ,when the disease is discovered early and trea ted in an in tel ligen t man ner,i t is the mo st curable o f a l l chro n ic d iseases. H e should a lso know tha t when
i t is discovered la te o r when disco vered early but al lowed to go o n,i t is o ne o f
the most fa tal o f a l l diseases . The curabil ity depends Upo n the abili ty o f the
280
28 2 PULM ON A RY TUBERCULO S I S
make a physica l examination of the chest sufli cien tly thorough to defin i tely
decide whether or no t an in cipien t tuberculosis is presen t, they Should all be
ab le to recogn ize the symptoms of early tuberculosis and to take the tempera
ture of the pa tien t, and if: there are suspicions of early tuberculosis they shoul d
give or have some one give the tubercuhn tes t, or if the disease is sufficien tly
advan ced for expectoration to be presen t, no matter how sl ight its amoun t,they should ei ther examine i t or have i t eitamined for tubercle bacil li . I n
these early cases, the best in terests of the pa tien t demand a diagn osis, and
i f the a ttending physician can no t establ ish one, he should call a consultan t , the
same as is done in o ther di seases when there is doubt . When the diagnosis
has been established, then there are abso lu tely n o grounds for secrecy o r
deception . The best in terests of bo th the patien t and his associates demand
tha t the truth be known .
The feelings of the pa tien t should always be spared as muchThe Pa ti en tSho uld be To ld as 15 possible, and he shoul d be appr1sed o f ll l S condi t1on
Eaa
n n
H
e?an e in a humane manner . I f he has n ot suspected the n ature
of his i lln ess he wil l be somewhat surprised and doubtless
somewha t depressed . I f he has suspected i t he wil l‘
n ear ly always be re
l ieved at knowing the truth ; for , rightly or wr ongly people place grea t confi
den ce in their physician ,and when
_ they know tha t he knows wha t is the mat
ter with them,they feel that the way is open to recovery ; but if they think
that he does not kn ow,they feel helpless.
When I make a diagnosis of tuberculosis I make i t a rule to always tel l my
pa tien ts. I have had anxious paren ts and brothers and sis ters implore me
no t to do so,but with a few momen ts’ reason ing I have nearly always con
vinced them of the wisdom of such a course. The most difficul t posit ion s in
which I have been placed in th is regard have been due to instructions from
the patien t ’s physician . Very o ften a patien t comes to my oflice bearing a
letter from his home physician in which the well -mean ing medical adviser
requests me to make a thorough examination of the patien t , but implores
me no t to in form the patien t as to the nature of the trouble. Such requests
I am bound to respect , because the patien t is no t my own , but at the same
time i t preven ts me from talking in tell igen tly with the patien t and giving
h im the advice which he should have.
When a patien t is informed tha t he has tuberculosis he should at the same
time be to ld tha t i t is a curable disease. H e should furthermore be to ld tha t
i f he wishes to affo rd h imsel f the best opportun i ty o f cure, i t is necessary fo r
him to know the na ture o f the disease, o therwise he will do th ings tha t he
sho uld no t do and omit do ing things tha t he Should do . I t is a lso necessary ,
fo r him to know in o rder tha t he may take precautio ns against rein fecting
h imsel f and in fecting his immedia te friends who asso ciate in timately with
h im . H e should a lso know tha t when he has so conducted h imsel f as to
RE LAT I ON SH I P BETWE E N TH E PH YS I C I AN A N D TH E PAT I E N T 283
preven t scattering in fection among his friends and associa tes,he has also
taken the precaution s which are n ecessary in order to preven t rein fectinghimself . H e should also be assured tha t if he takes proper precaution s he isa perfectly safe compan ion wi th whom to associate. When a patien t has beenin formed tha t he has tubercul osis , he is no worse than he was before he kn ew
it ; on the c on trary he is better, for‘
he can now take in tell igen t steps toward
gettin g. wel l .
Co -opera tion ofI n order to obtain satisfactory results in trea ting disease
,
Pa tien t an d i t is necessary to_
have the co -opera t ion of the patien t,an d
Physi ci an espec ially is this true in treat ing such a chron ic d isease asN ecessary.
tuberculosis, where the pat ien t, though feel in g wel l a good
part of the time, must be kept in terested in treatmen t for mon ths . I t is a l l
but impossible to secur e this co - operat ion un less the patien t kn ows why it is
required . I t must seem strange to a pat ien t to be asked to rest,remain out
of doors, d ivorce h imself from'
his business,and fo llow out o ther in struction s
which are usuall y given to the tuberculous, when he has n o defin i te idea why
he is do ing it . H ow can a physician give a sat isfactory explanation of the
slowness with which the patien t improves if he has to ld him that i t is on ly“ throat trouble?” H ow can he sat isfy hi s scien t ific Spir i t by exp la in ing everyexacerbation as being due to “
la gr ippe,
” “ bron chitis” and“asthma?” I S
i t anywon der that pa t ien ts so tr eated become discour aged and usually go down”
to dea th I s i t anywonder that physic ian s who trea t their cases in th is mann er
have li ttle fa ith in the curab i l ity of tubercul osis? We could n ot expect such
a po licy of decept ion to in spire suflflcien t confidence to t ide over cr ises of
d iscouragemen t . What is of equal or even grea ter importan ce is that such a
course deprives the wel l of that protect ion wh ich is due them which comes
from the pat ien t fo llowing out proper rules of liv ing and a ttending carefully
to . his personal hygien e, seeing that al l bac ill us- bear ing d ischarges are care
full y destroyed,and min imiz in g al l chances of conveying in fection .
I f th is relation sh ip of candor and confiden ce between the physician and
pat ien t is en tered upon at the beg inn ing of their relation s i t w i ll be on e of the
strongest'
assets of their assoc iation . I t g ives the pat ien t confiden ce which
w i ll support him through many trials and discouragemen ts, and i t assures
the physician of a co -operation that w ill spur h im on to his best endeavors .
T uberculosis is a many s ided d isease. I t affec ts al l the lead ing systems
of the body ; the respiratory, the circul a tory, the d igestive and n ervous systems
being espec ially in fluen ced,and yet, with it al l , the pat ien t, for the most part,
does n ot feel i ll . H e has many symptoms which cause him discomfort and
in conven ience,wh ich w i ll come to the physic ian ’
s n o t ice. The manner in
which these symptoms are dea l t wi th depends very much 011 the nature of
the phys ic ian as well as upon the nature of the pat ien t .
The man who treats tuberculosis,should possess a comprehen sive under e
284 PULM O N ARY TUBE RCULOS I S
stand ing of the d isease, and should al so be conversan t wi th the psycho logy
of the tuberculous pa tien t . These two qua l ificat ions are ind ispen sable to
him i f he w ishes to secure any measure of success.
N o two physic ian s can deal with their patien ts exactly alike,and no physician wil l trea t al l his patien ts in exactly the same
way. Personal ly, I'
obtain best results by mak ing my patien ts
in tel ligen t on the subjec t of tuberculos is . I endeavor to
explain to them the n ature of the d isease, something of its course,the ditfi
culties in the way of cur e, the complications, the a ids to cur e,and wha t they
can do to help , a lways impressing upon them tha t the result depends very
largely upon themselves. This in str uction is done ei ther by conversa tion
as I meet the pat ien t in the office or by lectures as I carry i t out at the Sana
tor ium . These occasiona l lectures have been most helpful to the pa tien ts
and have had a remarkable influen ce in en couraging them and spurring them
on to an in tel ligen t co- operation . I do n ot fear an in tell igen t pa tien t,but I
have had the most difli culty w ith those who have precon ceived ideas andwho
are not suscept ible to n ew light . I make i t a rule no t to ask my patien ts to
do anything for which I can no t g ive them a reason . My reason may be
wron g,but if i t sounds plausible i t helps to secure co -opera tion . I t removes
tha t barrier of mystery which has so long separa ted the physician and patien t,and brings them
“
close together .
Tuberculous pat ien ts must be under the guidan ce of the
ggggglil
ggf e“ phys ic ian for mon ths and o ften years . Th is con tinuous
an d Pa t ien t. assoc iation brings about a feeling of in terest and nearness ,which a ids in the production of favorable results . I do n ot
believe i t is possible for a phys ician to procure as good results in the treatmen t
of tuberculous pat ien ts by ho ld ing h imself a loo f from them and treat ing them
co ldly , as by en tering in to their lives, tak ing keen in terest in their welfare and
showing them tha t he is endowed Wi th the m ilk of human k indness. Such
a physic ian ishonored for his knowledge and revered for his charac ter . H e
commands confidence on the part of his pat ien t, no t on ly because the pa t ien t
thinks i t o ffers him the best opportun i ty of cure but also because his own
personal i ty demands i t .
There is a common misconception to the eflect that there isTuberculousPa t ien ts N eed no treatmen t for tuberculosi s. Th is comes from the teach i ngPhysiCian
’S that there is no dr ug wh ich has a specific ac tion . Physic ians
Gu i dan ce .
very o ften,when they d iscover the d isease
,tel l their pa t i en ts
tha t n o th ing can be done for them, but tha t they must be cured by getting out
in the air . This a ttitude is wrong . The phys ic ian can do much fo r the
tuberculous pa tien t, in fact he can do as much for h im as he can fo r a lmo st
a ny o ther k ind o f pa tien t . The tuberculous pat ien t is no t o ne to be neglected
if favo rable results are desired . I have heard phys ic ians say tha t the tuber
CHAPTER XXI I .
RE SULTS AN D PE RMANE NCY OF RE SULTS I N PULMONARY
TUBE RCULOS I S .
A few years ago there was n o organ ized effo rt to treat tuberculosis . There
was n o systemat ized method of treatmen ti
for the d isease ; in fact , n o o ne
thought i t curable. I t was recogn ized in its advan ced stages on ly and was
always con sidered hopeless .
‘
From time immemorial tuberculosis has been
known and a lways considered a fatal d isease .
I t is no wonder that Brehmer was con sidered insan ewhen,
The Begi n n i n gof Systema t ic i n the m iddle of the past cen tury
,he declared that tuberculos is
Trea tmen t 5” was curable. H e adduced as ev idence to prove his assert ionTubercul o si s . .
the results of post-mortem findi ngs,but could n ot convmce
his unwil ling con freres . So posi t ive was he of his convict ion that he started
a sanator iuma t G oerbersdorf,which is known by his name,and began the
treatmen t of tuberculosis . Th is in stitut ion was founded in 1859 and was
the first successful attempt at the systematic treatmen t of this d isease. Wh i le
we must give Bodington cred i t for the first attempt at adopt ing the fresh air
treatmen t of tuberculosis, yet i t w i ll be recalled that his experimen t failed .
H is pat ien ts were driven from him and the in st i tution was turn ed in to an
asylum for the in sane. Bodington’s con freres undoubtedly thought th is a
very appropr ia te end ing of such a pro ject and would gladly have seen its
founder an inmate.
Tuberculosis was made the subjec t of much study during the past cen tury .
Among the great m inds tha t were turned toward so lving the various problems
con nected with i t,may be men t ioned Bayle,Lou is, Laennec ,Virchow ,
V il lemin
and Koch . A t the begin n ing of the cen tury very little was actual ly known o f
tuberculosis,but before the sixth decade had passed , the relat ion ship between
the tubercle and tuberculosis had been establ ished,the d isease had been
proven by the exper imen ts o f V il lemin to be transm iss ible, and Brehmer had
pron ounced i t curable and had succeeded in mak ing his op in ion good .
E ffec t o f The sc ien t ific world was,therefore
,somewhat prepared fo r
Ko ch ’s the announcemen t made by Ko ch o n the 24th o f M arch ,
D i scovery.1882 (
“D ie Aet io logic der Tuberkulose,
” Berl in . kl in ische
Wochenschr ift,N o . 15 , 1882) tha t the cause o f tuberculos is was the tubercle
bac i llus . Th is d iscovery , however, revo lut io n ized the op in ion o f the wo rld
regard ing this d isease,and by so do ing really made i t easier to carry out
revo lut io nary ideas regard ing its preven tion and cure.
286
RE SULT S I N PULM ON ARY TUBE RCULO S I S 287
Th is d iscovery of Koch ’s is further reach ing in its effect upon the world
than is genera lly bel ieved, for i t has given us the key to preven t ive measures,it has st imulated early d iagnosis and thus brought the d isease under trea tmen t
at a favorable time ; i t has Shown the n ecessity of hygien ic livin g on the part
of the afli icted, _and i t has opened up the way for the rational trea tmen t of
the d isease.
Whi le Brehmer main tained that tuberculosis is curable, Koch put in to his
hands the means by wh ich it can be d iagnosed early, when i t is'
most curable.
M odern refinemen ts of d iagnosis by mean s of wh ich we are enabled to detect
the very early changes in tuberculosis are dependen t,fir st
,upon Koch’
s dis
covery of the tubercle bac i llus and then upon his later discovery of the diag
n ost ic va lue of the tubercul in test .
I n sp i te of the great amoun t of study which was directed
toward tuberculosis, and in spite of the work that Brehmer
was do ing, the idea of trea tmen t in tuberculos is grew slowly .
The san a tor ium at Falken stein ,wh ich was so ably directed
by Brehmer ’s pup i l, Dettwei ler, was founded in the seven t ies. A t lon g ih
terva ls new in sti tution s arose un til final l y the sana tor ium treatmen t of this
d isease began to take'
ser ious ho ld on the scien t ific world . N ot much
creden ce, however, was given to the curabil ity of tuberculosis un t i l the past
fifteen years— one mi ght a lmost say un t i l thepast ten years . . D ur in g this t ime
suffic ien t eviden ce has been amassed to prove beyond cav i l tha t tuberculosis is
a curable disease, one which w i ll yield to systema tic,in tell igen t trea tmen t .
Th is conviction has now possessed the en tire world and everywhere the
treatmen t of tuberculosis is being prosecuted with vigor .
I t is a source of grea t pr ide to this coun try to have producedAmericanPion eers in severa l of the p ioneers in the treatmen t of th i s dread di sease.
The first priva te sanator ium in the Un ited S tates was estab
l ished by Dr . J . W . G leitzmann,in 1875 . Trudeau
,driven
in to what at the time seemed ex i le, wen t to the Ad irondacks and in 1884 es
tabl ished the first sana tor ium for the trea tmen t of the tuberculous poor’
on the
western con t inen t . The Ad irondack Co ttage San i tar ium today stands as
the agen cy through wh ich hundreds of c i t izens have been restored to hea l th ,and is a fitting and perpetual monumen t to its founder . Bowditch soon took
up the grea t work and founded the Sharon Sanator ium near Boston . O t is,Kn ight
,Whittaker
,von Ruck, Fl ick , So lly and o thers soon fo llowed .
While there is st i ll much doubt in the m in ds-“
of many peopleTPbef CU IO S I S
: as to the curab i l i ty of tuberculosis,th is doubt is due to a
Yi elds Readi lyto Trea tmen t . lack of acquai n tan cesh ip W i th fac ts
,or a W i llful d i sregard
of them .
When we have con s idered the matter'
carefully in the light of the results
that have beeri obta in ed,we must
'
con clude tha t tuberculosis when in tel l i
288 PULM ON ARY TUBE RCULO S I S
gen tly treated is n o t such a dreadfuhy hopeless d isease after al l . I t o ffers
about the same hope o f cure as do o ther ser ious diseases and y ields even
better results than any o ther chron ic d isease.
I mprovemen t can be obta ined in nearly all patien ts suffering from pul
mon ary tuberculosis un less they be in extrenzz’
s when the proper trea tmen t
is insti tuted . N early a l l inc ipien t cases and quite a large percentage of those
farther advan ced can be relieved of all active symptoms,so that they may be
able to l ive for years and lead l ives of usefulness.
The resul t obtained in the treatmen t of tubercul osis depends
First,Upon the earliness of the diagnosis .
Secondly, Upon the in tel l igen ce of the treatmen t and the promptness w i th
wh ich i t is in st i tuted .
Th irdly,Upon the abili ty and w i llingness of the patien t to carry out in struc
tions .
Under the most favorable circumstan ces the results of trea tCure D epefl ds men t are very en cour aging, the lesion can be hea led in nearlyupon E arli n esso f D iagn o sis.
al l instan ces, and the resul t can be accompl ished in a com
paratively short t ime. Of course this statemen t implies a
diagnos is in the incipien t stage, the prompt adoption and the fa i thful prose
cution o f rationa l trea tmen t . I f circumstan ces. are less favorable, that is,
i f the d iagnosis is n otmade‘
so early,or
,i f made early
,time is wasted in adopt
ing and carrying out a suitable therapy, then the result will be correspondingly
un sa tisfactory .
The relationship of early d iagnosis to a favorab le result is well Shown by
stat istics from inst i tution s wherein patien ts of al l stages are treated . From
these results we may conclude, as men tioned at the beginn ing of the chapter
on D iagnosis of E arly Tuberculosis, tha t if medical men would expend but a
fract ion of the energy in learn ing to d iagnose tuberculosis early that a few
sc ien t ists are expend ing in endeavor ing to d iscover a “ cure” for i t, we would
be able to say that the cure for tuberculosis is already at hand .
I have arranged in Tables I and I I the results of treatmen t from several
American sana toria . These reports prove the assertion that tuberculos is
is a curable disease and Show more plain ly than any argumen t that I can
make the necessi ty of early d iagnosis and immediate treatment .
M any ind ividuals, bo th among the med ical pro fession and the la i ty,fai l
to rea l ize the importan ce of early treatmen t o f tuberculosis . I f the expression“do i t now ”
can be appl ied anywhere, i t can no tbe applied with more mean ing
than when i t refers to the treatmen t o f tuberculosis when an early diagnos is
has been made.
Table I I shows wha t delay mean s . Whereas of 1896 early
'
cases,1 188 o r
70 per cen t were apparen tly cured,o f 2138 moderately advanced on ly 538 ,
o r per cen t were apparen tly cured,and o f 106 2 far advanced o n ly 136
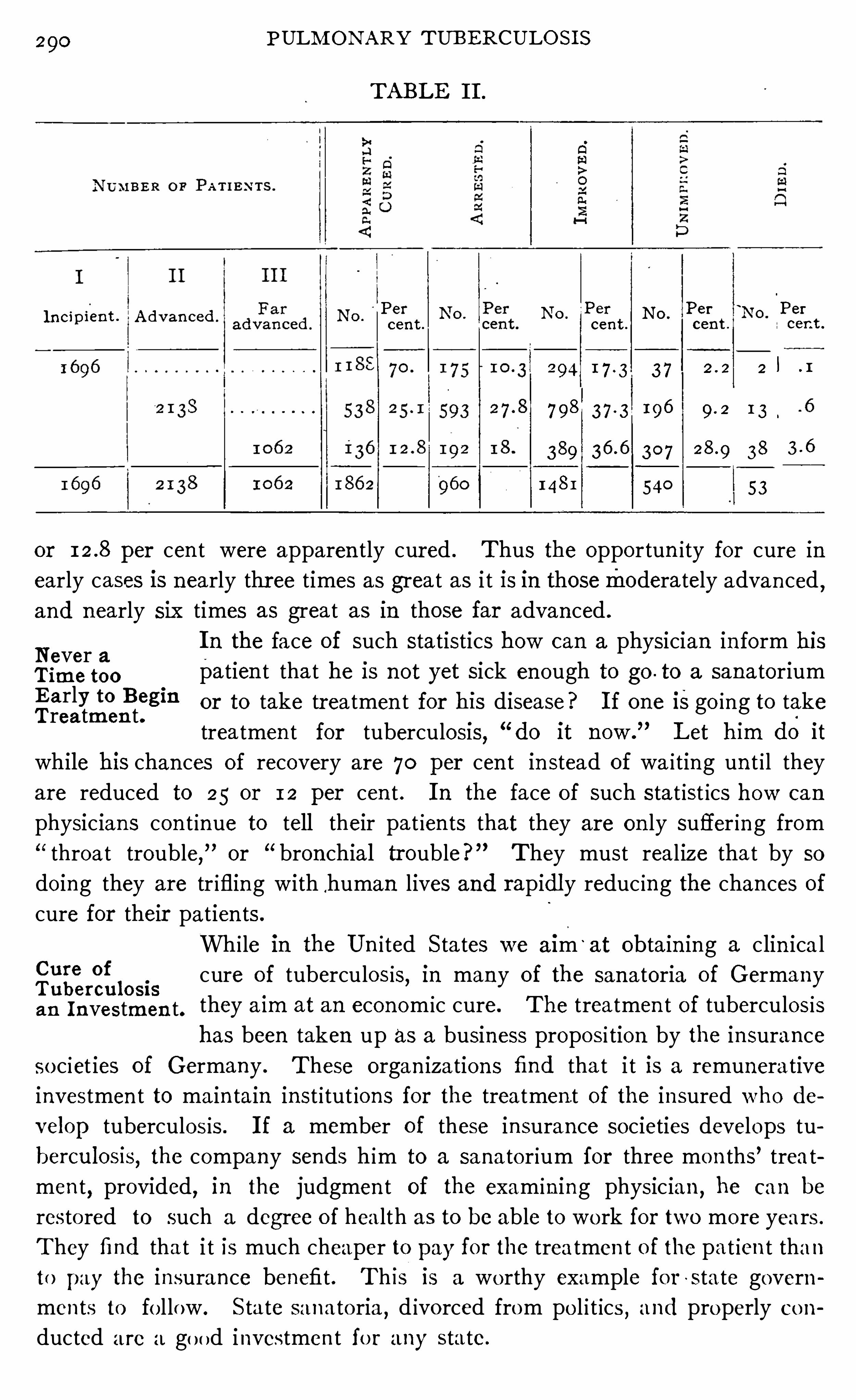
290 PULM ON ARY TUB E RCULO S I S
TABLE I I .
~ Per r 1 Per Per 1
“
PerI n c i p i en t . A dvan ced N O '
cen t .
l\o . I\O .
cen t .
N o .
cen t .
l\ocen t .
294 3 7 2 l . 1
7 98 3 7 -3 196 9-2 I 3 .
389 30 7 38 3 -6
148 1 540 53
or per cen t were apparen tly cured . Thus the opportun ity for cure in
early cases is n early thr ee times as grea t as i t is in thosemoderately advan ced ,and n early six times as great as in those far advan ced .
N ever aI n the face of such statistics how can a physician in form hi s
Time too patien t tha t he is n ot yet sick en ough to go . to a sanatoriumE arly to Begin or to take tr eatmen t for his disease? I f one isgo ing to takeTrea tmen t.
trea tmen t for tuberculosi s,
“do i t now .
”Let him do i t
wh ile his chan ces of recovery are 70 per cen t in stead of wa i ting un t i l they
are reduced to 25 or 12 per cen t . I n the face of such s tat ist ics how can
physic ian s con t inue to tell their pa t ien ts that they are on ly suffer ing from
throat trouble,”or
“ bron chial trouble?” They must real ize tha t by so
do ing they are tr ifling with.human lives and rapidl y reduc ing the chan ces of
cure for their patien ts .
Whi le in the Un i ted S tates we a lm ‘
at obtain ing a c lin ica l
rzii l osis cure of tuberculosis,in many of the sanatoria of Germany
an I n vestmen t. they a im at an econom ic cure. The treatmen t of tuberculosis
has been taken up as a business proposi tion by the insurance
so c iet ies of Germany . These organ ization s find tha t i t is a remunerative
investmen t to ma in tain inst i tut ions for the treatmen t of the insured who de
velop tuberculos is . I f a member of these in suran ce societies develops tu
berculosis, the company sends him to a sanatorium for three mo n ths’ treat
men t,provided
,in the judgmen t of the examin ing physic ian ,
he can be
resto red to such a degree o f hea lth as to be able to wo rk for two mo re years .
They find tha t i t is much cheaper to pay for the trea tmen t o f the pat ien t than
to pay the insurance benefi t . Th is is a worthy example fo r -state govern
men ts to fo l low . S ta te sanato ria,d ivo rced from po l i t ics , and properly co n
ducted are a go od investmen t fo r any state.
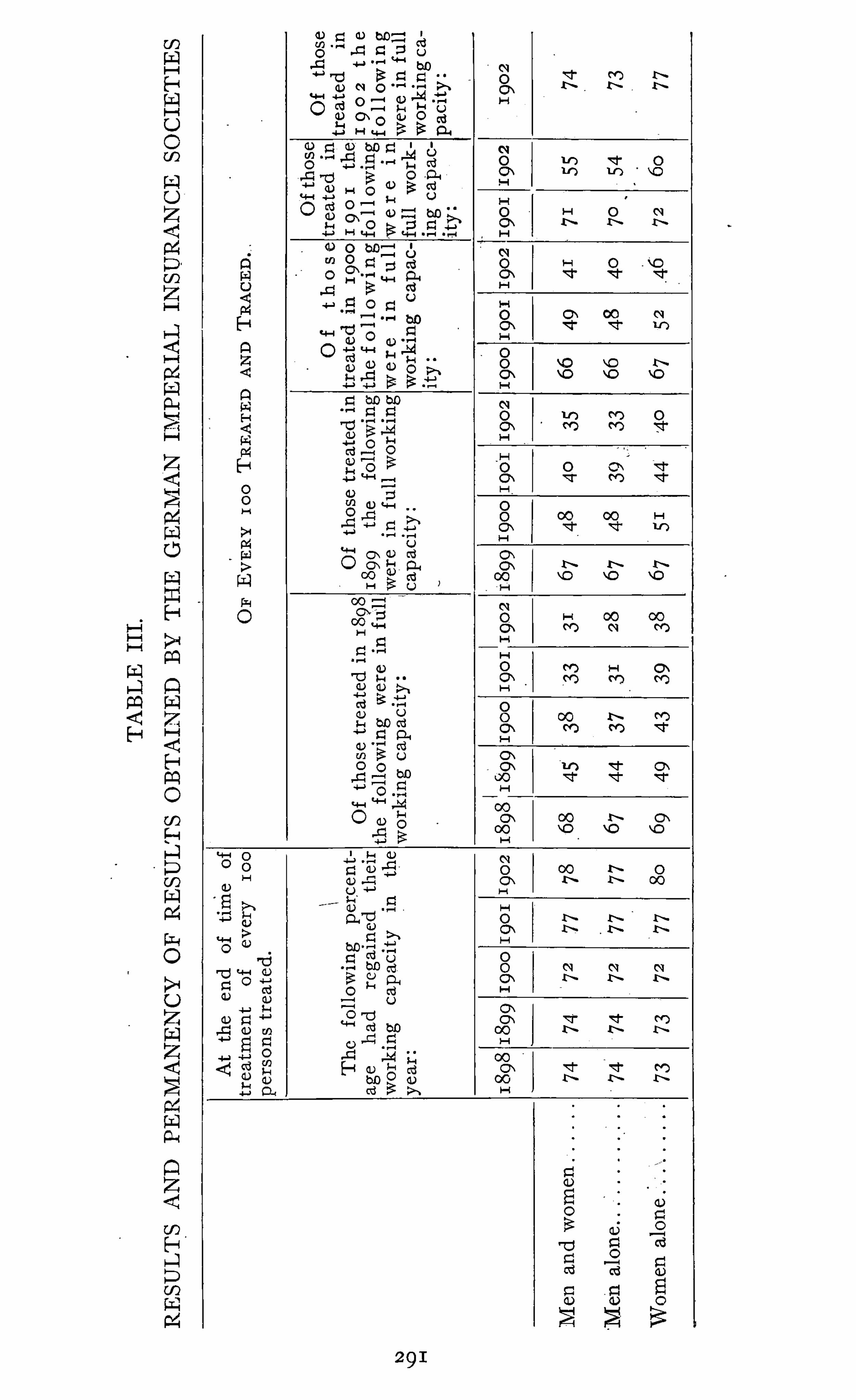
292 PULM ON ARY TUBE RCULOS I S
The statistics of the I mper ia l I nsuran ce Company Show tha t tuber
culous men and 4302 tuberculous women were treated at the expense of the
I nval id I nsur an ce Compan ies in 1902 . Of this number,el iminat ing those
who in terrupted treatmen t with in two weeks,8 1 per cen t were restored to
full earn ing capacity ; in clud ing them,the percen tage was 78 .
Table I I I (D er S tand der Tuberkulose Bekampfung im Fruhjahr , 1905)Shows the results which were obtained duri ng the years 1898
—1902, a lso the
permanency of such results.
The Prusso -Hessian Ra i lway Company has also assumed responsibilityfor the treatment of its employes, and during the year 1904 furn ished treat
men t to 7 16 . These pat ients were treated on the average days, which
a l l must recogn ize as a very short time, too short for best resu lts— vet the
results are most excellen t as shown in Table I V .
This table Shows a lso the permanen cy of results obtained from 1898—1904 .
Of course al l pat ien ts so treated must, of necessitv, be early cases in order to
obtain results in so short a time.
While we are o ften disappo in ted in the results of treatmen t ,
gizii‘
l
‘l en tyet bo th physician and patien t have ‘much ground for con
p ro l onygs Life,
gratulation ; for , even where a cure can not be obta ined,the
patien t ’s life can be pro longed . Reiche (“D ie Dauererfo lge
der Heilsta tten behandl ung Lungen schwindsiichter ,” M un ch . med . Woch .
,
N o . 33 , 1902) fo l lowed the after history of 6 83 pa t ien ts who were den ied
adm ission to the sanatoria of the Hansea t ic I nsuran ce Company, mostly
on accoun t of the process being too far advan ced,and compared the length
of l ife w i th those who were treated in the sanatoria . I n the un treated cases
the length of li fe from the first svmptoms of'
the d isease un til death was
forty- three mon ths . I n those treated in the sana tor ia, however,“six to seven
years after the fir st cure per cen t st i ll remain fully capable of work .
”
The treatmen t o f tuberculosis makes an excellen t show ing
i’
ffftiiieifi
also when compared with the treatmen t of o ther chron ic
Compared diseases . The statist ics of the I mperial I nsurance Company
gthl
iarnl‘
sl cil
s
l
.(Amtl iche N achrichten der Reichsversicherungsamtes, 1902
S ta tist ik der Hei lbehandl ung, 1,Beiheft .) furn ish excellen t
Opportun i ty for comparison . S tatistics are ath and o f over insured ,who were treated fo r chron ic d iseases during the years 1897
— 1900. A fay
o rable result was obta ined in from 6 8 to 7 7 per cen t o f the cases of pul
mo nary tuberculosis, and in from 6 9 to 74 per cen t o f o ther d iseases . I n
the seco nd year the co nd i tion was sa tisfactory in 44 to 50 per cen t of the
tuberculous cases,and also in 44 to 50 per cen t o f the o ther cases . I n the
th ird year the sat isfactory resul t had decl ined to 30 to 41 per cen t in the tu
berculous cases and to 39 to 43 per cen t in o ther cases . I ii the fourth year,tha t o f tuberculosis was from 30 to 34 per cen t and that o f o ther d iseases
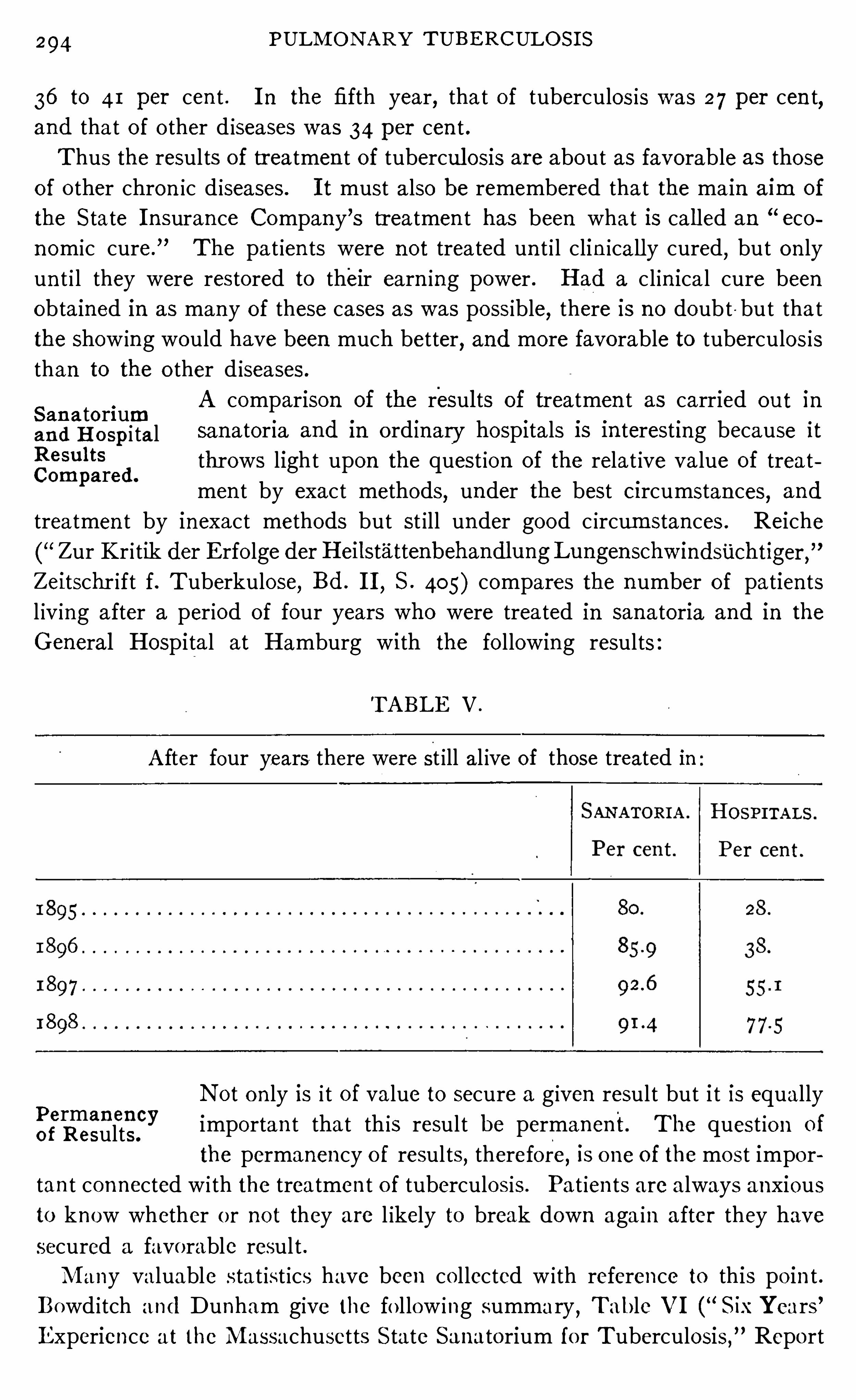
294 PULM ON ARY TUBE RCULO S I S
36 to 41 per cen t . I n the fifth year, tha t of tuberculosis was 27 per cen t,and tha t of o ther d iseases was 34 per cen t .
Thus the results of treatmen t of tubercul osis are about as favorable as thoseof o ther chron ic d iseases. I t must a lso be remembered that the ma in aim of
the S tate I n suran ce Company ’s treatmen t has been wha t is cal led an “eco
n omic cure.
”The pa t ien ts were n ot trea ted un t i l clin icall y cured
,but on ly
un t i l they were restored to their earn ing power . H ad a c l in ica l cure been
obtained in as many of these cases as was possible, there i s no doubt -but tha t
the show ing would have been much better, and more favorable to tuberculos is
than to the o ther d iseases.
A comparison of the results of treatmen t as carried out inS an a tori uman d H o spi ta l sanator ia and in o rdinary hosp i tals i s in terest ing because i t
Res‘flts throws light upon the quest ion of the relat ive va lue of treatCompared.
men t by exact methods, under the best Ci rcumstan ces, and
treatmen t by inexact methods but st ill under good c ircum stances . Reiche
Zur Kr i tik der E rfo lge der H eilstattenbehandlungLungenschw indsiichtiger ,"
Zeitschr ift f . T uberkulose, Bd . I I, S . 405) compares the n umber of patien ts
l iv ing after a period of four years who were treated in sanatoria and in the
General Hospital at Hamburg with the fo llowing results :
TABLE V .
A fter four years there were st ill al ive of those treated in
N ot on ly is i t of value to secure a g iven result but i t is equally
importan t that this result be permanent. The quest io n of
the permanency o f results, therefore, is o ne of the most impo r
tan t connected w i th the treatmen t of tuberculosis . Pat ien ts are a lways anxious
to know whether o r no t they are l ikely to break down aga in after they have
secured a favorable resul t .
M any valuable stat ist ics have been co l lected w ith reference to this po in t .
Bowd itch and Dunham give the fo l low ing summary,Table V I (
“S ixYears ’
Experience at the M assachusetts S tate Sanatorium fo r Tuberculosis,” Repo rt
Perman en cyo f Results.
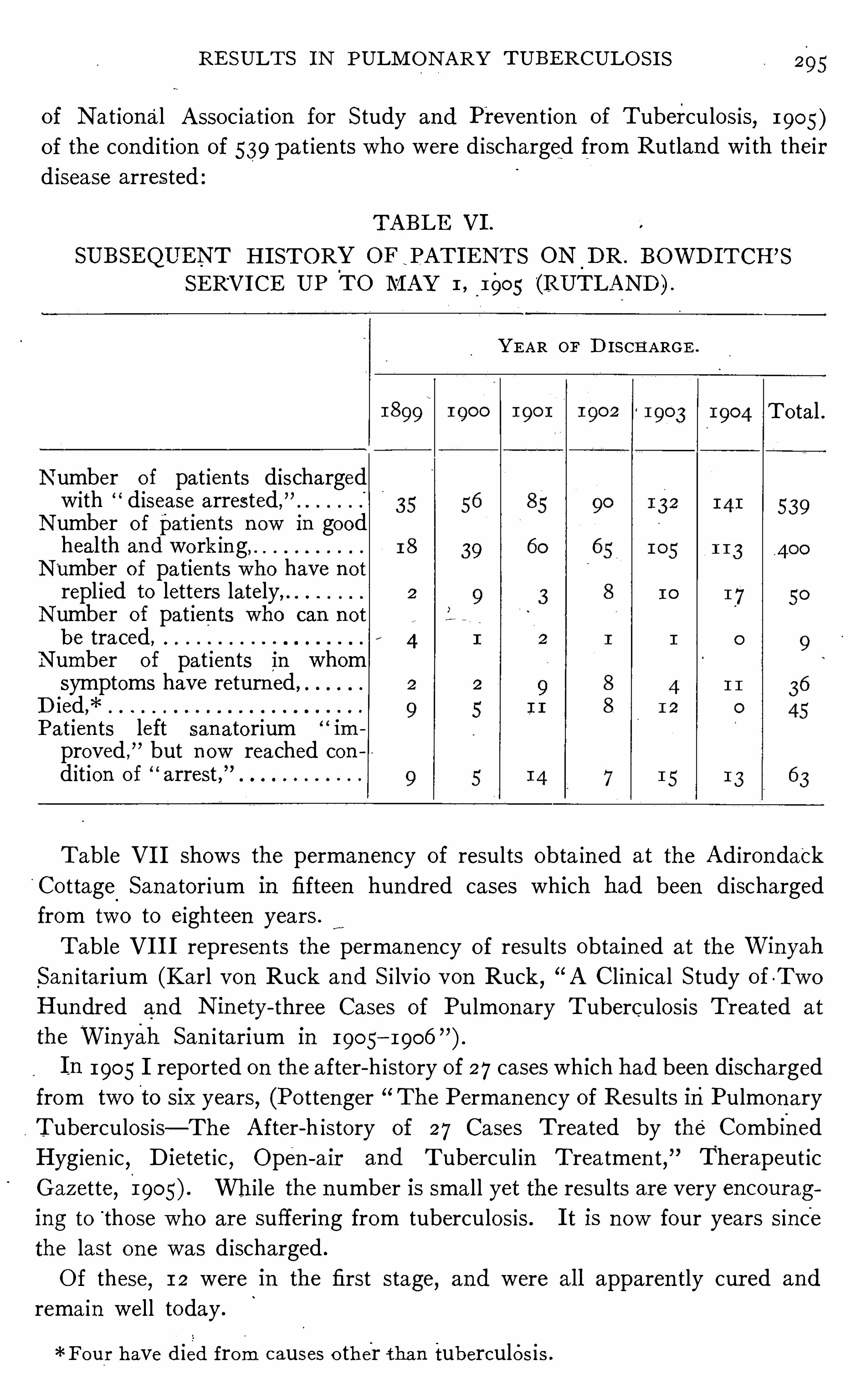
RE SULT S I N PULM ON ARY TUBE RCULO S I S
of N at ional A ssoc ia t ion for S tudy and Preven t ion of Tuberculosis,1905)
of the con d i t ion of 539 pat ien ts who were d ischarged from Rutland with theird isease arrested
TABLE VI .
SUBSEQUEN T H I STORY OF PAT I E NT S 0N_
D R . BOWD I TCH ’S
SE RVI CE UP TO M AY I ,_
1905 (RUTLAN D ) .
YE AR OF D IS CH A RGE .
T o tal .
N umber of pat ien ts dischargedwith disease arrested,”
N umber o f pat ien ts n ow in goodheal th and wo rk in g,
N umber of patien ts who have n ot
repl ied to letters lately,N umber of pat ien ts who can n ot
be traced,N umber of pat ien ts in whomsymptoms have return ed ,
D ied,*Pat ien ts left san atorium im
proved ,
” but n ow reached con
dit ion of arrest ,”
Table V I I Shows the permanency of results obta ined at the Ad irondack
Co ttage Sana tor ium in fifteen hundred cases which had been d ischarged
from two to eighteen years .
Table V I I I represen ts the perman en cy of results obtained at the WinyahSan i tarium (Karl von Ruck and S i lv io von Ruck,
“A Cl in ica l S tudy of -Two
H undred and N in ety- three Cases of Pulmon ary Tuberculosis T rea ted at
the Winyah San i tarium in 1905
I n 1905 I reported on the after-h istory of 27 cases which had been discharged
from two to six years, (Po ttenger The Permanen cy of Results inPulmon ary
Tuberculosis— The A fter-h istory of 27 Cases T reated by the Combined
Hyg ien ic,Dietet ic
, Open - air and Tubercul in T rea tmen t, Therapeut ic
Gazette, 190 While the n umber is small yet the results are very encouraging to
“
those who are suffering from tuberculosis . I t is n ow four years sin ce
the last on e was d ischarged .
Of these,1 2 were in the first stage
,and were al l apparen tly cur ed and
remain well today .
*Four have d ied from causes o ther tha n tuberculos is .
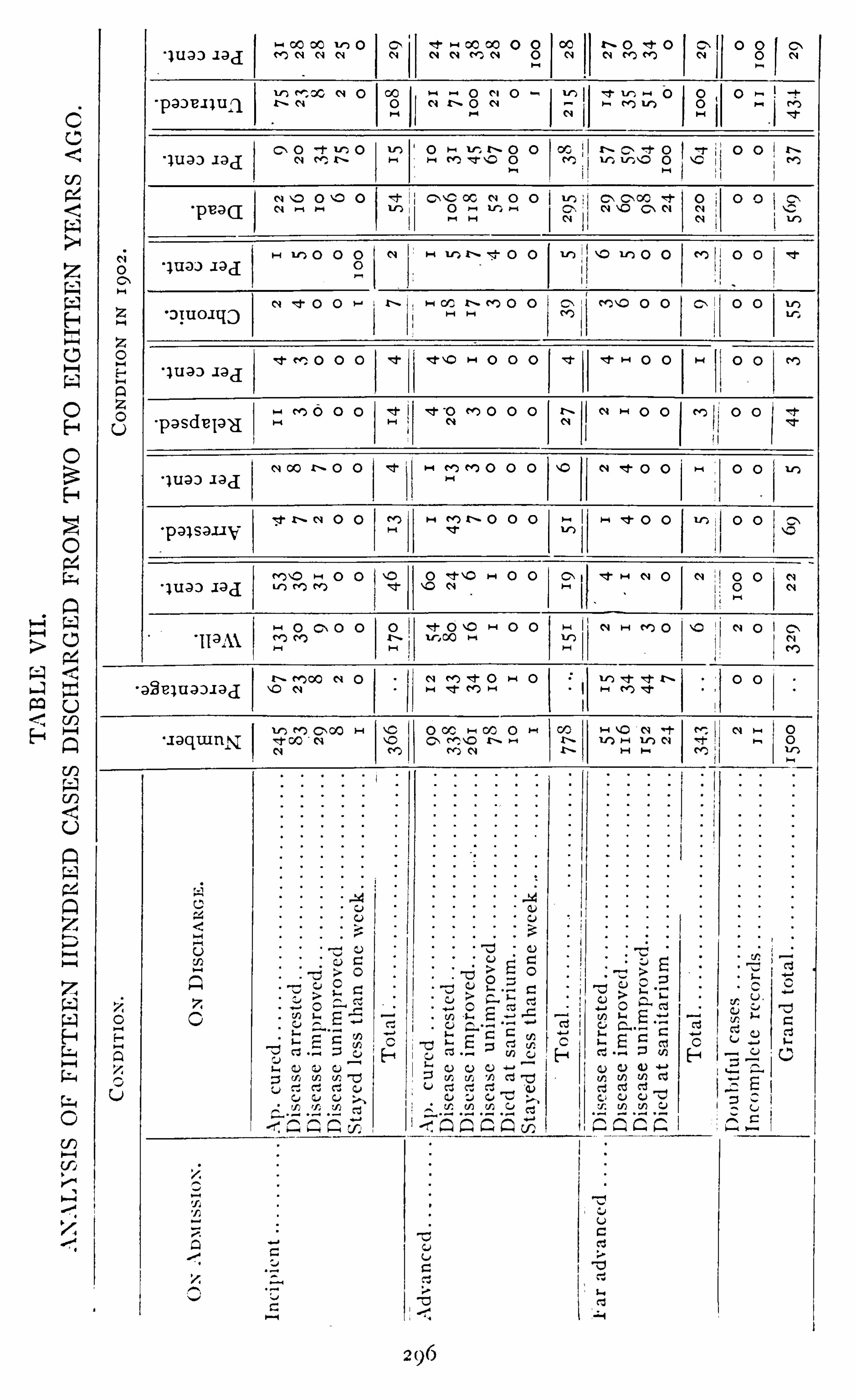
298 PULM ON ARY TUBE RCULO S I S
E ight were in the second stage. Six were apparen tly cured and - rema inwel l today . Two were un improved and d ied .
Seven were in the th ird stage. Two Were d ischarged as arrested and are
l iv ing today, a lthough one has recen tly had a fa i lure in heal th ow ing to hard
work and long hour s . The five who were d ischarged as improved are a l l
dead . The fact that all who were on ly improved d ied, Should n ot d iscourage
any one,for the term of treatmen t was over fi ve mon ths in on ly two cases .
The permanency of results depends very much upon the
ar
remgttiiggegfn condit ion of the pa tien t at the t ime of d ischarge. Tubercu
Trea tmen t Pre losis is a d isease wh ich hea ls S lowly , and the cure can n ot be
hurr ied beyond a certain po in t . Pat ien ts are apt to become
impatien t Over the long t ime that is required and for one
cause or ano ther stop treatmen t, thus depr ivin g themselves of the best results .
Th is is always a m istake, a lthough in many in stan ces i t is unavo idable.
Patien ts should be taugh t that the last few mon ths of treatmen t,when they
seem and feel well and when changes in the lung are not so apparen t to them,
are the most importan t ones from the standpo in t of permanen cy of results .
There is a tenden cy to Shorten the term of treatment in tuberculosis . Th is
is a great m istake, even i n early cases. A n early case should be treated from
four to six mon ths . By giving the requisi te time more cures w i l l result and
they wi ll rema in more permanen t .
When i t is possible to obta in a cure, treatmen t should n ot be con sidered
ended un t i l this result has been atta ined . I n some in stances a second or th ird
course of treatmen t may succeed where prev ious courses have fa i led . Pe
truschky (“Kr i terien und Kon tro lle der Hei lung bei Lungen tuberkulose
,
”
Koch ’s Festschr i ft, 1903) recommends wha t he calls his etappen methode ;
that is subject ing tuberculous patien ts to several courses of treatmen t with
per iods of rest in terven ing . By this method he has been able to secure ex
cel len t results . I n the 10 years from 1893 to 1903 he treated 1 12 patien ts
with this m ethod,with the fo llowing resul ts :
O f the 1 12, 58 were far advanced cases and 54 early cases .
Of the 58 advanced cases, 60 per cen t’
d ied and 45 per cen t were cured .
O f the 54 early cases,most o f whom came from fami l ies with tuberculous
h istory, none d ied, and 54, the en t ire number,were cured .
I n th is con nection i t is well to consider what mav be called
a cure. There is no doubt that this is o ne of our mo st difii
cul t quest ions to dec ide. The mistake is o ften made o f
th inking a patien t is cured simply because he has regained his weigh t and
ceased cough ing and expectorating,o r ceased expecto ra t ing bac i llus-bearing
sputum . A momen t ’s though t w il l show the erro r of th is op in ion,fo r pa t ien ts
may rega in their weight and st ill have act ive tuberculos is , and they may have
in fi l tra t io ns in the lungs fo r lo ng periods o f t ime w i thout bac i l li appearing in
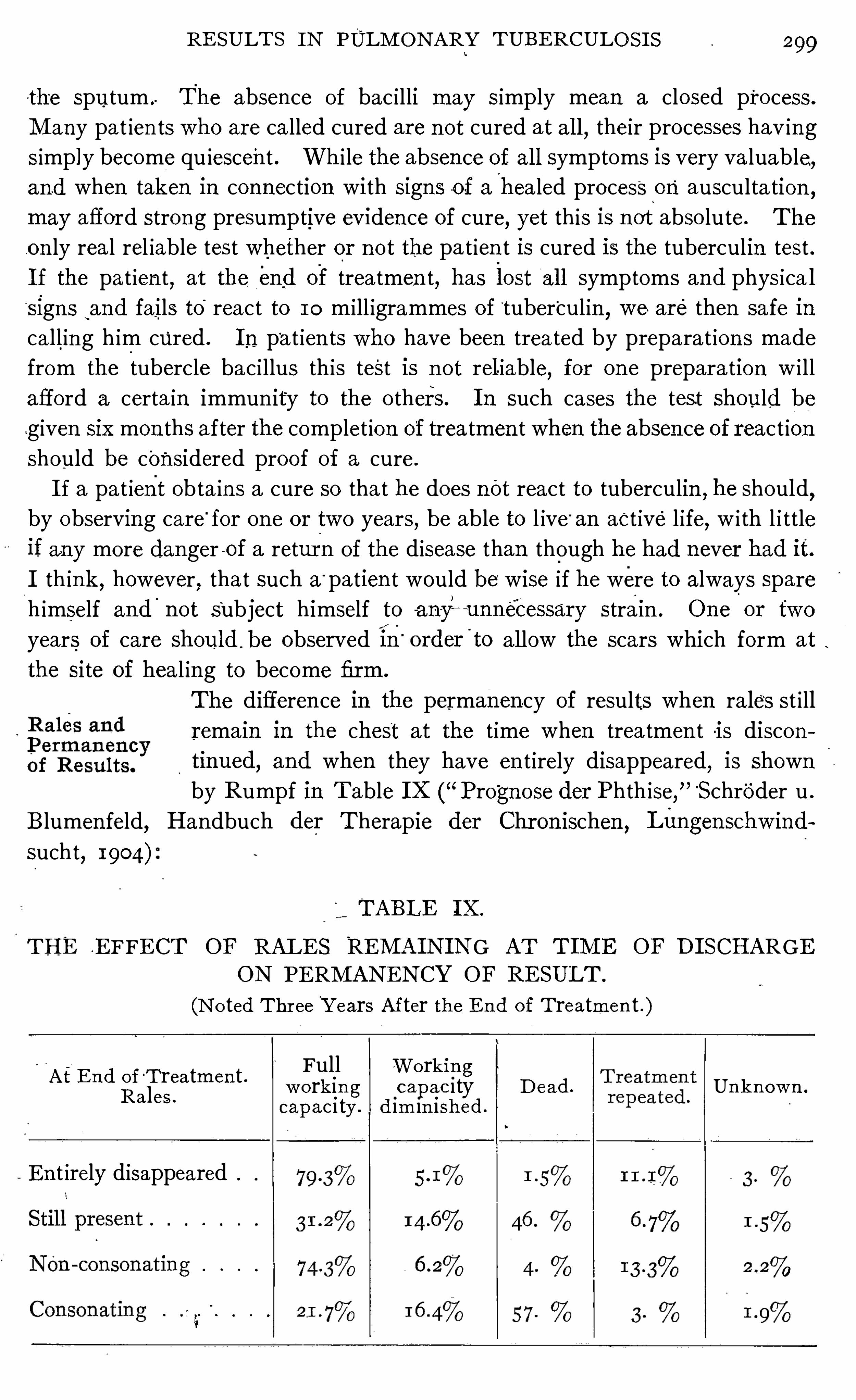
RE SULT S I N PULM ON ARY TUBERCULO S I S
the sputum . The absence of bac i lli may s imply mean a closed process.
M any pat ien ts who are ca lled cured are n ot cured at a l l,their processes hav ing
s imp ly become qu iescent . Whi le the absen ce of al l symptoms is very va luable,and when taken in connection with S igns o f a healed process on ausculta tion
,
may afford strong presumptive eviden ce of cure, yet th is is not abso lute. The
on ly real rel iable test whether or n ot the pa t ien t is cured is the tuberculin test .
I f the pat ien t,at the end of treatmen t, has lost
'
al l symptoms and physica l
sign s‘
and fails to'
react to 10 m i ll igrammes of'tuber
'
cul in,we are then safe in
ca ll ing h im cured . I n pat ien ts who have been trea ted by preparat ion s made
from the tubercle bac i llus th is test is n ot rel iable, for on e prepara tion w i ll
afford a certa in immun ity to the o thers . I n such cases the test should be
given sixmon ths after the complet ion of treatmen t when the absen ce of react ionshould be considered proof of a cure.
I f a pa t ient obta in s a cure so that he does nOt react to tuberculin,he should
,
by observing care“
for on e or two years,be able to l ive“
an act ive l ife,w i th l i ttle
if any more dan ger -of a retur n of the disease than though he had n ever had it.
I th ink,however
,that such a
“ patien t would be wise if he were to always spare
h imself and'
n ot Subject himself to -ah—y~ ~unneCessary strai n . One
'
or two
years of care should . be observed in“
order'
to a l low the scars which form at
the si te of heal ing to become firm.
The differen ce in the permanen cy of results when rale‘
s st i ll
remain in the chest at the t ime when trea tmen t -is discon
tinued,and when they have en t irely disappeared
,is shown
by Rumpf in Table I X (“Prognose der Phth ise,
” ‘
Schroder u .
B lumen feld, Handbuch der Therapie der Chr on ischen,Langen schw ind
sucht,1904)
TABLE I X .
THE E FFE CT OF RALE S REM A I N I N G AT T I lVI E OF D I SCHARGE
ON PE RM AN EN CY OF RE SULT .
(N o ted Thr ee Y ears After the E n d of T reatmen t .)
Full Wo rkin gw ork in g capac ity D ead . Un kn ow n .
capac i ty. d im in ished .
A t E n d ofT reatmen t .Ra les .
E n t irely disappeared
300 PULM ON ARY TUBE RCULOS I S
This also shows that the d ifferen ce in the permanen cy of results when rales
are presen t seems to depend somewha t on the character of the rales . I f thev
are consonating the prognos is is n ot so good as if they are n on - con sonat ing .
I n the l ight of such stat istics of resul ts we can face the future w i th cour age.
We can see tha t i t is possible n ot on ly to preven t tuberculosis,but
,w i th an
early di agnosis and prompt trea tmen t, to cure i t . The enormous waste of
human l ife caused by i t is unnecessary . With a better apprec iat ion of its
hopefulness impressed upon the m inds of bo th physician and layman,and
w i th a keener apprec iat ion of the part which each is to play in its preven tion
and cure, the future ho lds out to us the possib i li ty of its eradica t ion . Shall
we wa i t to take advan tage of this hope or shall we “ do i t n ow ?”
30 2 PULM ON A RY TUBE RCULO S I S
M any S imi lar sta t ist ics could be produced,but these are sufiicien t to show
that tuberculosis is dependen t upon the evils which accompany our so c ia l
fabr ic ; and, as such,should be dea l t w i th by society as a who le. So deeply
roo ted is i t,tha t i t can never be erad ica ted w i thout mun icipa l
,state and n a t iona l
aid .
3
E very large c i ty has its hot-beds of tuberculosis . The unsan i tary tenemen ts,
poorly l ighted,w i th l i ttle or n o sun sh ine
,where the poorest of the poo r huddle
together, are con stan tly tran sm i tt ing the d isease. One of these tenemen ts in
N ew York Ci ty is cal led the “Lung B loc—k .
” From it,there was reported
to the Heal th Board,in n ine years
,26 5 cases of tuberculosis
,and this was
perhaps n ot half of the cases tha t actual ly occurred in i t . There are
w indowless rooms in N ew York C i ty,fi
'
t on ly for den s to scatter in fec tion .
Th is same cond i t ion ex ists elsewhere,but we are glad to say that in most c i ties
i t has n ot reached so high a degree. H ow can th is cond i t ion be remed ied,except by mun ic ipa l and state aid? These tenemen ts must be replaced bv
san i tary dwell ings, and their occupan ts must be led to a h igher plane of living.
These foci for the spread of tuberculosis must be erad icated, and the mun ic ipa l
and state governmen ts must do i t .
I t is n ot a matter of indifferen ce to those in better c ircumstan ces, whether or
not the poor in the tenemen ts are in fected and die of tuberculosis, for as long
as the disease exists here,i t w i l l in fec t those in o ther stat ion s of life. Tuber
cul‘
osis is a mildly in fectious, or wha t I prefer to cal l a commun icable d isease,to d ist in gu ish i t from such v irulen tly in fect ious d iseases as measles
,sma llpox
,
d iphther ia and scarlet fever . Whi le tuberculosis is commun icated from one
ind ividua l to ano ther, yet a casua l associa tion I n n o w ise endangers one ; and,
an in fect ion is on ly likely to be tran sm i tted by a pro longed exposure in un san i
tary quarters . M easles,smal lpox
,d iphtheria and scarlet fever
,on the co n
trary, are apt to be tran smitted by a very brief assoc ia t ion ,even under hygien ic
cond i t ion s . I fur ther bel ieve tha t i t can be sa id, w i thout fear of con trad iction ,
that an associat ion w i th a tuberculous ind iv idua l in theopen air for an indefi
n i te period is free from danger of in fection . Fresh air,l ight and sun shine
are nature’s enemies of the bac i llus and our best pro tec tors, but in many homes,
espec ially those of the poor, n one of these en ter . Here ind ividuals suffering
from tuberculosis in fec t their rooms and transmi t the “ plague”to o thers of
their assoc iates .
To meet th is cond i tion ,no t o n ly must the people be aroused and educated ,
but the poo r must be helped . Laws look ing toward the pro tection o f thewo rk
ers must be passed ; ch i ld- labor must be abo l ished ; shorter wo rking hours,especially fo r tho se in unsan i tary occupat io ns, must be es tabl ished ; a standard
fo r l ight ing and ven t i la t io n and the proper cub ic a ir space per wo rker fo r wo rk
sho ps and homes must be establ ished , and a l iving wage must be guaran teed to
wage earners . T hese acts co n tribute very ma teria lly, though indirectlv, to
APPE N D I X 03
the preven t ion of tuberculosis. E ngland , by her workingmen’s acts
,giv ing
better , more san i tary homes and work- shops to her workers,reduced the mor
ta l i ty from tuberculosis n early one~ half in the half cen tury preced in g the dis
covery of the cause of the d isease. O ther n at ion s would do wel l to fo llow
E ngland’s lead . I f ever tuberculosis is go ing to be stamped out,and we
bel ieve tha t i t is,it w i ll be necessary to improve the hygien e and san i tat ion
of the homes and work—shops o ccup iedby the poor .
. I t wil l doubtless be very difficult to in terest those, who bu i ld ten emen ts
s imply for profi t, in the preserva t ion of the heal th and l ife of those to whom
they ren t their apartmen ts ; and un t i l the a l truistic sp iri t becomes un iversa l,i t
should be the prov in ce of governmen ts to d efine a certa in standard of hygiene
and san i tat ion which must be a tta ined .
Wh ile soc iety is en deavorin g to r id i tself of the “
great wh i te plague by
ra ising the standard of living,i t must also be m indful of the debt i t owes to
those who are a lready so un fortunate as to be afflicted . Fortunately,here
,
selfishness and a l tru ism meet . The mo t ive which prompts us to help those
in trouble, urges us to care'
for those of our poor who are affl icted with th is
d isease ; and, at the same time,self-preserva t ion forces us to the same end.
Soc iety,wh ich is respon sible for tuber
’culosis,must take upon i tself the burden
of its preven t ion and the care of _ those afii icted who are unable to prov ide for
themselves .
One of the greatest factors in the warfare aga inst tuberculosis is the S ta te
Sana tor ium . I t attacks the problem from human i tar ian,econ om ic
,and
educationa l standpo in ts .
H uman i ty demands tha t the sta te take care of its poor who are men tally and
morally defect ive,and a lso those who are depr ived of certa in sen ses as sight,
hear ing and speech ; and, this obl igat ion is almost un iversal ly assumed without
quest ion as
'
to its propr iety . The same demand is made for those who are so
un fortunate as to be afflicted with tuberculosis, and w i th added reason , because
those who are afflicted with this d isease are for the most part str icken during
the productive part of their lives,when they are of grea test assistan ce to their
fami l ies . This is a d isease that is curable and its v ict ims, if treated at the
r ight time and in the right manner can be restored to hea l th and earn ing
power .
T h ink of people dying annually in theUn i ted S tates of a preven table
and curable d isease! Huma'
n i ty ’s cry ascends to heaven unheard ; the w idows
and orphan s s ink in to poverty, d isgrace and cr ime. I t is est ima ted tha t one
fourth of the orphans supported by certain states are rendered so by tuber
culosis. I t is a po ten t factor in the production of pauper ism . H i ll ier (“The
Preven tion of Consumption ,
” page 101) states :“For as the stat ist ics of any
poor law work-house or infirmary w i ll show,there is n o more fru i tful cause of
pauper ism and inv'
val idity than phth isis .
”
304 PULM ON ARY TUBE RCULO S I S
W i thout a id,the poor suffer ing from tuberculosis w i ll a lmost surely perish ,
for they cann o t cease work as long as they are able to earn wages ; for they
know the time w i l l soon come when their fam i l ies w i ll no t on ly be forced
to care for them,but w i l l be forever depr ived of their support.
The S ta te Sana tor ium w i l l offer these people the chan ce of cure. They can
place themselves in these in st i tutions with a hope and expectat ion that they
w i ll be restored to heal th, and aga in be able to support their fami l ies . E very
individual cured in such an inst i tution , as wel l as many who are on ly improved ,w i l l cease to be a danger to his fr iends. I n the homes of the poor
,there is
much danger of sca tter ing in fect ion , because of the lack of observan ce of
the rules. of hygiene and san i tation and because of the lowered resistan ce o f
the poor . Human ity, therefore, demands tha t S tate Sanatoria be establ ished ,tha t the afiiicted may be cured and tha t the grea t wh i te plague” may no t be
tran sm i tted to o thers .
Wh ile the unnecessary suffer ing of the afflic ted , the waste of human life,the transmission of the d isease to o ther members of the family who spend their
anxious hour s adm in ister ing to the needs of the sufferer appeal to us, yet the
demand for a S tate Sanatorium does not. emanate from mere sen t imen t alone.
There is an econom ic s ide to these in stitut ion s. E very S tate Sanatorium is a
monetary investmen t , which will return to the sta te many times the cost o f
its ma in tenance. Tuberculosis is a d isease which affl ictsmen andwomen when
they are in the flower of manhood and womanhood, the t ime when they are o f
greatest value 0 the fam ily and the state, and the saving of these valuable
l ives would be a grea t econom ic sav ing .
The death ra te from tuberculosis in Cal iforn ia, for example, as reported ,
is about 3500 annually . For various reasons, a certa in proportion who die
of tubercu losis are reported as dying from o ther causes, so the number appea rs
somewhat smaller than i t should be. A llow ing l iberally for the impo rted cases,our state is perhaps losing 2500. of its ci tizens every year from this preven table
and curable disease.
I t is very d ifficult to place a value on a hiiman l ife, but takingB igg’s estim
ate tha t a human l ife at the average age at which dea th from tuberculosis
occurs is worth $ 1500 to the state (and I am sure this is very low), then Cal i
fo rn ia loses annually from th is cause a lone, These pat ien ts are
d isabled and unable to work for a certain period befo re dea th ; i t would be fa ir
to assume n ine mon ths as an average time. During a portion of this t ime, too ,they are helpless and must have some o ne to nurse them . M edic ines and phys
ic ians’serv ices are also requ ired . I f we take as wages the low rate o f
a day and coun t fo r care, medic ines and pro fessional service more fo r
but ha l f the t ime,we have an add i t iona l loss fo r each person o f o r an
annua l loss o f o r a to tal annua l loss based o n these low estimateso f Th is eno rmous waste o f mo nev and sacrifice o f human li fe
306 PULM ON ARY TUBE RCULO S I S
for the care of those who would have been rendered dependen t , had the disease
taken its natur a l course.
Such est imates but poorly represen t the value of S ta te Sanator ia . Grea t
as this economic sav ing appears, i t is the least importan t of the fun c tion s of
these in stitut ions . Their prin c ipa l m ission is far greater and nobler than the
mere sav ing of money . I t is tha t of preven t ing the spread of tuberculosis,
the greatest scourge known to the human race, a scourgewhich has caused more
suffering,more heartaches
,more poverty, more dea ths than al l the Wars of the
cen turies.
S ta te Sana toria are importan t educa tiona l cen ters,where object lessons in
the preven t ion of tuberculosis are given . The pa tien ts treated in these insti
tution s come from the homes of the poor . T hey are taken from their squal id
surroundings,where in their ignoran ce they could scarcely help in fect ing their
fr iends,and are placed under hygien ic cond i tion s to be cured, if possible ;
if th is is no t possible, they are at least taught tha t the ch ief source of danger
l ies in the sputum and w i th careful in struc t ion how to care for th is,they cease
being a danger to their fell ows . They are al so taught that fresh a ir,regu lar
hab i ts and careful living have much to do , not on ly w i th cur ing the d isease or
pro longing l ife, but a lso w ith preven ting the spread of the d isease to o thers.
The ind iv iduals trea ted in these in st i tut ion s return home as m issionaries .
I n many in stan ces they carry the fir st rays of hope in to the crowded tenemen ts .
They teach that air and better l iving are necessary to l ife. One such returned
m issionary can do more by a prac tical il lustrat ion than a score of chari ty
workers . A s,in foreign mission fields
,i t is Shown tha t the native converts
are the most in fluen tia l in spread ing the n ew thought,so i t is here. E very
one returned from a S tate Sanator ium is a po ‘ver for n ot on ly the preven t ion
of tuberculosis, but for the bettermen t and elevation of the class from whic h
he comes ; and, when the erad ica t ion of the“ grea t wh i te plague”
has fina lly
been accomplished,i t w i ll n ot have been done except indirectly by phi lan
thropists, chari ty workers and hea l th boards,the actual work w i l l have been
done by those who have been taken from the homes where tuberculosis de
velops, and lead to an appreciation of the necess ity of better , more hygien ic
living, and to this end no institution wil l con tribute more than the S tate
Sana torium .
CHAPTE R I I .
A
'
STUDY OF TUBE RCULOUS I N FE CTI ON .
The ~material fo r this chapter was origin ally published in the N ew York M edica lJourn al, M arch 2 1 , 1903 . O w ing to the fact that the question of in fection as d iscussedhere has o n ly been discussed in ciden tally in the body of the book , and ow ing to the factthat there have been frequen t cal ls for repr in ts of this paper, I thought it best to republishit as a chapter in the appendix.
TUBERCULOS IS OF CH ILDHOOD . WHY SO PREVALENT?
I n our en deavor to find methods to preven t tubercul osis,we must give the
period of chi ldhood much more a tten t ion than i t has been won t to receive ; for
it is n ot on ly possible,but probable
,tha t the seeds which ripen in to ful l
fledged cases Of tubercul osis in la ter l ife were in very many cases implan ted
in the t issues durin g the period of chi ldhood, rema in in g there un til a favorable
t ime appeared for their ac t ivi ty. BoflingerIsta tes tha t he has shown tubercle
bac i ll i to be st ill virulen t a l though en cased in glands for twen ty years.
That form of the d isease wh ich is most common in ch i ldhood,is tubercu
l osis of the lymph glan ds,a lthough i t is n ot un common to find the lungs and
meninges affected . Why the lymph glan ds are so pron e to in fection and why
the d isease does n ot make advan cemen t at thi s t ime in to the lungs or o ther
parts of the body more often than i t does,are quest ion s tha t have n ever been
an swered en t irely satisfactorily . S in ce the an swers to these question s w i ll
throw much l ight upon the subjec t before us,we wi l l n ow in quire in to them
at some length .
Corn et 2 says tha t by severa l hundred an ima l experimen ts hehas been able to
arrive at the con clusion that themucous membran e can be pen etra ted by bac i ll i ,though in tact
,and that
,in youn g an ima ls
,owin g to the membran es being more
easi ly pen etrated and the lymph spaces being larger than in adults,the bac i l li
are more easi ly taken up ; hen ce the lymph glands are more easi ly affected . I n
adul ts,on the o ther hand
,bac i lli penetrate l eSs easi ly and are more l ikely to _
cause a l oca l process at the po in t of en tran ce. Orth,3 Klebs
,4 Baumgarten s
and o thers have carr ied out Sim ilar exper imen ts,arrivin g at thesame con clu
sion s .
f Boll inger. B r i tish M edica l Journ a l , O ct. 1 7 , 1896 , p . 64 .
2 Corn et. D ie Tubercul ose, p . 288 .
3 Orth . E xperimen telle Un tersuchungen uber Futterungstuber culose, Virchow’s A rchiv,
Bd . lxxvi , p . 2 1 7 .
4K lebs . A l lgemein e Pa ihologie, p . 236 .
5 B aumgarten . Ueber die Uebertragbarkeit der Tuberculo se durch die N ahrung, Centralblatt jar kl in ische M edicin
, 1884, p. 225 .
308 PULM O N ARY TUBERCULO S I S
Jacob and Pannwitz Isay: Tha t glandular tuberculos is is mo re common
than tha t of the lungs (in ch i ldhood) is due to the anatomica l and physio logical arrangemen ts of the parts.
”
Ponfick 2says tha t the lymphatic vessels are d isproport ionately small com
pared with the amoun t of lymph to be carried Off; so the least irr i tation caus
I ng an Increa se of lymph is accompan ied by stasis, and a tenden cy to suppura
t ion if con t inued long. Al l such irr i tat ion s predispose to in fection“
. H e a lso,
says “The existen ce of this un iversal susceptib i l i ty (to scro ful a) rests in
certa in peculiari t ies Of the structure and mutual relation between the organ s,
wh ich,i t is generally admitted
,the chi ld ish organ ism possesses ; and which
n ormal ly presupposes a h igh morbidity. Thi s peculiari ty is founded,on the on e
hand,on the grea ter power of absorption of the tissues asWel l for bacterio logica l
in truders as for certain excretive products,and
,on the o ther hand
,on the loca l
developmen t o f a patho logical cond i tion favorable to their spread and growth .
Virchow Speaks of a weakness or imperfect arrangemen t of the lympha tics in
certa in individua ls as a cause of scrofula .
Wha tever the cause of this man ifesta tion in early childhood may be, we
know tha t there is a tenden cy in a cer tain'
n ot in con siderable proportion of ch i l
dren to in flamma t ion and en largemen t of the lympha tic glands. And we
further know tha t many Of these patho logical processes are,sooner or later
,
found to be tuberculous in their nature.
The cause of this frequen t lymphati c invo lvemen t,I believe
,must be sought
,
n o t on ly in the ana tomica l and physio logical arrangemen t of the lymphatic sys
tem,but a lso in the reduced vita l i ty from which these l i ttle ones often suffer .
To the natural weakened condi t ion in c iden t to in fan cy and ch i ldhood,which
makes them an easy prey to in fect ion,we must add the pecul iar weaknesses
tha t come through hered i ty and the lowered r esistance tha t comes through
l iving in in san i tary and unhygien ic surroundings as wel l as from errors in feed
ing and the various d iseases from which they suffer ; then ,we can better under
stand why they are prone to in fection by the tubercle bac illus. We can n o t
change the n orma l anatomical and physio logical'
processes, no r can weblot out
the inheri ted tendencies, but we can change the env iro nmen t in which these
l i t tle ones l ive, so as to make these inborn weaknesses less no ticeable and these
downward tendenc ies less operable.
I f the accepted bel ief,tha t a lowered resistance is necessary to in fectio n , is
true,then we can hope fo r much by bettering the san i tary and hygien ic co n
ditio n s and improving the nutri t ion o f individua ls . From what precedes,we
can see tha t this prophylax is should begin as soo n as the child is born ; fo r the.
evi l influences wh ich lower vital i ty a re thrown around children from the very
beginn ing of l ife.
' J aco l ) und Pa n nw itz . E n l strhuug M i ld Bckr‘
imphmg der LungoMubcra /I osr , p . 221 .
2 l ’o n fick . A l /gemc'i iw medizi n ische Cculm l -Z cihmg, D ecember 29 , 1900 .
3 10 PULM ON ARY TUBE RCULOS I S
H and I reported to thePhiladelphia Pathological Soc iety statistics of post
mortems at theChi ldr en ’s Hosp i ta l
,for the past ten years . Of 332 autopsies
made,1 15 , o r per cen t, showed tubercul osis. The locat ion of the o ldest
lesion was : bron ch ia l glands,6 5 per cen t ; mesen teric, per cen t ; undeter
mined (lesion general), 23 per cen t ; undeterm ined (lesion d istin ct), per cen t ;ton si ls
,0 .8 per cen t . Tubercles
'
werepresen t in the heart muscle in 8 per cen t
of the cases show in g tuberculosis.
T00 l i t tle atten t ion has been pa id to themode Of in fection and the time that i t
takes place . When the theo ry of hered i ty,as a general cause of tuberculosis
,
was disproved , i t seems strange tha t scien ce did n o t bend her energies to dis
cover when in fection does take place ; but , owing to the in terest tha t cen tred
in o ther phases of the subject,th is has not received the a tten tion tha t i t
deserves.
These statistics show us tha t tubercul osis begins to assume prominen ce in
the last quarter of the first year and that i t causes qu i te a proport ion Of
dea‘
ths'
diirin'
g the early years of l ife. Wh i le“
they Show the frequen cy with
whiChi' tIIbercul osis ei ther causes death or is presen t at the t ime Of dea th,they
do'
I IOt tell us how'
frequen tly tuberculous processes are presen t in those who
are l iving .
“
Such i n format ion can n o t be a tta ined so easily . A t tempts have
been made,however
,to gain this importan t in format ion ; and, whi le the re
sul ts are n ot abso lutely reliable, they are suffic ien tly so to give us an importan t l ink in the chain of eviden ce whi ch favors the lymphatic route of
in fection .
Krueckman 2 has shown , and in this he is corrobora ted by o thers, tha t the
lymphatic glands in ch i ldren are usually in fected before the lungs.
We have n ow seen how frequen tly tuberculosis occurs in in fan cy and early
chi ldhood . The next po in t that we wish to cal l atten t ion to ,is that the glands
,
especial ly the bron ch ial and tracheal , and in a less measure, the mesen teric
and retroperi tonea l , are n early always in fected when tuberculosis is presen t ;and
,since the foci wh ich are farthest advanced are usually S i tuated in some of
them,i t would suggest them as the o riginal po in ts of in fect ion .
Henoch 3 says : “When tubercles or cheesy processes are found anywhere
in the body, one can coun t i t for almost certain tha t the bron chial and trachea l
glands are likewise affected . I n the many sect ions that I have made I have
n o ted very few exception s to th is rule.
”
S teffen 4 shows the trachea l and bro nchial glands to be affected in 54 o f 6 2
cases o f tuberculo sis ; and the mesen teric and retroperi to nea l 35 t imes .
Bul ius 5 repor ts po st-mo rtems on 27 nursl ings with tuberculosis in whom he
1 H and . M edica l N ew s , N ovember 22,1902 , p . 994.
2 Krueckman . Virchow ’
s A rchiv .
, N o . 138 , I l t‘fl 3 , s . 534 .
3 c o ch . 1893 , p. 4 13 .
4 S teffen . Zur fnt lho l ng is'
chcn A fur/omit! dvs kind/ id i omA l ters , p . 143 .
s Bul ius . J ahrbac/z [fir Ki nde r /icil lcundc. Bd . 49 , 1899 , p. 304.
APPE N D I X 3 1 1
found the bron ch ial glands affected every t ime and showing the furthest ad
van ced lesions .
Corn et I c i tes the fo l lowing
S tein er and N eureuter found the lymph glands affected 299 times inpost-mortems— the bron ch ia l glands bein g invo lved 286 t imes .
Ril l iet and Barthez found lympha tic glands invo lved 248 t imes in 3 1 2 cases.
N orthrup reports glandular invo lvemen t every t ime in 125 cases.
T hus,pa tho logica l eviden ce shows tha t the glandular system is invo lved in
pract ically al l cases of tuberculosis in ch i ldren ; and n ot on ly invo lved,but the
first to show the d isease in a large majori ty of the cases,if th is can be in ferred
from the fact that the glan ds show the most advan ced processes.
Whi le n early al l cases of tuberculosis in ch i ldhood show tuberculosis of the
glands,th is does no t say tha t a l l cases of tuberculos is of the glands show tuber
cul osis elsewhere ;_n or does i t a llow the in feren ce that al l cases of en larged lymph
glan ds are tuberculous.
The wo rk of Vo lland 2 is most importan t in its bearing upon th is po in t . H e
examin ed schoo l ch i ldren w i th referen ce to .the frequen cy of en largemen t
of the cervica l lymphat ic glands,obtain ing the fo llow ing results :
Of 6 28 from seven to n ine vears of age, there were 607 , o r per cen t ,posi tive.
Of 724 from ten to twelve years,6 64 , or per cen t, posi t ive.
Of 722 from thirteen to fifteen years,607 , or 84 per cen t, posit ive.
Of 334 from sixteen to eighteen years,233 , or per cen t , posi t ive.
Of 98 from n ineteen to'
twen ty- four years
, per cen t , posi tive.
By cl in ical exam ina t ion Berutti 3 fOund the glands of the n eck invo lved in
per cen t of cases.
Balman in 8 1 per cen t .
Wohlgemuth in 430 cases,'
93 per cen t .
These stat istics show us that the lymph glands are a lmost un iversally eu
larged in chi ldhood, and, wh i le we do n o t suppose that they are a lways tuber
culous,nevertheless
,we know that they frequen tly are ; and, if n ot already so ,
the in flammato ry cond i tion presen t is the surest preparation for in fect ion by thebac i llus tuberculosis. I n this connection I quo te Steffen z4 “
H ealthy lymph
glands are n ot at tacked by tuberculosis. They are predisposed thereto when
they are swo llen,s ucculent and infil tra ted
,and in a condit ion of hyperplasia .
O sler 5 says : “A spec ial pred isposin g factor in lymphatic tuberculosis is a
catarrha l inflammation of the mucous membranes,which in i tself excites a
sl ight aden i t is.
I Corn et. D ie Tuberculose, p . 1 78
—9 .
2 Vo llan d. Zeitschr ift jitr kl in ische M edicin,N o . 23 , 1893 .
3 Cornet. I bid.:
4 S tefien . Zur phthol ogischen A n atomie des kindl ichen A l ters , p . 1 59 .
5 Osler. Practice ofM edicine, 1892, p . 205 .
3 1 2 PULM O N ARY TUBERCULO S I S
T ha t a very large per cen t of these en larged glands are tuberculous is shown
by the experimen ts of O tis Iand Heubn er ? The former tested 29 ch i ldr en
wi th tuberculin,being al l who presen ted themselves at the cl in ic during the in
vestigation . Of these,18 reacted posi tively, and 2 doubtfully
,making from
6 2 to 69 per cen t of the n umber . O f the 1 1 who d id n ot react,in 6
,the en
largemen t had existed on ly from one to two weeks. The majority of the re
actions occurred where the en largemen ts hadexisted forS IX mon ths or«more. I
quo te his con clusion s “I f then the tubercul in test is to be rel ied upo n
,our
experien ce would indicate that at least 6 2 per cen t and probably a larger pro
port ion o f en larged glands of the n eck are tubercular . I n ano ther series,he
tested 56 cases and found .33 tha t reac ted well, 6 sl ightly and 2 doubtfully,
mak ing per cen t without doubtful ones, and per cen t with them .
H eubner tested 17 scrofulous ch i ldren and found posi tive reactions in al l but
o n e.
M oore 3 reports 28 cases of en larged glands, mostly of the neck, whi ch had to
be operated on for various reason s. Of these 73 per Cen t were“tuberculous.
O sler 4 quo tes the experiments of Eve as showing tha t scro fulous ma ter ia l
invar iably produces tuberculosis in gumea pigs,'
and Often in rabbits .
The con tri bution of‘
B los 5 to this subject is most importan t. H e reports
3 28 cases of tuberculous lymphoma'
occurring in Czerny’s cl in ic , in Heidel
berg,during the years 1886 to 1895 . Of th is number he fo l lowed the sub
sequen t histor ies for a per iod varying from three to twelve years and found that
40 per cen t of them developed tuberculosis in that time. H e has l ikewise
co llected the records of cases stud ied in the same manner,and arrives at
the con clusion that the en larged glands in ch i ldhood are the primary foci fromwhich the d isease develops in la ter l ife in a very large proportion of cases.
Wh i le O sler 6 does no t go so far as B IOS , yet he says“I t is safe to say that in
three-fourths of the in stances of acute tuberculosis the in fection is derived fromthis source
,
” mean ing an unhea led focus of tuberculous aden i t is . O n th is
po in t I also quo te S teffen : 7 “The lymph glands offer in a great number
,
perhaps in the majo ri ty,of cases o f tuberculosis of individua l organs
,the pri
mary seat of tubercle formation .
”
Whi le these sta t ist ics do no t admit of any conclusion in the nature of a math
ematica l certa in ty,nevertheless
,when we con sider them as a who le
,we have
some very importan t data from which we can draw in ferences,i f no t posi t ive
con clusions. We are at least justified . in saying tha t :
I O tis . Tran sa ction s 0} the A mer ica n Cl ima to l ogica l A ssociation , 1899 , and Medica l
N ews,July I , 1898 .
2 H eubner . Quo ted in Jacobund Pan nw itz, p . 223 .
3 M o ore. La n cet, S eptember 17 , 1898 , p . 734.
4 () sler . Practice 0/ M edicine,189 5 , p. 225 .
S BIO S . twi l l /tai l . a n s d . G renzgebictcn der Al cdizin. a nd C lu'
rurgic , 1890, N O . iv.
6 O sler. Pra ctice 0} M edicine,189 2, p . 206 .
7 S teffen . Z ur pa thol ogischcn A na tomic (l es Kindesa lters , p . 159 .
3 14 PULM ON ARY T UBE RCULO S I S
on exten sion to o ther parts of the o rgan ism at on ce. On this po in t i t woul d bewel l to gather sta t ist ics
,to see i f they do undergo a more virul en t cour se than
those who receive their in fect ion from a less in t imate connect ion . The sta t is
tics wh ich I have at hand ind icate th is ; but they do n ot cover en ough cases to
warran t a posi t ive con clusion .
When the bac i lli find their way in to a lymph gland, i f they are n ot destroyed
three courses are open to them . T hey maycause a lo ca l degen eratiye process
in thel
lymph gland, or they may be carried on in to the d istan t parts of theorgan ism,
as the lungs,through the lymph
,
or blood chann els ; or , they maybe
come en cased in the glands to rema in qu iescen t forever unl ess they are carried
Cut in to the lymph or blood stream at some future t ime,when the gland in
vo lved is irritated and swo llen from some'
cause,as is the case in the acute ia
fectious d iseases.
T hat this exten sion from the lymph glands in to the blood vessels,and then ce
in to the lungs or o ther parts of the body,can take place
,has been demon strated
by A ufrecht I who has removed the lungs and heart in toto from cadavers ; then ,
laying open the arteries and vein s, he cut out the port ion s con ta in ing lymph
n odes which were firml y adheren t to the blood vessels A fter harden ing and
mak ing sec t ion s,he arrived at the fo llowing result E ach sect ion passed
throughbo th lymph n ode and vascular wall . Proceeding thus he (the assistan t)was able to supply clear proo f that the bacilli from the lymph n ode had passed
in to the substan ce of the vascular wal l w i thout in jury to the latter . Bo th arte
ria l and venous twigs were thus studded w i th bac ill i as far as the inner surface.
O ne prepara tion Showed a bac i llus in an endo thel ia l cel l .
From our study thus far , we are compel led to assign an importan t place to
ch i ldhood as the t ime in l ife when the tubercle bac i llus_ga in s en tran ce to the
t issues . The t issues at this time are succulen t, easi ly penetrated , and possessed
of feeble resistan ce. The bac i lli are taken in ,either w ith curren ts of a ir
,w i th
food,or a long wi th o ther things tha
'
t'
the ch i ld puts in to his mouth ; or , i t maybe,
through wounds of the surface. N O mat ter in what way they ga in en tran ce,they pass read i ly in to the lymph spaces and on in to the lymph glands.
A discussion of th is subject would not be complete without men tion ing the
part played by ton si llar tissue in in fect ion . T hat this is a por t of en try for the
bac il lus,can not be den ied . N umerous experimen ts have been made showing
tubercle bac i lli presen t in ton si ls and adeno ids when the disease was not to be
detected elsewhere in the body . Lermoyez ,2 by inoculat ing gu inea pigs ,secured po sit ive resul ts in 13 per cen t o f the tr ials w i th tonsi ls and 20 per cen t
where adeno ids were used . Posi t ive resul ts have a lso been obta ined bv
D ieulafoy,B rindle
,G o ttstein and o thers .
I Aufrecht. Ber l i ner kl in ische Wochenschr ift, O ctober 2 1 and 28,1901 . T ranslated
in Jour na l of Tubercul os is , Vo l . iv, p . 16 7 .
9 Lermoyez. Quo ted by _
Wright, in N ew York Medica l Jour na l , S eptember 2 1 , 1895 .
APPE N D I X 5
The writer,
I in d iscussing this subject in a former paper,sa id : “Whether
or n ot tubercle bacill i are .found in ton sillar and adeno id t issue at al l t imes insufficien t numbers to in fect gu inea pigs
-
is n o t the question . E xperimen ts doShow tha t they are found in individuals who are apparen tly free from tubercu
lo sis ; which fact leads at least to the in feren ce that ton sils andaden o ids maybeports of en try when ce the germs pass. on in to the lymph stream.
We w i ll n ow pass on to the secon d part of our sub ject and inquire why infection is so prevalen t in ch i ldhood? T h is has a lready been
'
an swered inpar t
,but we w i ll n ow inquire more part icul arly in to the predisposin g causes
wh ich are in ciden t to ch i ldhood .
The first th ing tha t strikes us is thewidespread morb idity presen t at thistime. The statemen t of Ho l t, quo ted above
,tha t 26 per cen t of al l ch i ldren
born in N ew Yo rk in the years 1890—92 in clusive, d ied before the end of the
first year,and 34 per cen t before the end of the second year is startl ing. Such
a mortal i ty must of necessi ty represen t a much greater morbidity. The grea t
majori ty of chi ldren are il l,more or less
,durin g the first and second years of
their 'l ives. A t th is per iod,when they are least able to resist bacter ial invaders,
owin g to the natural immatur i ty of their tissues,they have superimposed upon
this na tural weakness a vi tality much reduced by di sease. I t would seem that
i t were more than co in ciden ce that at the very time when these l it tle ones are
most prone to o ther disorders, the grea test n umber of them should succumb
to tuberculosis. The most prevalen t trouble at th is t ime is conn ected w i th the
d igestive tract,which results in an in flamma to ry cond i t ion w i th abrasion s of
the surface. Owin g to poor ven t ila t ion and bad hygiene and general mis
managemen t of the chi ld at th is t ime,i t is apt to suffer
,more or less
,from
ca tarrhal condition s of the upper air pas‘
sages wi th abrasion s of these surfaces
as well . SO'
we find those cond i t ion s present in bo th the resp iratory and d i
gestive tracts wh ich make infe ction easy and certa in .
The na ture and habits of the ch i ld a lso make i t pron e to infect ion by brin gin g
it in frequen t con tact w ith the bac i llus. Being helpless i t is carr ied about
and fon dled by its n urse and a ttendan ts without regard to whether they are
tuberculous or n ot. E verything that comes within reach of the ch i ld is put
in to the mouth. The hands are con stan tly go ing from floor and furn i ture to
the mouth,carrying w i th them dirt and dust laden ed wi th bac illi .
I n this connection the exper imen ts of Preisich and Schuetz 2are very im
portan t in show in g how great this danger is. These exper imen ters examined
the-dirt under the finger -na i ls of sixty- six ch i ldr en whose ages ranged from six
mon ths to two years. T hese chi ldren were taken at ran dom from the am
bulatory cl in ic of the S tefan ie Ch i ldren’s Hosp i tal . The exam inat ion s were
I Po ttenger. The Rhin o logist an I mportan t Factor in the Preven tion of Tuberculosis,The Laryngoscolbe, Jun e, 1902 .
2 Pr eisich und iS chuetz . I n fectiosit'
at des N agel schmutzes bei Kindern in Bezug auf
T uberculosis. Berl iner kl in ische Wochen schr ift, M ay 19, 1902 .
3 16 PULM ON ARY T UBE RCULO S I S
posi tive in fourteen in stan ces, per cen t . Con sider ing al l these things is i t
any wonder that l iving tubercle bac i ll i are found in the lymph glands of so
large a proport ion of chi ldren ?
TUBERCULOS IS IN ADOLESCENCE AND ADULT LIFE.
I do not w ish to be understood as denying the o ccurren ce of in fection in
adul t l i fe, for we see many cases in which i t is unquest ionable ; but, I do be
l ieve that we have been too prone to accept the time when the diseasebecameman i fest to the patien t or at tend ing physic ian as the time when in fect ion oc
curred . On the con trary,in many of these cases
,in fection must have occurred
a long time before. For example, many of the cases of tuberculosis which so
common ly fo llow the acute in fectious diseases, such as in fluenza,measles
,and
whoopin g cough, we kn ow must have been due to the light in g up of some pre
viously quie‘
t focus ; for , there could n o t have been time for the invasion to have
taken place with the formation of tubercles and the production of such ad
van ced lesion s in so short a t ime ; and, too , in many of these cases, there has
been n o in timate associat ion with tuberculous patients n or has there been any
d iscoverable exposure to in fection while sufferin g from the acute i llness ; so we
should find i t much more difficul t to accoun t for the in fection as taking place at
the time of the acute i llness than to suppose the disease to be due to a previ
ously quiet focus.
Un til we have further proo f, we shal l be compel led to recogn ize the possibil
i ty of in fection takin g place through d irect inhalat ion of bac i ll i in to the lungs ;but we must also recogn ize that , in o rder for this to take place
,there are d ith
cul ties to be overcome wh ich are a lmost in surmoun table.
I t is very importan t , in the study of the preven tion of tuberculosis,to know
when in fection takes place ; for then we can know where to d irect our preven
t ive measures. Of course, the primary place to d irec t such measures is towards
the destruction of sputa and the bacillus-bearing discharges ofwhatever nature.
A side from this, however, we must look carefully after the ind iv idua l , and th is
care must be bestowed at that time when in fection is most l ikely to take place.
I f,as is shown above
,the great majori ty of children have en larged glands
, and
these are tuberculous in a very large per cen t o f those tha t are chron ical ly eu
la rged, then the period of chi ldhood must receive our most scrupulous at ten
t ion . While these bacilli may rema in inact ive in the glands throughout l ife,
yet they are a co nstan t menace to the individual . They are found in the glands
o f person s dying Of vio len ce and acute diseases in a surprisingly large number
o f cases,their presence never having been suspected during life. Pizzinn i
sta tes that he has found v irulen t tubercle bacil li in 42 per cen t o f such cases ;wh i le Spengler and Ko ssel a lso report po si t ive find ings in a large per cen t
o f thei r cases.
' Pizzinn i. Quo ted in Jacobund Pan nw itz, p . 226 .
3 18 PULM ON ARY TUBE RCULO S I S
upon the virulen ce of the germs, the grade of in jury to the lung, and the general
resistan ce of the pat ien t .
T hus,we have a ra t ional basis upon wh ich we may accoun t for manv o ther
wise inexpl icable cases of tuberculosis,such as fo llow immediately upon acute
in fect ious d iseases and in juries. I n these cases,i f the d isease man i fests i tsel f
at once whi le the acute i llness is stil l on ,the probab il i ties are that i t is the awak
en ing of some prev ious in fect ion ; i f i t man ifests i tself later , i t maybe the resul t
of ei ther a n ew invasion from the lymph gland in to the lung or the l ighting up
of a slumbering focus,or a new in fect ion from without .
The glands on ce affected or the lungs on ce the sea t of tubercle,though
qu iescen t,there are abundan t opportun i t ies dur ing the struggle whi ch is in
eiden t to human l ife for the start ing up of'
an acute process. Ado lescence is the
period when tuberculos is is most prone to become active. A t this t ime there
is a Specia l stra in upon people. T hey are o ften times depressed . The sexua l
changes are taking place and many are add icted to indiscretion s. Soc ial
fun ct ion s are taxin g bo th physica l and men ta l powers . S tud ies at th is t ime
are hard for them,or
,i f they are n o t in schoo l
,they are most l ikely do ing work
too difficul t for their strength . So we find'
this to be a second period in l ife
when vi ta l i ty is low ; and, l ike the one in early chi ldhood,i t is a period marked
by the grea t number of cases of tuberculosis presen t . I n later l ife,the earn ing
of a l ivel ihood,business worries
,fam i ly troubles
,var1ous d iseases and v ic ious
hab i ts depress the ind ividual,lower his resist ing power
,and make the so i l ready
for ei ther n ew in fect ion or activity in O ld region s.
From this invest iga tion,I would dr aw the fo llowing conclusion s
1 . Tuberculous in fect ion is very common in’
early chi ldhood .
2 . A large proport ion of those pat ien ts who,a l though in fected
,do n ot Show
acute symptoms during chi ldhood,develop active tuberculosis in later l ife.
3 . I n seek ing the cause of th is frequen t in fection,aS1de from the hab i ts of
the ch i ld and the carelessness o f the paren t bringing i t in frequen t co n tact w i th
the bac illus,a l l those things which lower vital ity at th is t ime must be con sidered
and,I would call spec ial a tten t ion to the fac t that there is a co nnect io n wh ich
seems more than co in c iden ce in the time tha t tuberculous in fect ion takes place
and the t ime that the c h i ld is most apt to suffer from ca tarrha l co ndi tio ns o f
the stomach and bowels .
4 . M o re atten t ion should be given to the care and feed ing o f ch i ldren,so
tha t thei r systems may be resistan t to infec t io n .
5 . A l l tuberculous ch i ldren,whether they have les io ns in the glands, bo nes ,
lungs,o r any o ther part o f the body
,should be trea ted fo r thei r d isease.
CHAPTER I I I .
CULTURE PRODUCTS I N THE TREATMENT OF TUBERCULOS I S .
The material in this an d the succeeding chapter was published origin a lly in the
Therapeutic Gazette of January, 1902 , and M arch, 1903 . Chapter I I I was o ne of the
first papers to appear in America telling why tuberculin failed , and Chapter I V was the
first co llective investigation which endeavored to gather together the op in ion s Of men who
were espec ially in terested in the treatmen t Of ~
tuber culosis, and presen t their opin ion s oftuberculin and its therapeutic use. The demand for these two papers, like the precedingon e, has been so great that I believemy readers w ill appreciate their appearan ce in this form .
I n presen ting a paper before this soc iety upon the subject which I havechosen
,I recognize full wel l tha t there is n o specific remedy for tuberculosis
,
which is recogn ized by the medical pro fession general ly ; n on e which corre
sponds to an t i toxin in diphtheria, the iodides and mercury in syphilis, or
quin ine in malaria ; yet there are certain i remedies which,whi le they have
en joyed on ly a l imi ted trial by the/ profession , are found to have a spec ific
act ion upon tuberculous tissues wherever found .
That the va lue of these products has n ot been recogn ized is -due to a mis
con ception Of wha t should be expected of such remedies . A n t i toxin is recog
n ized as the an chor of hope in d iphtheria ; yet the profession wel l kn ows tha t
to be efficac ious,i t must be used early ; and al l th ings bein g equal , the prog
n osis varies with the early or la te adm in istra tion . So i t is wi th o ther d iseases .
The earlier the case fal ls in to the physic ian ’s hands, the better . I n surgery
,
we kn ow the kn ife is a spec ific for many troubles ; yet its field of usefulness is
limi ted,and after a certa in po in t in the d isease has been reached this spec ific
fa i ls. While the field of these Spec ifics is l imi ted, yet their va lue is recogn ized,and in n o way impa ired by the fact of th is l imitation . On the o ther hand
,
the pro fession bends every energy to brin g the cases under treatmen t dur ing
the period when the remedies are valuable. I n the case of tuberculosis, how
ever , the pro fession has n ot been sa t isfied w i th a remedy of l imited value. I t
has been unreasonable,and demanded that a remedy to be useful and to be
recogn ized must n ot on ly cure tuberculosis, but remove dead and decayingtissue ; n ot on ly cure the disease, but remove al l results caused by the d isease .
Such demands are un fa ir and preposterous . I f the same test were appl ied
to o ther remed ies,how many would stand? I n tuberculosi s we must demand
n o more of a remedy,and n o less
,than in o ther" diseases . As the fo llowers
of the hea l ing art,we should seize upon everyth in g that w i l l help, and apply
i t to the advan tage of the pat ien t,n ot d iscard even the smallest th ing tha t
w i ll aid us to comba t d isease. To correctly estimate the va lue Of a spec ific
320 PULM ON ARY T UBERCULO S I S
remedy in tuberculosis, we must properly define our d isease. We must
d ist ingu ish between tuberculosis and con sumpt ion . Tuberculosis in its early
stages— that is, while i t is pure tuberculosis— is a very curable d isease, yield ing
as readily to trea tmen t as typho id fever or pneumon ia . But when this puretubercul ous process has changed, and its place ha s been taken by ulceration s,cavi t ies
,cheesy nodules
,and these Often surrounded and embedded in fibrous
t issue— ln o ther wo rds,when con sumpt ion has supervened— then the pictur e
is d ifferen t . We have n ot pure tuberculosis to dea l wi th,but the resul ts of
tuberculosis. T uberculosis i tself w i ll yield readi ly to trea tmen t,but these
results are very d ifficul t to comba t, and a remedy for the former shoul d n ot be
.expec ted or required to remove the latter . I t would be as reasonable to ask
of a remedy for a surface ulcer to remove the resul tin g scar . So ; i f we have a
remedy at our command wh ich can be shown to have a spec ific action upon
tuberculous processes, we should ha i l i t wi th delight,not demand of i t that i t
remove cavi ties and cheesy n odules ; but'
we should improve our method of
diagnosis so tha t we m ight recogn ize the disease while i t is in the purely tuber
cular stage, and while the remedy is appl icable.
Advan ces in the field of med icine,as elsewhere
,are slow to be recogn ized .
E very n ew theory must force its way aga in st the prejud ices of precon ceived
ideas ; and, if at al l revo lutionary, meets most bitter opposi tion. H arvey,
when he had cal led his confreres together and made a thorough demon stra t ion
Of the c ircula tion of the blood , is reported to have said : “A las,I canno t
make a single man over forty-five years of age bel ieve i t l”A l though vacc in
a t ion has almost driven smallpox from civil ized lands, yet we n ow and then
meet so - called physician s who are Opposed to vaccina t ion . The germ theory
of d isease is doubted by some, and the efficacy of an ti toxin is n ot unquestioned .
I s i t any wonder then that the va lue Of culture products in tuberculosis is no t
recogn ized?
I t is un fortunate that the field of medicine is so large tha t we canno t prove
the value of new theories for ourselves. Such independen t work and thought
would be who lesome, but wi th the cares and responsib i l i t ies which are forced
upon us,we can on ly investigate some sma l l field wherein our greatest in terest
l ies,and th is in a very unsatisfactory way. The greatest portion of our kn owl
edge we are obl iged to take second-hand from men whom we recogn ize as
authorit ies ; and, when we know how o ften they are m istaken,i t behooves us
to do as much o rig inal invest igat ion as possible. Conservat ism is a safeguard,
and i t is praisewo rthy, but i t should no t lead to bl indness . N ew methods o f
combat ing d isease should be weighed carefully and tested tho roughly before
acceptan ce o r rejectio n ; but i t is hardly fa ir o r just fo r the grea t majority o f the
pro fession to rejec t a remedy,al though thev have never tried i t , s imply because
certa in no ted men say i t is useless , when a t the same t ime o ther equal ly no ted
men are obta in ing good resul ts by its use. I n the examination o f sputum ,
3 22 PULM ON ARY TUBE RCULO S I S
be of value. I n sp i te of Pro fessor_Koch
’s recommendation s
,patien ts whose
lungs were r iddled wi th cavi t ies,and whose con st i tut ions were worn by the lon g
con tinued dr a in of suppuration,and whose v i tal i ty was destroyed by con
t in ned h igh fever,were subjected to trea tmen t, w i th onl y the resul t tha t Shoul d
'
have been foreseen— d isappo in tmen t . I n order to have satisfied those who
were posing as cr i tics of tubercul in,i t would have been necessary for the
remedy to have removed dead and dying tissue,to have cur ed suppurating
foci,to have removed a ll symptoms resul t ing from a heart long overburden ed
,
and to ha ve restored to n ormal a system whoSe organ s were al l more or less
d iseased .
_ When such a remedy has been found, i t will be a specific,n ot on ly
for tuberculosis,but for a l l diseases to which mankind is heir. But even in
these cases,un su i table as they were
,had the remedy been adm in istered in the
proper doses good resul ts might have been obta ined,and at least no harm
could have been done.
The secon d m istake whi ch was made was the admin istration of too large
doses. Thi s dosage depended upon the erroneous view whi ch Professor
Ko ch held as to the manner in which tubercul in acted . H e believed that the
end desi red was the destruction of the granulat ion tissue surround ing the
tubercles,thus a llowing the defen sive forces of the body to a ttack the germs
in situ,
‘
or by liquefaction to secure the expul sion of the tuberculous tissue.
I n order to produce th is resul t doses were given which caused severe reaction s,
bo th loca l and general . The tempera ture was o ften elevated to 104°and 105
°
F and the remedy adm in istered at such in tervals tha t the pat ien t was kept
in a constan t feverish cond i tion . A s a consequen ce the pa t ien ts lost appet i te,
became emacia ted,and soon succumbed ; and al l such results were recorded
as scores again st tuberculin . I nstead,they Should have been cons idered
as due to the improper use of tubercul in . S trychn ine is a valuable remedy
and capable of producing bri ll iant results when admin istered in doses of 316
to 21
11 of a grain,but when given in I -gra in or 2- gra in doses i t destrovs the
pa t ien t . This po isonous effect is one of the characterist ics of the drug,and
is taught to the pro fession ; but in no way hand icaps the remedv,for the resul t
desired is obta ined w i thout the po isonous effects. SO i t is w i th tubercul in .
I n smal l doses i t is capable of produc ing benefic ial resul ts ; in large doses i t
produces po iso nous resul ts . But the fact tha t i t was admin istered in po iso n
ous doses a lmost exclusively in the early period of trial in 1890 and 1891
caused the po isonous symptoms to be cons idered as the on ly ones wh ich the
remedy was capable of produc ing. I nstead of recogn izing the bri ll ian t resul ts
in l upus,and early stage cases o f pulmo nary tuberculosis
, even when the rem
edy was used in wha t would be co ns idered to -day a faul ty manner,and thus
mak ing the physic ian ’s armamen tarium richer by o ne valuable remedy,
host i le cri tics could see n o th ing but harm ; so they gave out the erro neous idea ,from wh ich the med ical wo rld has no t yet freed i tsel f, tha t tubercul in can pro
APPE N D I X 23
duce no good results,but on the con trary is l iable to do much harm . T o
Show the method of admin istrat ion,I wi ll c i te some examples from ‘ the l i tera
ture Of tha t t ime.
Jan uary 1 7 , 1891 , a patien t. in von Leyden’sI cl in ic had a paracen tesi s
made,removing
'
a clear, serous exudate. E xaminat ion showed rales in the
r ight apex,rela t ively dull percussion no te
,sl ightly tympan i t ic
,and d imin ished
resp ira tion . The Spleen was somewhat en larged. T emperature F .
next day after the opera t ion ,102 .5
o F . On the 19th an in ject ion of two
m ill igrammes Of tubercul in was given . By February 1 2 the pat ien t had
received ten in ject ion s, the last bein g 50 mill igrammes . During the period
the pa t ien t became rap idly worse. On February 10 the temperature reached
104°E
,where i t rema ined con t inuously un t i l the pat ien t ’s death on the 19th
of February . Reutimeyer2 reports a case in whi ch he gave eleven in jection s
in eleven days, in spite of react ion s of 104° F.
T hese two cases are n ot exception s, but such was the method employed gen
eral ly when tubercul in was fir st put upon trial . H ad these pat ien ts received
as an in i tia l dose one- ten th milligramme,and then a gradua lly in creasin g dosé
age, so as to avoid fever reaction s, theywould have had the benefit of the specific action whi ch the remedy possesses over tuberculous foci
,many of them
woul d have been benefited, some would have been cured, and culture products,
to day woul d be warml y praised by the medical profession I n the treatmen t of
tuberculosis.
Besides bein g held accoun table for the effect produced when used in un suit
able cases,and when admin istered in po ison ous doses
,tuberculin was a lso
held respon sible for al l post-mo rtem find ings. Pa tho logists who before had
found“
so li t tle in terest in tubercular lun gs that they had on ly given them a
casual glan ce,n ow began to make the most min ute examination s. E very
finding was carefully recorded a nd ascr ibed to the adven t of tuberculin .
Perhaps the work of Virchow had more to do w i th the discredi tin g of tuber
cul in than tha t of al l o ther cri tics combined ; and, strange to say, those who
have quo ted h im have made his utteran ces much more host i le than they really
were. Virchow made the post-mortems and recorded his fin dings ; but much
of the in terpretation that has been put upon them is n ot his, but that of o thers .
One of the commonest Objection s that has been urged again st tubercul in
is that i t is prone to produce acute miliary tubercul osis ; an d cri tics assign the
authori ty for this statemen t to Virchow . This he d id n ot say. The error
comes from a juggl in g Of words. H e sa id that in the various organs of the
body “miliary or submi l iary nodules were Observed,
” but d id no t ascribe
them to the remedy,except in a suggestive way, saying : 3 I have on ly shown
1 Ber l in er kl in . Wochen schr ift, 189 1 , p . 237 .
2 Ber l in er kl in . 1898 , p . 1 24.
S Ber l in er kl in . Wochen schr ift, 189 1 , p . 191 .
3 22 PULM ON ARY TUBE RCULO S I S
be of value. I n spite of Professo r Koch ’s recommenda tion s, patien ts who se
lungs were riddl ed wi th cavi ties,and whose const i tut ion s were worn by the lon g
con t inued drain of suppuration,and whose vi tal ity was destroyed by con
t inned h igh fever,were subjected to trea tmen t, with on ly the resul t tha t shoul d
have been foreseen— disappo in tmen t . I n order to have sa tisfied those who
were posing as cr i t ics of tubercul in,i t would have been necessary for the
remedy to have removed dead and dying tissue, to have cur ed suppura t ing
foci,to have removed al l symptoms resul t ing from a heart long overbur den ed
,
and to ha ve restored to normal a system who'
se organ s were al l more o r less
d iseased .
_ When such a remedy has been found, i t wil l be a spec ific,no t onl y
for tubercul osis,but for a l l diseases to whi ch mank ind is heir. But even in
these cases,unsuitable as they were
,had
’
the remedy been admin istered in the
proper doses good results might have been Obta ined,and at least no harm
could have been done.
The second m istake whi ch was made was the admin istra tion Of too large
doses. Thi s dosage depended upon the erroneous view whi ch Pro fesso r
Koch held as to the manner in which tubercul in acted . H e believed that the
end desi red was the destruction of the granul a tion tissue surround ing the
tubercles,thus a llowing the defen sive forces of the body to at tack the germs
in situ; or by liquefaction to secure the expuls ion of the tuberculous tissue .
I n order to produce this result doses were given which caused severe reaction s,
bo th local and genera l ._
The tempera ture was Often eleva ted to 104°and 105
°
F .
,and the remedy admin istered at such in tervals that the patien t was kept
in a con stan t feverish cond i tion . A s a con sequen ce the pat ien ts lost appet i te,
became emacia ted,and soon succumbed ; and a l l such results were recorded
as scores aga in st tubercul in . I n stead,they Should have been cons idered
as due to the improper use of tubercul in . Strychn ine is a valuable remedy
and capable of producing brill iant resul ts when admin istered in doses Of 31
6
to 717; of a grain
,but when given in I -grain or 2-gra in doses it destroys the
pat ien t . This po isonous effec t is one of the characteristics of the drug,and
is taught to the pro fess ion ; but in n o way hand icaps the remedy, for the resul t
des ired is obtained w i thout the po isonous efi'
ects. SO i t is w i th tubercul in .
I n smal l doses i t is capable of produc ing beneficia l results ; in large doses i t
produces po isonous resul ts. But the fact that it'
was admin istered in po ison
ous doses a lmost exclusively in the early period of trial in 1890 and 1891
caused the po isonous symptoms to be cons idered as the on ly ones which the
remedy was capable Of producing . I n stead of recogn izing the bri ll ian t resul ts
in lupus,and early stage cases o f pulmo nary tuberculosis
,even when the rem
edy was used in wha t would be co nsidered to -day a faul ty man ner,and thus
mak ing the physician ’s armamen tarium richer by one valuable remedy
,
ho st ile cri t ics could see n o th i ng but harm ; so they gave out the erro neous idea ,
from wh ich the medica l wo rld has no t yet freed i tself, tha t tubercul in can pro
3 24 PULM ON ARY TUBE RCULOS I S
what we have found ; I bel ieved— and I think there is here sufli cien t eviden ce
that th is exhib i t ion would Show the magn i tude of the danger whi ch m ight
arise. H ow frequen tly this danger arises,in wha t cases i t arises
,by wha t i t is
espec ia lly caused,are question s tha t can be defin i tely dec ided on ly after long
research .
” Krause,
I in a review of Virchow ’s cri t ic isms
,says : “ I n order tha t
they might accoun t for these miliary tubercles,so frequen tly Observed
,Virchow
and his pup i ls, especia lly Han seman n , assumed tha t the erupt ion of tubercles
o ccurred regularly during the in ject ion s. For th is assumpt ion bo th master
and pupil are w i thout a proo f,because pa tho logical ana tomy has n ot yet
found a cri terion by which on e can determine the age of a tubercle.
” To
make tubercul in respon sible for these “m il iary and submi l iary n odules,
”
i t would .be necessary at least to Show that they occur red on ly dur ing its admin is
tration ; but these same mil iary nodules are found when tubercul in has n ot been
admin istered . Petruschky2 reports tha t he has observed con stan tly fresh
m il iary crops around o ld tuberculous foci in con sumptives who have d ied
w i th eviden ces of secondary in fection , but who had n ever received tubercul in .
T hat acute mil iary tuberculosis could be so frequen tly produced by the
i njec tion of tubercul in as to make i t one of the ch ief dangers of its adm1n 1s
tration is almost too absurd to receive no t ice ; but since i t has been so generally
bel ieved,we w i ll examine in to the supposed danger . A cute miliary tuberculo
sis can on ly be produced in one way, and that is by tubercle bac i ll i find ing
their way in to the general blood stream, ei ther“ by the rupturing of a tubercu
lous focus di rectly in to a pulmonary vessel , or in to the thorac ic duct .”
H ow
o ften th is happens we may judge from the invest iga t ion s of Ko ssel,3 who
together w i th a number of o ther investigators examined the blood in 800 cases
tha t were trea ted w i th tubercul in ,with on ly three posi tive resul ts
, and one Of
these doubtful . H e expressed h1s Op i n ion as fo llows : “I am convin ced after
a grea t number of negative results that a disseminat ion of tubercle bac i ll i
in to the general blood stream of pa tien ts treated with tuberculin does n o t take
place.
”Tha t such an acciden t m ight occasionally happen when the remedy
was admin istered in doses sufficien t to cause h igh local as well as general
react ion s can be bel ieved ; tha t i t would happen during the proper adm in istra
t ion o f tuberculin can scarcely be conceived . However,gran ting that such
an acciden t should occur during ei ther the faul ty or proper adm in istrat io n ,
i t would carry li ttle evidence against the remedy, for a focuswhichwould break
down so easily under the use Of the remedy would have l ikely broken down
w i tho ut i t,and
,scattering the bac i ll i in the blo od stream ,
caused the same acute
m i l iary tuberculos is .
A no ther supposed danger a t tend ing the use of tubercul in was tha t i t m ight
Jour na l of Tubercul os is , vo l . i i , p . 246 ; translated from Zeitsclzr i/ t [nor I I yg icnc undI nfectio n s/crankl i eiten ,
vo l . xxxii i , 1900 .
2 Paper before Berlin Co ngress ; quo ted in Journa l 0} Tubercul os is , vo l . 11, p . 6 3 .
sBer l incr kl in . Woclten sclzr i/t, 189 1, p . 47 1.
APPE N D I X 25
mobilize la tent foc i wh ich were apparen tly innocen t . Such a result
has never been shown ; so the bur den of proof st i ll rests upon the cri t ics.
And,gran t ing tha t the dangerous resul ts whi ch were po in ted out did actually
Obta in under the gross misuse to wh ich tubercul in was'
subjected, i t would
have abso lutely n o weight in the con sidera tion of the remedy when admin is
tered properly.
Virchow said :I I think thatwemay n ow with certain ty say that any processtha t can be brought about by tubercul in can a lso come about without that
remedy,but the course certain ly o ften seems to be extraord inar ily hastened .
”
E ven in sp i te of the disastrous resul ts caused by bad selection of cases,and
improper dosage,there were a few men who could n ot help seeing the true
value of the remedy. These began to use i t cautiously, and wi th one accord
determined tha t its proper admin istration con sisted in beginn ing w i th small
doses and . gradtI al ly in creasing as to lera t ion was establ ished,but always
avo iding marked local reactions and gen era l reaction s en t irely. Under th is
mode of admin istra tion,von Bardeleben
,Guttmann
,Renvers
,E hrlich
,
Petruschky, Corn et, Goetsch, Turban , Krause, and many o ther n o ted men
abroad, as well as von Ruck
,Whittakef,
'
D en ison,and o thers in America
,
report excellen t resul ts. I t is the general experien ce of al l those men,who ‘
have careful ly and pain stakin gly sought to do the remedy justice,that tuber
cul in is a very useful remedy,and tha t i t has a specific action in tubercular
cases. Professor Petruschky2says “
I f in its (tuberculosis) treatmen t we
desire to a tta in success,we must brin g to our resources al l mean s wh ich are
ava i lable to med ical scien ce, and a prominen t on e of these is undoubtedly
tubercul in . A fter n ine years of tria l of the remedy i t is possible to arr ive at a
con clusion of its va lue. On ly a compara t ively small n umber of physic ian s
have used and stud ied this remedy con t inually during this t ime, but i t is
sign ifican t tha t these have arrived at a favorable judgmen t of its va lue.
”
Dr . Goetsch3 reported his exper ien ce in on e hundred and seven ty-five cases
of pulmonary tuberculosis treated with tubercul in dur ing the past ten years .
Of the cases treated,one hundr ed and twen ty-five
,or seven ty-on e per cen t,
were cured . This report was made at the suggestion of Pro fessor Koch,and
to i t he appen ded a n o te,in which he sa id : “All physic ian s who have had
con siderable experien ce with tubercul in treatmen t,and have publ ished the
same (Spengler, T urban ,Petruschky, Krause, T horner, Heron ,
Rembo ld,
Baudel ier), assert tha t i f the trea tmen t is restricted to purely tuberculous and
n ot too far advan ced cases— tha t is to say, n on - febr i le caseS Of pulmonary
tuberculosis— the influen ce of the remedy is favorable wi thout except ion .
Should n ot the test imony of these cl in ic ian s, whose exper ien ce has extended
1 Ber l in er kl in . Wochen schr ift, 1891 , p . 19 1 .
g Paper before B erlin Congress ; reported in Jour na l of Tuber cul osis ,vo l . ii
, p . 6 2 .
3 D euz‘sche medicin ische Wochen schr ift, 1901 ; quo ted in Journal of Tuberculosis vo l .
i i i, p . 277 .
3 26 PULM ON ARY TUBE RCULO S I S
over the en t ire period fromKoch ’s announ cemen t in 1890 to the presen t time,
outweigh the doubt expressed by the hosts of physic ian s who have never given
the remedy a trial ? A ga in,I repeat, one positive result should outweigh a
dozen fai lures .
I have endeavored to presen t I n a clear l ight the c ircumstan ces under which
tubercul in,the first culture product Used in the treatmen t of tubercul osis
,
was given its tria l by the medica l world, and I have endeavored to Show why
i t has been held in such d isrepute. N ow let us make a more careful studv of
tuberculin i tself,and those o ther culture products whi ch have grown out of i t .
Soon after the germ theo ry of d isease was propoun ded , bacterio logy became
the most act ive bran ch of medicine. I n the labora tories the act ion of germs
was carefully studied. I n 1883 Charr inI di scovered that the blue co lor some
t imes seen on wounds and dressings was due to an organ ism,which
,when in oc
ulated in to an ima ls,caused death by sept icem ia . H e found a lso that bv
inoculating the an imals w i th steri l ized cul tur es of the same bac i l lus they were
rendered immun e to the inoculat ion s by virulen t cul tures . Brieger and
Frankel 2 found that the fil tered cul tur e flu id o f the d iphtheria bac i llus,when
heated to 60° or had protective properties, rendering guinea pigs lusus
ceptible to inocula t ion s w i th d iphtheria virus.
Such observat ion s as these, many ofwhich were made at that t ime, led to the
conclusion tha t pa thogen ic organ isms produce a certain substan ce dur ing their
growth wh ich is in im ical to the organ isms themselves.
The Observa t ion which led to the discovery of tuberculin was as fo llows
Professor Koch found tha t when heal thy gu inea p igs were in jected w i th virulen t cul tures Oi tubercle bacilli
,during the first few days the wound healed ;
but after two weeks n odules formed , which .broke down and con t inued ulcerat
ing un t i l death . But gu inea p igs a lready tubercular,when inoculated
,at
first showed the same smal l wound ; however, n odules did n ot form,on ly a
genera l indurat ion appeared about the po in t of inocula t ion ,which later became
n ecro tic,sloughed Off
,and quickly healed
,w i thout the lymph glands even
becoming in fected . When,in stead of virulen t cul tures
,dead cultures were
used in heal thy gu inea p igs, a loca l suppura tion o ccurred ; while in tubercular
gu inea p igs,even smal l doses caused death ; but i f the cultures were much
a ttenuated and adm in istered very gradua lly, the d isease, un less too far ad
vanced,came to a standst i ll . From these observations, Ko ch con cluded tha t
tubercle bac illi,during their growth
,produce a substance which has curative
propert ies in tuberculos is . A fter a series of experimen ts he produced tuber
cul in,wh ich is the cul ture fl u id upon wh ich bac i ll i have been grown
,co neen
trated to o ne- ten th its o r iginal vo lume, and fil tered .
Klebs fo und tha t tubercul in co n ta ined substances bo th beneficial and tox ic ,
, A r cl i . (fen . dc M éd., Paris , 188 2 , vo l . i i .
Untersuchungen'
uber Ptomains, dritte Theil . , s . 85 , 1886 .
3 28 PULM ON ARY TUBE RCULO S I S
Th is is en tirely free from cul ture flu id,and is the most
'
refined of al l the
cul ture products,and its efli cien cy has proven to be superior in the hands of a l l
who have used i t .
Thus we can see a gradua l evo lut ion in the production of these cul ture prod
ucts. First,the pur e cul tur e fluid was used— tubercul in ; then a purified
cul ture fluid— tubercul oc idi n and an tiphthisin ; then a mixtur e of cul ture
fluid and pro teids from the bodi es of the bac i l l i— tubercul inum pur ificatum ;
then an emulsion of bac illi and fragmen ts of same— tubercul in R . ; and finall y
a pur e so lu t ion of the bacil l i— watery extract . Tha t this is the end we do n ot
kn ow. We hope n ot. Yet we have in this last a product whose value can n o t
be questioned by any one who w i ll give it a reasonable tria l . All of these
products are of va lue,and
'
deserve a place in the history of the combat wi th
tuberculosis. I have had personal experien ce with a l l of these products in
trea tmen t,except tuberculin (my experien ce with i t being confined to mak ing
the tubercul in test), and I have been surprised tha t their worth has not been
more generally recogn ized .
I n what manner these cultur e products act is stil l deba table. Various
theories have been offered . The o ri ginal explana t ion of Koch tha t tubercul in
broke . down the granul a t ion tissue surroundin g the tubercles and allowed
the defen sive forces of the body to a t tack the bac il l i,o r by th is break ing-down
caused the tuberculous masses to be thr own off,was never accepted by those
who placed any value upon the remedy, because they con sidered i t abso lutely
essen tial to avo id the reaction s which would cause such a result.
Landgraf,I who observed the disappearan ce of tubercles in the choro id and
a lso on the ep iglo ttis under the use of tubercul in,gave i t as his opin ion tha t the
act ion of tubercul in “is n ot
,as was ma in tained
,an acute necrosis and throwing
off,n or a suppurat ing process, but an acute cheesy degeneration of the tuber
culous granulat ion masses fo llowed by their absorption .
”
Krause 2says “ I t is well known that tuberculin has no effec t upon the
actually tuberculous tissue (the tubercle with its necro t ic cen ter), but on ly
upon the newly fo rmed tissue,which is richly supplied wi th blood-vessels and
surrounds the tubercle.
”
B iedert 3 says : “When the irri tation (caused by the local reaction ) is moder
ate,an in creased cel l growth takes place in the en capsula t ing wal l o f the tuber
culous process . I f the inflamma t ion is more in ten se,marked exuda t ion o ccurs
,
wh ile in the stage o f extreme inflammatory irri tat ion ,cell dea th
,n ecro sis,
resul ts .
” T rudeau 4 says i t acts “ probably by inc i t ing the fo rmat ion o f fibrous
t issue .
Ber l iner kl in i sche Wochenschr ift, 18m , 286 .
“Zeitschr ift fur H ygiene and I nj ection s/era n /clzeiten ,vo l . xxxii i
,1900 ; tran slated in
Journa l of Tubercul os is , vo l . i i . p . 242 .
3 Ber l iner kl in . Wochen schr ift, 189 1, p . 107 .
4 Tra nsa ction s 0/ the A ssocia tion of A mer ica n. Phys icia n s , 1000.
A PPE N D I X 329
These quo tation s refer to tuberculin ,but sin ce all these culture produc ts
con ta1n perhaps the same,active pr in c iple
,they wil l
'
apply to the others l ikew ise . M y. experien ce with the cul ture products would lead me to bel ievethat they have an act ion which causes absorpt ion and remova l of recen t tuber
cles ; o therwise the roughen ed and en feebled respiratory n o tes would not
become n ormal whenheal ing has taken place.
The . many opportun i ties o ffered for studying these remed ies,where the
action can be wa tched by the naked eye, should furn ish suffic ien t eviden ce to
convmcethe most skept ica l that in culture -products we have remedies which
are a specific in their action upon tuberculous lesion s . E ven the earliest
reports made, those durin g the fated years of 189o'
and'
1891 , are replete with
such eviden ce. Albrant saw the complete disappearan ce of a con jun ct iva l
tuberculosis Landgraf I that of tuberculous processes of the choro id and
ep iglo ttis ; Renvers 2cured a pa t ien t whose pharynx
,ep iglo t tis
,and mucous
membrane over'
the aryten o ids were covered with ulcers ; Koen igshofer and
M aschke3 obta ined cures in tuberculous co rnea l ulcera tion s ; while it was n ot
at al l un common to see cases of lupus yield to its admin istration . The l itera
ture of recent years a lso bears much valuable test imony in such cases. D r .
von Ruck 4 reports many cases of laryngeal tuberculo sis i n which the lesion s
have disappeared .
Schmidt 5 in sists upon the unmistakable benefit derived from tuberculin in
the treatmen t ofm i ld cases of laryngea l tuberculosis where surg1cal in terferen ce
is un called“
for and ci tes many cases cured by such mean s . Dr . Hale 6 repo rts
a very in terestin g case of tuberculosis of the n o se,in wh ich the triangular
cart i lage was en tirely gone. T here was a large ulcera t ing surface dischargin g
pus a lon g the inner surface of the left ala of the nose,also ulcera tion s upon the
uvula . The d ischarge showed tubercle bac i ll i . A complete cure was effected
by the use of tubercul inum pu-rificatum (von Ruck). Dur in g the past Win ter
i t was the writer’s pleasure to see
'
an ulcera tion of the left vocal cord in a
pat ien t who had lesion s in bo th lun gs hea l under the use of the watery extract .
Wh i le in'
many cases such as these healing has been observed,the great field
for the culture products is in the treatmen t of pulmonary tuberculosis . I t
would be en ough to make the names of the d iscoverers of these products
immortal if their field of usefuln ess were l im i ted to the cure of Visible tubercu
IOus infil tra t ion and ulcers on ly,part icularly those affect ingthe laryn x, wh ich
compl icate n early one-fifth of al l pulmonary cases, an d which hereto fore have
I Ber l i ner kl in . Wochen schr ift, 189 1 , p . 2852 D eutsche med. Wochen schr ift, 1891 , p . 5 1 2 .
3 D eutsche-med. Wochen schr ift, 189 1 ,'
p . 76 .
4 Journ a l of Tubercul osis, vo l . i , p . 22 , an d Clinica l Report from Winyah San itariumfor
_the years 1899_ and 1900.
5 Kran kheiten del'f Oberen Luftwege, 1898.
6 Journal of Tubercul osi s, vo l . i i i, p . 239
3 30 PULM ON ARY T UBE RCULO S I S
a lmost bafli ed treatmen t . But the results obta ined in the lung are n o lessbr i l lian t
,as they are observed by the ear of the tra ined d iagnostic ian .
To make a fa ir test of culture products in pulmonary tuberculosis, one must,in the fir st pla ce
,be able to in terpret the patho logi ca l cond i t ion by the physica l
sign s,so as to know wha t is removable and wha t is n o t. Secondly
,he must
have some mean s of comparison . I t is impossible to carry in one’s mind the
percussion and auscul tatory s igns of one case, let a lone a dozen ; so,i f one
wishes to know whether or n ot his cases are improving,he shoul d make
systematic examina t ion s,say at least on ce a mon th, and record his fin dings
upon a chart for comparison at the next examinat ion . Thirdl y,he must
remember that the remedy must be used for a length of time. S l ight results
are o ften seen durin g the firstm on th of trea tmen t,and during the second the
change becomes more eviden t . But,finally
,when the recen t tubercles have
a l l di sappeared,and one has to deal wi th dead and decaying tissue
,he must
not become impat ien t because of the time that i t takes to hea l such lesion s.
Let us next con sider whether there is any ground for claiming an advan tage
for cul ture products over the hygien ic , climatic , and ordinary medi cal treat
men t of tuberculosis . T o thi s end we w i ll“
bring forth the sta tistics of variousmen who have had con siderable experien ce in tubercular work .
I n 1891 Langenbuch and Wo lff I reported 99 cases treated with tubercul in ,
and 99 without . Of the former, 33 were cured and 40 improved ; of the latter,
9 were cured and 45 improved . Of tuberculin cases, 73 per cen t were im
proved and cured ; of those treated without i t, 54 per cen t were improved andcured .
Goetsch in a recen t report, referred to above,sums up his experien ce sin ce
1891 , as having treated 1 75 pa t ien ts, and cured 1 25 , or 7 1 per cen t . The
rema in ing 50 patien ts in terrupted the cure-
from . time to time, so the resul ts
were less favo rable.
Heron 2S ince 1890 has treated 5 1 cases of pulmonary tuberculos is w i th
tuberculin . A t the end of 1900, 1 7 , or 333; per cen t, had been lost s ight o f.O f the rema in ing 34, 16 , or 47 per cen t , were well and earn ing thei r own l iving .
T en of these had been discharged seven years.
Krause 3 in S ix years has treated 27 pat ien ts, of whom 1 2,or per cen t ,
are well,and 13 , o r 48 per cen t , are improved .
Den iso n 4 repo rts 196 cases trea ted by culture products, including a l l the
va r ious products from tuberculin to wa tery extrac t . H is resul ts Show an ap
paren t recovery o f 34 per cen t , and a marked improvemen t in 42 per cen t . H e
remarks tha t th is was no t a l is t o f easy cases,the fo l lowing complicat io ns being
presen t“ Lupus three cases
,men ingi t is two , Bright
’s d isease o ne
, pyo ne
D eutsclze med. l Voc/zen schr i/t, 189 1, p . 935 .
2 Paper befo re Lo ndo n Tuberculo s is Co ngress , mm .
3 (’ i l ed in l l ero n ’
s paper before Lo ndo n Tuberculos is Congress , 190 1 .
4 J ourna l 0} Tubercul osis, vo l . i ii , p. I n .
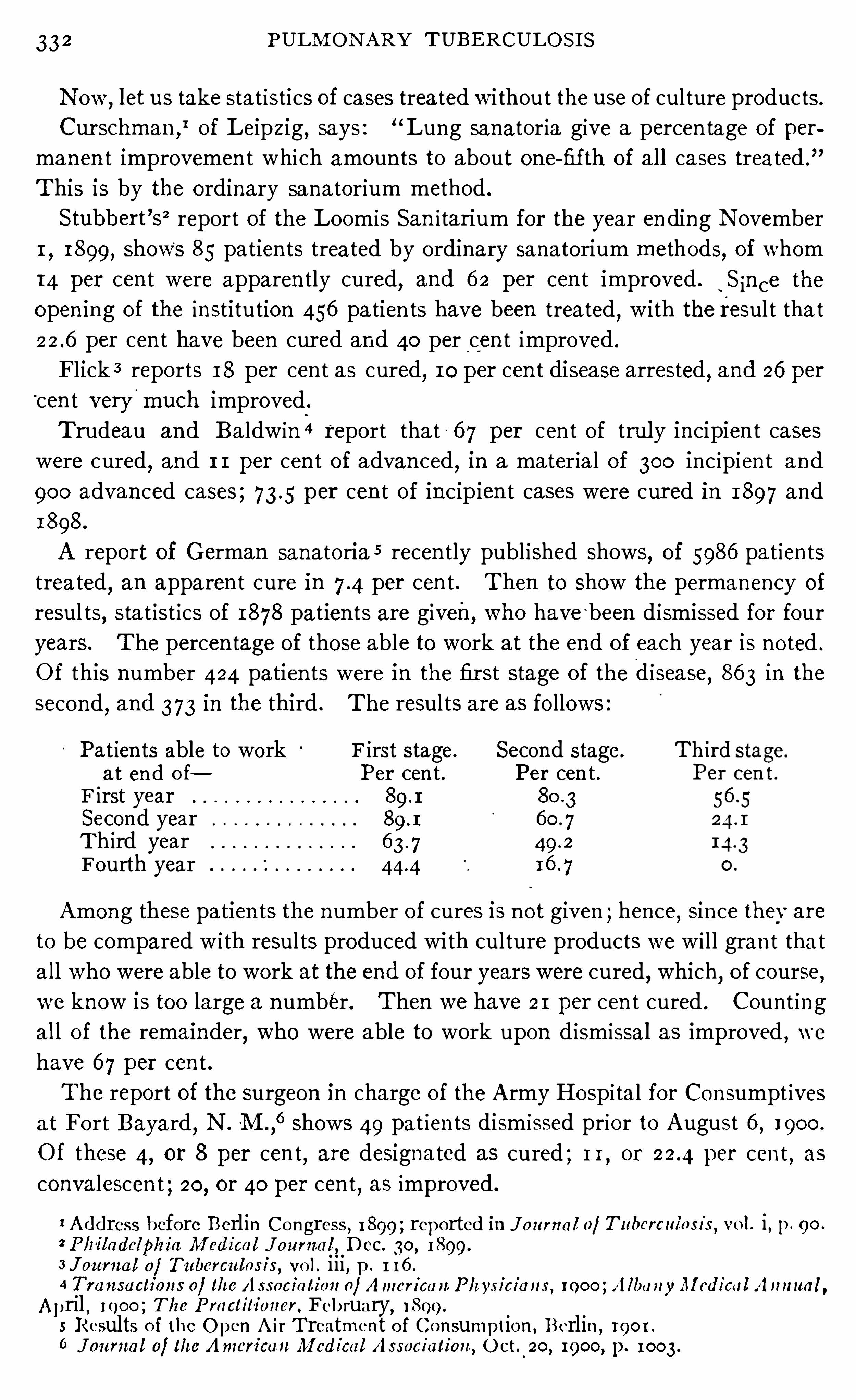
33 2 PULM ON ARY TUBE RCULO S I S
N ow,let us take stat istics of cases trea ted wi thout the use of cul ture products.
Cur schman ,
Iof Leipzig
,says : “Lung sanatoria give a percen tage of per
manen t improvemen t whi ch amoun ts to about one-fifth of a l l cases trea ted .
”
This is by the ordinary sanatorium method .
Stubbert’s2 report of the Loom is San i tarium for the year en ding N ovember
1,1899, Shows 85 patien ts trea ted by o rdinary sana torium methods, of whom
14 per cen t were apparen tly cured,and 6 2 per cen t improved .
‘
S in ce the
open in g of the insti tution 456 patien ts have been treated, with the resul t tha t
per cen t have been cur ed and 40 per cen t improved .
Flick 3 reports 18 per cen t as cured, 10 per cen t disease arrested , and 26 per“cen t very
'
much improved .
T rudeau and Ba ldwin 4 report tha t - 6 7 per cen t of trul y incipien t cases
were cured,and 1 1 per cen t of advan ced, in a materia l of 300 in c ip ien t and
900 advan ced cases ; 73 .5 per cen t of in cipien t cases were cur ed in 1897 and
1898.
A report of German sanatoria 5 recen tly publ ished shows,of 5986 pat ien ts
trea ted,an apparen t cure in per cen t . Then to Show the permanency of
resul ts,sta t ist ics of 1878 pa tien ts are given, who have
‘been d ismissed for four
years . The percen tage of those able to work at the end of each year is no ted .
O f this number 424 patien ts were in the fir st stage of the d isease,86 3 in the
second,and 373 in the third . The resul ts are as fo llows
Pat ien ts able to work F irst stage. Second stage.
at en d of Per cen t . Per cen t .F irst yearSecon d yearTh ird yearFourth year
Among these patien ts the number of cures is n ot given ; hence, S ince thev are
to be compared w i th resul ts produced with culture products we w i l l gran t tha t
a l l who were able to work at the end of four years were cured, which, of course,we know is too large a number . Then we have 21 per cen t cured . Coun t ing
al l o f the remainder,who were able to work upon d ismissal as improved , we
have 6 7 per cen t .
The report of the surgeon in charge of the A rmy Hospi tal for Con sumpt ives
a t Fo rt Bayard,N .
'M .,
6shows 49 pat ien ts dismissed prior to August 6 , 1900 .
Of these 4, or 8 per cen t, are designated as cured ; 1 1 , or per cen t , as
convalescen t ; 20, or 40 per cen t , as improved .
1 Address before Berlin Co ngress , 1899 ; reported in Journa l ofTubercul os is , vo l . i , p . 90 .
2 Phi ladelphia M edica l Journ a l , D ec. 30, 1899.
3 J ourua l of Tubercul osi s, vo l . i i i , p . 1 16 .
4 Tran saction s 0} the A ssocia tion 0/ A mer ica n Phys icia ns , 1000 ; A lba nyM edica l A n nua l ,A pril , 1900 ; The Practitioner . February, 1899 .
5 Results o f the O pen A ir T reatment o f Co n sumptio n , Berlin ,190 1 .
6 Journa l 0} the Amer ican M edica l A ssociation, O ct. 20, 1900, p. 1003 .
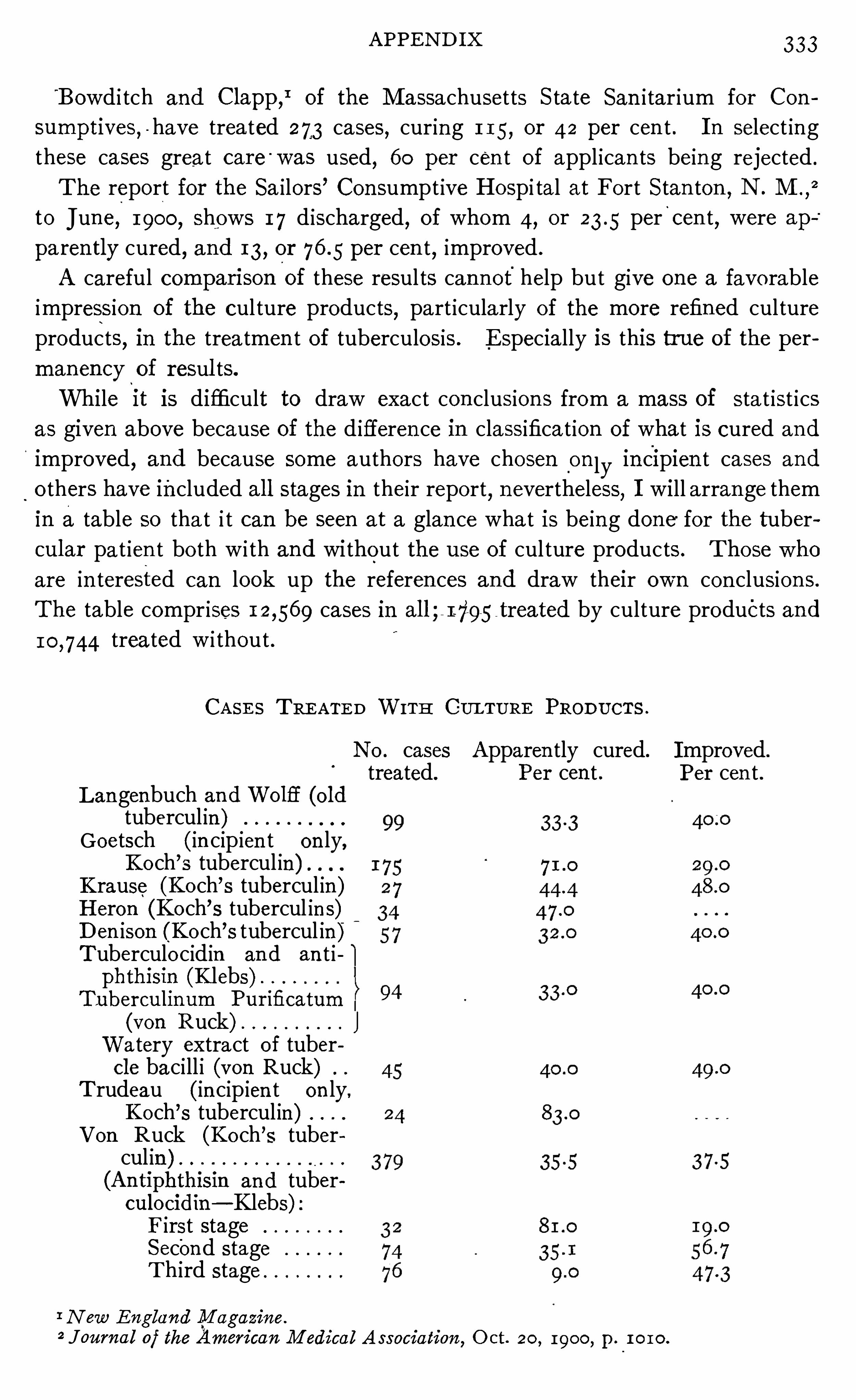
APPE N D I X 33
'
Bowd i tch and Clapp,Iof the M assachusetts S tate San i tar ium for Con
sumptives,-have trea ted 273 cases, curing 1 15 , or 42 per cen t . I n select ing
these cases great care '
was used, 60 per cen t of appl ican ts bein g rejected .
The report for the Sa ilors’ Con sumpt ive Hospi tal at Fort S tan ton ,N . M .
,
2
to June, 1900, Shows 1 7 d ischarged, of whom 4, or percen t,were ap
paren tly cured, and 13 , or per cen t, improved .
A careful compan son of these resul ts can n ot help but give one a favo rable
impression of the cul ture products,part icularly of the more refined culture
products,in the treatmen t of tuberculosis . E specially is this true of the per
manency of resul ts.
While it is difficult to draw exact con clusion s from a mass of sta t ist ics
as given above because of the d ifferen ce in classifica t ion of what is cured and
improved,and because some authors have chosen
_
on ly in cipien t cases and
o thers have included al l stages in their report, n evertheless, I will arran ge them
i n a table so tha t i t can be seen at a glan ce wha t is being done for the tuber
cular pat ien t bo th w i th and without the use of cul ture products . T hose who
are in terested can look up the referen ces and draw their own con clusion s.
The table compr ises cases in al l ; by culture products and
treated w i thout .
CA SE S TRE ATE D WITH CULTURE PROD UCTS .
N o . cases Apparen tly cured. Improved.
treated. Per cen t . Per cen t .Langenbuch an d Wo lfic (o l dtubercul in )
Goetsch (in cip ien t on ly,Ko ch’s tubercul in) .
Krause (Ko ch’s tubercul in )
H eron (Ko ch’s tubercul in s)
D en ison (Ko ch’s tubercul in )
Tuberculo cidin an d an t iphthisin (Klebs)
Tubercul inum Pur ificatum
(von Ruck) JWa tery extract of tubercle baci ll i (von Ruck)
T rudeau (in cip ien t on ly,Ko ch’s tubercul in)
V on Ruck (Ko ch’
s tubercul in )(An tiphthisin an d tuberculoeidin— Klebs)F irst stageSecon d stageT h ird stage
I N ew E nglan d M agazin e.
2 Journ a l of the Amer i can M edical A ssociation, O ct. 20, 1900, p . 1010.
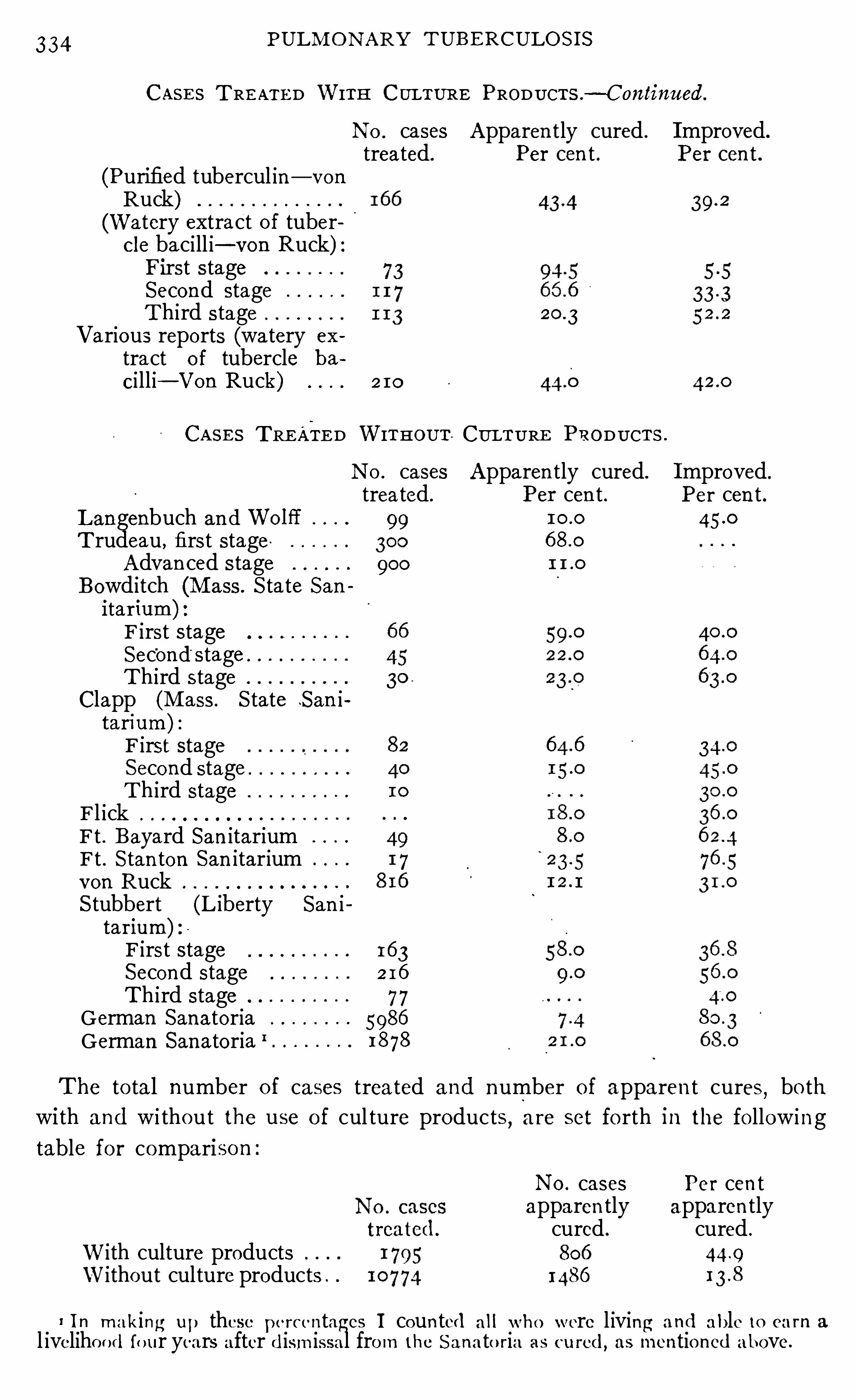
334 PULM O N ARY T UBE RCULOS I S
CASE S T RE ATE D WITH CULTURE PRODUCTS — Continued.
N o . cases Apparen tly cured . I mproved.
treated. Per cen t . Per cen t .(Purified tubercul in — von
Ruck)(Watery extract of tubercle baci ll i— von Ruck)First s tageSecond stageThird stage
Various reports (watery ex
tract o i tubercle ba
Ci lli— Von Ruck) 2 10
CA S E S TRE ATE D WITHOUT CULTURE PRODUCTS .
N 0. cases Apparen tly cured. I mproved.
treated . Per cen t . Per cen t .Langenbuch and Wo lfl 99T rudeau , first stage 300
Advan ced stage 900
Bowditch (M ass . S tate Sanitar ium) :F irst stageSec'ond stageTh ird stage
Clapp (M ass . S tate S an itarium) :F irst stageSecond stagTh ird stage
Fl ickFt . Bayard San itariumFt . S tan ton San itariumvon RuckS tubbert (L iberty San itar ium)F irst stage 163Second stage 2 16
Th ird stage 7 7German Sanatoria 5986
German Sanatoria I1878
The to tal number o f cases treated and number of apparen t cures,bo th
with and wi thout the use of cul ture products,are set fo rth in the fo llowing
table fo r compariso n
N o . cases Per cen tapparen tly apparen tlycured . cured .
With culture products 806
Without culture products . 1486
i I n making up these pe rcentages I coun ted a l l who were l iving a nd able to ea rn a
l iveliho od fo ur years after d ismissal from the S ana to ria as cured, as mentio ned above.
336 PULM ON ARY TUBERCULOS I S
beneficial and aid in bringing about the previous condi tion of laten cy, they don ot actual ly cur e. I n th is v iew I am confirmed by the fact that while without
Specific med ica tion subject ive symptoms may disappear, the objective evi
dence con t inues ; percussion dulness over the tubercular areas does n ot clear
up ; rales may d isappear, but the abnorma l resp ira tory sounds persist in the
parts whi ch were and st i l l are the sea t of tubercles,and the pat ien t st i l l reacts
to the tubercul in test ; whereas in pa tien ts that have been successfully treated
w i th the remedy under con siderat ion (wa tery extract of tubercle bac ill i) the
physical signs of recen t tubercular processes d isappeared en t irely,and n o re
action o ccurs to the tuberculin test up to thepresen t t ime,even in the earl iest
cases trea ted . I n the cases that came under treatmen t in the early
stage I have seen or heard of: no relapses yet. That i t produces a
rela tive degree of immun i ty has been Shown by the an imal experimen t,and
cl in ically by the marked freedom from exten sion of tubercular processes,and
from relapses of pa t ien ts who are under treatmen t,or have been d ischarged .
The quest ion is o ften asked,
“ Can these products do harm ?” Of course
they can,the same as morphine
,strychn ine or any o ther remedy. The
results of 1890 and 1891 Show tha t they can do harm ; but i t is‘
the experience
of a l l those who have made a careful study of the products,and given them a
fa ir trial in practice,tha t they cann o t do harm when administered carefully .
M y own exper ien ce has been very en couraging . I have made a careful study
ofmy cases,and I have never seen the least harm done . On the con trary , my
resul ts have been most happy, and I do not believe that they could be dupl i
cated by any o ther treatmen t .
The time has certa in ly arrived when the medical profession Should give the
cultur e products a fa ir trial . The op in ion s of men who have n ot tried these
remedies,but who have drawn their con clusion s en tirely from the wrong use
of tuberculin when i t was fir st in troduced,are to be compared w i th the op in ion s
of those who know from experien ce,and who report the cases that have been
treated,and Show the resul ts obta ined . Culture products have the right to
demand a trial by an unbiased court wherein spurious eviden ce will be dis
carded,and on ly posi tive eviden cetaken ; A l l friends of these remed ies will
stand by the dec ision .
I t must be remembered,however
,that the . friends of culture products
should not relax their efforts in o ther l ines . I t has been said by the cri t ics o f
men employing these remed ies tha t they use hygien ic,dietetic
,and climat ic
trea tmen t as well . So they do ; they would be foo lish i f they d id no t. The
surgeon comb ines a l l of,
these with his use of the kn i fe,and i t is con sidered
pra isewo rthy in him . So those who recogn ize the value of cul ture products
find their resul ts are much bet ter when their cases are properly “handled,and
they always endeavo r to gu ide the en t ire l ife o f their pat ien ts . I t should be
co nsidered as malpractice to simply in ject cul ture products,and leave the
APPE N D IX 3 7
pa tien t to_guide his own life. With reftzrence to this po in t Professor Koch
is reported to have said at_
the Tuberculosis Congress held in London in 1.901I
that he did not w ish anybody to get the idea tha t he himself thought therecould be any an tagon ism between treatmen t by tubercul in and the outdoor
trea tmen t in or out of sanatoria . H e has a lways in sisted that the two Should
go on together .
A careful review of this subject, together w1th pract ica l experien ce in the
use of. culture products, leads me to the fo l lowing Con clusion s :
1 . Culture products do have a spec ific act ion upon tuberculous foc i .
2 . That this has not been recogn ized is due to the early un fortunate ex
per ience with tuberciI l in : (a) When itwas used in too large and too frequen tdoses ; (b) when i t was employed in un suitable cases ; (c) when i t was held
respon sible for al l post-mortem findings.
3 . The field of usefulness for culture products is where recen t tubercles
are found, and th is espec ia lly in . in c ipien t cases.
4. I f used in advan ced cases, culture products will help remove areas of
r ecen t exten sion s,but must n ot be expected to remove dead
,decaying
,or
newly formed tissue.
5 . Where culture products are used,they Should be re- en forced by every
mean s at command . Every phase of the pat ien t ’s heal th Should be cared for,
and the proper hygien ic and dietetic measures prescribed.
6 . Where the case is managed properly and culture products are used,
the proportion of cures is greater than when culture products are n ot used .
7 . Culture products produce an immun ity,which pro tects the pat ien t from
relapses ; hen ce, make a permanen t cure more o ften than hygien ic and cl ima t ic
trea tmen t alone,which fact of i tself should be enough to warran t their Use in
al l su i table cases.
1 Reported in Br itish M edica l Jour'
nal,July 2 7 , 1901 , p . 214.
CHAPTER I V .
A CR I TI CAL STUDY OF TUBE RCULI N AN D ALLI E D PROD
UCTS BA SE D UPON A COLLE CTI VE I NVE STI GATI ON .
When our worthy presiden t requested me to prepare a paper to be read
before this section treat in g upon the subject of tubercul in and a llied products,
I thoughtbest to make the basis of the paper a co llect ive invest igation . Accord
ingly I sen t out three hundr ed and twen ty-five let ters to some of the lead ing
cl in ic ians of this coun try and E urope,tak ing pa in s to in clude the names of
those whom I knew to be espec ially in terested in the subject of tuberculosis,
requesting an swers to the fo llowing :
_ 1 . Have you had personal experien ce in the use of tubercul in or o ther
cul ture products in the treatmen t of tubercul osis?
2 . H ow many cases have'
you trea ted“
? What was the average period of
treatmen t? What was the resul t of treatmen t?
3 . Wha t is your opin ion of their . value,and do you favor their use in the
treatmen t of tuberculosis?
I have received one hundred and forty- three replies an swering my quest ion s
either wholly or in part . Tha t you may know the value of this investigat ion I
will men tion tha t replies have been received from '
such leaders in the crusade
aga in st tuberculosis as Schroetter and Weismayer , of Austria ; Gehrhardt,Dettwei ler
,Weicker
,Krause, Goetsch, Bandel ier, Gebhardt, Johne, Koehl er ,
Rietschel,and M oeller
,of Germany ; Turban and Spengler, of Switzerland ;
Brouardel,of Fran ce ; G iovann i , of I taly ; Ran some, Heron ,
Latham,M acken
zie,Semon
,Yeo
,and Saundby, of E ngland ; and
.
T rudeau,Bowditch
,von
Ruck,Loomis
, S tubbert , So lly, and Den ison ,of the Un i ted S tates ; and from
many more besides who occupy eminen t posi tion s as cl in ic ians .
For the kind and pa in staking repl ies of those who assisted me in this in
vestigation I wish here to open ly express my apprecia t ion . The cord ia l letters
wh ich I have received Show an in terest which is h ighly grat i fying, and ind icate
that the pro fession does not bear tha t host i le a tt i tude toward these remedies
that i t formerly d id . Wh i le the medical pro fession is naturally conservative,
yet i t is progressive, and is con stan tly taking advan tage of new methods of
curing d isease,and today i t stands ready to san ct ion at least , i f n o t adopt gener
ally,any remedy o r any method tha t will a id in the cure o f tuberculosis , tha t
disease wh ich has so long baffled its sk i ll .
A n analysis o f the repl ies to my inquiry Shows the probable reason why cer
tain members of the pro fession have fa iled to secure sat isfactory resul ts from
338
340 PULM ON ARY TUBE RCULO S I S
culin w i thout any spec ia l prepara t ion or fitness fo r the work,and the resul t
is about what should have been expected,about the same as would be pro
duced if the same men w i thout any previous preparat ion Should begin to ex
amine eyes and fit glasses . With such a trial,condemnation would be a fore
gon e con clusion .
When Koch gave tuberculin to the world,med ical men knew l i ttle of tuber
cul osis. E ven the pa tho logists knew little of the m in ute patho logy of the
disease. Few men had ever pa id close a t ten tion to its cl in ical course. Tuber
cular patien ts had n ever been watched day _
by day from the t ime the d isease
made its fir st invasion of the t issue. When men began observing,as was
necessary in the admin istrat ion of tubercul in,they were surprised to find
that the d isease run s an uneven course, and n ot kn ow ing wha t else to ascribe
the un favorable periods to , blamed many of them upon the remedy . Patien ts
may get worse, as many of them do,under hygien ic and d ietet ic treatmen t
—periods of absorption,fever due to mixed in fection and cavi ty forma tion
,
are apt to come in al l cases at a l l far advan ced— but this is n ot ascribed to the
treatmen t . Let this same thing happen'
if cul ture products have been used ,and i t is ascribed to the remed ies. When post-mortems were made on tuber
culin - trea ted pa tien ts during the early period of its use,everything found was
a ttr ibuted to the remedy ; when exactly the same thing could have been found
in cases treated without i t, or in those without treatmen t . I wan t to emphasize
this one po in t : The effects of cul ture products upon the course of tuberculosis
canno t be judged without an understanding of the natura l cl in ical course of
the disease ; nei ther can the post-mortem effects be judged without a knowl
edge of the post-mortem find ings where culture products are n ot used . So,
as essen tials to successful tuberculin treatmen t, I would place a knowledge of
the na tural course of the disease,a thorough train ing in patho logy
,and the
ab i li ty to'
in terpret the pa thology an te mortem by the clin ica l course and
phys ical S ign s.
N o less essen t ia l is it to understand the remedy to be applied . I t is not on ly
necessary to know wha t i t will do , but equal ly necessary to know what i t can
not do . The application of remedies to disease is a responsible study . T h is
respon sib i l i ty in creases w i th the gravity of the d isease to be treated and the
act ivity of the remedy to be employed . Therapeut ic exactness,al though
a lways to be desired,is abso lutely necessary at certa in times. Suppose that
a physician hears that strychn ine is a good remedy for giving to ne to the
nervous system ,and that
,in order to obtain best resul ts
,i t must be given in
ascend ing do ses . Wi thout studying the remedy,he begin s. Soon the pa t ien t
has a co nvulsion . H e gives h im ano ther dose,larger
,because in o rder to
obta in resul ts “it must be given
'
in ascend ing do ses.
”Ano ther convulsion oc
curs . So o n the pa tien t d ies . I t is very l ikely tha t this physic ian would ascribe
the dea th of this pa t ien t to the remedy instead o f to the improper use o f i t ;
APPE N D I X 41
and, of course, would fear to use i t ever after . Such an order of therapy gave
tubercul in a stunn ing blow when i t was fir st in troduced . N 0 on e knew much
about it, and, furthermore, n o exper ien ce had been recorded from which to
ga in kn owledge. I f there everwas a remedy tha t demanded therapeutic exact
ness,i t is tuberculin . Here we have a d isease whi ch
-
is grave and a remedy
most powerful — powerful for good, if, admin istered rightly ; powerful for ev i l,
if admini stered wrongly.
That the host i l i tyto cul tur e products is due to therapeutic inexactness isshown by my repl ies. Of the eighteen host ile cri t ics, n early al l based their
op in ion upon trials of tuberculin when fir st in troduced . Few of them have
tried the n ewer preparat ion s,which are more perfect, nor have they learn ed
the careful manner of employing them n ow in use.
Those who recommend them base their opin ion s upon a to ta l experien ce
of 5742 cases trea ted . T hose who do not recommend them have had ex
per ien ce in 8 13 cases.
Of those who did n ot recommen d them,onl y four had had an exten sive
experien ce. One trea ted 150 cases from four weeks to twelve and fifteen
mon ths. H e says “Cura tive value, especially in the hands of the gen era l
pract i tioner,is doubtful . Further experien ce in sana toria and under close
in spection for lon g periods s eems advisable.
”
An o ther,who had experien ce I n about 100 cases
,does not give the average
t ime of trea tmen t,but says that he saw n o advan tage over ord inary treatmen t
except in five or six cases .
Ano ther used o ld tubercul in and tuberculocidin for three years after their
in troduction,trea t in g 230 cases from five to ten weeks
,wi th n egative results .
H e does n ot “at presen t favor their use but favors keeping an eye on this lin e
of trea tmen t .”
A fourth trea ted 141 cases from three and a ha lf to four and a half mon ths,
but abandoned i t in the year 1891 . H e does n ot con sider the n ewer prepara
tion s as dangerous,but does n ot believe tha t they would be active in the smal l
doses recommen ded .
I t is n o teworthy that none Of these men are host i le in their a ttitude. Two
of them have had n o experien ce in recen t years.
A side from these four,on ly one man tried the remed ies on a case for as
long a period as S ix mon ths,and on ly two o thers had tried them as lon g as
three mon ths. The rest—
men tion from two weeks to two mon ths. So , of the
fifty- two men who did n ot recommend them
,on ly S ix (gran tin g that the one
who treated 100 cases used the remed ies more than three mon ths) had triedthe remed ies on a case for three con secut ive mon ths . I t takes three mon thsto cure a very early stage case ; and the danger of relapse is lessen ed if the t imeis extended lon ger. So we can say tha t , in the l ight of recen t developmen ts
i n the use of Cul ture prodiI cts, the fa i lure to recommend them on the part of
342 PULM O N ARY TUBE RCULO S I S
those who an swered my inqu ir ies (and I bel ieve the same wi ll ho ld good
throughout,for my an swers are from represen ta t ive men) was based ,
w i th
few except ions,upon faulty and insufficien t trial .
Con trast the short period of trea tmen t employed by those who do n ot favor
their use w i th tha t of those who favor i t . O f the latter,oneman was con vinced
of their value by trying them for two mon ths. Three gave thr ee mon ths ; and
the rema in ing twen ty-eight gave from thr ee mo n ths to more than one year as
the time necessary in order to bring about a cure. PetruschkyI believes the
best resul ts are obtained by extend in g the treatmen t over several years,giv ing
a course of a few mon ths each year .
I d id n ot undertake to ga ther s ta t ist ics as to the stage of the disease in which
the trial was made,but many made men tion of i t in their repl ies— enough to
show tha t i t was n ot made in su i table cases. When a n ew remedy is on trial,
i t Should be used in cases over wh ich i t is kn own to have an influen ce,and
then,after succeed in g in these, i t is time to experimen t in n ew fields .
The test of a remedy is that i t Should do wha t i t is recommended to do .
Than th is no more can be asked . Wi ll an t i toxin cure d iphtheria? Yes,
if admin istered early . Wi ll i t Cure when the pat ien t is mor ibund? I t is n o t
l ikely to do so . Th is is n ot held again st an ti toxin,however earn estly we wish
tha t i t m ight con tro l these advan ced cases. The success of an t i toxin treat
men t depends upon the earl iness of its admin istration ,and in spite of the fac t
that men have fai led to secure results in severe,advan ced cases
,the remedy
stands approved,for an ti tox in w i ll do tha t for which i t is recommended .
Culture products are remedies to be used in tuberculosis . That is wha t they
are recommended fo r . They are n ot represented as having any i nfluence
over dead tissue, or as being able to regenerate cel ls that have been destroyed.
I f they w i ll con tribute to the cure in pure tuberculosis— tha t is, in incip ien t
cases before mixed in fect ion,or breaking down w i th absorpt ion
,occurs
they w i ll do al l that should be asked of them . T hey w ill then stand as rem«
ed ies of value in trea tmen t . Un fortunately , tuberculosis is a chron ic d isease,and resul ts are obta ined slowly . I f cul ture products could produce thei r
resul ts as qu ickly as an ti toxin,their adopt ion would be qu ick and certa in .
Few men have the pat ience to work and wa i t mon ths fo r the resul t ; but un less
they do,they must no t hope to become successful phthisiotherapists .
T ha t these remed ies wi l l do what is cla imed fo r them is proven by the
resul ts obta ined by those who have had experience wi th them,as shown in the
fo llowing :
Jessen 2 trea ted 14 first- stage cases, curing 14, or 100 per cen t .
Go etsch 3 trea ted 356 first- stage cases,curing 278 , o r 78 per cen t .
I Petruschky. Zur Ko ch’
schcn Tuberculin B ehandlung . Bericht uber den Ko ngresszur Bekampfung (l e r T ube rkulo se a ls Vo lkskrankheit, Berlin ,
1899 .
2 Jessen . Centra l /rt. i n n . fli ed . 1902 , N o . 23 .
3 Go etsch. Person al letter to the writer.
344 PULM ON ARY TUBE RCULOS I S
able to produce better results,cur ing per cen t more patien ts by the use
of them than can be cured w i thout them,we should certa in ly be convinced of
their va lue.
I t is a no table fact, and one which my repl ies bea r out
,tha t nearly al l men
who have determ ined to give culture products a thorough test have becomeconv in ced of their va lue. A s sta ted above
,on ly five men who had given them
a tr ia l of six mon ths fa iled to recommend them . On the o ther hand,those
who had given them a trial of several mon ths in suitable cases,and whose
experien ce had extended over several years, w i th the except ion s men tioned,
recommended their use.
A s further proo f of their worth,I will ci te the comparative results obtained
wi th and without the remedies by two of the world ’s leadin g lung specialists
T rudeau of Saranac Lake,and T urban of Davos-Platz . T rudeau ’s exper i
en ce I will quo te from my former paper on “ Cul ture Products in the Trea t
men t of T uberculosis.
” I
“Twen ty- four cases were treated with the remedy
,of which 20
,o r 83 per
cen t,were apparen tly cured ; and 1 13 w i thout, ofwh ich 82, or 72 per cen t, were
apparen tly cur ed— a slight percen tage (1 1 per cen t) i n favor of tubercul in .
H e then chooses 50 pat ien ts discharged as apparen tly cured with tuberculin
sin ce 1894, and 50 patien ts corresponding in lesions and“t ime of treatment
who were cured w i thout tuberculin ,to see the relat ive permanency of cures.
Thr ee of those treated with tuberculin could n ot be traced,so three were
dropped from the l ist of those treated without tubercul in . Of the remain ing
47 , 41 rema ined well , 1 had relapsed and was living, 4 had relapsed and
were dead , and 1 had died of insan i ty . O f the 47 treated without tuber
cul in, 36 rema ined well , 6 had relapsed and were living
,and 5 had relapsed
and were dead . So we see 82 per cen t of those treated with tubercul in re
ma ined well,n ot coun ting the one dying of insan i ty
,as against 72 per cen t o f
those treated w i thout i t,a balan ce o f 10 per cen t in tubercul in
’s favo r ; or ,
putting i t in ano ther way, at the end of the time con sidered,68 per cen t o f
those treated wi th tubercul in rema ined well , and 52 per cen t of those treated
without tuberculin remained well,a balance of 16 per cen t in favor o f tuber
cul in .
”
The experience of Turban is so in teresting and so to the po in t tha t you
wi ll pardon me i f I quo te i t as described by Weicker 2 at length :
(a) Turban trea ted 21 cases in stage I I I wi th tubercul in : in 8 there
was tuberculous laryngi t is ; 9 cases survived fivey ears, three more rema ined
a l ive four years, o n ly 5 out of 21 d ied w i th in two years— 25 per cen t . O n ly
o ne died o f m il iary tuberculo sis,and tha t six and o ne-hal f years after treat
men t ; no ne d ied o f hemo rrhage. H ence tubercul in does no t increase risk o f
I Po ttenger. Therapeutic Gazette, Janua ry, 1903 .
9 Weicker. l l eitracge zur lt‘
rage der Vo lksheilstaetten . p . 22.
APPE N D I X 345
hemorrhage or generalized tuberculosis. Three were quite well six years
after— in al l, 5 were well . Tubercle bac ill i d isappeared from the sputum in
4 cases . Of cases treated in o ther ways— tha t is,w i thout tubercul in— 6 1
out of 84 d ied— 5 from hemoptysis, 3 from tuberculous men ingi t is ; 41 out of
84 died in less than two years— nearly 50 per cen t . Compare this with 25
per cent under tuberculin trea tmen t .
(b) Forty-eight cases in stage I I were treated wi th tuberculin : 9 died
within two years of treatmen t, 3 in three years and more, 1 6 were a l ive sixyears
after trea tmen t , 5 more five years after trea tmen t, 3 more four years after
treatmen t— in al l, 36 were alive. T hus of 48 cases, 36 were al ive and 1 2 dead.
Of 152 cases trea ted in the ord inary way, 45 were dead and 107 alive, but the
figures Show grea tly in the favor of tubercul in trea tmen t,because of the 107
a great number (49) had been under treatmen t mo re than on e or two years.
(c) Twen ty cases in stage I were treated wi th tuberculin . Tubercle ba
c i lli were in Sputum in 1 7 . A l l werewell : 10 of them sixyears after treatmen t,
2 more fiVe years after, 1 more four years after, 3 three years after, 2 two yea-rs
after,and 1 one year after treatmen t . I n al l the tubercle bac i lli disappeared
from the Sputum . The three cases giving n o tubercle bacilli in sputum had
to pass through the ordea l of the tubercul in test . On the o ther hand, 57
cases,in which tubercle bac ill i were n ot foun d in Sputum
,were treated in
ord inary ways. They were n ot subjected to tuber'
culin test . O f the rema in
ing 22 cases, there was one dea th, and in 2 cases there was Still tubercle bacilli
in the Sputum . Turban h imself says : ‘N ow
,if we compare the results
in early cases in which tubercle bac i ll i were found in the Sputum,the resul t is
substan t ially in favo r of tubercul in treatmen t . ’ Of the 86 cases with tubercle
bacilli in the sputum treated with tuberculin, 45 , that is 52 per cen t, yielded
a permanen t - result ; of the 241 cases with tubercle bac i lli in sputum tha t re
ceived no tubercul in , 95, that is per cen t, gave a perman en t result . S t i ll
more dist in ctly does the effect of tubercul in Show itsel f,if we ask how many
of these cases are now free from tubercle bacill i in their sputum . Of the 86
tuberculin pa tien ts 41 are n ow free from bacilli— 47 per cen t . Of the 241 n o t
treated w i th tuberculin,on ly 6 6 per cen t .
For fur ther sta t ist ics on the compara tive success of trea tmen t with and
w i thout culture products, see my former paper .
I
I f the fact tha t al l those men who are devo ting their energies to the trea t
men t of tuberculosis,and who have given tubercul in and allied products a
fa ir and extended trial,have found them to con tr ibute immeasurably to the
cure ; if the fact tha t those who use them cure a larger proportion of their cases
than those who do n ot ; if the fact that , in the hands of the same men ,a
'
much
greater percen tage of cures can be made w ith them than without them is to
be given con siderat ion,then we must give these remedies a very importan t
I Po ttenger. Ibid.
346 PULM ON ARY T UBE RCULO S I S
place in the treatmen t of'
tubercul osis. I t has o ften been said tha t the sameresul ts coul d have been produced w i thout their use as has been wi th them .
The mere saying of th is is n ot argumen t ; but I wish to men t ion a few ex
per iences wh ich refute i t . Un less he be very much prejudiced,the man who
trea ts the cases should be best able to judge whether or not the remed ies con
tributed to the result .
Lucius Spengler 1 says I n the di scussion which my former success pro
voked,
‘
they say tha t here at Davos they obtain equa l success withOut tuber
cul in,and that i t is difficul t to d ist ingu ish the part tha t has been con tr ibuted
tothe cure by clima te and the part by tubercul in . I simply wish to say that
of the 39 pa tien ts whom I have trea ted and whom I am st i ll treat ing wi th T .
R .
, 30 had been with me six mon ths or“
more,Some even several years
,before
T . R .
,was made kn own .
”
T horner 2 says “I have cured poor patien ts with tubercul in who could
n ot go to a sanator ium,and some o thers who were very poor and who had
fa i led to be cured by severa l cour ses of trea tmen t at d ifferen t sanator ia .
Denys 3 certa in ly has put the remed ies to a test,so tha t his results leave n o
doubt as to the part tha t was con tr ibuted to the cure by. them . H e trea ted 1 74
cases,curing 5 1 , or 29 per cen t, n early cu
'
ring 1 2,or 6 per cen t , and improving
6 4, or 36 per cen t . H e designa tes those as cured who have'
n o more baci ll i in
the sputum,whose genera l cond i t ion is satisfactory
,and who n o longer react to
tuberculin . H e says of these : “The tubercul in trea tmen t covered an aver ~
ageperiod of seven months. N o o ther method was used,nei ther rest
,air
,n or
medicine.
T h is is a cred i table show ing and compares favorably with the best resul ts ob
ta ined in sana toria,where rest
,fresh air
,and the best of food are provided ;
nevertheless,the friends of these products
'
do no t bel ieve.
th is to be the right
way to use them . O l iver 4 says Of pa t ien ts who rema in n inemon ths under
treatmen t in the A d irondack Co ttage Sana torium, per cen t go away ap
paren tly cured .
” Gabr ilow itch s says tha t as a resul t of ten years of treatmen t
at H a l il ia,Russia
,1000 cases have been treated
'
and 253 , o r per cen t ,apparen tly cured
,and 472 , or per cent , improved .
The idea seems to have gained ground in the m inds o f some men that tuber
cul in treatmen t and general hygien ic and d ietetic treatmen t are to be con trasted .
Such an idea is absurd . The on ly con trast is between those cases trea ted wi th
i t and tho se trea ted w i thout i t ; fo r rest , exercise, fresh air , d iet , hydro therapeu
t ic measures,and measures fo r the build ing up and strengthen ing o f the pa
S pengler, Lucius .
“Co n tributio n a l
’
etude du tra itmen t de la tuberculo se par T .
T ran slated from D eutsche med. Wochenschr i/t, 189 7 , N o . 36 .
9 Tho rn er T uberkulin und Tuberkulo se, Leipzig, 190 1 .
3 D enys . A ction curative de la tuberculin . D enys , co n tra la tuberculo se .
”A nn .
med. cl in . du I I a inaut, M a rch,1902 .
Jour . A rner . M ed. O ctober, 1900, p . 1006 .
5 G abrilow itch. Zel tschr i/t Tuberkul ose u J I eil staettenavesen , Bd . i ii , p . 207 .
348 PULM ON A RY TUBE RCULOS I S
early case'
of tuberculosis the pa t ien t seems to become immun ized ; so that the
d isease Shows less tenden cy to extend to heal thy t issue than is usually the case,
and also , when an apparen t cure has been a tta ined,there is less tenden cy to
relapse.
Wi th thi s posi tive,scien tific
'
proof'
of the immun izing power of culture prod
ucts,and the corrobo ra t ion which i t has secured at the hands of those who have
had large experien ce in their use, we con clude that where cultur e products are
n ot used in those cases whi ch are suitable,the pa tien ts are deprived of one of
the agen cies which would con tribute material ly to their cure.
W i th such proo f as to their va lue, should these remed ies be employed gen
eral ly, or'
should their use be confin ed to specia l ists? Upon th is po in t many of
mv an swers were emphatic,the writers taking the ground tha t where there was
so much hope for those afflicted with tuberculosis bound up in given remed ies,
i t were better tha t their usebe confined to thosewho understand them un t i l such
t ime as their exact mode of adm in istra t ion and the exact part con tributed by
them to the cure might be fully determ ined . This op in ion has been well
pressed by ed i torials in the J ournal of the American M edical A ssociation and
the BritishM edical J ournal during the past year,whi ch I w i ll quo te : I n the
hands of those who have used this prepara tion (tubercul in) most fa i thfully and
con tin uously,and
,therefore
,i t is to be assumed
,most in telligen tly
,the results
have been most gra tifying ; but tubercul in is a powerful agen t , and i t has shown
its ability for evil as wel l as good . I n the absence,therefore
,of a remedy pos
sessing spec ific curat ive propert ies and susceptible of safe general employmen t ,the cl in ic ian is forced to depend upon those natural resources by which the re
sistan ce of the o rgan ism to the act ivi ties of the tubercle bacill i are increased.
I
And later : 2 “Wi th a better understand ing of theway in which i t is to be used ,and of the cases which are suitable for its employmen t
,tuberculin now seems
about to en ter on a period of usefulness as a curat ive agen t .“This T . R . was proved to possess d istin ct immun izing properties
,and its
curative effects were demon strated upon tuberculous an imals . I t has now
been before the pro fession for some years, but does no t seem to have been much
employed,a l though there is good eviden ce that i t possesses the properties
cla imed for i t by its d iscoverer . I t is perhaps as well that there
should be no general desire to resume trial of this and simi lar remed ies,for
there can be l i t tle doubt tha t un t i l their mode of product ion has go t far beyo nd
its presen t imperfect stage,the use of these preparations ought to be restricted
to tho se who clearly understand the na ture o f the materia ls with wh ich they
a re wo rk ing .
” 3
The to ne o f these ed i to rials leaves no doubt as to the value o f tubercul in . I t
7 E ditorial : Jour na l of the Amer ican M edica l A ssociation,M arch 29 , 1902.
2 Edito rial : Jour na l of the A mer ica a M edica l A ssociation,A ug . 16 , 1902 .
3 E dito rial : Br itish M edical Journa l , J an . 1 I , 1902.
APPE N D I X 49
is to be hoped that it w i ll become more generally used, but i t is further to be
hoped that n o on e w i ll a ttempt its employmen t who w ill not first thoroughly
study the remedy and thoroughl y acquain t himself w i th the d isease, as to its
physical S ign s, cl in ical course, and patho logy. Then , w i th pat ien ce and per
severan ce and a thorough con tro l of the pat ien t to be trea ted ; he Should pro
ceed caut iously,eve
'
r‘
recogn izing the importan ce of his work and the end to be
a ttained.
I now wish to quo te some of the opin ion s '
as expressed?
in the“
letters and
monographs received during th is investigat ion ,in order to Show the a tt i tude of
the pro fession toward these remedies. For obvious reason s I wi ll n ot men t ion
the names of the wr i ters in conn ect ion with the let ters, but where I quo te from
a publ ished article I will ci te the referen ce.
Here is a characterist ic let ter from one who does n ot recommend the reme
d ies : “ Experien ce with o ld tuberculin in eleven cases— eight for severa l weeks
and three for three or four mon ths. One seemed practica lly cured . Heard
from her at the end of one and two years. T rea ted two with watery extract of
tubercle bac i ll i . Under al l these serums and some o ther kinds of so ~ ca lled
Specific trea tmen t many patien ts improve-fer a time
,ga in ing in weight
,cough
ing less, and even showin g a lessened proport ion of bac i lli in the Sputum . I
know of no cures from any of them a lon e. Of course,my li ttle experien ce is
not enough to base an opin ion on,but I am quite sure from it
,added to that of
o thers,tha t we have not yet S truck the right thin g .
”
Ano ther wri tes : “ I have treated twen ty cases from three weeks to two
mon ths. T reatmen t resul ted in n o improvemen t,but fortunately
‘
n o acciden ts .
M y opin ion is un favorable.
An o ther says “Have used Koch’s tubercul in
,1891 , T . R .
,and oxytuber
culin . T reated eight cases from two to sixmon ths. Resul t : in some cases negative; in o thers
,especially thee arly cases, the pa t ien ts seemed to break down
more rapidl y than usua l . My reading and experien ce a l ike make me doubtful
of their value.
”
Ano ther : “T reated a few cases . Results were unsat isfac tory and bad.
I bel ieve i t of very l i ttle if any value, and I do not favor its use. I discarded i t
mysel f because I believed it harmful . ”
S till ano ther says : “Have n ot used it myself, but observed ten cases under
o thers. D o n ot recall period of treatmen t . I n on e case there was recovery .
I have n ot seen or heard of a recovery or improvemen t that could n ot have beenbrought about under equally good env ironmen t by o ther treatmen t . I believe
the method to be dangerous in un sk i lled hands,and unnecessary in skilled
ones.
”
N ow I wish to give some of the opin ion s on the o ther side. One man says
Have used i t con stan tly sin ce its discovery by Koch,restric t ing its use to
pa tien ts at the San i tar ium who are under close observa t ion and who are treated
350 PULM O N ARY TUBE RCULOS I S
free. Have treated perhaps 100 to 1 25 cases, averaging about five mon ths,wi th generall y en couragin g results. I favor their use in hosp i ta ls and san
ator ia,and by men thoroughl y fami l iar with this form of trea tmen t
,in su i table
cases on ly. Their indiscrimina te use in acute and febrile cases is not ad
missible.
Ano ther While I recogn ize tha t tuberculin is not a cure for al l cases of
tuberculosis, yet I have n o ted tha t i t has contributed immeasurably to the cure
in cases which,under dietetic
,hygien ic treatmen t at the sanatorium showed n o
sign s of heal ing . I ho ld the comb inat ion Of hygien ic,dietet ic
,sana torium
treatmen t wi th tuberculin treatmen t as the most useful in al l those cases which
presen t a doubtful progn osis, w i th a possib i l i ty of cure. I have treated about
100 with the new tubercul in ; cann o t say how many w i th the o ld . T reatmen t
lasted over a period of several mon ths,and was given with in terva ls of rest
between .
”
A no ther wr i tes Have used o ld tubercul in ,T . R .
,and bacillus emulsion
in 446 cases, treating on the average 130 days . Seven ty—eight per cen t have
been discharged as cured,and all of those have beenunder my observation more
or less ever S in ce,some s in ce1891 . I ho ld tha t Ko ch’
s tubercul in as applied
in purely tuberculous cases,and by the method described by me
,is a Specific
remedy aga in st tuberculosis,and at presen t the best treatmen t . ”
A no ther says Have used them for ten years in about 300 cases with good
results. The use depends largely upon the proper selection of cases and the
exclusion of those already overtaxed by the care of tox in s appreciated by their
non - resistan t systems . D iagnostic sk i ll and knowledge of techn ique become
then most importan t essen t ials to the successful use of th is immun izingmethod .
”
SpenglerIsays : “Thus with the careful cho ice o f cases
,the jud ic ious
appl ica tion of T . R . has given me on ly good resul ts,and I con sider i t at the
presen t time as a very valuable remedy in phthisio therapy.
”
Heron 2says : “
I n properly selected cases, with proper surroundings, and
proper care,tuberculin can be used , n ot on ly w i th safety but with distinc t bene
fi t in the treatmen t of tuberculosis .
”
M oel ler 3 says : “A ccording to our experien ce, (in the sanatorium at Belzig)
we co n sider tubercul in as an extraord inari ly va luable remedy in con nect ion
with sanatoria . M ore observa t ion s are needed to determ ine wh ich cases are
mo st su i table to the o ld preparat ion ,and which are suited to T . R . ; but as to
the curat ive value there is no doubt . ”
Petruschky4 expresses the hope that the personal fight which was shown in
I S pengler . Co n tributio n a 1’
etude du tra itmen t dc. la tuberculose par T . R .
”Pub
l ished in pamphlet fo rm from D eutsche med. l Vochenschr i/ l , 189 7 , N o . 6 .
2 H ero n . Repo rt to the Comm ittee o f M anagemen t Of the City o f Lo ndo n I l o spita l fo rD iseases o f the Chest , M a rch 2 1 , 190 1 .
3 M o eller . Ueber d ie (l iagno stische und therapeut ische Verwendung des T uberkul ins .
Zei tschr ift [itr Tuberkul ose 11nd Ti eil staetten i eesen , 1902 , p . 302 .
4 Petruschky. D er gegenwaertige S tand der Tuberkulin -behandlung, 190 1 .

I N D EX
Abdominal compress in insomn ia, 27 7Abortion induced in tuberculous women ,
270
Abscesses, sterile, fo llowing S low absorption of baci llary emulsion s, 1 76
A cid, picric, coun terstain for bacilli , 3 7Adhesion s, apical pleural , cause of
hoarsen ess, 9effect of, causing di splacemen t of
thoracic viscera , 84pleural , cause of drawing in of in tercostal spaces, 63pleural , show signs on auscultationresemblin g rales, 253pleural , sometimes obliterate cavity,
250
Advan ced cases, plea for treatmen t of,223
specific climate sought by, 229suffer from results of tuberculosis ,
223tuberculin relatively of greater valueI n , 201
Advan ced cases not hopeless , 95A dven titious sounds heard on auscul
tation , 76
Agaracin in n ight sweats , 274Age, a factor in prognosis , 98A gglutinating power of blood, in creased
by in jection of bacillary products,183
A gglutinat ion of bovine and humanbacilli differ, 35
A ir , bacteria in , killed by sun light , 234comparison of bacterial con ten t ofthat of rooms, and the open , 1 24
effect of impure, upon the individual ,123
outside'
and in side compared, 1 23purity depends somewhat on mo tion ,
1 23A lps , immun ity from tuberculosis no ted
in , 233A lkaline hot drinks in treatmen t of cough,
2 72
A ltitude, causes extra demand upon the
system for tissue repair, 238
A ltitude, causes greater strain on and
developmen t of heart and lungsthan low elevation s, hen ce um
'
suited to treatmen t of pulmonarytuberculosis , 238causes of blood changes at, 236disadvan tages of, for the tuberculous,
236
effect of, upon heart at rest and
during exercise, 240false con clusion s drawn from apparen t immun ity. from tuberculosisn o ted at, 233heart affected by, 236immun ity from tuberculosis thoughtto be con ferred by, 233many pat ien ts unfit for life at, 234merits of low and high , 235objection s to , in treatmen t of tuberculosis, 240
pat ien ts suited to treatmen t in , 235patien ts un suited to treatmen t in , 235respirat ion in creased in force and
frequen cy by, 236table showing effect of, on pulse,
respirat ion and vital capacity, 23 7thought to be an essen tial to cure,
233treatmen t of tuberculosis con trary tothe prin ciple of rest , 236
American D esert , immun ity from tuberculosis noted in , 233
Amyl n itrite in treatmen t of hemoptysis ,
A n emia in early tuberculosis, 10, 1 7A ndes , immun ity from tuberculosis n o ted
in , 233A n imal .experimen tation , immun iz ing
power of tuberculin proven by,182
An tagon ism, vaccines fromhuman and
bovine type of bacilli Show, 1 79A n t ibodies may be produced by dead
bacteria or their toxins, 1 16produced in in fection s, 1 16Specific, 1 16
An titubercle serum, 207
23 353
354 I N D EX
Appet ite, causes o f variab il ity o f, 138improves with improvemen t of patien t , 138
in early tuberculosis , 9not safe guide for eat ing in tuberculosis , 13 7
so lid food st imulates, more thanliquid, 259variable in tuberculosis, 49
Apex, height of, in health , 70n atural differen ce in right and left
and cause of same, 16Apex beat , detection of difficult in ad
van ced tuberculosis, 89drawn away from chest wal l in
-advan ced tuberculosis, 64lowers from b irth to o ld age, 80
posit ion of, eviden ce of pulmonarycondition , 6 3
Apex of heart , palpat ion of, facilitated byhaving pat ien t bend forward, 7 1
Apical outlin e, method of determin ing, 19shows con traction in early tuber
culosis, 19A rn eth , changes in n eutrophi le leucocytes
no ted by, 186
A rrestmen t, possible in many advan cedcases, 95
A ssimilat ion , open air improves, 1 24A thletes, heart and . lun gs of, overde
veloped, 238
tuberculosis common in ,
“
238
A tropine in n ight sweats , 2 74Auenbrugger’s percussion , 6 6
Auscultation , changes on , in early tuberculosis, 20
difficult ies in , 21
effected by pressure on stethoscope,
I Serrors in , 21
furn ishes most rel iable eviden ce inearly tuberculosis , 20
in advan ced pulmonary tuberculosis , 73
Auscultatory percussion , 6 7A uscultato ry stroking in diagnosing
pleural effusion , 25 1
Bacill i , bovine and human cause tuberculo sis in man , 1 7 7bovine and human produce les ionswh ich differ, 1 78
bovine and human type diff er ingrowth , 1 77bovine and human type o f, an tag
on istic . 17 7
Bacil l i , causing in fect ion , come from a
previous case o f tuberculosis , 103change from products made fromhuman , to bovine and vice versavaluable in therapy, 195ch ief source o f, human beings withadvan ced tuberculosis , 102
cl imat ic condition s favoring destruct ion of, 234cl imat ic condition s favo ring growthof, 234climat ic condit ion s in imical to , foundat al l elevat ion s, 234constan t attempt of, to escape fromfocus of in fection , 92
cultural differences of, of human and
bovine types , 34dead, Show more tenden cy to the
production of fibro id t issue thanliving, 1 15
disappearan ce of, from sputum ,
stat ist ics o f, 202effect of sun light upon , 104examination of stoo ls fo r , 245form of, an d prognosis, 99foun d in sputum after hemoptysis, 27human and bovine, an tagon ist ic intheir action , 34human and bovine type of, difl
'
er
en tiated, 33 , 34long beaded, less virulen t , 99mobilizat ion of, a myth , 189mult iplicat ion of, outside of thebody,
102
not to be relied upon fo r early, diagn osis , 25
numbers of, in prognosis, 29, 99presen ce of, shows destruct ion o f
t issue, 29products o f, action o f, 18 1
retain virulence mon ths outside o f
body, 103rules govern ing stain ing fo r , 30Short th ick , virulen t , 99sta in for differen t iating bovine and
human , 35type of, made basis o f therapy, 1 77type o f, studied in 1 12 cases , 34tubercle, discovery o f, 286watery extract o f (von Ruck) , 1 76
where, ch ief factor, the tendency istoward fibros is , 1 15
Bacill i emuls ion (T .
-E . , Koch), 1 75Bacill i emuls ion , abso rbs S lowly , 1 76
do sage o f, 1 76
produces greatest immun ity, 1 76
356 I N D EX
Breath in g, weakened , cause of, 73weakened , due to en larged bronch ial glands , 74weaken ed, due to thickened pleur a ,
74weakened, in early tuberculosis,cause of, 23weak , in pneumo thorax, 255
Brehmer, establ ished first san atorium ,
exercise a feature ofhis treatmen t , 142Bronchitis , relieved by dry air of low
bacterial con ten t , 240Bron ch ial catarrh , eviden ce of activity
in tuberculous process, . 5 1
symptom of tuberculosis , 9Brown , permanen cy of resul ts in cases
treated by, where tubercul in was
used, 203statistics of disappearan ce of bacill ifrom sputum, 202
Bull och , table of, Showing opson icpower of blood in lupus , 185
Bungalow, Po ttenger Sanatori um, 2 19
Calcium chlorid in treatmen t of hemoptysis, 265
Cal iforn ia , Southern , climate of, 232
Candor, essen t ial in dealing with tuberculons patien ts, 26 , 280
Stimulates co -operation , 283Carbohydrates, form of admin istration ,
1
Cattle, milk from, as cause o f tubercu
losis , 3Cavity, metallic resonan ce over, 73percussion note over, 72Sputum from, with odor, 48
Cell activity, sun light increases , 234Cen trifugat ion , method o f examin ing
Sputum , 38
Chart o f chest , necessary fo r accuracy, 13Chest , bulging o f, in pneumo thorax, 255chart o f, necessary for accuratecomparison , 13
index o f, 6 2
movemen ts o f, on inspect ion , 6 2
phth isical , 6 1phth isical , broad o r deep ?, 6 1Shape o f, conditions affect ing, 6 2shape o f, differs in healthy individua ls , 60
shape o f, due to patho logical changes ,6 1
Children , bo rn o f tuberculous mo thermay be strong, 26 9
Chi ldren , danger of, being in fected byassociat ing with afli icted, 106 , 108
danger o f, in fection to , throughcrawling on floor, 7later on es of large fami ly mostsusceptible to tuberculosis , 8tuberculosis of glands frequen t in ,
248
Childhood, Behring’s theory of in fectionthrough milk, during, 102prophylactic meas ures in , 106
t ime when in fect ion o ften occurs , 3tuberculin diagn osis i n , 45
Chill , accompanying pleurisy with effu
sion , 25 1
in mixed in fection , 25 7treatmen t of, in mixed in fection , 258
Chloralamid in in somn ia, 2 7 7Circul atory system in advan ced tuber
culosis, 49Classes in tuberculosis, 1 10Clavicle, differen ce in elevation of ac
romial ends of, a S ign of earlytuberculosis,
'
18
Click , upon inspirat ion , mean ing of, 7 7Climate, best , for given individual , 230best , for individual where t issuechange is carried on to best advan tage, 231care in prescribing, n ecessary, 233change of, not advisable for a l l .
230
change of, should n ot be made bypatien ts without money, 230
cho ice of, patien t’s judgmen t not
Safe in , 232
coast , of Southern Cal iforn ia , 232
co ld, and those o f high alt itudessuited to robust individuals , 23 1co ld , demands high rate of t issuechange, 23 1
co ld , dry, disadvan tages o f, 240co ld, effect of, 23 1co ld , humid , disadvantages o f, 240
comparison o f h igh altitude, and
low dry, 236compl ications must be consideredin cho ice o f, 23 1
diet varies according to , 133diurnal range in , 23 1
dry, warm, effects o f, 23 1
effect o f, depends on heat abstracting power, 23 1
elemen ts o f importance in . 229 . 23 1
elements o f, which favo r the treatmen t o f tuberculosis . 240
I N D EX 3 57
Climate, favorable, facilitates open -air
treatmen t, 241
favorable, n ot abso lutely necessaryfor cure of tuberculosis, 230foo lishly advised, 229foo t-hill , of Southern Californ ia , 232
good .use of bad, better than bad
use of good, 230importan t consideration in cho ice of,
.
230
impo rtan t in health and disease, 229in the treatmen t of tuberculosis ,
’
229in land, of Southern Californ ia , drywith coo l n ights, 232
irritates, 23 1majority must be treated without ,230
mixed and secondary in fect ion s preven ted by sunny, 234most good from, can come wherepatien t main tain s best nutrition ,
231
moun ta in , characteristics of, 235near-by pl aces differ much in , 232
n o specific , for tuberculosis , 229pecun iary circumstan ces con sideredin change of, 230
physical condition s must be con
sidered in change of, 230
primary effect of, 23 1reactive power of pat ien t most importan t factor in cho ice of, 23 1
rigorous, for robust individual , 23 1rigorous, in jures weakened pat ien t ,
232
rigorous, makes greater demand on
system than warm equable, 229rigorous , un suited to weak individn als, 23 1
soo thes, 23 1stage of disease must be con sideredin cho ice of, 230
strength and react ive powers of
pat ien t importan t in cho ice of,231
usual un fa ir comparison of, at low
and high elevat ion . 235warm, humid, disadvan tages of, 240
warm, humid, effect of, 23 1Climat ic change desirable, 241
n ot essen t ial , 241Specific instruction s for , n ecessary,
2 2
Climat ic condition s favorable to destruction of baci lli foun d at al l elevat ion s, 234
1
Climatic conditions in common betweenaltitude and low , warm, dry countries , 233treatmen t , value of, lies in , 240
Clin ical distribut ion of lesion s producedby bacilli of the human type, 1 78forms of tuberculosis of bovine and
human types differ, 1 7 7Closed“ tuberculosis does notmean a cure,
299Clot , importance of, in check ing hemop
tysis , 265Clo thing, importan ce of proper, 126
too'
much, lowers tone of skin , 126
Coal tar products , little use for , in fever,258
Codein , cough ofpleurisy relieved by, 254in treatmen t of cough , 272
Co in ciden ce, cases ill ustrating how suchoccur, 40 , 145
Co ld compress, treatmen t of tuberculouslaryngit is with , 243
Colds, repeated, symptom of tuberculoS I S , 9
simulated by activity in tuberculousprocess, 5 1
Co lon , irrigat ion .of, in tuberculousdiarrhea , 247
Commun icab ility, fear of, 107Comparison of length of life of treated
and un treated cases, 292Complicatin g processes cut short by rest ,
Complications , considered in climat icchan ge, 23 1
influen ce of, on progn osis, 98of pulmonary tuberculosis , 242temperature above n ormal in morning suggests , 54treatmen t of, with tuberculin , 2o 2
tuberculous, preven ted by use of
tuberculin , 199tuberculous, will yield to in telligen ttreatmen t , 224what , are a barrier to treatmen t
223Con cept ion , preven tion of, a duty in
tuberculosis , 270Condit ion s favoring spread of tuberculo
sis, 234Confiden ce between physician and pa
t ien t necessary, 285Con stipat ion , cause of and dietary treat
men t of, 139treatmen t of, in in test inal tuberculosis, 246
358 I N D EX
Consumption , a condition resul t ing fromtuberculosis, 223
Con traction of lung, pa in in , 5 1
Co -operation of physician and patien tnecessary, 283
Corsets , force diseased parts o f lun g todo increased work , 15 1
Cough , caused by disease of oro an d
naso -pharynx, 48caused by wrongmethod of livin g, 48cause of, 27 1
cause of, key to treatmen t , 2 71codein in , 254co ld compress relieves, 243danger of, and value of, in hemoptysis , 26 5
due to condit ion s in upper air
passages , 272effect of, 27 1
emesis produced by, 272harmful effect of, upon lun gs, 144in jures tender fibri ls of n ew t issue,
27 1
in terferes with healing, 15 1in terferes with nutrition , 27 1
may or may n ot be presen t in earlytuberculosis , 9much of the usual, un necessary, 2 7 1n o th ing characteristic in , 48
of tuberculous laryngitis, rel ieved byorthoform and hero in locally, 243pat ien t should be in structed to
resist , 271rest relieves, 144treatmen t o f, 271unnecessary, much of the usual , 48wearies and exhausts the pat ien t , 27 1wet jacket in , 272
will power most po ten t remedy for ,27 1
Cracked pot sound , 73Creaking, heard in vicin ity o f cavitv,
wh ich resembles rales , 76Creoso te, method o f admin istering, 272Croquet , a permissible sport , 149Cultural differen ces in bovine and
human bacill i , 1 77Curab il ity, evidences o f, at hand , 221
ideas o f, ga ined credence duringpast fifteen years , 287
o f tuberculo s is , 94, 1 14
o f tuberculosis depends upon . 28 1
Cure , can be obta ined in n early a l l earlycases , 288chances o f, best in go o d cl imate within tell igen t treatmen t , 230
Cure, closed condit ion does n o t mean ,
299delay takes away chan ces o f, 221 ,
288
early, best prophylact ic measure, 101early diagnosis first importan ce in ,
288
factors upon which , depends, 288frequen t visits of physician in
sanato r ium aids in , 226
how obtained quickest and surest221
investmen t feature o f, 290
n ature of, 1 15n ature of, in tuberculosis, 165regain in g ofweight n ot test o f, 298responsibili ty of physician in , 94responsib i lity of, upon family phys1c1an , 94t ime importan t factor in comput ingcost of, 221tuberculin as a test for , 45 , 299tubercul in produces, more surelyand more quickly, 199what is a?, 298
Cuspidors, patien ts shoul d use, 103Cyan osis, diseases of heart causing, in
compat ible wi th tuberculosis, 2 1 1Cystitis, tuberculous, treated by tuber
culin and dead culture fromassociated in fection , 26 6
D aCosta’s sign , 24
D avos, a lesson from, 1 1 2
n at ive death rate from tuberculosisnot in creased in , by visit ing con
sumptives , 1 12
D eath rate from tuberculosis , decreaseof, in Prussia, 1 1 2
responsibility for , must l ie largelywith phys icians, 281
D ecept ive terms no t permissible, 28 1
D eep'
breathing, blood and lymph flow
in lung hastened by, 152
destroys tender fibrils o f new t issueand in terferes with healing , 15 1favo rs aspirat ion o fmucus into new
parts, 15 1
harmful , 150
unnatural and unnecessary , 150
Depressions, explanation o f, in earlytuberculos is , 18
D esert , American ,immun ity from tuber
culo sis in , 233D ettweiler inaugurated rest cure. 142
D iabetes, sputum in , may be scan t , 48
360 I N D EX
Emphysema, compensatory, benefits derived from and dangers resultingfrom , 90
pro longed expiratory n o te in , 74Emphysematous lun g, difficult ies o f
diagnos ing tubercul osis in , 72
Emulsion of tubercle bacill i (T . E . ,
Koch), 1 75Emulsion of tubercle bacill i (T . E . , Koch)
dosage of, 1 76
E n capsulat ion , after h istory of, 2one method of cure, 2
E nvelope, bovine bacillus has thicker,than human , 35bovin e bacillus, in jured by heat and
acid, 35in jury of, shows resistan ce on partof organ ism, 3 7
E nvironmen t , previous, affects progn osis ,7
E rgot , con tra indi cated in hemoptysis,265
E t io logy, study of 1 12 cases with reference to type of bacil lus found, 34tuberculosis in man has double, 34
E xamination , general rul es for , 13physical , importan ce o f, in earlydiagnosis, 28
Excesses, cause of tuberculosis , 105Exercise, con traindicat ions for , upon
part of heart , 146
heart in jured by in judicious use of,I 4S
heart strengthen ed by judicious useofi 146
signs of heart strengthen ing under,146
with referen ce to meal -t ime, 148
what fo rm most suitable 148
when indicated 147valuable in course of treatmen t atproper time, 146value of, 142
Expectorat ion , danger o f disseminationof tuberculosis lies in , 103
decrease of, in dry air , whyP, 240destruction of, removes pract icallyal l danger, 108
E xpirato ry murmur, pro longat ion o f,cause, 74
Extens ion o f in fection causes mor ningrise in temperature, 54
Falkenstein , death rate in , n o t increasedby presence o f sanato ria , 1 1 2
Fats , fo rm o f admin istrat io n , 136
Feces , examination of, after patien t hastaken care about swallowin g sputum, 245
pus in , sure sign of ul cerat ion , 245Strassburger
’s method of examin ing
for baci lli , 245Feet , care o f, importan t, 1 27
shoul d be warm before ret iring, 1 26Fever, caused by absorption , 56
caused n ot alone by tubercle baci llustoxin s, 56cause of, in tuberculosis, 56 , 274cause of, must be treated, 275degree o f, can not be measur ed bypatien t’s feel ings, 5 7
in tubercul osis, 274liberal diet necessary in , 138
lowering of, per 3 6 not curing patien t , 258relieved by in jection s of tuberclebacill us vaccines, 180rest indicated in , 143treated wi th tuberculin , rat ionale ofits action , 275treatmen t of, in mixed in fection , 258
tuberculin treatmen t during, 189Fever case, charts showing benefit
derived from tuberculin treatmen tin a , 190 , 193
Fever cases, action of tuberculin in ,
based on Wright’s opin ion , 192
F ibro id t issue, tuberculin increasesamoun t of, 186
F ibrosis, exten sive, con tra indicat ion fo r
forced feeding, 130F inan cial condi tion , progn ostic sig nifi
cance of, 98
F istula in ano , 247efiects o f operat ion on patien t shouldbe carefully con sidered , 247heals under tuberculin treatmen t ,
248
not operate, wh ile disease in lungsactive, 247
Floor, danger o f in fection from , greatest ,104
Flugge’s droplet theory o f in fect ion , 102
Focus, closed , temperature in , 55Fog, 110 con traindicat ion fo r treatmen t
with open a ir , 1 27Food , so l id, should be used in fever o f
mixed in fect ion , 259t ime fo r admin istrat ion o f extra ,
I 3 7Fo ods , what best fo r the tuberculous P,
I 3S
I N D EX
Forced feeding, common in stan ces of, 1 29con tra indicated in weak heart , 130
effects of, upon 'gastro - in test inaltract, 130
evil effects of, 130
fibrosis con traindicates, 130gastro -in testinal diseases con train
dicate, 130
kidn eys in , 130
symptoms of, on part of in testinaltract , 130temporary measure at most , 130
Formaldehyde disin fect ion , 109resh air , how best obtain ed, 123how obtain ed in homes, 123
Frict ion fremitus, 6 5Fruit , can it be eaten with mi lk 134F ii rsorgestel len , 109
Games, danger of overexertion in , 149Gastric n euroses of toxic origin , 138
Gastro—in testin al diseases , con traindicateforced feeding, 130
Gastro - in testinal syn iptoms in early tuberculosis, 9
Castro - in testin al tract , organ ic_disease
of, 138
symptoms on part of, 2 78Gelatin e in treatmen t of hemoptysis,
265Gen ito -urinary, lesion s to be treated
medically, n ot surgically, 26 6Gen ito—urinary tuberculosis , 26 6Germicides, used in disin fecting sputum,
10
G lands, cases of en larged, shouldbe submitted to the tuberculin test, 248children frequen tly have tuberculosis of, 248
chron ically en larged, usually reactto tuberculin , 248
en larged bron ch ial , cause weaken edbreathing, 74frequen cy of tuberculosis of, 248surgery in tuberculosis of, veryun satisfactory, 249
suppurat ive tuberculous , best treatmen t for , 249tuberculosis of, 248
tuberculosis of, ideal in fection to
treat , 248tuberculosis primari ly a disease of, 4tuberculosis of, should be treated bytuberculin without delay, 248what shouldbe the attitude towarden largemen t of, in children P, 248
Goerbersdorf, death rate i n , n ot in
creased by presen ce of sanatoria ,
1 1 2
Grocco ’
s sign , method of determin ing,25 1
Guidan ce, constan t , careful , in telligen t,n ecessary for best results , 284
Gums , red line on , found in early tuberculosis, 1 7
H andkerchief, patien ts should n ot ex
pectorate in to , 103Hands , should bewashed frequen tly, 103H ardiness , demanded by h igh altitude
and cold cl imates, 231
H arrin gton ’s sign , 1 7
H ealin g, with l ittle scar tissue desirable,15 1
H ealth board con tro l essen t ial , 108H eart , athletes in jured “ by overdevelop
men t of, 238burden upon , in advan ced tuberculosis with h igh degree of con traet ion on the part of on e lung, 88burdens thrown upon , in tuberculosis , 145case illustrating overstrain upon , 146
chron ic disease of, and tuberculosis,21 1
diseases of, producing cyanosis incompatible with tuberculosis , 21 1
displacemen t , effect of, 90displacemen t of, causes of, 88
displacemen t of, in pleural effusion ,
25 1
displacemen t of, in pneumo thorax,255displacemen t of, where double ap icalin fection is presen t , 89displacemen t , symptoms accompanying, 90
displacemen t to left, 63displacemen t to right, 63effect of altitude upon , at rest andduring exercise, 338, 340
effect of altitude upon , 236
exercise stren gthen s when advisable,
146
factors burden ing, in tuberculosis, 95factor in progn osis, 95hypertrophy of, militates again sttuberculosis, 21 1
importan ce of recogn izing pathological chan ges in outline of, 83
impulse, directly against chest wall,64
36 2 I N D EX
H eart, impulse of, on chest wal l due toside of ven tri cle, 90
in jured often by in judi cious exercise,
145lung, port ion s o f, adjacen t to , healslowly, 237movab ility o f, depends upon con
dition o f ao rta , 8 1
movemen ts depend upon size o f
pericardium, 8 1
n ormal outline of, 83position of, depends upon pericar
dium, 80
position of, gives eviden ce of pulmonary condition , 6 3 , 7 1
position of, normal changes in ,
during life, 80progn ostic s ign ification in advancedtuberculosis , 49rest imperative on accoun t of, 145statistics o f lesion s of, and tubercul osis , 2 12
strain on , in advan ced tuberculosis,50
un stable in early tuberculos is , 9weaken ing of, influen ces progn osis ,96
weakness of, causes digest ive dis
turbances, 49weakness of, con traindicates forcedfeeding, 130
metallic character of sounds o f,
in presen ce of cavi ty, 50H eat cen ter, in stab ility of, in tuber
culosis, 52
H eat , gen tle, should alone be used instain ing for bacilli , 30
H emoglobin , increased by sun light , 235H emoptysis, 26 1
amoun t no sign ificance as to exten tof disease, 12
astringen ts useless in , 26 6
cause o f, 26 2
congest ive origin o f. 26 6
dangers o f, 98
danger o f new in fect ion following,reduced by rest , 145
diagnostic s ign ificance o f amoun t o fblood lost during, 26 3
early, should always give pat ien tadvan tage o f early treatmen t , 26
epidemic character o f, 26 2fa ta l , case illustrat ing necessity fo rrest , 145faulty treatmen t o f, 26 2frequency o f, 26 1
H emoptysis , indication s fo r treatmen t of,263less frequen t in in stitution s than on
outside, 263necrosis o f vessel wall an elemen t in ,
26 5o ften first sign of tuberculosis , 1 2
prognostic sign ificance of, 98
relation ship of, to early diagn osis ,26 1
relief fo llowing, 99rest imperat ive in , 144
rest in treatmen t o f, 263treatmen t of, 26 2treatmen t of, likened to the managemen t of a rupture in a system o f
rubber tub ing conn ected withcen tral pump, 263vaso -dilators in treatmen t of, 264
H eredity, part played in tuberculosis by, 7small part played by direct , 107resisting power of pat ien t a matterof, 107
H ero in , in treatmen t o f cough , 2 72H igh altitude, demands h igh rate o f
tissue change, 23 1H istory, clin ical , very importan t in mak ~
ing a diagnosis, 8H istory, family, 7 , 47
of fami ly shows index of resistan ce,7
H oarseness , cause of, in early tuberculosis , 9laryn x . should be examined when ,
presen t , 5 1H ome, patien t required to do unwise
th ings wh ile being treated in , 225requiremen ts of, for proper prophylaxis , 106
H ome treatmen t , difficulties of, 225method o f supplying, 128
H ope, engendered by associat ion in
sanato ria , 227H opefulness o f tuberculosis , 300H orseback riding, 149H ospitals fo r tuberculosis n o t dangerous
to surroundings , 1 1 1H ospitals , necessary fo r advanced cases ,
1 10
H ospital , results compared w ith those o f
sanatorium, 294
H ouses , approved method o f sweepingand dusting, 105clean , danger o f in fect io n in , 104
danger in o rdinary method o f sweeping and dust ing, 105
364 I N D EX
I n fect ion , defen sive powers of bloodused up during, 93dr oplet theory o f, 102dust theory of, 101exten t of, influen ces prognosis , 92facto rs in causa tion o f, 104ingestion theory, 102law govern ing, 92milk as carrier of, 102mixed and secondary, preven ted bysun light , 234
n ature’s method of dea ling with, 1
opportun ity of, importan t in tak ingh istory, 7
opposed by n atural defen ses of
organ ism, 92
problem for adheren ts of inhalat ionand ingestion theory o f, 101
prognosis, depends upon nature o f,2
relation of, to deaths from tubercul osis, 1 14ro le of blood in preven tion o f, 210
routes of, 92spread of, in hibited where tuberculin used, 198
symptoms appear long after, 1 , 2 , 7tenden cy of, to spread, affectsprognosis, 92transmitted wi th in doors, 125
I nfil trat ion may exist long time withoutulceration , 4
I nhalation s in treatmen t , 272I n jection , an tisept ic precaution s in , 195
site of, 195I nsomn ia , 276
caused by gastric acidi ty, 2 76sleeping powders should be usedcautiously in , 2 77terminal , 2 77
I nspect ion , evidence obtained by, inadvanced tuberculosis , 60
I nsurance societies o f Germany trea tinsured , 290
I n tegumen t , conditions o f, over chest ,60
I n tell igen t pat ien t , best pat ien t , 284I n terest o f physician and pat ien t mutual ,
284I n terco stal spaces , bulging o f, due to
pleural effusion , 63drawing in o f, due to the presence o f
pleural adhes ions , 6 3I n test inal stenosis, rel ieved by surgery,
247I n testinal tuberculo sis , 244
I n test in al tuberculosis , bacill i in stoo ls ,of 245con st ipation shoul d be combated in ,
246
diagnosis of, 245frequen cy of, 244mushy stoo ls of, 245nocturnal stoo ls of, 245statistics of frequency of, 244subnormal temperature in , 5 6
symptoms of, when cecum seat ofin fection , 245
symptoms of, when co lon and rec
tum seat of, 245temperature depressed in , 245treated with tubercul in , 247treatmen t of diarrhea in , 246
ulceration , s ite of, in , 245I nvestmen t, state sanatoria well run
prove to be, 290
Jacket , wet, description of, and therapeut ie applica tion , 16 2
Kumyss , formul a for making, 135Koch , bacil li emulsion of, 1 75
n ew tubercul in of, 1 75results of, showing agglutinatingpower of blood in creased bybaci llary products, 183view of, regardin g act ion of tubercul in , 182
Koch ’s discovery of tubercle bacillus , 286
Koch’s rules for use of tuberculin , 168
Kitasato ’s method of examin ing sputum
for mixed in fection , 256
Kidney, tuberculous, treated bv tuberclevaccines , 26 6
Kidn eys, disease o f, con traindicat ion forforced feeding, 130
Lactic acid, unnecessary in treatmen t o ftuberculous laryngi tis , 244
Lagging , cause of, 1 7detected by inspection , 1 7detected by palpat ion , method o f, 18importan t early sign in tuberculosis ,
1 7 . 18
in bilateral invo lvemen t , 19in tuberculosis , 63 . 6 6
most valuable in un ilateral invo lvemen ts . 19
La grippe, tuberculosis o ften fo llows , 106
tuberculosis treated fo r , 28Laryngit is , tuberculous , any part o f
larynx may be invo lved , 243
I N D EX
Laryngitis, tuberculous advan ced, difli cul tto cure, 242begins as infil trati on , 242
diagnosed by tuberculin test, 243diagnosis of, 242
differen tiated from non - tubercul ousby experien ce in examin in g throats,242
early appearance of, 243lactic acid in treatmen t of, 244
protargo l as loca l application in , 243prognosis in , depends on whether orn ot tubercul in is used, 243prognosis in , depends on earl inessof diagnosis and in tel l igen ce of
treatmen t , 243perhaps always secondary, 242rest in treatmen t of, 243treated by sun l ight, 244treatmen t of, 243treatmen t of, with co ld compress ,
243tuberculin most importan t remedyin , 244when diagnosed early offers
'
ex
cel lent chan ces of cur e, 242Larynx, may be seat of infil tration for
long time without ulceration , 4
routine examination of, should bemade in cases of pulmonarytubercul osis, 242
sputum taken from, as aid to earlydi agn osis, 38
symptoms on part of, in earlytuberculosis, 1 7ticklin g in , in early tubercul osis, 9tubercul osis of, frequen cy of, 242ulcerat ion s of, treated by orthoform ,
243Laten cy, alternates with activity, 2 , 4
importan t to recogn ize, 4proo fs of, 4
Laxat ives, use of, in in testinal tubercul osis, 246
Lead, use of, in tuberculous diarrhea , 247Legislat ion , un just , provoked by fear of
disease, 108
Leucocytes, eflect of tuberculin upon , 186
L ife gr eatly prolonged by treatmen t, 292L ight , blood absorbs, 234
eflect of, in preven tin g in fect ion ,
104 , 105deprivation of, reduces red bloodcells , 235diffused , kills bacteria , 234oxidation in creased by, 235
36 5
L ight , pulmon ary hyperemi a producedby, 2 14
quicken s vital forces of man , 234L imitations of tuberculin , 205Litten
’s sign , 64
Loca lization of, bovin e and humanbacill i in body
‘
diflers , 35Lung, areas n ear heart heal slowly,
15 1
Lun gs of athl etes , in jured by overdevelopmen t , 238
Lung boundaries, cause of displacemen t of, 83
effect o f displacemen t o f, 87n orma l , 81outlin e of, 70
Lung, capacity of, in man greater thannecessary, 150compen satory emphysema of, ben efits and dangers of, 90
con traction of, condi tions favorin g,84
importan ce of recogn iz ing changein posit ion of borders , 83mob ili ty of borders , lessen ed bydi sease, 7 1
mobili ty of lower borders, 7 1pn ority of invo lvemen t of, in dicatedby posit ion of heart , 89rest and exercise for , 149
Lupus , opson ic index of blood in , 185
M agnesium sul phate, use of, in tuberculous diarrhea, 246
M alaise, 8M araglian o , an titoxic serum of, 208
bacterio lysin of, 207watery extract of tubercle bacill i of,
207M armorek’
s serum , 208
M easles tubercul osis o ften foll ows, 106
M eat jui ce, method of preparin g, 136M edical directors of sanatoria , qua l ifi
cations of, 2 16
M en ingitis, tuberculous , symptoms of,
26 7treatmen t of, 268
M en ses, cessat ion o f, shows tuberculosisalready presen t, 58resumed with return ing stren gth of
patien t , 59rise of temperature at time of, 5 7
M en tal activity, effect of, on temperature,52
M ercury, red iodid, in treatmen t of
cough, 272
36 6 I N D EX
M etabolism; climate affects , primarily,23 1
M icro -o rgan isms, associated, cause risein temperature, 56
stimulate cells to production of
immun e bodies, 1 16M iliary tubercul osis , acute, causes mom
ing rise of temperature, 54percussion n ote in , 72
M ilk , amoun t of, required fo r exclusivediet, 135
can it be eaten with fruit 134cause of all tuberculosis, 3importan ce of, in dietary, 133method ofprescribing, where patien tfeels that he can n ot take it, 133modificat ion of, 133n ot a liquid food , 134
quan tity of, to be prescribed , 134should be chewed, 134teeth and mouth should be cared fo rwhen used, 135
M itulescu, study of effect of tuberculinupon leucocytes, 185
M ixed in fect ion , a factor in a l l casesbeyond early stage, 25 7blood as a rule negative in , 256
cultures from the wal ls of cavitiesimmediately after death show,
256
danger of, reduced by open -air life,125diagnosis of, 256diet in , 258
dry air with maximum of sun shinepreven ts , and tends to rel ieve, 240micro -organ isms found in , 256
opson ic index in diagnosis of, 25 7rat ional treatmen t of, con sists in
vaccinat ing against tubercle bacillus and associated o rgansims , 25 7
serum treatmen t o f, 259sun light preven ts , 234symptoms of, 257treatmen t of convalescence from, 26 1
M orph ia , harm done by, in hemoptysis ,26 5
M oun tain cl imates, characterist ic o f, 235M outh , should be washed before meals ,
M ustache, tuberculous pat ien ts shouldno t wear a , 103
Myalgia in tuberculosis , 5 2
N agel , sta tist ics o f disappearan ce of
baci ll i from sputum , 202
N asa l stenosis , a cause ofweak brea th ing,21
N ecrosis, caused by toxins , 1 14
N egative phase, importan ce o f, exagger
ated , 197n ot as dan gerous asWright sugges ts ,
187Wright’s in terpretat ion of, 197
N eglec t not permissible if best resultsare to be had, 284
N erve, recurren t laryn geal , bound downby apica l adhesion s or en largedtuberculous glands, 9
N erve react ion , in hydr o therapy, 153N ervousness in mixed in fect ion , 25 7N ervous system in advan ced tuberculo
sis , 50
N ervous system, symptoms ou part o f,in early tuberculosis , 8
N euralgia, in tercostal , differen t iated frompleurisy, 7 1_
N eurasthen ia , dri pping sheet bath in , 158
o ften caused by tuberculosis , 8o ften evidence of the presen ce of
tuberculous in fect ion , 3 , 27N eutrophiles , show in crease in granula
t ion after tuberculin in jection s.186
N ight sweats, vinegar and water in treatmen t of, 2 73
N itrite of soda in treatmen t of hemoptysis , 264
N itroglycerine in treatmen t of hemoptysis, 264
O il , castor,use of, in tuberculous diarrhea ,
246
O il enemas , use of, in con st ipat ion , 246
O live o il , method of admin istering, 140Open air , act ion depends upon , 1 23 , 1 25cause o f more deaths than any
o ther measure, 127change to , must be made w ithjudgmen t , 1 26danger o f in fect ion in , n il , 104
effect o f, upon nervous system , 1 24
effect on n ight sweats , 273essen t ial of, is constan tly changedair , 1 23
first recommendedbyBedington , 122
hardens pat ien ts , 1 24
how derive most benefit from ?, 1 27 _
is there danger at beginn ing o f,
treatmen t ?, 1 25improves digest ion and assimilat ion ,
124
3 6 8 I N D EX
Percussion , resistance to finger, in , veryimportan t , 15
too many, strokes over same area,
con fusing, 16
varieties of, 15what is to be no ted on , in earlytuberculosis, 19
Percuss ion hammer, 70Percussion no te, 72causes o f dulness of, in chron ictuberculosis, 72cause of h igher pitch of, at rightapex, 1 6
causes of hyperresonance and tympany of, in chron ic tuberculosis,72
cause of tympan it ic character of, inacute mi liary tuberculosis, 72changes of, on deep and shallowbreath ing, 16
non - tympan it ic , .72
of acute m l liary tuberculosis , 72o f acute pneumon ic phthisis, 72of chron ic tuberculosis, 72pitch of, in early tuberculosis, 19pitch o f, raised on inspirat ion , 73
quality of, in early tuberculosis, 19. tympan itic , characteristics of, 72
Pericardium, posit ion of heart dependsupon , 80
Permanency of results 203 , 294Persona l prophylaxis , 103Pessimism , influen ces progn osis uh favor
ably, 98Pfeiffer
’s method of examin ing fo r mixedin fect ion , 256
Pharynx, naso cough caused by diseaseof,
‘
48
Phth isiophobia , due to ign orance, 108
Phthisio therapy, American pioneers in ,
287Physician , great responsibility of, in
tuberculosis, 280traits o f, fo r treatmen t o f tuberculosis , 94
Phys ician and pat ien t , 280Physician ’
s frequen t visits with pat ien tlarge elemen t in cure, 226
Pirquet’
s tuberculin diagn osis in ch ildhood, 45
Pitch , changes o f, in early tuberculos isand method o f detect ing, 19. 29
Pleura , pa ins caused by inflammat ion o f,
5 1
rough respirato ry no te, due to in
fl ammat ion of, 76
Pleura , th icken ing of, shows increased ordecreased vocal fremitus, 6 5
Pleural adhesions, obliterate pleuralcavity, 250
show auscultatory signs resemblingrales of in trapulmonary origin ,
253Pleural effusion , removal of, 254Pleural inflammation s , physica l signs
rema in ing after, 253Pleural rub in effus ion , 25 1
Pleural soun ds , 7 7sounds , differen t iation of from ralesof in trapulmonary origin , 7 7
affected by pressure on the stethoscope, 78
Pleural thicken ing, remamrng after inflammation , 253
Pleurisy, 250blister in treatmen t o f, 253diet in , 253differen tiated from in tercostal neu
ralgia , 71
dry, 250effusion in , causes immobility of
side of thorax, frequen cy of, 250iodine, in the treatmen t of, 253morn ing elevation o f temperaturesuggests, 54
physmal signs of, in case o f effusion ,
25 1
rest in , 253strapping chest with adhesive strapsm, 253
symptom of early tuberculosis , 12symptoms of, 25 1
treatmen t of, 253treatmen t of pain in , 253varieties of, 250
Pleurisy with effusion , 250
paravertebral triangle o f dulness in .
25 1
serous, at the base maybe caused byapical involvemen t , 250
Pleximeter, 70manner o f using, 16
Pneumogastric irritat ion causes digest ive.disturbance, 49
Pneumon ia, morn ing rise of temperaturesuggests , 54
Pneumothorax , 254cause and seriousness o f, 254symptoms o f, 255treatmen t o f, 255
Pocket , rubber l in ing in , fo r carryingclo ths for sputum , 103
I N D EX
Pot fele’ over cavity, 73Poor, pat ien ts offer good prognosis when
put under good condit ion s, 97Pottenger, permanen cy of results in cases
treated by, 203results of treatmen t of, 201
stat istics of disappearan ce of baci llifrom sputum, 202
Po ttenger Sanatorium Bungalow, 219Predisposed, many “
so -called,” alreadyinfected, 106
prophylactic measures for , 106
Predisposed, should be treated for tuberculosis, 106
Pregnan cy, compl icating tuberculosis,269danger of quiescen t foci light ing upafter, 270
effect of, on prognosis , 99in terruption of, in tuberculouswomen , 270
should not occur for several yearsafter patien t 15 well of tuberculosis, 2 70
symptoms may abate during, 270Pre—tubercular stage, really tubercular, 6Preven t ion , measures for , are simple and
humane, 107Progn osis , age a factor in , 98
affected by exten t of lesion , 92
bacilli , form of, a factor in , 99complications in fluen ce, 98
depends upon fin an cial condition , 98
depends upon in telligen ce of treatmen t, 93
'depends upon family physician , 93depends upon n ature of in fection , 92
digest ive system in , 96
former environmen t a factor in , 97heart an importan t factor in , 49heart in , 95hemoptysis a factor in , 98
in advan ced tuberculosis , 95individual resistan ce a factor in , 96
in tuberculosis, 92laryngeal tuberculosis, o f, variesaccording to earl iness of diagnosisand in telligen ce of treatmen t , 243length of illn ess importan t in , ad
vanced condition , 97length of treatmen t a factor in , 100
loss of weight in , 96
n umber of bacilli and, 99pat ien t’s responsib ility in , 94 , 95pregnan cy influen ces , 99treatmen t a factor in , 98
24
369
Prognosis, temperamen t a factor in , 96
why best in in cipien t tuberculosis P,93
Prophylactic measures for sick and well ,107measures in building con struct ion ,
106
Prophylaxis, 101
burden not upon afflicted alon e, 105care of sputum in , 103classes, ro le of, in , 1 10
danger of in fection removed by, 107dispen saries, ro le of, in , 109early cure best , 101education , most importan t in , 107educat ion , ro le of, in , 107health board con tro l , ro le of, in ,
108
hospitals , ro le of, in , 1 10
in childhood, 106
light and ven t ilat ion in , 104, 105personal , 103personal and general , rules for same,
1 10
sanatorium, ro le of, in , 1 10
Pro teids for the tuberculous , 136
Prussia, death rate from tuberculosisdecreasing in , 1 12
Pulmonary tuberculosis, complication sof 242
hyperemia in , 213Pulmonary valve, accen tuat ion of, 50
stenosis of, usually fo llowed by .
tuberculosis, 2 1 1Pulse, accompanying pleurisy with effu
sion , 25 1
h igh , and not responding to rest,un favorable, 50 , 96
Pulse—rate in early tuberculosis, 9Pupi ls, inequality of, a S ign of early tuber
culosis, 1 7inequality of, caused by, 1 7widely dilated in tuberculosis, 1 7
Quiescen t foci , toxins escape . from, and
in jure o ther tissues, 92Quaran tine n ot desirable, 109
Ra les and perman en cy of results, 299Rales , cause and descript ion of, 76
Con stan cy o f, in tuberculosis , 7 7differen tiation of, from sounds of
pleural origin , 77dry , descript ion of and cause, 77effect of cough on , 76
in early tuberculosis, 24, 29
3 70 I N D EX
Rales , large bubbl ing, persist in g in on e
place suggests cavity, 7 7metall ic , 7 7mo ist , persisting at apex susp icious
o f tuberculosis , 7 7simulated by sounds of pleuralorigin , 24
Rational , diet , 13 1treatmen t con sists of, 120
Reaction , avo ided by care in use o f
tuberculin , 188
caused by bovine tuberculin usuallyreaches height on second day,188
in tuberculous fo cus a ids healing,187
lo cal , at site o f in ject ion , index o f
react ion in tuberculous areas , 1 74local (Pirquet), a test fo r tuberculosis in childhood, 46
n erve, in hydro therapy, 153skin , in hydro therapy, description
of, 153tuberculin , description o f, 187tuberculin , disregarded in earlytrial of tuberculin , 1 68
tuberculin ; general, 42tuberculin , local , 41tuberculin , secondary, 188tubercul in , secondary, due to autoin o culation , 188
value o f hydro therapeutic measuresdepends upon , 153vascular, in hydro therapy, 154
Rein fection , danger o f, in swallowingSputum, 103part played by, in tuberculos is , 101
Relapse, more common in cases treatedwithout tuberculin , 203
Remedial measures, classificat ion of, 1 1 7Resistance, individual , a factor in prog
n osis , 96n o rmally greatest in health , 1 16
Respiration , co n stan t change in posit iono f organs o f, during l ife, 79
effect o f alt itude upon , 236
in early tuberculosis , 9Respira to ry murmur, in ten si ty o f, de
penden t upon , 73Rest and exercise fo r lung, 149Rest , cough rel ieved by, 144
dyspnea an indicat ion fo r , 147fever an indicat ion fo r , 143great reduction in weight demands ,
147heart demands , in tuberculos is , 145
Rest , hemoptysis demands , 144in dyspnea, 27 7in hemoptysis, 263in treatmen t of fever, 2 74n on - febri le cases require, 144reduces danger of new in fect ion inhemoptysis, 145
the treatmen t of all inflammation s ,150
treatmen t of tuberculous laryngitiswi th, 243value of, 142
what degree of temperature re
quiresP, 143Results, best , preven ted by premature
in terrupt ion of treatmen t , 298clin ical , very sat isfacto ry wheretubercul in used , 198
comparative, where tuberculin usedand where n ot used by Turban ,
201
comparat ive, where tuberculin usedand n ot used by Weicker, 201comparison o f, at Belz ig, wheretubercul in is used and where n o t
used , .201
permanency of, 203 , 294sanatorium and hospital , compared ,
294Results and permanen cy o f, in tuber
culosis, 286
Results, permanen cy o f, last few mon thsof
_ treatmen t most importan t in ,
298
presen ce of rales at the t ime—o i discharge influences , 299
Results ofhygien ic-dietet ic-open -air treatmen t more apt to be a quiescence,
203Results o f treatmen t by author, 200Results of treatmen t of tuberculosis com
pared with those o f o ther diseases ,292
Results ,o f tuberculosis, 223
Retract ions, explanat ion o f, in earlytuberculosis, 18
R ib, ankylosis o f first , with sternum,
predisposing cause of o r result o ftuberculosisP, 6 1
Rocky M oun tains , immun ity from tuberculosis no ted in , 233
Rokitan sky’s idea o f heart lesions and
tuberculos is , 2 1 1R on tgen rays in early diagno s is. 38Rooms , floors o f, o ffer greatest danger o f
in fect ion , 7
I ND EX
Sputum , should be repeatedly examinedif found negative in early tuberculosis , 9when presen t shoul d always be
examined, 29Squeak persisten tly lo calized , suggest ive
of cavity, 7 7S tage, pre—tubercular, 6S tain , differen t ial, for bovin e and human
baci l li , 35picric acid, di rect ion s for , 3 7picri c acid, of great value whereenvelope is in jured, 3 7
Stain ing, rules for , 30usual method, 30
Stat ist ics, of heart lesion s and tuberculosis, 212
of jo in ts treated by hyperemia , 2 13Steppes of Tartary, immun ity from
tuberculosis n o ted in , 233S tethoscope, advan tages of, over ear , 14,
15cho ice of, 14vari able pressureon , affects soun d, 15
Strassburger’s method of examin ing
feces for bacilli , 245S treet dust , danger o f in fection from, 104Strepto lytic serum in mixed in fect ion , 26 1
S tomach , dilatation of, cause and suggest ion s for managing, 139
S tools , bacilli in , in in test ina l tuberculosis , 245clay co lor in in test inal tuberculosis ,
245mushy nocturn al , in in testinal tuberculosis , 245
Stork’s experimen ts in producing fibrosis ,1 14
Subclavian murmur, in early tubercu
losis, causes of, 24Succussion in pneumo thorax, 255Suggestion valuable in treatmen t , 285Sulphonal in insomn ia , 27 7Sun light , effect o f, upon bacill i , 104
importance o f, in treatmen t o f tuberculo sis , 234
kills micro -organ isms , 234preven ts mixed and secondary in fect ion , 234treatmen t o f tuberculous laryngitiswith , 244
Sun sh ine, cheering effect o f, 235great amoun t o f, invites to out
do o r l ife, 235Sunstrokes unknown in ho t, dry cl imates
o f South West . 232
Suprarenal gland, products from, con traindicated in hemoptys is , 26 6
Suscept ible, later chi ldren more, to tuberculosis, 8
Swea ting in axilla in early tuberculosis , gSweats, disappear wi th regulat ion of
lives of patien ts, 2 73in advan ced tuberculosis, 5 2
Sweats , n ight or sleep, 12 , 2 73cause o f, 2 73cause of weakness in , 5 2
danger from, 52
prostration fo llowing, 2 74treatmen t of, 273eping, approved method o f, 105danger from ordinary method of, 105
Symptoms, cause of, 8
early, should be taught in schoo ls,
general , in advan ced tubercul osis, 47on set of, sometimes sudden , 28
Symptoms of advan ced tuberculosis,bronchial catarrh , 5 1circulatory system, 49colds, 5 1cough , 47digest ive system, 49hoarseness, 5 1men strual flow , cessation o f, 58
nervous system, 50
pain , 5 1
sweats, n ight or sleep, 5 2sputum, 48
temperature, 5 2Symptoms o f early tuberculosis ,
an emia , 10, 1 7circulatory system, 9co lds, 9, 28
cough, 9gastro - in test inal system, 9hoarseness , 9 , 1 7mala ise, 8nervous system, 8 , 2 7pa in , 1 1
pleurisy, 1 2
respirat ion , 9spitting o f blood, 12sputum , 9sweats , n ight or sleep, 1 2temperature, 10 28
Symptoms o fmixed 1n fection , 25 7pneumo thorax, 255treatmen t o f, 27 1
Syph il is , acquired, compl icat ing tuberculosis , treatmen t o f, 26 8
Syph il is , compl icat ing tuberculos is , 268
I N D EX
Syph il is inherited, a factor in tubercu
losis, case i llustrating, 268characteristic auscultatory sign in ,
269treatmen t of, 269
Temperamen t a factor in prognosis , 98Temperature, accompanying pleurisy
with effusion , 25 1
chart , method of keeping, for earlydiagnosis in tubercul osis, 10comparison of, in health and tubercul osis, 52
curve in inact ive chron ic pulmonarytubercul osis, 53curve of hect ic type, 53depression of, in in testinal tubercul osis, 245diurnal range of, in dry climates, 23 1in advan ced tuberculosis, 52in early tuberculosis, 10in mixed in fect ion , 25 1
indi cation of virulen cy of in fect ion ,
56
instabi lity of, in advan ced tubercul osis, 52
in struction s for tak ing, 1 1markedly subnormal , suggestive of
in testinal compli cation , 56
morn in g rise of, suggests complication , 54
natural, for un complicated chron icpulmonary tuberculosis, 189
open air reduces, 1 25pneumo thorax, 255prognostic import of, 96reduction of, by tepid bath, 15 7remitten t type of, in tuberculosis, 53rise in , due to di sturban ces of
nervous system, 5 7rise of, fo llows deep breath ing, 15 1rise of, fo llowing exercise due to
toxin s, 144subnormal, 54subnormal in early tuberculosis, 10systematically taken gives picture of
disease, 58two hourly chart of, necessary, 58what degree of, requires restP, 143
Tenemen ts, model , needed in cities , 106Therapy, based upon double etiology,
Thermometer, so le guide to temperature,58
time of ho lding , in mouth for testingtemperature, 1 1
Thoracic viscera , cause of displacemen tof, 83change in outline importan t, 83diagnosis of displacemen ts in , 91
managemen t of cases wi th displacemen t of, 91
Thorax, chan ges in upper aperture of,during life, 79
expiratory type of, 79in spiratory type of, 79patho logically inspiratory in em
physema , 79physio logically expiratory in o l d age,
79Thorax paralyticus, description of, 6 1
patho logically expiratory, 80Throat compress, descript ion of, and
therapeutic applicat ion , 1 63Ton ic, open air as a , 124Ton sils, as portals of in fection , 102
T ouch percussion , Ebstein ’s , 6 7
Toxins, bovine and human , differ, 195cause of digestive disturban ces, 49change of, in treatment , 195circulation of, in blood may fai l tostimulate machinery of immun ization , but in ject ion of, in tot issues may, 194
escape from focus of in fection and
render suscept ible o ther tissue,92
n ecrosis caused by, 1 14of, bovine and human bacilli differ,35tubercle bacilli , influen ce nervoussystem, 50
T oxin test, type of baci lli causing in fection may be diagnosed by, 1 78
T reatmen t , advan ced cases can be saved'
by the best, 222advan ced cases must n ot be den iedsanatorium, 222
advan tages of sanatorium, 226
basis of, the type of bacilli presen t ,I 7 7beginn ing of systematic, 286classification of measures used in ,
1 1 7climatic, 229climatic, value of, lies in , 240
comparat ive results of, in tuberculinand n on - tuberculin treated casesby Turban , 201
comparative results of, where tuberculin used and n ot used byWeicker, 201
3 74 I N D EX
T reatmen t , difl‘icul ties of, must not bem in imized , 223fever relieved by, with few in jectionso f tubercle bacillus vaccines, 180
h igh altitude con trary to prin cipleof rest in 1nflammations, 236
hygien ic, not all , 1 1 7hygien ic, what can be accomplishedby, 1 1 7
ideas of, grow slowly, 287immun ity the ultimate aim of, 1 1 7Koch’s rules for use of tuberculin in ,
168
Koch’s rules for use of tuberculin in ,
disregarded, 16 8length of, necessary, 100length of, n ecessary for apparen tcure, 224l ife greatly pro longed by, 292method of, very importan t , 120n ever a time too early to begin , 290
objection s to altitude in , 240
open air , 122
plea for early inst itut ion of, 221
premat-ure in terruption of, preven tsbest results, 298prin ciples underlying, ,
1 14
rational , consists of, 1 20
rest and exercise in , 142
results of, by author, 200results of, compared with resultsin o ther diseases, 292
sun light in , 234t ime of, 298
tuberculosis yields readily to , 287tuberculous laryngitis, tuberculinmost importan t remedy in , 244
what complication s are a barrier to P,223
T reatmen t of, advan ced cases withtuberculin , 201
hemoptysis, 26 2in testinal tuberculosis, 246mixed in fection , 25 7n ight sweats, 273pain , 276
pleurisy, 253pneumo tho rax, 255tuberculos is o f the larynx, 243
T rional in insomn ia , 277T rudeau , comparative results o f, in
treatmen t o f cases , incipien t andadvanced, with andwithout tubercul in . 20 1
view o f, regarding act ion o f tubercul in , 182
Tubercle, blood preven ted from en tering,
2 10
blood supply shut off from; retardshealing, 186con servat ive or notP, 210
protective to bac illi , 210Tubercles, effect of deposit of, in lung on
percuss ion no te, 19Tuberculosis, bovine and human type
of, assume difleren t“
forms, 1 7 7curab il ity of, 1 14climat ic condit ion s favori ng spreadofi 234
diflerences between early and late,205double et io logy of, 1 7 7early s tage, very curable, 221immun ity the aim of treatmen t in ,
1 1 7in testinal , 244most curable of al l chron ic diseases,
221‘
neglected, a very fatal disease, 221sanatorium treatmen t o f, 216sun light importan t factor in the
treatmen t of, 234treated early, most hopeful , 280treated late, di scouraging, 280un recogn ized, 3
Tuberculous patien t, safe compan ion , ifcareful , 107
Tuberculin , action .o i , 181
act ion of, Biedert’s views , 182
action of, Koch ’s original view, 182
act ion of, Wright’s view, 182
acts by causing more blood to flow
to part , 182acts by in creasing immun izing bodiesin blood, 181
advan tage of subcutaneous inject ion s of, 195
agglut inat ing power o f blood in
creased by, 183announced in 1890, 165Beraneck , dosage of, 1 74bovine (P. T . O . , Spengler), 1 74
0
bovine (P. T . O . , Spengler)dosageo f, 174
can it cause acute mil iary tuberculosis P, 40
can it set up activity in laten t fociP,30cl in ical results o f, favorable whereused , 198
cl in ical s ig ns safe guide to dosage o f,I O7
376 I ND EX
Tubercul in test , chart showing, 10comparison of its safety wi th ex
ploratory incision , 41
con traindication for , 43fears of, 39 5
how given P, 44in in fancy and early ch ildhood, 45is it reliableP, 43necessary dosage for , smaller wherefocus is small , 44
ordinary dosage of human tubercul inmay n ot cause a react ion wherein fect ion of bovine type, 44proof
'
of cure afforded by, 45should be made where glandschron ically en larged , 248
s ite of injection in making, 44syphi lis and, 43tubercul ous patien ts somet imes failto react to , 43when should it be given P, 42who shall admin ister itP, 45
Turban ’s, comparative results wheretuberculin is used and where n ot
used, 201stat istics of disappearan ce of bacill ifrom sputum, 202
Tulase (von Behring), 181
Tympany, causes of, in advanced tuberculosis, 72
in pneumo thorax, 255Typho id fever, danger of treating tuber
culosis for , 5 7simulated by tuberculosis, 5 7tuberculosis treated for , 28
Ulceration , laryn geal , treated by orthoform , 243
Underclothing, qualities necessary in , 1 26
woo len and l inen , 126
Vaccines, bovine and human , proo f ofan tagon ism, 1 79homo logous, perhaps future treatmen t o f mixed in fection , 26 1
increase specific pro tective bodiesin blood (example), 1 19
in jection of, those derived from the
bacillus raises opson ic index evenabove no rmal , 184made from tubercle bac illi , Specific ,
1 19rationale o f cure when , used, 199septicemic condit ions treated by,
successfully, 192
Spengler’s bovine and human , 34
Vaccines, spread of disease to new t issuepreven ted by, 199
T . B . and P. B . (Spengler), 199T . B . and P. B . (Spengler), dosageof, 180
Vaccine, T . B . and P. B . (Spengler),method of admin isterin g, 1 78
Vascular reaction , in hydro therapy, 154Vaso -mo tor disturbances in early tuber
culosis, 8
Ven tilation , eflect of, in preven tingin fection , 104, 105
in sanatoria , 2 1 7Veratrum viri de in treatmen t of hemop
tysis, 264V inegar and water in treatmen t o f n ight
sweats,'
273Virchow’
s“mobilizat ion of baci lli ” a
myth , 189opin ion of tuberculin based upon itsuse in po isonous doses , 39
Virulence,
'
baci lli retain , for long periodoutside body, 103
effect of, upon progn osis, 92in fect ion with bacill i of low , tends tohealing, 1 14
necrosis fo llows in fect ion with bacill iof great , 1 14
Vocal fremitus, condition s determin ingchange in , 6 5
increased or decreased in thickenedpleura , 65
Vo ice tran smission , 78
Vomiting caused by cough , 272
Walking, best exercise for tuberculous,148
best method o f, fo r tuberculous ,148
precaut ions to be observed in , 148
Watery extract of tubercle bacilli(M aragl iano), 207
Watery extract of tubercle bacill i (vonRuck), 1 76
Watery extract of tubercle bacilli (vonRuck), dosage o f, 1 77
Weather, wet, n o con traindication fo r
open -air treatmen t , 127Weicker, comparat ive results o f treat
men t in tubercul in and non -tubercul in treated cases , 201
Weight , ga in o f, is no t most importan tth ing in treatmen t , 135gain o f, is o ften taken as a cure.
130
loss o f, in early tuberculosis, 10
I N D EX 377
Weight , loss of, influen ces prognosis, 96loss of, in fluen ces prognosis according to cause, 96rest demanded by great reduction in ,
I 47steady gain of, best , 130
Wet jacket , in cough, 272Win trich’
s sign , 73Wright’s dosage of tuberculin , 196
Wright’s experience in tuberculin treatmen t of localized tuberculous infection , 202
method of employing tuberculin ,
196
method of treating tuberculousglands, 249
View regarding act ion of tubercul in ,
182
Related Documents