Pulmonary Pulmonary Tuberculosis Tuberculosis http:// http:// crisbertcualteros.page.t crisbertcualteros.page.t l l

Pulmonary Tuberculosis
May 07, 2015
ptb diagnosis, management and updates.
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Pulmonary Pulmonary TuberculosisTuberculosishttp://crisbertcualteros.page.tlhttp://crisbertcualteros.page.tl

Pulmonary TuberculosisPulmonary Tuberculosis
Etiology:Etiology:
1.1 1.1 Mycobacterium tuberculosisMycobacterium tuberculosis
1.2 1.2 Mycobacterium bovisMycobacterium bovis, rarely, rarely

EpidemiologyEpidemiology
Philippine Statistics: FHSIS –DOH 2001Philippine Statistics: FHSIS –DOH 2001o Respiratory TB, 6Respiratory TB, 6thth leading cause of leading cause of
morbidity with 110,841 cases and rate of morbidity with 110,841 cases and rate of 142.2/100,000 population 142.2/100,000 population
o TB meningitis with 466 cases or rate of TB meningitis with 466 cases or rate of 0.6/100,000 population0.6/100,000 population
o Other forms of TB, 11,494 cases with a Other forms of TB, 11,494 cases with a rate of 14.7/100,000 populationrate of 14.7/100,000 population
EpidemiologyEpidemiology
Source:Source:o Usually sputum form an infected adult; occasionally Usually sputum form an infected adult; occasionally
exudate from draining sinuses and urineexudate from draining sinuses and urine
Mode of transmission:Mode of transmission:o Inhalation of droplet nuclei as a ruleInhalation of droplet nuclei as a ruleo Occasionally, by ingestion of contaminated milk (M. Occasionally, by ingestion of contaminated milk (M.
bovis)bovis)o Direct contamination of open wounds (pathologistDirect contamination of open wounds (pathologist
and lab personnel)and lab personnel)
EpidemiologyEpidemiology
Period of communicability:Period of communicability:o Only if associated with open lesions of PTB, draining Only if associated with open lesions of PTB, draining
sinuses or renal involvement; as long as tubercle bacilli sinuses or renal involvement; as long as tubercle bacilli are found in sputum, exudate or urine, respectivelyare found in sputum, exudate or urine, respectively
o Children with active PTB are rarely contagious Children with active PTB are rarely contagious because of the nature of pulmonary lesion, the low because of the nature of pulmonary lesion, the low baterial output and because sputum is often baterial output and because sputum is often swallowed.swallowed.
o A patient is non-infectious within 2-4 weeks of starting A patient is non-infectious within 2-4 weeks of starting adequate therapy adequate therapy

Risk FactorsRisk Factors
1.1. Age: infants and adolescents are at highest risk of Age: infants and adolescents are at highest risk of diseasedisease
2.2. Close contact with an untreated sputum positive Close contact with an untreated sputum positive patientpatient
3.3. Impaired host defenses: immunodeficiency states, Impaired host defenses: immunodeficiency states, particularly that associated with HIV infection; particularly that associated with HIV infection; immunosuppression related to accompanying viral immunosuppression related to accompanying viral infection, or drug induced; malnutrition.infection, or drug induced; malnutrition.
4.4. Other disease staes: Hodgkin’s lymphomas, diabetes Other disease staes: Hodgkin’s lymphomas, diabetes mellitus, leukemia, malignancy (head and neck) mellitus, leukemia, malignancy (head and neck) severe kidney disease, silicosis, prolonged treatment severe kidney disease, silicosis, prolonged treatment with corticosteroidswith corticosteroids

Risk FactorsRisk Factors
5. Persons whose tuberculin skin test 5. Persons whose tuberculin skin test results converted to (+) in the past 1-2 results converted to (+) in the past 1-2 yearsyears
6. Persons who have CXR suggestive of 6. Persons who have CXR suggestive of old TBold TB

Portal of EntryPortal of Entry
o Usually respiratory tract (inhalation of Usually respiratory tract (inhalation of aerosolized particles containing 1-3 aerosolized particles containing 1-3 tubercle bacilli); rarely, skin, tubercle bacilli); rarely, skin, gastrointestinaltract, mucous membrane, gastrointestinaltract, mucous membrane, transplacentally from mother to fetus or transplacentally from mother to fetus or via infected amniotic fluidvia infected amniotic fluid

Incubation PeriodIncubation Period
o From 3 to 8 weeksFrom 3 to 8 weeks
CLASSIFICATIONCLASSIFICATION
Class I (TB exposure)Class I (TB exposure) (+) exposure(+) exposure (-) Mantoux tuberculin test(-) Mantoux tuberculin test (-) signs and symptoms suggestive of TB(-) signs and symptoms suggestive of TB (-) chest radiograph (-) chest radiograph

CLASSIFICATIONCLASSIFICATION
Class II (TB infection)Class II (TB infection) (±) exposure(±) exposure (+) Mantoux tuberculin test(+) Mantoux tuberculin test (-) signs and symptoms suggestive of TB(-) signs and symptoms suggestive of TB (-) chest radiograph (-) chest radiograph
CLASSIFICATIONCLASSIFICATION Class III (TB disease)Class III (TB disease)
Has three or more of the ff. criteriaHas three or more of the ff. criteria (+) history of exposure to an adult/adolescent with active TB (+) history of exposure to an adult/adolescent with active TB
diseasedisease (+) Mantoux tuberculin test(+) Mantoux tuberculin test (+) signs and symptoms suggestive of TB(+) signs and symptoms suggestive of TB
Cough/wheezing > 2 weeks; fever > 2 weeksCough/wheezing > 2 weeks; fever > 2 weeks Painless cervical and/or other lymphadenopathyPainless cervical and/or other lymphadenopathy Poor weight gain; failure to make a quick return to normal after Poor weight gain; failure to make a quick return to normal after
an infection (measles, tonsillitis, whooping cough) or failure to an infection (measles, tonsillitis, whooping cough) or failure to respond to approriate antibiotic therapy (pneumonia, otitis respond to approriate antibiotic therapy (pneumonia, otitis media)media)
Abnormal Chest radiographAbnormal Chest radiograph Laboratory findings suggestive of TB (histological, Laboratory findings suggestive of TB (histological,
cytological, biochemical, immunological or molecular)cytological, biochemical, immunological or molecular)
CLASSIFICATIONCLASSIFICATION
Class IV (TB inactive)Class IV (TB inactive) A child/adolescent with or without history of A child/adolescent with or without history of
previous TB and any of the ff:previous TB and any of the ff: (±) previous chemotherapy(±) previous chemotherapy (+) radiographic evidence of healed/calcified TB(+) radiographic evidence of healed/calcified TB (+) Mantoux tuberculin test(+) Mantoux tuberculin test (-) signs and symptoms suggestive of TB(-) signs and symptoms suggestive of TB (-) smear/culture for M. tuberculosis(-) smear/culture for M. tuberculosis
Clinical Forms of Clinical Forms of TuberculosisTuberculosis Pulmonary/endothoracicPulmonary/endothoracic
Asymptomatic or Latent TB infectionAsymptomatic or Latent TB infection Primary TB/primary complexPrimary TB/primary complex
Primary focus, lymphangitis and regional Primary focus, lymphangitis and regional lymphadenitislymphadenitis
Most common clinical symptomsMost common clinical symptoms Non-productive coughNon-productive cough Mild dyspneaMild dyspnea Cervical lymphadenopathiesCervical lymphadenopathies
Clinical Forms of Clinical Forms of TuberculosisTuberculosis
Pleurisy with effusionPleurisy with effusion Accompanies primary focusAccompanies primary focus Considered a component of the primary complexConsidered a component of the primary complex Onset is usually abruptOnset is usually abrupt Fever, chest pain, shortness of breathFever, chest pain, shortness of breath Dullness to flatness and diminished breath soundsDullness to flatness and diminished breath sounds Obliteration of costophrenic sulcus on CXR Obliteration of costophrenic sulcus on CXR
(minimal)(minimal) Layering of fluid density (moderate effusion)Layering of fluid density (moderate effusion) Occupy one hemithorax (massive effusion)Occupy one hemithorax (massive effusion)

Clinical Forms of Clinical Forms of TuberculosisTuberculosis
Progressive primary tuberculosis Progressive primary tuberculosis More severe fever, malaise, cough, weight lossMore severe fever, malaise, cough, weight loss Classical signs of cavitationClassical signs of cavitation Crepitant rales, diminished breath sounds, Crepitant rales, diminished breath sounds,
lymphadenopathylymphadenopathy
Endobronchial TBEndobronchial TB Bronchial obstruction due to enlargement of Bronchial obstruction due to enlargement of
peribronchial lymph nodesperibronchial lymph nodes Sudden death by asphyxiaSudden death by asphyxia EmphysemaEmphysema AtelectasisAtelectasis

Clinical Forms of Clinical Forms of TuberculosisTuberculosis
Miliary TB Miliary TB Generalized hematogenous tuberculosis due to Generalized hematogenous tuberculosis due to
massive invasion of the blood stream by the massive invasion of the blood stream by the tubercle bacillitubercle bacilli
Arises from a discharge of a caseous focus often Arises from a discharge of a caseous focus often from a lymph node into the blood vessel from a lymph node into the blood vessel (pulmonary vein)(pulmonary vein)
High fever, cough, dyspneaHigh fever, cough, dyspnea Crepitant rales, splenomagly, hepatomegaly, Crepitant rales, splenomagly, hepatomegaly,
signs of menigeal irritationsigns of menigeal irritation
Clinical Forms of Clinical Forms of TuberculosisTuberculosis
Chronic TBChronic TB Reinfection or adult TBReinfection or adult TB Apical or infraclavicular infiltrates often with Apical or infraclavicular infiltrates often with
cavitation and no hilar lymphadenopathycavitation and no hilar lymphadenopathy Persistent cough, prlonged fever, chest pain, Persistent cough, prlonged fever, chest pain,
hemoptysis and supraclavicular adenitishemoptysis and supraclavicular adenitis
TuberculomaTuberculoma Pericardial TBPericardial TB

Clinical Forms of Clinical Forms of TuberculosisTuberculosis
Extrapulmonary TBExtrapulmonary TB TB of the cervical lymph nodes/ScrofulaTB of the cervical lymph nodes/Scrofula
Involved LN are painless, firm, discrete, movable Involved LN are painless, firm, discrete, movable becoming adherent to each other and anchored to becoming adherent to each other and anchored to the surrounding tissues and skin as they enlargethe surrounding tissues and skin as they enlarge
Scofuloderma (when left untreated and ruptures Scofuloderma (when left untreated and ruptures resulting in a draining sinus tractresulting in a draining sinus tract
TB of the CNSTB of the CNS TB meningitisTB meningitis TB abscessTB abscess

Clinical Forms of Clinical Forms of TuberculosisTuberculosis Skeletal TBSkeletal TB
TB of the bones and jointsTB of the bones and joints TB of the spine or Pott’sTB of the spine or Pott’s
GI TBGI TB TB enteritisTB enteritis TB peritonitisTB peritonitis Hepatobiliary TBHepatobiliary TB TB of the pancreasTB of the pancreas
Cutaneous TBCutaneous TB Ocular TBOcular TB GUT TBGUT TB TB of the Middle EarTB of the Middle Ear
Diagnostic TestsDiagnostic Tests Mantoux Testing/Tuberculin skin testMantoux Testing/Tuberculin skin test
Most widely used method to determine latent Most widely used method to determine latent TB infection TB infection
Standard method for screeningStandard method for screening positive if ≥ 8 mm induration sizepositive if ≥ 8 mm induration size A dose of 0.1 ml of 2-TU PPD-RT23 or 0.1 ml A dose of 0.1 ml of 2-TU PPD-RT23 or 0.1 ml
of 5-TU PPD-Sof 5-TU PPD-S Provides a general measure of a person’s Provides a general measure of a person’s
cellular responsecellular response
Diagnostic TestsDiagnostic Tests
Mantoux Testing/Tuberculin skin testMantoux Testing/Tuberculin skin test Features of reaction Features of reaction
Delayed course reaching a peak of more than 24h after Delayed course reaching a peak of more than 24h after injection of antigeninjection of antigen
Indurated characterIndurated character Occasional vesiculation and necrosisOccasional vesiculation and necrosis
A pale wheal of 6 to 10mm in diameter should A pale wheal of 6 to 10mm in diameter should be evident after injectionbe evident after injection
Read within 48-72hrs from the time of Read within 48-72hrs from the time of administrationadministration
Diagnostic TestsDiagnostic Tests Mantoux Testing/Tuberculin skin testMantoux Testing/Tuberculin skin test
False positiveFalse positive Nontuberculous mycobacteriaNontuberculous mycobacteria BCG vaccination BCG vaccination
Reaction develops 6-12 weeks after vaccinationReaction develops 6-12 weeks after vaccination Wanes after 5 years from immunizationWanes after 5 years from immunization
False negativeFalse negative AnergyAnergy Very young age (< 6 months)Very young age (< 6 months) Recent TB infection or overwhelming TB diseaseRecent TB infection or overwhelming TB disease Live-virus vaccination Live-virus vaccination
postpone for at least 4 – 6 weeks after immunization or postpone for at least 4 – 6 weeks after immunization or do it on the same day of vaccinationdo it on the same day of vaccination

Diagnostic TestsDiagnostic Tests AFB smears (microscopic examination)AFB smears (microscopic examination)
Provides presumptive diagnosis of active TBProvides presumptive diagnosis of active TB Gives a quantitative estimation of the number Gives a quantitative estimation of the number
of bacilli on the smear of bacilli on the smear Implies infectiousness of the patientImplies infectiousness of the patient Low sensitivity (51.8 – 53.1%)Low sensitivity (51.8 – 53.1%) High specificity (97.5 – 99.8%)High specificity (97.5 – 99.8%) 10104 4 bacilli per ml of sputum : lowest bacilli per ml of sputum : lowest
concentration that can be detectedconcentration that can be detected

Diagnostic TestsDiagnostic Tests
Culture : gold std. Culture : gold std. Solid media: 4-6 weeks for isolation and another 2-Solid media: 4-6 weeks for isolation and another 2-
4 weeks for susceptibility testing4 weeks for susceptibility testing Middlebrook 7H-11 7H-10 (agar-based)Middlebrook 7H-11 7H-10 (agar-based) Lowenstein-Jensen (egg-based)Lowenstein-Jensen (egg-based)
Liquid mediaLiquid media Bactec : as few as 7 to 10 days; carbon-14 (marker of Bactec : as few as 7 to 10 days; carbon-14 (marker of
bacterial growth)bacterial growth) Middlebrook brothMiddlebrook broth Septi-check AFBSepti-check AFB BBL mycobacteria growth incubator tubeBBL mycobacteria growth incubator tube
Diagnostic TestsDiagnostic Tests Specimens collected for demonstration of Specimens collected for demonstration of
tubercle bacillitubercle bacilli Sputum Sputum
for older children able to expectorate for older children able to expectorate Series of three early morning specimens on Series of three early morning specimens on
different days before starting chemotherapydifferent days before starting chemotherapy Make sure brought up from the lungsMake sure brought up from the lungs

Diagnostic TestsDiagnostic Tests Specimens collected for demonstration of Specimens collected for demonstration of
tubercle bacillitubercle bacilli Gastric aspirateGastric aspirate
For infants and children who cannot expectorate For infants and children who cannot expectorate even with aerosol inhalationeven with aerosol inhalation
5-10 ml of gastric contents aspirated early in the 5-10 ml of gastric contents aspirated early in the morning after the person has fasted for at least 8 – morning after the person has fasted for at least 8 – 10 hours preferably before the child arises and 10 hours preferably before the child arises and peristalsis empties the stomach of respiratory peristalsis empties the stomach of respiratory secretions swallowed overnightsecretions swallowed overnight
Diagnostic TestsDiagnostic Tests Specimens collected for demonstration of Specimens collected for demonstration of
tubercle bacillitubercle bacilli Bronchial washingsBronchial washings UrineUrine
First morning-voided midstream specimenFirst morning-voided midstream specimen
Other body fluids and tissuesOther body fluids and tissues Bone marrow, lung and liver biopsy in patients with Bone marrow, lung and liver biopsy in patients with
hematogenous spread/disseminated disease must be hematogenous spread/disseminated disease must be consideredconsidered
Diagnostic TestsDiagnostic Tests Radiographic FindingsRadiographic Findings
No pathognomonic findings in childhood TBNo pathognomonic findings in childhood TB Lateral projections are important wherein Lateral projections are important wherein
partially calcified mediastinal nodes may be partially calcified mediastinal nodes may be visiblevisible
Most common cause of calcification in children Most common cause of calcification in children Uniform stippling of both lungs found in miliary Uniform stippling of both lungs found in miliary
tuberculosistuberculosis Lobar or lobular consolidationsLobar or lobular consolidations Common findings: Enlarged retrocardiac Common findings: Enlarged retrocardiac
lymphadenopathy (70%), hilar adenopathy with lymphadenopathy (70%), hilar adenopathy with pulmonary infiltrates (20%), and pleural effusionpulmonary infiltrates (20%), and pleural effusion

Initial Empiric Therapy of Tuberculosis Initial Empiric Therapy of Tuberculosis in Infants, Children and Adolescentsin Infants, Children and AdolescentsCategoryCategory RegimenRegimen RemarksRemarks
Class I TB Class I TB ExposureExposure <5 years<5 years 5 years5 years
3 months INH3 months INH Immediately Immediately prophylaxis prophylaxis controversial for controversial for those 5 years, but those 5 years, but is recommended by is recommended by some experts some experts specially if with risk specially if with risk factors e.g. factors e.g. malnutrition, malnutrition, immunocom-immunocom-promised statespromised states
Initial Empiric Therapy of Tuberculosis in Initial Empiric Therapy of Tuberculosis in Infants, Children and AdolescentsInfants, Children and Adolescents
ExtrapulmonaryExtrapulmonary
(a)(a) Severe, life-Severe, life-threatening threatening disease: disease: disseminated/ disseminated/ miliary, meningitis, miliary, meningitis, bone/joint diseasebone/joint disease
(b)(b) Other Other extrapulmonary extrapulmonary sitessites
2 months HRZ + E or S 2 months HRZ + E or S ffd by 10 months HR ± ffd by 10 months HR ± E/S given once daily or E/S given once daily or as DOT 3x weekly as DOT 3x weekly
Same regimen as Same regimen as pulmonary diseasepulmonary disease
Corticosteroids Corticosteroids (usually prednisone at 1 (usually prednisone at 1 mkday for 6-8 weeks mkday for 6-8 weeks with gradual tapering) with gradual tapering) beneficial for the beneficial for the following: meningitis, following: meningitis, pericarditis, pleuritis, pericarditis, pleuritis, endobronchial TB, endobronchial TB, miliary TBmiliary TB
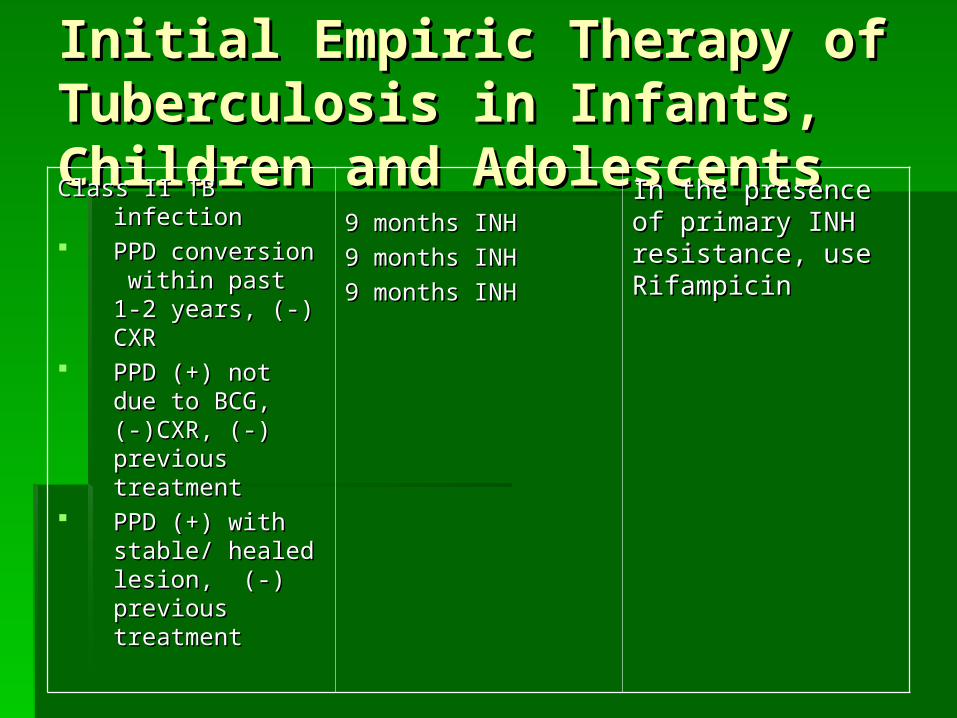
Initial Empiric Therapy of Tuberculosis in Initial Empiric Therapy of Tuberculosis in Infants, Children and AdolescentsInfants, Children and AdolescentsClass II TB infectionClass II TB infection PPD conversion within PPD conversion within
past 1-2 years, (-) CXRpast 1-2 years, (-) CXR PPD (+) not due to PPD (+) not due to
BCG,(-)CXR, (-) BCG,(-)CXR, (-) previous treatmentprevious treatment
PPD (+) with stable/ PPD (+) with stable/ healed lesion, (-) healed lesion, (-) previous treatmentprevious treatment
9 months INH9 months INH
9 months INH9 months INH
9 months INH9 months INH
In the presence of primary In the presence of primary INH resistance, use INH resistance, use RifampicinRifampicin
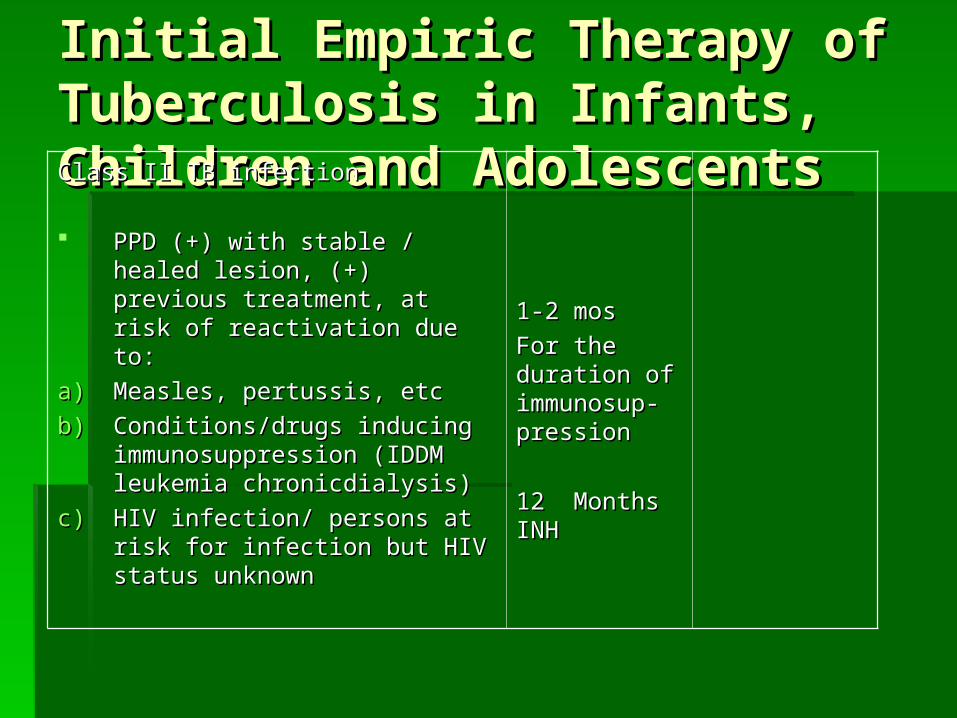
Initial Empiric Therapy of Tuberculosis in Initial Empiric Therapy of Tuberculosis in Infants, Children and AdolescentsInfants, Children and AdolescentsClass II TB infectionClass II TB infection
PPD (+) with stable / healed lesion, (+) PPD (+) with stable / healed lesion, (+) previous treatment, at risk of reactivation previous treatment, at risk of reactivation due to:due to:
a)a) Measles, pertussis, etcMeasles, pertussis, etcb)b) Conditions/drugs inducing Conditions/drugs inducing
immunosuppression (IDDM leukemia immunosuppression (IDDM leukemia chronicdialysis)chronicdialysis)
c)c) HIV infection/ persons at risk for infection HIV infection/ persons at risk for infection but HIV status unknownbut HIV status unknown
1-2 mos1-2 mosFor the duration of For the duration of immunosup-immunosup-pressionpression
12 Months INH12 Months INH

Initial Empiric Therapy of Tuberculosis in Initial Empiric Therapy of Tuberculosis in Infants, Children and AdolescentsInfants, Children and AdolescentsClass IIIB TB DiseaseClass IIIB TB Disease PulmonaryPulmonary(a)(a) Fully susceptible: based Fully susceptible: based
on culture results of on culture results of index case,index case,
(-) previous treatment, <10% (-) previous treatment, <10% local prevalence of local prevalence of primary INH resistanceprimary INH resistance
(b) Susceptibility unknown or (b) Susceptibility unknown or initial drug resistance initial drug resistance suspected because of suspected because of big bacillary population, big bacillary population, previous treatment (1 previous treatment (1 month), close contact month), close contact with resistant source with resistant source case, residence in area case, residence in area with >10% primary INH with >10% primary INH resistanceresistance
2 months HRZ once daily, ffd 2 months HRZ once daily, ffd by 4 months HR given once by 4 months HR given once daily or as DOT 3x weeklydaily or as DOT 3x weekly
2 months HRZ plus E or S 2 months HRZ plus E or S once daily, ffd by 4 months HR once daily, ffd by 4 months HR ± E/S given once daily or as ± E/S given once daily or as DOT 3x weeklyDOT 3x weekly
Streptomycin preferred in Streptomycin preferred in children < 6 years of age, children < 6 years of age, where visual acuity/color where visual acuity/color perception cannot be perception cannot be monitored reliablymonitored reliably
In immunocompromised In immunocompromised patients, continuation phase patients, continuation phase extended to 7 months (total extended to 7 months (total duration of therapy:9 months) duration of therapy:9 months) or for at least 6 months after or for at least 6 months after sputum conversion (if sputum conversion (if applicable) whichever is applicable) whichever is longer. If susceptibility results longer. If susceptibility results anavailable, continue E/S for anavailable, continue E/S for the entire duration of therapythe entire duration of therapy
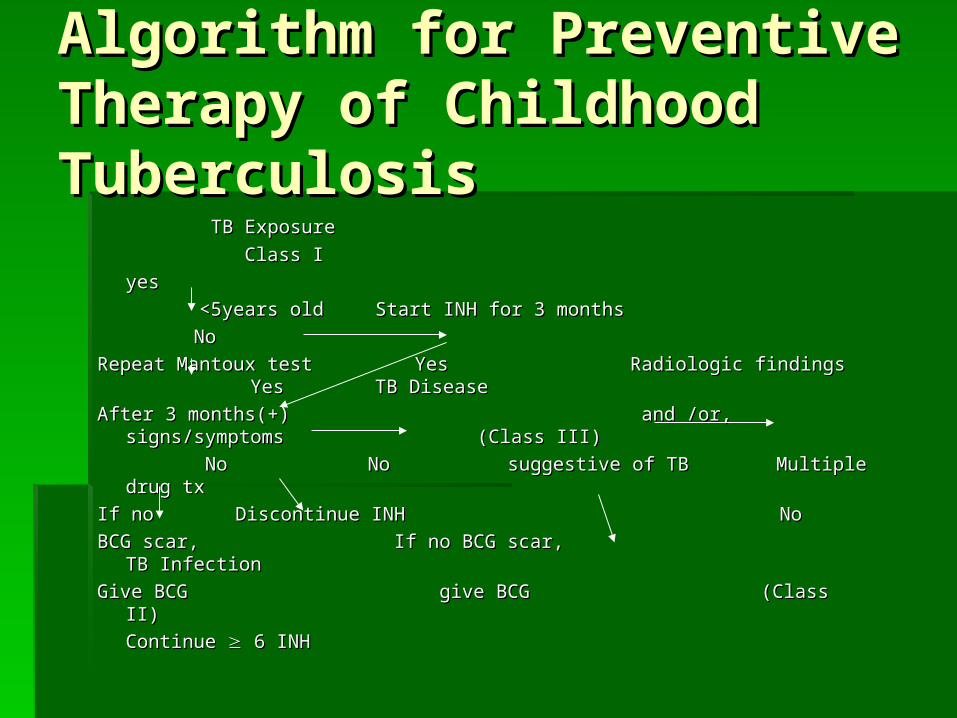
Algorithm for Preventive Therapy of Algorithm for Preventive Therapy of Childhood TuberculosisChildhood Tuberculosis
TB ExposureTB Exposure Class IClass I
yesyes <5years old<5years old Start INH for 3 months Start INH for 3 months
NoNoRepeat Mantoux test Yes Radiologic findings Yes TB DiseaseRepeat Mantoux test Yes Radiologic findings Yes TB DiseaseAfter 3 months(+) and /or, signs/symptoms (Class III)After 3 months(+) and /or, signs/symptoms (Class III)
NoNo No No suggestive of TB suggestive of TB Multiple drug tx Multiple drug txIf no If no Discontinue INH No Discontinue INH NoBCG scar,BCG scar, If no BCG scar, TB Infection If no BCG scar, TB InfectionGive BCGGive BCG give BCG give BCG (Class II) (Class II)
Continue Continue 6 INH 6 INH
Related Documents











