PULMONARY PHYSIOLOGY Gary L. Weinstein M.D. Director of Pulmonary and Critical Care Medicine Presbyterian Hospital of Dallas

PULMONARY PHYSIOLOGY Gary L. Weinstein M.D. Director of Pulmonary and Critical Care Medicine Presbyterian Hospital of Dallas.
Dec 31, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
PULMONARY PHYSIOLOGY
Gary L. Weinstein M.D.
Director of Pulmonary and Critical Care Medicine
Presbyterian Hospital of Dallas
Physiology for Dummies
“Good Air In, Bad Air Out”
Physiology for Psychologists
Take Slow, Deep, “Cleansing” Breaths
Physiology for Internists
• Remember (review ?) your little orange book from 1st year med school on Respiratory Physiology by Dr. West
• You MUST understand normal physiology to understand abnormal physiology
• You may BORROW my tape on normal lung sounds (especially if you have insomnia)

Physiology
• The respiratory system is composed of – the conducting airways (nose, mouth, larynx,
trachea, bronchial tree)– the lungs (terminal bronchioles, alveoli)– the parts of the CNS concerned with control of
the system (pons, medulla, cortex, Vagus…)– the chest wall (muscles of respiration, rib cage)
Physiology
• Functions of the respiratory system include– O2 extraction from the external environment– CO2 elimination from the body– maintenance of acid-base balance (along with
other TRIVIAL organs)– phonation– defense from the outside world– metabolism (e.g. ACE I ACE II)

Physiology
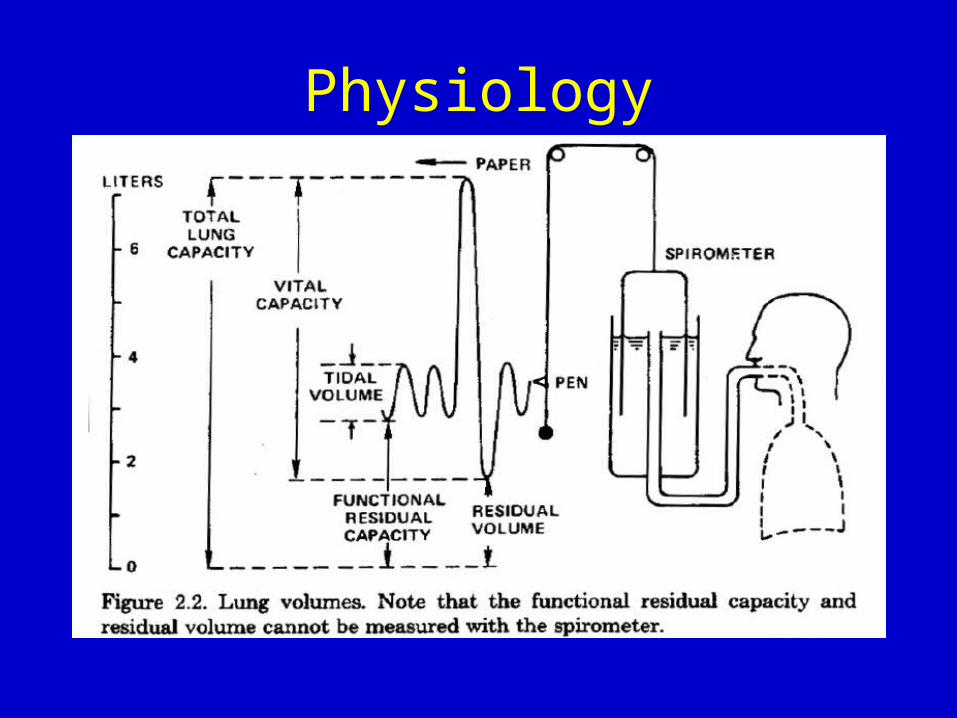
Physiology
Physiology
• Defense: each day about 10,000 liters of air is inspired along with dust, pollen, ash, microorgansims, toxic gases, particulates…
• Jobs include– air conditioning - by the time air reaches the
alveoli, it is at body temp and 100 % humidified– olfaction - a shallow sniff bring air to the nose
but not to the lung allowing “retreat”

Physiology• Jobs (cont’d)
– filtration• nasal hairs trap 10 - 15 um particles
• in addition, particles > 10 um impact onto the septum and turbinates as well as the nasopharynx
• tonsils and adenoids provide immunologic defense against biologically active materials
• particles 2 - 5 um sediment via gravity in the smaller airways and become trapped in the mucous that lines the airways, then are transported up and out
• particles 0.1- 0.5 um mainly stay suspended as aerosols and about 80 % of them are exhaled
Physiology
Physiology

Physiology
Physiology
Physiology
Physiology
Physiology
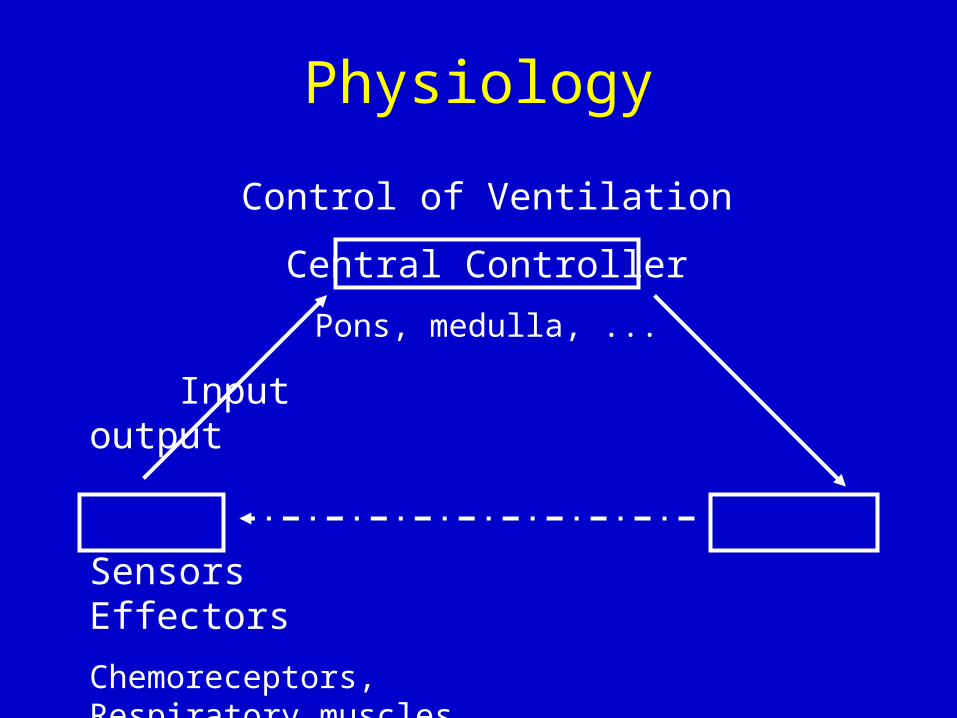
Control of Ventilation
Central Controller
Pons, medulla, ...
Input output
Sensors Effectors
Chemoreceptors, Respiratory muscles
lung and other receptors
Physiology
Physiology
• Lung and other receptors1) pulmonary stretch receptors
– lie within the airway smooth muscle
– impulses travel in the vagus nerve
– result in a slowing of respiratory rate
2) irritant receptors
– lie between airway epithelial cells
– stimulated by noxious gases, cigarette smoke, inhaled dusts and cold air
– impulses travel up the vagus and the reflex effects include bronchoconstriction and hyperpnea

Physiology
3) J receptors (juxta-capillary)– impulses pass up the Vagus and result in rapid,
shallow breathing– may play a role in the dyspnea a/w left heart
failure and ILD
4) Nose and upper airway receptors– respond to mechanical and chemical stimulation
with sneezing, coughing and bronchoconstriction
Physiology
• 5) Joint and muscle receptors– Impulses from moving limbs are believed to be
part of the stimulus to ventilation during exercise
Physiology• Fun Facts
– Alveolar surface area is 50-100 square meters– There are approx. 300 million alveoli, each 1/3
mm in diameter– The blood-gas interface is approx. 0.5 microns– O2 and CO2 move by simple diffusion– Anatomic dead space is approx. 1 ml/lb. body wt– Each RBC spends about 1 sec in the capillary
network and transverses 2 - 3 alveoli– Surfactant, made by type II pneumocytes,
dramatically lowers alveolar surface tension
Related Documents











