Theme: "Pulmonary Emphysema. Pathomorphology, outcomes, complications " Done By: Myrzakhanov Yerik 3course GMF 348 group Checked By: Abishev Zhasulan Zhumataevich Semey 2013

Pulmonary Emphysema. Pathomorphology, outcomes, complications
Jul 15, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Theme:
"Pulmonary Emphysema. Pathomorphology, outcomes,
complications "
Done By: Myrzakhanov Yerik3course GMF 348 group
Checked By: Abishev ZhasulanZhumataevich
Semey 2013
Plan
Introduction
Pulmonary Emphysema
Pathological anatomy of chronic diffuse
obstructive emphysema
Introduction The main cause of the disease - chronic bronchitis, which
implies a chronic infection. Chronic bronchitis usually develops between the ages of 30 and 60 years and occurs more often in men than in women. In fact, the result is the formation of chronic bronchitis emphysema.
Smoking, air pollution by various dust particles and some working conditions, such as those associated with the constant inhalation of coal dust or asbestos particles and silicon, also contribute to the development of the disease.? At the same time, emphysema, leading to severe respiratory failure may develop without preceding respiratory disease, i.e primary.
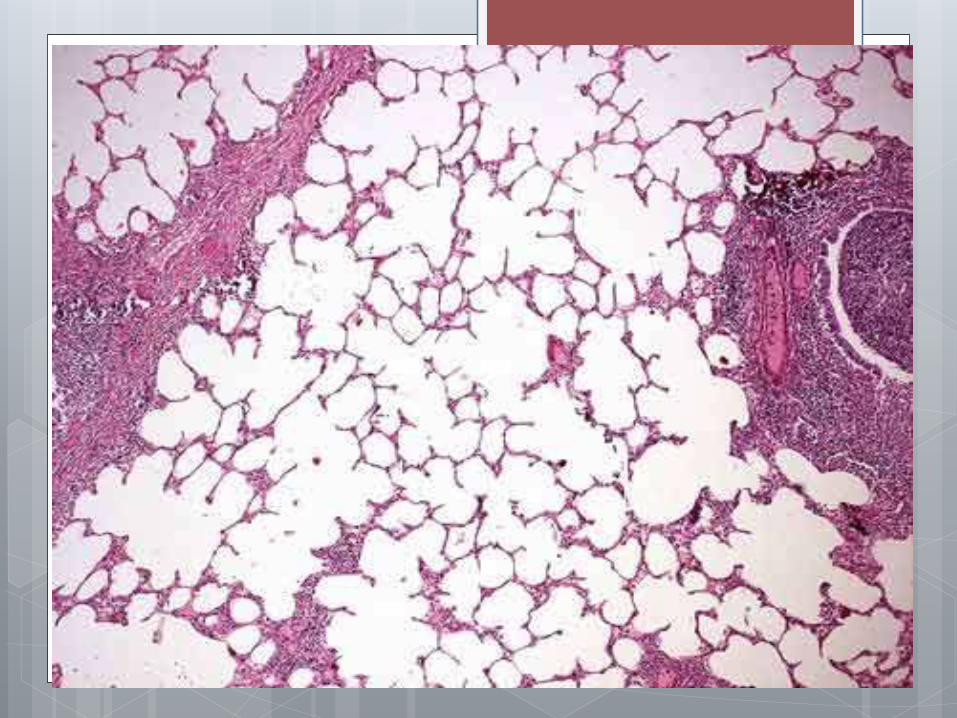
Pulmonary Emphysema - (from the Greek. emphysao – swell, inflated)respiratory disease characterized by abnormal enlargement of airspaces distal bronchioles accompanied by destructive morphological changes of alveolar walls, one of the most frequent forms of chronic nonspecific pulmonary diseases.
The following types of emphysema:
Chronic obstructive diffuse
Chronic lobular (perifocal, scar)
Vicarious (compensatory)
Primary (idiopathic)
Senile (emphysema in the elderly)
Interstitial
Etiology and pathogenesis There are two groups of causes leading to the development of
emphysema The first group includes factors that violate the elasticity and
strength of the structural elements of the lung: pathological microcirculation, changes in the properties of surfactant, congenital deficiency of alpha-1-antitrypsin, gaseous substances (cadmium compounds, nitrogen oxides, etc.), as well as tobacco smoke, dust particles in inhaled air. These causes may lead to the development of primary always diffuse emphysema. The basis of the pathogenesis of pathological reorganization of the entire respiratory lung; weakening of the elastic properties of the lung leads to the fact that during exhalation and therefore increase intrathoracic pressure small bronchi without their cartilaginous skeleton and devoid of elastic recoil of the lung, passively fallen down , thus increasing bronchial resistance and expiratory pressure increase in the alveoli . Inspiratory bronchial permeability in primary emphysema is not violated.
Factors contribute to the second group of high pressure in the lungs and respiratory department reinforce stretching alveoli, alveolar ducts and respiratory bronchioles. The highest value among them is airway obstruction that occurs in chronic obstructive bronchitis. This disease is becoming a major cause of secondary or obstructive pulmonary emphysema, as it was when it created the conditions for the formation of the valve mechanism of distension of the alveoli. Thus, the reduction in intrathoracicpressure during inspiration, causing passive stretching of the bronchial lumen , reduces the degree of bronchial obstruction available ; positive intrathoracic pressure during exhalation causes additional compression of bronchial branches and exacerbating already existing bronchial obstruction , helps delay the inspired air in the alveoli and hyperinflation . Important to the spread of the inflammatory process to the adjacent bronchioles alveoli with the development of alveolitis and destruction of interalveolar septa .
In the context of the insolvency of the stromaof the lung (particularly elastic) included the so-called valve mechanism.
It boils down to the fact that the mucus plug formed in the lumen of the small bronchi and bronchioles in chronic diffuse bronchitis, inspiratory air passes into the alveoli, but do not let him out when you exhale.
The air accumulates in the acini of the cavity expands, which leads to diffuse obstructive emphysema.
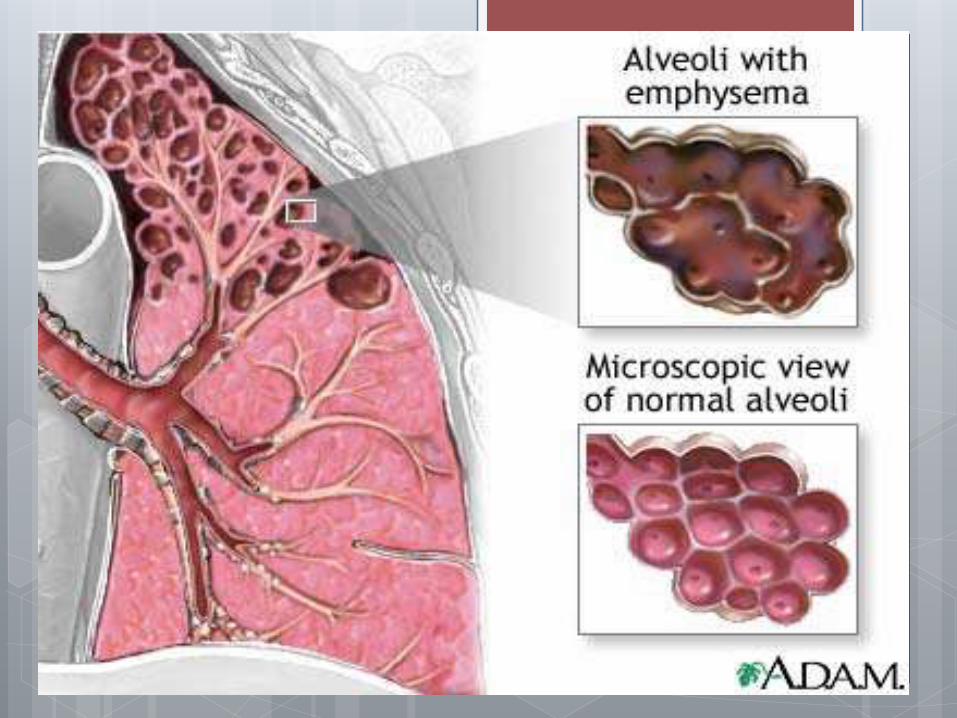
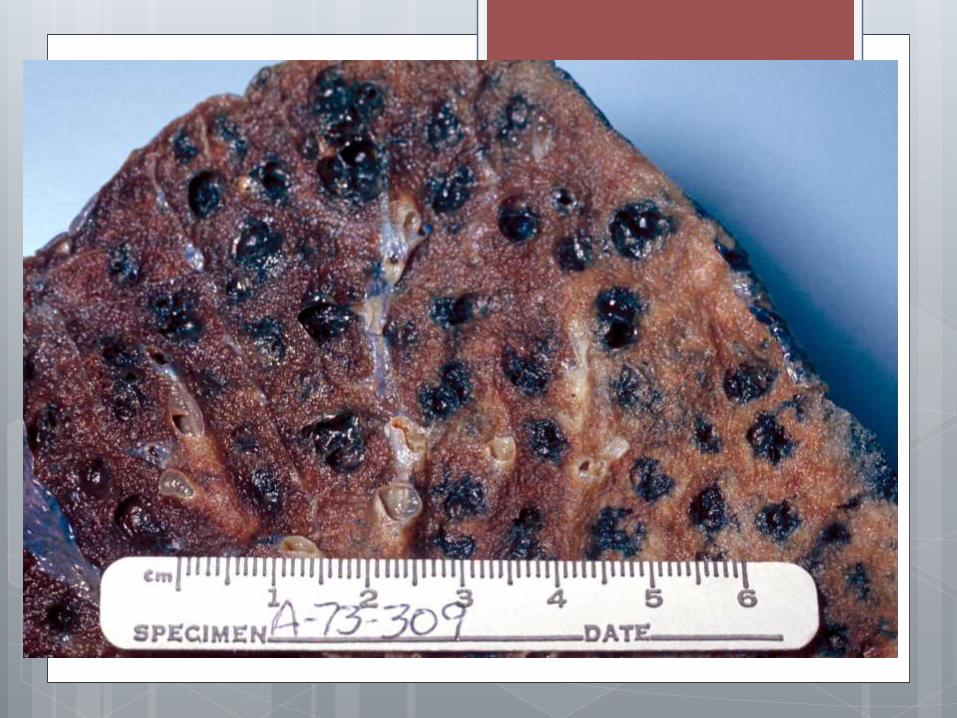
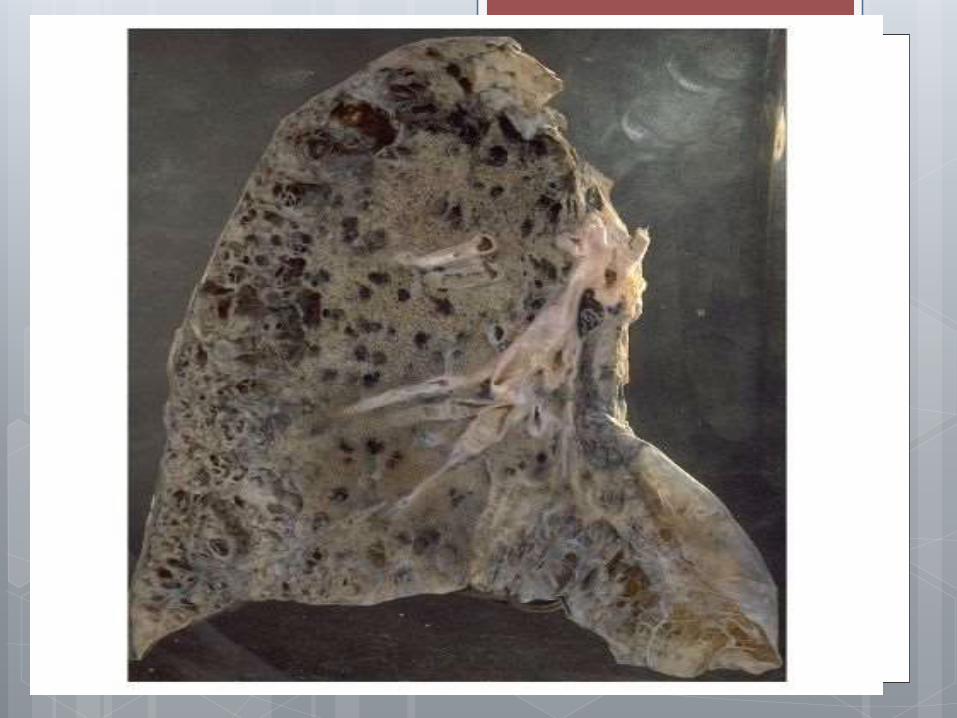
Pathological anatomy of chronic diffuse obstructive emphysema
Lungs increased in size, cover their edges anterior mediastinum, swollen, pale, soft, do not collapse, can be cut with a crunch.
Of the bronchi, the walls of which are thickened, squeezed muco-purulent exudate.
Bronchial mucosa full-blooded, marked hypertrophy of the muscular layer of uneven terminal bronchioles and small bronchi, the appearance of the mucosa of the last large number of goblet cells.
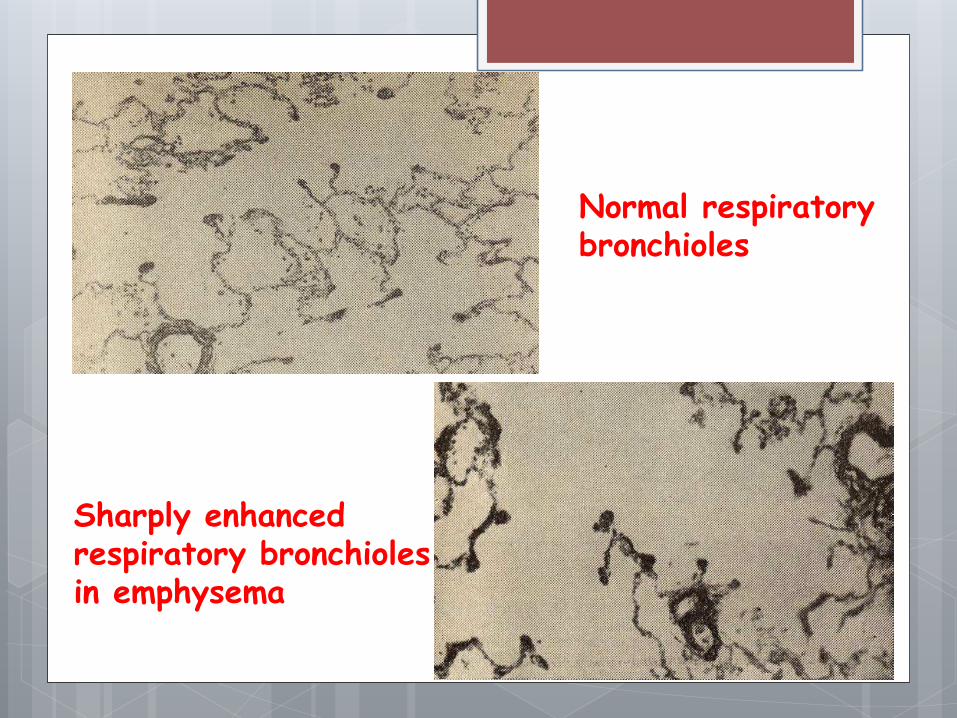
Normal respiratory bronchioles
Sharply enhanced respiratory bronchioles in emphysema
If the overall picture is dominated by changes in the bronchioles, the expanded proximal acinar(respiratory bronchioles 1st and 2nd order).
This is called emphysema centeracinar.
In the presence of inflammatory changes mainly in the larger bronchi (eg, intralobular) bloating and expansion affect the whole acinus and then talk about panatsinarnoy emphysema.
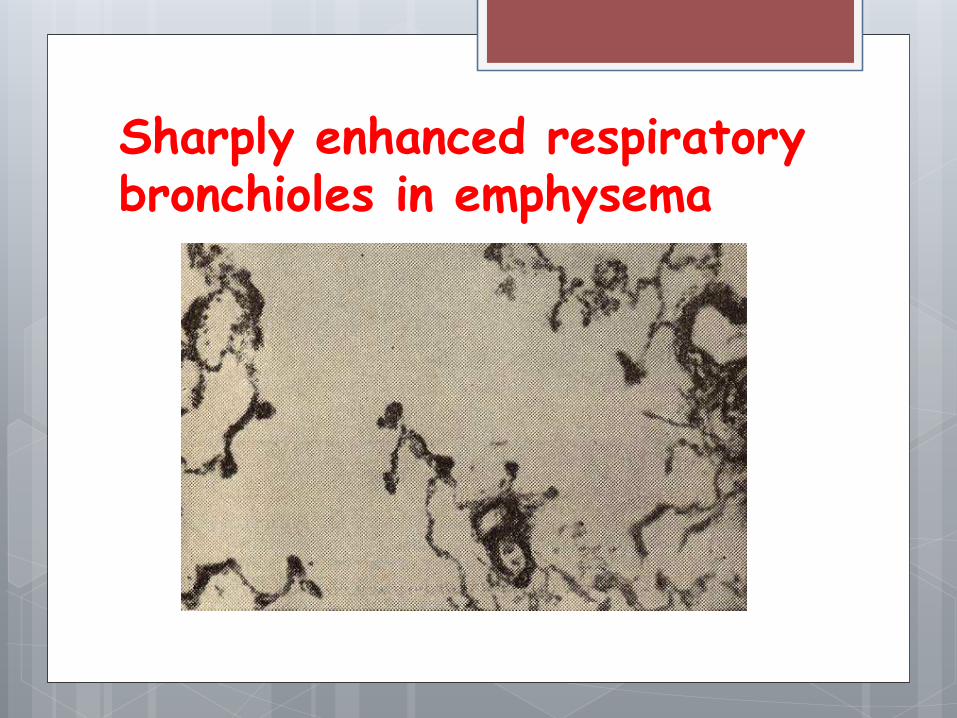
Sharply enhanced respiratory bronchioles in emphysema
Acinar walls stretching leads to stretching and thinning of the elastic
fibers, expanding alveolar ducts, alveolar
septa change.
Alveolar walls become thinner and
straightened, *Kohn pores dilate capillaries
zapustevayut.
*This so-called alveolar pores Kohn, creating the possibility of penetration of air from the alveoli into one another.
There is a strong expansion of conducting air and flattening of the respiratory bronchioles
and alveolar sacs shortening.
Consequently there is a sharp decrease in the
area of gas exchange and ventilation disturbed
lung function.
The capillary network in the acinus of respiratory reduced until the complete disappearance of capillaries, resulting in the formation of the capillary unit.
Overgrowth occurs mezhalveolyarnyhcapillaries collagen fibers and the development of intracapillary sclerosis.
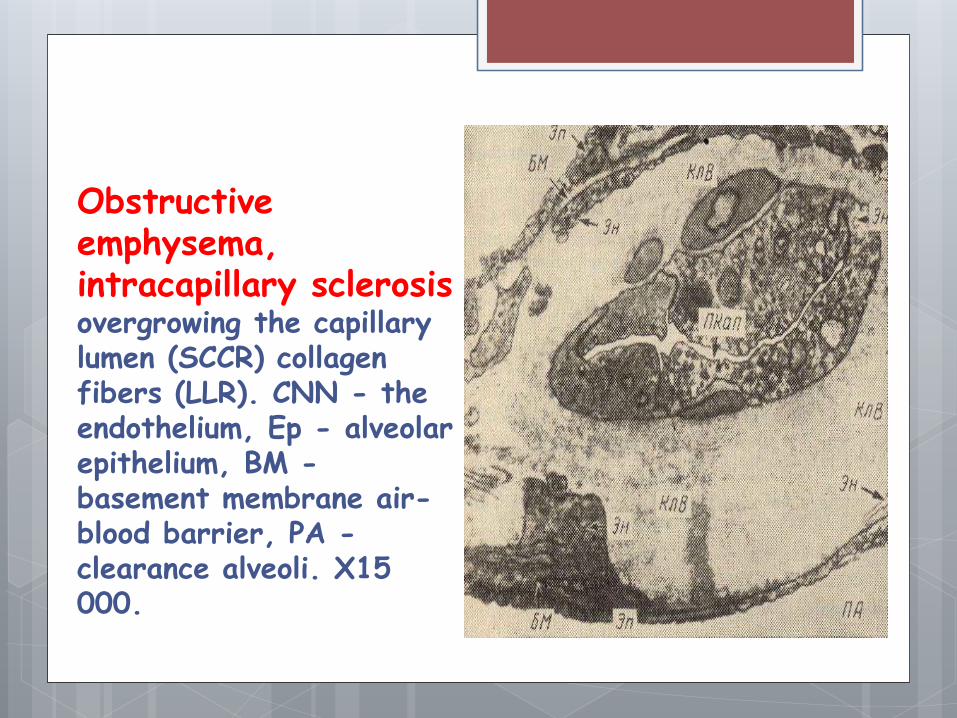
Obstructive emphysema, intracapillary sclerosisovergrowing the capillary lumen (SCCR) collagen fibers (LLR). CNN - the endothelium, Ep - alveolar epithelium, BM -basement membrane air-blood barrier, PA -clearance alveoli. X15 000.
It is sometimes observed the formation of new I not typical built capillaries, which has adaptive value.
Thus, in chronic obstructive pulmonary emphysema occurs prekapilljarnyh the pulmonary hypertension leading to cardiac hypertrophy (cor pulmonale). Patients suffering from chronic emphysema, at a certain stage of the disease become cardiopulmonary patients.
Complications
- Respiratory failure;
- Heart failure;
- Pneumothorax (air to the chest).
Any of the complications leading to disability of the patient.
Conclusion The term "emphysema" refers to pathological processes in the
lung, characterized by a high content of air in the lung tissue, a chronic lung disease characterized by respiratory failure and pulmonary gas exchange. In recent years, the frequency of emphysema increases, especially among the elderly.
Pulmonary Emphysema, along with chronic obstructive bronchitis and bronchial asthma refers to a group of chronic obstructive pulmonary disease (COPD). All these diseases are accompanied by bronchial obstruction, which accounts for the similarity of some of their clinical picture.
Reference
http://www.medchitalka.ru/patologicheskaya_anatomiya/kollagenovye_bolezni/17852.html
http://www.eurolab.ua/encyclopedia/morbid-anatomy/33164/
http://ru.wikipedia.org/wiki/%D0%AD%D0%BC%D1%84%D0%B8%D0%B7%D0%B5%D0%BC%D0%B0_%D0%BB%D1%91%D0%B3%D0%BA%D0%B8%D1%85
Легкие // Энциклопедический словарь Брокгауза и Ефрона: В 86 томах (82 т. и 4 доп.). — СПб., 1890—1907.
Related Documents











