WHEN PRESCRIBED ACTION HAS BEEN TAKEN, FILE THIS TRANSMITTAL WITH BASIC DOCUMENT. HPOD CHANGE 32 6010.61-M FEBRUARY 8, 2019 PUBLICATIONS SYSTEM CHANGE TRANSMITTAL FOR TRICARE REIMBURSEMENT MANUAL (TRM), APRIL 2015 The Defense Health Agency has authorized the following addition(s)/revision(s). CHANGE TITLE: REIMBURSEMENT & CODING UPDATES 18-004 CONREQ: 19892 SUMMARY OF CHANGE(S): See pages 3 and 4. EFFECTIVE DATE: See pages 3 and 4. IMPLEMENTATION DATE: March 8, 2019. This change is made in conjunction with Apr 2015 TPM, Change No. 41. Jose L. Lozoya Chief, Manuals Change Section Defense Health Agency (DHA)

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

HPOD CHANGE 326010.61-MFEBRUARY 8, 2019
PUBLICATIONS SYSTEM CHANGE TRANSMITTAL FORTRICARE REIMBURSEMENT MANUAL (TRM), APRIL 2015
The Defense Health Agency has authorized the following addition(s)/revision(s).
CHANGE TITLE: REIMBURSEMENT & CODING UPDATES 18-004
CONREQ: 19892
SUMMARY OF CHANGE(S): See pages 3 and 4.
EFFECTIVE DATE: See pages 3 and 4.
IMPLEMENTATION DATE: March 8, 2019.
This change is made in conjunction with Apr 2015 TPM, Change No. 41.
Jose L. LozoyaChief, Manuals Change SectionDefense Health Agency (DHA)
WHEN PRESCRIBED ACTION HAS BEEN TAKEN, FILE THIS TRANSMITTAL WITH BASIC DOCUMENT.

CHANGE 326010.61-MFEBRUARY 8, 2019
REMOVE SECTION(S) INSERT SECTION(S)
CHAPTER 11
Addendum A (FY 2016) ★ ★ ★ ★ ★ ★★ ★ ★ ★ ★ ★ Addendum A (FY 2019)
Addendum B (FY 2016) ★ ★ ★ ★ ★ ★★ ★ ★ ★ ★ ★ Addendum B (FY 2019)
Addendum C (FY 2016) ★ ★ ★ ★ ★ ★★ ★ ★ ★ ★ ★ Addendum C (FY 2019)
2

CHANGE 326010.61-M
FEBRUARY 8, 2019
SUMMARY OF CHANGES
CHAPTER 2
1. Section 1. This change updates cost-shares and deductibles. EFFECTIVE DATE: 10/01/2018.
CHAPTER 6
2. Section 4. This change updates DRGs. EFFECTIVE DATE: 10/01/2018.
3. Section 7. This change updates DRGs. EFFECTIVE DATE: 10/01/2018.
4. Section 8. This change updates DRGs. EFFECTIVE DATE: 10/01/2018.
CHAPTER 7
5. Section 1. This change updates the TRICARE Manual Health Reimbursement System for FY 2019. EFFECTIVE DATE: 10/01/2018.
6. Addendum A. This change updates the TRICARE Manual Health Reimbursement System for FY 2019. EFFECTIVE DATE: 10/01/2018.
7. Addendum B. This change updates the TRICARE Manual Health Reimbursement System for FY 2019. EFFECTIVE DATE: 10/01/2018.
CHAPTER 10
8. Section 1. This change provides updated 2018 and beyond Birthing Center Non-Professional Component Rate and replaces DRG-775 with DRG-807 2. EFFECTIVE DATE: 04/01/2018.
9. Addendum A. This change provides updated 2018 and beyond Birthing Center Non-Professional Component Rate and replaces DRG-775 with DRG-807 2. EFFECTIVE DATE: 04/01/2018.
CHAPTER 11
10. Section 4. This Change provides the updated national hospice rates, cap amount and wage indexes for care and services provided on or after October 1st, 2018 through September 30th, 2019. EFFECTIVE DATE: 10/01/2018.
3

CHANGE 326010.61-MFEBRUARY 8, 2019
SUMMARY OF CHANGES (Continued)
CHAPTER 11 (Continued)
11. Addendum A (FY2016). Deleted. This Change provides the updated national hospice rates, cap amount and wage indexes for care and services provided on or after October 1st, 2018 through September 30th, 2019. EFFECTIVE DATE: 10/01/2018.
12. Addendum A (FY2019). Added. This Change provides the updated national hospice rates, cap amount and wage indexes for care and services provided on or after October 1st, 2018 through September 30th, 2019. EFFECTIVE DATE: 10/01/2018.
13. Addendum B (FY2016). Deleted. This Change provides the updated national hospice rates, cap amount and wage indexes for care and services provided on or after October 1st, 2018 through September 30th, 2019. EFFECTIVE DATE: 10/01/2018.
14. Addendum B (FY2019). Added. This Change provides the updated national hospice rates, cap amount and wage indexes for care and services provided on or after October 1st, 2018 through September 30th, 2019. EFFECTIVE DATE: 10/01/2018.
15. Addendum C (FY2016). Deleted. This Change provides the updated national hospice rates, cap amount and wage indexes for care and services provided on or after October 1st, 2018 through September 30th, 2019. EFFECTIVE DATE: 10/01/2018.
16. Addendum C (FY2019). Added. This Change provides the updated national hospice rates, cap amount and wage indexes for care and services provided on or after October 1st, 2018 through September 30th, 2019. EFFECTIVE DATE: 10/01/2018.
4

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 2, Section 1
Cost-Shares And Deductibles For TRICARE Services Received Prior To January 1, 2018 And For TRICARE Services Received On Or After January 1, 2018 By TRICARE For Life (TFL) Beneficiaries
1.3.1.3.4 Adjustment of Excess. Any beneficiary identified under paragraphs 1.3.1.3.2 and 1.3.1.3.3 who paid any deductible in excess of the amounts stipulated is entitled to an adjustment of any amount paid in excess against the annual deductible required under those paragraphs.
1.3.1.3.5 The deductible amounts identified in this section shall be deemed to have been satisfied if the catastrophic cap amounts identified in Section 2 have been met for the same fiscal year in which the deductible applies.
1.3.2 Deductible Amount: Inpatient Care
None.
1.3.3 Cost-Share Amount
1.3.3.1 Outpatient Care
1.3.3.1.1 The cost-share for ADFMs for outpatient care is 20% of the allowable amount in excess of the annual deductible amount. This includes the professional charges of an individual professional provider for services rendered in a non-TRICARE-approved ASC or Birthing Center. For family members of active duty members of the armed forces of NATO/PfP foreign nations who are eligible for outpatient care under TRICARE per DEERS, see paragraph 1.1.5.
1.3.3.1.2 Other Beneficiary. The cost-share applicable to outpatient care for other than active duty and authorized NATO/PfP family member beneficiaries is 25% of the allowable amount in excess of the annual deductible amount. This includes: partial hospitalization for alcohol rehabilitation; professional charges of an individual professional provider for services rendered in a non-TRICARE-approved ASC.
Note: Per paragraphs 1.3.3.10 and 1.4.3, annual deductible amounts do not apply to the preventive care services described in the TPM, Chapter 7, Sections 2.1 and 2.5.
1.3.3.2 Inpatient Care
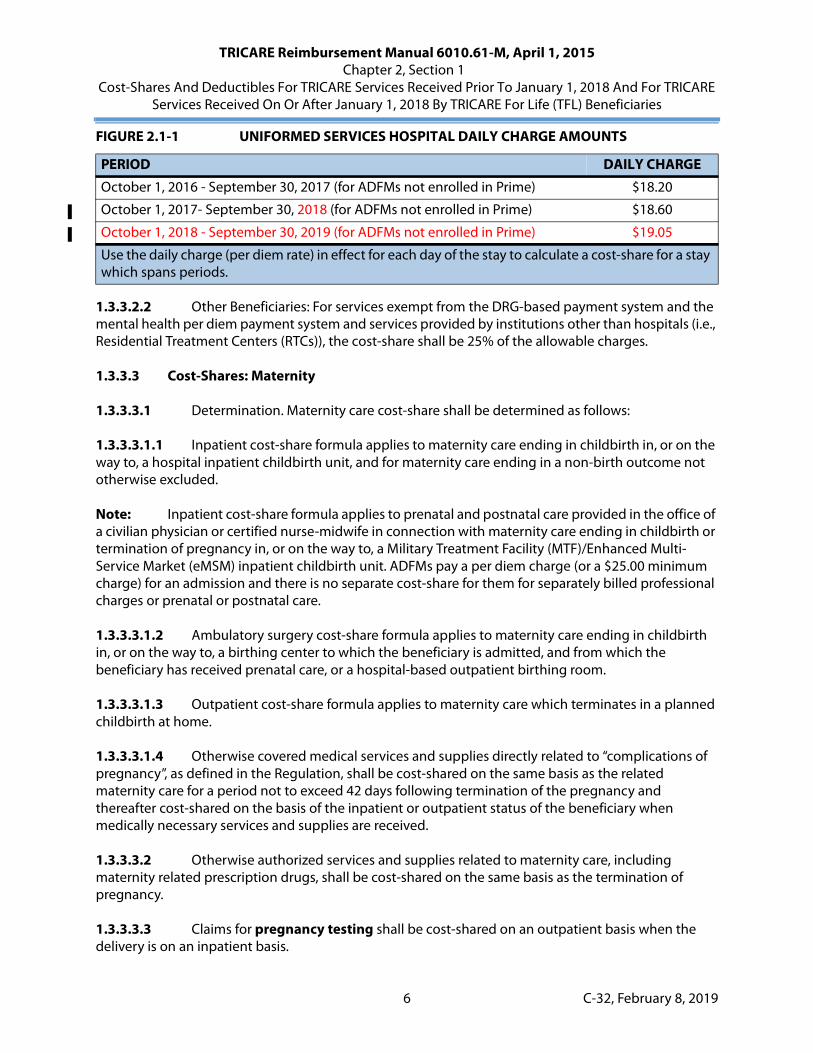
1.3.3.2.1 ADFM: For services prior to October 3, 2016, except in the case of mental health and Substance Use Disorder (SUD) services, ADFMs or their sponsors are responsible for the payment of the first $25 of the allowable institutional costs incurred with each covered inpatient admission to a hospital or other authorized institutional provider, or the daily charge the beneficiary or sponsor would have been charged had the inpatient care been provided in a Uniformed Service hospital, whichever is greater. (Please reference daily rate chart below.) For services on or after October 3, 2016, the following applies to all services (to include mental health and SUD services) for ADFMs or their sponsors.
FIGURE 2.1-1 UNIFORMED SERVICES HOSPITAL DAILY CHARGE AMOUNTS
PERIOD DAILY CHARGE
October 1, 2015 - September 30, 2016 (for ADFMs not enrolled in Prime) $18.00
Use the daily charge (per diem rate) in effect for each day of the stay to calculate a cost-share for a stay which spans periods.
5 C-32, February 8, 2019
TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 2, Section 1
Cost-Shares And Deductibles For TRICARE Services Received Prior To January 1, 2018 And For TRICARE Services Received On Or After January 1, 2018 By TRICARE For Life (TFL) Beneficiaries
1.3.3.2.2 Other Beneficiaries: For services exempt from the DRG-based payment system and the mental health per diem payment system and services provided by institutions other than hospitals (i.e., Residential Treatment Centers (RTCs)), the cost-share shall be 25% of the allowable charges.
1.3.3.3 Cost-Shares: Maternity
1.3.3.3.1 Determination. Maternity care cost-share shall be determined as follows:
1.3.3.3.1.1 Inpatient cost-share formula applies to maternity care ending in childbirth in, or on the way to, a hospital inpatient childbirth unit, and for maternity care ending in a non-birth outcome not otherwise excluded.
Note: Inpatient cost-share formula applies to prenatal and postnatal care provided in the office of a civilian physician or certified nurse-midwife in connection with maternity care ending in childbirth or termination of pregnancy in, or on the way to, a Military Treatment Facility (MTF)/Enhanced Multi-Service Market (eMSM) inpatient childbirth unit. ADFMs pay a per diem charge (or a $25.00 minimum charge) for an admission and there is no separate cost-share for them for separately billed professional charges or prenatal or postnatal care.
1.3.3.3.1.2 Ambulatory surgery cost-share formula applies to maternity care ending in childbirth in, or on the way to, a birthing center to which the beneficiary is admitted, and from which the beneficiary has received prenatal care, or a hospital-based outpatient birthing room.
1.3.3.3.1.3 Outpatient cost-share formula applies to maternity care which terminates in a planned childbirth at home.
1.3.3.3.1.4 Otherwise covered medical services and supplies directly related to “complications of pregnancy”, as defined in the Regulation, shall be cost-shared on the same basis as the related maternity care for a period not to exceed 42 days following termination of the pregnancy and thereafter cost-shared on the basis of the inpatient or outpatient status of the beneficiary when medically necessary services and supplies are received.
1.3.3.3.2 Otherwise authorized services and supplies related to maternity care, including maternity related prescription drugs, shall be cost-shared on the same basis as the termination of pregnancy.
1.3.3.3.3 Claims for pregnancy testing shall be cost-shared on an outpatient basis when the delivery is on an inpatient basis.
October 1, 2016 - September 30, 2017 (for ADFMs not enrolled in Prime) $18.20
October 1, 2017- September 30, 2018 (for ADFMs not enrolled in Prime) $18.60
October 1, 2018 - September 30, 2019 (for ADFMs not enrolled in Prime) $19.05
FIGURE 2.1-1 UNIFORMED SERVICES HOSPITAL DAILY CHARGE AMOUNTS
PERIOD DAILY CHARGE
Use the daily charge (per diem rate) in effect for each day of the stay to calculate a cost-share for a stay which spans periods.
6 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 2, Section 1
Cost-Shares And Deductibles For TRICARE Services Received Prior To January 1, 2018 And For TRICARE Services Received On Or After January 1, 2018 By TRICARE For Life (TFL) Beneficiaries
1.3.3.5.4.2.1 A fixed daily amount multiplied by the number of covered days. The fixed daily amount shall be 25% of the per diem adjusted so that total beneficiary cost-shares will equal 25% of total payments under the inpatient mental health per diem payment system. This fixed daily amount shall be updated annually and on the DHA website at http://www.health.mil/rates. This fixed daily amount will also be furnished to contractors by the DHA. The following fixed daily amounts are effective for services rendered on or after October 1 of each fiscal year.
• FY 2017 - $235 per day.• FY 2018 - $241 per day.• FY 2019 - $248 per day.
1.3.3.5.4.2.2 Twenty-five percent (25%) of the hospital’s billed charges (less any duplicates).
1.3.3.5.5 Claims which span a period in which two separate per diems exist. A claim subject to the inpatient mental health per diem payment system which spans a period in which two separate per diems exist shall have the cost-share computed on the actual per diem in effect for each day of care.
1.3.3.5.6 Cost-share whenever leave days are involved. There is no patient cost-share for leave days when such days are included in a hospital stay.
1.3.3.5.7 Claims for services that are provided during an inpatient admission which are not included in the per diem rate shall be cost-shared as an inpatient claim if the contractor cannot determine where the service was rendered and the status of the patient when the service was provided. The contractor shall examine the claim for place of service and type of service to determine if the care was rendered in the hospital while the beneficiary was an inpatient of the hospital. This would include non-mental health claims and mental health claims submitted by individual professional providers rendering medically necessary services during the inpatient admission.
1.3.3.6 Cost-Shares: PHPs And Intensive Outpatient Program (IOPs)
1.3.3.6.1 For care rendered prior to October 3, 2016, cost-sharing for partial hospitalization is on an inpatient basis. The inpatient cost-share also applies to the associated psychotherapy billed separately by the individual professional provider. These providers shall identify on the claim form that the psychotherapy is related to a partial hospitalization stay so the proper inpatient cost-sharing can be applied. The cost-share for ADFMs enrolled in Prime for inpatient mental health services is $0. For retirees and their family members, the cost-share is 25% of the allowed amount. Since inpatient cost-sharing is being applied, no deductible shall be taken for partial hospitalization regardless of sponsor status. The cost-share for ADFMs shall be taken from the PHP claim.
1.3.3.6.2 For care rendered on or after October 3, 2016, cost-sharing for PHPs and IOPs is on an outpatient basis. The outpatient cost-share also applies to the associated psychotherapy billed separately by the individual professional provider. These providers shall identify on the claim form that the psychotherapy is related to PHP or IOP care so the proper outpatient cost-sharing can be applied. Cost-shares for standard beneficiaries can be found in paragraph 1.3; cost-sharing requirements for prime beneficiaries can be found in paragraph 1.2.
11 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 2, Section 1
Cost-Shares And Deductibles For TRICARE Services Received Prior To January 1, 2018 And For TRICARE Services Received On Or After January 1, 2018 By TRICARE For Life (TFL) Beneficiaries
1.3.3.7 Cost-Shares: Ambulatory Surgery
1.3.3.7.1 For non-TRICARE Prime ADFMs, for all services reimbursed as ambulatory surgery, the cost-share shall be $25 and shall be assessed on the facility claim. No cost-share shall be deducted from a claim for professional services related to ambulatory surgery. This applies whether the services are provided in a freestanding ASC, a hospital outpatient department or a hospital emergency room. So long as at least one procedure on the claim is reimbursed as ambulatory surgery, the claim shall be cost-shared as ambulatory surgery as required by this section. For family members of active duty members of the armed forces of NATO/PfP foreign nations who are eligible for outpatient care under TRICARE per DEERS, see paragraph 1.1.5.
1.3.3.7.2 Other Beneficiaries. Since the cost-share for other beneficiaries is based on a percentage rather than a set amount, the cost-share shall be taken from all ambulatory surgery claims. For professional services, the cost-share is 25% of the allowed amount. For the facility claim, the cost-share is the lesser of:
1.3.3.7.2.1 Twenty-five percent (25%) of the applicable group payment rate (see Chapter 9, Section 1); or
1.3.3.7.2.2 Twenty-five percent (25%) of the billed charges; or
1.3.3.7.2.3 Twenty-five percent (25%) of the allowed amount as determined by the contractor.
1.3.3.7.2.4 The special cost-sharing provisions for beneficiaries other than ADFMs will ensure that these beneficiaries are not disadvantaged by these procedures. In most cases, 25% of the group payment rate will be less, but because there is some variation within each group, 25% of billed charges could be less in some cases. This will ensure that the beneficiaries get the benefit of the group payment rates when they are more advantageous, but they will never be disadvantaged by them. If there is no group payment rate for a procedure, the cost-share shall simply be 25% of the allowed amount.
1.3.3.8 Cost-Shares and Deductible: Former Spouses
1.3.3.8.1 Deductible. In accordance with the FY 1991 Appropriations and Authorization Acts, Sections 8064 and 712 respectively, beginning April 1, 1991, an eligible former spouse is responsible for payment of the first one hundred and fifty dollars ($150.00) of the reasonable costs/charges for otherwise covered outpatient services and/or supplies provided in any one fiscal year. Although the law defines former spouses as family members of the member or former member, there is no legal familial relationship between the former spouse and the member or former member. Moreover, any TRICARE-eligible children of the former spouse will retain a legal familial relationship with the member or former member and shall be included in the member’s or former member’s family deductible. The former spouse cannot contribute to, nor benefit from, any family deductible of the member or former member to whom the former spouse was married or of that of any TRICARE-eligible children. In other words, a former spouse must independently meet the $150.00 deductible in any fiscal year.
1.3.3.8.2 Cost-Share. An eligible former spouse is responsible for payment of cost-sharing amounts identical to those required for beneficiaries other than ADFMs.
12

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Diagnosis Related Groups (DRGs)
Chapter 6 Section 4
Hospital Reimbursement - TRICARE Diagnosis Related Group (DRG)-Based Payment System (Applicability Of The DRG System)
Issue Date: October 8, 1987Authority: 32 CFR 199.14(a)(1)Revision: C-32, February 8, 2019
1.0 APPLICABILITY
This policy is mandatory for reimbursement of services provided by either network or non-network providers. However, alternative network reimbursement methodologies are permitted when approved by the Defense Health Agency (DHA) and specifically included in the network provider agreement.
2.0 ISSUE
What providers and services are to be reimbursed under the TRICARE DRG-based payment system?
3.0 POLICY
3.1 Areas Affected
3.1.1 The TRICARE DRG-based payment system shall apply to hospital services in the 50 United States (U.S.), the District of Columbia, and Puerto Rico. The DRG-based payment system shall not be used with regard to services rendered outside the 50 U.S., the District of Columbia, or Puerto Rico.
3.1.2 State waivers. Any state which has implemented a separate DRG-based payment system or similar payment system in order to control costs may be exempt from the TRICARE DRG-based payment system under the following circumstances:
• The following requirements must be met in order for a state to be exempt.
• The state must be exempt from the Medicare Inpatient Prospective Payment System (IPPS);
• The state must request, in writing to DHA, that it be exempt from the TRICARE DRG-based payment system; and
1 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 6, Section 4
Hospital Reimbursement - TRICARE Diagnosis Related Group (DRG)-Based Payment System (Applicability Of The DRG System)
• Payments in the state must continue to be at a level to maintain savings comparable to those which would be achieved under the TRICARE DRG-based payment system. DHA will monitor reimbursement levels in any exempted state to ensure that payment levels there do not exceed those under the TRICARE DRG-based payment system. If they do exceed that level, DHA will work with the state to resolve the problem. However, if a satisfactory solution cannot be found, DHA will terminate the exemption after due notice has been given to the state.
3.2 Services Subject To The DRG-Based Payment System
Unless exempt, all normally covered inpatient hospital services furnished to TRICARE beneficiaries are subject to the TRICARE DRG-based payment system.
3.3 Services Exempt From The DRG-Based Payment System
The following hospital services, even when provided in a hospital subject to the TRICARE DRG-based payment system, are exempt from the TRICARE DRG-based payment system and shall be reimbursed under the appropriate procedures.
3.3.1 Services provided by hospitals exempt from the DRG-based payment system as defined in paragraph 3.6.
3.3.2 All services related to TRICARE covered solid organ transplants for which there is no DRG assignment.
3.3.3 All services related to solid organ acquisition, including the costs of the donor’s inpatient stay for TRICARE covered transplants by TRICARE authorized transplantation centers. Acquisition costs related to solid organ transplants shall be paid on a reasonable cost basis and are not included in the DRG.
3.3.4 All services provided by hospital-based professionals (physicians, psychologists, etc.) which, under normal TRICARE requirements, would be billed by the hospital. This does not include any therapy services (physical, speech, etc.), since these are included in the DRG-based payment. For radiology and pathology services provided by hospital-based physicians, any related non-professional (i.e., technical) component of these services is included in the DRG-based payment and cannot be billed separately. The services of hospital-based professionals which are employed by, or under contract to, a hospital must still be billed by the hospital and must be billed on a participating basis.
3.3.5 Anesthesia services provided by nurse anesthetists. This may be separately billed only when the nurse anesthetist is the primary anesthetist for the case.
Note: As a general rule, TRICARE will only pay for one anesthesia claim per case. When an anesthesiologist is paid for anesthesia services, a nurse anesthetist is not authorized to bill for those same services. Services which support the anesthesiologist in the operating room fall within the DRG allowed amount and are considered to be already included in the facility fee, even if the support services are provided by a nurse anesthetist. Charging for such services is considered an inappropriate billing practice.
2 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 6, Section 4
Hospital Reimbursement - TRICARE Diagnosis Related Group (DRG)-Based Payment System (Applicability Of The DRG System)
3.3.6 All outpatient services related to inpatient stays.
Note: Payment for trauma services (e.g., revenue code 068X), is included in the TRICARE DRG-based payment system.
3.3.7 All services related to discharges involving pediatric (beneficiary less than 18 years old upon admission) bone marrow transplants which would otherwise be paid under the DRGs for such transplants.
3.3.8 All services related to discharges involving children (beneficiary less than 18 years old upon admission) who have been determined to be Human Immunodeficiency Virus (HIV) seropositive.
3.3.9 All services related to discharges involving pediatric (beneficiary less than 18 years old upon admission) cystic fibrosis.
3.3.10 For services provided before the mandated date, as directed by Health and Human Services (HHS), for International Classification of Diseases, 10th Revision (ICD-10) implementation, an additional payment shall be made to a hospital for each unit of blood clotting factor furnished to a TRICARE patient who is a hemophiliac. Payment will be made for blood clotting factor when one of the following hemophilia International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) diagnosis codes is listed on the claim:
3.3.11 For services provided on or after the mandated date, as directed by HHS, for ICD-10 implementation, an additional payment shall be made to a hospital for each unit of blood clotting factor furnished to a TRICARE patient who is a hemophiliac. Payment will be made for blood clotting factor when one of the following hemophilia ICD-10-CM diagnosis codes is listed on the claim:
286.0 Congenital Factor VIII Disorder
286.1 Congenital Factor IX Disorder
286.2 Congenital Factor XI Deficiency
286.3 Congenital Deficiency of Other Clotting Factors
286.4 Von Willebrand’s Disease
286.5 Hemorrhagic Disorder Due to Circulating Anticoagulants
286.7 Acquired Coagulation Factor Deficiency
D66 Hereditary Factor VIII Deficiency
D67 Hereditary Factor IX Deficiency
D68.0 Von Willebrand’s Disease
D68.1 Hereditary Factor XI Deficiency
D68.2 Hereditary Deficiency of Other Clotting Factors
D68.31 Hemorrhagic Disorder Due to Intrinsic Circulating Anticoagulants
D68.4 Acquired Coagulation Factor Deficiency
3 C-32, February 8, 2019
TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 6, Section 4
Hospital Reimbursement - TRICARE Diagnosis Related Group (DRG)-Based Payment System (Applicability Of The DRG System)
Note: Since the costs of blood clotting factor are reimbursed separately, for these claims all charges associated with the factor are to be subtracted from the total charges in determining applicability of a cost outlier. However, the charges for the blood clotting factor are to be included when calculating the cost-share based on billed charges.
3.3.12 Contractors shall make payment for blood clotting factor using Average Sale Price (ASP) plus 6%, using the Medicare Part B Drug Pricing file. The price allows for payment of a furnishing fee and is included in the ASP per unit.
3.4 Hospitals Subject To The TRICARE DRG-Based Payment System
All hospitals within the 50 U.S., the District of Columbia, and Puerto Rico which are authorized to provide services to TRICARE beneficiaries are subject to the DRG-based payment system except for those hospitals and hospital units below.
3.5 Substance Use Disorder Rehabilitation Facilities (SUDRFs)
SUDRFs are subject to the DRG-based system.
3.6 The following types of hospitals or units which are exempt from the Medicare IPPS, are exempt from the TRICARE DRG-based payment system. In order for hospitals and units which do not participate in Medicare to be exempt from the TRICARE DRG-based payment system, they must meet the same criteria (as determined by DHA, or designee) as required for exemption from the Medicare IPPS as contained in Section 412 of Title 42 CFR.
3.6.1 Hospitals within hospitals.
3.6.2 Psychiatric hospitals.
3.6.3 Rehabilitation hospitals.
3.6.4 Psychiatric and rehabilitation units (distinct parts).
3.6.5 Long-term hospitals.
3.6.6 Sole Community Hospitals (SCHs).
3.6.7 Christian Science sanitariums.
3.6.8 Cancer hospitals. Any hospital which qualifies as a cancer hospital under the Medicare standards and has elected to be exempt from the Medicare IPPS is exempt from the TRICARE DRG-based payment system.
3.6.9 Hospitals outside the 50 U.S., the District of Columbia, and Puerto Rico.
3.6.10 Satellite facilities.
4 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Diagnosis Related Groups (DRGs)
Chapter 6 Section 7
Hospital Reimbursement - TRICARE Diagnosis Related Group (DRG)-Based Payment System (Adjusted Standardized Amounts (ASAs))
Issue Date: October 8, 1987Authority: 32 CFR 199.14(a)(1)Revision: C-32, February 8, 2019
1.0 APPLICABILITY
This policy is mandatory for reimbursement of services provided by either network or non-network providers. However, alternative network reimbursement methodologies are permitted when approved by the Defense Health Agency (DHA) and specifically included in the network provider agreement.
2.0 ISSUE
What are the Adjusted Standardized Amounts (ASAs) under the TRICARE DRG-based payment system, and how are they used and calculated?
3.0 POLICY
3.1 General
The ASA represents the adjusted average operating cost for treating all TRICARE beneficiaries in all DRGs during the database period. Rural hospitals and hospitals located in other areas shall receive the same ASA payment rate as large urban hospitals.
3.2 Calculation Of The ASA
The following procedures will be followed in calculating the TRICARE ASA.
3.2.1 Apply the Cost-to-Charge Ratio (CCR)
In this step each charge is reduced to a representative cost by using the Medicare CCR. Effective FY 2017, the CCR is 0.2541. Effective FY 2018, the CCR is 0.2566. Effective FY 2019, the CCR is 0.2514.
1 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 6, Section 7
Hospital Reimbursement - TRICARE Diagnosis Related Group (DRG)-Based Payment System (Adjusted Standardized Amounts (ASAs))
3.2.2 Increase for Bad Debts
The base standardized amount will be increased by 0.01 in order to reimburse hospitals for bad debt expenses attributable to TRICARE beneficiaries. Effective FY 2013, the base standardized amount will be increased by 0.0065.
3.2.3 Update for Inflation
Any recalculation of the ASA will use an inflation factor equal to the hospital market basket index used by the Centers of Medicare and Medicaid Services (CMS) in their Inpatient Prospective Payment System (IPPS).
3.2.4 Preliminary Non-Teaching Standardized Amount
At this point Indirect Medical Education (IDME) costs have been removed through standardization in the weight methodology and direct medical education costs have been removed through the application of the Medicare CCR which does not include direct medical education costs. Therefore, a non-teaching standardized amount will be computed by dividing aggregate costs by the number of discharges in the database.
3.2.5 Preliminary Teaching Standardized Amounts
A separate standardized amount will be calculated for each teaching hospital to reimburse for IDME expenses. This will be done by multiplying the non-teaching standardized amount by 1.0 plus each hospital’s IDME factor.
3.2.6 System Standardization
The preliminary standardized amounts will be further standardized using a factor which equals total DRG payments using the preliminary standardized amounts divided by the sum of all costs in the database (updated for inflation). To achieve standardization, each preliminary standardized amount will be divided by this factor. This step is necessary so that total DRG system outlays, given the same distribution among hospitals and diagnoses, are equal whether based on DRGs or on charges reduced to costs.
3.2.7 Labor-Related and Nonlabor-Related Portions of the ASA
The ASA shall be divided into labor-related and nonlabor-related portions according to the ratio of these amounts in the national ASA under the Medicare IPPS. Effective October 1, 2013, and subsequent years, for wage index values greater than 1.0, the labor related portion of the ASA shall equal 68.3%, and the non-labor related portion shall equal 31.7%. For wage indexes less than or equal to 1.0 the labor-related portion for the ASA shall equal 62% and the non-labor-related portion shall equal 38%.
2 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 6, Section 8
Hospital Reimbursement - TRICARE Diagnosis Related Group (DRG)-Based Payment System (Adjustments To Payment Amounts)
hospital.
3.2.6.3 Short-Stay Outliers
The TRICARE DRG-based payment system uses short-stay outliers and are reimbursed using a per diem amount. All short-stay outliers must be identified by the contractor when the claims are processed, and necessary adjustments to the payment amounts must be made automatically.
• Any discharge which has a LOS less than or equal to the greater of 1 or 1.94 standard deviations below the arithmetic mean LOS for that DRG shall be classified as a short-stay outlier. In determining the actual short-stay threshold, the calculation will be rounded down to the nearest whole number, and any stay equal to or less than the short-stay threshold will be considered a short-stay outlier.
• Short-stay outliers will be reimbursed at 200% of the per diem rate for the DRG for each covered day of the hospital stay, not to exceed the DRG amount. The per diem rate shall equal the wage-adjusted DRG amount divided by the arithmetic mean LOS for the DRG. The per diem rate is to be calculated before the DRG-based amount is adjusted for IDME. Cost outlier payments shall be paid on short stay outlier cases that qualify as a cost outlier.
• Any stay which qualifies as a short-stay outlier (a transfer cannot qualify as a short-stay outlier), even if payment is limited to the normal DRG amount, is to be considered and reported on the payment records as a short-stay outlier. This will ensure that outlier data is accurate and will prevent the beneficiary from paying an excessive cost-share in certain circumstances.
3.2.6.4 Cost Outliers
3.2.6.4.1 The following steps shall be followed when calculating cost outlier payments for all cases other than neonates and children’s hospitals:
Standard Cost = (Billed Charges x CCR)
Outlier Payment = 80% of (Standard Cost - Threshold)
Total Payments = Outlier Payments + (DRG Base Rate x (1 + (IDME))
Note: Noncovered charges should continue to be subtracted from the billed charges prior to multiplying the billed charges by the CCR.
3.2.6.4.1.1 The CCR for admissions occurring on or after October 1, 2016, is 0.2541. The CCR for admissions occurring on or after October 1, 2017, is 0.2566. The CCR for admissions occurring on or after October 1, 2018, is 0.2514.
3.2.6.4.1.2 The National Operating Standard Cost as a Share of Total Costs (NOSCASTC) for calculating the cost-outlier threshold for FY 2017 is 0.921, for FY 2018 is 0.923, and for FY 2019 is 0.925.
9 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 6, Section 8
Hospital Reimbursement - TRICARE Diagnosis Related Group (DRG)-Based Payment System (Adjustments To Payment Amounts)
3.2.6.4.2 For FY 2017, a TRICARE fixed loss cost-outlier threshold is set at $21,710. Effective October 1, 2016, the cost-outlier threshold shall be the DRG-based amount (wage-adjusted) plus the IDME payment, plus the flat rate of $21,710 (also wage-adjusted).
3.2.6.4.3 For FY 2018, a TRICARE fixed loss cost-outlier threshold is set at $24,494. Effective October 1, 2017, the cost-outlier threshold shall be the DRG-based amount (wage-adjusted) plus the IDME payment, plus the flat rate of $24,494 (also wage-adjusted).
3.2.6.4.4 For FY 2019, a TRICARE fixed loss cost-outlier threshold is set at $25,479. Effective October 1, 2018, the cost-outlier threshold shall be the DRG-based amount (wage-adjusted) plus the IDME payment, plus the flat rate of $25,479 (also wage-adjusted).
3.2.6.4.5 The cost-outlier threshold shall be calculated as follows:
{[Fixed Loss Threshold x ((Labor-Related Share x Applicable wage index) + Non-labor-related share) x NOSCASTC] + (DRG Base Payment (wage-adjusted) x (1 + IDME))}
Example: Using FY 1999 figures {[10,129 x ((0.7110 x Applicable wage index) + 0.2890) x 0.913] + (DRG Based Payment (wage-adjusted) x (1 + IDME))}
3.2.6.5 Burn Outliers
3.2.6.5.1 For admissions on or after October 1, 2008, the DRGs related to burn cases can be found at http://www.health.mil/rates.
3.2.6.5.2 Burn cases which qualify as short-stay outliers, regardless of the date of admission, will be reimbursed according to the procedures for short-stay outliers.
3.2.6.5.3 Burn cases which qualify as cost outliers will be reimbursed using a marginal cost factor of 90%.
3.2.6.5.4 For a burn outlier in a children’s hospital, the appropriate children’s hospital outlier threshold is to be used (see below), but the marginal cost factor is to be either 60% or 90% according to the criteria above.
3.2.6.6 Children’s Hospital Outliers
The following special provisions apply to cost outliers.
3.2.6.6.1 The threshold shall be the same as that applied to other hospitals.
3.2.6.6.2 Effective October 1, 2016, the standardized costs are calculated using a CCR of 0.2760. Effective October 1, 2017, the standardized costs are calculated using a CCR of 0.2781. Effective October 1, 2018, the standardized costs are calculated using a CCR of 0.2719. (This is equivalent to the Medicare CCR increased to account for CAP/DME costs.)
10 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 6, Section 8
Hospital Reimbursement - TRICARE Diagnosis Related Group (DRG)-Based Payment System (Adjustments To Payment Amounts)
3.2.6.6.3 The marginal cost factor shall be 80%.
3.2.6.6.4 For admissions occurring during FY 2015, the marginal cost factor shall be adjusted by 1.18. The marginal cost factor for FY 2016 and beyond is posted to the DHA web site at http://health.mil/Military-Health-Topics/Business-Support/Rates-and-Reimbursement.
3.2.6.6.5 The NOSCASTC for calculating the cost-outlier threshold for FY 2017 is 0.921. The NOSCASTC for calculating the cost-outlier threshold for FY 2018 is 0.923. The NOSCASTC for calculating the cost-outlier threshold for FY 2019 is 0.925.
3.2.6.6.6 The following calculation shall be used in determining cost outlier payments for children’s hospitals and neonates:
Step 1: Computation of Standardized Costs:
Billed Charges x CCR
(Non-covered charges shall be subtracted from the billed charges prior to multiplying the charges by the CCR.)
Step 2: Determination of Cost-Outlier Threshold:
{[Fixed Loss Threshold x ((Labor-Related Share x Applicable wage index) + Non-labor-related share) x NOSCASTC] + [DRG Based Payment (wage-adjusted) x (1 + IDME)]}
Step 3: Determination of Cost Outlier Payment
[{(Standardized costs - Cost-Outlier Threshold) x Marginal Cost Factor} x Adjustment Factor]
Step 4: Total Payments = Outlier Payments + [DRG Base Rate x (1 + IDME)]
3.2.6.7 Neonatal Outliers
Neonatal outliers in hospitals subject to the TRICARE DRG-based payment system (other than children’s hospitals) shall be determined under the same rules applicable to children’s hospitals, except that the standardized costs for cost outliers shall be calculated using the CCR of 0.64. The CCR used to calculate cost outliers for neonates in acute care hospitals shall be reduced to the same CCR used for all other acute care hospitals.
3.2.7 IDME adjustment
3.2.7.1 General
The DRG-based payments for any hospital which has a teaching program approved under Medicare Regulation Section 413.85, Title 42 CFR shall be adjusted to account for IDME costs. The
11 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 6, Section 8
Hospital Reimbursement - TRICARE Diagnosis Related Group (DRG)-Based Payment System (Adjustments To Payment Amounts)
adjustment factor used shall be the one in effect on the date of discharge (see below). The adjustment will be made by multiplying the total DRG-based amount by 1.0 plus a hospital-specific factor equal to:
• For admissions occurring during FYs 2008 and subsequent years, the same formula shall be used except the first number shall be 1.02.
3.2.7.2 Number of Interns and Residents
TRICARE will use the number of interns and residents from CMS most recently available Provider Specific File.
3.2.7.3 Number of Beds
TRICARE will use the number of beds from CMS’ most recently available Provider Specific File.
3.2.7.4 Updates of IDME Factors
3.2.7.4.1 TRICARE will use the ratio of interns and residents to beds from CMS’ most recently available Provider Specific File to update the IDME adjustment factors. The ratio will be provided to the contractors to update each hospital’s IDME adjustment factor at the same time as the annual DRG update. The updated factors provided with the annual DRG update shall be applied to claims with a date of discharge on or after October 1 of each year.
3.2.7.4.2 Other updates of IDME factors. It is the contractor’s responsibility to update the IDME factor if a hospital provides information (for the same base periods) which indicates that the IDME factor provided by TRICARE with the DRG update is incorrect or needs to be updated. An IDME factor is updated based on the hospital submitting CMS Worksheet showing the number of interns, residents, and beds. The effective date of these other updates shall be the date payment is made to the hospital (check issued) for its CAP/DME costs, but in no case can it be later than 30 days after the hospital submits the appropriate worksheet or information. The contractor shall notify DHA of such IDME updates.
3.2.7.4.3 This alternative updating method shall only apply to those hospitals subject to the Medicare Inpatient Prospective Payment System (IPPS) as they are the only ones included in the Provider Specific File.
3.2.7.5 Adjustment for Children’s Hospitals
An IDME adjustment factor will be applied to each payment to qualifying children’s hospitals. The factors for children’s hospitals will be calculated using the same formula as for other hospitals. The initial factor will be based on the number of interns and residents and hospital bed size as reported by the hospital to the contractor. If the hospital provides the data to the contractor after
1.04 x [(1.0 + number of interns + residents
number of beds ).5795-1.0 ]
12 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 6, Section 8
Hospital Reimbursement - TRICARE Diagnosis Related Group (DRG)-Based Payment System (Adjustments To Payment Amounts)
payments have been made, the contractor will not make any retroactive adjustments to previously paid claims, but the amounts will be reconciled during the “hold harmless” process. At the end of its fiscal year, a children’s hospital may request that its adjustment factor be updated by providing the contractor with the necessary information regarding its number of interns and residents and beds. The number of interns, residents, and beds must conform to the requirements above. The contractor is required to update the factor within 30 days of receipt of the request from the hospital, and the effective date shall conform to the policy contained above.
3.2.7.5.1 Each year, the contractor shall send a notice to each children’s hospital in its Region, who have not provided the contractor with updated information on its number of interns, residents and beds since the previous October 1 and advise them to provide the updated information by October 1 of that same year.
3.2.7.5.2 The contractor shall send the number of interns, residents, and beds and the updated ratios for children’s hospitals to DHA, Medical Benefits and Reimbursement Section (MB&RS), or designee, by April 1 of each year to be used in DHA’s annual DRG update calculations. These updated amounts will be included in the files for the October DRG update.
3.2.7.6 TRICARE for Life (TFL)
No adjustment for IDME costs is to be made on any TFL claim on which Medicare has made any payment. If TRICARE is the primary payer (e.g., claims for stays beyond 150 days) payments are to be adjusted for IDME in accordance with the provisions of this section.
3.2.8 Present On Admission (POA) Indicators and Hospital Acquired Conditions (HACs)
3.2.8.1 For services provided on or after ICD-10 implementation:
3.2.8.1.1 Those inpatient acute care hospitals that are paid under the TRICARE/CHAMPUS DRG-based payment system shall report a POA indicator for both primary and secondary diagnoses on inpatient acute care hospital claims. Providers shall report POA indicators to TRICARE in the same manner they report to the CMS, and in accordance with the UB-04 Data Specifications Manual, and ICD-10-CM Official Guidelines for Coding and Reporting. See the complete instructions in the UB-04 Data Specifications Manual for specific instructions and examples. Specific instructions on how to select the correct POA indicator for each diagnosis code are included in the ICD-10-CM Official Guidelines for Coding and Reporting.
3.2.8.1.2 There are five POA indicator reporting options, as defined by the ICD-10-CM Official Coding Guidelines for Coding and Reporting:
Y = Indicates that the condition was present on admission.
W = Affirms that the provider has determined based on data and clinical judgment that it is not possible to document when the onset of the condition occurred.
N = Indicates that the condition was not present on admission.
U = Indicates that the documentation is insufficient to determine if the condition was present at the time of admission.
13 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 6, Section 8
Hospital Reimbursement - TRICARE Diagnosis Related Group (DRG)-Based Payment System (Adjustments To Payment Amounts)
3.2.8.2 HACs. TRICARE shall adopt those HACs adopted by CMS. The HACs, and their respective diagnosis codes, are posted at http://www.health.mil/rates.
3.2.8.3 Provider responsibilities and reporting requirements. For non-exempt providers, issues related to inconsistent, missing, conflicting, or unclear documentation must be resolved by the provider. POA is defined as present at the time the order for inpatient admission occurs. Conditions that develop during an outpatient encounter, including emergency department, observation, or outpatient surgery, are considered as present on admission.
3.2.8.4 The contractor shall accept, validate, retain, pass, and store the POA indicator.
3.2.8.5 Exempt providers.
3.2.8.5.1 The following hospitals are exempt from POA reports for TRICARE:
• Critical Access Hospitals (CAHs)• Long-Term Care (LTC) Hospitals• State Waiver Hospitals, e.g., Maryland• Cancer Hospitals• Children’s Inpatient Hospitals• Inpatient Rehabilitation Hospitals• Psychiatric Hospitals and Psychiatric Units• Department of Veterans Affairs (DVA) Hospitals
3.2.8.5.2 The contractor shall identify claims from those hospitals that are exempt from POA reporting, and shall take the actions necessary to be sure that the TRICARE grouper software does not apply HAC logic to the claim.
3.2.8.6 The DRG payment is considered payment in full, and the hospital cannot bill the beneficiary for any charges associated with the hospital-acquired complications or charges because the DRG was demoted to a lesser-severity level.
3.2.8.7 Claims will be denied if a non-exempt hospital does not report a valid POA indicator for each diagnosis on the claim.
1 = (Definition prior to FY 2011.) Signifies exemption from POA reporting. CMS established this code as a workaround to blank reporting on the electronic 4010A1. A list of exempt ICD-10-CM diagnosis codes is available in the ICD-10-CM Official Coding Guidelines.
1 = (Definition for FY 2011 and subsequent years.) Unreported/not used. Exempt from POA reporting. (This code is equivalent to a blank on the CMS 1450 UB-04; however, it was determined that blanks are undesirable when submitting this data via 4010A.)
14

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015
Chapter 7
Mental Health
Revision: C-32, February 8, 2019
Section/Addendum Subject/Addendum Title
1 Hospital Reimbursement - TRICARE Inpatient Mental Health Per Diem Payment System
2 Partial Hospitalization Program (PHP) And Intensive Outpatient Program (IOP) Reimbursement: Mental Health And Substance Use Disorder (SUD) Treatment
3 Inpatient/Residential Substance Use Disorder Rehabilitation Facilities (SUDRFs) Reimbursement
4 Psychiatric Residential Treatment Center (RTC) Reimbursement
5 Opioid Treatment Programs (OTPs) Reimbursement
A Table Of Regional Specific Rates For Psychiatric Hospitals And Units With Low TRICARE Volume - FY 2017 - FY 2019
B Guidelines For The Calculation Of Individual Psychiatric Residential Treatment Center (RTC) Per Diem RatesFigure 7.B-1 DHA Form 771
1 C-32, February 8, 2019


TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 7, Section 1
Hospital Reimbursement - TRICARE Inpatient Mental Health Per Diem Payment System
3.3.3 Request for Recalculation of Per Diem Amount
Any psychiatric hospital or unit which has determined DHA calculated a hospital-specific per diem which differs by more than five ($5) dollars from that calculated by the hospital or unit, may apply to the appropriate contractor for a recalculation unless the calculated rate has exceeded the cap amount described in the previous paragraph. The recalculation does not constitute an appeal, as the per diem rates are not appealable. Unless the provider can prove that the contractor calculation is incorrect, the contractor’s calculation is final. The burden of proof shall be on the hospital or unit.
3.4 Regional Per Diems for Lower Volume Psychiatric Hospitals and Units
3.4.1 Regional Per Diem
Hospitals and units with a lower volume of TRICARE patients shall be paid on the basis of a regional per diem amount, adjusted for area wages and IDME. Base period regional per diems shall be calculated based upon all TRICARE/ lower volume hospitals’ and units’ claims paid (processed) during the base period. Each regional per diem amount shall be the quotient of all covered charges (without consideration of other health insurance payments) divided by all covered days of care, reported on all TRICARE claims from lower volume hospitals and units in the region paid (processed) during the base period, after having been standardized for IDME costs, and area wage indexes. Direct medical education costs shall be subtracted from the calculation. The regions shall be the same as the federal census regions. See Addendum A, for the regional per diems used for hospitals and units with a lower volume of TRICARE patients.
3.4.2 Adjustments to Regional Per Diem Rates
Two adjustments shall be made to the regional per diem rates when applicable.
3.4.3 Wage Portion or Labor-Related Share
The wage portion or labor-related share is adjusted by the DRG-based area wage adjustment. See Addendum A, for area wage adjustment rates. The calculated adjusted regional per diem is not to be rounded up to the next whole dollar.
3.4.4 IDME Adjustment
The IDME adjustment factors shall be calculated for teaching hospitals in the same manner as in the DRG-based payment system and applied to the applicable regional per diem rate for each day of the admission. For an exempt psychiatric unit in a teaching hospital, there should be a separate IDME adjustment factor for the unit (separate from the rest of the hospital) when medical education applies to the unit.
CAP PER DIEM AMOUNT FOR SERVICES RENDERED
1,126 October 1, 2016 through September 30, 2017
1,156 October 1, 2017 through September 30, 2018
1,190 October 1, 2018 through September 30, 2019
3 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 7, Section 1
Hospital Reimbursement - TRICARE Inpatient Mental Health Per Diem Payment System
3.4.5 Reimbursement of Direct Medical Education Costs
In addition to payments made to lower volume hospitals and units, the Government shall annually reimburse hospitals for actual direct medical education costs associated with TRICARE beneficiaries. This reimbursement shall be done pursuant to the same procedures as are applicable to the DRG-based payment system.
Note: No additional payment is to be made for capital costs. Such costs have been covered in the regional per diem rates which are based on charges.
3.5 Base Period and Update Factors
3.5.1 Hospital-Specific Per Diem Calculated Using Date of Payment
The base period for calculating the hospital-specific and regional per diems, as described above is federal FY 2018. The base period calculations shall be based on actual claims paid (processed) during the period July 1, 2017 through May 31, 2018, trended forward to September 30, 2018, using a factor of 1.1%.
3.5.2 Hospital-Specific Per Diem Calculated Using Date of Discharge
Upon application by a higher volume hospital or unit to the appropriate contractor, the hospital or unit may have its hospital-specific base period calculations based on TRICARE claims with a date of discharge (rather than date of payment) between July 1, 2017 through May 31, 2018, if it has generally experienced unusual delays in TRICARE claims payments and if the use of such an alternative data base would result in a difference in the per diem amount of at least $5.00 with the revised per diem not exceeding the cap amount. For this purpose, the unusual delays mean that the hospital’s or unit’s average time period between date of discharge and date of payment is more than two standard deviations (204 days) longer than the national average (94 days). The burden of proof shall be on the hospital.
3.5.3 Updating Hospital-Specific and Regional Per Diems
Per diems shall be updated by the Medicare Inpatient Prospective Payment System (IPPS) update factor. Hospitals and units with hospital-specific rates shall be notified of their respective rates prior to the beginning of each federal fiscal year by the contractors. New hospitals shall be notified by the contractor at such time as the hospital rate is determined. The actual amounts of each regional per diem that will apply in any federal fiscal year shall be published in the Federal Register prior to the start of that fiscal year. Medicare has determined a market basket and subsequent update factor specific to psychiatric facilities. Beginning in Fiscal Year (FY) 2017, the update factor shall be published on the TRICARE web site at http://www.health.mil/rates prior to the start of the fiscal year. The rates will no longer be published in the Federal Register.
FISCAL YEAR UPDATE FACTOR
2017 2.7%
2018 2.7%
2019 2.9%
4 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 7, Section 1
Hospital Reimbursement - TRICARE Inpatient Mental Health Per Diem Payment System
3.6 Higher Volume Hospitals and Units
3.6.1 Higher Volume of TRICARE Mental Health Discharges and Hospital-Specific Per Diem Calculation
3.6.1.1 In any federal fiscal year in which a hospital or unit not previously classified as a higher volume hospital or unit has 25 or more TRICARE mental health discharges, that hospital or unit shall be considered to be a higher volume hospital or unit during the next federal fiscal year and all subsequent fiscal years. All other hospitals and units covered by the TRICARE inpatient mental health per diem payment system shall be considered lower volume hospitals and units.
3.6.1.2 The hospital-specific per diem amount shall be calculated in accordance with the above provisions, except that the base period average daily charge shall be deemed to be the hospital’s or unit’s average daily charge in the year in which the hospital or unit had 25 or more TRICARE mental health discharges, adjusted by the percentage change in average daily charges for all higher volume hospitals and units between the year in which the hospital or unit had 25 or more TRICARE mental health discharges and the base period. The base period amount, however, cannot exceed the cap described in this section. Once a statistically valid rate is established based on a year in which the hospital or unit had at least 25 mental health discharges, it becomes the basis for all future rates. The number of mental health discharges thereafter have no bearing on the hospital-specific per diem.
3.6.1.2.1 The TRICARE contractor shall be requested at least annually to submit to the DHA Office of Medical Benefits and Reimbursement Section (MB&RS) a listing of high volume providers.
3.6.1.2.2 Percent of change and Deflator Factor (DF).
3.6.2 New Hospitals and Units
3.6.2.1 The inpatient mental health per diem payment system has a special retrospective payment provision for new hospitals and units. A new hospital is one which meets the Medicare requirements under Tax Equity and Fiscal Responsibility Act (TEFRA) rules. Such hospitals qualify for the Medicare exemption from the rate of increase ceiling applicable to new hospitals which are DRG-exempt psychiatric hospitals. Any new hospital or unit that becomes a higher volume hospital or unit may additionally, upon application to the TRICARE contractor, receive a retrospective adjustment. The retrospective adjustment shall be calculated so that the hospital or unit receives the same Government share payments it would have received had it been designated a higher volume hospital or unit for the federal fiscal year in which it first had 25 or more TRICARE mental health discharges. This provision also applies to the preceding fiscal year (if it had any TRICARE patients during the preceding fiscal year). A retrospective payment shall be required if payments were originally made at a lower regional per diem. This payment will be the result of an adjustment based upon each claim processed during the
FOR 12 MONTHS ENDED: PERCENT OF CHANGE DF
September 30, 2013 243.52% 3.4352
September 30, 2014 258.27% 3.5827
September 30, 2015 279.73% 3.7973
September 30, 2016 300.21% 4.0021
September 30, 2017 314.70% 4.1470
5 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 7, Section 1
Hospital Reimbursement - TRICARE Inpatient Mental Health Per Diem Payment System
retrospective period for which an adjustment is needed, and will be subject to the claims processing standards.
3.6.2.2 By definition, a new hospital is an institution that has operated as the type of facility (or the equivalent thereof ) for which it is certified in the Medicare and or TRICARE programs under the present and previous ownership for less than three full years. A change in ownership in itself does not constitute a new hospital.
3.6.2.3 Such new hospitals must agree not to bill beneficiaries for any additional cost-share beyond that determined initially based on the regional rate.
3.6.3 Request for a Review of Higher or Lower Volume Classification
Any hospital or unit which DHA improperly fails to classify as a higher or lower volume hospital or unit may apply to the appropriate contractor for such a classification. The hospital or unit shall have the burden of proof.
3.7 Payment for Hospital Based Professional Services
3.7.1 Lower Volume Hospitals and Units
Lower volume hospitals and units may not bill separately for hospital based professional services; payment for those services is included in the per diems.
3.7.2 Higher Volume Hospitals and Units
Higher volume hospitals and units, whether they billed separately for hospital based professional services or included those services in the hospital’s or unit’s charges, shall continue the practice in effect during the data base period used for calculating the hospital’s or unit’s per diem, except that any such hospital or unit may change its prior practice (and obtain an appropriate revision in its per diem) by providing to the appropriate contractor notice of its request to change its billing procedures for hospital-based professional services.
3.8 Leave Days
3.8.1 No Payment
The Government shall not pay (including holding charges) for days where the patient is absent on leave (including therapeutic absences) from the specialty psychiatric hospital or unit. The hospital must identify these days when claiming reimbursement.
3.8.2 Does Not Constitute a Discharge
The Government shall not count a patient’s departure for a leave of absence as a discharge in determining whether a facility should be classified as a higher volume hospital.
6 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 7, Section 1
Hospital Reimbursement - TRICARE Inpatient Mental Health Per Diem Payment System
3.9 Exemptions from the TRICARE Inpatient Mental Health Per Diem Payment System
3.9.1 Providers Subject to the DRG-Based Payment System
Providers of inpatient care which are neither psychiatric hospitals nor psychiatric units as described earlier, or which otherwise qualify under that discussion, are exempt from the inpatient mental health per diem payment system.
3.9.2 Services Which Group into Mental Health DRG
Admissions to psychiatric hospitals and units for operating room procedures involving a principal diagnosis of mental illness (services which group into DRG 876 on or after October 1, 2008) are exempt from the per diem payment system. They will be reimbursed on the basis of billed charges.
3.9.3 Non-Mental Health Procedures
Admissions for non-mental health procedures that group into non-mental health DRG, in specialty psychiatric hospitals and units are exempt from the per diem payment system. They will be reimbursed on the basis of billed charges.
3.9.4 Sole Community Hospital (SCH)
Admission prior to January 1, 2014, (the effective date of the SCH reimbursement methodology described in Chapter 14, Section 1), any hospital which has qualified for special treatment under the Medicare Prospective Payment System (PPS) as a SCH and has not given up that classification is exempt. For additional information on SCHs, refer to Chapter 14, Section 1.
3.9.5 Hospital Outside the 50 States, the District of Columbia, or Puerto Rico
A hospital is exempt if it is not located in one of the 50 states, the District of Columbia, or Puerto Rico.
3.9.6 Billed Charges and Set Rates
The allowable costs for authorized care in all hospitals not subject to the DRG-based payment system or the inpatient mental health per diem payment system shall be determined on the basis of billed charges or set rates.
- END -
7 C-32, February 8, 2019


TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Mental Health
Chapter 7 Addendum A
Table Of Regional Specific Rates For Psychiatric Hospitals And Units With Low TRICARE Volume - FY 2017 - FY 2019
Revision: C-32, February 8, 2019
Note: This table reflects maximum rates.
For FY 2017: For wage index values greater than 1.0, the wage portion or labor related share subject to the area wage adjustment is 69.6%. The non-labor related share is 30.4%. For wage index values less than or equal to 1.0, the wage portion or labor related share subject to the area wage adjustment is 62%. The non-labor related share is 38%. Utilize the appropriate year DRG wage index file for area wage adjustment calculations.
UNITED STATES CENSUS REGIONS
FY 2017REGIONAL RATES
10/01/16 - 09/30/17
FY 2018REGIONAL RATES
10/01/17 - 09/30/18
FY 2019REGIONAL RATES
10/01/18 - 09/30/19
NORTHEAST:
New England(ME, NH, VT, MA, RI, CT)
$895 $919 $946
Mid-Atlantic(NY, NJ, PA)
$863 $886 $912
MIDWEST:
East North Central(OH, IN, IL, MI, WI)
$746 $766 $788
West North Central(MN, IA, MO, ND, SD, NE, KS)
$703 $722 $743
SOUTH:
South Atlantic(DE, MD, DC, VA, WV, NC, SC, GA, FL)
$887 $911 $934
East South Central(KY, TN, AL, MS)
$949 $975 $1003
West South Central(AR, LA, TX, OK)
$808 $830 $854
WEST:
Mountain(MT, ID, WY, CO, NM, AZ, UT, NV)
$807 $829 $853
Pacific(WA, OR, CA, AK, HI)
$955 $981 $1009
Puerto Rico $609 $625 $643
1 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 7, Addendum A
Table Of Regional Specific Rates For Psychiatric Hospitals And Units With Low TRICARE Volume - FY 2017 - FY 2019
For FYs 2018 through 2019: For wage index values greater than 1.0, the wage portion or labor related share subject to the area wage adjustment is 68.3%. The non-labor related share is 31.7%. For wage index values less than or equal to 1.0, the wage portion or labor related share subject to the area wage adjustment is 62%. The non-labor related share is 38%. Utilize the appropriate year DRG wage index file for area wage adjustment calculations.
For FY 2017/Beneficiary Cost-Share: Beneficiary cost-share (other than active duty members) for care paid on a basis of a regional per diem rate is the lower of $235 per day or 25% of the hospital billed charges effective for services rendered on or after October 1, 2016.
For FY 2018/Beneficiary Cost-Share: Beneficiary cost-share (other than active duty members) for care paid on a basis of a regional per diem rate is the lower of $241 per day or 25% of the hospital billed charges effective for services rendered on or after October 1, 2017.
For FY 2019/Beneficiary Cost-Share: Beneficiary cost-share (other than active duty members) for care paid on a basis of a regional per diem rate is the lower of $248 per day or 25% of the hospital billed charges effective for services rendered on or after October 1, 2018.
- END -
2 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 7, Addendum B
Guidelines For The Calculation Of Individual Psychiatric Residential Treatment Center (RTC) Per Diem Rates
4.2.1 Prior to April 6, 1995, the capped per diem amount was set at the 75th percentile of all established TRICARE RTC rates nationally and weighted by total TRICARE days provided at each rate during the base period (July 1, 1987, through June 30, 1988). The capped amount was adjusted annually by the designated update factor (currently the Medicare update factor as noted in Chapter 7, Section 1). The following are the capped amounts in effect for the past three fiscal years:
4.2.2 The 70th percentile of the day-weighted current (Fiscal Year (FY) 1995) per diems was used in establishing a new cap amount for services rendered on or after April 6, 1995. The following methodology was used in establishing the RTC cap and floor amounts:
4.2.2.1 RTC institutional claims data from the period October 1, 1993 to March 31, 1994 were used (the first half of FY 1994).
4.2.2.2 The FY 1994 per diems were merged onto the claims (from the RTC per diem list in the TRICARE Policy Manual (TPM)) and updated by 1.046 (the CPI-U) to represent FY 1995 per diems.
4.2.2.3 The 30th and 70th percentiles of the day-weighted FY 1995 per diems were calculated as $429 and $515. Any RTC per diem above $515 was cut to $515 as of April 6, 1995.
5.0 ADJUSTMENT OF BASE YEAR RATE
5.1 The base year rate is adjusted by the following annual inflation factors to bring it forward to the current fiscal year. See Section 1, paragraph 3.5.3 for the update factors for FY 2006 and forward.
RTC CAPPED AMOUNTS
DATES OF SERVICE CAPPED AMOUNTS
October 1, 2016 - September 30, 2017 914
October 1, 2017 - September 30, 2018 939
October 1, 2018 - September 30, 2018 967
UPDATE FACTORS FOR RTC PER DIEM RATES
TIME PERIOD CPI-U INFLATION FACTORS
July 1, 1988 - November 30, 1988 2.6%
December 1, 1988 - July 30, 1989 4.9
October 1, 1989 - September 30, 1990 9.2
October 1, 1990 - September 30, 1991 8.6
October 1, 1991 - September 30, 1992 7.4
October 1, 1992 - September 30, 1993 6.0
October 1, 1993 - September 30, 1994 4.6
October 1, 1994 - September 30, 1995 4.4Note: The FY 1997 CPI-U for medical care is 2.6%. This inflation will be used in adjusting FY 1995 RTC rates falling below the 30th percentile of all established FY 1995 rates ($429.00). See also Chapter 7, Section 1, for FY 2006 and forward.
5 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 7, Addendum B
Guidelines For The Calculation Of Individual Psychiatric Residential Treatment Center (RTC) Per Diem Rates
5.2 If the RTC’s base year falls within the previous year’s reporting period, the inflation factor is prorated for the remaining time in that period. The updating process can best be demonstrated through the following example:
Example: RTC E is submitting reimbursement information as a final step in its authorization process. The data was collected over the facility’s first 12 months of operation (April 1, 2013 - March 31, 2014). Since the RTC’s base period extended six months (or 180 days, based on 30-day months and a 360-day year) into the inflation reporting period, the inflation factor for the subsequent update year (October 1 - September 30) was prorated for the remaining time period of April 1, 2014 - September 30, 2014 (six months or 180 days). The following are the calculations used in updating the RTC’s all-inclusive base year per diem to FY 2015 (current year per diem amount):
October 1, 1995 - September 30, 1996 3.6
TIME PERIOD MEDICARE UPDATE FACTOR
October 1, 1997 - September 30, 1998 2.4
October 1, 1998 - September 30, 1999 2.4
October 1, 1999 - September 30, 2000 2.9
October 1, 2000 - September 30, 2001 3.4
October 1, 2001 - September 30, 2002 3.3
October 1, 2002 - September 30, 2003 3.5
October 1, 2003 - September 30, 2004 3.4
October 1, 2004 - September 30, 2005 3.3
October 1, 2005 - September 30, 2006 3.8
ADJUSTMENT OF BASE YEAR PER DIEM RATE
Derived rate at 33.33% of total patient days during base period of April 1, 2013 through March 31, 2014.
$500.00
Plus:
An adjustment for the annual update factor, as listed in Chapter 7, Section 1, paragraph 3.5.3
For 6-month period ending September 30, 2014 (2.5% x 6/12 = 1.25%) 6.25
Adjusted Rate $506.25
For 12-month period ending September 30, 2015 (2.9%) 14.68
Adjusted Rate $520.93
TRICARE all-inclusive per diem rate for services on or after October 1, 2015 $521.00
UPDATE FACTORS FOR RTC PER DIEM RATES (CONTINUED)
Note: The FY 1997 CPI-U for medical care is 2.6%. This inflation will be used in adjusting FY 1995 RTC rates falling below the 30th percentile of all established FY 1995 rates ($429.00). See also Chapter 7, Section 1, for FY 2006 and forward.
6 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 7, Addendum B
Guidelines For The Calculation Of Individual Psychiatric Residential Treatment Center (RTC) Per Diem Rates
5.3 In a Final Rule published in the Federal Register (60 FR 12419) on March 7, 1995, TRICARE imposed a two-year moratorium on the annual updating of RTC per diems rates subject to the following provisions:
5.3.1 TRICARE payments will remain at FY 1995 rates for a two-year period beginning in FY 1996, for any RTC whose 1995 rate was at or above the 30th percentile of all established FY 1995 rates ($429).
5.3.2 For any RTC whose FY 1995 rate was below that of the 30th percentile, the rate will be adjusted by the lesser of the CPI-U, or the amount that brings the rate up to the 30th percentile level.
5.3.3 For fiscal years after FY 1997, the individual facility rates and cap amount will be adjusted by the Medicare update factor for hospitals and units exempt from the Medicare prospective payment system at the discretion of the Director, DHA or designee.
Note: The above provisions will lead to aggregate expenditures which approximate average facility costs. The 4.4% update factor was used in the RTC rate computation since its FY 1995 rate ($368) was below the 30th percentile level ($429).
6.0 CALCULATION OF RTC PER DIEM RATE
6.1 Array the rates accepted by other third-party payers (Item #9) in descending order from lowest to highest in the first column of the Reimbursement Information Work Sheet (see Attachment).
6.2 Place the number of days paid at each of the rates listed above in the second column of the work sheet.
6.2.1 If there is more than one rate with an individual third-party payer during the base period, the RTC shall provide the total number of patient days paid by the payer at each rate. Total patient days will be used in determining the most favored rate for the facility. The following is an example of multiple rates paid by an individual payer during the RTC’s base period:
Example: RTC F has negotiated three separate rates with a third-party payer over its base period. The three rates were reported as follows:
1. $295/day from July 2013, through October 31, 2013 - 2,000 patient days;
2. $315/day from November 1, 2013, through February 29, 2014 - 3,000 patient days;
3. $330/day from March 1, 2014, through June 30, 2014 - 2,000 patient days.
6.2.2 Each of the above negotiated rates shall be reported separately in Item #9 of the DHA Form 771 representing a blending of payments made by a particular payor over a facility’s base period.
6.2.3 Patient days will be combined in those situations where third-party payers were paying the same rate for RTC care. This will represent the cumulative frequency of payments made at each reported reimbursement level in Item #9 of the data collection form.
7 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 7, Addendum B
Guidelines For The Calculation Of Individual Psychiatric Residential Treatment Center (RTC) Per Diem Rates
6.2.4 The following examples represent the methodology used in calculating the TRICARE base year facility rate from data provided under Item #9 of the DHA Form 771:
Example: RTC G provided the following third-party reimbursement data under Item #9 of the DHA Form 771 as part of the certification process:
Step 1: Array the rates in descending order from lowest to highest with corresponding patient days paid at each rate:
ITEM #9 OF DHA FORM 771 (MODIFIED FOR EXAMPLE)
THIRD-PARTY PAYERS RATE ACCEPTED PATIENT DAYS
AA $253 312
BB 527 207
CC 402 163
DD *** 212 198
EE 454 371
FF 603 118
GG 317 446
HH 489 538
II 552 319
JJ 503 132
*** - State or local Government agency.
(1)
RATES
(2)PATIENT
DAYS
(3)CUMULATIVE
PATIENT DAYS
(4)PERCENT CUMULATIVE
PATIENT DAYS
$212 198 198 7.1 %
253 312 510 18.2
317 446 956 34.1
402 163 1,119 39.9
454 371 1,490 53.1
489 538 2,028 72.3
503 132 2,160 77.0
527 207 2,367 84.4
552 319 2,686 95.8
603 118 2,804 100.0
Total 2,804 Patient Days
8 C-32, February 8, 2019
TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 7, Addendum B
Guidelines For The Calculation Of Individual Psychiatric Residential Treatment Center (RTC) Per Diem Rates
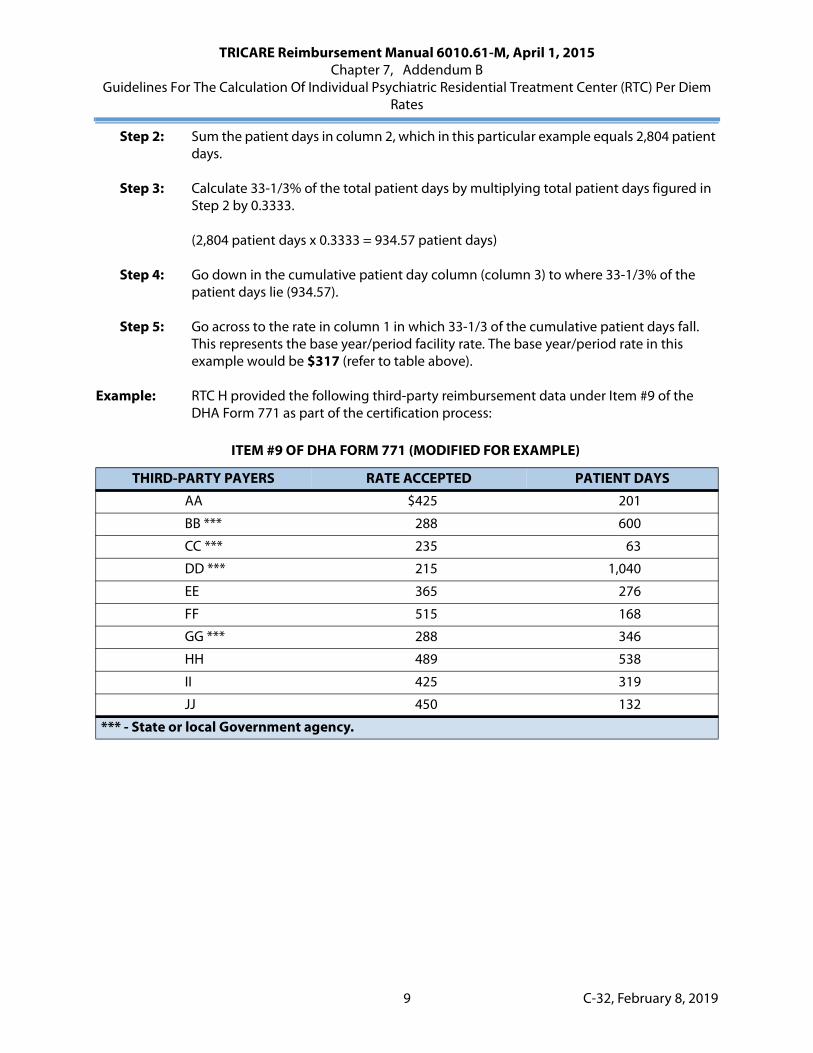
Step 2: Sum the patient days in column 2, which in this particular example equals 2,804 patient days.
Step 3: Calculate 33-1/3% of the total patient days by multiplying total patient days figured in Step 2 by 0.3333.
(2,804 patient days x 0.3333 = 934.57 patient days)
Step 4: Go down in the cumulative patient day column (column 3) to where 33-1/3% of the patient days lie (934.57).
Step 5: Go across to the rate in column 1 in which 33-1/3 of the cumulative patient days fall. This represents the base year/period facility rate. The base year/period rate in this example would be $317 (refer to table above).
Example: RTC H provided the following third-party reimbursement data under Item #9 of the DHA Form 771 as part of the certification process:
ITEM #9 OF DHA FORM 771 (MODIFIED FOR EXAMPLE)
THIRD-PARTY PAYERS RATE ACCEPTED PATIENT DAYS
AA $425 201
BB *** 288 600
CC *** 235 63
DD *** 215 1,040
EE 365 276
FF 515 168
GG *** 288 346
HH 489 538
II 425 319
JJ 450 132
*** - State or local Government agency.
9 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 7, Addendum B
Guidelines For The Calculation Of Individual Psychiatric Residential Treatment Center (RTC) Per Diem Rates
Step 1: Array the rates in descending order from lowest to highest with corresponding patient days paid at each rate:
Step 2: Sum the patient days in column 2, which in this particular example equals 3,683 patient days.
Step 3: Calculate 33-1/3% of the total patient days by multiplying total patient days figured in Step 2 by 0.3333.
(3,683 patient days x 0.3333 = 1,227.54 patient days)
Step 4: Go down in the cumulative patient day column (column 3) to where 33-1/3% of the patient days lie (1,227.54).
Step 5: Go across to the rate in column 1 in which 33-1/3 of the cumulative patient days fall. This represents the base year/period facility rate. The base year/period rate in this example would be $288 (refer to table above).
6.3 The above methodology for deriving the rate at 33-1/3 of the total patient days will only be applicable under the following conditions:
6.3.1 If the rates in Item #9 were all-inclusive for payment of RTC care (i.e., included all payments for institutional and professional services), no additional charges will be added on to the facility rates from Item #10 of the data collection form. The rate established in Step 5 of the above examples will represent the all-inclusive base year rate prior to the inflationary adjustment.
6.3.2 If the charges for additional services listed in Item #10 applied to all of the third-party payers identified in Item #9 (i.e., all of the third-party payers listed in Item #9 allowed payment for additional services outside the facility rate- rate derived at 33-1/3% of total RTC patient days during the base period-- at the charges PPD established in Item #10), the sum of these charges are added to the facility rate prior to inflationary adjustment.
(1)
RATES
(2)PATIENT
DAYS
(3)CUMULATIVE
PATIENT DAYS
(4)PERCENT CUMULATIVE
PATIENT DAYS
$215 1,040 1,040 28.2 %
235 63 1,103 29.9
288 946 2,049 55.6
365 276 2,325 63.1
425 520 2,845 77.2
450 132 2,977 80.8
489 538 3,515 95.4
515 168 3,683 100.0
Total 3,683 Patient Days
10

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015
Chapter 10
Birthing Centers
Revision: C-32, February 8, 2019
Section/Addendum Subject/Addendum Title
1 Freestanding And Hospital-Based Birthing Center Reimbursement
A Birthing Center Rate Non-Professional ComponentFigure 10.A-1 2016 Rate YearFigure 10.A-2 2017 Rate Year
1 C-32, February 8, 2019


TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Birthing Centers
Chapter 10 Section 1
Freestanding And Hospital-Based Birthing Center Reimbursement
Issue Date: February 14, 1984Authority: 32 CFR 199.6(b)(4)(xi)(A)(3) and 32 CFR 199.14(e)Copyright: CPT only © 2006 American Medical Association (or such other date of publication of CPT).
All Rights Reserved.Revision: C-32, February 8, 2019
1.0 APPLICABILITY
This policy is mandatory for reimbursement of services provided by either network or non-network providers. However, alternative network reimbursement methodologies are permitted when approved by the Defense Health Agency (DHA) and specifically included in the network provider agreement.
2.0 DESCRIPTION
A birthing center is a freestanding or institution affiliated outpatient maternity care program which principally provides a planned course of outpatient prenatal care and outpatient childbirth service limited to low-risk pregnancies; excludes care for high-risk pregnancies; limits childbirth to the use of natural childbirth procedures; and provides immediate newborn care.
3.0 POLICY
3.1 A freestanding or institution affiliated birthing center shall be considered for status as an authorized institutional provider.
3.2 Reimbursement for all-inclusive maternity care and childbirth services furnished by an authorized birthing center shall be limited to the lower of the TRICARE established all-inclusive rate or the billed charge.
3.3 The all-inclusive rate shall include the following to the extent that they are usually associated with a normal pregnancy and childbirth: laboratory studies, prenatal management, labor management, delivery, postpartum management, newborn care, birth assistant, certified nurse-midwife professional services, physician professional services, and the use of the facility. The rate includes physician services for routine consultation when certified nurse-midwife is the attending professional.
Note: The initial complete newborn examination by a pediatrician is not included in the birthing center all-inclusive fee and shall be cost-shared as a part of the maternity episode when performed within 72 hours of the delivery.
1 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 10, Section 1
Freestanding And Hospital-Based Birthing Center Reimbursement
3.4 TRICARE maximum allowable birthing center all-inclusive rates for services provided prior to April 1, 2018.
3.4.1 The TRICARE maximum allowable all-inclusive rate is equal to the sum of the CHAMPUS Maximum Allowable Charge (CMAC) for total obstetrical care for a normal pregnancy and delivery (Current Procedural Terminology (CPT) procedure code 59400) based on the appropriate class of the professional provider submitting the claim plus the DHA supplied non-professional price component amount. DHA will supply each contractor with non professional price components for each state annually to be effective for the forthcoming rate year (see Addendum A).
3.4.2 Claims for professional services and tests where the beneficiary has been screened but rejected for admission into the program, or where the woman has been admitted but is discharged from the birthing center program prior to delivery, shall be priced as individual services and items, subject to current policies for obstetrical care professional services and reported as appropriate CPT procedure code with either Place of Service code “22” or “25”.
3.4.3 Claims from birthing centers shall be processed as outpatient hospital claims using revenue code 724 and the following CPT procedure code with either Place of Service code “22” or “25”.
59400 - Obstetrical care
3.4.4 The cost-share amount for birthing center claims is calculated using the ambulatory surgery cost-share formula.
3.4.5 The maximum allowable all-inclusive rate shall be updated on April 1st each year to coincide with the Outpatient Prospective Payment System (OPPS) quarterly update.
3.5 TRICARE maximum allowable birthing center all-inclusive rates for services provided on or after April 1, 2018.
3.5.1 The all-inclusive rate requirement shall not preclude reimbursement of the individual components of covered services (both professional and non-professional) furnished by the birthing center that would otherwise be included within the all-inclusive rate. Therefore, birthing centers shall be paid an all-inclusive rate for services (professional and non-professional) that they actually provide. If the birthing center only provides part of the professional services because the beneficiary moves and gets the remaining services elsewhere, DHA will pay only for that part of the services (namely, the professional services) they provided as part of the all-inclusive rate for the birthing center. Likewise, if the birthing center does not provide facility services for the actual delivery, the all-inclusive rate shall not include the facility component payment.
3.5.2 The facility component of the birthing center all-inclusive rate shall be the one-day Diagnosis Related Group (DRG) Short-Stay Outlier (SSO) for DRG 775 (uncomplicated vaginal birth) adjusted for geographic cost variations. Since DRG 775 has been deleted by the Centers for Medicare and Medicaid Services (CMS) starting in Fiscal Year (FY) 2019, DHA is replacing DRG 775 with the one-day SSO for DRG 807 (uncomplicated vaginal birth without sterilization/D&C) adjusted for geographic cost variations, effective for service dates on or after October 1, 2018. This facility rate more accurately reflects the costs associated with a normal vaginal delivery and will be consistent with TRICARE reimbursement rates currently in use for inpatient institutional services. The DRG zip-to-wage index files shall be used for adjusting the facility component rate for geographical labor cost variations.
2 C-32, February 8, 2019
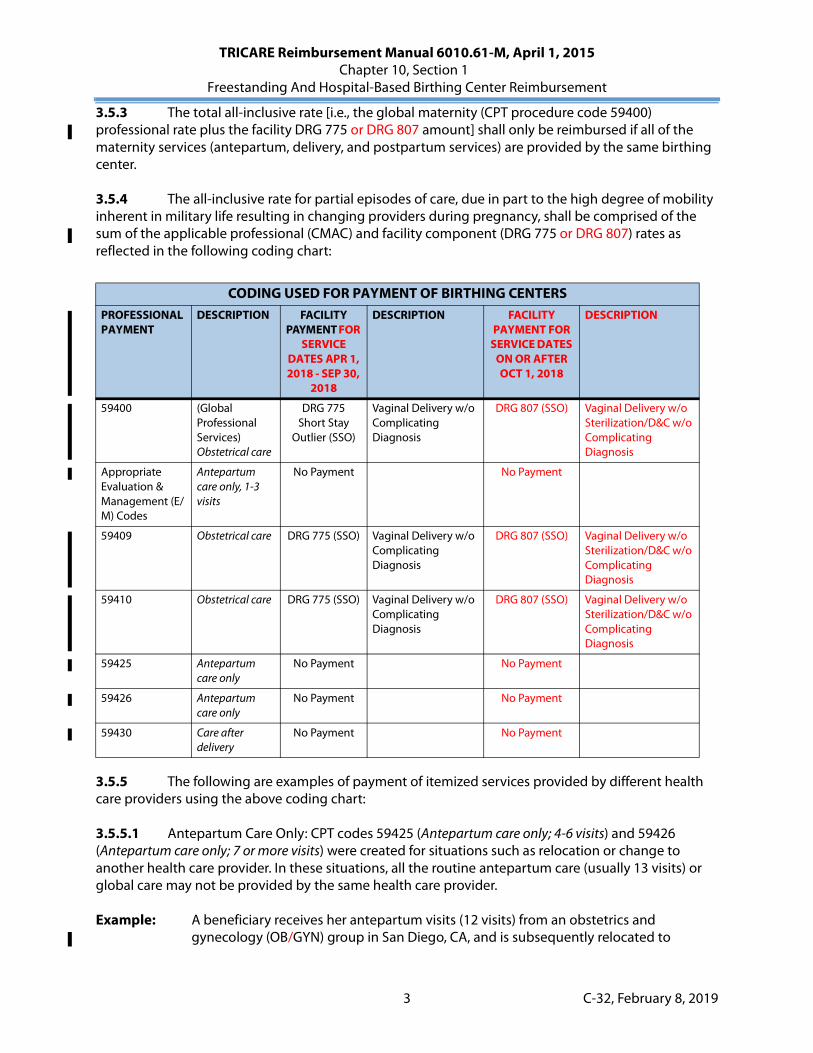
TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 10, Section 1
Freestanding And Hospital-Based Birthing Center Reimbursement
3.5.3 The total all-inclusive rate [i.e., the global maternity (CPT procedure code 59400) professional rate plus the facility DRG 775 or DRG 807 amount] shall only be reimbursed if all of the maternity services (antepartum, delivery, and postpartum services) are provided by the same birthing center.
3.5.4 The all-inclusive rate for partial episodes of care, due in part to the high degree of mobility inherent in military life resulting in changing providers during pregnancy, shall be comprised of the sum of the applicable professional (CMAC) and facility component (DRG 775 or DRG 807) rates as reflected in the following coding chart:
3.5.5 The following are examples of payment of itemized services provided by different health care providers using the above coding chart:
3.5.5.1 Antepartum Care Only: CPT codes 59425 (Antepartum care only; 4-6 visits) and 59426 (Antepartum care only; 7 or more visits) were created for situations such as relocation or change to another health care provider. In these situations, all the routine antepartum care (usually 13 visits) or global care may not be provided by the same health care provider.
Example: A beneficiary receives her antepartum visits (12 visits) from an obstetrics and gynecology (OB/GYN) group in San Diego, CA, and is subsequently relocated to
CODING USED FOR PAYMENT OF BIRTHING CENTERSPROFESSIONAL PAYMENT
DESCRIPTION FACILITY PAYMENT FOR
SERVICE DATES APR 1, 2018 - SEP 30,
2018
DESCRIPTION FACILITY PAYMENT FOR
SERVICE DATES ON OR AFTER OCT 1, 2018
DESCRIPTION
59400 (Global Professional Services) Obstetrical care
DRG 775Short Stay
Outlier (SSO)
Vaginal Delivery w/o Complicating Diagnosis
DRG 807 (SSO) Vaginal Delivery w/o Sterilization/D&C w/o Complicating Diagnosis
Appropriate Evaluation & Management (E/M) Codes
Antepartum care only, 1-3 visits
No Payment No Payment
59409 Obstetrical care DRG 775 (SSO) Vaginal Delivery w/o Complicating Diagnosis
DRG 807 (SSO) Vaginal Delivery w/o Sterilization/D&C w/o Complicating Diagnosis
59410 Obstetrical care DRG 775 (SSO) Vaginal Delivery w/o Complicating Diagnosis
DRG 807 (SSO) Vaginal Delivery w/o Sterilization/D&C w/o Complicating Diagnosis
59425 Antepartum care only
No Payment No Payment
59426 Antepartum care only
No Payment No Payment
59430 Care after delivery
No Payment No Payment
3 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 10, Section 1
Freestanding And Hospital-Based Birthing Center Reimbursement
Norfolk, VA, where she receives the remainder of her maternity care (i.e., delivery and postpartum care) from a birthing center. The OB/GYN group shall receive payment for the antepartum visits only (CPT procedure code 59425) while the birthing center shall receive payment for the remaining professional services related to the delivery and postpartum care (CPT procedure code 59410), along with DRG 775 or DRG 807 for the facility delivery services.
3.5.5.2 Postpartum Care Only: CPT procedure code 59430 (Care after delivery Postpartum care only (separate procedure)] was created for situations where postpartum care is not provided by the same health care provider that performed the actual delivery. The American Congress of Obstetricians and Gynecologists (ACOG) considers the postpartum period to be 60 days following the date of the vaginal delivery.
Example: A beneficiary receives her antepartum visits (13 visits) and delivery from a birthing center in Denver, CO, and is subsequently relocated to San Antonio, TX, shortly after delivery where she receives her postpartum care from an OB/GYN group. The birthing center shall be reimbursed for the antepartum visits (CPT procedure code 59426), the professional delivery services (CPT procedure code 59409), and the delivery facility services (DRG 775) while the OB/GYN group shall receive separate payment for the postpartum care (CPT procedure code 59430).
3.5.5.3 Vaginal Delivery Only, No Postpartum Care: Delivery services include admission to the birthing center facility, the admission history and physical examination, and management of uncomplicated labor and vaginal delivery. CPT procedure code 59409 (Obstetrical care vaginal delivery only, with or without episiotomy and/or forceps) was created for delivery services only; i.e., where only the delivery component of the maternity care is provided and antepartum and postpartum care are performed by other health care providers.
Example: A beneficiary receives her antepartum visits/care from a birthing center in Colorado Springs, CO, and is subsequently relocated to Augusta, GA, where she delivers at a birthing center, and after which she moves back temporarily to Colorado Springs to be with family and friends. She receives her postpartum care from the birthing center in Colorado Springs. The birthing center in Colorado Springs shall receive separate payment for the antepartum (CPT procedure code 59426) and postpartum (CPT procedure code 59430) care, while the birthing center in Augusta, GA, shall receive payment for both the facility (DRG 775 or DRG 807) and professional (CPT procedure code 59409) delivery services.
3.5.6 The maximum allowable all-inclusive component (professional and facility) rates shall be updated to coincide with the annual DRG and CMAC updates.
3.5.7 The cost-share amount for birthing center claims for which there is a facility component (DRG 775 or DRG 807) shall be calculated using the ambulatory surgery cost-share formula. That is, claims from birthing centers processed as outpatient institutional claims using Revenue Code 724 and the following CPT procedure codes with Place of Service “25” for birthing center shall be cost-shared the same as an Ambulatory Surgical Center (ASC). Separate cost-sharing shall not be deducted for professional services as long as there is a facility component billing (DRG 775 or DRG 807) on the claim.
59400 - Obstetrical care
4 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 10, Section 1
Freestanding And Hospital-Based Birthing Center Reimbursement
59409 - Obstetrical care59410 - Obstetrical care
3.5.8 Freestanding birthing center claims for which only the following professional services are billed shall be subject to the standard outpatient cost-share provisions; i.e., a separate cost-share shall be deducted for professional services for which there is no corresponding non-professional (facility) component billed on the claim.
59425 - Antepartum care only59426 - Antepartum care only59430 - Care after delivery
3.6 Extraordinary maternity care services (services in excess of the quantity or type usually associated with all-inclusive maternity care and childbirth service for a normal pregnancy) shall be cost- shared as part of the birthing center maternity episode and paid as the lesser of the billed charge or the allowable charge when the service is determined to be otherwise authorized and medically necessary and appropriate.
3.7 Claims for birthing centers shall be submitted on a CMS 1450 UB-04 claim form. Claims not submitted on the appropriate claim form shall be denied.
3.8 Both the technical and professional components of usual tests are included in the all-inclusive rate.
3.9 Excluded services when billed separately.
99071 - Patient education materials99078 - Group health education
- END -
5 C-32, February 8, 2019


TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Birthing Centers
Chapter 10 Addendum A
Birthing Center Rate Non-Professional Component
Revision: C-32, February 8, 2019
FIGURE 10.A-1 2016 RATE YEAR
These state specific non-professional component amounts are to be used in creating the maximum allowable all-inclusive TRICARE-authorized birthing center prices during the 2012 rate year (i.e., April 1, 2016 - March 31, 2017). The all-inclusive prices are to be updated on April 1st each year to coincide with the Outpatient Prospective Payment System (OPPS) quarterly update. (See Section 1, for instruction for the use of these amounts.)
2016 RATE YEARTRICARE-AUTHORIZED BIRTHING CENTER PROVIDER
NON-PROFESSIONAL COMPONENT FOR ALL-INCLUSIVE PRICING FORMULA
Alabama $4,324.06 Montana $2,989.28
Alaska $5,199.64 Nebraska $3,208.72
Arizona $3,314.39 Nevada $6,377.82
Arkansas $7,088.18 New Hampshire $4,397.25
California $5,545.26 New Jersey $5,553.59
Colorado $4,250.03 New Mexico $4,193.49
Connecticut $6,313.36 New York $2,323.34
Delaware $4,720.91 North Carolina $4,026.43
District of Columbia $7,059.48 North Dakota $2,654.37
Florida $5,282.39 Ohio $5,180.16
Georgia $4,884.28 Oklahoma $4,422.62
Hawaii $3,658.48 Oregon $2,954.86
Idaho $3,983.03 Pennsylvania $4,770.33
Illinois $4,268.78 Puerto Rico $868.89
Indiana $4,892.74 Rhode Island $5,139.17
Iowa $3,923.07 South Carolina $4,676.38
Kansas $5,179.01 South Dakota $2,556.59
Kentucky $3,287.92 Tennessee $3,631.33
Louisiana $3,414.76 Texas $4,425.49
Maine $4,175.41 Utah $2,377.76
Maryland $3,254.58 Vermont $3,493.23
Massachusetts $4,532.72 Virginia $3,433.93
Michigan $3,554.68 Washington $3,672.69
Minnesota $4,026.35 West Virginia $2,913.36
Mississippi $5,322.57 Wisconsin $3,126.70
Missouri $4,170.78 Wyoming $4,937.25
1 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 10, Addendum A
Birthing Center Rate Non-Professional Component
FIGURE 10.A-2 2017 RATE YEAR
These state specific non-professional component amounts are to be used in creating the maximum allowable all-inclusive TRICARE-authorized birthing center prices during the 2017 rate year (i.e., April 1, 2017 - March 31, 2018). The all-inclusive prices are to be updated on April 1st each year to coincide with the Outpatient Prospective Payment System (OPPS) quarterly update. (See Section 1, for instruction for the use of these amounts.)
2017 RATE YEARTRICARE-AUTHORIZED BIRTHING CENTER PROVIDER
NON-PROFESSIONAL COMPONENT FOR ALL-INCLUSIVE PRICING FORMULA
Alabama $4,498.83 Montana $3,156.29
Alaska $4,823.88 Nebraska $3,072.27
Arizona $3,393.89 Nevada $6,760.56
Arkansas $7,072.78 New Hampshire $4,369.86
California $5,762.19 New Jersey $5,336.08
Colorado $4,524.52 New Mexico $4,239.63
Connecticut $6,751.59 New York $2,612.86
Delaware $5,133.16 North Carolina $4,405.72
District of Columbia $7,274.87 North Dakota $3,100.27
Florida $5,595.41 Ohio $5,428.50
Georgia $5,249.76 Oklahoma $4,631.94
Hawaii $3,744.24 Oregon $2,893.58
Idaho $4,015.52 Pennsylvania $5,086.33
Illinois $4,392.88 Puerto Rico $658.00
Indiana $5,253.38 Rhode Island $4,725.58
Iowa $4,368.57 South Carolina $5,020.77
Kansas $5,362.90 South Dakota $2,747.16
Kentucky $3,413.35 Tennessee $3,728.32
Louisiana $3,741.41 Texas $4,699.01
Maine $3,586.18 Utah $2,572.90
Maryland $3,466.07 Vermont $3,768.11
Massachusetts $4,443.08 Virginia $3,554.41
Michigan $3,895.53 Washington $4,036.80
Minnesota $4,277.05 West Virginia $2,694.33
Mississippi $5,737.93 Wisconsin $3,091.87
Missouri $4,324.98 Wyoming $4,915.51
2 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 10, Addendum A
Birthing Center Rate Non-Professional Component
2018 RATE YEAR AND BEYOND
For services provided on or after April 1, 2018, the non-professional component or facility component of the birthing center all-inclusive rate is now the one-day Diagnosis Related Group (DRG) Short-Stay Outlier (SSO) for DRG 775 (uncomplicated vaginal birth) adjusted for geographic cost variations. Since DRG 775 has been deleted by the Centers for Medicare and Medicaid Services (CMS) starting in Fiscal Year (FY) 2019, Defense Health Agency (DHA) is replacing DRG 775 with the one-day SSO for DRG 807 (uncomplicated vaginal birth without sterilization/D&C) adjusted for geographic cost variations, effective for service dates on or after October 1, 2018. The DRG zip-to-wage index files shall be used for adjusting the facility component rate for geographical labor cost variations. The FY 2018 and FY 2019 DRG rates are available on the DRG Rates page of the Military Health System (MHS) web site at https://health.mil/Military-Health-Topics/Business-Support/Rates-and-Reimbursement/Diagnosis-Related-Group-Rates. The birthing center rates information for subsequent future FYs will no longer be published in this manual (Chapter 10, Addendum A) since the rates are located on the DRG Rates page of the MHS web site.
- END -
3 C-32, February 8, 2019


TRICARE Reimbursement Manual 6010.61-M, April 1, 2015
Chapter 11
Hospice
Revision: C-32, February 8, 2019
Section/Addendum Subject/Addendum Title
1 Hospice Reimbursement - General Overview
2 Hospice Reimbursement - Coverage/Benefits
3 Hospice Reimbursement - Conditions For Coverage
4 Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care
A (FY 2017) Hospice Care Rates - FY 2017
A (FY 2018) Hospice Care Rates - FY 2018
A (FY 2019) Hospice Care Rates - FY 2019
B (FY 2017) Hospice Rate Information - Hospice Wage Indexes For Urban Areas - FY 2017
B (FY 2018) Hospice Rate Information - Hospice Wage Indexes For Urban Areas - FY 2018
B (FY 2019) Hospice Rate Information - Hospice Wage Indexes For Urban Areas - FY 2019
C (FY 2017) Hospice Rate Information - Hospice Wage Indexes For Rural Areas - FY 2017
C (FY 2018) Hospice Rate Information - Hospice Wage Indexes For Rural Areas - FY 2018
C (FY 2019) Hospice Rate Information - Hospice Wage Indexes For Rural Areas - FY 2019
D Participation Agreement For Hospice Program Services For TRICARE Beneficiaries
1 C-32, February 8, 2019


TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 11, Section 4
Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care
3.1.9.2.1 The contractor shall be given discretion in developing its own recoupment letter/notice as long as it includes the data elements used in establishing each of its calculations and informs the hospice of the reconsideration provisions allowed under paragraph 3.1.10.
3.1.9.2.2 Refund checks will be sent to the DHA CRM Directorate. If the hospice fails to submit the refund, the contractor shall issue two additional demand letters which will be sent out at appropriate intervals as required by the TOM. Copies of the demand letters will not be sent to the beneficiary, and providers will not be placed on offset to collect overpayments. If the providers do not voluntarily refund the indebtedness in full, or do not enter into an installment repayment agreement, recoupment cases will be transferred to DHA in compliance with the TOM.
3.1.10 Reconsideration of Cap Amount and Inpatient Limit
A hospice dissatisfied with the contractor’s calculation and application of its cap amount and/or inpatient limitation may request and obtain a contractor review if the amount of program reimbursement in controversy -- with respect to matters which the hospice has a right to review -- is at least $1000. The administrative review by the contractor of the calculation and application of the cap amount and inpatient limitation is the only administrative review available. These calculations are not subject to the appeal procedures set forth in 32 CFR 199.10. A request for reconsideration must be filed no later than the 180th calendar day following the date the hospice received notice of the contractor’s determination.
Note: The methods and standards for calculation of the hospice payment rates established by TRICARE, as well as questions as to the validity of the applicable law, regulations or TRICARE decisions, are not subject to administrative review (the appeal procedures of 32 CFR 199.10).
3.1.11 Billing Procedures
Completion of the CMS 1450 UB-04 for hospice care. The following is information needed for completion of those items required for the billing of hospice care. Items not listed need not be completed unless otherwise required in double coverage situations.
3.1.11.1 Item 1 - Provider Name, Address, and Telephone Number Required
Enter name, city, state, and zip code. The post office box number or street name and number may be included. The state may be abbreviated using standard post office abbreviations.
3.1.11.2 Item 4 - Type of Bill (TOB) Required
This three digit code gives three specific pieces of information. The first digit identifies the type of facility. The second digit classifies the type of care. The third digit indicates the sequence of this bill in this particular episode of care (referred to as a “frequency” code).
CODE STRUCTURE
FIRST DIGIT - TYPE OF FACILITY
08 - Special (Hospice)
15 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 11, Section 4
Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care
3.1.11.3 Item 5 - Federal Tax Number
Enter Tax Identification Number (TIN) or Employer Identification Number (EIN) and the sub-ID assigned by the contractor.
3.1.11.4 Item 6 - Statement Covers Period (From-Through) Required
Show the beginning and ending dates of the period covered by this bill in numeric fields (MM-DD-YY). Do not show days before the patient’s eligibility began. Since the 12-month hospice “cap period” ends each year on October 31, hospice services for October and November cannot be submitted on the same bill. Use October 31 as a cutoff date. Submit separate bills for October and November.
Note: If the hospice bills for services that cross the cap period split the bill and process the October portions through the cap period cutoff date of October 31. Return the November portion of the bill uncontrolled.
3.1.11.5 Item 12 - Patient’s Name Required
Show the patient’s name with the surname first, first name, and middle initial, if any.
3.1.11.6 Item 13 - Patient’s Address Required
Show the patient’s full mailing address including street name and number or RFD, city, state, and zip code.
SECOND DIGIT - CLASSIFICATION
1 - Hospice (Nonhospital-Based)2 - Hospice (Hospital-Based)
THIRD DIGIT - FREQUENCY DEFINITION
1 - Admit Through Discharge Claim Use this code for a bill encompassing an entire course of hospice treatment for which you expect reimbursement; i.e., no further bills will be submitted for this patient.
2 - Interim - First Claim Use this code for the first of an expected series of payment bills for a hospice course of treatment.
3 - Interim - Continuing Claim Use this code when a payment bill for a hospice course of treatment has been submitted and further bills are expected to be submitted.
4 - Interim - Last Claim Use this code for a payment bill which is the last of a series for a hospice course of treatment. The “Through” date of this bill (Item 6) is the discharge date or date of death.
7 - Replacement of Prior Claim Use this code to correct (other than late charges) a previously submitted bill. This is the code applied to the corrected or “new” code.
8 - Void/Cancel of a Prior Claim This code indicates this bill is an exact duplicate of an incorrect bill previously submitted. Submit a code “7” (Replacement of Prior Claim) to show the corrected information.
CODE STRUCTURE
16

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 11, Section 4
Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care
3.1.12.3 Type of institution codes 78 and 79 along with the special processing code # (TSM, Chapter 2, Addendum D) will allow hospice institutional claims to by-pass all cost-sharing edits.
3.1.12.4 The revenue code 0657 will be used to identify the charges for services furnished to patients by physicians employed by, or receiving compensation from the hospice.
3.1.12.4.1 Physician procedure codes (CPT procedure codes) will be entered in Item 44 of the CMS 1450 UB-04 to the right of the revenue code 0657 (Item 42). The CPT procedure codes are required in order that the contractor shall make allowable charge (CMAC) determinations when reimbursing hospice physicians.
3.1.12.4.2 Hospice professional services will be paid at 100% of the allowed charge.
3.1.12.4.3 Place of service code 34 (TSM, Chapter 2, Section 2.7) along with the special processing code number will allow hospice non-institutional claims (hospice physician charges) to by-pass all cost-sharing edits and to be paid at 100% of the allowed charge (CMAC).
3.1.12.5 Institutional services (i.e., routine home care-651, continuous home care-652, inpatient respite care-655, and general inpatient care-656) will be reported on an institutional claim format while hospice physician services (revenue code 657 and accompanying CPT procedure codes) will be reported on a non-institutional claim format. The claim will be split for reporting purposes.
3.1.12.6 Patient care services rendered by an independent attending physician or NP (physician or NP who is not considered employed by, or under contract with the hospice) are not considered a part of the hospice benefit, and as such, will be billed in his/her own right.
3.1.12.6.1 Independent attending physician or NP services will be subject to standard TRICARE allowable charge methodology (i.e., subject to standard deductible and cost-sharing provisions).
3.1.12.6.2 The physician specialty code (TSM, Chapter 2, Addendum C) will be reported on the TED.
3.1.13 Billing for Covered TRICARE Services Unrelated to Hospice Care
3.1.13.1 Any covered TRICARE services not related to the treatment of the terminal condition for which hospice care was elected, which are provided during a hospice period, are billed to the contractor for non-hospice reimbursement.
3.1.13.2 Non-hospice services are billed by the provider in accordance with existing claims processing procedures under the TRICARE program.
3.1.13.3 The contractor shall identify and review all inpatient claims for beneficiaries who have elected hospice care to make sure that for:
• Nonrelated hospital admissions, nonhospice TRICARE coverage is provided to a beneficiary only when hospitalization was for a condition not related to his or her terminal illness; and
• Conditions related to a beneficiary’s terminal illness, the claims were denied.
21

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Chapter 11, Section 4
Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care
Note: Many illnesses may occur when an individual is terminally ill which are brought on by the underlying condition of the patient. For example, it is not unusual for a terminally ill patient to develop pneumonia or some other illness as a result of his or her weakened condition. Similarly, the setting of bones after fractures occur in a bone cancer patient would be treatment of a related condition. The treatment of these related conditions is part of the overall hospice benefit, and as such, cannot be billed as a non-hospice TRICARE claim, except for services of an attending physician who is not employed by, or under contract with, the hospice program.
3.1.14 Frequency of Hospice Billing
While inpatient billing is generally deferred until discharge, hospice programs may bill patient stays requiring longer than 30 days in 30-day intervals. This requirement applies to both the institutional and hospice-based physician claims.
3.1.15 Updated Hospice Rates
• The rates in Addendum A (FY 2017) shall be used for payment of claims for services rendered on or after October 1, 2016, through September 30, 2017. The hospice cap amount applies to the cap year ending October 31, 2016.
• The rates in Addendum A (FY 2018) shall be used for payment of claims for services rendered on or after October 1, 2017, through September 30, 2018. The hospice cap amount applies to the cap year ending October 31, 2017.
• The rates in Addendum A (FY 2019) shall be used for payment of claims for services rendered on or after October 1, 2018, through September 30, 2019. The hospice cap amount applies to the cap year ending October 31, 2018.
3.2 Beneficiary Cost-Sharing
There are no deductibles under the hospice benefit. TRICARE pays the full cost of all covered services for the terminal illness, except for small cost-share amounts which may be collected by the individual hospice for outpatient drugs and biologicals and inpatient respite care.
Note: The collection of cost-share amounts is optional under the hospice program.
3.2.1 The patient is responsible for 5% of the cost of outpatient drugs, or $5 toward each prescription, whichever is less. Additionally, the cost of prescription drugs (drugs or biologicals) may not exceed that which a prudent buyer would pay in similar circumstances; that is, a buyer who refuses to pay more than the going price for an item or service and also seeks to economize by minimizing costs.
3.2.2 For inpatient respite care, the cost-share for each respite care day is equal to 5% of the amount TRICARE has estimated to be the cost of respite care, after adjusting the national rate for local wage differences.
3.2.3 The cost-sharing provisions established under paragraph 3.2 are applicable to all beneficiaries regardless of the sponsor’s status (active duty or retired).
22 C-32, February 8, 2019

TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Hospice
Chapter 11 Addendum A (FY 2019)
Hospice Care Rates - FY 2019
Revision: C-32, February 8, 2019
The payment rates were increased by the market basket update of 1.8%.
Effective January 1, 2016, two separate payment rates will be applicable for Routine Home Care (RHC). A higher RHC rate for days 1 through 60, and a lower RHC rate for days 61 and beyond of a hospice episode of care, will replace the single rate.
The following national hospice rates are for care and services provided on or after October 1, 2018, through September 30, 2019. The hospice rates applicable to the above period are:
- END -
REVENUE CODE DESCRIPTION FY 2017 PAYMENT RATE LABOR SHARE NON-LABOR SHARE
0651 RHC (days 1-60) $196.25 $134.84 $61.41
0651 RHC (days 61+) $154.21 $105.96 $48.25
0652 Continuous Home Care (CHC) Full Rate =
24 hours of care = $41.56
FY 2018 hourly rate
$997.38 $685.30 $312.08
0655 Inpatient Respite Care
$176.01 $95.27 $80.74
0656 General Inpatient Care
$758.07 $485.24 $272.83
Allow the provider to split bills if they span the effective date. Use the previous year’s rates if the provider chooses not to split the bill.
Hospice Cap Amount
The hospice cap amount for the 2018 cap year is $29,205.44.
1 C-32, February 8, 2019


TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Hospice
Chapter 11 Addendum B (FY 2019)
Hospice Rate Information - Hospice Wage Indexes For Urban Areas - FY 2019
Revision: C-32, February 8, 2019
Source: 82 FR 38622. Medicare Program; FY 2019 Hospice Wage Index and Payment Rate Update and Hospice Quality Reporting Requirements; Final Rule.
The hospice urban wage indexes applicable for FY 2019 are available on the Centers for Medicare and Medicaid Services (CMS) web site at http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/Hospice/index.html. The urban wage index values for FY 2017 and subsequent fiscal years will no longer be published in this manual (Chapter 11, Addendum B). The urban hospice wage index for FY 2019 will be effective October 1, 2018, through September 30, 2019.
- END -
1 C-32, February 8, 2019


TRICARE Reimbursement Manual 6010.61-M, April 1, 2015Hospice
Chapter 11 Addendum C (FY 2019)
Hospice Rate Information - Hospice Wage Indexes For Rural Areas - FY 2019
Revision: C-32, February 8, 2019
Source: 82 FR 38622. Medicare Program; FY 2019 Hospice Wage Index and Payment Rate Update and Hospice Quality Reporting Requirements; Final Rule.
The hospice rural wage indexes applicable for FY 2019 are available on the Centers for Medicare and Medicaid Services (CMS) web site at http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/Hospice/index.html. The rural wage index values for FY 2017 and subsequent fiscal years will no longer be published in this manual (Chapter 11, Addendum C). The rural hospice wage index for FY 2019 will be effective October 1, 2018, through September 30, 2019.
- END -
1 C-32, February 8, 2019

Related Documents











