PTSD Abnormal Psychology Chapter 5.2 Anxiety Disorder

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
PTSDAbnormal Psychology
Chapter 5.2
Anxiety Disorder
What is PTSD PTSD is an anxiety
disorder that develops in response to a stressful event or situation of exceptionally threatening or catastrophic nature

What are the core features?
Type Name HereType Title Here
Type Name HereType Title Here
Type Name HereType Title Here
Type Name HereType Title Here
Reexperiencingof the
Traumatic event
Avoidance of associated stimuliand numbing of
general responsiveness(last more than 1 month)
Symptoms of extreme arousal

The Symptoms The symptoms of PTSD can start after a
delay of weeks, or even months. They usually appear within 3 months after the traumatic event.
Some people get better within 6 months. Others may have the illness for much longer.
For ABCS see p. 158

WHAT
CAUSES
P T S D ?

Natural disasters
PTSD can occur at any ages exhibit the symptoms varies:
• acute: less than 3 months• chronic: 3 months or longer• delayed onset: more than 6 months (DSM-IV)

TerrorismWar
The facts of child with PTSD experienced……… • traumatic events by age of 6: 68%• physical problems and emotional difficulties: 20%• more than one traumas: 50% (NCTSN http://www.nctsn.org/ )

Physical abuse
•A recent review of research on children exposed to specific traumas found wide ranges in rates of PTSD• 20 percent to 63 percent in survivors of childmaltreatment• 12 percent to 53 percent in the medically ill• 5 percent to 95 percent in disaster survivors (NCTSN)
Post Traumatic Stress Disorder (PTSD) – is considered a normal reaction to a potentially traumatic event such as war, torture, rape, natural disasters, etc.
However, it is still classified as a “mental disorder” within the DSM system.
Please Read: Research in psychology on p. 158 about
the case of Rwanda and answer the three questions afterwards

PTSD Symptom Prevalence: Several studies, including those in post-conflict settings,
indicate that approximately 25-33% of persons exposed to an extreme stressor/ violence experience will go on to develop PTSD symptoms (Breslau et al 1991, Kilpatrick et al 1992).
Aprox 70% of persons exposed to a traumatic stressor will NOT develop PTSD symptoms. This may point to a certain level of inherent resilience/ coping skills among the majority.

The two most frequently comorbid (occurring at the same time) disorders with PTSD are substance abuse and major depression, both of which may be accompanied by a high risk of suicide.
80% of persons with long-term PTSD suffer from depression, another anxiety disorder, or substance abuse (International Society for Traumatic Stress Studies, 2000).
Etiology (why do some develop PTSD more than some…) Biological Twin research has shown a possible
genetic predisposition for PTSD (Hauff and Vaglum 1994)
Higher levels of noradrenaline (Geracioti 2001)

Etiology Cognitive If individual cognitions could make a difference
to people who develop PTSD Intrusive memories – flasbacks – cue-dependent
memories (Brewin et al 1996) Virtual reality as a therapy: flooding which will
lead to habituation (Albert Rizzo) Attributional style (Beck): Focusing on Personal
responsibility or not/ emotion or problem makes a difference (Sutker et el. 1995)

Etiology Sociocultural Majority of research Experiences of racism and oppression are
predisposing factors for PTSD (Vietnam war, Roysircar 2000)
Threat of death, Bosnia (Dyregrov 1998) Social learning – domestic violence (Silva
2000)
Cultural Considerations in PTSD Several studies and existing biological
research suggest there is a universal biological response to traumatic events (A. Marsella et al 1993).
For example, intrusive thoughts/memories or “flashbacks” may transcend culture.
Cultural… However, Avoidance/ numbing and arousal symptoms
may be more specific to various cultural groups;
Some cultural groups may be more likely to describe physical symptoms (somatic complaints);
Gender Considerations There is significant gender difference Breslau et al (1991) longitudinal study of 1007
young adults exposed to community violence Found prevalence rate of 11,3 % in women
compared to 6% in men According to Horowitz et al 1995, women have a
5 times greater risk of developing PTSD after a traumatic/violent event
Why do you think?
Gender Considerations Women are raped more than men and rape
carries the highest risk of producing PTSD
50%!
Sexual abuse as well
Socialization could be a factor – lead to how the girls and women deal with their traumas to internalize them compared to men who externalize them (Nolen-Hoeksema 1994 and Achenbach 1991)

War Veterans Suffer from PTSD http://www.youtube.com/watch?v=z0DMNpYa3dg
PTSD: What is it? http://www.youtube.com/watch?v=H_H_mAm4a4s
The Virtual PTSD Treatment http://www.youtube.com/watch?v=eHmXYhS4HQI&feature=related
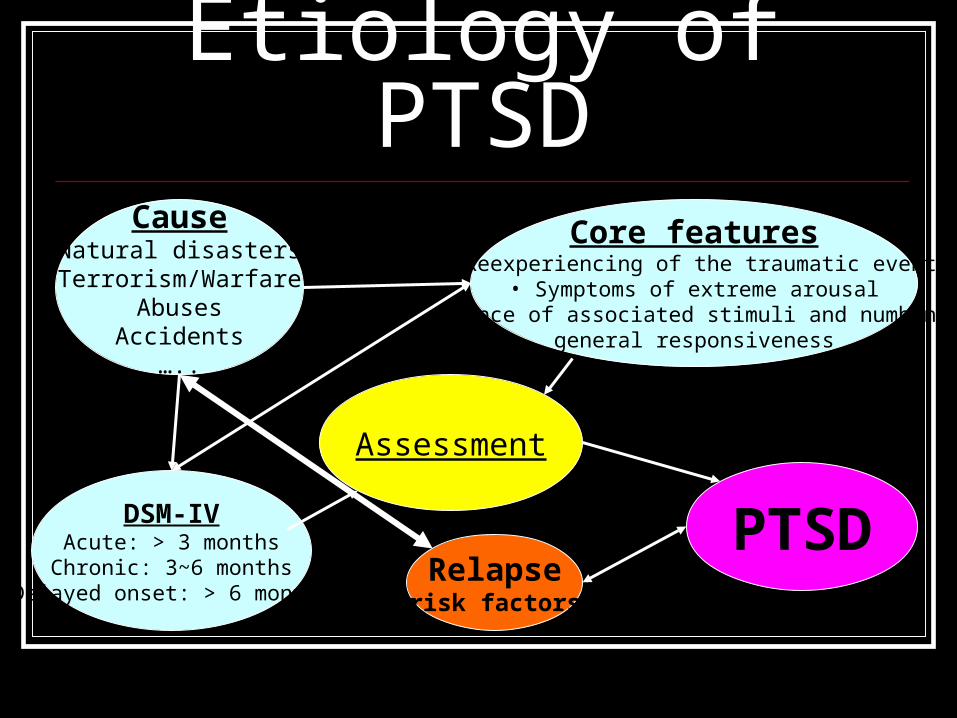
Etiology of PTSDCause
Natural disastersTerrorism/Warfare
AbusesAccidents
…..
Core features•Reexperiencing of the traumatic event
• Symptoms of extreme arousal•Avoidance of associated stimuli and numbing of
general responsiveness
Assessment
DSM-IVAcute: > 3 months
Chronic: 3~6 monthsDelayed onset: > 6 months
PTSDRelapse
(risk factors)
TreatmentsEMDR http://www.youtube.com/watch?v=gZ5MLn1Cc94&feature=related (2:57)
Video Game Tetris Used to Treat PTSD http://www.redorbit.com/news/video/technology/7/video_game_tetris_used_to_treat_ptsd/26700/index.html (0:50)

April, 2 2009The Department of Veterans Affairs (VA) will spend more than $1.4 billion as part ofPresident Obama’s economic recovery plan ofPTSD to improve services to America’s Veterans.
NO MORE FEAR!!
Related Documents