Psychotropic Medication in Foster Care Version 1.0 | April 2017 Trainer’s Guide

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

PsychotropicMedicationinFosterCare
Version1.0|April2017
Trainer’sGuide

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017
2
TableofContentsTableofContents.................................................................................................................................2
BackgroundandContext......................................................................................................................3
TipsforTrainingThisCurriculum..........................................................................................................6
Agenda.................................................................................................................................................8
LearningObjectives..............................................................................................................................9
LessonPlan........................................................................................................................................10
Segment1:WelcomeandIntroductions............................................................................................12
Segment2:LawsandRegulations......................................................................................................15
Segment3:CourtForms....................................................................................................................20
Segment4:Trauma...........................................................................................................................26
Segment5:AccessingMentalHealthServices.....................................................................................31
Segment6:PsychotropicMedication..................................................................................................37
Segment7:UsingtheCaliforniaGuidelinesDocuments.....................................................................49
Segment8:SummaryandEvaluation.................................................................................................56
Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 3
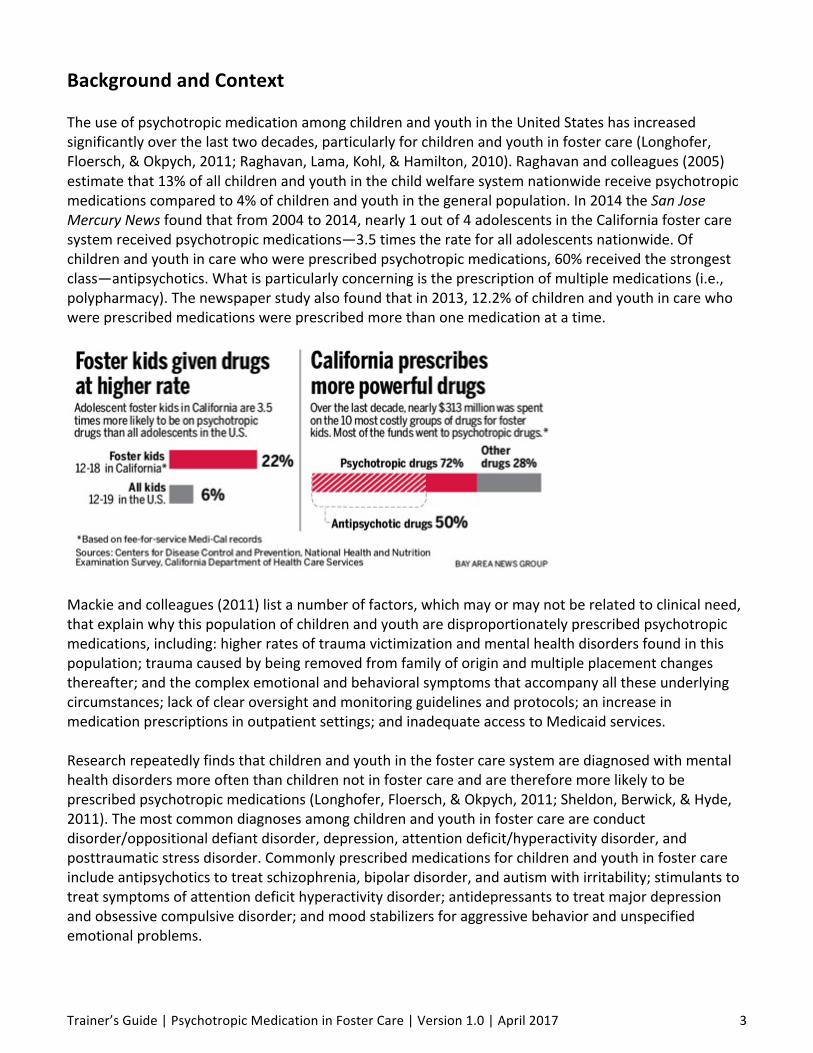
BackgroundandContextTheuseofpsychotropicmedicationamongchildrenandyouthintheUnitedStateshasincreasedsignificantlyoverthelasttwodecades,particularlyforchildrenandyouthinfostercare(Longhofer,Floersch,&Okpych,2011;Raghavan,Lama,Kohl,&Hamilton,2010).Raghavanandcolleagues(2005)estimatethat13%ofallchildrenandyouthinthechildwelfaresystemnationwidereceivepsychotropicmedicationscomparedto4%ofchildrenandyouthinthegeneralpopulation.In2014theSanJoseMercuryNewsfoundthatfrom2004to2014,nearly1outof4adolescentsintheCaliforniafostercaresystemreceivedpsychotropicmedications—3.5timestherateforalladolescentsnationwide.Ofchildrenandyouthincarewhowereprescribedpsychotropicmedications,60%receivedthestrongestclass—antipsychotics.Whatisparticularlyconcerningistheprescriptionofmultiplemedications(i.e.,polypharmacy).Thenewspaperstudyalsofoundthatin2013,12.2%ofchildrenandyouthincarewhowereprescribedmedicationswereprescribedmorethanonemedicationatatime.
Mackieandcolleagues(2011)listanumberoffactors,whichmayormaynotberelatedtoclinicalneed,thatexplainwhythispopulationofchildrenandyoutharedisproportionatelyprescribedpsychotropicmedications,including:higherratesoftraumavictimizationandmentalhealthdisordersfoundinthispopulation;traumacausedbybeingremovedfromfamilyoforiginandmultipleplacementchangesthereafter;andthecomplexemotionalandbehavioralsymptomsthataccompanyalltheseunderlyingcircumstances;lackofclearoversightandmonitoringguidelinesandprotocols;anincreaseinmedicationprescriptionsinoutpatientsettings;andinadequateaccesstoMedicaidservices.Researchrepeatedlyfindsthatchildrenandyouthinthefostercaresystemarediagnosedwithmentalhealthdisordersmoreoftenthanchildrennotinfostercareandarethereforemorelikelytobeprescribedpsychotropicmedications(Longhofer,Floersch,&Okpych,2011;Sheldon,Berwick,&Hyde,2011).Themostcommondiagnosesamongchildrenandyouthinfostercareareconductdisorder/oppositionaldefiantdisorder,depression,attentiondeficit/hyperactivitydisorder,andposttraumaticstressdisorder.Commonlyprescribedmedicationsforchildrenandyouthinfostercareincludeantipsychoticstotreatschizophrenia,bipolardisorder,andautismwithirritability;stimulantstotreatsymptomsofattentiondeficithyperactivitydisorder;antidepressantstotreatmajordepressionandobsessivecompulsivedisorder;andmoodstabilizersforaggressivebehaviorandunspecifiedemotionalproblems.

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 4
Inresponsetothisdata,Californiahastakenstepstobuilduponpreviouslegislationandexpandanddevelopnewguidelinesthatcontinuetopromotethebasicprinciplesofsafety,permanency,andwellbeing,withtheaddedgoalofreducingshort-andlong-termharmcausedbyinappropriateprescriptionsanduseofpsychotropicmedications.AspartoftheFosterCareQualityImprovementProject,TheCaliforniaDepartmentofHealthCareServices(DHCS)andtheCDSSreleasedtheCaliforniaGuidelinesfortheUseofPsychotropicMedicationwithChildrenandYouthinFosterCare,2015.Thenewguidelinescreateasharedunderstandingofoversightandmonitoringofpsychotropicmedicationpracticesforbothchildwelfareservicesandmentalhealthservices.Theguidelinessetexpectationsforphysicians,socialworkers,maturechildrenandyouth,parents,caregivers,Tribalmembers,andallotherpsychotropicmedicationstakeholderstocollaborateinstrengtheningtheoversightandmonitoringofpsychotropicmedications("Californiaguidelines,"2015).All-CountyInformationNoticeNo.1-05-14providesdetailsaboutsharingrequiredinformationwithcaregiverstofacilitatetheirinvolvementinprovidingcareforchildrenandyouth.SenateBill238,signedintolawbyGovernorBrownonOctober6thof2015stipulatesthatcertainprofessionalsandotherswhoworkwithchildrenandyouthinfostercareshouldbeprovidedtrainingaboutimportanttopicsrelatedtotheadministrationofpsychotropicmedicationtothosechildrenandyouth.Specifically,trainingaboutpsychotropicmedicationandtraumaasrelatedtochildrenandyouthinfostercareistobeprovidedtogrouphomeadministrators,fosterparents,childwelfaresocialworkers,probationofficers,publichealthnurses,dependencycourtjudgesandattorneys,courtappointedcounselandspecialadvocatesalongwithinformationaboutbehavioralhealthandsubstanceuse.Severalmediasourcesandotherstudieshaverecentlyrevealedthattherateofpsychotropicmedicationprescriptionsforchildrenandyouthinfostercareishigherthanthegeneralpopulation.Analarmingnumberofchildrenhavebeenprescribedmultiplepotentclassesofdrugstobetakensimultaneously.Thiscoverageandothermovementstoimprovementalhealthservicesinfostercareproducedseveralreformlaws.Theselawsmakeexplicitthatchildrenandyouthinfostercare,alongwiththeirfamiliesandrepresentatives,mustbeallowedtoprovideinputintowhetherornotpsychotropicmedicationispartoftheirtreatmentplan.Ratherthanworkingfromtheassumptionthatsymptomsandbehaviorsarenecessarilyindicativeofmentalillness,thesereformsencouragetheuseofatrauma-informedlenstoviewthechild’senvironmentandexperiencesaspossiblesourcesofbehaviororsymptomsandtoexploreabroadrangeoftreatmentoptions.Psychotropicmedicationsareonetoolamongmanythatmaybeusedtoaddressbehavioralhealthconcerns.Theymustbeconsideredverycarefullyasthelong-termeffectsofthesemedicationsondevelopingbrainsisunknownandpotentialsideeffectscanbesevere. Atthetimeofthiswriting,theCaliforniaDepartmentofSocialServicesisengagedinthedevelopmentoftheCaliforniaChildWelfareCorePracticeModel,whichsubsumesthePathwaystoMentalHealthServicesCorePracticeModelwithinalargerpracticeframeworkthatintegratesthechildwelfaresystemwithotherchild-andfamily-servingsystemsinthepublicsectorandtheirpartners.Inturn,theCaliforniaChildWelfareCorePracticeModelispartofatripartite“SharedApproachtoCalifornia’sChildren,Youth,andFamilies”withthepublicsystemsofbehavioralhealthandjuvenilejustice,whicharealsoinprocessofdevelopingpracticemodelsfortheirrespectivefieldsofpractice.An“Integrated

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 5
StatewideTrainingPlan”iscurrentlyunderwaywhichwillreflectthepracticeandservicedeliveryenvironmentsofthechildwelfare,behavioralhealth,andjuvenilejusticesystemsunderthe“SharedApproach.”ThiscurriculumiscongruentwiththedevelopingCaliforniaChildWelfareCorePracticeModelandwiththeforthcoming“IntegratedStatewideTrainingPlan.”TheCorePracticeModel(CPM)setsthefoundationforacommonpracticeframeworkthatintegratesbehavioralhealthscreenings,referrals,serviceplanning,servicedelivery,andoverallcoordinationandcasemanagementamongallthoseinvolvedinworkingwithchildrenwhoreceiveservicesfromchildwelfareandbehavioralhealthsystemsinthepublicsector.Theeffectiveengagementoffamiliesinthereferralandtreatmentprocessfortheirchildrenisintegraltothismission.TheCPMdescribesstandardsandexpectationsforpracticebehaviorsbychildwelfareandbehavioralhealthstaffthatensuresandsupportsmeaningfulparticipationbyfamiliesinthecareandtreatmentoftheirchildren.ChildandfamilyteamingisaservicerequirementforchildrenwhoqualifyforIntensiveCareCoordination,andwillsoonbethestandardthroughoutchildwelfare.Forchildrenandyouthwithidentifiedmentalhealthissues,childandfamilyteamingisstronglyrecommended.Childrenandyouthforwhompsychotropicmedicationisbeingrequestedfromthecourtwilllikelyfallintooneofthesecategories.AudienceTheintendedaudienceforthePsychotropicMedicationinFosterCareclassroomtrainingislinestafffromchildwelfare,juvenilejustice,andchildren'sbehavioralhealthagenciesthroughoutCalifornia,aswellaspublichealthnurses,caregivers,youth,andcommunitypartnerswhohaveaninterestinlearningaboutpsychotropicmedicationandhowitcanbeusedtoservethementalhealthneedsofchildrenandyouthinthechildwelfaresystem.

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 6
TipsforTrainingThisCurriculumDuration:OneDay(9:00am-4:00pm,anhourlunchbreak,two15-minutebreaks)Thiscurriculumprovides:
• Anoverviewoftheuses,benefits,andrisksofpsychotropicmedication;• Informationabouttraumaandhowitcaninformcareandtreatmentdecisions;• Guidanceforprofessionalstotomakeandmonitortreatmentdecisions;and• HowtolocateandusetheformsandinformationalmaterialsintheApplicationforPsychotropic
MedicationprocessintheCourts(JV-220Process).ThetrainershouldbefamiliarwiththeCaliforniaGuidelinesfortheUseofPsychotropicMedicationwithChildrenandYouthinFosterCarethemostrecentversionofwhichcanbefoundhere:http://www.dhcs.ca.gov/provgovpart/pharmacy/Documents/QIP_Guidelines.pdfThisGuidelinesdocumentoutlines:
• Basicprinciplesandvalues,• Expectationsregardingthedevelopmentandmonitoringoftreatmentplans(emotionaland
behavioralhealthcare,psychosocialservicesandnon-pharmacologicaltreatments),• Principlesforinformedconsenttomedication,and• Principlesgoverningmedicationsafety.
Mostimportantly,itisdesignedtobeusedasanadvocacytooltohelpguideprescribersandotherswhoareworkingwithchildrenandyouthinfostercare.ItisonewayformembersofatreatmentteamtoreferencethestandardsofpracticeandexpectationsoftheCaliforniaDepartmentsofSocialServicesandHealthCareServicesregardingtheuseofpsychotropicmedicationwithchildrenandyouthinfostercare.Itisintentionallycreatedsothatprofessionalscanrefereachothertoitforguidanceinmakingtheseimportanttreatmentdecisions.
Further,thetrainershouldknowandunderstandCalifornia’sPathwaystoMentalHealthpracticemodel.Themostrecentversionofwhichmaybefoundhere:http://www.dhcs.ca.gov/Documents/KACorePracticeModelGuideFINAL3-1-13.pdfAswellastheCaliforniachildwelfarecorepracticemodel(CPM).Themostrecentversionofwhichcanbefoundhere:http://calswec.berkeley.edu/california-child-welfare-core-practice-model-0ThetrainershouldbefamiliarwithandsupportiveoftheFosterCareYouth’sMentalHealthBillofRightswhichcanbefoundhere:http://www.fosteryouthhelp.ca.gov/PDFs/FosterYouthBillOfRights.pdf
AlamedaCountyTransition-AgeYouthandshareddecisionmakingtoolswhichcanbefoundhere:http://www.acbhcs.org/MedDir/decision_tools.htm

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 7
Practiceandlocalrulesofcourtvaryacrosscounties.Knowingthespecificsofthecountyorcountiesforwhichyouareprovidingtrainingwillhelpthetraininggosmoothly.Trainersshouldbefamiliarwithcountyprotocols,procedures,forms,andtoolsrelatedtotheprovisionofbehavioralhealthservicesforchildreninfostercare,andcourtauthorizationprotocolswheretheyaretraining.Ifparticipantsarefromseveralcountiesbesuretoallowinformationandfeedbackfromthegroupaboutthesevariations.AdditionalResources
• CalSWEChostsatoolkitforthechildwelfare/mentalhealthlearningcollaborativethathasanarrayoftrainingandimplementationresourcesregardingthedeliveryofbehavioralhealthservicestochildreninfostercare.Thetoolkitalsoprovidescontactinformationforpartneringorganizationsthatprovidetrainingandtechnicalassistance.ThetoolkitwasdesignedforusebyCaliforniacountiesandregions,andisalsoaccessiblebythepublic:http://calswec.berkeley.edu/toolkits/child-welfare-mental-health-learning-collaborative-katie.Withinthistoolkit,thetrainermayhaveparticularinterestintheresourcesfoundinthewebpagesfor“TeamingTools”and“EngagementTools.”
• TheChildren’sBureaupublishedMakingHealthyChoices:AGuideonPsychotropicMedicationsforYouthinFosterCarein2012https://www.childwelfare.gov/pubs/makinghealthychoices/andthecompanionguideforcaregiversandcaseworkerscalledSupportingYouthinFosterCareinMakingHealthyChoices:AGuideforCaregiversandCaseworkersonTrauma,Treatment,andPsychotropicMedicationin2015https://www.childwelfare.gov/pubs/mhc-caregivers.Theyarebothvaluableresourcesonthetopicsmostrelevanttothistraining.
• SubstanceAbuseandMentalHealthServicesAdministration’sConceptofTraumaandGuidanceforaTrauma-InformedApproach,July2014http://store.samhsa.gov/shin/content/SMA14-4884/SMA14-4884.pdf
• AmericanAcademyofPediatrics’HelpingFosterandAdoptiveFamiliesCopewithTraumahttps://www.aap.org/en-us/advocacy-and-policy/aap-health-initiatives/healthy-foster-care-america/Documents/Guide.pdf
• TheNationalChildTraumaticStressNetwork’stoolkitswww.NCTSN.org
• TheCaliforniaInstituteforBehavioralHealthSolutions(CIBHS)offerstrainingresourcesthatsupportKatieA.implementation,includingwebinarsforpreparingyouth,parents,andprofessionalsforparticipationintheChildandFamilyTeam(CFT)andteammeetings:http://www.cibhs.org/katie-implementation-technical-assistance-and-training
Thiscurriculumisdevelopedwithpublicfundsandintendedforpublicuse.Useofcurriculumcontentshouldbecitedas:CaliforniaSocialWorkEducationCenter.(Ed.).(2017).PsychotropicMedicationinFosterCare.Berkeley,CA:CaliforniaSocialWorkEducationCenter.
Forquestionsregardingthecurriculum,contactShayK.O’Brien,[email protected].

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 8
AgendaSegment1 WelcomeandIntroductions 9:00–9:15am
Segment2 LawsandRegulations 9:15–9:45am
Segment3 CourtProcessandForms 9:45–11:00am
BREAK 11:00–11:15am
Segment4 Trauma 11:15–11:45pm
Segment5 AccessingServices 11:45–12:30pm
LUNCH 12:30-1:30pm
Segment6 PsychotropicMedication 1:30-2:30pm
BREAK 2:30-2:45pm
Segment7 UsingtheCaliforniaGuidelines 2:45-3:45pm
Segment7 Wrap-UpandEvaluations 3:45-4:00pm
Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 9
LearningObjectives
Knowledge
K1:TraineeswillbeabletonameatleastthreekeypointsinthelawsandregulationsthatgovernadministrationofpsychotropicmedicationstochildrenandyouthinfostercareinCalifornia.
K2:Traineeswillbeabletonameatleastoneofthebasicprinciplesoftrauma-informedcareastheyrelatetouseofpsychotropicmedicationinfostercare.
K3:Traineeswillbeabletonameatleasttwocommonbehavioralhealthdiagnosesandtherelatedtreatmentoptions(bothpsychosocialandmedical)forchildren,youth,andyoungadultsinfostercare.
K4:Traineeswillbeabletodescribewhatdotoifsideeffectsarenoticedorreportedbyachild,youth,oryoungadultinfostercarewhoistakingprescribedpsychotropicmedication.
K5:Traineeswillbeabletolocateandutilizethecorrectstaterequiredforms(JV-217throughJV-224)whenamedicalproviderisstartingorcontinuingapsychotropicmedicationforachildoryouthinfostercare.
K6:Traineeswillbeabletodescribethenotificationprocessesusedinrequestingandmonitoringadministrationofpsychotropicmedications.
Skills
S1:Usingsampleplans,traineeswillutilizetheCaliforniaGuidelinesfortheUseofPsychotropicMedicationwithChildrenandYouthinFosterCareandthetoolsinitsappendicestoevaluateandmodifytreatmentplansthatincludepsychotropicmedicationdecisions.
a. PrescribingStandardsbyAgeGroup,b. ParametersforUseofPsychotropicMedicationforChildrenandAdolescents,c. ChallengesinDiagnosisandPrescribingPsychotropicMedication,andd. Algorithm/DecisionTreeforPrescribingPsychotropicMedication.
S2:Usingavignette,traineeswillbeabletoidentify:• Therelevantpartiesanddocumentationtobeincludedinthecourtprocess,• Thoseparties’rightsandobligations,and• Thetimelineforcourtrequests,decisions,andnotifications.
Values
V1:Traineeswillvaluebuildingonchildandfamilyresilienceandstrengthsinbothformalandinformalservicesusedtoamelioratethenegativeeffectsof
• abuseand/orneglect;• emotional,cognitive,and/orbehavioraldysregulations;and• potentialmentalillness.
V2:Traineeswillvalueensuringthatthevoicesofchildren,youth,andyoungadultsareincorporatedintotreatmentplansandmedicationdecisions.
V3:Traineeswillvalueworkingwithamulti-disciplinaryteamtounderstandandmanagetheuseofpsychotropicmedicationbychildren,youth,andyoungadultsinfostercare.
Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 10
LessonPlan
Segment MethodologyandLearningObjectives
Segment1
15minutes
9:00-9:15am
WelcomeandOrientation
Introductionsandreviewoflearningobjectives.
Groupagreements.
Segment2
30minutes
9:15-9:45am
LawsandRegulations
Reviewofapplicablelaw,regulations,policy,andprocedureswithafocusonrecentchanges.Videoclips.
LOs:K1
Segment3
75minutes
9:45-11:00am
CourtProcessandForms
Locatingandaccuratelycompletingtheappropriateform(s)forcourtapprovalof,monitoringof,and/orinputabouttheadministrationofpsychotropicmedication(s)toachildoryouthinfostercare.
Whoisinvolved,whentheyneedtobeinvolved,andtheirrightsandobligations.
Timelinefordecisionsandnotificationsandcourtapprovalprocessflow.
Applicationactivities:Matchinggame.Reviewofforms.
LOs:K5,K6,S1,S2,V1,V2,V3
BREAK11:00-11:15am
Segment4
30minutes
11:15-11:45
Trauma
Overviewoftrauma.Presentationofthebasicprinciplesoftrauma-informedcarerelatedtotheadministrationandmonitoringofpsychotropicmedicationinfostercaresettings.Challengesandbenefits.
Trauma-informedandstrengths-basedviewofsymptomsandbehaviorscommonlyincludedinmental/behavioralhealthdiagnosesincludingsubstanceusedisorder.
Applicationactivity:Sharingpracticeexperience.
LOs:K2,V1,V2

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 11
Segment MethodologyandLearningObjectives
Segment5
45minutes
11:45-12:30
AccessingServices
QuickoverviewofMental/BehavioralHealthServicesavailabletofosteryouthandhowtoaccessthem.
Choosingbestwaystotreatsymptomsandaddressbehaviors:a. utilizingformalandinformalinterventions,b. ensuringtrauma-informedandculturallyappropriateapproaches,andc. combiningpsychotropicmedicationsandnon-pharmaceutical
therapies.
Applicationactivity:Planningtowardquality,diverse,trauma-informedservices.
LO’s:K2,K3,V1,V2,V3
12:30-1:30pm
LUNCH
Segment6
60minutes
1:30-2:30
PsychotropicMedications
ReviewtheFosterYouthMentalHealthBillofRights.
Overviewofcommonbehavioralhealthdiagnosesandthemedicationsthatmaybeprescribedtotreatthem.Howtofindreliableandcurrentinformationaboutmedicationsideeffectsandadversereactions.
Howtoassistfosteryouthwithself-administration,trackingsideeffects,andothermonitoringissues.
Applicationactivity:Roleplayconversationsaboutevaluatingprescriptions,sideeffects,andsafetyplanning.
LOs:K3,K4,S1,S2,V1,V2,V3
BREAK2:30-2:45pm
Segment7
60minutes
2:45-3:45pm
UsingtheCaliforniaGuidelines
OverviewoftheGuidelinescontent.
Howthatcontentcanbeusedwithinateamtohelpmonitor,assess,andmodifytreatmentplansthatcontainpsychotropicmedication.
UsingtheGuidelinesandcourtprocesstoadvocateforbestinterestofthechild.
Applicationactivities:HowtousetheGuidelines.IncorporatingtheGuidelinesintoregularpractice.
LO’s:K3,K5,S1,V3
15minutes
3:45-4:00pm
Wrap-UpandEvaluations
Activities:Debrief/QuestionsandCourseEvaluations

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 12
Segment1:WelcomeandIntroductions
SegmentTime: 15minutes
Materials: LearningObjectivesFlipchartforGroupAgreements
Slides: 1–5
DescriptionofSegment:Facilitateintroductions,groupagreements,andreviewoflearningobjectives.
BeforetheSegment
p Activity1A:Ifpossible,beforetrainingbegins,useplacecardstoarrangetheseatingsothatsocialworkersandotherprofessionalsaresittingtogether,andmixupfolksfromdifferentcounties.
p Activity1C:Prepareyourchartpadinadvanceforthegrouptodeveloptheirownagreements.Bepreparedtofillingapsiftherearestandardsyouneedeveryonetoagreeto(confidentiality,silentphones,etc.).Somesuggestedstandardstogetstartedorfillinarelistedbelow.
DuringtheSegment
p Activity1A:Welcome
Slide1Coursename,Slide2BeginsSegment1Welcometheparticipantstothetraining,introduceyourself,andreviewanyhousekeepingmaterials(parking,bathrooms,cellphones).
p Activity1B:IntroductionsSlide3—IntroductionsandGroupAgreementsFacilitateparticipantintroductions.Introductionsshouldbesimpleself-introductionsthatinclude:
• Participant’sname• Thedepartment,unit,ordivisionwhereparticipantworks• Theirrolerelatedtopsychotropicmedicationinfoster
care.
Considerinvitingparticipantstostatetheirpreferredgenderpronouns*
p Activity1C:GroupAgreementsFacilitategroupagreements.Askthegrouptoprovidesomeguidelinesforinteractionandconductduringthetraining.Somesuggestedagreementsarelistedbelow.Thisactivityprovidesamodelforparticipantsfortheworktheydowithchildandfamilyteams,whichisaconnectionthatyoucannoteforthegroup.
SuggestedGroupAgreements
• Respecteachother’sperspectivesandexperience.
PsychotropicMedicationandFosterCareinCalifornia
WelcomeandOrientation
Segment1
3
Introductions
•Name•Department•Role
GroupAgreements
Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 13
• Mindfullyparticipatebykeepingtheenvironmentcollegialandproductive.
• Ifanissuearises,addresstheinstructorontheside,one-on-one,ratherthaninfrontofthewholegroup.
• Avoidinterrupting,ridiculing,ortalkingovereachother.• Considerprivacyandconfidentialityconcernscarefullybefore
youdiscussanycaseoruseacurrentorformercaseasanexample.
p Activity1D:Overview
Slide4—Whythistraining?SenateBill238,signedintolawbyGovernorBrownonOctober6thof2015stipulatesthatcertainprofessionalslistedhereandotherswhoworkwithchildrenandyouthinfostercareshouldbeprovidedtrainingonimportanttopicsrelatedtotheadministrationofpsychotropicmedicationtothosechildrenandyouth.Specifically,trainingabout• psychotropicmedication(uses,benefits,risks)• trauma• mental/behavioralhealthservices• substanceabuse• asrelatedtochildrenandyouthinfostercareistobeprovidedto• grouphomeadministrators• fosterparents• childwelfaresocialworkers• probationofficers• dependencycourtjudgesandattorneys• courtappointedcounselandspecialadvocates.
p Activity1E:LearningObjectivesSlide5—LearningObjectivesQuicklyreviewthelearningobjectiveslocatedonthenextpageandonpage8intheTraineeBinders.Goaroundtheroomandhaveparticipantsreadtheobjectivesonebyoneoutloudtothegroup.
*Youmayconsideraskingthegrouptomakeothersawareoftheirpreferredgenderpronounwhentheyintroducethemselves.Thisisgoodpracticewhetherornotthereappearstobeany“question”becausegender-identityisn’talwaysperfectlyinterpretable.Thispracticehelpstocreateaninclusiveenvironment,andwillhelpavoidmis-genderinganyparticipants.Italsomodelsanapproachthatparticipantscanuseininteractionswithyouth.
5
Whythistraining?
SenateBill238requirestrainingbeprovidedto:• Grouphomeadministrators• Fosterparents• Childwelfaresocialworkersorprobationofficers• Dependencycourtjudges• CourtappointedcounselandCASA• Publichealthnurses• Othersupportpeople
Aboutthesetopics:• Psychotropicmedication• Trauma• Mental/Behavioralhealthandsubstanceuse
5
LearningObjectives
ü Knowledge
ü Skills
ü Values

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 14
LEARNINGOBJECTIVES(onpage8ofthetraineebinder)
KnowledgeK1 Traineeswillbeabletonameatleastthreekeypointsinthelawsandregulationsthatgovern
administrationofpsychotropicmedicationstochildren,youth,andyoungadultsinfostercareinCalifornia.
K2 Traineeswillbeabletonameatleastoneofthebasicprinciplesofperson-centeredandtrauma-informedcareastheyrelatetouseofpsychotropicmedicationinfostercare.
K3 Traineeswillbeabletonameatleasttwocommonbehavioralhealthdiagnosesandtherelatedtreatmentoptions(bothpsychosocialandmedical)forchildren,youth,andyoungadultsinfostercare.
K4 Traineeswillbeabletodescribewhatdotoifsideeffectsarenoticedorreportedbyachild,youth,oryoungadultinfostercarewhoistakingprescribedpsychotropicmedication.
K5 Traineeswillbeabletolocateandutilizethecorrectstaterequiredform(s)whenamedicalproviderisstartingorcontinuingapsychotropicmedicationforachild,youth,oryoungadultinfostercare.
K6 Traineeswillbeabletodescribethenotificationprocessesusedinrequestingandmonitoringadministrationofpsychotropicmedications.
SkillsS1 Usingsampleplans,traineeswillutilizetheCaliforniaGuidelinesfortheUseofPsychotropicMedication
withChildrenandYouthinFosterCareandthetoolsinitsappendicestoevaluateandmodifytreatmentplansthatincludepsychotropicmedicationdecisions.
• PrescribingStandardsbyAgeGroup,• ParametersforUseofPsychotropicMedicationforChildrenandAdolescents,• ChallengesinDiagnosisandPrescribingPsychotropicMedication,and• Algorithm/DecisionTreeforPrescribingPsychotropicMedication.
S2 Usingavignette,traineeswillbeabletoidentify:• Therelevantpartiesanddocumentationtobeincludedinthecourtprocess,• Thoseparties’rightsandobligations,and• Thetimelineforcourtrequests,decisions,andnotifications.
ValuesV1 Traineeswillvaluebuildingonchildandfamilyresilienceandstrengthsinbothformalandinformal
servicesusedtoamelioratethenegativeeffectsof1. abuseand/orneglect;2. emotional,cognitive,and/orbehavioraldysregulations;and3. potentialmentalillness.
V2 Traineeswillvalueensuringthatthevoicesofchildren,youth,andyoungadultsareincorporatedintotreatmentplansandmedicationdecisions.
V3 Traineeswillvalueworkingwithamulti-disciplinaryteamtounderstandandmanagetheuseofpsychotropicmedicationbychildren,youth,andyoungadultsinfostercare.

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 15
Segment2:LawsandRegulationsSegmentTime: 30minutes
Materials: Internetconnectiontoshowvideos
Slides: 6-13
DescriptionofSegment:Lecture:Providebackgroundofpsychotropicmedicationandintroducethethreenewlawsandthenewregulationstheyputinplace.Watch:VideoclipsofStateAuditor’sReportandFosterYouthTestimony
Note:Keepcarefultrackoftimeinthissegment.Questionsthatmightariseherewilllikelybecoveredinlatersections,soit’sgoodtokeepmoving.Considerassigningatimekeepertoalertyou.
DuringtheSegment
Slide6beginsSegment2
p Activity2A:Lecture—BriefintroductiontodefinitionandbackgroundSlide7—DefinitionofPsychotropicMedication
FromtheWelfareandInstitutionsCode,psychotropicmedicationsaredefinedas
“Thosemedicationsprescribedtoaffectthecentralnervoussystemtotreatpsychiatricdisordersorillnesses.Theymayinclude,butarenotlimitedto,anxiolyticagents,antidepressants,moodstabilizers,antipsychoticmedications,anti-Parkinsonagents,hypnotics,medicationsfordementia,andpsychostimulants.”
TheCaliforniaDepartmentofSocialServicesandtheDepartmentofHealthCareServicesusethissamedefinitionintheirGuidelinesfortheUseofPsychotropicMedicationwithChildrenandYouthinFosterCaredocument,whichwewilluselaterintheday.
Slide8—BigPicture
Problemsthathavebeenraisedbyresearchstudies,governmentreportsandthemediacoverageinclude:over-medication,off-labelmedication,multipleprescriptionsinsufficientmonitoring,andveryyoungpatients.
Researchandmediasourcesrevealthattherateofpsychotropicmedicationprescriptionsinfostercareishigherthanthegeneralpopulation,childrenhavebeenprescribedmultiplepotentclassesofdrugstobetakensimultaneouslyandwithoutascheduletoevaluateeffectiveness(inotherwords,permanently).Thiscoverageandothermovementstoimprovementalhealthservicesinfostercareproducedseveralreformlaws.
LawsandRegulations
Segment2
7
Section1:PsychotropicMedication
“Thosemedicationsprescribedtoaffectthecentralnervoussystemtotreatpsychiatricdisordersorillnesses.Theymayinclude,butarenotlimitedto,anxiolyticagents,antidepressants,moodstabilizers,antipsychoticmedications,anti-Parkinsonagents,hypnotics,medicationsfordementia,andpsychostimulants.”
7
8
BigPicture
• Researchstudies,governmentreports,andmediacoverage• Inputfromchildren,families,andtheirrepresentativesabouttreatmentdecisions• Reformsencourageuseoftrauma-informedlensandteamingwithfamily• Psychotropicmedicationsareonepossibletooltobecarefullyconsidered• Supportservices
8

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 16
Federallawrequiresstatesfigureouthowtheywilladdresstheseissues.AdministrationofChildrenandFamiliesissuedIM-12-03.Inthebinder.Input:Theselawsmakeexplicitthatchildrenandyouthinfostercare,alongwiththeirfamiliesandrepresentatives,mustbeallowedtoprovideinputintowhetherornotpsychotropicmedicationispartoftheirtreatmentplan.Refusalandprotection:Theselawsalsoemphasizethechild’srighttorefusemedicationandtheirrightnottobepenalizedordisciplinedforthatrefusal.Trauma:Ratherthanworkingfromtheassumptionthatsymptomsandbehaviorsarenecessarilyindicativeofmentalillness,thesereformsencouragetheuseofatrauma-informedlenstoviewthechild’senvironmentandexperiencesaspossiblesourcesofbehaviororsymptomsandtoexploreabroadrangeoftreatmentoptions.Broadarrayofservices:Psychotropicmedicationsareonetoolamongmanythatmaybeusedtoaddressbehavioralhealthconcerns.Theymustbeconsideredverycarefullyasthelong-termeffectsofthesemedicationsondevelopingbrainsisunknownandpotentialsideeffectscanbesevere.Goalistogetappropriate,quality,accessiblemental/behavioralhealthservicestochildrenandyouthincare.
p Activity2B:VideoclipsSlide9—Expertvideos
ShowtheshortvideoclipfromStateAuditor.• StateAuditor’sReportis4:16minuteslong—Takeafew
momentsafterthisvideotoreviewthekeypointsandanswerquestions.Thefollowingvideosareemotional,solettheparticipantsknowthattheywillbehearingstrongtestimonyfromformerfosteryouthwhohadnegativeexperiences.
Besuretointroducetheformerfosteryouthbytheirnames(TishaOrtizisfirstandShanequaArrington).Thesefolksaretheexpertsinthistopic,andtheyrepresentthe“why”behindtheentiretraining.
• Tisha’stestimonyis4:10• Shanequa’stestimonyis2:28
p Activity2C:Lecture—Overviewofnewlaws(Slides10-13)
Slide10—SenateBill238
Courtauthorizationprocess:
• Onlyajuvenilecourtjudicialofficercanordertheadministrationofpsychotropicmedicationstoachildoryouthinfostercare(exceptrarecaseswe’llcoverlater)
• Thatofficermayonlydosobaseduponarequestfromaphysician.
9
ExpertVideos
StateAuditor’sReporthttps://youtu.be/8XLA5stjYgY
TishaOrtiz’stestimonyaboutSB1174https://youtu.be/bEEO83wMb5Q
Shanequa Arrington’stestimonyaboutSB1291https://www.youtube.com/watch?v=wWXP8tjxNw4
10
SB238:PsychotropicMedication
Providesforthefollowing:• Courtauthorizationtoadministermedication• Caregiverreceivesacopyofthecourtorder• Childandteamprovideinputaboutmedicationdecisions• Publichealthnurseparticipation• Dataandinformationsharing• Trainingrequirements
10

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 17
• Thatphysicianwillprovidereasonsfortherequestandadescriptionofthechild’sdiagnosisandsymptoms.
• Thecourtwillreceiveinformationaboutthechild’soverallmentalhealthassessmentandtreatmentplan,andtheprocessforperiodicoversightandevaluationtobefacilitatedbythesocialworker,publichealthnurseorothercountystaff.
• Caregiverreceivesnoticewithintwodaysofcourt’sdecision
ChildandFamilyInputProvidesopportunityforthechildandhisorherfamilyandcaregiver,court-appointedspecialadvocate,thechild’stribe,orotherstoprovideinputonthemedicationsbeingrequested,andrequiresthatthechild’scaregiverreceiveacopyofanyresultingcourtorder.
PublicHealthNursesSB238clarifiesthepublichealthnursingprograminchildwelfarewiththepurposeofpromotingandenhancingthephysical,mental,dental,anddevelopmentalwell-beingofchildreninthechildwelfaresystem.PHNswillcollectanddocumentmedicalrecords,assistwithreferrals,andparticipateinmedicalcareplanningandcoordination.WEWILLTALKMOREABOUTTHISTHROUGHOUTTHEDAY.
MonthlyStateDataRequirestheCaliforniaDepartmentofSocialServicestoissueamonthlyreportwhenredflagsarepresent.Forexample,• whenmultiplemedicationsareprescribedforthesamechild,or• whenunusuallyhighdosesareindicated,or• whenprescriptionsareforchildrenwhoare5yearsoldoryounger.Countiesaresubsequentlyrequiredtosharerelevantinformationwithappropriatejuvenilecourt,attorneys,countydepartmentofbehavioralhealthandCASAs.Countydata-sharingagreementsdiffer,sonoteveryonereceivesthesamereports.
MandatesthistrainingSB238alsorequirestrainingabouttheauthorization,uses,risks,andbenefitsofpsychotropicmedicationaswellastrainingonself-administration,oversight,andmonitoringofthosemedications.Thistrainingrequirementalsoincludesinformationabouttrauma,substanceusedisorderandmentalhealthtreatments.That’sthistrainingwe’reinrightnow.

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 18
Slide11—SenateBill319
NOTE:ThislawandtheissuessurroundingtherolesandresponsibilitiesofPHNscanbecontroversialand/orconfusing.IftherearePHNsattendingyourclass,taketimetoacknowledgetheirconcernsandreassurethemthatwewillbecoveringthisinmoredepthlaterintheday.ClarifythatthespecificpracticesandprotocolsforPHNactivitieswillvaryaccordingtocountydecisions,sosomespecificquestionsandconcernsareoutsidethescopeofthistrainingasitisdesignedprimarilyforchildwelfareworkers.Encouragethemtotalktoeachotherandtheircountyadministrationforclarificationandsupport.SenateBill319addressestheroleofFosterCarePublicHealthNurses.ItdoesnotfundamentallyCHANGEtheirrole,itjustoutlinesactivitiesspecifictopsychotropicmedicationoversight.PHNsareto:
o monitoruseofpsychotropicmedicationbychildrenandyouthinfostercare,
o documentinitialandfollow-uphealthscreenings,o collecthealthinformationtodetermineappropriatereferral,o helpchildrenandfamiliesconnectwiththeservicesthey
need,o assistwithtreatmentplanning,o assessprogresstowardtreatmentgoals,ando advocatetoensurethatthehealthneedsofthechildare
metandthatthechildandfamilycanmakeinformeddecisionsabouttheirownmedicaltreatmentandhealthcaregoals.
Makesuretolistentotheconcernsofnurseshere.Wewillgooversomeoptionsforhowtheseactivitiesmightoccurintheafternoonsectionofthistraining,anditwillbeimportanttocovertheirspecificconcernsandquestionsasmuchaspossible.RefertoACL16-48fordetails.Also,inthefuture,theremaybeaclassonthistopicespeciallydesignedfornurses.Anotherfutureoptionisthatitwillbeco-taughtbysocialworker/childwelfareworkerandanurse..Slide12—SenateBill484ThislawappliesprimarilytoGroupHomes.Runawayandemergencysheltersareexemptedfromtherequirementsofthisbill.Grouphomesarerequiredtousepsychotropicmedicationinaccordancewiththewrittendirectionsoftheprescribingphysicianasauthorizedbythejuvenilecourt.GroupHomesaretomaintainspecificinformationinthechild’srecords
• Acopyofthecourtorderthatauthorizestheadministrationofprescribedmedicationand
• Aseparatelogforeachmedicationthatincludes:ü thenameofthemedication,ü thedateofprescription,
11
SB319:FosterCarePublicHealthNurses
PHN’sroleisclarifiedto• Monitorandoverseepsychotropicmedication• Documenthealthscreenings• Makereferralsandlinkages• Playkeyroleinplanningandassessment• AdvocateforhealthneedsofthechildSB319allowssharingofhealthinformationbetweenspecificpartiesfortheexpresspurposeofaccessinghealthcareandmedicalservices.
11
12
SB484:GroupHomes
• Methodologyforidentifyingandinspectingfacilitieswithconcerningmedicationusage• Allowsforinformationsharingaboutinspections• AnnualreporttobepostedonCDSSwebsite• Requiresmaintenanceofcourtrecordsandmedicationlogs• Newperformancestandardsandoutcomemeasures
12

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 19
ü thequantityofmedicineandthenumberofrefills,ü dosageanddirections,andü thedateandtimewhenthechildtookeachdose.
Thestatewillidentifygrouphomesthatwarrantadditionalreviewandconductvisitsatleastonceayeartoidentifiedfacilities.GrouphomeswhohavehadavisitorreportwillbeallowedtosubmitimprovementplanstoCDSSwithin30daysofthatvisit.SB484authorizesCDSStoshareinformationaboutthesevisitswithcountyplacingagencies,socialworkersandprobationofficers,thecourtanddependencycouncilortheMedicalBoardofCalifornia.Grouphomeswillberequiredtoadheretonewperformancestandardsandoutcomemeasures.Slide13—LegislativeUpdatesSenateBills
• 1174—prescriber-oversightbillallowingMedicalBoardofCaliforniatoexamineprescriptionpatterns
• 1291—improvestransparencyandtrackingofmentalhealthservicesforchildrenandyouthinfostercare
InformationaboutnewCalifornialawsconcerninghealthcanbefoundhere:http://www.dhcs.ca.gov/formsandpubs/laws/Pages/LawsandRegulations.aspxNote:TraineeBindercontainsthecompletetextofeachoftheselawsshouldanyparticipantswanttoknowmore.
13
LegislativeUpdates
SenateBills• 1174—prescriber-oversightbillallowingMedicalBoardofCaliforniatoexamineprescriptionpatterns• 1291—improvestransparencyandtrackingofmentalhealthservicesforchildrenandyouthinfostercare

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 20
Segment3:CourtForms
SegmentTime: 75minutes
Materials:PacketsofblankcourtformsandJV-220HandoutsFlipchartsheets(7foreachteam)CopiedandcutsetsofStepcardsandFormcardsArolloftapeperteam
Slides: 14-33DescriptionofSegmentTrainerfacilitatesanoverviewoftheformsusedintheJV-220process,andguidesthegroupthroughtwoskill-buildingactivitiesforusingtheseforms.
BeforetheSegment
Createsevenflipchartpagesforeachgroupbywriting“Step1”through“Step7”andWhatForm(s)?halfwaydowneachpageasshownbelow.HangeachsetonadifferentwallinnumericalorderStep1-7.Itisprobablyeasiestifthisisdonebeforethetrainingbegins.
ThroughStep7
CopyandcuteachgroupasetofStepcardsandasetofFormscards(asincludedintheTrainerMaterialspacket).
DuringtheSegment
Slide14Introducesthissegmentp Activity3A:LectureontheCourtProcess
Slide15—CourtProcess
Theprocessofapplyingtothecourtforjudicialreviewofaplantoadministerpsychotropicmedicationtoachildoryouthinfostercare,andtheformsthatareusedinthatprocessaresometimesreferredtoasthe“JV-220Process.”ThenewprocessbecameeffectiveonJuly1st,2016.Itstrengthensthecontinuity,quality,andcoordinationofcare.• Continuityisimprovedbythesharingofmedicalandtreatment
historyacrossagencies,• qualityofcareisenhancedbyimprovedmonitoringandclear
expectations,and• coordinationiseasierbecausesocialworkersandpublichealthnurses
haveeasieraccesstonecessaryinformation.
CourtProcessandForms
Segment3
15
CourtProcess
•Continuity•Quality•Coordination
• JudicialReview• JV-220Forms
15
STEP1:WhatForm(s)?
STEP2:WhatForm(s)?
STEP3:WhatForm(s)?

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 21
MuchoftheworkdonebytheCFTorothertreatmentteamespecially1. thehealthhistory,2. pasttreatmentsdocumentationand3. risk/benefitanalysis,
willbeusefulforthecourtifpsychotropicmedicationisselectedaspartofthetreatmentplan.
Slide16—JudicialReview
Bylaw,achildwhoisawardordependentofjuvenilecourtorinfostercaremaynotreceivepsychotropicmedicationwithoutacourtorder.TheJudicialCouncilhascreatedaseriesofformsusedtorequestthisorderfromthecourt.Theymakeupthe“JV-220Process.”Thereareonlythreeexceptionstothismandate.
• Ifthechildoryouthlivesinanout-of-homefacilitythatisnotconsideredfostercare(e.g.juveniledetentionorvoluntaryplacement).
• Whenthereisapreviouscourtorderthatgivesthechild’sparentstheauthoritytoapproveorrefusethemedication.
• Inthecaseofanemergency.Adoctormayadministerpsychotropicmedicationtoachildiftheyposeaseriousrisktothemselvesorothers,topreventdeathorseriousharm,orifwaitingwouldcreatesignificantsuffering.Afteremergencyadministrationofmedication,thedoctorhasnomorethan2daystoseekcourtauthorizationthroughtheJV-220process.
Judicialreviewisinitiatedbythesocialworkerorprobationofficerwiththechild’sprescribingphysician.Theyworkincollaborationwiththechild,hisorhercourtandtribalrepresentatives,alongwithfamilymembersandcaregivers.PublicHealthNursesarekeymembersoftreatmentteamsforchildrenandyouthinfostercare.CivilCodesection56.103statesthatmedicalinformation,barringpsychotherapynotes,andotherrestrictedhealthinformationmaybesharedwithPublicHealthNursesorPHNs.CountieswillvaryintheapproachtheytaketoincorporatingtheroleofPHNsandthesedatasharingactivities.
Slide17—ExceptionsJudicialapprovalisrequiredexceptinthesecircumstances.
• Continuationofmedicinefrombeforetheywereinfostercare.• Parent/legalguardianremainstheonlypersonallowedto
consenttotreatment.• Emergency—rareandshort-term• Non-minordependentshavetheirownconsenttograntordeny,
theCourthasnoauthority
16
JudicialReview
• ApplicationforPsychotropicMedication• The“JV-220Process”• MandatedbylawunlessüOtherout-of-homefacilityü Previouscourtorderü Emergency
• Collaborationwiththechild,hisorhercourt,andTribalrepresentatives,family,andcaregivers• PublicHealthNurses
16
60
Exceptions
•Medicationiscontinuationofprescriptionbeingtakenbychildbeforetheyenterfostercare• Pre-disposition—parent/legalguardianconsentisrequired• Emergency• YouthwhoareNon-MinorDependents.Thesesyouthgranttheirownconsent(unlessemergencyornon-voluntaryhospitalization).

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 22
Slide18—RequiredFormsGiveaquickintrototheforms.Detailswillcomelater.JV-220isthebasicinformationformthatinitiatestherequesttoadministerpsychotropicdrugstoachildoryouthincare.JV-220(A)isanattachmenttotheJV-220andcontainsthephysician’sstatement.ItmustaccompanytheJV-220,unlesstherequestistocontinueanongoingtreatmentwithoutchangesandisrequestedbythesamedoctor.Inthatcase,JV-220(B)shouldbeattached.TheseJV-220formsarecommonlyreferredtoastheApplication.JV-221istheformthatshowstheCourtthatallpartieswitharighttoreceivenoticewereservedacopyoftheApplicationandattachments.Wewillcoverthesepartiesmorethoroughlyinafewmoments.JV-223istheOrderontheApplicationandistheformtheCourtusestoeithergrantordenytheApplication.JV-224istheCountyReportFormandisfiledwiththeCourtbythesocialworkerorprobationofficeratleast10calendardaysbeforeeachprogressreview.JV-217INFOisaGuidethatprovidesbriefdescriptionsofalltheformsrelatedtotheApplicationforPsychotropicMedication.ItissentalongwithnotificationsofapendingApplication.
Slide19—OptionalForms
Inadditiontotherequiredforms,therearesomethatthefamilyandtreatmentteammaydecidetouse.Itisimportanttonotethatwhiletheseformsarelistedas“optional,”thatdoesnotmeanthatseekingtheinputoftheseindividualsisoptional,justthattheuseofthesespecificformsisnotrequired.Involvedpartiesmaycommunicatetheirthoughtsandfeelingsusingothermeans,buttheirinputshouldalwaysbesought.
• TheJV-218formcanbeusedbythechildtoprovidetheirinputtotheCourtaboutthemedicationplan.
• JV-219isasimilarformthatmaybeusedbythecaregiver,CASA,orTribetoprovideastatementrelatedtotheApplication.
• JV-222formisfiledwhenoneofthespecifiedpartiesdoesnotagreethatthechildshouldtaketherecommendedmedication.
p Activity3B:MatchingGame—Slide20
NOTE:Thisslideisanimatedsothatyoucanrevealthecorrectanswerstothegameoncethegroupshavefinishedplaying.Thestepswillappearclockwiseasyouclickthrough.
1. Dividetheroomintoatleasttwogroups.Ifthegroupswillbelargerthan10persons,thenathirdgroupmightbeagoodidea.
2. Showthegroupsthesetofflipchartpagesyoucreatedandhungonthewallalready.EachgroupwillhaveasetofsevenflipchartpageswithStep1-7indicatedasdescribedabove.
61
RequiredForms
• JV-220 ApplicationforPsychotropicMedication• JV-220(A)Physician’sStatement• JV-220(B)Physician’sRequesttoContinueMedication• JV-221 ProofofNoticeofApplication• JV-223 OrderonApplicationforPsychotropicMedication• JV-224 CountyReportonPsychotropicMedication• JV-217INFOGuidetoPsychotropicMedicationForms
62
OptionalForms
• JV-218Child’sOpinionAbouttheMedication• JV-219StatementAboutMedicationPrescribed• JV-222InputonApplicationforPsychotropicMedication
Note:Itisnotoptionaltoseekinputfromthechildand/orfamily;itisoptionaltousethesespecificformstoprovideit.
20
JudicialProcessActivity1.Application
JV-220 2.Physician'sStatementJV-220 A
JV-220Bforrenewalofsameplanbysame
Prescriber
3.NotificationsAnnouncementofpendingApplication
BlankJV- 218,219,&222ProofofNotification
JV-221
4.Input/StatementsJV-218, JV-219,
JV-222Filedwithin 4 Court
DaysAndoptionalagainbeforeProgress
Reviews
5.Ruling/CourtOrderJV-223
Ifapproved,last2pagesofJV-220Aandmedication
informationsheetsFiledwithin7CourtDaysof
completeApplicationToCaregiverwithin2Court
Daysofruling
6.CountyReportJV-224
BlankJV-218&21910calendardaysbeforeeveryhearingorreview
7.ProgressReviewand/orStatusReviewAllrelevantformsand
information
20

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 23
3. Explainthattheywillbeputtingonesetofcards(helpfultodescribethesewithwhatevercoloryoucopiedtheStepcardsonto)intheproperorderfromStep1toStep7.Andthatthentheywillplacetheothersetofcards(again,whatevercoloryoucopiedthesecards,ideallyadifferentcolorthantheStepcards)willbeusedtomatchtheformswiththeappropriateStep.Forexample,”
4. Giveeachgroup• acopyofJV-217INFO,• theirsetofStepcards,• theirsetofFormcards,and• arolloftape.
5. Afterbothgroupshavefinished,clickthroughtheanimationtorevealtheanswers.Thisisthebig-pictureprocessoverview.Lettheparticipantsknowthatwewillbegoingintodetailabouteachofthesenext.
6. QUICKDEBRIEF:RemindtheparticipantsthattheJV-217INFOformisoftentheonlyinformationthatfamilies,caregivers,andotherfolksreceivetohelpthemnavigatethissystem.Isitenough?
CorrectAnswers:
STEP1:ApplicationForm(s):JV-220STEP2:Physician’sStatementForm(s):JV-220A(QuicklyexplainthatJV-220Bisonlyforsamemedicationplanwithsameprescriber)STEP3:NotificationsForm(s):JV-221,JV-217INFO,BlankJV-218,BlankJV-219,andBlankJV-222STEP4:InputandStatementsForm(s):JV-218,JV-219,andJV-222STEP5:Ruling/CourtOrderForm(s):JV-223STEP6:CountyReportForm(s):JV-224STEP7:ProgressReviewForm(s):JV-224(ongoingmonitoringandeval)BlankJV-218andBlank219providedbeforehand(sometimesthiswillcoincidewiththeCountyReport)p Activity3C:Lecture—ReviewofJudicialProcessForms.
Afterthegame,passoutthecopiesoftheactualblankformsandtheaccompanyingJV-220handouts.Showandreviewthedetailedslidesforeachform.Theyshouldcorrecttheirflipchartpagesandmovethingstotheproperplaceifmistakesweremadetovisuallyreinforcethroughouttheday.

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 24
JV-220ApplicationforPsychotropicMedication[Slide20]JV-220(A)Physician’sstatementandJV-220(B)Physician’sRequesttoContinueMedication[Slides21-25]JV-221ProofofNoticeofApplication[Slides26and27]JV-222InputonApplication[Slide28]JV-223OrderonApplication[Slide29]JV-224CountyReportonPsychotropicMedication[Slide30]Group7—JV-218Child’sOpinionabouttheMedicine[Slide31]Group8—JV-219StatementaboutMedicinePrescribed[Slide32]RequiredForms:
63
ApplicationforPsychotropicMedicationJV-220• Usuallycompletedbysocialworkerorprobationofficer• Functionslikeacoversheetfortheattachments• Providesthecourtwith:ü Basicinformationaboutthechildü Contactinformationforsocialworkerorprobationofficer
üMedicationandothertreatmenthistoryüWhowillbeprovidinginputandinwhatform
22
Physician’sStatement—JV-220(A)
Threeuses:1. aninitialrequesttoadministermedication2. arequesttostartadifferentmedicationor3. arequesttocontinuemedicationatdifferent
doseorfromdifferentPrescriber• Prescribingphysician’sinformation• Assessmentofchild’soverallmentalhealth• Descriptionofsymptoms,theirduration,andthetreatmentplan• Descriptionofchild’sresponsetocurrentmedicationifapplicable• SignedbythePrescriber(PhysicianorPsychiatrist)
22
65
Physician’sStatement—JV-220(A)(cont’d)
• Outlineofprevioustreatments:ü Listofpharmacologicalandnonpharmacological
treatmentsandthechild’sresponsetothemü Listofpreviousmedicationsandchild’sresponseü Descriptionofsymptomsnotimprovedbypast
treatments• Symptomsexpectedtoimprovewithrequestedmedication• DiagnosisfromDSM-5andrelevantmedicalhistory• Othertherapeuticservicesfornextsixmonths
66
Physician’sStatement—JV-220(A)(cont’d)
• Whetherornotthechildandcaregiverhavebeeninformedof:ü Recommendedmedicationü Anticipatedbenefitsü Possiblesideeffectsü Thatheorshemayopposetherequest
• Whetherthechild’sandcaregiver’sresponsestothisinformationwereagreeableornot
67
AttachmentstoPhysician’sStatement—JV-220(A)
• ListofmedicationcurrentlyadministeredüName,class,andtargetüDose,duration,andschedule
• Listofmedicationsthisorderwouldstop
• Mandatoryattachmentsü SignificantsideeffectsüWarnings/contraindicationsüDruginteractionsüWithdrawalsymptoms
68
Physician’sRequesttoContinueMedicationJV-220(B)
• ShorterversionofJV-220(A)• SamedoctorwhocompletedthemostrecentJV-220(A)• Samemedication• Samedosage,duration,andschedule
ProofofNoticeofApplication—JV-221
Parent/Guardian• Noticeofphysician’srequest• AnApplicationispending• Thenameofeachmedication• TheJV-217-INFOdocument• BlankJV-219(Statement)• BlankJV-222(Input)
Child’sAttorney/GAL• CopyofcompletedJV-220andJV-220(A)or(B)• CopyofJV-217-INFO• BlankJV-218forchild’sopinion• BlankJV-222forinput
Note:InconsistenciesexistbetweenthisformandCARulesofCourt5.640
Caregiver• SameasParent/Guardianexcept• Nomedicationinformation• NoJV-222(Input)
ProofofNoticeofApplication—JV-221
CASA• Noticeofphysician’srequest+pendingApplication• Nameofeachmedication
Child’sTribe• Noticeofrequest+pendingApplication• Nameofeachmedication• CopyofJV-217-INFO• BlankJV-219(Statement)• BlankJV-222(Input)
Note:InconsistenciesexistbetweenthisformandRulesofCourt
OtherAttorneys• Noticeofphysician’srequest• PendingApplication• Nameofeachmedication• CopyofJV-217-INFO• BlankJV-222forinput

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 25
OptionalForms:
JudicialProcessHandouts(locatedinHandoutFolder):AlltheBlankJVformsandthefollowinginfosheets:JV-220ApplicationforPsychotropicMedicationJV-220(A)Physician’sstatementandJV-220(B)Physician’sRequesttoContinueMedicationJV-221ProofofNoticeofApplication(IncludesnoteonJV-217-INFO)JV-223OrderonApplicationJV-224CountyReportonPsychotropicMedicationJV-218Child’sOpinionabouttheMedicineandJV-219StatementaboutMedicinePrescribedJV-222InputonApplication
71
OrderonApplicationforPsychotropicMedicationJV-223HearingsetwithinsevendaysCaregiverreceivesacopywithintwodays• ThedocumentsandformsthattheCourtconsidered• Noticerequirements• HearingDate/Time/Department• Application(pages5&6ofJV-220(A)attached)
ü Grantedü Grantedandmodifiedü Denied
• Resubmitwithmissinginformation• Progressreview
72
CountyReportonPsychotropicMedicationJV-224Completedbysocialworkerorprobationofficer:• Child’sinformation• Listofmedicationsanddosage• Caregiver’sobservationsabout:
ü Behavior/symptomchangeü Sideeffectsü Concerns
• Child’sobservationsaboutthesame• Datesofmedicationmanagementappointmentssincelasthearing• Datesandreasonsforotherappointments• AnyotherrelevantinformationFiledatleast10daysbeforethehearing
73
Child’sOpinionabouttheMedicineJV-218
Childcanusethisform,or:• Talktothejudgedirectly• Writealettertothejudge• Asktheirlawyer,socialworker,probationofficer,orCASAtotalktothejudgeforthem
Theformconsistsofashortquestionnaireaboutwhatthechildknowsaboutthemedicineandothertreatmentsandactivitiesandtheiropinionaboutthem. 74
StatementaboutMedicinePrescribedJV-219Caregiver,CASA,orIndianTribemayusethisformor:• Talktothejudgedirectly• Writealettertothejudge• Asktheattorneyofrecord,socialworker,probationofficer,orCASAtotellthejudgeforthem• TheCASAmayfileareportdirectlyTheformisaquestionnaireabout:• thechild’sbehavior• treatmentandfollow-upplans• descriptionsofcurrenttreatmentandcurrentmedicationifapplicable
70
InputonApplicationforPsychologicalMedicationJV-222
Thefiler’scontactinformationandoneofthreereasonsforfiling
1. OpposetheApplication2. Inputforthecourt(ifnotopposed)3. Attorneyneedsmoretimeand/ormore
information
• MustbefiledwiththeclerkoftheJuvenileCourtwithinfourdaysofreceivingnotice•Thecourtmayormaynotsetahearingduetooppositionorinput

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 26
Segment4:TraumaSegmentTime: 45minutes
Materials: DiscussionPrompts
Slides: 34-42
DescriptionofSegment:
Lecture:Traumaanditseffects,commonsymptoms/behaviorsthatmayresultfromtrauma,howtheserelatetofostercaresettinginparticular;howresilienceisprotective;andessentialelementsoftrauma-informedpractice.
Groupdiscussion:traumapracticeexperience,trauma-informedtoolsandservices,andadvocatingfortrauma-informedservicesintheirsmallgroups.
DuringtheSegment
p Slide34beginsSegment4:Trauma
p Activity4A:Lecture—TraumaasitrelatestoPsychotropicMedicationinFosterCare(Slides15-22)
Slide35—DefinitionofTrauma
SubstanceAbuseMentalHealthServicesAdministration’sdefinitionoftrauma:
“Individualtraumaresultsfromanevent,seriesofevents,orsetofcircumstancesthatisexperiencedbyanindividualasphysicallyoremotionallyharmfulorthreateningandthathaslastingadverseeffectsontheindividual’sfunctioningandphysical,social,emotional,orspiritualwell-being.”
Slide36—Thisdefinitionisspecialbecauseitincludes“setofcircumstances.”
Theinclusionof“setofcircumstances”incorporatestheexperienceofneglect,whichisthemostfrequentreasonthatchildrenandyouthareremovedfromtheirhomes.Therefore,thisdefinitionisimportantforworkwiththefostercarepopulation.Itdoesn’tcompletelyalignwiththediagnosticcriteriaforPTSD,sothisisanareathatrequiresattention.Thetrauma-informedapproachisofparticularimportancewhenwearediscussingmentalandbehavioralhealthinterventions.Often,thesignsandsymptomsoftraumacanresemblethoseofmentalillnessorbehaviordisorders.Thesesymptomsandbehaviorsmightthenbetreatedasamentalillnessorchemicalimbalanceand/orwithpsychotropicmedications,thuscausingmissedopportunitiestoaddressthetraumaaswellasincreasingthelikelihoodofaddingunduestressorevenre-traumatizingtheindividual.
Trauma
Segment4
15
Trauma
TheSubstanceAbuseandMentalHealthServicesAdministration(SAMHSA)definition:
“Individualtraumaresultsfromanevent,seriesofevents,orsetofcircumstancesthatisexperiencedbyanindividualasphysicallyoremotionallyharmfulorthreateningandthathaslastingadverseeffectsontheindividual’sfunctioningandphysical,social,emotional,orspiritualwell-being.”
36
Trauma
•Traumacanresultfroma“setofcircumstances”notonlyfromspecificevent(s)—includesneglect•PosttraumaticStressDisorder(PTSD)diagnosisrequiresexposuretoaspecificeventorseriesofevents,somaynotcoverfosterchildrenandyouthwhohavehistoriesofneglect.•Trauma-informedcareandservicesareespeciallyimportantwhenassessingandtreatingmentalorbehavioralhealthconcerns.•Traumaandmental/behavioralhealthconcernscanoverlap• Signsandsymptomsaresimilar• Canco-existandbeinter-related
36

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 27
Slide37—ThethreeE’softrauma
Thisdefinitionhighlightsthethreecomponentsoftrauma:THEEVENTORCIRCUMSTANCE:Thesourceofpotentialtraumaisan
eventorcircumstancethatcausessignificantstress.Noteverychildexposedtostresswilldeveloptrauma.Examplesmayincludetheactualorextremethreatofphysicalorpsychologicalharmorsevere,life-threateningneglect.(abuse,caraccident,murder,disaster).Theseeventsandcircumstancesmayhappenasasingleoccurrenceorrepeatedlyovertime.Traumacanalsooccurwhenanindividualwitnessesextremethreatsorstressfulcircumstancesexperiencedbysomeonetheycareabout(domesticviolence,abuseandneglectofothers).
EXPERIENCE:Thesingularexperienceanindividualhasoftheseeventsorcircumstancesdetermineswhetheritisatraumaticevent.Aparticulareventmaybetraumaticforoneperson,butnotforanother(i.e.siblingsremovedfromthesameenvironmentofneglectmaynotalldeveloptraumaresponse).Feelingsofpowerlessness,humiliation,guilt,shame,betrayal,orsilencingoftenshapetheexperienceoftheevent.Howtheeventisexperiencedmaybelinkedtoarangeoffactorsincludingtheindividual’spersonality,culturalbeliefs,availabilityofsocialsupports,ordevelopmentalstageatthetimetheeventoreventsoccurred.
EFFECTS:Acriticalcomponentofdeterminingifanexperiencewastraumaticforanindividualisthepresenceoflong-lastingandadverseeffects.Theymayoccurimmediately,ornot.Sometimesadverseeffectsarenotnoticeduntilmuchlater,butarenonethelesscausedbythepreviousEventsandExperiences.Itmaytakemanyyearsforsymptomsoftraumaticexperiencestobecomeapparent.Itisnotuncommonforadolescencetobeatimewhenchildhoodtraumaisrevealedinphysiologicaland/orbehavioralsymptoms.Individualresponsesvarywidely,soitisimportanttocarefullyandcompassionatelyassesssymptomsandbehaviorsthroughatrauma-informedlensevenifnothingobviouslytraumatichashappenedrecentlyinthechild’slife.
Slide38—TraumaandFosterCare
Childrenandyouthcurrentlyorformerlyinfostercarehavelivedthroughatleastonecircumstancewhichcouldbetraumatic:• theywereremovedfromtheirhome.Theylostaccesstotheirfamily
foratleastsometime.• Theyalsoexperiencedthesignificantloss,abuseand/orneglectthat
leadtotheirremoval.
Fostercareservices,whicharedesignedtoprotectchildrenfromharm,canbetraumatizing,
17
TheThreeE’sofTrauma
•TheEventorseriesofevents,orcircumstance
•TheExperiencedeeplypersonalandindividualized
•TheEffectlong-lastingandadverse
38
TraumaandFosterCare
• Removal,loss,abuse,and/orneglect• Evensystemsdesignedtoprotectcantraumatize
• Similarsymptomsü Sleepproblemsü Toiletingproblemsü Angerandaggressivebehaviorsü Depressionü Difficultysustainingattention
• Negativeeffectsoftraumaareoftensimilartomentalhealthsymptomsandbehaviors
• Maybeimmediateordelayed
38

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 28
• removalfromhome,neighborhood,community• separationfromsiblings,pets,andfamiliarenvironment• changeinroutineandexpectations• chaotic/unreliable(i.e.turn-overinsocialworker,placements)
Therefore,itmakessensetoviewthispopulationthroughthelensofpotentialtraumaanditseffects.TheAmericanAcademyofPediatricsidentifiedsymptomslike• sleepproblems,• toiletingproblems,• angerandaggressivebehaviors,• depression,• ordifficultysustainingattentionaspossiblepresentationsfromchildrenwithahistoryofadverseandpotentiallytraumaticexperiences.
Thesebehaviorsmaybeadaptiveandprotectivewhenthechildisinthestressfulenvironment,butcanbemisunderstoodaspathologicwhentheyareremovedfromthatenvironment.Noteverydysregulationisindicativeofadisease.That’swhyitisimportanttocarefullyscreenforandevaluatetraumawhenassessingtheneedsofchildrenoryouthandtokeepinmindthatchildrenaredoingthebesttheycanwiththecircumstancesthey’vegot.
Allthesesymptomsresemblesymptomscommonlyassociatedwithmentalorbehavioralhealthconcernsordiagnoses.Traumaandmentalhealthoftenoverlap.Traumacanhavenegativeeffectsonachild’spsychologyand,conversely,mentalhealthissuescanincreasevulnerabilitytotrauma.Traumashouldbeconsideredatallpointsinmentalhealthandsubstanceuseservicesincludingprevention,treatment,andrecovery.Negativeeffectsoftraumacansometimesalsoleadtomisdiagnosisand/orinappropriatetreatment(forexample,prescriptionofmedicationintendedtotreatamentalillnessratherthantreatmentfortrauma).Asmentionedbefore,theeffectsoftraumamaybeimmediateordelayed,whichisonereasonwhyongoingassessmentissoimportant.
Slide39—TraumaandResilience
Unaddressedtraumasignificantlyincreasestheriskof• mentalhealthconcerns,• substanceusedisorders,and• chronicphysicaldiseases.
Thesepotentialoutcomescanbemitigatedbyresilience.Resilienceiscomprisedofthreeinteractiveinfluences:
• Individualdifferencesintemperamentandcognitiveabilities• Qualityofsocialrelationships—doesthechildhavepeersand
adultstheycantrustandwhocareaboutthem?
39
Trauma andResilience
Resiliencehasthreeinteractiveinfluences:• Personaltemperament• Qualitysocialrelationships
andlovingconnections• Supportiveenvironment
Strength-basedapproachcanimproveresilience.
GroupDiscussion:Anyexamplesofresilienceand/orstrength-basedworkhelpingtoaddresstrauma?
39

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 29
• Qualityofthebroaderenvironment,suchasschoolandneighborhood
Resiliencecanbenoticed,heightened,andcenteredbytheuseofastrengths-basedapproachtoworkwithchildrenandfamilies.Focusingontheassetsandtoolsthatindividualsalreadypossessratherthanperceiveddeficitscanempowerindividualsandminimizelabelsandstigmas.Identifyingandbuildingonthestrengthsoftheindividual,theirsupportnetwork,andtheirenvironmentincreasesresilienceandcanimprovetheprotectivefactorsindealingwithpastandpotentialfuturetraumaandhelptomitigatenegativeeffectsfromstress.
Slide40—NegativeEffectsofTrauma
Examplesofnegativeeffectsincludethelimitedordisruptedabilityto:• copewiththenormalstressesandstrainsofdailyliving,• formrelationshipsorbeabletotrustinorbenefitfromthem.• managecognitiveprocesses,suchasmemory,attention,
thinking;• regulatebehavior;and/or• controltheexpressionofemotions.
Thiscansometimeslooklike• anger,violence,self-harm,distrustfulness• hypervigilanceornumbness• avoidanceorhopelessness• nightmaresorflashbacks• useofalcoholorotherdrugs• neurobiologicalmake-upandongoinghealthandwell-beingmay
bepermanentlyaltered.Theseeffectscaneventuallywearapersondownphysically,mentally,emotionallyandspiritually—survivorsoftraumahavehighlightedtheimpactoftraumaonspiritualbeliefsandthecapacitytomakemeaningoftheirexperiences.
Slide41—TraumaandSubstanceUse
Interrelatedandrisksgobothdirections• Substanceuseasanattempttomanagetraumasymptoms• Traumaoccursasresultofsubstanceuseandmaybemorelikely
(youngpeopleusingsubstancesaremorelikelytoengageinriskybehaviorsandbenearpotentiallyabusiveordangerouspeople,mayberequiredtodoillegalthingstosupportaddiction,etc.)
• Similarpatternsanddysregulationinaddictionandtraumaticstress
40
NegativeEffectsofTrauma
•Stress•Relationships—pushingawayortesting•Reducedcognitivefunctioning•Behaviorregulation—violence,self-harm•Expressionandregulationofemotion—anger,distrust
•Violenceorself-harm•Hypervigilanceorfear•Numbnessandavoidance--hopelessness•Nightmaresorflashbacks•Alcoholordrugs•Chronicphysicalillness•Spiritualimpact
40
41
TraumaandSubstanceUse
Interrelatedandrisksgobothdirections• Substanceuseasanattempttomanagetraumasymptoms• Traumacanberesultofsubstanceuseandmaybemorelikely• Similarpatternsanddysregulationinaddictionandtraumaticstress
Lookforintegratedservices• Canbechallengingtolocate• Integrationandresource-sharingcanoccurontreatmentteam• Acknowledgingtraumaanditsrelationshipwithsubstanceusecanbeanempoweringaspectoftreatmentandrecovery
41

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 30
Prioritizeintegratedservices:• Canbechallengingtolocate,butareamandatedcomponentof
MediCalviaEPSDT(SeeMHSUDSInformationNotice16-063).• Integrationandresource-sharingcanoccurontreatmentteam.• Acknowledgingtraumaanditsrelationshipwithsubstanceuse
canbeanempoweringaspectoftreatmentandrecovery.• Someserviceswon’tacceptfolkswhoareusingintotheirmental
health,andPTSDissometimesanexclusioncriterionforsubstanceusetreatment.
• Treatmentteamswithprofessionalsfrombothareascanhelpmakesuretheservicesarecomplimentary.
Self-medicatingtheory—substanceuseasacopingstrategyfortraumaYouthengageinriskybehaviorsasaresultofuseandexperienceatraumaticeventand/ormaybelessabletocopewithatraumaticeventduetosubstanceusethantheirnon-usingpeers.
Slide42—Trauma-InformedToolsandServices
• Awarenessthatsymptomscanbecopingmechanismsoradaptiveresponses,isanimportantpartofprovidingtrauma-informedcare.
• Carefulassessmentandtrauma-informedservicesarecrucialtoeffectivetreatment
• Thelongertraumaticstressgoesuntreated,thegreatertheriskofdevelopingmaladaptiveandpotentialdangerouscopingmechanisms
p Activity4B:SmallGroupDiscussionandReportOut(Slide42)Givethetraineesafewminutestodiscusstrauma-informedpracticeintheircountyoragency.Questionsareonpage19oftheirbinders.
Usethesediscussionpromptswiththeentiregroup:
1.Whataresomeexamplesofachild’sresilienceinthefaceoftraumaoratimewhenastrengths-basedapproachwasusedsuccessfully?
Oneexamplefromthepilot—ayoungadultinagrouphomewasactingoutatbedtime.Aftersomecarefulquestioning,herevealedthathedidn’twanttodo“lightsout”becauseheisafraidofthedarkduetotraumaticevents.So,thegrouphomeallowedhimtosleepwiththelightonratherthancontinuingdisciplinaryaction.
2.Doesanyoneinyourgroupuseformaltraumaassessmentsorothertrauma-specifictools?Whatabouttrauma-informedserviceproviders?
Ifso,howaretheyused?Whatarethesuccessesandchallengesofhavingthisinformation/approach?
Ifnot,doyouthinkitwouldbeusefultohavethesetools?Howwouldyouusethem?Howcanyougettheminyourcounty/agency?
42
Trauma-InformedToolsandServices
• Symptomscanbecopingmechanismsoradaptiveresponses.•Ongoingassessmentandtrauma-informedservicesarecrucialtoeffectivetreatment.• Thelongertraumaticstressgoesuntreated,thegreatertheriskofdevelopingmaladaptiveandpotentialdangerousresponses.
Smallgroupdiscussion—• Examplesofworkingwithtraumainfostercare.• Useoftrauma-informedtoolsorservices.Successes&challenges.• Ideas/nextstepforincorporatingmoreT-I.Getspecific.
42

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 31
Segment5:AccessingMentalHealthServices
SegmentTime: 30minutes
Materials: Flipchartandmarkers
Slides: 43-51
DescriptionofSegment:Lecture:Quickoverviewofmental/behavioralhealthcareservicesprovidedbyCountyMentalHealthPlansandMedi-CalManagedCarePlansandtherightsofchildren,youth,andfamilieswithinthoseplans.Activity:Brainstormingforbestmental/behavioralhealthcareservices.
BeforetheSegment
Flipchartreadytocapturebrainstormedideas.
DuringtheSegment
p Activity5A:LectureSlide43beginsSegment5
Slide44—Person-CenteredApproachBecausetraumaandstrengthsaresouniquetoeachindividual,assessmentandtreatmentplanningrequiretheuseofaPerson-CenteredApproach.Thisapproachcanbedefinedas:
“ahighlyindividualizedcomprehensiveapproachtoassessmentandservicesthatisfoundedonanunderstandingoftheperson’shistory,strengths,needs,andvisionofhisorherownrecoveryandincludesattentiontoissuesofculture,spirituality,trauma,andotherfactors.”
Forchildrenandyouthinfostercare,somefactorstoobservearegriefandloss,sexualorientation,genderidentityandexpression,andanythingelsethatthechildoryouthtellsyouisimportant.Thisapproachsharestheplanning,development,andmonitoringofserviceswiththepersonforwhomtheservicesareintended.
Slide45and46—AccessingServices
EPSDT:AllchildrenandyouthinfostercareareeligibleforEarlyandPeriodicScreening,Diagnosis,andTreatment(EPSDT).ComprehensivefederalbenefitpackagewithinMedicaidspecificallyforchildrenuptoage21.Itincludes• medical,• dental,• substanceusetreatment,and• mental/behavioralhealthcareservices.
AllchildreninvolvedwiththefostercaresystemareeligiblefortheseMedicaidbenefits(Medi-CalinCalifornia).
AccessingMentalHealthServices
Segment5
44
Person-CenteredApproach
“Ahighlyindividualizedcomprehensiveapproachtoassessmentandservicesthatisfoundedonanunderstandingoftheperson’shistory,strengths,needs,andvisionofhisorherownrecoveryandincludesattentiontoissuesofculture,spirituality,trauma,andotherfactors.”
¾InstituteofMedicine(CrossingtheQualityChasm,2001)
Sharedplanning,development,andmonitoringcare.
44
45
AccessingServices
Early&PeriodicScreening,Diagnosis,&Treatment•FederallymandatedserviceforMedi-Caleligiblechildrenandyouthuptoage21•CoversALLnecessarytreatmenteveniftheserviceisnotcoveredunderthestateplanSpecialtyMentalHealthServices•Covereddiagnosis•Conditionnotresponsivetophysicalhealthcare•NecessarytocorrectoramelioratementalillnessandconditionsdiscoveredinscreeningbyMCP
45
Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 32
Emphasizespreventionandearlyintervention,andrequiresthatchildrenreceivecomprehensiveexaminationstoidentifyandaddresstreatmentneeds.
Slide46—AccessingServices(con’t)SMHS:ChildrenandyouthwhomeetmedicalnecessitycriteriaareeligibletoreceiveSpecialtyMentalHealthServices(SMHS).AccordingtotheMentalHealthandSubstanceUseDisorderServices(MHSUDS)InformationNotice16-061,inordertoreceiveSMHS,childrenandyouthmustmeetthefollowingcriteria:1. Haveacovereddiagnosis(listedintheTraineeBinder)2. Haveaconditionthatwouldnotberesponsivetophysicalhealth
carebasedtreatment;and3. Theservicesarenecessarytocorrectorameliorateamentalillness
andconditiondiscoveredbyascreeningconductedbytheManagedCarePlan,theChildHealthandDisabilityPreventionProgram,oranyqualifiedprovideroperatingwithinthescopeofhisorherpractice,asdefinedbystatelawregardlessofwhetherornotthatproviderisaMedi-Calprovider.
SpecialtyMentalHealthServicesunderMedi-CalareprovidedthroughthecountyMentalHealthPlans(MHPs)MHPsmayprovideservicesdirectlyand/orthroughanetworkofproviders.Everycountyhasatoll-freenumbertocontacttheirMHP--listisonpages25-27intheTraineeBindersOthermentalhealthservicesinMedi-Cal--
• TherapeuticBehavioralServices/Coach• IntensiveCareCoordination• IntensiveHome-BasedServices• TherapeuticFosterCare
(TheMHSUDSInformationMemosNo.16-061andNo.16-063areintheTraineeBinder)Slide47—InitialMentalHealthScreeningFlowChart(alsoonpage23ofthetraineebinder)
ThefollowingflowchartoutlinesthebasicprocessofbehavioralhealthscreeningandassessmentaccordingtotheCorePracticeModelScreeningdeterminesemergencyornot(childwelfare)EmergencyreferstoMHwhothendetermines5150statusandeitherarrangesassessment/hospitalizationormeetswithCFTtostabilizeandsafetyplan.Non-emergencygoestoCFTtodeterminenextsteps.Screeninghappensatleastatintakeandannually,butcouldbemoreoftenifneeded.
46
AccessingServices
• SpecialtyMentalHealthServicesunderMedi-CalareprovidedthroughthecountyMentalHealthPlans(MHPs)
• MHPsmayprovideservicesdirectlyand/orthroughanetworkofproviders
• Everycountyhasatoll-freenumbertocontacttheirMHP--listisinyourbinders
• OthermentalhealthservicesinMedi-Cal--ü TherapeuticBehavioralServices/Coachü IntensiveCareCoordinationü IntensiveHome-BasedServicesü TherapeuticFosterCare
46
ChildWelfareConductsScreening
Intake+Annually
EmergencyNeeds
CWreferstoDept.ofMentalHealthforWIC5150evaluation
YesDMHnotifies
legalguardianandarranges
assessment
NoMentalHealthmeetswithChildandFamilyTeamtostabilizeandsafetyplan
Non-EmergencyNeeds
ChildandFamilyTeamdeterminesbestassessment.
ANYqualified MediCalmentalhealthclinician
canassess.Then,countyMHPorMediCal ManagedCarearrangefor/provide
services.
NoCurrentBehavioral Health
Needs
CorePracticeModelBehavioralHealthScreeningFlow
47

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 33
Slide48—Beneficiaries’RightsAllcountymentalhealthplansmusthaveatoll-freenumber(listedbelow).Beneficiarieshavearighttoreceive:1. Ahandbookthatoutlineshowtofileagrievanceand/oranappeal
andwhatservicesareavailabletothem,and2. Anelectronicversionofaproviderdirectorywithcontact
information.
Ifnecessaryservicesaredenied,terminated,reduced,ordelayedanappealmaybefiled.Contactyourcounty’sMHPortheHealthConsumerAllianceat888.804.3536orwww.healthconsumer.org.
Slide49—InformalMentalHealthServices
InformalMentalHealthServicesareactivitiesdeliberatelyintroducedtopromotehealingandalleviatesymptoms,andtoprovidethechildoryouthopportunitiesfor:
• positivepeerinteraction,• self-discipline,• toleranceforfrustration,• enhancedself-esteem,• masteryofskills,• beingpartofsomethinglargerthantheirowncurrent
circumstance.
Theycanalsoprovideasupportiveadultwhomaybecomeamemberofthetreatmentteamorcanofferinsighttotheteam,likeacoachoraninstructor.Someinformalmentalhealthservicesthattheteammaychoosetoincludeinachild’streatmentplanarethefollowing:
• Exerciseorparticipationinorganizedorinformalsports,• Musicaltraininglikemusiclessons,choir,orband• Artorwritingclassesorindividualartisticexpression.• Participatingincommunitytheaterproductionsordrama
activitiesatschool• Interactingwithanimalscanbeverytherapeutic,ascan
volunteeringtohelpothers.• Meditation,changesindietandcookingorparticipatingin
foodpreparationandgardeningcanallhelpchildrenmanagestressandfeelconnected.
Involvementintheseactivitiesshouldnotbethreatenedorremovedaspartofdisciplinaryactionsastheyareimportanttothechild’sresilienceandwell-being.Usecreativityandtheuniqueneedsanddesiresofeachindividualwhendevelopingthisportionofthetreatmentplan.Developingideasfor
48
Beneficiaries’Rights
• ChildrenwhoareassessedforservicesunderEPSDT,shouldreceiveaNoticeofActioninformingthemoftheresults.
• Ifservicesaredenied,terminated,reduced,ordelayedanappealmaybefiled.
• Familieshavearighttoreceive:ü Ahandbookthatoutlineshowtofilea
grievanceandanappealandwhatservicesareavailable
ü Aproviderdirectoryinelectronicform
48
49
InformalMentalHealthServices
• Exerciseandteamsports• Musicaltraining• Joiningacluboractivity• Artandwriting• Dramaanddance• Workingwithanimals• Volunteeringtohelpothers• Meditation• Healthyeating/cooking• Gardening
49

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 34
managingstressandenjoyingactivitiesispartoftreatment,sothechildoryouth’sengagementisvital.
Slide50—FormalMental/BehavioralHealthInterventions
Dependingupontheneedsofthechildandtheavailabilityofservicesinthecommunity,thetreatmentteammightconsiderthefollowing:
• MedicationSupportServices;• oneofthemanytypesoftherapy,suchasindividual,
family,orgrouptherapy;• medicalcasemanagement,• therapeuticbehavioralservices;• wraparoundservices;• intensivedaytreatment;or• residentialcare.
Alldecisionsshouldprioritizetheneedsofthechildabovewhatismerelyconvenient.Aclearlinetothegoalsofthetreatmentplanshouldbeevidentinanyinterventionselected.
Activity5B:HowtoselectservicesHaveparticipantsturntopage28intheirbinders.ThereisaMental/BehavioralHealthServiceBrainstormingForm.Thisisjustabrainstormingtool,notanofficialpieceofpaperwork.Instructions:Havetheparticipantsfilloutthisformascompletelyastheycanjustoffthetopoftheirheads.Writedownanyoneoranyservicesthattheythinkmightbeusefulforachildoryouthinneedofmentalorbehavioralhealthcare.Reportout—Askthelargegrouptodiscussthesetogetherusingthefollowingprompts:
• Whatresonated?• Wasthisuseful?(Theymightthinkaboutkeepingitupdatedor
addingelementstoresourcedirectoriestheyalreadyuse.)• Whataresomewayswecanincreasethequalityanddiversityof
careinourareas?• Didanyonecomeupwithnextstepsiftherearen’tanygood
serviceoptions?Suggestionstostart:CallyourCountyMHPContactandaskAskotherfolksinyourdepartmentBesureyoursupervisorknowsabouttheservicegapKeeptalkingaboutthegapuntilthereisaplantofillit
Thereisanotherform,similartothisone,inthehandoutfolderthatcanbeusedtobrainstormaboutoneparticularcase.Itisdesignedtohelpidentifystrengthsandresourcesinthechild,family,andtreatmentteamtobuildon.
50
FormalMentalHealthInterventions
• MedicationSupportServices• Therapy—behavioral/cognitive/relational• Counseling—individual/family/group• Medicalcasemanagement• Therapeuticbehavioralservices• Wrap-aroundservices• Intensivedaytreatmentservices• Residentialcare• Psychotropicmedication
50

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 35
Mental/Behavioral Health Services Brainstorming Form County or Agency:
Role in Mental/Behavioral Health for foster children:
County MHP Provider’s Name and Contact Info: Other Useful Partners’ Names and Contact Info: Agency strengths and resources:
Strengths and resources outside the agency:
What gaps/needs are left after considering these strengths and resources?
Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 36
What informal treatment options are available to children and youth served by your agency?
Are these options culturally sensitive? Safe for potentially traumatized children? Diverse?
What informal treatment options do you wish you had access to for your children and youth?
What formal treatment options are available to children and youth served by your agency?
Are these options culturally sensitive? Trauma-informed? Diverse?
What formal treatment options do you wish you had access to for your children and youth?
What can you do to increase the quality and diversity of treatment options? Who can you ask to help develop needed resources/services? Can you partner with another agency/entity already engaged in this work? What is your next step?

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 37
Segment6:PsychotropicMedicationSegmentTime: 60minutes
Materials: Dice—oneforeachgroupoftwotraineesFlipchart
Slides: 52-68
DescriptionofSegmentWatch:Videoclipofformerfosteryouthdescribingtheirexperienceswithpsychotropicmedications.Read:FosterYouthMentalHealthBillofRights.Lecture:Someusesforpsychotropicmedications,aswellaspotentialrisks/benefitsofthesemedications.Watch:Videoclipsaboutsideeffects.Lecture:Howtofindinformationaboutsideeffectsandadversereactionsandhowtomonitortheseeffects.Activity:Roleplaysideeffectconversationsandsafetyplanning.
BeforetheSegment
Makesureyouhavediceforeachgroupoftwoparticipants.Ifyoudonothavedice,youcancalloutanumberbetweenoneandsixforeachgroupateachfive-minuteinterval.
DuringtheSegment
Slide52beginsSegment4
p Activity4A:ShowvideoSlide53—FosterYouthVoicesVideo
Watchvideoclipofformerfosteryouthsharingtheirthoughtsonpsychotropicmedication.5minutes.
Quicklydebriefasalargegrouptoansweranyquestionsorprocessthecontent.
Thesevideosservetwopurposeshere:tooutlinethemostdangerousissuestobeavoidedwithPsychotropicMedication,butalsotore-centerthegroupafterthelunchbreakontothechildrenandyouthwhoseoptimalhealthandwell-beingarethepurposeofthistraining.
PsychotropicMedication
Segment6
52
Video
FosterYouthVoices
52
Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 38
p Activity4B:Slide54—Locatedonpage30intraineebinders.Havetheparticipantsreadovertheseoutloudasagroup.
53
FosterYouthMentalHealthBillofRights
53
Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 39
p Activity4C:Lecture—uses,benefits,andrisksofpsychotropicmedicationinfostercare
Slide55—Psychotropicmedicationinfostercare
• Non-pharmacologicalinterventionsarefirst-linetreatmentapproach.Medicationistobeconsideredonlywhenotheroptionsarenotsufficient(outsideofemergencies).
• Medicationcanbeprescribedafterthoroughassessmentidentifiesneedandcleartreatmentgoals.Keepinmindthatitmaytakemorethanonemeeting/session/cliniciantoconductathoroughassessment.
• Whennecessary,medicationisbestused:o withothersupportiveinterventionsando aspartofacomprehensivetreatmentplan
• Respectforthedignityofthechildandfamilyisaprerequisiteforalltreatment.
Sciencehasyettofullydeterminetheeffectsthatpsychotropicmedicationmighthaveonthedevelopingbrainsandbodiesofchildrenandyouth,butitisclearthatsomesideeffectscanbequiteseriousandlong-lasting.Consequently,thedecisiontousepsychotropicmedicationshouldbeconsideredverycarefully.Dependinguponthesymptomsachildisexperiencing,therearethreegeneralpathsforusingmedicationoutsideofemergencies:1. Medicationmightnotbeusedatallintheexampleoflearned
defianceorifsymptomsaredeterminedtobetheresultoftraumaratherthanmentalillness.
2. Theteammaydecidetoincludemedicationafterotherinterventionsweretriedbutfailedtoaddressallthesymptoms.Moderateanxietyordepressionmightbeanexampleofthisscenario.
3. Medicationmaybepartofaninitialtreatmentplan,forexample,ifthechildwereexperiencingsevereAttentionDeficitHyperactivityDisorder,acutesymptomsofdepression,orpsychosis.
Ifthephysicianandchildandfamilyhavedecidedthatmedicationisnecessary,itshouldbeusedinconjunctionwithotherinterventionstosupporttheholistichealthofthechildexceptinrareemergencysituations.Inafewcases,psychosocialinterventionsarenolongerrequiredwhentheyhavealreadybeensuccessfullyemployed,butcontinuingmedicationisneededtopreventrecurrenceofsymptoms.Regardlessofwhattreatmentplanisdesigned,respectforthedignityofthechildandfamilyisaprerequisite.Alltreatmentplansshouldincludetheinputandconsentofthechildandfamily,identifyandutilizetheirstrengths,aimtoincreasetheirresilience,andprioritizetheirneeds.
54
PsychotropicMedicationinFosterCare
•Non-pharmacologicalinterventionsarefirst-linetreatmentapproach.Medicationconsideredonlywhenotheroptionsarenotsufficient.•Medicationprescribedafterthoroughassessmentidentifiesneedandcleartreatmentgoals.•Whennecessary,medicationisbestused:
• withothersupportiveinterventionsand• aspartofacomprehensivetreatmentplan
•Thechildandfamilyshouldbeinformedandinvolvedateverystageofdecisionmaking.
54

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 40
Slide56—InformedConsentforMedication
• Childrenandyoutharetobeincludedintheconsentandassentprocesstothemaximumextentappropriatebasedontheirdevelopmentalstage.
• Child,family,andcaregiverareinformedoftherisksandpotentialbenefitsof:
o Proposedmedication(name,dose,effects),and
o Alternativetreatmentsincludingtheabsenceoftreatment.
• Thoroughdiscussionofanyseriousadverseeffectstowatchforandwhenandhowtocontacttheprescriberifanythinghappens.
• PrescribersconsultwithSW/POaboutwhocanprovidelegalconsent,andreleaseofHIPAAinformation.
Slide57—Limitsonpsychotropicmedicationinfostercare
• ContinuumofCareReformTitle22makesitclearthatpsychotropicmedicationsshouldnotbeusedforthepurposesofdisciplineorchemicalrestraint.Inacutepsychiatricemergencies,chemicalrestraintmaybenecessary.Thisshouldbeextremelyrare,andveryshort-term.
• Youtharenottobecoercedintotakingmedicationasaconditionofgettingintoorstayinginafostercareplacement.
• Safeandconsistentadministrationofmedicineattheprescribedtime,frequencyanddosageisasafetyissue,andmustbeaddressedinthetreatmentplan.Ifsafeadministrationcannotbeachieved,theCourtshouldbenotifiedandmedicationshouldbereconsidereduntilsafetyconcernshavebeenaddressed.
• Safeandaccurateself-administrationofmedicationisideal.Ifitisnotpossibleforthechildoryouthtoadministertheirmedsthemselves,itisnecessarytoassistthem.
• Whenassistingachildoryouthwithadministrationofmedication,itisimportanttoconsidertheirpreferencesregardinghowandwhenheorshewouldliketotakethemedicineaslongasthosepreferencesareinlinewiththeprescriber’sinstructions.Assistonlyonechildatatimeoutsidethepresenceofotherchildren.Thishelpsprotecttheirprivacyandconfidentialityaswellaspotentiallyreducingstigmaandshamethatmayaccompanytakingmedication.
• Documenttheappropriateprocedureforadministrationandeveryoccurrenceinthechild’srecordincludingdate,time,anddose.
• RemindtraineesthatthefullBillofRightsdocumentwithadditionalresourcesisinthesupplementalmaterialsintheirbinder.
55
InformedConsentforMedication
• Childrenandyoutharetobeincludedintheconsentandassentprocesstotheextentfeasiblebasedontheirdevelopmentalstage.• Child,family,andcaregiverareinformedoftherisksandpotentialbenefitsof:• Proposedmedication• Alternativetreatmentsincludingtheabsenceoftreatment
• Anyseriousadverseeffectstowatchforandwhenandhowtocontacttheprescriber• PrescribersconsultwithSW/POaboutwhocanprovidelegalconsent,andreleaseofHIPAAinfo.
55
57
LimitsonMedicationinFosterCare
• Medicationisnottobeusedfordiscipline,coercion,orchemicalrestraint.• Youthcannotbeforcedtotakemedicationasaconditionofgettingintoorstayinginafostercareplacement.• Monitoringschedule/dosageandarrangingcorrectadministrationarepartoftreatmentplanning.• Self-administrationshouldbesupportedwheneverpossible.
57

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 41
Slide58—AssistingwithSelf-Administration
Self-administrationofmedicationistheidealtreatmentplan.Itensuresresponsibilityandownershipoftheprocessandcanhelpempoweryoungpeople.Sometimesthiswillbeasimpleprocess;forotheryouth,itmaybemoreofachallenge.Asalways,utilizethewholeteamtohelp.Herearesomeideastoassistwithself-administration:
§ Makesurethattheyoungpersonisawareofandthoroughlyunderstandstheprescriber’sinstructionandhowtogetadditionalinformationifthereisconfusion.Goovertheplanthoroughlyandmakeparticularnoteoftheanticipatedeffects,bothpositive¾suchaspossiblesymptomrelief¾andnegative¾likepotentialsideeffects.
§ Regularlyreiteratetheimportanceoftakingthemedicationaccordingtotheinstructions.Itisnotenoughtosaythisonceatthebeginning.Itisimportanttoreinforcethismessagethroughoutthecourseoftreatment.Inparticular,makesuretheyouthunderstandsthatitcouldbequitedangeroustomissdosesorstoptakingmedicationwithoutthesupportofadoctor.Also,explainthattheywon’tbeabletotellifthemedicationisworkingornotunlesstheytakeitasinstructed,andthattheymaynotgetanybenefitfromthemedicationatallifitisn’ttakencorrectly.
§ Storethemedicationinasecurelocationthattheyouthcanaccesswhentheyneedto.Itisimportanttokeeptrackofmedicationandtobeawarewhenrefillsarecomingup.TheCommunityCareLicensingDivisionhasspecificguidelinesforgrouphomesandotherfacilitiesregardingmedication.
§ Becreativeaboutsupportingyouthtostayonschedule.Colorfulcalendarsorpillboxescanhelpmaketheprocessseemlessdullorclinical.Iftheyouthisusingacellphoneorcomputeranyway,somehelpfultoolscansupporttheirself-administration.
MangoHealthisamedication-trackingappthatisdesignedlikeagame.Participantscanearnpointsforstickingtotheirschedule,andtheycanevenwinreal-worldprizes,likegiftcards,forreachingtheirgoals.
MedHelperandMedCoacharetwoothermedication-trackingappsthatmighthelpkeepyouthontrackandprovidetheircaregiveranddoctorwithinformationabouthowtheyaredoing.Someyouthmayevenwanttokeeptrackoftheirsymptomsandsideeffectsusingthenotesfunctionwithintheappitself.
§ Whensymptomsimproveandthechildisfeelingbetter,itcanbeparticularlychallengingtokeeptakingmedication.Itisveryimportantthatthetreatmentteamandthecaregiverhaveregularlyscheduledcheck-insaboutsymptomsandmedication.Youngpeopleneedsupportthroughoutthecourseoftreatment,notonlywhenthingsaredifficult.Itisimportanttolistencarefullytowhattheysayabouthowtheyfeelandwhattheywantwhenitcomestotheirownhealthcare.
57
AssistingwithSelf-Administration
• Ensureyouthunderstandstheinstructions• Regularlyreiteratetheimportanceofinstructions• Usecalendars,pillboxes,textreminders,orappstohelpMangoHealth–earnrewardsforkeepingonscheduleMedHelper—freeappthatallowsusertotakenotesMedCoach—canproducereportforcaregiverordoctor
• Symptomimprovementcanbeachallengingtimetostayonschedule• Listentothedesiresandopinionsoftheyouth
57

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 42
§ Youngpeopledon’talwaysknowwhatisbestforthem,buttheyarealwaystheexpertsinhowtheyfeel.Buildingatreatmentplanthatwillworkbestforeachspecificpersonrequiresthattheybepartoftheplan.Everypersonisunique,soremainopentoalltheoptions.Continueaskingquestionsandexploringuntilyoufindtherightfit.
§ Scheduleregularcheck-inswiththeyouthandmembersoftheteamabouttreatmentandsymptoms.Anddiscussallchanges,notjustthetargetsymptoms.Bereliableandconsistent.
Slide59—Risks
Psychotropicmedicationsareassociatedwithanarrayofpossiblerisks.Theyvarywidelydependingupontheageanduniquecharacteristicsofindividualswhotakethem.Someoftheserisksarecalledsideeffects,meaningthatmedicationcancauseeffectsotherthanorinadditiontotheintendedones.
Individualshaveexperienced:• increasedsuicidalideation• sleepdisturbance• sleepinessandlethargy• difficultymovingaround• rapidweightgainleadingtoobesity• pronouncedchangesintheirbloodsugarandmetabolismsometimes
leadingtodiabetes• nervousness• restlessness• irritability• headaches• upsetstomachorchangesinappetitearealsopossible.Alltheserisksshouldbemadecleartothechildandfamilywhentreatmentdecisionsarediscussed.Childrenandfamiliescannotmakeinformeddecisionswithoutbeingawareofthesepotentialrisks.TheCaliforniaGuidelinesdirecttheprescribingphysiciantoinformthechild,family,andothersinvolvedintreatmentplanningabouttherisksandbenefitsofthemedicineandofothertreatmentoptionsincludingtherisksandbenefitsofnotreatment.Rarely,individualsmayhaveadversereactions• Chronicphysicaland/orneurologicalillness• Permanentfacialorbodyticsandtremors• DisabilityanddeathItispossibleforchildrenoryouthtobecomeaddictedtocertainmedications,andthisriskshouldbeincludedindecisionmaking.Additionalrisksarepresentwhenmedicationsarenottakenaccordingto
58
RisksofPsychotropicMedication
• Increasedsuicidalideation• Sleepdisturbance• Sleepinessandlethargy• Rapidweightgainandobesity• Bloodsugarandmetabolism• Nervousnessandirritability• Headachesandupsetstomach
Otherissues:• Adversereactionsandchronicillness• Addiction• Usingandstoppingcorrectly
58

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 43
theinstructions.Treatmentplansshouldincludedetailsaboutsafeandconsistentadministrationofthemedication,ensuringanadequatesupplyofmedication,andasafetyplanforhowtostoptakingthemedicationshouldthatbenecessary.
Slide60—SubstanceUseandMedication• Carefulconsiderationofthechild’soverallhealthandneedsiscrucial
totreatmentplanning.Ifthechildoryouthusesun-prescribedmedications,otherdrugs,oralcohol,itisimportanttoassesstheriskofaddingapsychotropicmedicationaccordingly.
• Interactionsbetweenmedicationsanddrugsoralcoholcanbepowerfulandtoxic,evenlethal.
• Sometimes,individualsareusingdrugsoralcoholtoself-medicateandtoessentiallytreatthesamesymptomsthatthetreatmentplanisattemptingtoaddress.
• Alternatively,substanceusedisorderitselfcanmimicthesignsorsymptomsofotherdysregulations.Ifthatisthecase,thatdisordermustbetreatedfirstinordertoaccuratelydiagnosisthechildoryouth.
• Ifbothsubstanceusedisorderandotherbehavioralhealthissuesarepresent,dualdiagnosistreatmentshouldbeprioritizedinthetreatmentplan.Thismeanstreatmentthatfocusesontheintersectionandoverlapofproblematicsubstanceuseandseriousmentalhealthneeds.Onewaytostartistomakesurethatsomeonetrainedinsubstanceuseisonthetreatmentteam.
Slide61—PotentialBenefits
Thebesttreatmentplanforanindividualmayincorporatemedication,whichhasthepotentialto
• improveschoolperformanceandabilitytoconcentrate• decreasetheexperienceofanxietyorworry• reducesymptomsofdepression• improveoreliminatefrequentphysicalpainorsomatic
complaints• reduceoreliminatenightmaresandothersleepdisturbance• limitexcessiveaggressionortempertantrums• improvemood
Thesepotentialbenefitsaretobeweighedagainstthepotentialriskswhendecidingwhetherornottoincludemedicationinachildoryouth’streatmentplan.Itisimportanttonotethatallthesebenefitsarealsopossibletoachievewithouttheuseofpsychotropicmedication—everythingdependsontheuniquecircumstanceofthechildandtheirenvironment.
59
SubstanceUseandMedication
• Drugsandalcoholcaninteractdangerously—evenlethally—withpsychotropicmedication• Substanceusecanmimicthesignsandsymptomsofmentalillness• Isoftenself-medicationfortraumaand/ormentalhealthissues• Dualdiagnosistreatmentispriority
59
60
PotentialBenefitsofMedication
• Betterschoolperformanceandconcentration
• Lessenanxietyorworry
• Decreasedepressionsymptoms
• Addresssomaticcomplaints
• Reducenightmares• ImprovemoodandmoodregulationNOTE:Allthesebenefitsarealsopotentiallyachievablewithouttheuseofpsychotropicmedication
60

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 44
Forchildrenandyouthinfostercare,notallofthesepotentialbenefitsarefullybackedbyevidence.Therefore,itisvitalthattheintroductionofmedicationsisincremental;beginningwithalowdose,andslowlyadjustedwhilecarefullytrackinganypositiveornegativeeffects.
Slide62—AttentionDeficitandAnxiety/DepressionMedications
AttentionDeficitandHyperactivityDisorderorADHD:Arelativelycommondiagnosisforchildrenandyouth.PsychomotorstimulantslikeRitalinandAdderallareoftenprescribedtotreatthesymptomsofADHD.Theycanhelpchildrentoconcentrateandcontrolhyperactivity.Commonsideeffectsincludedecreasedappetiteorstomachdiscomfortandpoorsleep.Non-stimulantssuchasStratterahavethesamebenefitsaswellasdecreasedcompulsivebehaviors.Thecommonsideeffectsarealsosimilar—stomachdiscomfortandpoorsleepalongwithheadache.AnxietyandDepression:Symptomsrelatedtoanxietyanddepressionmayalsobeaddressedwithmedication.SelectiveSerotoninReuptakeInhibitorsandAtypicalAntidepressantssuchasProzac,Zoloft,Celexa,WellbutrinorLexapromaydecreasedepressivesymptoms,improvemood,anddecreaseanxiety.Theycancausenausea,anddisturbsleep.Theyalsoposeanincreasedriskofseizureandanincreasedriskofsuicidalideationespeciallyinadolescents.Thesesideeffectsmayincreasewithirregularadministration,soshouldbecarefullyconsideredifproperadministrationisdifficultorunlikely.
Slide63—MoodandPsychoticDisorderMedications
Mooddisorders:ToaddressthesymptomsofmooddisorderssuchasBipolarDisorder,doctorsprescribemoodstabilizerslikeLithiumorAnticonvulsantslikeDepakote.Thesemedicationsmayimproveorstabilizemoodsymptomsandimproveimpulsecontrol.Lithiumcancausedrymouth,tremor,stomachdiscomfort,weightgain,memoryproblems,thyroidandkidneyproblems.Anticonvulsantsalsohaveseriouspotentialsideeffectssuchasdrowsiness,nausea,seriousrashes,liverproblems.Periodiclabtestsandcarefulmonitoringbyaphysicianisnecessarywhilechildrenoryoutharetakingthesemedications.Psychoticdisorders:Antipsychoticmedicationsareapotentclassofpsychotropicmedications.Theyaredividedintotwocategories,NewerandOlder.Theyareusedtotreatveryserioussymptomssuchashallucination,delusions,anddisorderedthinking.Theycancauseextrapyramidalsideeffects(EPS)suchasshakiness,drooling,andstiffness.Theyoftencauserapidweight
30
UsesofPsychotropicMedication:MentalHealthDiagnoses
AttentionDeficit/Hyperactivity• Psychomotorstimulants• Non-stimulantsü Bothcanhaveanegativeeffectonappetiteandsleep
AnxietyandDepression• SelectiveSerotoninReuptakeInhibitors(SSRIs)• Atypicalantidepressantsü Increasedriskofsuicidalideationandseizure
31
UsesofPsychotropicMedication:Mood,PsychoticDisordersMooddisorderslikebipolardisorder•Moodstabilizers• Anticonvulsantsü Bothimprovemoodandimpulsecontrolü Bothhaveserioussideeffectstobemonitoredclosely
Psychoticdisorders• Antipsychotics—newerorolder• Neuroleptics/Tranquilizersü Decreasepsychoticsymptomsü Cancausemovementdisordersaswellasweightgain
andseriousphysicalhealthproblems

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 45
gain,heartandbloodirregularities,permanentticsandtremors,anddiabetes.
Slide64—Medicationstoaddresssideeffects
Sleep:Manypsychotropicmedicationshavethepotentialtocausesleepdisturbance.Doctorsmayprescribesedativesorhypnotics,andsometimessleep-promotingmedicationslikeBenadryltohelpchildrensleep.Thesemedicationshavethepotentialtobehabit-formingandcancauseadditionalsideeffects.Extrapyramidal(EPS):Theseveresideeffectsfromantipsychoticscanbetreatedwithanticholinergicmedications.Thesecanreducetheshakiness,drooling,andstiffnessassociatedwithEPS.Multiplemedications:Itisimportanttonotethatmultiplemedicationsandusingmedicationtotreatsideeffectsofothermedicationisnotrecommendedpractice,butdoesoccur.Aswithallmedication,thesedecisionsshouldbecarefullyanalyzedbytheentiretreatmentteamtoensurethebestoutcomesforthechild.Childrenwithseveralsimultaneousprescriptionsareatincreasedriskforadverseeffects.Useofmultiplemedicationsshouldbecarefullymonitoredbythefamilyandthephysician.
Slide65—Watchvideoclipsofformerfosteryouthdescribingthesideeffectstheyexperiencedwhileonmedication.
Rochelleclipis29secondsSadeclipis49seconds
Theseclipsareareminderofwhythistrainingmattersandwhatthelong-termresultscanlooklike.NOTE:ThemonitoringofsideeffectscanbeachargedsubjectforPHNsandchildwelfareworkers,manyofwhombelieveitisonlywithinthescopeoftheprescriber’sroletodothatmedicalportionofoversight.
Usethistimetoencouragethemtoapproachthetopicofsideeffectsandotherchangesthatresultfrommedicationassomethingtheentireteammustbevigilantaboutintheinterestsofthechild.
Again,theydon’tneedtobemedicalexperts,theyonlyneedtousetheresourcesattheirdisposalintheGuidelinesandontheirtreatmentteam(includingandespecially)thechildandfamily)toadvocateforthechild.
32
MedicationstoTreatSideEffects
Sleepdisturbance• Sedatives,hypnotics,orothersleep-promotingmedicationsü Cancausedependencyandtheirownsideeffects
Extrapyramidal(EPS)• Anticholinergicmedicationsü DecreaseEPSsymptoms—shakiness,drooling,
andstiffnessü Drymouth,blurredvision,anddrowsiness
34
SideEffects
Rochelle• https://youtu.be/qQ7sUvIKzvs
Sade• https://youtu.be/kwp8i7mhNRs

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 46
Slide66—SideEffectsSafety:Ifsideeffectsaresuspectedoridentified,safetyisthepriority.Followallemergencymedicalproceduresifnecessary,andtakenecessarystepstoensurethesafetyofthechild.
• Consultwiththeprescribingphysicianimmediatelytodetermineifchangesneedtobemade.
• Donotallowthechild/youthtosimplystoptakingmedication.Thereisusuallyaprotocolforweaningoffpsychotropicmedications,anditisvitaltofollowthosedirections.
• Ifdoseorschedulechanges,followupwiththerequiredCourtdocumentsanddocumentthechangeinthehealthrecordandthechild’sfile.
Planahead:Findoutwhatsideeffectsarepossiblewhenthetreatmentplanwithmedicationismade.Haveasafetyplancreatedintheeventthatsideeffectsemerge.Itisimportanttobeawareifthereareanyknowninteractionswithotherdrugsoralcoholaswellasstepstotakethatmightreducethelikelihoodofsideeffects.
• AppendixBoftheCAGuidelinesistheprimarydocumentCDSShasidentifiedforreferenceaboutspecificmedicationsandtheparametersfortheiruse(dosage,sideeffects,potentialinteractions,etc.)LACountyiskeepingthisdocumentup-to-dateandpubliclyavailableontheirwebsite.
• Youcanlearnmoreaboutpossiblesideeffectsbyresearchingonsiteslikemedlineplus.govorfindingthepackageinsertfortheprescribedmedication,whichareusuallyavailableonline.
Slide67—DocumentingSideEffects• Socialworkersandprobationofficersmustensurethat
monitoringoccurs.ItmaybethePHNorcaregiverwhodospecifictasks,butthesocialworkerisresponsibleformakingsureithappensasoftenandthoroughlyasnecessary.
• Socialworkersandprobationofficersdon’tneedtobetheexpertsinknowingallthedetailsofthisinformation,buttheymustcollectitfromthedoctorsandhealthprofessionalswhoareexpertsandmakesurethatthechildandcaregiverandfamilyhavereceivedtheinformationandunderstandit.
• Regularlyaskthechildoryouthtodescribetheirexperiences—bothphysicalandemotional—sincetakingthemedication.Askthemtocomparethoseexperiencestohowtheyfeltbeforetakingmedication.Thisassessmentshouldoccurthroughoutthedurationofthetreatmentassideeffectscandevelopatanytime.
• Ifdevelopmentallyappropriate,thechildshouldbeawareofeffectstowatchoutforandwhotheyshouldtelliftheyexperiencesomethingnew.
38
SideEffects
• Followallemergencyandsafetyprotocols• Consultwiththeprescribingphysician• Documentationandcourtformneededifchangingmedicationordose
• Beprepared• Safetyplan• Gotomedlineplus.gov fordetailedinformation• Readthepackageinsertfromthemedicine(usuallyavailableonline)
• Possibleinteractionswithalcoholorotherdrugs• Howtoreducepotentialsideeffects
37
DocumentingSideEffects
• Socialworkerisresponsible,butnotexpectedtobetheexpert• Askthechildoryouthdirectlyandfrequentlyabouttheirexperiences—physicalandemotional• Reportanddocumentanychanges• Ensuredoseisappropriate• Speakwithfamily,caregiver,andothers(schoolpersonnel,churchandcommunitymembers)aboutchangesinbehavior,mood,orphysiology

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 47
• Theprescribingphysicianshouldmakecleartothetreatmentteamhowtheycanbecontactedshouldsomethingarise.
• Therecommendeddoseshouldbeageappropriate.• AppendixAoftheCaliforniaGuidelineshasageparameters.Even
ifthedosefallswithinacceptableguidelines,itmaybetoomuchortoolittleforaspecificindividual,soitisimportanttomonitortheirresponses.
• Itisalsoimportanttocheckwiththefamilyandcaregiversofthechildoryouthtoseewhethertheyhavenoticedanychangesinthechild’smood,behaviororappearance.Schoolpersonnel,friendsfromchurchandthecommunitymayalsobeabletoidentifyiftherearechangesinthechild’sbehaviorintheseotherenvironments.
• Collectivevigilanceandfrequentcommunicationcanhelpidentifyandaddresssideeffectsfrompsychotropicmedications.
p Activity4D:Quickroleplay(Total20minutes,4scenariosat5mineach)
Slide68—Conversationtopicsrelatedtomedication
Pairtraineesintogroupsoftwoandletthemdecidewhowillplaytheroleofsocialworker/probationofficer/orPHNfirst.Theothertraineewillplaytheroleofthechildorfamilymember.
Eachpairofparticipantsrolltheirdietodeterminewhichscenariotheywillworkonfirst.
Letthemroleplayforfiveminutesbypracticingtheconversationsthataccompanyrisks/benefits,sideeffects,andsafetyplanninginthatscenario.
ThenthepairwilltradewhoistheSO/PO/PHNandrollthedieagaintoidentifythenextscenariotheywillroleplay.
Repeatsteps2-4fourtimesuntileachparticipanthasplayedthehelperroletwice.
Walkaroundtheroomtoobservefordevelopmentallyappropriateconversation,useofthesafetyplanningtool,andtoanswerquestions.Ifitcomesup,remindfolksthattheyaren’texpectedtobetheexpertsonthemedicalaspects,butinsteadtoaddresstheneedsandcontext.ActasLINKtoresources,notBEalltheresources.
Havethegroupreportback—
Whatresonated?
Whoelsewouldbeinvolvedintheseconversationsinrealsituations?
68
PracticeConversations
• Risks/benefits
• Assessingandmonitoring
• Safetyplanning
• Advocacy
68

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 48
SIXSCENARIOS(locatedonpage37ofTraineebinder):1.Six-year-oldElizabethhasrecentlybeenprescribedRitalintoaddressrestlessness.Hertreatmentplancallsforevaluationofsymptomsandsideeffects.
2.Juliusis17yearsoldandabouttotransitionoutoffostercare.HecurrentlytakesaSelectiveSerotoninReuptakeInhibitor(Celexa)foracuteanxiety.Hisfostermotherisconcernedthathewillstoptakingitonceheleavesherhome,andwouldlikehimtohaveasafetyplan.
3.Afterherappointmentwiththedoctor,Phoebehassomequestionsabouttherisksandbenefitsoftakingtheantipsychotic(Zyprexa)thatherdoctorisrequestingfromthecourttoaddressherimpulsivityandaggression.Sheis15yearsoldandlivesinagrouphome.
4.CharlotteistenyearsoldandshehasbeentoseehertherapistweeklyforthreemonthsandistakingVistariltohelphersleep.Shefeelsthathersleepisbetter,butthetherapyismakingthingsworse,andtheconversationsshehasmakehermoreupset.Shewantstostopgoing.
5.Derrickisafosterparent.Hewastoldbythedoctorathisfosterson’slatestappointmentthatAdderalldoesnothaveanysideeffects.Hiseight-year-oldfostersonwasalreadytakingitwhenhecametoDerrick’shome.
6.TheJV-220ApplicationforSamtostarttakingZolofttoaddresssymptomsofseveredepressionwasapprovedbythecourt.Samis13yearsold.Discusstheriskofsuicidalideationrelatedtothisdrugandaboutsafetyplanning.
Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 49
Segment7:UsingtheCaliforniaGuidelinesDocumentsSegmentTime: 60minutes
Materials ScenariosCaliforniaGuidelinesdocumentandappendicesCopiesoftheAnswerKeyforUsingtheGuidelines
Slide: 69-81
DescriptionofSegmentLecture:WhataretheGuidelinesforandwhatisincluded.Activity:GetfamiliarwiththeGuidelines
BeforetheSegment
InstructtheparticipantstoretrievetheircopyoftheGuidelinesfromthebackpocketoftheirbinder.Thisisacopyofthemostrecentdocumentandallappendices.Makesuretoinformthemthatitwillberevisedatleastyearly,sotheyshouldplantoretrievenewcopiesregularlyfromtheCDSSwebsiteortheircountyagency.
DuringtheSegment
Slide69beginsSegment7p Activity7A:LectureSlide70—WhataretheGuidelines?CreatedcollaborativelybyCDSSandDHCS.Itoutlines:
Sharedvalues,expectations,andprinciplesofpsychotropicmedicationuseinfostercare.Itisdesignedtobeanadvocacytooltohelpguidenon-medicalprofessionalswhenworkingwithdoctorsandpsychiatristsandothermedicalpersonnelorserviceproviders
Ithasseveralimportantgoals:1. Increasedvisibilityofstrengthsandneedsofchildrenandyouth
withemotional,cognitive,and/orbehaviordysregulation2. Reductionofsocialstigmaduetodysregulation3. Promotingbestpracticesinthestate’scommitmenttoprovideboth
formalandinformalmental/behavioralhealthservicestochildrenandyouthincare.
Slide71—WhataretheGuidelines?(con’t)Expectationsabout:
• Treatmentplans,assessment,anddiagnosis• Whatprescribersshouldconsiderforcertainactivities• Beforeprescribing• Whenprescribing• Whenevaluatingwhetherornotatreatmentiseffective• Prescribinginanemergency
FourAppendicesA:PrescribingStandardsbyAgeGroupB:Parametersfordoserangeandschedule(LACounty’sParameters3.8)
69
UsingtheCaliforniaGuidelines
69
Segment7
70
WhataretheGuidelines?
• Sharedvalues,expectations,andprinciplesasagreeduponbyCDSSandDHCS• Tooltousewithprescribers,thecourt,servicedeliveryagencies,caregivers,andotherstoreachoptimaltreatmentdecisions• Goals:ü increasingvisibilityofthestrengthsandneedsof
childrenandyouthwithemotional,cognitive,and/orbehavioraldysregulation,
ü eliminatingsocialstigma,andü promotingbestpracticesintheprovisionofformal
andinformalmentalhealthservices70
71
WhataretheGuidelines?
Theyoutlineexpectationsabout:• Treatmentplans,evaluation,anddiagnosis• Prescribers’considerationsforcertainactivities
ü Beforeandwhenprescribingü Evaluatingtreatmentefficacyü Prescribinginanemergency
Fourappendices:• PrescribingStandardsbyAgeGroup• Parametersfordoserangeandschedule(3.8)• ChallengesinDiagnosisandPrescribingwithrecommendations• PrescribingAlgorithm(DecisionTree)
71

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 50
C:ChallengesinDiagnosisandPrescribingincludingrecommendationsD:DecisionTreeforPrescribingSlide72—PrinciplesandValuesTheGuidelinesoutlinethesharedprinciplesandvaluesofCDSSandDHCSregardingtheuseofpsychotropicmedicationwithchildrenandyouthinfostercare.
• Alwaystopromotesafety,permanence,andwell-being• Realpartnershipswiththeimportantpeopleinthechild’slife• Workingfromachild-centered,strength-basedperspectiveto
createtrulyindividualizedtreatment• Providingthehighestqualityofcarethatisintegratedwithinthe
child’scommunityandincollaborationwithanyhelpfulpartners.• Psychotropicmedicationisnottobeemployedasthesole
intervention(exceptinextremelyrarecaseswhentreatmentwithmedicationissuccessful,butneedstobecontinued),butratheraspartofarobustoveralltreatmentstrategyemployingbothformalandinformalinterventions.
Slide73—TreatmentPlan
Atreatmentplanisthedetaileddescriptionofservices,supports,andtreatmentsthatwillbeemployedtoeliminateorreducethechildoryouth’sidentifiedsymptoms,emotionaldistress,and/orproblematicbehaviors.Itisthedocumentthatdescribeshowtheteamwillattempttoimprovethingsforthechild.Treatmentplanningisalwaysdonecollaborativelywithchildrenandtheirfamilies,whetherornotaChildandFamilyTeamiscreated.Amulti-disciplinaryteamfunctionsverysimilarly,oranevenless-structuredsupportivegroupcanbesuccessfulincreatingaqualitytreatmentplan.Theimportantthingistoincorporatediverseperspectivesthatbuildaroundtheuniqueresources,abilities,strengths,andneedsofeachspecificchildandhisorhernaturalsupportnetworkandcommunity.Ifachildistooyoung,oriftherearedevelopmentalorprotectiveissuesinthecasethatpreventcollaboration,everyeffortshouldbemadetoinvolvearepresentativetospeakonbehalfofthechildindecisionmakingmeetings.Toeveryextentpossible,thechildortheirrepresentativeshouldbeincludedinalltheplanning,review,andre-assessmentofthetreatmentplan.Treatmentplansshouldseektoutilizeavarietyofinterventionstoaddresstherootcausesofdysregulationwhetherthatcauseistraumaormentalillnessoracomplexinteractionofmultiplefactors.Alleviationofspecificsymptomsisimportant,butisonlyPARTofacomprehensivetreatmentplan.Includinginterventionsthatarebackedbyevidencewheneverpossibleisideal.Plansshouldseektobecomprehensiveandtreatthewholechildnotsimplyperceived“problems”withthechild’s
72
PrinciplesandValues
• Promotesafety,permanency,andwell-being• Partnershipswithpeopleandagenciesinthechild’slife• Child-centered,strength-based,individualizedcare• High-quality,integrated,collaborativeservices• Psychotropicmedicationisonlypartofanoveralltreatmentstrategy
72
73
TreatmentPlan
•Developedincollaborationwiththechildandfamilyaroundtheiruniquestrengthsandneeds• Individualized,flexible,robust•Varietyofinterventions•Addressrootcause(s)ofdysregulation•Notlimitedtosymptomrelief•Evidence-based•ComprehensiveandHIPAACompliant
73

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 51
behaviororfunctioning.HIPAAcomplianceisasimportantintreatmentplanningasitisinallareasofhealthcare.
Slide74—What’sIncludedinaTreatmentPlanTheCaliforniaGuidelinesindicatethecomponentofatreatmentplanthatadherestobestpracticestandardsshouldcontainthefollowing:
1. Thechild’sdiagnosisand/oroutlineofemotional/cognitive/behavioraldysregulationbasedonthechild’shistoryofabuse,neglect,and/orremovalfromthehome;
2. Adescriptionofthechild’sbaselinestrengthsandneeds;3. Targetsymptomsasagreedtobythechild,family,andteam
membersandexpressedinclear,everydaylanguage;4. Short-andlong-termtreatmentgoals;5. Interventions,includingevidence-supportedtreatments,
psychosocialinterventions,substanceabusepreventionortreatment,casemanagement,informalmentalhealthservices,educationalorbehavioralservices,extracurricularandrecreationalactivitieswithstartdatesandanticipatedduration;and
6. Aclearandspecificplanforperiodicreviewandreassessment.KatieA.plansmustbereviewedatleastevery90days.Ifreassessmentinvolveschangesinpsychotropicmedication,thoseplansmustbecommunicatedwiththeCourtasanattachmenttoformJV220,whichwediscussfurtherinthenextsectionofthistraining.
Slide75—Assessmentofneeds
Childrenwhohaveemotional,cognitive,and/orbehavioraldysregulationfromtrauma,mentalhealthconcerns,orforotherreasonsrequireanddeserveatreatmentplanthatcontainsavarietyofinterventionstoalleviatetheirsymptomsandtopromotetheirsafetyandwell-being.Thefirststepinthatprocess,isahigh-quality,trauma-informed,child-centeredassessment.
Childrenwhohaveemotional,cognitive,and/orbehavioraldysregulationfromtrauma,mentalhealthconcerns,orforotherreasonsrequireanddeserveatreatmentplanthatcontainsavarietyofinterventionstoalleviatetheirsymptomsandtopromotetheirsafetyandwell-being.Thefirststepinthatprocess,isahigh-quality,trauma-informed,child-centeredassessment.
Aswementionedbefore,anyassessmentofchildrenoryouthinfostercareshouldbeconductedbyalicensedpractitionerwhoisinformedabouttheconditionsandeffectsoftrauma.Andshouldthoroughlycoveralloftheseitems:• PhysicalANDmentalstatusexaminations,• Identificationoftargetsymptomsandthegoalsoftreatment,
74
TreatmentPlan
Documentationshouldinclude:• Diagnosisordysregulation• Strengthsandneeds• Targetsymptom(s)• Measurabletreatmentgoals• Interventionswithstartdates• Ifpsychotropicmedicationisoneoftheinterventions,thedosageandmonitoringschedule*
• Reassessment/monitoringscheduleandwhoisresponsible
*MedicationtreatmentplansmustbecommunicatedasanattachmenttotheJV220aswellassharedwiththechild/youth,family,caregiver,andsocialworkerand/orprobationofficer.
74
45
NeedsAssessment
• Trauma-Informedandchild-centered• Assessmentshouldcover• PhysicalandMentalHealth• Identificationofwhatthechildandfamilywantaddressed(targetsymptomsandgoals)• Planforre-assessmentandmonitoring• Clearrisk/benefitoutlineofpotentialtreatmentoptions
• Oftenwillrequiremorethanonesession
45

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 52
• Aclearplanandtimelineforre-assessmentandhowmonitoringprogresswilloccurandwhoisresponsibleforwhichpartsoftheplan,and
• Aclearrisk/benefitanalysisofeachtreatmentintheplanincludingtherisksandbenefitsofnotreatment
Slide76—PhysicalExam
Theresultsofthemostrecentphysicalexaminationofthechild—withinthepastyear—shouldbereviewedaspartofthetreatmentplanningprocess.Theseresultswillbeusedtoruleoutmedicalconditionswhentheymaycontributetoorcausethepresentingsymptoms,andtoprovidebaselineinformationformonitoringpotentialsideeffects.Asappropriate,thetreatmentteammayconsiderapregnancytestorsubstanceusescreen,asbothcouldhaveseriousimplicationsforwhetherornottoprescribepsychotropicmedication.Theseinitialexaminationsareparticularlyimportantforfollow-upandmonitoringsideeffectsbecausewithoutabaseline,itmaytakelongertonoticechangesthatmayindicatedangerousdevelopmentsorsideeffectsthatneedtobeaddressedquickly.
Slide77—MentalHealthExam
Theexaminationofthechild’smentalstatusshouldbedevelopmentallyappropriate.Anyapplicablediagnosisshouldbeinlinewithprofessionalstandardsandbesupportedbysufficientdocumentationtoruleoutotherpossiblediagnoses.Theassessmentshouldidentifythetargetsymptomsandgoalsoftheselectedtreatment,alongwithatimelineforwhenresultsshouldbeexpectedandhowlongthetreatmentisintendedtolast.Itisimportanttosharetheresultsofthisassessmentwiththechildandtheirsupportnetwork,butitisespeciallyimportanttosharethegoalsandtargetsymptomswiththem.Inthisway,everyonewillunderstandwhatthetreatmentisforandwhattoexpect.Itisalsoimportanttoconsiderifthegoalsarefocusedontreatingtheunderlyingemotionaldistressthatthechildisexperiencing,andtorefocusthemontoalleviatingthatdistressifnecessary.Regularre-assessmentisanexpectedactivity.Thetreatmentteamshouldmonitorsymptoms,sideeffects,andthechildandfamily’sneedsanddesires.Alltreatmentplansshouldexplicitlyincorporatearisk–benefitanalysisthatcomparesatreatmentplanwithoutmedicationtothepotentialbenefitsandrisksofaddingaprescription.
76
PhysicalExamination
•Reviewpastexam(withinpastyear)•Baselinelabtests•Pregnancytestifappropriate•Screenforsubstanceuse•Useformonitoringchangeovertime
76
77
MentalHealthExamination
•Sensitivetoage,developmentalstage,andtrauma•Diagnosisoftenrequiresmultiplesessions• Ideallyinterviewchildwithandwithoutparentsorcaregiver
Diagnosis•Usingaccepteddiagnosticcriteria•Reconcileifnotconsistentwithpreviousorothers•Allprofessionalsworkwithsamediagnosisandcaseconceptualization
77

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 53
Slide78—GoalsandTargetSymptomsTremendouslyimportanttothequalityofthetreatmentplanistoidentifyspecificsymptomsthatthetreatmentisintendedtoaddress.Thisiswherethevoiceandopinionofthechildiscrucial.Treatmentplansshouldnotjusttargetthebehaviorsthatacaregiverfindsproblematic,butattempttoaddressthecoreissuesandsourceofdysregulation.Ideally,NOTjustmedicationwillbeusedtoreachthegoalsstatedhere.
Slide79—InformedconsentforANYtreatment
Itisimportanttoobtaininformedconsentforanyandalltreatment,notjustformedication.Theroleofthesocialworker,publichealthnurse,and/orprobationofficeristoensurethatthechildunderstandstheirrightsandtherisks/benefitsoftheproposedplan.Useterminologythatisclearandeasytounderstand.Informationshouldbeprovidedinthechildandfamily’sprimarylanguageandinwrittenform,ifpossible.InCalifornia,achildtheageof12andoverhastherighttoconsenttotreatmentandtherighttorefuseconsent.Theassent,oragreement,ofchildrenyoungerthan12isveryimportant.Thesocialworkerisresponsibleforknowingwhoisandwhoisnotabletoprovidelegalconsent.
Slide61—GuidelinesforPrescribing
• StartLow,GoSlow—tobestmonitoreffectivenessandsideeffects,itisimportantthatpsychotropicmedicationsareintroducedoneatatime,andstartingfromthelowestrecommendeddose.Thedosecanbeincrementallyincreaseduntilthelowesteffectivedoseisidentified.
• On-labelUse—preferenceshouldalwaysbegiventomedicationsthatareFDAapprovedfortheagegroup,diagnosis,anddoseforwhichitisbeingprescribed.Medi-Calhasalistofbrandsandgenericsthatshouldbeusedwhenpossible.
• Ifchangesarenecessary,theyshouldbemadetoonemedicationatatime.Itisverydifficulttodeterminewhatisworkingandwhatisn’tifmultiplechangestakeplaceatonce.
• Ifyouthinktheremaybetoomuchinaprescribeddoseortoomanymedicationstotal,talktoapsychiatricspecialistatyourcounty.Donotassumethatthedoctorisright.It’sokaytogetasecondopinion.
78
GoalsandTargetSymptoms
•Dysregulation•Focusonunderlyingemotionaldistressratherthanbehavioralone•Reassessoften•Whatmeasuresofpsychosocialfunctioningwillshowimprovement?(i.e.improvedgrades,peerrelationships)•Evaluatemedicationprosandcons•Prioritizewhatthechildandfamilyreportanddesire
78
79
InformedConsentforANYTreatment
•Alltreatmentrequiresinformedconsent,notjustmedication.•Goalistoinformthechildandfamily,andtoensuretheyunderstandandagreewithproposedplan.•Nota“formality”justtogetthemtoagree.•Useclearandunderstandabletermstoexplaintreatment,risks,andpotentialbenefits.•Provideinformationinthefamily’sprimarylanguageandinwrittenform,whenavailable.•Aminorage12andovercanconsent(ornot)totheirowntreatment.
79
80
GuidelinesforPrescribing
• Startlow,goslow• PreferencegiventomedicationthatisFDAapprovedfor
üAgegroupüDiagnosisüDose
• Usebrand/genericspecifiedinMedi-Callist• Trysinglemedicationfirstbeforeaddingothers• Changeonemedicationatatime• Consultwithpsychiatricspecialistwhenconsidering
üMorethanonemedicationfromthesameclassüUseofthreemedicationsconcurrently
80
Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 54
p Activity7B:Slide81GetfamiliarwiththeGuidelines
HaveparticipantsturntotheCaliforniaGuidelinesfortheUseofPsychotropicMedicationwithChildrenandYouthinFosterCaredocumentintheirbinders.Theyareattheendofthissegment.
GivethemafewminutestogetfamiliarwiththelayoutoftheGuidelinesbutnotreallytryingtoreaditallasthereisnottime.
Then,havethemcompletetheGetFamiliarwiththeGuidelinesworksheetonpage42oftheirbinder.
Thegoalistohavethemlookingthroughthecompletedocumentandappendicestobecomefamiliarwithhowtheymightusethemintheirpractice.
Reviewtheworksheetwiththewholegroup,callingonindividualstoanswerandaddressingquestionsastheyarise.
Spendtimeonthefinalquestion,andtrytogetparticipantstoreallyconsiderspecificwaysthattheGuidelinesdocumentandAppendicescanbeusedasatoolwithinteams.
Whenyou’vefinishedreviewingallthequestions,passaroundtheAnswerKeyHandoutforthemtokeepasareference.
GuidelinesAnswerKey(thisoneisforTraineruse,theAnswerKeyhandoutisincludedintheHandoutPacketandshouldbecopiedbeforehand)
1. Whatpagewillhelpyoudeterminetheprescribingstandardsforachildwhois13yearsold?
AppendixA,pages1and2outlinetheprescribingstandardsforyouthwhoare12-17yearsold.
2. WhatareallthepotentialcomplicationsandsideeffectsforSerotonergicAntidepressants?
AppendixB,page11indicatesthatSerotonergicAntidepressantshavethefollowingpotentialcomplicationsandsideeffects:
• Agitation,restlessness• Bipolar(manic)switching• Withdrawalsymptomsondiscontinuation• Serotenergicsyndrome• Obesity• Headache• Sweating• Sleepdisturbance• Gastrointestinalproblems• Sexualdysfunction• AndthefollowingCautionsandContraindications:• Allergytodrug,liverfailure,pregnancy/breastfeeding,donot
usewithMAOI’s
***BESURETODRAWATTENTIONTOTHESOMEWHATHIDDENWARNINGATTHEBOTTOMOFTHEPAGETHATREADS:“Antidepressantsmayincreasesuicidality(thoughtsorbehaviors)in
81
Worksheet
Getfamiliarwiththe
CaliforniaGuidelinesfortheUseofPsychotropicMedicationwithChildrenandYouthinFosterCare
andAppendices
81

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 55
children,teenagersandyoungadultsduringinitiation.(Idon’tknowwhyintheworldthisisn’tinthesideeffectssection.)Usethistore-inforcethattheyreadalltheinformationgiven.
3. AccordingtotheGuidelines,whoisresponsibleforobtaininginformedconsent?
TheInformedConsentsectiononPage11indicatesthatthe“..theprescriberinformsthechild,family,andcaregiveroftherisksandbenefitsoftheproposedtreatmentandtherisksandbenefitsofalternativetreatments,includingabsenceoftreatment.”However,itisimportanttorememberthatitisthesocialworker’sresponsibilitytobesurethishappensandthattheychild,family,andcaregiverunderstandwhattheyhavebeentoldbytheprescriber.
4. Sometimesdoctorsprescribemedicationtotreatasymptomotherthanthemedication’sindicateduse.Thisiscalledofflabelorblackboxprescription.WhereintheGuidelinescanyoufindinformationaboutthechallengeofoff-labelor“blackbox”prescription?
Thedocumentrecommendsthatall“off-label”prescribingshouldhavepeer-reviewed,publishedevidenceavailabletosupportitsuse.FoundonPage4ofAppendixC.Thisdocumentdescribesmanyofthechallengesthatoccurinpsychiatricdiagnosisandprescribingforfosteryouth.Itisagoodresourcefordeterminingwhenconsultationoradditionalsupportshouldberequested.
5. WhatarethethreesectionsofthePrescribingAlgorithm(DecisionTree)?Follow-upquestion,whatisSectionCactuallyusedfor?
• Beforeprescribing,havethefollowingconcernsbeenconsidered
• Whenprescribing,considerthefollowing
• Ifthisisnotthefirstprescriptionforpsychotropicmedicationforthischild,periodicevaluationoftreatmentefficacyandtolerabilityshouldoccur,asdescribedabove.Ateachsubsequentappointmentformedicationmanagement,thisevaluationincludesthereviewofthefollowing
SectionCintheDecisionTreeisachecklistofitemstobeevaluatedatmedicationmonitoringappointments.Itcanbeusedbytheclinicianwhoprescribedthemedication,butisalsoausefulguideforgatheringmuchoftheimportantinformationforProgressReviewsintheJV-220process.
6. HowdotheGuidelinesdocumentsconnectwiththeJV-220Process?
TheGuidelinesandthetoolsintheAppendicesaresupportiveofalltheinformationrequiredintheJV-220Processforms.TheGuidelinescaninformtheentiretreatmentteamregardingexpectationsandbestpractices.

Trainer’sGuide|PsychotropicMedicationinFosterCare|Version1.0|April2017 56
Segment8:SummaryandEvaluationSegmentTime: 10minutes
Materials:
Slide:
Evaluations
82-85
DescriptionofActivityDebriefandreflectionontheinformationcoveredthroughouttheday.Activity:Courseevaluations.
DuringtheActivity
Slide83—SummaryandEvaluations
p Activity8AIfthereistimeforadebrief,facilitateagroupconversationusingthequestionsbelow.Askparticipantsthefollowingquestions,alsolocatedonpage43oftheirbinders:
o IsthereanythingmissingfromtheGuidelinesthatyouthinkmighthelpyouwiththeissuesofpsychotropicmedicationandchildrenandyouthinfostercare?
o Whatresonatesmostwithyouaboutworkingfromatrauma-informedperspective?
o Anyquestions?
Slide84—Ombudsperson’sOffice
RemindparticipantsthattheycancontacttheFosterCareOmbudspersonaboutthistopiciftheyhavequestions,orneedresourcesorrecommendations.Contactinformationisprovidedhereandintheirbinders.
p Activity8BInstructparticipantstocompletethecourseevaluation(notincludedinthisguide).
WrapUpandEvaluations
Segment8
83
SummaryandEvaluations
• IsthereanythingmissingfromtheGuidelines thatyouthinkmighthelpyouwiththeissuesofpsychotropicmedicationandchildrenandyouthinfostercare?
•Whatresonatesmostwithyouaboutworkingfromatrauma-informedperspective?
• Anyquestions?
83
77
QuestionsorConcerns?
Ifyouhaveanyquestionsorconcernsaboutpsychotropicmedicationinfostercare,theFosterCareOmbudswomanofCaliforniahasagreedtohavehercontactinformationincludedinthistraining.
Herofficeisavailableforsupportandresourcesonthistopic.
Toll-freephone:1.877.846.1602E-mailaddress:[email protected]
Thankyou.
Related Documents











