This article was downloaded by: [Dr Francisco José Eiroa-Orosa] On: 26 August 2013, At: 18:02 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK International Journal of Psychology Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/pijp20 Psychosocial wellbeing in the Central and Eastern European transition: An overview and systematic bibliographic review Francisco José Eiroá Orosa a a Department of Psychiatry and Legal Medicine, Universitat Autònoma de Barcelona, Barcelona, Department of Psychiatry , University Hospital Vall d’Hebron, Barcelona, and Community Action Group , Madrid , Spain Published online: 23 Apr 2012. To cite this article: Francisco Jos Eiro Orosa (2013) Psychosocial wellbeing in the Central and Eastern European transition: An overview and systematic bibliographic review , International Journal of Psychology, 48:4, 481-491, DOI: 10.1080/00207594.2012.669481 T o link to this articl e: http://dx.doi.org/10.1080/00207594.2012.669481 PLEASE SCROLL DOWN FOR ARTICLE T aylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publicati ons on our platform. However, Taylor & Franc is, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by T aylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. T aylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content. This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. T erms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

Psychosocial wellbeing in the Central and Eastern European transition: An overview and systematic bibliographic review
Oct 05, 2015
This paper presents the results of a systematic review of literature on the psychosocial wellbeing of populations in Central and Eastern Europe during the transition period subsequent to the fall of the Soviet Bloc. A revision of research addressing emotional wellbeing trends in this period and theoretical models was carried in order to verify their validity in the analysis of empirical studies. Hence, a systematic bibliographic review was conducted, aiming to find possible subjective mediators between social variables derived from changes and emotional wellbeing. The results of the review show that subjective mediators such as locus of control, perceived control, self-efficacy beliefs, perceived familial support, and the subjective evaluation of social change explain part of the relationship between macrosocial changes and emotional wellbeing. Results appear coherent with proposed multidimensional models of social change and mental health, although further research should be conducted to determine the specific weight of these phenomena in individual emotional wellbeing.
Cet article présente les résultats d'une revue systématique de la littérature concernant le bien-être des populations de l'Europe centrale et de l'Europe de l'Est durant la période de transition suivant l'effondrement du bloc soviétique. Un examen de la recherche portant sur les modèles théoriques et les tendances du bien-être émotionnel durant cette période est fait pour vérifier leur validité à travers l'analyse d’études empiriques. Donc, une revue bibliographique systématique est menée pour trouver de possibles médiateurs subjectifs entre des variables sociales venant des changements et le bien-être émotionnel. Les résultats de cette revue montrent que les médiateurs subjectifs comme le locus de contrôle, le contrôle perçu, les croyances d'auto-efficacité, le support social perçu, la perception du soutien familial et l’évaluation subjective du changement social expliquent en partie la relation entre les changements macrosociaux et le bien-être émotionnel. Les résultats semblent cohérents avec les modèles multidimensionnels du changement social et de la santé mentale, bien que d'autres recherches devraient être menées pour déterminer le poids spécifique de ces phénomènes dans le bien-être émotionnel individuel.
Este trabajo presenta los resultados de una revisión sistemática de la literatura sobre el bienestar psicosocial de las poblaciones de Europa Central y del Este durante el período de transición posterior a la caída del Bloque Soviético. Se llevó a cabo una revisión de investigaciones sobre las tendencias de bienestar emocional durante ese período, así como de modelos teóricos con el fin de verificar su validez en el análisis de estudios empíricos. Para ello se realizó una revisión bibliográfica sistemática con el propósito de encontrar posibles mediadores subjetivos entre las variables sociales derivadas de los cambios y el bienestar emocional. Los resultados de la revisión muestran que mediadores subjetivos tales como locus de control, control percibido, creencias de autoeficacia, el apoyo famliar percibido, y la evaluación subjetiva de los cambios sociales explican parte de la relación entre los cambios macrosociales y el bienestar emocional. Los resultados parecen coherentes con los modelos multidimensionales de cambios sociales y salud mental ya propuestos, sin embargo nuevas investigaciones deberían llevarse a cabo para determinar el peso específico de estos fenómenos en el bienestar emocional individual.
Cet article présente les résultats d'une revue systématique de la littérature concernant le bien-être des populations de l'Europe centrale et de l'Europe de l'Est durant la période de transition suivant l'effondrement du bloc soviétique. Un examen de la recherche portant sur les modèles théoriques et les tendances du bien-être émotionnel durant cette période est fait pour vérifier leur validité à travers l'analyse d’études empiriques. Donc, une revue bibliographique systématique est menée pour trouver de possibles médiateurs subjectifs entre des variables sociales venant des changements et le bien-être émotionnel. Les résultats de cette revue montrent que les médiateurs subjectifs comme le locus de contrôle, le contrôle perçu, les croyances d'auto-efficacité, le support social perçu, la perception du soutien familial et l’évaluation subjective du changement social expliquent en partie la relation entre les changements macrosociaux et le bien-être émotionnel. Les résultats semblent cohérents avec les modèles multidimensionnels du changement social et de la santé mentale, bien que d'autres recherches devraient être menées pour déterminer le poids spécifique de ces phénomènes dans le bien-être émotionnel individuel.
Este trabajo presenta los resultados de una revisión sistemática de la literatura sobre el bienestar psicosocial de las poblaciones de Europa Central y del Este durante el período de transición posterior a la caída del Bloque Soviético. Se llevó a cabo una revisión de investigaciones sobre las tendencias de bienestar emocional durante ese período, así como de modelos teóricos con el fin de verificar su validez en el análisis de estudios empíricos. Para ello se realizó una revisión bibliográfica sistemática con el propósito de encontrar posibles mediadores subjetivos entre las variables sociales derivadas de los cambios y el bienestar emocional. Los resultados de la revisión muestran que mediadores subjetivos tales como locus de control, control percibido, creencias de autoeficacia, el apoyo famliar percibido, y la evaluación subjetiva de los cambios sociales explican parte de la relación entre los cambios macrosociales y el bienestar emocional. Los resultados parecen coherentes con los modelos multidimensionales de cambios sociales y salud mental ya propuestos, sin embargo nuevas investigaciones deberían llevarse a cabo para determinar el peso específico de estos fenómenos en el bienestar emocional individual.
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
-
This article was downloaded by: [Dr Francisco Jos Eiroa-Orosa]On: 26 August 2013, At: 18:02Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: MortimerHouse, 37-41 Mortimer Street, London W1T 3JH, UK
International Journal of PsychologyPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/pijp20
Psychosocial wellbeing in the Central and EasternEuropean transition: An overview and systematicbibliographic reviewFrancisco Jos Eiro Orosa aa Department of Psychiatry and Legal Medicine, Universitat Autnoma deBarcelona, Barcelona, Department of Psychiatry , University Hospital Vall dHebron,Barcelona, and Community Action Group , Madrid , SpainPublished online: 23 Apr 2012.
To cite this article: Francisco Jos Eiro Orosa (2013) Psychosocial wellbeing in the Central and Eastern Europeantransition: An overview and systematic bibliographic review, International Journal of Psychology, 48:4, 481-491, DOI:10.1080/00207594.2012.669481
To link to this article: http://dx.doi.org/10.1080/00207594.2012.669481
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the Content)contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensorsmake no representations or warranties whatsoever as to the accuracy, completeness, or suitabilityfor any purpose of the Content. Any opinions and views expressed in this publication are the opinionsand views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy ofthe Content should not be relied upon and should be independently verified with primary sources ofinformation. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands,costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly orindirectly in connection with, in relation to or arising out of the use of the Content.
This article may be used for research, teaching, and private study purposes. Any substantial orsystematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distributionin any form to anyone is expressly forbidden. Terms & Conditions of access and use can be found athttp://www.tandfonline.com/page/terms-and-conditions
http://www.tandfonline.com/loi/pijp20http://www.tandfonline.com/action/showCitFormats?doi=10.1080/00207594.2012.669481http://dx.doi.org/10.1080/00207594.2012.669481http://www.tandfonline.com/page/terms-and-conditions
-
Psychosocial wellbeing in the Central and EasternEuropean transition: An overview and systematic
bibliographic review
Francisco Jose Eiroa Orosa
Department of Psychiatry and Legal Medicine, Universitat Autonoma de Barcelona,Barcelona, Department of Psychiatry, University Hospital Vall dHebron, Barcelona, andCommunity Action Group, Madrid, Spain
T his paper presents the results of a systematic review of literature on the psychosocial wellbeing ofpopulations in Central and Eastern Europe during the transition period subsequent to the fall of the SovietBloc. A revision of research addressing emotional wellbeing trends in this period and theoretical models wascarried in order to verify their validity in the analysis of empirical studies. Hence, a systematic bibliographic
review was conducted, aiming to find possible subjective mediators between social variables derived from changesand emotional wellbeing. The results of the review show that subjective mediators such as locus of control,perceived control, self-efficacy beliefs, perceived familial support, and the subjective evaluation of social change
explain part of the relationship between macrosocial changes and emotional wellbeing. Results appear coherentwith proposed multidimensional models of social change and mental health, although further research should beconducted to determine the specific weight of these phenomena in individual emotional wellbeing.
C et article presente les resultats dune revue systematique de la litterature concernant le bien-etre despopulations de lEurope centrale et de lEurope de lEst durant la periode de transition suivantleffondrement du bloc sovietique. Un examen de la recherche portant sur les modeles theoriques et les tendances
du bien-etre emotionnel durant cette periode est fait pour verifier leur validite a travers lanalyse detudesempiriques. Donc, une revue bibliographique systematique est menee pour trouver de possibles mediateurssubjectifs entre des variables sociales venant des changements et le bien-etre emotionnel. Les resultats de cette
revue montrent que les mediateurs subjectifs comme le locus de controle, le controle percu, les croyances dauto-efficacite, le support social percu, la perception du soutien familial et levaluation subjective du changement socialexpliquent en partie la relation entre les changements macrosociaux et le bien-etre emotionnel. Les resultats
semblent coherents avec les modeles multidimensionnels du changement social et de la sante mentale, bien quedautres recherches devraient etre menees pour determiner le poids specifique de ces phenomenes dans le bien-etreemotionnel individuel.
E ste trabajo presenta los resultados de una revision sistematica de la literatura sobre el bienestarpsicosocial de las poblaciones de Europa Central y del Este durante el perodo de transicion posterior a lacada del Bloque Sovietico. Se llevo a cabo una revision de investigaciones sobre las tendencias de bienestar
emocional durante ese perodo, as como de modelos teoricos con el fin de verificar su validez en el analisis deestudios empricos. Para ello se realizo una revision bibliografica sistematica con el proposito de encontrarposibles mediadores subjetivos entre las variables sociales derivadas de los cambios y el bienestar emocional.
Los resultados de la revision muestran que mediadores subjetivos tales como locus de control, controlpercibido, creencias de autoeficacia, el apoyo famliar percibido, y la evaluacion subjetiva de los cambios
Correspondence should be addressed to Francisco Jose Eiroa Orosa, Department of Psychiatry, University Hospital Vall dHebron,
Passeig Vall debron, 119-129, 08035 Barcelona, Spain. (E-mail: [email protected]).
A previous version of this study was presented at the first conference of the Central and Eastern European Society ofBehavioral Medicine. I would like to acknowledge the support of the staff of the Autonomous University of Madrid, theWarsaw School of Social Psychology, and the Semmelweis University in Budapest.
International Journal of Psychology, 2013Vol. 48, No. 4, 481491, http://dx.doi.org/10.1080/00207594.2012.669481
2013 International Union of Psychological Science
Dow
nloa
ded
by [
Dr
Fran
cisc
o Jo
s E
iroa
-Oro
sa]
at 1
8:02
26
Aug
ust 2
013
-
sociales explican parte de la relacion entre los cambios macrosociales y el bienestar emocional. Los resultadosparecen coherentes con los modelos multidimensionales de cambios sociales y salud mental ya propuestos, sinembargo nuevas investigaciones deberan llevarse a cabo para determinar el peso especfico de estos fenomenos
en el bienestar emocional individual.
According to George Rosen (1968), the first workaddressing social change and mental health wasperformed by Benjamin Rush in 1774. ThisAmerican physician, and signer of theDeclaration of Independence, researched fertilityin American women during the revolutionaryperiod. Since then, hundreds of studies havesought to address if and how social changesinfluence the psychosocial wellbeing of individuals,although under very heterogeneous methodologi-cal approaches and ideologies.More than 200 years after this pioneer work,
as a result of the fall of the Iron Curtain,massive political, economic, and social changesdrove Central and Eastern Europe to a pre-viously unknown situation of transformation.Six months after the fall of the Berlin Wall, aneditorial of the American Journal ofPsychotherapy, written by Stanley Lesse (1990),announced that the situation offered as neverbefore, magnificent opportunities to observe theinterrelationships between these transitions andtheir macro-psychosocial effects. Neumann(1991) goes further, stating that Communismin Eastern Europe has failed mainly because thedeteriorating psychosocial conditions pushed themajority of the population into a state of social,psychological, and, in many cases, somaticdisorder approaching disease.Twenty years after these statements, the real
impact of the rapid changes in collective psycho-social wellbeing remains unclear. Although manyresearch projects attempted to address this topic,they did so under a heterogeneous set of dis-ciplines, methodologies and ideologies. Whatseems clear is that the transition brought aboutfactors of collective wellbeing such as democraticchanges, more respect to human rights, and adeinstitutionalization process of mental healthfacilities, but focused attention away from therole of society as a provider of care, promotingindividualism (Lewis et al., 2001). Hence, manyindividuals adjustment to the process, especiallythat of the most vulnerable such as children or theunemployed, was very poor (World HealthOrganization (WHO) Regional Office forEurope, 2003).WHO established a network of mental
health professionals in the member states,
who provided specific information for everycountry. According to the report of itscommittees 53rd session (WHO RegionalOffice for Europe, 2003), the reasons for theincreasing prevalence of mental disorders espe-cially in these societies and populations under-going stressful change are connected withdifferences in life expectancy related to societalstress and risky lifestyles. The cluster of stress-related factors includes depression and suicide,addiction, violence, risk-taking behaviors andlifestyles, and cardiovascular and cerebrovascu-lar morbidity and mortality.Overhospitalization and problems with theprocess of deinstitutionalization are majorproblems in these countries as well (Jenkins,1991; Jenkins, Klein, & Parker, 2005). Theslow improvement of community-based servicesand prevention programs is another factor totake into account.
Our objective within this work is to review andorganize the existing evidence, giving readers abroader point of view when analyzing thisphenomenon. Specifically, we try to address twoquestions: (1) Was there a generalized reduction inemotional wellbeing during the transition period?(2) What matters when analyzing this? (Or, intechnical terms: Which subjective mediators/con-founders can explain the poor adjustment ofcertain individuals in this period?
DEFINITION OF TERMS
We use two principal concepts in this paper: (1)Emotional wellbeing in this study is defined interms not only of mental health (incidence andprevalence of psychiatric comorbidity, depression,anxiety, mental hospital admission rates, andsuicide) but also of subjective measures of well-being such as self-rated physical health, enjoymentand interest in life, positive attitudes, and self-esteem (Grob, Wearing, Little, & Wanner, 1996;Pinquart & Silbereisen, 2004) in contrast with ill-being (Smith, 1996). (2) Psychosocial wellbeingrefers to an outcome within mediating factors andcontexts which includes social and emotionalwellbeing (Larson, 1996; Martikainen, Bartley, &Lahelma, 2002).
482 EIRO OROSA
Dow
nloa
ded
by [
Dr
Fran
cisc
o Jo
s E
iroa
-Oro
sa]
at 1
8:02
26
Aug
ust 2
013
-
WAS THERE A GENERALIZEDDECREASE IN EMOTIONAL
WELLBEING? EPIDEMIOLOGICALSTUDIES
Assessing the real variation in psychosocial well-being in the ex-communist Central and EasternEuropean area during this special period is not aneasy task. Psychiatric comorbidity could be used asa proxy for emotional wellbeing. However, thefirst problem arises when one tries to establish abaseline of psychiatric comorbidity before thechanges. Institutional data in the ex-communistcountries seems unreliable according to the evi-dence of the use of psychiatry by the state as a toolfor repression (Bonnie, 2002). Furthermore, fewauthors faced the task of comparing in observa-tional studies Western and Eastern psychiatriccomorbidity before the Iron Curtain collapsed.Temkov, Jablensky, and Boyadjieva (1975) esti-mated the incidence and prevalence of psychiatricdisorders in formerly socialist economies and inestablished market economies in the 1970s.Slightly lower but comparable rates can beobserved in the formerly socialist countriesduring that period. Another study carried out byRathner el al. (1995), before the political changes,shows a very similar picture for Western andEastern societies regarding eating disorders,although Hungarians had more minor psychiatricmorbidity than East Germans and Austrians did.The authors discuss these results in light of theprocess of Westernization that had begun in thelate 1980s. Regarding suicide, research carried byMakinen (2006) concluded that suicide changed itssocial nature during the Communist period,becoming more normal, and more equally dis-tributed among social classes and geographicallocations in the whole Warsaw Pact area.
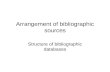
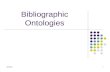
Data extracted from the European Health forAll Database (WHO Regional Office for Europe,2011) gives official epidemiological figures for thewhole process in the region. We can see higherfigures for both prevalence of mental disorders andmental hospital discharges in the group ofcountries that joined the European Union (EU)in 2004 and 2007 (Poland, Estonia, Latvia,Lithuania, Czech Republic, Slovakia, Hungary,and Slovenia in 2004; Bulgaria and Romania in2007) and in the Commonwealth of IndependentStates (CIS) than in the European Region as awhole, as shown in Figures 1 and 2. Figures ofincidence of mental disorders and suicide followdifferent patterns. While incidence (Figure 3)seems much higher and increasing in the new EUmembers than in the European Region and the
Figure 2. Hospital discharges, mental behavioral disorders
(per 100,000).
Figure 1. Prevalence of mental disorders (%).
Figure 3. Incidence of mental disorders per 100,000 population.
PSYCHOSOCIAL WELLBEING 483
Dow
nloa
ded
by [
Dr
Fran
cisc
o Jo
s E
iroa
-Oro
sa]
at 1
8:02
26
Aug
ust 2
013
-
CIS, suicide (Figure 4) increased dramatically inthe 1990s among CIS members (although itdecreased at the beginning of the third millen-nium), while patterns in the new members of theEU are similar to those of the whole EuropeanRegion.Although World Health organization data come
from heterogeneous sources in each country,research carried out employing observationalmethodology show similar results. A decreasingpattern in psychological wellbeing was found inBulgaria (Beshkov & Gerdgikov, 1999; cited inTomov, Mladenova, Lazarova, Sotirov, &Okoliyski, 2004), Czech Republic (Bobak,Pikhart, Rose, Hertzman, & Marmot, 2005),Estonia (Reinap, Lai, Janno, Tamme, & Tamm,2005), Hungary (Kopp, Csoboth, & Rethelyi,2004), Lithuania (WHO Regional Office forEurope, 2001), Poland (Czapinski, 1999; WarsawInstitute of Psychiatry and Neurology, 2004; WHORegional Office for Europe, 2001), Ukraine(Bromet et al., 2005), and Russia (Bobak et al.,2005; Charman & Pervova, 1996). An internationalpoll reports unhappiness and dissatisfaction withhealth, and decrease of satisfaction with life andhealth with aging in the whole of Eastern Europeand the former Soviet Union area compared withWestern countries (Deaton & National Bureau ofEconomic Research, 2007). To our knowledge, noempirical study claims a reduction in psychologicaldistress or psychiatric comorbidity in the areastudied during the political transition.Makinen (2000) studied suicide patterns in all
the countries of the former Soviet Bloc. No generalpattern was found, but the author divided thecountries regarding the basis of their suicide
mortality profiles (the level of suicide and itsage/sex distribution). No possible universal deter-minants of suicide were included among theindependent variables studied. He was, however,able to construct a model in which the changes inlife expectancy, alcohol consumption, democrati-zation, and homicide explained more than 92% ofthe variation in the changes in suicide rates in morethan half of the countries during two periodssubsequent to democratization, retaining its poweracross time.
Taken together, all this information seems topoint to a reduction of collective emotional well-being in the area. Identifying the profiles ofindividuals experiencing this reduction constitutesthe next objective of this work.
WHAT MATTERS WHEN ASSESSINGTHE IMPACT OF SOCIAL CHANGE IN
EMOTIONAL WELLBEING: SYSTEMATICBIBLIOGRAPHIC REVIEW OFSUBJECTIVE MEDIATORS
Different theories can be applied to the study ofhuman development in times of social change, asPinquart and Silbereisen (2004) reviewed, with afocus on the effects of the breakdown of thecommunist system. Using as frameworkBronfenbrenners (1979) ecological paradigm, thetransactional stress theory (Lazarus, 1966), andrecent developments of lifespan theories of controland coping, they introduce a behavioral model ofdevelopmental outcomes concerning abrupt socialchange, in which social support and individualresources such as internal locus of control,self-efficacy beliefs, problem-solving abilities, orsecure attachment buffer the effect of negativeconsequences of social change on psychologicaldistress.
In addition to these cognitive mediators, the wayin which the subjective perception of social changeinfluences individuals psychological wellbeing wasexamined in South Korea during the economiccrisis experienced as a result of the collapse of thefinancial market between 1997 and 2000 (Kim,2008). In this study the subjective perception ofsocial change was shown to mediate between theperceived scope and pace of social change, copingresources, and individuals psychologicalwellbeing.
METHODS
Following these models, a systematic bibliographicreview was conducted with the objective of testing
Figure 4. SDR, suicide, and self-inflicted injury (all ages,
per 100,000).
484 EIRO OROSA
Dow
nloa
ded
by [
Dr
Fran
cisc
o Jo
s E
iroa
-Oro
sa]
at 1
8:02
26
Aug
ust 2
013
-
whether Pinquart and Silbereisen (2004) and Kims(2001) hypothesis about social change and psy-chosocial wellbeing are applicable to the Centraland Eastern European transition. Inclusion cri-teria were as follows: English-language empiricalstudies concerning the Central and EasternEuropean transition or carried out between 1989and 2010, which included subjective mediatorsbetween any social outcome of sociopoliticalchange and emotional wellbeing.
We used a syntax that selected the names of atleast one ex-communist country of Central andEastern Europe (Russia, Ukraine, Moldova,Belarus, Estonia, Latvia, Lithuania, Poland,Czech Republic, Slovakia, Hungary, Slovenia,Bulgaria, Romania) or any of these terms: post-communist, Iron Curtain, political transition,Eastern Europe, Central Europe, Soviet Union;accompanied by at least one term referring toemotional wellbeing (psychiatric morbidity,mental health, psychological wellbeing, psycholo-gical distress, psychopathology, depression, anxi-ety, stress, affective, subjective health, self-ratedhealth, suicide, or emotional wellbeing itself).Databases explored included PsycINFO,PsycARTICLES, Medline, ERIC, Social CitationIndex and Sociological Abstracts. Titles were readfrom an initial pool of over 8000 articles; about500 were chosen for abstract review. Articlescentered in clinical facilities, addressing economicwellbeing, not including socioeconomic variablesderived from changes, or not including anysubjective mediator were excluded (some of thelast category are included in the introduction asepidemiological studies). A total of 14 studies metinclusion criteria.
RESULTS
A comprehensive description of the bibliographicreview is given in Table 1. Subjective mediatorscould be classified into three specific clusters:(1) perceived locus of control and self-efficacy,(2) subjective evaluation of social conditions andchanges, (3) familial social support.
Self-evaluation: Perceived locus ofcontrol and self-efficacy
Locus of control is a concept first developed byRotter (1954) in the framework of his sociallearning theory of personality. It is defined bythe extent to which individuals believe that theycan control events that affect them. Self-efficacy aconcept first developed by Bandura (1977) as part
of the social cognitive theory; it has been claimed
to be strongly related to, or even to be a part of,
the construct of perceived control (Ajzen, 2002).
Furthermore, the learned helplessness paradigm
(Seligman, 1975; Seligman & Maier, 1967) explains
how the perceived absence of control over the
outcome of a situation can result in depression and
related mental illnesses. These concepts appear to
be largely used and successfully tested as subjective
mediators between consequences of abrupt social
change and physical and emotional wellbeing.Poor control over life was associated with
chronic illnesses in an urban population in
Poland (Stelmach, Kaczmarczyk-Chalas, Bielecki,
& Dryga, 2004). Perceived control was strongly
associated with self-rated health, and appeared to
mediate the effects of deprivation and inequality in
several countries of the area (Bobak, Pikhart,
Rose, Hertzman, & Marmot, 2000). This construct
was also found to be correlated with depression,
mediating socioeconomic circumstances along
with social support (Aluoja, Leinsalu, Shlik,
Vasar, & Luuk, 2004). External locus of control
and emotional distress seem to mediate between
sociodemographic variables (structural dimensions
according to the authors) and poor self-rated
health (Leinsalu, 2002).The comparison of control over life between
Eastern and Western cultures gives interesting
results. Carlson (1998) found higher rates in
Western countries among adults; Grob et al.
(1996) found higher rates in Eastern countries
among adolescents and Wardle et al. (2004) lower
scores among Eastern university students.Regarding microsystems as workplaces, low
control at work and depression was found to be
a mediator between general morbidity and mor-
tality and the majority of risk consequences of a
low socioeconomic situation among men in two
national representative surveys of the Hungarian
population conducted in 1988 and 1995 (Kopp
et al., 2004). Nevertheless, the imbalance of
effortreward at work (which could be considered
an objective measure of working conditions) but
not job control (which could be considered a
measure of subjective control) was associated with
depressive symptoms and increased alcohol intake
and problem drinking in a transnational study in
three Eastern European urban populations
(Bobak et al., 2005).Self-efficacy beliefs were found to mediate
between commitment to the old political system
and distress over time in a study of Eastern
German adolescents (Pinquart, Silbereisen, &
Juang, 2004)
PSYCHOSOCIAL WELLBEING 485
Dow
nloa
ded
by [
Dr
Fran
cisc
o Jo
s E
iroa
-Oro
sa]
at 1
8:02
26
Aug
ust 2
013
-
TABLE
1Systematicbiblio
graphic
review
(mediatorvariables)
Reference
Participantcountries
Socialvariables
Mentalandperceived
physicalhealth
variables
Subjectivemediators
Resultsandconclusions
Aluoja
etal.(2004)
Estonia
Sociodem
ographic
data
(income,
occupational
status).
Depressiveness(sad-
ness,loss
of
interest,worth-
lessness,hopeless-
ness,self-
accusations,
thoughts
ofsui-
cide,
feelingsof
lonelinessand
impossibilityof
enjoyment).
Indices
ofsocial
adjustment(sense
ofcontrol,self-
ratedhealth,per-
ceptionofthe
future,perceived
socialsupport
andsatisfactionin
nineareas).
Strongrelationship
betweendepressivesymptomsand
sociodem
ographic
factors.
Depressiverespondents
hadconsiderably
poorersubjective
socialadjustmentthanrespondents
withanorm
almood
state.They
reported
lower
self-ratedhealthandexperienced
less
satisfactionin
most
importantareasoftheirlives.
Lesssatisfied,depressivesubjectsalsoexhibited
less
perceived
control.Thisisin
linewithstudiesstressingthe
role
oflow
perceived
controlin
depressionaseither
an
independentfactororamediatorofsocioeconomic
circumstancesandsocialsupport.
Bobaket
al.(2000)
Russia,Estonia,
Lithuania,Latvia,
Czech
Republic,
Hungary
and
Poland
Socioeconomic
fac-
tors
(education,
maritalstatus,
material
deprivation).
National
mortality
rates
Self-rated
health.
Perceived
control.
Consistentlywithmortality
rates,theprevalence
ofpoor
self-ratedhealthishigh,particularlyin
theform
erSoviet
UnionandHungary.
Educationandmaterialdeprivationare
importantpredic-
tors
ofself-ratedhealth,andthesocioeconomic
gradients
are
large.
Ecologicalmeasuresofinequalities
werenotsignificantly
relatedto
self-ratedhealth,andanypotentialeffectswere
removed
bycontrollingforindividualsmaterialdepriva-
tion.
Perceived
controlwasstrongly
associatedwithself-rated
health,andappearedto
mediate
theeffectsofdeprivation
andinequality.
Bobaket
al.(2005)
Russia,Poland,and
Czech
Republic
Deprivation,effort
reward
atwork.
Alcoholism
,
depressive
symptoms.
Jobcontrol.
Theim
balance
ofeffortreward
atwork
isassociatedwith
increasedalcoholintakeandproblem
drinking.Jobcontrol
waspositivelyassociatedwithallproblem
drinkingindices,
butnoneoftheassociationsreached
statisticalsignificance.
Theassociationappears
tobepartly
mediatedbydepressive
symptoms,whichmightbeeither
anantecedentora
consequence
ofmensdrinkingbehavior.
Carlson(1998)
10ex-communist
countriesand15
Western
countries
Country,age,
sex,
level
ofeducation
(ageatcomple-
tion)andoccupa-
tionalgroup,
mem
bership
of
nonpolitical
association.
Self-perceived
health
Lifecontrol,job
satisfaction,and
freedom
tomake
decisions,satis-
factionwitheco-
nomic
situation,
politicalinterest,
importance
of
familyand
friends.
Theaveragelevel
ofself-perceived
healthisgenerallyworsein
form
ercommunistcountriesthanin
Western
Europe,
for
both
men
andwomen.Theresultsindicate
thatpeoples
participationin
civic
activitieshasapositiveeffect
ontheir
health.Peopleslife
controlwasim
portantfortheirself-
perceived
healthin
alm
ost
everyEuropeancountry,both
in
theWestandtheEast.In
theform
ercommunistcountries,
however,people
did
notfeel
thatthey
hadthesamecontrol
over
theirlives
asdid
peoplein
theWest.Peopleseconomic
satisfactionwasthemost
powerfulpredictorof
self-perceived
health,in
both
theEasternandWestern
parts
ofEurope.
486 EIRO OROSA
Dow
nloa
ded
by [
Dr
Fran
cisc
o Jo
s E
iroa
-Oro
sa]
at 1
8:02
26
Aug
ust 2
013
-
Carlson(2000)
Russia
Objectivematerial
prosperity,
education.
Self-ratedhealth.
Familialsocialsup-
port,subjective
view
ofmaterial
prosperity.
Lesseducatedsubjectsreported
poorhealthtw
iceasoften
asa
higher-educatedgroup.Subjectivematerialprosperityand
relationswithin
thefamilywereim
portantforself-rated
healthandpartiallyexplained
theeducationalhealth
differences.
Forkel
&Silbereisen(2001)
East
andWest
Germany
Socioeconomic
con-
ditions(w
ork
sta-
bility,income,
incomechange,
materialneeds
...).
Depressed
mood.
Familialsocial
support
Familialsocialsupport
tested
inamediationmodel
predicted
interindividualdifferencesin
adolescentsdepressed
moodin
WestGermanybutnotin
East
Germany.Thisresultis
interpretedin
lightofdifferentattributionsandpublic
attitudes
tothecause
ofhardship.
Grobet
al.(1996)
8ex-communist
countriesand6
Western
countries
Gender,age,
region,
comparative
socialstatus.
Wellbeing.
Perceived
control
(controlexpec-
tancy,control
appraisal),sub-
jectivewellbeing
(positiveatti-
tudes,
self-esteem).
Themeanlevelsofwellbeingandperceived
controlvaried
along
stable
Western
vs.unstable
Easternsociohistoricalcontexts:
Easternadolescents
showed
(a)lower
levelsofwellbeing
(perhapsrelatedto
economic
aspects
ofchange)
and(b)
higher
levelsofperceived
control(perhapsrelatedto
perceived
freedomsim
plied
inthedirectionofchange).
Notably,however,theindividual-difference
relationsamong
theconstructswereveryuniform
across
the14settings,
suggestingthattheadaptivepsychologicalinterface
between
wellbeingandpersonalcontrolisrelativelyrobust
against
sociopoliticalinfluences.
Koppet
al.(2004)
Hungary
Gender,personal
andfamily
income,
education.
Severityofdepres-
sivesymptoma-
tology,anxiety,
BMI,tabaquism,
consumptionof
alcoholandself--
reported
morbidity.
Hostility,socialsup-
port
andcontrol
inwork.
Within
asocietyin
transition,theabsolute
economicindicators
are
inclose
relationship
withmorbidityand,withcertain
limitations,withmortality,mainly
amongmen.Theresults
alsoindicate
thattheseverityofdepressivesymptomscanbe
regarded
asaseriousrisk
factorofgeneralmorbidityand
mortality
andthatthemajority
ofrisk
consequencesofalow
socioeconomicsituationare
mediatedbydepressionandlow
controlatwork
amongmen,andbydepressionandanxiety
amongwomen.
Leinsalu
(2002)
Estonia
Maritalstatus,edu-
cation,economic
activity,occupa-
tionalstatus,per-
sonalincome.
Self-ratedhealth,
physicalhealth
status,em
otional
distress.Health
selection.
Locusofcontrol.
Thestudyrevealedsubstantialdifferencesin
self-ratedhealth
bydim
ensionsofsocialstructure
thatwerethoughtto
be
importantin
presentdayEstoniansociety.A
low
level
of
education,Russianethnicity,lowincome,and,formen
only,
ruralresidence
werethemost
influentialdim
ensionsin
predictingpoorhealth.Thisstudyshowed
thatpoor
self-ratedhealthwasstrongly
associatedwiththreecorre-
latesofem
otionaldistress,locusofcontrol,and,in
particular,self-reported
physicalhealthstatus.However,
thesecorrelatescould
notexplain
theethnic
oreducational
differencesin
self-ratedhealth.
Pikhart
etal.(2004)
Russia,Poland,
Czech
Republic
Socialcharacteristics
(education,mate-
rialdeprivation,
Depressive
symptoms.
Effortreward
imbalance
model,
jobcontrol.
Strongassociationsbetweendepressivesymptomsandeffort
reward
imbalance
atwork,materialdeprivation,andmarital
statuswerefound.Therewereweakassociationsbetween
depressionscore,education,andhistory
ofunem
ployment
(continued
)
PSYCHOSOCIAL WELLBEING 487
Dow
nloa
ded
by [
Dr
Fran
cisc
o Jo
s E
iroa
-Oro
sa]
at 1
8:02
26
Aug
ust 2
013
-
Table
1.Continued.
Reference
Participantcountries
Socialvariables
Mentalandperceived
physicalhealth
variables
Subjectivemediators
Resultsandconclusions
experience
of
unem
ployment).
butdepressionwasnotassociatedwithjobcontrolafter
controllingforsocioeconomic
factors.TheRussiandata
did
notshowsuch
arelationship.Itispossiblethatmeasurement
ofjobcontrolwithin
therapidly
changingem
ployment
practices
inRussia
isproblematic.
Piko&
Fitzpatrick(2001,2007)
Hungary
Socioeconomic
status:Objective
socialclass
(status
oroccupation,
andeducationof
thestudents
mother
and
father),typeof
school.
Psychosocialhealth
(self-perceived
health,psychoso-
cialwellbeing,
andfrequency
of
psychosomatic
symptoms).
Subjectiveevalua-
tionofsocioeco-
nomic
status.
Classicalorobjectivesocialclass
indicators
werenotlikelyto
playaveryim
portantrole
inpredictingadolescents
psychosocialhealth,even
inapostcommunistcountrysuch
asHungary.Onthecontrary,SESself-assessm
ent,a
subjectiveevaluationofonesownsocioeconomiccondition,
showed
asignificantassociationwithpsychosocialhealth,
even
after
controllingforother
variables.
Pinquart
etal.(2004)
East
Germany
Commitmentto
the
old
political
system
.
Psychological
distress.
Self-efficacy
beliefs.
Adolescents
whowerehighly
committedto
theold
East
Germanpoliticalsystem
showed
astronger
increase
in
distressafter
unification,butonly
ifthey
hadlow
preunificationself-efficacy
beliefs.In
adolescents
with
averageandhighlevelsofpreunificationself-efficacy,
previousidentificationwiththeEastGermansystem
wasnot
relatedto
changein
psychologicaldistress.In
addition,
higher
self-efficacy
predictedadecrease
inpsychological
distressover
time.
Stelm
ach
etal.(2004)
Poland
Personaldata,
familystatus,
education,
income,
employment.
Frequency
ofdoc-
torsvisits,medi-
calhistory,
chronic
diseases
diagnosedbya
specialistin
the12
monthspriorto
thesurvey.
Controlover
life
Poorcontrolover
life
wasassociatedwithchronicillnesses.The
studysuggests
thathigher
educationandhigher
incomein
theperiodofsocioeconomic
changes
are
theexplanatory
variablesforgoodhealth.Theincidence
ofcoronary
heart
disease
andback
illnesseswasverystrongly
relatedwithlow
education;low
incomewasrelatedless
strongly
with
hypertension,back
illnesses,andcoronary
heart
disease.
Wardle
etal.(2004)
5ex-communist
countriesand5
Western
countries
Sex,age,
region
(East
vs.West).
Depressive
symptoms.
Lifesatisfaction,
perceptionsof
controlandmas-
tery
over
life,
healthlocusof
control.
Depressionscoreswerehigher
inCentralEasternthanWestern
Europeansamples.Theprevalence
oflow
life
satisfaction
wasalsogreaterin
CentralEasternEuropeans,butratings
ofself-ratedhealthdid
notdiffer.Ratingsofperceived
controlweredim
inished,butsense
ofmasteryandinternal
healthlocusofcontrolwerehigher
inCentralEastern
Europe.Depressionandlowlife
satisfactionwereassociated
withlow
perceived
controlandmasteryandwithstrong
beliefsin
theinfluence
ofchance
onhealth.However,taking
thesefactors
into
accountdid
notexplain
theEastWest
difference
indepressivesymptomsandlow
life
satisfaction.
488 EIRO OROSA
Dow
nloa
ded
by [
Dr
Fran
cisc
o Jo
s E
iroa
-Oro
sa]
at 1
8:02
26
Aug
ust 2
013
-
Subjective evaluation of socialconditions and changes
Pinquart et al. (2004) found that adolescentshighly committed to the old East German politicalsystem had a stronger increase in distress afterunification, but only if they had had low pre-unification self-efficacy beliefs. Furthermore, Pikoand Fitzpatrick (2007) showed that subjectiveevaluation of ones own socioeconomic conditionshows a higher association with psychosocialhealth than objective social class indicatorsamong students enrolled in secondary schools ofthe Southern Plain Region of Hungary. Likewise,subjective material prosperity and familial socialsupport explained self-rated health and educa-tional health differences in a study carried out inRussia (Carlson, 2000).
Familial social support
Two studies tested the mediating role of familialsocial support. As cited in the previous section(Carlson, 2000), familial social support mediatesthe relation between education, material prosper-ity, and self-rated health. By contrast, Forkel andSilbereisen (2001), using a meditational analysis,show how familial social support influencesdifferences in adolescents depressed mood inWest but not in East Germany according tomaterial conditions.
DISCUSSION
On one hand it seems clear that the sociopoliticalchanges in Central and Eastern Europe had astrong impact on emotional wellbeing.International reports, official figures, and observa-tional studies agree on the reduction of emotionalwellbeing in large portions of society. According tothe reports reviewed, it seems that vulnerableindividuals such as children with low socialsupport or adults affected by the labour marketreform, may represent specific affected groups.
Cognitive and subjective mediators appear askey factors to understand how changing macro-systems affect emotional wellbeing. The concept ofperceived control has received extensive attentionalong with other possible explanators such asself-efficacy or the subjective evaluation of thepolitical process. As addressed in the Korean study(Kim, 2001) and the model proposed by Pinquartand Silbereisen (2004), these factors could help to
explain how these relations are mediated in
individuals.Comparisons of perceived control over life
between Eastern and Western cultures are in line
with Pinquart and Silbereisens (2004) model,
which expects age variation in the impact of
social change because of age-associated change in
individual resources and different views of the
direction of change. The few studies addressing
subjective evaluation of changes are line with Kim
(2001).The role of social support seems more con-
troversial. While the results of Carlson (2000)
clearly support the role of familial social support,
the study of Forkel and Silbereisen (2001) failed to
do this among East German adolescents. These
results could be interpreted in the frame of a
collective process in which economic hardships, at
least in the first steps of transition, did not give rise
to stigmatization and thus did not influence
adolescents emotional wellbeing.From a social constructionist point of view,
assessing changes in collective narratives could
explain how this process is developed. Some
previous work has been done in this direction.
The concept of collective identity has been used as
an analysis instrument on the East Germany
revolutionary mobilization (Pfaff, 1996).
Furthermore, under a social constructionist orien-
tation, Sztompka (2004) outlines an ideal-typical
sequence through which individual traumas
unfold, and applies it to the period of economic
and social collapse in Eastern and Central Europe.Study limitations should be addressed, especially
regarding the heterogeneity of the concept of social
change and how social outcomes of sociopolitical
change were defined. Future research should focus
on objective and subjective measures of social
change, which could be applied to different
contexts in order to allow comparisons among
studies.Although in this study we did an overview of the
individual factors that mediate the influence of
macrosocial changes in Central and Eastern
Europe on mental health, further research is
needed. Despite the fact that the research on the
subjective vision of changes has been carried out
from a sociopolitical perspective (Orkeny &
Szekelyi, 2000), psychosocial studies should inves-
tigate in depth the possible implications for
emotional wellbeing of the evaluation of social
environment in times of social change. These
studies, using larger and stratified samples,
should address short-term as well as long-term
developmental outcomes, taking account of both
PSYCHOSOCIAL WELLBEING 489
Dow
nloa
ded
by [
Dr
Fran
cisc
o Jo
s E
iroa
-Oro
sa]
at 1
8:02
26
Aug
ust 2
013
-
individual and social resources (Pinquart &Silbereisen, 2004).
Manuscript received June 2011
Revised manuscript accepted January 2012
First published online April 2012
REFERENCES
Ajzen, I. (2002). Perceived behavioral control,self-efficacy, locus of control, and the theory ofplanned behavior. Journal of Applied SocialPsychology, 32(4), 665683.
Aluoja, A., Leinsalu, M., Shlik, J., Vasar, V., & Luuk,K. (2004). Symptoms of depression in the Estonianpopulation: Prevalence, sociodemographic correlatesand social adjustment. Journal of Affective Disorders,78(1), 2735.
Bandura, A. (1977). Self-efficacy: Toward a unifyingtheory of behavioral change. Psychological Review,84(2), 191215.
Beshkov, N., & Gerdgikov, I. (1999). Psychiatric care inthe Republic of Bulgaria. Sofia, Bulgaria: Ministry ofHealth.
Bobak, M., Pikhart, H., Kubinova, R., Malyutina, S.,Pajak, A., Sebakova, H., et al. (2005). The associa-tion between psychosocial characteristics at work andproblem drinking: A cross-sectional study of men inthree Eastern European urban populations.Occupational and Environmental Medicine, 62(8),546550.
Bobak, M., Pikhart, H., Rose, R., Hertzman, C., &Marmot, M. (2000). Socioeconomic factors, materialinequalities, and perceived control in self-ratedhealth: Cross-sectional data from seven post-communist countries. Social Science & Medicine,51(9), 13431350.
Bonnie, R. J. (2002). Political abuse of psychiatry in theSoviet Union and in China: Complexities andcontroversies. Journal of the American Academy ofPsychiatry and the Law, 30(1), 136144.
Bromet, E. J., Gluzman, S. F., Paniotto, V. I., Webb, C.P., Tintle, N. L., Zakhozha, V., et al. (2005).Epidemiology of psychiatric and alcohol disordersin Ukraine: Findings from the Ukraine WorldMental Health survey. Social Psychiatry andPsychiatric Epidemiology, 40(9), 681690.
Bronfenbrenner, U. (1979). The ecology of humandevelopment. Cambridge, MA: Harvard UniversityPress.
Carlson, P. (1998). Self-perceived health in East andWest Europe: Another European health divide.Social Science & Medicine, 46(10), 13551366.
Carlson, P. (2000). Educational differences in self-ratedhealth during the Russian transition. Evidence fromTaganrog 19931994. Social Science & Medicine, 51,13631374.
Charman, T., & Pervova, I. (1996). Self-reporteddepressed mood in Russian and U.K. schoolchildren:A research note. Journal of Child Psychology andPsychiatry, 37(7), 879883.
Czapinski, S. (1999). Niekliniczne wskazniki zdrowiapsychicznego spoleczenstwa [Non-clinical indicatorsof mental health of society]. Unpublished report,Warsaw [in Polish].
Deaton, A., & National Bureau of Economic Research(2007). Aging and wellbeing around the world:Evidence from the Gallup World Poll. In D.A. Wise (Ed.), Research Findings in the Economicsof Aging (pp. 235263). Cambridge, MA: NationalBureau of Economic Research.
Forkel, I., & Silbereisen, R. K. (2001). Family economichardship and depressed mood among young adoles-cents from former East and West Germany.American Behavioral Scientist, 44(11), 19551971.
Grob, A., Wearing, A. J., Little, T. D., & Wanner, B.(1996). Adolescents well-being and perceived controlacross 14 sociocultural contexts. Journal ofPersonality and Social Psychology, 71(4), 785795.
Jenkins, J. H. (1991). The state construction of affect:Political ethos and mental health among Salvadoranrefugees. Culture, Medicine and Psychiatry, 15(2),139165.
Jenkins, R., Klein, J., & Parker, C. (2005). Mentalhealth in post-communist countries. British MedicalJournal, 331(7510), 173174.
Kim, J. (2001). Social change and psychological well-being: A structural equation model. Ann Arbor, MI:ProQuest Information & Learning.
Kim, J. (2008). Perception of social change andpsychological well-being: A study focusing on socialchange in Korea between 1997 and 2001. Journal ofApplied Social Psychology, 38(11), 28212858.
Kopp, M. S., Csoboth, C. T., & Rethelyi, J. (2004).Psychosocial determinants of premature health dete-rioration in a changing society: The case of Hungary.Journal of Health Psychology, 9(1), 99109.
Larson, J. S. (1996). The World Health Organizationsdefinition of health: Social versus spiritual health.Social Indicators Research, 38(2), 181192.
Lazarus, R. S. (1966). Psychological stress and the copingprocess. New York, NY: McGraw-Hill.
Leinsalu, M. (2002). Social variation in self-rated healthin Estonia: A cross-sectional study. Social Science &Medicine, 55(5), 847861.
Lesse, S. (1990). The political and economic changes incentral and eastern Europe: Possible macro-psycho-sociologic implications. American Journal ofPsychotherapy, 44(2), 157159.
Lewis, O., Sargent, J., Friedrich, W., Chaffin, M.,Cunningham, N., & Cantor, P. S. (2001). The impactof social change on child mental health in EasternEurope. Child & Adolescent Psychiatric Clinics ofNorth America, 10(4), 815824.
Makinen, I. H. (2000). Eastern European transition andsuicide mortality. Social Science & Medicine, 51(9),14051420.
Makinen, I. H. (2006). Suicide mortality of EasternEuropean regions before and after the Communistperiod. Social Science & Medicine, 63(2), 30719.
Martikainen, P., Bartley, M., & Lahelma, E. (2002).Psychosocial determinants of health in social epide-miology. International Journal of Epidemiology, 31(6),10911093.
Neumann, J. (1991). Psychiatry in eastern Europe today:Mental health status, policies, and practices.American Journal of Psychiatry, 148(10), 13861389.
Orkeny, A., & Szekelyi, M. (2000). Views on socialinequality and the role of the state:Posttransformation trends in Eastern and CentralEurope. Social Justice Research, 13, 199218.
490 EIRO OROSA
Dow
nloa
ded
by [
Dr
Fran
cisc
o Jo
s E
iroa
-Oro
sa]
at 1
8:02
26
Aug
ust 2
013
-
Pfaff, S. (1996). Collective identity and informal groupsin revolutionary mobilization: East Germany in 1989.Social Forces, 75(1), 91117.
Pikhart, H., Bobak, M., Pajak, A., Malyutina, S.,Kubinova, R., Topor, R., et al. (2004). Psychosocialfactors at work and depression in three countriesof Central and Eastern Europe. Social Science& Medicine, 58(8), 14751482. doi:10.1016/s0277-9536(03)00350-2.
Piko, B. F., & Fitzpatrick, K. M. (2001). Does classmatter? SES and psychosocial health amongHungarian adolescents. Social Science & Medicine,53(6), 817830.
Piko, B. F., & Fitzpatrick, K. M. (2007). Socioeconomicstatus, psychosocial health and health behavioursamong Hungarian adolescents. European Journal ofPublic Health, 17(4), 353360.
Pinquart, M., & Silbereisen, R. K. (2004).Human development in times of social change:Theoretical considerations and research needs.International Journal of Behavioral Development,28(4), 289298.
Pinquart, M., Silbereisen, R. K., & Juang, L. P. (2004).Changes in psychological distress among EastGerman adolescents facing German unification.Youth & Society, 36(1), 77101.
Rathner, G., Tury, F., Szabo, P., Geyer, M., Rumpold,G., Forgacs, A., et al. (1995). Prevalence of eatingdisorders and minor psychiatric morbidity in CentralEurope before the political changes in 1989:A cross-cultural study. Psychological Medicine,25(5), 10271035.
Reinap, M., Lai, T., Janno, S., Tamme, T., & Tamm, M.(2005). Cost-effectiveness of mental healthinterventions in Estonia. Tallinn, Estonia: HealthcareSociety.
Rosen, G. (1968). Madness in society: Chapters in thehistorical sociology of mental illness. Chicago, IL:University of Chicago Press.
Rotter, J. B. (1954). Social learning and clinicalpsychology. New York, NY: Prentice Hall.
Seligman, M. E. (1975). Helplessness: On depression,development, and death. New York, NY: W. H.Freeman.
Seligman, M. E., & Maier, S. F. (1967). Failure toescape traumatic shock. Journal of ExperimentalPsychology, 74(1), 19.
Smith, G. C. (1996). Caregiving outcomes for oldermothers of adults with mental retardation: A test ofthe two-factor model of psychological well-being.Psychology and Aging, 11(2), 353361.
Stelmach, W., Kaczmarczyk-Chalas, K., Bielecki, W., &Drygas, W. (2004). The association between income,education, control over life and health in a largeurban population of Poland. International Journal ofOccupational Medicine and Environmental Health,17(2), 299310.
Sztompka, P. (2004). The trauma of social change:A case of postcommunist societies.In E. R. Alexander et al. (Eds.), Cultural traumaand collective identity. Berkeley, CA: University ofCalifornia Press.
Temkov, I., Jablensky, A., & Boyadjieva, M. (1975).Use of reported prevalence data in cross-nationalcomparisons of psychiatric morbidity. SocijalnaPsihijatrija, 3(2), 111117.
Tomov, T., Mladenova, M., Lazarova, I., Sotirov, V., &Okoliyski, M. (2004). Bulgaria mental health countryprofile. International Review of Psychiatry, 16(12),93106.
Wardle, J., Steptoe, A., Gulis, G., Sartory, G., Sek, H.,Todorova, I., et al. (2004). Depression, perceivedcontrol, and life satisfaction in university studentsfrom Central-Eastern and Western Europe.International Journal of Behavioral Medicine, 11(1),2736.
Warsaw Institute of Psychiatry and Neurology (2004).Psychiatric and neurological care institutions.Warsaw, Poland: Statistical Yearbooks.
World Health Organization Regional Office for Europe(2001). Mental health in Europe: Country reports fromthe WHO European Network on Mental Health.Copenhagen, Denmark: WHO.
World Health Organization Regional Office for Europe(2003). Mental health in WHOs European Region.Copenhagen, Denmark: WHO.
World Health Organization Regional Office for Europe(2011). Health For All Data Base. Copenhagen,Denmark: WHO.
PSYCHOSOCIAL WELLBEING 491
Dow
nloa
ded
by [
Dr
Fran
cisc
o Jo
s E
iroa
-Oro
sa]
at 1
8:02
26
Aug
ust 2
013
Related Documents