PSYCHODERMATOLOGY 0733-8635/96 $0.00 + .20 PSYCHOPHYSIOLOGY OF STRESS IN DERMATOLOGY The Psychobiologic Pattern of Psychosomatics Emiliano Panconesi, MD, and Giuseppe Hautmann, MD In 1878, Bernard5first recognized the physi- ologic response of animals to environmental stimuli when he described the "milieu in- terieur" of the animal, characterized by its constancy, and the external environment, characterized by its variability. Cannon'O later redefined this concept as "homeostasis," in which a steady state is obtained by the opti- mal interaction of counteracting processes within the host. He also defined the flight- fight reflex of animals exposed to undue stress and identified the potentially damaging effects of stress on the individual. The physio- logic basis of the stress response was attrib- uted to activation of endocrinologic factors involving the sympathetic adrenomedullary axis." Selye106 then described the response of laboratory animals experimentally exposed to noxious stimuli, which he classified as the "general adaptation syndrome." The syn- drome was classified as having three distinct phases: (1) an alarm reaction, (2) a resistance phase, and (3) if stress was not dissipated, exhaustion of the biologic system. Because different noxious stimuli produced an appar- ently similar physiologic response, involving activation of the pituitary-adrenal-cortical axis, he concluded that the response to stress was "nonspecific." This led to the widely held view that stress largely involved nonspe- cific production of corticosteroids, and it sub- sequently has led to the measurement of glu- cocorticosteroids as the primary indicator of stress and animal well-being. As the field of neuroendocrinology evolved, Selye's concept of the nonspecific response was refuted. Ma- son68 has shown that different types of stress such as fasting and heat shock produce dra- matically different corticosteroid levels in ex- perimental monkeys. He showed characteris- tically different responses and produced characteristic responses to the different stres- sors. It now is accepted widely that there are unique but different endocrine responses to different physical, chemical, and psychologi- cal stressors and that these responses vary from one species of animals to another and from one individual to another within a spe- cies. Stress currently can be defined as an abnor- mal or extreme adjustment in the physiology of an animal to cope with adverse effects of the environment and management. In this article the adverse effect is designated the stressor. The term stress has been qualified further by other workersz3, Io5 to include the From the Department of Dermatology, University of Florence, Florence, Italy DERMATOLOGIC CLINICS VOLUME 14 - NUMBER 3 * JULY 1996 399

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
PSYCHODERMATOLOGY 0733-8635/96 $0.00 + .20
PSYCHOPHYSIOLOGY OF STRESS IN DERMATOLOGY
The Psychobiologic Pattern of Psychosomatics
Emiliano Panconesi, MD, and Giuseppe Hautmann, MD
In 1878, Bernard5 first recognized the physi- ologic response of animals to environmental stimuli when he described the "milieu in- terieur" of the animal, characterized by its constancy, and the external environment, characterized by its variability. Cannon'O later redefined this concept as "homeostasis," in which a steady state is obtained by the opti- mal interaction of counteracting processes within the host. He also defined the flight- fight reflex of animals exposed to undue stress and identified the potentially damaging effects of stress on the individual. The physio- logic basis of the stress response was attrib- uted to activation of endocrinologic factors involving the sympathetic adrenomedullary axis." Selye106 then described the response of laboratory animals experimentally exposed to noxious stimuli, which he classified as the "general adaptation syndrome." The syn- drome was classified as having three distinct phases: (1) an alarm reaction, (2) a resistance phase, and (3) if stress was not dissipated, exhaustion of the biologic system. Because different noxious stimuli produced an appar- ently similar physiologic response, involving activation of the pituitary-adrenal-cortical axis, he concluded that the response to stress
was "nonspecific." This led to the widely held view that stress largely involved nonspe- cific production of corticosteroids, and it sub- sequently has led to the measurement of glu- cocorticosteroids as the primary indicator of stress and animal well-being. As the field of neuroendocrinology evolved, Selye's concept of the nonspecific response was refuted. Ma- son68 has shown that different types of stress such as fasting and heat shock produce dra- matically different corticosteroid levels in ex- perimental monkeys. He showed characteris- tically different responses and produced characteristic responses to the different stres- sors. It now is accepted widely that there are unique but different endocrine responses to different physical, chemical, and psychologi- cal stressors and that these responses vary from one species of animals to another and from one individual to another within a spe- cies.
Stress currently can be defined as an abnor- mal or extreme adjustment in the physiology of an animal to cope with adverse effects of the environment and management. In this article the adverse effect is designated the stressor. The term stress has been qualified further by other workersz3, Io5 to include the
From the Department of Dermatology, University of Florence, Florence, Italy
DERMATOLOGIC CLINICS
VOLUME 14 - NUMBER 3 * JULY 1996 399
400 PANCONESI At HAUTMANN
term distress. This term is used to identify the extreme response to adverse stimuli that cause a damaging pathophysiologic reaction in the host, producing associative changes in behavior, physiology, and disease susceptibil- ity. It also has been recognized that other forms of stimuli potentiate the physiologic responses of the host without producing any adverse effect, and such responses are said to involve eustres~.~~, lo5
There are two main types of host factors that can influence y2 They are genetics and perception.
GENETICS
Evolutionary changes have led to marked differences in the adaptative physiologic re- sponse of different species exposed to stress. This is reflected in variations in the endocrine response of species to individual stressors and in the variable effects of specific endo- crine factors on the target cells in different animal species. Variations of response also are found within species and may be accentu- ated by selective breeding, age, sex, and con- ditioning.
PERCEPTION
The most important factor that influences stress is the individual’s perception of the challenge posed by the specific stimulus. Fac- tors that influence the individual’s perception of stress include bonding during rearing, the novelty or predictability of the stimulus, and training that frustrates the avoidance re- sponse and evokes a state of learned help- le~sness .~~ Conditioning to stimuli also may occur in which the association between an aversive chemical stimulus and an immuno- modulating agent, given in combination, can evoke a conditioned state of immunosuppres- sion or immunoenhancement when the aver- sive stimulus is applied in the absence of the immunomodulating agent.
There are numerous types of stressors. Stressors include a variety of environmental stimuli that evoke significant homeostatic al- terations in the host. They may result from
natural changes in the environment or from artificial changes imposed by management constraints or be caused by a range of experi- mental stimuli that have been used to study stress physiology. The effect produced by ex- posure to stress may be influenced by the severity of the stressor, the time of applica- tion (acute versus chronic), or whether the animal can escape the stressor if it is applied repeatedly (escapable versus inescapable).
Environmental
Natural exposure to extremes of heat or cold under climatic conditions or artificially in animal housing or holding facilities is among the most common stressors. Physical restraint associated with separation, treat- ment, or transport of animals is another im- portant stressor. Environmental changes that produce strange or novel sounds, sights, odors, or tastes also can evoke stress. Drugs or chemicals used in the management or treatment of animals can act as stressors, and toxic products released by infectious agents, environmental pollutants, or inadequate ven- tilation can have a similar effect. Shearing, docking, and castration carried out during routine management also cause stress.
Behavioral
Overcrowding, hierarchic challenge, wean- ing, exposure to unfamiliar surroundings, or isolation can have a major behavioral impact on animals and evoke stress. Changes or re- strictions in diet also can act as stressors, alone or in combination with other stressors such as physical restraint.
Psychological
In animal species, the capture of wild subjects or the exposure of domesticated ani- mals to restraint, transport, or management extremes may evoke adaptative stress in the host. In the context of Selye’s general adapta- tion syndrome, the response is recognizable initially as anxiety, which may progress to

PSYCHOPHYSIOLOGY OF STRESS IN DERMATOLOGY 401
fright or terror. Failure of the animal to ex- press the flight-fight response results in the expression of anger or rage and, if the stimu- lus persists, frustration or helplessness. Be- cause stress results largely from the individ- ual’s perception of the threat posed by a stimulus rather than its nature per se, a cogni- tive or psychological component is central to all stress.y2
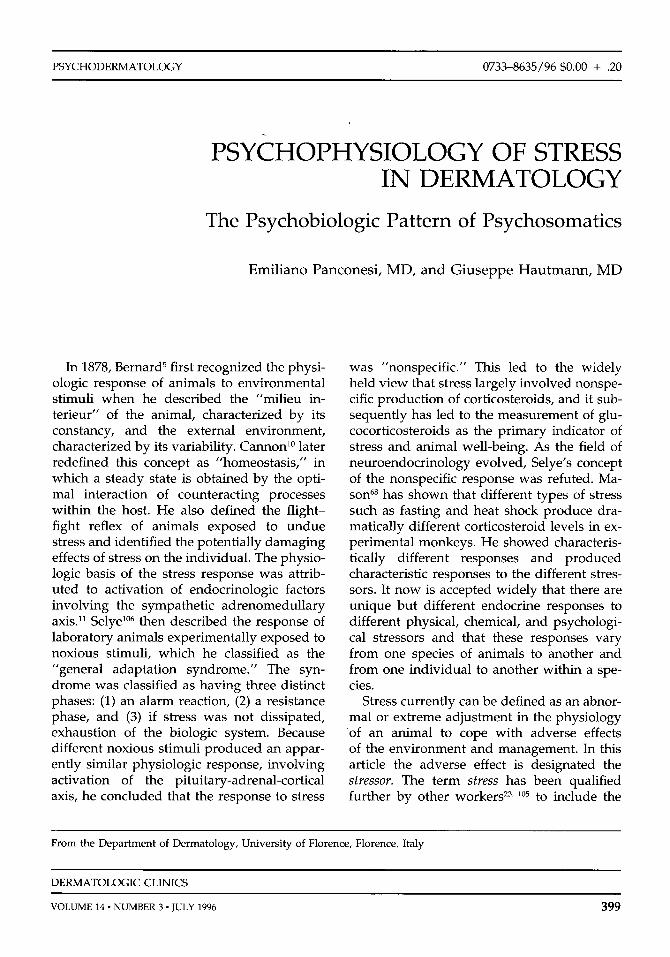
The biologic response within the host that results from exposure to stress is outlined in Figure 1. This response produces an impact on many of the organs within the affected
Behavioral and psychological experiences involving stress, documented in animals, are what our patients propose to us every day. Overcrowding, hierarchic challenge, wean- ing, exposure to unfamiliar surroundings, isolation, anger and rage, frustration, and helplessness, even without the precise flight- fright response, seem to be a normal condi- tion of life for modern humans. Isolation, deprivation, fasting, starvation, and religious and mystic passions can be proposed as eq~ivalents .~~
Because stress can be caused by environ- mental factors just as well as psychic re-elabo- ration, it is easy to perceive the relationship
y2
perception
activation CNS recognition
Autonomic nervous stimulation
Endocrine response
cardiovascular
multiorgan Flight-fight Systemic reactivity
immune system
Physiologic I -1 Conservation reactivity adaptation withdrawal
Pathologic Exhaustion reactivity
Figure 1. Organized multisystem response to stress. CNS = central nervous system.
between everyday stress and defense mecha- nisms and disease susceptibility, on one hand, and the involvement of the physical and psychological sphere on the other. The result is a unitary concept of human pathol- ogy, and the problem is to determine the entity of the emotional component in any dis- ease. The body (soma) and the mind (psyche) constitute a single unit. Separating the two and treating them individually should be con- sidered only reductive necessity or abusive operative simplification for the investigator or doctor.
Psychosomatic medicines3, 92 proposes the examination of psyche and soma as a unit “in sickness and in health” and, in the former case, useful intervention in the attempt to reestablish equilibria that have been altered. The fortunate term psychosomatic by now has become a part of current medical terminology incorporated into everyday language, and it was inevitable that any organ (including the skin) and its diseases become the object of medical observation and interpretation from a psychosomatic point of view.83 Neverthe- less, in the American dermatologic literature the term psychosomatic is resisted (in the author’s opinion, unjustifiably) and the term psychocutaneous is preferred.
Experimental studies done during the last 20 years have seen the marriage of psychol- ogy, neuroendocrinology, and immunology into a new subspecialty called psychoneuroen- docrinimmunology. Research in this multifac- eted system has identified and integrated the physiologic factors produced by the neuro- logic and immunologic systems. Soluble fac- tors produced by the neurologic and immu- nologic tissues in normal or pathologic conditions include neurotransmitters, neuro- peptides (NP), adrenocorticotrophin, cate- cholamines, corticosteroids, opioids, and cytokines, including lymphokines and mono- kine^.^ These bidirectional loops between the CNS and the immune system occur as a con- sequence of neurohormones acting on cells of the immune system, while cytokines or antibodies secreted by lymphocytes and mac- rophages influence neuroendocrine function. Nevertheless, the newly recognized similari- ties between the immune and neuroendocrine systems include the observation, in both sys-
402 PANCONESI & HAUTMANN
tems, of an increasing number of peptides and proteins that are used as intercellular messengers. These substances usually are called neuropeptides. These NPs represent a heterogeneous group of molecules; the small- est ones containing only two amino acids, with larger peptides consisting of 40 or more amino acids. In the nervous system, NPs ful- fill many of the criteria of a neurotransmitter and neuromodulator. Many have been stud- ied in other contexts as hormones, "gut peptides," or growth 65, 85 Recent evi- dence strongly supports the notion that NPs are endogenous to the immune system and are used for intraimmune system regulation, as well as for bidirectional communication between the immune and neuroendocrine
64, 91 NPs may exert their regulatory influence in one or more of the following ways: (1) as components of the autonomic nervous system, acting locally at peripheral sites; (2) as brain peptides, acting on central regulatory centers; and (3) as neurohormones, reaching their target organs via the hypo- physial portal vessels (such as the releasing factors) or via the general circulation (such as oxytocin or vasopressin).
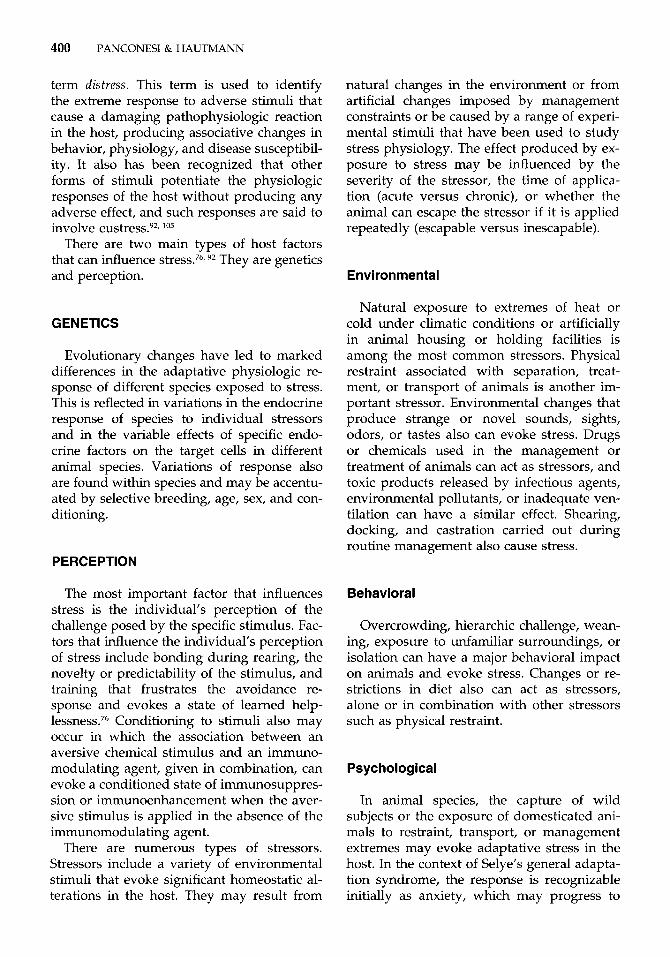
The number of NPs described exceeds 50, and most, if not all, alter behavior and mood states." Figure 2 shows a suggested schematic illustration of a possible NP-behavior rela- tionship. Relationship A illustrates how an NP can regulate different behaviors by acting differently or at different neural loci. This statement is supported by the findings that many individual NPs are widespread in the nervous system, exercise multiple neural ac- tions, and are involved in the regulation of many different and often unrelated behav- iors.
Relationship B in Figure 2 indicates that neurons mediating a given behavioral effect of an NP are distributed across anatomic boundaries in the CNS.
Different NPs act on the same population of neurons but through different cellular mechanisms to regulate a given mechanism. It is obvious that most of the behaviors are regulated by more than one NP.
They affect the same behavior through a similar neural locus, suggesting that different NPs act on the same population of neurons
to exert their effects on a behavior; moreover, in vitro studies suggest that some NPs act through modulation of neuronal responses, whereas other NPs probably act as stimula- tory or inhibitory neurotransmitters, as sche- matized in relationship C in Figure 2.
Finally, relationship D in Figure 2 shows that an NP that activates a behavior peripher- ally often also may serve as a neurotransmit- ter at each synapse in the central pathway mediating that behavior; thus, it has been suggested that a given behavior tends to be mediated by a pathway consisting of a chain of neurons containing the same NPs and that an NP could induce a given behavior at sev- eral neural loci. An infusion in the cerebral ventricles often would be more effective than a local microapplication for an NP to induce a given behavior.48
The skin and CNS are related embryologi- cally because the epidermis and neural plate derive from the embryonic ectoderm. The neural plate gives rise to the neural tube and neural crest, from which the central and pe- ripheral nervous systems develop. The mela- nocytes and, possibly, the Merkel cells in the skin also originate from the neural crest.h This embryologic association between the skin and the CNS is the most likely basis for the find- ing that various neuroectodermal syndromes often are associated with CNS abnormalities such as mental retardation and seizures. The clinical implications of this embryologic asso- ciation may be more far reaching because the skin and the CNS share various hormones, neurotransmitters, and receptors. The gener- ous primary sensory neuronal innervation of the superficial dermis should ensure a wide distribution of NPs in the skin. During the last decade, numerous studies have shown that many of these peptides, including sub- stance P (SP), calcitonin gene-related peptide (CGRP), vasoactive intestinal peptide (VIP), neuropeptide Y (NPY), neurokinin, and neu- rotensin A, are present in the skin, where they may play roles as neurotransmitters and trophins. Cutaneous NPs are contained in myelinated A-delta fibers and small unmy- elinated C fibers, including sensitive and au- tonomic fibers. It is well known that the skin is innervated by primary afferent sensory nerves, postganglionic cholinergic parasym- pathetic nerves, and postganglionic adrener-
PSYCHOPHYSIOLOGY OF STRESS IN DERMATOLOGY 403
CNS Locus a + behavior a CNS Locus b + behavior b CNS Locus c
behavior c € mediating action
modulatory action - I CNS Locus d A CNS Locus e _.+ behavior d
A Neuropeptide a
CNS Locus a CNS Locus b behavior a CNS Locus c CNS Locus d
B Neuropeptide a
C
Neuropeptide c -
D Neuropeptide a + CNS - NPa + CNS - NPa + CNS - NPa - behavior a , (NPa) , , puss Locus b Y u s c ,
Neuropeptide a - (modulation) Neuropeptide b - (mediation)
Neuropeptide d - (mediation)
a single population of CNS neurons + behavior a
c periphery
.) CNS
Figure 2. A-D, Possible neuropeptide-behavior relationship.
gic and cholinergic sympathetic nerves.48, 64, 91
It must be emphasized that sensory nerves not only function as an afferent system to conduct stimuli from the skin to the CNS but also act in an efferent "neurosecretory" fashion throughout their branches. In addi- tion to the classic role of the neuroendocrine and autonomic systems in the stress response, the sensory nervous system also plays a role in this response. Specialized cutaneous recep- tors (nociceptors) sense and transmit sensory signals, including noxious stimuli, by unmy- elinated afferent C fibers to the dorsal root ganglia and the dorsal horn of the spinal
Ascending nerve tracts transmit this sensory information to the thalamus, which transmits it to higher cortical centers involved in processing cognitive information.101 De- scending pathways relay the sensory infor- mation back down the spinal cord, resulting in peripheral autonomic responses (e.g., vaso- dilation and sweating).'O'
Stimulation of cutaneous nociceptors by noxious stimuli (mechanical, thermal, or chemical injuries) influences nerve endings that are depolarized, and impulses are con- veyed centrally and peripherally (antidromi- cally). These peripheral effector functions provided by afferent sensory neurons under-
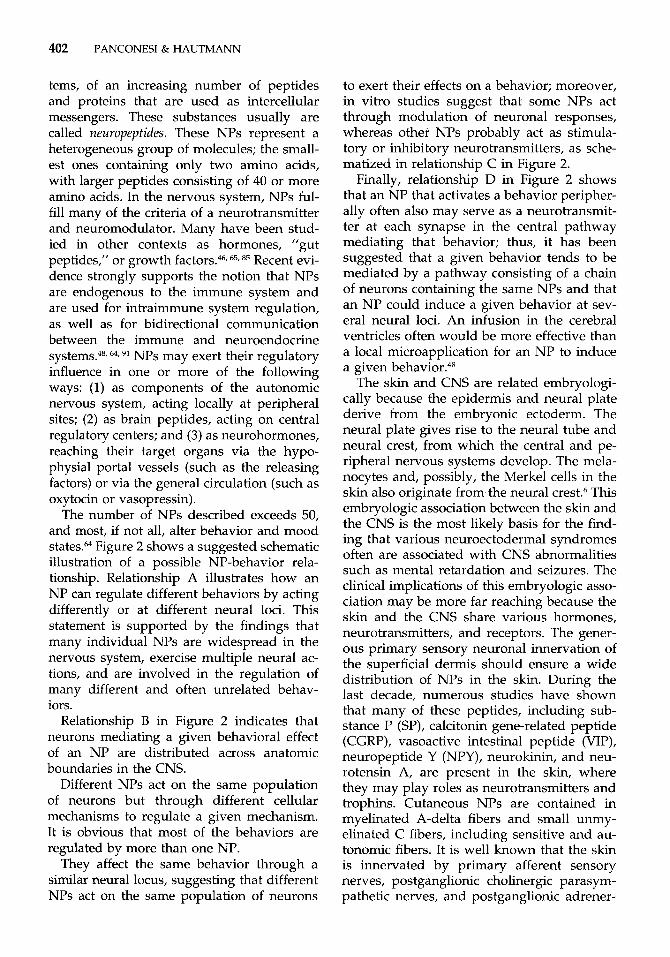
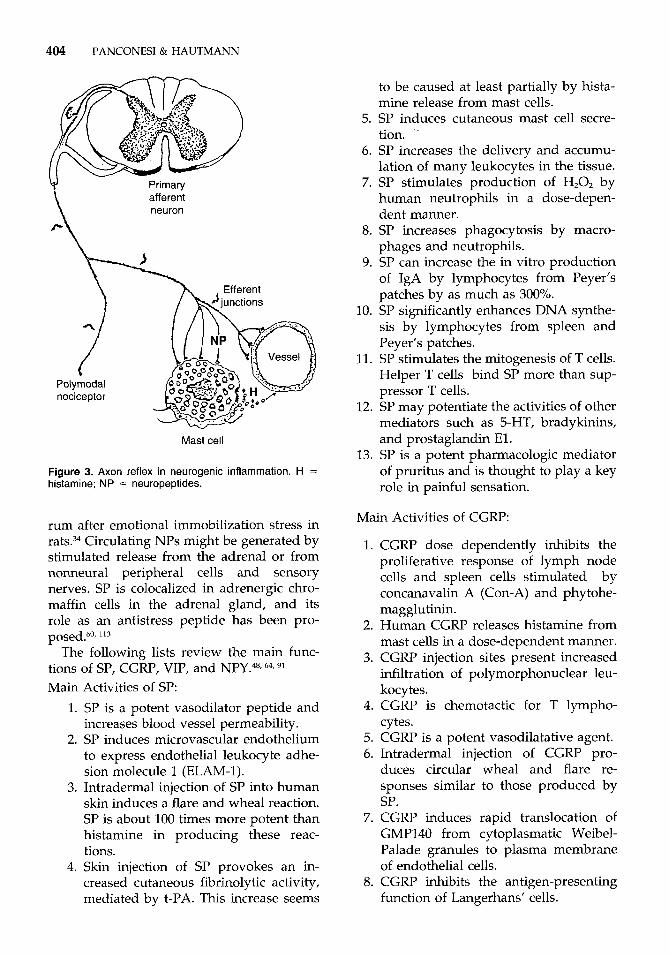
lie so-called neurogenic inflammation, which is based on the release of NPs, including SP, CGRP, and VIP, from collateral sensory nerve branches.'O' Stimulation of cutaneous nocicep- tors also causes activation of ascending path- ways, resulting in enhanced electrical activ- ity'02 and decreased levels of SP3I in several higher cortical CNS regions. Local release of NPs from sensory nerves in the skin, how- ever, has not been measured in response to stressful stimuli in animals or humans. Acti- vation of higher cortical areas during stress results in altered release of SP from the adre- nal gland by descending autonomic fibers."' Because some of these descending fibers in- nervate opioid interneurons in the dorsal horn63 and these interneurons are connected anatomically to SP-containing nerves in the spinal cord, it is possible that descending au- tonomic nerves can trigger antidromic release of NPs in the skin. In Figure 3 the authors present schematically the mechanism of axon reflex in neurogenic inflammation. Such a novel possible mechanism would explain the effects of emotional stress on skin physiology. Several experimental findings support this hypothesis.62, 82 In addition to stress-induced alterations in SP levels in the CNS, increased concentrations have been reported also in se-
404 PANCONESI & HAUTMANN
Primary afferent neuron
Polymodal nociceptor
Mast cell
Figure 3. Axon reflex in neurogenic inflammation. H = histamine; NP = neuropeptides.
rum after emotional immobilization stress in rats.34 Circulating NPs might be generated by stimulated release from the adrenal or from nonneural peripheral cells and sensory nerves. SP is colocalized in adrenergic chro- maffin cells in the adrenal gland, and its role as an antistress peptide has been pro-
The following lists review the main func- tions of SP, CGRP, VIP, and NPY.48* 64, 91
Main 1.
2.
3.
4.
Activities of SP: SP is a potent vasodilator peptide and increases blood vessel permeability. SP induces microvascular endothelium to express endothelial leukocyte adhe- sion molecule 1 (ELAM-1). Intradermal injection of SP into human skin induces a flare and wheal reaction. SP is about 100 times more potent than histamine in producing these reac- tions. Skin injection of SP provokes an in- creased cutaneous fibrinolytic activity, mediated by t-PA. This increase seems
to be caused at least partially by hista- mine release from mast cells.
5. SP induces cutaneous mast cell secre- tion. .
6. SP increases the delivery and accumu- lation of many leukocytes in the tissue.
7. SP stimulates production of H,O, by human neutrophils in a dose-depen- dent manner.
8. SP increases phagocytosis by macro- phages and neutrophils.
9. SP can increase the in vitro production of IgA by lymphocytes from Peyer’s patches by as much as 300%.
10. SP significantly enhances DNA synthe- sis by lymphocytes from spleen and Peyer’s patches.
11. SP stimulates the mitogenesis of T cells. Helper T cells bind SP more than sup- pressor T cells.
12. SP may potentiate the activities of other mediators such as 5-HT, bradykinins, and prostaglandin El .
13. SP is a potent pharmacologic mediator of pruritus and is thought to play a key role in painful sensation.
Main Activities of CGRP:
1. CGRP dose dependently inhibits the proliferative response of lymph node cells and spleen cells stimulated by concanavalin A (Con-A) and phytohe- magglutinin.
2. Human CGRP releases histamine from mast cells in a dose-dependent manner.
3. CGRP injection sites present increased infiltration of polymorphonuclear leu- kocytes.
4. CGRP is chemotactic for T lympho- cytes.
5. CGRP is a potent vasodilatative agent. 6. Intradermal injection of CGRP pro-
duces circular wheal and flare re- sponses similar to those produced by SP.
7. CGRP induces rapid translocation of GMP140 from cytoplasmatic Weibel- Palade granules to plasma membrane of endothelial cells.
8. CGRP inhibits the antigen-presenting function of Langerhans’ cells.

Main Activities of VIP:
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
PSYCHOPHYSIOLOGY OF STRESS IN DERMATOLOGY 405
life cycle. It long has been recognized that
VIP is a vasodilator agent on the small blood vessels. VIP has high affinity binding to human lymphoid cells through specific cell surface receptors for this neuropep- tide. VIP inhibits the response of murine lymphocytes to Con-A and phytohemag- glutinin but not lipopolysaccharides. VIP inhibits natural killer activity of large granular lymphocytes. VIP increases IgA synthesis by Peyer’s patches. VIP stimulates histamine releases in rat peritoneal connective tissue mast cells. VIP activates mast cells in a IgE-inde- pendent pattern. Mast cells and eosinophils can release VIP. VIP enhances monocyte migration in chemotaxis chambers. VIP often is present in cholinergic neu- rons. In the skin, VIP has mitogenic proper- ties on keratinocytes, stimulating their proliferation. Intradermally injected VIP provokes a slight but statistically not significant re- duction in weal and flare reaction.
Main Activities of NPY:
1. NPY is one of the most potent vasocon- strictor agents.
2. NPY often is present in adrenergic neu- rons.
3. NPY produces vasoconstriction and in- creases blood pressure.
4. NPY evokes coronary vasoconstriction and has a negative inotropic effect in some species.
5. NPY decreases glomerular filtration and inhibits renin secretion.
6. NPY can modulate the release of CGRP.
7. NPY is one of the most abundant pep- tides found in the CNS in all mamma- lian species studied.
The skin occupies a powerful position as an organ of communication and plays an im- portant role in socialization throughout the
psychosomatic factors play a role in dermato- logic disease. In agreement with I ron~ide ,~~ the authors believe that an organ system is vulnerable to psychosomatic ailments when (1) several etiologic factors, including genetic and constitutional predisposition, are opera- ble, (2) emotional factors mediated by the CNS are in play, ( 3 ) intrapsychic processes such as self-concept, identity, or eroticism are involved, (4) the organ system is likely to be the object of ”conversion” and conditioning because of emotional arousal related to intra- psychic problems, and (5) social values and standards are linked with the organ system. Rook and Wilkins~n,’”~ in the well-known Textbook of Dermatology, open the chapter on ”Psychocutaneous Disorders” with the af- firmation that “the role of emotional factors on diseases of the skin is of such significance that if they are ignored the effective manage- ment of at least 40% of the patients attending departments of dermatology is impossible.” These percentages are even higher for the psycho-influenced dermatoses; Obermayer8I reported 66% and for Medansky and Hand- ler73 “almost 80% of dermatologic patients had a psychogenic overlay.” The patient may use the skin to communicate emotional dis- tress, and there may be a full range of per- sonal and family problems underlying the presenting dermatologic problem. For exam- ple, women whose complaint of hair loss seems disproportionate to the objective de- gree of alopecia have been reported to have marital difficulties and depression.’Y Patients with immature psychological coping mecha- nisms may not be able to obtain nurturing or attention from others by other means and therefore may derive secondary gain from a visible skin condition. Alternately, develop- ment of a cosmetically disfiguring condition can result in social disapproval and increased self-consciousness. This can result in social withdrawal, academic underachievement, and even serious psychological problems, es- pecially when the skin disorder occurs during a developmentally critical period such as ado- lescence. In psoriasis, for example, the cos- metic disfigurement and consequent social stigma (real or imagined) can have a pro- foundly adverse effect on the patient’s quality
406 PANCONESI & HAUTMANN
of life and result in significant disease-related stress. This disease-related stress may exacer- bate the psoriasis and adversely affect the course of the disease.
Various clinical observations suggest that psychoneuroimmunologic factors may have important applications in dermatology. Psy- chological stress has been associated with in- creased CNS levels of opioid neuropeptides and also has been reported to exacerbate cer- tain dermatologic conditions that have a psy- chosomatic and an immunologic component, such as chronic idiopathic urticaria, atopic dermatitis, and psoriasis.48, 64, 91, 92 These are only a few examples, because the authors be- lieve that some stressing factor can be indi- viduated in almost all dermatoses, in major or minor degree.
PSORIASIS
Psoriasis is a frequent, chronic, erythema- tous dermatosis with squamous accumula- tions. It may be circumscribed or dissemin- ated with preferential sites (elbows, knees, scalp). It is presumed to be determined genet- ically, and it has typical histologic markers (capillary dilatation, sterile epidermal mi- croabscesses, parakeratosis) and accelerated epidermal turnover. In the vessels of the der- mal (”squirting”) papilla, Munro-Sabouraud epidermal microabscesses (formed by poly- morphonuclear cells squirted out from the vessels), and accelerated turnover of keratino- cytes, the authors hypothetically identify the key points of the disease influenced or influ- enceable by acute or chronic emotional stress. Arnetz et a12 studied psychoendocrine and metabolic reactions during standardized stressor exposure (color-word conflict test and forced mental arithmetics) in psoriatic patients and in matched healthy subjects. Un- der resting conditions, the groups were simi- lar with regard to psychological and biochem- ical variables, whereas during stressor exposure, the psoriatic group reported sig- nificantly higher strain levels. Blood pressure, pulse rate, plasma glucose, and urinary adrenaline excretion increased in both groups during exposure, with more pronounced in- creases in the latter two in the psoriatic
group.2 Serum cortisol, prolactin, progester- one, and urinary cortisol decreased in both groups during stressor exposure. The de- crease in serum cortisol was more pro- nounced in the psoriatic group. In contrast, during standardized stressor exposure, psori- atic subjects reported higher levels of strain, which was accompanied by higher levels of urinary adrenaline and lower levels of plasma cortisol, suggesting the hypothesis that psori- atic patients perceive certain challenging situ- ations as more stressful than do nonpsoriatic control subjects and react accordingly in their different psychoendocrine reaction pattern.2 Because in 60% of patients psoriasis starts before the age of 30 years, the nature of the skin disease (its visibility and the need for consistent care) becomes a crucial factor in these persons’ psychological development. Updike,Il2 one of the most important contem- porary American writers, writes of his feel- ings about his psoriasis: “One hates one’s abnormal, erupting skin. . . . The skin was my enemy . . . ,” and he refers to his mother, who had psoriasis, and her protec- tiveness of her ”defective cub. . . . Strategies of concealment ramify, and self-examination is endless.” Many studies have specifically indicated that feelings of being stigmatized by psoriasis are important in how patients perceive themselves. Jowett and Ryan55 re- ported that the majority of psoriatic patients indicated that the worst thing about their dis- ease was the appearance and consequent embarrassment; 89% reported shame and embarrassment, 50% anxiety, 42% lack of con- fidence, and 24% depression. Twenty-six per- cent said that psoriasis caused family friction. Almost half curtailed athletic activities, espe- cially ~wimming.’~, 52, 55, h1
Several studies support the importance of psychosocial factors in the onset or exacerba- tion of psoriatic symptoms in 39% to 80% of patientsz4 It also has been suggested that there is a subset of psoriasis patients charac- terized as high stress reactors who suffer more clinically disfiguring lesions and more frequent disease flare.43
Although there is evidence that heredity has a recognized role (probably multifactorial inheritance with a polygenic mechanism) in the case of psoriasis, it also has been shown
PSYCHOPHYSIOLOGY OF STRESS IN DERMATOLOGY 407
by studies on monozygotic that envi- ronmental factors are important in triggering the disease. Vast amounts of the literature and our personal experience allow‘us to in- clude acute and chronic emotional stimuli in the general group of environmental factors. There is a great diversity of exogenous and endogenous factors that can trigger the onset of psoriasis, possibly via the strategically lo- cated tumor necrosis factor-alpha producing dermal dendrocyte. Koebner’s phenomenon refers to the development of psoriatic lesions in traumatized skin, whereas endogenous fac- tors that may precipitate psoriasis include certain drugs and bacterial and viral infec- tions.
The importance of emotional shock was at the base of historic observations by Hardy, Leloir, Brocq, Bodin, and Andry, mentioned by Bolgert et a1,8 who answer affirmatively to the question posed in the title of their work: ”Le psoriasis est-il une psycho-dermatose?” (Is psoriasis a psychodermatosis?). Other au- thors are more cautious in affirming the rela- tionship between emotional events and psori- asis, but, with time, psychosomatic research has passed from reference to ”significant” an- amnestic episodes (the ”anedoctal” period) to reference to “personality profile” held to be specific for the various dermato~es.~, 297 99 Nu- merous studies have attempted to identify a specific personality profile, but have failed to show any reproducible personality type; however, several emotional features and reac- tions have been identified in samples of psori- asis patients. They have been found to have increased levels of anxiety and depre~sion,2~ increased tendencies for obsessiveness,M and increased expression of aggre~sion.~~ Feelings of stigmatization and other emotional se- quelae have been suggested as well.36 Despite these and other studies, it remains unclear whether these emotions precede and precipi- tate psoriatic flares or whether they are a consequence of having a chronic, sympto- matic, disfiguring illness. It is the authors’ opinion that hereditary factors constitute in all likelihood the fundamental predisposing condition on which various stressors, not the least of which psychosocial (psychobiologic) ones, activate the emotional stress mecha- nism, provoking onset or exacerbating the
disease. Much significance recently has been attributed to an understanding of the psycho- neuroimmunology of psoriasis.28 Neuropep- tides have been suggested to be of pathogenic importance in psoriasis,28, 4R, 64, 91 as a neuro- modulatory factor underlying psoriasis flare or responsible for the maintenance of psori- atic lesions. According to this theory, the oc- currence of a psoriasis flare after stress is related to the release of certain neuropep- tides, and the symmetry of psoriatic lesions would be caused by bilateral distribution of cutaneous peripheral nerves.2R There is a sig- nificant increase in SP-containing nerves in psoriatic skin, and psoriatic lesions are inner- vated more densely.
An abundance of neuropeptides such as SP and VIP has been shown in psoriatic lesions. The neuropeptides locally released, such as SP, VIP, and CGRP, can act as a neurotrans- mitter in neurogenic inflammation mediated by antidromic pathways. SP interacts in vitro with the functions of most dermal and epider- mal cells, including keratinocyte prolifera- tion.ls, 25, 27, 787 96 SP can influence inflammatory response by stimulating lymphomononuclear cells, altering endothelial cells, and degranu- lating mast cells.22, 95 VIP also can stimulate proliferation of keratinocytes. This effect is accentuated in the presence of leukotriene B4.98 Keratinocyte proliferation, a hallmark of psoriasis, can be triggered by SP and VIP. SP-induced lymphocytic proliferation may be responsible for the altered cell-mediated im- mune response in patients with psoriasis. In- duction of ELAM-1 on endothelium by SP and even more so by CGRP and VIP, could explain the initiation and maintenance of the lesional infiltrate.’O
Therapeutic efficacy of neuropeptide-mod- ulating drugs is more indirect evidence that supports the role of neuropeptides in psoria- sis. Capsaicin, an SP-depleter, has been re- ported to improve psoriasis partially, and peptide T, a VIP analogue, recently has been observed to be effective in the treatment of psoriasis. All these findings are consistent with the hypothesis that cutaneous nerves to- gether with their neuropeptides play a key role in the pathogenesis of psoriasis.47, 48 Con- sidering the influence of the previously men- tioned neuropeptides on the mechanisms of
408 PANCONESI & HAUTMANN
inflammation and immunity, as well as their trophic and stimulating effects on cell growth, certain pathogenetic mechanisms in psoriasis might indicate neuropeptide action in this disease.
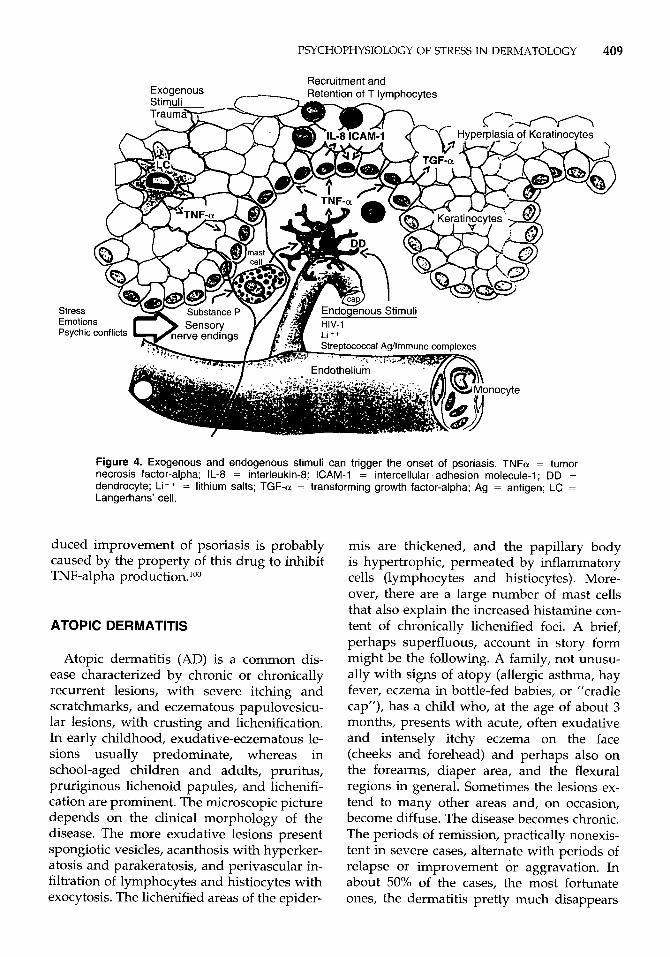
A plausible immunopathogenetic mecha- nism for psoriasis involves the reciprocal in- teractions between mononuclear cells within the dermis, including activated T cells, mac- rophages (Langerhans’ cells and dermal den- drocytes), and the overlying hyperplastic ker- atinocytes. Such a complex and reciprocal interaction between keratinocytes and immu- nocytes probably includes the cytokines in- terleukin-8 (IL-8), tumor necrosis factor-alpha (TNF-alpha), and the adhesion molecule ICAM-1.80 The results of in vivo studies, combined with others in vitro, delineate im- portant spatially coordinated cytokine-con- trolled interactions between TNF-alpha-pro- ducing dermal dendrocytes and overlying keratinocytes, which have increased IL-8, ICAM-1, and transforming growth factor- alpha (TGF-alpha) expression. IL-8 is known as a potent T-cell chemotactic factor, and ker- atinocyte-drived ICAM-1 is able to mediate the recruitment and retention of T cells, as characteristically observed in the squirting papilla zone of the psoriatic epidermis. The increased keratinocyte production of TGF- alpha induced by TNF-alpha may be an im- portant contribution to keratinocyte hyper- plasia because TGF-alpha is a potent mitogen for keratinocytes.21 It also has been suggested that the dermal dendrocyte plays an im- portant central role in cutaneous inflamma- tory reactions4I because anatomically it is sit- uated immediately between the basal keratinocyte layer of the epidermis and adjacent to the endothelial cells, permitting the monitoring of the external and internal microenvironmental milieu. Dermal mast cells, although increased in psoriatic lesions, do not appear to produce TNF-alpha or IL-8. The dermal mast cells, however, are associ- ated intimately with TNF-alpha-containing dendrocytes. This close association may have functional significance because stimulation of dermal mast cells in short-term skin cultures has been observed to induce TNF-alpha- mediated adhesion molecule expression on endothelial cells.57
It has been shown that SP stimulates mast
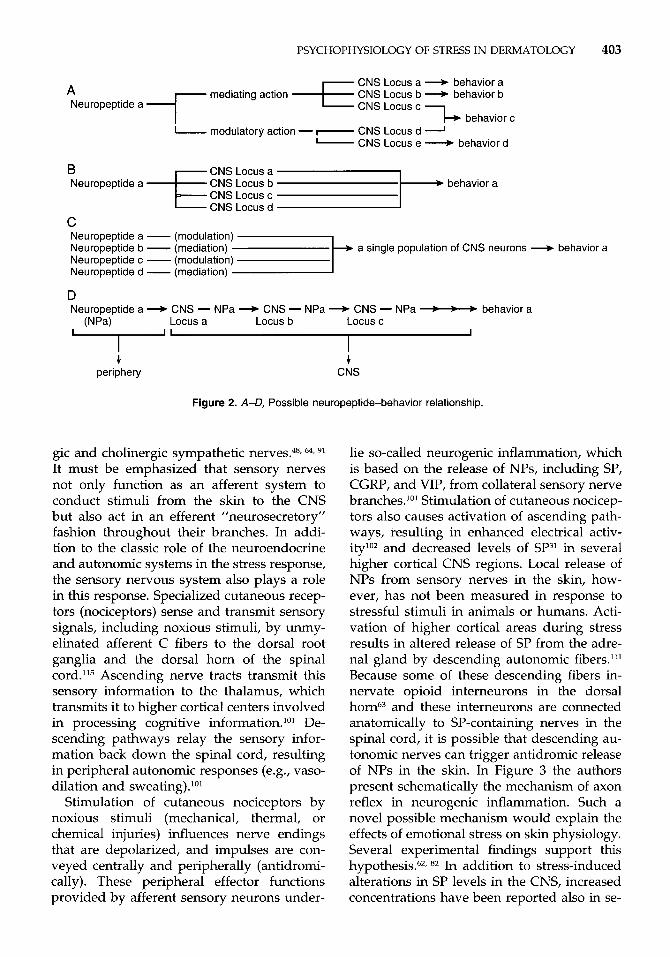
cell degranulation in foreskin cultures, which is associated with rapid induction of ELAM-1 on adjacent postcapillary venular endothelial cells.” The mast-cell inhibition blocks the ability of SP to induce ELAM-1. The dermal microvasculature is associated intimately with small, predominantly unmyelinated fi- bers and mast cells in the immediate perivas- cular space, and frequently axons are in direct proximity to mast cell membrane^."^ These associations raise the possibility that neuro- genic triggering of mast cells might be im- portant physiologically and in certain patho- logic settings such as psoriasis. The cytokine network in psoriasis involves production of TNF-alpha and IL-8 and expression of ICAM- 1 by resident and recruited cells. These data may explain several clinical and pathologic observations involving psoriasis, including that many different exogenous and endoge- nous stimuli can trigger the onset of psoriasis (Koebner phenomenon), possibly via the stra- tegically located TNF-alpha-producing der- mal dendrocyte. The stimuli illustrated in Fig- ure 4 (modified from 80) include exogenous factors that affect the skin directly, such as trauma, which may damage the increased numbers of sensory nerve fibers in psoriatic skin, leading to the release of SP. SP con- tained within dermal nerve fibers also may represent a critical initial mediator of a cas- cade of cellular events involving mast cell degranulation, with subsequent induction of ELAM-1 on adjacent venular endothelium. This would facilitate the local accumulation of blood leukocytes during early, vascular phases of the inflammatory reaction. This neuropeptide also may be produced by in- creased stress or during intrapsychic conflicts, then interact with the mast cells, and via the dermal dendrocyte, produce TNF-alpha. Other than stress, endogenous stimuli, that is, indirect stimuli delivered to the skin from the blood stream, capable of inducing psoriasis, include HIV, which would stimulate the der- mal dendrocyte via CD4, ICAM-1 cell surface molecules, lithium, which can potentiate the effects of macrophage-derived TNF-alpha, and immune complexes, perhaps formed by streptococcal antigen-antibody interaction. In psoriatic plaques, there are elevated levels of interleukin-6 (IL-6) because TNF-alpha in- duces its p rod~ct ion~~; the cyclosporine-in-
PSYCHOPHYSIOLOGY OF STRESS IN DERMATOLOGY 409
Stress Emotior Psychic
Figure 4. Exogenous and endogenous stimuli can trigger the onset of psoriasis. TNFa = tumor necrosis factor-alpha; IL-8 = interleukin-8; CAM-1 = intercellular .adhesion molecule-1; DD =
dendrocyte; L i t+ = lithium salts: TGF-a = transforming growth factor-alpha; Ag = antigen; LC = Langerhans’ cell.
duced improvement of psoriasis is probably caused by the property of this drug to inhibit TNF-alpha production.’00
ATOPIC DERMATITIS
Atopic dermatitis (AD) is a common dis- ease characterized by chronic or chronically recurrent lesions, with severe itching and scratchmarks, and eczematous papulovesicu- lar lesions, with crusting and lichenification. In early childhood, exudative-eczematous le- sions usually predominate, whereas in school-aged children and adults, pruritus, pruriginous lichenoid papules, and lichenifi- cation are prominent. The microscopic picture depends on the clinical morphology of the disease. The more exudative lesions present spongiotic vesicles, acanthosis with hyperker- atosis and parakeratosis, and perivascular in- filtration of lymphocytes and histiocytes with exocytosis. The lichenified areas of the epider-
mis are thickened, and the papillary body is hypertrophic, permeated by inflammatory cells (lymphocytes and histiocytes). More- over, there are a large number of mast cells that also explain the increased histamine con- tent of chronically lichenified foci. A brief, perhaps superfluous, account in story form might be the following. A family, not unusu- ally with signs of atopy (allergic asthma, hay fever, eczema in bottle-fed babies, or “cradle cap”), has a child who, at the age of about 3 months, presents with acute, often exudative and intensely itchy eczema on the face (cheeks and forehead) and perhaps also on the forearms, diaper area, and the flexural regions in general. Sometimes the lesions ex- tend to many other areas and, on occasion, become diffuse. The disease becomes chronic. The periods of remission, practically nonexis- tent in severe cases, alternate with periods of relapse or improvement or aggravation. In about 50% of the cases, the most fortunate ones, the dermatitis pretty much disappears
410 PANCONESI & HAUTMANN
when the child is just older than one year old. There may be minor signs of delicate or dry skin and some itching or redness in flexural areas. In the other 50%, the less fortunate cases, the dermatosis boldly persists, localiz- ing almost anywhere but preferentially on the face (eyebrows, eyelids, around the mouth), the backs of the hands, and the cervical and malleolar regions. As the years of childhood and adolescence go by, the youngster lives with the torment of lichenified dermatitis. The skin generally is pale, grayish, cold, dry, and anhydrotic with raised, keratotic follicles. When this child becomes an adult, the charac- teristics are similar to those described pre- viously, but with more evident signs of licheni- fication in the most severely affected areas, in particular the flexural areas, face, and hands.
Important dermatologists of the past asso- ciated the AD with neuropsychic factors, as is evidenced by the use of the term neuroder- matitis in the nineteenth century, whereas the term prurigo of Besnier, still used in Scandina- via, seems to emphasize that this strange af- fection comports also a strange and suspi- cious persistence of the itching, which is the most ambiguous and the most psychosomatic of all symptoms. Moreover, the itch appears to be the leitmotif of the disease, perhaps the cause of its continuati~n.~~. 4y, 65, 85-87
Cutaneous stimulation during infancy ap- pears to be an important factor for cell growth and differentiation and CNS maturation.30, 94
In the rat model, handling and cutaneous stroking in early life also appear to enhance humoral immunity in later life.30 In pre- weaned rats, temporary interruption of active tactile stimulation or maternal deprivation is associated with reduced ornithine decarbox- ylase activity, which is a sensitive index of cell growth and differentiation and CNS mat- ration.^^ It has been shown that human pre- term neonates who received tactile and kines- thetic stimulation gained weight more rapidly and exhibited more mature neurologic re- flexes than did controls; they were also more alert.'O' in a series of famous experi- ments involving monkeys, showed that depri- vation of touch, or contact comfort, in early life results in the development of inappropri- ately aggressive behaviors and other psycho- logical problems. All these findings underline
the relevance of cutaneous perception and stimulation in physical and psychological de- velopment. The awareness of the psychobio- logic unity of the human being and of the impossibility to consider the child's develop- ment separated from the environment obliges us to evaluate not only items concerning the child but also items of the parent-child sys- tem with the goal of creating interactive se- meiotics. This means that the operators try to bring out the most positive, significant, and functional choices of the child and family in that particular environment and moment.
Obermayer;' one of the fathers of psycho- somatic dermatology, in reviewing the ample series studied by Gruber and Sanford, em- phasized that many babies were separated early from their mother's breast, a truly trau- matizing event in the psychological develop- ment of the child and one that can cause severe damage to emotional stability. Many investigators have studied psychodynamics and the mother-child relationship, so often altered in the case of a child with AD. The extreme is the mother who rejects the atopic child, even refusing to touch him or her, with consequent anger, anxiety, or hostility of the child toward the mother herself or mother substitutes. In 1950, it was reported that up to 98% of children with AD had rejecting mothers, whereas few children in a control group without AD suffered maternal rejec- t i~n. '~, 85* 86 In some instances, the maternal rejection is a reaction to the child's dermatitis, that is, once the skin condition erupts, the mother tends to reject the ~ h i l d . ~ ~ , ~ ~ ~ The dis- turbed parent-child relationship aggravates the existing dermatosi~.~~ With scratching and self-excoriation the child makes himself or herself ugly and unlovable, unworthy of love; the excoriations modify the self-image, and they are also the results of disobeying the regular request not to scratch. As reported by Slany,lo8 children with AD frequently are in conflict with an unattentive, unaffectionate, and inadequate mother; this results in an un- conscious triggering of the psychosomatic mechanism, leading to onset of the disease. This model would work as follows: a small child or infant is unable to defend himself or herself from a psychic conflict except by removal, which provokes internal tension,
PSYCHOPHYSIOLOGY OF STRESS IN DERMATOLOGY 411
leading to anguish, depression, and hostility followed by conversion and regression. It has been hypothesized that in the phase of de- tachment from the mother, the subject with AD does not invent or find a transitional object and that the dermatitis substitutes the object; thus, the child's difficulty or inability to progress along the normal path of develop- ment is expressed in the form of a somatic cutaneous pathology.84, 86
It has been noted in general that patients with AD experience more emotional upsets than normal subjects. Parental separations, psychiatric illness, and skin disorders fre- quently are noted in the family history. Pa- tients with AD also tend to be more irritable, resentful, guilt ridden, and hostile than per- sons who do not have eczema.54
There have been many reports that refer specifically to the personality of the infant with AD. He or she is typically irritable, de- manding, and unhappy and needs more cud- dling and skin contact than the average baby. The parents' pride and joy in their offspring becomes compromised by the persistent and highly visible eczematous eruption. When the need to follow a complicated medical regi- men is compounded by the child being diffi- cult and unattractive, some degree of parental resentment, embarrassment, and withdrawal occurs. A bad fit (difficult interpersonal rela- tionship between parent and child and subse- quently with the rest of the world) begins, and the infant responds to unmet needs with self-stimulation and abusive ~cratching.~~ A vicious cycle is created in which anxiety pro- vokes itching, and itching and scratching ag- gravate the patient's anxiety.
As the child grows older, the problems as- sociated with AD increase. Other persons tend to avoid the child, seemingly fearful of contamination (the leper effect), and devel- oping peer relationships suffer. School prob- lems include increased absenteeism, impaired performance because of sleep deprivation, and decreased ability to concentrate as self- consciousness intrudes on learning ability.32
A subject with cutaneous atopy often is found to be tense, insecure, and aggressive and to have most or all of the following char- acteristics: feelings of inferiority and inade- quacy, repressed hostility toward parental
figures, affective hypersensitivity, emotional instability, sexual difficulties with masochistic tendencies and cutaneous eroticism, and a fairly high level of intelligence."" No con- stant, specific personality type, however, was found in patients with AD.77 What has been noted throughout all the investigations is that most patients with AD display some form of emotional disturbance?, 81 They usually are repressed persons who internalize their prob- lems and express their anxious and hostile emotional conflicts by scratching.56* 72 Whit- lock116 and Champion and ParishI2 have indi- cated that atopic subjects have "conflicting" personality profiles.
Atopic subjects are more likely than others to respond with itching and scratching to fairly minor signals and stimuli, and some of those signals are more profoundly significant in psychodynamic terms than would appear on the surface.56 Excitability and arousal of the CNS from an emotional upset can inten- sify the vasomotor and sweat responses in the skin and lead to the itch-scratch response. This is compatible with the observation that many patients experience an emotionally dis- turbing event before an attack of AD.116 The emotional upset lowers the itch threshold and triggers the scratch res~onse .~
Excessive anxiety is known to correlate with ease of conditioning, and patients with AD are conditioned more readily to scratch responses than are their matched control counterpart^.^^, 53 It is probably relevant that in moments of frustration or embarrassment many normal persons also tend to scratch at sites that are typically affected by AD.
AD also alters the personality. Because of the unsightly skin changes, difficulties en- countered in personal relationship are under- standable. The patient is judged unfairly be- cause of an unsightly appearance, which can be an emotional threat. Nighttime awakening because of violent itching also takes its toll on the patient's disposition and per~onality.~~
The pathway from the emotional phenom- ena, which the authors have tried to describe, to the triggering of the various phases of the disease phenomenon typical of AD still re- mains to be clarified fully. There may be glimpses of the basic structure in the experi- mental acquisitions of modern psychoneu-
412 PANCONESI & HAUTMANN
-1- (scratching) 4
roendocrinimmunology; its multifactorial pathogenesis makes AD a good model for the preparation of an integrated hypothesis of biological psychos~matics.~~~ 48, 49* 85, 86
A further essential step toward specifica- tion of the relays between psyche-emotion- stress (simplistically summarizing in this term the complex psyche-emotion factors characteristic of the psychological evolution of the patient with AD) and peripheral re- sponse was mastered with the findings of experimental studies on neuropeptides and their receptors, specifically their identification and involvement in the CNS and peripheral organs, including the 84-86
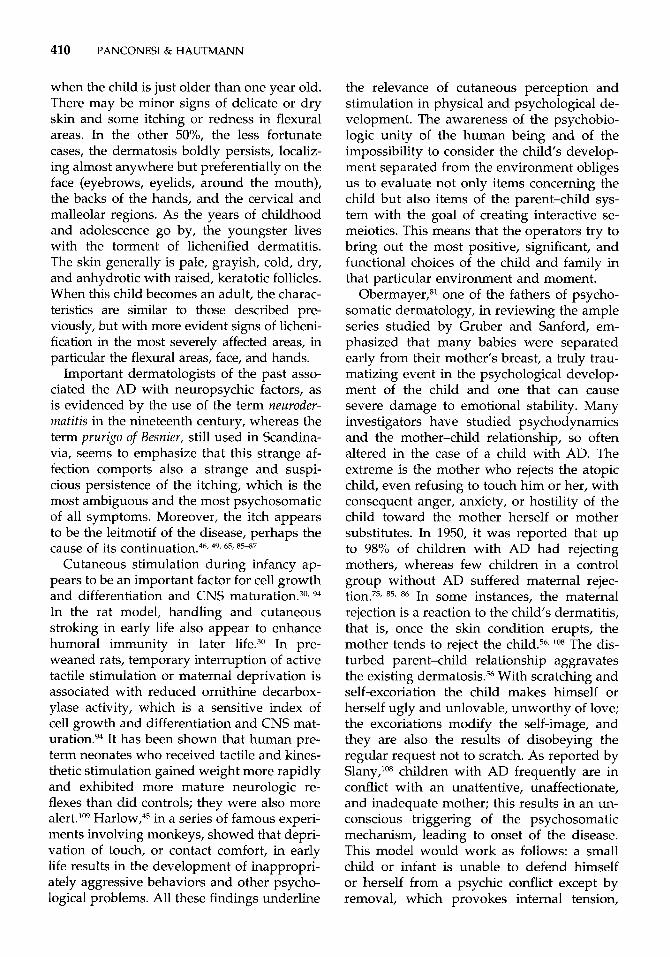
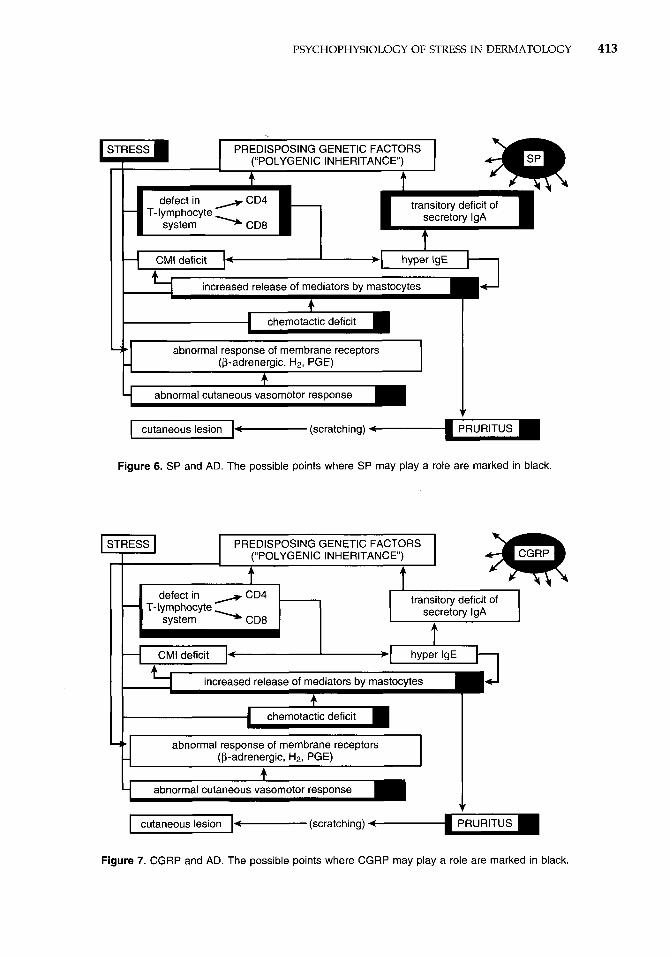
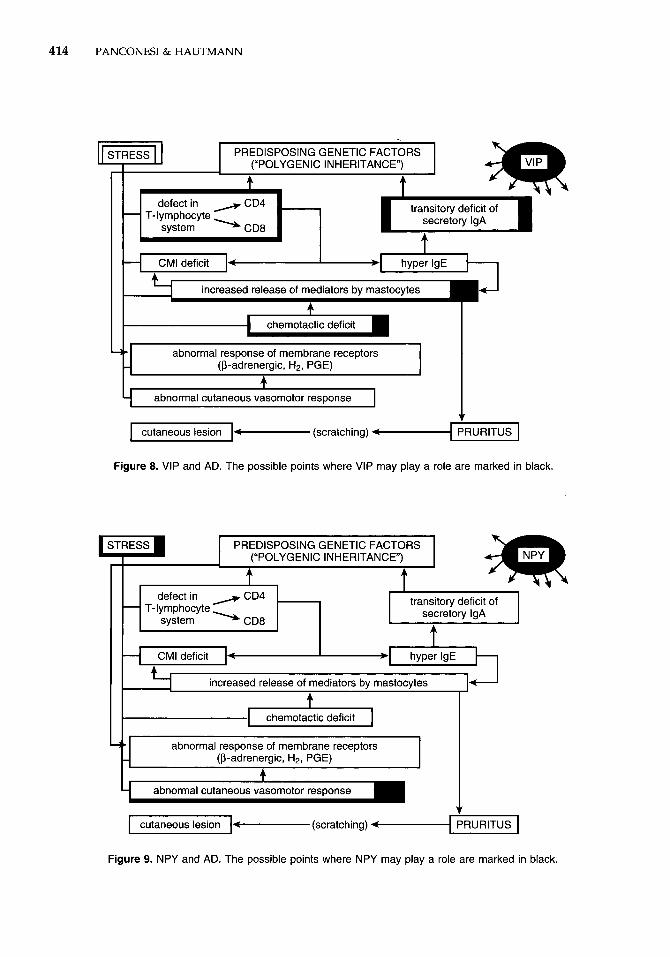
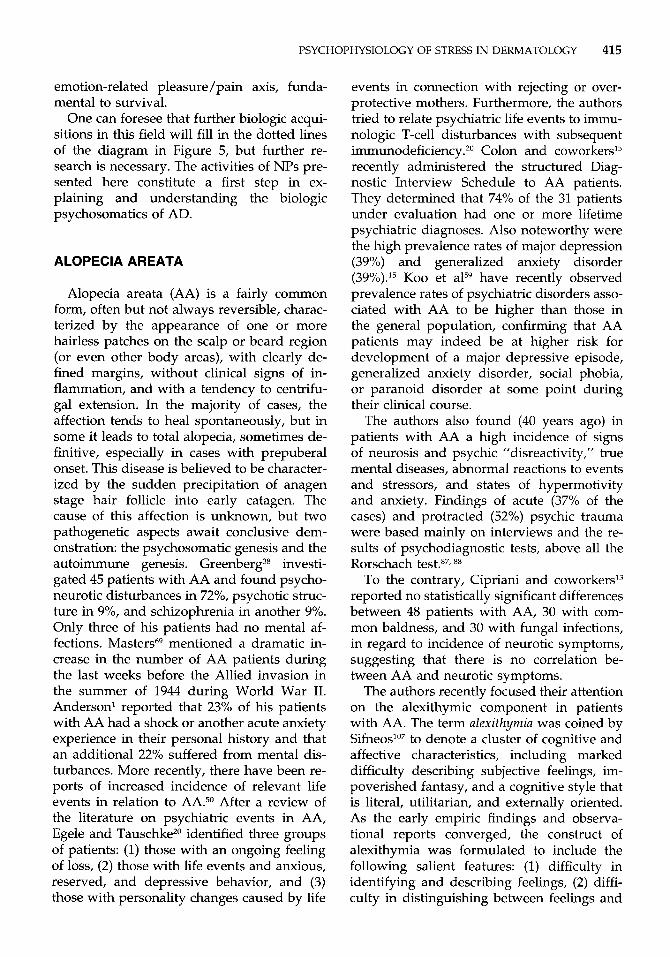
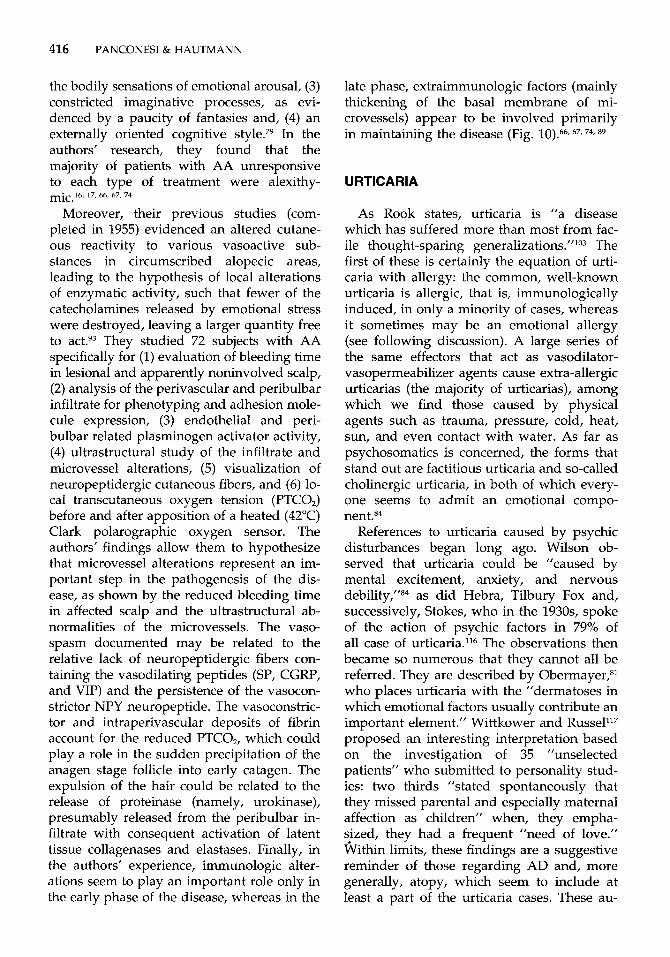
The most significant findings regarding AD in this field are presented in Figures 5 through 9. Figure 5 shows a hypothetic out- line of the pathogenesis of AD correlated with the possible influence of emotional stress (dot- ted lines) that was presented in 1984.84 Figure 6 illustrates the presumed influence of SP in the pathogenesis of AD (see also previous lists for functions of SP, CGRP, VIP, and NPY). SP has been shown in lichenoid infil- trate in the perivascular papillary dermis of
PRURITUS
AD subjects. Figure 7 shows the presumed influence of CGRP on the pathogenesis of this disease. CGRP-like immunoreactivity consis- tently is observed as free endings in the papil- lary dermis close to the dermoepidermal junction, with the same pattern and staining intensity in patients with AD and control subjects. A presumed influence of VIP on the pathogenesis of AD is presented in Figure 8. Levels of VIP are increased in lesional skin of patients with AD. Figure 9 presents a pre- sumed influence of NPY on the pathogenesis of AD. NPY-like immunoreactivity has been detected in Langerhans’ cells in 6 of 11 pa- tients with AD but not in normal control subjects; this NP is one of the most potent vasoconstrictor peptides (arteries and arteri- oles but not venous vessels) identified up to
Other peptides presumably involved, but without experimental evidence, in AD are the endorphins and somatostatin. Endorphins ex- ercise various effects in different phases of the hypothetic outline shown in Figure 5, and
now.35, 37. 97
. . the endogenous opioids also represent neuropeptidergic system involved - in
the the
Figure 5. Hypothetic outline of the pathogenesis of AD correlated with the possible influence of emotional stress (dotted lines). CMI = cell-mediated immunity; H, = type 2 receptors for histamine; PGE = prostaglandin E.
PSYCHOPHYSIOLOGY OF STRESS IN DERMATOLOGY 413
PREDISPOSING GENETIC FACTORS
transitory deficit of
I
chemotactic deficit
9. abnormal response of membrane receptors - (P-adrenergic, HP, PGE)
4 abnormal cutaneous vasomotor response - cutaneous lesion - (scratching)
Figure 6. SP and AD. The possible points where SP may play a role are marked in black.
f t STRESS PREDISPOSING GENETIC FACTORS
(“POLYGENIC INHERITANCE)
transitory deficit of secretory IgA
defect in CD4
system - CD8 - T- lymphocyte - I 4 . .
chemotactic deficit I
I abnormal response of membrane receptors (B-adrenergic, H2, PGE)
I I -~ I
4 abnormal cutaneous vasomotor response
cutaneous lesion 7 (scratching) <
Figure 7. CGRP and AD. The possible points where CGRP may play a role are marked in black.
414 I'ANCONESI & HAUTMANN
- abnormal response of membrane receptors (P-adrenergic, HP, PGE)
PREDISPOSING GENETIC FACTORS
defect in A CD4 - T-lymphocyte System - CD8
cutaneous lesion
I
chemotactic deficit
- (scratching) PRURITUS
Figure 8. VIP and AD. The possible points where VIP may play a role are marked in black.
PREDISPOSING GENETIC FACTORS
transitory deficit of secretory IgA
defect in CD4 - T-lymphocyte System - CD8 -
increased release of mediators by mastocytes
++ abnormal response of membrane receptors - (P-adrenergic, HP, PGE) A I
abnormal cutaneous vasomotor response
cutaneous lesion -(scratching) 4 PRURITUS
Figure 9. NPY and AD. The possible points where NPY may play a role are marked in black.
PSYCHOPHYSIOLOGY OF STRESS IN DERMATOLOGY 415
emotion-related pleasure/pain axis, funda- mental to survival.
One can foresee that further biologic acqui- sitions in this field will fill in the dotted lines of the diagram in Figure 5, but further re- search is necessary. The activities of NPs pre- sented here constitute a first step in ex- plaining and understanding the biologic psychosomatics of AD.
ALOPECIA AREATA
Alopecia areata (AA) is a fairly common form, often but not always reversible, charac- terized by the appearance of one or more hairless patches on the scalp or beard region (or even other body areas), with clearly de- fined margins, without clinical signs of in- flammation, and with a tendency to centrifu- gal extension. In the majority of cases, the affection tends to heal spontaneously, but in some it leads to total alopecia, sometimes de- finitive, especially in cases with prepuberal onset. This disease is believed to be character- ized by the sudden precipitation of anagen stage hair follicle into early catagen. The cause of this affection is unknown, but two pathogenetic aspects await conclusive dem- onstration: the psychosomatic genesis and the autoimmune genesis. Greenbe~-g~~ investi- gated 45 patients with AA and found psycho- neurotic disturbances in 72%, psychotic struc- ture in 970, and schizophrenia in another 9%. Only three of his patients had no mental af- fections. mentioned a dramatic in- crease in the number of AA patients during the last weeks before the Allied invasion in the summer of 1944 during World War 11. Anderson' reported that 23% of his patients with AA had a shock or another acute anxiety experience in their personal history and that an additional 22% suffered from mental dis- turbances. More recently, there have been re- ports of increased incidence of relevant life events in relation to AA.50 After a review of the literature on psychiatric events in AA, Egele and TauschkeZ0 identified three groups of patients: (1) those with an ongoing feeling of loss, (2) those with life events and anxious, reserved, and depressive behavior, and (3) those with personality changes caused by life
events in connection with rejecting or over- protective mothers. Furthermore, the authors tried to relate psychiatric life events to immu- nologic T-cell disturbances with subsequent immunodeficiency.*" Colon and coworkers'5 recently administered the structured Diag- nostic Interview Schedule to AA patients. They determined that 74% of the 31 patients under evaluation had one or more lifetime psychiatric diagnoses. Also noteworthy were the high prevalence rates of major depression (39%) and generalized anxiety disorder (39Y0).'~ Koo et alS9 have recently observed prevalence rates of psychiatric disorders asso- ciated with AA to be higher than those in the general population, confirming that AA patients may indeed be at higher risk for development of a major depressive episode, generalized anxiety disorder, social phobia, or paranoid disorder at some point during their clinical course.
The authors also found (40 years ago) in patients with AA a high incidence of signs of neurosis and psychic "disreactivity," true mental diseases, abnormal reactions to events and stressors, and states of hypermotivity and anxiety. Findings of acute (37% of the cases) and protracted (52%) psychic trauma were based mainly on interviews and the re- sults of psychodiagnostic tests, above all the Rorschach test.87,
To the contrary, Cipriani and coworkers'3 reported no statistically significant differences between 48 patients with AA, 30 with com- mon baldness, and 30 with fungal infections, in regard to incidence of neurotic symptoms, suggesting that there is no correlation be- tween AA and neurotic symptoms.
The authors recently focused their attention on the alexithymic component in patients with AA. The term ulexithymiu was coined by S i f n e o ~ ' ~ ~ to denote a cluster of cognitive and affective characteristics, including marked difficulty describing subjective feelings, im- poverished fantasy, and a cognitive style that is literal, utilitarian, and externally oriented. As the early empiric findings and observa- tional reports converged, the construct of alexithymia was formulated to include the following salient features: (1) difficulty in identifying and describing feelings, (2) diffi- culty in distinguishing between feelings and
416 PANCONESI & HAUTMANN
the bodily sensations of emotional arousal, (3) constricted imaginative processes, as evi- denced by a paucity of fantasies and, (4) an externally oriented cognitive style.79 In the authors’ research, they found that the majority of patients with AA unresponsive to each type of treatment were alexithy- mic.16, 17, 66. 67, 74
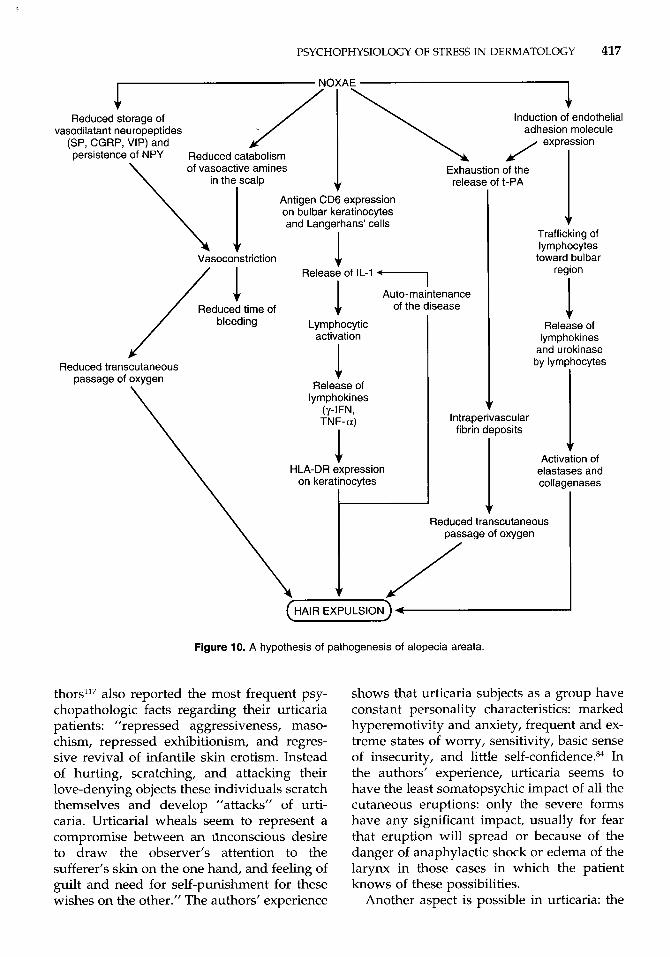
Moreover, their previous studies (com- pleted in 1955) evidenced an altered cutane- ous reactivity to various vasoactive sub- stances in circumscribed alopecic areas, leading to the hypothesis of local alterations of enzymatic activity, such that fewer of the catecholamines released by emotional stress were destroyed, leaving a larger quantity free to act.93 They studied 72 subjects with AA specifically for (1) evaluation of bleeding time in lesional and apparently noninvolved scalp, (2) analysis of the perivascular and peribulbar infiltrate for phenotyping and adhesion mole- cule expression, (3) endothelial and peri- bulbar related plasminogen activator activity, (4) ultrastructural study of the infiltrate and microvessel alterations, (5) visualization of neuropeptidergic cutaneous fibers, and (6) lo- cal transcutaneous oxygen tension (PTCO,) before and after apposition of a heated (42°C) Clark polarographic oxygen sensor. The authors’ findings allow them to hypothesize that microvessel alterations represent an im- portant step in the pathogenesis of the dis- ease, as shown by the reduced bleeding time in affected scalp and the ultrastructural ab- normalities of the microvessels. The vaso- spasm documented may be related to the relative lack of neuropeptidergic fibers con- taining the vasodilating peptides (SP, CGRP, and VIP) and the persistence of the vasocon- strictor NPY neuropeptide. The vasoconstric- tor and intraperivascular deposits of fibrin account for the reduced PTC02, which could play a role in the sudden precipitation of the anagen stage follicle into early catagen. The expulsion of the hair could be related to the release of proteinase (namely, urokinase), presumably released from the peribulbar in- filtrate with consequent activation of latent tissue collagenases and elastases. Finally, in the authors’ experience, immunologic alter- ations seem to play an important role only in the early phase of the disease, whereas in the
late phase, extraimmunologic factors (mainly thickening of the basal membrane of mi- crovessels) appear to be involved primarily in maintaining the disease (Fig. 67, 74, 89
URTICARIA
As Rook states, urticaria is “a disease which has suffered more than most from fac- ile thought-sparing generalization^."'^^ The first of these is certainly the equation of urti- caria with allergy: the common, well-known urticaria is allergic, that is, immunologically induced, in only a minority of cases, whereas it sometimes may be an emotional allergy (see following discussion). A large series of the same effectors that act as vasodilator- vasopermeabilizer agents cause extra-allergic urticarias (the majority of urticarias), among which we find those caused by physical agents such as trauma, pressure, cold, heat, sun, and even contact with water. As far as psychosomatics is concerned, the forms that stand out are factitious urticaria and so-called cholinergic urticaria, in both of which every- one seems to admit an emotional compo- nent.84
References to urticaria caused by psychic disturbances began long ago. Wilson ob- served that urticaria could be “caused by mental excitement, anxiety, and nervous debility,”84 as did Hebra, Tilbury Fox and, successively, Stokes, who in the 1930s, spoke of the action of psychic factors in 79% of all case of urticaria.’16 The observations then became so numerous that they cannot all be referred. They are described by Obermayer?’ who places urticaria with the “dermatoses in which emotional factors usually contribute an important element.” Wittkower and proposed an interesting interpretation based on the investigation of 35 “unselected patients” who submitted to personality stud- ies: two thirds ”stated spontaneously that they missed parental and especially maternal affection as children” when, they empha- sized, they had a frequent ”need of love.” Within limits, these findings are a suggestive reminder of those regarding AD and, more generally, atopy, which seem to include at least a part of the urticaria cases. These au-
PSYCHOPHYSIOLOGY OF STRESS IN DERMATOLOGY 417
Reduced storage of vasodilatant neuropeptides
(SP, CGRP, VIP) and persistence of NPY Reduced catabolism
of vasoactive amines
Induction of endothelial
release of t-PA
Antigen CD6 expression on bulbar keratinocytes
Vasoconstriction
Reduced transcutaneous passage of oxygen
and Langerhans’ cells
1 Release of IL-1 *-
I I Auto-maintenance of the disease J.
Lymphocytic activation
1 Release of
lymphokines (./-IFN, TNF-a)
I ’ HLA-DR expression
on keratinocytes
.). Trafficking of lymphocytes
toward bulbar region
1 Release of
lymphokines and urokinase by lymphocytes
1 Intraperivascular fibrin deposits
Activation of elastases and collagenases
1 I I Reduced transcutaneous I
Figure 10. A hypothesis of pathogenesis of alopecia areata.
thors117 also reported the most frequent psy- chopathologic facts regarding their urticaria patients: ”repressed aggressiveness, maso- chism, repressed exhibitionism, and regres- sive revival of infantile skin erotism. Instead of hurting, scratching, and attacking their love-denying objects these individuals scratch themselves and develop ”attacks” of urti- caria. Urticaria1 wheals seem to represent a compromise between an tinconscious desire to draw the observer’s attention to the sufferer’s skin on the one hand, and feeling of guilt and need for self-punishment for these wishes on the other.” The authors’ experience
shows that urticaria subjects as a group have constant personality characteristics: marked hyperemotivity and anxiety, frequent and ex- treme states of worry, sensitivity, basic sense of insecurity, and little self-~onfidence.~~ In the authors’ experience, urticaria seems to have the least somatopsychic impact of all the cutaneous eruptions: only the severe forms have any significant impact, usually for fear that eruption will spread or because of the danger of anaphylactic shock or edema of the larynx in those cases in which the patient knows of these possibilities.
Another aspect is possible in urticaria: the
418 PANCONESI & HAUTMANN
Eliciting Factors Modulating Factors Exogenous Endogenous
1
environment, temperature, foods, hormones, stress
(Neuropeptides)
IgE, C activation I I \ \ I
H Lymphocytes 1
Cytokines HRFs
Histamine-releasing Substances
Physical Stimuli temperature, water, trauma, vibration, physical exercise
Inflammatory Factors
eosinophil cationic proteins histamine, PGs, LTs, LTB4, PGs, 02, enzymes -
Psychic Conflicts
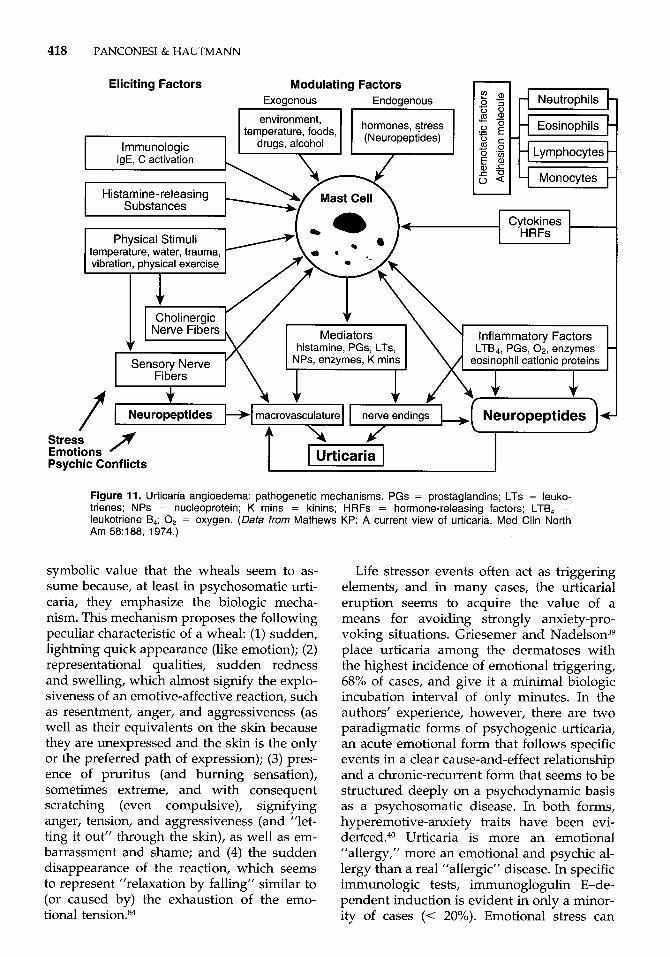
Figure 11. Urticaria angioedema: pathogenetic mechanisms. PGs = prostaglandins; LTs = leuko- trienes; NPs = nucleoprotein; K mins = kinins; HRFs = hormone-releasing factors; LTB, = leukotriene B,; 0, = oxygen. (Data from Mathews KP: A current view of urticaria. Med Clin North Am 58:188, 1974.)
symbolic value that the wheals seem to as- sume because, at least in psychosomatic urti- caria, they emphasize the biologic mecha- nism. This mechanism proposes the following peculiar characteristic of a wheal: (1) sudden, lightning quick appearance (like emotion); (2) representational qualities, sudden redness and swelling, which almost signify the explo- siveness of an emotive-affective reaction, such as resentment, anger, and aggressiveness (as well as their equivalents on the skin because they are unexpressed and the skin is the only or the preferred path of expression); (3) pres- ence of pruritus (and burning sensation), sometimes extreme, and with consequent scratching (even compulsive), signifying anger, tension, and aggressiveness (and "let- ting it out" through the skin), as well as em- barrassment and shame; and (4) the sudden disappearance of the reaction, which seems to represent "relaxation by falling" similar to (or caused by) the exhaustion of the emo- tional tension.84
Life stressor events often act as triggering elements, and in many cases, the urticaria1 eruption seems to acquire the value of a means for avoiding strongly anxiety-pro- voking situations. Griesemer and N a d e l ~ o n ~ ~ place urticaria among the dermatoses with the highest incidence of emotional triggering, 68% of cases, and give it a minimal biologic incubation interval of only minutes. In the authors' experience, however, there are two paradigmatic forms of psychogenic urticaria, an acute emotional form that follows specific events in a clear cause-and-effect relationship and a chronic-recurrent form that seems to be structured deeply on a psychodynamic basis as a psychosomatic disease. In both forms, hyperemotive-anxiety traits have been evi- d e r f ~ e d . ~ ~ Urticaria is more an emotional "allergy," more an emotional and psychic al- lergy than a real "allergic" disease. In specific immunologic tests, immunoglogulin E-de- pendent induction is evident in only a minor- ity of cases (< 20%). Emotional stress can

PSYCHOPHYSIOLOGY OF STRESS IN DERMATOLOGY 419
stimulate mast cells and IgE activity and in- fluence release of vasoactive substances, the protagonists of urticaria, with the involve- ment of certain neuropeptides such as SP, CGRP, and VIP. In the schematized patho- genesis of urticaria-angioedema (Fig. ll), the relevance of neuropeptides is seen; they could be endogenous-modulating factors acting di- rectly on mast cells and eliciting factors re- leased from sensory nerve endings acting on micro~asculature.~~
References
1. Anderson NP: Alopecia areata: A clinical study. Br Med J 4691:1250-1252, 1950
2. Arnetz BB, Fjellner B, Eneroth P, et al: Stress and psoriasis: Psychoendocrine and metabolic reactions in psoriatic patients during standardized stressor exposure. Psychosom Med 47528-541, 1985
3. Bassi R, Lazzerini E: La psoriasi: Nuove indagini in senso psicosomatico. Chron Dermatol 51735-70, 1974
4. Beerman H: Etiology and mechanisms of develop- ment of neurodermatitis. In Nodene JH, Mayer JH (eds): Psychosomatic Medicine. London, Henry Kimpton, 1962, pp 134156
5. Bernard C: Les Phenomenes de la Vie. Paris, Li- brairie J.B. Bailliere et Fils, Vol. 1, 1878, pp 879-893
6. Bernstein JE: Neuropeptides and the skin. In Gold- smith LA (ed): Biochemistry and Physiology of the Skin. New York, Oxford University Press, 1983, pp
7. Besedowsky H, Del Rey AE, Sorkin E: Immune- neuroendocrine interactions. J Immunol 135:750s- 754s, 1985
8. Bolgert M, Poisson R, Soul6 M: Le psoriasis esti-il une psychodermatose? Ann Dermatol Syphil3:273- 291, 1951
9. Brown DG: Emotional disturbance in eczema: A study of symptom-reporting behavior. J Psychosom Res 11:2740, 1967
10. Cannon WB: The emergency function of the adrenal medulla in pain and major emotions. Am J Physiol
11. Cannon WB: Stresses and strains of homeostasis. Am J Med Sci 189:l-12,1935
12. Champion RH, Parish WE: Atopic dermatitis. In Rook A, Wilkinson DS, Ebling FJG (eds): Textbook of Dermatology. Oxford, Blackwell Scientific Publi- cations, 1979, pp 349-361
13. Cipriani R, Veller Fomasa C, Peserico A: Symptom questionnaire and alopecia areata. G Ital Dermatol Venereol 118:281-282, 1983
14. Coles RB, Ryan TJ: The psoriasis sufferer in the community. Br J Dermatol93111-112, 1975
15. Colon EA, Popkin MK, Calliess AL, et al: Lifetime prevalence of psychiatric disorders in patients with alopecia areata. Comp Psychiatry 32245-251, 1991
16. Cossidente A, Figini-Simoncini R, Danesi A, et al: Alopecia areata: Casistica clinica "psicosomatica." 67" Congress0 Nazionale SIDEV. Stresa June, 5-8, 1991
1217-1233
33:356-372, 1914
17. Cossidente A, Sarti MG, Danesi A, et al: Test psico- diagnostici nei soggetti con alopecia areata. 67" Con- gresso Nazionale SIDEV. Stresa June, 5-8, 1991
18. Eady DJ, Johnston CF, Shaw CS, et al: Neuropep- tides in psoriasis: An immunocytochemical and ra- dioimmunoassay study. J Invest Dermatol 96:434- 439, 1991
19. Eckert J: Diffuse hair loss and psychiatric distur- bance. Acta Derm Venereol (Stockh) 55:147-149, 1975
20. Egele UT, Tauschke E: Die Alopezie: Ein psychoso- matisches Krankheitsbild. Psychoter Psychosom Med Psychol 3731-35, 1987
21. Elder JT, Fisher GJ, Lindquist PB, et al: Overexpres- sion of transforming growth factor-alpha in psoria- sis epidermis. Potential role of phospholipase C. Science 243S11-814, 1989
22. Ejavac F, Lembeck F, Irman IF: Release of hista- mine by substance P. Naunyn Schmiedeberg's Arch Pharmacol 31767-70, 1981
23. Ewbank R Behavioral responses to stress in farm animals. In Moberg GP (ed): Animal Stress. Bethesda, Waverly Press, 1985, pp 71-80
24. Farber EM, Nall ML The natural history of psoriasis in 5600 patients. Dermatologia 148:l-18, 1974
25. Farber EM, Lanigan SW, Rein G: The role of psycho- neuroimmunology in the pathogenesis of psoriasis. Cutis 46:314316, 1990
26. Farber EM, Nall ML, Watson W: Natural history of psoriasis in 61 twin pairs. Arch Dermatol 109:207- 211, 1974
27. Farber EM, Rein G, Lanigan SW: Stress and psoria- sis: Psychoneuroimmunologic mechanisms. Int J Dermatol 30%-12, 1991
28. Farber EM, Nickoloff BJ, Recht B, et al: Stress, sym- metry and psoriasis: Possible role of neuropeptides. J Am Acad Dermatol 14:305-311, 1986
29. Fava GA, Perini GI, Santonastaso P, et al: Stress, alessitimia e nevroticismo in alcune malattie derma- tologiche: psoriasi, orticaria cronica e micosi. In Der- matologia psicosomatica. Roma, Edizioni Internazi- onali, Gruppo Editoriale Medico, 1980, pp 277-282
30. Field TM, Schanberg SM, Scafid F, et al: Tactive kinesthetic stimulation effects on preterm neonates. Pediatrics 77654658, 1986
31. Foreman JC: Peptides and neurogenic inflammation. Br Med Bull 43:386-400, 1987
32. Fritz GK: Psychological aspects of atopic dermatitis. Clin Pediatr 18:360-364, 1979
33. Garrie EV, Garrie SA, Mote T: Anxiety and atopic dermatitis. J Consult Clin Psychol 42:742, 1974
34. Gerhart KD, Yezierski RP, Wilcox TK: Inhibition of primate spinothalamic tract neurons by stimulation in periaqueductal gray. J Neurophysiol 51:450-466, 1984
35. Giannetti A, Girolomoni G: Skin reactivity to neuro- peptides in atopic dermatitis. Br J Dermatol 121:681- 688, 1989
36. Ginsburg IH, Link BG: Feelings of stigmatization in patients with psoriasis. J Am Acad Dermatol 20:53-63, 1989
37. Girolomoni G, Giannetti A: Neuropeptidi e cute. G Ital Dermatol Venereol 124:121-140, 1989
38. Greenberg SI: Alopecia areata: A psychiatric survey. Arch Dermatol 723454457, 1955
39. Griesemer RD, Nadelson T: Emotional aspects of cutaneous disease. In Fitzpatrick IM, Eisen AZ, Wolff K, et a1 (eds): Dermatology in General Medi- cine. New York, McGraw-Hill, 1979, pp 1353-1363

420 PANCONESI & HAUTMANN
40. Griffin JFT: Stress and immunity: A unifying con- cept. Veter Immunol Immunopathol 20:263-312, 1989
41. Griffiths CEM, Nickoloff BJ: Keratinocyte intercellu- lar adhesion molecule-1 (ICAM-1) expression pre- cedes dermal T lymphocyte infiltration in allergic contact dermatitis (Rhus dermatitis). Am J Pathol
42. Grossman M, Krueger J, Yourish D, et al: Interleu- kin-6 is expressed in high levels in psoriatic skin and stimulates proliferation of cultured human ker- atinocytes. Proc Natl Acad Sci 8663674371, 1989
43. Gupta MA, Gupta AK, Kirkby S, et al: A psychocu- taneous profile of psoriasis patients who are stress reactors: A study of 127 patients. Gen Hosp Psychia- try 11:16&173, 1989
44. Hardy GE, Cotterill JA: A study of depression and obsessionality in dysmorphophobic and psoriatic patients. Br J Psychiatry 140:19-22, 1982
45. Harlow H F Primary affectional patterns in pri- mates. Am J Orthopsychiatry 30676-677, 1960
46. Hautmann G, Panconesi E: Neuropeptidi e derma- tite atopica. 14" Congresso Nazionale della Societi Italiana di Medicina Psicosomatica. Firenze, 12-15 maggio, 1993
47. Hautmann G, Panconesi E: Psychoimmunology in Dermatology. In Ich und die Haut (Kongress Arbeit- skreis Psychosomatische Dermatologie), Giessen, Germany, September 23-25, 1994
48. Hautmann G, Lotti T, Panconesi E: Neuropeptides and skin inflammation. In Getting in Touch, 6th International Congress on Dermatology and Psychi- atry, Amsterdam (Olanda), April 20-22, 1995, Ab- stract Book, p 44
49. Hautmann G, Tsampau D, Lotti T Stress, neuropep- tides and skin. XI1 Convegno di Immunopatologia Cutanea, Genova, October 9-10, 1992
50. Invernizzi G, Gala C, Russo R, et al: Life events and personality factors in patients with alopecia areata. Med Sci Res 15:1219-1220, 1987
51. Ironside W: Eczema, darkly mirror of the mind. Aust J Dermatol 15:5-9, 1974
52. Jobling R: Learning to live with it: An account of career of chronic dermatological illness and pa- tienthood. In Davis A, Horobin G (eds): Medical Encounters, the Experience of Illness and Treatment. New York, St. Martin's Press, 1977, pp 35-43
53. Jordan JM: Atopic dermatitis: Anxiety and condi- tioned scratch responses. J Psychosom Res 18:297- 299, 1974
54. Jordan JM, Whitlock FA: Emotions and the skin. The conditioning of scratch responses in case of atopic dermatitis. Br J Dermatol 86:574-585, 1972
55. Jowett S, Ryan T: Skin disease and handicap: An analysis of the impact of skin conditions. SOC Sci Med 20425-429, 1985
56. Kirshbaum BA: Eczema and emotions. Kalamazoo, MI, Upjohn Company, 1982
57. Klein LM, Lavker RM, Matis WI, et al: Degranula- tion of human mast cells induces an endothelial antigen central to leukocyte adhesion. Proc Natl Acad Sci 863972-8976, 1989
58. Kontou-Fili K: Anti allergic drugs in urticaria. In Indiveri F, Canonica GW (eds): Highlights on Anti- allergic Drugs. Genova, September 24, 1993
59. Koo JY, Shellow WVR, Hallman CP, et al: Alopecia areata and increased prevalence of psychiatric disor- ders. Int J Dermatol 33:849-850, 1994
60. Lebouleng AG, Charnay Y, Dubois PM: The coexis-
135: 1045-1 053, 1989
tence of neuropeptides and catecholamines in the adrenal gland. Ann Endocrinol (Paris) 45:217-227, 1984
61. Leichtman SR, Burnett JW, Robinson HM Jr, et al: Body image concerns of psoriasis patients as re- flected in human figure drawings. J Pers Assess 45:478-483,1981
62. Levine JD, Lane SR, Gordon NC: A spinal opioid synapse mediates the interaction of spinal and brain stem sites in morphine analgesia. Brain Res 236:85- 91, 1982
63. Lisoprawski A, Blanc G, Glowinski J: Activation by stress of the habenula-interpeduncolar substance P neurons in the rat. Neurosci Lett 25:47-51, 1981
64. Lotti T, Hautmann G, Panconesi E: Neuropeptides and skin. J Am Acad Dermatol, 1995
65. Lotti T, Cappugi P, Hautmann G, et al: Neuropep- tides: A meeting point between biological and men- tal. 3rd International Congress on Dermatology and Psychiatry, Florence, September, 20-21, 1991
66. Lotti T, Modesti P, Meo AL, et al: I1 passaggio transcutaneo di ossigeno nell'alopecia areata. 67" Congresso Nazionale SIDEV, Stresa, June 5-8, 1991
67. Lotti T, Palleschi GM, Benci M, et al: Studio ultra- strutturale, immunopatologico e biochimico dei mi- crovasi nell'alopecia areata. 67" Congresso Nazio- nale SIDEV, Stresa, June 5-8,1991
68. Mason JW: Over-all hormonal balance as a key to endocrine function. Psychosom Med 30:791-808, 1968
69. Masters R Psyche and skin. In Soter N, Baden HP (eds): Pathophysiology of Dermatologic Diseases. New York, McGraw-Hill, 1984, pp 441453
70. Matis WL, Lavker RM, Murphy GF: Substance P induces the expression of an endothelial leukocyte adhesion molecule by microvascular endothelium. J Invest Dermatol 94:492497, 1990
71. Matussek P, Agerer D, Seibt G: Aggression in de- pressives and psoriatics. Psychother Psychosom
72. McLaughlin JT, Shoemaker RJ, Guy WB: Personality factors in adult atopic eczema. Arch Dermatol 68:506-516, 1953
73. Medansky RS, Handler RM: Dermatopsychosomat- ics: Classification, physiology, and therapeutic ap- proaches. J Am Acad Dermatol 5:125-136, 1981
74. Meo AL, Fedi AM, Hautmann G, et a1 Passaggio transcutaneo di ossigeno in corso di alopecia areata, prima e dopo terapia: un marker di remissione clin- ica della dermatosi. I1 Incontro Italo-Francese "Della Riviera" di Dermatologia Clinica. Sanremo, Septem- ber 15, 1990
75. Miller H, Baruch DW: A study of hostility in allergic children. Am J Orthopsychiatry 20:506-519, 1950
76. Moberg GI? Biological response to stress: Key to assessment of animal well being. In Moberg GP (ed): Animal Stress. Bethesda, Waverly Press, 1985, pp 2749
77. Musgrove K, Morgan JK: Infantile eczema: A long- term follow-up study. Br J Dermatol 95:365-372, 1976
78. Naukkarinen A, Nickoloff BJ, Farber EM: Quantifi- cation of cutaneous sensory nerves and their sub- stance P content in psoriasis. J Invest Dermatol 92:126-129, 1989
79. Nemiah JC, Freyberger H, Sifneos PE: Alexithymia: A view of the psychosomatic process. In Hill OW (ed): Modem Trends in Psychosomatic Medicine. London, Butterworths, 1976, pp 430439
43:120-125, 1985
PSYCHOPHYSIOLOGY OF STRESS IN DERMATOLOGY 421
80. Nickoloff BJ, Karabin GD, Barker JNWN, et al: Cel- lular localization of interleukin-8 and its inducer, tumor necrosis factor-alpha in psoriasis. Am J Pa-
81. Obermayer ME: Psychocutaneous Medicine. Spring- field, IL, Charles C Thomas, 1955
82. Oehme P, Hecht K, Piesche L: Substance P: New aspect to its modulatory function. Acta Biol Med Ger 39:469477, 1980
83. Panconesi E: Commentary. In Panconesi E (ed): Stress and Skin Diseases: Psychosomatic Dermatol- ogy. Philadelphia, JB Lippincott, 1984, pp VIII-XIV
84. Panconesi E: Stress and Skin Diseases. Psychoso- matic Dermatology. Philadelphia, JB Lippincott,
85. Panconesi E, Hautmann G: Aspectos psychosomat- icos de la dermatitis atopica. Monografias de Der- matologia 5:428439, 1992
86. Panconesi E, Hautmann G: Neuropeptides in Psy- chosomatic Dermatology. In Burgdorf WHC, Katz SI (eds): Dermatology: Progress and Perspectives. The Proceedings of the 18th World Congress of
tho1 138~129-140, 1991
1984, pp 94-179
Dermatology. New York, 12-18 giugno 392, pp 904-907
87. Panconesi E, Mantellassi G: Fattori psichici nella eziopatogenesi della area celsi. Rass Dermatol Sifil
88. Panconesi E, Mantellassi G: Ulteriori risultati di in- dagini psicodiagnostiche sulla alopecia areata. Rass Dermatol Sifil 3:205-243, 1956
89. Panconesi E, Ghersetich I, Lotti T Nuove acquisizi- oni sulla patogenesi della alopecia areata. Ann Ital Dermatol Clin Sper 4755-62, 1993
90. Panconesi E, Giannotti B, Fabbri P: L’orticaria fisica e le orticarie cosiddette extra-allergiche. Folia Aller- gia Immunol Clin 4373-401, 1975
91. Panconesi E, Hautmann G, Lotti T: Neuropeptides in skin: The state of the art. JEADV 3:109-115, 1994
92. Panconesi E, Hautmann G, Lotti T: Stress, stigmati- zation and psychogenic purpura. Int Angiology, in press
93. Panconesi E, Sertoli A, Reali UM: La reattivita del cuoio capelluto alle sostanze neuroorminche ed ai polipeptidi biologicamente attivi nell’alopecia are- ata. Rass Derm Sifil 27:55-61, 1964
94. Pauk J, Kuhn CM, Field TM, et al: Positive effect of tactile vs kinesthetic or vestibular stimulation on neuroendocrine and ornithine decarboxylase activ- ity in maternally deprived rat pups. Life Sci
95. Payan DG, Brewster DR, Goetzl EJ: Specific stimula- tion of human T lymphocytes by substance P. J Immunol 131:1613-1615, 1983
96. Pincelli C, Fantini F, Giardino L, et al: Autoradio- graphic detection of substance P receptors in normal and psoriatic skin. J Invest Dermatol 101:301-304, 1993
97. Pincelli C, Fantini F, Massimi P, et al: Neuropep-
3~121-146, 1955
39:2081-2087, 1986
98.
99.
100.
101.
102.
103.
104.
105.
106.
107.
108.
109.
110.
111.
112.
113.
114.
115.
116.
117.
tides in skin from patients with atopic dermatitis: An immunohistochemical study. Br J Dermatol
Rabia M, Wilkinson DI, Farber EM: Neuropeptides modulate leukotriene B4 mitogenicity towards cul- tured keratinocytes. Fifth International Psoriasis Symposium, San Francisco, 1991, p 77 Rebora A, Savigni G: La personalita psoriasica. Chron Dermatol 7599412, 1976 Remick DG, Nguyer DT, Eskandarl ME, et al: Cyclosporin A inhibits TNF production without de- creasing TNF mRNA levels. Biochem Biophys Res Comm 161:551-555, 1989 Rexed B: A cytoarchitectonic atlas of the spinal cord. J Comp Neurol 100:297-380, 1954 Reynolds DV, Sjoberg A1 Neuroelectric Research. Springfield, Charles C Thomas, 1971 Rook A: Foreword. In Warin RP, Champion RH (eds): Urticaria. Philadelphia, WB Saunders, 1974, PV Rook A, Wilkinson DS: Psychocutaneous disorders. In Rook A, Wilkinson DS, Ebling FJG (eds): Text- book of Dermatology. Oxford, Blackwell Scientific Publications, 1979, pp 2023-2035 Selye H: The evolution of the stress concept. Am Sci 6L692-699, 1973 Selye H: The general adaptative syndrome and dis- eases of adaptation. J Clin Endocrinol 6:117-230, 1946 Sifneos PE: The prevalence of “alexithymic” charac- teristics in psychosomatic patients. Psychother Psy- chosom 22:255-262, 1973 Slany E: Kinderpsychoterapie im Rahmen der Der- matologie. Hautartz, 26:419422, 1975 Solomon GF, Levine S, Kraft JK: Early experience in immunity. Nature 220:821-822, 1968 Stokes JH: The personality factor in psychoneuro- genous reactions of the skin (AMA). Arch Dermatol Syphilol 42:780-801, 1940 Sweet WH: Cerebral localization of pain. In Thomp- son RA, Green JR (eds): New Perspectives in Cere- bral Localization. New York, Raven Press, 1982, pp
Updike J: Personal history: At war with my skin. The New Yorker 2339-57, 1985 Vaupel R, Schlomer H T Differential response of substance P containing subtypes of adrenomedul- lary cells to different stressors. Endocrinology
Wiesner-Menzel L, Schulz B, Vakilzadeh F: Electron microscopical evidence for a direct contact between nerve fibers and mast cells. Acta Dermatovenereol
Willis WD, Coggeshall RE: Sensory Mechanisms of the Spinal Cord. New York, Plenum Press, 1983 Withlock RA: Psychophysiological Aspects of Skin Disease. Philadelphia, WB Saunders, 1976 Wittkower E, Russel B: Emotional Factors in Skin Disease. London, Cassel and Co, 1953
122:745-750, 1990
205-242
123:2140-2145, 1988
(Stockh), 61x296-299, 1981
Address reprint requests to Emiliano Panconesi, MD
Department of Dermatology University of Florence
37, Via Alfani 50121 Florence
Italy
Related Documents











