Psychopharmacology Antipsychotic drugs Dr. Layali Abbasi Psychiatrist AL-Balqa Applied University 5th year/Faculty of Medicine 2019-2020

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Psychopharmacology Antipsychotic drugs
Dr. Layali Abbasi Psychiatrist
AL-Balqa Applied University
5th year/Faculty of Medicine 2019-2020

• Typical antipsychotics
• Atypical antipsychotics
Antipsychotic drugs
Antipsychotic drugs
• Conventional antipsychotics
Also called classical antipsychotics, or typical antipsychotics, or first-generation antipsychotics.
These drugs share the primary pharmacological property of D2 antagonism.
q
q
q
q
q
q
q
q
Found post-synaptic in limbic system, basal ganglia, prefrontal cortexG protein coupledD1–> increase cAMPD2–>Decrease cAMP so when blocked increase cAMP

Typical antipsychotics
• Haloperidol
• Chlorpromazine
• Perphenazine
q

Haloperidol
• High potency FGA
• High risk of causing EPS
• Available as LAI
q
q
q
q
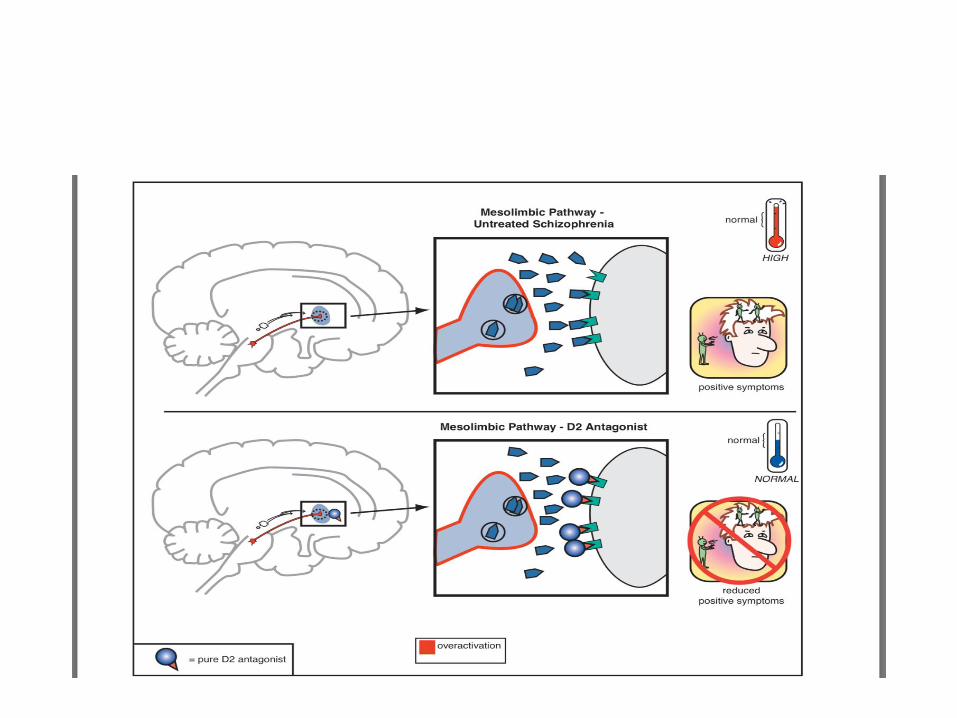

• D2 receptors in the mesolimbic dopamine system are postulated to mediate not only the positive symptoms of psychosis, but also the normal reward system of the brain, and the nucleus accumbens is widely considered to be the “pleasure center” of the brain. It may be the final common pathway of all reward and reinforcement, including not only normal reward (such as the pleasure of eating good food, orgasm, listening to music) but also the artificial reward of substance abuse.
• If D2 receptors are stimulated in some parts of the mesolimbic pathway, this can lead to the experience of pleasure.
q
q
q
q
q

• Thus, if D2 receptors in the mesolimbic system are blocked, this may not only reduce positive symptoms of schizophrenia, but also block reward mechanisms, leaving patients apathetic, anhedonic, lacking motivation, interest, and joy from social interactions, a state very similar to that of negative symptoms of schizophrenia.
• The near shutdown of the mesolimbic dopamine pathway necessary to improve the positive symptoms of psychosis may contribute to worsening of anhedonia, apathy, and negative symptoms, and this may be a partial explanation for the high incidence of smoking and drug abuse in schizophrenia.
q
q
q
q
q
q
q


• Antipsychotics also block D2 receptors in the mesocortical DA pathway, where DA may already be deficient in schizophrenia.
• This can cause or worsen negative and cognitive symptoms even though there is only a low density of D2 receptors in the cortex.
• An adverse behavioral state can be produced by conventional antipsychotics, and is sometimes called the “neuroleptic induced deficit syndrome” because it looks so much like the negative symptoms produced by schizophrenia.
q
q
q
q
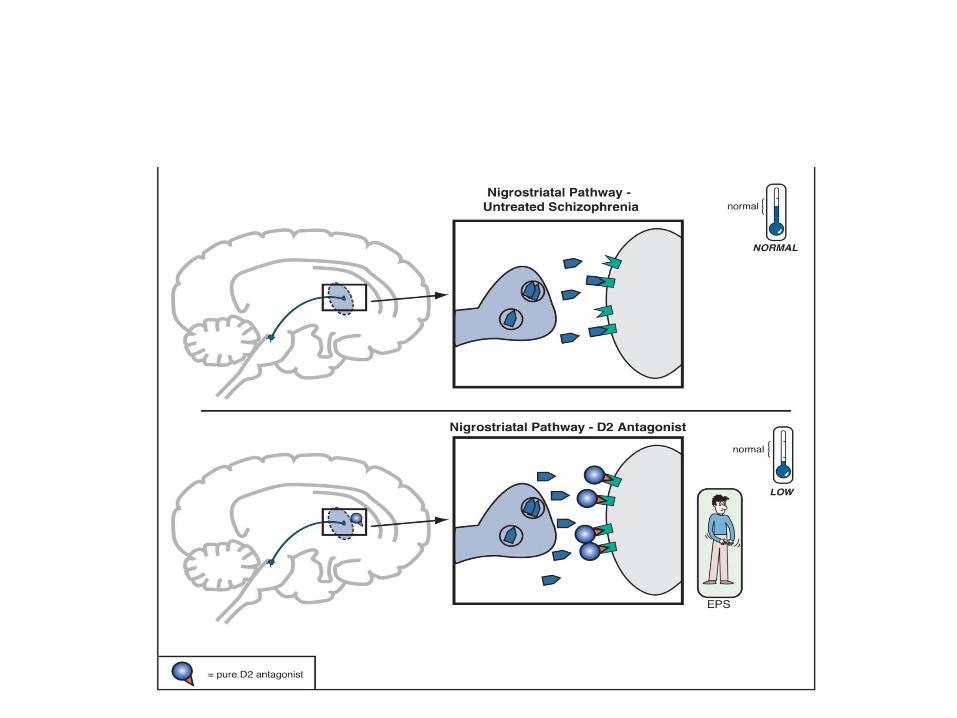
• When a substantial number of D2 receptors are blocked in the nigrostriatal DA pathway, this will produce various disorders of movement that can appear very much like those in Parkinson’s disease; this is why these movements are sometimes called drug-induced parkinsonism.
q
q
q
q

• Since the nigrostriatal pathway is part of the extrapyramidal nervous system, these motor side effects associated with blocking D2 receptors in this part of the brain are sometimes also called extrapyramidal symptoms, or EPS.
q
q

EPS -Acute dystonia
Intermittent and sustained contractions of muscles of tongue, face, neck and back.
Very frightening.
Typically occur during the first 5 days of treatment.
Mechanism: acute D2 antagonism.
Highest risk among young men treated with high potency agents.
q
q
q
q
q
Types of dystonia
• Oculogyric crisis (eyes rolled back in a locked position).
• Torticollis (spasm of cervical muscles of the neck).
• Laryngeal or pharyngeal dystonias.
• Macroglossia and tongue protrusion.
q
q
q
q
EPS -Acute akathisia Clinical features
-” Inability to sit still”, urge to move. - Subjective distress. - Akathisia can be confused with agitation. - Shifting the weight from foot to foot, walking on the
spot, inability to keep the legs still, feelings of inner restlessness.
- Onset: frequently after 5 days of treatment.
q
q
q
q

Akathisia- Management
• Reduce or change antipsychotic.
• Beta blockers (propranolol).
• High potency benzodiazepines (clonazepam).
q
q
q

EPS- Pseudoparkinsonism Clinical features
Masklike facies
Resting tremor
Bradykinesia
Cogwheel rigidity
Shuffling gait
Psychomotor retardation

Management of antipsychotic induced parkinsonism
• Dose reduction of antipsychotic agent.
• Anticholinergic agents:
Procyclidine
Biperiden
• Amantadine
q
q
q
q
q

EPS - Tardive dyskinesia
(TD)
• Hyperkinetic movement disorder that appears after prolonged use of dopamine antagonists (FGAs).
q

Tardive dyskinesia Clinical features
• Abnormal, repetitive, stereotyped, involuntary, painless, choreiform movement.
Ex: Sucking, smacking of lips
Tongue movements
Lateral jaw movements
q
q

Biological mechanism of Tardive dyskinesia
• Chronic blockade of D2 receptors in the nigrostriatal pathway induce up regulation of D2 receptors.
• Dopamine hypersensitivity.
q
q
q

Risk of TD
• Greater risk: elderly population, especially women (less likely to remit)
q
q

Pharmacological treatment of TD
• Most cases are not severe enough to warrant special treatment.
• There is no effective or standard treatment.
• Some strategies include:
- Taper antipsychotic.
- Switch antipsychotic.
- Drugs: clozapine.
q
q
q
q
q

Neuroleptic Malignant Syndrome
“ NMS is an acute disorder of thermoregulation and neuromotor control carrying a mortality
rate of about 21% when untreated”
q
NMS - Epidemiology
• Estimates of incidence were once around 3%
• Recent statistics suggest incidence of 0.01 -0.02%
• The syndrome has been described in all age groups (most are young adults)

NMS - Associated Drugs D
op
amin
e an
tago
nis
ts
Antipsychotics FGA
High potency
Low potency SGA
Antiemetics
q

NMS - Risk Factors
• Dehydration is present in about 92 % of patients ( risk factor or early complication?)
• Concomitant lithium use
• Use of high potency agents
• Long-acting injections
• High antipsychotic dose (not dose dependent)
q
q

NMS - Clinical Manifestations
Hyperthermia
• Higher than 38°C, even higher than 40°C
Rigidity
• Typical: “lead pipe rigidity”
Mental Status Changes
• Agitated delirium with confusion
Autonomic Instability
• Tachycardia, tachypnea, labile or high BP
NMS
Lab Testing
- Serum CK - Other abnormalities
- Leukocytosis - Electrolyte abnormalities

Management of NMS
• General
– Stop causative agent
– Supportive care
• Specific agents (limited evidence)
– Dantrolene
– Bromocriptine
– Amantadine
• ECT
q

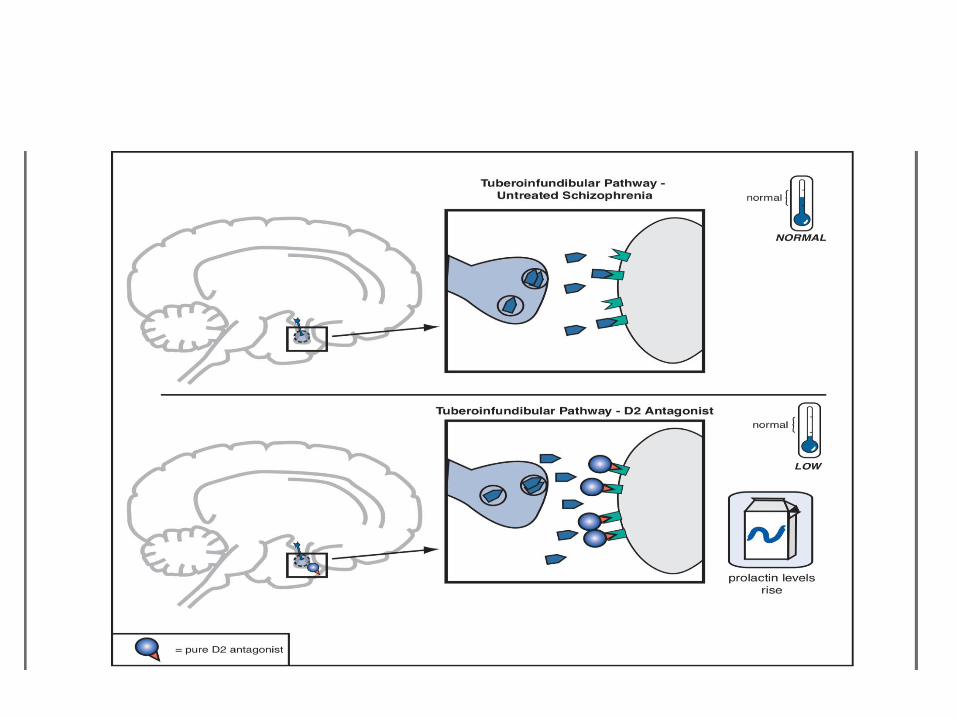
• Dopamine D2 receptors in the tuberoinfundibular DA pathway are also blocked by conventional antipsychotics, and this causes plasma prolactin concentrations to rise, a condition called hyperprolactinemia.
• Hyperprolactinemia may cause: Galactorrhea (i.e., breast secretions) Amenorrhea (i.e., irregular or lack of menstrual periods). Interfere with fertility, especially in women. More rapid demineralization of bones, especially in
postmenopausal women who are not taking estrogen replacement therapy.
Sexual dysfunction and weight gain, although the role of prolactin in causing such problems is not clear.
q
q
q
q
q



Muscarinic cholinergic blocking properties of conventional antipsychotics
• Differing degrees of muscarinic cholinergic blockade may also explain why some conventional antipsychotics have a lesser propensity to produce extrapyramidal side effects (EPS) than others.
• That is, those conventional antipsychotics that cause more EPS are the agents that have only weak anticholinergic properties, whereas those conventional antipsychotics that cause fewer EPS are the agents that have stronger anticholinergic properties.
q
q

Atypical antipsychotics
• Also called second-generation antipsychotics (SGAs).
• Serotonin–dopamine antagonists, with simultaneous serotonin 5HT2A receptor antagonism that accompanies D2 antagonism.
• Agonist actions at 5HT1A receptors and partial agonist actions at D2 receptors.
• All SGAs purportedly block 5-HT2A receptors. • SGAs provide greater blockade of 5-HT2A than D2
receptor blockade.
q
q
q
q
q
q
q
q
q
q
q
q
q

Atypical antipsychotics (SGAs)
• Risperidone
• Aripiprazole
• Amisulpride
• Quetiapine
• Ziprasidone
• Olanzapine
• Clozapine

Atypical antipsychotics (SGAs)
Although all atypical antipsychotics share a class warning for causing weight gain and risks for obesity, dyslipidemia, diabetes, accelerated cardiovascular disease, and even premature death, there is actually a spectrum of risk among the various agents.
High metabolic risk – clozapine, olanzapine
Moderate metabolic risk –risperidone,quetiapine
Low metabolic risk – aripiprazole, ziprasidone
q
q
q
q

Clozapine
• First of the SGAs
• Unique therapeutic benefits
• Unique side effects profile

Clozapine: Binding Profile
- D3 and D4 antagonist - 5HT1A partial agonist
q
q
q
q
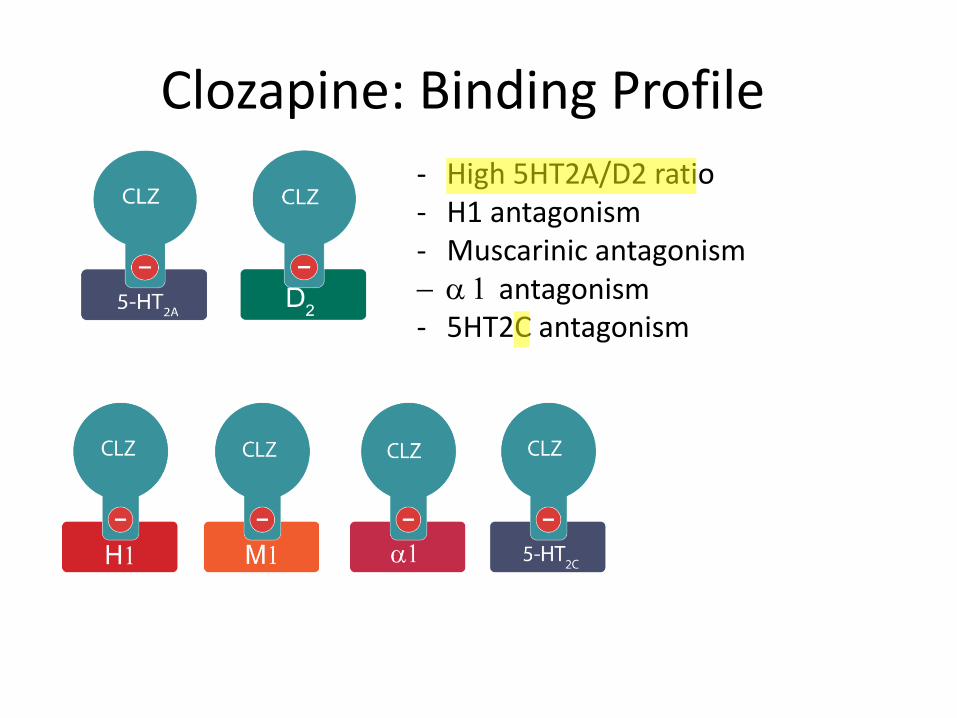
Clozapine: Binding Profile
- High 5HT2A/D2 ratio - H1 antagonism - Muscarinic antagonism a 1 antagonism - 5HT2C antagonism
q
q

Clozapine: Clinical Profile
• Effective for treatment-resistant schizophrenia.
• Reduces violence and persistent aggression in schizophrenia.
• Long-term treatment associated with reduction of risk of suicidal behaviors.
q
q
q
q
q

Treatment-Resistant Schizophrenia
Treatment-Resistant
Schizophrenia
clozapine is the one and only clearly effective option
30%-45% of patients with schizophrenia
q

Clozapine: potential advantages and disadvantages
• Advantages
May benefit treatment-refractory patients
May reduce suicidal, aggressive, or violent behavior
May increase life expectancy
Has diminished extrapyramidal side effects
Minimizes risk for or improves tardive dyskinesia
Avoids hyperprolactinemia
q

Clozapine: potential advantages and
disadvantages
• Disadvantages Box warnings Agranulocytosis Seizures Myocarditis Orthostasis Increased mortality in dementia Other adverse effects Weight gain/metabolic syndrome Diabetic ketoacidosis Gastrointestinal hypomotility Sialorrhea
q
q
q
q
q
q
q
q
q

Clozapine – Adverse Effects Profile
• One of the antipsychotics with the lowest EPS risk
• One of the antipsychotics with the highest metabolic risk
• Risk of agranulocytosis
• Dose-dependent seizure risk
• Can be very sedating
q
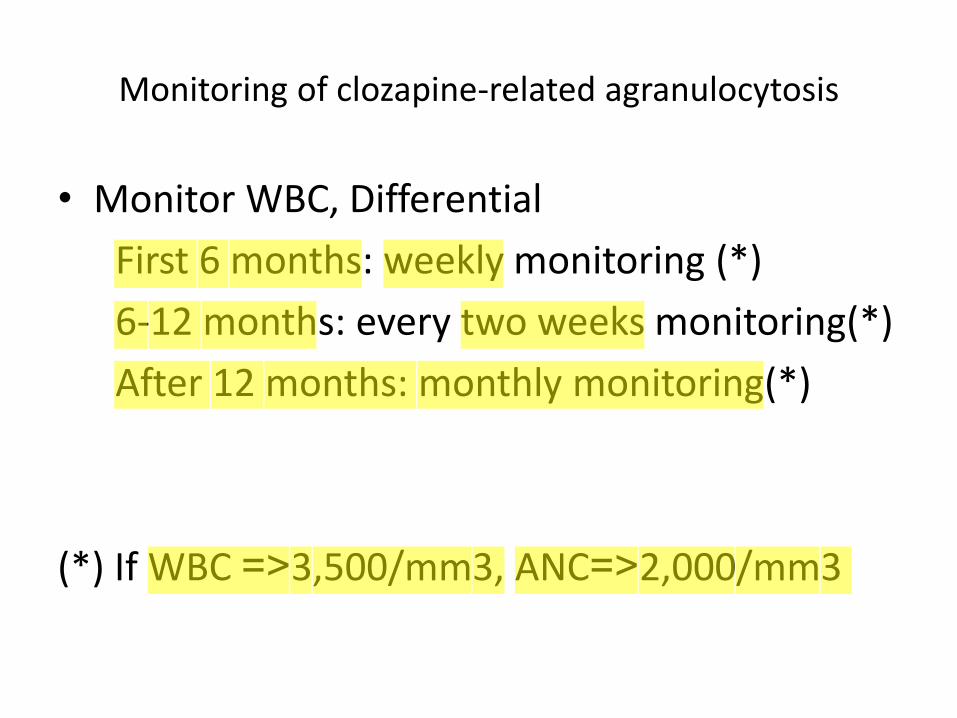
Monitoring of clozapine-related agranulocytosis
• Monitor WBC, Differential
First 6 months: weekly monitoring (*)
6-12 months: every two weeks monitoring(*)
After 12 months: monthly monitoring(*)
(*) If WBC <= 3,500/mm3, ANC <= 2,000/mm3
q
q
q
q
q
q
q

Olanzapine: side effects
Severe weight gain and metabolic
effects Even one dose:
Insulin resistance
Endocrine/ inflammatory dysfunction
q
q
q
q
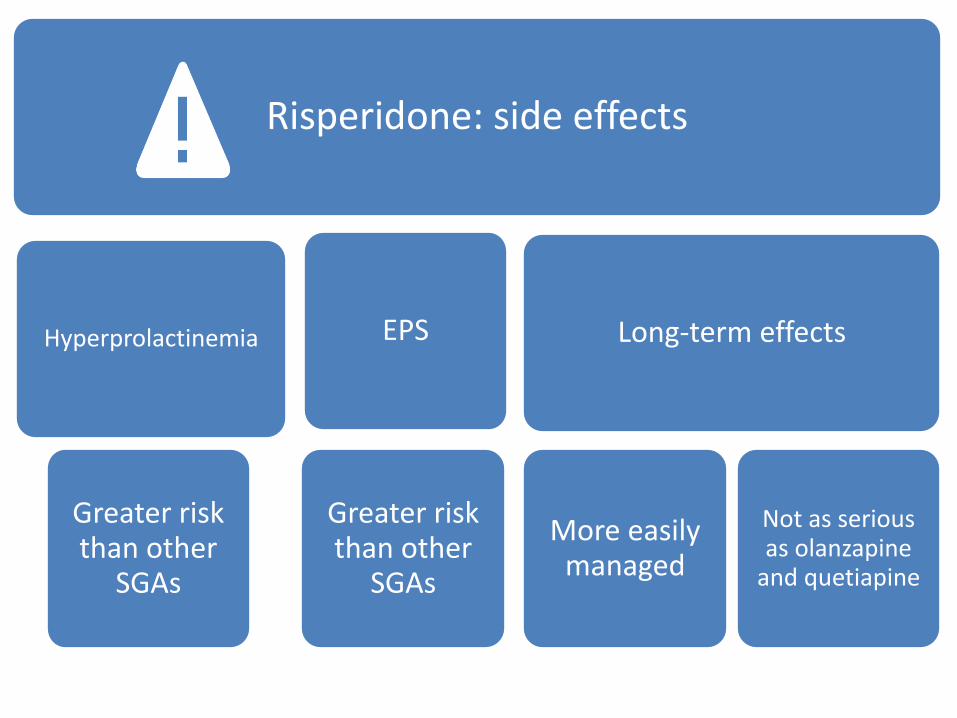
Risperidone: side effects
Hyperprolactinemia
Greater risk than other
SGAs
EPS
Greater risk than other
SGAs
Long-term effects
More easily managed
Not as serious as olanzapine
and quetiapine
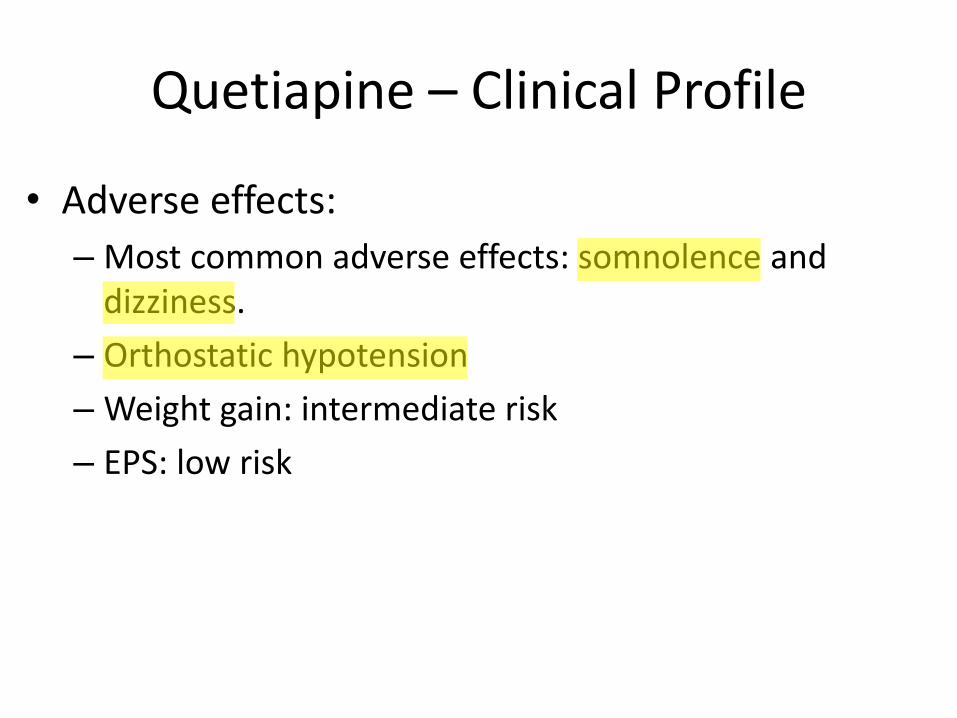
Quetiapine – Clinical Profile
• Adverse effects:
– Most common adverse effects: somnolence and dizziness.
– Orthostatic hypotension
– Weight gain: intermediate risk
– EPS: low risk
q
q
q
q

Aripiprazole – Binding Profile
- Partial D2/D3 agonist (pre and postsynaptic receptors)
- 5HT2A antagonist - 5HT1A partial agonist - Modest affinity for H1,
M1 and a 1 receptors
q
q
q
Schizophrenia Psychopharmacology Algorithm

Duration: 4-6 week trial
Adequate trial
Lower than usual doses
First-episode: First antipsychotic trial
Start with SGA
• No difference with FGAs in acute efficacy
Long-term advantages
• Increased time to first relapse
• Better treatment retention
• Greater probability of staying in remission
FGAs
• Adjunctive anticholinergic use
• Adverse cognitive and central anticholinergic effects

THE END
Related Documents











