Psycho-social Health in Fragile States: The Forgotten Emergency Willem van de Put General Director HealthNet - TPO Discussant: Amy Bess Senior Practice Associate, Human Rights and International Affairs National Association of Social Workers Chair: Isabel Guerrero Vice President South Asia Region, World Bank

Psycho-social Health in Fragile States: The Forgotten Emergency Willem van de Put General Director HealthNet - TPO Discussant: Amy Bess Senior Practice.
Dec 22, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Psycho-social Health in Fragile States: The Forgotten Emergency
Willem van de Put General Director HealthNet - TPO
Discussant: Amy Bess Senior Practice Associate, Human Rights and International Affairs National Association of Social Workers
Chair: Isabel Guerrero Vice President South Asia Region, World Bank
Structure of argument1. Mental health & social suffering: defining the field
– Cases: two examples illustrating that effects are on individual and community levels
2. Intervention in ‘recovery’ phase: stretching from relief to development3. A multisectoral approach:
– Health includes well-being and there is a clear need for mental health care– Integration of mental health is proven to be effective and cheap – yet it remains
to be done.4. But the issue is not limited to the health sector. The core of psychosocial
interventions is linking between sectors.5. Examples of how dynamics can be brought back in communities following
simple and cheap interventions.6. Work is done on developing the methodology to measure their cost-
effectiveness – but this can be said: costs are limited to building basic capacity for action in existing public services and community levels.

How common are mental disorders in fragile states?
• Many epidemiological studies have been done in last 10 years – mental disorders 15-18%, psychological distress 50-70% [1-29] – but validity of current data and applied methology are too easily contested [30-35].
• Patterns are seen:– Methods: higher quality surveys show lower rates– Geography : rates are relative low in Asia, relative high in Americas– Risk factors: life events (eg loss, trauma) and unsupportive environment are
among risk factors for wide range of disorders
• Given importance of environment, it is a fair assumption that rates are elevated in fragile states compared to what they would have been if the same state had been stable
• Fact is, that even a small percentage of people with burdensome disorders would still imply an enormous public health problem
Thanks to Mark van Ommeren, WHO

Psychosocial consequences of collective trauma
Mild and moderate mental disorders
5-10% increase 15%
after years
Severe mental
disorders 3-4%
Moderate or severe psychological distress
30-50%
Mild psychological distress20 -40%
IASC Guidelines on Mental health and Psychosocial support
The Inter-Agency Standing Committee (IASC) issued Guidelines to protect and improve people’s mental health and psychosocial well-being in the midst of an emergency.
Populations affected by emergencies frequently experience enormous suffering. Humanitarian actors are increasingly active to protect and improve people’s mental health and psychosocial well-being during and after emergencies.

IASC Guidelines on Mental health and Psychosocial support
Mental health and psychosocial problems in emergencies are highly interconnected, yet may be predominantly social or psychological in nature. Significant problems of a predominantly social nature include:
• Pre-existing (pre-emergency) social problems (e.g. extreme poverty; discrimination, exclusion)
• Emergency-induced social problems (family separation; disruption of social networks; destruction of community structures; increased gender-based violence)

Similarly, problems of a predominantly psychological nature include:
• Pre-existing problems (e.g. severe mental disorder; alcohol abuse);
• Emergency-induced problems (e.g. grief, non-pathological distress; depression and anxiety disorders, including post-traumatic stress disorder (PTSD))
IASC Guidelines on Mental health and Psychosocial support
From mental disorders to psychological distress
How bad is psychological distress?
Sorrow, grief, loss, sadness, in combination with poverty, ongoing crises, inability to cope, insecurity, destruction of social networks and loss of material possessions leads to hopelessness and despair.
Not only individuals are touched, but the relations between individuals, the community as such, may be broken.
"Social suffering" and “Structural violence” are interesting concepts – apart from their rhetoric value, they break down boundaries between specific scholarly disciplines, and offer a cross-disciplinary perspective.

The effect on families and groups
In Sri Lanka, fundamental changes in the functioning of the family and the community were observed. While the changes after the tsunami were not so prominent, the chronic war situation caused more fundamental social transformations.
At the family level, the dynamics of single parent families, lack of trust among members, and changes in significant relationships, and child rearing practices were seen [1].

Effects on communities and society
Communities tended to be more dependent, passive, silent, without leadership, mistrustful, and suspicious.
Additional adverse effects included the breakdown in traditional structures, institutions and familiar ways of life, and deterioration in social norms and ethics.
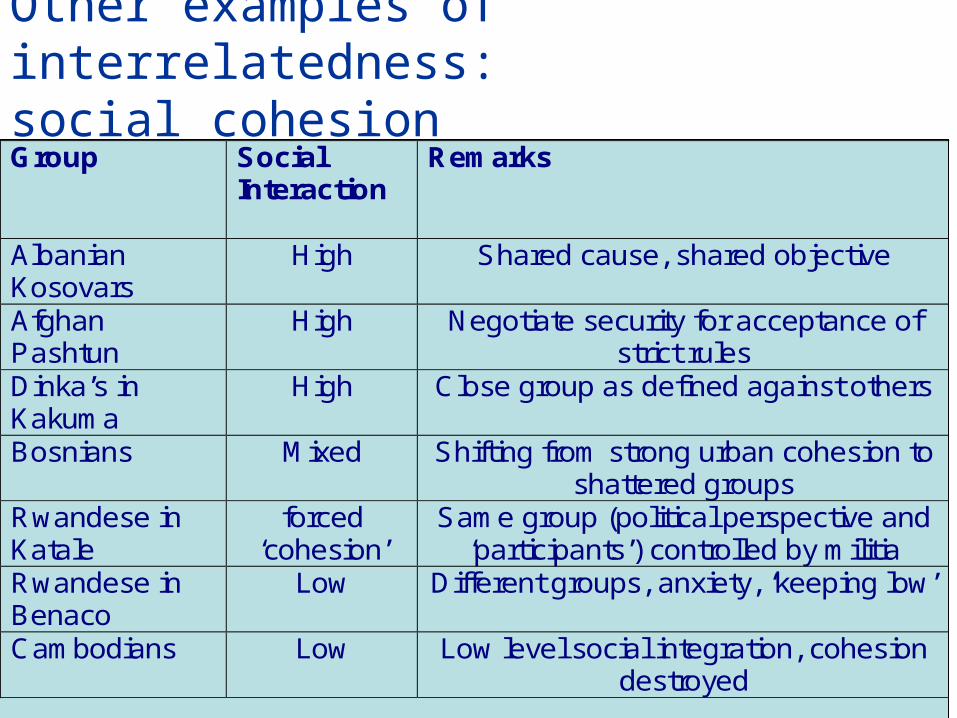
Group Social Interaction
Remarks
Albanian Kosovars
High Shared cause, shared objective
Afghan Pashtun
High Negotiate security for acceptance of strict rules
Dinka’s in Kakuma
High Close group as defined against others
Bosnians Mixed Shifting from strong urban cohesion to shattered groups
Rwandese in Katale
forced ‘cohesion’
Same group (political perspective and ‘participants’) controlled by militia
Rwandese in Benaco
Low Different groups, anxiety, ‘keeping low’
Cambodians Low Low level social integration, cohesion destroyed
Other examples of interrelatedness: social cohesion
Workfield: fragile states
• Fragile states have a disproportionately high disease burden compared to other low-income countries [1].
• Home to only 15% of the developing world’s population, more than a third of maternal deaths and half of the children who die before the age of five occur in fragile states.
• Poverty and exclusion remain most visible manifestation of ‘structural violence’ in fragile states;
• So that ‘fragile states’ now underpin the concept of ‘state security’

Where are 10 million children dying every year?
Black et al 2003


What needs to be done
• Integration of (primary) mental health in the (primary) health care system;
• Addressing psychosocial problems;
• Starting immediately when disaster strikes, working into the development phase.
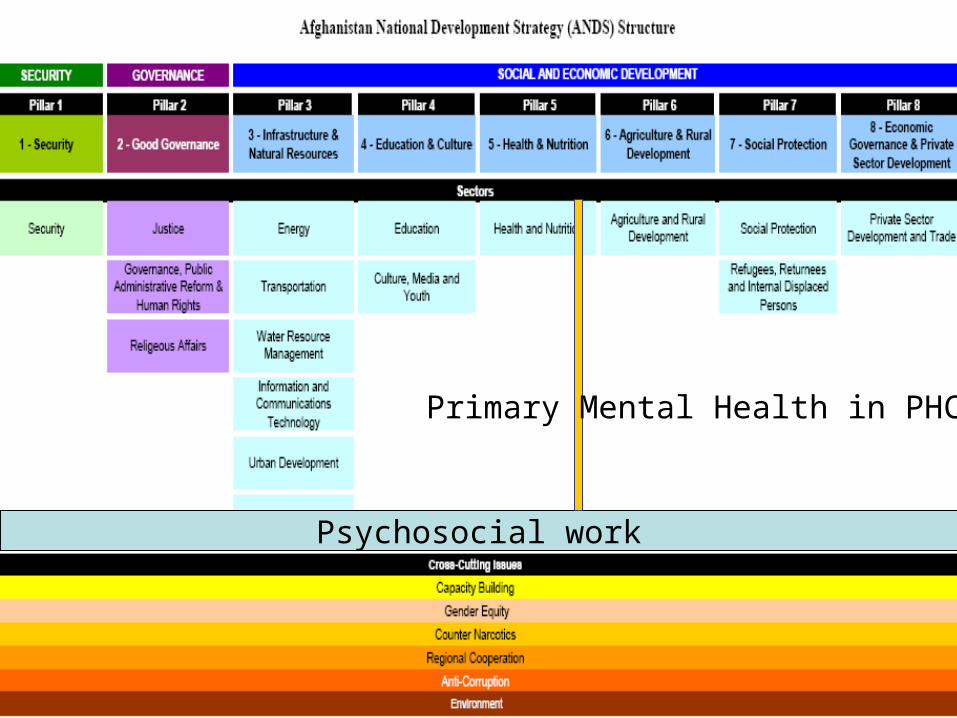
Psychosocial work
Primary Mental Health in PHC

Early Recovery
Development
Emergency Response
Reconstruction
Development
Thanks to Egbert Sondorp, LSHTM

Primary interventions on community and
family level • Creating self-help groups• Connect to income-generating models, e.g. rural
development activities• Organize public (health) education • Through community mapping, preservation of social
infrastructure• Support community empowerment and capacity-
building• Training, education and sensitization of health
workers, social workers, and teachers• Support for community leaders • Family reunion and family tracing

Intervention in the community
Source: Green, Friedman, De Jong et al. (2003)
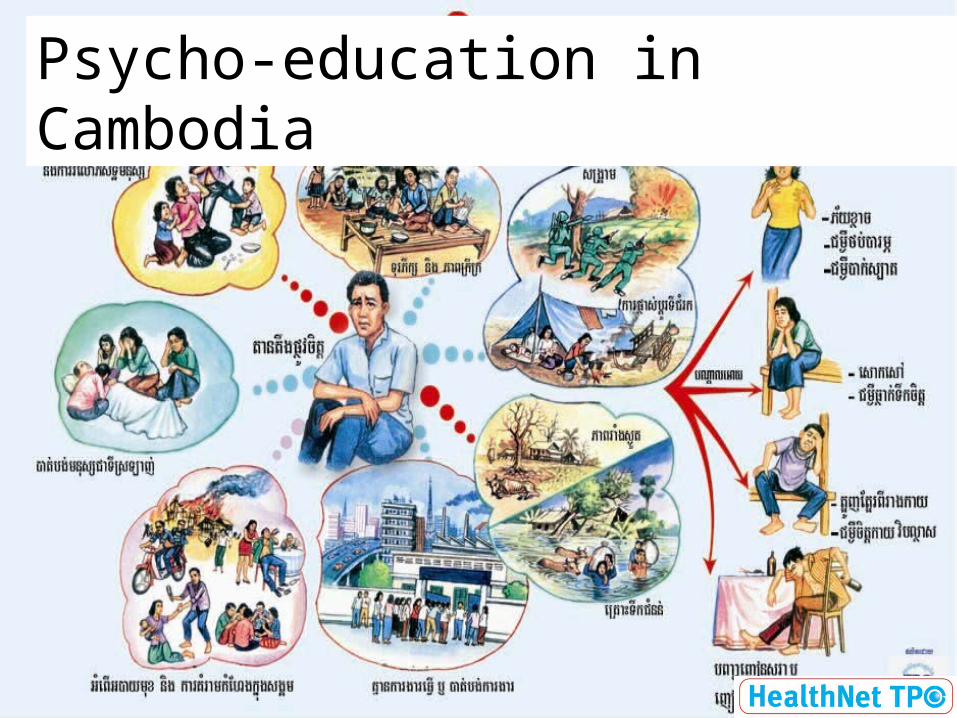
Psycho-education in Cambodia

Self-help groups

Under-stand local
values

Reaching out to people in distress

Is there an evidence base for interventions?
• In terms of successful treatment, yes.• In terms of cost-effectiveness, a beginning
evidence base for mental health.• Confusion on how to measure the impact and
cost-effectiveness of psychosocial interventions.

In 2002, mental and substance use disorders accounted for 13% of the global burden of disease, defined as premature death combined with years lived with disability. [1]
When taking into account only the disability component of the burden of disease calculation, mental disorders accounted for 31% of all years lived with disability.
And this figure is rising. By 2030, depression alone is likely to be the second highest cause of disease burden. In high-income countries, depression will become the single highest contributor to the overall disease burden.[2]
Mental disorders impose a substantial burden if left untreated

Cost of scaling up mental health care in low- and middle-income countries
DAN CHISHOLM, CRICK LUND and SHEKHAR SAXENA, 2007
Question: To estimate the expenditures needed to scale up the delivery of an essential mental health care package over a 10-year period (2006^2015), a core package was defined, comprising pharmacological and/or psychosocial treatment of schizophrenia, bipolar disorder, depression and hazardous alcohol use.
Current service levels in12 selected low- and middle income countries were established using the WHO^AIMS assessment tool. Target level resource needs were derived from published need assessments and economic evaluations. Results: The cost per capita of providing the core package at target coverage levels (in US dollars) ranged from $1.85 to $2.60 per year in low-income countries and $3.20 to $6.25 per year in lower-middle income countries, an additional annual investment of $0.18^0.55 per capita.
Conclusions: Although significant new resources need to be invested, the absolute amount is not large when considered at the population level and against other health investment strategies.

Cost effective mental health
Depression: In resource-poor regions, each DALY averted by efficient depression treatments in primary care costs less than1year of average per capita income,making such interventions a cost effective use of health resources.However, current levels of burden can only be reduced significantly if there is a substantial increase intreatment coverage [1] .
Schizophrenia: In Chile, Nigeria and Sri Lanka the most cost-effective interventions were those using older antipsychotic drugs combined with psychosocial treatment, delivered via a community-based service model.By moving to a community-based service model and selecting efficient treatment options, the cost of substantially increasing treatment coverage is not high (less than I$ 1 investment per capita). Taken together with other priority-setting criteria such as disease severity, vulnerability and human rights protection, this study suggests that a great deal more could be done forpersons and families living under the spectre of this disorder [2].

Cost effective mental health
Epilepsy: A significant proportion of the current burden of epilepsy in developing countries is avertable by scaling up the routine availability of low-cost antiepileptic drug (AED) treatments. Across nine developing WHO subregions, extending AED treatment coverage to 50% of primary epilepsy cases would avert between 150 and 650 DALYs per one million population(equivalent to 13–40% of the current burden), at an annual cost per capita of I$ 0.20–1.33. Critical factors in the successful implementation of such a scaled-up level of service delivery, apart from renewed political support and investment, relate to appropriate training and continuity of drug supply [1].

Treatment to prevention
The Global Burden of Disease study ranked depression as the fourth leading cause of burden among all disease, accounting for 4.1% of total burden. By 2020 it will rise from the fourth to the second leading cause of DALYs. It will then be second only to ischaemic heart disease for DALYS among both sexes.
Taking the example of ischaemic heart disease, risk factors such as smoking and high blood pressure have been identified, and public health interventions target those risk factors and try to reduce their frequency in the population.
We need such public health oriented research into depression that will then lead on to primary preventive programmes and to improved access to efficacious treatment for people with depression.

Is there an evidence base for psychosocial interventions?
Psychosocial interventions: the relatively modest additional cost of adjuvant psychosocial treatment is expected to reap significant health gains, thereby making such a combined strategy for schizophrenia and bipolar disorder treatment more cost-effective than pharmacotherapy alone. For people with depression or anxiety, psychotherapy is expected to be as cost-effective as newer (generic) antidepressants. Clearly, however, there remains a major human resource constraint in making psychosocial interventions more widely available [1].
Financial and human resource needs: Based on the use of efficient interventions, the financial implications of scaling-up the effective coverage of key mental health care strategies need not be overwhelming (less than US$ 10 in middle-income countries, and well below US$ 5 per capita in low-income countries; in countries such as Nigeria or Sri Lanka, for example, it is expected to be in the range of just US$ 1 per capita) [1]. HealthNet TPO has estimated the cost to install basic capacity for psychosocial interventions on the community level at 0.28 USD/per capita/year.
Is there an evidence base for psychosocial interventions?
A worldwide panel of experts on the study and treatment of those exposed to disaster and mass violence assembled (…) to gain consensus on intervention principles that should be used to guide and inform intervention and prevention efforts at the early to mid–term stages [1].
These are promoting these five principles: • a sense of safety, • calming, • a sense of self– and community efficacy, • connectedness, and • hope.

What is hope?
…Nevertheless, what is amazing aboutthe human spirit is that many people, whohave been down so long that everything elselooks like up, often do retain a sense of optimism,self–efficacy, and belief in both strongothers and/or a God who will intervene on theirbehalf (Antonovsky, 1979; Lomranz, 1990; Shmotkin, Blumstein, & Modan, 2003).
Five Essential Elements of Immediateand Mid–Term Mass Trauma Intervention:Empirical EvidenceStevan E. Hobfoll,

Psychosocial rehabilitation…
• Helps families care for their dysfunctional members;• Helps people cope with loss, regain resilience, and
find strength to ‘go on’;• Stimulates groups to take care of themselves;• Restores community ties, brings back dynamic in
communities;• Links services of different sectors to the people who
need them most;• Connects various public sectors with community
dynamics;• Creates a platform for human security and
willingness to participate in rebuilding society.
…and all these opportunity costs should be included

Model approach in…Afghanistan

Questions?
36
Related Documents











