OBSERVATIONS Identification of the Source of Androgen Excess in Hyperandrogenic Type 1 Diabetic Patients W e recently reported that the prev- alence of hyperandrogenic dis- orders is markedly increased in women with type 1 diabetes (1). The polycystic ovary syndrome (PCOS) de- fined by endocrine criteria was found in 18.8% of the type 1 diabetic women who followed-up in our hospital (1), as com- pared with the 6.5% prevalence in nondi- abetic women from similar ethnic and genetic backgrounds (2). The prevalence of hirsutism in type 1 diabetic women was 30.6% (1), which is markedly higher than the 7.1% prevalence of hirsutism found in nondiabetic women (2). In the present study, we evaluated the adrenal and ovarian steroidogenic pro- files of hyperandrogenic and nonhy- perandrogenic type 1 diabetic women and compared them with those of nondi- abetic hyperandrogenic women and healthy control subjects. A total of 24 women with type 1 dia- betes were recruited for the study (1). Fourteen diabetic patients (age [mean 6 SD] 20.6 6 4.0 years, BMI 24.8 6 2.9 kg/m 2 ) were considered to have hyperan- drogenism. The other 10 women with type 1 diabetes (age 19.0 6 3.0 years, BMI 23.3 6 2.6 kg/m 2 ) had no evidence of clinical or biochemical hyperandro- genism and had regular menstrual cycles. Both groups of type 1 diabetic patients had similar HbA 1c levels (7.4 6 1.2 vs 7.8 6 1.2% in nonhyperandrogenic and hyperandrogenic diabetic patients, re- spectively, F 5 0.591, P 5 0.450), and there were no differences in the mean daily insulin dose used for their treatment (0.82 6 0.27 vs. 0.66 6 0.28 U z kg 21 body wt z day 21 in nonhyperandrogenic and hyperandrogenic diabetic patients, F 5 1.875, P 5 0.185). A total of 86 nondiabetic women were included as control subjects. Nondiabetic women were matched for BMI and age with the diabetic patients to avoid any in- fluence of age and obesity on the results. Thirteen regularly menstruating women (age 23.2 6 3.2 years, BMI 24.6 6 5.1 kg/m 2 ) without signs or symptoms of hy- perandrogenism served as healthy control subjects; 73 untreated nondiabetic hyper- androgenic patients (age 20.6 6 3.8 years, BMI 23.7 6 3.2 kg/m 2 ) were included as hyperandrogenic control subjects. Basal and adrenocorticotropic hor- mone (ACTH)-stimulated samples were obtained and assayed as previously de- scribed (1,3). The study was conducted according to the principles expressed in the Declaration of Helsinki. The group of hyperandrogenic type 1 diabetic patients comprised seven women with PCOS and seven women with hirsut- ism and regular menstrual cycles. The percentage of patients with PCOS was not different among the groups of diabetic and nondiabetic hyperandrogenic patients (50.0 vs 38.4%, x 2 5 0.662, P 5 0.553). Both groups of hyperandrogenic pa- tients had higher hirsutism scores com- pared with nonhyperandrogenic diabetic patients and healthy control subjects (Fig. 1), but the hirsutism score was higher in nondiabetic hyperandrogenic patients compared with hyperandrogenic type 1 diabetic women (Fig. 1). Compared with healthy women, both hyperandrogenic type 1 diabetic patients and nondiabetic hyperandrogenic women had increased basal serum total and free testosterone concentrations, as well as basal D 4 -androstenedione con- centrations (Fig. 1). Nondiabetic hyper- androgenic patients had increased free testosterone levels and decreased sex hor- mone– binding globulin concentrations compared with all of the other groups (Fig. 1). No differences in sex hormone– binding globulin concentrations were found be- tween the groups of diabetic women and healthy control subjects (Fig. 1). Nonhyperandrogenic type 1 diabetic women had intermediate values of total testosterone, free testosterone, and D 4 - androstenedione that were not signifi- cantly different than those of hyper- androgenic diabetic patients and healthy control subjects (Fig. 1). No differences were observed among the groups in the serum concentrations of dehydroepi- androsterone-sulfate, luteinizing hor- mone, follicle-stimulating hormone, and estradiol (Fig. 1). Hyperandrogenic type 1 diabetic pa- tients had higher ACTH-stimulated D 4 -an- drostenedione levels than healthy control subjects, whereas ACTH-stimulated D 4 - androstenedione and 17-hydroxyproges- terone levels were higher in nondiabetic hyperandrogenic patients than healthy control subjects and nonhyperandro- genic diabetic patients (D 4 -androstenedi- one 12.3 6 3.0, 15.7 6 3.1, 12.4 6 4.3, and 16.1 6 4.4 nmol/l, F 5 4.84, P , 0.005; 17-hydroxyprogesterone 6.1 6 1.5, 9.2 6 5.2, 6.7 6 1.9, and 10.1 6 5.4 nmol/l, F 5 3.30, P , 0.05, in nonhy- perandrogenic diabetic patients, hy- perandrogenic diabetic patients, healthy control subjects, and nondiabetic hy- perandrogenic patients, respectively). However, the net increments in D 4 - androstenedione and 17-hydroxyproges- terone after ACTH stimulation were not statistically different among the groups (D 4 -androstenedione 1.4 6 2.2, 3.3 6 2.3, 3.1 6 2.5, and 3.4 6 2.6 nmol/l, F 5 1.904, P 5 0.134; 17-hydroxyprogester- one 3.5 6 2. 1, 6.3 6 4.3, 4.4 6 2.2, and 6.2 6 4.6 nmol/l, F 5 1.761, P 5 0.159 in nonhyperandrogenic diabetic patients, hyperandrogenic diabetic patients, healthy control subjects, and nondiabetic hyperandrogenic patients, respectively). Basal and ACTH-stimulated cortisol and 11-deoxycortisol levels were not dif- ferent among the groups (data not shown), whereas basal 17-hydroxypro- gesterone concentrations showed a near- significant tendency ( P 5 0.056) to higher levels in nondiabetic hyperandro- genic patients. Finally, because ovulation may nor- malize many reproductive variables, we used analysis of covariance to rule out a significant impact of the presence or ab- sence of oligomenorrhea on the differ- ences in hormone analyses described above. None of these differences were in- fluenced by oligomenorrhea (data not shown). Our present results demonstrate that hyperandrogenic type 1 diabetic women have increased serum levels of total and free testosterone and D 4 -androstenedione comparable with those found in nondia- betic hyperandrogenic women. Consider- ing that hyperandrogenic type 1 diabetic women had normal dehydroepiandros- terone-sulfate concentrations and that the increase in ACTH-stimulated D 4 - androstenedione levels found in these patients possibly reflects a normal adre- L E T T E R S DIABETES CARE, VOLUME 24, NUMBER 7, JULY 2001 1297

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

OBSERVATIONS
Identification ofthe Source ofAndrogen Excess inHyperandrogenicType 1 DiabeticPatients
W e recently reported that the prev-alence of hyperandrogenic dis-orders is markedly increased in
women with type 1 diabetes (1). Thepolycystic ovary syndrome (PCOS) de-fined by endocrine criteria was found in18.8% of the type 1 diabetic women whofollowed-up in our hospital (1), as com-pared with the 6.5% prevalence in nondi-abetic women from similar ethnic andgenetic backgrounds (2). The prevalenceof hirsutism in type 1 diabetic women was30.6% (1), which is markedly higher thanthe 7.1% prevalence of hirsutism found innondiabetic women (2).
In the present study, we evaluated theadrenal and ovarian steroidogenic pro-files of hyperandrogenic and nonhy-perandrogenic type 1 diabetic womenand compared them with those of nondi-abetic hyperandrogenic women andhealthy control subjects.
A total of 24 women with type 1 dia-betes were recruited for the study (1).Fourteen diabetic patients (age [mean 6SD] 20.6 6 4.0 years, BMI 24.8 6 2.9kg/m2) were considered to have hyperan-drogenism. The other 10 women withtype 1 diabetes (age 19.0 6 3.0 years, BMI23.3 6 2.6 kg/m2) had no evidence ofclinical or biochemical hyperandro-genism and had regular menstrual cycles.Both groups of type 1 diabetic patientshad similar HbA1c levels (7.4 6 1.2 vs7.8 6 1.2% in nonhyperandrogenic andhyperandrogenic diabetic patients, re-spectively, F 5 0.591, P 5 0.450), andthere were no differences in the meandaily insulin dose used for their treatment(0.82 6 0.27 vs. 0.66 6 0.28 U z kg21
body wt z day21 in nonhyperandrogenicand hyperandrogenic diabetic patients,F 5 1.875, P 5 0.185).
A total of 86 nondiabetic women wereincluded as control subjects. Nondiabetic
women were matched for BMI and agewith the diabetic patients to avoid any in-fluence of age and obesity on the results.Thirteen regularly menstruating women(age 23.2 6 3.2 years, BMI 24.6 6 5.1kg/m2) without signs or symptoms of hy-perandrogenism served as healthy controlsubjects; 73 untreated nondiabetic hyper-androgenic patients (age 20.6 6 3.8 years,BMI 23.7 6 3.2 kg/m2) were included ashyperandrogenic control subjects.
Basal and adrenocorticotropic hor-mone (ACTH)-stimulated samples wereobtained and assayed as previously de-scribed (1,3). The study was conductedaccording to the principles expressed inthe Declaration of Helsinki.
The group of hyperandrogenic type 1diabetic patients comprised seven womenwith PCOS and seven women with hirsut-ism and regular menstrual cycles. Thepercentage of patients with PCOS was notdifferent among the groups of diabeticand nondiabetic hyperandrogenic patients(50.0 vs 38.4%, x2 5 0.662, P 5 0.553).
Both groups of hyperandrogenic pa-tients had higher hirsutism scores com-pared with nonhyperandrogenic diabeticpatients and healthy control subjects (Fig.1), but the hirsutism score was higher innondiabetic hyperandrogenic patientscompared with hyperandrogenic type 1diabetic women (Fig. 1).
Compared with healthy women, bothhyperandrogenic type 1 diabetic patientsand nondiabetic hyperandrogenicwomen had increased basal serum totaland free testosterone concentrations, aswell as basal D4-androstenedione con-centrations (Fig. 1). Nondiabetic hyper-androgenic patients had increased freetestosterone levels and decreased sex hor-mone–binding globulin concentrationscompared with all of the other groups (Fig.1). No differences in sex hormone–bindingglobulin concentrations were found be-tween the groups of diabetic women andhealthy control subjects (Fig. 1).
Nonhyperandrogenic type 1 diabeticwomen had intermediate values of totaltestosterone, free testosterone, and D4-androstenedione that were not signifi-cantly different than those of hyper-androgenic diabetic patients and healthycontrol subjects (Fig. 1). No differenceswere observed among the groups in theserum concentrations of dehydroepi-androsterone-sulfate, luteinizing hor-mone, follicle-stimulating hormone, andestradiol (Fig. 1).
Hyperandrogenic type 1 diabetic pa-tients had higher ACTH-stimulated D4-an-drostenedione levels than healthy controlsubjects, whereas ACTH-stimulated D4-androstenedione and 17-hydroxyproges-terone levels were higher in nondiabetichyperandrogenic patients than healthycontrol subjects and nonhyperandro-genic diabetic patients (D4-androstenedi-one 12.3 6 3.0, 15.7 6 3.1, 12.4 6 4.3,and 16.1 6 4.4 nmol/l, F 5 4.84, P ,0.005; 17-hydroxyprogesterone 6.1 61.5, 9.2 6 5.2, 6.7 6 1.9, and 10.1 6 5.4nmol/l, F 5 3.30, P , 0.05, in nonhy-perandrogenic diabetic patients, hy-perandrogenic diabetic patients, healthycontrol subjects, and nondiabetic hy-perandrogenic patients, respectively).
However, the net increments in D4-androstenedione and 17-hydroxyproges-terone after ACTH stimulation were notstatistically different among the groups(D4-androstenedione 1.4 6 2.2, 3.3 62.3, 3.1 6 2.5, and 3.4 6 2.6 nmol/l, F 51.904, P 5 0.134; 17-hydroxyprogester-one 3.5 6 2. 1, 6.3 6 4.3, 4.4 6 2.2, and6.2 6 4.6 nmol/l, F 5 1.761, P 5 0.159 innonhyperandrogenic diabetic patients,hyperandrogenic diabetic patients,healthy control subjects, and nondiabetichyperandrogenic patients, respectively).
Basal and ACTH-stimulated cortisoland 11-deoxycortisol levels were not dif-ferent among the groups (data notshown), whereas basal 17-hydroxypro-gesterone concentrations showed a near-significant tendency (P 5 0.056) tohigher levels in nondiabetic hyperandro-genic patients.
Finally, because ovulation may nor-malize many reproductive variables, weused analysis of covariance to rule out asignificant impact of the presence or ab-sence of oligomenorrhea on the differ-ences in hormone analyses describedabove. None of these differences were in-fluenced by oligomenorrhea (data notshown).
Our present results demonstrate thathyperandrogenic type 1 diabetic womenhave increased serum levels of total andfree testosterone and D4-androstenedionecomparable with those found in nondia-betic hyperandrogenic women. Consider-ing that hyperandrogenic type 1 diabeticwomen had normal dehydroepiandros-terone-sulfate concentrations and thatthe increase in ACTH-stimulated D4-androstenedione levels found in thesepatients possibly reflects a normal adre-
L E T T E R S
DIABETES CARE, VOLUME 24, NUMBER 7, JULY 2001 1297

nocortical response taking place in addi-tion to an increased basal secretion ofthis steroid (the net increment of D4-androstenedione was not different com-pared with that of healthy controlsubjects), a significant contribution ofthe adrenal gland to the androgen excessof these patients is not supported byour present results. Nevertheless, becauseof the small sample size, we cannot ex-clude that lack of statistically significantdifferences in dehydroepiandrosterone-sulfate concentrations and in the net in-crement of D4-androstenedione afterACTH-stimulation could reflect a type IIerror.
Virdis et al. (4) recently reportedfunctional ovarian hyperandrogenism(defined by an exaggerated response of17-hydroxyprogesterone to the gonado-tropin-releasing hormone analog leu-prolide) in five of nine type 1 diabetic
adolescents with oligomenorrhea, whichis in conceptual agreement with the mainovarian source for androgen excess intype 1 diabetic patients suggested by ourpresent results.
Surprisingly, serum sex hormone–binding globulin levels were normal inhyperandrogenic type 1 diabetic patients.The regulation of serum sex hormone–binding globulin levels depends on theinhibitory influence of insulin and andro-gens and the stimulatory effect of estro-gens (5). The hyperinsulinism resultingfrom insulin resistance together with in-creased androgen levels explains the de-crease in sex hormone–binding globulinlevels found in most nondiabetic hy-perandrogenic patients (5). On the con-trary, as stated above, sex hormone–binding globulin levels were normal inhyperandrogenic type 1 diabetic women.
Sex hormone–binding globulin con-
centrations are mainly regulated by portalvein insulin concentrations (6). However,in type 1 diabetes, insulin is administeredsubcutaneously instead of being releaseddirectly to the portal circulation, as ininsulin-resistant patients.
This difference may help to explainthe normal sex hormone–binding globu-lin levels in hyperandrogenic type 1 dia-betic patients. In addition to amelioratingthe increase in free testosterone levels, anormal sex hormone–binding globulinconcentration may decrease the tissueavailability of circulating testosterone.This mechanism might contribute to thelower hirsutism scores found in hyper-androgenic type 1 diabetic women com-pared with nondiabetic hyperandrogenicpatients, despite similar serum total tes-tosterone concentrations in both groups.
In summary, our present results sug-gest that the ovary is the main source ofandrogen excess in hyperandrogenic type1 diabetic patients. The normal serum sexhormone–binding globulin levels foundin hyperandrogenic type 1 diabetic pa-tients might partially protect these patientsagainst androgen excess by reducing thedelivery of androgens to tissues.
BELEN ROLDAN, MD, PHD
HECTOR F. ESCOBAR-MORREALE, MD, PHD
RAQUEL BARRIO, MD, PHD
HERMENEGILDO DE LA CALLE, MD
MILAGROS ALONSO, MD, PHD
RAFAEL GARCıA-ROBLES, MD, PHD
JOSE SANCHO, MD, PHD
From the Departments of Endocrinology and Pedi-atric Endocrinology, Hospital Ramon y Cajal, Ma-drid, Spain.
Address correspondence to Hector F. Escobar-Morreale, MD, PHD, Department of Endocrinology,Hospital Ramon y Cajal, Carretera de Colmenar Km.99100, 28034 Madrid, Spain. E-mail: [email protected].
Acknowledgments— Supported in part byGrant FIS 00/0414 from the Fondo de Inves-tigacion Sanitaria, Ministerio de Sanidad yConsumo, Madrid, Spain.
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
References1. Escobar-Morreale HF, Roldan B, Barrio R,
Alonso M, Sancho J, de la Calle H, Garcia-Robles R: High prevalence of the poly-cystic ovary syndrome and hirsutism inwomen with type 1 diabetes mellitus.
Figure 1—Comparison of the serum androgen and gonadotropin levels among nonhyperandro-genic diabetic women (NHD, n 5 10), hyperandrogenic type 1 diabetic patients (HD, n 5 14),healthy control subjects (C, n 5 13), and nondiabetic hyperandrogenic women (H, n 5 73). Dataare represented as means 6 SEM, and the dot scattergram shows the individual data. The meanvalues of all groups were compared by one-way ANOVA followed by the least-significant differ-ence test for multiple comparisons. Hirsutism score 5 modified Ferriman-Gallwey score; T 5total testosterone; FT 5 calculated free testosterone; SHBG 5 sex hormone–binding globulin;D4-A 5 basal D4-androstenedione; DHEAS 5 dehydroepiandrosterone-sulfate; LH 5 luteinizinghormone; FSH 5 follicle-stimulating hormone;. E2 5 estradiol. *P , 0.05 vs. nonhyperandro-genic type 1 diabetic women and healthy control subjects; †P , 0.05 vs. hyperandrogenic andnonhyperandrogenic type 1 diabetic patients and healthy control subjects; ‡P , 0.05 vs. healthycontrol subjects.
Letters
1298 DIABETES CARE, VOLUME 24, NUMBER 7, JULY 2001

J Clin Endocrinol Metab 85:4182–4187,2000
2. Asuncion M, Calvo RM, San Millan JL,Sancho J, Avila S, Escobar-Morreale HF:A prospective study of the prevalence ofthe polycystic ovary syndrome in unse-lected Caucasian women from Spain.J Clin Endocrinol Metab 85:2434 –2438,2000
3. Escobar-Morreale HF, Serrano-Gotarre-dona J, Varela C, Garcıa-Robles R, SanchoJM: Circulating leptin concentrations inwomen with hirsutism. Fertil Steril 68:898–906, 1997
4. Virdis R, Zampolli M, Street ME, VanelliM, Potau N, Terzi C, Ghizzoni L, Ibanez L:Ovarian 17 alpha-hydroxyprogesteroneresponses to GnRH analog testing in oli-gomenorrheic insulin-dependent diabeticadolescents. Eur J Endocrinol 136:624–629, 1997
5. Pugeat M, Crave JC, Tourniaire J, ForestMG: Clinical utility of sex hormone-bind-ing globulin measurement. Horm Res 45:148–155, 1996
6. Yki-Jarvinen H, Makimattila S, UtriainenT, Rutanen EM: Portal insulin concentra-tions rather than insulin sensitivity regu-late serum sex hormone-binding globulinand insulin-like growth factor bindingprotein 1 in vivo. J Clin Endocrinol Metab80:3227–3232, 1995
The Use ofContinuous InsulinDelivery Systems inSeverely Insulin-Resistant Patients
Obese type 2 diabetic patients withsevere insulin resistance tend to de-velop chronic hyperglycemia, de-
spite maximal treatment with diet,physical exercise, and oral hypoglycemicagents. Insulin therapy in these patientsusually does not lead to satisfactory glu-cose control, even when the insulin dos-age is very high. High doses of insulin alsocause weight to increase, which aggra-vates insulin resistance and exacerbatesother cardiovascular risk factors.
Continuous subcutaneous insulin in-fusion (CSII) provided by an insulinpump reduces the incidence of both post-prandial hyperglycemia and severe hypo-glycemia. To determine whether CSII hasa beneficial effect on insulin resistance inobese type 2 diabetic patients with severe
insulin resistance, a trial of CSII was ini-tiated in this group.
A total of 10 severely obese (BMI .30 kg/m2) type 2 diabetic patients withsevere insulin resistance (insulin doseof . 1 U z kg21 z day21) were recruitedfrom a hospital-based practice. Subjectswho qualified for the study had an HbA1c
. 8.5%, despite strict diet and compli-ance with the insulin regimen. After re-ceiving training, patients were started onan insulin pump (Minimed 507) . Bloodglucose levels were monitored with a glu-cometer and patients were instructed tomeasure their blood glucose at least fourtimes a day. Insulin dosage was optimal-ized by the study physician. Weight, in-sulin dose, and HbA1c levels weremeasured at baseline and throughout thestudy.
The patients’ age (mean 6 SD) was59 6 10 years. The duration of the studywas 40 weeks. All subjects in the studyhad a reduction in insulin requirements(in units per kilogram per day) from1.46 6 0.43 (mean 6 SD) at week 0 to1.19 6 0.42 at week 40. Concomitantly,there was a slight decrease in weight (inkilograms), from 95.9 6 13.2 at week 0 to93.4 6 12.7 at week 40. Most signifi-cantly, glycemic control improved, with adecrease in the percentage of HbA1c levelsfrom 12.34 6 1.74 at week 0 to 9.56 60.76 at week 40.
These findings suggest that CSII maybe an effective therapy to reduce insulinresistance in obese type 2 diabetic pa-tients without the deleterious side-effectsassociated with increasing insulin dosage.To further determine the effectiveness ofCSII, the Israeli Diabetes Research Groupis now conducting a randomized clinicaltrial with a cross-over design comparingCSII with intensive multiple-injection in-sulin treatment in this population.
JULIO WAINSTEIN, MD1
MURIEL METZGER, MD2
ISAIAH D. WEXLER, MD, PHD2
JOSEPH COHEN, MD3
ITAMAR RAZ, MD2
From the 1Diabetes Unit, Wolfson Medical Center,Holon; the 2Diabetes Center, Hadassah Ein Kerem,Jerusalem; and the 3Macabbi Health Care Services,Jaffa, Israel.
Address correspondence to Itamar Raz, HadassahUniversity Hospital, P.O. Box 12000, Jersusalem91120, Israel.
Postprandial LeptinResponses After anOral Fat ToleranceTest
Differences in type 2 diabetes
T he finding that circulating leptinconcentrations exhibit a diurnal pat-tern (1,2), with peak nocturnal con-
centrations up to two times higher thannadir levels, raised the hypothesis that theevaluation of fasting leptin levels mighthave underestimated the effect of foodsecretagouges on postpradial leptin regu-lation and action. This variation in diur-nal leptinemia is related to insulinexcursions in response to meals (2), andshifting mealtime by 6.5 h without chang-ing the light and sleep cycles will shiftplasma-leptin rhythm by 5–7 h (3). In arecent study (4), it was reported thatmeals with high fat content result in theproduction of lower 24-h leptin concen-trations compared with meals high in car-bohydrates, a phenomenon attributed tolower insulin excursions after fatty meals.However, the impact of reduced insulinsensitivity on short-term leptin produc-tion in response to meals has not been in-vestigated in subjects with similar degreesof obesity. We hypothesize that patientswith type 2 diabetes (a well-establishedinsulin-resitant state) show lower post-prandial incremental leptin production inresponse to an oral fat tolerance test.
A total of 18 type 2 diabetic male pa-tients and 14 control subjects werematched for age and anthropometric pa-rameters. After a 14-h fast, a test meal of700 kcal/m2 (consisting of 4.75 g protein,24 g carbohydrates, and 65 g fat) (5) wasingested. Blood samples were drawn atfasting and at 2-, 4-, 6-, and 8-h after themeal to determine the levels of glucose,total cholesterol, triglycerides, HDL-C,insulin, and leptin.
Triglycerides increased significantlyfrom baseline only in diabetic patients(P 5 0.001 vs. P 5 0.066, respectively),with peak concentrations attained at 6-h.Postprandial total cholesterol, LDL cho-lesterol, and HDL cholesterol levels didnot differ significantly between groups orfrom levels at fasting. Insulin levels in-creased postprandially in both groups(P 5 0.001 and P 5 0.002), with peak
Letters
DIABETES CARE, VOLUME 24, NUMBER 7, JULY 2001 1299
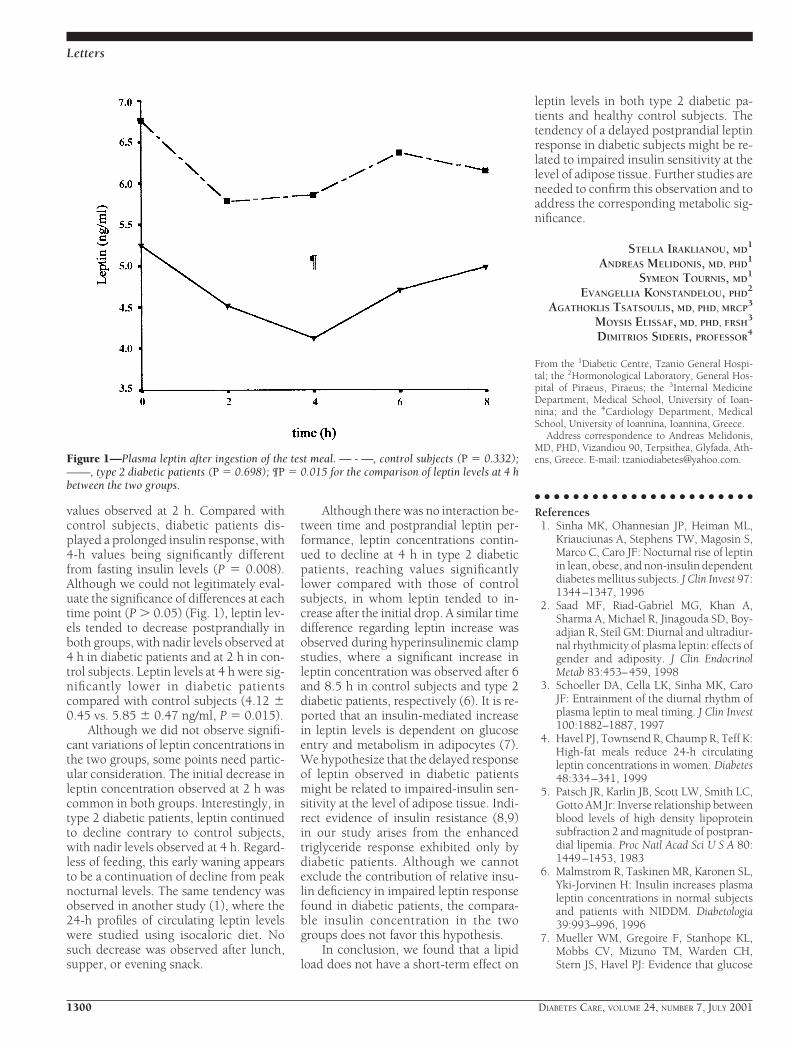
values observed at 2 h. Compared withcontrol subjects, diabetic patients dis-played a prolonged insulin response, with4-h values being significantly differentfrom fasting insulin levels (P 5 0.008).Although we could not legitimately eval-uate the significance of differences at eachtime point (P . 0.05) (Fig. 1), leptin lev-els tended to decrease postprandially inboth groups, with nadir levels observed at4 h in diabetic patients and at 2 h in con-trol subjects. Leptin levels at 4 h were sig-nificantly lower in diabetic patientscompared with control subjects (4.12 60.45 vs. 5.85 6 0.47 ng/ml, P 5 0.015).
Although we did not observe signifi-cant variations of leptin concentrations inthe two groups, some points need partic-ular consideration. The initial decrease inleptin concentration observed at 2 h wascommon in both groups. Interestingly, intype 2 diabetic patients, leptin continuedto decline contrary to control subjects,with nadir levels observed at 4 h. Regard-less of feeding, this early waning appearsto be a continuation of decline from peaknocturnal levels. The same tendency wasobserved in another study (1), where the24-h profiles of circulating leptin levelswere studied using isocaloric diet. Nosuch decrease was observed after lunch,supper, or evening snack.
Although there was no interaction be-tween time and postprandial leptin per-formance, leptin concentrations contin-ued to decline at 4 h in type 2 diabeticpatients, reaching values significantlylower compared with those of controlsubjects, in whom leptin tended to in-crease after the initial drop. A similar timedifference regarding leptin increase wasobserved during hyperinsulinemic clampstudies, where a significant increase inleptin concentration was observed after 6and 8.5 h in control subjects and type 2diabetic patients, respectively (6). It is re-ported that an insulin-mediated increasein leptin levels is dependent on glucoseentry and metabolism in adipocytes (7).We hypothesize that the delayed responseof leptin observed in diabetic patientsmight be related to impaired-insulin sen-sitivity at the level of adipose tissue. Indi-rect evidence of insulin resistance (8,9)in our study arises from the enhancedtriglyceride response exhibited only bydiabetic patients. Although we cannotexclude the contribution of relative insu-lin deficiency in impaired leptin responsefound in diabetic patients, the compara-ble insulin concentration in the twogroups does not favor this hypothesis.
In conclusion, we found that a lipidload does not have a short-term effect on
leptin levels in both type 2 diabetic pa-tients and healthy control subjects. Thetendency of a delayed postprandial leptinresponse in diabetic subjects might be re-lated to impaired insulin sensitivity at thelevel of adipose tissue. Further studies areneeded to confirm this observation and toaddress the corresponding metabolic sig-nificance.
STELLA IRAKLIANOU, MD1
ANDREAS MELIDONIS, MD, PHD1
SYMEON TOURNIS, MD1
EVANGELLIA KONSTANDELOU, PHD2
AGATHOKLIS TSATSOULIS, MD, PHD, MRCP3
MOYSIS ELISSAF, MD, PHD, FRSH3
DIMITRIOS SIDERIS, PROFESSOR4
From the 1Diabetic Centre, Tzanio General Hospi-tal; the 2Hormonological Laboratory, General Hos-pital of Piraeus, Piraeus; the 3Internal MedicineDepartment, Medical School, University of Ioan-nina; and the 4Cardiology Department, MedicalSchool, University of Ioannina, Ioannina, Greece.
Address correspondence to Andreas Melidonis,MD, PHD, Vizandiou 90, Terpsithea, Glyfada, Ath-ens, Greece. E-mail: [email protected].
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
References1. Sinha MK, Ohannesian JP, Heiman ML,
Kriauciunas A, Stephens TW, Magosin S,Marco C, Caro JF: Nocturnal rise of leptinin lean, obese, and non-insulin dependentdiabetes mellitus subjects. J Clin Invest 97:1344–1347, 1996
2. Saad MF, Riad-Gabriel MG, Khan A,Sharma A, Michael R, Jinagouda SD, Boy-adjian R, Steil GM: Diurnal and ultradiur-nal rhythmicity of plasma leptin: effects ofgender and adiposity. J Clin EndocrinolMetab 83:453–459, 1998
3. Schoeller DA, Cella LK, Sinha MK, CaroJF: Entrainment of the diurnal rhythm ofplasma leptin to meal timing. J Clin Invest100:1882–1887, 1997
4. Havel PJ, Townsend R, Chaump R, Teff K:High-fat meals reduce 24-h circulatingleptin concentrations in women. Diabetes48:334–341, 1999
5. Patsch JR, Karlin JB, Scott LW, Smith LC,Gotto AM Jr: Inverse relationship betweenblood levels of high density lipoproteinsubfraction 2 and magnitude of postpran-dial lipemia. Proc Natl Acad Sci U S A 80:1449–1453, 1983
6. Malmstrom R, Taskinen MR, Karonen SL,Yki-Jorvinen H: Insulin increases plasmaleptin concentrations in normal subjectsand patients with NIDDM. Diabetologia39:993–996, 1996
7. Mueller WM, Gregoire F, Stanhope KL,Mobbs CV, Mizuno TM, Warden CH,Stern JS, Havel PJ: Evidence that glucose
Figure 1—Plasma leptin after ingestion of the test meal. — - —, control subjects (P 5 0.332);——, type 2 diabetic patients (P 5 0.698); ¶P 5 0.015 for the comparison of leptin levels at 4 hbetween the two groups.
Letters
1300 DIABETES CARE, VOLUME 24, NUMBER 7, JULY 2001

metabolism regulates leptin secretion fromcultured adipocytes. Endocrinology 139:551–558, 1998
8. Mekki N, Christofilis MA, CharbonnierM, Atlan-Gepner C, Defroot C, Juhel C,Borel P, Portugal H, Pauli AM, Vialettes B,Lairon D: Influence of obesity and bodyfat distribution on postprandial lipemiaand triglyceride-rich lipoproteins in adultwomen. J Clin Endocrinol Metabol 84:184–191, 1999
9. Ida Chen YD, Swami S, Skowronski R,Coulston A, Reaven GM: Differences inpostprandial lipemia between patientswith normal glucose tolerance and noninsulin-dependent diabetes mellitus. J ClinEndocrinol Metabol 76:172–177, 1997
Use of Nicotinic Acidin the Managementof RecurrentHypoglycemicEpisodes in Diabetes
Chronic administration of nicotinicacid (NA) has been shown to cause adeterioration in glycemic control in
diabetic patients (1,2). Acute use of NAinhibits lipolysis in adipose tissue sup-pressing circulating nonesterfied fattyacid (NEFA) levels. Once the effect of NAabates, NEFA levels increase above base-line (3). According to the Randle cyclehypothesis, when NEFA availability in-creases, NEFA oxidation occurs at the ex-pense of glucose oxidation with aresultant reduction in glucose uptake byskeletal muscle and an increase in bloodglucose levels (4).
Some patients with type 1 diabeteshave frequent and often unpredictablehypoglycemic episodes. We hypothe-sized that the addition of regular oral NAto deliberately induce insulin resistanceand increase blood glucose levels wouldresult in an increase in insulin require-ments and reduce the propensity to severehypoglycemia. We report the cases of twopatients with long-standing poorly con-trolled diabetes in whom NA has beenused to decrease the occurrence of hypo-glycemic episodes. Both patients under-stood and agreed to the use of NA in anexperimental fashion.
Case 1A 49-year-old woman with a 30-year his-tory of type 1 diabetes complicated by a
painful peripheral neuropathy and auto-nomic neuropathy (gastroparesis andchronic constipation) reported a long-standing history of erratic blood glucosecontrol and daily hypoglycemic episodesinterspersed with marked hyperglycemia.Her insulin requirments were 30–35 Udaily. Following an addition of 1.25 g NAdaily, insulin requirments increased to70–75 U daily. There was a more predict-able pattern to her glucose levels; the pa-tient felt better and reported a reductionin hypoglycemic episodes to less thanonce a week. After several months, thepatient withdrew from use of NA becauseof recurrent nausea and vomiting. Bloodglucose control again became erratic withmore frequent hypoglycemic episodes.Insulin requirements returned to 30–35U per day. The patient recommencedNA at 1.25 g daily with subsequent im-provement in the rate of hypoglycemicepisodes and an increase in her insulinrequirements.
Case 2A 46-year-old woman with secondary di-abetes resulting from chronic pancreatitisalso suffered from recurring major hypo-glycemic episodes. In addition to havingchronic low back pain and coronary ar-tery disease, she had exocrine pancreaticinsufficiency that required the use of pan-creatic enzymes, and she used methadonefor the management of chronic narcoticdependency. The introduction of NA at1.5 g daily did not change her insulin re-quirements but did cause a reduction inthe reported frequency of major and mi-nor hypoglycemic episodes.
The problems encountered by thesetwo patients occur in a small number ofpatients with long-standing diabetes.Other potential causes of severe recurrenthypoglycemia were excluded, such as hy-pothyroidism, adrenal insufficiency, andceliac disease. Attempts to regulate bloodglucose control through strict control ofdiet, physical activity, and changes to in-sulin regimens (including the use of lisproinsulin and a return to bovine insulin) allfailed to provide relief from symptoms.Both patients benefited from a reducedrate of hypoglycemia, and in the firstpatient there was an increase in insulinrequirements. The malabsorption syn-drome in the second patient may havehad an impact on her response to thetreatment.
We feel that NA therapy as a preven-
tative treatment of recurrent hypoglyce-mia warrants further investigation in alarger group of patients with a formal ran-domized controlled trial.
FADIL HANNAN, MBBS
PETER DAVOREN, FRACP
Address correspondence to Dr P. Davoren, GoldCoastHospital,108NerangSt.,Southport4215,Aus-tralia. E-mail: [email protected].
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
References1. Molnar GD, Berge KG, Rosevear JW,
McGuckin WF, Achor RP: The effect ofnicotinic acid in diabetes mellitus. Metab-olism 13:181–189, 1964
2. Garg A, Grundy SM: Nicotinic acid astherapy for dyslipidemia in non-insulin-dependent diabetes mellitus. JAMA 264:723–726, 1990
3. Fuccella LM, Goldaniga G, Lovisco P,Maggi E, Musatti L, Mandelli V, SirtoriCR: Inhibition of lipolysis by nicotinicacid and acipimox. Clin Pharmacol Ther28:790–795, 1980
4. Randle PJ, Garland PB, Hales CN, News-holme EA: The glucose fatty acid cycle.Lancet 1:785–789, 1963
Metabolic ControlMatters: Why Is theMessage Lost in theTranslation?
The need for realistic goal-setting indiabetes care
The scientific evidence is clear: meta-bolic control matters. The questionis, why doesn’t this message per-
suade most patients? In this letter, we ad-dress one important consideration: goal-setting and its role in promotingbehavioral change and improved glyce-mic control.
The conclusive evidence from the Diabe-tes Control and Complications Trial(DCCT) (1) and the U.K. Prospective Di-abetes Study (UKPDS) (2) that estab-lished causality between glycemic controland the microvascular complications ofdiabetes has highlighted the importanceof the glycohemoglobin level as a criticalpredictor of future health. Inevitably, the
Letters
DIABETES CARE, VOLUME 24, NUMBER 7, JULY 2001 1301

focus of diabetes care and the interactionbetween the patient and clinician has in-creasingly become directed around self-monitoring of blood glucose (SMBG)records and glycosylated hemoglobinmeasurements (3). However, despite thisevidence for the efficacy of tight glycemiccontrol, as pointed out in a recent articlein Diabetes Care by Narayan et al. (4),translation of these goals into clinicalpractice has generally been unsuccessful.
The Clinical Practice Recommenda-tions of the American Diabetes Associa-tion (ADA) suggest a treatment HbA1cstandard of ,7% and a blood glucoseself-measurement target of 80–120 mg/dlbefore meals and of 100–140 mg/dl atbedtime in patients who do not have se-vere or unrecognized hypoglycemia (5).These targets are similar to those recom-mended by the American Association ofClinical Endocrinologists (6). For the pa-tient in the earlier pathogenic stages oftype 2 diabetes who has residual b-cellfunction and is focused on exercise andfollowing a diet, these can be attainableand realistic goals (2). However, even themost conscientious type 1 diabetic patientusing a complex regimen of multiple in-jections or the insulin pump can face afrustrating battle in trying to keep theirdaily blood glucose fluctuations in theprescribed “idealized” target ranges. Forthe vast majority of patients, especiallythose with type 1 diabetes, these “stan-dards” are unattainable “goals.” The medianHbA1c levels achieved by the intensivetreatment cohort in the DCCT were high-er than the currently recommended targetgoals. Furthermore, annual capillaryblood glucose measurements drawn fromthis group also exceeded these targets:postbreakfast measurements were highestat 195 6 50 mg/dl, and the calculated meanblood glucose level for this intensivelytreated group was 155 6 30 mg/dl (7).
As evidence from clinical trials (suchas the DCCT and the UKPDS) have clari-fied the impact of risk factors on the prob-ability of developing long-term diabetescomplications, recommended clinicalstandards, often inappropriately de-scribed as “treatment goals,” have beenspecified. As a first step in discussing“goal- setting in diabetes care,” we want tosharpen the distinction between stan-dards and goals, terms often used inter-changeably.
One of the first steps in clarifying thegoal-setting process with our patients is
differentiating and reconciling recom-mended clinical treatment standards andthe patient’s own personal goals. Whydoes the scientific evidence about the im-portance of metabolic control not per-suade most patients? We propose that thecurrent practice of imposing recom-mended standards, without first workingwith the patient to incorporate their per-sonal goals, undermines patient motiva-tion and engagement in treatment and thussabotages “the message” that metaboliccontrol matters. As the originators (8) ofthe “empowerment paradigm” have em-phasized, mutual frustration frequentlydevelops between patient and clinicianwhen externally recommended standardsare imposed on patients with diabetes.
In addition to distinguishing stan-dards from goals, we want to clarify twofundamental assumptions about the useof insulin replacement therapy in type 1diabetes and the more advanced patho-genic stages of type 2 diabetes with severe-ly compromised b-cell function. First, fromour perspective, despite tremendous re-cent technological innovations, the cur-rent tools for managing diabetes withexogenous insulin are imperfect. Second,blood glucose levels are not under theexclusivecontrolofpatientbehaviors.Tak-en together, these two assumptions pre-clude the achievement of consistently idealblood glucose control, even in the mostmotivated and conscientious patient withtype1diabetesor themoreadvancedpath-ogenic stages of type 2 diabetes (9,10).
An exclusive focus on clinical treat-ment standards within diabetes createsa vulnerability to perfectionism in bothpatients and clinicians. We know frombehavioral science research that perfec-tionism is frequently associated with se-vere behavior and mood disorders (11).Therefore, in the context of diabetes man-agement, the price of perfectionism isdangerously high. Yet this does not meanpromoting unhealthy glycemic goals.Rather, with respect to biological goals, itmeans we must encourage patients tomonitor their own personal progress interms of individual movement toward im-proved blood glucose levels, rather thanin terms of ideal and often unrealistic clin-ical standards. Changing behavior doesnot necessarily result in a commensurateimprovement in biological goals. How-ever, behavior change is the only goal re-alistically in reach of the patient, andkeeping this distinction between behav-
ioral and biological goals in focus is a keyelement in fostering engagement of thepatient in their self care. When concertedpatient motivation and behavior changedoes not result in the expected biological(glycemic) change, clinicians need to helppatients problem-solve the situation andencourage and reinforce them in their ef-forts in striving toward improvement.
Having standardized glycosylated he-moglobin treatment targets is importantfor disease management programs andserves a useful role as trigger points toprompt clinicians to action. As profes-sionals, we must strive for the ideal, andin view of the compelling evidence of theDCCT and UKPDS, we must have in ourminds the ideal HbA1c level of ,7% (oreven lower). But translating this ideal intoreality in the care of the individual withdiabetes is complex. For the individualpatient, SMBG and HbA1c levels are morethan just objective measures of glycemiccontrol; they translate into a judgment oftheir performance, competence, and self-worth. By setting goals for the individualpatient that are too ambitious and thatoverlook the complex difficulties of man-aging diabetes and the realities of life, wemay end up tripping up our best inten-tions; too often the patient will try, fail,and then disengage.
The ultimate goal in diabetes care (assupported by the scientific evidence andoutlined in the ADA guidelines) should betight glycemic control. However, in trans-lating these targets into clinical practice(4), it is important to recognize the criticalrole that goals can play in the complexprocess of promoting behavioral changein the patient, thus highlighting the needfor incorporating the concept of individ-ualized realistic goal setting into the ac-cepted standards of diabetes care.
HOWARD A. WOLPERT, MD1
BARBARA J. ANDERSON, PHD2
From the 1Section of Adult Diabetes and the 2Behav-ioral Research and Mental Health Unit, Joslin Dia-betes Center, Boston, Massachusetts.
Address correspondence to Dr. Howard A. Wol-pert, Joslin Diabetes Center, One Joslin Place, Bos-ton, MA 02215. E-mail: [email protected].
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
References1. The Diabetes Control and Complications
Trial Research Group: The effect of inten-sive treatment of diabetes on the develop-ment and progression of long-term com-
Letters
1302 DIABETES CARE, VOLUME 24, NUMBER 7, JULY 2001

plications in insulin-dependent diabetesmellitus. N Engl J Med 329:977–986, 1993
2. U.K. Prospective Diabetes Study (UKPDS)Group: Intensive blood-glucose controlwith sulphonylureas or insulin comparedwith conventional treatment and risk ofcomplications in patients with type 2 di-abetes (UKPDS 33). Lancet 354:837–853,1998
3. Butler C, Peters J, Stott N: Glycated hemo-globin and metabolic control of diabetes:external versus locally established clinicaltargets for primary care. BMJ 310:784–788, 1995
4. Narayan KMV, Gregg EW, Engelbau MM,Moore B, Thompson TJ, WilliamsonDE, Vinicor F: Translation research forchronic disease: the case of diabetes. Dia-betes Care 23:1794–1798, 2000
5. American Diabetes Association: Standardsof medical care for patients with diabetesmellitus (Position Statement). Diabetes Care24 (Suppl. 1):S33–S43, 2001
6. American Association of Clinical Endo-crinologists: AACE Medical Guidelines forClinical Practice. Jacksonville, Fl, AACE,2000
7. Diabetes Control and Complications TrialResearch Group: Implementation of treat-ment protocols in the diabetes controland complications trial. Diabetes Care 18:361–376, 1995
8. Anderson RM, Funnell M: The Art of Em-powerment: Stories and Strategies for Diabe-tes Educators. Alexandria, VA, AmericanDiabetes Association, 2000
9. American Diabetes Association: Implica-tions of the diabetes control and compli-cations trial (Position Statement). DiabetesCare 24 (Suppl. 1):S25–S27, 2001
10. American Diabetes Association: Implica-tions of the United Kingdom ProspectiveDiabetes Study (Position Statement). Dia-betes Care 24 (Suppl. 1): S28–S32, 2001
11. Burns DD: The Feeling Good Handbook.New York, Plume, 1990
High Incidence ofMaternalTransmission ofDiabetes in ObeseUruguayan Children
M etabolic experiences in utero, asreflected by a high amniotic fluidinsulin concentration, may condi-
tion diabetes-associated risk factors suchas high BMI (1).
As part of our survey (performed be-tween June and September 2000) of over-weight and obese Uruguayan children(age 9–12 years) and the contributing fac-
tors of their condition, we evaluated theincidence of maternal transmission of di-abetes.
The cross-sectional survey comprised886 children (452 boys and 434 girls),living in Montevideo, Uruguay, and othercities in Uruguay with .10,000 inhabit-ants, who were interviewed at home in thepresence of at least one parent. The sam-ple was stratified, aleatory, polyetapic, andsystematic according to the last nationalsurvey (2) and represented an urban pop-ulation (total 3,200,000: 91% living in ur-ban zone, 88% Caucasian, 8% crossbred,and 4% black). The children were weighedand measured in light clothes and withoutshoes using equal balances and scales. BMIwas calculated according to tables (3) forage and sex. Three subgroups were estab-lished: normal weight (NW) (BMI # 85thpercentile), overweight (OW) (BMI 85thto 94.9th percentiles), and obese (OB)(BMI $ 95th percentile). Incidence of an-tecedent diabetes was inquired and re-corded for both the mother and father.
A total of 17% of the children wereclassified as OW and 9% as OB. No dif-ferences in BMI were found between sexesat the age interval studied. All of themothers in the OB group had type 2 dia-betes, 1% of the mothers in the NW andOW groups had type 1 diabetes, and nodifferences were found between diabeticand nondiabetic fathers. This maternaltransmission of type 2 diabetes was ad-dressed in a recent study (4).
These are the first data regarding Uru-guayan children that emphasize the sig-nificance of intrauterine environmentwith respect to exceeding transmissionobesity and insulin resistance (a predia-betic condition). Recent reports have sug-gested that early consequences of anadverse in utero environment do not seemto be attenuating with time (5). Consider-ing the vertiginous increase in type 2 dia-betes among adolescents (6) and thepivotal role that obesity plays in the dis-ease (7), we feel these data are very im-portant for the prevention of type 2diabetes in our clinical practice.
RAUL PISABARRO, MD
ALICIA RECALDE, MD
YENICA CHAFTARE, MD
From the Department of Endocrinology, College ofMedicine, Montevideo, Uruguay.
Address correspondence to Dr. Raul Pisabarro,Universidad de la Republica Domingo Cullen 693,
Montevideo, CP 11300, Uruguay. E-mail:[email protected].
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
References1. Vohr BR, McGarvey ST, Tucker R: Effects
of maternal gestational diabetes on off-spring adiposity at 4–7 years of age. Dia-betes Care 22:1284–1291, 1999
2. Seventh General Uruguayan Population Sur-vey. Montevideo, Uruguay, National De-partment of Statistics and Surveys, 1996
3. Must A, Dallal GE, Dietz WH: Referencedata for obesity: 85th and 95th percentilesof body mass index (wt/ht2) and tricepsskinfold thickness. Am J Clin Nutr 53:839–846, 1991
4. Karter AJ, Rowell SE, Ackerson LM;Mitchell BD, Ferrara A, Selby JV, NewmanB: Excess maternal transmission of type 2diabetes: the Northern California KaiserPermanente Diabetes Registry. DiabetesCare 22:938–943, 1999
5. Lindsay RS, Hanson RL, Bennett PH,Knowler WC: Secular trends in birthweight, BMI, and diabetes in the offspringof diabetic mothers. Diabetes Care 23:1249–1254, 2000
6. Rosenbloom AL, Joe JR, Young RS, WinterWE: Emerging epidemic of type 2 diabe-tes in youth. Diabetes Care 22:345–354,1999
7. Colditz GA, Willett WC, Rotnitzky A,Manson JE: Weight gain as a risk factor forclinical diabetes mellitus in women. AnnIntern Med 122:481–486, 1995
Risky Delay ofHypoglycemiaDetection byGlucose Monitoringat the Arm
S everal devices for self-monitoring ofblood glucose (SMBG) (e.g., AtLast,Amira; OneTouch Ultra, LifeScan;
FreeStyle, TheraSense, Alameda, CA;G lucome te r -E l i t e XL1Mic ro l e t -Vaculance, Bayer; and Sof-Tact, Abbott)recently received Food and Drug Admin-istration approval for alternative sitemonitoring of capillary blood glucose.These alternatives are marketed with con-siderable efforts under the assumptionthat capillary blood glucose measure-ments, e.g., those taken at the forearm, donot differ from the results obtained byclassic finger pricking. Diabetic patientsusing different devices for SMBG reported
Letters
DIABETES CARE, VOLUME 24, NUMBER 7, JULY 2001 1303

discrepancies between clinical symptomsof hypoglycemia and normoglycemicSMBG values at the forearm. Neither stan-dardized quality control assessments oftechnical performance of such SMBG de-vices (1,2) nor patient device handlingresulted in any obvious explanation of thereported discrepancies. Because of this,we examined whether or not fast blood glu-cose changes over a larger range of bloodglucose concentrations could result inclinically relevant blood glucose differ-ences between forearm and fingertip.
Capillary blood glucose samples weretaken from the fingertip and the forearmof six male type 1 diabetic patients on in-tensified insulin treatment (age 26–54years, diabetes duration 0.1–25 years) us-ing the FreeStyle system (TheraSense) be-cause it required the smallest bloodglucose amount: 0.3 ml/sample. To avoidany disturbance of the normal regionalblood flow, the forearm skin was notrubbed before blood glucose sampling, asrecommended by the manufacturer. Thefollowing protocol was applied: after anovernight fast the usual prebreakfast in-sulin was omitted and the breakfast wasreplaced by oral Dextro O.G.T. (Roche,Mannheim, Germany), equivalent to 75 gglucose, in order to achieve blood glucosevalues of 300–400 mg/dl. Then the pa-tient’s usual short-acting insulin wasgiven intravenously at an individualdose (6 –15 U/injection). The blood glu-
cose decrease was followed every 5–15min until either steady state or hypoglyce-mia (,60 mg/dl) was reached. Hypogly-cemia was compensated by oral glucose.For control purposes, additional bloodglucose samples from the fingertip wereanalyzed by the Gluco-quant method(Roche, Mannheim, Germany).
The capillary blood glucose decrease(mean 6 SD) at the forearm (208 6 38mg/dl) was significantly smaller than atthe fingertip (295 6 16 mg/dl) (Student’spaired t test: P , 0.01) within 111 6 26min for all patients. An example is shownin Fig. 1. For the two patients with hypo-glycemic unawareness, the first asymp-tomatic hypoglycemic values at thefingertip (51 and 53 mg/dl) were accom-panied by normoglycemic values at theforearm (142 and 159 mg/dl). Comparedwith the fingertip, it took an additional27–34 min until the capillary blood glu-cose levels at the forearm reached hypo-glycemic values.
Despite the preliminary state of ourinvestigation, the consistency of clinicallyrelevant delays of blood glucose changesat the forearm prompted us to draw atten-tion to a potentially very dangerous situ-ation. Our results raise the possibility thatthe delayed glucose concentrationchanges at the forearm occur physiologi-cally. To our knowledge, this has not beenfully recognized as a potential problem by
the certifying administrations in the U.S.or Europe.
Even a few delays of hypoglycemiadetection could unnecessarily endangerthe life of diabetic patients. Because ofthis, we strongly recommend providingsufficient evidence that the suggested useof SMBG at the forearm and other alter-native sites does not result in a risky delayof hypoglycemia detection. Meanwhile,SMBG at the forearm should only be usedwhen ongoing fast blood glucose changescan be excluded.
KARSTEN JUNGHEIM
THEODOR KOSCHINSKY, MD
From the Clinical Department, German Diabetes Re-search Institute, Heinrich-Heine University of Dues-seldorf, Duesseldorf, Germany.
Address correspondence to Theodor Koschinsky,MD, Auf’m Hennekamp 65, D-40225 Duesseldorf,Germany. E-mail: [email protected].
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
References1. Koschinsky T, Dannehl K, Gries FA: New
approach to technical and clinical evalua-tion of devices for self-monitoring of bloodglucose. Diabetes Care 11:619–629, 1988
2. Koschinsky T, Heidkamp P, Vogt H: Free-Style: technical evaluation of a new bloodglucose meter for off-finger testing (Ab-stract). Diabetes 49 (Suppl. 1):A114, 2000
COMMENTS ANDRESPONSES
Response toJungheim andKoschinsky
Glucose monitoring at the arm
In this issue of Diabetes Care, we readwith interest the letter of Jungheim andKoschinsky (1) comparing glucose
measurements using blood extractedfrom the finger versus blood extractedfrom the forearm. The phenomenon theydiscuss is not a simple function of mea-surement technology, but a complexfunction of circulatory physiology. Ourcognizance and study of the phenomenonresulted in the explicit instruction to theusers of the TheraSense FreeStyle blood
Figure 1—Effect of a fast blood glucose decrease (3 mg z dl21 z min) on capillary blood glucosevalues at the fingertip (F) and at the forearm (E) using the FreeStyle system in a type 1 diabeticpatient. Control blood glucose values from the fingertip measured at the laboratory are indicated(‚).
Letters
1304 DIABETES CARE, VOLUME 24, NUMBER 7, JULY 2001
glucose monitoring system to rub the testsite before drawing blood. The increasedperfusion from rubbing significantly re-duces the difference in fingertip and fore-arm blood glucose measurements (seediscussion below). It is significant thatJungheim and Koschinsky did not rub thetest site. In addition, their protocol, whichinvolved a glucose tolerance test followedby intravenous insulin, created physio-logical extremes and influenced the ob-served differences in study subjects.
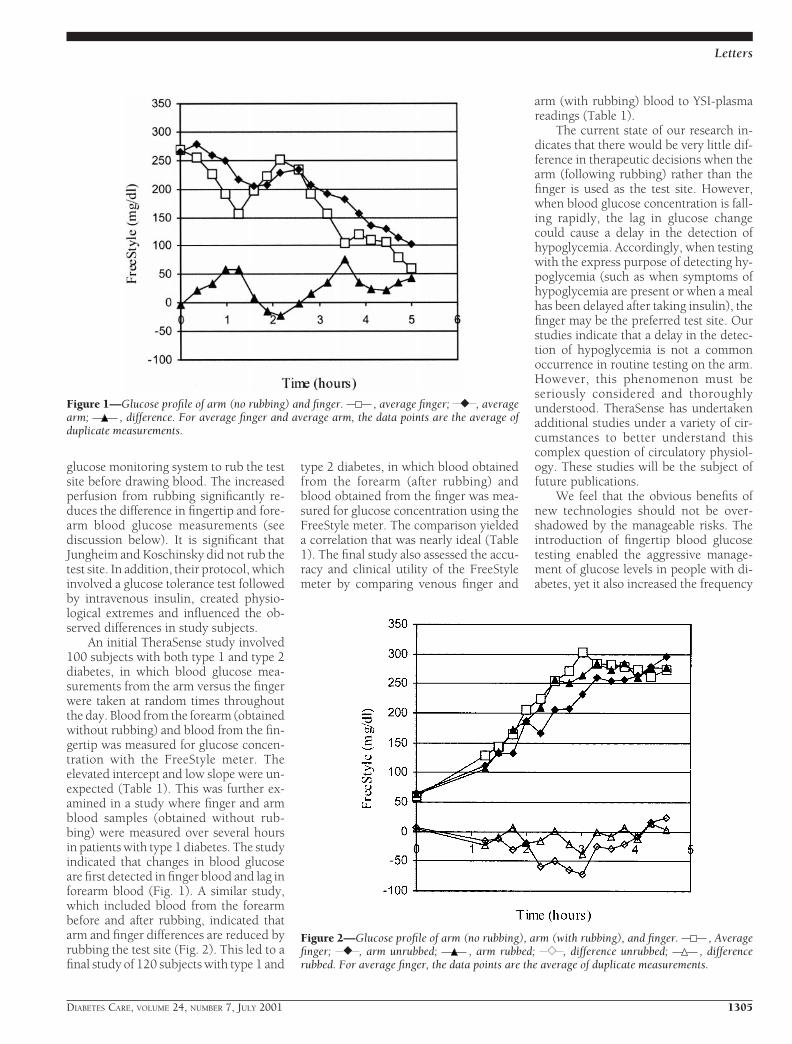
An initial TheraSense study involved100 subjects with both type 1 and type 2diabetes, in which blood glucose mea-surements from the arm versus the fingerwere taken at random times throughoutthe day. Blood from the forearm (obtainedwithout rubbing) and blood from the fin-gertip was measured for glucose concen-tration with the FreeStyle meter. Theelevated intercept and low slope were un-expected (Table 1). This was further ex-amined in a study where finger and armblood samples (obtained without rub-bing) were measured over several hoursin patients with type 1 diabetes. The studyindicated that changes in blood glucoseare first detected in finger blood and lag inforearm blood (Fig. 1). A similar study,which included blood from the forearmbefore and after rubbing, indicated thatarm and finger differences are reduced byrubbing the test site (Fig. 2). This led to afinal study of 120 subjects with type 1 and
type 2 diabetes, in which blood obtainedfrom the forearm (after rubbing) andblood obtained from the finger was mea-sured for glucose concentration using theFreeStyle meter. The comparison yieldeda correlation that was nearly ideal (Table1). The final study also assessed the accu-racy and clinical utility of the FreeStylemeter by comparing venous finger and
arm (with rubbing) blood to YSI-plasmareadings (Table 1).
The current state of our research in-dicates that there would be very little dif-ference in therapeutic decisions when thearm (following rubbing) rather than thefinger is used as the test site. However,when blood glucose concentration is fall-ing rapidly, the lag in glucose changecould cause a delay in the detection ofhypoglycemia. Accordingly, when testingwith the express purpose of detecting hy-poglycemia (such as when symptoms ofhypoglycemia are present or when a mealhas been delayed after taking insulin), thefinger may be the preferred test site. Ourstudies indicate that a delay in the detec-tion of hypoglycemia is not a commonoccurrence in routine testing on the arm.However, this phenomenon must beseriously considered and thoroughlyunderstood. TheraSense has undertakenadditional studies under a variety of cir-cumstances to better understand thiscomplex question of circulatory physiol-ogy. These studies will be the subject offuture publications.
We feel that the obvious benefits ofnew technologies should not be over-shadowed by the manageable risks. Theintroduction of fingertip blood glucosetesting enabled the aggressive manage-ment of glucose levels in people with di-abetes, yet it also increased the frequency
Figure 1—Glucose profile of arm (no rubbing) and finger. , average finger; } , averagearm; , difference. For average finger and average arm, the data points are the average ofduplicate measurements.
Figure 2—Glucose profile of arm (no rubbing), arm (with rubbing), and finger. , Averagefinger; } , arm unrubbed; , arm rubbed; { , difference unrubbed; , differencerubbed. For average finger, the data points are the average of duplicate measurements.
Letters
DIABETES CARE, VOLUME 24, NUMBER 7, JULY 2001 1305

of hypoglycemic events. Clearly, the ben-efits of intensive insulin therapy out-weighed the risks of hypoglycemia.Similarly, greatly reducing the pain asso-ciated with blood glucose testing by per-mitting testing on the forearm and othersites is likely to have a significant positiveimpact on compliance with monitoringregimens.
GEOFF MCGARRAUGH
From TheraSense, Alameda, California.Address correspondence to Geoff McGarraugh,
TheraSense Inc. 1360 South Loop Rd., Alameda, CA94502. E-mail: [email protected].
G.M. is employed by and holds stock in Thera-Sense, which manufacturers and markets the Free-Style blood glucose monitoring system.
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
Reference1. Koschinsky T, Jungheim K: Risky delay of
hypoglycemia detection by glucose mon-itoring at the arm. Diabetes Care 24:1303–1304, 2001
How Cost–Effective Isthe Treatment ofDyslipidemia inPatients WithDiabetes but WithoutCardiovascularDisease?
A response to Grover et al.
In the January 2001 issue of DiabetesCare, Grover et al. (1) reported on thecost-effectiveness of dyslipidemia
treatment in patients with diabetes butwithout cardiovascular disease. Althoughthe article was interesting and relevant, fur-
ther review of the assumptions of the study’sMarkov model raise several questions.
First, in the cost-effectiveness model,the choice of years of life saved (YOLS)rather than quality-adjusted life years(QALYs) is debatable. Diabetes is knownto have a significant effect on morbidity,mortality, and quality of life. In addition,other aspects of diabetes (including car-diovascular disease) are known to influ-ence the quality of life of people withdiabetes. Therefore, the use of YOLS as ameasure of effectiveness may be simplisticand insufficient as an outcome measurebecause it usually counts as less than onefull QALY (2). What effect would the useof QALYs have had on the study resultsand conclusions?
Second, the assumptions that lipidlevels and the effectiveness of simvastatintherapy were similar to that observed inthe Scandinavian Simvastatin SurvivalStudy trial appear problematic in light ofcurrent evidence. The assumptions in-clude LDL cholesterol of 188 mg/dl (4.87mmol/l) and HDL cholesterol of 46 mg/dl(1.18 mmol/l). Expected effects of simva-statin therapy based on a decrease in LDLcholesterol of 35% and an increase inHDL cholesterol of 8% would be 122mmol/dl (3.15 mmol/l) and 50 mmol/dl(1.29 mmol/l), respectively. However,these targets run contrary to the AmericanDiabetes Association (ADA) practiceguidelines for 2001 (3). The goals of lipidtherapy include LDL cholesterol of #100mmol/dl (#2.60 mmol/l) and HDL cho-lesterol of 45 mg/dl (1.15 mmol/l) and 55mg/dl (1.40 mmol/l) in men and women,respectively.
Very few patients were likely to meetcurrent standards of lipid treatment basedon the assumptions of the study. There-fore, to achieve ADA goals, higher dosesof simvastatin or longer duration of lipid
treatment may be required. The implica-tion is that the cost calculations are likelyto yield higher figures, which may alterthe cost-effectiveness ratios. What effectwould varying the cost calculations toachieve ADA end points have had on thestudy results?
These questions and comments shouldnot undermine the importance of thework of Grover et al. Rather, they are im-portant clinical questions that may needconsideration in future studies on cost-effectiveness, particularly on primary pre-vention of cardiovascular disease inpeople with diabetes.
LEONARD E. EGEDE, MD
From the Department of Medicine, Medical Univer-sity of South Carolina, Charleston, South Carolina.
Address correspondence to Leonard E. EgedeMD, Medical University of South Carolina, Divisionof General Internal Medicine and Geriatrics, Mc-Clennen-Banks Adult Primary Care Clinic (4thFloor), 326 Calhoun St., P.O. Box 250100, Charles-ton, SC 29425. E–mail: [email protected].
Acknowledgments— L.E.E. is a recipient of aCareer Development Award from the Ameri-can Diabetes Association.
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
References1. Grover SA, Coupal L, Zowall H, Alex-
ander CM, Weiss TW, Gomes DRJ: Howcost-effective is the treatment of dyslipi-demia in patients with diabetes but with-out cardiovascular disease? Diabetes Care24:45–50, 2001
2. Gold MR, Patrick DL, Torrance GW, Fry-back DG, Hadorn DC, Kamlet MS,Daniels N, Weinstein MC: Identifying andvaluing outcomes. In Cost-Effectiveness inHealth and Medicine. 1st ed. Gold MR, Sei-gel JE, Russell LB, Weinstein MC, Eds.New York, Oxford University Press, 1996,p. 82–123
3. American Diabetes Association: Stan-dards of medical care for patients with di-abetes mellitus (Position Statement).Diabetes Care 24 (Suppl. 1):S33–S43, 2001
Response to Egede
W e thank Dr. Egede (1) for his let-ter in this issue of Diabetes Careand for taking the time to read
our study (2) and provide us with histhoughtful comments. He raises severalimportant points.
The first point concerns the choice of
Table 1—Linear regression statistics and Clarke Error Grid Analysis
ComparisonIntercept(mg/dl) Slope r
Clarke Error Grid Zones(% of readings in the zone)
A B C D
Arm (no rubbing) vs. finger 19.4 0.913 0.956 NA NA NA NAArm (rubbing) vs. finger 20.5 1.027 0.971 NA NA NA NAVenous vs. venous YSI 7.1 0.923 0.992 99.6 0.4 0 0Finger vs. finger YSI 6.6 0.934 0.982 98.3 1.7 0 0Arm (rubbing) vs. finger YSI 9.0 0.945 0.967 87.7 11.4 0 0.8
NA, not applicable.
Letters
1306 DIABETES CARE, VOLUME 24, NUMBER 7, JULY 2001

years of life saved rather than quality-adjusted life years in the cost-effective-ness analysis. Dr. Egede’s point that bothdiabetes and cardiovascular disease mayhave a significant impact on quality of lifeis well taken. We agree with him that itwould be desirable to include quality-of-life issues in our analyses. We have re-cently completed a study evaluating thequality of life of individuals with andwithout cardiovascular disease, and webelieve this study could provide utilitymeasures suitable for part of the analysis.
Second, in our study, we comparedthe effects of simvastatin therapy for indi-viduals with diabetes or cardiovasculardisease based on the results of the Scan-dinavian Simvastatin Survival Study (4S)trial (3). Dr. Egede argues that the lipidtargets currently recommended by theAmerican Diabetes Association are lowerthan the mean LDL cholesterol levels ob-tained in the 4S study. We note that this isalso true of the lipid targets recom-mended by the American Heart Associa-tion for individuals with cardiovasculardisease. However, the focus of our analy-ses was on the benefits of lipid therapyamong various groups of patients ratherthan on the benefits of following expertguidelines. As a first step, this approachallows for a level playing field so that thebenefits of treatment and treatment aloneare being compared. We also note that thecurrently recommended lipid targets rep-resent levels that are not often achieved incurrent clinical practice. Finally, we areunaware of any data describing the costsof successfully treating groups of individ-uals to a specified target lipid level. With-out such cost data, it is impossible tocalculate the associated cost-effectivenessratios. We chose the 4S study because itprovided the necessary data on statin uti-lization and the largest reductions in LDLcholesterol associated with long-termclinical outcomes.
Third, the availability of results fromthe Heart Protection Study, which is ex-pected later this year, should provide awealth of additional information and fi-nally help to resolve any remaining ques-tions regarding the cost-effectiveness oflipid therapy in diabetic patients withoutcoronary heart disease (4).
Dr. Egede has raised important re-search questions for future analyses. Webelieve that with the availability of resultsfrom ongoing studies, as well as the com-pletion of additional research, the neces-
sary pieces will eventually be available toadequately complete the puzzle.
STEVEN A. GROVER, MD
LOUIS COUPAL, MSC
HANNA ZOWALL, MSC
From the Division of Clinical Epidemiology, theMontreal General Hospital, McGill UniversityHealth Center, Montreal, Quebec, Canada.
Address correspondence to Steven A. Grover,MD, The Montreal General Hospital, McGill Univer-sity Health Center, Division of Clinical Epidemiol-ogy, 1650 Cedar Ave., Montreal, PQ H3G 1A4,Canada. E-mail: [email protected].
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
References1. Egede LE: How cost-effective is the treat-
ment of dyslipidemia in patients withdiabetes but without cardiovascular dis-ease? A response to Grover et al. DiabetesCare 24:1306, 2001
2. Grover SA, Coupal L, Zowall H, Alex-ander CM, Weiss TW, Gomes DRJ: Howcost-effective is the treatment of dyslipi-demia in patients with diabetes but with-out cardiovascular disease? Diabetes Care24:45–50, 2001
3. Haffner SM, Alexander CM, Cook TJ, Boc-cuzzi SJ, Musliner TA, Pedersen TR, Kjek-shus J, Pyorala K: Reduced coronaryevents in simvastatin-treated subjectswith coronary heart disease and diabetesor impaired fasting glucose: subgroupanalyses in the Scandinavian SimvastatinSurvival Study. Arch Intern Med 159:2661–2667, 1999
4. MRC/BHF Heart Protection Study of cho-lesterol-lowering therapy and of antioxi-dant vitamin supplementation in a widerange of patients at increased risk of cor-onary heart disease death: early safety andefficacy experience. Eur Heart J 20:725–741, 1999
PseudonormalDiastolic FillingUnmasked WithGlyceryl Trinitrate inPatients With Type 2Diabetes With PoorMetabolic Control
Poirier et al. (1) report very interest-ing data regarding pseudonormaldiastolic filling in men who are free
of clinical heart disease and have well-controlled diabetes. Specifically, 28% of
their subjects had a pseudonormal fillingpattern, which was detected using a Val-salva maneuver and/or pulmonary ve-nous Doppler (PVD). We conducted asimilar study in 34 high-risk type 2 dia-betic patients (16 men, 18 women) whowere middle-aged (mean age 55.8 years),obese (BMI 30.6 kg/m2), and had poormetabolic control (HbA1c 10.6%, fastingblood glucose 13.4 mmol/l). None of thepatients had a history of heart failure ormyocardial infarction, and we includedpatients with controlled hypertension.The patients underwent echocardiogra-phy methods similar to those used by Poi-rier et al. (1), although preload reductionwas achieved with sublingual glyceryltrinitrate (GTN) (400 mg). PVD was sub-optimal in one-third of the subjects andthus not included in the analysis.
Diastolic filling pattern was assessedat baseline, and 14 (41%) of the subjectshad a normal filling pattern (E-to-A ratio1.0–1.7, deceleration time 0.14–0.23 s);the remainder had an abnormal fillingpattern. However, after administration ofGTN, all of the patients had an abnormalrelaxation pattern; 20 (58.8%) were clas-sified as having abnormal relaxation and14 (41%) as having pseudonormal relax-ation.
A total of six subjects in the abnormalrelaxation group had left ventricular (LV)dilatation (M mode: LV end-diastolicpressure .58 mm). In all but one of thesesubjects, LV size was normal when ad-justed for body surface area (BSA) LVend-diastolic dimension [LVEDD]/BSA,32 mm/m2). All patients had normal LVfunction as assessed by M mode fractionalshortening (.25%) and subjective as-sessment of ejection fraction from the api-cal views. Compared with the abnormalrelaxation group, the pseudonormal fill-ing group was younger (52.6 vs. 58.1years, P 5 0.03) and had lower fastingblood glucose (12.1 vs. 14.3 mmol/l, P 50.03). However, there were no differencesin the levels of HbA1c (10.3 vs. 10.8%,P 5 0.14), duration of diabetes (6.8 vs.7.9 years, P 5 0.48), LV size (LVEDD:50.4 vs. 54.1 mm, P 5 0.16) or LV mass(143.9 vs. 156.6 g, P 5 0.38).
Our group of patients had higherHbA1c levels than those reported byPoirier et al. (1), none displayed a normaldiastolic filling pattern, and 41% dis-played a pseudonormal pattern in the ab-sence of LV dilatation, hypertrophy, orsystolic dysfunction. Our findings sup-
Letters
DIABETES CARE, VOLUME 24, NUMBER 7, JULY 2001 1307

port the conclusions of Poirier et al. (1),highlighting the need for thorough echo-cardiographic evaluation in type 2 diabe-tes and, in particular, assessment of mitralfilling under different loading conditionsfor thorough assessment of LV diastolicfunction.
In our study group, PVD was subop-timal in many subjects and thus may notbe widely applicable in type 2 diabeticpatients. Poirier et al. (1) found that whilepreload reduction always identifiedpseudonormal filling, PVD did not.Pseudonormal filling detected by preloadreduction is related to LV diastolic pres-sure (2) and has been used to differentiatebetween true and pseudonormal fillingpatterns in both disease and healthy con-trol subjects (3,4).
Traditionally, the focus of echocardi-ography has been to assess LV hypertro-phy and systolic function. However, thepresence of diastolic dysfunction in thesetting of normal systolic function and noother structural heart disease may be im-portant for long-term cardiovascularprognosis in diabetes. The pseudonormalgroup may represent a separate subgroupof patients who are at particular risk ofdeveloping a restrictive diabetic cardio-myopathy. A thorough evaluation using alongitudinal study is necessary to mea-sure the natural time course of diastolicfilling changes in diabetes, which wouldrequire the follow-up of a large cohort ofpatients.
GILLIAN A. WHALLEY, MHSC
WARWICK BAGG, FRACP, MB, BCH
ROBERT N. DOUGHTY, MD, MRCP, FRACP
GREG GAMBLE, MSC
GEOFF BRAATVEDT, MD, MRCP, FRACP
NORMAN SHARPE, MD, FRACP, FACC
From the Division of Medicine, Faculty of Medicaland Health Sciences, University of Auckland, Auck-land, New Zealand.
Address correspondence to Gillian A. Whalley,Cardiovascular Research Laboratory, Division ofMedicine, University of Auckland, Private Bag 92019, Auckland, New Zealand. E-mail: [email protected].
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
References1. Poirier P, Bogaty P, Garneau C, Marois L,
Dumensil J: Diastolic dysfunction in nor-motensive men with well-controlled type2 diabetes. Diabetes Care 24:5–10, 2001
2. Dumesnil JG, Gaudreault G, Honos GN,Kingma JG Jr: Use of Valsalva maneuver tounmask left ventricular diastolic functionabnormalities by Doppler echocardiogra-phy in patients with coronary artery dis-ease or systemic hypertension. Am J Car-diol 68:515–519, 1991
3. Brunner-LaRocca HP, Rickli H, Jost CHA,Jenni R: Left ventricular end-diastolicpressure can be estimated by either changesin transmitral inflow pattern during Val-salva maneuver or analysis of pulmonaryvenous flow. J Am Soc Echocardiogr 13:599–607, 2000
4. Hurrell DG, Nishimura RA, Ilstrup DM,Appleton CP: Utility of preload alterationin assessment of left ventricular fillingpressure by Doppler echocardiography: asimultaneous catheterization and Dopp-ler echocardiographic study. J Am CollCardiol 30:459–67, 1997
Response to Whalleyet al.
W e would like to thank Whalley etal. (1) for their letter in this issueof Diabetes Care and for their in-
terest in our work (2). For the most part,the results they describe are in agreementwith the conclusions of our article. How-ever, the authors report a higher inci-
dence of diastolic dysfunction, perhapsbecause their subjects constituted ahigher risk group with poorly controlledtype 2 diabetes. Interestingly, the groupwith a pseudonormal pattern of diastolicdysfunction was younger than the groupwith an abnormal diastolic function (onaverage, 4 years younger than our group).
These results further emphasize theimportance of using preload reducingmaneuvers, such as the Valsalva maneu-ver, to unmask left ventricular diastolicdysfunction in type 2 diabetic subjects.Clearly, erroneous conclusions about car-diac function may be drawn if such ma-neuvers are not used. This must be aconsideration in the design of prospectivefuture studies dealing with type 2 diabeticsubjects. Finally, in our experience, theValsalva maneuver is much easier, morerapid, and more sensitive than the use ofglyceryl trinitrate, particularly when pa-tients remain in the supine position.
PAUL POIRIER, MD, FRCPC, FACC
From the Quebec Heart Institute/Laval Hospital,Sainte-Foy, Quebec, Canada.
Address correspondence to Paul Poirier, MD,FRCPC, FACC, Quebec Heart Institute/Laval Hos-pital, 2725 Chemin Sainte-Foy, Sainte-Foy, Quebec,Canada, G1V 4G5. E-mail: [email protected].
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
References1. Whalley GA, Bagg W, Doughty RN, Gam-
ble G, Braatvedt G, Sharpe N: Pseudo-normal diastolic filling unmasked withglyceryl trinitrate in patients with type 2diabetes with poor metabolic control. Di-abetes Care 24:1307–1308, 2001
2. Poirier P, Bogaty P, Garneau C, Marois L,Dumesnil JG: Diastolic dysfunction innormotensive men with well-controlledtype 2 diabetes. Diabetes Care 24:5–10,2001
ErratumKrampl E, Kametas NA, Nowotny P, Roden M, Nicolaides KH: Glucose metabolism in pregnancy at high altitude, DiabetesCare 24:8172822, 2001
The first sentence of the first full paragraph in the third column of page 818 should read, 0Plasma proinsulin concentrations werebelow the lower limit of detection of 2 pmol/l in 26 pregnant subjects (28.0%) at high altitude and in 3 subjects (2.4%) at sea level.0
Letters
1308 DIABETES CARE, VOLUME 24, NUMBER 7, JULY 2001
Related Documents










![Vaticanism Unmasked [1878]](https://static.cupdf.com/doc/110x72/577cd0ed1a28ab9e7893488a/vaticanism-unmasked-1878.jpg)
